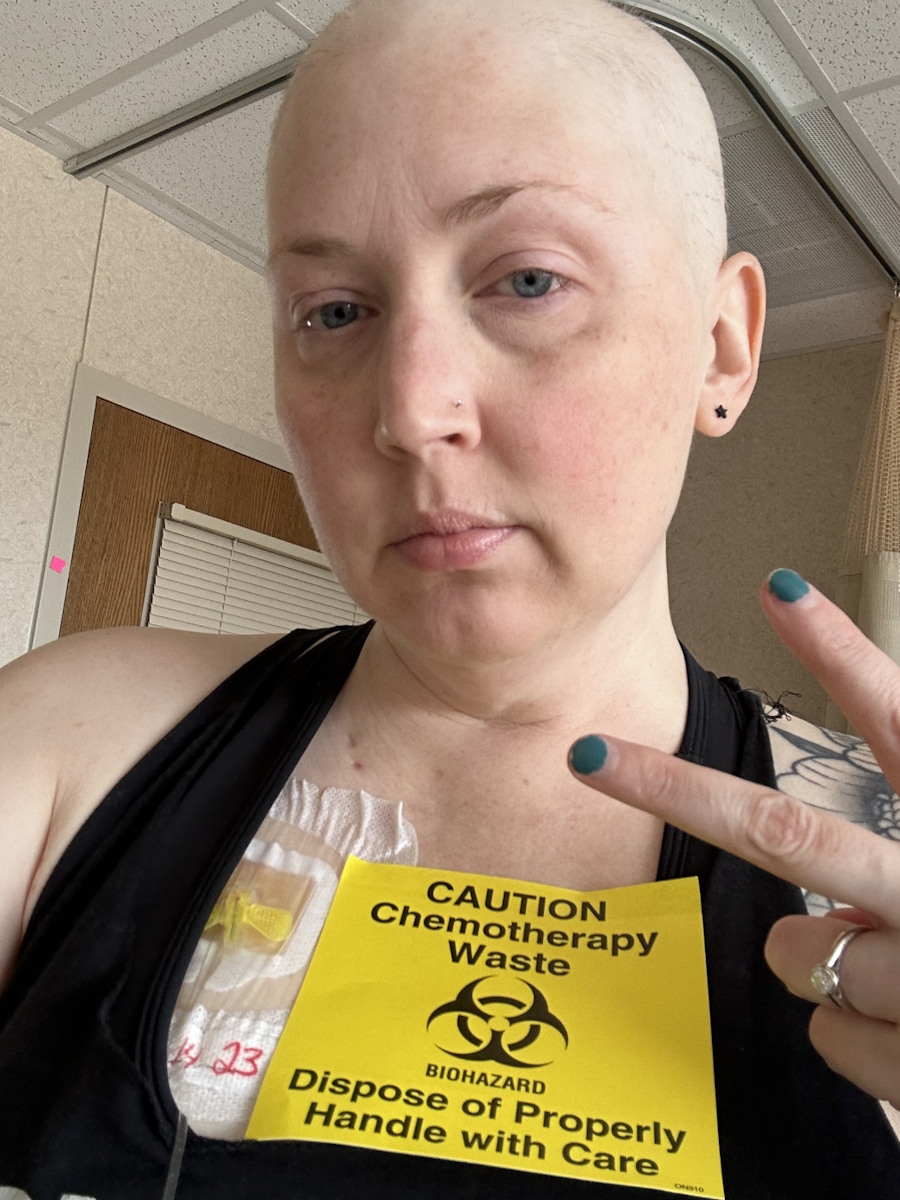
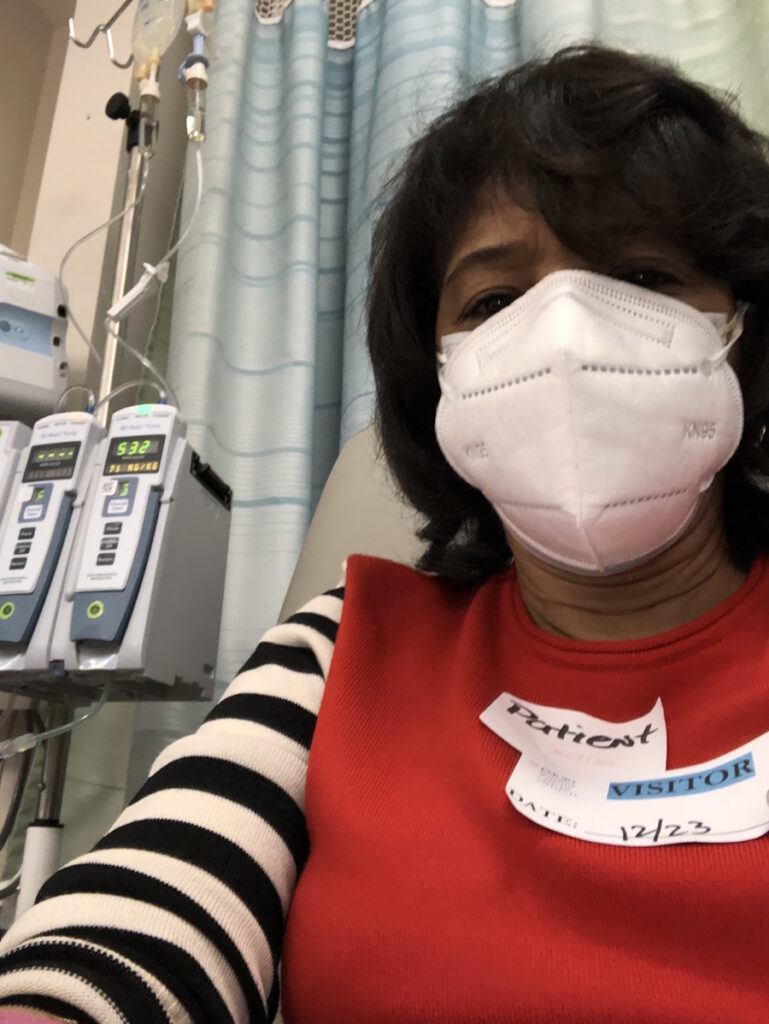
Not Just a Miscarriage: The Rare Cancer Shannon Never Saw Coming
When Shannon found out that she was pregnant, it was supposed to be a joyful chapter in her life. But within weeks, things began to feel off. Spotting led to a heartbreaking miscarriage and a D&C (dilation and curettage procedure) followed. Her doctor mentioned a possible molar pregnancy, but pathology came back negative so she was told to try again. Only, she never really felt better. It would be months before she was told she had a choriocarcinoma.
Even as her symptoms — persistent bleeding, clotting, stomach discomfort — continued to raise red flags, Shannon was repeatedly reassured it was “normal” following a D&C. Deep down, though, she felt something just wasn’t right and things weren’t improving. Months later, she visited a walk-in clinic where a concerned provider decided to look deeper. Another ultrasound led to a second D&C, and this time, pathology confirmed a molar pregnancy. From there, things escalated: she was referred to an oncologist, where she finally heard the word choriocarcinoma (a rare cancer most often occurring in the uterus).
Choriocarcinoma is a rare and aggressive cancer that can arise from placental tissue. Shannon was diagnosed with gestational trophoblastic neoplasia, which later turned into choriocarcinoma. After a series of scans, the cancer was found to be contained in her uterus. Weekly HCG blood tests tracked her progress. At first, the numbers dropped, but when they started to climb again, chemotherapy became inevitable.
She opted for the aggressive five-drug regimen, which required hospitalization. The toll was significant, especially emotionally. Losing her hair was devastating. Life outside of her diagnosis stood still. Shannon described feeling like the world kept spinning without her, while she was stuck trying to reclaim a version of herself she wasn’t sure existed anymore.
Eventually, remission brought relief, but four years later, her symptoms returned. A bloated stomach and a heavy gut feeling turned out to be a second encounter with choriocarcinoma — this time bigger, stronger, and more emotionally draining. Shannon underwent a full hysterectomy and another round of brutal chemo. She preserved her ovaries, which helped her hormonally, but the decision not to have children had long since been made due to the risks.
Throughout it all, Shannon leaned on happy distractions — laughter, humor, connection — and clung to her ability to find light in dark places. She speaks openly about losing parts of her identity, especially her mental state, but is also reclaiming herself piece by piece. Most of all, she urges others to advocate for themselves. If your gut says something is wrong, listen to it. Push for answers. You deserve to be heard, supported, and believed.
Watch Shannon’s full video to find out more about her story:
She knew something was wrong and she was right.
What happens when your body says “stop” and no one listens?
Laughing through chemo? How Shannon found joy even in the hardest moments.
What it’s like to lose part of yourself and slowly build something new.
Why she didn’t ring the bell after beating cancer a second time.
Name: Shannon W.
Age at Diagnosis:
35
Diagnosis:
Choriocarcinoma (gestational trophoblastic neoplasia initially, recurred as choriocarcinoma)
Symptoms:
Molar pregnancy
Vaginal bleeding
Overall feeling of unwell
Cramping
Weight loss
Elevated HCG level
Feeling bloated
Treatments:
Chemotherapy
Surgeries: dilation and curettage (D&C), total hysterectomy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Thriving with Multiple Myeloma: Yvonne’s Story of Strength Through Advocacy
Yvonne’s story is one of resilience, hope, and determined self-advocacy. Diagnosed with multiple myeloma in August 2008, Yvonne refused to let her diagnosis define her. She continued living fully, even earning her doctorate while undergoing treatment. Her life wasn’t paused by cancer; it evolved, grew, and took on new meaning.
It all started with sharp pain in her hip after a family trip. What seemed like a sudden injury led to a life-changing diagnosis. Instead of dwelling on fear, Yvonne focused on understanding multiple myeloma and moving forward. Her family was her motivation, especially her daughter, who was just starting college at the time and whom she was determined to watch graduate.
Throughout her experience with multiple myeloma, she prioritized learning and staying engaged. The Winship Cancer Institute of Emory University gave her access to educational materials early on, while she and her family took an active role in researching and understanding treatment options. This curiosity and courage eventually led her to CAR T-cell therapy, one of the most advanced treatments available.
Even when treatment became intense, such as during her stem cell transplant, Yvonne stayed grounded. She was scared, yes, but she asked questions, made informed decisions, and didn’t let fear take over. She delayed one of her treatments to walk across the stage and accept her doctoral degree. That moment represented more than academic success — it was proof of her persistence and belief in living fully despite the diagnosis.
Yvonne also found meaning and healing through advocacy. As a volunteer with The Leukemia & Lymphoma Society, and in particular its Myeloma Link program, she helped spread awareness in her community. She became a role model for those newly diagnosed, showing them that survivorship with multiple myeloma is not just possible, it’s vibrant.
Her advice is to stay positive, ask hard questions, know your options, and be your own advocate. “You can move through it,” she says, “with a sense of pride.” Yvonne’s strength isn’t in never feeling afraid — it’s in showing up, speaking up, and continuing to live with purpose and grace.
Watch Yvonne’s full video to find out more about her experience:
Learn how Yvonne earned her doctorate while navigating treatment.
What she told her doctor when facing her first stem cell transplant.
The surprising support system that helped her graduate during hospitalization.
How CAR T-cell therapy changed her approach to treatment.
Why she believes self-advocacy is the most powerful tool in managing multiple myeloma.
Name: Dr. Yvonne D.
Age at Diagnosis:
52
Diagnosis:
Relapsed/Refractory Multiple Myeloma
Symptoms:
Severe hip pain
Trouble walking (due to a broken pelvis)
Extreme fatigue
Bone pains
Treatments:
Chemotherapy
Stem cell transplant
Radiation therapy
Surgeries
CAR T-cell therapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
One symptom that stood out was the pain in my hip.
Introduction
I’m Yvonne and I was diagnosed with multiple myeloma on August 25, 2008.
My husband and I are retired, so we’re involved with a lot of volunteer organizations. We’re busy with activities at home. We like entertaining, traveling, gardening, and cooking. Outside of illness, we try to expand our interests in different areas. We watch plays and visit museums. We live our everyday lives. It’s about living with the disease and not succumbing to it.
How My Symptoms Started
One symptom that stood out was the pain in my hip. We went to a family reunion and were flying back from Delaware. When I stepped down from the shuttle, this pain exploded. My family got a wheelchair for me. That week, I was in the doctor’s office and the process of getting the diagnosis began.
How My Family Motivated Me
It has been 17 years. My daughter was starting college and I was determined to see her graduate. I have since seen her graduate four times. My family needed me and I needed them. I was determined not to have a defeatist attitude. I wasn’t woeful at the beginning. I never was. I needed to understand what I had and how to navigate this.
They were encouraging and supportive with every treatment. I learned that through illness, you build some resilience. You have to build resilience. I had things to look forward to. I had life to look forward to.
Even though the diagnosis was bleak initially, there have been advances in therapies and I continued to be positive about it. As such, I’ve continued to be involved. I went back to school and did all the things that you do when you’re not thinking about what’s going to happen. I never thought about whether the end was near.
I didn’t share my story with too many people. I was working for an airline at the time. They knew that I was ill. I would go for my treatments and go back to work. I kept one foot in front of the other and went about the business of living and not thinking about the alternative.
I took the resources that were presented to me and continued to learn about the new therapies.
What Resources Helped Me at the Beginning of My Diagnosis
My involvement with Myeloma Link took me into the community as a community volunteer at different events. They were in churches, in sorority and fraternity meetings, explaining what myeloma was and how you should continue to take care of your health. I became involved with another organization as well.
I took the resources that were presented to me and continued to learn about the new therapies. I spoke with my oncology team as well, who helped me through this process.
Materials were available to patients at Emory. I remember picking up a pamphlet. My initial involvement didn’t come until 2018 to 2019, but I had the material and I continued to research and read.
I decided after my stem cell transplant that I needed to become a little bit more engaged with my health as well as the community. I went to a conference, spoke with one of the representatives about volunteering, and the rest is history. I went through some training and shadowed a couple of volunteers.
They froze the cells, but I didn’t receive my stem cell transplant until 10 years later.
How I Found Out About CAR T-cell Therapy
I’ve only had two oncologists. My first doctor retired. He was slated to introduce one of his patients to CAR T-cell therapy. He had discussed this treatment with my family years prior. It was still in the developing stages then.
During a consultation visit, he talked to my husband and me about this new therapy and we agreed to it. We scheduled it after one of my graduations. I pushed it back a little bit because I wanted to walk across the stage, which I did.
I was in the hospital for about a week. I was fine for about two to three years and then I had to go back into treatment. It was explained to me that this treatment is the latest and greatest. I felt fine and still do. I’m back in therapy now getting a different treatment, but I’m nowhere near as ill as I was.
What It Felt Like to Do New Treatment Therapies
The only anxiety that I experienced throughout my experience was getting the stem cell transplant. I was receiving three different drugs twice a week for six months. In week 6 or 7, I went to the hospital to get the stem cell transplant. I reacted positively to the treatment initially. I distinctly remember that my stem cells were extracted on my birthday in 2008.
After all the paperwork and the discussions about how this was going to play out, I was downright scared of this treatment. It was explained that I was going to the hospital and would get a massive dose of chemotherapy. I remember asking my oncologist what this would do. He looked at my blood work and said, “It will get you to where you are now,” where the count was zero and the myeloma count wasn’t showing up. I said, “I don’t want it.”
They froze the cells, but I didn’t receive my stem cell transplant until 10 years later because I reacted so positively to the treatments that were being administered to me. I was happy about that, but that was the only time that I was scared about receiving some form of treatment.
I wanted to prove to myself that, despite all the different moving parts, I can still get this done.
I Earned My Doctorate Before My Second Stem Cell Transplant
It was fulfilling for me to earn my doctorate. It was something that I challenged myself with. At the end of the road, I was going to walk across the stage. I was going to go back to treatment at the same time I was going to graduate. I said, “This is something I want to do. Is that possible?” They said absolutely, so they rescheduled all the preliminary work for about three weeks. I was able to graduate and then go back to the hospital.
I wanted to do that also because when I finished my master’s degree, I was in the hospital. I was going to miss my last two classes. I was in my second-to-last class and I had to go to the hospital. My professor gave me a grade because I had done the work.
She was so instrumental in my graduating with my master’s degree. She came to my house and tutored me for my last class so I’d catch up. I’ve had a support system from the least likely of people, which gave me the drive to survive and say that I could do this.
I graduated with honors in my doctoral degree, and I was proud of myself. My family was proud of me. That speaks to being determined to do your best and not succumbing to the myeloma. Just because I don’t feel well doesn’t mean I’m not going to do this or that. That’s never been how I am. I wanted to prove to myself that, despite all the different moving parts, I can still get this done. And I did.
What I Learned About Life
You move past pettiness. When you’re diagnosed with cancer, you look at the bigger picture and what’s important. You look at what life is about. Sure, there’ll be ups and downs, heartaches, and all the things that one would experience when you’re not afflicted with a disease, but you learn to appreciate the beauty of small things.
I’ve learned to discover what else I can do, how I can help, and how I can give back. When I was at different events with The LLS and the public would come up to the table, I was the example of how you can continue to move through the disease.
Positivity is key. You don’t want to come into this journey with a defeatist attitude.
I was being asked questions, so I shared, but I didn’t go in depth. I let them know that I’m a myeloma patient and have been for X number of years. You can move through it. Not necessarily past it, but you can move through it with a sense of pride. I’m a survivor and I will continue to keep on surviving for as long as I can.
What I Want Other Multiple Myeloma Patients to Know
Remain positive. Be your own advocate. Understand what you’re going through. Ask the tough questions, even if you don’t want to hear the answers. Learn what may be available to you.
Positivity is key. You don’t want to come into this journey with a defeatist attitude. You need to keep your chin up. Strive for something. Appreciate life and its beauty. Love your family. Tell everybody you love that you love them. Live your life.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
Symptom: None; found through blood tests Treatments: Total Therapy Four, carfilzomib + pomalidomide, daratumumab + lenalidomide, CAR T-cell therapy, selinexor-carfilzomib
Why Showing Up Matters: Nat’s Caregiver Role in His Wife’s Muscle-Invasive Bladder Cancer Story
When Nat’s wife, Ebony, was diagnosed with muscle-invasive bladder cancer, life shifted dramatically for their entire family. As Ebony’s primary bladder cancer caregiver, Nat found himself navigating not only the physical demands of caregiving but also the emotional complexities of supporting a fiercely independent woman through something so life-altering.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
He wasn’t just present for her treatments — he became a constant, steady source of reassurance, encouragement, and strength, even when his own heart was breaking. Early signs were subtle, which included frequent bathroom trips and unexplained abdominal bloating. Ebony brushed them off at first, and like many people, she hesitated to push harder for answers.
When the diagnosis finally came, it hit like a punch. Despite medical appointments and proactive efforts, no one expected bladder cancer. Nat remembers the moment clearly, experiencing shock, disbelief, then anger, but he quickly moved into action mode, determined to be there every step of the way.
Throughout the experience, Nat stayed grounded. He didn’t try to predict the future or let fear take over. Instead, he focused on “conquering the day,” one at a time. His presence at every appointment spoke volumes. Even when words fell short, just showing up was a lifeline. That’s something every bladder cancer caregiver should know: being there matters more than having the right thing to say.
Navigating stigma was another layer of challenge. Bladder cancer isn’t always widely discussed, and Ebony didn’t fit the typical profile. Nat and Ebony leaned on bladder cancer support groups and online communities but were cautious, as too much information sometimes did more harm than good. Nat often had to remind Ebony to unplug from Google and focus on her story, not someone else’s.
Decisions about treatment — chemo, surgery, and eventually a neobladder — were daunting. But they approached everything as a team, asking questions, doing the research, and advocating for the best care possible. As a muscle-invasive bladder cancer caregiver, Nat learned how critical it is to be informed but not overwhelmed, to stay involved without letting fear drive every choice.
Nat and Ebony also had to help their sons understand what was happening without scaring them. That meant honest, age-appropriate conversations and plenty of reassurance. They were careful to preserve a sense of normalcy while allowing space for emotional reactions.
Now, years later, Ebony is doing well, and their relationship is stronger than ever. They celebrate the small milestones, like the first post-surgery walk or a day without pain. Nat says the experience taught him to cherish every moment and let go of the small stuff. He encourages other caregivers to do the same: stay present, speak love often, and make space for joy, even amid hardship.
Name:
Ebony G.
Diagnosis:
Muscle-Invasive Bladder Cancer
Staging:
Stage N2
Symptoms:
Microscopic amount of blood in the urine, which increased to a visible amount of blood
Pain when urinating
Weight gain in the midsection
Treatments:
Chemotherapy
Surgeries: removal of the bladder & bladder reconstruction (neobladder)
Thank you to Johnson & Johnson for supporting our independent patient education content. The Patient Story retains full editorial control.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
She never lost her beauty. She even became more beautiful after having experienced the ashes of her life.
Introduction
My name is Nat. I’m Ebony’s husband. My wife was diagnosed with muscle-invasive bladder cancer and I was her caregiver during that time. I’m not her caregiver now, but I still provide that support because it is needed even after recovery. I’m a father of three boys and a dedicated husband.
She would probably say that I’m an easygoing person. I don’t go from 0 to 100 easily. She would probably say I have a sense of humor. I’m definitely a jokester. I love to have fun. She’d describe me as pretty easygoing and laid back.
Ebony is a champion. Being there beside her and seeing everything that she had to go through, overcoming the internal challenges of the disease, as well as the external evidence of the disease, which played a big part emotionally and mentally.
She loves her hair and she knew that I loved her hair, so one of her biggest first concerns — and it may sound vain —was losing her hair. I know that played a big part in her daily walk through the cancer experience. She’s always had her hair. Some people don’t care about hair like that, but she did. I knew that was a big challenge for her.
She’s a very independent person, so having to rely on someone to help her do things that she used to do on her own was a big challenge.There were times when she was in the hospital and her heart rate was out of control, but she still needed to walk. She’s a determined individual as well. She could be stubborn, but stubbornness can work to your advantage, too.
In this battle, she was definitely stubborn. She was not going to lie there and die, and not do what needed to be done to become better. When I see her, I see her as a champion, a warrior, someone who overcame, and a good, stubborn person. I see all of those things.
She never lost her beauty. She even became more beautiful after having experienced the ashes of her life. She grew into something different and better.
She started going to the restroom frequently… My antenna started going up a little bit, but I still did not think it was cancer.
How Ebony’s Muscle-Invasive Bladder Cancer Symptoms Started
Initially, she didn’t share with me the symptoms that she was experiencing. Like many of us, when we experience something that isn’t such a huge red flag or shocks us into getting checked, we don’t move, so that’s probably why she didn’t initially. If she did, it was probably very casually done, so it wasn’t alarming.
As time went on, I recall her beginning to share more of her gaining weight in her stomach, which wasn’t an area where she gained weight.
I’m very observant, so I noticed she started going to the restroom frequently. As soon as she came home, she would go to the bathroom immediately. My father had prostate cancer and I saw the frequency and urgency that which he would have to go. My antenna started going up a little bit, but I still did not think it was cancer.
She said, “I’m going to go to the doctor because something is not right. I don’t gain weight here. I frequently have to go to the bathroom.”
Getting to the Diagnosis was Frustrating
It was frustrating for somebody to tell you that nothing is wrong when you know that something is wrong. I can’t diagnose myself. I can’t open my body up to find what’s going on, but I know that something’s going on inside.
When she went to the doctor, she called me and said, “They’re saying it’s just normal. This could just happen with age or being a mother.” You go on with your day because you want to lean into what the medical professionals are telling you. You want to believe that.
The process of getting the diagnosis was a challenge. Then, to get the muscle-invasive bladder cancer diagnosis, suddenly, everything is zoom zoom zoom. As you’re thinking about what’s to come, you’re thinking about what happened.
How did we get here? We checked the boxes. She was going to the doctor. She was seeing the urologist. She was going to the gynecologist. She was doing everything right, yet here we are.
To worry is to have already given an end to a beginning that has never started.
How I Supported Ebony in That Year and a Half to Diagnosis
I try not to think so much ahead. I’m not a worrier, but it’s not because I’m such a strong person. To worry is to have already given an end to a beginning that has never started. I know that if I go into that headspace, then it’s going to cause stress and spill over from that.
I’d say, “You’re good. Everything’s fine. It’s going to work out.” I didn’t have a medical answer, so I could not speak to that. I just had a faith answer that it was all going to work out. You were going to be fine. It wasn’t going to be that bad.
The Moment Everything Changed
When he uttered those words, I could not believe it. I was in a state of disbelief. I looked over at Ebony and instantly saw her eyes. I asked the typical questions: What are we looking at? What’s the next step? What do we need to do? Where do we go from here? How bad is it? You think about all of those things very quickly.
Then I felt a sense of anger because she’s been getting checked, and now this is what they tell us. The doctor just blurted it out.
Ebony was crying, walking out of the doctor’s office. It seemed like the world stood still because you’re trying to process everything. It was not until we pulled into our driveway and I parked the car that I began to cry.
Going through the cancer experience and the healing journey, you have to be careful of the environment that you keep and what you take in.
Nobody wants to hear those words. It was already a delicate time for me. My father had passed away in 2020 and 30 days before him, my older sister had passed. My heart was delicate.
I know I said earlier that I had faith answers for things, but I’m not the individual who does not understand. I’m human and I have human thoughts and emotions. When you hear the word cancer, you automatically think death sentence.
You automatically think, “How much time do I have?” That’s where your mind goes when you’ve had people who have passed away from cancer. After I got over that moment, it was, “This is what we have to do. What’s the schedule? Here we go.” It was time to do that. Now it’s time to compartmentalize because we have things to do to kick this cancer’s behind.
How We Learned More About Bladder Cancer
Bladder cancer was unique to us. We didn’t know anybody to call up and ask. She didn’t fit the mold of what they said a bladder cancer patient should look like, so we didn’t know where to go or who to ask.
My wife is a researcher. She was going to Google. The medical practice gave a manual of support material. The resources they gave her were helpful.
There were support groups that we didn’t even know existed. I found a support group on Facebook that we joined. But because it’s the Internet, you have to be very careful. Going through the cancer experience and the healing journey, you have to be careful of the environment that you keep and what you take in.
You have to be careful what you read and what you process because some people will quickly make it a death sentence. Some people will share with you how they had a friend who had the same sickness and died within two years. It’s not their intent to hurt you, harm you, or make you afraid. Now, because that’s what you see, that’s what you accept, so we had to be careful of that.
There weren’t a lot of options and we didn’t have time to decide what we were going to do.
I had to tell her to put her phone away and say, “Don’t read that today. I don’t need you scrolling through the comments. That may be their reality, but that doesn’t mean that it has to be your reality.”
She’s a very smart person. She’s a chemical engineer, but I have to tell her to stop Googling, “You’re not a doctor, so you may not understand the verbiage that they’re using. It causes extra stress on you that you don’t need for your healing process.” You don’t want to walk in ignorant concerning your diagnosis or what the physicians have told you, but you still have to be careful.
Discussing the Treatment Plan
The options were chemotherapy and surgery. When we got the diagnosis, he said, “It’s very aggressive. We have to start now.” There weren’t a lot of options and we didn’t have time to decide what we were going to do. It was this or that.
She underwent chemotherapy and surgery. There were more options with the type of surgery than for the treatment plan per se. You can get the neobladder that she has or have the bag attached for life, which she definitely did not want. Being in her mid-40s, she was still in her prime. She didn’t want the bag.
I give the team kudos. They were phenomenal. They never made you feel like a burden. They were very empathetic and professional. It made the decision to go with the neobladder, the chemotherapy, and the surgery very easy.
My first concern was, “How does your body function without a bladder?” When I was a kid, all the way up through a portion of high school, I wanted to be a doctor. This was interesting. He’s explaining what it will look like. I’m thinking, “No bladder. That’s not pretty. We need a bladder. You have to have one. How does this happen?”
If you want to support someone as a caregiver, your presence matters.
Then he talked about creating a bladder out of your intestines. I asked him, “Can you not do a bladder transplant? You can transplant hearts, lungs, and kidneys. Can’t you transplant a bladder?” He said, “We’re not there yet, but this is the next best option.”
We researched and were ready to go with it. You’re nervous about it, of course, because if he’s not the only one, he’s one of the very few who specializes in neobladders. I thought it was amazing, but at the same time, it was pretty risky. I was between impressed and scared.
Ebony was pretty calm, but because I know her, I knew she was nervous. She had her questions ready. I don’t think we went into an appointment where she did not have her questions ready. She had the research that she had done on different options. She was nervous, but she never cried. She wanted to get the facts. Whatever she needed to do to survive, she was ready to do that.
How We Continued to Communicate
It wasn’t hard because you have a big elephant in the room that you cannot ignore. You have to talk about it. You have appointments almost five days a week. You may have three appointments in one day. You have to talk about it because it’s not just the two of you. We have children. We have careers. There’s a lot of communication that has to be done for things to keep moving.
As soon as she was notified of an appointment, she would automatically send it to me so I could put it on my calendar. Everything would be scheduled that way. There wasn’t an appointment that she went to that I did not go to, which was very important.
If you want to support someone as a caregiver, your presence matters. Your words may not always matter, but your presence matters, and that was a way of communicating through this experience. Even today, that’s our way of communication.
If you conquer the day, you’ll be okay, and that’s what we continue to do.
Looking Back at Ebony’s Story with The Patient Story
I remember the headspace that she was in. I told her, “You don’t have to worry about that,” and she started saying, “But…” “There are no buts. I’m not going anywhere. You don’t have to worry about that. I’m going to be here. Let that be the least of your concerns.”
Sometimes, she can be stubborn. Here is where you have to watch what you read. She would say, “This person said this,” and I’d tell her, “I’m not that person. You know how I feel about being compared to anybody. I’m not them and we’re not going there, so let’s move on.”
What’s interesting is I didn’t even think about it. Even when we were talking to the nurse and the nurse brought that up, I was not thinking about that. We’ve been together almost 20 years. If you cannot control yourself in moments like this, you have a bigger problem in your marriage.
I even saw some of the comments in her interview where wives were saying their husbands left. My mind did not go there. It doesn’t mean that you are less of a man; that means you’re more of a man because you can now place the need for healing of your spouse over the need for a few moments of pleasure.
You’re trying to have a lifetime of pleasure. You’re trying to have more pleasure in your life with the person you say you love. Surely, I can put that on the back burner and focus on my spouse getting back to a place of wholeness because right now, she’s experiencing some brokenness. That’s where my mind was.
Where We Are at With Survivorship
You would not even know that anything happened. We celebrate the anniversaries, if you will, of that experience because it helps you appreciate where you are.
One of the things that I did right before her surgery was to take her and the family to the beach. She loves the beach and so do I. Being a travel business owner, I researched where we could go. We went to the beach and had an amazing time. I knew it would be a while before we could go anywhere and I knew she was very worried.
We were approaching a surgery that was about to change her life forever. I wanted to do that for her. We continuously celebrate the milestones — the day when she was in the hospital, the time when she couldn’t walk by herself — and that helps that wholeness be there.
Physically, I know she knows and probably thinks within herself that there’s still something different. Her body was not designed this way. She has to self-catheterize. But the wholeness of her emotions and her mental space is what it is. Even when she was concerned about her hair, her hair grew back better than it was before she lost it.
My thing for her was to conquer the day. If you conquer the day, you’ll be okay, and that’s what we continue to do.
The outpouring of support, love, prayers, and gifts was unreal. I believe that made an impression and an impact on our sons to see that we were not in this by ourselves.
How We Told Our Sons
Talk about communication. That was a big piece of communication because you are concerned with how you’re going to tell your children something that they should know without scaring them. Ebony said, “Nat, you tell them because you are good at that. I will probably start crying, but you know how to communicate and bring some assurance to them.”
We brought them all together on the couch. I told them what she had been diagnosed with, what she’s going to experience, and the changes that they’re going to see, such as her hair. But I told them she’s going to be fine. Ebony and I did our very best to make every day as normal as it could be.
The boys’ demeanor is like mine. They’re not going to worry. After we told them, they went on about their day. Sometimes, she would wonder if they’re worrying because teens have a way of not expressing themselves in front of you, but it comes out through other channels.
We think it affected our middle son as far as his studies. We met with his counselor as his grades dropped during that period and we told them what was going on during that time. We needed to communicate with our children and be as prepared as we could for any questions that they had. I told them if they had any questions or felt any type of way, they could ask and talk to me about anything.
The outpouring of support, love, prayers, and gifts was unreal. I believe that made an impression and an impact on our sons to see that we were not in this by ourselves. We had our parents or close friends come and look after them when we couldn’t be here or running around a lot. That’s how we navigated with our sons.
One of our good friends organized a meal train. People were dropping off food for dinner. When she was having chemo, I was at the hospital with her. They were even bringing food for me to the hospital. It was a breath of fresh air. Humanity may not be as bad.
You look at life through a different lens.
How I Was Taking Care of Myself During That Time
Honestly, I don’t think I did anything different. I had to be present and positive. I did have a few moments, but when I did, it was never in front of her or the children. Maybe because I was present, doing what I should do, so I didn’t feel like I needed to do anything extra to take care of myself.
People asked me, “Are you okay?” The wife of a good friend of mine, who was also my pastor back home, was going through cancer at the same time, so he and I would communicate. I remember calling to tell him the news once we made it public. When I shared it with him, we almost had the same story, just different types of cancers.
What Changed in Our Relationship
We enjoy more moments together and life in general. You look at life through a different lens. You don’t start majoring in minor stuff. There’s a saying about protecting your peace. You do adopt that. I am not about to deal with drama and this, that, and the other. I’m about to enjoy my life because you see how quickly life can change.
Just because she went through cancer doesn’t mean that we never disagree. It doesn’t mean that we don’t have arguments. It doesn’t mean that she doesn’t get upset with me and I don’t get upset with her. What it has done is make us not sit there and be angry forever, which I never did anyway. We can’t be doing this. It shifts and changes.
Every loss should make you appreciate the game. Every challenge should make you appreciate overcoming. Every day is a literal blessing to be alive. I tell people that the last four years of my life are one of the hardest periods, which included the losses and Ebony getting diagnosed with cancer. It shifts your thinking.
We now live in a space of living. She loves flowers. If you want to go outside and pick hydrangeas, go ahead and do that. Who cares? Nobody cares. If you want to roll around and frolic in the grass, who cares? As long as you are enjoying the time that you have.
For my birthday, she took me to San Francisco to watch a Golden State Warriors game versus the Lakers. I’m not a Lakers fan, but she took me there. It was amazing. It all speaks to enjoying the moment and enjoying life. That’s what I tell everybody. While you have the time and the opportunity, enjoy life.
I’m a person of faith, so I pray… It will get hard and you want to be there for that person in the best way that you can.
What I Want Caregivers/Partners to Know
Be present and be supportive. Be informed because it’s not a cancer that, from what I’ve seen, has a lot of information out about it. It’s becoming more discussed now than it was a few years ago, but do your best to stay informed.
As a caregiver, be present and remain positive. You’re not living in a space of untruth. Yes, this is your truth. This is the reality, but you have to become selfless as a caregiver. You have to assure that person that you are there for them. No matter how unattractive they may feel they are, they are the most beautiful thing that has ever walked this earth.
When Ebony came out of surgery, she was swollen. Nobody told us she was going to be like that. As I walked in, she had come to and was somewhat alert. She knew it was me. I was taken aback, but I couldn’t show that. You have to become selfless.
I’m a person of faith, so I pray and that is one thing I would definitely say to do. It will get hard and you want to be there for that person in the best way that you can. There were times when she was in the hospital and I couldn’t say anything. All I could do was be there and hold her hand. That was it.
There were times when she was in pain, moaning and groaning throughout the night. She doesn’t even remember that, but I couldn’t do anything. Nothing. That’s how you realize how little we are, when you cannot control the pain or the situation. It was the presence that contributed to her wholeness.
To anyone who is a caregiver to someone with bladder cancer, be a reassuring individual and a force in their life. Things may change, but let them know that you’re not going anywhere and they’re going to be all right. Let them know you’re going to live life to the fullest and conquer the day.
I believe God is always there, even in those moments of fear, doubt, and questioning. You’re never alone.
My Message of Hope
I know that my presence was there with her. I was not the one with cancer. Your friends can love on you, call you, be supportive, and be there for you, but you can still sit there and think, “I’m the only one. They don’t have what I have. They haven’t been diagnosed with what I have. They have a full bladder. I have one that’s been created out of my intestines.”
You may feel alone, even in a crowd. However, you’ve got to know that you’re never alone. There’s somebody who is going through the exact same thing as you or even worse. There were periods when she discovered somebody else who had bladder cancer, but their story was not turning out the way hers was. It made her and me even more appreciative and grateful for it being better than what it could have been.
I believe God is always there, even in those moments of fear, doubt, and questioning. You’re never alone. This may be a stretch for some people, but lean into your peace.Conquering the day is what I told her every day of chemo because she had to lean into that. That brought peace not only to her but to me.
None of us knew what the outcome would be. We hoped for it and prayed for it to be a certain way, but we didn’t know. Guess what? If I’m going to go through this, I can’t go through it spinning out of control. I don’t know what’s going to happen and I can’t put death as my today. We’re just going to conquer this day, this moment.
That’s my message of hope to anyone going through the situation. Conquer the day and you will find out that you’re stronger than you thought you were. There’s a little angel somewhere rooting for you, pushing for you, and clapping their hands like our little son did. He was sitting at the table, then he looked and started clapping because he saw his mom walk with me for the first time without her walker. There’s always an angel somewhere.
The Power of Holly’s Self-Advocacy in Rare Cancer Detection
When Holly started feeling a nagging pressure in her jaw back in 2021, she never imagined it would lead to a diagnosis of stage 1 adenoid cystic carcinoma. The pain was subtle at first, almost like a pinch, but persistent. Like many, she turned to Google. She initially suspected a temporomandibular joint (TMJ) disorder and saw her dentist, but he said it wasn’t and thought it was stiff muscles or tension.
Due to Holly’s history of vertigo and dizziness, she saw her ENT. After a thorough exam, he said it didn’t seem to be anything to worry about. He offered to do a CT scan, but Holly thought it might be an inner ear issue, so she didn’t pursue that path. She even went to see a rheumatologist in case it was an autoimmune issue.
Holly knew something wasn’t right. Her inner voice kept nudging her, so she continued pushing for answers. The rheumatologist suggested that she see a maxillofacial surgeon, who ordered an MRI, revealing a 0.5 mm mass in her parotid gland.
The mass was originally thought of as a lymph node, but Holly pressed forward. She found a specialist who finally offered a needle biopsy, a decision that changed everything. The pathology report came back with the official diagnosis of stage 1 adenoid cystic carcinoma. The news felt overwhelming. Holly had never heard of this rare cancer before.
Researching online only amplified her fears. What stood out most wasn’t the medical terminology, but the realization that many people discover this disease far too late. Holly caught it early, which her surgeon said was almost unheard of, especially given the tumor’s minuscule size.
Surgery followed, but the first attempt missed the tumor. Undeterred, Holly advocated for a second surgery with an ultrasound used in real-time. It worked. The tumor was finally removed and margins were clear.
Because it was stage 1 adenoid cystic carcinoma, her team decided against radiation due to the clean surgical outcome and the harsh side effects of facial radiation. Instead, they began a rigorous scan schedule. She now gets checked every six months, and so far, everything’s been clear.
Through her entire experience, Holly emphasizes one powerful message: self-advocacy is everything. She was persistent. She didn’t doubt the professionals, but she trusted herself, too. Her story is a powerful reminder that knowing your body, trusting your instincts, and refusing to settle for vague answers can make all the difference, especially with a rare diagnosis like stage 1 adenoid cystic carcinoma.
Today, Holly works full-time, volunteers, and spends every possible moment with the people she loves. She’s not taking anything for granted. Her gratitude is real, her perspective is grounded, and her story might just empower someone else to speak up — and speak out — when something feels off.
Watch the full video of Holly’s interview to find out more about her story:
What to do when every doctor says wait and see, but your gut says to keep pushing.
How Holly spotted stage 1 adenoid cystic carcinoma before anyone else even suspected cancer.
Why she chose to skip radiation and what gave her the confidence to say no.
What convinced her to keep advocating when the scans looked “normal.”
Name: Holly A.
Age at Diagnosis:
49
Diagnosis:
Adenoid Cystic Carcinoma
Staging:
Stage 1
Symptom:
Persistent jaw pain
Treatment:
Surgeries: two parotidectomies (second with intraoperative ultrasound guidance)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: Sore on the tongue, which caused pain during eating and speaking; changes in the color and texture of the tissue where the sore was located Treatments: Surgery (partial glossectomy, radical neck dissection, reconstruction), radiation
...
Jackson’s Stage 3 Colon Cancer at 26: Difficult Days While Trying to Keep a Routine
When Jackson was diagnosed with stage 3 colon cancer, right before his 26th birthday, it came out of nowhere. He had only been experiencing abdominal pain for a couple of weeks, which led to a trip to the ER for dehydration, only to discover something far more serious. The shock of hearing “colon cancer” at such a young age was overwhelming, especially with no family history and no warning signs.
What followed was a whirlwind: emergency scans, a colonoscopy, a biopsy, and a surgery all within days. Even before the official diagnosis of stage 3 colon cancer, Jackson had already undergone a transverse colectomy. It was fast, intense, and life-changing. But through it all, Jackson found strength he didn’t know he had.
There’s been a concerning rise in colon cancer in young adults, and Jackson’s experience highlights why awareness and timely attention to symptoms, no matter how seemingly minor, are critical. At an age when most people are focused on careers and relationships, Jackson was juggling chemotherapy with prepping for the bar exam. Instead of slowing down, he pushed through with grace, humor, and a lot of grit.
What stood out most in Jackson’s story is his mindset. He didn’t sugarcoat the hard days — like the allergic reactions to chemo, the side effects that made him feel decades older, or the anxiety of waiting for scan results — but he emphasized the power of keeping a routine, doing “normal” things with friends, and finding ways to enjoy life even during treatment. Reclaiming small parts of normalcy helped him feel human again.
Jackson also credits a lot of his resilience to his support system: his fiancé, family, friends, and coworkers, who helped keep him grounded and encouraged. Their presence gave him something to lean on during the hardest moments. Jackson wants others facing stage 3 colon cancer to know that they’re never truly alone.
Today, Jackson’s cancer-free, grateful, and looking forward to all the parts of life that once felt uncertain. His message? Believe you can get through it. Lean on people. Stay hopeful. Live your life. And never be afraid to speak up when something feels off.
Watch Jackson’s interview to find out more about his story:
How Jackson didn’t let cancer stop him, even if he was diagnosed with stage 3 colon cancer just before taking the bar exam.
How he found hope, balance, and even joy in the middle of treatment.
How subtle symptoms led to a life-changing diagnosis.
From chemo infusions to hanging out with friends, Jackson made living through cancer feel possible.
How he used mindset, support, and routines to power through cancer treatment.
Name: Jackson A.
Age at Diagnosis:
25
Diagnosis:
Colon Cancer
Staging:
Stage 3
Symptom:
Sharp abdominal pain
Treatment:
Surgery: emergency transverse colectomy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Advancements in Metastatic Breast Cancer Treatment & What They Mean for You
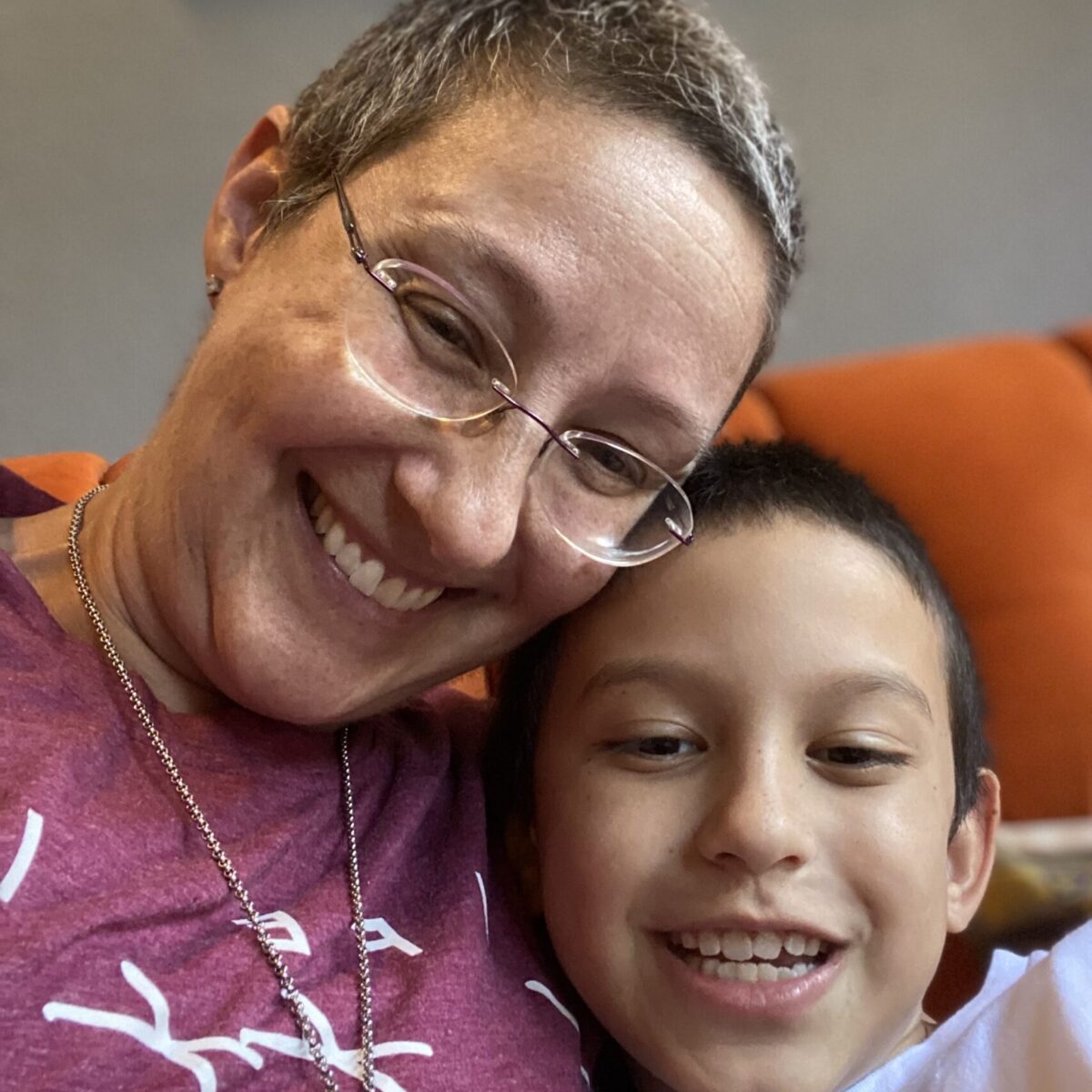
Abigail Johnston was a successful lawyer and mother of two young children, living a fulfilling life before being diagnosed with stage 4 metastatic breast cancer in 2017. Her diagnosis, with a prognosis of just 12 to 36 months, was devastating, but she chose to take an aggressive approach to treatment.
Abigail shares the emotional toll of her diagnosis, how she focused on being present with her family by closing down her law practice, and then highlights the power of how understanding more about her disease would change her life, specifically in understanding her cancer biomarkers.
As she reflects on the incredible advancements in metastatic breast cancer treatments and the hope she holds for long-term survival, she brings in another top expert voice, breast cancer specialist, Dr. Neil Vasan from Columbia University, to discuss the latest updates from the largest breast cancer meeting in the world, San Antonio Breast Cancer Symposium.
They talk about the most promising treatments that may be close to FDA approval, how getting tests to understand your disease can completely change your life, and even how the weight loss drugs like GLP-1s have entered the conversation in breast cancer.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
Some live for 15, 20, and even 25 years with stage 4 metastatic breast cancer.
Introduction
Abigail Johnston: I have been living with stage 4 metastatic breast cancer. At the age of 38, I was told I had 12 to 36 months to live. As a young person in the middle of my career with two young children, hearing that was devastating and overwhelming.
I chose to be more aggressive and have my treatments happen in a certain way because I’m always thinking of being present with them. I closed my law practice about a week after my diagnosis because if I was going to have limited time, I wanted to spend all that time possible with my kids and not in the office. I count those times with my kids and my husband as so much more valuable.
Some live for 15, 20, and even 25 years with stage 4 metastatic breast cancer. We need to understand why they live for a very long time. Is it a particular medicine? Is it a particular biomarker? Is it something about their genetics? That’s where precision medicine comes in.
Dr. Neil Vasan: Breast cancer is multiple diseases. It can be estrogen receptor-positive, triple-negative, and HER2-positive. This discussion is for women and patients with metastatic breast cancer, but of course, we have a lot of advancements happening in the curative breast cancer setting.
We think about screening and genetic mutations, and the advances there, which straddle all types of breast cancer. Especially for this audience, three important trials were either initially presented or updates were presented at the 2024 San Antonio Breast Cancer Symposium.
According to the National Cancer Institute: “Clinical trials test new ways to find, prevent, and treat cancer. They also help doctors improve the quality of life for people with cancer by testing ways to manage the side effects of cancer and its treatment.”
For a lot of metastatic trials in the past, we have used tissue biopsy, which is obviously more invasive and takes time to analyze. This trial utilized liquid biopsies in approximately 93% of patients, which was remarkably high. It also enabled this trial to report results quickly.
Dr. Vasan
INAVO120 Clinical Trial
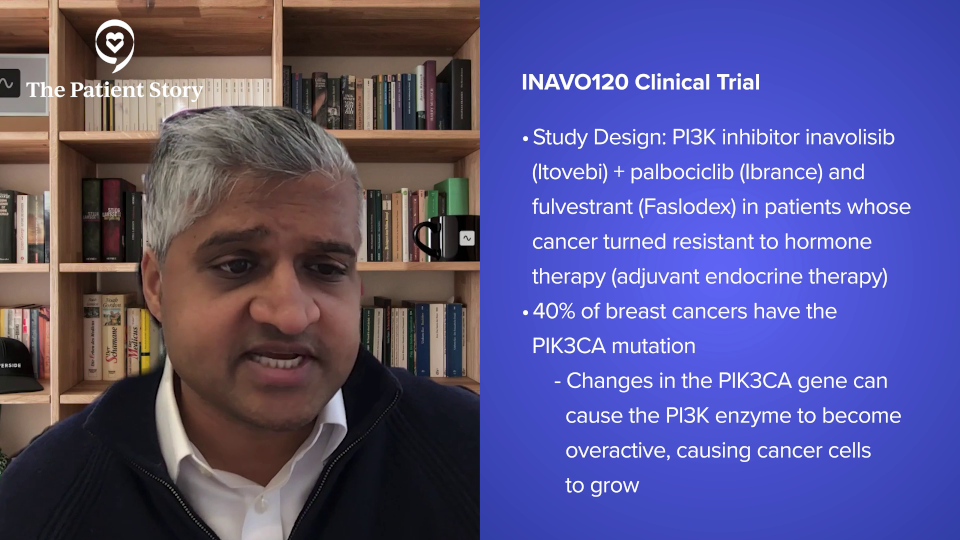
Dr. Vasan: The first clinical trial is INAVO120, which is a trial testing PI3 kinase inhibitors in the first-line setting in women who have progressed on adjuvant endocrine therapy. Thankfully, this is very rare, but we do see it. We do know that there are women who only get one or two years of mileage out of these therapies. Sometimes, these therapies can just stop working. This is a hard discussion with patients because the therapies that we think are supposed to cure you didn’t work.
This was a trial that looked at a type of drug that we give in the later line setting of breast cancer. This is called a PI3 kinase inhibitor. This is based on the fact that 40% of breast cancers have mutations in PIK3CA, which is the main engine of this pathway.
What was interesting about this trial was that they investigated this drug in combination with palbociclib, a CDK4 and CDK6 inhibitor, and fulvestrant in women who had either progressed on adjuvant endocrine therapy or progressed one year with infection. This patient population has very resistant disease.
There are a couple of interesting things about this trial. When this trial was initially reported, it doubled progression-free survival. Very recently, we had a press release stating that it improved overall survival. We don’t yet know the numbers for the overall survival improvement, but this is a significant achievement in the field. It’s the first time for a PI3 kinase pathway inhibitor to have improved overall survival in metastatic breast cancer, so that is a huge deal.
We’ve had drugs like everolimus that have targeted this pathway for decades, but we’re only now starting to see the fruits of that. The reason why overall survival has improved is because of a combination of factors. First of all, we’re using this drug in the first-line setting, so we’re putting all the weapons in one go in trying to eradicate breast cancer.
Second, we, as a field, have made a lot of progress in monitoring toxicities and making sure that these therapies have manageable toxicities. That was another important part of this trial. It was a drug that’s better tolerated than alpelisib, which is FDA-approved.
Lastly, this trial enrolled quite quickly because it used liquid biopsies. For a lot of metastatic trials in the past, we have used tissue biopsy, which is obviously more invasive and takes time to analyze. This trial utilized liquid biopsies in approximately 93% of patients, which was remarkably high. It also enabled this trial to report results quickly.
Some of the things I’ve mentioned have to do with the science, but some of them have to do with implementation issues and toxicities, which are science as well, but in a different way. All of these variables matter. This trial is practice-changing and I’m looking forward to hearing about the overall survival data.
Editor’s Note: This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
EMBER-3 Clinical Trial
Dr. Vasan: The second trial was looking at a drug called an oral selective estrogen receptor degrader (SERD). The EMBER-3 trial was investigating a drug called imlunestrant, which is sort of an oral version of fulvestrant that degrades the estrogen receptor. There’s already an FDA-approved drug called elacestrant, which is for women whose breast cancers have mutations in the estrogen receptor or in a gene called ESR1.
We see these mutations in about 15 to 20% of patients. I would say that number is a little bit all over the place if you look at the literature. We know that this mutation arises because it is a drug-resistant mutation to aromatase inhibitors. Women whose breast cancers progressed on adjuvant aromatase inhibitors often can get this mutation.
Imlunestrant was tested in combination with abemaciclib or a CDK4/6 inhibitor. This was a trial that looked at a complicated trial, but the gist is that in women whose breast cancers harbored an ESR1 mutation, those women had a longer progression-free survival if they took imlunestrant versus an endocrine therapy of their physician’s choice, which might be fulvestrant or an aromatase inhibitor monotherapy.
There were other more complicated arms of the trial where they looked at the combination of imlunestrant and abemaciclib in patients who had progressed on CDK4/6 inhibitors in the second line. Those resulted in positive data. They had improved progression-free survival. I’m not going to delve into the details of that because, honestly — and I say this as a breast oncologist — it’s challenging to understand exactly. The comparator arms were not necessarily what we would use in the second-line setting.
For any average patient in the second-line setting, we would obtain their genomics, figure out the exact targeted therapy, and then give them that therapy. This trial did not test that particular question. It showed that this combination has efficacy, but it’s hard to understand who the right patient population is. I look forward to seeing how the FDA weighs in on the combination. I anticipate that imlunestrant as a monotherapy is going to be a drug that we see being approved.
I was impressed by the imlunestrant side effect data. If this drug gets approved, I think it will be the preferred drug compared to elacestrant. The reason I say that is not because of the efficacy data, because the efficacy was pretty similar across both trials. It’s more because of the toxicities.
Elacestrant is a drug we give in the clinic. The nausea is very real for these patients. Imlunestrant looks like a cleaner drug. That being said, with all of these drugs, we don’t know how they work until they get deployed in the real world. That’s where a lot of you are very helpful. You can raise awareness for certain types of side effects that we either know about or may not get a lot of publicity, but then in later years, we find out that it’s a big deal.
An example of that side effect is inflammation of the lungs from CDK4/6 inhibitors. That was something that didn’t bear out in the phase 3 clinical trials, but it was patient advocates who noticed these side effects. Oncologists noticed these side effects in small numbers. The FDA did a big analysis where they pooled all of this data together and found out that this was actually a safety signal. This is where you all can be very helpful, as these drugs get newly launched into the real world to help us figure out the toxicities.
PATINA Clinical Trial
Dr. Vasan: The third trial is PATINA, which is an exciting trial and speaks to the fast-moving pace of this field. This hasn’t been published yet, but it is amazing and groundbreaking. The science is one part of it, but the dissemination of the information is another very important part.
Again, this is where patients can advocate. You want these data as soon as possible. Oncologists have already started to implement these results into clinical practice before the paper has been published.
This trial looked at women with HER2-positive metastatic breast cancer who are also ER-positive. HER2-positive breast cancer comprises about 20% of breast cancer and about 70 to 80% of that 20% is estrogen receptor-positive. We sometimes call this triple positive. Generally, we treat these cancers as we treat the HER2 component and then we tack on hormonal therapies in the adjuvant setting and metastatic setting as well.
This trial investigated the addition of CDK4/6 inhibitors, which we know improve overall survival in estrogen receptor-positive, HER2-negative metastatic breast cancer. What about testing it in estrogen receptor-positive, HER2-positive metastatic breast cancer?
It’s a little more complicated because the therapy is a combination of chemotherapy (paclitaxel or docetaxel) with anti-HER2 antibodies trastuzumab and pertuzumab. This is the THP regimen, which is the CLEOPATRA trial. It has been our standard of care for many years now and improves overall survival. It’s the best combination we have in this disease.
They gave the THP therapy. Normally, we give chemotherapy for six cycles, stop chemotherapy, and then patients will be on just trastuzumab and pertuzumab. That’s a great moment in any patient’s disease trajectory and treatment trajectory because once they’re off chemo, the HP (trastuzumab and pertuzumab) has very very few to no side effects.
Patients tell me it’s like getting water. Again, not to minimize anyone who’s had side effects from these drugs, but in large populations, they’re very well tolerated. At that point where we would normally drop the chemo, we would oftentimes add hormone therapy in these patients who are ER-positive, so also adding a CDK4/6 inhibitor, adding palbociclib.
They found that when they did that versus without adding palbociclib, the progression-free survival improvement was gigantic. It went from 29 months to 44 months. One chestnut about this data, if anything, that makes this underappreciated or underrated is the delta or the change between the therapy arms.
You want a big delta. That shows your therapy works. The delta of 12 months is higher than the delta in progression-free survival in ER-positive metastatic breast cancer, meaning that the addition of the CDK4/6 inhibitor is, by these data, maybe even doing more than what we thought it was doing in ER-positive, HER2-negative breast cancer, where CDK4/6 inhibitors transform the landscape.
This is exciting from a therapy point of view. I hope with all my heart that this results in an overall survival improvement. We still need to see, but this is exciting. I think the data blew everyone out of the water. When the progression-free survival curves were shown, there were audible gasps in the audience. We don’t get moments like that a lot and that’s wonderful, so I’m excited about this data.
Taking a big step back, the way that they conducted this trial was interesting because there are other targeted therapies that we use in ER-positive breast cancer, like Akt inhibitors and PI3 kinase inhibitors. PIK3CA is mutated in HER2-positive breast cancer in about 40% of women. Unfortunately, we already know that the antibodies don’t do very well in PIK3CA mutant cancers; antibody-drug conjugates (ADCs) seem to do better.
This is an interesting area to start putting in some of these targeted therapies that we only give in ER-positive breast cancer into the ER-positive, HER2-positive space. We’re going to see a lot more trials doing this paradigm.
That’s something for patients who may have ER-positive, HER2-positive metastatic breast cancer. This is going to be a very fast-moving area. We’re going to see a lot of trials by many companies and even cooperative groups combining all of these therapies.
There’s still a lot of complexity because you could imagine, this is now going from three drugs to four or five drugs. We have to think about toxicity, but this is incredible data. I was floored when I saw this because I was not expecting it as well. Again, that’s wonderful for all of you.
That’s an interesting example where these important questions that you raise, Abigail, form the hypotheses for clinical trials that are tested rigorously and prospectively, which can help change or guide future treatments.
Abigail: In that context, we know this information, but nothing’s been published yet. Is that correct?
Dr. Vasan: Nothing’s been published yet. Many of us have already started to change our recommendations based on this. Of course, this is a conversation with patients. We have an initial glimpse into the data, but we don’t have all the answers right now. This is such an amazing improvement. We hope that insurance companies and oncologists will advocate for you to try to get this and work their hardest to get this drug if this applies to you. Again, this speaks to the fast-moving nature of this field and how it’s so imperative that we get these results out as soon as we can for everyone.
Abigail: We talk about lines of treatment and how, with each line of treatment, usually you can’t go back once you’ve been on a line of treatment. When we talk about these combinations, is there a concern that we’re potentially taking up two lines of treatment in these triplets? What are your thoughts on that?
Dr. Vasan: Our thoughts on that have evolved. There were discussions five years ago about whether patients whose disease progresses after a CDK4/6 inhibitor in the first-line setting should switch to two different therapies, or if we should keep the CDK4/6 on and change the endocrine therapy, or vice versa. These are studies that have been reported.
We know now that switching the CDK4/6 inhibitor in the second line in large populations of women improves progression-free survival. That’s an interesting example where these important questions that you raise, Abigail, form the hypotheses for clinical trials that are tested rigorously and prospectively, which can help change or guide future treatments.
I do think it’s an important question. With INAVO120, this triplet regimen, you’re using three good drugs all in the beginning. There’s clearly going to be more toxicity, which is also something that has to be dealt with. But is that the best thing to do for these patients? I would argue that the overall survival is positive. We don’t know what the numbers are yet, but that’s a great sign and rationale for why you would want to give all of those drugs.
These are the academic discussions we have as oncologists and with patients as well. Sometimes, there are discussions about adjuvant CDK4/6 inhibitors. We know that these drugs improve disease-free survival. They prevent breast cancer from coming back, but we don’t know if they improve overall survival. They may, but it’s possible that they may not. The trials were not necessarily powered to answer that question. They were smaller trials, so we don’t know.
Should we offer this drug or give this drug? Offering versus giving in shared decision-making are two different issues. Should we be offering this drug to all women who meet these criteria? We don’t know if it helps them live longer. These are questions that we wrestle with every day.
For this triplet therapy, the fact that it improves overall survival is a great win for patients. It’s a complex decision because it adds more side effects in the first-line setting. Normally, patients in the first-line setting are not used to having lots of side effects in general.
Abigail: Thank you for that overview. It can be a little complicated for patients to look at these statistical analyses and graphs. They’re a little Greek to those of us who don’t have that background, so it’s always good to have a doctor interpret. It’s also important to see the evolution of science. We know what we know today, but we’re going to know more tomorrow because of clinical trials and ongoing research.
The Impact of Antibody-Drug Conjugates (ADCs)
Abigail: You mentioned ADCs. There were some conversations about antibody-drug conjugates and sequencing.
Dr. Vasan: Antibody-drug conjugates have changed the landscape in the treatment of breast cancer. We now have antibody-drug conjugates that are approved in all three subtypes of breast cancer. For HER2-positive, we have trastuzumab emtansine (TDM1) and trastuzumab deruxtecan (T-DXd). For HER2-positive and triple-negative breast cancer, we have sacituzumab.
For HER2-low, which was triple-negative/ER-positive but HER2-low, we have trastuzumab deruxtecan (T-DXd). For ER-positive metastatic breast cancer, we have sacituzumab and datopotamab deruxtecan (Dato-DXd), which is like sacituzumab, a similar target in ER-positive metastatic breast cancer.
In my opinion, it’s always good to have options on the table. I applaud the FDA. As an oncologist, given the data that that’s been shown so far, it’s hard for me to imagine for estrogen receptor-positive metastatic breast cancer recommending Dato-DXd over sacituzumab. This is my opinion, but it is an option, and it may be the best option for you.
It will be interesting to see how it’s progressed in other breast cancer subtypes and triple-negative breast cancer. It’s being investigated in lung cancer as well. ADCs are here to stay. They’ve changed how we think about drugs and targets. I think about it like next-generation chemotherapy, which is how I communicate it with patients as well.
From my point of view, it’s a helpful metaphor for a couple of reasons. These drugs have side effects that are more similar to chemotherapy. I would argue they’re more muted but similar. And they’re similar in genre. They can cause hair loss, diarrhea, and neuropathy, which are side effects we associate with chemotherapy. Generally, they’re less than what we see with chemotherapy. These drugs are also given in cycles, the same lingo and parlance as chemotherapy. For that purpose, it’s a helpful metaphor.
In the trials testing these drugs, they’re always comparing them to chemotherapy of the physician’s choice. It’s always a head-to-head versus chemo. We’re now seeing T-DXd moving earlier into the neoadjuvant setting and in the ER-positive metastatic breast cancer space. There was an approval for HER2 ultra-low, but it’s moving up.
It’s very likely that soon, with the INAVO120 regimen, if it stops working for those patients, we may be talking about ADCs even in the second-line. These would be patients who are fit and able to tolerate these therapies. That’s a different discussion, but I think that’s where the puck is heading, into the second line. It’s going to be an option. Maybe not for everyone, but it will be an option.
ADCs are changing the game because they’re changing the way we think about toxicity and efficacy, and they’re moving up. More options are always better for patients, but it’s going to be a complicated landscape.
Improving How to Get Medicine to People
Abigail: You’ve talked about toxicities, which is mostly in the context of side effects. What about time toxicity? How do you talk about that with your patients? For example, the difference between taking an oral therapy at home versus going to the infusion center every three weeks for an ADC.
Dr. Vasan: In the HER2-positive metastatic breast cancer space, there has been a lot of emphasis and research on subcutaneous formulations. PHESGO (pertuzumab, trastuzumab, and hyaluronidase-zzxf ) is the drug I’m thinking of, which is given in a shot in the fat. Biosimilars are also a relevant part of the conversation because of cost.
Most of the time, the trastuzumab and pertuzumab that we’re giving in big academic centers are biosimilars now because they’re generic drugs, cheaper, and better for the system. But I do think that this emphasis on the drug getting approved and becoming generic, but with a new formulation, is a very relevant conversation.
This is where your input is very helpful as patients and patient advocates. There may be a world in the distant future where patients, even with metastatic disease, might be taking these drugs at home. I do think that’s a possibility. During the COVID pandemic, when coming into the infusion center was risky for so many patients, those were options that were deployed in trials or feasibility studies. We know it’s possible, feasible, and safe.
Again, this is an area where the puck is moving. Can we come up with better models of getting drugs to patients? The concept of coming in every three weeks versus taking a drug every day have pros and cons. Obviously, a pro about taking an oral pill is that it’s in your control as a patient. You’re taking the medication. It doesn’t necessarily mean that the drug is less toxic. I would argue we have plenty of oral drugs that are more toxic than certain IV chemotherapies. It’s apples versus oranges.
This is where oral SERDs are interesting drugs. We give fulvestrant. Many patients tell us that no one wants to get shots in the buttocks every month. Interestingly, oral SERDs have come along. We thought as a field that oral SERDs were going to replace fulvestrant, but that’s not what we’re seeing because they only seem to have activity in patients whose breast cancers have ESR1 mutations, which is a small piece of the pie.
With every conversation around changing formulations, you have to reinvestigate these questions because some of our assumptions turn out to be wrong. This is an important change in the field. I would even go a step further. Breast cancer has led this in oncology because now we’re starting to see subcutaneous formulations of other antibodies.
These are the things where patients need to be savvy and know everything about what’s going on. If that’s something that gives you solace and lessens your anxiety, these are questions to ask your oncologist. What are the drugs available to me? What are the targeted therapies, antibody-drug conjugates, chemotherapies, antibody therapies, and clinical trials? Which of these drugs are given intravenously? Can we give this in a way that makes more sense for my life? These are all important questions that you should feel empowered to ask because we do have answers.
Abigail: Thank you for bringing up quality of life type discussions and how important it is to have with your doctor.
With obesity, we know that it is a known risk factor for estrogen receptor-positive breast cancer, but less so for other breast cancer subtypes.
Addressing Obesity in the Context of Breast Cancer
Abigail: There was some data that came out at San Antonio about obesity, which is always a sensitive or complicated subject to talk about. How are you having that conversation with your patients, Dr. Vasan?
Dr. Vasan: I’m sure you are aware of the prior Surgeon General’s declaration about multiple cancer types being linked to alcohol intake, and this is important. We’re always interested in trying to find out if there are modifiable risk factors that can decrease the risk of cancer. We know that the warnings on cigarette packs have decreased the rates of lung cancer and the smoking rates are much lower now than they were 20 years ago. But are there other modifiable risk factors that can decrease the risk of breast cancer?
I mentioned obesity in line with alcohol because those two are a little linked. The National Academies of Sciences, Engineering, and Medicine (NASEM) released a concurrent report that argues that if you look at alcohol in the absence of obesity, the risk of breast cancer is a lot lower than we thought. It’s 1% over someone’s lifetime, which is the absolute increase in risk. The relative risk, of course, is higher.
The bottom line is it’s a hard discussion. If there’s a 1% increase in absolute risk, how are you going to decrease that by alcohol cessation, which can be hard and complicated for people? I put that out there.
With obesity, we know that it is a known risk factor for estrogen receptor-positive breast cancer, but less so for other breast cancer subtypes. The way that I talk about it with patients is that this is a modifiable risk factor. If you’re on some sort of active therapy, we’ll put it out on the table and talk about this issue, but we won’t intervene until you’re done with the hardest parts of therapy.
This is something that comes up all the time in the adjuvant setting. It’s natural for women to want to lose weight. You get ambushed with breast cancer, so you want to investigate all the avenues of your life. How can I do better? How can I change things? I always say to patients, “Let’s get through the hardest part. Let’s get through chemotherapy. Let’s get through surgery first. Then, let’s talk about these issues.”
We are starting to see changes in the world of GLP-1s. There’s a lot of interesting work being done looking at these drugs and their anti-cancer effects. These are anti-cancer effects regardless of their effects on diet and weight loss, which is fascinating as well.
This is a fast-moving space. What I recommend to patients is that when we’re talking about weight loss, talk about the real specifics of an exercise regimen and food intake. These are great conversations that are happening in your doctor’s office. This is also something we’re seeing at the national level, even politically. We’re seeing a lot more discussion about lifestyle and changes that can be made.
There’s a lot more awareness now, even in the last couple of years, about what we’re putting into our bodies and our kids’ bodies. The big question is trying to understand if making a change affects your risk of breast cancer. Does that improve your survival with metastatic breast cancer? These are all questions that we’re hoping to find answers to.
They’re very hard studies to design. Certainly, weight loss is going to help anyone, myself included, with all aspects of life: cardiovascular disease, cardiovascular risk factors, etc. But I don’t want someone to become a vegetarian overnight. That’s a pretty drastic change. What’s that going to give you at the end of the day?
These are all important conversations to have, but I do think we’re going to start to see more research done in this area.
Abigail: It’s so important for patients to remember that this isn’t about patient shaming. It isn’t about saying that they’re responsible for anything, but about looking at how to improve the quality of life while reducing risk at the same time. I just wanted to make sure we talked about that.
Editor’s Note: This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
The Importance of Understanding Side Effects
Abigail: You were part of a discussion about a case-based clinical approach to ER-positive metastatic breast cancer at one of your presentations in San Antonio. Would you like to talk about that?
Dr. Vasan: ER-positive metastatic breast cancer is a fast-moving field with a lot of new therapies approved within the last two years and with new things in the pipeline. We get into a lot of clinical scenarios. This is very common and happens all the time in the clinic.
Patients who have multiple alterations that we have targetable drugs for, patients who have unusual comorbidities — these are scenarios we see all the time. We’re trying to understand what the best drug is for this patient that will help them live the longest and have the best quality of life. This was a great discussion. It’s wonderful to have a patient advocate on the panel. This is important because a lot of these drugs have side effects that mean different things to different people.
Side effects mean different things to different people. They also mean different things, I would argue, for oncologists compared to patients. The way that we grade and rate side effects can mean a lot of different things. Grade 3 diarrhea is 10 episodes a day, which is insane. Grade 3 is usually the red flag, but grade 1 and grade 2 is still a lot of diarrhea.
Stomatitis is something I think about a lot. It’s a side effect that we’re starting to see more now with Akt inhibitors. There was a reasonable percentage of women who had grade 3 stomatitis, which is inflammation of the mouth. Grade 3 means that stomatitis is so bad that you’re losing weight. Grade 1 means it’s there and grade 2 means it’s painful.
Those are big side effects. You could argue that grade 3 side effect X might be very different from grade 1 side effect Y, if Y is bad. The toxicities and communication of the toxicities are so important to make sure that everyone is on the same page. If you’re having a side effect that you feel is not getting the time that you need to talk about it, you need to talk about it. I always tell my patients, “If something doesn’t feel right, I want to hear from you. I’d rather hear from you than not hear from you.” These are important discussions.
The Importance of Sharing Side Effects with Your Doctor
Abigail: Patients talk about their fear of bringing up a side effect that they’re struggling with because it might mean they can’t stay on the medication. How do you handle that in the clinic?
Dr. Vasan: I always try to make it clear that we have a lot of doses that we can give of drugs. They’re generally for targeted therapies. Patients have multiple options. One of the biggest challenges is trying to communicate that there is no one optimal dose. For whatever reason that we don’t understand, some doses are much better tolerated than others. Certain doses for certain individuals are the perfect range.
It’s very hard to understand and hard to accept. If your doctor recommends a dose reduction, do not equate that with not being as hard enough on yourself or not being as strong. I always tell patients, “I don’t want you to feel the side effects of the therapy. The goal is to see it working on the scans and not have any side effects. That’s not what this is about.”
It’s hard. If I were a patient, I could understand feeling less than if my doctor said I need a lower dose. But I want patients to understand that there’s been so much rigorous analysis of every one of these FDA-approved drugs, looking at lower dose levels, and trying to understand if you are attenuating if you lower the dose. Are you decreasing the benefits of survival, the response rate, etc.? The answer for the vast majority is you’re not, which is so important for patients to understand.
There are a lot of initiatives being done at the American Society of Clinical Oncology (ASCO) level and the Patient-Centered Outcomes Research Institute (PCORI), looking at CDK4/6 inhibitors and changes in doses. Some of these drugs — but not all — are approved in the adjuvant setting. A big reason for that is that some doses were modified, and they used a lower dose in the adjuvant setting.
I want patients to know that doctors are always thinking about this, but that’s a perfect example where it’s baked into how we give the drug. With CDK4/6 inhibitors, we give them three weeks on, one week off. It’s not dose reduction per se — it’s dose intensity — but it’s the same idea. People need to know that if your doctor recommends a lower dose, it’s not because of anything you did or did not do; it’s just because that dose is the right dose for you.
There are a lot of people doing research into pharmacogenomics. There are aspects about different races that may change the way that you metabolize drugs. It’s been known for a very long time that Asians have certain metabolic enzymes that change the way their bodies process capecitabine.
That’s something in the GI (gastrointestinal) cancer field and in certain types of GI cancers, like stomach cancer, that are very prevalent in Asian countries. These are important parts of the conversation. There are biological reasons that we may not know yet that could explain why this dose is not the right dose.
Abigail: Yet another reason why diversity in clinical trials is so important. If we don’t have enough of each group of people, we’re not going to necessarily know if something is specific to that group. Thank you for raising that.
What are You Most Excited About in Breast Cancer Research & Development?
Abigail: What is new and exciting that you’re looking forward to?
Dr. Vasan: I’m very excited about the three trials that I talked about earlier. I think in HER2-positive, T-DXd has already changed the world. There are still many more scenarios that I think T-DXd will find an approved role in. Moving drugs into the neoadjuvant adjuvant setting is always wonderful and I think that’s going to be where that field heads.
The PATINA trial, where we’re starting to integrate targeted therapies into that complicated regimen, is going to be an interesting move that the field heads into.
In estrogen receptor-positive breast cancer, there are still a lot more interesting targets that are being investigated in phase 1 trials. One target I have my eye on is something called KAT6A, an epigenetic target. It’s the idea that your DNA can get modified in lots of different ways. The proteins that modify that DNA are called epigenetic proteins, writers, and erasers. There are lots of different classes and one of those is the protein called KAT6A. It’s going through clinical trials right now. The response rates are very high for patients who have progressed on lots of different therapies. There is also a lot of toxicity, so those will have to be managed.
Mutant-selective PI3 kinase inhibitors are exciting drugs. They seem to have little to no hyperglycemia. They are mutant-selective, so they’re ultra-targeted in a way. They’re only targeting the mutated PI3 kinase in cancer cells and not targeting the normal PI3 kinase in all the other cells in your body, like the liver and fat cells, which can cause all these bad side effects.
Triple-negative breast cancer is still the hardest disease. I do think that some interesting advances are being made in optimizing chemotherapies with immunotherapy. I don’t think we’ve quite cracked that yet. There’s always work being done with BRCA and trying to find the patients who benefit from those therapies.
I think ADCs are going to find a huge traction in TNBC, as they already have. As an example, sacituzumab is a better drug in triple-negative breast cancer than it is in ER-positive breast cancer. There’s still more to be seen there.
I love talking to people who know a lot about breast cancer and people who are outside the field because it’s such a fast-moving field. It’s a privilege to take care of patients who have breast cancer and to be able to talk about all these therapies and communicate. I hope you can tell how excited I am when I talk about this. It’s such an amazing field because everyone is so united and mission-oriented to keep moving faster.
Dr. Vasan: We were inspired by the lung cancer patient advocacy group. There have been targeted therapies for decades now against a slew of genes that are mutated in lung cancer. There have been these incredible groups that have formed around the target. EGFR Resisters is one of them. These amazing groups have changed the world. They have changed patient advocacy. They changed how oncologists think about designing trials. The people in these organizations have seats at the table with pharma companies as they design their trials with regulatory agencies as they’re approving these drugs. It’s incredible.
Breast cancer doesn’t necessarily have a genomically-directed targeted therapy, i.e., a gene that’s mutated that we find on a sequencing report, until PI3 kinase. That’s something that’s lacking in the field.
Abigail and I, together with two other incredible patient advocates, Marlena Murphy, who unfortunately passed away in 2024, and Melanie Sisk, have formed an organization called PIK3CA Pathbreakers. We’re a patient advocacy group formed around patients with PIK3CA-altered breast cancers.
We now have three FDA-approved drugs, two in the last year and a half for this patient population. We’re invested in trying to increase awareness around clinical trials in this space, increase knowledge about side effects through the lens of patients but articulated by oncologists, and try to make sure that we have strategies to mitigate these side effects.
What’s Exciting About Next-Generation Sequencing (NGS)?
Dr. Vasan: The education and landscape around next-generation sequencing have changed dramatically in the last two years. When to get sequencing? What to get sequencing on? How often to get sequencing? These areas are very fast-moving. We’re still trying to make sure that insurance companies are approving these drugs. I do think that these are bigger conversations that we need to have at a national level, but that’s another big area.
What are the mutations? There are thousands of mutations seen in patients. Some are very common, but we get questions all the time about these rare mutations. Do these rare mutations predict response to these drugs? We don’t know.
As an oncologist and someone who specializes in PI3 kinase, I get emails all the time from oncologists all over the country. They see this rare mutation. Does this predict the response for capivasertib? We don’t know.
What are Your Recommended Patient Resources?
Abigail: Thank you, Dr. Vasan, for your time, your insights, and your excitement. As a patient, it’s always good to see that there are doctors, researchers, and clinicians as invested in our care as we think everybody should be. Very much appreciated. The Patient Story has a YouTube channel with all these videos, which is wonderful. But, Dr. Vasan, where do you point patients to get more information?
Dr. Vasan: Every patient is so different. Sometimes you find something online that’s not right or relevant. Sometimes I hear from patients, “I saw this,” and I have to tell them, “That’s not relevant for you because of X, Y, and Z. It might be something we talk about later, but now, this is why it’s not relevant.”
There can be a lot of information and it’s hard to know how to interpret the data. Breast cancer is such a fast-moving field. When anyone gets diagnosed, they’re going to talk to family members. More often than not, how breast cancer was treated in your loved one five years ago might be radically different. It might not even be an option now because there are newer and better things. It doesn’t mean you should talk to everyone in your life, but you’re going to get a lot of information and sometimes it’s discordant.
Wikipedia and Twitter are not great places to start. That being said, Twitter is a great place to find your tribe, find your network, and link with people. I highly encourage people to reach out on Twitter. I’ve been humbled and awed by the groundswell in patient advocacy.
The PIK3CA Pathbreakers has a huge Facebook group, as do all of the other patient advocacy groups.
Find your tribe. Get anecdotes and stories from all of those people, but be judicious about what information you take in about your own cancer. Don’t necessarily extrapolate everything you hear to your own.
Conclusion
Abigail: The most important thing that patients who are living with breast cancer and their loved ones need to know is that there’s no one right way to do it. What makes you comfortable, what makes you able to handle it, and what makes you able to put cancer into your life, not your life into cancer — that is the right way to live with cancer.
Kyle’s Journey as a Care Partner Through Love and Loss
Jenny Appleford was a beloved YouTube creator who bravely shared her stage 4 lung cancer journey with the world – not just to raise awareness, but to help others feel less alone. Diagnosed at just 33 with no history of smoking, she used her platform to document everything from treatment updates to quiet family moments, offering a powerful glimpse into life with terminal illness. Her honesty, faith, and fierce love for her family inspired thousands.
In 2023, Jenny passed away – but her voice lives on, not only through her videos, but through her husband, Kyle. In this deeply personal interview, Kyle opens up about what it was like to care for Jenny through her illness, the heartbreak of losing her, and the challenges of navigating parenthood and grief without her by his side. He shares how he’s finding strength, honoring Jenny’s legacy, and learning to live again – one moment at a time.
Jenny was diagnosed with non-small cell lung cancer at 33, despite having no history of smoking. Initially, she was diagnosed with stage 3A but even after different treatments that gave her a good quality of life, they found metastases in her brain. She was later diagnosed with stage 4 lung cancer.
Losing Jenny was an experience filled with unimaginable heartbreak, quiet strength, and enduring love. As her husband and care partner, Kyle tried to remain strong for her and their two young kids, even when inside he was falling apart. In her final days, although confused at times due to the brain metastases, Jenny never stopped being Jenny — full of love, faith, and resilience. She was positive until the very end, always reminding them that she never gave up and that she loved her family deeply.
After Jenny passed, the grief was overwhelming. Kyle had to find a way to balance his pain while supporting their children through theirs. The house was quieter, lonelier, and full of memories, but the responsibilities of being a single parent didn’t stop. He leaned heavily on family and friends, and slowly, found moments of healing.
Grief isn’t linear. Some days, Kyle felt numb; other days, he felt too happy and guilty for it. Therapy, community support, faith, and exercise helped him start to move from just surviving to living again. He misses everything about Jenny — her voice, her parenting, her presence — but he’s learned that it’s okay to grieve at your own pace.
Parenting without Jenny is the hardest. Kyle can’t lean over and laugh with her about what the kids just said or ask her advice in the moment. But he still talks to her, and sometimes, he feels like she answers. Kyle tries to be the best parent he can be, not to replace her but to honor her.
Jenny’s legacy lives on in the way Kyle parents, in the milestones he celebrates with their kids, and in the love she left behind. She was selfless, even in her final days — writing letters for future birthdays and life moments for their kids. Her strength, kindness, and fight to the end left an imprint on everyone she met. She wanted people to enjoy the moment, to fight for more lung cancer research, and to share their stories to help others feel less alone. And that’s exactly what Kyle and their kids are doing.
Watch Kyle’s full interview to hear the raw, emotional story behind these moments:
Hear how Jenny’s final act of love included writing letters for her children’s future birthdays, weddings, and milestones.
Learn what it was like to sit bedside in the final days, holding on to every breath and every second together.
Discover why grief isn’t a straight path and why feeling “too happy” or “too sad” is part of healing.
See how parenting without Jenny has been both heartbreaking and beautiful, with conversations that still include her voice.
Find out how Jenny’s legacy continues through advocacy, everyday moments, and the promise to never let her be forgotten.
Name:
Jenny Appleford
Age at Diagnosis:
33
Diagnosis:
Non-Small Cell Lung Cancer (NSCLC)
Staging:
Stage 4
Symptoms:
Rib pain
Shortness of breath
Treatments:
Chemotherapy
Radiation therapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Kristen Opens Up About Crohn’s Disease, Her Ostomy, and Owning Her Story
Kristen was diagnosed with Crohn’s disease at just 12 years old. For anyone wondering what does Crohn’s disease look like, her story offers a vivid picture. Living with this chronic illness so young meant navigating growing pains and medical challenges simultaneously. She talks about how her world shifted from being a sports-loving, active kid to someone grappling with daily pain, blood in her stool, and emotional isolation. Her story is a heartfelt reminder that chronic illness changes more than your body — it affects how you relate to the world.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Throughout her teenage years, Kristen faced mounting symptoms and emotional struggles. By high school, her condition had worsened significantly. She bounced between treatments and doctors, often feeling let down. When she was in college, everything changed during an appointment when a doctor told her she needed an ostomy.
With her health deteriorating, Kristen agreed. That surgery, though overwhelming and unknown to her at the time, saved her life. She had no prior education about ostomy care and struggled initially, but she and her mom figured it out together.
Kristen is honest about the mental health toll of chronic illness, including medical PTSD and anxiety. She didn’t always advocate for herself, but she learned how to speak up. That shift empowered her. She realized that her voice mattered, especially when navigating multiple surgeries, including a total colectomy that made her ostomy permanent. While that decision was emotionally heavy, especially after being told it would be temporary, she eventually accepted it as necessary for her well-being.
Instead of letting shame or misinformation define her, Kristen started sharing her story online to educate and empower others. She uses Instagram as a blog, breaking stigmas around ostomy bags and showing the reality of life with one. She answers common questions about intimacy, product use, and body image. Kristen keeps it real but is always supportive, encouraging others to ask questions and never feel ashamed.
Body positivity plays a huge role in Kristen’s story. She’s chosen to love and appreciate her body for all it has endured. Even with an ostomy, she’s traveled the world, held full-time jobs, enjoys paddleboarding and rollerblading, and continues to thrive. She’s all about hope, mental health awareness, and creating inclusive spaces for people with invisible illnesses. Her message is clear: don’t be afraid to advocate for yourself, embrace your body, and know that even in the hardest moments, you’re not alone.
Watch Kristen’s video to find out more about her story:
What products she swears by for stoma care, and which ones she skips.
Her reaction when she found out that her ostomy, which she was initially told would be temporary, was going to be permanent.
What does Crohn’s disease look like and life with an ostomy, and how she lives fully and freely.
From hospital anxiety to medical PTSD, how Kristen’s mental health was impacted and how she’s healing.
How a single doctor changed Kristen’s entire life trajectory.
Name: Kristen F.
Age at Diagnosis:
12
Diagnosis:
Crohn’s Disease
Symptoms:
Fatigue
Abdominal cramps
Blood in stool
Loss of appetite
Frequent, painful bathroom visits
Perianal disease (open wound)
Mouth sores
Joint pain
Treatments:
Multiple medications
Surgeries: Temporary ostomy, total colectomy (permanent ostomy), Barbie butt surgery (proctectomy)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Blood Work Basics: Making Sense of Your Test Results
What do your cancer blood test results really mean and how do they help doctors detect or monitor cancer?
Join hematopathologist Dr. Kamran Mirza and cancer advocate Stephanie Chuang to break down the most common diagnostic cancer blood tests, including the CBC (complete blood count) and the CMP (comprehensive metabolic panel). Learn how pathologists interpret results, what those ranges mean, and how small changes in your numbers can offer big insights into your health.
Blood Work Basics: Making Sense of Your Test Results
Hosted by The Patient Story
What do your blood test results really mean — and how do they help doctors detect or monitor cancer? Learn about the most common diagnostic tests, including the CBC and the CMP.
Why doctors order cancer blood tests: What they’re looking for and how to prepare.
Making sense of the CBC: Understand what each number represents — and what it doesn’t.
How blood results guide treatment: From diagnosis to tracking remission or recurrence.
Whether or not you should be worried: When out-of-range numbers matter and when they don’t.
What’s next in the series: Learn how this session leads into condition-specific follow-ups for six different blood cancers.
We would like to thank Blood Cancer United for their partnership. They offer free resources, like their Information Specialists, who are one free call away for support in different areas of blood cancer.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
Stephanie Chuang: Hi, everyone! Blood Work Basics is part one of a multi-episode program designed to empower you with the information you need for your next blood work appointment. While the other episodes will be about specific blood cancers, this episode is more focused on the initial tests that you may deal with as you try to get a diagnosis or following your initial treatment.
I’m the founder of The Patient Story. I have gone through a myriad of blood tests, poked and prodded constantly, when I was getting diagnosed, which ultimately would be a non-Hodgkin lymphoma, diffuse large B-cell lymphoma, and all through treatment.
I remember having to wait to get my blood drawn. First, it was through my veins; then I got my PICC line and a port. They needed to make sure that my white blood cell counts were okay for me to be able to withstand the next round of chemotherapy. Each round of chemo lasted for about six days at the time, which was definitely not short or easy.
During that time, I started imagining what would eventually become The Patient Story. I felt so lost. There were so many things that I wanted to know the answers to, but I wanted to know them in a humanized way — don’t give me the medical jargon. That’s what The Patient Story focuses on.
We help curate humanized information to help you navigate life at and after diagnosis. We do this through in-depth patient stories, educational programs, and discussions to amplify the voices and concerns of patients and care partners.
I want to give a shout-out to our friends at The Leukemia & Lymphoma Society. They have so many fantastic resources, including their Information Specialists, who can help talk about things like blood tests if you need.
While we hope that this discussion is helpful for you, keep in mind that this is not a substitute for medical advice, so please consult with your team about your decisions. Hopefully, you’ll have some questions from this discussion that you can ask.
I’m excited to introduce someone I now consider a friend whom I met as a patient advocate: Dr. Kamran Mirza, the Godfrey Stobbe Professor of Pathology Education, Professor of Hematopathology, and Assistant Chair for Education at the University of Michigan.
Dr. Mirza also shares medical insights online to help people like us, patients and care partners, understand the science of diagnosis. You may know him from social media as @kampathdoc. Dr. Mirza, welcome again. It’s so good to see you.
Dr. Kamran Mirza: It’s always a pleasure to see you. Thank you very much for having me, Stephanie.
What Does a Pathologist Do?
Stephanie: Dr. Mirza, before we kick off this discussion, we want to humanize the word pathology. A lot of patients, their families, and friends may not see a pathologist during their experience at the hospital or at a clinic. Can you break down what a pathologist does?
Dr. Mirza: I always say to my patients that the pathologist is the doctor you never see or usually don’t see 99% of the time. A pathologist is a physician. They work in the medical laboratory, where all of the human body tissues and fluids go for any type of diagnostic work.
Whenever your physician orders any kind of testing, which could be blood tests, urine tests, or other types of tests like biopsies, they always come to a physician behind the scenes who is a pathologist. The work we do is pathology.
Like other parts of medicine that you might all be aware of, pathology is also subspecialized. I’m a specialist in blood pathology. My diagnostic area is leukemia, lymphoma, anemia, etc. Similarly, I have colleagues in pathology who deal with disorders of the brain or disorders of the liver, etc. Every part of medicine has a pathologist associated with it. We are physicians who will provide the diagnosis, which is what your patient-facing provider uses in order to treat you.
Stephanie: Thank you. I know there are a lot of things that you do as a pathologist and I’ve learned a lot from that already.
Initial Testing Before a Diagnosis
Stephanie: When we’re talking about blood cancer and the reason why pathologists are so focused on different blood tests at different times, could you give a generalized overview? If someone has a suspected diagnosis, what is the usual testing done at the very beginning, before people know exactly what they have?
Dr. Mirza: Whenever you present to a doctor, whether it’s a well visit or an urgent care visit, doctors are trying to piece together from your clinical history. They ask about how you’re feeling, how long you’ve been feeling this way, and your family’s health. They’re trying to ascertain whether these symptoms are short-term, long-term, from an ominous cause, or a more benign cause.
When you give a sample of blood, that is a snapshot of your internal health.
Once they’ve established in their mind what path they’re going down, they need to have some backing from diagnostic testing in order to clarify what it is. Typically, diagnostic tests include radiology, which is a visual imaging of the body. If they’re worried that there might be a mass lesion, they may send patients for X-rays or CT scans. The radiologists take a look at a particular part of the body and give you a report.
Similarly, the diagnostic laboratory is the pathology part. What we can provide you in the simplest way is a blood test. When you give a sample of blood, that is a snapshot of your internal health. Your blood can tell you so many things. Because we’re talking about blood cancers, it’s one of the simplest ways for your physician to find out if something is wrong in your blood or in the factory where all of the cells of the blood are made, which is the bone marrow.
All of us have bone marrow, which is the factory producing all of the cells. It’s inside our long bones, so it’s in the bones of our arms, our legs, and the pelvis. All of these bones are producing marrow, which is going to make all the cells in the blood.
A very simple way to figure out if the factory is working is to take a snapshot of the blood. In the blood, you have different types of cells. You can look at their numbers. Are they going up or down? There are a variety of other things that we can pick up from the blood as well. It can tell you things, whether it seems like an infection or cancer, or if everything seems okay.
All physicians need the next step of diagnostics to move things ahead. Whether it’s radiology or pathology, that’s where you will end up if you’re presenting symptoms to your physician.
Stephanie: Thank you for walking us through that. The stage we’re talking about is a period that’s very hard for people. It’s hard to wait because there are a lot of questions and uncertainty, and there’s no plan of action yet.
What is a Complete Blood Count (CBC) Test?
Stephanie: In the initial stage, one of the most commonly ordered tests is the CBC or complete blood count. I was diagnosed with non-Hodgkin lymphoma, but I don’t know if any numbers were flagged in my CBC results. What is the CBC? What is it looking for? Can go down each blood cancer area and what the focus may be for pathologists?
Dr. Mirza: The CBC is the complete blood count. There are three different aspects of the CBC that you can start thinking about, which go back to what the blood does.
Our blood carries oxygen. That oxygen is the oxygen we inhale into our lungs and the red blood cells in our lungs pick up all of that oxygen.
If you don’t have enough red blood cells, that might be anemia, for example. Associated with red blood cells is your level of hemoglobin, which is your oxygen-carrying protein. The RBC or the red blood cell count, the hemoglobin, and the hematocrit are used to look for your red blood cell component. Numbers going up or down may indicate that something is wrong with your red blood cells.
Another thing that your blood does is fight off infections, which are fought off by a variety of cells known as your white blood cells. You have different types of white blood cells. Your white blood cell count is an indicator of inflammation, infection, and a variety of things. The numbers going up or down can also indicate what may be happening to you as a patient.
The last number that you look for is the platelet count. Platelets are tiny fragments of cells that are floating around. Typically, these are in high numbers. Platelets help you clot or stop bleeding anytime bleeding occurs. For example, when a person who has a normal, healthy bone marrow has a small cut on a finger, that cut clots pretty quickly because the platelets are doing their job and the bleeding will stop. Similarly, you could have internal bleeding and not even know, but normal platelet counts and normal platelet function take care of all of that for you.
The CBC has a variety of numbers on it, but primarily, it’s looking for these three aspects of your bone marrow that produce cells and come out into the blood. It’s a snapshot of how those three things are performing.
What Happens if Your Blood Counts are Abnormal?
Stephanie: I love that you put it into these buckets for people to understand: red blood cell count, white blood cell count, and platelet count, and their different functions. This is not about any specific case but a generalized conversation. As a pathologist, can we go into each area? Let’s say there is an abnormal red blood count, white blood count, or platelet count. What might that generally indicate? How would you suggest further testing, or what are the next steps for the patient?
Dr.Mirza: If white blood cell counts go up, typically the most common reason will be an infection. This can be either a viral infection or a bacterial infection. When you look at the white blood cell count, it may also be associated with a differential count.
Typically, if a patient has a bacterial infection, neutrophils go up. If they have a viral infection, lymphocytes may go up.
A white blood cell count gives you the total number of cells, but that number won’t tell you what the cells are, so we need to figure them out. Either machines or human beings, who are medical laboratory professionals, look at the blood and then count how many different types of white blood cells there are.
There are different types of cells: neutrophils, lymphocytes, and monocytes. These are the words that you would potentially be coming across if you see a differential count. Depending on what is going up, you may have an idea of what it might be. Typically, if a patient has a bacterial infection, neutrophils go up. If they have a viral infection, lymphocytes may go up.
But then, abnormal cells might start showing up in the blood as well and the differential count might flag abnormal cells. These are what we typically call immature cells and by immature, we mean that they came out of the bone marrow too soon. They needed to cook in the bone marrow a little bit longer, but they didn’t and came out.
Now, having immature cells come out can also be part of an infection. It can be normally seen in an infection, but depending on how the patient is presenting, it could be something more ominous or even be part of leukemia, which is a cancer of the blood.
If the blood cancer is just presenting in the lymph nodes… chances are that the blood may not show anything abnormal.
You mentioned before that patients with non-Hodgkin lymphoma sometimes may not have any abnormalities in the blood and that’s absolutely true, like what you experienced. If the blood cancer is just presenting in the lymph nodes, which are all over the body, and you can feel them as masses, then chances are that the blood may not show anything abnormal and you need to take a look at the lymph node in order to diagnose what the lymphoma is.
However, there are other times when lymphoma can be floating around in the blood as well. There are many lymphomas that float around in the blood. They will be picked up in the white blood cell count and differential count as an increase in the number of lymphocytes because lymphocytes are the cells that constitute the blood cancer lymphoma.
Normal lymphocytes in all of us are floating around and they’ll be within a normal number. But if they go up, it can either be because of a viral infection, or if they’re really, really high, it could also be because of a lymphoma that’s floating around. It’s very context-dependent. These are just numbers. You have to put your story and your history. Every patient will have their own presentation. What we do as pathologists, as your physicians, is put all of that together in order to give a diagnosis.
With red blood cells, often the problem is a decrease in red blood cells. This could be either because of simple things, like a patient not having enough iron in their diet. If they don’t have enough iron, they may not make enough hemoglobin and then their red blood cell count goes down because they have anemia.
Anemia is a decrease in the oxygen-carrying capacity of the blood. This could be in patients who have been in an accident and lost blood, which can lead to anemia. The red blood cell count goes down because you’ve lost so much blood. It could also be because of nutrition or something more ominous, like a blood cancer. A blood cancer taking over your bone marrow could decrease the number of red blood cells that are being produced and also show up as an anemia.
Context makes a huge difference. If a patient is known to be nutritionally deprived or if it’s a female patient who has very heavy menstrual periods or losing blood regularly, that anemia will most likely be because of iron deficiency. But if there is no history of blood loss, the patient has been doing well nutritionally, and they’re still anemic, then you start worrying why there is anemia. Normally, patients should not be having anemia.
Lastly, platelet counts can go up or down. Usually, what happens is that the platelet count goes down, which will hinder the ability of the patient to clot properly. For example, a cut happens and they keep bleeding when it should have stopped, or they may have bruises. Under the skin, they see splotches of bruising, even with the smallest amount of trauma and that could indicate that their platelet count is low.
In all of these three cell types, things can go up or down and all of that could be part of a reactive process, which could be benign, or it could be part of a more ominous process, which could be malignant. Again, it all depends on how the presentation has come to the physician and a variety of things that the physician will likely ask you before coming to a conclusion and ordering a test.
Stephanie: Thank you. Even after all these years of advocacy, it was helpful to have them spelled out and learn what they all mean. What I’m hearing is there are signs and signals of your internal health by the CBC, but also, context is important. What you and other healthcare team members are doing is putting together the entire story.
CBC Tests for Non-Hodgkin Lymphoma Patients
Stephanie: Our audience comes from across a lot of different blood cancers, primarily non-Hodgkin lymphoma. We have aggressive and slow-growing Hodgkin lymphoma, chronic leukemia, acute leukemia, multiple myeloma, and myeloproliferative neoplasms. CBC is a very basic test start off with. With non-Hodgkin lymphoma, is it the same with aggressive versus indolent? What are you looking for in the CBC that might be a flag?
Dr. Mirza: Let’s talk about lymphoma in general. I’m sure patients like you are familiar with the fact that we divide them into Hodgkin and non-Hodgkin.
An increase in the number of lymphocytes by itself does not make it lymphoma.
Hodgkin lymphoma by itself typically does not show up in the blood. It will show up usually as masses or lymph nodes that you can palpate, which can be all over the body.
Non-Hodgkin lymphoma can also present with no abnormalities in the blood and just show up as masses or lymph node enlargement in different areas. When it does show up in the blood, that is what we call lymphoma in the blood or lymphoma in a leukemic phase.
Leukemia means there are white blood cells in the blood. Leukemia is a historic term. When people look at blood, they see red because red blood cells have a pigment. Next to them, they saw clear, colorless cells, which looked like they were white. White blood cells are not white at all. It’s just the contrast that they’re not red.
When you see white blood cell counts go up in a lymphoma, which is a non-Hodgkin lymphoma, what we’re typically looking for is an increase in the number of lymphocytes. An increase in the number of lymphocytes by itself does not make it lymphoma. You need to make sure that the lymphocytes that are increased are, for lack of a better term, malignant. They’re all being driven by a genetic problem that is causing a proliferation of lymphocytes that’s not normal. Abnormal lymphocytes are being created and propagated and continue to propagate.
If you are a patient with a lymphoma that did present in the blood, an example of which is chronic lymphocytic leukemia (CLL). Often, CLL is a disease seen in middle-aged to elderly patients. They might feel well, go to their PCP, and get a CBC done, which then shows that their lymphocytes are increased. Then they might do some additional testing, which will confirm that this is part of a lymphoma process. Typically, one of the tests that they do is called a flow cytometry test, a test that confirms that these lymphocytes are lymphoma cells that are floating around.
If we talk about non-Hodgkin lymphomas, you will see an increase in the number of abnormal lymphocytes floating around in the blood. The CBC will only give you the number. You will need extra testing in order to confirm that it’s a non-Hodgkin lymphoma.
Now leukemia can be of multiple types. You can have a myeloid leukemia or a lymphoid leukemia. This all goes back to the bone marrow, which produces all types of cells, including lymphocytes and other types of cells. If a patient has an acute leukemia, then that primarily means that their blood has a very high number of very immature cells.
If we see patients who have lots of blasts in the blood, then we immediately think of an acute leukemia.
What’s happening is that the most immature cell from the bone marrow is not undergoing any differentiation or growing up that it normally does and it’s coming out directly into the bone marrow. These immature cells are called blasts. If we see patients who have lots of blasts in the blood, then we immediately think of an acute leukemia. Very different from non-Hodgkin lymphoma, which are mature lymphocytes but are abnormal and proliferating. Acute leukemia is when blasts are coming out and are very immature.
Flow cytometry studies would be done to figure out whether those blasts are from the myeloid line or the lymphoid line. If they’re from the myeloid line, it’ll become an acute myeloid leukemia and if they’re from the lymphoid line, it becomes an acute lymphoblastic leukemia. But in general, the blood will show you very high numbers of immature cells or blasts.
When a patient looks at the CBC, the WBC count will be increased, but by itself, that doesn’t mean anything. Then you look at the differential count, where they will have counted the number of neutrophils, lymphocytes, and monocytes. There’ll be another one there that will be labeled “other” or “blasts,” and that will be increased. That’s how we will be able to tell the PCP that your patient likely has an acute leukemia.
The bone marrow is throwing out lots and lots of a particular type of cell. Depending on what that type of cell is, we can look at that and figure out what the disease entity is.
With a myeloproliferative neoplasm, it’s when the bone marrow is producing a lot of cells in the myeloid lineage, but they are not blasts. It’s not an acute leukemia, but there can be a high number of red blood cells, which we know as polycythemia vera, or there can be a very high number of platelets, which is known as essential thrombocythemia.
There are different types of myeloproliferative neoplasms. What’s happening there is that the bone marrow is throwing out lots and lots of a particular type of cell. Depending on what that type of cell is, we can look at that and figure out what the disease entity is. Often, patients will need to undergo bone marrow biopsies for that.
You also mentioned myeloma or plasma cell diseases. Plasma cell diseases usually are diagnosed by a bunch of blood tests that look at the number of proteins in the blood, but you also need to have a bone marrow examination. There are times when we can look at the blood and see slightly increased numbers of plasma cells, which are the abnormal cells for myeloma. But again, you have to put into context a bunch of things for myeloma.
You have to take into account any radiological lesions the patient may have. Typically, these patients have lytic lesions in their bones. You also have to take into account their kidney function, how much protein they have in their blood or urine, and how many plasma cells are in the bone marrow. You have to put all of that together to make a diagnosis of myeloma.
The blood and the numbers in the blood going up and down can start pointing us towards what could be happening within the blood cancer world.
To characterize the blasts, you need to study where the cells are coming from and what makes up that cell.
How Do You Process the CBC?
Stephanie: When you talked about the acute leukemias and the blasts, you said that you’re looking at different numbers as you do with all of these. But after the CBC, to confirm for AML or ALL, what is typically the next step in terms of testing? Is there one go-to?
Dr. Mirza: Yes, absolutely. When the blood is drawn, the phlebotomist takes the blood and brings it to the laboratory. The laboratory will immediately run the numbers. When the numbers are off, the machine starts flagging the sample as abnormal.
A medical laboratory professional, another hidden hero in the diagnostic journey, will make a blood smear quickly and start looking at the cells. If abnormal cells are there, we’ll be paged as a pathologist. I will look at it and confirm whether there are abnormal cells.
Typically, in high-resource settings like in the United States, the tests that are done are tests that will characterize the blasts. To characterize the blasts, you need to study where the cells are coming from and what makes up that cell. Is it a myeloid cell or a lymphoid cell?
The DNA of the cell might have some abnormalities that either gives a good prognosis or a bad prognosis.
The first test would probably be a flow cytometry analysis. Imagine if you’re going to a party and you don’t know who anyone is and everyone is wearing name tags. The name tag tells you who you are, where you’re coming from, etc. My tag says I’m Kamran and I’m from Pakistan.
Similarly, blasts have tags on them that can be studied by flow cytometry analysis. What flow cytometry analysis does is it shines a light on all of these cells and identifies what tags these cells are wearing.
When the tags are saying myeloid, we can say acute myeloid leukemia. When their tags are saying lymphoid, we can say acute lymphoblastic leukemia. Flow cytometry analysis is a study of the tags. In high resource settings, we don’t stop there because that’s important from a diagnostics perspective, but we also go forward and help the hematologist-oncologist by giving a prognosis.
Often, prognosis is associated with what is inside the genes of the cell. The DNA of the cell might have some abnormalities that either gives a good prognosis or a bad prognosis. We know, over decades of looking at this, that there are some leukemias that have a better prognosis and some that have a worse prognosis, and usually that stems from DNA. You have to figure out either mutations or looking at chromosomes.
If you are in the United States and you went to a tertiary care center and got a diagnosis of leukemia, you’ll often find a karyotype report, which are your chromosomes. Every human cell has pairs of chromosomes and those will be studied. The DNA in those cells will also be studied.
You’ll get a report with mutations, potentially a report of how chromosomes were affected, and that will all come together in your final pathology report. It won’t just be acute myeloid leukemia; it will be acute myeloid leukemia with translocation 821 or something. It will be a long report that can be very confusing.
It’s telling the hematologist that not only is it leukemia, it’s an acute leukemia, it’s an acute myeloid leukemia, and it’s an acute myeloid leukemia with a particular translocation. All of that will be put together and then that will help guide the hematologist in the treatment, if that makes sense.
What’s the Difference Between CLL and SLL?
Stephanie: You started talking about non-Hodgkin lymphoma and then went into CLL. I know that when we talk about CLL, there’s also SLL. Usually we hear CLL more often, but is there anything that you want to add as to how you look at things on the pathology side?
Dr. Mirza: CLL/SLL is actually one disease entity. You’re absolutely right. CLL is chronic lymphocytic leukemia and SLL is small lymphocytic lymphoma.
What happens is that in this particular disease state, the blood is full of lymphoma cells but lymph nodes are involved as well. When it’s just presenting in the lymph nodes, it’s called small lymphocytic lymphoma. If it’s just presenting in the blood, it’s called chronic lymphocytic leukemia, but it’s the same disease. Often, we’ll call it CLL/SLL. It’s the same disease; it just depends on where you’re picking it up on.
Because the blood is a very easy tap — all you need to do is find a vein and get a little bit of blood out — it’s much easier than doing a lymph node biopsy. Often, it will be diagnosed in the blood. But if a radiologist does a scan and sees a bunch of lymph nodes everywhere, most likely it’s part of the same process. In our classification schemes, it’s all lumped under one: CLL/SLL.
What are the Symptoms I Should Be Looking Out For?
Stephanie: You’ve done a great job laying out some of these signals. We’re talking very generally and in a vacuum, but you’re looking at signals that other people are providing individually. On that note, people might think how they can start to match some of this for themselves.
You talked about anemia, which is something that people are more likely to be familiar with. But what about some of these larger symptoms of things that might be wrong? Could you translate how they might manifest in the body? Could you laundry list and go through the major symptoms, starting with anemia?
When the numbers are off, then their functions are also off. If the function is off, then typically the three buckets are infection, tiredness or breathlessness, and bruising.
Dr. Mirza: Anemia reduces our ability to carry oxygen in the blood. Think about what we need oxygen for. We need oxygen for energy. We burn oxygen for energy, so patients will be tired and feel fatigued. They might be out of breath because they’re trying to breathe in more oxygen because they can’t carry it.
They might look pale. When you look at your hands and you press and get redness, that’s because of the hemoglobin. Under the eyes where you can see redness might be pale. If patients are pale, tired, are out of breath or have increased breathing, those might all be because of an underlying anemia.
For platelets, when they are decreased, you might see prolonged bleeding or bruising. They might accidentally hit their arm against the door and all of a sudden, they have a huge bruise. That’s probably because the platelet count is low.
With white blood cells, because what they’re primarily doing is fighting infections, the patient may present with recurrent infections if the white blood cell count is low.
All of these, when the numbers are off, then their functions are also off. If the function is off, then typically the three buckets are infection, tiredness or breathlessness, and bruising. Those will be the three that relate to the function of the three main types of cells.
What Recurring Tests Will Patients Need to Have Done?
Stephanie: Shifting over to chronic blood cancers, what are the typical recurring tests that patients will likely be undergoing? Also, could you give a little bit more detail of why that’s what they’re looking at?
Dr. Mirza: What your physician wants to know is real-time updates, especially if you have an indolent disease, which means it’s either slow growing or not giving you that many symptoms. For example, there might be situations where if a patient has CLL, they don’t treat it because the number is low, not giving them any symptoms, and was identified by chance. They may give a drug that decreases the number of lymphoma cells, which isn’t heavy chemotherapy.
Ultimately, what we want to do is monitor how the cell numbers look over time. Repeating your CBC may be a very common thing for your physician so that they can keep check to make sure that everything is stable. It isn’t as much about one value; it’s about trending over time.
Take a patient who has CLL. When they presented, the only abnormality was an increased WBC count. There were lymphocytes but no anemia and no thrombocytopenia, which means that the red cells and the platelets were good. They chose no therapy or very minimal therapy and the patient’s fine.
But then when they present the next time, you see that there’s anemia associated. There was no anemia before and there is anemia now. Could this be because the lymphoma is getting worse and it’s disrupting the red blood cells? Or is it all OK? Is their platelet count OK, etc.?
Routine testing can take a variety of shapes accordingly.
I would think of them as real-time updates. You need to figure out whether things are progressing, staying the same, or improving. It could be that the lymphocyte count is totally normal. They got a drug and it took care of many, if not all, of the lymphoma cells. Even though it didn’t cure it, the number is so low that now it’s barely abnormal. It’s more a matter of follow-up.
In some cases, the disorder might be identified genetically. For example, chronic myeloid leukemia has a particular type of mutation or rearrangement in our chromosomes that can be detected by molecular testing. The patient is treated with therapy and can go into remission. All they need is that molecular test to tell the hematologist whether they are in remission or still have the disease.
It depends on what the disease is, how it presented, and what types of tests we have available for it, but routine testing can take a variety of shapes accordingly.
Using Blood Work to Identify Minimal Residual Disease
Stephanie: I don’t want to get too in the weeds, but there’s more and more conversation in the last few years about getting more precise with detection of disease. I don’t know if there’s anything you could talk about with minimal residual disease and in what areas people might be more part of the conversation than others.
Dr. Mirza: That’s excellent. You are so deeply thoughtful; it’s amazing.
Minimal residual disease is our ability to take a look at a very tiny amount of residual disease left after treatment. Our detection methods have become so good that we can potentially detect that.
We want to know before a transplant if the patient free of disease or if the patient has minimal residual disease left.
When we think about minimal residual disease, the two types of diseases that come early to mind are myeloma and B-cell acute lymphoblastic leukemia. We have good mechanisms to figure out if there’s a very tiny amount of disease left. We’re talking about one cell in 10,000 cells.
It’s harder for minimal residual disease studies to be done in acute myeloid leukemia and there are a variety of reasons for it. We can do MRD testing in AML, but it’s harder.
Minimal residual disease can be very helpful in a variety of ways. For some blood cancers, the curative treatment is a bone marrow transplant or hematopoietic stem cell transplant. We want to know before a transplant if the patient free of disease or if the patient has minimal residual disease left. It’s an indicator of their disease status before they go for a transplant.
Minimal residual disease testing can be by PCR or molecular testing, or by flow cytometry testing, depending on what the disease is. There are a variety of tests.
Precision-based therapies target a particular molecular alteration in the disease. We talked about CML. The molecular problem in chronic myeloid leukemia has a drug that you can treat with, but if that problem doesn’t exist, the drug is not going to work.
Patients get cured of CML by using this drug. It’s miraculous. There will be certain mutations that have specific drug targets. There will be certain chromosomal rearrangements that have targets. All of those are important when it comes to longer-term monitoring of testing.
Why Would My Doctor Order a Comprehensive Metabolic Panel (CMP)?
Stephanie: We focused a lot on the CBC. What role does the comprehensive metabolic panel (CMP) play? Those are generally the two tests that patients probably see the most or have ordered the most.
Dr. Mirza: The comprehensive metabolic panel, like the name suggests, looks at the metabolic status of the body. The CBC is looking at the numbers and the differential will look at the types of cells, etc. But the CMP is going to give you a better understanding of the patient’s kidney function, liver function, and electrolytes.
All of this balance is effectively given to us as a snapshot in the CMP.
Electrolyte imbalances are not going to be picked up by the CBC. Blood sugar levels are not picked up by the CBC. When you think of metabolism in the body, you’re trying to figure out how the body is managing the different byproducts of what we eat.
The way we do that is by controlling blood sugar and keeping electrolytes balanced, and those are due to liver function. The liver is a huge player in the metabolism of what we eat. The kidneys are a huge player in what we excrete in the urine. All of this balance is effectively given to us as a snapshot in the CMP.
How Doctors Decide Which Blood Tests You Need
Stephanie: In the blood cancer space, is CMP a complementary test always given or not necessarily? And in what case is it a must?
Dr. Mirza: If it’s an initial diagnosis and we’re still trying to figure out what’s happening to the patient, I don’t know if it’s a must, but I definitely would order it. I would want to know. Indirectly, it can tell you a variety of things that are happening with different organ systems. It’s reassuring if it’s normal. But it depends on how the patient is presenting.
These are reasonable tests because what they provide you versus the cost is a good cost to benefit ratio.
The patient can have concurrent diabetes and the CBC isn’t going to pick that up. Patients can have CLL and diabetes, but the CBC is not going to pick up the diabetes component. Because CMP is a snapshot of overall health, it’s helpful. Would you need to do it every single time if everything else was normal? Unlikely.
I don’t want to be flippant about it, but in the context of how expensive health care is, the CBC and the CMP are relatively cheap tests. I don’t know the cost, but they’re not very expensive. We’re not talking about thousands of dollars or even hundreds of dollars. The hemoglobin by itself is a very cheap test. These are reasonable tests because what they provide you versus the cost is a good cost to benefit ratio.
Conditions That are Monitored More with CMP Tests
Stephanie: For blood cancers, is there something where the CMP is more frequently utilized as a complementary test?
Dr. Mirza: Myeloma is a disease where the cancer cell is the plasma cell and the job of a plasma cell is to make proteins. It makes antibodies to fight off infections, but in myeloma, it’s all abnormal. You will need more than the CBC to figure out how much protein there is. That could be a urine test, but it could also be a blood test.
What you find is that in the blood, the normal protein ratio is all out of whack because you have all these abnormal proteins, so you’ll get another test to figure out what type of protein it is. But again, you can think of the CMP as a screening tool, a first test that will give you a big picture and then you can do a more specific test.
Both the CBC and the CMP in that sense are quick screens. For example, when you get a CBC and the lymphocyte number is up, you need a flow cytometry to figure out what’s happening. Flow cytometry is more expensive. You don’t want to do that for every single person. Similarly, the CMP can guide you and say the liver function is off, so you may want to do a whole other panel of liver function tests, which you don’t want to do upfront.
Should Patients Check Their Lab Results Online Before Talking to a Doctor?
Stephanie: We’re in the age where many patients get the test result notifications even before they hear from the doctor. Would you recommend that patients take a look at their results online or that they wait? How should they interpret these different values over time?
Dr. Mirza: I’m not hesitating because I don’t know the answer. It’s very nuanced and very patient-specific. It also depends on your level of health literacy in general and your personality.
Some people like to go to the airport early. Some people like to go to the airport late. Some people think knowledge is power, but some people think knowledge is not power and they get stressed out about it.
By law, tests and diagnoses that we write are immediately transferred to the patient portal. There are some scenarios where there is a small pause of a couple of days for whatever reason, like if we feel that the patient may not understand it, giving the physician an opportunity to look at it.
The patient has the full right to know what is happening to them. But it’s tricky to think about how that process unfolds.
Let’s say it’s a Friday evening and the patient went to the clinic and had their blood drawn. I look at the blood, do the flow cytometry, and conclude that they have acute myeloid leukemia. I write acute myeloid leukemia and sign it out. Meanwhile, the patient’s physician is still seeing patients in the clinic, but by the time the patient gets home, they’ll get a result on their patient portal, which says they have acute myeloid leukemia.
Think about this patient. Do they want to know this diagnosis? Do they understand what this diagnosis is? What will happen is that their physician who is going to treat them hasn’t had a chance to talk to them about any of this yet.
But that said, all of the information that we provide in reports is the patient’s material. We’re not gatekeeping anything. The patient has the full right to know what is happening to them. But it’s tricky to think about how that process unfolds.
There needs to be a conversation with your patient-facing provider to make sure that you understand the details of the information that can be bombarded to you.
Now, you can have a patient who is very up in their health literacy, understands exactly what all these things mean, can manage the stress or anxiety associated with this information, and can manage looking online where all sorts of opinions will be there. You need to have trust in your provider. There are so many nuances here.
Ultimately, though, it’s not our information to gatekeep. It is the patient’s information. Broadly speaking, it is correct that the patient gets access to that information, but there needs to be a conversation with your patient-facing provider to make sure that you understand the details of the information that can be bombarded to you.
Remember that even if it’s monitoring of tests, there might be variations of fluctuations. If I look at them, I can say that it’s a tiny fluctuation and no big deal, but the patient might think the worst.
Within the world of testing, what’s complicated is that in certain situations, certain tests being a little bit flagged is not such a big deal. With hemoglobin, for example, if it’s off by one point or half a point, it may not be such a big deal, especially if it’s in the normal range. But if it’s a creatinine value and it’s off by 0.6, which can go from 0.8 to 1.2, that’s a huge change. It all depends on what the test is and what it’s being monitored for.
A variety of these things will be different based on what was happening with the patient. Was the patient dehydrated? Some numbers might be off. Is the patient on a completely new drug that is making some changes? Did the patient run a marathon before they got the test? All of these things make a big difference in the way the laboratory test results can be interpreted.
At the University of Michigan, we have a Patient and Family Advisory Council, which I co-chair. Patients are actively involved in a bunch of these decisions. Many of the faculty at Michigan are working on things like patient-centered reporting. They’ve looked at patients reading their pathology reports and have figured out that patients don’t even know what the diagnosis is. There’s so much scientific jargon, which can be difficult to write out.
Similarly, we have a pathology clinic where breast cancer patients talk to their pathologists who show them their cancers. There’s national literature now on patients, by and large, who are feeling value in speaking to their pathologists. This is something that is happening in only a few places, but it’s certainly happening now.
As a pathologist, I went to medical school. No one took away my license to speak to patients. It’s just that we are in a system where that typically does not happen. But it can be valuable to speak to your pathologist.
Your laboratory pathologist’s name is at the bottom of every pathology report. You can call them. Typically, patients don’t, but I have received calls from patients and I try my best to explain their test results. I obviously can’t talk about the treatment as I’m not that well versed on that aspect, but I do know what their biopsy is showing or what their blood test is showing.
It’s complicated because you want the information to be delivered to the patient in a way that will benefit the patient. Ultimately, it is their information. Let’s say no one follows up on it and it’s been a couple of days. At least the patient will know that something happened. Let’s say you’re in a very remote part of the country. There aren’t that many providers. Nobody’s checking the reports. That would be horrible if the patient didn’t realize that they have something wrong with them.
We have many checks and balances, but sometimes, the checks and balances don’t come through. It is important for the patient to know what their report was. I’m glad in a way that they get it, but that whole process is nuanced.
Stephanie: It’s a necessarily nuanced answer that you have to give because there are so many different situations. I also appreciate that you’re part of that Patient and Family Advisory Council. Thank you for doing all the patient-led work.
Dealing with Delays in Getting Test Results
Stephanie: You talked about being in the middle of the country versus somewhere, like Michigan, where it’s highly resourced. You have lots of research there and people like you. What are the reasons why people wait sometimes longer than other places for results? Does that have something to do with who they have on staff or whether they have to outsource the reading? How does that work?
Dr. Mirza: We always talk about low-middle income countries or low-resource settings, but there are some areas in remote parts of the United States where they may not have ready access to a laboratory or a pathologist that, for example, you may have in Chicago, New York, or San Francisco.
Often, if it’s a complicated case, then all of these places have contracts, affiliations, and agreements with pathology departments. Ultimately, everybody finds a place for their pathology to be read. But that said, sometimes it can be delayed because of several reasons.
Primarily, anything that’s delayed is because the test has a turnaround time of a particular amount of time. For example, some molecular tests can take up to two weeks. It can take up to a month in some settings.
It can be delayed because of several reasons. Primarily, anything that’s delayed is because the test has a turnaround time of a particular amount of time.
Think about when the blood was drawn. I hate to give this very negative example, but let’s say the blood was drawn in the middle of a state and the closest laboratory is a three-hour drive away. A patient got the blood drawn at 4 p.m. on Friday and the cutoff for the van was 3 p.m. To them, they’ve given the blood at 4 p.m. on Friday, but the actual pick up for the blood won’t be till Monday morning.
On Monday morning, the blood will be picked up. That’ll go to the laboratory three hours away. It’ll be put on the machine. It might be a little bit complicated. They may not have an answer until Tuesday morning. But in their mind, they gave the blood on Friday, but the laboratory only got it on Monday. I’m not defending the laboratory. I’m just saying that sometimes, these things happen.
On Monday, they might get the specimen and say, “Oh, before we give a real answer, we need some specialized tests,” and then somebody like me will probably call their physician and say, “I have to run a few more tests.” They’ll say, “OK, fine.” But then it’ll be Wednesday by the time the answer comes. It can be a little bit complicated. But by and large, if it’s a simple test, it’s pretty quick.
Conclusion
Stephanie: Thank you so much, Dr. Mirza. We appreciate you joining us. Let’s continue the conversation as this is beneficial to so many people out there.
Dr. Mirza: It’s a pleasure always talking to you. Thanks, Stephanie.
Stephanie: We want to point out some incredible resources from our friends at The Leukemia & Lymphoma Society, including their Information Specialists. You can reach them via phone call, email, and live chat. They also have regional support groups and peer-to-peer connection called First Connection®.
Thank you for joining. I know that there’s a lot to go through. We hope to see you at another program because hopefully, today was helpful for you. Thank you and take good care.
Blood Work Basics: Making Sense of Your Test Results
Hosted by The Patient Story
What do your blood test results really mean — and how do they help doctors detect or monitor cancer? Learn about the most common diagnostic tests, including the CBC and the CMP.
We would like to thank Blood Cancer United for their partnership. They offer free resources, like their Information Specialists, who are one free call away for support in different areas of blood cancer.
How Brittany Chooses Quality of Life in Her Stage 4 Rhabdomyosarcoma Treatment Decisions
Brittany received a life-altering diagnosis of stage 4 rhabdomyosarcoma in July 2024. What started as a small lump on her jaw quickly escalated into a whirlwind of hospital visits, major surgeries, and tough decisions. But throughout it all, Brittany has remained grounded in her values, fiercely committed to preserving her mental health, self-worth, and autonomy.
When Brittany first noticed the lump, doctors thought it might be a cyst. But after it rapidly swelled during a biopsy, further testing confirmed it was cancer. That moment, she recalls, shattered her sense of normalcy. Getting that phone call was a deeply painful turning point. From there, she had to quickly learn how to advocate for herself.
Initially, Brittany’s first oncologist didn’t offer many choices. She sought a second opinion, and that’s when things began to shift. Despite being a young adult, Brittany learned that stage 4 rhabdomyosarcoma is often treated as a pediatric condition, which brought its own emotional weight. But the new oncologist gave her options, including fertility preservation, which was emotionally and physically taxing but important to her.
Brittany started chemotherapy and endured severe nausea, weight loss, and exhaustion, only to find out that the treatment wasn’t effective. In October, doctors removed the tumor surgically, replacing her jaw with titanium and using bone and muscle from her leg for reconstruction. She lost some facial movement in the process, a harsh reminder of the physical toll this diagnosis has taken.
Radiation therapy came next, damaging her salivary glands without improving her condition. Then the cancer spread to her lungs. After more chemo and even a clinical trial, Brittany made the decision that her treatments and their impact on daily life were stealing the quality of life she wanted. She bravely chose to stop her clinical trial treatments and take a more holistic approach, focusing on diet, lifestyle, and emotional healing. She is monitoring her lungs and scheduling a second surgery to work on her jaw.
Mental health has been the toughest part. Losing her physical strength, independence, and even pieces of her identity has been crushing at times. But Brittany has also grown immensely. With unwavering support from her boyfriend and his community, she’s learning to trust herself again, reclaiming her life on her own terms.
Brittany wants others to know they aren’t alone. Stage 4 rhabdomyosarcoma is terrifying, but fear doesn’t get to make the rules. You do. And she’s living proof that, even in the darkest hours, hope and strength can coexist.
Watch Brittany’s video to find out more about:
How Brittany found clarity and control after a devastating diagnosis
Why she has a titanium jaw
The emotional toll of stage 4 rhabdomyosarcoma
Why Brittany walked away from treatment to protect her quality of life
What it means to find your voice when the world tells you what to do
Name:
Brittany C.
Age at Diagnosis:
22
Diagnosis:
Rhabdomyosarcoma
Staging:
Stage 4
Symptom:
Small, sharp lump on the right side of the jaw
Treatments:
Surgeries: tumor removal & planned corrective jaw surgery
Chemotherapy
Radiation therapy
Clinical trial
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: Pain behind left knee, needle-like sensation in left foot Treatments: Surgery to remove what was thought to be benign tumor, chemotherapy, final surgery, radiation (36 sessions)
...