Your Follicular Lymphoma Questions, Answered by Dr. Peter Martin
Living with follicular lymphoma often comes with more questions than answers. That’s why we’re turning directly to the community — and a leading follicular lymphoma expert — to help.
For a limited time, we’re collecting your most important questions about living with and treating follicular lymphoma for Dr. Peter Martin from Weill Cornell Medicine. We’ll present his expert answers in a special webinar hosted by The Patient Story.
Program Topics
- We’re gathering questions from the follicular lymphoma community for a limited time.
- Dr. Martin will answer as many as possible during the webinar.
- Please note: Due to the number of registrants, not every question can be addressed individually.
- Answers will be provided in general terms and not as personalized medical advice. For your specific situation, always consult your own physician and care team.
Program Expert
Program Partner

A special thanks to our friends at the Living with Follicular Lymphoma Facebook Group for their partnership. Their private Facebook group is dedicated to supporting individuals with follicular lymphoma, their families, and supporters. They offer a safe space to share personal experiences and learn about the latest research, trials, and treatments.
This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
- Introduction
- What’s your advice for newly diagnosed patients?
- Should a PET scan be used to determine staging after treatment?
- How will I know when to start treatment?
- Is “R2” (Rituxan + Revlimid) a good first treatment for follicular lymphoma?
- Do I need maintenance therapy after bendamustine and rituximab (B + R)?
- Should mosunetuzumab be used as maintenance?
- Can you explain the EPCORE FL-2 clinical trial?
- How close are we to finding a cure for follicular lymphoma?
- What’s the longest you’ve seen a patient stay in remission?
- What can somebody expect if follicular lymphoma is found in their lungs?
- Can follicular lymphoma change into another form of cancer?
- Can supplements help lower the chances of lymphoma coming back?
- Can treatment of follicular lymphoma cause side effects, like excessive sweating?
- What are the risks if pleural effusion happens with follicular lymphoma?
- What are the chances my kids might also develop follicular lymphoma?
- Should I get the COVID vaccine?
- Conclusion
- Hear from people living with follicular lymphoma
Edited by: Katrina Villareal
Introduction
Hi, I’m Peter Martin. I’m a lymphoma doctor in New York City. Welcome to Ask Me Anything About Follicular Lymphoma.
What drew you to treating lymphoma?
I’ve been a lymphoma doctor for the past 20 years in New York City. I started taking care of people with lymphoma at a time when everything was changing in the world of cancer research. It was especially changing quickly in lymphoma, so I got excited and wrapped up in that. I wanted to be part of the new generation of people who were moving new treatments forward and helping to take care of people better and better than they ever had been before.

I had also just finished my residency in internal medicine at McGill University in Montreal. I liked the idea of continuing to be a “real doctor” and getting to know people for years or decades, which turned out to be the case in my career.
What’s your advice for newly diagnosed patients?
The number one piece of advice I’d give is to bring somebody to your doctor’s appointments and write down your questions in advance. There’s a lot of information that goes back and forth during these discussions, especially at the very beginning, that it’s hard to keep track of it all.
It took me years and years and years. In fact, I’m still learning about cancer every single day. The expectation that you could possibly learn that much in half an hour or 45 minutes is very difficult. Having somebody else with you to help you ask questions and take in all of that information is helpful.
Should a PET scan be used to determine staging after treatment?
Let’s talk a little bit about imaging and then we’ll transition to staging.
For most imaging in follicular lymphoma, we use two treatment modalities. One of them is called CT imaging, which is effectively a fancy form of X-ray. CT is computed tomography. Essentially, a machine sends X-rays through a body and then a computer is used to integrate all of those X-ray images into a two-dimensional form that allows you to see changes in density at different places in the body. There are a few densities that we see. We see bone, air, water, and fat, and that contrast allows us to effectively visualize anatomy. When we do a CT scan, we’re visualizing anatomy.
The other imaging modality that we use is called PET imaging. PET is positron emission tomography. Almost all PET scans that we do in lymphoma right now include F18-FDG. FDG stands for fluorodeoxyglucose PET imaging. In this case, a glucose molecule, which is a kind of sugar, is labeled with radioactive fluorine, F18, and injected intravenously in advance of the scan. That glucose is then carried around the body by the bloodstream.
All cells in our body, in differing degrees, use sugar or glucose for energy and metabolism. Turns out, cancer cells, for a variety of reasons — and this was described a long time ago, something called the Warburg effect — use very high amounts of glucose to produce energy, as well as to create other molecules for synthesis of proteins, in terms of helping the cell to grow and divide.
Cancer cells take up this fluorodeoxyglucose molecule and then it’s phosphorylated by an enzyme inside the cells, which essentially traps it inside the cells where it’s taken up. Then that F18 decays into an oxygen molecule and as it decays, it releases a positron. That positron then collides with an electron in the immediate area of the cancer cell where that glucose molecule is and that high-energy collision essentially releases two photons in opposite directions.
Again, there’s a scanner that’s going around a person with a detector that detects those photons and the computer puts it all together in an image. But instead of imaging anatomy, what we’re imaging is physiology. How much sugar is being used? Again, it relies on contrast between different tissues using different amounts of sugar. But essentially, you can see how much sugar a specific tissue uses at that particular time. Cancer cells in general are using more sugar and active cancer cells, which are cells that are growing faster, will use more sugar.
Using these PET and CT images, we can get an idea of where the tumor is, how big it is, how much of it there is, and how metabolically active it is.
Now let’s talk a little bit about staging. For most lymphomas, we use something called the Ann Arbor staging system. This is an old staging system that was invented decades ago for evaluating how much lymphoma there is in a lymphoma called Hodgkin lymphoma. That information was used to determine where to radiate and whether or not somebody else needed chemotherapy in addition to that.
We’ve obviously moved beyond those particular questions in most cases. Although we still use the Ann Arbor staging system, staging in lymphoma has become less relevant for a variety of reasons. In fact, it’s far less relevant than staging in solid tumors, like breast cancer, where an early-stage breast tumor could be removed surgically and cured, and stage 4 breast cancer is another story.
In the case of lymphoma, it has much less prognostic or treatment-related information. Where PET/CT scans do continue to play a role is at the very end of a specific treatment, so we can assess their response to that treatment. In general, better responses correspond to longer intervals between treatments.
How will I know when to start treatment?
The first task is to think about our goal of starting treatment, which is to help somebody live a life that’s as close to the life that they would have lived had they never been diagnosed with lymphoma. Most people with follicular lymphoma — over 80% — will live a normal lifespan as long as somebody without lymphoma.
We start treatment when we think that the potential symptoms related to the lymphoma can be mitigated, and the potential side effects of any treatment might be warranted.
There are rules for this that we see in clinical trials. These are the GELF criteria, which refer to the number of lymph nodes, the size of lymph nodes, blood counts, LDH, and other symptoms. We’re thinking: is it likely that my treatment is going to help somebody feel better than if we were not treating them at all? That depends on what symptoms somebody might be having, when we might be expecting somebody to have symptoms, but also, importantly, what treatment we might be planning to use.
Is “R2” (Rituxan + Revlimid) a good first treatment for follicular lymphoma?
R2 refers to the treatment of lenalidomide (Revlimid) plus rituximab (Rituxan). It has been studied in a lot of clinical trials in follicular lymphoma. That regimen is, in fact, approved by the FDA for people with follicular lymphoma that has been previously treated. It has been studied in multiple phase 2 trials, in single-arm trials in people with follicular lymphoma.
We published one of those called CALGB 50803. But then, there was a big randomized clinical trial called RELEVANCE that compared the R2 regimen to other chemotherapy regimens. In effect, it showed that they are relatively similar in terms of how well they worked. In terms of side effects, there were some differences, but for the most part, those differences were fairly modest.
Is it a good treatment for untreated follicular lymphoma? I guess it depends on what you define as good. Again, I would go back to the idea that treatment should be individualized for somebody with follicular lymphoma based on the goals, their symptoms, expected safety profile, and what we’re hoping for. For some people, it’s an appropriate choice. For other people, there are other choices that might be better.
Do I need maintenance therapy after bendamustine and rituximab (B + R)?
BR is bendamustine (Bendeka, Treanda), which is an old chemotherapy drug, and rituximab (Rituxan), a kind of immunotherapy. These two drugs are frequently given as treatment for follicular lymphoma, either for people who have never received prior treatment or people who have received prior treatment, and they work very well to get rid of a lot of lymphoma cells.
One question that comes up is if somebody does very well with this regimen, can we potentially prolong their time to next treatment by giving an easy drug, rituximab (Rituxan)?
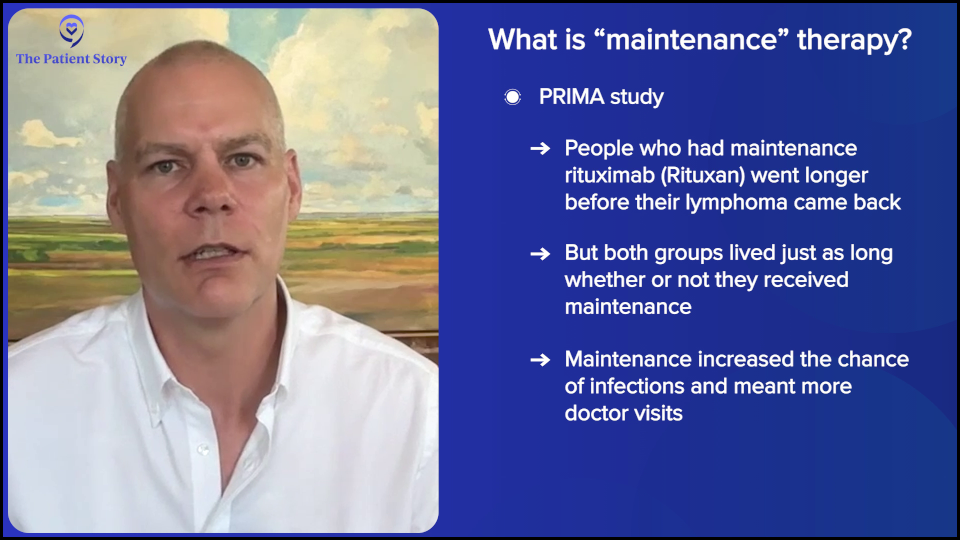
There are a couple of key clinical trials. One of them is called the PRIMA clinical trial. In that trial, everybody received immunochemotherapy — different regimens, not including bendamustine (Bendeka, Treanda) and rituximab (Rituxan) — and then they were randomized to receive rituximab (Rituxan) or observation. In that trial, the people who were randomized to receive rituximab (Rituxan) had about a 40-50% reduction in the probability of progression at 10 years compared to people who were randomized to observation.
That increase in remission duration came at the expense of some side effects, mostly infections. But obviously, there are things that are not measured, like the hassle of having to go back and forth for treatment for two years, in the case of that trial. If you look at the big results or the most important question, the proportion of people who were still alive at the end was the same in both treatments.
Looking at the big picture, there wasn’t a big difference, but people who received maintenance had a longer period of time without other treatment that didn’t include bendamustine (Bendeka, Treanda) and rituximab (Rituxan).
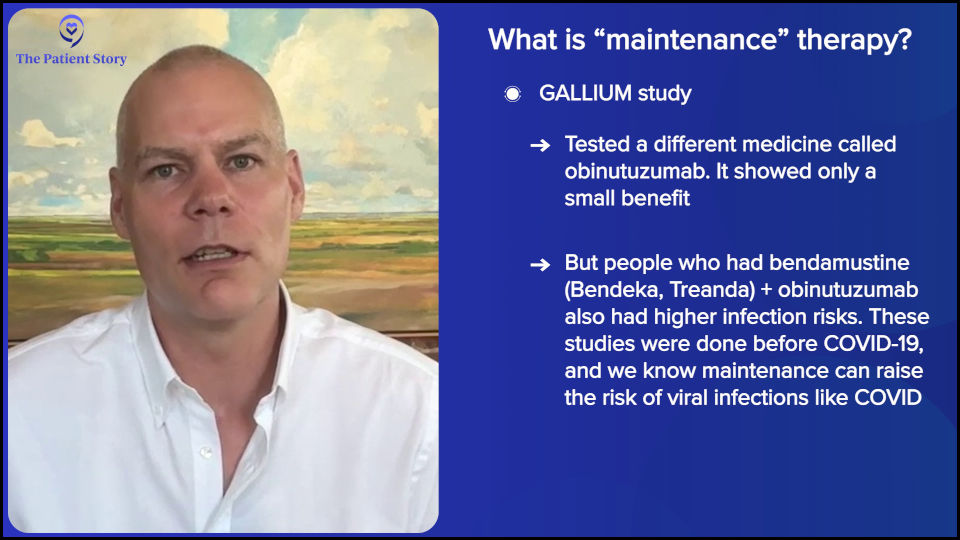
Bendamustine (Bendeka, Treanda) and rituximab (Rituxan) were included in a later clinical trial called GALLIUM. In that clinical trial, people received immunochemotherapy — again either rituximab (Rituxan) or obinutuzumab (Gazyva), plus chemotherapy. In this trial, bendamustine (Bendeka, Treanda) and rituximab (Rituxan) were a common backbone, and then people received either obinutuzumab (Gazyva) or rituximab (Rituxan) maintenance.
That trial showed a small benefit for obinutuzumab (Gazyva) over rituximab (Rituxan), about a 4-5% reduction in the risk of progression by two or three years. Interestingly, it showed that people who received bendamustine (Bendeka, Treanda) followed by obinutuzumab (Gazyva) maintenance had an increase in risk of some side effects, especially infections.
Both trials were done before the COVID-19 pandemic. What we do know, as I mentioned, is that maintenance rituximab (Rituxan) does increase the risk of some infections, including viral infections like COVID.
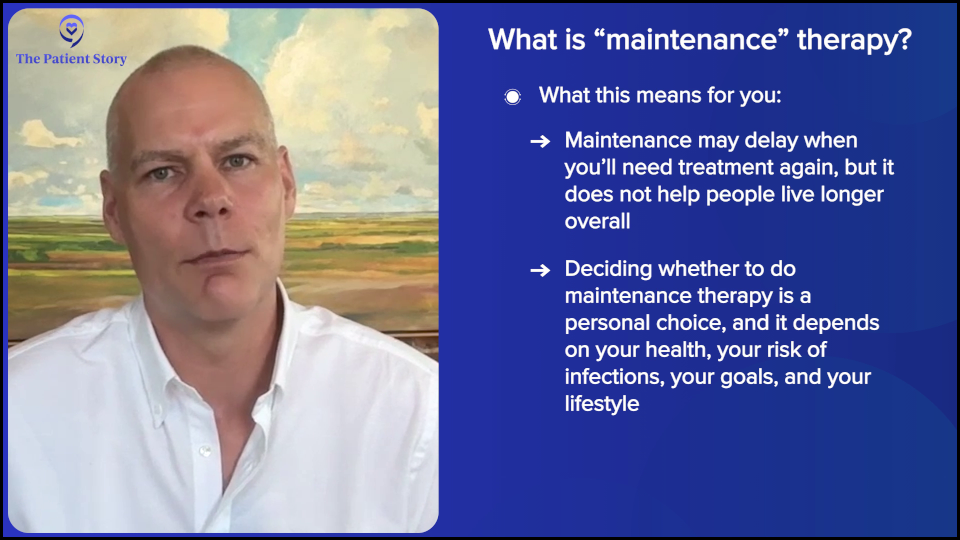
Unfortunately, the answer again is, as you’ll probably hear many times, it depends. Is maintenance a good treatment? It’s definitely an option to prolong time to progression. Maintenance, as far as we know, does not increase overall survival rates, which is the most important big-picture question, and it comes at the expense of increased risks of infection. It’s a very personal decision.
Should mosunetuzumab be used as maintenance?
Mosunetuzumab (Lunsumio) is a bispecific antibody that targets CD20 on B cells, including B-cell non-Hodgkin lymphomas, and CD3 on T cells, which is a part of our immune system. These antibodies bring the T cells in very close proximity to the B cells and activate those T cells to kill the B cells that they’re also bound to. It’s a very effective form of immunotherapy.
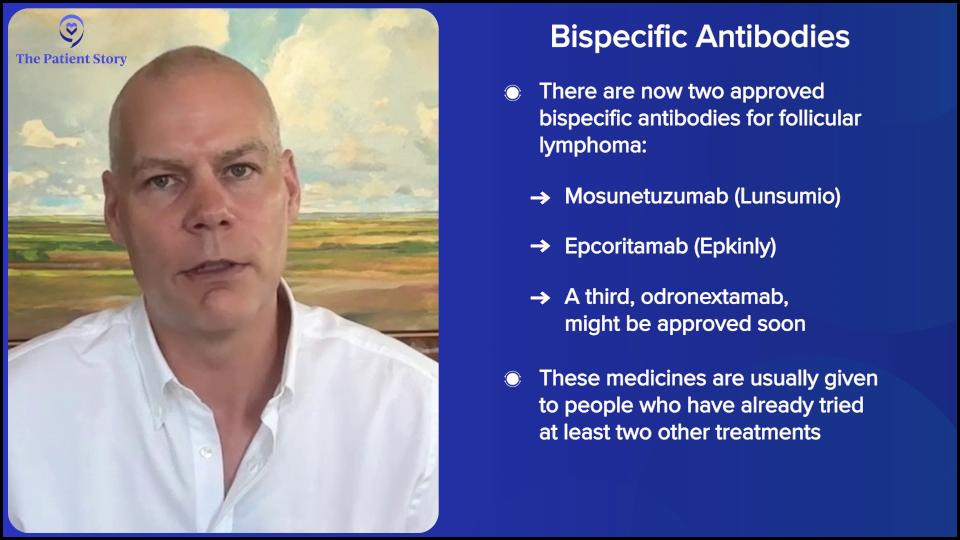
There are currently two bispecific antibodies approved for treatment of follicular lymphoma: mosunetuzumab (Lunsumio) and epcoritamab (Epkinly). There’s a third that will likely be approved in the near future called odronextamab. All of them produce pretty similar effects with similar overall and complete response rates.
They’re approved for people who have had at least two prior treatments for lymphoma. Interestingly, there are small differences in how they’re administered and in their duration.
The side effect profile is pretty similar amongst all of them. These include a potential risk of cytokine release syndrome (CRS) in the first month, which includes fever and chills. Effectively, it looks like an infection without one. This is mitigated by starting slowly and ramping up the dose of the drugs over time.
One of the issues relevant to this question is the longer somebody is on these drugs, the more immunosuppressive they become, so we start to see other infections. This is similar to other kinds of immunotherapy, but more profound.
Is it a form of maintenance? Again, it depends. My personal bias is probably not to overdo it with bispecific antibodies, but to get to a point where we’re confident that someone is responding well and then consider stopping. But there might be some scenarios where continuing would be attractive.
Can you explain the EPCORE FL-2 clinical trial?
The EPCORE FL-2 clinical trial is an ongoing study in follicular lymphoma using the bispecific antibody, epcoritamab (Epkinly). In this clinical trial, people with follicular lymphoma who have had at least two prior lines of therapy will receive either the R2 regimen, lenalidomide (Revlimid) and rituximab (Rituxan), plus epcoritamab (Epkinly), or the R2 regimen alone without epcoritamab (Epkinly), or chemoimmunotherapy.
They’ll be followed for efficacy outcomes, essentially how well it works, as well as side effects. The trial has been going on for a while now. It’s an interesting clinical trial and we’ll see the results when they’re available.
How close are we to finding a cure for follicular lymphoma?
This is a short question to ask, a long question to answer. It’s an interesting one.
On some level, semantics come into play because we have to accept a couple of things.
One of them is that, again, most people with follicular lymphoma will live a normal lifespan, equivalent to people without lymphoma. Two, in general, the treatments we give for people with follicular lymphoma are not given with the intention of curing the lymphoma, but instead are administered with the intention of helping somebody to live a life that’s as close to the life they would have without lymphoma, so we choose treatments according to that.
But in general, the intention is not to cure the lymphomas. It’s because, over time, we’ve learned that most of these treatments don’t specifically cure follicular lymphoma.
That said, there probably are several people with follicular lymphoma who are cured by these treatments. They will get one treatment, may never again require treatment in their lifetime, and may never have evidence of lymphoma in their lifetime.
Were they actually cured? If they had lived another 50 years, for example, would it have come back? We don’t know, but I think this is a concept of functional cure. Many people experience functional cure from all kinds of lymphoma therapies for follicular lymphoma.
We don’t typically think most of these treatments will be curative. We’ve seen over time that whether we’re choosing chemotherapy, immunotherapy, or newer targeted drugs, like kinase inhibitors, in general, we don’t see most people with follicular lymphoma experiencing cure from these treatments.
I do think that in my lifetime, we will have a cure for more people with follicular lymphoma, but I’m not sure whether that will be through combinations of more treatments together or more likely related to understanding some of the underlying biology in people with follicular lymphoma. In other words, if we can understand why some people get follicular lymphoma, we might be able to turn that switch the other way.
What’s the longest you’ve seen a patient stay in remission?
I’ve been taking care of people with lymphoma for 20 years. Since I started, there are some people with follicular lymphoma I’ve seen who have never required treatment, and there are other people who I’ve treated their lymphoma early on who have never required treatment again after. Ask me again in another 10 years.
What can somebody expect if follicular lymphoma is found in their lungs?
Most people with follicular lymphoma will live a normal lifespan. I guess the question here refers specifically to certain parts of the body. There are a couple of lymphomas. The word lymphoma literally means tumors in the lymph nodes. It’s an old word.
For the most part, cancer cells like to grow in lymph nodes because they get all of the signals that they need for growth and survival in those lymph nodes. They float around between the lymph nodes through the bloodstream and lymphatic channels in those areas, but they don’t grow. They grow in tissues like lymph nodes.
But they do pass through all of these other organs in our body and can be found in various organs as a result. Interestingly, they prefer to be in lymph nodes than anywhere else. For example, it’s exceptionally uncommon to find follicular lymphoma in the brain, even though it’s probably floating through the brain all the time.
There are a couple of exceptions to that. One is cutaneous follicular lymphoma, which for some reason starts to grow in the skin and prefers to be in the skin. Another is called duodenal follicular lymphoma, which starts in a part of the small intestine next to the stomach called the duodenum and prefers to grow there.
Both of those forms of follicular lymphoma are remarkably indolent. You may hear that word indolent. It basically means lazy, which is a very accurate description of these two follicular lymphomas. However, secondarily, any follicular lymphoma can involve other organs, potentially including the lungs.
In general, it would be fair to say that when lymphoma starts to prefer to grow outside of the lymph nodes, it might mean that biologically, it’s become a little bit more challenging. But still on average, most people with follicular lymphoma, regardless of wherever it is, are still going to do very well with most of the current treatments that we have today. And treatments keep getting better.
Can follicular lymphoma change into another form of cancer?
Yes and no. Follicular lymphoma can undergo something called transformation. That’s essentially where one follicular lymphoma cell acquires additional biological changes that increase its growth rate and we call this transformation. In effect, most of these transformations are follicular lymphoma to another lymphoma called diffuse large B-cell lymphoma. That happens at a rate of roughly 2% per year. Somewhere in the range of about 10% of people may experience a transformation from follicular lymphoma to diffuse large B-cell lymphoma over the first decade. In general, if it hasn’t happened within that first decade, it seems to become less likely.
When that happens, the diffuse large B-cell lymphoma component of this transformed lymphoma is treated with curative intent. Even if we manage to cure the diffuse large B-cell lymphoma component, we don’t typically cure the residual follicular lymphoma component, although the treatments for diffuse large B-cell lymphoma are also very effective for follicular lymphoma and continue to be well controlled.
Can follicular lymphoma evolve into other lymphomas? There have been cases of it evolving into more of a lymphoblastic lymphoma, which is a very aggressive lymphoma. I don’t believe there are cases of follicular lymphoma evolving into mantle cell lymphoma or Burkitt lymphoma. That said, just because somebody has follicular lymphoma doesn’t mean that they’re never going to develop other cancers.

Can supplements help lower the chances of lymphoma coming back?
Mostly, the answer to this question is no, but I’ll give a couple of caveats.
We’ve done a lot of studies in the research community about what’s causing follicular lymphoma. Outside the exception of nuclear disasters, for the most part, we don’t have a lot of data that there are strong environmental factors driving most follicular lymphomas, which includes diet and other lifestyle changes. Taking this into account, if it’s uncommon for lifestyle changes likely to impact the development of lymphoma, then it’s even less likely that lifestyle is going to impact the behavior of lymphoma once it’s already taken place.
That said, it’s important to remember again that just because somebody has follicular lymphoma doesn’t mean that their health is frozen at that point in time. People with follicular lymphoma will go on to live years or decades. One of the strange paradoxes of living a very long period of time is that we can also develop other health related issues, like cardiovascular disease or diabetes, for example.
In general, what I tell people is to try to live as healthy a lifestyle as possible because the easier you are, the easier it is for me to do my job now and in the future. For example, imagine somebody develops a cure for follicular lymphoma 15 years from now, but it requires that you have to have super healthy kidneys. Then you want to be the person that has super healthy kidneys 15 years from now. Do supplements do that? Not necessarily, but a healthy diet and exercise especially probably do.
There might be rare scenarios where somebody has some malabsorption syndrome and under those circumstances, taking vitamins or minerals might be beneficial.
Can treatment of follicular lymphoma cause side effects, like excessive sweating?
There is something called night sweats that you may read about. These are what we call B symptoms or constitutional symptoms. In this case, we typically define excessive night sweats as somebody who is drenching their bed to the point where they have to change their sheets once or twice in the middle of the night. It’s common for all of us periodically to have sweating during the day or even at night. But if you’re not waking up to change your sheets in the middle of the night, we wouldn’t say that that is a B symptom or constitutional symptom.
What are the risks if pleural effusion happens with follicular lymphoma?
I mentioned follicular lymphoma grows in lymph nodes, which are tissues that are part of our lymphatic system. The lymph nodes are connected by a series of channels called lymphatic vessels. Within those lymphatic vessels is lymphatic fluid plus white blood cells. The lymphatic fluid basically picks up fluid that has drained into other tissues elsewhere in our body, has basically leaked out of the bloodstream, and has to be returned to the heart. It accumulates in the lymphatic vessels and then gets returned to the heart.
When we have lymphoma, sometimes lymph nodes can become enlarged and can block those lymphatic vessels or sometimes even veins, and then the fluid essentially is not able to travel as efficiently back to the heart. Sometimes, people with follicular lymphoma can have lymph nodes that are in the chest — usually the middle of the chest, but sometimes anywhere in the chest — and those lymph nodes could block lymphatic vessels. The fluid that should be returned to the heart can sometimes leak out and layer out into something that we call a pleural effusion.
This is generally not very common. Typically, the treatment for it is to try to shrink those lymph nodes, essentially relieving the blockage and allowing the fluid to return to the heart. However, sometimes while we’re waiting for those lymph nodes to shrink and for the fluid to start moving back in the right direction, we have to remove the fluid through other ways, including putting a needle in there and taking it out. In terms of the frequency of drainage, that depends on how much fluid there is and how quickly we can shrink the lymph nodes and get things moving in the right direction.
What are the chances my kids might also develop follicular lymphoma?
Follicular lymphoma occurs somewhere in 3 to 5 per 100,000 people per year, so it’s pretty uncommon. That means every year, for every three people with follicular lymphoma, there are 99,997 without follicular lymphoma.
Epidemiological studies, including cohort studies and case-control studies, have tried to evaluate whether there’s a familial link. While there is a measurable familial link when you study thousands and thousands of people, this is generally pretty rare or it’s a weak link. It’s roughly a two-fold or maybe three-fold increase in risk.

If you have a first-degree relative with follicular lymphoma, your relative risk of having follicular lymphoma goes up by about two times. In other words, instead of 3 out of 100,000 people per year, now it’s 6 out of 100,000 people a year. That means your children are much more likely to be in the 99,994 people without follicular lymphoma. There’s a measurable risk, but effectively, on a personal level, it means almost nothing.
Should I get the COVID vaccine?
In general, we recommend vaccines for people where the risk of having any sort of significant morbidity or mortality from an infection is likely to be significant. Under those circumstances, it’s reasonable to take a vaccine.
If we look at the rates of COVID in the United States, they typically continue to spike on a six-month frequency. This information could change at any point in time, but if we look at the past two years, we typically saw spikes in August and September, then six months later in the mid-winter, and then again in August and September. The prevalence of infection tends to go up and down during the year.
We also see rates of COVID-related deaths in the United States in general go up from very low up to maybe 1-2% of all deaths being attributed to COVID during these periods where the prevalence is very high. If somebody has a very high risk of having any significant morbidity or mortality from a COVID infection during one of these periods of high prevalence, then it would be reasonable to get the vaccine. Does everybody need it? That’s debatable.
The same thing goes with the flu vaccine. I recommend everybody should get the annual flu vaccine.
I also recommend that everybody should get the Prevnar 20 vaccine against pneumococcus and most people should also consider getting the shingles vaccine called Shingrix. It’s currently recommended for people over age 50. For people above age 60 or 65, there’s an RSV vaccine that’s available as well.
Prevention can go a long way and it’s particularly valuable in people who are likely to have major symptoms or potentially die from certain infections.
Conclusion
That’s it for this Ask Me Anything. Hopefully, it was interesting. If it was, let us know and we’ll do it again.
This interview has been edited for clarity and length. The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story. This content does not replace professional medical advice.
Hear from people living with follicular lymphoma
Real experiences with diagnosis, treatment choices, side effects, and life beyond follicular lymphoma — in their own words.







