Robin’s Zest for Life Helped Him Overcome Stage 4 Melanoma
Robin, an architect born and raised in France and now based in the USA, shares his experience with stage 4 melanoma. In 2023, he discovered a tiny bump on his chest. He showed it to his dermatologist, who thought it was just a cyst. After closer inspection, the doctors discovered that the bump was actually melanoma and it had already metastasised to Robin’s liver.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Robin was overwhelmed, confused, and numb all at once, but he refused to cave in. He didn’t isolate himself; instead, he looked for the right support. He understood that facing such a situation would be easier with a strong community behind him.
Robin found that the hardest things for him to face weren’t the treatments for stage 4 melanoma (which is a type of skin cancer), but the weeks of uncertainty before he was fully diagnosed and could receive proper treatment. This uncertainty left him struggling to maintain his footing. However, the moment that his oncologist introduced the option of a clinical trial, his fear, anxiety, and numbness faded, and his perspective shifted for the better.
Robin passionately advocated for himself. He emphasized the power of making informed decisions. He dove headfirst into understanding the trial and kept asking questions so he could regain control over his health.
Under the clinical trial, Robin’s treatment included three months of chemotherapy combined with immunotherapy, followed by 18 months of immunotherapy maintenance. He’d read about all the potential side effects in the clinical trial booklets and braced himself for a rough experience. Happily, the side effects he ended up experiencing turned out to be minimal.
His positive mindset bolstered his psychological well-being. Instead of viewing his treatment days with fear and dread, Robin approached them like regular activities, for instance, like going to the office or visiting friends. This made a significant difference in his healthcare.
Throughout his stage 4 melanoma experience, Robin kept up his active lifestyle. He continued working, traveling, and spending quality time with his loved ones. His zest for life and people gave him strength, and he stayed true to himself even in the thick of his health challenges.
Today, Robin is thriving. His recent scans show no signs of tumors or metastasis. He looks forward to having regular check-ups every six months for the next five years, then annually.
Watch Robin’s video and:
Discover how his love for life helped him through stage 4 melanoma.
Learn how a little bump changed his life, but couldn’t dampen his spirit.
Discover the moment Robin’s fear turned into fearless patient advocacy.
Find out the unexpected reason he found joy in hospital visits.
Learn why Robin views clinical trials with gratitude, not fear.
Name:
Robin A.
Diagnosis:
Melanoma
Staging:
Stage 4
Symptom:
Appearance of a small bump on the chest
Treatments:
Chemotherapy and immunotherapy (under a clinical trial)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Sam Chooses Hope in the Face of Grade 2 Brain Cancer
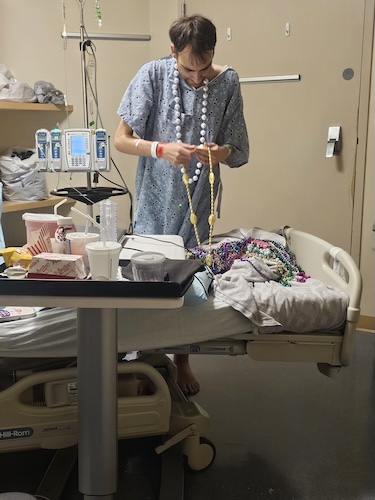
Sam is a passionate photographer and a proud mom to a six-year-old boy named Felix. Her life took a terrifying turn when a series of seemingly minor symptoms led to a diagnosis of grade 2 brain cancer (astrocytoma with IDH1 mutation).
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
Sam’s experience began subtly, with feelings of being “off.” She attributed this feeling to holiday stress and the hustle of running her business. She also experienced occasional fatigue and what she thought was food poisoning. But little did she know that things would soon escalate.
One night, Sam collapsed in her bathroom and suffered what would be the first of many seizures. Her husband acted swiftly, calling 911. She woke up in the ER to the shocking news that they had found a mass in her brain that was causing her seizures. An MRI confirmed the diagnosis, and Sam had to undergo emergency brain surgery.
Grade 2 brain cancer (astrocytoma with IDH1 mutation) had more than just physical effects; it also deeply impacted Sam and her family’s mental well-being. (Editor’s Note: An astrocytoma is a tumor that develops in the brain or spinal cord and grows from star-shaped or astrocyte cells. An IDH1 mutation is a mutation in the enzyme-making IDH1 gene, which can result in cancer.) Sam spoke with her son Felix honestly, aiming to teach him about what was happening to her instead of making him afraid. Her husband was overwhelmed by the sudden shift in their family dynamics. Sam realized the importance of open and honest dialogue, emotional check-ins, and seeking professional support in helping her family maintain its mental health.
After her surgery, Sam had to have radiation treatments and chemotherapy. She found the treatments grueling, given the lifestyle adjustments, dietary restrictions, and emotional hurdles she had to deal with as a result. But through it all, she was still able to find light in the darkest moments, whether through joking with medical staff or cherishing time with her son and husband.
Sam’s message is clear: seek medical advice when something feels off, prioritize self-care, and embrace support from those around you. Watch her video and find out more about:
How a seizure led to a completely unexpected diagnosis.
The subtle symptoms Sam thought were due to holiday and work stress.
How she prepared her young son Felix for really tough news.
The surprising realities of being awake during brain surgery.
Why mental health is so vital in cancer care.
Scroll below to read the full transcript from Sam’s interview!
Name: Sam D.
Age at Diagnosis:
37
Diagnosis:
Brain Cancer (Astrocytoma with IDH1 Mutation)
Grade:
Grade 2
Symptoms:
Consistently feeling overwhelmed
Seizures
Treatments:
Surgery: awake craniotomy
Radiation therapy
Chemotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I am a mom to an amazing six-year-old boy. He is the light of my life. I own a photography business that brings me so much joy.
I remember going into the bathroom and brushing my teeth afterward. And I remember setting my toothbrush down, and I very vaguely remember falling backwards. But I don’t remember anything beyond that.
I was so stunned at the entire event. And I think, knowing that when you hear you have a mass in your brain, I don’t think I registered immediately that that meant I have a brain tumor.
When I first noticed something was wrong
I started feeling a bit off. The weekend before I was admitted to the hospital, I started just feeling off, and I thought it was compounding stress. We were in the closing window to Christmas, and we hosted Christmas. My initial thought was that I was just stressed to get to the end of the year. And I had said something to my husband, we were snowboarding that day, and I said, I just don’t feel 100%. I don’t feel like myself. I feel like I’m just too stressed to make commitments. And I think he brushed it off like, yeah, we’ve got a lot going on. And as did I. And then we went back to Denver and stayed. We’re getting ready for the week, the weekend to end into the beginning of the week.
And on Sunday night into Monday we I ended up experiencing what I thought was food poisoning. And I was experiencing that every once in a while for the last few years, and I just assumed that I was maybe developing an allergy to something or developing a food intolerance. But what led me to be sick for a solid four hours? The last time I got up, I fell in my bathroom and fell into a seizure. Thankfully, my husband was home and caught it immediately and called 911 when he realized I was seizing. And that it was a very short time, I think, in the grand scheme of things. And I don’t know if I would have ever assumed that food poisoning like symptoms, and maybe not being able to bear the weight of stress was causing me to, or showing me that I had something going on internally.
What happened next
I got admitted to the hospital. The newest and greatest one, actually, which was really lucky timing for me. I had my seizures around 4:30 in the morning, and I came to between 730 and eight in the morning. And by that time, I was in an emergency room. I was admitted into an emergency room, an actual room. And my husband and son were sitting on the waiting room chair there. And when I woke up, my husband said, Sam, you had several seizures this morning. They did a CT scan when you got here. They found a mass in your brain. They’re prepping you for an MRI, and a neurosurgeon is coming to talk to you.
So that was the first thing I heard when I woke up. And I believe, or I feel like I asked him to repeat that because I was so not only out of it, but extraordinarily confused that I was in an emergency room and had zero recollection of how I got there and the events that led up to it. I went in for my MRI. Very shortly after, the neurosurgeon was in the office or in the emergency room with me. And he said, You have a mass in your frontal right lobe. It is putting pressure on your brain, which is now causing these seizures. You need to have surgery immediately in order to survive.
The moment everything changed
I was so stunned at the entire event. And I think knowing that when you hear you have a mass in your brain, I don’t think I registered immediately that that meant I have a brain tumor. It did take me a little bit of time to become more cognitively aware later that day, and just really sit with the fact that I have a brain tumor and they’re just going to remove it and everything’s going to be fine. And that’s really where my head and positivity came from. And that’s far from the reality of what having a brain tumor really is. And it was a little bit disheartening knowing that reality later.
And as things went on, I think it took me a while to really process what it meant to have a brain tumor and to hear that you have a brain tumor. I had just turned 37 the month prior, so I was just recently I was hitting my late, late 30s and making jokes about getting older. But I believe that getting older is a blessing, and I wasn’t quite prepared to be the youngest person in a treatment center for the condition that I have.
How I prepared for surgery
It was an emergency call to my lawyer to make sure my will and my living will were up to date. And that was really where my stress was. I was making sure that my son Felix was just taken care of if something were to happen to me. His dad’s passing when he was two is incredibly tough. And just him having to go through all that, and him and I together, and then now getting married again last year, just a few months before I found out I had a brain tumor.
I wanted to protect Felix. Even while being in the hospital and being tended to by the nurses and doctors, Felix was there too. I really wanted to make it positive and that being in the hospital wasn’t always scary, and that they are there to help fix the problem, and that that’s what they went to school for. So I’m trying to use that with him to be positive. But I was terrified for him. And later, we had those conversations too. He’s pretty in touch with his emotions and seemed pretty scared. My husband also did. And I think just the burden and weight.
I hate to say burden, but the burden of taking on our entire household and our life all of a sudden at four in the morning, I was suddenly not in the home. I wasn’t able to drive for months and everything, and we had no idea going into it that that was it. But I felt the fear in his voice when he told me, and I can just tell I had felt it over the last few months as we’ve digested and talked about the initial moments and being in the hospital and how much stress that and a burden that he took on himself to go ahead. Just taking it in stride together has been the most positive part.
I was awake during my brain surgery
They admitted me to the ICU and monitored me. And he said that very kindly and humbled me in the thought that I was I could leave and come back. I spent the first part of the week in the ICU taking various medications to make sure I didn’t have any more seizures and doing all the bloodwork, etc. to make sure I had I was properly set up for the procedure. And one thing that came up, because it’s on my right side and I’m left-handed, was that I had to be awake for the craniotomy as well. So I spent he prepped myself that it was going to be two hours for the surgery, that I would be in and awake for the entire surgery for two hours, and then I would be done and on my way. The surgery ended up being about 5.5 hours, and I was awake for the entire surgery.
I was a bit surprised to have surgery awake, as I mentioned. But I also was a bit surprised that I was sitting up the whole time, too. They have your head in a vise, and they kept me sitting upright. And what I remember was the anesthesiologist. I was sedated on my right hand side, and the surgeon was on my left hand side. I’m assuming he was kind of coming this way directionally. If I remember correctly, barely. Thankfully, there was enough sedation that I was lucid in that way. So sitting up, and I could hear everybody talking and you know, reacting to things and their interactions as well in terms of the frustration that I could. I could hear the initial grabbing of the tumor. And that’s why it took a little bit longer. They were hoping to also have initial pathology results back during surgery, and make sure they got as much of the tumor as they could. Generally, you can’t, because it does. If they go too far into the brain matter, they can certainly hurt you more than they can help you at that point, too. And that’s where people end up having dysfunction. I do remember him getting frustrated, and maybe he said that I got a little anxious because I reminded him that the Broncos were still playing every hour.
And they did call my husband and told him. Sam’s still saying that the Broncos are on tonight, so she’s in good spirits and really looking forward to this game. But the surgery itself was a bit shocking to be in and awake and alert for the actual procedure. The most jarring part was actually getting the incision of the bone out, like you’re sawing the bone, because I was awake for that. And there’s no way you can really make that not painful. So that was the most painful part. And my incision goes all the way. I have hair now. All the way around. I have some great pictures of my incision. But it was much larger than I expected. And the picture I took the night before. They did little shaved spots around where they mapped, where the vise was going to hold my head together. Really lovely photos of that, too. I wish I could capture how sad I felt about losing little tiny bits of hair there, where I did lose a large chunk of hair. With it, they shaved this the during surgery, and I lost more with treatment later.
I got my results five weeks later
A little bit of relief came when the doctor came in and he said, You have a grade two astrocytoma and a few mutations with it, one of them being IDH1. And that can be hereditary or it can be environmental. I found out after thinking that I had the hereditary one, that I actually have the environmental one. It can be stress or exposure to toxins and things like that. And there’s no way of knowing when or what toxins or what you can do to avoid that exposure. And the other mutation I have is that it has a very slow-growing brain tumor. I’ve had the actual tumor for years, if not decades. And the astrocytoma, at one point, mutated into that grade of tumor. And that’s likely what the stress and the IDH1 mutation are.
I was in shock. Yeah. And I felt like at that point, especially along the way, and the months following and the weeks before that, I had zero alone time. I most frequently hear that nobody wanted me to be alone if I did fall into a seizure or something happened, or I needed something that I was not able to do yet because I wasn’t able to, like, lift anything heavy or, you know, do a lot of normal, functioning things within the day. So I think the shock was a bit of biggest part of it for me was that I just was like, okay, I do have cancer. Like what’s next? And that I was really more focused on what the path forward is. Like, am I going to die, or is this like what is going to happen? And that is a very hard thing to hear, regardless. I found myself. Later on, any moment that I would be alone, especially in those first few weeks of really processing, I would find my little times to just like, have a little cry, or just shed a few tears just to feel like just to feel. But I didn’t want to. I didn’t feel like I was the doom and gloom, and I didn’t want people to feel sorry for me in that way. I did try to hold it to be a little bit more of a private grieving on that side.
I told my son a few days after I found out that I wanted to make sure it was an educational opportunity for us. I don’t think that when I was six years old that I understood or knew what cancer was or understood the impacts on the close circle. I kind of prepped everybody, and I said, Please don’t cry like I have cancer and have brain cancer. And encapsulated what my treatment plan was going to look like. And the positive side of extending my life and the quality of life. But the hopes that this doesn’t come back. And my husband. That’s a good question. But we were together, and I think he just really held a lot of space for me and just really wanted me to kind of lead with what emotions we wanted. We’ve had some cries. It’s been a hard year. First year of marriage. That’s been compounded on that.
What my treatment options were
One option that I did not get in the hospital before the surgery was you do nothing. Because I believe that before the surgery. And they did believe, too, that if I did nothing, my chances of surviving within days were probably a little to nothing. So, thankfully, my oncologist did say you can do nothing. And live with post-surgery and the chances of recurrence for the brain tumor to grow back, and to be more aggressive, and to ultimately take over. My chances of survival for five years were under 20%. Statistically, and for astrocytoma specifically, they generally have two types of chemo treatments along with radiation. So they do one that’s one, a single pill, and a radiation combination. And the other one is a cocktail of three different types of chemo and a radiation combination. The one with the three different chemos that you take has been around a little bit longer, and they’ve seen a lot of people live into multiple decades. And that one has a lot of research and positive results because it’s been around longer. The other new chemo, like single chemo and radiation, has not been around as long. And that one doesn’t have as much in terms of longevity that they know about yet, because it hasn’t been around long enough that they’ve used it on brain cancer patients.
But the other one seemed a little bit more positive. And I’ve since joined a bunch of brain tumor support groups and specifically for astrocytoma. And several people have lived for multiple decades with astrocytoma and have had the same treatment. So it made me feel much more comfortable going with that route. The oncologist did recommend the chemo route, which I went over the other one, just due to research, but he said both he felt very comfortable saying and hearing your life expectancy going up to 70 percent for over ten years. I measure the time with my son. If I were to pass in under five years, he would lose both of his biological parents before he’s 11 years old. And how was that fair to him? And that’s really what was making me most emotional. Was that fight for him and not putting him in a place in his life that he deserves? Hearing that and just mentally preparing to go through radiation and chemo was a big lift. I did call and make that decision about a week after I found out. And it moved pretty quickly. I was a week later getting fitted with my mask that they put on your face for radiation. And I was in radiation very shortly after. And chemo followed.
My treatment plan
I did kick off my treatment plan with 27 rounds of radiation. It was supposed to be 30, but the doctor had said that that was the higher end of treatment for me. But the way my resection for the brain tumor went and the way my scan looked right before, they felt comfortable reducing the session. I went five days a week, Monday through Friday, into these sessions, which were relatively easy for what they sound like. I enjoyed the nurses and the staff there. We had a good time, and I was coming in with funny jokes instead of saying my birthday every day because we all knew it. We were all friends there. Now that I would say, oh, did you know on my birthday this happened or that this happened that year? Or what was the top song in America? It was a fun way to bring things together in that way.
And about four weeks post, I started chemo. They did break that up. And I do a mixture of three different medications. Day one, it’s four cycles, and each cycle is 42 days long. And within those 42 days, I take three different medications.
One is an IV into our oral pills that I’m able to take at home. Day one is a single medication that I take. And it makes you kind of sick for a few days after. And I experienced quite a bit of nausea. I do manage through nausea, medication, and things that make it a little bit easier. And then I go in and do an IV infusion, and I start another medication for two weeks. And that one’s the most aggressive. I am not allowed to eat cured meats, aged cheeses. Most sauces or soy sauces. Anything that has any alcohol or soy, like any source. In general, I can’t touch rubbing alcohol. So there are a lot of restrictions, and it’s very difficult to eat out. I’ve utilized AI to upload different menus at restaurants and asked, “What can I eat at this restaurant with this medication that I’m taking?”
The plan moving forward
I’ve not had any clinical trial discussions. And my plan moving forward after this, for my understanding, is just to monitor. I’ll be getting MRIs every three months. My last one was in May and had positive signs of progress from the radiation treatment. My next one in three months should be this month in August. And I’ll have one more at the end of the year. So every three months for the foreseeable future, I’ve heard anywhere from 5 to 10 years. So that’s going to be a big stretch of that. But I’m hopeful that is something, and being patient with going every three months, that if anything does happen or anything does recur, we’re able to find it quickly, and maybe mitigate it from being too invasive. I would love not to have brain surgery again. But another fun fact that I found out is that once you find out you have a brain tumor, the chances of recurrence are high. No matter what you do. So I’m hoping that if that does happen, I’m 105 years old and it will be okay. But my other hope is that it just doesn’t. And this is maybe a one-time blip in my earlier life than expected.
The challenges of my diagnosis
My biggest challenge has been being able to live with it comfortably. I have had a full head of hair my whole life, and I think it just changed my appearance so much, especially at the beginning when I was missing all my hair. And I had a very noticeable scar that I couldn’t cover. That I had to really become comfortable with that, or who I was. I found myself very often justifying, like I have brain cancer, or just telling that to somebody. My son even said it to people at school. They’re like, You look so different. Felix’s mom, what’s different about you? And he would even say it. She has brain cancer. Leave her alone. So, whether I want this to be a traumatic event for everybody, it kind of is. I think it’s been hard to come to terms with and hard to keep private, as it’s so physically obvious in my appearance. But I’ve gotten a little bit better, and I’m trying to own it now.
I feel like initially, maybe it’s going to take a little bit of time in this drastic change in my life. Is it just being treated a little bit differently? People started treating me differently or acting as if I were more delicate or needed extra padding around me. I’m very much independent, but I’m also going to push myself in every way I can, and I think the bubble around me, or people hoping to give me the ability or to protect me, has become a big change in my life. Improving that has been a little bit challenging as well. Just being like, I can do this. I’m good. I’m. They said I can do my normal activities. I’m not trying to be extreme by any means. I only got one day of snowboarding in last year, and I’m hopeful that that is not the end of it for me. They promise that I can do all that, but it’s a little bit hard to overcome that aspect as well. Just hearing that somebody had brain surgery. Even my mom, when I called her, said, Wow, I can’t believe how well you’re talking. I just assumed you wouldn’t be able to talk if you had your brain operated on, which I can see is a very valid deduction, but I don’t know if it’s something that we know enough about.
My message of hope
We all go through extraordinarily hard times in life, and if we want to live in or ruminate in the negative and live in that, and it can make us sick, we can go under and live in the stress and the the disheartening feeling of being like, I have a brain tumor, I’m going to die, and this is what’s going to kill me, and it’s the end of the world and living in that is so toxic and so bad for you that living within the positive side of things, or feeling positive and optimistic that you can overpower this and that it’s mind over matter everywhere. And I try to be as mindful of that for myself all the time, losing my husband and becoming an only parent, and then finding out I have brain cancer four years later. I cannot let the burdens and the hurdles in my life take over. What is more positive? And seeing the joy on my son’s face and giving him the best experience in life together, and making memories that last.
I would say if I had one piece of advice for anybody, it would be to take care of yourself. Know that if you’re feeling overwhelmed or stressed, or if something’s not right, it’s okay to just go and get a checkup and look. And maybe that stress can be something else. What most often do we hear? Don’t give yourself an ulcer. Don’t get so stressed. You get an ulcer. But in my world, I’m wondering if I got so stressed that I gave myself a brain tumor. I made my existing brain tumor worse. So. Self-care. Taking care of yourself in every way you can. And that would be my best advice. And finding out and being preventative.
Heart and Humor: Jeanine’s Stage 3 (T3bN0M0) Rectal Cancer Story
Jeanine found out she had stage 3 rectal cancer (stage T3bN0M0) in January 2025, but her health experiences goes much further back. She had been experiencing rectal bleeding in her mid-20s. She had a colonoscopy back then, but it found nothing more serious than hemorrhoids. This made it easy for her to attribute these recurring symptoms over the years. As time passed, there were new symptoms and they worsened, including urgency to use the restroom, mucus in her stool, and stool that was narrower than usual.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Her intuition told her that she was experiencing something far more serious than just hemorrhoids now. Jeanine looked up her symptoms online, and based on her research, began to suspect cancer even before she was properly diagnosed. She consulted doctors, and her research paid off when a new colonoscopy revealed that she had stage 3 rectal cancer (T3bN0M0). (Editor’s Note: A T3bN0M0 tumor has grown into the outermost layers of the rectum, but hasn’t spread to nearby lymph nodes or distant sites.)
Jeanine didn’t feel overwhelmed by this diagnosis. She instead felt that it validated her concerns and knew that this was a big step forward in helping her get better. She tirelessly and fearlessly advocated for herself, pushing for answers, seeking second opinions, and switching medical teams to feel more understood by a team that also understood another medical condition she had. Her experience shows how important it is to feel comfortable with healthcare providers and communicate effectively with them.
Her treatment for stage 3 rectal cancer included chemotherapy (with adjustments to manage severe side effects) and radiation therapy. Although Jeanine may need to undergo the surgical procedure known as abdominal perineal resection or Barbie butt surgery, there’s a chance she won’t need it if the tumor responds well.
One of Jeanine’s biggest strengths is her positive outlook. It shines through her creative coping mechanisms, like naming her tumor “Chester McButt Sprout” and sharing funny updates on social media. These approaches not only help her process her experience but also help her loved ones stay informed, amused, and connected.
Jeanine’s identity has evolved through her diagnosis and treatments. It’s not defined by cancer, and is enriched by her perspectives regarding life, joy, and connection. She draws strength from her late mother’s resilience and tries to live authentically through all of the challenges she faces.
Watch Jeanine’s video for more on:
How she transformed her stage 3 rectal cancer diagnosis into a story of empowerment
Jeanine’s surprising (and funny) creative approaches to coping with cancer
Why self-advocacy can be life-saving — her bold healthcare decisions
From confusion to clarity: Jeanine’s 20-year health puzzle
How her resolve and resilience helped her take her cancer experience forward
Name:
Jeanine B.
Age at Diagnosis:
46
Diagnosis:
Rectal Cancer
Staging:
Stage 3 (T3bN0M0)
Symptoms:
Rectal bleeding
Pain in the tailbone
Urgent need to use the restroom
Unusually narrow stools
Presence of mucus in stools
Fatigue
Treatments:
Chemotherapy (FOLFOX)
Radiation therapy (coming soon)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
The Patient Story Podcast: I’m a Young Cancer Patient
(Ep. 01) From Cancer Caregiver to Patient: Taylor’s Story
What do you do when you get a cancer diagnosis? Where do you go? Whom do you call? How do you become your own patient advocate?
There are so many overwhelming questions that hit the people who’ve been diagnosed and those in their closest circles. Here is the first-ever episode of a new video podcast hosted by The Patient Story founder and lymphoma survivor Stephanie Chuang.
This inaugural episode features a special guest: Stephanie’s colleague at The Patient Story and fellow former TV journalist, Taylor Scheib, who shares her experience navigating a cancer diagnosis, shifting from her role as a patient advocate and the daughter of a cancer survivor — her mom, Kelly — to becoming a cancer patient, herself.
Interviewed by: Stephanie Chuang Edited by: Chris Sanchez, Stephanie Chuang
Taylor shares the moment she discovered her diagnosis. She was sitting on her couch and casually checking her MyChart when the words “oncocytic carcinoma of the thyroid gland” appeared. (Editor’s Note: Oncocytic carcinoma of the thyroid gland is a rare, aggressive kind of thyroid cancer. It’s also known as Hürthle cell carcinoma.)
She was devastated by the diagnosis, but her background in patient advocacy helped her regain her footing. Her experience and knowledge built from working closely with both patients and caregivers helped her recognize symptoms and push for answers. This reinforces a crucial message: You are your own best advocate.
Taylor’s ability to listen to her body played a pivotal role in her experience. She had first noticed a nodule in her neck three years before her diagnosis, and had continued monitoring it through regular check-ups. When the nodule grew, she trusted her instincts and insisted on further evaluations, even when her concerns weren’t met with urgency. This underscores the vital lesson of trusting your body and speaking up when something feels off.
Taylor experienced further challenges when she tried to navigate the healthcare system. Her patience was tested by insurance hurdles, delays in scheduling surgeries, and having to wait for tumor board evaluations. She candidly discusses the frustration of feeling like just another case number. But her experience and resilience won through as she managed both the system and the mental toll of cancer. She found strength in support from her husband, family, and friends.
Taylor’s patient advocate experience also underscores the power of storytelling. At the start, it wasn’t easy for her to share her story publicly, but when she did so, she found it cathartic. Through opening up, she not only helped herself heal but also offered enlightenment and hope to others with similar struggles. Taylor’s authenticity is a good reminder that behind every social media highlight reel, real struggles do exist, and sharing them can be profoundly empowering.
Please scroll below to read the full transcript from The Patient Story Podcast Episode 1!
Name:
Taylor Scheib
Age at Diagnosis:
30
Diagnosis:
Thyroid Cancer (Oncocytic Carcinoma of the Thyroid Gland)
Staging:
Stage 1
Symptom:
Appearance of neck nodule that grew over three years
Editor’s Note: This transcript has been edited only for simple clarity.
Podcast Summary
When It Rains, It Pours
Taylor shares her mom’s own brush with cancer and how this was her first touch point in joining The Patient Story.
Taylor and Stephanie talk about the unpredictability of medical challenges, including those faced by cancer patients.
Introducing Taylor: A Patient Advocate Becomes the Patient
Taylor discusses her role at The Patient Story and how it made her more aware of cancer and its impact.
Taylor and Stephanie delve into the unexpected turn Taylor’s cancer experience took.
The Shock of Diagnosis: Getting News from MyChart
The moment Taylor learned about her diagnosis and the emotions that welled up.
The challenges associated with getting life-changing news like she did over a digital platform like MyChart.
Emotional Fallout: Processing a Cancer Diagnosis
The immediate emotional impact when Taylor heard the word “carcinoma.”
The questions that surfaced afterwards.
Self-Advocacy: Trusting Your Instincts and Pushing for Answers
Taylor discusses the importance of self-advocacy and being a patient advocate in healthcare, as well as the power of listening to one’s body.
She also opens up about her persistence in getting her nodule checked and how it helped her get results.
Barriers and Delays: Navigating the Healthcare System
Taylor and Stephanie delve into the problems many patients experience when they try to navigate the healthcare system, including systemic delays and provider shortages.
They also explore the frustration patients can experience when urgent concerns face logistical roadblocks.
The Waiting Game: Coping with Uncertainty and Lack of a Plan
Taylor and Stephanie discuss how difficult it can be to wait for clear next steps post-diagnosis.
They outline and explore strategies to help manage mental health during periods like these.
Community and Connection: Reaching Out and Trauma Bonding
Taylor shares how reconnecting with old friends and the support from her community have been vital during her journey.
“Give yourself grace, but also do it on your own time.”
Telling Others: Navigating Reactions and Support Systems
Taylor and Stephanie reflect on how to talk about a new diagnosis, the variety of reactions from others, and maintaining boundaries in relationships.
Supporting a Loved One: Tips for Friends and Family
They offer tangible advice for supporters: what to say, what not to say, and how to truly show up.
“The small stuff means more.” — Some of the most thoughtful and meaningful gifts aren’t the most expensive ones.
Sharing the Journey Publicly: The Power and Healing of Storytelling
Taylor explains why she chose to be open on social media and the cathartic role of storytelling.
She offers advice for those who are also considering sharing their experiences.
Give Yourself Grace: Final Reflections and Words of Wisdom
In closing, Taylor and Stephanie share uplifting thoughts on the importance of being a patient advocate, self-compassion, and owning one’s narrative.
Introducing Taylor: A Patient Advocate Becomes the Patient
Stephanie Chuang: Hi, everyone. It’s Stephanie here with The Patient Story. I’m just starting something new here. Wanting to be able to touch base more with everyone out there who’s finding us. If you remember, I had my own cancer experience when I was diagnosed suddenly with a non-Hodgkin lymphoma. Diffuse large B-cell lymphoma. I was 31 at the time, two months from getting married, and it was a complete whirlwind, to say the least.
But joining me today, I’m so excited to introduce someone who many people may be familiar with on our channel, Taylor. Taylor is on our team at The Patient Story. An amazing leader. And Taylor’s joining us for not-so-great reasons, but I am so grateful that she’s coming on to share her story. So, Taylor, do you want to share a little bit about yourself first, of course, outside of the cancer diagnosis?
Taylor Scheib: Stephanie, thank you so much for the warm welcome. So crazy being on this side instead of being the one guiding the conversation. I live in the Pacific Northwest with my amazing husband Justin and our dog Sage. She is our world. She’s our Chocolate Lab. And we love to hike. We love to be outdoors, and we love to camp. I’m originally from Illinois, from a really small town. My high school graduating class was 30 people, and so I’m from a very rural area. And I’m so grateful where I grew up, though I have amazing friends and family back home, I’ve lived away from home for a long time, so that’s been an interesting part of navigating my situation. But yeah, my mom is a colorectal cancer survivor. She was diagnosed with stage 3 colon cancer in November of 2023.
Stephanie Chuang: Taylor has been someone who’s led so many of these conversations with people, with patients, caregivers, care partners, and you know, the first personal touch point in joining The Patient Story was you introducing your mom, Kelly, to the process. She shared her story of going through colorectal cancer. And I’m so grateful again to both of you for being so open about that. But you may see that Taylor has a throat scar. Yep. And that her voice sounds hoarse. She doesn’t normally sound like that. I was on a work trip, actually, and then, got a late text from Taylor, and that was, of course, not usual. So, Taylor, just walk us through what was happening at the time.
The Shock of Diagnosis: Getting News from MyChart
Taylor Scheib: Yeah, it was a Monday night. 5:15 p.m.. I was about two weeks post partial thyroidectomy for a nodule on the right side of my thyroid. And that night, I just got a message from MyChart with my pathology results. And when I got the pathology results, it was out of sight, out of mind, from my surgery. Because not once did anyone say, “Hey, be on the lookout for your pathology.” I knew that the nodule and the mass were going to be sent off, of course, but I never thought that when I got those results, it would read anything but benign. And unfortunately, when I got those results, I was sitting on my couch, my husband’s cooking dinner. I get into MyChart, and the first thing I see is “oncocytic carcinoma of the thyroid gland.”
I immediately shoot up. I’m crying. My husband is like turning off the burners in the kitchen because I just bluntly, out loud go, “I’m pretty sure I have cancer.” And my husband goes, “What? What do you mean?” And that word ‘carcinoma’. I know what that means. And I don’t know if, before starting at The Patient Story and dealing with my mom’s diagnosis that I would have known what carcinoma meant. And so, because I am educated, because I’m privileged to work for such an amazing company where I’m learning so much every single day, I knew carcinoma meant cancer. We immediately came to this very spot, right where I’m sitting. We got on my laptop, we started researching, and the word oncocytic was a word I had never heard. I’d never seen or heard anything. Yeah, you start to Google. And that’s where my patient advocate story began, with my diagnosis.
Stephanie Chuang: Oh, wow. Yeah, there’s a lot there, I know. When I got the message, and then I got on the phone with you and you told me, first of all. I mean, it just took me right back to that feeling of, wait a minute. What’s going on? Right. And cancer and all the things.
And of course, my diagnosis was years previous. I was diagnosed back in December of 2016 and into January 2017. So it’s been a minute, which I’m very grateful for. But really, no matter how long the time, I remember that feeling of, What the hell just happened? And in your case, to spell it out for people, they would go, “Oh, you have this nodule, and you need to get it removed.” It’s benign, though, and nowhere, never did anyone ever say it might be something.
Now, I can understand, by the way, why, without the information of a biopsy and without other, maybe contextual clues that they might say this is benign. But at the same time, there’s this whole thing of, oh, my God, you said the results had actually been in for a while, and then it just popped up on MyChart. What was hitting you in that moment about your life? What were the thoughts and the emotions?
Emotional Fallout: Processing a Cancer Diagnosis
Taylor Scheib: Yeah. I already have tears in my eyes thinking about this answer. Because when you work for an amazing organization like The Patient Story, you’re hearing these stories every single day. You’re writing scripts and you’re creating this beautiful content. The underlying thing is tragic, and that is a cancer diagnosis. And so I would be lying if I said I never thought I’d get cancer. I’ve thought it. And you become just so much more aware of your body and the feelings that you’re feeling, and going to the doctor and getting your checks, getting your women’s health exams when you’re listening to these incredible people every single day.
And then when your mom goes through it as well. So I was shocked. But when the dust settled, I wasn’t that shocked because cancer can happen to anybody. And so being so young, I had just turned 30. My husband and I just came back from this incredible trip to Puerto Vallarta that he planned for my 30th birthday.
And this year was going to be filled with amazing trips and celebrating friends who are getting married. And you know, we’re doing all of those things still, of course. But in that moment, I just thought, what are the next six months going to look like? I’m such a planner, as Stephanie knows.
And I just kept thinking, what is this going to look like for me? And then the unknowns started. That started the spiral of, How do we know for sure that it’s all gone? But, going back to the emotional part of it, it was devastating for my husband and me. We have heard about cancer a lot in our families, so cancer was not new to us even before starting my job. But it was still just heartbreaking, devastating.
How could cancer be growing in my body for three years and I not know it, because I found the nodule three years ago? And so it was a hard moment. But because of my husband and his personality, and how just fun and outgoing and level-headed he is. It didn’t take me long from the initial spiral to come down and realize, this is not going to be my whole life. This is hopefully going to just be a moment in time. That was sad and devastating, but we’re going to look back at the beauty of it.
Stephanie Chuang: Yeah, that is so beautifully said. Thank you, Taylor. What I’m hearing you say is a few things. And by the way, I think this applies to people outside of cancer diagnoses. It’s like anything, anything in general, but definitely with healthcare, something that is about your body, maybe feeling like I’ve heard people, including myself, you know, talk about betraying us, you know, in a way. And you have the initial shock. There’s a lot of sadness, and there’s a lot of, how did this happen?
And then for you, what I’m hearing is that you went, okay, well, now it’s time to tackle this. This is not going to be my life. This is one thing that I’m just going to look at and get and get through. Right. And one of the things I know you exemplify, and I think you did before you started here, and maybe even more so now. But this idea of self-advocacy, which we hear so much about for you, started really early on because no one was really that concerned about your nodule except for you. And I think there’s a message in there. And what is that message for other people?
… you know your body best, and you know how comfortable you are with something inside your body or making a decision.
Self-Advocacy: Trusting Your Instincts and Pushing for Answers
Taylor Scheib: Yeah, that message would be, you know your body best, and you know how comfortable you are with something inside your body or making a decision. And for me, when I found the nodule. It was after my 27th birthday. We had just karaoke all night. It’s one of my favorite pastimes.
And I immediately went to the doctor, got bloodwork, got an ultrasound of the lump, and from there, it was my choice, what I would do with that information. So I continued getting my yearly exams, getting full blood work done. And last year was when I was like, okay, this is getting bigger. People are starting to notice it.
And I want to say this part as well, because I had a friend who, and this is where advocacy comes in many different ways, not only for yourself, but other people doing it for you. She noticed the lump, and her dad had thyroid cancer. So she asked me, “Have you gotten that checked out?” And I said, “Yes, I have.” But at that point, I realized that it’s been a year since I had done it previously. Why not get it done again? So I started the process all over. Routine blood work, ultrasound, you know, did that. And then I just wanted to get it out at that point because it was really large. It ended up being 5.7cm.
And so after that ultrasound, it was up to me to schedule the ENT appointment. You know, getting into the ENT took months. As we all know, those specialty appointments just take a long time to get into. So I finally got into the appointment in November, and my ENT was very casual about it. Looked at the ultrasound.
At this point, no one ever said, “Let’s do a biopsy,” and we don’t know if the biopsy even would have caught it anyway, so I’m not going to dwell on that. But she went, “Yeah, this is benign. The features are all normal. It’s your choice to get it out. Are you ready to have a scar? And I said, “Yeah, let’s go.” I just couldn’t do abs anymore. Like working out without it choking me. Being in bed, lying on it. I could feel it all the time at that point. So I advocated to get it out because I knew that was the best choice of action for me. It was also something my mom was telling me, “Maybe you should just get it out.”
But at this point, it had compromised that whole side of my thyroid. So I was going to have to get a partial thyroidectomy. So I was a little scared. But coming back to the self-advocacy part of this, you know your body best, and it’s okay to push and not necessarily get it removed. Did I push because they got me on the schedule, but I was non-emergent, so very limited spots to get. Surgery was scheduled for surgery in January. My insurance referral did not go through in time. So the morning of that original surgery in January, I’m on the phone with my ENT, and they’re like, well, you could just chance it. And I’m like, facing a large medical bill without the correct referral.
Stephanie Chuang: Right.
Taylor Scheib: And my husband’s in the military, so I knew there were a little bit more hoops to jump through with that type of insurance. And so I was on the books for April. It just automatically got pushed back three months.
Barriers and Delays: Navigating the Healthcare System
Stephanie Chuang: Yeah. So I just have to interject there because I feel like that part of the patient advocate story, right, is like it’s one of the parts of the experiences that we all experience to some degree, but isn’t talked about a lot, which is when you’re dealing with cancer. I remember, you know, getting told that this might be cancer and then being like, but it’s probably mono. And I was like, mono? And then it was like, but you need an ultrasound to one here, one here.
I got on the call to get it scheduled. And they said, “We don’t have an appointment for weeks.” And I’m thinking, you can’t tell me that there’s this thing and that I have to wait. So my point is that there’s the system, there’s like our situations, and this message of self-advocacy is, it truly is the squeaky wheel gets the grease or whatever, because you know, you know your body best what you just said and also you I mean, there’s some things that are out of our control. But you see, the system we’re working with and the unexpectedness of being like, how come I’m the only one who’s concerned about this? Did you feel that?
Taylor Scheib: Yes, I felt that. And it was. That’s been the whole thing over the last six months of seeing the NT. Getting the surgery scheduled is why there is no sense of urgency behind this. Every time I’ve seen my ENT. She’s so busy. When I had my follow-up for my surgery, it was not her. It was her [physician’s assistant] PA.
And it continued past my diagnosis. First of all, I found out through MyChart, which is a story I’ve heard, unfortunately. And every time someone I’m talking to tells me that story, instant goosebumps. Instant. Just feeling what they’re feeling through the screen. Then it was okay. Your case is going to be presented to the tumor board, and I want to make sure that I’m explaining what a tumor board is correctly.
So Stephanie, please help me with this color. But basically, when you have a unique case like mine, where we thought it was benign for three years, the mass was 5.7cm. And then on top of that, it is a less common subtype of thyroid cancer. It’s being presented to the tumor board. Well, they only meet once a month. So and it was at the end of the month when this happened in April, so it wasn’t going to be until a month for the tumor board.
Stephanie Chuang: You talked about self-advocacy, which we’ll talk about throughout the entire conversation. But this idea of waiting, waiting for your appointment, waiting for insurance to approve or not approve, waiting for a tumor board. For me, it was like getting a diagnosis on the phone and then being told by a family friend. You know, oncology is going to take forever at your large academic institution, so just go to the emergency department.
So that’s another tip for people, by the way: just get into the system. So you get seen, and then they put you somewhere that you’re supposed to be. But I was waiting to understand. I remember they did so many procedures, I had biopsies and bone marrow biopsies and lymph node extractions and blood tests upon blood tests. And then it was the whole week in the hospital. What is it like? We know it’s lymphoma. Is it Hodgkin or non-Hodgkin? Are we talking about, you know, aggressive or indolent? Are we talking… So? Not this period, and you’re still in it. That’s what I want to acknowledge, is you’re still in it, is it feels like there’s still no plan of action.
And I think for different people who are dealing with a diagnosis that it varies. Like sometimes it’s very short and, you know, right away for other people like you, you’re waiting weeks to understand, well, what are we going to do about this? So how have you been able to manage the mental part of that, the waiting part of it?
I have my good days. I have my bad days, more good than bad days, which is good. But it’s just about occupying your mind.
The Waiting Game: Coping with Uncertainty and Lack of a Plan
Taylor Scheib: It’s so hard, honestly, and I have my good days. I have my bad days, more good than bad days, which is good. But it’s just about occupying your mind. And when I was diagnosed and I started telling my close friends and family, I think, like trauma bonding, it’s very powerful. I have some friends that I don’t talk to every day, of course, but they’re your best friends no matter what. You pick up right where you left off.
So, as crappy as this was to get this diagnosis, it gave me a chance to actually kind of get closer with some of my friends. That has been such an amazing distraction since my diagnosis, catching up with old friends, catching up with your family again. My dad is calling me so much more, he calls all the time in general, but even more so now, my grandparents are reaching out like every so often. So I would say that’s been one solid thing.
Then the other part has been my husband. He has been my rock, of course, through this. Then we’re super active people. So we went and bought really expensive bikes to get on the trails. Stay active. And we’re just trying to find ways to continue living our lives. And for us, that is planning a trip. So, sorry, Stephanie, in the next year or so, I’m going to be going on some trips.
Stephanie Chuang: Oh, 100%. And you should go out and live your life 100%. No apologies. That’s 100% what you should be doing. And it makes me so happy to hear that. Those are the steps that you guys are taking. So many things came up when you were talking about that. You know, when you talk about trauma bonding, I’ll talk about the flip side of some of the experiences I’ve had, too. But this is the question of why we need a reason? But we do. I love that it just automatically gave this a thumbs up.
Community and Connection: Reaching Out and Trauma Bonding
Stephanie Chuang: People come from different places, whether you’re close. My friends started a campaign called #SpicyStrong. And I think it’s because when I was in my delirium, when they put me under for the lymph node biopsy, I had to go under full anesthesia, and I don’t know if I was going in or coming out, but I was super loopy. And so I was talking to the nurse. And I went, “I’m so spicy and strong,” or something, I mean, ridiculous. And then that just became the hashtag.
They printed shirts, and it got to people, and they were posting on social media. This is making me remember a lot of things I forgot. But people who are super close to me, people who I hadn’t seen in years. And that is such a beautiful part of this, right? One of the silver linings. I’d rather not have this, but the fact that I do and people like me are showing how much they think about me. I mean, what was the most powerful? I mean, I know you had lots of people reach out, but is there one situation where it took you by surprise, or a message that came from someone you hadn’t talked to in a while?
Taylor Scheib: Yeah, there’s one example where, and I’m sure you can relate to this, being formally in the news. You bounce around all these towns and cities, and you have friends everywhere, like I mentioned. And even when I just had the partial thyroidectomy, a group of friends in Denver sent me a care package, and that was before I even got my diagnosis. And so I was just so taken aback and just so thankful for them sending that. And so that was one thing. And then the other has been again, when I was in sports broadcasting, and I’ve heard from so many people from the little towns that I was covering, you know, seven, eight, nine years ago. And they’re commenting on my post, just saying, you know, we’re supporting you. This community is supporting you.
That’s just meant the world to me. And so those have been instances where it kind of stops you in your tracks. I don’t know if you’ve felt that way, but you just think, humanity is good. Yeah, yeah. Decency still. And there is a way to break through the screen. There’s a way to break through the phone call, the FaceTime, the message. And so I’m not sure if you felt that same way in those instances, but it stops you in your tracks, and you just realize, I have so many amazing people in my life.
Stephanie Chuang: Yes, 100%. It does resonate. Taylor. It’s 100% humanity is amazing. These are the beautiful moments of humanity when people come out. And, you know, I think a lot of the social stuff might be we are scared to, you know, reach out to someone from before because we think, well, what if they think I’m weird or they don’t even remember me or whatever? And these situations just take us completely out of that. Right. It’s like, no, I care about this person, or I just want them to know that I’m thinking about them, and it’s okay if they don’t reply or all those things. I think that is beautiful, and I wish more of us could get to that.
Yes, 100%. It does resonate. Taylor. It’s 100% humanity is amazing. These are the beautiful moments of humanity when people come out. And, you know, I think a lot of the social stuff might be that we are scared to reach out to someone from before because we’re like, well, what if they think I’m weird or they don’t even remember me or whatever? And these situations just take us completely out of that. Right. No, I care about this person, or I just want them to know that I’m thinking about them, and it’s okay if they don’t reply or all those things. I think that is beautiful, and I wish more of us could get to that.
… whatever other people’s reaction is, it is not about you. It is, of course, about concern for you and what you’re going through for the people who love you.
Telling Others: Navigating Reactions and Support Systems
Stephanie Chuang: I do want to touch on just because, for anyone who’s tuning in who is dealing with something again, it could be a diagnosis, cancer, or otherwise. It could be something else. When you have something to tell other people that they’re not familiar with. So I don’t know, sometimes I’ve found that military people find that with civilians. It’s like a walking-around language with sickness. Or maybe if someone’s announcing, say, a divorce and other people aren’t familiar with it, it could be any of those things.
I think the way other people react is very – it can be very jarring. And so I’d like to spend some time here, which is that, you know, people have different kinds of people in their lives. Some people have tons of friends, some people have a tighter circle and and all these things. I’ll start with an example, which is a newer friend, but I’d known her for a few years at least. More of a social friend, maybe.
But when I was diagnosed, she kind of disappeared, and she was one of the people I saw more often in that time frame. You know, a lot of my friends, to your point, are scattered around the country. And so it was very disappointing, and it was hurtful because here I am thinking about my mortality, not sure about what I’m going to do, worried about my hair loss, and all these things. I’m 31, and she just dropped off.
I just want to say this, not to harp on her as a person, but really to say, I think what I learned in that is whatever other people’s reaction is, it is not about you. It is, of course, about concern for you and what you’re going through for the people who love you. But for any of the weird stuff or the things that might be surprising, I would just say, broad strokes, the reaction is about their discomfort. They don’t know how to show up. They do care about you, but they’re worried about how they’re going to come across.
Maybe they think other people are talking a bunch to you, and so they’re trying to be respectful of you. Not right or wrong. But I do feel like that’s something I’d want to share with other people who are going through something, because it can be very tough when it’s unexpected. I don’t know if there’s something that resonated for you there a lot.
Taylor Scheib: It is. When I first started telling people, I realized very quickly, the way you present it will help determine how they react. So in the first couple of conversations I had, it was kind of very emotional. A lot of information, whoa, what is going on? But then the more I told people, the more I started setting the precedent of, right at the beginning, I’m going to be fine. I’m going to be okay. And then that’s when I think people went, okay, she’s she’s she’s going to be okay. And I have been very positive throughout this whole situation. And I think that has helped the way people are reacting.
Now, I will say on the positive side, kind of the opposite of what you experienced was I’ve gotten a lot closer to one of my high school best friends, like my childhood best friends. We have been friends literally since kindergarten. Wow. And we talk every once in a while. And when we see each other, we pick up right where we left off, like I’ve said. But we’ve talked more since this happened to me. And even when I just did the partial thyroidectomy, she called me that weekend, and I sounded like crap. Did not have a voice.
Taylor Scheib: She was crying on the phone. And it makes me emotional because that’s an experience where she’s showing up for me. And that, and her mom, and her. They are like my OGs, but I don’t see them very often. And so it’s kind of the flip side of what you experienced. But what you experienced with someone dropping off like that is likely going to happen for me in the next six months or however long this process ends up being.
But my mom experienced that. She was shocked by the people who she didn’t hear from again, or they didn’t show up for, you know, she had a benefit. They didn’t show up for that, or just a text message or a phone call. She was shocked by the couple of people. And you don’t forget those things, but I think it makes you become a better human in a way, and it makes you check up on your people a little bit more. That’s how I’m trying to spin it, at least.
Stephanie Chuang: And knowing you from what I know of you, Taylor, I don’t even think it’s a spin. I think you have that. That’s just the way you approach life. And I appreciate that. Yeah. No, 100%. I would say that was the only example of that. And everything was largely positive. I think I do want to call out that it may not happen to you, by the way. Right. I think it’s good to understand that if it does, though, that it’s normal and it’s not about you. It’s about them. And the other drop off, someone had warned me when I was just going through it, and she had gone through the same cancer just six months before I did. And she said, “Look, I’m struggling now that I’m done with treatment. People are like, you’re fine now.”
And then, the medical help drops off, and then the support also, because, well, you’re all good. And so that’s another conversation for another day. But I think my point is that at different parts of this, you know, it doesn’t mean, oh, I’m past this now. It’s that there’s different versions depending on where we are as patients, as people supporting other people, that these same emotions can come up or these same situations can come up. I also want the chance to drop in this video of my best friend in New York, she flew out with her husband, and at the time, I had to give myself blood thinner injections every day.
And those are freaking large. You know, I did IVF shots to freeze embryos at the same time. So I had to do the little needles and then the spring needles for the blood thinners. And, oh my God, it was terrible. And there’s a video of the way they supported me, trying to make fun sometimes. So, you know, the song that goes, shots, shots, shots, shots, shots, shots, shots. Yeah. So I was about to give one, and they go, “Oh, we’re just gonna sing the song for you.” And those are moments for sure where this is me getting loved on by people who are trying to lighten the situation for me in the way that they think might be helpful. So anyway, I think that’s awesome.
Stephanie Chuang: I want to ask about your mom. I know other people may not have this specific example where it’s like their parent also went through a similar diagnosis, but in terms of other people’s reaction to when you’re telling people what that was like, what’s your guidance to other people who feel like there’s an extra layer there? Whatever the reason is for you, it was that your mom had gone through her cancer recently, even. But for anyone who feels like there’s an added pressure in making sure the other person’s okay, what is your guidance there?
Taylor Scheib: Yeah, I would just say the biggest thing is give yourself grace, but also do it on your own time. That is so important. Yes, there’s pressure to tell people and update people and do all the things. I totally get that. But do it on your own time. You and I also think that what helped as well is I just I’m a very factual person. I’m blunt. I’m not going to sugarcoat things. So I think it was my messaging to them. These are the facts, I know. I don’t know anything else. And then I think that helps with them asking a bunch of questions.
You know, like deep dive spiraling. I think it’s just about giving yourself grace and giving the situation grace and not feeling like you have to always be giving updates to your friends and family or talking to them. Or it can take about a day to respond to someone. And my friends and family know that. They know that I’m very busy. My husband and I, Justin. We live a very active life. We are always doing something. And so yeah, I think it’s also if you get a text message, don’t feel like you have to respond right away or call them back or anything, right? This is on your own time, and that goes beyond just your friends and family. I’ve heard this so many times from people that I interview. You are the CEO of your life, of your body, of what you do. You are the leader of your own life. And I think that’s just so important.
Stephanie Chuang: Yeah. I mean, in the future conversations, I’m going to be pulling up from our patient advocate interviews because they have so much wisdom in what they’re saying. I mean, there are so many things that I want to talk to you about. Let’s talk for three hours. No, that’s fine with the audience. No. But I think, you know, whatever way you want to look at it. In terms of tips. There are some tips for the person who’s dealing with the diagnosis. Diagnosis? I agree with you, Taylor. 100% of the give yourself grace. I think in life in general, we could stand to hear that more often anyway, right? We give other people the compassion we don’t give ourselves. But on that note, give yourself grace and do not worry as much as you can about the other person’s reaction. You don’t have that space to carry that burden. So don’t tip on the other side.
Supporting a Loved One: Tips for Friends and Family from a Patient Advocate
Stephanie Chuang: I would give to people who are looking to support patients, because I’ve heard that a lot. Right? They might go, “Oh my gosh, my friend, my family member was just diagnosed. How can I support them?” I think in terms of messaging, I would always lead with whatever. If it’s an email or a text or whatever, or a voicemail.
No pressure to respond. I just wanted to, and that just takes off the pressure. So you get to send the message, and you’re letting them know. I get that you’re super busy and you’re occupied, and I’m not trying to take away your bandwidth. Another tip would be people ask about, “What can I send someone who’s just been diagnosed with cancer?” I’m going to ask you about this, too, so you can brainstorm. But I’ve often thought, if you can figure out if they know their treatment, I would base the care package on that. So if you know that they’re going through radiation, you can look, and we’re going to create this online to have some guides at The Patient Story, but it is to really look at what that modality of treatment is, and then try to send stuff. So, you know, I’ve sent organic lotions to people because they were going to get dry skin, blankets because one of the side effects was going to be feeling cold, things like that. I don’t know if there are things that you feel would be great advice for people trying to help people dealing with the new diagnosis.
Taylor Scheib: Yeah. You made such a great point. Blankets, things like that. But then I also think, like anything, that the person who’s going through the treatment or diagnosis, self-care, they should just put self-care out there.
So yeah, if it’s maybe organic products or maybe it’s a bath bomb, or of course, depending on their treatment, like we said. But for me, everyone knows I’m going through the waiting period. So I think a lot of people went, “How does she want to relax and sew face masks and bath bombs and electrolytes and different things like that?” So I would say anything that you can think of that person likes, that is self-care.
Books, a journal. You can never have enough journals. Something to preoccupy them, too, whether that’s like a coloring book or, you know, crossword puzzles. Not that I do any of that, I’m not going to lie. But if you know that person enjoys that kind of pastime. Right. Or maybe something like, this is old school, but a CD with their favorite songs on it.
Stephanie Chuang: Right, right.
Taylor Scheib: And I also think, too, when it comes to what you could give that person or send them in these moments, it does not have to be elaborate. The small stuff means more. And so maybe it’s a Spotify playlist, maybe it’s a $15 Amazon gift card, maybe it’s a gift card to their favorite restaurant. The self-care food.
Don’t overthink it. When you want to give something to that person. It can be something very small, even just a Venmo. I had a good friend, one of my best friends from home, send me a Venmo the day of my follow-up ENT appointment, and the caption was, Go get a cheeseburger after this.
Stephanie Chuang: Oh no, I love that it is. It’s the small things. It is that thought that counts. It is true. I think there are a couple of things that came to mind, too. And then we’ll and then we’ll wrap this conversation, which, by the way, I’ve enjoyed having with you. I think one quick note is if people are waiting. You’re not in the hospital. I know when I was waiting, and I was in the hospital for a shorter period of time, the nurses at one point said, “Don’t send flowers, or we’re telling people, don’t send flowers.” And that’s for when people are immunocompromised.
The knee-jerk sometimes is like beautiful flowers, but just to make sure.
… why I decided to share my story so openly was because at the core of who I am, I’ve always been very transparent, very honest, and I am an empath. I need empathy at the core of who I am, and that’s where the storytelling part of my life, like my whole life, has been storytelling at the core.
Sharing the Journey Publicly: The Power and Healing of Storytelling
Stephanie Chuang: The other point that happens to matter both in terms of support, but also in terms of talking about messaging and not having to respond to text messages right away. What was helpful for me was to designate people who knew the information, and if other people needed to know or wanted to know about the diagnosis or where I was in that, specifically, they would go through those people. You know, it’s funny, we both were on TV before, but we were also very private people, actually, and I never imagined that I would bare my soul online or continue to have a presence after my news career.
But I had a blog, and the initial point of the blog was a it just helped. It was cathartic to get stuff out on, like just journaling, essentially. But then it was like, well, two things: if I can help other people not feel alone. And also then it helped in terms of people getting updates without me having to like constantly. But then that slowly became cathartic as a storytelling mechanism.
And by the way, you know, we’ll have like the storytelling, you could share yours. There are the prompts below in the description. But for you, Taylor, what has it been? This is my last question to you. What has it been like? I guess, how did you decide to want to share? I didn’t even realize you were going to share your story on social media. And it happened. But like what? What drove you to want to do that? And what has been maybe the most cathartic part of the process, especially a message for people who do feel like I’m private. I don’t think this is for me. Right?
Taylor Scheib: Yeah. I resonate so much with when you get out of a job that is so public, like we were in in TV, I don’t find myself posting at all anymore, but why I decided to share my story so openly was because at the core of who I am, I’ve always been very transparent, very honest, and I am an empath. I need empathy at the core of who I am, and that’s where the storytelling part of my life, like my whole life, has been storytelling at the core. I’ve always been a storyteller. You know, I can get along with anyone, and I just am amazed and mesmerized by other people.
I just love people so much, and they teach me so much about life and about the way you should live life. You know, there’s no guidebook to that, of course, but when I decided to share it publicly, I just wanted people to know that we say it all the time, that they’re not alone. They might be going through anything, and they’re like, “Wow, this person feels just a little bit like I do.” And that’s what keeps people going. And so behind sharing my story and trying to keep people up to date, I just. It’s kind of. It’s hard to explain. I just wanted people to know that everyone is going through something that is a big part of it, and to social media.
If you look at my Instagram, you will see my husband, my friends and family, my dog, and you go, wow, that girl has a really good life, and I do. We live an amazing life. But behind the curtain, behind social media. I’m going through something that really sucks, and I’m still finding ways to navigate that. So why not be open about that conversation? Let people in. I have a big tribe. I have a lot of people in my corner. I’m so thankful for that. But. Those strangers. Those are the strangers who come to you. Those are so impactful. Just the little comments of, “Wow, I thank you so much for sharing your story.” I’ve had so many people say, “Thank you so much for sharing your story.”
Taylor Scheib: And it’s not even about the cancer. It is about making sure you are getting your physical exams, that you are getting your women, your women, health, health exams, your PAP smears, your full blood work, whatever it may be.
I’m getting emotional about it because I feel like people get so lost in how they’re feeling, and they don’t know if it’s something, if it’s their life, because they’re really busy, or if it’s something underlying. And so I just want people to know that it’s okay to go to the doctor. It’s really scary. I totally get it. I was so scared to get this surgery, and now I’m dealing with voice loss, and I can’t get my voice back. So trust me.
Oh my gosh, it’s so, so scary. But it doesn’t have to be. And find your partner, find your friend. Find your family. Find someone like The Patient Story who can hold your hand through that. So that was really the ‘why’ behind sharing the story publicly. The most therapeutic thing for me in this process, honestly, has been talking freely like this. When I posted those videos, they were maybe 15 minutes long, and I had to cut them down.
But talking so freely about it has been so cathartic and so therapeutic for me. Those are like my blogs, like you did. I’m just doing it as a vlog. And after I get done, I go, “Wow, I kind of look cute.” I’m going to take a couple of selfies, you know? Yeah, go do things anymore.
You know, like those moments. You go, “Wow, I just feel so stinking good.” Yeah. And so that’s been super helpful. And then just keeping the lines of communication open with me, with my partner, with my husband, with my friends and family. You know, I just want to say this one part fast. My mom and I are best friends. We talk all the time, but recently we haven’t been able to talk a whole lot because she’s two hours ahead of me. We don’t work the same hours, or we do work the same hours. So, we’re constantly working. We’re not finding time to talk.
And last night, I told her, I said, “I’m sorry. I have not been able to call you. I have just been so busy. There’s been so much going on.” And she goes, “It’s okay.” And I go, “But it’s not okay.” She goes, “I know, but I don’t know what to say.” And so it’s there, that balance of course, she knows I’m busy. She’s not pressuring me, but she just wants to have a conversation like this. She wants to just openly have the conversation. And we did talk today, and it was very therapeutic for me. So open communication and just kind of setting up my phone and talking. But that’s also because I’ve been doing that for so long, and I’m a storyteller by nature.
Stephanie Chuang: So you are. You really are.
Give Yourself Grace: Final Reflections and Words of Wisdom
Stephanie Chuang: Taylor, I thank you so much for opening up, being vulnerable. You are such an empath. I know you bring it to your life and also to work every day, and I’m so grateful that you’re part of The Patient Story team doing that. Yeah. For anyone who’s you know, wants to hear the tips that were part of this conversation, I think we can come up with something that you can download. We’ll put it into a link somewhere on the description, not at the time of this discussion. Thank you for being such an open book. And looking forward to being able to share more of your incredible voice throughout all of this. So thank you.
Taylor Scheib: Yes. Thank you. And I’ll just leave this here. We’ll talk about it more, of course. But when I got my diagnosis, I didn’t feel overwhelmed. And that’s because, of course, in moments I did, but I didn’t overall because of The Patient Story. And I’ve said this so many times to my friends and family and to people who I’ve told my story to when I’m interviewing them, because now I’m openly sharing my story, is that when someone gets a diagnosis, I never want them to feel overwhelmed, and I want them to have a place like The Patient Story where they can go and think, wow, okay, I have someone, I have an organization that can support me. So when I got that diagnosis, I didn’t feel overwhelmed. And I want other people to feel that way. And that’s why I’m so passionate about our work at The Patient Story.
Stephanie Chuang: Yay! I couldn’t say that better. That was amazing. Thank you. Taylor. All right. And this was like the first of many conversations that will happen with Taylor with different folks. Really looking forward to this. All right. Great. So for The Patient Story, that’s Taylor. I’m Stephanie. Gift yourself grace. Take care. And we hope to see you next time.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Will’s Experience with Stage 4 Liver Cancer is Marked by Moments of Joy
Will found out that he had stage 4 liver cancer in December 2022. Before that, his life felt like a blur. He struggled with unexplained exhaustion, frequent diarrhea, sporadic vomiting (especially after eating pork or rich food), and a sense of discomfort he couldn’t put his finger on.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
One day, in the middle of a badminton game, Will felt an unusual hardness in his abdomen. This led him to seek medical advice. He ended up going to a hospital, where doctors ran tests and procedures and eventually uncovered a massive tumor that took up nearly 70% of his liver.
The ER doctor compassionately delivered the grim news that Will had liver cancer, and this thoughtfulness and consideration helped him find his footing despite the overwhelming odds. He also found solace in actionable steps. He initially underwent immunotherapy and targeted therapy. These treatments weren’t successful, but he and his medical team didn’t stop there. Clinical trials offered Will hope and insight into medical advancements. These trials were grueling, but they supported his resilience and determination to get better.
Stage 4 liver cancer introduced a new rhythm to Will’s life. He learned to accept his situation, which became his basis for adaptation and also formed a surprising foundation for moments of joy. He found that physical activity helped him feel free and helped him reclaim his autonomy. Despite Will’s physical limitations, sports, including swimming and cycling, became a refuge and source of comfort. His ambitions grew bolder: he aimed to complete a triathlon. Every move he made, further emboldened his defiance against any thoughts of despair and helped him enjoy life’s simple freedoms.
Will’s tumor shrank significantly, and his health stabilized remarkably, thanks to treatment, which was made available through applying for compassionate-use medication or using a new treatment not yet approved even if you are not taking part in the clinical trial. Uncertainties linger regarding his stage 4 liver cancer, but he remains laser-focused on living fully. He urges fellow patients to be proactive regarding their health management and to ask questions, prepare for medical appointments, and embrace discomfort as part of the process. He’s found that happiness isn’t dependent upon one’s health status; one can enjoy meaningful moments even during times of adversity.
Watch Will’s video to find out more about:
How badminton led him to uncover a stage 4 liver cancer growing right under the surface of his abdomen
The unexpected role that swimming and cycling played in his health transformation
Why a dead phone during Will’s diagnosis became an oddly pivotal moment
How he found happiness amid treatment for advanced cancer
The power of asking the right questions during medical appointments and pushing for compassionate use medication
Name:
Will M.
Age at Diagnosis:
29
Diagnosis:
Liver Cancer
Staging:
Stage 4
Symptoms:
General uneasiness
Exhaustion
Diarrhea
Hard mass in the abdomen
Worsening abdominal pain in the upper right quadrant
Treatments:
Surgery: kyphoplasty
Chemotherapy
Targeted therapy
Transarterial chemoembolization (TACE)
Radiation therapy
Clinical trial
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Maria’s Self-Advocacy and a 2nd Opinion Found Her Stage 4 Breast Cancer
Maria’s experience being diagnosed with stage 4 breast cancer began when her young nephew accidentally kicked her breast while they were playing. She checked her breast afterwards and found a marble-sized lump. She first dismissed it as a cyst, partly because she has a history of ovarian cyst issues, and the doctors she’d seen before had told her that hormone fluctuations could cause benign growths.
Part 1: Diagnosis
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
Over the next few months, Maria started to experience more serious symptoms, including burning sensations, skin changes, the inversion of her nipple, and night sweats. After several ER visits and numerous tests, including ultrasounds, she was given a diagnosis of granulomatous mastitis, which was later found to be inaccurate. (Editor’s Note: Granulomatous mastitis is a rare, benign breast cancer condition that can cause symptoms like pain, tender lumps, and nipple inversion.)
Finally, Maria had an accidental encounter with a breast cancer survivor, who suggested the Every Woman Counts program, which offers free breast and cervical cancer screening and diagnostic services in California. Maria’s persistent self-advocacy paid off when she was correctly diagnosed with stage 3 ductal carcinoma, which later progressed to stage 4 breast cancer when it metastasized to her bones and lungs.
While Maria found her first chemotherapy sessions manageable, she experienced intense side effects during the next sessions: hair loss, severe nausea, neuropathy, skin changes, and emotional distress. Maria faced these challenges head-on, focusing on practices like meditation to help promote positivity and mindfulness.
Although Maria’s family has been there to support her, she has still felt lonely facing breast cancer without a partner or children of her own. A part of that is struggling with the harsh realities of the effect of illness on daily life and finances — dealing with evictions, having to live with family members, and missing her sense of self. She was also affected by the physical changes she experienced, including those due to surgical scars.
Maria wants to emphasize that stage 4 breast cancer patients and others in situations like hers should never lose hope. There are many helpful things that they can do for themselves, like self-advocating fiercely, trusting their instincts, and surrounding themselves with supportive people. She adds that cancer doesn’t determine whether one deserves love, rest, or joy.
Have a look at part 1 of Maria’s video and:
Discover how a playful moment led to her life-changing stage 4 breast cancer diagnosis
Learn why Maria’s persistence saved her life
Feel the emotional impact of metastatic cancer
Explore the struggles of living with stage 4 breast cancer and its treatments
See how Maria’s strength and positivity shine, even in her most painful moments
Stay tuned for Part 2 where Maria tells her treatment story including chemo, radiation, surgery, and targeted therapy.
Name:
Maria S.
Age at Diagnosis:
30
Diagnosis:
Breast Cancer
Staging:
Stage 4
Symptoms:
Intermittent but severe pain, including a burning sensation on the side of the breast
Appearance of a cyst and a lump
Abnormally warm and pink-colored breast
Nipple inversion
Strangely liquid menstrual periods
Unusual underarm odor
Darkening and dimpling of the nipple
Severe fatigue
Night sweats
Treatments:
Chemotherapy
Surgeries: mastectomy, lymphadenectomy
Radiation therapy
Targeted therapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Life Without a Stomach? Graham’s Stomach Cancer Surgery Story
At 61, Graham found out that he had stomach cancer. He’d been vigilant for years due to his family’s history with Lynch syndrome, and so he started having annual screenings. These reassured him, but eventually also brought him the life-altering news about his health.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Graham discovered he was positive for Lynch syndrome, a commonly inherited cancer syndrome that increases cancer risk, after his cousin was diagnosed with colon cancer and his family underwent genetic testing. Two decades followed, during which he had regular screenings. Nothing turned up suspicious, but everything changed in 2023. A routine endoscopy revealed something worrisome and, soon after, Graham was told he had stomach cancer, specifically early-stage diffuse gastric adenocarcinoma with signet ring cell features, poorly differentiated. (Editor’s Note: Signet ring adenocarcinoma is a rare and aggressive subtype of adenocarcinoma. Diffuse stomach cancer is a rare form of stomach cancer. Poorly differentiated adenocarcinomas spread faster than other carcinomas whose cells are better differentiated.)
Graham was devastated by his stomach cancer diagnosis. Thankfully, his wife, Christina, was with him when he had that fateful conversation with his doctor. She absorbed all the crucial information and helped him stay calm when his mind drifted due to shock, fear, and uncertainty.
Dealing with everything after diagnosis involved coming to grips with stomach cancer and his treatment, which included adjusting both emotionally and physically. Graham underwent a total gastrectomy, which meant that he needed to learn to live without a stomach. Recovering from surgery wasn’t just about physical healing; it also involved redefining what was normal for him. Graham’s weight plummeted while he struggled to deal with the loss of his stomach. He also worked to find foods that his digestive system could manage, and he had to make do without the usual hunger cues.
Graham’s consultations with dietitians were crucial. Their guidance helped him learn to focus on nutrient-dense foods and supplements that could counter dietary deficiencies. He found that emotional support was also important. Graham found solace in counseling and an online support group where he connected with others, exchanged practical tips, and found mutual encouragement.
When Graham attempted to re-enter his social environment, he found new challenges. Because food is part and parcel of social gatherings, he faced “food anxiety” and thought twice about joining even friendly gatherings. Over time, though, he gradually became more confident as he found new ways to engage with his friends and family and became less pressured by eating norms.
Graham’s advice regarding stomach cancer is clear: talk to your doctor about screenings, regardless of your age. Early detection saved his life, and it may well save others’ lives, too.
Watch Graham’s video to learn more about:
How does one live without a stomach? Graham’s story reveals the answer
Graham’s candid reflections on life after stomach cancer
The unexpected challenges of social life after a total gastrectomy
The vital role of emotional support in Graham’s recovery from stomach cancer
Why talking to your doctor about screenings could save your life: Graham’s heartfelt plea
Name:
Graham L.
Age at Diagnosis:
59
Diagnosis:
Stomach Cancer (Diffuse Gastric Adenocarcinoma with Signet Ring Cell Features, Poorly Differentiated)
Staging:
Stage T1bN0
Symptoms:
None; a stomach polyp discovered during his annual screening tested positive for cancer
Treatments:
Surgeries: total gastrectomy, lymphadenectomy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Devon found out she had stage 4 rectal cancer in March 2023, when she was only 30 years old. She started to experience her first symptoms a month before that: frequent bathroom visits (up to 20 times a day), discomfort that became pain, and, in some instances, passing mucus instead of stool. She initially thought she had irritable bowel syndrome, but her gut feeling (literally and figuratively) convinced her to look for medical advice.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Devon took a proactive approach to her diagnosis. This included closely tracking her symptoms and how they progressed, as well as persistently communicating with doctors. Thanks to her approach, she was able to land a quick appointment with a gastroenterologist. Within just 20 minutes of meeting her and conducting an exam, the doctor detected something amiss and recommended that she undergo a colonoscopy immediately. The diagnosis? Stage 4 rectal cancer.
Devon was shaken by her diagnosis. Because she had neither a family history of rectal cancer nor any of the typical risk factors, it felt surreal. However, she didn’t fixate on asking, “Why me?” Instead, she asked, “What’s next?”
Devon’s doctors conducted a flurry of tests and scans and referred her to other doctors, but she ended up returning to Seattle for comprehensive care. However, her symptoms worsened while she was making her way back, resulting in an emergency ostomy surgery in San Francisco. It was a painful procedure, but she felt better afterwards.
After surgery, Devon’s stage 4 rectal cancer treatment plan included six weeks of daily pelvic radiation, low-dose chemo pills, and four months of traditional chemotherapy. Although she initially responded well to these treatments to the point of being declared no evidence of disease, the cancer returned. She then started a more intense second round of chemotherapy. But Devon has refused to buckle despite this setback and has managed this new phase of her treatment with courage and support from her loved ones.
Devon and her doctors now rigorously and closely monitor her health. She offers simple but powerful pieces of advice to others: listen to your body and find your community. Because the adolescent and young adult cancer community played such a crucial role in her emotional recovery as a young adult who faced cancer, thanks to offering understanding and solidarity that’s hard to find elsewhere, she recommends that other patients find their people, too.
Watch Devon’s video and:
Learn how the “small” but ominous symptoms she struggled with led to a big discovery
See what it’s like to face stage 4 rectal cancer, which is usually associated with older people, at just 30
Rethink what you think you know about rectal cancer — Devon has neither family history nor risk factors for it
Find out how she navigates life with rectal cancer: from symptoms to survival
Name:
Devon B.
Age at Diagnosis:
30
Diagnosis:
Rectal Cancer
Staging:
Stage 4
Symptoms:
Pain when trying to move bowels
Increased frequency of bowel movements, alternating with periods of constipation
Passing mucus instead of feces
Narrow stools
Treatments:
Surgery: ostomy surgery
Radiation therapy
Chemotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Tor is from the UK, but she lived in Taiwan for a little while, an experience made more memorable by a jolting diagnosis of appendix cancer. For years before that point, she had been struggling with baffling symptoms, including sporadic, stabbing stomach pains that doctors thought were due to overexercising or food allergies.
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
In 2022, all of a sudden, Tor’s discomfort turned unbearable. She sought help at a Taiwanese hospital where she had ultrasounds and blood tests, all of which were clear. She kept insisting on more checks, though, because something inside her screamed that her condition was serious. She begged for and finally got a CT scan, which revealed a mass near her bowel.
The medical team initially suspected a twisted bowel, but they conducted an emergency surgery. It unveiled the true culprit: appendix cancer — specifically, a low-grade appendiceal mucinous neoplasm or LAMN. (Editor’s Note: A LAMN is a rare, low-grade, mucus-producing tumor of the appendix.) Tor was terrified by this diagnosis, all the more since she was byherself in a foreign hospital, far from family, with few friends who could drop by to comfort her.
Tor felt better when the doctors told her the mass was benign. She flew back to the UK to recover, only to be blindsided when she found out that the mass was, in fact, malignant. The revelation hit her hard, filling her with confusion and fear, especially since her pain and uncertainty contrasted with the happiness of friends celebrating birthdays and other milestones. Since she was single, she also had to deal with fears about being unable to meet someone and her desire to have children.
Tor was determined to reclaim control over her health, so she focused on regaining her fitness. She used to be into running, and, after surgery, she struggled to return to her old routines. But while waiting for the results of MRI scans, she decided to take a personal training course, a long-time goal of hers. It kept her mind occupied, but also gave her a fresh sense of purpose. Through it, she discovered a course in cancer exercise rehabilitation, which gave her an avenue to help others within the appendix cancer community by offering them physical guidance and emotional comfort.
Tor’s appendix cancer experience highlights the power of self-advocacy. Her story might have ended quite differently if she had simply accepted what her first set of doctors had told her. She also underscores the importance of staying physically active. Because she had been into sports before surgery, she was able to recover faster afterwards, and it also gave her a way to help others.
Watch Tor’s video to take a deeper dive into:
How a gut feeling and insisting on it despite what others said saved her life
What it’s like facing an appendix cancer diagnosis alone and miles away from home
From half-marathons to healing: Tor’s fitness-fueled recovery
The emotional toll of cancer when your friends are celebrating life milestones
How self-advocacy became Tor’s most powerful health tool
Name:
Tor K.
Age at Diagnosis:
29
Diagnosis:
Appendix Cancer (Low-Grade Appendiceal Mucinous Neoplasm or LAMN)
Symptoms:
Sporadic stabbing pains in the abdomen and groin after meals, occurring over several years
Fatigue
Treatment:
Surgery: appendectomy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Curiosity and Self-Advocacy Shaped Ian’s Stage 3C Colon Cancer Experience
Toward the end of November 2022, Ian was diagnosed with stage 3C colon cancer. This diagnosis came after he experienced subtle but worrying signs: fatigue, strange blood test results during his annual physical, and the appearance of blood in his stool.
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
Ian’s family has a history of cancer (his father also had colon cancer), which has made him extra vigilant. Additionally, his wife and sister, both strong advocates for his health, supported him and encouraged him to seek prompt medical help. Ian advocated for himself from the start, insisting on having diagnostic procedures done immediately, including a colonoscopy he refused to delay.
Ian was emotionally devastated after receiving his stage 3C colon cancer diagnosis, especially after he learned that it had spread to some lymph nodes. The timing of the diagnosis worsened his emotional burden, as his wife was pregnant with their second child at the time. But Ian refused to back down in the face of these challenges. He not only had a can-do approach; he was also determined to understand every aspect of his condition. This gave him the strength, clarity, and confidence to navigate through his complex healthcare decisions.
Ian’s experience shows how crucial it is to have a medical team that’s aligned with one’s values. In his case, it was paramount that they focused on his quality of life during treatment. He was happy to find an oncologist who didn’t just prioritize effective cancer treatment but also considered his well-being key. This included undertaking strategies to minimize debilitating side effects like neuropathy. Ian was also able to take part in a clinical trial that aimed to reduce chemotherapy-induced neuropathy.
Through his stage 3C colon cancer experience, Ian has remained a staunch self-advocate. He firmly believes in being the “squeaky wheel” — outspoken, persistent, and informed — to help ensure that one receives timely, appropriate medical care. As a survivor, Ian takes his role as a husband and father to heart, actively participates in cancer support communities, and shares his story to help inspire and support others facing similar challenges.
Watch Ian’s video to get a better grasp of:
How Ian’s innate curiosity and intellectual approach turned out to be his greatest strength in facing stage 3C colon cancer
Why being a “squeaky wheel” can make all the difference in healthcare
How Ian balanced cancer treatment with family life, including a new baby on the way
Choosing an oncologist based on far more than just credentials
How clinical trials helped Ian maintain his quality of life during chemotherapy
Name:
Ian D.
Age at Diagnosis:
38
Diagnosis:
Colon Cancer
Staging:
Stage 3C
Symptoms:
Fatigue
Unusual blood test results during annual physical
Blood in stool
Treatments:
Surgery: partial colectomy
Chemotherapy
Clinical trial
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: Abdominal pressure, fatigue, small amounts of blood in stool Treatments: Surgery (colon resection), chemotherapy (FOLFOX: folinic acid, fluorouracil, and oxaliplatin)