Empowering Your Voice: Signs of Medical Gaslighting as a Cancer Patient
Nadia was repeatedly told, “Nothing was wrong with her.” Amy’s symptoms were consistently attributed to anxiety. Nick was told that he was too physically fit to be sick. Sadly, all three were eventually diagnosed with various types of cancer.
The term “gaslighting” has gained significant popularity in recent years, often used to describe situations where individuals manipulate others into questioning their own reality.
As a cancer patient, you likely trust your doctors and healthcare providers to provide the best care. Unfortunately, some patients experience medical gaslighting, a phenomenon where doctors or healthcare providers downplay a patient’s symptoms or dismiss their concerns.
Medical gaslighting can be devastating for patients and can lead to delayed diagnoses, inadequate treatment, and even death.
Dr. Jennifer Kilkus, Ph.D., ABPP, is a board-certified clinical health psychologist with a special interest in oncology. She is also the owner of Grounded Behavioral Health, an organization with a mission to improve the quality of life of healthcare consumers and providers through evidence-based consultation and intervention.
For a deeper understanding of the topic and how to manage it, we sat down with Dr. Jennifer Kilkus, a board-certified clinical health psychologist and an Assistant Clinical Professor within the Department of Psychiatry at Yale School of Medicine. Specializing in the mental health of oncology patients, she sheds light on gaslighting in the medical field and its impact on cancer patients.
In conversation, she discusses the origins of the term and how medical gaslighting manifests as a dismissal or minimization of cancer patients’ concerns. We explore medical gaslighting in the patient experience, its underlying biases, and the importance of slowing down, listening, and advocating for oneself in the face of dismissive medical encounters.
Medical gaslighting is based on the concept of gaslighting, which originates from the movie Gaslight, where a husband manipulates his wife’s reality to make her doubt her own judgment.
Dr. Kilkus describes medical gaslighting as, “A minimization or a dismissal of people’s concerns. I think there are a lot of different contributors to it, but that’s kind of the general gist of it, is just a dismissal or minimization of what someone’s saying that they’re having an experience within a medical context.”
“I was so angry and resentful while starting treatment that my oncologist continued to gaslight me and ignore all of my cries for help. I felt like a crazy person. I often wonder, what stage would I have been, and would my journey have been different had the doctor believed me.”
To further clarify that medical gaslighting might not necessarily be attributed to malicious behavior, Dr. Kilkus says, “I wouldn’t put so much intent behind it.” She explains that as humans, we all have biases, misunderstandings, and time constraints that may lead to unintentionally gaslighting someone else.
Despite intentions, there are ways to spot medical gaslighting when you’re experiencing it.
Five Signs You’re Experiencing Medical Gaslighting
By understanding the signs of medical gaslighting, you can assert your needs, seek additional opinions, and ensure that you receive the care and respect you deserve. Here are a few situations that might clue you into medical gaslighting.
Chronic pain dismissal: You’re experiencing pain, but your healthcare provider tells you that it’s “all in your head” or that “you’re exaggerating your symptoms.” Dr. Kilkus emphasizes that “people have wisdom about their bodies,” and patients should be persistent if something doesn’t feel right.
“I got an appointment with my primary care. I said, ‘These symptoms aren’t going away. In fact, everything seems to be getting worse. I’m really concerned.’ He said, ‘You don’t look sick. If you had cancer, Amanda, you would be losing weight at a rapid pace. Your face would be sunken in.’ I just couldn’t believe he said that to me.”
Unexplained symptoms dismissal: You’re experiencing symptoms that your healthcare provider cannot explain, but they insist that there’s nothing wrong with you. Dr. Kilkus encourages patients to educate themselves about their condition and seek a second or third opinion if necessary.
Dismissal based on age: You’re experiencing concerning symptoms or pain but your healthcare provider asserts that you are too young to get cancer. “That is a really common thing that I hear is ‘you’re too young to have cancer’,” says Dr. Kilkus. “You’re too young to have this kind of pain. You’re too young to have these kinds of problems. It must be anxiety or it must be X, Y, or Z thing.” She explains that people experience pain at all ages so this phrase is a really big sign. Again, Dr. Kilkus recommends getting a second opinion.
Immediately blaming symptoms on mental health issues: You’re healthcare provider quickly attributes your symptoms to anxiety or stress. “If somebody is having a symptom that is medically concerning to them, of course, they’re going to be anxious about it,” explains Dr. Kilkus. “And it is true that anxiety can exacerbate symptoms or kind of mask what is really going on. But that doesn’t mean, that it shouldn’t be followed up on, because we also know that there are medical conditions that can cause symptoms that look like mental health concerns.”
“When I went back to that doctor for the follow-up, he said to me, ‘Yeah, there’s nothing wrong with you. You must have just had an infection.’ I tried to tell him, ‘No, wait, there’s more I’m concerned about.’ These rashes and things were starting to cause alarms to go off. Anyway, he cut me off, and he said, ‘I can tell that you’re just one of those anxious patients who needs a little more coddling.'”
According to Dr. Kilkus, “One of the things that is fairly common is that women and people of color are more likely to experience medical gaslighting.” She further explains that this is due to societal narratives and stereotypes surrounding how women and people of color present with pain.
Dr. Kilkus highlights the bias that “women might be more anxious and they’re saying they’re in pain, but actually maybe, maybe it’s anxiety and it’s not actually pain.”
She also addresses the harmful stereotype that “people of color have a higher pain threshold than white people.” A 2016 study found that some medical students still think black patients feel less pain than white patients.
Dr. Kilkus emphasizes the need for awareness and self-compassion, stating that “it’s not conscious, it’s sort of unconscious biases that we all hold” and that experiencing medical gaslighting is not exclusive to certain individuals.
“The other thing I want to make sure that people hear is that this doesn’t just happen to women and people of color. It happens to everyone,” explains Dr. Kilkus, “It’s just more likely to happen to those populations or for people who have certain disabilities, people have certain chronic health issues, people who have difficulties with their weight. These are all sort of more vulnerable to medical gaslighting. But it can happen to anybody. It can happen to the most well-educated white male person that there is. It just can.”
“It was a little intense because I feel like I could feel him saying it’s so unlikely that this is colon cancer, especially colon cancer that’s causing you to bleed. But the alarms in my body and my mind were going off. I remember there was a point where it was like, ‘Either put me on the schedule or just call your security and they can escort me out because I need this colonoscopy.’”’ He was like, ‘Whoa, whoa, whoa, Miss. It’s okay. I will give you the colonoscopy.'”
If you find yourself being gaslit in a medical setting, Dr. Kilkus suggests simple ways to get your doctor to listen.
Ask your doctor for documentation: “It’s perfectly okay for you to say, ‘If you’re not going to follow up on this, then I would like you to document that in my medical record,’” says Dr. Kilkus. She explains that it might clue in the doctor that there may be a negative consequence of them not acting on your symptoms. For follow-up, Dr. Kilkus recommends looking at your medical notes to make sure it’s been added.
Keep a diary: “To keep track of symptoms and that could be duration, intensity, and frequency of symptoms,” says Dr. Kilkus “And that way you have that data to provide the physician. So they also know what has changed since the last time you came to them.”
Find a doctor you trust: I’m a huge fan of people finding other physicians if they don’t feel supported because there’s no point if you don’t have a doctor you can trust,” says Dr. Kilkus. “I really feel like that’s a foundational component of health care. And if you don’t have that, then you need to find a way to at least get as close to that as you can.”
Download 5 Tips For Overcoming Medical Gaslighting
One of the most effective ways for cancer patients to protect themselves from medical gaslighting is through self-advocacy. This means being an active participant in your own healthcare, asking questions, and speaking up if you feel like something isn’t right. Dr. Kilkus also recommends reaching out to your community or support network to find doctors who others have connected with.
“You’re not just a number. These doctors have a lot of patients, but you’re a human. You go in there and let them know you’re not a number. You have concerns about your health, and your doctors should be concerned about you..’
A crucial component of self-advocacy is education according to Dr. Kilkus. “The more information that you have, the more seriously you’re taken to in a health care setting,” says Dr. Kilkus. To better understand your rights as a patient, you can explore the Patient Bill of Rights. These also vary from state to state.
In addition to education, taking a compassionate approach can be helpful in your patient journey. “We all share challenges and experiences that we often feel like we’re walking with alone,” says Dr. Kilkus. “And I really feel like the more that these things are voiced, the easier it is for everyone to just slow down and be kind to one another because we’re all suffering. That’s part of being human.”
It’s cancer. How should you be feeling? That’s a complex question without a single answer. Hear from real cancer survivors about how they reacted to their diagnoses...
There’s no clear way to know what is best to say to someone with cancer, but there are some basic guidelines to help make your words and actions matter. Hear what helped and what didn’t from the patients themselves...
If you’ve been diagnosed with cancer and are unsure how to go about telling your friends and family, read stories from real cancer survivors who share their experiences on how they broke the news...
Marriage is wonderful, but a cancer diagnosis can create a disconnect for some couples. Here are three things to keep in mind in order to keep your relationship healthy after a diagnosis...
Scanxiety is the you have about any scans that will update you on your current status as a cancer patient or survivor. Most patients report feeling this particular kind of anxiety at least once. Find out how real cancer patients and survivors cope with scanxiety...
Cancer treatments save lives, but they also come with side effects. Hear straight from patients who’ve been treated for cancer - what they experienced and what helped them get through it...
Cancer affects people of all ages. What can Medicare do for older cancer patients? How is Medicare changing in 2020? Guest writer Danielle K Roberts shares her expertise...
Gifts can be a great way to show your support for a loved one with cancer, but it can be tough to know what to give. Here are gift ideas from real-life cancer survivors - from physical gifts to volunteering your time...
Whether you continue working or take time off during treatment, there are many questions new cancer patients face when it comes to their job. Here's what survivors had to say about dealing with work during chemo, radiation, and more...
Hear how patients facing cancer navigated diagnosis and treatment while balancing their role as a parent. Hear their advice from how to talk to your kids about cancer to when to ask for help with childcare...
Leaving the hospital after a surgery or course of treatment can evoke a variety of emotions. Hear from real cancer patients about how they were feeling when they went home and the support that’s available when you leave the hospital...
It can be hard to stay healthy and in balance when you're going through chemotherapy. Here are some ways you can optimize your eating habits to alleviate some common chemotherapy side effects...
Sometimes the content we need is to read journals from patients and caregivers, themselves. Here’s a list of wonderful blogs by cancer type curated by The Patient Story...
Unlike THC, CBD does not make a person feel “high.” Read on to learn more about CBD, its potential uses for cancer patients, and tips on finding the right product...
Wondering how a yoga or meditation practice can help in cancer treatment? Read the benefits of starting a practice, both for your mental and physical health, and get tips on how to start...
Read real genetic counselors and patients explain how genetic testing works, how it affects treatment and outcomes, and other important information to know...
Choose from over 40 cancer organizations and nonprofits for any cancer type and location Find where to get help for financial, housing, transportation and more...
Leukemia is a cancer of the white blood cells. Lymphoma affects lymphocytes–a type of white blood cell. What are the similarities and differences of leukemia and lymphoma? How are they diagnosed? How are they treated?...
October is Health Literacy Awareness. Health literacy is when the information and health services you need align with your ability to process, understand, and use that information and those services. Why does it matter?...
Medicaid is a federal and state-run program that assists its patients with healthcare costs. Read how updates to the program in many states might make it easier to receive Medicaid coverage for your cancer...
Dr. Babis Andreadis of UCSF shares his approach with patients, the importance of patient self-advocacy, whether to ask for a second opinion, and more on shared treatment decision-making...
Chef Ryan Scott’s Cancer Story You may have seen him compete on Top Chef or on network TV morning shows like The Today Show, but in this special clip, Chef Ryan Scott does more than share a recipe. He shares his own personal colon cancer story, describing how he was just a kid when he...
From egg harvesting to retrieval, making the decision between freezing eggs or embryos, the process of giving herself shots daily, paying for the procedures, and the paperwork that brought up so many unanticipated questions, Kimberly shares every part of this intimate journey...
Mark Lewis, MD, is not just an oncologist, he's a cancer survivor, himself. This gives him a unique perspective as both physician and patient. Hear more about his thoughts on second opinions and importance of self-advocacy...
Read 10 acts of service and emotional support to help a loved one who's been diagnosed with cancer. These are suggestions from real former cancer patients who share what was most helpful for them...
Finding power through the words of other patients can make a world of difference when you're going through cancer treatment. Reader quotes about diagnosis, hair loss, survivorship, and more...
Diarrhea is an unpleasant condition that can be mild and easy to treat, but in rare instances, it can be a sign of cancer. It's also a common side effect for many cancer treatments...
From 1st symptoms of cancer to how we communicate with our doctors, the importance of patients advocating for themselves is key to getting through diagnosis and treatment in the best way possible.
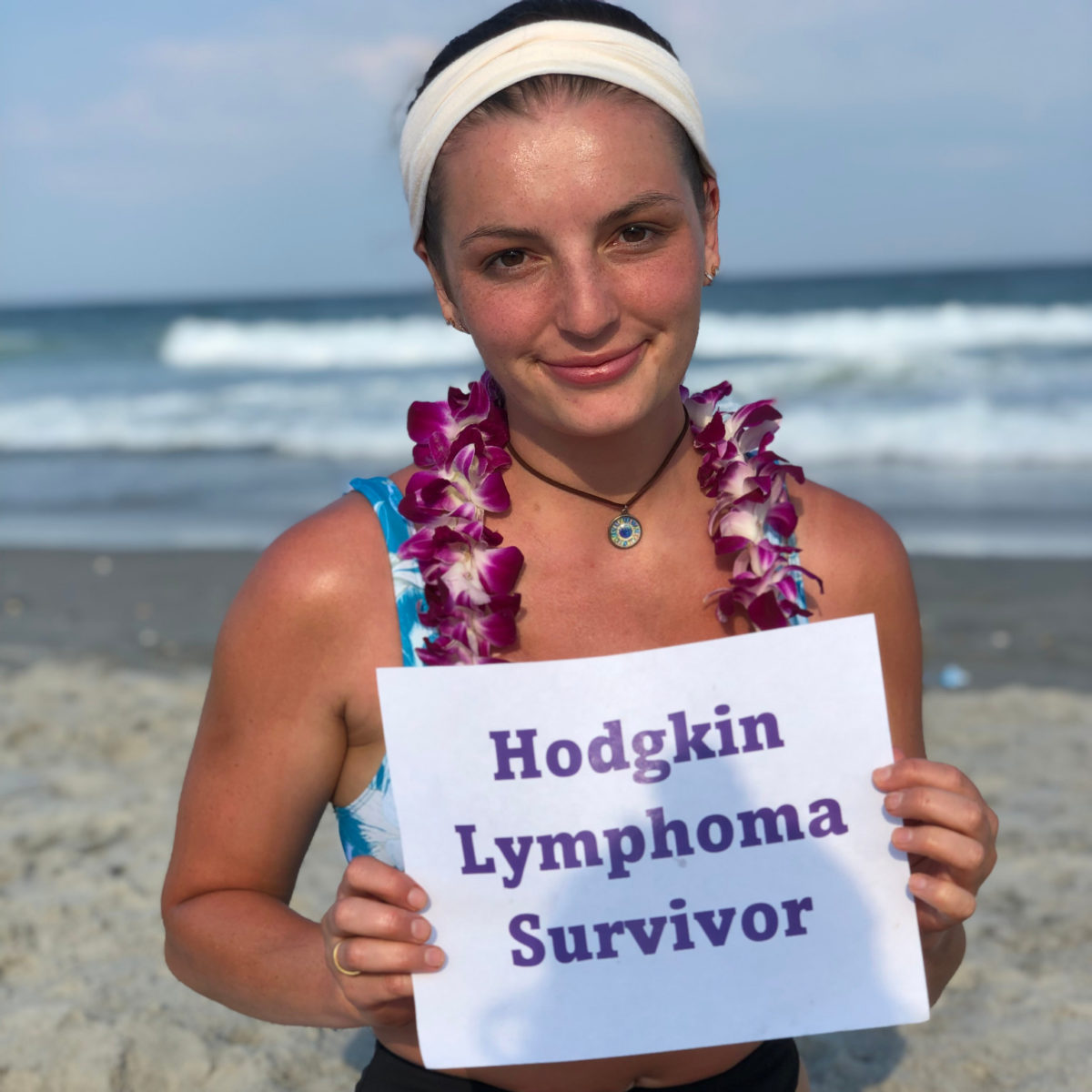
Hodgkin lymphoma patients/survivors share how they were able to advocate for themselves throughout their cancer care...
Empowering Your Voice: Signs of Medical Gaslighting as a Cancer Patient Nadia was repeatedly told, “Nothing was wrong with her.” Amy’s symptoms were consistently attributed to anxiety. Nick was told that he was too physically fit to be sick. Sadly, all three were eventually diagnosed with various types of cancer. The term “gaslighting” has gained...
Navigating Life with an Ostomy: Tips from Patients and Medical Experts Undergoing an ostomy procedure involves major changes. To offer guidance, The Patient Story hosted a live discussion with colorectal cancer patients Amy Hart and Jason Randall, who both have ostomies, along with Dr. Vanessa Wookey, a gastrointestinal oncologist from Fox Chase Cancer Center. From...
Cancer patient panelists Nick Mundy, Lainie Jones, and Matt Ode share their real-life experiences and offer practical tips and strategies for managing scanxiety and maintaining emotional well-being throughout the cancer journey.
...
What is the Difference Between Lymphoma and Leukemia? A leading oncologist offers clarity on leukemia vs. lymphoma In this discussion, we delve into the distinction between two types of blood cancer: leukemia and lymphoma. Confusion often arises because both are blood cancers. Leukemia typically occurs in the bone marrow, while lymphoma originates in the lymphatic...
Navigating the Sweet and Bubbly as a Cancer Patient Dr. Urvi Shah Shares the Impact of Sugar and Soda on Cancer Patients As you navigate your cancer journey, questions about diet often bubble to the surface. Dr. Urvi Shah, is a board-certified hematologist-oncologist at Memorial Sloan Kettering and a Hodkin lymphoma patient. Dr. Shah led...
A Guide to Cancer Survivorship Care Plans for Hodgkin Lymphoma Patients
Expert insights from Dr. Matthew Matasar
Written by:
Jenna Jones
Survivorship care plays a vital role in your cancer journey, helping you feel less alone and more prepared to receive the necessary support and guidance through Hodgkin lymphoma and beyond.
To offer a real-life understanding of cancer survivorship care plans, we talked to Dr. Matthew Matasar, the chief of blood disorders at the Rutgers Cancer Institute of New Jersey and RWJBarnabas Health. He emphasizes the significance of survivorship care and offers practical advice.
This article will explore Dr. Matasar’s expert insights and provide a comprehensive guide to cancer survivorship care plans for Hodgkin lymphoma patients.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
“Everybody who’s gone through Hodgkin lymphoma deserves to receive compassionate, thoughtful, wise survivorship care as they survive and live with their history of Hodgkin lymphoma,” says Dr. Matasar.
To facilitate effective survivorship care, it can help to have a cancer care plan template, often referred to as a survivorship care plan. This straightforward document outlines your diagnosis, treatment details (including medications, doses, and radiation therapy), as well as recommendations from your oncologist and their team for your ongoing care.
“When someone is in charge of saving your life, you want them to actually care about your life and find it interesting and important.”
Dr. Matasar reassures patients by stating, “That simple document can then go with you, which you can then share with your other doctors, your primary care providers, your other providers so everybody’s on the same page. Everyone understands what you went through and what everybody should be attentive to protecting your health going forward.”
Creating Your Personalized Survivorship Care Plan
If you’re not sure where to start on your cancer survivorship care plan, visit Penn Medicine’s Oncolife. The program offers a quick questionnaire to help you outline your plan which you can later personalize with your healthcare team.
What Should Your Cancer Survivorship Care Plan Include?
1. Diagnosis and Treatment History: Your care plan should clearly document your Hodgkin lymphoma diagnosis, stage, and subtype, including any specific details or variations that may be relevant to your ongoing care.
2. Treatment Summary: Provide a detailed summary of the specific treatments you have received, including the medications administered, radiation therapy, and the number of cycles or rounds completed.
3. Side Effects and Potential Long-Term Effects: Address any potential side effects or long-term effects associated with your treatments. This may include details about potential risks and suggested steps for regular check-ups to detect any issues early on and ensure proper management to stay proactive about your health.
4. Recommendations for Ongoing Care: Outline the recommendations from your oncologist and their team regarding your future care. This may include details about follow-up visits, screenings, lifestyle modifications, diet changes, and other proactive steps to safeguard your health.
5. Supportive Care Services: Include information about supportive care services that can assist you in addressing your physical, emotional, and psychosocial needs. This may involve counseling, rehabilitation, survivorship programs, and other resources that can support your overall well-being.
Dr. Mattazar mentions that cancer survivorship clinics, often found within cancer centers, can provide specialized care for individuals.
He emphasizes their unique value stating, “Patients who are survivors at the highest risk for complications from treatment can be followed in a more multi-disciplinary, thoughtful, data-driven way so that we can really do the very best job at protecting our survivors.”
Additionally, cancer survivorship clinics often take a “whole person” approach to health and treatment. They can help you navigate the healthcare system, address your diet and exercise regime, and refer you to other services.
Expert Advice on Self-Advocacy
Preparing for your Hodgkin’s journey with cancer survivorship care can help quickly communicate your health status but Dr. Matasar also emphasizes the value of self-advocacy.
“Don’t be afraid to ask questions,” he says. “So often I have patients come in and they are overwhelmed — and of course. There’s so much relief to hear a plan, to hear good news that there [are] treatment options, and that cure is attainable that there’s a reluctance to want to rock the boat, to advocate for yourself, to ask questions, and to learn more.”
“It could be a spouse, relative, primary doctor or an organization that can advocate for you when the process becomes stressful. This trusted companion ensures that you are able to ask the questions we may easily ignore or miss because we are processing our own emotions.”
For patients unsure where to start with the overwhelming number of questions that may be circling their minds, Dr. Matasar offers a few to get started.
“What I tell my patients is that this is not my journey, he says. “This is your journey. You’re the one climbing the mountain. I’m the Sherpa. I’ll drag your bags alongside you. But this is your journey and I need you to be as prepared and ready, as informed and engaged as possible so that we can do this together.
“Just check with yourself. When you do not feel anything, or if you feel like everything — everything is valid. Even the smallest thing that might be off, tell your doctor so they can know. It might be significant later on.”
Cancer details: Most common and most treatable form of Hodgkin lymphoma 1st Symptoms: Shortness of breath Treatment: 3 rounds (6 infusions) of ABVD chemo
Cancer details: Diagnosed at age 25 1st Symptoms: Swollen lump on right side of neck/chest area, continued to grow Treatment: ABVD chemotherapy (3 cycles = 6 infusions)
Cancer details: Found lymphoma cells in adenoid tissue 1st Symptoms: Difficulty breathing with blockage in nose, surgery to remove tissue resulted in discovery of Hodgkin lymphoma cells Treatment: ABVD chemotherapy (4 cycles), radiation (20 sessions)
Cancer details: Diagnosed at 23 years old with nodular sclerosis, relapsed after 6 months of 1st-line treatment 1st Symptoms: Itchy body, enlarged lymph node over collar bone Treatment: ABVD chemotherapy and ICE, radiation, and stem cell transplant for relapse
Cancer details: Diagnosed at 18 years old 1st Symptoms: Enlarged lymph nodes (around neck), diagnosed at 18 years old Treatment: ABVD chemotherapy (2 cycles), AVD chemotherapy (4 cycles)
Cancer details: Accidentally found in x-ray after months of symptoms 1st Symptoms: Night sweats, fatigue, extreme itchiness, persistent cough Treatment: AAVD chemo, clinical trial w/brentuximab (Adcetris) + nivolumab (Opdivo) immunotherapy
Cancer details: Mother is a nurse practitioner; suspected cancer 1st Symptoms: Swollen lymph nodes in neck Treatment: Clinical trial; Chemotherapy, BMT
Cancer details: Possibly misdiagnosed the first time; later diagnosed as grey zone lymphoma 1st Symptoms: Pulled muscle in chest Treatment: ABVD chemo, radiation, high-dose chemo, stem cell transplant
Cancer details: Staged 2 then 4 after second opinion 1st Symptoms: Extreme fatigue, persistent itching on lower half of legs Treatment: 6 cycles (12 infusions) chemo, ABVD then AVD (dropped bleomycin)
Cancer details: Diagnosed at 29, misdiagnosed as mono 1st Symptoms: Achiness, extreme fatigue, reactive rash on chest and neck. Later: chills, night sweats Treatment: ABVD chemotherapy (6 cycles)
Symptoms: Loss of menstrual cycles, iron deficiency, itching, night sweats, tiredness, night terrors, trouble breathing, difficulty concentrating, enlarged lymph nodes Treatment: ABVD chemotherapy, radiation, ICE chemotherapy, bone marrow transplant
What its like to get a Colonoscopy: Patient & Doctor Perspectives
What it’s really like to get a Colonoscopy
Patients and doctors share their real-life experiences
Written by:
Jenna Jones
Knowing what to expect from a colonoscopy can help you feel more prepared and comfortable about the procedure. To demystify the experience, we discussed colonoscopies with experts and patients.
In this article, we will delve into what it’s really like to undergo a colonoscopy, including its purpose, duration, and preparation. We’ll also explore why more young people are being diagnosed with colorectal cancer.
To provide expert insights and, we spoke to Dr. Wookey, a colorectal cancer specialist from the Fox Chase Cancer Center.
To get the patient’s perspective on colonoscopies, Amanda G. shares her first-hand experience. She received a colonoscopy in 2020 and was diagnosed with stage 2A colon cancer.
“The colonoscopy was an interesting experience,” says Amanda. “I’ve never had one before.”
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Simply put, a colonoscopy is a medical procedure that plays an important role in the early detection and prevention of colorectal cancer, one of the most common types of cancer.
Dr. Wookey explains, “A colonoscopy is our gold standard for colorectal cancer screening. It not only detects cancer early but also prevents it by removing polyps that may eventually turn into cancer.”
The procedure involves using a colonoscope, a long, flexible tube with a light and camera on the end. By gently inserting the colonoscope through the rectum, doctors can see the entire colon, examining its inner lining for abnormalities. In some cases, your doctor may remove polyps (abnormal growths) or tissue to examine.
How Long Does a Colonoscopy Take
According to Amanda, “The procedure itself was so easy and quick. I was in and out in a couple of hours, and there was no pain afterward.”
The duration of a colonoscopy can vary, but typically it takes around 30 minutes to an hour. Factors such as the complexity of the case or the need for polyp removal can influence the duration. According to the Mayo Clinic, a colonoscopy typically takes about 30 to 60 minutes.
“It’s a very quick routine procedure and really nothing to be too nervous or scared about in my opinion.”
Preparing for a colonoscopy is key to an accurate and effective examination. “You have to be on an all-liquid diet,” says Amanda. “You can’t eat any food the day before so you’re hungry. You’re given this prep that you have to drink the day before your procedure. It cleans you out.”
The preparation typically involves following a clear liquid diet and taking a prescribed bowel prep, usually a liquid laxative, to flush out stool from the colon according to UCLA Health. Amanda suggests having candies or lemonade to help with the taste of the prep, and she advises, “Don’t skimp on it because you don’t want to do this again.”
“The day before, as you’re prepping for a colonoscopy, you are fasting and just on clear liquids. I do a lot of chicken broth, popsicles, clear sodas, and hydrate all day.
That evening, you start your preparation and drink a lot of different solutions that clear out your system. Up until about 11 p.m., you’re having a lot of bowel movements and some cramping. Your body is clearing out your colon so that the next day, when you go in, you’re ready for your scope.”
To be further prepared, you may want to stock up on wet wipes, diaper cream, clear sodas, and low-fiber foods you enjoy according to the American Society of Anesthesiologists.
Dr. Wookey also recommends talking to other people who have had a colonoscopy to create a clearer picture of the experiences.
As for the level of sedation, you can discuss options with your doctor. Your health history, age, and risks all factor into what level of sedation your doctor may recommend.
“I know some people are awake, just groggy.,” says Amanda. “I was completely sedated. Best nap of my life. It felt great but I know that’s not the case for everybody but that was just my personal experience. It was super easy.”
“The worst part — or the challenging part of the prep — is drinking gallons of this liquid that they make you drink to clear out your bowel. It doesn’t taste the best, and you have to frequently use a bathroom to clean out your system, for about 24 hours.”
Before your colonoscopy, ask your medical team for a list of approved foods and drinks to have after the procedure. After the colonoscopy, it’s important to ease back into regular eating gradually.
Start with light, easily digestible foods and gradually reintroduce your regular diet. Amanda recommends, “I stuck with soups, smoothies, and soft foods for the first day or two and then gradually went back to my normal meals.”
Why are Colorectal Cancer Rates Rising Among Younger Adults?
According to the American Cancer Society, more people under 55 are diagnosed with colorectal cancer than 10 years ago. There are a few theories as to why there has been a jump in diagnosis. “it may be related to environmental exposures or even kind of the normal bacteria that we all have in our gut,” says Dr. Wookey. “Maybe it’s related to some changes in that. A lot of research is going on to try and figure out why younger patients are having this cancer more often.
“What we think is good for your heart is also good for your colon. So a diet high in fruits and vegetables, low and processed meat, and probably low in red meat is the best for us. But our diet is going in the opposite direction. People don’t sit down to have a good meal. It’s always on the go. [Some food] has a lot of preservatives and that’s one component. I see rectal cancer in young adults as the canary in the coal mine. Our lifestyle is catching up to us.”
Additionally, Dr. Wookey emphasizes that it’s important to understand your own personal risk factors. “Young patients can have certain conditions that may run in their family like Lynch syndrome is one, for example, where younger people are more likely to get cancer at young ages,” she says. “But most young patients who have colorectal cancer, don’t have anything.”
Screening for colorectal cancer is recommended at age 45, for people who have an average risk level, according to the American Cancer Society. Dr. Wooky adds, “It’s very important to talk to your doctors if you may have had family members that have had colorectal cancer because that recommended age for screening might be even younger.”
Cancer Details: Diagnosed 2 weeks after 5 years remission from testicular cancer 1st Symptoms: Inflamed bowel Treatment: Subtotal colectomy, immunotherapy
Cancer Details: The sigmoid colon (or pelvic colon) is the part of the large intestine that is closest to the rectum 1st Symptoms: Stomach discomfort, nausea, bloating, blood in stool Treatment: Colectomy
Cancer Details: Discovered Lynch Syndrome after genetic testing 1st Symptoms: Found the cancer as a result of family history, early colonoscopy Treatment: Partial colectomy
Cancer Details: Family history wasn’t flagged, should have had colonoscopy earlier 1st Symptoms: Stomach discomfort, difficult to process food Treatment: Colectomy, Chemo (FOLFOX, CAPOX)
Cancer Details: Had no usual first symptoms, found as a result of routine colonoscopy and endoscopy 1st Symptoms: None Treatment:Partial colectomy, chemotherapy (FOLFOX)
Cancer Details: Diagnosed at 32, cancer spread to ovary and lung 1st Symptoms: Lump in pelvic area, funny-smelling food, weight loss Treatment: Chemotherapy, colectomy (surgery)
Symptoms: Abdominal pressure, fatigue, small amounts of blood in stool Treatment: Surgery (colon resection), chemotherapy (FOLFOX: folinic acid, fluorouracil, and oxaliplatin)
Kelly B.Diagnosis: Stage 3 Colon CancerSymptoms: Blood in stool, cramping, bloating Treatment: Chemo, surgery
Courtney H.Diagnosis: Stage 1 Colorectal CancerSymptoms: Blood in stool, fatigue Treatment: Chemo, oxaliplatin, capecitabine, surgery
Reclaim Your Energy: Effective Strategies for Fatigue Relief in CLL
Expert advice from Dr. Shazia K. Nakhoda
Written by:
Jenna Jones
Living with chronic lymphocytic leukemia (CLL) brings its own set of challenges, and one of the most prevalent and exhausting symptoms is CLL fatigue.
Fatigue is often described as having a complete lack of energy, despite getting enough sleep. For people with cancer, fatigue is incredibly common. Between 80% and 100% of people with cancer report having fatigue according to the American Cancer Society.
For CLL patients on watch-and-wait, understanding the degree of your fatigue may be a sign to start treatment. “I started treatment when my doctors discovered that my fatigue had become so debilitating that I couldn’t do the normal things I needed to do in my daily life,” says Jeff Folloder, CLL patient and advocate. “I couldn’t lift certain things. I couldn’t stay awake long enough.”
As a CLL patient, it can help to understand the impact of diet and lifestyle on managing fatigue and optimizing overall well-being. While specific dietary changes may not alter the course of CLL, adopting a healthy lifestyle can play an essential role in supporting your journey toward more vitality.
In this article, we explore dietary tips and wellness for CLL patients with Dr. Shazia Nakhoda, an Assistant Professor at the Department of Hematology/Oncology at Fox Chase Cancer Center. She also shares ideas about how to manage the psychological toll of CLL and promising new treatments on the horizon.
Remember to chat with your medical team before making any dietary or lifestyle changes based on this article. Everyone’s situation is unique, and healthcare professionals can offer personalized guidance that suits your specific needs.
Dr. Nakhoda explains that the amount of fatigue CLL patients feel is often linked to the degree of the disease circulating in their bloodstream. In addition, having an enlarged spleen and swollen lymph nodes can also contribute to the level of fatigue experienced.
Anemia in CLL is also a common cause of fatigue according to Dr. Nakhoda, “This happens because the CLLs are taking up too much room in the bone marrow and not allowing the healthy red blood cells to grow or because of an autoimmune phenomenon where the red cells are getting destroyed in circulation.”
For her patients who have very early CLL, Dr. Nakhoda typically advises them to rule out other causes of fatigue like cardiovascular disease or pulmonary diseases.
She adds, “We know that CLL is primarily driven by dysregulation of the immune system, which leads to unchecked inflammation and seems to be a major cause of fatigue.”
Using Diet to Manage CLL Fatigue
There is growing recognition that dietary choices and physical activity, can play a significant role in managing CLL.
According to Dr. Nakhoda, “While there is no specific nutrient or herbal supplement identified that can change the normal disease course for people with CLL, maintaining a healthy lifestyle through diet and exercise is crucial for patients with CLL.”
Dr. Nakhoda’s Diet Recommendation Summary
Choose a heart-healthy diet to minimize the risk of cardiovascular disease.
Include a variety of nutrients from fruits and vegetables in the diet, which is beneficial for cancer patients.
Opt for whole grain products and low-fat dairy options instead of processed foods high in salt and sugars.
Reduce inflammation in the body and enhance tolerance to CLL-directed therapies through dietary choices.
Follow a Mediterranean diet to improve rates of cardiovascular disease and achieve healthy weight goals.
Include healthier fats from extra-virgin olive oil, nuts, and fish in the diet, replacing unhealthy meats and fats.
She emphasizes the importance of choosing a heart-healthy diet to minimize the risk of cardiovascular disease and keeping blood sugars in check, particularly among patients with diabetes.
Dr. Nakhoda further urges, “Getting a variety of nutrients derived from fruits and veggies is beneficial for patients with cancer in general. Choosing whole grain products and low-fat dairy options over processed foods with high salt and sugars are also recommended.” These dietary choices can help reduce inflammation in the body and generally allow patients to better tolerate CLL-directed therapies.
Regarding specific diet recommendations, Dr. Nakhoda adds, “We have some great data showing a Mediterranean diet can improve rates of cardiovascular disease and achieving healthy weight goals. And there are some large epidemiology studies that show this may also benefit patients with cancer risk in general.” Again, she encourages a diet that includes healthier fats from extra-virgin olive oil and nuts and fish in place of unhealthier meats.
Finding Balance with CLL Fatigue
When it comes to managing CLL-related fatigue, Dr. Nakhoda recommends several approaches. She says, “In some patients who meet criteria for CLL-directed therapy, treating the CLL can make a huge difference in fatigue.”
However, for patients in the Watch & Wait phase or without clear indications for therapy, she highlights the importance of lifestyle modifications. “We have found exercise to make a huge impact on improving fatigue,” she says.
Starting with small activities like a 15-minute walk or yoga session and gradually increasing activity levels over time can be beneficial. “Overtime, the more activity patients are able to do, we see fatigue symptoms often improve,” says Dr. Nakhoda.
She also suggests optimizing sleep patterns and addressing any underlying medical conditions that may contribute to fatigue. She adds, “We know that patients with other medical conditions like cardiac disease or pulmonary disease can also contribute to fatigue so addressing any risk factors like coronary arterial disease or sleep apnea, for example, are important.”
Psychological Impact of Watch-and-Wait: Connecting with Others
Living with chronic lymphocytic leukemia (CLL) can be an emotional rollercoaster, especially during the Watch & Wait period when patients face uncertainty about their treatment timeline.
Dr. Nakhoda acknowledges the psychological toll that the watch-and-wait period can take on CLL patients. She says, “The stress of a new diagnosis of cancer, not knowing if or when you may need therapy, and grappling with the unknowns that come with this type of disease can be really tough.”
To cope with these challenges, she recommends connecting with other patients who have CLL through support groups and online networks. The CLL Society offers a guide to helpful support groups. Dr. Nakhoda notes that support groups can provide valuable encouragement and make a significant difference in managing the emotional fatigue associated with the waiting period.
Promising CLL Treatments
As CLL patients continuously seek new avenues for treatment, Dr. Nakhoda highlights the dynamic nature of managing chronic lymphocytic leukemia, with ever-evolving therapies and approaches that are reshaping the CLL landscape.
“The way we treat CLL is rapidly evolving. The survival data we had from even 5 years ago is now outdated. We have new drugs approved every couple of years that are quickly changing the way we treat patients.”
She highlights the emergence of non-covalent BTK inhibitors as a promising new class of drugs. “This type of drugs works similarly to the first and second-generation BTKi inhibitors (ibrutinib, acalabrutinib, zanubrutininib) but binds in a different way to the receptor.”
She also mentions pirtobrutinib, which was recently approved by the FDA for patients with mantle cell lymphoma. “Hopefully, it will receive approval for other B-cell lymphomas like CLL in the near future. It seems to be effective in patients who previously were intolerant or resistant to another BTK inhibitor, and has a very favorable side effect profile,” she says.
Minimal Residual Disease Testing
Another important aspect of patient care is the restorative space between treatments. “I hear from patients that getting time off of therapy is really important as well. There is exciting data about using minimal residual disease testing, which is a method of detecting very small levels of microscopic disease in the blood or bone marrow as a marker of deep response. We are trying to understand how to use these tests to help identify which patients may be spared from continuous use of certain drugs and get more time off of therapy.”
While specific dietary changes may not alter the disease course of CLL, Dr. Nakhoda emphasizes the importance of maintaining a healthy lifestyle through diet and exercise. Fatigue is a common symptom of CLL, and managing it involves a combination of treating the disease itself and incorporating lifestyle modifications. Connecting with other CLL patients through support groups and staying informed about promising new treatments can also be beneficial for patients and their overall well-being.
Easy Mediterranean-Inspired Recipes For CLL Patients
Here are five super simple recipes that align with Dr. Nakhoda’s dietary recommendations for CLL patients:
1. Mediterranean Quinoa Salad:
– Ingredients:
– 1 cup cooked quinoa
– Assorted chopped vegetables (such as cucumber, cherry tomatoes, bell peppers)
– Kalamata olives, pitted and halved
– Feta cheese, crumbled
– Fresh parsley, chopped
– Extra-virgin olive oil and lemon juice (as dressing)
– Instructions:
1. In a bowl, combine cooked quinoa, chopped vegetables, olives, and feta cheese.
2. Drizzle with extra-virgin olive oil and lemon juice.
3. Garnish with fresh parsley. Mix well and serve.
2. Veggie Stir-Fry with Brown Rice:
– Ingredients:
– Assorted vegetables (such as broccoli, carrots, bell peppers, snap peas)
– Tofu or lean protein of choice
– Low-sodium soy sauce
– Garlic, minced
– Ginger, grated
– Cooked brown rice
– Instructions:
1. In a wok or skillet, heat a small amount of olive oil over medium heat.
2. Add minced garlic and grated ginger, and sauté for a minute.
3. Add the vegetables and tofu (or protein) to the pan and stir-fry until cooked but still crisp.
4. Stir in low-sodium soy sauce to taste.
5. Serve over cooked brown rice.
A Simple Fish Recipe
3. Grilled Lemon Herb Salmon:
– Ingredients:
– Fresh salmon fillets
– Lemon juice
– Fresh herbs (such as dill, parsley, or basil)
– Extra-virgin olive oil
– Salt and pepper to taste
– Instructions:
1. Preheat the grill to medium-high heat.
2. In a small bowl, combine lemon juice, chopped fresh herbs, olive oil, salt, and pepper.
3. Brush the mixture onto the salmon fillets.
4. Grill the salmon for about 4-6 minutes per side, or until cooked through.
5. Serve with a side of steamed vegetables or a mixed green salad.
4. Chickpea and Vegetable Curry:
– Ingredients:
– 1 can chickpeas, drained and rinsed
– Assorted vegetables (such as cauliflower, sweet potatoes, spinach)
– Curry powder or paste
– Coconut milk (light or full-fat)
– Fresh cilantro, chopped
– Instructions:
1. In a large pan, heat a small amount of olive oil over medium heat.
2. Add the vegetables and sauté until slightly tender.
3. Stir in curry powder or paste to taste and cook for another minute.
4. Add the chickpeas and coconut milk to the pan and simmer for about 10-15 minutes, or until the vegetables are cooked through.
5. Garnish with fresh cilantro and serve with brown rice or quinoa.
1. In a glass or bowl, layer Greek yogurt, fresh fruits, and a drizzle of honey or maple syrup if desired.
2. Repeat the layers until the container is filled.
3. Top with a sprinkle of granola or nuts.
4. Enjoy as a nutritious breakfast or snack option.
These simple and delicious recipes incorporate the key principles of a Mediterranean diet, providing CLL patients with a variety of nutrients from fruits, vegetables, whole grains, and healthier fats. Remember to consult with your healthcare team or a registered dietitian for personalized dietary recommendations based on your specific needs and preferences.
1st symptoms: Tightness, lumps in left side of neck, severe pain in left shoulder, enlarged spleen Treatment (CLL): 6 cycles of EPOCH, clinical trial for DuoHexabody-CD37
When it comes to managing DLBCL (Diffuse Large B-Cell Lymphoma), physical activity can play a crucial role in enhancing overall well-being. In this article, we delve into the valuable benefits of exercise for DLBCL patients and provide practical tips to help integrate physical activity into your daily life.
Drawing upon the expertise of Dr. Joshua Brody, the Director of the Lymphoma Immunotherapy Program at The Tisch Cancer Institute at Mount Sinai, we gained insightful perspectives on addressing patient concerns, emphasizing a healthy lifestyle, and debunking common misconceptions.
Dr. Brody’s extensive experience and groundbreaking research in lymphoma treatment offer guidance for patients seeking optimal outcomes and improved quality of life.
According to Dr. Brody, it is natural for patients to have questions and concerns driven by fear upon receiving a diagnosis. He empathizes, stating, “How did I get this? What did I do? As though someone wants to blame themselves for this. I guess it’s natural.”
Offering reassurance, Dr. Brody explains, “There’s nothing you did. You got this for the same reason that people get hit by lightning. Nothing that they did. You got this, primarily for most patients, because of one cause and one cause only: bad luck. That’s why you got this.”
Patients often inquire about diet and supplements’ impact on the condition. Dr. Brody advises, “You should eat [healthily] and be healthy. Being healthy is not just about eating; it’s about physical activity and exercise.”
While numerous studies support the benefits of physical activity and a healthy lifestyle for cancer and lymphoma patients, Dr. Brody clarifies that micromanaging specific details is unnecessary. He highlights, “We don’t micromanage and have a specific, ‘Oh, you need these blueberries, this green tea, this antioxidant.’ Healthy eating [and] healthy living is critical, but the details [are] probably not critical.”
Before starting any exercise routine, be sure to discuss physical activity with your healthcare team. Listen to your body when you need to rest or relax. Start small and keep it fun.
Easy Exercise Ideas for DLBCL Patients
To help DLBCL patients incorporate physical activity into their daily routines, we’ve outlined simple ways to add some exercise in.
1. Take short walks: Begin with short walks around your neighborhood or nearby park, gradually increasing duration based on energy levels. Walking is a low-impact exercise that enhances cardiovascular health and overall well-being.
2. Stretching and flexibility exercises: Engage in gentle stretching exercises to improve flexibility and joint mobility. You can perform these exercises at home or with the guidance of a physical therapist. The American Cancer Society offers a helpful resource on stretching exercises.
3. Chair exercises: If mobility is limited, consider chair exercises that can be done while sitting. These exercises focus on strengthening muscles and increasing circulation. To perform the heel/toe raises exercise, have a chair with armrests and a pillow nearby. Start by placing both feet flat on the floor. Point your toes up towards your nose while keeping your heels down. Then, point your toes down towards the floor and try to lift your heels off the ground. Repeat these steps for about 30 seconds, if comfortable. For more, check out this Chair Exercise Guide by Memorial Sloan Kettering Cancer Center.
4. Yoga or Tai Chi: Incorporate gentle forms of exercise like yoga or Tai Chi, which improve balance, and flexibility, and reduce stress. In a study involving 14 patients with malignant lymphoma, a home-based yoga program was found to be safe and feasible during chemotherapy treatment. The program also showed improvements in health-related quality of life, fatigue, sleep, depression, and anxiety. However, further validation through randomized studies is necessary.
5. Household chores and gardening: Engaging in light household chores and gardening not only provides physical activity but also a sense of accomplishment. Simple tasks like sweeping, vacuuming, or light gardening contribute to daily activity levels. If you’re heading outdoors, The Leukemia & Lymphoma Society emphasizes sun safety, especially while in treatment. Plan ahead and seek shade when you can.
Stephanie Chuang, founder of The Patient Story, celebrates five years of being cancer-free. She shares a very personal video diary with the top lessons she learned since the Non-Hodgkin lymphoma diagnosis.
Cancer details: Characteristics of both subtypes 1st Symptoms: Lower abdominal pain, blood in stool, loss of appetite Treatment: Chemotherapy (Part A: R-CHOP, HCVAD, Part B: Methotrexate, Rituxan, Cytarabine)
Watch-and-wait strategies can be confusing for both cancer patients and their care partners. The Leukemia and Lymphoma Society defines this approach as “closely monitoring a patient’s condition without administering any treatment until symptoms appear or change.”
But how does this approach affect the day-to-day life of a cancer patient? In this live discussion held in May 2023, we explore everything you need to know about the watch-and-wait strategy, including red-flag symptoms, safe activities, and tips for maintaining good health.
Michele Nadeem-Baker: I am a CLL patient, but I’m also a medical journalist and a really passionate CLL patient advocate trying to help all of us understand better just what CLL is and SLL in everyday language.
So probably like the majority of you, I was pretty surprised when I was diagnosed with CLL and thrown into something called watch-and-wait, which made absolutely no sense to me. It was pretty illogical. The doctor walked in. I had no clue there was anything wrong with me and he said, “You have the C word, but it’s the best you can have.” Doesn’t that kill you when they say that? Nothing made sense to me. How anything with cancer could be the best. And then he told me that he’d see me in four months and then I’d be fine. So all of this was pretty illogical to me, having to grasp all of this at once and understand.
But during this time of watch-and-wait, what I did is I got a second opinion and then I started what you would call front-loading information. I was trying to find out the most credible places to go for information, but also the most current. And that’s something we have to watch out for with Dr. Google. So I learned Dr. Google is not necessarily the doctor, you want to listen to and also to go to find where we can find some credible answers. And so in that time, I also found great CLL specialists, the latest in treatment, and it’s good to stay on top of what those treatments are.
I made sure that I took a lot of stress out of my life. My job was a 24/7 job and when I tell you that, that’s not an exaggeration. I slept 2-4 hours a night — Dr. Rogers, can you believe this? — for years because that was my job. I thought, “I think I need to get a little healthier.” I upped my game on working out and on eating healthy and I started doing yoga and meditating and trying to do everything I could to be the healthiest I could be for when it was time to start treatment. And in treatment didn’t happen for some years.
Jeff Folloder: I am a passionate patient advocate. And there’s a reason for that. The reason is I am living an excellent life with CLL. And my goal, my mission is to make sure that others know it is possible to live a great life with CLL. A little bit about me. I love fast red cars, I love expensive whiskey, and I love sharing stories and learning about this ugly journey of cancer that I’m dealing with and helping people figure out better ways to deal with it.
Catherine Ferguson: My name is Catherine Ferguson.
I live just outside of Boston and am a retired college professor. I’m a vet tech and I work in surgery. And I’m also a CLL thriver — not only surviving but thriving.
Dr. Kerry Rogers: I just love doing this type of thing and I really enjoy talking to my patients in the clinic and I enjoy talking about CLL in general. I’m a hematologist, I’m a physician-scientist, and I’m an associate professor in the Division of Hematology at the Ohio State University. I see people with both CLL and hairy cell leukemia in my clinic and do research mainly in investigational therapeutics. And I enjoy talking about CLL with people, but I also really enjoy college football and was just reminded it’s only three and a half months or so until we have college football back.
Why is watch-and-wait used for CLL Treatment?
Dr. Kerry Rogers: The majority of people diagnosed with CLL won’t need treatment right away. And, in fact, with people getting routine blood work now so often, the most common way to be diagnosed is getting a blood test and then finding out you have CLL without any symptoms. It is very confusing for people when you’re told you have a cancer and most of the things you hear about all forms of cancer is that you have to treat it, catch it early, and be aggressive with treatment, and that’s not really the scheme in CLL.
The reason for that is that we know that treating it earlier doesn’t help people live any longer or any better. So way back when we used to use chemotherapy to treat CLL, there was more than one randomized study where they took people who were recently diagnosed with CLL that did not have any of the traditional reasons to treat it, like symptomatic lymph nodes or blood counts that were abnormal enough to need treatment. So they took people who were asymptomatic or minimally symptomatic with no issues that required treatment and randomized them to either be observed and then get treatment when they needed it or to get treatment right away with chemotherapy. And there was more than one study and this is, again, back when chemotherapy was the thing we used.
Does immediate treatment for CLL/SLL improve overall survival compared to the watch-and-wait approach?
Dr. Kerry Rogers: And, actually, there was no difference in overall survival, which is how long people were living between the two groups. People treated when they needed it or people treated immediately had the same survival so we know it doesn’t help you live longer. And, actually, it looked like there was a slight trend towards shorter survival in people treated immediately because chemotherapy is not overly good for people and they got chemotherapy they didn’t need yet.
The way I like to view it is CLL is not something that we can currently cure with conventional treatments. We expect people to live a very long and rich lifespan with it. And so given that, why expose someone to side effects from treatment earlier? Because the sooner you take it, the sooner you get side effects from treatment. And why expose he CLL cells earlier to agents they could become resistant to, shortening the amount of someone’s lifespan, where they might be expected to have their CLL controlled by targeted agents?
So if you think about it, there are a couple of reasons not to do early treatment because of side effects and the risk of resistance to the treatment. And we know it doesn’t help people live any longer in fact, it might help them live worse if they’re getting side effects. So that’s the rationale on the science side behind watch-and-wait, which I like to call observation.
Is there a percentage of patients that go immediately into treatment?
Dr. Kerry Rogers: That’s a good question. I do think that percentage is probably decreased over the years so I’m sure someone has looked at that as a straight percentage, but I’m not sure that really applies anymore. But it is really the vast majority of people that are in watch-and-wait, at least for some time. It’s a much, much less common thing to need treatment immediately.
Are there ongoing studies with newer drugs to determine if treating early improves survival?
Dr. Kerry Rogers: As a scientific question, they are repeating some of these studies with the newer drugs to see if this is still true, that it doesn’t improve survival for people, which is how long they live with their CLL, to treat early. Those studies are being done. The German CLL study group has one with ibrutinib as an early intervention. And then there’s one that’s occurring in the United States called EVOLVE that’s looking at venetoclax-obinutuzumab either immediately or delayed. We will get more information about that. Because people live so long, it will take over a decade or more to see if there’s a survival difference because people don’t die, which is great. I think that when you think about other types of cancers, like colon cancers or breast cancers, the reason to find them early is that you can cure them. And if you don’t find them and treat them earlier, people die of them.
When you’re looking at CLL, you’ve got a lot of people who, even though they have it, are unlikely to die of it — that’s not everybody, but a lot of people are unlikely to die of it — and we can’t cure it so you don’t get to do treatment and go back to whatever indefinitely, right? If you do treatment now, even with our newer drugs, these still have side effects.
What are the potential risks and drawbacks of treating CLL/SLL early with targeted treatment?
Dr. Kerry Rogers: Anyone that thinks they’re getting treatment with no side effects, you never get anything for free, right? Why expose someone to risks of high blood pressure, diarrhea? And then also we know that once you start exposing CLL cells to these targeted agents we use, there’s an amount of time that the disease will respond before the cells become resistant and their CLL comes back. If you start treatment 5 years before you had to, that’s 5 fewer years where someone’s CLL could be controlled by that drug so you might actually shorten someone’s lifespan by giving them a drug that you didn’t have to by either causing a severe side effect or causing their cancer cells to become resistant earlier.
Understanding the challenges of diagnosing and treating CLL/SLL
Dr. Kerry Rogers: And those schemes for screening, treat early — and I get asked this all the time, “But what if my cancer has spread? What if the CLL has spread? How will I know if it’s spread?” And I’m like, “Okay, this is really hard because it’s a blood cancer, right? So it goes everywhere the blood goes.” And they’re like, “Well, that’s everywhere.” And I was like, “I know,” and it’s so upsetting to think that. I can just see how upset people are by this idea. But for CLL, it’s actually okay. We expect it to be everywhere the blood can go and that doesn’t make it any less treatable or make our therapies any less effective.These conventional things that apply to solid tumors are not really the same as applied to these blood cancers and then there’s a huge difference between aggressive cancers that can be cured or cause symptoms immediately and some of these cancers.
And just for context, I have some patients that were diagnosed with CLL when I was in high school and have never needed treatment and it’s been over 20 years — actually over 25 now; I’m getting old.It’s hard to say that you can improve someone’s life by treating early and aggressively when the last two-plus decades have been them living their lives without anything hurting them from the CLL. So when you see that, then you think. it’s not a good idea to expose these people to things they don’t need. You can’t improve on feeling well, right?
Mental and emotional health effects
Jeff Folloder: The most debilitating part of CLL for me is the mental burden of this. We can be candid with each other. watch-and-wait is not a normal thing for anyone. And when you’re told you have cancer and you’re told you’re going to watch, you’re going to wait, you’re going to have to be vigilant, you’re going to have to go into observation mode, that becomes a mental burden. I will admit that I did not deal with that mental burden very well when I first went through watch-and-wait.
Michele Nadeem-Baker: Jeff had been through treatment. I’m like, “How did you do this? I didn’t have control over what my own body was doing and that is really difficult, especially for someone like myself who really likes to be in control of things. I think I’m doing everything I can. Is there anything more I can do? No, there really isn’t and it just doesn’t matter and that is so difficult.
And also my dad passed away from mesothelioma, a lung cancer. He was diagnosed and in two weeks, he died. So it’s just like, to me, that’s like, “You don’t treat? Oh my gosh, that’s what happens.”I got all worked up there from when I was going through it the first time because you really don’t know what it looks like. You don’t know what it’s like.
Catherine’s experience before front-line treatment
Catherine Ferguson: I dealt with it about the same as you guys initially. When I was diagnosed, I was at one of the top hospitals in Boston, but when they said they weren’t going to treat it, I was like, “Oh my God, I’m going to have to go to Dana-Farber.” So I went for a second opinion over to Dana-Farber and they told me pretty much the same thing.
My personality is I’m a go-getter. I want the plan. I want to get it done. I want to get it started and I want to get it ended. So for the first couple of weeks, it was probably all-consuming for me, honestly. I could have gone down the rabbit hole really quickly.
I look at my dogs and I’d think, “Am I going to outlive them or are they going to outlive me?” But pretty soon thereafter, I had an epiphany where one day, I thought,” I could go walk off the curb tomorrow and get hit by a car,” and then I spent my last days on this earth worrying about when I might die somewhere down the line.
For me, that set something off in my head that life is for living right now and none of us know what tomorrow brings. It’s not a guarantee for anybody. So for me, I try and just live my life. I’m basically an optimistic person in general, by nature. So for me, I try and just believe that] I do the things that I can do for myself and stuff like that. I take care of myself. I listen to the doctors. I get my screenings. I do all the things I’m supposed to do in watch-and-wait. And then I just continue to live my life. I have to say, the second time around, it’s been much better.
How did you cope with the emotional toll?
Catherine Ferguson: When I was first diagnosed, I was diagnosed with intermediate markers. I wasn’t high risk, I was intermediate on the genetic markers and so I knew I was going to likely need treatment. What the doctor couldn’t tell me is when. So I knew that sooner or later, I wasn’t going to be one of those people that was going to go forever without needing treatment.
And so around the 4-year mark, I started to get really anemic. I started getting really, really tired. I had a couple of nodes that were big, but that was it. Everything else — my platelets, my white blood count — was perfectly fine. We found out I was iron deficient so I did iron infusions. It helped initially, but when we rechecked it again two months later, it had dropped again.
Because I didn’t have any other symptoms other than I was anemic, we kind of assumed that it might be the CLL progressing at that point. I had a bone marrow biopsy done and it came back as Hodgkin’s lymphoma from a Richter’s transformation. So Richter’s transformation is when the CLL transforms into something much more aggressive. Usually, it’s not a Hodgkin’s, usually it’s something worse so I actually got the better of the two, if you want to see that. See, that’s the optimism.
I had to do a regular six months of chemo every other week. High-dose chemos. And for me, I’ve been in remission since I finished that chemo and that was five years ago. I have never had any more issues with the Hodgkins or the Richters.
What are some tips for guys dealing with watch-and-wait and how can they learn to talk to people about it?
Jeff Folloder: We’re at a point where I’m supposed to give some pro tips about how guys deal with watch-and-wait. And we’re going to go straight to a poll that Stephanie’s going to introduce in just a second. I’m going to give you a sliver of the pro tip because it’s part of dealing with this whole mental health aspect that we’re going to be focusing on a bit here.
Michele talked about it. She talked about being in control.] Guys, we all try to be type A and we try to always be in control. The answer is not always, “I’m fine.” The answer is not always, “I’m good.” You’re going to need to learn how to talk to people.
How do patients and care partners cope with watch-and-wait from an emotional and mental health standpoint?
Dr. Kerry Rogers: As you were saying that don’t just say, “Oh, I’m okay,” I have people’s partners all the time say, “Will you just go ahead and tell her what’s on your mind? You need to actually tell people what’s happening.” And I was like, “I’m here to listen to you about what’s happening.” I observe that quite a bit. We get so many people now diagnosed at a time when they have no symptoms — their blood tests are abnormal, they get diagnosed with CLL, they don’t need treatment, and they had no symptoms and say they felt perfectly fine and had no idea something was wrong until this happened —for this group of people, sometimes I think the hardest aspect of having CLL is knowing that they have it.
I see people where the worst part of it for them is not physical symptoms, but it’s living with knowing you have it. And I try to tell people, “You’re feeling well from this.” I’ve said, “Based on the disease features, I don’t expect this to be something that shortens your lifespan, even though you might need treatment at some point. Please don’t let knowing you have this ruin your life] Don’t let just knowing you have this fear in your life.”
We have great programs here at Ohio State at the James, like psychosocial oncology, which is mental health professionals that can help with this. I try to offer what I can, but this is something that I don’t have formal training in helping people cope with some of these aspects, which really can be much more impactful on their lives than the physical symptoms of CLL.
I think people knowing they have it can actually be much harder for them than any physical symptoms they’re experiencing. I can see sometimes people that have spouses or partners or caregivers or people in their lives that come to the clinic with them, it’s really helpful because sometimes, something, their friends, family, or loved ones are observing is something they choose to share during the visit and that helps me know that there’s something else that needs to be addressed.I think sometimes it can be hard for other people to know how to support their loved one that has CLL. I find that the majority of people help facilitate some of the communication in clinic and have been good.
Jeff’s experience with watch-and-wait: learning to communicate with healthcare team
Jeff Folloder: I want to share just a little bit about my experience with watch-and-wait I learned through going through all the questions and answers at the hospital that I chose that I wasn’t being candid with my healthcare team. I believe the military says I was exhibiting a lack of candor.
Well, the problem was I didn’t know how to answer their questions. I didn’t know what was important when they said, “So what’s going on? How are you dealing with things? Is there anything that we need to know about?” Things like night sweats. I associated it with my love of Thai food. You eat too much hot chili, you’re going to sweat at night, right? No. Going through all of this watch-and-wait was learning how to communicate with my healthcare team and not knowing what was going to be the tripwire for treatment meant that I was learning new things about communication.
I started treatment when my doctors discovered that my fatigue had become so debilitating that I couldn’t do the normal things I needed to do in my daily life. I couldn’t lift certain things. I couldn’t stay awake long enough. I couldn’t do this. I couldn’t do that. That was the tripwire for, “Okay, watch-and-wait is now over. Now it’s time to move into treatment.”
Dr. Rogers, explain to us what you’re doing with all these questions and answers. What are you looking for? What is happening during this period? And what should the patients and their caregivers be looking out for?
How to determine symptom severity and potential causes
Dr. Kerry Rogers: There are a few things that we always look for. We always check people’s lymph nodes. But just because we found some lymph nodes, it’s okay. It doesn’t mean you need treatment. But if people notice a bunch of lymph nodes everywhere that’s bothering them and keep getting bigger, then that might be important that we should do something to improve that for them. And then we look at the blood counts, which people don’t usually see their blood counts between visits that often and so that’s something that’s really important.
But in terms of what people tell us, it’s always good to hear about how people are functioning. If they have things that are interfering with their professional, leisure, or preferred activities, if it’s fatigue, if it’s something else, we always ask about night sweats. And then if someone’s like, “Yeah, I’m going through menopause,” I’m like, “Right, so that’s cool.”
The difference between normal night sweats and abnormal night sweats
Dr. Kerry Rogers: There are people with night sweats where everyone in bed with them is wet. They’re wet, their wife is wet, and the dog is wet. They had to change all the sheets. That’s actually a problem. And it’s hard because people don’t know that that we think there’s a difference between, “Oh, yeah, my neck got sweaty at night,” because they got hot versus, “Everyone in the entire bed with me is soaked because I’m so sweaty.” Those are the things we try to figure out by asking questions when people like to come to see us. Finding out about night sweats is fine and we can help people determine what might be normal like you were saying, the Thai food versus not really normal, right?
The significance of reporting severe fatigue and sleep issues
Dr. Kerry Rogers: Fatigue is the hardest because there are so many things that can add to someone’s fatigue. Every once in a while, we get someone that has fatigue that’s really quite severe and it’s actually sleep apnea. So we get their sleep apnea treated and they’re like, “Oh, I feel like a million bucks.” And you’re like, “I’m glad we didn’t treat your CLL because of that,” because that’s not going to fix your sleep apnea, right?
Part of what we do when symptoms are reported is not like, “Oh, you have fatigue, you need treatment,” but have more questions about what’s going on, and what might be causing that. One patient I talked to said, “I have fatigue, but I haven’t slept.” She only slept 2 to 4 hours a night. People are tired when they’re busy and they have something going on. A lot of the stuff we look for is not only asking those questions but severity and follow-up questions about some of those symptoms.
What is the average watch-and-wait period for intermediate and high-risk CLL/SLL patients, and does it vary by mutation type?
Dr. Kerry Rogers: The answer is yes, there is. This has been done in more than one study where they’ve looked at the time from diagnosis to first treatment. It’s hard to pinpoint from these studies what will happen to any one person though. So these are studies that look at a group of people diagnosed with CLL and how long between the time they are diagnosed and treated. Then they look at different disease features — so high-risk features like deletion 17p in the CLL,ow-risk features like IgHV mutated status, and then they look at the median. You can think of the median as a little bit like the average. It’s not exactly the same thing, but the median number of times for the 100 people in that group to start treatment.
Dr. Kerry Rogers: For things like deletion 17p, the median in one study was around a year and a half between diagnosis and needing treatment. But within that group, some people needed treatment right away, some people didn’t need treatment for five years. There’s a staging system called Rai staging that can help predict the time to the first treatment. But you never know what’s going to happen for an individual person so I try not to get people too wrapped up in that because you don’t know how it’s going to turn out for them.
Activities, supplements, and exercise
What activities can you do during watch-and-wait?
Dr. Kerry Rogers: I’m going to go with all of them that are recommended for people. People ask me this all the time, “Can I do this? Can I do that? Can I do the other thing?” I’m like, “Yeah, do all of it.” And then they’re like, “Can I do something crazy that really nobody should be doing?” I’m like, “No, don’t do that.”
“Can I drink beer because I have CLL? I like drinking beer and watching football.” I’m like, “Me too. That’s the best.” And they say, “I want to drink one beer watching football.” I’m like, “Okay.” Or they say, “Sometimes I like to drink two beers while watching football.” I’m like, “Yeah, that’s fine. Really just don’t get drunk every day and that’s not because of the CLL, that’s just general advice.”
If you think of someone with CLL, people in observation do live with a higher risk of infection and other forms of cancer. So I do think the COVID-19 pandemic was much more limiting for people with CLL in observation than for the rest of the public so there are a few things like that. But aside from going somewhere where you can’t access medical care if you’re about to need treatment or some really dangerous activities that are not recommended for anybody, I tell people to just go ahead, enjoy their lives, and do whatever they want to do.
How can we extend the watch-and-wait period and slow down CLL or SLL progression?
Dr. Kerry Rogers: Not that I’m aware of. There are a couple of things, right? There’s a study with green tea extract tablets like a high dose that can lower the white count, but I don’t know that there’s any data that really help people live longer or really prolonged watch-and-wait.
There are things that I’m sure help people in general. You were saying you did some things to make sure you’re fit and rested and eating healthier. Those things can make people feel better and be better with their overall health. But I don’t know of anything people can do specifically to increase the amount of time before they need treatment.
Matcha green tea and supplements: Are they effective in managing CLL or SLL?
Dr. Kerry Rogers: Not that I know of for CLL. Vitamin D does have a variety of health benefits. If you’re deficient, getting that replaced is important for other health metrics. But I don’t know of anything specific that will help the CLL. [Supplmenents] aren’t regulated so it’s helpful to go on the Internet and look at some of the companies that rate the quality of supplements before you buy them.
Green tea, it was an extract used in a study. You’d have to drink more than one can physically drink in a day to get the same benefit if you’re going to drink the tea. So if someone wants to try that, I strongly recommend finding a high-quality green tea supplement because it’s just physically not possible to drink that much green tea in a day.
Can jumping rope be beneficial for managing CLL/SLL?
Dr. Kerry Rogers: Exercise is good for people, right? But there’s no data that jump rope actually helps CLL. Probably won’t help your joint health but will help your cardiovascular health. But it doesn’t do anything to impact the CLL specifically.
Managing CLL/SLL Comorbidities
Jeff Folloder: One of the things that I have learned through my 13 years of dealing with CLL, I finally believe my first CLL specialist. He said, “I’m more worried about the comorbidities than I am about the CLL. If you will actually put time and effort into taking care of those comorbidities, you’ll actually make my job easier.” So I have embraced that.
I know it’s going to sound pedantic, but you can exercise more, you can eat better, you can eat less, and you can do all the things that you need to do to reduce your comorbidities. And, truthfully, there is no upper ceiling for it. I’m currently training for a marathon. I’m relapsed and training for a marathon, so yay.
Dr. Kerry Rogers: Modifying your other risk factors for your other health conditions because that is something everybody can do in watch-and-wait. And I would say more people with CLL my clinic die of heart attacks than die of CLL. So just please keep that in mind. And, of course, keeping up with cancer screenings and vaccines is very important.
When to start treatment for CLL/SLL
What are the indicators that it’s time to end watch-and-wait and start treatment for CLL/SLL?
Dr. Kerry Rogers: There’s a group of people where they have no symptoms, lymph nodes aren’t big, blood counts look fine, and you say absolutely there’s no reason whatsoever to treat this person. There is no cut-off on white blood cell count where you need to do treatment. I do think if you get above 400 or 500, usually other reasons develop and it’s about time, but there’s no cutoff like, “Oh no, my white count hit 50. We need treatment.” That’s not a thing. And yes, there is a thing with doubling, but that’s only with higher white counts. So it’s not like, “Oh, it went from 10 to 20, I need treatment.” That’s not a thing. You can actually be very flexible with the white blood cell count. Don’t think of a hard number there.
There are people who I think could be ready for treatment.] The blood counts are going in the wrong direction so you can see the hemoglobin and platelets are dropping, white counts going up, and lymph nodes are getting big, but they’re not actually really problematic for the person. Maybe they’re having some fatigue so there’s a window where you could say like treatment’s reasonable.
The span from, “We shouldn’t do treatment,” to “We should have done this sooner,” especially for a first treatment can be over a year. You’ve got a very long window and that gives you some time to decide, along with your doctor, what treatment’s best for you and things like that. It’s uncommon that you hit something and you need treatment tomorrow. It’s more like an ongoing discussion for a while.
The things I see that I notice sometimes are, “The white count shooting up pretty fast, along with the hemoglobin and platelets kind of dropping.” Or every time people come back, there are more lymph nodes and they’re losing some weight. There are a lot more lymph nodes and you see this trend happening. And then I do see some people that develop a lot of fatigue that suddenly starts to interfere with their personal and professional activities and that would be a reason to say, “We should really do something before this really impairs your life more.”
Are there any specific signs to watch for?
Dr. Kerry Rogers: Every once in a while, I have a patient who develops a significant health concern that they think is in another area, like severe diarrhea or chest pain, that’s not addressed by going to like their cardiologist or something else. When people develop health concerns, weird symptoms — and not like, “Oh, my toe is itchy one day and then it’s not the next day,” that’s fine; that happens to everybody – something significant, impacting their life, weird that maybe other doctors they thought might help them with this can’t figure it out, that is always something to check in and ask, “Hey, could this be related to CLL?”
Because there are some weird things that happen to people with CLL and certainly the physician caring for anyone with CLL should be able to figure it out. If anyone develops weird health concerns that are really symptomatic or problematic that other doctors can’t figure out, always a good chance that it could be CLL related and you should check in.
Does CLL increase the risk of other cancers?
Dr. Kerry Rogers: Yes, it is true. CLL is a cancer of immune system cells called B lymphocytes so it changes the way the immune system works because the CLL cells are there. By the way, treatment to reduce the CLL cells doesn’t fix this — only makes the problem worse. Your immune system is what protects you from other cancers by killing abnormal cells that your body forms as it makes new cells over time so cancer screening is important.
The top ones we see are actually skin cancers and, of course, lymphomas, as was pointed out earlier, do occur in people with CLL but those are kind of related types of cancers. But skin cancer’s actually one of the top ones so I try to get everyone’s skin cancer screening.
Side effects of treatments
Fatigue caused by CLL treatment
Catherine Ferguson: That was the worst part of it for me, honestly. I could deal with any of the other side effects even when I just finished a clinical trial a year ago. I’ve been undetectable MRD and in remission now for a year and I feel so much better. But that fatigue, even during treatment. Everybody said once you start treatment, the fatigue goes away, but I still had the fatigue even during treatment till I got off of the meds.
I work out a lot and I went to the gym every day and I tried to just keep up my routines. I’m generally an active person anyhow so I try not to give into it.
For a time period there, I would fall asleep while I was working on the computer with my hand on the mouse and my wife would look over and say, “Cathy,” and then I just wake up and I’d start to keep on moving again like I didn’t do anything. But I didn’t decide I was going to take a nap; I would just fall asleep. It’s just really hard.
How do new CLL/SLL treatments differ from traditional ones and what are some of the latest options available?
Dr. Kerry Rogers: I like to say that about a decade and a half before this kind of chemotherapy or chemoimmunotherapy, which is chemotherapy with an antibody works real well. In last decade and a half have been all about targeted agents. We actually no longer use chemotherapy to treat CLL. We do use it to treat other lymphoma successfully, but the whole name of the game is oral targeted agents and these are drugs that interfere with proteins in the CLL cells that make them behave like cancer cells.
The two main classes of drugs are something called BTK inhibitors and venetoclax, and they are extremely successful with virtually everyone achieving a remission, and just work very well.
The field is currently looking at newer generation agents of these different dosing schemes or different combinations to try to make treatment more effective but also easier to do for people and to have fewer side effects.
Is it crucial to see a CLL specialist immediately after diagnosis, or can it wait?
Dr. Kerry Rogers: It’s actually an individual decision. There are some reasons that people actually definitely need to see a CLL specialist. One is just if things aren’t going well, right? So not responding to treatment, developing side effects, not being offered acceptable options from your general hematologist oncologist — things aren’t going well, always see an expert.
Some other good times are planning a treatment, any treatment, because, usually, the CLL specialist will be able to have a good and, hopefully, more detailed discussion about treatment options or even offer participation in a clinical trial, which has a lot of advantages. But this doesn’t always have to be done at the time people are diagnosed just because if you’re in watch-and-wait and you’re happy with what’s going on,] it doesn’t mean you have to run out and see a CLL specialist right away, especially if you don’t live near a CLL specialist.
If you live in Boston, it’s very easy to go see one of my colleagues at Dana-Farber and other excellent doctors in that area. But if you live in rural Ohio or West Virginia, we get people that come from West Virginia. It’s like a three-hour drive so it’s a big burden to do that right away
And then I guess at diagnosis, one of the main reasons to see a CLL specialist is to get questions answered and to learn about CLL, which I think benefits all people. Most people do want to learn more about it, but there’s] a group of people that cope by putting CLL from their mind and they can certainly delay seeing a CLL specialist until there’s a reason like needing treatment.
Cancer details: IDC is most common kind of breast cancer. 1st Symptoms: Lump found during self breast exam Treatment: TC chemotherapy; lumpectomy, double mastectomy, reconstruction; Tamoxifen
Cancer details: IDC is most common kind of breast cancer. Stage 1B. 1st Symptoms: None, caught by delayed mammogram Treatment: Double mastectomy, neoadjuvant chemotherapy, hormone therapy Tamoxifen
Cancer details: IDC is most common kind of breast cancer. 1st Symptoms: Lump in right breast Treatment: Neoadjuvant chemotherapy, double mastectomy, targeted therapy, hormone therapy
Cancer Details: ER/PR positive = estrogen and progesterone receptor positive 1st Symptoms: Lump found on breast Treatment: Lumpectomy, AC/T chemotherapy, radiation, and hormone therapy (Lupron and Anastrozole)
Cancer details: Triple negative doesn’t have any receptors commonly found in breast cancer making it harder to treat 1st Symptoms: Lump in breast Treatment: Chemo, double mastectomy, hysterectomy
Cancer Details: ER positive = estrogen receptor positive 1st Symptoms: Dimpling/lump found on breast Treatment: Mastectomy, AC/T chemotherapy, hysterectomy, reconstruction
Cancer details: IDC is most common kind of breast cancer. Triple positive = positive for HER2, estrogen receptor (ER), progesterone receptor (PR) 1st Symptoms: Lump in breast Treatment: chemotherapy, lumpectomy, radiation
Cancer details: IDC is most common kind of breast cancer. Triple positive = positive for HER2, estrogen receptor (ER), progesterone receptor (PR) 1st Symptoms: Lump in left breast Treatment: Neoadjuvant chemotherapy (TCHP), lumpectomy, radiation
Cancer details: Triple negative doesn’t have any receptors commonly found in breast cancer making it harder to treat 1st Symptoms: Lump in left breast Treatment: Mastectomy, chemotherapy, 2nd mastectomy
Cancer details: Triple negative doesn’t have any receptors commonly found in breast cancer 1st Symptoms: Lump in left breast Treatment: Chemotherapy, surgery
Cancer details: Triple negative doesn’t have any receptors commonly found in breast cancer making it harder to treat 1st Symptoms: Pain in breast Treatment: Surgery, chemotherapy, radiation
Cancer details: IDC is most common kind of breast cancer. DCIS means cancer has not spread into surrounding breast tissue 1st Symptoms: Pain in left breast, left nipple inverting Treatment: Double mastectomy, chemo (AC-T), Radiation
Symptoms: Lump in breast Treatment: Chemotherapy, double mastectomy, radiation
Cynthia J., IDC, Stage 2B Diagnosis: Stage 2B Breast Cancer Symptoms: Architectural distortion on mammogram Treatment: Double mastectomy, radiation
Nikki M., Stage 3 HER2+ InflammatoryDiagnosis: Stage 3 Inflammatory Breast Cancer Symptoms: Centralized pain around the nipple, inverted nipple, swollen breast, differences in nipple color, warm-feeling breast Treatment: Chemotherapy, single mastectomy, radiotherapy
Cancer details: IDC is most common kind of breast cancer. DCIS means cancer has not spread into surrounding breast tissue 1st Symptoms: Pain in left breast, left nipple inverting Treatment: Double mastectomy, chemo (AC-T), Radiation
Cancer Details: Only 1-4% of breast cancer cases also includes Paget’s 1st Symptoms: 2cm lump found in right breast Treatment: Lumpectomy, double subcutaneous mastectomy, hormone therapy
Cancer details: IDC is most common kind of breast cancer. DCIS means cancer has not spread into surrounding breast tissue 1st Symptoms: Pain in left breast, left nipple inverting Treatment: Double mastectomy, chemo (AC-T), Radiation
Cancer details: Both ductal and lobular, estrogen receptor positive. Different than breast cancer Tina’s mom was diagnosed w/ twice. 1st Symptoms: Sunken in nipple of right breast Treatment: Double mastectomy, chemotherapy, radiation, hormone therapy
Cancer details: IDC is most common kind of breast cancer. DCIS means cancer has not spread into surrounding breast tissue 1st Symptoms: Pain in left breast radiating from lump Treatment: Bilateral mastectomy, chemotherapy
Cancer Details: Previvor 1st Symptoms: Family history of breast cancer, no physical symptoms Treatment: Preventative double mastectomy, direct implant reconstruction
...
Ruth Fein: Myeloproliferative Neoplasms (MPN) Story
Ruth shares her Myeloproliferative Neoplasms (MPNs) story, a rare blood cancer, and builds awareness to help bridge the gap in a world where so little information exists.
In her story, she shares her experience in navigating her rare disorder, self-advocacy, how her life and outlook evolved with her diagnosis, why she chose to join a clinical trial and her hope in the ever-growing research toward rare cancers such as hers.
Myeloproliferative Neoplasms (MPN) Cancer Diagnosis & Evolution
What was your initial diagnosis?
I was 38 years old when I was diagnosed first. That was with something called Essential Thrombocythemia (ET). And about 15 years later, that transformed to PV, which is Polycythemia Vera.
But when I was first diagnosed, and this was a number of years ago, it was called a blood disorder. Then a number of years went by and the World Health Organization reclassified it as a blood cancer.
Today, it’s called a group of rare blood cancers and Essential Thrombocythemia is basically an overproduction of platelets and Polycythemia Vera is like this little switch that goes off and says, “Oh no, you’re bone marrow. Listen to me, you don’t need extra platelets. You need more red cells.” So your platelets go down, but your red cells go high.
The third disease in that category is something that I’ve also progressed to over the years called myelofibrosis.
“What happens in myelofibrosis, which is very rare – only about 10% of people with either ET or PV progressed to myelofibrosis. I’m just one of the lucky ones.”
What happens in myelofibrosis is your bone marrow starts to produce fibrosis, which is scar tissue or scarring of your bone marrow. And what that does is it prevents your blood cells, or your stem cells, from producing healthy blood cells, red cells, white cells, and platelets.
You become anemic, among other things, and so your high risk for clots and also for bleeding sort of live between this vicarious place between a risk of bleeding and a risk of clotting. That’s a very strange place to sit because the treatments, of course, are exactly the opposite.
How did you process your chronic cancer diagnosis?
It’s a great question because I really think it’s important to make the distinction between chronic and acute cancer. You hear the diagnosis, you hear that “big C” word and I think a lot of times people don’t hear anything beyond that.
“So they then walk out of the office saying, ‘I have a rare blood cancer.’ And that’s how they feel it and that’s how they communicate it and that’s how they research it. They jump to the Internet where they get old, outdated information.”
With any rare disease, particularly with myeloproliferative neoplasms, the research has just accelerated at such a rate in the last five to ten years. Even in the last three years, if you go on the Internet, you’re going to get very different information if you just do a generic search, then if you go to a trusted source like Patient Power and lots of others.
Living with Myeloproliferative Neoplasms
Describe life after your cancer diagnosis
When I was first told that I had Essential Thrombocythemia, I basically lived my life. Five years later I ran the Dublin Marathon. I was on an aspirin a day. I was raising two children. I honestly didn’t think about it often.
But what it did do, and I think that this is something I can share, even though it wasn’t supposed to affect the longevity or quality of my life, they thought at the time, it still made me face my mortality in a way that a 38-year-old doesn’t usually have, what I call, “privilege” to do that. Right? We go on with our lives and we raise our children if we have children, and we work furiously.
I think most people, unless they have a scare, a health scare, don’t face that mortality in the way that gives us the benefit of saying, “Hey, you know what? Let’s slow down and [ask] what’s really important to us.”
As I used to say…”I could get hit by a truck tomorrow.” That was my way of saying “I could also die tomorrow.” But it’s more comfortable to say I might get hit by a truck. It definitely has an effect and it can be a positive effect.
Then when the disease changed to Polycythemia Vera, there were totally different treatments. It comes with much higher risks. I had life-threatening blood clots [and was] hospitalized a couple of times. You know, it did change things and by then they were calling it blood cancer.
Did you tell people that you had cancer?
At that point, I still really didn’t tell very many people in my life, which is a conversation that I often also think is important to have. We can have that.
Everyone deals with a cancer diagnosis and even living with cancer, very differently. And for me, I wasn’t in chemotherapy every day. I wasn’t in a situation that people could see my hair falling out and some of the other things that people live with who are being treated aggressively. I was on daily chemotherapy – an oral drug that was probably the oldest chemo drug available to men or women. But it wasn’t visible.
For me, I didn’t want to be a person who everybody looked at as someone living with cancer and “Oh, how are you and how are you doing?” And all the things that go along with that, and people bringing meals to my doorstep.
However, I don’t want to minimize the importance of all of that. People need different things. I’m just suggesting that we think that people want or people should – there’s a “should” word – tell people, express themselves, share how they feel, and tell their community so their community can reach out to them.
“I’m bringing it up because I think it’s important to acknowledge that everyone doesn’t react the same. Everyone doesn’t have the same needs, and they can change, which is what happened to me.”
Describe your secondary cancer diagnosis
What happened is I had a bout with early colon cancer, which we now think is probably secondary cancer, which is common to have with Myeloproliferative Neoplasms.
I have eaten healthier than anybody I know for my entire life. So when I got colon cancer, my children actually laughed out loud. Not in a cruel way, but saying “How could you have colon cancer?” But it probably was secondary.
The point is they took eight inches of my colon out. I didn’t need additional therapies because it was very early. I was walking around the hospital on day three like Superwoman. I’m feeling great and “You’re doing great. We’re sending you home.” And I went home.
Twenty-four hours later, I had a massive bleed that put me in the ICU for five days, and really recovery for multiple months where I couldn’t really get out of the recliner.
How did colon cancer change your outlook on living with blood cancer?
At that point, I decided to take my disorder, then a blood cancer, to a different level. My acknowledgment of it, my treatment of it. I sought a super-specialist. I was already seeing a hematologist oncologist in the community and I saw a specialist – which, when I was first diagnosed, there was no such thing.
That changed everything, you know? So from there, I realized the high risk that I was at. They did a bone marrow biopsy and found I had myelofibrosis, which is dreaded of the three MPNs because it’s the most life-threatening. And it was offered to me to be on a clinical trial.
Clinical Trial
Why did you choose a clinical trial?
It’s a great question. I think in our society, and maybe around the world, we’ve come to look at clinical trials as a last resort. And for me, that’s so wrong. And I know in your experience that’s so wrong as well, particularly with a rare disease.
“The research is happening so quickly. We have very, very few treatments that are approved. The only way we’re going to get better drugs and better treatments is through clinical trials.”
And so I hadn’t ever thought about it before, quite honestly, but I have a great physician specialist in New York. And she said to me, “You know, there’s a new trial and you would be a perfect candidate. What do you think?” And I, of course, said, “What do you think?”
Because another very important thing with a rare disease, or any disease, is to have a practitioner that you really trust. And that might take a second opinion and a third opinion, but find that person who knows your disease and knows it in and out, and that you trust their judgment. So when she thought I was a perfect candidate. I said, “Okay, I’ll go for it.”
Weighing the risks and benefits of clinical trials
When you go into a clinical trial, you look at the risks, you look at the benefits and you weigh them and you always have the ability to do one of two things. If you’re not doing well, you have the ability to get out. This was, for instance, a two-year trial. You’re not committing to two years.
And the first six weeks were really rough. Really, really rough. And I think a lot of people do walk away. For me, I was encouraged by my practitioner that she was watching me carefully every week and that I was probably going to get past this very early stage of side effects.
So the other option with a clinical trial is if you do well, which I’m doing extraordinarily well after three years, you could stay on that trial. So I’m still on that trial, even though it was a two-year trial. I still meet all the protocols and get my magic drugs, and I’m doing better than anybody expected me to be.
What was the transition from your local oncologist to a clinical trial like?
It was me who was uncomfortable because I felt as if I was second-guessing his expertise, but he did not feel that way. With a rare disease, he had a handful in a lifetime. His entire life of practicing, he had a handful of patients like me, and he didn’t have access to the information at his fingertips or experience as you would find in an academic center.
Myeloproliferative Neoplasms survivor Ruth, with her two sons.
Being A Patient Advocate
Bridging the gap between community practitioners and specialists
Now, that said, I think one of the things that we can do as people living with rare blood cancer – or whatever conditions we have – and also as a patient advocate, I think one of the things we can do is to help educate our community practitioners.
I think we need to do a much better job as an organization, as individuals and organizations, advocacy organizations, research organizations, and even the media, to bridge that gap between the community practitioners and the specialists. because I was on a drug that [my doctor] was very happy keeping me on that was just controlling my symptoms. But in the process, I got sicker.
And we now know that in particular for myelofibrosis, it’s not just about symptom management. You need to look at more than just your blood counts, which is the typical thing that someone outside of an academic institution is going to do – they’re going to look at your blood counts.
I would go to see [my doctor] and he would say, “Wow, you look great. Your blood counts are great. See me in another three months.” And of course, that’s not the answer, because all that time my bone marrow was producing fibrosis.
I was lucky that you know, while I had episodes, I was lucky that I saw someone when I did.
Describe your experience with bone marrow biopsy
Bone marrow biopsy is a very common procedure for blood cancer patients. It is, in my opinion, and in a lot of experts’ opinions, overused. And particularly in clinical trials, it has become an endpoint, or at least a measurement, if not an endpoint, of how a person is doing and they build it into protocols for clinical trials.
The [clinical trial] I’m on, I had to have a bone marrow biopsy every six months. When in fact, after the first one, at six months I was doing better. [After] the second one, I was doing great. I probably didn’t need to have them every six months continuously unless something changed.
So most super specialists that you speak to will want to do a bone marrow biopsy at the beginning of diagnosis and [again] if there are any changes or they’re concerned about something that may be different.
And the experience of a bone marrow biopsy makes me want others to advocate for themselves because it’s not fun. I know I’ve spoken to many people who say it’s not at all for them – their experience was not terrible. For me, it was.
I had two terrible bone marrow biopsies where the anesthesia didn’t work and they’re basically drilling into your bone. Just visualize that.
Discovering a better option for bone marrow biopsy
What I did is I had one after I had two bad [biopsies], it was suggested to me by someone that they could do this with – you know, under no anesthesia, but like sedation– with interventional radiology. Someone mentioned to me that they always have their bone marrow biopsies with interventional radiology, and that was total news to me.
So I asked for it and they did the first one and the next one that way. And I said quite clearly, “I am never ever having one without again.”
I think [bone marrow biopsies are] barbaric. And I think any practitioner who does them needs to have one themselves before they do it on their patients. And I don’t say that to scare people. Many people have them and they’re fine.
“I know [interventional radiology is] expensive, but we spend our health care costs on lots of things. Why shouldn’t it be on something that’s so directly related to comfort and pain?”
We do it for other procedures. Just because there isn’t a large patient population that needs a bone marrow biopsy, it should not keep us from doing it in the best way we know how.
Reflections
Well, I’m a health and science writer, so one of the things I did is I used that tool to start to write about MPNs, and that’s because others weren’t. It’s a rare disease, and what I started to hear through a very small grapevine, is that people didn’t have materials to share with their friends and families to explain what they had.
How did you share your cancer story with others?
Again, it comes back to “I have blood cancer” and that’s so frightening. Likewise, practitioners didn’t feel as though they had great consumer-level materials to share with patients to explain it. So it happened by accident.
I actually wrote a story. I’ve written on and off for the New York Times for a number of years, but I wrote a first-person story that they accepted and published. That was in 2021, and it’s the first time I really told my story publicly.
The outpouring of support, even still, is amazing to me. Not to pat myself on the back at all, but to make me recognize how large the need was and still is for people to talk about and write about and read about rare cancers.
And so I started using my tools to do that and I started writing more about it. I started doing webinars for Patient Power, which I’ve really enjoyed. I started working with the Research Foundation and writing for their newsletters and various other publications.
“Little by little, I’ve become involved as a patient advocate along the way, and that’s been really good for me and that’s not how I initially saw it. I saw it as my way to help others.”
How did your lifestyle change?
I’m probably a little outside the norm in many things, but in this as well.
I’ve eaten healthy my whole life – probably as close to the Mediterranean diet as is now prescribed for anti-inflammatory issues such as [Myeloproliferative Neoplasms} and so many other cancers. So it wasn’t about diet, it wasn’t about exercise – I’ve been active my whole life. Some of that had been taken away from me.
I went from, for a while, not being able to walk up the street without holding on to a lamppost at the end of one block to having to sit in a recliner and not do much some days because the fatigue just made it impossible.
I then had to become active again, and that’s a long haul. People who have gone through that, for all kinds of reasons, know that that’s a slow process. So for me, it was relearning rather than learning.
Probably more than all of those things, in terms of lifestyle, was me learning to share my own feelings and experiences. And my dear, sweet husband would tell you I had to learn how to ask for help, which I’m not good at. And his main frustration, which you as a care partner know, is that he wants to help and I don’t always allow him to because I want to do things myself. Those things are where the changes came in for me personally.
What advice do you have for someone diagnosed with Myeloproliferative Neoplasms (MPNs)?
I think number one on my list is, to find a specialist. And it’s a shame that has to be at a major academic center. Because for so many people it has nothing to do with geography as much as it does socioeconomic status and every other thing that defines us or surrounds us. But there are ways.
If anything positive came out of the pandemic for us – a patient population – is that most of the super specialists I know, that I speak to in my work, are very happy to have a remote consult.
It doesn’t mean you need to give up your local hematology oncologist or whoever you see in your community. It means that you need a bridge to a specialist who can work with that physician and make sure that they’re seeing, not just the whole you and the whole picture, but also the latest and greatest of what’s happening there in the academic centers that they can do in their clinic.
Clinical trials, again, are a misnomer. Clinical trials don’t have to be done in an academic setting. They can be done by community physicians. They just don’t always take that opportunity or know about those opportunities. So finding a specialist, no matter where you live. You can do it remotely. Do the research, and get your answers.
Number two. I think you have to believe – and this is about learning and educating yourself so that you can educate others. You have to believe in the difference. As I said before, it’s sort of like fact-based hope, as I like to call it. The facts are different now than they were even three years ago.
This is a chronic condition. This is not an acute condition where you can cut it out, radiate it out, be in remission, and go through life. This is something you’re likely to live with, and because of that, you need to be educated and your hope comes from the education.
Ruth and her husband, Danny during their wedding.
What hope do you want to share with those with Myeloproliferative Neoplasms (MPNs)?
Your hope will come from how fast things are changing and how many new answers there are out there. New medications. New treatments. The more you learn, I think you will start to believe that there really is a difference between chronic and acute cancer. And that many cancers today, because of our advancements in science, many cancers that were known as killers just a few decades ago are now chronic because people can be treated and live a good, long life.
What is your top tip for those with cancer?
The last thing on my list is advocacy, and I touched on that before.
Be your best patient advocate. Advocating for yourself is your best patient advocate. The on bone marrow biopsy is a perfect example. You have to say that that’s what you want. “I want my bone marrow biopsy with interventional radiology.”
The other thing is, I have very tiny veins and they roll. Just getting blood work done, which I have to do every three weeks, is an emotional chore because sometimes it takes six or eight sticks. It’s not the pain of it, it’s the stress of it. So an IV is always really stressful for me. When I go into any procedure, I say right from the get-go, “I want an IV Specialist because I don’t want you to feel the stress of having to stick me eight times. It’s going to hurt you more than me.” Which it does, you know?
“You need to learn the things to advocate for. It’s not about being a bothersome nuisance. It’s about getting what you need, using the resources that are at hand to everyone’s benefit, and using the great science that we’ve advanced to, to make life easier, less stressful, and healthier.”