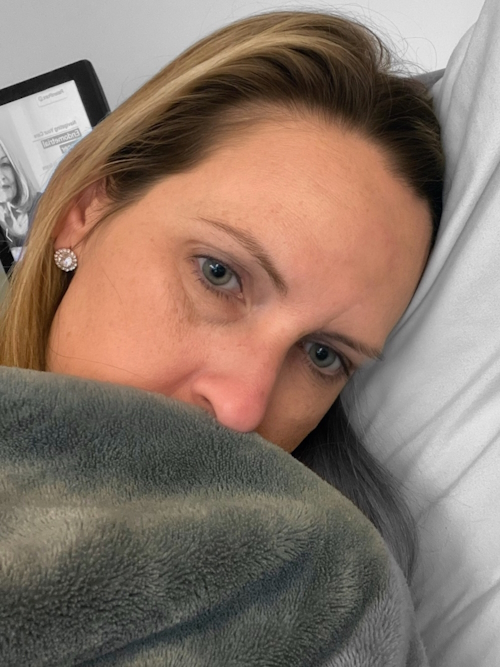
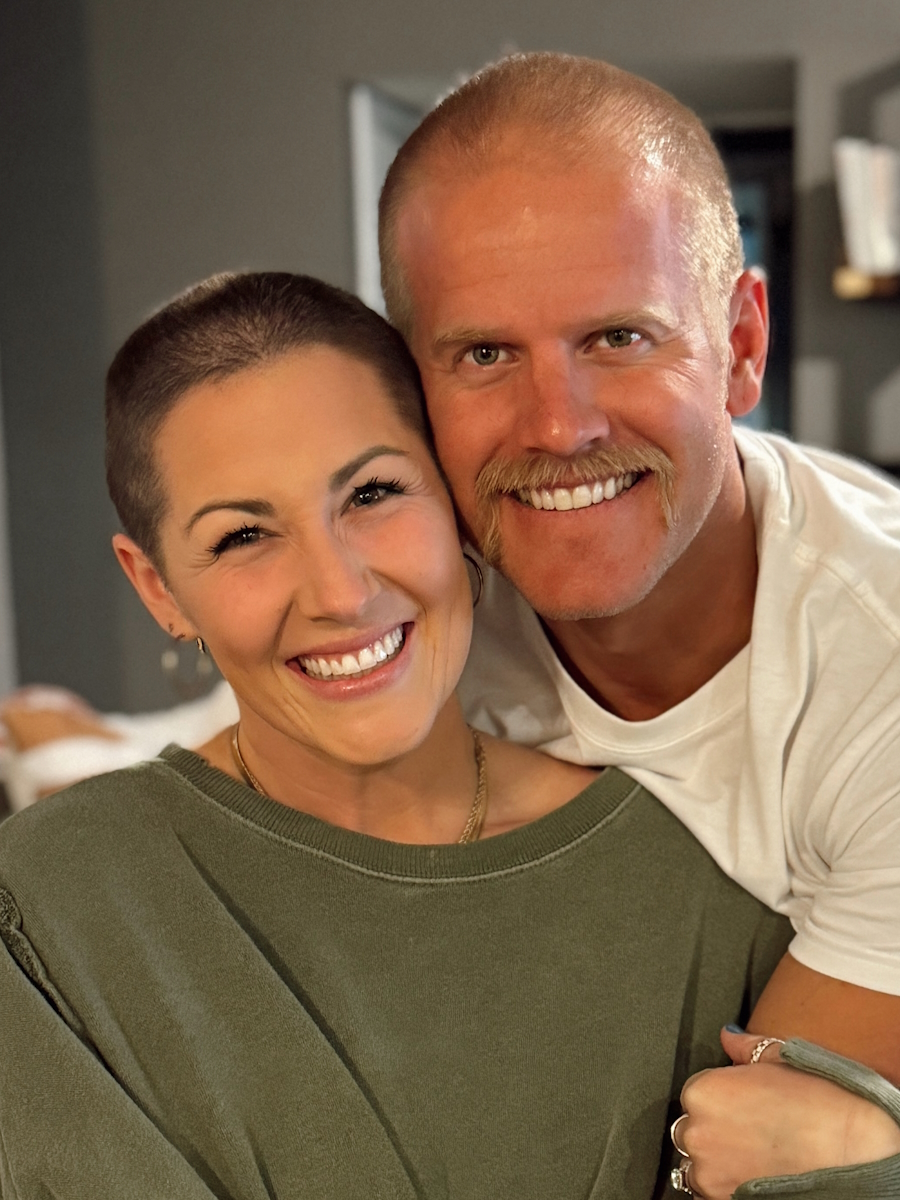
Nicole, a nurse and single mother of three from Florida, was diagnosed with chronic lymphocytic leukemia (CLL) a week before her 39th birthday. She initially attributed her symptoms—extreme fatigue, night sweats, and persistent lumps on her neck—to the demands of her job during the pandemic or possibly pre-menopause. After a series of misdiagnoses, including post-COVID fatigue and infections, Nicole’s OB/GYN referred her to an ENT, triggering a series of tests that led to her leukemia diagnosis.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Despite the emotional and logistical challenges, Nicole adopted a pragmatic approach, focusing on understanding her disease and navigating her treatment plan. Nicole underwent an initial six-month treatment with a BCL-2 inhibitor and monoclonal antibody. While the therapy brought her into remission temporarily, symptoms such as night sweats and fatigue resurfaced, prompting renewed treatment of the BCL-2 inhibitor.
Financial struggles and logistical hurdles with insurance and medication access compounded the difficulties of her chronic lymphocytic leukemia diagnosis. However, Nicole relied on support from family, friends, and her children, alongside advocacy and connection with others facing similar challenges, to maintain her resolve.
Throughout her experience, Nicole emphasized the importance of self-advocacy, understanding her diagnosis, and not comparing her circumstances to others. Her coping mechanisms included leveraging social media to share her experiences, seeking guidance from a CLL specialist, and shifting her perspective on life to prioritize meaningful moments with her children. Nicole’s ultimate hope is for greater awareness and resources for CLL and blood cancers, and encourages others facing similar situations to advocate for themselves, seek help, and live in the moment.
Name: Nicole B.
Age at Diagnosis:
38
Diagnosis:
Chronic Lymphocytic Leukemia
Symptoms:
Extreme fatigue
Night sweats
Lumps on neck
Rash
Shortness of breath
Treatments:
BCL-2 inhibitor
Monoclonal antibody
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
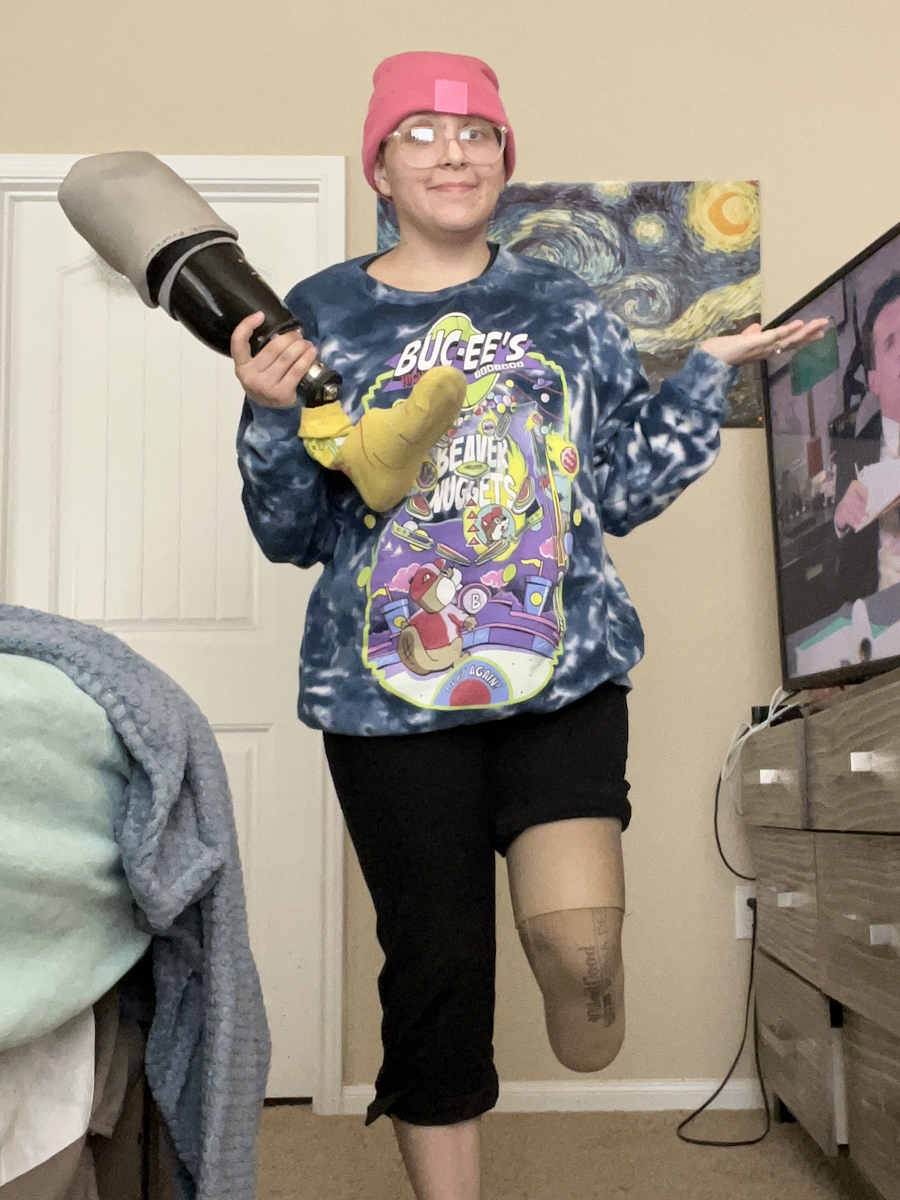
Marisa shares her experience living with stage 4 synovial sarcoma. Diagnosed initially with stage 3 in 2017, Marisa’s symptoms began in high school when she noticed a small bump on her foot. Despite consultations with podiatrists over the years, the bump was misdiagnosed as a benign cyst until after its removal in 2017. By that time, the lump had grown significantly during her pregnancy. The devastating cancer diagnosis came when her daughter was six weeks old, marking a life-changing moment.
Marisa’s treatment included chemotherapy, a below-knee amputation in 2017, and multiple surgeries for lung metastases, starting in 2020. She underwent four pulmonary wedge resections, a segmentectomy, and later, radiation therapy to target residual cancer. Unfortunately, the cancer became more aggressive, spreading to her bones and lungs by early 2023. Despite numerous treatments, including 27 lung radiation sessions and systemic chemotherapy, Marisa remains optimistic and continues to monitor her health closely.
Mentally and emotionally, the impact of cancer has been profound. Marisa finds it challenging to balance parenting, work, and being a stage 4 cancer patient. She’s candid about the toll it takes on her and her family, especially explaining her illness to her young daughter. However, Marisa has chosen to focus on small joys—mundane daily tasks and moments with loved ones that now hold deeper meaning.
Marisa emphasizes the importance of self-advocacy in health care, urging others to trust their instincts and pursue answers when something feels wrong. She shares her story to provide hope to others battling sarcoma or cancer. She aims to raise awareness about the disease and inspire others with her determination to live fully, even while managing ongoing health challenges. Her message is clear: life with stage 4 cancer is not the end—it’s an opportunity to cherish each moment and look forward to advancements in medical science.
Name: Marisa C.
Age at Diagnosis:
24
Diagnosis:
Synovial Sarcoma
Staging:
stage 3 (2017)
Stage 4 (2021)
Symptom:
A small bump on the foot (stable for years, then grew during pregnancy), pain when pressed, difficulty wearing closed shoes
Treatments:
Surgeries: below-knee amputation, pulmonary wedge resections, and segmentectomy
Chemotherapy
Radiation: lungs and hip
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: Pain behind left knee, needle-like sensation in left foot Treatments: Surgery to remove what was thought to be benign tumor, chemotherapy, final surgery, radiation (36 sessions) ...
Bella, an Australian living in the UK, shares her experience with malignant paraganglioma, diagnosed after years of medical gaslighting and misdiagnoses. Her symptoms began when she was 15 with severe vomiting, chronic cough, dizziness, a neck lump, and extreme weight loss. Misdiagnosed with anorexia and bulimia, she endured invasive and ineffective treatments for years. Her condition deteriorated until a general physician recognized the seriousness of her symptoms, leading to an ultrasound and eventual diagnosis of a paraganglioma.
Surgery to remove a large neck tumor was extensive, lasting eight hours, and left Bella with stroke-like symptoms, paralysis on one side of her face, and difficulties swallowing and speaking. Subsequent testing revealed the tumor was malignant and had spread. Bella underwent six weeks of intensive radiotherapy, during which she suffered severe pain, hearing loss, and isolation.
Her treatment revealed a genetic mutation in her family that predisposes them to certain cancers. Although she has faced recurring health scares and complications over the years, Bella has worked to rebuild her life. Struggling with identity and mental health post-treatment, she initially turned to partying as a coping mechanism. The COVID-19 lockdown, however, marked a turning point, leading her to seek deeper healing through community support. Bella found solace and strength in a women’s cancer survivor group, which helped her realize the importance of connection in healing.
Now, Bella emphasizes the power of community and advocates for understanding that the challenges of cancer extend far beyond treatment. She encourages others to find support networks and validates the emotional toll of living with and recovering from cancer.
Name: Bella J.
Age at Diagnosis:
19-20
Diagnosis:
Malignant Paraganglioma
Symptoms:
Severe vomiting
Chronic cough
Dizziness
Swelling in the neck
Low heart rate
Extreme weight loss
Hair loss
Dental issues
Vocal strain
Persistent pain and exhaustion
Treatments:
Surgeries: approximately 15 procedures, including an eight-hour tumor removal
Radiotherapy
Physical therapy: for arm mobility and swallowing techniques
TW // Suicidal ideation
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Kristin was diagnosed with stage 3A melanoma in April 2008 at the age of 38. Her diagnosis came unexpectedly during her attempts to conceive. While recovering from a fertility procedure, she noticed a change in a lifelong mole on her leg. Prompted by her family history of basal cell carcinoma and her dermatologist’s biopsy, she was diagnosed within days.
Kristin underwent extensive treatments, including two surgeries to remove the melanoma and affected lymph nodes, followed by a challenging year of interferon therapy, which left her with flu-like symptoms and required regular interruptions due to blood count drops. Despite the physical and emotional toll, she worked throughout her treatment and planned a celebratory trip to Alaska once her therapy concluded.
The stage 3A melanoma diagnosis had profound effects on Kristin’s personal life. Her inability to continue trying for children led to a period of depression, but she eventually found emotional resilience through activities like skydiving and advocacy. She began raising awareness about melanoma prevention and promoting the importance of early detection.
Kristin also navigated the complexities of being a caregiver when her mother battled cancer. This experience deepened her understanding of the patient-caregiver dynamic and strengthened her resolve to advocate for improved support and research in oncology.
Sixteen years after her stage 3A melanoma diagnosis, Kristin continues to educate and inspire others, emphasizing melanoma’s preventability and the importance of self-advocacy in healthcare. Her story underscores the critical role of research, the availability of modern treatments, and the emotional challenges survivors face while redefining their purpose.
Name: Kristin M.
Age at Diagnosis:
38
Diagnosis:
Melanoma
Staging:
Stage 3A
Symptom:
Change in color and border of a mole on her leg
Treatments:
Surgeries: melanoma and lymph node removal
Immunomodulator: interferon
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Building Bonds Episode 2: How to Find and Partner with a Doctor for Better Waldenström Care
Finding a doctor is important in your Waldenström macroglobulinemia care. A strong partnership leads to more informed decisions, personalized care, and a greater sense of control. Patient advocate Pete DeNardis, hematologist-oncologist Dr. Jonas Paludo from Mayo Clinic, and patient advocate Lisa Ramirez discuss how her decisions led to being treated by Dr. Paludo and forming a trusted patient-doctor relationship.
Edited by: Katrina Villareal
Discover the importance of second opinions and how even top specialists recommend them. Understand how a Waldenström macroglobulinemia specialist can provide a unique perspective having seen more cases. Learn about shared decision-making in Waldenström treatment. Hear first-hand experiences of navigating a chronic cancer with your doctor by your side. Get practical tips for advocating for yourself or a loved one in the treatment process.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Tiffany Drummond: I’m a patient advocate with over 20 years of experience in cancer research. My journey as a care partner began when my mother was diagnosed with endometrial cancer in 2014. I quickly realized the challenges of finding reliable information to support her care, so I am committed to helping others avoid similar difficulties.
At The Patient Story, we create programs to help you figure out what’s next. Think of us as your go-to guide for navigating the cancer journey. From diagnosis to treatment, we’ve got you covered with real-life patient stories and educational programs with subject matter experts. I’m your personal cheerleader, here to help you and your loved ones best communicate with your healthcare team as you go from diagnosis through treatment and survivorship.
We want to give a big thank you to The Leukemia & Lymphoma Society for its partnership. The LLS offers incredible free resources, like their Information Specialists who help you communicate with members of your healthcare team and provide information about treatment options.
The Patient Story retains full editorial control over all content. While we hope you find this helpful, please keep in mind that the information provided in this program is not a substitute for medical advice. Pete, a patient advocate and Waldenström’s survivor, will lead the conversation.
Peter DeNardis, IWMF Chair Emeritus
Peter DeNardis: I’m currently the chair emeritus of the International Waldenström’s Macroglobulinemia Foundation. I have been a long-time volunteer for the organization and a patient myself. I was diagnosed 20 years ago and I’m well aware of the importance of a strong patient-doctor relationship. I look forward to learning from our esteemed panelists about how best to build and maintain that relationship.
With us is Dr. Jonas Paludo, a hematologist-oncologist and assistant professor of medicine and oncology at Mayo Clinic in Rochester, Minnesota. His research interests include studies to understand the biology, genetics, and therapy of lymphoma and plasma cell disorders, and he is also a noted researcher in Waldenström’s.
Lisa Ramirez, Patient Advocate
Lisa Ramirez: I was diagnosed in 2021. I was getting into a doctoral program and had to do some routine testing and physical exams, and in the process, I was diagnosed with Waldenström’s macroglobulinemia. The diagnosing oncologist was retiring, so he passed me on to another doctor in his practice.
I did a lot of research on Waldenström’s immediately and read Dr. Gertz’s recommendation on getting a second opinion, which I appreciated. I looked for the doctor who I thought would be best in getting a second opinion from and that was Dr. Paludo since he specialized in Waldenström’s in young people. I got another opinion from a physician at a major cancer center in the state in which I live as well.
I had a great rapport with Dr. Paludo immediately, but I initially thought I would only see him for a second opinion since I lived in Texas and he was at Mayo Clinic. I made it work and secured Dr. Paludo as my primary oncologist. I was very pleased about that.
Proactively Participating in Your Care
Peter: It’s good that you immediately did research and also went for a second opinion. Is it appropriate to say that you were an involved patient from the start?
Lisa: Yes. I work in public health. I’m a natural researcher and a very curious person. I wanted to learn as much as I possibly could and as quickly as I could about Waldenström’s to plan out my course of treatment and to be a well-informed patient.
I listened to all the lectures I could get my hands on and tried to understand the philosophies of the different cancer institutes. They seem to have differing philosophies about treatment and I tried to find one that fit with my personal philosophy and how I wanted to approach treatment.
I wanted to learn as much as I possibly could and as quickly as I could about Waldenström’s to plan out my course of treatment and to be a well-informed patient.
Lisa Ramirez
Signs and Symptoms
Peter: Looking back, do you think you had any symptoms that you weren’t paying attention to at the time?
Lisa: I was having night sweats, but I didn’t I thought I was experiencing early pre-menopause symptoms. Now I know the difference between hot flashes and night sweats. There’s a big difference.
I had some testing done because of other reasons and there was a note to rule out lymphoma and to check in six months after. Right at the six-month mark, my primary physician had me see a hematologist because of those test results. I had zero symptoms then. I felt great.
Looking back, I had some input from other oncologists that perhaps I had the disease for so long that I thought I felt good. That small incremental change in a negative way can go unnoticed, but I thought, “Does it matter? If I believe I feel good, then I feel good.”
Insurance Concerns
Lisa: The average time between diagnosis and treatment is about two and a half years and that’s about how long it took for me, so I was right on pace with the average.
Peter: You got a second opinion in a different state. You live in Texas while Mayo Clinic is in Minnesota. Did you have any financial or insurance issues trying to see Dr. Paludo?
Lisa: Surprisingly not. I received some treatment in another city in Texas. When you break down the costs, that treatment was more expensive.
Different institutions have different priorities in terms of testing and the amount of testing at checkups. In my case, the cost of the additional testing outweighed the cost of travel to Minnesota. It ended up being more cost-effective and worth it to travel to receive treatment at Mayo Clinic.
Peter: You’re very fortunate in that regard. I’m glad that worked out for you. You’re under great care and it appears that right from the start, you’re a very involved, proactive patient, so I applaud you for that and hope that other patients can take your lead.
WM at a Glance
Peter: Dr. Paludo, many of us patients have a general idea of what Waldenström’s macroglobulinemia is, but can you give a 30,000-foot view explanation of what the disease is?
Dr. Jonas Paludo: Waldenström’s is a rare type of blood cancer. It’s a form of an indolent or slow-growing subtype of a B-cell non-Hodgkin’s lymphoma. It’s a disease that has some overlapping features between lymphoma and myeloma, but it’s a type of blood cancer.
Common WM Questions
Peter: You see patients either coming initially to see you or for a second opinion. They probably have similar questions, but in your experience, what are the more common questions that patients ask?
Dr. Paludo: I can group the most common questions into three specific categories. In one shape or another, they’re trying to understand: What is Waldenström’s? What is this disease? Then the next one is: what do we do about this? Do we have to do anything about it right now? What it will look like? And then the third one is: what is my prognosis? What can I expect out of this disease?
Peter: Those questions are pretty common for Lisa and me when we were first diagnosed, so it’s good to see those questions are still being asked.
Diagnostic parameters, treatment options, follow-up testing, and surveillance are not as well-established in rare diseases as they are in more common diseases.
Dr. Jonas Paludo
Getting a Second Opinion
Peter: Many in the medical community and even the IWMF itself encourage patients to get a second opinion in certain circumstances. Dr. Paludo, as a healthcare provider, what are your thoughts on patients getting second opinions?
Dr. Paludo: Waldenström’s is a rare disease and like any rare disease, a second opinion should always be considered. Diagnostic parameters, treatment options, follow-up testing, and surveillance are not as well-established in rare diseases as they are in more common diseases or more common forms of cancer, like breast cancer or colon cancer, for example. That’s where a second opinion can help.
In addition, the familiarity of physicians with the disease or the current evidence and data of the disease can be quite variable. It’s part of reality. We can’t keep up with all the information generated daily for all diseases. Getting a second opinion from someone who has more experience or more interest in that specific type of rare disease is very important and adds a lot to the treatment and management.
I always encourage second opinions. To be honest, with most patients I see with Waldenström’s, I’m the one giving the second opinion. But for the patients who we see that are local, I encourage asking for another opinion elsewhere to have different points of view. I don’t think a second opinion would ever hurt a patient. It can only add information and help with the treatment and plan.
Peter: That’s a good point and hopefully they’re not trying to juggle three different opinions. In Lisa’s case, it was the one that she felt more comfortable with, which is appropriate.
Dr. Paludo: That’s a potential downside, but the benefits of a second opinion outweigh that downside.
Lisa: Waldenström’s is so different in terms of it being a cancer because you want to time treatment perfectly and take into account your quality of life. With a lot of other cancers, there’s a rush to treat and there are very specific treatment regimens. With Waldenström’s, you’re playing a very long game of chess.
You want your partner to be someone who you trust and who understands your quality of life and your age as you’re moving along the course of treatment. You’re going to want someone who understands you well enough, to keep pace, and who has a similar philosophy and approach to treatment. With Waldenström’s in particular compared to other cancers or other diseases, it’s important when selecting an oncologist that there’s a good fit.
Different cancer centers can appeal to different types of people. Mayo Clinic and Dr. Paludo were the perfect fit for me.
Dr. Jonas Paludo
Knowing Your Options
Peter: How did you know where to go for a second opinion? You mentioned Dr. Gertz’s presentation, but how did you figure out what your options were?
Lisa: The resources from the IWMF immediately pointing to Dr. Gertz and understanding Mayo Clinic’s philosophy led me there and looking into physicians there. I found Dr. Paludo in relation to Waldenström’s and other aspects of Waldenström’s that were of particular interest to me. I immediately sought him out for a second opinion.
I seem to resonate more with the philosophy of Mayo Clinic. They seem to have an approach that is slower to overreact. Their approach feels more strength-based rather than fear-based and I respond to that. When I need to embark on an intimidating treatment like chemotherapy, I want my partner to be able to reassure me that I’m strong enough, that I’ve prepared enough, and that it is the right time.
I understand that people have different motivations for starting treatment and some people can be more motivated by fear-based approaches. I don’t respond well to that. I respond better to a strength-based approach and the reassurance that all my questions are answered and that there’s enough time spent understanding the procedure or what’s happening with the progress of the disease. I find direct information very reassuring.
I have had oncologists who took a different approach where they feel nervous about my condition and then I start to feel very nervous and anxious. I know that it’s best to time treatments correctly and wait a little bit longer. It’s a fine line. Different cancer centers can appeal to different types of people. Mayo Clinic and Dr. Paludo were the perfect fit for me.
Finding a WM Specialist
Peter: Dr. Paludo, you mentioned that some patients come to you initially while others come for second opinions. If you’re telling a patient to get a second opinion, where do you direct them to? And for the patients who come to you initially, how did they find out about you in the first place?
Dr. Paludo: I also rely a lot on the IWMF resources to help patients decide on where to go next. There are so many factors, like insurance coverage and cost of travel, that are so particular to each patient, so I try not to be very specific. I point them to resources that they can look at to see which one makes more sense based on insurance, cost, travel, timing, family members, where they are, and things like that.
As with most rare diseases, you find more experience in bigger centers because they tend to see more patients with their rare diseases. It doesn’t necessarily mean that’s the only place you can find experience and expertise. It’s just the more common place where you can find expertise for rare diseases. The IWMF helps with pinpointing areas with more expertise or experience with Waldenström’s than other sites.
Peter: Because of my involvement with the IWMF, I’m well aware of the services they provide. On their website, they have a list of top doctors to go to for a second opinion regardless of what part of the world you’re in. The IWMF also has online discussion groups and Facebook groups where you can ask other patients who they go to. Granted, that’s word of mouth from one patient to another, but you can form an idea of who are the more noted doctors and who you could see if you want a second opinion.
The biggest challenge that I see is often related to indications to start treatment… sometimes it’s better if we don’t jump into treatment and instead sit tight and watch very closely.
Dr. Jonas Paludo
Building Bonds Ep. 2: How to Find and Partner with a Doctor for Better Waldenström Care
Hosted by The Patient Story
Finding a match is important in your Waldenström care. A strong partnership leads to more informed decisions, personalized care, and a greater sense of control. Join host and patient advocate Pete DeNardis, Dr. Jonas Paludo from Mayo Clinic, and patient advocate Lisa Ramirez as she discusses how her decisions led to being treated by Dr. Paludo and forming a trusted patient-doctor relationship.
Peter: Dr. Paludo, what do you see that some healthcare professionals don’t get right about a WM patient?
Dr. Paludo: Waldenström is such a unique disease that the biggest challenge that I see is often related to indications to start treatment. Because of the uniqueness of this disease with overlapping features with other indolent lymphomas, sometimes I see more of a generalization of what we do for similar diseases applied to Waldenström’s. I understand where they’re coming from, but it doesn’t always fit with our best practices for Waldenström’s.
They haven’t seen a lot of cases and sometimes it can be difficult for a provider to sit tight on a patient who has a very high IgM level and hold off on doing something. It’s often easier to do something, but sometimes it’s better if we don’t jump into treatment and instead sit tight and watch very closely when patients are asymptomatic or not having significant symptoms.
Peter: I hesitate to say this, but back when I was first diagnosed, there was something called the 10,000 IgM Club. There were a handful of patients who felt that they were okay and feel fine. Their IgM level is 10,000, but their symptoms are fine. In hindsight, that may have not been, but every patient is different. You’re exactly right. It depends on a patient’s symptoms and how they’re feeling along with the blood values. It’s critical to go to a specialist if you can.
I’m Newly Diagnosed. What Now?
Peter: Let’s turn to the important role of the doctor-patient relationship in managing your disease course, both short- and long-term, especially about WM. It’s considered incurable, but with the more novel agents that have come around in the last 5 or 10 years, it’s much more treatable.
Lisa, you mentioned your path to getting a second opinion. What advice would you give to a newly-diagnosed patient who’s looking for care and what do you think is most important?
Lisa: What we’re talking about here is building rapport. You have to be able to trust your oncologist 100%. There are some scary moments and you question yourself. You want to have the reassurance of an oncologist who has expertise in this area, understands you, and has a sense of how uniquely your disease is manifesting.
Every WM patient is a little bit different, so find a physician who you can trust and sees you. Sometimes that’s not something tangible. It’s what occurs during a conversation and a sense that you feel shared insights or philosophies. During my visits with Dr. Paludo, he would ask, “And what else?” I loved that he always left room for all of my questions and he was always very direct with me.
You want to have the reassurance of an oncologist who has expertise in this area, understands you, and has a sense of how uniquely your disease is manifesting.
Lisa Ramirez
Do your research. Understand what it is that you want in terms of your quality of life and what’s important to you.For example, I was going to start treatment under the care of a different oncologist, which would have put at risk my ability to dance ballet on my toes because there was a higher risk of peripheral neuropathy with that particular treatment. At my age, I thought the first treatment I should do perhaps shouldn’t be that one. I was able to have that conversation with Dr. Paludo and talk about things that are important to me.
Oncologists see a lot of different patients and their priority is to save your life and get you treated, which is understandable, but it’s a little bit different with WM. My quality of life includes being able to dance on my toes, so losing feeling in my toes was a big deal. It would have negatively impacted my quality of life had I started with that particular treatment if I had the unfortunate side effect of being unable to feel my toes.
Find an oncologist who understands who you are as an individual, what your quality of life is based upon, what’s important to you, who you feel comfortable sticking with throughout your life, and who will map out a course of treatment that’s going to work for you. One time, Dr. Paludo said, “You’re probably going to have to do all the treatments. We just have to figure out what works for you when.” Everyone’s different, so that’s important.
Deciding to Stay Local or Travel for Your Care
Peter: You have a good rapport with Dr. Paludo. Do you still see a local oncologist in Texas?
Lisa: No, I see Dr. Paludo exclusively. I was already scheduled for treatment somewhere else, but I got cold feet at the last second. The first step in treatment is so critical. It impacts the next move and the next move and the next move. Even though those moves are spaced out—hopefully many years apart—it still sends off a ripple effect.
You want to feel very comfortable with your provider and the institution you’re receiving care from is critical. I had to advocate for myself and say, “I know it doesn’t make sense to seek treatment in a different state and to get my primary care from an oncologist so far away, but we’re going to Minnesota.”
How Often Do You See WM Patients?
Peter: Dr. Paludo, Mayo Clinic is a world-renowned medical institution, but, hopefully, many people with Waldenström’s also understand that it’s world-renowned for Waldenström’s macroglobulinemia. Out of curiosity, can you say how many patients you maybe see a day or in a week that have Waldenström’s?
Dr. Paludo: It’s variable these days, but I estimate about two to three patients a week with Waldenström’s and sometimes as many as five patients a day. We looked at this a few years back and to give some context, if you were to consider all practicing doctors in the US and all newly-diagnosed Waldenström’s patients in a year, each doctor will see a new case of Waldenström’s once every eight years. This gives you a sense of how rare diseases are very, very difficult to come across.
I want the patient to feel empowered that they can ask any question, no matter what it is, and bring up any concerns or fears that are important to them.
Dr. Jonas Paludo
Approaches to Personalized Care
Peter: You and Lisa have a very good doctor-patient relationship. In your experience, does each patient approach you differently? Do you have a different approach depending on what kind of interaction you have or what works best for that patient?
Dr. Paludo: My approach is different for each patient. The things that we always try to discuss and focus on are the main concerns that each patient brings to the visit, which can be different. If someone was recently diagnosed with Waldenström’s versus someone who’s reviewing, studying, researching, and now we’re talking about treatment, there would be some differences in how I approach each patient.
Managing Your Life with WM
Peter: Given that Waldenström’s is becoming more of a manageable disease, what is your guidance to patients when they first come to you as far as dealing with having a disease like ours? You have periods of requiring active treatment and periods of watching and waiting for the next shoe to drop, in a sense.
Dr. Paludo: It depends on the situation, but I’m always trying to discuss the key concepts related to Waldenström’s. We talk about follow-ups and treatment indications. I like to address that because they’re important for the patient, especially if they’re not coming to Mayo for their care.
At the end of the day, we always try to establish trust and an open space. I want the patient to feel empowered that they can ask any question, no matter what it is, and bring up any concerns or fears that are important to them. It’s difficult to do everything in one visit, although we do try, but sometimes we need several visits to discuss all of these.
Peter: That’s very commendable. That should be the model for all clinicians. Unfortunately, a lot of them are pressed for time or dealing with a large patient load, so they don’t make the extra effort, and you should be applauded for doing that.
WM Treatment Options
Peter: Lisa, you had some choices to make concerning treatment. Were you aware of the treatment options before you spoke to Dr. Paludo?
Lisa: Yes. The second oncologist I saw was supposed to be my first treatment opinion. When I started talking to her about the treatments, she said, “Gosh, you sure do know a lot about this. What do you think?” I didn’t get the first opinion that I was hoping for because I had done so much research that the oncologist felt that maybe I had a better sense of what treatment I should start with, which ultimately led me to a second opinion with Dr. Paludo.
I have done a lot of research, which I enjoy doing. It’s not a situation you want to be in, but I work in public health and public health strategy, so I enjoy strategy and research. I wanted to find out as much as I could about the treatment options. From the scientific papers, it’s not always clear. Actual patient experiences are something that’s missed in very scientific journal articles, which can only be shared through patient-to-patient experiences.
With Waldenström’s, that can be additionally challenging because we are each so unique. It’s a full-body disease that manifests differently. The symptoms are different from person to person. There are also fewer females with the disease and fewer people my age, so it can become more difficult to know exactly what to expect even though you do a lot of research.
What reduced my anxiety was talking to Dr. Paludo about being vulnerable about parts of the treatment that I thought were most concerning.
Lisa Ramirez
The Emotional Impact of a WM Diagnosis
Peter: You did a lot of research, but how were you dealing with it emotionally? How did it affect you when you were first diagnosed and how did you deal with the enormity of it?
Lisa: When I was first diagnosed, I was shocked. I knew I couldn’t have the conversation with my daughter that day, so she had a sleepover that night.
After that, I felt somewhat calm about it, even though I do have a history of anxiety disorder. I knew going into treatment that my outcomes would be better if my anxiety was reduced. Stress plays a huge role in your physical health in general, but especially as you undergo something as stressful as chemotherapy where you have a lot on the line.
I made sure to take care of my mental health through exercise and seeing a therapist weekly. What reduced my anxiety was talking to Dr. Paludo about being vulnerable about parts of the treatment that I thought were most concerning. I was able to talk in-depth about how I was concerned about a recurrence of my anxiety and eating disorders in the course of treatment.
Dr. Paludo was able to reassure me that, at any point in time, if I was having concerning symptoms, we could talk about it, but most of all, we could always stop treatment and take a different course of action. That option was never presented to me before by any of the oncologists I had seen. Having that way out and knowing that I had that autonomy was so reassuring and helped me get through a lot of rough times throughout treatment.
I had a pretty good treatment experience. It wasn’t always easy, but it was a lot easier knowing that I had the support of my oncologist to pivot, redirect, and find a different course of treatment that worked better for me. My quality of life was most important to both of us.
Peter: Thatfocus on quality of life is critical. Every patient’s different, both physically and mentally, and it’s important to treat both aspects of how a patient approaches their disease.
Important Takeaways from Initial Consultation
Peter: Dr. Paludo, when you see a patient, what do you want patients and care partners to take away from that initial visit with you? What do you want them to understand?
Dr. Paludo: One of my priorities is to have patients understand that treatment for Waldenström’s is not a sprint but a marathon. It’s a long-term process that involves long-term planning, and we have to consider all short- and long-term strategies for treatment.
I usually say that when you’re getting treatment, you’re not in a long-term commitment. You can always stop and find a different option. I also like to discuss, usually in broad terms, that what we have today for treatment options has an overall similar efficacy. They are different in potential side effects, logistics, duration, and frequency. That often allows patients to focus on the implications of the treatment on their quality of life and their goals.
Once we remove the efficacy piece from the discussion, we can talk more about side effects and logistics. We can focus on how the treatment can help patients achieve what they want at the end of the day, which is improved quality of life, and accomplish what’s important to them. Those are things that I always like patients to take away from those initial discussions about treatment options before even we decide on which treatment to go next.
Lifestyle Changes in the Face of a WM Diagnosis
Peter: Lisa, you wanted to make sure you had a good quality of life. After you were diagnosed and started treatment, did you do anything different? Did you make lifestyle changes to help you emotionally and physically?
Lisa: Absolutely. Dr. Gertz said that frailty is the enemy, so I immediately got a personal trainer and hit the gym. People train for marathons. This is the rest of my life. I don’t want chemotherapy to knock me down. I need to be as fit as possible.
I also participated in an educational session on nutrition through The Leukemia & Lymphoma Society and met with a nutritionist. I changed my diet to reflect some of the recommendations based on those talks. I’m eating more of a plant-based diet and building up my strength as I approached treatment knowing that treatment was inevitable.
I saw a therapist weekly, which ultimately helped. During chemotherapy, I didn’t miss any work. I remained very active. I was still able to dance. I wasn’t allowed to skateboard anymore, but I was still exercising as much as I could to fight the fatigue and it paid off. That makes a big difference in terms of how one feels during the course of treatment and your ability to be resilient and make good progress in treatment.
Peter: I agree completely. It’s important to move. A lot of patients say that their treatment has debilitated them, but I tell them to try to move a couple of feet and take a couple of steps a day and build on it. It does make a difference.
Maximizing Your Quality of Life
Peter: Dr. Paludo, do you have any follow-up advice for Waldenström’s patients on how to deal with quality of life issues? Can they continue to live like they did before they had WM?
Dr. Paludo: Absolutely. It’s always difficult to cope with a new diagnosis of any cancer, including Waldenström’s. Every patient is a little different on how they try to cope. I try to understand what’s important for each patient and focus on what we can do to control what we can.
With Lisa, dancing was very important. We couldn’t control when treatment was needed, but we could control that she could continue to dance. It would be a form of exercise that helps her cope and keep some form of normalcy. Life can be disrupted with diagnosis and treatment, so trying to keep as much of a normal life as possible after diagnosis or when you’re going into treatment is very important. As you go through the watch and wait period with Waldenström’s before treatment or in between treatments, it’s very possible to live life like before as much as possible.
I’m not a mental health expert, so I also look for help. I refer my patients to cancer therapists and psychologists. The team we have at Mayo Clinic helps. I play within my limitations and always look for help from others who know more than I do about topics that are very important for every patient.
Patient Advocacy
Peter: Lisa, you’ve advocated for yourself right from the start. What would your advice be to newly-diagnosed patients or even those who are even in remission?
Lisa: For newly-diagnosed patients, get connected with IWMF. I was so impressed with the resources available for such a rare disease. It’s honestly very impressive how well IWMF is organized.
If you’re a young person or under 50, it can be more challenging because it’s almost a different disease. When you have young kids at home, there are a lot of different things to consider. Getting connected with the IWMF support group for young people was helpful. Find support with people in your community.
Watch lectures and read all the resources available sooner rather than later. You have some time to figure everything out. If you’re newly diagnosed and you don’t have symptoms that require immediate treatment, you have time to research.
It’s necessary, I would say also, to look at the different cancer institutes that have different philosophies. When you’re listening to lectures from different experts, find who resonates with you and what makes sense to you. Who do you seem to align with in terms of what feels right for you and what you value?
Take time to consider all that’s important to you so that you can locate the physician and your team that you’re hopefully going to be with for the rest of your life, working on achieving a good quality of life while living with this disease. Take in all the information, talk to your support network, and connect.
At first, I thought that having Dr. Paludo as my primary oncologist was not possible, but you may be surprised at what is possible so have hope and advocate for yourself.
It’s great to have an external brain to help process the information and to reflect back to you.
Lisa Ramirez
The Role of Care Partners
Peter: You approach each appointment with knowledge beforehand, you do your research, and you advocate for yourself. Do you go to your appointments on your own or do you take a care partner with you? You read that someone should always have someone else with them because they can mishear something. How do you manage that?
Lisa: I have a great partner and support. You’re absolutely right. Sometimes it can be overwhelming. When I would go to appointments with a different provider, I’d walk out sweating and notice I was so nervous during the appointment. Having someone there can be helpful. When I went to treatment, my partner would go with me. One time, my sister went with me.
Sometimes, you get disappointing news. I oddly got disappointed that I couldn’t do chemo a couple of times and I got upset and emotional, so to have someone to provide emotional support is helpful. It’s much better to not have to do it alone.
But if you are alone, there are people who are there to support you. At Mayo Clinic, there’s a whole team. Everybody there is supportive, so you can do it alone. It’s great to have an external brain to help process the information and to reflect back to you. Maybe you didn’t even notice that you weren’t feeling comfortable with a certain provider. It’s helpful to have someone to bounce off, so it’s important to have someone with you.
Peter: Dr. Paludo, what’s your advice in that regard? Do most patients come with someone to the appointment? And do you suggest it to patients if they don’t?
Dr. Paludo: Most patients come to their appointments with someone else. That’s very helpful and very important, if possible, of course. It’s difficult to take people away from their normal day-to-day lives, but it helps to have someone else also listening. We usually don’t remember everything that is discussed. Each person may remember different parts of the discussion. It helps, so I encourage that if possible.
Living with WM
Peter: Lisa, you’ve been living with Waldenström’s for a few years now. How do you not let Waldenström’s consume your everyday life? What’s your approach to living with it?
Lisa: In the beginning, it was difficult to not let it consume my life. For me, planning out a theoretical course of treatment to last my whole life was helpful. What helped was having that plan in place and also having a plan when I didn’t have symptoms or symptoms that I thought were bothersome to me.
Having those things mapped out in advance allows me to trust the plan and not have to think about it in my daily life. Once those decisions are made for the future, I can always change my mind at any point, but to have that mapped out for myself allows me to forget that I have Waldenström’s and live my life. It might take a minute to get there.
At first, it’s consuming. You’re consumed with the research. Don’t overreact. Take your time. Talk with your oncologist about a plan, put a plan in place, and then put it aside and live your life. Ultimately, treatment is all about having a good quality of life and living your life normally. You want to be able to do that and not add any additional stress to yourself. Putting a plan in place, putting it aside, and referring back to it when you need to is important.
Talk with your oncologist about a plan, put a plan in place, and then put it aside and live your life. Ultimately, treatment is all about having a good quality of life and living your life normally.
Lisa Ramirez
Waldenström: The Patient-Physician Relationship
Peter: Right from the start, you had a good relationship with Dr. Paludo. How has that evolved over the past few years? Is it different now than it was initially?
Lisa: Dr. Paludo has been very consistent. Initially, I met with him before I even met with who I thought was going to be my primary oncologist. I walked away from that conversation saying, “Gosh, I met the right oncologist for me. Too bad. I can’t possibly get treatment in Minnesota.”
It felt like a good fit from the beginning and we’ve built upon that trust. I instantly felt comfortable and felt trust. He engaged with me in a way that was strength-based and not over reactive. He’s very steady. Our relationship hasn’t changed much other than we’ve been through this treatment together and there’s a deepening of trust.
I’ve talked about my next treatment episode with my partner and when I have to do the weekly treatment, we’re going to live in Minnesota for six months. There’s no question about that. I know Dr. Paludo’s there for me and he’s my oncologist until the end, so I feel very comfortable with that.
Key Takeaways
Peter: Dr. Paludo, do you have any key takeaways for patients or healthcare providers in building and sustaining a strong relationship through the cancer journey?
Dr. Paludo: Advocate for yourself. Go after what you think is important for you. Lisa and I are on the same page. For the healthcare providers, what’s very important is to actively listen to each patient’s priorities. Listen and not just hear. Pay attention and focus on what’s important for each patient, like their main concerns and fears.
As providers, we have to be frank and honest with the limitations of what we know and what we don’t know about Waldenström’s. There are a lot of things that we know now that we didn’t know before, but there are a lot of questions that we can’t answer yet. Being honest with our limitations, paying attention, and focusing on what is important to the patient help build that trust, which is important in a relationship. We’re all going together through good and not-so-good moments in this long journey of Waldenström’s.
Being honest with our limitations, paying attention, and focusing on what is important to the patient help build that trust, which is important in a relationship.
Dr. Jonas Paludo
Peter: It’s good to see you’re both in agreement. You’re both following the proper path and I applaud both of you, especially for taking the time to share your experience with healthcare providers and patients.
Lisa mentioned that she first did a good bit of research through the IWMF website. I did that myself 20 years ago. I was a youngster back then and the services and support they provided meant so much to me that I started volunteering for the organization and I’ve been with them since then.
Waldenström’s is a rare disease, so you don’t encounter many people who have it, so finding an online community was of great benefit. Sharing stories with them, joining support groups, taking part in discussions, viewing webinars, and going to their annual educational forum are key components of becoming a more knowledgeable patient.
Before we had the technology, I would have my own chart that I would give to my doctor and say, “Here are my trends.” He would laugh at me, but he would look at it. We had a great relationship and that’s important to have. Be educated about your disease, know your options, what your preferred lifestyle, and what you want in quality of life, and pick a doctor who fits well.
Lisa: My therapist thinks Dr. Paludo is great.She’s convinced he took some classes in psychotherapy. She’s got great admiration for him. I’m also trained as a therapist and I would say Dr. Paludo has those skills, but please don’t leave the work you’re doing to be a therapist, although you’d be a great one.
Mayo Clinic is huge and yet after every visit, I would think, “How is it possible that each person on my care team was able to spend that much time with me?” I’ve never encountered that anywhere else. How is it that nurses remember me? People remember me. We had little inside jokes. Those things matter so much.
Our healthcare environment is changing. There’s limited time with patients. We’re speaking to healthcare institutions and I don’t know how providers get reimbursed and what expectations are in general.
Physicians want to have these kinds of relationships with their patients and perhaps there’s a larger pressure that prevents them from doing so. I hope that we can get back to that. Institutions like Mayo Clinic and physicians like Dr. Paludo give me the hope that it’s possible to have those kinds of relationships with patients in the current healthcare environment somehow.
Dr. Paludo: I don’t think I can say it better. It’s important to keep in mind what the priority is, which is the patient and what matters to that patient. Always keeping that in mind is the goal at the end of the day.
Conclusion
Peter: I enjoyed this discussion. It’s always good to meet with a fellow WMer and a noted, world-renowned Waldenström’s clinician and researcher. I’m very grateful for both of you for sharing your time. I hope others find this information very useful and beneficial as much as I did. Thank you both and thanks to The Patient Story.
Tiffany: Thank you, Pete, Lisa, and Dr. Paludo for an engaging discussion. It is so crucial to be empowered so that you and your caregivers can make informed decisions about your care.
Amber’s Stage 4B High-Grade Serous Ovarian Cancer Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Amber’s symptoms began subtly with bowel irregularities, night sweats, missed periods, unintended weight loss, fatigue, and pain, but she initially rationalized these as related to stress or her active lifestyle. With her mother battling stage 3 colorectal cancer at the time, she feared a similar diagnosis but delayed seeking medical help. By the fall of the same year, her symptoms had worsened significantly, including blood in her stool and severe discomfort, prompting her husband to schedule medical appointments.
After a colonoscopy revealed a mass, a subsequent emergency surgery determined Amber had stage 4 ovarian cancer, with the tumor spreading to both ovaries and her colon. This led to initial chemotherapy and the placement of an ileostomy bag. She later transferred care to a specialized center, where treatment included more chemotherapy to shrink the tumor before undergoing a radical hysterectomy and removal of other affected tissues. Genetic testing revealed she was BRCA1 positive, which shaped her treatment plan and ultimately led to the decision for a preventive double mastectomy two years after achieving remission.
Despite multiple allergic reactions to treatments and procedures, she persevered, completing six rounds of chemotherapy, a surgical recovery phase, and several years on a targeted PARP inhibitor. Though she mourned the loss of her fertility, she and her husband pursued fostering and adopted their daughter, who brought new purpose and joy to their lives. Now in remission, Amber reflects on the challenges of cancer, the trauma it caused, and the blessings that emerged through her resilience and determination.
Name: Amber C.
Diagnosis:
High-Grade Serous Ovarian Cancer
Staging:
Stage 4B
Symptoms:
Bowel irregularities (urgency, alternating constipation, and diarrhea)
Night sweats
Unintended weight loss
Irregular periods
Fatigue
Pain while sitting or going to the bathroom
Blood in stool
Treatments:
Surgeries: Debulking surgery, radical hysterectomy, oophorectomy, ileostomy placement, preventive double mastectomy with breast reconstruction
Chemotherapy
Targeted therapy: PARP inhibitor
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
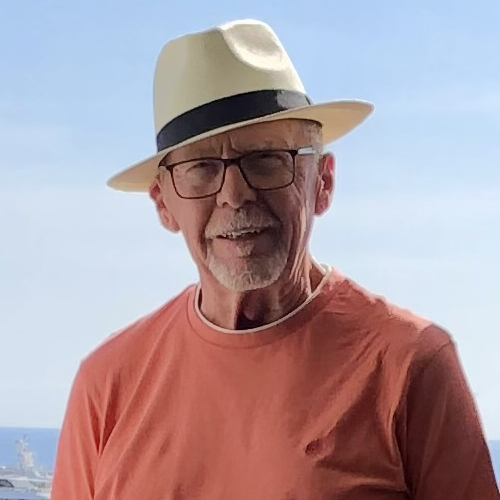
In 2014, Jim was diagnosed with myelofibrosis after an X-ray for kidney stones revealed an enlarged spleen. Follow-up tests showed elevated white blood cell counts, leading to a bone marrow biopsy and confirmation of the disease. Initially asymptomatic, he monitored his condition through regular blood work.
Four years later, in 2018, he began experiencing severe fatigue and breathlessness. These symptoms led to a diagnosis of myelodysplastic syndrome (MDS), a serious condition that could progress to leukemia. His prognosis was grim without a stem cell transplant, giving him potentially only months to live. Despite his age of 70, a medical committee deemed him a suitable candidate for the transplant due to his overall health. He underwent chemotherapy and numerous blood transfusions to prepare for the procedure.
A matching stem cell donor was found in Germany, and the transplant occurred in October 2018. The process involved intensive chemotherapy and total body radiation, followed by a stem cell transplant. Post-transplant recovery was challenging, with prolonged hospitalization, physical weakness, and isolation to protect his immature immune system. However, he avoided severe complications such as graft-versus-host disease, experiencing only a manageable rash.
This experience reshaped his outlook on life. Gratitude became a central theme, as he embraced moments with family, trips to the beach, and future travel plans, including a visit to meet his donor. He credits his recovery to the unwavering support of his wife, who served as his full-time caregiver, and his confidence in his medical team.
Looking ahead, he hopes for advancements in treatments to eliminate the need for stem cell transplants and alleviate complications. He encourages others facing similar challenges to maintain faith in themselves, their medical teams, and support systems.
Name: Jim C.
Age at Diagnosis:
70
Diagnoses:
Myelodysplastic syndrome (2018)
Myelofibrosis (2014)
Symptoms:
Enlarged spleen
Fatigue
Shortness of breath upon exertion
Treatments:
Chemotherapy
Blood transfusions
Allogeneic stem cell transplant
Thank you to Sobi, Karyohpharm, GSK, and Novartis for supporting our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
My myelofibrosis was discovered accidentally. I didn’t experience symptoms.
Introduction
I’m a retired lawyer. I was a prosecuting attorney for 10 years and then a corporate litigator for about 20 years. Nearing the mid-2010s, we moved west of downtown St. Louis. We live with our daughter and her three children, so they help us and we help them. We have horses, donkeys, and chickens. Most of the time, I’m the pool boy, the stable boy, the groundskeeper, and the handyman, but most importantly, I’m grandpa.
I was diagnosed with myelofibrosis in 2014 and myelodysplastic syndrome in 2018.
Pre-diagnosis
Initial Symptoms
My myelofibrosis was discovered accidentally. I didn’t experience symptoms. I had kidney stones, so I would get an X-ray every year. In late 2013 when the X-ray results came back, I also had a slightly enlarged spleen, which I didn’t think was important.
Luckily, my wife’s a nurse and our doctors thought it was important. They started doing some follow-up and more blood work. My white count was too high, which was suggestive of a problem.
I had no symptoms, no discomfort, and no treatment. We kept track of it by doing blood work fairly often.
Getting a Blood Cancer Diagnosis
My family doctor recommended that I see an oncologist, who my wife and I knew well. He ordered a bone marrow biopsy. I still remember the day he came in and said, “We’ve got a diagnosis. You have blood cancer.” He indicated that it was not his area of expertise, so he recommended either Saint Louis University or Washington University. Since WashU’s where I’d gone to law school, I figured their medical school was probably good too, so I chose Washington U.
I met a doctor there who is a leader in that area of cancer. He told me about myelofibrosis, where you had 7 to 10 years on average before you run into trouble, and at that point, it might morph into leukemia or something. I had no symptoms, no discomfort, and no treatment. We kept track of it by doing blood work fairly often.
In the spring of 2018, I began to get very short of breath at the slightest exertion. I was 70 years old at the time and I thought that maybe it was my age, but it was worse than that. Fatigue set in, so we did more tests.
We had a conversation with the doctor and he said, “Jim, this is serious. You have myelodysplastic syndrome. With your situation, you might go six months, a year, or a little longer if you’re lucky unless we can find a donor and get a transplant.”
We walked down the hall to the transplant doctor to begin the process. When we first talked, she used the word cure, that stem cell transplant is a possible cure. It was encouraging. She also said, “When I saw your picture, I knew that you were a good candidate for this,” so that gave me comfort and hope.
Because I was 70, a special committee had to meet to determine my eligibility. I was otherwise a healthy person, so her acknowledging that and saying I was going to be okay for the transplant made me feel good.
I was very confident in the medical treatment that I was getting and the support I had from my wife and my family.
Reaction to the Diagnosis
I don’t remember panicking or getting too distressed. When the doctor from Washington said 7 to 10 years, I thought, well, I’m already 70. When you tell a 70-year-old that he’s got 7 to 10 years, he’s probably going to say that’s not too bad and so that didn’t upset me too much.
What it did do is that instead of my wife and I talking about doing something someday, we scheduled it for the following month or year. We started to travel a lot and did a variety of other things that kept getting pushed back. You say that you’ll do something someday and so we did.
When the doctor came in and gave me three months, that was a little more unsettling. The worst moment was being told you’ve potentially got a few months to live. It was a combination of being an optimistic person and a person of faith. I was very confident in the medical treatment that I was getting and the support I had from my wife and my family.
The other possibility is I’m oblivious to it. What am I going to do? I can shout and throw things; that’s not going to help. I don’t ever remember feeling down.
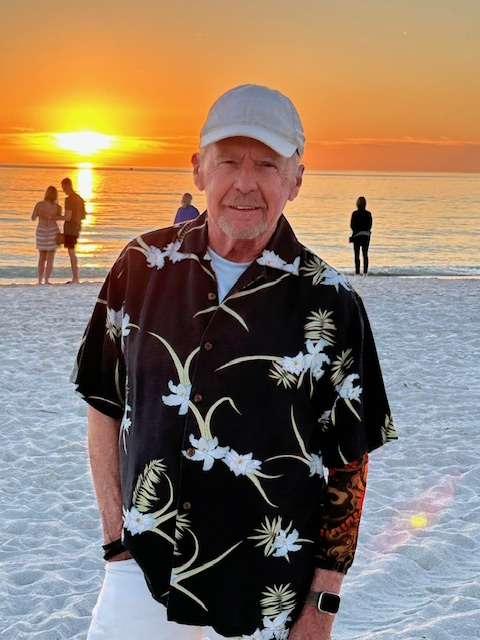
Shortly before I went into the hospital, I said I’ve got to get to the beach again. Living in St. Louis, there are no beaches nearby, so we took a quick trip down to Destin. It was still warm enough where you could walk along the beach and that was relaxing.
There was one time when I thought this might be the last time I was going to be at the beach. I guess it’s part of my faith. I thought if I was going to die six months from now, after that, I probably wouldn’t miss the beach. I hope where I’ll be is a lot better than the beach anyway, so that’s not an issue.
They found a donor and it was a perfect match… My donor is from Germany.
Getting a Stem Cell Transplant
For the myelofibrosis, we watched and waited. Once the myelodysplastic came in, we immediately started a pretty serious regimen of chemotherapy and blood transfusions. In June 2018, I had a week of chemo every day, probably one or two transfusions during that week, a couple of weeks off, and then repeat. I don’t know how much chemo I had, but I counted 15 or 16 blood transfusions during that time. Thankfully, I did not react poorly to the chemo. I don’t remember being sick at all. I usually felt better after getting blood.
In late September, I was told that they found a donor and it was a perfect match. Before the scheduled transplant, I went to the hospital and received heavier chemo for about a week and then I had total body radiation, which I referred to as being microwaved. You sit on a table, clutch your knees, they measure your body, you stay in one position for about 10 minutes, you turn around, and do it again. That was the only time I felt sick after.
I was weak. It’s do-or-die at this point. They scheduled the transplant for the evening of October 11, which was cool because that’s my oldest granddaughter’s birthday and I’ll get my new birthday on the same day. My donor is from Germany. We discovered later that the courier missed the train, so it was delayed. The transplant finally happened a little after midnight on the next day, October 12.
The doctor came in and it was in a small bag, smaller than a typical blood bag. I already had a port in my chest. I suspect the doctor was there in case I had an immediate bad reaction for some reason, which I did not. It’s pretty anticlimactic. You wait for the stem cells to drain out of that bag. After a while, I went to sleep and that was it.
I don’t know how I would’ve felt if this hit me at 29… I’ve had a good life already. If something happens, it’s unfortunate, but at 70, it’s not terrible.
Post-Transplant
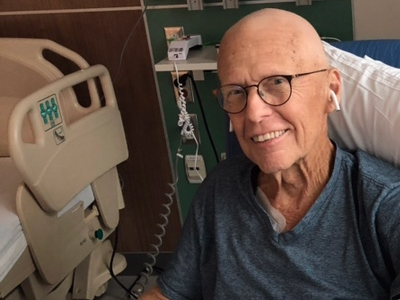
I was in the hospital for a month. My wife was with me 24/7. Thank goodness she’s also a nurse, so that helped. Fairly soon, I started taking antibiotics, antifungals, and antivirals. I didn’t have graft versus host disease, except for a rash that we treated and went away.
I was very weak. When I came home, I very slowly got my strength back. I had physical therapy and occupational therapy. I stayed away from other people for a good bit because I had a very immature immune system. I’m still taking various medications.
Renewed Appreciation for Life
I didn’t and don’t wake up every morning saying thank you to God for another day; my wife does. Other times, it will hit me, like when I’m watching my grandson do something, being able to go to a baseball game, or going back to the beach, I would think, “I almost missed this,” and that makes me feel good.
I don’t know how I would’ve felt if this hit me at 29. One of the first times that I felt sorry for myself was when I was getting chemo and a kid next to me learned that he had leukemia a week before. He was around 20 and you know how different and how difficult that must be. I’ve had a good life already. If something happens, it’s unfortunate, but at 70, it’s not terrible.
If you’ve got a caregiver who’s impatient or gets tired easily, that can be a problem. It requires dedication and love. Having a caregiver makes a difference.
I have a renewed appreciation for life. It comes at the weirdest times, but almost every day, something comes to mind and I say to myself, “Oh, I almost missed this.”
We’re planning a vacation for the summer. We already planned a trip to Scotland with our church group. I’ve been in contact with my donor, who was 24 at the time. He recently turned 30 and said that we would have to find each other if I were ever in Europe. We decided to spend a few extra days to go to Germany to meet him and his girlfriend.
The Importance of Having a Care Partner
I hit the jackpot with my caregiver. My wife’s an RN and a retired hospital administrator, so she knew who to call if there was an issue and who to talk to, and was not shy about doing it. There weren’t that many issues, but she also literally stayed in the hospital room with me 24/7, except for one time, but my sister substituted for her.
At home, I couldn’t do much for myself. If you’ve got a caregiver who’s impatient or gets tired easily, that can be a problem. It requires dedication and love. Having a caregiver makes a difference. I don’t know how you could do it without someone, even if they can’t stay 24/7. It’s hard to describe how important it is.
Connect and look for help. Don’t give up.
The Future of the MPN Landscape
It would be great if there could be some treatment that would be as good as a transplant but didn’t require a transplant. White Caucasians have a pretty good chance of finding a good match. If you’re Black or Latin American, there aren’t that many donors. I don’t know if it’s a lack of education or effort to spread the word or how important it is. If there could be something other than a transplant that would work, that would be great.
A lot of work still needs to be done on graft versus host disease. One of the doctors in the team had 2 or 3 transplants himself and had terrible graft versus host disease. A gentleman down the hall from us had terrible mouth sores that made it almost impossible for him to eat or drink. Now, I think that eventually cleared up, but it’s still a difficult time to have to go through. Work needs to be done and an alternative to transplants would be great.
Words of Advice
Have faith. Have faith in yourself, in God, and in your medical team. If you don’t have faith in your medical team, find another one. It’s easy for me to say being in St. Louis because we have a variety of excellent medical facilities around, but there’s help out there.
Finding organizations that will help you find the help you need would be worth looking into. If you’re not happy with your doctor, find another one. Luckily, that’s not been my experience at all. It’s important to connect and look for help. Don’t give up.
Special thanks again to Sobi, Karyohpharm, GSK, and Novartis for their support of our independent patient education content. The Patient Story retains full editorial control.
Shayla was diagnosed with metastatic colorectal cancer at 33 years old after years of experiencing unexplained digestive issues. Initially, symptoms like stomach sensitivity, exhaustion, and food intolerances were attributed to a sensitive stomach. Over time, she sought medical attention, including multiple gastroenterologist consultations but received inconclusive diagnoses. She was diagnosed with celiac disease, but despite cutting out gluten, she continued to feel unwell.
After more months of fatigue, Shayla noticed blood in her stool, which persisted for several weeks. When her husband insisted she seek medical help, a colonoscopy revealed polyps. While initially told that they weren’t cancerous, a biopsy later confirmed that one was malignant. Further tests revealed lesions in her liver and lungs, prompting additional biopsies. The lesions in her lungs were clear, but the cancer had metastasized to her liver, resulting in a stage 4 colorectal cancer diagnosis.
Her treatment plan included four rounds of chemotherapy, followed by a hepatectomy or liver resection to remove 25% of her liver. After the surgery, Shayla began her chemotherapy again, with plans for more rounds to finish her treatment. Although she initially struggled with side effects, such as hot flashes, nausea, and fatigue, her doctors adjusted her treatment plan to help her manage better. However, cold sensitivity, neuropathy, and physical weakness persisted.
Despite these challenges, Shayla remained focused on her healing and recovery, even as the emotional toll of her diagnosis began to weigh on her mental health. She shared that the isolation during recovery and the struggle with seeing her children react to her illness was particularly difficult.
Shayla advocates for others to take their symptoms seriously, stressing the rising rates of colorectal cancer in younger adults. She encourages others to seek second opinions and advocate for themselves if they’re not satisfied with their medical care. Through her experience, she has seen the importance of a strong support network and the need for proactive health care, urging others to catch cancer early to increase treatment success.
Name: Shayla L.
Age at Diagnosis:
33
Diagnosis:
Colorectal Cancer
Staging:
Stage 4
Symptoms:
Stomach sensitivity
Food intolerances
Exhaustion
Blood in stool
Treatments:
Chemotherapy
Surgery: hepatectomy (liver resection)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Jim began experiencing alarming symptoms one day when his head and neck swelled up suddenly due to backed-up blood flow, causing his face to turn purplish and his neck veins to bulge. After the swelling subsided, he was rushed to the ER at the University of Pennsylvania, where initial tests revealed a severe narrowing in his superior vena cava.
Doctors were baffled by his condition. Over four days of hospitalization, various specialists attempted to diagnose the cause of the obstruction, but no clear answer emerged. Even though lymphoma was mentioned early on, it was dismissed because lymphoma typically doesn’t present in veins. The situation grew more critical as the narrowing worsened, leading to a second hospitalization, but still, no one could identify the cause.
As hope dwindled, a heart and lung transplant surgeon proposed an innovative surgery: removing the entire superior vena cava and replacing it with a graft made from pig intestine. Jim underwent the surgery, which was more complicated than expected due to the extent of the tumor. The pathology report later revealed that the obstruction was caused by diffuse large B-cell lymphoma.
Following the surgery, Jim faced additional challenges as his surgical site began to narrow again due to natural healing and scarring. The doctors debated whether to insert a stent to keep the vein open, but Jim opted to endure the discomfort, trusting that his body would heal over time and develop new collateral veins. After weeks of uncertainty, he started chemotherapy to address the lymphoma.
Name: Jim Z.
Age at Diagnosis:
41
Diagnosis:
Diffuse Large B-cell Lymphoma (DLBCL)
Symptoms:
Sudden and severe head and neck swelling
Purplish facial discoloration
Bulging neck veins
Treatments:
Surgery: resection and reconstruction of the superior vena cava
Chemotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
Suddenly, my head and neck began to swell up… if this was going to continue at the rate it was going, I wasn’t going to be around for much longer.
Introduction
My wife Vanna and I are parents to two terrific boys, Nikitas and Victor. We live in the suburbs of Philadelphia, where I also teach. I’m a high school English teacher and a writer. I also paint and coach Little League.
How the Symptoms Started
I was getting ready to go to a Phillies game when, suddenly, my head and neck began to swell up with backed-up blood flow. It was so alarming. I looked in the mirror and saw my head puffing up like a balloon filling up with water.
I called out to my wife, who came rushing and immediately saw me. My father is a doctor, so I called him. It was pointless to call 911 because if this was going to continue at the rate it was going, I wasn’t going to be around for much longer.
My wife and I stared at myself in the mirror while my father very amazingly and gently told me to breathe. This went on for two or three minutes. You can imagine the swelling and purplish appearance of my face and neck with neck veins bulging
As dramatically as it started, it stopped. My blood flow reached equilibrium and I began to feel normal. I even joked that we were going to go off to the Phillies game after that. My father said no and that I was going to the emergency room.
She pointed to the narrowing and said, ‘We don’t know what this is, but it could be fatal.’
Going to the Emergency Room
When I went to the ER, I appeared normal, but when I described what happened to me, I could tell from their reaction that something serious was going on. In a matter of hours, I had blood draws and X-rays taken. I waited in a room very patiently and watched the entire Phillies game on the TV.
Around midnight, I went to the front desk and asked the attending doctor if she was as surprised as I was that we still hadn’t heard any results. She looked at me with tender eyes and said she would see me in a minute.
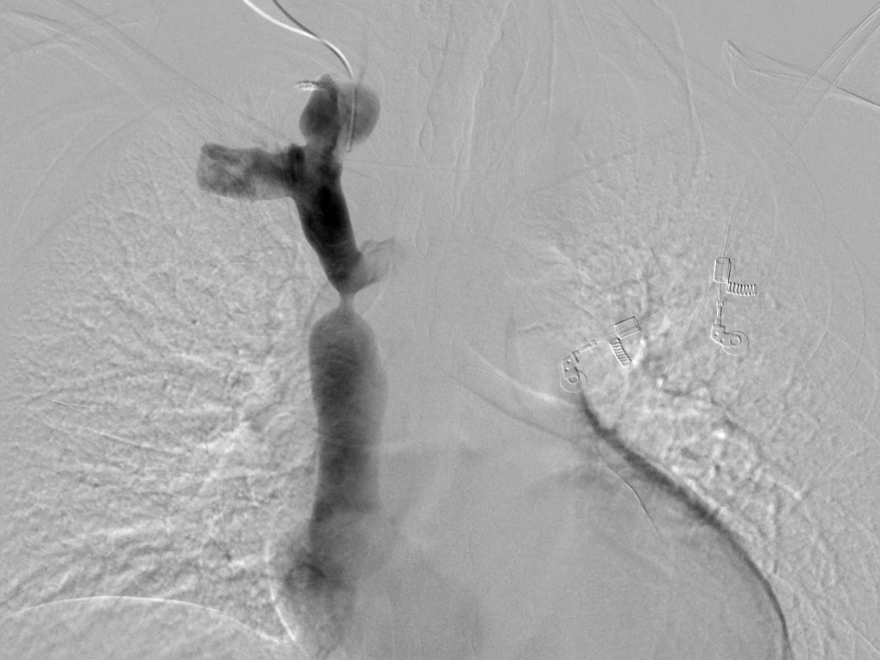
She came into my room, sat next to me, held a pretty fuzzy X-ray image up, and pointed to what looked like an hourglass. She pointed to the narrowing and said, “We don’t know what this is, but it could be fatal.” Those were the first words that I heard from a doctor about whatever was going on inside of me.
As shocking as that sounds, it wasn’t entirely surprising because of what had happened to me. The force of the earlier incident of whatever seemed to be obstructing my blood flow was stunning. I understood that it was game on.
A couple of hours later, I was getting an MRI. I had never gotten an MRI before and it’s not something anyone feels comfortable doing. As claustrophobic as I am, it didn’t even occur to me because it was my first time and I didn’t know any better, so I just lay there in that tube. I was in survival mode and if this is what’s necessary to get to the bottom of things, I can do this. I went back to my father’s advice to breathe and tried to stay calm.
The irony is that every department had somebody come to see me to speculate on what might be ailing me—every department except oncology.
What the Doctors Could See From the Scans
There was some blockage or obstruction in my superior vena cava, the main vein that descends to the heart and the last and most crucial vessel that brings blood back to the heart. In retrospect, that would explain why all of a sudden, I had backed up blood in my head and neck. At some point, the blood managed to get through the superior vena cava, so my blood flow returned to normal.
I was admitted to the hospital for four days. The cardiovascular surgeon was appointed as the head of my team. A young attending doctor was trying to round up the best people. At one point, he told me, “You’re the talk of the hospital. Everybody wants to be the guy who figures out what’s going on in your chest, but we don’t know.”
The irony is that every department had somebody come to see me to speculate on what might be ailing me—every department except oncology. Early on, the theory was cancer or lymphoma, but it does not present this way. It’s rarely in the chest and never in veins and this was clearly in a vein. Six months later, my oncologist told me, “We do find lymphoma in veins occasionally, although rarely and only in an autopsy,” so this was not in anybody’s working diagnosis and it was disqualified almost from the get-go.
The one guy who might be able to do something would be the interventional radiologist to do a biopsy, but he was determined to avoid doing that because he would have to put a needle into my superior vena cava. Not only was there some obstruction in there, but it appeared to be in the wall of the vein. He explained how he would have to pierce a needle through the wall of the vein and somehow extract a piece of whatever was in there. He said, “I’m not doing it. It would be catastrophic and I don’t want to kill you.”
We saw a narrowing so severe that it was hard to imagine how any blood was getting through to my heart.
After four days, a cardiac surgeon proposed to open up my chest completely to get to the vein, but we were still left with a catch-22. The interventional radiologist said, “Even if I had your superior vena cava in the palm of my hand and my best needle in my other, I would not dare try to get a piece out of the wall of your vein to do a biopsy.” We were stuck. I wasn’t having dramatic inflamed symptoms but I was still uncomfortable.
On day four, a cardiovascular surgeon came in and said, “It may be some idiopathic thing that we can’t explain. There are medical mysteries. We’re going to send you home without a diagnosis. If you have another flare-up, if you continue to have worsening symptoms, we’ll have you come back in a month and we’ll do more imaging.”
I left and I was not confident because you feel the sensations in your own body. I was hopeful, but my gut said something was happening inside of me.
Symptoms Returned After Leaving the Hospital
Over the next few days, it got worse. It was backing up. Again, with the benefit of hindsight, what was happening was the tumor was growing and the narrowing was becoming more severe. The blood flow to my heart was decreasing by the day.
I packed my bag. My parents happened to be at our townhouse that afternoon. I showed up in the doorway and said we had to go back. We went back to the hospital and I was readmitted.
The cardiovascular surgeon and the interventional radiologist decided that I was going to get a venogram, where they put the dye into the bloodstream to get a more vivid image. We saw a narrowing so severe that it was hard to imagine how any blood was getting through to my heart.
It was supposed to be 15 mm at its maximum and it was narrowed down to about 3 mm — that’s how much blood flow was going to my heart.
Three or four doctors were looking at the gigantic triptych of images that showed my superior vena cava and the narrowing that came nearly closed and then opened again. They shook their heads and said, “We don’t know what this is.” The cardiovascular surgeon came in and somberly said, “I’m sorry. We’ve tried to do everything and there’s nothing left that we can do.” We all knew what that meant.
My father, who’s a doctor and is always inquisitive and never at a loss for hope, was quiet. That gives you some indication of all the conversations, research, and investigations that had gone on for the last 10 days had come to this moment and we accepted it.
I hugged my wife. My parents went over to the window and I went over and hugged them. Very strangely, I was more equipped to handle the news than anybody. I had been living with that first thought on the night I went to the ER and was told this could be fatal. We didn’t know what this was, so I had been preparing for this possibility.
When I hugged my dad, he said, “I’m sorry, son,” and I said, “I’m sorry, dad,” and the next thing that he said was, “Tomorrow, more research.” That was a profoundly hopeful, illogical moment, but it shows you the balance of this man of science who, even after all of that, was still determined that there might be something, but he was also my dad, going through this with me and all of us.
Not Giving Up Hope
A couple of hours passed and there was a new young attending doctor on call that day. I said to her in passing, “I would love to sit with the head of radiology and be able to look at all the images from the first day to the most recent venogram.” A lot of imaging had been done and I was trying to understand the anatomy of the superior vena cava and the brachiocephalic veins that go up into the jugular veins. I learned all this anatomy and I wanted to understand it better.
I was looking at these spectacular 3D images. It was supposed to be 15 mm at its maximum and it was narrowed down to about 3 mm — that’s how much blood flow was going to my heart.
The doctors looked at each other and shook their heads. The interventional radiologist was convinced more than ever that he wasn’t going to stick a needle in there. They both said, “It’s got to come out since we can’t get to it.” But nobody knew what the surgical strategy would be.
‘I’ve got an idea. I propose that I open you up and take out your entire superior vena cava and replace it with a graft.’
Six hours or so later, a man I had never seen before walked in. He’s a heart and lung transplant surgeon at UPenn. He said, “I know you don’t need a heart or lung transplant, but I’ve got an idea. I propose that I open you up and take out your entire superior vena cava and replace it with a graft that I’m going to craft out of this material that I’ve been using to patch hearts and lungs. I’ll make a vein for you and attach it at both ends. I think I can do it.”
My wife and I were alone with him, stunned and giddy, happy and amazed, and slightly skeptical. My wife Vanna ran to the hallway, grabbed my parents, brought them back in, and said, “Repeat what you just said.”
We listened to him describe the surgery that he had planned. He had been using an organic material made out of pig intestine. He’d been using it to patch hearts and lungs, but he thought he could make a cylinder out of it and make a vein that would replace my superior vena cava. He said he would do this. I said, “So there’s still hope?” And he said, “There’s always hope.”
Surgery Day
I went into surgery feeling good and confident. I woke up on the other side and it worked. When the surgeon came to visit, he said, “It ended up being a little more complicated than we were anticipating. It wasn’t just a tube after all.” He described it as black muck that he’d never seen anything like before. It went up into the brachiocephalic vein. He took more of that material and had to make a Y shape, did the surgery, and attached my superior vena cava to the brachiocephalic vein, which is even narrower. A brilliant surgery to say the least.
They sent the whole thing off to pathology to find out what it was all along. Five days later, while I was still in the hospital recovering, a young man from hematology came to see me and said, “You’ve got diffuse large B-cell lymphoma.” Everybody’s mind was blown because it defied all expectations.
We would give the graft a month to heal and then start chemo. Fortunately, I was able to get the chemo through a vein in my arm.
Doctors Couldn’t Believe It Was Cancer
My oncologist, one of the great lymphoma doctors, said he had never seen anything like it. In a month, I started chemotherapy and that’s when I met my oncologist.
That was the first time I ever heard about cancer or lymphoma. But I had a graft in my chest that needed three months to heal. That was the plan.
My surgeon said, “I don’t know what chemotherapy is going to do to Jim’s graft made out of pig intestine and we’re certainly not going to stick a port in his chest into his superior vena cava. Hopefully, the chemo will go well into a vein in his arm.”
On the other hand, my oncologist, said, “We’re not waiting three months for this graft to heal. We called the company that makes the graft and asked how chemotherapy interacts with the material. They had no idea.
The doctors compromised and agreed that we would give the graft a month to heal and then start chemo. Fortunately, I was able to get the chemo through a vein in my arm and we went from there.
Despite everybody’s certainty that lymphoma doesn’t present that way, a lymphoma tumor was growing inside the wall of the vein of my superior vena cava.
The obstruction that was originally in my superior vena cava was a lymphoma tumor. Despite everybody’s certainty that lymphoma doesn’t present that way, a lymphoma tumor was growing inside the wall of the vein of my superior vena cava.
I tolerated some great discomfort but in time, I trusted that the body would do its magic and heal itself, and other tributaries would form as these guys described to me. Presumably, that’s what happened because I’ve had scans since and I still have this dramatic narrowing. Even though you can’t see in any of these images that other collateral veins have formed, everybody thinks that the only scientific explanation is that’s what happened.
I am sure I am one of the very rare cases where the cancer and the chemotherapy were always secondary to the healing of the surgery.
Cancer Responded Well to Chemotherapy
While it was an aggressive cancer lymphoma, it responded well to chemotherapy. These were all very promising signs and that gave me optimism. As long as I could withstand the symptoms, my body tolerated the chemotherapy, and the healing could continue, we’d get to the other side of this and hopefully, the chemo cocktail would do its work.
I maybe had six rounds of chemo every three weeks. I had one reasonably tolerable week and one week of debilitating nausea. But all the while, I was also recovering from surgery.
By the sixth round, I was in remission. There was no lymphoma showing up on the PET scans.
When we got to the fourth round or so, I got tested and it appeared that there was no growth. Eventually, by the sixth round, I was in remission. There was no lymphoma showing up on the PET scans.
At the time, I couldn’t wait to get back to normal. There was only one marking period left in the year. I teach English and writing to seniors and wanted to be in this atmosphere of dynamic conversation, kids, and vitality.
When I came back at the beginning of April, my colleagues were thinking, “Are you crazy? Take the year off at this point and see you in September.” But I couldn’t have been happier to be back. My hair was growing back. I was still bald, but it felt great to be back.
How I Survived
As a patient, I was the unluckiest guy on the planet because nobody could detect what I had. I reached a low point where doctors told me there was nothing else that could be done. Then the surgeon said the magic words: there’s always hope.
I take that with me into everything that I do. Even after all seems lost, you don’t know what you don’t know. You’ve got to stay awake for every moment of your life because if you’re full of anxiety and despair, you might not see an opportunity that could point you down a positive path to good health.
I was fortunate to grow up with a doctor as a father and live in a city with institutions, like the University of Pennsylvania. I had faith in the doctors and the institution, and I don’t take any of that for granted. It’s easy for me to tell others to have faith and hope because I was born with that.
Keep the faith. Stay hopeful. Be your best self-advocate.
What came from my experience as the son of a doctor was confidence in having conversations with my doctors, the expectation that they were listening to me, and that they wanted to hear my story because that’s the kind of doctor my dad was.
My dad was a family doctor and he made sure to make eye contact to hear the patient’s story and to be there emotionally not just clinically. Again, it’s easy for me to say to a patient who might be going through these things who didn’t have the good fortune that I had with all these other lucky things that I had going for me.
Words of Advice
Keep the faith. Stay hopeful. Be your best self-advocate because you never know and the doctors don’t always know either. They need to hear your story.
Willow’s Rare Grade 1, Stage 2.5 Pelvic Cancer Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Willow was diagnosed with a rare stage 3 pelvic cancer that was a combination of endometrial and cervical cancer. Initially, she had persistent flu-like symptoms, fatigue, a scratchy throat, and chills. Despite requesting cancer tests from her gynecologist, her concerns were dismissed as symptoms of aging. Eventually, more alarming symptoms like post-orgasm pain, heavy bleeding, and severe cramping led her to fabricate symptoms to expedite care because she couldn’t find answers. Multiple tests yielded no results until a naturopathic gynecologist ordered advanced imaging, which revealed a hidden tumor masked by scar tissue from her cesarean section nine years prior.
The diagnosis confirmed she was on the brink of stage 3 pelvic cancer. Willow underwent a radical hysterectomy, followed by six weeks of radiation and chemotherapy. Despite the rigorous treatments, she felt fortunate to have the tumor removed first, which alleviated her symptoms. Recovery, however, was daunting due to the internal nature of the surgery and the emotional toll of transitioning from intensive care to self-reliance. Post-treatment, Willow suffered from angioedema and the abrupt onset of menopause, leading to brain fog, brittle bones, and balance issues, causing several falls and broken bones.
Despite these challenges, Willow adopted hormone replacement therapy (HRT), which significantly improved her quality of life. She emphasized the importance of conventional cancer treatments, advocating against relying solely on holistic methods. During her treatment, Willow reached out to her community and received crucial support.
Her identity transformed post-cancer; she embraced a fearless, purpose-driven life. Willow’s candid discussion about intimacy post-surgery highlighted that recovery and fulfilling sex life are possible with proper care, including pelvic floor therapy. She encouraged others to pursue their passions without waiting for life-threatening circumstances, emphasizing that cancer is not a death sentence but a call to fully engage with life.
Name: Willow B.
Diagnosis:
Pelvic Cancer (Endometrial-Cervical Hybrid)
Staging:
Grade 1, Stage 2.5
Symptoms:
Persistent fever-like chills
Scratchy throat
Fatigue
Post-orgasm pain
Heavy bleeding
Severe cramping
Treatments:
Surgery: radical hysterectomy
Radiation
Chemotherapy
Hormone replacement therapy (HRT)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: Heavy periods, abnormal bleeding, large blood clots, severe cramping, severe abdominal pain, pain radiating down the left leg, loss of mobility in the left leg, loss of appetite, fatigue
Symptoms: Intermittent spotting during or after sex, unpredictable menstrual cycle, abdominal pain particularly under the rib cage Treatments: Chemotherapy (cisplatin & paclitaxel), immunotherapy (Keytruda), surgery (total abdominal hysterectomy with bilateral salpingo-oophorectomy & omentectomy) ...