Joseph, a 76-year-old man who maintains an active lifestyle, shares his journey with myelofibrosis, a rare bone marrow cancer.
Initially unaware of his condition, his low hemoglobin levels prompted a visit to a hematologist and a gastroenterologist, which eventually led to a hospital admission when a nurse noticed that he was symptomatic.
After his oncologist diagnosed him with myelofibrosis, he found out that there was no cure. Hesitant about undergoing a transplant, Joseph explored alternative options, eventually joining a clinical trial at Mount Sinai. The trial, which involved the drug pacritinib, became a vital part of his treatment plan.
Despite initial challenges, Joseph’s health started to improve. His hemoglobin levels stabilized and he found success on the clinical trial. The treatment being studied was pacritinib, later known as VONJO, which later received FDA approval.
Throughout his journey, Joseph experienced changes in spleen size and fluctuations in appetite. Despite these challenges, his hemoglobin and platelet levels improved significantly.
Joseph emphasizes the importance of seeking specialized medical care, encouraging others to research and choose healthcare providers wisely, and stressing the importance of self-advocacy and education in navigating medical challenges.
In addition to Joseph’s narrative, The Patient Story offers a diverse collection of myeloproliferative neoplasm (MPN) stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
Name: Joseph C.
Diagnosis:
Myelofibrosis
Initial Symptoms:
None; caught at routine blood work
Treatment:
Clinical trial: VONJO (pacritinib)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I’m 76 years old. I go to the gym seven days a week. I ride a bicycle for two hours every day then I come home.
I’ve always run and walked my whole life. I’ve been in sports for decades. I’ve played football, basketball, tennis, and ran track. I do all of these things to keep myself active.
Pre-diagnosis
Initial Symptoms
When we came back from a vacation, I got a call from my primary physician who said my hemoglobin was 6. I didn’t know what that meant. He told me to make an appointment with a hematologist and go to a gastroenterologist to see if I could get a colonoscopy.
At the appointment with the gastroenterologist, the nurse looked at me and said, “You look symptomatic. I think you should go to the hospital.”
I went home, picked up my wife, and went to the hospital. By the time I got admitted and got into a bed, my hemoglobin was 5. They gave me a couple of pints of blood and I stayed overnight.
Diagnosis
Getting the Official Diagnosis
I met Dr. Samir Patel of New York Cancer & Blood Specialists. He told me I had myelofibrosis. When I went home, I looked it up and found out that there was no cure.
When I went back to see him, he said, “Make an appointment to go to Mount Sinai Hospital in Manhattan and talk to a surgeon regarding a transplant.”
They told me I was in good enough shape to do the transplant, but I didn’t want to put my family through all of that.
Treatment
Discussing Treatment Options
I shied away from a transplant. I knew a little bit about it so it wasn’t something I wanted to entertain. I asked him, “What’s the alternative?” He said, “Another part of the team has a trial program that you can try.”
I told myself that the trial program is the nucleus. I’m going to roll the dice and see what happens. I don’t know what the answer will be.
They told me I was in good enough shape to do the transplant, but I didn’t want to put my family through all of that.
We were going to Mount Sinai once every three months and it was a headache. If we had to do that 3 or 4 times a week, I don’t know what would’ve happened. It’s too much pressure.
I know from my experience that a trial is what it says, it’s a trial. They don’t know what the answer is going to be.
Enrolling in a Clinical Trial
I saw Dr. John Mascarenhas, who introduced me to the trial. He told me that this is about the third trial they’ve had so far and 70% of the people do well. I didn’t ask how the other 30% do, but I said, “I’m going to try it.”
He asked me a bunch of questions, which was always interesting because they asked me these questions all the time. Do you have bone pain? Do you have sweats? Do you have this? Do you have that? I said, “I don’t have anything. If you didn’t tell me I was sick, I would just think I’m old.”
The drug seems to be working for 70%, is what he told me and 70% is pretty good if you ask me.
Deciding to Join a Clinical Trial
I know from my experience that a trial is what it says, it’s a trial. They don’t know what the answer is going to be. They’re going to take the results and compare it at the end. That’s what it means to me.
I said, “The transplant is not the answer. I don’t want that. What other option is there?” They said this is the option and this is what I did.
The paperwork was pretty much done by Mount Sinai. I had to sign at the end. I don’t remember what the details were.
Everybody’s going to be different. The trial is a trial. The drug seems to be working for 70%, is what he told me and 70% is pretty good if you ask me.
Joining the Pacritinib Clinical Trial
I started to do the trial. For the first year or so, the medicine was working but not working. I was producing red blood cells, but they weren’t staying.
I would get a transfusion and my hemoglobin would go up maybe one point per pint. If I went there with a 7, I come out and have a 10, but in 10 days, I’d be back to 7. That was what happened for a while.
All of a sudden, I had my last transfusion on September 15, 2021. Things started to kick in. My hemoglobin is now 14.9 and has been pretty steady between 13 and 14. Dr. Mascarenhas said I was famous in Mount Sinai and was like a poster child.
Pacritinib Receives FDA Approval
He told me the trial was going to end in January 2023. The drug got approved and is now known as VONJO. Everything was great. “But as of January 23rd, you’re off the trial,” he said.
Getting Financial Support for Treatment
I didn’t know how much the drug cost. I found out that it costs $22,000 a month. I got in touch with Mount Sinai and they gave me a grant.
Then I got in touch with the drug company and I qualified for an exemption. In case the grant isn’t good, the drug company will pick up the rest.
I’m under the assumption it’s for the rest of my life. This pill is keeping me alive so to speak.
Side Effects
For whatever reason, at one point in time, my spleen was getting bigger. I took this and then it shrunk by 65%. I don’t feel any different anywhere. He said I didn’t have to do anything. Maybe it’s the medicine. I couldn’t tell you, honestly. They told me it was large and then it shrunk.
They asked me about my food intake. I said it depends. Even up to now, some food tastes good and some food doesn’t taste so great to me. My appetite is good if it’s something that tastes good. If it’s something that I’ve had before and it was good then, sometimes it’s not so good now so I don’t eat as much.
I have a big appetite, but there are days when it doesn’t interest me to eat anything. It’s hard to say. Give me Italian food, I’ll sit and eat all day. Give me something else, maybe not.
With the hemoglobin and the platelets, my hemoglobin was at 5 and my platelets were at 2. Now my hemoglobin is at 14.9 and my platelets were 186 the last time I checked. But the platelets fluctuate. They’re not as steady as hemoglobin for some reason.
For whatever reason, at one point in time, my spleen was getting bigger. I took [pacritinib] and then it shrunk by 65%.
Being on Pacritinib Long-Term
This is my third year on pacritinib. They haven’t said, but I’m under the assumption it’s for the rest of my life. This pill is keeping me alive so to speak. My red blood cells have been pretty steady for almost a year and a half now so I’m thinking that the pill is the answer.
If I needed to have a transplant, I probably would have done it.
Importance of Seeing a Specialist
My primary care physician sent me to see an oncologist. I picked somebody based on somebody else’s experience who gave me some feedback as to where to go.
The oncologist and I discussed the scenario. He said, “You need to speak to a surgeon who does transplants,” and laid it on the line that this is what you need to do if you want to stay alive.
When I went and spoke to the surgeon, who was part of Dr. Mascarenhas’ team, he gave me a booklet to read and told me how the transplant works.
If I needed to have a transplant, I probably would have done it, but they gave me the clinical trial option and I decided to take it.
Be educated with what you have.
Being Physically Active
I do a Marcum Workplace run through my employer. I’ve also done a run for breast cancer. My wife had breast cancer so I’m all for the walk.
I’ve done a Michael Murphy Run in Long Island. I’ve done that for the last eight years. He was in the Navy and passed away in Afghanistan. He’s from our high school. Both sons went there and that place is loaded with Michael Murphy memorabilia.
I don’t run; I walk. I don’t walk as fast as I used to. I get there at 6:00 a.m. and park in the handicapped spot. I walk from the bus stop to the lake and go back and forth until I reach the four-mile mark on my watch then I stop. By then, it’s 8:00 a.m. The race hasn’t started yet and I’m already done. I can’t leave because all the roads are closed so I sit and wait, listen to music, or have a bagel.
Do exercise. Diet is another issue, but I think exercise is key to being in shape. If that helps you with this issue, God bless you.
Importance of Self-Advocacy
Go and check out the doctor that you go to see. Check out their credentials. Read the reviews. You might find some things that you don’t want to know or things that you want to know. It’s good to compare before making these decisions.
It’s important to be active. If somebody tells you something, you need to look it up and see what you can find. There are a lot of things out there. There are a lot of people out there who don’t know much about medical stuff and they listen to what somebody tells them. You need to be educated with what you have.
A Practical Approach to Disputing Cancer Care Expenses, Backed by Experts and Real Patient Experiences
Edited by: Katrina Villareal
Navigating the costs of cancer treatment can be overwhelming. This live conversation provides practical tips from experts and real cancer patients on understanding your health insurance, finding financial assistance programs, knowing your rights to appeal insurance decisions, and reducing financial toxicity.
In this conversation, we’ll explore the fundamentals of health insurance, emphasizing the importance of reading and understanding your policy, including basic insurance terms. Discover your rights as a cancer patient, learn strategies for appealing insurance decisions, and explore avenues for applying for financial assistance.
Hear from Abigail Johnson, a stage 4 metastatic breast cancer patient advocate, and attorney, Gregory Proctor, a multiple myeloma patient advocate, and Monica Fawzy Bryant, a cancer rights attorney and co-founder of Triage Cancer, as they share real-world experiences, health insurance tips, and strategies for tackling financial toxicity to help you navigate the financial aspects of cancer treatment. This live conversation took place in November 2023.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Abigail Johnson: Hello, everyone, and welcome to a discussion of how to dispute cancer care costs sponsored by The Patient Story and including representatives of patients experiencing this individually, as well as a representative from Triage Cancer.
The Patient Story’s tagline is Human Answers to Your Cancer Questions. Founded by a cancer survivor who took her love of storytelling and producing videos, they assist people in the cancer community to get that all-important peer support and information about how other people have handled something that you as an individual might be facing yourself.
Without further ado, I want to get to the amazing people that we have talking about this very human issue, which is getting your cancer care costs covered.
Gregory Proctor: My name is Gregory Proctor. I’m a multiple myeloma survivor diagnosed back in July 2021. In the early stages, it was very overwhelming and very impactful not only emotionally but physically. Coming from a project management background, one of the things was trying to figure out how to navigate.
Information is not easily found in a lot of cases because if you Google things, you tend to get the bad before you get the good. But overall, my professional experience as well as having friends and family to help me move this forward has provided an overall successful outcome.
I’m proud to say that I’m still MRD negative, thriving, in remission, and continuing to flourish and be an advocate.
Monica Bryant: My name is Monica Bryant. I’m a cancer rights attorney and co-founder and chief operating officer for Triage Cancer, which is a national nonprofit dedicated to providing free education on legal and practical issues that arise after a cancer diagnosis. We provide education to the individuals who have been diagnosed, their caregivers, and healthcare professionals who are often on the front lines of getting these questions.
Abigail: Thank you, Monica. Y’all wrote the book on cancer and the law. What’s the name of that again?
It isn’t written for lawyers because we wanted to make sure that it was written in a way that was accessible for anybody to be able to access it — whether it’s the person who’s been diagnosed, their caregivers, lawyers who are trying to help out, or healthcare professionals. It’s written in a way that anybody should be able to pick it up, regardless of whether or not they have a law degree.
Abigail: I enjoyed reading it very much.
Like Monica, I’m also a lawyer, and in 2017, I was diagnosed with stage 4 metastatic breast cancer. I was 38 and it was, to put it nicely, a bombshell that went off in our lives and has changed everything since that has happened.
I’m working on getting into a clinical trial, which will be my sixth line of treatment. With breast cancer, because it’s a solid tumor, we don’t go into remission. That’s not necessarily a status or a goal for us. It doesn’t necessarily apply to our experience.
There can be no evidence of disease or, in my case, no evidence of active disease. I have been able to get to that point at least once in the last six years but I’m back getting a new treatment. For us with metastatic breast cancer, we go from treatment to treatment to treatment. There are a few that can go off treatment for some time.
I’m learning to adjust to being a professional patient, I like to call myself, because managing cancer itself can be a full-time job and that’s why discussions like this are very important because our quality of life, and Gregory alluded to this, is very much tied to not just how the cancer cells are being controlled in our bodies by the medication but also impacted by how we can get to that treatment, whether it’s literal transportation to get to that treatment or being able to afford cancer treatment.
Here in the US, cancer is quite the machine in a lot of ways. There are a lot of different players and moving parts. Our goal is hopefully to illuminate some of those moving parts, at least when it comes to covering the cost of cancer care.
Managing cancer itself can be a full-time job.
Abigail Johnson
Health Insurance
Abigail: This concept of covering cancer care a lot of times boils down to insurance. In my experience, being on a private insurance plan through my husband’s employment as well as Medicare, the first thing that I always talk to people about is getting a copy of the insurance contract. That can be daunting for a lot of people because these contracts can be 200 or 300 pages long. They are written by lawyers and many clauses can be super complicated.
If this seems daunting, intimidating, and confusing, it is. It absolutely is. It is for the professionals that are working in this arena. Getting your insurance contract, whether you have a government-sponsored insurance policy, whether you’re working with the Veterans Affairs and have coverage there, whether it’s Medicare, some documents explain what is covered.
When it’s private insurance, it is a literal contract between you and the insurance company, and it spells out what they’re going to do and not do. In my experience, there are about 10 pages that are vital for me to know out of the 300-page long contract. I have those pages highlighted, bookmarked, saved, and written all over.
I continually go back to those pages to see the clauses and the language that govern what my insurance company is supposed to do. I set my expectations based on what my insurance company is supposed to do, and then I know if they have or not.
It’s important to know what tier your medication falls in because that impacts the cost of your copay.
Abigail Johnson
Many times, a medication, a surgery, or a procedure has to have prior authorization. The medical professional has to get with the insurance company and say, “We want to do X,” and the insurance company has to look over that and opine whether or not that is medically necessary. I won’t get started about how that is practicing medicine on the part of the insurance company, but that’s the system that we have.
My insurance company has 24 hours to respond to a prior authorization request from my medical team. That’s important for me to know because if there’s a delay, I can call the insurance company and say, “My doctor sent you a fax 48 hours ago. You had 24 hours to respond. This needs to rise to the top. You need to deal with this right away because you’ve not responded in the timeline that we anticipate.”
That’s one example of how knowing what my policy says, who’s supposed to do what, and when they’re supposed to do that helps me set my expectations. I’m not fussing at my doctor’s office if it’s not their responsibility and I’m not fussing at the insurance company if my doctor hasn’t done what they’re supposed to do. Knowing when they have not done what they’re supposed to do, I can bring that to their attention and that means that will become more of a priority for my insurance company.
It’s important to know what tier your medication falls in because that impacts the cost of your copay. These are examples of things that are important to know about your insurance policy so that you know how to navigate that.
Gregory: I’ve worked with a lot of attorneys in my professional career, but I’m not one. I have always been a professional. I make my premium payment and expect that coverages are going to be there when I need them. Until something traumatic or something like cancer knocks on your door, you don’t realize the implications that you’re faced with.
We contacted my insurance company and they said, “Okay, we’re going to be able to help you move and navigate through this,” with all of the empathy and compassion that they try to give.
I’m 2 ½-3 months into treatment. I’m paying my $1,000 premium and doing everything I need to do, but I’m burning $22,500 a week. The billing department for my oncologist calls and says, “Mr. Proctor, we’re at a point where you’re a quarter of $1 million. We’re going to have to stop your treatment. Your insurance company hasn’t paid.”
I’m sitting here flabbergasted. I’m trying to fight for my life. I’m several months into my treatment and my doctor hasn’t received a single dollar from my private healthcare insurance. At that moment, I realized it wasn’t just about me fighting cancer. Now I’ve got to engage in something that you expect would be covered.
For me and my family, we had to turn the switch on and get laser-focused. Now it’s not just about the financial implications, insurance, and survival. We’ve got to look at all three with a critical eye.
Having the knowledge and knowing what to do with that knowledge to be able to save your life, save money, and avoid some of those pitfalls is extremely important.
Gregory Proctor
I had to contact the insurance company and say, “I need to see the full contract. I need to understand why you guys are not paying my doctor.” Their reason at that time was, “We have to go through an audit, Mr. Proctor. You’ve been healthy. You’ve never had any type of circumstance like this come along and then all of a sudden, now you go from 0 to $22,500 a week.”
To me, that wasn’t an excuse. I said, “I’ve never missed a premium. I’ve never missed a payment. I need this to occur for me on my behalf because I’ve done what I needed to do.”
Everyone comes from a different walk of life and sometimes knowing what to do as well as knowing how to do it becomes extremely important. One of the things that was formidably important for my wife and me was taking all of my project management experience and applying it to myself as the project so that we could cover all of the gaps.
As they always say, knowledge is power. In this particular case, having the knowledge and knowing what to do with that knowledge to be able to save your life, save money, and avoid some of those pitfalls is extremely important.
In most cases, those are not things that you think about when you’re thrown into the tsunami of cancer. You’re thinking how to get from day to day, from week to week. There’s a lot more involved and it all embodies getting yourself educated.
Abigail: Thank you for all of that, Gregory. You’re coming to this with all of the information and experience that you have. You’re going to do it as a project manager because that’s your background. Who you are, your strengths, and how you solve problems is going to be key.
Understanding Insurance Terms
Abigail: Monica, what are the top things that patients need to know when they’re looking at their insurance contract or how to get cancer care covered?
Monica: There are some things that people really should understand about their insurance long before there’s ever a diagnosis or a serious medical situation. But the unfortunate reality is that in this country, health insurance is confusing. There are going to be differences depending on the source of that insurance, whether that’s government insurance, through an employer, or a policy someone purchased on their own.
Based on studies that have been done, only about 4% of Americans understand the four most common terms used in health insurance policies. People don’t even understand the words. We’re not even talking about complex legalese here. We’re talking about the basic words because we’re never taught what those words mean.
There is an amount someone pays monthly to have health insurance and that’s the monthly premium. They’re going to pay that amount whether they go to the doctor or not. It’s like having car insurance all year but never getting into an accident.
Once someone starts utilizing their health care, there are going to be some additional costs and those costs are going to depend on the policy. Most policies have an annual deductible, a fixed dollar amount that someone has to pay before health insurance kicks in. Someone could have a $500 deductible or a $5,000 deductible. It’s all going to depend on the plan.
Once they’ve met that deductible, insurance kicks in and pays a percentage. That percentage is referred to as the cost share or the coinsurance. Here’s where it gets tricky because we have multiple names for the same thing. Cost share and coinsurance are the same thing, and that’s a percentage. If someone has an 80/20 plan, once they meet their deductible, insurance kicks in at 80%, but they’re still responsible for 20%. And when the treatment is expensive, 20% is still a huge dollar figure.
Based on studies that have been done, only about 4% of Americans understand the four most common terms used in health insurance policies.
Monica Fawzy Bryant
In addition to that percentage, many plans have copayments, which is a fixed dollar amount that is going to depend on the policy and also potentially on the service. Someone could have a $25 copayment to see the doctor, a $35 copayment to see a specialist, or a $250 copayment to go to the E.R. Figuring that out could be complicated.
The most important thing for every single person to know about their health insurance policy is if there’s an out-of-pocket maximum and what is it. Because in theory, that’s the most that someone is going to pay out of pocket for their care if they go to in-network providers for the year.
Understanding that allows us to figure out what you are going to have to be responsible for out of pocket in a worst-case scenario. The way you get to your out-of-pocket maximum depends on the plan, but often it involves adding up everything you’re paying towards your deductible, your copayments, and your coinsurance. It’s everything you’re paying out of pocket except the monthly premiums.
The reason this is so important on the front end is when people are making choices around their health insurance. We have the opportunity to do that every single year now, thanks to the Affordable Care Act and a whole bunch of other laws.
To be an effective shopper and consumer of health insurance, you have to understand those terms and be able to do the math concerning your out-of-pocket maximum.
Gregory: For me, that’s key. I always maintain a pretty healthy lifestyle. I don’t want to have to come up with $15,000 as a deductible. If I’m healthy and I still feel pretty good, I can go with a little less coverage. You take a little bit more risk.
I was diagnosed at the age of 50, which was not the best year to be diagnosed with multiple myeloma. The older I got, I began to get laser-focused in my mindset as it relates to my family of four and my insurance.
At the age of 50, I’m more susceptive to all of these things that maybe I don’t want to think about, but I need to be in a position to ensure that I’m covered holistically without any repercussions.
Abigail: It’s amazing how expensive everything is. One of the things about cancer treatment is the medication and prescription drug costs, which can be complicated. When you’re put on medication by your doctor, they don’t always tell you the price tag upfront. In the breast cancer world, many of the medications that we take will cost our insurance companies between $14,000 and $20,000 per month.
Copay Assistance Programs
Abigail: In the context of private insurance, there are often copay assistance programs, which pharmacists will often help patients apply for. These programs are offered by the drug manufacturers or pharmaceutical companies. They will also have foundations sometimes. But depending on your insurance, these programs apply differently.
For myself, having a private policy means I’m eligible for copay assistance programs. Those copays go from hundreds of dollars a month to zero, oftentimes depending on which tier of medication you’re on.
My friends who transitioned to Medicare are surprised to notice that those copay assistance programs are not always possible when you’re on Medicare and that’s where those foundations do come into play as well.
Gregory, how has that affected you in terms of paying for your medication and working with the VA, where your primary insurance is?
Gregory: I was in a unique category. I had private healthcare insurance with a national provider when I was first diagnosed. I had been away from the government programs for many years. Since I’d gotten out of the Navy, I hadn’t utilized any of their benefits.
I started going through this process and all of this funding that you don’t account for starts to show up at my doorstep. Blood work for $16,000, a test for $15,000, and I wondered what insurance is truly covering if these bills are showing up.
I was very lethargic and incoherent for five days a week for three and a half months because I was on chemo for five days a week, 6 to 8 hours per day, which was tough.
Once I finally got to the point of reckoning and saying it was time to get a hold of this situation, I found out that there are subsidy programs. Sometimes they’re publicly known, other times they’re not, particularly if you don’t ask. We started pulling our energy into how could we tap into maybe a program to be able to give us a grant and move forward.
On record today, I’ve spent $2.65 million. Navigating that journey was not easy… It’s overwhelming. You’ve got to get other people involved to help be your eyes and ears
Gregory Proctor
With private healthcare, there’s a little bit of leniency. By the time I was approved for government healthcare being a prior veteran, I couldn’t utilize those programs. It was a very delicate balancing act to ensure that going forward, I would be able to reap all of the potential benefits that I could not afford out of my pocket to maximize my overall primary care going forward.
Because on record today, I’ve spent $2.65 million. Navigating that journey was not easy. But certainly, you have to get laser-focused because no one is going to do it for you.
It’s overwhelming. You’ve got to get other people involved to help be your eyes and ears, to help address the questions of who, what, where, when, and how. Sometimes when you’re getting information from the doctors, you don’t want to accept the reality. Acceptance is always the key to making the first step in the progress of being able to battle and weather the storm.
Abigail: You have personally spent $2.65 million or your insurance company has spent that?
Gregory: I love to throw that number out there because people always say, “Oh my, what happened?” For clarification, that’s the running total. When you think about that number and go back to what Monica said. Whether you’re 70/30, 80/20, or 60/40, part of that expense is coming from you as the patient.
When you step into the throes of dealing with cancer, these are the things that you have to get laser-focused on very early on. Are you going to be successful coming out of the back side of this? Are you going to be bankrupt or dealing with the overall financial toxicity of what it does to you and how it changes your life?
Abigail: Thank you for that. Those are big numbers. Mine’s a little over $3 million so I’m tracking with you. I have not spent $3 million keeping me alive, but certainly between my family and the insurance company.
Monica: Thank you for your service, Gregory. I’m glad that the VA was helpful in this process for you because it’s deserved.
Financial Assistance for Cancer Patients
Abigail: Monica, would you like to talk a little bit more about financial assistance and how patients can go about getting help to cover their portion of these costs?
Monica: With respect to getting financial assistance, I would say don’t start there. That should not be step one when you see the big bills come in because there isn’t a whole lot to go around. As you both alluded to, there are some barriers depending on the type of insurance that somebody has.
Before someone goes down the path of trying to apply for financial assistance, there are some steps to take. Did the insurance company cover what they’re supposed to cover? That requires making sure you’ve waited until you’ve gotten your explanation of benefits, which is the letter from the health insurance saying this is what we’re going to cover and this is what you potentially owe. It’s about keeping track of your out-of-pocket maximums.
If someone understands what their out-of-pocket maximum is and what’s included in their out-of-pocket maximum, it can help them figure out how much they need from financial assistance. A lot of times, people get those prescription drug bills and don’t realize the prescription drug benefits are included. It doesn’t matter what their insurance company will pay or not. If you’ve hit your out-of-pocket maximum, they’re responsible for 100% of it.
Unfortunately, some additional steps fall into the laps of patients and family members before getting financial assistance.
Do a deep dive into what’s out there and what’s available. Even among the pharmaceutical companies, there might be different programs.
Monica Fawzy Bryant
With financial assistance, oftentimes people get tunnel vision when they’re thinking about sources of help. Abigail, you mentioned how expensive your monthly prescription drug is.
How am I going to get money? How am I going to get assistance to pay for that prescription drug? I’m on Medicare so I don’t have access to the same pharmaceutical programs that I did. What am I going to do now?
Are there other places you could potentially get help? Could you get mortgage assistance, utility assistance, or other types of financial assistance and then shift the money around? Anything that you set aside to pay for the mortgage or student loans can get shifted to help pay for prescription drugs.
Do a deep dive into what’s out there and what’s available. Even among the pharmaceutical companies, there might be different programs. Some companies can provide free drugs, some companies can provide assistance to pay copays. They all have different programs. Figuring that out is daunting.
AtTriageCancer.org, we have a chart that lists most of the major cancer drugs, the pharmaceutical companies that make those drugs, and the various programs that they have to try to make it a little less daunting to go down the Google rabbit hole because that is stressful by itself.
You can look for other types of financial assistance or grants that might be out there based on the type of cancer you’ve been diagnosed with. Sometimes there’s even financial assistance for family members who might be acting as caregivers. We have a tool called Cancer Finances that has pulled those resources from trusted sources to make it a little easier. It’s still not easy but a little easier for people who are trying to seek out those sources of financial support.
Abigail: Great resources. I have sent so many people to Triage Cancer. If you have a Sam’s or a Costco membership, you don’t even use insurance when you go to your wholesale clubs. For a medication that I was previously on, my copay was $15, but if I got it without using my insurance company, it was $20, which boggled my mind. Unfortunately, that puts a whole lot of burden on the family to figure out some of those things.
Gregory, did you ever get assistance from a social worker to help you figure some of these things out? Was that something that was offered in your oncologist’s office?
The life that you know before and after cancer is totally different. Asking questions could be the differentiator in a lot of the things that we’re talking about.
Gregory Proctor
Gregory: Not in my oncologist’s office but as I was getting prepped for a stem cell transplant. As a patient, it is important for you to ask.
Seek out and ask as many questions as possible. What do I need to do? How do I need to do it? What resources? What assets? Even if your doctor doesn’t want to give you the answers, you need to continue to perpetuate that going forward because it’s your life. The importance of survival doesn’t have a price tag.
I looked at everything. My wife and I flipped everything upside down because, at that point in time, your life is already flipped upside down. The life that you know before and after cancer is totally different. Asking questions could be the differentiator in a lot of the things that we’re talking about.
Abigail: Thank you for saying that. I talk to so many patients all the time who are worried that asking questions might be offensive or upset their healthcare providers. While that is certainly a good human thing to think about, in a situation like cancer, it’s your life on the line so ruffling a few feathers doesn’t seem to be as important as getting the answers.
Appealing Insurance Decisions
Abigail: I want to talk more about denials or when the insurance company is asking for your doctor to jump through some hoops. I talked about prior authorizations. What happens when an insurance company says, “No, we don’t think that that is medically necessary,” or like in Gregory’s situation, “We need to examine this a little bit more,” that sort of thing?
I want to throw out a couple of things that I’ve learned along the way in dealing with private insurance. Typically, when a doctor gets prior authorization, the insurance company says no. Usually, you, as the insured, get a letter that says why they denied it. Your doctor typically gets the same letter. And then what?
Besides changing your mind and doing something different that your insurance company goes along with, in my experience, what’s next is your doctor has the opportunity to do a peer-to-peer discussion. This is covered in all the insurance contracts that I have seen, along with the definition of what a peer is.
Very early on in my cancer treatment, my doctor wanted to do a PET scan. For those of us with solid tumor cancers, PET scans are often the gold standard in terms of seeing where the cancer is and how metabolically active it is. This is a tool that doctors need to be able to make good decisions.
A doctor employed by my insurance company, who was a family doctor about five years out of medical school, deemed the PET scan not medically necessary.
By looking at my insurance policy, I learned that my insurance company was required, upon my asking, to provide a peer to my doctor. I realized that somebody who’s five years out of medical school, who has a small amount of experience, and who is in a specialty that has nothing to do with oncology does not meet the definition of a peer.
I learned that I could say to my insurance company, “I require you to provide a peer to talk to my doctor.” That conversation took five minutes.
In the first conversation where it was denied, my doctor spent 40 minutes trying to convince this doctor employed by the insurance company that what she was doing was standard of care. When she was able to talk to an oncologist — not an oncologist that had 30-plus years of experience, but somebody in the cancer world — it was a five-minute conversation and it was approved.
The first person that my doctor talked to was looking at a chart and the wrong category. She was looking at somebody who was stage 3 versus stage 4.
I’ve let my doctor’s offices and their staff know as they are scheduling that they can ask for a peer. Make sure it’s a peer who’s talking to your doctor.
By looking at my insurance policy, I learned that my insurance company was required, upon my asking, to provide a peer to my doctor.
Abigail Johnson
By looking at your insurance policy and understanding the definition of a peer, that one small thing can save your doctor time. That 40-minute conversation took my doctor away from seeing patients. The five-minute conversation was a whole lot more effective and efficient.
As an insured, you also have the option of filing an appeal. It can get involved and it’s a really heavy lift when it comes to attempting to explain to your insurance company why they are not following the contract.
Gregory, what experiences have you had in getting something covered, especially when you got that initial no?
Gregory: After burning $22,500 a week and hitting a cap, hearing the words, “We will cover this, but we won’t cover that,” meant, “We’ll cover you for the period of your transplant. However, if there are any complications, then that’s on you, Mr. Proctor.”
Going from my private healthcare and trying to get the VA to pick me up had already been denied by the VA. It was very frustrating very early on knowing that I would want it to go through the VA from the beginning, but I was denied and that’s just how the system works.
Their rationale was there was no service-related tie that could tie back to me being diagnosed with cancer. I had to get attorneys involved and justify what my job and MOS (military occupational specialty) was in the military. Going through that took a tremendous amount of time.
You can’t ever give up. You have to continue to push.
Gregory Proctor
For me, one of the things that I had to sink into throughout this whole journey is don’t ever give up. Find a will. Find a way to navigate. I had to go back through all of the tests to prove that I had multiple myeloma.
Once we proved that, I was able to get 100% coverage but that took approximately five months from the time that I was diagnosed up until I was getting ready to go into a stem cell transplant.
The best Christmas gift that my wife and I could have ever received in December 2021 was that letter from the VA saying they are now my primary healthcare provider and they will cover not only my stem cell transplant but all post-maintenance costs. We’re talking, “Hallelujah!”
That was well worth all of the effort, the headache, the anxiety, the concerns, and the worries to get to that point. But like I said, you can’t ever give up. You have to continue to push.
Abigail: Thank you for those reminders. It’s easy to give up, especially when there are a lot of roadblocks. I love how you mentioned that you realized you needed help and that getting a professional involved was important.
Legal Rights as Insurance Consumers
Abigail: Monica, would you talk a little bit about the legal rights that we each have as consumers and talk about those appeals and what services might be available to patients?
Monica: Gregory did a little bit of my job for me in that we don’t have to take no for an answer. The details around that will certainly depend on the type of insurance we’re talking about, whether it’s the VA, Tricare, Medicare, or Medicaid.
If we’re talking about private insurance, at the bare minimum, every single consumer is entitled to at least two levels of appeal. The first level is an internal appeal and that’s essentially where we go back to the insurance company and say we’d like you to reconsider.
The internal appeal can take a couple of different forms. It could be a written internal appeal where you’re providing documentation. It could also be what Abigail was referring to, which is a peer-to-peer conversation between two healthcare providers.
There are time limitations on when we as consumers get to file internal appeals. We usually get 180 days. Then there are time limitations on the insurance company to give a response depending on where somebody is.
In Abigail’s example, it was a denial of a prior authorization so the insurance company has to answer within 30 days. If you’ve already received the service and they’ve come back and said, “Nope, we’re not covering that,” then they get 45 days.
Here’s the problem. When we’re talking about cancer care specifically, a lot of times we don’t have 30 or 45 days to wait for an answer. What we as consumers need to understand is that we have the right to ask for an expedited appeal when the need for care is urgent, which it is in most cases when we’re talking about cancer care. The insurance company then has to answer within 72 hours. But people don’t know this. People don’t understand that they have this right.
If the insurance company ultimately comes back and still says no, we have the right to an external appeal and that’s where we go to an independent entity. It’s going to vary from state to state, but an independent entity will look at all the facts and all the medical evidence, and then make a decision as to whether or not the care is medically necessary.
People need to understand those words, medically necessary, are the legal standard on which the appeals will be decided. Is it medically necessary for you to get that service? The decision of the independent entity at these external appeals is binding on the insurance company.
We don’t have to take no for an answer. The details around that will certainly depend on the type of insurance we’re talking about
Monica Fawzy Bryant
I made it overly simplistic for this session. I understand that requires a lot of legwork and effort to get the doctors involved. I’m not minimizing any of that, but here’s what we know to be true.
Of the millions of claims that are denied every single year, 99.9% of them are never appealed. Yet we also know that when people do appeal, somewhere between 40 and 60% of the time is decided in favor of the patient.
When we’re talking about how to help people afford cancer care, I want to talk about appeals long before we get to financial assistance. If insurance is coming back and saying, “We’re not going to cover that,” for whatever reason, “You’ve hit your max,” “We think you’re too expensive,” “We don’t think you need your PET scan,” if you’re not appealing those denials, you’re essentially leaving money on the table.
Abigail: That is such a great point. When your insurance company knows that you will appeal and will not take their decision lying down, in my experience, they’re much less likely to deny things in the future. It’s really important to make it hurt and make it difficult for them.
I’m not talking about doing anything drastic. Take up a lot of their time. Be bold in saying what you need and in filing those appeals. In my experience, they typically won’t be as likely to deny something in the future.
Thank you for giving us those numbers, Monica, because those are shocking numbers, like the millions of dollars that Gregory and I were talking about earlier.
I’m going to do whatever it takes because I’m all about living. I still have a lot more life to live than to let cancer dictate and determine how that’s going to be for me.
Gregory Proctor
Monica: It’s also helpful to put into context for people who are already overwhelmed. They’re reaching capacity in what they can handle. They’re trying to survive. Now the lawyer is saying to go through this burdensome appeals process. The numbers are helpful, particularly around the number of successful stories, to make that additional burden almost worthwhile, so to speak.
Gregory: That’s the main reason why my mantra going through this was don’t ever give up. There’s got to be a will. There’s got to be a way. It may not be door A, it may be door B or door C, but you’ve got to keep asking those questions and ensure that you’re getting the answer that you need to move forward.
When my life’s at stake, it doesn’t matter to me if it’s $1 billion. I’m going to do whatever it takes because I’m all about living. I still have a lot more life to live than to let cancer dictate and determine how that’s going to be for me.
Financial Toxicity
Abigail: I want to talk about financial toxicity. We’ve thrown that word around a couple of times. I didn’t realize this, but in 2013, it was researchers at Duke University that coined the term financial toxicity to describe the financial hardship and distress that can result from the high cost of cancer treatment.
Their research showed how the burdensome out-of-pocket expenses associated with cancer care, such as copays and deductibles, can negatively impact a patient’s mental health and quality of life, leading to increased anxiety, stress, and depression.
We hear all the time that stress is not good for patients. Stress is not good because it changes chemical things in your body. It makes your quality of life more difficult when you are stressed out. Then here comes our medical system that causes stress on us.
Gregory, how have you handled the mental toll of those bills and the financial stress? How do you handle that emotionally, too?
At one point in my life, I was questioning whether or not I would be able to afford groceries that week. That’s when you know the toxicity has gotten hold of you.
Gregory Proctor
Gregory: You’ve got to be willing to accept that this is your reality. That’s the first step in going forward with any type of traumatic or life-altering things that are happening.
The other aspect that became very, very important for me personally was stepping away from the notion of dealing with cancer 24 hours a day, seven days a week. One of the most therapeutic things that I did during my cancer battle was getting out in nature, walking on the trails, and separating my mind from the overall objective of having this wreak havoc on me.
With all of the debt and bills coming in, your life still goes on. You still have your normal expenses and now you’ve got cancer expenses and all these other things that happen. At one point in my life, I was questioning whether or not I would be able to afford groceries that week. That’s when you know the toxicity has gotten hold of you. You’ve got to navigate and weather the storm to figure out how to maneuver and move forward.
I’ve done a lot of things to get through that and find assets and various other elements in my life that I could move forward without having so much of the burden of the debt wreak havoc on me.
Abigail: Thank you for sharing that. I tell my medical teams all the time that I have to fit cancer care into my life not fit my life into cancer care. It’s a paradigm or a different way of looking at things that I think makes us as patients address some of these things a little bit differently.
Monica, would you talk a little bit about resources that Triage Cancer has or strategies for managing medical bills and finances so that people can have a good quality of life?
Monica: It’s at the core of what Triage Cancer is about. We have tons of educational resources in a variety of formats because we’re trying to meet people where they are and how they learn. Some people are big readers and that’s how they’re going to absorb information so we have quick guides and longer practical guides that can be downloaded and read off our websites.
We have live events that people can join for free, both in person and virtually. We also have worksheets, animated videos, and other materials to help people with things that can contribute to financial toxicity.
Health insurance status and navigation are only one piece of the puzzle. Certainly, employment changes that can occur after a diagnosis are going to impact somebody’s finances. Everything that normally happens in life that impacts finances keeps happening. You don’t get a pause button on paying the mortgage.
When you look at TriageCancer.org, you will see a variety of topics around health insurance, employment, and disability insurance to address holistically the financial impact that cancer and cancer care can have on people. When thinking about how to maximize health insurance, people need to remember a couple of things.
Every single year, we have the opportunity to make choices. If someone is experiencing high out-of-pocket expenses due to their insurance this year, there may be opportunities to pick a different source of insurance for the coming year.
Open enrollment for Medicare is coming up at the end of the year and that’s an opportunity to make some different choices — whether that’s finding a plan with a lower out-of-pocket maximum, a plan that has more of your providers in their network so they’re being covered at higher rates, or has a different prescription drug formulary so any prescription drugs you’re taking may be covered at a better rate.
You may be experiencing high financial toxicity right now based on the type of insurance you have, but there may be opportunities to make those changes for the coming year. We have resources at Triage Cancer to help you make those determinations.
When you look at TriageCancer.org, you will see a variety of topics around health insurance, employment, and disability insurance to address holistically the financial impact that cancer and cancer care can have on people.
Monica Fawzy Bryant
We also have a legal and financial navigation program where people can fill out a form and they’ll get a calendar link where they can schedule a call with one of our staff. We’ll talk through their situation and the sources of financial toxicity. We’ll try to provide them with personalized education and information about what they need to know and understand, point them in the right direction, and give them action steps. You can read quick guides all day long, but you may still have questions about your situation.
Abigail: Those are wonderful resources. I’ve sent all kinds of people to Triage Cancer and they’ve helped them figure things out and navigate those things.
Since Monica was talking about open enrollment and the possibility of adjusting your coverage, working with a good insurance broker can also be a tremendous help, especially when you’re going on Medicare. There are all these supplements and different options. Working with somebody who can take your situation, your doctors, your medication, and your diagnosis, and help you back into those policies that would meet some of those needs.
Typically, brokers are paid by the companies so you are not out of pocket any amount of money when you work with an insurance broker. That’s one thing that I suggest to a lot of people, especially those transitioning from private insurance to Medicare because it can be complicated with all of the different supplements.
Monica: I actually would give the opposite advice to somebody and that’s based on reports that have come out of the U.S. General Accountability Office. Over the last several years, many insurance agents and brokers have misbehaved in several ways. Now, certainly, that is not all of them. There are wonderful insurance agents and brokers out there so I’m not disparaging the profession as a whole by any stretch of the imagination.
Oftentimes, people can be led down a path that may not be the best for them. Those agents and brokers are paid by the insurance companies so they have a vested interest in enrolling people in specific insurance policies, even if those aren’t the best policies for that patient.
For the cancer community, where there is a heightened importance of making sure they are in the right plan for them, we would suggest unbiased sources of support and there are different places that people could go.
You might get a very different answer from an insurance broker versus a social worker who is employed by your cancer center. Getting different input can be important.
Abigail Johnson
If someone is transitioning to Medicare for the first time, every single state has a SHIP program, which is the State Health Insurance Assistance Program. They’re called different things in every single state. They are trained to help people navigate their Medicare options and they are unbiased. They do not get paid by enrolling people in one plan over the other.
For people who are buying insurance in the marketplace, there is a similar entity called In-Person Assistors. Again, they are paid by the government not by the insurance companies so they don’t have any bias as to putting people in one plan over the other. I agree with your sentiment about seeking help and support in picking those plans, but I’m not sure that’s the place I would send someone for support.
Abigail: That’s why we’re having this conversation to talk about different perspectives. I work with a handful of insurance brokers who I have personally vetted and are now familiar with metastatic breast cancer because they’ve assisted a lot of people that I have worked with. Having those connections and knowing if there are people in your community who are doing some of these things can be key.
But thank you for that caution, Monica, because that’s also important to remember who you’re talking to and who they’re employed by. You might get a very different answer from an insurance broker versus a social worker who is employed by your cancer center. Getting different input can be important.
Gregory: You have to educate yourself. You have to go through due diligence to ensure that you understand your situation. I’m more aware of my needs now going forward as opposed to before because it was something that I wasn’t interested in. Make sure that you educate yourself and do your due diligence because those two things can save you thousands of dollars going forward.
As we’re navigating this system, how we embody that power can make a big difference in navigating cancer treatment.
Abigail Johnson
Empowerment
Abigail: The word empowerment gets thrown around a lot. We need to understand how we’re looking at empowerment because there are multiple definitions of empowerment.
One definition, that makes me itchy, is that somebody is giving you power. The second definition, which doesn’t make me as itchy, is that we all have inherent power as people and as patients. As we’re navigating this system, how we embody that power can make a big difference in navigating cancer treatment.
Gregory, how do you look at empowerment? How have you gotten in touch with your power as an individual and as a patient?
Gregory: When I was diagnosed, I realized the importance of my purpose in life and the importance of rekindling my faith in the Lord Jesus Christ. My empowerment came back through not only my connectivity to my spirituality but also through my family, friends, and the congregation of people who follow me on social media who were there to lift me.
I took that empowerment and tried to be a beacon of hope and inspiration, uplifting people’s minds and souls when they go through a horrific experience, and letting them know that they’re not in this alone. There’s unconditional love out there, even if you get that unconditional love from a stranger who gives you power and uplifts you to be able to weather the storm and be able to move forward.
Abigail: Thank you for that, Gregory, that was beautiful. Monica, would you like to chime in on this whole idea of empowerment and how that fits in with what Triage Cancer does?
Monica: It’s not my job as a cancer rights attorney to give somebody else power because that power is theirs. But what I can hopefully give people is the knowledge that they need. Knowledge is power.
You shouldn’t have to have a law degree, a project management background, or a million people surrounding you and lifting you to be able to survive this disease with your homes intact, your jobs intact, your insurance, and overall financial health. Yet, unfortunately, because of our system, sometimes that is what’s needed. We want to walk side by side with people and support them through education and providing information so that they can then take that and use their power.
I took that empowerment and tried to be a beacon of hope and inspiration, uplifting people’s minds and souls when they go through a horrific experience, and letting them know that they’re not in this alone.
Gregory Proctor
Gregory: That’s very, very powerful. As we talk about education, you need to seek others who have endured and weathered the same storm that you’ve gone through. A lot of times, people say that may not be a good idea or maybe that is a good idea.
For me, that became one of the circumstances that my wife and I were able to glean from others who are five-year survivors, 10-year survivors, and 20-year survivors and understand how they made it that far. Of course, now drugs and everything has changed, but knowing how they weathered the storm became a tremendous, valuable lesson for us.
Abigail: That’s a wonderful comment, Gregory, this idea of seeing examples of other people, which is what we’re doing and what The Patient Story does all the time as well.
Key Takeaways
Abigail: Know who you are. Allow your strategies and how you figure out how to pay for cancer to flow from who you are. You’re doing something that’s not you. It’s not going to work so well so know who you are.
Knowledge is power. Knowing how to navigate things, knowing the right things, and sticking to your guns in that context can be extremely helpful.
Don’t take no for an answer. Keep going. Keep pushing. Keep asking questions.
Don’t forget to ask for help and collect those people who you can ask so make sure that you’re saving the link to Triage Cancer, which is TriageCancer.org.
Watch for other patients who are navigating this, jot their names down, and know that you might be able to reach out to those people for help. That list can include social workers, nurse navigators, and professionals who do these things that you’re trying to do.
Vote with your feet. When your insurance policy doesn’t cover what you need, vote with your feet. If your doctor is not going to bat for you and not going to do that peer-to-peer discussion, vote with your feet. If you know that medication is way too costly and there’s an alternative, vote with your feet.
We have these choices and to vote with our feet can be extremely helpful and maintain that quality of life to fit cancer care into our lives versus the other way around.
Knowledge is power. Knowing how to navigate things, knowing the right things, and sticking to your guns in that context can be extremely helpful.
In 2019, Paul received a shocking diagnosis of prostate cancer after a routine check-up uncovered a Gleason score of 4+3. Reeling from the news, he underwent radical prostatectomy surgery.
After connecting with a prostate cancer support group, Paul was able to make sense of treatment options and find emotional support. But two years later, a follow-up PSA test revealed rising levels, indicating his prostate cancer had returned. This relapse encouraged Paul to research integrative medicine techniques and shift his mindset with mindfulness practices as active parts of his healing journey.
Now in remission following radiation and hormone therapy, Paul took to writing for Medium where he shared his cancer journey and the lessons he learned along the way. He now shares his story with us and discusses how changing his mindset and focusing on positivity has helped him on his healing journey.
Paul’s story is part of the “Our Voices, Our Power” series by The Patient Story. Discover more of the series by exploring Tim’s stage 1 prostate cancer story.
Thank you to Janssen for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I grew up outside New York City, in suburban New Jersey. I was an athlete and an editor of my school paper.
I decided I wanted to go to college in California, so I went to UC Santa Cruz, 2,000 acres of rolling meadows and redwoods overlooking Monterey Bay. I invented my own major called The Politics of Mass Media. I was a disc jockey and had a sports show on the radio station.
After graduating, I realized there were no media jobs in Santa Cruz, so I went back to New York City to start my career.
I was highly motivated. This was the 70s, so there were plenty of other highs as well. I wanted to explore different things. I knew what I liked. I loved sports and I liked writing.
Being a Storyteller
I jumped from the radio to CNN when it was first starting. I went down to Atlanta where it was going to be the first 24/7 station. I was hired as a writer. Within a week, I became a producer and a producer anchor within two weeks. At the time, that was the way CNN was because they didn’t have enough people.
I learned to become a storyteller in the video medium. I ended up doing high-end corporate videos and nonprofit videos, so I had to learn how to tell those stories as well.
After 40-plus years of being in media, I consider myself — and I say this with humility — a master storyteller. I’m still working on my craft.
I was probably telling stories when I was a child, too.
The great gift is not only being loved but giving love.
Meeting My Wife
In 1988, I was in Central Park riding my bike approaching Strawberry Fields at 72nd Street. I saw this young woman, Wendi Messing, lacing up her roller skates and when she got up, I sidled up next to her and said, “Are you going to Disco Heaven?” This was a place near the volleyball courts where everybody skated around with giant boom boxes. She’d never been there before. It wasn’t a truth or dare moment, but I pushed her a little bit, so she went up there and skated around having a grand old time.
I was riding my bike around, but I was watching. When she left, I rode behind her and threw out a line. She bit and I reeled her in.
We sat and talked. She was an advertising producer. We were both cutting videos to the song Hot Together by the Pointer Sisters. Talk about serendipity!
We made a date to get together. As the months went on, the other thing we found out was we didn’t want to live in New York anymore. We ended up in San Francisco and started from there.
I had been a serial dater. I was in my mid-30s at that point. They said she was the kind of girl I wanted to marry. She was hard-oriented, sweet, and really cute. We were in the same business. We were both Jewish. A lot of things lined up.
The great gift is not only being loved but also giving love. I think in some ways, we want that even more. I feel that with my dog. As much as they say, “Dogs give unconditional love,” we also give them unconditional love back.
I won’t use the word “caretakers.” We’re givers. I tell Wendi, “I never come home without something for you.” I’m always thinking, What could I bring her? I know she was always looking out for me.
When I was diagnosed with prostate cancer, I realized that I had gone from living a normal life to now all of a sudden, I’m in a club I never wanted to be a member of.
I realized that I had gone from living a normal life to now all of a sudden, I’m in a club I never wanted to be a member of.
Pre-diagnosis
Initial Symptoms
I went to a regular checkup and during the rectal examination, the doctor said he felt something. I didn’t know what to think. I didn’t think it was good, but I didn’t think it was terrible. He sent me to a urologist and said, “I feel something there. Let’s do a biopsy.”
I started to worry a little bit. Biopsies are not fun. They’re very invasive. They go in through your urethra and take samples. I was really sore afterward.
Diagnosis
Getting the Official Diagnosis
About a week later, I was in my car after a workout. I got a phone call from the urologist and he said, “You have prostate cancer.” That’s the minute your life switches.
Reaction to the Diagnosis
I was in shock. I was 63 years old, super healthy, and ate relatively well. I have a sweet tooth, but I didn’t have a lot of high-risk factors. There wasn’t a lot of cancer in my family.
Later on, I found out that two of my uncles had prostate cancer. It was like a kick in the balls, no pun intended. I was stunned. When I told Wendi, I knew immediately that she would be there for me 100%.
I had gone from living a normal life to all of a sudden being in a club I never wanted to be a member of. I’m young, I’m healthy, I eat well, and I exercise. How is this happening? It doesn’t sink in right away. You know that life will never be the same again.
I figured that, for now, I’m going to keep this to myself.
Choosing Who to Share a Cancer Diagnosis With
I’m a very private person. I have a few really good friends that I will tell almost anything, including women, friends, and couples. Unfortunately, both my parents had passed by then. Actually, that was probably fortunate because I know they would have worried so much.
My older brother had frontal temporal dementia and had passed, so it was only my younger brother who knew. I didn’t want to go through it with Wendi’s family. My thing is once you tell everyone, it’s out. You can always decide later on who you want to share it with and how.
I remember reading an article in The New York Times that said the way people react to news about cancer can be very draining for the person who’s sharing the news. They may ask a lot of questions, including a lot that you don’t know the answer to. They may offer advice that you really don’t want to hear.
Everybody knows somebody other than their family or friends who’s had cancer, but if someone’s had breast cancer, leukemia, or lung cancer, it doesn’t relate to prostate cancer. Sometimes people say things that are inappropriate and I didn’t want to go through that.
I figured that, for now, I’m going to keep this to myself because my Gleason score was 4+3. That’s a whole thing in itself. You start learning all these numbers — Gleason scores, quadrants of your prostate capsule, different kinds of reports, and genomic tests. It’s overwhelming.
They couldn’t find anything. That was encouraging… On the other hand, if you don’t know where it is, how are we going to treat it?
What the Numbers Meant
One of the first things I heard was that prostate cancer is a “good cancer.” I would never put those two words together. The reason they call it a good cancer is because it’s very treatable if it’s caught early. Not necessarily cured, but very treatable.
I didn’t feel like I was one of the lucky ones. I got prostate cancer. The word cancer is what you hear. I found that it gets very matter-of-fact with doctors. They’re compassionate, but their job is to tell you the facts and the statistics.
We were getting all these numbers, the Gleason scores, and I was a 4+3. There’s low risk, medium risk, and high risk. I fell right on the cusp of intermediate, but I was on the wrong side of it. 3+4 and below are considered good candidates for active surveillance where you’re watching your PSA levels. That made it a little challenging, too, because I wasn’t high-risk. I was on the cusp. But then they told me the genomic tests showed that it was aggressive, so that put me in another category.
PSMA PET Scan
I had a PSMA (prostate-specific membrane antigen) PET scan, which is a highly sophisticated PET scan. They shoot you with radioactive isotopes and iodine. They couldn’t find anything. That was encouraging because it meant things were small and they hadn’t moved into my organs or bones. On the other hand, if you don’t know where it is, how are we going to treat it?
I didn’t want to share other than with Wendi. That’s how scared I was.
Breaking the News to the Family
I was somewhat obsessed with thinking about it. It was always in the back of my mind. It’s hard to avoid that when you have cancer.
I told our children a month or two after I found out. I didn’t want to worry them. As I was approaching surgery, I knew that I needed to tell them what was going on.
I also wrote an email to Wendi’s family telling them what was going on. I was going to have surgery, but I was very clear about my boundaries and that I didn’t want to discuss it.
At some point, I would share information as it came up. I might have gone overboard with this, but I was very firm about my boundaries. I know they care and they love me and want to support me, but I didn’t want to go down that road of getting lots of questions and phone calls, so I played it pretty close to the vest.
Processing the Emotions of Having a Cancer Diagnosis
When you hear you have prostate cancer, there’s a lot of fear because it’s a sexually related thing. You’re talking about your internal plumbing and the unknown side effects, which can be incontinence or sexual dysfunction. You don’t want to talk about those things. You also think about dying.
I didn’t want to put that burden of fear on other people. If I couldn’t project overwhelming confidence that I got this, I didn’t want to share it other than with Wendi. That’s how scared I was. I like to be in control as much as possible.
I also grew up in a household where there was a lot of emotional chaos. I’m sure that made me even more of a person who wanted to have control. Suddenly, I was thrust into this situation where I felt like I had no control. I did share it once I knew I was having surgery.
I was tortured during that time by not wanting to make the wrong decision.
Treatment
Treatment Options
I had one of the top surgeons in the country, so I was confident that I was in good hands, but you have to make a decision early on.
Are you going to do radiation or are you going to do surgery? The catch-22 is if you choose radiation, you can’t do surgery later on. If you choose surgery, you can do radiation later on.
I’m in limbo. We can’t find it, I’m on the intermediate to low risk but on the wrong side of it and it’s aggressive.
I wanted more opinions. I didn’t want just a second opinion, I wanted a third opinion. The doctors kept saying, “We think it’s confined to the capsule based on what your Gleason score is and your PSA levels,” but they couldn’t guarantee it.
My initial diagnosis was in January. Over the next months, I was tortured not wanting to make the wrong decision. I had the surgery in April.
Surgery
One of the big concerns of surgery is nerve sparing because there are all these delicate nerves around the prostate. You’re anesthetized and you know that this robot is being controlled by a surgeon. I came out of surgery very groggy. The surgeon said, “I was able to spare your nerves and didn’t see anything outside the capsule.” I felt like that was good, but I was also wounded to the core.
The surgery was a traumatic shock to my system. It was good that it was confined to the capsule. It gave me some relief. Having a catheter is weird. You walk around with this bag.
For someone who liked to be in control and make things happen, it felt like things were happening to me and they were out of my control. That’s a tough one to crack.
Support
Finding a Cancer Community
I joined the prostate cancer support group at MarinHealth. They offer so much information. It’s the guys who’ve been in the trenches. I don’t want to say they knew more than my doctors, but they’d all been to so many doctors. Some had surgery, some had radiation, and some were on active surveillance. They knew all the drugs.
I was 63. I never thought of myself as old. I thought of myself as young. Part of me still feels 18 or 25. You get a cancer diagnosis and a prostatectomy and you start to feel a little old fast because you’re wounded. There’s no certainty that you’re ever going to be whole again.
You wonder if you’re ever going to get your old life back. For someone who liked to be in control and make things happen, it felt like things were happening to me and they were out of my control. That’s a tough one to crack.
When you get a cancer diagnosis, you’re a member of a club. One thing that’s really positive about that is every man that I met who has gone through this wanted to support me. They’d call and say, “I’ll be happy to talk to you about it.” A lot of them say, “You’re going to get through this. It’s going to be okay.”
They talk about what happened after surgery, incontinence, drugs, shots, pumps, and all the sexual things that you think, I don’t even want to know about, but you do want to know about it. I felt like I was in a community, but at the same time, it was a community club I didn’t want to be in.
It was not pleasant to have to discuss the fact that my body had felt like it betrayed me.
Once you’ve been diagnosed with prostate cancer, all of a sudden this community opens up to other men who’ve gone through this and they all want to pay it forward. They all want to tell you about their experience and support you through yours to reduce the worry and to give you information you may not get from your doctors. There’s so much information from doctors that it’s overwhelming. To have more practical terms broken down step by step makes a huge difference.
When you’re one of the new guys in the cancer support group, you can feel the fear in the room. There’s a separation between people who’ve just found out who sometimes bring their wives with them, people who are trying to make a decision on how to be treated, and men who’ve been there and keep showing up over and over again to support you.
It was not pleasant to have to discuss the fact that my body had felt like it betrayed me. That was not an easy thing to talk about. I tried to be matter-of-fact about it, but I was definitely under a lot of pressure and stress.
These were now my people. It was healing in one sense, especially all the information they had that was easy to understand. But sometimes, there were people in there who were terrified. I had a hard time being around that energy.
As I went to more groups and more sessions, I realized it’s geared toward men who are just finding out they have prostate cancer. There’s a lot of that initial overwhelm.
Your doctors are great, but the support group provides things that the doctors don’t.
The Power of Having a Cancer Support Group
It was a safe space to talk because everybody in that room either has it or had it. It is important to unburden yourself however much you’re comfortable doing. The unspoken question for everybody is: how is this going to affect me as a man? That’s what people want to know. The cancer support group provides a place to share however much you want to share and ask any question you want to ask.
You’ll find out that your doctors are great, but the support group provides things that the doctors don’t. It provides emotional support. My doctors are compassionate, but it’s not their job to hold your hand. It’s their job to take care of you medically and to give you the facts.
Sometimes the facts are pretty scary — the percentages of survival, the percentages of when the disease could come back. I encourage men to go to prostate cancer support groups and decide for themselves. Is this for me? How much do I want to share? Are there men I want to stay in touch with during this or afterward? There are a lot of men who come there.
If they’re not done with prostate cancer, they’ve been dealing with it for a long time. They’ll tell you almost anything you want to know. It’s a chance to be around experienced veterans. You can always call someone outside of the meetings. I called the person who leads our group, Stan Rosenfeld, my prostate cancer rabbi because I could call him anytime. There wasn’t anything I couldn’t ask.
Having Someone to Answer Your Cancer Questions
It took some of the angst out of it. It made it accessible. The information was accessible whether or not I liked hearing it. Cancer is not fun. You’re not at a men’s group to talk about work and family. You’re dealing with your mortality, but there’s no other space quite like it. You’re amongst your peers and they’re going through the same thing you are.
I didn’t get into saying I’m really scared. You don’t hear me say things like that, but you can feel it. I’m sure they can feel it. The sense of empathy and caring and wanting to make men feel informed, that’s part of being a little bit more in control if you really understand your options.
They know we’re scared. I didn’t feel the need to say, ‘I’m really, really scared.’
Not Discussing Feeling Afraid
It’s not my nature. I’m not going to say I’m scared shitless. I’m afraid I’m going to die. I have no control over this and my life will never be the same. That’s not what I wanted to share with them.
I wanted them to give me some information and hear some solutions. Sometimes that’s what we’re looking for, solutions. You have a big problem and sometimes there aren’t solutions other than looking for second opinions and third opinions. Facts are facts. You’ve got prostate cancer, this is your Gleason score, and you have to deal with that.
It’s a foreign experience to be in a group. All of a sudden, you found out you had prostate cancer and you’re in a group of 20 men who also either had or have prostate cancer.
Oncologists use the term “no current evidence of disease,” but they never use the word “cure.” It’s really strange at first to be in this room with all these other people going through the same crisis. They know we’re scared. I didn’t feel the need to say, “I’m really, really scared.”
I did express a lot that I didn’t know what to do. I have two choices: surgery and radiation. Ideally, I’d like to find a way not to have to do either. Radiation also involves hormone deprivation therapy and that’s a whole thing in itself.
I felt comfortable in the sense that there wasn’t anything I couldn’t share. I honored my feelings about it. This is as much as I do want to share. I know I can say anything I want and they will support me and give me information and advice. You have to decide what your comfort level is. You have to become your own medical advocate.
It’s a very different energy to be around men in the same boat.
Discussing a Cancer Diagnosis
I’ve dealt with a lot of doctors. I have a team. It’s double figures of how many doctors I have. Part of that is because there were complications.
I didn’t talk to my doctors about my emotions. I said to my main oncologist, Dr. Terry Friedlander, “I’m scared. I don’t know what to do.” He was very compassionate and said, “I understand. It’s really hard.” But he hadn’t had the surgery. He was dealing with it every day as a doctor. It’s a very different energy to be around men in the same boat.
Wendi was there with me the first or second time. It was good to have her support, but I think she became more scared. When she heard about some of these stories, the reality started to hit.
That’s one of the things about a support group; it’s all about reality. This is what you’re going through, these are your options, here’s what a lot of us have learned, here are some of the doctors we recommend, and here are medications or things you can try. It’s like going to a diner with a big menu with pages and pages to choose from.
Not Being Informed About the Medical Situation
The ball was dropped a couple of times. The first time was when I wasn’t told that one-third of men who have a prostatectomy will need salvage radiation later on. I’m going into my healing stage thinking it’s done, it was confined to the capsule. I did have side effects from this wound in my body that took a while to heal. When you’re practicing your Kegels and doing all these things like the catheter for 2 weeks, that was really weird and very uncomfortable. It was a relief when I got that out.
I thought I was done. They said I got it all. All these feelings came rushing back, except this time, they were stronger.
Relapse
The other thing was because of the pandemic, I wasn’t getting regular PSA tests and I thought I’d been cured. I wasn’t told that I needed to get one every 3 months. It probably wasn’t until almost a year and a half later, maybe 2 years later, that I took a PSA test and it wasn’t 0.002, which is what they say no evidence of disease. That’s 0 because they always put the 2 there because it’s immeasurable at some point.
I thought I was done. They said I got it all. All these feelings came rushing back, except this time, they were stronger. It’s back. You may never get rid of it at this point. That’s what it felt like to me. I looked for all these different ways to not have to go into radiation hormone therapy.
I had two pretty serious complications. There was a history of frontal temporal dementia in my family, which was genetic, so I had to get tested with the psychiatric oncology program, and that took a while. When they tell you to see a specialist, it can take months. My doctors made things much easier. They put a word in.
I asked for a routine EKG when I was ready to start hormone therapy. As it turned out, there were some issues, like ischemia and an enlarged heart. Now I had to go through cardiology oncology. That was also resolved as not an issue with ADT and radiation.
Having a Good Medical Care Team
UCSF has some of the best doctors in the world. I was very fortunate to be near a teaching hospital. There are three in California – UCLA, Stanford, and UCSF. I was lucky I had access to some of the best doctors in the world, but I was knocked for a loop. I went into this I can’t believe this is happening mentality.
I did four PSMAs because I don’t want to get radiated because in my mind, if we don’t know where we’re radiating, that’s like carpet bombing versus guided missiles.
PSMAs are good at seeing clumps or tumors where cells congregate. Individual cancer cells are microscopic. In my case, they couldn’t find them. I’m going to have to make a decision in good faith. This is when I found my mind-body medicine person. That was when the whole cancer experience shifted.
The closer you are to people, the more it affects them. It shocks and scares the people who love you.
Reaction to the Prostate Cancer Relapsing
I was even more closed-mouthed when it came back. I did not want to share that news.
I had made a decision about treatment, so I didn’t need any questions about what I was going to do. I did tell my confidants and our kids. I can feel it when I tell somebody it’s not good news.
The closer you are to people, the more it affects them. It shocks and scares the people who love you. It hits home for them. If you’re talking to medical professionals or a support group, it’s more matter-of-fact. I didn’t want to talk about it. I even skipped a family reunion.
I decided I was going to work with a cancer coach. What I found was there’s work for me to do that makes me feel like I do have some control over this and it can change my outlook on what’s happening now and what’s going to happen next. This was a game-changer.
I was so fortunate to have a partner who I knew would be there and would provide the support and confidence.
Telling Loved Ones About Relapsing
I knew I could tell Wendi and that the reaction would be we’re going to get through this. I was so fortunate to have a partner who I knew would be there and would provide the support and confidence that I couldn’t feel right away and for some time, actually. My good friends also supported me.
My children stepped up. They didn’t break down crying. It was more, “I’m really sorry. We’ll be there for you, whatever you need.” I know that not everybody has that in their lives. Some people are alone with this, so I was fortunate.
I went back to the prostate cancer support group and they’re very matter-of-fact.
They talk about hormone therapy, different hormone therapy drugs, and different kinds of radiation. I felt like I’ve been there once before, so I know what I can get from the prostate cancer support group. I know I can go there and get some answers and very solid information from people who’ve been there and done that. I felt like I could ask anything.
Hormone therapy and radiation are tough on the body. Men aren’t prepared for menopause.
Effects of Hormone Therapy
Hormone therapy affects everyone differently, as does radiation. Surgery is very straightforward. They cut out your prostate. Now that I was entering into this more nebulous treatment, you hear about hot flashes, loss of libido, weight gain, and reduced bone density.
You alter your diet, increase your exercise routine as much as you can, and do focused meditations to help balance the treatment you’re getting. Hormone therapy and radiation are tough on the body. Men aren’t prepared for “manopause.” We suddenly develop a lot of empathy for middle-aged women at that point. It’s a whole new ballgame.
If I had a question about treatment, radiation, or hormone therapy, I felt like I could get really solid information and things I didn’t necessarily even hear from my doctors. Not that my doctors aren’t super knowledgeable, but I think doctors and radiation oncologists stay in their lane. When you go to a cancer support group, there are no lanes. It’s whatever you need.
Do you want to talk about hormone therapy? We’ll talk about it. Do you want to talk about sexual function? We’ll talk about it. Do you want to talk about radiation effects? We’ll talk about it.
There are things some of these men have been doing for decades and decades. They know all the doctors. They know all the different symposiums, papers that are out there, and the statistics.
There was no sign of disease. I admit it’s a struggle for me to fully accept that’s great news when I know that I’m going to have to keep testing for years to come.
Navigating Cancer Statistics & Survival Rates
I asked my oncologist, “What are the chances we’re going to get this eradicated and I’ll be done with this?” What really shocked me was it’s not 100% based on your age, your Gleason scores, Decipher scores, and genomic scores.
I got different numbers from different doctors. Some would say, “Based on statistics and studies, you have a 25% chance of living 10 or 15 years. This is what the studies show for men with your Gleason score, with your surgery, and with your Decipher score. These are what the statistics show.” That’s sobering because now you’re talking about death and that’s something nobody wants to talk about.
You’re in uncharted territory. You don’t know and they don’t know. Every time you take a PSA test, there’s no current evidence of disease.
The good news is I had my first 3-month past treatment PSA test and there was no sign of disease. I admit it’s a struggle for me to fully accept that’s great news when I know that I’m going to have to keep testing for years to come.
This is where the mind-body medicine comes in. I changed my attitude. I got this. I’m going to keep this cancer out of my body and I’m going to do everything I can to stay healthy. That was a turning point in my treatment.
I had oncology tumor boards meet twice about my case because, between neurology and cardiology, it’s a little more complicated. They all said the same thing: hormone therapy and radiation.
I wanted someone who was totally in my corner, but who was going to support me and push me.
Coping with Your Cancer Diagnosis
Having a Cancer Coach
I know the value of a coach. I used to work with the top coaches in professional basketball, so I know we need teachers, mentors, and particularly coaches. Coaches provide not only expertise but also support. They will call you on things that you need to address with the goal of getting better. You’re improving and gaining new skills. The term cancer coach appealed to me because I’d done enough personal therapy over the years that I was talked out.
There are therapists you can talk to. There are a lot of people at UCSF. I talked to palliative care and counselors. They’re great, but they weren’t going to be there for me day in and day out. That’s not their job and they’re busy, so the idea of having a coach appealed to me. He was filling a role that I needed.
I wanted someone who was totally in my corner, but who was going to support me and push me. At that point, I was not feeling optimistic. I was scared and pessimistic. Maybe skeptical, but I was not feeling optimistic.
I learned I could gain practical tools like meditations, cancer visualizations, writing in a gratitude journal, and self-hypnosis. All of a sudden I realized that this is something I’m in control of. When you also focus on gratitude, your life perspective changes. It shifts from what isn’t working to what’s working in my life. We know what’s not working with cancer. What’s working and how can I make it work even better? How can my mindset work even better?
Mind-body medicine sounds confusing to people. What does that really mean? It means using the power of our minds to lift us up into not necessarily being in control but playing our part, being in the game, and not just counting on our doctors.
I embraced the concept that I had a role in my healing. I signed up for it. I was doing hormone therapy, practicing these tools, and using my mind and spirit to become a part of my healing.
Fear was going to make things worse. Fear wasn’t healthy.
Letting Go of Fear
I was letting go of a lot of the fear and feeling like I could be in charge of what was happening to me. That shifted everything.
When you’re diagnosed with cancer, you have this feeling that the doctors are in control, the universe is in control, and you’re not in control. There are practical things I can do to support my doctors and to push it to another level where I’m part of the healing.
I would wholeheartedly recommend people consider having a cancer coach or somebody who’s going to be there to push you to be your highest, most positive, and most powerful self.
Being part of my own healing was new for me. I learned that the fear was going to make things worse. Fear wasn’t healthy for me. Optimism and practical everyday tools helped me feel like I was attacking the cancer.
I used visualization exercises. When I was underneath the linear accelerator, I would envision drones zapping the cancer cells in my body. I swim laps 3 or 4 times a week. When I was in the water, I visualized dolphins zapping my body with sonar. Other times, it was waves washing the cancer cells out.
I focused on being part of my healing and that was really powerful. I kept to my gratitude journaling. I wake up in the morning and ask: what am I grateful for? I go to bed at night and ask: what am I grateful for? And that’s a different mindset than what am I scared of.
Practical Things to Improve Cancer Journey
There is integrative oncology. There are departments in integrative oncology, so it’s not just surgery and radiation. UCSF has an integrative oncology department.
You also have the Internet, which is actually a Pandora’s box because it can scare the living daylights out of you. You can find out things that you might not have known on your own.
With this kind of medical crisis, you can decide who you really want to be in your life. You can see who you really are and how you want to live.
The Power of Sharing Your Cancer Story
I never thought I’d write about my prostate cancer. Then I got to the point where I wanted to pay it forward. As a storyteller, I realized that’s how I could pay it forward. I knew I could share my experience in a way that was very accessible.
I started to write it knowing that I didn’t have to share it with anyone. I’m an inveterate rewriter and that’s what I think makes great writing. People are willing to rethink and rewrite. I’ve been an essayist for decades, so I know how to tell that kind of story.
I started writing it and kept it to myself. I’d come back and write some more. I’d come back and go at it again. I have a friend who’s a writing coach and editor. She looked at it and gave me suggestions. I kept working at it. I showed it to my cancer coach and after a while, I thought, I will tell this story. I will take that huge leap of faith — and when I say huge, I mean huge.
I tried to put some humor in it. It was dark humor, but I felt like this was a way for me to make the best possible use of my experience by sharing my story with other people. I still feel like that’s my gift to give and my way of paying it forward.
I don’t wish this cancer on anybody. I know what it’s like to be diagnosed with prostate cancer not once but twice. Even though there’s a lot of fear, angst, and uncertainty, there can also be a silver lining to having cancer. With this kind of medical crisis, you can decide who you really want to be in your life. You can see who you really are and how you want to live. That’s what these life crises often give you the opportunity to do.
I didn’t want to live in fear and be tagged as the cancer guy. I wanted to live fully. I wanted to do things in life that I may be putting off. I felt like I’d been given a gift. Now it’s time to share this gift with others. I can’t cure their cancer, but I can tell them things that, from my experience, changed everything.
I do recommend that people ask their family, including those who’ve passed, if there was a history of cancer.
Talking About Family Medical History
What happens with families is when someone passes, they take their stories with them. Unless you’re one of these people who’ve done interviews or videos of the elders, you’re not going to know directly from them because they’re gone. Their kids, my cousins, are mostly on the East Coast. I’m not really close with my cousins, so I’ve never asked them. I never asked what their fathers passed away from.
Turns out both of my uncles died of prostate cancer. I believe they were in their late 70s or early 80s. That was a real surprise. It was one of those things I probably didn’t want to know about because that made me worry even more. It would have helped to know because my doctors would have wanted to know. My brother had anal cancer, but that’s not related to prostate cancer.
I do recommend that people ask their family, including those who’ve passed, if there was a history of cancer and, with men, prostate cancer. It does give your doctor information that will help in the long run.
It’s the same thing with the genetic disposition of dementia in my family. You want to tell your cousins about this. We think my father had it. He was the one who started with it or it could have been his grandfather, but who knows? If they’re my uncles, they’re brothers, part of that same family, so they should know about it too because it could be passed on to them and to their children.
Laughter is the Best Medicine
To me, the old adage that laughter is the best medicine is true. It’s scientifically proven. It raises your endorphins and dopamine levels, and your blood pressure lowers. It’s all the good stuff. It’s so much fun and so bonding with other people.
When you’re in a group of people, it can be very healing. It can be very powerful because it opens your heart. Having prostate cancer, your heart tends to close down. You clench in your body, your heart, and your mind. Anything that can unclench your mind, body, and spirit, anything that can relax, release, and bring pleasure and joy, that’s big medicine.
Prostate cancer is not the only thing going on in your life. Find other things to balance it out.
Focusing on the Positive
My dog is some of the most powerful medicine I can have by being around her, loving her all the time, and feeling that affection coming back. Things that make you smile are important.
Cancer is not funny. It’s not happy. But there are still things in life that are joyful. I urge men who are dealing with cancer to find joy or at least something they’re grateful for. It could be that you’re alive, that the sun is out, you have a roof over your head, food, family, or a good job, whatever it is.
While this is going on, it’s not the only thing in your life. Prostate cancer is not the only thing going on in your life. Find other things to balance it out. I’m still living, I’m still here, and I’m going to make the best of this. I’m going to trust my doctors. I’m going to trust my mind and my body to help me heal. Again, laughter was one of them for me and still is.
Don’t think about it as a death sentence. Prostate cancer is the second leading cause of cancer deaths in men, but if you read the statistics, that’s only about 35,000 men a year. That’s a very small number. Hundreds of thousands are diagnosed with various types of cancer each year.
Doctors will tell you that most men die with prostate cancer, not of prostate cancer. You may get into your 70s or 80s and have prostate cancer and they may say, “Your Gleason scores are low. We don’t need to treat you unless you really want to be treated. Go on and live your life.”
Don’t go down with the ship. Shit happens, things happen, life happens. Deal with it. As much as I didn’t want to hear, “It’s a good cancer,” prostate cancer is a lot better than some of the others. There are resources and there is hope. That’s all we want. We want hope.
A man talking to women about prostate cancer is a little strange because you’re talking about the most private part of your body and what could be permanent side effects.
Why Story Resonates with Women
Women open their hearts and deal with cancer in a different way. They’re in touch with their emotions. They talk to other women about their deepest, most private feelings, not even hesitating sometimes, and even with strangers. I wasn’t totally surprised that women were the ones who were commenting and highlighting my essay on Medium because women are naturally focused on healing, communication, compassion, and love.
That’s not to say men aren’t. We’re more like onions. You have to peel away the layers. I always think of Shrek, where the donkey says, “You’re like an onion. You got to peel away the layers to get to the good parts.”
A man talking to women about prostate cancer is a little strange because you’re talking about the most private part of your body and what could be permanent side effects. I had a lot of reactions to hormone therapy from women saying, “Welcome to my world.”
I’m very comfortable with women. I’ve always had really strong friendships with women. I wasn’t surprised by the support I got from women about sharing my story.
With prostate cancer, it’s like, ‘What kind of man am I going to be after this?’ That’s a pretty tough question for someone to deal with.
Words of Advice
When you’re first diagnosed with prostate cancer, it’s a shock and it’s easy to feel terrified and out of control. You have no control. When you talk to other men who’ve been there or who are there, you realize you’re not alone.
In my support group, there was nothing I couldn’t discuss. I could ask the most personal, private, emotional, mental, and physical questions. There was a sense of relief that I wasn’t in this alone. I have a resource outside of my doctors. Doctors are busy. They’ve got appointments left and right. The support group was, “You need us, call us.”
I was able to pay it forward to other men. If someone needed to talk about prostate cancer, they could call me. Some people are going to think of gratitude journaling and visualizing drones zapping the cancer away.
What you would hear from a support group is, “There are no guarantees, but here’s what we know, and here’s what worked for me.” There’s a big difference between saying, “You ought to,” and someone saying, “This was my experience,” and then you can ask them about their experience.
Get out of your head. My mind was spinning and spinning with the same old questions and worries.
Go somewhere where you can get answers if you have questions and you’ll get support immediately as long as you need it. You can go for years if you have to. There’s no limitation.
They meet in person once a month. Men are more solitary creatures than women. I’m always amazed at women. They get together and within two minutes, they’re talking about the most personal parts of their lives. Men are more comfortable talking about what’s happening in our business, sports, and politics.
Sometimes, during a conversation about prostate cancer, I’ll say to some men that I know who’ve been diagnosed, “Let’s drop deep. Let’s cut the bullshit and get right to it.” With men, we’re in a place we’re not used to being. We’re feeling weak and scared. With prostate cancer, it’s like, “What kind of man am I going to be after this?” That’s a pretty tough question for someone to deal with.
It’s hard to get a diagnosis of prostate cancer, but there’s hope and there’s healing. There’s a silver lining.
I’m taking on this role. It’s not something I thought I’d do. I was lucky to find great doctors. I also had a coach that opened up a whole new world for me of self-healing. It was total serendipity and luck that I happened to find him through a Google search.
Every man has his own journey, his own path, and has to be his own medical advocate. You can’t just count on your doctors. You’ve got to ask questions.
You’d be well off to get second opinions and go to cancer support groups. You’ll hear things there that you won’t hear anywhere else. I came out of the cancer closet and felt like I had to pay it forward to other men and participate in something like this. I’ve been through this now. I’m still going through it, but I’ve been through this, and it’s an act of selflessness to want to help other people go through this.
It’s hard to get a diagnosis of prostate cancer, but there’s hope and there’s healing. There’s a silver lining in this. You can see parts of your life and ask: is this how I want to live? Is this who I really am? What do I want to do now? Not only do I want to be cured of cancer, but how do I want to live? What have I learned through this process?
Time is precious. We’re not guaranteed anything. We all go at any time. You read the newspaper every day and someone can die at 20. My dad lived to 98, but there are no guarantees in life.
If you’ve been diagnosed with prostate cancer, don’t waste your time and energy on the negative part of it. Trust your doctors. Trust whatever healers you end up with. Trust your men’s support group and most of all, trust yourself. Trust that you will find a way through this journey.
There’s no guarantee that you’re going to be cured. But listening to other men talk about this, you can see that you’re not alone and that there are happy endings or at least life changes that you didn’t know were possible. I put my story out there and I can continue to expand that story. I felt that I was doing something noble by taking that leap of faith and coming out of the cancer closet.
Special thanks again to Janssen for its support of our independent patient education content. The Patient Story retains full editorial control.
When Joseph was diagnosed with prostate cancer, the news came as a shock and forced him to face questions about his health, future, and faith. He shares how he navigated his diagnosis, chose robotic surgery, and learned to open up to his loved ones about his health.
Stephanie was diagnosed with stage 3 colon cancer when she was 32. A mom to a 15-year-old son, she shares her journey from pre-diagnosis to recovery.
Before the diagnosis, she experienced stomachaches, bloating, fatigue, and low energy. Despite seeking medical help, doctors brushed off her symptoms. Various attempts to address the issues, including dietary changes and birth control, proved unsuccessful.
Her symptoms worsened and eventually led to an emergency room visit. A CT scan revealed a mass, leading to a hospital admission. Unable to perform a colonoscopy due to the obstruction caused by the tumor, the surgical oncologist recommended immediate surgery. Steph feared the worst, but the surgery went well, and she avoided having a colostomy bag.
The official diagnosis of stage 3 colon cancer came after a PET scan, revealing no spread beyond the colon. She underwent chemotherapy, surprisingly experiencing minimal side effects. She underwent regular monitoring, including periodic lab tests and CT scans. Despite insurance hurdles, a PET scan confirmed her cancer was in remission.
Engaging in activities and maintaining connections with friends was crucial for her mental health throughout the journey. Dealing with anxiety post-treatment, she emphasized the importance of self-advocacy, trusting one’s intuition, and having a positive mindset.
In addition to Stephanie’s narrative, The Patient Story offers a diverse collection of colorectal cancer stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
Name: Stephanie K.
Diagnosis:
Colon cancer
Staging:
3
Initial Symptoms:
Very bad cramps
Bloating
Indigestion
Burping
Treatment:
Surgery
Chemotherapy: CAPOX (capecitabine and oxaliplatin)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I felt that something was wrong. There was no blood so I never thought of colon cancer.
Introduction
I’m 33 years old. I’m a nanny and I work occasionally as a server in restaurants.
I have a 15-year-old son. He’s a sophomore in high school.
Before I was diagnosed, I went to the gym. I like to lift. I had a bunch of gym friends and we lifted a lot of weights.
Pre-diagnosis
Initial Symptoms
I was getting stomachaches and felt very bloated. I was tired and didn’t have much energy. I felt that something was wrong.
There was no blood so I never thought of colon cancer. I had bowel movements but felt bloated and had terrible pains that would come and go pretty much every day.
I went to the doctor and said, “I’m getting these terrible stomach pains. I feel like something’s not right.” They said, “You’re active, you’re healthy, and your labs look good,” but I always had low iron so they said, “Maybe change something with your diet and see if that takes away the cramps and the bloating.”
I was driving myself crazy. I would eat a lot of broccoli and look up online, “Does broccoli cause bloating and stomach pains?” I started thinking, Am I crazy? Because I would go to the doctor and he’d say everything’s good.
One weekend, I was out to lunch and couldn’t even stomach a bite because that’s how bad my stomach was hurting.
Gynecology Appointment
I went to the gynecologist. I wasn’t on birth control, but she said, “Maybe due to your heavy menstrual cycles, the birth control will help lessen the cramps and all the things that come with your menstrual cycle, like tiredness and headaches.” She said it could make the flow lighter. We went the whole route of doing birth control to see if that would help, but nothing seemed to help.
One weekend, I was out to lunch and couldn’t even stomach a bite because that’s how bad my stomach was hurting. I couldn’t eat. I knew something was wrong. I said, “I need to go home and lie down.”
I had that feeling like I was going to throw up. I called my mom and she said, “Maybe you caught a stomach bug. Take some Pepto-Bismol,” so I did that.
The next morning, the pain was still there. It was pretty bad and I knew. I called my mom and said, “I should go to the ER.”
Emergency Room Visit
She dropped me off at the ER. When they were checking me in, I said, “I’m getting terrible stomach pains. I’m sick.” COVID is going on so they said, “Maybe you have COVID. We’ll do a COVID test.” Negative for COVID.
The physician said, “I’m going to order a CT scan to see what’s going on in your abdomen.” We got the CT scan and he came back and said, “We found a mass in your stomach area so we’re going to have to admit you.”
I’m 32. I was thinking of the worst-case scenario. I’m scared. I called my mom and said, “They found something in the CAT scan. They’re going to admit me to the hospital. You have to come down.”
My mom came down. When they took me into a room, the nurse said, “We’re going to have a gastro doctor come down and check you out.” He came down and said, “We can’t tell you what it is until we go inside and do a colonoscopy.”
I called my mom and said, ‘They found something in the CAT scan. They’re going to admit me to the hospital. You have to come down.’
Preparing for a Colonoscopy
They tried to prep me for the colonoscopy. All night, I couldn’t drink. It was coming back up. I was very nauseous. They tried every nausea medicine, but nothing was working. The nurse said, “I’m going to call the physician on call and see what he suggests.”
He must have gotten in touch with the gastro doctor and they took me as the next case first thing in the morning. I had an endoscopy and was supposed to have a colonoscopy. All I remember is being wheeled down.
Finding a Mass
When I woke up, there were a ton of doctors around. They couldn’t do the colonoscopy because the tumor was causing an obstruction. They couldn’t get through.
They said, “We found a mass. It’s probably cancer. We’re going to have to get a surgical oncologist in to see you.” They took me back up to my room and when the surgical oncologist came in, he said to my mom, “If this was my daughter, I would do surgery now.”
Surgery
They wheeled me down to the OR. He explained, “You could have a colostomy bag when you wake up. We don’t know until we get in there.” I’m scared. I’ve never had major surgery. I was thinking, Cancer. Chemo. I’m going to lose my hair.
I don’t remember anything, but when I woke up, the first thing I looked for in recovery was if I had a colostomy bag. Thankfully, I didn’t. The surgery went well.
I had an idea of what a colostomy bag was, but no other information like what it would make me feel like or what I would have to do if I woke up and I had one.
I had no time to process anything because everything happened so fast. It put things in perspective. I knew that something wasn’t right in those two years when my stomach was hurting, but the doctors kept on saying, “Oh, you’re young,” and then it turned into a horror story.
I don’t remember anything, but when I woke up, the first thing I looked for in recovery was if I had a colostomy bag.
Recovering from Surgery
When I woke up in the recovery room, the doctor wasn’t there but my parents were. They took me up to the oncology floor until I could heal. The doctors came in, but they couldn’t tell me until the results came back from pathology.
My mind is in a million places. I have cancer. Did it spread? Am I going to live? Everything comes crashing.
Diagnosis
Getting the Official Diagnosis
Once I was discharged from the hospital, I had a follow-up appointment with the surgical oncologist.
Both my parents came to that appointment. He said stage 3 or 4 because the CT scan picked up a spot on my liver and lung and he wouldn’t know exactly until I had the PET scan.
The PET scan results showed that it was just in my colon. It did not spread.
After the surgical oncologist, I went to see the general oncologist and he went over my treatment plan, the pathology results, and all that.
Breaking the News to the Family
I honestly didn’t know what to say because I was probably as scared as my son was and I didn’t want to show that to him. My parents, my two older sisters, and my brother reassured him that things would be okay. I’m sick, but I’m on the path to get better.
Treatment
Discussing the Treatment Plan
Both my parents came with me. I remember being so nervous and scared to death. I was thinking, I’m going to have to get a port and get chemo. I’m going to lose my hair. I didn’t know the side effects or how it was going to feel.
I remember him telling my parents the cancer had gone into some of the lymph nodes. They cut them out during surgery, but I will have to do chemo to make sure. I would do a chemo regimen of oxaliplatin and Xeloda (capecitabine).
I got a port placed in my chest. Once every two weeks, I would go in for a chemo infusion. Every day for two weeks, I would take two chemo pills — one in the morning and one in the evening.
It was very hard for me to relax because I wanted to keep on living life as normal as possible. That’s what helped me the most.
Side Effects of Chemotherapy
My side effects were very minimal. My oncologist was very surprised.
I had a little bit of hair thinning. I had neuropathy in my fingers and feet. I had a ton of cold sensitivity. After I would get the chemo infusion, for about a week, I couldn’t have cold water. Everything had to be at room temperature.
I was very tired. I would get nauseous. I took a lot of nausea pills from the oncologist.
Managing the Side Effects
I’m very outgoing. I love to socialize so it was very hard for me to relax because I wanted to keep on living life as normal as possible. That’s what helped me the most.
This is sad to say, but I was the youngest patient getting chemo. Everyone else was probably 50 and older. I’m coming in, this young girl, and I still have my hair while a lot of these patients are sick.
I tried to be very positive. I would bring in little note cards and hand them out to patients. I brought in a lot of word searches and positivity coloring books because they helped take my mind off of everything else that going on. There are also these little crafts that I would buy. They’re little sticky coloring pages and you put the gem to the number and they make very beautiful pictures.
I also bring music. Anything to distract you and keep you occupied.
Follow-up Monitoring
When I was going through chemo, I usually went in the morning. Every morning, they would draw my blood, check my cancer markers and all that, and make sure I was on the road to recovery.
If I had low iron or if they saw a red flag within my labs, they would check with the oncologist. I had iron transfusions a few times. If I needed potassium or sodium, they would give that to me. I didn’t have any scans until after my chemotherapy ended.
After my treatment, my insurance kept denying a PET scan. I couldn’t have a PET scan so I had a CT scan. I didn’t know any of the results until I saw the doctor. I followed up with the doctor and he said, “Things look great. Your cancer is in remission.”
But I wanted to get a PET scan because it scans your whole body and it would help me sleep better so I pushed for that. He said, “I don’t think you need it. Labs look good. The CAT scan looked good.”
After my treatment, my insurance kept denying a PET scan… But I wanted to get a PET scan because it scans your whole body and it would help me sleep better so I pushed for that.
I said, “I really want to get a PET scan,” to ease my mind. The nurse navigator was able to contact insurance and get authorization so I was able to get a PET scan.
I still have the spot on my liver and lung, but it did not grow in size so they’re not very concerned, but they’ll continue to monitor. Every three months, I go in for a CT scan and lab work. Every eight weeks, I get my port flushed.
My last scan was in October 2023. The scans came back clear and the doctor says my cancer is in remission.
Dealing with Scanxiety
Since my diagnosis, my anxiety is pretty bad. Every little ache and pain, I think, Oh, is something wrong? The oncologist told me that’s normal.
I try not to think too much about it, but if I have a test coming up, I do take anxiety medicine prescribed by the oncologist to help put me at ease so I’m not too stressed out.
The oncologist reassured me. At my last oncology appointment, he said, “Your cancer is in remission.” I thought, Then what? What if I feel a pain? But he said, “You’re going to get stomach aches. You’re going to get the stomach flu. Try to not think worst-case scenario every time you feel something.”
Words of Advice
Trust your intuition. When you feel as though something isn’t right and you need further help, you need to advocate for yourself. “I’m not going to leave this doctor’s office until you do a test.” I would hate for someone to end up in my shoes, but I didn’t know then.
I was going to the doctor and at one point, I felt like I was crazy. My friends and I would have plans to go out to dinner and I would cancel because my stomach was hurting. I didn’t want to be the girl who has terrible stomach aches all the time. I thought it was social anxiety. It was driving me insane.
What I’ve learned through my experience is to advocate for yourself when your intuition is telling you something’s not right. Fight to get your voice heard.
I knew something was not right. Unfortunately, I’m young. I was 32 at the time of my diagnosis. How often do you hear of a 32-year-old female getting diagnosed with stage 3 colon cancer?
Advocate for yourself when your intuition is telling you something’s not right. Fight to get your voice heard.
Colonoscopies aren’t necessary until you’re a certain age and that I think should be changed because I’m proof. Stomach pains for two years and the doctors said I was fine because I was young, but I knew within me that something was not right.
You have to be positive. Cancer is a scary diagnosis and your world can come crashing down. Think positively and try to keep pushing forward. You’re going to have bad days, but take those bad days and turn them into good days.
Go for a walk. Get outside. Try to stay involved in activities. Hang out with friends. My friends called to check in and sent text messages, asking if I needed anything.
Do things to keep your mind off of what’s happening, even though it’s so hard to do. That was my saving grace.
Dania, a 35-year-old mother of three, shares her journey of being diagnosed with stage 4 colon cancer that spread to her liver and peritoneum.
She experienced stomach issues since childhood but didn’t seek medical attention until her symptoms intensified. A visit to the emergency room revealed the shocking diagnosis of colon cancer. The news was initially overwhelming, but her faith and acceptance helped her face the challenging road ahead.
She began immunotherapy with Keytruda, responding well and experiencing minimal side effects. However, she faced complications, including a blockage that required an emergency ostomy.
During this time, Dania and her family made significant life changes, moving closer to her husband’s family for additional support. Her husband played a crucial role as her advocate, utilizing his medical knowledge to navigate the complexities of cancer care.
She emphasizes the importance of not taking health for granted, urging others to be proactive about their well-being. She advocates for increased accessibility to colonoscopies and encourages individuals to speak up and be persistent in seeking medical attention if something feels wrong.
In addition to Dania’s narrative, The Patient Story offers a diverse collection of colorectal cancer stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
Name: Dania M.
Diagnosis:
Colon cancer
Staging:
4
Initial Symptoms:
Stomach issues like constipation & diarrhea, depending on the food
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I’m 35 years old. I have three kids, ages 17, 12, and three.
I’m married. My husband works in the medical field. He used to be an oncology nurse, but he’s a case manager now so he’s still in the medical field but in a different branch.
I was in school prior to being diagnosed. Now I’m volunteering. I love volunteering at my church. I teach catechism and found that I really love working with children, especially adolescents.
I didn’t have alarming symptoms that made me think of cancer.
Pre-diagnosis
Initial Symptoms
I have always had stomach issues since I was little. Food wouldn’t sit right. I would eat carbs or bread and it would hit me hard in my belly then it would take days for my belly to go back. I’ve dealt with it for years and learned to live with it.
I learned what food would hurt me. If I ate it, I knew I was going to suffer later. I never thought to have it checked out or think that wasn’t normal. I didn’t have alarming symptoms that made me think of cancer, not until September.
Symptoms Intensified
We went to a wedding where I ate a lot of carbs and drank wine. At the end of the night, I felt a strange pain in my stomach, but I thought, It’s the food. I ate a lot today. Not the best, not the healthiest. I knew the process. It would take a few days of cutting out foods that hurt me and sticking to a clean diet so my stomach would get back to normal.
Only this time, it didn’t. The following day, I woke up feeling very bloated and uncomfortable so I thought, Maybe one more day, but it went that way the whole week. My husband, being a nurse, said, “This is strange. You shouldn’t be feeling this way. Not after a week.” He kept telling me to go to the ER, but I was hesitant because my idea was that the ER is for life or death and I didn’t feel like this was such a situation.
Scheduling a PCP Appointment
I made an appointment with my regular doctor. This was September. They didn’t schedule it until October. My husband said, “No, you need CT scans. You need additional testing.”
Finally, Saturday came and this was a week from the prior Saturday when I felt that sharp stomach pain. I woke up and was still feeling really uncomfortable. By then, my tummy looked a couple of months pregnant. It was so bloated and uncomfortable.
‘Everything looks good. Your blood work looks good. The real way to find out what’s going on is through a CT scan.’
Emergency Room Visit
I turned to my husband and said, “You know what? I should probably go to the ER.” He asked if I wanted him to come with me and I said, “No, it’s fine. I’m sure I’ll be back by noon.” We were having this conversation at around 8 or 9 o’clock. I even said, “Be ready. Maybe we can go out for breakfast or late brunch after.” I was thinking they were going to diagnose me with gastritis or some type of stomach issue.
I went to the ER and checked in. I even felt bad because there are other people who are sicker and here I don’t even have pain. I was bloated. Luckily, it wasn’t busy so they admitted me quite quickly. They did all the regular testing and blood work. Everything came out fine.
The doctor comes in, starts examining me, touches my belly, and we start talking. He was feeling the bottom portion of my belly and he said, “You know why I’m feeling there, right?” I said, “Yeah, in case my appendix is doing something.”
He said, “Yeah. Everything looks good. Your blood work looks good. The real way to find out what’s going on is through a CT scan. The only thing is that you’ll be exposed to radiation.” I said, “That’s fine. Let’s do it.”
Getting a CT Scan
He does the CT scan. I was still waiting by myself. I have the app for that particular medical group so I can get my results before the doctor can come in and tell me.
I had been looking at my blood test results, taking screenshots, and sending them to my husband who was home with my two girls. My 17-year-old son was out of town at the time. I thought, Maybe my CT scan results are in, so I check and they were.
Getting the Results
Everything was broken down. I didn’t understand the medical terms so I scrolled to the bottom because I knew it would have a conclusion where they give you the bigger picture.
I felt like a bucket of water had been thrown my way. I felt my heart skip a beat and drop. I don’t remember the exact words, but all I remember are the words “cancer” and “tumor.”
All I remember is him saying, ‘This is going to be a long road. There are so many things being done for cancer now.’
Diagnosis
Reaction to the Diagnosis
I froze. I took a screenshot and sent it to my husband. He immediately called me and I could hear the panic in his voice. He said, “Calm down. Everything will be okay.” I remember shaking. I was in shock.
At that moment, the doctor comes in. Poor guy. I’m sure that the last thing he wanted to do at that moment was tell a 33-year-old that she had colon cancer. I actually felt sorry for him. I’m sure it was hard.
I had my husband on speaker and I remember the doctor showing me my file. He asked, “Is this you?” I nodded. My eyes were glassy. I wasn’t crying yet, but I was about to.
He pulled up a chair and sat next to me. I honestly don’t even remember what he told me. All I remember is him saying, “This is going to be a long road. There are so many things being done for cancer now.”
Processing the Diagnosis
I was trying to process what I read. At that moment, my husband raced over to the hospital. He started calling my mom, my dad, and my siblings, and they all arrived and were very supportive.
Looking back, I don’t know if this was a symptom, but my stomach was so irregular. If I ate something like carbs, I would get constipated. If I did have blood in my stool, I thought it was constipation because it was so hard to go to the bathroom. It wasn’t something that would scare me or be a red flag.
Cancer never went through my mind. Nobody in my family has had cancer, any type of cancer. I’m the first one so it was a shock to everybody in my family.
I remember having a conversation with God and saying, ‘I give this all to you. I don’t know what my journey will be like, but I hand it all over to You. Whatever happens, let me have peace. Let my family have peace. You’re completely in control.’
Looking Back
Around that time, I remember being frustrated with everything and being uncomfortable with my stomach. I remember saying, “I’m going to make an appointment and get to the bottom of this. Maybe it’s a food allergy. Maybe I have something. Food isn’t sitting right. It’s hurting me. I shouldn’t be having this much pain or struggles with food. I should be able to eat normally and not have a bloated tummy immediately after eating.”
I remember saying, “I’m going to schedule an appointment. Maybe a nutritionist. Maybe I’ll see my doctor and she can run some tests or refer me to a specialist to see what it is that I have.”
They say that it’s such a silent killer. It doesn’t get diagnosed until it’s causing damage. At this point, it was already causing issues with my colon.
Admitted to the Hospital
After that, I was hospitalized for three days where they did a colonoscopy, a biopsy, and everything. I remember being on cruise control. I never really broke down and cried. I feel like I accepted it.
Leaning on Faith
I’m a practicing Catholic so my faith is a big part of my life. I don’t remember what procedure it was. It might have been my colonoscopy because I was going to be put to sleep.
I remember the countdown and having a conversation with God and saying, “I give this all to you. I don’t know what my journey will be like, but I hand it all over to You. Whatever happens, let me have peace. Let my family have peace. You’re completely in control.”
As I fell asleep, I felt so much peace. It helped me stay calm. At that time, I didn’t know what the stage was and where I was with the diagnosis. All I knew was I had a tumor and I had colon cancer, but I had a lot of peace after that.
I decided that I wasn’t going to be angry because being angry was going to feed this monster. I wanted to do what I needed to do. I gave it all up to God and I felt a freedom after that.
My children were going to see me at my sickest and that’s the only thing that tore me, but I was at peace.
Treatment
Discussing the Treatment Plan
At the ER, when the doctor came in to talk to me, he asked if I had any questions. At the time, I only had one. I asked, “Is it going to hurt?” I wanted to be prepared. I’m the type of person where I like to know.
I don’t remember exactly what he said, but he said, “That’s a very interesting question you’re asking. I usually get that a lot from older patients.” I don’t know what he meant by that.
I wanted to know what I was about to go through to prepare myself. I kept thinking my children were going to see me at my sickest and that’s the only thing that tore me, but I was at peace. I said, “Let’s go with it and see where I’m heading.”
Pathology Report
I was diagnosed on September 17th when I went to the ER. The next day, I received the pathology report, which confirmed the cancer. My tumor was at the top of my colon.
I don’t even remember them telling me. I remember briefly hearing conversations that it was stage 3 or 4. Finally, in one of my appointments and through seeing in my app, I saw stage 4 colon cancer with liver and peritoneal carcinomatosis.
Realizing the Gravity of the Situation
My husband was an oncology nurse and worked years in that department so he has been my biggest advocate. I understood that that was pretty late, but I didn’t understand the gravity of it.
I try not to Google because online, they will tell you the worst-case scenario and I didn’t want to know so much. I don’t think I understood what that meant until I had a conversation with my oncologist a few months down the road.
I was under the understanding that I would have surgery to remove the tumor and start treatment and all that. I asked the doctor when we would start thinking about surgery. She wouldn’t straightforwardly say we’re not looking at surgery, but the conversation led to that. Surgery was not on the table because my cancer had spread.
That’s when it hit me. My heart dropped. My husband was right next to me during the video call. After we hung up, I looked at him and asked him for clarification to see if I understood right and that’s when I broke down. I understood then that it was a lot more serious than I thought.
The CT scan confirmed that my tumor was blocking 98% of the colon. He said I would need an emergency ostomy.
Keytruda Immunotherapy Treatment
When I was diagnosed and while they were doing all those tests, they wanted to give me a first dose of chemo before leaving the hospital so they put in my port. My husband started talking to the doctors to see if I would be a good candidate for immunotherapy. The oncologist decided that they would wait for the pathology report to come back to see if I was indeed a good candidate and, thank God, I was.
I went home with the goal to start immunotherapy as soon as possible. I had my first immunotherapy on September 29th and that has been the only treatment I’ve been receiving.
I’ve been doing Keytruda. I haven’t had any side effects at all. I do feel a little tired, but compared to what chemo does to you, I’ve been so blessed. I am so thankful.
New Stomach Pains
I ended up going to the emergency room again at the beginning of October. It started with horrible stomach pain. It felt like contractions. I could not eat anything. The smallest thing I would vomit back up. My husband made me a smoothie, begging me to eat something.
I spent the whole Saturday in bed, in pain and extremely nauseous. We thought it was a reaction to the immunotherapy because I just had my first dose. But it was horrible. The pain was so excruciating.
On Sunday morning, my husband turned to me and asked how I was feeling. I said, “I don’t feel good. What do we do?” He said, “ER.” We headed to the ER. The same doctor that diagnosed me was there. As soon as he saw my name, he rushed into my room. After reading my symptoms, he had an idea of what the issue was.
He looked at me and said, “Remember that first day when I told you this would be a long journey and there would be some bumps in the road? This is just a bump.”
He thought it was a blockage. The tumor was already blocking the passage so I was eating, but nothing was coming out. The only way to confirm this was to have another CT scan and it confirmed that my tumor was blocking 98% of the colon. He said I would need an emergency ostomy.
My quality of life wasn’t good. I couldn’t do much. I couldn’t do basic tasks because I felt so tired. It hurt. I couldn’t lift.
Emergency Stoma Surgery
Having an emergency ostomy was harder than my cancer diagnosis because all of a sudden, I was pooping through a bag.
I had to learn how to clean it and how to take care of it. I’m a very squeamish person so this was a challenge for me. It was painful. To see part of my organ outside of my body was an adjustment.
But I have so much support. I would see my ostomy nurse two days a week. She would come to my house, help me change it, and educate me more on it. She was the sweetest lady. Love her. She was amazing.
She gave me my space. She understood that it was hard for me and let me drive this situation. She knew that I was struggling. She gave me time and, eventually, after baby steps, I was able to clean it. By the time we were done, I was doing it on my own and I learned to take care of it.
Prolapsed Stoma
Immediately after, I started having issues with my ostomy. It prolapsed so it was starting to come out. Mine started protruding. Eventually, it would get really big and would hang out. It was very painful. I started developing a pretty good-sized hernia right behind it. Once I lay down, it went back into my body.
It’s a blessing because, without this, I could have lost my life so I was very, very thankful for it. But it was very uncomfortable. I had to use a waistband to keep everything in place.
My quality of life wasn’t good. I couldn’t do much. I couldn’t do basic tasks because I felt so tired. It hurt. I couldn’t lift.
I said to my oncologist, “We have to fix this because this is not a good way to live. My future is so unknown. I want to be able to go to the park. I want to be able to do stuff with my kids. I want to make memories.” The conversation started happening about referring me to another oncologist for a second opinion to see what we could do.
We were heading in the right direction. This is from surgery being off the table to removing this tumor. It was such a blessing.
Getting a Second Opinion
The goal was to see if I could have surgery to replace the ostomy. I was referred to UCSF and I spoke to a doctor there via video chat. He saw my chart and said, “I don’t see why we couldn’t have surgery for this.” He said that we could pause immunotherapy and then have surgery, but he said that he would refer me to a surgeon there because they would know best.
I was referred to a surgeon and she was amazing. She gave me the worst-case scenario and the best-case scenario. After seeing everything, she said that she would try to see where the tumor was, and if everything wasn’t in my favor, she would remove the tumor or do a colon redirection and repair my hernia.
But if she goes in there and everything looks worse than what the CT scans have shown, then she would close up the stoma and place it somewhere else where it wasn’t likely to prolapse or cause another hernia. She said that as long as I had the tumor, the ostomy had to stay in.
I have been responding really well to treatment. Everything had shrunken significantly. But because of scar tissue and not knowing, we didn’t want to risk reversing the ostomy, having to go to the emergency room again with the same problem, and then having emergency surgery.
We scheduled surgery for June 12th. She came in, took a last look, and made markings. She was so amazing and so thorough. She wanted to cover her bases before going into surgery. She decided on a new stoma placement should we have the worst-case scenario.
Surgery
Colon Resection, Ostomy Reversal & Hernia Repair
Thank the Lord, everything came out great.
The first night was horrible. I had so much pain because it was a pretty big opening. She took out the main tumor and a big chunk of my colon, and she repaired my hernia.
I went back for my follow-up appointment to remove the drainage. She told me that the doctor had taken out everything. She focused on the colon. She gave me the great news that from stage 4, it had gone to stage 1. If the cancer hadn’t spread, that would have been the end of my cancer journey. We still had the liver and the peritoneal area.
The amazing news was that we were heading in the right direction. This is from surgery being off the table to removing this tumor. It was such a blessing. She also took out my appendix because it was connected somehow. She said that they went through it and they studied it and had no cancer, which is amazing news. The cancer stopped spreading.
I still needed to have PET and CT scans to confirm. But he said that everything looked great and that the immunotherapy and surgery were successful.
Seeing a New Oncologist
Another blessing of my husband working in the medical field was that he knew people and started asking for an oncologist referral. I got a new oncologist where we moved and he is amazing.
At my first appointment, he was very proactive. He said, “Let’s see what we can do with your liver,” because that was the next step. Immediately, he referred me to a surgeon at USC.
He explained that I was responding perfectly to immunotherapy. Everything was shrinking. The cancer could shrink a lot with immunotherapy, but there are still cancer cells there and the risk of it coming back is greater. He said that the best thing to do was to have surgery and remove that part of the liver so that’s what we did.
Partial Hepatectomy (Liver Resection)
We scheduled surgery again for September 20th. I mentioned to him about the lining of the stomach and he said he would look into it. He would check that out, too. The surgery date came, I had surgery, and it was successful. Thank God.
He said that everything looked great based on what he saw, but I still needed to have PET and CT scans to confirm. But he said that everything looked great and that the immunotherapy and surgery were successful.
Follow-up Appointment
I saw my oncologist recently, who scheduled me for a PET scan to see where we’re at, but he said that I look good and that everything looks great.
We decided to move, which was scary because I had to look for new doctors and everything.
Getting Support from Family
Moving Closer to Family
Around that time, we made a life-changing decision. We lived in Northern California and decided to move to Southern California to be closer to my husband’s side of the family.
My family had been great, but we needed a little more support with appointments. My in-laws are retired and they’ve been amazing. We decided to move, which was scary because I had to look for new doctors and everything.
Husband as Biggest Advocate
I knew nothing about cancer, just little things that my husband would tell me when he would come home. He would get close to patients that he cared for and when they would pass away, he’d come home sad and we’d talk about it.
Things would be different if my husband didn’t have the knowledge that he did. He’s been my biggest advocate. He understands so he can have conversations with the doctors and surgeons. I don’t know what my situation would have been like otherwise.
I saw a palliative care doctor and she would ask me how he was doing. She said that knowing works like a double-edged sword because he knows too much. He knew stage 4 was serious. He knows that this can go south fast so I can’t imagine what he feels being my husband and knowing all this information.
In a way, sometimes I feel like ignorance is bliss. I didn’t know much, which helped me because I didn’t realize the extent of my illness until I had that conversation with my doctor that one day. But having somebody who knows is big.
Things would be different if my husband didn’t have the knowledge that he did. He’s been my biggest advocate.
Words of Advice
Don’t take your health for granted. If you feel that something is wrong, have it checked out. I never thought in a million years I would be on this journey.
Be proactive and push. The day I went into the ER, the doctor didn’t want to do the CT scan because I looked fine, but I said, “It’s okay if I’m exposed to radiation. Let’s do this. I want to know what’s going on.”
Colon cancer is happening to a lot of younger people. This is not an old person’s disease anymore. I’ve read about people as young as in their 20s being diagnosed with colon cancer.
For some reason, it is so hard to schedule a colonoscopy. Whatever the reason is, that needs to change. It should be more accessible.
So many people are dying because they’re being diagnosed at such a late stage. It’s so silent at the beginning and you don’t know that there’s something wrong until it starts creating havoc in your body and that needs to change.
We need to have a colonoscopy or whatever testing is available at a younger age. My siblings were able to schedule a colonoscopy immediately because I have cancer. They became high risk. My sister had such a hard time scheduling an appointment because of insurance. That should change.
You have to advocate. Speak up and be firm. If something is wrong, don’t stop because the more you wait, the more this monster can mess with your health.
Don’t take your health for granted. If you feel that something is wrong, have it checked out.
Tim, a non-Hodgkin lymphoma & prostate cancer survivor, father of two, and basketball coach, shares his journey from the shock of a cancer diagnosis to his recovery and newfound passion for cycling.
Prior to his non-Hodgkin lymphoma diagnosis, he wasn’t feeling well, was very tired, and had swollen lymph nodes.
His prostate cancer was discovered months after finishing treatment for non-Hodgkin lymphoma when his primary care doctor noticed his rising PSA levels. Given the different treatment options, he chose to have his prostate removed, despite initial reservations about the robotic surgery involved.
Dealing with cancer, he emphasizes the importance of a strong mindset and having a support system, drawing strength from his faith, support group, and friends. Facing the diagnosis alongside his mother’s battle with breast cancer, Tim hopes that his experience can inspire others.
Despite the challenges, Tim’s positive mindset and faith played a crucial role in his recovery, encouraging others to persevere through difficulties with the belief that tomorrow will be better.
Tim’s story is part of the “Our Voices, Our Power” series by The Patient Story. Discover more of the series by exploring Paul’s prostate cancer story.
Thank you to Janssen for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Name: Tim J.
Diagnosis:
Prostate cancer
Initial Symptom:
None; caught rising PSA levels
Treatment:
Surgery: prostatectomy
No matter how tough it is today, tomorrow is going to be better.
I’m a cancer survivor, a father of two awesome sons, and a basketball coach. I recently discovered a passion for cycling.
I grew up in North Carolina. I was the son of a Pentecostal minister. My father was also a farmer so I definitely know the meaning of hard work.
First Cancer Diagnosis
Initial Symptoms
I wasn’t feeling well and was very tired. My lymph nodes behind my ears, my armpits, and my groin area were swollen. I couldn’t sleep.
I finally decided to go to the doctor. My primary care doctor was pretty sure that I had cancer.
They did the first biopsy in the office. They cut behind my ear to remove some tissue. It wasn’t good enough so they had to do another biopsy where they sedated me and took more tissue. I had to wait about two weeks.
I received a phone call one morning. “We need to see you as soon as possible.” When I walked in, I had a feeling that the news wasn’t going to be positive. It was a very uneasy feeling not knowing how that visit would go, but I knew that it wasn’t good news.
There have been moments in the past when I was feeling the same way, but it didn’t linger. It disappeared. This time, the pain progressively got worse and very uncomfortable.
Getting the Lymphoma Diagnosis
My doctor started by saying, “I have good news and bad news. Which one would you like to hear first?” I asked him for the bad news first. He said, “You have cancer.” At that time, he didn’t know was lymphoma because the test results hadn’t come back yet.
Then I said, “Give me the good news.” He said, “The good news is this is the best cancer you can have.”
Once I found an oncologist, we did a spinal tap, which was very painful but a process that must be done to see if the cancer got into my bones. I was very relieved that it didn’t.
In a few days, I found out I had non-Hodgkin lymphoma.
Reaction to the Diagnosis
I didn’t know how to take that. Cancer is cancer. I was in shock, but had a sense of relief, in a way because now I knew the reason why I wasn’t feeling well. Now that we are here, we can start the process of what would be the next step for me.
I wanted to be proactive. If there’s something that I need to do, the more information I have will help me know how to deal with it to get to a place where this is no longer an issue. But I knew there was something wrong.
After receiving the initial diagnosis, I wasn’t worried about myself. I was worried about how to tell my family. How do you start that conversation?
I wasn’t worried about the future. My faith kicked in at that point. I wanted a plan of attack to get started with the process of healing.
The Impact of Faith
There’s no such thing as a perfect life. How boring would that be?
Growth comes from going through storms of life. My diagnosis was a chance to grow. It definitely gave me a more sense of awareness and appreciation for life that was much different than I had before.
Treatment
I went to treatment three times a week and had blood tests every week.
After my first treatment regimen, the cancer was still active in my lymph nodes so we started another treatment regimen. My doctor thought that would work best for me.
Side Effects of Treatment
I lost my hair. It affected me in a much different way.
Throughout treatment, I continued coaching and working. I continued being a part of my honor guard team, which was very important to me.
I maintained my lifestyle and activities as much as possible to help me not focus on my circumstances and what I was going through. Of course, there were days when I wasn’t feeling like this, but they weren’t as often as I thought they would be.
In Remission
I had my last cancer treatment in April, two days before my birthday. A few weeks later, I saw my doctor for a routine visit and he informed me I was in remission. He also told me that remission doesn’t mean that you’re necessarily cancer-free. It does mean that you will have flare-ups occasionally.
I never had that explained to me that way; that was a shock. But on days that I don’t feel that well — and I do have those days — I have something to relate it to.
Second Cancer Diagnosis
Initial Symptoms
In January 2020, I relocated from Long Beach, California, to Savannah, Georgia, for work. In the era of COVID, it was a very isolated time moving to a new city.
There, a primary care doctor noticed that my PSA counts were continually rising. He suggested I go to a urologist and have them run some tests. It was discovered that I had prostate cancer.
Getting the Prostate Cancer Diagnosis
It was a shock. I had been feeling very uncomfortable after riding a bike for numerous miles. This pain was different than being on a bike for 2 or 3 hours.
Reaction to the Diagnosis
It was hard to accept at first, especially knowing that a robot was going to be operating on you. I knew it wouldn’t be an easy recovery process.
I didn’t feel sorry for myself. If I could go through three years of treatment for lymphoma, I would be able to make it through this with no problem.
It’s a very painful recovery process, but I made it through and I knew I would. I just had to be patient. The healing process takes time. It doesn’t happen overnight.
Receiving that news for the second time, I was better prepared because I had already gone through that process of treatment for three years. But even then, I didn’t feel sorry for myself. My thought process was, Why not me? This will be part of my story to let someone else know that they would be okay. They can do it. You can come out of this storm stronger as well.
Breaking the News to Family & Friends
It was very difficult, but I knew I couldn’t keep it to myself because having a support team is very important.
As a father, we want to protect our children. But without sharing the news with them, we hurt them at the same time. It definitely brought us together and made our relationship much stronger.
My son was playing basketball in Finland at the time, but I knew that was a phone call I had to make. It was very difficult for me to share the news with him being in another country.
They were in shock. They felt sorry for me. It was hard for them to come and sit with me during treatment, but as I progressed and went into remission two times, they saw strength, confidence, and resilience.
Talk to your sons about your cancer experience and what they should be keeping an eye out for. I know more about my family history so I pass it on to them. It’s something that they should stay on top of and not be prideful about.
My circle of friends is very small, but a lot of my friends now are in the cycling community. I’m riding with a group I’ve never ridden before. They’re having a meeting and a doctor is going to be present. One of the things they’re going to be talking about is the stigma in the community of men and prostate cancer.
I share my story with them very briefly. My words are very short and to the point. I tell them, “I’m a cancer survivor and I’m blessed to ride with you guys today. It’s no joke. If you’re not feeling well, you should go get checked out. It may be something that’s not going to go away. It’s better to find out now. I’ve lost friends because they were too shy or too proud and didn’t want to tell anyone.”
Talk to your sons about your cancer experience and what they should be keeping an eye out for. I know more about my family history so I pass it on to them. It’s something that they should stay on top of and not be prideful about.
Sharing that news with my mother was very difficult because she was battling breast cancer in North Carolina at the same time.
I was diagnosed with cancer for a second time. My son was in Finland playing basketball. There was a lot going on, but I knew I had my faith to fall back on and I could see myself assuming my normal daily life.
Unfortunately, I couldn’t sit down for more than 5 minutes at a time. I was allowed to work from home, but it meant standing up as soon as I could. A friend was nice enough to drive with me to North Carolina to see my mother. Unfortunately, that was the last time that I saw her. She passed away the following week.
My mother’s very strong. Being strong, knowing that you’re going to be okay, and falling back on your faith came from her. She was more worried about how I was doing than what she was going through.
Dealing with a Cancer Diagnosis
Cancer is not something you can plan for. Cancer can affect you at any age. When it affects you personally, there’s a choice you have to make. How do you deal with it?
Having a strong mindset from the beginning can make a difference. From the day I received my diagnosis, I could see myself after the process and the healing process was over.
I didn’t focus on my circumstances at the moment because I knew this was something I would recover from. However, that would be a process that I would have to go through, but it was one that I wasn’t afraid of. I knew I would be okay.
Prostate Cancer Treatment Options
I was given three options. I could have my prostate frozen, undergo radiation treatment, or have my prostate removed. I asked my doctor what choice would he make if he were in my position. He said he would have it removed so I made the same choice.
After three years of immunotherapy treatment, I didn’t want radiation because of what it does to your body. For me, the best choice after getting advice from my doctor was to have my prostate removed and deal with the process of recovery and healing.
I had a chance to discuss my options with the surgeon as well as my primary care doctor. A team of doctors gave me what they thought the best options were and what the side effects would be.
Recovering from Surgery
It was difficult at times not being able to sit, not being able to sleep the way you wanted to, and being confined home a lot. Your whole approach to your body functions is a lot different.
It’s a very long, painful process, but I’m blessed it was found early because I could have had a much different diagnosis.
Follow-up Protocol
I see my oncologist every six months. There were blood clots in my lungs that were discovered during a routine check in August 2022 so I was placed on a blood thinner.
I continue to cycle. I didn’t let that stop me. After four months, they took me off blood thinners. We still don’t know the reason why the blood clots were there, but life goes on.
Importance of a Strong Support System
My high school basketball head coach had my initials along with our trainer who was also going through cancer treatment put on the jerseys for that season. They had us come up. To have a high school cheer for you made a big difference.
A good support group comes in handy. You can pick up the phone and say, “Hey, I’m not feeling well. I have this test coming up.” To have someone to reassure you that everything’s okay makes a big difference.
My faith was first and foremost. That was my go-to. I also had my support group and my friends from church.
It’s very important to have a first responder, someone you can go to when you receive bad news.
My circumstances don’t control who I am, but at the same time, I have a core support group that I can reach out to when I’m not feeling my best. They reassure me that I’m okay and I can reassure them that they’re okay.
Stigma of Prostate Cancer
I feel there’s a stigma. Part of the stigma could be not having the financial coverage that should be available to everyone. Pride is a factor.
Men are very proud. I’ve got this. Nothing’s wrong. I’m going to be okay. Even if I feel uncomfortable for a week, it’ll go away. If I tell my friends about this, they’re going to think less of me. my friends are going to laugh at me. They aren’t going to understand. My kids aren’t going to understand.
When your body is telling you that there’s something wrong, don’t ignore it.
I’ve had conversations with my sons and told them if they’re not feeling well, go to the doctor. It’s important to know your family history.
Unfortunately, I grew up not knowing my family history. My father was a Pentecostal minister and they didn’t believe in doctors. As a young man growing up and you don’t know your family history, it puts you in a high-risk category. The only time I went to a doctor when I was younger was for my physical for sports.
I believe everyone’s given a gift in life. When you’re not feeling well, your body tells you. It’s very important to listen to your body and go to a doctor rather than trying to diagnose yourself.
My story can be used to cheer someone else on. I became stronger, more generous, and more understanding of others. There’s nothing more powerful than when you’re going through treatment.
I’m blessed to sit here and tell my story and have that opportunity to bless someone else.
Words of Advice
I’m human. I allow myself to have those thoughts but not stay there. We have freedom of choice, especially with the way we think. I would welcome that thought but never let a negative thought control who I am because that’s not who I am.
Storms of life are going to happen. How you choose to navigate through them is up to you. I became stronger for my children.
Share the news with your family as soon as possible. You will have good days and bad days, but when you have a core group of people who love you and care about you, they will be there for you on those bad days.
Listen to your body. If you’re not feeling well, go get checked out. Don’t wait to have tests done. They’re vital because they’re very important to staying on top of your health.
Be strong for someone else who may be going through the same thing.
Cancer is part of my life story, but fortunately, I’m blessed to share this story with other men who may not want to get checked out. Even women ask me how I’m able to do what I do. First, my faith. Second, I didn’t let my circumstances control who I am.
Having a very strong mindset from the beginning is the key. See yourself not where you are now, but where you will be when you go into remission. Realizing that through that process there will be days when you’re not feeling your best. But remember, those days won’t last for long.
New Motivation
Cycling gave me an outlet during COVID. I could get out and ride in Savannah for 10, 12, 15, 20 miles to clear my head. It gave me a new sense of purpose and not let what was going on around me and the world affect me.
Cycling is a process. It starts with being mentally tough, just like going through treatment. I feel empowered. I’m doing something that I never thought I would be doing, but I’m blessed to do that.
Cycling has given me a second chance, another option to be active. It also allowed me to tell my story. I met an awesome young man who is going through treatment and he told me about The Patient Story and how he thought it would be an awesome opportunity for me to share my story.
I have a sense of gratitude that I can ride 50 miles at 25 miles an hour. I can push it to 30 miles an hour.
As a cancer survivor, I hope that what I’ve gone through can give someone else hope to hang in there. No matter how tough it is today, tomorrow is going to be better.
I’m blessed to tell my story. I didn’t know when that process started that a bike would be my saving grace. But it was and I could use that as part of my journey to help someone else.
Special thanks again to Janssen for its support of our independent patient education content. The Patient Story retains full editorial control.
When Joseph was diagnosed with prostate cancer, the news came as a shock and forced him to face questions about his health, future, and faith. He shares how he navigated his diagnosis, chose robotic surgery, and learned to open up to his loved ones about his health.
Lena was diagnosed with stage 1 diffuse large B-cell lymphoma (DLBCL) and shares her journey from pre-diagnosis to life after cancer.
Initially, she had blood in her urine, which she thought meant a UTI. After being treated with antibiotics, her symptoms first alleviated and then worsened, which eventually included clots in the blood. Further tests revealed a bladder tumor. Despite having no typical signs of DLBCL, the diagnosis came unexpectedly after she had surgery to remove the bladder tumor.
Lena recounts the challenges of chemotherapy, including severe reactions to certain medications and the emotional toll of losing her hair. Following chemo, she underwent a month of radiation, which she found relatively easy compared to the previous treatment.
She highlights the various side effects faced during and after treatment, such as neuropathy, loss of taste, and early menopause. She also emphasizes the importance of managing emotional well-being, seeking support during and after cancer treatment, and staying strong throughout the cancer journey.
She shares her positive approach, acknowledging the support received from family, friends, and medical professionals. She encourages open communication with doctors, advises against excessive online research, and advocates for finding the right medical team and support groups.
In addition to Lena’s narrative, The Patient Story offers a diverse collection of diffuse large B-cell lymphoma (DLBCL) stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
Name: Lena V.
Diagnosis:
Diffuse Large B-cell Lymphoma (DLBCL)
Staging:
1
Initial Symptom:
Blood in urine
Treatment:
Surgery
Chemotherapy: R-CHOP
Radiation
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I’m 53 years old. I’m a wife, a mother, and a grandmother. I enroll students for a university in Arizona. I live just outside of Phoenix in Mesa.
My husband has a motorcycle. We like to go motorcycle riding in the winter when it’s cooler because it’s so hot in the summer.
We have lots of kids around us and grandkids that we like to spend a lot of time with. We are a blended family of six children, ages 32 to 14. The 14-year-old lives with us. He’s our last one in high school.
We have learned to be very grateful and live our best life. Every day is a blessing.
Pre-diagnosis
Initial Symptoms
I had no symptoms that are typically involved with diffuse large B-cell lymphoma. I didn’t have any pain, fever, night sweats, or weight loss. I was told after the fact that it typically affects men who are over 65.
I thought I had a UTI. I had a little bit of blood in my urine. I went to urgent care and they did the routine test, gave me an antibiotic, and sent me home. That alleviated the blood in the urine for a few days then it came back heavier and with clots in it. That’s when we knew there was a problem.
It was completely out of the blue. I was healthy. We were newlyweds. We were about a year and a half into our marriage. We sold a house that we had as a rental and we were doing some work on the inside of it. We were celebrating my son’s birthday the next month.
I remember going to the bathroom at the restaurant three times. I thought I was getting a period. I wasn’t sure, but I had no pain. The next couple of days, it seemed like there was always blood and I thought I had a UTI or it was in my kidneys. The reason I went to urgent care was to make sure there was nothing else going on.
I took the antibiotic they gave me for a week and the blood had alleviated. There was no blood for about 3 or 4 days then it started to come back slowly and I thought, Maybe this infection is coming back. Maybe it’s farther into my kidneys than I thought. I still didn’t have any pain, fever, or any other symptoms but the blood.
There were clots in the blood so it was getting harder to urinate because the clots were blocking the way. I was trying to use the bathroom and it hurt. I couldn’t go at all because there was a blood clot blocking the way. I didn’t realize that at the time, but I figured with everything that had happened that was the issue.
I was crying and my husband said, “We’ve got to get you to somebody.”
Trying to Get a Urologist Appointment
The next day, I called a urologist and told them what my symptoms were. I had to call six of them because they were so busy. One of them was backed up for about six months and I thought, I can’t wait that long. That’s a long time.
I found an opening the next day, but it was with a nurse practitioner. I said, “I’ll take it. I will absolutely take it. That’s fine.” I saw her and gave a urine sample, but it looked like a cup of blood. She said, “Everything that we’ve tested looks very interesting so I’m going to send you over and we’re going to get a scan done.” That’s when I went, “This is not good.”
Getting Referred to a Cancer Center
I went over the same day to check in and I drove into the parking lot and it was Ironwood Cancer & Research Center. That’s when I thought, Oh boy, is this cancer? I didn’t know because she didn’t know and she didn’t tell me it was. She said, “We’re going to take a look at it because we don’t know what’s going on.”
The urologist was amazing. He took out most of the tumor. He couldn’t remove all of it because it was attached to the wall of my bladder.
Getting a CT Scan
I had the scan done on Valentine’s Day. On Monday, which was President’s Day, I got a phone call and they said, “We’ve looked over your scan. You have a tumor in your bladder.” It was about 5 cm, which is the size of a lime. They said, “We’re going to have to remove it immediately so we’re scheduling you for surgery on Thursday.” This went from zero to surgery.
Surgery to Remove Tumor
I had the surgery done and the urologist was amazing. He took out most of the tumor. He couldn’t remove all of it because it was attached to the wall of my bladder. He said if he removed it all, it would have perforated my bladder and that’s a whole different lifestyle for me so he opted to leave part of it there to protect my bladder.
Going in, they thought I might have bladder cancer and he said the tumor looked nothing like bladder cancer, which typically resembles a flower. We thought maybe it was a cyst. At that point, we thought, Wow, it’s not cancer! That’s great! We didn’t even think it could be a different kind of cancer.
After my surgery, the doctor spoke to my husband and my mom who had flown from Montana to help. He said, “We’re going to send this off for a biopsy.” I went home with a catheter for a week to help my bladder heal.
Had we not caught it when we did in February, I would not have made it to my birthday in September. It probably would have killed me before then.
Diagnosis
Getting the Official Diagnosis
The day I had my catheter removed, the doctor accidentally called my husband on his way home from work, thinking it was my number. He ended up telling my husband my diagnosis and my husband had to tell me, which I can’t imagine being in his shoes.
He came home and pulled me away from my mom to take me into the other room and said, “Dr. Matthews called me accidentally, but he told me what’s going on. You have diffuse large B-cell lymphoma.”
I was trying to be so optimistic. I said, “I have no idea what that means.” He said, “It’s a type of cancer in your blood and he’s very thankful that we caught it because now you can get treated for it. You’re going to do six rounds of chemo and a month of radiation possibly.”
Thankfully, it was caught because Dr. Matthews told me this type is very aggressive. Had we not caught it when we did in February, I would not have made it to my birthday in September. It probably would have killed me before then.
I knew nothing about staging. I was stage 1, which means it didn’t spread to any other areas of my body so that was why they did the bone marrow biopsy. They wanted to make sure it wasn’t in my bones.
The scans were to make sure it wasn’t in any of my organs that were around my bladder. My bladder pretty much contained it all, luckily, because it could have spread to my liver, to my stomach, and all of those organs right there. My bladder held it in and that’s what saved me.
Reaction to the Diagnosis
My mom is a breast cancer survivor. She was on hormone replacement therapy, which is what caused her to have breast cancer. She had a mastectomy done. She’s a fighter. She’s tough, she’s fierce, and she’s feisty. She’s a little Thai woman and she’s hilarious. I take after her quite a lot in that area.
I sat there in shock after my husband Dave told me and thought, Wow, really? Are you sure? I got upset a little bit because my dad wasn’t there. We shared the news with my mom and she had this look on her face. She stood up, slapped my arm, and said, “You’ll be fine,” and walked out of the room. I said, “She’s right,” and that was the attitude I had the whole time. This isn’t over. I’m just starting.
‘I have a lot of life to live. Can we get started ASAP?’
Treatment
Discussing the Treatment Plan
After we had determined my steps, I was referred to an oncologist at Ironwood Cancer & Research Center, which was a mile and a half from our house. I met with Dr. Monique Chang. I had my mom and my husband with me.
The minute I went in there, I said, “Look, I have a lot of life to live. Can we get started ASAP?” She said, “Oooh, you’re a spitfire.” And I said, “I am. This is not going to get me. We’re going to do this.” And she said, “Absolutely.”
We set up the appointment for chemo, but I had to have an echocardiogram, a port placed, and a bone marrow biopsy. They wanted to make sure that it wasn’t in my bones. Those were the next steps before my first treatment.
Chemotherapy
I did R-CHOP, which is a very common treatment for DLBCL, but I also have the Neulasta device on my arm. The device itself didn’t hurt. It helps rebuild your bone marrow so it’s very painful when you’re healing from that.
The injection is the day after chemo. It injects you for about 30 minutes and it’s painful the next couple of days out. It was probably about a week after that that you ache. Your bones ache because it’s regenerating all those white cells for you.
I did chemo every three weeks from March to July 2nd. My very last treatment was on my husband’s birthday.
Radiation
After chemo, I did a month of radiation. The doctor wanted to make sure they got everything. It was one treatment daily for the whole month of August 2018.
Radiation was a piece of cake for me because I didn’t feel anything. They made a pillow that fit my body in the area where they were scanning it and I would just lay there. It was under 30 seconds every day and I was out of there. The wait in the waiting room was longer than the radiation itself.
After chemo, I had a stutter so it took me a while to be able to talk again to where I could piece a sentence together.
Side Effects of Cancer Treatment
R-CHOP was difficult. On my very first chemo day, we went at 7:30 in the morning and they told us it was roughly 5 to 6 hours. For us, it was almost 11 because I reacted to vincristine, which they call the Red Devil.
It was brutal. The first time I had it, I turned red and felt like my insides were made of lava. I felt like I was melting. It was that bad of a reaction. They slowed down the drip for that and that helped so I never had a reaction again.
In between each medication, they gave me Benadryl so I was completely groggy by the end of the day. Honestly, I’m not sure how my husband got me out of the car and into the house. I remember that being a very, very long day.
I had to take prednisone as well, which is not my friend. I know that it’s very helpful for a lot of people and it’s part of the regimen for this particular type of cancer.
I was taking five doses of prednisone a day for five days each time I had the treatment. I gained a lot of weight because of it. Normally, cancer patients lose weight because of chemo and being sick and nauseous. That may be the case, but the prednisone started packing on the pounds.
I had bad neuropathy. I still suffer from neuropathy. Five years later, I still have some issues. Not as bad as they were, obviously, but with every chemo session, I would get a headache right at the base of my skull and nothing would make it go away. It would go all the way down my arm.
By the end of chemo, I couldn’t tell the difference between hot and cold. My fingers and toes were numb. My hands and feet were a different color. They were grayish. I heard it’s a typical change. There was another patient there who she said all her toenails and fingernails fell off. They turned black and fell off from chemo.
Many different things can happen to you. I tried acupuncture to alleviate some of the pain, but it did not work for me. They tried to put me on gabapentin and other antidepressants, but the side effects from those were so bad that I didn’t want to do them.
I never regained a period so I got pushed into early menopause and had heavy, heavy hot flashes. I would have them for minutes at a time for probably about six months, midway through chemo until the end of that year.
I still have hot flashes, but they’ve slowed down. I didn’t take any hormone replacement therapy after my mom went through what she did. I said, “Absolutely not. I’m not going to do it. I’ll naturally let my body figure it out.”
After chemo, I had a stutter so it took me a while to be able to talk again to where I could piece a sentence together. I would try to talk and it would not come out. That took me close to a year to feel like I could speak normally again.
My very last chemo treatment was almost as bad as the first one. I was disappointed because it’s your very last one and you’re thinking, Oh, I’m done. This is great! I’m finished! It kicked my butt and I was down for about a week. Typically, after each treatment, I would be out of it. It was never the day after. It was the day after that for 2 or 3 days when I didn’t feel right at all.
I lost my sense of taste for almost two years. It’s still off. I love coffee, but it does not taste the same as it did at the beginning of 2018. It’s not the same.
I didn’t have any side effects from radiation. They told me, “You could have blood in your urine.” I freaked out when I heard that, thinking, I don’t ever want to see blood in my urine ever again. They said I could be fatigued. They said I could have burn marks. I had none of those so I was very lucky.
I’m not going to sit here and feel sorry for myself because it’s hair. It’s going to grow back. My mom’s came back after her treatments. It will come back.
Hair Loss Due to Chemo
My son was eight when I was diagnosed. We honestly weren’t going to tell him. I said, “We can hide it. I’ll be okay.” I told the nurse, “I’m not going to lose my hair.” And she said, “Oh no, sweetie, you’re going to lose your hair. You don’t have a chance to keep any of it.” I thought, I’ll be the one that does. It’s okay. I’ll be the one, trying to psych myself up.
I woke up one day and our white bedding had a big pile of hair. I started brushing it and the sink was full of hair. That was after my first treatment.
I cried for about an hour and a half, sitting there, pulling it, and combing it. I could feel where I had little patches and thought, I’m not going to sit here and feel sorry for myself because it’s hair. It’s going to grow back. My mom’s came back after her treatments. It will come back.
That night, my husband shaved my head. Not gonna lie, it was hard. It was hard for him. He didn’t want to do it. I said, “I need you to. I can’t do it by myself.” At the time, our son came in and said, “You shave my head, too,” so we all shaved our heads together.
It’s tough. It does grow back. My hair grew back weirdly. Initially, it grew back white and stubbly. That all fell out and then it grew back to salt and pepper, which was appropriate for my age, but it was curly like I had a perm. That lasted about a year. Then as it grew out, it returned better than it was. It’s thicker and healthier than it was before.
Managing the Side Effects
The neuropathy is much better. I use CBD oil; that was the only thing that relieved the pain. I take CBD gummies to help me sleep.
I’ve been suffering from neuropathy for about a year and a half. I was trying Tylenol, ibuprofen, and Aleve, and nothing was working. I thought, This is something I’m going to have to deal with. I’m alive. If this is the worst of it, I accept it. I’m still alive.
One of my friends and I were standing and having a conversation and she said, “Have you ever tried CBD?” I said, “No, I never really gave it a thought.” She said, “You should try these.” I thought no because in my mind, you’re going to smoke weed and I didn’t want all those weird side effects either. I thought, No, it was never my thing. I’m not that girl. I don’t want to do that.
She said, “There’s no weed in it. Let’s try it.” She had a little tincture bottle in her purse and she put two drops under my tongue. Within an hour and a half, the pain was completely gone and it never came back.
It’s not going to work for everybody. I got lucky that she suggested it because I probably would have never done it on my own.
Once you reach the five-year mark with this particular type of cancer, you are considered cured.
Monitoring with Scans
I was pretty good about keeping a journal. I’m very organized. I kept every piece of information because I still have chemo brain. There are things that I’ve forgotten that people remind me of and I can’t remember.
I had the CT scans and PET scans often when I was going through treatment. I had one at the beginning, one at the midpoint, one right before my final treatment to make sure it was going to be my final treatment, and one after my final treatment.
I’ve had to have a cystoscopy where they go up into your bladder with a camera. My urologist at the time was wonderful. He has since retired, but I never felt any pain and he was amazing. He was a good source of positivity.
I don’t have to have a cystoscopy or scans anymore. If I start to feel anything off, they told me to come back and they’ll check me out completely.
At the end of chemotherapy, they said that everything looked clear. November 6th was my final cystoscopy after chemo. That was when Dr. Matthews said there’s no evidence of disease so that is what I count as my anniversary date.
Dr. Chang told me that once you reach the five-year mark with this particular type of cancer, you are considered cured. I was thankful that she removed my port when she did because many patients have to keep a port in for at least a year or two after treatment. She was confident enough to let me get mine removed.
I said, “I can sleep on my stomach again. I don’t have this object protruding out of my chest and I don’t have people staring at me.” I don’t care if you stare at me now. This is a badge of honor, honestly. It was a good feeling to hear that there was nothing left.
When I saw Dr. Chang not long ago, she said, “You did it.” I said, “You helped me do it because there’s no way I could have done it alone.” She’s amazing. She’s in the Phoenix top 100 physicians and she’s incredible.
Even on my worst, worst, worst day when I was miserable and in bed crying because I was in so much pain, I knew there was light at the end of the tunnel.
Managing Scanxiety
I know it’s not realistic for all people, but if you can, have somebody go with you. My husband typically would go with me and wait with me. I would go in there with a positive attitude.
I know it’s hard. It is hard. Even on my worst, worst, worst day when I was miserable and in bed crying because I was in so much pain, I knew there was light at the end of the tunnel. I had to keep going because if I gave up, what good would I be to my kids, my grandkids, and my family who were watching me struggle and were helpless?
You’re the one in charge of your emotions every day. You have to get a hold of that and stay positive. Because if you let go of that and you sink into this hole, it’s really hard to get out of it.
I wanted my normal life back and it was never going to be like that again.
Life After Cancer
I had a hard time after treatment because I went into a bad depression, which made no sense. I’ve been used to this routine and being taken care of by these specific people. Then when you’re done and you don’t have that routine anymore, even your friends fall by the wayside. They check in once in a while. This is pretty common from all the people I’ve talked to so it’s not their fault.
When you think about somebody going through cancer and then they’re done with their treatment and they’re in remission, a lot of times people think you’re okay. We’re not okay.
I went through a lot of mental struggles. I had to go see an integrative oncologist. She was like a counselor. She tried to get me back to my new normal, which I was sick of hearing. I wanted my normal life back and it was never going to be like that again.
If you have a doctor that is not listening to you, it’s not the right doctor for you.
Shared Treatment Decision Making
I had a terrible family doctor who had the worst bedside manner and who wasn’t sympathetic. I’ll never go to another doctor who doesn’t understand and listen to me first of all.
A lot of times, people need a second opinion if they’re not comfortable with their doctor. With the surgeon whom he referred me to, I researched on her before I even saw her. When I talked to her, I thought, If I’m not comfortable when I talk to her, I don’t care what kind of accolades she has, I will find another doctor, because I’m very much one that will speak out and advocate for myself.
She listened to me and my needs. When I told her I was going through the pain with neuropathy, she was the one who sent me to the integrative oncologist who then asked, “Lena, what do you need most? I can put you on antidepressants. I can put you on this.” I said, “I don’t want to take medicine. I’ll do lion’s mane to rebuild my brain. I’ll do whatever it takes. I don’t want to take any more pills.”
She worked with me. She suggested acupuncture. She suggested lots of other things that were great. If you have a doctor that is not listening to you, it’s not the right doctor for you.
If you’re going through something, you have to reach out and let someone know. There is a ton of support.
Words of Advice
I shared a lot of information on social media not because I wanted attention for what I was going through. I wanted to share my feelings and be honest with people. I had people messaging me, saying, “Hey, my mom just got diagnosed.” “My brother got leukemia.” I’m able to use what little voice I have to try to help those people get through it.
I’m a big advocate for speaking up for yourself. If you’re going through something, you have to reach out and let someone know. There is a ton of support. I found that out after the fact because I lost friends with cancer through my journey. You have survivor guilt plus depression plus not going to treatment anymore. I miss my nurses who were fantastic in my recovery.
You’re in a whole new cycle of life that you’re trying to navigate and you still have it in the back of your head. Every doctor’s appointment, every time I go for a scan, every time I have blood work done, I think, Something’s going to go sideways.
Talk to somebody, even if it’s a stranger. LLS has all kinds of resources and support. They were huge in helping me find support. My oncologist had a list. They had support groups at Ironwood Cancer & Research Center. They were supportive. They had mental health checks.
I wish people would reach out. It’s important. If you’re feeling any type of way, do something about it because sitting there is not going to help. You’ve got to talk to somebody.
When you get diagnosed, do not Google anything. Don’t have family members do it. Don’t have friends do it. I was told that immediately and I listened. Had I done it, that would have probably put me down a rabbit hole of despair and giving up. Everyone’s journey is completely, completely different so stay on track.
Listen to your doctors. If they’re not listening to you, find a new doctor
Find support groups. There are tons of them out there. That’s how I found The Patient Story. I was posting about Light The Night when Instagram suggested The Patient Story.
There is hope. Don’t give up. Stay fighting. Stay strong.
Cindy was diagnosed with stage 4 diffuse large B-cell lymphoma (DLBCL) in April 2021 and concurrently battled COVID.
About a month before getting diagnosed, the palms and soles of her feet started getting itchy. Later on, her skin started turning yellow and she was feeling sluggish. Since she never got sick, she didn’t think anything of it until her eyes turned yellow as well.
She took herself to the ER and there found out that her bile duct was completely blocked, in which they performed surgery to put a stent in.
Not long after, she tested positive for COVID and had double pneumonia and super pneumonia. To give her lungs a break, she had to be intubated, not realizing the severity of her condition.
Her oncologist was so relieved upon seeing her in his office since not all patients have the same outcome as her. Once she started treatment, the tumors started shrinking immediately.
She shares her journey going from being extremely healthy to getting diagnosed with cancer and getting COVID, how she had to relearn breathing, swallowing, walking, and talking, and her spiritual journey while she was in the ICU.
In addition to Cindy’s narrative, The Patient Story offers a diverse collection of diffuse large B-cell lymphoma (DLBCL) stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I am retired so I’m no longer working. I have a couple of kids and six grandkids.
I have a couple of dogs that keep me as companions. I’m in remission now from the diffuse large B-cell cancer.
Pre-diagnosis
Initial Symptoms
I was diagnosed in April 2021. The skin on my palms and soles of my feet started to get itchy maybe a month before. I thought it was dry skin because it was still winter. I ignored it because I was in extremely good health. I never get sick.
My skin started turning yellow a couple of weeks later. I made an appointment with my primary care physician. I was a little sluggish and tired, but I wasn’t sure why. I thought I was working too hard so I ignored those. I told myself, “If my eyes turn yellow, I’ll go in.”
They turned yellow so I took myself to the ER, called my kids, and let them know. My daughter came to join me. They did blood tests and CAT scans. They came up with this horrible diagnosis that I was going to die from some rare type of cancer. They didn’t even know what it was.
I didn’t have time to process. I didn’t realize I was that sick.
They called a GI specialist who came in and did an endoscopy. That’s when they determined I needed to do surgery immediately because my bile duct was completely blocked.
They asked for a urine sample. The urine was red so it wouldn’t have been much longer and I would have been dead in the next couple of days.
Diagnosis
Reaction to the Diagnosis
I didn’t know anybody in my family who got diagnosed with what I exactly had. There was one tumor around the bile duct and one in the liver hiding.
It was surreal. I’d been extremely healthy. I didn’t get colds, flu, or anything. It was a shock.
I didn’t have time to process. I didn’t realize I was that sick. I went to the ER, got the surgery, got blood work, saw the oncologist, and started treatment the following week.
I didn’t know what to expect. I didn’t even know what this cancer was. I couldn’t sleep so I watched TV a lot at night. I saw an infomercial about the type of cancers that Roundup was causing and they said, “Call one of our lawyers.” They took my case like nothing.
It’s been an interesting journey getting that sick. Honestly, even when I got out of the hospital, I never really thought I was that sick. It wasn’t until maybe six months later that it sunk in. Even when I had to learn how to walk, talk, and all that, I thought it was normal, but it’s not.
Those were challenges that I had to go through, but I stayed positive. I didn’t question anything and did what I was told. The way I looked at it, I’ll be okay by Christmas and be able to be with my family. That was my goal and that’s what I cared about. That’s what got me through everything.
I didn’t know what to expect. I didn’t even know what this cancer was.
Biliary Stent Placement
After they put the bile stent in, I started to get my color back.
Appointment with Oncologist
They scheduled me for an oncology appointment. When I saw the oncologist, he was very real. He said, “I can cure this hopefully in 6 to 8 treatments.”
He asked if I had any questions. My daughter, poor thing, was crying her eyes out. I felt bad for her. What I heard was that I can be cured. What she heard was a death sentence because she heard chemo.
I asked if I was going to lose my hair. He said yes. She cried more. I said, “It’s just hair. It grows back. It’s not a big deal. Who cares?”
My other question that she couldn’t believe I asked was, “Can I still drink beer?” I like beer. He said, “Yeah, two a week.” He knows once you get on chemo, who wants a drink? You’re sicker than a dog.
They did blood work the week before I saw the oncologist and he explained what type of cancer it was and what type of chemo they were going to do. They have you watch videos, give you pamphlets, get the port put in, and start getting you hooked up.
My daughter asked, “If she doesn’t do chemo, how long will she last?” He said, “She’ll be dead by July.” It was that aggressive and I didn’t know. I was always against chemo, but when you’re in that position, you change your mind real quick. If that’s what’s going to save my life, so be it.
Testing Positive for COVID
I tested positive for COVID. My lungs were acting up, but they still sent me home only to come back three days later and be admitted for a month. I was intubated in between that time because the COVID was so bad.
If I never had chemo, I could have been okay with COVID. I never got sick. This is new to me so I didn’t know I was that sick.
I was rolling with the punches. I slept all the time. That was all I could do. I had no energy.
My lung capacity was going way down and I was on oxygen, but it didn’t concern me. I thought that I’d snap out of it sooner or later. Even when they said they needed to do a transfusion, it didn’t concern me.
Getting Intubated
On my daughter’s 40th birthday, they woke me up and said, “We need to intubate you. We need to give your lungs a break.” As far as I was concerned, it had to sign the document and that’s all it has to be.
I could barely talk. My daughter planned a trip to Mexico and I kept trying to tell her, “Go on your trip. There is nothing you can do for me.” She was so emotional that I didn’t think she could hear what I was saying.
The next thing I know, I’m intubated. I remember waking up and being tied because I tried to pull it out, but I don’t remember that.
I remember waking up one time and biting it nervously. It’s an ordeal to be on a breathing tube. Nobody wipes your saliva so it goes down the back of your neck. Your nose runs and nobody cleans it. Your lips are severely chapped.
They do bathe you. Thank God for the port because that’s how they fed me.
My lung capacity was going way down and I was on oxygen, but it didn’t concern me. I thought that I’d snap out of it sooner or later.
Spiritual Journey
The things that I remember were crazy. During one of those times, I believed I was going to die because I saw my body float past the stars to the universe. I could see around the world.
I saw people from Saudi Arabia praying. I saw my friends and relatives who were Catholics praying with candles and my other cousins who were in two different congregations. My kids’ dad, who was Native American, was doing a ceremony in a teepee. All of these people were praying.
Seeing those woke me up to the things that I took for granted like breathing, walking, talking, and swallowing, which I all had to relearn.
When I felt myself slipping, I prayed. All that came back to me. Am I religious? No, I’m more spiritual. But I was asking the universe, God, anybody, “Just let me live. I’ll figure it out from there.”
I begged for my life that night.I woke up and the sun was out. I was so grateful. I wasn’t out of the woods.
When I could talk, the first thing I asked my daughter was, “Did your dad do a ceremony for me?” She said, “How did you know?” I said, “Because I saw it.” I asked my two cousins, “Were you guys praying for me? Each one of your congregations?” They said yes.
The one that stumped me was Saudi Arabia. I don’t know anybody there. I told my father about it and he said his wife’s daughter married Saudi Arabian. They live there and they told them so their whole congregation was praying. That’s what I saw.
When I felt myself slipping, I prayed. All that came back to me.
Getting Off the Ventilator
They tried to get me off the ventilator. I couldn’t talk, but they put me on a Zoom video call with my daughter. They put the phone on my chest and all I could hear was, “You breathe the same air that we breathe, Mom. They’re going to take you out tomorrow. Take deep breaths. You’re going to be fine.”
The next day, they said, “We’re going to take you off. Honestly, the worst thing is the stickers on your face that hold the breathing tube.” I didn’t feel the breathing tube coming out. They were too busy sticking their fingers in my mouth and checking that I didn’t crack my teeth.
The nurses loved my bald head. They’d come by and rub it all the time.
Recovering from COVID
It’s been an interesting journey being shut in because COVID was really bad. I had no immune system. I didn’t dare go to a store. I didn’t go anywhere out of the house except to the doctor’s visits or blood work. I was very cautious. I never want to be that sick again.
I had a double pneumonia and a super pneumonia from COVID so my lungs are scarred. Can I handle another pneumonia? I don’t know and I don’t want to find out.
My mother was very sick when I was a child. She had heart disease so she was intubated several times. We saw that and she came out of it every single time. To me, when he said they were going to intubate me, it didn’t scare me. I thought I’d be fine.”
My kids couldn’t understand that. You hear people dying from COVID, but in my mind, I’m going to come out of it. I’m going to be okay somehow.
Treatment
Getting back to the oncologist, I was determined to get off the walker and walk into the oncologist’s office with no cane and I did do that. He was so incredibly happy to see me. He kept saying, “So good to see you, my friend. So good to see you. I watch your chart every day hoping you weren’t going to die. When do you want to start chemo?” I looked at my daughter, “Why is he asking me that?” She said, “Do you not have anybody like my mom?” He said, “No, they all died.”
I want to get on with treatment as soon as possible because I want to get on with my life. His being concerned that the cancer was so aggressive scared me a little. I figured I had already gone through the worst. Plus I was trying to get my strength back.
I’m grateful to my children for being here, taking care of me, cooking my food, and helping me. You lose so much strength and muscle. Taking a shower is horrendous. It’s an energy sucker. I had to learn all these things a little at a time.
Side Effects of Treatment
Five days after treatment, I got neutropenia. I ended up in the hospital for a week.
I only had one chemo after coming out of the hospital so it did make me tired but not more tired than what I had already been through.
I never got nauseated, which was a good thing. I did get neuropathy so now I have chronic neuropathy. I have chronic lower back pain. I don’t know what to contribute that to other than being in the hospital for so long and staying in the same positions plus the shortage of nurses to turn you when you’re in ICU.
The last chemo kicked my butt. That left me weak for weeks.
I want to get on with treatment as soon as possible because I want to get on with my life. His being concerned that the cancer was so aggressive scared me a little.
Follow-up Scans
The tumors were starting to shrink very fast. They were almost gone on the first treatment, but he wanted to do two more to make sure.
Right now, their only concern is a small lesion on my liver. They don’t know what it is. It’s staying steady, but it’s still there.
Some of my blood work for the liver is still high and we don’t know why. The liver could be damaged, probably from the chemo. I don’t know how long it takes to recover. The last scan I had still shows the lesion.
He may want to do a liver biopsy if it shows up again in six months. It might be scar tissue.
Life After Cancer
I hadn’t been out in so long that I didn’t even know what’s what anymore. There’s so much new development.
I went to play darts once and in the back of my mind, I got freaked out that I was around a lot of germs, but my counts were pretty good so I felt okay. It’s summertime and the doors are open.
In the fall, I’m not going anywhere. I do believe that my immune system is better. My granddaughter comes over and she’s been sick twice but I didn’t so I must be doing okay.
I don’t want COVID again. That put the fear of God in me. I don’t even know if I can handle the flu. It’s an interesting journey going from being extremely healthy to this crazy cancer because that never ran in my family.
They said I had to relearn to swallow; that’s part of having the breathing tube. I thought they were kidding me, but they didn’t lie because I tried to swallow Jell-O and it freaked me out. Even today, I have problems swallowing.
I have to chew my food in tiny little bites because I’ll choke. They can stretch it if they want to, but I don’t want to do that because I’ve had so many surgeries and procedures.
Staying Positive
Being positive is the key to anything, regardless of what you do in life. I never asked why me because why not? Why not me?
Words of Advice
Stay positive. It’s okay to get angry, but don’t dwell on it.
Try not to feel sorry for yourself because it’s not going to do any good. You’re going to give cancer the advantage. Go in with the attitude that you’re going to kick its butt. They give you all the tools to kick its butt.
Know that you’re not alone. It’s unfortunate, but you’ll get through it. There’s no reason not to.
I had a rare cancer. They told me I was going to die, but I thought to myself, No, I’m not because you don’t know me.I’m not going to die. I don’t care what kind of cancer you say I have. It’s not going to happen.
Be positive and know yourself. I’m pretty stubborn so that helps.
I’m alive and kicking. My grandkids and my dogs are happy. I get so excited to see a full moon or the leaves change. I appreciate life.
Patients, care partners, and a panel of CLL experts including Dr. William Wierda, MD, Ph.D. from MD Anderson, Dr. Nicole Lamanna, MD from the Columbia University Medical Center, Dr. Adam Kittai, MD from the Ohio State University, and Jackie Broadway-Duren, PhD, DNP, APRN, FNP-BC from MD Anderson gather to share the latest in CLL research, clinical trials, treatments, and comprehensive care strategies.
Guided by the insights of patient advocate moderator Jeff Folloder, the discussion will bridge the gap between medical expertise and patient perspectives, creating a truly comprehensive dialogue.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Navigating Clinical Trials for Lung Cancer: A Patient’s Guide
Is a Clinical Trial Right for Me?
Edited by: Katrina Villareal
Understand the different lung cancer types and the significance of biomarker testing through this recorded conversation. Learn about the evolution of biomarker testing inclusivity for all patients. Know more about KRAS and EGFR biomarkers, available treatments, and ongoing clinical trials.
This program was produced in close collaboration with our partner KRAS Kickers. We thank them for their time, expertise, and passion.
Get expert insights on current and promising clinical trials. Find out the importance of proactive patient engagement in finding suitable clinical trial opportunities.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Stephanie Chuang, The Patient Story: Hi, everyone! I’m Stephanie Chuang, founder of The Patient Story and a cancer survivor myself.
The topic of clinical trials can be pretty daunting. Some may know a lot and some may not even know what a clinical trial is. We’ll try our very best to cover as much ground as possible with our incredible panelists.
We’re collaborating with KRAS Kickers, a grassroots nonprofit led by patient advocate leader Terri Conneran, who will lead the discussion devoted to KRAS: knowledge + research + advocacy = survivorship. Their focus is on any KRAS oncogene or cancer type with the mission of connecting people to the latest research resources and community.
We’re co-hosting with them here at The Patient Story. I founded the patient and care partner organization after my own cancer experience, going through hundreds of hours of chemo, and feeling really alone.
Our mission is to humanize cancer so you know that you are not alone. We also invest in educational programs to help empower you and your loved one in your own care. We cover cancers across the board, including lung cancer, with a focus on biomarkers and clinical trials.
We want to stress that The Patient Story and KRAS Kickers retain full editorial control of this entire program. This program is not meant to be a substitute for medical advice. We want you to walk away knowing more, but please consult with your own medical team before making decisions.
Terri Conneran
Stephanie: Many of you may have already seen or heard our patient advocate moderator, Terri Conneran, who shared her story on our platform. I’m very lucky to call her a friend now.
Terri, a lot of us know how passionate you are as an advocate. You’re out there making sure people know how to be empowered in their care. Can you share more about your personal story and what led you here?
Terri Conneran: It’s such a blessing to be anywhere after you get diagnosed with lung cancer. I was diagnosed with non-small cell lung cancer, went through chemo and surgery, and had no evidence of disease.
I connected with other lung cancer groups and heard about biomarkers. Not getting the information I needed or wanted from my doctor, I eventually, after about two years, got a second opinion. The second opinion doctors told me I had KRAS.
I wanted to connect with other people so that we can all learn what this means and how we can make it better to live with KRAS cancers. We need to take KRAS and turn it into knowledge + research + advocacy = survivorship. We’re all here together to kick cancer’s KRAS so I’m delighted to be here. This is all about the hope that we’ve learned over the years.
Dr. Estelamari Rodriguez
Terri: We have Dr. Estelamari Rodriguez, a hematologist-oncologist at Sylvester Comprehensive Cancer Center at the University of Miami Health System. She specializes in early detection and treatment of lung cancer.
Dr. Estelamari Rodriguez: Thank you for the invitation. Delighted to be here.
Dr. Jason Porter
Terri: We also have Dr. Jason Porter, a hematologist-oncologist at the West Cancer Center Research Institute in Memphis, Tennessee. He’s the director of the Lung Cancer Disease Research Group and specializes in treating patients with molecularly-altered lung cancers and lung cancers with no actionable driver mutations.
Dr. Jason Porter: I’m super excited. Estela, it’s so good to see you again and I look forward to the discussion.
Different types of lung cancer
Terri: We’ve got a lot of ground to cover. Dr. Porter, what are the different types of lung cancer?
Dr. Porter: When somebody is new in my clinic, they want to know, “Do I have the really bad one or the one that’s not so bad?” Most people have heard that small cell lung cancer (SCLC) is more aggressive so that’s in the back of people’s minds. Basically, what it means is when we look under the microscope, how do the individual cancer cells look? Are they big or small?
Non-small cell (NSCLC) is the same thing as saying large cell or cells that aren’t as small under the microscope. We divide that into three categories: non-squamous, squamous, and large cell neuroendocrine carcinoma. Outside of those three, there are other rare histologies that we don’t see quite as often, but those are the more common ones.
Adenocarcinoma is the most common type of lung cancer and the most common non-small cell lung cancer then it’s squamous cell carcinoma. Large cell neuroendocrine is a different type of tumor.
When we look at the patient’s body, the trachea breaks off to the left and right lungs and squamous cells line the the epithelium; that’s the type of tissue that we see in the upper airways. Adenocarcinomas happen more peripherally in the lung fields. Small cells can pretty much happen anywhere.
Biomarkers are genes that drive cancer. We have been successful at identifying at least 10 of those.
Dr. Estelamari Rodriguez
Different lung cancer biomarkers
Terri: Dr. Rodriguez, what are the different biomarkers?
Dr. Rodriguez: When I started my training, we only knew about lung cancer as non-small cell and small cell. Now we really need to dig deeper into the genes that caused the cancer because today, we have 10 biomarker-driven treatments for specific types of cancers.
We know that a lot of these genes, mutations, and oncogenic drivers first described adenocarcinoma, but there are mutations in any type of cancer.
If you have a diagnosis of advanced lung cancer or even earlier stage lung cancer, it is important not only that you get a biopsy so that you understand the histology and how it looks under the microscope, but that you get that test about the genes that caused cancer.
Biomarkers are genes that drive cancer. We have been successful at identifying at least 10 of those, although a lot of them have been seen in adenocarcinoma.
Initially, they were in never smokers. We see them on people who have smoked a long time and who stopped smoking a long time ago so it really has nothing to do with smoking history. It has nothing to do with gender. It just has to do with the cancer.
It’s part of the information that’s critical to get at the beginning of the treatment so that you can pick the best treatment for the patient. A patient that gets started without that information may not be started on the right treatment. It’s important to do that test. It’s usually ordered in the tumor specimen or through a blood test called liquid biopsy.
Tissue biopsy vs. liquid biopsy
Terri: Is there a difference in what comes back from the liquid biopsy compared to a tissue biopsy?
Dr. Rodriguez: The gold standard of where we think we are most likely to find a source of the genes is going to be the tumor. But many times when you do a biopsy, you get part of the tumor that is very necrotic or dead tissue so the actual DNA inside that tumor is not good enough to get all the information that you need. You learn more from the blood.
The opposite can also happen. You can have a blood test that’s completely negative in terms of actionable mutations, but there’s a lot in the tumor specimen.
A lot of centers, mine included, try to do both tests because they can be complementary and specific. You can identify some mutations through the blood, especially RNA fusions where two genes come together.
With the blood test, we can do that in the office and get results in 7 to 10 days. Technology has allowed us to treat patients faster with the right treatment that we didn’t have available 10 years ago.
We’ve now discovered that we need to do biomarker testing in all lung cancers.
Dr. Estelamari Rodriguez
Most common types of lung cancer biomarkers
Terri: What are the most common types of biomarkers in lung cancer, Dr. Porter?
Dr. Porter: A long time ago, we found EGFR as a biomarker and then we have also the KRAS mutations. We actually found KRAS a long time ago and couldn’t target it for such a long time. It can serve as a biomarker that we can use to target for treatment and also a prognostic biomarker that gives us some information about how a tumor may behave.
We have both prognostic and diagnostic biomarkers outside of KRAS as well. We have PD1 and PD-L1, which are proteins that we can study to give us an idea about how our immune checkpoint therapies may work when we treat non-small cell lung cancer.
We also have BRAF, ALK, ROS1, and all these different proteins that may be driving the cancer or giving us information on how different cancers may respond to treatment.
We used to associate these biomarkers with non-smoking and now we have drivers that are actually associated with smoking.
Testing biomarkers is becoming very important for all patients regardless of their smoking history. BRAF is one of those biomarkers that we can see present in smokers as well as KRAS. MET exon 14 is another biomarker that’s also an actionable biomarker that we can target in therapy that may be associated with smoking.
We’ve now discovered that we need to do biomarker testing in all lung cancers.
Terri: Dr. Rodriguez, with the biomarkers, are you either one or the other?
Dr. Rodriguez: The world has become more complex as technology has allowed us to really dig in. It’s an alphabet of different mutations that are in each of these genes.
For example, with EGFR, the more common mutations are deletion 19 or exon 21 changes. But when you look at that whole protein, there are a lot of insertions and atypical mutations that we used to ignore because we didn’t identify them very commonly and we didn’t think that they mattered. But they do matter.
We have drugs developed, for example, for EGFR 20 insertion, which is something that was there all along and unrecognized. Those patients were not responding to the traditional treatments for EGFR because they had a different configuration of that protein so they needed a different type of drug to work.
The same thing with KRAS. There are a lot of KRAS mutations and it can be a whole alphabet of different KRAS mutations. KRAS G12C, which is a bigger proportion of those KRAS mutations, has two newly approved targeted therapies that we can offer.
We also see patients who have other types of cancers in other parts of the body who share these KRAS mutations and they may be of a different variety.
Because they’re all different, we have to invest in research to really define the best treatment for each of these parts of the mutation that the patient is encountering.
Testing biomarkers is becoming very important for all patients regardless of their smoking history.
Dr. Jason Porter
Latest clinical trial updates
Terri: We just came out of the big annual World Conference on Lung Cancer. Can you tell us some of the excitement that happened around KRAS or EGFR?
Dr. Rodriguez: Two things are happening. We’re getting more data from patients who have been treated for a long time in whatever option we had, like osimertinib, which is the first drug used for EGFR. We’re learning that people progressed. The next question is: how can we treat those resistant clones earlier?
One of the exciting data that came out was FLAURA2, a trial that used the same backbone of osimertinib, which is the targeted therapy that we use for most patients, and added chemotherapy. The question was: would patients do better if they had proper targeted therapy along with chemo? Will they be able to decrease the burden of disease and be managed better to prevent resistant clones in the future? That’s one of the theories.
I was happily surprised that it made a big difference. I always used to think that osimertinib works very well. You get a lot of responses. Then when it stops working, you can try chemo. However, I didn’t expect that patients would have almost nine months of improvement in disease. They were less likely to relapse if they were getting chemotherapy upfront.
With that same concept of making the treatment upfront more aggressive, there were other antibody-drug conjugates that were presented. We’re going to see a lot of exciting data with these new drugs that bind our receptors and inject chemotherapy into cells.
For EGFR, we saw a trial called HERTHENA that used patritumab, which is an antibody to HER3, which is another antibody similar to EGFR. It basically would inject chemotherapy into those cells that have become resistant. We saw data for that and there’ll be trials adding that antibody-drug conjugate to the first-line therapy.
We also saw the MARIPOSA trial, which is a drug approved for EGFR 20 insertion, trying to use that drug, which is an antibody-type drug, upfront with an EGFR inhibitor called lazertinib.
There’s a lot of excitement about combining drugs, not sitting back and waiting for things to happen, but trying to be more proactive. The data that was more mature was the FLAURA2 trial in EGFR.
Dr. Porter: KRAS, as I talked about earlier, is a very interesting biomarker because we’ve known about it for such a long time. One of the clinical trials in KRAS is the KRYSTAL-1 clinical trial. We have two drugs that are approved right now by the FDA for second-line use for KRAS G12C: sotorasib and adagrasib.
The KRYSTAL-1 clinical trial is a phase 1/2 clinical trial of patients with different tumor types that had KRAS G12C mutations and the non-small cell lung cancer cohort was included. We have data that continues to mature and we see response rates of around 35% in the non-small cell lung cancer cohort. These were patients with both smoking and non-smoking histories, mostly male patients.
As the data continues to mature, particularly in non-small cell lung cancer, it’s now been FDA-approved for use in the second line after patients progressed on an immune therapy-based treatment, so an immune therapy plus or minus chemotherapy.
Very interesting to see that, as Dr. Rodriguez alluded to with the FLAURA2 trial where we’re adding chemotherapy to targeted therapies, what the tolerability is going to look like and whether it is really going to cause benefit.
In KRAS G12C targeting in clinical trials, we have further study with adagrasib, which is looking to add chemotherapy to adagrasib with an immune checkpoint inhibitor.
It’s becoming a much more robust combination of therapies in the more advanced setting for KRAS G12C patients, where we’re familiar with the fact that KRAS G12C patients are more likely to be smokers so they’re probably having other co-mutations that may additionally be driving the tumor outside of KRAS G12C. This is where it becomes particularly interesting for me to see the addition of chemotherapy to the KRAS G12C inhibitor so that we are covering clones or parts of the cancer that are not actually being driven by the KRAS G12C mutation.
It will hopefully increase not only the outcomes for those patients, but also the response rates will hopefully be higher as we see with the EGFR inhibitor plus chemotherapy, and then the duration of response and survival for those patients.
Starting out with sotorasib and adagrasib now approved in the second line and then adding chemo and immune therapy to those drugs in more advanced settings upfront to hopefully improve outcomes, durations of response, and survival for those patients.
Terri: Essentially, it’s not like I only have one biomarker and that’s it. There’s a little bit more to it. There may be a biomarker that comes on down further or not as a result of treatments or what have you, but that makes a difference. Am I tracking with you?
Dr. Porter: Absolutely. It makes a huge difference. In the case of EGFR, as Dr. Rodriguez talked about, it’s more likely to be that one single biomarker that we need to focus on, maximize response, and benefit from targeting that pathway. But when it comes to KRAS, we know that there can be so many other drivers along with it.
Essentially, when I think about it, I think about if this patient were a smoker or if they had environmental exposures, they wouldn’t have one single driver. They may have other carcinogenic consequences from being exposed to cancer-causing agents like what we have in smoking or the environment like radon so more than one gene may be affected as opposed to these single gene-driven tumors like EGFR, ALK, and ROS1.
Dr. Rodriguez: The other thing that has become clear to me is that patients need to empower themselves with this information. There have been many cases in which I have seen second opinions or patients whom I have gotten to know where the information was there, but it wasn’t acknowledged.
They had a test earlier on in their disease and it was ignored because it wasn’t what the doctor was doing at the time. Either the patient went to surgery and they had a KRAS G12C mutation that wasn’t recognized or the patient had chemotherapy-immunotherapy and then that was not acknowledged and the patient missed an opportunity to get treatment earlier that we know can work.
Another part of this is understanding that science moves and there are new options and new combinations, but that you can’t make any decisions until you have the information in front of you.
We really need to be very strategic about what the treatments are. If you don’t have all this information going into it upfront, you can’t be strategic at all.
Terri S.
Terri: It is an exciting time. I’d love to drill down a little bit deeper into some of the clinical trials and what you guys are hearing and seeing.
Dr. Porter: For me, particularly with KRAS, the excitement got a little bit curtailed with the toxicity that we see sometimes when we add G12C inhibitors with immune checkpoint inhibitors. We may see a little bit more immune-mediated side effects like hepatitis, pancreatitis, and type 1 diabetes development.
The tolerability with the combinations was a little bit unnerving initially, but I think we felt the same way about immune checkpoint inhibitors when we first started using those, even in monotherapy. Imagine the experience with that first pneumonitis and the first dermatitis. I had a patient the other day who had some mucosal issues from immune checkpoint inhibition alone.
When we first encountered these, it was very unsettling. But now we feel so much more comfortable with these side effects. It’s really, really exciting to see the combinations of KRAS inhibitors with chemo, plus or minus immune therapy.
Right now, the unlikelihood of KRAS inhibitors being used in front-line monotherapy, to see those, explore the toxicity, and figure out how to use them in combination, modify doses, and do all of these things is very exciting. I assume, like we see with EGFR, that it’s going to improve outcomes when we’re able to bring them in combinations.
Any combination is very exciting. G13 is exciting to me, too. Again, I’ve only seen two in clinical practice and the first one was really a surprise to me. As we develop these pan-RAS inhibitors, again, more excitement for me.
Dr. Rodriguez: It was also seen in EGFR, but this whole message of treating patients earlier with chemo and targeted therapy really got my attention. In our practice, we have seen patients who have this mutation but have to wait for second line. We have to go through chemotherapy and immunotherapy and some of them get very sick. It’s very sad to me that they never got to see that targeted therapy.
In the trial that combined carboplatin-based chemotherapy with adagrasib, they saw responses of over 60%. They were able to bring up the responses that you wouldn’t see with chemotherapy.
Patients sometimes get a good chance to decrease the burden of disease. We know that some patients with KRAS mutations have a lot of burden of disease. It’s very aggressive. They have a lot of symptoms so if we’re able to help them with all our drugs upfront and we can find a way to deal with the toxicity, we’ll be able to help more patients.
Dr. Porter: Earlier, they’re more likely to tolerate a more robust regimen. It’s also exciting to get to do that a little bit earlier. We suppress the subclones that are being driven by the driver that we’re targeting.
When we aren’t able to use chemo and/or immune therapy upfront, those other clones that grow through are resistant to our therapy and may even be more resistant to chemotherapy later so we see lower response rates.
Where we have these drivers in the second line, it’s really sad to see those patients come to that point and be clinically unable to tolerate whatever the therapy is.
I had a patient with a G12C mutation who wasn’t a candidate for a clinical trial in the front line. When we got to the second line, his effusion was refractory, even loculated, and not amenable to easy drainage. He was definitely not a candidate for VATS (video-assisted thoracoscopic surgery) where we go in and clean that out so trying to get him onto the G12C inhibitor wasn’t possible. He couldn’t tolerate it.
He spent most of that time hospitalized and eventually went into hospice. When I first met him, he was walking into the clinic and still robust. Being able to target at that time would have really been nice for him.
Terri: We really need to be very strategic about what the treatments are. If you don’t have all this information going into it upfront, you can’t be strategic at all.
We want to forget the actual stigma but remember that stigma is a problem.
Dr. Jason Porter
Smokers & non-smokers
Terri: You mentioned that the EGFR group of patients is equal to the amount of KRAS G12C patients and yet they’ve had a whole lot more studies and a lot more drugs that have been going on.
We’re not there yet when it comes to other KRAS subtypes, let alone some of the others as well. You both brought up smoking. Is it that important where it got here from or is that one of those things that keeps getting reported out?
Dr. Porter: For me, it’s not important where we got here from, but what we have to remember is stigma. We want to forget the actual stigma but remember that stigma is a problem.
The reason I always bring up smoking is because I was sitting in a room with a very, very smart oncologist who told me, “This patient was a smoker so they’re less likely to have an oncogene driver.” I said, “Twenty years ago or 30 years ago, that would have been true.”
I like to use smokers, next-generation sequencing (NGS), and studies in the same sentence so that people start to make the association that you can definitely have a driver that’s actionable even with a history of smoking. You’re more likely to find BRAF, MET exon 14, and even KRAS with FDA-approved therapies in smokers.
Where it becomes relevant for a never smoker is we know they’re less likely to respond to immune therapy by itself. But for smokers, I like to keep saying that and putting NGS testing in the same sentence so people stop having this association that the oncogene driver patient is a young female, Asian, never smoker. That’s what we learned in medical school. We need to really change that narrative.
I don’t want it to seem like I’m harping on smokers. I’m harping on the fact that smokers can have drivers and that we have to study everybody. We have to.
Terri: Thank you for clarifying that because that’s exactly what I was hoping you would say. We definitely need to test and it’s important for what’s next.
We have two fantastic patients who went through clinical trials.
I highly recommend a clinical trial to anybody, but do your homework. Have an exit strategy in the event something happens or a side effect you cannot tolerate.
Mike S.
Mike’s lung cancer story
Mike S.: I have stage 4 lung cancer. I was diagnosed in 2016 and like most people, I was stunned, particularly since I was a non-smoker.
It’s been an uphill roller coaster ride, depending on what kind of medications I’m on, the side effects of those medications, or the availability of certain alternative treatments that I’ve been on for the last couple of years, including a clinical trial drug.
My initial diagnosis put me on the standard of care treatment and that lasted about 27 months. The efficacy rate was about 24 to 26 months.
In discussion with my oncologist and also with what treatments were available, I was presented with TAGRISSO, an FDA-approved drug, or I could go on a clinical trial.
Our thinking here was that if I went on a clinical trial drug that was supposed to work as well or better, then I could perhaps extend my life. They’re proposing that this clinical trial drug had an efficacy drug of two years versus an FDA-approved drug that had an efficacy rate of about three years. This particular drug was thought to be better than the FDA-approved drug.
I’m going to get scanned more frequently. I’m going to get a report card of my tumors. There’s a lot more testing, monitoring, and scanning that takes place because you’re on a clinical trial.
The additional monitoring was what prompted me to say yes to the clinical trial. I may have the benefit of getting additional months added to my life with the efficacy rate of a potential clinical trial drug working for a period of time.
Before I started the clinical trial, I met one of the nurses who was going to be assigned to me. She was great and explained the whole process. She also helped facilitate the scans, progress reports, meetings, and discussions.
I was one of the earlier ones to get in, but there weren’t a lot of people in the clinical trial. There was no drug name. I believe it was in phase 2 when I got involved.
Initially, I did really well. I had a reduction in tumor size. I was just astonished. I was getting monthly progress reports showing tumors shrinking so I was flabbergasted.
I made the right decision because the benefit of this is I got on a clinical trial that’s working. Even if it fails at some point, I’ve got a reduction in tumors. I’ve got an extension of life.
That lasted for about 10 months then the worst happened. I had a brain scan and it showed five brain mets. I reached out to several people in the lung cancer community who had similar situations but not from the use of a clinical trial drug.
Because they had brain mets, they switched to Tagrisso, which I had put off moving to because I wanted to try the clinical trial drug. Tagrisso was supposed to ward off any type of brain mets but also eliminate them if you had them.
I knew exactly what was going to happen if the clinical trial drug failed, which was to go on Tagrisso, in discussion not only with my oncologist previously but also with about 5 or 6 different lung cancer patients I knew.
I was pretty calm about this even though the placement of some of these brain mets was not good. I had one of my brain stem, which essentially made it inoperable.
When I went in, I saw the oncologist, the oncologist nurse, the nurse navigator, the social worker, and the nurse assigned to the trial. I thought this couldn’t be good because I don’t usually meet with a parade of people like this.
The discussion centered on some of the results and the five brain mets. I said, “What we’re going to do is move to Tagrisso, correct? When you tell me it’s inoperable, you can’t do anything. You can’t do radiation, right? I’m out of the trial. The intent is that this drug is going to eliminate these brain mets.” He said, “That’s correct. That’s our hope.” I said, “Okay, well, then that’s what we’re going to do.”
They were all looking at me like, “Wow, does this guy have nerves of steel or something or is he crazy?” I wasn’t reacting in the way they thought I was going to react. I was informed at the start of the trial what may happen. When I got negative results, I did the research, too, before I met with my oncology team.
After we met, everybody left the room and then a moment later, the nurse came in, gave me a big hug, and said, “Are you okay?” I said, “Yeah, I am. I know it’s what I was in for when I signed up for this. You are working to save my life and we’ve got a plan. I’m fine as long as we have a plan.”
What I don’t like is when something happens in the roller coaster journey of having lung cancer and you don’t have an established plan and you’re waiting for something. That’s when it gets a little bit more nerve-wracking.
There’s a lot of paperwork associated with the clinical trial because there’s the acknowledgment of the risks associated with going on a drug that you don’t know what it’s going to do to you. There’s an assignment of a lot of pages to read through and sign.
The nurse associated with the clinical trial did a very good job of explaining the risks associated with being on this drug. I didn’t have any problems with understanding the risks.
Prior to getting on the clinical trial drug, you had to do tests. I got off the prior drug for maybe a week or so before I started the trial to make sure I didn’t have any prior drugs in my system.
There are some attestations that you didn’t use the drug or any other drugs prior to starting the clinical trial. The attestations are pretty straightforward. They ask a lot of other questions.
For anybody who’s considering a clinical trial, do your homework not only at the front end but also at the back end. It’s not just about getting on the clinical trial drug. At some point, you’re going to get off the clinical trial drug. Generally, there’s an exit strategy.
I got out early because I developed brain mets. How the trial ended or not is confidential information. I had some conversations with my oncologist and the nurse associated with the study because they had to provide information to the clinical trial provider.
I highly recommend a clinical trial to anybody, but do your homework. Have an exit strategy in the event something happens or a side effect you cannot tolerate. You have an entry plan and an exit plan. Make sure you’re covering your bases with all those questions before you get on the drug and then be prepared for what may happen.
I had an extension of life for 10 months, but had I not gone on it, I would have gone on some other drug that had a different efficacy rate. I would wholeheartedly do it again in the availability of a clinical trial drug that meets my particular criteria.
It’s more important to get the right treatment than it is to get a treatment quickly. Ask as many questions as you can and don’t be afraid.
Joann J.
Joann’s lung cancer story
Joann J.: I was diagnosed in November 2021 with stage 4 non-small cell lung cancer KRAS G12V. I had several standard-of-care treatments, all of which resulted in progression. Luckily, I got on a clinical trial in February 2023. It was a targeted therapy and it was a daily pill, which was wonderful. No more infusions.
I had a great quality of life for six months with very minimal side effects. I was able to go back to work. I was in a really good place.
Unfortunately, my last scan showed progression and new growth, which is unusual for a targeted therapy. I have an upcoming biopsy on the liver, which is where the new growth is, and based on the results, we can figure out how to move forward.
My biomarker is KRAS G12V. We’re doing this liver biopsy to make sure that it’s the same cancer. I think the next step is another clinical trial, probably immunotherapy.
Through KRAS Kickers and Terri, it’s definitely something that I researched and looked into. The first time this particular clinical trial was mentioned to me was through my oncologist in New York. I was put on a waiting list.
I traveled to Dana-Farber in Boston and to MD Anderson in Houston to hopefully get on the trial sooner. Interestingly, Dana-Farber and MD Anderson would not allow me because I had a history of pneumonitis.
MD Anderson was going to put me on a different trial. I was all set to get an Airbnb and move to Texas for six months when, all of a sudden, they had a spot for me in New York for the RMC-6236 trial.
I definitely feel like my knowledge of the clinical trials and my aggressiveness in the whole process certainly helped me.
My only fear was whether or not I was going to get a drug or a placebo. From what I gathered, they don’t give placebos to cancer patients. It’s just cruel. Once I understood that, I was and still am very willing to go on any trial. It’s the future of cancer treatment so I have no problem.
I had a good experience and I know other people have not. When I went to MD Anderson, my insurance company paid for my airline ticket plus my husband’s. Things like that are very difficult. The financial toll is significant. In that respect, I feel very lucky. But I also feel like KRAS Kickers has definitely given me knowledge and, with that knowledge, strength.
For someone who may be considering a clinical trial, I would say go for it. Ask as many questions as you could possibly think of. A second opinion is always a good idea. It’s never a bad idea.
In fact, even if they don’t give you a different direction, the peace of mind you get is invaluable, knowing that the direction you’re going in now is the right way to go.
The first thing I learned in the cancer community is it’s more important to get the right treatment than it is to get a treatment quickly. Ask as many questions as you can and don’t be afraid.
Terri: Those are some powerful stories. These are real people who are doing these clinical trials. Pretty amazing.
Dr. Porter: It really is. To hear Mike’s excitement about the clinical trials and to hear how he thought about what the possibilities were as it was being presented to him, it’s really exciting. He really captured some of the things that our patients ask us when we bring up clinical trials and what they can expect.
Dr. Rodriguez: We don’t hear enough from people who have a good experience in a clinical trial. We have a lot of patients who think that they’re going to be experimented on and that they’re going to be getting a placebo.
I work in an experimental therapeutic clinic where everybody gets a drug. We’re not giving placebo drugs for phase 1 trials or phase 2 trials. They’re all about testing a drug.
We don’t know how well those drugs would work, but one of the things that has really changed in oncology is that we’re getting results faster and drugs faster for patients. Sometimes not as fast as you will need them, but much faster than they used to be.
Biomarker testing has allowed us to do better trials because now we can find the right patients who are more likely to respond to some of these treatment options. In the past, we will have a new drug and it will be given to everyone with or without chemo. The responses were obviously very low because you were not looking for patients who were more likely to benefit.
As a provider in one single location with limited resources, if I open the network and use everything out there, I exponentially increase the chance that my patient’s going to find something that’s tolerable and may be very effective for them.
Dr. Jason Porter
Importance of getting a second opinion
Dr. Rodriguez: I would encourage patients to think of second opinions as a good thing, not a bad thing. I have patients who come to me and say, “I’m sorry, I’m going to go speak to so-and-so.” I say, “I am delighted that you’re going to speak to someone else.”
We’re all friends. If you have a doctor that gets upset about this, it’s kind of odd. If I were going through this, I would want to learn from other people and get a different perspective. Maybe another doctor can see something that was missed. It is good to do that. You’re not going to hurt your doctor’s feelings and they’re not going to stop treating you.
Dr. Porter: Coming back from the World Conference on Lung Cancer in Singapore, I had a patient who was progressing. He said two letters to me, “MD,” and I was already typing an email to one of my colleagues at MD Anderson, saying, “Hey, my patient’s progressed and I don’t have a trial that’s right for him. Would you look at it?”
He’s going to see my colleague and it’s not about me or my feelings. I love my patient and I want him to be okay. I want to make sure he gets access to whatever is out there that may benefit him.
As Dr. Rodriguez said, if we get upset, it’s probably something odd about us. There’s really no reason to get upset. It takes a village and as a provider in one single location with limited resources, if I open the network and use everything out there, I exponentially increase the chance that my patient’s going to find something that’s tolerable and may be very effective for them.
Clinical trials sometimes give you the best therapy before it’s even available for general use.
Dr. Jason Porter
Clinical trials are NOT a last-ditch effort
Terri: It really is different than I thought it was because I’m not a doctor. I didn’t know anything about this. The surprise was that you don’t do clinical trials as a last-ditch effort. I had no idea there was an actual order to it, you qualify for it, and it matters a lot what your biomarkers are.
Dr. Porter: We don’t want to take it as a last-ditch effort because when we get ready to go on clinical trials, we have to control for as many variables as possible. Are the kidneys functioning okay? If something happens on the trial and the kidneys aren’t functioning well, it could be a complication of kidney dysfunction and then the drug gets associated with that unfortunate outcome. We have to control those things.
Earlier in a disease like lung cancer, you’re less likely to have some of those other disease issues that may exclude you from the clinical trials. Doing it earlier is better.
I came into my clinical practice around the time that immune therapy was starting to come into second-line FDA approval. I thought about the people who went on immune checkpoint inhibitor clinical trials, the ones who are still responding from 2013/2014. There are still some survivors. For those patients who went on early, the clinical trials sometimes give you the best therapy before it’s even available for general use.
Our guideline compendium says that the best therapy for a patient with lung cancer or with any cancer is in a clinical trial. If you end up getting in early, you have long-term benefits. Definitely not a last-ditch effort and sometimes access to the most effective thing available.
Identify the biomarkers early so you can get on the right track.
Dr. Estelamari Rodriguez
New immunotherapy trials
Terri: We had a question that was asked about new immunotherapy trials. Will previous trial patients be able to participate?
Dr. Rodriguez: That’s the beauty of earlier phase trials. The patients didn’t fail; the treatment didn’t work. You want to find a different way to treat them.
A lot of the trials that we do after immunotherapy is a new immunotherapy that is in a different way, a vaccine trial, or a different mechanism to try to wake up the immune system because, in a way, most tumors can possibly be treated with immunotherapy. They become what we call hot tumors that are more likely to activate the immune system. Some tumors lose that capacity. You have an innate resistance that is not a tumor that is very hot in that end and you can do something to it.
We have tried different things, like radiation followed by immunotherapy. There are a lot of exciting vaccine trials that are trying to push that immune response.
What we have seen success of is the memory of the T cells in a longer way, infiltrating T lymphocytes, which are white cells of your own body that get activated against the tumor and then given back to you to do a more directed immune therapy. Those are treatments that immunotherapy can possibly help patients with many different biomarkers.
Biomarker-driven research and treatment is very exciting because sometimes you get very deep and long responses.
Another exciting development is in the ROS1 and NTRK space. We had a new drug, repotrectinib. When we understand how you can bind these receptors and do better, then the next drug can have an even higher response. Some of these drugs have responses of 70% with intracranial responses that are over 40%. That means that we get better at the next generation of the drug.
That’s what I hope for KRAS G12C. We already have seen adagrasib and sotorasib have intracranial activity that is real.
I had a patient who I was getting ready for our next-generation KRAS inhibitor and I thought she was progressing. I did all the studies to get her ready for the trial. The one she was on was working very well. She had a response in the brain and the pleural disease she had went away. Identify the biomarkers early so you can get on the right track.
Terri: What a great problem to have that she was responding so well that she didn’t have to join the clinical trial.
Dr. Porter: Right, that’s exciting.
Patients can get a copy of their own biomarker testing. A lot of times, the results will list out the clinical trials that are relevant to that particular biomarker.
Dr. Jason Porter
Looking for clinical trials
Dr. Rodriguez: Patients who are most likely to go into trials are patients who have been on trials before. We have a lot of patients who had a good experience and that opens a whole new door of options for them. I would encourage people to look.
Fortunately, everything’s consolidated in ClinicalTrials.gov, a website where you can put in your mutation and your state, and get a readout of trials that are open. All of those trials have an email of an investigator and a nurse coordinator.
I do that for my patients. I say, “We’re going to write an email and you’re going to find out if this trial is open.” Sometimes there’s a trial right next door that you hadn’t even known about. You just have to do the work.
Dr. Porter: There is a lot of work.
If you are patient and your doctor is not really considering or giving you the option to discuss clinical trials, you may need to consider reaching out on your own, maybe get in touch with Terri or us, and see about what options may be there.
An amazing resource for finding a clinical trial is your doctor and that’s where you need to start. But obviously, you can’t wait in case that’s not presented as an option for you.
If a patient has access to their biomarker analysis or if they know they have any particular mutation, you may just search that mutation + clinical trials on the Internet and see what comes up. You may even type in your city to see what comes up in your city.
Patients can get a copy of their own biomarker testing. A lot of times, the results will list out the clinical trials that are relevant to that particular biomarker and even give you a listing of where those trials are.
We assume patients don’t want the information from the actual report of their next-generation sequencing but as we educate and get advocates out there, letting patients know how important biomarker testing is, they can find often a list of the relevant clinical trials for their biomarker right there on the report and that can guide them in their initial searches for clinical trials for their biomarker.
Dr. Rodriguez: We can forget that crowdsourcing for clinical trials is really one of the most effective ways. I have patients who have found trials because they were part of a patient support group. Someone in another state was in a trial and that opened up an opportunity to really look at a trial that was in the same state.
I had a patient who came from Jacksonville, which is pretty far from us, but she found the trial through the patient support group. You can reach out. People who have gone through other trials already have made connections and that can be very helpful.
Dr. Porter: A lot of patients want to know the purpose of a trial and if there are any risks associated with being in a trial. It’s a little counterintuitive, but if you think about it, you’re monitored so closely. Any risks are much more likely to be discovered while you’re on a clinical trial.
If there’s going to be any trouble with your kidneys or your liver while you’re on the clinical trial, which could happen with chemotherapy that’s already approved anyway, you’re going to be getting labs more frequently. You’re going to be coming in to see the nurse a little bit more frequently and possibly even phone calls from the clinical trial coordinators. You’re monitored a little bit more closely so I feel like it diminishes the risks that may be associated with the clinical trial.
Crowdsourcing for clinical trials is really one of the most effective ways. I have patients who have found trials because they were part of a patient support group.
Dr. Estelamari Rodriguez
Different stages of a clinical trial
Dr. Porter: As we get to the different stages or phases of the clinical trial, we have more experience with that particular drug so there’s even more information about what risks may be out there.
There’s a phase 1 clinical trial that Dr. Rodriguez mentioned that she helps facilitate at her clinic. That is pretty much the first time that these drugs are being used in a single agent or in combination with another chemotherapy or agent.
In phase 2 clinical trials, we have already established that it’s effective or that we can see responses so we want to study a bigger population. We’re seeing more patients now being exposed to the medication to confirm that it works.
In phase 3, we’re doing a much larger trial where we’re comparing it to what’s already considered to be the standard of care. This is the way we treat this, but now we have this new option, and let’s compare the two to see if one is better.
Those eligibility criteria are there to make it safe, although we do know that sometimes they’re too safe that they’re excluding patients who need treatment.
Dr. Estelamari Rodriguez
Eligibility criteria for clinical trials
Terri: Carina asks, “What are the typical eligibility criteria? My mom can’t do trials near her because of her poor ECOG PS and she’s on oxygen.” Give us some guidance.
Dr. Rodriguez: We need to develop trials for real-world patients. Because of their disease, some of them will be on oxygen. Patients will have brain metastases. They’re going to need clinical trials and many trials have excluded them in the past.
I’m very excited about the Pragmatica trial by SWOG; that has no lab requirements. They don’t need to look at your oxygen status. They just need a doctor who has a patient in front of them and they just want to evaluate their response.
We need to encourage more trials that are for patients who need them and have a lot of symptoms. Sometimes, these patients are too sick to go into a trial because they’re new drugs and we really don’t know how they’ll tolerate them or we have serious concerns about toxicity.
You have to trust your doctor that those eligibility criteria are there to make it safe, although we do know that sometimes they’re too safe that they’re excluding patients who need treatment. There is a big movement by the NCI to make trials for real-world patients.
Terri: That’s the direction we need to really go in because we’re real people and we need to have real-world access.
This is the fight of your life. If you’re not open to clinical trials, you’re closing your eyes to opportunities.
Dr. Estelamari Rodriguez
Final takeaways
Terri: What is the top takeaway that you hope our audience members leave with when it comes back to clinical trials in lung cancer?
Dr. Rodriguez: Don’t be afraid to ask about clinical trials because if you have a diagnosis of lung cancer where a lot of patients are going to progress, this is the fight of your life. If you’re not open to clinical trials, you’re closing your eyes to opportunities.
I always tell patients about those patients who went on immunotherapy trials and are alive 10 years later. It was as scary as the trials that we’re talking about now, too. No one knew that drug would work and look what happened. That drug worked and made a difference. It changed lives.
I want to give people the sense of hope that clinical trials offer hope. People who do clinical trials do get better outcomes because they’re monitored very closely for risks. Clinical trials give you an opportunity to do better and really push the envelope in a disease that can be relentless.
Dr. Porter: Clinical trials are very important. I would love for patients and caregivers to take away the need for biomarker testing. I know that we’ve heard it over and over again, but I don’t think we can express that enough because most of the clinical trials are biomarker-driven trials.
In order to find out if a patient is going to be a candidate for a trial, we have to have their initial biomarker testing done. Not only do we increase the likelihood of them getting a relevant first-line therapy, but we also increase the likelihood that at the time of progression, we will have a good clinical trial that may be available for them.
As patients, make sure you’re asking, “Did you do my biomarker test? What does my biomarker test say?” We can’t ask that enough. If you’re at the clinic with someone who’s been diagnosed with lung cancer or any cancer, ask, “Have you done any biomarker testing?”
As providers, it holds us accountable so that we make sure that we’re doing that for patients. We can then give them a good first line of standard of care and good clinical trial options when a clinical trial is not appropriate in the first line.
Terri: You need to know what you are so that you can take charge of what you’re doing because you’re the patient in this and it’s your skin in the game.
Stephanie: Thank you, Terri, Drs. Porter and Rodriguez. It’s so clear you’re so driven to help patients and their families. Thank you for the amazing conversation. We hope to see you at a future program.
























































































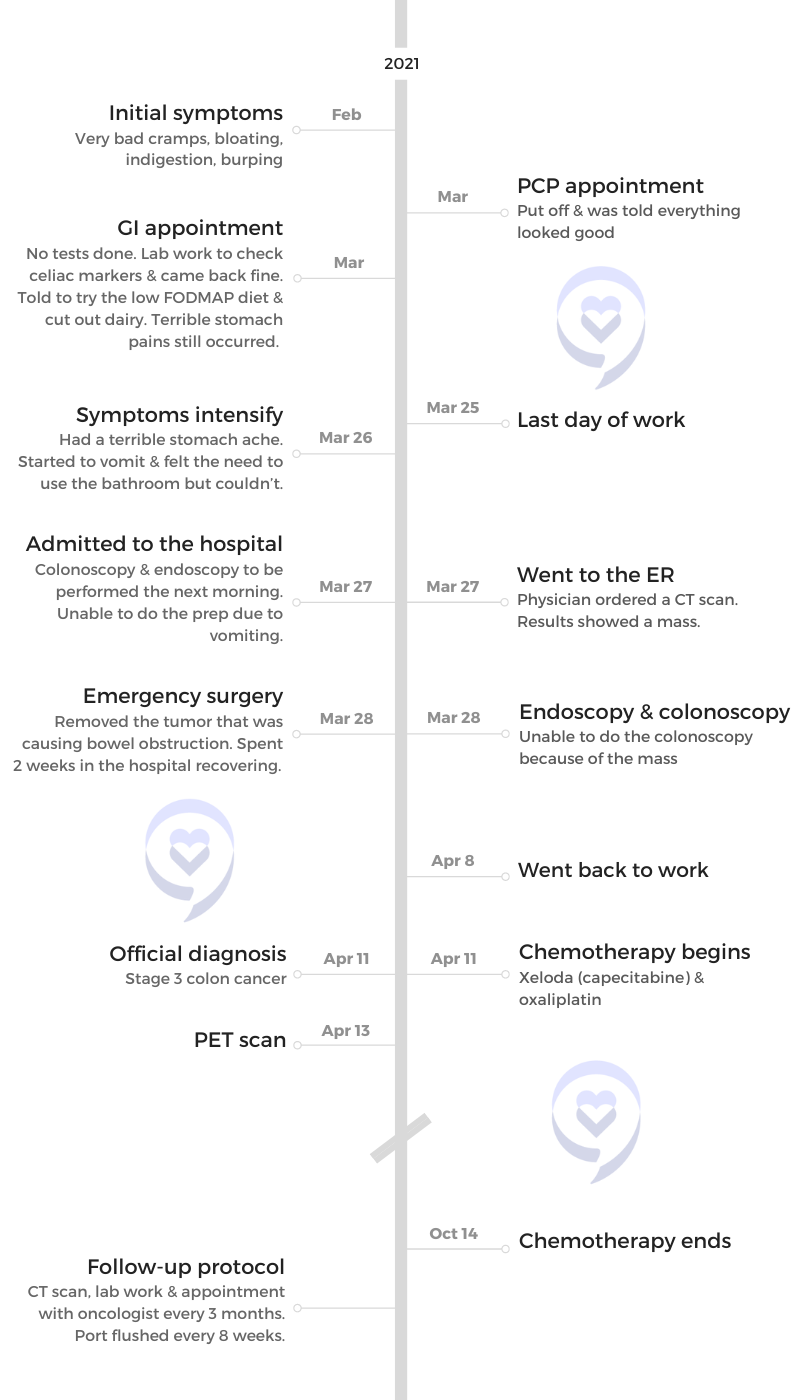



































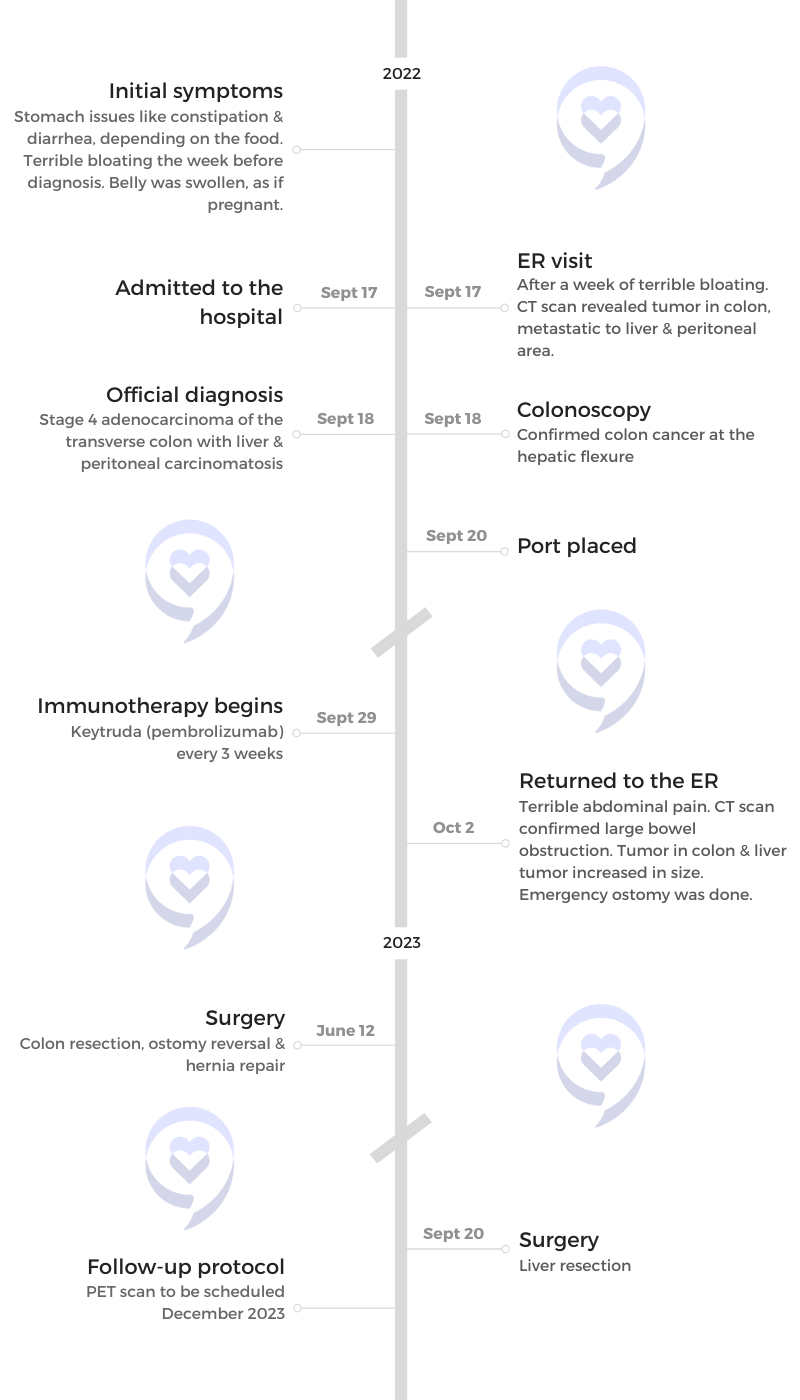























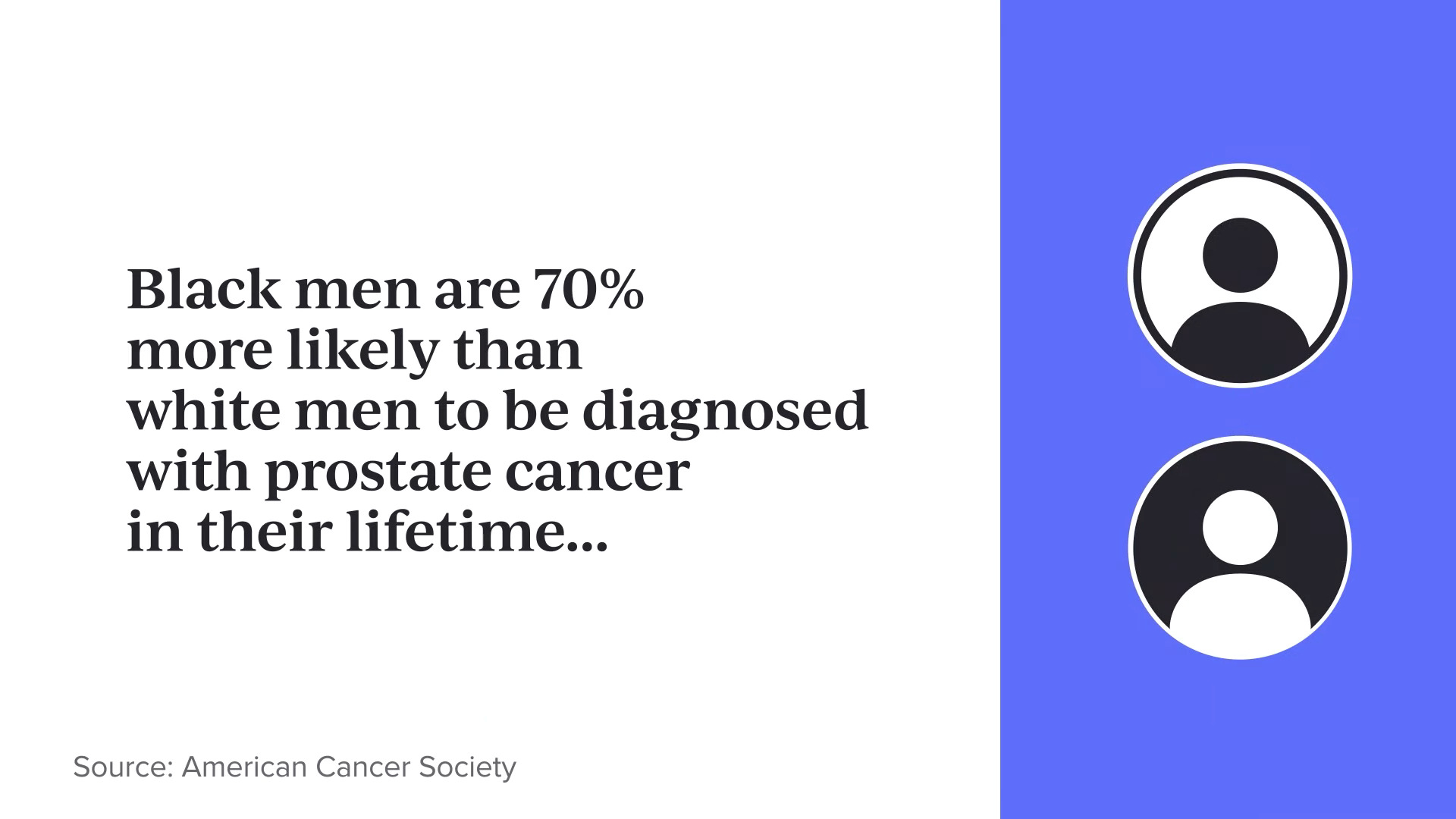















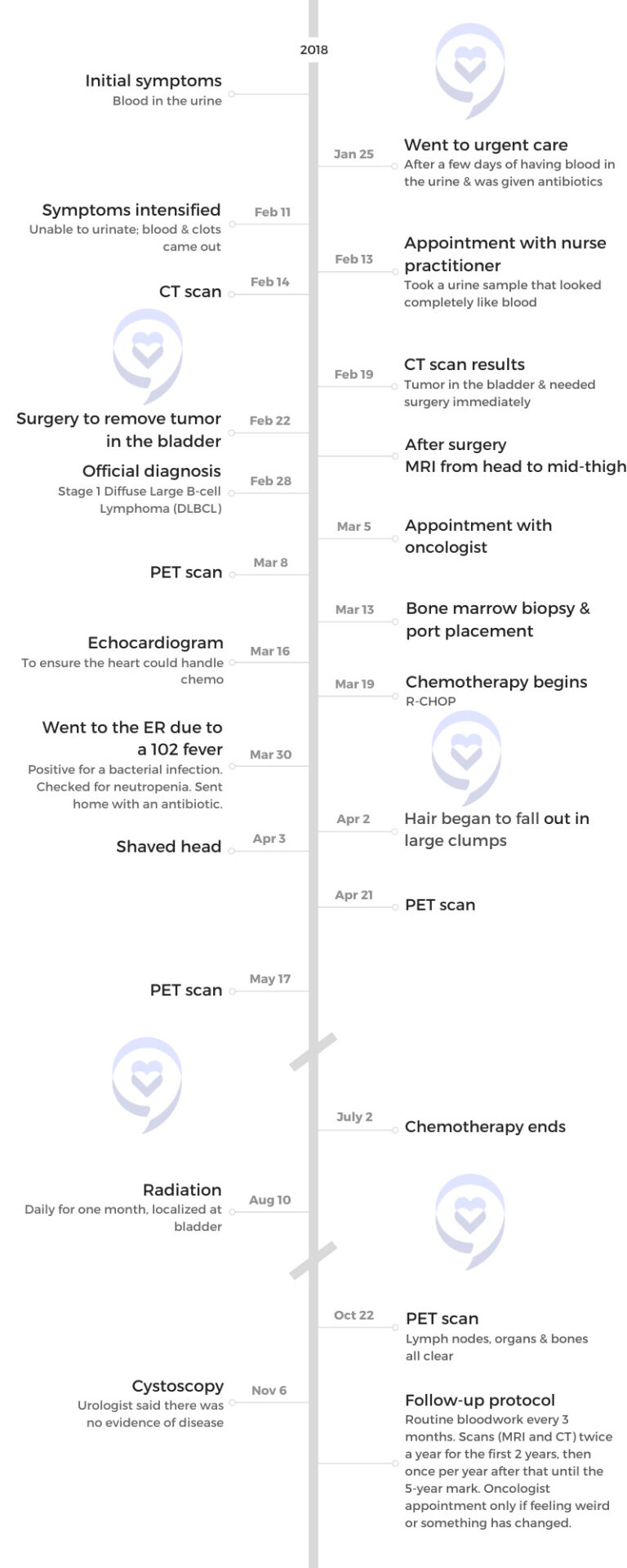






















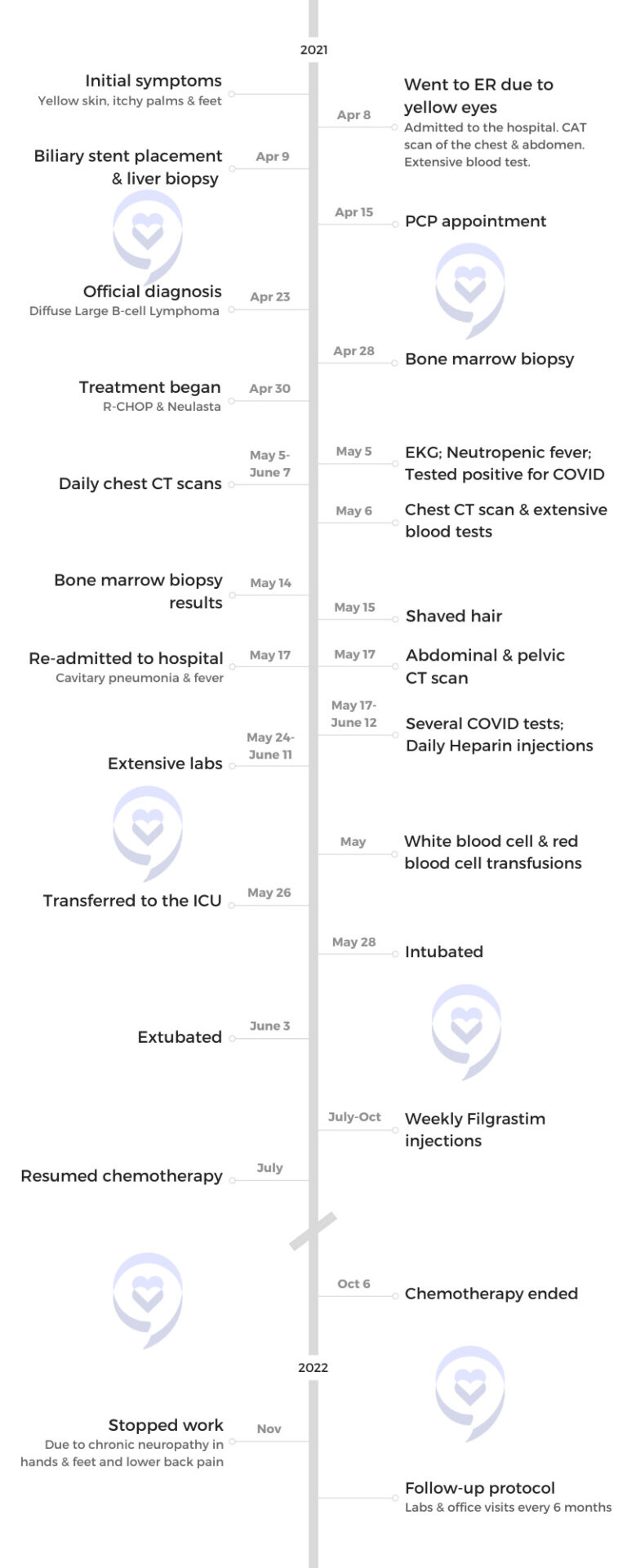

























































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}