“Not Me. That’s Not My Story.”: Haley’s Rarest of the Rare Diagnosis – Breast-Primary Neuroendocrine Carcinoma
Haley was 36 years old when neuroendocrine carcinoma, one of the rarest and most silently aggressive cancers, arrived in her life without warning. A healthcare professional, Haley had been going to the gym every morning and had no family history of cancer, no genetic predispositions, and no alarming symptoms that would have raised a red flag. The fatigue she felt, the night sweats, the gradual dip in her workout performance: all of it had quietly become her new normal. It wasn’t until jaundice appeared and coworkers noticed she’d turned yellow that the cascade toward diagnosis began.
Interviewed by: Taylor Scheib
Edited by: Chris Sanchez
What followed was a whirlwind that most patients couldn’t navigate even with years to prepare. In the span of a single week, Haley went from thinking she needed her gallbladder out to sitting in a Buc-ee’s parking lot in Baytown, Texas, crying on the phone with her doctor, and refusing to leave Houston without being seen at MD Anderson. Her physician called in every connection he had. Within 14 days of her diagnosis, she was at one of the country’s premier cancer centers, where an even more startling discovery awaited: her neuroendocrine carcinoma was breast-primary. It was so rare that her oncologist had seen only three patients like her before. Positive for estrogen and progesterone receptors, but not breast cancer — she was, as she put it, “a zebra among zebras.”

The treatment road has been demanding. Haley underwent weekly chemotherapy for nine months with no breaks, navigated a septic episode requiring stent replacement, and received an initial prognosis of six months or less. She shaved her head in response to hair loss, cried in the shower, then made a deal with herself and with God to let go of what needed to go to keep fighting.
Thirteen months later, Haley still goes to work. She walks when she can’t lift weights. She lets her mother clean her house and says yes when dinner is offered. And her scans? They are showing regression, not just stability, with the word “remission” appearing on some of her liver and lung spots as of her most recent visit to MD Anderson. The medical team that once braced for the worst is now simply shocked.
Haley shares her experience because this cancer is quiet, often dismissed as hormonal fluctuations, perimenopause, or ordinary exhaustion, especially in women. She wants every person reading this to know: listen to your body, advocate for yourself, and do not wait.
Watch Haley’s video and browse the edited transcript of her interview below for the details of her story.
- Neuroendocrine carcinoma can be invisible for months or years. Symptoms like fatigue, night sweats, mood changes, and disrupted sleep are easy to attribute to stress, aging, or hormonal shifts, especially for women near 40. Haley’s experience is a powerful reminder that “normal” symptoms still deserve a conversation with your doctor.
- A trusted medical team can move mountains. The speed of Haley’s diagnosis and referral to MD Anderson, within seven days, was made possible by a physician who knew her, advocated fiercely for her, and leveraged every resource available. It’s vital to build relationships with your care team before a crisis.
- Advocating for yourself at a major cancer center is worth it. When MD Anderson’s first available appointment was two weeks away, Haley refused to leave Texas. Her insistence, and one more phone call from her doctor, changed the timeline of her care. Pushing for urgency is not a burden; it is your right.
- A rare diagnosis may require a rare level of persistence. Haley’s cancer was not only neuroendocrine carcinoma: it was breast-primary, hormone-receptor positive, and unlike anything her oncologist had seen in nearly all of her career. Seeking specialists, tumor boards, and multi-institutional consultation saved Haley from a one-size-fits-all treatment plan.
- Allowing others to support you is not a weakness; it is wisdom. Perhaps Haley’s most universal truth: the people who love you need to feel useful. Saying yes to help, such as dinner, housecleaning, and company, is not giving up independence. It is giving the people who love you the gift of purpose.
- Transformation is possible even inside a devastating prognosis. Haley entered this experience as a fiercely independent, gym-every-morning, one-trip-with-the-groceries person. She emerged as someone who walks gently, prays with intention, lets her mom clean her house, and shows up to share her story; not despite what she has been through, but because of it.
- Name: Haley K.
- Diagnosis:
- Neuroendocrine Carcinoma
- Age at Diagnosis:
- 36
- Symptoms:
- Dark urine
- Extreme fatigue
- Loss of appetite
- Constipation
- Poor-quality sleep
- Mood swings due to hormonal changes
- Treatment:
- Chemotherapy: carboplatin and paclitaxel





This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
- Who I am
- The early signs and symptoms
- My complete list of neuroendocrine carcinoma symptoms mistaken for normal life
- The moment my coworkers noticed I had jaundice
- Unexpected lab results and CT scan findings that changed everything
- What happened next
- Receiving the neuroendocrine carcinoma diagnosis and the urgent referral to MD Anderson
- Arriving at MD Anderson in Houston
- PET scan and CT scan results
- Rare breast-primary neuroendocrine carcinoma diagnosis: “A zebra among zebras”
- My treatment plan
- Stent replacement, blood transfusions, and managing side effects during treatment
- Thriving against all odds
- Navigating hair loss during chemotherapy: finding acceptance and unexpected strength
- Why I share my neuroendocrine carcinoma story
- Letting people help you: A lesson in accepting support through cancer
Who I am
My name is Haley, and I was diagnosed with neuroendocrine carcinoma in February of 2025.
The early signs and symptoms
Initially, there were no red flag symptoms. That’s the beauty and the beast of neuroendocrine carcinoma — its symptoms are very normal, everyday life symptoms: fatigue and things like that. The thing that sent me to the doctor was that I became jaundiced. My pallor became yellow, and my friends noticed it at work. So we did some blood work. I worked for a physician, and we did some blood work. My bilirubin — which, as people hear of infants having high bilirubin, it’s the same thing in adults — was high. We thought I needed my gallbladder taken out because I was having some right-sided pain. Come to find out, that was not the case once we did a CT scan.
There was never a red flag symptom. That’s why it’s so important that I get my story out there — to not brush off fatigue. Come to find out, fatigue, hot flashes, night sweats, things like that are all part of this cancer that is easily pushed under the rug. I was someone who was going to the gym every single day for two hours before work every morning, so it was easy for me to push my fatigue under the rug.
But looking back now, I do see that I started to decline in not being able to progress in my workouts the way I had been in the previous months. I noticed it probably around July of 2024. Looking back, that was probably the first time I could correlate feeling different in my workouts — so that was probably when it started affecting me physically.
It’s crazy, and it’s weird, because there’s nothing significant to point to and say, “That right there is where it started,” or, you know, an emergency room visit because of a sudden, acute pain, the way people sometimes have. This cancer is not very red-flag-ish. It’s very, very silent.
My complete list of neuroendocrine carcinoma symptoms mistaken for normal life
It would be: fatigue, night sweats, waking up suddenly in the middle of the night at the same time every night consistently — I started waking up around 3 a.m. I was having an overall decreased strength and endurance in my workouts, as well as a decreased appetite toward the end. That would probably be about it. Maybe some emotional changes as well, because it is a hormone-driven cancer. Some hormonal changes were going on that I wasn’t used to — I was having mood swings and things like that.
I started to go off-topic from the list, but I honestly thought I was in perimenopause. That was a thought that crossed my mind in the months leading up to my diagnosis. I’m almost 40, I’ve not had any children, and my mother had menopause early, so it was reasonable that that was something going on for me.
Other than that, that’s literally the list. Nothing crazy — until literally four days before my diagnosis. And then it was a waterfall.
The moment my coworkers noticed I had jaundice
I always go back to the Thursday prior. I noticed that my urine was darker than normal. Being someone who exercises, goes to the gym, and eats healthy, I drink tons of water, so I’m used to seeing clear urine. When I used the bathroom, and it was dark, I thought, “Wow, I’m dehydrated — have I not been drinking as much water?” And so there was a whole process: I even went to one of the IV bars around my town and got an IV infusion that weekend. We have those available around town, and one of my coworkers works there part-time.
But that Monday, I was just not feeling well — not enough to go to the doctor or anything. I was literally sitting in my physician’s office talking to him and his wife, who is a nurse practitioner at our clinic. One of my coworkers walked in, looked at me, and said, “Haley, you’re yellow — what is wrong with you?” I told her, “I’m not feeling good,” and I mentioned I had been constipated that morning. I said I hadn’t paid close enough attention to my bathroom habits.
I had to digitally disimpact myself that morning. I said, “That’s so odd that you say that because I noticed my bathroom habits this morning were different.” Being in the medical field for the last 18 years, I know that pallor change and those other symptoms all go together, and so it all just snowballed from there.
When she said that, the doctor — who had been at his computer, listening but not looking at me — whirled around in his chair. His wife, whose desk is back-to-back with his, swirled around at the same time. They both looked at me and said, “Oh my goodness, you are significantly yellow.” My coworker said, “You were not that color this morning — when you walked in, you were not that color.” This was later in the afternoon. So I started telling them what had happened over the weekend.
They said, “Okay, you might need your gallbladder taken out.” I said, “Yep — I still have it.” The doctor said, “You’ve mentioned a couple of times having little random twinges in your right side, and we’ve joked amongst ourselves about, ‘Hey, you might need your gallbladder taken out.’” It just escalated from there. He said, “I’m going to order some lab work on you,” and his wife said, “Go ahead and order a CT scan and ultrasound of her liver as well — let’s get ahead of this.” He said, “I’m going to call Dr. Palmer, our GI doctor, who is a close colleague, and she’s female, so I know you’ll be comfortable with her — and I’m going to call the surgeon too.”
It’s good to have people. It’s good to know people. Before I had any blood drawn, he had everything lined up to have my gallbladder taken out. He said, “Because it’s late in the evening and the lab is closed, go first thing in the morning before you come to work and get your labs. By the time you get here, we’ll have the results because we have access to our hospital’s internal medical records.”
Unexpected lab results and CT scan findings that changed everything
When the results came back, my bilirubin was 5.3 — normal is less than 1.2. My AST and ALT, which are my liver enzymes, were about five and six times what they should have been. But otherwise, all other lab work was normal: kidney function, blood counts, no infection, white cells — all normal. So we were still thinking there was a gallbladder obstruction.
The plan continued: “I’m going to admit you to the cardiac unit so I can have control over your care — it’ll get you fast-tracked for your CT scan. You can have your gallbladder taken out tonight or tomorrow morning, be done, and be back at work on Monday.” I was like, “That sounds fantastic — let’s get this taken care of.”
So I left work, got my dog settled, took a shower, and grabbed some things from the house. My mom had actually had surgery on the Monday when all of this was going on — this was Tuesday morning, and she was getting ready to be discharged. I called her and my stepdad and said, “Don’t freak out — I just think it’s my gallbladder. It explains everything that was going on this weekend. I’m going to get a CT scan.”
I got admitted, got settled, and went for my CT scan. I had previously been an employee of the hospital — I was a scrub tech in the cardiac cath lab and did monitoring in cardiac cath — so I had many coworkers still at that facility. My room was full of people continuously while I was there. But then they all had to go back to work, and Dr. Hemstreet came back.
When the results came back from my CT scan, I could tell by the look on his face when he walked in. I said, “It’s not good. Something’s wrong.” And he said, “It’s not good.” He sat down on the edge of the bed, grabbed my hand, and started telling me what they saw. We hugged, and he said, “Do you want me to call your mom?” Because he knows my mom — we were coworkers before he became my employer, and we have a very close relationship. He said, “Where’s your phone? Do you want me to call her on yours or mine?” I said, “I don’t know where mine is.” So he called her, put her on speakerphone, and told her everything. He said, “We’re going to order an MRI. I’ll try to get it done tonight.”
He explained: “She does have some growth around her common bile duct, in her pancreas, and in her liver. That’s what caused the blockage. That’s why she’s sick. We’re going to do the MRI and then an ERCP tomorrow to try to get that bile duct open and put a stent in so that everything can drain — the bilirubin, the bile — and get it out of her system.”
We had the MRI that night because of who he is in our town. I always joke with him that before the new administration at the University of Alabama, it was God, Nick Saban, and George Hemstreet in Tuscaloosa. He has all these connections, and so he got them to do the MRI for me. One of my coworkers was actually my CI when I was in radiology school — he took one look at me and said, “What are you doing here?” I told him, and he was devastated. He did my scan. I could tell by the look on his face when it was over — he came to my room afterward. He couldn’t technically tell me what he saw, but I could tell. Being an X-ray tech, a radiology tech, and an MRI tech — we see everything before anybody else does, but we can’t say anything. He just said, “If you need anything, you let me know,” gave me his cell phone number, and said, “I’ll be here until 11 tonight.”
The MRI confirmed everything the CT scan had shown.
What happened next
The following morning, we prepared, and I had an ERCP. Dr. Palmer is fantastic — she tried for almost five hours to get a stent in for me so they wouldn’t have to place a drain and do more dramatic interventions. But she was unable to do it because of my anatomy and all the growth that was present. After trying so hard for so long, I remember waking up from anesthesia and her almost in tears, saying, “I tried. I wanted to do this for you so badly, but I can’t.”
She said, “I have to send you to Grandview,” which is a larger, upper-level facility about an hour up the road. We’re a Level II trauma center; they’re Level I — a step up in specialty. She said it might take until later in the week to get in with the specialist there because he is in such demand — “It takes months for people to get in with him. But I’m going to do everything I can.”
This was at about 7 p.m. on Wednesday. At 1:00 a.m., my nurse woke me up and said, “The ambulance is here to get you — they’re going to place the stent tomorrow.” Everything was just happening so fast. I took the ambulance up to Grandview. They settled me in, let me go back to sleep, and said, “We’ll check on you in the morning. We’re going to give you a couple of hours before we come back. Sometime after lunch is when we’re expecting he’ll be able to work you in.”
True to their word, around noon, they came and got me. They took me to pre-op. At this point, we were all thinking I had pancreatic cancer, based on everything we had seen — while Dr. Palmer was in there trying to do my ERCP, she did take some samples for biopsy, but those hadn’t come back yet.
The physician came to me and said, “Haley, I’ve looked at the films. I want you to know — I’ve diagnosed pancreatic cancer before, and this is not what this is. I don’t know what it is, but that’s not what it is.” That gave us a little bit of comfort. To most of us, hearing “pancreatic cancer” is a death sentence. Everybody watched Patrick Swayze — he’s a perfect example. That was in the back of our minds the whole time. But hearing him say that gave us a little hope.
In less than an hour, he had the stent in, and I was back in my room, waking up. I remember waking up in the post-procedural area and feeling what I recognized as reperfusion pains — because I hadn’t been in pain before they opened it back up, and that release of pressure was intense. It happened so fast. I asked my stepdad what time I got back to my room, and he said around 2:00 — and it was only 1:00 when they took me back. He also took additional samples at that point.
Receiving the neuroendocrine carcinoma diagnosis and the urgent referral to MD Anderson
That Thursday night — the night after I got my stent placed — the biopsy results from Tuscaloosa came back showing neuroendocrine carcinoma. Dr. Hemstreet, of course, got the results before anybody and called me. He screenshotted the results on his computer, texted them to me, and called me. He said, “I’ve already spoken to two oncologists, and we need to get you to MD Anderson. That’s where we need to go next. This is a very rare cancer.”
He told me, “I spoke to one of my colleagues that I went to medical school with, who is the head of oncology at a facility in South Alabama, and I’ve spoken to one of the oncologists here in our town. Both of them said you need to go to MD Anderson first — because if they have any trials or anything, they don’t want to start you on treatments that may negate you or put you out of those trials.”
I said, “All right, then.” This was Thursday. All of this had only started on Monday. By Thursday, we had a diagnosis, and we were going to MD Anderson.
I got discharged on Friday. Dr. Hemstreet texted me that morning asking for my driver’s license, insurance card, and everything else so the office staff could get my referral together. He was calling people and making things happen. We spent the weekend with family and friends, and my mom and I packed up. Even though she had had surgery the prior Monday, the two of us were on the road the very next Monday. Within seven days of my diagnosis, I was on the road to MD Anderson.
Arriving at MD Anderson in Houston
Mom and I basically got there, and they were scrambling a bit. They said, “We got you an appointment for February 27th,” — and this was February 11th. We said, “Well, we’re here. We were told to come, so we came.” They said, “Let’s see what we can do.”
I called Dr. Hemstreet, and I was crying. We were sitting in a Buc-ee’s parking lot in Baytown, Texas. My mom was like, “It’s okay. We’ll figure it out. We’ll go home and come back. We’ll do whatever we need to do.” And I said, “I’m not leaving. I’m not leaving. I’m not leaving. This is where I need to be.”
Dr. Hemstreet called me back and said, “I know the person who is the head of cardiology at MD Anderson. Give me five minutes, and you’ll have an appointment.” He called me back in about ten minutes and said, “Go to your hotel. They’re getting your stuff together. You’re going to have an appointment before the end of the week. Don’t worry — it’s fine.” And he was right. Within 14 days of being diagnosed, I was at MD Anderson.
PET scan and CT scan results
They did my PET scan, and we also did a chest, abdomen, and pelvis CT. I had only had a pelvic and abdominal CT and MRI up to that point — nothing of my chest yet. That CT scan showed nodules in my lungs and spots on my lungs, adding to what had already been seen on the abdominal and pelvic imaging. Then the PET scan showed a hot spot on my right breast.
We were all like, “That is very odd — why is that there?” Because normally neuroendocrine carcinoma originates and stays within the GI tract and the GI system, and sometimes in the reproductive organs — that’s mainly where it originates. Based on everything we could see up to that point, the working diagnosis was that mine was originating from the pancreas. But again, not all of the biopsies had come back yet because everything was happening so fast.
MD Anderson’s radiologist, after reading the PET scan, said, “I really think we should biopsy the right breast — not only because of fewer potential complications post-procedure, but it was a hotter spot.” Those were his exact words. I said, “Whatever you think is best. I don’t care if you do both spots — whatever you need to do. As a medically minded person, I want to know exactly what this is so we can deal with it the right way. I don’t want anything left in question.”
Rare breast-primary neuroendocrine carcinoma diagnosis: “A zebra among zebras”
The right breast biopsy came back showing that it was breast-primary neuroendocrine carcinoma, which is very rare. The oncologist told me she had only ever seen three people [with that presentation]; I would have been the fourth. She has only seen three people with breast cancer as the primary site for a neuroendocrine carcinoma.
Then they continued to test the biopsy slides for other mutations and markers — they had gotten a much better biopsy from my breast than from the pancreas, so they had a lot more tissue to work with. Over the course of the next week, while I was in Houston, I kept getting phone calls: “It was breast-primary — and it’s also positive for progesterone. It’s also positive for estrogen. But it’s HER2-negative.” They started testing it for all the breast cancer markers and genes, and it was positive for those. They had never seen anyone who had a positive hormone receptor with this presentation but whose disease was not breast cancer.
The ribbon for neuroendocrine carcinoma is zebra stripes — because it is so rare, that’s what the ribbon is. I was a zebra among zebras because mine was so different. My oncologist said, “I have colleagues at NIH, at Vanderbilt, and in Florida who are NET specialists,” and she was consulting other specialists at other hospitals to figure out the best treatment plan.
My treatment plan
We changed the treatment plan slightly, but we still planned to have my first treatment before I left Houston. The oncologist did all of that. I had my first treatment at MD Anderson, and the next day, my mother and I got in the car and drove home. We stopped in Mississippi to spend the night and got home the next day.
I went to the cancer center here in Tuscaloosa. Dr. Hemstreet had them ready for my next shot. I met my new local oncologist, who would be managing my treatment here — we are affiliated with MD Anderson, so everyone is in communication with one another.
Then I had to also get in with the breast oncologist at MD Anderson. So I see both a GI oncologist and a breast oncologist out there, and then I have our regular oncologist at home. They put me on a tumor board because the breast oncologist felt the treatment plan should be adjusted.
Initially, they had me on carboplatin — a platinum-based drug — and paclitaxel, which is typically a three-hour infusion on day one of a 21-day cycle, with 20 days to recover. But once everybody on the tumor board reviewed my case, they determined I should have a 21-day cycle with carboplatin on day one, followed by a one-hour infusion of paclitaxel the following week, then another one-hour infusion of paclitaxel the week after that. So I was getting chemotherapy every single week — no breaks.
I did that for nine months.
Stent replacement, blood transfusions, and managing side effects during treatment
In those nine months, I did have to have my stent replaced. One Sunday morning, I had what I thought was anxiety — just a tightness in my chest. I took some medication I have for that, and it didn’t go away after an hour. I took more, and nothing happened. Then I got up to use the restroom, and my urine was dark, and I took my temperature and had a fever. I said, “Okay, I know exactly what’s going on — I’ve been here and done that.” But this time I had pain I hadn’t had the first time. My stent was blocked. I was septic and needed it replaced.
Dr. Palmer was able to do it this time without me having to transfer, since the Grandview specialist had already made a tract in there for her. I had a little one-week hospital stay in September of 2025 for that. Other than that, I’ve had no major hiccups besides having to get blood infusions from time to time when my blood counts get low.
I was given a diagnosis and a prognosis that was devastating. Initially, we thought this cancer was more like the dormant, slower type — that’s the neuroendocrine tumor side, called NET. Those cells do not proliferate or reproduce quickly. They’re very, very slow. People often have them their entire lives and never even need treatment — they just watch them. But on my side, mine was the carcinoma. My gastrointestinal oncologist called it “the ugliest of cancers.” She told me my prognosis was six months to a year — maybe — if I was lucky; likely less. She said some outliers are very lucky and make it two to three years, but mine was six months or less initially.
But of course I was like, “No. Not me. That’s not my story. That’s not how this is going down.”
Thriving against all odds
When we came home, we locked down on diet, keeping things positive, doing all kinds of different things to keep my body healthy so it can tolerate my chemo. I’m doing things that help make my chemo more effective. I keep my body moving — I go for walks; I can’t go to the gym and lift weights like I used to, but I keep moving. And here we are, 13 months later.
I still go to work every day except for the day I have chemo and the day after — I keep that day after to recover, nap a little, and get ready to go back. I do as much as I can and want to. This past weekend, my mom, her best friend, and my best friend went to a little place in North Alabama near the Tennessee line — kind of like a miniature Gatlinburg, a very small-town feel.
So it’s basically treatment indefinitely — until it stops working or I become intolerant to it. In January, on my last visit to MD Anderson, we decreased the carboplatin a little because I needed blood transfusions more often. We also added an extra week at the end of my cycle, making it a 28-day cycle with an extra week between treatments. They said, “We have never seen anybody take a full year of chemo like you have. We’re going to let your body have a little bit of a break.”
Over the last couple of months, that plan has been great — I’ve only needed a blood transfusion once since the Tuesday before Christmas. That’s been nice. It keeps me on a more even plane; I don’t have the same large dips in how I’m feeling with that extra week in between.
And all of my scans — regardless of what we were told — have shown nothing but regression since we started. Not even just stability. Regression. The word “remission” was used for some of the spots on my liver and some of the spots on my lungs on my last scan at MD Anderson in January. We are just exceeding expectations. We are doing the opposite of what we thought we would do.
They are just shocked every time I go out there. The last time I went, my hair had just started growing back, and the same nurse who had seen me before said, “Oh my gosh, your hair is growing back!” I was like, “I know — I thought I was just going to stay bald for the rest of my life.” I had bought a bunch of wigs, and then my hair started growing back.
So we’re just being a unicorn — a zebra — being different and doing the things they said we probably wouldn’t do. I’m very in tune with my spirituality and my religion. Between God and the extra things I’m doing and my medical team, I literally could not ask for more, because He’s already given me more than they told me I would have.
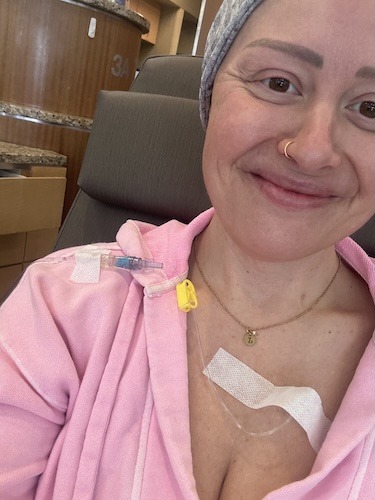
Navigating hair loss during chemotherapy: finding acceptance and unexpected strength
The hair loss, I would say, was the hardest thing from the initial diagnosis. I think I was still in shock then. My hair started falling out less than two weeks after my first treatment — and we weren’t expecting that. We expected to have at least another treatment before it started coming out, but that was not to be the case.
I had taken a shower and was running my hands through my hair with conditioner — it’s so long and curly that I don’t brush it between washes; I just make sure I get the tangles out before I get out. And it was just coming out — all over my hands. I just stood there in the shower and cried.
I had a conversation with God, and I said, “If you ever asked me my favorite thing about myself before this, I would say it was my hair. I love my hair. But if I have to lose my hair to save my life, I will gladly give that up.”
I said, “Whatever you need to take from me to help me get through this — to fulfill whatever purpose needs to come from this — I’m here, and I will do it.” I went the next day and got my hair cut, and by the end of that week, I shaved my head because it was coming out so much that it was matting, itching, and hurting. So I just embraced it. I said, “I always wondered what I would look like with a shaved head — I’ve always had to deal with so much hair.” And now, with it growing back, I’m like, “This is really cool. I’m getting to experience something I was always afraid to do because it was an unknown.” I’ve never had short hair before. So it’s a new experience.
We saw what I looked like with a shaved head, we saw what I looked like with a bald, shiny head, and now we’re seeing what I look like with hair growing back.
Why I share my neuroendocrine carcinoma story
I want to share my story because this came so out of nowhere. I have no family history. I had genetic testing, and I do not have any genetic predisposition for any type of cancer. I was 36 years old, and it snuck up on me so silently.
I want to be so aggressive about this awareness because of how easy it is for people to overlook small things — small changes in the way their body is reacting and behaving — outside of their normal. It was just such slight changes over time that each one became my new normal. And then that became my new normal. And then that became my new normal.
We are all so busy and in such a rush that we brush everything under the rug because it is an inconvenience to stop and take a look at it. I want people to stop and listen to their bodies and tell their doctors. And I want them to push — push for, “Something isn’t right.”
Even at your yearly physical, they are not checking you for possible cancer markers. They’re not checking you for possible genetic mutations. They’re not checking you for any of that. So I encourage people to ask their physician about this kind of stuff. I’ve started telling friends and family, every time they mention something — “Hey, I’ve been having GI upset,” or “This really odd symptom happened the other day” — I say: tell your doctor. Let somebody know that’s going on. Because a blood panel, a chest X-ray, something small could save your life.
The sooner they find any cancer — regardless of how rare or how resistant to treatment — the sooner they find it, the better. So it’s all about paying attention to your body, even to the slightest, smallest change. Let somebody know, just to be on the safe side. Don’t think you’re being annoying or a bother to your physician. Because I promise you, when the day comes that somebody gives you a diagnosis, you are going to look back and wish you had said something sooner.
Mine was so incognito that I had had a gynecological appointment in August of 2024 with a breast exam, and neither my physician nor I felt anything. It wasn’t a solid tumor in my breast. So it’s the small things you need to pay attention to — anything outside of your normal that doesn’t have a solid reason for the change.
Letting people help you: A lesson in accepting support through cancer
I do have one more thing that has actually been very difficult for me, because I am a very independent person. I have never asked for help. I live in an apartment upstairs, and I make one trip with the groceries. I don’t ask for help unless I literally cannot physically carry something up the stairs myself. But I have learned over the course of the last year to allow people to help me.
Allow people to bless you. Allow people to get joy from helping you — because that’s what it is for them. The people who love you don’t know what to do, and they don’t know how to help you. So if somebody calls and asks, “Can I bring you dinner?” say yes. Let them bring you dinner. If somebody wants to come over and clean your house, let them. I’ve sat and talked to my mama while she cleaned my house because I was too tired that day, and she said, “Just sit there. You’re okay. You don’t have to help me.”
And somebody said it perfectly early on, when my mom and I were in Houston and my stepdad, my dad, my brother, and everybody back home was trying to help manage things and telling us not to worry: one of them said, “Stop taking the joy from us to be able to do something and take the weight off your shoulders.”
So let people get joy from helping you through your journey. Let people in. Let people support you, because you are going to need it. That would be the other major thing I would say: let people help you. Let people in. Let people support you.
Inspired by Haley’s story?
Share your story, too!
More Neuroendocrine Carcinoma Stories

Regina J., Lung Neuroendocrine Tumor
Symptoms: Wheezing, back pain, coughing that sometimes produced blood
Treatment: Surgery (partial lung resection)
…

Tabbie V., Pancreatic Neuroendocrine Tumor (pNET)
Symptoms: Abdominal pain, unusual organ “inflammation” feeling when walking, fatigue
Treatments: Chemotherapy (oral and IV), surgeries (Whipple procedure or pancreaticoduodenectomy, liver resection or partial hepatectomy)
…

Hayley O., Pancreatic Neuroendocrine Tumor (pNET)
Symptoms: Severe right-sided pelvic pain, nausea, diarrhea
Treatment: Surgery (pancreaticoduodenectomy or Whipple procedure)
…

Drea E., Gastric Neuroendocrine Tumor (gNET), Stage 3, Grade 1
Symptoms: Fainting spells, fatigue, dizziness, anemia, shortness of breath, absence of menstruation, unexplained weight loss, night sweats
Treatment: Surgery (total gastrectomy with a Roux-en-Y reconstruction)
…

Leave a Reply