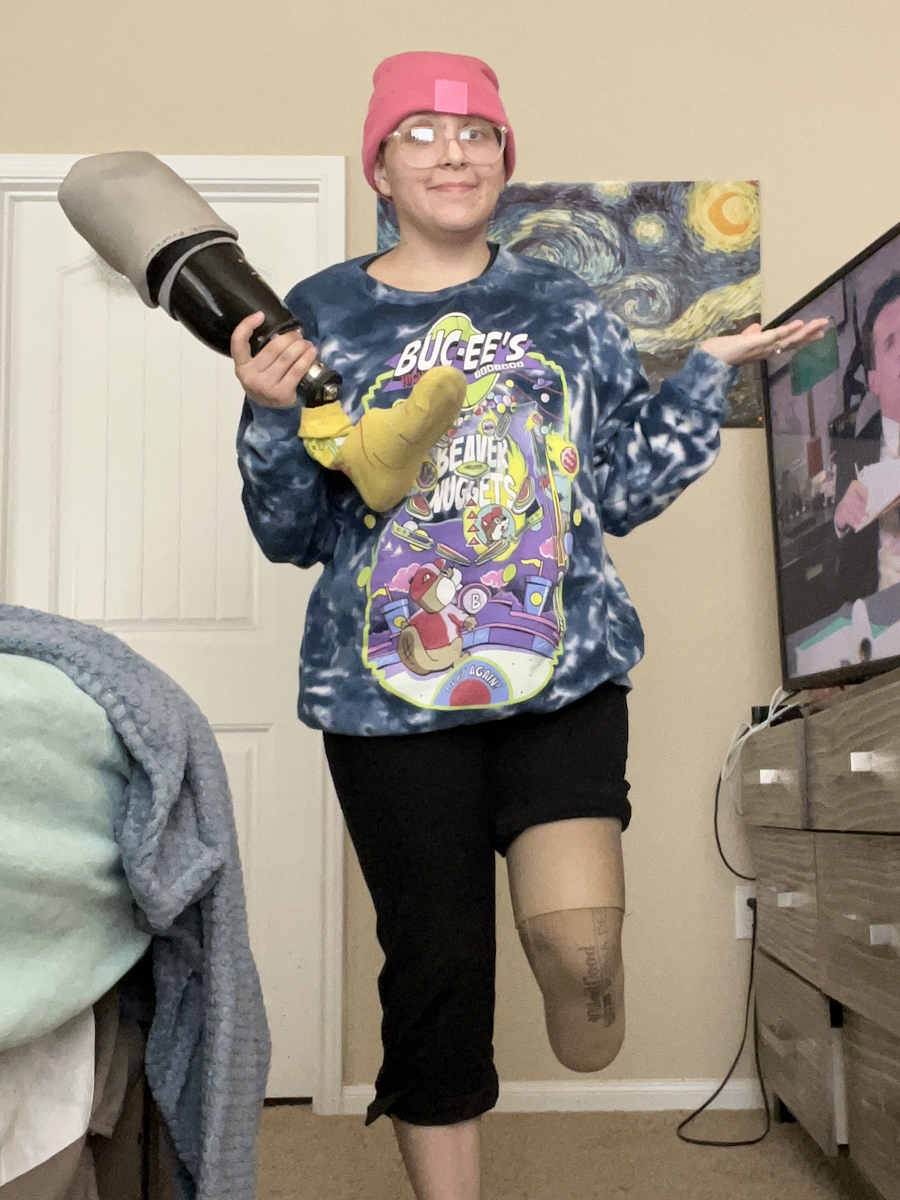
Emily, from Richmond, VA, was diagnosed with stage 4 Burkitt non-Hodgkin lymphoma in November 2022.
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
Emily’s journey began with unexplained symptoms, including prolonged sickness, speech changes, and an inability to stick her tongue out straight. Initially, doctors misdiagnosed her with Eagle syndrome and anxiety. She also experienced night sweats, petechiae, and severe weakness, but struggled to find a diagnosis until an ENT referred her to palliative care, urging immediate action.
Emily visited the ER, where specialists quickly recognized the severity of her condition. A lymph node biopsy confirmed stage 4 Burkitt lymphoma, affecting her bone marrow, spleen, and central nervous system. She was also found to have hemophagocytic lymphohistiocytosis (HLH).
Emily began aggressive treatment involving 6 rounds of chemotherapy. Chemotherapy caused severe side effects, including mucositis, rapid weight loss, and extreme fatigue. Despite the challenges, Emily remained determined, knowing the transplant could cure both her cancer and HLH.
In May 2023, Emily underwent an autologous stem cell transplant. Afterwards, she endured an intense isolation period, followed by extensive physical therapy to regain strength and mobility. By August, scans confirmed remission, yet Emily found survivorship mentally and emotionally taxing. Returning to her job in special education only 4-5 months post-transplant proved difficult, as her immune system remained compromised. She continues to manage her health with frequent medical appointments, immunotherapy, and physical recovery.
Emily’s journey was not without complications. For instance, she suffered a small stroke during treatment, caused by an oversight in managing her blood thinners. Despite the challenges she faced, she emphasizes the crucial role of self-advocacy, community support, and compassionate medical professionals, particularly her nurses, who provided emotional and practical support during her hospitalization.
Emily actively raises awareness about young adults facing late or misdiagnoses, stressing the need for better medical attention for this demographic. She also highlights the impact of genetic factors and Epstein-Barr virus on her cancer, urging the importance of thorough family history and testing.
Now, Emily finds healing through therapy, volunteering at an animal shelter, and reintroducing physical activity. She plans to explore trauma-focused therapies like eye movement desensitization and reprocessing (EMDR) therapy and continues to engage with online communities for support, including on Instagram. While the fear of relapse lingers, Emily focuses on building a new normal and empowering others to advocate for their health and seek community connections during and after treatment.
Name:
Emily S.
Age at Diagnosis:
28
Diagnosis:
Burkitt non-Hodgkin lymphoma
Staging:
Stage 4
Symptoms:
Constant fatigue
Tongue deviated to the left
Abscess in right breast
Petechiae on legs
Night sweats
Nausea and vomiting
Persistent cough
Treatments:
Chemotherapy
Stem cell transplant
Immunotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Tiffany, a 38-year-old mother of 4, has stage 4 bile duct cancer or cholangiocarcinoma, also known as liver cancer. In April 2024, she experienced severe left flank pain, which led her to seek medical attention. A CT scan at the hospital revealed a mass on her liver, initially suspected to be colon cancer. Further tests, including an MRI, PET scan, and liver biopsy, confirmed the diagnosis of cholangiocarcinoma that had spread to her spine.
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
Following the diagnosis, Tiffany began receiving treatment. Her oncologist initiated a combination of chemotherapy and immunotherapy, alternating between therapies weekly, with a rest period every 3 weeks. Despite initial radiation treatments failing to shrink the tumor on her spine, targeted radiation was applied to her liver, followed by spine surgery to remove most of the tumor. Recovery was challenging, requiring a week-long hospital stay, physical therapy, and the use of a walker and cane at home.
Subsequent treatment involved ablation surgery to address new lesions on her liver. Tiffany resumed chemotherapy and immunotherapy, experiencing side effects such as back pain, headaches, and nausea. As her treatment continued, she received support from her medical team, including a liver specialist in Baltimore.
Mentally, Tiffany struggles with anxiety and the fear of leaving her family. She takes anxiety medication to help cope, though the emotional toll remains significant. She stresses the importance of self-advocacy, sharing her story to raise awareness about cholangiocarcinoma and stressing the importance of regular medical check-ups.
The ongoing battle with cancer challenges Tiffany physically and emotionally, but she remains determined to see her children grow up. Her story serves as a reminder to pay attention to one’s health and advocate strongly for oneself in the face of medical challenges.
Name:
Tiffany J.
Age at Diagnosis:
38
Diagnosis:
Liver cancer (cholangiocarcinoma)
Staging:
Stage 4
Initial Symptoms:
Left flank pain
Treatment:
Radiation
Chemotherapy
Surgery
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Rachael, a 34-year-old mother of three, shares her experience with stage 4 sigmoid colon cancer, which has spread to her ovaries and liver. Her journey began unexpectedly when she visited the emergency room due to severe stomach pain. After undergoing a CT scan, she was abruptly informed of her diagnosis, a moment that left her in disbelief and shock. Despite this, Rachael quickly shifted her focus to taking control of her treatment, scheduling procedures like a liver biopsy and partial colectomy. She underwent emergency surgery with the help of robotic technology, which included a total hysterectomy and the placement of a colostomy bag.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Rachael describes the difficult emotional decision to undergo a hysterectomy, knowing it meant she would no longer be able to have more children. However, she prioritized her health and the need to be there for her 3 children. She talks about her intense chemotherapy regimen, which was both physically and mentally challenging. One of her greatest fears was not being able to be the same mother to her children during this time, but with the support of family and friends, she was able to manage her treatments and maintain a sense of normalcy for her kids.
Rachael reflects on the strange and sudden symptoms she experienced before her diagnosis of sigmoid colon cancer, including the loss of taste, appetite, and intense stomach pain. She also recalls how her dog seemed to sense something was wrong, constantly staying close to her in the months leading up to her diagnosis.
Rachael expresses a determination to keep moving forward despite the numbness and emotional difficulty of the situation. After completing her chemotherapy, she now faces the uncertainty of whether her tumors will grow again. She is awaiting further scans and potential liver surgery as well as HIPEC treatments. While she feels anxious about the future, she remains resilient and has accepted that she cannot control everything. She now possesses a sense of peace and a more positive outlook on life.
Despite moments of frustration and asking, “Why me?”, Rachael has found strength in her acceptance of her condition. She is grateful for her family, friends, and support system, and continues to focus on spending quality time with her children, making the most of the present while preparing for any challenges that may lie ahead.
Name:
Rachael M.
Age at Diagnosis:
33
Diagnosis:
Colorectal cancer
Staging:
Stage 4
Initial Symptoms:
Loss of sense of taste and smell
Loss of appetite and vomiting
Stomach pain
Bloating
Headaches
Fatigue
Treatment:
Surgery (total hysterectomy, sigmoid colon removed, tumor removed in colon, stoma configuration, port placement)
Chemotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Marisa shares her experience living with stage 4 synovial sarcoma. Diagnosed initially with stage 3 in 2017, Marisa’s symptoms began in high school when she noticed a small bump on her foot. Despite consultations with podiatrists over the years, the bump was misdiagnosed as a benign cyst until after its removal in 2017. By that time, the lump had grown significantly during her pregnancy. The devastating cancer diagnosis came when her daughter was six weeks old, marking a life-changing moment.
Marisa’s treatment included chemotherapy, a below-knee amputation in 2017, and multiple surgeries for lung metastases, starting in 2020. She underwent four pulmonary wedge resections, a segmentectomy, and later, radiation therapy to target residual cancer. Unfortunately, the cancer became more aggressive, spreading to her bones and lungs by early 2023. Despite numerous treatments, including 27 lung radiation sessions and systemic chemotherapy, Marisa remains optimistic and continues to monitor her health closely.
Mentally and emotionally, the impact of cancer has been profound. Marisa finds it challenging to balance parenting, work, and being a stage 4 cancer patient. She’s candid about the toll it takes on her and her family, especially explaining her illness to her young daughter. However, Marisa has chosen to focus on small joys—mundane daily tasks and moments with loved ones that now hold deeper meaning.
Marisa emphasizes the importance of self-advocacy in health care, urging others to trust their instincts and pursue answers when something feels wrong. She shares her story to provide hope to others battling sarcoma or cancer. She aims to raise awareness about the disease and inspire others with her determination to live fully, even while managing ongoing health challenges. Her message is clear: life with stage 4 cancer is not the end—it’s an opportunity to cherish each moment and look forward to advancements in medical science.
Name: Marisa C.
Age at Diagnosis:
24
Diagnosis:
Synovial Sarcoma
Staging:
stage 3 (2017)
Stage 4 (2021)
Symptom:
A small bump on the foot (stable for years, then grew during pregnancy), pain when pressed, difficulty wearing closed shoes
Treatments:
Surgeries: below-knee amputation, pulmonary wedge resections, and segmentectomy
Chemotherapy
Radiation: lungs and hip
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: Pain behind left knee, needle-like sensation in left foot Treatments: Surgery to remove what was thought to be benign tumor, chemotherapy, final surgery, radiation (36 sessions)
...
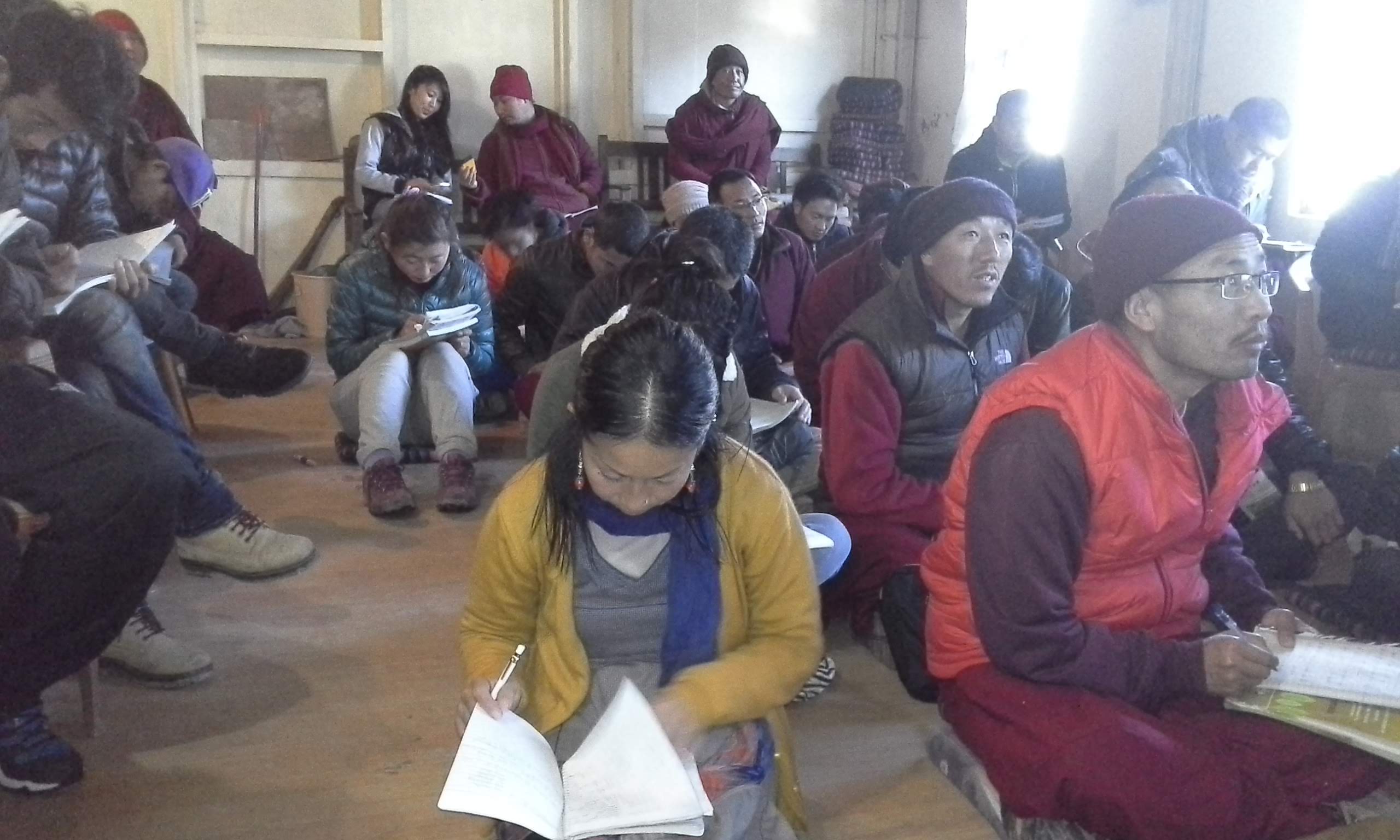
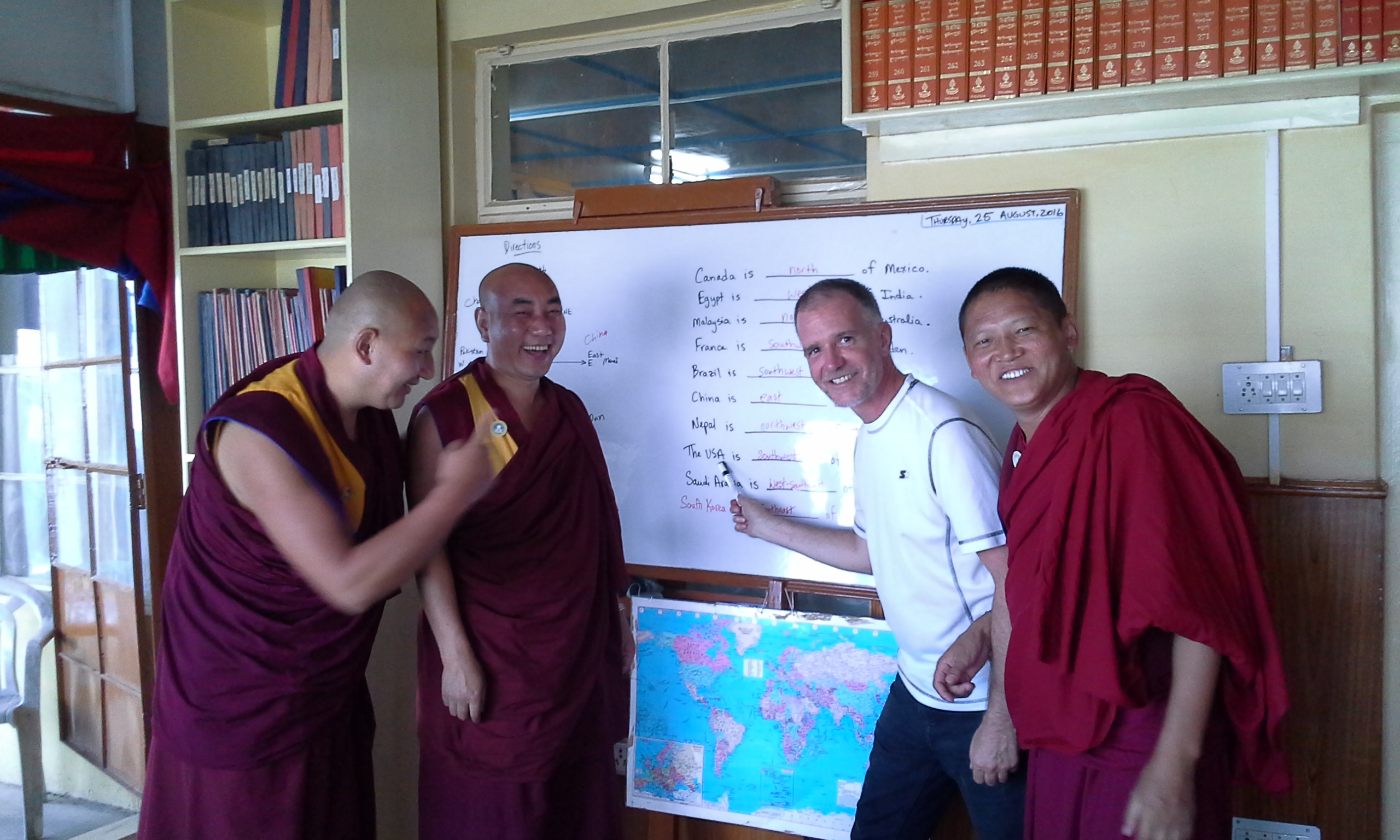
Ken, 59, from Minnesota, shares his journey battling stage 4 colon cancer, which he was diagnosed with in October 2022. His life prior to diagnosis included an adventurous career as a meteorologist and storm chaser, followed by a long stint as a volunteer English teacher in the Himalayas. However, in 2020, the COVID-19 pandemic forced a change of plans, and he settled back in the U.S. with his family.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Initially, Ken ignored concerning symptoms like intermittent bowel changes and blood traces, attributing them to minor issues. His symptoms diversified and intensified in late 2022, with frequent fevers, weight loss, and fatigue. After visiting urgent care, he received a CT scan revealing thickening of the sigmoid colon and metastasis to his liver [making it a stage 4 colon cancer diagnosis]. His oncologist warned him that without treatment, his life expectancy was limited to under a year. Though chemotherapy was initiated promptly, Ken faced immediate complications, including endocarditis, which halted his treatment temporarily and required a PICC line and weeks of antibiotics. The chemotherapy’s side effects left him drained and underweight, sinking to his lowest point emotionally and physically by early 2023.
A critical moment came when Ken experienced an intestinal blockage. Doctors recommended palliative care and hospice, as his heart was too weak for surgery. However, Ken’s cousin, a liver specialist at MD Anderson, connected him to the Mayo Clinic, where surgeons conducted a life-saving colectomy and liver resection, removing 68% of his liver. This marked a turning point in his recovery, as he began to regain weight and strength.
In 2024, after successfully undergoing a heart valve replacement and prostate procedure, Ken faced new challenges as scans revealed minor cancer regrowth. His oncology team pursued aggressive treatments, including ablations for liver and lung spots, as well as new medications, all of which proved highly effective. Despite persistent health challenges and skin reactions, Ken’s latest scan in mid-July 2024 showed that his treatment was working remarkably well.
Throughout this ordeal, Ken’s faith and positive outlook and his strong support network of family and medical teams helped him navigate his complex diagnosis and treatment, underscoring his resilience and determination to overcome each new hurdle.
Name:
Ken S.
Age at Diagnosis:
59
Diagnosis:
Colon cancer
Staging:
Stage 4
Symptoms:
Intermittent appearance of blood in stool
Occasional diarrhea
Increase in bowel movement frequency
Fevers and chills
Fatigue
Weight loss
Treatments:
Chemotherapy
Surgery
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Roshonda shares her story as an “ostomy warrior” after she was diagnosed with rectal cancer in 2022. Her initial symptoms included blood in her stool and a sensation of incomplete bowel movements in 2021. When she first visited a doctor, she attributed the symptoms to hemorrhoids. As her symptoms progressed, including seeing blood after sexual activity and worsening discomfort, she switched to Medicaid and a new healthcare provider, eventually leading to a colonoscopy in March 2022. The procedure revealed a mass and 3 polyps in her rectum, resulting in a rectal cancer diagnosis that devastated her, as memories of her late father’s battle with cancer resurfaced. She also had a spot on her lung which brought her diagnosis to stage 4.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Following her diagnosis, Roshonda met her team of specialists and began 6 weeks of daily radiation and oral chemotherapy. Despite the challenges, including burning pain, skin darkening, and intense discomfort, she persevered. Unfortunately, she lost her longtime job, and her unemployment benefits ended shortly after her diagnosis, complicating her financial situation. Thankfully, her mother and grandmother provided support, covering bills and easing some of the burden.
Despite the intense treatment, Roshonda’s tumor did not initially shrink enough. Her oncologist advised further treatment with intravenous chemotherapy, which involved 8 sessions over 4 months. These sessions were grueling, leaving her nauseated and exhausted. Reflecting on the mental toll, Roshonda stresses the importance of maintaining a positive outlook, which she believes helps many cancer patients manage their journey.
Facing surgery to remove her rectum and anus due to the tumor’s location, Roshonda had to decide between keeping the anal area, risking potential recurrence, or opting for a complete removal with a lifelong colostomy bag. She chose the latter, enduring significant pain after the procedure, with limited mobility and initial difficulty sitting.
Roshonda joined an online ostomy support group before surgery, learning from others’ experiences and finding comfort in a community of people facing similar challenges. This network has been invaluable, especially since she is the only one in her family with an ostomy bag.
Sharing her rectal cancer journey on TikTok and Facebook, Roshonda aims to raise awareness about colorectal cancer, particularly within the Black community, which faces higher incidence rates. She encourages early screenings and prompt medical attention for symptoms. Gospel music and faith have helped her find peace, especially a song that resonated deeply with her, helping her surrender her worries before surgery.
Adjusting to life with a colostomy bag, Roshonda emphasizes listening to her body and finding what works best for her. Though the journey has been painful and challenging, she remains grateful for her support network, faith, and the resilience she’s developed throughout her battle.
Name:
Roshonda C.
Age at Diagnosis:
37
Diagnosis:
Rectal cancer
Staging:
Stage 4
Initial Symptoms:
Blood in stool
Blood from rectum after intercourse
Sensation of incomplete bowel movements
Treatment:
Chemotherapy
Surgery
Radiation
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Ashley’s Stage 4 ROS1+ Non-Small Cell Lung Cancer Story
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Ashley, a mother of 2 young children, shares her journey with stage 4 lung cancer. Initially experiencing a persistent cough post-COVID, Ashley also began to experience shortness of breath and sharp pains that led her to seek help at a hospital. While the first hospital misdiagnosed her ailment as pneumonia, a second hospital found a life-threatening pulmonary embolism. Further tests confirmed stage 4 adenocarcinoma (non-small cell lung cancer). Ashley and her husband, Jason, deeply felt the impact of her diagnosis, particularly given past family losses to cancer.
Determined to seek comprehensive care, Ashley pursued a second opinion from MD Anderson. There, she learned about her ROS1 biomarker, which allowed her to undergo targeted therapy. This approach has been successful, putting her in remission.
Ashley sought refuge in her faith and combines traditional treatment with holistic methods, emphasizing the importance of integrating both to support her immune system. She has taken proactive steps to improve her well-being, including leaving her full-time job to focus on her health and spend more time with her family.
Ashley underscores the significance of self-advocacy in her treatment, highlighting instances where she challenged medical advice and conducted her own research. Through therapy and a positive mindset, she combats the mental health challenges associated with her illness. Ashley advises others to maintain hope, advocate for themselves, and support their emotional and physical health integratively. Her story emphasizes the importance of seeking answers and living fully despite her prognosis, as she cherishes her time with loved ones and continues making memories.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I’m such a data-driven, logical, realistic person.
But cancer has taught me that I have to live in the space where optimism and hope are.
Introduction
Hi, I’m Ashley. I was diagnosed at 35 years old with stage 4 lung cancer, adenocarcinoma, non-small cell with the genetic mutation of ROS1.
I am a mom of 2, a little boy and girl who were 5 and 2 respectively when I fell ill. I love being outside, going on nature trails and hiking.
Also, we have a pool in our backyard and swimming laps for exercise is definitely a hobby and something I was doing a lot leading up to my diagnosis.
I was also working out with a personal trainer and lifting weights, all up until the day my initial symptoms started.
Pre-diagnosis
Initial symptoms
Before all this began, I struggled with a persistent cough that lasted for maybe 8 or 9 months.
I’d had COVID in January, and by September I was still coughing. On a daily basis, it would start out mild, but would worsen as the day progressed, and then I would be hacking by bedtime. But I wouldn’t allow it to interrupt my day; I would still be going 100mph as a mom.
I saw a doctor in May, and he chalked it up to allergies. I just kept getting my daily stuff done because it wasn’t so disruptive anyway.
Later on in the year, my husband Jason and I were working out with a personal trainer, and I was weightlifting, deadlifting heavy weights. We started HIIT workouts, high intensity interval training.
One morning, we were swimming laps in our backyard pool to the point that we were trying to huff and puff. And I noticed that I really couldn’t be underwater for a very long time.
I went on about my day and began work by 2:00 p.m. that day. I started having a sharp pain in my right abdominal area, the rib cage area. I powered through and ignored it.
That evening we were hosting a small group, so we had roughly like 20 or so people over, and were in the middle of a meal when I started having another bout of sharp pain in my right abdomen again and my right shoulder area too.
I thought, man, was it something I ate? Could it be gallstones? It’s unbearable, just a lot of pain. But I decided I would get to it after everybody left. The group laid hands on me and prayed over me, and we went about our night after they went home.
The next day, the pain got even more intense. I couldn’t walk from my bed to the bathroom without hunching over in agony. So we decided it was time to head to the ER.
We went in, and they did a workup. And they found that I had a lung full of fluid. They told me I had pneumonia and sent me home with literally 12 prescriptions, like muscle relaxer, pain relievers and inhaler and everything you could think of for pneumonia.
That weekend, I spent in my room away from my kids because I didn’t want them to catch anything from me. And that evening, my lips started to turn blue. And at this point I was having trouble breathing, but at no point did I think that it had anything to do with my lungs — I just thought that the pain was so intense that it was affecting my breathing.
First hospital admission
Jason rushed me to a hospital where I got admitted this time. They took my blood oxygen level using a pulse oximeter and the reading was 70 or so, which was unbelievably low.
I had them retest me 3 times, with the same result each time. They rushed to provide me with supplemental oxygen, and I ended up staying at that hospital for 4 days.
At that hospital they conducted a workup and scans, including a CT scan with contrast. And that’s when the 6-letter word entered the conversation.
They said they had seen lesions on my spine, and said that they could be either calcium deposits or cancer. And since I wasn’t anywhere near 60 years old, calcium deposits were unlikely.
They did 2 biopsies — the first one was around the sternum and completely missed the area. I could feel it, feel the drill, feel everything. They were nervous about proceeding because they could hit my heart if I moved.
So the next day they drained the fluid from my right lung and conducted a second biopsy, for which they completely put me under. It was in a whole different location this time. And then they started working on getting my oxygen back.
So it was a bit of a jarring hospitalization for me. I was thankful to have been supported by my family and my church during my stay.
After 4 days, I was ready to be discharged me and to be sent home with oxygen. But they spoke with me and said that since cancer has entered the conversation, they recommended that I transfer to a second hospital, in Dallas.
You have to lead your treatment process in your journey.
You can feel like you’re just a number, given the number of patients doctors have to see.
But of course you’re more than just a number.
Second hospital admission
The second hospital was 45 minutes away by car, and my husband took me there right after I was discharged. We got in pretty quickly and told them what the first hospital had said — that we needed to have a PET scan double-time.
Lo and behold, this second hospital discovered that I had a really large pulmonary embolism, caused by a huge blood clot in my lung, which the first hospital had missed completely.
So only by the grace of God did I manage to survive. I’ll never forget the expression on the faces of the doctors.
They immediately put me on a blood thinner, and I had some great specialized care courtesy of amazing nurses and specialists like physical therapists. But cancer continued to be the main topic of conversation at this hospital.
I had to undergo scans that required me to be wrapped up like a mummy. I was terrified and claustrophobic, but I just had to go in that machine. I just had to talk to the Lord and try to be courageous, and also focused on scripture and thought about my kids.
I ended up spending 8 days in that Dallas hospital.
Non-Small Cell Lung Cancer Diagnosis
While I was in Dallas, the results had come back from the tests the first hospital had run.
They were positive for adenocarcinoma.
Reaction to the diagnosis
Initially, during those 12 really long, jarring, shocking days before my diagnosis, we just kept holding on to the hope that I didn’t have cancer. We kept praying and hoping that they really were just calcium deposits or just something else, something benign. But all the signs were always pointing towards cancer.
And so the moment that the doctor came in and confirmed it was cancer, I completely lost it. I bawled my eyes out and shook uncontrollably. It felt so, so unbelievable. And what’s worse, it wasn’t just cancer, it was lung cancer.
Because the doctor had told me that since I was a nonsmoker, if I did have cancer, it would probably be breast cancer. So I was so taken aback that it was cancer. It was lung cancer. It was stage 4 non-small cell lung cancer. It was inoperable. It was terminal. And he told me that some people in my situation would live, say, 5 to 10 years.
So a tremendous amount of fear rushed over me, and I was shaken. But I clung to my faith and knew that the ultimate physician is the one who has the final say.
As for my husband, he’s a bit of an introvert, and processes things very differently from me. I think he did a lot of his grieving outside the room. He wanted to remain strong and steady and full of faith and constant. He’s already lost his dad and brother — the latter to cancer, just in 2020, and in the low 40s, so I think there’s some PTSD there. And I think he kind of shut down.
So quite apart from me, he sat in his chair and didn’t express too much emotion. And that’s been in character with how he’s been grieving, like when the kids are asleep, we’ll lie down and sometimes cry together.
You may have big decisions to make really fast, and to do that — and to advocate for yourself — you need to be prepared.
Second opinion
I decided to get a second opinion with MD Anderson, based on their reputation.
While I still do have an open file at the Dallas hospital and can get treatment from them if I need to, the quarterback of my care team, the decision maker, would be MD Anderson.
MD Anderson had a lot to teach me. For instance, I had already heard that a particular drug I was about to take, if I were to respond well to that treatment, would work for a couple of years.
But then I learned from talking to MD Anderson that the cancer was likely to come back, that I might grow resistant to the drug in a couple of years. I didn’t know that coming into that appointment.
ROS1 and biomarker testing
I also have the ROS1 biomarker.
The topic of me possibly having a biomarker was brought up at my first appointment. Ever since then, I was really hoping that I had a genetic mutation, because I don’t want to do traditional chemotherapy at all.
So I was very happy to learn that I do have the ROS1 biomarker. And my having it has informed my treatment.
So I’ve been undergoing a targeted therapy. I’m taking a TKI drug and it’s been working really well.
Treatment, remission, and further steps
Targeted therapy for non-small cell lung cancer
I’m now in remission thanks to my first-line treatment.
Every single night, I take my TKI drug. I’ll be on it for the rest of my life.
I can’t actually handle a full dose — I didn’t even start out on the full dose, I began with three-fourths of a dose — and now I’m just taking half a dose every time.
My medicine is heavy on my kidneys and my liver, which makes it imperative that I get them to be in tiptop health.
Holistic approach
My total approach, though, is actually more integrative and holistic. I augment the solution MD Anderson has given me with solutions from integrative doctors.
I had actually quit my job so I could spend more time with my family, my kids. But another big reason I did that was also to free myself up to do things that are going to help my immune system. A lot of holistic care and integrative treatment.
I don’t think it’s all Western or all traditional medicine that helps. I believe it’s a blend of both, like you take the best of both worlds. And so I do seek out the opinions and inputs of both oncologists and experts in integrative medicine.
When your mortality is on the table and you see so many people across the board struggling with and passing away from cancers like this [ non-small cell lung cancer ], it’s like you want to throw a hundred things at the disease and not just 1. If I were to depend on MD Anderson alone, that would just be like placing all my eggs in only 1 basket. And so I would rather have multiple experts weighing in.
I think the integrative world does great at looking into root causes. They say that cancer isn’t just this tumor that appears 1 day and out of nowhere; it’s something that has been building in one’s body for maybe a decade, for example. And it’s like a perfect storm, like glucose in the body, the diet, the microbiome, the immune system, and so on.
And so I do things like taking IVs of sodium bicarbonate — which is alkaline and helps make my body alkaline too, so that cancer cannot survive in it. I think my whole mentality as far as integrative medicine goes is that I create an environment within me that cancer is unable to return to.
I went to an integrative cancer center in California for 6 weeks through Thanksgiving and Christmas last year. I entered with my oxygen tank in tow. I left without it.
Self-advocacy
Sometimes, these approaches I go for and experts I consult clash and don’t agree with each other, or with me. And, moreover, sometimes they miss things. And this is where I have to be my own advocate and discern and ask God which direction I should go.
I’ve already mentioned earlier that the first hospital I went to completely missed my pulmonary embolism, and that’s no less than life-threatening. I also have a run-in with a particular doctor to share.
So I did a blood panel and checked out my B12 levels, which were way off the charts at over 2,000. The doctor just shrugged it off, saying that it was water-soluble and thus not worth looking into. He said, it’s probably from your diet. So I paused drinking this plant-based protein shake I’d been taking, and it had no effect on the super high B12 levels.
So I self-advocate. For every doctor’s appointment I go to, I craft bullet points and an agenda to help guide our discussion. And sometimes I’ll send this agenda ahead of time and tell the doctor, hi, I’d like us to address these concerns and I want you to know ahead of time what we’ll be discussing.
You have to lead your treatment process in your journey. You can feel like you’re just a number, given the number of patients doctors have to see. But of course you’re more than just a number.
Do your research, learn from other people. At the start I was like, it’s a full time job to learn everything. But that’s how I know what kind of questions to ask. You may have big decisions to make really fast, and to do that — and to advocate for yourself — you need to be prepared.
So I’m living life.
I’m doing all the things and making all the memories.
Improving mental health
I’ve also found that there are steps one can and should take to improve one’s mental health.
After my non-small cell lung cancer diagnosis, I literally was walking in depression. I was literally preparing to die. For the first year or so, I experienced so many days and nights where I thought about dying a lot. I would just see my husband and our 2 kids continuing life. My mind would even go to events like my daughter’s future wedding taking place without me, or my funeral with my family grieving.
But I couldn’t succumb to that.
Some people in cancer groups online, for example, are preparing to die and doing things like writing their kids books so that they’ll read them in the future and get to know or remember their parents.
Sure, I’d want to write a book of my own down the line. But I’d like to do it from the standpoint of being NED.
And so I think that a lot of therapy has been necessary.
Living life
So I’m living life. I’m doing all the things and making all the memories.
I’m literally not saying no to anything, just trying to do all the fun things I can with my husband and kids.
We’re having a whole lot of fun.
Advice for others
Place your trust and have hope
The first piece of advice I would like to offer is definitely to have hope. And for me, this is based in faith.
My faith is everything to me. My experience has taught me that placing my trust in God and something bigger than myself is crucial.
I’m such a data-driven, logical, realistic person. But cancer has taught me that I have to live in the space where optimism and hope are.
Think positively and act like you’re healed
Positive thinking is massive. It may seem silly to some, but from all the research I’ve done, I’ve found that there’s so much truth to it.
It’s like our brain is telling our body what to do.
So act like a healed person. Keep living your life like you’re healed.
Advocate for yourself
I’ve said this already earlier — it’s so important to advocate for yourself, and to do so you must prepare properly.
Don’t just trust one doctor. Go get a second opinion, seek the help and inputs of other experts. Get as many eyes on the glass as you can. Especially if you have other people like kids who love you and depend on you.
And if their opinions and advice clash, seek guidance to resolve it. But build your own knowledge base too.
Support yourself both physically and emotionally
I think it’s also crucial to support yourself integratively, holistically, as you’re going through this. And emotional work is extremely important.
I’ve learned in the integrative space that emotional work matters just as much as physical work does. And not only dealing with the emotions you’re managing at present, but also with any emotional backstory, like childhood traumas, that might have contributed to your situation at present.
I’ve heard from more than one integrative provider that deals with cancer patients and has been doing so for decades. The ones who don’t survive are the ones who aren’t doing the emotional work.
Get to the root cause
If you experience a suspicious symptom just like I did with my cough, don’t shrug it off. Investigate it and get to the root cause.
I didn’t have allergies year-round — so why was I having a cough for 9 months?
I didn’t want to take time away from my work and family to do so, and besides, I thought, my cough was livable. It wasn’t really interrupting my daily life. But look at how things developed.
My cough was in itself a small thing, but it was persistent. It wasn’t allergies. It wasn’t long COVID. It wasn’t pneumonia. It was a sign that I had stage 4 non-small cell lung cancer.
Interviewed by: Nikki Murphy Edited by: Chris Sanchez
At age 34, Shirley, a translator from Southern California, faced the unexpected news that she had stage 4 lung cancer with an ALK mutation.
Shirley’s journey began in 2021, during the height of the COVID-19 pandemic, with a persistent cough that refused to go away despite multiple rounds of antibiotics and testing. Her doctors reassured her it was likely a minor infection, even though her symptoms grew to include severe back pain. Finally, a CT scan revealed a mass, but doctors still downplayed the likelihood of cancer due to her young age and history. Initially undiagnosed, she faced months of additional procedures, including 2 bronchoscopies and a wedge resection surgery. Only after extensive testing did she receive the staggering news: she had adenocarcinoma, initially suspected to have originated elsewhere in her body. Despite various scans showing otherwise, she spent weeks fearing widespread cancer.
Determined to take control, Shirley switched hospitals, explored different insurance options when she got married to her longtime boyfriend, and underwent chemotherapy. The side effects were brutal, including severe hair loss, swallowing difficulties, and infections that required hospitalization. Finally, genetic testing revealed she had an ALK mutation, allowing her to switch to a targeted therapy in pill form, providing 2 years of relative stability and an improved quality of life. Then, in 2023, the cancer began progressing again, necessitating further procedures and consultations. When her initial targeted therapy became ineffective, Shirley bravely enrolled in a clinical trial for a 4th-generation ALK inhibitor in July 2024. This new medication has had minimal side effects, with her tumor currently stable. Although she initially hesitated to join a clinical trial, Shirley realized its promise and now appreciates the thorough monitoring and regular scans.
Living with an incurable cancer has profoundly affected Shirley’s outlook on life. “It feels like I have a bomb inside of me,” she says, expressing the constant awareness of her tumor’s presence. With humor as her coping mechanism, Shirley shares darkly comedic memes and gives villain names to her tumor. Her husband and fellow cancer patients have become her pillars of support, as she finds comfort and laughter within her community of ALK patients, appreciating the unique understanding they bring.
Despite the trials of cancer, Shirley finds solace in sharing her experience, including on her Instagram, to help others. Her advice to newly diagnosed patients is heartfelt: avoid over-Googling statistics and connect with others who understand the cancer journey. “You’re not a statistic,” she insists. “See yourself as an individual.”
Shirley’s journey is one of resilience and transformation, where she now cherishes connections and purpose. By sharing her story, she aims to support others, proving that even amid uncertainty, there is value in embracing life with hope and humor.
Name:
Shirley M.
Diagnosis:
Lung cancer
Staging:
Stage 4
Initial Symptoms:
Persistent cough
Wheezing
Back pain
Shortness of breath
Treatment:
Chemotherapy
Targeted therapy
Radiation
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Shayla was diagnosed with metastatic colorectal cancer at 33 years old after years of experiencing unexplained digestive issues. Initially, symptoms like stomach sensitivity, exhaustion, and food intolerances were attributed to a sensitive stomach. Over time, she sought medical attention, including multiple gastroenterologist consultations but received inconclusive diagnoses. She was diagnosed with celiac disease, but despite cutting out gluten, she continued to feel unwell.
After more months of fatigue, Shayla noticed blood in her stool, which persisted for several weeks. When her husband insisted she seek medical help, a colonoscopy revealed polyps. While initially told that they weren’t cancerous, a biopsy later confirmed that one was malignant. Further tests revealed lesions in her liver and lungs, prompting additional biopsies. The lesions in her lungs were clear, but the cancer had metastasized to her liver, resulting in a stage 4 colorectal cancer diagnosis.
Her treatment plan included four rounds of chemotherapy, followed by a hepatectomy or liver resection to remove 25% of her liver. After the surgery, Shayla began her chemotherapy again, with plans for more rounds to finish her treatment. Although she initially struggled with side effects, such as hot flashes, nausea, and fatigue, her doctors adjusted her treatment plan to help her manage better. However, cold sensitivity, neuropathy, and physical weakness persisted.
Despite these challenges, Shayla remained focused on her healing and recovery, even as the emotional toll of her diagnosis began to weigh on her mental health. She shared that the isolation during recovery and the struggle with seeing her children react to her illness was particularly difficult.
Shayla advocates for others to take their symptoms seriously, stressing the rising rates of colorectal cancer in younger adults. She encourages others to seek second opinions and advocate for themselves if they’re not satisfied with their medical care. Through her experience, she has seen the importance of a strong support network and the need for proactive health care, urging others to catch cancer early to increase treatment success.
Name: Shayla L.
Age at Diagnosis:
33
Diagnosis:
Colorectal Cancer
Staging:
Stage 4
Symptoms:
Stomach sensitivity
Food intolerances
Exhaustion
Blood in stool
Treatments:
Chemotherapy
Surgery: hepatectomy (liver resection)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Lindy was diagnosed with stage 4 colon cancer when she was two months postpartum at age 34. During her pregnancy, Lindy experienced severe abdominal pain, changes in bowel movements, blood in her stool, and significant discomfort, all of which she initially attributed to pregnancy. Unbeknownst to her, these symptoms were indicative of colon cancer, which was eventually discovered during a routine full-body MRI for a previous benign brain tumor and spinal tumor.
Doctors identified malignant cancer had spread to her colon, lymph nodes, liver, and lungs. The shock of her diagnosis came at a time when Lindy was navigating the challenges of new motherhood. She took an active role in researching her diagnosis, and while the news was overwhelming, it helped her process the information before meeting with her oncologist.
Lindy’s treatment began swiftly with chemotherapy in January following her December diagnosis. Although surgery was not considered an immediate option due to the cancer’s spread, chemotherapy has been her primary treatment. She transitioned to maintenance chemotherapy, as her body responded well to the treatment with minimal side effects. While she still experiences some numbness from neuropathy, she considers herself fortunate for not facing more severe symptoms.
Throughout her experience, Lindy has been grateful for her medical team, who never dismissed her concerns despite her young age. While colon cancer is typically seen in older individuals, Lindy’s case is part of a growing trend of younger people being diagnosed with the disease. This has prompted her to encourage friends and family to undergo early screening.
Lindy is realistic about her prognosis, understanding that while her cancer is not curable, it is treatable, and she remains hopeful for potential advancements in treatment. She has made practical preparations for the future while focusing on enjoying life with her son and husband. Lindy’s strong support system has helped her navigate both motherhood and cancer.
Lindy emphasizes not spiraling into despair. Instead, she encourages others to seek out a supportive care team, possibly including palliative care to manage pain symptoms, and to focus on living in the moment. Lindy’s outlook remains positive, bolstered by the progress she’s made and the hope for future treatment developments. Despite the challenges, she is determined to live as fully as possible, enjoying time with her loved ones.
Name: Lindy A.
Age at Diagnosis:
34
Diagnosis:
Colon Cancer
Staging:
Stage 4
Symptoms:
Blood in stool
Changes in bowel movements
Pencil-thin stool
Severe abdominal pain
Loss of appetite
Rapid weight loss
Anemia
Fatigue
Treatments:
Chemotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.