Navigating a rare blood cancer diagnosis like an MPN can feel like being lost in a thick fog of medical jargon and “what-ifs.” Whether you are struggling with the relentless fatigue of Myelofibrosis or the anxiety of “watch and wait” with ET or PV, you deserve answers that make sense. In this “Office Hours” session, we sit down with a leading specialist to translate complex science into actionable steps for your daily life.
Topics:
Understanding the “Why” Behind Your Symptoms: Discover why your bone marrow’s “thermostat” is stuck in the “on” position and how that leads to common challenges like fatigue, “brain fog” (difficulty concentrating), and that classic “hot shower itch.”
Expert Answers on Your Diagnosis: Get the facts on why certain tests—like Next-Generation Sequencing (a highly sensitive genetic test) or bone marrow biopsies—are essential to identifying the specific “driver mutations” (genetic changes) like JAK2, CALR, or MPL that guide your care.
Managing Your Daily Life & Wellness: Learn the “middle ground” of weight management—why losing weight can be a red flag in Myelofibrosis, while maintaining a healthy weight is vital in PV to reduce the risk of blood clots.
Getting What You Need from Your Care Team: Master the use of “Symptom Assessment Forms” to track how you feel, ensuring your doctor sees the full picture of your quality of life, not just your blood counts.
Actionable Next Steps for Specialized Care: Walk away with a clear plan on how to access an MPN specialist via telehealth, even if you live far from a major medical center, to ensure you are receiving the most “state-of-the-art” guidance.
Expert:
Dr. Kristen Pettit Assistant Professor of Hematology and Oncology University of Michigan, Ann Arbor, MI
Move from overwhelmed to empowered as you listen in to leading experts answer patients’ most pressing questions.
This webinar has been completed!
This webinar has not yet been completed.
Understanding MPNs: Expert Answers to Your Most Pressing Questions with Dr. Kristen Pettit
Hosted by The Patient Story Team | 31m 34s
Tackle the complexity of MPNs with Dr. Kristen Pettit. Discover a grounded, honest approach to managing your condition and partnering with your care team.
Living with an MPN (myeloproliferative neoplasm) brings challenges that aren’t always visible—but tracking your symptoms can make a powerful difference.
This webinar has been completed!
This webinar has not yet been completed.
Take Charge of Your MPN: Tracking Symptoms & Advocating for Better Care
Hosted by The Patient Story Team | 44m 55s
Living with an MPN (myeloproliferative neoplasm) brings challenges that aren’t always visible and tracking your symptoms can make a powerful difference. In this free patient-led discussion, MPN advocates Ruth, Nick, and Demetria open up about what it means to live proactively with ET, PV, or MF.
Webinars in this series must be completed in order.
Pick up where you left off →
Thank you to Incyte and Karyopharm Therapeutics for supporting our patient education program. The Patient Story retains full editorial control over all content.
Ruth Fein: This conversation is focused on living with myeloproliferative neoplasms, or MPNs, and how tracking symptoms can empower you to advocate for the care that you need or the care of a loved one.
My story spans over 30 years. I was initially diagnosed with essential thrombocythemia (ET), which transformed into polycythemia vera (PV), and then eventually became myelofibrosis (MF), which is what I have now. I’ve had several symptoms and I’ve been on a few different drug therapies along the way. I’ve had life-threatening clots and life-threatening bleeds, which, of course, conflict with each other.
Now, I’m on a clinical trial and doing great. They call me the poster child for this clinical trial and it’s been five and a half years. I’m always proud and happy to speak to other people living with MPNs, particularly since I didn’t know anyone else living with an MPN for the first 20 years that I had this disease.
This discussion is brought to you by The Patient Story, where our mission is to humanize cancer. We’ve had more than 100 million views of our in-depth story videos that mostly feature patients, sometimes caregivers, care partners, and, of course, physicians, clinicians, and other care professionals. Our goal is to help promote self-advocacy and connection.
We want to thank our sponsors, Incyte and Karyopharm, for their support of our independent educational program. This allows us to create more content like this for free. The Patient Story retains full editorial control. While we hope this is helpful, this is not a substitute for medical advice. Please still consult your healthcare team when making treatment decisions.
Meet Our Panel
Ruth: I’m joined by two other amazing people who also advocate for those living with MPNs.
Nick Napolitano: Hi, Ruth. My name is Nick. I’m a polycythemia vera patient. I was diagnosed in 2016, so I’m approaching the 10-year mark, which is a big deal. Like you, Ruth, I’ve experienced a range of symptoms throughout my journey — everything from itching to bone pain. I have experienced different treatment options and am currently on a drug, doing very well.
I’m a husband to my beautiful wife, Kara. I have two boys, Jake and Nick. They keep me very active.
Demetria J: I’m a wife, a mother, a mother, a business owner, and a coach and mentor. I’ve been a business owner for nearly 20 years. I initially started in the beauty industry and owned a nail salon. Then in 2021, I pivoted to salon suites and an event space. And then life happened.
I received a diagnosis of ET in 2018. I went through a series of different doctors and ended up at Emory in Atlanta, where the oncologist put me on a new medication that had just come out of clinical trials and was showing positive results. He believed that, at that point, I would benefit better from that.
Eventually, my levels began to level out. My platelet counts went down tremendously, so I thought we were in the clear. Then in 2023, I found out it had progressed to myelofibrosis. I was experiencing different symptoms, such as fatigue and stomach pain. I went to the emergency room, was given some pints of blood, and a diagnosis of myelofibrosis after having a bone marrow biopsy.
Ruth: Thank you both for being here. Let’s dive in.
What Were the First Symptoms of Your MPN?
Ruth: We’re talking about understanding symptoms and what to track. One of the main challenges with MPNs is that the symptoms are often subtle and can easily be mistaken for normal aging or other conditions, like menopause. Nick, what symptoms did you notice first? You alluded to a few, but what was the first symptom that prompted you to start tracking?
Nick: The itching, for sure. Like you mentioned, a lot of symptoms can be dismissed, like headaches and fatigue, but the itching stood out. It wasn’t something I experienced before, so that raised the red flag and made me start tracking and monitoring the details around when it would happen.
Demetria: Probably the fatigue. I have a high pain tolerance level and the fatigue that I experienced would probably get to most people, but it wasn’t getting to me. My adrenaline was running, being a mom, a wife, and a business owner. I had a very demanding life, so I was going and going, and not paying attention to my body as much as I probably should have been.
It wasn’t until the day before I went to urgent care. I was having bad stomach pain, which I now know was because of my enlarged spleen. My doctor informed me that when your bone marrow is not making enough white blood cells that the spleen will kick in and try to do the job of the bone marrow and that’s not its job. In the process, your spleen gets enlarged because it’s doing something that it is not designed to do.
That day, I also had some shortness of breath, which was very unusual for me because I usually don’t get out of breath. My body was sending me signs and I ignored them until it gave me a dire warning. “We can’t go anymore. Something needs attention.”
I want to know every little detail about what I’m feeling and then I use that as part of my conversation with my doctor.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
Tracking Your MPN Symptoms
Ruth: What kinds of things do each of you track now to manage your MPN and how has that been helpful?
Nick: I track everything, but that’s me personally. I want to know every little detail about what I’m feeling and then use that in conversation with my doctor. I let my doctor tell me whether I’m crazy or not with respect to the symptoms I’m feeling. But I think it’s important to track everything.
So much of our disease is a journey over time. Things pop up and go away. I think you need to track everything and have the details around it. Make sure you’re communicating with your doctor because you never know what part of the journey or what symptoms you’re experiencing at any given time actually matter until you look at everything.
Demetria: I didn’t track symptoms until towards the end, maybe that last week before I received my myelofibrosis diagnosis. Each day, I was saying, “Wait a minute. I am really, really tired.” I would go to the grocery store, come back home, lie down, and would need to sleep for like an hour and a half.
The other thing I dismissed was a little bit of dizziness because I had just had a sinus infection, so they were thinking it was vertigo from the sinus infection. I thought everything was isolated and not related to one diagnosis. I thought they were all individual symptoms of something else.
The last week before receiving my diagnosis, I was noticing a little bit of progression. The fatigue was feeling a little bit more intense each day until that last day when I had severe stomach pain.
Ruth: How do you track symptoms? Is it through an electronic app or do you use a notebook?
Nick: It’s a combination of an app and a spreadsheet. I would say the most basic and useful tool for me is the notes app on my phone. I open it up almost daily and log stuff there. Then I use that as the basis for my conversations with my doctor. Everything is there between visits, so I can go over questions and things I notice.
It’s the fear of missing something that may play a role in changing the course of my disease or progression.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
What Motivates You to Track Your Symptoms?
Ruth: Nick, what’s helped you be consistent with your tracking? What’s made it easier and what helps you remember to keep it up?
Nick: It’s fear, to be honest with you. It’s the fear of missing something that may play a role in changing the course of my disease or progression. I’m very fearful of not tracking something, going to a doctor’s appointment, and being asked, “Have you experienced this before?” And then having to say, “I don’t know. I haven’t been tracking it.” Then, realizing that it’s too late. Quite literally, it’s fear.
Ruth: That’s real.
Noticing Your Symptom Patterns
Ruth: Let’s talk about symptom patterns. Do you ever notice your symptoms come and go, get worse at certain times, or come in waves?
Demetria: I don’t know that I necessarily noticed any patterns. It was an everyday thing. I was starting to notice that the fatigue was increasing every day. I don’t necessarily know the time of day, whether it was in the morning or the evening. I just knew that when I woke up, I was fatigued. When I went to bed, I was fatigued. Throughout the day, I was fatigued.
It’s unpredictable… You don’t know what’s going to happen from one day to the next when it comes to symptoms.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
Ruth: What about you, Nick? I assume that’s why you started tracking, because our symptoms do come and go. Do you ever notice that they get worse at certain times of the day or on certain days? What have you found in your tracking?
Nick: Yeah, I think that’s probably the most important part of tracking. I’ll give an example with itching. Itching was dormant for a while and then it popped up over the last couple of years. It’s not just random — it happens at certain times of the day. It pops up in the morning and at night, and then it goes away in between. When I take a shower, whether hot or cold, it pops up. When I roughhouse with my kids, the rubbing of my skin activates it. I used to have a lot of bone pain, but that’s gone.
One of the challenging parts of the disease is that sometimes it’s unpredictable. Things come and go. You don’t know what’s going to happen from one day to the next when it comes to symptoms.
Now I feel better prepared because I understand how important it is to pay attention to everything concerning your body.
Ruth: I think that uncertainty is palpable. A lot of us experience anxiety and stress related to that. Does tracking ease some of that anxiety because it helps make sense of things, or is it the opposite? Do you see those ups and downs and worry more because of it?
Nick: That’s a great question. It helps me because I feel like I’m educated and prepared when I go to my meetings. I call them meetings with my doctor and I treat it very much like a work meeting. I want to have all the information I possibly can when walking into that meeting. I feel a little more prepared. Having the knowledge of the ups and downs, and maybe the reasons why, is very, very important for me.
Demetria: Yeah, absolutely. One of the things my transplant surgeon pushed for was for me to be very observant of my body, like skin changes, because not only in terms of cancer coming back, but also graft versus host disease with having the transplant. Sometimes your body can reject the transplant. They were huge proponents of me making sure that I am paying attention to everything — not just how I’m feeling, but any changes in my skin, my eyes, my throat, my ears, or my range of motion.
Now I feel better prepared because I understand how important it is to pay attention to everything concerning your body and to make sure that I am letting my care team know, so that we can be ahead of it to be more proactive instead of reactive. Sometimes those subtle things that we don’t pay attention to could absolutely be the start of something. If you catch it early enough, you can stay ahead of it.
Don’t think, ‘Oh, this is probably not related to this.’ Express everything that’s going on in your body.
How Tracking Symptoms Can Inform MPN Treatment Options
Ruth Fein: Now we’re tracking our symptoms and thinking about when it’s important to share with our care teams. Has that directly led to any action or changes in your treatment? I’d love to hear any examples. We’re not talking about specific drugs, but has it led to a change in your treatment or your activities, Nick?
Nick: Yeah, for sure. I talked about the itching and brought that up with my doctor. We talked through the details of when it happens and when it doesn’t. He recommended a couple of different options and one in particular that has worked. I very much appreciated the dialogue and brainstorming. That’s one of the aspects I want from my doctor is brainstorming and idea generation. That’s been a life changer, to be honest with you.
Ruth: Tracking your symptoms and bringing that information to your health team can make a big difference. What tips do you have for talking openly, honestly, and clearly with your doctor and your entire care team about how you’re feeling? Do you have any specific tips? What helps you maintain an open conversation with your care team?
Demetria: One of the things, looking back, is I wish I hadn’t seen my symptoms as isolated incidents. I wish I had known to say to somebody, “I’m having these symptoms,” and list them all out, instead of thinking, “This may be related to the sinus infection. Maybe this is related to this.”
I wasn’t sharing with my oncologist or different people early on about other symptoms that seemed random. I didn’t mention those things when they could have been related to the progression of the disease. When working with your care team, it’s important to tell them everything that you’re feeling. Don’t think, “Oh, this is probably not related to this.” Express everything that’s going on in your body.
Ruth: Nick, do you have anything to add or something that specifically works for you to have an open and honest conversation with your practitioners?
Nick: I make sure that at the beginning of the appointment, we talk about how I’m feeling — mentally, physically, and symptom-wise. I try to talk about how I’m feeling in between visits. I’ve learned that doctors and caregivers want details. They’ll ask about what you’re experiencing and how you’re experiencing it. Coming prepared to the conversation right up front to talk about some of the details of what you’re feeling creates a nice dialogue with your doctor.
Ruth: It sounds like you have a perfect doctor because we’re always talking about how to have productive conversations with your doctor and care team. You’ve got it down and I’m sure our audience will learn something from that.
Nick: Ruth, I learned that over time. Believe me, I learned that over time. It’s not always perfect.
You can learn so much from other people’s experiences and gain real courage and support that way.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
Ruth: Same here. And it’s not easy for everyone. You’re communicative, I’m communicative, but some people aren’t. We always encourage bringing a care partner, someone who can interact on their behalf or listen closely, especially if they might miss something the doctor says. For those who aren’t as outgoing or find it hard to share how they’re feeling, that care partner can step in and say, “Remember last week, when…” or add important details. All of that helps. Thanks for sharing that!
Nick: I totally agree. That’s exactly why programs like this are so important. Connecting with the patient community makes such a difference. You can learn so much from other people’s experiences and gain real courage and support that way.
How Has Tracking Symptoms Changed Your Treatment?
Ruth: As one more follow-up to that, has any of your tracking changed not just your treatment, but raised new concerns that you then brought to your doctor? Questions and answers that perhaps would not have come up before?
Nick: It was the tracking of phlebotomies when I was being treated solely with phlebotomies and the impact that was having on me physically. For a while, I was able to deal with them well, but over time, they affected my overall health and well-being. I wasn’t tolerating them as well as I had in the past, so we started talking about different options. Not only were they not making me feel well, but I was also getting them too often, which is usually a red flag with MPNs. That changed the conversation toward exploring different treatment options for my care.
Ruth: That speaks to how important it is, as a patient or patient advocate. Sometimes doctors ask us yes-or-no questions, like, “Are you doing well with your phlebotomies?” and it’s either yes or no. But if you expand on that and say, “Yes, I’m going, and yes, they’re helping my blood counts, but I’ve been experiencing this or that.” If a person living with MPN or their care partner doesn’t step in to add to that yes-or-no question, we don’t progress in our knowledge and, therefore, better care. Thanks for going there. It’s important for others living with MPNs to hear different experiences.
I’m a woman of faith, so I rely heavily on my belief in God. It has anchored me throughout my journey.
Dealing with Fears About Your MPN Symptoms Returning
Ruth: Now, let’s talk about progression. It’s a topic nobody wants to face. Or maybe we all want to talk about it, but we don’t want to go there. We know MPNs can progress over time — for example, ET to PV, or for me, PV to MF, and MF can progress to acute myeloid leukemia (AML). That can bring up a lot of emotions, stress, and sleepless nights.
Sometimes we hear that sleeplessness is a side effect of living with an MPN, but I believe it’s not always a biological or molecular response from the disease itself. A lot of it is the stress. Personally, I don’t think about these things during the day, unless I’m doing a webinar like this. But when I close my eyes at night, that’s when everything starts swirling and it keeps me from sleeping.
It’s important to talk about the balance between facing reality, staying present, and being grounded in daily life. We don’t want anxiety or stress to take over, but it’s also important to acknowledge that it’s real. I believe it’s equally important for others to acknowledge that it’s real because sometimes we feel misunderstood. Demetria, are you worried about MPN symptoms coming back?
Demetria: I’m a woman of faith, so I rely heavily on my belief in God. It has anchored me throughout my journey. I don’t believe in crossing over into fear. It’s healthy to have concern and caution about things, but I try not to go too far into the future because that’s when anxiety sometimes can arise, because you’re thinking about the what-ifs. And sometimes the what-ifs never happen.
For me, I rely on my track record that God has always pulled me through. I believe that if something else were to arise, because I’m anchored in that belief that I’m taking care of spiritually, that it’s going to be okay. Sometimes we do have to go through journeys and valleys, but it’s how you respond to those valleys that makes the difference.
Ruth: Nick, what about you? How do you balance living in the moment and not worrying about progression? I also wonder: have you talked with your doctors about this? Because some doctors don’t always ask about mental health or make that connection, while others do.
Nick: I’ve been very open and public about some of the mental health struggles that I went through, especially early on. It was a very shocking and confusing diagnosis. I kept everything inside. I didn’t communicate at all with my wife or my family, and it was deteriorating my mental health.
What helped me was communicating. I communicated a little bit better with my wife. I did that through a documentary that I did, which was life-changing, to be quite honest with you. It wasn’t necessarily about the documentary, but it was about getting involved in the cause. It made me feel like I was doing something to help. You quickly realize that it’s not about you. There’s a greater cause out there. There are other people that you can help by sharing your story and communicating, and that was the turning point for me.
Connect with other patients. It’s so life-changing to speak with someone who is going through something similar and may have a different perspective.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
I did seek professional help. I remember going to the emergency room a couple of times because of the anxiety pains that I had, which I thought then was a heart attack. At that point, everything was all bottled up inside. Again, that was another pivot point to seek professional help.
Both of those things were life-changing. I talk about this all the time: don’t be afraid to communicate. You have to communicate because it is a release point. Get help and also connect with other patients. It’s so life-changing to speak with someone who is going through something similar and may have a different perspective. It is valuable.
Ruth: All of that is thanks to the internet. Obviously, when I was diagnosed 30 years ago, the internet was in its infancy. I didn’t have resources like The Patient Story, which are invaluable for those of us living with any chronic disease, particularly chronic cancer and an MPN.
Primarily my husband and then my mother… With both of them on my team, things that I didn’t say, didn’t know to say, or forgot to say, they would jump right in to say those things for me.
Ruth: Let’s move on to the role of care partners in symptom tracking. Do either of you have someone helping you track symptoms or notice changes that you might miss?
Demetria: Primarily my husband and then my mother. My mother has a background in the medical field. Sometimes she would accompany me on my visits and would ask questions that I may not have known to ask because of her background.
When I had my bone marrow transplant, I had to have a caregiver with me. My mother and my husband alternated because I had to go to another city to have the bone marrow transplant, which was two hours away from where we lived. My daughter at the time was 10, so he had to navigate caring for her as well as caring for me.
They were some of my biggest supporters. I remember one doctor visit. I was starting to itch a little bit. I hadn’t said anything to my oncologist about it and he said, “You need to tell him about the itching.” The doctor asks, “What about the itching?” I said, “Yeah, I’m having a little bit of itching.” With both of them on my team, things that I didn’t say, didn’t know to say, or forgot to say, they would jump right in to say those things for me.
Kara, my wife, is my caregiver and I don’t know where I’d be without her… She’ll ask me questions to make sure that I’m being honest about what I’m going to talk to the doctor about.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
Ruth: I know a lot of times people will go to their doctor and say, “No, I’ve been fine.” “Are you fatigued?” “No.” “Have you been tired?” “No.” Then the care partner says, “Well, we’ve had to rest a lot when we’ve gone on our two-mile walks every morning or when going up the stairs.” People in our lives play a role that I think is important. Have there been times when your caregiver noticed something you hadn’t picked up on at all yet?
Nick: Kara, my wife, is my caregiver and I don’t know where I’d be without her. We do a lot of communicating now. I’ve mentioned that I treat the doctor appointments like business meetings, so I will prep with her by going over my notes and what I’m feeling. She’ll ask me questions to make sure that I’m being honest about what I’m going to talk to the doctor about. Then we’ll do a debrief about what the doctor said, what the numbers looked like, and everything in between.
I give her a lot of credit for this. I was having trouble with my vision. I’ve had blurry vision before, but all of a sudden, I was having issues seeing. Everything was coming up blurry and she says, “You’ve been on a certain drug for a while. Do you think that has any effect? Why don’t you bring it up to your doctor?” Lo and behold, it does. There is an impact taking certain drugs with your vision. She’s fantastic. She’s a lot smarter than I am, so I rely on her a lot.
His presence and being willing to sacrifice to go through the journey with me were enough for me.
Ruth: Demetria, how does your care partner support you emotionally, particularly when you’re dealing with anxiety?
Demetria: Surprisingly, my husband and I have had these kinds of conversations, and he said that the way that I was so calm and remained calm through all of this helped him to stay calm. People look at the husband as the protector, as the one to shoulder the emotional burden to keep the household calm. But he shared that he watched me and how calm I was, which helped him. He felt as if there was nothing he could do to help me in terms of getting through this. We had to work through the process.
There is an emotional and mental component to someone simply being there. It makes you feel confident. It feels like you are seen. He sees me. He sees that I’m going through this. I feel secure because he’s here. He’s not leaving me by myself to go through this journey. Even though he may not have offered any specific emotional or mental help in the traditional sense, his presence and being willing to sacrifice to go through the journey with me were enough for me.
I heard from an MPN doctor that if we ask every person living with MPN if they were willing to participate in a study, 90-something percent would probably say yes.
Ruth: We’re moving on to clinical trials and looking ahead, which is important because some of the best drugs for MPNs are still in clinical trials. I like to say that clinical trials are no longer a last resort and I’m a perfect example of that. I’ve been in one for five and a half years, and I’m doing extraordinarily well on that trial.
There are challenges, however. I have to go back and forth 3.5 hours each way to the major academic center where I’m being seen, but I’m having a life-changing result, and to me, that’s worth it. By the same token, not everyone has access to clinical trials, which is difficult, and we acknowledge that.
Has your doctor ever brought up the idea of clinical trials as part of your treatment plan? I heard from an MPN doctor that if we ask every person living with MPN if they were willing to participate in a study, 90-something percent would probably say yes. The only obstacle is that they’re not asked. What about you, Demetria? Have you ever been offered a clinical trial?
Demetria: I haven’t ever been asked. But I have been told about them, especially when I was at Emory, because they do participate in a lot of clinical trials. The conversation was, “If this medication does not work well for you, then we could look at putting you in a clinical trial.”
He heard of a diet study that Dr. Angela Fleischman was doing to take a look at the Mediterranean diet and the impact that it has on MPNs. He thought that would be of interest to me.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
Ruth: What about you, Nick? Is that something you’ve been asked about?
Nick: I will answer this a little bit differently. When I first got diagnosed, I focused on my diet. I tried to take out a lot of the inflammatory foods I was eating and made that a focus of my overall care. My doctor knew that at the time because I talked about that openly with him.
He heard of a diet study that Dr. Angela Fleischman was doing to take a look at the Mediterranean diet and the impact that it has on MPNs. He thought that would be of interest to me, so I participated in it and it was nothing short of fantastic. It validated some of the things that I was doing were correct, but also exposed some of the things that I wasn’t doing, and some of the nutrients and proteins that I wasn’t getting based on my diet, and iron. We don’t need too much iron as MPN patients, obviously, but we need a base level of iron.
It was great and it was educational for me. It’s important for people to know that those kinds of studies are out there, outside of the drug clinical trials that we typically see.
Ruth: Thanks for mentioning that. Dr. Fleischman’s studies are interesting. We can learn a lot, not just from the Mediterranean diet, but from the Mediterranean diet’s influence, if you will — picking and choosing what works for us, but understanding inflammation’s effect on MPNs.
Have an open dialogue throughout your care with your doctor. I never want to feel complacent with where I’m at in my care.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
Considering Clinical Trials in the Future
Ruth: If you were asked, whether it’s today or when things change, what would your care team be able to do to make you feel comfortable exploring a clinical trial?
Nick: For me, it starts before talking about the clinical trial. I feel like you need to have an open dialogue throughout your care with your doctor. I never want to feel complacent with where I’m at in my care, so I’m constantly challenging my doctor. What’s out there? What can we be doing differently, if anything? What’s on the horizon? What if this happens, what do we do? Those are the type of questions that I ask my doctor, maybe every other appointment, and brainstorm.
If you’re having those discussions, it makes that conversation about clinical trials a little bit easier and more comfortable because you’ve already talked about it. Starting with having a regular cadence of talking about the what-ifs and what we could do if things change will help with the conversation about clinical trials and ultimately participating in them.
Ruth: Totally agree. Sometimes we have that conversation long enough that the clinical trial becomes an approved drug, and we don’t have to have that conversation anymore.
If there were newer things out there or that are coming, I want to be in the know and figure out how I can benefit.
Ruth: Have either of you ever come across a clinical trial in your own research that seemed interesting, but you didn’t know how to move forward or how to talk to your doctors about it?
Nick: I would say I think that’s where the communication part comes in with the patient community. Also, with organizations like The Patient Story, they can get you resources and someone to talk to to further vet that out, and then ultimately maybe find an MPN expert to talk through that in a little bit more detail.
Demetria: Initially, when I was diagnosed with ET, I was very young. I was about 34 when I was diagnosed. I did some research on the medication that she put me on and said to her, “My husband and I may still want to have children, and this medication is not going to fare well if that is the case.”
I researched some new medications and clinical trials that were out. There was one particular doctor whom I mentioned to her that I saw was making headway and introducing new concepts and treatment plans. I asked her, “Is there a way that you can see if these things would work for me?” I didn’t feel like she was willing to do anything other than what she suggested, so that’s how I ended up at Emory.
This is my life. I have to be an advocate for my life. I have a husband and a daughter. I want to live. And if there were newer things out there or that are coming, I want to be in the know and figure out how I can benefit from the newer things that could be better than what she was offering.
All options are on the table. I want to live as long as I possibly can and I will do whatever is necessary to make that happen.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
Ruth: If things change, Nick, are you open to participating in a drug clinical trial, if at some point that becomes the right choice for you?
Nick: Of course. The way I look at my disease and the care is that all options are on the table. I want to live as long as I possibly can and I will do whatever is necessary to make that happen.
Ruth: Thank you for sharing that. I will just add that science is advancing at unprecedented speeds. Thirty years ago, things were so different. Twenty years ago, ten years ago, even five years ago, for that matter. Within the last two or three years, our options have expanded exponentially. The longer we’re well enough to live a good quality of life while we wait for new and better treatments to come along, those decades add up, and that’s a good thing.
Do not think that any symptom is too insignificant. Track everything and let your doctor tell you whether you have to worry about a particular symptom or not.
Nick Napolitano, Polycythemia Vera Patient & MPN Patient Advocate
Final Words of Advice
Ruth: To move on to final reflections, what advice would you give to someone who was just diagnosed with an MPN about tracking symptoms specifically? Is there anything you’ve learned over time about how to talk to your doctors so they hear what’s going on and see that you’re a knowledgeable patient?
Nick: I would say track it all. Do not think that any symptom is too insignificant. Track everything and let your doctor tell you whether you have to worry about a particular symptom or not.
Be prepared for your doctor’s appointments. Do the research. Communicate how you’re feeling. Be open-minded with treatment options. Be open-minded in getting the care that you need, whether it’s an MPN expert or a mental health expert, if you’re struggling with that. But be open-minded, please.
Demetria: I would say to pay attention. Life is fast. I call this the microwave generation. We do everything fast. We want everything fast. And sometimes when you’re moving as fast as I was, you don’t get a chance to pay attention to what’s going on inside of you. Sometimes when you’re driving on the highway, you’re going so fast that you can’t see anything. But if you’re on the back roads, you have to slow down. You can’t go fast, but you’re able to see the scenery. When you slow down, you can pay attention to see what’s going on.
Sometimes, we need to slow down to pay attention and be intentional about looking at ourselves, looking at our bodies, and evaluating how we feel. How long have I been feeling this way? Don’t discount it as a fluke or an isolated incident. Take it seriously. Take it to your doctors and find out what’s going on so you can live.
Sometimes, we need to slow down to pay attention and be intentional about looking at ourselves, looking at our bodies, and evaluating how we feel.
Ruth: Thank you so much, Nick and Demetria, for sharing so openly.Your stories are powerful reminders of how even small steps, like tracking symptoms and writing them down, can have a big impact and make a real difference in managing your health.
We’d like to also thank our audience. If you’re living with MPN or caring for someone who is, we hope that this discussion has left you feeling more informed, supported, and empowered, and a little less invisible and misunderstood.
We want to thank our sponsors, Incyte and Karyopharm, for their support of our independent educational program. This allows us to be able to do more content like this one and at no cost to you. The Patient Story always retains full editorial control. While we hope that this is helpful, this is not a substitute for medical advice. Please still consult your own healthcare teams when making your healthcare decisions.
We want to hear from you. Please share your feedback on this discussion and also what you want us to cover next. Thanks so much from The Patient Story.
Thank you to Incyte and Karyopharm Therapeutics for supporting our patient education program. The Patient Story retains full editorial control over all content.
“I underwent a lot of sadness, hardship, and difficulty, and all that entails. But I pressed forward in hope for sure. There was a lot of hope that just kept me going all those years.”
Symptoms: Extreme fatigue, stomach pain (later identified as due to an enlarged spleen), dizziness, shortness of breath Treatments: Spleen-shrinking medication, regular blood transfusions, bone marrow transplant
Symptoms: Extreme fatigue, stomach pain (later identified as due to an enlarged spleen), dizziness, shortness of breath Treatments: Spleen-shrinking medication, regular blood transfusions, bone marrow transplant
Jeremy Smith and Dr. Angela Fleischman share empowering insights on living well with polycythemia vera, from symptoms to treatment and patient advocacy.
Dr. John Mascarenhas of The Tisch Cancer Institute at Mount Sinai and patient advocate Andrew Schorr share the latest breakthroughs in MPN care.
Get clarity on your AML journey. Dr. Alice Mims shares expert insights to help you understand your diagnosis and feel better equipped to engage in your care.
Role: Director, Clinical Research Center for MPNs at MD Anderson; Section Chief, MPNs; Prof., Dept. of Leukemia Focus: Myeloproliferative neoplasms (MPN) Institution: MD Anderson
Dr. Serge Verstovsek and Dr. Naveen Pemmaraju discuss cutting-edge treatments and therapies, and combination therapy as a focus in treating myelofibrosis.
Understanding MPN Biomarkers: JAK2, CALR, MPL and More
What Mutations Reveal About Your Diagnosis, Prognosis, and Treatment Options
Biomarkers can be confusing. This program makes them clear. Well-known MPN patient advocate, Andrew Schorr, interviews Dr. Angela Fleischman (UC Irvine) about how common mutations (JAK2, CALR, MPL) help confirm an MPN and what they can (and can’t) predict about symptoms and clotting risk. They discuss when “watch and wait” is right and when to consider medicines like interferon or JAK inhibitors.
You’ll also learn how high-risk mutations (ASXL1, IDH1/2, EZH2) may affect transplant discussions, why results can change over time (clonal evolution), and how NGS is shaping more personalized monitoring. Practical takeaways help you talk with your care team and explore clinical trials with confidence.
Program Topics
Biomarker Basics: What JAK2, CALR, and MPL show and how blood tests find them
Treatment Decisions: When watch-and-wait, interferon, or JAK inhibitors make sense
High-Risk Mutations: How ASXL1/IDH1/2/EZH2 can guide closer follow-up or transplant talks
Clonal Evolution & NGS: Why results change over time and how sequencing tracks it
Personalized Care & Trials: Using risk scores (e.g., DIPSS/MIPSS) and clinical trials to tailor options
This program has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Table of Contents
Edited by: Katrina Villareal
Introduction
Stephanie Chuang, The Patient Story: Hi, there! I’m so glad you could join us. This program is part of The Patient Story’s continued commitment to empower you with the information you need to know when your doctor orders blood work or other tests. You may have already have seen our Blood Work Basics series, including part one on complete blood count and part two on the blood tests that are essential to managing treatment for myeloproliferative neoplasms (MPNs). In this program, we will dive deeper into blood work with a look at something that many of you have asked questions about: biomarkers.
My name is Stephanie Chuang. I’m the founder of The Patient Story but more importantly, I’m also a former blood cancer patient. I had lymphoma and I remember how alone I felt and how hard it was to get humanized information that felt relevant and good for me, which is what we focus on at The Patient Story. In the space of a diagnosis like MPN where you have to get tests done regularly, there is a lot that goes along with it, so we build programs like this conversation and hundreds of patient stories, all to amplify your voice.
This discussion features someone who’s been advocating for patients with blood cancers for a very long time and who I’m lucky to consider a good friend: Andrew Schorr. His story is almost three decades in the making. First, he entered a clinical trial for chronic lymphocytic leukemia (CLL) in 2001. Then he started treatment for myelofibrosis (MF) in 2011. He’s a very passionate advocate, always helping educate and empower other patients, and has been advocating for us at The Patient Story.
We’re also incredibly lucky to have again Dr. Angela Fleischman from UC Irvine, who is so committed to patients beyond her clinic walls, which is evident in everything that she participates in. She’s regularly leading clinical trials to understand what drives MPNs and all of that is to try and develop new therapies to treat or prevent MPNs.
While we hope that this discussion will be helpful, keep in mind that it’s not a substitute for medical advice, so please consult with your healthcare team about your decisions.
Lastly but importantly, we want to hear from you. Your voice matters. We want to know what we can do to make the experience better. We want to know what you’re looking for, what topics you’d like discussed, which guests you’d like featured, and what has worked well so we know to do it again.
Andrew, I’m going to send it over to you.
Andrew Schorr: I’m Andrew Schorr and I’ve been living with primary myelofibrosis since 2011 and, believe me, I closely follow everything about the characteristics of my illness.
We’re going to talk about biomarkers and see how biomarkers affect the management and monitoring of MPNs. Joining me is an expert in MPNs from the University of California at Irvine, Dr. Angela Fleischman, who is both a clinician and a researcher. Dr. Fleischman, welcome to our program.
Dr. Angela Fleischman: Thank you, Andrew. It’s always great to see you and talk with you both in person and on these online forums.
Andrew: Thank you. It’s a delight. And we have a lot to talk about.
What are Biomarkers?
Andrew: Dr. Fleischman, you’re a hematologist who specializes in MPNs. Let’s understand the term biomarkers. Where do they fit in with helping you give patients the treatment that’s right for them?
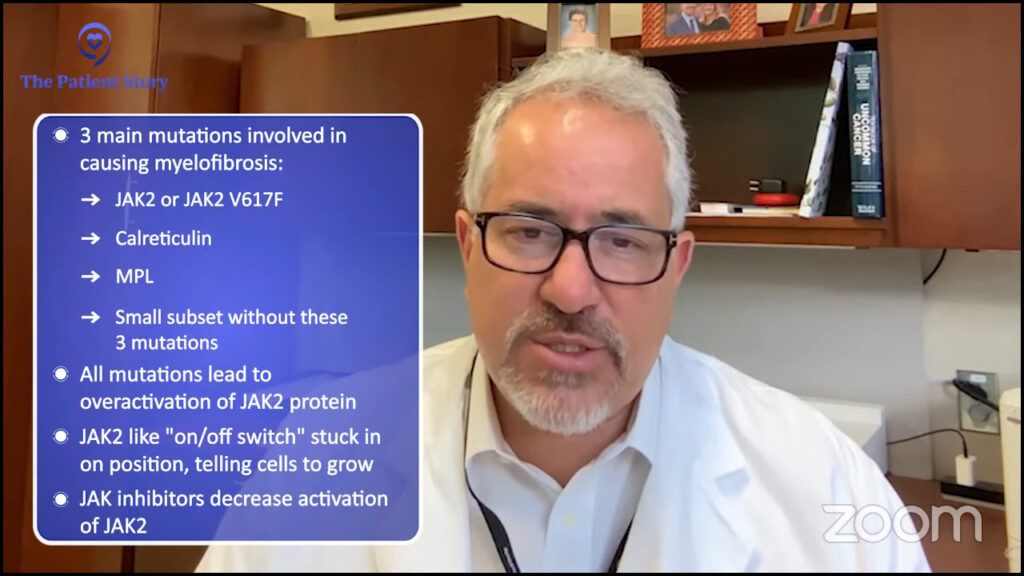
Dr. Fleischman: The actual term biomarker could be very broad in terms of something that we can see in the lab that would give us some information about the biology of the disease of a person. In myeloproliferative neoplasms (MPNs), the biomarkers that we use are the mutations.
Almost everyone with an MPN will have one of three driver mutations: JAK2, calreticulin (CALR), or MPL. But MPN patients can have additional mutations on top of their JAK2, MPL, or CALR, which may help prognosticate or predict what their disease course will be.
But as the word says, they’re simply a biomarker. It can help us predict but not necessarily 100% tell the future. It can, however, help us with treatment decision-making as well as how closely we would monitor a patient.
Are We Born with Mutations or Do They Develop Later in Life?
Andrew: Let’s try to understand the word mutation for a minute. From a healthy person to someone who has one of these conditions, did they always have these genes or did they develop and get out of whack?
Dr. Fleischman: In a myeloproliferative neoplasm, the genes that we’re talking about are acquired at some point in the person’s life, specifically in blood stem cells. We do know now that a JAK2 mutation is usually acquired about 20 to 30 years prior to someone’s diagnosis, so if you’re diagnosed with an MPN, you probably have been living with these JAK2 mutant cells for years.
A good proportion of an older population will come up with mutations in their blood. It’s a common consequence of normal aging.
Dr. Angela Fleischman
A mutation means a change in the DNA, so cells in your blood have this change in the DNA. We know that if you screen the general population for these mutations, including JAK2, a good proportion of an older population will come up with mutations in their blood. It’s a common consequence of normal aging that these cells with mutations expand to a level that we can see them with our testing.
Andrew: Okay. And the mutations cause bad things to happen in the blood?
Dr. Fleischman: Not necessarily bad. For example, a JAK2 mutation can cause blood count abnormalities. Yes, that is bad, but they become obvious or viewable by the medical system because they cause abnormalities in people’s blood counts that we can identify.
However, for other mutations that are commonly seen in the general population and in myeloproliferative neoplasms, such as TET2, DNMT3A, or ASXL1, which is the third most common clonal hematopoiesis, those people are walking around with mutant cells in their blood with no real detectable abnormalities in their blood counts. Do you say that’s bad? There can be some negative health consequences of having these mutant cells, but everything’s a spectrum.
The variant blood cells are in the person’s blood, so it’s easy just to take a blood sample and quantify.
Dr. Angela Fleischman
What Blood Tests are Used to Identify Abnormalities?
Andrew: JAK2 is typically the most common biomarker and it was identified a number of years ago. JAK2 V617F to be technical. Then a few years later, it was CALR. How do you know what somebody has? What tests do you do to know what genes are in an individual?
Dr. Fleischman: Usually, if a patient is found to have some abnormal blood count, such as high platelet count or high red blood cell count, the first diagnostic step is to screen for these mutations. Different labs will do it differently in terms of whether they do all of them at the same time or start with JAK2, which is the most likely one. If that’s negative, then they’ll go down to CALR and then if that’s negative, go down to MPL. But at the present time, these are standard tests that are easily available across the US.
Andrew: From a blood test and not necessarily a bone marrow biopsy?
Dr. Fleischman: Correct. The variant blood cells are in the person’s blood, so it’s easy just to take a blood sample and quantify. You can do two different tests. Usually for diagnosis, you want a yes or a no. Is it there or not? But JAK2 can also be quantitative. So if it’s there, what percentage of the cells have that mutation? But usually for a diagnosis, you want a yes or a no answer.
Even though there are JAK inhibitors, they do not get rid of JAK2 mutant cells.
Dr. Angela Fleischman
How Do You Decide When to Start Treatment?
Andrew: Then if it’s there, the next question is: do you need to treat it? How do you decide that? If somebody is JAK positive, you have medicines for that now. What leads to saying that the JAK is of such an extent that we need to do something about it?
Let’s talk about polycythemia vera (PV) patients first. Our primary objective with what we define as our treatment goals in PV and essential thrombocythemia (ET) are to reduce the risk of blood clots because these patients have an increased risk of blood clot and to improve symptoms.
There are risk categories of blood clotting based on age, whether the patient is older or younger than 60, and whether they’ve had a blood clot in the past. Depending on the risk profile, one can choose different treatments per se.
In polycythemia vera, we want the hematocrit below 45 because those people have been shown to have fewer blood clots, so the treatment is however the person can achieve that. Potentially, there’s therapeutic phlebotomy, aspirin, or something to reduce the blood counts like hydroxyurea, interferon alpha (IFNα), or ruxolitinib (Jakafi). It depends on the person’s age, whether they have a blood clot, whether they have an enlarged spleen, or whether they’re symptomatic. It’s very personalized for each person in terms of what they want to achieve.
To be clear, in terms of the JAK2 mutation, although we have JAK inhibitors, none of our treatments that we have reduce the JAK2 percentage of cells — potentially after years and years, but not initially. I want to emphasize that even though there are JAK inhibitors, they do not get rid of JAK2 mutant cells. Realistically, the only drug that we have that can actually bring down the JAK2 cells in a good proportion of patients — in some cases down to zero — is interferon alpha.
Andrew: You’re watching the patient and looking at their situation. Then you may bring in different medicines. Is CALR different? Are there different medicines for that?
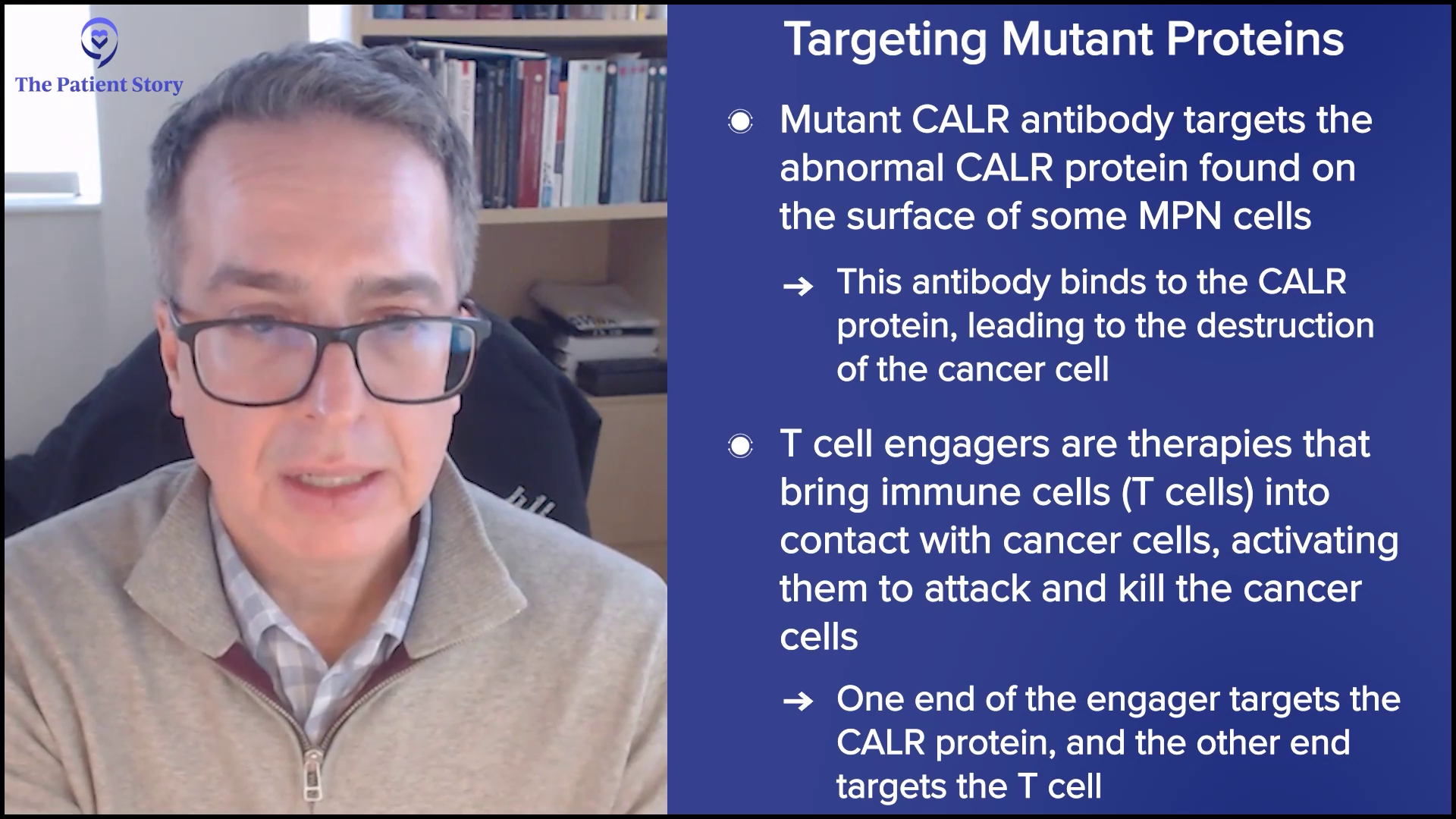
Dr. Fleischman: CALR is a very interesting topic. There are CALR-specific drugs being tested in clinical trials, so at present time, we don’t have CALR-specific drugs on the market that you can get a prescription for. The mutations change the protein such that it looks very different than the normal protein, which is a great opportunity for things like immunotherapy where we utilize our immune system to recognize things that look different than our normal proteins that our body should have.
It’s too early to predict because they’re all in very early stages of clinical trials. But potentially in the future, there could be a whole slew of calreticulin-specific drugs. CALR is never seen in PV. It’s seen in ET and MF.
Interestingly, people with the CALR mutation have a lower risk of blood clots. Theoretically, a very young person is categorized as very low risk with calreticulin. If they’re under the age of 60 and haven’t had a blood clot, they don’t even need aspirin — absolutely no treatment whatsoever. Low risk would be somebody over the age of 60, but no blood clot. Those people can just have aspirin.
One thing I want to emphasize, which I feel is the most common misconception, is that platelet count correlates with blood clotting risk. Despite studies, there has been no correlation between platelet count and blood clotting risk. There’s realistically no medical rationale for reducing a platelet count.
The only medical rationale for reducing a platelet count is if the platelet count is super high because it actually causes bleeding. We reduce the platelet count to reduce bleeding, not clotting. Or if the patient is symptomatic from their platelet count, that would be a reason to reduce the platelet count. But the platelet count itself does not correlate with blood clotting risk. I want to emphasize that and I can’t emphasize that more strongly.
High platelet counts can basically sponge up those clotting factors that it looks like you have a bleeding disorder.
Dr. Angela Fleischman
Andrew: One quick question. I’ve thought of low platelet count as a bleeding risk.
Dr. Fleischman: Correct.
Andrew: But high platelet counts are also a risk?
Dr. Fleischman: Yes. Because when platelet counts get to over 1,000 or 1,500, they can sponge up your clotting factors. The person can have acquired von Willebrand disease (AvWD), which is usually a genetic disorder where you have defects in your blood clotting. But high platelet counts can basically sponge up those clotting factors that it looks like you have a bleeding disorder.
Andrew: Oh, I’ve never heard that before. There’s one other biomarker we didn’t comment about: MPL. Do we have a treatment related to people with MPL?
Dr. Fleischman: Of the three common mutations, it’s the least common. There are fewer people with MPL-mutated ET or MF. We lump them together in terms of risk in ET as a non-JAK2. We lump CALR and MPL together in terms of criteria for risk, as we say JAK2 and non-JAK2.
Theoretically, they’re treated less aggressively in terms of thrombotic risk compared to JAK2. However, because it’s a less common mutation, we don’t have hordes of people that we can observe and clearly say what their risks are.
Andrew: Dr. Fleischman, over the last few years, you have had these scoring systems — DIPSS (Dynamic International Prognostic Scoring System) and MIPSS (Mutation-Enhanced International Prognostic Score System) — where you can put in a patient’s situation and their biomarkers, and have some picture of where they are and where they may be headed. Are these routinely used? What is the impact of these scoring systems?
Dr. Fleischman: Yes, it is routinely used in particular for somebody with myelofibrosis, which can have a wide range of expectations in terms of what the disease trajectory would be and the prognosis. It’s important if you’re diagnosed with myelofibrosis.
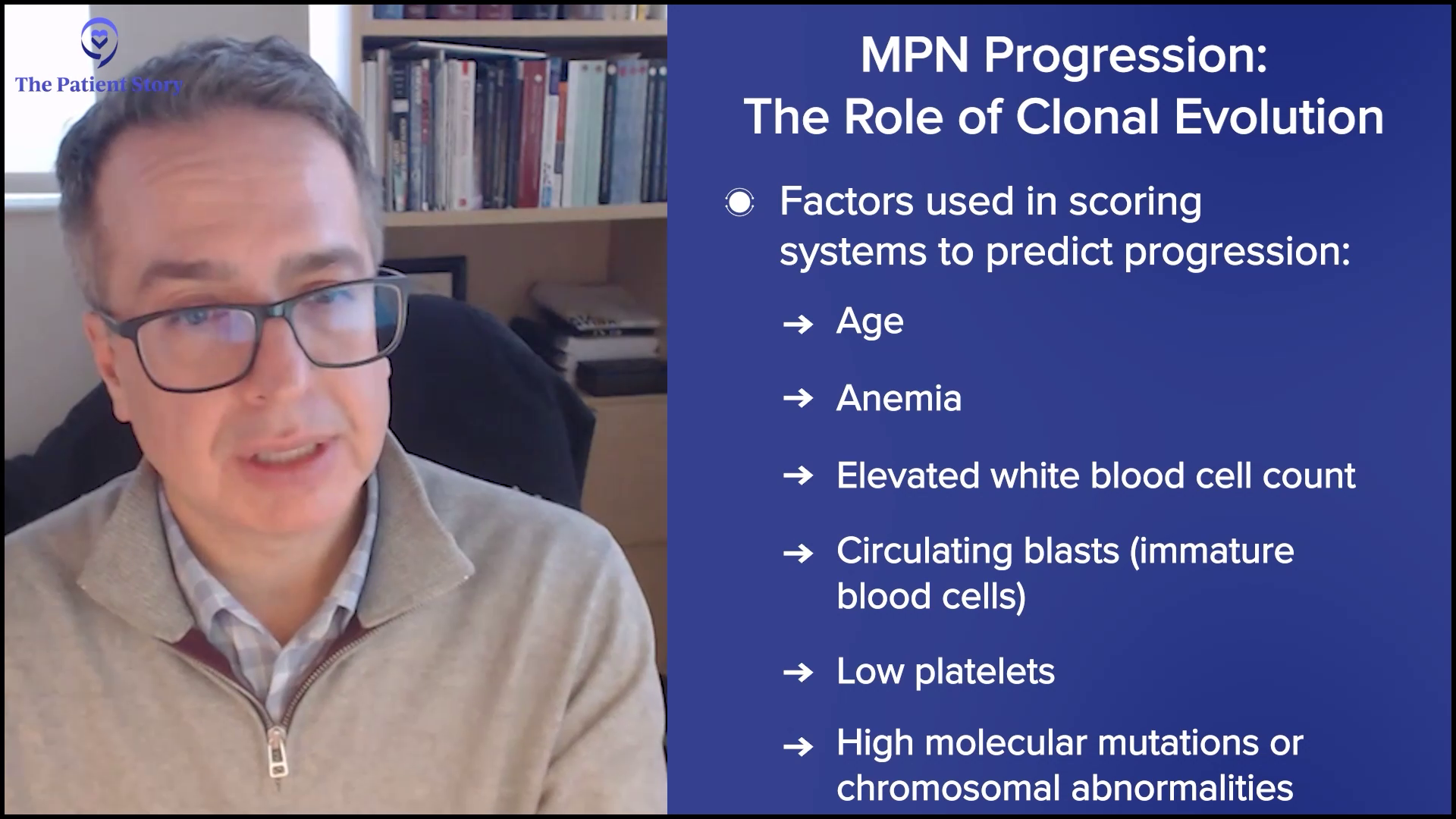
One myelofibrosis patient can be extremely different from another based on their risk factors. For example, somebody with very mild anemia, their white blood cell count looks fine, nothing abnormal, and don’t have an enlarged spleen, that person is very low-risk. It’s going to be different for somebody who has transfusion-dependent anemia, very low platelet counts, or have blasts in their blood. You’re going to have very different situations between those two patients.
These risk scoring tools help us assign points for each hit against the person, like bad anemia or blasts in their peripheral blood, and allow us to have a scoring tool that helps us predict the person’s outcome.
It’s probably most important with the decision on transplant. Transplant is the only cure for a myeloproliferative neoplasm, but it’s a difficult procedure and comes with significant risks. We don’t want to give a person a treatment that could make them worse off than they are from their underlying disease. That’s why it’s important for us to predict how bad the disease is going to be or how quickly it’s going to progress to a serious situation to help us determine if it’s worth the risk of a transplant now or not.
There are obvious things, like if the person is anemic, that the patient can realize that it’s a bad situation if they need transfusions. But other things that we may not be able to see from our general labs, such as genetic tests, are the additional mutations, which may portend a higher risk. Those are very beneficial in helping to predict what may happen to a person later on that may not be clearly obvious from their outward clinical situation.
Andrew: We mentioned ASXL1 in passing and it’s supposedly a higher risk mutation. Is that an example?
Dr. Fleischman: That would be an example. ASXL1, IDH1/ 2, and EZH2 are genes that would make a physician concerned that the patient would have a higher risk of progression. How to address a higher risk mutation in somebody who clinically looks pretty good is a little bit of a conundrum.
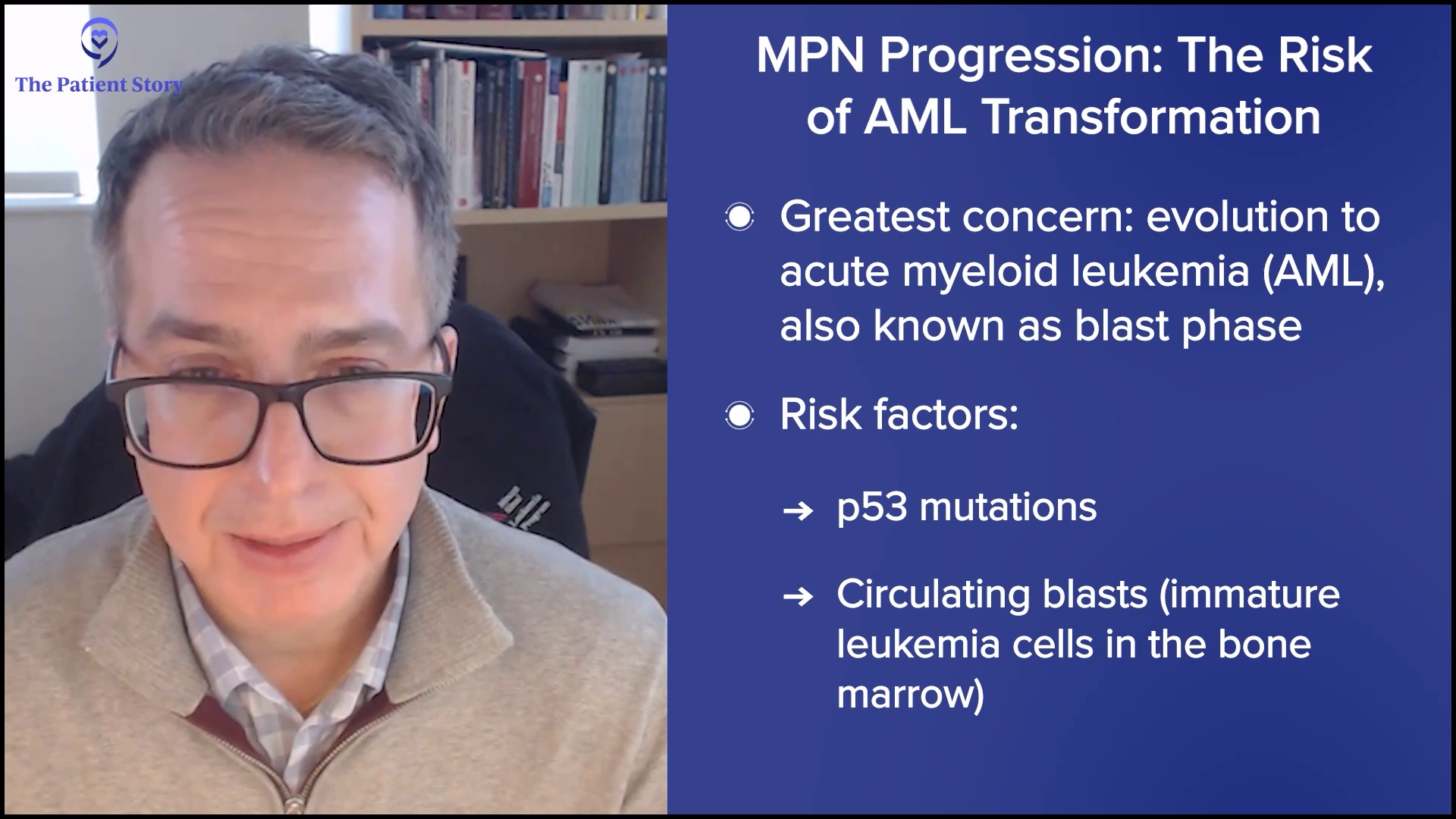
If you have somebody who looks clinically very ill and has high-risk mutations on top of that, that makes the decision easy to say that this person needs a transplant because there are a lot of things that are quite concerning about this person’s situation that makes us worried. This person may be on their way to getting a leukemia.
Transplant is the only cure for a myeloproliferative neoplasm, but it’s a difficult procedure and comes with significant risks.
Dr. Angela Fleischman
However, if the person looks clinically very well in terms of their blood counts looking good and feeling well, yet they have some high-risk mutations, it’s a bit of a more difficult situation. You have some data that makes you think that something isn’t quite right, but by looking at them, they look very healthy and look good. That’s a tough situation.
In those situations, it’s a personal decision for the patient. What usually can occur is they’re watched extremely closely. We have some information that something might not be right, but we need a little bit more information that something isn’t going well in this person. We’re going to closely monitor and see if we get other clues that something is moving in the wrong direction. Again, you don’t want to put too much weight on one specific piece of data. It’s more of a whole picture.
Understanding Clonal Evolution
Andrew: There’s a term that comes up called clonal evolution. Where does that come into play? In other words, if at the outset of a diagnosis, you see JAK2 and don’t see all the other stuff, but now you’re following somebody for an extended time and then when you do a blood test, ASXL1 or one of these other ones come up. Am I right that this stuff can pop up or can change?
Dr. Fleischman: That’s the definition of clonal evolution. Things are changing over time. That’s also helpful in terms of prognostication. If you had just JAK2 to begin with and then you’re developing another mutation — for example, ASXL1 — and some other clinical features are coming with it that are concerning for progression, then you’re getting information that the disease is moving in a different direction.
Whereas five years before, they had the same mutation and it hasn’t changed. Things are looking pretty stable. It’s sort of common sense. If you see things moving and changing, that’s probably not a good sign. If new mutations are popping up, particularly if they’re high-risk mutations, then that’s likely not a great sign in that the disease is moving in a direction that you probably don’t want it to be moving in.
Talking to Your Doctor About Clinical Trials
Andrew: Happily, based on your research and those of your peers around the world, research and clinical trials have been moving forward.
Dr. Fleischman: Correct. Yes.
Andrew: As you see a change in patients, is it appropriate for the patient to discuss clinical trials with their physician as to whether they apply to where their change is headed? Like when you talked about CALR medicines or MPL medicines.
Dr. Fleischman: Yes, it’s very appropriate and important, particularly in rare diseases where we need clinical trials in order to come up with new treatments.
They can ask the physician what clinical trials they have available for their scenario, whether at their institution or elsewhere.
Dr. Angela Fleischman
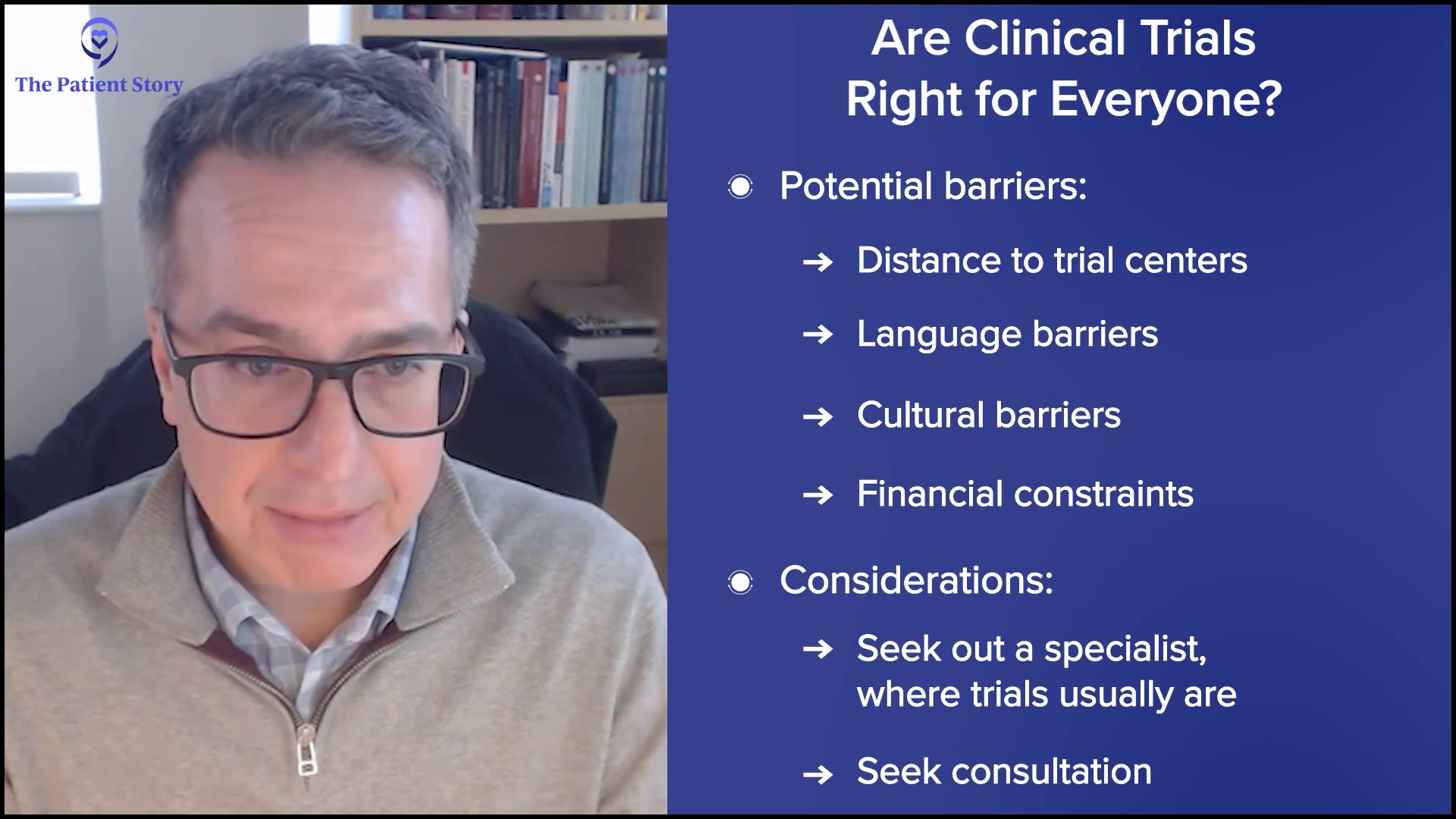
Each person is different. Every patient is not required to be on a clinical trial. If your interest is not in clinical trials, you don’t have to join. But if there’s an interested patient, it’s very appropriate for the patient to research online before they visit their doctor and bring a printout to discuss. Or if they’re at a large university, they can ask the physician what clinical trials they have available for their scenario, whether at their institution or elsewhere.
Usually at large institutions, it’s built in, particularly when a new patient is evaluated. They’re looked at while thinking what clinical trials they’re eligible for. But given that this is a rare disease, it’s important that patients participate to help develop the treatments of the future.
Andrew: Right. And this is an ongoing discussion. You talked about when they’re newly diagnosed. But with clonal evolution, maybe they’ll have the discussion a few years later if things have changed.
Should I Get Tested for Biomarkers Over Time?
Andrew: Which brings us to monitoring. As we have blood tests as patients, you’ll be looking at biomarkers over time, right?
Dr. Fleischman: Correct. What’s exciting is that sequencing, meaning detection of the mutations, is becoming more and more economical and widespread. Realistically, around five years ago or even 10 years ago, if you had a bone marrow biopsy, you wouldn’t have next-generation sequencing (NGS). You wouldn’t know your mutational profile. It wasn’t widely available and quite prohibitive in terms of cost.
But with costs coming down, it’s incorporated into general bone marrow biopsies. Because we can identify most of these mutations in the blood or probably all of them in the blood, one could envision in the future that you could go in at a specific frequency, but maybe not as not as frequent as a complete blood count (CBC). At some sort of routine frequency, mutational analysis could be done to see if that may predict changes before we would identify any changes in your CBC.
In some places, serial screening of the mutational profile is routine, but it’s still too expensive for general medical care. But maybe in the future, as things get cheaper, that will become standard.
At some routine frequency, mutational analysis could be done to see if that may predict changes before we would identify any changes in your CBC.
Dr. Angela Fleischman
But with costs coming down, it’s incorporated into general bone marrow biopsies. Because we can identify most of these mutations in the blood or probably all of them in the blood, one could envision in the future that you could go in at a specific frequency, but maybe not as not as frequent as a complete blood count (CBC). At some sort of routine frequency, mutational analysis could be done to see if that may predict changes before we would identify any changes in your CBC.
In some places, serial screening of the mutational profile is routine, but it’s still too expensive for general medical care. But maybe in the future, as things get cheaper, that will become standard.
Developing More Personalized Treatments
Andrew: Dr. Fleischman, you’ve been at this for a few years and work hard on this. Are you encouraged by the direction that things are going as far as your ability to give personalized medicine based on the biomarkers and the other input you have for what’s right for an individual patient?
Dr. Fleischman: I think so, yes. We can get at that through multiple ways, particularly through clinical trials. You could rationally think. If this person has a mutation, biologically, we know what this mutation does, so let’s try to design treatments around that or predict what treatments might be helpful for a person with this particular mutation.
Another approach, which may be a little bit less direct but a more luck-based, would be in clinical trials. In most cases, we’ll take patients with all mutations. Retrospectively, you could say, “We enrolled 200 patients into this study and found a subset where the drug was perfect for these people. Did those people have a particular mutation? A group of people did well or a group of people didn’t do well. What was different about the people who did well?” You could identify things that way.
With regard to the JAK2 allele burden, we don’t know its clinical relevance, whether or not a rising JAK2 allele burden is bad.
Dr. Angela Fleischman
Should Patients Ask Their Doctors About Biomarker Testing?
Andrew: When a patient comes to see their MPN specialist, should they ask, “How’s my biomarker?” Or should they ask, “Based on my biomarker and other input you’re getting, how am I doing?” How would you evaluate it? It sounds like it’s a constellation, with biomarkers being part of it.
Dr. Fleischman: Correct. With regard to the JAK2 allele burden, we don’t know its clinical relevance, whether or not a rising JAK2 allele burden is bad. There are certain things associated with an increased JAK2 allele burden, such as the risk of blood clots. But realistically, with regard to progression, we don’t know what to do with the percentage number of the JAK2 allele burden. If it’s going up, we don’t know what to do with that.
So why test it in the first place? I don’t know why, but for some patients, particularly if they’re on interferon for the purpose of reducing their JAK2 allele burden, it would be a reason to check. If the stated purpose is to reduce the JAK2 allele burden, you’d like to know if it’s doing that.
We’re all working together for a central goal, which is to improve the lives of patients living with MPN. Although we have good treatments today, we have a long way to go.
Dr. Angela Fleischman
The Future of MPN Research
Andrew: I wanted to make an analogy. You probably remember the famous hematologist, Dr. Kanti Rai, who was an expert in another condition. I have CLL — and this goes back years — and he talked about the knowledge or the indications of different signals they were getting in the disease. We talked about it like furniture in a room and how we didn’t know where to place the couch, the armchair, and the other stuff.
It sounds like with MPNs, you’re getting a lot of furniture and signals about things, but as you just said, we don’t know. But that’s happening. You also mentioned the National Comprehensive Cancer Network (NCCN). I’m on a panel for that and, folks, that’s where experts like Dr. Fleischman from different institutions from around the country get together and put their heads together to come up with guidelines for treatment. I think that’s very exciting how the collegiality is going on in MPNs where you’re trying to figure things out together. Wouldn’t you agree?
Dr. Fleischman: I love being part of the MPN community. We’re all working together for a central goal, which is to improve the lives of patients living with MPN. Although we have good treatments today, we have a long way to go. There are a lot of improvements that can be made, which is why it’s so exciting to be in this field. We have hope. We’ve already made some good strides, but there’s so much more work to do. It’s satisfying to know that potentially, we can make some good impact in the future.
Andrew: Right. But as you pointed out, particularly related to clinical trials, patients are in partnership with specialists, such as yourself, whether it’s clinical trial participation or active dialogue on our situation and what’s right for us. We’re partners in this and hopefully for over many years.
Conclusion
Andrew: Dr. Fleischman, thank you so much for your time in helping us understand biomarkers and where they can fit in in this ongoing, personalized treatment for MPNs.
Dr. Fleischman: Thank you very much. As always, it was great to talk with you. The time just flew. You are so great to talk to, so thank you.
Stephanie: Thank you so much to two tireless patient advocates, Andrew Schorr and Dr. Angela Fleischman from University of California, Irvine, for this discussion. Thank you for helping us to break down what could be a very complicated topic and making it understandable.
We want to keep this discussion going. We want to hear what you enjoyed and, more importantly, what we can do even better. What educational programs and what kinds of patient stories are you’re looking for?
Thank you so much for joining. We hope that you’re able to walk away knowing more and feeling more empowered in your care. We hope to see you at another program soon. Thank you and take good care.
Updates from ASH: How New Discoveries Will Impact Personalized Care in MPNs
Treatment News from the American Society of Hematology on Myeloproliferative Neoplasms
Hear about cutting-edge research and new therapies presented at the 2024 American Society of Hematology meeting. Learn how individualized treatments can improve your outcomes and quality of life. Get practical strategies for handling common side effects of MPN treatments. Discover innovative therapies, including JAK inhibitors and combination treatments. Find out how to stay informed and participate in promising clinical trials. Learn the key questions to ask your healthcare team to ensure you’re receiving the best, most current care.
Whether you’re newly diagnosed or managing ongoing care, learn how the latest findings impact your myeloproliferative neoplasms (MPN) treatment options and quality of life.
Dr. John Mascarenhas of The Tisch Cancer Institute at Mount Sinai and patient advocate Andrew Schorr share the latest breakthroughs in MPN care. Explore personalized treatments, cutting-edge therapies, and groundbreaking research that are changing how MPNs are treated. Learn how new discoveries can improve your treatment options, help manage side effects, and enhance your quality of life.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
Tiffany Drummond: As a clinical researcher and patient advocate, I am excited to talk about some very exciting developments in MPN treatment, including important breakthroughs and promising new combination therapies. Many of these advancements were highlighted at the 2024 American Society of Hematology meeting, better known as ASH, where leading doctors and researchers from around the world gather to share the latest findings.
Our goal is to provide patients and care partners with valuable information to help in their healthcare journey. We want to empower you to have informed conversations with your medical team so you can better understand your treatment options and how to balance effective care with maintaining your quality of life.
We want to thank all of our promotional partners for their support. It is because of you our programs reach the audience who needs it. While we hope you find this program helpful, please keep in mind that the information provided is not a substitute for medical advice.
Let’s kick off another engaging conversation with amazing patient advocate Andrew Schorr and leading hematologist-oncologist Dr. John Mascarenhas.
Andrew Schorr: Welcome to this program about the latest in MPNs. I’m with a friend and leading scientist-physician Dr. John Mascarenhas at The Tisch Cancer Institute at Mount Sinai in New York. John, you have many titles. You’re a noted hematologist and subspecialist in MPNs. Thanks for joining us.
Dr. John Mascarenhas: Andy, thanks for inviting me. I always enjoy connecting with you.
There has been a lot of interest as we understand the disease biology even greater than we did in 2005 when the JAK mutation was first discovered.
Dr. John Mascarenhas
Is There Encouraging Progress for Myelofibrosis Patients?
Andrew: It’s very personal for me. I’ve been living with primary myelofibrosis since 2011 and it’s somewhat progressed. I’ve been on two JAK inhibitors and maybe I’ll switch to a third. Will I have combination therapy with a JAK inhibitor and something else? We all wonder about that.
Some of us are concerned. Should we have a transplant or can medical therapies take the place of a transplant? If you have polycythemia vera or essential thrombocythemia, you ask if you’re going to progress to myelofibrosis and at what rate. How is our situation different from the next person?
John, you were a speaker at the 2024 ASH meeting in San Diego, and you were involved in lots of studies. I want to talk about what’s significant for patients. We have the current therapies and a lot of drugs that many of us have never heard of that are in development. You’re involved in a lot of the development. Which way is the wind blowing? Are you encouraged for us? We saw progress in other blood cancers. Is it now starting to blossom in MPNs, specifically for myelofibrosis?
Dr. Mascarenhas: The short answer is yes, I am encouraged. That’s a fundamental defect that I have, continuing to be optimistic no matter what we’re looking at. That optimism has been maintained over almost 20 years that we continue to move in the right direction, but unfortunately, often not fast enough for our patients.
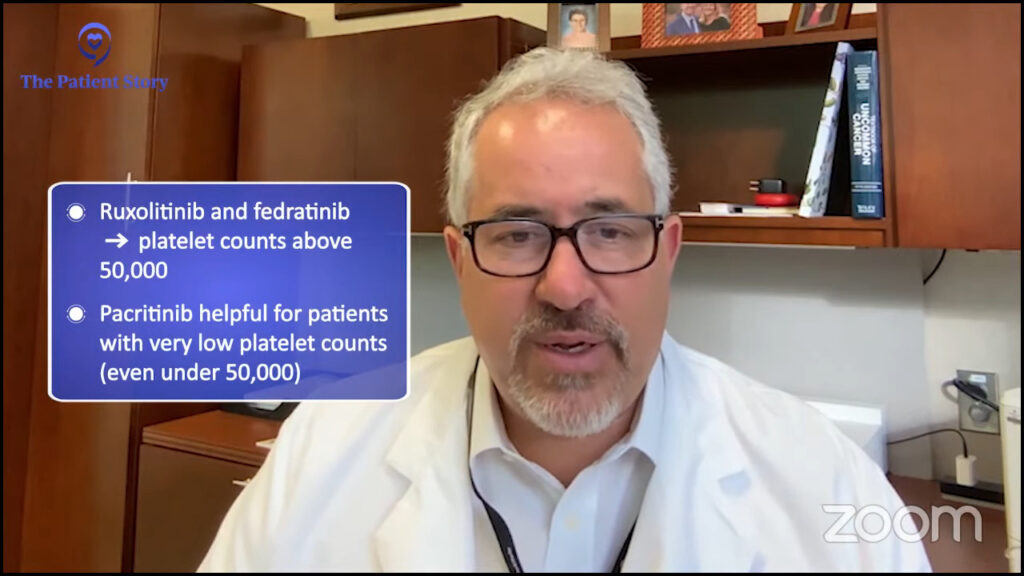
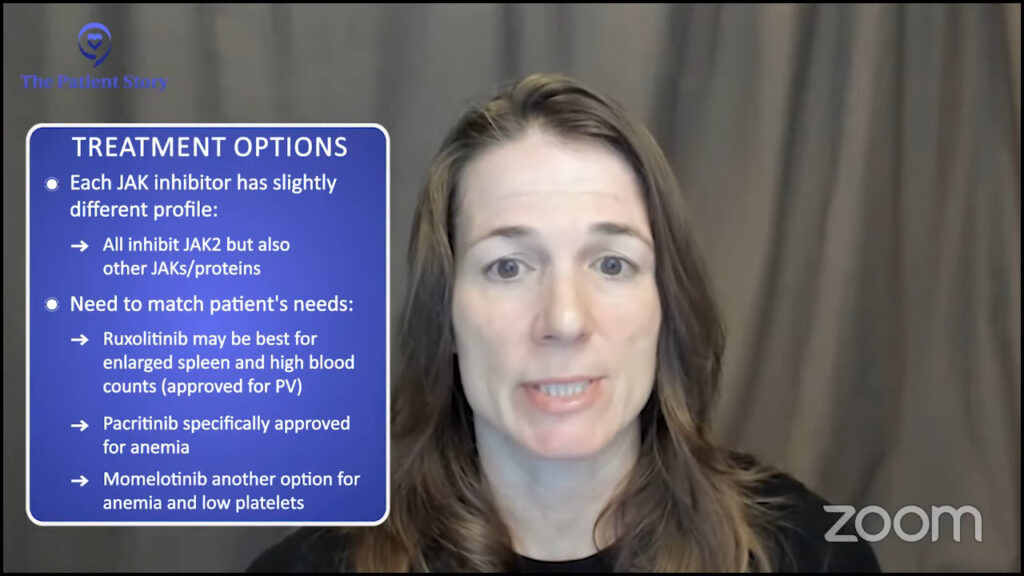
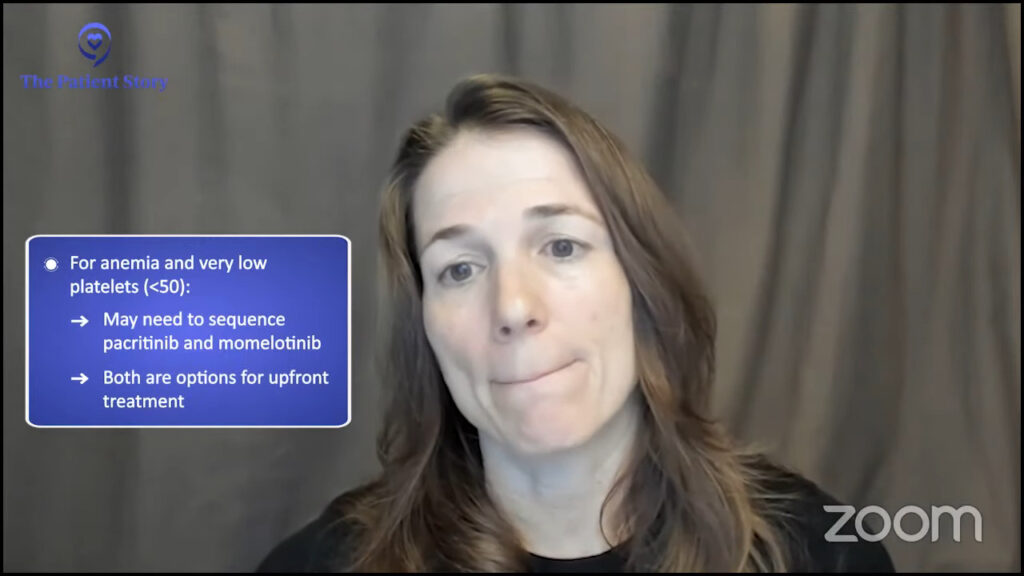
What I’ve seen is the evolution of the JAK inhibitor era, which you alluded to. We have four JAK inhibitors that are approved that allow us to tailor and personalize the therapy to patients based on their profile and blood counts, and even provide serial sequencing of JAK inhibitors. But that isn’t enough.
There has been a lot of interest as we understand the disease biology even greater than we did in 2005 when the JAK mutation was first discovered. We now recognize that there’s a greater degree of complexity and heterogeneity among patients. There are a lot of different pathways that appear to be very important and relevant to the physiology and pathophysiology of this disease.
There is a real interest in targeting the grandfather/grandmother cell in which the disease originated. We are looking for vulnerabilities in those pathways in that cell population that would allow us to ultimately delete that cell to provide deeper responses and even curative approaches. Outside of transplantation, the therapies we have don’t cure patients. They address issues that are not unimportant, like spleen size and cytopenia or low blood counts, and improve how patients do and ultimately prolong survival. But we’re looking to leverage these findings from the lab to find therapies that change the disease course and improve outcomes like survival and progression-free survival.
Many agents are leading us in that direction. These agents turn on the p53 pathway, like navtemadlin, an oral drug that binds a protein called MDM2 and relieves repression on p53, allowing for the natural cell processes to be induced, which is cell death of the malignant cell. It’s a fascinating concept. Navtemadlin is at the forefront of doing that. We showed data in the relapsed/refractory setting of using that as a single agent. We’re now going to move it up to combinations.
Drugs like that are telling. They’re hitting pathways that can induce malignant cells at their core to die, to synergize, and be practical with it. We want to create therapies and approaches that capitalize off the benefits we have, like JAK inhibitors, which can be well-tolerated but can provide deeper responses than what we’ve seen thus far. Navtemadlin is a great example of that.
What Have We Learned from MPN Gene Mutations?
Andrew: We’re going to go through a laundry list as we dig into different drugs, but I want to go over what you said. You’re trying to go back to the very basics of cancer, what went haywire in a patient who ends up with a bone marrow problem that leads to one of the MPNs. Can you shut it down at the earliest stage by understanding it?
Over the last few years, your scientific community has identified different oncogenes (cancer genes) that have been responsible for that. You talked about the heterogeneity or the differences. Some of us have CALR, some have JAK2, and some have MPL. Is that understanding helping?
Dr. Mascarenhas: I do think it helps because we recognize that it’s not a monolithic disease. The driver mutations and the different amounts of those mutations that are understood to be present in the bone marrow cells as well as the sequence in which the mutations arose all tell a picture. They paint a picture of complexity at the molecular and cellular level that explains why there’s heterogeneity at the clinical level — why some patients have very high white counts and some patients have very low platelet counts; why some patients have very big spleens and some patients have a lot more anemia and transfusion dependence. It can all be explained relative to the biology, these mutations, and the effects of these mutations.
Once we’ve realized that, the next step is how to take all of that complex data and distill that to help us understand how best to target those cells based on that genomic complexity. That’s where things like artificial intelligence and machine learning will help us move the field forward as it’s doing with other sciences. We’re moving in this direction of a deeper understanding of the biology from the molecular standpoint that informs us with prognostication, which is important, but most importantly, therapeutic implications.
There is substantial data that would suggest that certain mutations likely influence outcomes and responses to treatment. Most patients will have had next-generation sequencing. You look at these gene panels and see if mutations exist in any given individual and what they mean. We know that some of these mutations can have influenced prognosis and outcome. Some of these mutations and the presence of more than one mutation could even predict a lesser response to drugs like ruxolitinib, a less robust spleen, a shorter duration of response, and a quicker time to failure of drugs. Knowing that upfront may be strategic in understanding how better to approach diseases rather than give the same drug to everybody.
The same drug for everyone is not going to be the right answer. At the forefront, drugs that target CALR, for example, are exciting. We’re taking out a subset of patients with myelofibrosis and ET with the mutant CALR protein expressed on the surface of the cell and saying these patients may be best served by a drug that specifically targets that protein on the surface. That wouldn’t make sense for a JAK2-mutated patient. A JAK2-mutated patient may be best served with a small molecule inhibitor that specifically and selectively targets the JAK2 mutation, which is under investigation. You’re seeing these mutations inform the clinical development of very selective and specific drugs.
Andrew: I almost think of next-generation sequencing like a modern art painting with red and blue splattered. Hopefully, with some consultation with an MPN specialist, you can find out how current therapies or investigational ones apply to your specific situation.
The genes that are driving our illness may evolve, so what the story is today may not be the same story in a year, two, or three.
Andrew Schorr
How Do Doctors Choose the Right JAK Inhibitor for the Patient?
Andrew: You also mentioned how the genes that are driving our illness may evolve, so what the story is today may not be the same story in a year, two, or three. I’ve been living with myelofibrosis since 2011. It has been pretty stable and has been driven by JAK2 V617F. You mentioned the four current approved JAK inhibitors. They have nuances and it would seem like the choice of which one or sequencing, as you said, may vary by patient based on their situation. How do you know where to start?
Dr. Mascarenhas: We are blessed that we have choices today because it wasn’t always the case. We have opportunities to select drugs that may be best suited for different subsets of patients. For example, patients with low platelets or those who have cytopenic profiles may be best served by drugs that are easily delivered and have rationale in that patient population, namely pacritinib over ruxolitinib, in which we know platelets often limit the ability to dose up on ruxolitinib. Fedratinib, even more recently, had some data providing some more security there. We know that platelets could be a determinant of which one of the JAK inhibitors you’re going to select.
Most patients will start with ruxolitinib. It’s the oldest, most familiar, and probably still one of the best drugs that I’ve ever seen in this field
Dr. John Mascarenhas
Anemia is another one that’s gotten a lot of attention. It can be a major issue for patients at presentation and can worsen over time. Ruxolitinib is a great drug, but it can worsen anemia for some patients, so it may not be the best therapy in that setting. However, drugs like momelotinib or even pacritinib that inhibit ACVR1, a different protein, can improve anemia in some patients.
We use patient profiles to help us understand which drugs to choose from, but for the most part, most patients will start with ruxolitinib. It’s the oldest, most familiar, and probably still one of the best drugs that I’ve ever seen in this field in terms of achieving its goals. But again, not every patient fits the bill, so you can tweak that as needed.
Is Combination Therapy the Next Step in Building on JAK Inhibitors?
Andrew: A lot of studies talk about building on ruxolitinib and I’m sure there’s discussion about building on the other JAK inhibitors as well. Is a one-two punch necessarily better? Is that where you’re headed?
Dr. Mascarenhas: It’s definitely what we’re interested in asking. We have JAK inhibitors that are disposable and beneficial, but they’re not sufficient. We have other drugs that have demonstrated clinical activity and are rational and validated in preclinical models, which are systems that help us understand whether it makes sense to take it into a patient. These are drugs like pelabresib, imetelstat, navtemadlin, and selinexor, but each drug has a rationale and is active even as a single agent in these diseases.
The question being asked now is: is it better to combine the two drugs? If you look throughout oncology, most of oncology is treated with combinations of therapy. It’s very rare to find an oncologic disease, whether it’s of the blood or of the solid malignancy, where we use one agent and then if it fails, we go to a single subsequent agent. Usually, combinations of therapy are more potent together.
If you put agent X — whether it’s selinexor, navtemadlin, pelabresib, or imetelstat — together with ruxolitinib, which tends to be the first drug you pick, you tend to see better efficacy and, in some cases, even better safety profile when the two are combined.
Dr. John Mascarenhas
A term we often use is synergize. If you take either drug alone in a lab and expose them to malignant cells, the combination of the two drugs works better than one plus one — it’s almost one plus one plus one. You get better effects in terms of killing or limiting malignant cells. We hope to replicate in humans what we see in the lab or in mice that are engineered to have these diseases.
The data in the field has taken us towards the route of combining novel agents that have shown activity in the relapsed/refractory setting with a single agent as combination therapy upfront. Most of the data would point that if you put agent X — whether it’s selinexor, navtemadlin, pelabresib, or imetelstat — together with ruxolitinib, which tends to be the first drug you pick, you tend to see better efficacy and, in some cases, even better safety profile when the two are combined. The natural question is: if we take two active agents, can we get deeper responses? What does deeper response mean?
At the most superficial, it could mean more spleen reduction — that’s a regulatory endpoint — and deeper symptom improvements, but we’re looking at other biomarkers to understand if we’re hitting the target that we want. Are we getting deeper reductions in the driver mutation amounts of the variant allele frequency (VAF)? Are we reducing those numbers to suggest that we’re reducing the burden of disease in the bone marrow? Since we can’t measure it with a CT scan, are we reducing the disease in the bone marrow from other viewpoints like fibrosis? Is the amount of circulating abnormal cells reduced, something called the CD34+ cell number? Are we also reducing cytokines or inflammatory markers to a deeper extent?
We look at all of these biological aspects and hallmarks of the disease. Are we getting even more profound effects on these biomarkers, suggesting that we’re modulating the disease more effectively? At the end of the day, MPN patients want to live better and longer, but we look for markers early in trials to understand if we’re getting there.
Andrew: These are very powerful medicines. Will the quality of life be diminished if you add this other big gun? We want to live longer, for sure, but we want to live well. Could you talk about the power of the combinations but the worry about additional side effects?
Dr. Mascarenhas: I’ll give you a prime example where one plus one can equal three from an efficacy standpoint but might still equal one from a safety standpoint. A great example is the MANIFEST-2 study. We took JAK inhibitor-naive patients with myelofibrosis and randomized them to the standard of care, which would be ruxolitinib, plus a placebo and ruxolitinib plus the study drug pelabresib, which is an oral BET inhibitor, a very rational drug that modeling has shown us should synergize very nicely with ruxolitinib. It’s a double-blinded study, so the patients and investigators don’t know what the person is getting; only a computer knows.
The answer is it did. Efficacy-wise, if you look at 24 weeks, there were very profound reductions in spleen size and very profound reductions in symptoms. If you look at the biomarkers — the bone marrow fibrosis, the inflammatory cytokines, and the JAK2 mutation — the reductions were far more significant. Everything aligned with the superiority of the combination.
But most intriguingly, if you looked at the safety profile, there were fewer grade 3 and 4 treatment-emergent side effects with the combination than with the single agent. I’ve never seen that before where two active agents combined got almost double the clinical activity and less toxicity. I hope it’s reassuring for patients that double the action doesn’t mean double the trouble. You can combine some of these drugs, get good activity, and not make patients feel worse but even make patients feel better and have less toxicity.
We have to acknowledge that we add toxicity sometimes when we add combinations. Sometimes that toxicity is in the form of gastrointestinal (GI) toxicity or lower blood counts. Sometimes it’s a trade-off. Are we getting deeper responses that could lead to better outcomes where we could be getting more cytopenia and more need for monitoring, or even transfusions? Is that reasonable for a given individual? Could we be adding some nausea and diarrhea by doing that?
What’s key to this conversation is: are we adding these toxicities continuously or periodically when some of these (MPN treatments) are dosed? For example, navtemadlin is a very active drug. When we looked at the data, it was very clear that you could get some GI toxicity. It was mostly low-grade and easy to manage, but it’s there. The drug is dosed for seven days in a row out of 28 days. The toxicity was mostly relegated to days two and nine.
This is an esoteric or personal question: for any given individual, if that deeper response could lead to better outcomes, is that period where you may have GI toxicity worth it? From a human perspective, I’m not sure. From a clinical investigation, we’re interested in trying to understand: are we providing full good at a price or is it going to be good and no price? Nothing comes for free, but these are important questions.
We rely on the patient community to tell us. We don’t simply ask patients how they’re feeling. There’s also a much-validated tool that we use called Patient Global Impression of Change (PGIC), which is simple. It asks: if you put everything together, all the toxicities that might ensue and benefits that you’re noticing or being told by the physician that you’re getting, do you feel like you are the same, a little better, a lot better, a hell of a lot better, or a little worse? The PGIC is a very valuable tool because patients will tell you if the whole thing is worth it or not. It’s key to making sure that globally, they believe that they feel that what they’re doing and what they’re going through is a net benefit at the end of the day.
Transplant vs. Medication: Where Do We Stand?
Andrew: You’ve mentioned a number of these drugs that are investigational on top of the four approved JAK inhibitors. I’m 74, so I don’t plan to do a transplant, but some patients are younger and it’s been recommended they have a transplant. As you say, it can be curative. It’s a big gun. I lived in Seattle for a long time where they developed it originally and I knew about the morbidity and mortality, and that continues for some people. Where are we now with transplant versus all these other treatments?
My hope and my goal in my lifetime and my career would be that we ultimately develop therapies that make transplants unnecessary.
Dr. John Mascarenhas
Dr. Mascarenhas: Fortunately or unfortunately, transplant remains the only modality that we have for a cure and, as you’ve pointed out, it’s not for everybody. If you’re advanced in age or have too many comorbidities, a transplant may be more dangerous and detrimental than it ever will be helpful. I’m an advocate for transplant, but it’s for a select group of patients. Patients who go into transplant are moving into an aggressive type of therapy, but it has to meet the aggressive nature of the disease. You would never take someone who has a low-risk version of the disease right into transplant because you could cause more harm earlier on than good.
It’s a complicated discussion that involves understanding where the patient is from a disease perspective, the nature of their disease, their goals, understandings, and expectations, and making sure they have a donor and support system to do a transplant. I encourage that conversation. It’s important, but it’s not going to be for everyone.
My hope and my goal in my lifetime and my career would be that we ultimately develop therapies that make transplants unnecessary. At its core, transplant is taking immune cells and using them to ultimately get rid of the grandfather or grandmother cell, which is what we call the stem cell that started the disease process, and that’s an immune-mediated elimination of the cell. If we can figure out how best to do that with medicinal therapies that may not be as intense, then we could get to a point where transplant may become historic.
At Mount Sinai, that’s what a lot of our translational research has been based on, and Ron Hoffman and others have taught me this. It’s a stem cell-directed approach to shut down or eliminate that pool of cells that allows the disease to persist. Even after you wipe out cells with a transplant, those cells can come back. Using science and collaborating with patients, targeting stem cells with rational therapies is the only way we’re going to do that.
If it weren’t for patients who show up at tertiary care centers like ours, meet physicians like me, and sign consent forms to allow us to take their blood, bank it, and use it to understand the biology, then we wouldn’t be able to move the field forward. It’s the science that we derive from our patient’s cells and their generosity, and allowing us access to their data that help us understand how to make the next generation of therapies that will target that stem cell.
Andrew: I’m a big believer in that. I go to a tertiary center as well. I’m willing to give the blood and I’d recommend that to people.
Will PV or ET Progress to Myelofibrosis? What Can Be Done?
Andrew: We have people who may not have myelofibrosis. They may have polycythemia vera or essential thrombocythemia. As they learn, they know that there can be a progression from one to another. They’re not on a JAK inhibitor, but they might be someday. What do we know about slowing progression or even knowing who will progress?
Dr. Mascarenhas: We know that the disease is chronic and progressive. Progression is not just a fear of the patient; it’s a reality that we as physicians try to risk stratify. When we meet patients, we try to understand if there are risk variables that may help us predict what that timeline might be to make treatment decisions.
We believe the rate of progression and the reason patients progress is due to clonal evolution. Blood cells acquire more mutations and alterations that allow that cell population to behave differently and change the clinical picture. We use variables, like age, anemia, white blood cell count elevation, presence of circulating blasts, low platelet count, and high molecular mutations or chromosomal abnormalities, and enter them into prognostic scoring systems, which can be found online.
Many patients will find one of these prognostic scoring systems, plug their information in, and get a sense of where they fall in prognosis. But I will caution patients: if you ever do that or speak to a physician, you must understand statistics. Please don’t make the mistake of assuming that the median survival you see is what your lifespan is. It doesn’t work that way. It’s a framework to understand where in the spectrum of patients you fall and help us make treatment decisions about the most appropriate therapy.
Our approach will evolve over time to a more refined, risk-adapted approach where we use mutations to guide us not just in the selection of therapies but the timing of when to use those therapies. From seeing enough patients, I understand that progression is a real concern for ET, PV, and myelofibrosis patients.
Progression to Acute Myeloid Leukemia (AML)
Dr. Mascarenhas: The ultimate concern about progression is the potential to evolve into acute myeloid leukemia (AML). Sometimes you might hear it called the blast phase. That’s an aggressive form of leukemia that is problematic and is a fear factor for patients and physicians treating patients with MPNs.
To see if that’s a concern, we look at mutations like p53, a type of mutation, or the presence of circulating blasts or blasts, which are immature cells in the bone marrow. That information can help us get a sense of what the risk may be of a patient transforming into an acute myeloid leukemia.
MPN-related AML is molecularly distinct from de novo AML… Unfortunately, it’s often more resistant or refractory to the traditional types of therapies that we give in that setting.
Dr. John Mascarenhas
Are We Making Progress with Secondary AML in MPN Patients?
Andrew: There’s a percentage of MF patients who traditionally would progress to AML. There’s been progress in what you’d call primary AML and there have been a number of drugs developed, but secondary AML that would come out of myelofibrosis, I understand, has been more difficult. Where are we with that now?
Dr. Mascarenhas: You’re right. For what we call de novo AML, we have a plethora of different agents. They’re still not enough, but we have agents that can be quite effective in trying to control that type of AML and induce a response. Those agents typically are not as effective and don’t have a very significant impact on the disease process in secondary AML or AML that arises out of an antecedent myeloproliferative neoplasm, whether that’s ET, PV, or myelofibrosis.
MPN-related AML is molecularly distinct from de novo AML. It looks different from a mutation profile and behaves differently. Unfortunately, it’s often more resistant or refractory to the traditional types of therapies that we give in that setting. There’s no benefit to an AML patient who had an MPN previously by giving them induction chemotherapy unless that’s followed by a transplant. Every study tells us that doesn’t improve patient outcomes, so we know that’s not effective.
We rely on drugs like hypomethylating agents, like decitabine, decitabine+cedazuridine, or azacitidine. These epigenetic therapies try to induce maturation of these immature cells, which is what leukemia is, or immature cells that don’t know grow up. We try to induce that maturation process so that they die a more natural death. It’s less intense, but it’s more effective with this type of AML.
There are a lot of other therapies under clinical investigation. Some of them are molecularly directed therapies. We’ve run trials with IDH inhibitors, oral drugs that specifically go after mutations that can be present in AML that arose out of an MPN, which can be quite effective. Understanding the molecular profile of that AML could inform treatment decisions. The reality is that’s an AML that’s problematic. Our real goal is to stop the process from evolving to AML because we know that treating that is complicated.
Role of Interferon for the Treatment of MPNs
Andrew: We’ve had interferon for a long time. Where does that fall in?
Dr. Mascarenhas: Interferon, which is a biologic that has been around a long time, is an interesting compound. There is a lot of data in the lab and in patients who’ve been treated on trials, particularly polycythemia vera and essential thrombocythemia, that this drug can be anti-cloning. You can see changes in blood count numbers with ET and PV, and reductions in mutation levels that are driving mutations like the JAK2 mutation. Groups have shown that a reduction in those levels correlates with better event-free survival (EFS). Events are clotting, bleeding, progression, and death in ET and PV. We see the value in that setting. Interferon’s increasing in its utility and use throughout the world.
Myelofibrosis is a little bit different. There’s probably some value there, particularly in treatment-naive early forms of the disease or prefibrotic forms. Interferon is under active clinical investigation in a global study, which is taking patients with lower-risk diseases that don’t have so much complexity and fibrosis in their bone marrow and have seen so many different types of therapies. Interferon works best early on in the disease course. Once the disease gets too complicated and too advanced, it may not be that effective.
New Drugs Being Studied in MPN Treatments Clinical Trials
Andrew: We mentioned the ASH conference. There are the European Hematology Association (EHA) meetings and other meetings that you attend as well. You mentioned selinexor and navtemadlin. There’s nuvisertib, elritercept, and DISC-071, an anti-hemojuvelin antibody. Help us understand this constellation of what’s going on.
Dr. Mascarenhas: You’ll notice certain themes. For the uninitiated, these names are somewhat frustrating because they don’t resonate. If one were to think about themes, they make sense.
What we’re trying to do in translating the understanding of the biology from the laboratory to the clinic is targeting signaling pathways. These pathways are inappropriately activated in malignant cells that continue to tell them to proliferate, secrete inflammation, and do things that they’re not supposed to do.
We have very intricate, complex, and overlapping signaling pathways in many malignancies, including myelofibrosis. Multiple signaling pathways are inappropriately activated or hyperactivated. For example, JAK inhibitors inhibit the JAK-STAT signaling pathway and you’ll notice those drugs end with “nib.” Those are small molecule inhibitors that inhibit enzymes in those signaling pathways.
Nuvisertib is a small molecule inhibitor which is a selective PIM-1 kinase inhibitor. It inhibits an enzyme in a signaling pathway that is very relevant to the biology of the disease. It has nice data so far that shows a reduction in symptoms, particularly spleen size and cytokines, as a single agent in patients who’ve already been on a JAK inhibitor.
Other drugs may try to turn on mechanisms that have been turned off, like navtemadlin and selinexor. These drugs are focused on different pathways but with one unifying theme, which is the p53 pathway. It’s the master regulator of cell fate. In a normal situation, your cells would get cues to commit suicide if they were infected or corrupted in some way and that is governed by the p53 pathway, an intrinsic pathway that limits the cell’s life. The problem is malignant cells have co-opted that system and turned it off. They turn it off in different ways. Navtemadlin and selinexor, through having different mechanisms, act on trying to turn that pathway on and encourage that cell to die.
You’ll see drugs that get into the cell that affect pathways, drugs that get into the cell that try to turn on pathways, and drugs that try to use the immune system in different ways to go after the abnormal cell.
Dr. John Mascarenhas
Then you might see a drug like a calreticulin antibody, which inevitably will get a name. You’ll notice early on that it’s just letters and numbers and as the development goes on, it becomes funny names that don’t make any sense and then ultimately, when it gets to the commercial space, it will be a catchy name that could be marketed. The mutant CALR antibody drug by Incyte is a perfect example of what will be a “mab,” a monoclonal antibody, which is targeted at the CALR mutant protein expressed aberrantly on the surface of the cell and is a marker for those abnormal cells. What better way to attack an abnormal cell than to have a selective marker? It’s like a handshake. It’s not even a drug; it’s a peptide. It’s a protein that binds that and by doing that, internalizes that protein complex, and that leads to the death of that cell selectively.
Approaches like that will be very fascinating. Those are immune-based approaches. They have BiTEs (bispecific T-cell engagers) that multiple companies are developing, which introduce T cells in a myelofibrosis patient to the abnormal cell by having two ends of that antibody — one that goes after the CALR, for example, and the other one that goes after CD3 on a T cell — and introduces the two cells together so that that T cell does what it should have done in the first place: recognize and create a response to that abnormal cell.
You’ll see drugs that get into the cell that affect pathways, drugs that get into the cell that try to turn on pathways, and drugs that try to use the immune system in different ways to go after the abnormal cell. These are the general themes.
Considering a Clinical Trial
Andrew: Some drugs are being studied at different levels. What would you say about considering enrolling a patient in a trial once there’s a clear picture of their case? Is there one of these that could line up with that? Take us through the thinking and discussion between a doctor and a patient about considering being in a trial.
Dr. Mascarenhas: I have to acknowledge that being on a trial is scary. I hear this all the time: guinea pig. You feel as though you may be experimented on. I always try to caution patients from that mentality because if you have a disease like myelofibrosis that is frightening to have in itself and can limit the quality of life and maybe even the time that you have, then it warrants consideration to do better than the MPN treatment standard of care. The standard of care, which is JAK inhibitors, has benefits for sure, but it’s incomplete for many patients.
The consideration for trials hinges on the patient’s goals and desires. Clinical trials may not be reasonable for every patient. Geography influences clinical trials. If you live in a rural area, the distance to a center offering a clinical trial may preclude you from participating. We know other factors may also get in the way of joining clinical trials, like language barriers, cultural barriers, and financial barriers.
I would encourage any patient who sees a specialist and goes to a tertiary care center to at least seek a consultation. This will help them understand what someone who does this full-time thinks about their disease, to clarify or classify their disease, and what clinical trial options exist.
Trials should make sense. You have to ask questions so that you understand what you’re getting involved in.
Dr. John Mascarenhas
I’ve been around long enough to know ruxolitinib as INCB18424 before it was Jakafi. The drug was used in the clinic and we prayed that it was going to make a big difference and it did. It wasn’t enough of a difference, but it made a big difference. I remember those brave patients who were the first patients to get on that study. They set the tone for the whole field and the development of other therapies because of what they put themselves into. Those patients needed the therapy, but what they did allowed us to prescribe the drug to a lot of patients. It has a profound impact way beyond that individual.
The reality is patients go on a clinical trial for themselves and that is what it should be, but you end up helping the greater good at the same time. You have to feel comfortable with joining a clinical trial. You have to read the consent form. You have to ask questions. What does it involve? What are the potential toxicities? What would be the consequences of participating in a trial?
I feel very comfortable saying that in 2025, any trial I’m aware of that’s offered to patients is an informed trial. These are not trials where we’re taking a random agent off a shelf, throwing it over there, and hoping that it works. These are drugs and agents that are vetted, have a rationale, and go through many layers of pre-testing before they go into humans. You have to trust your physician because if your physician is working with you, then the trial that’s offered to you would hopefully make sense. Trials should make sense. You have to ask questions so that you understand what you’re getting involved in.
Getting the Test Drug vs. a Placebo
Andrew: You mentioned that people ask if they’re going to be a guinea pig. They also ask if they’re going to get the “good stuff.” In other words, they want to know if they’re getting a sugar pill or a placebo. Could you talk about that concerning these trials for drugs that are investigational now?
Dr. Mascarenhas: If you’re in a phase 3 study that’s randomized, a computer randomizes you to arm A or arm B. Arm A may be the active clinical trial agent and arm B could be a placebo, but that has to be disclosed in a consent form. That’s essential. You can ask the physician, “Do I get the study drug or is it going to be randomized? Is it going to be a placebo?”
But a placebo is not always bad. For example, in the MANIFEST-2 study or what’s currently enrolling in the SENTRY study with selinexor, you get randomized as a JAK inhibitor-naive patient with myelofibrosis to either Jakafi plus a placebo, so you’re still getting active therapy, versus Jakafi plus selinexor.
It would be unethical to give nothing to someone who needs treatment.
Dr. John Mascarenhas
The idea is: can we build upon the success of the standard of care? That becomes important. It would be unethical to give nothing to someone who needs treatment. It’s not unethical and it’s practical to give someone who needs treatment the standard of care plus a sugar pill, which is blinded, versus the standard of care plus the study drug to ask which treatment regimen is better.
You can ask your physician, but you’ll notice that most trials will allow crossover and that becomes important. If you get the placebo, which only the computer knows, at some interval, most trials will allow you to cross over to the active compound. It becomes a question of: do I get the active combination upfront or is it delayed? That’s a nuance that I want to stress. If you’re participating in a phase 1 or phase 2 study, you’re going to get the drug. Those are not placebo-controlled studies. You should always be getting the drug in those settings.
What If I Have Other Chronic Conditions?
Andrew: Some of us have other conditions, like diabetes, high blood pressure, or a heart condition — for me, it’s chronic lymphocytic leukemia, which is fortunately pretty well-controlled— but we’re often excluded from trials depending on the condition. We understand the worry of the investigators. Is our data clean? Can you extrapolate from that? Can you talk about exclusion criteria and compassionate use?
Dr. Mascarenhas: The reality is there are biases in the way we do trials. We avoid patients who may be inappropriate and these are real patients who might be in need, but the trial may not be appropriate. These can be patients who have very significant kidney or heart dysfunction or a competing malignancy. Interestingly, CLL, which is more frequently seen in patients with MPNs, has different stages. Sometimes a study will allow patients who have a very indolent type of CLL to go on the study. But often, trials will be very particular, especially registration studies where they’re going for approval.
The last thing a study needs is to have confounding data where they’re unclear whether they’re making something unrelated to the myelofibrosis worse or that condition is making the assessment of the drug harder to appreciate. There is a tendency to exclude patients who have extremes of comorbidities so not all comorbidities. If you have grade 1 heart failure, that’s often allowed in a study because that’s a reality of life.
There is a very strict inclusion and exclusion criteria, what we call eligibility criteria, which determine the ability to put someone on a study. Most of those are there for safety reasons to avoid causing additional problems with a drug because it’s not intended for that reason. Another reason why they’re there is if you have a very messy, patient population with lots of diversity and heterogeneity in organ function, etc., it can be very difficult to assess whether the treatment we’re giving is safe or effective. To some extent, out of necessity, we create some homogeneity out of the heterogeneity.
Compassionate use… requires a lot of regulatory oversight, approval, and effort, which is not provided by a company or anyone.
Dr. John Mascarenhas
Andrew: How about compassionate use? If somebody would otherwise be excluded, could their doctor make a plea for a late-stage patient?
Dr. Mascarenhas: Compassionate use is often not that compassionate. It’s trying to get access to a drug under an investigational new drug (IND) and creating a protocol for one individual. What is not always appreciated is while that sounds great, many steps go into that and it requires a lot of regulatory oversight, approval, and effort, which is not provided by a company or anyone. It’s the physician and whatever team members he can assemble to try to do that.
Although compassionate use is an opportunity to get a drug, it’s often an opportunity plagued by the realities of a very cumbersome bureaucratic system that doesn’t make it very easy and timely to get to that drug. Although it’s there and in some cases helpful, it’s not always practical or realistic for people to get compassionate use and sometimes the access to those drugs is restricted by the FDA and/or the sponsor.
But compassionate use can sometimes be an opportunity to get a drug that wouldn’t otherwise be eligible and that’s key. If there’s a trial that allows the patient to get access, they often will not provide compassionate use because it would be felt unethical to allow someone to get access to a drug while all other patients would have to go through the normal routine of the clinical trial. This has to fit very strict criteria and is not always achievable.
The Future of Treatments for MPN Patients
Andrew: We have ASH in the rearview mirror. You have other conferences during the year and you’re speaking at a number of them. You’re actively involved in research and seeing patients as well. I want to get where your head’s at as far as promise in the field, how you feel about it, and what people can do about it.
Dr. Mascarenhas: We are way further ahead than we were in 2005, 2010, and 2015. I’ve watched the field grow in terms of our understanding, the amount of attention and support that’s provided to this rather small area of hematology from the federal government in terms of NIH grants — in which we indulge in getting to try to help move the field forward independent of pharmaceutical interests — but as well as pharmaceutical interest and philanthropy. They all help grease this machinery of translational research and understanding. We have cadres of smart, well-intentioned PhDs, MDs, and MD-PhDs that are helping us understand the biology and that is directly translating into the clinic to help us fine-tune our treatment.
We’re trying to understand how to get access to and develop multiple therapies that could be used in different subsets of patients or different combinations.
Dr. John Mascarenhas
You look at ASH or EHA and see endless abstracts of agents that we didn’t even know about or targets that we didn’t even understand 10 years ago. I have to believe that’s going to translate ultimately to better therapies and multiple therapies. I don’t think it’s going to be one therapy fits all. We’re trying to understand how to get access to and develop multiple therapies that could be used in different subsets of patients or different combinations and that is something that I do feel optimistic about. I would say we’re moving forward in 2025 and beyond in rational combinations and allowing science to drive the advancements.
You’ve known me for a long time. I always feel positive. I walk to work and I’m enthusiastic every day I come in because I believe in the mission. We’re making strides. I see it in the patients that I treat, but I believe it for the future.
What Patients Can Do to Alleviate Symptom Burden
Andrew: For a patient who has significant anemia, declining platelet counts, an enlarged spleen, or whatever symptom they’re experiencing, what can they do that could make a difference in the short term?
Dr. Mascarenhas: If you’re having symptom burden, particularly if it’s interfering with your quality of life and activities of daily living, you should see a physician who specializes in hematology and, ideally, someone who has expertise in this area.
The longer one delays starting therapy, the less likely that therapy will be effective and that the effects of that therapy will be durable.
Dr. John Mascarenhas
A JAK inhibitor is the front-line therapy to try to address those aspects. It doesn’t preclude one from looking at clinical trials that might even be combinations upfront of a JAK inhibitor plus an active agent to see if one can get even better, deeper, and earlier responses. But at the very least, a JAK inhibitor to try to address symptoms because you don’t get extra points for suffering through symptoms. It’s harder to rescue if one delays treatment. The data is very clear about that. The longer one delays starting therapy, the less likely that therapy will be effective and that the effects of that therapy will be durable.
Andrew: You may live at a distance from one of the major centers where there is an MPN specialist, but there are MPN specialists. You refer to cadres of researchers and physicians who are working in this area and it makes sense to have a consultation with somebody like Dr. Mascarenhas at Mount Sinai or my doctor, Dr. Jamieson at UC San Diego. Fortunately, many others are studying this and working on it and understand these nuances, so you get personalized care for where you are now and where you may be headed.
Final Takeaways on MPN Treatments
Andrew: This has been a helpful discussion. Is there anything you wanted to add, John, that we didn’t cover?
Dr. Mascarenhas: We covered all the major points and I conveyed my continued optimism. One boon that we have is it’s a very collaborative field. When you look at the abstracts, trials, and studies, you will see all the names that are listed, which reflects our collaborative nature. These are rare diseases. You can’t work in a silo. We’re all friends and colleagues. We all have a unified mission. We’re focused on that as an international team and that’s why I remain enthusiastic that we’re going to make the progress.
Andrew: Thank you for your collaboration and people. I’m seeing a lot of younger physicians and scientists interested in this area, so that gives us a great deal of hope. Dr. Mascarenhas, thank you for your devotion to us. We appreciate your time. We’re all bonded in this together. Remember: knowledge can be the best medicine of all.
Conclusion
Tiffany: That discussion [ on MPN treatments ] was the definition of news you can use. Thank you, Dr. Mascarenhas and our patient advocate and moderator Andrew, for taking the time out of your busy schedules to keep The Patient Story community informed. If you are a patient, caregiver, partner, or advocate, consider being a voice leader in your community or with us at The Patient Story.
To be empowered is to be inspired. We want you to make informed decisions about your care and that includes being educated about the latest treatment options.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Ruth Fein Revell: Hi and welcome to our program, Clinical Trials Update: What to Know in Myelofibrosis Care. My name is Ruth Fein Revell and I’ve lived with a myeloproliferative neoplasm (MPN) for nearly 30 years.
I was diagnosed with essential thrombocythemia in 1995, polycythemia vera about 20 years later, and myelofibrosis in 2018. I’ve also lived with a number of complications from dangerous blood clots and hemorrhages that put me in the ICU to debilitating headaches, bone pain, and extreme fatigue.
I’m a health and science writer and very fortunate to be in a clinical trial for the last four years with amazing results, eliminating my symptoms, and significantly reducing my bone marrow.
We want to note that The Patient Story retains full editorial control of this entire program. This is not meant to be a substitute for medical advice.
Joining us is Dr. Naveen Pemmaraju, a top expert in MPNs and myelofibrosis from MD Anderson. Dr. Pemmaraju, it’s so nice to see you. Thanks for joining us and for being a part of this program. Can you tell us more about yourself and what drew you to MPNs?
Naveen Pemmaraju, MD
Dr. Naveen Pemmaraju: Thanks for having me. I’m a professor of leukemia at MD Anderson in Houston, Texas. I serve as the executive director for cancer medicine and as the director for our rare disease program, including blastic plasmacytoid dendritic cell neoplasm (BPDCN).
Ruth: It’s always great to see you and to speak to you. You offer so much to the MPN community and we really thank you.
JAK inhibitors are not JAK2 mutant-specific inhibitors, so that’s why they work in patients whether they’re JAK, MPL, CALR, triple-negative, or have no mutations.
Dr. Naveen Pemmaraju
Standard of Care: JAK Inhibitors
Ruth: We now have four JAK inhibitors and one one of them was just approved. Walk us through this. First of all, how does a JAK inhibitor work?
Dr. Pemmaraju: The basic premise is that MPN cells signal through a specific pathway called the JAK/STAT pathway.
A regular cell uses the JAK/STAT pathway for normal blood cell growth, differentiation, and lifespan. Now take an MPN cell and that pathway is hijacked and used in a malignant way, so those cells keep growing and dividing. It’s like a light switch that’s turned on that doesn’t go off.
Interestingly, the JAK inhibitors are not JAK2 mutant-specific inhibitors, so that’s why they work in patients whether they’re JAK, MPL, CALR, triple-negative, or have no mutations.
JAK inhibitors are based on the principle that the JAK/STAT pathway and the cells are overactive and not working properly. JAK inhibitors aim to block that malignant activity and restore normal growth.
Ruxolitinib was the first-ever approved JAK inhibitor. Since 2011, three JAK inhibitors have been US FDA-approved: fedratinib in 2019, pacritinib in 2022, and momelotinib in 2023. The four currently approved JAK inhibitors have some interesting similarities and differences.
[Ruxolitinib] works very quickly in relieving the symptom burden for our patients with MPNs.
Dr. Naveen Pemmaraju
Ruxolitinib
Dr. Pemmaraju: Ruxolitinib, the first and longest in class, is a JAK1/JAK2 inhibitor. This drug was simply amazing in the original clinical trials, which were COMFORT-I and COMFORT-II, led by Serge Verstovsek and Professor Claire Harrison.
In those studies, we learned a few things about ruxolitinib. One is that it works very quickly in relieving the symptom burden for our patients with MPNs. It can shrink the spleen rather quickly as well, so quickly that the hallmark ended up being at week 24 by six months.
Some side effects to look out for over time in this otherwise well-tolerated drug have been the development in some patients of opportunistic infections, such as herpes zoster or shingles, weight gain, and non-melanoma skin cancers.
Basal cell and squamous cell cancers of the skin are already common in our patient population, so a lot of our patients end up seeing a dermatologist. Most of our patients don’t necessarily discontinue for those side effects, but we need to watch out for them.
All patients who are going to get treated with fedratinib should have their thiamine level checked.
Dr. Naveen Pemmaraju
Fedratinib
Dr. Pemmaraju: Fedratinib improves symptoms and decreases spleen size, but it has a very notable toxicity or side effect, which garnered an FDA black box warning. It’s a very serious potential side effect called encephalopathy. Some have seen it to be Wernicke’s encephalopathy, but on later analysis, not exactly.
Wernicke’s encephalopathy is a name for a syndrome that can cause problems with thinking and even balance and can result from severe nutritional deficiencies. For fedratinib, it appears that it displaces vitamin B1 (thiamine) so what we see is the linking of those. All patients who are going to get treated with fedratinib should have their thiamine level checked because the encephalopathy can be related to that.
Patients can have GI side effects with fedratinib, like nausea, vomiting, and diarrhea, so we have to watch out for that, particularly in our older and more frail patients.
The unique thing with pacritinib is for several years, it was being watched for the development of cardiac and/or bleeding signals.
Dr. Naveen Pemmaraju
Pacritinib
Dr. Pemmaraju: Pacritinib is an interesting agent. Again, all these are trying to hit the JAK/STAT pathway, but this hits other pathways outside of that and that may be part of its benefits and toxicities.
It helps to shrink down the spleen and improve the symptom burden of patients, but the unique thing with pacritinib is for several years, it was being watched for the development of cardiac and/or bleeding signals.
I and others have done a lot of evaluation and analysis, including post-approval. We’re not seeing a high signal for that, but that’s something you have to be aware of if the patient is on a blood thinner, having chest pain, or having heart surgery.
Not only did [momelotinib] show improvement in the spleen size and symptoms, but what’s interesting — and pacritinib is showing this as well — is having an improvement in anemia.
Dr. Naveen Pemmaraju
Momelotinib
Dr. Pemmaraju: Momelotinib is the most recently approved JAK inhibitor. Again, not only did it show improvement in the spleen size and symptoms, but what’s interesting — and pacritinib is showing this as well — is having an improvement in anemia. Now that’s important.
Ruxolitinib and fedratinib don’t necessarily do that and, in some cases, it can make it transiently worse. Momelotinib has ACVR1 inhibition. Pacritinib also showing that as well unleashes a new era for our patients of JAK inhibitors having beneficial side effects, such as improvement of anemia and potentially, thrombocytopenia.
You have to watch out for GI side effects with fedratinib, pacritinib, and even momelotinib. In the earlier studies of momelotinib, there was a signal for peripheral neuropathy. I want to put those forward as an overview. There are some subtleties and differences, if one reads further.
Ruth: Thanks for that explanation. I’ve heard a lot of people say that they have a different mutation, so a JAK inhibitor isn’t going to help them, but we know that that’s not the case, so thanks for your explanation of how they work.
There isn’t a single molecular test. The decision is based on clinical factors and the art of medical decision-making.
Dr. Naveen Pemmaraju
Switching JAK Inhibitors
Ruth: How do you know which JAK inhibitor might or might not work and which one to try first? How is that decision made?
Dr. Pemmaraju: The decision to switch JAK inhibitors is not scientific. We’re not there yet. At some point, I envision that we’ll have a decision tree, like our colleagues in CML. But right now, there’s no molecular test, so it is the art of medicine. It is clinical decision-making.
There are some factors, if one looks up in the NCCN and other guidelines. One is platelet count. Ruxolitinib and fedratinib should be given to patients who have a certain amount of platelets and that’s where pacritinib was able to get its approval.
Pacritinib is specifically approved in the front-line setting for patients whose platelet count is less than 50, for example. The NCCN guidelines and other groups say that once you use pacritinib in later lines, maybe you don’t have to pay attention to the platelet as much, but that’s obviously for debate.
Another factor is the GI signal. If you have someone who has a known encephalopathy syndrome or thiamine deficiency, then fedratinib is not going to be one that you would choose.
Finally, you have to look at some of these subtle side effects that we mentioned earlier, such as GI and neuropathy, to help you choose.
The bottom line is there isn’t a single molecular test. The decision is based on clinical factors and the art of medical decision-making.
Switching can have financial cost repercussions, new toxicities when a patient was otherwise doing ‘okay,’ problems with access to the drug, and could uncover idiosyncratic side effects that may be specific to that patient and weren’t seen in the studies.
Dr. Naveen Pemmaraju
Ruth: So it’s possible that somebody could start on one JAK inhibitor and at some point switch to another. Is that an issue if you change?
Dr. Pemmaraju: This is a great important point about switching JAK inhibitors and what are the indications. There are several buckets here.
First is clear disease progression in terms of the spleen. If you have a patient who’s been on a certain JAK inhibitor for a sufficient amount of time and you have a spleen that previously shrunk but now starting to rise again, that could be considered disease progression and an indication to switch.
Second is worsening MPN symptom burden to the point where the patient’s quality of life is affected.
Third is blast count, peripheral blasts or bone marrow blasts, going up.
Fourth is the progression of the disease to an outright higher level of disease, what we call an accelerated blast phase.
The development of these clinical factors, such as the platelet count, may matter if you have a patient who’s on ruxolitinib, for example, and you consistently have platelets below 50, then that’s an indication to switch, for example, to pacritinib. If you have a patient who has anemia, you may think about momelotinib.
These are some of the reasons to think about switching. But again, there isn’t a molecular test or a definitive moment to switch. Switching can have financial cost repercussions, new toxicities when a patient was otherwise doing “okay,” problems with access to the drug, and could uncover idiosyncratic side effects that may be specific to that patient and weren’t seen in the studies.
Finally, you have a question about withdrawal and overlap, so these are things I think we’ll all work out together over the coming years as we have these JAK inhibitors in the clinic.
The story of JAK inhibitors is an evolving story and it’s evolving at three levels.
First is the science of it alone. In 2005, I was at Johns Hopkins with Alison Moliterno and Jerry Spivak, and I remember the day that the JAK2 mutation V617F was elucidated. From that time to now, we have JAK inhibitors that are amazing, so science is still evolving.
Second is the clinical part, as we’ve discussed. When to switch, how to switch, what are the factors, etc.
Third is the future. How do we combine these drugs with a second agent and potentially a third agent? What are those cross-reactivities? How does that benefit the patient to start those upfront rather than later on? You have this evolving area that’s quite exciting but also quite daunting not only for the patients and the clinic but for researchers.
This is preliminary data, but it was so encouraging that they are now moving on to a phase 3 randomized global study.
Dr. Naveen Pemmaraju
Clinical Trials: Combination Therapy
Selinexor & Ruxolitinib
Ruth: We’re seeing some really exciting updates as far as combination therapy. Let’s talk about clinical trials, starting with selinexor plus a JAK inhibitor and then move on to other combinations.
Dr. Pemmaraju: At ASH 2023, Dr. Sri Tantravahi from Utah presented the first public data of front-line combination, updated I should say, of selinexor with ruxolitinib. This is untreated patients with myelofibrosis, intermediate to high risk, who were given the combination rather than ruxolitinib, which would be considered the standard or JAK inhibitor.
Although it was early on and only a few patients, very surprisingly and amazingly, the group showed that there’s a high rate of activity in spleens being reduced as well as symptom burden being increased.
Now, this is preliminary data, but it was so encouraging that they are now moving on to a phase 3 randomized global study. The combination selinexor-ruxolitinib, so the XPO1 inhibitor plus JAK inhibitor, versus JAK inhibitor alone. Those data will be eagerly awaited.
This is also, if I may say, a fascinating study.
Dr. Naveen Pemmaraju
Navitoclax & Ruxolitinib
Ruth: What about the BCL inhibitor navitoclax?
Dr. Pemmaraju: A second combination is that of the BCL-XL inhibitor navitoclax with ruxolitinib, which I presented as an oral presentation at ASH on behalf of my colleagues. This is also, if I may say, a fascinating study.
We globally enrolled 252 patients into a randomized, double-blind, placebo-controlled study of ruxolitinib plus navitoclax, which is not yet approved for any indication, versus ruxolitinib alone. Again, we had intermediate to high-risk patients, around 80-plus percent of intermediate-2 patients.
What we found is a very outstanding rate of 60-plus percent of patients in the combination arm having an SVR35 at week 24, so spleen volume reduction of 35% or more, versus only 30-plus percent in the control arm, which was ruxolitinib alone. The waterfall plot showed that almost all patients benefited from the combination.
In terms of statistical analysis, the primary endpoint of spleen reduction was met with a high statistical significance, but the symptom burden difference was not yet found to be statistically significant. Both groups had reductions, so there was a numerical reduction of the symptoms in both the combination and the ruxolitinib alone, but there was no statistical difference.
The study is ongoing for collecting for maturity and overall survival duration, so this was a preliminary presentation at 15 months follow-up. We’ll stay tuned to see how it gets updated over the next congresses.
Great safety, but you have to watch out for thrombocytopenia, which is low platelets, and watch for that signal very closely.
Luspatercept & Ruxolitinib
Ruth: Another combination being investigated is the use of a shot called luspatercept to boost hemoglobin or fight anemia, and that also is being used with ruxolitinib. Can you tell us more about that one?
Dr. Pemmaraju: Luspatercept is a fascinating molecule. It’s already FDA-approved in the myelodysplastic syndrome setting. In the MPN setting, we think it has a similar activity to improve hemoglobin and anemia, which is an urgent, unmet medical need.
The initial studies have shown positive data, which is either luspatercept by itself, usually given every three weeks, or in combination with the JAK inhibitor ruxolitinib. Those studies are ongoing and we eagerly await those results in the coming year or two.
When the group looked back at certain subsets, including the intermediate-1 patients and others, it appeared that there was a benefit in both spleen size and symptoms.
Dr. Naveen Pemmaraju
Pelabresib & Ruxolitinib
Ruth: We’ve also had the MANIFEST trial, which is the trial that I happen to have been on for the last four years, and that’s a different drug, s pelabresib. Could you talk about that combination and what you think the potential is?
Dr. Pemmaraju: Another exciting combination presented at ASH 2023 was that of the MANIFEST-2, which is ruxolitinib plus a new agent pelabresib, a bromodomain or BET inhibitor, which is not yet FDA-approved for any indication.
This encouraging data set was presented by Dr. Raajit Rampal from Memorial Sloan Kettering. It’s the second-largest study ever conducted in the myelofibrosis front-line space, which included 430 patients. They also randomized ruxolitinib-pelabresib versus ruxolitinib alone in the control, mostly intermediate-1 to intermediate-2 patients, so a slightly different population.
They showed a very similar profile. A highly statistically significant primary endpoint was met, which is SVR35 at week 24. The symptoms in all comers, although showing a numerical decrease in both groups, did not quite meet statistical significance.
When the group looked back at certain subsets, including the intermediate-1 patients and others, it appeared that there was a benefit in both spleen size and symptoms.
The supposition is the same as navitoclax. These two are the first ever in our field, resulting in phase 3 global, double-blind, placebo-controlled, front-line, untreated myelofibrosis patients with a novel combination of pelabresib and navitoclax, neither of which are FDA-approved for any indication.
I would say my editorial comment is super exciting for the field that we even did it. Both were international studies largely conducted during the pandemic and involved lots of patients and investigators.
The primary endpoint was met for both of them. The symptoms were not quite met in either study in terms of statistical significance so the question asked is three-fold.
What is the utility of following the symptom burden scale in combination studies, something that was designed 15 years ago for a single-agent JAK inhibitor?
Do we expect a combination to improve symptoms over ruxolitinib alone, or because you’re introducing a second drug, you’re going to introduce new toxicity?
On behalf of my colleagues, maybe it’s time to reevaluate: what are the endpoints for our patients with myelofibrosis? Perhaps in addition to reducing spleen size and improving symptoms, we should be factoring in overall survival, progression-free survival, and bridging to stem cell transplant. This is the time to talk about it because these combination studies are difficult, if not impossible, to judge based on the COMFORT-I and COMFORT-II studies.
Imetelstat is in an ongoing phase 3 trial, which is in the second-line setting and beyond, against the best available therapy (BAT).
Dr. Naveen Pemmaraju
Telomerase Inhibitors
Ruth: Let’s go beyond JAK inhibitors. There are other drugs being studied. Can you help us understand other approaches?
Dr. Pemmaraju: There’s an exciting alphabet soup of clinical trials and drug molecules out there. It’s exciting for our patients to know that there are people around the world who care about MPNs, so it’s good to know that despite COVID, we have a lot of innovation.
We’re adding a new trial once a week, so it’s almost impossible to keep up, but I do want to give some sampling of what’s going on.
Imetelstat is very important for everyone to know. It’s a first-in-class telomerase inhibitor. Some people have heard of telomeres. They are the little ends on the ends of chromosomes that help to determine aging and possibly even cancer biology.
Imetelstat is in an ongoing phase 3 trial, which is in the second-line setting and beyond, against the best available therapy (BAT). I praised this trial because it’s the first and, to my knowledge, only phase 3 trial that has overall survival as its primary endpoint. Hopefully, it will give us a readout in the next year or two.
MDM2 Inhibitors
Dr. Pemmaraju: MDM2 inhibitors have gotten a lot of press in all MPNs. This is a key pathway that has to do with guarding the cell TP53. It’s an oral drug that has been studied before. As a class of drugs, there may be some GI side effects to watch out for, but in the later trials we’ve seen, the groups have figured out a way to address that by either adjusting the dosing schedule or dosing frequency.
I’m excited to see where that area goes. Right now, the lead trials are MDM2 inhibitors with ruxolitinib as an add-on approach or a suboptimal approach. You’re already on a JAK inhibitor. You have an okay response, not a great one, but not quite ready to come off of it, and then you add the MDM2 inhibitor. Those studies are actively ongoing and I think we’ll be excited to see those results.
The good thing about myelofibrosis is whether you’re JAK, CALR, MPL, or triple negative, you respond to JAK inhibitors and novel agents alike.
Dr. Naveen Pemmaraju
Genetic Mutations in Myelofibrosis
Ruth: What if someone’s myelofibrosis isn’t driven by a JAK mutation but a different mutation, is there a different approach? We’ve also been hearing about a cancer vaccine related to CALR, so could you walk us through both?
Dr. Pemmaraju: There’s a two-part answer to the question of molecular mutation targeting in MPNs. Historically and in the clinic right now, there is no difference at the moment.
The good thing about myelofibrosis is whether you’re JAK, CALR, MPL, or triple negative, you respond to JAK inhibitors and novel agents alike. That’s an interesting thing that suggests that there’s a common pathway.
But for the future, yes. Already in the clinic in 2024, we expect a new era to begin, which is, for the first time, to have mutant-specific approaches for both JAK2 and CALR. I expect that we’ll see multiple different drugs targeting mutant JAK2 specifically. The hypothesis is: could that be better and more specific than targeting the whole pathway? Let’s see. You’ll see phase 1 trials there.
CALR turns out to be a really good target, especially for immune therapy targeting. That’s only new science in the last five years. There are vaccine approaches either by themselves or with other immune drugs, such as ipilimumab. There’s an exciting bispecific molecule, which is a mutant CALR x CD3 bispecific antibody that I and others will be working on.
There are also going to be other ways to target CALR. You have multiple different ways of targeting mutant-specific approaches, but let me highlight these are phase 1 clinical trials. They’re backed by animal preclinical data. Now we need to see how they do in the initial trials.
For the first time, I’m seeing sustained improvement in the anemia of MPN, specifically myelofibrosis. We have three different categories trying to address this for our patients.
Dr. Naveen Pemmaraju
Anemia in Myelofibrosis
Ruth: Dr. Pemmaraju, you mentioned that many people suffer from anemia when hemoglobin is low. We know they can feel extremely fatigued so much that it interferes with their quality of life, which I know from personal experience, unfortunately. With what you’ve described, do you feel like we’re getting better tools to fight anemia and hopefully avoid people needing more frequent transfusions?
Dr. Pemmaraju: Yes. For the first time, I’m seeing sustained improvement in the anemia of MPN, specifically myelofibrosis. We have three different categories trying to address this for our patients and it’s simply exciting.
First is the JAK inhibitors themselves. As we mentioned earlier, the first initial ones did not improve and may have worsened the anemia transiently in some patients. Now these second- and third-generation JAK inhibitors are improving the anemia and possibly through the inhibition of ACVRL1, so that’s exciting.
Second is the additional agents, such as luspatercept. You can add on an agent that works outside of the JAK inhibitor that aims to stimulate the hemoglobin and improve the anemia.
Third is these novel agents. When you look closely at the navitoclax and pelabresib data sets, in those two particular instances, you have some people who get anemia as toxicity, but you also have patients who have anemia improvement with the combination, maybe better than with ruxolitinib alone. These three approaches, we’re already seeing in the clinic in phase 1, 2, and 3 clinical trials.
Out of all of these theoretical things, a lot of times what our patients are suffering from is anemia. When the hemoglobin gets below 7, 6, 5, or 4, it’s not even compatible with life, much less quality of life. Anything we can do to reduce the burden of getting transfusions, missing appointments, and missing life events is going to be a big breakthrough, and I’m starting to see that.
If a transplant is available and indicated, it is the only curative approach for myelofibrosis.
Dr. Naveen Pemmaraju
Role of Stem Cell Transplant in the Treatment of Myelofibrosis
Ruth: Typically, a doctor will tell a patient that the only cure for myelofibrosis is having a stem cell transplant. With these new medical therapies, my question is always the same: do you see a changing role for transplants?
Dr. Pemmaraju: The role of stem cell transplant in myelofibrosis is one of great importance still. While I’m personally excited about all of these drugs in development, two things are important.
First, none of these have been shown to create a long-term cure in and of themselves for myelofibrosis. Second, if a transplant is available and indicated, it is the only curative approach for myelofibrosis.
Having said that, the realistic problem with allogeneic transplants is that it’s not available for everyone because of their comorbidities, how frail versus how fit they are, matching, the infection rate, and the mortality rate. As patients get older, it may be tougher at some centers and for some folks to do it. There are some real limitations.
The other problem is that out of all of our patients, the vast majority are not going to transplant. Improvements are being made with transplants every day. Haploidentical transplant, which is a half match, is becoming more of a standard, so that gives the donor pool exponentially more options.
Trying to reduce graft versus host disease, which are complications after the transplant, with medicines are revolutionizing the field.
As I’ve traveled all over the world, people can do stem cell transplants in economically diverse situations. The transplant procedure itself can be highly expensive. Interestingly, even though cost-effectiveness is an issue, in some locales, if you can do a transplant and potentially cure the disease, it can lead to an improvement in socioeconomic status overall.
There are some cool, important things happening. But it’s an important point that even with all the excitement of these medicines and medicine combos, we’re still not at the point where we’re talking about a cure, so if you have the availability and indication for transplant, you have to pursue that consideration.
We have brand new approaches that we didn’t have a few years ago. There is a lot of data and science, so there’s hope.
Dr. Naveen Pemmaraju
Final Takeaways
Ruth: Let’s put all of this together. For those of us living with myelofibrosis or others who are concerned about progressing to myelofibrosis, what do you want to leave them with? When you total up everything we’ve talked about, how do you want to leave the conversation?
Dr. Pemmaraju: This discussion was very exciting because it left me with even more hope than when I started the day. I would leave our patients, caregivers, family members, advocates, and stakeholders with a message of hope and positivity. It’s not blind hope and positivity. It’s not based on hunches or ideas. It’s based on data.
The last three years in particular, I would call it — and I do not use this phrase lightly — a golden era for research for the MPN, specifically including myelofibrosis.
There are four areas to highlight and to be very excited about for our patients and families. First is the development of new JAK inhibitors. We mentioned the four that are already approved in the US, so let’s get them available all over the world. There are several more in clinical development.
Second is the JAK inhibitor combinations. Very exciting data from ASH. Let’s see the new combinations. Maturing data for navitoclax, pelabresib, and selinexor.
A third area of excitement and hope is that of anemia-improving agents.
Finally, the delineation, description, and demonstration of brand-new molecular pathways inside the cells that were never known before. New insights and ways of approaching. We mentioned potential immune therapy approaches, like the CALR mutation. It’s exciting that we have brand new approaches that we didn’t have a few years ago. There is a lot of data and science, so there’s hope.
Ruth: Dr. Pemmaraju, thanks so much for being with us today. You’re always a pleasure to talk to and so informative to our guests. We really appreciate your time.
Dr. Pemmaraju: Thank you so much for having me. This was a very thought-provoking and stimulating discussion.
Interested in myelofibrosis clinical trials? We’ve gathered the leading experts to explain emerging clinical trials, misconceptions, and how to find the treatment best for you.
Gain invaluable insights into upcoming exciting clinical trials, the purpose and benefit of trials, and navigating trials and treatments. Optimize communication with your healthcare team and empower yourself with extra support and resources.
We try to help patients and their supporters navigate a diagnosis and we do this through in-depth conversations with patients, care partners, and top specialists across different cancers.
It’s important to have these educational programs, especially when it comes to topics like clinical trials, which are daunting and overwhelming, so we’re trying to humanize your options.
We’re so proud to be co-hosting this with The Leukemia & Lymphoma Society, the world’s largest non-profit health organization dedicated to funding blood cancer research as well as offering patient services and education.
They have great resources, including information specialists who are a phone call away to help answer your questions. We’ll be highlighting the Clinical Trial Support Center, a very critical free resource that offers one-on-one support to enroll in and stay in clinical trials.
This is not meant to be a substitute for medical advice. We want you to walk away and be able to ask your own doctors and medical teams questions about clinical trials in myelofibrosis.
I know how fortunate I am as many people suffer so much more than I ever have.
Ruth Fein Revell
Ruth Fein Revell, Patient Advocate
Stephanie: I’m thrilled to introduce someone who’s not only a big MPN and myelofibrosis patient voice and leader in the community but also someone I’m lucky to call a friend and who will be leading the conversation.
Ruth, I know that you’re going to share more about your own myelofibrosis cancer story and how you became a passionate advocate. But first, can you share more about yourself outside the cancer context? Because as we know, we are so much more than a diagnosis.
Ruth Fein Revell: Thanks so much, Stephanie. Professionally, I’m a health and science writer who now writes primarily about cancers, blood cancers in particular. I also host patient programs. I have the privilege of speaking to many of the world’s most prominent researchers and clinicians.
In many ways, I think cancer has attracted many of us because we feel we can make a real difference in a difficult disease.
He’s globally recognized as a leader in the MPN space and we are so fortunate to have him with us. Our audience would love to know you beyond that white coat of yours. What drew you to work in cancer and research?
Dr. Ruben Mesa: Cancer is such a terrible disease. It impacts and steals from an individual’s length of life and quality of life. I myself have been touched by cancer as so many have. My father passed from cancer and my mother is a cancer survivor. I was able to witness the impact of cancer research, developing new therapies, and the value of really compassionate care and how important these things were.
In many ways, I think cancer has attracted many of us because we feel we can make a real difference in a difficult disease. It’s also an exciting time when scientific progress is really making a genuine impact.
There are many aspects of myeloproliferative neoplasm that I find extremely rewarding to take part in.
Dr. Angela Fleischman
Dr. Angela Fleischman, Hematologist-Oncologist
Ruth: Dr. Angela Fleischman is a hematologist-oncologist at UC Irvine Health, where she leads the Fleishman Lab with a special focus on MPNs and improving the options and care for patients.
As a physician-scientist, Dr. Fleischman not only treats patients but also actively researches hematological malignancies. She’s passionate about translating findings from the lab bench to the patient’s bedside.
Dr. Fleischman, we’d love to know a little more about your passions as well. What drew you to blood cancers and research?
Dr. Angela Fleischman: I have always been extremely interested in blood cell development. I started out as a Ph.D. student prior to my MD and focused on normal blood cell development and what determines whether a blood stem cell goes one direction or the other.
When I decided to go to medical school and first learned about myeloproliferative neoplasms, I was extremely fascinated by them because I felt that it was an opportunity to learn what happens when blood cell development goes awry.
Another extremely interesting aspect of myeloproliferative neoplasm that I was extremely drawn to is the ability to make connections with patients throughout the years because it’s a chronic disease. As a physician, I’m able to travel with them through their journey as a patient. There are many aspects of myeloproliferative neoplasm that I find extremely rewarding to take part in.
I help patients navigate the complicated clinical trial landscape, and provide them with education and potential treatment options to take back to their care team.
Melissa Melendez: I’ve been in the oncology field for almost 20 years and it was a happy accident how it happened. While in nursing school, I started my first clinical rotation in the oncology unit. I was pretty apprehensive and concerned that I was being plunged into caring for such complex patients with extreme highs and extreme lows of treatment outcomes.
I instantly fell in love with not only helping patients on their journeys throughout their treatment but also the privilege of caring for their families who were going through the journey as well. I decided that oncology was going to be my career path.
I started as a patient care assistant then a registered nurse, a division supervisor, and currently a nurse practitioner. Working for The Leukemia & Lymphoma Society in the Clinical Trial Support Center has been such a blessing for me as a nurse and it was a pretty easy transition from my previous occupation.
I help patients with clinical trials and throughout their journey. Not only do I work with intelligent, caring, and selfless colleagues but also with a population of patients and families that I truly love.
On a daily basis, I get to see the impact that the LLS has on patients and families, help patients navigate the complicated clinical trial landscape, and provide them with education and potential treatment options to take back to their care team to discuss so they can make informed decisions about their care. I get to build relationships with patients and family members that last for years.
It wasn’t until I was taken off hydroxyurea before starting a clinical trial that I realized how severe my symptoms were without treatment.
Ruth Fein Revell
Ruth’s MPN Story
Ruth: What is myelofibrosis? Myelofibrosis is one of the MPNs, a myeloproliferative neoplasm, and a very personal topic for me. I’ve lived with an MPN for nearly 30 years, originally diagnosed with essential thrombocythemia or ET at age 38 while I was raising two young boys.
I was taking an aspirin a day, which was stopped because I developed an ulcer. I ended up with clots in my portal and splenic veins. After a week in the hospital, I was put on an anticoagulant or a blood thinner. Several years later, my bone marrow flipped a proverbial switch and instead of producing too many platelets, it now produced too many red blood cells.
The diagnosis was changed to polycythemia vera and I lived with periodic phlebotomies and daily hydroxyurea. That was part of my life, as with many people who live with polycythemia vera and the different MPNs.
In 2018, I had surgery for early colon cancer. The surgeon was so focused on avoiding any more clots that I had the opposite happen. A major bleeding episode put me in the ICU for nearly a week, followed by several months of healing.
I finally sought out an MPN specialist and began to see Dr. Ellen Ritchie at Weill Cornell in New York. I had an updated bone marrow biopsy, which confirmed a diagnosis of myelofibrosis.
I used to say I was mostly asymptomatic but I’ve lived with severe migraines, a few TIAs (transient ischemic attacks), and other constitutional symptoms my whole life. It wasn’t until I was taken off hydroxyurea before starting a clinical trial that I realized how severe my symptoms were without treatment.
I experienced both life-threatening clots and bleeding episodes. I had such extreme fatigue that I couldn’t walk up the street without stopping to lean or sit on a neighbor’s step. Of course, I also know how fortunate I am as many people suffer so much more than I ever have.
Fibrosis does not always equal the MPN myelofibrosis.
Dr. Angela Fleischman
What is Myelofibrosis?
Ruth: Let’s dig right in. Dr. Fleischman, what exactly is myelofibrosis?
Dr. Fleischman: People may interpret the word myelofibrosis as having some fibrosis in the bone marrow. What we’re talking about is the myeloproliferative neoplasm myelofibrosis, which also can have some fibrosis in the bone marrow. However, I want to emphasize that fibrosis in the bone marrow does not always equal myelofibrosis.
MPN myelofibrosis is a chronic blood cancer that stems from the proliferation of some abnormal mutant cells in the bone marrow. Exactly what causes the fibrosis is unclear. The abnormal megakaryocytes or the cells that are producing platelets have been implicated as the bad cells in myelofibrosis and causing the fibrosis.
Patients also tend to have an enlarged spleen, which can also be seen in ET and PV but is more prevalent in myelofibrosis.
Blood counts can look very different. There’s a wide variety of what a myelofibrosis patient’s blood counts look like, but a classic myelofibrosis patient may have some anemia. They may have a little bit of a high white blood cell count. They may also have immature cells in their blood so their bone marrow cells are not maturing fully before going into the blood, indicating that there’s some stress going on in the bone marrow.
Myelofibrosis patients can have some significant constitutional symptoms. ET and PV can also, but in myelofibrosis, they tend to be more severe.
I do want to emphasize that because somebody has a bone marrow biopsy that says fibrosis does not necessarily always equal the MPN myelofibrosis. Other things, like autoimmune diseases, can cause some fibrosis in the marrow. Infections can cause fibrosis in the marrow. Other blood cancers can cause fibrosis in the marrow. What I want to emphasize is fibrosis does not always equal the MPN myelofibrosis.
Ruth: That’s a really good reminder and not something that people focus on much so thank you for that.
We’ve seen an explosion in many different types of therapies. Over the last three years, we’ve seen a rapid increase in FDA-approved options.
Dr. Ruben Mesa
Advances in Myelofibrosis Treatments
Ruth: The world of MPNs, in particular myelofibrosis, is changing before our eyes as clinicians, researchers, and people living with these conditions. Dr. Mesa, would you tell us how the landscape of treatments for MF patients has changed so dramatically in the last 2 to 3 years?
Dr. Mesa: I first saw patients with myelofibrosis at the beginning of my training almost 30 years ago. In the first half of those 30 years, the medicines we had for myelofibrosis were really limited because we had a very limited understanding of the biology of the disease.
What happened about 15 years ago is we identified important genetic changes, such as JAK2, CALR (calreticulin), MPL, and others that lead downstream to a patient having a myeloproliferative neoplasm.
With that, we’ve seen an explosion in many different types of therapies. Over the last three years, we’ve seen a rapid increase in FDA-approved options, now four different JAK2 inhibitors. They’ve made a real impact in patients with myelofibrosis regarding the enlargement of the spleen, perhaps helping to slow down the course of the disease to some degree and, for some individuals, dramatically so.
The next step we’re launching into is combinations of therapies where we use more than one drug and look at treating different aspects of the disease or different targets in terms of the biology of the disease to make a deeper impact.
Wearing my cancer center hat, as I look at how therapies are advancing in many different diseases, both blood cancers as well as non-blood cancers, most of the time we’re now using more than one therapy where medicines complement each other.
Different blood diseases, such as multiple myeloma, use up to four different drugs at a time. The explosion went from really very little understanding to multiple drugs, a much greater understanding of the biology of the disease, and hopefully a deeper and deeper impact.
For the majority of individuals, probably over 90%, based on a variety of factors, we start with medicines.
Dr. Ruben Mesa
Standard of Care: First-Line Treatment
Ruth: Dr. Mesa, what is the standard first-line treatment for myelofibrosis?
Dr. Mesa: When patients come in with a diagnosis of myelofibrosis, their doctor first gets a sense of the risk of the disease, how likely is the disease to be life-threatening, and the burden that the patient is facing from an enlarged spleen, from symptoms, or from the risk of progression.
We discuss whether we should pursue the potentially curative option of bone marrow transplant or stem cell transplant; we use those terms interchangeably. That’s a very complex therapy, but it’s something that we consider throughout for individuals up until their 70s, depending on the risk of the disease and other factors.
For the majority of individuals, probably over 90%, based on a variety of factors, we start with medicines. The only approved medicines for myelofibrosis are the JAK inhibitors. Transplant either in the near future, delayed, or we’re not going to pursue transplant and then consideration of a JAK inhibitor.
JAK inhibitors help to decrease the activation of JAK2. Regardless of which mutation a patient has or even if they don’t have one of the three mutations, they all seem to benefit from JAK inhibitors.
Dr. Ruben Mesa
How JAK Inhibitors Work
Ruth: We currently have four FDA-approved JAK inhibitors, including momelotinib, which was approved in September 2023. How do JAK inhibitors work? For each of the approved JAK inhibitors, would you explain what their benefits and limitations are?
Dr. Mesa: In myelofibrosis, there are three main mutations that we believe are involved with causing the disease. The JAK2 or the JAK2 V617F, the mutation in calreticulin, and the mutation in MPL. There’s even a small subset of people who do not have one of those three.
All of those mutations lead to the same outcome: an overactivation of the protein JAK2. JAK2 is one step. It’s an on-off switch stuck in the on position telling cells to grow.
JAK inhibitors help to decrease the activation of JAK2. Regardless of which of those mutations a patient has or even if they don’t have one of those three mutations, they all seem to benefit from JAK inhibitors.
Ruxolitinib has been approved since 2011. It improves the spleen and symptoms, may help patients who respond live longer with the disease, and in many ways has long been the standard. It’s frequently been used as the base in combination trials.
Fedratinib has been approved since 2019. It can be used to improve the spleen or symptoms. It may be used in the front-line setting instead of ruxolitinib or in the second-line setting if someone has had ruxolitinib already.
Pacritinib was approved in 2022 and this one has a little distinct profile. It’s particularly helpful for decreasing the spleen and symptoms but for individuals with a very low platelet count.
Both ruxolitinib and fedratinib are approved for individuals with a platelet count above 50,000. Pacritinib can be helpful in anyone, but its particularly unique niche is in individuals under 50,000 and we certainly will consider it for individuals with lower blood counts.
Momelotinib was approved in September 2023. This can improve the spleen symptoms and anemia. It showed the strongest improvement in anemia compared to the other three. Pacritinib sometimes can have an improvement in anemia. Unfortunately, both fedratinib and ruxolitinib sometimes can have anemia as a side effect or worsen anemia and rarely would improve anemia.
There are some differences among the four of them, but they overlap in many ways in terms of improving the spleen and symptoms and can be beneficial regardless of the mutation profile that a patient with myelofibrosis has.
Ruth: It’s very exciting for the MPN community to finally have so many treatment options. People often think that because they have mutations other than JAK2, a JAK inhibitor won’t help them so thanks for noting that that’s not necessarily the case.
It’s really exciting now that we have four different JAK inhibitors so we can try to tailor the best JAK inhibitor for the person upfront.
Dr. Angela Fleischman
Navigating Treatment Options
Ruth: Dr. Fleischman, here’s a loaded question. How do you know which JAK inhibitor may or may not work and which one to try first?
Dr. Fleischman: This is an evolving topic. It’s really exciting now that we have four different JAK inhibitors so we can try to tailor the best JAK inhibitor for the person upfront. Sometimes it’s a hit or miss but, as Dr. Mesa described, each JAK inhibitor has a little bit of a different profile.
All of the JAK inhibitors inhibit JAK2 but each one has “off-target” effects and some different proteins and that may explain why they have their own unique profile.
Each myelofibrosis patient is quite unique so they have different needs. For example, for somebody who has an enlarged spleen, with symptoms, and pretty robust blood counts, ruxolitinib would be a great option, which is also the only JAK inhibitor currently approved for PV, in which the purpose is to bring down blood counts.
If the person’s primary problem is anemia, which is unfortunately a very common problem in myelofibrosis, it’s very exciting that we have an option that’s specifically designed for patients with anemia. That’s a patient population very, very appropriate to start pacritinib first.
Many patients with anemia also have a low platelet count. What do you do for somebody who has both anemia and a very low platelet count? We’re going to have to learn how to sequence and make decisions between pacritinib and momelotinib. For a myelofibrosis patient with both anemia and thrombocytopenia or low platelet count, the two options that exist upfront are momelotinib and pacritinib.
Different tiers of needs as we talk about individual clinical trials.
Dr. Ruben Mesa
Combination Therapy Clinical Trials
Ruth: Some of the most exciting clinical trials for MF patients are for combination therapies. Dr. Mesa, can you explain the idea behind combination drug approaches and who might benefit?
Dr. Mesa: We think about different populations of patients. We have those who are JAK inhibitor naive or individuals who have not had a JAK inhibitor yet. This may be at the time of diagnosis or individuals who have had the disease for a while, have been observed, and now, based on spleen symptoms or changes, need to begin therapy.
There are individuals who have been on a JAK inhibitor and have had some benefit, but we feel that there’s an opportunity for further benefit. Some of these individuals are participating in add-on studies where you have a JAK inhibitor that they’ve been on for a while, they have a partial response, and a second drug is added.
The third type of patient is an individual who was on a JAK inhibitor and now no longer has a benefit from that medication so you are switching them to a different therapy altogether. Different tiers of needs as we talk about individual clinical trials.
Selinexor + JAK Inhibitor
Ruth: Let’s talk about some of those combination trials. There are a number of them where JAK inhibitors are given with the addition of a new agent with a different mechanism of action. Let’s talk about selinexor plus JAK inhibitor.
Dr. Mesa: There’s a whole constellation of different agents that have an impact on different mechanisms of action that are being looked at in combination with JAK inhibitors. This one is a little bit earlier in its development.
It’s an approved drug for multiple myeloma and has been approved since July 2019. It’s an anti-cancer medication. It’s a selective inhibitor of nuclear export. It works on some of the processes within the cell in a different way that we feel may be beneficial in combination.
Data from early studies suggest that there is benefit and it may be more with two drugs than the single drug itself. Whether this will become an option for patients with myelofibrosis, the trials will demonstrate, but it has made an important impact for individuals with myeloma so we’re hopeful that it’ll be helpful in this group of patients as well.
Ruth: It’s great to see when we borrow from different areas of research.
Navitoclax + JAK Inhibitor
Dr. Mesa: This works against a process within cells called apoptosis or programmed cell death. Navitoclax is a cousin of a drug that’s approved for acute leukemia called venetoclax.
In studies with myelofibrosis, navitoclax has shown real activity for decreasing spleen symptoms and potentially impacting the disease and, in combination, to a greater degree than JAK inhibitor alone. We have had patients on large phase 3 trials who have been newly diagnosed as well as other situations so those data are anticipated with great interest.
It may take further time for us to identify which combination is a better fit for a patient. These trials are not necessarily designed to answer that itself.
Dr. Ruben Mesa
Pelabresib + JAK Inhibitor
Ruth: Let’s talk about pelabresib, a drug very close to my heart. That’s the trial I’ve been on for more than three and a half years used in combination with a JAK inhibitor. I understand the results have been very promising. At Weill Cornell, they’re calling me the poster child for this study so I’m very grateful for that. Dr. Mesa, tell us about the MANIFEST-2 trial.
Dr. Mesa: This is probably the furthest along of the combination approaches. Pelabresib is an inhibitor of another cellular process called BET. There’s reason to believe that it may have a very complementary role in inhibiting JAK2.
In the early studies, it appeared very promising in terms of having an impact, perhaps more than JAK inhibition alone or in combination when individuals had failed a JAK inhibitor.
We now have phase 3 trials of patients newly diagnosed or who are JAK inhibitor naive receiving this combination versus ruxolitinib alone. We are looking for information to see the net benefit of using the two drugs.
Are the responses more profound? Do they last longer? Are patients better off? We always weigh any downsides to being on two drugs versus one. There are multiple combinations being tested in parallel. It’s possible that multiple of them may be beneficial. It’s possible that multiple of them could become FDA-approved.
It may take further time for us to identify which combination is a better fit for a patient. These trials are not necessarily designed to answer that itself. They’re designed to answer if they are better than a JAK inhibitor alone.
Downstream, we’ll have a better understanding based on specific patient features or other aspects of their health whether one of these combinations may be a better choice for one patient versus the other.
Ruth: Dr. Fleischman, what should patients be asking their doctors to understand if one of these combination therapies might be best for them?
Dr. Fleischman: Entering into a clinical trial is a personal decision for the patient and deserves deep thought. There are many reasons why somebody may want to do a combination therapy. It’s not only because your current therapy isn’t working or that you want something “new” but also to help other people.
Clinical trials are not necessarily only supposed to be for the benefit of the patient themselves, but by participating in a clinical trial, the patient is increasing our knowledge of whether specific combinations work, the appropriate dosing, and the side effects. You’re helping other patients who will come after you.
Cancers are pretty smart that if you target one, they’re going to find a way to get themselves around that medicine you’re giving them.
Dr. Angela Fleischman
Trials Beyond JAK Inhibitors
Ruth: We go into clinical trials often because we were on Jakafi or another treatment and it wasn’t effective, caused side effects that were serious and needed to be discontinued, or maybe it worked for some time and then stopped. Dr. Fleischman, can you talk more about aiming to introduce non-JAK inhibitor treatments?
Dr. Fleischman: JAK inhibitors are very good in terms of reducing inflammation and reducing spleen size and, in some patients, can work very well for a period of time.
Patients could get “resistance.” Resistance with JAK inhibitors is very different than what we think about with other cancers. People on JAK inhibitors don’t develop new mutations that make them “resistant” to the JAK inhibitor. They start to not work as well so that would be one reason to add on and target different pathways.
Myelofibrosis is very heterogeneous. Each patient is very different. Each patient may have different mutations. They may have either JAK2, calreticulin, or MPL, but some patients will have additional mutations that make them look a little bit different than other myelofibrosis patients.
Trying to target multiple pathways, as Dr. Mesa had mentioned, is a very common technique. Cancers are pretty smart that if you target one, they’re going to find a way to get themselves around that medicine you’re giving them. They’re quite ingenious and able to grow despite our single treatments. Each myelofibrosis patient is very different so identifying what the appropriate second agent would be is really on a case-to-case basis.
Part of the challenge that we have with medicines against blood cancers or cancers is finding ways to deliver medicines solely to the cells affected by the disease without harming normal cells.
Dr. Ruben Mesa
Ruth: What’s exciting to see is that we’re more forward-thinking in our endpoints of clinical trials so we’re looking more at survival and not just symptom relief.
All of the clinical trials that we’ve talked about so far are exploring new drug treatments. There are also trials that look at lifestyle issues like exercise or the benefits of yoga and meditation.
Dr. Fleischman is renowned for her work studying inflammation and diet. She and her collaborators recently published the results of a clinical trial that tested the feasibility of the Mediterranean diet for MPN patients.
For those of us living with an MPN, anything we can do ourselves to potentially control our symptoms is very welcome. In fact, it helps us feel in control of our own blood disorder. Even if it’s only a little bit, it’s important.
Dr. Mesa, let’s move on to an area of treatment that the MPN community is very excited about exploring, which is a novel therapy targeting calreticulin, the CALR mutation, one of the most common drivers of essential thrombocythemia and myelofibrosis. People are calling this a potential vaccine. What can you tell us about this that explains it best?
Dr. Mesa: About a third or more of patients with myelofibrosis have a mutation in the protein called calreticulin. This is a little different from JAK2 and MPL because calreticulin might be on the surface of the affected cells and we may be able to target the abnormal calreticulin in a specific way.
Part of the challenge that we have with medicines against blood cancers or cancers is finding ways to deliver medicines solely to the cells affected by the disease without harming normal cells. In the bone marrow, that’s particularly important.
There has been a great interest in seeing if we can target calreticulin in a specific way. A vaccine trial has been done in Europe and is in its infancy.
There’s a theme of multiple different approaches being developed, both cellular-based therapies, such as CAR T or vaccines, or a monoclonal antibody against calreticulin. That is creating great interest but has not yet started in human trials. In the laboratory, it appears to be a very promising medicine.
We’re very hopeful, but we also recognize that until we’ve started treating patients, we never know how good a fit it’s going to be, if there’s going to be an unexpected side effect, or if it will have the benefit that we hope that it has.
I certainly hope that this medication is successful. Even if it is not, I suspect there will be others behind it that hopefully will be. We learn from trials whether they end up being a home run or not. This theme of us trying to selectively target the cells involved is really key.
As we think about anemia, there are JAK inhibitors that can have an impact on the spleen and symptoms, but they may either worsen anemia or not improve anemia.
Dr. Ruben Mesa
Treatment for Patients Who Suffer From Anemia
Ruth: Dr. Mesa, as we know, anemia is very common in myelofibrosis and many people need regular transfusions so this isn’t something that’s likely to go unnoticed. There can be severe fatigue associated and MF patients will have regular blood tests so in theory, it should be seen and diagnosed early on. Tell us about some of the new hopeful treatment options for MF patients who suffer from anemia.
Dr. Mesa: Anemia is when an individual has fewer red blood cells than they’re supposed to. Red blood cells carry oxygen from our lungs to the rest of the body so that’s key for us in terms of our muscles to work well and for us to feel well. That’s why we can have issues in terms of anemia.
Myelofibrosis anemia has multiple aspects. There can be baseline anemia because the bone marrow is not producing enough red blood cells. There can be other contributors if they’ve had baseline iron deficiency that contributes to that. If the spleen is very enlarged, it can hold on to many red blood cells.
Historically, we’ve had a range of options. None of them have been overly dramatic in terms of their impact, but they can help. Injections such as erythropoietin-stimulating agents and androgens like testosterone help to produce red blood cells in both men and women.
There are medicines that are in development. Luspatercept, a medicine that can help with anemia, is currently in phase 3 clinical trials for patients with myelofibrosis. Momelotinib, which was most recently in September 2023, is a JAK inhibitor that can also help to improve anemia.
We look for that medicine to improve both spleen symptoms and anemia. As we think about anemia, there are JAK inhibitors that can have an impact on the spleen and symptoms, but they may either worsen anemia or not improve anemia. Both things can be present.
Momelotinib is an important advance. I hope that as we see other combination therapies, we may see broader improvement in spleen symptoms and anemia.
Should momelotinib or those agents that are more helpful with anemia, perhaps even pacritinib, be that JAK inhibitor to be used with other medications in combination? That has yet to be answered with some of these combinations.
Some real progress in anemia and improving anemia can clearly have a benefit, in terms of the patient’s quality of life and their ability to have enough energy to do their daily activities or things they enjoy, as well as being easier on the body.
One area that we’re intensely working on is trying to identify surrogates for survival or something that we can capture with data amenable to a clinical trial that will be a marker for disease impact.
Dr. Angela Fleischman
Symptom Control While Being on Treatment
Ruth: Dr. Fleischman, what I find very exciting in today’s clinical trials is that we’re moving beyond symptom management and moving more toward progression-free survival, living longer with a high quality of life. When evaluating clinical trials, it’s important to understand the goal of the study. Where do you think we are with this?
Dr. Fleischman: That’s a very important point. For a clinical trial, you need to have an endpoint, a defined thing that you’re going to test. Ideally, something that you anticipate that your drug of interest is going to achieve better than the comparator.
Classically, in myelofibrosis, we’ve focused on spleen volume reduction and symptom burden because those are two things that we can quantify and expect to see a change in a short period of time. Although spleen size reduction and symptom burden are extremely important, they just don’t capture the whole picture of myelofibrosis.
The endpoint of survival obviously is extremely important to myelofibrosis patients. Survival is extremely important to everybody. But because, in general, myelofibrosis patients live a long time, it’s not a feasible outcome for clinical trials.
One area that we’re intensely working on is trying to identify surrogates for survival or something that we can capture with data amenable to a clinical trial that will be a marker for disease impact.
There are some clinical trials such as the imetelstat clinical trial in which survival is the actual endpoint, which is a unique and forward-thinking endpoint. One of the key areas of need in myelofibrosis is identifying markers that can be used in clinical trials that indicate a significant impact on the disease that goes beyond reducing spleen size and symptoms.
Ruth: We’re definitely getting into a very exciting time that will make such a difference therapeutically once we have those answers.
A transplant itself is an extremely risky procedure that can lead to significant side effects or even death.
Dr. Angela Fleischman
The Best Time to Get a Stem Cell Transplant
Ruth: When is the best time to get a stem cell transplant? I know there isn’t a black-and-white answer, but Dr. Fleischman, how do you answer this common question?
Dr. Fleischman: That is another million-dollar question in myelofibrosis and I think the most difficult decision for a myelofibrosis patient as well as for the physician.
As we know, at this point in time, a bone marrow transplant is the only curative option for patients with myelofibrosis. You may say, “If it’s curative, why doesn’t everybody just get a transplant?”
Transplants themselves can be quite risky. The media may miscommunicate transplants. You always see on the news that somebody’s looking for a donor so it may seem that the only problem with transplants is you can’t find a donor. That’s not necessarily the case.
A transplant itself is an extremely risky procedure that can lead to significant side effects or even death. We don’t want to give somebody a transplant if the transplant is going to make them sicker or potentially lead to their death earlier than would be the case if they just treated their myelofibrosis through other means.
The ideal time to transplant is when you get clues from this myelofibrosis patient that with standard treatments, they are very likely going to have an extremely bad outcome or will have an outcome that will lead to their death very quickly. That’s the time going forward with a transplant is worth the significant risk.
The safer the transplant becomes, the greater the consideration of when it is used.
Dr. Ruben Mesa
Dr. Mesa: There is a balance between a patient undergoing a stem cell transplant and a medical treatment. They have very different dynamics. A stem cell transplant can potentially be curative but can come with significant risks, including upfront risk.
The benefits of medication depend on many things, like how much benefit, how long is that benefit, and the impact on the patient. I would certainly view it as a success if we are able to have medicines that are sufficiently impactful that it leads us to either be able to skip a bone marrow transplant or delay it further.
We have precedent in other areas and the most successful example is in chronic myeloid leukemia. At the beginning of my career, most young patients had a stem cell transplant. Now, with the impact of medications, it is rare for patients to have a stem cell transplant because of the effectiveness of medications.
Currently, we are not there yet. A patient who clearly needs a transplant still will go for a transplant. Over time, there may be more combinations of both. Can the medicines help to decrease the burden of the disease and make the likelihood of success with the stem cell transplant greater? That is also a win.
In parallel, there’s tremendous research from our colleagues who do stem cell transplants to try to make that process safer. The safer the transplant becomes, the greater the consideration of when it is used.
It continues to evolve. We reevaluate every option we have. Does that change the dynamic in terms of transplantation as well as how the two things work together? With our current medicines, we are not changing our decisions for transplant, but increasingly, almost all patients that go to transplant have had at least one or more of the JAK inhibitors ahead of time.
The data would suggest that the outcomes with transplant are better in part because of JAK inhibitors but also because of improvements in the processes, antibiotics, other medications, and expertise of our colleagues who run transplant centers.
Asking About Clinical Trials
Ruth: When should a patient ask about clinical trials? How and when do you introduce the idea of considering a clinical trial to your patients?
Dr. Mesa: Clinical trials may exist in any aspect of the disease, from diagnosis to initial treatment to treatment downstream. It’s always a fair question for patients to ask. Is there a clinical trial that may be appropriate for me? It is not limited to one segment of the disease.
Clinical trials are how we make progress. They are highly regulated and always have the needs of the patient front and center. At a minimum, a patient is always getting the option that is at least as good as the standard of care.
It’s a fair question to ask at any point along the way. Truly, all the options we currently have have only been possible because of patients’ willingness to participate in clinical trials.
As physicians, we are happy to have another set of eyes look at the patient and hear another person’s thoughts. That is in no way hurting your physician’s feelings by seeking out a second opinion.
Dr. Angela Fleischman
Dr. Fleischman: This may be a different answer than one may get in a community practice. When I approach a new patient and we talk about treatments, I’ll always talk about standard-of-care treatments first and give people their options, and the pros and cons of each of the standard treatments.
Afterward, we’ll discuss potential clinical trials that the patient might be eligible for. I talk about clinical trials at my own university or elsewhere that I think would be appropriate for the patient. If there was something specific that I thought the patient would be ideal for, we’d talk about that trial first.
Because I want to give the patient all of the information, I would talk about other clinical trials that the person may be eligible for. I would give them reasons why they might be a good idea but also why I don’t think that clinical trial would be ideal for them and give them specific reasons why.
I highly recommend second opinions or even third opinions. Sometimes patients feel bad going for a second opinion. Their primary oncologist may think that they are not happy with their approach. That is not the case.
As physicians, we are happy to have another set of eyes look at the patient and hear another person’s thoughts. That is in no way hurting your physician’s feelings by seeking out a second opinion.
I highly recommend a second opinion or a third opinion, even if it’s just, “I want to learn more about my disease. I’m happy with my treatment now, but I want to get somebody else’s point of view, learn about my future, and what might the options be if this happens or that happens.”
All drugs must move through the steps or phases to ultimately be approved by the FDA.
Melissa Melendez
Trial Knowledge #1: Phases of Clinical Trials
Ruth: Melissa, clinical trials try to see if we can improve the standard of care and give more and better options to more people.
There are different phases of a clinical trial. What are they and what do they mean?
Melissa: I like to think of clinical trials as steps to drug approval. All drugs must move through the steps or phases to ultimately be approved by the FDA. If drugs are studied in new combinations or in diseases outside of their approved indication, they still need to go through all the phases.
For phase 1 trials, the treatment is tested in a very small number of patients. It could range from 20 to 40 patients. We’re testing dosage and looking at the safety and side effects.
Phase 2 trials typically build on phase 1 results. They try to determine the effectiveness and safety of the drug in a specific population. We’re trying to answer the questions of whether a treatment works and how well it works.
For example, there may be a phase 1 trial that tests a drug in blood cancer patients or MPN patients. After the phase 1 results, they determined that myelofibrosis patients showed the best response to the drug. The phase 2 trial now might only include myelofibrosis patients and they’ll be testing it in a larger subset, like 100 to 300 patients.
Researchers continue to monitor patient safety throughout the phase 2 trial and phase 2 studies with positive results will then move into the phase 3 trial.
Phase 3 trials are often referred to as randomized trials, comparing a new treatment against the best standard treatment. These trials can be done with anywhere from 300 to 3,000 participants. Researchers are trying to see if a new treatment has better survival outcomes and fewer side effects.
When a trial is completed and shows that the drug is in fact better than the standard of care or the best standard treatment, that’s when the newly investigated drug becomes a standard of care and will become FDA-approved.
By the time a clinical trial enters phase 4, the FDA has already approved the treatment. These trials are done in thousands of patients and they usually go on for many years.
Placebos are not typically used with patients in cancer clinical trials. But if a placebo is used, the person will also receive the standard treatment for their specific cancer.
Melissa Melendez
Trial Knowledge #2: Use of Placebos in Clinical Trials
Ruth: This one needs myth-busting. A lot of patients and care partners say, “I wouldn’t want to risk getting a placebo.” Are placebos used in myelofibrosis clinical trials?
Melissa: Ruth, I’m really glad you asked that because federal regulations require patients to know if a placebo, which is an inactive substance that looks the same as the one used as treatment, will be incorporated into a trial. An example of a placebo could be a sugar pill.
Placebos are not typically used with patients in cancer clinical trials. But if a placebo is used, the person will also receive the standard treatment for their specific cancer. In our case for myelofibrosis patients, the placebo will be in combination with active drugs so patients are receiving at least the standard of care. No one with active cancer would be treated with only a placebo because that is unethical.
When researchers do use a placebo, they must tell the patient that they have a chance of getting a placebo and that they will receive an experimental treatment at some point in the clinical trial, if not right away. For example, you may be assigned to the placebo group, but if your cancer gets worse, researchers will switch you to a study drug or new treatment.
The more you ask and open up the lines of communication with your team about potential treatment options, the more you learn.
Melissa Melendez
Trial Knowledge #3: Finding Clinical Trials
Ruth: For people who want to explore clinical trials, what can they do to find one for themselves? The ClinicalTrials.gov site isn’t the most user-friendly and that’s why the LLS Clinical Trial Support Center is in existence and is so important. Tell us about that.
Melissa: I agree that ClinicalTrials.gov isn’t the most user-friendly and can be difficult to use. ClinicalTrials.gov is a searchable registry and database of clinical trials conducted in the United States and around the world. It can be overwhelming and this is where the patient’s healthcare team and the CTSC can come into play.
Patients can talk to their doctors and learn more about clinical trials done at their home institution or outside of it. The more you ask and open up the lines of communication with your team about potential treatment options, the more you learn. This can help you better understand what options are available to you and feel more comfortable moving forward with a treatment plan.
The LLS created the Clinical Trial Support Center to arm patients with information to take back to their healthcare team. The CTSC provides a free service to patients. It usually takes under five minutes to fill out a form online. Don’t get overwhelmed. If you’re worried that you haven’t filled out enough information, please submit it anyway.
We reach out to patients within 1 to 2 business days; typically, on the same business day that we receive the referral. When you connect with one of the nurses, you can expect a teammate who will join you on your cancer journey.
We take your individual needs into account. We learn about your treatment goals. We educate the patient about trials and conduct a clinical trial assessment. This includes addressing barriers, such as travel, and discussing financial assistance through LLS or even outside organizations.
We search for trials and go through each one individually, which is a little bit different than other online services. We take an individualized approach and only send trials to patients that they’re likely eligible for. We send the results to the patient and encourage them to take them back to their doctors to discuss the results.
We provide patients with a non-biased, patient-friendly list of appropriate clinical trials. Ultimately, we work in collaboration with the patient’s healthcare team to decide if a clinical trial is right for them. We offer to reach out to the trial sites if there’s anything on the trial list that they would like to learn more about.
We have many patients that we’ve worked with for several years and developed a personal connection with them. We really strive to provide continuity of care throughout their journey. I always tell my patients that I’m just a phone call away and they can always reach out to me at any point with questions or if their disease or treatment changes.
Over time, trials may change. Additional trials may open up or some may have closed so I want to make sure that I can provide them with an updated search any time.
Our services are available to myelofibrosis patients as well as other blood cancers ranging from pediatric patients to adult patients. We even encourage healthcare providers to reach out to us. We do clinical trial searches for physicians in large centers and smaller community centers where they don’t have as many resources or staff.
The clinical trial landscape is pretty complicated. CTSC nurse navigators are here to break down the barriers to clinical trials that patients face to help them make informed decisions. We’re here to help and welcome any patient referrals.
We learn about each patient and take a personal approach to find out their treatment goals, their physician’s goals, and what they’re looking for in a trial.
Melissa Melendez
Trial Knowledge #4: Staying in a Clinical Trial
Ruth: What are the top three things that you do at LLS to help people stay in a trial? Talk about the challenges and the solutions.
Melissa: We learn about each patient and take a personal approach to find out their treatment goals, their physician’s goals, and what they’re looking for in a trial.
Barriers are the first challenge. Nurse navigators are proactive during those conversations on breaking down barriers that patients might face. Are these barriers financial? Will they have to travel if we find one that they’re interested in? Our solution to these issues is to find out if a trial offers financial assistance in addition to what we may offer at LLS.
We email trial coordinators and principal investigators and inquire about the treatment schedule. How many visits may the patient expect? Can they get labs at their home institution?
This is also dependent on what phase the trial is in. This may not be possible for phase 1 trials, but more possible for phase 2 or phase 3 trials. Can any of the long-term follow-up visits be virtual?
Communication is also another challenge. Our solution in the CTSC is to help break down the intimidating medical language or trial jargon. We try to use the simplest explanations and if patients want more in-depth or complex information, we can definitely adjust and provide that as well.
We always check on a patient’s understanding. When we’ve explained something or provided information, we may ask the patient to repeat what they understood and listen as they walk through that process with us. The more they understand, the more comfortable they feel when they’re making the decision.
Trial awareness is a challenge and we can help raise awareness through programs like this. We talk about trial myths and help patients understand the clinical trial landscape better. We help patients be more well-informed about trials that may be available to them and about personalized trial services like ours and the Clinical Trial Support Center at LLS.
At the LLS, our main hub is our information resource center through our information resource specialists, nurses, and social workers. You can call the 1-800 number Monday through Friday, 9 a.m. to 9 p.m. Eastern Standard Time.
We also have a chat option where you can do a live chat online, and that’s Monday through Friday, 10 a.m. to 7 p.m. Eastern Standard Time.
If for some reason you reach out to us outside of our business hours, you can always leave a message 24/7 and we’ll give you a call back.
We’re in a very exciting time for myelofibrosis… We can personalize FDA-approved JAK inhibitors for each myelofibrosis patient.
Dr. Angela Fleischman
Final Takeaways
Ruth: If you could leave people with just one message, what would that be?
Dr. Mesa: I would leave them with a message of hope. We have made a tremendous amount of impact and a much greater understanding of the biology of the disease, the genetic mutations, and why people progress. We are building on a base of very good medicines that have made an impact with the JAK inhibitors but to a new era of multiple different approaches.
I would heavily encourage patients to consider clinical trials where appropriate. Clinical trials will build on the base of these medications to try to drive progress further and further. We need your help and together we will continue to improve the therapy of diseases like myelofibrosis.
Dr. Fleischman: We’re in a very exciting time for myelofibrosis. In the past few years, we’ve moved from a single FDA-approved JAK inhibitor to four JAK inhibitors. We can personalize FDA-approved JAK inhibitors for each myelofibrosis patient.
There are a lot of opportunities for combination treatments that are moving forward in clinical trials as well as going beyond JAK inhibitors, trying to identify other key pathways to target myelofibrosis.
Melissa: In the CTSC, we educate, support, and empower myelofibrosis patients as well as other blood cancer patients to be active participants and have control over their treatment decisions with their healthcare team.
The Leukemia & Lymphoma Society wants to make a difference in patients’ lives through research, advocacy, education, support, and financial assistance. We want to see a future without blood cancers. We have a lot of free information for patients, caregivers, and healthcare providers to check out.
We’re a phone call away and we are here to help make clinical trials less overwhelming for patients and to help healthcare providers.
Ruth: We have covered an awful lot of information and invaluable insight from our experts. I know I speak for people living with ET, PV, and MF, their loved ones, and care partners when I offer our very sincere gratitude to you all for everything you do for our community.
Stephanie: Thank you so much, Ruth. I always appreciate the way you bridge the conversation for us.
Thanks so much to Drs. Mesa and Fleischman for the work that you do in the clinic and in research to help patients and families who are trying to navigate a myelofibrosis diagnosis and treatment, and all the decisions that come in between.
Thank you to our LLS clinical trial nurse Melissa Melendez for being there day to day and helping people who are overwhelmed by the topic of clinical trials.
We really hope that you walk away with a greater understanding of clinical trials in myelofibrosis. We hope to see you at a future program.
Myelofibrosis experts Dr. John Mascarenhas (Mount Sinai) and Dr. Tania Jain (Johns Hopkins Medicine), and Clinical Trial Nurse Ashley Giacobbi (The Leukemia & Lymphoma Society) explain cutting-edge therapies. Hosted by The Patient Story Founder Stephanie Chuang and featuring insights from patient advocate Mary Linde, this empowering discussion will help you navigate all aspects of clinical trials.
The myelofibrosis panelists discuss momelotinib, navtemadlin, selinexor, pelabresib, navitoclax, imetelstat, and other myelofibrosis treatments.
I had a different blood cancer, non-Hodgkin lymphoma, and I went through treatment a few years ago, but I’m so passionate about these discussions. So many things are happening in the landscape of changing treatment options and they start with clinical trials.
We hear about clinical trials but the term is so daunting and overwhelming. Our goal is for you to have a much better understanding of what they are in human terms. Maybe some might be right for you that you can ask your own doctors about.
The Patient Story features hundreds of in-depth, authentic patient stories across cancers and we also feature top cancer specialists. Our goal is to humanize cancer and help you navigate life after a diagnosis, whether you’re a patient or a caregiver. You can join our community and you’ll get first access to programs like these with new updates and new stories.
We’re so proud to be co-hosting this with The Leukemia & Lymphoma Society. It is the world’s largest nonprofit health organization dedicated to funding blood cancer research as well as offering patient services and education.
They have great resources if you haven’t checked them out yet. Their information specialists are just a phone call away to help you answer some cancer questions. They also offer help to pay for cancer costs through a co-pay assistance program, like travel to CAR T-cell therapy or clinical trials.
Dr. Mascarenhas, really appreciate you being here. I heard you describe yourself as being tireless and working nights and weekends to help patients in this space. We really want to understand what drew you to MPNs and to continue to do this work for patients.
Dr. John Mascarenhas: Thanks for having me join you. My interest began in the laboratory doing leukemia research many years ago. It evolved over time into clinical research in which I was introduced to MPNs and I really gravitated towards it. This was at a point where we didn’t have JAK inhibitors.
I was at the right time when the discovery of the JAK2 mutation came out. I got involved in the early development of JAK inhibitors and watched the field blow up. It’s been really exciting and rewarding to see this transition from how we used to treat patients with myelofibrosis and other related MPNs to what it looks like today so I’m very enthusiastic and optimistic about the future.
Stephanie: Thank you, Dr. Mascarenhas. We know that the landscape has shifted very quickly in a short amount of time. Excited to talk about it.
Dr. Tanya Jain
Stephanie: We’re also really excited to have Dr. Tanya Jain here tonight, another MPN specialist. She is an assistant professor of oncology at Johns Hopkins Medicine and director of the Adult CAR-T Cell Therapy Program at the Sidney Kimmel Comprehensive Cancer Center with myeloproliferative disorders as a top area of interest and studying newer drugs in the early phase of development.
Dr. Jain, thank you for joining our discussion. We’d also love to understand what drew you to the MPN space. What’s the driver of doing this work for patients and their families?
Dr. Tania Jain: Thank you so much for having me. I’m absolutely delighted to be a part of this panel.
I don’t think it was a specific event. It was a natural transition during my fellowship under the mentorship of Dr. Ruben Mesa and Dr. Jeanne Palmer, who’ve obviously done a lot of work and continue to do so.
How that transitioned me was to recognize the significant unmet need in the space and the opportunity that existed to contribute to improve outcomes for patients and to improve the lives of patients and their families so that’s what we try to do.
Stephanie: Thank you so much. That means a lot for all of us who’ve gone through cancer.
Ashley Giacobbi
Stephanie: Speaking of incredible work, we have Ashley Giacobbi representing The Leukemia & Lymphoma Society’s Clinical Trial Support Center. It’s a really great resource because as we know, clinical trials can be very daunting and seem like a lot to wade through.
Ashley, thank you for being here. I have such a special place in my heart for nurses. I remember going through my treatment and nurses being such a lifeline so I really appreciate the work that you do. We’d love to understand more about yourself and what drew you to this calling.
Ashley Giacobbi: Thank you so much. I’m really honored to be here.
I have been a nurse for almost 20 years now and have enjoyed all of my time at the bedside.
I get extra excited when talking about new changes and how much has changed in the world of oncology over the last 20 years. It’s exciting to be able to help patients find clinical trials when they’re seeking the newest and next level of care and some of these new developments and advancements that we’ve had.
Stephanie: Thank you, Ashley. We’ll be talking about some of the top topics you’re getting from patients and care partners who are calling you and asking for your help in the clinical trial space.
Mary Linde
Stephanie: Finally, we’ve got Mary Linde, who I’m really blessed to be able to call a friend now. Mary, you’re a myelofibrosis patient advocate. You lead a group on Facebook with myelofibrosis patients and care partners. We’re so lucky to have you share your perspective as well. Can you describe yourself a little bit outside of cancer? As we know, we are so much more than a diagnosis.
Mary Linde: Thank you for that. I’m almost 61 years old. I’m a nurse as well and have both a bachelor’s and a master’s degree in nursing. I stopped clinical nursing for 25 years.
I’m currently the CEO of a small nonprofit foundation that mostly runs a retirement community here in San Francisco. I have always had a heart to serve the elderly.
I’m a mom to two amazing adult sons who are launched and living on their own. One is married and one is about to get married. I’m really hoping for grandchildren soon and to live long enough to really enjoy those grandchildren.
I have a three-year-old Coton de Tulear puppy who gets me out and moving. I walk 3 or 4 miles a day with him.
Mary’s myelofibrosis diagnosis
Stephanie: Like so many of us experience, a diagnosis changes our lives. What led you to figure out that something wasn’t right and how did you get your primary myelofibrosis diagnosis?
Mary: It wasn’t easy. I was about 54 1/2 when I started with vague symptoms. I had fatigue, dizziness, and sometimes vertigo to the tune of whoosh and then I fell. I felt like I needed to nap more frequently. I felt like if I walked up any incline, I needed to rest.
I knew something was wrong. I thought I had mono or Lyme disease. I kept complaining to my primary physician about these symptoms. He kept telling me I had menopause, which had long been through at that point.
I would repeatedly go back to my primary physician and say, “Please, let’s investigate what this is,” and even told him that my father had a rare blood cancer at around this same age.
Finally, six months into begging, I reached out my arm to the doctor and said, “I’m not leaving your office till you do a chem 7 and a CBC,” and he did.
Three days later, I got the results that I had platelets in the 800,000. Of course, Google became my friend. I called the doctor and he refused to talk to me. He said, “I’m sending your blood off for special testing. I don’t want to tell you because I don’t want to scare you.”
I started Googling and I was pretty certain I had an MPN. Three months later, I found out that I had the JAK2 mutation. I didn’t find out from my primary care physician; I found out when I got a call from the oncology center admitting me to services.
When I walked into the oncology center, I had a very strange experience. The introductory oncologist said to me, “I know you’re probably really afraid of the C-word so we’re not going to talk about it. Let’s talk about it like a blood disease.” I told her that I was a nurse so she didn’t have to do this. Then she said, “The other C word is an evil drug so we’re not going to talk about that either.”
I kindly asked her to get me another doctor and then sought a second opinion. At that time, I wasn’t so afraid of dying as much as I was afraid of not having the information I needed to live well. I didn’t know if my life was going to be shortened and I wanted as much information as I could get.
Stephanie: I really appreciate you sharing all that, Mary. I also love the message of self-advocacy and empowerment. It’s your life, you know your body, and you certainly didn’t let that fall through the cracks.
What is myelofibrosis?
Stephanie: Dr. Jain, what is myelofibrosis in layman’s terms? What are some of the more common first signs or symptoms?
Dr. Jain: What we heard from Mary’s story is something that I hear in the clinic fairly commonly. Having that fatigue and tiredness is something that often takes people to physicians to get tested. Delays are not uncommon either because fatigue or tiredness have several possible reasons. Some may be more common than others.
Mary also mentioned the JAK2 mutation, which is of relevance here. The premise of myelofibrosis starts with the overactivation of the JAK/STAT pathway, which is supposed to be a normal functional pathway that’s supposed to do regular stuff and make blood cells.
When it’s over-activated or activated without any restrictions, that’s when undesirable things happen, which can include affecting the bone marrow function in a negative way.
You could be making too many cells or you could alter the bone marrow function in the way that there is more scarring in the bone marrow, which is the fibrosis in the term myelofibrosis, which again affects the ability of the bone marrow to function normally whose job is to make a normal quantity and quality of blood cells.
As a result, patients can get anemic or have low hemoglobin, which can cause tiredness, fatigue, difficulty breathing, and related symptoms.
By virtue of the JAK/STAT pathway activation, this systemic or generalized inflammation that we often notice or patients leads them to a workup. What that results in is what we in our clinic call constitutional symptoms or symptoms that could be nonspecific or vague as sometimes labeled.
Those can include things like night sweats, low appetite, or other symptoms resulting from an enlarged spleen like abdominal discomfort, which are other symptoms that can sometimes lead to further investigations clinically.
Stephanie: Thank you. I know that’s a lot to cover in a short amount of time. We do hear lots of stories about how long it can take to figure out a myelofibrosis diagnosis so that’s not unique to Mary’s situation.
Landscape shifts in myelofibrosis treatments
Stephanie: Dr. Mascarenhas, you alluded to how optimistic you are because there are so many developments happening. How would you describe the landscape shifts that have happened in myelofibrosis treatments, especially in just the last few years?
Dr. Mascarenhas: Myelofibrosis is a stem cell-derived blood cancer and it could affect people in different ways. You don’t meet two people that walk the same path. They all come in different forms and fashions. Their clinical picture can be really varied and their course can be quite heterogeneous and variable, too. You have to understand the patient that you’re dealing with and the patient-specific goals of therapy.
For some patients, it could be alleviation of anemia. For other patients, it could be systemic symptoms like fevers, night sweats, weight loss, bone pain, and profound fatigue that can be quite debilitating. For many patients, it can be an enlarged spleen or liver that’s causing a lot of discomfort and challenging normal activities like bending over and doing things that would be normally easy to do.
Knowing how the disease is affecting the patient really informs and dictates how best to approach the patient. It’s typically trying to alleviate the symptomatology and reduce the spleen, and that’s usually using JAK inhibitors.
JAK inhibitors
Dr. Mascarenhas: Over the years, we’ve grown to have three clinically or commercially available JAK inhibitors: ruxolitinib since 2011, fedratinib since 2019, and pacritinib since 2022. And a fourth one, momelotinib, later in 2023.
This provides a lot of opportunities to try to address those symptoms. Those cytokine-driven symptoms that Dr. Jain explained are a result of this JAK/STAT pathway. These drugs are great in reducing a lot of that inflammatory cue that makes patients feel terrible, improving their sense of well-being and functionality, and reducing their spleen.
In doing so, patients have a better quality of life and, by virtue in most cases, will live longer because they can do the simple things that we need to do. They can move and eat. People who move and eat will simply live longer and do better than patients who cannot and that’s just generally true in oncology.
They have really revolutionized the quality of life aspect. As Dr. Jain pointed out, she worked with Dr. Mesa who was really instrumental in measuring quality of life and making that an endpoint for clinical trials and bringing attention to symptomatology and quality of life.
We have a great armamentarium that covers lots of different types of patients to improve their symptoms and quality of life.
We are developing drugs that are looking to try to improve anemia. Historically, we use drugs like epoetin alfa or darbepoetin alfa, which are erythropoiesis-stimulating agents, to try to improve hemoglobins, get patients out of the transfusion suite, and give them some more energy back, or drugs like danazol, a synthetic male androgen.
There are drugs that we repurpose, which is a common theme in oncology, from other diseases like multiple myeloma. We use drugs called IMiDs or immunomodulatory drugs like thalidomide, lenalidomide, or pomalidomide. These can all be used in myelofibrosis off-label to improve hemoglobin with responses of about 20 to 30%.
The reality is we can improve hemoglobin in some patients, we can improve symptoms in the spleen, but there’s still really a lot left to do.
How JAK inhibitors work
Mary: Dr. Mascarenhas, could you tell us how JAK inhibitors work? What are their benefits and limitations?
Dr. Mascarenhas: JAK inhibitors are a class of agents interestingly invented in the setting of this disease and now have applications to a lot of different diseases that are not even malignant.
They intermittently reduce the JAK/STAT pathway that is inappropriately activated in the bone marrow cells. This pathway is responsible for causing the proliferation of blood cells and elaborating inflammatory mediators.
JAK inhibitors intermittently quell this cascade of events. That reduces the propensity to have this inflammatory state, this overproduction of blood cells, and seems to improve symptoms by reducing cytokines, which are inflammatory byproducts.
Patients feel better and can move and eat. It restores vitality for reasons that I personally don’t understand and I’ve never seen a good explanation for.
It also reduces the spleen. It’s a phenomenon I don’t really understand. It’s an interesting aspect of the drug. It reduces symptoms by reducing the activity of this pathway.
Unfortunately, these drugs don’t induce remissions. They don’t kill what I would call the maternal stem cell that gives rise to all of these abnormal cells. It doesn’t get rid of that cell.
It quiets down what’s happening in the bone marrow and the spleen allows for some degree of normalcy. The malignant cell population still remains in the body, in the bone marrow, and in the organs.
Unfortunately, we don’t see changes in the bone marrow that would lead us to believe that we’ve remitted the disease. Myelofibrosis is in the name. You have scarring in the bone marrow that typically remains even while patients enjoy the clinical benefits of the drug.
Then there’s the potential for downsides of the drugs. They often will exacerbate cytopenia or low blood count. Anemia and thrombocytopenia (low hemoglobin and low platelet) count can often get lower with these drugs.
We’ve pivoted to try to develop drugs that may not be as myelosuppressive, as count reducing and may even improve some of the blood counts.
Pacritinib can be delivered in patients with low blood counts and can improve hemoglobin in about 25% of patients. Momelotinib has also been associated with improvements in blood counts.
What we now know, which we didn’t know when we started off in all of this, is these drugs are not just JAK inhibitors. They interfere with a lot of different pathways that may be relevant and irrelevant and cause toxicity.
For example, inhibiting ACVR1, which is another pathway that’s important for iron availability, might explain why pacritinib and momelotinib improve hemoglobins and why maybe ruxolitinib and fedratinib.
There are a lot of nuances with these drugs that help us understand why they may fit niches and help certain people in certain ways and why you can provide serial JAK inhibitors.
If you fail one, it doesn’t necessarily mean that you wouldn’t enjoy some response to another. You can go from one to the other. The tailoring of the JAK inhibitor is somewhat of an art more than a science in some cases and requires knowing the patient, what the goals are, and trying to match the potential goals and potential toxicities to that patient.
Mary: Thank you for that. I’ve often heard that we’re not getting rid of our JAK2 but maybe turning the volume down on it a bit with the use of these drugs.
Determining the sequence of treatment
Mary: Dr. Jain, how do you know which JAK inhibitor might or might not work and which one to try first for a patient?
Dr. Jain: I’m going to piggyback on what Dr. Mascarenhas said and emphasize the point that no two patients with myelofibrosis will be the same. Everybody will have their own presentation or different things that you need to address.
Everybody will have a different trajectory in terms of their disease course and that’s what’s important to recognize as you’re thinking about what you’re going to start a patient on in terms of your choice of JAK inhibitor. We don’t have the same treatment for everyone. We’re looking at what we need to address in you as a patient.
If we’re trying to address high counts, a JAK inhibitor makes sense. If they have a big spleen and/or symptoms that will need to be addressed in combination with that, a JAK inhibitor would make sense based on the fact that we have the longest experience with it.
Ruxolitinib has been our first go-to. It was the first approved and we feel more comfortable with it. We know how to adjust the dose and move things around with it. If that doesn’t work, then the go-to next step in an ideal world would be a clinical trial.
If we don’t have one that would fit, it would either be fedratinib or pacritinib. The choice would depend on where the blood counts stand. If the platelets or the cell counts are on the lower side, pacritinib would probably be a better choice.
There are patients who have anemia as a major presenting symptom. In those situations, options such as epoetin alfa, danazol, pacritinib to some extent, and hopefully momelotinib in the future are some of the options. Luspatercept is in clinical trials; we’ll see how that pans out. Those will be some of the options.
The third set of patients is those who come with more advanced disease in the way of more excess or a higher fraction of blasts or leukemic cells or very, very early cells in the bone marrow that indicate that these patients are headed towards the pathway of a more aggressive pattern of disease like leukemia.
In those situations, either in combination with JAK inhibitors or without something like hypomethylating agents could be considered usually en route to a bone marrow transplant, if that makes sense in terms of eligibility.
Stephanie: What’s clear is this is very individualized. There are so many considerations.
What are clinical trials?
Stephanie: Mary, can you bring us back to the day when you got the diagnosis? What was that like for you learning about cancer?
Mary: When I was initially diagnosed, it was over a long period of time so it wasn’t shocking exactly as I grew into it.
I thought back to my own father, who had a rare blood cancer in the late 1980s, had it for five years, and died at age 60. In fact, we were both diagnosed at age 55. I felt like I was somewhat prepared for how to manage this because I’m in the health field.
I had a bird’s eye view of it with my own father and I knew how to advocate for myself, especially since my dad had to advocate at a time when there really weren’t a lot of options for this cancer.
There’s a lot of fear and a lot of wondering. Will I be around to see my grandchildren? Will I finish my career? Will I make the contribution to society that I had hoped? Will I have a painful death?
I’m grateful over the years to have learned that I have so many treatment options available to me that I don’t look at the future as something grim at all. I just see it as my normal life.
I’m so grateful to learn of combination therapies because not all of us can make it to stem cell transplant, which is ultimately our cure.
There’s a whole lot more hope on the horizon for us with MPNs, particularly primary myelofibrosis. I’m just grateful for the research and the amount of research that’s being churned out these days, the clinical trials, and the combination therapies.
I’m so excited to be able to talk to experts in the industry about research and development towards not only treatment but cure for myelofibrosis.
Stephanie: We’ve talked a little bit about some of the drugs and combinations that are being studied now.
The first time I heard the term clinical trials, it felt a little daunting. There are lots of misconceptions about clinical trials. We do know that different stakeholders are trying to research what can be better to improve the standard of care for different patients and patient groups. One of the challenges is that people view clinical trials as a last resort.
Ashley, we know clinical trials might not be right for everybody, but they are an access to tomorrow’s treatment today. We’re sure you get lots of questions in your role at the LLS. What are clinical trials in layman’s terms and what are some of the top questions and misconceptions you hear from people?
Ashley: Clinical trials are carefully controlled research studies, which are conducted by doctors, researchers, and scientists. They may be investigating new therapies or therapies used in the past in a slightly different way or in combination with other therapies to find out which works better or might have fewer side effects. They’re looking at both tolerability as well as effectiveness of the treatments.
There are so many misconceptions out there, but one of the largest is that it’s for patients who have exhausted all options. That’s simply not the case. There are clinical trial options at all stages of diagnosis.
There are interventional trials, which test treatment options, as well as observational or registry trials, which help us learn more about myelofibrosis as a diagnosis but may not involve specific treatments.
Another concern that we regularly hear about is the use of placebos. Placebos have definitely gotten a bad rap. A placebo can be known as a sugar pill. They’re not very commonly used in cancer clinical trials because it just wouldn’t be right for us to use a sugar pill in place of somebody who needed active therapy for a serious or life-threatening disease.
When placebos are used, it would be in a setting where a patient doesn’t require any type of treatment at that particular moment or in combination with another therapy so that the patient is continuing to receive active therapy for the disease that they have.
Logistical concerns may come up as well. We always like to chat with patients about travel for clinical trials and what that might entail. We’ve talked about some of the academic medical centers and how important it is to have an MPN specialist.
Very often, investigators who are looking at clinical trials for myelofibrosis are in academic centers. We’re always encouraging and pushing for those clinical trials to be available in the community setting because traveling to and from those academic centers can be a real challenge for patients.
In addition to the logistical travel considerations, there are some misconceptions that clinical trial participation is free or that patients may even receive money for participating. Unfortunately, that’s not always the case. It’s really important that we explain that to patients.
Parts of the clinical trial that are investigational or are not approved will be provided by the clinical trial. Physician visits and lab work are things that we would expect patients to undergo if they were receiving standard care. Those will still get billed back to the insurance company or may have to be paid for in another manner.
Each clinical trial is structured a little bit differently and it’s hard to know from an overview, but really it’s important to have a general understanding before diving into the specifics of any clinical trial.
If you are participating in a clinical trial, occasionally, there can be stipends available to support the patient or caregiver and that’s why it’s so important to reach out and find out more and make sure that you have all the information you need as you make a decision about participating.
Mary: Thank you, Ashley. It’s so important to hear that we do have access to medication, not necessarily the placebo. A lot of us do worry about that. We also need to check in to find out what is available to us in terms of financing.
Momelotinib, a new drug
Mary: Dr. Mascarenhas, let’s talk about single-drug therapy. There’s a new drug that was recently FDA-approved, momelotinib. What patient might it benefit?
Dr. Mascarenhas: Momelotinib is a JAK inhibitor so it’s much like ruxolitinib except as I mentioned before, there are some nuances that make these drugs a little bit different. It also inhibits ACVR1, which is another pathway that regulates iron availability for red blood cell production. In its long development history, it’s differentiated itself from other drugs in large part by its ability to improve hemoglobins in a subset of patients.
It went to the FDA based on a study called MOMENTUM. The expected approval was in late June. It was delayed by the FDA, which is not uncommon, to September for re-review. My expectation is it will probably be commercially available in the pharmacies and available for prescription likely by mid to late September.
I encourage patients to discuss with their physicians if that drug might make sense for them or any of the other drugs that we’ve talked about, whether it’s fedratinib, ruxolitinib, or pacritinib. As we’ve said, it really has to be tailored to the patient.
I’m excited to see momelotinib come up. For a physician, it’s great because it gives us different options and allows us to tailor the treatment for each patient. That might be a great opportunity for some patients to either embark on that therapy or switch.
The clinical trials set the tone for the interactions with the FDA about what that label would look like based on the way the clinical trial was designed and run. We can only guess that there may be stipulations.
It may only be available after the use of a first-line JAK inhibitor or it might have to have certain requirements for depth of anemia level. There are some nuances that sometimes play into the decision-making and these are based on the clinical trials that led to the approval.
Best drug combination therapies
Mary: Dr. Jain, there’s combination therapy to think about. June F. asks, “What are the best drug combinations at present?” Can you introduce us to combination therapies?
Dr. Jain: I’m not sure if I can answer what the best drug combination is right now, but hopefully that is a question we will learn more about and address in the future.
There are drug combinations that are promising. It brings options that we can offer to patients. They’re mostly in clinical trials but hopefully, some will move the field forward.
Historically, we addressed the JAK/STAT pathway, which we have learned the most about in the last couple of decades. That is the primary pathway involved in the occurrence of myelofibrosis.
As we have learned more over the years, there are other pathways that are critical to the development of myelofibrosis and that is where the rationale for drug combinations comes in.
We’ve seen several clinical trials that have addressed that or used combination therapy in patients who don’t have a good response to ruxolitinib itself and need more than that. Many of those drugs have been tested in the first-line setting to see if patients would do better with combinations upfront rather than ruxolitinib alone, which has been the long-standing go-to first-line treatment for over a decade now.
Some of the drugs that you’ll hear about are navtemadlin, for example, which is an MDM2 inhibitor. Dr. Mascarenhas presented data at EHA that showed a 35% spleen reduction in about one-third of patients in patients who weren’t responding to ruxolitinib itself.
There are BET inhibitors like pelabresib that I heard Dr. Mascarenhas talk about at ASH, which also is being tested in the first line in patients who are starting upfront treatment.
There are BCL-xL inhibitors like navitoclax, which have shown some improvement in the second-line setting. We’re awaiting a public announcement on the data for the first-line trial.
The premise is that you’re combining two mechanisms that have shown to work such that you do not have overlapping toxicities. That’s an important piece to remember.
JAK inhibitors can cause some decrease in blood counts; we’ve seen that with ruxolitinib. You want to add a drug that may not do that as much or may not do that to an extent that makes it prohibitive of a combination.
With pacritinib, for example, patients often would get gastrointestinal toxicity so don’t combine a drug that may also have gastrointestinal toxicity. That’s important to remember as we think about combinations, which we will see more and more in the future.
Logistics are certainly important to consider as we’re thinking about clinical trials, what the trial offers, the frequency of visits to the center, and whether that makes sense in terms of continuing to be on it or not.
When to consider combination therapy
Mary: Dr. Mascarenhas, what should patients ask when considering a combination therapy like Dr. Jain just talked about? How do we know when it’s right or the right time to start one?
Dr. Mascarenhas: The first question to ask is: Why is this combination for me? What would be the advantage in my case in terms of addressing my goals of therapy? Importantly, what are the potential risks?
As physicians—and I’m definitely included when I say this—we often focus on what we think is going to be the advantage of participating in a clinical trial. The reality is there are disadvantages sometimes. There can be toxicity associated with approved drugs and unapproved drugs that are in clinical trials.
Patients want to understand expectations of results and the potential toxicities that one could incur. What does the patient need to be aware of in terms of mitigating and reporting?
A trial is not really a passive experience. Patients are active participants. They’re not simply receiving a drug. They have to be very willing and engaged to report all symptoms and not just what they think might be important. They need to report everything to the study team.
That might involve calling ahead of their visit to let the team know what’s going on, making sure that all their medications are accounted for, and they’re following up. It’s an opportunity to assess whether a drug is active and adequately characterize the toxicities of a drug. As the drug moves along, it’s optimized in the delivery for future patients.
There are two objectives. How is this drug going to help me and what is my role in this whole process? It really should be a joint venture. It’s not a one-sided experience. We learn from the patients. Hopefully, the patient community learns from what we’re doing and everyone benefits.
Stephanie: Dr. Jain had set up the landscape of combination therapies and talked about different options. Dr. Mascarenhas, it’d be great to run through a few specific combinations.
Dr. Mascarenhas: Clinical trials today to a large degree are unlike what clinical trials were historically. These drugs are all rational with supporting pre-clinical data. People don’t always realize that they go through enormous amounts of testing through various aspects before they ever enter a human being.
There’s an enormous amount of regulatory burden that exists that’s really annoying but really important because it provides that sense of confidence in the investigators but also in the patients that what we’re introducing makes sense. We’re not just taking something off the counter and saying, “I wonder if this is going to work,” and throwing it into a clinical trial. These are rationally developed drugs.
An example is selinexor. Selinexor is a really interesting drug. It’s already approved for blood cancers that are not myeloid cancer like multiple myeloma and other B-cell lymphomas. This drug affects the shuttling of proteins in different compartments in the blood cell, in the nucleus, and in the cytoplasm.
Why does that matter? Because if you can affect where proteins are in a cell, you can ultimately affect the functioning of these proteins. Selinexor inhibits this shuttling protein and affects the way certain proteins exert their function, which might be important to the pathophysiology of the disease. This might even turn on other proteins and put them in an area where they can actually induce a good effect.
For example, there is probably a multitude of different changes when you use a drug like selinexor that shifts the cell’s functioning from one in which it’s acting inappropriately and nefariously into one in which you try to induce it to die through normal mechanisms.
There are normal mechanisms that are built into our cells that if they get corrupted by a virus or by cancer, they turn on this mechanism called apoptosis and undergo programmed cell death. Cancer cells have ingeniously figured out ways to get around that. We struggle each day to figure out ways to get them back on track, to encourage them to recognize that they’re inappropriate and to undergo this programmed death.
Selinexor is a great example of a drug that affects multiple pathways and induces myelofibrosis, perhaps even the primordial cells, to undergo this process of death. It works best in combination with ruxolitinib and that’s a common theme that we’ve seen.
In oncology, it’s very rare, except for maybe CML or some other diseases, that we use monotherapies. In most of oncology, we use combination therapies to synergize together to get deeper responses and avoid overlapping toxicities.
That’s what we’re seeing with drugs like selinexor or navtemadlin, which has a great wealth of data at this point. These drugs are active as single agents, but they seem to be even more active in combination.
This is supported by studies that are done in mice that are engineered to have myelofibrosis with primary cells from people who have been generous enough to donate their blood cells. We experiment and figure out how we are going to make better drugs in the future.
I thank those patients. Seems like a small thing, but it’s a huge, huge aspect of how we move this whole machine forward in clinical research. All of that information allows us to say this combination really looks effective.
We’ve got JAK inhibitors that are commercially available. We’re going to add this drug that synergizes nicely in preclinical models and cells in the dish. We think it’s going to work better than each drug alone and we’ll figure out how to dose them and schedule them to minimize toxicity. That’s really where we’re seeing it.
Selinexor, navtemadlin, pelabresib (BET inhibitor), and navitoclax (BCL-xL inhibitor) all look good in combination with ruxolitinib. As Dr. Jain said, ruxolitinib has been around the longest and that’s the go-to drug that we combine drugs with.
We’re not even waiting anymore for patients to have failed the first line of therapy. We’re introducing the drugs earlier on. We get confidence in their ability and their toxicity profile. Why wait for patients to do worse? Why not try to get deeper responses earlier on?
The deeper we can reduce the disease burden, we believe that the better the patient will be overall. They will not simply feel better but have smaller spleens, which is important. Fewer disease cells in their body will hopefully mean longer progression-free survival.
Navtemadlin, selinexor, pelabresib, navitoclax, imetelstat — there’s a whole host of drugs that are aiming to really hit the clone and induce deeper responses.
Second-line treatment after Jakafi
Mary: For people who have been on ruxolitinib and, for whatever reason, the treatment wasn’t effective, what treatment options are available?
Dr. Jain: That’s a common situation we run into because as Dr. Mascarenhas pointed out, ruxolitinib has a very strong role. There are a lot of things that it does do, but there are a few things that it doesn’t do. Based on registration studies and clinical practice, if it works, it works for a few years and then we start losing that response.
A clinical trial available that would be a combination of a JAK inhibitor with something else or something added to ruxolitinib itself would be my go-to to consider. There are several of those going on at this time. There are also trials with single-agent drugs.
The way drug development goes is there’s testing of efficacy by using the drug alone. Then once we are comfortable with their efficacy and safety profile, we add it onto a ruxolitinib or a JAK inhibitor backbone.
If we see efficacy and safety in that combination, we move it up the ladder a little bit more and try to investigate if that would be a better option in the front line compared to ruxolitinib itself.
There are non-JAK inhibitor combinations that get added to ruxolitinib. Navtemadlin, an MDM2 inhibitor, has data. It restores the natural cell-killing pathway that should happen but is not working very well for some reason. We’ve seen patients respond in a post-ruxolitinib setting in terms of their spleen and symptoms.
There are other drugs like navitoclax, a BCL-xL inhibitor, that show responses in about one-third of the patients who were not having a good response to ruxolitinib by itself.
Pelabresib is a BET inhibitor. There are other BET inhibitors in the pipeline that are being developed with slightly different nuances to their conformation and how they inhibit the pathway. These are some of the categories of drugs that look promising and worth looking forward to.
Imetelstat has emerging data. It’s slightly different in the way it works. It inhibits the telomerase activity. It’s one of what we think happens in myelofibrosis or leads to that, even though the telomerase length may be not as long or in fact short. The telomerase activity tends to be high and that’s what imetelstat inhibits.
I’m sure I’m missing some here and that’s not for the lack of preference. Selinexor is another one that Dr. Mascarenhas already mentioned.
I would tell my patients that if we can get our hands on one of these combination clinical trials at that time, that would be my first go-to option.
If for any reason there are no clinical trial options available after ruxolitinib, then obviously there are other JAK inhibitors like fedratinib, pacritinib, and hopefully soon momelotinib. Patients may still benefit even though they stopped responding to or did not achieve benefit from ruxolitinib as a front-line JAK inhibitor.
When to get a second opinion
Mary: When is it right for a patient to seek a second opinion during this time of figuring out the right treatment options?
Dr. Mascarenhas: The right answer always is now. I don’t think it ever hurts to seek a second opinion at the time of diagnosis to confirm the diagnosis. There is a lot of heterogeneity in the way these diseases can present. There are overlaps and nuances.
It’s important to seek a second opinion because you may be a patient who should be considered for a bone marrow transplant, which is the only curative option we have. Sometimes that’s delayed too late and the patient misses the window of opportunity. For some patients, that may not be on their plate but having that discussion is really important.
I don’t recommend seeing lots of different people; that can be problematic. Getting a second opinion at each stage never hurts — at the time of diagnosis, if you’re not doing well on your first therapy, and when there’s consideration of second therapy.
If you have a physician who gives you pushback about getting a second opinion or comes across negatively, you might want to find another physician because it shouldn’t be an ego thing.
It’s your life. You’re dealing with cancer. You should feel free and confident that a second opinion is not a reflection of your treating physician. It’s getting more information and the more information you have, the better the outcome.
Dr. Jain: I agree with that 100%. The MPN community is small but also very well knit and I think we work very closely together. I’ve asked my patients to get second opinions and I’ve set them up for them if they need to go. I’ve sent patients to Dr. Mascarenhas and to others if there is, for example, a clinical trial opportunity that we may not have and they may have.
Sometimes it’s better for them to hear it from more than one person. We do a lot of things similarly, but there are some that we may have different perspectives about.
A common joke is if you ask 10 MPN experts, you’ll get 12 different opinions, and not because anything is right or wrong. There just may be a slight difference in our prior experience with a particular strategy or what our perspective about a particular strategy may be. All those are important things.
The role and timing of the transplant may benefit from a second opinion. Get another perspective as to what their center’s experience has been and how they may do something different. There are nuances to every transplant center and some of it may be more beneficial to you. Geography obviously plays a big role.
How to look for myelofibrosis clinical trials
Stephanie: We’ve talked about treatment options in myelofibrosis, but when you actually come down to needing to find one or stay on one, there are so many questions that we all encounter. We know that ClinicalTrials.gov is out there, but it’s a little bit difficult to navigate and that’s why the LLS’ Clinical Trial Support Center is so important. Ashley, what are your top recommendations in terms of looking for clinical trials?
Ashley: Often, people try to go about it on their own. ClinicalTrials.gov is the most comprehensive database of all clinical trials. In addition to cancer clinical trials, there are also clinical trials for all types of disorders and diagnoses.
It’s not always easy to hone in on what you need depending on past treatments you’ve had or medical history so it can be a challenging situation to find clinical trials that are actually applicable to you as an individual.
It’s a free service staffed by nurses who have expertise in blood cancers and clinical trials. Nurse navigators connect one-on-one with patients, caregivers, or even other healthcare providers who may need to learn more about potential clinical trial options.
We find out more about the patient’s diagnosis. We learn about any past treatments they may have had and find out about their medical history because all of those factors will play into a patient’s eligibility to participate in a clinical trial.
We also take a long time to find out about patient preferences and any unique obstacles that could hinder or drive participation in clinical trials. We help tailor some of the support and resources that we’re able to provide so that patients can overcome some of those barriers that may be in place.
After we’ve generated all of that information and really taken the time to get to know the patients, we produce an individualized clinical trial search. That could be related to geography and preferences. What matters most to the patient? Is this something that they’re really not interested in spending a long time in the hospital if they can avoid it?
We definitely look at all of those and produce a list that can be taken back and reviewed with their treatment team so that that can be part of the informed decision-making with the patient’s next steps.
We are available for all blood cancers, including myelofibrosis and other MPNs. It’s important to know that patients can reach out.
Half of the ongoing clinical trials are cancer clinical trials, but sadly, only about 5% of cancer patients actually enroll or participate. There’s so much opportunity out there and we’d really love to help overcome any barriers that patients might have so that they can consider participating.
The role of stem cell transplant
Stephanie: Transplant is such a huge topic for so many people and they hear so much about it. In the context of the landscape changing so quickly, do you feel that you and other specialists in the field will be recommending transplants less to people? This is probably a very individual response, but with everything happening, what’s the trend?
Dr. Jain: I actually think of it the other way. By virtue of having more effective treatment strategies to improve the spleen and symptoms, and get a disease response, we may be able to take more patients to transplant as a curative therapy.
A lot of times, lack of spleen response, poor performance by virtue of a lot of symptoms, or disease advancement into a more aggressive disease pattern become barriers to transplant. Having more options in the future will allow us to take more of these patients to transplant.
We’ve seen a lot of advances with a lot of these options. What we have not seen so far is the curative potential. Hopefully, we will in the future. All of these drugs have a lot of advantages in terms of improving spleen symptoms and cytopenias but we have not had definitive improvement or getting rid of the abnormal stem cell clone. That’s something that at least so far we’ve only achieved with a stem cell transplant.
At some point, as long as patients are eligible for transplant and that is something that would fit their life wishes in general, that would be a curative option to consider. Better non-transplant treatments will only get more patients to something more curative like a transplant.
Dr. Mascarenhas: I couldn’t have said it better myself.
Final takeaways
Stephanie: We’ve covered a lot of ground in a short amount of time. If there’s one thing you’d like for our audience of patients and care partners to walk away with, what would that be?
Dr. Mascarenhas: I hope to share my enthusiasm and optimism that we are making advances. There is a brighter future and I’m really genuinely excited about that.
Embrace the opportunity of clinical trials. Clinical trials are looked at for other people, but they may be important for you. Talk to your physicians. You may not go through with it but learning about it and exploring it is important for each patient.
Dr. Jain: It’s never a wrong time to see a specialist or to see someone else if something is not working out. Some symptoms are nonspecific. Never hesitate to be an advocate for yourself, to get things done, and to seek a second opinion.
As a transplanter, I’m obliged to pitch in that getting an opinion about transplant and at what course in your disease that makes sense is important to address. You don’t have to wait until you’re progressing or not responding to drugs. That needs to be addressed and outlined in an early appointment rather than waiting for too long.
Ashley: I really want to echo what’s already been said. It’s so important to consider clinical trials as part of the treatment plan. Even if they may not be an option at that particular moment, it’s important to be informed and look at all of those components as you’re making an informed decision about the treatment plan with your providers.
As a representative of The Leukemia & Lymphoma Society, I would really encourage any patient with myelofibrosis or any MPN to reach out. The Leukemia & Lymphoma Society has so many resources available, including clinical trial support but also so many others that we would really enjoy the opportunity to connect and provide those resources to patients.
Mary: Continue to have hope. Continue to want to thrive and live.
At the beginning of my journey with myelofibrosis six years ago, I was told I’d be dead by 72. Now they’re saying you could outlive this. You could die with this, not of it. Hearing both Dr. Jain and Dr. Mascarenhas talk about all these combination therapies and how they actually might get us to the cure was very exciting.
Conclusion
Stephanie: Thank you so much, Mary. Your story is so powerful. It’s also on our platform so feel free to check out Mary’s story.
Thank you to Ashley from The Leukemia & Lymphoma Society and to Dr. Jain and Dr. Mascarenhas for the work that you’re doing to push forward research and help patients and family members better understand their options in myelofibrosis and MPNs altogether.
I hope you’re able to take away something that was really key for you, because that’s our goal, to empower you in your own care. We look forward to seeing you at a future program.












 Stephanie Chuang, The Patient Story: Hi, there! I’m so glad you could join us. This program is part of
Stephanie Chuang, The Patient Story: Hi, there! I’m so glad you could join us. This program is part of 
 We’re also incredibly lucky to have again Dr. Angela Fleischman from
We’re also incredibly lucky to have again Dr. Angela Fleischman from  Andrew Schorr: I’m Andrew Schorr and I’ve been living with
Andrew Schorr: I’m Andrew Schorr and I’ve been living with