How Lauren Found Clarity Beyond T-cell Acute Lymphoblastic Leukemia (T-ALL) and Treatment Challenge
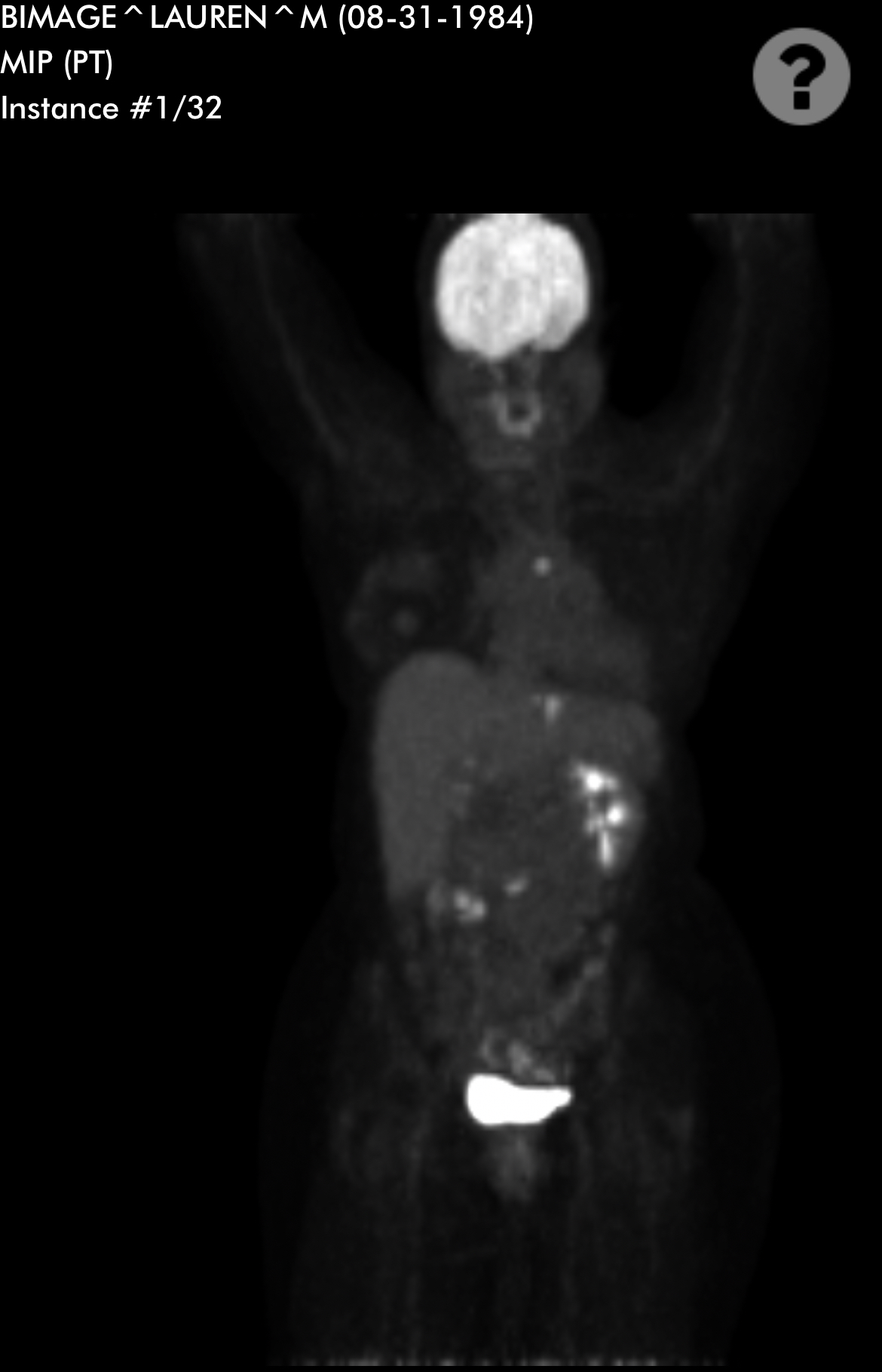
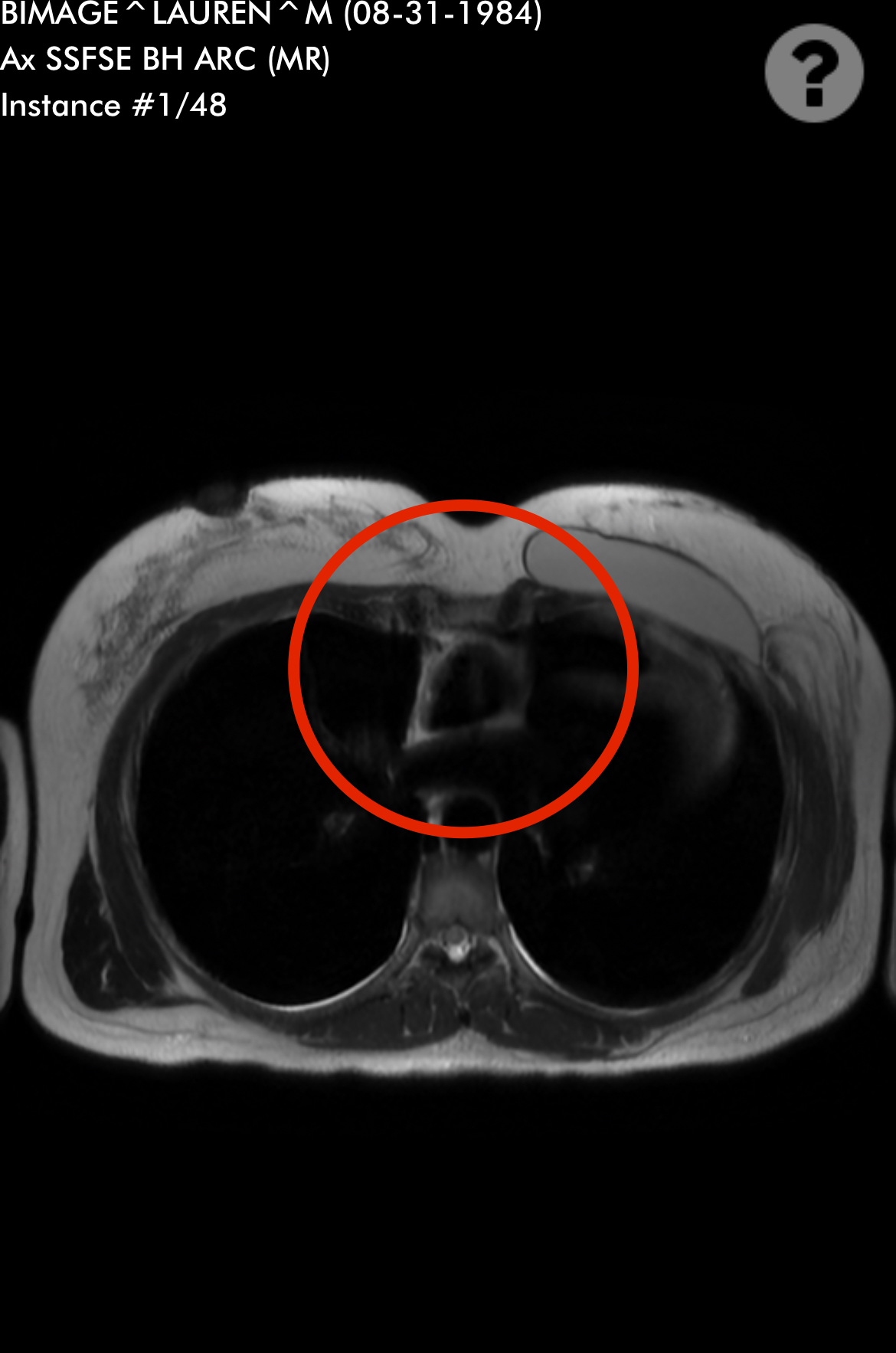
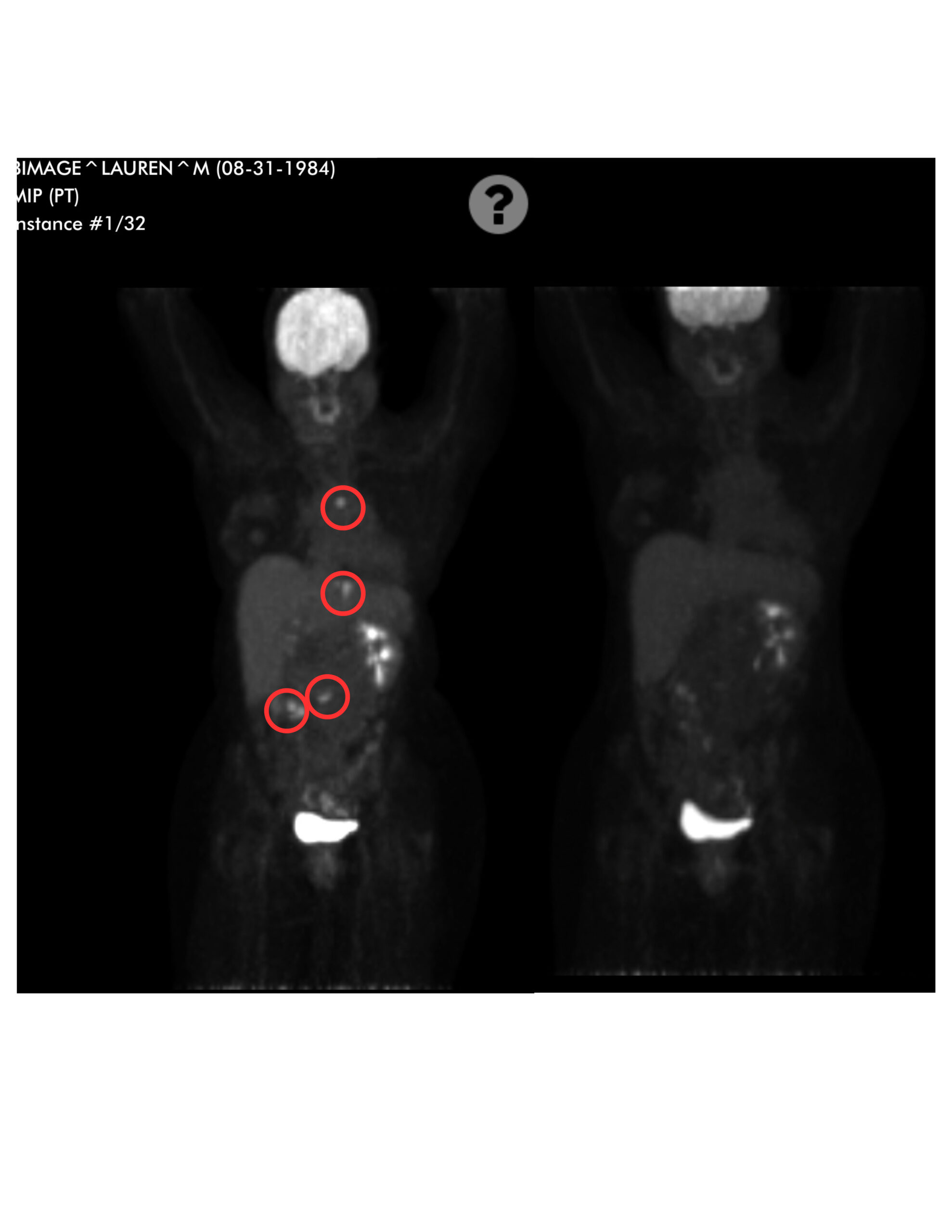
Lauren, who hails from Ohio, was diagnosed with T-cell acute lymphoblastic leukemia (T-ALL) in May 2022, a twist she never saw coming. What started as a typical cold spiraled into severe symptoms, including persistent cough, chest pain, and fever, which led to multiple doctor visits and misdiagnoses. Eventually, a chest X-ray and CT scan revealed an enormous mass near her heart, which rocked Lauren’s world. Her cancer diagnosis came swiftly, delivered bluntly by an oncologist who had little bedside manner.
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
Adjusting to life with cancer was overwhelming. Lauren faced intensive treatments, including lumbar punctures, rounds of brain radiation, and weekly chemotherapy. The treatments caused dramatic physical changes, including hair loss, neuropathy, and severe nausea, which challenged her daily comfort. Yet, amidst the chaos, Lauren found clarity. She decided to stop drinking alcohol, embraced a more balanced approach to health, and left a business venture that no longer aligned with her values.
Mental health played a significant role in Lauren’s recovery from T-cell acute lymphoblastic leukemia. She sought help from a palliative medicine doctor, not just for physical symptoms but for emotional support, too. Accepting this help was transformative, providing better management of her anxiety, depression, and physical side effects.
Lauren’s message is powerful: healing isn’t linear, and facing tough days is okay. She encourages others to focus on one day at a time, embrace the good moments, and reach out for support when needed. Her story underscores the importance of advocating for oneself, mentally and physically, during and after cancer treatment.
Watch Lauren’s video to discover:
How a common cold led to a life-changing T-cell acute lymphoblastic leukemia diagnosis.
Why Lauren says cancer became an unexpected blessing.
The role of mental health and palliative care in cancer recovery.
How leaving a business she co-owned helped Lauren find clarity during treatment.
How Lauren coped with T-cell acute lymphoblastic leukemia, one day at a time.
Name:
Lauren M.
Age at Diagnosis:
33
Diagnosis:
T-cell Acute Lymphoblastic Leukemia (T-ALL)
Symptoms:
High fever
Trouble breathing while lying flat
Bad cough
Headaches
Treatments:
Chemotherapy
Radiation
Lumbar puncture
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Spenser’s Stage 4 Oral Cancer Story: Turning Trauma into Triumph Against All Odds
Spenser was diagnosed with stage 4 oral cancer. He had always been athletic and was training to be a professional bodybuilder. But in 2022, he experienced an excruciating toothache, which led him to visit the ER. Although he had the tooth removed, he still felt something was off.
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
As time progressed, Spenser started to feel very tired and kept having canker sores. He powered through and continued his rigorous workout routines. By January 2024, though, he could no longer dismiss his symptoms. A dental visit revealed a jarring sight in his mouth, leading to a referral to an oral surgeon, who immediately suspected cancer.
The surgeon’s suspicions proved true when Spenser was diagnosed with stage 4 oral cancer (squamous cell carcinoma of the tongue), which had spread to his neck and throat lymph nodes. To deal with a massive tumor, he underwent a grueling seven-hour surgery. The surgeon removed part of his tongue and numerous lymph nodes. The surgery was life-threatening, and his communication abilities were seriously jeopardized.
Recovering from surgery, Spenser next had to consider undergoing chemotherapy and radiation. He initially refused, but his doctors ultimately won him over. His treatment and its side effects were grueling, but Spenser’s resilience shone through. He defied expectations and refused to let his cancer defeat him.
Although Spenser survived stage 4 oral cancer, he experienced permanent kidney damage from chemotherapy and psychological scars, including PTSD and severe depression. Work became difficult, and he struggled under the pressure of his thoughts.
But Spenser rose to the occasion yet again. He found solace in boxing and embraced a new perspective on life. His story is about fighting against the odds, transforming trauma into strength, and never giving up.
Watch Spenser’s story for more about:
The importance of health and nutrition in cancer recovery.
How he remained resilient even during the hardest moments.
Listening to one’s body and seeking medical help if something feels wrong.
What he’d like other people to learn from his experience.
Name:
Spenser S.
Age at Diagnosis:
33
Diagnosis:
Oral Cancer (Squamous Cell Carcinoma of the Tongue)
Staging:
Stage 4
Symptoms:
Severe toothache
Excessive fatigue
Persistent canker sores
Appearance of a large cyst in the mouth
Treatments:
Surgery: partial removal of tongue, neck dissection with flap
Chemotherapy
Radiation
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Symptoms: Sore on the tongue, which caused pain during eating and speaking; changes in the color and texture of the tissue where the sore was located Treatments: Surgery (partial glossectomy, radical neck dissection, reconstruction), radiation
...
Small Changes, Big Impact: Easing Myeloma Treatment Side Effects
Multiple myeloma advocate Valarie Traynham is joined by Donna Catamero, Associate Director of Myeloma Research at the Icahn School of Medicine at Mount Sinai and a nurse practitioner specializing in the treatment of multiple myeloma patients, and Abbey Reiser, a dietitian/nutritionist and board-certified specialist in oncology nutrition from the Ruttenberg Treatment Center The Tisch Cancer Institute, to share practical strategies for handling side effects, optimizing nutrition, and improving quality of life.
Tiffany Drummond: I’m a patient advocate with over 20 years of experience in cancer research. My journey began as a caregiver when my mother was diagnosed with endometrial cancer in 2014. I quickly realized the challenges of finding resources, support, and shared experiences, and now I’m committed to helping others, no matter the condition.
At The Patient Story, we create programs to help you figure out what comes next. Think of us as your go-to guide for navigating not only the cancer journey but your overall health journey. From diagnosis to treatment, we’ve got you covered with real-life patient stories and educational programming with subject matter experts. I’m your personal cheerleader to help you and your loved ones best communicate with your healthcare team as you go from diagnosis through treatment and survivorship.
The Patient Story retains full editorial control over all content. We want to thank all of our promotional partners for their support. Because of them, our programming reaches the audience who needs it. I hope that you find this program helpful, but please keep in mind that while the information provided is encouraging, engaging, and insightful, it is not a substitute for medical advice.
Donna Catamero ANP-BC, OCN, CCRC
Abbey Reiser MS, RDN, CDN, CSO
Valarie Traynham Patient Advocate
We are joined by two experts from The Tisch Cancer Institute at Mount Sinai in New York. First up is Donna Catamero, Associate Director of Myeloma Research at the Icahn School of Medicine at Mount Sinai and a nurse practitioner specializing in the treatment of multiple myeloma patients. We also have Abbey Reiser, who has a unique role as part of the multidisciplinary team at the cancer institute’s Ruttenberg Treatment Center. She is a dedicated dietitian/nutritionist and is also board-certified as a specialist in oncology nutrition. Valarie Traynham, a multiple myeloma survivor and thriver and an inspiration to many, will moderate this conversation. Your journey is one of inspiration. I’m excited about this engaging discussion.
Valarie Traynham: I’m a myeloma and breast cancer thriver. I’ve been on the myeloma journey for about nine years and the breast cancer journey for about five years. I can understand the issues when it comes to treatment side effects, so I am so excited to be here and have this conversation with these two ladies.
Difference Between Relapsed and Refractory Multiple Myeloma
Valarie: Donna, can you explain the difference between relapsed and refractory disease? I get this question a lot and it can be confusing to some of the patients.
Donna Catamero: Most patients are both relapsed and refractory. Relapsed is when a patient has an initial response to therapy, so they’re either in complete remission, partial remission, or very good remission, and then their disease starts coming back, which means they’re relapsing from their response.
Refractory is when patients are on therapy and start to relapse, so that means they’re refractory to that therapy. Most myeloma patients are on continuous therapy, so when they start to relapse, they’re going to be a relapsed patient and then refractory to the current treatment thereon. Most patients past their first line of therapy are going to be relapsed/refractory.
Common Symptoms of Relapsed/Refractory Multiple Myeloma
Valarie: When we think of relapsed/refractory, what are some of the common symptoms? Is it just like when we are first diagnosed with myeloma? Is it some of those same symptoms or is it totally different when it comes to the relapsed/refractory setting?
Donna: Patients fall into two categories. Some patients have a biochemical relapse, which means only their numbers are going up. We monitor myeloma patients through their labs. We look at their protein levels and see an increase, but otherwise, the patient feels fine. On paper, we see that their cancer is coming back.
On the other hand, a patient can have a symptomatic relapse, so they’re either more anemic (A), have new bone disease (B), new renal (R) insufficiency or kidney disease, or elevated calcium (C) in their blood. These are the typical CRAB symptoms of myeloma, so they either have those or none at all and we’re seeing the cancer in their blood work.
Current Treatment Options for Relapsed/Refractory Multiple Myeloma
Valarie: What are some of the current treatment options for relapsed and refractory multiple myeloma?
Donna: The landscape of treating relapsed/refractory myeloma is so quickly evolving. We have so many new therapies. In the past five years, we’ve had so many approvals for multiple myeloma patients in the relapsed setting, so it’s a very exciting time.
We have more targeted approaches with proteasome inhibitors, like kyprolis and bortezomib, that we can use in the relapse setting. We have more novel mechanisms of action, so more targeted towards the immune system, like bispecific antibodies for patients who’ve had four prior lines of therapy and then CAR T-cell therapy, another immunotherapy, which is very exciting for patients. It was initially approved for patients who had four prior lines of therapy, but now we can use CAR T-cell therapy in patients after one prior line of therapy.
Valarie: That’s awesome. I always get excited when I think of the therapies that we have since I’ve been diagnosed and even the therapies in the pipeline. It’s given us so much hope as patients.
Easing Multiple Myeloma Treatment Side Effects
Valarie: Abbey, how can a well-balanced diet specifically benefit multiple myeloma patients undergoing treatment?
Abbey Reiser: Diet recommendations often change throughout treatment based on how patients feel and if they experience any side effects that affect their appetite and/or their ability to eat. For multiple myeloma patients who are feeling an eating well, the nutrition recommendations are the same for most other cancers, which is also consistent with the recommendations for the general population.
Plant foods, like fruits, vegetables, whole grains, beans, nuts, and seeds, contain a variety of cancer fighters, including vitamins, minerals, fiber, and phytochemicals. Phytochemicals are naturally occurring compounds in plants that have the potential to stimulate the immune system, reduce inflammation, and fight infection, making these foods especially beneficial for patients to consume while undergoing treatment.
Protein can also help to boost the immune system, promote healing, and build cells, tissues, and muscles. We encourage choosing a variety of lean, animal-based and plant-based proteins, including chicken, fish, turkey, tofu, beans, and nuts. The current plant-based eating model recommends filling two-thirds or more of your plate with plant-based foods and one-third or less of your plate with animal protein to create a well-balanced meal.
Valarie: Are there certain nutrients or dietary patterns that can help manage side effects like fatigue and anemia?
Abbey: Definitely. Patients who experience side effects from treatment may find it difficult to follow a plant-based diet to a tee. Fatigue is one of the most common symptoms among myeloma patients and one of the most common side effects of treatments. I typically recommend staying as active as you can, eating often, and adequately drinking plenty of fluids. Try planning ahead by asking for help with meal prep, trying meal delivery services, and keeping ready-to-eat snacks on hand, like nuts, granola bars, or pre-made protein shakes.
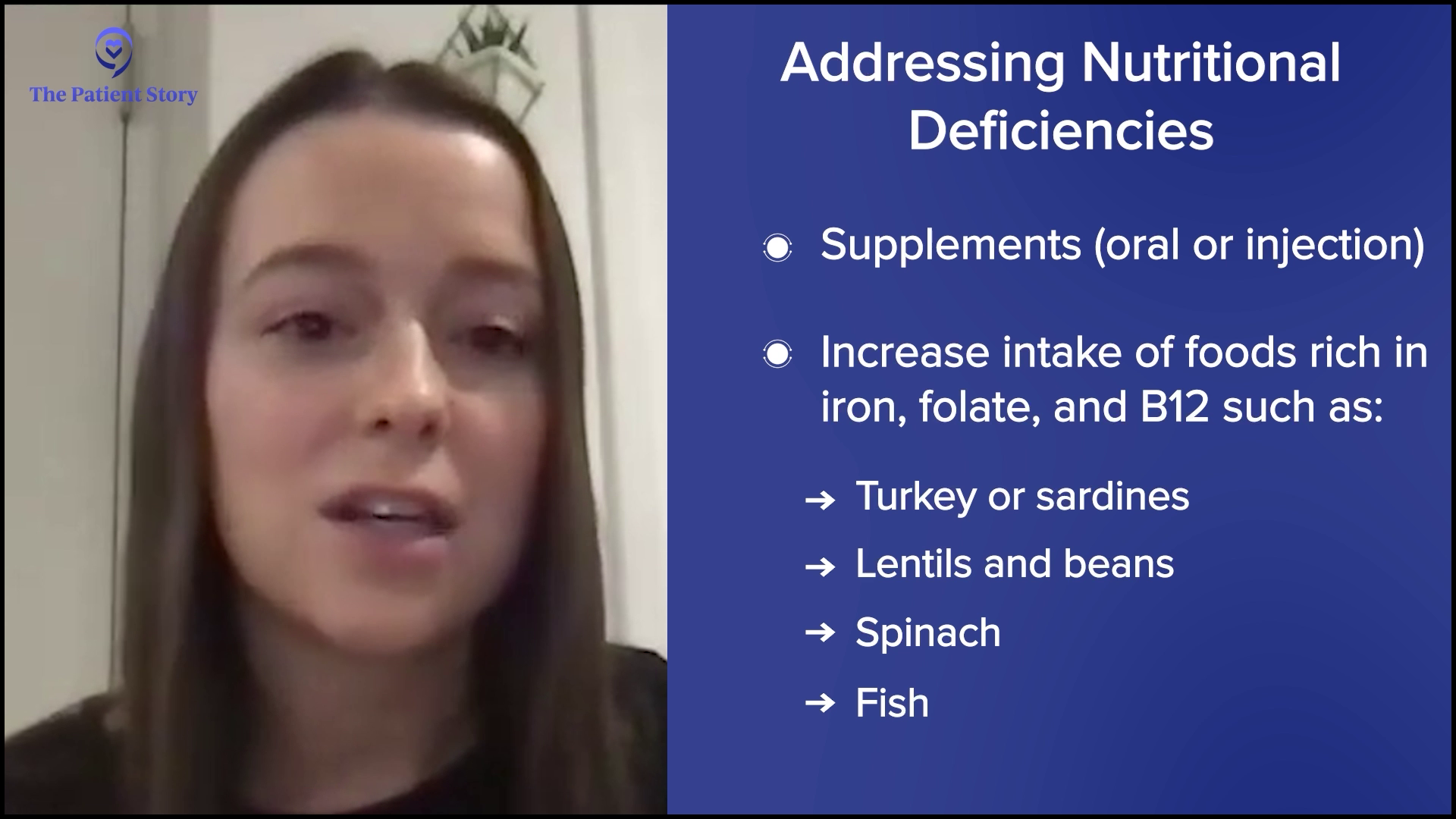
Anemia is commonly caused by the disease, treatments, or kidney dysfunction caused by multiple myeloma and cannot be improved by diet. However, nutritional deficiencies such as iron, B12, or folic acid can also be a cause, and this can be improved by supplementation either orally or by injection. It also couldn’t hurt for patients with these deficiencies to increase their intake of foods rich in these vitamins and minerals, such as turkey, sardines, lentils, and beans for iron, lentils, beans, and spinach for folate, and fish and dairy for B12.
Typically, I encourage patients to talk to their doctor about the cause of and plan of care for anemia before making any significant changes to the diet or starting a new supplement.
Eating the Rainbow
Valarie: As a patient, we’re often told to eat the rainbow. Is that something you recommend?
Abbey: Yes. If their appetite is good, they’re feeling well, and they can eat a variety of fruits and vegetables, I’m all for it because they’re going to get different nutrients from different colors. That’s definitely a recommendation that’s still staying strong to this day.
The Role of Hydration in Managing Kidney Function and Oral Health
Valarie: We often hear about the role of hydration. Can you discuss that role in managing side effects of multiple myeloma treatment, such as kidney function and even oral health?
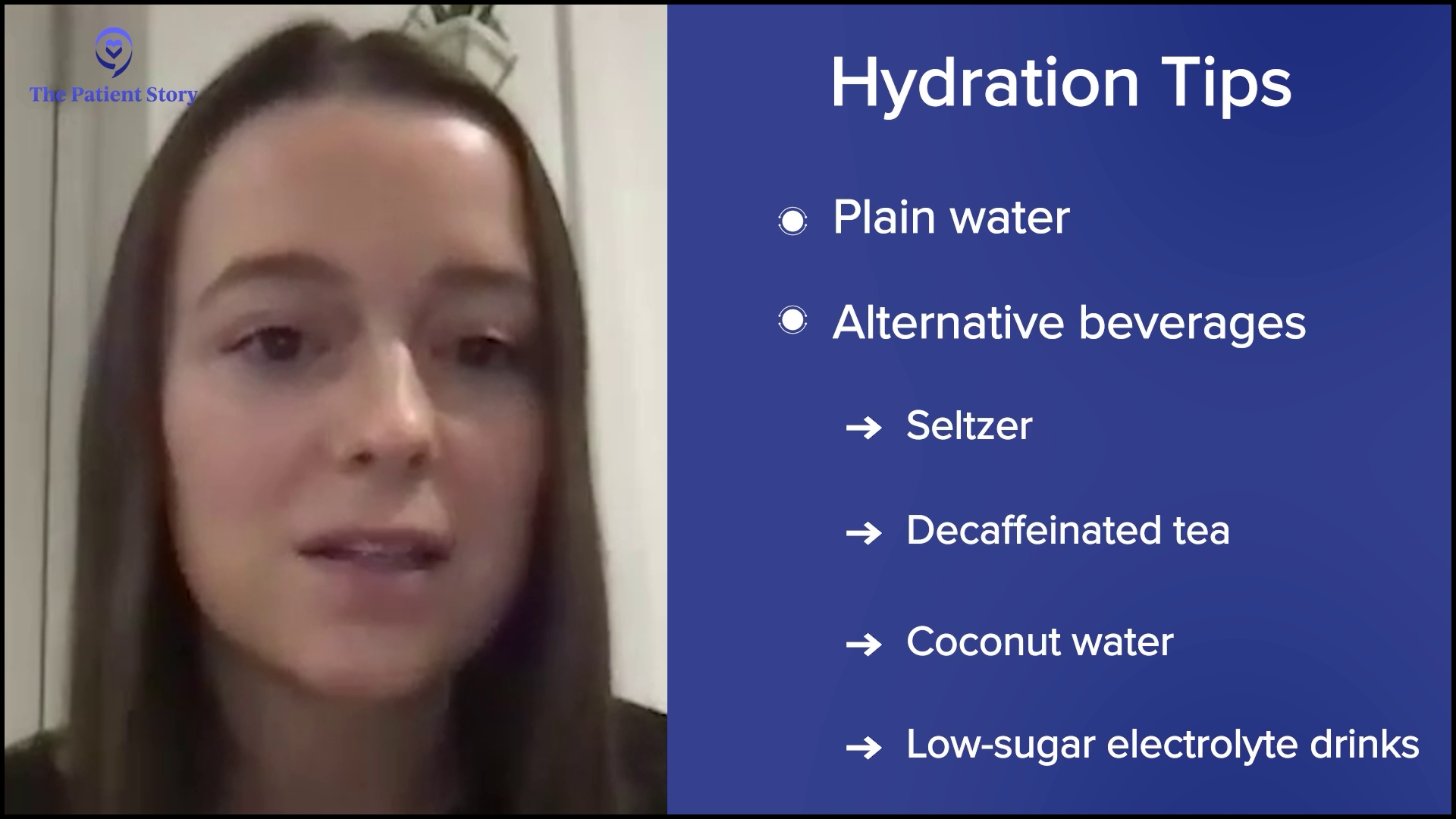
Abbey: Staying hydrated during myeloma treatment is essential, especially because dehydration can worsen kidney function, which is a common concern due to the disease’s impact on the kidneys. Drinking sufficient fluids helps to flush out waste products and manage potential complications, like high calcium levels, which can occur with myeloma. Bispecific treatments, like talquetamab, can cause oral toxicities including dry mouth, mucositis, and taste changes, and good fluid intake plays an important role in managing these side effects.
I recommend aiming for at least 8 to 10 8-ounce glasses of low-sugar fluids per day. Plain water is the gold standard and the preferred beverage for hydration, but other beverages such as seltzer, decaf tea, coconut water, and lower-sugar electrolyte drinks can also promote adequate hydration. Caffeinated beverages, like coffee, tea, and colas, as well as alcohol may worsen side effects like dry mouth, so I recommend limiting those.
Foods and Drinks That Multiple Myeloma Patients Should Avoid
Valarie: Are there any specific dietary considerations or restrictions that myeloma patients should be aware of? You mentioned alcohol and caffeine, but are there certain foods or drinks that they should strictly avoid?
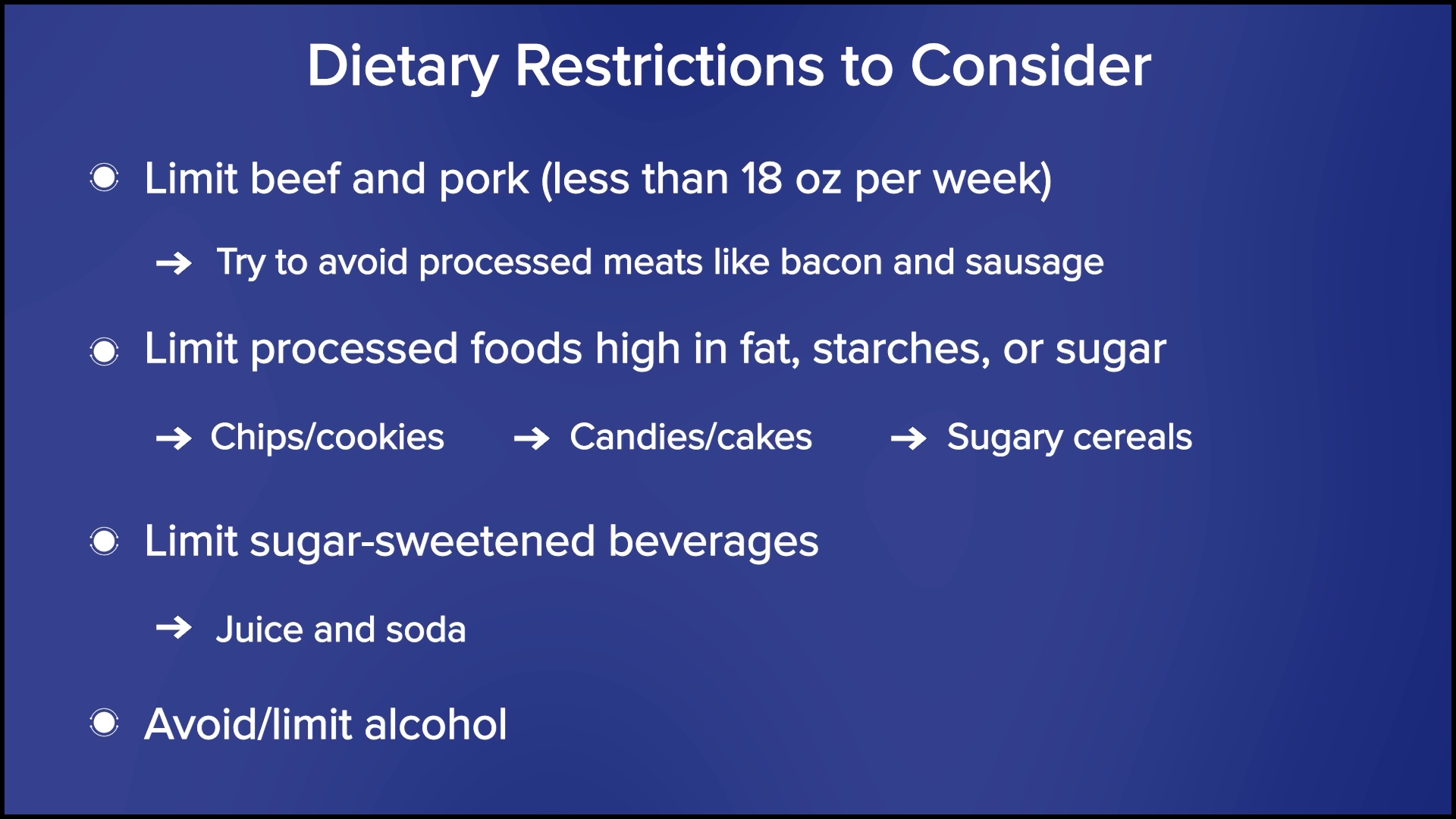
Abbey: A couple of limitations apply to every type of cancer. We recommend limiting red meat, such as beef and pork, to less than 18 ounces per week, and avoiding processed meats, like bacon and sausage, as much as possible.
I also recommend limiting processed foods that are high in fat, starches, or sugars, such as chips, cookies, candies, cakes, and sugary cereals. Patients should also limit sugar-sweetened beverages, like juice and soda, and avoid or limit alcohol. General guidelines recommend no more than two alcoholic beverages per day for men and one drink per day for women, but I typically defer questions regarding alcohol to the doctor.
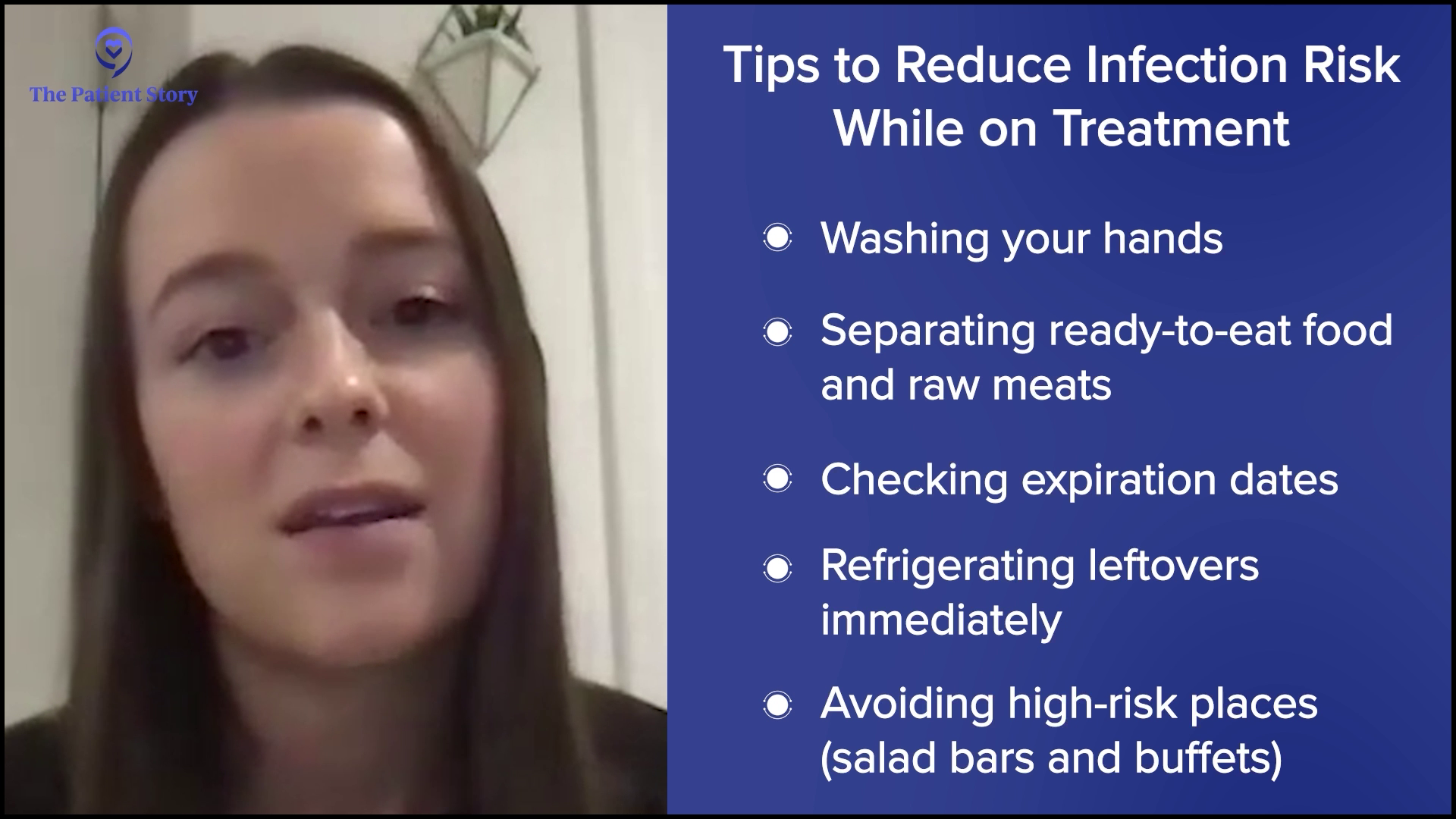
Multiple myeloma and its treatments can weaken the immune system and increase the risk of infection, which can make patients more susceptible to foodborne illness, which we often call food poisoning. Therefore, it’s important to follow food safety guidelines while on treatment in an effort to reduce infection risk. General tips include washing your hands well, separating ready-to-eat food and raw meats, checking expiration dates, refrigerating leftovers immediately, and avoiding high-risk places, like salad bars and buffets, and high-risk foods, like raw and rare meats, runny eggs, unpasteurized dairy, sushi, and unwashed fruits and vegetables.
I also discourage the use of supplements, unless you have a deficiency or are told otherwise by your medical team. Supplements don’t offer the same benefits as eating whole foods. They’re typically not regulated by the FDA, and research tends to be limited in terms of how they may interact with treatment. For patients who are hoping to start taking a supplement, make sure to check with your doctor before doing so.
Avoiding Green Tea Supplements
Valarie: What advice can you provide about green tea? With some treatments, they say to avoid green tea on the day that you’re getting treatment and a few days after. Is there anything you can say about that?
Abbey: That’s usually discussed if they’re on bortezomib. Donna, you and I talked about this before. I believe it’s the green tea supplement that they need to avoid entirely.
Donna: It’s the high-dose green tea extract that’s available as a supplement, which is contraindicated when on a regimen containing bortezomib. I advise patients who love green tea to not consume it on treatment days. The beverage itself is fine for patients. It’s the supplement that can get patients into trouble.
Managing Weight Changes
Valarie: How can a nutritionist help patients manage weight changes? I experienced a lot of weight gain taking steroids. Some patients deal with weight loss, which can be a common side effect of treatment. What can we do from a nutrition standpoint?
Abbey: Treatment side effects, especially oral toxicities, often lead to decreased appetite and weight loss. If a patient is experiencing unintentional weight loss, I recommend having small, frequent meals every 2 to 3 hours and choosing high-calorie foods as tolerated. I will emphasize healthy fat sources, like nuts and nut butters, avocado, and olive oil, because fat contains more calories per gram than proteins and carbs. I also encourage them to make homemade smoothies and shakes, and to drink oral nutrition supplements because sometimes it is easier to drink your calories than eat them when your appetite is low.
Low-impact physical activity as tolerated can also help to increase appetite and maintain muscle mass. For patients who are struggling to eat and whose appetite has been consistently low, it could be worth asking the doctor if starting an appetite stimulant is appropriate.
On the other hand, I also see patients experience weight gain while in treatment. Oftentimes, this is in part due to steroids or fluid retention. To maintain a healthy weight, we recommend following a Mediterranean-style, plant-based diet, which emphasizes having lots of fruits and vegetables, lean proteins, whole grains, and legumes. We also emphasize watching calorie intake, monitoring portion sizes, and eating slowly and mindfully. It takes 20 minutes for your brain to get the message that your body is getting food before you stop feeling hungry. The slower and more mindfully you eat, the sooner you should realize that you’re full.
I also recommend being physically active as tolerated, specifically to engage in at least 150 minutes of moderate-intensity physical activity per week, which can equate to 30 minutes, five days per week. Moderate-intensity physical activity could be a brisk walk or biking.
Common Skin Conditions Multiple Myeloma Patients Experience
Valarie: I’ve dealt with severe dry skin and hyperpigmentation. What are some of the common skin conditions that multiple myeloma patients experience as a result of treatments?
Donna: A lot of multiple myeloma treatments are subcutaneous injections, which means they go right underneath the skin, so we often will see injection site reactions. Around the area where we administered the medication, it gets inflamed, red, and itchy.
Another side effect we see is dry skin. For patients who experience this and if I know a regimen will cause dry skin, I tell patients to use heavy barrier moisturizing creams at the initiation of therapy, especially during long winter months. Our skin dries out fairly quickly with the heat. You want to use heavy barrier creams to help retain the moisture and start at the initiation of therapy.
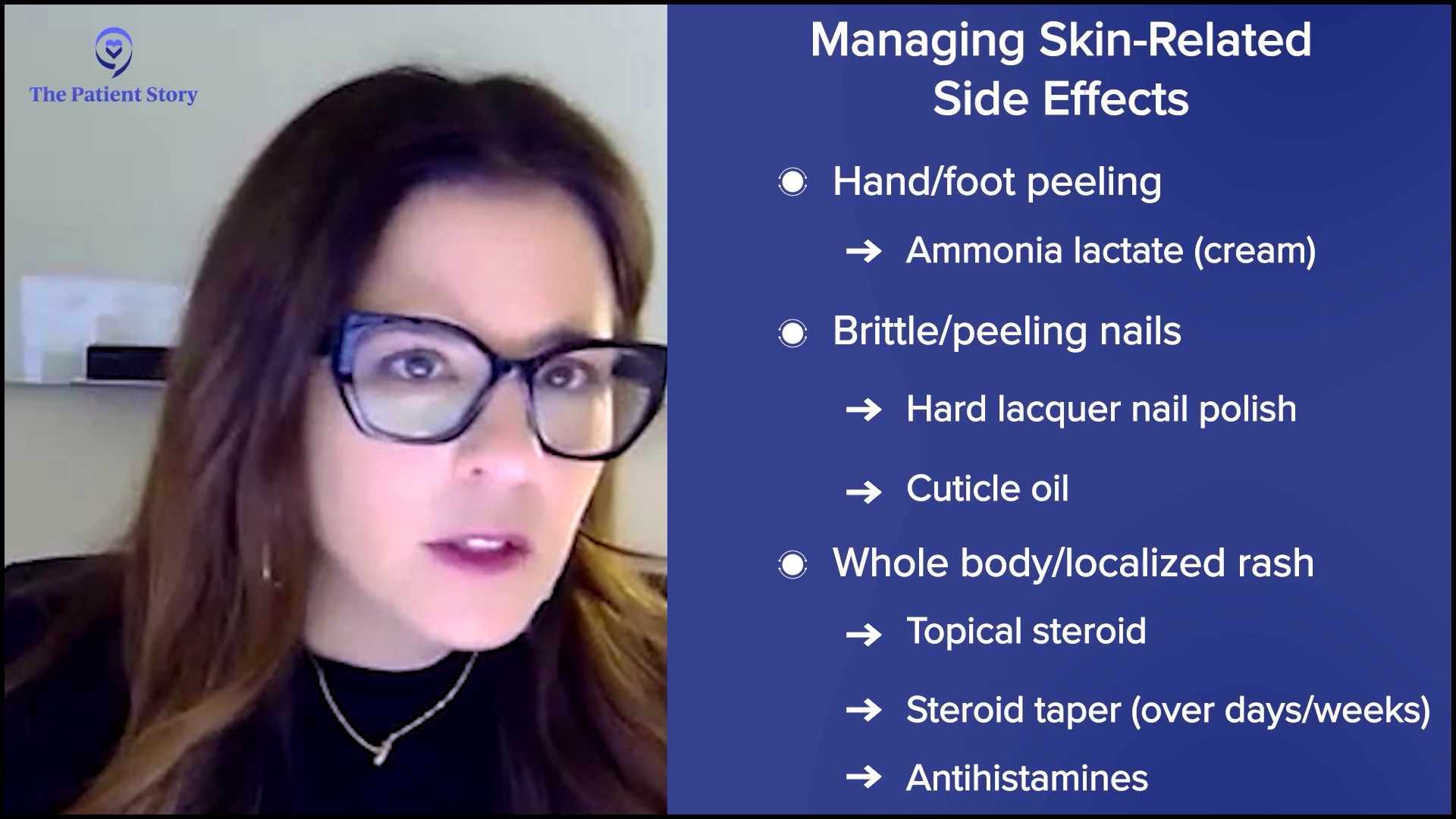
When we see on-target, off-tumor side effects with talquetamab, for example, the skin on the palms of the hands and the soles of the feet start to peel. These side effects can be self-limiting and we can manage them well. We use lotions, like ammonia lactate, on the area. We’ll do that twice a day and this typically will resolve in 2 to 3 weeks for patients.
We also see nails that get brittle and peel. Unfortunately, there isn’t something we can give patients to eliminate brittle, peeling nails, but we can suggest nail polish hardener lacquers to make the nails stronger so they’re less likely to break. We recommend cuticle oil around the cuticle bed. We look for signs and symptoms of infection because we don’t want to have any nail infections.
Another side effect that patients can experience is a whole-body rash or a localized rash. Depending on the size of the rash, we can manage it quite well with topical steroids or lotions. If a rash is more generalized, we’ll add a steroid taper. A course of steroids over several days will tamper down the whole-body rash, which will typically be resolved in several days.
A rash can be itchy or a patient could feel itchy in general, so we can use antihistamines for several days to help with any itchiness. If the itchiness is drug-induced and depending on the severity of the skin reaction, I’m going to hold off on the medication until these symptoms resolve before resuming therapy. If the rash is severe enough, I would consider either a dose reduction or a look at how frequently treatment is administered.
Valarie: Do you often refer to a dermatologist or treat them within your cancer center?
Donna: Early on, when we look at these new treatment modalities, we weren’t typically seeing these side effects. We work very closely with our dermatology colleagues, but we can manage these side effects quite well. I will definitely refer to our colleagues in dermatology, but for the most part, we can manage these symptoms quite well within our own practice.
Bispecific Antibodies for Relapsed/Refractory Multiple Myeloma
Valarie: Bispecific antibodies are emerging as a promising treatment option for relapsed/refractory myeloma. Donna, can you explain how these antibodies work? Have you seen an increase in this approach with patients?
Donna: This is a new and very exciting treatment modality. We had several drug approvals within the past few years with this new class of drugs. It’s similar to daratumumab where it will bind to a receptor on the myeloma cell. One arm of the bispecific antibody will grab the myeloma cell and the other arm will grab the receptor of a T cell.
Our T cells are little soldiers of our immune system. T cells will do surveillance and get rid of anything that looks bad in our system, so that includes infections and cancer cells. What a bispecific antibody does is grab onto the myeloma cell, grab onto the T cell, and bring that T cell close to the myeloma cell so that the T cell can recognize the myeloma cell and kill it
In essence, it mimics the mechanism of action of CAR T-cell therapy, but the benefit of a bispecific antibody is it’s off the shelf, so there’s no downtime unlike waiting for manufacturing CAR T cells. If I need to start a patient tomorrow, we can initiate therapy quickly. We’re harvesting the patient’s immune system to attack the myeloma cells. This is an exciting new treatment approach.
Common Side Effects Associated with Newer, Targeted Therapies
Valarie: As a patient, I’m very excited to hear about bispecific antibodies. What are some of the common side effects associated with these newer targeted therapies?
Donna: We’re activating that immune system, so the immune system gets revved up and what happens is it releases cytokines. Cytokines are little immune substances that can cause havoc. It can affect everybody’s system. Typically, when a patient gets a bispecific antibody, they’ll have a fever. This can progress to low blood pressure or difficulty with breathing, but these are so well-managed now.
The patient will typically complain of a fever, almost like when we get our flu shots where we feel a little achy and get a low-grade fever. As a provider, I know this patient is probably having cytokine release syndrome (CRS). The immune system is getting revved up, so I will tap the brakes. We have treatments that will simmer down the immune system and within 24 to 48 hours, the patient’s symptoms will resolve and allow us to continue treatment.
We try to mitigate this side effect by giving premedication, so we’ll give acetaminophen, diphenhydramine, and some steroids, but the majority of patients are going to experience CRS. Typically, we manage this inpatient, but more and more institutions are learning to manage these side effects as outpatients. We monitor patients very closely by checking their vital signs and intervening at the first sign of a fever. If a patient has a drop in their blood pressure or difficulty with breathing, we intervene very quickly.
The majority of patients will have cytokine release syndrome and to a much, much lesser extent, we see neurotoxicity. If patients have cytokine release syndrome, typically we see neurotoxicity immediately after. A patient might present with some confusion and maybe a little disoriented. They can name the hospital and their name, but instead of saying that it’s winter, they’ll tell you it’s spring.
Also, we see patients with a change in their handwriting and this can be quite drastic. Before starting these therapies, we obtain a handwriting sample and monitor the handwriting sample throughout treatment. We’ll see a change from one 12-hour shift to the next where a patient will write a beautiful sentence and then a few hours later, will scribble across the paper. This patient is experiencing a neuro event. This can be scary, but this is reversible. We manage this very well. This is self-limiting, so it won’t reappear.
Care partners are very important when we give these types of treatment because if the patient is at home, they might not understand that they’re confused. It’s very important to have a care partner to monitor the patient to see if there’s any alteration in their mental status. We manage this quite well with steroids.
Specific Strategies for Managing Cytokine Release Syndrome and Neurological Side Effects
Valarie: Are there specific strategies for managing cytokine release syndrome and neurological side effects?
Donna: To mitigate some of these potential side effects, like cytokine release and neurotoxicity, we do two things. First, we’re going to do a step-up dosing approach. We’re going to give a small dose for that first dose, a slightly higher dose for that second dose, and then the full dose. We ease the patient into that medication.
The second thing we do is to have premedication on board to mitigate the severity. Most patients are going to have cytokine release syndrome, but it’s typically mild like a fever, which we can manage quite well. Neurotoxicity happens in a very low percentage. Less than 7% of patients will have this neurological event. Step-up dosing and medications can help, but that’s something we will manage when the symptoms arise.
Dietary Changes to Help Manage Loss of Taste
Valarie: Abbey, we talked about diets and how having healthy snacks can help manage the side effects. For patients experiencing loss of taste, how can they change their diet to help manage that particular side effect?
Abbey: Taste change is one of the most common side effects that I talk about and it’s definitely one of the most difficult to manage. There’s no one-size-fits-all approach, not one miracle food that everyone enjoys, and no medication that provides total relief. It’s tough for patients to find foods they enjoy, let alone tolerate.
Something I emphasize to everyone, regardless of their experience, is good oral hygiene. Patients are often prescribed a mouth rinse, but if this doesn’t help, I recommend trying a homemade rinse made with baking soda, salt, and water, or an over-the-counter, alcohol-free mouthwash. Brushing the tongue and teeth after meals and before bed is also important to keep the mouth clean. It also doesn’t hurt to try sugar-free gums or mints to see if that improves any unpleasant taste in the mouth.
When patients describe taste changes, I hear a wide range of statements, including everything tastes too bitter, too sweet, too metallic, has no taste, tastes like cardboard, or everything tastes bad. If food tastes too bitter or too sour, I recommend adding something sweet to food, like honey or fruit. Or, if food tastes too sweet, try adding an acid, such as vinegar, lemon, or other tart, tangy, or acidic flavors. If everything tastes metallic, I recommend using nonmetal utensils and cookware, such as plastic, glass, or ceramic. Try fresh or frozen foods over canned and serving meat cold or at room temperature.
For bispecific therapies, the most common statement is everything tastes bad or has no taste. For this, I emphasize the importance of experimenting with different flavors, textures, temperatures, herbs, spices, seasonings, and sauces because you never know what might work for you. I often hear that adding acids like lemon, lime, vinegar, and tomato can make foods more enjoyable. I’ll often recommend adding fresh lemon or lime juice during and after cooking, and adding citrus to water, such as lemon packets or sliced lemons and oranges, if plain water tastes unpleasant.
Taste is the combination of not only the taste but also the smell and touch of food. If you can’t get any pleasure from taste, don’t underestimate the power of texture and smell. Soft, moist foods like oatmeal, soups, and mashed potatoes are usually more tolerable since they’re easier to chew and swallow, which means they spend less time in your mouth.
Smoothies and oral nutrition supplements are my go-to recommendations because they’re quick and easy ways to get in calories. Protein and smoothies allow a patient to experiment. Fruit is one of those foods that are often tolerable, so I recommend blending different fruits into smoothies to see if that makes them easier to get down. Animal proteins tend to be tough for patients to tolerate, so I typically recommend choosing softer animal proteins, like egg salad or fish, or marinating and cooking meats in acidic dressings or sweet juices.
Many patients report that they maintain their sense of smell despite losing their taste. I’ve had a patient say that certain foods, like cucumbers, cantaloupe, and coffee smelled good, which helped them taste good too, so it’s definitely worth experimenting in this way.
An important point that patients should take away when it comes to taste changes is that everyone is different. A recommendation that works for one person may not work for the other, so it’s important to keep trying and retrying foods because you never know what may end up working for you. Even though everyone is different, if patients are experiencing these side effects, they should know that they’re common and they’re not alone.
Coping with the Emotional Challenges of Relapse
Valarie: Let’s talk about the emotional side, such as anxiety and depression. Donna, how can patients cope with these types of challenges?
Donna: In the relapsed/refractory setting, every relapse causes a lot of anxiety and fear. When starting a new treatment, there’s a lot of fear, which can then increase anxiety and can lead to depression. Having a good support network is important for patients. We’re very fortunate in my institution to have a wonderful social work team that can help patients. We have support groups. Support groups work for some patients but not for others, so have care partners on your team to help patients through these challenging times. Each relapse becomes challenging for patients. The good news is that we do have great therapies for patients to provide support for patients to get through their therapies.
Abbey: From a nutrition standpoint, a patient experiencing side effects from treatment that affect their ability to eat can significantly impact a patient’s quality of life. It can cause patients to feel isolated because it’s hard for anyone to fully understand what they’re going through. On top of that, they might feel pressure from family and friends to eat more even when they don’t feel well and I’ve seen that cause resentment. Eating is such a social and cultural activity, and many patients feel like they don’t have a place at the table to help cope with these challenges.
I encourage patients to ask for a referral to a dietitian. Our job is to provide tips and tricks to help patients eat despite these side effects. I also encourage them to try to continue living their lives as much as possible, to go out to eat, and to attend social events when they have the energy and when it is safe for them to do so. When people are experiencing side effects and they go out to eat, they feel embarrassed or afraid to advocate for themselves. I encourage them not to hesitate to ask for their food to be prepared a certain way if it makes it easier for them to eat. If they want to bring their own food when they go out, that’s completely okay. I’m sure their friends and family would prefer to see them enjoying their meal and feeling supported, rather than feeling embarrassed or ashamed.
Valarie: As a patient and as somebody who’s been on that side of it, you have to look out for yourself. If that means taking something to a restaurant to spend time with your loved ones and be able to enjoy a meal, then do it.
Support groups are not for everyone, but there’s also one-to-one support available. You can talk with a myeloma coach or a mentor angel in various programs. Know that you’re not alone as you’re dealing with these side effects. Others are going through them as well and you always have someone to support you.
Final Takeaways
Valarie: Thank you, Donna and Abbey, for taking the time to speak with me and The Patient Story audience. Do you have any final remarks?
Donna: We have some great therapies we can offer patients. The important thing is getting patients through that therapy. There are side effects, but we’re going to help manage those so that patients can have the best possible outcomes.
Abbey: I encourage patients who are experiencing any side effects to speak up, advocate for themselves, and let their teams know. The sooner their team is aware, the sooner they can provide supportive care or treatment to help manage those side effects. If the side effects they experience make it difficult to eat, don’t hesitate to ask for a referral to a dietitian if their team has not referred them to one already.
Valarie: Yes, I agree with you wholeheartedly. Speak up and don’t suffer in silence. There’s no need for that.
Conclusion
Tiffany: Thank you again, Donna, Abbey, and our patient moderator and advocate Valarie, for taking the time to discuss mitigating side effects, especially to Valarie for sharing her myeloma experience. I am grateful that she shared her story with us. It takes a village and I know that your story, Valarie, will resonate.
It is important to be empowered so that you and your caregivers can make informed decisions about your care. That includes being educated on the latest on the side effects, mitigating those side effects, and getting the support that you need.
Symptom: None; found through blood tests Treatments: Total Therapy Four, carfilzomib + pomalidomide, daratumumab + lenalidomide, CAR T-cell therapy, selinexor-carfilzomib
Sandy was diagnosed with stage 4 non-Hodgkin lymphoma in 2024. Her initial symptoms included persistent coughing, weakness, and shortness of breath. After weeks of worsening symptoms and ineffective treatments, an MRI revealed a large mass in her chest, which eventually led to the collapse of her left lung due to a massive tumor. A biopsy confirmed the diagnosis of lymphoma, a cancer that Sandy later described as a blessing in disguise due to its responsiveness to chemotherapy.
Treatment began immediately, consisting of six intense rounds of chemotherapy, each lasting five days in the hospital followed by two weeks of recovery at home. The process was physically and emotionally grueling, marked by extreme fatigue, weight loss, and hair loss. Despite these challenges, Sandy focused on mental resilience, which she believes was critical to her survival. She emphasized the importance of maintaining movement, even during the most debilitating moments.
To cope mentally with stage 4 non-Hodgkin lymphoma, Sandy turned to spirituality, meditation, and writing. She frequented a meditation garden where she found solace. Writing became a therapeutic outlet, leading to the creation of her book, Cancer Ramblings. Writing helped her process her experience and turn her pain into purpose.
Sandy celebrated her remission as a profound moment of liberation and gratitude, describing it as a second chance at life. She plans to monitor her health closely while maintaining a conscious lifestyle. She views sharing her story as a way to inspire others, providing hope and comfort to those facing similar challenges. Her key advice is to visualize a positive outcome and hold onto it as a guiding light through the darkest moments. Sandy’s enduring image was of herself running on the beach—a vision she ultimately realized.
Name: Sandy D.
Age at Diagnosis:
45
Diagnosis:
Non-Hodgkin lymphoma
Staging:
Stage 4
Symptoms:
Persistent coughing
Weakness
Shortness of breath
Treatment:
Chemotherapy (six rounds)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: Severe fatigue, deep shoulder pain, ear pain with inflammation, abdominal and pelvic pain, bloating, early fullness, nausea, difficulty eating, inability to urinate despite feeling an urgent need, internal bleeding, delayed period/bleeding, intense whole‑body pain leading to collapse
Treatments: Surgeries (emergency laparoscopic surgery with left ovary removal), chemotherapy (R‑CODOX‑M/IVAC), immunotherapy, hormonal therapy (to protect the remaining ovary)
...
Symptoms: Feeling like holding breath when bending down or picking up objects from the floor, waking abruptly at night feeling “off,” one episode of fainting (syncope), presence of a large mass in the breast
Treatments: Chemotherapy, bridge therapy of chemotherapy and radiation, CAR T-cell therapy
...
Symptoms: Constant fatigue, tongue deviated to the left, abscess in right breast, petechiae on legs, night sweats, nausea and vomiting, persistent cough
Shayla was diagnosed with metastatic colorectal cancer at 33 years old after years of experiencing unexplained digestive issues. Initially, symptoms like stomach sensitivity, exhaustion, and food intolerances were attributed to a sensitive stomach. Over time, she sought medical attention, including multiple gastroenterologist consultations but received inconclusive diagnoses. She was diagnosed with celiac disease, but despite cutting out gluten, she continued to feel unwell.
After more months of fatigue, Shayla noticed blood in her stool, which persisted for several weeks. When her husband insisted she seek medical help, a colonoscopy revealed polyps. While initially told that they weren’t cancerous, a biopsy later confirmed that one was malignant. Further tests revealed lesions in her liver and lungs, prompting additional biopsies. The lesions in her lungs were clear, but the cancer had metastasized to her liver, resulting in a stage 4 colorectal cancer diagnosis.
Her treatment plan included four rounds of chemotherapy, followed by a hepatectomy or liver resection to remove 25% of her liver. After the surgery, Shayla began her chemotherapy again, with plans for more rounds to finish her treatment. Although she initially struggled with side effects, such as hot flashes, nausea, and fatigue, her doctors adjusted her treatment plan to help her manage better. However, cold sensitivity, neuropathy, and physical weakness persisted.
Despite these challenges, Shayla remained focused on her healing and recovery, even as the emotional toll of her diagnosis began to weigh on her mental health. She shared that the isolation during recovery and the struggle with seeing her children react to her illness was particularly difficult.
Shayla advocates for others to take their symptoms seriously, stressing the rising rates of colorectal cancer in younger adults. She encourages others to seek second opinions and advocate for themselves if they’re not satisfied with their medical care. Through her experience, she has seen the importance of a strong support network and the need for proactive health care, urging others to catch cancer early to increase treatment success.
Name: Shayla L.
Age at Diagnosis:
33
Diagnosis:
Colorectal Cancer
Staging:
Stage 4
Symptoms:
Stomach sensitivity
Food intolerances
Exhaustion
Blood in stool
Treatments:
Chemotherapy
Surgery: hepatectomy (liver resection)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Follicular Lymphoma: Latest Advances in Precision Medicine and Emerging Therapies
Dr. Peter Martin, a leading lymphoma expert at Weill Cornell Medicine, and Laurie Adami, a follicular lymphoma patient discuss the latest advancements in follicular lymphoma treatment. This conversation talks about precision medicine and emerging therapies, addressing how to manage side effects and improve quality of life, and is designed to empower patients with practical knowledge and support as they navigate their diagnosis.
Understand current and emerging options, including targeted therapies and bispecific antibodies, and how they address treatment challenges. Gain actionable strategies to manage side effects and improve quality of life. Explore how precision medicine tailors treatment plans to individual needs, including chemo-free options. Get answers to common and critical questions about follicular lymphoma. Be part of a conversation that brings the patient experience front and center to inspire hope and informed decision-making.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
Tiffany Drummond: I’m a patient advocate with over 20 years of experience in cancer research. My journey as a care partner began when my mother was diagnosed with endometrial cancer in 2014. I quickly realized the challenges of finding resources, support, and shared experiences, and now I am committed to helping others avoid similar difficulties, no matter the condition.
At The Patient Story, we create programs to help you figure out what comes next. Think of us as your go-to guide for navigating not only the cancer journey but your overall health journey. From diagnosis to treatment, we have you covered with real-life patient stories and educational programs with subject matter experts and inspirational patient advocates and guests. I genuinely am your personal cheerleader, here to help you and your loved ones best communicate with your healthcare team as you go from diagnosis through treatment and survivorship.
The Patient Story retains full editorial control over all content as always. We also thank all of our promotional partners for their support. It is because of you our programming reaches the audience who needs it. I hope you’ll find this program helpful, but please keep in mind that the information provided is not a substitute for medical advice.
I had access to great cancer centers. I went to four different big cancer centers and that’s where I was able to join clinical trials.
Tiffany: I have the pleasure of interviewing Dr. Peter Martin and it so happens that we have much more in common than you might think. I will also be speaking with a follicular lymphoma patient, Laurie Adami. It’s so important to get a patient’s perspective and I’m sure her experience will resonate with you and your loved ones. Let’s learn about Laurie’s journey before deep diving into the latest treatment options.
Laurie Adami: I was diagnosed in 2006. My son was in kindergarten. There was one treatment I did right away. We thought I was in remission, so I merrily went back to work, which entailed traveling internationally. Three months later, my cancer was back on the first follow-up scan. That prompted 12 years of treatment. From 2006 to 2018, I was in continuous treatment and underwent seven different lines of therapy, including three clinical trials.
The first six treatments didn’t work, but thankfully, the seventh line of treatment did. I live in Los Angeles, so I had access to great cancer centers. I went to four different big cancer centers and that’s where I was able to join clinical trials.
Dr. Peter Martin, Hematologist-Oncologist
Tiffany: Dr. Peter Martin serves as the professor of medicine and chief of the lymphoma program at Weill Cornell Medicine. He is a hematologist-oncologist who specializes in caring for patients with lymphoma at NewYork-Presbyterian Hospital. His research focus, which is very dear to my heart, is on clinical investigation of new and promising therapies. Dr. Martin, how are you doing today?
Dr. Peter Martin: It’s great to see you again, Tiffany. I don’t know if everybody else knows this, but we worked together long ago.
Tiffany: You could say how long ago. It was about 15 years ago. I used to call him Peter, that’s how far we’ve come. I’m glad to see that we both have stayed the course, which is fighting cancer and finding a cure. I know that you made great strides, so thank you for being here.
[Follicular lymphoma] typically grows slowly over months, years, or decades, and that’s why we call it indolent, which means lazy.
Dr. Peter Martin
What is Follicular Lymphoma?
Tiffany: I’m a patient advocate for many types of cancer, but for those who aren’t as familiar, can you break down follicular lymphoma? We know that it’s considered an indolent lymphoma. Can you walk us through that characteristic? What makes follicular lymphoma distinct from more common types of non-Hodgkin lymphoma, such as DLBCL or diffuse large B-cell lymphoma?
Dr. Martin: Follicular lymphoma is pretty common from the lymphoma perspective but not common from a cancer perspective. In the United States, about 20,000 people every year will be diagnosed with follicular lymphoma. Depending on your perspective, there are up to 130 different kinds of lymphoma, which is hard to keep track of. Each subtype is a little bit different biologically in how they’re defined and how they behave clinically.
Follicular lymphoma is based on the way it looks under the microscope. They look like little follicles in the lymph node. It typically grows slowly over months, years, or decades, and that’s why we call it indolent, which means lazy. I like the word lazy because it’s a lymphoma that can’t be bothered to cause problems.
Once diagnosed, we’ll often talk about the goal of treatment, which is to help somebody live a life that’s as close to the life they would live without lymphoma. It hangs around for a long time and we keep managing it and kicking the can down the road.
How is Follicular Lymphoma Diagnosed?
Tiffany: If someone is living with follicular lymphoma for years or even decades, how is it diagnosed? Do they come in for some other type of symptom that usually makes them get referred to a specialist? How does that work for a patient who doesn’t even know that they have it?
Dr. Martin: It can vary a little bit. Ultimately, to diagnose follicular lymphoma, you have to look at it under the microscope. The word lymphoma means tumors of the lymph nodes, so most of the time when we meet somebody with follicular lymphoma, they’ll have an enlarged lymph node. Typically, it’s a painless, enlarged lymph node in the neck, armpit, or groin.
It might be picked up accidentally while getting tested for other reasons, which is pretty common because follicular lymphoma is often asymptomatic. Although it’s called lymphoma, sometimes it’s not in a lymph node. It might be present in the bone marrow or some other organ, like the gastrointestinal tract or the skin. Ultimately, though, somebody has to look at it under the microscope and that’s how we make the diagnosis.
All of my doctors dismissed me. I would specifically tell them, ‘I’m very worried I have lymphoma,’ and they would say, ‘Your bloodwork is all normal, so you don’t have cancer.’
Laurie Adami
Symptoms of Follicular Lymphoma
Tiffany: Laurie, did you experience any symptoms before your diagnosis or was it something you noticed but didn’t read into it enough to get it checked right away?
Laurie: When my son was three years old, I started to get frequent sinus infections and couldn’t get rid of them. I also developed a dry eye. I was a long-time contact lens wearer and suddenly, I couldn’t wear my right contact lens. I was very tired. I had a lymph node on my neck that was concerning me and I felt something in my abdomen.
All of my doctors dismissed me. I would specifically tell them, “I’m very worried I have lymphoma,” and they would say, “Your bloodwork is all normal, so you don’t have cancer.” I told my husband that they wouldn’t listen to me and he didn’t believe me, so I took him to my appointments and he couldn’t believe how I was dismissed. He was mortified. This went on for three years.
I wanted to believe these doctors. I wanted to believe that allergies were causing these sinus infections. I was also at the age where I could be starting to get perimenopausal symptoms, so my symptoms were attributed to my hormones. It was aggravating.
I kept feeling worse and worse. The exhaustion was incredible. One of the doctors I saw said, “Laurie, you’re president of a software company. You’re traveling internationally. You’re traveling a week a month. You’re running a household. You have a young boy. I’m exhausted just listening to what you do.”
Finally, someone I knew referred me to a diagnostician who took me seriously. I went in to see him and explained everything. I said, “People think this node is from allergies.” He said, “Did you get tested for allergies?” I said, “Yeah, and there was nothing.” He said, “Okay, that doesn’t make sense then.”
I explained the possibility of a hernia and he said, “It could be, but Laurie, we don’t guess. We have CT machines and I’m going to send you to a hernia specialist. We’re going to do imaging.” That week, they imaged me and it was scary because I was supposed to go in for a simple imaging. They expected to find a hernia and I wasn’t supposed to have contrast. Suddenly, this lady brought in the bottles of contrast because they had to get a better image. My heart began to sink as I was sitting there.
Two days later, on Good Friday of 2006, the doctor’s office called and said I needed to come in. My mother and brother were in town for the Easter weekend, but they didn’t tell me to bring anyone, so I went by myself and they told me I had either lymphoma or a mesenchymal tumor. The imaging also detected lesions on my lungs, so he said, “You may also have lung cancer.” That’s when I found out that I had some type of cancer.
I knew a little bit about lymphoma because when I had this node and I put in my symptoms online, lymphoma kept coming up. But 90% of lymphoma patients are diagnosed at stage 4 because most patients don’t have symptoms. I did, but I didn’t have anybody listening to me, so they dismissed my concerns.
As it turned out, it was good that they didn’t listen to me because the only treatment that existed at the time was a monoclonal antibody, multi-chemo, prednisone treatment. If I had it earlier, it wouldn’t have worked and I would have had nothing else.
I had autologous stem cell transplant as an option, but it was not a good option, especially if you relapse after the first line of chemo and monoclonal antibody treatment. In a way, it ended up being a blessing because, by the time they were pushing me to do the transplant, I managed to find a trial of a histone deacetylase (HDAC) inhibitor, which is what I did as my second line of therapy.
Dr. Martin: Oftentimes, somebody will say, “I’ve had this lump for five years and finally my friend told me that I should have it looked at.” That’s a testament to how it behaves. It hangs around for a long time, so people often get accustomed to it being there before they decide to bring it to somebody’s attention.
Traditional Treatments for Follicular Lymphoma
Tiffany: Before we get into the novel approaches, can you walk me through the traditional treatments for follicular lymphoma? What factors determine a more or less aggressive approach in your practice?
Dr. Martin: The job of a hematologist-oncologist is to learn as much as we can about the lymphoma and that’s changing all the time as we get more sophisticated. We recognize that this lymphoma isn’t happening in a petri dish in a lab somewhere; it’s happening in a real live person, so we have to learn as much as we can about that person. That includes not only their medical issues but also all of the things that are important to them. What are their values? What is their support network like? There are 8 billion of us on the planet and we’re all different, so there’s even more heterogeneity among people than there is amongst the 130 different lymphomas.
We bring all of that information together and come up with a plan that makes the most sense for that person. Treatments are constantly evolving and we have new treatments available today that we didn’t have in the past. In general, the goal of treatment is to try to give somebody the life that’s the closest to the life that they would have if they didn’t have lymphoma.
We have to learn as much as we can about that person. That includes not only their medical issues but also all of the things that are important to them.
Dr. Peter Martin
Approaches can vary. In some cases, you say, “Look, this is not causing you any problems. It’s not going to cause problems hopefully for a long time — on average, multiple years — and so we watch it and it sits there.” That can be a little bit counterintuitive. In the Western world, you want to catch and deal with cancers early. That’s certainly the case for breast cancer, lung cancer, or colon cancer, so the initial discussion around follicular lymphoma can be a little bit awkward sometimes. You say, “Oh, great. No problem. Let’s do nothing about it.” But it’s a proven strategy to help people live a good quality of life without dealing with any of the side effects of treatment.
On the other end of the extreme, we might propose using more aggressive therapies, including chemotherapy if we need to shrink something quickly and help them feel better. There are options in the middle where we use immunotherapies that may shrink the tumor, may help somebody to feel better, and may prolong the time between that and other kinds of therapies by months or years. There are vast options and more new treatments are being approved.
Bispecific Antibodies for Treatment of Relapsed/Refractory Follicular Lymphoma
Tiffany: Let’s talk about some of the data that came out of the 66th American Society of Hematology (ASH) annual meeting. Bispecific antibodies are changing the way that we look at and treat cancer, especially when it comes to immunotherapy. What benefit may they contribute to our relapsed/refractory follicular lymphoma patients?
Dr. Martin: Bispecific antibodies are a type of monoclonal antibodies. Antibodies are proteins that our immune system makes to fight against bacteria. A few decades ago, clever people figured out how to make antibodies that would fight not against infections but against cancer. That moved quickly from the lab to people and, for the past 25 years, has revolutionized the way many cancers are managed. It started with lymphoma. We’ve been leading the way for a long time.
Bispecific antibodies are a natural evolution of trying to come up with ways to make this kind of immunotherapy work better. They’re very cleverly engineered. They bind to tumor cells the same way an antibody would bind to a virus or bacteria, but in addition, they also bind to other parts of our immune system called T cells and they activate them. When those T cells are activated, they secrete chemicals called granzymes and perforins that poke holes in cancer cells and cause them to die. This is a clever way of using our immune system to kill cancer cells and it does it remarkably effectively.
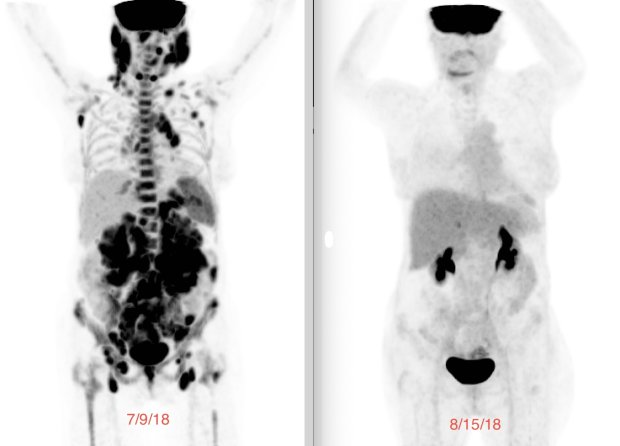
The vast majority of people will have not only responses to this treatment, meaning the tumor shrinks, but in many, if not most, cases, the tumor will disappear on a CT scan. It might be completely gone — we’ll find out as the years go by — but it disappears on a CT scan in a lot of people.
Bispecific antibodies are attractive in that it’s a non-chemotherapy approach and it’s a proven form of immunotherapy. It’s an evolution of the kinds of immunotherapies that we’ve been using in the past and it’s more effective.
The other thing that’s nice about it is that it’s off the shelf, so you order it from a pharmacy. It doesn’t have to be engineered specifically for each patient the way something called chimeric antigen receptor T cells or CAR T-cells have to be.
I did a monthly infusion of a third line monoclonal antibody… but as soon as I stopped, it came back, so it was a race against time.
Laurie Adami
Experience with CAR T-cell Therapy
Tiffany: Laurie, I believe you’re familiar with CAR T-cell therapy. How was that experience and where are you currently in your cancer journey? Are you also familiar with bispecific antibodies? I would love to get your perspective on this immunotherapy versus CAR T-cell therapy.
Laurie: I heard about CAR T-cell therapy six years before I could get it. I heard about it in 2012 when I attended an LLS event where they showed Emily Whitehead’s film. I went to my college that week and asked about it because I didn’t know about CAR T-cell therapy. He said, “They’re not trying it for follicular lymphoma. They’re doing it for more aggressive tumors. We have to wait. You’re on a PI3 kinase inhibitor. We’re going to ride this horse.” That took me through 2016 when the cancer finally outsmarted that pill.
A new monoclonal antibody had been approved. It was a nine-month course, so I did a monthly infusion of a third-line monoclonal antibody, obinutuzumab. It immediately started shrinking my tumors again, but as soon as I stopped, it came back, so it was a race against time.
In 2018, my tumors were huge. While I was out hiking in April, my oncologist called and said, “We finally got the trial for follicular lymphoma. It’s going to open at UCLA. We’re going to have five patients enrolled in the first cohort and you will be patient number one.”
When you’re in a clinical trial, you have to review the paperwork to sign. It discloses all the side effects of patients in the phase 1 study. This was a phase 2 study, so it wasn’t completely bleeding edge. Then they have to do biopsies and imaging. They had to make sure I didn’t have anything in my brain. They weren’t allowing patients with central nervous system involvement to get CAR T-cell therapy because they didn’t know how it would work and what it would do. Now they know, so they do it for people with involvement in the central nervous system.
It was amazing because, within days, the tumors were shrinking.
Laurie Adami
I had a sinus infection again because my cancer was coming back. My oncologist said, “You can’t get CAR T-cell therapy with an active infection,” so I went to my ear, nose, and throat specialist. I explained, “I need to get this treatment, but I can’t do it with an active infection.” He called his scheduler and said, “Clear the schedule tomorrow. I have an urgent patient.” They operated on me the following day and it ended up being a major surgery with general anesthesia because there were so many blockages everywhere. He cleaned me out and got rid of the sinus infection so I was good to go.
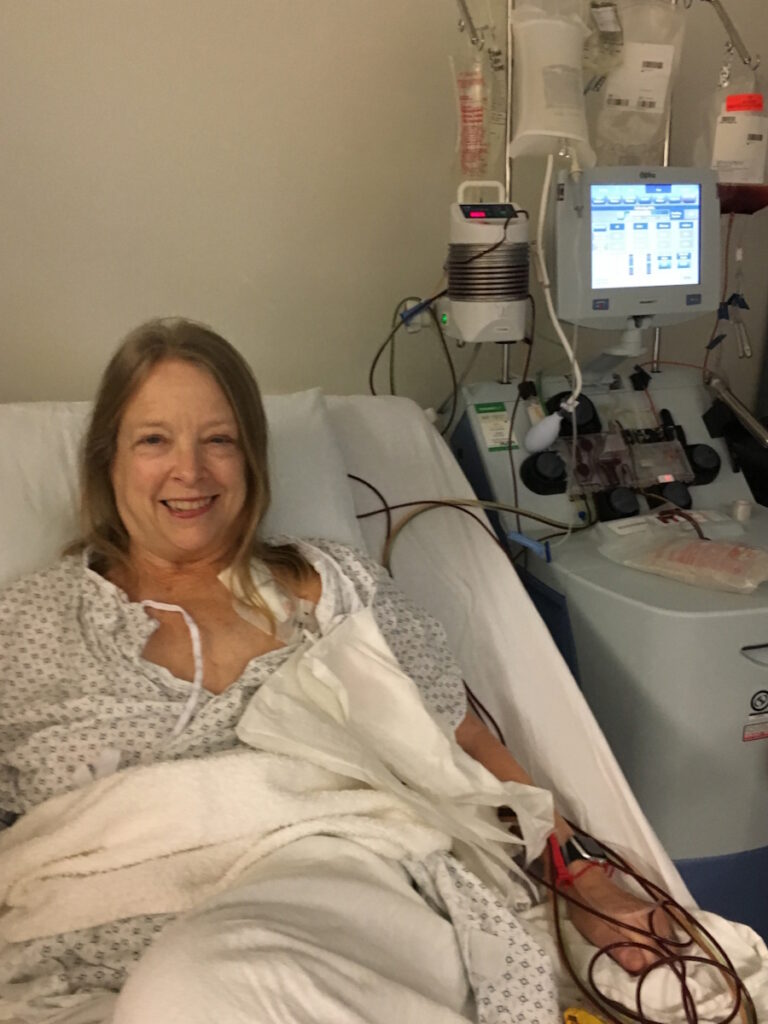
About a month before you get your cells back, they do apheresis. They harvest your T cells. It’s a very easy process that takes half a day outpatient. The courier ships your bag to the CAR T company, which happens to be down the highway in LA. I remember the courier came to pick it up in the apheresis center and I said, “Do not let my cells fall out on the freeway. Please make sure the van door is tightly sealed.” He said, “Don’t worry. We’ll get it there, Laurie. No problem.”
CAR T-cell therapy is about an 18-day process. They shaved off a couple of days and shortened it even more, so the patient didn’t have to wait that long. They take your cells, put the target on them, and grow them in the lab. They harvested about a million cells from me and after they became CAR T cells, there were a billion cells that would get infused.
Before you get your CAR T cells, you go through lymphodepleting chemotherapy, which is chemo light compared to the 18 cycles that I had. It makes room in your bloodstream for you to get your CAR T cells back and gives them room to expand. After three days of lymphodepleting, you get the cells back on day zero, your CAR T birthday. It was amazing because, within days, the tumors were shrinking.
FDA-Approved Bispecific Antibodies for Follicular Lymphoma
Tiffany: Are bispecific antibodies available to patients outside of a clinical trial? Is there anything we can use now straight from a pharmacy without having to go to our investigational one?
Dr. Martin: Two bispecific antibodies are approved for follicular lymphoma: mosunetuzumab and epcoritamab. There probably will be a third one very soon called odronextamab. They’re all pretty similar in terms of how they work and the proteins they target on the surface of the B cells.
There are more coming that we will continue to see in lymphoma and across all cancers. They’re all administered in the clinic or the hospital, so these are not pills that you take at home the way a lot of cancer therapy has transitioned. They’re administered either through an intravenous injection or a subcutaneous injection.
Why are Bispecific Antibodies Administered in the Clinic or Hospital?
Tiffany: Is there a reason for that? Is it because we want to watch for any side effects immediately or is it because of the toxicity and potency of the drug itself?
Dr. Martin: A little bit of both. These are big proteins. They have to be administered by needle because they have to bypass the gastrointestinal tract.
There are some side effects. The side effects that somebody might experience during the infusion are minimal. That said, somewhere in the range of hours to even a couple of days after the treatment, there can be cytokine release syndrome, which happens in up to a third of patients getting these antibodies.
Cytokine release syndrome sounds complicated, but… it’s very manageable.
Dr. Peter Martin
Cytokine release syndrome sounds complicated, but it’s what I described. T cells secrete these chemicals, the same chemicals you experience when you have an infection, including fever, feeling rundown, muscle aches, and what you feel when you have the flu. But in some cases, it can be a little bit more severe. Not very common, but it can happen. We’re often able to manage it with acetaminophen. Sometimes we have to use steroids, like dexamethasone, and rarely do we even have to use other medications.
Because of that, there’s very careful preparation at the facility level, the physician and nursing level, and the patient and caregiver level. It’s all about preparation, helping people to know what to recognize and what to do if something like that happens. It’s very manageable, but it’s a little bit more complicated than taking a pill.
Side Effects of Bispecific Antibodies
Tiffany: Patients are concerned about side effects in general and we know when it comes to cancer, a lot of these drugs are toxic, even though we’ve drastically reduced that over time. In your experience, how do bispecific antibodies differ from traditional chemotherapy and CAR T-cell therapy in terms of side effects? Are they more severe, less severe, or not as long? And does the impact on quality of life determine which avenue they want to take for their treatment?
Dr. Martin: It’s not such a straightforward question to answer because everybody’s different and everybody’s situation is different. Where better-tolerated treatments might be appropriate for one person, more aggressive treatments with more side effects might be appropriate for another person. In most cases, we have options among all of these and oftentimes, there are no wrong or right answers. We try to pick one, but in some cases, we’re driven to say this is the right answer. It’s the job of the whole team — the patient, the caregiver, the physician — to try to pick the right treatment.
Where better-tolerated treatments might be appropriate for one person, more aggressive treatments with more side effects might be appropriate for another.
Dr. Peter Martin
Bispecific antibodies are straightforward in that they can be administered in an outpatient setting or at least partly in an outpatient setting. They don’t cause a lot of the side effects of traditional chemotherapy, like hair loss and nausea, which aren’t major issues with a lot of chemotherapy that we use, but we’re understandably scared of them. Hair loss is a particularly interesting one in that it’s a signal to the rest of the world about something you’re undergoing privately. It tells them publicly that something’s going on, so I understand why that’s not attractive.
Personal Experience with Side Effects
Tiffany: It’s important to get a patient’s perspective regarding side effects. Laurie, can you give us an overview of your experience with side effects? Were there any that you found particularly taxing on you or that affected your quality of life? Were you able to manage your symptoms relatively well?
Laurie: It was a mixed bag. With the first chemo, I lost my hair and got mouth sores. With the second treatment, which was a targeted therapy, I was very, very fatigued. I also lost my hair. They told me that it wasn’t from the trial drug, but when I dug into it, I saw a very small percentage of patients lost their hair.
White counts typically would get depleted, which made me prone to getting infection… so I was a real early adapter of mask-wearing.
Laurie Adami
My fourth treatment was radioimmunotherapy and I had very, very low counts for a long time. My platelets dropped. I never had to get an infusion of platelets, but I had to go in every day to get it checked. I had to be very careful not to fall because I had no clotting ability with low platelets.
White counts typically would get depleted, which made me prone to infections, so I had to be careful. When I went back to work after my first chemo treatment in 2006 and had to start traveling again, I asked my oncologist, “Is it okay if I travel to New York, Boston, London, etc.?” She said, “Yes, but you have to wear a mask,” so I was a real early adapter of mask-wearing.
Precision Medicine as an Approach to Follicular Lymphoma
Tiffany: Something that was also talked about at ASH (American Society of Hematology annual meeting) in general is the idea of precision medicine and how it’s a relatively new approach to cancer treatment. Is precision medicine being used as an approach to follicular lymphoma? What are your thoughts on precision medicine?
Dr. Martin: It depends how much of a fan of science fiction you are. To some degree, we’ve always practiced precision medicine. What do I know about this lymphoma? What do I know about this person? What do I know about all of the different treatment options? How do I put it all together?
Over time, treatments are becoming more specific in some ways, so you can apply them under certain circumstances. Our ability to understand more about cancer changes with new technologies. We’ve always been trying to personalize medicine in the sense of sequencing the entire genome of a cancer cell and saying this is the right treatment for you according to lab testing, but we’re not there yet for follicular lymphoma.
Over time, treatments are becoming more specific in some ways, so you can apply them under certain circumstances.
Dr. Peter Martin
There’s one treatment, a pill called tazemetostat, which has modest activity but is generally well-tolerated. It’s an inhibitor of an enzyme called EZH2, which is mutated in about 20% of people with follicular lymphoma. It’s approved for the treatment of people with mutated EZH2 enzyme, but it’s also approved for people with wild-type unmutated EZH2 if they don’t have other treatment options. Realistically, it works reasonably well in both groups, so it’s a precision medicine approach, but you don’t necessarily have to have the mutation to use it. That’s the closest we have right now, but this is coming. It will continue to change and there are other examples where we’ll see more of that.
Long-Term Implications of Chemo-Free Treatments for Follicular Lymphoma
Tiffany: I know you can’t read the future, but what do you think the long-term implications may be for follicular lymphoma, specifically for chemo-free treatments? What I hear a lot is that I’m living with cancer, not that I have cancer. What do you see with that in terms of chemo-free treatments?
Dr. Martin: People with lymphoma want treatments that work and are well-tolerated. Whether you call them chemotherapy, immunotherapy, or something else, if it works and is well-tolerated, that’s already great. They also want options that conform to where they are in life.
Different treatments that work in different ways have the advantage of potentially allowing us to mitigate some of the short-term and long-term issues that can come up.
Dr. Peter Martin
Every year, we have more and more options available to us. We always try to pick the right treatment for that moment, thinking about the here and now. We also try to think about how what we do today impacts what the patient’s life is going to be like 10 to 20 years from now.
More than chemotherapy, these new treatments potentially have a lesser impact on the body in the longer-term setting. With multiple lines of chemotherapy back to back, people will get through them for decades without major issues but over time, it catches up. Different treatments that work differently have the advantage of potentially allowing us to mitigate some of the short-term and long-term issues that can come up. Having more options is always better.
Clinical Research and Follicular Lymphoma
Tiffany: Both of our backgrounds are heavy in research. I like to talk about clinical research anytime I do a program to get the point out there because oftentimes, people think that a clinical trial is one of their last resorts, they’re not at least getting a standard treatment, or they’re not getting treated at all for their cancer. I know that at Weill Cornell Medicine, you have a robust research program. What does your research program look like and how receptive are your patients to joining clinical trials?
Dr. Martin: I appreciate your disclosure that we both come from a research background, so people should take that into account knowing that we have those biases. The number one barrier to entrance into clinical trials is not patient refusal. It’s because they don’t know that there’s an opportunity. The real burden is having physicians let patients know that this is something that they could do, not patients saying that it’s something they don’t want to do. It’s us. We’re probably the bigger part of the problem.
There are different reasons why somebody might want to participate or not want to participate in clinical trials. They offer new opportunities to access new treatments that might be more effective or better tolerated. In some cases, that might be when other treatments have been exhausted, but in a lot of cases, it might be when a new opportunity has already been well-studied in another setting and you’re looking to apply it in a new setting. There are also some downsides to research, a little bit more of a hassle often.
Tiffany: I’m a proponent of decentralization. Patients can get labs locally without having to track things like that. I’m a little biased when it comes to clinical research, but I do think it has so many benefits, so I’m always promoting it.
Dr. Martin: It can’t be understated that historically, there have been a lot of questionable research practices that were not always in the interest of participants. The medical community on the whole has tried to grapple with this. We’ve got multiple committees, like hospital and patient advisory committees, which try to minimize that and make research as ethical as possible.
There are going to be some people who are distrustful, which is their prerogative. I’m never the person who’s going to twist somebody’s arm to participate in a study that they’re not comfortable with, but I’m also not going to shy away from proposing a study because I’m afraid that somebody is not going to go for it. That’s not respectful to their autonomy either. You propose every option that exists and talk about the pros and cons then people will decide what’s right for them.
Tiffany: Absolutely. I always say too that we don’t give patients enough credit. We always talk about patient education. They need to know that clinical trials are out there and they’ll be more than willing to make that informed decision themselves.
Fertility preservation is also a highly charged issue, but it’s like research: if you don’t talk about it, people don’t have the opportunity to consider it.
Dr. Peter Martin
Fertility Preservation and Follicular Lymphoma
Tiffany: Something that is less talked about in general when it comes to cancer is fertility preservation. An abstract I saw at ASH talked about fertility. For younger patients with follicular lymphoma, does that discussion come up? From what I saw from the abstract, a lot of patients don’t bring it up. They don’t want to discuss it. What has your experience been in terms of having a fertility discussion with your follicular lymphoma patients?
Dr. Martin: Fertility preservation is also a highly charged issue, but it’s like research: if you don’t talk about it, people don’t have the opportunity to consider it. It’s important from the physician’s perspective to ask people about where they are and what they’re thinking about, but it’s also something that patients should advocate for themselves if it’s something they’re thinking about.
In general, follicular lymphoma happens as we get older, but a significant number of people get follicular lymphomas while they are younger and some of those may be considering having children in the future. We’ll get away from the reasons why somebody might choose to have or not have children in the setting of cancer; that’s a whole other complicated discussion.
It needs to be discussed early so that we can think about all of the treatment implications now and longer term, and how we sequence things.
Dr. Peter Martin
Many big hospitals, including Weill Cornell Medicine and NewYork-Presbyterian, have fertility teams that help people consider all of their possible options and how to preserve fertility. Fortunately, even the chemotherapy regimens that we typically use in follicular lymphoma don’t have a major impact on fertility and a lot of the newer treatments have no impact on fertility. The caveat is that you don’t necessarily want to be treating the lymphoma when somebody’s pregnant, although that becomes necessary in many cases and, depending on the treatments used, it often turns out to not be a problem either. It needs to be discussed early so that we can think about all of the treatment implications now and longer term, and how we sequence things.
Tiffany: Thank you for saying that. That’s a conversation you want to have whether you are considering children or not. If you’re younger and considering children, advocate for yourself. If your physician doesn’t bring it up, don’t be afraid to bring it up.
Bridging the Gap Between Academic Research Centers and Community Hospitals
Tiffany: In my experience talking to patients, they don’t get their diagnosis until after they see their primary care physician or go to the emergency room for something different. Because you’re from a large research center, you have multidisciplinary teams, which many people don’t have. They could be going to their community clinic. Patients may not know to go to an academic research center because they haven’t been referred to a specialist. Do you work with any community clinicians or community hospitals? What are your thoughts on working with community doctors to bridge the gap?
Dr. Martin: Even in New York where we have multiple academic medical centers, the majority of people with cancer are managed outside of those academic medical centers, so that’s a reality that we have to acknowledge. I also work in Brooklyn a couple of days a month. People must have access to medical care in their community.
We have to bring better medical care to the communities that people live in rather than vice versa.
Dr. Peter Martin
It took me a few years to come to this conclusion, which is embarrassingly slow, but it’s probably not fair to expect people and their caregivers to travel a couple of hours to see somebody when they have access to medical care in their community. We have to bring better medical care to the communities that people live in rather than vice versa. There are a lot of excellent oncologists practicing in communities and that’s where the majority of people can and probably should receive their care.
One caveat I’ll say is that all of cancer is becoming increasingly complicated, so I don’t think that people should feel uncomfortable seeking a second opinion. I have friends who work in community medicine throughout the whole tristate area in New York and I work with them and help them to manage their patients. Telemedicine has made that easier as well.
This is where patient advocacy comes in. You have to advocate for yourself and speak up about it. If your physician is uncomfortable with that, that might be a sign that they’re thinking about more than your best interests. You’ll find that almost all academic oncologists will encourage second opinions. I certainly do that and help arrange them when I can.
It comes down to a balance. What do you get out of it, what do you have to give to get that benefit, and is it worth it?
Dr. Peter Martin
Key Takeaways from ASH
Tiffany: The ASH annual meeting is a big conference. Was there anything for you that stood out?
Dr. Martin: Bispecific antibodies are going to be a major part of treatment for follicular lymphoma. Exactly how they fit in, which line of therapy, and which combinations get used is interesting to think about. They’re not going anywhere for a while, so that’s pretty cool.
Another interesting study that came out was a late-breaking abstract looking at tafasitamab combined with lenalidomide and rituximab. This was a randomized controlled trial that showed that the addition of tafasitamab to lenalidomide and rituximab improved time to progression. Effectively, it doubled it compared to lenalidomide and rituximab, which is probably one of the more common second or third-line treatments for follicular lymphoma, so that’s a pretty significant benefit.
In some ways, it’s a no-brainer to say that’s something we should do. On the other hand, tafasitamab is a little bit of a hassle. People have to come into the clinic frequently for it, so it’ll be interesting to see where this plays out everywhere. I don’t necessarily know how I’m going to use that information. Again, it comes down to a balance. What do you get out of it, what do you have to give to get that benefit, and is it worth it? But it’s a strikingly positive trial.
Tiffany: I’m going to be following that trial as well.
Conclusion
Tiffany: Thank you so much for this engaging and insightful conversation. I always learn something on the other end of these educational programs.
Dr. Martin, thank you for taking the time to speak with us at The Patient Story. It was so good to catch up with an old colleague and know that we both have remained dedicated to improving cancer care and finding a cure. I’m optimistic about the future as long as we have physicians and researchers around like Dr. Martin.
Laurie, thank you for sharing your story. Lived experiences are very personal and I’m forever grateful to patients who are open and transparent because I believe that it helps the next person and the next patient.
It’s so important to be empowered so that you and your caregivers can make informed decisions about your care. That includes being educated about the latest treatment options for your cancer.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
Symptoms: Intermittent feeling of pressure above clavicle, appearance of lumps on the neck, mild wheeze when breathing and seated in a certain position Treatments: Surgery, chemotherapy
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
Michelle is a survivor of stage 2 primary mediastinal large B-cell lymphoma (PMBCL)non-Hodgkin lymphoma. In her early thirties, she began experiencing symptoms such as neck pain, which she initially dismissed as a pulled muscle. This was around the anniversary of her mother’s passing from stomach cancer, and Michelle felt a growing sense that something was wrong. Following a series of inconclusive medical exams, an x-ray ultimately revealed a large tumor in her chest, leading to her diagnosis of non-Hodgkin lymphoma. Michelle’s diagnosis and subsequent journey marked a significant and transformative chapter in her life.
The discovery of the tumor stunned and terrified Michelle, particularly given her recent experience losing her mother to cancer. Genetic testing revealed no hereditary links to her illness, suggesting it was likely environmental, further compounding her sense of the unknown. Her treatment plan included 6 rounds of intensive chemotherapy, which involved 5-day hospital stays on a continuous drip. The treatment was effective but came with a host of side effects, including severe nausea, fatigue, appetite and weight loss, and hair loss, which further traumatized Michelle. She recalls how losing her hair and eyebrows created a “loss of identity,” as she struggled to recognize herself. Her physical transformation added to the emotional toll, which was exacerbated by continuing to work full-time.
Ringing the bell at the end of Michelle’s successful chemotherapy treatment marked the start of a difficult recovery journey rather than closure. She found that, contrary to popular belief, the end of treatment brought a new set of challenges: trauma from the experience, persistent health issues from chemotherapy, and anxiety about recurrence. Additionally, her body struggled to absorb nutrients due to chemotherapy’s impact on her digestive system. Despite these challenges, Michelle committed herself to her recovery, focusing on nutrition and mental well-being.
This experience led Michelle to change her career path, eventually becoming a certified integrative nutrition health coach to support other cancer survivors in recovery. She emphasizes that recovery is an ongoing process, requiring tools to manage stress, anxiety, and long-term side effects like lymphedema and scar tissue.
Michelle has found purpose in helping others navigate the post-treatment journey, hoping to bridge the gaps in aftercare support. Through her own trials and transformations, she has emerged with a renewed sense of identity and dedication to holistic health, embracing the perspective and purpose she found on the other side of her battle with cancer.
Name:
Michelle P.
Diagnosis:
Primary mediastinal large B-cell lymphoma (PMBCL) non-Hodgkin lymphoma
Staging:
Stage 2
Initial Symptom:
Severe neck pain
Treatment:
Chemotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Stephanie Chuang, founder of The Patient Story, celebrates five years of being cancer-free. She shares a very personal video diary with the top lessons she learned since the Non-Hodgkin lymphoma diagnosis.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Michelle’s experience with recurrent stage 1 bladder cancer started with intermittent blood in her urine, which led to multiple urgent care visits, where she was initially misdiagnosed, and eventually a diagnosis of papillary urothelial carcinoma. Upon diagnosis, she underwent TURBT surgery to remove the tumor and then chemotherapy.
Despite multiple rounds of chemotherapy, Michelle’s cancer recurs within three to six months after stopping treatment. Her doctor suggests ongoing monthly maintenance chemotherapy, but she negotiates for less frequent sessions due to the harsh side effects. She became vigilant about recognizing symptoms of recurrence, helping her manage the chronic nature of her cancer.
Facing the possibility of losing her bladder, she expresses a preference for an Indiana pouch, influenced by her friend’s experience and her desire for a better quality of life. She has already undergone surgery to improve her chances of adapting to the Indiana pouch, demonstrating her proactive approach to managing her health.
Michelle emphasizes the importance of self-advocacy in medical care, seeking multiple opinions, and making informed decisions. She acknowledges the emotional toll of living with cancer and stresses the importance of mental health care and self-care.
Name: Michelle R.
Age at Diagnosis:
43
Diagnosis:
Bladder Cancer
Staging:
Stage 1
Symptoms:
Irregular occurrences of seeing streaks of blood in urine
Specific type of pain when bladder is full
Unexplained weight loss
Urinary urgency
Malaise
Fatigue
Treatments:
Chemotherapy: gemcitabine
Surgery: transurethral resection of bladder tumor (TURBT)
Thank you to Johnson & Johnson for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I had been experiencing some streaks of blood in my urine… It was very random and not consistent at all.
Introduction
I live near Atlanta, Georgia. I’m a mother to an adult son and an auntie to my nieces and nephews. I have two brothers and a sister. I’m a genetic genealogist. If I’m not working my full-time job, I’m working my side business, Bless Your Vibes LLC.
I have recurrent stage 1 non-muscle-invasive bladder cancer (NMIBC). I’ve had nine recurrences, countless surgeries, and chemotherapy. As long as I catch it before it invades the muscle, I’ve been told I can deal with this for the rest of my life.
Pre-diagnosis
Initial Symptoms
I had been experiencing some streaks of blood in my urine. It would happen for a day or two and then nothing for a month, and then it would happen again. It was very random and not consistent at all. I already had a hysterectomy several years prior, so I knew it wasn’t related to that. I didn’t have any pain nor symptoms of a urinary tract infection, so I immediately thought about kidney stones.
Going to Urgent Care
When I went to urgent care, they did a culture and said, “You don’t have any infection, so it’s probably kidney stones. We’re going to give you antibiotics and send you on your way.” I went to urgent care a total of four times from June 2017 to February 2018.
She said, “I want you to demand to see a urologist. You’ve been experiencing this for quite some time. Tell them painless bleeding.’
The last time, I did a televisit. I knew they were going to give me antibiotics because it was the same old story, so I planned to call them during my lunch break. The doctor I spoke with during my televisit was more thorough than any other doctor I’ve ever had in my life.
She asked me questions and didn’t allude to any infection or kidney stones. She said, “I want you to demand to see a urologist. You’ve been experiencing this for quite some time. Tell them painless bleeding. Don’t say ‘blood without pain.’” She stressed that to me for whatever reason.
Seeing a Urologist
The urologist still didn’t indicate anything. They said, “We’ll try to figure out what’s going on.” I had a CT scan and some urine tests, but that was about it.
Diagnosis
Getting the Diagnosis
The urine test results came back through my patient portal and said I was positive for papillary urothelial carcinoma. I knew what carcinoma was, but I didn’t know what papillary urothelial meant. I panicked. It was Friday afternoon and everybody’s gone. The only person I told was my boss at work because I had to leave early.
First thing on Monday morning, I called the office and left a message. They called back and said, “We can’t tell you anything. You need to come in to see the doctor.” I couldn’t go in until later that week, so I had to sit with it for a whole week.
When I went in, the doctor was so matter-of-fact and cold. He started talking about treatment. I said, “Stop. Do I have cancer?” He looked at me like I should already know. I was numb. He said, “Based on the CT scan, it looks like there’s a large mass. Normally, we would go in with a scope and then proceed with surgery. But since we know that it’s cancer, can we bypass the scope and go into surgery?” I said yes because I wanted this out of me, so he scheduled it for two weeks after.
I had one friend… She wasn’t that close of a friend but for her to drop what she’s doing to help me, stay with me, and bring me home meant the world to me.
Treatment
Discussing the Treatment Plan
With bladder cancer, you have high-grade or low-grade, muscle-invasive or non-muscle-invasive. My doctor pulled out a treatment chart and it showed everything. It was pretty clear-cut. It showed the schedule of treatment, which starts from removal or transurethral removal of bladder tumor (TURBT), and then it goes through the surgeries and the types of chemotherapy.
Preparing for Surgery
I remember trying to prepare myself. I was freaking out because up until the night before, I had no ride to my surgery. My son didn’t have his license yet and all of my friends worked. I didn’t have any family to help. I literally had no one. I started calling people that I casually knew and nobody stepped up.
Then I had one friend who I called and I was telling her about it when she said, “Why didn’t you ask me?” I didn’t even think about it because she’s disabled and she turned out to be the one who would step up. She wasn’t that close of a friend but for her to drop what she’s doing to help me, stay with me, and bring me home meant the world to me. It humbled me. I didn’t even know then all the friendships that I was about to lose over this, but from back home, she’s the only friend I have left. I’ve lost all of them.
I went into surgery and at the time, I felt like I had a lot of people depending on me, so I told the doctor, “I’m not just another patient. Treat me well. Do me right because I have a lot of people who depend on me.” I felt he was offended by that because he said, “I treat all my patients the same.” He was very dry.
I asked, “What’s the best-case and worst-case scenario?” He said, “Best-case scenario is I get it all, you go home today, and you rest. Worst-case scenario is you wake up and have a bladder bag.” He told me this right before going in and I was in complete shock. I couldn’t do anything else but pray.
I had a follow-up after surgery and there was another growth. It was the first time I got to see it inside of me.
Surgery
After surgery, my friend was the first person to greet me coming out. She was in the recovery room and as I was waking up, I felt that he got it all and I was going home. I believed it in my head. After I got more coherent, I asked the nurse, “Did he get it all?” And she said yes.
I went home to recover, took the next day off, and went back to work the following day. It was like I had cancer and then I didn’t have cancer in that short time. I didn’t know at the time that it was going to happen nine more times over 6 ½ years.
One of the first things this doctor told me was, “I have patients who have been coming to me for 20 years. I go in and get it out, and they go about their way for 20 years.” At first, I was upset that he said that, but later, I was glad because that prepared me. He indicated that it was going to be normal to keep coming back.
Not every case is chronic, but I like to know things because I like to be prepared. It helped me put it into my head that I’m going to have to deal with this. On one hand, it helps me. But on the other hand, I don’t feel like I’ll ever have that winning moment. It’s going to be a lifetime thing to deal with.
Recurrence
I had a follow-up after surgery and there was another growth. It was the first time I got to see it inside of me. It looked like a succulent flower because it was so tiny and had little shoots. I’m lying there looking at the screen, thinking, “How could something so beautiful be so deadly?” Then he said, “We can take care of this right now.”
I asked him, “What does this entail?” He said, “We pluck it off.” Then through the screen, I saw this little grabber thing come through and he plucks it. It was very surreal. You go from cancer to no cancer because once that’s gone, you have no evidence of disease.
If I have to do a cystoscopy or a procedure, that takes priority because in order to keep my bladder, I have to stay on top of everything and not wait.
Moving to Atlanta
I was moving from Ohio to Atlanta, so I asked him what I needed to do. He said, “Come see me one more time before you go.” I did that and I was clear, so I was okay.
I started searching for the top urologists, top oncologists, and the hospital networks in the area. I did a lot of research and called some of the hospitals, which included Emory because they were in my insurance network. I asked, “If you had a serious problem with your bladder and you needed a urologist, who would you go to?” They told me about this doctor and as soon as I connected with the office, it was so different.
This doctor is a urologic oncologist and supposedly the best in the network. I explained my situation and gave my brother’s address since I didn’t have my new address yet. They emailed me papers and everything. There was such an urgency to be seen and that made me feel very comfortable and that I would be taken care of.
When I went, they said, “We’re not even going to have a consultation. We’re going right into cystoscopy. I want to see what’s going on there.” I’m glad they did because that was my fourth growth and it had taken off. It was very large and from the pathology report, it was high-grade.
After that scope, they said, “We’re going to do the surgery and we’re going to do your chemo,” so I did that.
During my follow-up, I didn’t see the doctor, but I saw someone else from his team. I had been taking cues from my first doctor that it wasn’t a big deal. She was the first one who looked me in the face and said, “Do not put this off because you can die from this,” and that was the first time anybody said that I could actually die from this.
Up until then, it was very casual. From that point on, I took everything very seriously. If I have to do a cystoscopy or a procedure, that takes priority because in order to keep my bladder, I have to stay on top of everything and not wait.
There are specific symptoms that I now recognize when I have active cancer.
Being Aware of Symptoms of Recurrence
I’ve had this nine times now, so I’ve paid attention to my body and my symptoms, and I started recognizing patterns. When I have active growth, there is a very specific pain that I feel in the morning when my bladder is full. Once I empty it, the pain goes away. When I feel that, I know I have a growth.
I’m a plus-sized person. I’m fairly large. But before I was diagnosed, I lost a lot of weight. I lost 60 lbs and that was one of my other symptoms before I was actually diagnosed. I had unexplained weight loss and I had been trying to lose weight my whole life.
Then I have a lot of sense of urgency to go to the bathroom, like when you have a UTI. I can’t wait for too long because the fuller my bladder, the more it hurts. Then I have a general feeling of unwell and being tired a lot. There are specific symptoms that I now recognize when I have active cancer.
One time, I was having bad pain in the morning. I had a cystoscopy not even a month prior and he said, “It’s probably because you’re still healing.” I said, “No, something’s going on.” He got me in and sure enough, it was another growth. This doctor trusts that I know my body and he’s fully on my team.
Maintenance Chemotherapy
For the last recurrence, we know that chemo worked. I got chemo for a whole year and didn’t have any growth, but when I stopped, I had another growth within three to six months, so I had to have another surgery and chemo.
I told him that it seems my growths occur between the three- and six-month mark, so he wants to introduce another chemo to mix with the original one I was taking and do monthly maintenance chemo probably for the rest of my life. I’m not down for that, so I said, “That’s hard on me. What if we go every two or three months?” That’s not even what the board recommends, but he’s willing to consider it.
He said I could stop and we’ll see how I do. In six months, it came back, so I’m going to be on chemo for the rest of my life.
Side Effects of Chemotherapy
The chemotherapy drugs are all different. I get nauseous, but I don’t get sick. I have a little thinning of my hair, but I don’t go bald. I feel overall icky and tired. I go through hot and cold flashes, low-grade fevers, and night sweats. Those last probably about five days before I start to feel a little bit better. But when I went for the whole year, the longer I was doing it, the worse I felt every month.
It started like I was having aphasia or problems with recalling certain words. My memory wasn’t as good. I was having trouble concentrating and trying to process things. It was more complicated. I still have that problem where I trip on my words sometimes. It got progressively worse the longer I was doing chemo.
Taking a Chemo Break
I was supposed to do it until the end of the year, but I asked him, “Can I take a break for a month?” Since I had the six-week course before the monthly sessions, he said I could stop and we’ll see how I do. In six months, it came back, so I’m going to be on chemo for the rest of my life.
It’s going to be a cat and mouse game, and the end result is a ticking time bomb. I’m going to do whatever I can to avoid losing my bladder and as long as I can tolerate the chemo. If it gets to the point where I can no longer take it, then I’ll probably have my bladder removed. There aren’t very many options for that.
Even if it meant I was going to lose the battle to not lose my bladder and choose quality of life over quantity of life, I made peace with that.
Facing the Possibility of Losing Her Bladder
There’s only one option that I would like. My best friend had urethral cancer, a rare form of it, and she got an Indiana pouch and that to me is the most tolerable. I don’t want to live with a bladder bag. It’s a decision I made before I met her. The only options I knew of were a neobladder or ileostomy bag, and I didn’t like either of those options because if the neobladder doesn’t work, then all you have is the bag.
I’m older and my child is grown and independent. I’ve suffered a variety of things throughout my life. I’m a chronic pain patient and with where I’m at in my life, I didn’t want to suffer, so I made the decision. Even if it meant I was going to lose the battle to not lose my bladder and choose quality of life over quantity of life, I made peace with that, and that was hard for other people.
I didn’t really talk about it, but I mentioned to people close to me, “Spend time with me now.” I didn’t come right out and say it, but I would drop hints. Then I met my friend and she showed me that and for the first time, I actually had hope that I could live with this little pouch and do the catheter. I could deal with that. Now that’s where I’m at. If I have to lose my bladder, I want the Indiana pouch.
When I was first diagnosed, I was fortunate to get involved with a cancer support center in my old town. I started going to support groups and would see there was only one other person with bladder cancer and he had a bag. He was pretty matter of fact about it and he was happy. He didn’t go through what I did, but his was found at a later stage.
You could tell which ones had a good support system and which ones didn’t. The ones who had a good support system wanted to fight and they fought until the very end.
At the time, I thought I had a good support system, so I was ready to fight. There was a woman who came in who had been diagnosed with stage 4 and it looked like there was no hope for her, but she had such a good support system. Her decision was to not do any treatment. She was going to live the rest of her days.
I remember that meeting because that’s where we got into quality versus quantity. She said, “Why would I prolong my life with the extra time I have being miserable, rather than have a shorter life and be absolutely happy and at peace with it?” That hit me so deeply because I wasn’t even nowhere near where she was as far as stage, but it put in my head that if I ever get to that point, that’s what I would do. It allowed me to process those choices and come to terms with it.
I knew people wouldn’t understand that. Even to this day, when I talk about it, people would say, “Why would you even think like that?” And these are people with cancer. You’re not me. You’re not going through what I do.
Everybody’s days are limited, whether you have cancer or not. We only have one life, so you have to do what you can in between the dashes.
Shared Treatment Decision-Making
My doctor is still pretty dry, but I’ve grown to appreciate him. I had a different surgery a few years ago and prior to that surgery, I let him know right away, “I’ll do whatever I need to do to keep my bladder, but if it comes down to losing my bladder, I will pass. I want you to know that’s where I’m at.” He respected that and said, “I’ll do whatever you want.” I appreciated that for a variety of reasons. He must have written it in my file, so he knows that when I come in, we have the surgery and then chemo. It’s become routine now.
When I had the high-grade recurrence, it got to the point where we weren’t sure and I was scared. I had met my friend by then and brought it up to him. I said, “Can I do the Indiana pouch if I have to lose my bladder?” He said, “Let me see your abdomen.” At the time, I had a B belly, so my waist dipped in and right where the crease was is where the stoma would be. I asked, “How would that work?” He said, “It probably wouldn’t.”
I had this discussion with him. My concern was if I had a bladder bag, every time I moved, bent over, or sat, it would fold over on itself, so it would pinch off the flow. The stickers for the bag wouldn’t stick. I would then have a higher risk for infection and leaks. It solidified why I wasn’t going to live with a bladder bag.
I thought about it and said, “What if I got a tummy tuck to smooth that out?” I’m a bariatric patient too and I had lost some weight. He felt around and said, “If you could get this smoother, I think you would have a better chance,” so I started on that journey to get that done.
I had a panniculectomy, so now I have a big round D belly and I’m comfortable with the fact that if I had an ileostomy bag, I wouldn’t crease anywhere. But then I met my friend and that made me feel even better. Now that I’ve had the surgery, I could live with that. It was important that I had that discussion with my doctor because if he blew me off, then I wouldn’t have made that decision.
At my last visit, I brought up that I’m coming up to seven years. He said, “If you want to remove your bladder, we can do that, but I don’t think you’re there yet. This is all superficial, but I understand that if the chemo’s getting to be too much and doing all this is too much, we can do that. But I remember what your decision was initially.” Whatever I decide, he’s comfortable with it.
Where we left off was, I have to let him know whether we’re going to introduce this other chemo and try a few rounds every three months to see if that keeps it away. I can live with that and that’ll buy me a little bit more time. Everybody’s days are limited, whether you have cancer or not. We only have one life, so you have to do what you can in between the dashes.
Importance of Self-Advocacy
Self-advocacy is absolutely critical. I talk about it on my social media and I have a lot of women sending me messages, not very many men, but I tell them that this doesn’t have to be a death sentence. It’s a health challenge, especially if you have the type that I have.
You have to advocate for yourself and understand what’s going on with you. Ask your doctor. Don’t feel like you’re putting him off. If he or she’s brushing you off, find another doctor. Get those answers and make those decisions.
Don’t let any doctor gaslight you. I’m a big proponent of that. I don’t think I would’ve been like this if it wasn’t for all the other experiences I’ve gone through in my life. It brought me to this point where I can advocate for myself and others.
A lot of people I talk to don’t know how to advocate for themselves. I’ve seen five oncologists, two different ones in the same week. There’s nothing out there that says you can’t go to another doctor. You have to fight for yourself and speak up for yourself.
Handling the Emotional Toll
I haven’t carried myself with grace. I’ve spent a lot of time crying and being angry at everything. Oddly, one thing I never felt was, “Why me? Why did this happen to me?” I don’t know why. I can’t tell you why, but I’ve not handled it very well.
There have been a lot of times that I get depressed. I shut down. I get gripe-y with people. I withdraw. I’ve always been a quiet person. Everybody says you have to remain positive and be positive. In a lot of aspects, that’s true, but you also have to be a realist and allow yourself to feel these feelings to get through them.
My counselor said, ‘Before cancer or any major health issue, you experience a grieving process over the life that you had before the diagnosis.’
Some things that I do that help me is seek mental health care. When I was first diagnosed, I was seeing a counselor and was on anxiety medication. When I moved, I didn’t need those anymore because back then, I had other situations I was dealing with that I wasn’t in anymore.
I practice a lot of self-care. I used to feel guilty about spending money on myself, especially as a parent, but I don’t anymore because it’s vital to my survival and helps me cope after years of dealing with my cancer.
You go through a grieving process too, much like a death. My counselor said, “Before cancer or any major health issue, you experience a grieving process over the life that you had before the diagnosis. You’ll never go back to life before that diagnosis, especially with cancer. You start grieving the loss of that life, so you need to go through all those steps and emotions to get through it.” For a lot of people, that’s hard.
The biggest stigma in the cancer community is to fight it and beat it. Either beat it or you lose. Normally, those are your only options. But when you have cancer that keeps on coming back, you don’t have that. You’re either sick or not sick. You never win. You never go the rest of your life not having to worry about it again. It becomes a part of you and you learn to deal with it. It’s like getting diagnosed with any other type of major illness. There’s before the diagnosis and after the diagnosis. You have to figure out how to live with it. Find a good support system and resources to help you.
Publishing a Cancer Care Book
When I was first diagnosed, there were different things that I had to keep track of. I had a little notebook where I was writing everything down on because I couldn’t keep track of everything, especially once I moved. I had to get new doctors, new patient portals, and new insurance. There was too much for me to keep track of. I found a group and talked to other people about it.
I’m a graphic designer by profession, so I thought about making a book for other people and created a guided journal called Cancer Care Book, which is available on Amazon (no commission is being earned with this link). It’s geared toward women, but men could use it too. It’s for anybody who has cancer but specifically for newly diagnosed people.
There are different sections in it where you can keep track of all your appointments and bills, write things out like a journal, or if you’re an artist, you can draw or doodle. There are coloring pages because I’m a big believer in art therapy.
There’s a section called The Tough Stuff where you can organize your bucket list items and final wishes. They may deny it, but everybody will think about what happens if they die and this is the perfect way. Nobody has to see this if you don’t want to.
If you get so sick and have a caretaker, you can keep track of all the information, like medication, and hand it off to a caretaker. There’s an emergency contact list on the first page, so if something happens to you, people will know who to reach out to. I put everything that I thought I would want when I was first diagnosed.
You can’t take care of anybody else if you don’t take care of yourself first.
Words of Advice
I made a video that showed six things that are key to your survival and the biggest one is early detection. Don’t wait. If you have any kind of symptom or you feel like something is wrong with your body, get it checked out. Don’t put it off. Early detection is key.
Advocate for yourself no matter what. Get those answers and get education.
Find your tribe. Find your support. They’re out there. On my website, I have a Resources page with over 500 websites for all cancers.
Take care of yourself because much like when you’re flying on a plane and they tell you to put the oxygen mask on first, you can’t take care of anybody else if you don’t take care of yourself first.
Anyone who has had a cancer diagnosis needs to get some kind of mental health care to process everything. You can find a lot of help in support groups and support centers, but they’re limited and can only help you so much. If you’ve never seen a counselor or a therapist before, once you get a diagnosis, they should be next on your list of doctors to see.
You have to come to terms with your mortality. A lot of people think they’re going to live forever. You have to shift your thinking. Cancer could take you out, a car accident could take you out, or a fire could take you out. Anything could happen. You need to reevaluate your life and make better choices of what’s important to you and your closest loved ones.
Special thanks again to Johnson & Johnson for its support of our independent patient education content. The Patient Story retains full editorial control.
Lauren’s Stage 4 Breast and Stage 4 Colon Cancer Story
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Lauren, from Houston, Texas, is living with stage 4 breast cancer and stage 4 colon cancer. Her journey began in 2014 when, after breastfeeding her second child, she discovered a lump in her breast. As her doctor initially dismissed it as fibroadenoma, Lauren did not undergo further testing. 2 years later, she developed pains in her breast and noticed that her left nipple looked strange, and upon further examination, doctors diagnosed her with stage 3 breast cancer. She underwent chemotherapy, a mastectomy, and radiation, followed by hormone therapy for several years.
In 2021, Lauren began experiencing stomach pains and noticed blood in her stool. Following a colonoscopy, she was diagnosed with stage 3 colon cancer after doctors discovered a cancerous lymph node. She underwent surgery and chemotherapy but struggled with side effects. Lauren also began to explore alternative treatments like high-dose intravenous vitamin C and fasting, inspired by research on treating KRAS mutation cancers, which are known to be particularly aggressive and difficult to treat.
In 2022, after experiencing further stomach pain, a PET scan revealed that the cancer had spread to Lauren’s abdominal lining and spine. Her oncologist gave her a terminal prognosis, estimating that she had around 10 months left to live. Desperate, Lauren intensified her vitamin C treatments, fasting, and other therapies. Remarkably, by December of that year, her PET scan showed no evidence of disease, although her doctor cautioned her to remain vigilant.
Lauren’s journey took another turn when a biopsy revealed that her spinal cancer was not colon cancer but a recurrence of her breast cancer, which had resurfaced and spread while her immune system was weakened. Although she has had to deal with recurring spots of cancer in her spine, Lauren has successfully managed her colon cancer, with her tumor markers remaining low. She credits her alternative treatments, alongside traditional therapies, for keeping her cancer at bay.
Now, Lauren undergoes PET scans every 3 months to monitor her condition. While managing cancer has become part of her daily life, especially with gastrointestinal side effects from her colon surgery, she remains proactive in her treatment and hopeful for the future. Despite the challenges, Lauren emphasizes the importance of staying informed, advocating for oneself, and maintaining hope, especially for those dealing with KRAS mutation cancers.
Name:
Lauren B.
Age at Diagnosis:
31
Diagnosis:
Breast cancer
Colon cancer
Staging:
Stage 4 for both
Initial Symptoms:
Lump in left breast that grew
Strange appearance of nipple
Treatment:
Surgery (radical left mastectomy, lymph node removal; removal of part of colon and appendix)
Chemotherapy (Doxorubicin and Taxol; Oxaliplatin and Xeloda)
Radiation therapy
Hormone therapy
Complementary treatments (fasting, high-dose intravenous Vitamin C)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: First instance: appearance of lump that later on increased in size, orange peel-like skin around inverted nipple, persistent ache under right arm; second instance: appearance of lump
Treatments: First instance: chemotherapy, targeted therapy, hormone therapy; second instance: surgery (mastectomy), chemotherapy, radiation therapy, CDK 4/6 inhibitor
Symptoms: Appearance of lump in right breast, significant fatigue, hot flashes at night, leg restlessness leading to sudden, unexpected leg muscle cramps
Treatments: Chemotherapy, hormone therapy, PARP inhibitor, integrative medicine
Symptoms: Intermittent but severe pain including a burning sensation on the side of the breast, appearance of a cyst and a lump, abnormally warm and pink-colored breast, nipple inversion, strangely liquid menstrual periods, unusual underarm odor, darkening and dimpling of the nipple, severe fatigue, night sweats Treatments: Chemotherapy, surgeries (mastectomy, lymphadenectomy), radiation therapy, targeted therapy
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Nick’s symptoms began a year or two before his diagnosis, including changes in bowel habits, size, and consistency, blood in the stool, and abdominal pain, which he initially attributed to aging or irritable bowel syndrome. After experiencing fatigue and escalating pain, he went to the ER where he was diagnosed with diverticulitis and sepsis. Despite initial treatment, he required a laparoscopic washout due to a perforated colon and subsequent complications, including an abscess.
During a follow-up colonoscopy, doctors found a mass, which was later confirmed as adenocarcinoma. He underwent a sigmoid resection, removing part of his colon. While clear margins were achieved, 19 of 49 lymph nodes tested positive for cancer.
Nick began CAPOX chemotherapy, experiencing severe side effects like fatigue, neuropathy, and an acne rash due to the addition of Avastin (bevacizumab). When they noticed an elevation in his tumor marker and growth in his lymph nodes, he was switched to Keytruda (pembrolizumab), an immunotherapy, to reduce the cancer to a manageable level.
Nick emphasizes the importance of mental health support to manage anxiety. He advises listening to your body, advocating for yourself, and using support systems. He encourages seeking thorough medical evaluation for unexplained symptoms and finding strength in support groups, hobbies, and loved ones, stressing perseverance and finding reasons to keep fighting.
Name: Nick S.
Diagnosis:
Colorectal Cancer
Staging:
Stage 4A
Initial Symptoms:
Change in bowel habits, size & consistency
Blood in stool
Abdominal pain
Fatigue
Treatment:
Surgery: sigmoid colectomy
Chemotherapy: CAPOX (capecitabine & oxaliplatin),
Immunotherapy: bevacizumab, pembrolizumab
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
My symptoms started a year or two before diagnosis. It started with a change in bowel habits, size, consistency, some blood in the stool, and abdominal pain.
Introduction
I’m a stage 4A colorectal cancer fighter. My wife and I live in Chippewa Falls, Wisconsin. We have a wonderful 28-year-old daughter.
I’m a full-time firefighter and critical care paramedic. I’ve been doing firefighting for about 16 years and paramedicine for about 13 of those 16 years.
Pre-diagnosis
Initial Symptoms
My symptoms started a year or two before diagnosis with stage 4A colorectal cancer. It started with a change in bowel habits, size, consistency, some blood in the stool, and abdominal pain. I had some acid reflux type of reactions that my wife and I chalked up to aging and not being as healthy as I could be. My wife has irritable bowel syndrome and I thought some of it was IBS because some foods would trigger some reactions in me.
I was working full-time for the department for about a decade and a couple of years later, I decided to change over to a neighboring department. For these jobs, we have to pass a physical agility test.
I have been working by myself daily. I was in pretty good shape. The test is a pretty rigorous test to be able to do what we do. I was 48. I was doing this at an older age than the 20-year-olds they were usually hiring.
I was diagnosed with diverticulitis and sepsis, so they started me on antibiotics right away.
A couple of months later, we responded to a house fire. At some point, my battalion chief pulled me off the line and said, “You look wiped out. I’m going to sit you out for a little bit to catch your breath.” I felt a little tired, but, again, I was getting a little older.
I sat out and went back in for another round. This time, the chief was on the scene and said, “Nick, take your gear off. You don’t look good. Go back to the ambulance. You’re going to be doing rehab, making sure everyone else is doing okay, but we don’t want you going back in.” I thought something was weird.
I called my wife to meet me in the ER. I didn’t know what was going on. I’ve got bad abdominal pain. I haven’t slept. I’m going to go get checked out.
Diverticulitis & Sepsis
I was diagnosed with diverticulitis and sepsis, so they started me on antibiotics right away. They weren’t sure if surgery was going to be necessary, but they transferred me to another hospital. At that point, I was stable.
When I got transferred, I met with a thoracic surgeon and started to realize that things were serious. He said, “We’re not going to go in right away. We’re going to keep an eye on you tonight. Hopefully, things will subside with some more antibiotics and some steroids, if we have to. But we’re going to keep an eye on you and evaluate you. We’d like to avoid surgery.”
The next day, when they were getting my vitals, the nurses said, “We see you’re slated for surgery.” That turned into a laparoscopic washout. They found that I had a perforated colon in the sigmoid area, the area right before the rectum, but that had healed itself.
All of a sudden, I heard the doctors say, ‘That’s not good.’ I remember seeing a black mass on the screen.
They went in through a couple of small incisions, washed everything out to make sure there was no fecal matter, and stitched me back up. I had a couple of surgical drains. I was in the hospital for five or six days and then I was sent home to heal.
I ended up getting readmitted a couple of days later because I had some drainage coming from my drain sites. After a CT scan, they found I had an abscess. I believe E coli was one of the culprits. There was something else too, so they needed heavy-hitter antibiotics.
After another two weeks of antibiotics, the PICC line was removed. I met with the surgeon and everything was looking great. He said, “Let’s do a follow-up colonoscopy to check how the diverticulitis is.”
Colonoscopy
I wanted to sleep through it. I was joking with them and we were all relaxed when all of a sudden, I heard the doctors say, “That’s not good.” I remember seeing a black mass on the screen. He tried advancing past it and I said, “Ow,” but I didn’t feel it. I said “ow” instinctively. He said, “We can’t get past this mass. We’re going to pull out.” The tone changed. You could have heard a needle drop in that procedure room.
They wheeled me back into the recovery room where my wife was waiting. On the way there, one of the nurses handed me a polished stone that had the word “hope” stamped on it. I didn’t think that choked me up, but I carry it wherever I go. In hindsight, it meant a lot and drove home the seriousness of the situation. We didn’t know exactly what was going on, but something wasn’t right. I have enough medical training and field experience to read the room and know it wasn’t good.
The doctor eventually came back in and said they couldn’t diagnose it yet. They took a small sample to send off for testing to confirm what they thought it was. He wouldn’t say whether it was cancer or not.
The good news was they got the tumor with clear margins. They felt it hadn’t spread far…
Diagnosis
Getting the Biopsy Results
I was waiting for the results at home. When I finally got the notification on my phone, I checked it and it said adenocarcinoma. Now we know what we’re dealing with. It’s cancer of some sort. I never thought about it as a possibility.
Treatment
Sigmoid Colectomy
During the colonoscopy, he said we were going to have surgery because what it was had to come out. He referred me to surgery right away. Luckily, it was the same surgeon who performed my earlier surgery who I trusted with my life.
I met with him about a week later. They were going to do an exploratory surgery until they knew exactly what it was in there and then do their thing.
I remember being in the room when my mother-in-law came out too. My wife was there, of course. They wheeled me in, put in the IVs, and told me to start counting back from 100. I don’t think I hit 95. Hours later, I woke up in my hospital room with a slightly sore throat. They performed a sigmoid resection. I can’t remember how much of my colon they took out, but I didn’t require an ostomy, thankfully. They were able to resect it and reconnect it right away.
The good news was they got the tumor with clear margins. They felt it hadn’t spread far, at least in the tissue of the colon. But the surgeon sampled some lymph nodes right next to the tumor site. They took out 49 and 19 of them tested positive for cancer.
I stayed positive. The whole reason I’m in this fight is my family.
CAPOX Chemotherapy
At that point, I was referred to oncology. I met with my oncologist. His nurse was a former ER nurse who I was familiar with and seeing a familiar face went a long long way.
He explained what he planned on doing based on the CT scans. They saw some inflammation in other lymph nodes and they weren’t sure if that was post-surgical. They wanted to do another CT scan to check, but they were happy about the margins being clear. I was staged at 3C then. It metastasized a little bit past the point of origin but not very far.
The first day of chemo was going to include labs and a CT scan to see where we were at. The plan was to do CAPOX: capecitabine, an oral medication, and oxaliplatin, an IV medication. I would do the oral chemo for two weeks and then on the third week, I would go in for the IV chemo. They would do labs on those days to make sure everything was okay.
Unfortunately, the doctor didn’t like what he saw on the CT. He wanted to get a little more defined imaging, so he set me up for a PET scan and delayed the chemo. A couple of days later, we came back to start chemo again and get the PET scan read.
The doctor confirmed that it had spread to the lymph nodes in the abdominal area, along my aorta, and up to my left shoulder. It had spread a lot further than we thought it had.
I felt like every time we made a plan to move forward, we were getting kicked back a couple of steps, but I stayed positive. The whole reason I’m in this fight is my family. I believe that someday, this cancer will get me, but I’m not going down without a fight. I’m stubborn, so it’s going to be a long fight. I won’t go down without swinging.
I have a four-day weekend so I tried to time my infusion, so I had a couple of days to recover post-infusion and feel somewhat human before returning to work.
Side Effects of CAPOX Chemotherapy
Chemo wasn’t fun. It knocks you out. I felt fatigued on the first day. For probably a week and a half, when you start getting the infusion, you can’t drink cold drinks. It felt like swallowing glass shards. A lot of fatigue and neuropathy kicked in.
I didn’t like being out in the cold and I love ice fishing. You’ll catch me outside at -20°F on a normal day, but with chemo, not a chance. I had to be bundled all the time.
My eyes were always drying out, so they hurt a lot. I had insomnia, joint pain, and muscle pain.
They added Avastin (bevacizumab), which is an immunotherapy, to my chemo routine. That caused a bad acne rash on my back from the waistline up to my neck. The doctor had never seen nor heard of it, but we can only attribute it to Avastin.
Working While in Treatment
I was able to go back to work full-time as a firefighter. I have a four-day weekend so I tried to time my infusion, so I had a couple of days to recover post-infusion and feel somewhat human before returning to work.
My work was very accommodating. We’re firefighters, so we don’t sleep all day, but the chief said if I needed to rest, I could go to the dorm, which I appreciate. I never took him up on it. I tried to stay with my brothers and sisters training or doing calls, and that worked great.
I was going to be on treatment for the rest of my life. I might get some time off if we get no evidence of disease at any point, but it will come back at some point and I’ll have to go back on treatment.
Switching to Immunotherapy
The initial plan was for six months or eight cycles of chemo and Avastin. Unfortunately, because of the restaging, I was going to be on treatment for the rest of my life. I might get some time off if we get no evidence of disease at any point, but it will come back at some point and I’ll have to go back on treatment.
My tumor marker was through the roof when this all started and it was dropping with chemo. We were seeing shrinkage in the lymph nodes. Chemo sucks, but it’s doing what it’s doing, so we stayed very positive.
When we got to cycle six, we noticed my CEA was going up a little bit. We were doing CT scans every three months and we noticed some growth in the lymph nodes. The doctor said, “We’re going to stop the chemo. It’s not working. You can only receive so much oxaliplatin before it becomes completely ineffective. This saves us a couple of cycles where if we need to go back to it, we can go back to it. We’re going to switch over to an immunotherapy called Keytruda (pembrolizumab).”
The side effects of immunotherapy are supposed to be much less than chemo and I’m all for that. I switched from chemotherapy to immunotherapy in August 2023. I still have very slight neuropathy every now and then in my toes and my fingertips. Nothing debilitating but a reminder that I was on chemo at one point and that probably won’t get any better or any worse, hopefully.
Keytruda is a half-hour infusion. Side effects are minimal. Between cycles two and three, while we were camping, I noticed that my resting heart rate was higher than it should be. I was not exercising as much and a little out of shape, but I shouldn’t have a resting heart rate of 130-140 beats a minute. I was sweating a lot without doing anything, so I couldn’t figure it out. I talked to the oncologist and they ran some thyroid tests.
One of the known side effects of Keytruda is thyroid burn. It’ll cause hyperthyroidism until the thyroid burns out and then it’ll cause hypothyroidism.
The support of my family, my work family, and my friends is what gets me through this.
Treatment Plan
We want to do Keytruda for 18 more months. It’s a two-year plan. We’ll see what it does and go from there. Hopefully, the response brings everything down to normal levels, I won’t have evidence of disease, and I can ride that out for a while.
Fingers crossed, maybe Keytruda is the cure for colon cancer, but realistically, I don’t think so. I think it’ll be a lifetime battle, but it’s going to be a long life. The support of my family, my work family, and my friends is what gets me through this.
Managing Scanxiety
As a paramedic, I’ve dealt with patients with panic attacks and anxiety. Anxiety’s a real thing. A lot of times, it doesn’t seem like it with the patients you’re dealing with, but now that I’m put in that position, it’s a real thing. I’ve dealt with it even before cancer through another set of unfortunate circumstances and luckily, I have a great support group in place.
We see a lot of things as paramedics and firefighters, so after a while, you realize things aren’t normal. I had to start paying closer attention to my mental health. I started seeing a therapist and she’s great. She taught me how to deal with stress, anxiety, and my feelings.
What we go through as cancer patients is not something most people go through nor is it something they understand.
Stay strong and recognize that the stress is real. What we go through as cancer patients is not something most people go through nor is it something they understand. Take a deep breath. Listen to what your mind and body are telling you.
Your feelings are valid. Don’t try to brush it off and try to be strong by pushing your way through it. Rely on your support team. If you have a therapist, talk to that therapist.
Most oncology teams come with a social worker. Use that resource. Rely on your family for strength. Tell your spouse what you’re feeling even when you don’t want to. Sometimes talking about it gets it out there and puts it away, as opposed to it weighing you down.
What helps me is retreating home, spending time with family, or staying busy with work. Rely on your hobbies if you have any. If you don’t, find some. I’m a big fisherman. I love fishing. You could put me on a lake and even if I couldn’t catch a fish for days, I would be in my happy place. Find something that helps you disconnect from the cancer and what you’re going through.
Words of Advice
For anyone who might be experiencing symptoms that you’re not quite sure of, listen to your body. Talk to your doctor. Advocate for yourself. If you feel something’s not right, push for tests to try and figure out what’s going on. The answer, “We don’t know what’s wrong with you,” is not acceptable. Push to find answers.
For cancer warriors who are going through this, keep going. You’re not alone. There’s support beyond your family, friends, and coworkers. There are a ton of support groups online. There are social workers available. There are platforms like The Patient Story.
You’re not in this alone. Some days, it may feel like it. Some days, I get down in the dumps, but I find something to get me back up. I find a reason to keep going. There are a million reasons to keep going and even if you find just one, that’s all it takes.
Listen to your body. Talk to your doctor. Advocate for yourself.