Stage 4 Non-Hodgkin Lymphoma Patient Story: I Said Yes to Bispecific Antibodies
At 42 years old, Meg considered herself a very healthy person. A mother of three children, she initially brushed off lower back pain during her daughter’s gymnastics meet as a suspected bout of kidney stones, which ran in her family. A routine CT scan to check for stones quickly turned into an emergency room referral, where she was blindsided by the news that she had cancer.
Edited by: Katrina Villareal
Suddenly, Meg was confronting a follicular lymphoma diagnosis, and her first terrified thoughts immediately went to her then 9, 11, and 13-year-old children and how they would cope if she only had six months to live. Fortunately, the panic was soon tempered by the reassuring presence of Dr. Tara Graff. She walked Meg through her treatment options without pressure, paving the way for Meg to make an empowered decision to participate in a clinical trial. Having watched her own mother navigate cancer treatments, Meg felt strongly about contributing to medical science and opted for a cutting-edge, chemotherapy-free approach.

The clinical trial involved an immunotherapy drug designed with bispecific antibodies to supercharge Meg’s own immune system to target the lymphoma cells. While the treatment itself has been highly effective, there was also monitoring for side effects such as cytokine release syndrome (CRS) and neurological toxicity. Since this was part of a clinical trial, Meg had to keep track of her temperature and blood pressure every three hours, fielding check-in calls from the trial team at 1 a.m. and 4 a.m. Despite the intense monitoring and the overwhelming exhaustion that inevitably hit her, Meg avoided the CRS side effects linked with these aggressive treatments.
In this conversation, Meg has a candid conversation with her own hematologist-oncologist, Dr. Tara Graff of Mission Cancer & Blood, an Iowa community oncology network partnered with University of Iowa. While Meg talks about how she navigated her treatment options and how she’s grappled with things like survivor’s guilt, and a lingering anxiety of waiting for the other shoe to drop, Dr. Graff talks about bispecifics in lymphoma and shares how her healthcare team monitors potential side effects like CRS.
Watch the video and/or read the edited transcript of the interview to find out more about Meg’s story:
- Understanding lymphoma staging can completely change your outlook. Hearing stage 4 immediately causes panic, but staging in lymphoma primarily indicates where the affected lymph nodes are located throughout the body. Recognizing this difference can shift a patient from terror to a place of actionable hope.
- Clinical trials can offer access to chemo-free, cutting-edge therapies. Meg chose a trial utilizing bispecific antibodies to supercharge her own immune system to target the lymphoma cells, bypassing traditional chemotherapy. By participating in research, patients can access highly monitored, innovative treatments while helping to advance medical science.
- Intense monitoring helps prevent severe cytokine release syndrome (CRS). A major concern with bispecific antibodies is CRS, a potentially severe immune reaction causing sudden, body-wide inflammation that harms your healthy tissues and organs. Following strict protocols allow doctors to intervene early. In Meg’s trial, this proactive approach meant she could be managed entirely as an outpatient without experiencing high-grade CRS.
- It’s okay to drop the strong front and let others care for you. As a busy mother, Meg was used to doing everything for her family, but the exhaustion of treatment eventually forced her to pause. Allowing yourself to cry, feel overwhelmed, and accept help is a necessary part of navigating a major health crisis.
- The emotional toll often surfaces in the quietest moments. Between the frantic medical appointments and managing family life, the reality of a diagnosis can feel delayed. For Meg, the shower became a safe space to finally catch her breath, release the pressure, and process the sheer weight of her experience.
Meg’s Diagnosis Facts
- Name: Meg L.
- Age at Diagnosis:
- 42
- Diagnosis:
- Follicular Lymphoma
- Staging:
- Stage 4
- Symptoms:
- Lower back pain
- General feeling of unwellness
- Treatment:
- EPCORE-FL-2 Clinical Trial: Bispecific antibody (epcoritamab) and immunotherapy (lenalidomide, rituximab)

Story Sponsor

Thank you to our sponsor for their support of our independent patient education story. The Patient Story retains full editorial control over all content.
This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
Editor’s Note: Below is the experience shared by one hematologist-oncologist, Dr. Tara Graff of the University of Iowa Healthcare, and her patient. This article does not represent all cases for follicular lymphoma and is meant for informational purposes only.
- Meg’s Diagnosis Facts
- Facing a possible terminal diagnosis as a mother of three
- Understanding what stage 4 lymphoma meant and the reassuring first steps
- For patients: what is follicular lymphoma?
- Typical symptoms of follicular lymphoma
- Presenting a follicular lymphoma clinical trial for newly-diagnosed adults
- Deciding to join a clinical trial
- Breaking down clinical trial “myths”
- Preparing for the clinical trial
- Talking about side effects on bispecific antibodies
- Demystifying cytokine release syndrome (CRS) symptoms and management
- Overcoming the fear of CRS and ICANS symptoms
- Can doctors predict levels of CRS?
- Bispecific antibodies on clinical trial
- Bringing cancer care closer to the local community
- Processing remission, survivor’s guilt, and moving forward
- Hear from people living with follicular lymphoma
How’s this going to affect my kids? Are they going to be okay in adulthood if I only have six months to live?
Meg L., stage 4 follicular lymphoma patient

Facing a possible terminal diagnosis as a mother of three
Meg: Honestly, my first thought was my kids. I have not lost a parent to cancer, but I know how that can affect somebody at a young age. My children were nine, 11, and 13 at the time. Losing a parent at any age is awful, but my thoughts were: How would a nine-year-old cope with losing their mom? How’s this going to affect my kids? Are they going to be okay in adulthood if I only have six months to live?
From suspected kidney stones to an emergency room cancer referral
Meg: It was like in the movies, where the character starts with not feeling well and, all of a sudden, they have cancer. We were at my middle daughter’s gymnastics meet when I started not feeling great and experienced some lower back pain. Kidney stones run in my family, so I thought it was my turn. Everybody thought it was kidney stones.
My primary care physician (PCP) said that if I wanted, we could do a CT scan to see how many stones there were. Two days later, I had a CT in the morning. By lunchtime, I got a call from my PCP and she asked, “Hey, can you sit down?” I sat down and she said, “I need you to go to the ER.” I remember asking, “Did you say I have cancer?” She said yes and to go to the ER. Panic started to set in a little bit. In my mind, I knew it was serious. If I needed to go to the ER, it’s probably pretty bad.
First of all, you’re going to be okay. The staging of lymphoma is very different.
Dr. Tara Graff, Univ. of Iowa, Hematologist-Oncologist
Managing family panic while heading to the ER
Meg: There were a lot of things being triggered in my mind, including the panic of going to the ER. I called my husband and tried as calmly as possible to let him know what was going on. At this point, my kids were getting home from school and I didn’t want them to panic. In hindsight, I was sorry I did that, called him and told him I had cancer and I was going to the ER. He handled it amazingly, though.

After talking to my husband, I called my mom, but she was also going through cancer treatment. Her journey has been much longer than mine and, unfortunately, she had to deal with more. With her being well-versed in medical terminology and very educated through her cancer experience, I called her and started explaining what was happening.
Understanding what stage 4 lymphoma meant and the reassuring first steps
Meg: I was very fortunate. One of the physician assistants (PAs) of Dr. Graff went down and talked me through all the medical jargon because I had no idea what the words meant. The staff was reassuring and Dr. Graff was amazing. I went to the ER right away and she got me admitted into the hospital to stay overnight. I had a biopsy the following day and met Dr. Graff that day as well.

Dr. Tara Graff: You must understand the patient because every single patient requires something different. Some patients want you to be very straight with them. Some patients want you to be a little bit more delicate. Some patients want you to be their friend. You have to know your audience. I feel that I have a pretty good sense of people when I walk into the room.
When I met Meg, she was in the hospital, so when I walked into her room, I treated her like my friend. I said, “Okay, I realize that this is going on, but you’re a mom, you’re busy, and you’re young, so I’m not keeping you in the hospital. First of all, you’re going to be okay.”
Whether it’s an outpatient clinic or a hospital room, I don’t think you need to walk in any of those areas and start rambling. Before you even start talking about disease, you need to tell the patient, “You’re going to be okay. Here’s what we’re going to have to do. We’ll figure it out.”
There are many different kinds of lymphoma, so the patient might have heard of a horrendous situation that is nothing like what they’re personally dealing with.
Meg: When Dr. Graff came in, she was reassuring me, “This is what we’re going to do. We don’t even know what kind of cancer you have or if you even have cancer. We’re going to take it one step at a time.”
I was in the ER and they put me on the cancer floor. I even had nurses ask, “Wait, are you the patient?” Because they weren’t expecting somebody young. Everything was happening so fast. She approached a complete stranger, was reassuring, and kept it simple. Emotions are already complicated in that situation, so it was amazing.
For patients: what is follicular lymphoma?
Dr. Graff: It’s important that you quickly put away the misnomers. In Meg’s situation, she was diagnosed with follicular lymphoma and it’s very important to explain that follicular lymphoma is a type of non-Hodgkin’s lymphoma, which is different from Hodgkin’s lymphoma. And even within the bucket of non-Hodgkin’s lymphoma, follicular lymphoma is considered one of our slower-growing lymphomas and is not highly aggressive.
Before you even get down to the stage, where things are at, and what PET scans look like, it’s important to separate all of that information and understand what the patient is dealing with. And then we could tackle the important things, like, “You have lymph nodes here or there. We need a bone marrow biopsy.”
When it comes to lymphoma, I make it a point to explain that lymphoma staging is very different from that of solid tumors. When I say to my patient, “You have stage 4 lymphoma,” that has to do with where the lymph nodes are. It doesn’t mean the same as stage 4 pancreatic cancer, for example.
But the minute a patient hears stage 4, their whole body composition changes, so I try to go near them and say, “Listen, I’m going to tell you something, but I need you to hear me. This is very different. You still have [up to] a 95% chance of having a complete remission.” You need to make sure, as best as you can, that they hear that and they hear the differences because if you say “stage 4,” the curtain goes down.
Typical symptoms of follicular lymphoma
Stephanie: Meg, what were some of those initial things you said? And then, Dr. Graff, if you could address it by widening the scope of the reasons people get diagnosed?
Meg L.: My initial symptom was lower back pain, mostly on the right side. Around a month after being in the hospital, I started getting night sweats, but it didn’t happen all the time. We took a trip before I started treatment. I hadn’t had any swelling in my lymph nodes before then, but on that trip, I had some swelling in my neck. Those were the only symptoms I had before I started treatment.
Dr. Graff: In Meg’s case, she was having back pain because of where her lymph node groups were sitting. Our bodies are anterior-posterior. We’re not a linear up-and-down figure. When lymph nodes sit in the back, in the posterior part where your kidneys and back muscles are, you can have discomfort. People will typically present if their lymph node groups are large enough and pushing on something, whether it’s their stomach, colon, or whatever their lymph node group is near. It has to be a pretty decent size. A 1-centimeter lymph node is unlikely to cause pain.
Some patients are like Meg, whose lymph node group was starting to cause issues. She had pain and then she developed B symptoms. When a person gets sick, they may have fever, chills, night sweats, loss of appetite, and severe fatigue. It’s because their immune system or the B cells of their lymph system are activated, so you’re supposed to feel those. In lymphoma, the lymphocytes are the same cells involved when we get sick. When those cells are having their own party, you will get fevers, chills, drenching sweats, fatigue, and loss of appetite. It’s not always about swollen lymph nodes, but the B symptoms too.
Now, there are some patients who don’t present with any pain. They get a scan for something and then, lo and behold, lymph nodes show up. The lymph nodes are there because they’re reactive from X, Y, and Z, or we diagnose follicular lymphoma and some of our other indolent lymphomas incidentally, because someone’s getting a workup for something else.
Sometimes it’s a silent presentation and sometimes patients are symptomatic, and that’s different from other forms of more aggressive lymphoma, when you’re usually presenting with symptoms. There are differences.
Presenting a follicular lymphoma clinical trial for newly-diagnosed adults
Dr. Graff: Meg’s a healthy, young female. It’s going to be very different if I had an 87-year-old who was on oxygen and in a wheelchair. You have to know your patient, first and foremost.
I run our clinical trials program and I’m a strong believer in clinical trials when they fit the situation. We were very fortunate that, at the time Meg was diagnosed, we had an amazing front-line follicular lymphoma trial. In fact, it’s still going on with only a few slots left because it’s enrolled so well globally.
Not only were we tackling a new diagnosis, but I also needed to present the treatment options. I come in, lay out my sheet of paper with Meg, and say, “Okay, here are the options. You can have standard of care, which is a fully-approved combination of chemotherapy and immunotherapy. You can have this option, which is immunotherapy and some pills. Or we can do this clinical trial, in which you may receive the experimental drug or one of the two options I just talked about. But here’s the deal: No matter what, you’re going to get good treatment. You’re either going to get the standard of care, which we use all the time and have a proven record that we know works, or standard of care in combination with another therapy that we have seen make a huge impact in later lines of therapy.”
Not only are you navigating a new diagnosis and trying not to scare the heck out of your patient by talking about chemotherapy and treatment cocktails, but you’re also bringing up the topic of a clinical trial and they’re worried about being made into a “guinea pig.” It’s about breaking down the walls of what that means as well.
As a clinician and lymphoma specialist, I need to lay out all of the options for the patient. Ultimately, it’s their decision. Walking in the room and telling them, “This is what you’re going to do,” isn’t going to work. You need to give them the options and let them decide for themselves and what makes the most sense for their lifestyle. Quality of life is important. Again, it’s different for a younger person versus an 85-year-old, but I still approach it the same way.
Deciding to join a clinical trial
Meg: Dr. Graff laid out all the options, but I distinctly remember her saying they’re all good options no matter what I choose. Again, it was reassuring. She wasn’t recommending a treatment that she doesn’t believe in, so how can you not trust her and her advice on that?
We’re not going to play around with your life. We’re going to give you something that’s already approved, plus the clinical trial drug.
At minimum, you’re going to get what we use every day and what we know works. We’re not going to monkey around at all.
Dr. Tara Graff, Univ. of Iowa, Hematologist-Oncologist
My mom had gone through clinical trials, so joining a clinical trial was a no-brainer for me. Why wouldn’t I want the best possible treatment out there? On the clinical trial side, you can’t help anything improve if we’re not willing to help science and help others. If I can do that, why wouldn’t I try to help others in this situation too?
Dr. Graff: Meg’s trial was for treatment-naive follicular lymphoma, which means patients who are newly diagnosed and haven’t received treatment. At that time, it was a three-arm trial. We don’t get to pick what people get. It’s a blinded randomization. I can’t cherry-pick.
Meg was fortunate to get the clinical trial arm, but the nice thing about the trial is that even if she had been randomized to one of the standard-of-care arms, they’re the exact therapies I would use. It wasn’t going to be subpar care, which is what’s important for patients to understand in the front-line setting. We’re not going to play around with your life. We’re going to give you something that’s already approved, plus the clinical trial drug. At minimum, you’re going to get what we use every day and what we know works. We’re not going to monkey around at all.
In Meg’s case, she received the standard backbone of rituximab and lenalidomide, paired with a new therapy that people are starting to learn about called the bispecific antibody. In her case, she received epcoritamab. Think of the drug like a matchmaker. You’re bringing your healthy T cells, so your healthy lymphocytes, together with the cancerous B cells causing the lymphoma. If it’s a perfect match, fireworks happen, and those fireworks are the proteins released by the healthy cell to kill the bad lymphoma cells.
It’s chemo-free. You’re literally enhancing your immune system to fight the lymphoma. We’ve seen this combination in second-line treatment for follicular lymphoma, which was approved in November 2025 with response rates and complete remission rates that are absolutely astounding.
We want to be able to offer that combination on the front line, in the hope that we don’t have to worry about a second line. That’s how I approached it. When Meg called, she said, “Are you serious? Can I come off early? Two years?” I said, “Yes. You have to stay on, because I don’t want you ever to have this come back.”
We have to break that barrier of clinical trials because they are amazing. Without them, we cannot advance cancer care.
Dr. Tara Graff, Hematologist-Oncologist, Univ. of Iowa
The number of patients we have today is due to clinical trials.
Breaking down clinical trial “myths”
Dr. Graff: What goes on with clinical trials is hard. My father lost his battle with cancer, but when a clinical trial was presented to him, he thought he had no other options. There’s this misnomer that you only qualify for a clinical trial if you’ve exhausted every option and some patients will hear that as they’re dying. They think, “I’m going on a trial. It’s experimental. It’s voodoo.” I’ve heard everything. I had to remind my mom, “Mom, do you think I do this every day for things that don’t work?”
For most of our patients, when you start talking about clinical trials, you scare them. And when you start talking about them in the front line or [who’ve never had treatment], they say, “Why would you put me on a trial? I have all these other options.” It’s because we’ve been using this drug in the third line or in the second line, and the response rates are 90-something percent, so why are we going to wait to use it? Let’s use it now and keep you from ever relapsing.
You have to break down the negative connotation around clinical trials because they change the treatment landscape. They’re the reason people live longer because people like Meg and other patients who participate are allowing novel therapies to be approved so patients don’t need to have chemotherapy at all.
Meg’s treatment is two-plus years, but the other six-month regimen includes chemotherapy, so there’s a trade-off sometimes. Novel therapy might be longer and chemotherapy will be shorter, but you’re dealing with different side effects and other things around those therapies.
We have to break that barrier of clinical trials because they are amazing. Without them, we cannot advance cancer care. The number of patients we have today is due to clinical trials.
Meg L.: I remember she drew it on a piece of paper. I think of Dr. Graff’s description of it as “supercharging.” I was going to be given the juice to supercharge my cells so I could fight this. She simplified it, so it’s understandable and not overwhelming with medical terminology.
Preparing for the clinical trial
Meg: My husband came for the first couple of appointments before I signed all the clinical trial paperwork, so he could hear it and ask any questions. I had all my questions ready in a little notebook.
I felt overwhelmed and needed other people to step up and take over.
Meg L., stage 4 follicular lymphoma patient
Letting others care for you
Meg: Medical jargon was more information overload. I would say after four to five months is when I remember being in the shower, exhausted. I went down the rabbit hole. Up until this point, I considered myself a fairly healthy person. I never had any health issues. I’d only been in the hospital for births.
The shower is my release. It’s my only moment of quiet. The kids aren’t in there. The husband isn’t in there. I don’t know what it is. It’s a moment where you can catch a breath, get a moment of relief, and then have it all come out.
Mostly, I felt overwhelmed and needed other people to step up and take over. I was always the one to do everything. It’s okay to not be the strong one all the time and to let people care for you. It’s okay to cry and to show weakness.
You’re at risk for a reaction called cytokine release syndrome (CRS), which we think about with CAR T-cell therapy.
Dr. Tara Graff, Hematologist-Oncologist, Univ. of Iowa
It’s a little bit different with bispecifics. It’s lower grade, so it’s not as intense, but it requires a lot of monitoring.
Navigating clinical trial monitoring calls
Meg: I was charting everything every three hours. It was a little bit more overwhelming because you had to check in so much. They were calling at 1 a.m. and 4 a.m. I didn’t want my husband to get woken up, so I would sleep in during that period so we could get some rest. Fortunately, I didn’t have any severe symptoms.
Dr. Graff: You try to explain to them that they’re going to be monitored and to not be scared that we’re calling every six hours. It’s a fine balance, but in a sense, it’s probably almost overkill sometimes. But it’s also better to be safe than sorry.
Talking about side effects on bispecific antibodies
Dr. Graff: With Meg’s therapy, working on your immune system can introduce side effects or potential adverse reactions that are different from chemotherapy. We think about hair loss, nausea, vomiting, and other typical side effects. Still, with bispecific antibodies, because you’re revving up the immune system, which you want to happen, you’re at risk for a reaction called cytokine release syndrome (CRS), which we think about with CAR T-cell therapy. It’s a little bit different with bispecifics. It’s lower grade, so it’s not as intense, but it requires a lot of monitoring.
You’re telling somebody, without making them think that their head’s going to explode, “You may have a fever, lower blood pressure, or shortness of breath, but don’t worry because we’re going to monitor these things. We’re also going to intervene if we have to. We’re going to call you every six hours to make sure that you’re not having this reaction. We’re going to give you a checklist to go through.”
It’s a commitment. Forget just committing to the clinical trial. It’s a commitment while you’re going through the loading of this therapy into your system. Meg’s a trooper. Our patients who go through this therapy are all doing amazingly, but they have to get through a month-long process of this therapy being introduced into their systems.
Demystifying cytokine release syndrome (CRS) symptoms and management
Dr. Graff: The rates of CRS with Meg’s treatment regimen are low. They’re all grades 1 and 2. There are no higher-grade events. Less than 30% of patients who receive epcoritamab have CRS. It received approval to be used in combination for second-line treatment in November 2025.
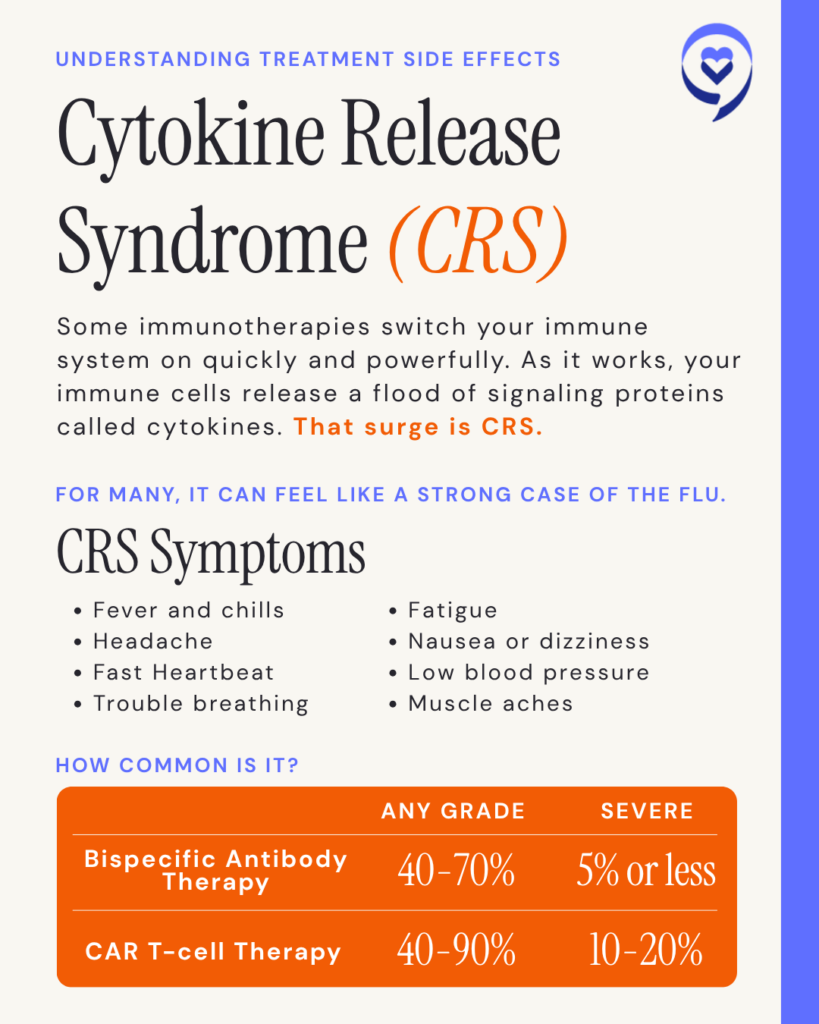
The rates of CRS are very low because of the other drugs involved. Epcoritamab is approved to be given by itself in third-line treatment for follicular lymphoma. Again, we have no grade 3 or 4 events and no neurotoxicity, but about 49% of patients will experience grade 1 or 2 CRS, with the majority being grade 1.
What does it look like? Other patients might have CRS. For the most part, our lymphoma patients don’t even have to come in most of the time. They’ll be monitored via calls. Let’s say they have a temperature of 101°F, but all their other vitals are stable. We’ll tell them to take 1,000 mg of acetaminophen and call them back in an hour.
If, when we call back, their temperature hasn’t quite broken or if their blood pressure is trending lower than their baseline, but they’re still feeling fine, we’ll have them take their steroids and call back an hour later. In most cases, the fever’s gone, you’ve put out the fire, and they’re back to normal. That’s grade 1, where a fever is the presenting symptom. We also see grade 2 CRS, but fortunately, not a lot with our lymphoma patients.
Editor note: CRS can range from a mild flu‑like reaction with fever (grade 1), to moderate symptoms needing IV fluids or low‑flow oxygen (grade 2), to more severe reactions needing ICU‑level blood pressure or breathing support (grades 3 to 4), and in very rare cases can be life‑threatening (grade 5).
With epcoritamab, the dosing schedule and being paired with other drugs decreases the risk of CRS compared to when we use the drug alone or when used in diffuse large B-cell lymphoma (DLBCL), which is a more aggressive form of lymphoma. We have managed every single patient exclusively as an outpatient the entire time; not one of them had to be admitted. Not to say that they didn’t have low-grade CRS, but they were always able to go home.
Now there are [also] patients we call hybrids. We have them inpatient for the first dose because they didn’t have a caregiver, were going to be out of town, or lived too far. I always hate to admit those patients, but social constraints dictate that. Those patients started inpatient, but finished their step-up dosing as outpatients.
We have managed every single patient exclusively as an outpatient the entire time; not one of them had to be admitted.
Dr. Tara Graff, Hematologist-Oncologist, Univ. of Iowa
Overcoming the fear of CRS and ICANS symptoms
Meg: The neurological side effect was the biggest thing, but as I said, the way Dr. Graff explains, she simplifies and reassures you, so it doesn’t seem as intense or as scary. And also, she has an amazing team. You’re constantly checking in at the beginning. I remember going in for blood draws, as well. They have all these safeguards in place, so it doesn’t feel scary in my opinion. They’re very strict. One time that my blood pressure was trending low, they told me to get my butt in there.
There are a lot of potential side effects that you can have when you’re getting cancer treatment. I’m not saying that CRS and immune effector cell-associated neurotoxicity syndrome (ICANS) aren’t severe, but they’re in the gamut of symptoms when you’re going through cancer treatment. I don’t remember feeling nervous about getting CRS again because we had check-ins, and I was checking my blood pressure and temperature regularly.
I don’t want to use the word guilt, but I don’t understand why my journey wasn’t as difficult as others’.
Meg L., stage 4 follicular lymphoma patient
Can doctors predict levels of CRS?
Dr. Graff: As an expert in the field, together with my colleagues at big institutions, we sit and try to predict who is going to have CRS. If you have 30 lymph nodes involved versus two, are you going to have CRS? I would have assumed Meg would have had CRS. If I were playing the lottery, I would have bet on her. But she didn’t.
Other things that we think about are inflammatory markers. Do higher inflammatory markers at baseline mean you’re going to have a higher risk of CRS? We don’t know. Sometimes yes. But I’ve had patients whose labs have been through the roof and they’re my best patients. This is not just on trial but also with the standard of care.
If someone has a higher-grade CRS, does that mean the impact is bigger and the drug is working? No. It’s just your immune system’s reaction, for whatever reason. Why does one kid get high fevers with every single minor virus they contract and another kid barely ever gets a fever? Why do our immune systems act the way that they do? We don’t know.
A grade 3 CRS versus a grade 1 CRS doesn’t mean that you’re going to have a better response. Meg had no CRS or neurotoxicity, and she was in complete remission by her first scan. She wasn’t even through her full induction therapy and she already had a complete remission.
Whether you have more or fewer side effects or whether you had CRS or not doesn’t correlate with your response to the treatment. You need to trust that the therapy is working. There are so many checks and balances along the way, especially when you’re treating a lymphoma patient. Whether it’s a clinical trial or standard of care, we’re doing scans after a few treatments. If everything is good, we’re continuing. We’re not going to close our eyes and let it roll. We’re keeping a close eye.
I wish there were a perfect correlative answer for people. I would love to have a predictive model, but [we are all] different for a reason, so it’s hard to predict and we just have to reassure our patients.
When I talk about this with other clinicians, advanced practice providers (APPs), nurses, and pharmacists, the important thing to note is that they’re part of a team. The caregiver and the patient are part of that team as well. It’s not just the doctor and nurses. You’re all part of the team, and you need to have communication in every direction. I will say this until I’m blue in the face: Without that team, this doesn’t work. If you have that team, you can do anything.
For every lymphoma patient I have had on these therapies, whether they’ve had to come into the clinic or been managed at home, it’s been positive for them because they feel they’re being taken care of.
Dr. Tara Graff, Hematologist-Oncologist, Univ. of Iowa
Dr. Graff: A dear patient who had follicular lymphoma and diffuse large B-cell lymphoma received the drug that Meg got, but as a monotherapy. He would do anything I asked. If I had signed him up for 30 clinical trials, he would have done anything. That’s who he is. As I was telling him about the reaction, he said, “Okay, so you know I’m going to have it because it’s me.” I said, “You don’t know that you’re going to have it.” He goes, “Oh no, no, no, no. I’m going to have it.”
True enough, with every single step-up dose, he developed CRS. I told him, “You’re not supposed to keep having this. Your percentage should be down by now. You’ve already had it.” No. Every dose. And he always did when I was at a meeting and I wasn’t there. He would always have it outside the window when it was supposed to happen. But he did great. He stayed at home with grade 1 and grade 2 events. He monitored his temperature every hour on the hour.
For every lymphoma patient I have had on these therapies, whether they’ve had to come into the clinic or been managed at home, it’s been positive for them because they feel they’re being taken care of. I know Meg can attest to this. She has direct access to our nurses and the research coordinator. They’re never alone. There’s always somebody they can reach out to, and that’s what’s different from other therapies. It’s not just about clinical trials; it’s the journey where they always have somebody. Our patients are never alone.
Yes, you worry about CRS and neurotoxicity, but because you’re worrying about those, it’s as if you’re having a slumber party together. You’re never alone in the journey. You’re scared because of the unknown, but you’re going through something with people who have your back. Our team is four-and-a-half years into this, so we don’t get wigged out over anything, but we still have to treat every patient like it’s the first patient.
Dr. Graff, being such an advocate for getting that type of care to people, is amazing.
Meg L., Stage 4 Follicular Lymphoma Patient
She is determined and that’s what’s so inspiring about it. It’s not only for people who live close to the care centers; it’s for anybody who needs it. Everybody should be able to have that option presented to them.
Bispecific antibodies on clinical trial
Dr. Graff: It’s a little different depending on what bispecific antibody therapy you’re getting. Four years ago, I started our all-outpatient bispecific program at Mission Cancer + Blood with a clinical trial patient. Bispecifics weren’t approved four years ago, but we started this on a trial. I wanted patients to be able to sleep on their beds. I didn’t want them to be admitted to the hospital inpatient if they didn’t have to be, so that took a lot of logistical planning. I had a giant plan that was published.
By the time Meg’s trial came along, we were two-plus years into our monitoring. What we do for patients, and Meg will tell you herself, is pretty in-depth. For them to be treated as outpatients while receiving that therapy, they all need their own medical equipment to monitor their blood pressure, heart rate, oxygen saturation, and temperature.
They need a caregiver with them for 24 hours. They need to have somebody, because if they’re super sick, they’re not going to know it. They need somebody who can help and make phone calls. They have to live within a certain distance of the treating center that has the medications they will need to break the reaction, if it comes to that.
It’s a commitment. You try to explain to them, “We’re going to monitor you. Don’t be scared when we’re calling you every 6 hours.” It’s a fine balance. It’s probably almost overkill sometimes, but it’s also better to be safe than sorry. It’s better to catch these in real time so you can intervene.
We make sure that all of our patients have acetaminophen in their medicine cabinets. We don’t let them start their therapy unless we know that they have them and they’re up to date. They all have steroids that they can take, should they have a reaction.
We’re in constant contact with them. We call on step-up dosing days, when they can have this reaction. Meg will attest to this. I have an amazing team of dedicated nurses who are literally the best humans I’ve ever met on this planet. They give up their time to make phone calls late at night and early in the morning. They come to the clinic. We open our clinic in the middle of the night if a patient has a reaction. Fortunately, Meg did not.
Bringing cancer care closer to the local community
Stephanie: Dr. Graff is clearly a believer in clinical trials, as are you, and in bringing treatments closer to more people, especially in the community. When you hear her talking about all these developments, what’s your reaction?
Meg L.: It’s amazing. We live in Iowa, where there are many rural communities, so people don’t have access to the care they would have in larger urban communities. Iowa has one of the highest rates of cancer, so Dr. Graff, being such an advocate for getting that type of care to people, is amazing.
She is determined and that’s what’s so inspiring about it. It’s not only for people who live close to the care centers; it’s for anybody who needs it. Everybody should be able to have that option presented to them.
Processing remission, survivor’s guilt, and moving forward
Dr. Graff: Whether it’s a clinical trial or standard of care, we’re doing scans after a few treatments. If everything is good, we continue. We’re not going to close our eyes and let it roll. We keep a close eye.
Meg: I went into remission fairly quickly after starting treatment. The trial I’m on is for two and a half years. Sometimes, I almost forget. Unfortunately, I’ve had people very close to me who have passed away from cancer. I don’t want to use the word guilt, but I don’t understand why my journey wasn’t as difficult as others’. I think, “When’s the other shoe going to drop? When’s it coming back?”
Honestly, I’m forever changed from going through this. There are so many mixed emotions. A year and a half into the trial, I didn’t want to talk about cancer anymore. While that’s always going to be part of my life, I try not to dwell on that. There’s more to my life than cancer.
Story Sponsor
Thank you to our sponsor for their support of our independent patient education story. The Patient Story retains full editorial control over all content.
This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
Inspired by Meg’s story?
Share your story, too!
Hear from people living with follicular lymphoma
Real experiences with diagnosis, treatment choices, side effects, and life beyond follicular lymphoma — in their own words.











Leave a Reply