follicular lymphoma top questions answered by Dr. Peter Martin Weill Cornell Medicine
Your Follicular Lymphoma Questions, Answered by Dr. Peter Martin
On Demand Replay Now Available
Living with follicular lymphoma often comes with more questions than answers. That’s why we’re turning directly to the community — and a leading follicular lymphoma expert — to help.
For a limited time, we’re collecting your most important questions about living with and treating follicular lymphoma for Dr. Peter Martin from Weill Cornell Medicine. We’ll present his expert answers in a special webinar hosted by The Patient Story.
What to expect:
We’re gathering questions from the follicular lymphoma community for a limited time.
Dr. Martin will answer as many as possible during the webinar.
Please note: Due to the number of registrants, not every question can be addressed individually.
Answers will be provided in general terms and not personalized medical advice. For your specific situation, always consult your own physician and care team.
A special thanks to our friends at the Living with Follicular Lymphoma Facebook Group for their partnership. Their private Facebook group is dedicated to supporting individuals with follicular lymphoma, their families, and supporters. They offer a safe space to share personal experiences, learn about the latest research, trials, and treatments.
Register for this informative program then invite a Friend or Care Partner.
This webinar has been completed!
This webinar has not yet been completed.
Your Follicular Lymphoma Questions, Answered by Dr. Peter Martin
Hosted by The Patient Story Team | 34m 29s
Living with follicular lymphoma often comes with more questions than answers. That’s why we’re turning directly to the community — and a leading follicular lymphoma expert — to help. For the next two weeks, we’re collecting your most important questions about living with and treating follicular lymphoma for Dr. Peter Martin from Weill Cornell Medicine. We’ll present his expert answers in a special webinar hosted by The Patient Story.
Looking to the Future: Treatment Paths for Relapsed/Refractory DLBCL
Plus: How Academic & Community
Hospitals Work Together for You
For people facing relapsed or refractory DLBCL, the path forward can feel uncertain and overwhelming trying to weigh treatment options.
That’s why this program brings together Dr. Joshua Brody from Mount Sinai and Dr. Amir Steinberg from Westchester Medical Center, two lymphoma specialists who coordinate closely across academic and community settings. Moderated by The Patient Story’s own founder and DLBCL survivor, Stephanie Chuang, they’ll share how new therapies are changing the landscape and how working together across systems helps ensure patients have access to the most up-to-date treatments and support.
Topics:
What relapsed/refractory DLBCL means for patients
Latest treatment advances and what they could mean for care
How academic and community oncologists collaborate on patient treatment
Clinical trial opportunities and why they matter
Practical tips for patients to advocate for themselves and ask the right questions
What the future may hold for people living with DLBCL
Thank you to Genmab and AbbVie for their support of our independent patient education program. The Patient Story retains full editorial control over all content.
This program has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Register for this informative program then invite a friend or care partner.
This webinar has been completed!
This webinar has not yet been completed.
Looking to the Future: Treatment Paths for Relapsed/Refractory DLBCL
Hosted by The Patient Story Team | 1h 9m 30s
Hear Dr. Joshua Brody and Dr. Amir Steinberg discuss new treatments for relapsed/refractory DLBCL and how academic–community collaboration helps patients access the best care. Moderated by DLBCL Advocate Stephanie Chuang.
Webinars in this series must be completed in order.
Pick up where you left off →
Table of Contents
Edited by: Katrina Villareal
Introduction
Stephanie Chuang, The Patient Story: Hi, there! I’m so glad you could join us for our discussion. Diffuse large B-cell lymphoma (DLBCL) can return or be difficult to treat. This conversation aims to help you, as a patient or care partner, to walk away with questions you can ask your healthcare team if the first treatment doesn’t work. I want to highlight that, as difficult as this situation is to be in, we keep hearing from DLBCL experts that there’s so much research and so many developments happening in terms of lymphoma treatments, and that’s what we’re going to dive into. We’re also going to talk about how you can work with different kinds of doctors who work at different centers, as well as busting clinical trial myths and sharing more of what they are.
My name is Stephanie Chuang. I’m the founder of The Patient Story, but more importantly, I had my own diagnosis of DLBCL. I went through hundreds of hours of chemoimmunotherapy and I’m lucky to have had no evidence of disease for eight years now. I started The Patient Story as a result of my experience of feeling isolated in trying to find other people who were dealing with the same diagnosis and trying to empower myself when all I was finding was a lot of medical jargon.
We would like to thank our sponsors, Genmab and AbbVie, for their support of this program, which enables us to host more programs like this at no cost to our audience. We want to note that The Patient Story maintains full editorial control. While we hope this conversation is helpful, this is not meant to be a substitute for medical advice. It’s informational, so please consult your healthcare team when making decisions.
Finally, but importantly, we want to hear from you. Your voice matters so much in helping us shape what we put out next. Was this helpful? What would you like to hear more about? What could we do better? Please let us know what your feedback is.
I’m so honored to be joined by two amazing experts. Dr. Joshua Brody, who’s a friend of The Patient Story, is the director of the Lymphoma Immunotherapy Program at The Tisch Cancer Institute at Mount Sinai in New York, a faculty member of the Icahn Genomics Institute, and the primary investigator at The Brody Lab.
We’re also so lucky to be joined by Dr. Amir Steinberg. He’s the director of the Cellular Therapy Program at Westchester Medical Center in New York and a professor of medicine at New York Medical College. Dr. Steinberg has been involved in research focused on lymphoma, quality of care, and nonmalignant transplantation. I got a rundown of how the two of you know each other, so there’s some history, which is wonderful. I’m so excited to have this discussion with you both.
But before we jump into this educational content for our patients and care partners, we would love to humanize you, doctors. You’re so great at what you do. You’re brilliant. But we’d love to understand more about the personal aspect. Dr. Brody, again, thank you for being here for the millionth time. You clearly spend a lot of time outside of the clinic and research to help patients who are not in your direct care. You’re very busy. Can you share what motivates you to continue dedicating your time?
All diseases are bad, but sometimes cancer feels like the most unjust.
Dr. Joshua Brody
Dr. Joshua Brody: Oh, you said this is going to humanize me and though this is going to make me sound like a saint, those who know me, like Amir, know it’s not true. There are things you could help people with. You could help people with all kinds of problems. But cancer just sometimes seems like the most unjust thing. People did everything right. They didn’t do anything bad. They were healthy. They tried everything. They have a family. They worked so hard. And then they get struck down seemingly out of nowhere.
All diseases are bad, but sometimes cancer feels like the most unjust. I come from a childhood background of comic books and superhero stories, so justice is a big theme. Folks like Amir and I are lucky to have access to opportunities to help people, and if we have an opportunity to help, how could we not take advantage of that opportunity when there’s a person in need? I don’t know if that was humanizing enough. I should have said something more about how I like baseball and beer, but you have to help people if they need help.
Stephanie: We like that. We got the comprehensive view: baseball, beer, and being a saint. I know how busy you are, so I’m appreciative and I know our community is as well every time you join us on a program like this.
The care I received and the academic physician who took care of me inspired me to emulate his career, so that’s why I went into the field of oncology.
Dr. Amir Steinberg
I’d like to welcome Dr. Steinberg for being here. This is the first time we’re able to meet you and we’re happy to. Speaking of humanizing, you have many personal reasons why you’re in the work that you do. I read a poem about how it affects us all and it details a lot of your connection to cancer, including your own. Could you share a little bit about that connection and how that’s motivated you to do what you’re doing today?
Dr. Amir Steinberg: I was a senior in high school, reading comic books and watching baseball — all those things that Dr. Brody was alluding to, as we come from the same stock in that regard — when I came down with Hodgkin’s lymphoma. I had these big lymph nodes in my neck that started to grow early in my senior year.
I had never heard of MD Anderson Cancer Center before, even though I grew up in Houston. We had a family friend who recommended that we go there. I enrolled in a clinical trial, but I didn’t know what I was signing up for. My mom and I signed the paperwork when I was 17 years old. I did well. I completed all my treatment. Our family friend did my radiation. The care I received and the academic physician who took care of me inspired me to emulate his career, so that’s why I went into the field of oncology.
Over time, other family members came down with cancer as well, particularly lymphoma. My father was diagnosed with follicular lymphoma in his late 70s and, subsequently, diffuse large B-cell lymphoma and then he was diagnosed again with follicular, so maybe that DLBCL might have been follicular lymphoma to begin with. Then my sister was diagnosed with gray zone lymphoma (GZL) a couple of years ago. She had chemotherapy. Stephanie, you mentioned that you got R-EPOCH and she got the same regimen as you. She was treated in Seattle, where she lives, and she’s doing fantastic now.
Cancer can affect anybody. Just like Dr. Brody was alluding to, we could be the healthiest people possible and yet cancer can still affect you — even if you didn’t smoke, ate healthy, or were a marathon runner.
Stephanie: It’s unfortunate, the number of connections to cancer there are. Thank you for joining us. I’m also very interested. I didn’t realize that you were a clinical trial participant at such a young age. We’ll be talking about clinical trials. We’ve talked over and over again about how unfriendly the term itself can be for people to hear. Our goal at The Patient Story is to try and help make it more accessible as a concept for people, so they can ask doctors like you about clinical trials.
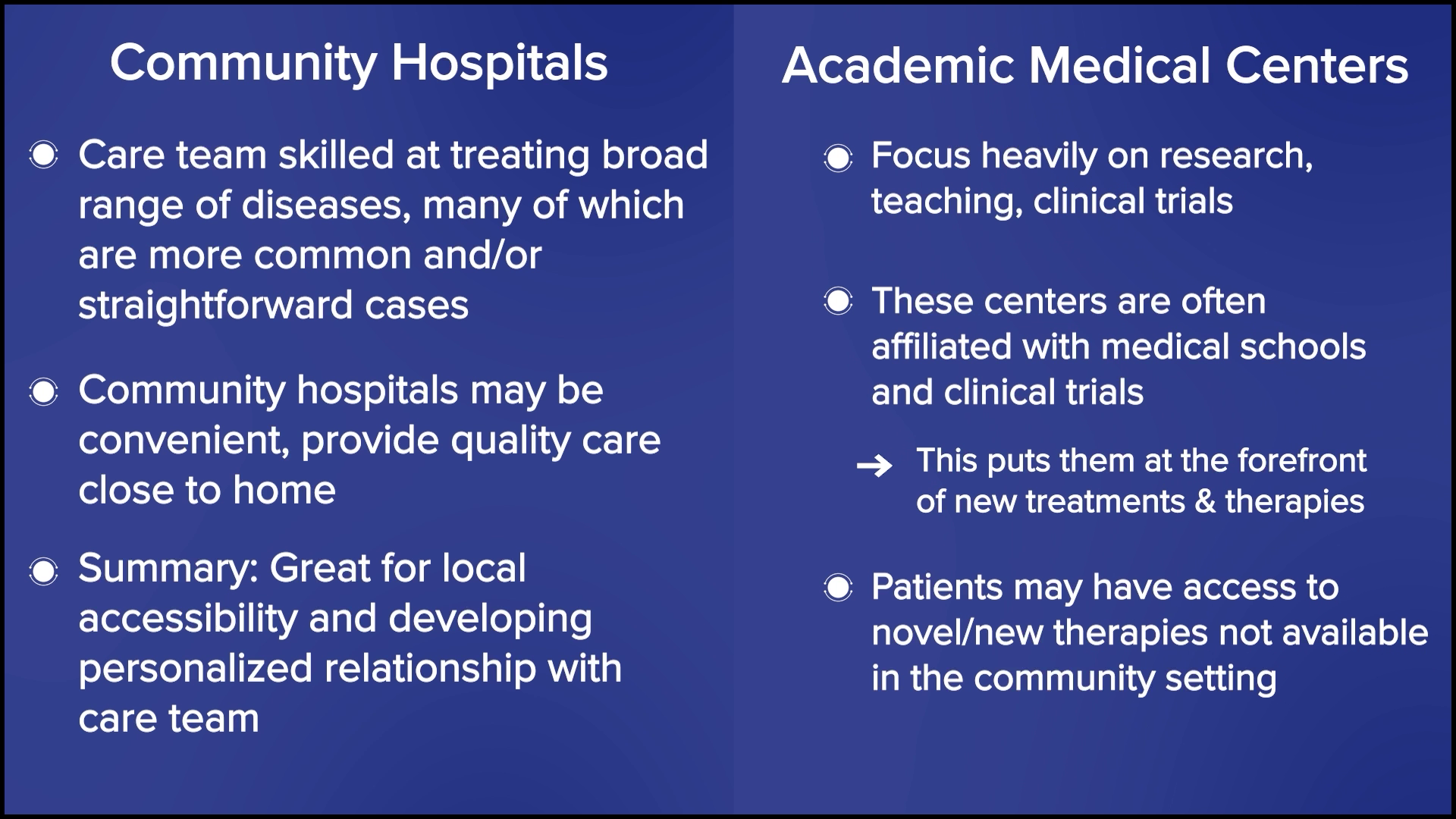
We’ll jump right in with the basics. For the relapsed/refractory diffuse large B-cell lymphoma population, we’re going to talk about some information that is going to go into clinical trials. Another thread is working with different kinds of doctors at different kinds of centers. Dr. Brody is at Mount Sinai, which is a huge academic center, and Dr. Steinberg, who is also an academic but also at a community center where you are all up to date on the latest. Also, you have referred people to see some specialists, like Dr. Brody, in some instances.
There’s information overload during that first discussion... A newly diagnosed DLBCL patient is barely hearing you.
Dr. Joshua Brody
Conversations with Newly Diagnosed vs. Relapsed/Refractory
Stephanie: Dr. Brody, what’s the first conversation you have with newly diagnosed patients when describing the situation and likely treatment options versus when you have to talk to people who’ve already gone through at least one line of treatment?
Dr. Brody: Although relapsed/refractory DLBCL is an objectively worse conversation to have because our statistics are not as amazing, somehow it’s an easier discussion. There’s information overload during that first discussion. “Wait, I have lymphoma?” A newly diagnosed DLBCL patient is barely hearing you. The audience may be too young to remember, but Charlie Brown had a teacher who, whenever the teacher spoke, it was just, “Womp womp womp womp.” Very little can get in because they’re sitting there thinking, “Wait, what? I have what? I’ve never heard of lymphoma. Is that rare?”
The conversation has to be, “Here’s all the information, but you don’t need to memorize any of this.” I’m going to hit a couple of bullet points, which are the key points. The emphasis is to try to convert it as quickly as possible from a didactic doctor talking to a patient to hopefully a conversation. You have to keep interrupting. “All right, I spoke for 35 seconds. Do you have any questions about that part?” Usually, patients will still be a little too shell-shocked to even have questions, so I’ll say, “As soon as I walk out the door, you will think of some questions. Here’s what you need to do. Write them down there in the Notes app on your phone or a notebook, so you can come back next time and ask those questions.”
Whereas with relapsed/refractory DLBCL, this person has probably been clicking and learning for the past year, two, or three about lymphoma, so we can get down to the nitty-gritty a bit more. There’s a very different conversation with a newly diagnosed patient and a relapsed/refractory patient for the patient’s emotional experience of what they’re hearing.
Stephanie: Thank you for that, Dr. Brody. I appreciate that you’re probably getting very similar questions, but that you provide space for people by saying that as soon as they walk out, it’s expected to have more questions; it happens. I know that patients have shared bringing somebody else to the appointment. You can ask the doctor. Sometimes they’ll let you record the appointment, so you can reference the notes later. I was a journalist and a researcher, so I loved information, but as a patient, it went in one ear and out the other for the very reasons that you explained.
Dr. Brody: It’s good to record it. If you didn’t think to bring a person with you, you can get someone on speakerphone as soon as the doctor sits down. Every doctor is open to that. No doctor gets offended or annoyed by recording or by a speakerphone. It’s all good.
Stephanie: That’s awesome to know. Thank you, Dr. Brody. Dr. Steinberg, how often are you talking to patients about treatment options? How different are the conversations between the newly diagnosed and relapsed/refractory DLBCL?
Dr. Steinberg: I see a little bit of 50/50 in terms of my patient population. I’ll have patients that are referred to me with lymphadenopathy (swollen lymph nodes), or when I’m on service in the hospital, they’ll be worked up for some symptoms that they’re having because they’re rather sick. We have to start from scratch because a lot of newly diagnosed patients have never even heard of lymphoma before. The cancers they hear about are lung cancer, prostate cancer, and breast cancer, so even though lymphoma is fairly common in the cancer world, for whatever reason, it’s not as prominent. There’s a lot of education. You’re going to have to repeat yourself many times so patients can better understand, and we have to repeat it to their family members and their loved ones, as Dr. Brody was saying.
With the relapsed/refractory population, in some respects, it’s an easier conversation because you don’t have to start from scratch in terms of explaining what lymphoma is. A lot of them may have already read up on what the next steps are. During the course of their initial treatment, I’m sure a lot of them were worried that they wouldn’t respond, so what happens next? They may already come in to see me asking about transplant or CAR T-cell therapy.
There’s a lot of education. You’re going to have to repeat yourself many times so patients can better understand.
Dr. Amir Steinberg
Stephanie: That makes perfect sense, also. I’m curious. For people who aren’t as familiar with Westchester Medical Center, can you describe the lymphoma program and what you usually advise patients to do when they’re relapsed/refractory? When do you refer them to an institution like Mount Sinai or introduce them to a specialist like Dr. Brody, and when do you treat them onsite at Westchester?
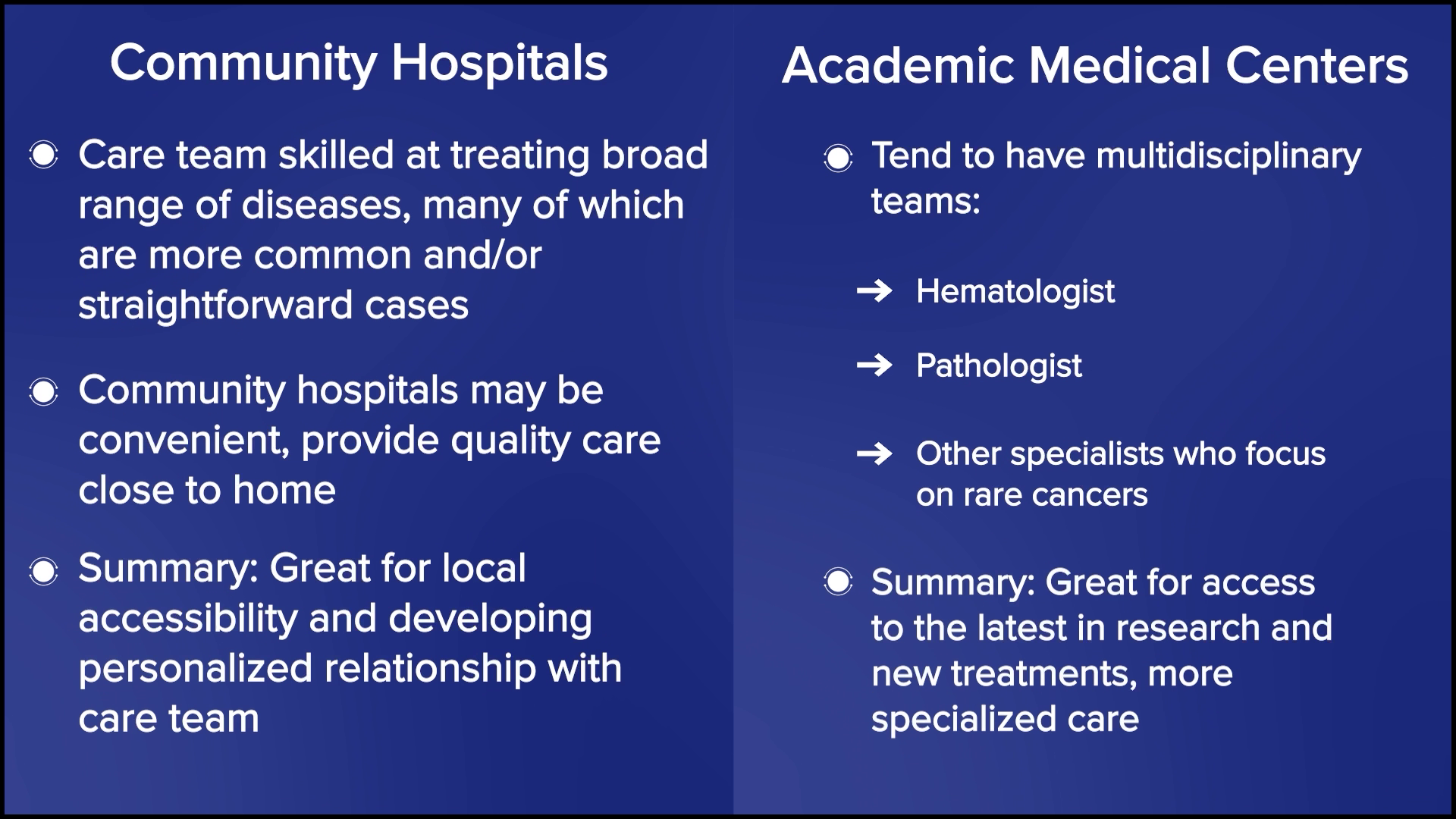
Dr. Steinberg: We have the resources here for cellular therapy, whether that’s CAR T-cell therapy or stem cell transplant. We have a couple of lymphoma studies here, but not to the same extent as Mount Sinai. There is a small group of doctors here who handle all the hematologic malignancies, whether that’s myeloma, leukemia, or lymphoma. Whereas at a big academic center like Mount Sinai, there are more disease-specific specialists, where you have someone who primarily treats leukemia or lymphoma, so that’s how we differ.
We work very closely with other community centers that lack inpatient chemotherapy and cellular therapy. We’re south of the Hudson Valley and north of that is Albany, so between Albany Medical College and University at Albany’s hospital and ours, there’s a lack of more cutting-edge or advanced clinical trials or cellular therapy. We sometimes serve as a bridge to those patients. If we don’t have a clinical trial that a patient is interested in, then I may connect with Dr. Brody or another center within Manhattan.
When do we do that? If a patient asks and wants another opinion, then I ask one of my former colleagues, like Dr. Brody, to see the patient. That’s the big trigger for me to refer to Manhattan. The other is if they’re not responding to their salvage chemotherapy. We try and bridge people to a transplant or CAR T-cell therapy, and if they’re just not responding at all and we think they might benefit from something new and different, then that’s when we’re going to refer out. Something that’s not available per se from the FDA alone.
What Makes for a Good Partnership Between an Academic Center and a Community Practice?
Stephanie: What looks good in terms of communication and making it work, whether Dr. Steinberg gets with the smaller community centers that rely on Westchester or Dr. Brody, any of the partners you have in the community setting? What we’ve heard from patients sometimes is, “Do they talk to one another? Is it trickier if we have multiple healthcare centers involved?” I would love your insights on how to make this a great partnership.
Dr. Brody: What you’re seeing here might be more the exception than the rule, and a good exception because Amir and I are buddies. In these large systems, we try to come up with a systematic way to have good communication and interaction. It turns out it’s mostly a personal way or nothing. Amir has my cell phone number, so as he’s seeing a patient, he can literally call me up right at that moment, and when I see it’s Amir and not some spam caller, I’ll pick it up and try to give him quick answers. If it’s about papers getting faxed and records getting signed, and “Oh, we can’t send those records there until that gets blessed,” then all of a sudden, the system starts to get more complicated, and delays build up at every level of it.
Unfortunately, it works best on a personal level, and the only way to improve upon that is to have more personalization and more interactions between community docs and academic docs. It would be great if we could get the systems working, but it seems that systems get more complicated, more cluttered, and more bureaucratic the more layers you add to them. If you’re a community doc, you need to have some academics that you have good access to and if you’re academic, you have to make yourself accessible. This is a huge obstacle for many. You have to make yourself accessible to as many docs in the community as possible.
If you’re a community doc, you need to have some academics that you have good access to and if you’re academic, you have to make yourself accessible.
Dr. Joshua Brody
Frequently, it’s not even about the patient having to be seen at the academic center. It’s just the community doc asking, “Hey, are you guys doing this the same way as before? Any new change updates? Or is there a critical trial that the patient needs to see you for?” And frequently, we say, “No, this patient would be as well served in the community as they would be here.” Or sometimes it’s, “Oh no, this is actually a high-risk patient for some subtle reasons and I would recommend having them at least get seen here once so they can hear about the options.” But that connection, unfortunately, seems like it works best when it’s personal.
Stephanie: Got it. That makes sense. Dr. Steinberg, any additions to that?
Dr. Steinberg: I agree. We know each other. We have each other’s phone numbers that we can text or we can email each other. One of the issues, for example, is that I have never even met a lot of people in the community who work near me, though we may communicate via email or phone calls. I wish we had a better connection and that I could see these doctors at some point in the future and see where they take care of patients.
Another barrier is the computer system. Epic, for example, is a computer system that a lot of hospitals use, where they have something called Care Everywhere and you can read what’s going on with the patients at another hospital. You just have to have a patient sign off to allow you to do that. My institution uses a different computer system, so they don’t have Care Everywhere, and what we use is not as prevalent as Epic, so that can create barriers in terms of communication.
Nonetheless, we try the best we can by talking to that clinician, sending records as best we can by email. Even the patients sometimes are our communicators. I had a patient who, when I mentioned, “We need a PET scan on you in about a month,” they said, “Okay, we’ll talk to our local doctor and have them order.” I trust this patient, so I feel like I don’t need to tell the referring doctor to order the scan because the patient will end up asking.
Stephanie: That’s great because a lot of times, patients will ask, “What can we do to help facilitate this?” It sounds like we can be quarterbacking some of the communication, if that’s helpful and can expedite some of this process. I appreciate that.
If it’s 70% likely to be cured, you’re wrong 30% of the time. But in our hearts, we may still have our suspicions, though.
Dr. Joshua Brody
Having Conversations About Future Treatment Choices
Stephanie: As we go into this idea that there are so many options right now, I would love to talk about one quick point. You both mentioned that when people are newly diagnosed, there’s so much information that they have to take in already, so it’s not an opportune time to add more. Once someone’s relapsed/refractory, is it a conversation that should have already happened? Where they’re told, “Hey, there’s a lot of development happening. Here are some clinical trials. If it ever gets to that point, know that there are options.” Is that something in your playbook? Or is that something you discuss only if that happens when it becomes a relapsed/refractory disease?
Dr. Brody: I’ll give an answer and it’s not a one-size-fits-all. Secretly, we tell people we don’t know the statistics. This is likely to occur, but you still don’t know. If it’s 70% likely to be cured, you’re wrong 30% of the time. But in our hearts, we may still have our suspicions, though. “This one feels higher risk to me.” For the ones we are worried about, you definitely don’t want to have these more difficult conversations all of a sudden, especially if they’re a newly diagnosed patient.
You can set that up, ideally multiple times. “Hey, we’re going to get a scan. If the scan looks great, then great. You can come back in six months. If the scan doesn’t look good, here’s how it might go.” If you have the luxury to set that up a few times, then if the scan looks great, you just wasted a minute of their time. And if it didn’t look great, now they’ve heard about this a few times, so it’s a little less shocking on whatever fraction of folks when you actually have to have that more serious discussion.
I think it’s extremely helpful to set it up. “If it goes well, then great. There’s nothing you need to think about. If it doesn’t go well, here are some things we are going to talk about. I’m not going to give you the details now. We’re going to talk about this. We’re going to talk about trials. We’re going to talk about some other options.”
Dr. Steinberg: I agree with Dr. Brody’s sentiments in that regard. To be honest, for me, part of it is also guiding them on what to plan for in the future based on their prognosis. Let’s say a Hodgkin lymphoma patient may have a better prognosis than someone with other lymphomas. I may be less likely to talk about what treatments to give them if they have a recurrence. Whereas if they have another kind of lymphoma that the statistics don’t favor as much as an average — not that specific patient, but just on average — I might mention to them, “By chance, if this happens to come back, we do have other great therapies that we can offer you, including this and this.”
Outlining Treatment Options for Relapsed/Refractory DLBCL
Stephanie: Now we can dive into the actual treatment conversation. Let’s talk about how you set up the conversation for people whose disease is refractory or they’ve relapsed. Dr. Brody, what is the first conversation? What are the considerations in laying out treatment options in terms of what’s already out there and approved?
Dr. Brody: Folks who think that oncologists don’t have silly things to say haven’t been around oncologists much. There’s a silly expression we say: “A lot more was known about that a few years ago,” meaning that we had clearer answers 10 years ago. Now they’re less clear. That sounds bad, but it’s very good.
Answers have evolved even more to make it even a bit more complex, but in a good way, because if you’re getting more options, then that can only be a good thing.
Dr. Joshua Brody
If you asked me this exact question two years ago, we would say, “Oh, it’s a fairly simple algorithm. If people relapse with DLBCL within 12 months of finishing their front-line chemo, the right and best answer is CAR T-cell therapy,” and it is for the vast majority of patients. Most patients could be eligible for CAR T-cell therapy, but not everyone, so that’s the right second-line treatment for early relapsing patients.
For later relapsing patients, it was a little more confusing. In 1994, we had a big trial proving that an autologous stem cell transplant, after some more platinum chemotherapy, was the right answer. But the field has evolved so much since then. Even though no one has rewritten that textbook, we don’t all believe that that textbook is necessarily the best way to go.
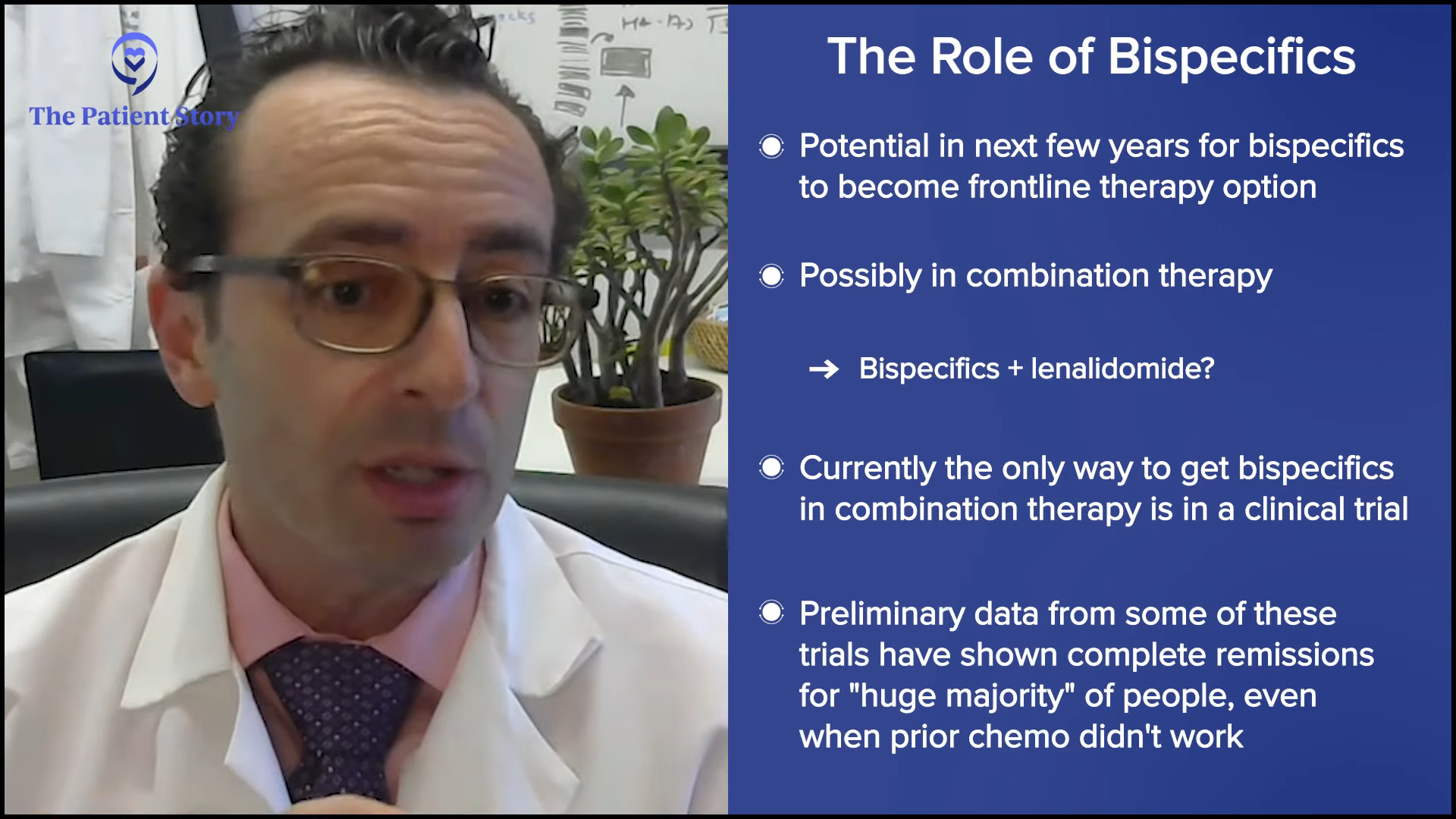
In 2024, those answers have evolved even more to make it even a bit more complex, but in a good way, because if you’re getting more options, then that can only be a good thing. People would rather have a clear answer. But they would rather have better therapies and better options. We have some remarkable data that adding bispecific antibodies to chemotherapy for patients in second- or third-line has a huge benefit in overall survival and progression-free survival.
There are a few studies like this, but the largest randomized study is the STARGLO trial. The study showed that the combination of bispecific antibody, platinum chemotherapy, and gemcitabine chemotherapy seems to put the majority of people into complete remission — about 60% — and many of those remission patients seem to have durable remissions for years, though we need more follow-up. The way that trial was written is that it’s only supposed to be for people who weren’t eligible for transplant or CAR T-cell therapy. But there’s little nuance now because there’s a gray zone of who exactly is eligible for CAR T-cell therapy, so now we have a more nuanced conversation.
Here, if you have relapsed within the first year, CAR T-cell therapy is probably the right answer for you. If you relapse later, it might be chemotherapy, maybe plus a bispecific antibody. But even for people who relapse in the first year or in their third line, there is great evidence for bispecific antibody plus chemotherapy. Overall, it certainly seems to be a bit safer than transplant, maybe even safer than CAR T-cell therapy, and it’s a lot more accessible to folks who are being treated in the community when they don’t have a CAR T-cell therapy center nearby. The contribution of bispecific antibodies plus chemotherapy is a huge advance. All of these are versions of immunotherapies — CAR T-cell therapy and bispecific antibodies — but there’s still a rapid evolution over the past few years.
The data showed that compared to transplant, within your first year of relapse or primary refractory disease, CAR T-cell therapy had a better outcome.
Dr. Amir Steinberg
Stephanie: That’s incredible. Dr. Steinberg, we were talking about how at Westchester, bispecifics were available before CAR T-cell therapy was. Can you share a little bit about how you have that conversation with relapsed/refractory DLBCL patients on what treatment options you think are best for them and what goes into that consideration?
Dr. Steinberg: Before we had CAR T-cell therapy, if you relapsed in your first year, I would have to refer you out. The data showed that compared to transplant, within your first year of relapse or primary refractory disease, CAR T-cell therapy had a better outcome. I had to refer patients out, but I would work with the academic center that I was referring to in terms of providing salvage chemotherapy or some kind of chemotherapy to keep the lymphoma under control until the whole process of CAR T-cell therapy could be arranged.
Now with bispecifics, with all these other therapies out there, we’re helping the community centers ourselves. For example, the community center may want CAR T-cell therapy or a transplant for their patient. They have access to bispecifics, but they may not be able to give, for example, inpatient chemotherapy. We help them by doing, let’s say, the first dose or two in the hospital. Like a lot of bispecifics, they need to be monitored closely, and then we hand the patient off to the community center and the community oncologist.
More and more, they’re showing that potentially, some of these patients who are getting bispecifics may not necessarily need to be admitted. It’s a moving target in terms of how that’s evolving. But if you have someone with a lot of disease and you want to monitor them for any kind of tumor lysis, then sometimes inpatient admission to monitor them for that, plus any other side effect,s may be required. There’s a little bit of help out to the community. Also, we sometimes would need help. Now with CAR T-cell therapy here, we don’t refer as much to the centers, unless it’s a special trial, which Dr. Brody and other oncologists and centers may have access to.
Deciding Between CAR T-cell Therapy and Stem Cell Transplant
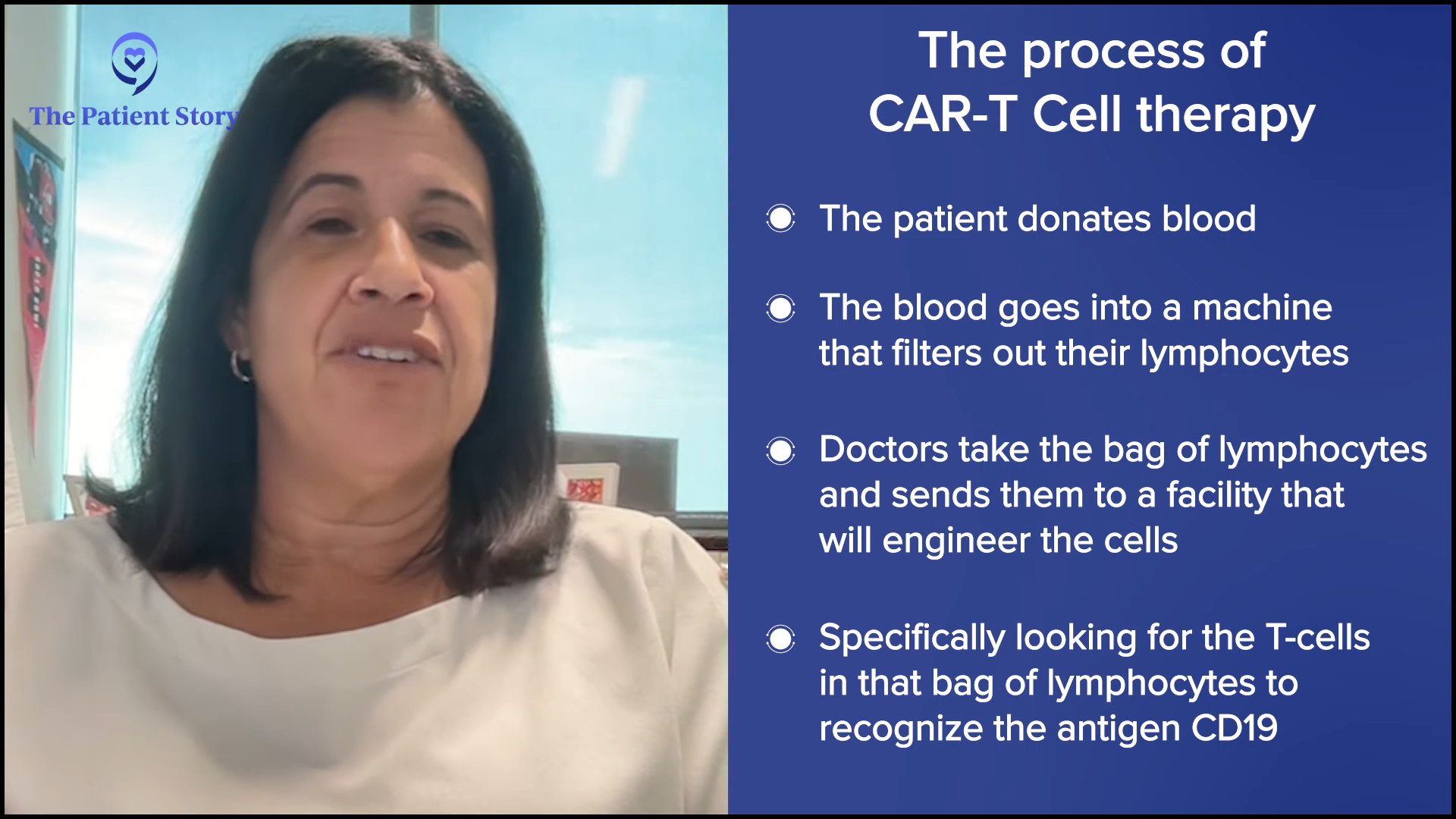
Stephanie: Can we zoom out a little bit? A lot of people have heard, of course, about CAR T-cell therapy and bispecific antibodies. Dr. Steinberg, I know that you had your first patient in 2023. Can you describe that process now that it’s available at Westchester? How many patients are typically undergoing CAR T-cell therapy versus a transplant, and why do you make that decision? What is it about the patient that you go either direction?
Dr. Steinberg: I believe it was the ZUMA-7 study that compared patients who had a recurrence of their lymphoma. They were randomized to either an autologous stem cell transplant, which is high-dose chemotherapy with stem cell rescue, or to CAR T-cell therapy. The first patients who had a recurrence within the first year of their initial treatment for the lymphoma did better if they went to CAR T-cell therapy. Whenever I have a patient who relapses within the first year of treatment, say R-CHOP or a similar regimen, or they had a primary refractory disease, meaning they did not respond well to R-CHOP, R-EPOCH, or pola-R-CHP, that’s when we think about CAR T-cell therapy.
There’s a lot of time and effort involved with talking to the insurance company and getting the CAR T-cell therapy approved, getting our administration to approve it, and going through all these hoops. In the meantime, while we’re doing all that, the patient would get a regimen to keep the lymphoma under control until all the ducks are in a row and everything’s approved for them to get the CAR T-cell therapy.
If they relapse after the one-year mark, as you know, CAR T-cell therapy is not approved for patients who relapse beyond the one-year mark, and the insurance companies are pretty strict about that. Could you get around it? I don’t know. You can do appeals with the insurance reviewer to see if you could get it if it progressed beyond a year, but typically, it’s difficult to get approval, so we usually try to head down the transplant road.
However, some patients are not fit enough to get a transplant. They may be fit enough to get CAR T-cell therapy, but not a transplant, so you may then head down the road of doing bispecifics, which have shown tremendously good results. Sometimes you could even use that as a basis. You could argue that they may not be fit enough for an autologous transplant as an argument for why they should get CAR T-cell therapy. With a transplant, you have to be stronger, fitter, and have fewer comorbidities.
Some patients are not fit enough to get a transplant... so you may then head down the road of doing bispecifics, which have shown tremendously good results.
Dr. Amir Steinberg
That’s how we make decisions when we see a relapsed/refractory diffuse large B-cell lymphoma patient. We can get into follicular lymphoma, mantle cell lymphoma, marginal zone, and all the indications for them in terms of CAR T-cell therapy and transplant.
Stephanie: Well, you just volunteered yourself for four different programs in the future. [Laughs] No, I appreciate that. This discussion is focused on DLBCL. There is so much to get into, but I know in so many other spaces, there’s a lot to talk about as well.
Using Treatments Earlier in Care
Stephanie: Dr. Brody, let’s zoom out even further on bispecifics. You talked about one of the clinical trials, STARGLO. If you were to lay out in simple language, which I know you’re really good at, for patients who are dealing with relapsed/refractory disease… There are different lines of treatment, obviously. You’re getting your second or third line. What is the matrix right now? There are different considerations based on a patient’s profile, but what are the general options for second-line and third-line treatment? This will help us set up to talk about other clinical trials because we know that when something is approved and doing well, there’s a tendency to try and get them to earlier lines, right?
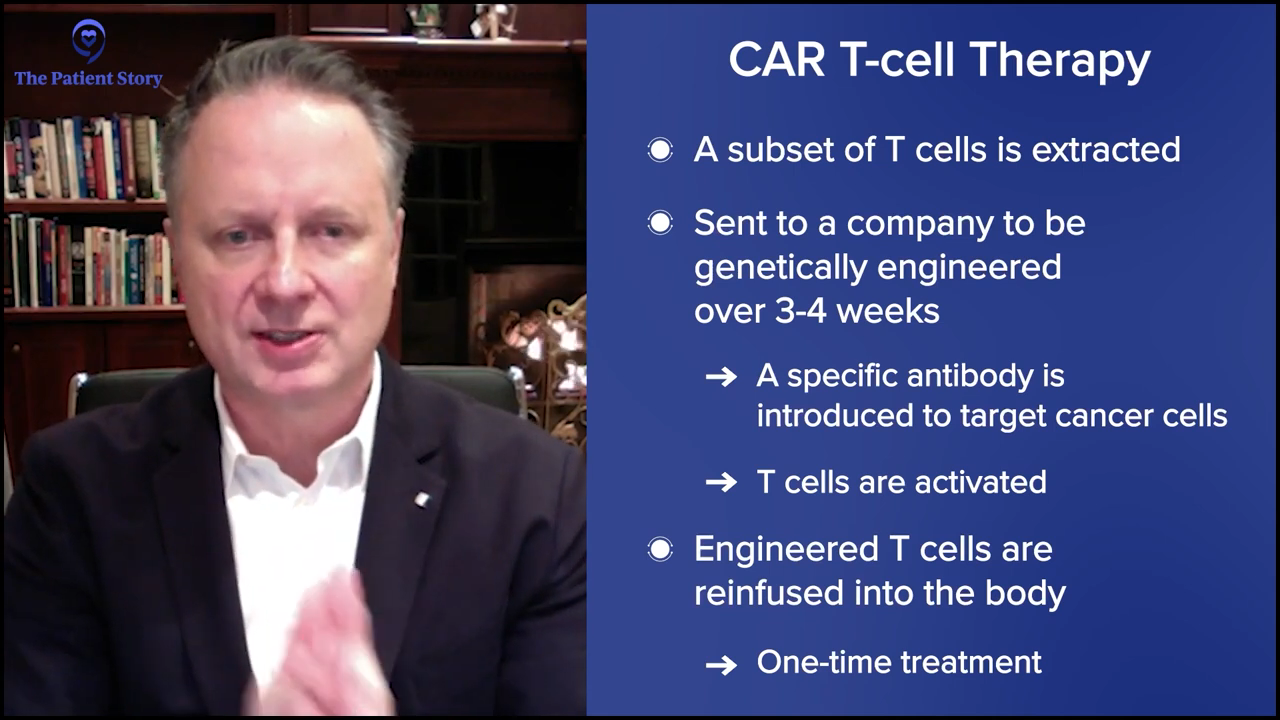
Dr. Brody: For the second line, one of the favored options is autologous CAR T-cell therapy. Axi-cel (Yescarta) and liso-cel (Breyanzi) are certainly a high priority for the folks who relapse after their first-line chemotherapy within 12 months, so it’s very high on the list.
Then again, the nuance is that some patients may not be great candidates because CAR T-cell therapy has some significant adverse events associated with it. We won’t get into the specifics. For some folks who are 85 years old and not running marathons recently, they may not be great CAR T-cell therapy candidates. There’s a spectrum of exactly how great a candidate someone is. There’s no absolute age cutoff and no number of miles you need to be able to run.
There’s a little bit of nuance there because, as Amir was saying, this is not just what we think is best, but what’s been proven and accepted by the FDA. Then there’s another overlap of what insurance payers are agreeing and willing to pay for. There are a lot of layers to that.
In 2025, the FDA has been extremely interesting. We’re just going to leave that as a blanket statement and say that we, Amir and I, go by what has been proven to be the best for patients, and our beliefs about that are based on very strong data. Bispecifics plus chemotherapy should be an option for second-line DLBCL patients, especially for those who aren’t eligible for CAR T-cell therapy. But I don’t want to put it as a blanket statement that that’s what everyone should be able to get access to. We have been able, fortunately, to get access to that option.
As Amir was saying, the old standard was platinum-based chemotherapy — and there are a few versions of that — followed by autologous stem cell transplant. But I’ll say that the third option I mentioned has been diminishing over the past few years for us, while those other two have been increasing.
In the third line, we have a lot of options. We’re very lucky because, even though lymphoma is technically the fifth most common cancer in America, we have more FDA-approved medicines for lymphoma than for any other cancer, even more than for breast cancer, which is so incredibly common. It’s awesome because it means we have more options for patients, but it also makes things a bit more complicated because we don’t always have the right and wrong answers. We have, “Here’s a bunch of options. They haven’t all been compared to each other.”
In third-line treatment for DLBCL, it’s like that. We have CAR T-cell therapy approved. We have bispecific antibodies approved, either by themselves or combined with other agents. We have antibody-drug conjugates (ADCs). It’s an antibody with a little bit of chemotherapy on the tail end. We technically have about three of those approved now — loncastuximab tesirine (Zynlonta) targeting CD19, polatuzumab vedotin (Polivy) targeting CD79, and brentuximab vedotin (Adcetris) targeting CD30.
I want to give a special shout-out to brentuximab because it had fantastic results in a randomized phase 3 trial called ECHELON-3, proving that with brentuximab combined with lenalidomide (Revlimid) and rituximab, compared to other standard therapies, those patients live longer than patients who got lenalidomide (Revlimid) and rituximab by itself. The reason that’s pretty exciting is that brentuximab was not thought about very much for DLBCL, even just a couple of years ago. This randomized trial showing that patients lived longer — with some of them having some pretty durable remissions — is a huge advance that I would not even have predicted two years ago.
I’ve hit most of the big categories of therapies for the second and third line. It’s a long discussion with your doctor, as you can imagine, but not impossible. It’s a lot, but happily, as Amir was saying, you don’t have to capture it all. It’s good to record the conversation or have someone with you, keeping track of it all for you, and having questions about all the things that are most promising.
Obviously, patients know the critical question: “Doc, if it were you or your family member, what would you do?” We give straightforward answers for that, so you don’t have to memorize all 20 things. You may want to hear about the two or three that the doctor says would probably be appropriate.
Questions to Ask Your Doctor About Treatment
Stephanie: What questions can patients ask their doctors if they’re not seeing specialists like the two of you? Are there other questions that you might suggest patients to ask to make sure that they’re on the right track and that the right considerations are happening, especially given all the options right now?
Dr. Steinberg: I can just say that there’s a question that a lot of patients do ask, which is about hair loss. That was a concern I had as a cancer patient. My dad lost his hair and my sister as well, so I know patients sometimes ask that. Unfortunately, sometimes the regimens we give cause hair loss. But one thing that you can point out to patients is that in these later lines of treatment, a lot of these treatments may not necessarily cause hair loss, such as bispecific antibodies and the antibody-drug conjugates that Dr. Brody brought up. They have different side effect profiles.
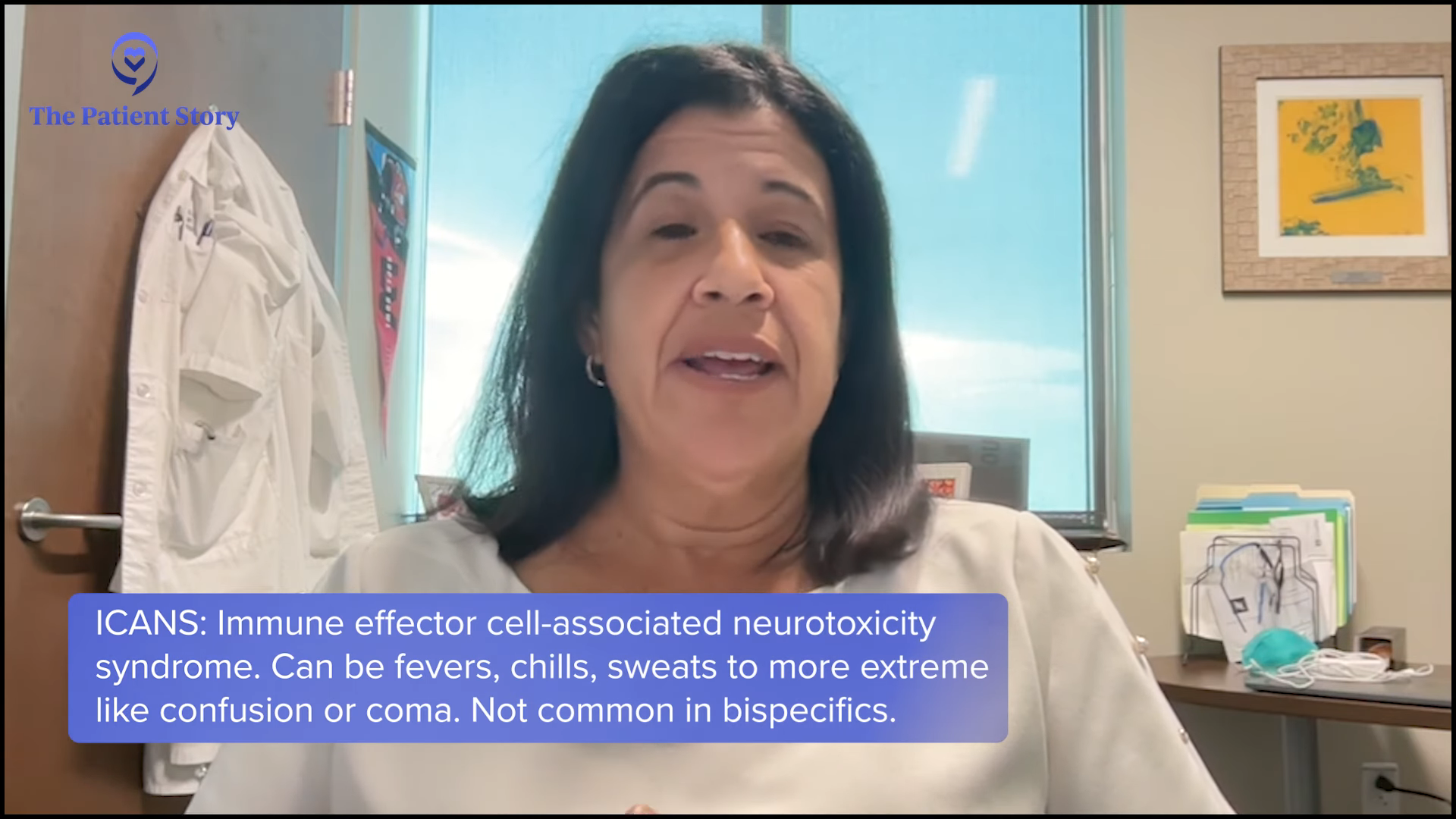
Asking about side effects should be focused on. They’re more focused on allergic reactions. Certainly, you still have to worry about infections, but it’s a different kind of side effect for allergic reactions and no hair loss, not necessarily nausea and vomiting. Sometimes, you have to worry about potentially fevers, but very rarely and that’s why we sometimes have to monitor these patients in the hospital. The bispecific antibodies altered mental status, which they call neurotoxicity. Those are the different side effect profiles for later lines of treatment or these newer agents.
Considerations When Taking a Bispecific Antibody
Stephanie: That’s a great addition to the context. There are a couple of questions about access. We’ve talked about it throughout the conversation. But before, when we started hearing about bispecific antibodies, it was about having more access to something like that in more places versus a CAR T-cell therapy, where — don’t even talk about insurance — logistically getting to a center that offers CAR T-cell therapy is a little harder. There’s a long process to getting certified or making sure you have all the right things to be able to execute CAR T-cell therapy. I would love to understand what that’s looked like for you. It may be a little bit different where you are, Dr. Brody, but Dr. Steinberg, you had bispecifics first. Has that been a big factor in what you suggest to patients?
Dr. Steinberg: I’ve been very impressed with bispecifics. The data speaks for itself, but also my personal experience treating patients with them. Again, the good news is that they’re not stuck in the hospital for weeks on end. You can primarily manage them outpatient and try to get the community oncologists to give those agents so that you can see them less frequently. That’s the big benefit of bispecifics now.
The question is: will the community hospital give the drug? I think they’re willing to give it, especially if it’s an outpatient medication. We’re there to help them start the medication if they need any inpatient monitoring. But once they get the show on the road, once the patient starts the drug, most community oncologists will probably be able to give these medications in the outpatient setting.
Stephanie: Awesome. Dr. Brody, anything to add there? I know you offer all of the above at a big center like Mount Sinai.
Dr. Brody: We shouldn’t totally shake a stick at CAR T-cell therapy because in this setting, they not only have great results, but also the best kind of precedent of how long we’ve seen these patients for. We have relapsed/refractory DLBCL patients who we used to think that if they weren’t transplanted, it was an incurable disease. Here we see CAR T-cell patients five years later and beyond, staying in remission. We must be curing 40 to 45% of them; we don’t know the exact number, so that’s awesome. No therapy has that much long-term follow-up to prove that patients are being cured.
At the same time, we have all these metrics, like survival, cure rates, and all that, but patients have their own metrics in their lives. I was talking about CAR T-cell therapy with a patient and they said, “You don’t understand. There’s no one else to take care of my mom except for me. I cannot be in the hospital for one, two, or three weeks. I can’t ask a friend to all of a sudden be my mom’s caretaker.” That is a metric for that person. Not just having an optimized cure rate, but being able to live their life, and sometimes, their lives are very practically complex. They have to do things.
The results with bispecifics have been so promising. They’re great by themselves because they’re simple and well-tolerated enough that you can combine them with chemo. Now, bispecifics plus chemo start to have complete remission rates that are getting quite close to CAR T-cell therapy. We don’t have enough follow-up yet, but we certainly have seen a lot of relapsed DLBCL patients in remission for two to three years and coming up on four years now. We cannot say the exact cure rate with chemo plus bispecific versus CAR T-cell therapy, but it’s getting closer. And as Amir was saying, it’s much more doable in the community setting.
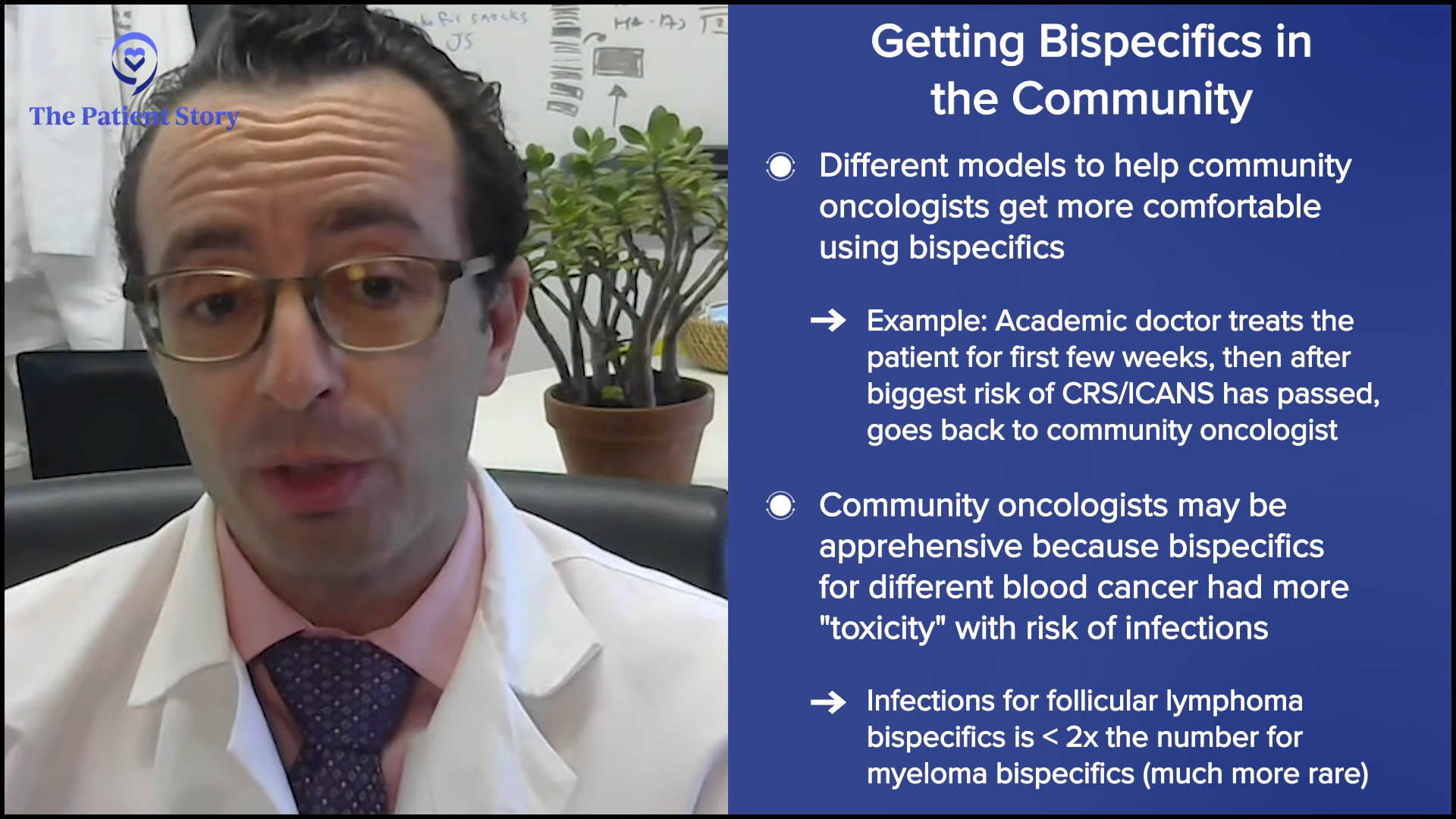
As you were asking about earlier, we do sometimes need that collaboration between the academic center and the community center because the first cycle of bispecifics can be tricky for some of the community centers. There are a few solutions, but one solution is doing the first cycle at the academic center in the big city, the subsequent cycles after that first month with the academic center, and the subsequent months with the community doc close to home, so it’s a lot easier. That model does exist. We do that sometimes. It might be doable for patients.
Dr. Steinberg: Bispecific antibodies may someday be approved in the front line in combination with chemo, so a lot of these community oncologists will be the ones treating the patients upfront. They’re getting their feet wet, so to speak, with these relapsed/refractory patients. In the future, who knows? Josh, do you have any thoughts on when they might be approved in the front line? I think it’s coming.
Dr. Brody: It’s coming soon because those trials are mostly fully accrued, so we’re waiting for the data. We cannot predict the weather in a year from now, but sometimes you can. If you’re in the Sahara Desert, it’s going to be dry. If you’re in the Amazon, it’s going to be wet. And these trials are going to be positive. That’s just me saying that with no secret insider information.
We’re talking to patients, but if there happens to be an oncologist in the audience, that oncologist is going to need to be able to be comfortable with these medicines. The oncologist might say, “I don’t see that much second-line or third-line DLBCL, so maybe I don’t need to learn about these bispecifics.” You do see first-line DLBCL. It’s the highest incidence lymphoma subtype, so if you’re going to be treating those patients, you will need to know about these a couple of years from now because they will be approved for the front-line, just as Amir was saying, so might as well learn about them now and solve some of these logistical issues about hospitalization.
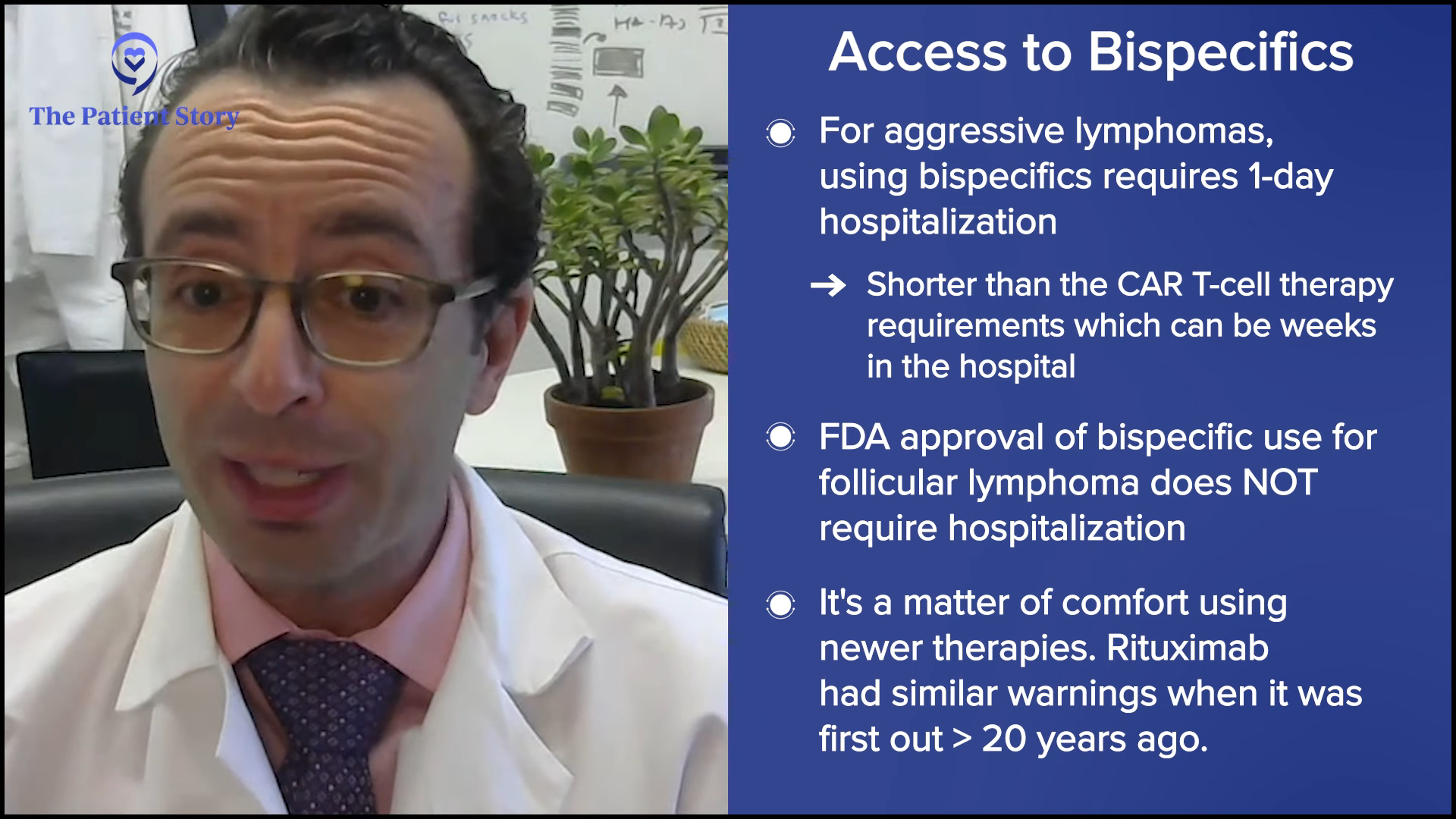
Also, some of the companies that make the medicines are helping solve these logistical issues, so we can maybe change it so that most patients don’t need to be hospitalized for a day. Usually, for most bispecifics for DLBCL, patients need a one-day hospitalization. We might be able to get rid of that for a lot of patients in the near future as well.
Stephanie: Can you synthesize what you just talked about? What does it look like for someone going through CAR T-cell therapy in terms of the logistics versus bispecifics?
Dr. Brody: Amir, do you want to give your center’s approach to how long folks are in for axi-cel or liso-cel?
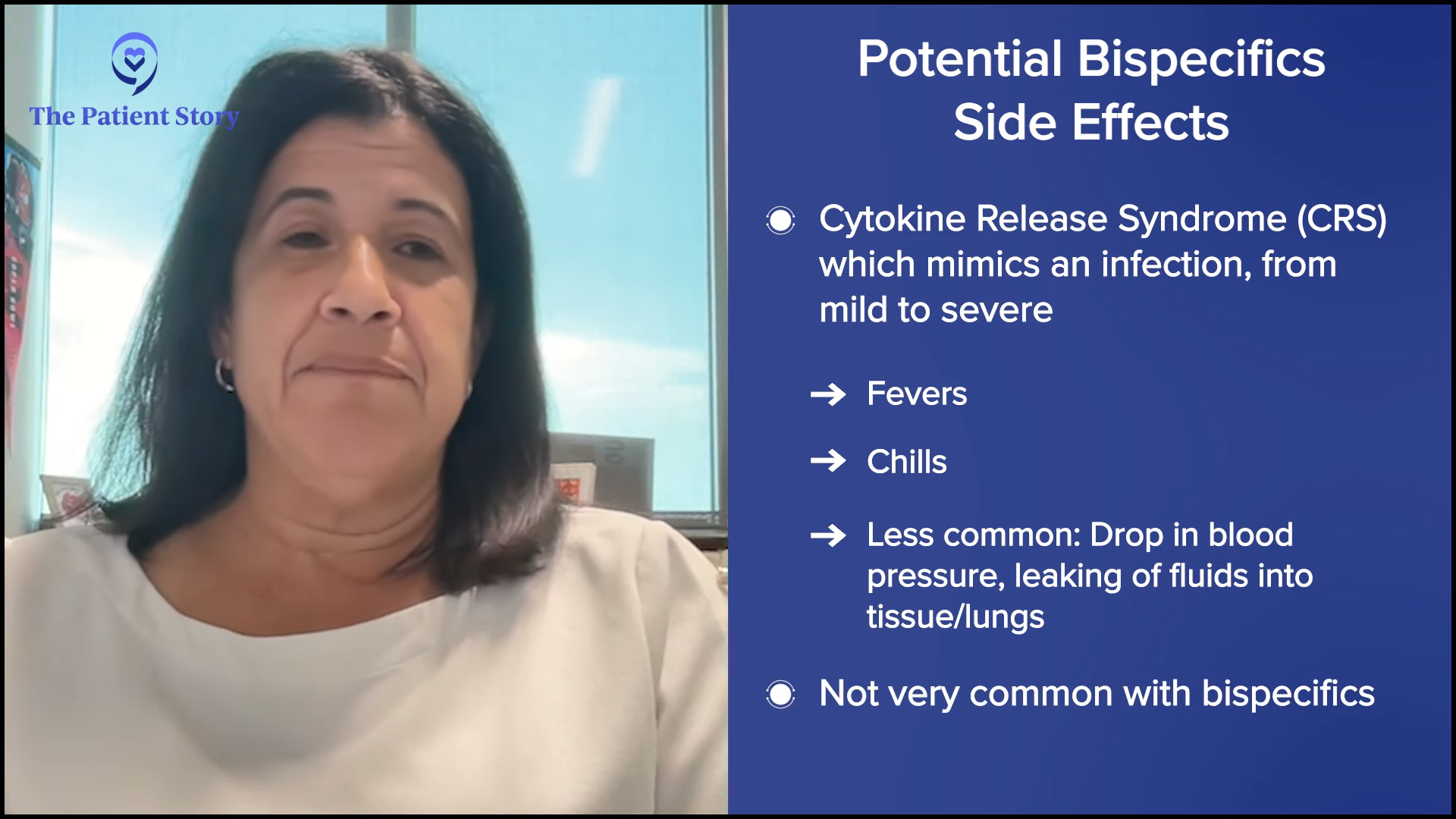
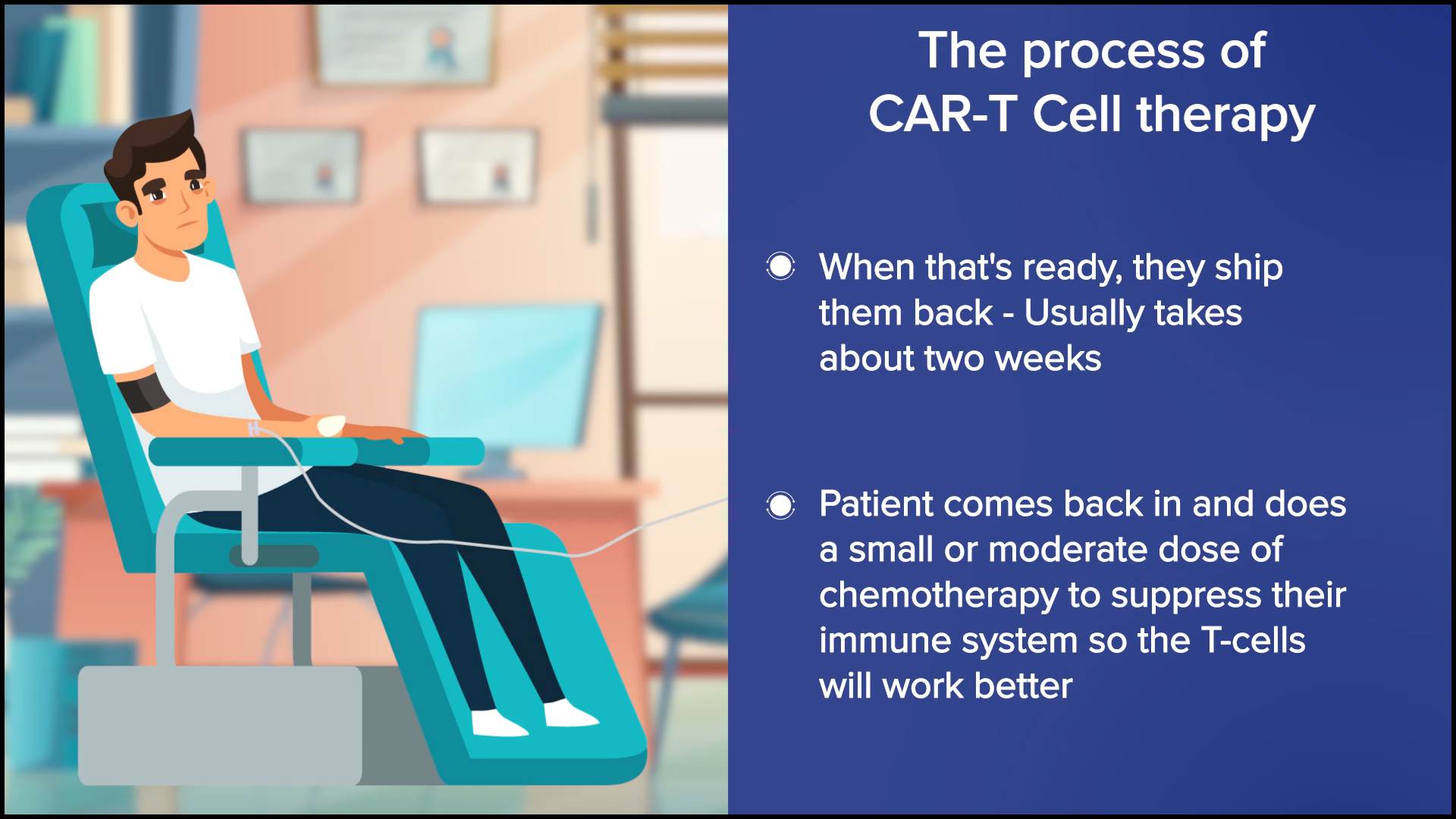
Dr. Steinberg: There are exceptions. Some centers may be doing outpatient CAR T-cell therapy, where they may give the infusion outpatient and then cross their fingers that the patient won’t be admitted or plan on the patient being admitted as soon as they exhibit side effects. But for the most part, I would say most centers will admit the patient and keep them there. We’re looking at a three-week hospital stay, with five days or so of chemotherapy, CAR T-cell therapy, and then an observation for two weeks or so until blood counts drop and then recover. You get them through all the toxicity and side effects, such as cytokine release syndrome (CRS) and neurotoxicity. That’s the typical CAR T-cell therapy story. That’s why Josh was mentioning the patient who was the mother’s caregiver and couldn’t commit to three weeks in the hospital.
Some centers may be doing outpatient CAR T-cell therapy... But for the most part, I would say most centers will admit the patient and keep them there.
Dr. Amir Steinberg
Dr. Brody: I totally agree. Some centers can do this outpatient, but that’s not the majority of centers. The reason is that it puts extra risk and concern when emergencies happen at midnight, unless you can set this up in such a way that the patient is across the street at a hotel and they have a great family member or someone who can keep a close eye on them and rush them across to the hospital. But that’s logistically difficult to set up in many centers.
At our center, it could be anywhere from a week and a half to three weeks on average — and that’s if everything goes pretty smoothly. If bad things happen, it could go much longer. It’s not nothing. CAR T-cell therapy is a super effective therapy, but these risks for adverse effects are not nothing.
Stephanie: And then versus bispecifics, can you spell that out? They’re coming into the hospital… What’s happening?
Dr. Brody: Overall, the standard for most patients should be a one-day hospitalization — literally overnight. We can do that in a few different ways. On average, it’s one day for most patients. It could be more for some, but usually it’s one day of observation.
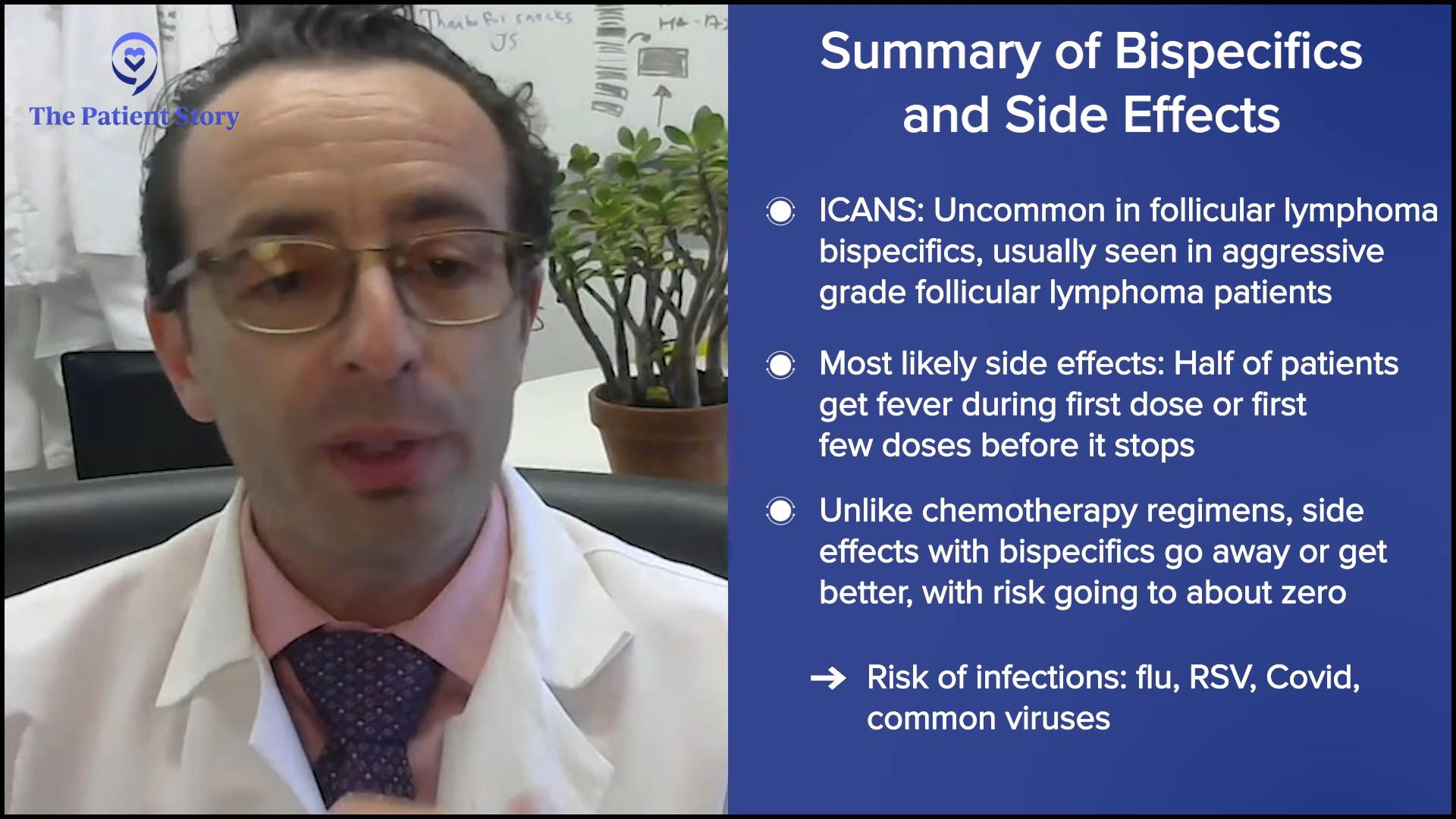
For most patients, it’s a pretty boring day. They got a fever, got some ibuprofen (Motrin) or acetaminophen (Tylenol), got some fluids, and then went home the next day. But maybe 3% of patients could end up in the ICU. Three percent is a lot, but for 97% of patients, it wasn’t that exciting. That’s for DLBCL bispecific antibodies.
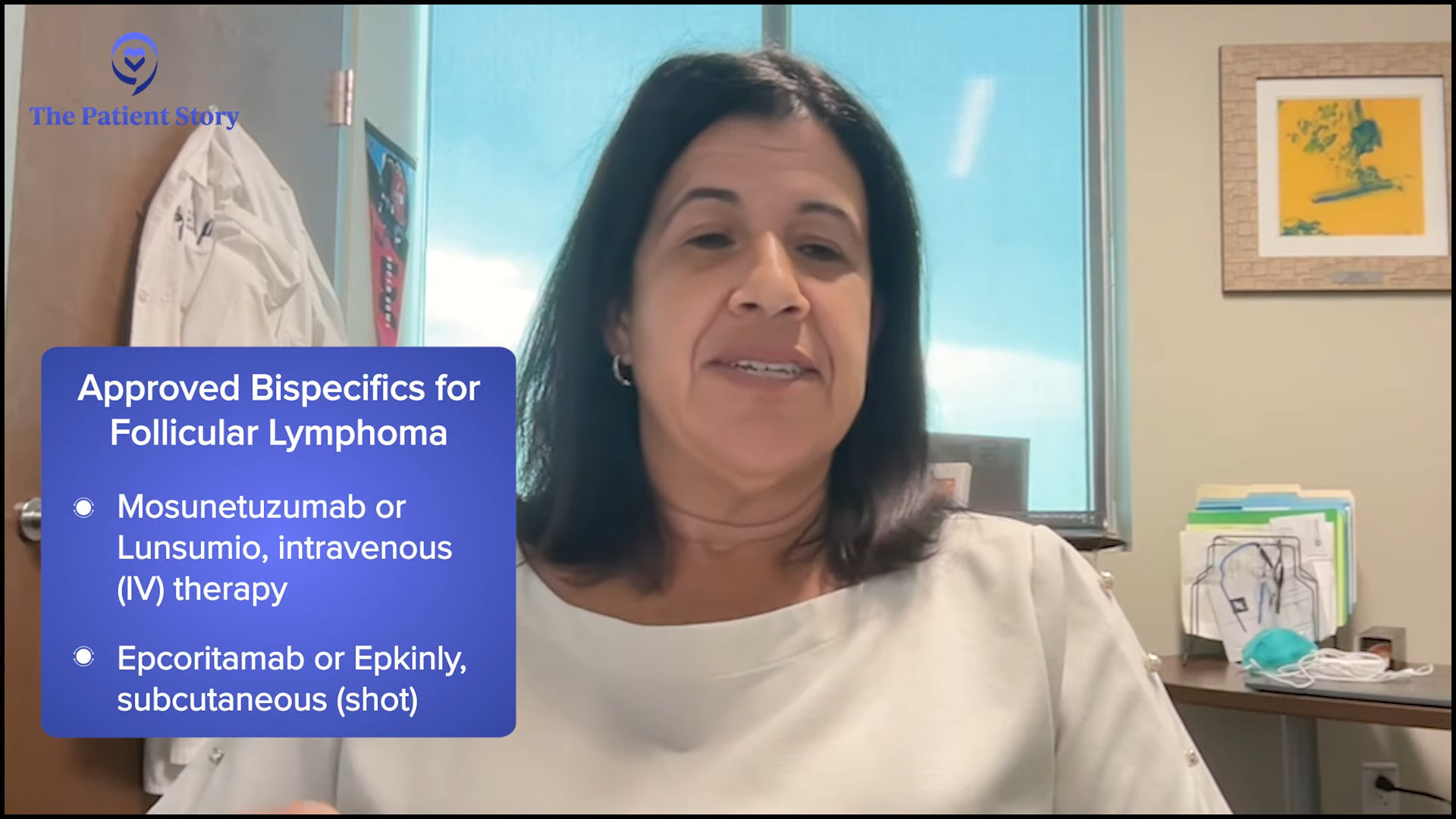
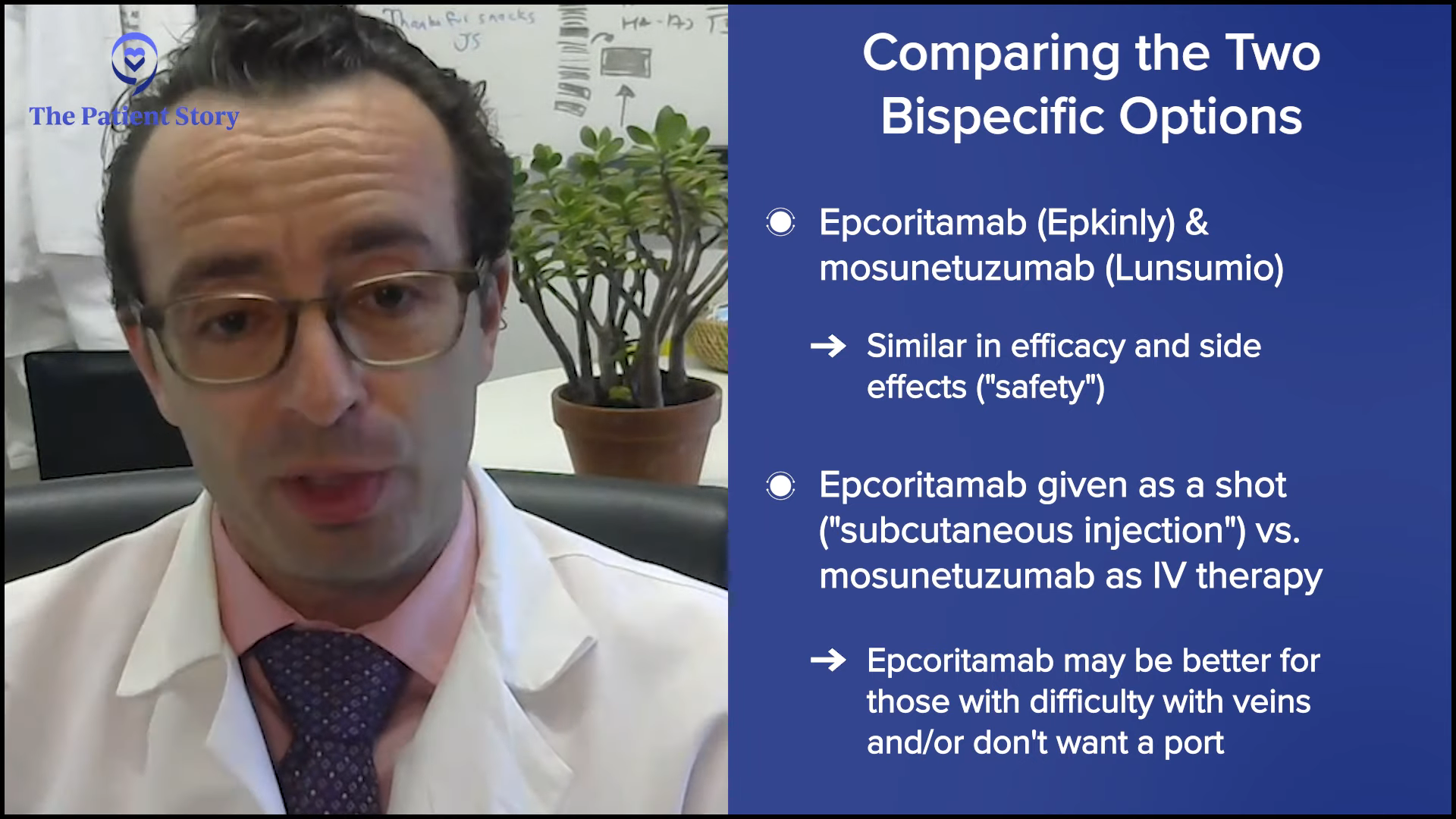
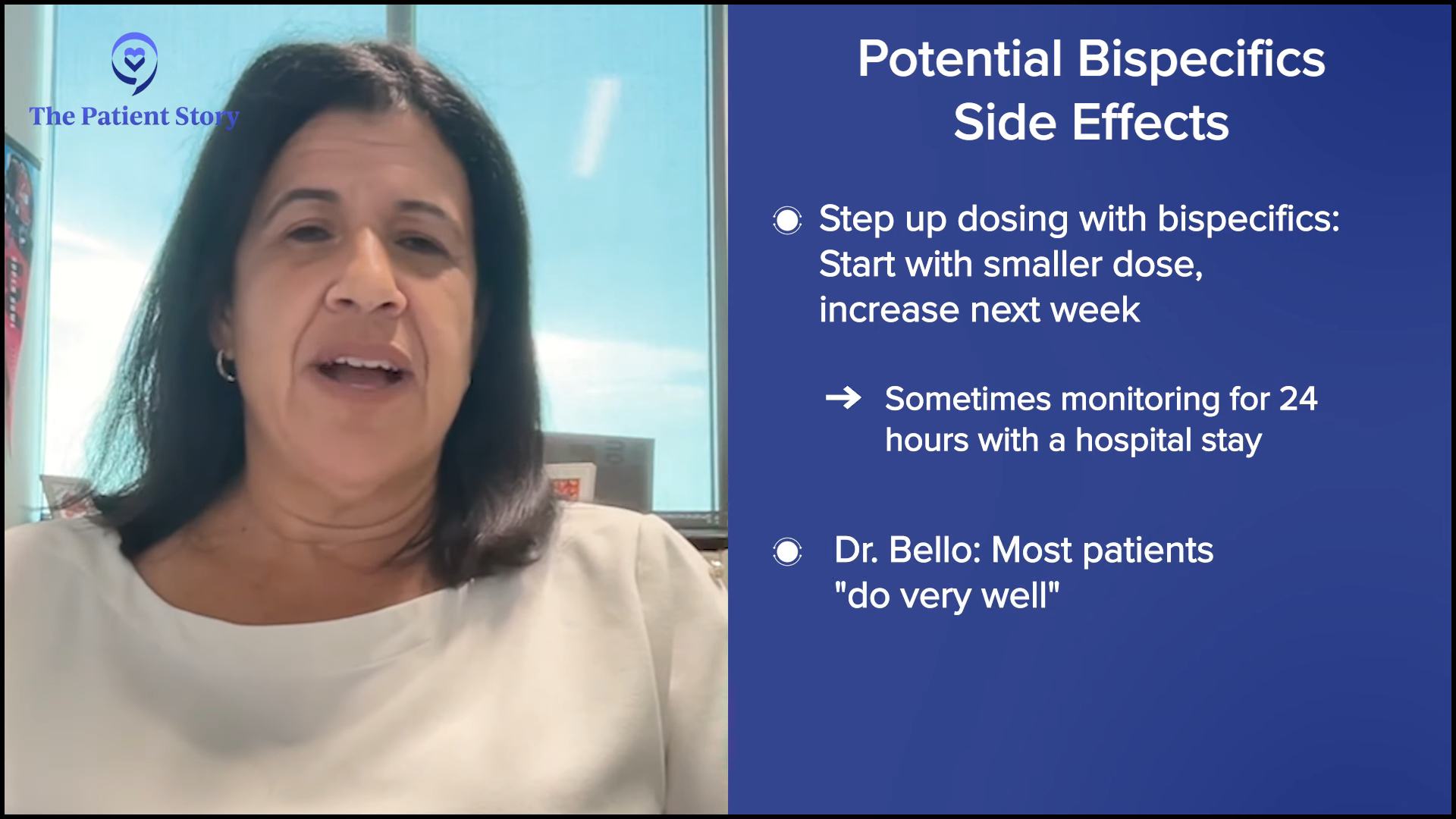
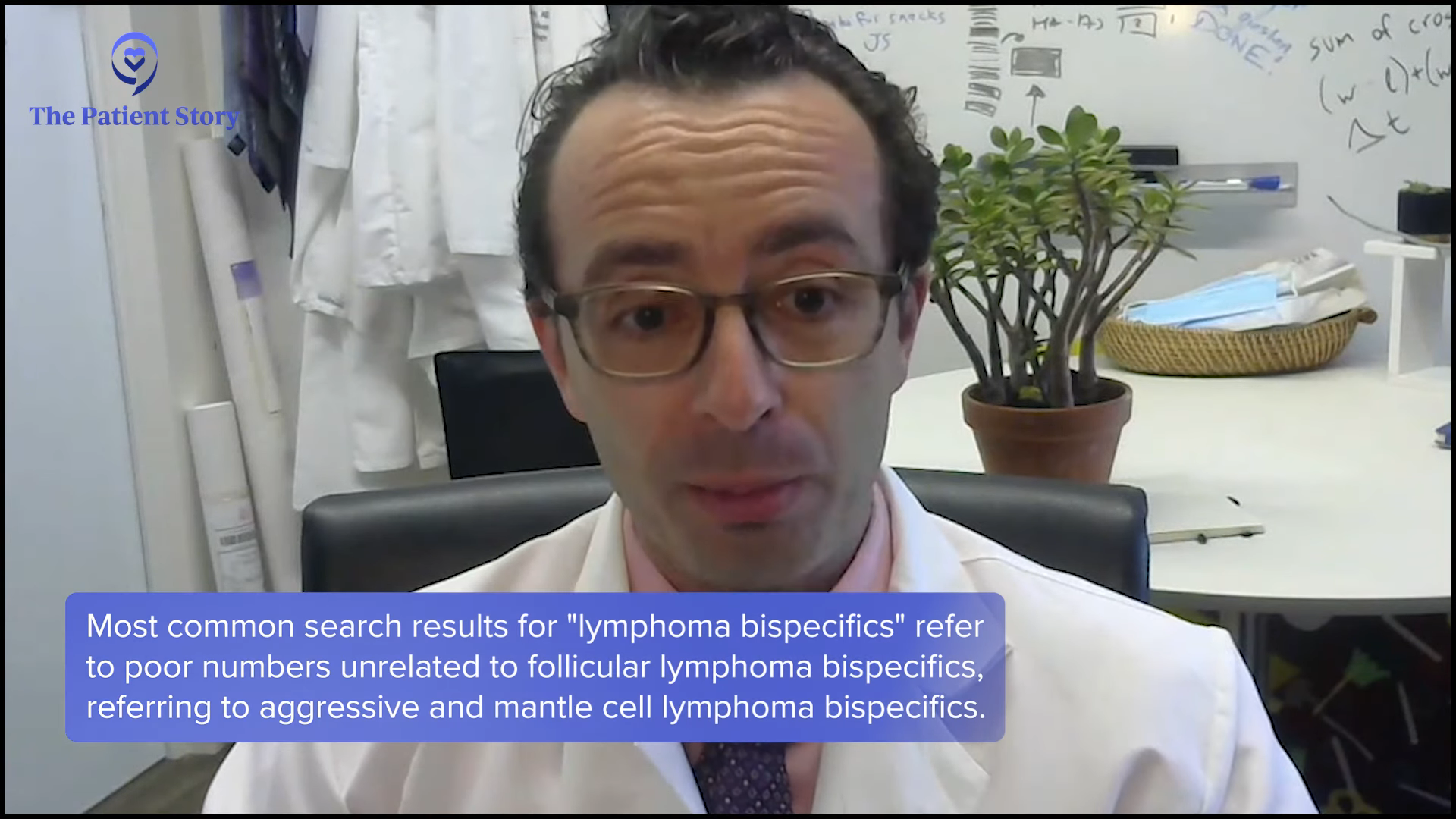
We should just say, since we’re talking about them, that we have bispecifics for follicular lymphoma as well. It’s the same idea but with slightly different recipes. Those do not require any hospitalization. Some patients might need to get hospitalized for other reasons, but for most patients, there should be no hospitalization for bispecifics for follicular lymphoma.
Overall, the standard for most patients should be a one-day hospitalization — literally overnight.
Dr. Amir Steinberg
Understanding Clinical Trials
Stephanie: How do you introduce the concept of clinical trials while you’re talking to patients and/or their family members? How do you help them understand what they are?
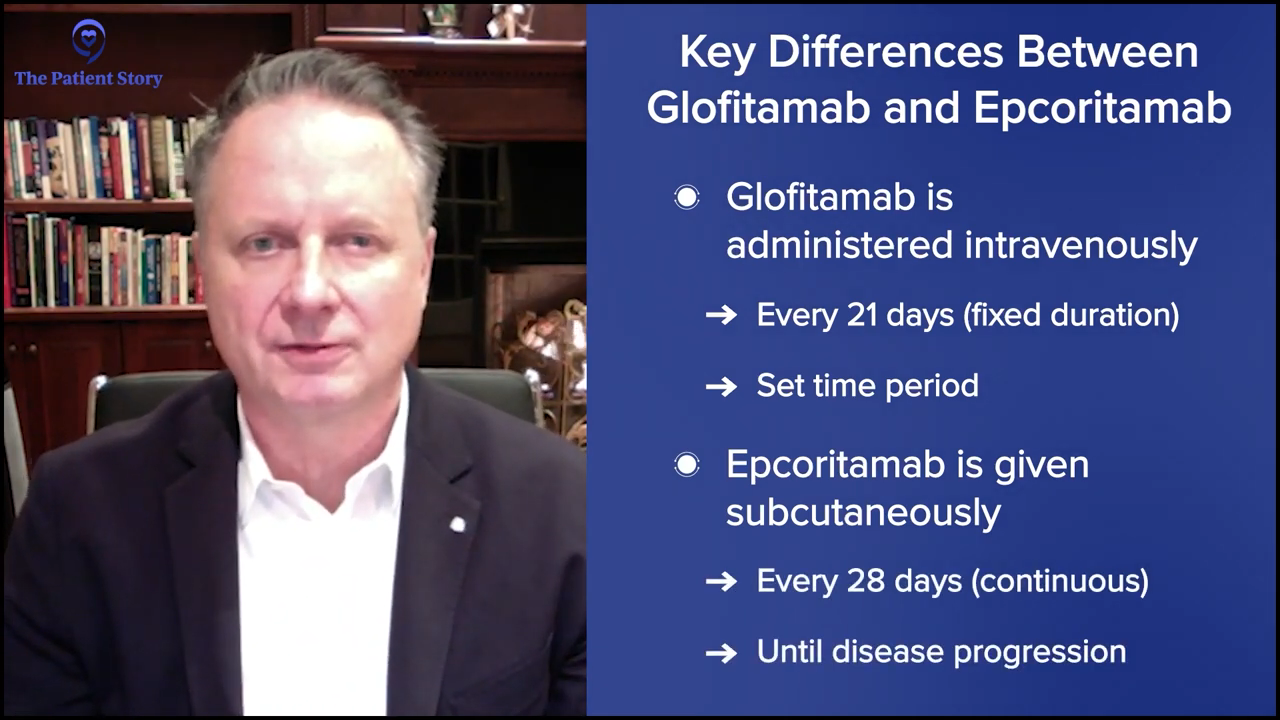
Dr. Steinberg: That’s a great question. We don’t have a clinical trial right now for front-line treatment for lymphoma. We do have two trials open for relapsed/refractory patients: one for epcoritamab (Epkinly) combined with traditional chemotherapy versus traditional chemotherapy alone, and another trial looking at zilovertamab vedotin, an ROR1 antibody-drug conjugate.
If I have a patient in those shoes, we always want to try and enroll them in a trial in the relapsed/refractory setting. This is not something where you can just say, “Oh, by the way, we have a trial.” I said it simplistically when I said I signed some papers when I joined a clinical trial. There’s a lot of time and attention that goes on behind the scenes. The doctor has to go through with a research coordinator and the institutional review board (IRB), which is a governing body that makes sure the study is safe in your institution and all the contracting that goes on. It involves a lot, and a lot of time and effort to discuss it with patients.
When the patients do get enrolled, it requires a lot of commitment on the patient’s part, which is why a lot of patients don’t enroll. Either we don’t think that they can make the frequent visits, or the patient doesn’t think that they can or want to commit to frequent visits and that’s sometimes the issue. I might refer a patient to the city from Westchester for a trial, but it’s too daunting for the patient to think about having to make multiple trips back and forth, sometimes even multiple trips a week. Maybe they live an hour away from my institution to enroll in a study that requires multiple visits.
But you weigh the difficulties of participating in a trial versus the potential benefits.But you weigh that negative aspect, the difficulties of participating in a trial, versus the potential benefits. What are the benefits? They may get early access to a medication that’s currently not approved in that line of treatment or a medication that may not even be approved, such as zilovertamab, the ROR1 antibody-drug conjugate, which has shown in studies to be an excellent medication, so now they’re trying to get it FDA-approved. That’s one of the benefits: getting early access.
I’ve had patients who, for whatever reason, didn’t have insurance, so they weren’t able to get these medications. Any of the regular medications would have cost them too much money, but they happened to have a clinical trial where I enrolled the patient in and were able to get access to a medication that otherwise would have cost a fortune. You have to factor that in. These clinical trials will pay for a lot of the treatments for the patients. Sometimes, we’ll pay for transportation, or they’ll give a small stipend for the time and effort that patients put in.
But you weigh the difficulties of participating in a trial versus the potential benefits.
Dr. Amir Steinberg
Dr. Brody: Those stipends where we pay for the travel costs have been very helpful for some patients because there can be more back-and-forth trips, as Amir was saying. Let me give a quick example of how clinical trials can work and, for many of them in lymphoma, how they do work.
I gave the example of chemotherapy plus bispecifics, which have been super effective and pretty well-tolerated for most patients because it tends to be gentler chemo and not super aggressive. Some of the combinations of gentle chemo plus bispecifics are just getting approved this year. As I was hinting, they were approved in Europe even before the U.S., so far, but are now getting approved in 2025, yet we have patients who got access to these medicines in 2021 and 2022. It’s like they had a time machine and were able to get future medicines years before they could have gotten them.
In lymphoma, we’re very lucky because there’s so much progress. Frequently, the newest medicine is the best medicine. In other cancers, that is sometimes the case. In pancreatic cancer, a very terrible cancer where our progress has been slow, the clinical trial may have something better than what’s already there, or it may not as they are not making as rapid discoveries as we happen to luckily be doing in lymphoma. But frequently in lymphoma, the newest medicines are the best medicines, so getting access to them four years ahead of time — if the goal is to live and to live well — is a huge opportunity.
We must always dispel myths about clinical trials. Patients always say, “Oh, wait, I could get some kind of placebo and get nothing.” There are no bizarre mysteries. As Amir was saying, we have ethics committees such as the IRB that oversee everything, so doctors and drug companies can’t do a trial just because they feel like it. They have to have everything approved and the ethics committees can be quite on top of it. They know all the details. They want the 167 pages to actually be 169 pages because they want you to put in more information so that the patients are well-informed. They are overseeing pretty rigorously. That’s the local IRB, and then you have the FDA as well. These local IRBs are either in the hospital or nearby, making sure that these things are, hopefully, healthy and safe for patients.
There is no mystery placebo where you may get something or not. Maybe there’s a placebo trial for toe cream or something. But in cancer, there are no random placebo trials because everyone is either getting the standard of care plus more. Should there be a placebo, you get the standard plus placebo. You’re already getting the standard treatment or the standard plus something new. That can exist. We tell you which one you’re getting, but sometimes, even we don’t know until the end. But you’re at least getting the standard therapy for sure.
Most trials are earlier phases, like phase 2 trials, where everyone gets the same treatment. There’s no mystery. Everyone knows what you’re getting. The doctor will explain to you before you get started. There are no surprises, which is an important myth to dispel for patients because that’s something that intimidates folks to ask about clinical trials.
Everyone is either getting the standard of care plus more. Should there be a placebo, you get the standard plus placebo.
Dr. Joshua Brody
Dr. Steinberg: Whenever possible, we try to offer trials because that’s how we advance the science and get higher cure rates. They’re essential. And as Josh alluded to, sometimes these medications are available a few years in advance.
When I first joined Westchester, I referred a patient to him who got access to a medication that wasn’t FDA-approved yet and that patient was able to receive it and did well. Otherwise, whatever other options were available weren’t quite as good as what this particular patient could have gotten through the trial. That’s what patients have to be aware of.
They’re not going to offer you some bogus medication that’s not going to work. When they’re testing, there are millions of dollars being invested in testing this medication, meaning there’s a high chance that they’re hoping that this is going to work and that this medication will work. Many years of time and effort have gone into researching these drugs. They’re not experimenting on people for the sake of it. They’re experimenting because they want patients to do better — because hey, capitalism — and if that drug is approved, then the company is going to do quite well, so there’s an incentive for that company to offer that medication.
There are non-company trials as well. There are trials that benefit the researcher. They’ve dedicated so much time and effort into developing a new treatment that, to them, it’s a passion, and it’s a passion that the medication or treatment they’re developing succeeds. Maybe they were devoting their whole life to lymphoma treatment because there was a family member who had lymphoma, or because they find that science so interesting and they want to do it for the joy of helping others.
It’s not always pharmaceutical. Sometimes, you could find investigator-initiated trials (IITs) where they’re making brand new medications that aren’t pharmaceutical-sponsored, so patients should be aware of that. They’re not randomly getting A, B, or C. There was a lot of thought put into this.
Stephanie: I appreciate the myth-busting.
Dr. Brody: Stephanie, just because Amir mentioned the money, let me say something about that because patients do ask us this frequently as well and we have to speak plainly about this. Patients will frequently ask, “Wait. The new medicine could be hugely expensive. And because it’s a trial, my insurance will not pay for it.” That’s an absolute myth.
Every medicine provided on trial, if it’s a new medicine and not the old standard, is 100% covered by whoever is doing the trial, whether it’s the investigators or the company, so they usually end up being cheaper. The patients may have had a copay if they were getting a pill of some type, like a BTK inhibitor or a BCL-2 inhibitor, and those will now be free instead of having a copay or whatever the patient was going to pay. Everything that is in any way nonstandard always gets paid 100% by the trial.
In addition, they also sometimes give a nice stipend to help the patients get back and forth. That’s another common misconception: “My insurance won’t pay for this because it’s in trial.” Your insurance doesn’t have to pay because it’s going to get covered automatically. Insurances sometimes still have to pay for routine scans and tests when they’re part of a trial, but anything nonstandard is free. That’s an important thing for patients to be aware of.
Don’t quickly dismiss a trial. Think about all the considerations and ask your doctor about the coverage.
Dr. Amir Steinberg
Dr. Steinberg: To piggyback off of that, I’m going to use my father as an example. He was enrolled in a trial that used lenalidomide (Revlimid). Had he not participated in the trial, it still would have been the standard treatment for him for follicular lymphoma, which would have cost him a fortune in copays. But because it was the standard arm option in the trial, even though it wasn’t the experimental arm, it got covered, so he got the Revlimid paid for, which he couldn’t have gotten otherwise. Don’t quickly dismiss a trial. Think about all the considerations and ask your doctor about the coverage.
Stephanie: I truly appreciate all this myth-busting because there are lots of misconceptions and I know there’s a lot of effort in trying to help support patients get to clinical trials, whether it’s the investigator or the pharmaceutical companies trying to cover costs. We have friends at Blood Cancer United (formerly The Leukemia & Lymphoma Society), where they have programs and grants to help cover things like travel or lodging.
Working with Your Care Team
Stephanie: There’s so much information available. You two are incredible specialists and anyone would be lucky to see either of you. Who else is also on the care team for patients and care partners? They have questions about insurance, coverage, lodging, logistics, side effects, and managing them. When I was going through it, I spoke with my nurse a lot about how to manage side effects in different ways. At your centers, how would you describe the care team to patients?
Dr. Steinberg: We call them transplant coordinators, but they’re really our cellular therapy coordinators. When it comes to discussions about CAR T-cell therapy or autologous stem cell transplant as a potential treatment option for relapsed/refractory diffuse large B-cell lymphoma, they’re great resources. They give our patients their cell phones, text with them all the time, and answer any quick, immediate questions they may have.
It’s a team — and it’s not just a diplomatic thing to say. If it weren’t a team, the whole thing wouldn’t work at all.
Dr. Joshua Brody
Also, the social worker is a fantastic resource in terms of finding housing and coverage for medications that patients might need. I will sometimes fill out Blood Cancer United (formerly The Leukemia & Lymphoma Society) grant forms for patients so that they can get these medications covered. Those are the two big people with whom I work closely. Sometimes even the fellow. If they happen to see a trainee hematologist-oncologist, they’ll sometimes develop a connection with that fellow who can help answer their questions as well.
Dr. Brody: As Amir was saying, it’s a team — and it’s not just a diplomatic thing to say. If it weren’t a team, the whole thing wouldn’t work at all. We have nurse practitioners, registered nurses, dietitians and nutritionists, social workers, and holistic therapists — a connected part of the team, but not built right into it because a lot of patients ask about that. We’re lucky to have easy access to all of these resources.
If it were just the doctor by themselves…, oh my. The patients depend heavily on communication with our nurses, nurse practitioners, and the rest of the team every day, sometimes.
Conclusion
Stephanie: Thank you both so much for your time. Is there anything you’d like to end with and share with patients and care partners on what’s happening in DLBCL?
Dr. Steinberg: Thank you for having me. Certainly, treating lymphoma patients is a passion of mine. There’s so much that’s changed in the last 20 to 30 years, most especially in the last five years. Things are changing for the better so rapidly for patients. As doctors, we have so much to catch up on and stay up on in terms of the knowledge out there, but it’s totally worth it because it will make patients’ lives better and more fulfilling.
Dr. Brody: Agreed, agreed. We’re very lucky to have you, Steph, and The Patient Story team as you try to get information out to patients. Information is power and the patients could use some power in this scary setting. In line with that, I’ll answer a question from before. What else should patients ask their doctors? Here’s the important thing: ask whatever you want. Do not in any way put doctors or nurses on a pedestal where you cannot ask a dumb question. People say there’s no such thing as a dumb question. There are, but don’t worry about it. Just ask them. It’s okay. If they go in the back room after and make fun of you, fine. At least you got your question answered. Don’t be shy to ask questions of your doctor and the nurses. That’s what they’re getting paid to do: to answer your questions.
Stephanie: I appreciate the humor, especially when we’re talking about something like this. Again, Dr. Amir Steinberg from Westchester Medical and Dr. Joshua Brody from Mount Sinai, thank you so much for being here.
We hope that this discussion has helped you consider all your treatment options, how to navigate different systems and centers, and walk away with questions for your healthcare team. On that note, while this conversation is meant to be helpful, it’s not a substitute for medical advice, so please still consult your doctor and healthcare teams.
We want to thank our sponsors, Genmab and AbbVie, for making this program possible. Their support helps us to host more of these. We want to note that The Patient Story maintains full editorial control of the program.
Finally, we want to know how you felt about this discussion. Was it helpful? How was it helpful? What would you like to hear more of? What could we do better?
I’m very glad that you were able to join us and we look forward to your feedback. I hope that you’re able to join us for another program in the near future. For now, thank you and take good care.
Thank you to Genmab and AbbVie for their support of our independent patient education program. The Patient Story retains full editorial control over all content.
This program has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Living Well Together with Follicular Lymphoma: Real Talk from Patients & Partners
How do you navigate living with follicular lymphoma (FL) as a couple from diagnosis, to treatment decisions, and life beyond?
In this heartfelt discussion, three couples share their personal stories and unique insights on living with FL. From the shock of diagnosis to finding emotional balance, hear real talk on what helped them move forward together.
Living Well Together with Follicular Lymphoma: Real Talk from Patients & Partners
Hosted by The Patient Story Team
How do you navigate follicular lymphoma (FL) as a couple — through diagnosis, treatment decisions, and life beyond? In this heartfelt discussion, three couples share their personal stories and unique insights on living with FL. From the shock of diagnosis to finding emotional balance, you’ll hear real talk on what helped them move forward together. Whether you’re a patient or a care partner, this program offers connection, validation, and hope.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
Thank you to Genmab for its support of our independent patient education program. The Patient Story retains full editorial control over all content.
Stephanie Chuang: The focus for today is living well with follicular lymphoma, navigating the healthcare system, staying informed and connected in the system, and so much more. We’ve got an incredible panel.
I’m the founder of The Patient Story and I had my own blood cancer diagnosis. When I was getting my 600-plus hours of chemotherapy — so much fun — I felt very isolated and confused. I wanted to hear from real people, experts who are not already being highlighted, and to me, that would be other patients and care partners. That’s when the idea came up to help others navigate life at and after diagnosis, which is what The Patient Story aims to do. We try to build community through in-depth patient stories, educational programs, and discussions to amplify your voices, the voices of patients, caregivers, and partners.
Living with Follicular Lymphoma also provides another community where you can chat in real time with thousands of people living with FL from around the world. It is the largest FL-dedicated Facebook group online.
We would like to thank Genmab for its support as our sponsor, which allows us to continue hosting these discussions and programs free for our community. I want to stress that The Patient Story retains full editorial control and while we hope that this is helpful, remember that this is not a substitute for medical advice. Please consult with your team as you’re making your decisions.
Joining me are follicular lymphoma patients and their care partners. We have Nicky and Craig from Perth, Western Australia, Hayley and Carl from St. Louis, Missouri, and Milissa and Andrew from Clear Spring, Maryland. I’m joining from just outside San Francisco, so we’re covering a lot of space.
Nicky & Craig
Nicky: I was diagnosed with follicular lymphoma in February 2014 at 32 years old. My kids were very young then, one and four. I also recently graduated from university and I’m now a clinical nutritionist. My passion is supporting cancer patients through their nutrition and lifestyle.
Craig: I’m Nicky’s husband and we’ve been together for a long time.
Nicky: 28 years, I think.
Craig: I’m Nicky’s caregiver, but it’s probably a lot more than that.
Nicky: We’re each other’s caregiver.
Craig: I’m a dad, I work, and I try to keep everything rolling.
Milissa & Andrew
Milissa: I was diagnosed with follicular lymphoma at the end of 2023. Andrew and I had been living together for a little over a year at that time. I’m also a nurse, so that put a different spin on everything that went on.
Andrew: Milissa and I have been together since August 2021 and have been living together since September 2022. She was diagnosed with lymphoma in November or December 2023 and started getting treatment in January 2024. It’s been a challenge since she seeks treatment in New York City, which is about a five-hour commute from where we are. But she gets good care where she goes, and right now — knock on wood — she’s doing well.
Hayley & Carl
Hayley: I got diagnosed with stage 3B follicular lymphoma in October 2024, which had already transformed to diffuse B-cell when we found it. We started treatment by November. I’m also a nurse and work in the emergency room, so that’s where I got my diagnosis, at work.
Carl: We’ve been together nearly two years. We’ve been together about a year and a half when she was diagnosed. Luckily, we had already lived together when that happened. I have two kids, so my role was to support her and try to stay healthy and present. I’m lucky that I work remotely, so I’ve been able to attend almost every appointment, be there for her as best as I can, and try to hold everything together. She’s done great and we’re happy to see the other side of this.
What Were Your First Symptoms of Follicular Lymphoma?
Stephanie: Let’s kick off with when you found out about all this. We know that for follicular lymphoma, many people don’t feel any symptoms, but some feel subtle symptoms, so there’s a bit of a range there. A lot of people get curious about this part of the story. How did this lead to a diagnosis? Nicky, you were diagnosed at 32. I was 31. We both mentioned fatigue, which, by the way, isn’t just tired. It’s beyond that. But you also just had your son, so there’s a feeling that the fatigue comes with that, doesn’t it? What moved you to become concerned?
I felt my neck and realized that it was like a corncob.
Nicky
Nicky: I didn’t notice any signs or symptoms. I was working, I just had a baby, and I had a toddler as well, so I thought that being tired and fatigued was normal. I used to be a mortgage broker. One of my colleagues was a bit of a hypochondriac who always thought she had any kind of illness that came. She mentioned that she always checks her neck for lumps because in her head, if you have a lump on your neck, it means that you have cancer.
I laughed it off, but I felt my neck and realized that it was like a corncob. It was very lumpy. I didn’t worry too much, but I went to the general practitioner (GP) and he said, “Oh, okay, we’ll do a blood test and see.” I never heard back. I went back about a month later and told him I still had lumps on my neck, and that’s when he said to do some more testing. It took a good two to three months for me to get my actual diagnosis. There was a lot of back and forth going to different doctors and getting tests done, so that was a little traumatic at the time.
Stephanie: Hayley, you shared that you felt pressure in your neck, but it didn’t feel like a typical sore throat and you were otherwise feeling healthy. What pushed you to listen more to your body and to seek medical help?
When I would sit slouched back on the couch and breathe out a few times, I felt a wheeze.
Hayley
Hayley: It originally started with a deep-set lump over my clavicle. It didn’t feel like a lymph node; it almost felt like a pulled muscle. It wasn’t bothering me all day and it wasn’t even every day. It was only in certain positions. When I would raise my arms above my head, I would feel the pressure. Now, looking back, I know exactly what that was. Every time I lifted my arms, it would push the mass. It deviated my trachea.
Besides those nodules, my only other symptom was a little bit of wheezing, which I didn’t think anything of at the time. It wasn’t alarming enough or often enough to spark concern. When I would sit slouched back on the couch and breathe out a few times, I felt a wheeze. I thought I only needed to change my position. I found out that I had a big mass right in the middle of my chest and that’s never happened since then, so now I know that’s what that was.
Getting a Doctor to Address Your Concerns
Stephanie: When you were seen by a doctor and voiced your concern, did you get any feedback like it’s nothing? Especially as young women, sometimes we hear stories about that.
Hayley: That morning, I called an ENT because at that point, I knew that it wasn’t something normal, and it came on overnight. I said, “I would like to get a scan.” The ENT said, “I’ll see you in six months,” and I said, “It came overnight, so in six months, I don’t think I’ll be here.”
When I went to my primary care doctor, she was pushing on my thyroid and having me swallow. She wasn’t quick to order a scan. I had to push for that. She was thinking along the lines of a thyroid issue and ordered an X-ray. Originally, the only thing that we had was the X-ray. They called me that night with the results showing widening of my mediastinum. I was shocked because I was under the impression that I might have some swollen nodules. I didn’t understand why she ordered an X-ray of my chest.
Stephanie: I’m so glad you pushed for what you needed. As a nurse, I can only imagine all that you know when it comes to this. Milissa, did that also show up for you in terms of self-advocacy, in trying to figure out the diagnosis? Did you have any red flags for symptoms that you experienced?
Milissa: I commonly had lymph nodes in my neck. I went to primary care doctor who also thought it was my thyroid. They did some ultrasounds, but they didn’t see anything. They did a CT scan and it came back with “possible lymphoproliferative disease.” I went to see an ENT doctor at a pretty big center and he said it was just inflammation. He didn’t know what it was, told me to get another ultrasound of my thyroid, and then said, “I’ll see you in six months.” I said, “Can we biopsy it?” And he said, “No, I don’t think it’s warranted.” I went on for another two years until I got another CT scan.
Stephanie: We’ve heard that sometimes, it does take time, especially when there’s not a more pressing symptom to flag something.
It’s a little hard to grasp the severity of it. You don’t have a lot of answers in the beginning.
Andrew
Helping a Patient Cope as a Care Partner
Stephanie: There are two very different perspectives when we enter a diagnosis: the person who’s diagnosed and the main care partner. For each care partner, what do you think your partner was thinking and feeling in terms of how to handle the diagnosis?
Andrew: It was a big shock for both of us. She’s always been very healthy, vibrant, and energetic, so you’re thrown back by it. It’s a little hard to grasp the severity of it. You don’t have a lot of answers in the beginning. Milissa knew that she needed to get more answers and she wanted to go to a facility where she would probably have the best chance of getting the best treatment. Being a nurse, she wants to research and look up symptoms, which is good because she’s educated in that respect and I’m not.
Stephanie: Milissa, what I heard was part of it was fear but being in the field of healthcare, you know a lot, which is good, but it brought some anxiety. When you heard him describe your reaction, was that spot on or is there anything else you’d like to add about what you were feeling?
Milissa: Yeah, that was spot on. I went down every bad road that there was.
I was feeling anxious about it and didn’t know what to do… If you’re diagnosed with cancer, your outlook on your future changes dramatically overnight.
Andrew
Stephanie: If you could list a couple of words for Andrew and how you think he was at diagnosis and moving forward into this new relationship, what would that be? How would you describe that?
Milissa: I think he was lost and terrified. He took one day at a time, whereas I took five years in advance, so it was probably better for him.
Stephanie: Andrew, did she nail that, or were there other things that you were feeling?
Andrew: No, I think she nailed it. I’m sure I was feeling anxious about it and didn’t know what to do. It’s a different role. If you’re diagnosed with cancer, your outlook on your future changes dramatically overnight. That’s hard to deal with and grasp right away for a person who loves you. It takes a little time to absorb those things.
Stephanie: Craig, could you talk about Nicky and her reaction and how she was during that time as you guys were trying to figure it out? What descriptive words would you use there?
Craig: Uncertainty, fear, being lost, and not knowing what tomorrow’s going to be. The information 10 years ago was a lot different compared to what it is now. It was very difficult. I don’t remember many days of my life other than my wedding day, but I do remember February 13th and the conversation. It was certainly a tough day.
Stephanie: Nicky, was there anything that Craig didn’t know at the time or did he pretty much capture all of that for you?
Nicky: It was pretty bang on. We live a little out of Perth and the doctor was a fair way away, so they called to give me the news. He was next to me and I said, “Is it cancer?” I didn’t know what lymphoma was. There wasn’t even that much information, but I remember the doctor said to me, “Google indolent.” Craig went off straight away and Googled indolent, then he came running back and said, “Don’t go on Google and don’t Google anything.” I was banned from Googling, but I don’t know what he read. It was a very shocking moment. We were very stunned because I didn’t expect to hear that. It was like a punch in the face.
Stephanie: When we talked, you mentioned the emotional response and that Craig felt something first, then when he was able to collect everything and move forward, then you got the chance to let go. Can you describe that?
Nicky: He came back and must have read something that scared him, so he broke down first. I said, “It’s going to be okay, love.” We called his mum to come over because she has breast cancer and we’re very close. When she arrived, that’s when it hit me and I broke down. We took turns supporting each other and as we started to get into it, the information came to light, but there was an initial shock.
After I had my bone marrow aspiration, we found out that it was stage 4. In our minds, hearing the words stage 4 for any cancer was the worst it could be, but for FL, it’s a bit different, which we didn’t know at the time. There’s a lot more information out there about FL than there was over a decade ago.
Craig: We went through the process before the diagnosis and went to numerous doctors’ appointments and procedures. I kept saying to Nicky, “You have nothing to worry about. It’s going to be fine. This is the process they go through and what they do to rule stuff out.” When we got the diagnosis, I felt awful that I was saying these things to her. I don’t know how to put it into words, but it was tough for me that I’d gone through that process with her, telling her everything’s going to be sweet, and then obviously it’s not. It’s like a bit of a bomb gets dropped.
Stephanie: Nicky, how is it hearing him describe that piece of it? Have you talked about that before?
Nicky: No, we haven’t spoken in depth about how he felt at the time of diagnosis, so it’s good to talk about it and get it out in the open, but I don’t think you should have any guilt about it. It’s nothing we could control. When you get a diagnosis like this, your whole mindset starts to change. Things that mattered before don’t matter anymore. Now I’m realizing what a blessing that is because it opened my eyes to take notice of things around me, make the most of every moment with our kids, and watch them grow. We don’t miss a moment anymore and I’m grateful for that.
Stephanie: Wonderful. Thank you both for sharing all of that. I know it’s a lot to remember back to 11 years ago, so thank you.
When you get a diagnosis like this, your whole mindset starts to change. Things that mattered before don’t matter anymore
Nicky
Stephanie: Hayley and Carl, I’m so interested to know if any of that resonated with either of you. Carl, what do you remember Hayley feeling and thinking at the time of diagnosis?
Carl: I was in the ER room when the doctor came in and gave her the diagnosis. I would say shock was the number one emotion, probably for both of us, because she was so young and healthy. We were active people, went to the gym quite a bit, and ate pretty well. Then it quickly turned to fear. Fear of the unknown and all the uncertainty, like Craig was talking about. She was quick to harness all that, bring it back, and hit everything head-on.
Carl and I had only been together for a year and a half, so I had a pit in my stomach. What was I signing him and his kids up for?
Hayley
Stephanie: Hayley, was there anything else that was going on for you? It wasn’t that long ago. Was Carl pretty right on with that? Was there anything else that you were feeling that he wasn’t able to see, maybe?
Hayley: Shock was the first emotion. I was pretty much in disbelief that it could be cancer. I also didn’t quite know what lymphoma was. When they said the word, I didn’t know that meant cancer. I asked, “Is this terminal? Is this something that can be treated?” Now I know there are over 180 forms of non-Hodgkin’s lymphoma.
I didn’t know what to think or what to expect. My doctor and I are close, so I asked, “Am I going to die?” He told me no, so that was helpful, even if he didn’t know. At least during that time, I knew it wasn’t a death sentence.
I was scared. Carl and I had only been together for a year and a half, so I had a pit in my stomach. What was I signing him and his kids up for? But he’s been good about being strong and not making me feel that anymore. I couldn’t help but think that. We’re 30 years old. When we got together, this wasn’t what he was thinking we were going to buckle up for. I had my last chemo recently, so it’s still new and there’s still fear percolating in there. It’s been a lot.
I needed to know if I had a future. I kept thinking, ‘Am I going to be able to have children? Am I going to get married? Do I tell him to go live his life and not wait for me?’
Hayley
Stephanie: I can only imagine. It was a while ago for me, but it’s still a lot coming at you and you’re still in it. Hayley, how about with Carl? You were in the room together that day. But for the days and weeks after, what did you notice about his reaction and what he was going through?
Hayley: He held it together pretty well. He was listening, very supportive, and understanding. We’re going to get through it no matter what happens. It was nice to know that he didn’t run away and wasn’t like, “I don’t want to get into this. This seems like a stressful time.” He stood by me and we’re going to get to the end of it, whatever that is going to be. Despite having two younger kids, we were going to get through it all together
It all happened so fast. After I got my diagnosis, I went to an oncologist the very next day then the day after that, I had surgery. Two weeks later, I started with treatment. I feel like my oncologist was trying to say as little as possible and not tell me much. He wanted me to focus on treatment. We’ll get there when we get there and talk about all that later. But for me, that wasn’t good enough. I needed to know if I had a future. I kept thinking, “Am I going to be able to have children? Am I going to get married? Do I tell him to go live his life and not wait for me?” That went through my head many times.
Stephanie: That hits home for me because that was where I was in my relationship, too. I thought all the same things. We imagine this life then cancer comes and it wasn’t part of the plan, obviously. Thank you for sharing that, Hayley, I appreciate it. Carl, was there anything that you feel Hayley didn’t see at the time or did she cover all of it?
Carl: No, she did a good job. None of those thoughts ever crossed my mind, but there was some underlying fear and things that I probably suppressed a little bit to be there for her. But a lot of the same emotions she was feeling, I was, too. I probably didn’t show them quite as much in the beginning.
I probably suppressed a little bit to be there for her. But a lot of the same emotions she was feeling, I was, too. I probably didn’t show them quite as much in the beginning.
Carl
Processing Your Emotions as a Care Partner
Stephanie: It sounds like you were feeling all those emotions but in order to support Hayley, you didn’t want to access them right away. Have you been able to process it more since then?
Carl: I feel like I have. We’ve been submerged in this for six months now. I’ve had my moments.
Stephanie: Can you talk about what those moments look like for you?
Carl: My first big one was when she went in for her biopsy. I stayed back while her parents went in to see her off. It was tough to see her go back. We’ve had a couple of difficult moments together around the house and some of the scary times where when she got sick during treatment, but my biggest one was while she was in surgery for her biopsy.
Stephanie: Andrew, how about you? Were you able to process early on, or did it also take some time? Do you remember the first time it hit you emotionally?
Andrew: It was when Milissa went up for her first treatments at Memorial Sloan Kettering. She didn’t feel well at all after her first treatment, so it worried me. She had to go to the ER afterwards. That’s when it emotionally hit home for me that this is very serious. We don’t know what the outcome is going to be and it’s going to be a fight.
Major Challenges Faced by Care Partners
Stephanie: Craig, what was the most challenging part of the role of care partner?
Craig: The hardest was when she was having treatment, seeing the wasting away of her body and what the drugs were doing to her. She went from a fit and healthy young lady to skinny and weak. It was tough. You’re looking from the outside in and it’s very difficult to see your partner go through that change. I said to her a thousand times that I’d swap places in an instant, but unfortunately, that’s not how it works.
Stephanie: Andrew, when we were chatting before, Milissa mentioned that she has been a nurse for over 30 years, so being the patient was a hard transition. Milissa, you called yourself a “bad patient.” Andrew, was that challenging for you? What was that like for you?
Milissa researching morphed into finding other people who were in the same situation. It became a support group for her, too, which was a good thing and continues to be a good thing for her.
Andrew
Andrew: It was very challenging. Milissa wanted to do a lot of research and that’s her nature. She would say that would help ease her mind, but I felt differently. I tried to accept that, but I felt that it would make her more anxious. I wanted her to try to put those things aside and still live her life, which is maybe a naïve way of looking at it. I couldn’t do much because I don’t have a medical background and have a limited understanding of the technical aspects of things.
In the end, Milissa researching morphed into finding other people who were in the same situation. It became a support group for her, too, which was a good thing and continues to be a good thing for her. She has taken that support group and given back to people who are going through the same experience with lymphoma. It’s been great for her because it helps her heal a lot.
Stephanie: What you’re speaking to, I’ve heard many times over. No matter how great the relationship is, there is something to be said about each person’s role and the understanding of what it feels like, which is why I’m glad we’re having this discussion with all of these perspectives.
I had what I thought was quite an unusual treatment because I haven’t met anybody else who had the same treatment as I did.
Nicky
Deciding on the Right Follicular Lymphoma Treatment
Stephanie: Could everyone share what treatment they’ve had and what that looked like, and then shift into the treatment decision-making conversation? Hayley, what treatment have you had and what’s ahead?
Hayley: I had R-CHOP chemotherapy and then Neulasta (pegfilgrastim). I’m doing at-home Neupogen (filgrastim) injections for 10 days to boost my white blood count. I took my last prednisone two days ago. I have a PET scan and labs in six weeks, but as far as meds go, I don’t have any more, nor do I want any more.
Stephanie: I hear you. Watch and wait, or active surveillance, is a big part of follicular lymphoma. Milissa, what have you had in terms of treatment?
Milissa: I had a research drug called mosunetuzumab, a bispecific antibody, which was a good decision. I had eight rounds of that.
Stephanie: Were you on that after some period of watch and wait?
Milissa: No. I was diagnosed in December 2023 and started treatment in January 2024.
Because of the radioactive iodine, I’m trying to stay away from radiation as much as I can.
Nicky
Nicky: I had what I thought was quite an unusual treatment because I haven’t met anybody else who had the same treatment as I did — and I know a lot of FL patients. They put me straight into a clinical trial, so we didn’t have decisions to make, but I wasn’t educated enough to know what I was going to get into.
They suggested I go on a clinical trial of rituximab coupled with radioactive iodine. I was radioactive and put under house arrest for a couple of weeks. I wasn’t allowed within five meters of anyone or 100 meters of children or pregnant women. That was quite confronting, being away from the kids and the whole family for a couple of weeks.
After the infusion of radioactive iodine followed a year’s worth of rituximab and it worked pretty quickly. The lumps melted away within a month or two. Three months into my treatment, I had a PET scan and it was clear. I was no evidence of disease (NED).
I haven’t had a scan since then. Because of the radioactive iodine, I’m trying to stay away from radiation as much as I can. I do have a couple of lumps in my neck that we monitor, but I haven’t needed any treatments since. Fingers crossed that I don’t need any more. But the treatment fractured my immune system, so I manage that, but I manage it pretty well.
Stephanie: I’m glad to hear it. That was a good background to understand if you had these long periods of waiting. To open this into a broader discussion about communication with the healthcare team, you have two people in this: the patient and the care partner. First, there’s the treatment decision-making part, if you had that conversation with your doctor, and then symptom management and reporting what people are feeling. Hayley and Carl, how did you feel you took on the roles when it came to making decisions about your treatment?
Hayley: As far as medical treatment decisions, what do you think, babe?
Carl: I stay in my lane. I stay quiet. I take notes so she doesn’t forget what the doctors say.
Stephanie: Taking notes is good because a lot is coming at you all at once.
I was looking for any glimmer of hope, even if it came with 50 bad things that I read. If I could find two supportive statements that made me feel better, that would be helpful.
Hayley
Hayley: When Andrew was talking about Milissa researching and he was thinking it would make her more anxious than not, I was trying to figure out where that was coming from because I did the same thing. I was looking for any glimmer of hope, even if it came with 50 bad things that I read. If I could find two supportive statements that made me feel better, that would be helpful. But with treatment, I made a lot of those decisions, but they didn’t give us any options because it had transformed.
Carl: Put a lot of trust in the doctors, too. We ask questions, even retrospectively, on why this and not this, and they had very detailed answers to everything. At the time, it was happening so fast. As she said, she didn’t necessarily have a choice, but it all worked out.
Stephanie: You said you stayed in your lane, which I think resonates with a lot of people. I wonder how you were able to do that because, of course, you care for Hayley, so you want to do something. Did you channel wanting to help in a different way, outside of taking notes? How did that manifest for you?
Carl: I helped with the day-to-day stuff as much as I could. She’s pretty strong-willed and independent, so I try not to make her feel like she’s being babied too much. We cleaned up the food around the house and did the typical things hygiene-wise to try and stay healthy and support her.
It was only a year and a half into knowing them, so the emotional connection was different because I couldn’t be as affectionate.
Hayley
Hayley: That was rough. He has an 11-year-old daughter and a six-year-old son. They were both a year younger when I got diagnosed, but I’m close with the 11-year-old girl. We’re buddies. It was sad because I knew that she would probably grasp a little bit. After all, her friend’s mom went through leukemia and it scared her badly. She started crying. She was scared for me. We try to let her know that it’s going to be okay without completely lying and saying I just have a cold, so that was a teeter-totter for sure.
With the younger boy, we try not to make him feel like he’s doing something wrong by continuously reminding him to wash his hands, change his clothes, or shower. Because all of a sudden, I’m like this bubble and he has to stay away from me when we used to lie on the couch together. “Does she not like me anymore? Why is she not being so lovey?” It was only a year and a half into knowing them, so the emotional connection was different because I couldn’t be as affectionate. I was stressed and, to be honest, I thought of them as little germ factories when they came home and I was scared. After I got diagnosed, I went into neutropenic fever and stayed in the hospital for a week. It was a lot to endure.
When they got a little bit older, we had a conversation with them. The emphasis was that when you hear the word ‘cancer,’ it’s not something to be immediately scared of.
Craig
Stephanie: You’ve gone through a lot, but I appreciate you bringing this up because there’s the obvious stuff and then there are all the other things that come with treatment that impact day-to-day life. Nicky and Craig, with the kids, did you play different roles in communicating the diagnosis?
Nicky: We didn’t tell them.
Craig: The kids were too young when Nicky was going through treatment. When they got a little bit older, we had a conversation with them. The emphasis was that when you hear the word “cancer,” it’s not something to be immediately scared of. There is a lot of information. There are different types and a lot of different scenarios. We wanted to reassure them that mum has a condition, but it’s something that we manage and something that we’re going to manage for the rest of her life, so that’s how we move forward with that.
Nicky: Our daughter was five when I finished treatment. When I went away, I told her it was for work and she was mad at me for going away. She noticed how it affected my mental health. For the whole year after finishing treatment, before I set up the Facebook group, I was absolutely miserable and she felt that. It wasn’t until I realized how much she felt that was when I knew I had to do something about my mental health.
Our youngest was very little. He wasn’t even one when I was diagnosed, but when we told them, like Craig said, we didn’t want them to be scared of the word cancer. We decided to tell them when we were doing some fundraising for the leukemia foundation. It was a lantern night, so we had fun. We explained why we were fundraising and why mum has a white lantern and everyone in the family has a blue lantern. We try to explain it in a way that wasn’t scary for them.
I didn’t know much about the clinical trial drug because it hadn’t been out very long, maybe two years, so there wasn’t much information, which was scary.
Milissa
How Care Partners Can Help with Treatment Decision-Making?
Stephanie: Milissa and Andrew, what were the roles that you played in treatment decision-making in the doctor’s office? Did you find that one was speaking up more than the other?
Milissa: I have a mini homestead, so I have several animals to take care of, so thankfully, he stayed back for that. I went by myself a couple of times and then my mom went with me for the decision-making. I was given two options for treatment: one was the clinical trial and the other was rituximab and Revlimid (lenalidomide). The doctor waited for the clinical trial. He pushed me into it creatively.
Stephanie: Can you talk about that more? What did he say and what resonated so that you decided to go in that direction?
Milissa: I, of course, researched both. I didn’t know much about the clinical trial drug because it hadn’t been out very long, maybe two years, so there wasn’t much information, which was scary. It seemed like my insurance would pay more for the standard treatment, so I was leaning more toward that.
My doctor told me that he would have the pharmacist talk to me about the standard treatment; the clinical trial nurse talked to me about the clinical trial. I’m glad I did it. He said that the clinical trial had fewer side effects and discussed those with me at length. He also discussed some of the side effects of the others. That’s when I decided to do the bispecific antibody.
From very early on, she knew that was the route she wanted to go, so that fell into place very quickly.
Andrew
Stephanie: Andrew, when Milissa is talking to you about these treatment options, did you agree? What thoughts did you have about the decision?
Andrew: I was a little concerned about the clinical trial, like how much is known about it and the success rate, but Milissa was concerned about the side effects of the more traditional treatments. If I remember, the insurance would cover her to receive these clinical trials at Memorial Sloan Kettering Cancer Center in New York City. I don’t know if she would have been able to receive that locally, but we had some unsatisfactory experiences with some of the local healthcare facilities. Memorial Sloan Kettering is world-renowned.
My only concern was her going to New York City by herself because she couldn’t go on public transportation or fly, so she needed somebody to take her. Fortunately, her mom stepped up and would take her to New York and I would stay behind and take care of the farm.
Stephanie: How important was it to have Milissa’s mom? Who else was part of the regular support circle and how important was that?
Andrew: Her mom was supportive. Sometimes she would get stressed with her mom because her mom had her thoughts about things and that’s normal. I know she would confide in some of her girlfriends and seek support from them as well. But from very early on, she knew that was the route she wanted to go, so that fell into place very quickly.
Stephanie: Hayley and Carl, and Nicky and Craig, were there additional major players in your support circle?
Hayley: Definitely both sides of our family, but I would say the next after Carl is my mom. She definitely has been there every step of the way. The only time she wasn’t was when she was sick and when my dad got sick. She was in tears over not being able to be at treatment with me. She definitely made it very clear that it doesn’t matter what’s happening or what time of day — she wants to be there and be able to help me.
We’re similar in some ways and opposite in a lot of ways. We butt heads at times, but she put everything to the side. There are things about her that drive me crazy and she can be a little overbearing, but whenever she’s at the doctor, she’s able to turn it off and let me do my thing.
One time, she begged to be in the room to see the doctor and I remember saying, “I have a lot of questions. It’s already a small room. We have the doctor, the nurse coordinator, me, and him (referring to Craig). There’s no room for you in there.” She asked the people at the front desk, even though I said no, and still came and knocked on the door. I let her in and said, “I have a lot of questions for the doctor and a lot of stuff I want to cover, so I need you to reel it in,” and she did. She sat there quietly and was grateful to be in there. But she’s been good throughout the whole thing.
She definitely made it very clear that it doesn’t matter what’s happening or what time of day — she wants to be there and be able to help me.
Hayley
Stephanie: It sounds like you were very clear with your communication in setting boundaries.
Hayley: Yeah. They needed to be set.
Carl: It’s one of Hayley’s strong suits.
Hayley: And she did a good job.
Carl: The web runs pretty wide with us. My parents were great in helping out with the kids. I have them 50% of the time, so we aligned our schedule with chemo. The first one got delayed, so all bets were off after that. We had to be fluid and flexible. We had help from both sides of the family all the way down the list at some point, whether it was with the dogs, the kids, or everything in between. It was pretty great. A lot of friends reached out. She received a lot of care packages and flowers. Those meant a lot in those times.
Hayley: You don’t realize how much they mean. Flowers have never meant more. They showed up at the door and my whole day became better. I wish that I didn’t know how people could make someone feel, but now I know moving forward for not if but when I know somebody that goes through this. I’m almost thankful that I know how to take care of them and I’m excited to pass along what people have done for me.
We had great support on both sides of the family… the people I am friends with are like family… Whatever I or Nicky needed, they were able to accommodate that for us and I’ll be forever grateful for that.
Craig
Stephanie: That’s beautiful because you’ve been in this position and now you’re paying it forward with all that empathy. Nicky and Craig, how about you? Did you have additional support and how important was it to have that?
Craig: We had great support on both sides of the family as well. We have an extra network of our friends who we’re close with; these were people we grew up with and stayed friends with. I don’t have a large circle of friends, but the people I am friends with are like family. It was good to be able to rely on them and fall on them when I needed to debrief and maybe forget about things for a while. Whatever I or Nicky needed, they were able to accommodate that for us and I’ll be forever grateful for that.
Nicky: We’re lucky that my parents live about 200 meters down the road from where we live. Although at the time of my diagnosis, my mum wasn’t well, so she couldn’t be there for me. But Craig’s mum was a pillar of strength, particularly for me. She lives about an hour away from us, but she took me to my first treatment. I stayed at her place because I had my treatment in Perth. She has metastatic breast cancer. At the time, it wasn’t metastasized, but she had been through breast cancer, so we connected on that level as well. She was probably one of our biggest supporters, as well as my parents and our close friends. We’re very lucky because when I went away for a couple of weeks, we had family support the kids so Craig could keep working and I was appreciative of that.
We got used to operating on a little bit of a higher stress level with dealing with treatments and the whole situation.
Carl
Biggest Emotional Challenges for Couples
Stephanie: For Hayley, Carl, Milissa, and Andrew, did anything resonate for you in terms of the emotions and what you found was the most challenging? Have you been able to talk about it with each other or did you talk to other people about it and preserve your relationship differently?
Carl: It was always the outside stresses that caused the most tension, like one of the kids getting sick or something like that. Going through treatments, Hayley was very lucky. She definitely had some bad moments, but she had more good days than bad days. I would think that would be fair to say. We still had a lot of normal, if you will, quality time together, even through treatments. But when something would go wrong, unforeseen challenges piled on top of everything else.
We got used to operating on a little bit of a higher stress level with dealing with treatments and the whole situation. We were already at our tipping point, so at times when something else would get introduced, it would put us over the edge, but we always got to settle down and bring it back. What helped us was being grounded and centered at home. Honestly, it’s one of the things that I see as a benefit and a net gain out of this. We got a lot of quality time in our house. All the running gets cut out. You trim back the activities, which can be hard but at the same time, it was definitely good for us and the kids.
I was too focused on making sure that Milissa was staying positive and trying to take care of things… I have my little hobbies and things that I do on the side to help ease my mind.
Andrew
Stephanie: There’s always attention on the patient but maybe a lot less so on the care partner — that was my experience at least. Everyone was worried about me. I remember telling my now husband, “Hey, what you need, you need. Make sure to take care of yourself.” How did that show up for you, Carl, or did it not?
Carl: It did in ways. I have some property about an hour away, so when it would build up, I’d escape there for a few hours and take time when I needed it. Luckily, I didn’t need a whole lot, but Hayley was always understanding of it. She’d be able to tell. We’re pretty in tune with each other, so it ended up working out okay on my end.
Stephanie: Andrew, how did that show up for you? Did you take care of yourself? Was it a thought that crossed your mind?
Andrew: No, I was too focused on making sure that Milissa was staying positive and trying to take care of things. I went with her a couple of times for her treatments, so it was comforting for me to be able to accompany her, feel what she was going through, and see how the process was. It eased my mind a lot. I felt that she was getting good care there, so that made me feel good. I’m the kind of person who stays busy and that helps. I have my little hobbies and things that I do on the side to help ease my mind.
Biggest Lessons Learned as a Patient and Caregiver
Stephanie: You shift from being partners in one way to this completely different dynamic of patient-care partner, so things like emotional health, mental health, intimacy, and the way that you look at one another in all these different ways can be impacted. I think that’s very natural. What is the biggest way that you saw that impacted the relationship and the biggest solution, too?
Nicky: It definitely brought us closer together, didn’t it?
It makes you realize how fragile life is… We’re more thoughtful with how we approach everyday things. You don’t sweat the small stuff anymore because it’s not worth it.
Craig
Craig: Yeah. It definitely made us a lot stronger and more resilient, and changed our perspective on everything. We definitely take a lot more care with the kids and make sure we soak up all the little moments. It makes you realize how fragile life is. To try and put a good spin on this, our lives changed dramatically with the diagnosis, but for the most part, our lives have changed for the better.
Nicky: Absolutely.
Craig: We take better care of ourselves. We’re more thoughtful with how we approach everyday things. You don’t sweat the small stuff anymore because it’s not worth it. Those insignificant things don’t matter because when you think about the big picture, what you’re trying to achieve, and the direction you’re heading and where you’re going, you don’t have time for the small stuff anymore. It’s the big stuff.
Nicky: The mental health aspect was probably the hardest for me. He was an incredible support for me during that time. As I was leaving the hospital, I remember them saying, “Expect it to come back in three to five years, but if it comes back in two years, your prognosis is worse,” so that stayed with me. When I realized I needed to do something about this, I felt like the only thing that would help me at the time was to connect with other people with the same diagnosis. At that time, we couldn’t find anybody. Craig suggested, “Why don’t you start a Facebook group and let them come to you?” That’s exactly what I did and they did. Instantly, all that stress just melted and I felt like I found my people.
Stephanie: Milissa and Andrew, what was the biggest shift for you and the biggest piece of guidance you have for others on that?
Milissa: It was finding people who have gone through the same thing. I joined another research study at Colorado State University where they did exercise afterwards and that changed my life. Now I lead a group that exercise online afterwards and we still stay together. It’s a national group, which is awesome. But for us relationally, it’s evolved. I feel like in the relationship, we’re in the infantile stages and we learned about each other, what our strengths are, and what each other can give, so that was a good thing.
Andrew: The diagnosis and going through the experience of treatment made our relationship evolve. We became a lot more emotionally mature as a couple. It’s still a growing process because you still have to maintain your care and your treatment, but we’re in a much stronger place than we were when we first got the diagnosis.
We learned about each other, what our strengths are, and what each other can give.
Milissa
Stephanie: Hayley and Carl, I know this happened not too far into your relationship and it was a lot to go through. What guidance do you have for other people?
Hayley: I feel like it pushed issues that we hadn’t even come across yet because it was only a year and a half into our relationship, so we had to learn a lot about how we dealt with things. I had never seen him be emotional. I am not an emotional person and then all of a sudden, we’re a wreck for a while and let all of our walls down at one time. It seemed like it would have taken 10 years normally to go through what we went through in 90 days. It escalated our communication and understanding a lot quicker than it normally would have in a relationship.
I know that follicular lymphoma will come back, but I’m ready and I’ve come to terms with that… I’m not nearly as scared as I was at the beginning.
Hayley
But I do think that some positives come of it in general. I can appreciate life more. The meaning of everything is a lot different and I feel like people don’t realize that they treat life as a disposable item, but they do. I’m more appreciative. Looking outside at the green grass seems different from last year. I can’t wait to sit on the beach. I told Carl, “I’m probably going to start crying sitting on the beach this year because I’m so grateful to be here,” especially whenever you think about the alternative that goes through cancer patients’ minds. It’s also new for me, so I’m excited to be on the other side right now.
I know that follicular lymphoma will come back, but I’m ready and I’ve come to terms with that. I’m okay with it being something like a condition, like Nicky and Craig said. It’s going to come back, but there are so many treatments for it. I feel like it’s moving at such a fast rate that I’m not nearly as scared as I was at the beginning.
Carl: I would say quality time was huge for us in terms of what helped us. Within that is obviously talking a lot, whether it was about cancer or not. While hanging out on the couch or in bed, I tried to make a point to get away from cancer talk sometimes. We’re goal-oriented, so we talk about short-term goals and long-term goals, reminding ourselves that there’s another side to this, which we’re starting to see now.
Conclusion
Stephanie: Thank you all for an insightful conversation. Because you’re all at different points of this experience, I think this discussion is going to help so many people who are experiencing different situations. It was so great to hear your perspective in-depth, so thank you so much for joining us.
Thank you again to our sponsor, Genmab, for its support of our independent patient program, again allowing us to be able to host more of these for you. The Patient Story always retains full editorial control.
We want to point out again some of our incredible resources from our friends at The Leukemia & Lymphoma Society and the Living with Follicular Lymphoma Facebook group. The LLS has a community section for people to meet and chat with other blood cancer patients and care partners. It also has free personal guidance through Information Specialists. The Living with FL Facebook group features an ongoing lively chat in real-time with thousands of people from across the globe. It is the biggest FL-dedicated Facebook group that there is.
We hope that this was helpful for you. Thank you so much and we hope to see you at another program soon. Thank you and take good care.
Living Well Together with Follicular Lymphoma: Real Talk from Patients & Partners
Hosted by The Patient Story Team
How do you navigate follicular lymphoma (FL) as a couple — through diagnosis, treatment decisions, and life beyond? In this heartfelt discussion, three couples share their personal stories and unique insights on living with FL. From the shock of diagnosis to finding emotional balance, you’ll hear real talk on what helped them move forward together. Whether you’re a patient or a care partner, this program offers connection, validation, and hope.
Symptoms: Intermittent feeling of pressure above clavicle, appearance of lumps on the neck, mild wheeze when breathing and seated in a certain position Treatments: Surgery, chemotherapy
Navigating Waldenström’s: Getting the Best Care Close to Home
Unlock Better Waldenström’s Care – Right in Your Community!
Waldenström macroglobulinemia (WM) patient advocate Pete DeNardis, expert hematologist Dr. Hussam Eltoukhy, and practice administrator Maria Lamantia discuss the latest in community-based cancer care, personalized treatment options, and effective communication strategies.
Whether you’re newly diagnosed with WM or managing ongoing treatment, learn how to optimize your care, navigate “watch and wait,” and access clinical trials without leaving your local support network.
Effective Community Cancer Care: Learn how local treatment options can be both effective and personalized for Waldenström’s patients.
Navigating Watch and Wait: Get emotional and practical support for managing the uncertainties of the “watch and wait” approach.
Advocate for Better Care: Discover communication strategies to ensure you’re getting the best care from your local oncologist.
Latest Treatment Options: Understand new therapies and clinical trials that are available even in community settings.
Access to Specialized Care: Find out how collaboration with larger cancer centers can enhance your treatment journey.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang: We know most Americans are getting their cancer care at their local hospital or clinic and not at the large academic institutions, maybe not regularly or not even at all. But you may also hear that for blood cancers like Waldenström’s, it’s important to see a specialist. What does this mean and how can patients and their care partners successfully get the best care?
I’m the founder of The Patient Story. I was diagnosed with a different kind of non-Hodgkin lymphoma, diffuse large B-cell lymphoma. When I was getting my 600-plus hours of chemoimmunotherapy, the idea came up: how can we help cancer patients and care partners navigate life at and after diagnosis? That’s what The Patient Story focuses on.
The LLS offers free resources like its Information Specialists, who are one free call away for support in different areas of blood cancer. The IWMF offers many support resources specifically for the Waldenström’s community, including dozens of in-person support groups around the world in addition to so many that are happening online.
I want to stress that The Patient Story retains full editorial control over all content as always. While we hope that this is helpful, keep in mind this is not a substitute for medical advice, so still consult with your own team about your decisions.
This is sure to be an incredible discussion led by friend of The Patient Story and long-time advocate with the IWMF, Pete DeNardis.
Pete DeNardis: I’m chair emeritus of the International Waldenström’s Macroglobulinemia Foundation and a long-time volunteer for the organization. I’m a patient myself, was diagnosed in October 2003, and have had multiple periods of treatment and watch-and-wait status over the years. My treatment has included chemotherapy, radiation, monoclonal antibodies, and targeted therapies. Most recently, my WM has been behaving itself.
I live in Pennsylvania and my care is directed by a hematologist at a cancer teaching hospital. Over the years, I have had overnight stays in a university-based hospital and at local community hospitals in emergency situations. I will be joined by Dr. Hussam Eltoukhy and Maria Lamantia.
Dr. Hussam Eltoukhy: I’m a clinical assistant professor with RWJBarnabas Health and the Rutgers Cancer Institute of New Jersey. I’m a hematologist specializing in blood cancers.
My role is interesting. I work out of a community-based setting but in close partnership with our academic center, the Rutgers Cancer Institute, which gives me a very different perspective on treating patients. I have many patients with Waldenström’s and other conditions, and I’m thankful to be here to talk more about that.
Maria Lamantia: I’m so happy to work alongside Dr. Eltoukhy. We work together as a team. We have a wonderful staff and we treat our patients like family. Working alongside Dr. Eltoukhy, I see him take the time with his patients to answer all of their questions. We treat them emotionally and physically, so we need to treat them as a whole.
Pete: That’s fantastic. Patients need to have a good relationship with their healthcare professionals, especially for people with rare cancers like Waldenström’s, and to have a very caring and a very productive relationship. It sounds like you’re doing a fantastic job.
The Most Common First Symptoms of Waldenström’s
Pete: We want to get your perspective on how you approach Waldenström’s patients. Dr. Eltoukhy, can you describe the typical diagnostic journey for a patient with WM? What are the initial symptoms you usually see? Do you run certain tests when a patient comes in?
Dr. Eltoukhy: The diagnostic journey for a patient with Waldenström’s often can be prolonged because the initial symptoms are quite nonspecific and can mimic other conditions. The most common symptoms patients report are fatigue and weakness, which are most often due to anemia. Some patients may also experience unintentional weight loss, night sweats, and peripheral neuropathy, which presents as numbness or tingling in the hands and feet. In more advanced cases, symptoms related to hyperviscosity, like headaches, blurred vision, dizziness, or even nosebleeds may develop.
Common Steps to Diagnose Waldenström’s
Dr. Eltoukhy: The diagnostic approach typically starts with a thorough history and physical exam, which is critical for identifying patterns of symptoms and any physical signs, like enlarged lymph nodes or spleen. From there, blood tests are usually the first step. A complete blood count might show anemia and serum protein electrophoresis can detect a monoclonal IgM protein, which is characteristic of Waldenström’s. Further testing with immunofixation and serum viscosity levels can provide more details.
Once Waldenström’s is suspected, a bone marrow biopsy is essential to confirm the diagnosis. It will show the infiltration of lymphoplasmacytic cells. The bone marrow can be tested for other things, like the MYD88 mutation, which is present in over 90% of Waldenström’s cases. Imaging studies like CT scans can be useful in assessing lymph node or organ involvement.
Diagnosing Waldenström’s requires piecing together clinical signs, lab results, and histologic findings. Because the symptoms can be subtle or overlap with other conditions, taking a comprehensive history and performing a thorough physical exam is foundational in guiding the diagnostic workup.
How to Communicate with Your Primary Care Physician the Need to See a Specialist
Pete: I can tell by your response that you have a lot of experience with Waldenström’s patients. You’re hitting all the high notes and the critical aspects of diagnosing someone with Waldenström’s. Sometimes the symptoms manifest over a longer time.
I had classic symptoms, but I didn’t realize it then. I kept on thinking it was something else and waited a long time before I saw my doctor. How can a patient best communicate their concerns to their primary care physician to ensure a timely referral to a specialist? How do we get people to understand that we should take this to the next level in terms of testing and analysis of what’s going on?
If something feels off… it’s crucial to report these symptoms accurately and thoroughly.
Dr. Hussam Eltoukhy
Dr. Eltoukhy: Interestingly, that happens a lot. When it comes to ensuring a timely referral to a specialist, one of the most important things patients can do is to be clear and proactive in communicating their concerns. First and foremost, patients should be their own advocates. If something feels off — like you’re having persistent fatigue, unexplained weight loss, night sweats, or any unusual symptoms such as numbness or frequent infections — it’s crucial to report these symptoms accurately and thoroughly. Even if the symptoms seem minor or unrelated, sharing the full picture helps the physician connect the dots.
It’s also helpful for patients to record their symptoms: noting when they started, how often they occur, and whether they’re getting worse over time. This level of detail provides valuable context that can prompt a physician to dig deeper and consider a hematologic cause like Waldenström’s.
In addition, there should be no hesitation to express concerns directly. If they feel their symptoms are not improving or are being overlooked, it’s perfectly appropriate to ask, “Could this be something more serious? Do you think I should see a specialist?” Open and honest communication ensures the primary care physician fully understands the patient’s level of concern and can make an informed decision about referring them to a hematologist. Ultimately, while I know that physicians play a key role in guiding care, patients who actively engage in the process and advocate for themselves help ensure timely, appropriate evaluations.
Deciding Whether to Go to an Academic/Research Center or Community Hospital
Pete: In many cases, an important aspect of receiving treatment is where you get treatment. Of course, what determines that could be where you’re located and what type of services are available to you. This brings up the conversation of cancer care in a community setting or a suburban/rural setting. What’s the difference between a community hospital versus an academic center or a cancer hospital? How can people best understand the difference between them? If it does make a difference, how do they know which one to go to?
Dr. Eltoukhy: When we talk about cancer care in general, especially for rare diseases like Waldenström’s, the setting where a patient receives treatment can be as important as the treatment itself. Broadly speaking, there are key differences between community hospitals and academic medical centers or more specialized cancer centers.
By design, community hospitals are designed to provide general health care services to the local population. They offer a wide range of medical care, from routine checkups to managing common conditions and even some cancers. The care teams in these settings are skilled at treating a broad spectrum of diseases. For patients with more common or straightforward cases, community hospitals are convenient and provide excellent care close to home. Accessibility is a big advantage because patients don’t have to travel far. They also often have a more personalized relationship with their care team.
On the other hand, academic medical centers and specialized cancer hospitals focus heavily on research, teaching, and clinical trials, so these centers are often affiliated with medical schools and are involved in clinical trials, so they’re at the forefront of new treatments and therapies. Patients treated at these centers may have access to novel therapies that aren’t widely available in the community setting. Additionally, these institutions have multidisciplinary teams, which include hematologists, pathologists, and other specialists who focus specifically on rare cancers providing a more specialized approach.
In terms of the patient population, your typical community hospital will manage more common cancers and straightforward cases, while academic centers are more in tune to see more complex, rare, or treatment-resistant cases. However, this does not mean that community hospitals cannot manage diseases like Waldenström’s effectively. Many do, such as ours, especially with proper collaboration and referral pathways.
Ultimately, the best approach may involve a balance between the two settings. Patients might receive specialized consultation at an academic center while continuing their routine care and follow-ups in the community, ensuring both accessibility and cutting-edge treatment options.
Stephanie: Dr. Eltoukhy, I want to jump in very quickly as we have two patient perspectives about how they were able to figure out the best Waldenström’s care for themselves. Annmarie was diagnosed a few years ago and heard right away to see a specialist. Bob, on the other hand, was diagnosed in 1997, which was a very different time, and says the IWMF was instrumental in helping him link between a local care team and a specialist. Bob, what was it like trying to figure out your care almost three decades ago?
Bob B.: First of all, my local oncologist didn’t know about how I should be treated. With IWMF, we were able to get Arnie’s advice. There was some research going on at Scripps, MD Anderson, Lombardi Comprehensive Cancer Center, Mayo Clinic, and a couple of others. We visited a few places to go through the discovery of what might seem to make the most sense to be treated, bring that information back to my local oncologist, and allow him to be my quarterback.
Annmarie S.: If you’re lucky enough to go to a place with specialized care, that’s crucial in terms of them understanding the disease, diagnosis, different treatments, what future treatments can look like, research, and all the positivity that comes along with that. What’s challenging with Waldenström’s is general practitioners and hematologists don’t understand what it’s all about in terms of care and the next level of getting treatment, so they look at it more broadly as a cancer.
When you go to the next level and get a Waldenström’s specialist, they treat it more as disease management if you will. A lot of times, people cannot do that. Sometimes people are comfortable with the practitioner that they have. Utilize a facility that treats Waldenström’s and if you have to use your primary care physician or a general hematologist, have a Waldenström’s team as part of your overall treatment plan.
The Biggest Challenge for Waldenström’s Patients Who Get Community Care
Pete: In my situation, I go to a local university-based hospital because it’s as convenient as going to a community hospital. My condition is a little unusual even among rare cancer patients. What would you consider is the biggest challenge to providing cancer care in a local community setting, like in a rural setting?
Dr. Eltoukhy: One of the biggest challenges in providing cancer care in the local community setting comes down to the availability of resources. It’s not about the knowledge or expertise. We have highly skilled specialists dedicated to treating complex conditions like Waldenström’s. The challenge lies more in the infrastructure and support systems compared to larger cancer centers.
For example, while I can offer phase 2 and 3 clinical trials in my community practice, phase 1 trials, which are often the first step in introducing new therapies, typically require more specialized resources and are more readily available at larger academic or dedicated cancer centers. This includes specialized monitoring, regulatory oversight, and more intensive support systems.
Another significant factor is personnel. Larger cancer centers tend to have extensive multidisciplinary teams with dedicated staff for clinical trials, patient navigation, and supportive care services. In the community setting, we operate with leaner teams, so it can be more challenging to coordinate the logistics of complex care or get patients enrolled in trials as quickly as we’d like.
One of the biggest challenges in providing cancer care in the local community setting comes down to the availability of resources… It’s not that care is any less thorough, but the resources to streamline and support those processes are more limited.
Dr. Hussam Eltoukhy
It’s not that care is any less thorough, but the resources to streamline and support those processes are more limited. That said, working closely with the cancer center, as I do, helps bridge some of those gaps. We can offer high-quality, specialized care locally while collaborating with larger institutions to ensure patients have access to the full spectrum of treatment options when needed. The goal is always to deliver the best possible care, whether it’s in the community or at a specialized center.
Pete: That’s great. I like how you touched on clinical trials. We try to encourage patients in the Waldenström’s macroglobulinemia community to seek out clinical trials whenever they can. It’s good to know that even in a community hospital setting, patients can participate in a clinical trial.
Referring Waldenström’s Patients to an Academic Center
Pete: From a community setting, collaboration is important with larger hospitals when the need arises. Are there circumstances where you refer your patients to a larger center or to another hospital setting where there are more people with more extensive knowledge or more facilities that can tend to their particular circumstances?
Dr. Eltoukhy: Yes. As a blood cancer specialist practicing in a community setting, I feel fully confident managing a wide range of hematological malignancies, including Waldenström’s. My knowledge and expertise are not limiting factors when it comes to providing high-quality care for these patients. However, collaboration with our main cancer center and other academic institutions is vital to ensuring patients have access to the full spectrum of treatment options when needed.
Typically, there are two main circumstances where I would refer a patient to a larger center. The first is when additional resources or specialized support are necessary. For example, if there’s a clinical trial, particularly an early phase trial, that could offer a promising new therapy not available in our community setting, I would absolutely refer a patient to take advantage of that opportunity. While we do offer phase 2 and 3 trials locally, phase 1 trials are very specialized research protocols usually housed in these larger academic centers with the infrastructure to support them.
The second scenario involves treatments that require specialized procedures we don’t currently offer at our center. While this isn’t specific to Waldenström’s, right now, therapies like bone marrow transplants or CAR T-cell therapy are examples of advanced treatments that require more dedicated facilities and more specialized teams with highly specific protocols. These are scenarios where I would refer to the academic center.
Referrals are part of a collaborative approach… This partnership allows patients to receive cutting-edge treatments without losing the personalized, accessible care they value in the community.
Dr. Hussam Eltoukhy
That said, these referrals are part of a collaborative approach, so even when a patient is referred out for a specific treatment or trial, I remain closely involved in their care, coordinating with the academic center to ensure a smooth transition and continuity of care when they return to the community setting for a follow-up. This partnership allows patients to receive cutting-edge treatments without losing the personalized, accessible care they value in the community.
Referring Waldenström’s Patients to Another Specialist for a Second Opinion
Pete: In line with that, the IWMF provides a list of several dozens of doctors who are considered second-opinion doctors because perhaps they work at an institution that focuses solely on Waldenström’s, like Dana-Farber Cancer Institute or Mayo Clinic. Have you ever referred a patient for a second opinion because their situation is so unusual? And is that a common practice?
Dr. Eltoukhy: Yes, that is. Typically in the community, a lot of oncologists would be what we consider generalists, which means they treat a lot of different conditions. The referral basis for these doctors would be a lot more than me. Being a blood cancer specialist, while I don’t do it as often as I would if I was a generalist, I absolutely do on a regular basis. These come back to the patients who are treatment-resistant or unusual cases when we send out pathology and the pathology comes back blurring the lines between two different diseases, which happens quite often in blood cancers.
In our center at least, I collaborate very closely with the Rutgers Cancer Institute. We have combined tumor boards and I will refer patients. For most patients, first-line treatment will be the standard of care. No matter where you go, there’s somewhat of an agreement about what the standard of care would be.
Once you get to the second, third, fourth, fifth, and so on lines of treatment, that’s when I in the community setting or other doctors in an academic center usually go to other colleagues to get their opinion. Seeing me in the community doesn’t mean you don’t get the opinions of the other doctors in the academic center. I’m always presenting on these two boards, sharing the cases, and getting other doctors opinions. This shouldn’t be an ego thing. It’s more about giving the best care possible to the patients.
Pete: I can tell by your responses that you obviously are a doctor who has the needs and the health of the patient as the number one priority and I commend you for that.
What Waldenström’s Patients Should Consider in Choosing a Community Hospital or Provider
Pete: For patients who don’t require specialized care, can you describe how going to a community hospital could be in their best interest and benefit them?
Dr. Eltoukhy: There is a common misconception that community cancer care isn’t as high quality as what you’d find at a larger academic center, but that’s simply not true. For many patients who don’t require highly specialized treatments, receiving care in a community setting can offer distinct advantages without compromising the quality of care.
First and foremost, being treated closer to home means patients are in a familiar environment surrounded by their support system, such as family, friends, and their local community. That comfort can play a huge role in how patients cope with a cancer diagnosis and treatment. It feels like you’re in your own backyard, which can make the entire experience less overwhelming. But it’s not just about convenience.
Our community cancer center is equipped with a multidisciplinary team, which is essential for providing comprehensive care. We have radiation oncologists, surgical oncologists, pathologists, radiologists, and medical hematologist-oncologists all working together. We regularly hold tumor boards where complex cases are discussed collaboratively, ensuring that multiple expert opinions shape each patient’s care plan.
For disease sites where we may not have a dedicated tumor board locally, we seamlessly collaborate with our main cancer center to ensure every patient benefits from the collective expertise. Even though patients are receiving care in a local familiar setting, they’re still getting the benefit of a specialized collaborative treatment. It’s not one doctor in isolation. It’s a coordinated team effort to provide the best possible outcomes. For many patients, this combination of high-quality care and the comfort of being treated closer to home is honestly the ideal scenario.
Maria: We offer also procedures in the clinic setting for those who are a little frightened to be in a hospital setting, like bone marrow biopsies. We have very skilled, qualified staff to assist Dr. Eltoukhy and we’re able to do those right in an office setting, which is helpful for patients who have that fear of going to the hospital.
We’re conveniently located right on the same campus as the Community Medical Center, so knowing that the hospital is close by is very comforting and convenient for our patients. The building that we’re in is comprised of oncology-based physicians, so it’s a one-stop shop as well and all of the doctors collaborate with Dr. Eltoukhy.
Pete: It’s great. That does sound like you have an ideal environment.
Financial Benefit of Going to a Community Provider
Pete: No offense, but people tend to think less of a community-based hospital when you’re providing the same quality of care as if they went directly to a university-based hospital. But then on the flip side, is there a cost savings for the patient for going the community-based hospital route? They’re getting the same standard of care, but is it more affordable for certain patients to do that?
Dr. Eltoukhy: I do think so. Care at a community hospital can be often more affordable and accessible for patients and that’s an important factor when considering treatment options. One of the biggest advantages is the reduced financial burden related to travel and lodging. When patients are treated closer to home, they don’t have to worry about the added expense of traveling long distances, taking extended time off work, or even arranging accommodations closer to a larger academic center. This alone can make a significant difference, especially for patients undergoing long-term treatments, such as patients who have Waldenström’s.
From a healthcare cost perspective, community hospitals can also offer more cost-effective care without compromising quality. Administrative and operational costs tend to be lower in the community setting and that can translate into lower out-of-pocket expenses for patients. Additionally, treatments and services provided locally often come with fewer facility fees compared to larger institutions.
Another important factor to consider is insurance coverage. Community hospitals are typically well-integrated with the local insurance networks, which makes it easier for patients to access care that is covered under their plan. This can help minimize unexpected medical bills or any out-of-network charges that might arise when seeking treatment at larger, more specialized centers.
From a healthcare cost perspective, community hospitals can also offer more cost-effective care without compromising quality.
Dr. Hussam Eltoukhy
Ultimately, by offering high-quality comprehensive care in a local setting, community hospitals provide patients with financial and logistical advantages, and this accessibility ensures that patients can focus on their treatment and recovery without the added extra stress of significant financial strain.
Pete: I was having significant issues early on. Because of my insurance and health situation, I had to decide whether I should go out of state for the next level of care to resolve my issues at the time. Fortunately, what’s in place is if it becomes serious enough, you have a very good support network in your local community hospital, but you can reach out for a second opinion to centers of excellence and that’s important for people to understand. You don’t have to travel, especially if you can’t do it physically because of your health situation. The resources are there. You just have to work with your medical staff and coordinate that.
Monitoring Waldenström’s Patients on Watch and Wait
Pete: From your perspective and your experience, what are key considerations in monitoring disease activity for patients who are on a watch-and-wait status? How often do you follow up with them? What do you typically do in your practice?
Dr. Eltoukhy: For patients with Waldenström’s who are on a watch-and-wait approach, regular monitoring is essential. This strategy is common because many patients are asymptomatic at diagnosis or have very slowly progressive disease. This disease usually doesn’t require immediate treatment. However, just because treatment isn’t starting right away doesn’t mean the disease isn’t being closely managed.
In my practice, follow-up appointments typically occur every three to six months, depending on the patient’s specific situation and how stable their condition is. During these visits, we focus on clinical assessments and laboratory monitoring. We look at hemoglobin levels to monitor for anemia. We monitor IgM levels to track monoclonal protein. We check serum viscosity if there are any symptoms suggestive of hyperviscosity.
We also check kidney function, calcium levels, and assess for any signs of organ involvement. A thorough physical exam is equally important. I look for signs like enlarged lymph nodes, enlarged spleen, enlarged liver, and ask about any new or worsening symptoms, like fatigue, night sweats, weight loss, neuropathy, or changes in vision that could signal disease progression.
Key signs that might indicate a need to move from watchful waiting to active treatment usually include worsening anemia, symptomatic hyperviscosity, significant weight loss, fevers, night sweats, organ enlargement, or the development of any kind of neuropathy that would affect your daily life. If any of these arise, we reassess and discuss the treatment options.
In addition to monitoring, I always like to emphasize the importance of maintaining a healthy lifestyle. Staying active, eating a balanced, healthy, and whole foods diet, and managing other health conditions, like high blood pressure or diabetes, can improve overall well-being and help patients feel more in control of their health.
Emotional support is also very important as living with chronic conditions like Waldenström’s, even in a watch-and-wait phase, can be stressful. Regular follow-ups not only track disease activity but also provide reassurance and a structured plan for managing the condition over time.
The watch-and-wait approach is not about doing nothing. It’s more of a proactive strategy based on solid data and extensive clinical experience.
Dr. Hussam Eltoukhy
Pete: Could you talk a little bit more about the emotional and psychological challenges in that aspect? How do you help a patient navigate through that part of having the disease?
Dr. Eltoukhy: Living with a chronic condition like Waldenström’s, especially under our watch-and-wait approach, can be emotionally challenging for many patients. There’s this uncertainty of knowing you have a cancer diagnosis but not needing immediate treatment. Many patients will relay that it creates a lot of anxiety and stress. It’s completely natural to feel this way, but there are several strategies that we try to do to help patients cope with this.
I try to emphasize that it’s important to remember that the watch-and-wait approach is not about doing nothing. It’s more of a proactive strategy based on solid data and extensive clinical experience. If we recommend monitoring rather than immediate treatment, it’s because we know from research and patient outcomes that this is the safest and most effective approach for certain cases. Sometimes, if you explain it to them this way, it can help alleviate some of this uncertainty and fear.
That said, managing the emotional side of this journey is as important. Stress management techniques like mindfulness meditation and deep breathing exercises can help reduce day-to-day anxiety. Regular physical activity is also excellent, even doing something as simple as walking, which I always advocate for my patients. If you ask any of my patients, I tell them, “Do you track your steps daily? If not, you should start tracking and start increasing.”
Start with small goals and try to work your way up. If you can get that to 10,000 steps, great, but start somewhere, even if it’s at a lower number. Increasing physical activity can have a profound impact on mental health by improving mood and reducing stress. I’ve seen it with my patients. I’ve had patients who have done this and say their energy level has increased.
By focusing on physical health and emotional well-being, patients can live full, active lives while feeling confident that their condition is being closely monitored.
Dr. Hussam Eltoukhy
Support groups are also important. They can be very valuable whether they’re in person or online. Connecting with others who are going through the same experience can provide a sense of community and shared understanding. It helps to know that you’re not alone in navigating these emotional ups and downs. Counseling or speaking with a mental health professional can also be very helpful. They can provide tools to manage anxiety and cope with uncertainty.
It’s very important to emphasize to patients the importance of staying connected with their loved ones. Family and friends can be an essential support system, offering emotional comfort and practical help when needed. Maintaining a positive outlook doesn’t mean ignoring the challenges but trying to focus on what’s in your control. Staying active, attending regular follow-ups, and trying to lead a fulfilling life despite having a diagnosis.
Ultimately, while the watch-and-wait approach can feel uncertain, it’s grounded in strong evidence and a deep understanding of the way Waldenström’s progresses and acts. By focusing on physical health and emotional well-being, patients can live full, active lives while feeling confident that their condition is being closely monitored. At RWJBarnabas, we offer many support groups and have a regular monthly calendar that we offer to patients.
Maria: As the supportive team to the provider and the patient, we do our best so that the patient doesn’t have to worry about anything as far as authorizations or appointments. We educate them on all of that because those can be also very stressful for them. We try to take all of that away from them so they can focus on their health.
However, we also use the resources that are on campus. There are plenty of groups, like Dr. Eltoukhy said. We also have resources that include dietary and social work that we can refer these patients to and support them.
The staff here is kind and empathetic and treats patients like family. They know that they can call us if they’re scared and we don’t rush them. They know if something happens or they’re having a little symptom in between, they can call, they will receive a callback, and we will take the time to listen and report it to Dr. Eltoukhy, who will then follow up. They know that even though there is a bit of a wait, they can reach out to us at any time.
We do our best so that the patient doesn’t have to worry about anything… so they can focus on their health.
Maria Lamantia
Pete: That’s great. Thank you to both of you. You touched on many aspects, much more than I even anticipated. Your advice is very sound and your practice is amazing and commendable. I know from personal experience that a lot of the things that you mentioned are important in helping a patient navigate through not only the physical health aspects but also the mental health aspects of dealing with the disease and living with a chronic illness.
I go to my local hospital. I take notice of what services they provide and if they have any special programs coming up, I take advantage of them. I’m deeply involved in volunteering for the IWMF, but they help me immensely. It’s always important whatever cancer you have to try and get together with patients who have similar cancers to learn from each other and share stories. There’s a healing aspect in sharing and understanding what someone else has gone through and the IWMF provides that capability.
The IWMF has support groups and affiliates all around the world that help patients. We have a weekly newsletter, online discussion groups, webinars, and an annual education forum. We answer any questions patients, their caregivers, or their family members may have at any point in time.
I encourage people to visit IWMF.com and check out their services. It’s an extra level of care that you can get besides what you’re getting from a very caring hematologist-oncologist and a very caring staff who works with them. I can’t speak highly enough of the very qualified medical community and medical staff and the IWMF. When you put those two together, you’re in very good hands.
How Waldenström’s Patients Should Talk to Their Healthcare Team About Their Symptoms
Pete: Another thing that comes up, especially when you’re dealing with a disease that is chronic and you’re in a watch-and-wait period, is odd manifestations that you think is the disease. How should a patient communicate those symptoms? Should they say something or not say something? What’s your advice for communicating any symptoms to their healthcare team?
Dr. Eltoukhy: Effective communication with your healthcare team is crucial when managing a condition like Waldenström’s, especially if you’re on a watch-and-wait approach. One of the most important things patients can do is to promptly report any new or worsening symptoms. You don’t have to wait for your next scheduled appointment, whether it’s in three or six months. I end every single visit with my patients by telling them that if anything comes up before the next appointment, they should call and come in. I don’t say that to fill in the gaps. I tell the patients over and over again, “Do not wait. Come in.”
Effective communication with your healthcare team is crucial when managing a condition like Waldenström’s.
Dr. Hussam Eltoukhy
It’s important for patients to understand that and to know that they can reach out to their doctor. You don’t have to wait. You’re not bothering anyone. We want you to do that. We want you to come in. I want to know if anything is going on because we want to catch some of these symptoms like hyperviscosity very early. Don’t wait. Call your team. If you can’t see the doctor, see one of their colleagues or their nurse practitioner. If something feels different or concerning, reach out right away. That’s what we’re here for.
Keeping a symptom diary can be a very helpful tool. By tracking how you feel on a daily or weekly basis, you can start to identify patterns or changes over time that might not be obvious at the moment. Note things like fatigue levels, changes in weight, night sweats, any new pains anywhere, or any new neurological symptoms like numbness or tingling. Detailed information can give your doctor and the rest of your team a clearer picture of what’s happening and can help guide decisions about whether it’s time to adjust your plan.
Listening to your body and trusting your instincts is also key. No one knows your body better than you. If your gut is telling you that something isn’t right, whether it’s a new symptom or a shift in how you’re feeling overall, it’s important to speak up. You’re not bothering anybody. No one’s going to think otherwise.
Your healthcare team is your partner on this journey. Open and ongoing communication ensures that we can address concerns early and adjust care as needed.
Dr. Hussam Eltoukhy
What’s the worst-case scenario? It wasn’t caused by Waldenström’s. As a patient, don’t think anything of it. We want you to tell us all the new symptoms. We want to know what’s going on because we’re here to help the patient.
Sometimes, subtle changes can signal that it’s time to reassess and take a different plan. If you were on the cusp of considering treatment, maybe it’s time to consider it or not consider it. Remember that your healthcare team is your partner on this journey. Open and ongoing communication ensures that we can address concerns early and adjust care as needed. Once again, don’t hesitate to reach out. This is why we’re here. We’re here to support you every step of the way.
Clinical Trials for Waldenström’s Patients
Pete: You mentioned that even in the community hospital setting, you participate in clinical trials. Are clinical trials being conducted in your setting? What kind of trials do you have your patients participating in?
Dr. Eltoukhy: Across all cancers, we currently have over 60 clinical trials available at our community cancer center, including many for hematologic malignancies. We offer phase 2 and phase 3 clinical trials. We’re not able to offer phase 1 clinical trials at this time.
Offering clinical trials in a community setting is a great way to provide patients with access to cutting-edge treatment without requiring them to travel to larger academic centers. When determining the feasibility of conducting trials in our center, one of the biggest considerations that we look at is resources. It’s not just about having the physical space or the equipment. We need to ensure that we have the right personnel and infrastructure in place to manage trials safely and effectively. This includes dedicated research coordinators, nurses, pharmacists, and regulatory staff who are trained in clinical trial protocols and patient safety.
Our goal is to offer trials that are not only scientifically valuable but also feasible and safe to administer in the community setting.
Dr. Hussam Eltoukhy
Clinical trials in the US are very heavily regulated and rightfully so. There are strict guidelines and oversight to ensure that every trial is conducted ethically, that patient safety is the top priority, and that data is collected accurately. We have to assess whether we can meet all those requirements from patient monitoring to data reporting while maintaining the highest standard of care.
Ultimately, our goal is to offer trials that are not only scientifically valuable but also feasible and safe to administer in the community setting. We want to make sure patients have access to innovative treatments while receiving the same level of care and oversight that they would expect from one of these larger academic centers.
Different Phases of Clinical Trials
Pete: For those who aren’t as knowledgeable about clinical trials, can you do a quick overview of the different phases of clinical trials?
Dr. Eltoukhy: Phase 1 is when a new drug starts to be administered. Once you move on to phase 2, you have already determined the safety of the drug and you’re starting to look at efficacy and how it could work. Once you move on to phase 3, you have a better understanding of how well it works and how safe it is, and you’re looking at a broader approach and getting the real data on efficacy and how well it works.
A phase 4 clinical trial is always ongoing. Any drug that’s out there is always being monitored to make sure that it continues to be safe because safety doesn’t end after phase 1 or phase 2. Safety is ongoing. In phase 1, they’re new drugs that need very close monitoring and you could have unexpected side effects. We don’t quite partake in phase 1 trials right now, but we have many phase 2 and phase 3 trials.
Busting Clinical Trial Myths
Pete: In a community clinical team, what can you do to ensure patients will learn about clinical trial options and whether they should be concerned about the potential side effects of being in a clinical trial? Am I going to be worse off by doing that or not? How do you educate them? How do they find out about the clinical trials?
Dr. Eltoukhy: That’s a very common concern. Ensuring patients learn about and understand clinical trial options starts with the clinical team, especially the physician. Physicians should take an active role in discussing these opportunities directly with the patients.
When I open a clinical trial at our community center, it’s because I believe it has the potential to benefit the patients. But offering a trial isn’t enough. We have to make sure that patients understand, are fully informed, and are comfortable with their options. For me, that means sitting down with each patient and having an open, honest conversation.
The right choice for one patient isn’t necessarily the best for another patient. It’s essential to personalize the discussion based on the patient’s health status, personal preferences, and lifestyle.
Dr. Hussam Eltoukhy
I explain what we can offer under the standard of care, what treatments are currently approved and routinely used, and lay out what the clinical trials could provide. I go through the potential benefits, the goals of the study, and also any limitations or uncertainties. Patients must understand not just the possibilities but also the risks and the level of commitment involved.
One of the most critical aspects of these conversations is avoiding bias. My role isn’t to push a patient toward one option or another but to provide them with all the necessary information to make an educated, confident decision. What might be the right choice for one patient isn’t necessarily the best for another patient. It’s essential to personalize the discussion based on the patient’s health status, personal preferences, and lifestyle.
Ultimately, patients should feel empowered to choose the path that’s best for them, whether that’s enrolling in a clinical trial or sticking with the standard of care. By fostering clear, transparent communication, we try to help patients navigate their options and ensure that they’re making decisions that align with their goals and values.
Our goal is to offer as many trial opportunities as we can in our setting but also to recognize when a referral is necessary for something more specialized.
Dr. Hussam Eltoukhy
Bringing Waldenström’s Clinical Trials to the Community Cancer Care Site
Pete: From a perspective of trying to make sure that your patients are aware of these clinical trials and wanting them to take advantage of them if it’s in their best interest, how do you ensure that they have access to the latest trials? How does it work for your hospital system to get involved in a clinical trial, especially for Waldenström’s patients? Do you seek them out yourself or are you approached by the people who are running the trial? How does the process work?
Dr. Eltoukhy: We recognize the importance of staying connected with larger academic centers that may offer these opportunities. A lot of times, we will open trials collaboratively with the Rutgers Cancer Institute. One of the key roles of community medical centers is to understand where we fit within the broader healthcare system. It’s not a one-size-fits-all approach. We need to be very clear about what we can effectively manage in our setting and when it’s in the patient’s best interest to refer them to an academic center for a clinical trial or more specialized treatment.
Once again, it’s not about limitations in expertise. It’s about ensuring patients receive the best possible care whether that’s locally or through a specialized trial at an academic center. Of course, whenever possible, we want to provide that care closer to home. It’s more comfortable, more cost-effective, and less burdensome. Traveling long distances to participate in a clinical trial can be incredibly challenging, especially when dealing with the physical and emotional toll of cancer care.
High-quality cancer care isn’t limited to large academic centers. Community hospitals like ours play a vital role in delivering comprehensive, patient-centered care that’s accessible, effective, and personalized.
Dr. Hussam Eltoukhy
Our goal is to offer as many trial opportunities as we can in our setting but also to recognize when a referral is necessary for something more specialized. Effective collaboration means maintaining strong communication with the academic center, letting them know what trials we have open, what we can manage, and as importantly, what we can’t. By advocating for our patients and fostering these partnerships, we’ve been able to create a seamless system where patients benefit from the convenience of local care and innovations of cutting-edge research when needed. It’s about working together to make sure patients have access to the best options, wherever they may be.
Pete: The IWMF, through the efforts of Dr. Jorge Castillo at Dana-Farber, has established the WM-NET, which is designed to become a network of hospitals across the United States that will participate collectively in clinical trials and have them at their sites. Not all of the participating organizations are going to do all of the trials, but they will try and distribute it more broadly to make it easier for patients to get access to these trials locally rather than having to travel to a major cancer center.
Final Takeaways
Pete: Thank you, Dr. Eltoukhy and Maria, for your time and perspective on providing care to Waldenström’s patients in your hospital setting and community-based hospitals. Do you have any final remarks you want to pass along to Waldenström’s patients?
Maria: It would be an honor to treat you and take care of you. Consider our establishment if you don’t want to go to the bigger facilities. It’s a more boutique-like atmosphere. If you come to see Dr. Eltoukhy, you will be in very good hands. It’s an honor to work alongside him.
At the end of the day, cancer care is a partnership between doctors and patients, between community hospitals and academic centers, and between healthcare teams and families.
Dr. Hussam Eltoukhy
Dr. Eltoukhy: Thank you so much for having me. It’s been a privilege to share my perspective on improving outcomes for patients with Waldenström’s, particularly within the community setting.
I hope it’s clear that high-quality cancer care isn’t limited to large academic centers. Community hospitals like ours play a vital role in delivering comprehensive, patient-centered care that’s accessible, effective, and personalized. Whether it’s through offering clinical trials, collaborating with larger academic centers, or simply being there for patients in their communities, the goal is always the same: to provide the best possible care tailored to each individual’s needs. It’s about open communication, staying informed, and making sure patients feel empowered and supported throughout their journey.
At the end of the day, cancer care is a partnership between doctors and patients, between community hospitals and academic centers, and between healthcare teams and families. By working together, we can ensure that every patient has access to the best treatments, latest research, and compassionate care that they deserve, no matter where they are. Thank you again for the opportunity to be part of this important conversation.
Pete: It’s been a pleasure speaking to both of you. I learned a lot and got a better appreciation, other than what I already have, of community care practitioners and the dedication and care they have, making sure that Waldenström’s patients are on the path to living healthier and fuller lives. You are instrumental in making sure that happens, so I commend both of you.
For Waldenström’s patients, caregivers, and families, it’s very important at the beginning to establish a good working relationship with a hematologist-oncologist who’s going to be managing your journey with Waldenström’s. It’s important to decide what practice or hospital setting you prefer to go to for periodic testing and treatments, or extended hospital stays if you should ever need them when you have some significant issues. All the doctors, nurses, physician assistants, medical staff, and clinical staff are to be commended for their commitment on a day-to-day basis to help all of us live fuller, healthier lives.
Establish a good working relationship with a hematologist-oncologist who’s going to be managing your journey with Waldenström’s.
Pete DeNardis
I want to encourage anyone around the world who’s affected by the disease to take advantage of opportunities that are out there to find the best local hospital systems that can cater to their needs but also to be involved with an organization devoted specifically to their disease, like the International Waldenström’s Macroglobulinemia Foundation. The IWMF is the only global organization dedicated specifically to the support, education, and research of Waldenström’s.
Stephanie: Thank you so much to Pete, Dr. Eltoukhy, and Maria for providing such incredible context. Self-advocacy is vital, especially for Waldenström’s where having long-term care and long-term doctor-patient relationships are so important. Don’t be afraid to speak up for yourself and ask any questions that are coming up for you, whether you’re a patient or a care partner. The keyword that Dr. Eltoukhy kept talking about was partnership. It doesn’t have to be one place or the other, as long as the medical team is working in partnership with you.
Thank you so much for joining our program. We hope that this was helpful for you and that you walk away with more knowledge and understanding and more questions. We hope to see you at another discussion. Take good care.
The Future of Lymphoma Therapy: Expert Perspectives on Breakthroughs and New Combinations
Explore advancements in non-Hodgkin lymphoma treatments with cancer experts, Dr. Andrew Evens from the Rutgers Cancer Institute and Dr. Tycel Phillips from City of Hope, and Stephanie Chuang, a non-Hodgkin lymphoma survivor and founder of The Patient Story. Dive into the latest research, treatments, and strategies to empower patients and caregivers. Gain valuable insights including promising clinical trial results, breakthrough therapies, and personalized treatment options.
Discover breakthrough treatments reshaping care for DLBCL and follicular lymphoma. Understand cutting-edge combinations like CAR T-cell therapy, antibody-drug conjugates, and bispecific antibodies. Learn to balance effectiveness and quality of life with insights into side effects and survivorship. Access guidance on clinical trials, emerging therapies, and personalized medicine. Hear directly from leading experts about what’s next in lymphoma research and care.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
Stephanie Chuang: Hi, everyone! We’re talking about the two most common subtypes of non-Hodgkin lymphoma: diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma. We recently had a meeting of minds from all over the world at the 2024 American Society of Hematology (ASH) annual meeting, where doctors and researchers present the latest updates on treatments and potential treatments with the most promise.
Our goal is that you, as patients, caregivers, and partners, walk away with a better understanding of how to approach your own decision-making with your medical team, specifically how to understand the options and balance effective treatment and quality of life.
We want to thank the LLS for its partnership. If you don’t know already, the LLS offers great free resources, like their Information Specialists and the Clinical Trial Support Center, which is staffed to provide one-on-one support in different areas for the blood cancer community.
The Patient Story retains full editorial control over all of this content as always. While we hope that this is helpful, keep in mind this is not a substitute for medical advice. Consult with your team about treatment decisions.
We have an incredible panel of experts to discuss the latest advancements in the field. Dr. Tycel Phillips is a hematologist-oncologist from the City of Hope National Cancer Center in Southern California. He’s an associate professor in the Department of Hematology and focused on treating patients with lymphomas, both Hodgkin and non-Hodgkin. Dr. Phillips lost his grandmother to pancreatic cancer and his mother to breast cancer while he was studying to become a doctor, and I’m sure that informs the way Dr. Phillips practices as a doctor.
Dr. Andrew Evens is a physician-scientist and clinical expert in lymphoid malignancies at the Rutgers Cancer Institute in New Jersey. He serves as associate director for clinical services and the associate vice chancellor for clinical innovation and data analytics at Rutgers Biomedical and Health Sciences. Over the past two decades, he’s been the principal investigator of more than 80 cancer clinical trials from phase 1 through phase 3 studies.
Our audience is cancer patients and the people around them. The goal is to translate for our audience what matters to them. The two of you are dedicated to the patients you see in your clinic and to the research happening in lymphoma. You go above and beyond outside the clinic walls, so thank you so much for that, especially as a former diffuse large B-cell lymphoma patient.
We’re covering two types of non-Hodgkin lymphoma: one is the most common aggressive form, which is diffuse large B-cell lymphoma, and the other is slow-growing or indolent and the most common form of that, follicular lymphoma. We often see a lot of research in these areas. Let’s go into DLBCL first.
Latest DLBCL Advancements in Front-Line Therapy Options
Stephanie: Dr. Evens, what’s been the standard of care for front-line therapy for DLBCL? What’s happening now with front-line therapy options after we have the POLARIX trial where, for the first time in decades, the FDA approved a new option for patients?
Dr. Andrew Evens: It’s evolved and you said it. R-CHOP chemotherapy had been the standard of care for more than 15 years after rituximab broke through around 2005, but it wasn’t for lack of trying. A multitude of randomized phase 3 studies over the ensuing 15 years tried to knock R-CHOP off the top of the hill.
Finally, one at least had some benefit. In a head-to-head study, polatuzumab vedotin replaced the O in CHOP and garnered FDA approval after a phase 3 randomized trial, which was POLARIX, and pola-R-CHP has broken through. Is it used in all patients? That’s open for discussion. It’s FDA-approved for patients who have a certain clinical risk score.
Ongoing DLBCL Studies in First-Line Treatments
Stephanie: Dr. Phillips, ASH is a big conference. What excited you the most about the ongoing studies for first-line treatments, specifically with R-CHOP and novel treatments?
Dr. Tycel Phillips: Surprisingly, a whole section was dedicated to R-CHOP plus X. The POLARIX study invigorated the field to explore more options to improve the front-line setting because, after so many negative studies, we had hit a point where there was very little interest in exploring a way to improve R-CHOP.
In the 2024 ASH meeting, there were a few studies. Venetoclax was added to pola-R-CHP for patients with aggressive B-cell features and this was presented by Dr. Diefenbach. This study looked at venetoclax at a dose of 800 mg given for five days, which indicated a very high response rate across the board, even in those with triple- and double-hit lymphoma, albeit only seven patients. It’s still a very short follow for all of these, but in this situation, a way to move the needle. Some drawbacks were higher rates of neutropenia and grade 5 CRS events. If that were to move forward, there may be some dose reductions to venetoclax because they went up to 800 mg. The question is whether it’s necessary.
Moving along the theme of adding a small molecule to a chemotherapy backbone, there was a study looking at parsaclisib, which is a PI3Kδ (PI3 kinase delta) inhibitor in patients with R-CHOP, which was presented by Dr. Yucai Wang from Mayo Clinic. Surprisingly, this showed a very high overall response rate for the patients enrolled. It’s a small study and didn’t appear to be subtype-specific, so it’s a little bit agnostic. But as Dr. Evens can tell you, the delta inhibitors have become a dirty word in our industry, so how that moves forward will be very interesting considering that for the most part, outside of CLL, these drugs have pretty much been killed off by the FDA.
Additionally, there was golcadomide plus R-CHOP in patients with large-cell lymphoma. This was presented by Dr. Jason Westin from MD Anderson. Again, this compared to lenalidomide, which is built off of, supposedly keeps cereblon in a more closed configuration, so more inhibition of Ikaros and Helios and more T-cell activity than what we saw with lenalidomide. This also had a very encouraging high overall response rate. We can all agree we can’t hang our hats on phase 2 studies anymore, but this one will move forward into a randomized phase 3 trial to try to see if this can improve on the R-CHOP backbone.
Dr. Lorenzo Falchi presented a study with epcoritamab, which is a bispecific antibody, and R-CHOP. Again, a very high overall response rate. We all suspect bispecifics will move forward in this space. There will be a phase 3 study looking at epcoritamab in this patient population.
Lastly, we had the COALITION study, which looked at glofitamab and R-CHOP or glofitamab and pola-R-CHP. Again, a high response rate in the phase 2 studies, very impressive complete response rates, and a high short-term duration of response; but again, more follow-up. As Dr. Evens can attest to, there’s a third bispecific. The OLYMPIA study is looking at odronextamab in this patient population.
It’s going to be a very, very difficult next couple of years teasing out the new standard of care for front-line large cell lymphoma if any of these phase 3 trials are positive. There are several ones that we didn’t even mention that will likely read out in that time frame. We’re in interesting times, but again, there’s a bit of confusion based on the backbone that’s being used — R-CHOP, pola-R-CHP — and the partner drug.
Stephanie: Dr. Phillips, thank you so much for going over all of that. You could characterize that as difficult and confusing because there are so many options now in a space that you’re looking at.
At the end of the day, whatever gets approved will be great for patients and that will be up to the providers, together with patients, to say what’s best for them.
Dr. Andrew Evens
How Long Until We See These Options? How Do We Choose?
Stephanie: Dr. Evens, how long until people could potentially see some of these treatment options? Let’s say they all get approved at some point. How would you decide for individual patients on recommendations for which way to go?
Dr. Evens: It’s a lot to digest and Dr. Phillips did a great job as he alluded to the tip of the iceberg, but it’s confusing. We say it’s a competitive landscape, but through the lens of the patient, it’s fantastic because it means we have a certain standard and a certain cure rate, and we’re trying to do better.
At the end of the day, whatever gets approved will be great for patients and that will be up to the providers, together with patients, to say what’s best for them. We always desire what’s called biomarkers to try to predict personalized therapy. Can we find a treatment or a regimen for particular patients? We’re certainly not there yet but that’s hopefully along with, in parallel, or, at worst, in sequence. We have a regimen approved for a large general patient population. Can we start to figure out who it works in?
To your point, the question always is how effective it is. It’s not just the initial response, but we want it to be stable and stay in remission. How is it tolerated? If it is as good or better tolerated, then that’s fantastic. If there are different or unique toxicities, is it balanced out by the efficacy? Then we think about the cost of care. We want to make sure it can be affordable for patients.
At the end of the day, whatever is approved down the road that builds upon R-CHOP and pola-R-CHP is all good news. Patient by patient, we’ll have to make smart, informed, personalized decisions.
Dr. Phillips: ASH in 2026 and 2027 will be quite interesting.
Dr. Evens: There’s going to be a lot. You know how it goes, Tycel. Most won’t break through, but maybe I’m wrong. As you mentioned, the bispecifics have the best chance.
With the bispecifics, part of the belief in how they will be upwardly mobile is that they’re built off the backbones of monoclonal antibodies, which have revolutionized how we treat patients with lymphoma.
Dr. Tycel Phillips
Questions for Patients to Ask Their Doctors
Stephanie: Bispecifics look like they might rise to the top. Can you share more about why that is? You talked about more personalized medicine. We’re certainly not there yet with biomarkers, but it’s a conversation that’s very hot for patient advocates as well. What guidance do you have for patients to ask their doctors? What can they ask about these different options?
Dr. Phillips: With the bispecifics, part of the belief in how they will be upwardly mobile is that they’re built off the backbones of monoclonal antibodies, which have revolutionized how we treat patients with lymphoma. As Dr. Evens mentioned, the major improvement was the addition of rituximab to a chemo backbone in CHOP. Ideally, if we look at glofitamab, epcoritamab, odronextamab, and mosunetuzumab, they’re still built off that same paradigm. In this sense, we’re encouraging the patient’s immune system to take more part in trying to fight off these cancers with the addition of chemotherapy drugs that are not necessarily immunotoxic.
In that sense, the combined ability and safety of these medications, especially when the patients get a few cycles of chemo first, support their addition to the front-line regimen. It’s that balance. If you have all these different options, we’re going to start going into the weeds and figuring out if there are any things that separate these regimens, like the safety, tolerability, and convenience of giving these to patients.
Is it more convenient to come in for an injection or infusion every couple of weeks or have to take a pill for a certain number of days? We already know that compliance with oral medications is not great. While you may get surveillance and pharmacovigilance on clinical trials, that doesn’t happen outside of a clinical trial setting. Quite frequently, patients will not be as adherent to these medications as they should be and that may impact clinical outcomes.
Echoing Dr. Evens again, it’s an exciting time. Another part we also want to look at is how they may impact certain subsets. With POLARIX, there’s the issue of subtype specificity, but do we have other treatments that may be agnostic to subtype? If we start getting more of these molecular tests that will divide patients into certain subtypes, how do these treatments broadly apply across the board? Do we need to play mix and match based on a person’s genomic profile? We’re still away from that, but that’s a place where everybody is trying to get to where it’s more individualized for the patient versus everybody who walks in gets the same treatment even though they’re not the same.
Dr. Evens: Dr. Phillips summed it up greatly. Clinical trials can be overwhelming. There’s not a better or the best clinical trial. To me, they’re all good options and that is one thing I would ask your doctor. What’s currently FDA-approved for my condition? Are there any new treatments? For newly diagnosed, there are very mature clinical trials taking the standard of treatment, like R-CHOP or pola-R-CHP, and trying to do better and looking at safety.
Long-Term Benefits/Risks of Bispecifics
Stephanie: There are clinical trials where we’re studying all these possibilities and then there are the approved options. The Patient Story set this conversation up backward in terms of clinical trials in that much of it is done for relapsed/refractory patients first and then works its way up to earlier lines of treatment.
We’re going to talk about bispecifics for relapsed/refractory patients. Dr. Evens, you talked about bispecifics rising to the top. Is there anything else in terms of long-term benefits and risks for what we understand so far when it comes to everything presented at ASH?
Dr. Evens: What about after treatment? Survivorship is very important. Yes, we want to cure with minimal side effects and fairly cost-effective treatment, but there are late effects that remain to be determined. Since these agents are not classical cytotoxic chemotherapy or radiation for the most part, the hope is that they’re going to have less late effects, whether it’s cardiac, pulmonary, or infections. But at the same time, we can’t assume anything. It needs to be studied.
My hope is that, whether through the pharmaceutical companies or academic institutions, it will be bolted on in some form or fashion to these studies to follow clinical trial participants for late effects whether it’s five or 10 years later because we certainly don’t want to cause harm down the road.
Dr. Phillips: When you have options, you could be a little bit more stringent about what’s the best thing moving forward. The more options there are, the better it is for our patients.
Dr. Evens: Tycel, I’m sure you have survivorship expertise at City of Hope.
Dr. Phillips: Yes, there is a survivorship clinic.
Dr. Evens: In the past, I wouldn’t say we minimized it, but maybe we didn’t appreciate or have the science associated with survivorship after treatment, so that’s also a valid question for your oncologist whether it’s two years or five years later. Can we talk more about my individualized survivorship? In most academic centers, even in some non-academic centers, there is survivorship expertise. Whether it’s led by nurse practitioners or physicians, it’s all good as we get into that important part of the rest of life.
Dr. Phillips: Yes, life after chemo.
Stephanie: I can’t tell you both how much I appreciate that you brought that up. I love how survivorship is becoming much more of a focal point. I went through hundreds of hours of chemo. I had dose-adjusted R-EPOCH in 2017 and the thought of being able to focus on survivorship and the things that I need to look out for because my body went through this is wonderful.
Dr. Evens: You look great and I’m hopeful you’re doing well, but it’s something to bring up. I don’t want to make it seem like it’s an epidemic or malady of late effects. They’re slight and subtle, but they’re real and we’re still learning a lot about them. We’ve learned a lot from Hodgkin’s lymphoma, which was one of the first curable cancers in man that we learned in the 1970s. But a lot of the medications, in particular anthracyclines, the vinca alkaloids, the alkylators they’re called, whether dacarbazine or cytoxan, are very similar, so they’re probably more similar than not and, frankly, regardless of age.
One other important pin to put in this point is when we hear about late effects, we sometimes think that’s 20 to 30 years down the road. What we’re learning, at least in Hodgkin’s and it’s probably true in large cell lymphoma if we take a close look, is within a few years and for sure by five and 10 years after treatment, we’re already seeing some of these late effects. It’s important to get that understanding from your local oncologist or survivorship expert.
Dr. Phillips: With anthracycline, a lot of times, we didn’t look and when you looked, you’d see a lot of cardiac effects, even within a year after completion of treatment.
Dr. Evens: You do. Now, it’s always tough. What do you do about it? But at a minimum, controlling your risk factors, like hypertension and cholesterol, certainly can’t hurt. It’s only going to do the body good.
Dr. Phillips: A lot of sites have cardiologists now that have taken an interest in oncology-related events. There are a lot of processes and steps, cardiac rehab per se, that have helped ejection fractions for a lot of patients.
Dr. Evens: There’s more funding. I’m working with a cardiologist at Tufts Medical Center who’s going to Beth Israel in Boston. She’s a cardio-oncologist and got a big grant funded to look at some cardioprotective agents early on, so thankfully, hopefully, they’ll be some resources.
It’s always hard, Stephanie. Whenever we talk about doing research, as you can imagine, you need funding and there tends to be a lot more from the pharmaceutical companies, which is understandable with the medications. With survivorship, there aren’t as many companies there, so we rely on the government through the National Institutes of Health or National Cancer Institute and philanthropy. There might be some other ways, but it’s such an important part of cancer care.
Stephanie: A hundred percent. Let’s get more funding for studying survivorship because that is so impactful for people.
With various agents, there’s always a small risk of secondary cancers that come from chemotherapy drugs. Whether you receive radiation or not is also a very important concern.
Dr. Tycel Phillips
Treatment Side Effects
Stephanie: Are there other late-term effects that people should be thinking about if they’ve undergone chemoimmunotherapy? Based on what you’re talking about from the R-CHOP plus X from ASH, is there anything else to call out specifically? People might think you’re adding a new drug, so does that mean they’re going to experience more side effects?
Dr. Phillips: It depends on the drug. With various agents, there’s always a small risk of secondary cancers that come from chemotherapy drugs. Whether you receive radiation or not is also a very important concern. We’ve learned long-term that some radiation risk factors don’t plateau and rather age with the patient. Those are all things to keep in consideration with some of these other drugs.
Thankfully, even with vincristine, which is a microtubule inhibitor, the biggest thing is neuropathy. The risk is the nerve damage is unpredictable and you may not get a resolution, so there’s always that concern and trying to prevent that from happening.
With some of the newer drugs, depending on their class, they all have unique side effect profiles. In the front-line setting, they’re given for a more limited time, which would hopefully prevent some of the side effects that we see in the relapsed/refractory setting, especially for drugs that are given until intolerance or progression, which is always a concern.
Looking at delta inhibitors in the relapsed/refractory setting, with indefinite use, you worry about liver irritation in some situations, diarrhea, and infection risk. With golcadomide, which is like a lenalidomide analog, reproductive risk is always a concern with that class, so if you’re a young woman, that’s always a concern in handling that medication. It can cause neutropenia, which may increase your infection risk when given with chemotherapy.
With the bispecifics, cytokine release syndrome is the biggest concern. Depending on when you give the chemo, you may mitigate a lot of higher-grade CRS, so you can potentially make that a bit easier to tolerate and less risky if you give a little chemotherapy to debulk the tumor and maybe blunt the immune response a bit.
Recent Data About Current FDA-Approved Bispecifics
Stephanie: Let’s move to relapsed/refractory DLBCL. There are two approved bispecifics for DLBCL: glofitamab and epcoritamab. Dr. Evens, can you talk about the most recent data? What’s relevant to patients about the two of them and the differences?
Dr. Evens: Generally speaking, it dovetails off of a lot of what we’ve already said. They’re very active. There are side effects, thankfully less than CAR T-cell therapy but similar, which is called cytokine release syndrome. Patients experience almost flu-like symptoms and some neurologic side effects as well. Thankfully, it’s less common, but it can still happen, so there certainly needs to be caution.
When we’re meeting a patient who received front-line therapy, whether it’s R-CHOP, R-pola-CHP, or dose-adjusted EPOCH and there’s a relapse, the historic standard was an autologous stem cell transplant. That’s gone down, but not away, with CAR T-cell therapy, commercial CD19.
I know your question was about bispecific antibodies, but there is a multitude of new CAR constructs. The current commercial CARs are CD19. More often than not, that’s the treatment of choice for many patients who relapse the first time, especially if it happens within 12 months, because bispecific antibodies for diffuse large B-cell have been after that. Not that it would be wrong to do it instead of CAR T-cell therapy; we just haven’t seen as much of the data. In some ways, that’s where bispecifics have tried to leapfrog and go to the front-line setting.
Whether it’s used in second-line or third-line, the bottom line is both medications are very active. They’re more similar than different, although there are some key differences. One is given intravenously, the other is given subcutaneously, and one has a few more doses than the other, but they’re largely much more similar than they are different.
Tycel, you don’t ever use standard before CAR, do you, in someone who can take CAR, right?
Dr. Phillips: That was a bridge.
Dr. Evens: Are you doing bispecifics as a bridge to CAR sometimes?
Dr. Phillips: Only in patients whose diseases rapidly progress and we need to stabilize before we can get them to the CAR product. But I agree with you. CAR equals cure. With bispecifics, we guess, but we don’t know for sure. Until we can be 100% certain, you’d be very hard-pressed to put a bispecific before a CAR in the second-line space.
Dr. Evens: Part of that is time. CARs have a several-year lead time and to say “cure,” two years in remission is a pretty good point. After five years, you feel good. That’s where we see CAR T-cell therapies. We saw some data at the meeting settling out around the 30% to maybe 40% range. We’re hopeful that we can say cure. We don’t have that lead time with bispecifics, although we’ll see over the next couple of years where those land.
Stephanie: CAR T-cell therapy came out first in research, so there’s more data and real-world evidence about how they perform. With clinical trials, it’s a different population, so it’s nice to be able to see what happens.
Dr. Phillips: CAR T-cell therapy has remained reproducible in the real-world space as it has in clinical trials, which is not the same as a lot of other drugs where you typically see a decline in efficacy once you move out of the clinical trial space. That hasn’t happened with CAR T-cell therapy.
Dr. Evens: Clinical trials are real world. Real world is a lingo that we use, meaning all comers, regardless of kidney function, age, etc., and not like the qualifications you need to join a clinical trial. He’s exactly right.
To put an extra point on that, for CAR T-cell therapy and bispecifics, there’s almost no upper age limit. With autologous stem cell transplant, you can do it up to patients in their 70s, maybe up to 80, but it gets a little tricky. Not to say CAR T-cell therapy and bispecifics in older age groups are a walk in the park, but they’re very manageable and doable.
Another part of science we hope to understand: which treatment works in which type of patient.
Dr. Andrew Evens
Bispecifics vs. CAR T-cell Therapy Mechanism of Action
Stephanie: Dr. Evens, could you summarize the mechanisms between CAR T-cell therapy and bispecifics in a way patients can understand?
Dr. Evens: It can be confusing for sure. I would frame them both under the rubric of immunotherapy. We talked about autologous stem cell transplant, which is also a fancy word. It’s not like getting a new liver or kidney; that’s called an allogeneic. Autologous transplant is one cycle: a very high-dose chemotherapy blasting hopefully the lymphoma away. But what about blasting your cells? We know that one of the most powerful anti-cancer agents is your immune system — your T cells in particular. We don’t know why, but in some cancer patients, lymphoma patients, they’re not doing what they’re supposed to.
CAR T-cell therapy cell is filtering out your T cells, sending them to a company, and over about a 3 to 4, sometimes five-week period, they’re re-engineering it by doing two things. They’re transfecting an antibody to tell it where to go when you put it back in and then in some ways, you supercharge it or activate it. When you re-inject it, it’s a one-time treatment several weeks later. It not only rapidly expands, but hopefully, it goes this supercharged T cell with the CD19 attached to it wherever the lymphoma is in the body.
What are bispecifics? It’s similar in concept in that it’s the patient’s immune system, but it’s an off-the-shelf treatment. The way to think about it most simply is a double antibody. It’s a CD20, which interestingly is rituximab. If rituximab in most patients stops working, why would this? Because the second antibody is CD3. When it’s off the shelf and injected, CD20 goes to where the lymphoma is, but the CD3 has T cells attached to it, so it delivers the patient’s endogenous or in vivo T cells to where the lymphoma is.
It’s remarkable. I’ve had a multitude of patients, as I’m sure Dr. Phillips has, where CAR T-cell therapy is given, it doesn’t work and we don’t honestly know why, but we’re thrilled when it happens, then you give bispecifics, and the lymphoma completely goes away. This is someone who has already failed regular CD20 single antibody, CD19 CAR, and then a different immunotherapy for one reason or another is effective. That’s another part of science we hope to understand: which treatment works in which type of patient.
Stephanie: There’s a lot of science to wrap up into this very abridged version, but I know the goal here is this more targeted. It’s engineered and using your immune system and it’s targeted with the goal being that we feel fewer side effects than blasting the whole body with chemoimmunotherapy. Dr. Phillips, is that how people can think about that?
Dr. Phillips: When I try to find the easiest way to compare chemotherapy to other treatments, I go back to the military where chemo is like napalm. It’s going to kill anything that’s growing rapidly because that’s what it’s designed to do. It isn’t specific for anything, one way or the other. A lot of these targeted treatments, such as bispecifics and CAR T-cell therapy, are more focused on directing your treatment toward the problem, which is, in essence, a malignant B cell.
There is still some ambiguity because normal B cells will be impacted. After all, we’re still targeting CD20. Hopefully, in the future, we’ll have some cancer-specific markers that may even spare normal immune cells. But to this point, we’re sparing a lot of other tissue because it’s directed toward a malignant B cell, which chemotherapy can’t do.
The closest we can get to that is antibody-drug conjugates, which will deliver a toxic drug directly to the tumor. The drug isn’t active until it’s internalized and then it can kill the tumor off. But even in that sense, you will get some spillage. As the cancer cells die and open up, that drug is also free to kill other bystander tumors but also any normal tissue that’s in the area, which explains some of the side effects we see.
Stephanie: I love it when there’s real-world verbiage so people can understand better.
Cytokine Release Syndrome
Stephanie: Dr. Evens, cytokine release syndrome was mentioned as a monitored side effect when it comes to immunotherapy. What does that look like in patients and what are the differences between what you’ve seen in the responses with CRS from CAR T-cell therapy versus bispecific?
Dr. Evens: It’s very similar as to when it happens. Thankfully, with bispecifics, it’s usually less frequent and less severe, although not zero, so you still have to have some caution. We don’t like to talk about it, but whenever we mention grade 5, that’s a fatal side effect and thankfully, it’s very uncommon, but we want to keep that 0%, as long as there’s the right training and the right medication on the shelves.
When I say the right training, it’s not the oncologists, doctors, nurses, and pharmacists. It’s making sure your emergency room and intensive care unit know. Like for many things in life, you’re preparing for the worst in case it happens.
For example, I gave a patient a bispecific antibody on a Friday. By Wednesday night, that patient had a very high fever, so he was experiencing a delayed cytokine release. He went to the emergency room. We have a protocol, so they know what to look for. We had a conversation and were able to mitigate it. The patient did not need to be admitted to the hospital. The fever quickly came down and he felt fine.
It’s a team sport as we’re managing some of the side effects and thankfully, almost always, it’s very manageable but it’s important to have that communication and collaboration across all specialties.
If a patient has cytokine release syndrome, the earlier you intervene, the better because you can mitigate and stop it from escalating to a higher grade, but your team has to be aware of what to look out for.
Dr. Tycel Phillips
Monitoring Side Effects
Stephanie: A huge topic for patients is the logistics side and considering what they have access to. Dr. Phillips, can you paint that picture for those considerations when it comes to patients? Do they have to be monitored? How long do they have to be monitored for potential CRS after CAR T-cell therapy and bispecifics? How can that impact the choices that they may have depending on where they live?
Dr. Phillips: In essence, CAR T-cell therapy is a little different. We typically think that the patient will be in and around the cancer center for about 30 days. You also are required to have a caregiver with you almost 24/7. Even in institutions where we can move patients to outpatient for CAR T-cell therapy, that still requires you to be on campus, have a caregiver, and go back and forth to the hospital. It requires more logistical hurdles to get over.
In some sense, CAR T-cell therapy is also akin to transplant centers. A lot of these things are in place as far as the inpatient portion because instead of admitting somebody for high-dose chemotherapy and then a stem cell rescue, you’re giving them CAR T-cell therapy with inpatient monitoring and very close follow-up. When you’re in the hospital, they’ll be monitoring you for neurological changes and vitals will be taken to monitor for any signs of cytokine release syndrome. These are done very closely.
Bispecifics, on the other hand, as Dr. Evens has eloquently elucidated, can be given in a community setting. The only real thing you need to have is education for the patient and the staff about what may happen if bad things happen. If a patient has cytokine release syndrome, the earlier you intervene, the better because you can mitigate and stop it from escalating to a higher grade, but your team has to be aware of what to look out for.
Normally, when a patient is on any oncologic treatment and they come in with a fever, you reflexively think it’s an infection and you give antibiotics and draw blood cultures. You don’t necessarily think cytokine release syndrome. With bispecifics, you need to think of cytokine release syndrome. Even if you are working up for an infection, you need to be putting those things in place to mitigate cytokine release syndrome.
Having certain medications on the formulary, like tocilizumab, can be difficult because it is cost-prohibitive, to be honest, so every hospital system doesn’t want to keep this on, especially if they’re not using it. These need to be in place. Most centers that have incorporated bispecifics have a designated champion, which is somebody who plays quarterback to organize the rest of the team. We have plans in place when patients come in. We have contact information and if anything goes awry, they’re there to fix and get everybody realigned, so when the next patient comes in, it doesn’t happen.
The timing depends on what you receive. IV medications tend to have an early onset of cytokine release syndrome with bispecific. With these subcutaneous formulations, sometimes these things happen at home, at which patient education becomes very important.
Make sure you have a thermometer at home to monitor for fevers. Some people have blood pressure monitors. Some people have advocated for other things to self-help. Make sure you have antipyretics at home, like acetaminophen or ibuprofen. Some physicians send patients home with a pill in a pocket, which is steroids, which in some situations can mitigate cytokine release syndrome or at least keep things stable until they can get to the hospital.
Can CAR T-cell Therapy Cure Some Patients?
Stephanie: Dr. Evens, you mentioned the word “cure,” but we need data. There was the five-year data for ZUMA and TRANSCEND trials. From a quick glance at that, is there anything more you want to add to this general feeling about CAR T-cell therapy and its ability to be curative? I know you talked again about needing more time.
Dr. Evens: It is time, though, Stephanie. It comes down to that. In the pre-CAR era, we tell patients that hopefully it doesn’t come back. In the minority of cases when it does, it most commonly happens in the first two years and then a little bit through years three, four, and five. It’s uncommon after five years with chemotherapy, but never impossible.
We expect that that dynamic should be the same because it is an aggressive cancer. How can it live around for five-plus years? These numbers we’re seeing at five years is what we call the plateau in the curve. It looks pretty darn flat once you’re getting out to three, four, and especially five years. I feel pretty confident we can use the word cure.
Anytime you have a treatment primarily anchored around academic medical centers when we know that over 80% of cancer care happens at nonacademic centers or community centers, there’s going to be a problem and a problem related to access.
Dr. Andrew Evens
Community Access to Treatments
Stephanie: Dr. Evens, widely discussed in patient groups is accessibility to CAR T-cell therapy. You both are at major academic centers. You’ve got all the tools and the latest, but for a lot of people who live in the community, this doesn’t seem to be very feasible.
Dr. Evens: That’s a major issue and Dr. Phillips aptly alluded to this. Depending on which data set you look at, in some cases, only 20 to 25% of patients who should receive it are receiving it. It will never be 100%, but it certainly should be more than 20. Anytime you have a treatment primarily anchored around academic medical centers when we know that over 80% of cancer care happens at nonacademic centers or community centers, there’s going to be a problem and a problem related to access.
What are ways to circumvent that? We don’t want to do anything haphazardly with any treatment. Can we try with certain community centers in collaboration with academic centers or maybe on their own and working with pharmaceutical companies or even foundations to be able to do it? You bet. In New Jersey, some strong, non-academic medical centers are giving CAR T-cell therapy carefully, so it definitely can be done. Better knowledge and prophylactic treatments, like steroids or tocilizumab. There was some data on this at the 2024 ASH meeting.
Maybe we can get to second- and third-generation CAR T-cell therapies that are engineered in a way that rapid overexpansion of T cells, which is driving a lot of the side effects, is more predictable or doesn’t happen. I’m hopeful that we’ll get there, but that’s part of the reason why bispecific antibodies have become a little easier.
Assuming the patients have access, some can’t wait four or five weeks. They don’t have enough time. It’s a big issue, but it’s top of mind and we’re thinking about all of these issues and how to remedy them. You guys have community centers don’t you, Tycel, not just in Duarte, right?
Dr. Phillips: We have a lot of community sites. They’re not doing CAR though.
Dr. Evens: They’re not? You know what we’re starting to do? We’re segmenting it. We loosened it to a little less than 30, but what we’re doing is having them do the pheresis. We have the New York Blood Center. It’s going to be tough with the current commercial CAR. Maybe in a bigger community, but it’s going to be tough in a small one.
We’ve had several data sets that show that you can still successfully harvest and administer CAR T-cell therapy in patients who’ve been exposed to bispecifics.
Dr. Tycel Phillips
Choosing Bispecifics vs. CAR T-cell Therapy
Stephanie: With bispecifics being more accessible in the community and in terms of wait time, when would you want to give bispecifics versus CAR T-cell therapy? Let’s say a patient has both as an option.
Dr. Evens: We’re not sure bispecifics are as effective as CAR T-cell therapy in the second-line setting. Let’s say for one reason or another, you can’t get CAR T-cell therapy. I don’t know what you think, Tycel. It wouldn’t be wrong to give bispecifics.
The only mild note of caution would be it’s not like rituximab. Even though most patients do well, you have to have some structure and organization in place before you even give the bispecific antibodies. They’re more doable for community oncology for sure than CAR T-cell therapy, but there still needs to be that note of caution.
Dr. Phillips: Thankfully, we know that limited use of bispecifics doesn’t appear to impact the efficacy of CAR T-cell therapy. We’ve had several data sets that show that you can still successfully harvest and administer CAR T-cell therapy in patients who’ve been exposed to bispecifics. That was a big concern that everyone had. But so far, based on a French and a US study, it doesn’t seem like that is much of an issue in that patient population.
Because they’re off the shelf, the accessibility of bispecifics is there. As these drugs move into other disease settings, such as solid tumors, you’ll likely see wider adoption and more incentive for community sites to use them because they won’t be doing them for the limited number of lymphoma patients. If they’re giving it for lung cancer, breast cancer, and prostate cancer, there are far more patients in that sense. Financially, it gives them more of a reason to have a structure in place for bispecifics and also the medication they need in case things go wrong.
Dr. Evens: There are two off-the-shelf CAR T-cell therapies in clinical trials, which are the so-called allo-CARs. The current agents we have FDA-approved are good, but there are still barriers and we need them to transcend more throughout the community for our cancer treatment.
Stephanie: For clarification, Dr. Phillips, there was some concern about bispecifics impacting the efficacy of CAR T-cell therapy given after, but that hasn’t proved to be the case. You were talking about bridging as well. What I’m hearing is it’s looking promising in terms of the optionality that is here at the fingertips and in research. Is that right?
Dr. Phillips: At this point, especially for the patients who Dr. Evens has talked about and those who maybe can’t get to CAR T-cell therapy for whatever reason, at least with these, we can maybe stabilize the disease enough to allow them the opportunity to get the CAR T-cell therapy if it’s feasible. In some patients, they won’t be able to get to CAR T-cell therapy because they need a lot more support than other treatments so that all has to be in place.
Latest Treatments in Follicular Lymphoma
Stephanie: Follicular lymphoma is very different in that it’s a slow-growing, indolent disease. Let’s start with the relapsed/refractory follicular lymphoma patient population. Can we set the stage by going over what’s available right now and some of the updates?
Dr. Phillips: In the relapsed/refractory phase, most people will use R2 (Revlimid and rituximab) based on the AUGMENT study, which showed a significant improvement over rituximab in this patient population. A lot of us are very comfortable with the use of that medication, and the efficacy and tolerability seem to justify it in the second-line space.
After that, it gets a little bit more variable. You have bispecific antibodies approved: mosunetuzumab and epcoritamab. CAR T-cell therapy is available in follicular lymphoma, albeit a little bit of a different argument. CAR T-cell therapy doesn’t necessarily have that curative label as it does in large cell lymphoma, so there’s a lot more variability about what you use in that space.
Recently, we had zanubrutinib and obinutuzumab based on the ROSEWOOD study, which is the first time a BTK inhibitor has shown any benefit for follicular lymphoma. Then there’s tazemetostat, which is an oral EZH2 inhibitor for patients with an EZH2 mutation or those who are deemed to be unfit for other agents, which are all approved in the relapsed/refractory follicular lymphoma space.
Top Developments in Relapsed/Refractory Follicular Lymphoma
Stephanie: Dr. Evens, there was a late-breaking abstract at the 2024 ASH meeting from the phase 3 InMIND study, which looked at tafasitamab plus lenalidomide and rituximab for the relapsed/refractory situation. Can you provide highlights from this and why patients should pay attention?
Dr. Evens: This was an important presentation and abstract, which was presented by Dr. Laurie Sehn from BC Cancer. It was built off the R2, Revlimid (lenalidomide) in combination with rituximab, which is commonly used in the second-line setting. It was a placebo-controlled study of R2 plus or minus tafasitamab, a CD19 antibody that is already FDA-approved for relapsed/refractory diffuse large B-cell and looking at its entry into follicular lymphoma. It was relapsed/refractory follicular lymphoma, so you had to at least have received rituximab therapy, second line, some somewhere beyond.
It was very effective. There are certain things we look at called hazard ratios and percentage points. Relatively speaking, there was a 57% improvement in progression-free survival, which was pretty significant. If you want to look at it by absolute months, it was on the median of about 12 months, a little bit less than 12 months benefit. This is a presentation. It doesn’t mean it’s FDA-approved although it’s pretty encouraging. I would hope and expect that soon, it will be submitted and eventually be an FDA-approved option for patients.
Dr. Phillips: I was surprised when I saw it and even more surprised about the results.
Dr. Evens: I like tafasitamab. There are no side effects and sometimes it works, but obviously, it’s a tougher patient population than diffuse large B-cell lymphoma. But it had very impressive efficacy and tolerability. We’ve known through the diffuse large B-cell approval that it’s a pretty tolerable medication.
Dr. Phillips: One key point also is that the standard of care arm performed worse than the AUGMENT study, but they enrolled patients with worse disease burden than AUGMENT did. It was a harder-to-treat patient population and they still had very good results that look better than what we got on AUGMENT, so hats off to them because they addressed the elephant in the room ahead of time and had data to support it.
How Should Patients Interpret the Results?
Stephanie: Compared to what’s approved for relapsed/refractory follicular lymphoma, Dr. Evens, how would you explain to patients one side’s already approved and the other side we’re talking about is promising data in research?
Dr. Evens: Like many clinical trials, it’s more than encouraging. It was a phase 3 head-to-head study and you’re not sure of the comparison. It’s a little bit of a waiting game. Sometimes what happens in the United States is there’s a panel called the National Comprehensive Cancer Network (NCCN) that will sometimes list it on its site before FDA approval, although usually they like to see a peer-reviewed manuscript and FDA approval. It emboldens the point of how important clinical trials are. For all of non-Hodgkin’s lymphoma and Hodgkin’s lymphoma for that matter, there are so many new and exciting treatments, but they have to be done with caution on a controlled clinical trial.
Bispecifics and Follicular Lymphoma
Stephanie: We talked extensively about bispecifics in DLBCL. What has the response been in follicular lymphoma and relapsed/refractory follicular lymphoma?
Dr. Phillips: It’s been good. The data has been very impressive. They have longer follow-up mosunetuzumab compared to epcoritamab, but that’s because it was approved sooner. I would think most people would prefer a bispecific over CAR T-cell therapy in a very similar patient.
There are some caveats. Some patients have more aggressive disease and more concerning features where you would probably go to CAR T-cell therapy. The safety of these drugs and lack of hospitalization are important. None of the ones approved in follicular lymphoma require patients to be hospitalized for observation and have very low rates of CRS. Mostly the ones that we see are grade 1, very few grade 2, and again, high overall response rate, high complete response rate, and very impressive durability of response.
Pending how things appear when the patient relapses, like if they still express CD20, it does offer the opportunity to retreat these patients with a bispecific, which is some of the stuff that future research is looking to determine whether they can still get very durable responses on second treatment. There have been very small data sets so far about the retreatment aspect, but that’s the opportunity that bispecifics can offer patients, even in a community setting without having to travel far from home.
Dr. Evens: Sometimes these diseases, even follicular lymphoma or other indolent lymphomas, can pick up ahead of steam and cause symptoms and that usually is where it gets large or becomes a trigger to start treatment. It’s treatable. We know now through randomized trials that life is extended with many of these therapies.
Generally speaking, it’s still not curable. We’re going to keep doing clinical trials and shooting for that cure. Not that quality of life is not important in diffuse large B-cell, but it’s ultra-important in follicular lymphoma. Hopefully, most if not all of these trials have some embedded quality-of-life measures to make sure that not only is the treatment effective, but it also allows patients to maintain their quality of life.
Over a 20-or 30-year period, some patients with follicular lymphoma may go through six, seven, or eight different treatments. Our hope is during that length of life, a good chunk of it is off-treatment and that’s why so many of these studies, thankfully, are being done with time-limited treatment. You treat for six months, a year, or even 18 months, pause, and hopefully patients can enjoy that remission off-treatment for as long as possible.
Dr. Phillips: He summarized the dilemma in follicular. You’re less willing to take toxicity because longevity and quality of life are paramount.
Dr. Evens: We presented a poster at ASH. Dr. Vaishalee Kenkre at the University of Wisconsin was the lead author. We have the Big Ten Cancer Research Consortium where we’re able to study. A study that Dr. Kenkre brought up is a common treatment, bendamustine-rituximab, in the front-line setting, given usually for six months. She brought tazemetostat, one of the medications Dr. Phillips mentioned, to the front-line setting and only gave three cycles of bendamustine-rituximab. There was a very early, response rate of 100% so far. But again, every trial in many ways is a good clinical trial. Hopefully, we can shift many of these novel and targeted treatments to the frontline that are more tolerable and time-limited, and garner long remissions without cytotoxic chemotherapy.
Dr. Phillips: Tazemetostat is one of the more tolerable oral medications I’ve ever seen.
Dr. Evens: It is and it’s remarkable. It’s very early. It was only 12 or 13 patients, but it’s a lead-in study, so you get tazemetostat and then concurrent taz-BR. It’s agnostic of the EZH2 mutation. We’ll have to see how that pans out, whether it matters or not in the front-line setting.
Dr. Phillips: The big point you said is no added toxicity, which we saw with a lot of other drugs. Lenalidomide is toxic with bendamustine. Even BTK inhibitors can cause some problems with bendamustine.
Dr. Evens: That’s right. It was investigator-initiated and thankfully, we were able to convince the company not to add it on to six of bendamustine-rituximab, but let’s try and do a short course of bendamustine. We’ll see how that pans out. Almost all of the medications in some form or fashion are being looked at in clinical trials in the front-line setting and that’s what we want — super-targeted, effective, incredibly well-tolerated, yet time-limited therapy for follicular lymphoma and other indolent lymphomas.
Key Takeaways
Stephanie: We’ve talked a lot about the research that’s happening and what’s already out there. What would you say to patients and their care partners in terms of the landscape over the next few years, both in DLBCL and in follicular? What are the trends and what are you excited by for patients and care partners?
Dr. Phillips: In large cell lymphoma, we are moving towards more personalized care. Even though we’re adding extra medications, it doesn’t necessarily mean we’re adding extra toxicity, which hopefully gives more efficacies without impacting quality of life or even adding long-term side effects to the patient profile. It’s all good news for the patients because everything for the most part is a specifically targeted treatment and not necessarily as generalized and causing a lot of side effects.
I’m excited to see where front-line large-cell lymphoma goes. Even in the relapsed/refractory space, as Dr. Evens alluded to, there are more and more treatments coming along. We are incrementally increasing the number of patients we’re curing from this cancer. The fewer patients there are in the relapsed/refractory space, the fewer patients we lose to this cancer, which is important and a big leap. Five years ago, you could routinely say that about 35% of patients would probably have very bad outcomes and there wasn’t much we could do about it.
Follicular lymphoma has become like what we see with Hodgkin’s without the ability to cure, but we’re trying to improve what we’re doing for patients with a very high recognition of tolerability. Anything moving up and being added are drugs that are safe and effective. Safety is paramount, so the quality of life that patients deserve and the extended survival will be time that they can enjoy with their family without worrying about side effects that come from these treatments.
We’ve already talked about tafasitamab, lenalidomide, and rituximab. We’ll have the bispecifics. Tazemetostat is being explored with R2. Eventually, some of these things may move into the front-line space and we can re-challenge the role of where chemotherapy fits in our patient population, even with time-limited therapies without cytotoxic drugs. It’s a very exciting time as we move forward. It may be more confusing for us as physicians because we’ll have more options, but that usually always equals good outcomes for patients.
Dr. Evens: Tycel did an amazing job of giving a summary, so I’m going to put a pin in a word he said: exciting. It’s an exciting time for investigators, like Dr. Phillips and myself, but also for patients and caregivers. There are a multitude of novel, targeted treatment options. We talked a lot about immunotherapy but also even some oral, targeted therapies that are on our shelves now as we speak and probably 100-plus new ones coming down the pipeline. What does that mean for patients? It hopefully means a lot of good things and a lot of more effective and tolerated therapy.
For patients and caregivers, always ask questions. Please never be hesitant to ask your oncologist a question. What are all of my treatment options, whether on the shelf or on a clinical trial? Never hesitate to bring up a side effect you have, whether it’s numbness, tingling, fever, or something more significant. Open lines of communication are paramount.
Patients have their family members and doctors, but there are so many good societies and foundations out there that can be a great anchor for patients to talk to other patients and get information. There’s a lot of great information in a fast-moving field but in all great directions.
Conclusion
Stephanie: Thank you so much, Drs. Evens and Phillips, for being here, for the work that you do, and for going way above and beyond treating your patients. We look forward to featuring you again soon.
With that, we wrap up another wonderful discussion at The Patient Story. I appreciate these doctors who take time out of their busy schedules to provide great insights for us in a way that we can understand better. It’s so important to be empowered, to lean into this communication, and to have more conversations about what’s impacting your quality of life so that you as patients, caregivers, and care partners can work together with the medical teams to stay on treatments that are effective and live life the way that you want to.
Thank you again to our partner, The Leukemia & Lymphoma Society. Check out the links to the LLS’ different parts of their website for their resources, like the information resource center, which provides free one-to-one support with questions across the board, and their Clinical Trial Support Center, where clinical trial nurses help you find trials, stay on trials, and answer all the questions in between.
We hope that this was helpful to you. Thank you so much for joining and we hope to see you at another program soon. Take good care.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
Symptoms: Intermittent feeling of pressure above clavicle, appearance of lumps on the neck, mild wheeze when breathing and seated in a certain position Treatments: Surgery, chemotherapy
Building Bonds Episode 2: How to Find and Partner with a Doctor for Better Waldenström Care
Finding a doctor is important in your Waldenström macroglobulinemia care. A strong partnership leads to more informed decisions, personalized care, and a greater sense of control. Patient advocate Pete DeNardis, hematologist-oncologist Dr. Jonas Paludo from Mayo Clinic, and patient advocate Lisa Ramirez discuss how her decisions led to being treated by Dr. Paludo and forming a trusted patient-doctor relationship.
Edited by: Katrina Villareal
Discover the importance of second opinions and how even top specialists recommend them. Understand how a Waldenström macroglobulinemia specialist can provide a unique perspective having seen more cases. Learn about shared decision-making in Waldenström treatment. Hear first-hand experiences of navigating a chronic cancer with your doctor by your side. Get practical tips for advocating for yourself or a loved one in the treatment process.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Tiffany Drummond: I’m a patient advocate with over 20 years of experience in cancer research. My journey as a care partner began when my mother was diagnosed with endometrial cancer in 2014. I quickly realized the challenges of finding reliable information to support her care, so I am committed to helping others avoid similar difficulties.
At The Patient Story, we create programs to help you figure out what’s next. Think of us as your go-to guide for navigating the cancer journey. From diagnosis to treatment, we’ve got you covered with real-life patient stories and educational programs with subject matter experts. I’m your personal cheerleader, here to help you and your loved ones best communicate with your healthcare team as you go from diagnosis through treatment and survivorship.
We want to give a big thank you to The Leukemia & Lymphoma Society for its partnership. The LLS offers incredible free resources, like their Information Specialists who help you communicate with members of your healthcare team and provide information about treatment options.
The Patient Story retains full editorial control over all content. While we hope you find this helpful, please keep in mind that the information provided in this program is not a substitute for medical advice. Pete, a patient advocate and Waldenström’s survivor, will lead the conversation.
Peter DeNardis, IWMF Chair Emeritus
Peter DeNardis: I’m currently the chair emeritus of the International Waldenström’s Macroglobulinemia Foundation. I have been a long-time volunteer for the organization and a patient myself. I was diagnosed 20 years ago and I’m well aware of the importance of a strong patient-doctor relationship. I look forward to learning from our esteemed panelists about how best to build and maintain that relationship.
With us is Dr. Jonas Paludo, a hematologist-oncologist and assistant professor of medicine and oncology at Mayo Clinic in Rochester, Minnesota. His research interests include studies to understand the biology, genetics, and therapy of lymphoma and plasma cell disorders, and he is also a noted researcher in Waldenström’s.
Lisa Ramirez, Patient Advocate
Lisa Ramirez: I was diagnosed in 2021. I was getting into a doctoral program and had to do some routine testing and physical exams, and in the process, I was diagnosed with Waldenström’s macroglobulinemia. The diagnosing oncologist was retiring, so he passed me on to another doctor in his practice.
I did a lot of research on Waldenström’s immediately and read Dr. Gertz’s recommendation on getting a second opinion, which I appreciated. I looked for the doctor who I thought would be best in getting a second opinion from and that was Dr. Paludo since he specialized in Waldenström’s in young people. I got another opinion from a physician at a major cancer center in the state in which I live as well.
I had a great rapport with Dr. Paludo immediately, but I initially thought I would only see him for a second opinion since I lived in Texas and he was at Mayo Clinic. I made it work and secured Dr. Paludo as my primary oncologist. I was very pleased about that.
Proactively Participating in Your Care
Peter: It’s good that you immediately did research and also went for a second opinion. Is it appropriate to say that you were an involved patient from the start?
Lisa: Yes. I work in public health. I’m a natural researcher and a very curious person. I wanted to learn as much as I possibly could and as quickly as I could about Waldenström’s to plan out my course of treatment and to be a well-informed patient.
I listened to all the lectures I could get my hands on and tried to understand the philosophies of the different cancer institutes. They seem to have differing philosophies about treatment and I tried to find one that fit with my personal philosophy and how I wanted to approach treatment.
I wanted to learn as much as I possibly could and as quickly as I could about Waldenström’s to plan out my course of treatment and to be a well-informed patient.
Lisa Ramirez
Signs and Symptoms
Peter: Looking back, do you think you had any symptoms that you weren’t paying attention to at the time?
Lisa: I was having night sweats, but I didn’t I thought I was experiencing early pre-menopause symptoms. Now I know the difference between hot flashes and night sweats. There’s a big difference.
I had some testing done because of other reasons and there was a note to rule out lymphoma and to check in six months after. Right at the six-month mark, my primary physician had me see a hematologist because of those test results. I had zero symptoms then. I felt great.
Looking back, I had some input from other oncologists that perhaps I had the disease for so long that I thought I felt good. That small incremental change in a negative way can go unnoticed, but I thought, “Does it matter? If I believe I feel good, then I feel good.”
Insurance Concerns
Lisa: The average time between diagnosis and treatment is about two and a half years and that’s about how long it took for me, so I was right on pace with the average.
Peter: You got a second opinion in a different state. You live in Texas while Mayo Clinic is in Minnesota. Did you have any financial or insurance issues trying to see Dr. Paludo?
Lisa: Surprisingly not. I received some treatment in another city in Texas. When you break down the costs, that treatment was more expensive.
Different institutions have different priorities in terms of testing and the amount of testing at checkups. In my case, the cost of the additional testing outweighed the cost of travel to Minnesota. It ended up being more cost-effective and worth it to travel to receive treatment at Mayo Clinic.
Peter: You’re very fortunate in that regard. I’m glad that worked out for you. You’re under great care and it appears that right from the start, you’re a very involved, proactive patient, so I applaud you for that and hope that other patients can take your lead.
WM at a Glance
Peter: Dr. Paludo, many of us patients have a general idea of what Waldenström’s macroglobulinemia is, but can you give a 30,000-foot view explanation of what the disease is?
Dr. Jonas Paludo: Waldenström’s is a rare type of blood cancer. It’s a form of an indolent or slow-growing subtype of a B-cell non-Hodgkin’s lymphoma. It’s a disease that has some overlapping features between lymphoma and myeloma, but it’s a type of blood cancer.
Common WM Questions
Peter: You see patients either coming initially to see you or for a second opinion. They probably have similar questions, but in your experience, what are the more common questions that patients ask?
Dr. Paludo: I can group the most common questions into three specific categories. In one shape or another, they’re trying to understand: What is Waldenström’s? What is this disease? Then the next one is: what do we do about this? Do we have to do anything about it right now? What it will look like? And then the third one is: what is my prognosis? What can I expect out of this disease?
Peter: Those questions are pretty common for Lisa and me when we were first diagnosed, so it’s good to see those questions are still being asked.
Diagnostic parameters, treatment options, follow-up testing, and surveillance are not as well-established in rare diseases as they are in more common diseases.
Dr. Jonas Paludo
Getting a Second Opinion
Peter: Many in the medical community and even the IWMF itself encourage patients to get a second opinion in certain circumstances. Dr. Paludo, as a healthcare provider, what are your thoughts on patients getting second opinions?
Dr. Paludo: Waldenström’s is a rare disease and like any rare disease, a second opinion should always be considered. Diagnostic parameters, treatment options, follow-up testing, and surveillance are not as well-established in rare diseases as they are in more common diseases or more common forms of cancer, like breast cancer or colon cancer, for example. That’s where a second opinion can help.
In addition, the familiarity of physicians with the disease or the current evidence and data of the disease can be quite variable. It’s part of reality. We can’t keep up with all the information generated daily for all diseases. Getting a second opinion from someone who has more experience or more interest in that specific type of rare disease is very important and adds a lot to the treatment and management.
I always encourage second opinions. To be honest, with most patients I see with Waldenström’s, I’m the one giving the second opinion. But for the patients who we see that are local, I encourage asking for another opinion elsewhere to have different points of view. I don’t think a second opinion would ever hurt a patient. It can only add information and help with the treatment and plan.
Peter: That’s a good point and hopefully they’re not trying to juggle three different opinions. In Lisa’s case, it was the one that she felt more comfortable with, which is appropriate.
Dr. Paludo: That’s a potential downside, but the benefits of a second opinion outweigh that downside.
Lisa: Waldenström’s is so different in terms of it being a cancer because you want to time treatment perfectly and take into account your quality of life. With a lot of other cancers, there’s a rush to treat and there are very specific treatment regimens. With Waldenström’s, you’re playing a very long game of chess.
You want your partner to be someone who you trust and who understands your quality of life and your age as you’re moving along the course of treatment. You’re going to want someone who understands you well enough, to keep pace, and who has a similar philosophy and approach to treatment. With Waldenström’s in particular compared to other cancers or other diseases, it’s important when selecting an oncologist that there’s a good fit.
Different cancer centers can appeal to different types of people. Mayo Clinic and Dr. Paludo were the perfect fit for me.
Dr. Jonas Paludo
Knowing Your Options
Peter: How did you know where to go for a second opinion? You mentioned Dr. Gertz’s presentation, but how did you figure out what your options were?
Lisa: The resources from the IWMF immediately pointing to Dr. Gertz and understanding Mayo Clinic’s philosophy led me there and looking into physicians there. I found Dr. Paludo in relation to Waldenström’s and other aspects of Waldenström’s that were of particular interest to me. I immediately sought him out for a second opinion.
I seem to resonate more with the philosophy of Mayo Clinic. They seem to have an approach that is slower to overreact. Their approach feels more strength-based rather than fear-based and I respond to that. When I need to embark on an intimidating treatment like chemotherapy, I want my partner to be able to reassure me that I’m strong enough, that I’ve prepared enough, and that it is the right time.
I understand that people have different motivations for starting treatment and some people can be more motivated by fear-based approaches. I don’t respond well to that. I respond better to a strength-based approach and the reassurance that all my questions are answered and that there’s enough time spent understanding the procedure or what’s happening with the progress of the disease. I find direct information very reassuring.
I have had oncologists who took a different approach where they feel nervous about my condition and then I start to feel very nervous and anxious. I know that it’s best to time treatments correctly and wait a little bit longer. It’s a fine line. Different cancer centers can appeal to different types of people. Mayo Clinic and Dr. Paludo were the perfect fit for me.
Finding a WM Specialist
Peter: Dr. Paludo, you mentioned that some patients come to you initially while others come for second opinions. If you’re telling a patient to get a second opinion, where do you direct them to? And for the patients who come to you initially, how did they find out about you in the first place?
Dr. Paludo: I also rely a lot on the IWMF resources to help patients decide on where to go next. There are so many factors, like insurance coverage and cost of travel, that are so particular to each patient, so I try not to be very specific. I point them to resources that they can look at to see which one makes more sense based on insurance, cost, travel, timing, family members, where they are, and things like that.
As with most rare diseases, you find more experience in bigger centers because they tend to see more patients with their rare diseases. It doesn’t necessarily mean that’s the only place you can find experience and expertise. It’s just the more common place where you can find expertise for rare diseases. The IWMF helps with pinpointing areas with more expertise or experience with Waldenström’s than other sites.
Peter: Because of my involvement with the IWMF, I’m well aware of the services they provide. On their website, they have a list of top doctors to go to for a second opinion regardless of what part of the world you’re in. The IWMF also has online discussion groups and Facebook groups where you can ask other patients who they go to. Granted, that’s word of mouth from one patient to another, but you can form an idea of who are the more noted doctors and who you could see if you want a second opinion.
The biggest challenge that I see is often related to indications to start treatment… sometimes it’s better if we don’t jump into treatment and instead sit tight and watch very closely.
Dr. Jonas Paludo
Building Bonds Ep. 2: How to Find and Partner with a Doctor for Better Waldenström Care
Hosted by The Patient Story
Finding a match is important in your Waldenström care. A strong partnership leads to more informed decisions, personalized care, and a greater sense of control. Join host and patient advocate Pete DeNardis, Dr. Jonas Paludo from Mayo Clinic, and patient advocate Lisa Ramirez as she discusses how her decisions led to being treated by Dr. Paludo and forming a trusted patient-doctor relationship.
Peter: Dr. Paludo, what do you see that some healthcare professionals don’t get right about a WM patient?
Dr. Paludo: Waldenström is such a unique disease that the biggest challenge that I see is often related to indications to start treatment. Because of the uniqueness of this disease with overlapping features with other indolent lymphomas, sometimes I see more of a generalization of what we do for similar diseases applied to Waldenström’s. I understand where they’re coming from, but it doesn’t always fit with our best practices for Waldenström’s.
They haven’t seen a lot of cases and sometimes it can be difficult for a provider to sit tight on a patient who has a very high IgM level and hold off on doing something. It’s often easier to do something, but sometimes it’s better if we don’t jump into treatment and instead sit tight and watch very closely when patients are asymptomatic or not having significant symptoms.
Peter: I hesitate to say this, but back when I was first diagnosed, there was something called the 10,000 IgM Club. There were a handful of patients who felt that they were okay and feel fine. Their IgM level is 10,000, but their symptoms are fine. In hindsight, that may have not been, but every patient is different. You’re exactly right. It depends on a patient’s symptoms and how they’re feeling along with the blood values. It’s critical to go to a specialist if you can.
I’m Newly Diagnosed. What Now?
Peter: Let’s turn to the important role of the doctor-patient relationship in managing your disease course, both short- and long-term, especially about WM. It’s considered incurable, but with the more novel agents that have come around in the last 5 or 10 years, it’s much more treatable.
Lisa, you mentioned your path to getting a second opinion. What advice would you give to a newly-diagnosed patient who’s looking for care and what do you think is most important?
Lisa: What we’re talking about here is building rapport. You have to be able to trust your oncologist 100%. There are some scary moments and you question yourself. You want to have the reassurance of an oncologist who has expertise in this area, understands you, and has a sense of how uniquely your disease is manifesting.
Every WM patient is a little bit different, so find a physician who you can trust and sees you. Sometimes that’s not something tangible. It’s what occurs during a conversation and a sense that you feel shared insights or philosophies. During my visits with Dr. Paludo, he would ask, “And what else?” I loved that he always left room for all of my questions and he was always very direct with me.
You want to have the reassurance of an oncologist who has expertise in this area, understands you, and has a sense of how uniquely your disease is manifesting.
Lisa Ramirez
Do your research. Understand what it is that you want in terms of your quality of life and what’s important to you.For example, I was going to start treatment under the care of a different oncologist, which would have put at risk my ability to dance ballet on my toes because there was a higher risk of peripheral neuropathy with that particular treatment. At my age, I thought the first treatment I should do perhaps shouldn’t be that one. I was able to have that conversation with Dr. Paludo and talk about things that are important to me.
Oncologists see a lot of different patients and their priority is to save your life and get you treated, which is understandable, but it’s a little bit different with WM. My quality of life includes being able to dance on my toes, so losing feeling in my toes was a big deal. It would have negatively impacted my quality of life had I started with that particular treatment if I had the unfortunate side effect of being unable to feel my toes.
Find an oncologist who understands who you are as an individual, what your quality of life is based upon, what’s important to you, who you feel comfortable sticking with throughout your life, and who will map out a course of treatment that’s going to work for you. One time, Dr. Paludo said, “You’re probably going to have to do all the treatments. We just have to figure out what works for you when.” Everyone’s different, so that’s important.
Deciding to Stay Local or Travel for Your Care
Peter: You have a good rapport with Dr. Paludo. Do you still see a local oncologist in Texas?
Lisa: No, I see Dr. Paludo exclusively. I was already scheduled for treatment somewhere else, but I got cold feet at the last second. The first step in treatment is so critical. It impacts the next move and the next move and the next move. Even though those moves are spaced out—hopefully many years apart—it still sends off a ripple effect.
You want to feel very comfortable with your provider and the institution you’re receiving care from is critical. I had to advocate for myself and say, “I know it doesn’t make sense to seek treatment in a different state and to get my primary care from an oncologist so far away, but we’re going to Minnesota.”
How Often Do You See WM Patients?
Peter: Dr. Paludo, Mayo Clinic is a world-renowned medical institution, but, hopefully, many people with Waldenström’s also understand that it’s world-renowned for Waldenström’s macroglobulinemia. Out of curiosity, can you say how many patients you maybe see a day or in a week that have Waldenström’s?
Dr. Paludo: It’s variable these days, but I estimate about two to three patients a week with Waldenström’s and sometimes as many as five patients a day. We looked at this a few years back and to give some context, if you were to consider all practicing doctors in the US and all newly-diagnosed Waldenström’s patients in a year, each doctor will see a new case of Waldenström’s once every eight years. This gives you a sense of how rare diseases are very, very difficult to come across.
I want the patient to feel empowered that they can ask any question, no matter what it is, and bring up any concerns or fears that are important to them.
Dr. Jonas Paludo
Approaches to Personalized Care
Peter: You and Lisa have a very good doctor-patient relationship. In your experience, does each patient approach you differently? Do you have a different approach depending on what kind of interaction you have or what works best for that patient?
Dr. Paludo: My approach is different for each patient. The things that we always try to discuss and focus on are the main concerns that each patient brings to the visit, which can be different. If someone was recently diagnosed with Waldenström’s versus someone who’s reviewing, studying, researching, and now we’re talking about treatment, there would be some differences in how I approach each patient.
Managing Your Life with WM
Peter: Given that Waldenström’s is becoming more of a manageable disease, what is your guidance to patients when they first come to you as far as dealing with having a disease like ours? You have periods of requiring active treatment and periods of watching and waiting for the next shoe to drop, in a sense.
Dr. Paludo: It depends on the situation, but I’m always trying to discuss the key concepts related to Waldenström’s. We talk about follow-ups and treatment indications. I like to address that because they’re important for the patient, especially if they’re not coming to Mayo for their care.
At the end of the day, we always try to establish trust and an open space. I want the patient to feel empowered that they can ask any question, no matter what it is, and bring up any concerns or fears that are important to them. It’s difficult to do everything in one visit, although we do try, but sometimes we need several visits to discuss all of these.
Peter: That’s very commendable. That should be the model for all clinicians. Unfortunately, a lot of them are pressed for time or dealing with a large patient load, so they don’t make the extra effort, and you should be applauded for doing that.
WM Treatment Options
Peter: Lisa, you had some choices to make concerning treatment. Were you aware of the treatment options before you spoke to Dr. Paludo?
Lisa: Yes. The second oncologist I saw was supposed to be my first treatment opinion. When I started talking to her about the treatments, she said, “Gosh, you sure do know a lot about this. What do you think?” I didn’t get the first opinion that I was hoping for because I had done so much research that the oncologist felt that maybe I had a better sense of what treatment I should start with, which ultimately led me to a second opinion with Dr. Paludo.
I have done a lot of research, which I enjoy doing. It’s not a situation you want to be in, but I work in public health and public health strategy, so I enjoy strategy and research. I wanted to find out as much as I could about the treatment options. From the scientific papers, it’s not always clear. Actual patient experiences are something that’s missed in very scientific journal articles, which can only be shared through patient-to-patient experiences.
With Waldenström’s, that can be additionally challenging because we are each so unique. It’s a full-body disease that manifests differently. The symptoms are different from person to person. There are also fewer females with the disease and fewer people my age, so it can become more difficult to know exactly what to expect even though you do a lot of research.
What reduced my anxiety was talking to Dr. Paludo about being vulnerable about parts of the treatment that I thought were most concerning.
Lisa Ramirez
The Emotional Impact of a WM Diagnosis
Peter: You did a lot of research, but how were you dealing with it emotionally? How did it affect you when you were first diagnosed and how did you deal with the enormity of it?
Lisa: When I was first diagnosed, I was shocked. I knew I couldn’t have the conversation with my daughter that day, so she had a sleepover that night.
After that, I felt somewhat calm about it, even though I do have a history of anxiety disorder. I knew going into treatment that my outcomes would be better if my anxiety was reduced. Stress plays a huge role in your physical health in general, but especially as you undergo something as stressful as chemotherapy where you have a lot on the line.
I made sure to take care of my mental health through exercise and seeing a therapist weekly. What reduced my anxiety was talking to Dr. Paludo about being vulnerable about parts of the treatment that I thought were most concerning. I was able to talk in-depth about how I was concerned about a recurrence of my anxiety and eating disorders in the course of treatment.
Dr. Paludo was able to reassure me that, at any point in time, if I was having concerning symptoms, we could talk about it, but most of all, we could always stop treatment and take a different course of action. That option was never presented to me before by any of the oncologists I had seen. Having that way out and knowing that I had that autonomy was so reassuring and helped me get through a lot of rough times throughout treatment.
I had a pretty good treatment experience. It wasn’t always easy, but it was a lot easier knowing that I had the support of my oncologist to pivot, redirect, and find a different course of treatment that worked better for me. My quality of life was most important to both of us.
Peter: Thatfocus on quality of life is critical. Every patient’s different, both physically and mentally, and it’s important to treat both aspects of how a patient approaches their disease.
Important Takeaways from Initial Consultation
Peter: Dr. Paludo, when you see a patient, what do you want patients and care partners to take away from that initial visit with you? What do you want them to understand?
Dr. Paludo: One of my priorities is to have patients understand that treatment for Waldenström’s is not a sprint but a marathon. It’s a long-term process that involves long-term planning, and we have to consider all short- and long-term strategies for treatment.
I usually say that when you’re getting treatment, you’re not in a long-term commitment. You can always stop and find a different option. I also like to discuss, usually in broad terms, that what we have today for treatment options has an overall similar efficacy. They are different in potential side effects, logistics, duration, and frequency. That often allows patients to focus on the implications of the treatment on their quality of life and their goals.
Once we remove the efficacy piece from the discussion, we can talk more about side effects and logistics. We can focus on how the treatment can help patients achieve what they want at the end of the day, which is improved quality of life, and accomplish what’s important to them. Those are things that I always like patients to take away from those initial discussions about treatment options before even we decide on which treatment to go next.
Lifestyle Changes in the Face of a WM Diagnosis
Peter: Lisa, you wanted to make sure you had a good quality of life. After you were diagnosed and started treatment, did you do anything different? Did you make lifestyle changes to help you emotionally and physically?
Lisa: Absolutely. Dr. Gertz said that frailty is the enemy, so I immediately got a personal trainer and hit the gym. People train for marathons. This is the rest of my life. I don’t want chemotherapy to knock me down. I need to be as fit as possible.
I also participated in an educational session on nutrition through The Leukemia & Lymphoma Society and met with a nutritionist. I changed my diet to reflect some of the recommendations based on those talks. I’m eating more of a plant-based diet and building up my strength as I approached treatment knowing that treatment was inevitable.
I saw a therapist weekly, which ultimately helped. During chemotherapy, I didn’t miss any work. I remained very active. I was still able to dance. I wasn’t allowed to skateboard anymore, but I was still exercising as much as I could to fight the fatigue and it paid off. That makes a big difference in terms of how one feels during the course of treatment and your ability to be resilient and make good progress in treatment.
Peter: I agree completely. It’s important to move. A lot of patients say that their treatment has debilitated them, but I tell them to try to move a couple of feet and take a couple of steps a day and build on it. It does make a difference.
Maximizing Your Quality of Life
Peter: Dr. Paludo, do you have any follow-up advice for Waldenström’s patients on how to deal with quality of life issues? Can they continue to live like they did before they had WM?
Dr. Paludo: Absolutely. It’s always difficult to cope with a new diagnosis of any cancer, including Waldenström’s. Every patient is a little different on how they try to cope. I try to understand what’s important for each patient and focus on what we can do to control what we can.
With Lisa, dancing was very important. We couldn’t control when treatment was needed, but we could control that she could continue to dance. It would be a form of exercise that helps her cope and keep some form of normalcy. Life can be disrupted with diagnosis and treatment, so trying to keep as much of a normal life as possible after diagnosis or when you’re going into treatment is very important. As you go through the watch and wait period with Waldenström’s before treatment or in between treatments, it’s very possible to live life like before as much as possible.
I’m not a mental health expert, so I also look for help. I refer my patients to cancer therapists and psychologists. The team we have at Mayo Clinic helps. I play within my limitations and always look for help from others who know more than I do about topics that are very important for every patient.
Patient Advocacy
Peter: Lisa, you’ve advocated for yourself right from the start. What would your advice be to newly-diagnosed patients or even those who are even in remission?
Lisa: For newly-diagnosed patients, get connected with IWMF. I was so impressed with the resources available for such a rare disease. It’s honestly very impressive how well IWMF is organized.
If you’re a young person or under 50, it can be more challenging because it’s almost a different disease. When you have young kids at home, there are a lot of different things to consider. Getting connected with the IWMF support group for young people was helpful. Find support with people in your community.
Watch lectures and read all the resources available sooner rather than later. You have some time to figure everything out. If you’re newly diagnosed and you don’t have symptoms that require immediate treatment, you have time to research.
It’s necessary, I would say also, to look at the different cancer institutes that have different philosophies. When you’re listening to lectures from different experts, find who resonates with you and what makes sense to you. Who do you seem to align with in terms of what feels right for you and what you value?
Take time to consider all that’s important to you so that you can locate the physician and your team that you’re hopefully going to be with for the rest of your life, working on achieving a good quality of life while living with this disease. Take in all the information, talk to your support network, and connect.
At first, I thought that having Dr. Paludo as my primary oncologist was not possible, but you may be surprised at what is possible so have hope and advocate for yourself.
It’s great to have an external brain to help process the information and to reflect back to you.
Lisa Ramirez
The Role of Care Partners
Peter: You approach each appointment with knowledge beforehand, you do your research, and you advocate for yourself. Do you go to your appointments on your own or do you take a care partner with you? You read that someone should always have someone else with them because they can mishear something. How do you manage that?
Lisa: I have a great partner and support. You’re absolutely right. Sometimes it can be overwhelming. When I would go to appointments with a different provider, I’d walk out sweating and notice I was so nervous during the appointment. Having someone there can be helpful. When I went to treatment, my partner would go with me. One time, my sister went with me.
Sometimes, you get disappointing news. I oddly got disappointed that I couldn’t do chemo a couple of times and I got upset and emotional, so to have someone to provide emotional support is helpful. It’s much better to not have to do it alone.
But if you are alone, there are people who are there to support you. At Mayo Clinic, there’s a whole team. Everybody there is supportive, so you can do it alone. It’s great to have an external brain to help process the information and to reflect back to you. Maybe you didn’t even notice that you weren’t feeling comfortable with a certain provider. It’s helpful to have someone to bounce off, so it’s important to have someone with you.
Peter: Dr. Paludo, what’s your advice in that regard? Do most patients come with someone to the appointment? And do you suggest it to patients if they don’t?
Dr. Paludo: Most patients come to their appointments with someone else. That’s very helpful and very important, if possible, of course. It’s difficult to take people away from their normal day-to-day lives, but it helps to have someone else also listening. We usually don’t remember everything that is discussed. Each person may remember different parts of the discussion. It helps, so I encourage that if possible.
Living with WM
Peter: Lisa, you’ve been living with Waldenström’s for a few years now. How do you not let Waldenström’s consume your everyday life? What’s your approach to living with it?
Lisa: In the beginning, it was difficult to not let it consume my life. For me, planning out a theoretical course of treatment to last my whole life was helpful. What helped was having that plan in place and also having a plan when I didn’t have symptoms or symptoms that I thought were bothersome to me.
Having those things mapped out in advance allows me to trust the plan and not have to think about it in my daily life. Once those decisions are made for the future, I can always change my mind at any point, but to have that mapped out for myself allows me to forget that I have Waldenström’s and live my life. It might take a minute to get there.
At first, it’s consuming. You’re consumed with the research. Don’t overreact. Take your time. Talk with your oncologist about a plan, put a plan in place, and then put it aside and live your life. Ultimately, treatment is all about having a good quality of life and living your life normally. You want to be able to do that and not add any additional stress to yourself. Putting a plan in place, putting it aside, and referring back to it when you need to is important.
Talk with your oncologist about a plan, put a plan in place, and then put it aside and live your life. Ultimately, treatment is all about having a good quality of life and living your life normally.
Lisa Ramirez
Waldenström: The Patient-Physician Relationship
Peter: Right from the start, you had a good relationship with Dr. Paludo. How has that evolved over the past few years? Is it different now than it was initially?
Lisa: Dr. Paludo has been very consistent. Initially, I met with him before I even met with who I thought was going to be my primary oncologist. I walked away from that conversation saying, “Gosh, I met the right oncologist for me. Too bad. I can’t possibly get treatment in Minnesota.”
It felt like a good fit from the beginning and we’ve built upon that trust. I instantly felt comfortable and felt trust. He engaged with me in a way that was strength-based and not over reactive. He’s very steady. Our relationship hasn’t changed much other than we’ve been through this treatment together and there’s a deepening of trust.
I’ve talked about my next treatment episode with my partner and when I have to do the weekly treatment, we’re going to live in Minnesota for six months. There’s no question about that. I know Dr. Paludo’s there for me and he’s my oncologist until the end, so I feel very comfortable with that.
Key Takeaways
Peter: Dr. Paludo, do you have any key takeaways for patients or healthcare providers in building and sustaining a strong relationship through the cancer journey?
Dr. Paludo: Advocate for yourself. Go after what you think is important for you. Lisa and I are on the same page. For the healthcare providers, what’s very important is to actively listen to each patient’s priorities. Listen and not just hear. Pay attention and focus on what’s important for each patient, like their main concerns and fears.
As providers, we have to be frank and honest with the limitations of what we know and what we don’t know about Waldenström’s. There are a lot of things that we know now that we didn’t know before, but there are a lot of questions that we can’t answer yet. Being honest with our limitations, paying attention, and focusing on what is important to the patient help build that trust, which is important in a relationship. We’re all going together through good and not-so-good moments in this long journey of Waldenström’s.
Being honest with our limitations, paying attention, and focusing on what is important to the patient help build that trust, which is important in a relationship.
Dr. Jonas Paludo
Peter: It’s good to see you’re both in agreement. You’re both following the proper path and I applaud both of you, especially for taking the time to share your experience with healthcare providers and patients.
Lisa mentioned that she first did a good bit of research through the IWMF website. I did that myself 20 years ago. I was a youngster back then and the services and support they provided meant so much to me that I started volunteering for the organization and I’ve been with them since then.
Waldenström’s is a rare disease, so you don’t encounter many people who have it, so finding an online community was of great benefit. Sharing stories with them, joining support groups, taking part in discussions, viewing webinars, and going to their annual educational forum are key components of becoming a more knowledgeable patient.
Before we had the technology, I would have my own chart that I would give to my doctor and say, “Here are my trends.” He would laugh at me, but he would look at it. We had a great relationship and that’s important to have. Be educated about your disease, know your options, what your preferred lifestyle, and what you want in quality of life, and pick a doctor who fits well.
Lisa: My therapist thinks Dr. Paludo is great.She’s convinced he took some classes in psychotherapy. She’s got great admiration for him. I’m also trained as a therapist and I would say Dr. Paludo has those skills, but please don’t leave the work you’re doing to be a therapist, although you’d be a great one.
Mayo Clinic is huge and yet after every visit, I would think, “How is it possible that each person on my care team was able to spend that much time with me?” I’ve never encountered that anywhere else. How is it that nurses remember me? People remember me. We had little inside jokes. Those things matter so much.
Our healthcare environment is changing. There’s limited time with patients. We’re speaking to healthcare institutions and I don’t know how providers get reimbursed and what expectations are in general.
Physicians want to have these kinds of relationships with their patients and perhaps there’s a larger pressure that prevents them from doing so. I hope that we can get back to that. Institutions like Mayo Clinic and physicians like Dr. Paludo give me the hope that it’s possible to have those kinds of relationships with patients in the current healthcare environment somehow.
Dr. Paludo: I don’t think I can say it better. It’s important to keep in mind what the priority is, which is the patient and what matters to that patient. Always keeping that in mind is the goal at the end of the day.
Conclusion
Peter: I enjoyed this discussion. It’s always good to meet with a fellow WMer and a noted, world-renowned Waldenström’s clinician and researcher. I’m very grateful for both of you for sharing your time. I hope others find this information very useful and beneficial as much as I did. Thank you both and thanks to The Patient Story.
Tiffany: Thank you, Pete, Lisa, and Dr. Paludo for an engaging discussion. It is so crucial to be empowered so that you and your caregivers can make informed decisions about your care.
Follicular Lymphoma: Latest Advances in Precision Medicine and Emerging Therapies
Dr. Peter Martin, a leading lymphoma expert at Weill Cornell Medicine, Laurie Adami, a follicular lymphoma patient and advocate, and Tiffany Drummond, cancer advocate and clinical researcher, discuss the latest advancements in follicular lymphoma treatment. This conversation talks about precision medicine and emerging therapies, addressing how to manage side effects and improve quality of life, and is designed to empower patients with practical knowledge and support as they navigate their diagnosis.
Understand current and emerging options, including targeted therapies and bispecific antibodies, and how they address treatment challenges. Gain actionable strategies to manage side effects and improve quality of life. Explore how precision medicine tailors treatment plans to individual needs, including chemo-free options. Get answers to common and critical questions about follicular lymphoma. Be part of a conversation that brings the patient experience front and center to inspire hope and informed decision-making.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
Tiffany Drummond: I’m a patient advocate with over 20 years of experience in cancer research. My journey as a care partner began when my mother was diagnosed with endometrial cancer in 2014. I quickly realized the challenges of finding resources, support, and shared experiences, and now I am committed to helping others avoid similar difficulties, no matter the condition.
At The Patient Story, we create programs to help you figure out what comes next. Think of us as your go-to guide for navigating not only the cancer journey but your overall health journey. From diagnosis to treatment, we have you covered with real-life patient stories and educational programs with subject matter experts and inspirational patient advocates and guests. I genuinely am your personal cheerleader, here to help you and your loved ones best communicate with your healthcare team as you go from diagnosis through treatment and survivorship.
The Patient Story retains full editorial control over all content as always. We also thank all of our promotional partners for their support. It is because of you our programming reaches the audience who needs it. I hope you’ll find this program helpful, but please keep in mind that the information provided is not a substitute for medical advice.
I had access to great cancer centers. I went to four different big cancer centers and that’s where I was able to join clinical trials.
Tiffany: I have the pleasure of interviewing Dr. Peter Martin and it so happens that we have much more in common than you might think. I will also be speaking with a follicular lymphoma patient, Laurie Adami. It’s so important to get a patient’s perspective and I’m sure her experience will resonate with you and your loved ones. Let’s learn about Laurie’s journey before deep diving into the latest treatment options.
Laurie Adami: I was diagnosed in 2006. My son was in kindergarten. There was one treatment I did right away. We thought I was in remission, so I merrily went back to work, which entailed traveling internationally. Three months later, my cancer was back on the first follow-up scan. That prompted 12 years of treatment. From 2006 to 2018, I was in continuous treatment and underwent seven different lines of therapy, including three clinical trials.
The first six treatments didn’t work, but thankfully, the seventh line of treatment did. I live in Los Angeles, so I had access to great cancer centers. I went to four different big cancer centers and that’s where I was able to join clinical trials.
Dr. Peter Martin, Hematologist-Oncologist
Tiffany: Dr. Peter Martin serves as the professor of medicine and chief of the lymphoma program at Weill Cornell Medicine. He is a hematologist-oncologist who specializes in caring for patients with lymphoma at NewYork-Presbyterian Hospital. His research focus, which is very dear to my heart, is on clinical investigation of new and promising therapies. Dr. Martin, how are you doing today?
Dr. Peter Martin: It’s great to see you again, Tiffany. I don’t know if everybody else knows this, but we worked together long ago.
Tiffany: You could say how long ago. It was about 15 years ago. I used to call him Peter, that’s how far we’ve come. I’m glad to see that we both have stayed the course, which is fighting cancer and finding a cure. I know that you made great strides, so thank you for being here.
[Follicular lymphoma] typically grows slowly over months, years, or decades, and that’s why we call it indolent, which means lazy.
Dr. Peter Martin
What is Follicular Lymphoma?
Tiffany: I’m a patient advocate for many types of cancer, but for those who aren’t as familiar, can you break down follicular lymphoma? We know that it’s considered an indolent lymphoma. Can you walk us through that characteristic? What makes follicular lymphoma distinct from more common types of non-Hodgkin lymphoma, such as DLBCL or diffuse large B-cell lymphoma?
Dr. Martin: Follicular lymphoma is pretty common from the lymphoma perspective but not common from a cancer perspective. In the United States, about 20,000 people every year will be diagnosed with follicular lymphoma. Depending on your perspective, there are up to 130 different kinds of lymphoma, which is hard to keep track of. Each subtype is a little bit different biologically in how they’re defined and how they behave clinically.
Follicular lymphoma is based on the way it looks under the microscope. They look like little follicles in the lymph node. It typically grows slowly over months, years, or decades, and that’s why we call it indolent, which means lazy. I like the word lazy because it’s a lymphoma that can’t be bothered to cause problems.
Once diagnosed, we’ll often talk about the goal of treatment, which is to help somebody live a life that’s as close to the life they would live without lymphoma. It hangs around for a long time and we keep managing it and kicking the can down the road.
How is Follicular Lymphoma Diagnosed?
Tiffany: If someone is living with follicular lymphoma for years or even decades, how is it diagnosed? Do they come in for some other type of symptom that usually makes them get referred to a specialist? How does that work for a patient who doesn’t even know that they have it?
Dr. Martin: It can vary a little bit. Ultimately, to diagnose follicular lymphoma, you have to look at it under the microscope. The word lymphoma means tumors of the lymph nodes, so most of the time when we meet somebody with follicular lymphoma, they’ll have an enlarged lymph node. Typically, it’s a painless, enlarged lymph node in the neck, armpit, or groin.
It might be picked up accidentally while getting tested for other reasons, which is pretty common because follicular lymphoma is often asymptomatic. Although it’s called lymphoma, sometimes it’s not in a lymph node. It might be present in the bone marrow or some other organ, like the gastrointestinal tract or the skin. Ultimately, though, somebody has to look at it under the microscope and that’s how we make the diagnosis.
All of my doctors dismissed me. I would specifically tell them, ‘I’m very worried I have lymphoma,’ and they would say, ‘Your bloodwork is all normal, so you don’t have cancer.’
Laurie Adami
Symptoms of Follicular Lymphoma
Tiffany: Laurie, did you experience any symptoms before your diagnosis or was it something you noticed but didn’t read into it enough to get it checked right away?
Laurie: When my son was three years old, I started to get frequent sinus infections and couldn’t get rid of them. I also developed a dry eye. I was a long-time contact lens wearer and suddenly, I couldn’t wear my right contact lens. I was very tired. I had a lymph node on my neck that was concerning me and I felt something in my abdomen.
All of my doctors dismissed me. I would specifically tell them, “I’m very worried I have lymphoma,” and they would say, “Your bloodwork is all normal, so you don’t have cancer.” I told my husband that they wouldn’t listen to me and he didn’t believe me, so I took him to my appointments and he couldn’t believe how I was dismissed. He was mortified. This went on for three years.
I wanted to believe these doctors. I wanted to believe that allergies were causing these sinus infections. I was also at the age where I could be starting to get perimenopausal symptoms, so my symptoms were attributed to my hormones. It was aggravating.
I kept feeling worse and worse. The exhaustion was incredible. One of the doctors I saw said, “Laurie, you’re president of a software company. You’re traveling internationally. You’re traveling a week a month. You’re running a household. You have a young boy. I’m exhausted just listening to what you do.”
Finally, someone I knew referred me to a diagnostician who took me seriously. I went in to see him and explained everything. I said, “People think this node is from allergies.” He said, “Did you get tested for allergies?” I said, “Yeah, and there was nothing.” He said, “Okay, that doesn’t make sense then.”
I explained the possibility of a hernia and he said, “It could be, but Laurie, we don’t guess. We have CT machines and I’m going to send you to a hernia specialist. We’re going to do imaging.” That week, they imaged me and it was scary because I was supposed to go in for a simple imaging. They expected to find a hernia and I wasn’t supposed to have contrast. Suddenly, this lady brought in the bottles of contrast because they had to get a better image. My heart began to sink as I was sitting there.
Two days later, on Good Friday of 2006, the doctor’s office called and said I needed to come in. My mother and brother were in town for the Easter weekend, but they didn’t tell me to bring anyone, so I went by myself and they told me I had either lymphoma or a mesenchymal tumor. The imaging also detected lesions on my lungs, so he said, “You may also have lung cancer.” That’s when I found out that I had some type of cancer.
I knew a little bit about lymphoma because when I had this node and I put in my symptoms online, lymphoma kept coming up. But 90% of lymphoma patients are diagnosed at stage 4 because most patients don’t have symptoms. I did, but I didn’t have anybody listening to me, so they dismissed my concerns.
As it turned out, it was good that they didn’t listen to me because the only treatment that existed at the time was a monoclonal antibody, multi-chemo, prednisone treatment. If I had it earlier, it wouldn’t have worked and I would have had nothing else.
I had autologous stem cell transplant as an option, but it was not a good option, especially if you relapse after the first line of chemo and monoclonal antibody treatment. In a way, it ended up being a blessing because, by the time they were pushing me to do the transplant, I managed to find a trial of a histone deacetylase (HDAC) inhibitor, which is what I did as my second line of therapy.
Dr. Martin: Oftentimes, somebody will say, “I’ve had this lump for five years and finally my friend told me that I should have it looked at.” That’s a testament to how it behaves. It hangs around for a long time, so people often get accustomed to it being there before they decide to bring it to somebody’s attention.
Traditional Treatments for Follicular Lymphoma
Tiffany: Before we get into the novel approaches, can you walk me through the traditional treatments for follicular lymphoma? What factors determine a more or less aggressive approach in your practice?
Dr. Martin: The job of a hematologist-oncologist is to learn as much as we can about the lymphoma and that’s changing all the time as we get more sophisticated. We recognize that this lymphoma isn’t happening in a petri dish in a lab somewhere; it’s happening in a real live person, so we have to learn as much as we can about that person. That includes not only their medical issues but also all of the things that are important to them. What are their values? What is their support network like? There are 8 billion of us on the planet and we’re all different, so there’s even more heterogeneity among people than there is amongst the 130 different lymphomas.
We bring all of that information together and come up with a plan that makes the most sense for that person. Treatments are constantly evolving and we have new treatments available today that we didn’t have in the past. In general, the goal of treatment is to try to give somebody the life that’s the closest to the life that they would have if they didn’t have lymphoma.
We have to learn as much as we can about that person. That includes not only their medical issues but also all of the things that are important to them.
Dr. Peter Martin
Approaches can vary. In some cases, you say, “Look, this is not causing you any problems. It’s not going to cause problems hopefully for a long time — on average, multiple years — and so we watch it and it sits there.” That can be a little bit counterintuitive. In the Western world, you want to catch and deal with cancers early. That’s certainly the case for breast cancer, lung cancer, or colon cancer, so the initial discussion around follicular lymphoma can be a little bit awkward sometimes. You say, “Oh, great. No problem. Let’s do nothing about it.” But it’s a proven strategy to help people live a good quality of life without dealing with any of the side effects of treatment.
On the other end of the extreme, we might propose using more aggressive therapies, including chemotherapy if we need to shrink something quickly and help them feel better. There are options in the middle where we use immunotherapies that may shrink the tumor, may help somebody to feel better, and may prolong the time between that and other kinds of therapies by months or years. There are vast options and more new treatments are being approved.
Bispecific Antibodies for Treatment of Relapsed/Refractory Follicular Lymphoma
Tiffany: Let’s talk about some of the data that came out of the 66th American Society of Hematology (ASH) annual meeting. Bispecific antibodies are changing the way that we look at and treat cancer, especially when it comes to immunotherapy. What benefit may they contribute to our relapsed/refractory follicular lymphoma patients?
Dr. Martin: Bispecific antibodies are a type of monoclonal antibodies. Antibodies are proteins that our immune system makes to fight against bacteria. A few decades ago, clever people figured out how to make antibodies that would fight not against infections but against cancer. That moved quickly from the lab to people and, for the past 25 years, has revolutionized the way many cancers are managed. It started with lymphoma. We’ve been leading the way for a long time.
Bispecific antibodies are a natural evolution of trying to come up with ways to make this kind of immunotherapy work better. They’re very cleverly engineered. They bind to tumor cells the same way an antibody would bind to a virus or bacteria, but in addition, they also bind to other parts of our immune system called T cells and they activate them. When those T cells are activated, they secrete chemicals called granzymes and perforins that poke holes in cancer cells and cause them to die. This is a clever way of using our immune system to kill cancer cells and it does it remarkably effectively.
The vast majority of people will have not only responses to this treatment, meaning the tumor shrinks, but in many, if not most, cases, the tumor will disappear on a CT scan. It might be completely gone — we’ll find out as the years go by — but it disappears on a CT scan in a lot of people.
Bispecific antibodies are attractive in that it’s a non-chemotherapy approach and it’s a proven form of immunotherapy. It’s an evolution of the kinds of immunotherapies that we’ve been using in the past and it’s more effective.
The other thing that’s nice about it is that it’s off the shelf, so you order it from a pharmacy. It doesn’t have to be engineered specifically for each patient the way something called chimeric antigen receptor T cells or CAR T-cells have to be.
I did a monthly infusion of a third line monoclonal antibody… but as soon as I stopped, it came back, so it was a race against time.
Laurie Adami
Experience with CAR T-cell Therapy
Tiffany: Laurie, I believe you’re familiar with CAR T-cell therapy. How was that experience and where are you currently in your cancer journey? Are you also familiar with bispecific antibodies? I would love to get your perspective on this immunotherapy versus CAR T-cell therapy.
Laurie: I heard about CAR T-cell therapy six years before I could get it. I heard about it in 2012 when I attended an LLS event where they showed Emily Whitehead’s film. I went to my college that week and asked about it because I didn’t know about CAR T-cell therapy. He said, “They’re not trying it for follicular lymphoma. They’re doing it for more aggressive tumors. We have to wait. You’re on a PI3 kinase inhibitor. We’re going to ride this horse.” That took me through 2016 when the cancer finally outsmarted that pill.
A new monoclonal antibody had been approved. It was a nine-month course, so I did a monthly infusion of a third-line monoclonal antibody, obinutuzumab. It immediately started shrinking my tumors again, but as soon as I stopped, it came back, so it was a race against time.
In 2018, my tumors were huge. While I was out hiking in April, my oncologist called and said, “We finally got the trial for follicular lymphoma. It’s going to open at UCLA. We’re going to have five patients enrolled in the first cohort and you will be patient number one.”
When you’re in a clinical trial, you have to review the paperwork to sign. It discloses all the side effects of patients in the phase 1 study. This was a phase 2 study, so it wasn’t completely bleeding edge. Then they have to do biopsies and imaging. They had to make sure I didn’t have anything in my brain. They weren’t allowing patients with central nervous system involvement to get CAR T-cell therapy because they didn’t know how it would work and what it would do. Now they know, so they do it for people with involvement in the central nervous system.
It was amazing because, within days, the tumors were shrinking.
Laurie Adami
I had a sinus infection again because my cancer was coming back. My oncologist said, “You can’t get CAR T-cell therapy with an active infection,” so I went to my ear, nose, and throat specialist. I explained, “I need to get this treatment, but I can’t do it with an active infection.” He called his scheduler and said, “Clear the schedule tomorrow. I have an urgent patient.” They operated on me the following day and it ended up being a major surgery with general anesthesia because there were so many blockages everywhere. He cleaned me out and got rid of the sinus infection so I was good to go.
About a month before you get your cells back, they do apheresis. They harvest your T cells. It’s a very easy process that takes half a day outpatient. The courier ships your bag to the CAR T company, which happens to be down the highway in LA. I remember the courier came to pick it up in the apheresis center and I said, “Do not let my cells fall out on the freeway. Please make sure the van door is tightly sealed.” He said, “Don’t worry. We’ll get it there, Laurie. No problem.”
CAR T-cell therapy is about an 18-day process. They shaved off a couple of days and shortened it even more, so the patient didn’t have to wait that long. They take your cells, put the target on them, and grow them in the lab. They harvested about a million cells from me and after they became CAR T cells, there were a billion cells that would get infused.
Before you get your CAR T cells, you go through lymphodepleting chemotherapy, which is chemo light compared to the 18 cycles that I had. It makes room in your bloodstream for you to get your CAR T cells back and gives them room to expand. After three days of lymphodepleting, you get the cells back on day zero, your CAR T birthday. It was amazing because, within days, the tumors were shrinking.
FDA-Approved Bispecific Antibodies for Follicular Lymphoma
Tiffany: Are bispecific antibodies available to patients outside of a clinical trial? Is there anything we can use now straight from a pharmacy without having to go to our investigational one?
Dr. Martin: Two bispecific antibodies are approved for follicular lymphoma: mosunetuzumab and epcoritamab. There probably will be a third one very soon called odronextamab. They’re all pretty similar in terms of how they work and the proteins they target on the surface of the B cells.
There are more coming that we will continue to see in lymphoma and across all cancers. They’re all administered in the clinic or the hospital, so these are not pills that you take at home the way a lot of cancer therapy has transitioned. They’re administered either through an intravenous injection or a subcutaneous injection.
Why are Bispecific Antibodies Administered in the Clinic or Hospital?
Tiffany: Is there a reason for that? Is it because we want to watch for any side effects immediately or is it because of the toxicity and potency of the drug itself?
Dr. Martin: A little bit of both. These are big proteins. They have to be administered by needle because they have to bypass the gastrointestinal tract.
There are some side effects. The side effects that somebody might experience during the infusion are minimal. That said, somewhere in the range of hours to even a couple of days after the treatment, there can be cytokine release syndrome, which happens in up to a third of patients getting these antibodies.
Cytokine release syndrome sounds complicated, but… it’s very manageable.
Dr. Peter Martin
Cytokine release syndrome sounds complicated, but it’s what I described. T cells secrete these chemicals, the same chemicals you experience when you have an infection, including fever, feeling rundown, muscle aches, and what you feel when you have the flu. But in some cases, it can be a little bit more severe. Not very common, but it can happen. We’re often able to manage it with acetaminophen. Sometimes we have to use steroids, like dexamethasone, and rarely do we even have to use other medications.
Because of that, there’s very careful preparation at the facility level, the physician and nursing level, and the patient and caregiver level. It’s all about preparation, helping people to know what to recognize and what to do if something like that happens. It’s very manageable, but it’s a little bit more complicated than taking a pill.
Side Effects of Bispecific Antibodies
Tiffany: Patients are concerned about side effects in general and we know when it comes to cancer, a lot of these drugs are toxic, even though we’ve drastically reduced that over time. In your experience, how do bispecific antibodies differ from traditional chemotherapy and CAR T-cell therapy in terms of side effects? Are they more severe, less severe, or not as long? And does the impact on quality of life determine which avenue they want to take for their treatment?
Dr. Martin: It’s not such a straightforward question to answer because everybody’s different and everybody’s situation is different. Where better-tolerated treatments might be appropriate for one person, more aggressive treatments with more side effects might be appropriate for another person. In most cases, we have options among all of these and oftentimes, there are no wrong or right answers. We try to pick one, but in some cases, we’re driven to say this is the right answer. It’s the job of the whole team — the patient, the caregiver, the physician — to try to pick the right treatment.
Where better-tolerated treatments might be appropriate for one person, more aggressive treatments with more side effects might be appropriate for another.
Dr. Peter Martin
Bispecific antibodies are straightforward in that they can be administered in an outpatient setting or at least partly in an outpatient setting. They don’t cause a lot of the side effects of traditional chemotherapy, like hair loss and nausea, which aren’t major issues with a lot of chemotherapy that we use, but we’re understandably scared of them. Hair loss is a particularly interesting one in that it’s a signal to the rest of the world about something you’re undergoing privately. It tells them publicly that something’s going on, so I understand why that’s not attractive.
Personal Experience with Side Effects
Tiffany: It’s important to get a patient’s perspective regarding side effects. Laurie, can you give us an overview of your experience with side effects? Were there any that you found particularly taxing on you or that affected your quality of life? Were you able to manage your symptoms relatively well?
Laurie: It was a mixed bag. With the first chemo, I lost my hair and got mouth sores. With the second treatment, which was a targeted therapy, I was very, very fatigued. I also lost my hair. They told me that it wasn’t from the trial drug, but when I dug into it, I saw a very small percentage of patients lost their hair.
White counts typically would get depleted, which made me prone to getting infection… so I was a real early adapter of mask-wearing.
Laurie Adami
My fourth treatment was radioimmunotherapy and I had very, very low counts for a long time. My platelets dropped. I never had to get an infusion of platelets, but I had to go in every day to get it checked. I had to be very careful not to fall because I had no clotting ability with low platelets.
White counts typically would get depleted, which made me prone to infections, so I had to be careful. When I went back to work after my first chemo treatment in 2006 and had to start traveling again, I asked my oncologist, “Is it okay if I travel to New York, Boston, London, etc.?” She said, “Yes, but you have to wear a mask,” so I was a real early adapter of mask-wearing.
Precision Medicine as an Approach to Follicular Lymphoma
Tiffany: Something that was also talked about at ASH (American Society of Hematology annual meeting) in general is the idea of precision medicine and how it’s a relatively new approach to cancer treatment. Is precision medicine being used as an approach to follicular lymphoma? What are your thoughts on precision medicine?
Dr. Martin: It depends how much of a fan of science fiction you are. To some degree, we’ve always practiced precision medicine. What do I know about this lymphoma? What do I know about this person? What do I know about all of the different treatment options? How do I put it all together?
Over time, treatments are becoming more specific in some ways, so you can apply them under certain circumstances. Our ability to understand more about cancer changes with new technologies. We’ve always been trying to personalize medicine in the sense of sequencing the entire genome of a cancer cell and saying this is the right treatment for you according to lab testing, but we’re not there yet for follicular lymphoma.
Over time, treatments are becoming more specific in some ways, so you can apply them under certain circumstances.
Dr. Peter Martin
There’s one treatment, a pill called tazemetostat, which has modest activity but is generally well-tolerated. It’s an inhibitor of an enzyme called EZH2, which is mutated in about 20% of people with follicular lymphoma. It’s approved for the treatment of people with mutated EZH2 enzyme, but it’s also approved for people with wild-type unmutated EZH2 if they don’t have other treatment options. Realistically, it works reasonably well in both groups, so it’s a precision medicine approach, but you don’t necessarily have to have the mutation to use it. That’s the closest we have right now, but this is coming. It will continue to change and there are other examples where we’ll see more of that.
Long-Term Implications of Chemo-Free Treatments for Follicular Lymphoma
Tiffany: I know you can’t read the future, but what do you think the long-term implications may be for follicular lymphoma, specifically for chemo-free treatments? What I hear a lot is that I’m living with cancer, not that I have cancer. What do you see with that in terms of chemo-free treatments?
Dr. Martin: People with lymphoma want treatments that work and are well-tolerated. Whether you call them chemotherapy, immunotherapy, or something else, if it works and is well-tolerated, that’s already great. They also want options that conform to where they are in life.
Different treatments that work in different ways have the advantage of potentially allowing us to mitigate some of the short-term and long-term issues that can come up.
Dr. Peter Martin
Every year, we have more and more options available to us. We always try to pick the right treatment for that moment, thinking about the here and now. We also try to think about how what we do today impacts what the patient’s life is going to be like 10 to 20 years from now.
More than chemotherapy, these new treatments potentially have a lesser impact on the body in the longer-term setting. With multiple lines of chemotherapy back to back, people will get through them for decades without major issues but over time, it catches up. Different treatments that work differently have the advantage of potentially allowing us to mitigate some of the short-term and long-term issues that can come up. Having more options is always better.
Clinical Research and Follicular Lymphoma
Tiffany: Both of our backgrounds are heavy in research. I like to talk about clinical research anytime I do a program to get the point out there because oftentimes, people think that a clinical trial is one of their last resorts, they’re not at least getting a standard treatment, or they’re not getting treated at all for their cancer. I know that at Weill Cornell Medicine, you have a robust research program. What does your research program look like and how receptive are your patients to joining clinical trials?
Dr. Martin: I appreciate your disclosure that we both come from a research background, so people should take that into account knowing that we have those biases. The number one barrier to entrance into clinical trials is not patient refusal. It’s because they don’t know that there’s an opportunity. The real burden is having physicians let patients know that this is something that they could do, not patients saying that it’s something they don’t want to do. It’s us. We’re probably the bigger part of the problem.
There are different reasons why somebody might want to participate or not want to participate in clinical trials. They offer new opportunities to access new treatments that might be more effective or better tolerated. In some cases, that might be when other treatments have been exhausted, but in a lot of cases, it might be when a new opportunity has already been well-studied in another setting and you’re looking to apply it in a new setting. There are also some downsides to research, a little bit more of a hassle often.
Tiffany: I’m a proponent of decentralization. Patients can get labs locally without having to track things like that. I’m a little biased when it comes to clinical research, but I do think it has so many benefits, so I’m always promoting it.
Dr. Martin: It can’t be understated that historically, there have been a lot of questionable research practices that were not always in the interest of participants. The medical community on the whole has tried to grapple with this. We’ve got multiple committees, like hospital and patient advisory committees, which try to minimize that and make research as ethical as possible.
There are going to be some people who are distrustful, which is their prerogative. I’m never the person who’s going to twist somebody’s arm to participate in a study that they’re not comfortable with, but I’m also not going to shy away from proposing a study because I’m afraid that somebody is not going to go for it. That’s not respectful to their autonomy either. You propose every option that exists and talk about the pros and cons then people will decide what’s right for them.
Tiffany: Absolutely. I always say too that we don’t give patients enough credit. We always talk about patient education. They need to know that clinical trials are out there and they’ll be more than willing to make that informed decision themselves.
Fertility preservation is also a highly charged issue, but it’s like research: if you don’t talk about it, people don’t have the opportunity to consider it.
Dr. Peter Martin
Fertility Preservation and Follicular Lymphoma
Tiffany: Something that is less talked about in general when it comes to cancer is fertility preservation. An abstract I saw at ASH talked about fertility. For younger patients with follicular lymphoma, does that discussion come up? From what I saw from the abstract, a lot of patients don’t bring it up. They don’t want to discuss it. What has your experience been in terms of having a fertility discussion with your follicular lymphoma patients?
Dr. Martin: Fertility preservation is also a highly charged issue, but it’s like research: if you don’t talk about it, people don’t have the opportunity to consider it. It’s important from the physician’s perspective to ask people about where they are and what they’re thinking about, but it’s also something that patients should advocate for themselves if it’s something they’re thinking about.
In general, follicular lymphoma happens as we get older, but a significant number of people get follicular lymphomas while they are younger and some of those may be considering having children in the future. We’ll get away from the reasons why somebody might choose to have or not have children in the setting of cancer; that’s a whole other complicated discussion.
It needs to be discussed early so that we can think about all of the treatment implications now and longer term, and how we sequence things.
Dr. Peter Martin
Many big hospitals, including Weill Cornell Medicine and NewYork-Presbyterian, have fertility teams that help people consider all of their possible options and how to preserve fertility. Fortunately, even the chemotherapy regimens that we typically use in follicular lymphoma don’t have a major impact on fertility and a lot of the newer treatments have no impact on fertility. The caveat is that you don’t necessarily want to be treating the lymphoma when somebody’s pregnant, although that becomes necessary in many cases and, depending on the treatments used, it often turns out to not be a problem either. It needs to be discussed early so that we can think about all of the treatment implications now and longer term, and how we sequence things.
Tiffany: Thank you for saying that. That’s a conversation you want to have whether you are considering children or not. If you’re younger and considering children, advocate for yourself. If your physician doesn’t bring it up, don’t be afraid to bring it up.
Bridging the Gap Between Academic Research Centers and Community Hospitals
Tiffany: In my experience talking to patients, they don’t get their diagnosis until after they see their primary care physician or go to the emergency room for something different. Because you’re from a large research center, you have multidisciplinary teams, which many people don’t have. They could be going to their community clinic. Patients may not know to go to an academic research center because they haven’t been referred to a specialist. Do you work with any community clinicians or community hospitals? What are your thoughts on working with community doctors to bridge the gap?
Dr. Martin: Even in New York where we have multiple academic medical centers, the majority of people with cancer are managed outside of those academic medical centers, so that’s a reality that we have to acknowledge. I also work in Brooklyn a couple of days a month. People must have access to medical care in their community.
We have to bring better medical care to the communities that people live in rather than vice versa.
Dr. Peter Martin
It took me a few years to come to this conclusion, which is embarrassingly slow, but it’s probably not fair to expect people and their caregivers to travel a couple of hours to see somebody when they have access to medical care in their community. We have to bring better medical care to the communities that people live in rather than vice versa. There are a lot of excellent oncologists practicing in communities and that’s where the majority of people can and probably should receive their care.
One caveat I’ll say is that all of cancer is becoming increasingly complicated, so I don’t think that people should feel uncomfortable seeking a second opinion. I have friends who work in community medicine throughout the whole tristate area in New York and I work with them and help them to manage their patients. Telemedicine has made that easier as well.
This is where patient advocacy comes in. You have to advocate for yourself and speak up about it. If your physician is uncomfortable with that, that might be a sign that they’re thinking about more than your best interests. You’ll find that almost all academic oncologists will encourage second opinions. I certainly do that and help arrange them when I can.
It comes down to a balance. What do you get out of it, what do you have to give to get that benefit, and is it worth it?
Dr. Peter Martin
Key Takeaways from ASH
Tiffany: The ASH annual meeting is a big conference. Was there anything for you that stood out?
Dr. Martin: Bispecific antibodies are going to be a major part of treatment for follicular lymphoma. Exactly how they fit in, which line of therapy, and which combinations get used is interesting to think about. They’re not going anywhere for a while, so that’s pretty cool.
Another interesting study that came out was a late-breaking abstract looking at tafasitamab combined with lenalidomide and rituximab. This was a randomized controlled trial that showed that the addition of tafasitamab to lenalidomide and rituximab improved time to progression. Effectively, it doubled it compared to lenalidomide and rituximab, which is probably one of the more common second or third-line treatments for follicular lymphoma, so that’s a pretty significant benefit.
In some ways, it’s a no-brainer to say that’s something we should do. On the other hand, tafasitamab is a little bit of a hassle. People have to come into the clinic frequently for it, so it’ll be interesting to see where this plays out everywhere. I don’t necessarily know how I’m going to use that information. Again, it comes down to a balance. What do you get out of it, what do you have to give to get that benefit, and is it worth it? But it’s a strikingly positive trial.
Tiffany: I’m going to be following that trial as well.
Conclusion
Tiffany: Thank you so much for this engaging and insightful conversation. I always learn something on the other end of these educational programs.
Dr. Martin, thank you for taking the time to speak with us at The Patient Story. It was so good to catch up with an old colleague and know that we both have remained dedicated to improving cancer care and finding a cure. I’m optimistic about the future as long as we have physicians and researchers around like Dr. Martin.
Laurie, thank you for sharing your story. Lived experiences are very personal and I’m forever grateful to patients who are open and transparent because I believe that it helps the next person and the next patient.
It’s so important to be empowered so that you and your caregivers can make informed decisions about your care. That includes being educated about the latest treatment options for your cancer.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
Symptoms: Intermittent feeling of pressure above clavicle, appearance of lumps on the neck, mild wheeze when breathing and seated in a certain position Treatments: Surgery, chemotherapy
Building Bonds Episode 1: Patient-Doctor Partnerships for Better Waldenström Care
The relationship between a patient and their doctor can make all the difference. A strong partnership leads to more informed decisions, personalized care, and a greater sense of control. Dr. Shayna Sarosiek, an expert in Waldenström macroglobulinemia, and patient advocate Jason Euzukonis discuss what makes their patient-doctor teamwork truly effective.
Learn how to build trust and open communication with your healthcare team. Understand the role of shared decision-making in Waldenström treatment. Hear first-hand experiences of navigating chronic cancer with your doctor by your side. Discover practical tips for advocating for yourself or a loved one in the treatment process. Explore how teamwork fosters a supportive environment for long-term care.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Tiffany Drummond: I have worked in cancer research for 20 years, but more importantly, I became a care partner and advocate when my mom was diagnosed with endometrial cancer in 2014. Her journey led me on a quest to find out as much information as I could to help with her care. Quite honestly, it wasn’t easy to find and that’s why we at The Patient Story put on programs to help people navigate life after diagnosis.
This program is hosted by The Patient Story, a multi-platform organization that aims to help people navigate life before and after diagnosis in human terms through in-depth patient stories and educational discussions, focused on how patients and care partners can best communicate with their doctors as they go from diagnosis through treatment in Waldenström’s.
We want to thank The Leukemia & Lymphoma Society for its partnership. The LLS offers incredible free resources, like their Information Specialists who can help you communicate with members of your healthcare team and provide information about treatment options.
The Patient Story retains full editorial control over all content. While we hope this is helpful, please keep in mind that this program is not a substitute for medical advice.
Jason Euzukonis: My name is Jason. I recently turned 50 years old. I’m married and have two children who are 13 and 10. I live on the North Shore of Massachusetts. I’m an avid runner and a sales rep in the athletic footwear industry, and I was diagnosed with Waldenström’s macroglobulinemia in June 2018.
Dr. Shayna Sarosiek, Hematologist-Oncologist
Stephanie Chuang: Dr. Shayna Sarosiek is someone whom we’ve had the pleasure of collaborating with before and have heard so many great things about. Dr. Sarosiek, can you tell us about who you are, what you do, and what drew you to this specialty?
Stephanie: We hear about shared treatment decision-making, being an empowered patient, or self-advocacy, and sometimes that concept can get a little bit lost in the mix. There’s a lot of conversation without specific examples. Our goal is to showcase not the only kind of communication and the relationship that can happen between a physician and a patient but also to showcase what a great relationship looks like.
Jason and Dr. Sarosiek have a great relationship and a lot of that is centered on communication and long-term relationship building. Having said that, Jason, what were the signs that something wasn’t right and who was the first physician you went to see?
Jason: I’m a runner and I know my body well. In the spring of 2018, I noticed signs that something wasn’t right. I can go for a run and feel tired but still slog through a few miles, but I started feeling some fatigue that felt off. Three or four minutes into the run, I would feel like my body was shutting down. It felt like blood and oxygen weren’t getting to my muscles.
After I learned my diagnosis, it turned out that’s exactly what was happening. It led me down the path of trying to figure out what was going on. I went to my primary care physician then to a hematologist then to a general lymphoma specialist. I went through multiple steps before I ended up at Dana-Farber with a team that specialized in my subtype of non-Hodgkin’s lymphoma.
Primary care physicians are not cancer specialists.
Stephanie Chuang
Stephanie: I want to dive into some of this because I think different parts of your story will resonate with different people. As we know, primary care physicians are not cancer specialists. Yours ordered blood work and saw something was wrong, but your self-advocacy started pretty quickly. Can you describe that?
Jason: The primary care physician was able to identify that something wasn’t right. I was very anemic and they had me come in within a day or two to make sure blood counts weren’t crashing in case there was some internal bleeding, in which case I would have needed to go to the emergency room. Things seemed stable, even though my blood counts were low, and that’s when they kicked me over to the hematologist.
I started doing more research and realized that I needed someone who knew the disease.
Jason Euzukonis
As I look back, there’s certainly a role for hematologists, but even then, especially for my situation with a rare type of non-Hodgkin’s lymphoma, you want to go to another level. That’s when I started doing more research and realized that I needed someone who knew the disease.
There were some things that the hematologist said that jumped out at me. When they were talking about treatment, they said, “We treat all these tough types of non-Hodgkin’s lymphoma the same way with chemotherapy.” I thought that didn’t sound right. I was fortunate that I knew someone who worked in a lab at another medical center in Boston and that’s when we started taking a deeper dive and getting the true diagnosis of Waldenström’s macroglobulinemia.
This is why I think it’s important for a patient to continue doing research. They were great over there, but during that time, if you search Waldenström’s macroglobulinemia, it’s not going to be too hard to find The Bing Center at Dana-Farber.
When I realized that there was a team there that truly specialized in my cancer, that’s when the real journey began of getting over to that team. I felt like the more I could work with doctors who truly know this disease inside and out, the better my chances of living a normal lifespan.
Doing Research & Asking Questions
Stephanie: Jason, you mentioned in a previous conversation that you love research. I was a professional journalist and a research geek myself. When I became a patient, I felt very self-conscious about being labeled as a problematic patient, which I defined as asking too many questions. Did you have to get over any hump like that, even though that’s your nature to ask questions, to want to know? Do you have guidance for those who have less of an affinity for asking questions or wanting to take up that space?
Jason: I didn’t have a problem getting over that. My life was on the line. I’m naturally curious anyway and when I get on top of certain topics, I like to take a deep dive and learn as much as I can, but I don’t have a problem asking questions.
That said, I know there are patients for whom that can be challenging. We’ve had to deal with that in our own family where an older relative got a difficult diagnosis. Their generation tends to be a little bit shyer about questioning the doctor, but I think good doctors have no problem with patients asking questions and probably prefer that.
Get your family or friends involved because there’s likely someone who will take the bull by the horns. Let them know the situation because there likely is somebody who will be more familiar with what to do and what questions to ask.
I’m naturally curious anyway and when I get on top of certain topics, I like to take a deep dive and learn as much as I can
Jason Euzukonis
Patient Demographics
Stephanie: Dr. Sarosiek, can you describe how many years you’ve been focused on Waldenström’s and how many patients you see on average?
Dr. Sarosiek: I’ve been focusing on Waldenström’s for about four years now since I came over to Dana-Farber. It varies a little bit, but I see about 30 to 40 patients a week and the vast majority of them have Waldenström. A few of those patients might be patients with a precursor to Waldenström called MGUS (monoclonal gammopathy of undetermined significance) or related disorders.
Navigating Your Way to a Specialist
Stephanie: You’re seeing 30 to 40 patients a week, the majority of them have Waldenström’s, some of them with MGUS. Whereas in the community, hematologist-oncologists are seeing everybody across the board, so they may only see one or two Waldenström’s patients a year.
Similar to Jason’s trajectory, most people are probably going to see a community provider and then end up with someone like yourself. Dr. Sarosiek, what is your guidance to people on how to get to a specialist and the importance of that?
Dr. Sarosiek: Because of what I do, it’s important to get to a specialist in whatever way you can. If you’re able to and have the means to see a specialist, that’s the best because you can have one-on-one dedicated time.
There are other ways of getting a specialist’s opinion. If you’re unable to travel, Dana-Farber offers grand rounds where you can send in your records and physicians can review them.
I give patients as much time as I can to dig deep into their disease knowing that it’s not possible in the community to specialize in Waldenström’s.
Dr. Shayna Sarosiek
Some employers have second opinion programs and it’s a good idea for patients to look into that. The employer provides the ability to give your records and a physician can give a second opinion. Those physicians are typically at large academic centers that specialize in the disease. You can also access some opinions of physicians as well through some support groups. It wouldn’t be exactly for your case, but it might be a way for the patient to inform themselves and learn a little bit.
But if possible, seeing a specialist is a good idea. Having practiced for a few years before I came to Dana-Farber, I saw a handful of Waldenström’s patients a year. I never could have known all the literature that there was to know about Waldenström’s then or any other particular disease. If you’re able to see a specialist, they might be able to better tailor your care around all of the literature on that one disease.
The other part that I try to do with my patients—and hopefully I’m okay at it—is to recognize that when patients come to see me, typically they’re seeing their local doctors who are excellent physicians but don’t know all the details. I give patients as much time as I can to dig deep into their disease knowing that it’s not possible in the community to specialize in Waldenström’s.
Decentralized Care
Stephanie: Many people hear, “Go see a specialist,” but logistically speaking, that might seem daunting for some people, especially if this is something that they’re going to have to be minding for a long while. How does that work? Do they have to travel every single time? Do you have relationships where patients see you as the specialist, but they’re getting their blood draws and some of the routine care closer to home?
Dr. Sarosiek: We have a lot of cases where patients do what works best for them. Patients who live nearby can travel to see us. We have an ongoing relationship with routine care and routine blood work at our center. But a lot of our patients can’t travel, so they have a local oncologist who we’re willing to work closely with and they can have their routine follow-up there.
Patients will see us once a year and then for the rest of the year, we remain available to them for questions or concerns. Sometimes we might do an initial consult and then tell the patient if something comes up in the future, now that we have a little bit of their background, their local oncologist can reach out to us with questions or concerns or they can come back if and when they have to make a big treatment decision. We can tailor it to what works best for the patients in terms of their ability to visit our center.
Stephanie: That’s wonderful. It sounds like you are as flexible as you possibly can to meet the different situations that patients and care partners have.
My gut was telling me that there should be more discussion between the patient and the doctor.
Jason Euzukonis
Your Doctors, Your Decision
Stephanie: Jason, the first place you were at, you were there for a year before you went to Dana-Farber and saw Dr. Sarosiek. Could you describe what the difference was between where you were before and Dr. Sarosiek?
Jason: With the doctor I was seeing before, there wasn’t as much back and forth in terms of decision-making. It was here’s what we’re going to do and that’s that. I felt like I didn’t know if that was the right approach. My gut was telling me that there should be more discussion between the patient and the doctor.
By the time I got to Dana-Farber, which was about a year after my diagnosis, I couldn’t believe the difference. At my first appointment, I worked briefly with another doctor before Dr. Sarosiek and that doctor was phenomenal. I remember him sitting back and saying, “What questions do you have?” He took more time than any other doctor I’d ever met with before and that seems to be the case with the whole team at Dana-Farber.
That’s something important for all patients to remember. If you feel like you’re getting rushed, if you feel like there’s not a good discussion with your doctor, then you might want to see if there are other options. It was just such a big difference not just between Dana-Farber and that one hospital, but also almost with any other doctor I’ve met with before.
How the Right Care Impacts Mental Health
Stephanie: Mental health is a huge part of every diagnosis, but because this is long-term, it’s a huge part of the consideration. Can you describe the daily impact and what shifted for you after you moved to Dana-Farber?
Jason: In that first year after my diagnosis, I had a massive amount of anxiety. I woke up every morning and I could feel it in my chest. I had to spend a good solid half hour in quiet meditation every day. Fortunately, I’m an early riser, so I’m up before the family and I get that moment of quiet.
Meditation was huge for me. Whether people believe that works or not, the point is to find things to help you get through your day. At the end of the day, we have to get used to living a long time with this cancer and at some point, once you start to feel better, you’ve got to get back to your routine in terms of work and, in my case, raising a young family.
A cancer diagnosis can feel very lonely and being around others who are going through something similar is helpful.
Jason Euzukonis
I felt like I lost control of my health, so I was trying to do whatever I could to reclaim that control. I changed the way I eat. I was able to get back to exercise. It doesn’t have to be an intense form of exercise. It’s simply moving, like going for a walk or gardening. It’s helpful that those were the things that I did.
Support groups are a critical component in moving forward with your mental health. There are a lot of people who have been through some difficult journeys in those groups. You can learn a lot. If you’re dealing with something, there’s a good chance that somebody else in that support group has been dealing with the same thing at some point. Another great way to help with your mental health is to talk to others who are on the same journey. A cancer diagnosis can feel very lonely and being around others who are going through something similar is helpful.
Stephanie: Absolutely. I know you lead a couple of support groups for the IWMF, so thank you for highlighting that.
It’s a journey for patients as they get used to living with this disease and restructuring their lives around the disease. I have to change a little bit of who I am for the patients depending on where they are in that journey.
Dr. Shayna Sarosiek
Approaches to Care from a Doctor’s Perspective
Stephanie: Dr. Sarosiek, hearing Jason’s journey to you, how often do you see patients who are in a very similar space where they’ve been told what to do? What are you noticing from the patients you’re seeing and how do you approach them when you first meet them?
Dr. Sarosiek: Patients will see me and say, “What would you do for my treatment? This is what I was told I have to do.” Luckily with Waldenström’s, we often have quite a few options. I lay out the options and some patients don’t know that they have other options and that’s an important part of seeing a specialist.
The longer I’ve been in Waldenström’s, the more I learn that a lot of patients face something similar to Jason. I can’t speak to this personally, but patients come to see me initially around the time of diagnosis and it’s an everyday, day-in, day-out thing where they’re thinking about the disease and worrying about the future.
It’s a journey for patients as they get used to living with this disease and restructuring their lives around the disease. I have to change a little bit of who I am for the patients depending on where they are in that journey. Initially, patients will have a lot of questions and a lot of anxieties. I even tell them that this is a time when you ask questions because relieving your anxiety or getting questions answered is important right now.
At one point, they’re going to learn to live with this and feel more relaxed, and it’s not going to be the only thing on the front of your mind all the time. I try to adjust to patients as they work their way through because it’s life-changing, but it also changes during the time that they’re living with the disease as well.
Approach with Different Kinds of Patients
Stephanie: You see different kinds of people with different personalities and preferences. I know that there’s so much more depth to this, but could you generalize the different kinds of patients and care partners who walk through the door? Jason is very research-oriented and has no problem asking questions. How about the other kinds of people who are not the same? What’s your guidance to them on how to approach a Waldenström’s diagnosis?
Dr. Sarosiek: That’s something that I try to feel out during an appointment. Who am I meeting with and what works best for them? Many of our patients who come to Dana-Farber for a second opinion tend to ask more questions and want more information. But as I talk to the patients in the first few minutes, some patients are overwhelmed by a lot of information, especially in the beginning. I try to tailor what I’m saying or what I’m offering in that first appointment in terms of information.
Then you might have someone who wants to learn more after they get over the initial shock or anxiety about the diagnosis. Sometimes after I give them the options, patients want more guidance from me rather than leaving the decision up to them. There are a lot of different people and a lot of different personalities and I try to feel that out, so hopefully I can best serve the patient in a way that would make them most comfortable with their disease.
Stephanie: Are there top questions you recommend that patients should ask their doctor after a Waldenström’s diagnosis that would be pretty key in helping them understand the disease and how the care is going to follow?
Dr. Sarosiek: A lot of patients want to confirm if they have the right diagnosis. Most of the time, they do but occasionally, that’s not the case. Part of what we do in that initial visit is walking through to confirm that a patient has Waldenström’s. No one wants to hear that they have cancer, but sometimes that helps patients to understand that this is the cancer that they have and they can move forward without having doubts.
It’s important to ask what treatment options are available. They should ask, “Are there other things that I could consider as my options? Are there alternatives?” Most cancers do; not all of them, but most have multiple options for treatment.
Knowing the key markers to watch closely empowers the patient to know what’s going on with their disease.
Dr. Shayna Sarosiek
Patients should ask about the differences in the treatments and that depends on the patient’s goals. What are the differences in side effects? How long am I going to be on treatment? The patient can help tailor their treatment to what their goals are in life.
Another key question is, “What do I need to look at going forward? What are the most important markers?” With Waldenström’s, we watch their IgM level and we watch for anemia. That’s another key thing that often helps patients to feel a sense of control if they know exactly when they should be following up and what they should be looking for. We always check labs and a hundred values will come up on any patient portal for any visit, but knowing the key markers to watch closely empowers the patient to know what’s going on with their disease.
You have a certain amount of time with a doctor and it’s a matter of being more upfront and telling them if you’re not comfortable with where things are at with the relationship.
Jason Euzukonis
Taking Back Control of Your Care
Stephanie: I’ve heard control come up a couple of times and that resonates with me as well, the sense of how to regain control. Like you said Dr. Sarosiek, some people are clearly overwhelmed and you recognize that they may not be able to or want to hear and digest a ton of information, so you tailor the conversation to them. What is your recommendation on anything else that can help them in the beginning? Jason, when you had some problems feeling heard or feeling like an actual participant and partner in the conversation, what is your recommendation?
Jason: In retrospect, with the doctor who I saw before I got to Dana-Farber, I probably should have been more upfront and said, “I’d like you to hear me out a little bit more. Are you okay with me asking more questions?” Because I think a lot of people have a hard time getting past that hurdle. I wish I would’ve been more upfront because for all I know, maybe they were more open to a back-and-forth.
The challenge that the doctor ran into was that particular center was overwhelmed. The healthcare system was very taxed. It was one patient after another and it felt like they didn’t have the time. I don’t think that was the fault of the doctor. But at the end of the day, it’s your life. You have a certain amount of time with a doctor and it’s a matter of being more upfront and telling them if you’re not comfortable with where things are at with the relationship.
Ask your physician, ‘What’s the best way for me to ask questions?’… You need to have a comfortable way to reach out to your provider and be able to ask those questions.
Dr. Shayna Sarosiek
Stephanie: Thank you for pointing that out. It’s true. The systems are quite inundated, unfortunately, and time is the biggest resource that is unavailable. Dr. Sarosiek, do you have anything to add?
Dr. Sarosiek: As a physician, I agree that there are a lot of time constraints in terms of seeing patients and other responsibilities. You could ask your physician, “What’s the best way for me to ask questions?” Maybe there isn’t enough time in that initial appointment or they have a full schedule.
They may say, “You can reach out to me through the patient portal or talk to my nurse who’s an excellent resource.” Some patients email and if they’re comfortable with that, that’s another avenue. You have to see with your physician the best way that they feel comfortable and a way that you feel comfortable communicating. If you can’t get all of that done in a clinic appointment, then is there another way? Because that’s a key part of the relationship.
As a physician, I feel like it’s important to be available if questions come up, particularly in the beginning when there are a lot of anxieties or questions surrounding a diagnosis. Even as time goes on, there can be things that pop up and the patient wants to know if it’s something they should worry about. You need to have a comfortable way to reach out to your provider and be able to ask those questions.
Navigating Conversations Between the Patient and the Physician
Stephanie: Dr. Sarosiek,you see so many Waldenström’s patients, family members, care partners, and caregivers. What’s your message to healthcare providers who don’t see so many Waldenström’s patients and who may not understand how to navigate the conversation? What are your top tips for them on how to navigate these conversations in the beginning?
Dr. Sarosiek: I don’t know exactly the secret to this, but I do think that as a physician, it’s important to know that we don’t know everything. I know a lot about Waldenstrom’s, but still, I don’t know everything and I certainly don’t know a lot about things outside of Waldenstrom’s. It’s important for us all to realize that we have limitations and to be open to hearing from other people.
Physicians who don’t have the expertise shouldn’t hesitate to reach out to specialists at larger academic centers and feel free to ask questions.
Dr. Shayna Sarosiek
We try to be available to other providers who might not have expertise. I usually tell my patients to tell their local doctor that I’m more than happy to answer questions and be available. Physicians who don’t have the expertise shouldn’t hesitate to reach out to specialists at larger academic centers and feel free to ask questions. People email us a lot and even if I don’t know who they are or I haven’t personally interacted with them before, we’re happy to answer questions. The goal for all of us is to provide the best care.
As a physician, it’s important to be open to learning. I do it all the time. I see patients who have other clinical questions or needs that I don’t know about, and I reach out to specialists in different fields to try to answer those questions. We all have to be open to learning and open to asking other people questions when we don’t know the answers.
Understanding Waldenström’s Treatment Options
Stephanie: It’s a rapidly shifting landscape of treatment options in lymphomas, non-Hodgkin lymphoma, including Waldenström’s, and there’s a lot of discussion we’re hoping can happen in the clinic between the physician and the patient. Jason, before you met Dr. Sarosiek, where was your mind in terms of wanting to understand treatment options and what was that first conversation like with the other physician?
Jason: That was a very difficult and very different time. I didn’t know even remotely as much as I know now, so I was still very much in the mindset of doing whatever the doctor said. As I got deeper into the journey, that’s when I realized that there were other options, but I initially pretty much did what the doctor said.
My treatment options are a tad more limited than the average Waldenström’s patient. Chemotherapy wasn’t a great option for me. In retrospect, the good news is that the previous hospital did put me on the right path, so I’m grateful for that. I didn’t know about the other options anyway and I likely would’ve started with the same option. As time went on, I got more informed and realized the right questions to ask, but I didn’t know them back then.
Stephanie: Dr. Sarosiek, how do you define what Waldenström’s is at the first meeting? What is top of mind for you as you try to lay out treatment options?
Dr. Sarosiek: I draw out the bone marrow and how the IgM comes out of the bone marrow. I usually try to explain it and do a little bit of a drawing because some people are more visual while other people like to hear it. I give a little background about Waldenström’s and ask what questions they have and what they want to know.
Usually, at a first appointment, patients have something that’s at the forefront of their mind or they have a list of questions. If I’m spewing out information about other things that they don’t care about before I answer the question that’s most burning, it’s not helpful. I often ask them what questions they have and that guides the conversation.
Ultimately, we often end up covering the same things at every new appointment that I have with a patient with Waldenström’s, but we might get to it in a different order or a different way, depending on what’s most important for them.
Stephanie: It sounds like during the initial meetings, you’re meeting people where they are. At what point do you lay out the treatment options? Whenever that happens, how do you lay out the options in a way that people will understand and the impact on quality of life?
Dr. Sarosiek: There’s a small percentage of patients that need treatment immediately. For those patients, in the first conversation, we go through the diagnosis and then we jump right into treatment options.
Stephanie: What’s that profile? Why do they need treatment? How do you explain to them why they need treatment faster than other patients with Waldenström’s?
Dr. Sarosiek: A lot of our patients present similar to what Jason described. They have pretty significant anemia, their disease was brought to their attention, and they have symptoms that need to be addressed right away. In the case of Waldenström’s, the reason most patients need treatment is because of anemia. They presented to their doctor to work up the symptoms of their anemia.
Another percentage of patients will have hyperviscosity or thickened blood and that’s causing symptoms related to their Waldenström’s. In those cases, patients typically need treatment right away, so we jump into treatment discussions.
Some patients come to us because their disease was incidentally diagnosed. They had a routine blood test for their annual checkup with their primary doctor and they were noted to have high protein or very mild anemia that’s not causing any symptoms. In those cases, we have the opportunity to discuss treatment later on. We often don’t get to treatment discussion on the first visit; that comes up months or even years later.
Stephanie: For the majority of patients, when you do talk about treatment decisions, how do you lay these out for them?
Dr. Sarosiek: I usually walk through the options. Often with Waldenström’s, we’ll have two or three different options. I typically write those out and give the big-picture details. Is this a treatment you stay on for years or is it a limited-time therapy? What are the main side effects that patients can experience? What are the biggest risks that we worry about with each of those treatments?
Next, I try to figure out what might be most important to the patient. Are they someone who doesn’t want to be on a pill every day? Are they someone who would hate to take a pill because they would miss it all the time? That information helps me to guide the patient on which treatment option might be better for them.
Stephanie: Can we go into specifics of the major courses of treatment that you would offer? You mentioned the continuous and time-limited therapies. What patient profile would you consider for one versus the other?
Dr. Sarosiek: For Waldenström’s, one of the main treatments that we talk about is chemoimmunotherapy, which is chemotherapy and immunotherapy together. It’s an IV therapy and it’s time-limited, usually four to six months. Some patients prefer to have a very time-limited therapy. There are risks associated with that, particularly infections. There’s a small risk of damage to the healthy cells in the bone marrow, so that’s an important conversation to bring up with patients
On the other end of the spectrum is another treatment option, which is oral therapy. Patients take pills every day and it’s continuous as long as your disease is responding, which is often for years. It’s a little bit easier because you’re not getting aggressive therapy upfront with all of the treatment at once. It’s low-level therapy all the time. There are risks associated with that as well. For example, a small risk of heart side effects, but in a patient with severe heart disease, I might stray away from using that as a first option.
Then there are some options in between, like targeted therapies that are injections and we use those in a small percentage of people. Luckily, Waldenström’s has a lot of different options.
Stephanie: What are some of the most common questions you get from patients? Are there some that rise to the top when you’re introducing these treatment options?
Dr. Sarosiek: An important question is: how will I be able to live my life during these treatments? Many of our patients are still working, have families to raise, and have other things that are important to them, so they ask, “What will my day-to-day life look like?”
Another important question is, “How will this treatment look to people around me? Will I lose my hair? Will I be constantly sick?” That’s a huge part of how patients can deal with and move forward with their disease. The biggest thing is what their lives will look like on the treatment.
The next important question that patients ask is, “How long is this treatment going to work for? What’s going to happen with my disease if I start this treatment? Am I going to need more treatment again in a year or two?”
They also ask, “What’s the worst thing that could happen to me from this treatment? What are the scariest risks associated with the treatment?”
Dr. Sarosiek and I did have to decide on treatment when I was starting to experience some side effects… That’s when Dr. Sarosiek led into the conversation about shared decision-making.
Jason Euzukonis
Stephanie: Jason, your first line of therapy was a BTK inhibitor. You had some rituximab infusions earlier on, but you were on the daily pill. What was that like for you? What were the considerations for you before you met with the Dana-Farber team?
Jason: At the time I was diagnosed, there weren’t quite as many options as there are now, so I’m a lot more at ease knowing that there are a lot of good options on the table for me when the time comes. I was already responding well to a BTK inhibitor. By the time I got to Dana-Farber, there wasn’t a need to change it, I guess.
Probably the more relevant question from someone in my shoes is: had chemotherapy been an option, which way would you go? That’s a common question with pros and cons, as Dr.Sarosiek mentioned for both approaches. Had both been an option for me, I likely still would’ve chosen the same path of the BTK inhibitor.
As a younger patient, there are some things to think about in terms of the long-term potential side effects of chemotherapy versus targeted therapy. I’m in pretty good health overall, younger, and don’t have heart issues, so I wasn’t all that concerned about any potential side effects surrounding my heart.
Dr. Sarosiek and I did have to decide on treatment when I was starting to experience some side effects; nothing overly threatening but more annoying. I approached her and asked, “What do you think about cutting the dose?” That’s when Dr. Sarosiek led into the conversation about shared decision-making and presented this newer version of the targeted therapy. I guess it’s the best example of the decision-making with Dr. Sarosiek that put me on the right path.
Stephanie: What I appreciate about this is you had clearly done enough research where you even knew to ask about lowering the dosage. What got you to that point? What were your considerations about staying on something that had been working versus shifting completely?
Jason: At the end of the day, part of it is a certain amount of trust in your doctor. I have my feelings on things, but I quite literally would trust Dr. Sarosiek with my life. But at the same time, this is where hopefully people do their homework and read up on what’s latest and greatest.
I had already read up a bit on the newer targeted therapy that Dr. Sarosiek presented and when she mentioned that, I was also fortunate that it had recently been approved. I was already aware of it and knew that the side effect profile was better on it, so I was very comfortable when she brought up moving to that.
Knowing the side effects I was dealing with, there was a good chance a lot of it was related to what I was on. With the newer version of that, based on the data, those side effects were improved. It’s a combination of doing your research, trusting your doctor, and asking them what they think.
Addressing Side Effects
Stephanie: Dr. Sarosiek, how many times are you seeing people who are nervous to even talk about the side effects and how do you address that? We’ve heard from other people who are hesitant to bring up side effects because they’re worried their doctor’s going to take them off of their treatment because they want to preserve as many options as possible.
Dr. Sarosiek: A lot of patients are comfortable discussing their side effects; that’s my experience, at least. They’re comfortable saying what it is that’s going on without having to worry that we’re going to adjust their treatments or change their outcomes because we stopped therapy or changed therapy. I would say most patients are comfortable saying if they have a side effect.
Although maybe I have some patients who are scared to tell me that they have side effects, on the other hand, I do have some patients who don’t want to know about potential side effects from treatment. A lot of patients want to know what they can expect so that if it happens, they’re aware and not worried. But once in a while, I’ll tell a patient this side effect might happen, but they don’t want to know because either they’re then going to worry it’s going to happen or they feel like they might manifest that for themselves if they know about it.
We can still have a conversation about if it’s a side effect they can live with or if we need to change their treatment because of it.
Dr. Shayna Sarosiek
Again, it’s trying to feel out what the patients are comfortable with hearing in terms of side effects. I hope I make patients comfortable to know that they can tell me about their side effects without me immediately making a treatment decision for them based on the reported side effects. We can still have a conversation about if it’s a side effect they can live with or if we need to change their treatment because of it.
Stephanie: Jason, what were the main key side effects that you were experiencing that brought this discussion up for you?
Jason: Mouth sores were probably the biggest one. I had a lot of mouth sores. They were brutal. I was starting to experience some joint pain. Sometimes it’s tricky to determine if I’m experiencing side effects from the treatment or if I’m getting a little older. But I was getting the sense that it was a sudden increase in joint pain.
The blood pressure was a little higher than I would’ve liked. The platelet count wasn’t dangerously low, but it was a little on the low side. From what I had been reading on the newer version, it seemed like a lot of those side effects had been improved, so I was pretty comfortable. I was responding well; it was just annoying side effects.
Stephanie: Dr. Sarosiek, how do you navigate the conversations? People have different preferences and there is that mental hurdle of not wanting to make too much of a deal about side effects.
Dr. Sarosiek: When patients have side effects, then I try to feel out if there is anything that they would like to do about them. If someone has mild, loose stool once every few weeks, they might say, “Oh, forget it. It doesn’t bother me. I’m telling you about it so that you know.”
My next approach is to try to find some supportive care measurement that we might be able to do. I have a lot of patients on the treatments we use for Waldenström’s who have loose stool or diarrhea and typically, adding fiber to their diet, like a fiber supplement once a day, is quite helpful. It treats it and they can continue on the same dose.
For a lot of the side effects, I ask if it bothers them, and if it does, we try some supportive measures. If the supportive measure doesn’t help, then it is a conversation about whether or not we want to decrease or change the dose. In that case, I try to bring up any data that we have in that setting to reassure patients that if we decrease the dose, the patients will still have very good outcomes. Often, we have data to help guide us if we should reduce the dose or not. We think about that, but usually, we try other supportive things first so that we can try to stick to the regimen that’s proven in the literature.
As Dr. Sarosiek knows, I typically will ask, ‘Hey, what are you seeing? What’s the latest and greatest? Any thoughts about the future?’ That’s been my approach.
Jason Euzukonis
Patient-Physician Relationships
Stephanie: This is a long-term relationship that’s happening. What are the other points where major discussion tends to happen? I imagine it’s talking about active surveillance or watch and wait, as well as at any point that treatment may need to come up. Is that the case? How do you both approach this as an ongoing relationship that’s different than other cancers?
I think about it because I get reminded twice a day when I take my pill. I try to stay up to date on what’s latest and greatest. Ultimately, the day will come when Dr. Sarosiek and I will have to figure out what the next best step is. The good news is there are a lot of good options, so that lessens my anxiety knowing that there’ll be a lot of good options on the table for me when the time comes.
Jason: I’m on treatment, but while I could potentially get many more years out of this treatment, the reality is at some point, I’ll start to slowly lose the response. From a mental standpoint, I’m pretty good at being able to compartmentalize. I’m fortunate enough that I can move through my day without it weighing on me.
We meet every three to four months. I’ll go in for blood work, which is helpful for me because we can get a pretty good idea of not just the disease itself but also my overall health to avoid any pitfalls there as well. As Dr. Sarosiek knows, I typically will ask, “Hey, what are you seeing? What’s the latest and greatest? Any thoughts about the future?” That’s been my approach.
If we’ve known them for months or years and they show up one day and seem a little bit different than they have been at every other visit, then something’s off with their disease and we should look into it.
Dr. Shayna Sarosiek
Dr. Sarosiek: From my perspective, part of what drew me to oncology and which I love about Waldenström’s is we have this luxury in most cases to get to know the patients and be able to sit down and talk about them outside of their diagnosis. That’s what I love about what I do. It’s great because I get to know the patients and that’s how I know how they are doing.
If I know a patient is a runner, loves to spend their time golfing, or loves to spend their time with their grandkids, then they come in and say, “I cut back on my running,” or “I’m not hanging out with my grandkids,” I don’t necessarily have to ask, “What are exactly your symptoms?” I know them well enough to realize that if they’re not doing what they love to do or what they’re usually doing, something has changed.
Part of active surveillance, watch and wait, or monitoring someone on treatment is getting to know them and being able to tell if they’re not able to do the same things that they were doing. If we’ve known them for months or years and they show up one day and seem a little bit different than they have been at every other visit, then something’s off with their disease and we should look into it. What I love about oncology and what I do now is getting to spend time with my patients and getting to know who they are.
Dr. Sarosiek wants to learn more about her patients and who they are beyond the diagnosis so that she can treat them as a whole person and not just the disease specifically, allowing her to understand how different options might impact them and their quality of life.
Stephanie Chuang
Jason: I’m confident that there aren’t many doctors in the world who know this disease and the science around this disease as well as Dr. Sarosiek, but she also knows me well and that’s critical in the doctor-patient relationship.
Stephanie: I love that you’re both highlighting that this is a long-term relationship that’s very different than other cancers. We talk a lot about survivorship in other spaces, but this is an ongoing conversation. You know that Dr. Sarosiek knows her stuff and she’s at the top of her game. You talked about the anxiety and mental load that you had to work through daily.
The difference is Dr. Sarosiek wants to learn more about her patients and who they are beyond the diagnosis so that she can treat them as a whole person and not just the disease specifically, allowing her to understand how different options might impact them and their quality of life. That’s such an amazing thing that’s happening and I do hope that patients, care partners, and physicians will take that away.
Is there anything else you want to mention that is important in the context of having patients and physicians be partners? Are there misconceptions? Are there any other things that people are missing that you think would benefit them?
Dr. Sarosiek: It’s important to find a physician who is open to learning and is willing to work with you within your space. We’re all different people, as we all know. We are born into families that have different personalities and we learn to work together. Sometimes, we find friends along the way who are more like family because they’re people you relate to. You want to find a physician like that who can meet you in your space.
Sometimes, you have different personality issues and maybe you want to find a different doctor who can work with you in a way that would make you most comfortable with your disease. It’s worth getting second opinions or meeting other physicians and finding someone that you feel can be your partner through the journey. I know I fail in some ways, but I try my best to be a partner with my patients and hopefully, patients can find someone who can do that with them.
Jason: Take care of your health, both physically and mentally. Join support groups. If you have Waldenstrom’s, go to the IWMF.com. Ask your doctor lots of questions. Don’t be afraid to seek multiple opinions. Find a doctor who you’re comfortable with and who knows this disease inside and out, if possible, or at least ask your doctor to be in touch with the doctor who knows this disease inside and out.
Waldenström’s Clinical Trials
Stephanie: Dr. Sarosiek, do you ever talk about clinical trials with your patients? It’s a huge topic and very important in a space where there’s so much development. What is your mindset in terms of the research? How and when do you bring them up to patients?
Dr. Sarosiek: I’m a huge advocate for clinical trials and in general, especially in academic institutions, we tend to use clinical trials a lot to be able to offer novel therapies to patients. As Jason mentioned, he’ll come in and ask about novel therapies, so often it comes up in conversation with patients when they ask what’s new and we’ll talk about clinical trials.
If there is a trial available that a patient would qualify for, I always bring it up as a potential option. Some patients can’t participate because of logistics and not being close to a center with clinical trials, but I will always bring it up because I think it’s the best way that we can move the field forward. If a patient is eligible for a trial, it will certainly come up in conversation with me.
There are so many options that doctors are trying to figure out the right order of treatments, which one is more effective and safer than the other, and the only way we can get the answers to those questions is by patients taking part in clinical trials.
Jason Euzukonis
Jason: I’m still responding well, so I’m not there yet. But as Dr. Sarosiek mentioned, I do make it known that I’m very much open to a clinical trial if and when the time comes.
The good news is that there are so many new options now and they’re making advances every day. The challenge is there are so many options that doctors are trying to figure out the right order of treatments, which one is more effective and safer than the other, and the only way we can get the answers to those questions is by patients taking part in clinical trials.
A lot of people think that with clinical trials, they’re guinea pigs, but no. There are a lot of great options and the doctors are looking to get answers.
Stephanie: From the patient’s perspective, what would be your major considerations on whether you would want to go on a particular trial?
Jason: I’d be very interested in a clinical trial that combines agents that aren’t chemotherapy and will eventually be able to give me a break from treatment. There’s a lot of progress being made on that front. I know that’s a priority for a lot of the centers and doctors out there.
At the end of the day, it’s a drug… Each one of us is different, so I don’t know how it’s going to impact me long-term
Jason Euzukonis
Stephanie: That makes perfect sense, for sure. But if we could dive in, can you share more about what it is that’s coming up for you? Chemotherapy sounds like it’s the side effects and quality of life. With time off treatment, who doesn’t want a break? Can you describe why that’s so important for you and what’s driven you to that point?
Jason: With the targeted therapy that I’m on now, there doesn’t seem to be a lot of risk long-term, but it’s still relatively new and we don’t know that. I also know that these treatments aren’t cheap and pretty taxing on the healthcare system to remain on these things, so I know that’s a consideration.
At the end of the day, it’s a drug. There are no free rides when it comes to these medicines. Each one of us is different, so I don’t know how it’s going to impact me long-term if I stay on this for 10, 15, or 20 years. I likely won’t be on it for 20 years, don’t get me wrong. But as we say in the Waldenström’s community, if you know one Waldenström’s patient, you know one Waldenström’s patient. That can be applied to a lot of different cancers, but the bottom line is I don’t know the long-term ramifications of continuous therapy, so it would be nice to not be on a drug for a period of time.
Stephanie: Dr. Sarosiek, is there anything else that you think would be helpful for patients to understand both in terms of guidance for them and questions that they can ask that might be helpful?
Dr. Sarosiek: Some concerns that patients bring up when they hear clinical trials include: Are you testing something that you don’t know anything about? Am I going to get a placebo so I won’t be getting any treatment for my cancer? Does this mean that this is the last option for me, that I’m going to be dying with this cancer soon?”
It’s important for patients to know that that’s not the case. Often, we have many trials for patients who have never been treated before and this is going to be their first treatment in decades of life that they’ll live with Waldenström’s. It’s important for patients to know that clinical trials are a way to get novel therapies.
While clinical trials may not be right for everybody, it’s great to have the conversation so people can choose what is right for them.
Stephanie Chuang
Currently, we have a clinical trial that uses two oral therapies that we know independently work very well in Waldenström’s and we use them as the standard of care. But the trial is trying those two together so that you can use them for a limited amount of time and get a better response. It’s a way to get novel therapies or advanced therapies that otherwise wouldn’t be available as a standard of care.
Stephanie: Sometimes you hear people say, “Tomorrow’s treatment today.” While clinical trials may not be right for everybody, it’s great to have the conversation so people can choose what is right for them.
Conclusion
Stephanie: Thank you, Dr. Sarosiek and Jason, for joining this conversation. You highlighted a lot of the nuances that come up in the conversations between the physicians and the patients. You’re a great example of how partnership can work well here, so thank you both so much.
Tiffany: Thank you, Jason, Dr. Sarosiek, and Stephanie for such a great discussion. It’s so important to be empowered and to lean into communication so that you and your caregivers can make informed decisions about your care.
The Latest Treatment Options for Relapsed/Refractory Follicular Lymphoma
Edited by: Katrina Villareal
Discover the latest in treatment options for relapsed/refractory follicular lymphoma from leading experts to help you or your loved one navigate this journey with confidence and hope. Dr. Joshua Brody from The Mount Sinai Hospital and Dr. Celeste Bello from the Moffitt Cancer Center discuss bispecific antibodies and CAR T-cell therapy, including their benefits and side effects.
Understand the role of watchful waiting and active surveillance. Gain valuable advice from lymphoma specialists on navigating treatment options and clinical trials. Discover the importance of support groups and resources for patients.
Stephanie Chuang: I’m the founder of The Patient Storyand a blood cancer survivor myself. I went through hundreds of hours of chemotherapy for my diffuse large B-cell lymphoma diagnosis. During that time, I realized how lonely it was and how hard it could be to get good information, and that was the genesis of The Patient Story.
Our goal is to help patients and care partners navigate life after a diagnosis and what it means in human terms. We do this primarily through in-depth patient stories and educational programs. This is especially important in spaces like follicular lymphoma. Patients and loved ones are being told by doctors that it’s highly treatable but not curable, so it’s great to know the latest therapy options and clinical research. We stand behind this message of self-advocacy, especially after diagnosis.
The Patient Story retains full editorial control of all content.
We’re bringing this to you in collaboration with Blood Cancer United, which has raised and invested over $1.5 billion in blood cancer research and provides free educational resources and support. Their information specialists provide one-on-one support on questions from treatment to social and financial challenges.
While we hope that you will walk away with more knowledge, we want to stress that this is not a substitute for your medical advice.
Our discussion focuses on the latest treatment options for relapsed/refractory follicular lymphoma. My co-moderator Dylan Lepak, another non-Hodgkin lymphoma survivor who became a patient advocate, will help lead the discussion.
Dylan Lepak, Patient Advocate
Dylan Lepak: I’m a diffuse large B-cell lymphoma survivor like Stephanie. I was diagnosed in 2021. I went to the hospital with stomach pain and came out with a horrible diagnosis, but luckily, I had a very standard treatment approach. I went through six cycles of R-CHOP and since then, I’ve been good. Since that time, I’ve done a ton of different charity work and moderated online discussion boards.
Dr. Bello, when you first see a patient with lymphoma, what message do you want them to take away after that first meeting?
Dr. Celeste Bello: I try to convey to them that they can relax and take a deep breath. In most cases, we can manage this quite well. Most of the meeting is trying to get everybody’s anxiety down a bit.
Dr. Josh Brody, Hematologist-Oncologist
Stephanie: Another amazing doctor and leader in this space is Dr. Josh Brody, a hematologist-oncologist, director of the Lymphoma Immunotherapy Program at Tisch Cancer Institute at Mount Sinai in New York, and faculty member of the Icahn Genomics Institute. Since 2011, he has developed The Brody Lab, a translational cancer immunotherapy lab that investigates the development of novel therapies, particularly for lymphomas, and specializes in how to use immunotherapy against treatment-resistant lymphoma.
Dr. Brody, I know that you’re very invested in patients beyond the clinic. When you see patients and family members in your office, what do you hope they walk away with from that first meeting?
Dr. Josh Brody: Aggressive lymphomas are a sprint and we need to get things going right away, but follicular lymphoma is a marathon. If you see someone starting a marathon by sprinting, they’re not doing it correctly. We don’t want to overwhelm people with information the first time we meet them. We give them the big picture that hopefully this is going to go very well.
There are a lot of great medicines for front-line therapy and second-line therapy. Some patients might need Plan C, Plan D, and Plan E, so how you develop Plan A and Plan B might impact those. Even though there’s no emergency for the vast majority of follicular lymphoma patients, Plan A and Plan B might affect Plan C, so you want to plan out the marathon thoughtfully and as best you can.
We have to be flexible because we’re going to have to change the plan depending on how things go. There are unique options available at some places that may not be available to others. We might want to do the smartest plan A so that we don’t burn bridges down the road.
What is Follicular Lymphoma?
Stephanie: Dr. Bello, could you summarize the nature of follicular lymphoma?
Dr. Bello: Follicular lymphoma is an interesting disease that’s broken down into different subtypes. We have low-grade indolent ones, which are slow-growing, and one subtype that’s a little more aggressive than the others. Most of the time, when we’re talking about follicular lymphoma, we’re talking about the low-grade, slow-growing one.
A lot of times, they’re picked up by accident on another diagnostic test, like a mammogram, which is a common one I see. Somebody had a screening mammogram and there’s no evidence of breast cancer, but there’s an enlarged lymph node in the underarm or axillary area.
Some can behave aggressively, so we have to keep an eye on these people and treat them differently, but as a whole, it’s a long-term disease that’s managed like a chronic illness. We try to keep it under control and if there’s a flare, we can manage that in most cases. It’s a cancer of lymphocytes, but one that sometimes doesn’t even need treatment.
Most Common Symptoms of Follicular Lymphoma
Dylan: Dr. Brody,if patients do have symptoms, what symptoms do you usually see with follicular lymphoma?
Dr. Brody: My grandma died at the age of 101. She didn’t have follicular lymphoma, but she had the next cousin over that we treated in a very similar way as other low-grade B-cell non-Hodgkin’s lymphomas. We did watchful waiting for 37 years and never needed any therapy.
Most people are asymptomatic, but some people can have symptoms. The most common symptom of follicular lymphoma is a painless lymph node. The B symptoms, which are fevers, night sweats, and weight loss of more than 10% of your body weight, are pretty rare for follicular lymphoma and happen in less than 10% of patients.
Terminology: Watchful Waiting vs. Active Surveillance
Stephanie: Some people don’t like “watch and wait” as a term. It can be tough for so many people to be told they’ve got cancer but they don’t need to be treated right away. How do you describe that period to your patients? What term do you use? How often are people told that they’re on watchful waiting or active surveillance? What is the plan that accompanies that?
Dr. Brody: I grew up saying watchful waiting. Dr. Mike Schuster, a lymphoma doctor at Stony Brook, told me he patented the phrase “active surveillance.” I’m not sure if he patented the phrase, but it sounds a lot better. We’re going to actively surveil you as opposed to watchful waiting, which sounds like we’re going to sit around and do nothing. It’s all about branding.
The reality is we’re going to keep a close eye on you and how close depends on what’s been going on with them, how well you’ve known the patient, and for how long. This concept is super freaky to patients and their families when they first hear it. Some patients don’t get surveilled for that long, but every patient who is still on active surveillance a year later loves the concept. But on day zero, “Wait, what? Why aren’t you treating me? Cancer and no treatment sound super freaky.”
I come in with my grandma’s story, so they can hear that sometimes this can go for decades without needing therapy. The only test that tells you if you’re going to go down the same course is the test of time. There’s no test as good as that, but we’re going to watch you closely as we give you that test.
Dr. Bello: I usually use observation or keep an eye. Some people say that’s what they wanted to hear. Others say they’re getting a second and third opinion. They can’t take it and I feel for them. You have people whose lymphoma was picked up incidentally and you tell them, “We’re just going to watch you.”
Since these are picked up by accident, I always wonder if it would’ve been better if we picked this up 20 years later. Are we doing a disservice that we diagnosed this little lymph node under their arm? Should we have left it alone to begin with? They were living life peacefully and blissfully, and now they’re going to have 20 years of anxiety instead. The anxiety can sometimes be the hardest part of the diagnosis.
Standard Treatment for the First Two Lines of Therapy
Dylan: We’re going to dive into the treatment options, but before we go into the novel treatments, can you give us a breakdown of the standard treatment for the first two lines?
Dr. Bello: The standard is there’s no standard. That’s always the first problem, but it’s a good problem because we have a lot of different options. You like to base it on the patient you’re treating and your goal with treatment.
Some people may have one large lymph node that’s causing them discomfort, so radiation to that spot may be the best option. Some people may have generalized symptoms, like severe fatigue that’s interfering with some of their daily activities, but don’t have a lot of disease. In that case, you may want to give them a less intensive treatment, like a monoclonal antibody like rituximab, put the disease into remission, and see if it corrects their symptoms.
Other people are very symptomatic. They come to you with rapidly growing lymph nodes and have fluid build-up in certain body cavities like in the abdomen. You want to treat them with something that’s going to work quite quickly and that’s usually a chemotherapy plus immunotherapy regimen.
There are a few options available. One of the more popular ones is bendamustine plus rituximab or bendamustine plus obinutuzumab, which is another monoclonal antibody. There are also milder or non-chemo approaches, like oral therapy with lenalidomide and rituximab. The treatment has to be geared toward the patient you’re treating, fitness level, and treatment goal.
What are Bispecific Antibodies?
Dylan: Dr. Brody, what are bispecific antibodies? How are they different than CAR T-cell therapy? What’s their mechanism of action?
Dr. Brody: Dr. Bello mentioned that one of our go-to therapies over the last 24 years is monoclonal antibodies, anti-CD20 antibodies, especially rituximab and obinutuzumab. Rituximab is certainly the most famous. It’s an anti-lymphoma antibody. CD20 is one protein marker on the surface of lymphoma cells. CD3 is a marker on T cells. Bispecific antibodies are two of those antibodies.
In Lady and the Tramp, when the puppies were sucking from the dish at the same time and ended up accidentally sucking on the same noodle, it brought the two of them together. Now instead of that, it’s the kiss of death where the lymphoma cell and the immune cell are brought together by the bispecific antibody and it activates the immune cell at the same moment so the T cell kills the lymphoma cell. I think it was Dr. Matthew Lunning at Nebraska who made up the Lady and the Tramp reference.
T cells are incredibly good at killing lymphoma cells, better than probably any other cancer. It’s the same idea as CAR T-cell therapy. The main difference is that we have to take the T cells out of the person, ship them somewhere, get the CAR T cell made, and have it shipped back. A bispecific antibody is in some ways an off-the-shelf version of that, so you can use it today.
They’ve been incredibly effective at melting away lymphoma cells, even when other therapies like chemotherapy, lenalidomide, and a few others have not been working, especially when rituximab has not been working. Still, these bispecific antibodies have been awesomely effective in inducing remissions in the great majority of follicular lymphoma patients. It’s been an absolute revolution. That is not an overstatement because we didn’t have anything nearly as effective and safe as this until bispecific antibodies came along.
Approved Bispecific Antibodies for Follicular Lymphoma
Stephanie: We have two FDA-approved options in follicular lymphoma so far. Dr. Bello, for what kinds of patients would you recommend bispecific antibodies? Is there anything practice-shifting for you?
Dr. Bello: For follicular lymphoma, we have mosunetuzumab and epcoritamab. Thankfully, the majority of these lymphomas are pretty indolent and respond very well to front-line treatment, whatever you use. You can use chemoimmunotherapy, like bendamustine and rituximab or obinutuzumab, both of which are monoclonal antibodies. We have the luxury of having a lot of patients who don’t end up needing to get a bispecific antibody.
But for patients who progress, we have these immunotherapies: bispecific antibodies and CAR T-cell therapy. I use bispecific antibodies in people who have progressed after two lines or more of treatment. I always try the other lines first, unless we have a clinical trial because they’re proven and have a great track record. I don’t skip straight to a bispecific.
Bispecific antibodies have some side effects that are very unique to them and may not be the best for everybody. They also require a little bit more skill in monitoring them. They are administered in the hospital at the beginning and in the office for the subsequent doses.
Stephanie: Dr. Brody, what about you? How do you approach bispecific antibodies and how do you decide to use one over the other?
Dr. Brody: We’re very lucky to have two FDA-approved options. Their roles are evolving very rapidly and will be evolving very rapidly over the next few years. I would expect that five years from now, bispecific antibodies will be an option for front-line therapy. They may be given as a monotherapy, but honestly, I don’t think that’s their future. I think the future is like rituximab, which is to become part of combination therapy.
Dr. Bello was doing some comparison between CAR T-cell therapy and bispecific antibodies, and I agree very much with what she was saying. But in the future, it may be an irrelevant comparison because it won’t be what’s better between CAR T-cell therapy or bispecific antibodies. It’ll be an apple and orange comparison. Who cares what’s better?
In the future, we probably won’t be giving bispecific antibodies by themselves. Today, they’re only FDA-approved to be given by themselves, so the only way to get them as part of a combination is through a clinical trial. The preliminary data from some trials of bispecific antibodies plus standard therapies have been awesome with the huge majority of people getting complete remissions in some cases, even when prior chemotherapy and such weren’t working.
Medically, mosunetuzumab and epcoritamab are pretty similar. They have pretty similar efficacy and pretty similar safety profiles. Epcoritamab is given subcutaneously and mosunetuzumab is intravenously. For many patients, it doesn’t make a difference. For some patients, especially those who have had multiple prior lines of therapy and whose veins have gotten beat up, it does make a difference to them. Some patients have a port that they don’t want to have anymore or they don’t want to get a port.
Another difference is that mosunetuzumab is a finite course of therapy, about nine months, while epcoritamab can be given until it stops working or until you have a bad side effect. We have a lot of patients who have been on it for a year or two and say they want to pause for now, and we’re okay with that. It’s not exactly the recipe as written, but we don’t feel like we’re burning any bridges because if the lymphoma were to grow back, we might be able to treat them again. Some patients prefer to keep going because they don’t like the notion of doing nothing.
Because it’s more about the total doses of epcoritamab, for me, it’s simple. If I have a patient who lives across the street and they don’t want any IV therapy, that patient gets epcoritamab. If the patient lives four hours away and feels strongly about not making too many trips and doesn’t mind getting IV therapy, that patient gets mosunetuzumab. Patients have a big role in that decision.
Dr. Bello: I still prefer CAR T-cell therapy over bispecific antibodies because I see more durable responses, but not everybody can wait to do the whole process. As Dr. Brody mentioned, you have to collect the T cells, send them to be manufactured, and wait for them to be sent back. By then, four to six weeks have gone by and if they’re having rapid progression, they can’t wait.
CAR T-cell therapy can have a little more toxicities with them. Patients are hospitalized a bit longer, so not everybody has a performance status that’s robust enough. That’s when I would use the bispecific antibodies.
Common Side Effects of Bispecific Antibodies
Dylan: Dr. Bello, you touched on the side effect profile of bispecific antibodies. If I was a caregiver or a patient, what should I be on the lookout for and what would my experience be like?
Dr. Bello: A lot of people are now familiar with cytokine release syndrome (CRS). It mimics the most severe infection you’ve ever had with symptoms including fevers and chills. Sometimes, it can be more severe. Patients can have a drop in blood pressure. There can be fluids leaking into the tissue and lungs.
Bispecific antibodies don’t cause much of CRS in most people, so it’s nice that we err on the side of caution. We do it in step-up dosing where we start with a small dose, have the patient come back a week later and give them an increase, then a week later, another increase. Sometimes we hospitalize them to monitor them for 24 hours, but the majority of the time, they do very well.
Neurologic toxicity or immune effector cell-associated neurotoxicity syndrome (ICANS) is more serious. It can present as confusion, word-finding difficulties, or as severe as being obtunded or in a coma. Again, we don’t see much of it with bispecific antibodies so fortunately, it’s not something we need to look for. We let patients know about the possibility, but we don’t usually see that.
Dr. Brody: Dr. Bello was very thoughtful in reminding people that this can be severe, so the patient and, even more importantly, the caregiver needs to know it can be severe. But then we also like to tell people about the reality and the statistics. If they read too much on Google, they’ll unfortunately also read about aggressive lymphoma bispecific antibodies and mantle cell lymphoma bispecific antibodies where the numbers are a little bit worse. But with the follicular lymphoma bispecific antibodies, almost all of these CRS incidences are low-grade.
Similarly for ICANS, in the biggest studies for follicular lymphoma patients, it was the high-grade version of that where people were confused. There was 0% in all of the recent studies, so we do have to tell people about that. At the same time, we want to tell them not just what might happen but what likely will happen. What likely will happen is about half of patients get a fever and they get it either on the first dose or the first few doses.
If a person is getting many more doses in the future, they rarely happen. Most side effects of cancer therapies get worse as you go, like with chemotherapy. Bispecific antibodies are the opposite. It’s the first couple of weeks that have the risk of fevers and then that risk goes down to about zero. I don’t want to say there are no risks because there still are some risks. The risk of infection from common viruses like the flu, RSV, and COVID are real, but they’re true for almost every therapy we give and even for some lymphoma patients who are not even on therapy. Those are the common risks that most of us are facing.
The main thing is cytokine release syndrome and neurological side effects mostly happen in the first few weeks or never happen at all. In that way, it’s a bit of a comfort to a patient because once they get through the first few weeks, I don’t want to say they’re in the clear, but they’re definitely in the easy running part.
Access to Treatment
Stephanie: When CAR T-cell therapy first came out, there were some issues with access in that it has to be done at very specific places. What are your thoughts about bispecific antibodies and access to them?
Dr. Brody: That’s supposed to be the main transformation and revolution about bispecific antibodies. They’re supposed to be accessible and they are or definitely will be. Let me make a little distinction.
For aggressive lymphoma bispecific antibodies, there’s one little speed bump: the ones that are approved now require a one-day hospitalization. One day in the hospital isn’t that bad, but that becomes a real pain for the doctors who have to coordinate that. Even though it’s not a big deal medically , it’s a logistical pain in the butt. Still a lot easier than CAR T-cell therapy, where the patient can spend weeks in the hospital sometimes, but it’s still not nothing.
By contrast, no hospitalization is required for the follicular lymphoma bispecific antibodies (epcoritamab and mosunetuzumab), based on the FDA label and the way that we do it. We occasionally will have an elderly patient we are worried about, so we’ll admit them to be safe, but for most patients, no hospitalization is required. That makes the accessibility hugely more doable than CAR T-cell therapy or even bispecific antibodies for aggressive lymphoma.
The main obstacle to accessibility is community oncologists getting comfortable with these. They’re recently FDA-approved, so they haven’t used them a lot before. Doctors like Dr. Bello and I have been using these for years as parts of clinical trials, so we’re pretty comfortable with them. Like Dylan said, rituximab sounded scary when it was first released and people having infusion reactions was a big deal. Now, no one’s surprised by infusion reactions and everyone’s comfortable with it.
I think it’ll be similar with bispecific antibodies. The hurdle to accessibility is community oncologists getting comfortable with them. There are different ways to facilitate that. One version is the academic doc treats the patient for the first few weeks until they get over that little hump of the risk and then we send them back to their community oncologist. They don’t have to drive back and forth so much. In a couple of years, community oncologists will be very comfortable with these, so it will be less of an obstacle.
Dr. Bello: I agree. Like all drugs, once they’re out for a few years and people have become more comfortable with them, they’ll become more readily available at multiple locations.
Differences Between Bispecific Antibodies and CAR T-cell Therapy
Dylan: CAR T-cell therapy is still a major player. We have three FDA-approved options—liso-cel, axi-cel, and tisa-cel—and tons in the pipeline targeting anything you can find. We talked about bispecific antibodies. What’s the difference between them and CAR T-cell therapy, and the mechanism of action for CAR T-cell therapy?
Dr. Bello: As Dr. Brody mentioned earlier, they’re similar, but the mechanism of action is obtained differently. CAR T-cell therapy is a much more complicated process. Patients come in, they donate blood, and a machine filters out their lymphocytes and gives them their whole blood back. Their lymphocytes are sent to a facility that will engineer the T cells to recognize a marker on the lymphoma cells. In the three products that you mentioned, the marker is an antigen called CD19, which is pretty much common in almost all B-cell lymphomas.
In addition to the T cell being able to recognize that antigen, the T cells are also programmed to be turned on. By nature, when T cells are in your body, they’re not attacking your body randomly. They need a trigger to turn them on. These T cells are engineered to recognize a certain antigen in the lymphoma cells and they’re activated already.
When they’re ready, they ship them back. Usually, it takes a couple of weeks for them to do this. The patient comes in and we give them a moderate dose of chemotherapy over a couple of days to suppress their immune system and then we give their T cells through a transfusion.
Once they get into the body, they immediately start to attack the lymphoma. A lot of times, we hospitalize people for this portion because now is when they start getting cytokine release syndrome or neurological toxicities. We monitor them in the hospital because there are tests we can do to see if they’re going to start getting more severe symptoms. We also have some medicines we can use to attenuate some of these if they start happening.
Patients are in the hospital anywhere from seven days to three weeks, depending on how long the inflammatory process lasts. It can start as soon as the cells are put in or it can start a couple of days later, so we don’t let them go home within 24 or 48 hours. There’s a peak in the symptoms and then you’ll start to see the inflammation lessen, the patients start to get back to their baseline or their normal status, and then we eventually let them leave the hospital.
Obviously, their work is not done because, at that point, their blood counts will be low. Even though it’s an immune therapy and we think that it’s attacking the lymphoma cells, it does cause quite a bit of a drop in the white cells, red cells, and platelets. Some of these patients require transfusion support during the first few weeks after and antibiotics because we see infections happen because of the low white cell count.
What I always found weird with CAR T-cell therapy is sometimes people get very sick for a few days and then it’s like a light switch is turned off. All of a sudden, the inflammation stops. Once the inflammation lessens, the patients start to get back to normal. I always tell them they’re going to have a week of hell and then they’re going to feel all right afterwards.
Dylan: I’m glad you said that because these neurological symptoms can be terrifying. For the patient, it’s going to be a blur most of the time, but for the caregivers, it’s the most terrifying thing in the world.
Dr. Bello: It’s good to let them know because there’s some misconception that CAR T-cell therapy and immunotherapies are benign. They come into the office saying, “I don’t want chemotherapy. I want CAR T-cell therapy.” No, we’re not going straight to that. There’s a misconception that because it’s not chemo, it must be easy. It’s an intense treatment. It’s not going to be a walk in the park.
The Role of Inhibitors
Dylan: Probably the most confusing for patients are the inhibitors. There’s BCL2, BTK, and SYK, and some of these are FDA-approved. Where do those fit into this new paradigm with CAR T-cell therapy and bispecific antibodies? Dr. Bello, how do you use them in your practice?
Dr. Bello: Unfortunately, the data with BTK inhibitors in follicular lymphoma has not been the greatest. BTK inhibitor stands for Bruton’s tyrosine kinase inhibitor. We use them a lot for other types of indolent lymphomas, like small lymphocytic lymphoma (SLL), chronic lymphocytic leukemia (CLL), and Waldenstrom’s, but with follicular, it hasn’t worked that well. There are some studies in development looking at BTK inhibitors in combination.
The other one is the BCL2 inhibitor venetoclax. That one is still a shocker to me. BCL2 is what’s mutated in 99% of follicular lymphoma and this drug that blocks the BCL2 pathway doesn’t work in follicular lymphoma.
The one that had the best results, PI3K inhibitors, was pulled from the market. Thankfully, we have these other options that I don’t miss them too much.
Cure vs. Longer Periods of Survival
Stephanie: Dr. Brody, there’s so much development happening in the immunotherapy space, like CAR T-cell therapy and bispecific antibodies. I know doctors don’t like using the word “cure,” but is there a discussion about that? And if not cured, what’s the consensus on the impact on longer periods of survival?
Dr. Brody: Doctors, especially academic doctors, are extremely diplomatic. We say to patients all the time that follicular lymphoma is incurable. Nothing’s incurable. We just have not found the cure yet. It’s not the disease’s fault. It’s us. There’s nothing magical about the disease. We haven’t been smart enough over the past 40 years, but we’re getting close. When my grandpa’s sister had Hodgkin’s lymphoma in 1949, it was 100% incurable. Now it’s 85% curable and that wasn’t that long ago.
We refer to follicular lymphoma as incurable. That’s how we write it in all of the papers. That sounds scary. It’s a terrible word. Whenever I say that, I have to say it’s incurable, like high blood pressure or diabetes. We don’t have a cure for high blood pressure, but we’ve got pretty good pills that can keep your blood pressure good for the next 50 years. We can’t give you one pill to cure it and that’s what we say for follicular lymphoma so far.
Bispecific antibodies have been the highest bang for the buck in follicular lymphoma in terms of efficacy versus toxicity. By themselves, they have some limitations. They’re good but not perfect. But in combination with standard therapies, like rituximab and lenalidomide, the complete remission rates have been huge in the first early studies. The big studies are getting done now.
Quite honestly, I wouldn’t be surprised if we look back in 20 years and find out that those who got bispecific antibodies plus combination standard therapies never relapsed. It will not hold for 100% of the patients, but it will be for a fraction. I don’t know that that will happen, but I absolutely would not be surprised because so many people are getting such deep remissions. We may be handing out curative therapies to people on those studies today. What’s the likelihood? Ask me again in 20 years, but it’s a real likelihood.
Clinical Trials in Follicular Lymphoma
Stephanie: When it comes to clinical trials, are there ones that are particularly exciting in the follicular lymphoma space?
Dr. Brody: Clinical trials are not always great. However, clinical trials are a time machine into the future. We have been giving people some of these bispecific antibodies in combination for about four or five years now, and some of them are just getting FDA-approved now. Some of these combination therapies are not FDA-approved yet, but they will be FDA-approved in the next year or in some cases, the next five years.
It’s a bit of a tragedy that Americans don’t get access to these mostly for lack of awareness. They’re available at many dozens or sometimes hundreds of hospitals around America, but maybe they didn’t think to ask or the person they asked wasn’t aware of them. That’s where resources like The Patient Story, The Leukemia & Lymphoma Society, and the Lymphoma Research Foundation can be helpful in guiding patients. There’s no absolute commitment to be part of a trial, but hear about it and get the information.
We were talking about front-line therapies for follicular lymphoma before and then hinting at later lines. The NCCN Guidelines are clear. They recommend finding out about clinical trials. Old therapies are considered non-curative, but it doesn’t mean we can’t get a curative therapy with some of these promising trials.
The first thing that patients need at the beginning of their journey is the awareness that there may be some self-advocacy involved. No doctor in America should ever be annoyed if a patient goes and gets a second opinion. My patients get second and third opinions beyond me and I always ask because I’m always interested to hear what they say.
People think of trials as a last-ditch effort and it’s such a bad branding. It shouldn’t be.We have trials for front-line therapy and second-line therapy. The trials for first-line therapy are what we’re super excited about. One example is getting immunotherapy instead of chemotherapy. We have trials of front-line therapy of bispecific antibodies where half the patients get that and half the patients get standard therapy.
Patients have concerns that they’re guinea pigs and don’t know what they’re getting or they’re getting a placebo. There’s no such thing as a placebo in cancer clinical trials. They may get the standard treatment plus a placebo. In most trials, people are aware of what they’re getting. There’s no mystery.
Some of the most exciting trials give patients the chance to skip chemotherapy, to get front-line bispecific antibodies, and combinations of the standard with or without the bispecific on top of it. Because bispecific antibodies have been pretty gentle and mostly safe, we can safely combine them with standard therapies.
The results from some of the early versions of those trials that have been presented at ASCO and ASH showed unparalleled remission rates. They’ve been awesome. Some of those front-line and even second-line trials of similar combinations are, for me, some of the most exciting trials out there right now.
Dr. Bello: I agree. For bispecific antibodies or immunotherapy treatments, the trials that are moving them up now to the second line and even to the front line are the most interesting. If you could get a non-chemotherapy approach, that would be great.
Again, we always have to be careful because when we find out years later that this drug caused this kind of malignancy or this kind of immunologic problem, maybe we should have stuck with the original treatment that we had. Immunotherapies are the wave of the future and the sooner we can move them up, the better, and those are the trials that I’m looking for the results in.
Dr. Brody: In many ways, it’s a rehashing of 20 years ago. Rituximab was approved as a monotherapy and now, we say that rituximab is like chocolate chips: add it on top of everything. There’s not a single B-cell lymphoma where you don’t add rituximab on top of whatever the standard was before and made it better.
CHOP was the standard of care then, but no one talks about CHOP anymore. R-CHOP is the only thing now except for some newer versions of R-CHOP as well. I do think that that will be the standard five years from now. Wait five years for the better stuff or get access to it now through clinical trials.
Recommended Online Resources
Stephanie: A follicular lymphoma patient, Donna P., said, “One of my first questions was how long will I live. Until I found a support group, I was so depressed and fanatical about my disease. Then I started seeing all the comments and how longevity was in my diagnosis, so many others then gave me hope.”
In the initial conversations with the patients when they’re dealing with so much, do you have any guidance for them, whether it’s support groups or resources?
Dr. Brody: My first recommendation always is The Patient Story and as Dr. Bello said, The Leukemia & Lymphoma Society (LLS) or Lymphoma Research Foundation (LRF). There are a few others as well, but those are the best for lymphoma patients.
We also sometimes have in-person groups. The stress of this can be a significant factor, especially for someone who already had stress as a problem before or anxiety as a diagnosis before, so we try to get them personalized counseling. At cancer centers, we’re very lucky to have counselors who have experience with cancer patients specifically or, in our case, with lymphoma specifically.
The LLS Clinical Trial Support Center
Stephanie: The Leukemia & Lymphoma Society has a Clinical Trial Support Center that offers free, one-on-one support. You get connected to an LLS Clinical Trial Nurse Navigator to help you throughout the clinical trial process from finding the right trial all the way through when you’re on a trial, making sure that you have all your questions answered.
Clinical trials aren’t a last resort. The terminology itself can be quite daunting. Patients need to understand more about what clinical trials are so that they can decide for themselves with their healthcare team. ClinicalTrials.gov isn’t necessarily the easiest site to navigate, but the Clinical Trial Support Center can help you navigate a resource like that.
The Right Time to Seek Lymphoma Specialists
Dylan: People often ask, “When’s the right time to get a second opinion?” If you or your loved one has follicular lymphoma, when is the time to get an opinion from a lymphoma specialist? Can you explain the difference between a lymphoma specialist and a hematologist-oncologist?
Dr. Brody: Let me first say that being a community oncologist is tough. Most of these folks are taking care of lung cancer, breast cancer, kidney cancer, bladder cancer, etc. It goes on literally all day. I’m buddies with dozens of them and I hear about what they do and how they stay on top of everything. It’s a very tough job.
Academic oncologists and community oncologists have a pretty good way of working together, which hopefully means they have my cell phone, and for any little thing, they’ll give me a buzz or give me a text. For most of those, the patient doesn’t need to come see us.
Compared to breast cancer, follicular lymphoma is rare. Your regular community oncologist knows about follicular lymphoma and has had a few patients with it. Every month, they see dozens and dozens of breast cancer and lung cancer patients, but probably zero follicular lymphoma. They’ll see maybe a few per year, so it would be impossible for them to stay on top of every little bit of data. There’s no way they could do that for every single type of cancer. Dr. Bello and I can barely do it for all the types of lymphoma, so you can imagine that plus other cancers.
The answer for when to see a specialist is always. However, most patients don’t need to keep seeing a specialist. They can have a back-and-forth where we share the patients. The most common intervention I make when there’s a difference in opinion between me and the community oncologist is to downgrade the therapy. They’ll come in and say, “My community oncologist said I need R-CHOP,” and I’ll say, “You don’t. You definitely do not.” They can get either nothing and undergo active surveillance or get something gentle. We make them aware of clinical trials where they may get access to something that won’t be available for years sometimes.
I don’t fault them for saying that. Even a hematology-focused oncologist sees acute myeloid leukemia (AML), myelodysplastic syndrome (MDS), myelofibrosis, and myeloma most of the day, and then a little bit of follicular lymphoma. As a lymphoma specialist, all we see is lymphoma, so we have to have a little more experience.
Final Takeaways
Stephanie: We’ve had an incredible discussion. Hopefully, many things have resonated, but if there’s one thing that you hope people would walk with, what would you like that to be?
Dr. Bello: One of the most important things is that it’s okay to not get treatment. There are a lot of times when people don’t need to have their lymphoma treated because a lot of low-grade follicular lymphomas can be observed. If that’s your doctor’s recommendation, come to terms with that and know that you’re being monitored. If something changes or happens, we have great options.
Lymphomas are very different than solid tumor cancers in that they all need to be treated and the sooner the better. You have to change your whole mindset with these kinds of conditions.
Dr. Brody: Dr. Bello said it beautifully and I agree with how she said it. If you get diagnosed with follicular lymphoma, thank God you got follicular lymphoma and not some horrible lymphoma because it could have been something else. Thank God you got lymphoma in the 2020s and not in the 1990s because the advances have been unparalleled. There’s no cancer where the advances have been as incredible as in lymphomas and B-cell lymphomas, like follicular lymphoma especially. I guarantee that the 2030s medicines will be better than the 2020s medicines, so some patients will be savvy enough to get access to those even now.
Conclusion
Stephanie: Thank you, Dr. Brody, Dr. Bello, and Dylan for this discussion. I really appreciate your time.
I hope that you enjoyed the discussion and we hope to see you in a future program. Take good care.
Symptoms: Intermittent feeling of pressure above clavicle, appearance of lumps on the neck, mild wheeze when breathing and seated in a certain position Treatments: Surgery, chemotherapy
Living with the Mental Health Aspects of Waldenström Macroglobulinemia (WM)
Edited by: Katrina Villareal
WM patient advocate Pete DeNardis leads the discussion as two experts in the field of cancer care, Dr. Jonas Paludo from the Mayo Clinic and Dr. Shayna Sarosiek from Dana-Farber Cancer Institute, dive deep into the crucial topics of watch and wait and mental health. Gain insights that could transform your understanding and approach to cancer treatment.
Thank you to Blood Cancer United for their support of our patient education program. The Patient Story retains full editorial control over all content
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang: I’m the founder of The Patient Story after my non-Hodgkin lymphoma diagnosis. The goal of our platform is to help patients, care partners, and anyone in the support circle navigate life after a diagnosis. The Patient Story does this primarily through in-depth patient stories and educational programs.
It’s especially important in a space like Waldenstrom’s where patients and families are told many times that there will be no immediate treatment and that they’ll enter a period known by most as watch and wait. This discussion is all about support and getting through something as difficult as hearing that.
We want to thank The Leukemia & Lymphoma Society for supporting this independent educational program, which helps us host more of these and always for free for our audience. The LSS has invested over $1.5 billion in blood cancer research and provides free educational resources and support, like information specialists on hand who provide one-on-one support on everything from questions about treatment to social and financial challenges.
While we hope you walk away with more knowledge, this discussion is not meant to be a substitute for medical advice. Please speak with your medical team about important decisions.
Stephanie: I’m lucky to know Pete DeNardis, who has been an incredible part of the IWMF as someone who was diagnosed with Waldenström’s and an advocate. Pete, thank you for taking the time.
Pete DeNardis, WM Patient Advocate
Pete DeNardis: I’m a WM patient myself. I was diagnosed in 2003 at the age of 43. I’ve been a volunteer for the International Waldenstrom’s Macroglobulinemia Foundation (IWMF) since 2005 and have been a board member for a long time and currently serving as the chair of the board of trustees.
I’ve been in multiple periods of treatment and watch and wait, so I understand the physical and mental impact of Waldenstrom’s when you’re navigating through those various periods.
Dr. Jonas Paludo, Hematologist-Oncologist
Pete: Dr. Jonas Paludo is a hematologist-oncologist at the Mayo Clinic and part of their lymphoma group, including Waldenstrom’s Macroglobulinemia. He also investigates the effectiveness of various treatments for WM, examines the outcomes of patients with the disease, and studies the genetic mechanisms associated with the development of this malignancy. Dr. Paludo, what drew you to becoming a doctor?
Dr. Jonas Paludo: I had the first-hand opportunity to experience the difference that a good doctor can make in the lives of patients and families when they go through a cancer diagnosis. I thought my calling was to help patients and people when they’re struggling with a difficult diagnosis. I always thought I was going to be an electric engineer because I enjoyed math and physics. I changed my mind, applied to medical school, and never looked back.
Dr. Shayna Sarosiek, Hematologist-Oncologist
Pete: Dr. Shayna Sarosiek is a hematologist-oncologist at Dana-Farber Cancer Institute, specifically at The Bing Center for Waldenström’s Macroglobulinemia, the largest center in the world dedicated to the study and development of new targeted therapies for Waldenstrom’s. She’s involved in clinical research focused on the use of immunotherapies and antibody treatments. She also sees patients on a day-to-day basis and deals with patients who have both WM and amyloidosis. Dr. Sarosiek, what drew you to becoming a doctor?
Dr. Shayna Sarosiek: I was very young when I decided I wanted to be a doctor. I was interested in biology. Instead of pictures of bands on my bedroom wall, I had a poster of every system in the body. I had anatomy setups around my room so that I could study the human body. I also had a close family member with cancer when I was a child and that’s what drew me to cancer care specifically. I’m very happy that I’m in this field.
Understanding Waldenström Macroglobulinemia
What is Waldenstrom’s Macroglobulinemia?
Pete: Let’s talk about understanding WM. Dr. Paludo, can you describe Waldenstrom’s Macroglobulinemia?
Dr. Paludo: Waldenstrom’s is a type of lymphoma. There are many different types of lymphomas, several dozen to be honest, and they behave in different ways. They come from different cell types and different classifications. Waldenstrom’s belongs to the non-Hodgkin’s lymphoma category, which has several dozen different lymphoma subtypes.
Waldenstrom is also sometimes called lymphoplasmacytic lymphoma as it involves the bone marrow of the patients. This type of cancer comes from B cells or B lymphocytes that are part of our immune system. For reasons that we don’t understand exactly why or how, when one of those normal B cells or B lymphocytes becomes a cancer cell, it starts to grow and take up space in the bone marrow.
But it does grow very slowly and that’s why we also classify Waldenstrom’s as indolent lymphoma or slow-growing lymphoma. It’s an indolent lymphoma that comes from B cells and belongs to the category of non-Hodgkin’s lymphoma.
Waldenstrom’s is very unique in that not only is the cancer cell in the bone marrow, but these cancer cells can go to other organs, like lymph nodes and the spleen. It also produces a protein called IgM protein that can circulate in the blood and can cause different types of symptoms along the way.
Most Common Symptoms of Waldenstrom’s Macroglobulinemia
Pete: Dr. Sarosiek, we know that WM is rare as Dr. Paludo just mentioned, but what are common ways people find out that they have Waldenstrom’s and what are the symptoms when they’re diagnosed?
Dr. Sarosiek: Patients find out that they have Waldenstrom’s in a multitude of different ways, but a lot of patients don’t have any symptoms and it’s picked up incidentally when they have other testing done.
One of the most common things I see in my clinic is that during normal primary care follow-up, patients are noted to have a high total protein on routine blood tests. The IgM antibody that you heard from Dr. Paludo is made in Waldenstrom’s and is a type of protein. Often, the protein level in a patient’s blood might be high if they’re making a lot of IgM.
For some patients, it’s picked up because they had an MRI done for other reasons and the bone marrow looks active or looks like it has some changes.
Some patients are noted to have anemia in routine labs. Even if they don’t have symptoms, their doctor notices that their hemoglobin or red blood cell level is a little below normal. Sometimes it’s picked up incidentally; other times, patients have symptoms.
The most common symptoms we see with Waldenstrom’s, both at the time of diagnosis and the time of treatment, are symptoms of anemia. Some patients notice that they’re feeling tired, weak, or getting short of breath doing their usual activities. More commonly, patients attribute their symptoms to aging when in reality, it’s because they’ve developed anemia and their disease has progressed. When symptoms of anemia are present, it might be a cause for a workup.
Another symptom that isn’t as common is hyperviscosity or thickened blood. They might have frequent nosebleeds or visual changes and their eye doctor notices some bleeding in the blood vessels in the back of the eye. Sometimes, they might have symptoms from thickened blood, but it can be a variety of different things that happen and lead to the diagnosis.
Pete: My diagnosis came as a result of a blood test I had for another reason. The doctor said I had elevated protein levels and I thought I needed to cut back on my red meat to lower the protein level. I didn’t know anything about it.
Watch and Wait Process
What is Watch and Wait?
Pete: I’ve had Waldenstrom’s for almost 20 years now, so the definition of watch and wait has evolved and continues to evolve depending on the stage of the disease that I’m at. Initially, it was to see how well the treatments were working but in between treatment periods, watch and wait turns more into a waiting process.
Each time there’s a blood test, you have a little bit of anxiety as to what the results will be. I learned over the years to watch the trends and not focus so much on one blip up or down and that’s helped me relax a little bit. It’s not easy and it can lead to a lot of anxiety on the part of the patient and the caregiver. It’s important to watch those trends and stay in close contact with your doctor.
From the doctor’s perspective, can you describe the watch and wait process?
Dr. Paludo: The watch-and-wait process is the time between diagnosis and when we have to do something or start treatment. It’s the period when you’re monitoring the disease and waiting for symptoms or changes that would require treatment.
Pete, as you mentioned, you were diagnosed when they found an abnormal protein level in your blood. I’m assuming you weren’t having any symptoms at that time and that’s the case for a good number of patients diagnosed with Waldenstrom’s. As Dr. Sarosiek mentioned, a patient could have a test done that eventually led to a Waldenstrom’s diagnosis, but they were feeling well and not having symptoms at that time. Because Waldenstrom’s is a very slow-growing disease, we know that a lot of patients can go for many, many years without having any symptoms from this disease.
During watch and wait, we are keeping an eye on things and monitoring labs, like the trends of the protein level, hemoglobin, and platelet count. Some people call it active monitoring because we’re doing frequent follow-ups with labs and doctor visits, looking for symptoms or changes that would suggest treatment has to be done.
Dr. Sarosiek: I agree with everything you said. Generally, the process of watch and wait, active surveillance, or active monitoring is keeping an eye on a few key things, most importantly patient symptoms. Often, symptoms will align with a patient’s lab results or physical exam, but sometimes they don’t.
We’re trying to maintain a patient’s quality of life, so during that period, we’re monitoring the patient’s symptoms and blood work because if there are changes that are concerning or could become dangerous, then that’s the other thing we want to watch. Sometimes patients develop enlarged lymph nodes or an enlarged spleen.
Pete, you hit the nail on the head by saying that watching the trend is important because there can be some natural fluctuations. The IgM might increase or decrease a little bit. If a patient had a viral infection, it could affect the lab results. It’s more about the trend over the course of time rather than one lab value.
The same thing is true for symptoms. If a patient is sick, they might feel more fatigued but feel better the following week. We like to see the trend over some time during watch and wait.
Pete: I used to keep a spreadsheet to track the trends. My doctor used to expect that and wait for me to hand the sheet that I put together so we could look at the trends together. Thanks to technological advancements, I don’t have to do that anymore.
How Often Do Patients See Their Doctors?
Pete: When someone is in watch and wait, is there a standard frequency of doing blood tests or does it vary?
Dr. Sarosiek: It varies from patient to patient. On average for most of my patients, we follow up every three months. A lot of patients have a very slow progression of the disease, but it depends on the patient. Sometimes we have patients who have been stable for years, so we might extend that follow-up to align with what we know is happening with their disease.
In the beginning, patients are adjusting to their diagnosis and learning more about the disease and probably have more questions, so more frequent follow-up sometimes happens. Even if we don’t feel like we need it from a lab perspective, more frequent follow-ups allow us to check in with patients and allow them to ask questions and get used to having this disease. It can be important from a mental health perspective.
I don’t want any of my patients to be at home thinking they wanted to check at two months and spending the last month of the three-month period waiting anxiously. Sometimes, we’ll check in a little more frequently, especially around the time of a new diagnosis, but on average, it’s every three months.
Dr. Paludo: We have a very similar schedule. We tend to follow up with watch-and-wait patients approximately every three months, especially at the beginning as we have a better idea of how the disease is changing and what the trends look like initially. Assuming that everything is stable or mostly stable, then we start to space those visits about every six months, sometimes even a little longer depending on the patient, what they might be experiencing, and where they’re coming from.
Pete: I hadn’t considered the mental aspect behind the timing. You’re not just focused on the physical aspects of what the patient’s going through but also mentally. Looking back, I guess that did happen to me also. I appreciate that that’s part of the art of being a doctor as it’s not just science, so I compliment both of you on your ability to do that.
Top Tips for Getting Through Watch and Wait
Pete: Are there mental health issues surrounding being on watch and wait? I’ve been in various phases of watch and wait as I’ve been through multiple rounds of treatment. Fortunately, I have a strong support network with my wife, my kids, and my family. Through my involvement with the IWMF, I’ve talked to a lot of patients and not every patient has that support. Patient support is important. Talking to other patients and being part of a support group helps.
All that being said, there are still periods where you have rough patches. You don’t know what’s going to happen next and you’re either anxious about where your disease is heading or when the other shoe is going to drop. It’s important to take advantage of your support network, talk to your doctors, and seek mental help if you need it. There’s no shame in seeking help. You’re to be commended for doing so because you’re taking active control of your disease and your condition.
Doctors, what are the most common questions and concerns you get from your patients when it comes to watching and waiting? What are the top tips you provide them when they’re going through that process?
Dr. Sarosiek: Mentally, for a patient who has cancer, something changes in terms of the way that you think about new symptoms that come up. If you don’t have cancer or haven’t had a major medical issue and you have a little bit of back pain, you might think you hurt your back and move on with your day. But once you have an underlying diagnosis, you start to interpret symptoms differently. I see that very commonly and it’s very normal for that to happen with patients with Waldenstrom’s and other cancers. You start to see your symptoms through a new eye.
From my perspective, it’s important to have an open line of communication with your provider to relieve your anxiety, especially at the beginning when you don’t know exactly what to expect. Many patients will reach out to me and say, “I know this probably isn’t related, but I want to reassure myself. I have this new pain or new symptom. Do you think it’s part of the Waldenstrom’s or something bigger to worry about?”
The important part of active monitoring and surveillance is having that open line of communication to be able to ask questions to put into the context of your Waldenstrom’s, which otherwise you might have ignored. Don’t be afraid to ask to allay your anxieties and be able to enjoy your quality of life without having to worry every day about the small things.
Dr. Paludo: Another common thing is being concerned about watching and waiting. A patient is told they have Waldenstrom’s and now that patient is told that we’re not going to do anything about it. I discuss the rationale and the quality of life component, and reinforce that we do not forget about it. We’re going to have frequent regular time points to check and monitor things.
As Dr. Sarosiek mentioned, have an open line of communication and tell the patients to ask questions. If you have any concerns, contact your doctor to discuss them because there could be a great deal of anxiety, especially at the beginning as patients are getting used to living with Waldenstrom’s and not starting treatment right away.
Dr. Sarosiek: It’s important to find support and resources that work best for you. A lot of people have families and friends to support them and though some patients don’t have that, they might find support in other places. A lot of institutions have great social work care or psycho-social teams that can help deal with anxieties and mental health issues surrounding a cancer diagnosis. There are resources like the IWMF.
Some patients benefit from talking with other patients and being active participants on online forums. Other patients may find that overwhelming and don’t want to necessarily get all that information in the beginning. They might want to learn on their own through patient-directed education. Patients should use the resources available to them and find support in ways that they find most helpful. They don’t need to feel like they have to use everything available. It’s about finding a balance of what they feel most comfortable in.
Pete: Those are very insightful responses and hopefully, people find some help and guidance. I’ve been on this journey for a long time and I’m at a point where my disease is behaving itself and has been so for a while. I’m at the point where I’m worried more about my children and my grandchildren. If they have a bruise or some strange thing, I think, Could it be Waldenstrom’s or something related? It’s a different level of anxiety and I hate to admit that, but it’s true.
What Factors Impact the Watch-and-Wait Process?
Pete: Do different patient profiles, like age, gender, geographic location, and other considerations, impact how you work with patients on the watch-and-wait process? Does it matter where they are in terms of what type of patient they are or even where they live?
Dr. Paludo: They certainly influence the approach to a certain degree. I think about the interaction of Waldenstrom’s and other medical problems patients may have. For example, am I concerned about a potential kidney problem in a specific patient because they may have other risk factors for kidney problems or am I concerned about something else, like a big spleen?
Depending on how a patient presents, depending on what other medical problems they may have that could interfere with Waldenstrom’s, I may look at that and adjust a little bit of how we watch and wait. At the end of the day, it’s all about the trends in their labs and how the patient is feeling, but depending on other medical issues they may have, we may keep a closer eye or adjust the watch and wait period.
Dr. Sarosiek: You mentioned urban versus rural in terms of where a patient resides. That also can impact continued care. Dr. Paludo and I are both very fortunate to work at larger academic centers where we get to have more experience with specific diseases. If a patient is in a rural area, their local doctor might not see as much Waldenstrom’s.
Connecting with someone at a larger academic center could be helpful in terms of continuing to follow the disease. I work with a lot of local oncologists in terms of developing watch-and-wait plans and seeing what they’re comfortable with and what the patient is comfortable with. In some settings, in terms of developing a plan for active monitoring, it’s not just me and the patient, but it’s me, the patient, and their local oncologist.
Approaching the Mental Challenges of Watch and Wait
Pete: If a patient’s going through a mentally difficult time, do you do anything different in the treatment? How do you work through that process when they’re on watch and wait and they’re particularly anxious?
Dr. Paludo: A component of our discussions at patient visits is talking about stressors and anxiety symptoms. I tend to meet more often with patients who may have a higher anxiety level, which is not uncommon. The shorter intervals between appointments allow us to monitor labs a little closer. I found that usually helps a lot with those patients.
More important than that, we’re fortunate to have a very large group of psychologists and psychiatrists at Mayo who are experts in cancer patients. We tend to make a referral earlier in the disease process, so patients would have other professionals to speak with. We also share the different resources available outside of our institution.
Dr. Sarosiek: Part of the beauty of Waldenstrom’s is since our patients do well and we get to know them very well, we can have open conversations when they’re feeling more anxious or when they would like to be connected to more support systems. Based on our conversations, if they have anxiety about specific things happening with the disease, we can connect them to resources or see them more often.
I have many patients who I would feel comfortable seeing less often from a medical perspective, but the mental health perspective is also very important, so I continue to follow them a little bit more closely to manage that part. Keeping both mental and physical health in mind is an important part of the follow-up.
Importance of WM Caregivers
Pete: I’m a patient, but I also happen to be a caregiver. My wife has a related blood cancer and it’s strange to find myself wearing the caregiver hat. Do you work with caregivers in this regard? Do you have advice for them, specifically when a patient is going through the watch and wait period?
Dr. Sarosiek: Caregivers carry a big portion of the burden of the disease. We have a great social work team and they’re quite wonderful in terms of working with the families and seeing what needs the caregiver or the family member might have.
A patient needs to bring someone to an appointment. I always try to address if the family member or caregiver has other questions too because they’re quite involved. They’re often an extra set of ears, help quell anxieties the patient may have later, and can report back information that might have been too overwhelming at the time of the appointment.
A key part of caring for the patient during a visit is whoever they bring along is someone important and involved in their care, so I make sure their questions are answered too.
Dr. Paludo: Caregivers are very important, especially in Waldenstrom’s. I include them and check with them because they might be experiencing different types of anxieties and concerns. Caregivers are also looking for other things that we may not discuss, like family, work, and finances, which are important topics that don’t take center stage in the discussions but are important to address. They provide a lot of support to the patient, so it’s important to make sure they’re supported as well.
Pete: Having to wear the caregiver hat, I had a newfound respect for what my wife had been through for years. In some respects, it’s harder than being the patient. I have a lot of appreciation for all the caregivers and physicians who are working with us, trying to help during these difficult periods, whether we’re in treatment or watch and wait.
Latest Treatment Options for Waldenström Macroglobulinemia
Pete: We want to touch on the current treatment landscape or what treatment is like for Waldenstrom’s patients and where we might be headed. When I was diagnosed in 2003, Rituxan (rituximab) was a fairly new treatment paradigm and there were concerns about whether it was safe to take long-term. We know much better now, but back then, we weren’t sure.
One of my initial treatments, which was fludarabine, cytoxan, and rituximab, isn’t used anymore. I have an unusual disease course, so I’ve had different courses of treatment. I’m currently on a BTK inhibitor, which is working well for me. Because I have a different manifestation of the disease, I also get monthly IVIG.
Every patient is different. What are the current treatment options for patients? If they’re newly diagnosed, what do they have to look forward to in terms of options?
Dr. Sarosiek: Over time, if a patient’s disease progresses or comes back, we have a lot of different treatment options, which is wonderful. Most commonly for a treatment-naïve patient, which means they’ve never had treatment for their Waldenstrom’s, we think of two big categories for first-line therapies.
We often think about BTK inhibitors, like zanubrutinib, ibrutinib, and acalabrutinib. There’s also chemotherapy with rituximab. There are quite a few different chemotherapies. Fludarabine is one of the older ones, but we don’t use that as frequently anymore. In the US, we often use bendamustine with rituximab, but there’s also another chemo called Cytoxan (cyclophosphamide) that can be combined with rituximab. I would say the two most common are rituximab with chemotherapy or BTK inhibitor.
There is another class of drugs called proteasome inhibitors, like bortezomib, or related drugs that we can also use. I tend to use those in younger patients. A lot of patients with Waldenstrom’s have neuropathy, so we don’t use those drugs as frequently because neuropathy can happen with that group of drugs.
There are other oral therapies like venetoclax or the newer BTK inhibitor ibrutinib. There are also different options available as well for patients who have had their disease come back. Clinical trials are also an option, which is the way that we move therapies forward.
We have so many different options and we’re lucky enough to have a conversation with our patients about what might fit their disease and their preferences. Some patients don’t want to take a pill every day, some people don’t want chemotherapy. In most cases, we can tailor therapies to patient preferences and what we might expect to be best for their disease.
Pete: Dr. Paludo, can you talk about fixed-duration therapy versus continuous therapy? What are the differences and what are the advantages and disadvantages?
Dr. Paludo: As Dr. Sarosiek mentioned, we are very lucky to have so many different options, a lot more options than we had 20 years ago, Pete, when you were diagnosed. We can divide the different treatments into fixed-duration treatments and continuous treatments.
With fixed-duration treatment, there’s a start date and an end date. Those include chemoimmunotherapy regimens, like bendamustine and rituximab, and cyclophosphamide, rituximab, and steroids. Treatment is usually given at frequent intervals for a specific amount of time.
Continuous treatments include newer drugs, like targeted therapy. They have a start date but they don’t have a predefined end date. Treatment is continued for as long as it’s working and not causing side effects that require us to stop treatment. That’s where BTK inhibitors come into play, like the one you’re currently taking, Pete. You’re going to continue on it for as long as it’s working and not causing enough side effects to impact your quality of life to justify stopping treatment.
We usually think of fixed-duration treatments as having more side effects at a higher intensity and that’s why they’re given for a certain duration. Continuous therapy tends to have a lower level of side effects so patients can continue on treatment for a long time. Patients can choose what fits them better, whether it’s fixed-duration treatment or continuous treatment.
Promising Clinical Trials in Waldenström Macroglobulinemia
Pete: What’s always interested me was when it was time to decide, the doctor would tell me my options and ask which one I wanted. We’re fortunate as WM patients to have so many different options available regarding treatment, which is a testament to the amazing research being done to move the ball forward.
We look forward to the newer agents down the road and better treatments in the future for improved quality of life for all. With that in mind and looking at the future of treatments, what’s exciting at this point? What are some of the studies you’re most interested in, and why should patients and care partners be interested in participating in a clinical trial specifically?
Dr. Sarosiek: Clinical trials are how we move forward in the field. We’re in an exciting time with the number of clinical trials that we have available for Waldenstrom’s and there are quite a few that I’m interested in. When I bring up Waldenstrom’s clinical trials to patients, there’s an initial hesitance because of concern that a patient would get a placebo and not get treatment for their disease.
An important thing to remember is that we’re certainly treating our patients and what the trials do is try some of the treatments in a new way. Maybe a specific treatment was effective for other types of lymphomas and we’re seeing if it would work in Waldenstrom’s or if a combination of two effective therapies has been used before, we’re studying if we could use both for a shorter duration.
Patients should always be open to asking questions about clinical trials if they have any hesitancy, are worried that they’re not going to get active therapy, or are worried about side effects. Some trials offer an opportunity to get something new and different that might be more effective based on some encouraging background data.
We have a couple of ongoing clinical trials for patients with Waldenstrom’s, a precursor of Waldenstrom’s, or who don’t quite meet the criteria for Waldenstrom’s but have an abnormal IgM antibody. Patients can develop neuropathy that affects the lining of the nerves We have a clinical trial open for exploring that neuropathy differently by treating the underlying abnormal IgM and then following the patient’s nerve damage over time and hoping to find something that’s effective. That trial used rituximab with acalabrutinib to see if that regimen can protect the patient’s nerves.
Another clinical trial we have is using a drug called loncastuximab tesirine, an antibody that delivers a toxin to the site where the abnormal cells are, and that’s a limited-time therapy of six months. The trial is ongoing and it’s for patients who have had at least two other types of therapy in the past.
We have another clinical trial that’s using two oral therapies, venetoclax and pirtobrutinib. We know both of those drugs are effective in Waldenstrom’s on their own, but this trial is using a combination of both for two years in hopes of deepening or getting better control of Waldenstrom’s, and also in hopes of allowing patients to come off treatment after two years.
I could go on and on about many other clinical trials available for Waldenstrom’s, but those are some of the more exciting ones that we’re talking about. Dr. Paludo, do you have other thoughts about clinical trials for patients with Waldenstrom’s?
Dr. Paludo: Participating in clinical trials is very important for patients and the community. Participating helps patients have new and other different treatment options available and that’s how we got where we are right now. Often, the first patients to benefit from a new treatment are the ones in the clinical trials, so the ones in the ibrutinib clinical trial are the first ones to benefit from that drug and become the standard of care. Hopefully, loncastuximab will become part of the standard treatment in those patients in clinical trials who are the first ones to benefit from that.
There are several clinical trials available for Waldenstrom’s. There are a few that are very interesting and seeing results and I hope they will be available soon. There are some trials comparing differences in the treatment regimens and classes that we were talking about earlier, trying to see if one is better than the other, or which situation to use one or the other.
We don’t have the specific trials yet, but I’m looking forward to seeing what novel types of immunotherapy drugs will bring to Waldenstrom’s field. I’ll be very curious to see what we’re going to find with bispecific antibodies in Waldenstrom’s. We have seen excellent results in different lymphomas similar to Waldenstrom’s and I’m hoping that we’ll have clinical trials soon that will be able to investigate if those treatments are helpful in Waldenstrom’s as well.
Pete: With the clinical trials, what it comes down to is that it’s an opportunity to be on the cutting edge in a sense of what treatments are out there and find something that will work well for you.
Correct me if I’m wrong, but the thing that people should take away is that if you are in a position where you need treatment, you will get treatment whether it’s from a clinical trial drug or another treatment.
Dr. Sarosiek: That’s correct. No matter what, patients need to understand that if their disease needs treatment, they will get treatment for their disease. If they qualify for a trial and want to participate, they can do that. We would never advocate for a clinical trial that wouldn’t provide the treatment that the patient needed.
Dr. Paludo: We also look for clinical trials that make sense for the patient. If the patient needs treatment, do the new drugs in clinical trials make sense for that patient or do they have potential side effects that will cause more trouble? If so, we would avoid those clinical trials. When looking for a clinical trial or treatment, it has to fit the patient.
Pete: Patients could always ask if there’s a clinical trial that they can participate in. Depending on where they’re located, they may have to reach out to people, like at Mayo Clinic and Dana-Farber, to see if there are trials available. They may have to travel, but they have an option. I encourage patients to always look at clinical trials and see if any of them are the right fit for them because you help yourself and you also help other Waldenstrom patients in the process. It’s a win-win situation.
Final Takeaways
Pete: Dr. Paludo, as a final message to any patient who’s in watch and wait, what would you tell them to alleviate their anxiety and mentally dealing with being on watch and wait?
Dr. Paludo: I always try to convey to my patients that being able to watch and wait is very positive. It’s an excellent situation to be in where you don’t need treatment. You want to kick that can down the road only when you have symptoms. Work with your hematologist. You need to follow up. Despite all the anxiety that comes with it, being on watch and wait is an excellent position to be in.
Dr. Sarosiek: Watch and wait or active monitoring is a personalized process. It can be adjusted and will be adjusted as needed for each patient in terms of what to follow up on and how often to follow up. I encourage everyone to find a physician who they’re comfortable with, who they can go through that process with, and who they feel is supporting them.
Pete: As a patient myself, I always appreciate my doctor and the advice that he gives me. Having a good working relationship with your doctor and having your caregiver involved is important, so make sure to have someone come to your appointments with you.
It’s okay to let your emotions out. Be upset, yell, and cry if you need to. Don’t hold it in. But if you find that that doesn’t help, reach out to your doctor, to your care professionals, to social workers, and to whatever support is available to you. Take advantage of that support network. You don’t have to suffer alone. There are people who can help you through the process.
The Leukemia & Lymphoma Society
Stephanie: Before we wrap up this discussion, I’d like to spend time on a very great hands-on resource at your fingertips, The LLS’ Information Resource Center, which features specialists who work with people one-on-one. Joining us is Jennifer Wilson, a senior information specialist with The LLS. Jennifer, can you share the basics of how you are helping patients and care partners in general?
Jennifer Wilson: We want to make sure that whether someone calls us for the first time or the 40th time that we hear what they need. Sometimes people can identify it, but sometimes they can’t. We want to make sure that they have good, up-to-date information on their disease and treatment options and how to get support because we know that what your needs are from day one can be very different over time.
Stephanie: For Waldenstrom’s patients and care partners in particular, what are some of the common questions and topics that come up, and how do you help the people who approach you?
Jennifer: When someone is newly diagnosed, oftentimes they may be told that Waldenstrom’s is a chronic illness so they’re going to watch and wait, but to hearing that can be completely overwhelming. We prefer to use the phrase “active surveillance” because that indicates that they’re keeping an eye on things. They’re not waiting to see what happens. They’re very deliberately monitoring to manage the disease.
Then we look at what supports are available. We have the First Connection® Program, a peer-to-peer program so that someone with Waldenstrom’s would have the opportunity to speak with someone else who has been in watch and wait to find out what that felt like and how to communicate with their friends and family.
A lot of times, we help patients figure out what they need to ask at their next appointment to ensure that when they leave the doctor’s office, their top five questions have been answered.
Conclusion
Pete: Thank you again to both of you, Drs. Paludo and Sarosiek. We look forward to future discussions and further advancements in the clinical trials and the future of Waldenstrom’s research.
Stephanie: Thank you, Jennifer, for the work that you’re doing to help patients and families everywhere, including those who are dealing with Waldenstrom’s. We want to thank both Blood Cancer United and the IWMF for being incredible partners.
Thank you, Pete, for leading an incredible discussion, spending the time, and your advocacy in general. You have made an immeasurable impact in this space.
Thank you, Dr. Sarosiek and Dr. Paludo, for the work that you’re doing both in the clinic with the people you’re helping directly in Waldenstrom’s and beyond, and also all the research that you’ve contributed to lifting the possibilities for everybody with Waldenstrom’s.
I hope that this discussion was helpful and that you walk away feeling more confident. We hope to see you at a future program.
If you read and/or watched our program, we encourage you to take our program survey to help us improve future programs and answer your questions.



 Stephanie Chuang, The Patient Story: Hi, there! I’m so glad you could join us for our discussion.
Stephanie Chuang, The Patient Story: Hi, there! I’m so glad you could join us for our discussion. 


 Dr. Joshua Brody: Oh, you said this is going to humanize me and though this is going to make me sound like a saint, those who know me, like Amir, know it’s not true. There are things you could help people with. You could help people with all kinds of problems. But cancer just sometimes seems like the most unjust thing. People did everything right. They didn’t do anything bad. They were healthy. They tried everything. They have a family. They worked so hard. And then they get struck down seemingly out of nowhere.
Dr. Joshua Brody: Oh, you said this is going to humanize me and though this is going to make me sound like a saint, those who know me, like Amir, know it’s not true. There are things you could help people with. You could help people with all kinds of problems. But cancer just sometimes seems like the most unjust thing. People did everything right. They didn’t do anything bad. They were healthy. They tried everything. They have a family. They worked so hard. And then they get struck down seemingly out of nowhere.
 I’d like to welcome Dr. Steinberg for being here. This is the first time we’re able to meet you and we’re happy to. Speaking of humanizing, you have many personal reasons why you’re in the work that you do. I read a poem about how it affects us all and it details a lot of your connection to cancer, including your own. Could you share a little bit about that connection and how that’s motivated you to do what you’re doing today?
I’d like to welcome Dr. Steinberg for being here. This is the first time we’re able to meet you and we’re happy to. Speaking of humanizing, you have many personal reasons why you’re in the work that you do. I read a poem about how it affects us all and it details a lot of your connection to cancer, including your own. Could you share a little bit about that connection and how that’s motivated you to do what you’re doing today?