-

·
Laura’s Stage 4 Kidney Cancer Story
Laura E., Type 2 Kidney Cancer (Papillary Renal Cell Carcinoma), Stage 4 Symptoms: Profound fatigue, hypertension, high red blood cell count, severe back pain, badly swollen legs Treatment: Chemotherapy (Cabometyx (cabozantinib) assigned under S1500 PAPMET clinical trial)
-

·
Raquel’s Stage 4 Colorectal Cancer Story
Raquel A., Colorectal Cancer, Stage 4 (Metastatic) Symptoms: Frequent bowel movements, pin-thin stools, mild red blood in stoolTreatment: Chemotherapy
-

·
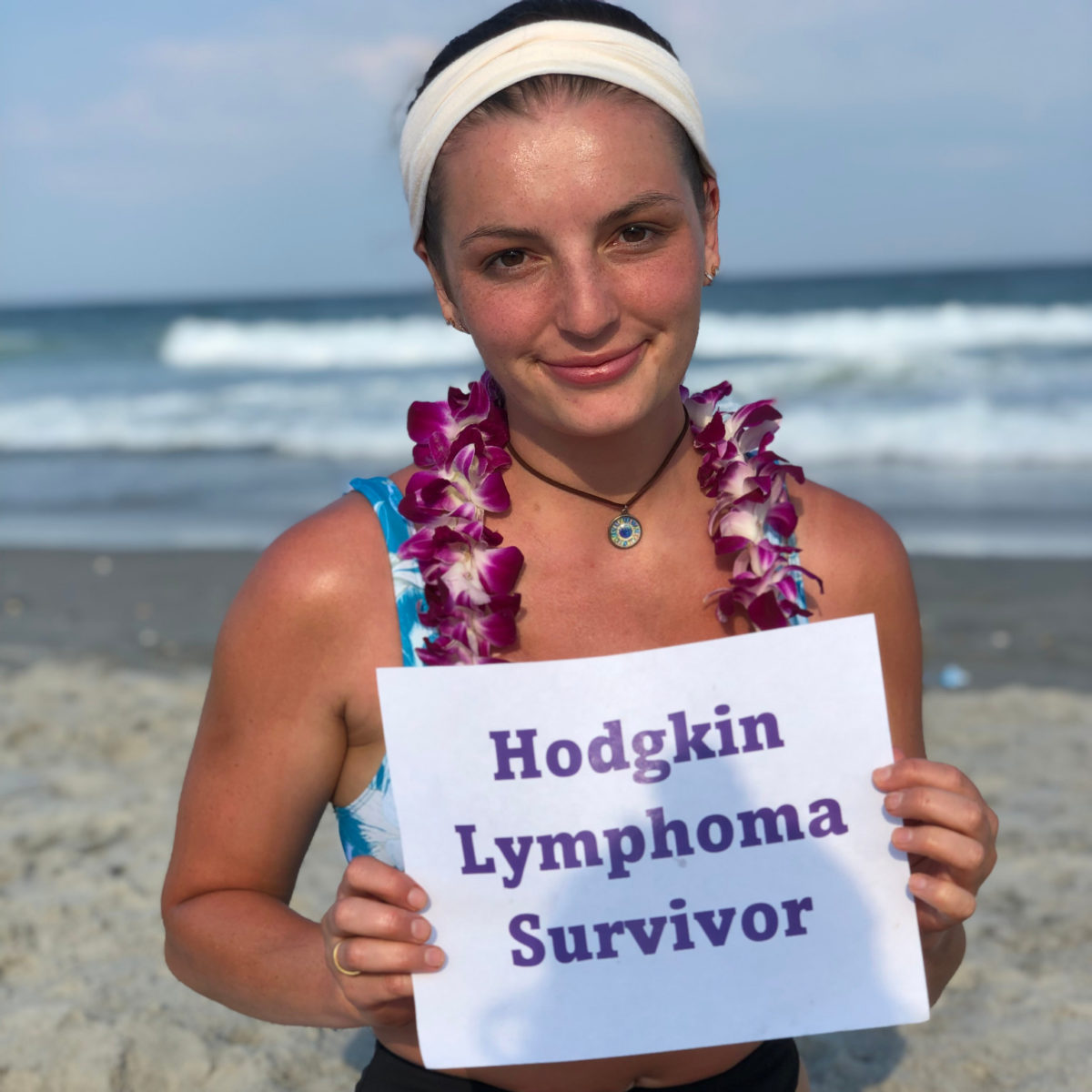
Rachel’s Stage 4 Hodgkin Lymphoma Story
Rachel E., Hodgkin Lymphoma, Stage 4 Symptoms: Extremely itchy rashes, nausea, nosebleeds, severe fatigueTreatments: ABVD chemotherapy, steroids, dexamethasone, acyclovir, antiviral therapy
-

·
Keith’s Stage 4 Colorectal Cancer Story
Keith H., Colorectal Cancer, Stage 4 Symptom: Abdominal painTreatments: Surgery, Chemotherapy
-
·
Danielle’s Stage 1 Classical Hodgkin’s Lymphoma Story
Danielle D., Classical Hodgkin’s Lymphoma, Stage 1 Diagnosis: Stage 1 Classical Hodgkin’s Lymphoma Symptoms: NoneTreatment: Chemo, ABVD, Immunotherapy, Nivolumab, Brentuximab, Bone Marrow Transplant
-

·
Jason’s Stage 4 Colorectal Cancer Story
Jason R., Colorectal Cancer, Stage 4 Symptoms: Abdominal pain, constipation, belly button dischargeTreatments: Liver surgery, chemotherapy, radiation
-
·
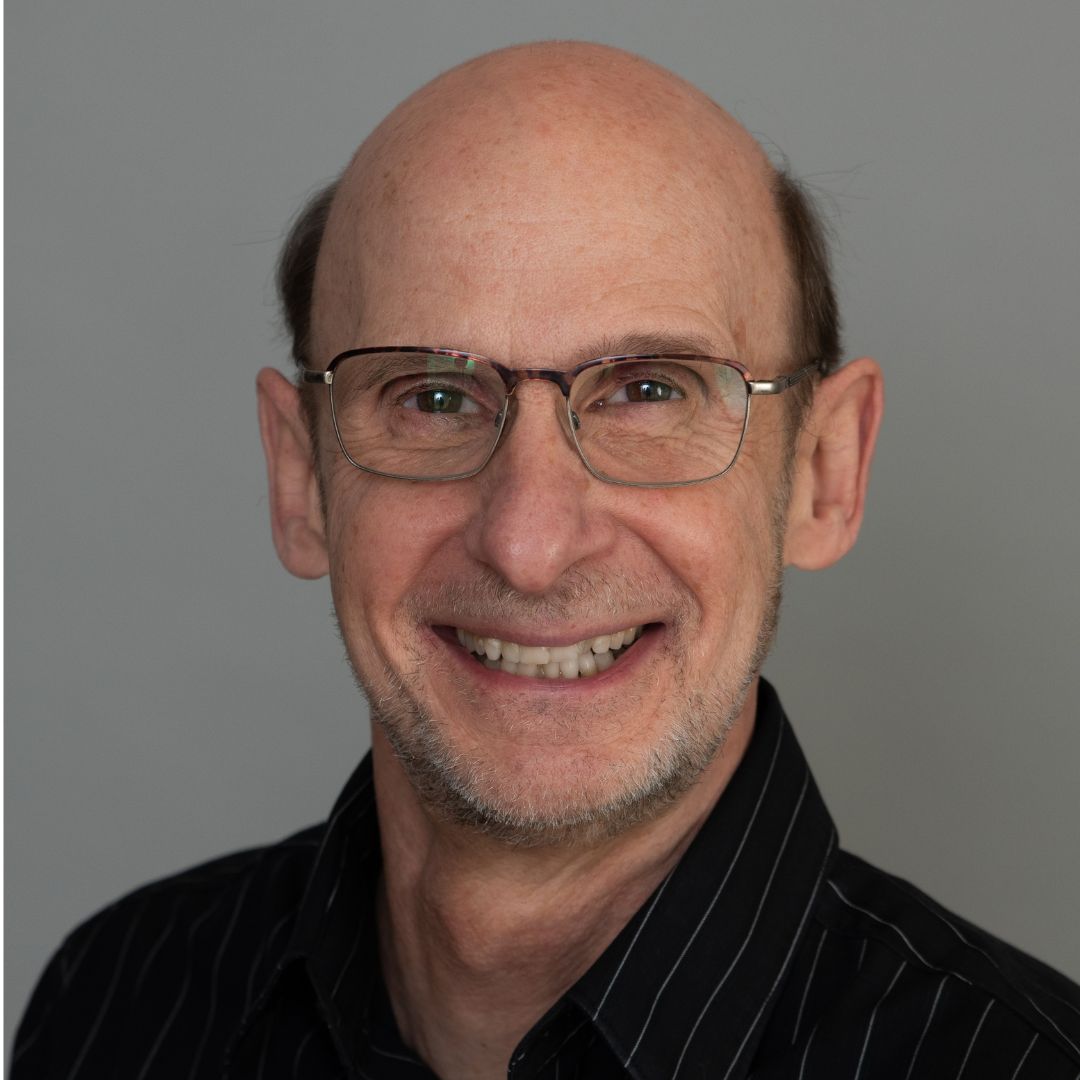
Steve’s Acute Myeloid Leukemia (AML) Story
Steve B., Acute Myeloid Leukemia (AML) Symptom: Low white blood cell count Treatments: 7+3 chemotherapy, pre-transplant conditioning, stem cell transplant