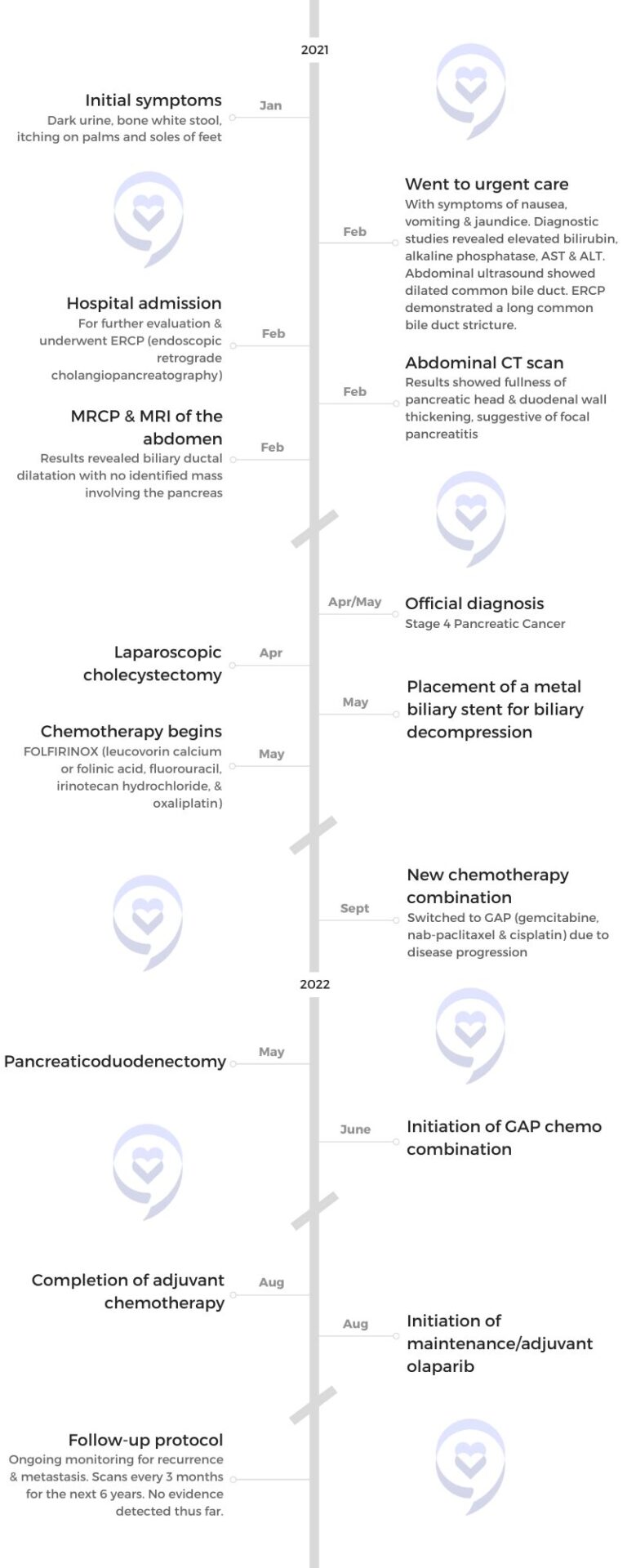
Initially misdiagnosed due to overlapping symptoms with his existing condition, Matthew experienced concerning symptoms such as dark urine, pale stool, and intense itching. Eventually diagnosed with metastatic pancreatic cancer, Matthew underwent different combination chemotherapy treatments, including FOLFIRINOX (leucovorin calcium or folinic acid, fluorouracil, irinotecan hydrochloride, and oxaliplatin) and GAP (gemcitabine, nab-paclitaxel, and cisplatin).
Despite setbacks and the grim prognosis associated with pancreatic cancer, Matthew’s tumor responded positively to the new chemotherapy regimen, leading to tumor shrinkage and the disappearance of metastases in the liver. Following a successful Whipple procedure, Matthew emphasizes the importance of not being defined by statistics and advises others facing similar challenges to live life to the fullest while also taking their health seriously.
His story highlights the unpredictable nature of cancer treatment, the importance of advocating for oneself in medical settings, and the significance of cherishing each moment, even in the face of adversity.
In addition to Matthew’s narrative, The Patient Story offers a diverse collection of cancer stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I live in Hazel Park, Michigan, with my girlfriend Natalie and our pug Monique. Because of the nature of my illness, I haven’t had a job in three years, but in my former life, I was finishing a PhD. I was going to be an academic.
Pre-diagnosis
Initial Symptoms
The most popular narrative surrounding pancreatic cancer is that not only is it very lethal but also very difficult to diagnose. The pancreas is deep in the body. The earlier symptoms are very nuanced, can go unnoticed, and can also be misdiagnosed as a multitude of other things. By the time you’re experiencing symptoms, the cancer has spread outside of the pancreas. I don’t want to say it’s too late, but that’s what conventional wisdom is.
I was diagnosed with Crohn’s disease when I was 25. Gastrointestinal distress, which is one of the more perceptible symptoms of pancreatic cancer, was par for the course for me. I probably wouldn’t have noticed even if I didn’t have Crohn’s. I lost some weight over the months, but it wasn’t until late January 2021 that I started to experience starkly distinct symptoms.
It was the COVID pandemic. I lost my job and moved to a different city to help my friend with his business. His business closed and he moved away, so I was alone when all this started.
I had dark urine and bone-white stool. I didn’t even notice the stool color for a while. At first, I thought I was hungover. I had a few beers the night before so I drank some Gatorade and lay in bed, but the urine did not get lighter.
My skin started to itch. The bathroom symptoms were pretty jarring, seeing urine that dark and poop that pale, but the itching was probably the worst. The palms of my hands and the bottoms of my feet itch. It was worse at night. I never felt anything like it before and those are hard places to scratch.
After a whole night of itching, I put my hands and feet in the tub under hot water to numb the sensation. In retrospect, it’s jarring to think about burning my hands and feet to alleviate the pain, but the itching was that significant.
Not everyone gets the itchiness. There seems to be some controversy because not every pancreatic cancer awareness campaign includes itchiness. I experienced it and it was horrible.
When something started to happen, I sat on it for 48 hours before I finally told someone. It wasn’t the most responsible, but in retrospect, not that bad. I was in a long-distance relationship with a woman I knew from graduate school. I told her and she said, “You should go to the doctor.”
I have a lot of medical anxiety. I have never been a good patient. For someone with such anxiety about doctors and hospitals, I needed someone to tell me.
Going to Urgent Care
I had recently moved to Durham and didn’t even have health insurance, but I went to an urgent care center. My blood test results showed that my bilirubin was high. We get some more tests back. The nurse said, “You don’t have a doctor here yet and these test results are troubling. You should go to the ER.”
Going to the Emergency Room
I went home to sleep because I hadn’t slept in three nights. I was so tired that despite the itching, I passed out. Early the next morning, I went to the ER and that was the beginning of my journey.
They admitted me to the hospital and ran some more blood tests to see what was going on with my liver enzymes. They did an ultrasound and an endoscopic ultrasound.
Bile Duct Stricture
They found that there was a stricture in my bile duct. Your liver produces bile, a digestive enzyme stored in your gallbladder and then released into your small intestine to digest fats and other foods. The tube that brings the bile down goes through the head of your pancreas. That tube had a stricture, so it was closed off. When bile can’t be distributed normally, you end up depositing it in your blood and your flesh, and that causes jaundice and elevated liver enzymes.
With the endoscopic ultrasound, they were able to place a stent in my bile duct in the hope that it would stretch it out. They told me to come back in a few weeks to have another endoscopy and remove the stent.
There was no sense of urgency. I was an otherwise healthy person with a history of colitis. They didn’t think that this was anything scary.
After they removed the stent, the symptoms came back, so they decided that it was my gallbladder causing the symptoms. With pancreatic cancer, it’s very common for people to assume that it’s a gallbladder issue. They decided to take my gallbladder out. After the surgery, the symptoms return.
It was late April. I went to my gastroenterologist’s office, who was the one who did the endoscopy. She said, “I don’t know what’s happening, but you for sure don’t have cancer. We have done so many brushings and you definitely don’t have cancer. If you have cancer, I will roll over in my grave.” I left her office feeling pretty confident.
Diagnosis
Getting the Official Diagnosis
Three hours later, I got an automatic notification on my phone from MyChart. One of my cytology reports came back. It said adenocarcinoma. I didn’t know what that meant, but I knew it wasn’t good.
I sat with that for about two hours. Then the surgical oncologist who did my gallbladder surgery called me. My case got automatically referred back to him. He was out of town and called me using his personal cell phone.
I told him, “This lady told me I definitely did not have cancer and now I do so I’m freaked out,” and he apologized. My surgeon is the salt of the earth. He calmed me down. I don’t know if he remembers it this way, but I’ll never forget this conversation. He said, “If this is cancer, the tumor’s very small and I should be able to get this. I’m confident.”
The area in which they found the adenocarcinoma is called the ampulla of Vater. Everything in this part of the body is pretty small and overlapping so pancreatic cancer could be an explanation. But given my age and, let’s face it, the taboo around death, no one was talking about that.
When pressed, the doctor told me ampullary cancer, which has a higher survival rate and is still incredibly rare for someone my age but less rare than pancreatic cancer in the same age category.
Treatment
Discussing the Treatment Plan
Because of the size and the layout of this part of the body, they do the Whipple procedure, also called the pancreaticoduodenectomy. They do the same surgery for ampullary cancer as they do for pancreatic cancer.
Five days after the phone call, I was in his office and he said, “I’m going to remove part of your pancreas and part of your small intestine.” I didn’t have a gallbladder, but that also would have gone including part of my stomach.
My surgeon told me that they cut me open and, contrary to what they thought, found a tumor on the head of my pancreas that had spread outside of the pancreas. Metastatic pancreatic cancer is considered inoperable so when they saw that, they closed me up.
Because of my age and because they suspect that I’m a BRCA2 mutation carrier, the surgeon said, “We have to confirm with genetic tests, but I’m pretty sure you have this particular genetic abnormality. If that’s the case, then there are targeted therapies that might work for you.”
He said, “This is a mean cancer. But because of your particular situation, after treatment, we might be able to try the surgery again in a year.” For pancreatic cancer, surgery is the only long-term survival solution. Chemotherapy and radiation are life-extending, but they’re not curative. He was pretty confident, at least in the context of a lethal diagnosis.
Later that day, he introduced me to my oncologist. He was not as confident. When pressed, he said, “With treatment, you might have 1 to 3 good years left, but that’s it.”
FOLFIRINOX Chemotherapy
This was at the beginning of May 2021. My wound had to heal. Three weeks later, I started chemotherapy. Like a lot of other people with metastatic pancreatic cancer, I was given FOLFIRINOX, which is five different drugs. It’s awful. Chemo combinations are all awful, but FOLFIRINOX was really, really abrasive.
I had a scan after three months on FOLFIRINOX. The oncologist said, “Your tumor shrank a little bit,” but you can tell from the way he’s telling me that it could be an imaging error or a minute retreat that it’s barely perceptible.
At my next CT and MRI three months later, the tumor grew. It had metastasized to my liver so things were not looking good. At this point, I was not confident that I would be a special case or a miracle. I thought this was it.
Switching Chemotherapy Regimens
My oncologist switched me to a different chemotherapy combination. He told me there was a combination that some researchers found was promising for people in my situation. It was gemcitabine, nab-paclitaxel, and cisplatin (GAP).
I was honestly relieved because after being on FOLFIRINOX for almost six months, the neuropathy had gotten so bad that I couldn’t get out of a chair by myself. I needed someone to hoist me up. I was pretty thin at this point. It was miserable.
On the new chemotherapy regimen, my quality of life improved dramatically. By the time my first set of scans came around three months in, some of the spots on my liver had started to disappear. I did three more months of chemo and made it through.
I didn’t lose my hair. I’m six feet tall. I was 215 lbs when I was diagnosed and miraculously maintained a healthy weight so I’m very thankful for that. At this point, I thought I was still dying sooner rather than later so I was trying to have fun and it certainly made having fun a lot easier.
Post-Treatment Scans
In March 2021, he looked at my scans and, if memory serves, they could not identify cancer outside of the tumor.
Almost a year to the day, they attempted to do the Whipple and, this time, it was successful. When Dr. Allen came into my hospital room, he said all of my margins were good and the lymph nodes they tested were negative.
Before this, they couldn’t see any cancer on the CT or MRI, but that didn’t mean that my peritoneum wasn’t covered in cancer. That just meant that they wouldn’t be able to tell until they got in there. They were pleasantly surprised that things had worked.
Follow-up Protocol
The last scan was a lot smoother than the others, but they’re incredibly difficult. I get a scan every three months for the next six years, but the chances of me living out those six years are astronomically small. Pancreatic cancer has a remarkably low five-year survival rate. It’s unlikely that I will see all of that time, at least on paper.
Words of Advice
It’s important to remember that you are not a statistic. I was diagnosed with something I wasn’t supposed to have at my age. It was very unlikely. It was supposed to kill me and I didn’t die so, in a sense, I beat the odds not once, but twice.
People think that pancreatic cancer is an old person’s disease. I think that’s why no one ever looked because no one ever even thought that I could have pancreatic cancer. I’ve heard over and over again that I’m too young. Statistically speaking, they’re correct. For people under 35, it’s incredibly rare, but there is a difference between statistical analysis and what statistics are for, and encountering a patient one-on-one.
Treatment is not linear. Pancreatic cancer is often thought of in linear terms as a quick, short trajectory to death. We assume that if treatment will work, it will work immediately. You don’t take one step back and one step forward. In my experience, that’s not true. Sometimes things get worse before they get better and it’s not a reason to lose heart.
Have a drink, eat the cheeseburger, and live your life to the extent that you can. That’s how I lived. Take your health seriously but also meet yourself where you are.
Courtney, a high school English teacher from Spokane, experienced symptoms such as fatigue and blood in her stool that led her to suspect she had colon cancer. Despite initial dismissals from multiple doctors due to her age and lack of family history, Courtney persisted in advocating for herself, ultimately undergoing a series of tests, including colonoscopies and scans, which confirmed her suspicions. Diagnosed with stage 3A colorectal cancer, Courtney underwent surgery to remove the tumor and lymph nodes, followed by chemotherapy as a precautionary measure.
Throughout her treatment journey, Courtney faced various challenges, including side effects from chemotherapy such as hand-foot-and-mouth sores and neuropathy. Despite these obstacles, she pushed forward, continuing to teach full-time and engaging in physical therapy to regain her strength. Three years into remission, Courtney emphasizes the importance of self-advocacy, listening to one’s body, and pushing for answers, especially when faced with medical dismissals or ambiguity. She encourages others to trust their instincts, seek support from loved ones, and persevere in navigating the healthcare system to ensure proper diagnosis and treatment.
Name: Courtney H.
Diagnosis (DX):
Colon Cancer
Staging:
3A
Symptoms:
Blood in stool
Fatigue
Treatments:
Surgery
Chemotherapy
Capecitabine
Oxaliplatin
Advocate for yourself, know your body, listen to your body, and keep pushing until you find answers.
Courtney H.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
My name is Courtney. I am a teacher. I teach high school English – specifically honors 9 English and mythology. I am a big lover of reading. I like to play outdoor volleyball, garden, and explore. I live in Spokane, in the Pacific Northwest. It’s so beautiful. We have four seasons and lots of activities and different things to do. I like to spend time with my niece and nephew.
What were your first symptoms?
I took an anatomy and physiology class in college, and one of the only things I remember from that was that the professor said, “Most often when you have internal bleeding of some sort, it is your body’s inability to heal itself, and that usually comes in the form of a tumor.”
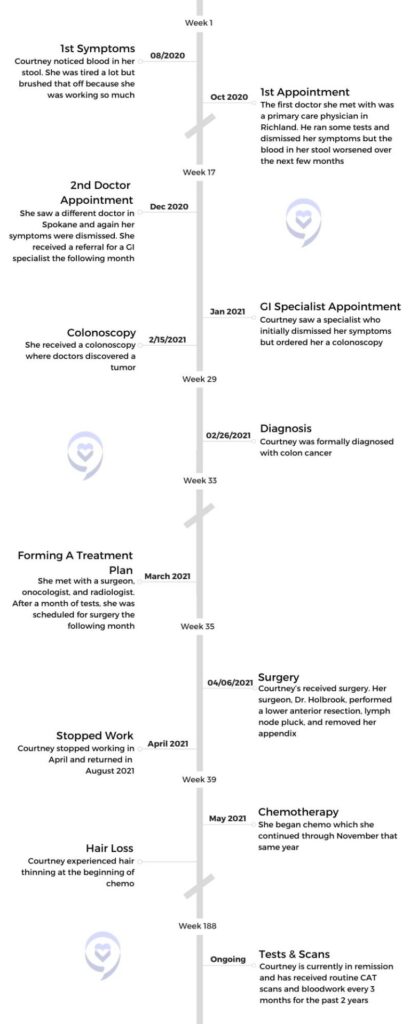
What had happened was I had gotten a teaching job in Othello, where I grew up, and I moved down there. This was August of 2020. I was a very busy new teacher. I was the head cheer coach for a cheer program. I worked a lot of jobs in grad school, and so I just was very used to being on the go all the time and having a busy and packed schedule.
I knew I was sick. I knew I had colon cancer, so I just kept pushing.
When I moved to Othello, I started showing one symptom – I had blood in my stool, and I instantly knew. I knew instantly that I had colon cancer. Moving down to Othello, I had to get all of my records and everything transferred down there, including all my medical stuff. So I wasn’t able to go in and see a doctor until October. My symptoms kept progressing, and I just knew when that started happening. I was trying to find somebody that could help me find the exact diagnosis. The answer.
Did you have any additional symptoms?
Just blood in the stool and fatigue. My friend’s mom, who’s a nurse, did a blood test on me and she said I was very anemic. What we ended up finding out when they had taken the tumor out is the blood flow was feeding the tumor, and that’s why I was so anemic.
The first general practitioner doctor I went to, he dismissed all my symptoms and said, “There’s nothing wrong with you. You’re thin, you don’t have a family history. You just need to make some dietary changes.” I was like, “Well, I’m going to keep trying to find answers.” It was in the middle of COVID, so everything was pushed back. Then symptoms kept getting worse. When I came home for Christmas break – home was Spokane – I saw a different doctor and it was the same thing. He spent about an hour with me, ran some tests, dismissed all my symptoms, but I knew I was sick. I knew I had colon cancer, so I just kept pushing.
The first doctor in Richland, he actually had put in a referral for me to see a GI specialist. I was able to see a GI in January of 2021 and [experienced] the same thing. She dismissed all my symptoms. Finally I said, “Listen, this isn’t about you being right or me being right. This is about figuring out what’s wrong. You’re speculating and I’m speculating.” They were all saying, “We think you have Crohn’s or diverticulitis, diverticulosis, or a bleeding hemorrhoid.”
One of the greatest skills that my parents ever taught me was the ability to advocate for myself and to know your body.
I said, “No, I think that I’m sick. What can we do?” She said, “Well, we can give you a colonoscopy. You’re too young and they’re very expensive.” I said, “Well, I’m a teacher. I have great health insurance. We need to do this. I think it’ll give me peace of mind knowing that we have tried everything.”
Receiving a colonoscopy
Months later, she did a colonoscopy and found the tumor. That was February of 2021. That whole month and a half that I went through 9 different tests. I did 3 colonoscopies, a sigmoidoscopy, 2 CAT scans, a PET scan, and an MRI. There’s another one I did but I can’t remember the name of it. All of those tests brought me to the diagnosis. Now what are we going to do? What’s the plan of action going to be? I got a team together.
What tests did the first doctors do?
He did a blood test and some general stuff. He felt my stomach to see if I had any lumps or bumps. Then he went through and looked at family history. Obviously, I don’t have a family history of it. He said, “You’re thin, you’re not pre-diabetic.” I was in Richland, Spokane, and then I went to Kennewick. So three different cities, three different doctors. The doctor in Spokane pretty much did the same thing. They didn’t do anything extensive because you can’t really diagnose it unless you actually get a colonoscopy.
The problem was, neither one of those two doctors could perform that. Then they just dismissed my symptoms. They said, “Well, we’re not going to put in a referral for you to have a colonoscopy because we don’t think, from our experience, that you have it. I really had to beg the GI specialist to give me one.
We did a blood test with the first doctor and he didn’t see anything abnormal. Then the doctor in Spokane didn’t really see anything abnormal. But my friend’s mom, who’s a nurse, knew what to look out for because I told her what was going on. She did her own test and said, “You are severely anemic. Something’s going on.”
Did your insurance cover the cost of the colonoscopy?
I paid a little bit out of pocket, but it was mostly covered. The problem was, and this is something that I think a lot of people run into when they’re getting tests done, especially a colonoscopy or sigmoidoscopy. My insurance company did not want to pay for the right type of drugs. I didn’t know that. I didn’t hear the confirmation. They actually had to tell my parents, and it took 8 hours for the drugs that they gave me to wear off. So I actually didn’t find out about the tumor until the next day. My parents waited to call because they tried to talk to me after the procedure and I was just bonkers.
Surgery
The importance of advocating for yourself
They dismissed the symptoms because I didn’t fit the profile, but one of the greatest skills that my parents ever taught me was the ability to advocate for myself and to know your body. I just knew I was sick. I had that feeling in my stomach. Sometimes science can only go so far, and sometimes you have to put it in your own hands and keep pushing for it. It was a unique set of circumstances, because when I did my colonoscopy, COVID cases were very light, so I was able to go in and get a colonoscopy. When I had my surgery, COVID cases were really light, so they didn’t push my surgery back. These were just perfect little windows where things ended up really working out in my favor.
Formulating a treatment plan
Because I didn’t have the right drugs, she couldn’t finish the colonoscopy. I would have to come back 4 days later and do another one. I came back that Friday. I had [the first one] done on a Monday, came back that Friday, and everything else looked clear. She said, “I’m 98% sure that this is a cancerous tumor. We’re going to send it off to have it biopsied.”
It took two weeks to get back. The next conversation, I said, “I know a surgeon who saved my dad’s best friend’s life. He had stage 4 rectal cancer and he’s been in remission for 20 years. I want that guy.” She was going to put in a referral for somebody else. I said, “No, I want this guy.” Then everything started to move, all the tests.
After all of the tests came back – because the original plan was to do some radiation, 6 weeks of chemo, and then do surgery after the MRI, – the radiologist called me and said, “This is miraculous, but your tumor is a lot smaller than we thought, so we’re going to operate. Nothing else is lining up in your body, so we’re just going to go for it and operate.” So they did.
Describe your surgery
Dr. Holbrook went in and did a lower anterior resection and took out part of my colon, 21 lymph nodes, and my appendix. He said, “I had a stage 4 appendectomy patient who’s 17 years old last week. I just thought I’d take your appendix out.” He spent about 4 hours in surgery. He just retired last year, but he’s one of the best in Spokane. I trusted him.
The prep work was I had to go onto a liquid diet about 48 hours before. They gave me some things that they wanted me to take prior. After I was in the hospital for about 4 days, I had a series of things that I had to go through to get out of there. I had round the clock bloodwork. They would come in at 2 a.m., they’d come in at 6 a.m.. They were checking fluids and different things like that.
As far as the procedure, he just went in. He didn’t tell me how much of my colon he took out, but he took out the sigmoid region of the colon. That’s the end. He took that part out and did the lymph node pluck. After that, I was on a liquid diet for about 3 weeks, giving my bowels a break and allowing things to heal. He was able to go in and do it minimally. The incision where he went in was about this big. He was able to go in right underneath my stomach and do it.
Chemotherapy
What stage were you in?
We got a really good prognosis back. I had a stage one tumor. There were just a few little cancer cells that had broken off and gone into one lymph node, so I had a really good prognosis.
Preserving fertility before starting chemo
I had my 3 week clearance from surgery, and then I actually harvested my eggs, and then I did chemo. It was boom, boom, boom. My body had been through some things. Harvesting your eggs is quite an interesting process. I didn’t know this. When you go through and you do all the things, they monitor you, they take your temperature, they do all the things.
The day before my procedure, they did a COVID test on me and it came back positive. I didn’t know I was asymptomatic. Seattle Reproductive had to fight with Seattle to advocate to harvest my eggs because it’s a $15,000 procedure. They ended up saying, we’re going to suck it up, risk it, and do her procedure. Then I started chemo right after I was cleared from COVID.
I didn’t have to do chemo because of my prognosis, but my surgeon and team recommended that I do it as an insurance policy. I was prescribed 2 different types. I had an infusion chemo which entered through a port and a pill chemo. I would do one infusion every 3 weeks. Then I was on pill chemo for 2 weeks at a time and I’d get a break at the end of it.
Which chemos were you on and did you have side effects?
Capecitabine. The infusion chemo was called oxaliplatin. I had side effects with each. With capecitabine, I had hand-foot-and-mouth, where you get really bad sores everywhere. The other chemo was oxaliplatin. It’s a platinum chemo. It had some really strange side effects. You couldn’t touch anything cold. You couldn’t ingest anything cold. I couldn’t drive in my car with the AC on or it could close my throat. Everything had to be room temperature or hot.
It was in the middle of the summer, so one of the biggest issues I ran into was I was dehydrated a lot. I was hospitalized 2 different times for dehydration which was scary. I lost a lot of weight. I think I lost about 25 pounds. I tried to eat when I wasn’t hungry. I had to watch what I ate. They tell you you can’t have raw fruits and vegetables while you’re on chemo, which is so weird because you should be eating healthy foods, and they said to eat what I could.
The first two days after infusion chemo and pill chemo, you’re the sickest, you’re nauseous. It’s really, really hard to get up and move around. With oxaliplatin, like I said, it’s a platinum chemo so it causes neuropathy. You have a lot of tingling going on in your body. It got to the point where my eyes were affected by it. I could taste it in my mouth. It was very all-consuming throughout my body.
Stopping oxaliplatin
I did my own research about my particular prognosis and I decided to stop oxaliplatin after 4 rounds. That’s the infusion chemo. A lot of patients push past that, and there are some patients that end up disabled from doing that chemo. I did not want to do that. I didn’t want to risk that. It was making me so sick that I could barely eat.
Did anything help alleviate your chemo symptoms?
When I was dehydrated, I would go in and get pumped with fluids. That helped. I did take Zofran to help with the nausea. You can’t be in the sun either when you’re on chemo. You have all these things that you can’t do.
The best thing that helped with the side effects was to get my mind off of it.
I think for me, the best thing that helped with the side effects was to get my mind off of it. I taught full time while I was on it. That was my choice. I didn’t want to lay in bed every day and dwell on it. That’s just my personality so I decided that I was going to work and let that be the thing that would help get my mind off of it. I did oxaliplatin for 3 months and capecitabine for 6 months.
When I went back to school to teach, I did physical therapy and that helped a lot. It helped me build up strength because I had lost so much muscle mass and lost so much weight and it helped with getting through those days.
Reflections
How long have you been in remission?
I am almost at the 3 year mark of being in remission. I count it as April. My oncologist counts it as November because that’s when I finished chemo, but I think that the surgeon got everything.
How often do you get scans and do you experience scanxiety?
I don’t think that it ever really leaves you. I think that it stays with you.
I just hit the 2.5 year mark, so now I go every 6 months. I think that’s one of the hardest parts. I was joking with a friend that I’m a part of an exclusive club now because it doesn’t really ever leave you. With scanxiety, I just do my best to just try and stay positive. It’s always quite exhausting because it’s a 4-day process – blood work, scan, and meet with your doctor.
My aunt is a phlebotomist, so she’s always encouraging, giving me tips on how to stay positive and hydrate, make sure you’re ready to go. But it is a real thing, and I honestly don’t think that it ever gets any better. I think that you learn how to manage, how to live with it. The farther out that you get, you feel better. But I don’t think that it ever really leaves you. I think that it stays with you.
What advice do you want to share with cancer patients?
Advocate for yourself, know your body, listen to your body, and keep pushing until you find answers.
You need to advocate for yourself and you need to be able to listen to your own body. Science only goes so far. Knowing, understanding, and listening to your body is really important. Because if you’re sitting in front of this doctor that doesn’t know you, you’re just a statistic. They’re trying to see where you fit, and if you don’t fit the category, you don’t fit the profile, of course they’re not going to suspect anything.
I also think that you have to hold on to your faith and keep pushing through roadblocks and things that are in your way. You just have to keep going until you find the answers that you really desire to have. For me, that was, I’m sick of hanging out in ambiguity. I know I have it. You are speculating, but that’s why we have science. That’s why we have these things. We shouldn’t be profiling people based on their age or the way that they look. We should be listening to the patient and to their concerns.
Advocate for yourself, know your body, listen to your body, and keep pushing until you find answers. That’s why I’m alive and well today, because I advocated, and I continued to push until I got the answers that I needed. I don’t blame any of them. They’re doctors, they’re human, but I do think that they need to listen to patients better. I think that they need to listen to their patients, listen to the concerns that they have, and really do a better job of putting something in place that is going to help. Help eliminate this ambiguity. For people that may not feel as comfortable to advocate, you just have to remember that you know your body. So even if it’s something that’s totally foreign, talk to somebody about it and try and find those answers that you are desiring to look for.
Interviewed by: Alexis Moberger Edited by: Chris Sanchez
Laura survived stage 4 kidney cancer.
Originally from south Louisiana, Laura now lives in Southern California. She splits her time between working full time in marketing in the gaming and hospitality industry, being a kidney cancer patient advocate, enjoying her sports and hobbies, and caring for her family.
Laura had been struggling with her health for at least two years before her symptoms were properly diagnosed as cancer. She suffered from elevated blood pressure and fatigue so significant that she would sometimes have to nap in her car during lunch breaks, and was also found to have a very high red blood cell count. But the doctors she would consult chalked her symptoms up to lack of sleep, stress due to her demanding job, excess weight, and so on.
Later on, Laura’s health took a turn for the worse. She started to experience back pain so bad that she sometimes had a hard time walking, and her legs became so swollen that she was unable to wear pants to a dinner out to celebrate her 29th birthday. She returned to the doctors, who started taking a closer look at her symptoms and ordered more procedures.
Blood work uncovered kidney issues. Her doctor told her to have a CT scan done that week, but she decided to take immediate action. That very night, just 5 days after her 29th birthday, she went to the emergency room. It was a pivotal and timely decision: the doctors discovered that she had stage 4 cancer and a massive 13cm tumor on her right kidney. The doctors also found that this tumor was what was causing her legs to swell, because it was blocking her vena cava–the main artery bringing blood back up to the heart from the lower parts of the body–making immediate treatment even more urgent. Laura was also diagnosed with the rare genetic disorder, hereditary leiomyomatosis and renal cell cancer (HLRCC), or Reed’s Syndrome.
Laura’s ER surgeon, a kidney cancer survivor himself, connected her with the UCLA-based surgeon who had operated on him years ago, and she ended up heading there for surgery. During a 5-hour session, the surgical team removed her right kidney, right adrenal gland, most of her inferior vena cava, and 7 lymph nodes. However, a checkup some weeks later revealed that the cancer was not only still present but had also spread to her lungs, liver, and nearly all the lymph nodes in her chest.
Laura started seeing another doctor in Las Vegas, who recommended that she take part in the S1500 PAPMET randomized clinical trial organized by the global cancer research community, SWOG Cancer Research Network. After some deliberation, she decided to join the trial, where she ended up taking the targeted therapy drug Cabometyx (cabozantinib).
The side effects of cabozantinib were crippling. But just a year after Laura started taking it, she was found to be in complete remission. Out of 147 patients who joined the trial, she was 1 of only 2 who had had a complete response to their treatment.
Laura continues to be healthy to this day; she undergoes scans every six months, and to date her status continues to be “NED” (no visible evidence of disease). But not only is she enjoying her life once again, she is also now a patient advocate, and actually works with the very doctors who concluded the clinical trial she joined.
Laura is sharing her story with us to show that a Stage 4 diagnosis does not have to be a reason to give up hope; to exhort cancer patients to advocate for themselves as a lifelong responsibility; and to urge them to get to know both their bodies and their disease, in order to be able to make the best possible choices for themselves.
In addition to Laura’s narrative, The Patient Story offers a diverse collection of stories about kidney cancer. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
Name: Laura E.
Diagnosis:
Genetic condition: hereditary leiomyomatosis and renal cell cancer (HLRCC) (Reed’s Syndrome)
Type 2 metastatic papillary renal cell carcinoma
Staging:
Stage 4
Symptoms:
Profound fatigue
Hypertension
High red blood cell count
Severe back pain
Badly swollen legs
Treatment:
Chemotherapy: Cabometyx (cabozantinib) assigned under S1500 PAPMET clinical trial
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I’m not the same person I was before I was diagnosed. There’s no way I could be.
I definitely look at life differently now…
I try my best to live as authentically as possible. Because I know time is a gift.
Introduction
I am 36 years old. I live in Southern California, and I’m originally from outside of Baton Rouge, in the south of Louisiana.
I’m a proud graduate of Louisiana State University, where I got a bachelors and masters from National University. I’ve been working in marketing in the gaming and hospitality industry for over a decade now. Just busy with my family when I’m not at work.
I also like to read and do Zumba and watch global reality TV. I’m actually am part of an all women’s Mardi Gras krewe; I ride in a parade in New Orleans every year and it’s one of my favorite things to do. I just rode earlier this year and I’m already ready for next year.
Pre-Diagnosis
I was having symptoms of my kidney cancer probably two years before I was officially diagnosed.
I had horrible fatigue and was actually going to my car in my lunch breaks to sleep. My blood work was really off. I would go get my blood work done and there would be this one level that I was like, why is it off? And actually had a doctor tell me, oh, if something was really wrong, it would be like hundreds off the charts.
My blood pressure was high, too. I talked to my primary care doctor and she said, well, hypertension runs in your family. And I said, I know, but I’m in my 20s. It’s usually people in their 40s and 50s in my family that have hypertension.
Everyone just kept telling me, lose weight, get more sleep, reduce your stress. And at the time I was working in marketing for a casino corporation that has multiple properties across the country. I was the marketing manager over three of their properties on the strip. And so I thought, okay, well, I probably am stressed.
You know, I was working a lot of hours and, and had a lot of responsibilities. My kids were in middle school at the time or late elementary school. And so I just thought that’s kind of how things were. And then it was about six months before my diagnosis.
Diagnosis: Type 2 metastatic papillary renal cell carcinoma
I went to get another biometric screening done, and they almost called an ambulance because my blood pressure was so high.
So I went to my primary care doctor. But she again said, lose weight, reduce your stress. I ran my blood work and my red blood cell count came back really high, which I later found out is an indicator of kidney cancer. But the doctor said, oh, you probably just had an infection or something.
I felt like a hypochondriac at that point. These are all specialists. These are all doctors. They know what they’re doing, who am I to question it? So that was December.
And then one day in May, ten days before my birthday, I woke up and I just had the most horrific back pain I’ve ever had in my life.
I was honestly struggling to walk. It felt like I was a puppet and someone was just pulling the strings, you know?
And so I went to urgent care because my primary care couldn’t get me in. But it was more of the same. They said, yeah, you probably pulled a muscle here. I was given some muscle relaxers. Of course, they didn’t work.
It progressed to the point that a few days later, for my birthday, we went out to dinner and I couldn’t even put pants on. I had to wear a dress because my legs were really swollen.
So my mom was in town at the time and I didn’t want to freak her out, so I waited until she left town a few days later to go to my primary care. And when I went there, the doctors did more blood work and said, something’s wrong with your kidneys. I’m going to send you for a CT scan. Go get it done within the week.
But I was really feeling that it couldn’t wait. Thankfully I didn’t listen. I went to the ER that very night after work.
The ER doctor diagnosed me with a 13 centimeter tumor on my right kidney and told me I needed to have surgery as soon as possible. He told me to go to a specialty hospital, not to just let any surgeon operate on me, which now that I know so much more about my disease than I did at the time, I realized it’s because it was a very complicated surgery they had to do.
And that was five days after my 29th birthday. I know my outcome would have most likely been very dramatically different had I not gone to the ER that night.
I was also diagnosed with a rare genetic disorder, known as hereditary leiomyomatosis and renal cell cancer (HLRCC), or Reed’s Syndrome.
Reaction to the Diagnosis
It took forever for me to get diagnosed, but once I did, everything lined up into place.
I think I just kind of shut down mentally after the ER doctor said, you have cancer. And I really struggled to process it. I almost felt for a minute there like if I said it out loud, it made it real, you know? I’m a very logical person, but it was hard to process.
I remember we got home from the emergency room, early the next morning because I had been there all night. I had to call my boss. It was a work day; I actually had a presentation that I was supposed to be giving that day. And so I’m thinking, oh my gosh, I have to call my boss and tell him I have cancer. And I actually sat in my chair in my living room and was practicing saying, “I have cancer” before I called him. I was trying to: one, make my experience a reality and, two, keep myself from crying while I’m telling him this. It just felt like a bad dream, honestly. It didn’t even feel real.
And there was about a month between my diagnosis and my surgery, and I was in terrible pain the whole month. You know, I just wanted to sleep and just not think about what was happening. So it took me a while, even after my surgery, to really come to terms with what was happening.
And I remember distinctly after my surgery, I was in ICU for, I think, about five days. And then they moved me to a regular room, and it was there that I finally went, I should probably look at my gown and see my doctors. I hadn’t even done that at that point. I think that was the moment that it really hit me, like, oh my God, my life is never going to be the same again. Like I knew that cognitively. But that was my emotional process. This isn’t just “I have surgery and I’m done with it and I move on with my life.” This is forever going to be something that I am now identifying as a cancer patient and cancer survivor.
It’s frustrating whenever I look back, because I know that at the time of my diagnosis, I had to have had cancer for at least a year, probably two plus. And the idea that had I not been diagnosed at stage four, I could have just had surgery and been done with it, I wouldn’t have reached a point where I’m being diagnosed with a terminal phase of this disease. It’s pretty heartbreaking and it’s really frustrating.
I went back and talked to my primary care doctor a few months after I was diagnosed. Obviously, I’d switched doctors at that point. But I talked to to her and the head of the clinic and I said, look, I know that you will probably never see another case like mine again, but, you know, there’s this phrase with rare cancer patients that they tell doctors at medical school to look for horses when you hear hoofprints, not zebras. And I’m a zebra.
Look, you’re going to go on and treat other patients. And you may never see another case like mine again, statistically speaking, but it doesn’t mean that you don’t have to see other cases that aren’t rare on their own. And I think that we are conditioned a lot of times, especially as women, to just accept diagnoses, if you’re telling me nothing’s wrong, nothing’s wrong, and I’m just going to believe that. But we know our bodies.
I really encourage people to trust their instincts when it comes to their health. You know your body best, you know if something’s wrong with you.
And I really wish I would have just kept listening to that little voice that I had in my head. You know, in my heart that said, Laura, something’s wrong.
I’m glad that I finally did, because that’s what encouraged me to go to the ER that night.
Surgery
The ER doctor told me that he’d already contacted a local urologist in Las Vegas, where I was living at the time, and that the urologist was going to help me get to either USC or UCLA in California for surgery. The ER doctor was very adamant that I needed to go to California for surgery.
I’m now realizing how extensive the tumor was. It’s not just that it’s 13cm, which is very large for a kidney tumor, but it was also blocking my vena cava, which is your main artery that brings your blood back up to your heart from your legs and all. Which is why my legs were so swollen. And so that’s a life threatening condition, which I’m glad I didn’t know at the time because I probably would have just completely shut down at that point.
I realize now that’s why the ER doctor was so insistent that he needed to go to California for surgery. And so the next morning we went to the urologist in Vegas, and he said there was one surgeon in town who may be willing to take your case. Didn’t want that. But he said, if you go to California, I’ll get you in at UCLA.
The doctor added, actually, I was you seven years ago, with kidney cancer. And if you go to UCLA, I will send you to the surgeon who operated on me. And sure enough, he did. He actually walked out of the exam room and called the surgeon on his cell phone and said, I’m sending you a patient from Vegas. And so I got into UCLA.
They did a phenomenal job with my surgery. I was incredibly lucky. I had two amazing surgeons and it was a five and half hour surgery, and they removed my right kidney, my right adrenal gland, most of my inferior vena cava, and seven lymph nodes. And we were hopeful that they’d removed all the cancer. And maybe I would need to do immunotherapy afterwards to keep it from coming back. So that was in June.
Cancer metastasized
But when I had my first scans in August, the cancer was spreading like wildfire.
And so at that point, the cancer was in my lungs and my liver and pretty much all the lymph nodes throughout my chest.
And the doctor at UCLA said, I could put you on this one treatment.
Again, I would just go back to if something doesn’t feel right, listen to your body.
I think even as cancer survivors, we tend to dismiss things sometimes, and so even if you’re in your cancer journey or you’re a survivor, you have to.
It’s advocating for yourself as a lifelong responsibility.
Treatment
Treatment Options
The doctor said, I don’t know if it’s going to work for you. I think you probably should look into clinical trials, but if you do that, you’re going to have to come back and forth a lot. And I know that’s going to be kind of a burden for you to do that. So there’s a doctor in Vegas who is a specialist in kidney cancer, and I would recommend you go see her.
And I was really nervous about switching my care back to Vegas because of the experiences I had before, obviously. I actually had debates with my family and friends on whether I was making the right decision to move my care from UCLA? And I said, you know what? I’m going to go ahead and try it.
And I wound up with the most wonderful oncologist, who, again, was a GU, a kidney cancer specialist named Doctor Vogelzang. And at the first appointment, he sat me down and said, look, here’s what you have. He was the first doctor to explain to me what specific type of kidney cancer I had, answered all my questions, said, I have these treatment options lined up for you. There were all clinical trials because at the time there was no standard of care for the type of kidney cancer I had.
And so he said, here’s the one I think is the best option for you. There were three other ones that he had lined up. And then he said, look, I’ll even do chemo if I have to. Chemo isn’t usually used for kidney cancer patients. But I was so young that he just was like, I’ll do whatever I can to try to give you as much time as we can.
So he explained the first trial and he said it’s four different types of treatments. It’s a randomized trial. I can’t promise you which one that you’ll get. We have no control over that. But there is one treatment on this trial that I think would be your best bet. He said, look, think about it. Let me know what you think in your next appointment, what you want to do.
Decision to Join a Clinical Trial
And I decided to join the clinical trial. The clinical trial that I was on was sponsored by a group called SWOG.
Even now people say to me, oh, that was so brave of you to choose a clinical trial. And I recognize now that it was a brave decision to do a clinical trial. And I’m really proud of my decision to do that. But at the time, it just felt like, what choice do I have? I have terrible choices to make. And, if I make the wrong decision, that’s my life in the balance. That’s how it felt.
I also remember having this conversation with a close friend on my next steps. I said, look, the doctor I met with in Vegas is saying he doesn’t think the treatment that UCLA recommended is going to work for me. And let’s be honest, I’m dying anyway.
So maybe this is a Hail Mary. Maybe this will help me to live a few years. My goal at the time was to see my kids graduate high school. But if not, at least I’ll be doing something that will help other patients at some point. And so that’s why I decided to do the trial.
Cabometyx (cabozantinib)
And I remember when they randomized my treatment. My doctor said, oh my gosh, you hit the jackpot. This is the drug I wanted you in. It was a drug called cabozantinib.
And, at the time, I didn’t know what that was. I thought I was going to be doing immunotherapy, which I’m now embarrassed to admit because I know the differences between the drugs now.
And so I’m like, I can’t believe I thought I was doing immunotherapy because I just didn’t know the difference. It was a targeted therapy drug. And I started it and I was just terrified. And of course, my doctor explained the side effects and I’m going like, wait, what’s going to happen to me?
But again, I was like, what choice do I have? I mean, I can’t die now. I knew at that point that I had no more than a year and I would be lucky if I had another year.
And so I actually pulled my kids out of school for my first day of taking my pills. They needed a mental health day anyway, I’m sure, they had been watching me go through this all summer. And so I brought them to this little hotel outside of Vegas. And they have a really nice pool and all and then I’m sitting here thinking gosh, this is probably dumb. What if I take the first pill and I have this terrible reaction and then my kids are, you know, even more scarred, because mom had to go rushing to the E.R., which thankfully didn’t happen.
Side Effects
The side effects of cabozantinib were rough, to say the least.
What’s hard about being a cancer patient who’s doing one of these newer forms of treatments, like targeted therapy or immunotherapy, is you don’t typically have the same outward side effects that people recognize, whether they think of cancer patients.
I didn’t lose my hair, but it actually turned white. That’s one of the typical side effects from this type of treatment. And that was heartbreaking for me because I’m 29, 30 years old. My hair is going white; even my eyebrows went white. And it’s just all those things that you try to tell yourself, okay, the prize is I live longer and it’s true. It worked for me. I don’t regret it for a second. I would do it all over again in a heartbeat. But, you know, it does a number on you. It changes who you are.
I always say, kidney cancer helped me take the best pictures of myself that I ever took, which is terrible. I mean, I lost an unhealthy amount of weight. Honestly, looking back at pictures now is honestly kind of painful because I go, oh my gosh, I looked sicker than I realized I did
And because you don’t look like people expect a cancer patient to look, when I got back to work and all, they’d go, you’re doing great now, right? And like, no, I threw up three times before I left the house and had to drag myself out of bed because I was so fatigued and also, these targeted therapy drugs actually create a lot of GI issues. You get horrible diarrhea.
I recall standing in the grocery store aisle like about six months into my treatment, trying to pick out what adult diapers I was going to wear. I’m 30 and I’m buying adult diapers. And then I go to check out, I’m thinking, oh my gosh, this woman’s going to know, right? And she probably thought I was buying it for a grandparent or a parent or something.
You get all these side effects like it’s almost shameful to talk about. Your body is crumbling. And, again, it’s things that with traditional treatment you don’t always encounter. And of course, the side effects from traditional treatment are also horrible, too.
… if something isn’t sitting right with you even once you’re diagnosed, you know, if your doctor is telling you, oh, you should do this and something’s just not sitting right, get a second opinion. Get a third opinion if you need to.
You have to feel comfortable with your care.
NED Status
I reached NED within a year of starting Cabometyx, which is, like, insane. Incredibly hard to come across, to say the least.
I had a very rare response where I was 1 of only 2 of the 147 patients who had a complete response to treatment.
I wound up staying on Cabometyx for another about three years, because we just didn’t know what was going to happen after I had that first med scan. And so in 2020, my oncologist said, look, I think the side effects will kill you before the cancer does. Let’s see how you do coming off of it, which was terrifying because at that point it was my security blanket, right?
But I did successfully transition off Cabometyx. I stopped treatment in April of 2020, and now I have scans every six months. And thankfully I have had NED scans ever since. I just had a scan last January: I’m still NED. So I’m really, really fortunate.
And now I’m actually a patient advocate for the GU committee. And so I’m now actually working with the doctors that concluded the trial that I was on that saved my life.
So it’s honestly one of the most meaningful things that I do in my advocacy work, because it’s just a complete full circle.
Knowledge is power in every sense of the word.
You are a better patient if you are knowledgeable about your disease.
Words of Advice
I really encourage people to trust their instincts when it comes to their health. You know your body best, you know if something’s wrong with you. And I really wish I would have just kept listening to that little voice that I had in my head. You know, in my heart that said, Laura, something’s wrong. I’m glad that I finally did, because that’s what encouraged me to go to the ER that night.
Again, I would just go back to if something doesn’t feel right, listen to your body. I think even as cancer survivors, we tend to dismiss things sometimes, and so even if you’re in your cancer journey or you’re a survivor, you have to. It’s advocating for yourself as a lifelong responsibility.
And, you know, I’ve had the unfortunate gift of being not just a patient, but also a caregiver to my mom who passed away five years ago from complications of kidney cancer and lymphoma.
Also, I really encourage you, especially if you’re a younger patient who has a rare cancer, get genetic testing done. I encourage my family members to get genetic testing done, and receive their carrier for it as well.
And I always encourage anyone who has any kind of outliers in their health history that would indicate maybe they could benefit from genetic testing to take the tests. I know it’s scary to have a genetic disorder diagnosed, but I really wish I would have had the opportunity to know I had my disorder before I had cancer.
Knowledge is power in every sense of the word. You are a better patient if you are knowledgeable about your disease, which is what I really try to encourage patients and caregivers to do, to understand their disease.
And also, if something isn’t sitting right with you even once you’re diagnosed, you know, if your doctor is telling you, oh, you should do this and something’s just not sitting right, get a second opinion. Get a third opinion if you need to. You have to feel comfortable with your care. And if you’re not, you know it.
So you’re the best person that’s most knowledgeable about yourself, your body. Honor that in all the ways.
Symptom: None; found the cancers during CAT scans for internal bleeding due to ulcers Treatments: Chemotherapy (capecitabine + temozolomide), surgery (distal pancreatectomy, to be scheduled) ...
Raquel first noticed symptoms in 2019, like pencil-thin stools, pain, bloating, and blood in her stool. She then started getting full quickly after eating.
When she finally went to the doctor after developing severe pain, she was dismissed and told, “It was just anxiety.” She then ended up in the emergency room and was later diagnosed with stage 4 colorectal cancer, which had spread to her liver, ovaries, and lungs.
In sharing her story, she aims to raise awareness about rising colorectal cancer rates in young people and the importance of listening to your body.
In addition to Raquel’s narrative, The Patient Story offers a diverse collection of colorectal cancer stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Name: Raquel A.
Diagnosis:
Colorectal cancer
Staging:
4
Initial Symptoms:
Frequent bowel movements
Pin-thin stools
Mild red blood in stool
Treatment:
Chemotherapy: oxaliplatin, 5-FU (5-fluorouracil), and irinotecan
I feel so confident that whether I can heal from this or not, I’m going to be able to handle it well. It’ll be okay. I’ve overcome other things in life and I hope that I can be an inspiration to people who are struggling.
I’m 33 years old with terminal colorectal cancer. It has been such a huge part of my life that I have to remind myself that there are other parts outside of that.
I currently work in the tech industry and I’m very blessed to be able to do so.
In my spare time, I like reading and drawing. I’m very artistic and very recently, I’ve been posting more. I’ve been finding great connections on social media with other people who are going through the same thing as me.
I didn’t take my symptoms more seriously because they would come and go.
Pre-diagnosis
Initial Symptoms
I first started noticing symptoms in 2019. I was roommates with my best friend and she started to notice how often I was going to the bathroom. At the time, I was working in restaurant management so I figured I was probably eating too much of the food at work or eating too many processed foods.
I started changing my diet, trying to eat healthier and more protein but also using fiber supplements. I figured I wasn’t eating enough fiber and that’s one of the first things you read online about how to resolve diarrhea or bowel issues. That did help. The symptoms went away, but they would come back to plague me again.
Symptoms Worsened
In 2022, I was working as a contractor in the tech industry. I made really good friends with people on my team. One of them noticed how often I was going to the bathroom and she said, “Raquel, are you okay?” I said, “Yeah, I’m fine. Maybe it’s the dairy in my coffee. Maybe I have a gluten sensitivity.”
At the time, I wasn’t concerned and wrote myself off. I dismissed my symptoms. But knowing what I know now, I was having classic colorectal cancer symptoms.
I experienced frequent bowel movements and pin-thin stools. In addition, any kind of blood in your stool is a huge red flag. It means something is wrong. The color, whether it’s dark or mild red, pinpoints where exactly that bleed is located. Mine was mild red. I didn’t have heavy bleeding, which is why I thought there wasn’t something wrong.
But another classic sign is getting full quickly after eating and that was a huge red flag that something was wrong. That happened from 2022 until when I got diagnosed in May 2023. Every time I took a couple of bites of something, I immediately felt so bloated.
I was actively dieting before my diagnosis, but despite how healthy I was eating, I could not lose weight, which I thought was strange. My stomach was so round and hard. I would later find out that the cause of some of my bloating was ascites. When you have cancer that is as advanced as mine, especially with colorectal cancer, the tumors start secreting free fluid. I had about a gallon of fluid in my stomach that they had to drain. That immediately relieved so many symptoms I was having with eating.
I didn’t take my symptoms more seriously because they would come and go.
They’re not going to think of cancer when they see somebody who visually looks very healthy and young so I don’t necessarily blame her. At the same time, this dismissal of people who are like me is widespread because I know I’m not alone.
Symptoms Dismissed by Primary Care Doctor
It’s important to note that as a millennial—and I have statistically looked into this—half of us don’t have a primary care provider. That was the story of my 20s. I was blessed to land a permanent role in the tech industry where I had good healthcare and was able to schedule my first physical in 10 years back in May of 2023.
When you don’t go to the doctor for that long, there is a lot to talk about. I let my primary care physician know all of my symptoms, especially my bowel symptoms, and that I had severe abdominal pain somewhat recently. It wasn’t in one spot and felt very abnormal.
When I was talking to her about this, I could tell that she thought it was in my head. She scheduled me for a psychiatric appointment after my physical because she thought I had anxiety.
But now that I know so much about my disease, I know that they were classic colorectal cancer symptoms. Because I was so young, a woman, and a minority, statistically speaking, even just one of those categories is going to make you more likely to be dismissed in a medical setting and that is absolutely what I experienced.
It was maybe three weeks after that physical when my cancer was found to be completely metastatic and had spread all over. I know that she probably felt some guilt because, after my diagnosis, they sent the information to my primary care provider before I was assigned to an oncologist.
I’m sure once she saw how bad it was, she felt guilty at the same time. She’s not the only doctor who has done that, especially when you’re young. Medical doctors are taught these statistics of colorectal cancer being an older person’s disease. They’re not going to think of cancer when they see somebody who visually looks very healthy and young so I don’t necessarily blame her. At the same time, this dismissal of people who are like me is widespread because I know I’m not alone.
It wouldn’t be until I had a liver biopsy that they would find the primary source of my cancer, which was colorectal, and I wouldn’t find out until later how incredibly it had advanced.
Diagnosis
Getting the Cancer Diagnosis in the Emergency Room
I finally went to the ER. I remember that day so clearly.
I had severe abdominal pain that was migrating to my lower back and I almost fainted in my apartment. My intuition was saying that something was wrong so I went to the ER.
They did a full blood panel on me, which included the cancer markers CEA, CA 125, and CA 19. Mine were elevated. My CEA alone was in the 700s and anything above 30 is already a sign of cancer activity in your body. For mine to be that high means that my cancer was so advanced.
When I was in the ER, I felt that they took me seriously that’s why my cancer was found. The doctor knew something was wrong so she did that blood panel. I had an MRI, a CT scan, and an ultrasound. They did all those tests immediately.
The ER doctor told me that I had ovarian cancer because that’s where they found it initially. Based on the CT scan, the cancer was pretty advanced in my ovaries and my liver. It wouldn’t be until I had a liver biopsy that they would find the primary source of my cancer, which was colorectal, and I wouldn’t find out until later how incredibly it had advanced.
The metastases are in my colon, ovaries, liver, lungs, peritoneal cavity, and omentum. They found them through those tests within a week.
Everything happened so fast. I feel truly blessed that when I went to the ER, my cancer and the type of cancer was diagnosed so quickly. They ran all these tests, found my cancer, and immediately referred me to an oncologist. The next day, I was talking to an oncologist who then referred me to have a liver biopsy. A couple of days later, they found the primary source of my cancer.
Even though it’s very, very unfortunate how late my cancer was found, what an incredible experience for them to take me so seriously and find out what was going on. Kudos to the hospital that I went to. They took me very seriously.
Reaction to the Diagnosis
I don’t think I reacted like a normal person would have and that’s because I’ve had a lot of things happen in my life. I have a very calm demeanor. When things go wrong, I’m your go-to person to think logically and that’s how I processed my cancer diagnosis.
Even the doctor seemed really surprised that she said, “Raquel, you’re not even crying. I’m so sorry I’m not telling you good news.” I said, “You know what? It’s okay because no matter what happens, I’m going to get through it.”
I feel so confident that whether I can heal from this or not, I’m going to be able to handle it well. It’ll be okay. I’ve overcome other things in life and I hope that I can be an inspiration to people who are struggling. I feel like everything’s going to be okay. I told myself that even at the beginning of my diagnosis.
My liver and lung metastases aren’t responding to chemo, but the metastases in my ovaries and colon are responding moderately well. My oncologist and I are trying to see what combination could help with wherever else my cancer is.
Treatment
The treatment protocol and how they’re going to approach your diagnosis depends on your hospital. When I first got diagnosed, I was at a different hospital but for insurance purposes, I had to switch to a different one.
My treatments would have been a little bit different if I stayed with the first hospital because they wanted to start surgeries right away. They said, “You’re going to have a full hysterectomy. I’m going to be doing this in collaboration with one of our very renowned liver surgeons and we’re going to do this at the same time.”
But then when I switched to a different hospital, they told me, “We’re going to focus on chemotherapy. Let’s see how you react, shrink what we can, and then talk about surgery.” I understand the reasoning for that because they want to shrink as much as they can to lessen things going wrong during surgery or make it a little bit less risky.
Because I ended up switching hospitals, I’ve just been primarily I’ve been chemotherapy.
Being on Chemotherapy for Life
I first started with oxaliplatin. The side effects are not pleasant. It causes neuropathy. Fortunately for me, we stopped that in December. I was on it for six months until the side effects started affecting my quality of life too much.
I have switched to 5-FU (5-fluorouracil) and irinotecan. They introduced irinotecan to see if that’s going to help my liver metastases because so far, I’m having a mixed response to chemotherapy.
My liver and lung metastases aren’t responding to chemo, but the metastases in my ovaries and colon are responding moderately well. My oncologist and I are trying to see what combination could help with wherever else my cancer is.
I have chemotherapy bi-weekly and for Christmas, I pushed back my chemotherapy because I didn’t want to be sick during the holidays. My CEA, one of my cancer markers, jumped when I wasn’t strictly on my bi-weekly regimen. If I ever stopped chemotherapy, decided I didn’t want to continue, or changed my protocol at all, my cancer would jump at that opportunity to be aggressive.
I don’t have a choice as of right now. Chemotherapy is keeping me alive so I’m going to continue being on it bi-weekly. Fifty percent of people who have chemotherapy might need what’s called GRANIX shots.
The white blood cell count gets so low with chemotherapy that medications are needed to boost the white blood cell count to continue treatment. I, unfortunately, fall under that category so not only do I have my chemotherapy, but I have to have those shots to even have chemotherapy because my white blood cells get too low.
I’m very actively looking to find and get second opinions from hospitals that are willing to touch me and get some of this out because I know it would help me in the long run.
Looking for Other Opinions
As of now, they’re telling me that they don’t want to do surgery because of how incredibly advanced my cancer is. They’re saying that it might not be worth it.
However, I’ve read and seen from other people with colorectal cancer that they have better survivability with surgery because the more cancer is in your body, the more opportunities it has to spread and be aggressive.
I’m very actively looking to find and get second opinions from hospitals that are willing to touch me and get some of this out because I know it would help me in the long run. I will be traveling to MD Anderson and Memorial Sloan Kettering, hoping that they can do surgery on me, which will help extend my life. Even though I know it’s risky, I’m willing to do it because the alternative is being on chemo forever.
Getting Help & Support as a Cancer Patient
Having the support of family and friends has been such a huge help and I give so much thanks to the incredible people in my life who have helped me through this.
Some things have personally made it a little bit easier, like trying to buy foods that are pre-cut or pre-chopped. I like getting frozen oatmeal because I can just microwave it.
I’m sicker some days than others and I have found that it helps to have plastic utensils so that I’m not thinking about washing the dishes. To alleviate some of the guilt of buying disposables, I buy the biodegradable kind. You never think about how much something like that would make your life a little bit easier, but it does.
Give yourself grace and find the little things that you deserve to make your life easier.
If I had advocated for myself sooner, my cancer would have been found sooner… Listen to your intuition. You know your body more than anybody else.
Importance of Self-Advocacy
Self-advocacy has been such a big part of my cancer journey because if I had advocated for myself sooner, my cancer would have been found sooner. A lot of people who are as young as me or even younger don’t have a primary care provider.
Maybe they don’t have health insurance and I understand that there is a money barrier to getting treatment for a lot of people. That’s why I’ve been speaking to people who are younger than me and are getting diagnosed with advanced colorectal cancer because of those barriers.
One of the reasons why I started to be so outspoken about my diagnosis is to encourage people to go to the doctor. It’s never normal to have blood in your stool, even if it’s a little bit. Something’s wrong.
Unfortunately, if you’re young, a woman, or a person of color, you have to advocate for yourself so much more than people in different demographics. I hope to inspire people to get the medical help that they need for their symptoms because I was invalidating myself.
I went to my primary care provider and had my physical. I told her all of my digestive issues and bowel symptoms, and she said it was all in my head and that it was anxiety.
Other young people say in the comments on my social media, “This happened to me, too.” That’s one of the reasons why I’m trying to be so outspoken and raise awareness. I want people who have had the same experience to hear my story and say, “I need to take this seriously. Even if a medical professional says that I have nothing to worry about, I need a second opinion. I need to go to a GI specialist.” That is my goal in sharing my story. Don’t let anybody write you off. Get seen. Go to a GI specialist.
All it takes is one who will listen to you and help you. They’re out there. We just have to find them.
Words of Advice
Listen to your intuition. You know your body more than anybody else. A medical professional is diagnosing you based on generalities, but you know yourself better than anybody so if you are having these problems, you deserve to see a specialist and get a second opinion. Don’t listen to the first doctor. Get opinions from a second or a third, especially if your symptoms are persistent.
If your symptoms are persistent and aren’t going away, then something is wrong, especially if you have blood in your stool. That should never be written off. Any kind of blood in your stool is a huge red flag. Pay attention to it.
You deserve to be listened to and taken seriously in a medical setting. If the first doctor isn’t taking you seriously, all it takes is one who will listen to you and help you. They’re out there. We just have to find them.
If you have been invalidated about your bowel health or your symptoms, follow your intuition. As much as we want to completely trust that they have our best interests, that they went to medical school and they’re knowledgeable, that doesn’t mean that they aren’t sometimes wrong and don’t make mistakes or misdiagnoses.
Go out there and fight for yourself. Fight for your health. I hope everybody who hears my story feels very validated to go and seek help.
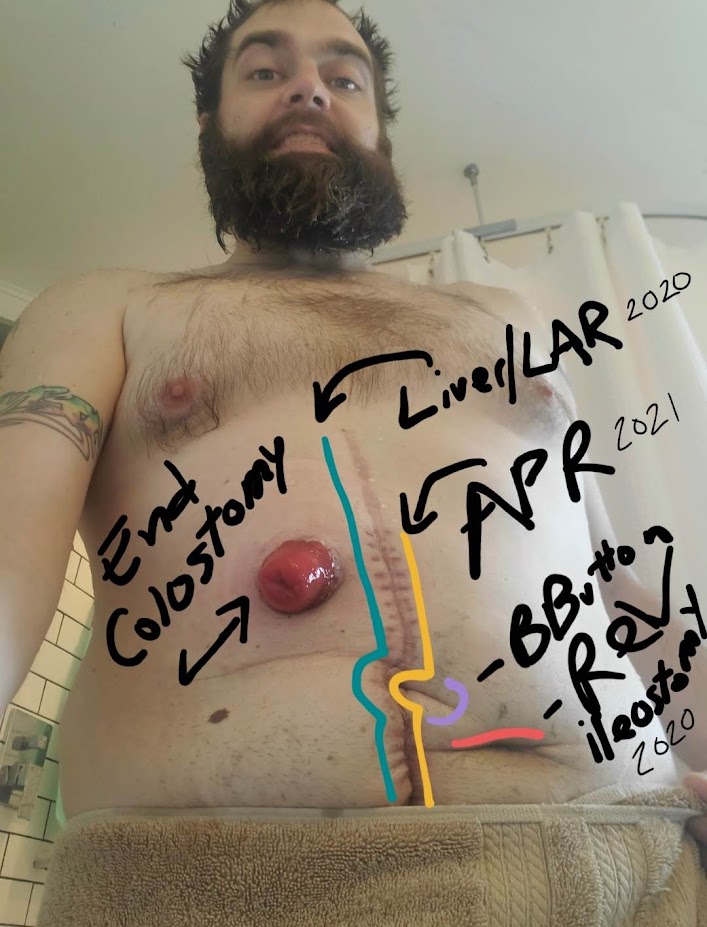
Jason Randall, A Stage 4 Colorectal Cancer Survivor
Jason’s Stage 4 Colorectal Cancer Story
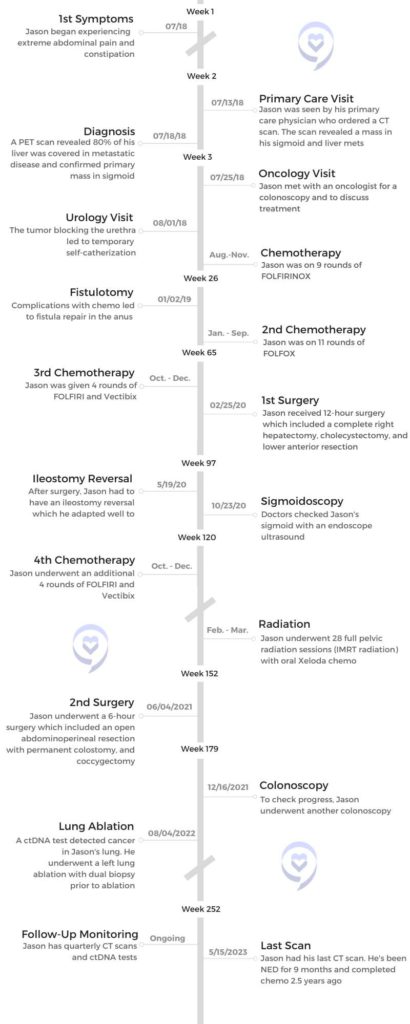
Jason’s cancer journey began in 2005, in the middle of his Navy service. He began experiencing stomach issues and was diagnosed with GERD. Much later, in 2018, he was seen by his doctor when he developed severe abdominal pain and infrequent bowel movements. A scan revealed 80% of his liver was covered with metastatic disease, which led to a stage 4 colorectal cancer diagnosis.
After years of fighting Veterans Affairs to prove his cancer was connected to exposure to cancer-causing chemicals during his Navy service, restitution was granted through the Pact Act – an Act that grants better healthcare and funding to veterans exposed to toxic chemicals.
Jason shares his cancer journey, his work with COLONTOWN – a colorectal cancer support network, and how he overcame liver surgery and chemo after doctors said it couldn’t be done.
Just this year, Jason and his wife launched Kohala House of Healing, a cancer retreat in Hawaii. The lush hideaway is designed for those affected by cancer to find hope, healing, and renewed purpose.
At the Patient Story, we feature the real voices of cancer patients to empower and offer hope. Explore more Colorectal Cancer Stories for further inspiration.
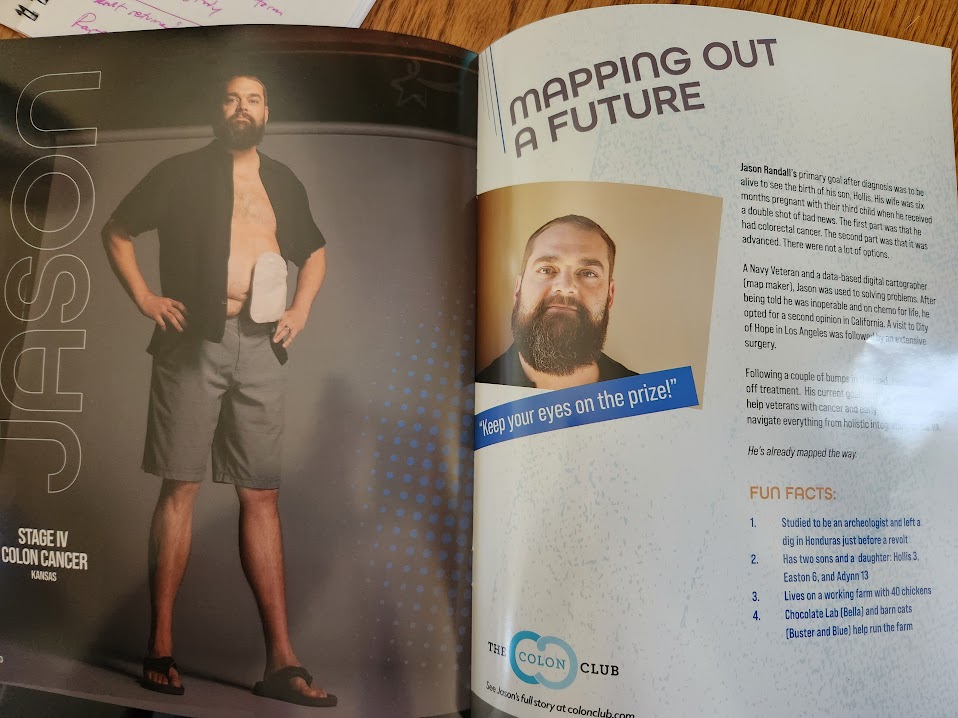
My name is Jason Randall. I live in Eudora, Kansas with my wife and 3 children. We live on a hobby farm. I was in the Navy for 5 years from 2003 to 2008. After that, I went to school.
My wife and I were best friends in high school. After the Navy and college, we reconnected. When I came back from Hawaii for a semester at the University of Kansas, we started dating. My wife has our daughter from a previous relationship, who I’ve adopted.
We’ve lived on this hobby farm for 10 years. I’m a cartographer by profession. Technically, a GIS analyst. We like to fish as a family. We go to the gym and swim quite a bit.
When did you first notice something wasn’t right?
In about 2005, right in the middle of my Navy service, I had some stomach issues that they tested. They came to the conclusion that I had GERD reflux disease, so they put me on omeprazole and Zantac-type medications. It was fine for years after that.
About 2018, I was diagnosed with stage 4 colorectal cancer. It blindsided us. I say us as in my family because I always include caregivers. They are often overlooked in this process.
They saw that about 80% of my liver was covered in what appeared to be metastatic lesions…It started me in this world of advanced-stage colorectal cancer.
Two weeks before, I had some severe abdominal pain that I’d never had before and 2 weeks before that, I’d noticed that I wasn’t going to the bathroom at a regular frequency. Then it just stopped and I started getting abdominal pain. That’s when I thought something was wrong. I need to go get this checked out.
My mom had diverticulitis quite a bit over the last couple of decades and they said, “It’s probably that. Let’s get a CT scan just to make sure so we can put you on antibiotics for it.”
I had that scan on July 16th. They saw that about 80% of my liver was covered in what appeared to be metastatic lesions. That prompted a PET scan on the 17th which confirmed it. My liver, the large majority of it, was covered in metastatic disease. It started me in this world of advanced-stage or stage 4 colorectal cancer.
Was there any connection between your GERD and colorectal cancer?
I brought that up along the way many times after I was diagnosed. The doctors never put them together because they generally think, anything in the upper esophagus or upper GI tract is Barrett’s disease or esophageal cancer instead of colorectal cancer.
My colon, where we found the tumor was at the sigmoid part of my colon, right before the rectum. So there really wasn’t a tie to it.
Ironically, after I had surgery to remove 30 cm of my colon, my GERD completely went away. It cued me to ask, what’s going on here?
If you look at the history all the way back to 2005, I was on ranitidine, which is Zantac. Then when I got out of the military into the Veteran Affairs (VA) system, I was on omeprazole for 10 years. My doctor mentioned that the advanced stage of my disease and the extent of it [means] it had been in me for about 10 to 15 years at a minimum. That squarely placed it right in my military service.
Did the VA take responsibility for your diagnosis after your exposure to cancer-causing chemicals?
Not definitively. Presumptively, yes. I was fighting the VA for about 3 years, trying to tell them that everything lines up with the exposures I had while I was in the Newport News Shipyard.
After I got out of my basic and my school training, I reported to the USS Eisenhower in 2004, in what they call an RCOH overhaul, where they take an aircraft carrier in the middle of its life and completely redo everything. They take it down to bare steel. They replace the reactor rods. I was in that environment for about 2 years.
We had all sorts of chemical and toxic exposures. You can use PPE and try to protect yourself, but you still inhale it once you take the equipment off. I was also within the burn pit zones in the Persian Gulf from 2006 to 2007.
Finding help through the Pact Act
They said you need to prove to us and provide a nexus that caused this, which is impossible. Even though statistically, 25-35% of all veterans of any service have an increased risk of multiple cancer types.
Jon Stewart was one of the biggest promoters of this law called the Pact Act for Toxic Exposures and Burn Pits. It finally connected my service to my cancer diagnosis.
Because of the way the laws were written before, the burden of proof was on the person having cancer. They said you need to prove to us and provide a nexus that caused this, which is impossible. Even though statistically, 25-35% of all veterans of any service have an increased risk of multiple cancer types, like prostate, breast cancer, colorectal cancer, and all sorts of different things.
The law was really good to help veterans who have been struggling to get this care and to have the military take responsibility for that within their service.
Did you have any other symptoms before your stage 4 colorectal cancerdiagnosis?
The only other symptom was, before diagnosis, I had something in my belly button that would appear every 4 to 5 months. By the time I could get in [to the doctor’s office], it would go away. They’d say, come back when you can. By the time I could get scheduled, it would go away.
It only lasted for a couple of days and it was like a little bit of discharge from my belly button and a little bit of hair follicles. It seemed like there were hair follicles that would come out. It’s hard to explain, but something wasn’t right.
It turns out that’s right where my primary tumor was, along the sigmoid colon. It was like, this could be a correlation to that.
What happens, happens but I wish I could have got in when they could have examined that a little bit better.
Did you have bleeding?
They say the number one symptom of colorectal cancer is no symptoms at all.
You hear a lot of people with colorectal cancer say they had blood in their stool. I think I’ve only had it at one point and it’s because I ended up having an emergency stent placed shortly after diagnosis because of the situation at hand. Even then, it was a couple of times.
They say the number one symptom of colorectal cancer is no symptoms at all.
How did you react to receiving your stage 4 colorectal cancer diagnosis?
No matter how much you think you know about cancer, unless you’ve experienced it firsthand or been a primary caregiver or even a secondary caregiver to someone, there are so many misconceptions about it.
It’s very vivid, even though in July, it’ll be 5 years now on this journey. I was diagnosed on July 17th, 2018. It was 2 days after my son’s second birthday, and my wife was pregnant with our third child.
I remember walking into the doctor’s office after the CT scan. They called about 15 minutes later and said, we need to see you tomorrow first thing. I go in and the doctor casually says, “I don’t know another way to put this, but you’ve got cancer and it spread to your liver.” I said, okay, took a minute, and then as soon as I walked through the doors leaving the place, it was like a rush of holy crap. I’m a dead man.
No matter how much you think you know about cancer, unless you’ve experienced it firsthand or been a primary caregiver or even a secondary caregiver to someone, there are so many misconceptions about it. I thought I was dead.
I come from a large breast cancer family. I carry a BRCA1 germline mutation. The women in my family, if they’re a carrier, they’re almost guaranteed to get breast cancer. It’s not as prominent in men. My mom had cancer, and her mother passed from cancer. I have had exposure to this, but it was emotionally devastating.
My wife was at the bowling alley with the kids and a friend. When I called her, she completely lost it. It was a bad, very dark time. We ended up coming home that night, my wife and I. We had my parents watch the kids, and we just held each other thinking, how much time do I have?
With 80% of my liver covered, that’s not a good situation. And I had a fully blocked sigmoid colon so they couldn’t go in and remove the primary tumor. I had to have that stent open me up before I could pass stool. Everything from there was a whirlwind getting into doctors, and getting the stent placed. It was emotionally devastating.
Treatment
What were the next steps in your treatment?
That’s a little more vague to me. I do remember [the doctor] saying, we’re going to have to get you in for a PET scan, which happened the next day to confirm it was stage 4 colorectal cancer. After that, I was at my local hospital system near Lawrence.
If you’re not used to it, it’s a lot to process, to listen to everything they’re telling you, and to absorb it.
Luckily, I have a doctor cousin who took me with his training. We called him and asked, “Do you have any advice?” He said, “I want you to go see Dr. Miranda at KU Medical Center,” which is the National Cancer Institute (NCI) here in the Kansas City area. It’s the only one in the Kansas City area.
He came with me to the appointment. That was a very pivotal moment in this. Going to one of the top centers in the area with that NCI rating, it’s important to have.
I work in the colorectal cancer support community and advocacy, and I heard the average time for people going from symptoms to starting chemotherapy is above 200 days, which is insane. I got in within 2 weeks. I was diagnosed on July 17th and I had my first chemo on August 1st, about 2 weeks later. I’m very blessed to have that team move that quickly.
A lot of it is very vague. It was just, go see this doctor, see this, get this scope. If you’re not used to it, it’s a lot to process, to listen to everything they’re telling you, and to absorb it.
I’m very grateful my oncologist never told me an expiration date. They did say, “You have a terminal prognosis of chemo for life and are inoperable due to your extended disease. You’ll never get off chemo and you’ll never be operated on for a curative intent. Palliative reasons, possibly, but we’ll do everything we can to extend your life.” That was a big pill to swallow
How did you come to terms with a terminal prognosis?
I don’t know if I ever fully digested it. I never believed I had cancer. It was all very surreal. I thought, is this happening? Did I get phase-shifted into some weird parallel universe? This has to be a bad dream. When am I going to wake up?
It was a lot to process. Every time I heard it, I would sigh and griff and say, “No, I don’t want to hear this. This is not my fate. I don’t foresee this being me.” It was really hard to swallow, especially every time my oncologist said, “We’ll do everything we can to extend your life, but you will be on this forever.”
I was put on what they call FOLFIRINOX. Sometimes they call it FOLFOXIRI. It’s basically how the drug is administered. With colorectal cancer, if you’re not a candidate for immunotherapy, irinotecan, and oxaliplatin are the 2 big drugs [that are given], and 5-FU which has been a standard since the 70s.
I had what’s called the kitchen sink. It was a combo of those 3 drugs. I started on August 1st and I started with what would have been the first of 30 initial cycles. I did 9 of the FOLFIRINOX, then we paused to do Y-90, which is Yttrium-90. It’s a radioactive isotope of the element yttrium.
They go through your hepatic vein and your groin and they send a catheter up into your liver. It’s a liver-directed therapy where they drop millions of radioactive resin beads right into your liver where the tumors generally form based on where the blood flows. I had 2 of those in November and December 2018, then I resumed 11 more treatments of what they call FOLFOX, which is the previous one, minus the irinotecan. They wanted to drop down the irinotecan because of the 2 Y-90. It’s a lot to take on with the radiation.
It’s targeted radiation, so I ended up having 6 of the 5-FU, largely driven by blood numbers – whether my white blood cells were up or my platelets were high enough. My big issue was low platelets, something I still suffer from today, from all those treatments.
Switching treatments due to lung spots
In September of 2019, I had some lung spots show up so we switched the drug oxaliplatin. A lot of the time, oxaliplatin causes severe neuropathy. Luckily, I never had too bad of that and I ended up taking 20 cycles with that in the mix, which is a lot. Some people dip out after 4. Usually, it’s between 8 and 12 of those.
Then I started back on the irinotecan drug through a combo called FOLFIRI. We added a biological drug called Vectibix or panitumumab, an epidural growth factor inhibitor that prevents blood vessels from growing. I did 4 more treatments through December 2019, and then I stopped to break for Christmas.
Getting a second opinion led to new treatment options
Even though they had my best interests in mind, I still sought that second opinion out at the City of Hope in California. It’s probably the best decision of my life.
My story started to change through COLONTOWN, an online colorectal cancer support community. I learned about Dr. Fong who’s a liver specialist and surgical oncologist. He doesn’t do just the liver, he does a lot of stuff in the abdomen area minus the colon itself.
People kept saying, you need to go see him. I had scans in December at my local center. Even though I had a really good response to chemo, they told me, you’re going to be on chemo for life and inoperable. They were scared that if I did have liver surgery, the liver would grow back. It’s the only organ that does that and the disease would progress with that regrowth.
Even though they had my best interests in mind, I still sought that second opinion out at the City of Hope in California. It’s probably the best decision of my life. It led to a surgery that was 12 hours long in February 2020.
They removed my entire right side and a right hepatectomy and then a lower anterior resection (LAR). They removed 30 cm of colon and a quarter of my rectum with curative intent and also took my gallbladder. I had 5 ablations on my left side at the time. I had lost 110 pounds prior to that surgery.
What inspired you to get a second opinion?
It was the support group COLONTOWN. People kept mentioning it. I was holding out on hope at my current NCI center. I still actually see them to this day, but I was hoping that with that next set of scans, they’d say, we’re going to try. They never did.
Ultimately it was my wife who said, “You need to go do this. Let’s go out to California. What is the worst they’re going to say? No, and you’re still the same?” I said okay, let’s rule it out. If one of the top people in the world says no, then it’s my fate. Thankfully it wasn’t.
Cancer recurrence and COVID caused changes to treatment
That’s not where the treatments ended. I stopped chemo after that because I had 30 cycles and 2 liver embolizations and they said my body needed a break. About 6 months later it returned, but not in my liver or colon. It returned in my tailbone in October 2020.
I started back on the FOLFIRI with the Vectibix for 4 more cycles. On my very last cycle, my 34th chemo, 2 days later I tested positive for COVID. That was a crazy week. COVID delayed my radiation treatment.
In February and March of 2021, I had 28 full pelvic radiation sessions to the entire pelvic region, which destroyed my rectum. For 3 months, it was pretty rough. I was sitting on the toilet for 3-plus hours a day, not really living life, just stuck.
Finding hope after his son’s birth
Throughout January and February 2019, I was on a lot of treatments. My son was still in my wife’s belly at the time. I caught him about 2 hours after my eighth round of heavy chemo. That gave me a lot of motivation, wanting to see my kids grow older.
It’s a very powerful moment in my life. Seeing my son born and being able to catch him. Both my sons were born at this house. My wife did a home birth, bless her soul. I didn’t think it would work out, but it did and it really changed me. It gave me a little bit more hope in October 2018 when that happened.
Then it got dark again. I had surgery in January 2019 because the chemo destroyed my anus and caused a fistula to bore through. It caused a lot of pain.
In early February, I found an integrative medicine doctor through my dentist of all people. I went to see him and he joined my team. That was one of the biggest moments of my stage 4 colorectal cancer experience. Not just diet and exercise, which are important, but he also helped mitigate the side effects, which helped get through it and process it.
I had hope, even though the hope was taken out from underneath me when they said you’re going to be on chemo for life.
One of the biggest things [he taught me] was the mind-body connection and meditation called Psychosomatic Wellness, which has a lot of science behind it. I wasn’t big into that kind of stuff. I thought, “This is heebie jeebie. This isn’t going to work.”
About a month into it, I connected to it. I went somewhere. I still don’t know what to call it. Some people may call it universal energy, God, chi, soul. Whatever you want to call it, I went somewhere and connected with something. It really helped me process things.
I was able to accept life, death, purpose, and what all this means. I was grateful for whatever was to come. I carried that into this second opinion. I had hope, even though the hope was taken out from underneath me when they said you’re going to be on chemo for life. What do I have to lose? I went out to California and sure enough, it happened and here I am still.
Getting an Ostomy
Describe getting an ostomy bag
Back during the big February 2020 surgery, I had a temporary ileostomy placed which is where the small bowel dumps into a bag with a stoma. That was reversed in May 2020.
Fast forward to the radiation. In June 2021, I had an abdominal perineal resection (APR). It’s a surgery that’s known as Ken or Barbie butt. Imagine a Ken doll or a Barbie doll. They just have a straight stitch on the backside. They took my anus, my rectum, and in my case, my tailbone and part of my sacrum to get clear margins. It was successful, and it left me with a permanent colostomy bag but it’s been a blessing in disguise.
Having it removed has been great for me. I don’t sit on the toilet for 3 hours a day. I spend 60-90 seconds messing with bowel function now. I still swim 3 to 4 times a day. I get to play with my kids. I lost 110 pounds and I wasn’t sure if I’d ever gain it back, and now I’m on the other end of it. It’s been so good to me that now I need to lose a few pounds.
What types of ostomy bags are there and which do you use?
There are several types of ostomy:
The ostomy that comes off your small bowel and avoids your large intestine.
A colostomy, which can be placed along your transverse colon all the way down to your sigmoid.
One-piece open bags which have a little cut-off valve that you can drain as needed.
Two-piece drainable bags.
Two-piece closed systems in one-piece closed systems.
I had a temporary ileostomy. At first, they tend to be more of a liquid output. They’re always on because the way the bowel works is your ileo dumps into your cecum and that’s when your stool starts to form. Before that, it’s all liquid as your small intestine absorbs nutrients. [Ileostomy is] common when people have a large surgery over a colostomy.
If you’re removing the lower part, you tend to get a stoma. That’s the medical name for the exit point. The stools tend to be more formed, it’s more predictable. I find that [colostomy] systems are a lot easier to use than the ileostomy systems.
Considerations when choosing an ostomy bag
Any closed system is not a good idea if you have an ileostomy, because you’d be changing it all day long. Whereas with a colostomy, it’s a little more predictable. It’s easier to manage. People tend to go with closed systems for convenience.
I used to be a 2-piece ostomy person for both my ileostomy and my colostomy. I’ve had about 2 years of colostomy and 3 months of ileostomy. With the colostomy, I’ve gone down to a 1-piece system.
There’s usually, a flange that adheres to your stomach. Once that gets on, a lot of people use either pastes, barriers, or protective rings to help hold that on to prevent leaking.
Leaking is the #1 thing that gets people flustered. It’s like crapping your pants and no one wants to crap their pants. It’s one of the big anxiety drivers with an ostomy. Am I going to leak? How am I going to manage this?
Also when you have a peristomal hernia. The creation of a stoma is a hernia in itself. That can cause more herniations so you want to be very careful with your abdominal wall and building your core back. When you get a herniation, you can feel it. It can lead to blockages.
With an ileostomy, you have to watch your diet a lot more than with a colostomy. Things tend to get blocked more with the ileostomy. From my experience and hearing from others’ experiences with a colostomy, people can still get it.
Leaking is the #1 thing that gets people flustered…It’s one of the big anxiety drivers with an ostomy.
If you have an ostomy, make sure you have a good hernia belt. I’ve got several. I have several Stealth belts. I also have one called a Stomaplex, which is like a stoma guard for impact. You don’t want things to hit it because it can bleed. Some people also use a Nu-Hope binder. It’s like a taller binder that goes around with a hole in it to support that and push your abdominal wall together so that you don’t herniate as often.
Is colostomy irrigation an option for some?
You cannot do it with an ileostomy, but with a colostomy, not many people are aware you can do irrigation. Instead of having to worry about having a bag going throughout the day and finding a frequency, people that are more active tend to go the irrigation route.
Imagine an enema but for your stoma. It goes all the way up your bowel track and basically gets behind the stool and you force water through it and then drain it over the next 30 minutes to an hour after that. When it drains, your bowel is empty and you can put a stoma cap on it. A lot of people are able to go hiking for 24 to 48 hours at a time [after irrigation].
Has your ostomy experience always been good?
Go out there and explore, call, get samples if you can, and find the system that works for you.
I’ve had a very good experience with my colostomy and my ileostomy. A lot of people do have struggles though, so if someone’s out there and they’re asking, “Why does this guy have such a good experience?” You’re not alone.
I struggled the first couple of months with mine before I found a nice rhythm and system. Don’t be afraid to call the 3 big companies – Hollister, Convatec, and Coloplast – and request samples. It can be very good to talk to one of their reps to find out what system works for you.
Having an option between a flat bag and a convex bag can be a game changer. A lot of people get stuck and say, “This is what the hospital gave me. How do I deal with this?” Go out there and explore, call, get samples if you can, and find the system that works for you. Because what works well for me may not work well for you.
Post-Treatment Tests & Scans
A circulation tumor DNA (ctDNA) test helped catch cancer recurrence
In June when I had the APR, I got the colostomy, and my Ken butt, I had about a year’s worth of no evidence of disease (NED). Then I had a recurrence in my lung. A spot that had been on CT scans since diagnosis, which they thought was scar tissue, initially never responded to any other thing. After all the chemo I went through, it decided to grow in May 2022.
I didn’t go on treatment because we caught it very early. I’m on a circulating tumor DNA test (ctDNA) called Signatera. Another company, Guardant, has one called the Reveal. It’s the same test, different companies. They sequence the biology of your tumor, specific to the person and no one else. The signature will never pop up in anyone else.
It can detect circulating tumor DNA in your body. It’s not cancer itself, it’s just junk DNA our body puts off, but it has that signature of your disease and they can detect if you have a recurrence. My tailbone recurrence was caught by September or October 2020.
After I went through the radiation, the chemo and more radiation, and the second major surgery, I was about a year clear. Then I had that Signatera test which detected an extremely low amount.
Is a ctDNA test for everybody?
It’s still in the testing phase. Not everyone responds the same. Their bodies aren’t as sensitive to the test.
There are also different areas of the body that put off more ctDNA like the liver, whereas the perineal may not. It’s still in flux, but it can be another tool because the normal marker for me was never above. It was always within range and it still is. It’s never varied more than a point, so it was never really a good indicator. The Signatera test has been really important for that.
COVID delayed a necessary treatment
In May 2022 when I had a spot come back in my lung that grew, COVID struck again. When I went in to get it ablated, I’d had COVID 3 weeks prior. Even though I felt better, my lungs still had some junk in them covering up the spot and they can’t ablate what they can’t see.
Then in August 2022, I had a biopsy that confirmed it was colorectal cancer in my lung and I had an ablation the same day. I was in at 6 a.m. and I was out by noon, working at 12:30. It was the least invasive. It allowed me to skip treatments by detecting them so early.
As of Monday, I had a negative Signatera test come back and I had my CT scans showing that I’m 9 months no evidence of disease and I’ve been off chemo for 2.5 years.
How does it feel to be done with chemo?
Surreal. They told me I’d never get off of it, and here I am. 2.5 years off of chemo.
How often do you have scans?
Right now it’s every 3 months until I hit 2 years. Then it should jump up to every 6 months. In 3 to 5 years, they’ll jump it up to either none at all or every year.
I plan on setting records. I’m going to be the longest person NED ever. At least that’s the way I’m setting my mind up for it.
Reflections
Describe the work you’ve done since being diagnosed
I’m blessed to be where I am, and if I can help alleviate someone’s symptoms, give them peace of mind, or just provide some hope, I won’t be quiet.
I do a lot of work within the colorectal cancer support space. I’ve worked for COLONTOWN since July 2020, after I had my Dr. Fong surgery. Dr. Kaiser was my colorectal surgeon.
PALTOWN, which is the nonprofit for COLONTOWN, asked me to be on their leadership cabinet. They were forming a new leadership cabinet, a new model. There are 7 of us. I’ve been there ever since.
I do a lot of support work. I reach out to a lot of people. I do work for Man Up to Cancer. A primary goal is keeping men from isolating during a diagnosis.
I also do early-onset colorectal cancer awareness through the Colon Club. Through that group, I was in their 2023 On the Rise magazine. It lays out where we’re at and our story to raise early-onset awareness. It came with a photo shoot. I never thought I’d become a model but here I am.
I’m blessed to be where I am, and if I can help alleviate someone’s symptoms, give them peace of mind, or just provide some hope, I won’t be quiet.
The importance of expressing your emotions
Meditation, I went somewhere with it and that was my first foray into the emotional side of [my diagnosis]. I learned to accept that it’s okay to be emotional. And we should be emotional because if you push it down, it does nothing but hurt your mental health. Other people are going through this, and at this point in the game, if you have cancer, who cares?
It’s so much easier said than done, but you need to talk. Tell everyone how you feel. Some people are quieter than others. If you need to join a group and listen to other people do it, you don’t have to be active in those communities. Seeing what other people are going through can help your mental and emotional health more than anything. Some of us happen to be a little more vocal about it, but it helps to get people out of that bubble, that survival mode that we get stuck in.
A trip to Hawaii led to new revelations
In 2021, my family was gifted a vacation. During this trip, we realized that we weren’t living. We were stuck in this deep survival mode, which is mental and emotional depression. You’re living between scans. You’re stuck in survival.
It woke something up in us. We asked, what have we been doing? I’m doing all this support work, but we’re just going through the motions. We’re not really living our own lives.
We came up with the idea of going back to the Big Island of Hawaii. Then we said, we should move back there.
We came back [home], I looked at my wife and said, “I have this crazy idea. Would you ever move back, get a secondary house and host people to experience what we did?” I was thinking she was going to say, “You’re nuts, Jason. No.” And she said, “Yeah. I think that would be great.” So we started developing this plan.
I went to school for a semester on Oahu at the University of Hawaii Manoa studying anthropology and geography. It’s a beautiful place. If you’ve never been, I highly suggest going.
We were stuck in this deep survival mode, which is mental and emotional depression. You’re living between scans. You’re stuck in survival.
Connecting with a cancer retreat center
About 6 months into [developing this plan], I was looking for health care on the Big Island or through the VA because I’ll always need to go see doctors. I found this cancer retreat on the north side of Hawaii on the Kohala Crater. We said, “Holy crap. These people are doing what we thought of, except it’s a whole retreat center.” We reached out to them and they agreed to become our mentors.
Life gets busy with 3 kids and I was still worrying about that lung recurrence. Two days before or after my lung ablation, I finally had my VA claim accepted which lifted a huge medical burden off of my back because they’ll cover all my medical expenses. That freed up some resources.
My wife and I flew out in December to visit them as a patient and a caregiver to see what they had to offer. We really bonded with the couple. We shared our story with them. She was a cancer survivor. Her husband was on chemo for 12 years before she got with her current husband. He was a disabled veteran as well, and we really bonded.
We told them our dream and they offered to sell us the place. I went back for 5 weeks in April and March of this year to see what they meant by that, get more details, figure it out, and work on the farm. It’s also a sustainable farm that teaches food as medicine, and it has a temple that aligns with the integrative practices that I was doing, which was so beneficial to me.
After that trip ended, we came back and we now have a purchase agreement with a timeline to make that happen. We’ve got a little more money to raise and we have a timeline to do that.
My wife and I want to move our family out there, live on-site, and host cancer patients. Ultimately, it would be if we can find enough funding where it’s no cost to other people, but we’ll see how it goes once we get the next steps in place. That’s pretty active right now. We’ve formed an LLC and our nonprofit to make that happen.
What’s helped you stay hopeful throughout your cancer journey?
It’s hard to think in terms of hope when you are told you have stage 4 colorectal cancer, you’re not going to have any other options or it’s a grave diagnosis. Sometimes it’s hard to remove yourself from thinking way into the future. You have to just take it day by day. Take every day, even if it’s minute by minute, hour by hour. Do what you can to help yourself get through the day. Join support groups. That’s been such a big, thing.
The first thing you need to do is never look at Dr. Google. It’ll send you down a rabbit hole of despair. I had my first mental breakdown ever because I was looking at Google and looking at different statistics, then I started thinking about my kids. Avoid that.
Find your people. Find people that will lift you up and support you. A lot of people lose their support networks, especially once they’re out of treatment. Everyone thinks, I’m cured or thinks, you’re done. You’re never really done. Whether the physical stuff is over and the treatments are over, there’s going to be mental and emotional damage. Don’t dwell on that. Everyone goes through this with a cancer diagnosis. It’s okay to not be okay.
What advice do you have for someone recently diagnosed with cancer?
If I have any advice for anyone starting a diagnosis is, once you get diagnosed, it’s going to be rough at first. But once you get through that initial despair and anxiety, start setting goals. Future goals.
Something my integrative medicine doctor told me and it’s been my mantra ever since, he said, “Jason, set a goal and reach it. And once you reach that goal, set another one. Always keep your eye on the prize.”
Symptoms: Sensitive stomach sometimes leading to vomiting after eating, bleeding during bowel movements, persistent fatigue, back pain, abdominal pain, anemia, significant symptom flare-up during second pregnancy
Treatments: Surgery (colectomy), chemotherapy, targeted therapy
Symptoms: Dull lower abdominal pain that sharpened and was focused on the lower left side, appearance of dark blood in stool, difficulty retaining food due to near-complete blockage of sigmoid colon