Follicular Lymphoma Lab Tests Explained: How Blood, Biopsy, and Imaging Tests Impact Treatment Decisions
Join an expert-led webinar - Pick the date and time that works best for you.
How do blood test results help guide care for follicular lymphoma (FL)? What do terms like CBC, LDH, beta-2 microglobulin, and FLIPI really mean—and how are they used in monitoring and treatment planning?
In this in-depth discussion, Stephanie Chuang speaks with FL expert Dr. Celeste Bello of Moffitt Cancer Center. Together, they walk through the most important blood work and imaging tools in FL, when and how they’re used. They cover what biopsy types matter most, and how criteria like FLIPI, POD24, and GELF help determine when to start treatment.
Topics:
What blood tests and scans reveal in FL—and when they matter most
Biopsies and diagnostic tools: flow cytometry, IHC, and imaging
Understanding prognostic tools like FLIPI, POD24, and GELF criteria
Monitoring during observation and treatment: labs, scans, and red flags
Why speaking up about subtle changes can shape your care plan
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and dedicated support through their Information Specialists.
Register for this informative program then invite a Friend or Care Partner.
This program is designed to empower patients and care partners with clarity around tests—and when to speak up.
Follicular Lymphoma: Your Lab Tests Explained
Hosted by The Patient Story Team
Explore how blood tests, biopsies, and scans guide follicular lymphoma care—from diagnosis and observation to active treatment. Dr. Celeste Bello breaks down what lab markers really mean and when to act on them.
DLBCL Tests Explained: How Blood, Biopsy, and Imaging Tests Impact Treatment Decisions
Join an expert-led webinar - Pick the date and time that works best for you.
Diffuse large B-cell lymphoma (DLBCL) is fast-moving, but often curable—especially when caught early. Blood work plays a key role throughout diagnosis, treatment, and remission, though many patients are left unsure of what their lab results really mean.
In this discussion, Dr. Robyn Stacy-Humphries, a three-time DLBCL survivor, moderates a conversation with lymphoma expert Dr. Tycel Phillips of City of Hope. Together, they unpack what blood tests can (and can’t) tell you, how biopsies and imaging are used, and what markers like LDH, neutrophils, and immunoglobulins mean during and after chemotherapy, CAR T-cell therapy, and beyond.
Topics:
Learn what your CBC, LDH, and metabolic panels really mean during treatment
Understand the role of imaging, biopsies, and why blood tests alone don’t diagnose DLBCL
Get clarity on neutrophils, immunoglobulin levels, and why some “abnormal” results are not dangerous
Find out how often blood work is done during and after treatment like R-CHOP, CAR T-cell therapy, or bispecifics
Hear what’s ahead in MRD and liquid biopsy research for DLBCL monitoring
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and dedicated support through their Information Specialists.
Register for this informative program then invite a Friend or Care Partner.
Whether you’ve just been diagnosed or have been living with diffuse large B-cell lymphoma for years, this conversation is for you.
DLBCL Tests Explained: How Blood, Biopsy, and Imaging Tests Impact Treatment Decisions
Hosted by The Patient Story Team
DLBCL is fast-moving, but often curable—especially when caught early. In this discussion, Dr. Robyn Stacy-Humphries, a three-time DLBCL survivor, moderates a conversation with lymphoma expert Dr. Tycel Phillips of City of Hope.
AML Labs Explained: What Blood and Bone Marrow Tests Reveal After Diagnosis
Join an expert-led webinar - Pick the date and time that works best for you.
After an AML diagnosis, treatment often begins right away—leaving little time to process what’s happening, let alone what your lab results mean.
In this discussion, AML survivor Steve Buechler speaks with Dr. Alice Mims from The Ohio State University Comprehensive Cancer Center about the key blood and bone marrow tests that guide treatment, track progress, and inform long-term decisions. From CBCs and blast counts to FLT3 and NPM1 mutations, they break down what you need to know moving forward.
Topics:
Learn what your CBC results mean—including white blood cells, hemoglobin, and platelet counts
Understand what blast cells are and why they matter in AML
Hear how bone marrow biopsies and genetic testing (like FLT3 or NPM1) shape your treatment
Get guidance on monitoring your bloodwork during treatment and remission
Know when to consider clinical trials and how MRD tracking may guide next steps
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and dedicated support through their Information Specialists.
Register for this informative program then invite a Friend or Care Partner.
Whether you’ve just been through induction treatments or have been living with acute myeloid leukemia for years, this conversation is for you.
AML Labs Explained: What Blood and Bone Marrow Tests Reveal After Diagnosis
Hosted by The Patient Story Team
Dr. Alice Mims from The OSU Comprehensive Cancer Center explains the key blood and bone marrow tests that guide treatment, track progress, and inform long-term decisions.
Monitoring Myeloma: How Blood, Urine, and Imaging Tests Impact Treatment Decisions
Multiple program dates to pick from! Join over the next 2 weeks or get the replay.
Lab tests play a central role in diagnosing and managing multiple myeloma, yet they can feel confusing and overwhelming.
In this expert conversation, Dr. Brandon Blue of Moffitt Cancer Center sits down with Bryon Daily, a multiple myeloma patient and community leader from The Leukemia & Lymphoma Society, to break it all down in real terms.
They share honest insights on:
Imaging tests explained: X-ray, MRI, PET
Find out how lab work helps guide treatment decisions
What labs indicate a relapse or treatment change
Using biomarkers in clinical trials
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and dedicated support through their Information Specialists.
From groundbreaking studies to insightful patient stories, MPN Research Foundation is at the forefront of making real change for those directly affected by essential thrombocythemia (ET), polycythemia vera (PV), and myelofibrosis (MF).
Register for this informative program then invite a Friend or Care Partner.
Whether you’re newly diagnosed or have been living with multiple myeloma for years, this conversation is for you.
Monitoring Myeloma: How Blood, Urine, and Imaging Tests Impact Treatment Decisions
Hosted by The Patient Story Team
Lab tests play a central role in diagnosing and managing multiple myeloma. Dr. Brandon Blue of Moffitt Cancer Center sits down with Bryon Daily, myeloma patient and community leader from The LLS, to break it all down in real terms.
Multiple Myeloma: Creating Personalized Treatment Options Through Clinical Trials
On Demand Replay Now Available.
Explore how clinical trials are creating more personalized, effective treatment options for people with multiple myeloma.
Select an “On Demand” session to watch right now.
Select a “Replay” session to have a link sent to you.
In this joint program with Blood Cancer United (formerly The Leukemia & Lymphoma Society), join an expert-led discussion with Dr. Ajai Chari (UC San Francisco) and myeloma patient advocate Bryon Daily (Blood Cancer United) as they discuss how clinical trials are changing the standard care options for relapsed and high-risk patients.
Key Topics:
Learn the differences between 3-drug vs. 4-drug regimens and when each is recommended
Compare the pros and cons of CAR T-cell therapy vs. bispecific antibodies
Hear real patient insights from Bryon Daily, myeloma patient advocate
Get expert tips on navigating disparities in access to treatment
Ask smarter questions at your next appointment by understanding your options
By registering, you agree to let us share your contact information with The Leukemia & Lymphoma Society.
We would like to thank Blood Cancer United (formerly The Leukemia & Lymphoma Society) for their support.
Visit their Multiple Myeloma Overview for information and a list of resources to help you navigate myeloma.
The LLS also offers free resources like its Information Specialists, who are one free call away for support in different areas of blood cancer.
Table of Contents
Introduction
Stephanie Chuang: I’m the founder of The Patient Story. More importantly, as someone who’s dealt with her own blood cancer diagnosis, I have spent a lot of time talking with patients, care partners, and doctors about how we can make the best treatment decisions, including figuring out when clinical trials enter the conversation, especially in multiple myeloma where so much development has happened. I know firsthand how confusing and overwhelming it can be trying to navigate those options. We’re here to try and give you the information and, hopefully, the confidence that you need to have those important conversations with your care team.
Before we dive in, I want to give a big shout-out to our friends at The Leukemia & Lymphoma Society (LLS). As you probably know, they offer so many fantastic resources, including the free one-on-one support in navigating clinical trials through their Clinical Trial Support Center. I have the pleasure of speaking with many of their nurses who are there for you on the other end of that line and they are fantastic. It’s clear that not only do they know about clinical trials and how to navigate them, but they also care about these relationships and the people they connect with.
For this discussion, we teamed up with The LLS, which supported and sponsored this program, and also one of its community outreach managers, to bring you a special conversation. You’re going to hear from Bryon Daily, who was diagnosed with multiple myeloma in 2018. He had a basketball injury that then led to the diagnosis. After years of navigating treatment, Bryon has been dedicating his time to helping other people find their way after diagnosis.
He’s going to sit down with Dr. Ajai Chari, one of the leading experts in multiple myeloma. Dr. Chari is from the University of California San Francisco (UCSF), which is where I got my care in lymphoma. They’re going to talk about the latest in treatments, research happening through clinical trials, and why knowing your clinical trial options matters so much for us as patients and care partners. It’s not a last resort. It can bring tomorrow’s treatment to you today and it’s about figuring out if this is the right trial for you.
While we hope that you find this discussion to be helpful, it is not a substitute for medical advice, so please talk with your healthcare team about what’s right for you.
Bryon Daily: Our discussion will be on treatment options for patients with multiple myeloma and the importance of clinical trials in battling this disease. I’m the National Community Outreach Manager for The Leukemia & Lymphoma Society’s Myeloma Link initiative. I’m also a six-year survivor of multiple myeloma, having been diagnosed back in 2018.
I have no history of cancer in my family that I’m aware of, so, needless to say, it was a surprise when I was diagnosed. The diagnosis was a result of my primary care physician being very diligent in following certain trends in my labs. I had escalating protein over the course of several months, but it wasn’t until about the sixth month when, while I was playing basketball at the gym, I caught the ball wrong, which hit my finger. I went home thinking it was a simple sprain.
Two weeks later, it didn’t heal; it was still as if it happened the day before, so I went to my doctor. We did imaging and it turned out to be a fracture. The fracture, paired with the escalating levels of protein, was a red flag for my primary care physician. Fortunately, he was able to refer me to several specialists.
About a month later, we ultimately went to see an oncologist who ordered a biopsy and I turned out to have myeloma. I went through several months of chemotherapy and, ultimately, had an autologous bone marrow transplant, which was successful. After several months of being out of the public domain, I began to recover.
I’m joined by Dr. Ajai Chari, a hematologist-oncologist at the University of California San Francisco. He is the Director of the Multiple Myeloma Program and Professor of Clinical Medicine. His research interests include the development of novel chemotherapy regimens, including phase 1 and 2 studies.
Look Ahead: Top Takeaway for Today
Bryon: Dr. Chari, our audience includes patients, caregivers, and partners. What is the number one takeaway you hope that they walk away with before we dive into details?
Dr. Ajai Chari: Thank you, Bryon, for having me. It’s a pleasure to be with you and thanks for sharing your story. The number one thing that patients are looking for is hope. They want to know that they’re going to be able to live as long as they want to live and with a good quality of life.
What is Multiple Myeloma?
Bryon: Doctor, what is multiple myeloma and how do we treat it?
Dr. Chari: Myeloma is a cancer of the plasma cells. The hallmark of any cancer is that one cell in the body grows out of control and when it’s myeloma, it’s a plasma cell. They live in the marrow, so we call it a bone marrow disorder, but the manifestations can be in the blood and outside the bone marrow.
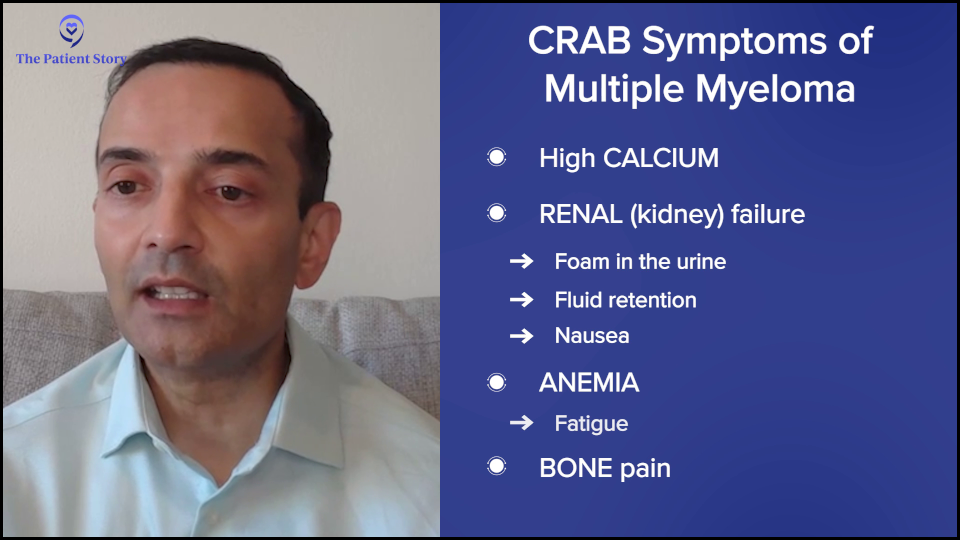
The symptoms of myeloma, when those plasma cells grow too much, are often summarized by CRAB: high calcium (C), renal failure (R) or kidney dysfunction, anemia (A), and bone disease (B).
If they’re hypercalcemic, they can present with confusion or bone pain. Kidney failure can often be subtle. They may see foam in the urine. In advanced kidney failure, they may see fluid retention or nausea. Anemia often presents with fatigue, which is one of the more common symptoms.
Because it’s usually a slow-growing condition, it’s not something that pops up right away, but patients may gradually notice that they’re not able to walk as briskly or go up hills or stairs as readily. Everybody can have bone pain, especially as we get older, but it’s persistent, severe bone pain, and not something that comes and goes or fractures.
Treatment for Multiple Myeloma
Bryon: Dr. Chari, how do we treat it?
Dr. Chari: At a high level, cancers can be treated theoretically by chemotherapy, radiation, or surgery. In myeloma, there’s not a role for surgery other than to fix a fracture because it’s a bone marrow cancer. Radiation can be used for spot welding of pain at a particular site. But the mainstay of therapy is systemic or whole-body therapies.
Sometimes, people get concerned about the terms chemotherapy and immunotherapy. I would say any drug that’s used to kill cancer theoretically could be called chemotherapy because it’s killing cancer. A good example of that is steroids, everybody’s least favorite drug. Dexamethasone technically kills myeloma.
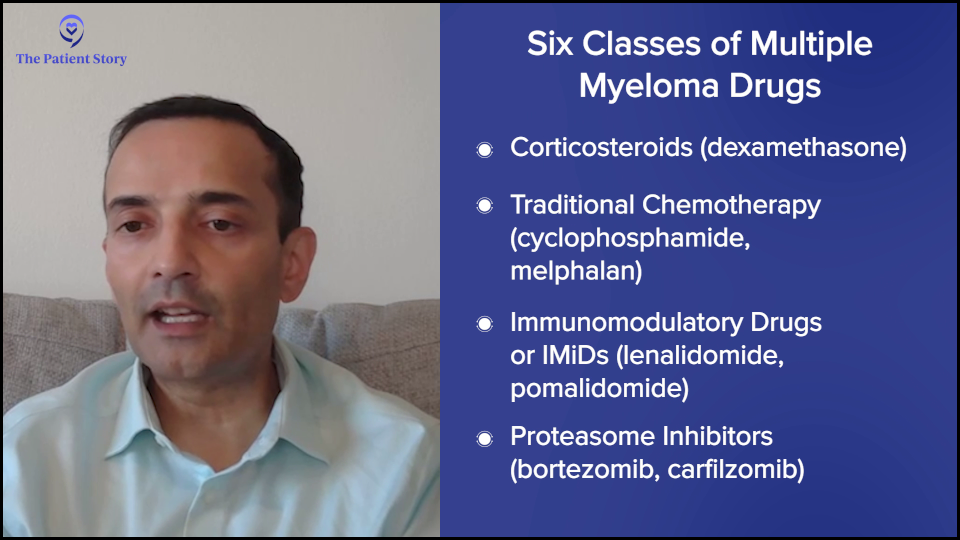
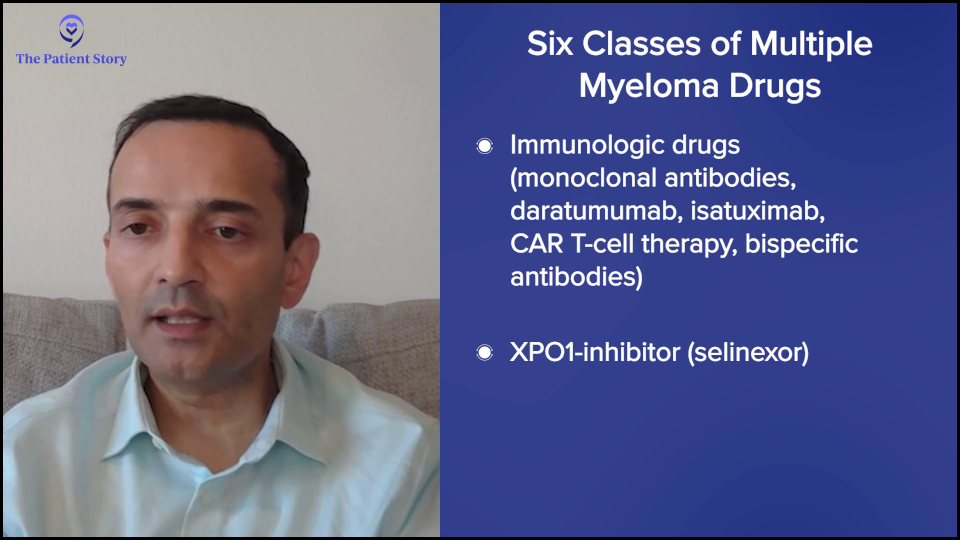
The classes of drugs in myeloma, which we can use in a newly diagnosed patient, are steroids, conventional chemotherapy (cyclophosphamide or Cytoxan, melphalan or Alkeran), immunomodulatory drugs (lenalidomide or Revlimid, pomalidomide or Pomalyst), proteasome inhibitors (bortezomib or Velvade, carfilzomib or Kyprolis), immunologic drugs (naked monoclonal antibodies, daratumumab or Darzalex, isatuximab or Sarclisa, CAR T-cell therapy, bispecific antibodies), and an XPO1 inhibitor (selinexor or Xpovio).
Those are the six classes of drugs and we can mix and match these based on efficacy and safety data, and how they will work and combine. For a newly diagnosed patient, the field has moved to, at a minimum, three drugs. Everybody gets steroids, at least at the beginning. Most people get lenalidomide (Revlimid), which is an oral drug, and CD38 antibodies, such as daratumumab (Darzalex) or isatuximab (Sarclisa).
There’s now a movement for younger patients and now even older patients to also get a fourth drug, which is a proteasome inhibitor, either bortezomib (Velcade) or carfilzomib (Kyprolis). The challenge there is that daratumumab (Darzalex), lenalidomide (Revlimid), and dexamethasone, which is called DRd or MAIA, is projected to give a five-year remission for the typical older patient even without a transplant.
To me, it’s not clear that every patient needs an extra drug because the fourth drug can come with additional side effects. But if it’s a fit older patient, certainly four drugs can be done. The other question is how long you need to continue. There are these movements of “down with dex.” Get the myeloma under control, but then drop it off, and then similarly drop the proteasome inhibitor.
For younger patients, there’s the question of whether or not to do the transplant. It’s not wrong to do the transplant, particularly for high-risk patients. The value added is even higher. For the typical patient, transplant adds about 16 months of remission. For high risk, it can be even up to three years.
Some people have an aversion to transplant and are more interested in CAR T-cell therapy, but we need those data sets to read out that CAR T-cell therapy’s better than transplant. Whether or not you do transplant, you go to maintenance therapy typically of three to four drugs. Lenalidomide (Revlimid) is the easiest drug to maintain because it’s a pill. Some people also get daratumumab (Darzalex). Very rarely, we also do the other drugs.
We hope these remissions last a long time. Some of the quadruplets are now projected to last, believe it or not, 90 or 100 months, so eight to nine years, which is amazing.
But unfortunately, many patients will relapse. When a patient relapses, you could go back to any of those drugs on that six classes, except you can’t go to drugs that the patient’s no longer responding to. For example, if somebody was on lenalidomide (Revlimid) maintenance, you wouldn’t use that. If somebody was on lenalidomide (Revlimid) and daratumumab (Darzalex), you wouldn’t use those.
There are a lot of options and it’s impossible to go through them in a short time, but at a high level, the more high-risk the patient is, meaning the earlier or the more aggressive the relapse, the more you might want to consider CAR T-cell therapy because it’s now approved for one to three lines of prior therapy.
The slower and more well-behaved a myeloma is, you may be able to get away, for example, with a combination a CD38 monoclonal antibody, carfilzomib (Kyprolis), and dexamethasone, like daratumumab (Darzalex), carfilzomib (Kyprolis), and dexamethasone (DKd), or isatuximab (Sarclisa), carfilzomib (Kyprolis), and dexamethasone (Isa-Kd). You could also use the other drugs that we mentioned, like pomalidomide (Pomalyst). At a high level, that would be the first relapse. There’s now data to even potentially use belantamab (Blenrep), but it’s not yet approved. It’s an antibody-drug conjugate that could also be used in this space.
Lastly, for those who’ve had more than one relapse — they’ve had initial therapy, first-line therapy, and they’re now in second line and beyond — it’s the same principle. You can’t use drugs that the patient’s no longer responding to and, of course, you wouldn’t use drugs that the patient didn’t tolerate in the past. Beyond that, you could come up with any other combination. For example, you could do carfilzomib (Kyprolis), pomalidomide (Pomalyst), and dexamethasone (KPd) if you haven’t had those drugs before. You use all the drugs that you can.
Currently, bispecific antibodies, which are also exciting, require four or more lines of prior therapy, so that’s how the sequencing works. If you’re going to consider CAR T-cell therapy, it needs to be done before bispecific antibodies and antibody-drug conjugates because those will adversely affect the CAR T-cell therapy outcome. That’s a high-level overview of how we approach myeloma therapy.
What Roles Do Age, Gender, and Race Play in Multiple Myeloma Treatment?
Bryon: What role do demographics like age, gender, and race play in treatment?
Dr. Chari: We would love to personalize myeloma. Our closest example is translocation t(11;14), which was targetable by venetoclax (Venclexta, Venclyxto), but it was very complicated. Part of the reason is that even though patients did better with that drug, the studies were not always clear and I think it has to do with how complex myeloma is. It’s not just the genetic component. There are also a lot of important patient factors.
One of the unmet needs in myeloma is for the frail elderly patients, people who are 70-plus with a lot of medical problems. We have to do better for them. It’s great to have all of these amazing regimens, but if you can’t give them safely, then that’s a problem. Younger patients typically do better.
Concerning gender, we’ve seen pretty balanced outcomes. One thing is that CAR T-cell therapy with the rare Parkinsonism seems to be seen more in men than women, but that’s also because that’s where the demographics of Parkinson’s are, in that men get it more than women.
With race, the biggest thing is disparities in outcomes. Not everybody’s getting access to therapy. For example, when you look at the veterans’ hospital where everybody has access to therapy, you don’t see the differences in race-based outcomes. It’s when you take away equal access that you start to see differences. There are some studies suggesting that African-Americans may have better disease biology, so they may even have better outcomes with the same therapies if everybody’s getting access equally.
I would add that not just race, but anybody underserved, which includes economically disadvantaged and people in rural communities. We’re such a large country and if you live in a rural part of the country, you may not have access to some of the novel, exciting therapies. We have a lot of work to do in transposing all of these amazing outcomes and exciting drugs to all patients in the U.S. with myeloma and, honestly, globally, too.
Deciding on the Best Treatment Options
Bryon: Doctor, when I was diagnosed, I had a sit-down visit with my oncologist to discuss next steps. We talked about clinical trials, of course, but that’s not always the case. I decided at the time that I didn’t know enough to decide on the spot, so I said, “What is the standard line of treatment? I prefer to follow that and then see what happens.” How do you decide what treatment options are best for a patient?
Dr. Chari:Myeloma is not one of the most common tumors. The most common cancers are breast, colon, prostate, and lung. If you’re a patient who’s diagnosed in the community, chances are your oncologist is very experienced with those cancers, but possibly not as much with myeloma.
Studies show that outcomes are better for patients who are affiliated in some way with an academic center. I always tell my patients that they don’t get points for suffering. You don’t need to drive hours to come see me or get the same treatment you’re going to get close to home.
However, you should have a connection with an academic doctor who knows and keeps up with the latest data. Myeloma publications are like drinking from a fire hydrant. Every year, there are multiple, high-impact publications. As a community oncologist who’s treating all those other cancers, how can you possibly expect one person to be an expert at everything?
If you’re a patient, you want expert opinion, but the convenience of getting it close to home. At a minimum, get that academic opinion, hear about the options that are being proposed, which may or may not include clinical trials, and then make a decision.
Remember that today’s clinical trials are tomorrow’s standard of care. Every treatment that you’re getting today was because people like you did studies before you. We found that these newer therapies often displace the older therapies. It’s important to get your options, but also to recognize that some patients may not be eligible. If you have kidney failure or your counts are too low, you may not be eligible for studies, but it never hurts to have the options.
Benefits and Challenges of CAR T-cell Therapy
Bryon: A lot of your research has been focused on CAR T-cell therapy. Can you explain how it works and some of the challenges with T-cell therapies?
Dr. Chari: People ask why they got myeloma. The short answer is we don’t know, but the fact that most people get it in their 60s and 70s suggests that perhaps the immune system gets lazy as we get older. Maybe we all have a little bit of cancer when we’re younger, but our immune system gets rid of it. As the immune system gets lazy, we can lose that ability.
One way to deal with that is you can take somebody’s T cells out, genetically modify them, and put them in the patient. Essentially, these supercharged T cells can then kill the myeloma.
Initially, I have to say we were not too excited about this. As with all clinical trials of new therapies, we typically test them in people who have exhausted all available options because that’s the only way to do it. If you don’t know the side effects of something, you first start with patients who have very limited options.
When you take patients who are older and have been treated with many chemotherapy regimens, you don’t necessarily think the new therapies are going to work, but guess what? These CAR T-cell therapies are working like gangbusters.
When we put these supercharged T cells into patients, we’re getting responses of 80 to 90% lasting from one to three years in patients where you would historically expect — at best — a new exciting therapy to give a 20 to 30% response rate lasting from three to four months.
It’s a paradigm-shifting time. CAR T-cell therapies have taken patients who are almost hospice-bound and now put them in stringent complete remission, off therapy, and enjoying their lives.
Bispecific Antibodies vs. CAR T-cell Therapy
Bryon: Another area of research is bispecific antibodies. What advantages do bispecific antibodies offer over CAR T-cell therapies?
Dr. Chari: CAR T-cell therapy has to be very personalized. You have to collect T cells, genetically modify them, and put them back, so it’s personalized therapy. There’s what’s called vein-to-vein time, which is the time from collection to administration, and that can be anywhere from four to six weeks.
I would add that there’s also a brain-to-vein time. It’s from the day patients who are in the community are evaluated by their doctor and referred to an academic center, to when they get insurance approval and have their T cells collected.
The problem is that some patients don’t have the luxury of time. Whether it’s four to six weeks or several months, if your myeloma is taking off, you don’t have the luxury of waiting, so you need an off-the-shelf product that’s ready to go and this is where bispecific antibodies come in.
Bispecifics are like all other myeloma medications. If there’s a side effect, you can stop the drug and wait for the side effect to get better.
With CAR T-cell therapy, you administer it once it’s manufactured and after you put it all in, you don’t have control. You can’t take it back. If somebody has severe side effects, you just have to manage them. You can’t pause or reverse the process. In patients who have a lot of medical problems, you have a little bit more control over bispecifics than you do with CAR T-cell therapy.
Those are the two main differentiations: off-the-shelf and the ability to stop the therapy.
What are Trispecific Antibodies?
Bryon: Can you elaborate on the development and potential impact of trispecific antibodies in multiple myeloma patients?
Dr. Chari: CAR T-cell therapies and bispecific antibodies have historically targeted one antigen or one protein, which is ideally overexpressed on myeloma and not on other cells. The reason you want to do that is if you’re going to activate your T cell, whether with a CAR or bispecific, you don’t want them to attack your heart, kidneys, lungs, or normal parts of your body. You want those T cells to be like snipers and go after the cancer. We do that by selecting proteins that are overexpressed in myeloma but not in normal body parts.
Bispecifics bind your T cell, which is your immune cell, and your myeloma cell. With CAR T-cell therapy, the T cells are supercharged to kill one protein. Trispecifics are saying, “Why do we have to stick with one protein? Why not have the snipers go after two different proteins to increase the specificity?”
Even though we try to pick proteins that are overexpressed in myeloma, some of the other cells that express these will also be hit. For example, many people know about BCMA or B-cell maturation antigen. When you target that protein, you kill the myeloma cell, but you also kill some other immune cells, which can then increase the risk of infections.
The other big protein that we target is GPRC5D, which stands for G protein-coupled receptor class C group 5 member D. A mouthful, but it’s basically a protein that’s overexpressed on myeloma. But this protein can also be overexpressed in tissues that have a lot of keratin, like the nails and skin, so you see some of those side effects. It also causes oral side effects, like affecting taste and weight loss.
The trispecific is saying, “What if we target both? Let’s take the T cells and attack GPRC5D and BCMA at the same time. Will that decrease some of these side effects? Can you get even better responses?” It’s a nuclear war. When we go after one protein, the myeloma cell stops making that protein. By targeting two at the same time, it’s harder for the myeloma cell to bypass that.
Those are some of the theoretical benefits, which are possibly fewer side effects and hopefully more efficacy and better activity, but we’ll have to see. Preliminary data will be presented at the 2025 American Society of Clinical Oncology (ASCO) meeting and there’s a lot of excitement about this approach.
Another difference is when you give bispecifics and CAR T-cell therapy, after the first dose, sometimes you have massive T-cell activation. We call that cytokine release syndrome (CRS), which can present with fever and low blood pressure, often requiring hospital admission. By doing this dual targeting, will that make the safety profile better?
Lessons from Clinical Trials
Bryon: These novel innovative treatments that you mentioned have emerged over the past few years at a rapid pace. Let’s talk about clinical trials. There have been a few trials recently looking at different combination therapies, such as the AURIGA trial, MajesTEC-5 trial, and DREAMM-7 trial. What are researchers hoping to understand about these treatment options?
Dr.Chari: When we start with the patient journey, most people are getting an initial therapy of a combination of three drugs, now often four, then many people get a transplant. What happens after a transplant?
AURIGA Trial
Dr.Chari: If you’ve gone through initial chemotherapy and transplant and you’re still not what I call the A+ of myeloma — which means not only have we eradicated all the myeloma in the blood, the urine, and the bone marrow, but even the minimal residual disease — can we improve your outcome to get you to an A+?
In the AURIGA study, you had to be MRD positive after a transplant and could not have had a CD38 monoclonal antibody, like daratumumab (Darzalex) or isatuximab (Sarclisa), in your initial therapy. You could have had chemotherapy and a transplant, and you were still MRD positive. In the study, half of the patients got lenalidomide (Revlimid) alone and the other half had the addition of daratumumab (Darzalex) as a shot.
What that study showed is that the A+ conversion was improved, so more patients got MRD negativity, which, more importantly, translated into doubling of the remission duration. That’s now a strategy that could be used. Although it’s a randomized phase 2, not a phase 3, there’s a lot of excitement about trying to improve outcomes.
MajesTEC-5 Trial
Dr.Chari: Similarly, the MajesTEC-5 trial takes patients who are post-transplant and asks, rather than just doing lenalidomide (Revlimid) maintenance as a minimum, can you do better than that? One of the ways they’re trying to do that is by incorporating a BCMA bispecific known as teclistamab (Tecvayli), which is why it’s called MajesTEC-5. The TEC in MajesTEC refers to teclistamab.
This is not a randomized study. It’s a small study of only about 30 patients in two different arms, but it showed dramatic responses where the MRD negativity achieving A+ was markedly increased. Pretty much everybody achieved MRD negativity in this study.
Now, of course, we haven’t talked a lot about side effects, but these bispecifics can increase the risk of infections when you’re targeting BCMA. We’re going to need larger data sets to understand how to put getting an A+ into context with the potential risk of infections and needing preventative drugs and intravenous immunoglobulin (IVIG). It’s hard to argue against an A+ for 100 % of patients and so I think that’s where a lot of excitement is.
DREAMM-7 Trial
Dr.Chari: With the DREAMM-7 trial, patients have had an initial therapy, they may or may not have had a transplant, and they may or may not have had maintenance, but now the myeloma has come back. What can you do?
Historically, because a lot of patients are getting lenalidomide (Revlimid) maintenance after transplant, you can’t use lenalidomide (Revlimid) anymore. You have to move on. We could use daratumumab (Darzalex) and bortezomib (Velcade), and dexamethasone (DVd), but can we do better than that?
In this study, they took bortezomib (Velcade) and dexamethasone, but swapped out the daratumumab (Darzalex) with a new BCMA antibody-drug conjugate known as belantamab mafodotin (Blenrep), or bela for short. Basically, it’s a three-drug versus three-drug combination and everybody got Velcade-dex. The question being asked is belantamab (Blenrep) versus daratumumab (Darzalex). What that study showed was, surprisingly, belantamab (Blenrep) beat the pants off daratumumab (Darzalex). This was a marked improvement in the remission duration.
Now, this drug does come with eye side effects. It can cause dryness of the eye, irritation, and blurry vision. Most of them are reversible and sometimes they can hold the belantamab (Blenrep). This is a great option because if you can beat daratumumab (Darzalex), then why not?
The only limitation is that very few people will be in this population. These are typically going to be older patients. For most people who are younger with relapsed myeloma, you’re going to want to think about CAR T-cell therapy. If you give drugs, like belantamab (Blenrep) or BCMA bispecifics, you’re going to impair the CAR T-cell therapy outcomes down the road, which we know from some clinical trials.
For example, cilta-cel (Carvykti) gives a three-year remission. If you give a bispecific that goes to five months and an antibody-drug conjugate that goes to nine months, we don’t want to impair that amazing CAR T-cell therapy outcome.
For those who may not be eligible for CAR T-cell therapy— either they don’t want to do it, or they’re perhaps old and have a lot of medical problems — DREAMM-7 could be a good and exciting option. The other big difference is that it could be done in the community. You don’t need to go to an academic center to get belantamab mafodotin (Blenrep).
Why Should a Patient Consider a Clinical Trial?
Bryon: Why should a patient consider a clinical trial?
Dr. Chari: I was in New York for about 18 years, including the time when CAR T-cell therapy and bispecific antibodies came. I remember patients had exhausted all the therapies at that point. They’ve had the big five: lenalidomide (Revlimid), pomalidomide (Pomalyst), bortezomib (Velcade), carfilzomib (Kyprolis), and daratumumab (Darzalex). What do you do for someone like that?
We’ve had hospice conversations with some people, but let’s try this study. Those patients are now in their deepest and most durable remissions in their entire myeloma journey, despite having had all those drugs, which is a clear example. If you’ve run out of options, then you should be looking for new strategies. Many people would understand the need for clinical trials there. Even if you’re newly diagnosed or have had an early relapse, it’s also important to think about a clinical trial.
Back when I was a fellow, our initial therapy was two drugs, lenalidomide (Revlimid) and dexamethasone. How would we know that we need to do three drugs, then four drugs, a transplant, and maintenance? That’s been incremental learning from every clinical trial and that’s how medicine progresses. It’s always good to think about how you can get the best care for yourself and how you can advance the science for everybody.
Fears About Participating in a Clinical Trial
Bryon: The results of those clinical trials helped to determine what’s best for any given patient based on the data that comes out of trials. There are a lot of myths about clinical trials, as you know. One of the concerns we address with Myeloma Link is the fear that people will be receiving a placebo and getting no treatment or that the participants will become guinea pigs. Think about the Tuskegee syphilis study or the harvesting of Henrietta Lacks’ cells. What do you tell patients about these fears?
Dr. Chari: Fear is understandable, especially when you’re dealing with a diagnosis of cancer. When I was a medical student, we had a class called “Is It Cancer and Can I Still Have Sex: The Two Questions Patients Had, But Were Afraid to Ask.” What you learn is that 50% of the information during that first cancer visit goes in one ear and out the other because not only are they dealing with the diagnosis and the intellectual questions, but also the emotional aspect. It’s always good to have a family member or friend with you to listen in on all of your conversations, so that they can help catch some of the things you might have missed or record the visit, if your provider allows.
It’s also important to understand that because of the Tuskegee syphilis study, Henrietta Lacks, and all of these other stories, there are a lot of protections built in. As an investigator, you can’t simply say that you want to test a new drug.
You have to write a protocol. You have to write a consent form, which independent doctors review on several committees. The FDA has to oversee it. If it’s sponsored by a company, the company has to oversee it. There are a lot of checks and balances within the institution, the pharmaceutical company, and the FDA. There are three different major stakeholders.
As a patient, you have to ask: What’s the question being asked? For example, it’s unethical to take somebody with advanced myeloma, who has active disease, and assign them to a placebo. That would never pass all of those various committees.
Where you might see a placebo is if you’re not sure if you need an extra drug. If the combination of three drugs is doing pretty well and you want to add a fourth drug, you might have to do a placebo arm. There is a placebo effect. When people take a drug, they’re going to feel better and think they’re getting a better outcome.
In my experience with myeloma, the placebo-based studies are very few and far between. Probably the only time you see that is in maintenance, where you don’t know if you should be doing something preventively or wait for the cancer to act up. Or perhaps in smoldering myeloma, where you don’t have symptoms and you’re trying to prevent the cancer, you might think about doing something like that. But even with those, the field is moving.
In cancer, the concern that you’re going to be a guinea pig is typically because of an admitted lack of knowledge. Otherwise, if we knew the answer, we wouldn’t be doing it, so there is an inherent unknown. We put a lot of safeguards in to mitigate that.
Managing Side Effects of Multiple Myeloma Treatment
Bryon: Let’s talk about managing treatment side effects. What are some of the common side effects people experience from treatment and what can be done to mitigate them?
Dr. Chari: This is a complicated question because it is very drug-specific and therapy-specific.
If we’re talking about steroids, everybody’s least favorite drug, the possible side effects include irritability, sleep, heartburn, and fluid retention. You can try to lower the dose and, if possible, even stop it. You could also take a sleep medication.
Conventional chemotherapies often cause a lowering of blood counts because they kill the myeloma cells. We’re talking about drugs like melphalan (Alkeran), which is part of the transplant. There’s some interest in cooling caps for reducing hair loss that are showing some activity at our institution.
For the IMiDs (immunomodulatory drugs), like thalidomide (Thalomid), lenalidomide (Revlimid), and pomalidomide (Pomalyst), they typically increase the risk of blood clots, so it’s important to take an aspirin to prevent those. If you’re on certain other drugs, have a history, or have a high risk, you might want to take something stronger.
With proteasome inhibitors like bortezomib (Velcade), carfilzomib (Kyprolis), and ixazomib (Ninlaro), there’s a risk of shingles, so you would want to take a preventative pill. Sometimes, bortezomib (Velcade) can cause neuropathy, and carfilzomib (Kyprolis) can cause heart issues, so you have to monitor blood pressure. Immunotherapy drugs can also increase the risk of infection, so you have to monitor that.
CAR T-cell therapy and bispecific antibodies can cause cytokine release syndrome, which has to be monitored and treated. With bispecifics, there is also the risk of infections and oral toxicity, which you have to do supportive care, like IVIG, or modify the dose.
When Would a Doctor and Patient Consider Switching Treatment?
Bryon: At what point would side effects lead to considering switching a patient from one treatment to another?
Dr. Chari: This is always a balance between efficacy and safety. What kind of myeloma is this? How well is it controlled? How bad are the side effects? If somebody has very favorable myeloma with very little disease, you’re not going to tolerate many side effects. If you have very difficult-to-control myeloma or very high-risk myeloma with multiple genetic abnormalities, there might be more willingness to take on side effects.
Ultimately, you have to give it a shot. This is why oncology is a specialty. You have to know this kind of risk-benefit balance and walk this tightrope. That’s why we have frequent visits and labs so that you can make treatment decisions. Am I happy with the myeloma control? How bad are the side effects that this patient’s having? Is the patient willing to continue with some modifications of dose and schedule or medications to offset side effects?
Quality of Life Concerns for Younger Patients
Bryon: Multiple myeloma is generally diagnosed in older patients. What are some of the quality of life considerations that you discuss with patients who are younger than 50?
Dr. Chari: My youngest patient was diagnosed below 18 and the oldest is over 100. It’s a very heterogeneous disease, so it’s hard to do a one-size-fits-all. There’s a movement in all of medicine, specifically in oncology, to not use a chronological age and to focus on how healthy that person is. Some 70-year-olds are going to be way healthier than 50-year-olds who might have multiple other medical problems.
For older patients, you have to look at their other medical issues. For young patients, you’re trying to walk that tightrope between preventing the disease from coming back and allowing them to live their lives. It’s important to talk about fertility preservation, maybe banking sperm or freezing eggs and embryos if possible, understanding what may or may not be feasible depending on the pace of the disease. Ultimately, it’s what we do in oncology. You have to personalize the therapy for each patient.
Promising Treatment Developments
Bryon: What are the most promising developments in multiple myeloma treatment that you foresee in the next few years?
Dr. Chari: The first is moving therapies that are currently in advanced myeloma to earlier and earlier lines of therapy. Initially, CAR T-cell therapy was for heavily treated patients; now it’s approved for patients who have had one to three prior lines. There are clinical trials that may lead to their approval in newly diagnosed patients and perhaps even smoldering myeloma. Similarly, bispecific antibodies are making their way up, showing 100% response rates and MRD negativity in earlier lines of therapy.
We also need new combination therapies. Let’s say somebody has had CAR T-cell therapy and bispecific antibodies. What do we do then? When you beat up all the T cells with all these therapies, you need non-T-cell-dependent strategies. Some new targets are promising, like bromodomain inhibitors and trispecifics that target different antigens.
Then we talked about dual CARs, triple CARs, and newer CARs that don’t have the same safety issues, some data that maybe we don’t see Parkinsonism, improving on existing therapies and moving them earlier, and having new targets.
Importance of New Immunotherapies
Bryon: How do you envision the integration of novel immunotherapies into standard treatment protocols for multiple myeloma?
Dr. Chari: Thankfully, the health authorities across the Atlantic, both our FDA and Europe, have allowed MRD negativity. The MAIA study had a median age of 73, who received daratumumab (Darzalex), lenalidomide (Revlimid), and dexamethasone (DRd). If you start at 73, those patients are going to get a five-year remission. If you’re going to try to improve on that combination, imagine how long you’re going to have to wait before hundreds of patients are accrued and randomized before we find out if they’re better.
The MRD negativity is a huge advancement in earlier lines of therapy because then, MRD negativity should translate into progression-free survival, which is how long the remission lasts. Ideally, that could lead to living longer. Sometimes people are looking for overall survival improvement, but as you get to newer and newer diagnoses of myeloma or less heavily treated, the number of drugs that we have to rescue myeloma can make it very difficult to show that the initial therapy is going to translate into living longer. MRD negativity is going to be a big one.
Honestly, we need these clinical trials, like CAR T-cell therapy versus transplant, which I think is super exciting. I don’t think anybody wants to go through a transplant voluntarily. If we can do new therapies that don’t cause hair loss, nausea, vomiting, diarrhea, weight loss, and fatigue, by all means, we should get rid of it.
But we need studies to show not just that they’re better, but remember, we also need to think about long-term side effects. Because myeloma patients are living longer, there’s an increased risk of getting other cancers, so we need to follow patients long enough to know that not only is the initial benefit there, but there are no unexpected longer-term side effects.
Advice for Newly Diagnosed Patients
Bryon: Dr. Chari, as we wrap up, if there’s one thing you want someone newly diagnosed with multiple myeloma to know about their treatment options, what would it be?
Dr. Chari: My passion is the personalization of therapy. No two patients are alike. You can read about a clinical trial, you can go to a patient support group, and you can talk to a friend, but that doesn’t mean that’s the right treatment for you.
There are patient factors to consider, like age, kidney function, heart history, diabetes, and neuropathy. There’s the disease, like your ISS stage and genetics. Do you have myeloma coming out of the bone marrow or extramedullary disease (EMD)? There are treatment considerations. What side effects are you willing to accept? Can you take time off work? Do you have a caregiver? What therapies have you had?
I see a lot of patients who come in the door so anxious that they just want me to give an immediate answer as to what I would recommend. You have to put all of those factors that I mentioned together. I need to know your medical history, your cancer, and what you want as a patient. Then I can give you an answer. But if you’re just asking for an answer, you’re not getting the best care, and that includes the options for clinical trials.
I would encourage everybody to speak to a myeloma consultant at an expert medical center and make sure that all of these factors are being considered to personalize a therapy for you.
Conclusion
Bryon: Dr. Chari, thank you so much for sharing your insights.
We hope this discussion has provided you with valuable information. We encourage you to follow or continue following the latest advancements in the field and to discuss your options with your healthcare providers. Please check out The Leukemia & Lymphoma Society’s Myeloma Link initiative and support for patients and caregivers.
Stephanie: Thank you so much, Bryon and Dr. Chari, for leading this incredible conversation. We’re so glad that you could be a part of this discussion about promising clinical trials in multiple myeloma. We hope that this leaves you with new information, fresh hope, and a reminder that you are not alone as you’re dealing with this.
Every patient and care partner deserves to understand all of their options. Clinical trials are not just for someone else. They’re not a last resort. They can open doors to the latest in treatments and care. It’s all about having the conversation with your team to know your options. It may not be the right one for you, but at least you have that at your fingertips.
If you need any support, don’t hesitate to reach out to The Patient Story or The Leukemia & Lymphoma Society. The LLS is deep and rich with resources. They have a Clinical Trial Support Center that offers free one-on-one support for clinical trial navigation, which happens even before the clinical trial. They can help you figure out the questions beforehand, including which clinical trial might be the right one for you. They also have a patient community and peer-to-peer support.
Remember, your voice and story matter. Keep advocating for yourself. Don’t be afraid to ask questions. Do your research. Talk openly with your team. Be curious. We hope to see you again at another conversation. Take good care.
We would like to thank Blood Cancer United (formerly The Leukemia & Lymphoma Society) for their support.
Visit their Multiple Myeloma Overview for information and a list of resources to help you navigate myeloma.
The LLS also offers free resources like its Information Specialists, who are one free call away for support in different areas of blood cancer.
Multiple Myeloma: Personalized Treatment Options through Clinical Trials
Hosted by The Patient Story Team
Explore how clinical trials are creating more personalized, effective treatment options for people with multiple myeloma in this expert-led discussion, Dr. Ajai Chari (UC San Francisco) and patient advocate Bryon Daily (Blood Cancer United).
AML Biomarkers: How Testing Shapes Your Treatment Options
Watch the Replay On DEMAND
Hear a Patient-Physician Perspective – Follow Joseph’s journey and learn how a doctor makes decisions when he’s the patient.
Listen in as AML expert Dr. Stephen Strickland from Sarah Cannon Research Institute, AML patient and doctor Joseph, and advocate Steve Buechler discuss how biomarker testing can unlock better options. Learn how understanding what mutation you have, like NPM1, IDH, KMT2A, and FLT3 can shape treatment choices—and how patients can work with their doctors to explore every option, including clinical trials.
Key Topics Covered:
Understand AML Biomarkers – Learn how FLT3, NPM1, IDH1/2, and KMT2A mutations impact risk and treatment choices
Test Early, Treat Smarter – See how early biomarker testing shapes decisions from day one
Explore Targeted Treatment Options – Understand how biomarker-driven therapies are changing care
Navigate Clinical Trials with Confidence – Learn how to evaluate opportunities and what trial participation really looks like
Partner with Your Care Team – Get tips to advocate for testing and align on a personalized treatment path
Thank you to Kura Oncology for its support of our patient education program. The Patient Story retains full editorial control over all content.
Table of Contents
Introduction
Stephanie Chuang: There’s so much going on at and around diagnosis. There’s a lot to digest and so much information coming at us. We hope that you walk away from this discussion empowered to improve your AML care by knowing more questions to ask your healthcare providers or maybe to advocate for yourself, to understand how to be more engaged in your care, and to know your treatment options from biomarkers through clinical trials.
I’m the founder of The Patient Story. More importantly, I’m a blood cancer patient advocate myself. While I wasn’t diagnosed with AML, I was diagnosed with non-Hodgkin lymphoma and I remember swimming in questions. Things were happening so quickly and it felt so difficult to understand what was what.
We don’t know what we don’t know and that’s why The Patient Story aims to build education and community through educational discussions and hundreds of in-depth patient stories, all with the goal of amplifying the voices of patients and care partners.
For this discussion, our patient advocate Steve Buechler talks with a leading expert in AML treatment, Dr. Stephen Strickland from Sarah Cannon Research Institute (SCRI) and one of his patients, Joseph.
We want to thank our sponsor, Kura Oncology, whose support allows us to share more educational content, editorially independent and free for our communities. While we hope that this discussion is helpful for you, keep in mind that this is not meant to be a substitute for medical advice, so please consult with your healthcare team about your decisions.
Steve is going to help guide this discussion, but we all agree that it would be helpful to understand his story first. Steve, as an AML patient advocate, we’d love to hear more about what brought you to this point in sharing your story.
Not only did I not have nonspecific symptoms, but I didn’t have any symptoms whatsoever… If not for that physical, I probably would have learned about my AML when I was in much rougher shape.
Steve Buechler, AML Patient
Steve Buechler: I was diagnosed in June 2016. I did what doctors tell you to do, which is to get an annual exam. I had no symptoms whatsoever and thought I didn’t need to do it, but I kept the appointment. As part of the routine annual physical, a complete blood count (CBC) test was performed, and it was found that my white blood cell count was dangerously low. They referred me to a hematologist-oncologist who did a bone marrow biopsy, which detected the AML with 50% blasts.
From there, we were off to the races. I was admitted to the hospital the next day and was hospitalized for 37 days with the initial 7+3 treatment and eventually, a stem cell transplant. Not only did I not have nonspecific symptoms, but I didn’t have any symptoms whatsoever. Maybe I was a week away from having symptoms, who knows? If not for that physical, I probably would have learned about my AML when I was in much rougher shape.
Now, more than ever, knowing your biomarkers, mutations, and genetic alterations is absolutely essential. I heard there are dozens of different subtypes of AML, based on how those are present or absent. Many of them respond to different treatments, so you have to know that information if you want to find a targeted treatment that’s right for you.
We’ll be talking about the importance of testing for biomarkers in AML treatment and how doctors and patients can work together to determine what options are best for them. We’re joined by Dr. Stephen A. Strickland, the Director of Leukemia Research for Sarah Cannon Research Institute. He’s an internationally respected leukemia researcher with more than 100 peer-reviewed scientific publications and abstracts. Also joining us is Joseph, one of Dr. Strickland’s patients. Joseph, can you tell us a bit about your journey with AML?
Joseph A., MD: My story started when I was coaching mountain biking two summers ago. I noticed that my legs were becoming very fatigued very quickly. During a mountain bike race, I started having chest pain, which led me to the emergency room and yielded a CBC test that showed extreme concerns for a blood cancer.
Immediately, I was flown to Sarah Cannon under the care of Dr. Strickland and it took off from there. It’s a wild ride to find out you have leukemia, then to find out that you don’t have months or even weeks to think about and weigh the treatment options. Over the course of several days, I had to make some pretty aggressive decisions and start treatment. It was a whirlwind.
What are Biomarkers in AML?
Steve: We’re going to start by looking into biomarker testing. Dr. Strickland, what are biomarkers and what are the different types? We hear about diagnostic, prognostic, predictive, and monitoring. It sounds pretty complicated. Can you sort it out for us?
Dr. Stephen Strickland: You hit it on the head. It’s complicated. Historically, as we looked at AML, it was diagnosed simply by looking at cells under a microscope. We know that those cells can look similar under the microscope, but the biology of AML is very heterogeneous and diverse. Looking at these biomarkers can help us understand the true heterogeneity of those cells and now help us to predict prognosis as potential therapeutic opportunities.
There are different biomarkers that have been developed over the years. Now, we have a broader spectrum of testing that we do on every patient as standard of care at the time of initial diagnosis to help guide us in our treatment decision-making.
What Biomarkers are AML Patients Tested For?
Steve: For AML in particular, can you describe what type of biomarkers you commonly test for?
Dr. Strickland: There are different types of biomarkers and what we’re looking at is the biology of the leukemia cell. There are tests where we look at the cytogenetics or karyotype, which is a chromosome analysis of the leukemia cell, to see if there are specific genetic aberrations. Those genetic changes may inform us if someone is going to be a favorable risk, intermediate risk, or high risk.
A patient’s risk classification can have implications for therapies that we may want to consider, including clinical trials that we may want to consider from the very beginning. But it also helps inform us, once we hopefully have the patient in remission, whether or not we need to consider something like a stem cell transplant to give them the best chance at a cure.
Several mutations are important and, ever since the early 2000s, have been encouraged to be tested at initial diagnosis, like the FLT3 mutation. We know that patients who have FLT3-ITD can often have higher-risk disease biology, especially before the availability of FLT3 inhibitors.
IDH inhibitors are now available for patients who have IDH1 or IDH2 mutations, which has been historically and predominantly in the relapsed/refractory setting. Data is now looking at the incorporation of IDH inhibitors into frontline therapy. More recently, understanding NPM1 as a prognostic factor, but with the advent of menin inhibitors, we look at the availability of NPM1 as a potential therapeutic target.
Recently, in the relapsed/refractory setting, we had the approval of revumenib (Revuforj), which is the first targeted therapy for patients with KMT2A-rearranged relapsed/refractory acute leukemia. We’re looking at combinations of this menin inhibitor with other menin inhibitors in the frontline space, which are known in more advanced leukemia and have activity. Can we do better for patients by incorporating them in the frontline setting?
There was recent data at the 2024 Annual Society of Hematology meeting where multiple menin inhibitors were presented in a relapsed/refractory setting with single-agent activity as well as in combination therapy in a relapsed setting and a frontline setting.
Two menin inhibitors, bleximenib and ziftomenib, had data presented in combination with conventional, intensive induction therapy in the frontline setting with very high response rates and more importantly, good complete remission (CR) rates and also MRD-negative CR, which is the deepest remission we can test for, being achieved at a high rate for NPM1-positive patients.
Also, in patients who have KMT2A rearrangement, which is a specific genetic rearrangement that can often confer higher risk, we’re seeing high response rates in combination with conventional, intensive induction therapy plus menin inhibitors. This specific area has been an area of struggle for us because many of these patients were resistant to conventional chemotherapy and now, it seems like we’re finally breaking down the door and helping more patients.
Do Age and Gender Play a Role in Biomarkers and Mutations?
Steve: Do any of these mutations or biomarkers cluster into specific groups of people, by age, gender, or other social factors?
Dr. Strickland: There are a variety of factors that we can see. NPM1 can occur across the age spectrum, but the other aspect is what mutations or other abnormalities are occurring simultaneously and that has an influence. By itself, NPM1 is thought to be a favorable risk feature. But there’s also data that suggests that when NPM1 co-occurs with an IDH mutation or a DNMT3A mutation, its positive impact may take a hit based on the co-occurrence of these other mutations.
Let’s take, for example, NPM1 that co-occurs with a FLT3 mutation. FLT3 by itself puts patients into a high-risk category, but FLT3 plus NPM1 puts them in an intermediate risk, whereas NPM1 patients by themselves go into a favorable risk. It’s not a single mutation that’s driving it. You have to look at the bigger picture of the molecular profile and the diversity within a patient’s leukemia to see the impact and open the door for additional therapies.
Historically, KMT2A rearrangement has been associated with patients who have received prior anthracyclines. Some patients who receive prior anthracyclines will have KMT2A rearrangement, which confers a higher-risk disease. The availability of these therapies for a traditionally high-risk patient population is going to be very important.
You have to look at the bigger picture of the molecular profile and the diversity within a patient’s leukemia to see the impact and open the door for additional therapies.
Dr. Stephen Strickland, AML Expert Oncologist
Steve: Interesting. My treatment was in 2016 and they ran me through the traditional 7+3. They tested for FLT3, which was not present and was a good thing, and NPM1, which was also not present. That’s what landed me in the intermediate risk category and made for a more complicated decision, along with a normal karyotype. None of which I understood at the time. I’ve since come to understand it, but it’s a lot to learn and take on.
How and When Do You Test for These Biomarkers?
Steve: How and when do you test for these biomarkers?
Dr. Strickland: Testing at diagnosis is critical to help inform prognosis, but as the treatment landscape has changed over the years, it can also inform treatment decisions from day one. It’s strongly encouraged and I’d say a necessity to do at the initial diagnosis. Even if we don’t get the information back, like when we have to start treatment in an emergent situation, that information can still be obtained. If the patient responded to the initial therapy and achieved remission, if we don’t have their biomarker information, we can’t always inform prognosis and/or recommendations, like whether or not they need to proceed with a stem cell transplant.
We check at the time of presentation to confirm the initial diagnosis and help us understand the characteristics of the disease. But for some of these tests, we’ll reassess, even when the patient is in remission, to help us understand the depth of remission. Are patients achieving a very deep remission, which is the goal of our therapy?
We can do some of this testing on peripheral blood, especially for interval follow-up to minimize the number of bone marrow biopsy procedures patients have to undergo.
Dr. Stephen Strickland, AML Expert Oncologist
Steve: Is this typically done through a bone marrow biopsy or some other technique?
Dr. Strickland: Typically, we would do it at the time of the bone marrow biopsy on the liquid portion that we achieved during that process, but it can also be done on peripheral blood. There are ongoing debates about one being more sensitive than the other, but bone marrow biopsies are not always the most fun to undergo repeatedly, though sometimes a necessity. We can do some of this testing on peripheral blood, especially for interval follow-up to minimize the number of bone marrow biopsy procedures patients have to undergo.
Because of my previous exposure to chemotherapy, we elected to go with a more aggressive chemotherapy regimen right out of the gate… the genetic markers guided his recommendations.
Joseph A., AML Patient
How I Processed My AML Diagnosis
Steve: Joseph, how long after your diagnosis before you were tested? Through that process, what were your thoughts? Did you have any fears or anxieties? What was it like to live through that phase?
Joseph: Mine was a little more complicated than average. I had a childhood malignancy for which I received chemotherapy. I fell into an atypical category in that mine could have been and may still be treatment-associated leukemia, which could fall into the higher-risk category.
I was admitted in the middle of the night after being helicoptered to Sarah Cannon. On day one, Dr. Strickland stepped into the room and said, “We’re going to look for markers. This is what I’m thinking. There are some newer drugs for these different markers.” We sat down and talked about those markers within a day or two of the bone marrow biopsy.
Because of my previous exposure to chemotherapy, we elected to go with a more aggressive chemotherapy regimen right out of the gate. My case is a little bit skewed, but the genetic markers guided his recommendations of newer medicines versus the overall course of my therapy and even the choice that we ultimately made about stem cell treatment.
Barriers to Biomarker Testing
Steve: Dr. Strickland, despite its importance, early biomarker testing is not universally standard. What kinds of barriers or limitations exist to implementing this as a routine practice and how can they be addressed?
Dr. Strickland: It’s gotten better over the past several years as we’ve tried to get the word out. It’s listed in the NCCN Guidelines to be able to get a baseline assessment on patients at the time of initial diagnosis. But it also has some implications as far as where a patient is presenting, where the initial bone marrow biopsy was done, and whether or not the hospital system has access to those tests.
It’s not uncommon to repeat the bone marrow assessment to ensure that we get the testing done. But all of the providers who are coming in contact with these patients advocate with the hospital system and the pathology laboratories to ensure that we get this testing done. It’s critically important in the decision-making process.
AML Standard of Care and New Treatments
Steve: We’re going to shift gears to treatment options for newly diagnosed and relapsed/refractory AML. Dr. Strickland, once a patient has undergone testing, what are their treatment options? Before we get into specifics, can you give a broad overview of what has been the standard of care and what we might be shifting to, including targeted therapies or other options?
Dr. Strickland: The conventional induction therapy that we use is a regimen called 7+3. It’s easy to remember because some of the first publications about it were in 1973. It’s seven days of backbone therapy of cytarabine and three days of an anthracycline, either daunorubicin or idarubicin.
[In the past] If patients were not fit enough to receive therapy, they were often not offered any chemotherapy and sometimes went directly to hospice.
Dr. Stephen Strickland, AML Expert Oncologist
For many years, that was the treatment of choice and it was a one-size-fits-all therapy. If patients were not fit enough to receive therapy, they were often not offered any chemotherapy and sometimes went directly to hospice. With a diagnosis that has a median age in the upper 60s, you can imagine that quite a few patients were sometimes not offered therapy if they weren’t fit for intensive induction.
But in 2017, with the approval of midostaurin (Rydapt), that started to change, at least for patients with FLT3 abnormalities that were identified at the time of their initial diagnosis. The approval of that drug added a targeted therapy, an FLT3 inhibitor. As a result, that began changing the landscape.
Now, that’s a subset of patients — about 25 or so percent of AML patients fall into that category. We’ve continued to work towards identifying other markers and developing new targeted therapies.
The landscape has changed with the approval and availability of medicines like gemtuzumab (Mylotarg) and other medicines that have come on the market to help guide us for favorable-risk patients who may get an additional antibody therapy. Gemtuzumab, in addition to conventional therapy, is for FLT3 patients who may get an FLT3 inhibitor. We also have midostaurin and quizartinib (Vanflyta), which are now approved in the frontline setting.
We’ve also had therapy advances for patients who are not fit for intensive therapy with the availability of hypomethylating agents (HMAs), like azacitidine (Vidaza, Onureg), decitabine (Dacogen), and even low-dose cytarabine (Cytosar) in combination with venetoclax (Venclexta), a BCL2 inhibitor.
Based on a patient’s fitness level and molecular or cytogenetic profile that the leukemia may possess, we have multiple agents to help us hone in and take advantage of those markers that are present to guide the patient to the most effective therapy.
Promising Areas of AML Research
Steve: What are some of the most exciting spaces that are either newer options that are already approved or those that are promising in research in phase 2b or 3 trials? Does it make a difference? Can you distinguish what’s for newly diagnosed patients as opposed to relapsed and refractory patients?
Dr. Strickland: There’s a lot of work that’s being done in this space and across different spectrums with different mechanisms of action. There are areas of opportunity in terms of how we can harness the power of the immune system with either antibodies or antibody-drug conjugates (ADCs).
We’re also developing cellular therapy options, whether it’s the patient’s immune system being educated to identify and attack the leukemia cells or whether a healthy donor donates immune cells that can be engineered to hopefully attack a certain characteristic of the leukemia cell. We’re seeing this across different tumor types and across the landscape of oncology in general.
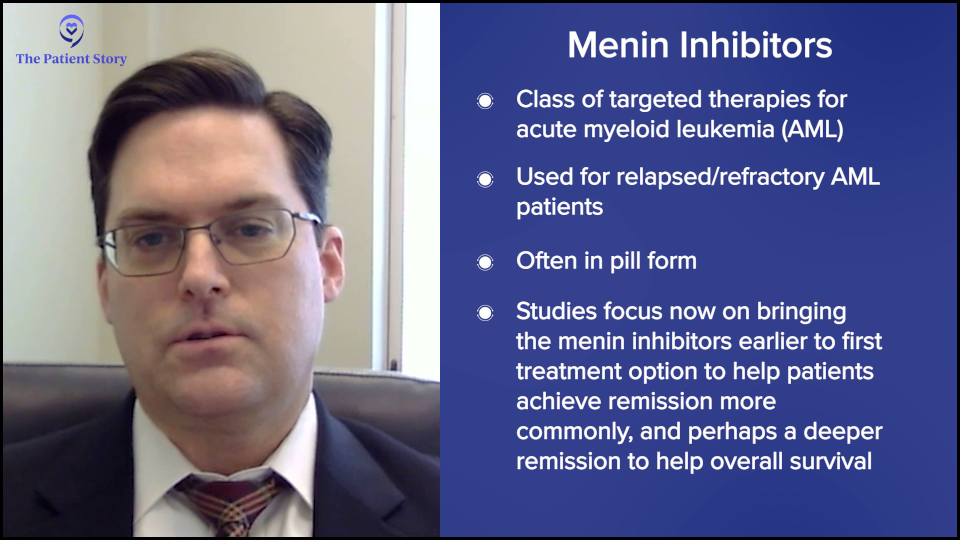
But one very exciting area that we’re dealing with is a new small molecule inhibitor called menin inhibitors. This is being looked at in the relapsed/refractory patient population and is showing activity as a single agent, being able to achieve deep remissions for some relapsed/refractory patients. Relapsed/refractory patients are those who have undergone prior conventional therapy and whose disease has persisted and/or relapsed despite the conventional therapy.
This opens up an opportunity. If menin inhibitors benefit relapsed/refractory patients, can we add these to conventional and frontline therapy? Can we get these medications to patients earlier on to hopefully help them achieve remission more commonly and achieve a deeper remission to hopefully impact overall survival?
Menin inhibitors are very popular nowadays in the world of leukemia. Every conference has a session with multiple companies that are developing menin inhibitors because it’s a very exciting space.
We’re trying to take advantage of the biological characteristics of a patient’s cancer, so there are a lot of studies that are biomarker-driven.
Dr. Stephen Strickland
The Role of Biomarkers in Clinical Trials
Steve: How do biomarkers play a role in clinical trials? Can they make you either eligible or ineligible for certain trials? How do those two things work together?
Dr. Strickland: It’s definitely been an evolution in the leukemia research space, the clinical trial space, and oncology research in general. We’re trying to take advantage of the biological characteristics of a patient’s cancer, so there are a lot of studies that are biomarker-driven.
If a patient’s malignancy has a specific marker, then we try to get them access to targeted therapies. Sometimes these drugs may be more effective on a broader scale. With the initial development, we’re also trying to enrich the population of patients who are truly going to, hopefully, benefit from the medications.
We’re trying to take advantage of the characteristics we now can better understand about one person’s leukemia that we didn’t know existed, say, 30 to 40 years ago. Now, we have the technology to help us identify these biomarkers and identify them relatively quickly, which can be instrumental in guiding us to either commercially available therapies or clinical trial participation where there may not be something that’s already FDA-approved.
How Biomarkers Guide Treatment Decisions
Steve: How does knowing someone’s biomarkers impact their treatment choices? Do biomarkers give you some idea about the potential effectiveness or potential side effects of treatments?
Dr. Strickland: Biomarkers can definitely help to guide the therapy decisions, not so much from a side effect profile but more so from an efficacy perspective. The way that I view traditional therapies is like going to battle with a tank. Tanks can be very effective, but they’re not very specific. Some of these newer therapies, these targeted therapies like FLT3 inhibitors, menin inhibitors, and IDH inhibitors, are like adding a sniper to the mix. Hopefully, by going to battle with both tanks and snipers, we can have a more effective outcome against this malignancy.
As the final testing came back, I found out that I might be a candidate for one of the new menin inhibitors, which was very exciting.
Joseph A., AML Patient
Working with a Doctor on Treatment Decisions
Steve: Joseph, how did you work with Dr. Strickland to decide on the best treatment options and how did it influence treatment choices?
Joseph: Right out of the gate, we knew that I was going to start in the high-risk category, so we started with the typical chemotherapy regimen. But as the results of my biomarker testing started to come back, every day during rounds, I would anticipate another conversation with Dr. Strickland and his team.
As the final testing came back, I found out that I might be a candidate for one of the new menin inhibitors, which was very exciting. I could start with a tank and a sniper right from the beginning. That’s the route that we elected to go.
When you’re starting to learn what the next three to six months of your life would look like, then you can settle in and realize the path that’s in front of you.
Joseph A., AML Patient
Addressing Fears and Concerns During Treatment
Steve: That does sound promising, but nonetheless, what were some of your biggest concerns during the process? It had to be an anxiety-provoking time.
Joseph: Anxiety doesn’t even cover it. Steve, you might know yourself. You go from somebody healthy, active, and surrounded by people you love, then you’re put in this unfamiliar environment, told you can’t leave the floor because you’re going to be neutropenic in several days, and can’t have contact with the world or your typical support network.
Every day, as you’re discovering a little more about your disease, there are very few familiar faces around you or familiar environments. It was a very anxious time. But at the same time, I found hope as we talked about some of these findings. I could have found out that I had multiple mutations and was a candidate for none of the new drugs and that we were going to try chemotherapy. If that didn’t work, here was the backup plan and here was the backup for the backup.
There was no end to the initial anxiety, if you will. About three to four weeks in, when you’re starting to learn what the next three to six months of your life would look like, then you can settle in and realize the path that’s in front of you.
Addressing Common Concerns from AML Patients
Steve: Dr. Strickland, on your side of this collaboration, what are some of the most common questions that you get from patients going through this process?
Dr. Strickland: It’s such an overwhelming time for many patients. Acute leukemia, in general, is cruel in the sense that patients don’t go into the hospital or the doctor’s clinic expecting to get that diagnosis. They walk in with nonspecific symptoms and often think there’s something else.
Then they’re told they’re going to be sent to a leukemia center and they’re going to undergo a biopsy. Before they even have time to digest the word leukemia or cancer in general, they’re being told they’re starting treatment in the next day or two, and we start talking about all of the side effects before many patients and their families have time to process the information.
We’re trying to navigate and walk hand-in-hand with the patient and their families as we get this information.
Dr. Stephen Strickland, AML Expert Oncologist
With other malignancies, patients and their families have weeks to digest the information and come to terms with it. But in the world of acute leukemia, we often have days to maybe a week, if we’re lucky, but often it’s less than a week when all of this happens. Then we talk to patients and their family members about a clinical trial or different therapies and what we have to offer. It’s a very overwhelming time.
We’re trying to navigate and walk hand-in-hand with the patient and their families as we get this information. What are we looking for? What is it going to mean? How are we going to use this information? In Joseph’s case, we understood that there was prior chemotherapy exposure, so there’s a possibility that this is a therapy-related leukemia, which guided our choice of induction therapy. Eventually, some of the biomarker testing came back and, as a result, we were able to access a particular trial with a menin inhibitor that allowed patients to start conventional backbone therapy.
If we had the information about the biomarker, then we could enroll the patient and get them access to this other targeted therapy, so to speak. It’s a huge effort to try and coordinate this. There’s communication and coordination even with the sponsors of the trial to set it up in a way that we have a little bit of flexibility on the front end. We didn’t burn a bridge for someone who we wanted to and felt the need for starting therapy quickly but yet still could have access to some of the more cutting-edge therapies that are coming up as well.
How Care Partners Influence Treatment Decisions
Steve: We’ve talked about providers and patients. Let’s bring in a third group here because at The Patient Story, we’ve often talked about getting loved ones involved in the process. Joseph, can you say a bit about who your caregivers or care partners are and how they help influence or inform your decisions?
Joseph: My wife is an office manager for a medical group. It was beautiful because they gathered together and said she could stay with me and manage the office remotely. She stayed by my side the whole time, which was phenomenal and honestly helped me make a lot of the tough decisions.
There was nothing left off the table. Here are the good and the bad. Here are all the options.
Joseph A., AML Patient
In addition to that, I’m a physician as well, so I had access to a lot of different doctors whom I could call and ask about certain things. I called a buddy of mine who’s a vascular surgeon when I was picking out whether I wanted to port-a-cath or a temporary line in my arm. I pulled some strings that way to make my decisions.
But ultimately, I felt so comfortable with Dr. Strickland. When he entered the room the very first time, he laid it all out. I felt like there was nothing left off the table. Here are the good and the bad. Here are all the options. Then, as more information came back, I felt like he immediately updated me on what the new information was and what the options were. My wife Heather and I felt like we had all the information we needed to make the best decisions for my care.
Since I had no basis for choosing one over the other, I agreed to join the trial.
Steve Buechler, AML Patient
How Can Patients Learn About and Navigate Clinical Trial Opportunities?
Steve: Let’s talk about clinical trials. I was in a clinical trial myself. We reached a point where I decided I wanted a transplant, but we had to select a donor. I had a half-matched sibling, my brother, and they said he’s a potential donor, but we should also consider umbilical cord blood donors. It sounded like science fiction to me, but they convinced me it was a plausible alternative. I asked which one’s better and they didn’t know, but there was a clinical trial to figure that out and I could join the trial.
Since I had no basis for choosing one over the other, I agreed to join the trial. They randomly assigned me to the cord blood option, so my brother, as a donor, was off the hook. My fate was in the hands of a mother and baby who donated their umbilical cord blood. All ended well, but ironically, years later, the results of that trial came out and they slightly favored half-matched siblings as opposed to umbilical cord. I was an n-of-1 and the umbilical cord blood worked for me.
Clinical trials are crucial to figuring out what works and who benefits from what works. Dr. Strickland, when and why are clinical trials a good option for a patient and how can patients find and evaluate trial opportunities?
Dr. Strickland: I’m going to be biased, but I will say that when available, clinical trials are going to be appropriate for any patient with acute leukemia and every patient with acute leukemia. We’ve had drugs that have been around since the early 70s or even earlier that we’ve utilized, but while some of these agents can be effective in getting patients in remission, we know that for many patients, a cure can be elusive.
Unfortunately, the majority of patients with acute leukemia end up relapsing, but that’s also because many of them fall into an intermediate risk or higher risk group. When that happens, we know we can get them in remission, but the question is: how do we keep them there? That’s where a lot of the effort is to try and modify frontline therapy to achieve deeper and hopefully more sustainable remissions.
If they have well-tolerated medications, maybe those medicines can be used as maintenance therapy. Those will allow the patients to stay on a low-intensity, well-tolerated therapy for a longer period and hopefully exhaust that leukemic clone altogether.
As we get the information about the biology of any patient’s leukemia, if we have a trial option, we want to try to swing the pendulum as much in their favor and give them a benefit.
Dr. Stephen Strickland, AML Expert Oncologist
I’m very passionate about the idea of clinical trials. I’m going to be biased because I’m a clinical trialist at heart. We want to offer the best available therapies to our patients. As we get the information about the biology of any patient’s leukemia, if we have a trial option, we want to try to swing the pendulum as much in their favor and give them a benefit.
But there are patients with leukemia who are treated throughout the country and the world without access to clinical trials. Sometimes, we also deal with patients in a relapsed/refractory setting. In that area, it’s even more crucial to try and gain access to clinical trials.
Historically, many of our relapsed/refractory therapies have about a 30% chance of getting the patient in remission, which means the majority of patients in a relapsed/refractory setting will not achieve remission with the salvage therapy. Better therapies, more effective therapies, and/or combinations of therapies to take advantage of the biology of the disease are crucial to be able to offer to patients.
How Can Patients Learn What Clinical Trials are Available?
Steve: Dr. Strickland, it sounds like your patients are going to hear about clinical trials, but for other patients who may not have a doctor who’s a clinical trialist, how should they go about finding and evaluating clinical trial opportunities? What’s a good source of information?
Dr. Strickland: There are plenty of resources out there, but with the Internet, you have to be cautious about what you Google. The Leukemia & Lymphoma Society is instrumental in trying to help provide patients with education about opportunities, and they obviously support quite a bit of research as well.
ClinicalTrials.gov is a website where all clinical trials in this country are registered. With its search engine, you can input a few keywords and your diagnosis to get information about trial opportunities available. There’s also additional information about the sites that are participating in each of the different clinical trials.
We’re here trying to offer them access to the most cutting-edge therapy that they can have access to and that’s where my passion is.
Dr. Stephen Strickland, AML Expert Oncologist
The information is out there if you know where to look, but the biggest thing is talking with your oncologist. Patients need to be informed and empowered to ask questions. Where is the nearest leukemia center near me? What are my trial options?
We’re trying to get away from people thinking that they’re guinea pigs when they go into a study. We’re not trying to experiment on patients. We’re here trying to offer them access to the most cutting-edge therapy that they can have access to and that’s where my passion is.
When we look at hundreds or thousands of patients who go on a study, we will be able to make informed decisions about patient populations. But when we’re meeting one-on-one with a patient, it’s about what we can do to help that individual patient and that’s where the offering for a clinical trial comes from.
What Role Does Age Play in Clinical Trial Eligibility?
Steve: Given that the typical AML patient is in their late 60s, does age impact the decision to encourage them for a clinical trial?
Dr. Strickland: It does. Age impacts it in several ways. We know that age is not the best determination of someone’s performance status or fitness, but it does play a role as far as the wear and tear of other organ systems and how well a patient can endure the side effects associated with an intensive therapy approach.
We also know that patients who are in their mid-60s and above tend to have higher-risk disease. Even if we have the opportunity to give them intensive therapy, the majority of those patients are not going to be cured with that therapy, so they’re going to be faced with potential relapse.
It does play a role as far as the wear and tear of other organ systems.
Dr. Stephen Strickland
If they’re a transplant candidate, we try to get them to a transplant. But again, as we get on the more mature range of the age spectrum, it makes the availability of something like a stem cell transplant and the intensity that goes along with it very challenging.
We need more effective therapies that can be used, for instance, as maintenance therapy. We do have that nowadays with patients who can receive hypomethylating agents plus venetoclax, which is approved for unfit patients in the frontline setting. But what do we do for patients when they progress after that therapy stops working? That’s another opportunity for clinical trial enrollment as well.
Patient Perspective on Clinical Trials
Steve: Joseph, you’re on the young end of the spectrum for AML, but how did clinical trials come up in your treatment? What did you know about them? If anything, how did you get familiar with them? How’d that go?
Joseph: Starting day one, the discussion about clinical trials was opened and what some of the possibilities were before we even knew my mutations. We immediately started talking about the opportunity of clinical trials. We talked about the whirlwind of the diagnoses, learning it, and trying to navigate and come to terms with it. I was in such shock that I was happy with any opportunity.
Unlike a traditional cancer course, there was such urgency in my case that to hear I had options, both in the traditional sense and a clinical trial, gave me comfort. They were going to be used simultaneously. We’re going to use traditional induction therapy, which we know has some efficacy, but in addition, I’m going to be considered for clinical trials and these are going to be parallel treatments. In no way did I feel like I was being experimented on. I felt very comfortable.
There are some impacts on your quality of life from being in a clinical trial… Overall, I’ve had a phenomenal experience.
Joseph A., AML Patient
As the trial went on, I loved it. There are some impacts on your quality of life from being in a clinical trial. There are checkboxes, if you will. I probably get to see Dr. Strickland’s clinic staff a little more often than the average AML patient who’s in remission. I have a bone marrow biopsy every three months, which is not ideal, but a small price to pay.
As far as side effects, I’m surprised that I’ve had minimal side effects with this drug. There was a little bit of variation in my clinical trial, almost as if they were trying to figure out the highest effective dose. There was a dose escalation partway through my trial where they tried a higher dose, but I didn’t tolerate it very well. Dr. Strickland’s team was very amenable, along with the company that runs the trial, in saying that I’ll go back down to the dose I was tolerating. That was the biggest bump in the road when they doubled and even tried to triple the dose to see if it could be tolerable and it wasn’t for me. Overall, I’ve had a phenomenal experience with this trial that I’m in.
Clinical Trials Happening Right Now
Steve: Dr. Strickland, can you describe the promising trials that are happening right now?
Dr. Strickland: We could spend a lot of time at different sites across the country with all kinds of different trial opportunities. I’ve been fortunate to be a part of several trials and also see colleagues present data on theirs as well.
The SAVE trial is looking at a triplet oral therapy for patients. It’s an oral decitabine plus venetoclax plus a menin inhibitor, revumenib, in a relapsed/refractory population that is taking away the need for daily trips back and forth to a clinic to receive chemotherapy. As some of these agents have oral formulations, being able to use a strictly oral formulation in combination therapy to hopefully impact patients and has shown very nice response rates, is opening the door for how we cater to patients as they live with this disease over time. We know that historically, they spend a lot of time in the hospital, away from work, and living their lives.
Other trials incorporate menin inhibitors into frontline chemotherapy, like the KOMET-007 trial. There’s a 7+3 plus ziftomenib that we have been fortunate enough to participate in. For patients who are NPM1 positive, the data that was presented in December 2024 suggested that 100% of patients who had NPM1-positive disease were achieving true CR and about 76% of those patients were achieving MRD-negative responses, which is very encouraging.
Now, it’s a small number of patients. We still have a lot of work to be done and we’ll see if that 100% holds up or not. Nevertheless, the fact that the majority of patients are seemingly benefiting from the therapy is very encouraging.
We also have access to relapsed/refractory studies and I briefly mentioned cellular therapy studies, like the SENTI-202 trial. We’ve been very fortunate to participate in some of these and provide access in Nashville and across our Sarah Cannon network. These therapies engineer immune cells from healthy donors to give to patients and they attack a certain characteristic commonly found on AML cells. We recently presented data that four of the seven patients who have ever received this cellular therapy product achieved deep MRD-negative remission. That’s very encouraging for patients who have had relapsed/refractory disease.
Again, a lot of this is still in its early stages, but it’s a testament to what we’re trying to do. Access to clinical trials can sometimes be better than what we have on the proverbial shelf and offer patients opportunities that they otherwise wouldn’t have.
Patient Perspective on Entering a Clinical Trial
Steve: Joseph, can you say something a bit more specific that might provide some guidance to patients who are trying to figure out whether they should think about a clinical trial? How do they decide about a clinical trial? How do they fight their way through the consent form? What’s it like from the patient’s perspective to go through the whole process of deciding and entering a trial?
Joseph: I had a good experience. Multiple staff members came to me and did a phenomenal job explaining the trial. They sent a representative to answer any questions about the potential side effects of the traditional treatment and the immunotherapy they were testing, so I thought that was great. Logistically, I found it easy to navigate the forms because there’s an expert sitting right beside you, explaining what everything means.
They want to see how efficacious it can be if they move it up in the treatment course, so I found a lot of comfort in that.
Joseph A., AML Patient
What gave me the best feeling on my trial is that I was on one of the menin inhibitors. NPM1-positive was my genetic makeup. When they presented the trial to me, they said that there isn’t half who’s getting the medicine and half who isn’t. The way it was presented was that there’s a medicine that they know works in refractory patients. The question in the trial is if it’s given at the very beginning, do you go into remission quicker and get a deeper remission?
Before I came into all of this, clinical trials were a black box. You don’t know what’s going to happen in them. The word experimentation is a daunting word. Am I going into something where they don’t even know what it does and what the side effects are? Am I going to get the real pill or the fake pill? It wasn’t like that. They know that what they’re giving me is efficacious. They want to see how efficacious it can be if they move it up in the treatment course, so I found a lot of comfort in that.
Best Advice for Newly Diagnosed AML Patients
Steve: Let’s focus on some key takeaways. I’m interested in your final thoughts. If there was one thing you wanted someone newly diagnosed with AML to know about testing and their treatment options, what would that be?
Joseph: The best advice that I could give to a patient who’s just been diagnosed, which is the advice that I followed myself and has served me very well, is to access great resources. I see that even in my practice as a neurologist. People come in after they’ve searched for their disease online with all this preconceived bad information, which is very scary.
There are great websites and professionals who can give you good information. When I headed into this dark time with a lot of confusion, I made a big promise to myself and my wife that we weren’t going to go online and search all these poor resources. We were going to trust in Dr. Strickland, his team, and his protocols. If he offered us different websites that we could look at, we would restrict our vision and our knowledge to those. I feel like you can get more solid ground under your feet by starting there, versus the huge cloud of misinformation that is the global Internet.
Access great resources… There are great websites and professionals who can give you good information.
Joseph A., AML Patient
Dr. Strickland: I would let people know that there are options. Too many times, when people hear the word leukemia, which I hear all the time, they come in very distraught. From what they know, there’s no cure. There are a lot of unfortunate predispositions or misnomers as far as what we can do. It may be because they had a family member from years ago who was told that they didn’t have any treatment options. But who knows what the specifics were?
We have many more opportunities available to us today. Approach this with an open mind. Try to understand what options are available. Hopefully, with this discussion and resources from websites like The Leukemia & Lymphoma Society and The Patient Story, you can put a wonderful face and story to this disease in the sense of what we can do and the success that we can have if we have the opportunity.
We want to empower patients. We want them to be informed. We try to inform them with our discussions early on.
I do think participation in clinical trials and getting the best available therapies as possible is going to open the door for more patients to do that.
Dr. Stephen Strickland, AML Expert Oncologist
Joseph’s story, to me, is incredible. He was living his life without any idea of what was going on underneath the surface until some symptoms developed and then the whirlwind of being transferred. One time when I called him to ask a few questions, he was very out of breath. At first, I was very concerned about what was going on. I asked, “Are you okay? What’s going on?” He said, “I’m at mountain bike practice teaching middle schoolers.”
The impact of the therapies we have nowadays and the access to a clinical trial to take someone who had to stop racing because of symptoms to the point of getting him back to doing what he loves was very gratifying. That’s the opportunity we want for all patients to have. We want them to get back to their lives and live their lives to the fullest. I do think participation in clinical trials and getting the best available therapies as possible is going to open the door for more patients to do that.
Conclusion
Steve: Thank you to Dr. Strickland and Joseph for sharing their insights. We hope this discussion has provided you with valuable information. We encourage you to continue following the latest advancements in the field and to discuss your options with your healthcare providers.
Stephanie: Thank you so much to Steve, Dr. Strickland, and Joseph for spending your time with us on this discussion that features so many perspectives. Hopefully, this was resonant with you.
We want to thank our sponsor, Kura Oncology, for supporting this program, which helps us make sure that we provide these more often and always for free for our communities. We want to remind you that this program is not a substitute for medical advice and that The Patient Story retains full editorial control.
We hope this was helpful for you and that you walk away feeling more empowered to ask questions. We hope to continue having more of these conversations and to see you at another program soon. Thank you so much and take good care.
Thank you to Kura Oncology for its support of our patient education program. The Patient Story retains full editorial control over all content.
Pamela Price: Saving Lives Through Awareness and Action
Pamela Price, Deputy Director of The Balm in Gilead, an organization focused on eliminating healthcare disparities, says she felt fine before she was hit by the news that flipped her world upside down. She was diagnosed with cervical cancer. It’s also not the first time Pamela has had to deal with cancer. She lost her mom and both grandmothers to cancer and has been a care partner to her husband, who’s living with a chronic blood cancer.
Pamela says it was her and her husband’s doctors who truly advocated for them, changing the trajectory of their care and their lives. Now she works every day to help save other lives through awareness and action. Her mission is to bring the conversation of healthcare and awareness to faith communities across the country.
Multiple myeloma disproportionately impacts Black Americans — 1 in every 5 people diagnosed is Black or African American. That’s why Pamela spent nearly two years working with fellow patients and advocates to identify the top ways to help cut through healthcare disparities for multiple myeloma patients. Pamela and her group were selected to present their findings at the largest gathering of top doctors and researchers in blood disorders and cancers called American Society of Hematology (ASH).
Watch this last episode of our series of three to hear about their top solutions for reducing healthcare disparities and serving as many people as possible who are dealing with the hardships of a cancer diagnosis.
Thank you to Pfizer for supporting our patient education program. The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
It was an amazing primary care physician who wasn’t his regular primary care provider who saw something off in his labs…
To us, she saved his life.
Introduction
I’m the Deputy Director of The Balm in Gilead, where public health and faith intersect.
I’m very extroverted and my husband’s very introverted. He served for over 22 years in the US Army. It was an amazing primary care physician who wasn’t his regular primary care provider who saw something off in his labs. She said, “Hey, you’re young and in shape. I doubt it’s anything, but I’m going to order some additional tests anyway.” To us, she saved his life.
He’s an awesome father. We have twins and an older one who will be graduating from college soon. Outside of the father and the husband that he is, which is why I could be here sharing his story, I’ve never met someone as disciplined, mentally strong, and resilient as he is. I see the physical toll that this takes on him, from the fatigue to the lethargy and the headaches, and I see him every day push through and show up for me and our kids.
He plans 10,000 things when we go on vacation every year, even though we know that 9 times out of 10, one of those days is going to be a day when he’s not going to physically be able to do it. Those are the things that I love about him so much because it’s a constant reminder of what this journey can be like for a person like him living with it but also for me as a spouse and care partner.
We both were in the military. He served much longer than I did. We met as a group of friends. It was interesting because when I first met him, I thought he was an attractive guy who knew he was attractive and was expecting a certain thing from the ladies, and I was not going to do that. I’m not that girl.
Lo and behold, our paths would cross again. He ran into a good friend of mine who mentioned that we were going to be back at the same duty station. He asked for my number and we connected. We talked on the phone probably daily for months because he was in another duty station until he had a permanent change of station. After about six months, we decided to move in and then six months later, we got engaged before his last deployment to Iraq. We got married once he came back.
I lost my mother unexpectedly in January 2018. I had my bout with cervical cancer the same time…
Then we get my husband’s diagnosis. This was all within January to July 2018.
How Cancer Has Impacted My Life
Cancer has impacted me in different ways. I lost my maternal and paternal grandmothers to breast cancer. My amazing husband was diagnosed with polycythemia vera, but he progressed even after treatment. We have been on his cancer journey since 2018, which was also the year I lost my mom, so that was a very trying year.
He’s a big part of my why. I try to carry the stories of my family, my background, and people from communities where I come from with me.
The first thing was that we realized that life is fragile.
Experiencing Personal Loss from Cancer
I lost my mother unexpectedly in January 2018. I had my bout with cervical cancer the same time. I had surgery and I was going through radiation, so we were of the mindset that I was going to be fine. Then we get my husband’s diagnosis. This was all within January to July 2018. At that time, our twins were still young. They were about to turn five.
Initially, I thought about the things that we wouldn’t be able to do. I had done the research and realized that we may not have as many years with each other as we had planned. Our initial conversation was about how to master the now. How do we live in a way that will still allow us to do the things that we had planned to do for however long we have? Then we had to sit down and explain to our oldest at the time. We had to wait a couple of years before we explained to the twins and that was difficult, as well.
The first thing was that we realized that life is fragile. We’re not going to have all the time. What do we do? What we came up with was that we were going to maximize every minute. We already had our wills. It’s the day to day. What are we going to do on this anniversary? What are we going to do this weekend? I usually would let it slide that we didn’t have our date night last month or the month before or the month before, because I was somewhere working, but now, how do we reprioritize that?
A small silver lining of his diagnosis is that it allowed us to refocus.
Between losing my mom, having my cancer diagnosis, and now having my husband be on this journey, it helped us focus and prioritize time, how we were going to spend it, and where we were going to channel our energy and focus. A small silver lining of his diagnosis is that it allowed us to refocus that without the diagnosis, we would not have done.
I had no symptoms, which was the crazy part. I went in for a wellness exam and a Pap smear, like I normally would. Then I got a letter that said I had to come in for follow-up testing. When I found out I had cervical cancer, I told my husband, “My reproductive system is literally trying to kill me.” I’ve lived with endometriosis my whole life.
I went to the doctor to find out the course of action, but I wanted to make sure it’s not keeping what I have. We have children, so I don’t need it anymore. I was able to work with my clinician and my oncologist to get a good form of care. Luckily, we caught it early. I had to have some radiation because of the issues with the endometriosis and I had cervical tissue in places it shouldn’t have been, but I was able to come through it well. I lost my hair, but it worked out well.
I had no symptoms whatsoever and I almost canceled that appointment because I had lost my mom. I said I’ll reschedule. Something in me said, “You already have a schedule. You know that with the VA, it’s hard to get an appointment. Keep the appointment.”
Luckily, I kept it and I got referred to a good OB-GYN and a good oncologist. We found a plan that worked for me. They didn’t try to convince me to keep things. I told them they could take it all. I welcomed menopause early. At this point, I didn’t want to risk that something else along this reproductive track would decide it doesn’t like me anymore. We’ve been on this with my husband since that same year. 2018 was a doozy.
You will always be your best advocate because you’re the one who knows your body the best.
Importance of Paying Attention to Our Health
One of the first things that I tell them is not to rely on the information given to them. A lot of times, you have to research and find that information yourself.
You will always be your best advocate because you’re the one who knows your body the best. You may pick up on telltale things that externally aren’t revealed. Maybe they won’t even show up on a lab, like they did with my husband.
Recognize that when you walk into a provider’s office, you have the most important voice in that appointment. I know we don’t always see it that way. We trust and rely on our providers and we do need them, but we also should make sure to keep that power dynamic equitable. Don’t relinquish your voice. Those are the key things that I constantly tell my family, friends, and the people I meet through the work that I do. I tell my daughter now that she’s having her doctor’s appointments without me.
Importance of a Patient’s Lived Experience
This research was patient-focused. I know we use that term a lot, but this was one of the rare opportunities that I’ve been able to participate in a committee where nothing was decided without the patient. Even in this abstract, our lead author is a patient, so it amplified the power of the lived experience of the patient.
There’s no amount of education that we can have academically or even in work that I do as an advocate that can rise to the level that lived experience provides. This project centered on that and we could see the fruit of what something could look like in a scientific conference like ASH that is, the patient on a poster in a paper. It’s useful not just for patients. This is something providers, clinicians, and other community organizations can use.
There’s no amount of education that we can have academically or even in work that I do as an advocate that can rise to the level that lived experience provides.
Multiple Myeloma Disproportionately Impacts Black and African Americans
The biggest problem was cost. That’s something that, even we as a group, we’re not necessarily equipped with to deal with insurers and payers. Eventually, the right stakeholders will have to get together to figure out how to address that because that’s a significant issue.
Another one is access. Even if we can educate the community about what multiple myeloma is, what MGUS (monoclonal gammopathy of undetermined significance) is, and all these other things, it’s all for naught if we don’t have access. By access, I mean rethinking and reimagining where healthcare is delivered, how healthcare is delivered, and making sure that access is no longer a barrier like it is today.
Reimagining Access to Healthcare & Information
The healthcare system, as it stands today, is very transactional. For better or for worse, that’s the system that we currently have. By reimagining it, how can we put something, let’s say, in a church that’s a trusted place?
Within the landscape of multiple myeloma, clinical trials are key and pivotal. We have so many new therapies coming to market, but we don’t have the representation that we need. Can we invest something in a church that has a community center and come out to them on a Saturday, like we typically do at The Balm in Gilead, and do some type of awareness event with them?
Even if we can educate the community about what multiple myeloma is… it’s all for naught if we don’t have access.
Then take it a step further. How can I work and train a couple of people in the church on the basics of a clinical trial or what cell therapy looks like for a multiple myeloma patient? How can I work with the church to establish a multiple myeloma peer support group?
For the African American community, our church has historically been our anchor. From the time we arrived on this continent, our faith has been an anchor for us and it drives our behavior. One of the biggest scriptures we use in our work is that faith without works is dead. We don’t ask people to abdicate their faith, whatever form it comes in. We don’t ask you to abdicate praying, but we do ask you to pair that with action. Make yourself a more informed individual, make your communities more informed, and break down some of the traditional silos of how and where we think this type of information and engagement can take place.
Importance of Talking About Our Health
Something that I’ve said to churches, faith leaders, and pastors is that we know and we teach in terms of the God that we serve that we are nothing but spiritual beings having this earthly encounter. But along this earthly encounter, it is this fleshly body that we must have this encounter through, so we have to make sure that we’re doing our part, whether it’s prevention or treatment.
God will do His part and do His work, but we have to make sure that we identify our work to make sure that we’re doing what we can to protect this vessel that we’ve been given, so that we’re not sending souls to see our Maker prematurely.
Sadly, we see it play out and that’s in the disproportionate rate of deaths. It’s in the disproportionate rates of individuals being diagnosed too late or inaccurately. How are we going to shift that paradigm? We know the social determinants of health, and that’s been something that’s been coined and raised for decades, but still, here we are and African Americans are bearing the burden for multiple diseases and conditions.
African Americans are bearing the burden for multiple diseases and conditions.
Can we afford as a community, as a people, and even collectively as a country, to not pause and take the time to get it right? Look at some of the solutions that this committee, led by patients and take some of those things to heart. Make the tough decisions. Be first, be bold, be innovative, be forward-thinking, and get outside of the box to not do something just because that’s the way we’ve always done it. The risk is that we will continue to lose lives that we don’t have to lose.
I know it seems ridiculous, but go get your wellness exams. We let so many things pass and get worse, and then we decide to go and it’s through the route of an emergency room. I know many of us have heard of someone who goes into the ER, then the next thing you know, they’ve got a triple bypass and it’s because of high blood pressure that has been running rampant for who knows how long.
How do we start to nurture this next generation to be able to not only move forward with the advocacy but move forward with the innovation that we’ve heard and learned about at ASH? That would be my thing. My passion is young people because they are going to be the future. I figured that if we can take care of you better, you will take care of us.
Special thanks again to Pfizer for supporting our patient education program. The Patient Story retains full editorial control over all content.
Oya Gilbert had always been full of energy. A father, a hip-hop lover, and a man who rarely got sick. But in 2015, his body started sending him signals he couldn’t ignore. But for two years, doctors dismissed his symptoms as anxiety. Watch Oya’s story from misdiagnosis to myeloma advocacy.
Brandon Blue knew at a young age that he wanted to help people. Decades later, he’s done that and so much more, changing and saving the lives of people who’ve been diagnosed with cancer.
Learn key tips on how people can make a difference for themselves and their health, and what can help save lives.
Symptom: None; found through blood tests Treatments: Total Therapy Four, carfilzomib + pomalidomide, daratumumab + lenalidomide, CAR T-cell therapy, selinexor-carfilzomib
Blood Work Basics: Making Sense of Your Test Results
Watch ON DEMAND
What does your cancer blood test results really mean — and how do they help doctors detect or monitor cancer?
Listen in as hematopathologist Dr. Kamran Mirza and cancer advocate Stephanie Chuang to break down the most common diagnostic cancer blood tests, including the CBC. Learn how pathologists interpret results, what those ranges mean, and how small changes in your numbers can offer big insights into your health.
Key Topics:
Why doctors order cancer blood tests: What they’re looking for and how to prepare.
Making sense of the CBC: Understand what each number represents — and what it doesn’t.
How blood results guide treatment: From diagnosis to tracking remission or recurrence.
Should I be worried?: When out-of-range numbers matter and when they don’t.
What’s next in the series: Learn how this session leads into condition-specific follow-ups for 6 different blood cancers.
The LLS offers free resources like its Information Specialists, who are one free call away for support in different areas of blood cancer.
Register now to get notified about the follow-up program tailored to your cancer type.
Blood Work Basics: Making Sense of Your Test Results
Hosted by The Patient Story
What do your blood test results really mean — and how do they help doctors detect or monitor cancer? Learn about the most common diagnostic tests, including the CBC and the CMP.
Shine a light on someone who’s helped you along the way.
We all have someone who lifted us up when we needed some support. Maybe it’s a loved one, a nurse, someone you saw online who inspired you, maybe even yourself.
Share who inspired you and why they mattered. Your words could help someone else feel a little less alone.
No script. No pressure. Just you and your story.
Answer a few short video prompts
Respond by video or text
Get featured on our website, YouTube, or social media to reach others who need to hear it.
Why We’re Asking This Question
In healthcare, it’s often the small acts of kindness that leave the biggest marks on our hearts. Whether it’s a doctor who listened a little longer, a nurse who offered comfort in a scary moment, a family member who stood strong beside you, or even a stranger who shared their story, these heroes help shape the experience of healing.
At The Patient Story, we believe every voice matters—and so do the voices that lift us up along the way. In this video request, we are asking you to share who made a difference in your healthcare journey. Your heroes could be anyone: a caregiver, a fellow patient, a community advocate, or even you yourself.
By celebrating these moments of inspiration, we help others see the power of connection, compassion, and encouragement. These videos honor those whose words, actions, or simply their presence made your healthcare experience feel more human.
Your story could inspire someone who is facing a new diagnosis, navigating treatment, or simply needing a reminder that good people exist.
Who made you feel seen, supported, or stronger? Tell us about them—and help pass that hope forward.
How do you practice self-care and what has that done for you? From rest to reflection, movement to mindfulness, or simply saying “no,” we want to hear what self-care looks like for you. Whether you’re a patient, caregiver, or care partner, your experience could inspire someone else to prioritize their own well-being.
You never know who needs permission to put themselves first.
Self-care isn’t selfish — it’s survival.
Answer a few short video prompts
Respond by video or text
Get featured on our website, YouTube, or social media to reach others who need to hear it.
Why We’re Asking This Question
Self-care isn’t selfish—it’s a critical part of surviving and thriving through health challenges. Patients, caregivers, and care partners often give so much of themselves to others that their own needs can easily be overlooked. At The Patient Story, we want to help normalize self-care as a vital, necessary act of strength.
In this video interview, we are asking you to share what self-care looks like in your life. Maybe it’s finding quiet moments to breathe, asking for help when you need it, making time for joyful activities, or setting healthy boundaries. No act of self-care is too small—each step is a powerful commitment to your own well-being.
Your experiences can light the way for others who may feel guilty prioritizing themselves. By speaking openly about self-care, we show that caring for ourselves makes it possible to better care for others, face challenges with more resilience, and stay connected to what makes life meaningful.
We hope these videos inspire people to honor their own needs, to listen to their bodies and minds, and to recognize that putting themselves first sometimes is not only okay—it’s essential.
How do you practice self-care? So when you’re ready, hit record. We’re here. We’re listening.