Latest Data on Newly Approved CLL Drug Pirtobrutinib Presented at ASH 2023
Top CLL doctors share their thoughts on pirtobrutinib
Edited by:
Jenna Jones
Accelerated approval was granted to pirtobrutinib (JAYPIRCA, Eli Lilly and Company) by the U.S. Food and Drug Administration (FDA) for the treatment of adult patients with chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (CLL/SLL) who have received at least two prior lines of therapy, including a BTK inhibitor and a BCL2 inhibitor.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
What makes pirtobrutinib distinct from other FDA-approved BTK inhibitors?
Dr. Joanna Rhodes: Pirtobrutinib is different from our other FDA approved BTK inhibitors because it’s something called a non-covalent inhibitor. It is a different drug entirely than our prior BTK, our covalent BTK inhibitors – ibrutinib acalabrutinib, and zanubrutinib. I consider it in its own class of drug, as opposed to lumping it into all BTK inhibitors because they do have different pathways and I think will be used in different scenarios.
Right now, the current FDA approval for pirtobrutinib is for patients that have received a covalent BTK inhibitor – so have gotten ibrutinib, acalabrutinib, or zanubrutinib – as well as a BCL2 inhibitor. And in usually in the United States, that’s venetoclax. It’s the one that’s commercially available. One of the challenging clinical scenarios that we were in before pirtobrutinib was if patients need more than two lines of therapy, what were we giving them? And we didn’t have a lot of great options.
Can you share your insights on the safety and effectiveness of pirtobrutinib?
Dr. Joanna Rhodes: Having participated in the BRUIN trial, I can tell you from a patient perspective that it is very few side effects. I think that’s really wonderful, and it’ll be exciting to see how pirtobrutinib moves into the treatment landscape of CLL
Can you provide an overview of the BRUIN trial?
Dr. Adam Kittai: So here at ASH, we saw an updated BRUIN trial analysis by my mentor, Dr. Woyach, at the CLL oral session that gave us a longer time follow up for patients on pirtobrutinib. But it also helped us know how patients do, whether they got BCL2 inhibitor venetoclax or not. In the trial, it was only mandated that you get a BTK inhibitor. 100% of patients received a BTK inhibitor. However, about 50% of received venetoclax as well. Dr. Jennifer Woyach showed us in the trial that if patients had received a prior BTK inhibitor and a venetoclax when they got pirtobrutinib, the median PFS was around 15 months, whereas if they did not give venetoclax, the median PFS is around 23 months.
Can you elaborate on the implications of this data for informing patients about the expected duration of treatment?
Dr. Adam Kittai: The reason why I bring this up, and why I think it’s important, is it helps us inform patients about how long we expect them to stay on drug. It also might have implications into the future about sequencing in terms of whether or not we should go from a covalent BTK inhibitor to venetoclax to a non-covalent or covalent BTK, better to non-covalent BTK orbiter to the nucleus. I think time will tell until we really know the answer to that question, but at least knowing this data is really informative.
Another thing that was presented by Doctor Jennifer Brown at Dana-Farber was the resistance mechanisms to pirtobrutinib. We got a better idea of how resistance forms in pirtobrutinib and how pirtobrutinib helps with resistance to covalent BTK inhibitors.
Once again, she showed that T474I and L528W are the primary resistance mutations for pirtobrutinib, and knowing those resistance mutations helps us as well. Knowing, sequencing, knowing and informing in the future whether or not we can go from covalent to non-covalent, which we know we can, or non-covalent to covalent, which is still a question that I think remains to be solved.
What can you tell us about pirtobrutinib’s side effects and clinical trials?
Dr. Joanna Rhodes: I can tell you from a patient perspective that it has very few side effects. I think that that’s really wonderful, and it’ll be exciting to see how pirtobrutinib moves into the treatment landscape of CLL.
There’s a lot of upcoming clinical trials using pirtobrutinib that we don’t have data from yet. They’re currently enrolling, and some have completed enrollment. Those are comparing pirtobrutinib to other covalent BTK inhibitors for patients who haven’t been treated with a BTK inhibitor. And then I think what’s interesting is we’re going to see it used in combination therapy for time-limited durations of treatment. And I think it’s going to be a safe and effective drug in that scenario as well, but we don’t have data from those trials yet. So definitely more to come from pirtobrutinib. But again, really exciting that for patients that have progressed or have received a BCL2 inhibitor and a covalent BTK inhibitor, we have this as a potential treatment option, commercially available and readily available outside of clinical trial.
Final thoughts
Dr. Adam Kittai: So really exciting to see this data, really exciting to see the evolution of pirtobrutinib. And I think the most exciting thing is now we just have another drug that’s approved for the treatment of CLL, which is just fantastic for our patients.
The Doctor Talk: Latest Relapsed Refractory Multiple Myeloma Treatments
Dr. Cristina Gasparetto, Duke Dr. Joshua Richter, Mount Sinai
The list of options of treatments for relapsed refractory multiple myeloma patients and their caregivers continues to grow, so much so that it can get pretty tough to keep track of every possibility out there.
To help sort through the newest drugs and combinations, how they work, side effects and managing through them, The Patient Story hosted top myeloma specialists in our latest event focused on relapsed refractory treatment options:
Thanks to Karyopharm for its support of our educational program. The transcript has been edited lightly for clarity.
Transcript
Introductions
Stephanie, The Patient Story: Hi, everyone. Good morning, good afternoon to you, depending on where you’re joining us from. I’m Stephanie with The Patient Story and incredibly excited to lead this program today with our two incredible guests. I’ll get to that in just one moment. Our topic today is treatment options for relapsed refractory multiple myeloma. And as we know, it’s a landscape that is constantly shifting, which is great news.
But that also means it’s a conversation I think that we should continue to have pretty frequently as the information keeps coming in. First, we’d like to give special thanks to Karyopharm for its support of our educational program today. Now, what I hope people you all take away from today’s conversation is more humanized sort of context of all this information that’s coming out. We’re going to have the medical jargon. Of course, it’s part of the conversation, but we’re going to have an incredible discussion that’s led by two top myeloma specialists.
We have Dr. Cristina Gasparetto, Director of the Multiple Myeloma program at Duke University. And we also have Dr. Joshua Richter, who’s the Director of Multiple Myeloma at the Blavatnik Family- Chelsea Medical Center at Mount Sinai. So welcome to you both.
Dr. Cristina Gasparetto: Thank you. Thank you. Pleasure to be here with you guys.
Dr. Cristina Gasparetto: I knew since I was very young, that I was going to become a doctor because my dad was a physician, and his father and his brother and everybody, so it is a long history. And of course, I wanted to emulate my dad.
But myeloma, I was in the first year of fellowship and just my first month rotation. I didn’t know anything about blood cancer, very little coming up on residency. And I was called for a consult, patients with newly diagnosed myeloma.
I tell you the truth that I really didn’t know anything about it. So I went to the library. Back then, because I’m quite old, we didn’t have Google and everything and I read about myeloma and the average age was about 70.
And I went to meet with this patient. And it was a young woman, 42 years old, and she had actually spent 20 years of her life in Italy. So we were conversing in Italian. I’m Italian, and I was fascinated by that, by the story. And I started to read everything and to make a proper recommendation at that time.
And do you know, at that time the autologous transplant was definitely increasing in terms of becoming almost a standard of care and allogeneic transplant. We didn’t have anything. We didn’t have the new agents.
And from that, it became a love hate affair, I guess, with this disease.
Dr. Joshua Richter: I’m the first doctor in my family. I was kind of drawn to this kind of romantic, noble notion of being a physician to help patients.
And I knew I wanted to do oncology hematology, but wasn’t sure about surgical or the medical side until I scrubbed into my first Whipple procedure in medical school.
Well, then, after 14 hours of holding retractors, I realized this is not for me. And then I did my internship in residency at a hospital that no longer exists called St. Vincent’s. And it was an epicenter of myeloma with people like Sundar Jagannath, Ajai Chari, David Vesole, Madhav Dhodapkar.
And my first day on the oncology ward, when I get up to the floor to see the admitted patients and understanding that myeloma is less than two percent of all cancer, the hospital is very known for HIV and myeloma.
And normally an inpatient floor will be lung cancer, colon cancer. But because it was HIV, the first three patients had Burkitt’s lymphoma, another rare disease, and every other bed was myeloma, which is just a very strange thing for an oncology floor.
And I got to see world class people treating a complex disease. And I find that fascinating that the field was in this earlier phase of evolving exactly as Dr. Gasparetto talked about.
The older days, there was little we could do. In the last 10, 15 years have been an explosion of options. And it just seemed like a place where you can make a huge impact. So I got hooked.
COVID-19
What is your guidance on the third vaccine shot?
The Patient Story: I’d like to kick off with some COVID-related questions, actually, just because it’s timely. You know, people are talking about with the CDC’s recommendation about hey, you’ve got to go get your booster shot, your third shot. For a lot of folks, they’re hearing more people talk about certain things.
So they want some clarification and we’re hoping that maybe you can provide some. One of the questions is about how some of the treatment immunosuppressive, might prevent a better antibody response from the vaccines. How bad is it?
Dr. Cristina Gasparetto: We don’t have a lot of data on safety but it looks like a lot of patients with myeloma already participated, they are participating. And the problem is that we don’t know, we don’t know if the third boost is going to protect them even more if they are taking special treatment.
When I talk with my patients, I always stress the importance of maintaining precautions – the masks, the social distance, and then at the first exposure, I think if they are exposed, very quickly to contact us to receive antibody treatment.
So we actually have at Duke infectious disease, we can move very fast on providing them with the infusion of the antibody infusions to minimize the risk of major symptoms with infection. So we don’t know. We’re learning about it and I think the Leukemia & Lymphoma Society are going to collect the data about the third shot, the boost.
And right now, do you start it? So we have some recommendations and we can provide recommendations to our patients in active treatment less than two years from transplant to go ahead with another booster. But we don’t have a lot of data on safety.
The Patient Story
Dr. Joshua Richter: A third booster may help some people, but there may be people whose immune system is so far down that if two didn’t do it, a third won’t do it. I think the best advice is exactly what Dr. Gasparetto said, which is until we are on the other side of these big waves, and we learn a little bit more, continue masking and social distancing.
What precautions should myeloma patients take in spending time with unvaccinated kids?
The Patient Story: Perfect, the message being, of course, you know, better to get the booster shot, especially if it’s been effective than to not, and then just take those extra precautions.
A second question comes from Jane L. who says her father was recently diagnosed with multiple myeloma. She’s worried because he spends a lot of time with his grandkids and one of them is six. So unvaccinated and going back to school now, so is masking up enough? Is there any sort of general guidance there? And we can start with you, Dr. Richter.
Dr. Joshua Richter: Yeah. I mean, these are the really, really tough questions that we always have a saying in myeloma: You ask three myeloma doctors a question, you will get five answers. So I don’t know that there’s a clear guideline. The likelihood is that there’s going to be vaccinations for two and up later in the year.
This is a really difficult time, especially with, they talk about this thing called the R nought (R0), which is how many people you’re likely to spread the infection to.
And the original Covid was more like an R0 of two. And now with the Delta variant, it’s like nine. So the concern is as kids get back together after the summer, they’ll share a little bit. Teachers may share and they may bring it back.
So I think the way I would approach it is I think everyone has been very diligent and it’s taken a huge toll on everyone, physically, psychologically. But early on in the next year, where we have more people vaccinated, including people potentially as young as one year old. I think it’s going to be a different story. So I would say still try to keep a little bit of distance.
Relapsed refractory multiple myeloma treatments
The Patient Story:Ok, perfect. Thank you so much for that. So as we shift now into talking about these treatment options and his shifting landscape, we do have to set the stage a little bit. Everyone knows in the space that myeloma, the experience ranges widely.
And Dr. Richter, you just said ask one question, get five answers. So we should expect that and want to remind everyone that today’s discussion is very much a discussion, it’s about this information, empowering patients and caregivers to take what they can from it, but that it is not medical advice.
When do you restart treatment?
So the first one is about deciding when and how to restart treatment. You know, what are those signals that you take in? And I know it varies, again, from patient to patient. And how much does it vary depending on the standard risk versus high risk? And maybe we’ll start with you, Dr. Gasparetto.
Dr. Cristina Gasparetto: Sure, it’s always a very difficult question because you are correct. Standard risk, high risk probably is a little bit different. If you have a patient, for instance, I’m going to give you some examples so it makes more sense.
Standard risk
If you have a patient with standard risk myeloma five years after transplant, remission, and now you check labs and you start to see a resurfacing of the protein marker. Do you need to treat the patient immediately? Probably not.
The first step that we do, we do staging to make sure that the myeloma is not causing any damage. And then we monitor the amount of care that protein and if the protein remains relatively stable.
Sometimes we postpone treatment because we know that as soon as we initiate treatment, we have to go with three drugs, a combination and we increase the risk of toxicity. So we don’t want to do any harm and we want to, you know, if every drug has a half life and the clock starts to tick when you start the drug, if you start the point, you have enough time.
So if you postpone the initiation, it may be beneficial. You may have something else to offer to your patient later on and decrease, improve. And particularly if the patient comes to you and says, I feel okay, I don’t have any symptoms. Why? And to follow that particular patient.
High risk
Now, if a patient progresses more rapidly, if they’re still on treatment or if it’s very quickly after the transplant, or a patient with high risk myeloma,that is a different story. Then we have to take that in account and probably initiate treatment a little bit sooner at that point.
And of course if a patient has symptoms, and we find out that the myeloma is already damaging then yes, absolutely, no question.
Dr. Joshua Richter: Perfect. Yeah, I couldn’t agree more. You know, I think one of the things you brought up, Stephanie, is this notion of high risk or standard risk. And typically when we talk about high risk, we talk about cytogenetic high risk.
So abnormalities in the DNA of the cancer cells, things like deletion of part of the 17th chromosome or extra copies of the first chromosome. But something that Dr. Gasparetto brought up, which is absolutely critical in deciding who needs retreatment, is something we call functional high risk.
So with many of our great drugs, we anticipate that initial response to induction or a transplant to last many, many years. If your disease relapse is much sooner than that, it doesn’t matter if your genetics don’t show any high risk. You’re demonstrating the biology of the disease to be functionally high risk.
So I completely agree with Dr. Gasparetto. We’ve had patients, a few months after the transplant, the numbers are coming up. That’s an omen of something bad. We may have to act on that sooner.
Using more aggressive treatment upfront
The Patient Story: I appreciate you both responding about that. I’d like to ask too now and we’ll start with you, Dr. Gasparetto. It’s generally said that the first line response tends to be deeper, longer than the second. I’m curious, what’s your opinion about starting with more aggressive treatment up front?
Dr. Cristina Gasparetto: Yeah, well, we have a lot of data on the achievement of the deep response, and we have a lot of data showing if a patient achieves that deep response, we probably have a better outcome or remain in remission longer.
It looks like we are trying to go to the same goal, even in second relapse we’re pushing the envelope more and more.
And, you know, actually, when I started, we were not bringing everybody to a complete remission. It was very difficult to explain to patients, because after transplant, some patients who still had residual myeloma, and we were saying, oh, it doesn’t matter. You know we’ll see if the myeloma is resurfacing sooner or not.
But now we’re pushing, we are becoming more and more aggressive like other cancers, right? At the beginning it didn’t make sense because if you treat any other type of cancer, you want to achieve a complete remission.
With myeloma, we were like, it doesn’t matter. But now we know it matters. And we are accumulating more and more data. And I think achieving a deeper response is important. Even in cycle maybe third line, and that correlates with a better outcome.
But what’s happened is sometimes, we can’t. Later on we cannot do that. It’s clear. And in fact, some of the new approaches, what is amazing to us, that we can reach the depth of response. We’ll talk later about the CAR T and other immunotherapy and even in later life of the myeloma. So we are learning about that. But, yes, we keep that as one of the goals earlier on. And then sometimes with time, unfortunately, we may not be able to achieve that.
Dr. Joshua Richter: It’s definitely been this push and pull, as we slowly develop more and more drugs. The question was:
What’s the best way to use them?
Do you give just one or two at a time?
This way you have something for later on. Combining different chemo drugs with using classical chemo. So old school chemotherapy drugs like melphalan and etoposide and adriamycin, the older generation of chemo. Combining multiple drugs can be very toxic. But many of the novel or newer drugs we use in myeloma could be combined much easier.
There’s been discussions of do you save things for further down the road or do you make these three and four drug combinations earlier and earlier on? And we now know that that’s probably the better way to go.
And now that we have more drugs, we have three unique drugs to give upfront, three unique drugs to give second, third and fourth line.
It’s really important to put your best foot forward, because despite the probably dozen or more drugs we have, the average patient in the United States only gets three or four total lines of treatment for both good and bad reasons.
The good reasons being that some people do so well with their first or second line. They can live for many, many years, and pass of something else, in complete remission.
Unfortunately, some people have higher risk disease and don’t make it beyond the first few lines because they’re so sick. But yeah, achieving deep remission now with multiple drugs is really key and we know that people get these deep responses, such incredible outcomes.
We used to talk about the entire journey from diagnosis to death being only two years where there was a recent study that looked at giving daratumumab, REVLIMID and dexamethasone to the older, frailer patients who were not eligible for transplant. And they just recently looked at the data.
And the average remission has not yet been reached, but across the five year line. So we’re talking about the older, frailer patients who can’t get transplant with their upfront therapy. What used to be the entire journey from diagnosis to death was two years. Now, the older, sicker patients get more than five years on average with their first line alone.
Dr. Cristina Gasparetto: Absolutely, I think some of these combinations are becoming so powerful and we are learning the early exposure of some of these agents is very important and the combination.
Definitely we’re treating the myeloma very differently from even five, 10 years ago.
The Patient Story: It is so promising and so energizing to hear about even these numbers. It just paints that picture for people. Perfect. Ok, I hear a lot of agreement there between the two of you, that’s wonderful.
Ok, so then without further ado, I think a lot of people are curious about these newer therapies, newer combinations. And in this context, there is a lot of information out there already I’ve seen about what it is and more of the medical jargon. We do have to talk about, you know, things like how it works just so people understand these different classes, they work differently.
But I’d love to get some color from the both of you in terms of your own experience with patients. The real world experience. And we got a lot of audience questions. I’m just going to sort of throw it all in general to say they wanted to know about side effects going through each one. And of course, the most important is how you try to reduce them, if possible.
Selinexor (XPOVIO)
What is selinexor and how does it work?
The Patient Story: So we’ll start with selinexor, trade name XPOVIO, just because it was more recently approved to be used earlier. And so I think there’s a lot of curiosity about that.
That approval was for selinexor, bortezomib or Velcade, and dexamethasone. Dr. Gasparetto, we’ll start with you. Can you talk about how it works and then experience with it?
Dr. Cristina Gasparetto: Selinexor, first of all, is another oral, by mouth, medication. So it’s always good to explain that to the patient. So for convenience, who doesn’t like an oral medication?
And it has a different mechanism of action, but it is not unique of myeloma. In fact, XPOVIO has been used for different type of malignancies, including solid tumor.
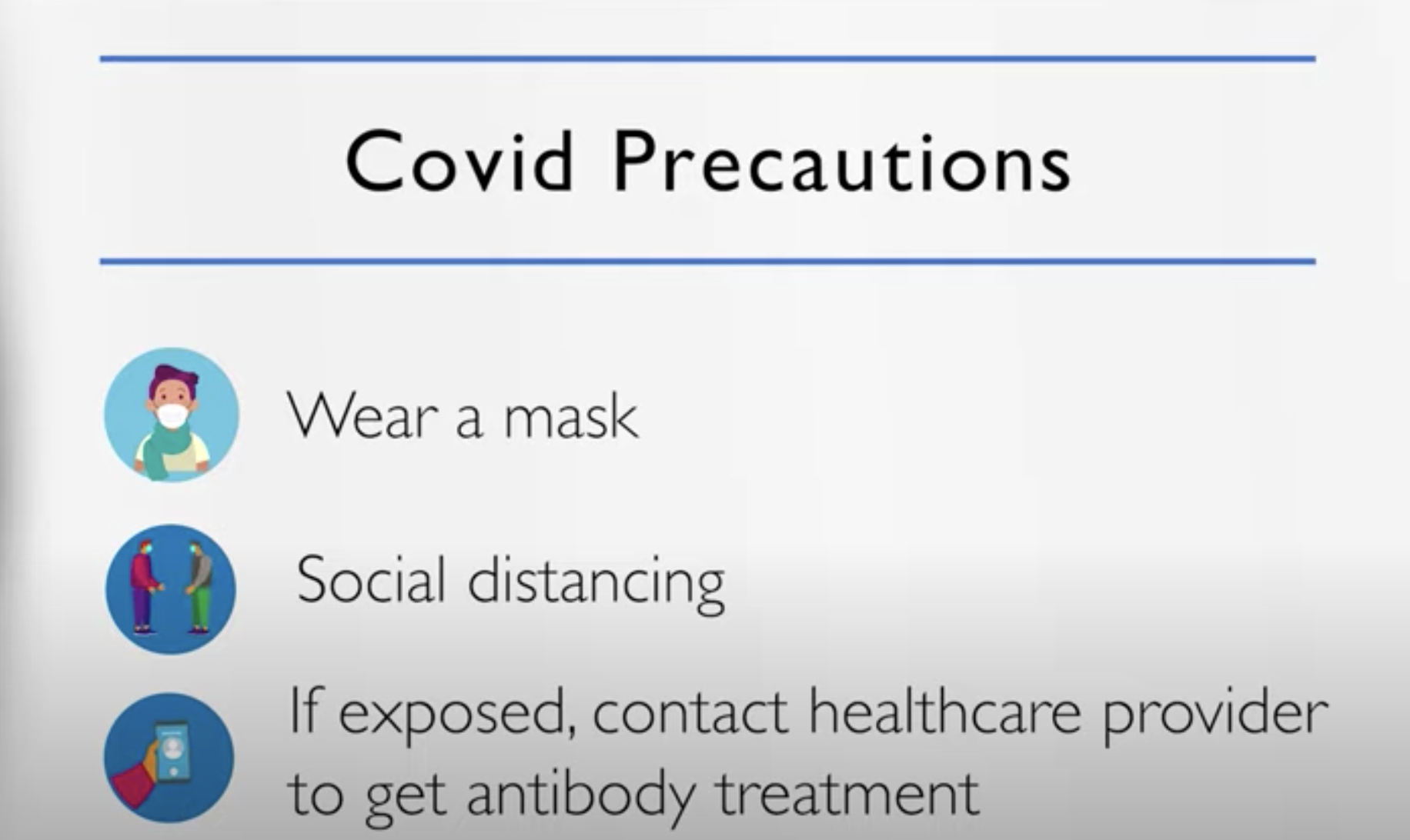
XPOVIO blocks a very important protein. It’s called exportin-1. And the reason why it’s important for cancer, because keeps the cancer cells going on, multiply and staying alive. And I’m trying to explain these very simplistically.
So XPOVIO blocks this protein. So the cells eventually, because this protein is blocked, they go what we call in apoptosis, they go to death. So they die. And these exportin-1 is over-expressed in myeloma and actually correlates with worse survival or worse prognosis in a way. And so it works very well.
Selinexor’s 1st approval
When XPOVIO was first approved, it was in combination with dexamethasone in heavily-pretreated patients. Joshua was part of the STORM study, XPOVIO was given twice a week to patients that we call refractory to everything, the penta-exposed, so very difficult to treat. And there was a signal.
However, very difficult to tolerate. I think you guys did a lot to work with the supportive care, the triple antiemetics anti-nausea medication to support the patient. And we don’t use XPOVIO like that anymore. That’s the passé, it’s old school.
Selinexor’s latest approval
The Patient Story
Now XPOVIO is once a week and when we use once a week in combination, we are able to mitigate some of these side effects. And that’s the reason why XPOVIO was recently approved in combination with bortezomib once a week. And patients are able to tolerate the agent XPOVIO much better.
In fact, we have a lot of data on the nausea, the fatigue that kind of dissipates with time. If patients are able to, I always tell patients that you just have to, in a way, toughen up for the first couple of cycles and then we can maybe be able to adjust the dosage and you’re able to tolerate.
So XPOVIO was approved in combination with dexamethasone twice a week. We don’t use that anymore. We use it in combination.
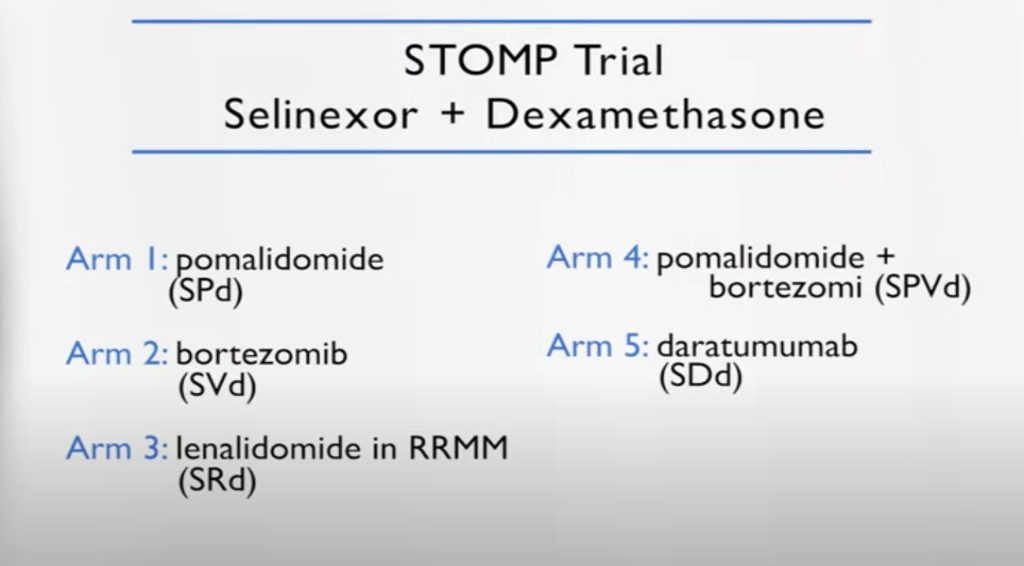
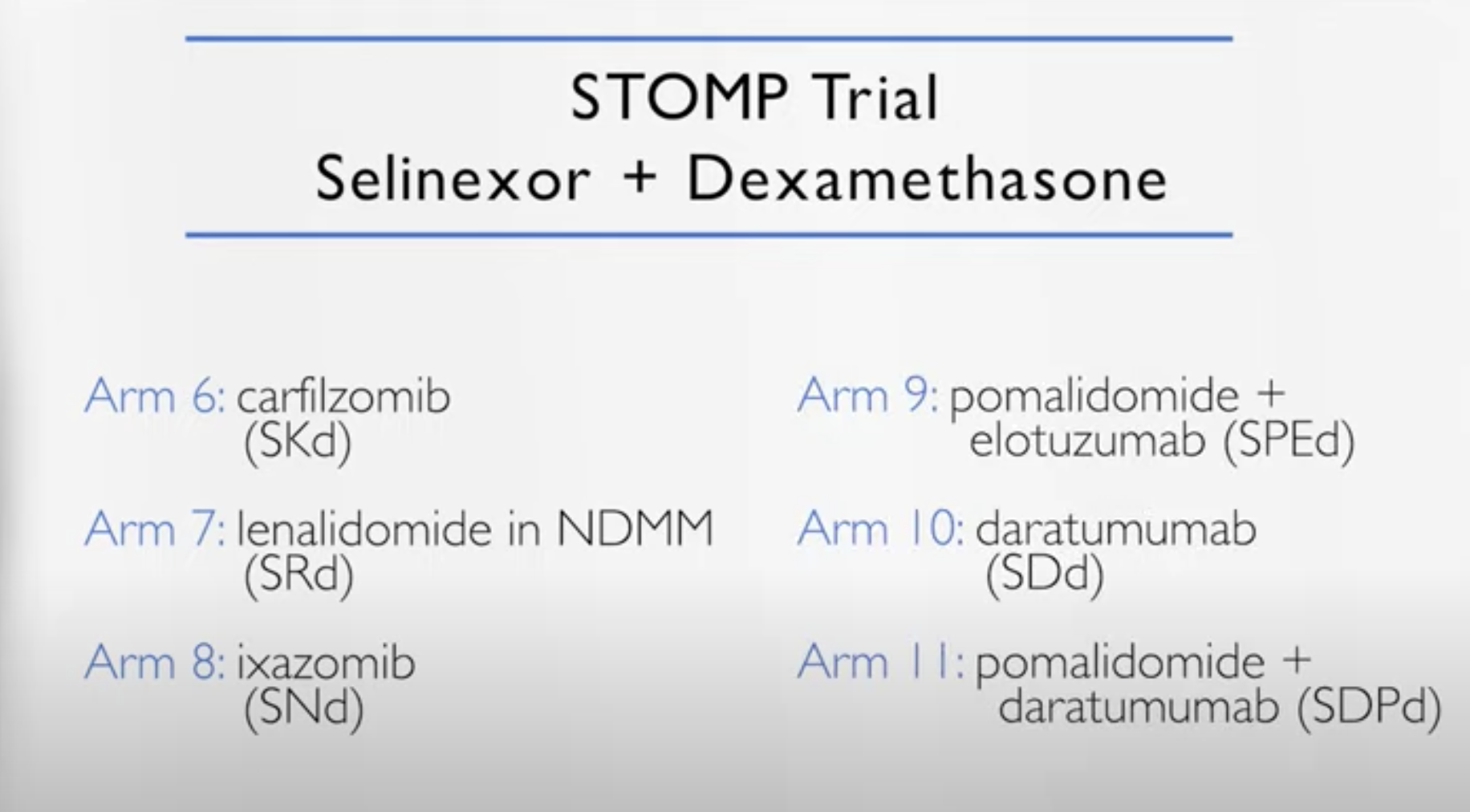
STOMP clinical trial
(Selinexor and Backbone Treatments of Multiple Myeloma Patients)
And I’m part of a study called the STOMP study, where XPOVIO is used in combination with everything else. So bortezomib, which led the launch of the BOSTON study and then carfilzomib, daratumumab, REVLIMID, pomalidomide – you name it.
We present, we channel the patient based on what they were exposed to before. So for example, in the carfilzomib XPOVIO they were naïve to carfilzomib and so forth. We discovered during the study that in certain combinations, it’s very effective.
Once a week we adjust the dosage and they’re relatively well-tolerated. In fact, I have patients able to sustain therapy for a few years. And everybody was like, how did you do that?
Because with adjusting the dosage and the proper supportive care at the beginning. It’s definitely a very powerful drug, and we have data on high risk myeloma. We have data that we learned from the BOSTON study on how to manage the toxicity.
So it’s a new drug and it went totally from the very heavily pretreated to the BOSTON in first relapse. There are some very interesting combinations that we launched from this STOMP study. And probably they are going to be becoming more established based on the early results of the STOMP study. So it’s a very interesting drug, it’s a new mechanism of action for myeloma, a new target.
Dr. Joshua Richter: I think this brings up something that’s absolutely crucial is that there have been studies to show that if patients at least see a myeloma specialist like Cristina, myself, or any of the number of places in the country and in the world, you will do better long term because you will take advantage of the expertise of someone like Dr. Gasparetto and be able to take that locally.
And I always talk about myeloma kind of like remember the movie The Matrix? They say some rules can be bent, others can be broken. You know, the more insights you have, the more you can navigate that.
You know, the fact that these regimens, some of the STOMP ones have NCCN guideline approval means that Medicare will cover them, but only if your practice team knows about them and knows exactly what Dr. Gasparetto was talking about – how to dose these drugs, because giving 80 milligrams twice weekly of selinexor is very complicated. And exactly what she said, we don’t do that anymore.
But doses between 60 and 100 once a week, especially with other drugs. So when it was by itself, it had to do all the heavy lifting. When it has other drugs to synergize with, you can bring the dose down, add supportive care and really get these much better outcomes.
Selinexor side effects and how to manage them
Nausea
dexamethasone
Zofran
olanzapine (Zyprexa)
rolapitant (Varubi)
Dr. Joshua Richter: The way that we really approach this is that old saying an ounce of prevention is a pound of cure and really being very aggressive in the early cycles with trying to prevent toxicity instead of waiting until it shows up, because then nausea is one of those complicated ones once it shows up, patients can then have anticipatory nausea.
So a lot of work was done with one of my colleagues as well, Dr. Ajai Chari, looking into different combinations of drugs to help prevent nausea and some of the standard ones we use, like dexamethasone and Zofran.
But two ones that are a little bit off the beaten path seem to really help. One is a drug called Zyprexa, which is olanzapine, which is a drug that’s been used in the psychiatric world. But it also really is good at preventing nausea.
The Patient Story
The other is a drug called Varubi or rolapitant. It’s a very poorly used drug in general. It’s the same class of drugs as things like Emend or aprepitant, but it doesn’t have the same drug interactions with selinexor that Emend might.
So I think that’s one thing I would encourage all patients, even if you love your local team, now especially in the days of COVID, where we have telemedicine, go out of your way to seek care at a place like Duke or Mt. Sinai, or one of the many advocacy groups that can help you get connected with one of the great myeloma centers in the country.
The Patient Story: Absolutely. Myeloma specialists. I mean, we are talking about just how many variations and presentations, and it’s tricky. And so being able to talk to someone who focuses just on this, I think is really important. This is part of why we do these things, to reach people who are in the community setting to help them out and get them going on the right path, hopefully.
I have olanzapine, I think, in my cabinet from when I was treated for the nausea. And it’s exactly right. Right. Like don’t start to chase as soon as you start to chase the nausea, it’s just like it’s impossible. It feels like. But I haven’t heard much about Varubi.
So I was going to ask you about, you know, all the work that you’ve done looking into the side effects and the management. Is there anything else? I mean, I think the nausea is a huge one. And anything else in terms of I know that sometimes they talk about loss of appetite, you know, things like that.
Weight loss
Dr. Joshua Richter: So loss of appetite, you definitely want to talk to someone more like me than Cristina, because she’s in phenomenal shape and you cannot see from here down but I eat a lot more than Cristina does. So I have plenty of tips for people to gain weight. One of them is really being ahead of the game again, helping prevent it. Small, frequent meals.
The Patient Story
Loss of or change in taste
lemon juice
sour candies
Carnation instant breakfast mix
The other thing is sometimes with chemotherapy, people’s taste may go off because the taste buds are not high on the pecking order for the body when they’re dealing with other things. So food often tastes bland or like paper.
Sometimes a little simple thing is taking that lemon juice bottle that looks like a plastic lemon we all have in our refrigerator for 100 years, squirting a little bit of that on the tongue or sucking on some sour candies prior to a meal may liven up the taste buds to help food taste better for people who are losing weight.
Remember Carnation Instant Breakfast? You can use Carnation Instant breakfast, but instead of mixing it with milk, mix it with ice cream so that even if you’re only taking a few small bites of food, each bite is very calorie dense.
Hypernatremia (low salt levels in blood)
The other side effect is selinexor can cause a little bit of what we call hypernatremia, low salt levels in the blood. Usually not very symptomatic, but again, recommending things like potato chips and pretzels can help along with that.
Blood platelet counts
The other thing is it can affect the blood counts, specifically selinexor seems to affect the platelets.People may get things like growth factors throughout their treatment course and people may be more familiar with drugs like Procrit or Retacrit which raises the red count or Zarxio or Neupogen (filgrastim) that raises the white count.
But there are drugs that raise the platelet count. The two big ones are eltrombopag or Promacta and romiplostim or Nplate. And our experience is that you need to titrate the doses of that up quickly and pretty high to overcome some of the low platelet count you’ll get with selinexor. But again, we see that more when we use selinexor. Towards the very end, less of it when we use it earlier on.
The Patient Story: Perfect. Thank you so much. I know that was a lot to get through, and I think that’ll be incredibly helpful for people – start Googling things. I’d like to shift over now to isatuximab or Sarclisa, a monoclonal antibody. We will start with you, Dr. Richter, if you want to talk about how it works and your experience with it.
Isatuximab (SARCLISA)
What is isatuximab and how does it work?
Dr. Joshua Richter: All right, so SARCLISA or isatuximab is a monoclonal antibody, and just like our body makes antibodies to fight infections, this is an engineered antibody to attack myeloma. All cells in the body have different markers on them to kind of interact with other cells and take out various actions.
And they all go by these names CD – CD1, CD2, CD583. CD just stands for cluster of differentiation. All cells have different groups. So lymphomas have CD20 and CD3. Myeloma cells universally have CD38.
This is a naked antibody, which means it doesn’t come along with any toxin or anything. It’s just the antibody. It seeks out anything that has that CD38 marker, grabs on to it, and can induce that cell to undergo what Cristina talked about earlier, apoptosis, through a number of different mechanisms, complement-dependent cytotoxicity, antibody directed. There’s a few different ways you can do it, and it directly kills the myeloma cells.
Current isatuximab FDA approvals
Isatuximab currently has two FDA approvals, one based on a trial called the ICARIA trial, which gave isatuximab, pomalidomide and dexamethasone to refractory patients, and the IKEMA trial more recently, isatuximab, Kyprolis and dexamethasone.
Although many people may be more familiar with daratumumab, which comes now in both intravenous and subcutaneous administration, isatuximab is only intravenous at the moment. There are ongoing studies with the subcutaneous version.
Isatuximab side effects & how to manage them
The biggest side effect is that the first dose can have an infusion related reaction, whereas as the drug is going into you, you can get shakes, chills, and flushing. We give medicines ahead of time to prevent that.
If you do get it, the nurses will have a protocol to give medicines to stop it immediately. And generally, after you get beyond the first or second dose, most people don’t have any side effects and is overall a very well tolerated drug and is definitely part of our treatment paradigm for relapsed and refractory myeloma.
Dr. Cristina Gasparetto: I’m jumping from one thing to the next. Over the next few years, hopefully soon that we are going to adjust tailor our treatment based on the patient, the age, comorbidity, genetics, type of myeloma. And so we are learning.
Our job as a myeloma expert is to learn the difference, the nuances between one regimen and the next. Am I going to choose isatuximab carfilzomib versus isatuximab pomalidomide based on the age again? And so relatively well tolerated in the elderly with the carfilzomib.So we are dissecting all this data. There is no doubt that these regimens are very effective. Now, the question for us is,sequencing.
Preference of how drugs are given
The Patient Story: I love all of that. And the goal, of course, the trend of more precision medicine and tailoring.Incredibly exciting. Another factor and you both brought it up. I mean, Dr. Gasparetto you talked about selinexor being the oral pill. Who doesn’t like just popping a pill?
And Dr. Richter, you also we were talking about how isatuximab right now it’s IV only. Sometimes there’s some reaction to that, whereas daratumumab, there is that shot. How often in your conversations with patients is that coming up in terms of how it’s given? So let’s not talk about the pill. I think that’s always pretty preferred. But the shot versus the IV, does that come up?
Dr. Cristina Gasparetto: Of course. Of course. In fact, one of the convenience, you know, the daratumumab with pomalidomide, when you go to dara monthly with pomalidomide becomes very convenient.
But a patient with high risk myeloma may in fact, benefit from the IV infusion and the consistency of the IV, the drug, with a different mechanism of action. So while we are talking about convenience, we are also talking about, you know, this is probably a better regimen for you or vice versa. So it’s part of the discussion, of course.
Melphalan flufenamide “Melflufen” (PEPAXTO)
What is melflufen and how does it work?
The Patient Story: Perfect. Wonderful. We will shift over now to melflufen, trade name PEPAXTO, and this is maybe a little bit later on for the patients who’ve had four or more lines of prior therapy. Let’s go to you, Dr. Richter, to talk about melflufen and your experience with it.
Dr. Joshua Richter: Sure. So, melflufen tries to marry one of the greatest drugs in myeloma history to the new way. So when we talk about chemotherapy or drugs, there’s kind of a dividing line.
There’s classical chemo that was invented around World War 2 that just kind of kills everything. And then there’s the newer therapies that better target the bad cells and less off target toxicity. Melphalan is the drug that has been given both orally and the majority of the way we use it in the US is to give high doses of melphalan as part of our stem cell transplant procedure.
What melflufen is is it’s a peptide driven melphalan and which basically because the peptidases are overexpressed in the cancer cells, the cancer cells will suck this up more than normal cells. And it delivers the melphalan more specifically to the cancer cells than to others. So think of it as a newer way of giving melphalan.
How is melflufen administered?
Dr. Joshua Richter: It’s a very interesting drug. It’s given once a month. So it’s nice to give a drug only once a month. It is an IV. However, at the current time, it requires a central line.
So a central line can either be a triple-lumen catheter or a PICC line or any other way to get central access. There is an ongoing study called the PORT study, which is evaluating giving the drugs for a peripheral IV, which will hopefully be out later this year, which will allow us to give the drug through a peripheral IV instead of a central line.
The Patient Story
Melflufen’s status (October 2021)
Dr. Joshua Richter: I’ve used the drug with some success. I think it’s a very powerful drug. At this very moment right now, there are a lot of issues at the FDA level. In July of this year, there was an independent review committee that looked at another study that was done that was head to head, melflufen versus pomalidomide.
And even though the progression free survival was still better with melflufen, patients stayed in remission longer, the overall survival was shorter with melflufen. So the FDA put a bit of a hold at the moment.The FDA and the company that makes this, Oncopeptides, are currently going through discussions of trying to tease out who was having the poor outcomes, who are having the better ones. So the future is a little complicated.
Melflufen side effects & how to manage them
Including, not limited to:
low blood counts
low platelet counts
Dr. Joshua Richter: The biggest side effect is it lowers the blood counts. Apart from cytopenias or low counts there are very few other toxicities, specifically thrombocytopenia and low platelet counts. So the patients that I have, I usually have to delay their next cycle a little bit because their platelets haven’t quite come up just yet.
And there’s some really great ongoing studies in the same vein of Cristina’s STOMP study of combining it with drugs already out there and the two most mature datasets are melflufen plus bortezomib, and melflufen plus daratumumab.
The good thing is in the study, that allowed the FDA to approve melflufen in combination with dexamethasone. There was a group of patients who had what we called extra medullary disease, meaning that the myeloma was kind of losing control a little bit and presenting with several tumor outside the bonds.
And there was a good signal. So it’s old fashioned chemotherapy, but it’s more targeted than chemotherapy. So we learned very quickly that can be used in these difficult to treat population of patients with extra medullary disease. And that was a good signal, a good response rate.
The Patient Story
The Patient Story: It’s all promising. What I’m hearing, of course, is we’re in the thick of things and all these different combinations. People are trying to tease out what is that right combination. Different people respond differently. I also like that you’re talking about, before you talked about different doses of selinexor for instance, that can help with side effects and you can play around after a couple of cycles. People tough it out. And then, Dr. Richter, you are talking this time about the schedule, right. So maybe you will have to delay for a few days so that it’s more palatable.
Dr. Joshua Richter: Maybe dose reduction in combination. We are, I guess, establishing the right dose in different combinations, and it may not be 40, maybe 30 or lower.
Belantamab mafodotin (BLENREP)
Belantamab mafodotin and how it works
The Patient Story: Perfect. Great. And so our last one for this section is the belantamab mafodotin or trade name BLENREP, which again is a little bit later, the FDA approval is for 4+ prior lines of therapy. Dr. Gasparetto, could you talk about how it works and again, your experience with it, with your patients?
Dr. Cristina Gasparetto: We call it a conjugated antibody. It’s like Joshua was explaining about the daratumumab. So the target now is different, it is not CD38, but it’s BCMA B-cell maturation antigen, which is becoming a very important target for myeloma, a new one. And so it’s conjugated, these are linked to a toxin, the mafodotin.
It kind of binds to the myeloma cells, the BCMAs mainly expressed on the myeloma and mature B cell. Then there is the delivery of these microtubule toxins. And so that is, again, the destruction of the cells, the cells’ death.
How is belantamab mafodotin administered
Dr. Cristina Gasparetto: So this drug is very convenient, is given in the outpatient setting. IV, but you don’t need a central line, it’s about a 30 minute infusion. It comes, though, with the big warning. The ocular, the eye, toxicity.
The drug is a single agent. Doesn’t have dexamethasone, doesn’t have steroids. It works. And some of the responses are very durable.
Even when patients are skipping the dosage because of the toxicity. But you really have to sit down with a patient in explaining what the ocular the eye toxicity involved, what it is.
The Patient Story
Belantamab mafodotin’s biggest side effect: Keratopathy
Dr. Cristina Gasparetto: Patients can have what we call keratopathy, which is the microcyst formation of the corneal epithelium. And at the beginning they don’t have any symptoms. 50% of patients don’t have any symptoms.
So the importance is to establish a partnership with the eye care, ophthalmology, optometrist. So patients are followed by both of us, by the eye ophthalmologist, optometrist so we can decide together if we can continue.
We can give the infusion every three weeks, because all these ocular toxicities in the clinical study were reversible because people would present with this keratopathy, decrease of the eye, the vision, blurred vision, dry eyes, and they are reversible.
As long as you don’t continue on the infusion, you don’t want to arrive at the severe keratopathy, the grade 4 with the ulceration. You want to stop it. And so the partnership and explaining to the patient that, of course, of these ocular toxicities is reversible.
They’re not going to get blind, but when we’re dealing with eye toxicity, we all get scared, and unfortunately it’s the deliveries, the toxin that is linked to BCMA, to the antibody that is causing directly that.
How can patients manage the keratopathy
Dr. Cristina Gasparetto:
A lot of studies are trying to prevent, trying to help patients, lubrication of the eye. Don’t use the contact lens and keeping a constant, you know, follow up with us, with the physician and the ophthalmologist or optometrist so we can guide. And the beauty of this drug is there are some patients who just skip one, two, three doses. And the responses were not changing. They were able to maintain their response.
I have patients that are continuing therapy and doing quite well. And I’m impressed by the durability of the responses. There is a lot of press and talk about the ocular toxicity. But when you are counseling the patient and explaining that we prevent, we don’t want the patient to develop the severe toxicity and they’re reversible, I think it is a very good drug.
And we’ll see the evolution also this drug in other combinations. But so far, I’m quite impressed with the drug and the efficacy of this drug.
Dr. Joshua Richter: I couldn’t agree more. It’s definitely an important tool that we have, and the really interesting thing about the drug is, Stephanie, you mentioned,in terms of melflufen, sometimes a dose reduction is going from 40 milligrams down to 30, but sometimes it’s going from giving it every four weeks to every five or six weeks.
Same thing with Velcade. When you have 1.3 as the starting dose twice weekly, you can go to one twice weekly or one point three once a week.
Belantamab dose schedule
Dr. Joshua Richter: And with belantamab, we have those options, the starting dose is 2.5. We can go down to 1.9, but probably the better way to dose reduce is to stretch out the frequency of dosing.
So it’s prescribed as an every three week drug. But my experience has been it’s mostly an every four to six week drug because you kind of have to space it out.
And that’s a dose reduction simply by reducing the frequency and the benefit of extending it out to every four weeks or every eight weeks is it starts to kind of jive better in combination, because most of our other drugs, like daratumumab, like Kyprolis, like the IMiDs, are on 28 day cycles.
So it’s probably better as a every four week drug. And earlier on, maybe in first or second relapse, some of those trials or even giving it every eight weeks. So basically once every other four week cycle when you’re giving it in combination. And the same thing there, you know, we may have to use a different drug.
DREAMM Clinical Studies
So all of the studies that are being done with belantamab are called DREAMM with two M’s. So the drug got approved by the DREAMM-2 study. The most robust data so far [00:59:30] that I’ve seen is from the DREAMM-6 study, which is mostly being led by Dr. Ajay Nooka at Winship at Emory. And it seems right now that when you give it with Velcade, it’s probably 1.9 is the dose.
So we learn so much more about these drugs after they’re approved, what the right supportive meds, what the right dosing levels, schedule. We all learn this as we use the drug.
Dr. Cristina Gasparetto: I agree. Also with a pomalidomide was presented with a longer interval. And those are new.
The Patient Story: It’s interesting to hear all these descriptions, and as you said, everyone has to stay tuned to see how the trials progress and then you get more data and know how to apply that to people, which is what we are all waiting for. But as Dr. Gasparetto was saying, when you talk about eyes, you know, it’s just..
Dr. Cristina Gasparetto: It is intimidating, right?
The Patient Story: Yeah, very intimidating. And I think, you know, people might have heard the term REMS, but it’s the risk evaluation and mitigation strategy. But really, you were both talking about, you know, you just have to have more of the follow up you have for safety.
Dr. Cristina Gasparetto: For safety. Absolutely.
CAR T Cell Therapy
Idecabtagene vicleucel or ide-cel (ABECMA)
The Patient Story: So that’s great to know. And now I’d love to shift over to a very exciting, of course, space. You talk about CAR T cell therapy and bispecific T cell engagers or bispecifics for short for now. So I’d like to set up first with CAR T.
What is ide-cel and how does it work?
I know that we’ve got ide-cel or ABECMA that’s been approved. Would love to know your experience with that. And I know there’s also a lot of excitement coming up with cilta-cel, which is expected to be approved hopefully shortly. So we’ll start with you, Dr. Richter.
Dr. Joshua Richter: Sure. So the old way of cancer treatment was just giving poisons to poison the bad cells and recognizing that along the way you would unfortunately poison some good cells.
What has really kind of evolved over the last period of time is this concept of immunotherapy or taking advantage of the fact that the best cancer fighter that exists is our own immune system. It fights cancer 24 hours a day.
The difficulty is that sometimes in an individual, parts of the system may break down. And what CAR T does is it tries to kind of rev it back up by collecting the T cells of a patient. And for many patients who’ve been treated, they may have gone through a similar experience collecting stem cells for transplant.
You need to get a catheter. You need to have your cells extracted on an apheresis machine. But the dial is switched. Instead of collecting stem cells, we collect T cells, which are some of the immune cells. In the lab, they’re engineered to all attack a specific target that’s on myeloma.
Ide-cel’s target
Dr. Joshua Richter: And right now, the main target is this BCMA, the same target for BLENREP, although there are other targets that are being explored in clinical trial.
Then we need to put these back into a patient. But before we do, we have to create what we call immunologic space, because people have a repertoire. They have all different types of T cells. And if you just infuse the new attacking ones in there, there’ll be a voice in the crowd, a drop in the ocean.
CAR T cell therapy process
Dr. Joshua Richter: So first we give something called lymphodepleting chemotherapy. Low doses of two drugs, cyclophosphamide and fludarabine. That clears out the T cells. And then we infuse the engineered T cells to attack the cancer.
This is a very effective and very powerful new tool. At the moment, we have one approved. It goes by the name of ide-cel, or idecabtagene vicleucel,ABECMA, and giving this drug or this therapy requires a two week admission into the hospital.
Ide-cel’s side effects and how to manage them
Dr. Joshua Richter: The major toxicity is something we call CRS or cytokine release syndrome. So when we infuse these T cells, they send out and they connect and communicate with other cells in the body through chemicals we call cytokines. And these cytokines activate the cells. And sometimes you can get an overactive immune system.
We have different techniques now to kind of quell to get kind of like the Goldilocks version. You don’t want the porridge to be too cold. You don’t want it to be too hot. You want just the right amount of immune activation where it kills the cancer cells but doesn’t get too active. So we try to walk that line.
And it’s interesting. Many of the ways we do that are similar approaches to how we manage COVID, because COVID can cause an overactive immune system. So there’s a lot of parallels there.
This was commercially approved in March 26th of this year. Another one is expected to be approved in November. And for patients who’ve had multiple lines of therapy, this type of technology is one of the best things that we can offer. And we’re just extremely excited about it.
The Patient Story: That was that was well described, Dr. Richter, I’d love to see if Dr. Gasparetto has anything to say with your experience.
Dr. Cristina Gasparetto: I think it’s a new way to treat myeloma. And one of the advantages of the current T cell is, it’s a one time deal. The last patient I treated, she unfortunately didn’t remain in remission for a long, long time. During that time, she was really active. She was happy that she was not receiving any additional therapy. And so that is definitely a plus.
Research on how to prolong response
Dr. Cristina Gasparetto: The problem is that unfortunately, because it’s a one-time deal patients eventually they lose the capability, the immune system. So now there is a lot of research involved on maybe designing these CAR T a little bit differently so there is more sustainability.
Maybe we need to do some maintenance. Maybe we can use it a couple of times. It will, of course, like all the other drugs that are entering the field of myeloma, initially, they are tested on very heavily pretreated patients.
So they are, of course, the first one to be approved. If you look at old patients the durability of response, they were a little shy of a year but quite impressive responses. So if we can move these approaches earlier and we saw that with the cilta-cel, with the CARTITUDE.
The CARTITUDE has a little bit different construction when it was used to treat the patients, the durability was maybe a little bit better, but similar to the KarMMa.
The Patient Story
Treating patients earlier with CAR T
Dr. Cristina Gasparetto: But now in patients treated earlier, we see amazing responses and the durability is getting longer and longer, particularly with patients achieving complete remission, the MRD that we were talking about earlier.
Can we use the MRD in this situation? And in addition, the CRS, we started to also get the feel of what we called neurotoxicity. There are different types of neurotoxicity. The earlier on that we can treat with steroids, tocilizumab, et cetera.
The overall response to ide-cel so far
I think we are making these CAR T cell safer and safer. I was impressed by the overall response, the MRD and the fact that the toxicity profile is becoming, you know, we’re testing now some of these CAR T cells exclusively in the outpatient setting.
Before when we started, Joshua said patients had to stay in the hospital to be monitored for these major side effects. But now we can manage them in the outpatient setting. So they’re becoming safer.
We’re moving them earlier. Maybe some maintenance may be a boost in a way. And so it’s a new way to treat myeloma. We’ll see, over the next few years, if we can use them up front for those at risk. If we can give them after transplant, etc. But very, very excited having these two major procedures available for all patients.
When should multiple myeloma patients and their doctors consider CAR T
The Patient Story: Thank you, Dr Gasparetto. You know, Dr Richter, as Dr. Gasparetto was saying, when you get CAR T will be used hopefully earlier in certain situations. But right now, I think there were some questions from the audience about how do I know when to talk to my doctor, especially if they’re not at a center like yours,about whether I should pursue one of these combinations, you know, and go in that direction versus when is CAR T right for me? So on a high level, how would you describe that?
Dr. Joshua Richter: The earlier, the better. And the reason why, the earlier the better is that right now there is one commercially available CAR T, but we still have many CAR T’s in clinical trials and slots in those trials come and they go. So being on someone’s list at an institution that does them is a really great thing.
The other issue is it’s worthwhile to have this communication between your local physician and the myeloma CAR T physician, because that’s right now CAR T’s are approved for four or more lines of therapy. But we’re starting to learn that the therapies you get leading up to that may affect the ability to collect and engineer those T cells.
For example, melphalan, which is a drug we absolutely love, if you get a good slug of melphalan prior to when we would need to collect T cells, we may not be able to collect enough to engineer.
So, you know, kind of making sure that is exactly as Cristina talked about earlier, that sequence that we’re all trying to figure out for each individual patient, trying to follow some relative do’s and don’ts so that if and when it’s time for a CAR T, you’re in the optimal position to do it.
The Patient Story
Bispecific T Cell Engagers (bispecifics)
The Patient Story: So I’d love to now go into an area a lot of people have been sort of hearing about, don’t know as much about, which is the bispecifics. So if we could just set it up again, in layman’s terms, what those are, what it means and maybe how patients can view them as a treatment option. And we’ll start with you, Dr. Gasparetto.
What are bispecifics and how do they work?
Dr. Cristina Gasparetto: These are the new antibodies. So, of course, like we were talking about the dara, the isatuximab, the belantamab, so they have different targets. And the reason why they are a little bit different, because in addition to the target, the myeloma and one of the most used targets is the BCMA. But we have different targets, actually different bispecific antibodies, different targets.
But the other one,they engage the T cells. So sometimes I explain to patients it’s maybe a way to do CAR T cell in vivo, in the person. So you don’t engineer, you don’t take the lymphocytes out but you’re trying to stimulate the lymphocyte in. So it is very important for this type of therapy to have a relatively good immune system.
We’ll see these therapies going a little bit earlier now and be tested. But we are all surprised, we’re all kind of excited by the preliminary results because I was involved with the elranatamab, I can’t pronounce it.
The Patient Story:Can I just say it’s very refreshing to hear that you can’t pronounce some of these things!
Dr. Cristina Gasparetto: No, I know, because we have all these names – elranatamab. I have to think about this. And it’s actually initially we are using these drugs. You know, again, engaging the T cells, attacking the myeloma. So that is the effect of the immune system directly.
Best administration for bispecifics
Dr. Cristina Gasparetto: They have other mechanisms of action, of course. And so what we’re learning is that we can give them IV in the vein, but the subcutaneous is becoming actually very for all these drugs, probably the better route of administration.
Bispecifics common side effects
Dr. Cristina Gasparetto: We are trying to find the right dosage. Also the toxicity of these drugs is very similar to the CAR T cells. So we see the cytokine release syndrome, we see the neurotoxicity. And so at the beginning, some patients in some trials are admitted to the hospital for observation for a few days, five days, and then they could continue the therapy in the outpatient setting.
So the difference with the CAR T cell, the CAR T cell is one time and then and you’re engineering your lymphocytes. With these bispecifics you have the continuation.
So which one is going to be better? The continuation versus or the convenience of doing one time.
The Patient Story
Elranatamab clinical trial response
Dr. Cristina Gasparetto: We see tremendous responses with the elranatamab. We had responses in about 70 percent of patients with one-third, 30 percent achieving a complete remission. Now, we don’t have long term follow up to see if these are sustainable.
We don’t know yet but we are very impressed by the early results. And so there are a lot of new bispecifics. They are being designed. Different targets engaging the T cells, it’s part of the immune system and definitely is going to change how we treat myeloma, in my opinion, over the next few years.
So very interesting results. Very similar toxicities with the CAR T cell, great responses. But we don’t know enough about durability. What do you think, Joshua? It is premature, but we are all excited.
Dr. Joshua Richter: I couldn’t agree more. I mean, to me, I think your statement of we don’t know which one is the optimal one for an individual patient is perfect. The one advantage that bispecifics have is a theoretical possibility of being given in the community.
The bulk of myeloma patients are treated in community setting
Dr. Joshua Richter:
In the United States, 70 to 80 percent of myeloma is treated in the community.
So despite the fact that Cristina earlier today probably had a quadruple booked clinic for every single time slot, within the United States, most people get treatment locally.
CAR T’s are probably always going to be reserved for the big centers, but as we get better at managing the CRS with these bispecifics, there may be a point in time where they can be given in the local community practice, which would be just available to more patients, which is an amazing thing.
Different bispecifics with different targets
Dr. Joshua Richter: The other thing is the different targets we have. So all bispecifics, they have two arms. One is CD3, which grabs onto the T cell and the arm that grabs onto the cancer cell. Right now in our clinic, we have four different targets. That’s the other part of it.
One is BCMA, which is the same target as the CAR T cell and as belantamab. One is CD38, So that same target as isatuximab or daratumumab.
Talquetamab and cevostamab
Dr. Joshua Richter: There’s a drug called talquetamab. Talquetamab has this arm here that targets something called GPRC5D, which is on all myeloma cells.
And then there’s another drug called cevostamab with this arm that has something called FcRH5 which is also on all myeloma cells.
And these different markers are independently expressed on the cancer cells. So there is a potential there to sequence these different drugs. We have no idea yet. Does BCMA go before CD38 or after GPRC5D? We don’t know any of that.
But the great thing is as we get these drugs approved, we will all, as a community, learn what the optimal strategies are.
Dr. Cristina Gasparetto: And there is also one that we’re participating with the CD38, so like the daratumumab target. And actually with the elranatamab we had about 20 percent of patients previously exposed to other BCMA targeted therapies, and we still had the response there.
So I think that another big question for us is:
Can I use belantamab?
Can I use the bispecific?
Can I use the CAR T cell with the same target?
So what are accumulating data information about?
Can we sequence these drugs and still maintain efficacy?
Because right now it’s a little bit all over the place. We don’t know.
The Patient Story: So much data coming out constantly. So what I’m hearing from you both is, you know, with bispecifics. Really importantly, Dr. Richter, the fact that I didn’t know it was 70 to 80 percent specifically for myeloma patients being treated in a community setting. That’s incredible. So that would help with that population, which would be huge.
There’s also the issue of sometimes with CAR T. Is it true that you have to bridge. Well, yeah, with another treatment. I mean, there’s variations as you’re waiting for the reengineering to happen and then infusing it back into the person. I mean, I guess maybe a summary of the pros and cons of both would be great. And we’ll start with Dr Richter.
Pros & Cons: CAR T vs. Bispecifics
Dr. Joshua Richter: The pros of CAR T’s is that it’s a one and done. But as you said, right now, all the CAR T’s that are either approved or about to be approved are what are called autologous. We have to have manufacturing of someone’s individual cells, which can take upwards of five weeks for some people. There are ongoing studies looking at allogeneic CAR T’s, which would be an off the shelf option, which would negate the need for bridging.
The pros of a bispecific is they, at some level, can be given in the community, which may make them more advantageous. And because it’s maybe a little more titratable in terms of the side effect profile. You could probably give a bispecific to a little bit of an older or frailer patient, but we don’t have all that information just yet. I don’t know if Cristina has any better way of putting it.
Dr. Cristina Gasparetto: I think that for now, the CAR T cell is limited to the larger academia large institutions. And you’re right that we may not be able to offer the CAR T cell to the frail, immunocompromised, very difficult patient to treat.
So the bispecific, out of the shelf. But you know, they have to sustain therapy, and most of them are given weekly or every other week or so. But maybe that will translate to longer durability of responses that, you know, we don’t know. So right now, we are still accumulating data. Can we use all of them?
You know, eventually our only type of combinations or so. But the good news is that we do have a lot of options available and that, when we are called to talk about the relapsed refractory myeloma, I don’t know if you have tried to make a slide deck recently, but is impossible because we have so much data, so many options.
And it’s impossible. I don’t want to talk about the relapsed refractory because it’s crazy to keep up with everything, which is great, right? It’s easy to talk about. No, I don’t know. Transplant, a one time shot. But there are lots of options. And, you know, we say a lot. But I think having a referral to a myeloma specialist, I agree with Joshua, is so important because we are aware of what’s going on, even behind the scenes.
And at least we know. And if we don’t have a particular trial available in our institution, you know, we know who does it, and we can refer patients to each other and continue the treatment.
What does it mean to be offered clinical trial participation?
The Patient Story: Perfect. And we’re going to end with an audience question. And you can just both respond and then that will be it for the day. And we’ll hopefully get some follow up questions later. But the question is from Richard D. His wife has been through a few lines of treatment. Another oncologist has brought up a new clinical trial.
I don’t have the details, but the question is, do doctors only bring up a clinical trial when the situation is hopeless? My wife is feeling upset and nervous about what this means for her/us.
I think what this brings us back to you is that there’s all this data and it’s great having these conversations. But when people hear certain phrases, sometimes it can be really overwhelming and very daunting, like what does this mean for me? So with that, maybe we’ll start with you, Dr. Gasparetto. What would you say to someone?
Dr. Cristina Gasparetto: I would say just keep it in perspective. I mean, so if they’re offering a clinical trial, it’s because the patient is still eligible for clinical trials. So that is good because we have stringent eligibility criteria, because the patient has to be in good shape, having good counts, good renal function so we can test a drug.
But I think about all these drugs that were just presented. They were all in clinical trials. And we have many success stories. We have patients in remission. A patient responded phenomenally.
I am pro clinical trial because it’s the only way that we can learn how to treat myeloma and other cancers. And so no it’s not a bad thing. It means that the patient is eligible for something that may be even more powerful.
We don’t know if we don’t test. We test a very powerful combination. So even if you are in a clinical trial comparing one old versus one new combination, they are very effective. We don’t design a clinical trial to have one of the combinations completely failing.
So I think that, you know, keep things in perspective. If the patient is eligible for a clinical trial, it may be a good thing. I mean, you know, a good marrow, sort of a good renal function and maybe new drugs, who knows? A new combination that can be really important for a cure for the patient and for other patients in the future.
Dr. Joshua Richter: I completely agree with Cristina. I am very pro clinical trial. And in fact, the earlier the better exactly as Cristina talked about. If you go through every treatment available, you may then no longer be eligible for any clinical trial.
The benefit of doing a clinical trial early on is that if it works, you get access to a standard of care. Five years from now, you get access to it now.
And the other benefit is that if it does not work, you have all of the currently approved drugs ready to go at a moment’s notice that you can salvage with if you need. And every moment you are on that clinical trial, the bucket you can reach into for new therapies grows and grows.
If she goes on that clinical trial today and is still in remission until December, we will have cilta-cel approved before then. If she stays in remission next year, we’re going to have CELMoDs approved and bispecifics improved. And that means that standard of care option bucket just grows larger and larger.
Cristina hit the nail on the head. Pro clinical trial involvement. We are all about it. It deepens our knowledge about how to treat an individual, how to treat everyone as a whole. And the simple fact is, the myeloma world is one big community.
If there is a trial, I do not have it, I know who it is and will refer them out. We have patients that move. So I had a patient that recently moved to Florida. I called up our colleagues at Sylvester Cancer Center in Miami. They’re going to see them. So taking advantage of the myeloma community that we all have for clinical trials is absolutely the right way to go.
The Patient Story: That is so well said. Thank you so much. And I want to thank you both for spending so much time with us today. Not only doing the work that you do in clinic and in research, but for things like this where you are reaching people who are not your own patients. And so very, very grateful for that. Doctor Cristina Gasparetto, Dr. Joshua Richter, thank you so much for joining us today.
Dr. Cristina Gasparetto: Thank you. Thank you for having us. And we love to treat patients that, you know, it’s a love hate affair, like I mentioned. So of course, this kind of discussion and conversation are always the best even for us.
Dr. Joshua Richter: Absolutely, it’s always a pleasure to work with community advocacy groups and to get to hear from the great Cristina Gasparetto.
Dr. Cristina Gasparetto: You, too. When, of course, when she told me that I was working with you, I was very happy.
Dr. Joshua Richter: So same here.
The Patient Story: Well, it’s been a great conversation. And for everyone who wants to watch this discussion again, just go to ThePatientStory.com where we give human answers to your cancer questions.
What are the emerging, most promising therapy options potentially available in 2022/2023?
Cindy Chmielewski (@MyelomaTeacher) talks with Dr. Saad Usmani, Chief of Myeloma Service at Memorial Sloan Kettering, about CAR T-cell therapy, bispecific antibodies, novel therapies and combination therapies, focusing on the relapsed/refractory patient population along with newly-diagnosed myeloma patients.
Thank you to Janssenfor its support of our educational program. The Patient Story has full editorial control of our content.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Cindy Chmielewski, @MyelomaTeacher: I’ve been living with myeloma since 2008 and more recently, became a research advocate in the multiple myeloma community.
Saad Z. Usmani, MD, MBA, FACP: I’m the chief of the Myeloma Service at Memorial Sloan Kettering Cancer Center in New York. I’ve been involved with myeloma research both on the clinical and translational side for well over a decade. I’m looking forward to so many exciting things that we have in the field and how things are moving forward for our myeloma patients.
CAR T-cell therapy
What is it & who are they for?
CC: There have been some meetings going on. There’s ASCO and EHA and the IMW is coming up. There are a lot of things happening in multiple myeloma.
Let’s start talking about the CAR Ts because CAR Ts have been around for a while. There are two approved CAR Ts. Can you talk a little about them and who they’re for?
Dr. Usmani: CAR T-cell therapies have been around for a while. They started early on in another disease — ALL in children, actually — but the ones that have been developed in myeloma are targeting a specific surface protein on the myeloma cells called BCMA.
There are two that are FDA-approved for patients who have had four or more prior lines of treatment — including a proteasome inhibitor immunomodulatory drug as well as anti-CD 38 monoclonal antibodies — people who have had a lot of prior therapy.
Those two products are called ide-cel and cilta-cel and they both target BCMA, but they are unique products. The general side effects are similar but tend to happen at different time points. Both products actually show good clinical activity.
The patient’s T-cells are taught to recognize the cancer cell and they’re grown outside the patient’s body in the lab.
Dr. Usmani
Where can you get CAR T-cell therapy?
CC: These CAR T-cells have to be given in a center of excellence, is that correct? I can’t just go to my doctor and say I want some CAR T treatment.
Dr. Usmani: These are cell therapy products so they need to be given at a center that does transplant and cell therapies. Many of our myeloma patients go for a transplant evaluation and end up getting a stem cell transplant during the early course of their treatment. The process is similar. Your doctor is going to refer you to a transplant center. They will do the evaluation and then get you those commercial products.
Typically, when you’re getting a stem cell transplant, you go through a process of getting growth factor shots and then getting the stem cells collected from your bloodstream through central venous access. In CAR T-cell therapy, we are selecting T-cells from the patient’s peripheral blood, but you don’t need growth factor shots so you can get those T-cells collected just off of the peripheral bloodstream.
Side effects of CAR T-cell therapy
CC: There are some unique side effects to CAR T-cell therapy that maybe myeloma patients haven’t experienced before. Can we talk a little bit about them?
Dr. Usmani: When you get these T-cells from the patients, you send them off to the specific company that’s manufacturing them. What happens is the patient’s T-cells are taught to recognize the cancer cell and they’re grown outside the patient’s body in the lab essentially; that production and expansion takes 3 to 4 weeks. When that product is ready, it’s shipped back to the center and patients get a certain lymphodepleting chemotherapy for three days before they get that product infused through the veins.
Those T-cells are active. They know how to recognize the cancer cells through the surface marker BCMA and they’re going to expand. There’s an expansion that happens in the patient’s bloodstream. These cells are growing and trying to go after the myeloma cells. It’s like introducing an inflammatory response in the patient.
The side effects are like the patient’s body is going through an inflammatory process. The two common side effects are what’s called cytokine release syndrome. These immune cells are releasing certain chemicals that enable them to go after the target. Due to that, patients can feel fevers [and] hypertension, as if they were infected with something. That tends to happen with ide-cel within the first two days. With cilta-cel, it tends to happen with a delay of 5 to 6 days typically.
We manage those side effects by giving antipyretics, fluids, sometimes steroids, or an antibody called Tocilizumab to patients. But for the most part, these side effects are grade one or two. They’re low-grade and are managed with those kinds of medications.
The other side effect that can happen because these T-cells are active is what we call neurologic side effects. Sometimes patients can feel loopy or have neuropathy. Very rarely, patients can have more serious neurologic side effects, such as seizures. Those tend to happen in a very low proportion of patients. Neurotoxicity tends to happen more commonly with ALL CAR T-cells rather than the myeloma CAR T-cells.
The side effects are like the patient’s body is going through an inflammatory process. But for the most part, these side effects are grade one or two. They’re low-grade and are managed with medications.
Dr. Usmani
Who might have a greater tendency for severe neurotoxicity?
CC: Are there any biomarkers that predict who might have a greater tendency for severe neurotoxicity? Or is that just up in the air?
Dr. Usmani: What we’ve observed is patients who have a higher burden of disease at the time of getting CAR T-cell therapy can be at a higher chance of developing these side effects. One can develop CRS and neurotoxicity independent of each other so it’s not that they come in as a package. In fact, CRS is more common. Neurotoxicity tends to happen in less than 10% of the patients. CRS tends to happen in almost all patients to some degree.
There aren’t typically specific markers that we can follow that are specific for CRS or neurotoxicity. There are certain markers that can give you a hint that there is a heightened sense of inflammation, like serum ferritin levels or CRP elevations in patients. We tend to follow some of those labs, but they’re not predictive. They’re just telling you that something is going on, just be careful.
Patients who have a higher burden of disease at the time of getting CAR T-cell therapy can be at a higher chance of developing these side effects.
Dr. Usmani
Are there any trials for more newly diagnosed patients or first relapse?
CC: The currently approved CAR Ts are for more heavily pre-treated patients who’ve exhausted many of the options. Are there any trials that have been reported for more newly diagnosed or first relapse? Are they coming closer?
Dr. Usmani: There are two randomized phase 3 studies that have looked at comparing each of these CAR Ts — both ide-cel as well as cilta-cel — in one to three prior lines of treatment comparing them to the standard of care triplet regimens. In fact, BMS (Bristol Myers Squibb) just announced that their phase 3 trial in one to three prior lines of treatment is coming out positive. Now, this was a company announcement so we haven’t seen the data but that is good news for our patients. I’m keen to hear more about this.
The key is the process [of] CAR T-cell therapy. It takes a while for that production time and so there are certain bottlenecks to the process.
Dr. Usmani
We do have smaller cohort studies that have reported out experience in one to three prior lines or early relapse patients with very high response rates of 80, 90% with Cilta-cel. In fact, well over 90% with Cilta-cel. We just need more updated data, though those are looking promising.
The key is the process [of] CAR T-cell therapy. It takes a while for that production time and so there are certain bottlenecks to the process. The big question is how applicable this technology will be to all patients that we treat.
Allogeneic CAR T-cell therapy
CC: What about allogeneic CAR Ts? Are they going anywhere? What are they? Can you explain? They seemed a little exciting.
Dr. Usmani: The idea of allo CAR Ts is you can take T-cells from a donor but knock out certain surface markers to make those T-cells more benign so that the recipient’s immune system is not recognizing them as the enemy and they’re not recognizing the recipient’s immune system as the enemy.
The advantage of having allo T-cells utilized to manufacture CARs is you can have one donor and make a product that can be given to a hundred different patients instead of taking the patient’s own T-cells. And those hundreds of products can be given in a very short duration of time. Essentially, if I see a patient today and I have an allo CAR T available, that patient can technically get that product three or four days from now. They can start getting lymphodepleting chemotherapy and they can get that product very quickly. Whereas if I were to see a patient today and try to collect their T-cells, even with everything aligning, it might take 5 to 6 weeks for them from today to get that product. That’s the major advantage of allo CAR T products, but they’re way behind in terms of clinical development and seeing the light of day.
The advantage of having allo T-cells utilized to manufacture CARs is you can have one donor and make a product that can be given to a hundred different patients… but they’re way behind in terms of clinical development and seeing the light of day.
Dr. Usmani
Efficacy of allogeneic CAR T-cell therapy
CC: Do we have any efficacy data? Are they working?
Dr. Usmani: They are working. We have seen some efficacy data. There’s an Allogene CAR product. In fact, Sham Mailankody from my program presented those data [in 2021] showing about 60% of the patients responding to that allo CAR product.
Now, the follow-up is short. We know that these patients, too, get CRS and neurologic side effects but the follow-up was only about three or four months so we need [a] longer follow-up to see. Is this activity long-lasting or just a short-duration activity? What kind of long-term side effects do we get from using this strategy?
Are there any CAR T-cell therapies that are looking at different targets on the myeloma cell?
CC: Right now, the approved ones go after BCMA. Are there any CAR T-cell therapies that are looking at different targets on the myeloma cell?
Dr. Usmani: Yes. Another target is called GPRC5D. That was a homegrown CAR T at MSK (Memorial Sloan Kettering) that Dr. Mailankody presented, showing good activity in patients who have had prior BCMA CAR Ts and BCMA therapies as well. The response rates, again, [are] in [the] high 60, 70% range looking at the various cell doses that the patients received. That CAR T is now being developed by BMS. There are other programs that are utilizing that CAR T.
We also have some very interesting dual CAR T data — BCMA and CD19 CAR T — that was presented by colleagues from China at the ASCO and EHA meeting showing high response rates.
The cool thing about that platform was the short production time. That product was manufactured within 48 hours. What we’re seeing is the new platforms are actually reducing the production time and that will be a good challenger to the allo CAR T strategy. If we are able to shorten that time, then there might not be as big an advantage for an allo CAR compared to [a] patient’s own T-cells.
Bispecific antibodies
Teclistamab
CC: Moving on to other types of T-cell redirection, there’s the bispecific antibody. There’s one that I hear it’s almost ready to be approved. Can we talk a little about Teclistamab?
Dr. Usmani: It got a favorable response from EMA, but it’s not yet approved. We’re waiting to hear from the FDA. I’ve been involved with Teclistamab from the very beginning. In fact, the first patient who was ever treated in the world was my patient. I’ve been with that program from cohort one, patient one.
CAR T-cell therapies are very effective, but bispecifics are therapies that will change how we manage patients in the community at large. They actually might challenge CAR T-cell therapies because they’re an off-the-shelf option, giving high response rates of, again, 60, 70% in relapse/refractory myelomas — [a] very similar patient population to CAR T-cell therapies — and it’s given subcutaneously.
Now, cytokine release syndrome is something that we see with the bispecific antibodies as well and that’s something that we have to watch out for.
The concept of this technology is very interesting. You’re going to hear TCE or T-cell engager as terminology. You’re going to hear bispecific antibody as terminology. The concept is the same. One part of that molecule recognizes the surface marker on myeloma cells. It could be anything. It could be BCMA, it could be GPRC5D, or something else. The other part of that molecule recognizes the T-cells. There is surface marker CD3 that recognizes.
The difference between [a] T-cell engager and bispecific antibody is the structure of that molecule. If it’s a whole antibody, then you call it a bispecific antibody. If it’s only a fragment of an antibody, you call it a T-cell engager.
Different companies and platforms have different molecule structures that are proprietary so the names are going to be different. Long explanation but a lot of excitement about that technology.
Teclistamab is the frontrunner. We might hear some good news about it later [in 2022] in the US and Europe. We’re all really excited about that platform.
Possibility of getting bispecific antibodies at a community hospital
CC: For patients, it’s exciting because it doesn’t involve having to probably relocate like the CAR T-cells. You have to go to a CAR T center and spend time away maybe from your home and family. Would the bispecifics be something that could be given maybe at [a] community hospital? Or is it something that you need to go away for?
Dr. Usmani: I think there will be a learning curve for our community physicians because giving bispecifics does require some education and comfort in managing cytokine release syndrome. It’s quite possible that they might ask the academic centers to give the first cycle of treatment.
Patients do need to be monitored during that first cycle as they’re going through the various step of dosing to full dose for that cytokine release syndrome. And because our community colleagues don’t see myeloma as frequently as some of the other solid tumors, they might ask us to give that first cycle.
Once patients are beyond that first cycle, it’s like getting any subcutaneous treatment so the short answer is yes, it will be possible for patients to receive this treatment out in the community. But I don’t see this happening during the first year of the FDA approval. It will be a steep learning curve for our community docs.
Side effects of bispecific antibodies
CC: Usually after the first cycle or two, the CRS and the neurotoxicity seem to go away?
Dr. Usmani: The likelihood of having those side effects is during the first three or four doses, so that first month. It’s really about engaging the T-cells.
Once the T-cells are active, they know exactly what to do, and they’re fine with the job assigned to them, it’s that early part where you’re trying to say go and kill the myeloma cells. They get revved up and release those cytokines. Once that process is done, the risk goes down to negligible.
Yes, it will be possible for patients to receive this treatment out in the community. But I don’t see this happening during the first year of the FDA approval.
Dr. Usmani
Frequency of subcutaneous injection
CC: For Teclistamab, is the infusion weekly [or] monthly? How often would I need to get this subcu injection?
Dr. Usmani: The subcu injection is on a weekly basis. [For] the first ten days, the step of dosing is given every fourth day for the first two doses before you get the full dose. That’s how it was done in the studies. I would be surprised if the FDA-approved label says something different. But again, we will know what the FDA says later [in 2022].
Very interesting and very encouraging data for our patients who have had triple-class refractory disease.
Dr. Usmani
Efficacy in comparison to CAR T-cell therapy
CC: What about the efficacy? How does it compare to CAR Ts?
Dr. Usmani: Response rates are around 63, 64%, which is very high. The median PFS (progression-free survival) is about a year, almost 12 months. The approvals for Carfilzomib, Pomalidomide, and even Daratumumab, the response rates were 25 to 30% for each of those products and the PFS for those products was about four months.
That gives you the context that you have this bispecific antibody, these are patients who have progressed on treatments like Carfilzomib, Pomalidomide, and Daratumumab, and you’re still seeing these high response rates and median PFS. In fact, the median PFS is similar to what was reported for ide-cel. Ide-cel’s PFS was less than a year and the response rates were over 70%, but median PFS was in a similar range. Very interesting and very encouraging data for our patients who have had triple-class refractory disease.
Talquetamab
CC: There are other bispecifics besides Teclistamab. There’s Talquetamab. Is that going after the same target or a different target?
Dr. Usmani: It’s in the same patient population, but the target is GPRC5D. GPRC5D is a unique target to plasma cells. Talquetamab appears to be active. Response rates are up in the 60% as well.
We don’t have the PFS data because the development of that particular bispecific is a little behind Teclistamab, but we’re seeing activity of Talquetamab even in patients who have had BCMA-directed treatments, including CAR Ts and bispecific. It’s looking very promising.
Bispecifics with other targets
CC: There are many others, not just these two. There are a lot of bispecifics out there. Are they all doing quite as well?
Dr. Usmani: Yes. For BCMA-directed bispecifics, there are several options. Elranatamab is very active. ABBV-838 is very active. There’s a Regeneron bispecific. There’s a BMS Celgene T-cell engager that’s targeting BCMA as well. All of them are showing very similar activity. I think there are some differences in the safety profile percentage of patients getting cytokine release syndrome when they’re getting it. Some of those issues will be the distinguishing factors.
There are some that are given less frequently. I think the AbbVie bispecific, which was actually developed by a smaller company called Teneobio, is given every three weeks. There will be some nuances or differences between these BCMA-directed bispecific.
It’s good to know that there are other targets where we can see good clinical activity in patients.
Dr. Usmani
For GPRC5D, we only have one, but there are others that are in early development.
We have another target called FcRH5. There’s an antibody called Cevostamab, which appears to be active, [with] response rates of about 50% in patients who have relapsed/refractory myeloma beyond four lines of treatment.
It’s good to know that there are other targets where we see beyond BCMA and even GPRC5D where we can see good clinical activity in patients.
CC: As a patient, that makes me feel good. Even though some people say you might be able to use another BCMA-directed therapy, for me, I would like to have another target in my back pocket.
Combination therapy
TRIMM-2 Trial
CC: TRIMM trials are not only using the bispecifics, but they’re combining them with things. Can you talk a little bit about those?
Dr. Usmani: Once the efficacy and recommended phase 2 dose of both Teclistamab and Talquetamab were ascertained, the next step was can we combine them with other myeloma treatments and see if we get better clinical activity.
The TRIMM-2 study is looking at the subcutaneous Daratumumab administered with Talquetamab as well as with Teclistamab. There is a combination study of adding Pomalidomide to those combinations as well. We haven’t heard about the Pom combos, but we know the subcu data combinations. They have been reported out by my colleagues — Drs. Krishnan, Ajai Chari, van de Donk — each of them presented these data at different congresses over the past six or eight months, and I’ve participated in those studies as well. The overall response rate with each of those combinations is about 80 odd percent, which is remarkable because most of these patients were Daratumumab refractory in a previous line of treatment.
Why are we seeing a higher response rate compared to what we would expect with Teclistamab and Talquetamab? Daratumumab also is inhibitory to regulatory immune suppressive cells by virtue of blocking CD38 so it’s really acting as an immune modulator and enhancing the effects of these. I feel that’s probably the reason why we’re seeing this activity.
Those are very high response rates. With both Teclistamab and Talquetamab, the responses are in the 60%, but you’re seeing a higher percentage. Very encouraging. It means that we can potentially use this combination in earlier lines of treatment, even for newly diagnosed patients. It would be really cool to have a non-chemotherapy approach just using antibodies.
CC: Right now, is it still in that triple-class refractory population?
Dr. Usmani: Yes, but there are clinical trials in earlier relapse and even in the newly diagnosed setting being planned. They’re not in the public domain yet, but they’re planned and we are probably going to have these bispecifics examined for newly diagnosed patients.
CC: Yes, that might be something to consider for the high-risk group, which is really still quite an unmet need here in myeloma.
Earlier lines of treatment
CC: There was a trial that was presented that talked about RVd plus or minus Elotuzumab. Was that correct?
Dr. Usmani: Yes, this was an update from the SWOG-1211 trial.
To give you a context about high-risk patients in general, myeloma is a very heterogeneous disease. Biologically, we have eight or nine different subgroups depending on how you classify it on a molecular basis. From a clinical behavior standpoint, the way that we classify myeloma is patients who are at a higher risk of relapsing early after getting front-line treatment compared to those who have standard risk; in those patients, we don’t expect the myeloma to relapse early.
High risk is defined by certain clinical features, such as circulating plasma cells or extramedullary myeloma, or certain stereotypic abnormalities, like translocation for 14, 14;16, 14;20 or deletion 17p as well as amplification of 1q21. The SWOG-1211 was the first clinical trial that I had the privilege of designing and running when I was a junior faculty within the US cooperative group setting focused on high-risk myeloma. If you look at all the clinical trials, all the major studies that have been reported, they take all comers — any myeloma patient can participate. What we recognized as clinicians is high-risk patients don’t do well.
The idea of the SWOG-1211 was [to] design a trial just for high-risk patients and see if we can make a difference for those patients; that was the first effort. The idea was [to give] RVd for induction and then [continue giving] RVd as maintenance — the dual PI/IMiD maintenance strategy. Then in the experimental arm, Elotuzumab was added to that same RVd backbone, both in induction as well as maintenance. It was a randomized phase 2 study and the study did not show a benefit of Elotuzumab adding anything to RVd. However, the trial showed better PFS than our historic control. The median PFS for just the RVd was about 34 months. Our assumption was that the median PFS for those patients would be about 26 months and that assumption was based on patients getting tandem transplant so this was from the total therapy time. The RVd arm actually performed better than the older therapy.
SWOG-1211 set up a benchmark for other high-risk trials to follow. At the ASCO meeting, we heard about a UK study looking at KRd-Dara for high-risk patients. There’s an IFM trial and there’s also a KRd-Isatuximab study from the German myeloma group. These are smaller single-arm studies that are trying to do the same thing — do enrichment design trials for high-risk patients.
I wanted to give the whole context of why that study is important. The results by themselves for SWOG-1211, it’s considered a negative study because Elo (Elotuzumab) didn’t add anything. But then it set up a very important benchmark for other studies to improve upon.
CC: That’s good to know. I really didn’t know that background and I’m glad to hear that more and more studies are just targeting that high-risk myeloma population. It’s so important to figure out how can we control that disease early on in that group of people.
DETERMINATION trial
CC: How about the DETERMINATION trial? I hear so much about it. I still haven’t quite figured out what the results mean. Can you try to clarify that?
Dr. Usmani: It’s very interesting. It’s a positive study. The primary endpoint for this particular trial was showing PFS benefit between doing an early transplant or delaying it at the time of the patient’s first relapse. There is a 21-month benefit in favor of doing [the] transplant early for that young myeloma patient.
The median age [in] this study for patients enrolled was 55 years so this is a young patient population. This is a sister trial to [the] IFM 2009 study that had already been reported out about five years ago.
The depth of response in terms of MRD (minimal residual disease) negativity and sustained MRD negativity appears to be higher in the transplant arm as well. The study has a median follow-up of about 70 months and, at that point, median OS (overall survival) has not been reached in either of the arms.
Some investigators, the way that they’re framing that is incorrect. They’re saying there’s no difference; that’s not how you read the statistics. You don’t say there’s no OS different at a time point when the median OS has not been reached in both arms because there’s not enough follow-up. If that was the case, we would be saying the same thing about the MAIA trial, the ALCYONE trial, the CASSIOPEIA trial… All of those trials had no OS benefit when they were reported out because the median OS had not been reached in those arms.
The new questions should be what about CAR Ts [and] what about bispecifics? We’re designing trials with that question in mind.
Dr. Usmani
The other important thing that we see is there is no difference between the two arms between second primary malignancies as well. The second primary malignancies that people get in one arm over the other are different, but the overall percentage is about 10-odd percent that was reported out. Again, that’s my take on the study. It really doesn’t add any new information. We already knew the IFM 2009 study data.
What it does augment is the use of Len (Lenalidomide) maintenance because the IFM 2009 study stopped maintenance after a year but the DETERMINATION trial continued maintenance for everyone until relapse, progression, or intolerance. The study really doesn’t add a lot more to what we already practice.
I hope that this is the last trial that we’re thinking about early versus late transplant because that is an old question. Now, the new questions should be what about CAR Ts [and] what about bispecifics? We’re designing trials with that question in mind. I think there’s a lot of hype around DETERMINATION but really it’s hype. I don’t think it adds much to what we are doing right now.
CC: Early transplant means transplant is part of your induction therapy. Late transplant means at first relapse. Is that what the trial was talking about?
Dr. Usmani: Yeah. Both arms did pretty good in terms of median PFS. Median PFS if you got [a] transplant was around 68 months. Median PFS if you just got RVd and delay transplant was about 47 months. There was a 21-month difference in favor of early transplants.
The follow-up is short on the study so you’re not going to have a lot of people even in the RVd arm relapsing to get their transplant.
Myeloma patients are doing so well today. The median OS is at least 10-plus years. You can just say after a four or five-year follow-up that we’re seeing OS differences. I’m hoping that by the time we get the DETERMINATION OS data, it’s going to be ten years from now. Because our patients are going to be doing so well that we’re going to be looking at this historic data and saying it was a good question at that time, but probably not relevant to us by the time that reads out.
CC: Exactly. In ten years, who knows what our induction therapy is going to look like? Much better, I’m thinking.
ENDURANCE Trial
CC: What about the ENDURANCE trial? Can you talk a little bit about what that was?
Dr. Usmani: The ENDURANCE trial ran side by side [with] the SWOG-1211 study and it was asking an induction question for standard-risk patients. Is KRd better or RVd better for induction?
ENDURANCE was a randomized phase 3 study. Half of the patients got Carfilzomib with Len-Dex (Lenalidomide-Dexamethasone) as induction. The other half got VRd or Bortezomib with Len-Dex as induction for eight cycles. Then everyone got Len as maintenance.
This study enrolled standard-risk patients because high-risk patients were going on the SWOG-1211. Translocation for 14 patients were enrolled [in] this study as well.
Trial readout [showed] no differences between PFS on either arm of the study. Essentially for standard-risk patients, it established RVd as the right treatment choice just like the SWOG-777 trial had shared with us.
The other interesting thing about the median PFS of RVd on the ENDURANCE trial is the median PFS was around 34 months. Again, the SWOG-1211 with the PI/IMiD maintenance showed the same thing. My colleague, Shaji Kumar, presents this slide saying what makes the difference in high-risk patients is the dual maintenance if you look at the ENDURANCE trial and SWOG-1211 together because both of these were enrolling at the same time.
CC: So dual maintenance is what’s happening now in high risk?
Dr. Usmani: For high-risk patients.
New & exciting studies
CC: Anything else that we should be talking about? Anything else new and exciting?
Dr. Usmani: There are a lot of new trials that are in the works. There’s the CARTITUDE-5 study, which is looking at patients getting RVd as part of induction. These are patients who either are transplant ineligible or they’re deferring their stem cell transplant to first relapse. Everyone gets RVd as part of induction treatment but then half of the patients get randomized to getting CAR T-cell therapy; [the] other half move on to their maintenance treatment. The people who get the CAR T-cell therapy don’t get any maintenance. That’s a really cool study. We’re hoping that it can provide a good answer for those patients.
The second trial is actually looking at transplant-eligible patients. Everyone gets the quadruple regimen of Daratumumab with RVd and then patients get randomized to either a transplant or CAR T-cell therapy. That’s a very exciting study. We’re hoping we can get a positive answer for our patients.
High-dose Melphalan and transplants have been a part of myeloma treatment for a long time but if we can replace them with another cellular therapy approach, which is more specific to the myeloma cells, I would really welcome that.
CC: I would welcome that, too.
CAR T-cell therapy for transplant-ineligible patients
CC: When you talk about transplant-ineligible patients — there’s that group of patients that really are not eligible for transplant for whatever reason — would those group of patients not be eligible for CAR T-cell therapy or would they be possibly eligible? I know you have to look at them individually, but as a group, is it just like you’re not eligible for this or you’re not eligible for that?
Dr. Usmani: We are a little bit more lenient in CAR T-cell therapy eligibility compared with stem cell transplantation because patients are not getting the same level of myelosuppression with high-dose chemotherapy like a stem cell transplant. There might be patients who are in their mid-70s or even late 70s who are able to get CAR T-cell therapy that we would not necessarily pick for transplantation. We’re thinking about CAR T-cell therapy in a more lenient way because of the safety profile.
CC: That’s good to hear. It’s just amazing all these new therapies. When I was diagnosed back in 2008, most of the things we talked about weren’t FDA-approved except Revlimid and Velcade.
Words of wisdom
CC: When you see a newly diagnosed patient or even an older patient who may be relapsed/refractory, how do you provide them with hope with all these new treatments? What are your words of wisdom to these patients?
Dr. Usmani: I give them the context. I tell them about the time when I was starting in the field in the early 2000s and how the outcomes were for myeloma patients. I walk them through how things have improved, what our goals and expectations are today for our patients, and the treatment options we have. I provide them with measured hope.
We do recognize that myeloma is still not a disease that we can cure, but we can control it for a long duration of time. Even for patients who have high-risk myeloma, we’re thinking about things in a different way and trying to be proactive in giving different strategies for those patients rather than just treating them in a vanilla, one-size-fits-all way. I provide that context to patients and then it’s really about individualizing treatments based on patient preference as well. This is really a partnership. Our job is to provide patients with as much information as they can gather to make good, informed decisions.
I give them the context. I provide them with measured hope. We do recognize that myeloma is still not a disease that we can cure, but we can control it for a long duration of time.
Dr. Usmani
What will cure myeloma?
CC: Good. Now, you did mention the word cure. Do you think we’ll be curing any myeloma patients any time in the future? What do you think that would look like?
Dr. Usmani: I would say, yes. This is something that I’ve shared on other forums as well. If we’re able to get patients to MRD negativity and maintain them in that negativity for a certain period of time and then stop therapy at that time, then we can functionally cure [a] majority of patients.
Myeloma is a disease that tends to occur later in life. There are other competing health issues that patients have so a true cure cannot be determined in that situation compared to someone who was 20, got diagnosed with cancer, and dies of a heart attack at 90. You can say this person was cured [of] cancer. You can’t say that about a myeloma patient who’s getting diagnosed in their sixth or seventh decade of life.
If you can kick myeloma down to undetectable levels, start treatment, and patients continue to thrive for years and cancer doesn’t come back, in my mind, that’s functional cure.
My answer is yes, we’re going to get our patients there. The key would be finding the right recipe to get patients to that sustained MRD negativity before stopping.
CC: Right, and now we have so many ingredients for that recipe that I’m sure we’re going to find it soon.
It’s really about individualizing treatments based on patient preference as well. This is really a partnership. Our job is to provide patients with as much information as they can gather to make good, informed decisions.
Dr. Estelamari Rodriguez and Dr. Ruben Mesa are respected oncologists in their fields, but in this video, they give a much deeper and personal look into their WHY for treating cancer.
They also detail the importance of having representation and diversity both in doctors and in patients, especially when it comes to clinical trials and research to ensure access to quality care for all patients.
Thank you, Dr. Rodriguez and Dr. Mesa, for sharing your stories and the work you two do!
The interview has been edited for clarity.
Dr. Estelamari Rodriguez, MD, MPH
I think what drew me to medicine is that I have in my family, like many other, people have experienced cancer.
My grandmother had endometrial cancer, my mother had breast cancer, and their experience in Puerto Rico — not really able to connect with doctors where doctors tell you what to do and this is what’s going to happen. They got these treatments but they didn’t understand them. I wanted to change that.
I’m the first college grad in my family and I don’t have any doctors in my family. When I applied to medical school, I feel like it was like a miracle that it happened. I went to a very good program.
I went to Columbia and I went to Penn with scholarships. I found great mentors who were non-Hispanics but they saw something that they wanted to promote.
High school graduation with her grandfatherCollege at Columbia UniversityWith other minority students at Univ. of BuffaloWith training fellows
My grandmother had endometrial cancer, my mother had breast cancer, and their experience in Puerto Rico — they got these treatments but they didn’t understand them. I wanted to change that.
I think that that’s one of the most rewarding parts of my day job — that I have patients that immediately when they see me, they can connect because we can speak the language. But not only is that a language issue, it’s really understanding the culture, the cultural nuances like understanding that their family is a big part of their health care decision group so you have to involve them and be respectful of their family.
Being able to connect with them on that level makes them feel that you took one of these barriers out. They don’t have to be overwhelmed about having that doctor connect with them.
I have patients that immediately when they see me, they can connect because we can speak the language… it’s really understanding the culture, the cultural nuances.
I think this space and this time where Latinos are coming together to support each other and recognize each other is letting other younger Latinos feel like this is a field where they can make a career, they can be happy, and they can make a difference.
If you have a dream, you should pursue it. Oncology can be a very intense field but it’s a very rewarding field. And we need you.
I think I’m only the first or second Latino NCI Cancer Center Director in the United States. It’s a neat connection with that community.
I had the chance this year to testify before Congress regarding changes in FDA regulations and legislation regarding diversity in clinical trials.
Diversity in clinical trials is both about social justice and good science. We want to know whether it is safe and effective. Diversity is powerful.
I was able to share when the first lady came to visit our cancer center that diversity in clinical trials in our care, it’s both about social justice — because we want everyone in our society to be able to benefit from the advances that we have — but secondly, it’s also good science.
As we evaluated treatment, whatever that is — that could be yoga, that could be a drug, that could be stem cell transplant — we want to know whether it is safe and effective. We wouldn’t know.
Is it effective in Asia? In Cuba? In Africa? Might we have worse side effects? Might we have no side effects? Diversity is powerful.
The problem with cancer is that it’s a thief. It steals from us.
I myself lost my father to lung cancer. He died at 62 and he passed away now 16 years ago. I think about it really in terms of all those things that he missed because of the disease that he had.
He won’t see my sister getting married this upcoming February. He didn’t see my brother get married two years ago. He won’t meet their children. He’s not seen my children grow up into adults. It is a loss that can’t be replaced.
The power not only to be able to care but to really make a difference.
The problem with cancer is that it’s a thief. It steals from us length of life and quality of life either from us, the patients we love, family members…
The power not only to be able to care but to really make a difference. What does that mean? People live longer, they live better. Deeply rewarding and deeply grateful to have that opportunity.
In segment 2 of our conversation with Srdan Vertsovsek, MD, PhD of MD Anderson, he shares the latest on research for polycythemia vera or PV treatments.
The Patient Story: For PV, polycythemia vera, you pointed out two drugs in particular. So I’d like to talk about those. One is rusfertide, which helps to possibly eliminate phlebotomy, which would be huge news for a lot of patients.
It’s a Phase 2 study, can you talk more about what this means? The shot that would help replace the phlebotomies?
Dr. Srdan Verstovsek: Polycythemia vera is different than myelofibrosis. We caught it earlier in the life of the myeloproliferative neoplasms. There are abnormalities that lead to uncontrolled cell growth. Polycythemia patients come with a very high red blood cell count, and many have also high white cells and high platelets. That’s why it’s called polycythemia. All the cells grow.
Some patients may have enlarged spleen or have some symptoms. That’s fine, too, but not as bad as myelofibrosis. So the life expectancy is much, much longer. We don’t really worry about much of the expectancy, but we worry about what is the main cause of death, and that is the blood clot.
There is a plan for a Phase 3 randomized study next year in people with PV that have too many phlebotomies.
Thrombosis (blood clot)
Thrombosis is a blood clot. We want to manage the patients for their thrombotic risk. What is the risk of having a blood clot? So we divide the patients into those that are the low risk for a blood clot, and in those patients, we just do phlebotomy.
Now, what is phlebotomy? It’s a bloodletting. You put the needle in the vein, and you let the patients bleed for some time, not for too long, though. You collect a couple of bags and you decrease with that red blood cell count because the red blood cell count is the number one problem that leads to a blood clot.
So it’s standard practice for many patients just to do phlebotomy occasionally to decrease the red blood cell number in the blood. And then you give them baby aspirin to decrease the stickiness. There is a plan for a Phase 3 randomized study next year in people with PV that have too many phlebotomies.
Now, some patients may have a problem with too many phlebotomies, With the phlebotomy, you eliminate iron from the body. The red color is in part of the item may have symptoms from the procedure. Symptoms from iron deficiency.
How rusfertide works
Rusfertide, in this case, may come as a choice because it cuts the iron supply to the bone marrow. That’s what it does. Very simple. It stores it in the liver or spleen and other parts of the organ of the body of the patients—no iron for the making of red blood cells.
Immediately, boom. And it’s safe. So that is being developed as a therapy in patients that are on phlebotomy regimens and have too many phlebotomies.
There are many other patients with PV that are already taking some medications. Hydroxyurea is the chemotherapy pill by mouth or an interferon is an injection under the skin. Or ruxolitinib that we talked about is also being used in PV. But maybe it doesn’t work.
Still, too many phlebotomies. Well, rusfertide works in this case, too, no matter whether you are on any pills or not, just phlebotomy, it works in the great majority of the patients. It’s quite amazing, actually, the new way of looking at the biology of the disease to cut the supply of the iron to the bone marrow biologically, physiologically, if you like in a body of the patients.
And there is a plan for a Phase 3 randomized study next year in people with PV that have too many phlebotomies. You can say, three or four are too many. We want patients not to have a need for phlebotomy at all, just to maintain the low number of red blood cells all the time decrease that blood clotting risk as much as you can. So these patients will be randomized between the placebo and the rusfertide for possible approval. Quite an exciting approach.
How often would PV patients get rusfertide (shot)?
The Patient Story: How often would someone have to get that shot just as many times as they would be instead of the phlebotomy would just be the shot instead?
Dr. Srdan Verstovsek: Once a week, people do it on their own at home, and they would occasionally come to check the blood and see whether there is any adjustments necessary in the dose, which is not usually a problem.
Rusfertide side effects
The Patient Story: I would be remiss not to ask about any notable side effects so far in terms of the shots?
Dr. Srdan Verstovsek: In fact, just a little bit at the site of injection in some patients, but nobody really stops because it goes away. You change the site in the belly or arm or a leg and not much anything else. It’s another biological principle of the disease that has been analyzed and discovered how to best approach it, and this is a very good example.
Ropeginterferon alfa 2b (BESREMi)
The Patient Story: There are different developments happening for PV, and I want to be able to shift now to another one that you talked about. What was the latest update with BESREMi or ropeg, with polycythemia vera patients responding better than to the hydroxyurea?
Dr. Srdan Verstovsek: We said that some patients with polycythemia vera are treated only with bloodletting, phlebotomy, and baby aspirin, but that’s actually a third of the patients.
Two-thirds of the patients are just to be at high risk for blood clotting, and phlebotomy alone is not good enough. So you give them chemotherapy by mouth. That’s hydroxyurea or injection under the skin, which is an interferon, a biological product. We all have interferon in our body, it’s an immune booster.
When you give it an extra injection, it can control the bone marrow growth of the cells, even normalize it sometimes, and affect the malignant clone. The number of cells with the mutations may decrease, and in some patients, you can give a ruxolitinib JAK inhibitor to decrease the growth and inflammation. But now interferon has been around for 50 years, actually different preparations of interferons.
On November 12, 2021, the first time ever in the United States, one of these interferons has been approved. And that’s the one that you are calling Besremi. It’s a commercial name. The real name is ropeginterferon. We call it ropeg.
Ropeg (BESREMi) administration and dose schedule
It’s slow-release interferon that is given under the skin every two weeks. Many patients apparently can get it even once a month. Fewer injection means better tolerance.
Ropeg (BESREMi) side effects
Because of the injections, it causes flu-type symptoms. If you give it any other week or every four weeks, that doesn’t happen many times. The tolerance goes up. With the tolerance, you can then expect efficacy.
In three-quarters of the patients, we normalized the blood count – completely normal red blood cells, white cells and platelets, not just the red blood cells. All three. It was approved in Europe two years ago, and now it’s approved by the United States.
No answers today, but the potential exists, and it appears to be safe and appears to be effective for years.
Learning from ropeg studies in Europe
So at this meeting here earlier this month, the American Society of Hematology meeting, we learned about five years of therapy on a study that was done in Europe.
More than half the patients are still on therapy. It can be given as a first-line, which would be my preference is the biological agents. It can be given after hydroxyurea as a second line and it works the same way. It doesn’t really make any difference. That’s the potential that I’m talking about.
It can change possibly the number of cells affected by the disease over time to non-detectable. This is very something unusual to see so far with any other therapy. We call this the molecular response. You can measure the number of cells in the blood affected by the disease.
We don’t really know what to do out of it, but it’s very instructive that, yeah, there is a therapy that possibly can aim forward to what you ask for myelofibrosis. No answers today, but the potential exists, and it appears to be safe and appears to be effective for years.
Major questions now
Can we eliminate disease?
Can we prevent progression?
Because some patients with PV do go to myelofibrosis. Can you prevent that when they go to myelofibrosis, the outcome is worse?
Some patients go to acute leukemia from PV. Not too many, but some do. That’s really not very good at all.
So if you can minimize or eliminate detectable malignant cells, does this mean you’re preventing progression?
Are we talking about the cure? These are open questions.
They’re all big questions. No answers today, but the potential exists, and it appears to be safe and appears to be effective for the years. So that’s at least the background where we now want to build on it.
Like we said, build on what we know about, JAK inhibitors in MF (myelofibrosis) here. Let’s build on the interferon. It’s just approved. Let’s learn about it. Lets utilize it to the maximum to optimal efficacy over many years for our patients with polycythemia vera.
The differences with ropeginterferon
The Patient Story: All very promising, although we need more data. It was interesting what you said about what it’s being studied for. It could be the first line. You can start with ropeg, or you could use hydroxyurea and then use ropeg after.
There are different administrations. So there’s one that’s a pill, one that’s the shot. But also it may have the ability, as a biologic, to actually not just control but help with the disease, itself.
Dr. Srdan Verstovsek: Yeah, change in natural history, that’s the big potential which we strive to prove or disprove over time. And the key is that you can actually provide the therapy for many years because so far in the past, we were not able to do that. Usually, it was maybe three to five years maximum that you can provide the old-fashioned interferons that you have to give much more often that much more toxicities.
This one is different. And so it’s really what we need to do is embrace the new therapy now that it’s approved and try it in everyday practice in many more patients and see whether we can give it for five or 10 or 15 years, and whether we can really change the natural evolution of the disease.
Ropeg (BESREMi) side effects
The Patient Story: My last question is about what you just brought up, which is the side effects, the quality of life issue because you can have great efficacy. But if people cannot stay on it, then it’s not very effective. So what is it with ropeg that in terms of side effects so far that we’ve seen?
Dr. Srdan Verstovsek: They are not as prominent, but they are the same types as in the past. So less often. But we worry about:
Depression
We worry about autoimmune problems making people have a condition where the body attacks on its own parts like autoimmune problems.
And we also want to make sure that there is no problem with too much suppression of the bone marrow causing anemia or thrombocytopenia.
But typically, it’s about this mental state, depression, autoimmune problems. You would actually exclude those patients from participation in such therapy because, you know, there is some small chance of a risk actually to cause some of these issues with depression and autoimmune problems.
How many people drop out of clinical trials from these side effects?
So these are known not as common. The dropout, meaning, how many people stop the therapy with peginterferon due to side effects, over five years of observation in this study that I described is very low – 10 percent, so it’s not very common.
In segment 2 of our conversation with Srdan Vertsovsek, MD, PhD of MD Anderson, he shares the latest on research for polycythemia vera or PV treatments.
Dr. Verstovsek gives a detailed overview of latest research involving myelofibrosis treatments, with a highlight on the recently approved MF drug pacritinib.
Dr. Fonseca has been a practicing hematologist for almost three decades, now interim executive director at Mayo Clinic. As a veteran specialist of the myeloma field, he shares his insights on the latest in emerging treatments and clinical trial studies.
The Patient Story:There were two big studies discussed at ASH focused on screening: iSTOP in Iceland, and the PROMISE study led by Dana Farber that started a couple of years ago, which focused on diverse populations. Can you describe the importance of those studies?
Why iSTOP Matters
This [iSTOP] is an incredibly important trial. Their goal was to do the whole screening for the country of Iceland. And what they went about to do was set up a system whereas people would be offered to be screened for the presence of monoclonal proteins. And they have a very robust partnership with the laboratory methodology to be able to test this at a high level and with great precision.
This is where phase III trials meet real world data, and really establishes some very interesting findings.
Dr. Rafael Fonseca
They went about to do a population based study, and at the end of it all, it was very, very large– 75,000 people. This is where phase III trials meet real world data, and really establishes some very interesting findings.
There were three or four key takeaways. One is that we know there’s a small fraction of the population with smoldering multiple myeloma, so they have established that through screening. It’s less than one percent that they estimated, but it’s still measurable. And that is important because as we have clinical trials where people are saying we should think about treating smoldering, we’re going to have to be more and more careful about that.
One of the randomizations was how to approach patients and then what to do afterwards. What they’re trying to see is if you have an early intervention, and you detect this early, then you can prevent some of the complications.
That’s very important because a myeloma patient who progresses to development of lytic bone lesions, especially if that results in a fracture, or renal problems, can have lifelong consequences. Then, as they live many years now after diagnosis, that’s very undesirable.
It also establishes the baseline for the prevalence of monoclonal gammopathy of undetermined significance (MGUS) in that population. So what we need to do is to think about how this extrapolates. I think there’s a susceptibility according to the various regions, but for what they tried to test, it was a remarkable study.
Why PROMISE Matters
PROMISE is a very large study led by the team of Dr. Ghobrial from Dana-Farber. And they’re able to show higher prevalence than expected for monoclonal gammopathy. In populations at risk, although the numbers will evolve, the number I keep in my head is about 10%. That’s in people who have family members who have monoclonal gammopathy or individuals of African-American ancestry, who have a higher incidence for this.
I hold the belief that many of us have slightly abnormal plasma cells somewhere in our body because we get exposed so many times through our lifetime that the opportunity for a mistake is actually quite high.
Dr. Rafael Fonseca
The other finding that was remarkable was that they found that a small fraction of patients that have abnormalities that would be a little bit more like a pre-MGUS, and some of those were reported as transient.
Now, there’s no reason to believe that humans don’t have some old clones. We know that for other tumors. So it was only logical that in time it would be found in patients who have things like MGUS. I hold the belief that many of us have slightly abnormal plasma cells somewhere in our body because we get exposed so many times through our lifetime that the opportunity for a mistake is actually quite high.
But you know, the studies are descriptive for the most part right now. But I really commend the efforts of the team of Dr. Ghobrial as well, too, in trying to establish this new baseline.
Takeaways for Current Patients
The Patient Story:What are the takeaways for current patientsregarding screening?
You know, there is no agreement at the moment regarding screening strategies or recommendations. And the reason for that is that these are conditions for which we don’t necessarily have treatments that will completely eradicate the process.
You screen for polyps because if you can excise those polyps, then you decrease the risk of colon cancer. But with the bone marrow, it’s very hard to do that because you can’t go in and just pull out the abnormal cells and then leave the rest of the bone marrow.
There is no question that, as time goes by and as the cells grow, there’s a greater likelihood that one might have a complication.
Dr. Rafael Fonseca
However, the question will change as was shown by the iSTOP study, because now the question is, “Can you do something to prevent a complication from happening?” There is no question that, as time goes by and as the cells grow, there’s a greater likelihood that one might have a complication.
So if you detect early, you might not be able to move on fully to the curative approach, although there are some clinical trials that are asking that question. But you might be able to establish a more careful monitoring strategy so that the next time you meet that person, it is for another laboratory testing, and not because the person has been admitted to the hospital with a fracture or with renal failure.
I think with most of the patients we see that have this condition, there’s somewhat surprise findings. You know, they’re going for a physical, and they’re found to have an elevated protein or someone orders a protein electrophoresis for other reasons, and now they know they have it. So we monitor them, but we don’t do this at large.
Genetic Screening
Now we get the question often from family members. “My mom or my dad has myeloma. What can I do to test?” So we give them the names of those tests, but without much information as far as what to do. And I feel like patients and families should know as well that we don’t have the best pathways yet defined, as it’s still early on.
[Testing] is a double-edged sword, because now you know you have it, then that creates a little bit of stress and anxiety. But on the other hand, you can prevent those complications.
Dr. Rafael Fonseca
But for instance, if you were in a family where there’s two or three members who have myeloma, that would be a pretty strong signal that there’s some familial clustering and then the person might want to test. And why not, if they find something to monitor? It’s a double-edged sword, because now you know you have it, then that creates a little bit of stress and anxiety. But on the other hand, you can prevent those complications.
Interestingly, at this meeting, we had a presentation by a team that looked for germline genetic changes that may predispose people to myeloma. They found that about 9% of patients have some genes that potentially could be contributing to the development of myeloma. Again, it’s very early, but that would be another path to explore as well.
Identifying Risk for Black Patients
The Patient Story: With PROMISE, there was a focus on Black patients, and a recognition that the high risk population over 50 years old was twice as likely as the general population to have MGUS. If you are a Black patient, what do you need to know about elevated risk, and do you need to talk to your primary care doctor?
You know, it could be right, but I don’t think we are ready yet to make recommendations. I think for readers in the audience who may have this question or that concern, it’s a fair request that your doctor does that testing if you are interested. As I mentioned earlier, we don’t have guidelines. I can’t pull them out and say, “This is what needs to be done.”
But I think people rightfully are concerned and would like to know. And the obvious question is, “Why?” And the “why” is so that you can have a good screening strategy. I hope that within the next five to ten years, we will have more specific guidance as far as what to do because again, if we can prevent complications, that would be pretty good.
Cancer treatments save lives, but they also come with side effects. Hear straight from patients who’ve been treated for cancer - what they experienced and what helped them get through it...
Hand of doctor giving plastic container with medicine
ASH 2021: Multiple Myeloma Screening
A Conversation With Joseph Mikhael, MD
In this segment on the American Society of Hematology (ASH) 2021 conference, Dr. Joseph Mikhael shares information about advances in multiple myeloma screening, including the iSTOP and PROMISE clinical trials.
The Patient Story:Is it true that iSTOP is the largest screening of any cancer project in the world so far?
We learned that it is feasible to do a huge screening study.
Dr. Joseph Mikhael
As far as I know. The numbers are jaw dropping when we think about it. There were over eighty thousand people in Iceland who consented to participate in the study. That in and of itself actually is one of the most important things. We learned that it is feasible to do a huge screening study. They’ve already collected over seventy-five thousand samples trying to detect myeloma at its earliest stages.
As we know, myeloma has a precondition called MGUS (Monoclonal Gammopathy of Undetermined Significance), and there’s a lot still to learn about it.
What is the true incidence of it?
How should we follow it?
Is there a way to detect it earlier?
Is there something that puts certain people at risk?
Does it mean something even if someone doesn’t ultimately develop myeloma?
Only a very small subset of people will develop myeloma. So these are some of the questions that only a screening study of that magnitude could answer.
I think we had four different oral presentations from the iSTOP study -from the Iceland screening study- to be able to start to answer some of these questions. We still don’t have anything definitive. We’re not suggesting that we now go and screen everyone, but we’re starting to learn who is at higher risk, what MGUS really means. Ultimately, we hope to be able to detect it not only sooner, but maybe even know who’s really at risk and possibly even prevent it.
Takeaways from iSTOP
The Patient Story:What are some of the biggest takeaways from iSTOP?
Well, I think some of the biggest takeaways are that, as I mentioned, it’s feasible to do a big screening study, and that when we use our most sophisticated techniques, which includes mass spectrometry, we really do find that this is a common condition. And we know that with the Caucasian background of patients in Iceland, their risk tends not to be as high. And that’s why we’ll come to the PROMISE study in a minute.
Although we have screening programs, for example, trying to detect things early in breast cancer and in colon cancer and many other areas, we really haven’t been doing that much in the hematology world.
Dr. Joseph Mikhael
But even then, in patients over the age of 40 or 50, we’re seeing around five percent of people with this. And interestingly, half of one percent have smoldering myeloma, which is a step between MGUS and true myeloma. So to see that high of a percentage -you might think half of one percent is small, but to actually have a diagnosed malignancy of that magnitude, you know, we always think of myeloma as being kind of rare disease that accounts for two percent of all tumors- you see that this is really quite common in its earliest stages.
And you know, although we have screening programs, for example, trying to detect things early in breast cancer and in colon cancer and many other areas, we really haven’t been doing that much in the hematology world. And so I think I stop is really starting to open the door towards that. We want to do it intelligently and appropriately. But it’s definitely taking us down that path.
Mass spectrometry
The Patient Story:Can you explain mass spectrometry?
Think of a mass spectrometer as just a really careful machine that can look at every tiny little protein in your blood and be able to quantify it very accurately.
Dr. Joseph Mikhael
So let me demystify it, because ultimately, I don’t think it’s going to be that expensive. I think it’s going to be cheaper in the long run. So when we look at a disease like myeloma, it’s a disease of proteins in the blood. And think of a mass spectrometer as just a really careful machine that can look at every tiny little protein in your blood and be able to quantify it very accurately.
If most myeloma patients or their caregivers saw how we measure some of the proteins in their blood or the M-spike, that monoclonal protein, we typically do it on what’s called a serum protein electrophoresis, which is just one way.
We put the blood on a plate and it runs over a period of time, and based on the weight of those different proteins, they kind of separate themselves out. And sometimes it’s like the hills here in Scottsdale, you know, they run into each other, and it’s hard to know how big one protein is versus the other.
Mass spectrometry is very precise, so it can detect low level proteins, which is really benefit number one– that it has that earlier detection. It measures them very accurately. It can also discriminate between different proteins sometimes.
Now, we use drugs in patients that themselves have a protein component, things like monoclonal antibodies, and they show up on a certain protein electrophoresis, and it can kind of confuse us. Like how much is the drug causing that, and how much is it actually the disease? The mass spectrometer is able to distinguish that difference.
Sometimes, unfortunately, in myeloma, proteins can change over time. And so mass spectrometry can know exactly which was the one that they had before and which is the one that they have now. So it’s really a fancy way of looking very carefully at these proteins.
With a mass spectrometer, we might be able to get people’s results literally within minutes.
Dr. Joseph Mikhael
And yes, the technology and the machine itself may be initially relatively expensive, but in the long run, as it may be able to replace some protein electrophoresis, it’ll be a lot cheaper because protein electrophoresis takes a lot of time in the lab and a lot of human effort.
With a mass spectrometer, we might be able to get people’s results literally within minutes. Right now, a lot of myeloma patients end up coming in a week before their visit or several days before their visit to get tested so that we can wait for all these results to cook in the lab. Here, we can do a much quicker turnaround.
Adoption of mass spectrometry vs. SPEP (serum protein electrophoresis)
It’s not been adopted universally yet. In fact, it’s not formally gone through the full FDA approval to be used yet. We anticipate, though, that it may be available as early as the first quarter of 2023, so in a little over a year from now.
There are some centers that are using it as we’re validating the tool more and more at Mayo Clinic and other places. So it’s not yet ready for prime-time. It’s being used in some of these clinical trials, like in iSTOP. It’s being used in the PROMISE study, but it really is, I think, going to be mainline and a little over a year from now.
iSTOP and measuring kidney function
The Patient Story:I read something about a special tracking system with the light chain levels, and that iSTOP was able to provide information on people with reduced kidney function. Can you expand on that?
So again, going back to how the mass spectrometer works. It can be much more precise, and we do have sometimes a little difficulty following patients who have light chain myeloma. The protein that’s made in myeloma is this big immunoglobulin, or an antibody, that’s composed of a heavy chain and a light chain. Sometimes the whole thing remains intact. Sometimes there’s the heavy chains, plus the light chains. And sometimes, there’s just the light chains.
We have a light chain measurement that we do in the blood, but that’s sometimes skewed a bit by kidney function because typically our kidneys clear those light chains out of our system. So if the kidneys are not working as well, those light chains hover in the blood for longer. So we’re now just trying to understand the best way to measure them and what the implications are of those measures. And only in big studies like iSTOP can we capture all of that information.
Severity of COVID in MGUS patients
The Patient Story:Is it true that covid outcomes aren’t more severe in people with MGUS than in the general population?
It did not appear that MGUS status by itself heavily influenced someone’s risk of developing or being very sick from COVID.
Dr. Joseph Mikhael
One of the abstracts that was presented was trying to look at this. And they hadn’t had a massive outbreak, so the numbers are relatively small. But there were so many patients that they had diagnosed with MGUS that it did not appear that MGUS status by itself heavily influenced someone’s risk of developing or being very sick from COVID.
Now, obviously, we all know this is a moving target now with different variants and so on, but it is very important for us to evaluate this because it’d been such a source of stress for our patients and their families because we know that myeloma is a cancer of the immune system.
We know that people with myeloma’s immune systems aren’t as robust to fight off infections, or even to fully respond to vaccines. But we have seen when our patients get their vaccines and their boosters, it clearly confers some protection. They may be still at high risk compared to the general population, but I urge anyone who may be reading to ensure that they have gotten their original vaccinations and their booster.
Answers with iSTOP
The Patient Story:What are you hoping iSTOP will answer? And how long will that take?
Well, it is going to take years to get all the answers, but I think we’re going to learn in the shorter term what the true incidence of these conditions are, and if there could be certain populations that we should begin to screen for in an earlier capacity.
Also, part of iSTOP was not just collecting this information. Patients were randomized to different groups with a more intense versus a less intense follow-up. So this may influence the field even in the short term. How frequently should we follow our MGUS patients? And when do we not do bone marrow biopsies, and when do we do x-rays? And what are the psychological impacts of having MGUS?
People are more comfortable understanding [MGUS] than fearing they may have something that hasn’t been diagnosed.
Dr. Joseph Mikhael
One of the things that I think is particularly important to the study is that they do surveys with patients. Would patients rather know that they have MGUS? And does that induce more stress? And initially, it does not appear to induce that.
People are more comfortable understanding it than fearing they may have something that hasn’t been diagnosed. So there are lots of things in the short term about the psychological impact of MGUS, how we follow MGUS, and whether or not we should be screening earlier in certain populations.
Diversity in Myeloma Care and Research
PROMISE study
The Patient Story:Can you tell us about the PROMISE study?
The PROMISE study is really a fantastic study, and I commend Dr. Ghobrial and her whole team. I happened to be a part of this program in the early days– we were planning it when I was still at Mayo Clinic.
PROMISE study goal of evaluating the impact of myeloma on diverse populations
I just think it’s a wonderful and important approach. In Iceland, obviously the numbers are massive, but we recognize that Iceland does not represent the diversity of what we see here in North America and in particular in people of color.
And so in the PROMISE study, they were looking to screen individuals and also use a large database that they have already existing in Boston to look at Black Americans and their true incidence of MGUS and myeloma, but also those individuals -independent of race and ethnicity- who are first degree relatives of myeloma patients.
This has always been a challenging question for us to know and really understand. ‘Familial myeloma’ is really quite rare, but are there ways to detect it more? And sure enough, we found that if, generally, MGUS is in about five percent of the population in patients over 40 or 50, that it really is double that in the African-American population and in those who are first degree relatives of myeloma patients.
But I’m very thankful that the country, if not the planet, is starting to put a spotlight on health disparities.
Dr. Joseph Mikhael
That it is in that 10 percent range, and maybe even higher when we use the more sophisticated techniques that I mentioned like the mass spectrometry. And so the numbers are still coming in.
Obviously, they’re not iSTOP numbers, and there’s still so much to learn, but I think it was really critical because in this group of individuals it demonstrates to us the greater incidence, and how these individuals are greater risk. And it speaks to us of the importance of health disparities in multiple myeloma that I know we’ll talk more about because there was great research presented within this field over the course of the meeting.
But I’m very thankful that the country, if not the planet, is starting to put a spotlight on health disparities. And the tragedy within the African-American community is that not only is disease more common, sadly, we do see that outcomes of survival are significantly reduced in this population.
And yet they don’t have to be, because there are studies that show that when African-Americans have the same access to therapies as Caucasians, their outcomes can be as good, if not better. So that tells us that there’s hope here, that there’s opportunity.
I think the PROMISE study is a step in that direction to really assess and understand the disease more fully as doctors. Diagnosis always comes before therapy, right? So if we can fully understand the issue, then hopefully we’ll be able to do more about it, so that we’re not just talking about these things, we’re doing something.
The Patient Story:This mass spectrometry that’s being used in both of these studies– that plays a big part in getting better, more accurate numbers, right? Being able to detect more minute amounts of the M protein– is that part of this?
That’s absolutely part of it. Mass spectrometry has that ability to detect proteins at lower levels than we’ve traditionally been able to look for.
Risks found with screening
The Patient Story:The follow-up four and a half years after showed a slightly higher mortality rate in patients that had that and protein detected versus not, and also a higher risk of myeloma, other blood cancers and possibly things like heart attacks. Is that right?
Something that’s emerging from both the PROMISE study and the iSTOP study that we’re starting to understand a little bit more of is that we tend to think of MGUS as being a precursor to myeloma. And so the worry about MGUS is that someone develops myeloma.
And that, of course, is the central concern. But we’re starting to notice something else– that patients who have MGUS may have other associated conditions and that their overall survival may be compromised. We still don’t fully understand this.
I don’t want to raise too much of an alarm yet, because we’re still sorting it out. But there may be greater connections to certain kinds of heart or kidney or other disease, and we’re trying to understand the mechanism of that– is it really driven by the MGUS, or is the MGUS just telling us something else that’s going on within the immune system or within the body?
And this is the kind of thing that really can only be fully assessed and understood in something like iSTOP. So that’s one of the things that we hope to have more answers about in the not-so-distant future.
Frequency of MGUS screenings in the US
The Patient Story:Can you talk about the frequency of MGUS screenings in the US?
So right now, whether it’s the International Myeloma Working Group, or our organization, the International Myeloma Foundation, or any other institution, no one is yet recommending that we just screen largely. I think the approach is that we’re learning more about this, and we’ll understand it better for the future.
I do, however, think it is really important for us to speak up when we identify people with signs and symptoms that could be consistent with myeloma. There’s a difference between screening the general healthy population and screening if someone has certain features.
The M-Power Initiative
This is part of the work that I do at the International Myeloma Foundation in our M-Power initiative, which is to educate the community and primary care docs about when to test for myeloma, how to recognize the signs and symptoms, and then what exact tests need to be done, which is the serum protein electrophoresis and the light chains like we talked about earlier.
So when people have a low hemoglobin count, or fatigue that is not otherwise explained, or bone or back pain in particular, that’s outside what we would expect, or their kidney functions off– there’s a whole series of things that kind of trigger this.
Thankfully, the majority of people with MGUS will not develop true myeloma. But now, as we have better techniques to measure it and better understanding of the disease, we want to keep an eye on it so that we can intervene when necessary.
Dr. Joseph Mikhael
Sometimes within the African-American community in particular, this isn’t thought of because these are many of the same things that we may see, for example, with diabetes. And some may say, “Oh, that’s just from your diabetes,” and not look a little bit deeper. But for those people who are reading and already have established MGUS, I think what it reminds us is that it’s important to continue to be followed.
Thankfully, the majority of people with MGUS will not develop true myeloma. But now, as we have better techniques to measure it and better understanding of the disease, we want to keep an eye on it so that we can intervene when necessary.
Follow-ups for MGUS patients
The Patient Story:What is the follow-up once someone has MGUS? And how long should it go on?
So the quick answer is that it depends on someone’s MGUS, and obviously they need to talk to their own physician about that. We have different groups that have provided different guidelines. In general, people with MGUS are seen either once or twice a year, so every six months or every 12 months. We have a sort of a grading system within MGUS of people who are higher risk and people who are lower risk.
This is also what we want to learn from iSTOP, because they have a strategy to look at how frequently people should be followed. Right now, it appears that people really do need to be followed indefinitely. It’s not like if you go five years and there’s no progression of MGUS to myeloma, you can stop looking. We see that people unfortunately can progress even after having MGUS for 19 years in their 20th year. It can happen, so it really is unfortunately a lifelong follow-up.
Future of screening
The Patient Story:What do you see for the future of MGUS screening?
I think it will take some time because the implications are huge, right? Massive screening programs are obviously very consuming and have to be done correctly if they’re going to be effective. And we don’t want to screen a whole group of people where it may not be necessary. So the day may come where we’ll say that at a certain age, or based on someone’s gender or ethnicity or race, that there may be a greater risk, and therefore it triggers the need to be screened.
That’s kind of how we do it now, right? We don’t screen everybody with mammography or with colonoscopies in their 20s and 30s. We set an age. If someone has family history, then their risk is increased. Someday, we’ll probably come to that. We’re just not there yet.
Hear from David Miklos, MD, Ph.D, an experienced and passionate specialist in blood and marrow transplants, as well as immunotherapy research.
As Chief of BMT & Cell Therapy, and Clinical Director of the Cancer Cell Therapy program at Stanford University Medical Center, Dr. Miklos spends his time not only seeing patients but also focusing on the latest science in cancer therapies.
Name: Dr. David Miklos
Specialty: Blood and marrow transplant
Roles:
Chief of BMT & Cell Therapy
Clinical Director Cancer Cell Therapy, Stanford University (2016 – Present)
Experience: 25+ years
Provider: Stanford Medical Center
We’d like to cure more and more diseases. What is cured?
People ask me all the time, ‘Am I cured?’ The difference between remission, where we have no measure of your cancer anymore on a scan or bone marrow or blood test, and a cure, is time.
Video: Dr. Miklos on Mantle Cell Lymphoma Treatment
Mantle Cell Lymphoma Treatments Have Improved
Mantle cell is kind of the story of my life. An interesting story. When I was training back at Harvard in 1995, mantle cell lymphoma was first being recognized because we needed some antibody test to be able to tell the difference of these immature lymphocytes.
The very first patient I actually diagnosed was a person who had lymphadenopathy in my internship clinic, where usually I was treating diabetes or hypertension. The therapy was terrible.
Using CHOP chemotherapy had only a three-year overall survival. Rituximab added very little benefits to those patients. But there was development of small molecule inhibitors that are interfering with the signal from the b-cell receptor to the division inside the nucleus.
Small molecule inhibitors
These are drugs your people have heard of like ibrutinib, a drug that targets the Bruton’s tyrosine kinase (BTK) inhibitor. There are also other drugs.
Ibrutinib was the first and certainly the most widely-used drug. A pill you take once a day that covalently links and binds and inhibits the BTK molecule. That cell was done. The importance of that therapy where everybody responds, and yet, there are patients with about a 20- to 25-percent risk per year of progression.
Once we lose that very special target, we can go onto some other medicines like venetoclax, which has also shown benefit in the mantle cells.
But we’ve been looking for something better.
We’ve tried high-dose chemotherapy. I’m a stem cell transplanter, so the notion of using high-dose chemotherapy with stem cell rescue or what your patients will know as an “auto transplant” has provided much benefit to the patients of mantle cell lymphoma.
It moves out the expected overall survival from three to six years or more. There’s a role for maintenance rituximab, FDA-approved, and has benefits in patients, and the small molecule inhibitors, ibrutinib, venetoclax, which we just discussed.
But where’s the home run?
Where’s the targeted immunotherapy that is going to eliminate this cancer and provide the patient a long term cure?
Role of allogeneic bone marrow transplants
Some of your patients may have had an allogeneic transplant which is truly the immune therapy of some else’s immune system.
Maybe it’s a brother or sister or HLA-identical donor whose blood destroys the white cells, red cells, and regrows and reconstitutes the normal blood system.
In the process of getting rid of the patient’s blood system, it gets rid of the white cells, the lymphocytes, the b-cells, and the mantle cell lymphoma.
The allogeneic transplant is an immune therapy. I am an allogeneic transplanter and will talk about the major side effect of allogeneic transplant which is graft-versus-host disease (GVHD).
That means the immune response is not only attacking the blood and cancer, but it’s also sometimes attacking the skin, the gut, the liver, causing detrimental, inflammatory problems that can be the real bane of the existence of the patient.
The quality of life and the difficulties with organ involvements across the whole body has been seen. Those patients are really dependent on immune suppression.
So where’s the home run? The home run is, again, CAR T.
The axi-cel therapy was the first FDA-approved treatment in large cell lymphoma. That company is called Kite. They were purchased by Gilead. They brought forward a very similar construct.
The actual molecule that is placed into the patient’s lymphocytes is exactly the same as what’s been used for the last three years in large cell lymphoma. So it binds the same CD19 again, same story, here comes the CAR. We’re going to bind and we’re going to then kill the cancer.
It’s prepared in a very special way because mantle cell frequently has lymphoma in the blood, so we have to separate the lymphocytes away.
That’s the unique difference between Tecartus and Yescarta. Otherwise, they’re nearly identical therapies.
And the prep to do this is the apheresis, the places where you’ll receive the therapy, the lymphodepletion chemotherapy, and the three days before we put the special cells in. It’s all the same. The follow-up stay in the hospital, seven to ten days, staying locally for 28 days, it’s all the same.
The expected toxicities of cytokine release syndrome, that’s the fever, achy, flu-like symptoms, or the confusion and neurological problems that can follow patients who have had the cytokine release syndrome, again, very similar incidents.
Newest study: ZUMA-2 clinical trial
Here’s the excitement: the excitement is in that study you addressed called ZUMA-2, which began in 2017, there were 60 patients treated and this overall response rate was 93-percent.
The overall complete response rate, couldn’t find the cancer, was 67-percent.
Two-thirds of the patients, 28 days after given this Tecartus infused in their body, had no measurable cancer, a complete response. That response has remained durable. The publication that is responsible for the FDA’s approval showed 27 months of follow-up in patients.
That’s just over two years, so let’s not get carried away. We have two years of follow-up and in that population, the response rate was 43-percent remaining in complete response and 67-percent overall response.
So it’s very durable. Probably even more durable than what we saw in the original treatment with axi-cel in large cell lymphoma. There are similar side effects and it still needs to be done inside the hospital at centers that have experience managing patients with CAR T therapy. The higher response rates and they appear to be very durable treatments.
These are for patients who had had three lines of therapy previously, so they probably had CHOP, or bendamustine and rituximab, they probably had ibrutinib as one of the therapies. That trial required they had a drug that targeted the Bruton’s tyrosine kinase (BTK).
The FDA, when they made the approval of this therapy in July, recognizing what a game changer the therapy offered patients, did not require patients go through three lines of therapy.
The FDA has authorized the treatment in second line and I think that’s because they really want to help patients achieve long-term disease-free survival and benefit.
Now, physicians will have to decide who should receive BTK inhibitors and who should go right on to CAR T-cells, and that’s discussion with the patients and the families. That really is still being worked out.
We’re going to be doing a new trial where we’ll be looking at patients who’ve had ibrutinib upfront or who have not had ibrutinib yet, and using the same therapy to see what the true incidents of benefit is in that second line.
But in the meantime, there are centers that can provide commercially-available therapy with Tecartus today. If somebody’s gone through all the available therapies, that’s a lifesaver.
As we decide whether we should use CAR T-cells in second line, that’s an individual decision at this point for the patients and their doctors.
What are the drawbacks of this newest therapy
I think we have to make sure the therapy does not cause more toxicity than the patient’s need warrants.
What I think is going to happen is we’re going to see less CHOP chemotherapy up front. We’ll probably be shifting more to the kinder, gentler bendamustine-rituximab, and maybe even in combination with ibrutinib in the first-line therapy.
The intent of that is to really clear the disease, make sure we get the highest response rate possible with the lowest toxicities, and frequency of going into the hospital with side effects like neutropenic fever. We want to avoid that.
I think that’s where the field is moving. Then the key decision, and I’m the Chief of Transplant (at Stanford) so I don’t want to malign my own therapy.
But whether or not auto transplant continues to be important in the management of mantle cell versus going right on to a targeted cellular therapy, is really the next question.
So that decision needs to be made. What we’re trying to judge is what’s the risk of the patient having cytokine release syndrome or really high-impact, really debilitating neurological toxicity.
Balance between therapy efficacy and adverse effects
A grade three neurological toxicity is when the patient is really unresponsive in the hospital, just lying there, eyes open, frequently having expressive aphasia, can’t talk, can’t find the words, can’t attend. That period of time lasts usually two to three days and patients are being treated with steroids.
Young people, like us, we may have the ability to have the reserve to get through something like that and easily bounce back.
But if you were 80 years old, having a similar treatment options, and trying to decide, I imagine the ibrutinib therapy would be the more appropriate, at least until it’s not working.
While patients are receiving those better-tolerated, maybe not curative therapies with very good efficiency or efficacy, we’re working on new therapies. We’re working on kinder, more gentler therapies, with less toxicities.
The companies we’re mentioning here are fully committed to trying to improve these treatments. Whereas maybe the drugs you took for your blood pressure and your diabetes are still the same drugs after 20 years, these drugs will not be the same drugs after five years.
We will be moving the development curve cycle into a very rapid change, because knowledge is what is going to drive the next therapy.
As we learn how to help the patients, how to improve the treatments, what happens as the universities will quickly disseminate through pharmaceutical companies to the patients’ care.
Why patients should consider clinical trials
It’s a very exciting time. It’s these small clinical trials that are able to demonstrate clinical benefit, but at the same time, we’re collecting blood samples and lymph node samples that allow us to test questions like:
How did it work?
How did the CAR expand?
Did it go into the lymph node?
Did the lymph node stop making the target?
How do we make this treatment better?
We call that the virtuous cycle of correlative clinical trials and that’s what these large academic centers are all about. We’re trying to turn that cycle as fast as we can.
That’s a partnership with our patients, so when your patients go to a cancer center and the doctor says, “We have a clinical research trial and we have the standard of care,” it’s important to listen closely.
There are very good treatments in the upfront use of tisa-cel, axi-cel, and soon, liso-cel, so we want to be able to offer those therapies to people with 60-percent complete response rates.
But if you are having a recurrence of disease after that therapy, or that therapy is not appropriate, then it’s important to consider participating on a clinical trial in order to get access to the more promising treatments.
That’s the hardest conversation. Bring all your friends, bring your family to the doctor’s visit. You’re going to need lots of ears to be listening to why you should do this or could consider these other options.
Your doctor should be making recommendations, but you, too, have to participate as you consider the benefits and the risks.
Role: Center Director Urologic Oncology Focus: Urological oncology, including kidney, prostate, bladder cancers Provider: Cleveland Clinic
...
Dr. Babis Andreadis of UCSF shares his approach with patients, the importance of patient self-advocacy, whether to ask for a second opinion, and more on shared treatment decision-making...
Oncologist: Specializing in breast cancer | HER2, Estrogen+, Triple Negative, Lumpectomy vs. Mastectomy Experience: 30+ years Institution: Stanford Medical
...
Role: Radiation oncologist Focus: Specializing in radiation therapy treatment for all cancers | Brachytherapy, External Beam Radiation Treatment, IMRT Provider: Salinas Valley Memorial Health
...
Featuring: CLL Patient & Advocate Michele Nadeem-Baker Dr. Nicole Lamanna, Columbia Univ. Medical Center Dr. William Wierda, MD Anderson
There are so many exciting developments in chronic lymphocytic leukemia or CLL treatment. But there is so much to wade through, how do we know what’s right for us and what we should be asking our doctors?
CLL patient and advocate, Michele Nadeem-Baker, guides us through the most promising trends in CLL treatment, spotlighting the voices of top CLL specialists who cover everything from new oral combinations to new drugs (pirtobrutinib) and so much more.
Michelle Nadeem-Baker: I’m Michele Nadeem-Baker, your Chronic Lymphocytic Leukemia Reporter for The Patient Story and a CLL Patient. There is so much happening in terms of new treatment research for us! There are more choices than ever for when it’s time to be treated and more in the pipeline. But how do you know what they are, how they’re different and which is best for you?
Our program will help new and not so new CLL patients learn today’s treatment landscape and the hottest drug trials from two leading CLL Specialists, Dr. Bill Wierda at MD Anderson in Houston and Dr. Nicole Lamanna at Columbia University Medical.
First, many patients think they need to start on chemotherapy. This is old school thinking.
Small molecular inhibitors > chemotherapy and chemoimmunotherapy
William Wierda, MD, Ph.D:: The targeted therapies BTKi, BCL-2 are superior to chemo and chemoimmunotherapy, so I don’t like to think about, or talk about, or plan for chemoimmunotherapy any longer because I think it’s inferior treatment for our patients and much more aligned with giving small molecule inhibitor based therapy.
I think for patients and moving that discussion a little bit further, what patients need to think about and have a discussion with their physician about is:
Do I want fixed duration or finite duration treatment?
Do I want to get in remission and get off treatment and have a reasonable period of time to expect off treatment in remission?
Or do I want to go on a maintenance and have medication that I take every day that is extremely effective at controlling the disease? But I continue on it and there are side effects associated with all treatments, including the continuous treatment.
Chemotherapy outcomes or outcomes with chemotherapy were inferior to outcomes for treatment with small molecule inhibitors, whether we’re talking about venetoclax-based therapy or BCL-2 inhibitor based therapy, or we’re talking about BTK-inhibitor based therapy or drugs.
Small molecule inhibitors
BCL-2 inhibitors
William Wierda, MD, Ph.D:: The small molecule inhibitors that we have are oral agents, and there are two category, three categories right now that we have of drugs that fall into the small molecule inhibitor category:
BCL2 inhibitors, we have one. There are several that are in clinical trial. The one that we have is called venetoclax. Very potent at eliminating disease, very potent at getting deep remissions. It’s the type of treatment that we give with the expectation of giving it for a set period of time and then stopping treatment once patients are in remission.
BTK inhibitors
William Wierda, MD, Ph.D:: The next category is BTK inhibitors. Those have been around longer than BCL-2 inhibitors. Examples of this drug that we currently have available are acalabrutinib and ibrutinib.
Ibrutinib has the most experience associated with it, and we have the most data and most patients treated so far on clinical trials with Ibrutinib. Acalabrutinib, though, is approved.
Zanubrutinib is not yet approved, but perhaps will be in the next within the next year probably. Those are drugs that are extremely effective at controlling the disease, but not as effective as, for example,
Venetoclax is in terms of getting the amount of disease down to the point where we’re comfortable with stopping treatment. So the best response, the lowest level of disease is usually still measurable with the BTK inhibitors like Ibrutinib or Acalabrutinib. So patients go on those medicines and they stay on them until they don’t work any longer. It’s more of a maintenance type treatment.
PI3K inhibitors
William Wierda, MD, Ph.D:: Third category of drugs are the P-I-3-Kinase-inhibitors. There’s two that we have currently available. One is called idelalisib. The other is called duvelisib. Those have a bit more side effects and toxicities associated with them, particularly Idelalisib and are used less frequently these days.
Ibrutinib and the BTK-inhibitors and the venetoclax or BCL-two inhibitors, are extremely effective and give very good and durable disease control. You can switch between those two if you develop resistance. So if you develop resistance to venetoclax, for example, you can switch to the BTK-inhibitors, one of the BTK-inhibitors, and expect a response and vice versa.
New BTKis
Michelle Nadeem-Baker: There’s another generation and category of BTKis – a new type – reversible and non-covalent. One of them in trial and getting much attention is pirtobrutinib. Until this trial, patients, and this includes me currently on one, hadn’t known about these BTKi differentiators – reversible and irreversible and non-covalent and covalent.
Pirtobrutinib is looking very promising.
William Wierda, MD, Ph.D
Pirtobrutinib
William Wierda, MD, Ph.D: So there’s a lot of things happening in CLL. There are a lot of new and exciting drugs that we’re studying that are in early development. There’s a drug called pirtobrutinib, which is a reversible inhibitor of BTK, which you would consider giving in a patient who has developed resistance to one of the irreversible inhibitors, such as ibrutinib, zanubrutinib or acalabrutinib.
Pirtobrutinib is looking very promising. It’s active in patients who are resistant to irreversible inhibitors, and those remissions are lasting a reasonable amount of time. It also is working in patients who are resistant to ibrutinib and venetoclax. So we’re excited about that.
Nicole Lamanna, MD: There are reversible and irreversible inhibitors. And so what’s different about pirtobrutinib or these non-covalent BTK inhibitors is that what we started to notice is that as patients who were on the covalent BTK inhibitors, such as ibrutinib or acalabrutinib, that there is no doubt that over time, some patients can develop resistant mutations to this class.
We can actually test for that in the lab so we can send somebody’s blood or their bone marrow sample and see that they might have, they might be starting to develop some resistance to the drug that they’re on, and we’ve identified some of these mutations.
Looking at pirtobrutinib, that certainly is a drug that might be able to reverse or overcome the resistant mutation that patients have developed on the other BTK inhibitors. And that may be useful to have another medicine. We know Venetoclax works for these individuals, but having yet another BTK inhibitor that works slightly differently may also be helpful.
Combination therapies
Acalabrutinib + ibrutinib + obinutuzumab (AVO)
Michele Nadeem-Baker: Combination therapies – means giving 2 or more treatments concurrently. Combining for treatment isn’t new – FCR, the former CLL go to treatment, was 3 drugs given all together: 2 chemotherapies: fludarabine and cyclophosphamide plus monoclonal antibody rituxan (rituximab).
Today, many CLL clinical trials are testing various drug combinations of individually approved drugs, such as acalabrutinib plus venetoclax plus obinutuzumab, AVO.
All eyes are on this important triplet trial as it could lead to more combination trials being approved. It’s currently in a trial and if approved, doctors say it will be “practice changing.”
Ibrutinib + venetoclax VS. chlorambucil + obinutuzumab
CLL trials are also comparing drug combinations with other drug combinations. A highly anticipated trial pitted ibrutinib plus venetoclax against chlorambucil plus obinutuzumab.
Ibrutinib plus venetoclax has better results giving a nice durable remission with the possibility of going treatment free for a while.
Nicole Lamanna, MD: So then can we take two orals – a BTK inhibitor and BCL-2 inhibitor and then do more of what they call a time limited approach, right? So then taking both of these oral agents for a period of time and then stopping, so, then they would be not, that you wouldn’t then be taking the BTK inhibitor chronically indefinitely. And so there were many trials producing very exciting results. The responses are very good with the oral-oral combinations, but we need longer follow up.
The role of venetoclax in combinations
Michele Nadeem-Baker: Both of these trials include venetoclax and many other trials using it are having great results.
William Wierda, MD, Ph.D: Right now, we’re seeing good responses for all patients independent of their risk features. If they have an unmutated immunoglobulin gene, their response is similar. If they have a 17p deletion, their response is similar to the non 17p. The challenge for the high risk is showing that they remain in remission and that their disease doesn’t come back and grow.
If we’re talking about achieving an undetectable-MRD state, venetoclax-based therapy is what we need to give to do that. Whether it’s the standard treatment which is venetoclax plus obinutuzumab, which is a CD20 antibody or a newer combination venetoclax plus ibrutinib, venetoclax plus acalabrutinib – those combinations, all of which include venetoclax, are intended to get into a deep remission, undetectable MRD and time off treatment.
Other CLL treatments
Michele Nadeem-Baker: And there are other types of treatments being studied for CLL patients.
Nicole Lamanna, MD: There are definitely some bispecific monoclonal antibodies that are also being looked at that also target the CLL cells. And so they’re early in development. And so that’s something that we’re going to see. Stay tuned.
CAR T Cell Therapy
And of course, many of us have also always talked about CAR T-cell therapy. So looking at different forms of immunotherapy to try to target the CLL cells in a different way. Manipulating the cells to then stay stimulated so that they attack your CLL cells. And so certainly there’s longer follow up on the CAR T-cell data as well.
Dr. William Wierda, MD, Ph.D: CAR T is an exciting topic. It’s an area that I’ve been involved in in development, and we will hear more about CAR T.
I have had many patients who have been treated with CAR T and who were resistant to standard treatments, who have had very durable remissions and who are doing very well. So for me, that holds a lot of promise for our patients.
Having multiple choices and having these conversations with your physician and team is great because there’s more than one option that is really good therapy for your disease
Nicole Lamanna, MD
Can treatments prevent relapse?
Michele Nadeem-Baker: Are there any treatments that can keep you from Relapsing?
Nicole Lamanna, MD: We know that patients can relapse even after these more aggressive therapies like CAR-T and allogeneic stem cell transplant. I think that it’s appropriate those conversations about where you are in your journey and your therapy and what you might need in the future are really good conversations to have with your physician team, for sure.
Having multiple choices and having these conversations with your physician and team is great because there’s more than one option that is really good therapy for your disease, which is very hopeful and great that you can. I think that the field has come a long way. Stay tuned. We’re doing a lot more, but there’s lots of lots of good things to look forward to.
Are we close to a cure?
Michele Nadeem-Baker: With so much research, are we close to a cure?
William Wierda, MD, Ph.D: In order for a patient to be cured, meaning no more leukemia period ever to be seen, they have to be undetectable MRD, whether that’s at the end of treatment or it’s three years or five years later.
I’m optimistic that we are curing some patients currently with our non-chemo treatment. Certainly, we know patients are being cured with chemo options. The problem is that chemo has side effects and toxicities associated with it, and we have exceptionally good treatments now with small molecule inhibitors to the point where I think despite the fact that we are able to cure some patients with with chemo, it doesn’t justify giving every patient who potentially could be cured the chemo because it’s only about half of those patients.
Nicole Lamanna, MD: I think that we’re going to need a lot more long term follow up to show that something is potentially curative in CLL. So stay tuned because some of this combination data, I think in some subgroups might render somebody with undetectable MRD for a really, really long time and albeit perhaps even cured.
But I never use that word. I use that word very cautiously. But I think that therapies have gotten so great that there’s no doubt a potential for some individuals. I think that we’re getting to a very good point, but we still have a lot of work to do.
Clinical trials
Michele Nadeem-Baker: Clinical trials are a great way to get tomorrow’s treatment today. If you’re interested in finding out more, ask your CLL team if they have any open trials or any in the future that would be a good match for you and for more trial information checkout clinicaltrials.gov
William Wierda, MD, Ph.D: I think clinical trials are important. They’re the only way that we’re going to make progress in the disease. They’re the only way we’ve made progress in treating the disease, and they’re very, very important.
Conclusion
I’m driven to share it to help you better advocate for yourself and to gain hope.
Michele Nadeem-Baker: Promising ongoing research continues producing more treatments for CLL patients with more on the way.
In the near term be on the lookout for news on potential FDA Approvals for:
Zanabrutinib (BTKi)
Ibrutinib and Venetoclax in combination
Importance – “could be practice changing – could lead to more combination approvals
Keep an eye on updates for pirtobrutinib and others in this new class of BTK inhibitors, as well as CAR T-cell therapy and the latest generations of BCL-2 drugs like venetoclax, and so much more.
As a CLL patient, seeing so much ongoing research and drug discoveries gives me so much hope! And I’m driven to share it to help you better advocate for yourself and to gain hope.
Dr. Farrukh Awan is an associate professor and hematologist-oncologist at UT Southwestern, who specializes in treating people diagnosed with leukemia and lymphoma.
Dr. Awan is also a member of several professional organizations, including the American Society of Clinical Oncology (ASCO) and the American Society of Hematology (ASH). He is also the recipient of the Young Investigator Award from ASCO and has published on many topics, including ibrutinib and acalabrutinib.
Dr. Awan shares about one clinical trial (phase 1) he’s a part of in exploring more treatment options for relapsed/refractory lymphoma patients – venetoclax-selinexor.
Hematologist-oncologists Dr. Satyajit Kosuri and Dr. Shernan Holtan, patient advocate Meredith Cowden, and LLS clinical trial nurse navigator Ashley Giacobbi discuss the role clinical trials play in advancing the GVHD treatment landscape.
...
Dr. Kulsum Bano, Dr. Nilanjan Ghosh, and Dr. Justin Favaro discuss the latest advances with 3-time DLBCL survivor and patient advocate Dr. Robyn Stacy-Humphries.
...