Multiple Myeloma: How Your Race and Age Can Affect Diagnoses and Treatment
Multiple myeloma is the most common blood cancer among Black patients in the U.S., but many of those patients have an entirely different experience.
Studies show that Black patients respond better to newer treatments but are still twice as likely to die from the disease.
Patient advocate Valarie Traynham speaks with Shakira Grant, MBBS, of the UNC Medical Center. They discuss the barriers many Black patients face, how it impacts their care, and what can be done to help improve their outcomes.

Newly diagnosed patients [need] someone [who] they can ask questions [and] find out information and where to go for good relevant resources.
Valarie Traynham
Introduction
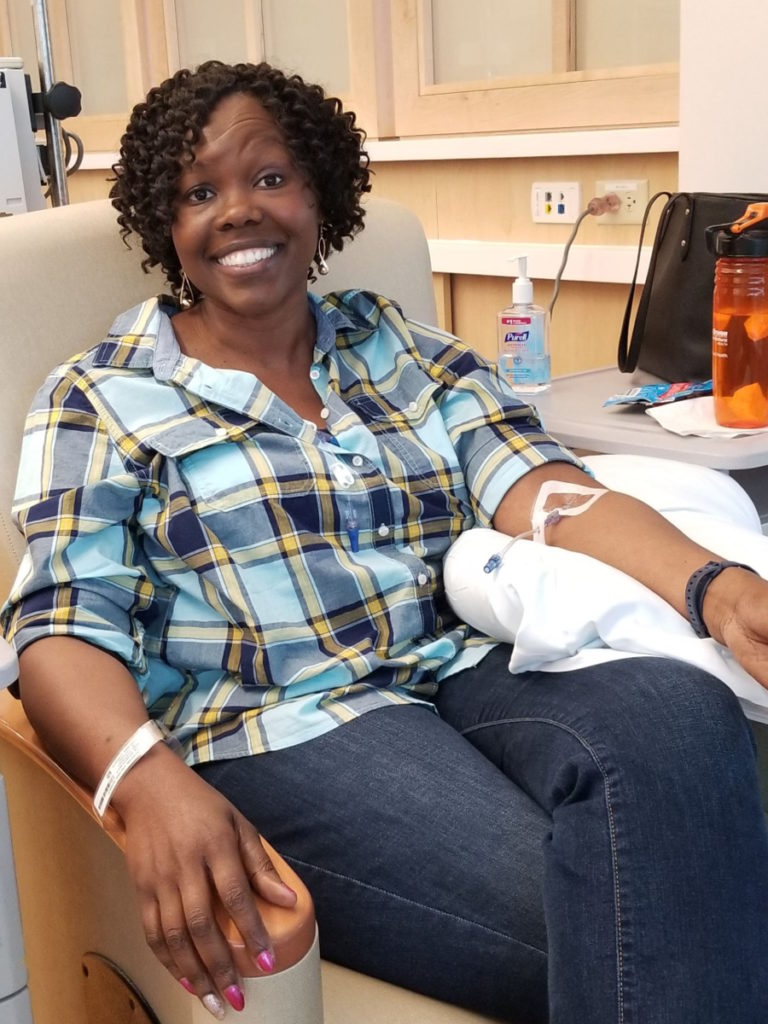
Valarie Traynham: I was diagnosed with multiple myeloma in 2015. Being a patient advocate, I want to be able to guide others through the process. When I was diagnosed, I did not have someone to go to and I think that’s very important. Newly diagnosed patients [need] someone [who] they can ask questions [and] find out information and where to go for good relevant resources.
I’m just so excited at the work that Dr. Grant is doing because it’s much needed. It’s an area that needs focus and she’s doing a wonderful job [of] getting that focus out there.
She focuses on a population of patients in the myeloma world that oftentimes [is] overlooked. It’s very important for that population of patients to be looked at and cared for and really understand what they are going through.
Dr. Grant is from the University of North Carolina and she focuses on geriatric multiple myeloma, health, and research.

Unfortunately, because multiple myeloma is also a disease that impacts older adults, we see this compounding effect, especially for Black older adults with multiple myeloma.
Dr. Shakira Grant

Dr. Shakira Grant: I’m primarily here to talk a little bit about our research and how this fits into sharing stories of patients and caregivers, which our team is really passionate about.
What really drew me to this type of work was this love for trying to bridge this gap in terms of the disparities that we see existing within not only outcomes but also survival for Black and white patients with multiple myeloma.
Unfortunately, because multiple myeloma is also a disease that impacts older adults, we see this compounding effect, especially for older Black adults with multiple myeloma. It’s really important for us as a research team to address some of these healthcare access barriers, which largely drive the disparate outcomes that we see in multiple myeloma.
We presented two studies. For the first one, we wanted to understand what barriers patients and their caregivers encounter when trying to seek care for multiple myeloma.
The top takeaway from that study is that many of our patients report that there’s really a delay in getting the diagnosis of myeloma and this results in them going to multiple specialists with their symptoms. Often, patients reported being dismissed by their doctors and being chalked up to just getting older and then repeating labs again in three months.
From this particular study, while we identified other barriers, including financial barriers, we do recognize that there is a need to focus on how we make the diagnosis, ensuring that patients are getting the diagnosis on time, which would allow them to enter into a care pathway where they can begin their treatment and minimize any chances that they will have any poor or adverse effects from multiple myeloma.
In terms of the other study, we wanted to look at factors that influence the participation in clinical trials for Black patients in particular. We did this by looking at the perspectives of patients with multiple myeloma as well as their hematologists.
One of our main takeaways from this is that the patient and their relationship with their doctor is really critical when trying to decide if a patient is going to be offered the opportunity to participate in a trial. Based on these findings, we do recognize that there is a need for more targeted interventions that address several steps in terms of communication between patients and their doctors to ensure that we have the best chances of offering clinical trials to a diverse patient population.
Many of our patients report that there’s really a delay in getting the diagnosis of myeloma and this results in them going to multiple specialists with their symptoms.
Dr. Grant
How do we get more diversity in clinical trials?
Valarie: I heard a lot about clinical trials. How can we get more minorities involved? What is that like for the older population that you see in the clinic?
Dr. Grant: Overall, when we think about increasing representation in clinical trials, we are coming up against two compounding factors. One is the older adult and then it’s the older adult who also identifies as having Black race.
For me, in clinical practice, one of the things that we try to do is to not only look at [the] patient’s chronologic age, but we also look at the functional age of patients. How well are they able to do their activity and to get around day to day? I believe that [is] probably better to assess eligibility for these particular patients for clinical trials in terms of Black representation or increasing representation of minoritized populations.
It is important for us to realize that myeloma does tend to affect an older adult population. We cannot really distill out and think about age and race separately, but we really should be thinking about these two things together. Our efforts to increase representation should be geared towards the older adult population, as well as thinking about the racial, ethnic, and minoritized populations.

We cannot really distill out and think about age and race separately, but we really should be thinking about these two things together.
Dr. Grant

How would you advise older multiple myeloma patients to stay positive?
Valarie: For a newly diagnosed older patient, how would you advise them? [There’s] so much going on. They’re getting the diagnosis. They’re trying to make it to the clinic. How would you advise them to stay positive and look for the good in the situation that they’re facing?
Dr. Grant: The thing that is really important that I’ve seen come out not only [from] our research but in my own clinical practice is the need to have a social support system. In our study, we looked at informal caregivers who were oftentimes spouses and, in some cases, adult children.
I really do think that having that support when you’re first diagnosed is really critical because you have, in essence, [a] second set of ears, [a] second set of eyes to help you with the amount of information that you’re getting, scheduling, [and monitoring] any potential treatment-related side effects.
I think [it’s] really important for patients to also seek knowledge about multiple myeloma from credible resources. Read as much as possible what you can about this disease, about things that you can expect, and then come to your provider’s visit prepared with those questions ready.
Having that support when you’re first diagnosed is really critical because you have, in essence, [a] second set of ears, [a] second set of eyes to help you.
Dr. Grant
Ask [about] things like clinical trial participation, if your doctor hasn’t mentioned it. It’s really important for patients to take that first bold step and say, “I’ve read about clinical trials. Do you think this could be a potential option for me?”
This really moves into this idea that we want our patients to not only have a really great social support system but also to be empowered to be able to ask the questions that they need of their physicians without feeling fearful or intimidated.
Valarie: I’m so glad you said that because that is one thing that I always try to tell newly diagnosed patients as a patient advocate. Find reputable material. Find out everything that you can about the disease. Don’t be afraid of it. It’s something that you’re going to be living with indefinitely.
We want our patients to not only have a really great social support system but also to be empowered to be able to ask the questions that they need of their physicians without feeling fearful or intimidated.
Dr. Grant
How do you build medical trust in Black communities?
Valarie: We know that trust in the African-American community is a big deal and that’s what we are focusing [on], too: raise trust and build trust in the community. As a physician, what are some of the things that patients are mainly dealing with?
I was listening to something and they talked about words matter — how you talk to patients, understanding patients, words that you use, words that the patient uses, and understanding and gathering information. Tell me [about] your thoughts on that.
Dr. Grant: What we’ve seen in our studies time and time again is that there is this legacy of medical mistrust that has been brought on by past research events where Black patients were intentionally harmed by the research enterprise and so it takes quite a while to be able to reverse those effects.
Things that we’ve learned from talking to patients [and] caregivers that can help close that trust gap is really working on our communication style as physicians, making sure that we’re using empathic communication, [and] letting our patients see that beyond the doctor title, we also are real people with real lives and lived experiences.
Don’t be afraid to pull back that curtain sometimes and let patients see that that relationship between patients and providers really helps to build up trust.

Find reputable material. Find out everything that you can about the disease. Don’t be afraid of it. It’s something that you’re going to be living with indefinitely.
Valarie
I think of a particular quote from one of our studies where a patient said that it’s all about [the] relationship and if we need to build trust, we really need to be focused on the relationship. That particular participant went on to say that really they believe that the physicians could benefit from relationship-building training.
That really stuck with me because I recognized that trust is so difficult to address. These are some strategies that, as a physician, we can do to at least start to build that and close that potential gap.
When it comes time to think about the research, there are different strategies that our team [uses] to really help foster trust and to help engage Black participants in our study. Some of those strategies have been described in the literature, but really it’s about having a team that is representative of the population that we’re trying to engage and helping them realize the value of this research and why we need to do this, especially for the Black community.

Trust is so difficult to address. These are some strategies that, as a physician, we can do to at least start to build that and close that potential gap.
Dr. Grant
We need to recognize that access to healthcare is dependent on several steps. This includes the patient’s ability to perceive their need for healthcare. Then they need to be able to seek out those services, reach the services, pay for the services, and engage with their healthcare provider.
I would encourage patients: if you are experiencing symptoms you’re concerned about and you’re seeing your provider and you don’t think your provider is necessarily answering or addressing those questions, don’t be afraid to talk to somebody else. Talk to another provider and do some additional research and see if there is potentially another option for you to have your symptoms examined.
They have to think about [the] costs of medications but also when they’re coming to the cancer center, the cost of parking, the cost of gas… all these things are really additive for patients, especially when they’re on a fixed income. This idea about having to pay twice was centered around the need to pay for all of these other healthcare services while also attending to the high cost associated with paying for parking at the health center.
In terms of other economic impacts, things like parking, don’t be afraid to tell your provider, “This is challenging for me to pay for parking,” or, “I’m having challenges just paying for my medications.” Because honestly, sometimes the visit time is so short that we don’t always have the time to ask if you are having financial concerns. We don’t want that. These financial challenges are a limitation to you getting your care on time.
Don’t be afraid to talk to your providers if you have concerns. Make those concerns known… If you’re having financial challenges, continue to share those concerns and ask about available resources.
Dr. Grant
Barriers patients face that prevent their care
Valarie: How often do you have patients that [face financial limitations?]
Dr. Grant: We actually see this, in my practice especially, quite often. It’s not uncommon at all for patients to be concerned about the cost of parking. Patients would express concerns about their ability to pay for parking. Sometimes it’s a bit of a challenge knowing what to do in those scenarios.
There are some efforts now at our cancer center to try to provide more accessible parking in terms of financial costs and reducing the cost of that, but it’s not always widely available to patients.
Don’t be afraid to talk to your providers if you have concerns. Make those concerns known. That goes from even when you’re first presenting, before you’re diagnosed and you’re concerned about it, keep sharing those concerns with your provider.
If you’re having financial challenges, continue to share those concerns and ask about available resources. There are more resources out there than sometimes patients may actually think or may actually have knowledge about.
Conclusion
Valarie: Thank you for joining us today and going over all of this. It’s so important what you do in the field of myeloma.
What we’re dealing with is meaningful. It’s life-impacting so it’s very important that you understand if you’re not being treated right or you feel that something is not right, say something because it’s not okay.
You have the right as a patient to have something done about that. You are in control of your health. Don’t settle. Without you, it would just be a missing piece.
Dr. Grant: Thank you for having me.

If you’re not being treated right or you feel that something is not right, say something because it’s not okay. You have the right as a patient to have something done about that. You are in control of your health. Don’t settle.
Valarie
Special thanks again to AbbVie for its support of our independent patient education content. The Patient Story retains full editorial control.
More Medical Expert Interviews

Using AI to Detect Lung Cancer Risks With Dr. Lecia Sequist

Trends in Cancer Research 2022

The Role of Bispecific Antibodies in the Treatment of Multiple Myeloma

The Latest in Multiple Myeloma: Understanding Promising Treatment Options

The Latest in Multiple Myeloma with Caitlin Costello, MD
The Latest in Multiple Myeloma Treatments
The Latest in Lung Cancer Treatments

The Latest in Hodgkin Lymphoma: Treatment Options in 2024

The Latest in Hodgkin Lymphoma

The Latest in Genetic Testing in 2023

The Latest in Breast Cancer Patient Research

Testicular Cancer: What Patients Need to Know

SABCS 2022 Highlights

Relapsed/Refractory Multiple Myeloma Highlights from ASH 2022

Pathologists: The Unseen Doctors of Your Medical Team
Optimizing Quality of Life: Reducing Toxicity in Hodgkin Lymphoma Care

Newly Diagnosed Multiple Myeloma Highlights from ASH 2022

Myelofibrosis Highlights from ASH 2022

Multiple Myeloma in 2023

Monsanto Roundup Trials Update
Lynch Syndrome: What Patients Need to Know

Lola Fayanju, MD, MA

Let’s Talk CLL: Patients & Doctors Discuss the Latest LIVE – Transcript

How to Work With a CLL Specialist

How Long Can You Live with Chronic Lymphocytic Leukemia
High-Risk Smoldering Multiple Myeloma Highlights from ASH 2022

Health Insurance and Cancer Treatment

Financial Toxicity of Cancer Treatment
DLBCL: The Latest in Treatment and Research
DLBCL in 2023

Colorectal Cancer in Young Adults

CLL Highlights from ASH 2022