Living Actively with Follicular Lymphoma
A Conversation with Experts About Active Surveillance
Nicky Greenhalgh, a follicular lymphoma patient advocate, and Dr. Jonathan Friedberg, Director of the Wilmot Cancer Institute, hold a special webinar diving into one of the most complex topics in the follicular lymphoma journey: active surveillance, also known as watch and wait.
Dr. Friedberg is a renowned expert in advanced therapies and a leading voice in the clinical argument for active surveillance. Get the latest, most balanced perspective on your care options, from managing anxiety after diagnosis to the newest treatment advancements, directly from a leading expert.
Program Topics
- The Rationale for Active Surveillance: Understand when active surveillance is a viable option for follicular lymphoma.
- Deciphering Your Diagnosis: Learn why Stage IV follicular lymphoma is less relevant to treatment decisions than in other cancers.
- The Latest Treatment Strategies: Explore individualized treatment, including chemo-immunotherapy and exciting new bispecific antibodies.
- Understanding Your Disease’s Behavior: Discover that the length of your response to any treatment is the most powerful predictor of your long-term outcome with FL.
- Tips for Being a Proactive Patient: Get expert advice on managing anxiety and using the active surveillance period to focus on overall health and learn more about your disease.
Program Panel
Program Partner
Thank you to the Living with Follicular Lymphoma Facebook Group for their partnership. Their private Facebook group is dedicated to supporting individuals with follicular lymphoma, their families, and supporters. They offer a safe space to share personal experiences and learn about the latest research, trials, and treatments.
Program Sponsor

Thank you to our sponsor for their support of our independent patient education program. The Patient Story retains full editorial control over all content.
This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
- Introduction
- Meet Dr. Friedberg: How a career in lymphoma begins
- What is active surveillance and why it feels tough not to start treatment right away
- Understanding stage 4 follicular lymphoma and why it’s not what you think
- Is it better to start treatment early or wait until symptoms develop and treat later?
- Biomarkers, predicting behavior, and how doctors make treatment decisions
- Lifestyle during watch and wait: What the evidence actually shows
- Staying engaged but not overwhelmed: Being a proactive patient
- Should I start follicular lymphoma treatment just to help my anxiety?
- Scanning, scanxiety, and how often you need to be imaged
- Caregivers and support: You’re not treating a patient, you’re treating a family
- When it’s time to treat: What are the follicular lymphoma treatment options?
- CAR T-cell therapy and bispecifics: Could this be a cure?
- Final thoughts: Tips for the newly diagnosed follicular lymphoma patients going into watch and wait
- Conclusion
- Hear from people living with follicular lymphoma
Edited by: Katrina Villareal
Introduction

Stephanie Chuang: Hi, I’m Stephanie Chuang, founder of The Patient Story. This conversation is “Living Actively with Follicular Lymphoma: All About Active Surveillance.” Some of you may call it watch and wait, or watchful waiting, which is the opposite of what most people are told to do when they hear, “You have cancer.” These are words I heard, but I had a different and aggressive form of non-Hodgkin’s lymphoma, so it’s something I can’t wrap my head around. Yet for many people with follicular lymphoma, it may be the right approach.
You’re going to hear from two people who know about this firsthand, but from different points of view.
Our moderator is Nicky Greenhalgh, a follicular lymphoma patient herself who also started the Living with Follicular Lymphoma Facebook group, one of the largest FL patient communities in the world.
We’re also so lucky to have our lymphoma expert guest, Dr. Jonathan Friedberg, Director of the Wilmot Cancer Institute at the University of Rochester. Dr. Friedberg is a leading lymphoma specialist who has spent more than 20 years carefully considering when to treat and when to wait.
Together, they’re going to walk you through what active surveillance actually means, what the research shows, what to watch for, and how to feel confident during this period.
This program is made possible with support from Genmab. Thank you for the support that allows us to do more in patient education. The Patient Story maintains full editorial independence on this program and content. Everything is for educational purposes only and is not medical advice, so please bring what you learn here to your care team.
Meet Dr. Friedberg: How a career in lymphoma begins
Nicky Greenhalgh: Welcome to this very special webinar with The Patient Story. I’m your moderator, Nicky Greenhalgh. We are diving into one of the most psychologically and clinically complex topics in the follicular lymphoma journey: watchful waiting.
I’m a follicular lymphoma patient myself. I was diagnosed in 2014 and was immediately put into treatment. At the time, I was extremely grateful to be doing something about it. But as I’m experiencing my first relapse, I’m on watch and wait or as many like to call it, active surveillance, and I cannot tell you how grateful I am for that.

Joining us is a true titan in the field: Dr. Jonathan Friedberg. As the director of the Wilmot Cancer Institute, Dr. Friedberg has spent over 20 years at the forefront of lymphoma research and treatment. What makes him the perfect guest is his balanced philosophy of care. He is an expert in the most advanced therapies and a leading voice for active surveillance.
Dr. Friedberg, thank you for being here. But first, how did you get into cancer research?

Dr. Jonathan Friedberg: First of all, it’s my pleasure to be here. It’s enjoyable for me to speak with patients and try to communicate as best I can.
I knew I wanted to do internal medicine, but I had some challenges choosing a specialty. It was an oncologist who I found very inspiring that led me into cancer. When I was a first-year fellow, Ernie Freedman at Dana-Farber Cancer Institute — himself a renowned expert in follicular lymphoma — was somebody who inspired me. I liked the way he took care of patients and incorporated research, and that’s how my career started.
Nicky: Oh, wow. Often, it’s somebody who inspires you, isn’t it? I’ve found I’ve been led to my passion through inspirational people, so it’s nice to hear.
Follicular lymphoma is very different from other cancers… Since follicular lymphoma is a blood cancer, it’s in many places at diagnosis.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
What is active surveillance and why it feels tough not to start treatment right away
Nicky: Let’s jump right into it. When a patient is newly diagnosed and told, “You need to go watch and wait,” the anxiety about not treating the disease can be debilitating. How have you dealt with that with your patients?
Dr. Friedberg: The decision to start treatment or to observe a patient for a period of time has to be individualized. It depends on many patient-related factors, clinical factors, and communication
The first thing I emphasize is that follicular lymphoma is very different from other cancers. We are programmed to find cancer early and cut it out. The reason you do mammograms is to find breast cancer early and treat it quickly to prevent it from spreading.
Since follicular lymphoma is a blood cancer, it’s in many places at diagnosis. There isn’t a concern about spreading. It’s already in many, many places. We know from decades of natural history studies that this disease can grow very, very slowly. I tell patients that they’ve probably had it for months to years before meeting me, without realizing it.
In order to better understand the rate of growth, as well as to more intelligently choose the right therapy, a brief period of observation can be very helpful. That often starts as a 3-to-6-month period. Then we repeat imaging and get a sense of how the disease is moving. If things haven’t changed much, patients often become much more comfortable with the concept that they’re being carefully observed. If things are growing, that’s when we revisit the strategy and think about starting treatment.
Nicky: What triggers treatment? Is it usually high tumor burden or bulky disease affecting organs, or are there other reasons?
Dr. Friedberg: We use a number of criteria. There’s an algorithm called the GELF criteria that is used to divide patients into those who need treatment and those who don’t.
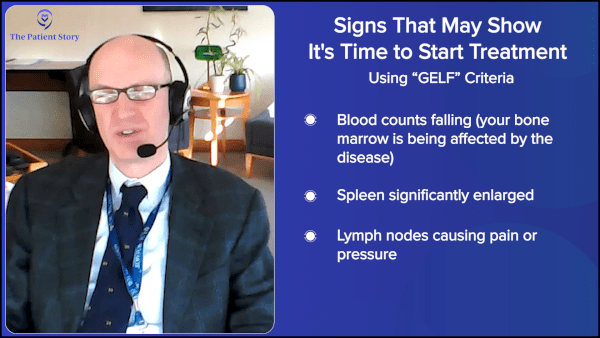
It includes blood counts. If normal blood counts start to get low because of the disease, that’s an indication for treatment. If the spleen gets very enlarged or lymph nodes are of a certain size, which may cause discomfort or other problems, those would be indications as well.
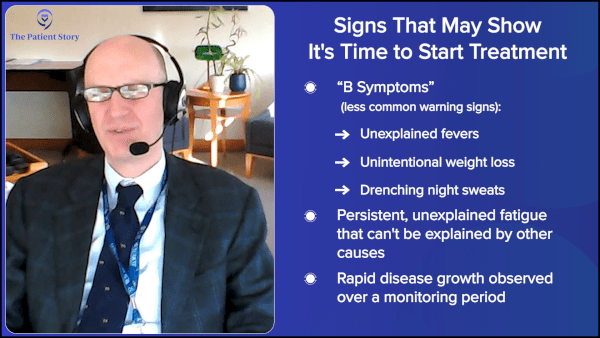
Very rarely, patients with follicular lymphoma have what we call B symptoms: fever, weight loss, and night sweats. But more commonly, some patients have fatigue. That’s a very vague symptom because lots of things can cause it, so you need to exclude other causes. But if you’ve excluded them, sometimes that’s a reason to start therapy to see if the patient may feel better after treatment.
Patients with advanced-stage follicular lymphoma, even those who are symptomatic, have survival measured in decades — not months or years — and that’s with stage 4 disease.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
Understanding stage 4 follicular lymphoma and why it’s not what you think
Nicky: When I was newly diagnosed, I was told I had stage 4, which was a terrifying moment because I thought stage 4 was the endgame. But in follicular lymphoma, it’s quite common for patients to be diagnosed at stage 4, isn’t it?
Dr. Friedberg: Yes. If you look hard enough — in the bone marrow, for example — you can almost always find some follicular lymphoma cells, but that doesn’t have the same dismal outcome as stage 4 in solid tumors. We know that patients with advanced-stage follicular lymphoma, even those who are symptomatic, have survival measured in decades — not months or years — and that’s with stage 4 disease. The concept of stage in follicular lymphoma is much less relevant to treatment decision-making than it may be in other cancers.
Nicky: I’m so glad that’s changing and patients are being told this. When I was first diagnosed, I was told my prognosis was 10 years, which was absolutely terrifying for a 32-year-old. New research is coming and the statistics are changing. It’s important from the get-go that patients are reassured this cancer is completely different from most cancers we know about.
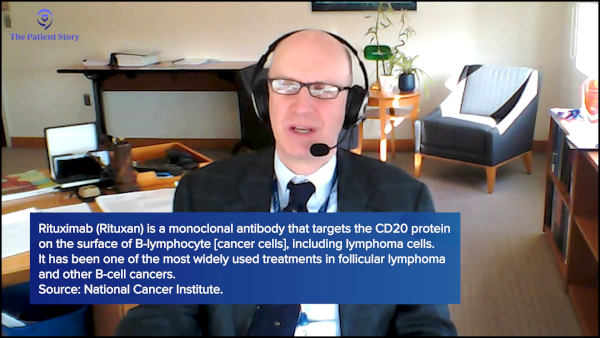
Dr. Friedberg: It’s far better than that now. It’s been one of the biggest success stories in oncology. When I trained in the ‘90s, we used to tell patients that six to eight years was the median survival. That was an era when rituximab was just being introduced and we didn’t know the impact that drug would have. Clearly, that’s changed.
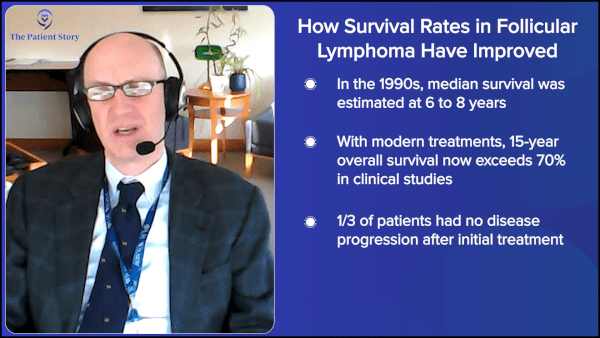
The SWOG study group, which I chair, published a 15-year follow-up of a clinical trial that started in the year 2000, looking at a combination of chemotherapy with monoclonal antibody treatment. We showed that overall survival at 15 years exceeds 70% and one-third of patients had no progression after their initial treatment.
Many patients with follicular lymphoma are older and may be dying of other causes, so the overall survival statistic includes deaths from other causes. It suggests that for a large number of FL patients, mortality from lymphoma is truly not going to be the issue.
Is it better to start treatment early or wait until symptoms develop and treat later?
Nicky: I’m an administrator of a large Facebook group called Living with Follicular Lymphoma, and in the last 12 months, there has been a lot of discussion about whether watch and wait is still a viable option. I believe this has come out of a study presented at the 2024 ASH meeting, the FLORA study. It looked at whether watch and wait was better than immediate rituximab monotherapy in patients with very low tumor burden. The findings were interesting. The study was actually terminated early because results were so clear that event-free survival was significantly better in the treatment group. But it’s not really all as it seems, is it?
Dr. Friedberg: Yes. This is one of several attempts to ask the important question: Is it better to start treatment early, or wait until symptoms develop and treat later? In a disease with a natural history of decades, that can be a very hard question to answer.
If you give active treatment and compare it to no treatment, patients are going to do better with treatment in the short term, unless the treatment has bad side effects. If the treatment is well-tolerated, like rituximab generally is, you’re going to see short-term benefit in progression-free survival and standard endpoints.
The best study that has tried to address this is a randomized trial comparing rituximab versus watch and wait, initially published in 2004, with long-term follow-up published in 2025. It took patients with low tumor burden follicular lymphoma and asked, from the start: Which is the better strategy?
What’s the trade-off between a relatively short course of rituximab given early versus watching and waiting, and giving that rituximab or chemotherapy later?
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
The short-term follow-up showed rituximab was a clear winner. Patients who got treated clearly needed less chemotherapy. With long-term follow-up, a subset of patients treated with rituximab has not needed any additional treatment. There was absolutely no difference in overall survival and transformation.
As we interpret these data, the question now becomes: What’s the trade-off between a relatively short course of rituximab given early versus watching and waiting, and giving that rituximab or chemotherapy later? That’s an individualized decision at this point.
Nicky: The key thing is there was no difference in overall survival. From my experience, I had rituximab over 12 years ago and I still have hypogammaglobulinemia. My immune system still hasn’t fully recovered. The way I think about it: Watch and wait allows your immune system to stay fresh for when the time comes to have more serious treatments. Would you agree?
Dr. Friedberg: Yes. There are both theoretical and active concerns about any treatment we give. We learned during the COVID pandemic that patients who had received extensive rituximab were in the group that had trouble with COVID; we saw some increased deaths in that group. There are definitely effects to the immune system that happen, even with relatively modest therapies like rituximab. And some patients, as it sounds in your case, do have prolonged immunosuppression after treatment.
Treating follicular lymphoma has to be considered a marathon, not a sprint… If you give all your treatment too early, over the decades you’ll have this disease, you may run out of options or the disease may become resistant.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
The other concern has been creating resistance. If you’re not curing patients with single-agent rituximab, it’s going to work for a period of time and then may stop. The question is: When is it most valuable to give the treatment?
The analogy I give patients is that treating follicular lymphoma has to be considered a marathon, not a sprint. If you sprint, you’ll be leading at mile two or three, but you’re not going to win because you’ll run out of energy. If you give all your treatment too early, over the decades you’ll have this disease, you may run out of options or the disease may become resistant. Because of all that and the lack of survival benefit, active surveillance remains a very viable option. I continue to encourage consideration of new clinical trials looking at whether we can intervene early and potentially cure a subset of patients.
Biomarkers, predicting behavior, and how doctors make treatment decisions
Nicky: When you’re deciding on treatment for someone who has been on watch and wait for a long time, are there biomarkers or lifestyle factors you look at? What guides your decision?
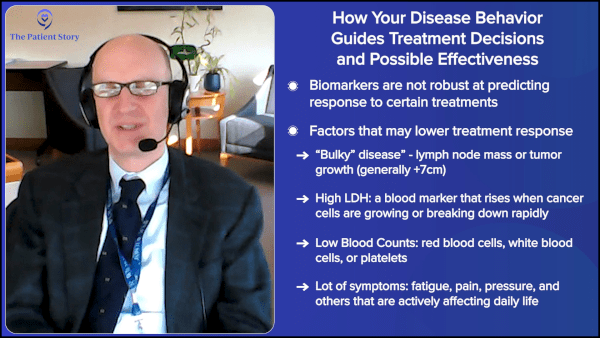
Dr. Friedberg: Unfortunately, in follicular lymphoma, we don’t have a lot of robust biomarkers that predict response to certain treatments. Certainly, if somebody has very large, bulky disease, high LDH, low blood counts, and a lot of symptoms, they may do a bit worse. But we don’t have the same genomic signals as some solid tumors, where you can define whether someone will respond to a certain treatment or not. Decision-making in follicular lymphoma is individualized and, ultimately, a bit of trial and error.
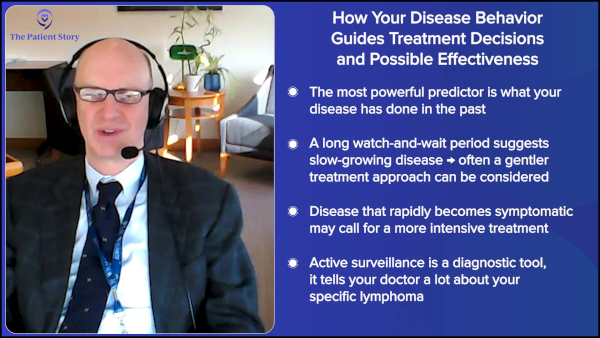
The most important predictor in my mind is what the disease has done before. What treatment or strategy have you had? Are you doing better or worse than the median expected response? You had radio-immunotherapy with an 11-year response — that’s better than the median in that situation. I wouldn’t necessarily be aggressive with the next strategy, because you’ve had a long-lasting response.
The most important predictor in my mind is what the disease has done before… The patient’s own history becomes the most powerful predictor of how they’ll do.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
You can use the same principle upfront. The median time on watch and wait in most trials or experiences has been in the 2-to-3-year range. If you’re observed and go eight years before needing any treatment, that’s a sign the disease is growing very slowly, so you’d probably choose something relatively gentle, like single-agent rituximab.
If you go on watch and wait, and within six to eight months your disease becomes symptomatic, I’d lean toward chemoimmunotherapy, because your disease has shown itself to be more aggressive.
That is one advantage of active surveillance. It allows you to monitor very carefully, and the patient’s own history becomes the most powerful predictor of how they’ll do.
Lifestyle during watch and wait: What the evidence actually shows
Nicky: Do you have any thoughts on lifestyle strategies that may extend a watch and wait period?
Dr. Friedberg: Almost every patient asks me that. Should I eat meat? Should I not eat meat? Should I take vitamins? The first principle is that there has been very little studied in a robust way that I could say either works or doesn’t work.
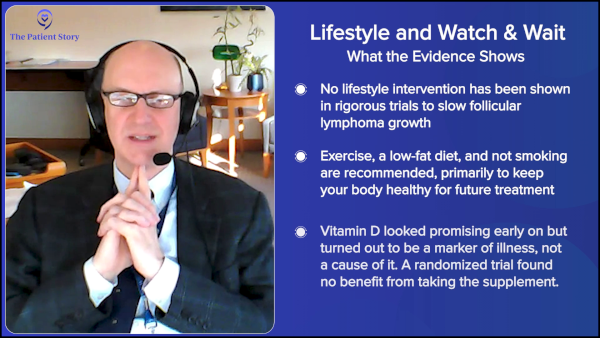
My advice is: Although we don’t have anything that specifically impacts follicular lymphoma, this is an opportunity to think about a healthy lifestyle to protect your heart and lungs, and to prevent other medical problems, so that if we ever need to treat the follicular lymphoma, you’re going to be healthy. Avoid smoking, exercise, and eat a low-fat diet. Even if there’s no impact on follicular lymphoma specifically, protecting your heart means all treatment options remain available to you when you need them.
A healthy lifestyle focused on general health is the advice, not chasing unproven supplements.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
I’ll give a cautionary tale about why clinical trials are so important. We observed that if you walk in the door with follicular lymphoma and you have a low vitamin D level, your outcome is worse. That was a fairly profound signal that was validated in two studies: one from the US and one from France and Australia. That quickly led some lymphoma specialists to supplement patients with vitamin D because it was an easy thing to do.
We then conducted a blinded randomized trial where half the patients got vitamin D and half got a placebo. We recently published those results: absolutely no difference in outcome.
The likely explanation is that vitamin D was a surrogate for illness. Patients with more advanced follicular lymphoma were going outside less, getting less sun, and having dietary changes because they were sick. Vitamin D was a marker of illness, not a modifiable risk factor.
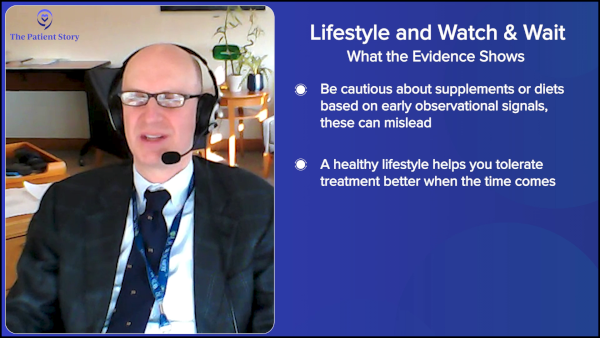
The message is: Just because you hear that something might be bad for cancer doesn’t mean changing it will impact things. A healthy lifestyle focused on general health is the advice, not chasing unproven supplements.
Nicky: I love to hear that you’re looking into those things. I think there needs to be more research around lifestyle and exercise particularly. In my last two visits with my hematologist, he has been drilling into me how much I need to exercise to prepare myself for treatment, because it’s true. With tolerability of treatment, the research is there that if you’re healthy and you exercise, your chances of tolerating treatment better are improved. Is that correct?
Dr. Friedberg: No question. Tolerability of treatment has been shown in many settings to be enhanced by exercise. There are even some provocative studies showing that cancer-related endpoints are better. In colorectal cancer, a formal exercise program incorporated as part of treatment led to better cancer outcomes. That hasn’t been studied in lymphoma specifically, but the principle is there.
Tolerability of treatment has been shown in many settings to be enhanced by exercise.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
It’s also where patients who are on active surveillance want to be doing something. It means trying to maintain good physical health. People end up feeling better for lots of reasons, including psychological benefits. If exercise were a pill, it would be prescribed all the time — and it would probably be pretty expensive, because it works so well. It becomes a little harder to study and control things to understand the benefits. But in many cases, it’s as profound as some of the treatments that we give.
Nicky: Absolutely. I do want to point out that when we say exercise, we don’t mean going for a walk. Get that heart rate up. Getting into zone two for a good half an hour a day makes a huge difference in so many areas of your life, including tolerating treatment when the time comes.
Part of the goal of watch and wait is to allow you to live your life, do the things you want to do, and not be consumed by anxiety about lymphoma progression.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
Staying engaged but not overwhelmed: Being a proactive patient
Nicky: I want to talk about being a proactive patient during active monitoring. A lot of patients start to panic and write down every symptom, which I think is great, but it can also cause anxiety. The main things I look out for are B symptoms: unexplained fevers, drenching night sweats, and unintentional weight loss. Would you agree?
Dr. Friedberg: That’s definitely true. But I try to reassure patients that I’m going to see them frequently enough that between visits, the likelihood of lymphoma coming back and causing a big problem is extremely low.
Part of the goal of watch and wait is to allow you to live your life, do the things you want to do, and not be consumed by anxiety about lymphoma progression. To a degree, we can carry some of that burden by seeing patients, examining them, and reviewing symptoms during office visits. Hopefully, that lifts some of that responsibility so that they can feel as normal as possible between visits.
For newly diagnosed patients, I encourage them over time to learn about the disease. It gives you confidence that you’re doing the right thing and that the messaging from your care team is resonating and being checked. It also gives you a feeling of control, because you understand why you’re doing what you’re doing, and you can participate in decision-making. When that happens, it’s best for everybody.
Nicky: I could not agree more. I mentioned earlier that being told that you’re going on watch and wait at initial diagnosis is terrifying, but it gives you time to educate yourself. The biggest benefit of that is finding other people who are diagnosed. See where they’re at and look for resources, like The Patient Story, and stories from other patients. We also have the Follicular Lymphoma Foundation, which has a support hub for follicular lymphoma patients, and they’re doing great things.
There’s so much out there now. When I was diagnosed, I couldn’t find much at all, but there are more resources available now. Do you have any particular resources, Dr. Friedberg, that you’d like to point out to patients?
Dr. Friedberg: The Lymphoma Research Foundation and Blood Cancer United in the US have very good resources for patients. They also have telephone lines where people can call in and speak to somebody, either someone who’s had a personal experience or someone who is very knowledgeable and can help direct them to clinical trials.
At initial diagnosis, some of the longest visits I have are the visits where we’re contemplating treatment for low-tumor-burden follicular lymphoma, including watch and wait, and trying to reassure patients that they’re not harming themselves by taking some time. Sometimes the second longest visits I have are when those same patients need treatment, and I have to convince them that it’s time to start because they’ve become so accustomed to the observation and don’t necessarily want to go off of it. Over time, people do become more comfortable with enhanced understanding and seeing that things aren’t moving quickly as they fear.
The number of times I have felt treating a patient because of anxiety is a very low number.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
Should I start follicular lymphoma treatment just to help my anxiety?
Nicky: Hypothetically, if you had a patient who was extremely anxious about going on watch and wait at initial diagnosis, would you consider a low-dose rituximab for them to help ease their mind?
Dr. Friedberg: I will, yes. That said, we have to be careful in medicine. Giving treatment is not a substitute for spending time with a patient and having them understand their options. It can be pretty quick to say you have lymphoma, so I’m going to give you this medicine and it’s going to shrink the lymphoma down. It almost always works. Everybody’s happy. You move on. It takes a lot longer to have a discussion and say, “We’re going to wait for a while and here’s why,” and monitor all of that.
But as you pointed out, for certain patients, that is probably the right thing to do if there’s concern about infection or other things, or if clinical trials are coming up and you want to try to maintain eligibility for some of those new treatments.
But I can say that the number of times I have felt treating a patient because of anxiety is a very low number. Most of the time, we’ll come to an agreement on treatment, but it’s not because of anxiety. It’s because of the way the disease is behaving or for that particular patient, it feels like the right thing to do.
A single CT scan does not have dangerous amounts of radiation. But if you’re going to have follicular lymphoma for 40 or 50 years and you’re getting scanned multiple times a year, then that starts to add up.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
Scanning, scanxiety, and how often you need to be imaged
Nicky: There’s another type of anxiety with watch and wait: scanxiety. How often would you tend to scan during watch and wait?
Dr. Friedberg: That’s changed quite a bit as far as recommendations over the years. Historically, we were doing more scans than we probably should and many were low-yield. Over time, there’s concern over radiation exposure. I’ll reassure people that a single CT scan does not have dangerous amounts of radiation. But if you’re going to have follicular lymphoma for 40 or 50 years and you’re getting scanned multiple times a year, then that starts to add up.
What I generally do is a fairly short-interval scan, maybe six to eight months after we decide on watch and wait to rule out early progression and understand how quickly the disease is changing. If that scan hasn’t changed much, it may be a couple of years before we need to repeat imaging, particularly if the disease is accessible and we can examine it.
More imaging isn’t necessarily better. If you have a small lymph node at 2 cm and we watch it grow to 4 cm, then 4.5 cm, then 5 cm, whether you start treatment at 4 cm versus 5 cm isn’t going to make any difference. But getting into that monitoring cycle creates a lot of anxiety that doesn’t help.
Caregivers and support: You’re not treating a patient, you’re treating a family
Nicky: Let’s talk about caregiver integration. How heavily involved are caregivers typically, and do you find them helpful?
Dr. Friedberg: One of the nice things about being a cancer provider is that you’re not just treating a patient; you’re treating a family. A patient’s journey impacts the family. Decisions to treat will have an impact on the children as well. You have to think about all of those things and provide support for families. Many patients come with family members who are understandably interested in the plan, and it’s important that they understand the rationale and feel supported.
From the symptom management standpoint, the patient is ultimately the important driver. Sometimes families can inadvertently contribute to anxiety if they’re worried about something. On the other hand, particularly once treatment starts, you need family to support you through all of that. There’s often a lot of caregiving that has to happen, so they are very important allies.
When it’s time to treat: What are the follicular lymphoma treatment options?
Nicky: Around treatment decision-making, when a patient is coming off watch and wait, what treatment options are there?
Dr. Friedberg: We’re in an era where we have so many different options for patients with follicular lymphoma. New treatments have come out faster than our databases have been able to inform us on what the best options are.
Standard approaches include single-agent monoclonal antibody, like rituximab, often used in low tumor burden situations or for patients with comorbidities that make chemotherapy difficult to tolerate.
For patients with higher tumor burden, the best chance to obtain a complete remission, which predicts the longest remission duration, is to combine chemotherapy with a monoclonal antibody, like rituximab or obinutuzumab. The chemotherapy regimens generally used are either bendamustine alone or a regimen called CHOP, which includes cyclophosphamide, vincristine, doxorubicin, and prednisone. Both of those regimens can give, on median, years of disease-free interval.
One of the most exciting things coming down the pike quickly is bispecific antibodies. I like to think of these as supercharged versions of rituximab. Rituximab is an antibody that binds to a protein called CD20 on lymphoma cells, activating your immune system to kill them.
When you have a bispecific antibody, it still binds CD20, but it also binds something called CD3, which is on your T cells. It physically brings the T cell up against the lymphoma cell and activates the killing. Early results are looking incredibly promising.
In our SWOG study group, we have a large randomized trial for patients with low-tumor-burden follicular lymphoma: half getting single-agent rituximab, the other half getting a bispecific antibody called mosunetuzumab. We’re following these patients for a very long time to get a signal as to whether giving the bispecific upfront might give us a chance at curing a subset of patients. The decision-making has to be individualized. The good news is that even if those options don’t work, we have many other options in the second and third lines. But that’s generally the approach when someone on watch and wait ultimately needs treatment.
CAR T-cell therapy and bispecifics: Could this be a cure?
Nicky: I know a few people who’ve had CAR T-cell therapy and consider themselves cured. Do you think CAR T-cell therapy could be a curative treatment for follicular lymphoma?
Dr. Friedberg: We definitely feel that CAR T-cell therapy has curative potential in diffuse large B-cell lymphoma (DLBCL) as it’s a very rapidly proliferative disease. With patients who were initially treated, it’s clear that if they hadn’t gotten CAR T-cell therapy, they wouldn’t be alive. And if you’re a year or two out from that treatment, the chances of it coming back are very, very low.
The question in follicular lymphoma is how durable the responses are. Similar to bispecifics, we probably don’t quite have long enough follow-up to say with conviction that it’s curative. But the number of events we’re seeing after about three years of getting CAR T-cell therapy for follicular lymphoma is very low. There’s certainly a signal that a reasonable percentage of patients are doing very well for a long period of time. But given the slow-growing, indolent nature of follicular lymphoma, I expect we’ll need at least 10 years of follow-up before we can say with certainty that people are cured.
Final thoughts: Tips for the newly diagnosed follicular lymphoma patients going into watch and wait
Nicky: Dr. Friedberg, before we finish up, what are the must-know tips for somebody newly diagnosed and going onto watch and wait?
Dr. Friedberg: Anybody newly diagnosed with cancer should get an opinion from a specialist in that cancer, even if it requires travel. In this disease, even though it sometimes feels rather ordinary, it’s important to ensure that the diagnosis is accurate and that the decision-making is correct.
Ensure that you have confidence in your care team… put some of the burden of follow-up on the care team… go on and live your life.
Dr. Jonathan Friedberg, Follicular Lymphoma Specialist
For patients considering watch and wait, it’s important that over time — and it doesn’t have to be immediate — they understand the rationale for it, what to look for, and develop a comfort level with it. The most resistant people I’ve had to the concept of watch and wait ultimately are people who didn’t want to give it up because they felt so comfortable with it.
Most important is to ensure that you have confidence in your care team. If you can put some of the burden of follow-up on the care team, and the care team is following you closely enough that you’re comfortable and can go on and live your life, that’s the best situation.
This is such an exciting time in follicular lymphoma. We’re using the word “cure,” which we never thought would be possible with several different modalities. For people on watch and wait, you can think about deferring treatment as we’re refining these approaches, so you’ll have access to some of the latest treatments when you need them.
Nicky: My tip is to make sure that you’ve got an amazing team around you. Not just the clinician, but also a nutritionist, a psychologist, and a nurse. If you’re not comfortable with your entire team, then look for the perfect team for you. Use the watch and wait phase to absorb all of the new information, because there’s a lot of it.
If you get the opportunity to go on watch and wait, it’s such a benefit as a patient. You have time to find your people, to learn about other patients’ stories on The Patient Story, and to use the resources of the Living with Follicular Lymphoma Facebook group. We have over 15,000 patients and carers in there, available 24/7. We also have the Follicular Lymphoma Foundation; excellent resources at theflf.org.
Conclusion
Nicky: Dr. Friedberg, thank you so much for joining us.
Dr. Friedberg: Thank you. It’s been a great conversation and I wish you the best of health.

Stephanie: Thank you so much for watching this program and a very special thank you to Nicky Greenhalgh for guiding this discussion and to Dr. Jonathan Friedberg for bringing his expertise and genuine care for patients to this conversation.
If there’s one thing I hope you take away today, it’s this: Active surveillance is not giving up. It’s not passive. It is a deliberate, evidence-based strategy, and one that can preserve your options, protect your immune system, and give you time to prepare for whatever comes next, which is great news.
As Dr. Friedberg said, we’re in one of the most exciting times in follicular lymphoma. Bispecifics, CAR T-cell therapy, and clinical trials are moving fast. Waiting may mean walking into better options when you truly need them.
Everything in this program is for educational purposes only. Please take what resonated with you and bring it to your doctor and medical care team. They know your specific situation and that conversation is where real decisions get made.
When I was going through my cancer diagnosis, I wanted better guidance on resources across organizations, so let me take a moment to highlight some great resources. The Patient Story has more follicular lymphoma content at thepatientstory.com and on our YouTube channel. The goal is to dive deep into real stories, so you know you’re not alone.
Nicky’s Living with Follicular Lymphoma Facebook group has more than 15,000 members. That’s a live and active community, which is great for conversation and real-time support.
If you’re looking for free, personalized support, Blood Cancer United is another great partner of ours. They have Information Specialists available by phone who are highly trained oncology nurses and social workers who can answer your questions, whether you’re newly diagnosed, on active surveillance, or preparing for treatment. You can find them at bloodcancerunited.org.
Nicky also mentioned the Follicular Lymphoma Foundation, which is dedicated to follicular lymphoma. You can find them at theflf.org.
Thank you for being part of The Patient Story community. Remember: You are not alone in this. I hope we get to see you more. Take good care.
Program Partner
Thank you to the Living with Follicular Lymphoma Facebook Group for their partnership. Their private Facebook group is dedicated to supporting individuals with follicular lymphoma, their families, and supporters. They offer a safe space to share personal experiences and learn about the latest research, trials, and treatments.
Program Sponsor
Thank you to our sponsor for their support of our independent patient education program. The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story. This content does not replace professional medical advice.
Hear from people living with follicular lymphoma
Real experiences with diagnosis, treatment choices, side effects, and life beyond follicular lymphoma — in their own words.







