Finding My Voice In the Healthcare System: Briana’s Stage 3 Colorectal Cancer Experience
This stage 3 colorectal cancer story follows Briana’s experience with persistent constipation, colostomy surgery and reversal, chemotherapy, and finding her voice in the healthcare system.
Interviewed by: Carly Knowlton
Edited by: Chris Sanchez
Briana was settling into a new chapter of life in San Jose. She had just found her footing in a new job, was deeply involved in her community, and felt like things were finally lining up. Then her body started sending signals she couldn’t quite explain including constipation, stomach discomfort, and a growing sense that something wasn’t right. The symptoms were subtle at first, but they lingered for months.
Doctors initially pointed to common digestive issues. Bloodwork came back, colonoscopy prep repeatedly failed because of an obstruction, and IBS remained the working assumption. It wasn’t until Briana pushed for answers during a final ER visit that a CT scan revealed the real cause: a tumor blocking her bowels. She was diagnosed with stage 3 colorectal cancer. “You don’t expect cancer,” she says. “It’s really unknown territory, so the shock was real.”

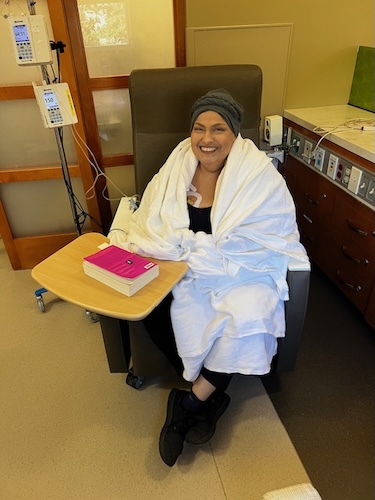
The path to diagnosis became a lesson in persistence. Briana’s refusal to back down, even when faced with skepticism, led to the truth. Her stage 3 colorectal cancer experience rapidly escalated: hospitalization, immediate surgery, and the sudden need to adapt to a colostomy bag all came with emotional and physical hurdles. Surrounded by supportive friends and family, with her best friend at her side and her mother flying in, Briana confronted a new reality marked by fatigue, wound complications, and infection in the initial recovery period.
Chemotherapy brought another layer of adaptation, with both IV and oral regimens producing hair loss, nerve pain, and unexpected side effects. After months of treatment, Briana celebrated “no evidence of disease” with milestones and new rituals, such as a new hairstyle and a tattoo. However, survivorship, she emphasizes, also brings anxiety and an ever-present uncertainty. She lives in six-month increments now, but is committed to staying present and trying new things.
Throughout her stage 3 colorectal cancer experience, Briana found strength in support groups, fellow young survivors on social media, and her own voice. She encourages anyone navigating similar paths to advocate fiercely for themselves. “Nobody knows your body the way you know your body, and if you feel something is off, keep finding someone who will listen,” she says.
Watch Briana’s video and browse the edited transcript of her interview. The video and transcript will provide insights, including:
- Why you should advocate for yourself persistently, especially when symptoms are dismissed or misdiagnosed
- How important it is to listen to your own body; self-knowledge can be vital for survival and diagnosis
- Why emotional adaptation is just as essential as physical recovery in cancer care
- How visibility and self-acceptance around medical changes, like a colostomy bag, can empower others and reduce stigma
- About Briana’s transformation: From self-doubt to vocal, resilient advocate for herself and her community
- Name: Briana H.
- Age at Diagnosis:
- 31
- Diagnosis:
- Colorectal Cancer
- Staging:
- Stage 3
- Symptoms:
- Periods of constipation initially lasting one week and then extending to two weeks
- Nausea
- Pain in lower left abdomen
- Lack of appetite
- Vomiting and inability to keep fluids down
- Treatments:
- Surgeries: colon resection, tumor removal, colostomy placement, colostomy reversal
- Chemotherapy











This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
- I am Briana
- Before my diagnosis
- When my early symptoms started showing up
- My situation escalated and I got diagnosed
- How I reacted to the diagnosis
- My surgery and the challenges I faced afterward
- Adapting to a colostomy bag
- Chemotherapy and its side effects
- Progress with chemo and colostomy reversal surgery
- I was declared no evidence of disease
- Personal celebration and moving forward
- Perspective and life changes after cancer
- My advice for others
- Cancer and diverse communities
I am Briana
I was diagnosed with stage three colorectal cancer in October 2024.
I love traveling, exploring new places, and being out in nature. I love going to concerts, always trying to see my favorite artists live. I enjoy hiking, camping, planting trees, and working in the environmental sector. I really try to stay connected with nature in every way possible.
My friends would probably describe me as the sarcastic one. I always give them a hard time, but I’m always present for them and always down for anything, whether it’s going out and trying new foods, attending a show, or an improv event. I am always one who’s ready to go out and do something.
Regarding the photos I’ve submitted, there’s one specifically from Seattle, which is one of my favorite cities to visit. I’ve been there twice, and if I were to move out of California, that’s likely where I would go. There’s also a photo from John Muir Woods, which represents what I like to do in my free time.
Before my diagnosis
Right before I was diagnosed, I had just started a new job in local government. I felt like I had finally reached stability in my life, career-wise and economically. I’m originally from Southern California, but I’ve built a home for myself here in the Bay Area. I felt like I was reaching that place where I could start working on other projects I’ve wanted to pursue.
I was beginning to look into organizations where I could volunteer my time as a board member or committee member. I was researching how to get more involved with organizations such as Latino Outdoors, which organizes outdoor outings for the community. Being active in that space is very important and dear to my heart. I was just starting to get more involved when I began having symptoms, which were very mild at first. I definitely did not think it was going to be cancer. It was unknown territory, so it was quite shocking.
When my early symptoms started showing up
My first symptoms were mild; you don’t expect cancer, and it was really unknown territory for me, so the shock was real.
The first symptoms appeared about ten months before my diagnosis. It started as mild constipation, and it felt like I wasn’t able to digest food. The day before Christmas Eve in 2023, I felt like I couldn’t process any food, ended up throwing up that night, and spent the whole night in the bathroom. That was my first trip to urgent care. They did a urine analysis and blood work, told me everything looked fine, and suggested it was just an upset stomach. I was told to stick to bland foods and given nausea medication.
The symptoms settled after that, but kept coming back in episodes. In April and May, the symptoms recurred and would last about a week at a time. I started visiting my primary doctor and repeatedly told him that, although it seemed like constipation, it didn’t feel normal. I was also having pain in my lower left abdomen. Blood work was done; I was found to be anemic and started on iron supplements, along with IBS medication. The initial thought was maybe it was IBS.
At the end of June 2024, my symptoms got much worse. Despite seeing my doctor, nothing got better. I remember driving to my appointment with a trash bag in my lap because the nausea was so bad. The symptoms were getting brushed off as IBS, and I was given stronger IBS medication and told to try Miralax, but there was no real solution.
Eventually, I was referred to gastroenterology and scheduled for a colonoscopy. By then, the tumor was already blocking my bowels, and I couldn’t do a proper bowel prep. The first colonoscopy was canceled because the prep made me very sick; I vomited the entire night. I got rescheduled with a different prep, but the same thing happened, as it was still blocked. Even after waking up from sedation at the clinic, they told me to go home, redo the prep, and come back tomorrow. Trying the prep again upset my stomach, and I couldn’t keep water or food down for days. I finally went to the ER at the end of August, received nausea meds, and was sent home. At that point, I didn’t want to schedule another colonoscopy. I wanted to talk to an actual doctor.
My situation escalated and I got diagnosed
In September, I tried to do a follow-up. By the second to last week of September, I was getting really sick again. The final week, I had to go home early from work and never returned. That Tuesday, I started throwing up again and couldn’t eat or drink. I went to the ER Thursday night after days without food or water, begging for a CT scan. The ER doctor advised me to go to my primary doctor the next morning for a scan request, but I was already in pain and didn’t want to wait.
By morning, I was throwing up again and couldn’t go to work, spending sixteen hours on the couch in pain until my friend showed up and insisted on taking me to the ER. A different doctor listened to me, took note of all my symptoms since December 2023, and said, “Let’s get you stable first, and then we’re going to start running tests.” They gave me a CT scan, and that’s when it was discovered.
How I reacted to the diagnosis
After the CT scan, the doctor explained they couldn’t definitively say it was cancer, but they were 95% sure and needed to do a biopsy for confirmation.
It was a sense of relief to hear the diagnosis, not because I wanted to hear those words, but because I knew I wasn’t going crazy; something was seriously wrong with my body. It has always been difficult for me to stand up and speak for myself, so this was a new experience. I wish I’d advocated for myself sooner, especially after my first colonoscopy, by insisting on alternative testing, since my body couldn’t process the prep for a proper colonoscopy.
I’ve been open about my cancer journey with friends and family, and I always emphasize that nobody knows your body the way you do. If you feel something is not right, and they’re brushing you off, keep looking for someone who will listen, because that person is out there. It’s important to listen to your body and find a doctor who listens, too. Sometimes we hold back from advocating for ourselves because we don’t want to be that squeaky wheel or rush the doctor, but when your life is on the line, it is crucial to speak up.
That’s why we pay into health insurance and have a healthcare system. It’s not perfect, but we have a right to use it and advocate for ourselves. Listen to your body, more importantly than anything. It took time for me to speak up, and I wish I had done it sooner. I learned during my hospital stay that learning to speak up for yourself is a whole different environment as well.
My initial thoughts were, “Okay, what’s next?” There was a lot to process. Because I had been in pain and brushed off for so long, my first response was, “Alright, we figured it out. I’m not crazy; something is wrong with my body. What do we need to do next?” The doctor told me surgery was imminent, and I was not going home, but was being admitted to the hospital.
The hardest part wasn’t hearing the diagnosis, but having to tell my loved ones what they found. Luckily, my best friend was with me when I was told, and my family was already making arrangements to come out and be with me.
My surgery and the challenges I faced afterward
Once admitted, I met the surgery team responsible for removing the mass and placing a colostomy bag. That was a big adjustment. It took about a week from surgery to get the official diagnosis from the lab. Once confirmed as stage 3, I was referred to the oncology team.
I did not get the surgery the night I arrived. That happened two days later, at that hospital. I arrived Friday night, the mass was discovered Saturday morning, and I had surgery Monday night. After surgery, I went home for a few weeks, then met with a new oncology team.
I spent about two weeks in the hospital after surgery because my body was in such poor condition. My heart rate was high, and I was transferred to the telemetry unit for continuous monitoring. I had a couple of blood transfusions, daily X-rays and blood draws, and spent a few days on oxygen. An additional procedure was required for a JP drain due to fluid buildup, causing infection. Even post-surgery, the hospital stay was rough.
I went home for about a week, but needed to be readmitted for another week because of a secondary fluid buildup. I required a second JP drain and then a wound vacuum for leakage into my wound from the colostomy bag. That first month was extremely difficult.
There was no time to process everything; it was very hard to compartmentalize. It wasn’t until a week after surgery, when I got the official diagnosis, that I broke down crying, and it became real. It wasn’t just surgery and done. There were many steps afterward, and this was only the beginning of recovery.
For the first week and a half, I was on autopilot, dealing with pain, nausea, adjusting to life with a colostomy, and the painful wound vacuum changes. There was no time to sit with my thoughts or emotions and really process what had happened.
Adapting to a colostomy bag
I remember the surgeon asking if I was ready to live with a colostomy bag. My answer was no; no one is ready for that. But when your life is at risk, you take the best outcome, even if it means living with a colostomy bag. They did let me know it could be reversible.
It took a while for me to even look at it and to process what’s normal or not regarding movement. You don’t know what to look for at first; you technically have your intestine outside your abdomen. Learning how to change it, maintain it, keep the skin healthy, and be in public with it was a huge learning curve.
I eventually learned to dress as I did before and found ways to style clothes for access to the bag. I reached a point where I didn’t care if someone saw it; it’s my body, and it is what it is. If someone asked, I told them.
I learned to change out the bag and the whole system by myself. My mom was my primary helper at the beginning, but we reached a good place.
It has since been reversed.
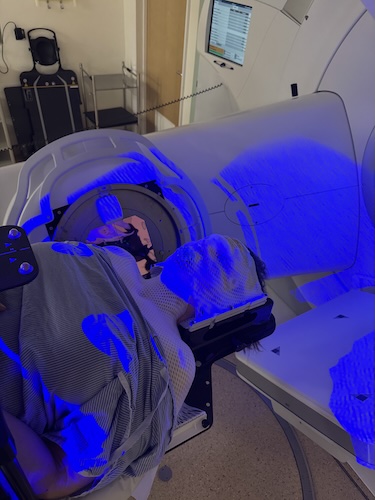
Chemotherapy and its side effects
Healing from surgery took longer than expected, so I started chemo about three months post-op, literally the day before Christmas Eve, a year from my first urgent care visit. I did eight rounds of chemo: four rounds of both IV and oral chemo, followed by four rounds of oral chemo. Oral chemo could be done at home.
The biggest side effect was hair loss. I lost about 50% of my hair, and it thinned significantly.
During my first chemo session, the first hour was bearable, but then my hand stiffened, pain set in, and I realized how painful the administration process was. My arm was sore for days after.
But the side effect that bothered me most was laryngospasms. The muscles of my throat would spasm with anything colder than room temperature or even slightly warm. I could only drink hot liquids, which was a challenge since I preferred iced coffee.
This side effect lasted for days and often recurred for two weeks, until the next round of chemo. For about four months, I only drank hot beverages.
Progress with chemo and colostomy reversal surgery
After about three or four months of chemo, we saw progress. My oncologist gave me the option of stopping chemo and starting monitoring, but I opted to continue oral chemo for another three months for my own peace of mind.
Once I finished chemo on June 1st, I was scheduled for my colostomy reversal at the end of August.
I had a colonoscopy to ensure I was ready for the surgery, and it was successful. There was no mass blocking my bowels. The first few days post-op were rough, and being back in the hospital brought back memories. The days felt endless, which was mentally challenging. It was hard getting used to my body again, but I went home about four days after surgery and monitored my recovery from there.
Eight weeks after surgery, I was back to work full-time and resumed almost all normal activity.
I was declared no evidence of disease
After chemo ended, I had a CT scan showing no evidence of disease.
I had already seen my results online before my doctor delivered the news, so it was somewhat less surprising but still very reaffirming to hear directly from my oncologist, “There’s no sign of disease.” We now move into monitoring for the future. It was a good conversation.
I also do quarterly blood work through Natera, a third-party company partnered with my hospital, checking for any traces in my bloodstream. All results have been negative.
Currently, I’m on a monitoring schedule for the next five years, with CT scans every six months for three years, then hopefully moving to annual checkups afterward.
I didn’t get to ring the bell for finishing treatment, as my hospital didn’t do that, and a lot was conducted virtually. My oncologist reiterated that they can’t guarantee zero cancer in my body, but now it’s about monitoring for recurrence. I celebrated in my own way.
Personal celebration and moving forward
This past week was my official first anniversary since my diagnosis.
It’s not really a day to celebrate; it’s not exciting, but when your life changes so completely, it shifts your perspective. There’s anxiety and depression, even in survivorship, so I did things to keep my spirits up: I dyed my hair, went to dinner, played trivia with friends, and got a tattoo for fun.
I am really trying to embrace this new chapter and not lose myself to the diagnosis. There is always some anxiety about recurrence, but I try to live in six-month increments, responsibly yet fully.
Perspective and life changes after cancer
I look at life differently now. I think about what I want to do every year, what impact I want to make, and how I want to show up in my community. Being present is a priority. I’m finally exploring grad school, having just started the application process. I try not to let my diagnosis stop me from doing things I’ve wanted to do.
When your mortality is in limbo, you realize many things aren’t as serious as you might think. I am more forgiving, both with myself and others, and more action-oriented. Long-term planning is difficult due to the unknowns, but planning for the future helps keep me present and moving forward.
Before my diagnosis, I struggled with anxiety, but not enough to seek help. When they changed my chemo regimen, the oral chemo side effects were less physically overwhelming, but that’s when the emotional weight set in. I began feeling depressed and anxious daily. With compromised health, going out in public caused anxiety; so did caring for my colostomy bag, thinking about returning to work, and worrying about getting better or what would happen if I didn’t.
Eventually, I sought help through regular therapy, which helped, but was still challenging. I searched for support groups for colon cancer and young adults, but could not find any locally. Connecting with others on social media helped, yet sometimes reminded me that not everyone has the same outcome. Finding a community that understands you, especially in such a challenging stage of life, is difficult.
My advice for others
I have a large red birthmark on my left arm, so I grew up used to stares. Adding the colostomy bag didn’t feel like a huge change from what I was already used to, but the struggle is internal. Looking in the mirror and seeing a bag takes adjustment, especially when you begin handling changes yourself.
Eventually, you become comfortable with yourself and your body, making it easier to go out in public and speak up for yourself. If you care for yourself, it doesn’t matter if others don’t understand—it’s not the end-all, be-all. My colostomy bag saved my life, so I am grateful for it. Even my young nephews understood the process, so adults can learn too.
Connecting with content creators and influencers with colostomy bags on TikTok and Instagram helped me immensely; seeing others being open about their journeys helped me accept mine.
Advocate for yourself, especially in medical settings. This journey isn’t easy, regardless of stage or prognosis. What also helped was having a friend who had been diagnosed a month before me; we constantly checked in. It’s important to unapologetically vent and be outspoken about what you’re feeling. Your feelings are valid. Sometimes you just have to ride out the motions before it gets better.
Cancer and diverse communities
Coming from a first-generation Latino household, I was the first in my family to be diagnosed with cancer at this age. One early struggle was being the main translator for my parents, since they were my main caregivers in the hospital. Navigating all the procedures, listening to doctors, and translating everything was a challenge.
For those who grow up translating for parents, it becomes routine, but repeating everything that’s happening to you is difficult. This was a real barrier during hospitalization. Having my mom as the main caretaker required me to help her as well.
Support within cancer communities is needed, not just by cancer type or age group, but also by ethnicity. More tailored groups could help address treatment barriers, translation services, fertility questions post-cancer, and life with colostomies. I’m still figuring out my place in support groups, especially now as a survivor and not in active treatment; there is still a lot of emotional turmoil.
Inspired by Briana's story?
Share your story, too!
More Colorectal Cancer Stories
No post found