Overcoming Racial Barriers in Clinical Trials from a Lung Cancer Oncologist
Marjory Charlot, MD, MPH, MSc, is a medical oncologist and health services researcher at UNC Lineberger Comprehensive Cancer Center. She primarily specializes in people who have lung cancer. Her research focuses on increasing awareness and access to clinical trials among Black communities and communities with low-income or persistent poverty.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Dr. Marjory Charlot: I’m a medical oncologist and health services researcher. I work at UNC Lineberger Comprehensive Cancer Center and primarily specialize in lung cancer patients. Part of my work is working in the hospital for patients who either have a suspicion of cancer or have a cancer diagnosis but are hospitalized for symptoms of their cancer or side effects from their treatment. As a health services researcher, my research focuses on increasing awareness and access to clinical trials among Black communities and communities with low-income or persistent poverty.
Outside of medicine, I’m a wife and a mom. I have two children, one in elementary school and one in middle school. I recently completed an aquathlon, a swim-run competition, which is a big deal for me because I don’t have a great relationship with swimming. I learned to swim as an adult, so it was a big accomplishment for me to be able to complete this duathlon, so that was exciting. I also love to travel and visit different places across the US or abroad. I also love to eat. I love various types of foods.
When I completed my medical training, I knew that I wanted to be an oncologist. There was no question about that.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
A Winding Path to Medicine
Nikki: What was your number one driver to becoming a doctor?
Dr. Charlot: I knew from a young age that I wanted to become a doctor. I grew up in Mattapan, a neighborhood in Boston, and I was privileged enough to have a Haitian pediatrician who had his practice in the community and did house visits. The Haitian community where I grew up was tight-knit and it was informative for me to be able to see someone who shared my heritage be a physician and be one with the community, so I wanted to be exactly like him.
My path to becoming a doctor was not straight and narrow. After I graduated from college, I spent a couple of years working in different types of advocacy work related to education and moved on to teaching middle school students about health professional careers. After that, I got my degree in public health and then after that, I went to medical school. It was a winding path to medicine, but I knew that’s where I would end up eventually.
Why Oncology Became Her Calling
Nikki: How did you end up specializing in lung cancer?
Dr. Charlot: When I completed my medical training, I knew that I wanted to be an oncologist. There was no question about that. I felt like it was the field where you develop close-knit relationships with your patients, so that was a no-brainer. Oncology was the way that I wanted to go.
Concerning lung cancer, I was influenced by my mentor. When I started my training, there weren’t that many options for lung cancer. There was chemotherapy and that was pretty much it. However, during my training, there were a lot of new therapies coming up, like immunotherapy and targeted therapy. The excitement in the field drew me to want to be a part of this growing field concerning options for our patients. The field was getting to a place where we had more options to offer our patients other than chemotherapy itself and that’s where my love and compassion towards lung cancer grew.
It was ingrained in me that we needed to think about the community and the circumstances that people are born in or the conditions they live in for the healthcare system to work.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
Growing Up in Mattapan
Nikki: What motivated you to go above and beyond and focus on helping an entire community get better access to health care and treatment options, including clinical trials?
Dr. Charlot: Mattapan is a predominantly Black community and interestingly enough, my street and pretty much my whole block were folks that immigrated to Boston. I have a Haitian background, so my interest in terms of thinking about communities draws from that experience.
I lived in two different worlds. I had the world where I grew up in Mattapan, but I also always went to Catholic school, which was outside of our neighborhood. I saw the dichotomy between the school in terms of the affluence of the area and some of the students who attended that school and my neighborhood where we’re very rich in culture and pride, and hardworking, but we didn’t have the same resources.
When I became a doctor, I did all of my training at a safety net hospital, so we cared primarily for people who were underinsured or had no insurance. It was the hospital where I was born, so it was ingrained in me that we needed to think about the community and the circumstances that people are born in or the conditions they live in for the healthcare system to work.
That’s where my whole approach comes from in terms of thinking about Black communities and the importance of ensuring that they have the knowledge and the awareness of all the resources available to ensure that they have access to care and can improve their outcomes through those connections. As a physician, I think about the Black community and understand ways how we need to make those connections together for us to thrive, do better, and live healthy lives.
I used my background concerning patient and community engagement to improve access to clinical trials, cancer care, and high-quality cancer care.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
Developing the CREATE Initiative
Nikki: How did you end up at UNC?
Dr. Charlot: I was recruited to UNC primarily to work as a thoracic oncologist, so my specialty in lung cancer, as well as develop a program that was focused on clinical trials and increasing equity in clinical trials. As a result of my research and clinical background, I ended up starting the CREATE initiative, which is Cancer Research, Equity, and Advocacy Through Engagement. This initiative speaks to the strong community focus and the work that we do with our community partners for the healthcare system to work and for the treatments to get to the people that they were designed to treat. I used my background concerning patient and community engagement to improve access to clinical trials, cancer care, and high-quality cancer care.
Most Common Lung Cancer Symptoms
Nikki: We understand that there’s a wide range of symptoms, but what are the most common symptoms of lung cancer? And what should people never ignore?
Dr. Charlot: Screening in general is meant to detect cancers early, before they cause symptoms. But generally speaking, by the time a patient is diagnosed with cancer, medical oncologists see patients after the cancer has spread or advanced and not in a stage where it could be cured with surgery. However, things have changed with cancer where we’re using chemotherapy and immunotherapy even for earlier cancer stages.
Common symptoms are generally related to shortness of breath, coughing (particularly coughing up blood), and sometimes weight loss. Those are the top three that patients describe in terms of things that they’ve noticed when they’re diagnosed with cancer.
If the cancer has spread, they could present with various symptoms, like a headache if the cancer has spread to the brain or pain in various areas, like in the bones or the joints. There could be a wide range of symptoms depending on where the cancer is.
The most important thing is to be aware that cancer screening is an option, particularly for people who have had a long history of smoking. Twenty pack-years is the recommendation. Screening is for those who don’t have symptoms, but if they do have symptoms, it’s another reason to see their doctors so they can get examined and evaluated for potential cancer.
It’s important to be able to test these drugs on a variety of people and understand how these treatments impact various groups.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
Demystifying Clinical Trials
Nikki: We know that trials aren’t for everyone. What would you say specifically to Black and African Americans to convince them to learn about clinical trials?
Dr. Charlot: Clinical trials are an opportunity to get access to new treatments that are not currently available. For the Black community in particular, we know that outcomes are worse when it comes to cancer survival and mortality rates. Clinical trials provide an opportunity to get access to new drugs, which ideally will prolong life.
It’s important for all patients, regardless of background, to have access. We don’t know how these drugs are going to affect people, whether it’s based on their environment, socioeconomic status, or race. It’s important to be able to test these drugs on a variety of people and understand how these treatments impact various groups.
A Patient’s Clinical Trial Success Story
Nikki: Can you think of a specific story that shows how impactful a trial can be for someone?
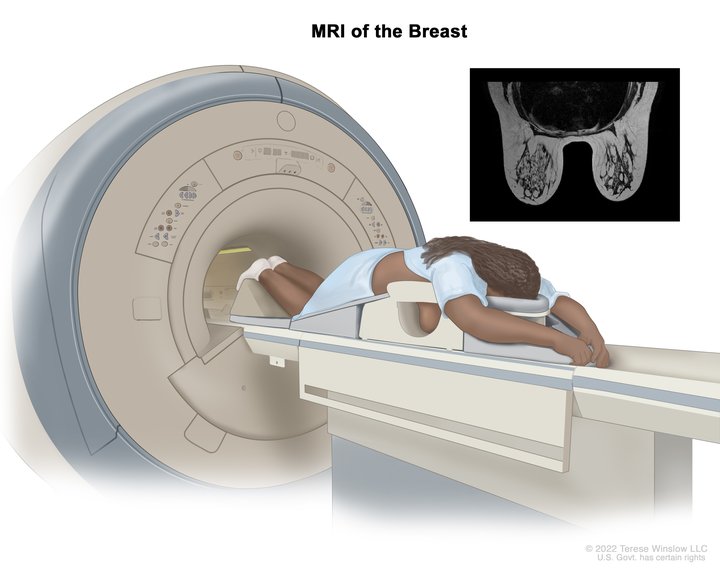
Dr. Charlot: I started the CREATE initiative at Lineberger and we’re in the process of completing a research grant that I have, which is building a mobile app for Black women with breast cancer to see if it can help increase discussions about clinical trials with their providers. One of our patient research partners shared her story about participating in a trial where the trial led to her being cancer-free for a very long time in that she’s been able to see this drug become a standard of care for breast cancer treatment.
It’s important to acknowledge the historical past and some of the mistreatment that Black communities and individuals often get within the medical care system.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
This goes to show that when going into a trial, we don’t know whether or not these drugs are going to work. What we do know is that when you’re in a clinical trial, you’re under such close follow-up, which gives you even an extra layer of eyes of people who are watching how you’re doing. If these drugs prove to be better than the standard of care, these drugs end up helping people live longer.
It’s fascinating and wonderful to be able to work with someone who’s been through this whole process of participating in a clinical trial and seeing that her participation led to the approval of a new drug that is now being used for breast cancer patients. There’s no better story than to live through the process of being in a clinical trial and to see how that participation led to the approval of a drug that more women and other people with breast cancer can benefit from.
Overcoming Barriers in Black Communities
Nikki: What would your message be to the Black and African-American community who are fearful of clinical trials?
Dr. Charlot: We know that our healthcare system and our research enterprise in this country have not been the best, particularly for our Black communities. At the same time, it’s important to acknowledge the historical past and some of the mistreatment that Black communities and individuals often get within the medical care system. Acknowledgment is at the forefront.
It’s also important to know that there are safeguards in place with clinical trials. It’s important for us, specifically as Black individuals, to be a part of clinical trials because it gives us opportunities that we would potentially not have to access newer drugs. Acknowledge the past and understand that we have a part and the right to have access to newer treatments and interventions.
We need to understand where our patients are coming from, know what their needs are, and partner with them.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
The Role of Black Physicians in Healthcare
Nikki: What do you think healthcare professionals can do better when building trust with the Black and African American community?
Dr. Charlot: As a Black physician and even for healthcare providers who are not Black, we need to be one with our community. We need to understand where our patients are coming from, know what their needs are, and partner with them. If we do these separately in our silos, it doesn’t help improve access to care. It doesn’t help our communities thrive and live healthy lives. Making connections is what’s helped me in the work that I do and hopefully helping the patients that I’ve had the privilege to take care of over these past couple of decades as a physician.
An internal medicine physician discusses healthcare access, preventative care, patient trust, and how both doctors and patients can improve relationships for better outcomes.
The Latest in Breast Cancer with Dr. Lola Fayanju at San Antonio Breast Cancer Symposium (SABCS) 2022
Interviewed by:
Stephanie Chuang
The San Antonio Breast Cancer Symposium (SABCS) provides the latest information in research, prevention, diagnosis, and treatment of breast cancer.
Dr. Oluwadamilola “Lola” Fayanju is the Helen O. Dickens Presidential Associate Professor in the Perelman School of Medicine at the University of Pennsylvania, the Chief of Breast Surgery for the University of Pennsylvania Health System, the Surgical Director of the Rena Rowan Breast Center in the Abramson Cancer Center, and an innovation faculty member at the Penn Center for Cancer Care Innovation (PC3I).
Dr. Fayanju’s focus as an academic breast surgical oncologist is on health disparities, patient-reported outcomes (PROs), and aggressive breast cancer variants.
Dr. Fayanju sat down with The Patient Story to discuss some of the latest news coming out of SABCS 2022.
discusses breast cancer, PROs, the language used around racial health disparities, and the importance of conferences like SABCS.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Introduction to Dr. Fayanju
Dr. Fayanju: I’ve always been interested in women’s health. [I was] one of those kids who always wanted to be a doctor and actually was really leaning towards OB-GYN. [I] was always interested in women’s reproductive rights.
Then when you go to medical school, you find out which parts of the body kind of attract you more. I have to admit, I was actually really attracted to surgical disease, found myself really gravitating towards surgical disease, and really got interested in general surgery.
As often happens, you are drawn into things because of the patients who move you and the mentors who inspire you. I was really moved by a patient who was a lot like me when I was a third-year medical student. She was about my age. She was actually also Nigerian.
She was presenting with a large triple-negative breast cancer, and she was alone. She had no family in the United States. I actually remember her starting to cry as I was examining her. I was seeing her in a safety net clinic. That is a clinic that was staffed primarily by trainees overseen by altruistic attendings at my medical school, who then connected those patients to tertiary care.
[I had] a wonderful couple of mentors, including Julie Margenthaler, who is the Chief of Breast Surgery at Washington University, and Ira Kodner, who was a colorectal surgeon but became very famous in the world of medical ethics, as well as care for the underserved.
Working with them, [I came] to realize that patients who presented through the safety net clinics were more likely to present with delayed care and more likely to present with a more advanced stage. That really launched, I would say, my career as a health services researcher and as someone interested in care that really reflected disparities in our society and our ability to provide equitable care.
I became interested in surgery because of the disease, I became interested in breast cancer because of the patients, [and] I also became inspired by having great mentors.
It all seems very linear, finding myself here now as a breast surgeon, but it was actually multifactorial and looks more clean and neat than it felt in the moment. But here I am today with the privilege of being a breast surgeon.
How did you feel meeting that patient who had delayed care?
I felt anger. I felt frustration. I felt the beginnings of despair, but then held myself back, thinking, “How could I make a difference?” Her experience and my experience working with the safety net clinic there actually led to a research project.
What was exciting about that [research project] is that it actually led to a change in the way that care was provided in St. Louis. It used to be the case that patients who were seen in one of the clinics that were treating patients who had no healthcare or who are underinsured — those patients often had to go back to their primary care providers to get referred to the tertiary clinic to get cancer care.
In fact, through research that we conducted, we were able to demonstrate that this led to delays because of having to redo imaging [and] because of missed appointments. It led to a change through the St. Louis Health Commission in the way that care is provided for these patients.
For me, it was a way to show that research didn’t have to be something that was localized to the ivory tower. It could actually be impactful. It could actually translate into policy and into real-world effectiveness. That was really exciting for me.
The importance of SABCS and other conferences
The importance of conferences like San Antonio, ASCO, ACR, or Society of Surgical Oncology is that we who are engaged in the scientific process take what we learn and implement it in our everyday care.
The tragedy of it is that often it takes too long. We know that the average amount of time it takes for our innovation to be implemented in routine clinical care is about 9 years.
One of the things that are really exciting [is] the field of implementation science, which at my institution, Penn Medicine’s Abramson Cancer Center, we actually have a funded implementation science center, which I’m a part [of].
That works to bridge the disconnect between discovery and delivery to ensure that what is found, what is discovered, and what is innovated by scientists actually makes it to patients.
What I would say is important about San Antonio is one, announcing new medications, devices, or approaches to care that will make a difference in the lives of patients with breast cancer. Two, updates on trials that were announced in the past that we now know more about. Then, three, ways in which we can take knowledge that has been kind of assumed to be standard and how we can actually apply that and update that in regular practice.
[Here are] examples of each of those 3 things. One, we are increasingly weighing the results of trials that will tell us how best to manage HER2-low disease. That is patients who have some HER2 expression, but where they don’t rise [to] the level of expression that we used to think was needed to benefit from targeted therapy.
An example of the middle one is the reporting of our understanding of Oncotype DX as both a prognostic and predictive tool for helping us better treat patients with estrogen-receptor-positive disease.
Then a third example is a talk that I’m giving today as part of a panel on patient-reported outcomes. [PROs] are opportunities for patients to describe how they’re feeling, what symptoms they’re experiencing, [and] what psychosocial challenges they might have that might prevent them from optimizing their breast cancer journey.
Those are 3 ways in which conferences like this allow us to communicate new findings, update knowledge we already have, and translate information and approaches we have into the clinical realm for the benefit of patients. Those are some examples of why San Antonio is important.
HER2-low breast cancer
The way to think about it is we’re looking for more opportunities for treatments. I think of HER2 targeted therapy as really an ideal within oncology because it really has changed our ability to achieve pathologic complete response — that is, eradication of tumor prior to surgery just through the use of systemic therapy.
It really has represented a gold standard that we’re trying to achieve for other types of molecular subtypes. Really, [what] we’re trying to figure out more and more is which types of HER2-low can be treated with systemic therapy. In whom can we deescalate other types of treatment? We know that some of the targeted therapy is very hard on the body, and so that’s something that we’re hoping to learn more about.
What are the new emerging treatments for breast cancer?
One of the big trials that came out several years ago was TAILORx, which allowed us to understand how well Oncotype DX, which is a genomic test that allows us to understand whether or not women with estrogen-receptor-positive breast cancer would benefit from chemotherapy in addition to endocrine therapy in the adjuvant — that is, post-operative setting.
Yesterday, an update on that was provided. It was very important in that it showed that women who had low or intermediate-risk Oncotype scores did not benefit substantially from additional chemotherapy beyond just getting endocrine therapy, except for women who were 50 years or younger. If they had an intermediate risk score, those individuals had some potential benefit from getting chemotherapy.
Worse outcomes reported for people of color
What was an unfortunate finding within the study was that Black women had worse outcomes even when you controlled for other factors. The way that was communicated was, I think, in a way that unfortunately is often communicated when trials are described.
Black race was communicated as an adverse factor, which is really not the way in which we want to describe these types of outcomes in minoritized groups. We know that race is a social construct.
As Dr. Lori Peirce, a very prominent radiation oncologist at the University of Michigan and former president of ASCO, described immediately before that presentation, race is a social construct that nonetheless has power and it is notable that in African Americans for many years, there was the one-drop rule in effect.
It was used to justify the enslavement of children of miscegenation in order to keep those children enslaved. It is also used to withhold rights from people of Native American ancestry by having it be that you have to have a certain minimal amount in order to claim Native American ancestry and take advantage of certain rights that are ascribed to them through the U.S. government.
Again, the use of ancestry is often political; it is not biological. When we ascribe risk or we describe disparities that are observed in certain groups, we need to really tease apart when we’re talking about genetic ancestry and when we’re talking about the systemic racism, bias, and the structures that contribute to seeing untoward outcomes in those groups. That, unfortunately, was not really described in the relaying of those results.
Language around racial disparities in healthcare
\We should never use language that Black race is an adverse factor or Hispanic ethnicity is an adverse factor. People’s identity is not an adverse factor, even if we find disparate results in that group.
The way I would describe those results is to say that, unfortunately, we continue to find worse outcomes amongst Black women. This is an important subject of future inquiry that hopefully will be better understood if we deliberately target Black women for enrollment in these trials, as they continue to be under-included and underrepresented in clinical trials.
Why is there a lack of diversity in clinical trials?
Many of the women who choose not to participate in clinical trials, who are African American, it’s not because they can’t afford to do so. It’s that they have a justified mistrust in the system, a system that has not earned the trustworthiness of people of color.
I think that descriptions of trial results matter. Words matter. As clinical trialists [and] as scientists, we need to think about how the words we put out there will influence [the] future behavior of the people we’re trying to attract to science.
Patient-reported outcomes
Dr. Fayanju: Patient-reported outcomes allow patients to communicate their feelings, sensations, [and] experience without the filter of the physician’s perspective. We know through some landmark work that it may actually improve survival, being able to communicate those experiences directly to their clinicians in a timely fashion.
We also know it is associated with improved shared decision-making, and improved quality of life. In vulnerable populations, it may even allow us to anticipate potential delays in receipt of care and receipt of treatment.
The difficulty is that there’s already a lot of pressure on the patient encounter with regard to what patients are trying to communicate and what doctors are trying to achieve. It’s not that doctors or clinicians as a whole aren’t trying to hear what their patients are trying to say. It’s often you have 15 to 30 minutes to accomplish all of those things.
What I’m hoping to communicate is how best to do that. What are some strategies for collecting that data prior to the patient encounter, during the patient encounter, and potentially afterward? Does it have to be limited to the cancer setting? Are there ways in which we can potentially engage primary care?
Additionally, what are the modalities in which we need to engage patients? How can we it feel less like work? One of the things that we need to think about is how to engage behavioral economics to make it feel easy, both for clinicians and patients. We need to make this not feel like homework, both for patients and for providers.
How can the patient-doctor experience be improved?
We need to be multifaceted. We need to recognize that our patients don’t all engage with patient portals. Many of them have smartphones, but levels of comfort vary. We also don’t want to exacerbate existing disparities by giving some patients a lot of opportunity to communicate with us and other patients the minimal opportunity to communicate with us.
Being able to use both smartphones and simple phones, being able to take advantage of opportunities to communicate in the waiting room, being able to sometimes rely on paper and pencil, and also making sure that we have culturally humble as well as linguistically diverse opportunities for collecting that data are really important.
Looking forward to future research on breast cancer
I’m really excited about the idea [of] precision oncology, which right now focuses on the kind of molecular milieu.
I think it also needs to think about the social milieu of the patients. How can precision oncology take into account the specifics of a patient’s social context and tailor their care to their lives, not just the cells in their body and the DNA of their tumor?
With the increased attention, the social determinants of health that COVID-19 really caused all of us to really focus on, I hope that there’s more research. I hope it’s sustained interest in making all of us believe that data that’s important to collect, act upon, and incorporate into our sense of what health should look like and how we can promote cures by incorporating the whole human into our care of the patient.
Multiple Myeloma: How Your Race and Age Can Affect Diagnoses and Treatment
Valarie Traynham
Multiple myeloma is the most common blood cancer among Black patients in the U.S., but many of those patients have an entirely different experience.
Studies show that Black patients respond better to newer treatments but are still twice as likely to die from the disease.
Patient advocate Valarie Traynham speaks with Shakira Grant, MBBS, of the UNC Medical Center. They discuss the barriers many Black patients face, how it impacts their care, and what can be done to help improve their outcomes.
Newly diagnosed patients [need] someone [who] they can ask questions [and] find out information and where to go for good relevant resources.
Valarie Traynham
Introduction
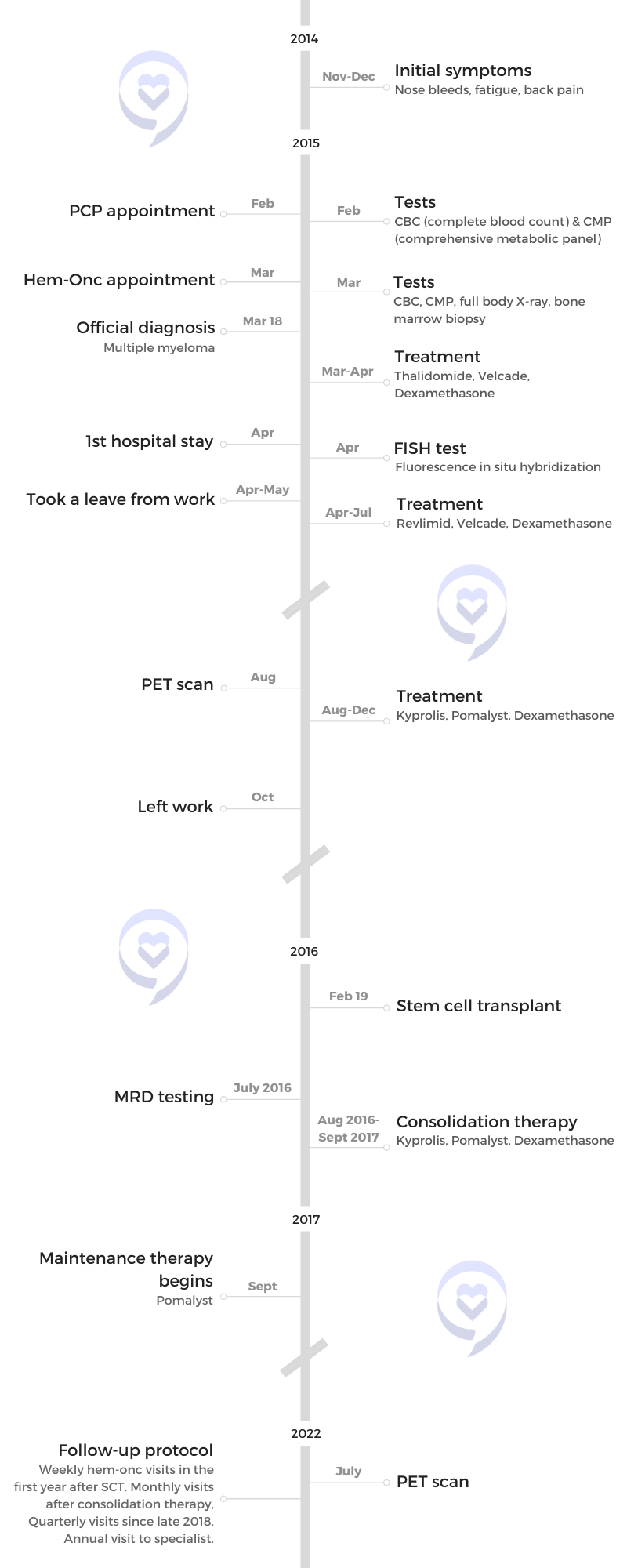
Valarie Traynham: I was diagnosed with multiple myeloma in 2015. Being a patient advocate, I want to be able to guide others through the process. When I was diagnosed, I did not have someone to go to and I think that’s very important. Newly diagnosed patients [need] someone [who] they can ask questions [and] find out information and where to go for good relevant resources.
I’m just so excited at the work that Dr. Grant is doing because it’s much needed. It’s an area that needs focus and she’s doing a wonderful job [of] getting that focus out there.
She focuses on a population of patients in the myeloma world that oftentimes [is] overlooked. It’s very important for that population of patients to be looked at and cared for and really understand what they are going through.
Dr. Grant is from the University of North Carolina and she focuses on geriatric multiple myeloma, health, and research.
Unfortunately, because multiple myeloma is also a disease that impacts older adults, we see this compounding effect, especially for Black older adults with multiple myeloma.
Dr. Shakira Grant
Dr. Shakira Grant: I’m primarily here to talk a little bit about our research and how this fits into sharing stories of patients and caregivers, which our team is really passionate about.
What really drew me to this type of work was this love for trying to bridge this gap in terms of the disparities that we see existing within not only outcomes but also survival for Black and white patients with multiple myeloma.
Unfortunately, because multiple myeloma is also a disease that impacts older adults, we see this compounding effect, especially for older Black adults with multiple myeloma. It’s really important for us as a research team to address some of these healthcare access barriers, which largely drive the disparate outcomes that we see in multiple myeloma.
We presented two studies. For the first one, we wanted to understand what barriers patients and their caregivers encounter when trying to seek care for multiple myeloma.
The top takeaway from that study is that many of our patients report that there’s really a delay in getting the diagnosis of myeloma and this results in them going to multiple specialists with their symptoms. Often, patients reported being dismissed by their doctors and being chalked up to just getting older and then repeating labs again in three months.
From this particular study, while we identified other barriers, including financial barriers, we do recognize that there is a need to focus on how we make the diagnosis, ensuring that patients are getting the diagnosis on time, which would allow them to enter into a care pathway where they can begin their treatment and minimize any chances that they will have any poor or adverse effects from multiple myeloma.
In terms of the other study, we wanted to look at factors that influence the participation in clinical trials for Black patients in particular. We did this by looking at the perspectives of patients with multiple myeloma as well as their hematologists.
One of our main takeaways from this is that the patient and their relationship with their doctor is really critical when trying to decide if a patient is going to be offered the opportunity to participate in a trial. Based on these findings, we do recognize that there is a need for more targeted interventions that address several steps in terms of communication between patients and their doctors to ensure that we have the best chances of offering clinical trials to a diverse patient population.
Many of our patients report that there’s really a delay in getting the diagnosis of myeloma and this results in them going to multiple specialists with their symptoms.
Dr. Grant
How do we get more diversity in clinical trials?
Valarie: I heard a lot about clinical trials. How can we get more minorities involved? What is that like for the older population that you see in the clinic?
Dr. Grant: Overall, when we think about increasing representation in clinical trials, we are coming up against two compounding factors. One is the older adult and then it’s the older adult who also identifies as having Black race.
For me, in clinical practice, one of the things that we try to do is to not only look at [the] patient’s chronologic age, but we also look at the functional age of patients. How well are they able to do their activity and to get around day to day? I believe that [is] probably better to assess eligibility for these particular patients for clinical trials in terms of Black representation or increasing representation of minoritized populations.
It is important for us to realize that myeloma does tend to affect an older adult population. We cannot really distill out and think about age and race separately, but we really should be thinking about these two things together. Our efforts to increase representation should be geared towards the older adult population, as well as thinking about the racial, ethnic, and minoritized populations.
We cannot really distill out and think about age and race separately, but we really should be thinking about these two things together.
Dr. Grant
How would you advise older multiple myeloma patients to stay positive?
Valarie: For a newly diagnosed older patient, how would you advise them? [There’s] so much going on. They’re getting the diagnosis. They’re trying to make it to the clinic. How would you advise them to stay positive and look for the good in the situation that they’re facing?
Dr. Grant: The thing that is really important that I’ve seen come out not only [from] our research but in my own clinical practice is the need to have a social support system. In our study, we looked at informal caregivers who were oftentimes spouses and, in some cases, adult children.
I really do think that having that support when you’re first diagnosed is really critical because you have, in essence, [a] second set of ears, [a] second set of eyes to help you with the amount of information that you’re getting, scheduling, [and monitoring] any potential treatment-related side effects.
I think [it’s] really important for patients to also seek knowledge about multiple myeloma from credible resources. Read as much as possible what you can about this disease, about things that you can expect, and then come to your provider’s visit prepared with those questions ready.
Having that support when you’re first diagnosed is really critical because you have, in essence, [a] second set of ears, [a] second set of eyes to help you.
Dr. Grant
Ask [about] things like clinical trial participation, if your doctor hasn’t mentioned it. It’s really important for patients to take that first bold step and say, “I’ve read about clinical trials. Do you think this could be a potential option for me?”
This really moves into this idea that we want our patients to not only have a really great social support system but also to be empowered to be able to ask the questions that they need of their physicians without feeling fearful or intimidated.
Valarie: I’m so glad you said that because that is one thing that I always try to tell newly diagnosed patients as a patient advocate. Find reputable material. Find out everything that you can about the disease. Don’t be afraid of it. It’s something that you’re going to be living with indefinitely.
We want our patients to not only have a really great social support system but also to be empowered to be able to ask the questions that they need of their physicians without feeling fearful or intimidated.
Dr. Grant
How do you build medical trust in Black communities?
Valarie: We know that trust in the African-American community is a big deal and that’s what we are focusing [on], too: raise trust and build trust in the community. As a physician, what are some of the things that patients are mainly dealing with?
I was listening to something and they talked about words matter — how you talk to patients, understanding patients, words that you use, words that the patient uses, and understanding and gathering information. Tell me [about] your thoughts on that.
Dr. Grant: What we’ve seen in our studies time and time again is that there is this legacy of medical mistrust that has been brought on by past research events where Black patients were intentionally harmed by the research enterprise and so it takes quite a while to be able to reverse those effects.
Things that we’ve learned from talking to patients [and] caregivers that can help close that trust gap is really working on our communication style as physicians, making sure that we’re using empathic communication, [and] letting our patients see that beyond the doctor title, we also are real people with real lives and lived experiences.
Don’t be afraid to pull back that curtain sometimes and let patients see that that relationship between patients and providers really helps to build up trust.
Find reputable material. Find out everything that you can about the disease. Don’t be afraid of it. It’s something that you’re going to be living with indefinitely.
Valarie
I think of a particular quote from one of our studies where a patient said that it’s all about [the] relationship and if we need to build trust, we really need to be focused on the relationship. That particular participant went on to say that really they believe that the physicians could benefit from relationship-building training.
That really stuck with me because I recognized that trust is so difficult to address. These are some strategies that, as a physician, we can do to at least start to build that and close that potential gap.
When it comes time to think about the research, there are different strategies that our team [uses] to really help foster trust and to help engage Black participants in our study. Some of those strategies have been described in the literature, but really it’s about having a team that is representative of the population that we’re trying to engage and helping them realize the value of this research and why we need to do this, especially for the Black community.
Trust is so difficult to address. These are some strategies that, as a physician, we can do to at least start to build that and close that potential gap.
Dr. Grant
We need to recognize that access to healthcare is dependent on several steps. This includes the patient’s ability to perceive their need for healthcare. Then they need to be able to seek out those services, reach the services, pay for the services, and engage with their healthcare provider.
I would encourage patients: if you are experiencing symptoms you’re concerned about and you’re seeing your provider and you don’t think your provider is necessarily answering or addressing those questions, don’t be afraid to talk to somebody else. Talk to another provider and do some additional research and see if there is potentially another option for you to have your symptoms examined.
They have to think about [the] costs of medications but also when they’re coming to the cancer center, the cost of parking, the cost of gas… all these things are really additive for patients, especially when they’re on a fixed income. This idea about having to pay twice was centered around the need to pay for all of these other healthcare services while also attending to the high cost associated with paying for parking at the health center.
In terms of other economic impacts, things like parking, don’t be afraid to tell your provider, “This is challenging for me to pay for parking,” or, “I’m having challenges just paying for my medications.” Because honestly, sometimes the visit time is so short that we don’t always have the time to ask if you are having financial concerns. We don’t want that. These financial challenges are a limitation to you getting your care on time.
Don’t be afraid to talk to your providers if you have concerns. Make those concerns known… If you’re having financial challenges, continue to share those concerns and ask about available resources.
Dr. Grant
Barriers patients face that prevent their care
Valarie: How often do you have patients that [face financial limitations?]
Dr. Grant: We actually see this, in my practice especially, quite often. It’s not uncommon at all for patients to be concerned about the cost of parking. Patients would express concerns about their ability to pay for parking. Sometimes it’s a bit of a challenge knowing what to do in those scenarios.
There are some efforts now at our cancer center to try to provide more accessible parking in terms of financial costs and reducing the cost of that, but it’s not always widely available to patients.
Don’t be afraid to talk to your providers if you have concerns. Make those concerns known. That goes from even when you’re first presenting, before you’re diagnosed and you’re concerned about it, keep sharing those concerns with your provider.
If you’re having financial challenges, continue to share those concerns and ask about available resources. There are more resources out there than sometimes patients may actually think or may actually have knowledge about.
Conclusion
Valarie: Thank you for joining us today and going over all of this. It’s so important what you do in the field of myeloma.
What we’re dealing with is meaningful. It’s life-impacting so it’s very important that you understand if you’re not being treated right or you feel that something is not right, say something because it’s not okay.
You have the right as a patient to have something done about that. You are in control of your health. Don’t settle. Without you, it would just be a missing piece.
Dr. Grant: Thank you for having me.
If you’re not being treated right or you feel that something is not right, say something because it’s not okay. You have the right as a patient to have something done about that. You are in control of your health. Don’t settle.
Valarie
Special thanks again to AbbVie for its support of our independent patient education content. The Patient Story retains full editorial control.
When it comes to cancer, the truth is different people need different approaches so equity refers to people getting what they need based on what they’re presenting with. That distinction is really important.
Dr. Kim Rhoads with her family, pre-pandemic
What drew you to medicine?
Stephanie Chuang, The Patient Story: What initially drew you to medicine and what drew you eventually to the area of cancer?
Kim Rhoads, MD, MS, MPH: Before we had the DEI language, I was in one of these pipeline programs in 1985 and 86. My mom happened to work at the School of Medicine at UC San Diego and she was in administration. They used to call her The Oracle. She was friends with the woman who started, I would argue, one of the first pipeline programs for underrepresented groups in medicine.
At 14, I worked in a lipid metabolism lab at UC San Diego for two summers in a row. I remember telling my mom, “Don’t get excited. I’m not going into medicine.” But the money was really good.
People in the lab took an interest in me and I liked science so it was fun for me to be in a laboratory. I already had a little bit of experience and the folks in my lab encouraged me to think about medical school. I was not thinking about that.
I majored in linguistics. I was not interested in being in the rat race. But as a junior in college and thinking about what a linguist does for a job, I decided to pursue the coursework to go to medical school.
I knew that it was a big commitment and that I needed to be making a conscious choice about going to medical school.
What personal experience really shaped you?
Stephanie, TPS: You were primed from a very young age, being in a lab at 14. You pursue medicine and, at some point, something personal happened that really shaped you.
Dr. Rhoads: I’d taken all the coursework [for medical school], but I decided to take a year off between college and medical school. Because I had worked in a lab, I was referred by my lab PI (principal investigator) to a lab in Washington, DC. I decided to move for a year [to] take some time and figure out, “Is this really what I want to do?” I wanted to take some time to make a decision [and] casually take the entrance exams.
I worked in an HIV lab at the time and my family is from Virginia, so I had a car. I would drive to Virginia on the weekends and spend time with my favorite cousin and my favorite aunt.
During that period, once I decided to apply for medical school, I was talking to them about interactions black people have with the healthcare system. My aunt was expressing that something was missing from her interactions with healthcare. I remember distinctly, she said, “I just want to be able to go to a clinic where when you walk in, people know your name.” But what I realized is she was asking for community. She wanted to feel like she was part of something, not like she was going into a situation where she would be judged for the choices she had made or how she lived her life.
I don’t want to be on a treadmill and then get to the end and find out that this isn’t what I really want.
What I didn’t know at the time was she had breast cancer. Nobody in the family knew. By my second year in medical school, the cancer had become so advanced she was not even offered surgery. She was treated with chemotherapy and died in the hospital. All contrary to having [a] choice, being supported, [and] feeling that warmth people need in a vulnerable time.
Because I’m [a] first-generation college graduate and [the] first doctor in my family, I thought, “Let me make a phone call. Maybe I could translate,” because I know that medicalese is being spoken and that people are probably not understanding what’s going on. When I called the hospital in Virginia, I was given a little bit of information. I asked if there was a specialist involved and was told, “General surgeons take care of breast cancer and we’re not operating anyway because the tumor is too large.” A lot of dismissive interaction.
By the end of the conversation, the person on the other end of the phone said, “Are you a nurse?” Because clearly, I had enough medicalese to get by as a second-year medical student. I said, “No, I’m a medical student,” and they hung up on me. That really stuck with me. This is not how it’s supposed to go, especially in that vulnerable time. That set me on a course of my original pathway in research, understanding the experiences of black women facing breast cancer and [their] relationship with surgeons.
What is that relationship like? Is it kind and caring? Did you feel taken care of and that somebody was looking after you? I remember one of the questions was, “Did your doctor make a U-turn at the foot of the bed?” It got me thinking about the fact that she never got radiation, which she needed based on the description of the tumor. That’s when I started to look into and think about it.
Many years into my surgical residency, comparing the different settings I had trained in — a Kaiser, a private institution, the academic center, the safety net hospital, the Veterans Administration — and seeing all kinds of different care provided for the same problem and making me wonder: Does this have anything to do with the difference in resources that are available? Going back to my aunt and asking the question: Was there radiation available at that hospital? As it turns out, there wasn’t so that’s why she wasn’t offered radiation. That started to form how I think about disparities because my suspicion was that you get the kind of care you get based on the institution that you select. And that brings us back to our question of inequities. Are people able to get what they need based on where they choose to get their care or where they’re forced to get their care based on their circumstances?
What is health equity?
Stephanie, TPS: What does health equity mean, Dr. Rhoads? We hear this now constantly. We hear about DEI in healthcare. What does that actually mean on a human level?
Dr. Rhoads: Health equity refers to everybody getting what they need. I think we started [with] liberation movements with the language of equality. But when it comes to cancer, the truth is different people need different approaches so equity refers to people getting what they need based on what they’re presenting with. That distinction is really important.
The word is now being overused. It is now being substituted for disparities. When we put the word inequity on top of disparities, what people are trying to refer to is the fact that these are addressable because if something is inequitable, it means it can be shifted towards equity. But by putting it over and covering over disparities, what we are effectively doing is trying to erase a state of being that exists as a result of inequity. It is the final common pathway of inequity. You end up with disparities. As long as we have inequities, we’re going to have disparities. But what we want to stay tuned for is the elimination of disparities by intervening to promote equity.
Stephanie, TPS: At the end of the day, words really matter and sometimes, it’s not really clear how powerful they are.
As long as we have inequities, we’re going to have disparities. What we want to stay tuned for is the elimination of disparities by intervening to promote equity.
What have you learned since then?
Stephanie, TPS: You were very conscious of this from the very beginning, even before you officially started seeing patients and becoming a surgeon. In the many years since then, what have you learned? Has it changed over time or are we still at the same place, depending on where you go for care?
Dr. Rhoads: Are we still there? Yes. The answer is yes. Most people don’t know because we don’t have a Consumer Report on what hospital you want to go to. There is website [for California] – CalHospitalCompare.org. You plug in your zip code, find the nearest hospitals, and look at their quality ratings. There were some efforts to try to promote better outcomes by ranking quality and letting providers know where the high quality is, letting the insurance companies know where is the high-quality care. There were several studies around 2005 [and] 2006 that came out showing that nobody was using those rankings. Referrals were being made based on personal networks.
My suspicion was that you get the kind of care you get based on the institution that you select… People don’t know that where you go determines what you get.
Whenever you talk about personal networks in [the] field of higher education, you know that those networks are going to be segregated. You can imagine how that can play out. Especially with the history in this country, for example, of black doctors only being allowed to train at certain institutions, only being allowed to practice in certain areas and in certain hospitals, [and] not being allowed to join professional societies with white physicians. That then is going to determine where your patients can go to get care.
California hospitals are still segregated by race [and] ethnicity but also by insurance status. That all came from policy, redlining, exclusion, and segregation in all of those layers — education and where you practice. That’s where patients are able to go.
Have things changed over time?
Stephanie, TPS: What you described, people might think, “Oh, that’s from before,” but what you’re saying is it’s very clearly still here.
Dr. Rhoads: It is. My aunt was treated in a safety net hospital and that’s the hospital that has to take you as a patient, regardless of your ability to pay. Your county has designated where those hospitals are. Those hospitals largely serve patients who have no insurance or Medi-Cal (when we’re talking California) [or] Medicaid (when you’re talking nationally).
If you rewind back to [the] ’64, ’65 civil rights era when Medicare and Medicaid legislation [was] being advanced at the federal level, the American Medical Association — which was very exclusive at the time, did not allow participants who were of color — [was] advocating against these policies. I don’t understand why, that doesn’t quite make sense to me. But the National Medical Association, a professional society created by black physicians out of exclusion, [was] heavily advocating for the passage of this legislation, in particular Medicaid, because they knew that those dollars were going to come to the hospitals where they were working and would have the opportunity for their patients to be covered by some kind of public insurance.
Dr. Rhoads with San Francisco Supervisor Shamann Walton
Now, what you’ve got across the country are hospitals that serve a disproportionate share of patients who have Medicaid or no insurance at all. What you’ll find is those tend to be your safety net hospitals so their revenues are not that high because they’re being paid by an insurer that doesn’t reimburse at a high rate. For example, Medicaid pays somewhere between $0.05 and $0.15 [per] dollar. If your total hospital bill is $10, you may get $1.50 back to the hospital to reinvest in their plants, property, and equipment.
Cancer care is expensive. A radiation machine costs money. A specialized CAT scanner costs money. If your revenues are low, those are not the investments you’re going to be making. That’s how you start to see a segregation of patients of color using high Medicaid hospitals for cancer care and then having to get whatever is available. That may not be the high-end PET scanner, may not be the CAT scanner that can slice the pancreas into thin enough slices that you can see a teeny little tiny tumor. If you need radiation and that hospital doesn’t have some kind of agreement with a place to provide radiation, you’re not getting radiation. That has a direct impact on outcomes.
When we looked back in about 2014 [and] 2015, we used publicly available data and asked which hospitals provide care to a high percentage of different racial and ethnic groups. We had what we called white-serving, Hispanic-serving, black-serving, [and] Asian-serving.
The one very notable thing is that white-serving hospitals do not overlap with black-serving hospitals and that they only overlap with Asian-serving hospitals. Hispanic- and black-serving hospitals are completely segregated. There are hospitals in California we can show you that have had zero black patients over a period of 10 years.
It really is segregated in a way that has not been amplified. We were looking at what was called minority-serving, so that was any non-white-serving hospitals. Those do not overlap with white-serving hospitals either. It is a pretty segregated system in California.
Across the country, minority-serving hospitals are black-serving hospitals. In California, minority-serving hospitals are Latino- or Hispanic-serving hospitals. Those are just some ways that we have looked at the data to understand the landscape of segregation that is still persistent in our healthcare system in a very liberal and very diverse state.
We used publicly available data and asked which hospitals provide care to a high percentage of different racial and ethnic groups… It really is segregated in a way that has not been amplified.
Why do people go where they go?
Stephanie, TPS: Sometimes, when we talk about these things, about race as a social construct and not just biology, I thought a lot of this is socioeconomic. If you live in a certain area and have limited means, you’re limited in terms of options. The most accessible hospital may be a safety net hospital. But you’re saying this is down racial lines. Can you talk about that? I know there’s another layer there. We talk about socioeconomic, but it’s very clear what you just described.
Dr. Rhoads: Socioeconomic factors — like income, education, [and] employment — track along racial lines as well. It’s hard to pull them apart.
We did publish a series of papers asking the question, “Why do people go where they go?” As you suggested, maybe you just live near the safety net hospital so that’s where you get your care.
We asked racial and ethnic minoritized communities [and] populations in California, “Would you use a National Cancer Institute-designated comprehensive cancer center?” That’s where the best outcomes, all the high-quality services, [and] all the specialists are. Then we also asked, “Would you use a high-volume hospital?” Because practice makes perfect, right? If you’re taking care of a lot of cancer, then your outcomes tend to be better. We’ve shown that that’s true.
We started off by asking, “What is the median travel distance that people will go in California to get colorectal cancer treatment?” We found that the median travel distance was five miles. Now there are all kinds of discussions that can be had about that. Five miles doesn’t seem like a lot. If you have a car, that’s short. If you’re on the bus, it might take longer. If you don’t have the access to either of those things, five miles is impossible.
We used that as a marker then we said, “What proportion of each racial and ethnic group lives within five miles of a National Cancer Institute comprehensive cancer center or a high-volume center?” It turns out that racial and ethnic minorities are the groups that live closest to these centers because they tend to be in non-rural areas in California. They live closer.
Then we said, “Of those who live within five miles, are you using them?” A lower percentage of racial and ethnic minorities who live within five miles of an NCI center or of a high-volume center were using them.
What’s going on here? Is it because some people are actually going where they can get better quality and going to a safety net hospital or high Medicaid hospital? Because that’s where the clustering of racial and ethnic minorities [is]. We asked, “Is this because of insurance?” The answer is no. Insurance did not move the needle. Insurance was not as statistically significant in its correlation. It did not explain this difference.
Then we asked, “Is it travel distance?” We counted everybody in because some people will be further than five miles out and travel distance did make a difference. So that was comforting because it makes sense. It has face validity.
But then we asked, “Is it possible that the neighborhood characteristics determine where you go?” We used education as the socioeconomic factor and it overrode travel distance. It neutralized the effect of travel distance. Travel distance did not matter. What mattered was [the] neighborhood education level. I know when I give this presentation on this series of papers, a lot of people will say, “I knew it.” They just don’t know better. But lots of people know better and still don’t pick the highest quality hospital, including insurers [and] referring providers.
The way I try to explain this is we looked at neighborhood-level education. It’s not the education of the individual; it’s the characteristics of the neighborhood. What we say is you are like your neighborhood. You’re like your neighbors in terms of your health behaviors because that is a marker of socioeconomics: What’s your neighborhood like? In your neighborhood, you’re in range with everybody else because you can afford to live there [and] you chose to live there. What we’re saying is neighborhoods develop patterns of where they get their care and that trumps quality and travel distance.
So that’s where my aunt went. If that’s where my grandma used to go, where my mom went, then that’s where we’re going because that’s our hospital. The problem is that if you peel back another social determinant — which is redlining and say, “Where are people allowed to live?” — then you become like your neighbors and you establish a relationship with the hospitals that serve that neighborhood. And those tend to be the safety net hospitals for racial and ethnic minorities.
Stephanie, TPS: Wow. You did ask all of the important questions. If not this, then what? While you were talking, I did think, “Oh, it must be the insurance.” And it’s not. The community events build a bridge of true understanding, not just, “You don’t know any better. You should be going here and this is why.” None of that.
What’s embedded in that history is a relationship and what that offers an opportunity to do is to have a different relationship.
Dr. Rhoads with her family
What are the solutions?
Stephanie, TPS: What are the solutions?
Dr. Rhoads: What’s happened is a relationship has been developed, whether that relationship is for better or for worse. You might not be aware that you could get better outcomes somewhere else because that’s always where everybody’s gone. The crazy things that happen there that don’t make sense are perfectly acceptable because that’s the relationship and that’s where you’re talking about history.
What’s embedded in that history is a relationship and what that offers is an opportunity to have a different relationship. But what about now? And what about going forward into the future? That is, I would argue, the foundation of Umoja Health — building a relationship and not building a relationship like it’s a destination. Understanding that relationships evolve over time.
Trust is the equity of relationships. You build it up as you go through good and bad things together. Not just all good things, but the bad things, too. I think [what] we have forgotten in medicine, in healthcare, is our own humanity. We’ve forgotten that we are also simply people. I don’t care if you’re green, purple, brown, [or] whatever. That’s the one thing I have in common with everybody. We need to be making relationships with communities that are around us in the same way we would be thinking about and making relationships with our friends.
We don’t have to tell them all our personal secrets but we shouldn’t be thinking about those relationships as, “I have all the resources and you do not.” There’s that way in which we otherize the patient. It happens in medicine, just in that doctor-patient interaction. The doctor is coming with some information. The patients come in with a lot more information than the doctor could ever have because they’re living in that body every day. But there’s some way in which we exalt the doctor, [as if] the doctor could never be the patient, which is a ridiculous proposition.
Similarly, as institutions, when we partner with [the] community, we otherize them. There’s a lot of paternalism. There [are] things that we want to hide and don’t want to say. Failing to recognize that.
If we came with transparency and said, “These are the hard parts. Let’s work on the hard parts together,” that is going to build trust faster. Then it all looks good and everything we do is great.
We need to be making relationships with communities that are around us in the same way we would be thinking about and making relationships with our friends.
How can we start the relationship on the right foot?
Stephanie, TPS: What are some things people could say to be more transparent and kick off the right conversation to lead to a good relationship?
Dr. Rhoads: First of all, it’s an acknowledgment that this one interaction is not our whole relationship. This is the beginning. I will see you again. In the process, as a human being, I will be making some mistakes. You will be making some mistakes. We will have some miscommunications. But the commitment to the relationship is that we will work through those together. I think that’s what can happen in the doctor-patient interaction.
In the institutional interaction, there also needs to be some humility. We talk about truth and reconciliation. We want to do the reconciliation; we don’t want to do the truth. That’s the hard part. Part of that is getting out of the building and being in community in whatever way you can. You don’t have to be in community as the doctor. Be in community just as an individual human, experiencing life in the same geographic territory as other people but obviously having a different experience. I think that’s what helped Umoja move along.
I also think people buy into Umoja and link into Umoja because even though it’s focused on COVID for the moment, it came out of our relationship with our partners around cancer. They asked us specifically to focus on COVID when the pandemic hit and we said we will do that because we committed ourselves. Year-round — not just when cancer is a problem. Non-transactional — we’re not here just because there’s a study and we need you to get in our study and diversify our study. We’re here because we want to be in partnership. It’s year-round, non-transactional community engagement.
I don’t think people really thought about the non-transactional part. They think about being nice. It’s not about being nice. It’s about being on a shared mission and sticking around when times get tough.
We need to build relationships and that’s where you’re going to get people wanting to be part of the solution.
When you get caught in a problem that gets posted on social media of your institution or a representative of your institution doing something that none of us want to see happen, what needs to be done is a confrontation of that behavior, an admission that that was not only wrong but is not what we are intending to do, and to sit with the community that’s impacted and listen as they express their frustration. Then figure out together how you can take action to avoid it in the future. It doesn’t mean that we’ll be perfect. Again, there’s a disclaimer. We’re going to continue to make mistakes. But what you’re committing to is continuing to work together. That’s the investment that is absent in all this DEI and DEIA conversation — the commitment to humility and transparency is what is always, always missing.
With Umoja, we’re out in the community. I’m wearing an Umoja T-shirt just like the volunteers who are there, just like any other medical provider volunteer who comes out — we all look the same. It gets me back to what my aunt was looking for. She’s looking for her neighbor to be at the clinic, to be the person to welcome her. When [you] take away that self-exaltation, holding ourselves more important than other people because we have special knowledge, you end up with the ability to connect with people. For the person coming into that setting, you also get rid of the feeling like they’re going to be judged for their life choices. If they feel like they’re judged, they’re going to lie about their life choices. They’re not going to be totally forthcoming. They’re not going to feel that they have permission to be fully who they are. And that’s where I think we’ve gone wrong with all of healthcare.
We do not train healthcare providers [to see] people in their full humanity without judgment. We provide rules of what’s good and what’s bad, and then you judge the people who are doing it wrong. Then if you layer racism in there, you have a quicker judgment [of] different people because there is a belief that they are inherently not good or inherently better than other people. Racism can go both ways. It’s not just thinking people are bad. It’s any judgment at all.
We need to build relationships and that’s where you’re going to get people wanting to be part of the solution, wanting to promote your study, wanting to participate in your study, because that’s not the primary thing you asked. The primary thing you asked them for was a relationship.
Racism can go both ways. It’s not just thinking people are bad. It’s any judgment at all.
How can small steps lead to big changes?
Stephanie, TPS: What you just said is really powerful. This piece about judgment is huge and that’s what you cut through when you started Umoja. You were in the community. You were leading. You were modeling. Something as simple as not wearing a UCSF shirt. It’s a simple decision but it sends a message.
Because of the timing, COVID is where a lot of the attention was paid. Can you give an example of how what seems like small steps and small decisions can actually really change someone’s mind if you really want to get them involved?
Dr. Rhoads: I’ve been doing community engagement work since 1993 and in 2020, I had a number of eye-opening revelations.
We started Umoja as United in Health District 10. It was an offshoot of Unidos en Salud and I always have to give credit to Diane Havlir for the brilliance of bringing COVID testing into the community when people didn’t have access. We were working in Bayview, southeast sector San Francisco — a large African American population, relatively speaking to the rest of the city — and then Sunnydale where we picked up Pacific Islander communities and then Latino population all throughout.
I remember having a conversation with my department chair and saying, “It really strikes me that the tents for the testing efforts were all just white tents. There was no signage anywhere that said Public Health Department or UCSF and I think that’s actually why people were willing to come.” That was my suspicion.
Then to bolster that, a participant I was speaking to — I had no idea she had gotten tested at our site — brought it up and said, “The only reason I answered your survey questions was [that] my neighbor was the person asking the questions.” Throughout setting these pop-ups, we would track the volunteers who are working the site: Do they match the demographic distribution in the neighborhood? Are we capturing the neighborhood people? Are we engaging the neighborhood people? So that was a big deal when she said, “I only answered because it was my neighbor. Otherwise, I wouldn’t answer any of those questions.” The trust was already there. The relationship was already there so that gives us an advantage.
Engaging people in the process changes how people perceive who you are.
Once we became Umoja Health in late 2020, people were coming out to work together who had never worked together before. I didn’t know because there were these community-based organizations [that] would come together under this umbrella. Thank you to the Brotherhood of Elders Network who opened the door.
We would get out into the field and I would have to say to people, “I know you’re really happy to see people, but please don’t hug each other.” It’s still COVID. There was joy inside of the pandemic and that joy was for us, by us, or FUBU work. Community saving the community. Community delivering the services. Community being valued for what they bring to the table, which is a relationship we don’t have.
That relationship translates because what you could see happening in the informational sessions we were doing in between the service events was people really understanding COVID in their own terms, in their own ability, to explain why social distancing mattered, why wearing a mask mattered, what is exponential spread… People just started to get it on their own. And that was huge. I realized these organizations suddenly are working together and have networks that we haven’t even seen.
By participating in delivering the services [and] setting up the site with COVID safety in mind, these people are going to go home to their families, they’re going to be in their social settings with their friends, and they’re going to be talking like this because it’s part of what they’re doing. It’s not because they’re now a doctor. It’s not anything formal. It’s the informal influence, the informal authority that they have within their groups that they could use to start promoting uptake and participation in COVID mitigation.
By the time we finished our first run of Umoja in the fall of 2020, African American people had gone from being the lowest testers in the county to being the highest testers in the county. We didn’t even work the entire county, but we had people in our informational meetings taking that information to their networks. People started really emphasizing and highlighting as credible messengers.
Those are examples of how engaging people in the process changes how people perceive who you are. Now, we get a lot of calls like, “Somebody has cancer. We need a second opinion. How can we get into UCSF?” People who would not have otherwise even considered talking to UCSF. These are people from our Umoja community, COVID-focused, calling us about cancer.
It just goes to show that the relationship is what matters. They perceive that we care because we’re willing to come out, to employ community people, [and] to make spaces for the community to be an active and primary part of the solution. We’re not looking at people as needing transportation and child care or you’re poor and you don’t know anything and we’re ministering to you. No, we’re saying we need what you know because that’s going to help us get the information out and that is what is going to help move us truly toward health equity.
Stephanie, TPS: Everything that you just described is so powerful. Those were really incredible examples. At the core of it, it’s about really building real relationships. People can feel it. They know. They know when you’re approaching them and they feel like, “Are you coming in thinking you’re going to save me?” Let’s go in equally because that’s what we are.
How can we avoid otherization?
Stephanie, TPS: For people who feel, “Well, that’s the other community,” what’s the message about why it’s so important for everybody? We’re not only talking about lifting black Americans or Latino Americans or Asian Americans or Pacific Islanders. What is that message to people who don’t get that part?
Dr. Rhoads: Otherization is really central to how I think about any of the work that we do in any community. You can be a short white man who is not aggressive and be otherized. There are a million ways to be otherized. What I go back to is the way to avoid otherization is to recognize your own humanity because that is the link you have to every single other person on the face of this earth. And I guarantee if you spend more time, you’ll find other similarities and other commonalities so you don’t have to separate yourself in that way. I think that’s core to what the problems are in healthcare.
What I would also point out is Umoja Health in Alameda County focuses on the African American community but in San Mateo County, it focuses on the Pacific Islander community and the Latino community. It’s whoever comes to the table. [It] really is people-powered. It is whatever resources. It is the actualization of stone soup. Whatever you can bring to the table, that’s the soup we’re making and that’s the soup that we’re having.
The way to avoid otherization is to recognize your own humanity because that is the link you have to every single other person on the face of this earth.
If what you’re bringing to the table is your ability to access resources from other spaces, even better, but it allows an opportunity for everybody to fully be who they are and not have to be other. We’re in this together. Everybody is susceptible to COVID. Everybody can actually come to the table and not be judged, “Well, you’re not bringing anything and so we’re here saving you.” No.
You can volunteer. You can encourage people to come to the site. You can educate people with what you’re learning in the meetings. You can invite people to the meetings. Everybody can contribute something. Until we get a handle on that, on believing that, and on operationalizing that, we’re going to be stuck.
For now, the paradigm we have is some people are better than others and have more than others and they need to give to or minister to those who have less. It discounts the importance of the other. Baba Arnold Perkins, who used to be the director of the Department of Public Health in Alameda County and who is now the chair of the Community Advisory Board for our cancer center, says, “Everyone is a piece of the puzzle and every piece is important.” And recently when I talked to him, he added to that. He said, “And every piece is equally important.” And that’s what I think we really need to recognize.
Dr. Rhoads with Baba Arnold Perkins (rightmost)
Think about doing a puzzle. Get a 5,000-piece puzzle. You’re just tooling along. It’s looking really good. A piece falls on the floor and you don’t notice until you’re done. When that piece is missing, it ruins the whole puzzle because it’s missing and it’s only one piece out of 5,000. So every piece is equally important.
Everyone is a piece of the puzzle and every piece is equally important.
Baba Arnold Perkins
How can we deal with the lack of trust?
Stephanie, TPS: Some people say this lack of trust or even distrust specifically when we’re talking about the black community, as the generations go on with younger people, slowly that’ll take care of that. In your experience, you met a range of people in terms of age with the same lack of trust.
Dr. Rhoads: Trust builds at the pace of the relationship. Think about this: If you don’t have a relationship, why would you expect to have any trust? You shouldn’t. Think about your own personal relationships. You just met somebody. You don’t automatically trust them. It takes some time of building up how you work together [and] how you relate to each other.
Over the generations, you might think [that] young people are unaware because this happened so long ago. But actually, the young people are where it’s at because their minds are flexible. They’re open. They’re willing to see disparate treatment, privilege, and access to opportunities. They can see it.
What I have observed is that for the younger people, it makes them uncomfortable. They want things to be different. We did hear the vaccine was developed too quickly. There [are] nanobots in it. Don’t trust the government. We saw that across age groups — no question. But I do think that there’s an opportunity because young people are now interested.
Climate change is another disaster that adults are creating for them. Racial discrimination. Killings of various kinds of people who are at a disadvantage at the hands of police. They’re seeing that for what it really is. I don’t hear from younger generations trying to smooth it over and say it’s just miscommunication. That’s definitely something that happens in generations who maybe don’t want to hold the responsibility for what we have created. The young people didn’t create it so it’s easy to critique it.
It’s not really a lack of trust; it’s an appropriate response to a history of untrustworthy behavior. There are reasons to be suspicious, which is why it matters to be in community, outside our walls, because that’s where you can start to break down things that happened in the past because now, something’s happening in real-time.
It’s not really a lack of trust; it’s an appropriate response to a history of untrustworthy behavior.
Dr. Rhoads with cancer survivor Norman Tillman
What are the next steps?
Stephanie, TPS: There are so many cancers that disproportionately impact black Americans compared to other groups. I know it’s across health care and life, really. But in cancer specifically, what do you see as the next real feasible steps? Bringing the hospital out into the community, really showing that we care, and trying to build real relationships. Are there additional steps that we can take collectively to help address the inequities and the disparities?
Dr. Rhoads: If you address the inequities, you’re going to get rid of the disparities. I’ve written some papers to look at [the] delivery of care and when you get the right care for the right stage of disease, the differences by race [and] ethnicity go away. We’ve shown it in colon cancer, acute myelogenous leukemia, gastric, and pancreas cancer. We know that if you address the inequities, you’re going to get back to differences. And differences are okay because innately, we are different from each other. We’re not going to live the same number of years. Those differences are acceptable. It’s the disparities where you didn’t get what you needed and therefore you’re dying early — that’s what we’re trying to eliminate. Addressing inequities is going to get us there.
There is a process that is in play. Building the relationship is the beginning of the process. What happens when you’re in relationship with [the] community is the questions start to be centered around the community instead of centered around institutionalists. Because we’ve made the barrier between the institution and the community more porous, we can actually receive input and guidance on what research questions should we be asking.
What are people observing on the ground that we’re unaware of and are assuming a sterile condition under which these disparities are happening? For example, higher rates of cancer in younger people. What do we know about what’s happening on the ground? Often, we don’t know anything. We assume everything’s equal.
The next step is having the community influence the research questions. We’re working with Cancer Grand Challenges, which is an international award to the United Kingdom and the US. The National Cancer Institute and Cancer Research UK combined to fund 11 projects. I’m involved with one of them and the question is about cancer promotion. Are there environmental exposures that cause a mutation you’re already carrying that your body is keeping in check? We are all carrying millions of mutations right now, but we’re not a million cancers. Are there environmental exposures that are selecting a mutation and saying now you’re going to start growing, you’re going to be a tumor?
I think that kind of research is going to be so importantly informed by advocates and community partners because they’re going to be able to tell you stories about what’s happening in their neighborhoods. When we see cancer clusters, we can start asking very specific questions about cancer promotion in those specific spaces. Again, that’s another example of centering the community in the research question. We can apply our scientific approaches, which are all very cutting-edge, but we’re applying them to questions that are directly relevant to people who are living regular lives outside of our institution. The next step is developing questions that really hit home so that our results are relevant to the people that we think we’re trying to serve and be in partnership with.
If you address the inequities, you’re going to get rid of the disparities… you’re going to get back to differences.
Differences are acceptable. It’s the disparities where you didn’t get what you needed and therefore you’re dying early — that’s what we’re trying to eliminate.
Before being diagnosed with multiple myeloma and breast cancer, Valarie Traynham worked in the human resources field. Since being on the cancer journey, her focus has shifted to patient education and advocacy.
As a cancer survivor, her goal is to learn more about the diseases, educate others and bring light to health inequity. She wants to use her voice for those who cannot speak up for themselves to ensure that they receive equitable access to good healthcare, clinical trials and proper treatment.
Valarie’s journey in patient education, mentorship and advocacy began when she became a support group leader. She is now a myeloma coach, mentor angel and leader of the Black Myeloma Health Community. She has had the opportunity to talk about disparities myeloma patients face and looks for solutions through partnerships with healthcare providers.
Name: Valarie T.
Primary Diagnosis:
Multiple Myeloma
Initial Symptoms:
Nose bleeds
Fatigue
Back pain
Treatment:
Chemotherapy
Stem cell transplant
Secondary Diagnosis:
Breast Cancer, Triple-Negative
Staging: 1A
Initial Symptoms:
None; caught at a regular screening mammogram
Treatment:
Chemotherapy
Mastectomy
Get educated about your disease. Understand what it is. Knowledge is power. When you get that knowledge, do something with it. Learn how to advocate for yourself. You have a voice. Your voice deserves to be heard so use your voice.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Pre-diagnosis
Introduction
I’m [a] pretty down-to-earth person. I enjoy the great outdoors when it’s warm [and] spending time with friends and family.
What I do is work that’s around myeloma and patient education. I also enjoy doing things at my church. I’m really involved with my church and that brings me great joy.
Initial symptoms
It was late 2014. The first incident happened around Thanksgiving. I went back to school. I was studying and working on some homework on my computer [when] I got a nosebleed. I didn’t think anything of it. I just stopped for a little bit, held my head back, and [it] kind of dissipated [so] I got back to doing what I was doing.
The exact same thing happened [again] a couple of weeks later but this time, it bled a little bit more, a little longer than the first time. I still wasn’t concerned. I thought it was the weather. I’d asked some of my friends, “What do you think’s going on?” And they’re like, “Oh, it’s changing seasons and you probably got just some dry sinuses.” They told me to “just put a little Vaseline in there. You’ll be okay and keep going.” I did that and I thought it was working.
When I got a bout of flu, it just wouldn’t go away.
About a month later, I got sick with the flu and I just felt tired, overly tired. At that time, I was working full-time in HR. I was overly tired when it came to work, but I didn’t think anything of it. I was working, doing schoolwork, [and] very involved in church, so I just chalked it up to just trying to do too much at one time.
But when I got a bout of flu, it just wouldn’t go away. I went to the doctor. I got all the things that you take [that] should [make you] feel better. It was Christmas Day [and] I couldn’t even celebrate because I was sick in bed so I knew something was going on. I went over to my local [pharmacy]. They gave me more meds and said, “If you’re not better by Monday, go see your primary care.” And that’s what I did.
I went to see my primary care physician. I told her what was going on with the tiredness. At that time, I did have some back pain. It was nothing major. I told her about the back pain and the nosebleeds. She listened to what I had to say. She ran a complete panel of blood work and that came back showing high protein so immediately, she sent me to see a hematologist-oncologist. That’s how things started.
When she sent me to the hematologist and I saw ‘oncologist’ tagged on, I knew something was not like it should have been.
Initial hematologist-oncologist appointment
When my primary care referred me to the hematologist, I didn’t think anything of that because I had been diagnosed with anemia many, many years ago and I was taking iron supplements.
It wasn’t until I went to see the hematologist and found out that he was an oncologist as well. I’m like, “Why would I need to see an oncologist?” It was something that snapped in my head at that moment. This is a little bit more than what I’m thinking, but I still didn’t think anything too drastic.
I make this joke all the time. I tell people, “I went to see my hematologist thinking I was going to get a prescription for iron and I came back with a cancer diagnosis.” That’s literally how it happened.
When she sent me to the hematologist and I saw “oncologist” tagged on, I knew something was not like it should have been.
I heard the term ‘biopsy’ and I’m like, ‘Okay, this is really serious.’
Testing
They were a little suspicious from the blood work. At this time, they were still doing the full body X-ray. It was when they did the full body X-rays and the bone marrow biopsy [that] all the pieces started to come together.
Another incident that let me know it was a little bit more serious [was] when they asked me to come back. I went and did blood work for the hematologist early one morning and before I had gotten home, the nurse called and said, “We need you to come back. The doctor wants to do some more tests.” I’m like, “Well, what does he see? What is he expecting?” She wouldn’t say anything so that was another thing. Something’s going on because I haven’t even gotten home and you want me to come back right away.
She told me to come back because they needed to do a bone test. I didn’t know what that was. Little did I know that that was a bone marrow biopsy. When I got there, I heard the term “biopsy” and I’m like, “Okay, this is really serious.”
Importance of a good support system
Luckily, my friend went with me. She said, “I’m not going to let you go back over there by yourself.” I did have some support when things started to unfold.
I remember the doctor talking to me and I heard the words, “You have myeloma. It’s incurable.” I went blank for a minute. It is always helpful to have someone with you [to] maybe ask some questions that you wouldn’t even think to ask [or be] a second set of ears, second set of hands. You want to have somebody there.
It wasn’t as shocking because I had just learned about my chart. I had been looking at every single test that had come back. If this is high, what does it mean? Multiple myeloma kept coming up and I’m like, “What in the world is that?” But I still put it out of my head.
It wasn’t until that moment I went into the office and was sitting there and heard those words. It was like somebody kicking me in the gut. What? Cancer? An incurable cancer? And that’s when the flood of fear came. I’m going to die. I’m too young to die. Why me? All of those range of emotions. How am I going to tell my family? What do I say? Where do I even start to talk about this?
My friend, Judy, went with me to that appointment. She’s a cancer survivor as well so she was like, “I’m not going to let you go by yourself.” That was very helpful to have someone who has heard those words before. She knew exactly what I could have been feeling so she was there to help me keep it together.
Breaking the news to loved ones
It was hard. I didn’t do it right away. It [took] a couple of weeks. I knew they would have questions that I didn’t know [the] answers [to] or where to even begin.
My friends see me every day and they want to know what’s going on. It was easier for me to say, “Hey, this is what’s going on,” and just left it at that because I didn’t know what to expect.
I don’t live near my family so it was a little difficult. It was hard because I didn’t know what to tell them. I didn’t know the answers. That was one of the most difficult things to do. I finally got the courage to just say, “I’ve got multiple myeloma and this is what it is. I don’t know where it came from. I don’t know anything, but this is what I’ve got. This is what I’m looking at.”
What was very helpful to me was the advocacy agencies… Places like that are very good to provide information.
Learning about multiple myeloma
It was tough to begin with because [of] the shock that you have myeloma. But I learned very, very early. I wanted to learn as much as I possibly could about whatever was invading my body. If I can learn about it, I can at least try to get one step ahead.
For me, I always say it was just a control thing. I felt the more I knew about it, at least I would have some control. That was my mindset so I went on this mission to find out whatever I could about the disease.
It just stuck with me, actually, this whole time. I’m always on a mission to find out a little bit more about the disease.
Finding the right information
It’s different for everyone. What was very helpful to me was the advocacy agencies. I went to the IMF (International Myeloma Foundation) website to find out what you’re going to need to know and some questions. They have some cool tip cards and brochures.
I utilized the MMRF (Multiple Myeloma Research Foundation) website [and] found out what was going on. Places like that are very good to provide information.
At that time, HealthTree was just coming up so I was looking to see what I could find that was going to help me figure out what to ask at what point in the journey.
I got diagnosed and they wanted me to start treatment the next day. I was like, “Okay, I guess I should go ahead and do this,” because what do you do when you get cancer? You want to get it out of you.
I didn’t start right away. It was probably a week or two later when I went in. I followed what they said because I didn’t know the right questions to ask. I went along with what the doctor [said]. I hadn’t sought a second opinion. I didn’t realize that I needed to see a specialist.
I was in really bad shape at this point. I had to have a wheelchair to get from the car to inside the facility.
Deciding to get a second opinion
About three treatments [in], I just felt horrible. At the urging of my family, they were like, “You got to get a second opinion. You have to. You’re up there where all those doctors are. You have the ability to do that.” I decided to get a second opinion and it’s one of the best things that I could have ever done.
I saw a hematologist at a local hospital. He treated other cancers as well so I realized that that was not the best thing for me.
They started me out with Thalidomide, Velcade, and Dex — that was my treatment regimen to begin with. I didn’t realize that was an old regimen that wasn’t being used and my doctor probably didn’t realize that either that’s why he gave me that. I did about three- or four-week cycles worth and by that time, I was able to get that second opinion.
I was in really bad shape at this point. I had to have a wheelchair to get from the car to inside the facility. I knew something was wrong because that was not me at all. Two months ago, I could still walk and was coherent.
Where I live, there is a facility called the Cancer Treatment Centers of America. Everyone was like, “You’ve got to go there. That’s all they do — cancer, cancer, cancer. You’re going to be in good hands.” I decided to go there.
It was[then] I started learning a lot more about myeloma and the different treatments available. It was through them that I got connected with the specialists.
I came to find out that my hemoglobin was at 4.6 so that’s why I was feeling horrible. I learned that [my regimen] was not the latest treatment. [It] was standard of care, but there was something better.
I also learned about stem cell transplant. We talked about [it] and what that looked like. I learned a lot more than what my local oncologist shared with me. I feel that with my local oncologist, [there] was a lack of communication. I was told, “You’re going to do four cycles of this, then you’re going to go for a stem cell transplant, then you may do a couple more cycles, and then you’ll be back to your new normal.” And I was like, “Oh, okay, so maybe [in] a year things will be back to normal?” And that was not the case.
When I got to the other doctor, he really explained what the process entailed and [that] there’s no certain time. It’s not like you’re going to do this and you’ll be back to your normal life. It was eye-opening because I wanted to believe what I had been told. It sounded so much better and it would have worked for me if that were the case. But life’s not like that.
At first, I was a little angry. How does this even happen? But it happens. It helped me understand that there has to be more done when it comes to awareness and letting people know about myeloma. Letting people know that this is what myeloma is, but also letting them know what treatments are out there, what you should be getting and what [is] probably not the best thing for you to be receiving either.
Side effects
When I switched from Revlimid to Pomalyst, it took a little bit of getting used to because my body was like, “Oh, I don’t think I like that.” I had major GI issues and most people don’t have GI issues with Pomalyst but that’s something that I was struggling with.
Taking those in combination, I had shortness of breath [which] slowed me down even further. I was concerned. There’s the risk of cardiac issues when you’re taking Kyprolis. I got afraid. I’m like, “I don’t want to take that because it may be doing something to my heart. I’m having shortness of breath already.” They sent me to see a cardiologist a couple of times just to make sure everything was okay and [it’s] one of the side effects. I eventually adjusted to that. That’s just part of the new normal so I adjusted and kept going.
I was very vocal. Even if I thought it was a side effect, I would say something because I didn’t know. I looked at the list of everything that could happen but maybe this is something that hadn’t been reported. It is possible.
With Velcade, I did have some neuropathy in my toe area to start with. My doctors would always ask, every week when I would come in to get it, “Are you feeling any numbness, tingling, or anything of that nature?” Even if it was a small amount, I would make sure that I said something so they could do something about it and that was very helpful.
Velcade is a subcu (subcutaneous injection) and I’m sure most people would have those little spots on their abdominal area wherever the shot was given. Sometimes it could be painful and I would tell them so they could guide me on what to do. [There] wasn’t a whole bunch they could do. It’s just unsightly. It’s a reminder of what you’re going through but still, I was very vocal in letting them know what was going on.
With Revlimid, one of the first things that scared me is I woke up itching one morning. It started as an itch on my legs. Did something bite me? Is it a mosquito bite? Before the end of the day, I was just itching all over uncontrollably. The more I scratched, the worse it got. Nothing would take it away. I called the doctor and they called in a prescription that would help. But people need to be aware of that. I didn’t know that could happen. I was surprised. What the heck is going on? It was really bad.
I realized that I’m not in control of this or anything else.
Dealing with treatment roadblocks
It was that word: control. It was then that I realized I’m not in control of this or anything else. I did all the things that I was supposed to do. I got my knowledge. I have no control.
All of those feelings, I just sat with them. I didn’t try to push them away. I just said, “You’ve got to deal with this. You’re going to have to deal with this.” And I just dealt with it.
My faith played a very important role. I had my prayer partners praying and that helped me tremendously. And I sought some therapy because I knew I can’t do this by myself. It’s not something that I can just pray away. I really needed some outside help.
I needed somebody that was going to listen and just listen. I couldn’t talk to my friends because they didn’t understand. They just hadn’t been there. They didn’t know. Therapy was one of the best things I could have done because my therapists helped me through the process.
My faith played a very important role… And I sought some therapy because I knew I can’t do this by myself.
Stem cell transplant
Preparing for stem cell transplant
I did four cycles of treatment thinking it was going to bring down the disease burden to where I could move forward with [the] transplant. At the end of my four cycles, I’m thinking, “Yes! It’s [the] transplant.” It didn’t happen. I hadn’t eliminated enough of the cancer cells in order to move forward.
Then comes the conversation of [needing] to do more therapy. We’re going to continue the induction therapy. That’s when I found out about myeloma clones. Never heard of that until I was about six months in. It’s those little things that if you know, then you can be better prepared.
I wasn’t prepared to be told [I] can’t go to transplant. It’s so funny because I went and shaved my head. I was like, “I’m going to shave it all off before it happens.” And they’re like, “No, you can’t. You’re not ready for that yet.” I was disappointed, a little angry, [and] just bewildered. What’s happening now? Another gut punch.
I got switched to Revlimid, Velcade, and Dex. I did four additional cycles. [When] it wasn’t working anymore, I was switched over to Kyprolis, Pomalyst and Dex, and I had [an] immediate response. That’s what really got me ready for the transplant.
Expectation setting
Going into the transplant, I was told what I could expect. I used to follow The Myeloma Beacon. I started following Pat Killingsworth and listened to what he said. I got his book about stem cell transplants. I read the book and I’m like, “I’m going to make sure I do everything that they say to do.”
Follow the advice of your doctors and nurses. They do this every single day. They can tell you how to prepare. I listened and followed some of the big names out there. These people know what’s going on and that helped me prepare for the transplant.
The week before the transplant, I found out my insurance was not going to cover [it] where I wanted to do it. That was something else that had to be worked out. Eventually, we got it taken care of but that was a very stressful time just trying to figure [it] out. What am I going to do if the insurance is not going to cover it here? What do I do?
Dealing with insurance issues
I was working with the stem cell transplant navigator at the hospital. She was such a godsend because I didn’t know what to do. I did not need the stress. She was like, “Hey, this happened. We’re going to take care of it,” and she just knew the right things to do.
I had everything in place. My family was coming out to spend time with me. A couple of my friends had taken off work. They had taken vacation time to be there for me. So when I heard this, I’m like, “Whoa, everything’s in place. It can’t just not happen because it’s going to affect other things.”
She helped me get it all worked out. Have somebody working on your behalf. Don’t try to do it all by yourself. If you’re one of those people [who thinks] you don’t need help, you do need help. Someone to help you with paperwork, to make phone calls for you, to do that type of work for you. People want to do that so let them.
The stem cell transplant navigator was excellent. My other friend, Karen, was excellent [at] making phone calls and doing things. I didn’t have to stress a lot because they made sure that things were taken care of. They [took] the pressure off of me.
Don’t try to do it all by yourself. If you’re one of those people that think you don’t need help, you do need help. People want to do that so let them. When things come up, let them.
Stem cell transplant process
It was a little scary at first. I was going into the unknown. I didn’t know what to expect. They told me, “On this day, you’ll go in. You’ll get the high-dose Melphalan. Make sure you chew ice chips. Then you’ll have a rest day and then you’ll get your stem cells back.”
A couple of weeks before, they give you shots that stimulate the stem cells. I had to give myself those shots in my stomach and that was a process because I never had to give myself shots before.
After four days of shots, I went to the facility to harvest the stem cells. They put this big catheter in your neck, which feels really, really weird. It was very painful for me to do the apheresis and get the circulating stem cells from the blood. That process was a little scary because you don’t know what to expect. You’re laying in bed hooked up to this machine and you see the blood going out of your body and being flushed back in.
I was very fortunate. I got all of the cells I needed in two days so I didn’t have to come back. They told me it could take four days to collect the cells.
I didn’t go for the transplant right away. I waited a couple of weeks and something was going on with my schedule and I wasn’t able to go.
Then came the insurance issue. My cells were frozen for a couple of weeks. I [went] back to the facility and had to reinsert the Hickman port — very uncomfortable to go through that process.
I’m admitted to the hospital. They test for C. diff (clostridium difficile infection) and lo and behold, I’m positive for C. diff so there’s another component that you don’t expect. That means I’ve got to be isolated in addition to the transplant. Other precautions had to be taken as well.
I remember it was a Wednesday evening. It was a very long day. I get the high-dose Melphalan and I’m chewing on ice chips. Thursday was my rest day. Bright and early Friday morning, the nurse comes in, checks all my vitals and she’s like, “This is it. This is the big day.”
A couple of hours later, the other nurse came in with this little bag of cells and I’m like, “This is the life-sustaining things that I’m going to get back.” At that time, a couple of members of my family had come up. My friends had taken off work to be there for me, supporting me. They kept a chart to let me know what was going on outside of the hospital.
I received my cells back. It was Friday morning [at] about 11:40, [I] celebrated my new birthday and the rest is just waiting to see what happens.
Recovering from the stem cell transplant
One of the most trying times was waiting for that engraftment period. I didn’t feel too bad the first couple of days. [On] the third day, I could start to feel something’s going on. The fourth day [was] okay.
On the fifth day, my head started to hurt. Every time I would run my fingers through my hair, it would just hurt tremendously. I’m like, “What the heck is going on?” Little did I know that was the beginning of the hair getting ready to fall out. And that was tough, even though I knew it was going to happen. It was still tough when it did happen.
Like clockwork, on day five, all my numbers bottomed out. I was feeling horrible [and] had the worst diarrhea that you can imagine. I felt that I was going to die. I woke up that morning and I was like, “Oh my God, I could die from this.” At that time, I was alone. My visitors hadn’t come in yet and I was just sitting there like, “I could die. If I get an infection, I could die. There’s no way I can fight it off.”
There was another patient undergoing stem cell transplant [who] had been there a few days before I’d gotten there, caught an infection and didn’t make it. Just knowing that on top of everything else, I was a basket case.
But I had great doctors, great nurses [and] a great team of people [who] took care of me and pulled me through it. They would come in every day, check on me, do what they had to do, and say, “Hey, you got to keep positive. You will get through this.” And I believed them because they do this every day. Why would I doubt them?
Recovery was really hard. The thing that surprised me most was the overwhelming fatigue. I would get up, sit on the side of the bed and go, “Oh, I can’t do this today,” and lay back down for a little bit. Then realize, “Okay, you’ve got to get up. You can’t just lay here in the bed. That’s not going to be helpful to you,” so I managed to get up. Then it was like, “Okay, let’s get to the shower,” so I would manage to get a shower, but I [got] out of the shower and I [had] to lay back down again. I’m like, “What in the world is going on? I can’t even hold my arm up.” That went on for a pretty good while.
I didn’t have to worry about cooking, cleaning, or anything like that. My friends were very good with making sure I was taken care of [so I could] take my time and get better. I made myself get out, walk to the mailbox, [and] walk around the block just to get some exercise. When I did that, I did feel better. There were times when it was 1:00 or 2:00 in the afternoon and I felt I needed a nap. I listened to my body.
Maintenance therapy post-SCT
We talked about what was going to happen after the transplant and we agreed on consolidation therapy. That was very popular at the time. Some doctors were doing it, some were [not]. We talked about doing consolidation for about two to three months after the stem cell transplant.
Consolidation therapy is just a continuation of the therapy you were on before you went for the transplant. You just do it a little bit longer to deepen the response to try and get rid of more of the disease burden.
When you look at that myeloma iceberg, consolidation therapy chips away at that iceberg a little bit more. We talked about doing that for two to three cycles more and that eventually turned into a 12-month cycle.
I really didn’t fully understand that at first. “We talked about two to three months. What are you talking about?” But when they explained to me how we want to deepen the response, I’m like, “Oh, okay. I guess I can go through this a little bit longer.” In my mind, that’s going to give me a longer remission, help me live longer, [and] help me live as much as normal life as I possibly can. I fought it at first but when I saw the risk-benefit, why not?
Consolidation therapy
We talked about what’s next long before the end of 12 months because I [didn’t] want any surprises. We talked about just doing Pomalyst, going on a single regimen for maintenance.
[While] I was going through consolidation therapy, I did MRD testing. I did find out I was MRD negative, which I was really excited about. I understood what MRD negative meant so I [asked], “Do I still need to do maintenance?” Because we had talked about going on maintenance indefinitely.
Side effects from Pomalyst
Once I completed the consolidation therapy, I went right into maintenance therapy. I didn’t have any problems with it [initially] but eventually, it did weaken my immune system to a greater magnitude to where my counts were always low.
I was doing monthly blood work. I had to do that in order to get Pomalyst. My counts were consistently low. I was having to get the Neupogen [and] Neulasta shots to build my ANC (absolute neutrophil count) up.
At that time, my hemoglobin was still borderline. I was still often fatigued. I had a conversation with my doctor about that and they were like, “Okay, maybe we can do a dose reduction.” We talked about that, what that meant and what it looked like. I did a dose reduction and that did help improve my numbers to where I was not as bad all of the time.
I stayed on that particular dose for a couple of years then the same thing started to happen. I was experiencing bone marrow suppression. It was really bad so we did another dose reduction. I told him what was going on, how I was feeling, [and] how it wasn’t improving. You could see it in my blood work. Every month, it was the same thing.
We decided to do another dose reduction and found a happy spot where I’m comfortable. I can live freely, so to speak. I’m comfortable doing things without fear my counts are low. And this is before COVID. You have to go out in a mask and it’s like, “I don’t want to do this.” You [can’t] participate in events because you’re afraid. If I get this least little thing, I’m going to be sick and down for days. It relieved that. It made things better.
Testing for minimal residual disease (MRD)
MRD stands for minimal residual disease. It is the test to determine if they can detect any myeloma cells after transplant or induction therapy. It wasn’t something they did on a regular basis back [then]. When I had that test done, I was very happy to hear that I was MRD negative.
My doctor and I had talked. “After you finish consolidation therapy, we’re going to put you on a single agent Pomalyst as maintenance.” My question was, “What if I’m MRD negative? You just said I don’t have any traces. Why should I take this? Why should I want to continue with the maintenance again?” They explained to me [that] the goal is to get rid of as much myeloma as possible, chip away at as much of that iceberg as possible.
When I saw the benefits, I made that [decision]. It was ultimately up to me if I didn’t want to do maintenance. All I had to do was say, “No, I don’t want to do that.” The doctors would have been okay with that.
That’s one thing I learned: shared decision-making. You have to have a say in it because ultimately, it’s your body, it’s your quality of life so make sure you have a say in what’s going on. Don’t just go along with it.
Receiving a second cancer diagnosis
I was doing well, trying to get back on track to my new normal and along came a breast cancer diagnosis. This was out of nowhere.
I was going for my yearly mammograms and always was told, “You have dense breasts. Just keep an eye out for things and we’ll see you back next year.” At this particular time, I went for my mammogram and got a callback. They [said] “We want you to come back. We need to do an ultrasound.” I didn’t think anything of it. I’m going to go back and they’ll do an ultrasound and tell me I’m good. That was not the case this time.
They picked up something on the screening mammogram [so] they pulled me back for a diagnostic mammogram and ultrasound. When they did the ultrasound, they did see a couple of things that were not on the previous year’s ultrasound so I was sent for a biopsy.
I’m not saying the treatment was easy — it wasn’t — but knowing the right questions to ask at the right time, I knew how to advocate for myself a lot better.
I was scared. At that point, I knew what biopsy meant. They’re looking for something. They don’t just send you for a biopsy. It was breast cancer. Here I am again, that whole gut kick. Again? Really? Where did this come from? What did I do to deserve this?
But I will say, having been on the myeloma journey and knowing a little bit more, it was a little easier to manage this. I’m not saying the treatment was easy — it wasn’t — but knowing the right questions to ask at the right time, I knew how to advocate for myself a lot better than I did going into the multiple myeloma. That’s been an added step to my journey. I’d like to say [that] myeloma prepared me for the things that I went through with breast cancer.
Dealing with a second cancer diagnosis on top of myeloma treatment
With the breast cancer diagnosis, I was terribly scared. I’m going to have to get treatment for this. Is that going to trigger something in the myeloma? That brought about this fear. Am I safe to do this?
The breast cancer diagnosis was very early stage — it was stage 1A. There was no lymph node involvement but the location of the tumors [meant] I [had] to have a mastectomy. That is a whole ’nother beast. The blood cancer was almost like an invisible cancer. It was something that was going on within your body.
With breast cancer, it was a lot different. It was harder. Having to have [my] breast removed was very difficult for me to accept in the beginning. This was just too much. I can’t go through this. I just can’t do this. It’s just the thought of amputation. I was very fearful.
Even though I was prepared as a patient, I was still very fearful because I didn’t know what the treatment would bring. I didn’t know [what] the side effects would be. Again, I tried to be positive about things and look for the silver lining.
My breast cancer was triple negative. There’s no pill that I can take to suppress anything. Again, I was very fearful. What if I go through all this — I have this chemo and I have my breast removed — what if it’s still there? What if it comes back because it’s triple negative and it’s not as easy to treat? I was dealing with a lot of fear in that instance as well, just like I was with the myeloma.
What helped me was I just sat there in the fear. I acknowledged that fear. I was thinking, Okay, you’ve gotten through myeloma. You can get through this, too. It’s very early stage. I was in a good position, if that makes sense. I don’t [think you’re] ever in a good position with any cancer, but I was in a good position where I wasn’t too concerned.
My doctor assured me early on. “We can take care of it. This will not take you out, Valarie.” That was very reassuring to hear. The oncologist said that the surgeon said the very same thing. Very supportive and [guided] me through that process as well.
How culture influences health care
There are so many things that vary from culture to culture. A lot of times, cultural beliefs prevent people from moving forward with a certain treatment. Not just stem cell transplants, but certain treatments. Receiving blood — certain cultures just don’t do that. Those things have to be acknowledged.
You have to understand someone’s culture in order to understand why they would make certain decisions. Culture is a big influence on decision-making in many instances.
Dealing with the healthcare system as a black woman in America
Being a myeloma coach, I get to talk to myeloma patients, many [of] who have been newly diagnosed and [have] been on the journey for a while. I get to hear a lot of what they have been through or how many times they had to go to the doctor to get a proper diagnosis.
I realize that I’m very fortunate. My primary care knew the tests to run, picked up on the high protein, and sent me to see a hematologist. I know that is not always the case. People may have to go to the doctor two or three times before they even are heard to say, “Hey, this is what’s going on.”
I talked to many people who, when they get to the doctor, find out that they’re in kidney failure. On top of having the disease, it’s the shock of how you are told that you have the disease. Those are the types of things patients deal with.
I was talking to this lady. She went to the doctor [and] finally got the diagnosis, but they wanted her to wait to start treatment. They didn’t want to start treatment right away. Why would they want you to wait? That doesn’t make sense. I see that that doesn’t make sense, but as a patient who doesn’t know how things are supposed to work, that may seem normal.
I was told about [the] stem cell transplant early on in the process. There are patients [who] are not told about that. They’re just told, “We’re going to utilize this treatment and if this doesn’t work, then we’ll go to something else.” This was before we had so many novel therapies so it’s not like you had a lot to choose from. It was just assumed you don’t want a stem cell transplant, you may not be able to get to the facility, or you may not have the support to go through a transplant. It’s just varying things that patients have to deal with when it comes to health inequities.
As a doctor, you have to talk to your patient and find out where there is hesitancy. You can’t make the assumption that someone just doesn’t want to do it because they just don’t want to do it.
Sometimes it’s not discussed simply because it’s not talked about. And that’s very unfortunate because of the bias. You’re making that assumption just because I live in a certain zip code that maybe I shouldn’t do this, I wouldn’t want to do this or I don’t have the ability?
A lot of it is just access to care. We [have] to make sure that we’re getting the patients to the right place at the right time. We have to break down those barriers.
I’m not a doctor, but as a doctor, you have to talk to your patient and find out where there is hesitancy. Let’s say you talk to someone about a stem cell transplant and they decide they don’t want to do it. You have to find out why. Is it that they don’t want to do it or [do] they have other things creating barriers [that don’t allow] them to do it?
Child care. If you have children, you can’t just say, “Hey, I’m going to shut down for two weeks to be in the hospital and then I’ve got 100 days of recoup time.” Who’s going to take care of things? Who’s going to take care of the house, particularly if it’s not a two-person home? Getting back and forth to the clinic [for] follow-up visits. All of those things need to be taken into consideration. You can’t make the assumption that someone just doesn’t want to do it because they just don’t want to do it. There may be underlying reasons.
People need to understand that they play a very important role in their treatment decisions. You don’t have to just go with the flow.
Importance of shared treatment decision-making
It’s a game changer, particularly for patients who are accustomed to just going along with what the doctors say. In the African-American community, that’s kind of the norm. The doctor knows best. He knows more than you do about the disease. You need to follow what you’ve been told. That’s just instilled in a lot of us. But that’s not the case. It doesn’t have to be like that.
People need to understand that they play a very important role in their treatment decisions. You don’t have to just go with the flow. You don’t have to follow what the doctor is saying blindly because you don’t think you can say anything. You can say something and you should. Because again, it’s your life. You have to live with the side effects. You have to live with the treatment schedule so you want to have as much say as possible in that.
All of those feelings that I was still in, I just sat with them. I didn’t try to push them away.
Words of advice
It was my faith that really pulled me through and knowing I’m going to get through this. I believe that I’m going to get through this. I’m trusting the process, as they say. Just trust the process.
You have to acknowledge those feelings that you have because if you don’t acknowledge them, they would just eat away at you. Tell somebody. I told my friend, “I felt like I was going to die this morning. I really felt that. I didn’t know what was going to happen, what could happen.” And that was very helpful when I let that out, when I released that and said something.
You can’t ignore your feelings because they are not going to go anywhere. They’re going to be there. They want to be acknowledged. I acknowledged every thought that came. I’m scared.I might die. It was just getting it out there and releasing it. Having that release was very helpful in my situation.
Find something that’s going to give you hope. Very early on with the myeloma, I got connected with others [who] were on the journey. Get connected with others that have been on the journey.
About six months into my diagnosis, I met a 26-year survivor and that just brought me so much joy. I was like, “26 years? You lived? I can do that, too! It’s possible for me, too.” Meeting that individual gave me so much hope.
Don’t think you’re alone in this. You’re not alone. There are so many people dealing with a lot of the same things that you’re dealing with. Reach out to those people. Get connected. Whether it’s through a support group or a group at your church, get connected.
One thing that you don’t want to do is shut yourself off from people. Don’t shut yourself off because that’s not going to do you any good.
Make your needs known. People don’t know what you need. They can speculate. “Oh, she’s going through cancer. She may need this,” or “Oh, she just got out of the hospital. She may need this,” but don’t make people guess. Let it be known because people want to help. They’re willing to help but a lot of times, they just don’t know what to do so you got to tell them.
Get educated about your disease whether it’s myeloma, breast cancer or any other kind of cancer. Find out about the disease. Understand what it is. Don’t just listen to what people tell you. I’m not saying you have to be this research advocate. Knowledge is power.
When you get that knowledge, do something with it. Don’t just sit on it. I think that’s where we make the mistake a lot of times. We have all this knowledge and then we don’t do anything with it. Learn how to advocate for yourself. You have a voice. Your voice deserves to be heard so use your voice.
Look for the positive. I try to be positive about everything. [There’s] a silver lining somewhere. Find that silver lining.
Listen to your body. Don’t think that you have to get back to life. You have to heal. You have to listen to your body and take the time that you need to get well.
Sometimes, people are afraid to speak up because of embarrassment. “I’ll just deal with it.” Don’t suffer through. There are things that can help you get through so take advantage of those things. Utilize those things. Communicate with your doctor. I know a lot of people are not comfortable talking to their doctors. Talk to the physician’s assistant. Talk with the nurse practitioner. That’s what they’re there for.
You [have] to speak up. If patients are heard or feel they are heard, that would change the whole dynamic. A lot of people, if they feel they’re not heard, they’re going to stop talking. It’s not going to benefit them.
Listening and understanding — listening for understanding and not just listening to say, “Well, I heard what they say. It still doesn’t make sense to me.” It may not make sense to you, but it’s still acknowledging what the patient said, what’s been said.
Find others on the journey. Connect with others. Educate yourself. Knowledge is power.
Don’t think you’re alone in this. You’re not alone.
Mical was initially diagnosed with stage 1 prostate cancer at 37. They learned after prostatectomy it was an aggressive stage 2.
He had no symptoms, and he wouldn’t have found out at an early stage if not for a guardian angel of a doctor who decided to include the PSA test in his regular blood work.
Now, Mical uses his voice and his story to advocate for prostate cancer awareness, especially in the Black community, conversations about family health history, and the importance of early screening.
Name: Mical R.
Diagnosis:
Prostate Cancer
Staging: 2
Symptom:
No symptoms, caught at routine physical with PSA test
Treatment:
Radical prostatectomy (surgery)
Since being diagnosed with prostate cancer, my focus has shifted, and I’ve become super passionate about spreading awareness and advocating for more awareness, certainly in the Black community.
As a Black man, I feel that if I had certain things on the awareness side, then my journey could have looked a little bit different.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Pre-diagnosis
Tell us about yourself
I have a twin brother. I’m a family man. I have two daughters. I’ve been with my wife for 18 years. We’ve been married 16 years.
I was a teacher for many years. I still work in higher education as an instructor. I’m passionate about reading and writing. That’s all I’ve ever taught, English language arts. Love writing.
Since being diagnosed with prostate cancer, my focus has shifted and I’ve become super passionate about spreading awareness and advocating for more awareness, certainly in the black community. As a black man, I feel that if I had certain things on the awareness side, then my journey could have looked a little bit different.
I’m doing my part so that men don’t have to go along not knowing the disparities and not knowing that black men are two times more likely to be diagnosed and 2.5 times more likely to die from the disease. It’s become my life’s work to do this.
I would have thought that if I had cancer that I would have been able to sense it.
Initial doctor’s appointment
[I’ve lived] in Houston my whole life aside from college. My whole family moved to Austin [when] I got a job promotion. That was 2017.
In 2018, we finally got settled. We [needed] to find a doctor because prior to moving, I went to the doctor every year. I was accustomed to going to my annual wellness visit at a minimum. My wife is from Austin. My in-laws recommended this primary care physician because they’ve been her patients for 15 to 20 years, so she came highly recommended.
My wife and I couldn’t get in. We kept calling to try to get an appointment. They were booked up. My mother-in-law said, “I’m going to text her and say, ‘Hey, I’m trying to get my son-in-law and my daughter.’” The doctor responded, “You tell the front desk that I said make it work.” That’s how I arrived at this doctor. This is key for me.
[On] my very first visit, she [needed] to know [my] family history. At that time, the only family history I knew was that my aunt, my mom’s only sister, had been diagnosed with breast cancer just weeks before. My paternal grandmother had recently died of stage four lung cancer — breast cancer that metastasized to her lungs.
This was a regular checkup. She did the blood work. But unbeknownst to me, she also tested my PSA levels. When the blood work came back, everything was great but she noted, “I’m concerned about your PSA levels.”
That was the first time I ever heard the word. I actually had to Google. What is that? I was just going for my annual physical, to establish this relationship. I had no symptoms at all, not one. I was very healthy [and] young.
I Googled it and I never got alarmed because I didn’t have symptoms. I always felt like whatever the concern is, it’ll be ruled out because I feel great. I would have thought that if I had cancer that I would have been able to sense it.
She told me, “I want to put you on an antibiotic for a month,” because she initially thought it was prostatitis, which is a prostate infection. I did the antibiotics for 30 days. She retested my PSA. She said, “I’m not satisfied. It came down a little but not enough. I want to put you on an antibiotic for another 30 days.” I did the 30-day round again. After that 30 days, when she tested my PSA, the levels had gone up higher than they were initially.
I cannot remember what the number was. It wasn’t crazily high but it was higher than it should have been. It was cause for alarm. In a period of two months, from whatever it was initially, it went up. It didn’t go down so that’s alarming.
At that point, she said, “I think we should send you to a urologist so that they can have a further look.” I did everything she told me to do. I went to the urologist that she referred me to.
They did a biopsy. A week later, I found out. At that time, they told me it was stage one prostate cancer. But we ended up finding out after the surgery that it was an aggressive stage two.
I always tell people that I used to think that I moved to Austin for a promotion, but I really think I moved to Austin to save my life.
What makes that doctor so good?
What makes her so great for me [is] that she comes highly recommended and they love her so that helps me feel more comfortable. [The] first time that I ever met her, I felt like [I’d] known this lady forever.
She’s intentional about being present, really listening and engaging, talking to me about other things, just getting to know me, and not making me feel like I’m one more [patient]. We know doctors are busy but I’ve been to so many doctors where I feel like [there’s] no time to connect so that’s what’s made her so special for me.
I call her my guardian angel. Essentially, she’s the person that diagnosed. She’s the reason that we’re here because I can almost bet that if I hadn’t met this doctor, there was no reason for me to get this PSA test if I wasn’t of age. I had no symptoms. It’s nothing but God.
If I didn’t meet this doctor, I can guess how things would have turned out.
I always tell people that I used to think that I moved to Austin for a promotion, but I really think I moved to Austin to save my life.
The night I found out my diagnosis, I called her and I said, “Hey, I just wanted to update you. It’s cancer.” She said, “Let’s pray,” and we prayed right then. She’s not a black doctor. She’s a white woman. Some people might assume maybe there was a cultural… no, she’s a white woman.
I call her mom, honestly. She 100% gives me that energy. I asked her, “What made you take my PSA levels? What made you do that?” She said, “I’ve just been noticing in the five years prior that younger and younger men are being diagnosed.” She’s probably just been reading literature. She’s up on the latest news and that’s what made her do it. And I’m grateful for it.
What did you know about prostate cancer?
I never thought anything. I’m sure I saw a commercial or something but a personal connection, never. I don’t know that I even knew anyone who had prostate cancer, besides maybe someone on TV.
It couldn’t hurt if you did the test and [if] it’s fine, then it’s fine.
Importance of knowing your family’s medical history
She said that because she noticed that younger and younger men [of color] were being diagnosed that it couldn’t hurt, which is true. It couldn’t hurt if you did the test and [if] it’s fine, then it’s fine. I also assumed that telling her about breast cancer on my mom’s side and my dad’s side may have just helped to make that decision.
This just goes into — and I can only speak for the black culture — we don’t discuss family history. We really don’t discuss things at all, but we certainly don’t discuss family history.
After I had surgery, I was back at work [and] I was on the phone with my dad’s only living brother. [I] found out that [he] had prostate cancer five years before me. My parents actually knew that he had it and they knew I had it. But even at the point [when] they found out I had it, they still didn’t tell me.
Men just don’t like to talk about this stuff, period. Men are not crazy about going to the doctor. Even if a man knows something’s going on, some men won’t go.
That also goes into why I choose to be such a big mouth about it because we’re just not doing ourselves any favor. This is not helping to move the needle forward by us keeping it to ourselves. We have to stop being such a taboo thing.
Men just don’t like to talk about this stuff, period. I’m just speaking for men. Men are not crazy about going to the doctor and this is a disease that affects men. I think specifically for prostate cancer that would be one of the leading reasons why most men feel like it makes them less of a man or they just don’t feel comfortable sharing it.
I’ve met so many men who I know have prostate cancer because I had it. But if I didn’t have it, they probably would have never told me that. I try to speak out for all of them because, at the end of the day, nothing is more authentic than an actual patient experience.
Doctors can get on here and they can say all of the amazing words. No one told me about this [and] I was going to the doctor. That’s a separate issue for some men because some men refuse. Even if a man knows something’s going on, some men won’t go to the doctor. But I was going to the doctor. And so for me, if I was aware of that health history, then I could have been advocating for it well before when this doctor just chose to do it.
If I didn’t meet this doctor, I can guess how things would have turned out. I would have still been going to the doctor but no one would have [chosen] to check it so it would have looked dormant until stage three or four. I’m so grateful for the way it happened and I have to do the work and be boots-on-the-ground grassroots because my life is essentially spared.
Getting a biopsy
Before this, the only surgery I’ve ever had was when I was in college to have a lymph node removed from [the] left side of my chest. When they said I needed to have a biopsy, I really didn’t understand what that was until I was there and it was happening.
They biopsy portions of my prostate. I can’t remember how many pieces they took, maybe four or five. Then based on that, they were able to see that cancer was present. At that time, it was stage one. But we later realized once they dissected my prostate after surgery that it was an aggressive stage two.
In black men, it can lie dormant and it can also be aggressive, which was exactly what happened to me.
Diagnosis
Getting the official diagnosis
It was seven days from the time I had the biopsy. The thing is, I don’t know if it was God keeping me sane, but I genuinely went through all of that — from the time that I met that first primary care physician all the way up to the results — whole time in between, I never ever got rattled. I never wondered, “Could it be?”
I consistently felt great. I felt good. I feel like I’m pretty in tune with my body. If there was something going on, I would have had a symptom, right? But it wasn’t until after learning more about this disease that it presents itself in different ways.
In black men, it can lie dormant and it can also be aggressive, which was exactly what happened to me. I had no symptoms but my cancer was an aggressive form, which is something that’s just wow.
I needed to go back to the doctor to get my results. Prior to that day, I had already gone to this urologist twice. The first visit was the consultation to talk to me about everything and then the second visit was the actual biopsy. Both times, I pay the co-pay.
On the third visit, I know that I’m simply going to pick up results. That morning at work, I was just talking to my colleagues. “I don’t think I should have to pay another co-pay because I’m really I’m not getting a service rendered. I’m just picking up results for a service.” They’re like, “No, I don’t think you should.” I’m like, “Yeah, I don’t think so either. I just want to call the doctor’s office just to make sure.”
I call the doctor’s office and the lady who I spoke with, I had a sense that she was a black woman. She reminded me of an aunt. I explained to her, “I’m just getting results today.” I don’t think I have cancer so this is also leading the way I’m dealing with it. “I just need to pick up my results today and I’m just trying to make sure if I have a co-pay.” She’s like, “No, you shouldn’t. You know what? This is what I’ll do. I’ll send an interoffice request for your results and then they’ll send them down to me. So call me back in an hour because I’ll have them by then.”
In an hour, to the minute, I called and she probably was so busy between the first time I talked to her and now that she hadn’t even checked her emails. She’s like, “Let me look. They haven’t sent it yet. That’s weird. I don’t know why they haven’t sent it. Listen, I’m going to go up there and get it and I’m going to call you back.”
She calls back and says, “Hey, I was just thinking you should probably just come in.” As soon as she said that, that’s when I got scared because I felt, even though I hadn’t talked to her that many times, we had just built this rapport where she agreed that she’s going to give me the results and now she’s calling me back and telling me to just come in. The inflection in her voice, the energy, all of it, just made me say, “Okay.” I didn’t ask her why. I didn’t say, “What made you change your tone?” I just said okay and I got scared then.
I came home that evening and I told my wife. We were actually driving to the urologist for that appointment. “Babe, I called earlier. I talked to a lady.” I said I was trying to make sure we shouldn’t have to pay another co-pay. She’s like, “Well, no, we shouldn’t.” I said, “Yeah. The lady was supposed to just be getting me my results. But then she just told me I should just come in. I don’t know why. That just felt weird to me.” That’s what I told my wife and that was the first time I got scared.
She calls back and says, “Hey, I was just thinking you should probably just come in.” As soon as she said that, that’s when I got scared.
Before that, I was just moving through whatever I was being told to do because, in my mind, we’re going to rule it out. All of this is going to rule it out. We get to the urologist’s office. When I walked back up [to the front desk], as I was approaching the counter, the lady says, “Okay, your co-pay for today is…” I don’t remember what the amount was. My wife [went] right up to the counter and she’s like, “I don’t understand why we have to pay a co-pay. We’re just getting results, that’s all we’re doing. Maybe we have to see the urologist but it’s not really a visit. We’re just getting results. The service was rendered.” The lady goes, “Let me go check.”
The lady comes back to the desk with a piece of paper and slides [it] under the little window. I looked at the sheet. It was graphs and charts. I don’t know what it was. She said, “Oh, that’s your results.” At that time, I’m certainly thinking now she’s sliding me my results that it’s got to be negative.
My wife demanded that the urologist at least come and hand us the sheet of paper himself. The lady at the front desk walked away, came back, and she said, “Okay, the urologist said he’ll see you in a moment.”
We sit in the lobby for about 15 to 20 minutes. A nurse came and got us, took us to a waiting room, and we waited there for about 10 more minutes. Then he walked in. It was me, my wife, and my daughters were with us too. We were all together so we were all in the room. My daughters were younger. They were playing at our feet. They were in their own little world.
He came in, he’s talking, and I don’t know if it was so traumatic that my mind just deleted it because I completely never heard him say it. One reason I knew he must have said something bad was because my wife was crying.
I looked at her. “What did I miss? Can you repeat what you just said?” He said, “Yes, you have stage one prostate cancer.” My immediate reaction to him was, “Wow. You knew that I had prostate cancer and you were going to let me take that sheet of paper home and figure that out on my own?”
I knew right then that on this journey, that wouldn’t be my urologist. He was very embarrassed. He was trying to explain it away. “I see so many patients every day and right before I came in here with you, I was seeing another patient and he was crying on the floor.” It’s terrible.
It’s amazing to this day, it just is… wow. I didn’t pay that co-pay.
‘Wow. You knew that I had prostate cancer and you were going to let me take that sheet of paper home and figure that out on my own?’
Looking for a new doctor
I came home that night [and] called my primary care because she’s the one that referred me to him. I said, “Hey, this is not going to work. I have cancer.” She referred me to a new urologist.
I think I’m [savvier] in that space because I’ve been going to the doctor so I immediately know I’m not going to be able to work with this urologist. I’m also going to make sure I file a complaint with the Board of Urology. Certainly people in my community, they’re not going to know those types of things. Some people in my community would actually still stay with that doctor just because they feel like I don’t have any choice.
I left that urologist. He’s in the rearview mirror. Met with the new urologist. My wife came with me. He was in a little rolling chair. He rolled it right up in my face and he’s talking to me, looking at me right in the eye. He’s just talking to me. The energy was just so tense. He needed to leave the room to get some paperwork and as soon as he walked out, my wife and I looked at each other. “That’s him.”
Treatment
Radical prostatectomy
I was diagnosed in November and I had surgery in June. When I was initially diagnosed, I was told it was stage one by that first urologist. Then after surgery, I was told that it was stage two so it could be one of two things. It could be that I was misdiagnosed at first or it could be that it just progressed during that time. What I’ve learned about the disease since then [is that] it’s plausible that it could have actually just progressed during that six-month period.
My team of urologists had actually advised me [that] because [of] my health and all these different factors, they wanted me to do it within a year from diagnosis. I chose to do it in six months. I probably could have done it sooner but that was during the summer, I was off from work, and that was the reason I chose to do June.
I could have done it later. I’m glad I did it but my urologist told me, “You’ll be fine. We don’t suspect that it’ll escape the prostate in this time and metastasize.” That’s why it wasn’t a real urgency to do it December or January because I was told that as long as I do it within a year, I’m good.
Deciding when to do the surgery
I’ve heard of many men who also found out they had it and they just waited even longer. They just didn’t want to confront it.
Do I want to lose my prostate? No. But I know that I have this disease and I want to get it out as soon as possible. I could have done it sooner. I just chose to wait until June specifically because I know I was going to be off. I wouldn’t have to use vacation time.
If I worked all year and didn’t have that as an option, I would have gotten it done soon.
Make sure you have people there to support you because that does help.
I don’t know if sometimes when things are just so traumatic or stressful, my mind doesn’t allow me to be as rattled as I probably could be. It’s not like I was going in there happy. I had my family with me. I felt comfortable. My parents were there. My brothers came. Everybody who I love was there so that helped a lot.
Make sure you have people, who you care about, there to support you because that does help. When I opened my eyes and saw those people around me, that did help because I knew I had a long journey ahead. They told me that I woke up cracking jokes.
The day of surgery wasn’t really stressful. It felt like everything moved fast. I had to go the day before to do registration. I remember my wife and my youngest daughter were out of town on a Girl Scout trip and they were coming back that night. My mother-in-law actually took me.
I remember getting there that morning. My daughters were with me and we were laughing. One of my best friends came into town [with] his wife from Houston and they were cracking jokes. My dad came.
Right up until the time when they told me we’re going back to surgery, I remember just laughing with my family. I know I was nervous but I just have to stay in that space.
Even before surgery, I just knew it was going to be a success because I knew, without a shadow of a doubt, I was in good hands.
Preparing for surgery
They really did a fantastic job preparing me. Up until the day of surgery, I had learned so much through them.
[During] the period between diagnosis and surgery, I connected with Us TOO, which is an organization for prostate cancer survivors, and they have a chapter in Austin. I learned a lot through them as well.
I felt so comfortable and I think that goes into the comfort level with your doctor or your HCP because I just had no doubt. Even before surgery, I just knew it was going to be a success because I knew, without a shadow of a doubt, I was in good hands.
I feel that changes the trajectory of the healthcare experience when the patient has that real, authentic connection with any doctor that they have to deal with.
Knowing you’re in good hands
I’m an intuitive person. I got my college degree in communications. I’m all about how we engage and how we deal with one another.
From the minute I met that second urologist, it was so evident that he was on my side. It almost felt like I was his only patient if I could just explain it that way, honestly. I felt like he didn’t have any other patients to see after me. I didn’t feel like he saw anyone before me. I didn’t get that feeling of next, next, next. Never. He seemed like his calendar was just open, like he didn’t have [anything] pressing. He was just really locked in and listening to me.
All of that really helped. I feel that changes the trajectory of the healthcare experience when the patient has that real, authentic connection with any doctor that they have to deal with.
Certainly in my culture, there’s nervousness there. It just comes from so many years of mistrust so more doctors need to be intentional about how they engage all patients but certainly patients who look like me because we know we need to get over that hill of mistrust. I just think that Dr. Giesler — who is my urologist, who I love and I talk to him to this day — did that so well.
I know a patient who actually feels like they never had prostate cancer. They feel they were being used as a project. I’m sure they did [have prostate cancer], but they feel this way and it’s primarily because they don’t trust the doctor. Stop the mistrust.
We know that that’s a real thing, like Tuskegee. In a lot of men’s minds, they still feel that that holds true today. I’m not here to say whether it does or doesn’t; I don’t believe it does.
My point with this patient is I’m pretty sure that the reason he feels this way is because he has a severe mistrust of his urologist and the team. I often wonder if he did have a trusting relationship with them, would that change how he felt? Would he still feel that he didn’t have prostate cancer? I’ve never heard someone say that and because I know that he has that mistrust, I’m pretty sure that’s what makes him feel that way.
If you do have cancer or anything else, it’s always better to know earlier than not.
Recovering from surgery
After surgery, I had to wear the catheter for seven days. For me, the catheter was the worst part. It wasn’t fun. Everything else, I could deal with. The catheter was terrible.
On the seventh day, I had to get the catheter taken out. I’m pretty sure it has a lot to do with the fact that I’m healthy and I’m younger. But when the catheter was taken out, I was at my daughter’s softball event that same day. Now, that’s not to say that I was just ready to go sail the seven seas but I was able to attend that. I had a little donut pillow that my wife bought me and I was sitting on that. I was able to walk from the car.
The catheter was the worst. It’s just so bad. They gave me two different bags. One bag I would wear when I’m at home, overnight when I’m asleep. Then another bag, I could be more mobile. It was attached to my leg.
I don’t think there’s anything that helped. I was just ready to get the thing off. All of the rest of it, it’s fine. But the catheter was not my favorite part.
I was back at work I would say six weeks. Maybe seven.
Every patient story is different. I’ve talked to other black men, patients who were maybe three or four years older than me and maybe weigh a little bit more, [and] their outcomes were a little bit different. I go days without remembering that I had prostate cancer. Everything functions on me the way it did. I don’t have issues with incontinence. I’ve never had to wear a diaper. None of those things.
I’m telling you all the positives about my specific scenario just to motivate you to go get checked because if you do have cancer or anything else, it’s always better to know earlier than not. We just have to get away from assuming that we can just ignore it and that it’s just going to resolve itself because that’s not the case.
You can still have an amazing life (wink, wink) after a diagnosis or after surgery. I’ve been disease-free since June of 2019 and I’ve never felt better.
It’s key that we talk about it in families. As a prostate cancer patient or survivor, I make sure everyone in my family knows that I have prostate cancer.
Prostate cancer awareness
If family health history have been discussed, then I would have known about prostate cancer. As a man, because I was going to the doctor, I could have just added that into the conversation.
My doctor visits, when health history is brought up, just like I was aware of my aunt having breast cancer and my grandmother having breast cancer stage four and I share that with the doctor, I could’ve also shared the prostate cancer.
It’s key that we talk about it in families. As a prostate cancer patient or survivor, I make sure everyone in my family knows that I have prostate cancer.
As a black man, as a prostate cancer survivor, I’m just here to tell men everywhere — but certainly, men who look like me — that doctors are here to help us.
I have a twin brother and an older brother who have still not gone to the doctor. I speak out for them. My brothers know I had prostate cancer and they came to my surgery. They know now that our uncle had it. My twin knows that because we’re genetically the same, that makes him at an even higher risk but yet they still haven’t gone.
I had people ask me before, “Why do you think that? Why do you think it is that men don’t wanna go to the doctor?”
When I think about it, the only word I can think of is fear. It could be a fear of the unknown or just don’t want to be poked and prodded. I don’t want people asking me personal questions. I don’t want to have anyone in my intimate space like that. It’s all these factors. Meanwhile, there are questions lingering with your health that go undealt with because of the fact that this fear continues to keep you frozen.
As a black man, as a prostate cancer survivor, I’m just here to tell men everywhere — but certainly, men who look like me — that doctors are here to help us. They are. If you go to a doctor and you don’t like the way they make you feel, I want you to know that you have every right to find another doctor. You shouldn’t have to go to a doctor that doesn’t make you feel comfortable.
It’s okay to speak up when you’re in doctor’s visits if you feel that the doctor is not meeting your needs and meeting you where you are. You need to know that you can certainly speak up and make the doctor aware of that.
If the doctor is still not being intentional about meeting your needs, you have every right to seek out another doctor. That’s something I really want to make sure that I hammer home because a lot of people don’t realize that as the patient, we actually have the power. We have more power than we think we do.
Let’s not be afraid to advocate for ourselves in the healthcare space and to speak up and ask questions so that we can change the narrative.
I used to go to doctor’s visits with my grandmother and the doctor would say something and I’d ask my grandmother, “Are you okay with it?” “Yeah, it’s fine, it’s fine. The doctor said it then that’s what it is.” I’m like, “But are you okay with it?” There’s just this thinking that the doctor knows it all. I don’t know anything.
I’m here to tell you no. You’re there to educate the doctor on who you are. I always say you have to teach people how to treat you and the same applies when you’re with doctors. Let’s not be afraid to advocate for ourselves in the healthcare space, speak up, and ask questions so that we can change the narrative.
If you go to a doctor and you don’t like the way they make you feel, you have every right to find another doctor. You shouldn’t have to go to a doctor that doesn’t make you feel comfortable.
How to address the fear
Two things. First, more unconscious bias training so that doctors and healthcare providers have the tools and know how to engage the black patient.
On the patient side, this is something that needs to be talked about in church meetings, fraternity meetings, in places where black people feel most comfortable because that’s going to essentially be what’s going to get them there. They also need to be hearing it from actual patients, actual black men who who who went through this, who are survivors and can speak to what it might look like in terms of the journey and speaks to the point of early detection.
Once we can get them there, we need to be assured that doctors are going to know how to engage them. It’s not just to start. It’s to stay.
You have to be very calculated. [If they feel like it’s falling on deaf ears again], it might even be worse. “Oh, you got me here and now, see? This is why I don’t even go to the doctor.” Then you will never hardly be able to get them to go after that. This is a combined effort for sure.
This needs to be talked about in places where black people feel most comfortable because that’s going to essentially be what’s going to get them there.
Engaging black patients in a better way
Understanding how we communicate and that connection is critical. Perhaps walking into the room with a black patient and choosing to just talk about regular things. I am not cancer.
I’m only speaking for black people because I’m a black person. We want that because that’s going to be the best way to help us feel comfortable. There is this cloud looming over healthcare when it comes to how black people perceive any capacity of healthcare. The HCPs and people on that side must be vigilant and diligent about making sure to flip that in their daily interactions when they’re meeting with patients.
That’s not just going to happen overnight that’s why training is so important because some doctors need to be trained [on] how to do this. When it comes to tactical recommendations, how would that look? Maybe pamphlets that are provided to HCPs so that they understand, little tips and tricks, and ways to engage the black community.
Getting them there is half the battle but keeping them there is probably the bigger part. “I like those shoes!”“Wow! I like your hair.” A rule of thumb is to treat patients like they’re your parents or your family members even if clearly we’re not of the same culture. Most black people in that healthcare space, we’re tense. We’re uptight. We don’t know what to expect.
My situation is a little bit different because I’ve been going to doctors longer but I’m always wondering. Is it going to be a good experience? Is the doctor going to treat me like a person or like a patient? Yes, we’re going to be a patient but we want to be treated like people. I think that goes for all of us.
When the doctor feels that this needs to be stated, [if] there’s still a little bit of a disconnect, it’s even okay to say, “Listen I know you may have had bad experiences before but not here.” Declaring that [and] then following through in your actions. That can be enough, honestly.
A lot of doctors might take it personally because they feel, “That’s not me.” Most people realize it’s probably not you. It’s the system but this is how you could separate yourself from the system and say, “You’re here with me now. I’m going to take care of you. I don’t know what happened to you previously but you won’t have that here.”
While Tuskegee did happen, we must do our part in ensuring that it doesn’t happen again and the best way to do that is to show up.
Information on and access to clinical trials
I knew what clinical trials were but I didn’t know how [they] all worked. I wasn’t up to date on all the particulars. I knew in general but there needs to be so much more work done in terms of educating the black community on clinical trials and providing access because they don’t even know.
There are so many clinical trials. You can go to clinicaltrials.gov and they’ll show you. But so many people don’t know that. I only learned that rather recently. You can just log on to clinicaltrials.gov, look through the list, and see what’s upcoming, what’s done, [and] what’s still open presently.
Providing access [and] making people aware that that website exists because, like many other things, it makes the black community feel like we’re being purposely left out of these clinical trials.
Efficacy comes into play because we haven’t been included in these. We might be taking the drug and then it doesn’t react the right way because we don’t have any data to show that that would happen.
I want black men and men in general to know that they can be an advocate for themselves. You have a voice because at the end of the day, you are the patient.
Clinical trial, that’s a big buzzword right now. There is a push to try because so much more awareness is being shed on prostate cancer that we may be moving the needle forward in that area.
I would say certainly at the HCP level, in the doctor’s offices, and [in] advertisements… “Did you know that clinical trials are available?” Providing the website so that people can look through that on their own.
I just think so many people don’t know that clinical trials are available and that black people can participate in them. It’s important that we have a seat at that table so that we are able to do our part in the research phase of these different medicines to show how they can help our community.
As a prostate cancer patient, as a black person, I would just tell black people in the community that, yes, Tuskegee definitely did happen. We honor that. But it’s important to know what clinical trials are, to understand how beneficial they are, and to know that that’s not a likelihood now. We’ve done so much better in terms of education and awareness. While Tuskegee did happen, we must do our part in ensuring that it doesn’t happen again and the best way to do that is to show up.
Early detection is the way you can ensure that you have the best quality of life. If my cancer wasn’t found as early as it was, my reality wouldn’t be what it is now.
Being an educator in a different space
When I was diagnosed in 2018, I could have never imagined that I’d be doing this work professionally. I’m meeting with doctors, talking to doctors, and working to spread awareness on a national level and that’s just a feeling that I can’t explain.
I’m able to transfer my skills into this space, having been a teacher for so many years and still actually teaching in higher ed. It feels good to merge my passions with my skills, to do this work, and to be alive and well enough to do it.
At the end of the day, the best thing you can do for yourself is to go to the doctor.
Words of advice
I wasn’t able to go in and advocate for prostate cancer necessarily. I did go to the doctor annually. Had I known about prostate cancer, I am sure that I would have.
At the end of the day, the best thing you can do for yourself is to go to the doctor. You have reasons to be around, whatever they are, whether it’s family or kids, or job. You have a reason to live and you have a reason to live your best life.
Early detection is the way you can ensure that you have the best quality of life. I know that if my cancer wasn’t found as early as it was, my reality wouldn’t be what it is now. I go many days without even realizing that I have prostate cancer and I think that’s just a testament to early detection, certainly because the cancer was able to be contained.
Early detection starts with going to the doctor. You’ve got to go to the doctor. You’ve got to move past those feelings of not being comfortable at doctor’s offices.
No one knows you better than you do so your best bet is to go to the doctor and speak up. If you feel something’s going on, then make sure you tell the doctor about it. But even if you don’t, I would advise all men. Nothing wrong with going in and requesting a PSA test.
Self-advocacy
For me, [the doctor] is going to have to be somebody that gets to know me in an intimate way. I want to feel comfortable with him. That goes along with why I speak out too. I want black men, and men in general, to know that they can be an advocate for themselves, that it’s okay. You can say, “No, I don’t agree with this.” You have a voice because, at the end of the day, you are the patient. That’s pretty much the story with the way I was diagnosed.
Black men are twice as likely to be diagnosed and 2.5 times likely to die. The disease presents itself in more aggressive ways and it remains silent in its earlier stages.
Importance of early screening
I was 37 [when I got diagnosed]. The truth is most doctors aren’t going to be screening for this until you’re 40. I tell men that are about my age that I run into. You can tell the doctor that you would like to have this blood test.
In all cases, if there’s a family history, you should certainly be getting screened. That’s why it’s so important to talk about things because if you don’t, then you’re not going to even know the history to be able to advocate.
Black men are twice as likely to be diagnosed and 2.5 times likely to die from the disease so just being a black man makes it much more important that you get this checked. In black men, the disease presents itself in more aggressive ways and it remains silent in its earlier stages.
For all those reasons, you need to go to the doctor. If you’re not 40, I would say still go to the doctor.
Another real barrier is this macho thing about the whole DRE, the digital rectal exam. First of all, if you have to get that done, you just need to do it. It’s for your life. With advances in technology, that’s not the first option now. The first option is the blood test and obviously, if the blood test reveals something, then that will be probably the next step. I try to make sure men know that because it seems minor, it seems trivial, but I promise you that a lot of men won’t go to the doctor for that reason. I’ve heard that so many times.
God wants you to depend on Him but he wants you to depend on people he’s placed here to do the job as well. The best thing I can tell you is quite simple. Go to the doctor.
While I’m talking about prostate cancer specifically, the overarching message is you need to be going to the doctor because you can’t get screened unless you go to the doctor. You need to be going to the doctor to get a baseline in terms of your health in general.
As a man, you definitely should be getting your PSA checked. If the doctor doesn’t do it, you should be requesting it. Even if you’re not 40. You could be 30. I would still say get your PSA checked because at least you have a baseline. You can do surveillance. It helps you to be more mindful and to be more vigilant about your health.
I still had a part to play in it because I went to the doctor. It was a blessing that it was this particular doctor but still, the fact that I went, I was able to be discovered.
You’ve got to get there. You have to get to the doctor.
Always look for support. If you don’t have any family support in terms of prostate cancer, there [are] support groups [and] mentors that can be provided to you. In terms of health care in general, you can jump on Google, you can research support groups that might be specific to something you’re dealing with. My reality is prostate cancer but I want to really reiterate that health care is of the utmost importance.
If you’re going to get your general health up, make sure that you’re aware of the latest as it relates to your general health. If that includes realizing that they need to do surveillance with regard to prostate cancer or breast cancer, do what the doctors tell you to do. Please don’t ignore what they’re telling you.
If you’ve got the diagnosis, don’t ignore it. We’ve got to get away from that.
I grew up in a Christian household. I love God. I know God. But I also know that God put doctors here to help us. God wants you to depend on Him but he wants you to depend on people he’s placed here to do the job as well. The best thing I can tell you is quite simple. Go to the doctor.
No one knows you better than you do so your best bet is to go into the doctor and speak up. If you feel something’s going on, then make sure you tell the doctor about it.
When Joseph was diagnosed with prostate cancer, the news came as a shock and forced him to face questions about his health, future, and faith. He shares how he navigated his diagnosis, chose robotic surgery, and learned to open up to his loved ones about his health.
My Dad Was Diagnosed with Prostate Cancer. Now I’m Fighting It.
Dr. Leanne Burnham: A Caregiver, Patient, and a Doctor’s Journey
Motivated by her father’s prostate cancer journey, Dr. Leanne Burnham, scientist and community program coordinator at the City of Hope, dedicates her time and expertise so that communities of people of color could better understand prostate cancer and its specific risk factors.
Not only has Dr. Burnham been been a caregiver to both parents with cancer, she’s a lymphoma survivor, herself.
Her mission has been to raise more conscious and open conversations among families about their risks of cancer. That makes her a perfect fit in her department: Division of Health Equities at City of Hope.
Dr. Leanne Burnham is doing such amazing and inspiring work, not just in prostate cancer diagnosis and treatment clinical trials but also in patient self-advocacy, support, and other important socio-cultural factors around cancer. Explore our entire conversation below.
I am Leanne Burnham. I was born and raised in Akron, Ohio. Home of Lebron, we like to say. I live in California now. I am a wife and a mom of three. I have a 17-year-old, a 12-year-old and a 10-year-old.
I’m a scientist at the City of Hope, that’s what I do. I do experiments at the bench for sure. We call it at the bench when we’re in the lab, but I also do a lot of community work and work in clinical trials.
Prostate Cancer
What is prostate cancer?
There’s a lot to unpack. But first of all, women don’t have prostate, so it’s just a male disease.
Another thing that seems silly to say, but the prostate and the colon are two separate things. A lot of times people think they’ve had a colonoscopy means they’ve gotten their prostate checked. But that’s not the case.
According to the American Cancer Society, prostate cancer is one of those diseases with a 100% cure rate at five years if you catch it when the disease is still localized or confined in the prostate.
That’s amazing because not a lot of cancers are like that. Many people would hear, “Prostate cancer is one of the better cancers to get,” or they hear, “Prostate cancer happens to older men,” which is true.
It’s a disease of age, and there have been some studies that by the time men reach their 70s and 80s, many men, if not most, have prostate cancer at some point. But prostate cancer isn’t what ultimately kills a lot of men that have it.
For that reason, a lot of people tend to not get so stressed when they think about prostate cancer and their risk of it.
But it’s important to realize that the second you have prostate cancer cells escape out of the prostate and spread in the body, you go from a 100% cure rate in five years to there is no cure.
There’s no in-between, so all of the treatments we have once the cancer cells have escaped are to prolong life or improve quality of life.
We’ve got some really great treatments out there. We’ve got cutting-edge treatments nationwide that are really extending the lives of many patients, and they’re living great lives. But I’m at the City of Hope, so, of course, I’m partial.
It is also important to point out that, yes, prostate cancer is very curable, it happens a lot to older men, but that doesn’t mean it doesn’t happen in younger men.
It doesn’t mean that there are no aggressive forms in younger men. It certainly doesn’t mean that if you have prostate cancer, you’re just going to be cured and be fine because it’s not that way for everyone.
Diagnosing and Staging
First of all, you start with a PSA test. That’s testing your prostate-specific antigen, which is a protein secreted by the prostate. It’s circulating in your blood, so that’s one of the first markers they can test and say, “Hey, something is going on with your prostate. It might not be cancer, but something is going on.”
After a PSA test, men will get a biopsy, then they get a Gleason score. Pathologists look at the tumor under the microscope and assign a score based on how cancerous the cells are looking.
The higher your Gleason score, the more aggressive your cancer is.
There are genetic mutations that not everyone has access to, but some physicians provide that for their patients. Especially if they have a lot of family members that have had prostate cancer.
You can look at the genetics and see if there are some mutations that make the tumors more aggressive. What makes it hard to pinpoint treatments for prostate cancer, and to find a cure ultimately, is that prostate cancer tumors are very heterogeneous.
If you’re taking a sample from one part of the prostate and another sample from another part of the prostate and you’re looking under the microscope, they look different. There are different genetic mutational landscapes in those tumors.
Prostate cancer cells are very smart. Every cancer cell is smart. I’ve had cancer but I also have tremendous respect for the cancer cell, its ability to navigate its way and go undetected by the immune system, its ability to receive treatments and figure out ways to resist those treatments and form mutations.
The ability of resistant cells to keep growing is truly amazing. Cancer cells find a way, I tell you, but the key to its science is when they find a way, we have to tackle that new way.
It was totally unfamiliar to me. I don’t really have a family history of cancer at all. My dad was relatively young. He was like 50 at the time. He worked out a lot, he ate very well, he was going to Mustard Seed (organic grocery store) and things like this.
One day, he called me as I walk out of a physics class. I picked up the phone but he wasn’t talking; he was just crying.
I was like, “What in the world is happening?”
I just heard him crying on the phone, and he said, “I have prostate cancer. You’re the first person I’m telling. I haven’t told your sisters, so if you can come to the house when you get out of class and I’m going to talk to all of you guys. I’m just letting you know.”
At the time, I was a premed student, so he was reaching out to see if I had any advice, which I didn’t know about prostate cancer at all.
That experience really kicked off my passion for understanding what was going on with him. But beyond his diagnosis of prostate cancer, I started to notice that Black men in our community were getting that, as well.
It was just something I hadn’t noticed before, so I’m like, “Oh wow, this person at church has it. Oh wow, this person at the grocery store has it.” Different men were getting prostate cancer in their 40s and 50s. It was younger than what I would have thought.
So since I was a student and I had some shadowing opportunities and some research opportunities, I decided to get those hours at Cleveland Clinic, which is number one in urology in the nation, and that’s where my dad is a patient.
I went, and I was able to spend quite some time there. I was with a physician one time when he walked into a room with a Black patient with prostate cancer, and when he walked in the hallway with me, he said, “I hate these cases.”
He said, “Because every time I see a Black man in their 40s, or 50s with prostate cancer, it’s almost like it’s a different disease than other prostate cancers.” He was like, “You have to treat it so much more aggressively. It’s just a different ballgame.”
That’s when I thought, “Wow. I never had thought about it. Was there a difference in race and all that?”
From that point, when I went on to Loma Linda University to get my doctorate, I decided that I was going to focus my dissertation on prostate cancer and Black men specifically, and looking at reasons why their tumors might be more aggressive.
Prostate cancer in Black men
There are so many reasons why that is, and there’s been a lot of research that goes into looking at the multifactorial reasons behind that. We do know that Black men are much more likely to get prostate cancer.
Different numbers float around.
The American Cancer Society says that Black men are 76% more likely to be diagnosed. We do know that Black men are much more likely to be diagnosed at younger ages. When they show up to the clinic, they’re at a more advanced stage.
We also know that they are more than two times more likely to die from prostate cancer.
But what’s new on the forefront that we have found in the past five years doing clinical trials that include Black men is that when Black men are given cutting-edge treatments that are out, they actually respond better to treatments than men of other ethnicities, which is really exciting for any disease that you look at.
You can look at breast cancer, colon cancer, or others. If you have a certain demographic that is most high risk and doing the worse, if you can show that if you give them medications, they’ll do better, that’s a win-win for everybody at the end of the day.
Disproportionate risk to prostate cancer
Watching him go through his surgery and radiation and seeing his medications and things that he was on made me realize how private prostate cancer can be.
I really have never even talked to him about this, so dad, don’t get mad when you watch. I noticed some issues come up that maybe men would be embarrassed about. That was the first time I saw it with him.
Now that I’ve worked with hundreds of men with prostate cancer, that appears as a common theme.
Men are scared of certain treatments. They don’t want to have the side effects and don’t necessarily feel comfortable talking to people. They feel isolated sometimes.
That was the first time I saw my dad not be such a superhero. He became more human at that moment. Maybe he was embarrassed or nervous. I wasn’t used to seeing him like that.
DNA and genetic component
In terms of different reasons why he got prostate cancer younger, or Black men in general, for sure, there is a genetic component. I’ll start with the things you can’t change.
You can’t change your DNA. The reason that Black men in the United States specifically are at increased risk for aggressive prostate cancer is because their DNA happens to trace back to the DNA of West African men.
This makes sense because, in the history of the US, the transatlantic slave trade, Black people in the US came from the western portion of Africa. Not surprisingly, men in West Africa have very high rates of aggressive prostate cancer as well, so that DNA matches.
There are certain variations on certain chromosomes that we know that are more likely to occur in Black men than other ethnicities that makes them more likely to get aggressive prostate cancer.
Role of Vitamin D
In addition to that, my boss, Dr. Rick Kittles, the Director of the Division of Health Equity at the City of Hope and an internationally known geneticist and prostate cancer researcher, has shown for a decade that there’s a link between vitamin D deficiency and prostate cancer risk.
People may have heard about COVID going on, like, “If you’re vitamin D deficient and have COVID, that’s not a coincidence.” Vitamin D deficiency leads to a lot of pathogenic trends.
With prostate cancer specifically, we know that vitamin D deficiency leads to tumor aggressiveness. But how that relates to Black men is that our bodies make vitamin D from the sun, and our bodies are dependent on sunlight.
The more melanin you have in your skin, the less vitamin D your body can synthesize.
If you have darker skin, and then in our lifestyles now, we’re not outside in the sun as much as we used to be, we’re much more likely to be vitamin D deficient.
In the African-American population, about 70% are vitamin D deficient or insufficient. There’s a vitamin D link to prostate cancer as well, then we know that there’s diet and lifestyle, of course.
It’s always good to have a healthy diet, of course. But we’re doing studies at the City of Hope right now where we’re looking at the link between charred foods, like barbecue or grilled foods, and the ability of the consumption of that to contribute to more aggressive tumors.
Socioeconomic factors
There’s also socioeconomic status, which goes a lot of different ways. But first of all, it controls your access to healthcare that you have.
Of course, if you have better access to healthcare, you’re going to have earlier screening, maybe a better team of doctors who will treat your case with a precision medicine approach, and you’ll have access to newer cutting-edge treatments.
But the other part of socioeconomic status that we’ve really dived into in 2020, given our nation’s culture, is looking at discrimination, especially in healthcare and medicine and in science really.
We know that stress kills, literally. And there are studies out there, and I published on it, on how much cumulative stress somebody’s taken on over their lifetime. We know it occurs more often in Black people.
If you have that cumulative stress, it dysregulates your HPA axis. It dysregulates how much cortisol your body is making and how your body responds to that cortisol and looks at glucocorticoid receptors. But that’s real science; we don’t have to go all into that.
Comparing cancer cells in Black and white men
Basically, what I’ve shown previously is that when I treated Black prostate cancer cells that I was growing in the lab with cortisol and compared them to Caucasian cells. I had Black cells and I had White prostate cancer cells.
The Black cancer cells grew more aggressively, and they upregulated these genes in these proteins that made them more likely to resist therapy. You could have this cumulative stress that would dysregulate your stress hormone system, making you more likely to get cancer. Then once you do get cancer, it makes you less likely to respond well to treatment.
That’s a very interesting concept that’s being studied right now. There’s a lot of research dollars going into that nationwide. I’m not working on that anymore, but I can’t wait to see like the results that come out of that.
Ignoring the risk factors
This is something that infuriates me, for sure. I’ve also published on this.
First of all, in Southern California, where I live, we did a study looking at more than 400 men and found that with 54% of Black men, their doctors never even talked to them about prostate cancer screening. We have to start with that.
A lot of men are not even getting screened when they should. That is because prostate cancer screening recommendations for a while we’re saying, “Okay, screen every man at 50,” and then in 2012, the US Preventive Taskforce said, “We’re not screening men at 50 anymore.”
The problem is that it really hurt Black men, and that recommendation was based on studies that looked at 200,000 men that did not have prostate cancer.
They had done the PSA test to see if it was indicative that they would get prostate cancer in the future, but the studies say over 95% were men of European ancestry.
This recommendation is applied to everyone, but it didn’t consider a racial difference in prostate cancer risk.
The American Cancer Society and Prostate Cancer Foundation says that if you’re Black, and you’re 45, you need to get your PSA tested. If you’re Black, and you have family members that have prostate cancer, you need to get tested at 40.
This is the recommendation, and then you go to the doctor and your doctor says, ‘Actually, no, you don’t need to be screened.’ That’s a big problem.
That happens so many times. Of course, if you go to the doctor and the doctor says you don’t need to test, who would want to get the test? You’re just like, “Okay, I’m good. I don’t need to get the test.”
That’s the first thing. But then once you do get the test and you get your PSA results back, there are differences in how those numbers should translate based on race.
For a while, the number that men would look at is four nanograms per milliliter of your PSA. If it’s higher than four, then maybe you want to do some follow-up.
It’s actually 2.5 for Black men, according to the American Cancer Society. Dr. Rick Kittles has published that, actually. You can look at numbers of 1.5 in Black men and it can be predictive years down the road that it’s going to transform into prostate cancer.
A PSA of 14 is quite alarming and then by the time he was diagnosed, it was 64, as far as I can remember.
When you go to the doctor, and you have an elevated PSA, and a high Gleason, I can’t tell you how many times where I’ve had people reach out to me and they’ll say, “Hey, my Gleason score is seven and my doctor says that I should do watchful waiting.” I say, “Did they look at you? Do they know that you’re Black? Did they get the memo?”
It’s not a one-size-fits-all blanket approach sometimes. You really want to make sure that your physician, first of all, is referring you to a urologist. I would definitely say, go to a urologist at that point and have them help you make the decision and hopefully with somebody that’s well-versed in how this disease affects men differentially.
Watching out your genetics and mutations
You hear about BRCA mutations of breast cancer. Not surprisingly, if you have a high risk of breast cancer in your family, that also translates to prostate cancer.
They’re both hormonal cancers, but particularly, if you have BRCA mutations that run in families, we can treat patients with those mutations with PARP inhibitors. There are different kinds of PARP inhibitors that are in clinical trials right now. You’d have to check and see what’s available for you.
Oftentimes, we know that these mutations lead to more aggressive tumors. But sometimes, it’s like hitting the jackpot because then you have access to an additional line of therapy compared other patients that don’t have those mutations.
Genetic Testing
I think it would be individualized, and that the urologist would discuss with the patient their family history and just get a sense of how high their risk is. I don’t believe that it’s offered to everyone. Just because you want it, I’m not sure that you can necessarily get it or your insurance would cover it.
You could always pay for it out of pocket, but not everybody has that luxury. But if you have multiple family members that have prostate cancer, it is definitely something worth looking into.
Ongoing studies on PARP inhibitors
Dilemmas and decisions
I love working on clinical trials, because to me clinical trials, how I try to explain it to people, is like a VIP access to cutting-edge treatment.
Many people can be afraid of clinical trials because you might think that you’re going to be a guinea pig. There’s a lot of mistrust in clinical trials in the Black community, for sure. Number one, because of the Tuskegee syphilis experiment that was just a trial gone completely wrong for 40 years.
There’s a lot of mistrust about clinical trials and who’s funding it and who’s behind it, and if I will be a guinea pig or get a placebo.
A lot of people have an idea that they’re going to get a placebo when in actuality, if you participate in a clinical trial, you are either going to get standard of care, which is what’s offered in the clinic to anybody that have your particular disease, or have the option get the VIP treatment on top of the standard of care or in place of the standard of care.
The VIP drugs don’t get to that stage just like that. It’s years and years in the making so by the time it’s to that point, we, scientists and physicians, feel very confident that this is going to work.
Thus, it is important to point where it’s at in a clinical trial and that there are different phases of clinical trials too. There’s phase 1, phase 2, phase 3. Obviously, the later the phase, the more people have used that drug in that disease setting before. So you can decide if you want to do a phase 1 trial or feel better with a phase 2 or phase 3.
Stratified Clinical Trials
With clinical trials, they typically, in the past, have not included a lot of minority populations—Black, Latino, Asian, Native American, for sure. So it really does a disservice to everyone because you need to know how a drug would work in the context of different genetic variations.
One drug may work really well in one demographic, and it might not work as well in another, so we really try to accrue.
This means recruiting and enroll Black men in prostate cancer clinical trials, which makes sense because they’re more likely to get the disease and die younger.
It’s important to look at these new VIP cutting-edge drugs and Black men could really benefit from them. As I mentioned before, some recent trials enrolled a lot of Black men. We call it race stratified clinical trials.
There were a few studies where one was looking at hormone therapy, one was looking at chemotherapy, and one was looking at immunotherapy. In all three of them, the Black men that participated in the trial had longer survival than men of other races and ethnicities.
When we looked at that, scientists like me who do health disparities research were like, “Wow, that’s so encouraging.”
At the City of Hope, we have a team of scientists and physicians and clinical research nurses, and statisticians who come together and think about diseases and ways to help people who suffer the most from that disease.
Talazoparib clinical trial
Alongside Dr. Rick Kittles, Dr. Tanya Dorff, who’s the Director of the Genital Urinary Program there, and Dr. Zijie Sun, who’s another prostate cancer researcher, we designed a clinical trial to use a PARP inhibitor called talazoparib. It’s a newer-generation drug that Pfizer makes.
This trial is also sponsored by Prostate Cancer Foundation and we’re going to be using PARP inhibitors in a racially diverse group of patients so we are going to have a third of the patients be white men, a third of the patients be Black men, and a third of patients be Asian-American.
The Asian population is very heterogeneous, so I just hate to throw it all into one.
Many Asian-American men actually do better with prostate cancer than white men. Black men do the worst. So we want to see how this drug works in different races. But we’re not just picking races just to see; there has to be some sort of a scientific reason.
Racial Differences in Androgen and Androgen Receptors
The reasoning there is an interplay at the cellular level between PARP and androgen receptor. Androgen receptor has some variations that affect its function.
Androgen and androgen receptors are crucial for prostate cancer cells to grow. That’s why if you get prostate cancer, one of the treatments is hormone therapy because we want to block androgen and the androgen receptor.
There are racial differences due to genetics where different trinucleotide repeats that exist in the antigen receptor. There’s different links, so they’re shorter repeat links and there’s longer repeat links.
Asian men, not just American, tend to have longer repeats, and African-American men tend to have shorter repeats. The repeat length may affect the men’s response to this PARP inhibitor with the talazoparib. We’re going to see.
The study just kicked off this past month and we’re starting to accrue patients. It would be one more drug in the arsenal because as I said, this is going to be offered to patients who already have metastasis.
They can do different drugs that are out there, but this PARP inhibitor could be something that’s extra added to their hormone therapy, and that’s what we’re looking at. We’re looking at the Talazoparib specifically with Abiraterone acetate at this point in time.
Developing targeted therapy according to race
That’s something that we could check in the future. We could look at their androgen receptor, look at your trinucleotide repeats, then we could say, look, you’ll be a great candidate for this drug in the future beyond clinical trials.
But it’s not going to target the shorter. It’s the same with everyone. We think that there may be differences in response in the androgen receptor and the trinucleotide repeats within that receptor, within that gene. But we don’t know what to expect.
It may work well for everyone, but if there is a difference, we want to tease that out.
This is a two-year study, and we assess the study. You don’t just start the study and then just let it go and check at the end. You’re constantly tracking your progress as it goes, so we should have a good idea by the end of the year.
Building trust in clinical trials
That to me is the most important part of it.
In the past 20 years, there has not been an increase in the number of Black physicians accepted into medical school. That’s the problem. It’s not making it through medical school; it’s getting accepted into it.
A study came out of Oakland last year that showed how much better the outcomes were and how much more the diseases were addressed when Black people went to Black physicians.
We look at it in Black maternal death rates and infant mortality, and we know that just by the presence of a Black nurse or a Black physician in the room, the mortality rates go down, just by them being in the room.
That is a lot to unpack on why that is, but there is a trust factor when you have cultural competency in the room. Race doesn’t have to match all the time as long as your physician is culturally competent and sensitive to different communication styles and cultural contexts. It can work just fine, but we know that there are still many barriers, for sure.
When they go into the office, the patients feel the bias going both ways. There’s bias on the part of the patient, and then there’s bias on the part of physicians.
First of all, increasing the number of minority physicians, in general, would help. But what we like to do is to have a diverse team—diversity, in terms of race, gender, age, and occupation. We have physicians, nurses, scientists, and many of us who work within the Division of Health Equities at the City of Hope have personal ties to how we even got into this.
I got into this because of my dad, and so I’m speaking to Black men, and they’re saying:
“Oh, I feel fine. I don’t have any symptoms.”
“Really? Because my dad didn’t have any symptoms either.”
“Oh, I don’t know if I get that done. I’m not going to have a normal life.”
“My dad had that, and he’s doing great.”
That works on these teams who have personal ties, and so it comes across as more genuine, for sure.
We’re not just going to collect samples for research and just leave. We are there to help the men. We do actual prostate cancer screening in the community.
I know people freak out. We don’t do digital rectal exams in the community, but we do the blood tests, we provide the men their results and then we offer follow-up care and it’s not just at the City of Hope.
We partner with community clinics for men who may not have insurance or under-insured to make sure that they get that follow-up care, especially if their numbers are low enough that we think it could be caught early.
That’s really the goal of everything that we do. But, yes, the mistrust is a real thing and we try to tackle it that way.
Another way to really increase minority enrollment in clinical trials is just to provide access in communities of color.
Not everybody can travel to your main clinical trial center. I know at the City of Hope, we’re very fortunate to have community sites in Pasadena, Antelope Valley, or Santa Clarita, Pomona.
There are different locations to make it easier for patients to go from their neighborhood to a closer location to get treatment, which helps.
There’s financial incentives as well, and that can be controversial for sure.
Some of our trials offer them, and some of them don’t. But a lot of times, when you’re a cancer patient, getting to clinical trials is expensive. You and your caretaker have to call off work, you might have to get lodging, have transportation costs, and so a clinical trial can provide some financial incentive to help overcome that. It can really open the door for a lot of people.
Telemedicine as a tool
Telemedicine definitely has its pros and cons we’ve all learned during quarantine, for sure.
That translates to prostate cancer as well. If you don’t live close and have the technology and the app you need to communicate with your provider, it can give you access to perhaps more than you were exposed to before.
City of Hope Work in Communities
It’s our community-based prostate cancer program directed by Dr. Rick Kittles. I am lucky and blessed that he allows me to be the project coordinator for that. I work under him to recruit licensed phlebotomists. We recruit volunteers.
It is not hard to recruit volunteers because these events are the highlight of our week. They’re so fun. We get so much more out of these events.
Anything that we give back, we receive back in the energy of the individuals that we meet and we touch.
First of all, we provide education.
Let’s say we’re at a church. Usually, the pastor will let us get on stage for five minutes to say what we are doing and why it is important.
We know in the literature that, unfortunately, the men who are most at risk for aggressive prostate cancer don’t think that they are. So the first piece is letting people know they belong to the high-risk group.
Then a lot of men are afraid of the digital rectal exam. We let them know that it’s the PSA test now. You can get the DRE when you go to the doctor, but since 2017, you lead with the PSA.
A lot of times, when they find that out, they say, “Oh, okay. You don’t have to do that. Then I’ll do the blood test.” That’s the next part of it.
We also let them know that most of the time, with prostate cancer, you don’t have any symptoms. Men will be at Taste of Soul or the Long Beach Jazz Festival and are sitting there with their drinks and their cigars, and they’re, “I feel great. I feel great.” On the other hand, you might frequently be urinating at night.
We go into the communities, educate, interact, do the blood tests, and then follow up within two weeks. And we tell them, “Don’t freak out. That doesn’t mean you have prostate cancer. But either way, you just want to stay on top of your prostate health.”
We send every person an individualized letter. By individualized, it’s an official letter from the City of Hope. It gives them their PSA level. Based on their race and age, we translate to them what that means for them. Not everybody’s letter is going to look the same.
If they are at a younger age but they are showing a 2.5 or a 3 PSA, we’re like, “You really want to follow up and get this double-checked.” We follow up within two weeks.
If a man has very high PSA levels, we will call to make sure they got that letter. We tend to follow up after a few weeks for everyone who has elevated PSA, anyway, just to see, “What have you done with that?”
Many men find out and haven’t told anybody and they’re nervous to take the next step. So we help them with that.
Then we have social workers that help to navigate them getting to their next follow-up person. Whether it’s at the City of Hope, we would love to offer the different treatments that we have there.
But not everyone can travel that far, or maybe their insurance doesn’t allow them to. We partner with community clinics in the LA area where patients can go there as well.
Lessons from Community Work
I’ve learned how much people trust their doctor without knowing their personal risk. They trust their doctor knows their risk. It’s scary how often it doesn’t necessarily seem to be the case.
I’ll talk to men sometimes, and they’ll say, “Oh, I had that test done.” Then I’ll say, “You went and got the blood test?” They’ll say, “No.” Then I find out they’re talking about the colonoscopy. That’s one thing.
A lot of times, I hear, “I got all my blood work. My doctor does all my blood work every year.” Then I’ll say, “Well, did they include that in your blood work?”
A lot of times, it’s not included. They’re checking your blood sugar and your enzymes but not the PSA. Now that you have medicine apps on your phone, they’ll say, “No, I did it. My doctor ordered it.” They’ll pull it up. I say, “If you don’t mind, let’s look and see. What was your PSA?” Then it’s not in there, and then they’re like, “What? My doctor was not testing?”
It’s endearing how a lot of people do trust their doctor. Then it is sad to see sometimes they’re let down, but it’s like, “Now you have the tools. Now you email your doctor, and next time you’re in there, you let them know that you want to have this test, but actually, you don’t have to because we’re going to do the test now, and we’re going to give you a letter, and you can show your doctor.”
Hopes and prospects in prostate cancer research
I think we’re so close. When I got into this when my dad was sick, his doctor told him at that time, “Oh, you have a set amount of years.”
He’s passed that amount of years, and he’s doing well. We know he’s not curable still, but I hope to change that. When I got into this, I said, “I’m going to find a cure for my dad,” many people say. That’s the goal of a lot of scientists. They have a loved one, and that’s why they got into it in the first place.
I’m at a place at City of Hope where we have so many clinical trials, so many cutting-edge treatments, and we’re seeing patients that are really doing well. I just feel like we’re just at the cusp of it.
I’m just like, “Dad, hold on. Just hold on. We’re at the cusp of it.” I do think that it’s around the corner. I don’t think that it’s something that’s decades away. I think it’s sooner than we think and I’m really hoping that’s the case.
Being on both sides: Survivorship and cancer research
I was in science before I got cancer. My dad had cancer first. Then I was in science. But I was walking around with cancer for six months myself, and then I had to do chemo in the whole nine yards.
After that, it just completely changed my thought process and my approach. It changed my outlook on life, first of all. Everything I did became urgent. I don’t know if I’ll be here tomorrow. Everything is urgent.
One in two men is diagnosed with cancer, one in three women. I walk through life like, “Listen, it’s morbid as it sounds.” I’m like, “It’s not a matter of if you’re going to get cancer. It’s just like, ‘When? At what age?'” It’s just so common. We really need to get a handle on something, and I’m so glad we have so many scientists really dedicated to that cause.
It changed my outlook on life, and then it changed my outlook on scientific approaches. I used to sit in scientific meetings, and it’s like, ‘Oh, we can use this drug. Let’s try this and that.’
Sometimes I would open my mouth and say, ‘These are people. Imagine what all of those drugs are going to feel like.’
I know with my lymphoma, I had four chemo drugs at each session. That just was not fun. The idea of like, “You really want to be able to treat your patients with the least invasive method. You don’t want to go so hard on the pain all the time. You want to find something that works, but it’s not so toxic to the patient.”
Then I also think I know what it’s like to walk around with cancer and not know that you have it. You think it could be anything else, and that applies to a lot of people.
When I’m out in the community and people will say, “Oh, I don’t feel like I have cancer.” Sometimes you don’t feel like it, but sometimes you get used to those nagging little symptoms that have formed over a few weeks or a few months. You never want to go off of how you feel when it comes to screenings.
Another thing, because I’m a cancer survivor, I have to go to my oncologist. But that’s always so weird to me. I’m in the lab and working in the hospital then, “Oh, it’s now my turn to go to the oncologist.” It’s just always weird.
When I went, they said, “Listen, we want to do a colonoscopy on you.” I was young. I wasn’t 40 yet. I’m like, “Fine. Another test.” So I did it. When I woke up, they said, “You know what? We found several pre-cancerous polyps.” I was like, “What?”
I was so happy that I did that colonoscopy that young. If I hadn’t had lymphoma, they wouldn’t have thought to do it that young. Now I know. I don’t wait as long as other people. Now I’ll be referred for a colonoscopy much more frequently than anybody else.
Don’t put off symptoms. If your doctor thinks that you have a reason to be screened for something, don’t be afraid because trust me, you want to be diagnosed at an earlier stage and save yourself some of the hassles, please.
Especially with prostate cancer because it’s curable if you catch it early. That’s literally life or death. You want to screen for that sooner rather than later.
Approaching conversations on cancer risks
I try not to freak out on him all the time. He’s 17 so it’s like, “Oh, everything’s fine.”
Just the other day, he texted me and said, “Oh mom, I’m having an allergic reaction to like 30 things.” Then I responded, “Oh my gosh, what are your symptoms?” Then he didn’t respond. Then I’m calling his girlfriend, calling every everybody to see, “Is he gone into anaphylactic shock?” I just assumed the worst all the time.
He’s used to, “Oh, mom’s just freaking out,” but I look at every symptom as like, “Oh my goodness.” He did have some swollen lymph nodes at one point. I thought it’s lymphoma because it’s hereditary. But it was not the case.
I don’t really talk to him because I take action. We’re going to see what happens when he becomes an adult and has to make decisions independently.
At that point, he knew his grandfather, who’s my dad. He was like, “Oh, well, he has cancer, and he’s okay.” I don’t know if he thought, “Oh, she has cancer. She’ll be okay.”
He saw my hair fall out and he saw me being sick and tired from the chemo all the time, and he seemed okay.
On my final PET scan, the day that I found out that there was no evidence of disease, I sat him on the couch, and I showed him the picture. Because at that point, my son is a little nerd like me, so he knew like, “Oh my mom. I’ve seen her cancer cells. There’s two nuclei instead of one.” He knew what the cancer cell looked like.
I said, “Let me show you the PET scan. This one, this is the before, and this is the after.” He said, “[gasps] there’s nothing there.” I said, “Yes.”
His shoulders just dropped. It’s like he sighed. I didn’t realize, in that moment, that he had been walking around like this for months.
I saw it, and I was like, “Oh my gosh. It’s the little boy Beck that I remember that’s worried for you.” I don’t think he worries about it anymore right now. It doesn’t seem like it. That’s going to be something interesting to navigate as he will not be missing any screenings.
Normalize these conversations
It’s super important. I hope it changes with younger generations because my sister-in-law just beat triple-negative breast cancer last year during COVID, and she’s only 40, the same age as me.
When she was asked about family history, it was difficult to think who had what cancer? I know it’s the same with me. People died, and you don’t really know what they died of.
I hope that really changes moving forward and we become more open to sharing. I know in my family and my husband’s family, prostate cancer is not limited to one person. It’s rampant. The more you talk about it, the more you normalize it.
It’s difficult because a lot of older generations may have had prostate cancer, treatments are not the same as they were then. Maybe you hear horror stories, and then the younger guys are like, “Oh, I really don’t want to do it.”
We really try to stress that the testing is different, the treatments are different, the outcomes are different. The side effects after the treatments are different because things are improving. It is important to talk about it as a family to know that your individual risks are based on your family members.
Patient Self-Advocacy
I am just so grateful that Al Roker shared his story like that. A lot of people know him, and they’re going to think, “Wow. He had this, and he’s doing well. I can get a screening for this. If I get that diagnosis, it’s not the end of the world. I can come through it on the other side.”
It’s important, and I recognize that importance. When we’re out in the community, I recognize my limitation. I’m a woman. I don’t have a prostate.
I can talk, turn blue in the face, but it’s not a one-person job. I make sure I show up with people who have been previous patients because men want to see somebody they can relate to that has been through and come out on the other side.
I really think support groups are a great thing as well for men who have been diagnosed with prostate cancer. Just seeing men talk about it and be open about it definitely helps with anything in life, for sure.
We see it with the COVID vaccine now, too.
One person in the family gets it, you talk about it, now the cousins get it. I was the first person in my family. Now everybody’s gotten it. But it’s taken weeks and weeks to get to that point. That’s an example of you just talk about it and then it normalizes it for everybody else.
Message to Black men cancer community
Well, that’s something I hear in the community a lot too. Men will say, “Oh, I don’t want to have this treatment because I’m afraid that I won’t be able to have sex anymore.” That is true for a lot of different treatments.
One thing I tell men, it’s funny, but it’s not, but I’ll say, “Listen, if you don’t treat it at all, you won’t be able to have sex anyway, and you’re definitely not going to have sex when you’re six feet underground. It’s just not going to happen.” I make sure that they know that, but that’s just more on the joking side.
There are nerve-sparing surgeries offered now where results are not the same as they were 10 years ago. Your chances of regaining that function are so much better. Al Roker spoke about how he was able to regain that function. So don’t let that hinder you.
At the same time, I’ve been a patient, and I firmly believe that it’s the patient’s choice. Some patients decide, “I don’t want to do any treatment.” It’s their life, and that’s totally fine.
I’ll never forget when I spoke to a man who had a very elevated PSA and a Gleason of 9, and he was like, “I don’t want to have anything done.”
He was in a support group, and other men—it was a room of all black men —were telling him, “Oh, I had this treatment, and I had that treatment,” and at the end of the day, he was like, “I just would rather just see what happens, and I’m just going to live with my decision.”
You just have to respect that at the end of the day. I don’t know if I could have done that before I was a patient myself.
That is an example of you just wanting somebody to be able to make an informed and educated decision.
If you know all that and that’s what you want to do, do you boo. Because you’re going to have to live with that. You should be allowed to make your own choice.
When Joseph was diagnosed with prostate cancer, the news came as a shock and forced him to face questions about his health, future, and faith. He shares how he navigated his diagnosis, chose robotic surgery, and learned to open up to his loved ones about his health.
Role: Center Director Urologic Oncology Focus: Urological oncology, including kidney, prostate, bladder cancers Provider: Cleveland Clinic
...
Dr. Babis Andreadis of UCSF shares his approach with patients, the importance of patient self-advocacy, whether to ask for a second opinion, and more on shared treatment decision-making...
Oncologist: Specializing in breast cancer | HER2, Estrogen+, Triple Negative, Lumpectomy vs. Mastectomy Experience: 30+ years Institution: Stanford Medical
...
Role: Radiation oncologist Focus: Specializing in radiation therapy treatment for all cancers | Brachytherapy, External Beam Radiation Treatment, IMRT Provider: Salinas Valley Memorial Health
...