Comprehensive Biomarker Testing
in Non-Small Cell Lung Cancer
Getting the Right Tests Can Help Find Your Cancer’s Weakness
If you or someone you love has been diagnosed with non-small cell lung cancer (NSCLC), you’ve likely heard the phrase ‘biomarker testing’ and the need to wait for results. This wait can feel unbearable, but the science is clear: knowing what is driving your specific cancer before you start treatment can change everything about the care you receive.
This program will explain why comprehensive biomarker testing is the foundation of the right treatment plan.
Program Topics
- What biomarker testing is and why it’s not inherited genetic testing.
- Why waiting for test results leads to better outcomes.
- Tissue vs. liquid biopsy: when and why both are needed.
- Common NSCLC biomarkers (EGFR, ALK, KRAS, ROS1, MET, PD-L1) and their treatment meaning.
- How targeted therapy, immunotherapy, and chemotherapy differ, and when to use each.
- What cancer progression means and why retesting is essential.
- How to advocate for yourself and be an active partner in your care.
Program Panel
Program Partner
EGFR Resisters is a grassroots patient-driven community dedicated exclusively to changing EGFR-positive lung cancer into a manageable chronic disease. Their community of survivors and caregivers shares knowledge and connects with others who are experiencing similar journeys. Find your community.
Program Sponsors

Thank you to our sponsors for their support of our independent patient education program. The Patient Story retains full editorial control over all content.
This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.


- Introduction
- What is biomarker testing and why does it matter?
- Waiting for biomarker results can help you live longer
- Tissue biopsy vs. liquid biopsy: Two tests, one strategy
- What “comprehensive” really means: Next-generation sequencing (NGS) and why one test isn’t enough
- Common biomarkers in NSCLC: Starting with EGFR and ALK
- Targeted therapy vs. chemotherapy: How they work differently
- Beyond EGFR: KRAS, ROS1, BRAF, RET, NTRK, and why rare still matters
- Protein markers and immunotherapy: A different kind of test
- MET: The most complex biomarker in lung cancer
- When treatment stops working: Understanding progression and resistance
- Does progression always mean changing treatments?
- With progression, what type of biomarker retesting do I need?
- Quality of life matters: What treatment looks like day to day
- Advocating for comprehensive biomarker testing: When to seek a second opinion
- Key takeaways: What to remember
- Conclusion
- Hear from people living with lung cancer
Edited by: Katrina Villareal
Introduction

Stephanie Chuang: Welcome to “Comprehensive Biomarker Testing in Non-Small Cell Lung Cancer.” We want to cover why this is important. Why do we need to find out more information about each person’s disease? Why does it matter? We have two incredible experts joining us to talk about that at The Patient Story, a multi-channel platform that I started when I was going through my cancer diagnosis.
At the time, I felt very alone. I wanted to understand, in human terms, not medical jargon, how to navigate life after diagnosis. We specialize in in-depth patient stories and informative discussions to connect you to each other and to information that’s useful when and where you need it.
We want to thank our sponsors for this program, AbbVie and Nuvation Bio, for their support of our educational content, which allows us to build more of this programming for patients and care partners. It’s important to note that The Patient Story retains full editorial control over all content. Also, this is not medical advice, so it should not take the place of conversations with your healthcare team, but we do hope that you walk away with better information and questions to ask.
Finally, we want to know what you think, so we can host more programs and content in the ways and on the topics that you want.
With all that aside, I’m so excited to introduce our two experts. Jill Feldman became a lung cancer patient advocate after she lost her grandparents, her aunt, and her parents to lung cancer, before being diagnosed with lung cancer in 2009.
She co-founded the EGFR Resisters, a global patient-driven grassroots advocacy group dedicated to supporting people with EGFR-positive lung cancer, and she serves on multiple advocacy and advisory boards. She’s told her story many times at The Patient Story. Honestly, I am so in awe of Jill.
Also, I’m a big fan of Dr. Eric Singhi, a medical oncologist at UT MD Anderson in Texas. He specializes in lung cancer, focuses on biomarker-driven treatment strategies inclusive of targeted therapies, and has become a very well-known clinical researcher and patient advocate with a social media following of his own.
Dr. Singhi and Jill, I want to thank you so much for joining us.
Jill Feldman: Thank you, Stephanie. Hi, everyone. My name is Jill Feldman and I’m a lung cancer patient and long-time advocate. I know firsthand that when you hear that you have lung cancer, your world begins to spin. Everything becomes urgent. You want answers. You want a plan and you want it now. Then you’re told you need to wait at least two weeks for biomarker testing. And you think, “Wait? Really?” Because that is the last thing you want to do.
We’re going to talk about why the wait matters and how biomarker testing helps make sure that you get the right treatment and not the fastest one. This is not only about finding the right treatment, but it is also about avoiding the wrong treatment. I’m thrilled to be joined by my friend, the amazing Dr. Eric Singhi from UT MD Anderson.
Dr. Eric Singhi: Thanks, Jill. I’m excited to be here and to reunite and unpack conversations with you. I’m looking forward to this conversation.
Jill: Me too. You are great at educating patients, and I’m so thrilled that you could join us.
When I meet patients and their families for the first time, I tell them, ‘I don’t just want to treat lung cancer. I want to treat your lung cancer.’
Dr. Eric Singhi, Thoracic Medical Oncologist
What is biomarker testing and why does it matter?
Jill: Let’s start at the beginning. When people hear biomarker testing, most of the time, what’s said is mutation or genetic testing, so patients often think genetics, ancestry, or something that they pass down to their children. But that’s not what this is at all. Can you explain what we’re talking about when we say biomarker testing?
Dr. Singhi: This is a great question. Honestly, it’s probably one of the most important questions in lung cancer care. At its core, biomarker testing is trying to understand what is driving your particular cancer. When I meet patients and their families for the first time, I tell them, “I don’t just want to treat lung cancer. I want to treat your lung cancer,” and that’s important. It’s honestly a privilege being a medical oncologist focused on lung cancer because now, we have the opportunity to try and personalize treatments for patients by personalizing the biology and going against what’s driving the lung cancer to grow.
If you think about it, every cancer has a reason it’s growing and we’re trying to find that reason. In lung cancer, we call that a driver mutation. There are different analogies.

One is the lock-and-key analogy. If your cancer is a lock, the biomarker is the shape of that lock, and the treatment is going to be the key that opens it. If we don’t know the shape of the lock, we might use the wrong key, which means that the treatment may not work or, even worse, could be unnecessary. It could cause toxicity and then patients get into trouble without getting any benefit. That’s an overarching explanation of what biomarker testing means and why we do it.
Jill: I love that lock-and-key analogy because it’s very visual and very universal, so everyone can understand it. I want to emphasize that most of what we’re talking about are changes in the cancer itself and not something that you were born with, inherited, or could be passed down to children.
Dr. Singhi: When we’re talking about genetic testing in lung cancer, we’re only looking at biomarker changes in the tumor cells themselves. All the testing that we do upfront for lung cancer testing is only on those tumor cells. We’re not looking at genetic changes in all the other cells in your body. Those are the ones that may be inherited from parents. We’re looking at genetic changes in the tumors and not genetic changes in you, and that’s an important point to emphasize.
There are unique circumstances where, if patients are symptomatic, having trouble breathing, and the cancer is growing quickly and causing trouble, we have to start treatment.
Dr. Eric Singhi, Thoracic Medical Oncologist
Waiting for biomarker results can help you live longer
Jill: Let’s talk about timing because this is where patients feel the most stress. You’ve been told you have lung cancer. You’re scared. Maybe you’re experiencing symptoms. Then you’re told to wait for biomarker results. To be quite honest, for patients in general, all you can think is that your cancer is growing bigger and bigger every day. You wonder why you’re waiting. The wait is heavy and can feel unbearable. I still feel it every single time I wait for biomarker results. But it’s important. Eric, can you talk about why it’s so important to get the biomarker testing results before starting treatment?
Dr. Singhi: When I meet patients and their families, usually it’s another physician who tells them that they have cancer. Now you have to see an oncologist. By that point, they’ve been waiting a week or even longer to come see me. They’ve already started thinking about questions. They’re anxious to get started. I want to acknowledge and validate that feeling.
But Jill, you’re right. In the ideal world, it’s important, particularly for non-small cell lung cancer, to get those biomarker testing results before we start treatment. However, there are unique circumstances where, if patients are symptomatic, having trouble breathing, and the cancer is growing quickly and causing trouble, we have to start treatment. We will typically start with chemotherapy by itself while waiting for the biomarker testing results. I’ll tell patients, “These are some red flags we need to watch for while we’re waiting. If A, B, or C happens, call me, but you also need to go to your local emergency center. We may need to pivot into giving chemotherapy sooner rather than later.”
We have real-world studies. Evidence now tells us that patients who waited to get their biomarker testing results before starting treatment actually lived longer and did better. We have data to say that the wait is worth it because it impacts your clinical outcomes. It gives you the opportunity to get more benefit out of the treatment that we choose and hopefully less toxicity.
These tests are complementary. They are not competing. If a liquid biopsy comes back negative, it does not rule anything out.
Dr. Eric Singhi, Thoracic Medical Oncologist
Tissue biopsy vs. liquid biopsy: Two tests, one strategy
Jill: When it comes to testing, we have two main ways to test, right? We have tissue biopsy and liquid biopsy, and both have their strengths and limitations.
Dr. Singhi: We throw around this buzzword called comprehensive biomarker testing, which we as a community are still trying to define. The way I describe it is that comprehensive biomarker testing is not just one test. It’s actually a strategy.
Sometimes biomarker testing is not just one sample. It can be a tissue, but it can also be a liquid. Tissue biopsy is our gold standard. That’s where we get tissue of the tumor, either from the primary location or if it’s moved to another site. We’ll run some tests in the lab and get those results back in about two to three weeks.
But there’s also an opportunity for a more noninvasive test, which is what we call liquid biopsy, and that’s a blood test. That can typically give us answers faster and sometimes even give us a broader snapshot of what’s going on.
What’s important to emphasize is that these tests are complementary. They are not competing. If a liquid biopsy comes back negative, it does not rule anything out. You need to use both so you don’t miss anything important. If something comes back positive, we go with it. But if it’s negative, you can’t always go with it. You have to wait for the tissue biopsy.
Jill: When it isn’t explained to patients exactly why they need to have one or the other or have both, you don’t understand what’s going on. It’s okay to talk to your doctor and ask questions. Did anything come back on the liquid biopsy? Should I have a tissue biopsy? Are there times you may not be able to get enough tissue? Asking those questions is important.
What “comprehensive” really means: Next-generation sequencing (NGS) and why one test isn’t enough
Jill: A lot of times, comprehensive biomarker testing is referred to as next-generation sequencing (NGS). If you hear NGS, they’re talking about comprehensive biomarker testing. Eric, can you talk a little bit about the different testing?
Dr. Singhi: What comprehensive means in comprehensive biomarker testing is that we’re not just checking one or two genes. We’re doing broad panel testing. We’re looking across many possible biomarkers all at once. We look at different DNA tests, but also RNA tests. There are a lot of nuances to this, but the emphasis is that you don’t want to be looking at one or two genes. You want to be looking at many genes at one time and that’s a big emphasis of comprehensive testing.
If you just throw EGFR out there, that’s like giving the zip code. You need to know more than just the zip code.
Dr. Eric Singhi, Thoracic Medical Oncologist
Common biomarkers in NSCLC: Starting with EGFR and ALK
Jill: We’ve talked about how we test and when we test. Let’s look into what we’re actually looking for, some of the most common biomarkers, and why they matter. We’ll start with the ones that we’ve known for the longest, which are EGFR and ALK.
Dr. Singhi: I know EGFR is very near and dear to you, Jill, especially with your EGFR Resisters organization.
We discovered EGFR mutations in lung cancer in 2004, so we recently celebrated 20 years of understanding that mutation in lung cancer, what it meant for patients, and what it meant for their treatment and their outcomes.

I’ll start with EGFR. Not all EGFR mutations are the same and that’s important to note. If you just throw EGFR out there, that’s like giving the zip code. You need to know more than just the zip code. You want to know the home address. What that means is that there are very common EGFR mutations. The two most common ones are exon 19 deletion and L858R, which make up the majority of EGFR-positive lung cancer. The good news is that these mutations respond quite well to many of our standard therapies, whether by themselves or in combination with other drugs.
But then there are also less common mutations with EGFR, including exon 20 insertions, G719X, and S768I. They can behave differently. As a result, your treatment team may talk to you about different treatments that may be more effective in that circumstance and may even have a different tolerability.
Jill: Yeah, definitely, and that’s why it’s important to get comprehensive testing.
Targeted therapy works by going after a very specific weakness in the cancer. This goes back to the biomarker testing.
Dr. Eric Singhi, Thoracic Medical Oncologist
Targeted therapy vs. chemotherapy: How they work differently
Jill: Can you talk about how targeted therapies are different than what people think of as old-school chemotherapy? Before you explain that, I want to emphasize that there is a role for chemotherapy, especially in EGFR-positive lung cancer. It does work. It may not be the right first treatment always, but it does work and there is a role for it. Could you explain the difference?
Dr. Singhi: There are different buckets of treatments. Chemotherapy is what people traditionally think of when they hear cancer and think about treatments. It’s a drug that’s typically given through the vein, but sometimes orally. It’s non-selectively killing very fast-growing cells, which definitely includes cancer cells, but also other normal cells, such as your hair (which is why you can have hair loss) and cells that line your gut (which is why you can have nausea or diarrhea).
Targeted therapy works by going after a very specific weakness in the cancer. This goes back to the biomarker testing. We want to identify that weakness and that signal that’s causing the cancer to grow. Targeted therapy very precisely goes after that signal that’s causing the cancer to grow and shuts it down.
The good news is that since it’s very precise, the response rates usually can be very high. Hopefully, because it’s going directly after those cancer cells, the side effect profile is better than chemotherapy and typically better tolerated.
Both a mutation and a fusion drive cancer growth, but they’re found and treated in different ways.
Dr. Eric Singhi, Thoracic Medical Oncologist
Beyond EGFR: KRAS, ROS1, BRAF, RET, NTRK, and why rare still matters
Jill: KRAS used to be the undruggable target, even though KRAS has been around much longer than EGFR and is common. But there are also some not-so-common biomarkers, such as ROS1, BRAF, RET, and NTRK. Can you talk about those and why it’s important to find out?
Dr. Singhi: What you’re highlighting is important. Not all cancer changes are the same. Two common types that we look for are mutations or fusions. Mutations happen within a change in a single gene. Then there are fusions, which are less common but still important. The way I think about fusions is that two different genes get stuck together.
Both a mutation and a fusion drive cancer growth, but they’re found and treated in different ways. They’re found at different frequencies as well in the population.
KRAS makes up almost a quarter of patients’ mutations if they have a mutation in non-squamous, non-small cell lung cancer. It’s a pretty big chunk of almost 25%. One specific KRAS sub-mutation is KRAS G12C. That last letter is important because it tells you the exact subtype of KRAS mutation that may be driving the disease.
Currently, what we have approved are drugs specific to the KRAS G12C mutation, but there are a lot of exciting clinical trials trying to go after other KRAS mutations. We’re seeing promise and hope, so we’re continuing to focus on targets and finding drugs to match those targets.
If you find this clue that’s driving that cancer cell to grow, we can find a drug that works very effectively.
Dr. Eric Singhi, Thoracic Medical Oncologist
Jill: Yeah, that’s exciting. It shows that science wasn’t wrong at the time. It was undruggable. But as science evolves, you learn more and that’s important to keep in mind. It’s not always so concrete. Again, it emphasizes the importance of biomarker testing. When you get to ROS1, RET, BRAF, and NTRK, they’re very rare. You could be talking about a small percentage of the population, but why are they important to find as well?

Dr. Singhi: Several of the ones that you mentioned are fusions, like the ROS1 fusion, for example. You’re right; it’s not very common, but it’s still very meaningful and critically important to find, because when we do find them, we have approved, highly effective targeted therapies that are being studied in clinical trials. If you find this clue that’s driving that cancer cell to grow, we can find a drug that works very effectively.
It not only targets the primary tumor in the lung, but many of these tumors will also go to the brain, even at the time of diagnosis. When we initially stage a patient, we find disease in the brain. These drugs can work well and go through the blood-brain barrier. They can have an impact on the disease in the brain and can work well, be very precise, and work in different areas.
Jill: That’s something very important to emphasize as well. Waiting for biomarker testing before treatment also means before radiation therapy for brain metastases. Of course, there are circumstances where you have to, but these drugs work so well in the brain. I’ve known people who have had dozens of brain metastases, go on the drug, and they all go away. Again, this is another reason why it’s important to wait for biomarker testing results.
The definition of biomarkers continues to evolve… There are multiple ways to check for biomarkers.
Dr. Eric Singhi, Thoracic Medical Oncologist
Protein markers and immunotherapy: A different kind of test
Jill: Let’s shift a little. We talked about targeted therapy. Now we’re going to talk about protein markers, which are a different kind of biomarker, and why they are important. I’ll let the expert explain it because he can do a much better job than I can.
Dr. Singhi: I’m learning a lot from you, Jill. I love learning from my patients because it allows me to take conversations back and translate them into a way that they can understand. You become a true partner in their care. What I will add to what you’re saying is that the definition of biomarkers continues to evolve. We talked about NGS, looking at the DNA and RNA, which is looking at the cancer’s blueprint.
What you’re talking about now is looking for proteins that the cancer may be expressing. We do that through a different testing method called immunohistochemistry (IHC). There are multiple ways to check for biomarkers. When we get into the weeds, you can look at proteins, but you can also look at the cancer’s blueprint, and that’s looking at the genes. The proteins are now becoming very important to understand for the treatment of lung cancer.
Jill: As you talk about these different tests, I want to emphasize that protein testing is not a substitute for comprehensive biomarker testing. It’s a piece of the puzzle, but not the whole picture. What do the results from protein testing mean?
Dr. Singhi: I’ll give you an example of one that we’ve been using for some time now that helps us think about what treatment we’re going to use for a patient with non-small cell lung cancer: PD-L1.
PD-L1 is not a mutation. It’s a protein. What this protein does is it helps cancer hide from the immune system. When we’re thinking about whether we can use immunotherapy, depending on how much this protein is expressed on the cancer cells, this can help guide our treatment decision-making. Is immunotherapy going to work well by itself or not? Do we need to add a partner to it, like chemotherapy?

Your cancer cells do a good job of wearing a cloak, so they can hide from the soldiers of your immune system, which are the T cells. The job of immunotherapy is to rip off that cloak and once we do, your immune system can finally recognize that there’s something foreign being cancer and something that’s not supposed to be in the body. Now the patient can use their immune system to go after the cancer cells. That’s what immunotherapy does; that’s why it’s so important in non-small cell lung cancer, and that’s why it’s a huge advancement for many patients.
Jill: Basically, you’re not targeting the cancer like you are with the other treatments. You are helping the immune system get back to what it’s supposed to be doing.
Dr. Singhi: Cancer is very smart. What we’re doing is exposing the cancer cells to the immune system and saying, “This does not need to be here,” and training the body to go after the cancer cells.
What PD-L1 does is tell us how likely immunotherapy is going to work, but it does not tell us what’s driving the cancer… That’s why it’s important to have all the pieces before making your decision.
Dr. Eric Singhi, Thoracic Medical Oncologist
Jill: I’ve heard stories — and you’ve probably experienced it as well — where people come in and ask for immunotherapy, but they don’t understand that there are different types of treatment and that not all lung cancer is the same. That’s one thing to emphasize. The other is that not every biomarker has an approved therapy in every setting, but it’s still important to get all the testing done for treatment planning, possible clinical trials, and understanding what may or may not be the next step.
Dr. Singhi: I like how you keep talking about the pieces of the puzzle. PD-L1 is an important test, but again, it’s only one piece of the puzzle. That piece can come back very quickly, often quicker than the results of NGS or some of the DNA and RNA testing.
What PD-L1 does is tell us how likely immunotherapy is going to work, but it does not tell us what’s driving the cancer. That’s what biomarker testing tells us, so you have to wait for all the different pieces of the puzzle to come back, because you need to put them all together. Initially, you might be fooled: If PD-L1 comes back high, you might think immunotherapy will work. But then, eventually, you get back your full results, and you find that you have an EGFR mutation, and immunotherapy doesn’t work very well with those. That’s why it’s important to have all the pieces before making your decision.
Jill: Because you’re talking about EGFR and immunotherapy, I want to stress that if you’re waiting for your biomarker results and have symptoms, you don’t want to start with immunotherapy. It can be dangerous to have immunotherapy and then start an EGFR-targeted therapy. We have data on that. As you said earlier, Eric, chemotherapy is usually the best place to start.
Dr. Singhi: Absolutely.
For MET, I would say the devil is truly in the details. You want to understand if you were tested and, if so, how.
Dr. Eric Singhi, Thoracic Medical Oncologist
MET: The most complex biomarker in lung cancer
Jill: We’ve covered the most common biomarkers. Let’s talk about one that causes a lot of confusion. MET can show up in different ways, and understanding that is important because you test for it differently and it has two different ways that it behaves. Can you help us break down the difference between MET exon 14 skipping and c-MET overexpression?
Dr. Singhi: MET is important in lung cancer. I’ll be honest: It’s one of the more complex biomarkers, so I’m going to try to simplify it.
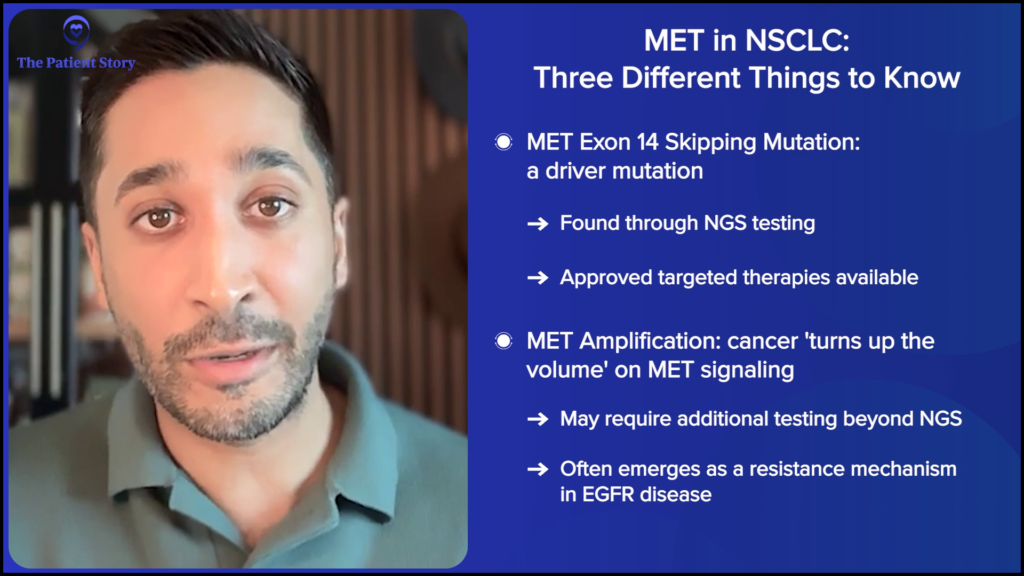
There are three ways that we think about how MET can show up in lung cancer. One is the MET exon 14 skipping mutation. It’s a very long name, but this is what we call the classic driver mutation, which means it’s what’s directly fueling the cancer. You can treat that with targeted therapy, which we have already approved.
The second one is a gene copy increase, which we call MET amplification. The easy way to explain it is that the cancer is turning up the volume on MET signaling. You test that in a very different way. You don’t actually do that, typically just with NGS. You can also do it with another form of testing. This one is important because, often, for patients who have EGFR disease, if they’re on a targeted therapy and that stops working, we want to understand why. We call that a resistance mechanism. In MET amplification, where you turn up the volume of the MET signaling, it can be the reason why, so you want to check for that as well.
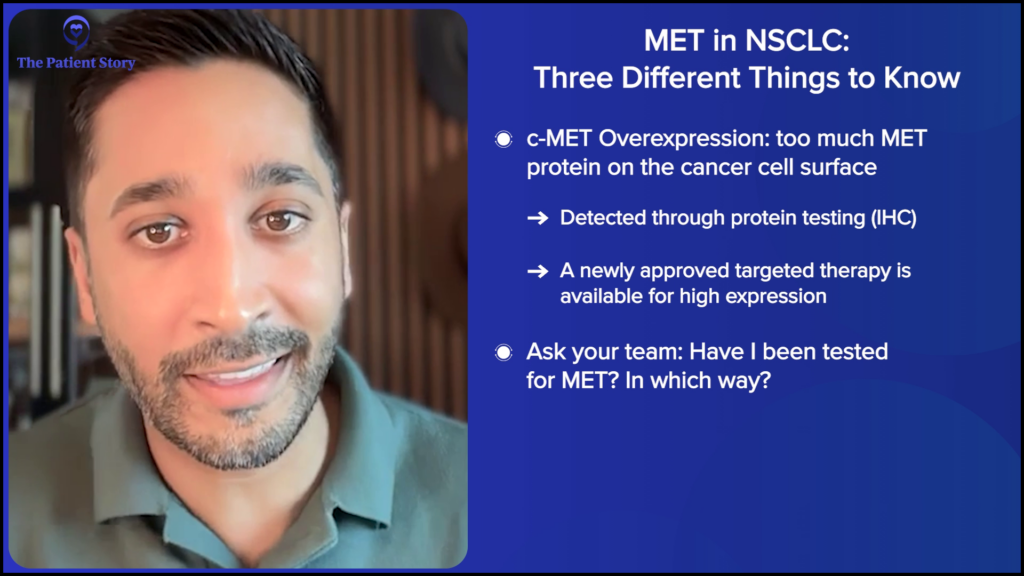
The third one is all about protein level expression, which we call c-MET overexpression. Sometimes you can have too much MET protein on the cancer cell surface, and you test that with protein testing, which we call IHC. This one is not about the gene. It’s about what the cell is expressing itself.
Those are three different ways of checking for MET, which don’t all necessarily mean the same thing. If you have one that’s positive, the others may not be positive, so it’s very complex. When you talk to your team, ask them: Have I been tested for MET? And if so, how? Because it’s important to understand.
Jill: So they’re not mutually exclusive?
Dr. Singhi: Yeah, they’re not always concordant in terms of the results. You may have one that’s negative, but if you check another way, that one could be positive. That’s why you want to understand. For MET, I would say the devil is truly in the details. You want to understand if you were tested and, if so, how.
Jill: Outside of MET exon 14 skipping, how do you treat the other two?
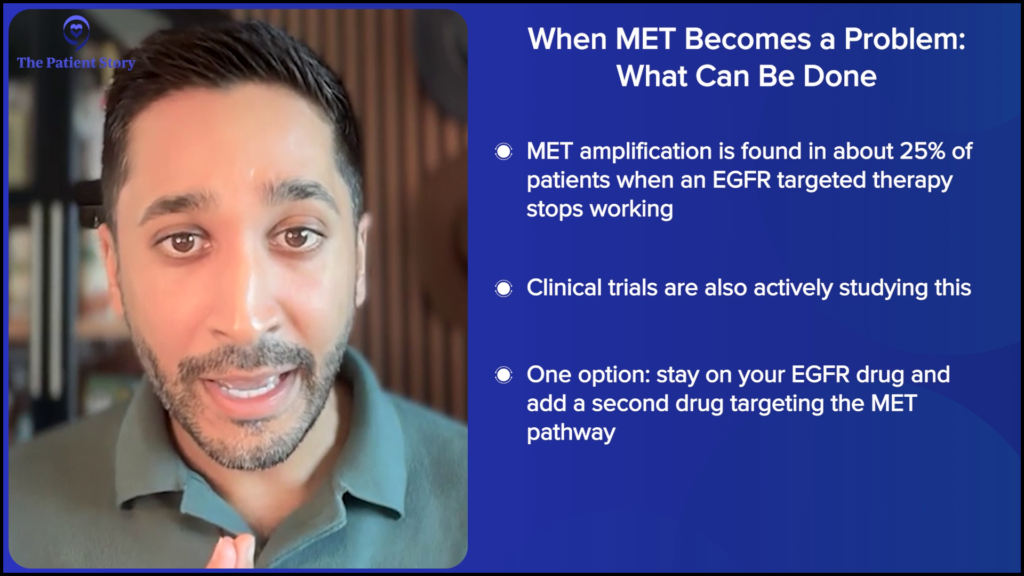
Dr. Singhi: MET amplification can emerge as a resistance mechanism for many patients who are on EGFR-targeted therapy and oral therapy. Sometimes, if they’re on an oral targeted therapy, 25% of the time, you can see this. It’s pretty common, so what do you do in those circumstances?
Clinical trials are looking at this, but there’s also clinical trial data that is read out where you can not only continue the EGFR-targeted drug but also add in another drug that goes against the MET pathway, so it’s a combination strategy. There are a lot of nuances to this. You should talk to your team. But there are some ways and there’s data to overcome that resistance mechanism.
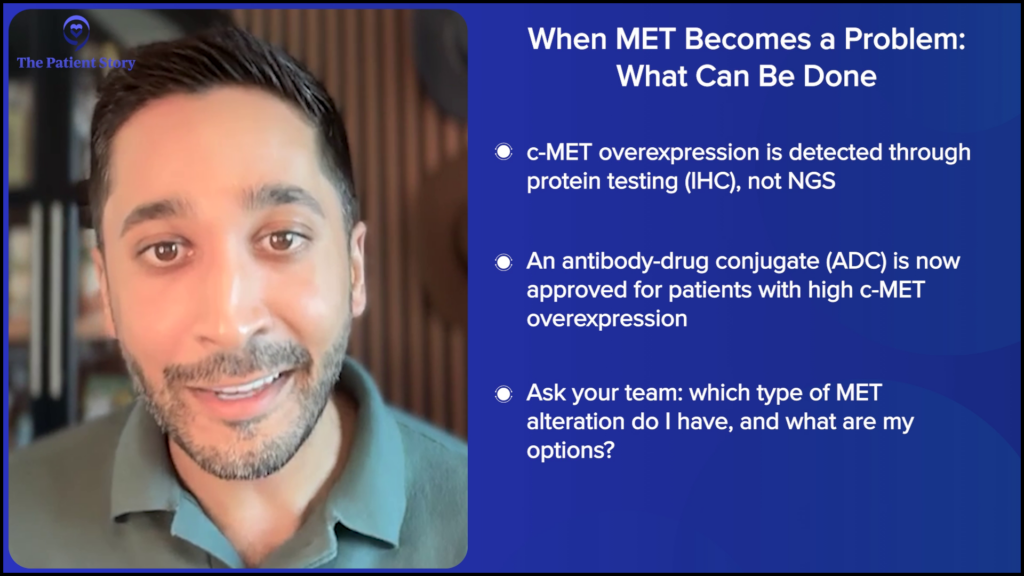
For the c-MET protein overexpression, we have a very recent approval of an antibody-drug conjugate (ADC). I call it sexy chemo or targeted chemo. We’ll go into what that means. If they have a high level of c-MET protein overexpression, an antibody-drug conjugate is approved for patients.
Jill: It wasn’t that long ago that there was chemotherapy only. The field is rapidly moving and it’s hard to keep up.
When I think about progression, I think about the time: How soon after starting a drug is the patient having sites of disease that are growing and no longer responding to the drug? Then I think about how many sites.
Dr. Eric Singhi, Thoracic Medical Oncologist
When treatment stops working: Understanding progression and resistance
Jill: Something every patient worries about is progression, because that’s when the cancer changes or starts to grow again. While we dread it, it’s something that we should understand enough to know that the cancer can do that. Sometimes, you can have progression where the treatment isn’t helping at all, or you could have progression in one little area where the treatment is still working everywhere else. It’s an important question to ask your team if you’re told that you’ve had progression.
Dr. Singhi: Yeah, and it’s probably one of the toughest conversations to have in the clinic. Unfortunately, cancer is not static. It often evolves. It’s something that we typically see over time and, unfortunately, start to expect. When this happens, we want to understand how it’s happening, how quickly, and where.
When I think about progression, I think about the time: How soon after starting a drug is the patient having sites of disease that are growing and no longer responding to the drug? Then I think about how many sites.
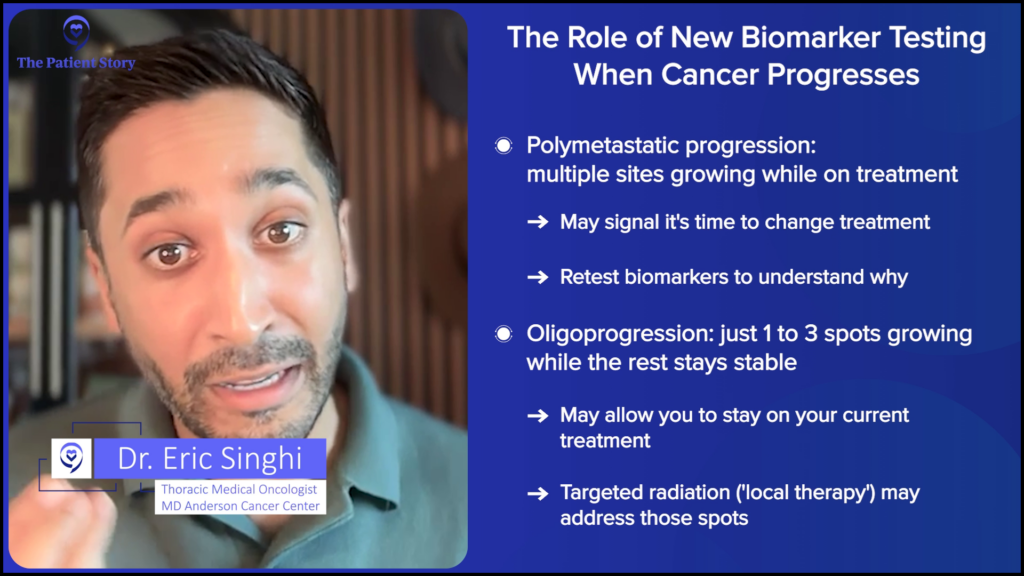
What you’re talking about is what we call polymetastatic progression, where multiple sites are growing all at once despite being on a drug. If that happens, we often need to switch our drug or think about a new treatment option. But you want to understand why that’s happening, which is what’s important.
We talked about biomarker testing at the beginning and not starting any treatment until you get the biomarker testing results. Another important takeaway is that you have to test again and try to understand why the cancer is growing. What changed? Did the actual cancer cells themselves change? Sometimes that can happen. It’s uncommon, but it can.

You can go from a non-small cell lung cancer (NSCLC) to a small cell lung cancer (SCLC), a much more aggressive, fast-growing type of lung cancer, or you can develop different mechanisms of resistance.

There are two categories of resistance that I generally think about. One is called on-target. Let’s say you have an EGFR mutation at the beginning. You’ve started on targeted therapy. It’s doing well. Then, unfortunately, the disease starts to grow. You repeat testing and now you have an on-target mechanism of resistance. It’s still going down the EGFR pathway, but the original mutation has changed shape.
Then there’s an off-target potential mechanism of resistance or what I call a bypass mechanism. That’s where the cancer finds a new route or a new pathway. One we already talked about was MET amplification. You want to understand why, because it has implications for thinking about the next treatment, combination treatments, and clinical trials. The key takeaway is to understand why the cancer is growing.
Jill: I know you don’t have the end-all, be-all answer, but a lot of people do ask: Why does resistance happen?
Dr. Singhi: There are two patterns of resistance. You can have primary resistance where you start a patient on a drug and the drug doesn’t work from the start. Then you have acquired resistance, where over time, the cancer drug starts to work less effectively. That’s more common. The reason why that happens is that you can get to a threshold of control of the cancer cells with a drug that you’re using, but it leaves behind some persistent cells, which stay there and start to cause problems. They start to get smart, evolve, build, and then build up to the size of a tumor, which then becomes visible on scans. That’s where you start to see that maybe the drug isn’t working. That’s the more common scenario and a general reason why that happens.
Jill: It’s important to get testing done once again so that you can make your plans for the next line of treatment. Again, you want to know what is driving that resistance. I want to point out what you said about the on-target mutation changing shape. I want to go back to your key-and-lock analogy. It’s like you’re getting a new lock for some reason, so your key no longer fits in that lock. Is that a good way to explain?
Dr. Singhi: Yes, absolutely right. We’re going back to the key and lock analogy. Exactly right.
Jill: It helps to visualize and understand it.
Does progression always mean changing treatments?
Jill: There’s progression where you may only have progression in one spot, but it’s still controlled and stable anywhere else, so the treatment is still working on those areas. Should you change treatments or are there other options?
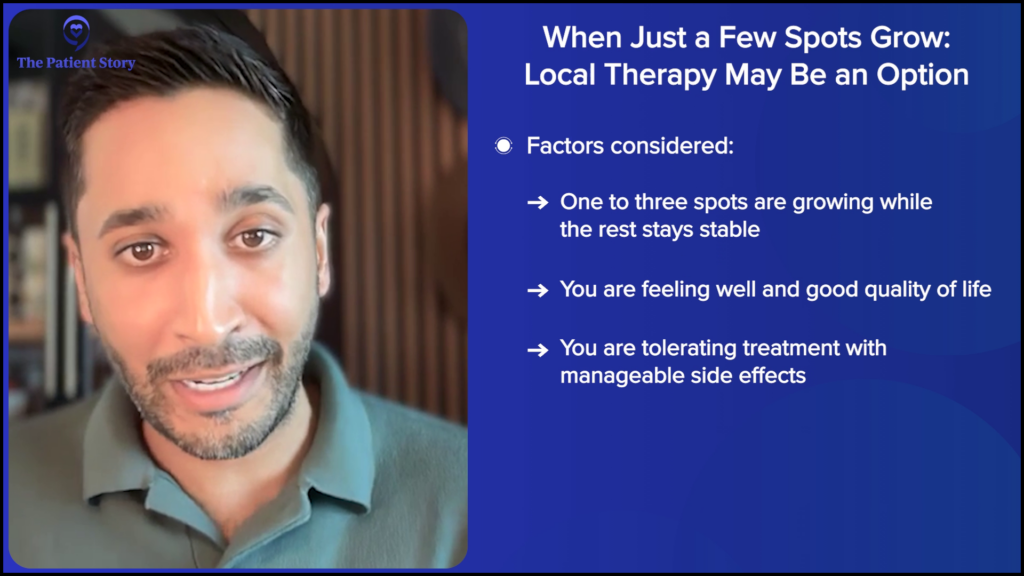
Dr. Singhi: We talked about many sites growing while on treatment. Now we’re talking about a few sites, maybe one to three sites, while the rest of the disease remains well-controlled. In these circumstances, if you have a drug that’s working well and overall controlling the disease burden, if the patient is feeling well, and importantly, if they’re tolerating the drug well, then we talk about using local therapies to try and control some of these bad-acting tumors that are starting to pop up.
What do I mean by local therapy? Radiation therapy is an option where you can call in a friendly radiation oncologist and say, “Hey, listen. I have a spot. Can we radiate it? Can we zap it, take care of it, and continue the drug that, for the most part, is working well?” That’s a very reasonable option. Many of us have had patients for whom we’ve done that. We’ve been able to continue the same drug for many months, even years. That’s a good opportunity to think about that.
Jill: Yeah, it is. I’ve had radiation, probably on seven different nodules, and it has allowed me to stay on the treatment I’m on. The radiation that you’re talking about is also very targeted and preserves healthy lung tissue. Two things to emphasize are that this is why you want to ask your team what type of progression you have so that you can advocate for yourself, depending on whether it’s one spot or whether multiple areas have grown.
An important rule is that if the liquid biopsy is negative, you should follow with a tissue biopsy, ideally. Right now, it’s the only way to understand if the actual cells have changed.
Dr. Eric Singhi, Thoracic Medical Oncologist
With progression, what type of biomarker retesting do I need?
Jill: This is where comprehensive biomarker retesting is important. We were talking about tissue biopsy versus liquid biopsy when someone’s first diagnosed. Upon progression, is this where liquid biopsy can be like a powerful first step? Do you use it first?
Dr. Singhi: This is important. We will often start with a liquid biopsy because it’s fast and minimally invasive. It can capture the whole body and what’s going on.
But an important rule is that if the liquid biopsy is negative, you should follow with a tissue biopsy, ideally. Right now, it’s the only way to understand if the actual cells have changed, if you’ve had a transformation of non-small cell lung cancer to small cell lung cancer, and to truly be comprehensive in figuring out if there’s a new biomarker that’s driving this progression.
Jill: That’s critical. The goal is to find out what’s driving the cancer now. When progression happens, I also encourage people to ask their team: Can we start with a liquid biopsy and, if it doesn’t provide information, consider a tissue biopsy? What are you testing for to understand why the cancer is growing? When you ask your team these questions, you’re not being confrontational. You are the CEO of your health. You want to know that everything’s being done and what the next steps are, so that you can understand it better. Knowledge is power.
Dr. Singhi: Three questions: What type of progression? Why the progression? And how are we going to deal with it? What, why, and how.
Quality of life matters: What treatment looks like day to day
Jill: It’s not a trade-off between quality of life and treatment. You should be able to live longer and live well. We talked about how some of the therapies have more acute side effects. Some of them have fewer side effects, but you’re on the drug longer, so they can be more persistent. It’s important to understand that low grade does not mean low impact. Any side effect can impact anybody. We respond in different ways. But if it impacts your daily life, you absolutely should talk to your team about it.
With the newer therapies, the treatment decisions aren’t just about how long something works. They’re about what your life looks like on that treatment. For many people on targeted therapy, they go every three months, so there is a real psychological relief in knowing that you could take a bit of a break and don’t have to go every few weeks for treatment. There’s also relief in knowing that there’s a tailored plan for your cancer. Do you see that a lot with your patients?
The mind-body-soul connection in cancer care is so important.
Dr. Eric Singhi, Thoracic Medical Oncologist
Dr. Singhi: Absolutely. We’re always so focused on the side effects that we can see, like skin changes and rashes, but there’s also the component of time toxicity. You highlighted it and said it so nicely. We need to weigh that in. How often can patients come to the cancer center? How often do they want to come? Do they have other obligations where they need to live their life outside the cancer center?
That’s the whole reason why we do what we do: to allow patients to live a life that has meaning and quality while taking care of their cancer. The mind-body-soul connection in cancer care is so important. That’s all I talk about with my patients. I talk about it with everyone, to be honest.
Jill: The other thing I would emphasize about quality of life is that it’s different for everybody. If you’re young and have young children, like I was when I was diagnosed, you’re worried about one thing: raising your children. If you’re older and retired, you may worry about certain side effects more, like neuropathy, especially if you play a musical instrument or love gardening. It depends on your preferences, your goals, your family, and how it will affect them. Those are all important pieces of the conversation to get the entire the whole picture.
We’re very privileged in our lung cancer treatments today because we have options and we’re able to personalize treatment for patients, but we do that with biomarker testing.
Dr. Eric Singhi, Thoracic Medical Oncologist
Advocating for comprehensive biomarker testing: When to seek a second opinion
Jill: When it comes to comprehensive biomarker testing, if you ask your doctor for it and your doctor says, “I don’t think we need to test for that,” do you think it’s okay to ask why?
Dr. Singhi: Absolutely, yes. I want to understand why and make sure we get into the details. The devil is in the details. We’re talking about repeating the DNA and RNA, but what about the proteins? Ask about those details. Ask why and why not.
Jill: Is there ever a good reason why not?
Dr. Singhi: Sometimes there are good enough reasons, like if there isn’t enough tissue sample to run the test. Sometimes we don’t expect changes necessarily happening in the tumor evolution to go looking for it. But any oncology team should be able to explain why.
What I’ll emphasize is that we’re very privileged in our lung cancer treatments today because we have options and we’re able to personalize treatment for patients, but we do that with biomarker testing. If your oncology team can’t exactly explain why we don’t need biomarker testing, then I would seek a second opinion. I would talk to another center and make sure we’re all on the same page.
Jill: Yeah, that’s a great point. A second opinion is important, especially if it’s going to help you feel better that everyone’s on the same page. But you also have to keep in mind that it’s not about mistrust. If that’s how the oncologist you’re with feels, then you need to think about the situation you’re in, the team you’re seeing, and whether you’ll be comfortable talking to them about everything that you need to talk to them about across this experience.
But it’s a way to make sure all options have been considered. You’re not being difficult. You’re being informed. When I have progression, my oncologist says, “Okay, I’ll talk to these people. You talk to these people.” That’s what you want: someone who is open to that.
Key takeaways: What to remember
Jill: Treating lung cancer is more complex and complicated than ever before, but no one has to navigate this alone. There are groups, like the EGFR Resisters, that exist because patients need a community that can provide information and support.
There are many groups for different biomarkers, different diagnoses, and specific treatments. In some ways, they are life-saving, but they are almost always life-changing for patients and caregivers. These communities help people understand their options, connect with others who truly get it, and feel less alone when everything else feels completely overwhelming. These communities help you get information and support and empower you, because these groups share important questions and best practices, allowing you to make more informed decisions and know you are not alone.
Let’s wrap up with some closing thoughts. Eric, what do you want people to remember?
Dr. Singhi: First of all, thank you for having me, Jill. I always love chatting with you. I learn so much every time I talk to you, so thank you for that.
Biomarker testing is incredibly important in lung cancer. We are not just trying to treat lung cancer. We’re truly trying to treat your lung cancer. I emphasize “your” in that sentence because the advancements that we’ve made for patients with lung cancer have been incredible. We have a long way to go, but we’ve definitely made strides. Having access to those advancements is important, which is achieved through clinical trials, research, science, and the guidance of biomarker testing.
We’ve talked about the buzzword of empowerment and being an empowered patient. Sometimes that can be overwhelming, but being an empowered patient doesn’t mean you have to know everything. What it means is that you should feel included, heard, and supported in your care. Support and communities can help do that. It’s important to feel like you’re heard and included by your team.
Jill: That’s a good point and such an important message. You don’t have to know everything. It’s okay to even tell your doctor, “I want you to make the decision.” I know people who have done that. That’s being heard and included. It’s so important, so thank you for pointing that out.
Test early and test broadly. Ask for your report so you can have discussions with your doctor. Find a community where you can connect with others who get it in a way that no one else can, who haven’t lived it.
You don’t have to know everything. You just need to know that there’s information out there. There are communities out there. There are people out there who will help you navigate this roller coaster ride, which is what I like to call it sometimes, because that’s what it feels like in the beginning.
Eric, thank you. I absolutely love working with you. I’ve known Eric since he was a fellow and it’s amazing. He’s a rising star and it warms my heart to see that his True North is still making sure that patients understand and that they’re heard. That is special, so thank you. And thank you to The Patient Story.

Conclusion
Stephanie: Wow. Thank you so much, Jill, and Dr. Singhi. I appreciate both of you for joining despite your very packed schedules and for leading a conversation not only with so much information but also in a way that’s so digestible.
Comprehensive biomarker testing can be a big tool in major treatment decision-making, both at diagnosis and again if the cancer progresses. It’s more than okay and important to advocate for yourself, which is something that I learned as a patient and in the many years now that I’ve been a patient advocate. I learned that you should ask if you’ve had tissue and liquid biopsies done, ask for a copy of the report, and ask your healthcare team to explain what was tested, what it means, why a treatment is being recommended now, and so many other things, so that you walk away from every conversation with your doctor understanding so much more.
Now, on that note, again, this conversation is not a substitute for medical advice and a conversation with your healthcare team. Consult with them as you make treatment decisions. We do, however, hope that you walk away with better questions to ask.
We also want to thank our sponsors, AbbVie and Nuvation Bio, for their support of our educational programming, over which The Patient Story retains full editorial control.
There are so many incredible lung cancer patient advocacy groups out there. Jill leads the EGFR Resisters. They have so many different resources and programs and educational information for people out there. There are also many others, like the ROS1ders, KRAS Kickers, ALK Positive, and The White Ribbon Project. They all have biomarker-specific resources for patients and care partners dealing with lung cancer in general.
Remember that your voice and opinions matter to us as we build more content for you. I hope we hear from you and get to see you again soon. For now, I’m Stephanie Chuang with The Patient Story. Take good care.
Program Partner
EGFR Resisters is a grassroots patient-driven community dedicated exclusively to changing EGFR-positive lung cancer into a manageable chronic disease. Their community of survivors and caregivers shares knowledge and connects with others who are experiencing similar journeys. Find your community.
Program Sponsors
Thank you to our sponsors for their support of our independent patient education program. The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story. This content does not replace professional medical advice.
Hear from people living with lung cancer
Real experiences with diagnosis, treatment choices, side effects, and life beyond lung cancer — in their own words.







