A Double Lung Transplant with Stage 4 Non-Small Cell Lung Cancer: Natalie’s Search for Hope
For more than five and a half years, Natalie has been living with stage 4 lung cancer as the backdrop of her everyday life, describing the experience as “part one, part two, and part three” of pure survival mode. She was diagnosed with no smoking history and no identifiable biomarkers, and yet her cancer progressed through multiple clinical trials and chemotherapy regimens. Eventually, one of her clinicians raised an option many people, including some clinicians, do not realize exists for certain stage 4 lung cancer patients: a double lung transplant.
Interviewed by: Taylor Scheib
Edited by: Chris Sanchez
By then, Natalie’s left lung function had dropped to around 3 percent, leaving her body functioning as if she had only one lung. She was told that chemotherapy options were essentially exhausted. Faced with ongoing non-small cell lung cancer progression and worsening day-to-day life, she chose to pursue lung transplant evaluation, relocate to a different state, and live within strict limits while waiting for “the call” that donor lungs were available. When that call finally came, she found herself rushing into surgery without her husband at her side, asking for medication to calm the fear as she was wheeled into an operating room full of people.

Recovery from the double lung transplant was far rougher than the discharge estimates suggested. Surgeons told her they had to “yank” her severely diseased lungs out through a clamshell incision, leaving her with intense pain and a chest that often felt like it had “bricks” sitting on it. She spent over a year in Chicago, navigating tube feeding, rehab, and the ongoing risk of rejection while trying to reclaim basic movement. Gradually, things improved enough that she could walk more, travel a bit, and eventually return home to Atlanta.
Just as she began to feel the payoff of the surgery, persistent back pain led to scans that revealed metastases to her spine only a few months after transplant. It was devastating to learn that after such a radical operation to treat her lung cancer, there were still four or five lesions in her spine that now required chemotherapy and radiation. Yet Natalie talks openly about allowing herself to cry, feel anger, and then ask, “What options do we have?” Her team is now exploring potential curative approaches to the spine, and she describes life today, with advocacy work, speaking, travel plans, and new lungs that allow her to stay active, as “actually pretty darn good.”
Through it all, Natalie has leaned on memories of her grandmother, her husband’s support, and a determination to help others understand that stage 4 does not always mean “no options.” She continues to share her experience to show that surgery may be possible for some people with stage 4 lung cancer, that biomarkers do not always appear, and that it is still worth seeking second opinions, staying close with your care team, and holding onto the possibility that miracles can still happen.
Watch Natalie’s video and read through her edited transcript below to learn more about her story. Read her previous interview about having been diagnosed with stage 4 lung cancer.
- Surgery, including a double lung transplant, may be an option for some people with stage 4 lung cancer when systemic treatments stop working, and it can open the door to more time and a better day-to-day life
- Even with no biomarkers and failed clinical trials and chemotherapies, it can be worth asking about additional options, relocation to centers with specialized programs, and ongoing retesting
- Recovery from a double lung transplant is often far more intense and longer than the estimates; pain, heaviness in the chest, and lifestyle adjustments can last many months or even years
- It is normal to feel anger, fear, and the urge to give up, but allowing those feelings, staying connected to your care team, and seeking other opinions can create new paths forward
- Natalie’s experience illustrates a powerful transformation from barely functioning with 3 percent lung capacity and no clear future to describing life with new lungs, advocacy work, and travel as “actually pretty darn good”
- Name: Natalie B.
- Age at Diagnosis:
- 33
- Diagnosis:
- Non-Small Cell Lung Cancer (NSCLC)
- Staging:
- Stage 4 (Metastatic)
- Symptoms:
- Extreme fatigue
- Severe cough
- Treatments:
- Chemotherapy
- Immunotherapy
- Clinical trials
- Radiation therapy
- Surgery: double lung transplant






This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
- Surviving five and a half years with stage 4 lung cancer
- Living life despite stage 4 lung cancer
- What keeps me going through cancer
- Why I keep sharing my lung cancer story
- The one thing I want people to know about lung cancer
- Cancer progression before my double lung transplant
- Hearing that a double lung transplant was my option
- Facing lung cancer with no biomarkers
- How I cope with not having biomarkers
- Deciding to relocate for a double lung transplant
- Waiting for “the call” for donor lungs
- Getting the call for donor lungs
- Being chosen for the lungs and heading into surgery
- My hope going into the double lung transplant
- Waking up with new lungs
- What recovery from a double lung transplant was really like
- How I feel about having someone else’s lungs
- When my back pain started after the transplant
- I lost my grandmother and father-in-law while in treatment
- Readjusting to life in Atlanta after Chicago
- Staying busy after transplant and treatment
- Continuing to do what I love, even with cancer
- How I look at the future now
- My message of hope to others with stage 4 lung cancer
- Why sharing my story matters
Surviving five and a half years with stage 4 lung cancer
I would say in the last five and a half years, it was a roller coaster. I would say part one, part two, and part three, but the last five and a half years have been about survival mode for me.
I’ve been trying to survive and get to a point where I’m never going to be comfortable, but getting to a point where I feel a little bit more confident in my living situation is the best I can describe it.
Living life despite stage 4 lung cancer
So I did actually have to take a step back. I recently started traveling, probably about three weeks ago. This hasn’t been anything that I’ve been doing regularly because I had to change my lifestyle for probably about, I would say, 12 to 15 months. I had to relocate to another state to get part two of this story done. So that actually put me down; it kind of held me back from doing what it is that I needed to do.
So in the past 12 to 15 months, I’ve been having to focus on rebuilding myself, not only from a physical standpoint, but I would say a mental standpoint as well.
What keeps me going through cancer
So I’m not one of those people who get to the end of their life, and they’re like 80 or however old they are, and they say, “Well, I’ve done everything. I’m okay with passing away,” and so forth. Well, I’m not quite 40 yet, and there are still a lot of things that I want to do. Other than travel, I want to hang around. I want to be around my family. I want to be around my friends.
Now, unfortunately, I do have this disease. But I want to try to make an impact on people’s lives. And not necessarily, most people say, “Oh, well, you can just start a foundation.” Well, I’ve already done that, and I did not want to continue doing it, so I’m not. But I want to continue to share my story, to try to give people hope. And I’m slowly realizing that I am actually helping people by sharing my story. So I want to continue to be able to do that. So as long as I can hang around here and share my story and travel and be with my family and friends, I think that’ll make life worth living.
Why I keep sharing my lung cancer story
I choose to do so for several reasons. Well, number one, especially with my new situation that has occurred, I want people to know that surgery can be an option for a stage 4 cancer patient. Well, let me not say cancer. Let me say lung cancer, because I don’t know about all cancers in general. But for a stage 4 lung cancer patient, if you qualify, surgery can be an option. And with this surgery, it’s an opportunity to help extend, save, or improve your life.
So I think that’s extremely important because so many people don’t even know that this option exists. A lot of medical professionals don’t even know about this, so that’s one reason. The second reason is that I want to show people what a stage 4 cancer patient and advocate can look like. Everyone does not look like me. Everyone doesn’t function like me. Everyone is different depending on treatment stages and all of that. But I want people to know that stage 4 is not always a death sentence. Are you going to have struggles and issues? Of course. Who isn’t? It’s stage 4 cancer.
But I want people to know, I’m sure you’ve heard this phrase a thousand times, but I’m going to repeat it a thousand more, that as long as you have lungs, you still can get lung cancer. You do not have to be a smoker. People also need to know, and which I don’t talk a lot about, which I’m actually focusing on more, is to talk about more things like radon. Radon causes lung cancer. I don’t hear a lot of people talk about that as much as it should be talked about, a lot of environmental factors. So I want to learn more about that and share my story more on that. And also, those are things that I’m working on for educational purposes as well.
The one thing I want people to know about lung cancer
It’s that no matter how healthy you think you are, and no matter how good you think you eat, and no matter how into fitness you are, you work out, you can work out three times a day or do something, something extreme, you can still get lung cancer. It does not matter. It doesn’t matter about anything, because a lot of people always say, “Well, you know, I eat well, and I don’t eat pork, and I don’t eat this and that.” Well, that’s great that you don’t eat a lot of these things. But I know people who literally have the cleanest diet in the world, or the best exercise routines, and they still end up catching something.
So it’s not all about what you do. Sometimes it just happens, unfortunately.
Cancer progression before my double lung transplant
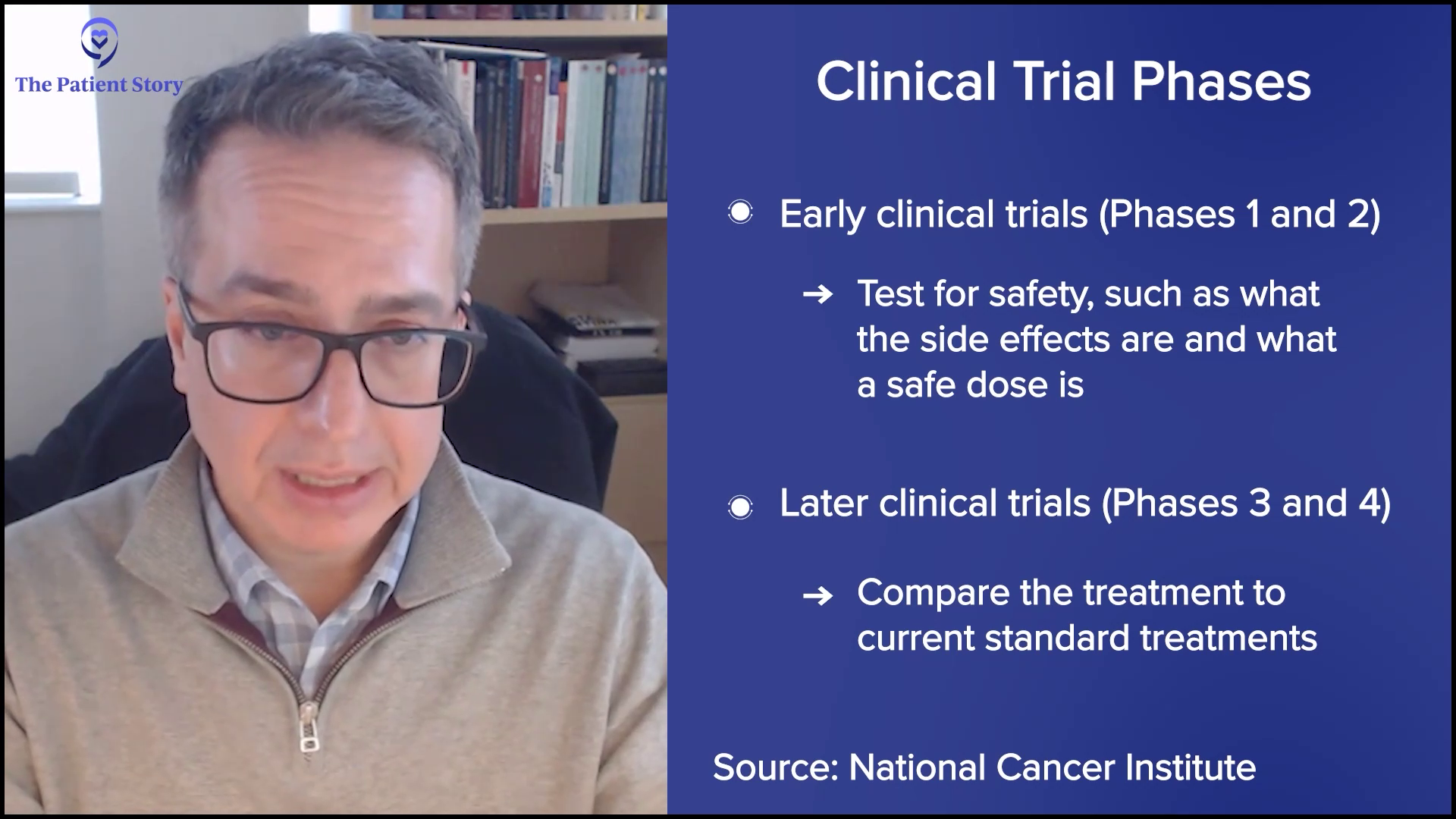
So before this was brought up for me, my cancer had started to progress, meaning, of course, it started to spread and/or get worse, however you want to word it. I had gone through two clinical trials already. They unfortunately failed. I tried two different chemotherapies after I started to progress, and they failed also.
So the idea behind this was, “Hey, well, let’s keep trying different chemos or different clinical trials and see if the progression stops.” Well, we don’t know if the progression is going to stop even if I continue to do these things. So that’s when one of my healthcare providers actually knew about this double lung transplant program, and she brought it up to me, because like I said, I was just going to continue to keep trying these things, but there was no guarantee that they were going to work.
And I was told, “Your disease is spreading slowly, but it is still spreading.” So on one hand, the fact that it was slow was great, but the fact that it was still spreading was not great. And then my health started to decline. So I think my left lung had dropped down to like 3% functionality. So basically, I had two lungs, but my body was only acting as if I had one. So my day-to-day started to get harder. I was not on oxygen or anything like that, but when it started to get difficult for me to do things, I said, “Okay, I think we do need to go ahead and fully entertain this.”
Hearing that a double lung transplant was my option
So my initial reaction was fear. I didn’t know what a double lung transplant was. I mean, obviously, I heard the words ‘double’ and ‘transplant’. If you put two and two together, you figure it out. But it just sounds really scary, like a double lung transplant. Excuse me, on this little itty bitty body. And I was just like, “Am I even going to be able to make this work?”
You know, I was on ChatGPT, and I was reading all this stuff, like the survival rates of transplant patients. And it was just saying all these things, and I’m just like, “Oh my goodness.” However, I thought about it. When I consulted with the surgeon at the hospital, he said, “Your lungs are trashed, and basically you can continue to try these trials and try these chemos.”
Let me back up for a second. We had pretty much run out of chemo options, so there were no more chemos that were really going to do anything. So we were only looking at clinical trials at the next point.
So he basically was saying, “You can keep trying these trials, but I mean, you either try the trial and go through it, or you just have the transplant if you qualify.” So I said, “Okay, well, let’s just go do the transplant.” So I was very afraid. But once I actually knew how, once I heard him say, “Your lungs are trash,” which I already knew that, I said, okay, let’s move forward with this testing.
Facing lung cancer with no biomarkers
I actually talk about that a lot to my husband and among the people I know. My mom specifically, I always tell her, ”It really sucks that I don’t have any type of biomarker.” And then every time somebody asks me this, they’ll say, “There’s no way that you don’t have one.” They’ll say, “Oh, maybe they missed it.” They didn’t miss anything.
And then, as of today, I still get tested every 90 to 120 days, and there’s still nothing there. So I feel some type of way about it, because I feel like if I did, that would give me, or open me up to, better options as far as treatment. I feel like maybe I wouldn’t have had to have the double lung transplant if I did have some targeted treatment. There are so many things that I think about, and sometimes I think, “Oh, wow, so-and-so is lucky.” And I mean, none of us are lucky because we have this.
But I think about it, just being transparent. It’s like, oh, well, this particular person does have a few more options than I do, just because they have a biomarker. And then they’ll get on the medication, and then maybe in a year or so they’ll say, “I’m no evidence of disease.” And of course, everybody still has their struggles, but sometimes it does make me feel sad because I don’t have that targeted option available. Not one bit. So that definitely still bothers me to this day.
How I cope with not having biomarkers
I just try to move forward. I sit in it for a second. I think about it. I get angry, or I cry, or whatever. When I’m angry, I just have to keep moving and think, “Since that option is not available, let’s talk about what option is available instead of just dwelling on what we have no control over.”
And then I always think, like, maybe one magical day a biomarker will pop up. I mean, anything is possible.
Deciding to relocate for a double lung transplant
I had to relocate for this procedure. That was the first thing that they told me. And I told my husband, “You know, I have to move.” Like, what? I was like, “It’s going to be so cold up there.” And I remember him saying, “You’re worried about the cold? Out of all the things to worry about? Like, girl, come on.” I said, “Yeah, you’re right.”
But yeah, I was thinking about cost, number one, because all the financials are on you. You don’t really get any help or anything for relocating. So that was something that I thought about. I thought about having people up there with me. How often would someone be able to be there? Would I be okay mentally? How long was it going to take me to recover?
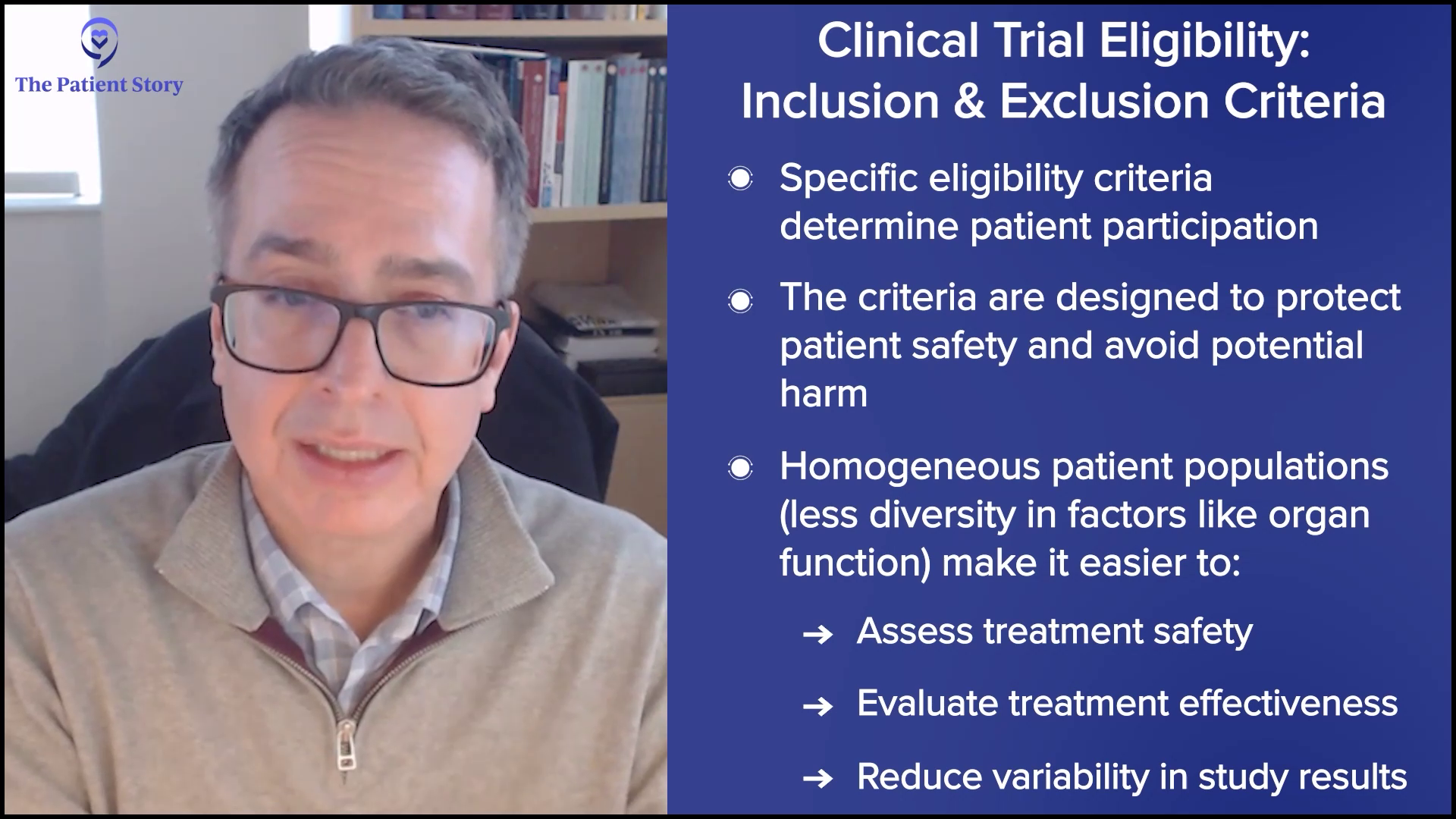
It was just so many things. Am I even going to meet the testing qualifications? Because you still have to go through about maybe two to three weeks of testing, maybe a little longer. So I’m thinking, “I still have to get past that.” And once you do that, it’s like the board has to meet to still decide whether or not you’re qualified, even though the results may say one thing.
So there were just so many things that I had to worry about, that I had to think about. I know this is not as important, but I’m thinking about my dog too. I’m going to have to leave my dog because I couldn’t take him, because I couldn’t care for him or anything while I was up there. So it was just so many things because this was like a life-changing surgery. It was risky. I thought about so many things.
Waiting for “the call” for donor lungs
You have to actually be in the state first. So once you actually get there, then that’s when they say, “We have officially put you on the list.” I think I was told that a call could take as quickly as 24 hours, which is unlikely, but it has happened. Or you could be waiting as long as 60 days.
And I’m thinking, “Oh, gosh, I don’t want to be a 60-dayer,” but you just never know how this thing is going to work. So, when I went up there, I had to prepare myself to get a phone call at any time. They said it could be the middle of the night, whatever it is. You gotta stop, drop, and go.
You have to be within X number of miles of the hospital. So this phone call was pretty much controlling everything that you do. So if I wanted to, let’s say, take a day trip somewhere, I couldn’t do that because I would be too far away. There were so many things. Once you actually get put on the list, it’s just basically the beginning of that story.
Getting the call for donor lungs
Yes, I was a little nervous. Well, for one thing, when you go through these procedures, they have what they call a dry run. So there’s a possibility that you could get a call, get to the hospital, and still not be a good match, and you’ll have to go home. So in the back of my mind, I’m thinking about the worst-case scenario anyway. “Hey, they’re going to call me, and then I’m going to get sent home.
Well, my situation was a little different. They called me on a Thursday night at around 8:00 pm, and they said, “We might have a pair of lungs for you, but we don’t know yet. So what you’ll have to do is come into the hospital on Friday morning. We’ll have to do testing for you and see if basically your lungs are going to be a fit. It’s going to be between you and somebody else.”
So, basically, it was me and somebody else at the hospital at the same time, just waiting on whoever was going to get the green light.
The only thing I knew was that the lungs were for a tiny person. So if they didn’t fit me, they were going to the other person, and then the other way around. But no, I didn’t know anything about them.
Being chosen for the lungs and heading into surgery
So they ended up telling me once I was at the hospital for like five hours before I even found out that I was the official person for the lungs. So they called me, and they came into my room and said, “Hey, just to let you know, the lungs go to you.” And I was like, “Yay!” I’m all excited.
And I said, “The next question is, how soon before surgery?” Because my best friend was there with me, but my husband was not there. He literally was getting on a plane, I think, as soon as I called him. So he was hanging out at the airport. And so they said, “We have, I think, three or four, maybe five hours.” And I was like, “Perfect, my husband will be here.” By the time I woke up, my family was there.
But that quickly changed. They came in, and they said, “Hey, we’re ready to go.” And I said, “Wait, my husband is not here yet.” And they said, “Well, you know, we can’t wait. We gotta go.” And I said, “You just told me I had a few hours.”
So my husband, at this point, I think, is about to take off, and I’m about to get wheeled out to start this prep, and he’s not going to make it before I get put to sleep. So I told my best friend, “Bye.” She was crying, and I’m just like, “Oh my gosh, this is really happening.” And I said, “Can you guys please give me some medicine? I’m so afraid.”
So they instantly gave me something to calm me down because I was about to jump out of bed at that point. And they wheeled me in. I talked to the anesthesiologist. They gave me some calming medicine. They rolled me into the room with like 50 other people, and I was just like, “Oh my goodness.” And the next thing I know, I wake up. It’s another day.
I was told it took between six and eight hours, a little longer than it was supposed to take, just because they had difficulty getting my lungs out.
My hope going into the double lung transplant
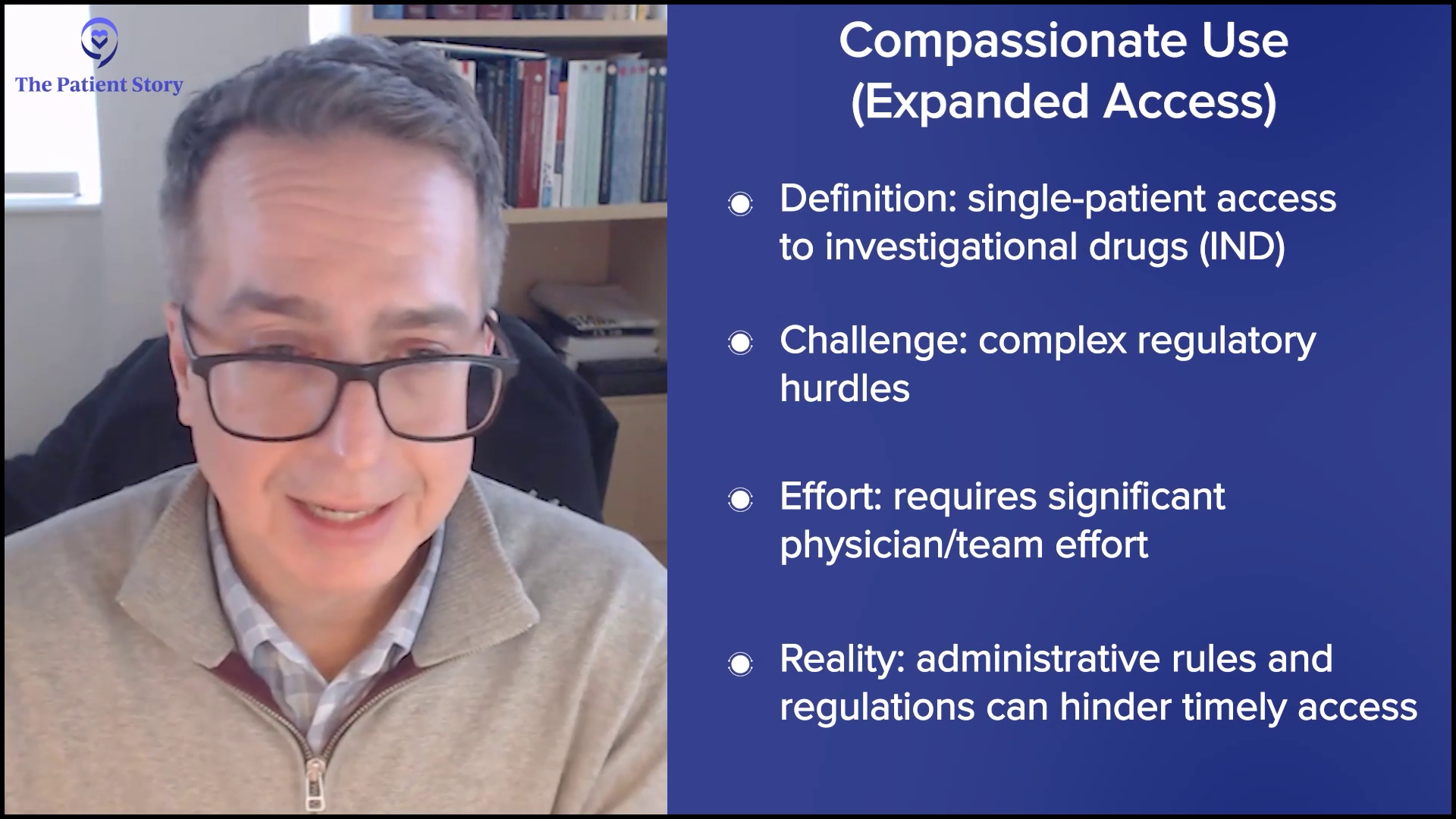
So my hope is based on what I was told. So first of all, the surgery is considered a clinical trial. So they let you know up front that there is a possibility that this may work, and that it may not work. Obviously, we’re doing this for the greater chance of it working.
But, you know, in my mind, I was thinking, “Hey, I’m going to get these diseased lungs that have lung cancer removed, and I’m going to get them replaced with some brand new lungs. When I wake up, I will no longer have lung cancer.”
Waking up with new lungs
When I woke up, well, first off, I woke up with a bunch of tubes in me, and another double lung transplant recipient had already told me kind of what to expect. So when I woke up, I was kind of freaking out. I couldn’t talk, but I was telling them to take the tubes and stuff off of me.
And so I remember requesting a sheet of paper and something to write with. And I remember saying, like, “Take this off of me,” or something I said. And I know my mom and my dad and everybody was freaking out and saying, “Please take these tubes off her, because she’s going to end up going crazy from them being in.”
And they were explaining to them that they had to keep them in because I wasn’t breathing on my own or something. And then I wrote on the paper again, “I can breathe on my own.” So finally, after going back and forth on the paper, they ended up taking them off, and they saw that I could breathe on my own.
But those tubes were very frightening for me. I had never had tubes before, so I was afraid.
What recovery from a double lung transplant was really like
So they want you to get out of the hospital quickly. They don’t want you to stay there long-term. They actually want you up and out of bed on day three, basically. So I was in the hospital for a total of two weeks: one week in the ICU and then one week on the stepdown floor.
I would have gone faster than two weeks if my pain weren’t so bad. They couldn’t get my pain under control, which is the only reason why I was there for two weeks. Because I know people who have only been in there one week, and they got released. So a combination of two weeks. I lost a lot of weight in the hospital, of course, because I was tube-fed for about a week and a half, which was awful.
I did really well in the hospital, though, towards the end of my two weeks, because I got out of bed more. I walked. They did have therapy coming to my room, but you can also request that your nurses, of course, walk you around the hospital. So I requested that. And then they determined that I still needed therapy. But instead of me actually staying in rehab, I could just go to rehab like two or three days a week. So that was the good part about it.
The worst, one of the worst parts about it, was the pain. I was told that they had to like, rip — I don’t want to use the word rip — or yank the lungs out. And they had to call in a second surgeon or backup surgeon to help because my lungs were so diseased that they couldn’t just pull them out like they normally would. So I was told that I would have more pain than the average person, just because of the way that they had to pull them out.
So I initially was told that my recovery would probably be about six months, when people started to feel better. But I disagree with that. I would say a partial recovery would take about eight months. As for full recovery, I’m not fully recovered still today, so I don’t know what a full recovery timeline is. I know I’ve talked to a few people who have had this done a while ago, and they said it took them a full two years to feel normal, whatever that is.
But I had to stay in Chicago. You have to do a one-year commitment to stay a part of the program. I was there maybe a little longer than a year, just because I had to go back and forth for testing, for about 12 to 15 months.
But as far as the recovery went, it was extremely rough. With this double lung transplant, they open you up clamshell-style, and a lot of times, your chest feels heavy. So sometimes, you know, I wasn’t able to wear anything under my shirt, no bra or anything like that, just so I could try to feel free. But there’s a heaviness that can come with the transplant. So sometimes, if you’re not even doing anything, it’s like you’re sitting there and you’ve just got bricks on your chest.
So it’s different. I had issues riding in cars. For instance, when I would take Ubers to the doctor’s office, the car had to be big because I had to be able to stretch or lie down across the back seat to get to the doctor’s office. Any bump in the road would make it hurt. There are so many things about the surgery.
A lot of people always say, “You look great.” Well, thank you, but it’s been a lot. My goal is to work out three days a week. But sometimes I can’t work out three days a week.
So I am back in Atlanta now. I got home about a month ago. Thank goodness I’m back home. So I started walking and working out when I first got back home. And then after that, I had some issues with my chest being like it had those bricks on it again, and I had to stop. I just started again yesterday.
So with this lifestyle, you kind of have to make adjustments according to how you feel. And nothing is wrong when your chest is heavy. It’s not what everybody faces; for me, it’s just what comes with the territory.
How I feel about having someone else’s lungs
I would say I don’t think it has bothered me as I heard it might. I heard a lot of people go through this mental situation where it bothers them that they don’t have their original lungs and, you know, they have a deceased donor and all that. God bless the donors.
I haven’t really had that issue that much. I’m extremely grateful for being able to get the lungs. Definitely sorry about how I had to go about getting them. But it doesn’t bother me, I don’t think that much because I think I try to focus on just making sure that the lungs are healthy. After all, these lungs can still go into rejection.
That’s a whole other part of it. You have to take these rejection meds your entire life. So instead of me thinking about the situation, I try to think about the situation this way: “Let’s try to make sure we keep these lungs healthy. Let’s try to work out. Let’s try not to be around certain things that will possibly cause rejection or make things worse.” So I try to focus on the quality of life of the lungs.
When my back pain started after the transplant
Probably about a month after I had surgery, my back started to hurt, and I kept telling them about it. And they would say, “It’s because you’re doing therapy and you’re stretching your muscles and you haven’t really moved.” And I would think, “Okay, that makes sense.” And then they were saying that it was because of the actual surgery.
And I listened to what they were saying for just a small amount of time, and I was just like, “No, something just does not seem right.” So I was already due for scans anyway, just because, still dealing with my history, I’m going to have to get scans for life anyway.
I already had a scan scheduled. So we were probably maybe two months after surgery at that point. And then I went ahead and had a scan, and they called me so quickly. And I already knew something was wrong because they called too quickly.
They asked me how soon I could come in. And I said, “The cancer is back, isn’t it?” They responded, “We really want you to talk to the doctor.” And then my phone went off. It was a MyChart notification.
So I was about to hyperventilate because at this point, I’m by myself right now. And I open it, just scanning it. I didn’t even want to read it in detail, but I saw enough words to say, okay. So I called my husband. I’m screaming. I’m like, “The lung cancer’s back.” I don’t really even know anything, but I’m just like, the cancer is back. And, you know, why did I have this surgery? I’m just, you know, he’s trying to calm me down. Obviously, he’s not there.
So I called a friend of mine who actually lived in the same building as me, and I was like, “Hey, I think my lung cancer is back. Can you go to the doctor with me?” And she’s like, “Wait, wait, wait, what?” So I was like, “I don’t know much. I just need you to go to the doctor with me.”
So we went to the doctor. A bunch of things lit up and this, this, this. “But what we’re mostly concerned about is your spine, your back area. So we need to do a biopsy of the spine.”
And fast-forwarding, we did, and it did come back and say that I have cancer in my spine. I have, I think, four or five lesions, which is why my back was hurting to the extent that it was hurting. So I was angry because at this point I’m like, you know, why did I even get this surgery done for the cancer to come back?
And I’m asking them, “Hey, please tell me why it came back. Just give me something.” And nobody really could give me an answer. We were kind of thinking that maybe this might have already been there, and it was hiding, and then something just made it come up to the surface, because I had been complaining about back pain for years, and we had been checking for years, and nothing ever came up.
So nobody to this day really knows where and how. But in the back of our minds, I’ve just had this major surgery to get rid of lung cancer, and now here we are again dealing with it. So I had to start chemo and radiation. So, imagine me only being two and a half, three months out from surgery, not only having to do chemo, but having to do. I mean, you know, I just had surgery. That was hard.
I lost my grandmother and father-in-law while in treatment
So I think I was thinking about two things at this moment. So I had another rough patch during all of this. Unfortunately, at the beginning of the year, my grandmother and my father-in-law actually passed away on the same day. So while I’m dealing with all this, I lost them, too.
And my grandmother, if anybody knows me, she does. Hands down, my best friend, best person. So that actually set me back mentally. But a lot of the time that I was going through things, I was always thinking about my grandmother. I basically feel like I got the ability to be strong from her.
So anytime any situation comes up, I’m always hearing her in my brain, “Hey, I know you’ve just overcome, you just have another obstacle, but, hey, let’s do this.” Literally, I feel like my grandmother was just always talking to me.
And so I always talk about my husband as well being a good influence, too. So I would think about him, and then I would think about my grandma, and I’m like, “Okay. All right, Grandma, I got this. I can do this.”
That’s the only way I think that I would have made it through. But I mean, obviously, if she had been here, that would have helped me too. But just thinking about her a lot helped me get through this. Definitely. Hands down.
Readjusting to life in Atlanta after Chicago
It’s been a slight adjustment. Number one, because I actually love Chicago. I wanted to leave, but I didn’t. I mean, that’s like my second home at this point. I love that place. But it has been an adjustment, especially coming back home. I have a lot of stairs in my home. So having all these steps has been a lot versus in Chicago, it’s mostly flat. So that’s been crazy.
But I’ve actually been really busy since I’ve gotten back between advocacy and speaking engagements. I’ve been to doctors’ appointments. At one point, I think I had one day where I literally had nothing to do, and that was last week. But every day since I’ve come home, there’s been something to do. And of course, you know, I want to see my friends and everybody else. So we’ve started to get together.
So I’ve been busy, and I haven’t had a lot of problems since I’ve been here. Things have been really good since I’ve been home.
Staying busy after transplant and treatment
I guess you can say I’ve really been busy, even prior to just coming back home. I will say that when I was in Chicago, it had gotten kind of hard for me because I was so involved in everything. I was so tired. It was at a point where I had to say, “I just can’t do it.”
Because Chicago was actually worse than Atlanta. When I was in Chicago, I mean, I was speaking. I was just completely busy in Chicago. And then when I found out when I was going home, I had like a little Chicago bucket list of things that I wanted to do, as if I wasn’t going back, but I wanted to check the box to try to do this, try to do that.
So when people were coming into town, I think the last three or four months of my being there, I had so many visitors. It was amazing. But every time someone came, we were never at my apartment. We were just out.
So it was very hard to try to entertain people, have fun, and go to doctors’ appointments, but still trying to worry about yourself. But once again, in the back of my mind, I’m thinking, “Hey, I’m still here. I’m in much better shape than I was before.”
Before the transplant, I had to take a nap to function. I do not take a lot of naps. As a matter of fact, I have issues going to sleep. That’s a whole other story. But I just have so much more energy now. It’s the strangest thing.
I mean, of course, if I work out, I’m going to be tired. But I know this is going to sound crazy when I say this, but life is actually pretty darn good. I would say that for me, from where I came from to now, there are so many things that have changed. I’m so much happier. Life is just really good.
I’m getting ready to go on vacation again. What did my husband tell me this morning? It’s in like 40 days. You’re ready to get ready. We’re going on vacation again, so of course that makes me excited. But things are just, things are just really good right now.
Continuing to do what I love, even with cancer
It makes me feel really good because I know a lot of people in my situation who are not able to do the things that I’m doing. I’m not even talking about traveling, just in general, because they’re sick and they can’t travel. I mean, not saying I’m not sick, but they just can’t do the things that I can do. Or mentally, they’re just not there. I mean, physically, you can be okay, but mentally, sometimes, if you’re not there, that can really throw things off.
But I’m just so glad that I can do these things and share my story. I’ve gotten more into advocacy. I wasn’t into advocacy as much. I’ve always done it since I got diagnosed, but something has driven me to go more into it. I think maybe last summer is when I started feeling a little better, and I started saying, “Since I feel better, let me go after it.” Because of course, you know, if you’re feeling good, then that’s when you want to try to do what it is that you can do.
So yeah, I don’t know how I’m actually doing it, but I am doing it, and I just feel good. Do I have issues? Yeah. I mean, to be honest, my back hurts right now. But I mean, I went to get a haircut today. I went and ran another errand. So, you know, I can’t just stop because of a little pain or a little something.
Obviously, if it’s drastic, I’m going to relax and not do as much. But overall, I know it sounds crazy, but as I said, I’m just a lot happier than I was before. But I mean, I do have new lungs, so I’d better be happy.
How I look at the future now
So before I had the double lung transplant, I didn’t think much of the future, just being completely transparent. I wasn’t even sure I was going to make it to five years. So the fact that I’m at five and a half just really means a lot to me.
But now I do look at the future differently. I don’t want to say hesitant, but I’m still kind of on the lookout. I still have anxiety, all of these things. But I’m not as scared or as fearful as I was before, because I feel like this surgery has opened up more healthy opportunities for me.
And I do feel like I’ve been talking to my team about my back, and we’re looking at some curative options for it. But that’s all I’ll say, because I don’t really know much about it. I actually have a meeting with them next week.
So things look like they are continuing to get better, or they do have options for me. Like, for instance, we’ve already talked about this particular chemo. Like, if this chemo doesn’t work, what’s next? So we already have another chemo lined up to try if something goes wrong. So the fact that my team is working with me to go to next steps if we need to makes me feel a whole lot more confident about the future.
As I said, I’m still a little shaky about things just because it’s cancer, and you know how that works. But I feel better. And then, with the lung transplant, I don’t want to use the word worry, but rejection is a possibility.
So not only are you thinking about lung cancer, but you’re thinking about rejection as well. So it’s basically like you’ve got two jobs with two different major medical conditions that you’re having to follow. So I do think about rejection a little bit more than I think about cancer, to be honest with you.
Just because, number one, I don’t want to have another double lung transplant. I don’t, even if I technically qualify, because that surgery was the worst one that I’ve done in my life. But you cannot control rejection. You can treat acute rejection, but you just never know when things are going to go wrong. So that does kind of bother me a little bit more than the cancer situation. So those are things that I still think about.
My message of hope to others with stage 4 lung cancer
I would say miracles do happen. It’s funny because I actually said that when I first had the surgery, and then, three months later, my lung cancer was in my spine. But still, piggybacking off of that, miracles still do happen because my doctors or my team have said, “We can look at curative options for you.” That has never been said before. So that’s something brand-new that gives me hope.
So I would just tell people that, try not to give up, because I know giving up is hard. At one point, I wanted to give up, so I’m not going to even act like I just have had it together all along because I haven’t. I wanted to give up.
But I would encourage people to be as close as possible with your medical team. I think that helps a lot. The better the relationship, the closer you are to them. I mean, I don’t mean you gotta bring them brownies every day or anything, but just try to establish a relationship with them so that you could have better options, better connections.
That’s what I do. I love my whole team in Chicago, in Atlanta. I’ve never had any major issues. Of course, you’re going to have some issues because it’s just healthcare, and then it’s the patient.
But I would just encourage people, don’t give up. Try not to give up and try to establish a good relationship with your healthcare team. It’s just extremely important. If you feel something’s not right, go get another opinion. I don’t know how many opinions I’ve had, but I’ve had enough of them. You know, I’ve had a lot. Let me just say that. I wouldn’t just go off one opinion.
So, I mean, there are so many things I could tell people all day, but just try not to give up because things do change. For instance, with the biomarker thing, I haven’t given up on biomarkers. I mean, I still get tested regularly, even though I don’t think anything is going to ever come up. But I still look for hope. Maybe one day.
Why sharing my story matters
As I said, I just try to encourage people not to give up. And then also, I would try to encourage people to share their story if they feel comfortable.
We all have lung cancer in the community, but our stories and our journeys are not the same. So, whereas I’ve had a double lung transplant, you might have somebody who’s been on targeted therapy for X amount of years or clinical trials. So sharing different versions of stories is very helpful and educational.
So if you feel comfortable and you want to, please share your story. You never know who it’ll help, is what I would finally say.
Inspired by Natalie's story?
Share your story, too!
Related Cancer Stories
More Lung Cancer Stories
Natalie B., Non-Small Cell Lung Cancer, Stage 4 (Metastatic)
Symptoms: Extreme fatigue, severe cough
Treatments: Chemotherapy, immunotherapy, clinical trials, radiation therapy, surgery (double lung transplant)
...

Stephanie K., Non-Small Cell Lung Cancer, ALK+, Stage 4 (Metastatic)
Symptoms: Persistent and intense cough, general feeling of sluggishness
Treatments: Chemotherapy, targeted therapy through a clinical trial, radiation therapy
...

Jennifer M., Lung Cancer, EGFR+, Stage 4 (Metastatic)
Symptoms: None per se; discovered during physical checkup for what seemed to be a sinus infection
Treatments: Radiation therapy (stereotactic body radiation therapy or SBRT), targeted therapy
...

Laura R., Non-Small Cell Lung Cancer, ALK+, Stage 4 (Metastatic)
Symptoms: Persistent cough, fatigue, bone pain
Treatments: Targeted therapies (tyrosine kinase inhibitors or TKIs, including through a clinical trial)
...

Ashley C., Non-Small Cell Lung Cancer, HER2+, Stage 4 (Metastatic)
Symptoms: Fatigue, breathlessness, persistent back pain, multiple rounds of bronchitis
Treatments: Chemotherapy, targeted therapy
...

Loryn F., Non-Small Cell Lung Cancer, HER2+, Stage 4 (Metastatic)
Symptoms: Extreme fatigue, persistent back pain, chest pain, joint pain in the feet, hips, legs, shoulders, and elbows
Treatments: Chemotherapy, radiation therapy (foot and elbow to help with mobility), antibody-drug conjugate
...
More Non-Small Cell Lung Cancer Stories
Natalie B., Non-Small Cell Lung Cancer, Stage 4 (Metastatic)
Symptoms: Extreme fatigue, severe cough
Treatments: Chemotherapy, immunotherapy, clinical trials, radiation therapy, surgery (double lung transplant)

Maggie M., Non-Small Cell Lung Cancer, EGFR+, MET Amplification & Overexpression, Stage 4 (Metastatic)
Symptoms: Ocular migraines (kaleidoscope vision), partial blood clot (DVT) in the leg, vision and balance problems, minor chest pain
Treatments: Targeted therapy (tyrosine kinase inhibitors or TKIs), radiation therapy (stereotactic body radiotherapy or SBRT), clinical trials, chemotherapy (combined platinum-based regimen)

Clara C., Non-Small Cell Lung Cancer, ALK+, Stage 4 (Metastatic)
Symptoms: Pelvic pain and discomfort, bladder issues related to pelvic tumors, incontinence, pain in the lower back and hip
Treatments: Chemotherapy, immunotherapy, radiation therapy, targeted therapy (lorlatinib)

Shira B., Lung Cancer, EGFR+, Stage 1B
Symptoms: None per se; discovered during a preventative full-body MRI
Treatment: Surgery (thoracotomy)

Phil P., Non-Small Cell Lung Cancer, ROS1+, Stage 4 (Metastatic)
Symptoms: Persistent cough, nasal drip, shortness of breath, inability to speak in full sentences
Treatments: Chemotherapy, targeted therapy, radiation therapy, next-generation ROS1 inhibitor (clinical trial)