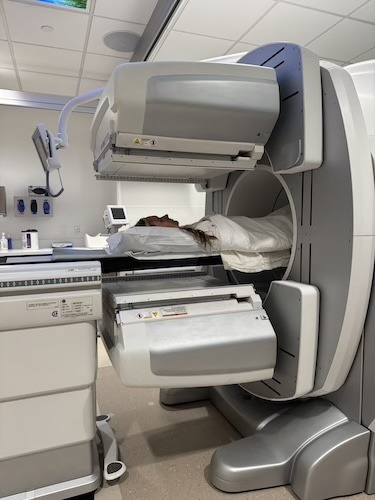
Self-Advocacy Saved Sydney’s Life: Diagnosed with Stage 4 Colon Cancer
Stage 4 colon cancer is a diagnosis that carries immense weight, especially when it comes at age 27. For Sydney, the path to discovering this reality began long before a doctor confirmed it. After years of dismissing chronic bloating and constipation as travel issues or normal digestive quirks, her symptoms escalated. Despite severe pain and an intuitive sense that something was wrong, she faced a barrier familiar to many young patients: being told she was too young for serious illness.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
The turning point came when Sydney, desperate for answers and unable to get a referral, made a bold decision to advocate for herself by fabricating a specific symptom — blood in her stool — to secure an appointment. This critical move led to a colonoscopy that revealed a massive blockage, resulting in an immediate colon cancer diagnosis. What followed was a whirlwind of emergency surgery, an unexpected ileostomy, and a move to a new city, all while processing the shock of a life-altering disease during the height of the pandemic.
Sydney’s experience has been defined not just by her diagnosis but by her resilience in navigating the medical system. After initially feeling written off by providers who offered no long-term hope, she sought multiple opinions and transferred her care to Siteman Cancer Center. There, she found a team that championed her quality of life, offering advanced procedures such as biomarker testing and various therapies. Today, Sydney balances ongoing treatment with her passions as a foodie and animal lover, finding strength in community and proving that a stage 4 colon cancer diagnosis does not mean the end of living fully.
Watch Sydney’s video and browse her edited transcript below to learn more.
Trust your intuition: When medical professionals dismissed her pain due to her age, she trusted her body’s signals enough to push for a screening, even when it required bending the rules to get in the door
The power of second opinions: Transitioning from a care team that told Sydney “we don’t know how to help you” to specialists at a research center opened new doors for treatment and renewed her hope
Quality over quantity: Her current care team prioritizes her ability to live a full life — traveling, eating well, and resting — rather than just focusing on aggressive treatment schedules at all costs
Community is vital: Finding specific patient groups, such as COLONTOWN and Fight Colorectal Cancer (Fight CRC), transformed Sydney’s experience from one of isolation to one of empowerment, connecting her with others who are walking the same path
Rest is productive: One universal truth she learned is that resting is not laziness; it is an active and essential part of the healing process that allows the body to recover from the trauma of treatment
Name: Sydney S.
Diagnosis:
Colon Cancer
Age at Diagnosis:
27
Staging:
Stage 4
Symptoms:
Constant stomachaches that only went away after bowel movements
Chemotherapy: FOLFOX, FOLFIRI, trifluridine and tipiracil
Monoclonal antibody: bevacizumab
Radiation therapy
Hormone therapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
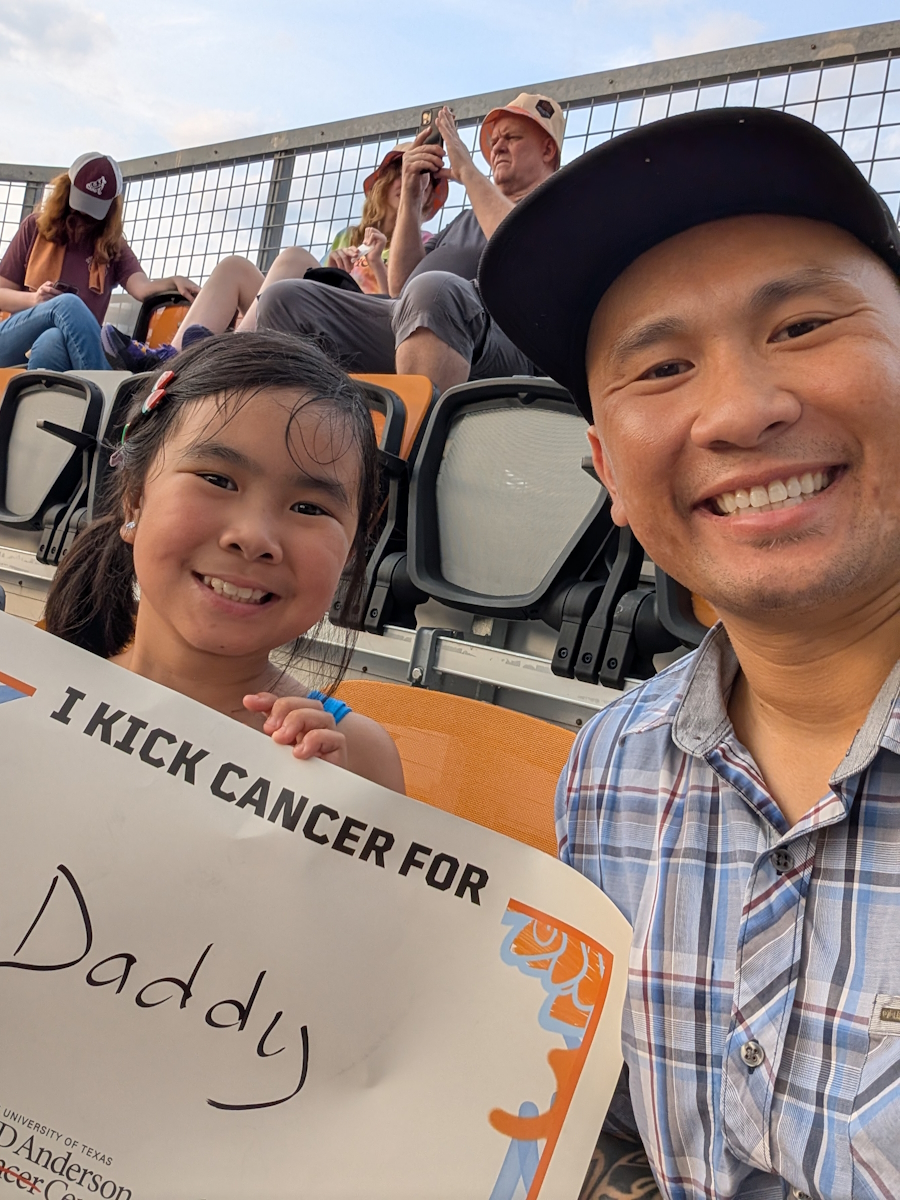
I am 32 now. I was diagnosed when I was 27, on September 28th of 2020, with stage 4 colorectal cancer. I’m from St. Louis. Well, actually, I’m originally from Arkansas, but right now I live in St. Louis.
I work in a cat cafe on my off weeks. I absolutely love animals and helping them. We get the cats adopted. I have two cats and a pit bull of my own right now. I love anything creative. Before I was diagnosed, I did a lot of professional theater work. I really like acting on stage, but I haven’t done that in a while.
I love Disney. I did the Disney College program in 2013, and so the obsession grew from that. I love food. My husband and I are really big foodies, so it’s really cool that we live in St. Louis because it has really great restaurants.
My early symptoms
I would always get what I thought was travel constipation because anytime we would travel, I could never go. Who knows when the cancer or a polyp started forming, but I remember always having trouble with constipation and bloating. Growing up, I never thought that there was an issue. It was just a normal thing because it would always work itself out.
Then, around the time my husband and I got married in 2018, things started getting worse. I was in pain more often. I thought I had IBS, and the doctors would just tell me, “No, you’re fine. All your labs look good. You’re too young for anything.”
In 2019, we went on a first anniversary trip to Riviera Maya. It was so bad. I was trying to read all these drug labels, and I was like, “I don’t know what this means, but I need something to help me get this out.” I think that maybe when the blockage started growing. I tried elimination diets, gluten-free, dairy-free, just to see if maybe it was the diet, because I used to do CrossFit four times a week. I would do spin classes. I love a sweet treat and a good burger, but I was eating pretty healthy. Every doctor would just be like, “You’re too young.” So I just never thought cancer would ever be the thing.
My path to diagnosis: advocating for care
Mid-summer in 2020, I was bent over at work in so much pain. I would only be relieved if I tried to go to the restroom, but after I ate, I was just always in so much pain. I finally called a gastroenterologist in Arkansas because I was still living there, and they wouldn’t see me just from the symptoms that I was telling them. They were like, “Well, you don’t have a referral.”
Then this thought came into my head. People always say, if there’s blood in your stool, they’ll see you hopefully. So I was like, “Oh, there’s blood in my stool,” even though I had never seen any. I lied, and she was like, “Okay, we can get you in.” I went in for my colonoscopy and endoscopy. I woke up in the middle of my colonoscopy because I heard them say “cancer.” They could not even get a foot inside my colon. Then they sent me straight for scans and surgery and everything from there.
I was just like, “I can’t be the one to figure out what’s wrong with me, right?” I have no experience in the health field, and people just continuously told me, “You’re too young, you’re fine.” I’m like, “I know something’s wrong inside my body.” For a little bit, you almost feel kind of crazy, or you just have these breakdowns of, “Is anyone going to believe me?” Thank God for that gastroenterologist for being like, “Okay, we can take you.” Even though I did have to lie because I was only 27 and didn’t have a referral, because my doctor at the time was like, “You’re too young.”
Receiving the colon cancer diagnosis and emergency surgery
It was 2020, the peak of the pandemic, so my husband was not allowed to come in with me. But I knew because, waking up after the colonoscopy, I didn’t remember them saying “cancer” at that moment. I just knew something was up whenever the doctor was like, “Okay, your husband’s going to come sit down in this room with us.” I was like, “Okay, well, that’s not a good sign.”
He was just like, “I’m 99.9% sure you have colon cancer… whether it’s cancer or not, you either way have a huge blockage that needs to be removed.” He said, “You cannot eat. You have to have smoothies and drink until your surgery because the blockage is so bad.”
On that weekend, I had a colonoscopy, and they scheduled surgery, but we had already scheduled to move to St. Louis. 2020 was a crazy year. So we move over that weekend, and I have to be back that Monday for surgery. But we had moved so much that I was like, “I need to eat, I have to eat something.” So I ate a little bit and was in pain. Then the prep for the surgery did not work. Nothing came out. On the way to the hospital, I’m crying because I’m like, “They’re not going to do the surgery because nothing came out.” But then I’m also trying not to throw up.
They did the surgery, and I woke up with an ileostomy that I did not know I was going to get because the prep did not work. They had to let my bowels rest. But I got it reversed after a little over a year.
Coping with the initial shock and chaos
I don’t really know how to describe it other than I was just like, “Okay, that’s what they told me to do. So that’s what’s going to happen.” I know nothing of this world. I had only known family members or friends who had cancer. I’ve never experienced it myself. I was like, “Well, these are the professionals, so I’ll just listen to what they do.”
Sticking to the matter-of-fact things was the only way that I was able to grasp what was going on. Even five years into it now, people still give you all of this advice, “You should try this,” or “Have you looked into this?” Or people would always ask, “Do you have an update?” or “What did your doctor say?” It’s just all the constant questions. For the first two years, I was just telling anyone, “If you have advice for me or if you have a question, please don’t, because I do not have the capacity to deal with that when I’m dealing with all these new things that have been thrown at me.”
I just pretty much stayed like, “This is what’s happening, and this is what I have to do. So this is what I’m going to do 100%.”
When we were sitting in that room, not when it was confirmed, but in the room after the colonoscopy with the doctor saying, “I’m 99% sure,” I was also still a little bit high from the anesthesia. I was just sitting there, and my husband was trying to comfort me, but he’s freaking out. He’s like, “How is she not freaking out?” I think I just froze. I just remember he was rubbing my back so hard. I was like, “Okay, that’s enough.” He was like, “I’m sorry, I’m just — how are you not freaking out right now?” I was like, “I think I’m just literally in shock. I’m a little frozen right now.”
When I woke up after surgery with the ileostomy, the doctor told me it was only stage 3B at that point. But then, when I got to St. Louis, and we did scans again, it was stage IV. I have never had a doctor give me a timeline or anything or tell me that I’m incurable. So that was very helpful. But I have had doctors tell me, “We don’t know how to help you anymore.” So that can be discouraging. To be told, “Hey, we don’t know how to help you anymore, you need to go elsewherer” was like, “No, what do I do now?”
Finding the right care team and second opinions
When we first moved to St. Louis, it was a year after being kicked off my parents’ insurance. My husband and I were trying to find insurance and then find a hospital that would take it. I started treatment at St. Louis University (SLU), and I had my first oncologist for one year, but she moved back to Texas to be with her family.
I applied for disability because I couldn’t work through treatment, especially Folfox or Folfiri, the heavy treatment. My husband’s a barber, so basically self-employed. I applied for disability, and I got it. I didn’t know that after two years, you get put on Medicare if you’ve been on disability for two years. So when I was able to be put on Medicare — which there was a whole awfulness about because I was on Medicare for eight months without knowing it and still paying for regular insurance — I was able to move to Siteman Cancer Center.
Being at Siteman has rejuvenated my hope – 100%.
Now, just always kind of telling myself, “It may happen, but I’m not going to die from this.” I believe that I will reach no evidence of disease, and then I will see it for five years, and they will tell me that I’m cancer-free. That’s what I believe. Of course, there are hard days, but really, it’s just what I keep telling myself. My husband likes to say I’m a little witchy, but I do my little manifestations, write in my journal, and put it under my pillow.
A look at my treatment
Initially, I did 12 rounds of FOLFOX. We waited because I was clear after the 12 rounds of Folfox. We waited for scans for two to three months. While scans were clear, bloodwork wasn’t. My doctor at the time said, “Well, we need to be aggressive.” So I started on 12 rounds of FOLFIRI.
After my first 12 rounds of FOLFOX, I did six rounds of radiation, three on this side of my lungs and three on this side. Then the blood work came back bad, and so then I did the FOLFIRI for 12 rounds, and then they put me on capecitabine, which is a chemo pill. That’s when they told me, “We can’t help you anymore. I don’t know what to do.”
So I went to Moffitt in Tampa to get a second opinion because they would take my insurance at the time. He was like, “No, I’d put you on trifluridine/tipiracil. You do have more options.” So we switched to that drug. I was on it for well over two years. It would be stable, then a little progression, and then go back down to stable.
Then I had a new spot show up in my liver, maybe in September or October of 2025. Now I’m on FOLFIRI again, but I’m at a low dosage, so it’s not as bad as the first time, but I am starting to experience a lot of the things — obviously, my hair is falling out again. My eyebrows are gone. Gotta draw them on. But that’s what makeup’s for.
I have two spots for sure on my liver, which significantly shrunk on scans after being on FOLFIRI. One almost went down a whole centimeter, or maybe it was cut in half. And then I have one that we’re not sure what it is on my liver. It’s not been confirmed. Then, on my lungs, I have numerous spots, too many for surgery.
Managing my colon cancer treatments and side effects
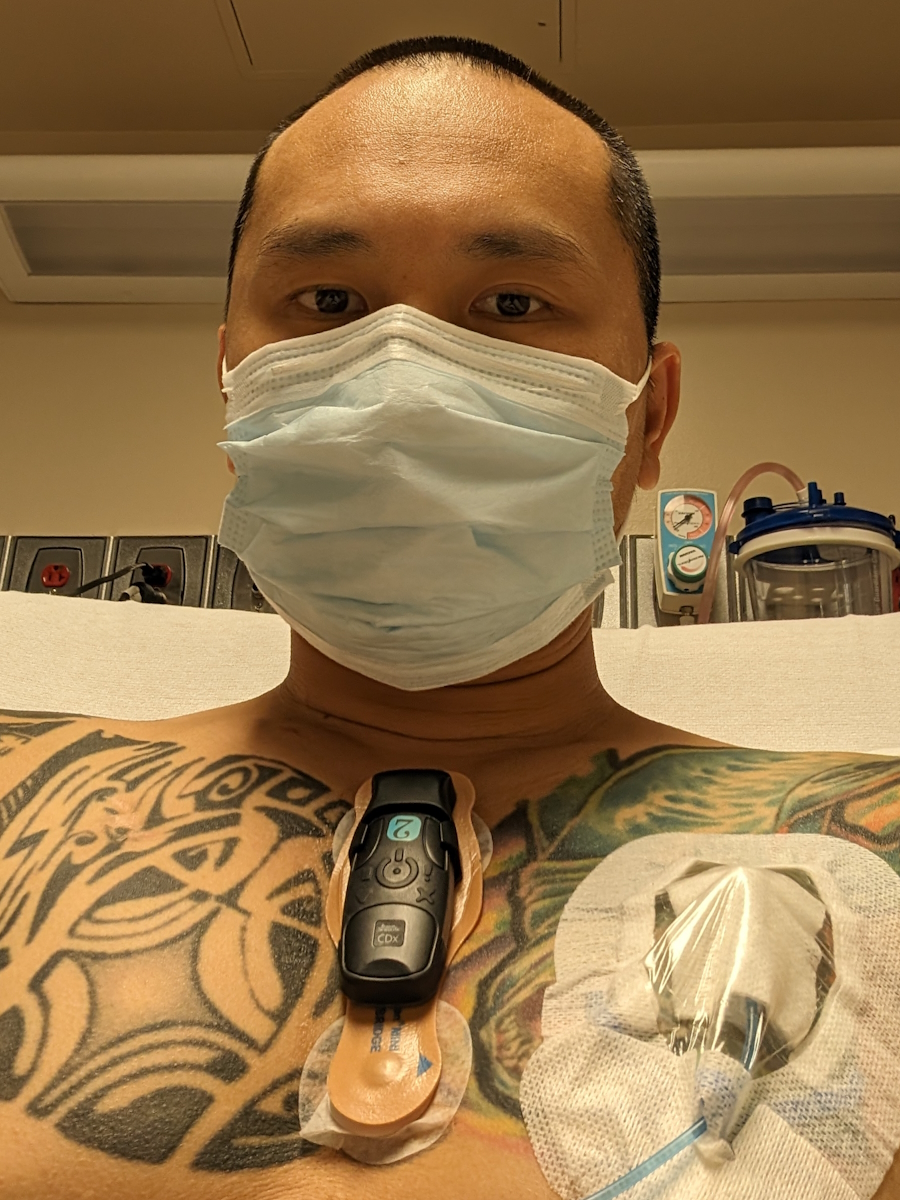
I have been on the schedule every other Tuesday for three years now. I’m on bevacizumab right now with FOLFIRI. So I go in, get labs drawn. They check my CEA every time. But I also have to do a urine sample to see if there’s protein in my urine from the bevacizumab. Unfortunately for me, I’ve been on bevacizumab for three years straight now, so my levels keep going up. I do have a kidney specialist who keeps track of it. We had to pause the bevacizumab on Tuesday because I had such high protein.
I am sent home on a 46-hour pump with my port right here. It’s affecting my vocal cords; my voice always goes out on these three days of treatment. Obviously, I get digestive issues, appetite, and fatigue, all of the things. But once I get unplugged on Thursday, I’m usually slowly coming out of that chemo fog. By about Friday night, I’m okay again. I tell my husband, “I’m sorry I was so lazy today.” And he’s like, “You’re not being lazy. What are you talking about? You’re on chemo.”
Maintaining quality of life during colon cancer treatment
My husband and I are both foodies, and so when I do have an appetite, I’m like, “Okay, we have to go find a good restaurant, or I need a good breakfast.” We also really love music. So we go to shows often, and we used to go to Music Fest all the time. We slowed down on the Music Fest, though, just because there are so many people and it’s a lot for a whole weekend. If the venue doesn’t have a chair, then I’m usually out.
I spend time with my pets, working at the cat cafe, my friends, and my family. We travel home to Arkansas pretty often. Especially with being at Siteman now, they are very much into the quality over quantity. My doctor told me, “If you want to take a trip and you want to pause for a week, we can pause for a week.” He was like, “I would rather you go live your life than just constantly be on treatment and not doing anything fun.”
How to support someone with cancer
When I got diagnosed, people didn’t really know what to say. How do you tell someone, especially after you get a stage 4 diagnosis — people hear that, and they think “terminal.” No shade to my sister, but she didn’t know how to handle it. She told my young nephew when I was getting treatments that I was going to get my nails done. I was like, “I mean, I wish.”
People really don’t know what to say, what to do. It can be really isolating. But I would tell people that it is going to be okay. There’s going to be a lot of hard times. But you find that if you can find community, especially in your specific cancer — like I found Fight CRC, then Colon Town — and I’ve met so many people who are going through the same thing as me.
You just have to find someone to champion you. My husband and my parents have learned so much. It’s night and day from when I got diagnosed to how people support me now. I do think cancer patients also need to let people know how to maybe readjust the speech. Maybe don’t tell me, “My grandma died from cancer,” as soon as I tell you I have cancer. Maybe don’t say those things.
I found The Patient Story on Instagram. There’s a colorectal cancer patient right now who has been given only a certain amount of time to live. But she said, “You know, as long as I can tell my story, and it saves one person’s life…”
The importance of hope and doctor-patient communication
I am so grateful that no doctor has ever told me my prognosis. No one’s ever called it terminal for me. My first oncologist would let me break down in front of her, and she would just put her hand on my back, and she’d be like, “Sydney, you’re going to be okay. We have these treatments, and yes, they’re difficult, but we have so much proof behind the first treatment that I did that it can be successful for you.” She would always point that out to me.
Being at Siteman, they’ll sit down and explain everything to me. I got pushed into menopause from chemo, and they sent me to a woman specialist who’s in the hospital. If something else is wrong, they’ll send me to this specialist. They just really, really care. Having a doctor who, while they have so many patients, can be so personable and say, “We care about you as an individual and not just another number,” has really helped.
My final advice: finding community and moments of joy
I don’t want to be cliché and be like, “Don’t give up,” but don’t give up. You can do it. I know people speak about how they don’t want to be called a warrior. I’m tired of people telling me that I’m brave because what other option did I have? But I mean it. We are fighting.
Take the time to rest. Don’t think you are lazy for resting, because resting is how you’re going to heal. Do the things that make you happy. You have to find those moments of joy, even in the heartache of everything. Find a community 100%.
I have friends all over the world, and I’ve only maybe met them through social media or maybe once in DC, and I know that I can message them and be like, “Hey, I need to have a breakdown, and I don’t want to put that on my husband right now. Can I please break down to you?” Find community.
It’s hard, but you can do it. If you decide one day, “I’m tired of treatment,” that’s your decision. And I fully support that as well.
Trust Your Body, Trust Your Care Team: How Aleeshia Faced Rare Burkitt Lymphoma at 33
Burkitt lymphoma and severe fatigue showed up in Aleeshia’s life long before anyone said the word “cancer.” Living in Milan but rooted in a multicultural family that spans Vancouver, Montreal, Egypt, and Italy, Aleeshia had always built a life around travel, food, and making every new place feel like home. When a strange, unrelenting fatigue settled in, she assumed it was stress, hormones, or lingering effects of polycystic ovary syndrome (PCOS), not an aggressive stage 4B blood cancer quietly growing in her abdomen and bone marrow.
Interviewed by: Nikki Murphy
Over a few weeks, subtle symptoms escalated into a cascade of red flags: deep bone-like shoulder pain that cortisone could not touch, severe ear pain, bloating, early fullness, nausea, and pelvic pain. One morning, the pain was so intense that she crawled from the bathroom to her bed. After an ambulance ride and emergency surgery came a shocking discovery: a 15-centimeter mass on her ovary, massive internal bleeding, and the first mention that this might be lymphoma.
While she processed the loss of her left ovary and the fear for her fertility, the full diagnosis came in stages: large B‑cell aggressive lymphoma, then Burkitt lymphoma, and finally, stage 4B disease with bone marrow involvement. Hospitalized, unable to walk on her own, and rapidly getting sicker, she started intense, inpatient chemotherapy and immunotherapy almost immediately. The protocol demanded month‑long hospital stays, repeated infections, brutal nausea, and near-constant IV lines including a catheter in her neck when a PICC line failed.
Amid the physical toll, the emotional weight was just as heavy. Aleeshia grieved the possibility that menopause and infertility might outlast treatment, and she weathered moments of rage and despair where she wanted to rip out the IVs and go home. Her hematologist‑oncologist and a hospital psychologist became anchors, normalizing her feelings and giving her space to speak honestly. Supported by her parents and her husband, she kept returning to one grounding belief: trust in her care team and in her body’s ability to heal.
At the end of November, she heard the words “no evidence of disease.” Survivorship now means scanxiety, new physical limits, and ongoing questions about fertility, but it also brought her back to a more spontaneous, authentic self — someone who no longer needs a perfect plan to feel like her life is meaningful.
Watch Aleeshia’s story or read the interview transcript below to know more about her story:
Fatigue that doesn’t improve with rest, deep bone-like pain, sudden changes in digestion, or pelvic pain can be meaningful signals that deserve thorough medical follow-up
A rare, aggressive cancer like stage 4B Burkitt lymphoma can be extremely chemosensitive
It is never a patient’s fault when treatment causes harsh side effects or long-term impacts; the burden belongs to the disease and the intensity of the therapy
Honest, compassionate communication can ground patients in moments of shock and fear.
Aleeshia describes a powerful transformation: from feeling trapped and powerless in the hospital to reconnecting with her spontaneous, joyful nature and considering advocacy around psychological care in cancer treatment
Name: Aleeshia T.
Age at Diagnosis:
33
Diagnoses:
Burkitt Lymphoma
Staging:
Stage 4B
Symptoms:
Severe fatigue
Deep shoulder pain
Ear pain with inflammation
Abdominal and pelvic pain
Bloating
Early fullness
Nausea
Difficulty eating
Inability to urinate despite feeling an urgent need
Internal bleeding
Delayed period/bleeding
Intense whole‑body pain leading to collapse
Treatments:
Surgeries: emergency laparoscopic surgery with left ovary removal
Chemotherapy: R‑CODOX‑M/IVAC
Immunotherapy
Hormonal therapy (to protect the remaining ovary)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
My name is Aleeshia. I’m from Vancouver, Canada, but I live in Milan, Italy, and I was diagnosed with stage 4B Burkitt lymphoma in May 2025.
I am quite passionate about traveling. I have been traveling my whole life. My dad worked in the airline industry for a big chunk of my childhood. My sister is a flight attendant and I also work in the industry; I work for a tour operator. I come from a very multicultural family. My dad is Italian-Canadian. My mother is Egyptian-American. They grew up going to a lot of places as well and passed that down to my sister and me.
I love exploring new places, but what I like is getting to a place and making it feel like home in a way. I have not been to the most countries or done the most things in the world, but I have spent a significant amount of time in places that I have been interested in. It has been 10 years since I came to live in Italy and I have moved around a lot, which is not typical of a North American expat who comes to Italy. They usually pick one place and stay. I love it because you see a slice of life in other parts of the world and how people live. I love to connect with people in that way.
A couple of other hobbies or things that I am passionate about are food and cooking. I actually came to Italy to get my master’s degree in food studies. Hand in hand with traveling, I am interested in understanding why people eat what they eat, how it gets to their table, traditional family recipes, and that kind of stuff. I cook a lot. Whenever I am at my grandmother’s house in Montreal, I’m usually writing down her recipes, cooking, and taking pictures so that I can preserve all of that knowledge.
I also read a lot. My undergraduate degree is in English literature. When I am not somewhere else in the world, I am usually on my couch reading a good book.
When I First Noticed Something Was Wrong
The fatigue was probably the very first symptom. I did not have night sweats. I was not losing weight. For most lymphomas, the classic B symptoms are rapid or unexplained weight loss, night sweats, and fatigue. I think I only had fatigue. It was a strange sensation because I felt tired, but sleep and rest did not make the fatigue go away. It felt more like my energy was completely depleted, and the effort needed to do certain basic things was almost non-existent. But I did not feel unwell.
Those very first signs of fatigue and energy loss did not register with me as anything wrong besides something potentially stress-related or health-related, but not cancer. At the time, my husband and I were trying to get pregnant. I had received a PCOS diagnosis the year before, so I thought something was going on there. It did not at all register that it could be a tumor.
My Path to Diagnosis
After the trip, I came back, and almost the day after I landed, I had this pain in my left ear. I thought I had picked up a little ear infection or a sinus infection that had traveled to my ear or something. I went to a walk-in clinic near my house, and the doctor did an exam and said it was definitely severely inflamed. I remember her saying that the lymph nodes in the area were not swollen but that the nerves were swollen. She said it was probably an infection, gave me some antibiotics, and I went on my way.
About five days into taking these antibiotics, I felt so much worse than I did originally. I had a fever and bad stomachaches, and that sense of fatigue and zero energy made it difficult to get out of bed. I called my GP and said, “I need to see you today. I cannot work. I am ill.” In Italy, you need your doctor to give you a note to say that you are sick so that your sick days get paid out. She said she had about a half-hour gap and if I could come at that time. This was the second week of April, and I dragged myself over to her studio.
In that visit, she looked at my ear and said she did not think those antibiotics were the right ones for the ear infection, so she switched the antibiotics. Given that I had a fever and stomachaches, she did an abdominal exam as well and chalked up the pain in my abdominal area to a bit of gastrointestinal inflammation because of the antibiotics.
The other thing is that my period was two weeks late. This is important for when I get to the hospital. I had been doing regular at-home pregnancy tests, and they were negative. She said, “I will prescribe you a blood test, and we will rule that out,” because I had cramping in the pelvic area. She said, “I think it is mainly due to the antibiotics, but we will rule that out if you do this blood test and then we can go from there.”
I changed antibiotics. I never made it to doing the blood test she prescribed. Three days later, the pain in my ear was through the roof, to the point where I thought maybe I needed to go to the emergency room. My husband said, “Why don’t you just go see an ENT?” I made an appointment with an ENT at the hospital. At that visit, he said, “You do not have an infection. It is severely inflamed. I am going to give you cortisone.” That was a bit of a switch in my mind because I thought, “Okay, it is not an infection. Why would my ear just randomly get inflamed?” But we decided I would take the cortisone and see what happened.
When I started on this course of cortisone, my ear pain went away almost immediately, but then my shoulder started acting up. I had this severe, very deep pain in the point of my shoulder, and it felt like it was coming from inside my bone. Stretching and exercising did not help, and it was worse at night. That was very worrisome for me because I could not understand why I would have a pain that would worsen during certain parts of the day and be more tolerable at other parts of the day.
I was still taking cortisone, which is an extremely powerful anti-inflammatory, so I thought if it was muscular or if there was an inflammatory response causing this pain, the cortisone would be knocking it out. Instead, it was not. I was quite worried about that, but I said to myself, “You have not been well this whole month, and you still have not had your period.” So there was still this potential underlying hormonal diagnosis brewing in my mind and in my doctor’s mind.
What Happened Next
I said, “Okay, I will finish the cortisone and we will see what happens.” I did finish the cortisone, but I could not hold out on the pain. About five days into the cortisone, near the end of April, the pain in my arm was so bad one night that I woke up around 3 a.m. and said to my husband, “You have to take me to the emergency room. It is searing. I cannot think about anything else.” I was seeing white from how bad the pain in my shoulder was.
We went to the emergency room, and they treated it like it was just a muscular situation. They gave me an injection of a high-dose painkiller, and I was sent home. That helped with the shoulder situation, but I was still having cramps, abdominal pain, and just feeling unwell in my belly in general. It was difficult to eat, and I would get full quickly.
During that last week of April, I was also noticing that I was very bloated all the time and eating had become difficult. I would get full almost instantly and feel nauseous after I ate. It was a lot of things all at once and very quickly.
The Weekend That Changed Everything
I went to the ER twice. The first time my husband brought me in the middle of the night for my shoulder was a Friday. That weekend, my sister was in Milan on a layover. My mom had been here; she had come for Easter. The three of us went on a little day trip. I was feeling all right. I could still feel this pain in my shoulder, but overall, I was feeling okay. We were out all day long and had a great time.
On Sunday, my mom and I had plans to do another day trip to Como, and I woke up and said, “Mom, I do not feel good. Do you mind if we stay home?” She said, “Yeah, sure, no problem.” We ran a couple of errands but stayed home for the rest of the day, and I slept most of that afternoon. What changed on Sunday was that I started bleeding. I thought my period had finally arrived a month late, which resolved the potential pregnancy situation. But it did not ease up any of the pain I was feeling in my pelvic area, which was strange because I normally do not have cramps or a difficult period.
My mom was a bit worried because she said, “I had an ectopic pregnancy, and it can be life-threatening. Is it painful?” I said, “No, I think it is just weird cramps. It is not that bad. I just feel tired. I will be okay.” I slept off most of the afternoon on Sunday, then had dinner, and went to bed super early. Around 5 a.m. on Monday, I woke up in pain that I do not even know how to describe. I was not in my body. The pain was so overwhelming that I felt like I had zero control over my body. The pain was controlling everything.
I got out of bed, went to the bathroom, and fainted. I was only passed out for maybe five or six seconds, but it was 5 a.m. My husband and my mom were in a deep sleep. I thought, “Something is wrong.” I had to crawl back from the bathroom to my bedroom. I could not stand straight. I was bent at a 90-degree angle, almost on all fours, because the pain was so bad.
When I got into my bedroom, I do not 100% remember what happened. But I was lying on my back and must have been screaming in pain because my mom and my husband both woke up and immediately asked what was wrong. I remember my mom screaming, “Call 911. Call 911.”
I Needed Emergency Surgery
My husband called an ambulance, and they arrived within about five minutes — super quick. I was awake but not super lucid. The paramedic helped me get onto the gurney, and when they picked me up, there were about three liters of sweat on the ground below me. My body was in shock. I was super pale, sweating profusely, and in so much pain that I could not walk or straighten my legs. They rushed me to the hospital. Thankfully, we live within a 10-minute drive of where I was treated.
They took me straight into the ER, and everything was very rapid-fire. It felt like an episode of a medical TV show. There were three or four nurses around me, stripping me, putting in IVs, and asking me questions. The emergency room doctor immediately had an ultrasound out. They called an anesthesiologist. With the ultrasound, they started saying there was a lot of fluid in my abdomen, which was the concerning bit. They said it looked like there was a shadow over one of my ovaries, and they were asking me if I had my period, if I was pregnant, and all of that.
In between all the pain, I was trying to explain that I was about a month late, that I had taken pregnancy tests and they were negative, and that I had just started bleeding the day before. They said, “This could be an ectopic pregnancy.” Everything my mom had said the day before was there on the table. They said, “We are going to have to go in for emergency surgery. We will go laparoscopically. We have to figure out what is happening, but we are going to call in a gynecologist.”
They explained everything to me as it was happening. They had me sign a bunch of consent forms. The anesthesiologist was prepping me for surgery because they said I was going to be put fully under. My husband was there, also signing consent forms so that if things happened during the surgery, he could make decisions on my behalf. It was full on. Within 25 minutes of being admitted into the ER, they had me moving toward an operating table.
The gynecologic surgeon came down and introduced himself. He had been briefed on the situation. They passed me off from emergency medicine into emergency gynecology because this hospital has an emergency obstetrics department and there was a suspected ectopic pregnancy. In the midst of being rolled into the operating room, this doctor said, “Hello, my name is Leonardo. I am going to be operating on you,” and I said, “Okay.” I was pretty much out of it, and that is the last thing I remember because they administered the anesthesia, and I was out right away.
I woke up around seven hours later in intensive care. My doctor was the first person there again. I said, “Hello, Leonardo,” and he chuckled a little bit because I was just waking up after anesthesia, with no idea where I was or how much time had passed. My husband was also there, and I did not realize that pretty much the whole day had elapsed. When I woke up, I thought maybe half an hour had passed. I said to my husband, “What are you still doing here? Are you not supposed to be at work?” He said, “The whole day has gone by. You have been on the operating table for hours. I have been here the whole time.”
Then the doctor said to me, “We had to remove your left ovary. It had died. It was not an ectopic pregnancy. Instead, we found a 15-centimeter mass. I have sent it for a full histology. I think it might be lymphoma, but I do not know which kind. The mass had caused massive internal bleeding. You had lost nearly three liters of blood. We had to do transfusions during the surgery. For right now, all seems well. You are going to spend the night in intensive care, and then you will probably be in the hospital for a bit of post-op recovery.” That was the very first time cancer was mentioned as a potential diagnosis.
The Moment Everything Changed
I was processing what he was telling me in a certain sense, but I do not think the cancer part stuck. I remember being most concerned about my fertility. I think the only thing I asked him was, “Will I still be able to have babies? I only have one ovary left.” He said, “We cannot say that for sure right now.” He was good in his responses. He said, “I did not remove the other ovary because it looked healthy enough. Given your age and the fact that you and your husband were trying, I wanted to give you a chance if there would be one.”
I was focused on that, and I do not think the cancer element did much that day. I remember thinking, “They found this mass; that is scary,” but because they found it on my ovary, I thought it might be a cyst, maybe something related to PCOS. I think there was a part of my brain that thought lymphoma was a possibility, but that there were many other possibilities. I do not think I understood how accurate his presumed diagnosis could be in that moment.
He was very careful to say, “I think it might be this, but I am not giving you this diagnosis. We have sent the mass for histology. I know that it is not a sarcoma because during the operation, we ran a rapid biopsy. If it had been sarcoma, I would have performed a complete hysterectomy because it would have been too dangerous.” I clung to that: it was not sarcoma, not that “dangerous cancer,” so it might be something completely unrelated. I was more focused on the loss of my ovary and what that would mean for my future fertility.
Waiting for Histology
I spent a week in the hospital after the surgery. I stayed one night in intensive care, and the next day, they said I was stable enough to be moved to gynecology. That first week, there was no more talk about cancer or histology. It was focused on post-op care. Every day, they checked my sutures. I still had a drainage bag, so they checked that, changed bandages, and so on.
That week in the hospital, the pain in my shoulder came back, and I started to dwell on it. They sent me for an X-ray to rule out any fracture. The X-ray came back totally normal. Because I was in the gynecological ward, I was only seeing gynecologists. Since the histology was still being performed, they were very careful about saying anything that could sound like a diagnosis. When I would bring up my shoulder, they would say, “The X-ray came back clean, but we are still waiting on the histology. It might be related. We do not know.” I think they were aware it was a symptom, but did not want to tell me it was related to cancer, because they did not want to give me a cancer diagnosis.
I was discharged and went home for a week. I had nothing planned that week. They told me we needed to wait for the histology report to come back. They set up an appointment a week after my discharge for a post-op check-in and said they would have the results at that point. This was the middle of May when I went back into the hospital.
I Was Getting Worse
The week at home, I deteriorated rapidly. During the week in the hospital, my shoulder had started acting up again, but coming off the anesthesia and painkillers was manageable. At home, the pain was through the roof again. I had been eating well enough in the hospital, but at home, I went from feeling okay — sore and tender from the operation — to being sick. I was throwing up everything I tried to eat. I could not go to the bathroom. I felt constantly like I needed to pee, but no urine was coming out. I was very thirsty and was drinking a lot of liquids.
I said to my husband, “I think we should go back to the emergency room,” and he said, “No, it is probably just your body reacting to a huge surgery. You were under anesthesia for at least five hours. They said there might be some tummy aches and stuff like that. You do not have a fever, your stitches have not ruptured, and you are not bleeding. Let us just wait until the 13th.”
On the 13th, we went back into the hospital. I was sick. I needed my husband to push me in a wheelchair. I went into the gynecologist’s office, and next to her was my hematologist-oncologist. At that point, I knew what I was going to be diagnosed with. He was there to tell me that the histology report had come back and that they definitely knew it was a large B-cell aggressive lymphoma. He thought it might be Burkitt lymphoma. He said, “You are going to be hospitalized today, and there will be a couple more diagnostic tests before we decide what your treatment plan will be.”
My diagnosis came in steps. It was discovered in the emergency room. It took two weeks from that emergency operation to a cancer diagnosis and then another week to the complete diagnosis with a treatment plan. In those three weeks, I spent two of them in the hospital.
Hearing My Full Diagnosis
The testing all happened while I was hospitalized. They would say, “Today you are doing an MRI; tomorrow you are doing a PET scan.” I had to do a bone marrow biopsy, which required a lumbar puncture. I had many lumbar punctures. It was probably the worst procedure out of all of them. It was extremely painful for me. I also had a CT scan.
I was hospitalized again. The very next day, I was sent to urology to have stents put into my ureters because the masses were basically blocking them, which is why I had not been able to pee. I had a diagnosis, but it was not the complete diagnosis. I spent another week in the hospital while all of these tests happened. I was very sick, so they wheeled me on beds into all of the different rooms in the hospital to get the CT, the PET, and all of these things. About five or six days after that, I had the Burkitt lymphoma diagnosis, and we had my treatment plan in place. I started chemo immediately the next day.
My first feeling was relief to have an answer, especially for the pain in my shoulder and how ill I had been. There was some release in finally not having to sit with the unknown. Now we knew, and that meant we could do something about it. At the same time, I was completely shocked, numb, scared, and bowled over by the fact that I was 33 years old and had just gotten a cancer diagnosis.
A small part of me was hyper-curious because I had never heard about Burkitt lymphoma. I knew, broadly, about Hodgkin’s and non-Hodgkin’s lymphoma. I have had relatives and other close people in my life who have had cancer or passed away from cancer, so you broadly know about breast cancer or colorectal cancer. Nobody is ever talking about Burkitt lymphoma. I thought, “What is this?”
There was a tiny part of me that was very curious to learn more and to think, “I guess I am going to be a human experiment in a way,” because it is a rare form of cancer. It has fewer than 100 diagnoses in Italy, fewer than 400 in the European Union, and around 200 in the United States, from what I remember looking up. It is classified as a rare cancer.
There was a small part of my brain that was intrigued by learning about something I would never have stumbled upon otherwise, but that was a very small part. It was mainly fear, shock, and a lot of “Why me? What did I do? Was there something I could have done?” It was a weird mixture of relief, fear, and curiosity.
I Thought I was Going to Die
The staging confused me. When I first heard stage 4, I panicked and thought, “I am going to die from this cancer.” My doctor said stage 4 for non-Hodgkin’s lymphoma is a very different diagnosis than stage 4 in other cancers, especially those with solid tumors. It is not that tumors do not grow with lymphoma, but you cannot simply cut lymphoma tumors out. They will keep growing because the cancer is in your blood. He said a stage 4 liver cancer diagnosis is very different from my diagnosis.
Ultimately, the staging was because they found masses all over my abdomen, both above and below my diaphragm, which made it stage 3. Then they also found it in my bone marrow, so it had traveled to one site outside of a lymph node area. Because it was in the bone marrow, it was hurting my shoulder so much. But my lymph nodes in my neck, behind my ears, and in my clavicle were not swollen. The lymph nodes that had swollen, where the masses originally grew, were deep in my abdomen. That is why I never saw a mass anywhere in my body.
Choosing My Care Team
I found my care team because I was already at this hospital. We have a national health service in Italy, so there was never an element of an insurance company needing to approve or not approve certain treatments. At the hospital where I was treated, they said, “Here is the standard of care. This is the protocol used pretty much everywhere in the world as the first-line care for Burkitt lymphoma. Your state of illness is so advanced that we need to start treatment immediately. It is extremely life-threatening, and that is what is going to happen.”
I did not have a chance to ask for a second opinion, shop around hospitals, or speak to other doctors. At one point, especially in that first week after we knew it was cancer but were waiting on the full Burkitt lymphoma diagnosis, I thought, “What if I fly home to Canada? Would the situation be better?”
My parents rapidly came to Italy to be by my side through all of this. My dad said, “We can make it happen if you want to.” It seemed comforting for a second, but the reality was that I was way too sick to travel. I had been living in Italy for nearly a decade; this is my home.
I was worried about doing care in Italian, but my doctor also spoke English quite well. I was nervous about things that were not going to impact my care. The hospital where I was treated is the number one in the country, and it is in the top five oncological centers in all of Italy. I was in good hands, and I happened to stumble into good hands. Once I realized that, I knew I did not need to go anywhere else.
My Treatment Plan
My doctor said, “Here is the main protocol. It is called R-CODOX-M/IVAC.” I thought, “Cool, I do not know what any of that means.” I wrote it down and later that evening did a bunch of Googling. He explained that it is administered in four cycles and that, given my age and the staging of my cancer, we were going to treat it very aggressively.
The good thing about Burkitt lymphoma, to my knowledge and from what my doctor shared with me, is that it is the fastest-growing blood cancer known to man. The masses can double in size in less than 24 hours. He said the good thing about it being so aggressive is that it is extremely chemosensitive. The faster and more aggressively we treat it, the quicker it dies.
He explained that because I was young and had no underlying health conditions, they thought my body could tolerate it, so we were going to go with the most aggressive version of this protocol. I had all high-dose chemotherapy. Because of that, I would need to be hospitalized every single time. I was not able to do day-hospital; I had to be in the hospital.
Each round of chemotherapy required me to be in the hospital for about a month to manage infections and the period of having no white blood cells. He said, “It will be four rounds. We will be done by the end of summer, beginning of fall.” I said, “Okay, fantastic. When do we start?” He said, “We will basically start tomorrow.”
I asked about side effects. I said, “I know what the typical side effects of chemo are. What can I expect here?” He said, “You are going to lose your hair. You are going to feel nauseous.” He told me that neuropathy was a potential side effect — thankfully, that did not happen to me. He said the higher-risk side effects with this chemo protocol, being so aggressive, were potential infertility and damage to other organs, and they would be monitoring that closely. He also mentioned tumor lysis syndrome (TLS), when the tumor rapidly dies and releases a lot of toxins into your bloodstream that make you ill. He said those were the side effects most concerning to them.
I Had to Submit Myself
I had to submit myself to what was happening and put my faith in my doctor’s hands. I did a lot of praying to God and thought, “We are going to get through this.” I think, especially in healthcare communications, being in a European country is very different from North America. I say this not having experienced care firsthand in Canada or the United States but having family members in both countries who have had serious hospitalizations. I think in North America, we are more prone to asking a lot of questions and talking about advocating for yourself.
Culturally, I think that is different in Italy and in Europe in general, where it is more like the doctor says something and you accept it. I asked a lot of questions, and my doctor was amazing and answered them all, but there was never space to say, “I am not going to do something.” He would say, “This is life-threatening, and you are not a hematologist or an oncologist. I am.” It was never in a condescending way, but that is how healthcare communication tends to work in Italy. I noticed that even with my roommates in the hospital. They would say, “Wow, you ask a lot of questions. You ask all these informed questions,” and it is just not the norm there. People accept what their doctor says and go with it.
I’m Worried About Future Fertility Issues
At the time, my husband and I had been trying to have kids. Hearing that the treatment could affect my fertility was not an easy thing to hear. It is probably the thing I asked about the most during the entire treatment. Every single round of chemo, I would ask, “Do we know? Is there any way we can know?” Now that I have finished treatment, Leonardo is still seeing me, and I have picked up visits with gynecology as well so we can monitor if my ovary will start functioning again.
As of right now, I am still in menopause. It was not medically-induced in the classical sense, but they did give me a medication that stopped the production of estrogen as a way to protect my ovary. It is not a fully medically-induced menopause, but it is something that suppressed hormone production to protect the remaining ovary. As it stands, it is still dormant. We do not know if this will be permanent due to the chemo or temporary. It has been the most difficult thing and the element I still need to process the most.
When it came to chemotherapy, immunotherapy, and beating this cancer, I was very much like, “Whatever we need to do, we will do it,” and I tried to stay positive. But my darkest moments through the whole treatment — and even now — are when I stop to think about the fact that my dream of becoming a mother might not come true in the way I imagined it before getting ill. I still do not know how I feel about it, to be honest. Some days I am positive and think, “If it is a permanent menopause, there are other options available. My husband and I can get informed about adoption or other options.” Other days I think, “Hopefully I will be able to get pregnant one day and it will happen exactly like I intended it to.” Every day is a little bit different in how I feel about it.
I did ask about freezing my eggs. I said, “This is important to me. Is it an option?” My doctor said, “I completely understand. I wish it were an option for you. I do. But feasibly, to do that, it is going to be at least three weeks. You have to go through a round of drugs. They have to do some testing and so on. You do not have three weeks. You will be dead in three weeks if we had to wait to do that.”
I think if I had not discovered this through an emergency room visit, I might have been a little incredulous about that and thought, “No, we have time.” But because we discovered it the way we did, and I had already gone through an extremely life-threatening situation — the tumor causing such bad internal bleeding that I would have died if I had not ended up in the emergency room that day — the second he said that, I understood. I thought, “It sucks for me, and I am going to have to work through how much that sucks for me, but obviously I want to live, so we will go forward with the chemo.”
My Treatment Plan was Aggressive and Painful
I was hospitalized for every single round, so treatment definitely affected my day to day because I was sleeping in the hospital. From the middle of April until the end of October, I would spend four weeks in the hospital and come home for 10 or 12 days between rounds. I was put on sick leave at work, so I could not work at all during this period. It meant huge changes to my day to day and my whole family’s day to day.
My husband and I had just brought home a puppy in January, so we had a four-month-old puppy at home that needed a lot of attention. I work from home, so it had been great because I could take him for walks during the day. My husband is a chef, so he is out of the house. Suddenly, we were rapidly trying to figure out how to deal with our puppy, his work, and my hospitalization.
Thankfully, my parents were able to spend extended periods of time with us. My dad came for three months and then my mom came for three months. That was an immense amount of support. They did a lot of the day-to-day stuff, like buying groceries, cooking, and taking the dog out for a walk. They also came every single day to visit me in the hospital.
Treatment itself was difficult. Immunotherapy for me was a breeze. The way the treatment cycles worked is that it alternated between one chemo protocol and then a second set of chemotherapy drugs. Then we switched back to the first set, and round four was the second set again. Each round, I also did an immunotherapy infusion. Those never caused me any side effects. They had told me there was a potential for severe allergic reactions, but I never felt anything. The only thing was they gave me an antihistamine beforehand, which made me drowsy, so the immunotherapy days in the hospital were actually nice because I would just sleep through them.
Chemotherapy was rough. I would get infusions every single day, varying between five and 10 days, depending on which round we were in. The infusions would go anywhere from two to 24 hours, depending on which chemotherapy, because it was basically a cocktail of different chemotherapies, and each had its own infusion times and administration.
I was always hooked up to something, instead of having a port or a PICC line. I did have a PICC line, but it got severely infected, so I ended up getting a catheter in my neck every single time. I still have the two little scars there; I call them my vampire bites. I was almost always hooked up to something in my neck.
When I was not receiving chemotherapy, they had me on an immense amount of fluids. That made mobility in the hospital difficult because I always had something attached to me. I spent a lot of time in bed. The reason I had to be hospitalized for a month at a time is that in the first week or week and a half when we would do the chemotherapy, my immune system would be destroyed. Because the drugs were so aggressive, the period afterward, when your immune system is suppressed, was more acute for me than for people who can go home at the end of the day. I would get severe infections. I got a bad infection every single round, so then I would be on antibiotics for five to 10 days.
My hemoglobin levels would drop low, making me feel dizzy. I would not be able to walk because I would feel so dizzy. The nausea was something out of this world. I had no sense of taste, and most food was disgusting to me. Then I would throw it up anyway, so eating was difficult. It was difficult because you need to eat, or the nausea gets worse. It was a bad cycle of eating to throw up but also needing to eat to not feel nauseous. That was not fun.
Some of the chemotherapy drugs caused severe mucositis in some rounds. I would get bad sores all along my tongue and down my esophagus, and I could not eat, swallow, or talk. During one round of chemotherapy, it got so bad that they put me on an IV drip of nutrition because everything was so swollen and covered in sores that it was impossible to swallow anything. The side effects were intense and debilitating.
How I Coped Mentally
Losing my hair felt almost like nothing compared to everything else. My blood pressure would get low afterward, which, along with the low hemoglobin, made me dizzy; even just sitting up felt uncomfortable. It does not matter if you are in the hospital or at home; when you feel so uncomfortable in your body, nothing is a distraction. You are just stuck there for hours, not feeling well. It was difficult, and that would bring me to a dark place.
I got good at recognizing the patterns that set me off feeling bad, because each chemo round followed a pattern. By the last two rounds, I went in prepared. During the chemo days, I was able to get up every day. I would do some stretching, read books, and call friends and family. In the post-chemo period, for two weeks, I would disappear, feel terrible, and only see my parents and my husband when they came to visit me every day. I did not even try to make myself feel better because I knew the second my white blood cell count went up, the infections passed, and everything stabilized, I would start to mentally feel better. So I accepted it. It took me the first two rounds to figure that out. It was a lot.
The Hardest Moment of My Journey
The hardest moment was during my first round of chemo. I was hospitalized again mid-May. There was that week of testing with all the scans, and the second week is when we started treatment. My first round of chemo did not go well. I ended up doing a fifth round because I had to recuperate some of the chemotherapy I was not able to do in the first round. Tumor lysis syndrome occurred on day two, and I got a raging fever and became very ill. They had to stop chemo.
The hardest moment was about a week or two after that. I was still in the hospital because I had gotten a bad infection and was on antibiotics. I just wanted out. Because everything had happened so rapidly and as an emergency response, I think that was the moment when my body finally started coming down from the shock and adrenaline that had kept me going since the ambulance.
I had a temper tantrum like a toddler. I just wanted out of the hospital. I did not want any needles in me. I did not want anything anymore. I thought, “I want all of this stuff out of my body right now. I want to go home. I do not care about any of this. This is not what I signed up for. I do not know what the universe has against me, but I need out.” My hair was also falling out in massive clumps, which did not help my mental health. I wanted to shave my head. I did not care about being bald, but I did not want to look like that anymore, with my hair looking bad.
Instead of feeling safe and taken care of in the hospital, I felt almost like I was a prisoner. It was a deeply emotional response to everything that was happening. My parents and my husband were thrown into this by surprise too, so none of us knew how to handle the situation. They were telling me to be patient, trying to make me feel better, and that was making it worse. I was crying and crying and crying. I was ready to yank everything out of my body and walk out of the hospital, even though I could not walk.
My doctor came in, put his hand on my arm, looked at me, and said, “Everything you are feeling is normal. It is okay. I cannot discharge you yet. You are too ill. But you will be okay.” I immediately calmed down. I was still crying, but I calmed down. He said, “We will talk more tomorrow,” and I said, “Okay, that is fine,” and left it at that for that day.
The next day, when he came in for the daily debriefs, I said, “I am sorry for my behavior yesterday. I do not know what came over me.” He said, “You do not need to apologize. It is normal. You have overcome so much trauma in such a short period of time. It is normal, and I want you to know that it is normal. I have requested that when you come in for the second round, you will have psychological support for the rest of your chemotherapy treatment provided by the hospital, because this is a lot. You are young, this is life-changing, and it is totally okay.”
A week later, after that moment, I was discharged. I was able to go shave my head, which made me feel a lot better. A lot of people are scared of that moment, but it made me feel better because pulling my hair out for weeks was bad. When I went back into the hospital for round two, I met with a psychologist. For every other round, a psychologist came and visited me every week. It was a moment for me to speak to somebody whose emotions were not tied up in the situation. That was extremely beneficial.
How Cancer Impacted Me
Psychologically, even now, this whole experience has impacted me a lot. My uncle had throat cancer and has been in remission for three years. We were talking about it over Christmas, and he said, “You are going to get a new lease on life.” I said to him, “I do not feel that. I do not feel a new lease on life. In fact, I feel like my quality of life has been decreased because of this.”
For the next five years, foreseeably, I will have regular checkups and scans, all of which bring a small set of anxiety. I had an MRI scan two weeks ago, and just a week of waiting for results brought a lot of stress and anxiety. I was worried about it, and I have never been a very anxious person. That is new for me. There is scan anxiety, the fear of it coming back, and a more heightened state of alertness about my body and how I feel. “Who would have ever thought shoulder pain was cancer?” That is something I am still working on with a psychologist.
At the same time, I feel like I came back to myself. In the few years before the diagnosis, I think I had lost touch with myself. When you make a big move to a new country, you usually do it because you deeply want to. You feel passionate, you are ready to risk a lot of things, and it is not the most traditional path forward. Right when I turned 30, we moved to Milan. It aligned with a more traditional path. My husband and I got steady work at that point and moved toward building a family, buying a house, and planning our wedding — all these stable elements of life that you think you are supposed to do and things we wanted to do.
With that came a new sense of responsibility to get there and be able to do those things. Before, it was, “I am just going to move to Italy,” or, “I am going to take this job because I feel passionate about it,” and it was not as much about long-term benefits. In the years leading up to the diagnosis, I do not think I was fully true to my slightly spontaneous nature.
Coming out of this, I feel like I have been able to reconnect with that version of myself. I have been reminded that you do not have to have a plan. You do not need to know exactly where you are going in life. As long as you stay open to what comes your way and are joyful about it, you will probably get where you want to go in the end. That has been nice. It has been liberating to let go of certain status quo norms I felt I needed to have in order to be successful in life. But there is still that element of increased anxiety that I never dealt with before.
I Was Declared NED Before the Holidays
Survivorship is still new. I was given the no evidence of disease or complete remission diagnosis at the end of November 2025. I almost do not believe it sometimes. When my doctor told me, I almost took it for granted. I thought, “Of course. We just did all of that horrible therapy, so this was the only outcome available.” I had never questioned that we would not get there. I was convinced from the very beginning that we would get there.
When he told me, I thought, “Fantastic.” Now, a couple of months out, I am starting to feel a little more like, “What if it comes back? What does this actually mean? I am now a cancer survivor, and I will be for the rest of my life.” I think I am still trying to figure out what that means. I am trying to understand my new limits, physically and mentally, and what rest looks like. I do not try to push myself as much. I love to travel. Before, I could spend most of the month out and about, between planes and trains and car trips, and I definitely cannot do that right now. I am trying to understand my new limits and be okay with constantly reassessing that.
The further out I go, most likely, the stronger I will get, and the more physically capable I will become. There are a couple of women in Italy who have also had cancer and do a lot of work sharing the importance of psychological care during cancer treatment. I am quite interested in that. If there is a way to get involved in promoting the importance of that, it might be something I want to do. For the most part, though, I think there is still a lot of processing left to be done.
What I Want Others to Know
Trust yourself and trust in your body’s ability to get better. One of the things hugely helpful for me was that from the moment we had the treatment plan, despite it being difficult, feeling horrible, and all the fear, I never once stopped believing in its ability to heal me.
I stayed quite positive — not in a way of forcing myself to be happy, because I was not happy about the situation. I did not want to be there; if this had never happened, that would have been fantastic. But I stayed positive about the power of being taken care of, of the treatment, and of having a care team. I stayed grateful for all of the support I had. My parents were able to leave Vancouver and come for an extended period of time. My work was extremely accommodating. My doctors and nurses were fantastic.
Staying extremely grateful for being able to get the care that I had and truly believing that it was going to make me better was the right mindset to get through something extremely difficult. Trust in your care team, but also trust in your body to get better. Accept the healing.
Symptoms: Constant fatigue, tongue deviated to the left, abscess in right breast, petechiae on legs, night sweats, nausea and vomiting, persistent cough
Symptoms: Severe fatigue, deep shoulder pain, ear pain with inflammation, abdominal and pelvic pain, bloating, early fullness, nausea, difficulty eating, inability to urinate despite feeling an urgent need, internal bleeding, delayed period/bleeding, intense whole‑body pain leading to collapse
Treatments: Surgeries (emergency laparoscopic surgery with left ovary removal), chemotherapy (R‑CODOX‑M/IVAC), immunotherapy, hormonal therapy (to protect the remaining ovary)
Navigating the “Good Cancer” Guilt: Taylor Scheib’s Story of Self-Advocacy and Finding Her Voice
Thyroid cancer wasn’t on Taylor Scheib’s radar when she first noticed a small lump on her neck at age 26. A sports broadcaster turned storyteller at The Patient Story, Taylor had watched her grandmother’s legacy and her mother’s recent battle with stage 3 colorectal cancer shape her understanding of cancer. But when she sought answers for the growing mass on her neck, she faced years of tests and dismissal. Doctors repeatedly assured her that the nodule was presenting as benign. Importantly, they were also advising her that surgery was optional and cosmetic. Even as it grew. It wasn’t until the lump began to physically impact her sleep and exercise, and she saw how visible it was in photographs, that she pushed for its removal.
Interviewed by: Herself (Taylor Scheib) Edited by: Chris Sanchez
The surgery Taylor underwent in April 2025 was supposed to be the end of a benign chapter. Instead, a MyChart notification delivered a shocking blow: the pathology report revealed oncocytic carcinoma of the thyroid gland, a rare and aggressive subtype of thyroid cancer. Taylor was traumatized by having to receive her diagnosis through a screen before speaking to a doctor, a system failure that ignited her resolve. She immediately sought a second opinion at the Fred Hutch Cancer Center in Seattle, which led to another thyroidectomy to remove the rest of her thyroid and subsequent radioactive iodine treatment.
Throughout her experience, Taylor has grappled with the complex guilt often associated with having a “treatable” cancer, especially while some of the patients she talks with face more ominous diagnoses. Yet, she realized that every patient’s experience is valid. Today, she uses her platform and The Patient Story’s platform to emphasize the critical importance of self-advocacy and second opinions. Her story is a powerful reminder that even when a condition presents as benign, patients know their bodies best and their stories are always worth telling.
Watch Taylor’s video and read the transcript of her interview below to take a deeper dive into her story.
Trust your instincts over “benign” labels. Even when medical tests suggest that a condition is harmless, persistent symptoms, like difficulty swallowing or physical changes, warrant further investigation. You are the expert on your own body
Be prepared for the possibility of getting shocking news electronically when checking test results online. Finding out a diagnosis via an electronic medical record (MyChart) before a doctor’s call is a devastating but increasingly common reality. This is the downside of new laws aimed at giving you access.
Second opinions are vital. Seeking a second opinion at a comprehensive cancer center can completely change your treatment plan and provide peace of mind, even if it requires travel
“Good cancer” guilt is real. It is common to feel guilty when facing a “treatable” cancer while others may be suffering more, but minimizing your own trauma doesn’t help anyone. Your pain and fear are valid
You must be your own biggest advocate. If you cannot fight for yourself, find a friend or family member who will ensure your concerns are heard
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I’m no stranger to cancer. It started really early for me, actually. That was when my Grandma Connie was diagnosed with breast cancer. It was actually before I was even born. My dad was a teenager, and unfortunately, she passed away before I was able to meet her. But I know that her legacy and her life live through all of us, especially my dad and his sisters, and through us grandkids. A lot of my family members actually say that I look a lot like her, and I agree.
I always knew what cancer was after my grandma, and as I got older. When I was old enough to really know and talk about my Grandma Connie, that’s when I really started to understand cancer. It was at a young age. Her death impacted a lot of my life in ways that I still don’t realize, and it would be a long time until cancer really directly impacted me again. But it came in November of 2023.
My mom was diagnosed with stage 3 colorectal cancer. I was living in Spokane, Washington. My mom was still back home in Illinois, and I remember she called me. I knew she had gotten a CT scan, but I didn’t know exactly what they were going to find when she called me that day.
She told me they found a mass, and I dropped everything to go and be with her. I think I knew deep down that it was cancer. That’s really because she had symptoms piling up: blood in her stool, fatigue, cramping, and bloating. All the signs really pointed towards colorectal cancer. I went home for a month from my mom’s diagnosis to her getting her treatment plan, to her having a major surgery to remove that tumor. It was really, really hard to see my mom go through that. Those were some of the hardest moments that I’ve had to see my mom go through. She is truly my best friend. To see her in so much pain… The surgery was really horrifying for me, my brother, and my sister. We’d never seen Mom look so tired and worn down, and she was on the verge of giving up.
I thought that would be the hardest time my mom and I would go through. But fast forward to April of 2025. My mom was about a year and a half out of chemo, and I had to call my mom and tell her, “You just beat cancer, but now I have it.” Different kind. Totally different treatment plan. But I had to tell my mom that I had cancer. That was one of the toughest phone calls.
Discovering the thyroid nodule: Initial symptoms and dismissal
There are thousands of miles between her and me, and my family and my closest best friends. But I had my husband. I had his family here and our chocolate lab, Sage, who is truly our daughter. In April 2025, I went in for surgery to have a 5.5-centimeter nodule removed from the left side of my thyroid. They would have to remove the whole left side of my thyroid because that mass had basically compromised it.
What happened, though, was that I thought it was benign. I thought it was nothing. I didn’t even think twice that it could be something like cancer. Even though I was connected to cancer in so many different ways, not once did I think it was anything but benign. That’s because multiple doctors told me that it was nothing, that it was just a benign thyroid nodule, and there was nothing I needed to do about it.
The mass was impacting my day-to-day. It was compromising the way I slept. If I was working out or doing a certain exercise, it was impacting that. It was getting so big that I felt, at times, it was choking me, and it had also become pretty noticeable. I would look at pictures of myself, and I would just be like, Oh my gosh. This thing is so huge. It’s getting so big.
It took me advocating for myself and pushing to get a surgery and get it taken out before I was ever taken seriously. Things were said to me like, “Are you ready to have a scar? It’s benign. Why do you want it out?” Not once did anyone say to me, “Oh, we should biopsy this,” or “Should we look further into this?” It was so frustrating to me at that time. I just wanted it out. Thankfully, I got it out. Before I even had time to process that there had been cancer in my body for multiple years, it was gone. The cancer was gone, essentially, before I even knew it was cancer. And that is why I have spent a lot of time thinking about other people.
From storyteller to cancer patient: The guilt of “the good cancer”
Less fortunate people are people who go through hours and hours of chemotherapy and radiation. The treatment that my grandma many years ago went through and suffered through. To me, having a cancer that is very treatable and has a very straightforward treatment plan… that guilt is something that I’ve carried ever since my diagnosis. And it’s not only what my grandma went through, or what my mom went through; it’s what hundreds of people I’ve talked to who’ve had cancer have gone through, because I’m a storyteller here at The Patient Story.
I went from telling stories, listening, and truly gaining so much knowledge and life lessons from people because they were brave enough to come to The Patient Story, reach out, or answer a message that we had sent them and share their stories. With that, for me, comes a lot of guilt. Because I’m so lucky. I’m so lucky that even though the cancer was in my body for a while and I didn’t know it, it still didn’t spread. But I talk to incredible humans every single day who have it so much worse. I’ve spoken to people who have passed away. People who have relapsed and their cancer has come back. People who have lost a loved one to cancer. People who are in active treatment and they’re still mustering up the energy to do an hour-long interview with me. These stories are so deep, so personal, that I struggled to figure out if my story was impactful enough or worth telling.
I’ve come to realize that everyone’s story is so special. Everyone’s story is different, and in every story, there’s a lesson. There’s something about life that you can take from that. So that’s why, for the first time, I’m sitting down, and I’m telling my story from the very beginning.
My life before cancer: A career in sports broadcasting
I’m originally from a really small town in Illinois. About 800 people, 30 kids in my graduating class. Yes, some are still my best friends to this very day. I have an incredible family. Some of them still live back in Illinois: my mom, my dad, my stepmom, and my siblings. I have an older sister who lives in Texas, a younger brother who lives outside of Omaha, Nebraska, with his fiancée, Mallory. And then I have two bonus siblings. One’s a freshman in high school, and one is a sixth grader. I’m so grateful for my family.
From a young age, I was always the girl who wanted to get out of the small town. That was no secret to anybody. I took school very seriously. I took extracurriculars and sports very seriously, and it led me down a path where I went to the University of Iowa. I became a sports broadcaster, and I really thought that that was going to be my life. It started in Iowa with The Daily Iowan, and then it transformed into my first real adult job in Grand Forks, North Dakota. Then I came to Spokane. That’s where I met my incredible husband, Justin. He is truly the light of my life, and I’m so lucky to have found him.
It’s a very typical story. He slid into the Instagram DMs. He was a coach; I was a sports reporter. I did a story on a team he was coaching, and next thing you know, it’s seven years later. After Spokane, though, I went on to Denver, and I covered professional sports, and I’m so thankful for that time because it really showed who I wanted to be professionally and where I wanted my life to go. I say this all the time, but my husband would have followed me to the ends of the earth if I had wanted to continue in sports broadcasting. But what I realized was I thought I was in love with sports — and I am — but I’m more in love with storytelling.
I wanted to just talk to people. I wanted to share their stories. I wanted to make an impact. That was the biggest thing for me. So I decided to get out of sports broadcasting. My husband and I moved back to Spokane, Washington. He grew up about two hours away, and we started creating our life here.
I could not be more grateful for where we’re at in our lives. We love the Pacific Northwest. We take our chocolate lab, Sage, hiking and swimming. We love camping. We also love showing people around the Pacific Northwest, with my brother and his fiancée, Mallory, being our biggest frequent fliers.
The lump appeared: Dismissed by doctors for years
When I was in sports, and I was in Denver at Fox 31, that’s actually when the lump appeared. I had just turned 26, and we decided to do a karaoke night — one of the greatest pastimes of my husband and me. We went out and karaoke’d, and the next morning, I found the lump. It was quite small, so I thought it might be a lymph node or something similar. But I immediately went to the doctor. Blood work. Ultrasound. No follow-up needed. The mass was presenting benign, so it was out of sight, out of mind.
I just continued with my life, and it wasn’t until a year later that my husband and I returned to Spokane. My girlfriends and I went out. My husband was our designated driver that night, and we’re on our way home, when one of my really good friends pointed out to me, “Hey, do you know that you have a lump in your neck?”
To be honest, it was kind of the first time someone had pointed it out to me. I know she did it just looking out for me and just wanted to make sure I knew. It hit really close to home for her because her dad had thyroid cancer. So she did it with the best intentions. I just said, “Yeah, I actually had it checked out a year ago.” But her bringing it up made me go and get it checked out again.
So, new doctor, new established care here in Spokane, because we had just moved back here. I went and got it checked out again. Blood work and ultrasound again came back. No follow-up needed. But at that point, I noticed that the lump was getting bigger. It was growing — not at a rapid rate — but it was growing, and it started to hinder my day-to-day life.
It was really strange. Then there’s this one picture. My dog and I are sitting on a log camping, and I looked at the picture, and I was so embarrassed. I was dumbfounded. I turned to my husband, and I’m like, “This thing is so freaking huge, and it’s embarrassing. How did I let this go on for so long? There is clearly a huge lump in my neck.” I was so mad at myself. I’m like, “Okay, we’re done. This is it. We’re getting this out.”
So I got a referral to an Ear, Nose, and Throat specialist. With specialty care, it took a while to get in. I finally get in, and I see this doctor. She brought up the ultrasound. She was like, “It presents benign. It doesn’t look like anything. It’s your choice to get it out.” And man, talk about pressure. It’s your choice to get it out. Keep in mind, I’ve never really had any major surgeries. Wisdom teeth? Yes. Broke my tailbone when I was younger, but I had not had a serious surgery, and it was just so casual. “It’s your choice to get it out.”
I’m like, “Okay, well, I’m getting it out. I can’t take pictures like this anymore. I can’t have it be super noticeable like this.” It’s not like people were pointing it out left and right, but if I pointed it out — if I was like, “Hey, I have this huge lump on my neck” — they’d be like, “Oh my gosh, I never even noticed.” That’s also at the point where my mom was like, “You need to get it out.” I don’t know if she had mom instincts or just cancer instincts, but she was also pushing me to get it out.
So I scheduled the surgery for January 2025. My referral from my insurance didn’t go through the morning I was supposed to have surgery. They were like, “You could just come in and have it done and just chance it.” I’m like, “No, no, medical bills are expensive. That’s not happening.” So, because it was non-emergent, it got pushed back to April 2025.
The surgery and the shocking MyChart discovery
The surgery was scheduled for April 18th. Two weeks before that, I had just turned 30. My husband planned this incredible trip to Puerto Vallarta, Mexico. We went and had the most incredible time. We stayed an extra day, and if I could go back and relive that day, every single day I would. The only thing that was missing was our dog. She obviously didn’t come with us, but if I could go back to that day, I would, because it was the most incredible day, and we had no idea what life was going to throw at us.
Granted, keep in mind, I still had this lump. It’s noticeable in the pictures. So in a way, I’d go back to that day, but then there’s also a part of me where I’m like, Oh, there’s cancer in your body. So you wanted to get it out. But again, I didn’t know at that time.
So we went home. We settled in. I had surgery on April 18th. My husband took me. It was an outpatient procedure. Very straightforward. But even before my doctor and surgeon came into the room, I told my husband, “She’s very nonchalant, she’s very casual, just heads up.” And she was. There was no indication this could be anything more. There was no talk of a pathology report. And I know why doctors do that. I know why care teams do that. I mean, it was presenting completely benign on an ultrasound. So what would make you think that it’s anything more than that? I don’t know. I wish that they had known that, or I would have gotten a biopsy, but I wasn’t that educated at that time. I mean, I was, but I wasn’t.
It was a very straightforward surgery. My husband said the surgeon came out and said everything was good. We got it all. She’ll be waking up soon. I went home so quickly after I woke up — it was like 20 minutes, and I went home. I was anxious to get back to working out and getting back into my routine. I just had a partial thyroidectomy, and it is a pretty straightforward procedure. I didn’t think about the pathology report. I didn’t think about any of that until my mom brought it up. She said, “When are you going to get your pathology report?” I said, “Oh, I have no idea.” I didn’t even really think about it.
That morning, the morning that I found out it was cancer, was a Monday. I had just been cleared to start working out again, and I started training for a seven-mile race known as the Bix. It’s this huge race near my hometown in Illinois, and my mom had asked all of us kids to come back and run the race with her to celebrate her being out of chemotherapy. No evidence of disease, and just celebrate her. So I started training that morning. I was so excited.
Then that night rolled around. I’m sitting on my couch, my husband’s in the kitchen cooking dinner, and I see a message in MyChart pop up. Human instincts: Open it. And for me, I didn’t know that opening it was going to be anything other than, “It was benign. It looks good. Glad you got it out.”
But I opened that MyChart message, and the first thing I see is carcinoma. I instantly knew what carcinoma meant. Cancer. The mass was freaking cancer. It wasn’t benign like I had thought for three years. It wasn’t benign. Like I was explaining to people and telling people so they wouldn’t freak out. It was f****** cancer. A cancer type that I had no idea about because there was this word “oncocytic” in the verbiage. I didn’t know what oncocytic meant. It said “Oncocytic Carcinoma of the Thyroid Gland.” So connecting the dots, it’s thyroid cancer. Oncocytic. What the heck does that mean?
I just burst into tears. My husband stops in his tracks, and I just yell it out: “It was cancer!” My husband drops everything, turns the burners off. He’s like, “What are you talking about?” I showed him the message. It was such a devastating moment. I felt like such a fool. I had taken videos before the surgery and even after, really honing in on the word “benign” because, again, I just didn’t want anyone to freak out. I didn’t want anyone to think anything else. But I was just saying the things that had been told to me for three years — that it was benign.
My husband and I — I mean, obviously, he’s so upset. We go into my office. The irony. I’m sitting in my office at my desk, The Patient Story sign behind me, and I am living in a moment that I’ve actually heard before. I’ve had people tell me in interviews, “I found out I had cancer through MyChart.”
No one — no one — should ever, ever find out that they have cancer through MyChart. It is so devastating. I know that it’s not the doctor’s fault. It’s the system. The system definitely has some things to work on. My husband and I sat in my office chair and we were googling words, and then I had to call my mom.
Navigating treatment: Second opinions and radioactive iodine
We went on a walk with that same friend who had said, “Hey, do you know you have a lump in your neck?” We went on a walk with her and her husband. We told them, and then we didn’t really tell anybody else. I did call Stephanie, the founder of The Patient Story, because I’ve always been so transparent with her about my mom’s situation. I started at The Patient Story two months after my mom was diagnosed with colorectal cancer. Then I’m working at this incredible healthcare organization that primarily focuses on cancer, when I myself am diagnosed with cancer. So why not go straight to someone who’s so well-connected and really gets it?
Stephanie and I had that conversation that night, and I felt relieved in a way, just knowing that my job was going to be there. I could have space. She was connecting with people she knew who specialized in endocrinology and thyroid cancers. So it was a tiny bit of relief that I felt.
The next day, I instantly started researching second opinions because I had had conversations with people who educated me on second opinions, who taught me that getting a second opinion is important. How blessed was I to be so privileged to know to get a second opinion, specifically at a comprehensive cancer center? I mean, that knowledge is invaluable. I can’t even describe how lucky I felt, even in a moment of crisis, trauma, and drama. It was very traumatic to be going through what I was going through, as it is for anyone who gets told they have cancer, regardless of the type.
I came across the Fred Hutch Cancer Center in Seattle. I didn’t care that it was 4.5 hours away. I just really wanted to have a second set of eyes on my pathology report, and just help me navigate what the next steps would be. I called Fred Hutch. I got connected with an incredible nurse navigator, and she was so kind. She got me an appointment without even a referral. She just put me on the schedule, and the wait times were pretty long. But it actually worked out because when you have a partial thyroidectomy, you have to wait a certain number of weeks to see if you have to start taking thyroid medication or not. Usually, you don’t — it’s like 15 to 20% who have to.
But it was going to be about four weeks from the surgery to finding out I had cancer to being seen at Fred Hutch. And the timeline was similar to providers here in Spokane. They were presenting my case to a tumor board, where they all get together and discuss special cases. Because of the size of my tumor — 5.5 centimeters — I wasn’t calling the mass a mass anymore or a benign nodule. I was calling it a tumor. They wanted to present it to the tumor board. They wanted to do genetic testing on the tumor to see what the next steps would be.
Those four weeks were so incredibly hard for me. My husband gave me so much grace, of course, but I can only imagine how he felt during that time because I was a mess. The waiting was horrific. I just wanted answers. I wanted a plan because I’m such a planner.
I went to Fred Hutch four weeks after my surgery. They were so kind. They provided incredible services. I met my endocrinologist, Dr. Roth, and she is incredible. All she had to do was look at my pathology report to know what the next steps were. And that was a full thyroidectomy and radioactive iodine treatment. That’s what I needed. I needed to just know what the next steps were and how I could just get past this. I really wanted it to be a chapter in my life story. I didn’t want it to overtake me, and that’s exactly what we did.
On June 10th of 2025, I got the rest of my thyroid removed. So, a complete thyroidectomy. At that point, they wanted to get rid of my thyroid, any remaining thyroid cells, because the subtype of thyroid cancer I have — oncocytic — is a rarer, less common subtype. It doesn’t happen in a lot of cases, and it can be aggressive. So it was: get the rest out.
During that time, though, I had lost my voice and was struggling to come back. So there was a little bit of how do we push this back more? My husband and I traveled to Fred Hutch — you know, that 4.5-hour drive — we’re so lucky to have the means to do that. I remember sitting with my surgeon, and she was laying it all out there. She was very honest, very kind, very gentle, but so honest about the possibilities, especially because my voice was gone. Come to find out, it was just like an inflamed nerve or something. It wasn’t my vocal cords, which was the fear.
During that wait — oh my gosh. Stephanie told me from the beginning, “The waiting is going to be the worst.” And something I’ve heard in interviews I’ve done is, “The waiting is going to be the worst.” It was agonizing to have all these wait times. I was just kind of sitting in it, and finally got the rest of my thyroid removed.
And then you have to wait eight weeks to do radioactive iodine therapy. So this is the midst of summer. My husband and I are very active. We’re very go-go-go. So I’m recovering from surgery. I’m trying to get back into my routine. I ran that seven-mile race that I had originally started training for before I found out it was cancer. I ran that race with my family and my mom, and it was so amazing and celebratory.
Then we get to radioactive iodine. That was in September of 2025. Again, that process is very straightforward. It’s just so lucky to have the care team I have. It’s a lot of appointments. It’s a low iodine diet. That’s not that fun. I couldn’t eat cheese for like three weeks. It was very sad. I make the jokes because I’ve just figured out that laughing and smiling through this has been kind of the best thing for me.
The mental toll: Body image, anxiety, and fertility
I’ve had moments, of course, of darkness and sadness, and just trying to figure out how to navigate this. So I get through radioactive iodine that involves a three-day isolation process. I was isolated from the outside world in a Fred Hutch facility for three days, and then I came out and got a scan and saw where the cancer was. It was contained in my thyroid bed, but it was more than they anticipated. So I did get a little bit of a higher dose of radioactive iodine.
Now I’m at this phase where it is follow-ups and blood work, and going to Fred Hutch for ultrasounds. What I’ve come to find out is that the surgeries were scary again. I hadn’t had a major surgery before; I had two in one year. And then radioactive iodine was a little sketchy. You know, you just take this pill. And I had a couple of side effects that were out of the ordinary.
Then you get to this part where I’ve been in, and that is processing what has happened to you and what you’ve gone through. In a way, I’ve had to kind of figure out who I am again. She was never really lost, but she’s gone through some things, as we all have. Cancer being a big one, being a caregiver to a parent, going through cancer, and then other life things.
I think after the radioactive iodine treatment, I found myself very anxious and struggling mentally. I couldn’t get myself into a good rhythm. I was living on a short fuse, using my husband as a punching bag, which is not fair at all. And all of this while keeping in mind I don’t have a thyroid anymore, which controls a lot of your hormones, your metabolism, different things like that. You’re taking a pill now. 5:00 a.m. every single day, my alarm goes off, and I’m taking my thyroid medication. That within itself is a total mind f***.
I just felt like I was slipping a bit. I was just not being my best self. And I’ve struggled with anxiety for a long time. I don’t know if anyone else feels this way, but I swear the older you get, the more anxious you become. It just becomes more apparent to the point where I would get numb, my hands would get numb. Sometimes, the side of my face — I was having physical symptoms of anxiety. I just felt… I didn’t like myself. I hated myself. And I would use that language on myself sometimes. Sometimes I’d say it out loud to my husband. “I hate myself. I hate my body.” It felt like body betrayal. What I went through. How did I not know? For three years, cancer was growing inside my body.
Then I got it out, and I started on this thyroid medication, and then I started having body image issues where I had gained weight. I would look at myself in photos, and I would speak so horribly to myself. So horribly to myself. And I hate that I did that. I hate that I was telling myself mean things about my body and about how I looked.
It was like an identity crisis in a way. When you’re a sports reporter and a sports broadcaster, and you’re on TV every single day, you’re looking at yourself, and you’re judgmental, and you’re being told things. And then you’re not on TV anymore, and you go through a big thing like cancer, and your body just is a little confused, and your mind’s confused. I don’t think I was giving myself enough grace in that moment. And it’s something I’m really trying to work on. I just hated the way I felt, the way I was treating my husband, my family, my friends. It was like a “fake it ’til you make it,” but my husband was seeing the real thing of how I was feeling, and that was really, really hard.
Another layer to this is that when you receive radioactive iodine therapy treatment, you can’t get pregnant for a year. And 2025 was the year my husband and I had discussed starting to explore the idea of starting a family.
It was at the point where early 2025, I was telling people, “Ooh, Justin and I are going to start trying. I’m going to be 30. We’re going to start trying. So excited.” Lesson learned: shouldn’t have done that. And it wasn’t like we were actively trying when I was diagnosed with cancer because we were not. But I wasn’t on birth control, and I had to go back on birth control because of radioactive iodine treatment. If I were to get pregnant in the next year, it would be very dangerous.
So I was also having a bit of a reality check; maybe Justin and I weren’t ready in that moment or in 2025, but it was taken away from me as a woman. Oh my God, it’s so hard. I’m so grateful to still have the ability to hopefully carry a child someday if we decide to do that, because I know not everybody gets that chance, and people struggle with fertility issues and that whole situation. My heart goes out to all of those people. To have it taken away from you, even for a year, was really, really sad. And you’re so happy for your friends who are getting pregnant for the first time, or with their second babies. Everyone knows I love being Auntie Taylor. But that dynamic was difficult. It really was difficult.
Healing and advocacy: Why your story matters
So I was processing all these emotions of hating myself, hating my body, body betrayal, not being able to start a family with Justin, and I got into a really deep, dark place. And then I started to climb out of it. At the start of 2026, I really committed to myself: to my body, to routine, and doing things that make me happy. I’ve started this morning routine that I’ve just lived and breathed by since the start of 2026, and I just feel really, really good.
Another big thing — and not something I’ve expressed a whole lot, though some of my friends and my mom, of course, my family knows — but I started taking anxiety medication. That was a huge step for me. So again, my body is going through a lot. Thyroid medication, I’m back on birth control, and anxiety medication. I’m really taking care of myself. Of course, I slip in a cheeseburger now and then. Everyone who knows me knows that I’m a sucker for a cheeseburger. But truly, I’ve shifted. And it’s not just physical for me. It’s truly mental. It is a mental game for me at this point, and I’m so proud of myself for taking care of my mind and my body and just recentering myself.
As I’ve recentered myself, one thing that I talked about at the beginning of my story was the dynamic of Is my identity… is my story important? Is it important enough to share? Is it worth sharing? Am I ready to just close this chapter? All those questions swirling around in my head, and thyroid cancer is looked at as “the easy cancer,” and yada yada.
I am fully aware that it is a very treatable cancer. It is very straightforward, and I’m forever grateful for that. It doesn’t mean that my story is not worth sharing, though. I’d be lying if I didn’t say I was terrified to share my story, especially on a platform where I interview so many people who have it so much worse than me, and I always keep that perspective in my mind. But those very people taught me to advocate for myself, to get second opinions, to share my story, and to be brave enough to share my story.
There are things in the story that I haven’t expressed out loud. So in a way, this is my own little personal diary. Looking back at the person who was diagnosed in April 2025, to the person I am now, she’s the same girl. She’s just grown up a little bit, and I’m really thankful for that. It’s truly a full circle moment to share my story and to continue sharing stories of others who are going through cancer, no matter what stage, no matter what type, no matter where you’re at in your story.
I’m so blessed to be able to have a voice and to have a platform like this. Timing is truly everything. And no matter what you believe in, everything does truly happen for a reason. At least I think. I found The Patient Story — or rather, they found me — three months after my mom’s colorectal cancer diagnosis. And then plot twist: I get cancer in the midst of working for a cancer company. I was exactly where I needed to be at the exact time of my diagnosis. And now what can I do? I can share my story. I can continue spreading that language and those words that people have taught me before about second opinions, about advocating for yourself, and making sure that you’re just truly taking care of yourself — mind, body, spiritually — however the dominoes fall.
One thing I’ve just been so lucky to do as well is because of The Patient Story. People in my personal life have come to me and been like, “Hey, I was diagnosed with said cancer,” or “Hey, I know someone who was diagnosed,” or someone sending me a message and saying, “Hey, I have the same subtype of thyroid cancer as you.” I mean, this is a domino effect. Sharing your story, sharing your light, sharing your truth is so incredibly important. You don’t know who it will reach or who it will impact. And I just think that’s really, really special.
What I want people to take away from my story and my experiences
There are three things:
One: Advocate for yourself. If you can’t find someone who will — a family member, a friend, a colleague — please fight for yourself and your body and your mind and what you’re feeling.
Two: Second opinions are so important. I know that comes with a lot of layers: insurance, travel, finances. But if you have the ability to get a second opinion or even just ask someone or try to connect with someone who can ask their oncologist, please explore a second opinion.
Three: Your story matters. If you are terrified, just like I was, to share your story fully, please don’t. Because I can promise you that your story is important and no story is the same.
Thank you so much for watching my patient story. It took a lot of guts, a lot of bravery to share this, but I’m so grateful to have this platform to do so. And if my story resonated with you at all, I’d love to introduce you to one of our team members, Ali. She shared her story, and it’s queued up for you right here. Please make sure you subscribe to The Patient Story community, where you’ll see me interviewing so many incredible people with their inspiring stories. We want you to join The Patient Story community because we’re humanizing cancer one story at a time, and always telling people and reminding people that you’re never alone.
The “Luckiest Unlucky Person”: Young Mom Laurel’s Kidney Cancer Experience
Clear cell renal cell carcinoma (ccRCC), the most common type of kidney cancer, can sound clinical on paper. For Laurel, however, it was anything but clinical. Her experience unfolded in the middle of new motherhood, sleepless nights, and Manitoba winters as chilly as -40°C (-40°F). At 33, Laurel was enjoying maternity leave with her baby when a sudden, excruciating gallbladder pain sent her to a rural emergency room. Imaging to confirm gallstones also revealed a tumor on her left kidney, leading to a diagnosis of early-stage clear cell renal cell carcinoma and a plan for partial nephrectomy.
Interviewed by: Carly Knowlton Edited by: Chris Sanchez
Before the diagnosis, life felt full and ordinary in the best way. Laurel describes how she finally loved being a mom after a difficult first few postpartum months, and savoring simple joys like skating, building backyard toboggan slides, and tending her white picket-fenced garden. That everyday joy made the call confirming that she had kidney cancer, which she received on her husband’s 40th birthday, all the more surreal. Her family doctor was direct about the likelihood of cancer, and a network of advocates, including an ER physician, nurse navigator, and urology team, moved quickly to get her into surgery.
Laurel underwent a laparoscopic partial nephrectomy with the understanding that she might need to have a full nephrectomy if necessary. Pathology later showed cancer cells close to one margin, but her urologic oncologist was confident that the extensive cauterization eliminated any remaining cells. While the clear cell renal cell carcinoma was addressed surgically, Laurel required emergency gallbladder removal and an endoscopic retrograde cholangiopancreatography (ERCP) to diagnose and treat issues in her bile ducts and pancreatic ducts. She ended up spending more time in the hospital for these complications than for the kidney surgery itself.
Emotionally, Laurel describes compartmentalizing to move through crisis — delegating research to her sister in clinical research, childcare to another sister, and advocacy to a cancer nurse navigator. The most painful moment came when she realized she needed to write a will and create memory albums for her young son, in case he grew up without remembering her. Over time, therapy helped her process the experience. Hearing “no evidence of disease” on an early CT scan brought profound relief and, unexpectedly, improved mental health; she now cares far less about others’ opinions and more about being present for her child and listening closely to her body.
Watch Laurel’s video and read through the edited transcript of her interview for more about her kidney cancer story.
Listening to new, severe, or persistent symptoms, like Laurel’s gallbladder attack, can sometimes reveal serious conditions such as early-stage kidney cancer and change the course of care
Delegating both the emotional and logistical load to trusted people, like family, nurse navigators, and clinicians, can make complex treatment and recovery more manageable
Taking symptoms seriously and advocating when “something doesn’t sit right” is not overreacting; it is an essential part of your health experience
Complications from treatment and other health issues, like gallstones, cholecystitis, and pancreatitis, can be more painful than kidney cancer surgery itself, and deserve equal attention and support
Laurel describes a powerful transformation: what she expected to be a long-term mental health burden instead became an experience that clarified her priorities, reduced worrying about others’ opinions, and deepened her focus on her son and her values
Name: Laurel M.
Age at Diagnosis:
33
Diagnosis:
Kidney Cancer (Clear Cell Renal Cell Carcinoma)
Staging and Grade:
Stage 1, Grade 2
Symptom:
Gallbladder attack resulting in extreme pain in sternum
Treatment:
Surgery: partial nephrectomy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I’m from Manitoba, Canada. At age 33, I was diagnosed with clear cell renal cell carcinoma. It was stage one and grade two.
This occurred in December 2024. I had my partial nephrectomy in January of 2025.
Hobbies, passions, and life in Manitoba
I really love just being outdoors any chance we get.
We get all four seasons here. It goes from plus 40 Celsius sometimes in the summer on really hot days to almost minus 50 Celsius on cold days in the winter. Any chance we get the in-between weather, we are outside, whether it’s on the skating rink or building a toboggan slide in our backyard, or we are just in the front garden. We live on a little river. I literally built a white picket fence around the garden at my house and attempt to garden when I have time. Some years are easier than others, but even when it’s weedy, I still find a little bit of joy in it.
I had a gallbladder attack that revealed I had kidney cancer
I was home alone with my son, who at the time was around nine months old, and I started getting this extreme pain in my sternum. It almost felt like a heart attack, to the point where it got so bad that I was afraid that if I called 911, they would not get to me in time. It was so extreme that I could not breathe. I live five minutes from a hospital that sometimes has an ER open. I took a chance and drove my son and myself there, basically hobbled through the door with him in one arm, and they ran to me, grabbed my baby, and immediately got me in. They did an EKG to make sure it was not a heart attack.
Thankfully, the ER doctor who was there that day had also had a gallbladder attack when she was postpartum after she had a child. It can be pretty common after pregnancy, and she recognized the symptoms right away and said, “This is a gallbladder attack.” Because I live in a rural area, that hospital did not have what they needed to do the ultrasound to confirm it. I had an appointment at a different hospital that I went to for that.
When they did the ultrasound to confirm the gallbladder attack and find the gallstones, which they did, they also found a tumor on my left kidney.
Hearing there was a tumor on my kidney
I have a really good family doctor, and he shoots it to me pretty straight. I am the kind of person who appreciates that. I do not like sugarcoating things that are not sugarcoated. If it is bitter underneath, do not try to trick me with sugar on it. So he was pretty honest with me and said that most kidney tumors end up being cancerous.
The ER doctor from our rural hospital, when she got the report, even though I was technically not a patient there anymore, gave me a call and said she was referring me for an urgent CT scan. She went above and beyond as well. Then my own doctor was looped in, and that is how the process went once I found out it was a tumor. It was actually my husband’s 40th birthday, December 5th, when I got the call saying it was cancerous. After the CT confirmed it as much as a CT scan can, they did it with dye and were basically 99.9% certain it was cancer at that point.
Life as a new mom before diagnosis
Life was really good. The first three months of postpartum were really rough, but I was finally in that stage where I was loving being a mom.
I was getting some sleep, and I was on maternity leave because in Canada, you can take up to 18 months. I had planned to take about 14 months, so I was getting close to the end of my maternity leave. I was really enjoying my time with my son, spending more time with family, and just really loving life.
Getting the exact kidney cancer diagnosis
Once I received the pathology report, they told me what type of kidney cancer it was, how aggressive it was, and were able to confirm it did not enter the vein there as well, so how likely it would be to spread. The pathology report gave those details. My family doctor got it before I even had my appointment with my urologist–oncologist. He gave me that printed-out report, which was really good.
By the time I went to see the urologist, the student there came in to try to give the report and misinformed me, telling me my margins were all clear. They actually were not, which I already knew because I had the pathology report myself. I just said, “No, they are not.” Then my oncologist came in and explained that, unfortunately, there was a little bit missed that did not look like a tumor. They had cut a really good size around it, and there were still some cancer cells found in one of the margins. He said that with the amount they had to cauterize my kidney, it is highly unlikely that any cancer cells were left. The cancer cells were still contained within the margin, so they did not hit the actual outside. He was pretty confident that, despite the margins not being clear, the cancer cells were all removed.
My kidney cancer treatment plan and surgery options
The first option was a laparoscopic partial nephrectomy. Based on the imaging they had, they said once they were in there, they might need to do a full nephrectomy and open surgery.
I signed off on all that ahead of time as well — basically, do what you need to do to get it out. The plan going in was always surgery based on the information we had.
Going in for kidney surgery
It was really an out-of-body experience because this all happened so fast, thankfully. Here, urology is really backed up. Most people have to wait months to get even cancer surgery. I had a lot of people on my team who pushed it forward more. They do not often see young moms come in with kidney cancer, so I think they were really empathetic to the fact that I am not an 80-year-old man. I am a young mom with a child at home. I had a baby in their office with me, and I think that had an impact.
There were numerous people. I had a nurse advocate who called offices, took the time to explain my situation, and really pushed forward for me to have that appointment sooner. I found out about the tumor at the end of November, got the call on December 5th about it likely being cancer, and by January 3rd, it was time for my surgery.
It all happened so fast that I think I was temporarily emotionally paralyzed and was just so excited that I did not have to wait. The worst stage of cancer is the wait between when you find out and when a solution starts to take action. I was very fortunate that I did not have to linger in that phase as long as a lot of people do.
Recovering after my partial nephrectomy and gallbladder surgery
I could not lift my baby for six weeks. That was really hard. They had not taken out my gallbladder yet because they were just kind of like, “Who cares about the gallstones? We need to get rid of this cancer.” They hoped the gallstones would not cause me trouble. Three days before my partial nephrectomy, I started projectile vomiting again and having episodes from the gallstones. Because the surgery for my kidney was on my left side and the surgery for the gallstones would be on the right side, they did not have the capacity to tackle both at the same time, and at the time, they did not think they needed to. They thought I was just having an episode and hoped I would not go through it again during recovery.
By mid-January, I started having severe gallbladder attacks, which compromised my comfort during recovery. I ended up back in the hospital needing emergency surgery to have my gallbladder removed about two weeks after my partial nephrectomy. They had wanted to wait at least three months to put me under general anesthesia again, ideally. There was no option at that point. I could not eat or drink fluids at all without getting severely ill. Because of the wait to remove my gallbladder, I developed cholecystitis, inflammation around the gallbladder. The gallstones had traveled outside of it. I developed jaundice and started turning yellow. I was like a Simpson at one point.
This was even after my gallbladder was removed. I ended up being in the hospital longer for that than I did for my partial nephrectomy, because I needed an ERCP to remove the gallstones and then developed pancreatitis. That was the month of January. The first bit of my recovery looked like a fluke situation where, wow, thank goodness this gallbladder attack helped catch my cancer, but it was very painful and compromised my recovery. I had two surgeries back-to-back and then, as I said, developed jaundice and pancreatitis because of the stent they had to put in because of the gallstones. I was not fully pain-free until about May.
Comparing pain: Kidney surgery vs. gallbladder complications
It is a tough call. The gallbladder issues were more painful in the moment than the partial nephrectomy. When I gave birth, I had to be induced without an epidural, which was highly painful. I do not recommend it. The gallbladder pain was up there with that, but for days and days and days. I would say the whole jaundice, pancreatitis, gallstone situation was a lot more painful than the partial nephrectomy.
Thankfully, they managed to do the partial nephrectomy laparoscopically. It was still very sore, and I had to regain muscle mass, deal with scar tissue, and pain from the cauterization they had to do on my kidney. I developed a bit of a hematoma from that.
Overall, the complications I had from the gallstones were more painful than the partial nephrectomy, but the pain specifically from the partial nephrectomy lasted until about May before it was fully gone. That was because of the hematoma, they said, mostly because they had to cauterize so much.
Processing a kidney cancer diagnosis after everything happened so fast
I did not process it until afterwards. When going through a crisis, I turn off the emotional side of my brain and think, “I have to think logically.” Because it was so extreme, I had moments where that would slip, and in those moments, I thought I was going to have a panic attack. Then I would collect myself and say I needed to focus on problem-solving: how can I get this fixed as fast as possible, and who can I delegate to?
I like to research a lot and know my stuff, but my sister works in research as a project coordinator, so I knew I could rely on her to read the studies and advocate for me. She came to a lot of my appointments with me. I delegated tasks to her to take care of a lot of that for me. My other sister was basically my nanny and took care of my son a lot.
The hardest part emotionally: Writing a will for my son
The hardest part emotionally, before surgery, was realizing I did not have a will and that I had to write that out for my son. I still get emotional about it, because no one wants to write that when they are faced with a really serious situation. It is something I wish I had done when life was fine. It puts you in a spot where you are thinking, “What if something does happen to me, and he will have no memories of me?”
I put together an album on my computer of a bunch of photos and memories for him. I wrote him a letter and put together a general will as well, making sure I had all my affairs in order. That was hard to do after such a serious diagnosis.
Coping with kidney cancer as a young mom
I manage by knowing what is in my control and what is not, and knowing that once I have the information, I can problem-solve and do the best I can with the cards I have been dealt. I cannot choose those cards. I am not the dealer, but I can choose what I do with them and how I manage them. I always joke that I am the luckiest unlucky person ever, because of the number of times I have heard the word “rare” the last couple of years, but then something miraculous always happens. Getting in for my surgery on January 3rd, even though I was told it would be months, is an example.
I manage by believing that it is going to work out, not just by relying on miracles, but by finding solutions to help push it along, and making sure that if there are miracles going to happen, I do everything in my power to assist that.
How cancer changed my outlook on life
I definitely look at life differently now. It is one of those “Be careful what you wish for” things. I used to think it would be nice not to care so much what other people think. I want to be the best mom I can be, and to be that, I need to make sure I am putting my son before other people’s thoughts. When you get diagnosed with cancer, it has a funny way of suddenly making you really not care what other people think, and realizing that your life is yours and that it can change rapidly, even overnight.
Imagine it being your last day and making decisions based on the thoughts of others — not even their actual thoughts, but your thoughts of what other people’s thoughts are, which are not always accurate. We always have this narrative in our head, especially as women, of what other people are going to think if we pursue this or if we do that. Often, it is a narrative we have made up ourselves. Even if it is not, who cares?
Seeing “No Evidence of Disease” on my scan
I found out I had no evidence of disease when I had a CT scan earlier than planned. My family doctor ordered it because of the pancreatic stent. Because of all the gallbladder issues, I ended up having an earlier CT in May, and it came back showing there was no cancer. There was no evidence of disease.
It was such a weight off my shoulders. It was such a good feeling. It gives you more mental freedom. I know that can change. I have my one-year follow-up coming up in January, but I am not really worried about it. The strange thing is, I thought this would impact my life in such a negative way mentally, and it has kind of had the opposite effect.
Mental health after cancer and the role of therapy
I thought I would live my life in worry and be so paranoid. There are moments of that — anytime something happens, or you get sick, you get worried, or you have pains. Nowadays, people see things on the internet and worry like that anyway. If anything, the cancer has helped my mental health in the long run. Once I went to therapy and processed a lot of it and addressed how I felt about it, that was important.
Overall, the negatives have not outweighed the positives. The negatives really do not outweigh the positives of it mentally, because it has released a lot of nonsense from my mind that did not matter.
Advocating for myself and support from my care team
I did have to advocate for myself, but I also had a lot of help. There was my doctor, my sister, myself, and then the cancer care nurse advocate. I forget the exact title, but it is a program in Manitoba for people recently diagnosed with cancer. Those nurses help bridge the gap to make sure no one slips through the cracks. Their job is to advocate for you and connect you with resources for you or your family, mental health resources, information, and someone you can reach out to with questions while you wait. She really advocated for me.
Even the receptionist at the urology office played a role in advocating for me because she was the one who talked to the nurse. Everyone played a part. My oncologist–urologist also advocated for me. When I had my initial appointment with him, he said it would probably be a couple of months until he could get me in. I said okay. A couple of hours later, when I got home, an unknown number called. I picked it up, and he said, “Laurel, it is Dr. Sharon.” I said, “Oh, hi.” He said, “How does next Friday sound?” I think it was about a week and a half from my first appointment with him to when he booked me in for surgery. A couple of hours earlier, he told me it would be months, and it ended up being days.
He and the team really played a role. I can only imagine he had to manage his schedule, call up anesthesiologists, and not overpromise in my appointment. This was right after New Year’s. For all I know, maybe he even had the day off. There were strings pulled, and they suddenly got me in within a couple of days.
Navigating motherhood while facing cancer and my son’s illness
There have been some hard times. My son had recently been sick. He is such a happy little guy. He makes being a mom so easy. He is so funny, and I truly enjoy his company. He is such a character. On October 6th, he spontaneously stopped walking out of nowhere. He went from being a super-active, typical toddler boy to not walking, irritable, having all these issues, and not eating.
I took him to the hospital five separate times. They said it was some form of post-viral illness and eventually thought it was post-viral arthritis. Something did not sit right with me. It just did not make sense. I kept advocating and took him to his pediatrician, who assessed him and agreed it did not seem like post-viral arthritis. I called rheumatology, where he was referred, talked to the nurse, and said I needed an immediate reevaluation. They got us in as soon as possible and referred him to a neurologist. There is only one pediatric neurologist who does these tests between Manitoba and Saskatchewan.
As soon as she was back in Manitoba, she saw my son, did the tests that were required, and confirmed he did not have post-viral arthritis. He had Guillain-Barré syndrome. It is a post-viral illness that attacks the nervous system. That was five weeks of him being unable to walk on his own, and he has recently started walking on his own again. He is such a trooper. She said he should have been immediately hospitalized and treated with a drug that calms down the immune system, and we are very fortunate that, miraculously, he just started recovering.
I was back at work for two weeks. I had taken time off work to process everything from the cancer and make sure mentally I was able to take that on again. I was back for two weeks when this happened, and then had to go back on unpaid leave to take care of him. I have been off since around October 6th, just caring for him at home until he is better.
Hearing “It’s so rare” again and again
They said those words again: “It is so rare.” It is so rare, especially in toddlers.
I would prefer not to hear that phrase anymore.
Advice for others facing cancer or supporting a loved one
Delegate to people you trust. Delegate the mental load and the physical load. People will hopefully step up for you and offer, and when they do, accept that help. I do not know what I would do without the people who helped me, whether emotionally or by taking care of my son. I could not hold him for six weeks, and my husband had to go to work because I was not working. We were not expecting me to be off work that long. Accept the help.
Another thing is to try to live within your means in case this happens to you. When something like this happens, it is going to be a financial burden. Having savings or making sure you are living within your means and not stretching too thin, even if you seem healthy, is important. You just do not know. That can mean life insurance or other insurance that covers you if you get cancer or need time off work. Find a way to prepare financially for emergencies like this.
Financial preparedness and the cost of cancer and caregiving
It is important. I do not know what I would do if I had to go back to work sooner than I did, or even now. I had to prioritize my health and then prioritize my son’s health. It is bad luck that all of this happened within one year, during which I could not work again. It is mind-boggling.
Had we not been in a financially safe space, the stress that finances can cause — I cannot fathom how much worse this would have been.
Listening to your body and not delaying care
Some topics feel almost too sensitive because you do not want to scare people. You hear how rare it is in young people for this to happen, but then you are also hearing how often it is happening now in young people. Do not delay if you notice serious, consistent changes in your body. Not every cancer will have signs, but sometimes whatever else is going on in your body might be trying to point you in a direction.
In my case, it was not my kidney cancer that made me go to the hospital, but I listened to my body and went to the emergency. In the past, I was not always good at that. I would go to the doctor too late for things. The timing lined up so that it helped catch something else. Even if cancer does not produce symptoms, something else might, and it can help save your life if you listen to your body.
Symptom: None; found the cancers during CAT scans for internal bleeding due to ulcers Treatments: Chemotherapy (capecitabine + temozolomide), surgery (distal pancreatectomy, to be scheduled) ...
Bill Faces Stage 4 Neuroendocrine Rectal Cancer With a Strong Community
Bill’s advanced neuroendocrine rectal cancer experience began most ordinarily: tiny, easy-to-dismiss drops of blood in his stool. He had just moved to Houston, started a new role in the pharmaceutical industry, and was settling into life as a new father when his primary care physician repeatedly attributed his concern to simple hemorrhoids. Even with a busy new life, Bill couldn’t shake the sense that something more serious was happening and kept pushing for answers. That insistence on being heard ultimately led to a colonoscopy and the news that he had neuroendocrine carcinoma in his rectum, diagnosed at stage 3 and later progressing to stage 4.
Bill describes the shock of waking up from the colonoscopy, still sedated, and hearing the word “cancer.” He also speaks frankly about being a younger adult whose symptoms were minimized and how he chose not to live in the land of “what if.” Instead of dwelling on missed opportunities for earlier diagnosis, he focused on the choices still in front of him.
Over time, he moved through multiple lines of treatment, a major surgery that left him with a permanent double ostomy, and several clinical trials after standard options were exhausted, including studies opened by a specific genetic mutation. The therapies included FOLFOX, FOLFIRI, and an 18-hour surgery.
As the treatments accumulated, so did the lifelong side effects and the mental gymnastics of facing each new drug, scan, and possible progression. Bill discusses how uncertainty became a constant alongside his determination to remain as physically and mentally prepared as possible. That meant tending to close relationships, nourishing his body, and embracing something he calls “practice suffering,” using endurance cycling and running to train his mind for the hardest days of treatment.
Throughout the advanced neuroendocrine rectal cancer experience, Bill also had to rewrite his identity as a man, a father, and a provider. He reflects on how cancer stripped away old concerns about status and appearances and sharpened his focus on service, advocacy, and time with his daughter. Sharing his story publicly has become part of that purpose. By speaking out about a rare, aggressive cancer, he wants future patients to have better options, more research, and the sense that they never have to go through this experience alone.
Watch Bill’s interview or read his transcript to learn more about his story:
How self-advocacy can be lifesaving
Why treatment response is not about personal failure
How cancer changed how Bill sees his identity, values, and priorities
What it has been like living with a serious illness
Why patients are encouraged to seek support, speak openly, and get involved in their care
Name: Bill T.
Age at Diagnosis:
33
Diagnosis:
Neuroendocrine Rectal Cancer
Staging:
Stage 4
Mutation:
ATM
Symptom:
Drops of blood in stool, recurrent over several months
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
My name is Bill. I’m from Houston, Texas. I was originally diagnosed with stage 3 neuroendocrine carcinoma of the rectum, which later progressed to stage 4. I was diagnosed in November 2018.
Life and Career Before My Cancer Diagnosis
I moved to Houston from Southern California in 2016. I was going to start a new role in the pharmaceutical industry in bladder cancer, which was a coincidence that I ended up getting cancer. I had recently started a new family, a new career, and built a new home. Everything that happened right after was a huge shock for me.
My Early Symptoms of Neuroendocrine Rectal Cancer
My symptoms were not very prevalent. There were drops of blood in my stool, but they were hardly noticeable. I always brushed it off because it would happen and then go away, but it would recur for about three months.
At the time, I was looking for a new job and when I did, I had benefits starting day one, which was great. I went in to see my primary care physician (PCP), who attributed the symptoms to hemorrhoids, but I didn’t accept that explanation since it was constantly coming back, so I pushed for blood work and a CT scan. They appeased me by doing what I asked, but when I came in for my follow-up, the PCP still brushed me off and said it was hemorrhoids.
Then I thought maybe it had something to do with my autoimmune issue. I have spondyloarthritis, which I’ve had for close to two decades. I went to see my rheumatologist to tell him my symptoms and he told me that this has nothing to do with that. He then referred me to a gastroenterologist, who scheduled me for a colonoscopy, which is how I discovered the tumor in my rectum.
How I Advocated for My Own Cancer Diagnosis
Part of it was a gut feeling. At the same time, I wasn’t satisfied with the answer I was getting. I already assumed that he was going to say hemorrhoids, but I did the research and this was not hemorrhoids. I needed confirmation and validation of what I was worried about. I needed additional testing to get an answer.
He didn’t even show me the images or go over my scan. He simply told me it was hemorrhoids. I said, “We need to go over the scan.” I sought out another clinician, who did what the previous clinician should have done, and that’s when I felt heard. But because of all this delay, I get my answer, which wasn’t a good answer.
Hearing My Colonoscopy Cancer Diagnosis
Getting the diagnosis was interesting. As you wake up from a colonoscopy, you’re somewhat drugged up, so you can’t fully feel the news. You have all these thoughts rushing through your mind. I was not expecting cancer. It was a shock and it took me some time to process.
Being Diagnosed With Cancer at 33
Automatically, I thought, “He’s a piece of s***. I can’t believe he missed this.” But over time, I thought that sinceI was so young, you don’t think cancer or even assume it, so they automatically think it’s hemorrhoids. I could understand his observation and way of thinking, but it also hurt because I wasn’t heard.
I’m glad that I advocated for myself in terms of finding another opinion. I wouldn’t say that opinion has saved my life, but it gave me enough room where it wasn’t stage 4 in the very beginning, so I had enough time to prepare for what was to come.
Coping Without Dwelling on ‘What If’ in Cancer
There’s no point in dwelling on the past. It’s easier to move on. I’m the type to not dwell on the past. I prefer to move forward and take on what’s in front of me. It’s helped me with my diagnosis to this day. I talk to so many patients who constantly question what-ifs and it destroys them psychologically, which can easily equate to physical effects. I didn’t want to go down that rabbit hole.
Telling My Family About My Neuroendocrine Cancer Diagnosis
It’s easier to be blunt. I didn’t know the severity of everything. When I finally got my pathology, I did what everybody does when they get diagnosed with cancer, which was consult Doctor Google. All the literature I read was bad: very short-term survival, very low percentage of survival rates past five years, not enough treatments offered, and majority of treatments failing.
Then I confirmed it with my colleagues. I would talk to them and they told me this wasn’t a good cancer to have. There’s no such thing as a good cancer, but having a rare aggressive cancer increases the anxieties brought upon the person. At the same time, I’m not the type who will basically bury myself in sorrow. I thought, “I need to do everything humanly possible to increase my chances of survival, regardless of whether it’s one, two, three, or whatever number of years. As long as I could survive as long as I could, that’s the best that I could do.”
Having Hard Conversations and Taking Ownership of My Health
It was difficult, but necessary. I understand that part of being an adult is having uncomfortable conversations. I understood the reality of my prognosis as well as the diagnosis, but at the same time, I understood the fact that I still had accountability in my survival. I would be accountable for my mental and physical health, what I put in my body, how much I moved, and everything beyond. We could easily fall into the trap of doing nothing and that wasn’t for me.
My Neuroendocrine Cancer Treatment Journey Through Nine Lines of Therapy
I’m fairly high up there in terms of the amount of treatments that I’ve had. I’ve been through nine different lines of treatment. My first line was carboplatin and etoposide. The next was 25 rounds of radiation and capecitabine. The next was FOLFOX. After that was FOLFIRI.
Following that, I had an 18-hour surgery that left me with a permanent double ostomy: a urostomy and a colostomy. Even after 18 hours, the surgeons weren’t able to get everything. I had four surgeons and a radiation oncologist, and they told me that they needed to bring me back in three months to get the residual tumors. We did a liver ablation and thought I had some breathing room.
Two months later, I had a recurrence in my liver. We had some biomarker testing done on my tissue and my blood, and found that I had a genetic mutation called ATM. Though the mutation is typically seen in breast cancer patients, it was great because it opened the doors to clinical trials because I had exhausted all standard of care treatment for my type of cancer.
I’ve been through four clinical trials. The first one was what’s now called olaparib and RP-3500, which is a PARP inhibitor and an ATR inhibitor, and lasted about 23 months. The following treatment was an immunotherapy clinical trial with vedolizumab. I did two cycles and had a bad adverse reaction that landed me in the hospital for 12 days. I had to be off treatment for about five months to recover from the adverse effects.
Then we moved to another clinical trial, ART6043, which was another PARP inhibitor. That didn’t last very long. I moved to another clinical trial, which was another PARP inhibitor, but that failed as well.
My oncologist looked back at my records when I was initially diagnosed. This was somewhat of a Hail Mary because he said that there was activity in my pelvis for somatostatin receptors. He moved forward with another dotatate scan and found my cancer lit up, which was interesting. Typically, those receptors aren’t seen in patients who have neuroendocrine carcinoma, so there’s a pro and a con. The pro was that we found it lit up. The con was that they were in even more parts of my body, so I had even more cancer than I thought.
At the time, I only had cancer in my liver, lungs, and pancreas, but the dotatate scan showed additional lesions in my chest, pelvis, and parts of my bones. We went through the insurance approval process for lanreotide and peptide receptor radionuclide therapy (PRRT), which has kept me stable until today.
I’ve had nine lines of treatment. For my type of cancer, I have to think two or three lines ahead because everything has a shelf life. The hardest thing about survival is that every drug that I jump on is a new accumulation of lifelong side effects. At the same time, the mental gymnastics of needing to jump on another drug, having the hope, anxiety, and understanding that to stay alive, I have to repeat this in a perpetual state of déjà vu.
How I Cope With Uncertainty and Ongoing Cancer Treatments
Uncertainty is a guarantee in life, just like death and taxes. I’ve learned to live with it by understanding that this is always going to be present. But at the same time, I could mitigate these anxieties by preparing myself physically and mentally through having good relationships, making sure that I’m eating and hydrating well, getting sunlight, leaning on community, and doing something I call “practice suffering.”
I engage in endurance activities where I’ll run and cycle. A lot of the time, I don’t want to because I feel the side effects of treatment. But being able to do things that make me feel uncomfortable, especially when I don’t want to do them, builds a level of resilience and makes me ready for unpredictable moments, such as going through all these treatments. When I come out on the other side, I continue to build on that resilience, which levels me up for anything that comes my way.
How Cancer Changed My Relationships and Support System
My family played a huge part. My mom has been with me through thick and thin. Even though she doesn’t know how to fully communicate with me on how for me to go through this, she has always made sure that if I needed something to eat, she makes it for me. If I needed someone to watch my daughter, she’ll do it. She’s unable to support me financially and in other ways, but she does what she can, which is all I need.
My brother and my sister have always been there for me, checking in on me. I’ve lost friends, but I’ve also gained a lot of friends. I feel that cancer simplifies life in that the relationships that you think you had that were great are put to the test. Cancer is one of those diseases that filters who is there and who isn’t there, who is superficial and who is only there to ride the wave with you. It’s a pleasant surprise finding new friends who I wasn’t very close with before but have become great friends in the long-term because they’ve been there, checking in on me, and constantly there to support.
There are people who have accepted the new me. Some people think that once I have stability with my disease, I could go back to being the old me, which is impossible because cancer changes a person — not for better or for worse, but because their outlook on life has completely changed. I hold those people very close to me now because they’ve seen me at my worst and can also handle me at my best.
Using Exercise and ‘Practice Suffering’ to Cope With Cancer
It helped that I already had a desire to be physically fit since the very beginning. I was already very into fitness. Over time, there were days when I couldn’t even get out of bed. Brushing my teeth and getting out of bed were probably the hardest things to do.
There were times during chemotherapy or when I’m on high-dose steroids that I experience pretty bad insomnia. I’m the type of person who can’t sit still, so I would walk around my room or around the house. Then it progressed to walking around the neighborhood at odd times of the day. Later, my dad shipped me a road bike, so I started riding my bike around the neighborhood. The distances kept getting longer.
I never liked running, which is funny. I’ve always viewed running as punishment because when I played sports, the consequence of doing something bad or not doing something correctly was to run a lap, so I would always hate running. But I also had a real curiosity because when I was on my clinical trial, I couldn’t run. After all, it would cause charley horses. It wouldn’t come from running, but when I tried running, it caused even more charley horses.
I would have three to five episodes a day because of the drug that I was on and none of my team could understand why. We did blood work and consulted multiple specialists, but no one could figure it out. I decided I would just continue cycling because the charley horses weren’t as bad. When that drug failed, I was curious to run, so I ran a mile and I was okay. I hated it, but at the same time, I practiced the suffering part, so I would continue increasing my mileage. I noticed I could go longer.
I heard about ultramarathons and thought I wanted to do one, which was funny because the longest run that I’ve done was a 5K with friends, a Turkey Trot. But being somewhat excessive in nature was a standard thing for me, so I decided to sign up for the Brazos Bend 50, an ultramarathon, which is a 50K. I started running in early January and the Brazos Bend 50 was going to be in April, so I was technically three months into running. It was one of those things where if I signed up, I was already committed and I don’t want to waste money.
But the other issue was that I was starting a new clinical trial, so I had to figure out the new side effects of this one. But I didn’t care. I ended up doing the ultramarathon and it was the most painful experience of my life. Once I hit marathon distance, it took me to a dark place. I had nothing but bad thoughts in my head because I was in so much pain. I’ve never run that kind of distance. Those moments when I was suffering and hated life taught me a lot about myself because I didn’t want to give up, but I also hated the fact that I was going through it.
It was a great reflection, as well as an introspection, of what an individual goes through with cancer. At the very beginning, they’re very excited. They’re very determined and will automatically say they’re going to do whatever is necessary to finish. But there are a lot of people who don’t finish the race. I see it in cancer as well. At the very beginning of a cancer diagnosis, you’re willing to do everything, but until you go through the treatment, the physical pain, the psychological pain, and when you’re hurting so badly, you think to yourself, “Can I get through this?” It’s a great comparison for me.
To go through that type of suffering daily helps me mindfully understand and be present with my thoughts and that this is only information for me to use in future moments. At the same time, it gives me accountability for my actions and how I follow through with anything. And that’s helped me to this day.
Running Marathons and Ultramarathons With Active Cancer
I haven’t run very many. Most of the time, I run on my own. The upcoming one I have is the Houston Marathon. My main goal for that event is to raise money for a cancer organization, to push the acceptance of people having cancer not going through it alone. This is the first marathon of one of my friends, Victor, so my only goal is to get him across the finish line. I couldn’t care less about my time. If I could help someone do something that they want to do, I’m happy. I’ve noticed that people always strive for a certain time, pace, or finish time. For me, it’s the experience. That’s all it is for me.
Training Through Chemotherapy and How Other Patients React
People don’t believe I have cancer because they say I can do a lot more than them, but there’s a lot of work involved. At the same time, people think about intensity, but for me, it’s about consistency. I always tell people I didn’t start here. I couldn’t get out of bed when I was first diagnosed. This is the result of seven years of consistent work and having no excuses. Everybody can easily have an excuse not to do something.
This has helped me psychologically and physically endure all the treatments that I’ve been on. You know what chemotherapy could do to you… I live with the fact that every time I sign my life on the dotted line, accepting this new treatment, I have to be prepared for the consequences. But that is part of trying to survive the disease that will ultimately kill us.
[Editor’s Note: Informed consent is a standard part of many medical treatments, including cancer care. These forms explain potential benefits, side effects, and rare but serious risks so patients can make decisions alongside their care teams. Treatments are recommended because doctors believe the potential benefit outweighs the risk for that individual. At the same time, signing consent forms can feel emotionally heavy, and this reflection speaks to the lived experience of making high-stakes decisions while living with cancer.]
From Feeling Betrayed by My Body to Learning From Cancer
Initially, I was very angry about my body, but at the same time, I was looking back at my lifestyle habits as well. I looked healthy, but I probably wasn’t healthy inside. Because I was young, I had a great metabolism. But when I look back and reflect, I didn’t have the greatest habits. I would binge drink. I would binge eat. I’d stay out late. I would constantly be exposing myself to radiation and everything, so I thought that, partly, that probably had something to do with it.
Over time, through introspection, I didn’t see my diagnosis as a death sentence. Cancer has been the ultimate teacher because it has narrowed my focus on what’s important. Some people never realize or understand what’s important in life. They think about what others think about them. They think about keeping up with the Joneses. They think about their superficial image to others. I no longer care about all of that.
I dress like a bum now. I don’t care if I have a stain on my T-shirt when I’m out. I will speak my mind. If I don’t like something, I will walk away from a person if I don’t feel that their conversation benefits me. I don’t care anymore. Before, I cared a lot about office politics, superficial images, and all those unnecessary things that make you unhappy. Now I care about my physical and mental health. I care about doing good and service. And I also care about making the next person who gets diagnosed with cancer make their journey less s*****.
How Cancer Changed My Identity as a Man, Father, and Provider
I constantly had to rewrite my identity through cancer. When I was initially diagnosed, I was a father, a brother, a son, and a provider. I was a person in this social circle. All that changed because of a diagnosis.
I no longer look like what I used to look like. I had to change careers multiple times. I had to rewrite my skill set. At the same time, I also had to surrender to the fact that life will never be what it used to be. And when I finally accepted that, things got better.
You have to give yourself grace in terms of what you’re going through. Cancer is something that I wouldn’t wish upon anyone because it’s one of the cruelest diseases that could be inflicted on a person. It destroys you on every level. It took years for me to understand that.
But at the same time, understanding that just because you get diagnosed with cancer doesn’t mean that it’s the end of your story. You could continue writing more chapters in your story to be who you want to be. Every day is a gift and every day is another day for you to become the person you want to be.
Parenting With Advanced Cancer and Talking to My Daughter About It
My daughter has seen me as normal as a person could be. She knows that I’m more physically fit than one of her friends’ parents. She also knows that I’m probably one of the most resilient people out there.
But I try to hide a lot of the struggle that I go through. As a parent, you don’t want your kids to see you struggle, but there’s also a danger in that because when they don’t see that, they don’t give the respect to the disease. I’m still figuring out how to discuss cancer with my daughter. She knows that I have it, but it’s one of those things where I struggle with trying to correctly explain it to an eight-year-old.
All she knows is that I have cancer. She was only five months old when I was diagnosed, so she has seen me go in and out of the hospital. She has seen me throw up. She has seen me so weak to the point where it causes anxiety and PTSD for her, so I try not to relive those moments for her.
It’s hard just because people think that because I can do what I do doesn’t mean that I’m not struggling psychologically and physically. I have so many side effects that some people would go crazy with all the side effects that I’ve had.
I have to see so many different specialists. People are surprised to learn that I see over 15 specialists. I’m only 40, but I have heart issues. Most people wouldn’t think that because I can run or cycle so much. But I do have heart issues. It’s one of those things where I tell everyone that, for a lot of people, cancer is an invisible disease, and they will never truly know unless they actually take the time to understand my story.
Why I Share My Rare Neuroendocrine Cancer Story Publicly
What I’m going through is not impossible, but at the same time, it gives light to people who are not comfortable with sharing their story that this is acceptable. It took me years to want to share my story because I was very private. But over time, I found that it’s part of the healing process in itself. It also gives a voice to other patients like myself.
I understood that there aren’t many people with my specific diagnosis telling their story or advocating for the disease. The majority of the people who have my diagnosis are struggling to survive. We don’t have a voice. I found that not having a voice equates to not having research dollars or any sort of awareness of the disease.
Many organizations are trying to find more treatments for my type of disease, but they don’t have patients stepping up. I found that by doing more advocacy within my field of cancer and within my subtype, having that voice and image outside in public is going to only help future people who get diagnosed with my cancer.
Life After Leaving Work and Becoming a Full-Time Cancer Advocate
I’m basically enjoying my retirement. I volunteer for different organizations in the advocacy space that focus on mental health as well as social and emotional support for men. I do research advocacy for Fight Colorectal Cancer. I serve on several research advisory panels.
I mainly want to use my time and efforts to make sure that the lives of future people who get cancer aren’t as bad and their struggles aren’t as rough as mine. I never saw the benefit of working through nonprofits, but when I received help and services from nonprofits, it totally changed my outlook.
My Hopes for the Future and Supporting Men With Cancer
I spend time with my daughter when I can, enjoying nature. I would love to visit more national parks and explore, meeting more cancer patients and helping them in their journey, furthering medical research in my type of cancer, and removing the stigma in men that they have to go through this alone.
Going through cancer as a male is very difficult because men tend to isolate themselves once they have a disease like this. The majority of the time, I see when men get cancer, their spouses or partners take the helm and do all the research, understand all the information, and the man basically has their head dug into the sand, knowing nothing about their disease.
I’m the exact opposite. I’m a very controlling person. I’m very type A. I need to know everything, so when I speak with my team, I know how to steer my conversation. But that is not what I see with the majority of the men out there. We need to remove the stigma that we could do this on our own — that’s what made me go crazy. When I finally accepted help, it’s no longer a weakness. It’s a tool. At the same time, it’s a way to make your journey and your progress in terms of your disease so much easier.
Redefining Strength for Men With Cancer and Embracing Emotion
Before, I was the typical man. Now, I’ve accepted and understood the fact that being able to talk about my emotions freely has been a game-changer in my life. I went to a retreat called Gathering of Wolves and saw a community where 100-plus other men were sharing their feelings and their anxieties, seeing that there’s no judgment. Being able to see that and experience that, and see that there is no judgment and fear of being ostracized and isolated into a different group, was empowering. It validated that everything I was going through sucked. And when I got a taste of that, I wanted to continue. I wanted to provide that to other men that I come across on my journey.
Man Up to Cancer has been a large part of my advocacy. They have helped me understand the role and benefit of what this can do for a person in their journey. I am part of the leadership team and one of my roles is to ensure that men of color are seen in this equation.
The majority of the time, men of color are diagnosed at a later stage in life, are less likely to seek out resources, and their prognosis and time of survival are shortened, and I’m making sure that I change that. I put in the effort to reach as many men of color as possible, as well as adolescents and young adults (AYAs), which is a very complex part of the equation for health systems because they have never seen this many young people getting cancer and they’re still figuring things out. Because I’m a man of color and an AYA, I want to further the progress of how medical institutions deal with this.
My Advice to Other Cancer Patients About Community and Survivorship
Being able to talk through your emotions, find community, and understand that your anxieties are information for you to process as well as implement in terms of how to deal with your disease are the most important things for a cancer patient to go through.
Survivorship after treatment is a very hard jigsaw puzzle to figure out. You need a team and a community to fall back on because, without them, you will basically be lost. Do not be fearful of seeking them out and trying as many as you can. Find a niche community that will help you navigate life, and you will never be alone.
Symptoms: Fainting spells, fatigue, dizziness, anemia, shortness of breath, absence of menstruation, unexplained weight loss, night sweats Treatment: Surgery (total gastrectomy with a Roux-en-Y reconstruction) ...
Drea Finds Identity and Strength with Stage 4 ROS1+ Lung Cancer
Drea is a video journalist who was only 26 when she was diagnosed with stage 4 ROS1+ lung cancer. It came as quite a shock. She never imagined that a physically active, young non-smoker who had never had any health issues, could ever get cancer.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Drea’s story began in early 2023. She began to experience some strange symptoms, including a swollen ankle from an unexplained deep vein thrombosis or blood clot, odd bruising, extreme weight loss, and persistent shortness of breath. She went to the ER several times, had some urgent care visits, and also saw specialists, but was reassured that what she was experiencing was due to stress or other such causes. She started to doubt herself even as her health began to deteriorate. Eventually, she succeeded in having a CT scan done. It revealed a large mass in her lung. Further tests confirmed that she had stage 4 non-small cell lung cancer that had already spread to multiple locations.
Drea’s experience has convinced her that self-advocacy is key. She explains why we always need to trust our instincts. “If you feel deep inside that something’s wrong, keep pushing,” she advises. Because she was persistent, she eventually had comprehensive biomarker testing, which identified the ROS1 mutation. This discovery opened the door to life-extending targeted therapies.
Living with stage 4 ROS1+ lung cancer has helped Drea redefine survivorship. It’s not just about existing; it’s about living fully. The targeted therapies she’s having allow her to enjoy climbing, biking, beach days, and gardening. She’s open and frank about her ups and downs, and acknowledges the chaos and struggle of having to navigate cancer in her 20s. But she’s decided to treat each day as an opportunity by focusing on what she can control rather than agonizing over the “what-ifs.”
Cancer didn’t strip Drea of her identity. Instead, it’s added new layers. She’s not just a video journalist anymore; she’s also an advocate, connector, and source of hope for others. She shares her story openly to help more people realize that “anyone with lungs can get lung cancer,” and, by doing so, to break the stigma that lung cancer is a smoker’s disease.
Drea urges others to be their own best advocate, seek second opinions, push for biomarker testing, link up with patient groups for support, and, most importantly, give themselves grace. Watch her video for more on:
Her diagnosis at such a young age and how she became her own health advocate against all odds
Drea’s struggle to be heard before her stage 4 ROS1+ lung cancer diagnosis
How targeted therapies gave her her life back
Why Drea names her cancer ‘Carl’, and how humor helps her thrive
The advice she offers young people who don’t feel heard by doctors
Scroll down for the transcript of Drea’s video interview!
Name: Drea C.
Age at Diagnosis:
26
Diagnosis:
Non-Small Cell Lung Cancer
Stage:
Stage 4
Mutation:
ROS1
Symptoms:
Swollen ankle resulting from a deep vein thrombosis or blood clot
Mysterious bruising
Extreme weight loss
Persistent shortness of breath
Rattling sound coming from the throat while breathing
Treatments:
Radiation therapy
Chemotherapy
Targeted therapies
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
My name is Drea. I was diagnosed with stage 4 non-small cell lung cancer at 26.
When I first felt something was wrong
I first started feeling off at the beginning of 2023. It began with the DVT, which is a blood clot that resulted in a swollen ankle, and at the time, it didn’t make sense to me because there were no known injuries; I hadn’t fallen, I didn’t trip or anything. I had gone to urgent care, which then sent me to the ER, and then they discovered that it was for sure a blood clot, so they put me on thinners. Following that, I kept having these sorts of mysterious symptoms, among them just bruising up and down my body, and extreme weight loss. It felt like I was in a pit of despair. I felt like there was something off, and I don’t know how to describe that feeling. And I think throughout the process of 4 or 5 months, the symptom that started scaring me the most was the shortness of breath. I think by the time they came around, I had this really weird, awful, rattling sound coming from my throat. Google scared me when I googled that one up. The entire five months of these symptoms, I had gone to urgent care a couple of times, I had gone to the ER, I had seen a specialist, and I kept getting sort of brushed off, getting told, “You’re young, you’re probably just needing a little more rest, you’re probably just tired or stressed.” Cancer or any sort of serious disease was never really mentioned. But then I remember in May, going back to that same urgent care that months earlier had prescribed me an inhaler for the shortness of breath, that same urgent care doctor had finally ordered a CT scan.
He gave me a call, and there was a sort of newfound sense of urgency in his voice. He told me I needed to go to the E.R. immediately. There was a mass that was found in the scan, and it did not look good. So I just drove myself over across the street and got admitted to the E.R. That was my first hospital visit that resulted in, I think it was like a 7 or 8 day stay.
They ran a swath of tests. My blood counts came back, not looking great, but nothing to signal cancer. But it was the imaging that scared doctors the most. They had found this huge lemon-sized mass on my right upper lobe, and sort of nodules scattered across it. They ended up doing a PET scan, and that’s when they found that there was also cancer up and down my spine and pelvis, and not even my noggin was spared, unfortunately. So they knew right away that this was serious and that it was likely cancer. And so I think it was maybe on day 4 or 5 of that hospital stay that they got me in for a bronchoscopy, and then I got the news.
The moment everything changed
Getting told that I had lung cancer at 26, as a never-smoker, never picked up a cigarette, or none of that, was shocking. I did not understand how that could even be possible. I never knew that non-smokers got lung cancer. My dad died of lung cancer in his 40s. He was a very heavy smoker, so I doubt he had any sort of mutations. But because of his lung cancer death, I had made the choice early on that I would never pick up a cigarette. I wouldn’t vape because I saw what it did to others. But then to find out that that didn’t save me from lung cancer was a shock.
Ten out of ten, I would not recommend getting your cancer diagnosis in the E.R. It is awful. So take that with you wherever you go. Try to establish care with the primary care physician who knows you and your history, because getting my diagnosis in the E.R. was not pleasant, to say the least. I think I was there anywhere between 5 and 7 days. It was complicated because after I got that diagnosis, I got discharged. I got sent home with no oxygen for some weird reason. Here’s a metastatic lung cancer patient who has cancer across both lungs, up and down the spine, in her noggin, and she still got sent home with no oxygen. And I just didn’t have anyone to check up on me in the way that I would imagine others would have if they didn’t get their diagnosis in the E.R.. It wasn’t until my at-home nurse noticed that my breathing was getting progressively worse, and she told me to head back to the E.R., that they found that my situation was getting even worse. And so the second time I got admitted, I had to get an emergency blood transfusion and start traditional chemo right away, the very next day, and that was the day that my oncologist told me, This doesn’t work.
We might have to put you in hospice. Because at this point, we had not gotten the biomarker testing results back. And so that was when things finally hit me that this was serious, that I don’t have my youth, I don’t have my young age to rely on, and that something needs to happen. And so I remember lying in bed with my mom by my side at this point, just panicking internally. And that was when I decided to just start calling around to see if there was a comprehensive cancer center that would take me right away, because I did not want to be put in hospice.
I took my health into my own hands
Hearing the word hospice just rattled me to my core. I knew that I had to do something to get myself from getting buried six feet under, and so I started crawling around trying to see what the next best option was. What is an option that is more familiar with these rare types of lung cancers? At the time, I didn’t know that I had ROS1 because we were still waiting on biomarker testing. But the oncologist at the time said that it was very likely, given the fact that I never smoked and I’m so young. I started calling around to this one major comprehensive cancer center in Florida. It was right after that conversation with the oncologist, and I think the call rep could hear the shakiness in my voice because I was trying to talk through tears, just trying to see if there was any sort of openings in the immediate couple of weeks. After all, things were serious, and as soon as I was discharged, I needed to seek care elsewhere to see what other options I had. Luckily, the lady found me in an appointment, and I was able to get in on time. I think it was two weeks later, and that’s how I ended up at my second hospital.
Learning my biomarker
I was actually very lucky that my oncologist at the time knew that there was a specific subtype of lung cancers that tend to impact younger nonsmokers. And he happened to be working that day and saw my case, and he ordered comprehensive biomarker testing right away. I think I got the results after just a couple of weeks. I consider myself very lucky because if it weren’t for biomarker testing, I don’t think I’d be here today.
It allowed me to take targeted therapies, which have been shown to work well with my specific type of cancer. Targeted therapies in general have truly revolutionized what it means to be metastatic and living with lung cancer. And it’s just unfortunate that there are people across this country, across the globe, who are not afforded that option because they’re doctors, or the hospital care system just may not be aware that comprehensive biomarker testing is a thing.
I was kind of all over the place, still trying to process the news. But when my oncologist at the time mentioned that comprehensive biomarker testing could open the window to newer forms of treatments, I was like, all right, let’s do it. And then when I finally got the news and I saw that I had ROS1, which tends to impact, I think it’s like 2 to 3% of all non-small cell lung cancer cases, I was like, great, so here’s to celebrating having a mutation, I guess, let’s do it. It was an interesting, interesting time. A couple of weeks later, my brother was doing some research on my behalf, and he found this incredible nonprofit advocacy group that does a lot to build community and share resources for people with ROS1. They’re called the Ross Wonders, and they have just been a godsend to me. They showed me how to be a better advocate for myself, they’ve connected me with those long-term cancer survivors, and they’ve shown me that you can still live a long and fulfilling life, although you have metastatic lung cancer.
My treatment plan
As soon as we found out that I had ROS1, it became very apparent that we had a better option than that platinum-based chemo that I had already gotten one round of. At the time, I had also gotten radiation. But there has been such incredible research out there about these targeted therapies that the best course of action at that time was to just stop chemo and go on a TKI pill, and so I was put on my first drug.
I got about three years of pretty great response, pretty great quality of life on what I like to call my beloved drug, and it was very good to me; it kept my cancer under control, and I was able to wrangle my control. And I was able to wrangle my life back from cancer in a way that I never envisioned, because I knew nothing about targeted therapies and what sort of quality of life that might have meant. It was great for me for about three years. Unfortunately, earlier this year, I had to switch to another drug, but thankfully, things have been going pretty well on this second TKI as well.
It’s gotten a pretty good control on some of the new lesions that have popped up, and I’m still able to live a relatively normal life. I have a couple of annoying symptoms, but they’re still manageable.
Everyone’s different. Everyone’s going to react differently to each drug. We may have the same cancer with the same lesions and other comorbidities, but we may still react differently to whatever drug we’re taking. I consider myself pretty blessed because I seem to be a fairly good responder to TKIs. I don’t deal with any sort of debilitating symptoms. I know that that’s not the case for a lot of other ROS1ers; unfortunately, I wish it were. But so far, everything that’s been thrown at me has been manageable. I’ve been able to get back to my old life. I climb a lot, I bike, I’m able to take my dog on long walks, I’m able to be out in the sun and garden, I’m a very big beach bum, true Floridian. And I have TKIs to thank for that.
How I feel about clinical trials
I will say a lot of people tend to fear the idea of clinical trials because they like to think, “I don’t want to be a lab rat, I don’t know what sort of outcomes I’m going to see if I join a clinical trial studying a very new drug.”
Editor’s Note: In cancer trials, no one is given only a sugar pill when an effective standard treatment exists. Instead, participants receive either the current standard-of-care treatment or the standard-of-care plus a new therapy being studied, and everyone is closely monitored for safety and benefit. Many of the oncologists we interview describe cancer clinical trials as "getting tomorrow's medicine today."
There are a lot of incredible treatments out there that are revolutionizing what it means to live with these sorts of subtypes of lung cancer, whether it’s ALK, EGFR, or ROS1, like what I have. These therapies are exciting; they’ve shown a lot of great promise. A lot of times, these drugs are being tested for years in a clinical trial setting, and there is early data that you can glean from and decide if that’s a good option for you at the time. If I’m ever at a point where I do run out of TKIs, I will gladly volunteer for science and to help the next lung cancer patient get access to even better drugs in the future.
How I’m navigating my diagnosis and being young
Navigating cancer in your 20s and 30s is incredibly messy; it is chaotic. It is a roller coaster you go through, so many loops, it’s complicated.
I’m not going to deny that, it’s not an easy feat. I’m metastatic, which has caused me to grow up in a lot of different ways. For people who have been diagnosed at earlier stages, it is life-changing. Just because treatment wraps up and your hair grows back and you’re in remission or you’re cured, does not mean that your life goes back to normal or that you’re even the same person you were the day that you were diagnosed. So it is complicated, and I try to remind every cancer patient that I meet to just give themselves grace. It is a work in progress. I am three years out, three years into survivorship, and I am still learning what it means to live with metastatic cancer, and to live each day as if I’m living, not as if I’m dying.
Honestly, I try to just make the most out of whatever time I have left. If it is three months, if it is three years, if it is six years. Let’s pray for six years, I will take six years happily. I like to treat every day like a new day.
And if I’m having a crappy day or just the type of day where you just don’t want to get out of bed and you’re just stuck doom scrolling on your phone, I try to remind myself that tomorrow is a new day.
I used to just get stuck on all the what-ifs. Like, what if I spoke up sooner? What if I pushed for answers sooner? Would my life have been different? Would my cancer have been when it was stage 2 or 3 instead of stage 4? But at the end of the day, what does that do for you? What are you thinking about, the crappy cards that you were dealt day after day? What does that do for you? And so I try to just remind myself to focus on the things that I can control. And that is what my life moving forward is going to look like. Whether that’s for three months, three years, or however long, I know that I just want to make the most of each and every day.
“Hope” is a complicated word for me
I am cautiously optimistic that I will be able to get a good chunk of time out of whatever TKI lines are currently available. And I hope that I will be able to respond well to those therapies until the next best thing comes out.
And there are a lot of really new and exciting TKI drugs currently being studied in clinical trial settings. I try to talk to my cancer from time to time and just be like, “Oh, Carl, can you give me three years of peace, until that next best thing comes out?” I know that next year there’s going to be another TKI out in the market, or at least that’s what my oncologist has said, and what we hope is that it’s going to get approved by the FDA. I try to count my blessings every day and try to beg Carl from time to time to just behave for a little longer, and just go from there.
I like to view my cancer as an insidious roommate that just does not pay rent, that has been uninvited. What is the most awful name you could give that imaginary roommate? And the first name that came to mind is Carl, so his name is Carl.
Carl used to be lemon-sized, around five centimeters. I think he’s down to two centimeters, and he’s been stable.
He’s been behaving this way this whole time. It’s just that I get random lesions outside of the primary tumor that pop up, but for the most part, he’s been good.
What I want others to know
My last piece of advice would just be not to take a lot of stock in survival statistics or prognosis. My first oncologist told me I likely had just three months to live; lo and behold, I’m still here. Three years later, and I’m still going strong, I’m still kicking.
And I hear it all the time in the lung cancer community, fellow patients who have been given months to live, a year to live, and they’re still doing well. And while that may not be true for everyone, there is reason to remain cautiously optimistic because newer therapies are coming out every couple of years, and science is advancing in a lot of incredible ways.
I want people to know that anyone with lungs can get lung cancer. You do not have to be smoking eight packs of cigarettes a day to get lung cancer. I was 26 when I was diagnosed, and I have not once picked up a cigarette or a vape or any of that stuff, but I still got diagnosed with stage four non-small cell lung cancer. It is something that is happening to more and more young people, year after year, and we don’t know why. It’s terrifying.
If you’re feeling out of breath, if you’re seeing a lot of troubling symptoms that don’t make sense, whether it’s back pain and then this weird rattling sound coming from your throat, and you’re getting told by your doctors you’re fine, it’s probably pneumonia or asthma, here’s an inhaler, don’t listen to them. Seek better care and keep pushing for answers, because lung cancer cases amongst nonsmokers are going up. And at the end of the day, you’re going to be your own best advocate.
Symptoms: Pelvic pain and discomfort, bladder issues related to pelvic tumors, incontinence, pain in the lower back and hip Treatments: Chemotherapy, immunotherapy, radiation therapy, targeted therapy (lorlatinib)
The Patient Story Podcast: I’m a Young Cancer Patient
(Ep. 01) From Cancer Caregiver to Patient: Taylor’s Story
What do you do when you get a cancer diagnosis? Where do you go? Whom do you call? How do you become your own patient advocate?
There are so many overwhelming questions that hit the people who’ve been diagnosed and those in their closest circles. Here is the first-ever episode of a new video podcast hosted by The Patient Story founder and lymphoma survivor Stephanie Chuang.
This inaugural episode features a special guest: Stephanie’s colleague at The Patient Story and fellow former TV journalist, Taylor Scheib, who shares her experience navigating a cancer diagnosis, shifting from her role as a patient advocate and the daughter of a cancer survivor — her mom, Kelly — to becoming a cancer patient, herself.
Interviewed by: Stephanie Chuang Edited by: Chris Sanchez, Stephanie Chuang
Taylor shares the moment she discovered her diagnosis. She was sitting on her couch and casually checking her MyChart when the words “oncocytic carcinoma of the thyroid gland” appeared. (Editor’s Note: Oncocytic carcinoma of the thyroid gland is a rare, aggressive kind of thyroid cancer. It’s also known as Hürthle cell carcinoma.)
She was devastated by the diagnosis, but her background in patient advocacy helped her regain her footing. Her experience and knowledge built from working closely with both patients and caregivers helped her recognize symptoms and push for answers. This reinforces a crucial message: You are your own best advocate.
Taylor’s ability to listen to her body played a pivotal role in her experience. She had first noticed a nodule in her neck three years before her diagnosis, and had continued monitoring it through regular check-ups. When the nodule grew, she trusted her instincts and insisted on further evaluations, even when her concerns weren’t met with urgency. This underscores the vital lesson of trusting your body and speaking up when something feels off.
Taylor experienced further challenges when she tried to navigate the healthcare system. Her patience was tested by insurance hurdles, delays in scheduling surgeries, and having to wait for tumor board evaluations. She candidly discusses the frustration of feeling like just another case number. But her experience and resilience won through as she managed both the system and the mental toll of cancer. She found strength in support from her husband, family, and friends.
Taylor’s patient advocate experience also underscores the power of storytelling. At the start, it wasn’t easy for her to share her story publicly, but when she did so, she found it cathartic. Through opening up, she not only helped herself heal but also offered enlightenment and hope to others with similar struggles. Taylor’s authenticity is a good reminder that behind every social media highlight reel, real struggles do exist, and sharing them can be profoundly empowering.
Please scroll below to read the full transcript from The Patient Story Podcast Episode 1!
Name:
Taylor Scheib
Age at Diagnosis:
30
Diagnosis:
Thyroid Cancer (Oncocytic Carcinoma of the Thyroid Gland)
Staging:
Stage 1
Symptom:
Appearance of neck nodule that grew over three years
Editor’s Note: This transcript has been edited only for simple clarity.
Podcast Summary
When It Rains, It Pours
Taylor shares her mom’s own brush with cancer and how this was her first touch point in joining The Patient Story.
Taylor and Stephanie talk about the unpredictability of medical challenges, including those faced by cancer patients.
Introducing Taylor: A Patient Advocate Becomes the Patient
Taylor discusses her role at The Patient Story and how it made her more aware of cancer and its impact.
Taylor and Stephanie delve into the unexpected turn Taylor’s cancer experience took.
The Shock of Diagnosis: Getting News from MyChart
The moment Taylor learned about her diagnosis and the emotions that welled up.
The challenges associated with getting life-changing news like she did over a digital platform like MyChart.
Emotional Fallout: Processing a Cancer Diagnosis
The immediate emotional impact when Taylor heard the word “carcinoma.”
The questions that surfaced afterwards.
Self-Advocacy: Trusting Your Instincts and Pushing for Answers
Taylor discusses the importance of self-advocacy and being a patient advocate in healthcare, as well as the power of listening to one’s body.
She also opens up about her persistence in getting her nodule checked and how it helped her get results.
Barriers and Delays: Navigating the Healthcare System
Taylor and Stephanie delve into the problems many patients experience when they try to navigate the healthcare system, including systemic delays and provider shortages.
They also explore the frustration patients can experience when urgent concerns face logistical roadblocks.
The Waiting Game: Coping with Uncertainty and Lack of a Plan
Taylor and Stephanie discuss how difficult it can be to wait for clear next steps post-diagnosis.
They outline and explore strategies to help manage mental health during periods like these.
Community and Connection: Reaching Out and Trauma Bonding
Taylor shares how reconnecting with old friends and the support from her community have been vital during her journey.
“Give yourself grace, but also do it on your own time.”
Telling Others: Navigating Reactions and Support Systems
Taylor and Stephanie reflect on how to talk about a new diagnosis, the variety of reactions from others, and maintaining boundaries in relationships.
Supporting a Loved One: Tips for Friends and Family
They offer tangible advice for supporters: what to say, what not to say, and how to truly show up.
“The small stuff means more.” — Some of the most thoughtful and meaningful gifts aren’t the most expensive ones.
Sharing the Journey Publicly: The Power and Healing of Storytelling
Taylor explains why she chose to be open on social media and the cathartic role of storytelling.
She offers advice for those who are also considering sharing their experiences.
Give Yourself Grace: Final Reflections and Words of Wisdom
In closing, Taylor and Stephanie share uplifting thoughts on the importance of being a patient advocate, self-compassion, and owning one’s narrative.
Introducing Taylor: A Patient Advocate Becomes the Patient
Stephanie Chuang: Hi, everyone. It’s Stephanie here with The Patient Story. I’m just starting something new here. Wanting to be able to touch base more with everyone out there who’s finding us. If you remember, I had my own cancer experience when I was diagnosed suddenly with a non-Hodgkin lymphoma. Diffuse large B-cell lymphoma. I was 31 at the time, two months from getting married, and it was a complete whirlwind, to say the least.
But joining me today, I’m so excited to introduce someone who many people may be familiar with on our channel, Taylor. Taylor is on our team at The Patient Story. An amazing leader. And Taylor’s joining us for not-so-great reasons, but I am so grateful that she’s coming on to share her story. So, Taylor, do you want to share a little bit about yourself first, of course, outside of the cancer diagnosis?
Taylor Scheib: Stephanie, thank you so much for the warm welcome. So crazy being on this side instead of being the one guiding the conversation. I live in the Pacific Northwest with my amazing husband Justin and our dog Sage. She is our world. She’s our Chocolate Lab. And we love to hike. We love to be outdoors, and we love to camp. I’m originally from Illinois, from a really small town. My high school graduating class was 30 people, and so I’m from a very rural area. And I’m so grateful where I grew up, though I have amazing friends and family back home, I’ve lived away from home for a long time, so that’s been an interesting part of navigating my situation. But yeah, my mom is a colorectal cancer survivor. She was diagnosed with stage 3 colon cancer in November of 2023.
Stephanie Chuang: Taylor has been someone who’s led so many of these conversations with people, with patients, caregivers, care partners, and you know, the first personal touch point in joining The Patient Story was you introducing your mom, Kelly, to the process. She shared her story of going through colorectal cancer. And I’m so grateful again to both of you for being so open about that. But you may see that Taylor has a throat scar. Yep. And that her voice sounds hoarse. She doesn’t normally sound like that. I was on a work trip, actually, and then, got a late text from Taylor, and that was, of course, not usual. So, Taylor, just walk us through what was happening at the time.
The Shock of Diagnosis: Getting News from MyChart
Taylor Scheib: Yeah, it was a Monday night. 5:15 p.m.. I was about two weeks post partial thyroidectomy for a nodule on the right side of my thyroid. And that night, I just got a message from MyChart with my pathology results. And when I got the pathology results, it was out of sight, out of mind, from my surgery. Because not once did anyone say, “Hey, be on the lookout for your pathology.” I knew that the nodule and the mass were going to be sent off, of course, but I never thought that when I got those results, it would read anything but benign. And unfortunately, when I got those results, I was sitting on my couch, my husband’s cooking dinner. I get into MyChart, and the first thing I see is “oncocytic carcinoma of the thyroid gland.”
I immediately shoot up. I’m crying. My husband is like turning off the burners in the kitchen because I just bluntly, out loud go, “I’m pretty sure I have cancer.” And my husband goes, “What? What do you mean?” And that word ‘carcinoma’. I know what that means. And I don’t know if, before starting at The Patient Story and dealing with my mom’s diagnosis that I would have known what carcinoma meant. And so, because I am educated, because I’m privileged to work for such an amazing company where I’m learning so much every single day, I knew carcinoma meant cancer. We immediately came to this very spot, right where I’m sitting. We got on my laptop, we started researching, and the word oncocytic was a word I had never heard. I’d never seen or heard anything. Yeah, you start to Google. And that’s where my patient advocate story began, with my diagnosis.
Stephanie Chuang: Oh, wow. Yeah, there’s a lot there, I know. When I got the message, and then I got on the phone with you and you told me, first of all. I mean, it just took me right back to that feeling of, wait a minute. What’s going on? Right. And cancer and all the things.
And of course, my diagnosis was years previous. I was diagnosed back in December of 2016 and into January 2017. So it’s been a minute, which I’m very grateful for. But really, no matter how long the time, I remember that feeling of, What the hell just happened? And in your case, to spell it out for people, they would go, “Oh, you have this nodule, and you need to get it removed.” It’s benign, though, and nowhere, never did anyone ever say it might be something.
Now, I can understand, by the way, why, without the information of a biopsy and without other, maybe contextual clues that they might say this is benign. But at the same time, there’s this whole thing of, oh, my God, you said the results had actually been in for a while, and then it just popped up on MyChart. What was hitting you in that moment about your life? What were the thoughts and the emotions?
Emotional Fallout: Processing a Cancer Diagnosis
Taylor Scheib: Yeah. I already have tears in my eyes thinking about this answer. Because when you work for an amazing organization like The Patient Story, you’re hearing these stories every single day. You’re writing scripts and you’re creating this beautiful content. The underlying thing is tragic, and that is a cancer diagnosis. And so I would be lying if I said I never thought I’d get cancer. I’ve thought it. And you become just so much more aware of your body and the feelings that you’re feeling, and going to the doctor and getting your checks, getting your women’s health exams when you’re listening to these incredible people every single day.
And then when your mom goes through it as well. So I was shocked. But when the dust settled, I wasn’t that shocked because cancer can happen to anybody. And so being so young, I had just turned 30. My husband and I just came back from this incredible trip to Puerto Vallarta that he planned for my 30th birthday.
And this year was going to be filled with amazing trips and celebrating friends who are getting married. And you know, we’re doing all of those things still, of course. But in that moment, I just thought, what are the next six months going to look like? I’m such a planner, as Stephanie knows.
And I just kept thinking, what is this going to look like for me? And then the unknowns started. That started the spiral of, How do we know for sure that it’s all gone? But, going back to the emotional part of it, it was devastating for my husband and me. We have heard about cancer a lot in our families, so cancer was not new to us even before starting my job. But it was still just heartbreaking, devastating.
How could cancer be growing in my body for three years and I not know it, because I found the nodule three years ago? And so it was a hard moment. But because of my husband and his personality, and how just fun and outgoing and level-headed he is. It didn’t take me long from the initial spiral to come down and realize, this is not going to be my whole life. This is hopefully going to just be a moment in time. That was sad and devastating, but we’re going to look back at the beauty of it.
Stephanie Chuang: Yeah, that is so beautifully said. Thank you, Taylor. What I’m hearing you say is a few things. And by the way, I think this applies to people outside of cancer diagnoses. It’s like anything, anything in general, but definitely with healthcare, something that is about your body, maybe feeling like I’ve heard people, including myself, you know, talk about betraying us, you know, in a way. And you have the initial shock. There’s a lot of sadness, and there’s a lot of, how did this happen?
And then for you, what I’m hearing is that you went, okay, well, now it’s time to tackle this. This is not going to be my life. This is one thing that I’m just going to look at and get and get through. Right. And one of the things I know you exemplify, and I think you did before you started here, and maybe even more so now. But this idea of self-advocacy, which we hear so much about for you, started really early on because no one was really that concerned about your nodule except for you. And I think there’s a message in there. And what is that message for other people?
… you know your body best, and you know how comfortable you are with something inside your body or making a decision.
Self-Advocacy: Trusting Your Instincts and Pushing for Answers
Taylor Scheib: Yeah, that message would be, you know your body best, and you know how comfortable you are with something inside your body or making a decision. And for me, when I found the nodule. It was after my 27th birthday. We had just karaoke all night. It’s one of my favorite pastimes.
And I immediately went to the doctor, got bloodwork, got an ultrasound of the lump, and from there, it was my choice, what I would do with that information. So I continued getting my yearly exams, getting full blood work done. And last year was when I was like, okay, this is getting bigger. People are starting to notice it.
And I want to say this part as well, because I had a friend who, and this is where advocacy comes in many different ways, not only for yourself, but other people doing it for you. She noticed the lump, and her dad had thyroid cancer. So she asked me, “Have you gotten that checked out?” And I said, “Yes, I have.” But at that point, I realized that it’s been a year since I had done it previously. Why not get it done again? So I started the process all over. Routine blood work, ultrasound, you know, did that. And then I just wanted to get it out at that point because it was really large. It ended up being 5.7cm.
And so after that ultrasound, it was up to me to schedule the ENT appointment. You know, getting into the ENT took months. As we all know, those specialty appointments just take a long time to get into. So I finally got into the appointment in November, and my ENT was very casual about it. Looked at the ultrasound.
At this point, no one ever said, “Let’s do a biopsy,” and we don’t know if the biopsy even would have caught it anyway, so I’m not going to dwell on that. But she went, “Yeah, this is benign. The features are all normal. It’s your choice to get it out. Are you ready to have a scar? And I said, “Yeah, let’s go.” I just couldn’t do abs anymore. Like working out without it choking me. Being in bed, lying on it. I could feel it all the time at that point. So I advocated to get it out because I knew that was the best choice of action for me. It was also something my mom was telling me, “Maybe you should just get it out.”
But at this point, it had compromised that whole side of my thyroid. So I was going to have to get a partial thyroidectomy. So I was a little scared. But coming back to the self-advocacy part of this, you know your body best, and it’s okay to push and not necessarily get it removed. Did I push because they got me on the schedule, but I was non-emergent, so very limited spots to get. Surgery was scheduled for surgery in January. My insurance referral did not go through in time. So the morning of that original surgery in January, I’m on the phone with my ENT, and they’re like, well, you could just chance it. And I’m like, facing a large medical bill without the correct referral.
Stephanie Chuang: Right.
Taylor Scheib: And my husband’s in the military, so I knew there were a little bit more hoops to jump through with that type of insurance. And so I was on the books for April. It just automatically got pushed back three months.
Barriers and Delays: Navigating the Healthcare System
Stephanie Chuang: Yeah. So I just have to interject there because I feel like that part of the patient advocate story, right, is like it’s one of the parts of the experiences that we all experience to some degree, but isn’t talked about a lot, which is when you’re dealing with cancer. I remember, you know, getting told that this might be cancer and then being like, but it’s probably mono. And I was like, mono? And then it was like, but you need an ultrasound to one here, one here.
I got on the call to get it scheduled. And they said, “We don’t have an appointment for weeks.” And I’m thinking, you can’t tell me that there’s this thing and that I have to wait. So my point is that there’s the system, there’s like our situations, and this message of self-advocacy is, it truly is the squeaky wheel gets the grease or whatever, because you know, you know your body best what you just said and also you I mean, there’s some things that are out of our control. But you see, the system we’re working with and the unexpectedness of being like, how come I’m the only one who’s concerned about this? Did you feel that?
Taylor Scheib: Yes, I felt that. And it was. That’s been the whole thing over the last six months of seeing the NT. Getting the surgery scheduled is why there is no sense of urgency behind this. Every time I’ve seen my ENT. She’s so busy. When I had my follow-up for my surgery, it was not her. It was her [physician’s assistant] PA.
And it continued past my diagnosis. First of all, I found out through MyChart, which is a story I’ve heard, unfortunately. And every time someone I’m talking to tells me that story, instant goosebumps. Instant. Just feeling what they’re feeling through the screen. Then it was okay. Your case is going to be presented to the tumor board, and I want to make sure that I’m explaining what a tumor board is correctly.
So Stephanie, please help me with this color. But basically, when you have a unique case like mine, where we thought it was benign for three years, the mass was 5.7cm. And then on top of that, it is a less common subtype of thyroid cancer. It’s being presented to the tumor board. Well, they only meet once a month. So and it was at the end of the month when this happened in April, so it wasn’t going to be until a month for the tumor board.
Stephanie Chuang: You talked about self-advocacy, which we’ll talk about throughout the entire conversation. But this idea of waiting, waiting for your appointment, waiting for insurance to approve or not approve, waiting for a tumor board. For me, it was like getting a diagnosis on the phone and then being told by a family friend. You know, oncology is going to take forever at your large academic institution, so just go to the emergency department.
So that’s another tip for people, by the way: just get into the system. So you get seen, and then they put you somewhere that you’re supposed to be. But I was waiting to understand. I remember they did so many procedures, I had biopsies and bone marrow biopsies and lymph node extractions and blood tests upon blood tests. And then it was the whole week in the hospital. What is it like? We know it’s lymphoma. Is it Hodgkin or non-Hodgkin? Are we talking about, you know, aggressive or indolent? Are we talking… So? Not this period, and you’re still in it. That’s what I want to acknowledge, is you’re still in it, is it feels like there’s still no plan of action.
And I think for different people who are dealing with a diagnosis that it varies. Like sometimes it’s very short and, you know, right away for other people like you, you’re waiting weeks to understand, well, what are we going to do about this? So how have you been able to manage the mental part of that, the waiting part of it?
I have my good days. I have my bad days, more good than bad days, which is good. But it’s just about occupying your mind.
The Waiting Game: Coping with Uncertainty and Lack of a Plan
Taylor Scheib: It’s so hard, honestly, and I have my good days. I have my bad days, more good than bad days, which is good. But it’s just about occupying your mind. And when I was diagnosed and I started telling my close friends and family, I think, like trauma bonding, it’s very powerful. I have some friends that I don’t talk to every day, of course, but they’re your best friends no matter what. You pick up right where you left off.
So, as crappy as this was to get this diagnosis, it gave me a chance to actually kind of get closer with some of my friends. That has been such an amazing distraction since my diagnosis, catching up with old friends, catching up with your family again. My dad is calling me so much more, he calls all the time in general, but even more so now, my grandparents are reaching out like every so often. So I would say that’s been one solid thing.
Then the other part has been my husband. He has been my rock, of course, through this. Then we’re super active people. So we went and bought really expensive bikes to get on the trails. Stay active. And we’re just trying to find ways to continue living our lives. And for us, that is planning a trip. So, sorry, Stephanie, in the next year or so, I’m going to be going on some trips.
Stephanie Chuang: Oh, 100%. And you should go out and live your life 100%. No apologies. That’s 100% what you should be doing. And it makes me so happy to hear that. Those are the steps that you guys are taking. So many things came up when you were talking about that. You know, when you talk about trauma bonding, I’ll talk about the flip side of some of the experiences I’ve had, too. But this is the question of why we need a reason? But we do. I love that it just automatically gave this a thumbs up.
Community and Connection: Reaching Out and Trauma Bonding
Stephanie Chuang: People come from different places, whether you’re close. My friends started a campaign called #SpicyStrong. And I think it’s because when I was in my delirium, when they put me under for the lymph node biopsy, I had to go under full anesthesia, and I don’t know if I was going in or coming out, but I was super loopy. And so I was talking to the nurse. And I went, “I’m so spicy and strong,” or something, I mean, ridiculous. And then that just became the hashtag.
They printed shirts, and it got to people, and they were posting on social media. This is making me remember a lot of things I forgot. But people who are super close to me, people who I hadn’t seen in years. And that is such a beautiful part of this, right? One of the silver linings. I’d rather not have this, but the fact that I do and people like me are showing how much they think about me. I mean, what was the most powerful? I mean, I know you had lots of people reach out, but is there one situation where it took you by surprise, or a message that came from someone you hadn’t talked to in a while?
Taylor Scheib: Yeah, there’s one example where, and I’m sure you can relate to this, being formally in the news. You bounce around all these towns and cities, and you have friends everywhere, like I mentioned. And even when I just had the partial thyroidectomy, a group of friends in Denver sent me a care package, and that was before I even got my diagnosis. And so I was just so taken aback and just so thankful for them sending that. And so that was one thing. And then the other has been again, when I was in sports broadcasting, and I’ve heard from so many people from the little towns that I was covering, you know, seven, eight, nine years ago. And they’re commenting on my post, just saying, you know, we’re supporting you. This community is supporting you.
That’s just meant the world to me. And so those have been instances where it kind of stops you in your tracks. I don’t know if you’ve felt that way, but you just think, humanity is good. Yeah, yeah. Decency still. And there is a way to break through the screen. There’s a way to break through the phone call, the FaceTime, the message. And so I’m not sure if you felt that same way in those instances, but it stops you in your tracks, and you just realize, I have so many amazing people in my life.
Stephanie Chuang: Yes, 100%. It does resonate. Taylor. It’s 100% humanity is amazing. These are the beautiful moments of humanity when people come out. And, you know, I think a lot of the social stuff might be we are scared to, you know, reach out to someone from before because we think, well, what if they think I’m weird or they don’t even remember me or whatever? And these situations just take us completely out of that. Right. It’s like, no, I care about this person, or I just want them to know that I’m thinking about them, and it’s okay if they don’t reply or all those things. I think that is beautiful, and I wish more of us could get to that.
Yes, 100%. It does resonate. Taylor. It’s 100% humanity is amazing. These are the beautiful moments of humanity when people come out. And, you know, I think a lot of the social stuff might be that we are scared to reach out to someone from before because we’re like, well, what if they think I’m weird or they don’t even remember me or whatever? And these situations just take us completely out of that. Right. No, I care about this person, or I just want them to know that I’m thinking about them, and it’s okay if they don’t reply or all those things. I think that is beautiful, and I wish more of us could get to that.
… whatever other people’s reaction is, it is not about you. It is, of course, about concern for you and what you’re going through for the people who love you.
Telling Others: Navigating Reactions and Support Systems
Stephanie Chuang: I do want to touch on just because, for anyone who’s tuning in who is dealing with something again, it could be a diagnosis, cancer, or otherwise. It could be something else. When you have something to tell other people that they’re not familiar with. So I don’t know, sometimes I’ve found that military people find that with civilians. It’s like a walking-around language with sickness. Or maybe if someone’s announcing, say, a divorce and other people aren’t familiar with it, it could be any of those things.
I think the way other people react is very – it can be very jarring. And so I’d like to spend some time here, which is that, you know, people have different kinds of people in their lives. Some people have tons of friends, some people have a tighter circle and and all these things. I’ll start with an example, which is a newer friend, but I’d known her for a few years at least. More of a social friend, maybe.
But when I was diagnosed, she kind of disappeared, and she was one of the people I saw more often in that time frame. You know, a lot of my friends, to your point, are scattered around the country. And so it was very disappointing, and it was hurtful because here I am thinking about my mortality, not sure about what I’m going to do, worried about my hair loss, and all these things. I’m 31, and she just dropped off.
I just want to say this, not to harp on her as a person, but really to say, I think what I learned in that is whatever other people’s reaction is, it is not about you. It is, of course, about concern for you and what you’re going through for the people who love you. But for any of the weird stuff or the things that might be surprising, I would just say, broad strokes, the reaction is about their discomfort. They don’t know how to show up. They do care about you, but they’re worried about how they’re going to come across.
Maybe they think other people are talking a bunch to you, and so they’re trying to be respectful of you. Not right or wrong. But I do feel like that’s something I’d want to share with other people who are going through something, because it can be very tough when it’s unexpected. I don’t know if there’s something that resonated for you there a lot.
Taylor Scheib: It is. When I first started telling people, I realized very quickly, the way you present it will help determine how they react. So in the first couple of conversations I had, it was kind of very emotional. A lot of information, whoa, what is going on? But then the more I told people, the more I started setting the precedent of, right at the beginning, I’m going to be fine. I’m going to be okay. And then that’s when I think people went, okay, she’s she’s she’s going to be okay. And I have been very positive throughout this whole situation. And I think that has helped the way people are reacting.
Now, I will say on the positive side, kind of the opposite of what you experienced was I’ve gotten a lot closer to one of my high school best friends, like my childhood best friends. We have been friends literally since kindergarten. Wow. And we talk every once in a while. And when we see each other, we pick up right where we left off, like I’ve said. But we’ve talked more since this happened to me. And even when I just did the partial thyroidectomy, she called me that weekend, and I sounded like crap. Did not have a voice.
Taylor Scheib: She was crying on the phone. And it makes me emotional because that’s an experience where she’s showing up for me. And that, and her mom, and her. They are like my OGs, but I don’t see them very often. And so it’s kind of the flip side of what you experienced. But what you experienced with someone dropping off like that is likely going to happen for me in the next six months or however long this process ends up being.
But my mom experienced that. She was shocked by the people who she didn’t hear from again, or they didn’t show up for, you know, she had a benefit. They didn’t show up for that, or just a text message or a phone call. She was shocked by the couple of people. And you don’t forget those things, but I think it makes you become a better human in a way, and it makes you check up on your people a little bit more. That’s how I’m trying to spin it, at least.
Stephanie Chuang: And knowing you from what I know of you, Taylor, I don’t even think it’s a spin. I think you have that. That’s just the way you approach life. And I appreciate that. Yeah. No, 100%. I would say that was the only example of that. And everything was largely positive. I think I do want to call out that it may not happen to you, by the way. Right. I think it’s good to understand that if it does, though, that it’s normal and it’s not about you. It’s about them. And the other drop off, someone had warned me when I was just going through it, and she had gone through the same cancer just six months before I did. And she said, “Look, I’m struggling now that I’m done with treatment. People are like, you’re fine now.”
And then, the medical help drops off, and then the support also, because, well, you’re all good. And so that’s another conversation for another day. But I think my point is that at different parts of this, you know, it doesn’t mean, oh, I’m past this now. It’s that there’s different versions depending on where we are as patients, as people supporting other people, that these same emotions can come up or these same situations can come up. I also want the chance to drop in this video of my best friend in New York, she flew out with her husband, and at the time, I had to give myself blood thinner injections every day.
And those are freaking large. You know, I did IVF shots to freeze embryos at the same time. So I had to do the little needles and then the spring needles for the blood thinners. And, oh my God, it was terrible. And there’s a video of the way they supported me, trying to make fun sometimes. So, you know, the song that goes, shots, shots, shots, shots, shots, shots, shots. Yeah. So I was about to give one, and they go, “Oh, we’re just gonna sing the song for you.” And those are moments for sure where this is me getting loved on by people who are trying to lighten the situation for me in the way that they think might be helpful. So anyway, I think that’s awesome.
Stephanie Chuang: I want to ask about your mom. I know other people may not have this specific example where it’s like their parent also went through a similar diagnosis, but in terms of other people’s reaction to when you’re telling people what that was like, what’s your guidance to other people who feel like there’s an extra layer there? Whatever the reason is for you, it was that your mom had gone through her cancer recently, even. But for anyone who feels like there’s an added pressure in making sure the other person’s okay, what is your guidance there?
Taylor Scheib: Yeah, I would just say the biggest thing is give yourself grace, but also do it on your own time. That is so important. Yes, there’s pressure to tell people and update people and do all the things. I totally get that. But do it on your own time. You and I also think that what helped as well is I just I’m a very factual person. I’m blunt. I’m not going to sugarcoat things. So I think it was my messaging to them. These are the facts, I know. I don’t know anything else. And then I think that helps with them asking a bunch of questions.
You know, like deep dive spiraling. I think it’s just about giving yourself grace and giving the situation grace and not feeling like you have to always be giving updates to your friends and family or talking to them. Or it can take about a day to respond to someone. And my friends and family know that. They know that I’m very busy. My husband and I, Justin. We live a very active life. We are always doing something. And so yeah, I think it’s also if you get a text message, don’t feel like you have to respond right away or call them back or anything, right? This is on your own time, and that goes beyond just your friends and family. I’ve heard this so many times from people that I interview. You are the CEO of your life, of your body, of what you do. You are the leader of your own life. And I think that’s just so important.
Stephanie Chuang: Yeah. I mean, in the future conversations, I’m going to be pulling up from our patient advocate interviews because they have so much wisdom in what they’re saying. I mean, there are so many things that I want to talk to you about. Let’s talk for three hours. No, that’s fine with the audience. No. But I think, you know, whatever way you want to look at it. In terms of tips. There are some tips for the person who’s dealing with the diagnosis. Diagnosis? I agree with you, Taylor. 100% of the give yourself grace. I think in life in general, we could stand to hear that more often anyway, right? We give other people the compassion we don’t give ourselves. But on that note, give yourself grace and do not worry as much as you can about the other person’s reaction. You don’t have that space to carry that burden. So don’t tip on the other side.
Supporting a Loved One: Tips for Friends and Family from a Patient Advocate
Stephanie Chuang: I would give to people who are looking to support patients, because I’ve heard that a lot. Right? They might go, “Oh my gosh, my friend, my family member was just diagnosed. How can I support them?” I think in terms of messaging, I would always lead with whatever. If it’s an email or a text or whatever, or a voicemail.
No pressure to respond. I just wanted to, and that just takes off the pressure. So you get to send the message, and you’re letting them know. I get that you’re super busy and you’re occupied, and I’m not trying to take away your bandwidth. Another tip would be people ask about, “What can I send someone who’s just been diagnosed with cancer?” I’m going to ask you about this, too, so you can brainstorm. But I’ve often thought, if you can figure out if they know their treatment, I would base the care package on that. So if you know that they’re going through radiation, you can look, and we’re going to create this online to have some guides at The Patient Story, but it is to really look at what that modality of treatment is, and then try to send stuff. So, you know, I’ve sent organic lotions to people because they were going to get dry skin, blankets because one of the side effects was going to be feeling cold, things like that. I don’t know if there are things that you feel would be great advice for people trying to help people dealing with the new diagnosis.
Taylor Scheib: Yeah. You made such a great point. Blankets, things like that. But then I also think, like anything, that the person who’s going through the treatment or diagnosis, self-care, they should just put self-care out there.
So yeah, if it’s maybe organic products or maybe it’s a bath bomb, or of course, depending on their treatment, like we said. But for me, everyone knows I’m going through the waiting period. So I think a lot of people went, “How does she want to relax and sew face masks and bath bombs and electrolytes and different things like that?” So I would say anything that you can think of that person likes, that is self-care.
Books, a journal. You can never have enough journals. Something to preoccupy them, too, whether that’s like a coloring book or, you know, crossword puzzles. Not that I do any of that, I’m not going to lie. But if you know that person enjoys that kind of pastime. Right. Or maybe something like, this is old school, but a CD with their favorite songs on it.
Stephanie Chuang: Right, right.
Taylor Scheib: And I also think, too, when it comes to what you could give that person or send them in these moments, it does not have to be elaborate. The small stuff means more. And so maybe it’s a Spotify playlist, maybe it’s a $15 Amazon gift card, maybe it’s a gift card to their favorite restaurant. The self-care food.
Don’t overthink it. When you want to give something to that person. It can be something very small, even just a Venmo. I had a good friend, one of my best friends from home, send me a Venmo the day of my follow-up ENT appointment, and the caption was, Go get a cheeseburger after this.
Stephanie Chuang: Oh no, I love that it is. It’s the small things. It is that thought that counts. It is true. I think there are a couple of things that came to mind, too. And then we’ll and then we’ll wrap this conversation, which, by the way, I’ve enjoyed having with you. I think one quick note is if people are waiting. You’re not in the hospital. I know when I was waiting, and I was in the hospital for a shorter period of time, the nurses at one point said, “Don’t send flowers, or we’re telling people, don’t send flowers.” And that’s for when people are immunocompromised.
The knee-jerk sometimes is like beautiful flowers, but just to make sure.
… why I decided to share my story so openly was because at the core of who I am, I’ve always been very transparent, very honest, and I am an empath. I need empathy at the core of who I am, and that’s where the storytelling part of my life, like my whole life, has been storytelling at the core.
Sharing the Journey Publicly: The Power and Healing of Storytelling
Stephanie Chuang: The other point that happens to matter both in terms of support, but also in terms of talking about messaging and not having to respond to text messages right away. What was helpful for me was to designate people who knew the information, and if other people needed to know or wanted to know about the diagnosis or where I was in that, specifically, they would go through those people. You know, it’s funny, we both were on TV before, but we were also very private people, actually, and I never imagined that I would bare my soul online or continue to have a presence after my news career.
But I had a blog, and the initial point of the blog was a it just helped. It was cathartic to get stuff out on, like just journaling, essentially. But then it was like, well, two things: if I can help other people not feel alone. And also then it helped in terms of people getting updates without me having to like constantly. But then that slowly became cathartic as a storytelling mechanism.
And by the way, you know, we’ll have like the storytelling, you could share yours. There are the prompts below in the description. But for you, Taylor, what has it been? This is my last question to you. What has it been like? I guess, how did you decide to want to share? I didn’t even realize you were going to share your story on social media. And it happened. But like what? What drove you to want to do that? And what has been maybe the most cathartic part of the process, especially a message for people who do feel like I’m private. I don’t think this is for me. Right?
Taylor Scheib: Yeah. I resonate so much with when you get out of a job that is so public, like we were in in TV, I don’t find myself posting at all anymore, but why I decided to share my story so openly was because at the core of who I am, I’ve always been very transparent, very honest, and I am an empath. I need empathy at the core of who I am, and that’s where the storytelling part of my life, like my whole life, has been storytelling at the core. I’ve always been a storyteller. You know, I can get along with anyone, and I just am amazed and mesmerized by other people.
I just love people so much, and they teach me so much about life and about the way you should live life. You know, there’s no guidebook to that, of course, but when I decided to share it publicly, I just wanted people to know that we say it all the time, that they’re not alone. They might be going through anything, and they’re like, “Wow, this person feels just a little bit like I do.” And that’s what keeps people going. And so behind sharing my story and trying to keep people up to date, I just. It’s kind of. It’s hard to explain. I just wanted people to know that everyone is going through something that is a big part of it, and to social media.
If you look at my Instagram, you will see my husband, my friends and family, my dog, and you go, wow, that girl has a really good life, and I do. We live an amazing life. But behind the curtain, behind social media. I’m going through something that really sucks, and I’m still finding ways to navigate that. So why not be open about that conversation? Let people in. I have a big tribe. I have a lot of people in my corner. I’m so thankful for that. But. Those strangers. Those are the strangers who come to you. Those are so impactful. Just the little comments of, “Wow, I thank you so much for sharing your story.” I’ve had so many people say, “Thank you so much for sharing your story.”
Taylor Scheib: And it’s not even about the cancer. It is about making sure you are getting your physical exams, that you are getting your women, your women, health, health exams, your PAP smears, your full blood work, whatever it may be.
I’m getting emotional about it because I feel like people get so lost in how they’re feeling, and they don’t know if it’s something, if it’s their life, because they’re really busy, or if it’s something underlying. And so I just want people to know that it’s okay to go to the doctor. It’s really scary. I totally get it. I was so scared to get this surgery, and now I’m dealing with voice loss, and I can’t get my voice back. So trust me.
Oh my gosh, it’s so, so scary. But it doesn’t have to be. And find your partner, find your friend. Find your family. Find someone like The Patient Story who can hold your hand through that. So that was really the ‘why’ behind sharing the story publicly. The most therapeutic thing for me in this process, honestly, has been talking freely like this. When I posted those videos, they were maybe 15 minutes long, and I had to cut them down.
But talking so freely about it has been so cathartic and so therapeutic for me. Those are like my blogs, like you did. I’m just doing it as a vlog. And after I get done, I go, “Wow, I kind of look cute.” I’m going to take a couple of selfies, you know? Yeah, go do things anymore.
You know, like those moments. You go, “Wow, I just feel so stinking good.” Yeah. And so that’s been super helpful. And then just keeping the lines of communication open with me, with my partner, with my husband, with my friends and family. You know, I just want to say this one part fast. My mom and I are best friends. We talk all the time, but recently we haven’t been able to talk a whole lot because she’s two hours ahead of me. We don’t work the same hours, or we do work the same hours. So, we’re constantly working. We’re not finding time to talk.
And last night, I told her, I said, “I’m sorry. I have not been able to call you. I have just been so busy. There’s been so much going on.” And she goes, “It’s okay.” And I go, “But it’s not okay.” She goes, “I know, but I don’t know what to say.” And so it’s there, that balance of course, she knows I’m busy. She’s not pressuring me, but she just wants to have a conversation like this. She wants to just openly have the conversation. And we did talk today, and it was very therapeutic for me. So open communication and just kind of setting up my phone and talking. But that’s also because I’ve been doing that for so long, and I’m a storyteller by nature.
Stephanie Chuang: So you are. You really are.
Give Yourself Grace: Final Reflections and Words of Wisdom
Stephanie Chuang: Taylor, I thank you so much for opening up, being vulnerable. You are such an empath. I know you bring it to your life and also to work every day, and I’m so grateful that you’re part of The Patient Story team doing that. Yeah. For anyone who’s you know, wants to hear the tips that were part of this conversation, I think we can come up with something that you can download. We’ll put it into a link somewhere on the description, not at the time of this discussion. Thank you for being such an open book. And looking forward to being able to share more of your incredible voice throughout all of this. So thank you.
Taylor Scheib: Yes. Thank you. And I’ll just leave this here. We’ll talk about it more, of course. But when I got my diagnosis, I didn’t feel overwhelmed. And that’s because, of course, in moments I did, but I didn’t overall because of The Patient Story. And I’ve said this so many times to my friends and family and to people who I’ve told my story to when I’m interviewing them, because now I’m openly sharing my story, is that when someone gets a diagnosis, I never want them to feel overwhelmed, and I want them to have a place like The Patient Story where they can go and think, wow, okay, I have someone, I have an organization that can support me. So when I got that diagnosis, I didn’t feel overwhelmed. And I want other people to feel that way. And that’s why I’m so passionate about our work at The Patient Story.
Stephanie Chuang: Yay! I couldn’t say that better. That was amazing. Thank you. Taylor. All right. And this was like the first of many conversations that will happen with Taylor with different folks. Really looking forward to this. All right. Great. So for The Patient Story, that’s Taylor. I’m Stephanie. Gift yourself grace. Take care. And we hope to see you next time.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.