Interviewed by: Taylor Scheib Edited by: Katrina Villareal
At 27, Kelsey was diagnosed with stage 2B estrogen-positive breast cancer in May 2023. When she felt a slightly tender lump, her primary care physician initially thought it was a cyst. However, an ultrasound and mammogram revealed otherwise. The diagnosis left her in shock and unable to process the information. All she could think about was her fear of dying.
Until her diagnosis, Kelsey had considered herself healthy. Cancer made her realize how precious health is. Being a mother to a toddler during treatment was challenging, but her child brought her joy and gratitude, giving her something to fight for.
Kelsey’s treatment began with AC-T chemotherapy (Adriamycin, cyclophosphamide, and Taxol) to target the fast-growing tumor. However, an allergic reaction to Taxol caused anaphylactic shock, leading to a switch to Abraxane. This experience underscored the importance of self-advocacy. Despite severe fatigue and nausea, she learned to accept her limitations rather than push herself.
A month after finishing chemotherapy, Kelsey underwent a double mastectomy with axillary lymph node removal on the left side and immediate reconstruction. Recovery was challenging, with constant nerve pain and cording, taking almost six months for her to raise her arm above her head. Nearly two months after surgery, she began 16 radiation sessions on the left side.
Currently, Kelsey is on tamoxifen, a selective estrogen receptor modulator (SERM), and will take the CDK inhibitor Verzenio (abemaciclib) for two years. She also receives Lupron shots to protect her ovaries from chemotherapy, as she couldn’t undergo fertility preservation.
Kelsey emphasizes the importance of self-advocacy, prioritizing medical concerns, and being more aware of one’s body. She hopes to inspire others and live a life of greater appreciation and gratitude, having gained a unique perspective from her cancer journey.
Name: Kelsey H.
Diagnosis:
Breast Cancer
ER+
Staging:
2B
Initial Symptom:
Slightly tender lump
Treatment:
Chemotherapy: Adriamycin, cyclophosphamide, Taxol switched to Abraxane
Surgery: double mastectomy with axillary lymph node chain removal
Alyssa was diagnosed with stage 4 stomach cancer after 2 ½ years of multiple doctor visits and normal test results. She initially experienced extreme fatigue and elevated resting heart rate. Subsequent symptoms like heartburn, weight loss, and difficulty swallowing prompted further medical consultations and tests, eventually leading to a GI specialist who performed an endoscopy and colonoscopy, where a biopsy revealed gastric cancer.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Upon diagnosis, Alyssa was shocked but sought a treatment plan. She was referred to a cancer specialist and a treatment center that acted promptly. She joined a support group, on which she relies heavily.
Her treatment involved chemotherapy and surgery, including a gastrectomy and oophorectomy. However, a laparoscopy revealed cancer spread to the peritoneum, changing the course of treatment to ongoing chemotherapy. She eventually joined a clinical trial that offered targeted chemo and surgery, but post-op results showed aggressive cancer with limited success from previous treatments.
Alyssa now waits for further scans and relies on a strong support system, faith, and therapy to cope. She emphasizes the importance of self-advocacy in healthcare, urging others to persist in seeking answers and appropriate care.
Name: Alyssa B.
Diagnosis:
Stomach (Gastric) Cancer
Staging:
Stage 4
Symptoms:
Fatigue
Elevated resting heart rate
Heartburn
Difficulty swallowing
Weight loss
Treatment:
Chemotherapy
Immunotherapy
Surgeries: total gastrectomy; partial esophagus removal; bilateral oophorectomy and fallopian tube removal
Clinical trial
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
It was not like me to have low energy, especially at my age and with my health history.
Introduction
I’m from Houston, Texas, and I was diagnosed with stage 4 stomach cancer in 2023.
Pre-diagnosis
Initial Symptoms
The first symptom I experienced was extreme fatigue. I was tired all the time. I didn’t have the energy to have a social life anymore. It was work, home, sleep, repeat, and that was not like me at all. I thought maybe there was something wrong. My family has a history of thyroid issues, so I wanted to have that checked out.
When I first saw my doctor, she agreed that it was not like me to have low energy, especially at my age and with my health history, so we ran some blood work to see if it was my thyroid or if we would uncover anything else.
Unfortunately, everything came back normal, so we didn’t get answers to what was causing the fatigue. She said maybe it was stress or I was exhausted from work. She wanted to do blood work every couple of months and keep checking in to see how my energy levels were.
A couple of months later, I started getting notifications on my smartwatch letting me know that my resting heart rate was over 100 bpm, which would happen when I was sitting down and relaxed. I thought it was a glitch, but after a few times of that happening, I thought it was something I needed to take back to the doctor to see what was going on. They did a quick EKG, which came back fine, but she didn’t want me to continue experiencing elevated resting heart rates, so she put me on a beta blocker. We redid the blood work and everything came back normal again.
A couple of months later, I experienced heartburn. I’ve never had heartburn, so I thought, “What is this burning sensation? Why is it so uncomfortable?” From the moment I got it, it happened every time I ate, no matter what I ate.
I went back to the same clinic but saw a different doctor because she had availability sooner. She told me, “It’s probably your age. You’re getting older, so maybe you can’t handle acidic foods anymore.” I told her I’ve never had it before and it’s happening constantly, regardless of what I eat. She said, “Let’s start this new medication and try to cut back on acidic foods.” I started the medication, but it didn’t do anything.
I was frustrated because I was taking more and more medications, but I wasn’t getting answers as to what was causing all of these symptoms.
I told her I wanted to figure out what was going on with my heart because I was taking medication, but we didn’t have answers. She said, “We can do a test, but it’s probably not going to come back with good results because you’ve been on the beta blocker for a couple of months.” I wanted to go ahead with the test to see and then we could go from there.
Sure enough, the results came back normal heart and she said, “It’s probably because it’s regulated by the beta blocker.” I was frustrated because I was taking more and more medications, but I wasn’t getting answers as to what was causing all of these symptoms. I’ve never had health issues before.
I told her I wanted to start over. I said, “I want to wean off of this medication. I don’t want to take this medication for heartburn anymore. Let’s do testing first, figure out what’s going on, and then we can go to medication if that’s what’s needed.”
Over the next couple of months, I slowly weaned off the pill that slowed down my heart rate because I didn’t want to have any adverse effects and within two months, I lost a lot of weight. I lost 15 lbs. I’m a very short person, so 15 lbs is a lot for my frame. Everyone noticed.
Then I started having difficulty swallowing. I would eat something and it felt like the food would get stuck halfway and I couldn’t breathe. When I would try to drink something, it would feel like I was drowning. I thought it was a one-off situation, but when it happened again, I said I wasn’t going to wait for a third time.
I booked the first appointment available. Again, my primary care doctor wasn’t available, but the other doctor at the clinic was and she told me, “We know that everything’s been normal. I don’t see any issues.” I told her I wanted to redo my blood work, but she was hesitant.
She started going through my chart, saw my weight loss, and said, “Oh, wow, you did lose a lot of weight in a short period. I don’t like what you’re saying about the difficulty swallowing, so let’s get you to a specialist.” I redid my blood work that day.
I was already two and a half years into this, spending all this money, but still had no answers.
Meeting with a GI Specialist
Two months later, I met with a GI doctor and she was concerned with the symptoms I was experiencing. She said, “I want to redo blood work. I also want to do a stool sample, an endoscopy, a CT scan, and possibly a colonoscopy.” I did all of that and the blood work came out great. The CT scan looked great as well. The only things left were the endoscopy and colonoscopy and they were going to be done on the same day.
By that point, four months had already passed doing these tests. I was already two and a half years into this, spending all this money, but still had no answers. Is it even worth it to do these last tests? If I get no answers, I’m still stuck in the same place. My spouse told me to stick with it. We needed to see if this could give us the answers that we’ve been looking for.
Biopsy
When I woke up from the procedure, the person who performed it told me, “We found one polyp in your colon. We removed it and it doesn’t look concerning, but you had a lot of inflammation in an area that we don’t typically see. It’s where your esophagus meets your stomach and the inflammation is pretty bad. I’m going to take a biopsy and send it off.” I asked, “Is that why I’ve been having difficulty swallowing?” He said it’s definitely why. I asked, “Will that also explain why I lost so much weight within a short period?” He said it could be.
Then he took a deep breath and said, “Does cancer run in your family?” I wondered where this was coming from. I had just woken up from the procedures, so I was trying to think and remembered two distant relatives but nothing stomach-related. He said, “Okay. Well, like I said, we’re going to send it off. I’ll call you back with the results in a couple of days.”
I had a million questions, but I didn’t even know where to begin.
Diagnosis
Getting the Official Diagnosis of Stage 4 Stomach Cancer
He called me back five days later and said, “Hey, it’s me. I performed your procedure,” so I called my spouse to hurry and come over. He was beside me right in time to hear that I had gastric cancer.
Reaction to the Diagnosis
We were both in complete shock. We didn’t react and were just staring at each other. It was like we weren’t in that conversation anymore.
I didn’t hear anything else said. I finally came back to what was going on when the person on the phone asked, “Do you have any questions?” I had a million questions, but I didn’t even know where to begin. The only thing I could think to ask was, “What’s next? Where do we go from here?”
He said, “Pretty hopeful that we caught this early. I know you’re scared, but you’re young and healthy. We’re going to take care of this and you’ll be okay. We’re going to do another scan higher up because we weren’t expecting to see that inflammation so high up. From there, we will get you with the oncology team and they will go from there.”
In addition, he told me that I had the bacteria H. pylori, which caused my gastric cancer. It looks like I got it when I was a child and because I never had symptoms, it went untreated and turned into gastric cancer. He said, “We need to clear that up first. You need to do the scan and then you can start treatment.”
After that, it was a little frustrating because I had another scan and the doctor said the scan looked good. He was going to call in my prescription and I said, “When do I talk with the oncology team?” He said they should be calling me but gave me the number. After that weekend, I went ahead and called them.
I found Stomach Cancer Sisters and it was specifically for women who have had or have stomach cancer. I joined and was immediately welcomed.
Referred to an Oncologist
They told me that they weren’t taking new oncology patients and I could be referred out, which turned out to be a blessing in disguise because the cancer specialist and the treatment center I was referred to was a complete 180. They moved with a sense of urgency. They said, “We book your appointments. We don’t call to confirm if it’s okay with you. If it’s not okay, call us back and let us know.”
Immediately, they made me an appointment with an oncologist and a surgical oncologist. They scheduled my blood work and scans. They were going to redo everything, which I knew was going to happen because it was a new provider.
Finding Online Support Groups
Before I got to those first appointments, I was searching for support. I knew I had cancer, but I didn’t know how to feel and I didn’t want to get lost in the emotions. I wanted to try to connect, especially since one of my friends told me her mom benefited from support groups.
I found some support groups, but I wasn’t getting what I needed. There were so many members and so many people talking about so many different types of cancers that it felt so overwhelming.
I found Stomach Cancer Sisters and it was specifically for women who have had or have stomach cancer. I joined and was immediately welcomed. I was asked about what type of stomach cancer I had and I had no idea. Someone asked if I could share my reports with her and so I did, and she told me we had the same type of cancer. She told me what was going to happen, including having to remove the entire stomach. Nobody’s told me this, but that empowered me so much that I felt ready to go to my appointments.
‘I have to do a laparoscopy. The type of cancer that you have doesn’t show up well on scans.’
Treatment
Meeting with the Surgical Oncologist
I met with my surgical oncologist first and he went through the plan. “We are going to do scans and blood work. We’re going to do another endoscopy. During the first one, they were looking around but now that we know you have cancer, we’re going to do it with an ultrasound as well.”
“We need to go ahead and implant your chemo port because you’re going to need to start chemo as soon as possible. We’ll have to do four rounds of chemo, then surgery to remove your entire stomach, and then four more rounds of chemo.”
“Before we can start that, I have to do a laparoscopy. The type of cancer that you have doesn’t show up well on scans, so we have to cut little holes in you, go in with cameras, look around, and look for signs of spread. We don’t want to see it spread to the peritoneum, which is very common. There’s no cure for it. At that point, you would be stage 4 and surgery would not be an option.”
There was a lot of information and a lot of steps, but I felt calm and confident because we had a plan in place.
Laparoscopy Results
I got a call from my surgical oncologist and he said, “Unfortunately, during the laparoscopy, I took some biopsies and they came back as cancerous. It has spread to your peritoneum. It’s stage 4 stomach cancer and, at this point, surgery is off the table.” That rocked my world because I knew that removing the stomach was the only cure for this type of cancer.
He said, “We’re going to pivot you back to your oncologist and you will work with her. You will do chemo and that’s it.” I asked him how I could get surgery back on the table. He said, “It’s not common for us to do that with stage 4 patients, but, in four months, we will check in with you. We could do a procedure called HIPEC (hyperthermic intraperitoneal chemotherapy) where we apply chemo directly to your stomach. But at that point, I want you to do four more months of chemo, so it depends on your progress. We will check in.”
I had two scans where one scan picked up a cyst on one of my ovaries.
Chemotherapy
My oncologist confirmed that I will have to do chemo essentially for the rest of my life to prolong my life. I said, “I understand that is your goal. However, my goal is to get surgery back on the table and I want you to know that’s important to me. I’m willing to do whatever you need me to do to get to that point. If there are any trials available, I would love to do that. I need to know how.”
At that point, there weren’t any trials available. I started chemo and did four months. During that time, I had two scans where one scan picked up a cyst on one of my ovaries. There weren’t any big notes on it, so we didn’t talk about it.
Joining a Clinical Trial
In October, my oncologist told me that there was a new trial available specific to the type of cancer I had (stage 4 stomach cancer) and the spread I had. She said, “With this, you would receive chemo directly to your peritoneum and have surgery to remove your stomach. They’re hoping to find a cure for the spread that you have.” It’s exactly what I wanted and needed so I asked her to sign me up. She said, “Okay. We have to do another scan to make sure there are no signs of spreading anywhere else because that would disqualify you.”
The scan showed that the cyst on my ovary got larger and she said, “Now we’re concerned. We need to make sure that that’s not cancerous. We need to do an ultrasound.” We did the ultrasound and after that, I met with my surgical oncologist.
During that appointment, he told me that the ultrasound came back as non-definitive, so they weren’t able to tell if it was cancerous or not, but I was okay to go forward with the trial.
I had a procedure to place the port in my abdomen and a few weeks after, I began the chemo to my peritoneum. I received three rounds of chemo. Everything was good. Then we started preparing for surgery.
They removed my stomach and attached my intestines to my esophagus.
Gastrectomy & Oophorectomy
I had a break and during that break, we did more blood work. We did the pre-ops. We did one final CT scan six days before the procedure. But also during that time, I had to meet with another surgeon who was supposed to remove my ovaries.
She told me, “Do you know that this is going to put you into menopause? Do you know that you will not be able to have kids anymore? You’re very young to be going through menopause.” I told her, “I completely understand. This is not a decision that we are making lightly. We know how big this is going to impact us and we want to continue having children, so it’s not an easy decision.”
She was upset with my decision. She wasn’t in agreement. We knew my type of cancer has a tendency to spread to the ovaries and they’re not able to tell us for sure if it’s cancerous or not. My surgical oncologist also feels like this is the best plan. He looked at my ovaries when he did the laparoscopy and said they didn’t look completely normal.
The day before surgery, I met with her again and she told me, “What are we doing?” I said, “We’re removing the ovaries.” I went in to have my surgery, which was a 7- to 8-hour procedure. They removed my stomach and attached my intestines to my esophagus. They also removed my ovaries.
I was supposed to be in the hospital for a week, but I was very determined to not have any complications. I knew the surgery had a tendency to have complications and it’s not 100% in my control, but I wanted to do everything that they wanted me to do to help with that.
They wanted me to walk around, so I walked around. They wanted to make sure that I was sitting up most of the day, so I sat up and hardly laid down. I ate the protein that they asked me to eat. I did everything that they asked me to do. Because of that and the way everything was looking, I was able to leave the hospital in four days versus a week.
‘The cancer is being very aggressive… we’re looking at distant spread. We didn’t get the results that we wanted.’
Post-Op Follow-up
I had a follow-up one week later with my surgical oncologist. He went over the pathology and that was a shocker for us because we had hopes that the trial was going to get me to no evidence of disease. Unfortunately, he wasn’t able to get clear margins. The cancer had gone further up my esophagus than it had before. He went as high as he could, that was safe to do so, but it was very high.
He also shared that the tumor had taken up half of my stomach and it wasn’t like that before. He removed 53 lymph nodes and 27 came back as cancerous. He said, “What this means is that the cancer is being very aggressive. It also signals distant metastasis, so we’re looking at distant spread. We didn’t get the results that we wanted to get. Even with the chemo that you did before the trial, it looks like you had a zero response to it.”
I was shocked. I didn’t know what to think and how to feel. He told me, “We still have you on the schedule to have three more rounds of chemo to your peritoneum, but I’m concerned with the results of the pathology. I don’t know if we can wait until you finish that to put you back on systemic chemo or if we need to jump right into systemic chemo to address anything in your body versus focusing on the peritoneum.”
We brought back in my oncologist and she shared that it’d be best to go ahead and finish the trial. After that, maybe we should move to observation.
That brings me to the present. I’m waiting it out. I have another scan to review what’s going on and if there’s anything else concerning anywhere.
My faith is very important to me. When I’m struggling, I put on my worship music, pray, and ask for guidance.
Having a Support System
I have a great support system. I have great family and friends who check in on me and make sure that I’m okay. I rely heavily on the support group. I bounce ideas off of them. They told me about the Signatera™ test that I wouldn’t have known about if it hadn’t been for that group.
My faith is very important to me. When I’m struggling, I put on my worship music, pray, and ask for guidance because some days are harder than others.
I also undergo therapy. Therapy is so important. I always felt like I was dealing with most of this relatively well, but I didn’t want to have too much confidence in myself, so I wanted to have someone I could talk to to make sure that I was dealing with everything okay.
For the most part, I feel okay, but there are times when things rock me and I want to make sure that I’m coping healthily. I don’t want to brush it off and think I’m being strong when I’m hurting myself more.
Importance of Self-Advocacy
Focus on your why. Why do you want answers? Why is it important? For me, it’s my family. I want to be here for my family. I have a son and want to be there for him and see him grow up. I want to be the cool, tatted grandma and witness my child grow up and be a husband and a father. I want to see all his big life moments and be there to support him. I want to spend the rest of my life with my spouse. We have so much more time and so many more memories to make.
Advocating for yourself is the most important thing when it comes to your health.
Feeling Different
My body is so exhausted. It’s not the body that I used to have. I always joke with my spouse and say I’m an old woman now because I get fatigued so easily. After doing one task, I feel like I did a whole day’s worth of running errands.
I have a lot of things that are going against my energy. Without a stomach, I’m not able to absorb B12, so I have to do B12 injections once a month, but those wear off. I’m not getting the maximum absorption of iron, so I’m anemic and struggling to absorb iron. That’s also making me exhausted. With my ovaries gone, I’m going through menopause and my hormones are going crazy.
Because of the after-effects of chemotherapy and immunotherapy, my body is tired and I can feel that. It’s a bit frustrating because I’m a very independent person and I like to take care of things.
Words of Advice
Self-advocacy is so vital. You have to make sure that you’re advocating for yourself at each appointment. You know your body. Unfortunately, doctors get a lot of patients and they’re very busy. It’s not all on them. Sometimes, we have to reiterate, “This symptom is concerning because of this. This is what I need from you.” We forget that we have that power.
We go into the doctor’s office wanting them to give us answers, but they don’t have all the information and that’s not their fault. Sometimes, we don’t have all the information but make sure that we are pushing for more.
If they can’t do something for you, then get a second opinion or ask them to put you in touch with someone who can do that for you. Advocating for yourself is the most important thing when it comes to your health to make sure that you are getting the right treatment that’s specific to you and your needs.
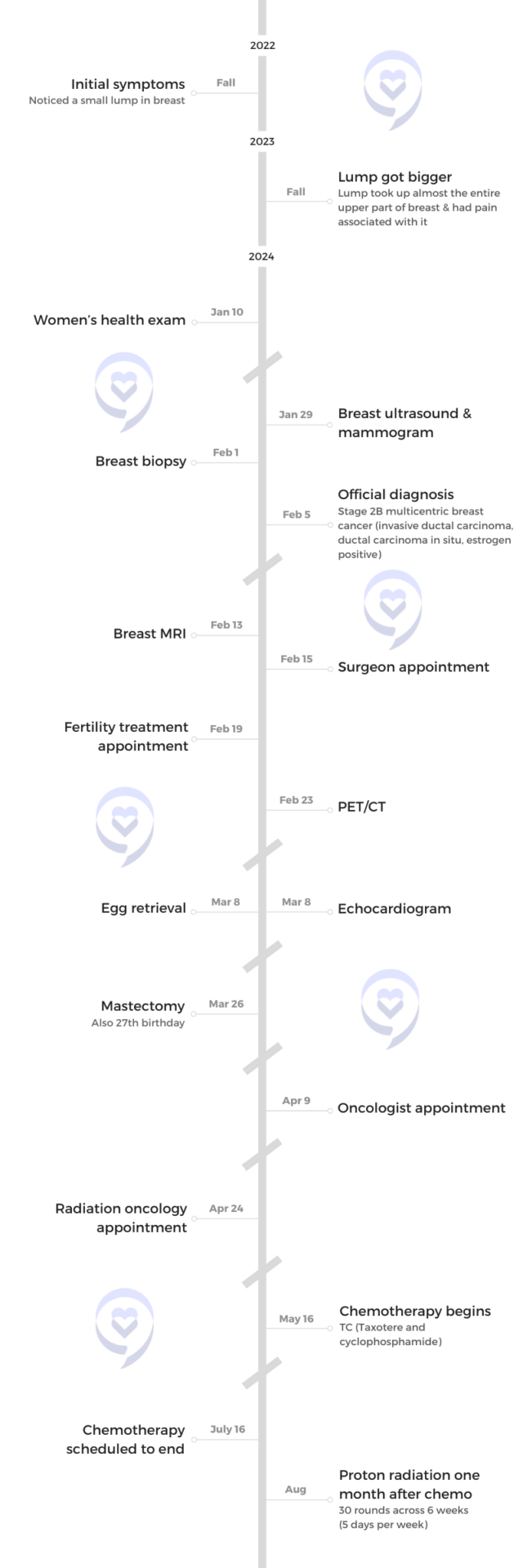
LaShae’s Stage 2B Multicentric ER+ IDC & DCIS Breast Cancer Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
LaShae, a PhD student in cancer prevention research, shares her journey with breast cancer. She initially dismissed a small, movable lump she found in her breast due to her busy schedule, but when the lump grew and she felt pain, she sought medical attention.
Her doctor referred her for a breast ultrasound and mammogram, revealing multiple masses and widespread calcifications. A biopsy confirmed cancer with a high likelihood of malignancy and a breast MRI revealed the spread in her breast and lymph nodes.
She had a mastectomy on her 27th birthday. Currently undergoing chemotherapy, she continues her fitness routine despite the side effects. Her experience has deepened her commitment to cancer research, particularly for adolescents and young adults (AYAs), highlighting the importance of self-advocacy and support groups.
Name: LaShae R.
Diagnosis:
Breast Cancer
Invasive ductal carcinoma (IDC)
Ductal carcinoma in situ (DCIS)
ER+
Staging:
2B
Initial Symptom:
Lump in breast
Treatment:
Chemotherapy: TC (Taxotere and cyclophosphamide)
Proton radiation (scheduled one month after chemo ends)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I found a small lump about a centimeter in size… I thought I had nothing to worry about.
Introduction
I live in Miami, Florida, but I was born and raised in Nassau, Bahamas, so I am a Caribbean girl.
I’m currently doing my PhD in cancer prevention research.
Pre-diagnosis
Initial Symptoms
I found a small lump about a centimeter in size. I didn’t think much of it. I did some research and found out that if the lump was movable, it had a lower likelihood of being cancerous. At that time, mine was movable so I thought I had nothing to worry about.
I hadn’t been doing much cancer research yet. I was looking at obesity research and now I’m at a parallel where we’re looking at exercise and diet and how they can impact cancer outcomes. I was still a baby when it came to cancer research, so that’s a big reason I pushed it to the side.
When my PhD started, a lot was thrown at me at once. Anyone who has done any graduate degree knows. I wanted to be the best student that I could be and the best person I could be for the new lab that I was in, so I prioritized those.
Sadly, like a lot of us, health was put on the back burner, so I forgot about the lump. I’m also a powerlifter. I bench press close to 300 lbs, so if I feel any tension or pain in my chest area, I attribute it to that.
In late 2023, I felt a lump again and wondered if it was the same lump. To this day, I don’t know if it was, but it grew in size so I thought that something was wrong.
I felt pain and that was what alerted me. I scheduled a wellness exam, but I had to keep postponing it because I had a lot of things coming up for my degree. I finally got in to do it in early January 2024 at the student center.
She said they were only going to schedule the ultrasound because I didn’t need a mammogram. I was too young.
Breast Exam
The doctor did a pap smear, vitals, and all the basic things done at a wellness exam, but she didn’t perform a breast exam. When she was about to leave, she asked, “Is there anything pressing that you want to discuss or want me to do for you?” I mentioned the lump and she immediately took it seriously. She put on gloves and performed a breast exam.
She wasn’t sure what it was, but she put “Mass?” on the paper and said, “I’m going to go ahead and be extra cautious. I’m giving you a referral to get an ultrasound and a mammogram.” She gave me instructions on the things that I needed to do and told me where to call, which was very helpful. To this day, that visit and that doctor were a part of the team that saved my life.
Breast Ultrasound
I called to schedule my ultrasound and mammogram. The person on the phone said I was young to be scheduling a mammogram and ultrasound. She asked if I had any symptoms. When I listed them off, I mentioned that I had a palpable mass and pain. She said they were only going to schedule the ultrasound because I didn’t need a mammogram. I was too young.
I’m very persistent and cautious. At this point, I was taking this seriously. You might think that I’m wasting your time because I’m too young and you probably think I can’t get cancer, but I’m going to waste your time.
When I went in for my ultrasound, I was filling out a form and it asked if I was of Bahamian descent. Women from the Bahamas have a higher likelihood of getting breast cancer and having more aggressive cancers due to the BRCA mutation, among other mutations.
They said it would probably going to take about 15 minutes. When the tech started the ultrasound, the moment she put the wand on, her eyes became wide and the same with the person assisting her. I knew that there was something there because it was palpable, but what was going on?
The radiologist came in and said, ‘You have multiple calcifications throughout all four quadrants of your breast.’
Every time they see something, they would take a picture and measure it. They did about 10 of those. Then they asked, “How long have you had these masses?” I replied, “Masses? Plural? As far as I know, I just have one lump.”
Before the ultrasound ended, they brought in someone to do the 360° view because they said they hadn’t done that. As someone who knows about cancer and who’s pursuing cancer research, I knew it meant that it’s spread all over the place. It’s in four quadrants.
When they went over to the left, there was nothing there. It was quick. Then they came back to the right and got another person to come in and help. What was supposed to take 15 minutes is taking 45 minutes now.
I started to gather my stuff to leave and they said, “No, no, no! You can’t leave. We’re about to do a mammogram now. You need to do a mammogram.”
Mammogram
I immediately got pushed to the top of the line and had a mammogram that same day. When I was done, I started gathering my things again and they said, “No! You can’t leave. The radiologist is going to talk to you right now. They’re going to talk to you today before you leave.”
They took me to a quiet room. The radiologist came in and said, “You have multiple calcifications throughout all four quadrants of your breast.”
I couldn’t believe what I heard. I started to get dizzy. I power lift daily. A couple of weeks prior, I bench-pressed 292 lbs, squatted 440 lbs, and deadlift almost 500 lbs that I had to get drug tested.
They start looking at you with that look of pity. After that, I asked what the next step was and they said I needed to do a biopsy.
When I found out the results, I felt a little better than having all of that anxiety trying to figure out what I had.
Biopsy Results
MyChart popped up and I saw the notes from the ultrasound and mammogram. It said fine calcifications throughout all four quadrants of the breast spanning 12.7 cm. Then it said it was in my lymph nodes and that I was BI-RADS 5. I looked it up and it meant at least a 95% chance of having cancer. I’m waiting for the biopsy results and now I’m stressed out.
Diagnosis
Getting the Results
Three days later, I got a call. They said, “Hi, I’m calling about your results,” and asked if I had a place to sit. Every time, they give you hints. I said, “Let me try to find a place,” and then they said, “We can call you back if you like.” I’m like, “No, no, no, no, no, don’t call me back. You already just made my brain explode. What’s going on?” Then the doctor lets me know that she doesn’t have good results. It was malignant.
Reaction to my Stage 2 Breast Cancer Diagnosis
When I found out the results, I felt a little better than having all of that anxiety trying to figure out what I had. Hearing that was a relief. After I got the phone call, the surgeon’s office called and I made an appointment.
Breast MRI
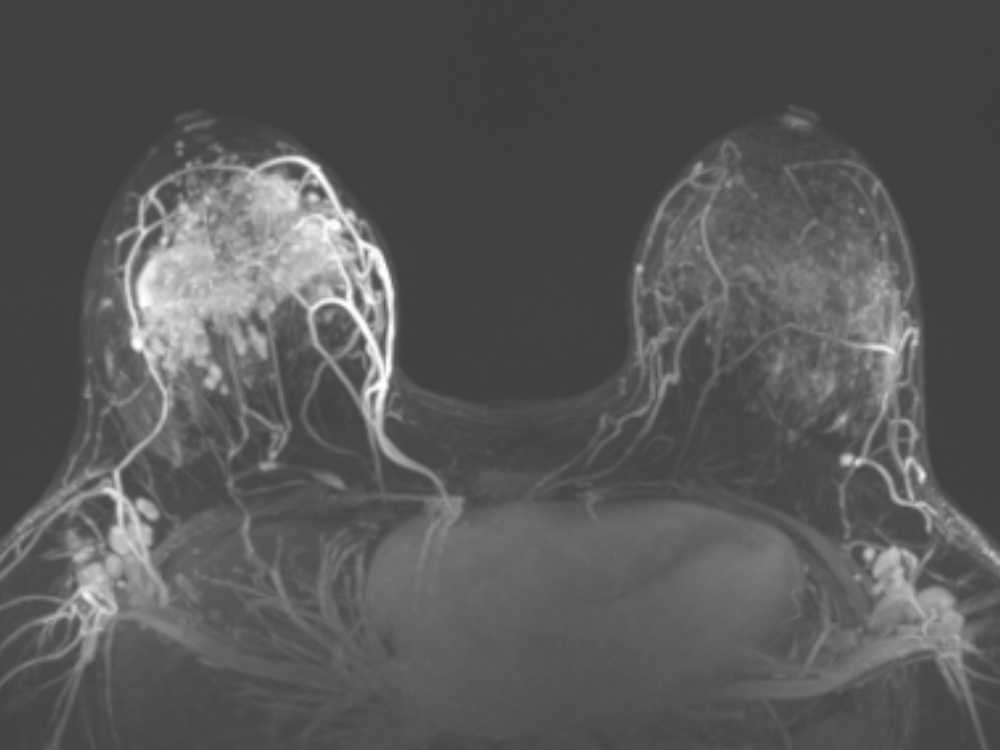
The breast MRI was very uncomfortable. Based on the results, they let me know that it was confirmed. I do have widespread, cancerous-looking things throughout my breast and in my lymph nodes.
I had my mastectomy on my 27th birthday. At first, I was upset, but I think it’s good because I would always celebrate when they took the cancer out of my body.
Mastectomy
After the MRI, the surgeon let me know that I didn’t have that many options because it was in all four quadrants of my breast. Usually, people can do a lumpectomy or certain types of mastectomies, like skin-sparing or nipple-sparing. I had to do a simple mastectomy, so it’s a flat closure along my sternum to my underarm or axilla. I think that was better than having to make a bunch of decisions.
She also told me I would be doing a PET scan. When I got the results, it was localized to my breast and nearby lymph nodes, so that was a big relief.
Pre-surgery Tests
I did a chest X-ray, EKGs, blood work, blood typing and cross-matching, and other tests before surgery.
I also worked out a lot because I wanted to prepare my body for the battle. One of the things I learned is that as you go through treatment, your body goes through a lot and you can lose muscle, which is detrimental to your outcome. I kept powerlifting and retaining muscle right up to the surgery.
I had my mastectomy on my 27th birthday. At first, I was upset, but I think it’s good because I would always celebrate when they took the cancer out of my body. After the mastectomy, my surgeon came in and explained that she removed the cancer. Two lymph nodes were positive and from what I know, that’s a hit or miss. Based on the final pathology, I can either have chemo or not, but I would definitely need radiation.
When I got home, that’s when the side effects kicked in. Fatigue was number one. I immediately had to shower and then I fell asleep for 18 hours.
Treatment
TC Chemotherapy
I was passed off to the medical oncologist. I met with her after my surgery and she’s the one who’s going to be spearheading the chemo, radiation, and hormonal treatments.
She let me know from the get-go that I would need chemotherapy and that’s the standard of care. I also would need radiation and hormone treatment because my stage 2 breast cancer was ER+, so I’m going to need to be on hormone treatment for 5 to 10 years.
It was a toss-up between A-CT (Adriamycin, cyclophosphamide, Taxol) or TC (Taxotere and cyclophosphamide). I needed chemo because of the lymph node involvement and my age. The longer you live, the higher the likelihood of recurrence simply because you’re around longer.
I’m currently undergoing chemo. We decided to do TC based on the results from additional testing. We did a MammaPrint® and I was found to be at high risk for recurrence.
Chemo was what I feared the most from the beginning. I had to get to my first chemo appointment early because I was doing scalp cooling. It didn’t take that long and it wasn’t as scary as I thought. They give a lot of pre-medications. I had never taken Benadryl at that dose so I was dizzy and sleepy. It knocked me out.
Side Effects of Chemotherapy
Less than 24 hours after chemo, I went to the gym and power lifted because I wanted to keep doing what I do. I felt solid, but when I got home, that’s when the side effects kicked in. Fatigue was number one. I immediately had to shower and then I fell asleep for 18 hours. It was brutal.
I had GI side effects. It wasn’t good. I got a headache and my whole body felt sore. I work out a lot, so I know what soreness feels like, but it had nothing to do with my workouts. It was a general, full-body soreness that even my bones were hurting. I had to take Zoladex to preserve my ovaries so that I’m able to have children after this. A lot was going on.
The side effects lasted for about five days. Over a week after chemo, I feel great. I was able to do a workout and not crash afterward.
This has opened my eyes to a new group that I had no idea was part of a disparaged group: AYAs or adolescents and young adults.
Cancer Research
I’m in a unique situation as somebody who wants to do cancer research for their entire career and is in the middle of a PhD focused on cancer prevention. It was very surprising, but it helped me get to my diagnosis. I would not have taken this seriously or even known I had alarming signs if I didn’t have that base knowledge.
When I think about what has happened, all I think about is how I’m going to be a much better researcher. I knew I wanted to work with marginalized and disparaged communities to help those who needed help the most. I’ve always believed in doing that and helping the less fortunate.
This has opened my eyes to a new group that I had no idea was part of a disparaged group: AYAs or adolescents and young adults. I’m going to include them in anything that I do in research and want to do community work with that group because being a part of that group, I understand now that these are unique circumstances.
When you’re a young adult, you are just starting your life. When you go to the doctor’s office, you’re the youngest. When I went to one of my appointments, the medical assistant asked where the patient was. I was right there, but she didn’t expect me to be the patient. Sometimes I go with my mom and they think she’s the patient.
This is very emotional and very isolating. Cancer in itself is isolating, but you may also be the only one in your age bracket going through this. When you go to the doctor’s office, people feel sorry for you more because of your age.
My experience is going to make me a much better researcher. It’s going to make me more invested and make me an advocate. I used to want to be an advocate, but now I want to be a research advocate and living proof.
Cancer is very emotional from when you get the diagnosis and throughout the whole process. This is a journey. You go through different emotions. I deal with it by taking deep breaths. That helped a lot.
I joined my AYA support group. Joining support groups is vital because they are going through the same thing. They’re at different stages of the journey, so they’re able to guide you and help you get on track because you’re pulled in so many directions and it’s overwhelming.
Caribbean people tend to have more aggressive cancers when it comes to certain types and they’re diagnosed at younger ages.
Genetic Mutations
Caribbean people tend to have more aggressive cancers when it comes to certain types and they’re diagnosed at younger ages. At the Sylvester Comprehensive Cancer Center in Miami, they asked me ahead of time if I was of Bahamian descent because they’re aware of this.
We’re known to have the BRCA mutation and other mutations. I got the comprehensive panel done and it turned out negative for all. I didn’t have all the common risk factors. I’m the first person in my family to ever get breast cancer, so I could not tell you at all why I got this.
Words of Advice
For patients undergoing chemotherapy, come in with an open mind. You’re going to be scared, but don’t stress out because stress is not good for you. It won’t help with your outcome.
Get some ice compression for your hands and feet to prevent neuropathy, depending on the type of chemotherapy that you’re going to have to get infused. Taxotere has been linked to neuropathy, so I did that.
Try to eat bland foods when you’re going through chemotherapy. If you don’t eat, you’re going to feel terrible. I know all these things are going on, but you’ve got to eat something. Whenever I didn’t eat, I would feel terrible. I started to feel better when I did. Nutrition is so important.
Advocate for yourself because only you know your body.
When you feel good enough, go outside and take a walk. I’m not saying do what I did 24 hours after chemo, but go out and move because it’s been linked to way better outcomes.
Advocate for yourself because only you know your body. There are a lot of professionals who are trained to diagnose. I do research and I know the statistics. But if we rely solely on the numbers, I’m not supposed to have cancer. I’m not even supposed to get screened.
No matter how young you are, make sure to go to your physical exam every year. Be in touch with your doctors. Eat well and exercise to be the strongest you that you can be.
Sophie’s Stage 4 Bowel Cancer with BRAF Mutation Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
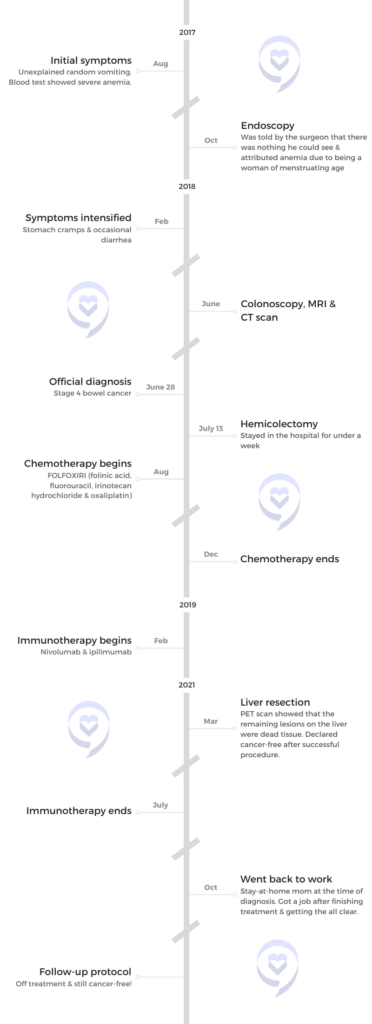
Sophie was diagnosed with stage 4 bowel cancer after experiencing symptoms for almost a year. Initially thought to have Crohn’s disease, her condition was finally identified after having a colonoscopy, a CT scan, and an MRI. The diagnosis revealed multiple lesions and a significant tumor, leading to a hemicolectomy.
Post-surgery, Sophie underwent aggressive FOLFOXIRI chemotherapy due to her BRAF mutation, enduring severe side effects like neuropathy, extreme fatigue, and significant weight loss. Despite the grueling treatment, the initial response was positive but when the chemotherapy failed, her oncologist pursued a different approach with immunotherapy drugs nivolumab and ipilimumab.
The immunotherapy had manageable side effects and led to significant improvement. After two years of treatment, Sophie was declared cancer-free following a PET scan and liver surgery biopsy confirming the absence of cancerous cells.
Name: Sophie U.
Diagnosis:
Bowel Cancer
BRAF
MSI
Staging:
Stage 4
Initial Symptoms:
Vomiting
Anemia (found in blood test)
Treatment:
Surgery: hemicolectomy
Chemotherapy: FOLFOXIRI (folinic acid, fluorouracil, irinotecan hydrochloride, and oxaliplatin)
Immunotherapy: nivolumab & ipilimumab
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I went to my doctor because I felt something wasn’t right.
Introduction
I’m from Warwickshire, England, and I was diagnosed with stage 4 bowel cancer in 2018.
I’m married with two kids and I currently work in Motorsport.
Pre-diagnosis
Initial Symptoms
It was a Monday night. I went up to bed and vomited all of a sudden. There was no reason for me to be sick. I’d eaten nothing suspicious, so it seemed a bit off.
It didn’t happen again until nearly the weekend. It was a bit strange because it was a single occasion both times. It happened again the week after, but it came out of both ends this time, so I thought I’d eaten something bad.
The following week, I went to my doctor because I felt something wasn’t right. I wasn’t vomiting a lot, but it didn’t seem normal. The doctor ran some blood tests and then we would go from there.
She called me the next day and told me that I was so anemic, she wondered how I was still walking. I was almost at the point where I needed a blood transfusion. My son was two then and wasn’t a good sleeper, so I was always tired.
In hindsight, they thought the tumor had gotten so big by that point that it was stopping food from going down. Before that, I hadn’t noticed anything.
Luckily, I had a great GP. She wanted to get to the bottom of things and was willing to go the extra mile.
Unfortunately, I didn’t have any typical symptoms, so that led us down a different path, thinking it was a stomach issue. We tried an elimination diet because we thought it might be an intolerance. She referred me to have an endoscopy, which showed nothing. We did all kinds of things, but that was it as far as symptoms for the first few months.
I was in a lot of pain. My stool wasn’t bloody, but it looked red.
Symptoms Intensified
When we went to Disneyland Paris in February, I was getting bouts of diarrhea. It wasn’t consistent, but I was in a lot of pain. My stool wasn’t bloody, but it looked red.
When I got back from the trip, I told my GP. I went to see her for something else but told her what I noticed while on our trip. She said, “Now I can refer you to the inflammatory bowel clinic because it’s moving towards that. It might be something like Crohn’s or colitis.”
It takes a while for the referrals to go through. That was February, but I didn’t see him until April or May. He was convinced it was Crohn’s disease, so he wanted to get all the tests done to get them out of the way and confirm the diagnosis so we could move on.
Colonoscopy & MRI
He ordered a colonoscopy and an MRI. That ended up happening in June. I had the colonoscopy on a Friday and then the MRI the following Monday. By this point, my stomach pains were getting worse. I couldn’t eat much because I wasn’t keeping anything down.
The colonoscopy was so painful. I didn’t realize what was going on at the time because I was under a lot of medication. I could see it on the screen, but I didn’t know what I was looking at although I knew something looked different. They said, “There’s a lesion and we can’t get the camera past it, so you have to talk to your doctor.” I didn’t know what lesion meant. I thought it was a cut or something. I started searching online, but cancer wasn’t in my mind at all.
It was a relief in some way to know that there was something wrong with me. I just didn’t want it to be that.
Diagnosis
Getting the Official Diagnosis of Stage 4 Bowel Cancer
They didn’t tell me at the time what it was. They called me the next day and said I need to have a CT scan before I see the doctor on Thursday. I thought it was another thing to get done.
I was really sick at that point, so I asked my husband to come with me. At no point had we’d been thinking it was cancer, so no one told me to bring him with me. He came because I couldn’t physically move. I had my CT scan then we walked to the IBD doctor and that’s when he told us.
They staged me at stage 4 bowel cancer. I did all the tests for Crohn’s disease, so they could see where it spread. There were multiple lesions in my liver, all throughout my torso, and a lot of my lymph nodes. No other organs. The tumor was tennis ball sized.
Reaction to the Diagnosis
To be honest, it was a massive shock for it to be cancer because I thought it was Crohn’s disease. It was a relief in some way to know that there was something wrong with me. I just didn’t want it to be stage 4 bowel cancer.
It wasn’t the IBD specialist’s area of expertise. He hadn’t had to give that kind of news before, so I don’t think he handled it in the best way because he didn’t know how to say it. It was delivered in quite a shocking way. He wasn’t an oncologist, so it wasn’t very sensitive, I guess.
The tumor was so large that it was almost cutting off my bowel and that’s why I was being sick.
Treatment
Hemicolectomy
I was told that I’d be assigned an oncologist and have a multidisciplinary (MDT) team. They were going to meet with me the following week and come up with a plan, so I didn’t get to speak to my oncologist until the week after. He said I was going to have surgery first because the tumor was so large that it was almost cutting off my bowel and that’s why I was being sick. Nothing was getting through. He said, “For you to get through any chemo, we’re going to have to get rid of this first.”
The surgery was called hemicolectomy and it happened the week after, around 10 days from when I was told I had cancer. I was in the hospital for about a week. It was quite “messy,” they said. It spread back towards my spine and wrapped around blood vessels. They removed a few lymph nodes and had to cut off part of my stomach because it attached itself to my stomach. It was quite a rough recovery, to be honest.
FOLFOXIRI Chemotherapy
I was told that I’d be put on the strongest chemo they could throw at it. Because of my age, they thought I could handle it. They were able to do a biopsy and found out that I had a BRAF mutation, which is very aggressive and has the worst prognosis of a bowel cancer diagnosis but because of that, they could also add another type of chemo.
The median survival rate of stage 4 bowel cancer is 8 to 12 months. My doctor didn’t know anyone with a BRAF mutation who survived. It’s known for not having good survival statistics, especially back then. More recently though, a lot of people have been living a lot longer because they’re finding out different treatments for it. It’s still not a great diagnosis, unfortunately.
I had a portacath fitted because they said the chemo was too strong to have in my veins. I had that done about three weeks after surgery and then a week after that, I started my chemo.
I was put on FOLFOXIRI, which is a combination of FOLFIRI (folinic acid, fluorouracil, and irinotecan hydrochloride) and oxaliplatin. I would go to the hospital and have an infusion for about six hours. I would come home with a pump attached to me that would stay on for the next 48 hours before I go back and have it removed.
Chemo was the most horrific thing I’ve had to go through… I was probably just surviving by the end of it.
Side Effects of FOLFOXIRI to Treat My Stage 4 Bowel Cancer
It was rough on me. During those 48 hours, I was horribly sick. The first cycle wasn’t too bad, but I was sick a lot. I also recently had bowel surgery, so they were expecting that. I had bad diarrhea. I was very tired all the time. It progressed because the side effects from the chemo were cumulative.
The oxaliplatin also gave me neuropathy. My feet weren’t so bad. I was having chemo over winter, so my hands were like needles and on fire. I couldn’t put them in the fridge.
They reduced the amount of chemo I was getting and extended my time, so I ended up being at the hospital for eight hours plus the 48 hours after. Honestly, chemo was the most horrific thing I’ve had to go through.
I lost my appetite and my taste of things. I lost a lot of weight. I was probably about 40 to 50 lbs lighter. I couldn’t eat anything. Nothing tasted like anything. Bread and pizza were like cardboard. I was probably just surviving by the end of it. I was living off nutrition drinks.
I had such bad brain fog that I couldn’t even talk to people anymore. I would try and say something, but I would forget what I was saying mid-sentence and be so exhausted that I couldn’t be bothered to correct myself.
I would sleep most of the time. My kids at the time were 6 and 3. My daughter was at school, but my son was at nursery. They were lovely enough to take him on for additional hours so I could sleep all day.
For the two days I had the pump at home, I would not be able to keep anything in my body. By the end of it, it was coming out both ends horrendously. I couldn’t leave the house because I had to be near a toilet all the time. I couldn’t even drink water at the end because it was like everything was being rejected.
I didn’t lose my hair, but it did thin quite a bit. I lost a lot of muscle. I melted away and became weak like an old lady. It was horrible because I couldn’t do anything for myself. I couldn’t look after my kids and that was the hardest thing.
One thing I wish I’d done is accept help more and ask for it… I was exhausting myself.
I wish I’d known that it affects everyone differently. If you go on social media, you see people dancing around their chemo poles. I couldn’t even stand up, let alone hold my phone to make a video or take a photo. I was asleep all the time. If I’d known that there were people like me, then I probably wouldn’t have felt so bad.
One thing I wish I’d done is accept help more and ask for it. People always offered to help. It’s hard to admit that you need help, but at the same time, I realized I should have done it because I was exhausting myself.
I only had eight cycles in the end. I was supposed to be on it indefinitely, palliatively. My first scan showed that it shrunk a lot. In bowel cancer, some of the CEA is measured and with me, it was a good indicator of how things were going. When I was first diagnosed, it was off the charts at around 7,000. The chemo got it down to 650 after my first scan. After that, I went downhill rapidly.
I had my last chemo session on New Year’s Eve 2018. The week after, I ended up in the hospital because I couldn’t eat anything or keep anything down.
Immunotherapy
We had time between having surgery and starting treatment, so my husband was looking into what else we could do. He read about immunotherapy and that it had been successful in the US. I was looking into it and we were seeing if we could go to Germany and get it done there.
We talked to my oncologist before I started chemo and my husband brought it up. He said he’ll look into it, but because of how far off in the distance it is treatment-wise, I wouldn’t be alive by the time it would be available. We would either have to go to Germany or see how we could afford it because it costs over $190,000 to get this treatment.
When the chemo failed, I met with him and he said he had been working behind the scenes with a different oncologist who was looking for someone like me with BRAF mutation and MSI. Most bowel cancer patients are MSS. I don’t know how it works and why immunotherapy works for people who are MSI, but that’s generally what they figured out.
The drugs were called nivolumab and ipilimumab. The plan was to have both for four cycles and then after four cycles move down to nivolumab alone.
They tested the immunotherapy in melanoma patients and there was something that we have similarly that it might work. They were working with Bristol Myers Squibb, so I could get the immunotherapy on compassionate use if all my other treatment options failed. My oncologist knew this, but he didn’t tell me until it did fail. At the time, that was the only treatment available for BRAF mutation. He said that now it’s failed, he can refer me to get the immunotherapy.
I had to transfer care to another oncologist, which was a further away hospital. The drugs were called nivolumab and ipilimumab. The plan was to have both for four cycles and then after four cycles move down to nivolumab alone. I had the first cycle every three weeks and then nivolumab every two weeks.
Because of the newness of the treatment, they didn’t know how it was going to affect me. I was having the dual drug, so they said I had double the chance of getting any autoimmune disease, which could happen at any point. They had to do blood work every time and check everything. If I noticed anything different about myself, I had to report it to them. They would then report back their findings to the drug company.
Side Effects of Immunotherapy
The immunotherapy compared to the chemo was night and day. I was only there for a couple of hours and that was it. The infusion was around an hour and a half to two hours for the first one and then it eventually dwindled to an hour. I could drive out of there when I was done. With chemo, I couldn’t drive out of the hospital. I was barely moving. With the immunotherapy, I felt a little bit sick and a bit tired, but that was it.
After I had the PET scan, he called me up the next day and said, ‘Nothing’s showing on your PET scan. No cancerous cells anywhere.’
Being Cancer-Free
I’d been on immunotherapy for two years. They didn’t know where to go with it because there weren’t many people in front of me, but they knew it was getting to the two-year mark.
I asked my oncologist if I could get a PET scan because they don’t do PET scans so much over here. He wouldn’t do it at first until he agreed eventually. After I had the PET scan, he called me up the next day and said, “Nothing’s showing on your PET scan. No cancerous cells anywhere. It looks like those are dead tumors and we think that your lymph nodes are probably filled with white blood cells and that’s where they’re showing on the CT scans.”
There wasn’t a defining moment of being cancer-free. The only moment I can say that did happen was after I had my liver surgery. My surgeon said they had the biopsy results back because he wanted to wait to make sure. Sometimes when they cut them out, there can still be cancerous cells in the middle. He said they didn’t find anything. He said, “I can tell you now that that means you’re cancer-free.”
It’s a great feeling. I was happy. When I got out of the hospital and sat in my car, I called my husband and cried. That was probably the first time I cried out of relief because it was unbelievable.
Words of Advice
Appreciate and enjoy life. We’re all so busy doing things and thinking that we’re living when we’re not. You don’t want something like a terminal cancer diagnosis to make you realize that, but sadly, it does take that for a lot of people. It’s not until you get to this point that you realize how much we’re not living and how much we should be enjoying everything and everyone. Be kinder to each other and enjoy what you have.
We’re all so busy doing things and thinking that we’re living when we’re not. You don’t want something like a terminal cancer diagnosis to make you realize that.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Erica, who lost her mother to breast cancer over 20 years ago, shares her stage 0 DCIS breast cancer journey. After a decade of concerning mammograms and due to her mother’s history, she remained vigilant despite negative BRCA results. Following her biopsy diagnosis, she was overwhelmed by the treatment choices but ultimately opted for a double mastectomy to minimize recurrence risk.
Choosing to undergo a double mastectomy including nipple removal provided Erica with confidence and a cancer-free peace of mind. She subsequently underwent reconstructive surgery and as she embraced her new body, she was more excited about having no fear of recurrence.
She completed her transformation with a 3D nipple tattoo from a specialized artist, providing closure to her journey. Leading a nonprofit for kids with cancer, Erica supports other women and caregivers, emphasizing the importance of trusting oneself and the process when navigating cancer treatment decisions.
Name: Erica C.
Diagnosis:
Breast Cancer
Ductal Carcinoma In Situ (DCIS)
Staging:
0
Initial Symptom:
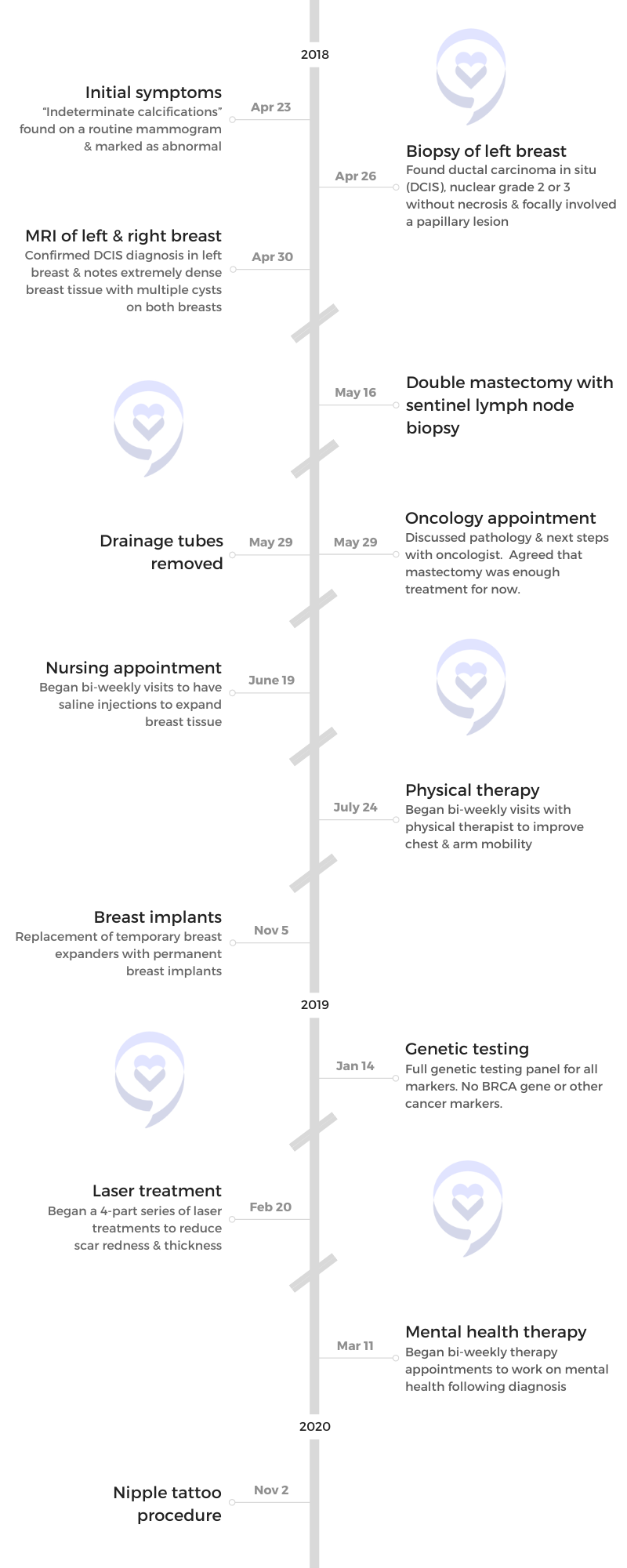
Indeterminate calcifications found on a routine mammogram
Treatment:
Double mastectomy
While cancer is a club you never want to join, once you’re in, there are some silver linings, like the people you meet and the life perspective that you get, and those are true gifts.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I had increasing scans over the years, but I’d never had a biopsy and that was when I thought this was going to get a little bit more serious.
Introduction
I live in Minneapolis, Minnesota. I’m a breast cancer survivor. I lead a nonprofit that helps children with cancer and their families. I’m also a cancer orphan because I lost my mother to breast cancer over 20 years ago. These multiple perspectives on cancer make me incredibly interested in other people’s journeys and sharing my journey to help other women who come after me.
Pre-diagnosis
I was diagnosed in 2018 and it came after about a solid 10 years of “scary mammograms.” Because my mother died of breast cancer, I was on high alert. I met with tons of doctors who said I have the same risk as any other human in the population. I underwent genetic testing and I wasn’t BRCA positive, but I still didn’t feel good about my health journey given my mother’s unfortunate diagnosis and death.
Over the years, I’ve had mammograms, ultrasounds, and MRIs. They would always see something a little bit scary, ask me to come back for a higher level of screening, and then say it’s fine. It built up this anxiety over the years because they started to see some abnormal things, particularly calcifications, which are potentially early signs of breast cancer.
It got to the point where I thought, When are we going to take this a little bit more seriously? I was getting routine mammograms every six months and one time, they said, “Let’s have a biopsy.” I had increasing scans over the years, but I’d never had a biopsy and that was when I thought this was going to get a little bit more serious.
While stage zero sounds great, it still requires a fair amount of intervention and a fair amount of choice.
Diagnosis
Looking back, I’m not sure if I was surprised by the diagnosis or if I felt like, “Finally.” After the biopsy, I received the diagnosis that it was DCIS, which is ductal carcinoma in situ. It’s an early-stage breast cancer. Many people can say that’s a good kind of cancer, but there’s no such thing as a good kind of cancer.
While stage zero sounds great, it still requires a fair amount of intervention and a fair amount of choice. Being presented with all those choices became the most overwhelming part because it was starting to come at me like a fire hose.
Treatment Decision Making
The choices that I had to make ranged from doing nothing to a double mastectomy and everything in between. I was given the choice of a lumpectomy to remove the part of my breast that showed early-stage breast cancer. I was also given the choice of hormone therapy. I was given a choice of radiation, even the choice of some chemotherapy. It all ranged amongst a spectrum.
My mother’s journey had been a painful one because hers also started as early-stage breast cancer. At the time, doctors said it wasn’t a big deal. As you know by the results, it became a big deal. She relapsed four times over her journey and it came back bigger, stronger, and more invasive every time.
I had all these choices of less aggressive treatment, but I wanted a double mastectomy because I didn’t want this to come back.
For me, it became this choice of how to rewrite the story. How do I advocate for myself in a way that maybe my mom didn’t? Maybe she didn’t have the right information at the time.
I felt more confident facing all these choices and because of what I’d seen with my mom, I went straight to a double mastectomy. I got a lot of eyebrows raised. I had all these choices of less aggressive treatment, but I wanted a double mastectomy because I didn’t want this to come back.
I had all the statistics and all the advice, but within about a week, I became pretty firm in my decision to choose a double mastectomy. People questioned me, but it was the best decision I ever made.
Double Mastectomy
A double mastectomy is a pretty radical choice. Once you choose a double mastectomy, they remove your breast tissue. A choice that you get to make is whether you want to also remove your nipples or if want to try to keep them through a nipple-sparing surgery.
For me, this was a fear-based choice. If I was going to do such an invasive surgery to essentially remove two near-lifetime body parts, I wasn’t going to leave anything to chance, so I chose to have my nipples removed as well.
I chose to go under the chest muscles, which is more painful but ensures the longer-term security of the implants.
Reconstructive Surgery
The other choice I had was whether or not I was going to have reconstructive surgery. I can buck the stereotype and say I don’t need breasts. I’ve already had children and was done breastfeeding. But I chose to have reconstructive surgery.
At the time, it was a very extensive surgery. It’s done in two parts, which is what I didn’t realize at first. I was in surgery for 8 to 10 hours. The first four were simply removing my breasts. I had a breast surgeon who was going to take out everything and some lymph nodes to test. Then the breast surgeon handed me off to a reconstructive plastic surgeon.
To me, plastic surgery sounded vain and unnecessary, but I had to get comfortable with having a breast plastic surgeon come in. For the next four hours, that surgeon cut into my muscles. I could have gone over my chest muscles, but I chose to go under the chest muscles, which is more painful but ensures the longer-term security of the implants.
My surgeon said, “It sounds like you’re all in and that you’re confident. This is going to be more painful, but you will have a better outcome with the implants. They’re not going to move around. They’re going to be secured into your chest. Trust me.” For somebody who I’ve just met to say, “Trust me,” is quite possibly the greatest leap of faith.
At the end of that surgery, not only did he cut underneath my chest muscles, but he essentially put two deflated balloons under my chest muscles and then sewed me up.
After that eight-hour surgery, my job was to heal and make the choice of what I wanted my breasts to look like afterward because, over time, he would fill those balloons with saline to expand my chest. If you’ve ever had dental braces, that’s the kind of soreness and pain you feel when they’re expanding your chest over time. It’s a wild ride and it was painful.
I didn’t realize how much I used my chest. When you raise your hand, that’s your chest muscle moving. I couldn’t touch my nose so when my nose itched, I had to have someone else scratch my nose for me. It was scary and painful, but I still stand by it being the best choice I ever made. I healed and have full mobility now. I can work out, do push-ups, and everything.
They look great. I can wear a bikini and you would never know.
Post-Mastectomy
Right after surgery, you start flat-chested with what looks like Frankenstein stitches. They are not pretty. What’s interesting is that every week, when I would go to the nurse or the doctor, they would say, “Oh, this is going to look amazing. I could see it.”
These sort of deflated balloons come with what seems to be a metal top that’s placed under my skin. Every week, they would put a magnet on my chest to find where that metal piece was and that’s where they would pierce my skin and inflate the balloon with saline a little bit at a time. This took about three months. It’s quite painful to stretch your skin and your muscles at the same time when this massive scar is healing.
As they’re slowly inflating these balloons with saline, I start to see what’s happening and start to see them look real. I’m still wearing loose tops and tops that zip up because I don’t have full mobility of my chest, but I was starting to feel normal again.
They were hard massaging my scars, which I couldn’t even believe. There are also certain oils you can apply. I even had a laser procedure done to reduce some of the scars. I ended up with this really beautiful chest—just without nipples.
I had to have another surgery, which was supposed to be easy but there’s no such thing as easy in this journey. They had to take out the temporary balloons and put in a permanent implant. They also did a fat graft by taking fat out of my belly and putting it around the implant so they looked natural. I walked out of the second surgery looking like someone attacked my breasts and my abs. Liposuction was so painful. I couldn’t even breathe. It’s not easy, but it was so worth it.
I wear the exact same bathing suit that I wore pre-surgery. I wear the exact same tight dresses. But here’s the kicker: I don’t have to wear a bra. My implants don’t move so I get to wear backless dresses with nothing. I get to wear fancy dresses that I wore before and not have that feeling at the end of the night when my bra is too tight and I can’t wait to take it off. They look great. I can wear a bikini and you would never know.
The biggest reason I’m so excited about this is because I have no fear. I have no fear of reoccurrence. The mental game that I had to go through to get here was hard. You heard about the physical pain. The procedures were challenging, but my mind is cancer-free and that is the most beautiful thing. I don’t worry about reocurrence. I can’t get breast cancer. I don’t have to get mammograms. I don’t worry about it and that to me is the greatest gift.
Between a lumpectomy and mastectomy, I’m confident in saying a double mastectomy.
I did get mental health therapy at the request of my breast plastic surgeon. He said, “You look great, but I’ve been around the block. I encourage you to get some therapy.” I’m a proud person and said I didn’t need it. I needed it. I absolutely needed it.
In the beginning, I had a fear of relapse. My therapist and I talked through some ways and some strategies to get around that. My body is cancer-free, my mind is cancer-free, and that is the greatest choice I made.
If I had had a lumpectomy, I’d be subject to continual mammograms and we all know that those are anxiety-inducing. I’d be subject to hormone therapy. I’d be on high watch. It would not be worth it.
A lot of people who are newly diagnosed reach out and ask what they should do between a lumpectomy and mastectomy, and I’m confident in saying a double mastectomy.
Lumpectomy vs. Mastectomy
A lumpectomy is a minimally invasive surgery where they take out the area that has the cancer and the surrounding tissue. It’s “easier,” although I’ve heard lumpectomies are still not easy.
A lumpectomy can be done outpatient, but depending on the diagnosis, there is typically some follow-up. For quite some time, you have to come in every day to have it taken care of.
With mastectomy, they remove the entire breast. Depending on whether or not that cancer has spread outside the breast, there could be chemotherapy as well.
You might need to have radiation to make sure they got everything and radiation can be painful. There’s also hormone therapy, which involves taking some drugs to make sure that some of your hormones are not feeding the cancer.
It was unclear whether or not I was going to get sensation back in my breasts and to be able to feel the pain of the needles of a tattoo was relieving.
Getting a Nipple Tattoo
I read an article about a tattoo artist who specialized in nipple tattoos. It was a beautiful article about how much compassion he had for breast cancer survivors so that’s where he dedicated his career.
I originally wasn’t going to see him because I’d have to fly across the country. It seemed to be a big hurdle and I was going to have it done at my plastic surgeon’s office where a nurse practitioner said she could do it. I kept hemming and hawing about it and I realized that I wasn’t ready for the journey to end because the last step of the entire journey was the nipple tattoo. I decided to get some mental health therapy first because I didn’t think the journey was over for me mentally.
On the day of my appointment, I canceled with the nurse practitioner. When I talked to my therapist, she said, “It sounds like this is a big thing for you. Tell me more about it.” I told her I had the dream about getting this fancy tattoo artist to do it for me. She said, “Well, then you go do that,” and so I did. It was the celebratory closure for me.
I drove up there and there was no fanfare. I was alone going to a tattoo parlor in a strip mall outside of Baltimore. I’ve never had a tattoo. I was afraid of needles and pain but here I am, about to get a tattoo, which was quite ironic.
Part of reconstructive surgery is that you lose sensation. I couldn’t feel my breasts. As I was sitting with the tattoo artist, he said, “You probably won’t feel a lot of this because you’re still in the reconstructive phase and your nerves are still healing.” Sure enough, it was painful. It was unclear whether or not I was going to get sensation back in my breasts and to be able to feel the pain of the needles of a tattoo was relieving.
The tattoo artist approached the process quite clinically. He looked at my breasts and said, “Okay, I think I’m going to do this. I think I’m going to do this.” He didn’t ask my opinion. He just asked, “You want 3D? You want it to look real?” I said, “Yes, I do,” and he went to town. Twenty minutes later, I put my shirt back on and it was over. It was truly over then.
My mission to support other women and caregivers because of the many gifts that I have been given by other cancer patients.
Life’s Mission
Cancer changed my life. I lead an organization that helps kids with cancer and their families, but that journey started when I was right out of college and didn’t have a lot of purpose. I didn’t love my first job and volunteered at a sleep-away summer camp for kids with cancer. I took a week off of work and would be the mom to these kids, whether they were seven-year-olds or teenagers. Those were some of the most life-changing experiences I have ever had.
When I was diagnosed, I realized it’s what I’m supposed to be doing. Not only is it my career now, but it is my mission to support other women and caregivers because of the many gifts that I have been given by other cancer patients.
I spent a lot of time with my mom in the hospital where I met other cancer patients. While cancer is a club you never want to join, once you’re in, there are some silver linings, like the people you meet and the life perspective that you get, and those are true gifts.
Words of Advice
Trust the process and trust yourself. No one better than yourself knows what’s right for you. While I recommend having a mastectomy or someone may have said something, ultimately, trust yourself and trust the process. That will get you through.
Discover the Latest Developments Used to Treat Advanced or Recurrent Endometrial Cancer
Edited by: Katrina Villareal
Patient advocate Tiffany Drummond and gynecological cancer expert Dr. Brian Slomovitz of the Mount Sinai Medical Center in Miami, Florida, discuss the latest treatments for endometrial cancer.
Develop a comprehensive understanding of advanced and recurrent endometrial cancer, enhancing your knowledge about the disease’s progression and challenges. Learn about the current treatment protocols and how they offer hope and recovery to patients dealing with this severe form of cancer.
Explore how immunotherapy is transforming the treatment landscape, providing new avenues for potentially more effective and personalized care. Discover cutting-edge developments in the field, including promising clinical trials that could offer new hope and treatment options for patients. Gain insight into advances in robotic surgery, including techniques using the da Vinci Surgical System, which offers precision and reduced recovery times.
Thank you to Karyopharm for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang: I’m the founder of The Patient Story and a cancer survivor. Mine was non-Hodgkin lymphoma. During that time, I realized how important connection was and that became the genesis of The Patient Story. This multi-channel community seeks to connect, educate, and empower patients and care partners. We do this primarily through in-depth patient story videos and educational programs with a thread of self-advocacy, asking questions, and sharing more about what you’re experiencing with your medical team, which is so important in cancers, especially like endometrial cancer where it’s critical people understand what is available to them and what to ask their doctors.
The Patient Story retains full editorial control of all content. While we hope you walk away with more understanding, this discussion is not meant to be medical advice or a substitute for your medical care.
The discussion will be moderated by Tiffany Drummond, who has more than 15 years of experience as a clinical research professional. Tiffany lost her mother Leonora Jean Drummond to endometrial cancer in 2016 and ever since, her mission has been to promote women’s health and wellness. Tiffany works with ECANA, the Endometrial Cancer Action Network for African-Americans, which is incredible in helping to create community.
Tiffany Drummond, Patient Advocate
Tiffany Drummond: As a clinical research educator, I’ve been doing hematology-oncology research for about 20 years, and most importantly, I’m a patient advocate and daughter of someone who I lost to endometrial cancer.
Dr. Brian Slomovitz, Gynecologic Oncologist
Tiffany: Dr. Brian Slomovitz is a gynecologic oncologist at Mount Sinai Medical Center in Florida. He’s a nationally recognized expert in robotic surgery, sentinel lymph node evaluation, and immunotherapy, and has led a number of clinical trials specifically in endometrial cancer. Dr. Slomovitz, what drew you to this field?
Dr. Brian Slomovitz: When I was thinking about which specialties to go into, I enjoyed surgery. I also enjoyed the why and the how of things and what we can do for the complete care of our patients not just surgical management, medical management, or preventative management.
As a gynecologic oncologist, I focus on complete patient care, including prevention or early diagnosis, initial treatment options, cure, and survivorship. I also focus on how to manage recurrent and advanced disease, improving one’s quality of life while trying to control cancer, and ultimately leading a woman through her disease course.
For me, it’s promising and rewarding. One of the things that was introduced to me in this area is clinical research and the importance of research in offering the best care for our patients.
What is Endometrial Cancer?
Tiffany: What is endometrial cancer?
Dr. Slomovitz: In gynecologic oncology, we deal with three major types of cancer: ovarian cancer, cervical cancer, and endometrial cancer. Endometrial cancer is the most common gynecologic malignancy. It’s much more common than ovarian cancer and cervical cancer.
Historically, we didn’t think about it as much because most women with endometrial cancer do well from their disease and will die of something else. But as we focus more attention on it, we’re learning that endometrial cancer has a subgroup of patients with metastatic or recurrent disease that represents an unmet need. We need to come up with better treatment options for them and that’s what I’m focusing a lot of my time on.
In 2024, the number of deaths from endometrial cancer will outnumber the deaths from ovarian cancer, which highlights the unmet need. We need to do better. We always thought about ovarian cancer as a “killer.” The fact that there are more deaths from this disease is something that frustrates us and something that we need to do something about.
Symptoms of Endometrial Cancer
Dr. Slomovitz: Abnormal bleeding is a symptom of endometrial cancer. A lot of times, people think it’s postmenopausal bleeding, which is true if you’re in menopause and have spotting. It would be best if you had an appropriate workup with a provider who does gynecologic exams. Some people see their family practice doctor or primary care doctor, but it’s important to see a gynecologist or someone who does gynecologic exams, which would include an endometrial biopsy as well as an ultrasound.
Other symptoms include pelvic pain, pelvic pressure, and abnormal pap smears. Any symptoms that last from 10 days to two weeks or get progressively worse need to get checked. We need to encourage women to see their healthcare provider, but abnormal bleeding is the number one issue that we worry about.
Tiffany: For my mother, it was postmenopausal bleeding and I’m not sure why, but she didn’t think it was something that needed to be looked at. She thought it was normal. I say this for women in general: our GYN care is going to help us throughout our lives. It doesn’t stop when you go through menopause. Always be aware of that.
Current Treatments for Endometrial Cancer
Tiffany: What are the current standard treatments for endometrial cancer?
Dr. Slomovitz: For women who are initially diagnosed, the first step is usually surgery. After we get imaging, like a CT scan, a lot of these patients will have clinical stage 1 disease surgical resection, which is a hysterectomy. Traditionally, we did these with an up-and-down incision. Patients would be in the hospital for a long period of time. Now we’re doing most things minimally invasive.
I do mine robotically with a da Vinci robot. We’ll remove the uterus, the tubes, the ovaries, and the cervix. The advantage there is less blood loss, less pain for the patients, and a quicker recovery. It’s a little easier for the surgeon too, which I don’t mind. It’s best for our patients. They can go home the same day or the next day.
We do a sentinel lymph node biopsy using the Firefly technology. It’s like using night vision goggles to identify nodes that are most likely involved.
Tiffany: I’m so glad that these advancements exist.
Advanced & Recurrent Endometrial Cancer
Tiffany: My mother had recurrent endometrial cancer and was diagnosed at stage 3. Can you talk to us about recurrent and advanced endometrial cancer and the current options for them? When we say advanced and recurrent, what do they mean in terms of endometrial cancer?
Dr. Slomovitz: Women who are diagnosed with stage 1 endometrial cancer will make up 80 to 90% of the patient population. It’s the patients with advanced disease that we’re worried about. Similar to your mom, lymph node positivity stage 3, widely metastatic disease stage 4, and the subgroup of patients with earlier stage disease that recur represent a diagnostic or treatment challenge and an unmet need.
Traditionally, we would use chemotherapy, but as we’re learning more and more about the disease and being able to look at the molecular subclassifications of endometrial cancer, we’re learning that different types of tumors can respond differently to different types of therapies.
Immunotherapy was originally found to work extremely well in non-small cell lung cancers and melanomas. When we learned more about endometrial cancer, not only did we find that there’s activity of immunotherapy in endometrial cancer, but there are distinct subgroups within patients with recurrent or metastatic disease that respond more favorably to immunotherapy. Those are areas that we need to exploit, taking knowledge that we have, and then pushing that forward into the clinical setting.
Not all patients are the same. We need to offer more unique, personalized medicine, and to do so, we need to better understand the biology of the disease to execute a better treatment strategy.
Biomarkers in Endometrial Cancer
Tiffany: We’re hearing about biomarkers and a lot of patients are becoming more familiar because they’re being told that they either have or don’t have certain biomarkers. Can you break down the biomarkers dMMR and pMMR and why they are important in guiding treatment decisions for our patients?
Dr. Slomovitz: When cells divide, normally there are errors in the process. Cell division isn’t a perfect process. The body normally recognizes the errors and corrects them. The team of proteins that does this is called the mismatch repair (MMR) proteins. If cells are proficient in mismatch repair proteins, they’re more likely to be able to repair those cells and move forward. That’s pMMR.
The dMMR is a different subgroup deficient in mismatch repair proteins. These are the ones that the body’s unable to fix. By not having these “fixed cells” or cells that look normal, these cells look like they shouldn’t be there. They look more like non-self instead of self, so they respond better to immunotherapy.
Immunotherapy is not a poison that we give cells. Immunotherapy is sort of a stimulant of the body’s immune system to fight off something that shouldn’t be there. When we think about tumors or cells that are more responsive to immunotherapy, it’s more of the non-self cells, cells with a high mutational burden, or cells that have some different molecular characteristics. DMMR is more responsive to immunotherapy. PMMR, while they still respond to immunotherapy, they don’t respond as well. We need to treat them differently.
Tiffany: I’m assuming the typical first-line treatment approach is immunotherapy. Are there other alternatives?
Dr. Slomovitz: For the dMMR population, the best treatment option for patients with advanced or metastatic disease is chemotherapy in combination with checkpoint inhibitors. Over the last year and a half or so, we’ve had landmark trials looking at drugs including pembrolizumab, dostarlimab, atezolizumab, and durvalumab, which are all checkpoint inhibitors. Given in combination with chemotherapy, they have shown unprecedented improvements in overall survival and progression-free survival in patients with dMMR tumors. There was a 70% reduction, which is remarkable.
Tiffany: What is a checkpoint inhibitor?
Dr. Slomovitz: A checkpoint inhibitor is a medication given to a patient that helps to stimulate the immune system to better fight off things that shouldn’t be there. When we give it to a patient to attack a tumor, the dMMR tumors are recognized by the body as something that shouldn’t be there more than the pMMR tumor, so that’s why checkpoint inhibitors work better in that setting.
Highlighting Endometrial Cancer Clinical Trials
Tiffany: Let’s talk about the changing treatment landscape. Immunotherapy is likely to become a more common treatment for women with advanced endometrial cancer. Following the results of these clinical trials that you were talking about, can you talk more about this and what these breakthroughs were with these results?
Dr. Slomovitz: The initial results showed that giving immunotherapy with chemotherapy works better. As we move forward, what we’re focusing on is to see if we can give combinations or single agents in the first-line setting before chemotherapy to eliminate the use of chemotherapy but to get the same effectiveness.
Recently reported was one trial looking at a combination of pembrolizumab and lenvatinib in the first-line setting. That didn’t meet its statistical endpoint, but that looked at all comers, pMMR and dMMR.
There are two ongoing trials now: one’s completed accrual but hasn’t read out and one’s still accruing, looking specifically at the dMMR population to see if a checkpoint inhibitor alone can work in those patients. I’m the global lead on one of those. We’re looking at pembrolizumab in patients with dMMR tumors and comparing it to chemotherapy to see if we can get rid of chemotherapy for that population. Now if we can, it’ll be amazing.
Tiffany: Very promising. This is why I’m such a proponent of clinical research and increasing diversity and participation, so we can get good data.
Tiffany: Let’s talk about adding immune checkpoint inhibitors, like pembrolizumab and dostarlimab. What is the conversation about this becoming the new standard first-line treatment for advanced or recurrent endometrial cancer patients with dMMR tumors? Is this something that needs more research or more data to fully understand the scope?
Dr. Slomovitz: I would say with certainty that for the dMMR population, unless there’s a contraindication to immunotherapy checkpoint inhibitors, those patients deserve or should get checkpoint inhibition as the standard of care based on the promising results. It’s not as much of a slam dunk for pMMR, but for the dMMR population, treatments should include a checkpoint inhibitor, without a doubt.
Maintenance Therapy Options in Endometrial Cancer
Tiffany: Let’s talk about some clinical trials that are actively enrolling in the advanced and recurrent setting, with late-stage endometrial cancer, such as selinexor as a first-line maintenance therapy. What trials are ongoing that people can learn about and be eligible for?
Dr. Slomovitz: In addition to leading the division of gynecologic oncology at Mount Sinai Medical Center in Miami Beach, I also serve in the GOG Foundation and lead the uterine cancer clinical trial portfolio. In that capacity, we have a lot going on in uterine cancer, which is exciting. Wearing my Mount Sinai hat, we’re excited that most of those trials are opened up at Mount Sinai.
Selinexor is a nuclear transport inhibitor. This is for pMMR, most likely p53 wild-type, which is a biomarker in the cell. The trial doesn’t require pMMR but knowing that they get checkpoints, it’ll probably all end up being the pMMR population. Chemotherapy versus chemotherapy and maintenance selinexor.
Now we did the preliminary trial, called the SIENDO trial, where we looked at all comers, whether they’re p53 wild-type or mutated, and found that the primary outcome didn’t benefit the selinexor group. But if we did a subgroup analysis, if we looked at patients with p53 wild-type tumors, there was a big difference in outcomes. Outcomes improved in patients treated with selinexor.
We then went to the FDA and said, “Wow, look at this outcome. This will be better for our patients.” The FDA agreed, but appropriately, they said we needed to do a separate study looking at that to see if it works and that’s one of the trials that we have open accruing globally. It’s called the XPORT-EC-042 trial. We’re looking to see specifically in chemo-naive, p53 wild-type patients if adding selinexor can help improve outcomes.
Other areas are taking off in endometrial cancer. There’s a class of drugs called antibody-drug conjugates (ADCs), which is a novel class of drugs. They have three components. They have an antibody that’s attracted to a protein on the tumor cells. Then there’s a chemotherapy kill, the part that helps kill the cell. The third and most important part is the linker.
When the drug is given, it travels throughout the body and only goes to the cancer cells because of the antibody-protein interaction. Once it gets there, the linker lets go of the chemotherapy, which then goes in and kills the cells.
In endometrial cancer, we recently got FDA approval in all comers for trastuzumab deruxtecan (T-DXd) based on the DESTINY-PanTumor02 data, which is an ADC that’s attracted to the HER2 protein on tumor cells. That had unprecedented response rates in the recurrent setting.
Tiffany: We have a lot going on in the clinical research world with endometrial cancer. I’m so excited because it wasn’t always as robust, so I’m glad to see researchers taking steps to improve that.
Endometrial Cancer Treatment Side Effects
Tiffany: Let’s talk about clinical trials in terms of side effects. We know that a lot of these drugs are toxic and have a lot of side effects.
Dr. Slomovitz: Clinical trials allow patients to get a drug that they normally wouldn’t be able to get, which hopefully, improves outcomes. New drugs can have new side effects that we need to be aware of. One of the things that I talk to my patients about when they go on a clinical trial is they get two teams of healthcare providers following them. It’s not only me and my team with our nurse practitioners and nurses, but the whole clinical research team.
Clinical research is like following a cookbook. To get FDA approval, we try to make treatment as homogeneous as possible without a lot of differences. We follow the cookbook to say dosing, when should things start, when to hold the dose, when to reduce the dose, how are the side effects being managed, and all those things. Between the research team and the clinical team, we communicate closely with our patients. We follow the side effect profile. We look for new signals.
Tiffany: That’s an excellent point you made. When I listen to the experiences of people in clinical trials, they tend to have the sentiment that they get more comprehensive care because they have this whole team of people including other providers outside of their GYN oncology. One of the benefits of clinical research that I think a lot of people don’t know because they’re afraid to jump into the unknown is that you’re getting looked at a lot more than you probably would.
Dr. Slomovitz: It’s important to highlight one of the fears patients have in going on clinical trials is not the side effects they’re going to get; it’s getting a placebo. Whenever patients are on a clinical trial, they’re at least getting the standard of care.
We do not experiment on patients. We do clinical research and study if the new treatment options do better, the same, or worse than the standard of care. Unless the standard of care is observation, we don’t give a placebo. I have to highlight this in every single talk I give.
I don’t want patients to think that if they’re going on a clinical trial, they’re actually getting worse care or they’re being studied incorrectly in a way we did historically. Over the last 20 years, the way we do research in the country has been completely revamped to be ethical, sound, and looking out for the best of our patients. There’s an understanding that we need to do better and make sure we give patients at least the standard of care. We need people to acknowledge that in the research community, we’ve changed. At worst, they’re getting standard of care, but even with the standard of care, they’re getting two teams watching.
Tiffany: I’m so glad that you brought that up. I drive that point home every time I’m talking as well because a lot of patients, specifically on cancer trials, do think that they don’t want to be experimented on. At the minimum, you’re going to get whatever the standard is. Thank you for driving that point home.
Diversity, Equity & inclusion (DEI) in Cancer Trials
Dr. Slomovitz: There’s something that we often mention in the last five minutes of these interviews that needs to be mentioned in the first five minutes. Diversity.
Once you talked about a patient signing on and not getting a placebo, patients need to know that they’re being represented on these trials and that they’re not the only person from their community from coming in on the trial. They’re equally represented. It’s crucial. We need to make sure that the results of the trial translate across different populations.
I’m going to throw the numbers out there, which are disturbing to hear but are facts. Black women are nearly twice as likely to die from endometrial cancer than white women. There’s no other way to say it. We need to do better.
In these research trials, we need to make sure that there’s an appropriate representation of all different diversities for the results to translate to those groups. If we have a clinical trial with 100% white women and it works, that doesn’t mean it’s going to work in Black patients, Hispanic patients, or Asian patients.
We must have this conversation at the beginning of the interview because we have to focus on it. We need to increase the diversity in our clinical trials and then we could ensure not only to get better outcomes but better outcomes across different populations.
Tiffany: A man after my own heart. This is something that I have a personal and professional passion for, increasing diversity in clinical trials and how important it is that when we look at these approvals, it’s representative across populations. The FDA came out with guidance that when you’re submitting investigational new drug applications, you need to have a diversity plan. I hope that researchers and investigators measure their success with that and not simply saying they tried but didn’t make it. Thank you for being a proponent of that.
Dr. Slomovitz: Patients need to reach out to their providers to talk about the option of clinical trials. As physicians, we want what’s best for our patients, even if it means taking care of a patient with the best standard of care at the hospital down the street if there’s a clinical trial available. We’re working towards having a community to be able to offer patients clinical trials. Fortunately, we have a lot going on at Mount Sinai Medical Center, which I’m able to offer to our patients.
Making patients aware of clinical trials is important. How do we do that? We have to go into different settings and different areas where we’re not used to. We used to put up a flyer on the wall that said, “Come to the hospital to learn about clinical trials.” We have to understand that certain populations either can’t get to the hospital, don’t want to go to the hospital, or don’t know what’s going on in the hospital. Going out to community centers, advocacy groups, churches, and places like that is extremely important to help overcome those barriers and biases against clinical research.
We don’t realize there’s not only the fear of research but there’s also the practicality of research. For example, sometimes we send our patients a questionnaire to fill out before an online visit. A lot of patients still don’t have access to Wi-Fi, so what do we do about that? Or we ask them to come to the hospital for a three-hour appointment. Who will take care of that person’s children or sometimes their grandchildren when they’re the primary caregiver? What if that person works and if they don’t, they can’t afford dinner? Those are things we need to do better at.
We’re working closely with sponsors to help overcome some of the things that we can overcome. We can’t do everything, but if it means having a sponsor pay for four hours of child care to get a patient on the research, it’s important to do that. The DEI plans that you mentioned include some of these ways to overcome the barriers associated with research to increase diversity, which will make the outcomes of trials better.
Setting Expectations for a Patient’s Clinical Trial Experience
Tiffany: Hearing the word “research” can be scary, but what can someone who has endometrial cancer expect when they go on a clinical trial?
Dr. Slomovitz: There needs to be an understanding that they’re going to get at least the best care if not better care than they would get off a clinical trial. They need to be comfortable in the environment.
Here in Miami, much of the population doesn’t speak English, so we need to educate patients about clinical trials in their language as best as we can. The cold comfort is the fear of the word research and fear of not being able to understand the information, so all of our consent forms and patient information are offered in multiple languages.
They need to understand that they’re watched closely. They may have some side effects that we’re not expecting, but just the same, they may have some outcomes that we’re not expecting either.
They need to know that it’s not a lifelong sentence. Part of the consenting process is if they decide to back out, they could back out. We’re not here to force people to do anything. We’re here to recommend. We’re not here to be paternalistic. Patients sometimes ask, “What would you do if it’s your family?” We’re honest with them about that, but we need to make it an experience that patients appreciate.
There are better rewards than a patient not responding to a trial, but a patient who’s not responding to a trial who says, “Doc, what’s next? What’s the next clinical trial for?” That means we’re doing a good job in offering that patient a trial. We knocked down barriers and that’s a patient who wants to do the best for herself.
Tiffany: I do tell people who are thinking about participating in a trial as well that they’re not only doing it for themselves, they’re doing it for future patients. If we’re altruistic, then participating in clinical trials is one thing that we can do to help others.
Requirements and Responsibilities of a Clinical Trial
Tiffany: Let’s talk about the actual procedures and tests that are done. People might be surprised that they already get these done anyway. What can someone expect?
Dr. Slomovitz: There are some similarities and some differences. Similarities include blood tests, appointments with doctors, signing consent forms, and answering questionnaires. These things take a bit longer, but they’re part of the process that we need to go through to get them on a trial. Those are things that we normally do but they’re a little bit more intense in a trial. It’s part of the standard of medical care not only of research care.
In addition, there are tests that we need to do that are outside the standard of care but important for a particular trial. For example, we don’t normally have to do a heart scan and an echo, but for a certain drug, we might have to do them.
The most annoying thing patients may need to do will be an extra biopsy. A lot of our trials now are biomarker-directed and some of these biomarkers are novel, so we don’t have that information unless we do a new biopsy. Any procedure you do has its risks and benefits. Fortunately, a lot of times, biopsies are relatively straightforward.
Improving Diversity in Clinical Trials
Tiffany: How can we improve clinical trial awareness and education in underserved communities?
Dr. Slomovitz: When we talk about a cancer that’s deadly and may end their life prematurely, it’s important to know all the options from the beginning, even if they’re not coming to the office from day one and thinking about or eligible for a clinical trial. Maybe not now but in the future. It’s the education process that says we have things on the standard of care and off the standard of care. It’s important to share the results with our patients so they see that we’re moving forward, knocking down some of the biases.
We talked about things like financial toxicity, time toxicity, and effort toxicity, and helping to overcome those barriers. There are resources out there. Sometimes patients can’t drive. Some of the car companies have different deals. The American Cancer Society supports that and things like that.
It’s a process. We’re getting better, but we still need to do better. I’m not going to be happy until we have a clinical trial option available for all of our patients with advanced recurrent disease to allow them to get the best standard of care before they are defeated by cancer.
Tiffany: The average life cycle of a clinical trial, from the time it starts to the time it gets market approval, could be anywhere between five-plus years. But if you are participating in that clinical trial, you get first-hand results on what’s going on in your care and that data is going to be used to push those approvals.
June is Uterine Cancer Awareness Month
Tiffany: You and I are very passionate not only about diversity in clinical trials but also about education and promoting clinical research. June is Uterine Cancer Awareness Month. Can you talk about that and why that’s important? What are you and Mount Sinai Medical Center doing to promote Uterine Cancer Awareness Month in June?
Dr. Slomovitz: We saw an unmet need. There’s Cervical Cancer Awareness Month in January, Ovarian Cancer Awareness Month in September, and Breast Cancer Awareness Month in October. We needed to make Uterine Cancer Awareness Month, so we started that in 2023.
Mount Sinai is making a big effort here and leading it in South Florida. They also have been supportive of my work with the International Gynecologic Cancer Society, the global leader in gynecologic cancers.
Final Takeaway
Tiffany: What is your takeaway for patients who are newly diagnosed and starting this journey?
Dr. Slomovitz: It’s important to describe why they got it or if we can know why. Sometimes these are obesity-related, hereditary, or caused by other factors. What can they do to get the best treatment options?
Make sure you’re comfortable with your care. Many patients can get a second opinion to make sure that they’re getting the best care. If they’re uncomfortable with the first opinion, seek out a second opinion because this is an important decision. It’s not only the surgery but the follow-ups. Not to say that the first doctor may have done something right or wrong, but when there are different options that patients weren’t made aware of from the beginning, it’s extremely frustrating.
Make sure that clinical trials are an option. If your doctor doesn’t do clinical trials, make sure that he or she is willing to send you to a center that has some of those clinical trials.
Create your medical team. That includes the patient, the patient’s family, friends, doctors, nurses, and navigators. It takes a team to defeat cancer.
Tiffany: Share this discussion with your family, friends, and loved ones. As Dr. Slomovitz said, don’t be afraid to have these discussions, especially when it comes to GYN care and health. A lot of times, we don’t want to talk about that as women and that’s something that we need to get around as well.
If you have a symptom that you know is not normal for you, speak up. Go to your provider and get the care that you need.
Dr. Slomovitz, thank you for the work that you do at Mount Sinai Medical Center in Florida and around the globe. Keep pushing the needle forward. I’m very hopeful that five years from now, we’re going to be in a whole different space with endometrial cancer, so I can only imagine where we’ll be 20 years from now.
Dr. Slomovitz: Tiffany, thank you so much. The future is bright and I’m excited about what it brings. I look forward to talking with you in the future when we talk about our victories too.
Stephanie: Thank you so much, Dr. Slomovitz. I couldn’t agree with Tiffany more. Thank you for being a global leader in this space. The rapid pace and shifting of the landscape of treatment options and all the research that’s happening is incredible. Please continue to do the great work that you do.
Thank you also, Tiffany, for leading this conversation to infuse that patient-care partner voice, which is so important for us here at The Patient Story and our community.
Check out ECANA: Endometrial Cancer Action Network for African-Americans and the work that they do. They create a community for African-Americans who have endometrial cancer or have been impacted by an endometrial cancer diagnosis.
Thank you so much for joining us. We hope to see you at another program.
Special thanks again to Karyopharm for its support of our independent patient education content. The Patient Story retains full editorial control.
Michael recounts his journey with diffuse large B-cell lymphoma (DLBCL) alongside his wife and care partner, Kimberly. He was initially diagnosed in 2016 but after experiencing pain in his lower back and leg coupled with severe itching, it led to a diagnosis of a relapse.
After undergoing chemotherapy, he faced severe side effects including weight loss, itching, and pneumonia. He then underwent CAR T-cell therapy, experiencing a brief remission. Michael tried a drug through a clinical trial but saw limited success. Eventually, he turned to epcoritamab, which has brought about significant improvement without notable side effects and improved his quality of life.
Michael emphasizes the importance of advocacy, seeking multiple opinions, and maintaining hope throughout the challenging journey. His wife Kimberly stresses the crucial role of care partners in managing and supporting treatment and well-being. She emphasizes the significance of self-care for caregivers and persistence in seeking answers and treatment options.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I was having lower back pain and an incredible amount of pain down the front of my right leg.
Michael
We knew two issues were going on, but we had no idea that they were pointing to the same thing.
Kimberly
Introduction
Michael: I was born and raised in Ravenna, Ohio. My wife Kimberly and I have six daughters and 10 grandchildren.
Kimberly: I didn’t know I would be a care partner when we got married, but it was a role I took on. I did it willingly, but it was a rough road.
Pre-diagnosis
Initial Symptoms
Michael: I was having lower back pain and an incredible amount of pain down the front of my right leg. I thought it was a pinched nerve or I’d done something wrong while working out.
Kimberly: We thought it was back trouble. That was coupled with severe rashes and itching. At that time, the two didn’t seem related. We knew two issues were going on, but we had no idea that they were pointing to the same thing.
Testing
Kimberly: The back and leg pain started around Labor Day and the rash started in October. By November, we noticed weight loss.
The Friday after Thanksgiving, he consulted with an orthopedic surgeon since we presumed it was back trouble and the surgeon ordered an MRI.
Michael: My wife pushed, so we got in sooner than scheduled.
They began treatment with the inclination that it probably was going to be diffuse large B-cell lymphoma.
Kimberly
Diagnosis
Kimberly: Based on Michael’s previous history, the doctor said, “We’re seeing enlarged lymph nodes. You have a lot of tumors pressing on your spine and that’s why you have this pain. We’re pretty sure your cancer is back.”
After the MRI, we saw the oncologist he had previously worked with.
Michael: I was diagnosed with DLBCL in 2016.
Kimberly: They ordered a biopsy, but because it was so severe, they began treatment with the inclination that it probably was going to be diffuse large B-cell lymphoma. They didn’t want to hold off on treatment. He had two rounds of chemo when the results of the biopsy came back and confirmed that it was DLBCL.
Michael: We didn’t find out what was going on until we went to Columbus. I will always be grateful to the oncologist in Akron because he had the wherewithal to say, “This is beyond me and I don’t know what to do with this.” He put us in contact with the hospital in Columbus and we met Dr. Voorhees, who took the ball and started running with it.
Kimberly: He was malnourished and dehydrated because of severe weight loss. The majority of the weight loss happened within three weeks.
Reaction to the Diagnosis
Michael: We were not expecting to hear that. When you hear something like that, it sets you back on your heels.
It’s scary because you don’t know what’s going on. Most people who get a cancer diagnosis start by looking for answers and don’t expect it to be serious. Most people think, I’ll get this taken care of and then we’ll move on the next day. Our next day turned into a 2 ½-year journey.
Kimberly: In the beginning, you don’t process because you’re on autopilot and doing everything you can for your loved one, like getting them to treatments and making sure they’re comfortable. Oftentimes, the reality of what’s happening doesn’t sink in.
An example is when we spent Christmas Day in the hospital. That was his initial stay from being dehydrated and malnourished and when he received his first round of chemo. I cooked him a quasi-Christmas dinner in the visitors’ lounge of the hospital.
Looking back at pictures of him, he was on the edge, but because I was so in the moment and going through everything a day at a time, I didn’t realize it then. A lot of the processing didn’t happen until later on.
One of the side effects I had was some of the worst itching of my life.
Michael
Treatment
Chemotherapy
Michael: We started with chemotherapy. I received a high amount of chemotherapy and I about died twice from it. Looking back, it was necessary to save my life.
I wasn’t in very good shape at all. I started at around 240 lbs. By the time we got to Columbus, I was down to 150 lbs. Being in that state physically is not a good place to start.
Side Effects of Chemotherapy
Michael: One of the side effects I had was some of the worst itching of my life to the point where it was causing me to have a different outlook on things. It was horrible. I’ve never experienced anything like that in my life.
Kimberly: When they started a second round, the reactions got worse. That’s when his skin started to blister and he was treated as a burn patient.
At that point, his doctor said, “This is way more than I can handle. I want you to go to the James Cancer Center.”
Michael: They had to come up with other treatment options. Thankfully, they got us through. It was like going through stages. Everything we went through got us to the next step. Then from there, we’d go to the next step. It went on down the line like that for a while. They kept me alive and kept me moving.
CAR T-cell Therapy
Michael: Our main goal was to get to CAR T-cell therapy, but we had to choose interim treatments in order to keep the cancer at bay long enough.
I asked Dr. Voorhees, “What do I have to do to be eligible for CAR T-cell therapy?” He said, “You have to be able to walk into my office.” Ten days later, by the grace of God, I was able to walk into his office. I went from being flat on my back to walking into his office.
I didn’t know anything about CAR T-cell therapy. We learned quickly, especially my wife. She’s a detail-oriented person and because of who she is, we learned quite a bit about how CAR T-cell therapy works. She has a curious mind and doesn’t accept not knowing things whereas I’m more of a big-picture guy. Tell me where we’re going and I’ll be there to do my part.
At the 100-day mark, I had a PET scan and they told us that my cancer had returned.
Michael
Post-CAR T-cell Therapy Monitoring
Michael: At that time, we thought CAR T-cell therapy was our cure-all. We believed that. But it turned out to be another step to get us to where we needed to be.
Relapse
Michael: At the 100-day mark, I had a PET scan and they told us that my cancer had returned. I didn’t feel any symptoms. My energy level was starting to increase. My weight was starting to come back. I was feeling good.
Reaction to the Relapse
Michael: When I receive information like that, I go quiet. I’m an internal processor and I think things through before I comment. I felt angry and frustrated. That was a bad day.
We believed that CAR T-cell therapy was a cure-all. We didn’t know that it only had a 47% success rate. Nobody told us. I don’t know if it was an oversight or nobody thought about it, but to be honest, there was some bitterness on my part because no one told us. But there comes a point where you have to accept things, move forward, and start looking at other options.
The next time we met with Dr. Voorhees, the first thing I asked him was, “Why didn’t somebody tell us that the success rate was less than 50%?” He said, “I don’t know why that didn’t happen.” He didn’t dodge the question. He was very honest with us about it. You don’t want to hear bad news, but you need to hear everything so that you can make good decisions.
I never allowed myself to think that there would be anything negative coming from that. We did everything that’s been asked of us. We trusted it and believed it would work. For 100 days, it was great.
Joining a Clinical Trial
Immunotherapy
Kimberly: We’re thankful that in today’s world, multiple options are available. His oncologist, who we started working with prior to and after CAR T-cell therapy, is always great at providing options. He felt that our best chance for controlling the lymphoma and giving Michael a quality of life would be to go on a trial.
There was a trial that he was aware of, which had some results, and he thought that would be best. We’re very adventurous and very aggressive, so we said, “All right, let’s do the trial.”
He was trying to keep my cancer under control until we could get to the point where we could find something that would work well.
Michael
Michael: I took eight pills a day and had to be monitored. Thankfully, I didn’t have any side effects.
Kimberly: Every day, I’d say, “Oh, you look a little better,” or, “Oh, you gained a little weight.” After several months, it was obvious that it wasn’t having an effect.
Michael: A PET scan showed that the disease progression slowed down but not to the degree that they had hoped. He was trying to keep my cancer under control until we could get to the point where we could find something that would work well. He said, “We’re going to try to move on to some other things because that wasn’t working.”
Kimberly: The good news is that it wasn’t necessarily worse, but there was no change, and there definitely still was active disease so we had to do something else.
Bispecific Antibody
Kimberly: Dr. Voorhees presented us with three options, but he felt that two of them were not viable.
His number one option—and the one I wanted Michael to pick—was another round of chemo because that’s a sure thing. We knew that it would control the lymphoma but not sure how it would play out.
A second option was to have a round of immunotherapy, which he responded to before but wasn’t a sure thing. Michael chose immunotherapy because he said, “Why would I want to be alive if I can’t have a quality of life and actually live?”
That was hard for me as a care partner because I wanted the sure thing. We knew that chemotherapy would knock out the lymphoma and keep it under control, but as a care partner, I also had to respect his wishes.
Michael: I love Dr. Voorhees dearly. He’s a good man. He makes you part of the process. If you start getting off the path a little bit, he’ll gently steer you back on, which I’ve always been grateful for and appreciated.
Kimberly: Based on Michael’s previous response to CAR T-cell therapy and the information from ongoing trials, epcoritamab seemed like it would be our best hope. Dr. Voorhees was confident that we would see at least some response.
Michael: He laid out the options. It was my choice. The choice I made was something that I thought would work best for me because of how my body handled CAR T-cell therapy. Bispecific antibodies were very similar so we went in that direction.
Kimberly: I read about the trial on epcoritamab and I felt that everyone who participated was identical to Michael. They had been through very similar things and that was very encouraging at that point.
We had to apply for compassionate use from the FDA because it was still waiting for approval. Michael had to have some additional treatment.
I thank God every day for the people who came up with the medication that saved my life.
Michael
Michael: I’m on epcoritamab (EPKINLY). One of my greatest hopes and prayers is that people have the opportunity to continue on to tomorrow, to enjoy life, and to enjoy their families.
Right now, I take epcoritamab once a month. I started with one a week and that went on for a while, then it went down to one every two weeks, and then we got to the point where I’m at now. The process takes 30 minutes. I used to take a couple of pills before I received the injection, but I don’t have to do that anymore. I go there, they give me my injection, then I go home.
From where we live, it takes between 2 ¼ to 2 ½ hours each way to drive to Columbus for a five-minute injection. It’s a very small price to pay for the results that we’re getting. Compared to everything else that we’ve been through, that is a very easy solution.
I thank God every day for the people who came up with the medication that saved my life. It was a very long ordeal for us and, thankfully, because of a lot of very intelligent people, epcoritamab was developed, is working for us, and makes a big difference.
Response to Epcoritamab
Michael: Within a month of receiving epcoritamab, my weight started coming back. My strength returned and I was able to do things that I hadn’t been able to do in quite a while. I’m back to 238 lbs and getting to do things that I never used to do.
I’m back to working out a lot, which I enjoy. My wife and I ride bikes, kayak, and play with the grandkids. We love to ride roller coasters and we like to travel. We live life and that’s something that was taken from us.
A lot of things were stripped from me when we went through cancer. I like to have the right to make my own choices and that was very hard for me to accept. To this day, when I think back on what happened, it doesn’t sit well with me. You have to learn to deal with it and get to the point where you find the goodness in things.
Kimberly: The immunotherapy did its job. It was almost as if I could see him transforming weekly. His energy level was up. He was able to resume his activities.
The day that I knew that we had hit a turning point was when he worked for about 10 hours in our yard. He loves landscaping. He’s an arborist by trade. He came inside and said, “I’m exhausted.” The red flags went up and I said, “Oh, no, here we go.” And he said, “No, I’m not cancer fatigued. I’m exhausted from working hard in our yard.” That was the moment I knew that we had turned a corner.
Side Effects of Epcoritamab
Michael: There were supposed to be some side effects, but I didn’t have any. It operates in a similar way as some of the medications that worked well for me, so I thought, If that worked really well, we’ll go ahead and have a go at this. It was a medication that my body accepted and that worked well. I have been at full tilt ever since. It’s a true blessing for us.
Don’t be afraid to ask all the questions that you want to ask. Make sure that you’re getting the information that you need.
Michael
Words of Advice
Michael: Part of the reason why my wife and I are doing what we’re doing is to help. We don’t want anybody to go through what we did. If there’s anything that we can do to help somebody look in another direction, hang on one more day, or give them a little hope that there is a better tomorrow out there, then that’s what we’re doing. We want to help and this is one of the ways that we’re doing it.
Don’t wait. Go see a doctor. If the physician that you are seeing now is not the right one for you, don’t be afraid to switch. At the end of the day, it wasn’t just about me. It was about my family and continuing on to be with them.
When you get to a hurdle that you need to cross, be your own advocate. Be involved in your own care. Find a doctor who will talk to you, not at you. Find a physician who will work with you.
The oncologist that we were seeing in Akron said that this was beyond him and what he was accustomed to dealing with. Once he got the PET scans, the test results, and the first attempt at chemotherapy, he said this was beyond him. I admire him for that because he could have said, “We can try this, this, or this,” but he cared enough about us to say, “This is beyond me.” I have always appreciated that about him.
I’ve always been grateful that he had the courage to say that he wasn’t the person who could do this for me. He could have been prideful and said, “I can handle this,” but he didn’t. He had my best interest at heart. We got pointed in the direction we needed to go, so I’ll always be grateful to him.
Before going to the James in Columbus, we did some research and, for us, it’s one of the premier centers in the United States for cancer treatment so we were very comfortable with that decision.
Everybody we met at the James was wonderful—the doctors, the nurses, the people who make the food, the people who clean the rooms. They were all wonderful people, very kind, very loving, very patient, and not afraid to answer questions. I can’t tell you what a really good organization they have down there so I have no regrets going there. Because they took care of me, I’m here today and I get to enjoy my wife, my family, and my friends. I get to enjoy life. Two years ago, that was not the case.
Don’t be afraid to ask all the questions that you want to ask. Make sure that you’re getting the information that you need. You owe yourself that much.
Don’t be afraid to change. Don’t be afraid to try things. Rely on your family and friends because they want to help. They may not always know how, but they want to help. Allow them to be part of the healing process. It makes a big difference.
There has been some goodness that came out of all this and we’re trying to focus on that now. I’ve tried to forget some of the things that happened because they were so bad. I’m trying to look toward the future and enjoy life the best way I know how.
Have things to hold on to, whatever it takes for you to hang on for one more day. For me, it was religion. If you’re a religious person, God is your rock. We’re a religious family and that was something that helped us get to the next day.
Have hope. I know that’s going to be hard at times, especially if you’re getting bad news after bad news after bad news. Sometimes that happens. Don’t give up. Everything that we did that didn’t work was a stepping point for us to get to the next step, to the next day, and to where we are today. Do everything in your power to not give up.
You and the people around you are a lot stronger than you realize.
Michael
There’s nothing to be ashamed of when it comes to talking to a mental health professional. They can help make a big difference. Sometimes you need to talk things out. You and your family are under a lot of pressure and stress.You have a lot of questions and maybe wondering if you’re going to have tomorrow. That is another avenue that you can take to help you clarify and focus on what you have to do to get to the next day. Being prideful that you don’t show your emotions is not a good thing. No one can do that. Sometimes things come out and that’s okay.
Value your family, the day that you have, and the life that God has given you. Be glad to get up in the morning and see the sun come up. Be happy with small things.
You and the people around you are a lot stronger than you realize. I learned that about my children. You try to protect your children by keeping things from them because you don’t want them to feel pain, but I learned that you don’t have to keep things from them to protect them. They’re there to help you and they will help you in ways that you never thought would happen.
My grandkids would always write me little notes and tell me, “You can do this!” They were right. Family is everything and everything like that matters. The things that used to matter to me are not very important anymore. It helps you focus on what matters.
It has been an experience, but at the end of the day, it’s been a good one. I’m grateful for everything that everybody has done for us and for where we are in life right now. It’s good to be alive, so I’ll do the best I can to enjoy life every day and be happy.
We want to help and that’s why we do what we’re doing. If this makes one person’s day a little better, then we’ve accomplished our goal.
Figure out a way to take care of yourself. It may look different to you than it does for other people, but it’s important and it’s okay to think of yourself.
Kimberly
Kimberly: Advocate for yourself and for the person who you’re going through this with. We all assume that medical providers know everything. They know a lot and we’re thankful for them. However, they’re not with our loved ones day in and day out. They don’t see the subtle changes that happen day in and day out. There are things that you can bring to their attention that they may not catch. It’s not that they don’t know their job. It’s not that they don’t care or that they’re in a hurry. They’re just not with them.
Ask questions. If something doesn’t seem right, ask. The worst thing that’s going to happen is the doctor is going to say, “No, this is correct,” or, “I’ve already taken that into consideration.” The best thing that’s going to happen is you’re going to bring up something that they were unaware of and that could make a difference in care.
I encourage care partners, whether you’re a spouse, a family member, or a friend, to figure out a way to take care of themselves. They say to get rest and ask for help because you can’t give if your tank is empty. All of those things are true, but no one tells you how to go about that.
It’s different for each person. Oftentimes, it’s difficult to think of yourself because you’re healthy and not the one going through treatment or constantly wondering what’s going to happen tomorrow. It’s important that you figure out a way to take care of yourself. It may look different to you than it does for other people, but it’s important and it’s okay to think of yourself.
We were dealing with a recurrence so there were things that we needed to be aware of that someone who is getting a first diagnosis may not.
All the little things matter. If something is persistent, you might think it will go away and it might, but it’s better to find out. If something is persistent and you can’t get any answers, keep asking and keep looking. Don’t defer to, “This is the best we can do,” “We’re not sure,” or, “Try this.” Keep asking.
On this side, it’s easy to say, “You have to have hope. Hope is what got us through.” It’s true. Having hope keeps you going. However, when your husband’s glucose levels are so low that he shouldn’t be able to open his eyes or breathe and you’re not sure how many more breaths he has, hope is hard, but you have to find something to hold on to.
With a terminal diagnosis, that hope may be that you get to spend five more minutes with that person. It might be that you get to spend one more day with that person. Our mantra through the whole thing is that life is good as long as we’re breathing the same air. It didn’t matter if it was hospital air, Hawaii air, bedridden air in our home, but as long as we were breathing the same air, there was hope and that’s what got us through. Find whatever hope is for you.
Special thanks again to Genmab for its support of our independent patient education content. The Patient Story retains full editorial control.
Kirsty’s Stage 4 Squamous Cell Kidney Cancer Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Kirsty, a single mother of two from East Yorkshire, England, was diagnosed with a rare and aggressive form of kidney cancer. Reflecting on her journey, she realized that she had been experiencing symptoms for years. During a 2021 check-up for endometriosis, fluid was discovered in her left kidney, but no further investigation was done. For two years, traces of blood in her urine were dismissed as part of her endometriosis.
In May 2023, Kirsty experienced constant flank pain on her left side after a bicycle fall. She also suffered from backache, fatigue, and significant weight loss. Persistent pain led to repeated visits to her general practitioner. In October, an ultrasound showed significantly more fluid in her kidney and a CT scan with contrast revealed the spread of cancer.
On December 1, 2023, Kirsty was diagnosed with stage 4 squamous cell kidney cancer that had spread to some lymph nodes. Though surgery was not a possibility, she began chemotherapy, which significantly reduced the tumor but came with severe side effects such as fatigue, nausea, and nerve pain. Despite the initial plan to do six cycles, she stopped after five due to the intensity of the treatment.
Kirsty was open with her children about her diagnosis, providing emotional support and encouraging them to express their feelings. Inspired by her mother’s battle with cancer, she focused on creating lasting memories with her children. Her approach to life shifted to prioritize meaningful experiences.
She advises others to listen to their bodies and seek medical attention when symptoms persist. She stressed not taking loved ones for granted and valuing time spent with family over work. Through her journey, Kirsty aims to inspire others to cherish every moment and prioritize what truly matters.
Symptom: None; found the cancers during CAT scans for internal bleeding due to ulcers Treatments: Chemotherapy (capecitabine + temozolomide), surgery (distal pancreatectomy, to be scheduled) ...
Margie shares her journey with stage 1B, grade 3 endometrial cancer. Initially attributing her symptoms to menopause, she experienced persistent irregular bleeding for years. After consulting her OB-GYN and undergoing a biopsy and ultrasound, she was diagnosed with cancer, leading to a swift progression from diagnosis to surgery, which confirmed the cancer had not spread beyond the uterine walls.
Margie’s treatment included surgery, chemotherapy, and brachytherapy radiation. Despite facing challenges with healthcare providers and navigating the medical system, she sought multiple opinions to ensure the best care. She managed side effects with essential oils and naturopathic remedies, emphasizing self-care and symptom documentation. Margie’s story highlights the importance of patient advocacy, thorough medical documentation, and compassionate healthcare providers, serving as an inspiration for others facing similar battles and advocating for awareness and proactive health management.
For more support in endometrial cancer, visit our friends at ECANA.
Thank you to Karyopharm for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I live in Seattle, Washington. I’m single and have two adult girls and five grandchildren. I work with my oldest daughter at home as a grandma nanny. I do a lot of driving, preparing meals, laundry, and help around the house.
I’m the program director of ECANA: Endometrial Cancer Action Network for African-Americans. I facilitate one program twice a month. Right now, it’s chair yoga and conversations where we meet with Black women who have been affected by endometrial cancer. We provide a space to talk, share, and ask questions, and then spend 15 to 20 minutes doing some physical exercises to help people get back on their feet after their cancer treatments. That is one of my passions as well. I’m a fitness instructor, so I teach classes when I can.
I didn’t do anything about the bleeding because I thought it was part of menopause.
Pre-diagnosis
Initial Symptoms
I first started questioning that something might be going on with me when I was in the middle of menopause. When you’re going through menopause, you have all these different symptoms, like hot flashes and mood swings. You could have a cycle for two months and then not have one for three, and then have one for four months and not have it again, but you have to go one whole year without having any signs of blood.
I didn’t pay attention to my cycles, so I don’t know if I ever went a whole year without seeing any blood. I didn’t document it, so my strong suggestion is to document when you start your cycle and when it starts being weird, document how it was. When you’ve gone 12 months with no blood and then now there’s blood, go to your doctor.
I didn’t do anything about the bleeding because I thought it was part of menopause. I felt like I had a cycle every day. Nothing for two days and then I’ll have bleeding for a week, then nothing for 2 or 3 days and then bleeding again for three weeks. It went on for 2 to 3 years, but I was quiet about it.
The spotting and bleeding became heavier. I had no pain, but I just got tired of it and thought, This has to stop. I need to do something about this. On one of my visits, I mentioned it to my OB-GYN. I said, “Shouldn’t I be done? I feel like I’m spotting or I’m bleeding still. Should I still be bleeding?” She said, “Yeah, you should be done.”
Biopsy
My OB-GYN requested an ultrasound. Before I went, she took a biopsy sample in her office. She said, “It’s not going to hurt. It’ll be fine. I need to pull out a piece so I can send it to the lab because I feel like there’s something going on in here, but I’m not sure.”
It lasted only 10 minutes, but I asked her, “Am I going to be able to walk to my car when you’re done?” She was digging in my vaginal area, trying to pull something out. It was so painful. There wasn’t any pain after, but the whole process was horrible. I hope that procedure is better today than it was before. She sent me home with antibiotics.
‘They’re sending you to an oncologist? … Mom, they think you have cancer.’
Ultrasound
When I went for an ultrasound, the tech said, “The lining of your uterus is thick. We need to check that out. I’m going to set you up for an appointment with an OB-GYN oncologist. Make sure you bring somebody with you to that appointment.”
When I got home, I told my daughter. She dropped what she was doing, stared at me, and asked, “They’re sending you to an oncologist?” I said, “I think that’s what she said. OB-GYN oncologist.” She said, “Mom, they think you have cancer.” I said, “How do you know that?” She said, “Because you’re going to see an oncologist.”
She then asked, “Who’s going with you?” I said, “My friend Holly’s going to come with me.” She said, “Okay. Make sure you take good notes and find out what’s going on.” That was my introduction to the possibility of having cancer. Even after hearing that, I thought, I don’t have cancer. Calm down, people.
Diagnosis
Getting the Diagnosis
When I went to see the OB-GYN oncologist, he saw my ultrasound and I thought that he had the biopsy results. He was fast talking and had no bedside manners at all. It was so bad. I’m still like a deer in headlights and you’re telling me something’s wrong with me.
He said, “You might have cancer, you might not have cancer. You might have a carcinoma or you might not have one. You’re 58. You don’t really need all those parts. We’ll take everything out. We’ll have a complete hysterectomy. If we see any signs of cancer in there — we might or we might not — then we’re taking everything out.”
My friend who was with me said, “Excuse me. Can you slow down? Can you tell her what that means? She doesn’t know what you’re talking about.” In 15 minutes, I was on the table getting checked then I was over in the other room, making an appointment for a surgery.
He said, “We’ll know for sure after surgery. It might be, but it might not be,” and then he started naming off different kinds of cancers that it could or could not be. That’s the part I thought was weird. My friend was totally put off by him and said, “She needs her female organs. What do you mean she doesn’t need them anymore?” After making the appointment, she said, “You know you can cancel this if you need to.”
The surgery was supposed to take 2.5 hours but it ended up taking 4 hours… the tumor was too big.
Reaction to the Diagnosis
I was in shock and couldn’t believe it. It all happened so quickly. I was numb for about two months. Everything was a blur.
My youngest daughter, who lives in Chicago, said, “Let’s get the email strings going. Let’s find out what we need for care.” My friends started mobilizing. Then I realized that everybody was talking about me. It was me who’s going through this. I couldn’t see myself at that moment.
I was diagnosed with stage 1B, grade 3 endometrial cancer. The tumor stayed inside the uterine walls, but it was already 80% of it, so 20% more and it would have been out. I got my lymph nodes checked including all the surrounding areas to make sure. All of that came back clear. Thank you, Jesus. I was happy about that.
Treatment
Surgery
The surgery was supposed to take 2.5 hours but it ended up taking 4 hours. They went in laparoscopically and saw that the tumor was too big. They couldn’t get it out, so they ended up having to cut me a little to get it out, which extended the length of time that I was in surgery.
When I woke up, my daughter and some friends were in my room. I was still pretty groggy when the doctor came in. He said, “It stayed inside the uterine wall. We feel like we got it all. We did take some lymph nodes and stuff all around to double-check. We’ll get that back from pathology in about a week.” He said it was like everything dissolved in their hands when they were taken out. It was a relief to hear that he felt like he got it all. When I came in for my 10-day appointment, we received good news: everything was clear. I healed well from the surgery.
He was very calm, kept eye contact, and talked to me like I was a person instead of a number.
Discussing Chemotherapy & Radiation
I didn’t get a second or third opinion until after the surgery because my doctor said, “Let’s get it done and we’ll research as we go.” After surgery, they talked about treatments. At that appointment, he started throwing out information about chemotherapy and radiation. My insurance did not cover the chemo with that hospital, so I had to go to another hospital. He was saying I needed 6 to 8 rounds of chemo and 6 to 7 weeks of radiation to make sure because uterine cancers tend to hide.
Getting a Second Opinion
I was referred to the Fred Hutchinson Cancer Center in Seattle, Washington, for radiation. When I talked to the doctor, who was my second opinion about chemotherapy and radiation, he said, “I’ve looked at all your files and it looks like we’re going to probably do 4 or 5 rounds of chemotherapy and maybe 4 or 5 weeks of radiation after.”
He was the complete opposite of the other doctor. I was in his office for probably an hour. I had people with me who were taking notes. He was very calm, kept eye contact, and talked to me like I was a person instead of a number.
I met Dr. Kemi Doll, who was my third opinion and became my chemo doctor. She asked me questions and gave me time to answer. She went back to repeat what she already said to make sure I understood everything.
Getting a Third Opinion
My daughter, who lives in Chicago, was working and doing research as a professor at the University of Washington and UW Medicine. She met a doctor who knows the doctor who was going to be my chemo doctor. She’s emailing and texting me, “Mom, I just talked to so and so who’s going to hook you up with so and so. They’re going to call the office and then call you. You’re going to go see them because she’s an expert in this area.” That’s how I met Dr. Kemi Doll, who was my third opinion and became my chemo doctor.
She asked me questions and gave me time to answer. She went back to repeat what she already said to make sure I understood everything. She drew pictures. “This is this, this is this. If you don’t do chemo at all, here are the percentages that your cancer may or may not come back. If you do this much chemo, this is the percentage.”
She said, “We’re not going to do pelvic radiation. We’re going to do brachytherapy.” She explained what brachytherapy was and why. She said, “At your stage and from looking at all your records, this is preventative. Your chemo and radiation is all preventative. We want to make sure it doesn’t come back.”
I finally agreed to do four rounds of chemo and then brachytherapy. Dr. Doll said, “You’re way too anxious about the chemo, so we’re going to get it started as soon as possible.”
She said, ‘I have a feeling you’re going to do great. This is not going to be what you think it’s going to be.’ I was grateful to hear that.
Chemotherapy
At my first session, I didn’t have my port yet so I did it through the arm. My daughter from Chicago flew in. Dr. Doll showed up too. She said, “I have a feeling you’re going to do great. This is not going to be what you think it’s going to be.” I was grateful to hear that. Then she said, “I think you’re going to handle it well, but if you don’t, then we’re done. We’ll do brachytherapy and we can be done with the chemo.”
You have to get blood work done two days before a chemotherapy session to make sure that your platelets and your blood count are up. Otherwise, they can’t give you chemo. Before my last session, mine were low. They called me and told me to come in so they can give me a shot to boost the cells up and have my last chemo the following week. Then she said, “By the way, your insurance doesn’t cover it and it’s about $2,000.”
I said, “I’m good.” She said, “Are you sure? We’ll show you how to do it and then you go home and do it over the weekend.” I said, “No, thank you.” She wasn’t happy. She said, “If your temperature goes up, go to emergency. You’re very vulnerable right now because your immune system is low.”
I wore a mask for a week and that was in 2017. I immediately went to my list of foods because there are foods that help boost your immune system. I looked like I’m already eating lots of them, so I made sure to eat more, like twice a day. I protected myself and made sure that in the environment I was going in, nobody was infected with anything. I didn’t ignore what she said.
The next day, my doctor called me and said, “I talked to the nurse. She told me about her conversation with you and she told me your decision. I want you to know that this is your body. You make decisions for you. When you come for your last chemotherapy, they’ll do blood work right before to check and make sure that it’s at the level it needs to be. But if not, then we’ll skip it and wait another week. Or we could be done. It’s totally up to you. You decide whether you want to do that last chemo or not, or we can just call it. Let me know. Keep doing the stuff that you like to do for your own health. If you have any questions, call me or text me.”
I didn’t have one bout of nausea. I dealt with neuropathy and brain fog, not being able to focus on something for long periods of time.
When I went in for my last chemo, my girlfriend who went with me and I had two plans. We said, “If I don’t do chemo, we’re going shopping. If we do chemo, we’re going to high five and say, ‘This is the last one.’” After you check in, you sit in this little room and either they call your name or they walk over to you. They called my name, so I went right back and did my last chemo.
The nurse heard us talking and she said, “You mean you didn’t get the shots?” I said no. She asked, “What did you do?” The whole time, she was talking about my diet. I believe that the body is made to heal itself. Not that I don’t believe in all the other stuff, but I believe that and I was just done. I couldn’t give anymore.
Managing the Side Effects of Chemotherapy
I use essential oils, so I immediately checked to see which oils help with nausea. Nausea is one of the possible major side effects you could have from chemotherapy. And you know what? I didn’t have one bout of nausea.
I dealt with neuropathy and brain fog, not being able to focus on something for long periods of time. It takes away from who you know yourself to be. For the neuropathy, I soaked my feet, rubbed my feet, and wore good, comfortable shoes.
I also saw a naturopath once a month. Acupuncture helped with the nausea too, so I was grateful to have different avenues.
Because I felt good, I was pretty okay, but in the back of my mind, it’s always there.
Brachytherapy
The radiation was scheduled 6 to 8 weeks after surgery because complete healing time is about eight weeks.
Brachytherapy is internal radiation. They take a tube and put it right in your vagina.
When I went to my first brachytherapy appointment, they got me ready and put my legs up in the stirrup. They had everybody in the room to look: the interns, the specialists, and all that. I sat mortified. I’m glad I took a pill to keep me calm. Then he said, “I still see some blood up here. You are not completely healed.”
My first appointment was a wash. He kept apologizing and asked, “Where do you live?” I said, “Just down the street.” He said, “Oh, good because some people have to travel. Let’s give this two more weeks because this needs to be completely closed before we do any radiation.”
I came back two weeks later and by the end of February, I was done. I didn’t have any major side effects from brachytherapy.
Follow-up Protocol
I ended my chemo in February 2017. I saw Dr. Doll every three months. In 2018, I saw her twice a year. I went in every six months for blood work and checkups. In 2019, I saw her once and then I was good.
Because I felt good, I was pretty okay, but in the back of my mind, it’s always there. A month or two before the appointment, if I knew I was going to see her again, I would have to do a lot of deep breathing and checking myself physically, thinking, You know the signs, you know what to look for, and being aware of my own body. If I hear from her within the next 24 or 48 hours after my appointment, I wonder why. Each year got better.
The work that I do with ECANA helps, but sometimes it doesn’t because I feel like I’m constantly reliving that hard season of my life.
The only thing that still happens that’s annoying me are the sharp pains that I sometimes get in my wrist, my hands, or my feet, which I believe are side effects from neuropathy. They say it doesn’t really go away, but that’s about it.
Don’t let a doctor dismiss you or tell you that what you’re experiencing is all in your head. If they don’t have an answer, find someone who does.
Words of Advice
If you start going through menopause and your cycle starts going crazy, document everything. If you have not had your menstrual cycle in more than 12 months and then all of a sudden, you have a cycle or see blood, go see your doctor. That is the strongest message from my journey that I speak loudly about because I didn’t know to do that. I didn’t keep a journal. I didn’t pay attention. I figured I was in menopause so when it’s done, it’s done.
Find a doctor who you like, who’s going to listen to you, and who’s not going to dismiss you. It’s not okay for a doctor to presume what you’re feeling and what you’re going through. They’re supposed to listen to you.
As the patient, you are the most important person in the room. When I was at the 2024 SGO Annual Meeting in San Diego, I saw a black and white picture on a screen that said: as a doctor, if you listen long enough to your patient, they’ll tell you what’s wrong with them. Make sure the doctor listens to what you have to say. You’re not just another number.
For years, I’ve thought that the doctor knows everything. No, the doctor doesn’t. All the doctor knows is the book. You know you. Don’t let a doctor dismiss you or tell you that what you’re experiencing is all in your head. If they don’t have an answer, find someone who does. If the doctor doesn’t have your respect, leave and find one you can. That’s so important. It’s you that you’re talking about, it’s your health. You have to be able to communicate in a way that’s clear and where you feel like you’re being heard.
Special thanks again to Karyopharm for its support of our independent patient education content. The Patient Story retains full editorial control.
Navigating the Latest Metastatic Colorectal Cancer Treatments and Clinical Trials
Edited by: Katrina Villareal
Please watch the above video replay then take our program survey.
Allison Rosen, a colorectal cancer patient advocate, talks with leading oncologist Dr. Cathy Eng from Vanderbilt-Ingram Cancer Center. Gain valuable insights into the latest advancements in the treatment of metastatic colorectal cancer and a deeper understanding of the current treatment landscape, including the most recent FDA-approved therapies that are making a difference.
Learn how biomarkers are revolutionizing the approach to treating metastatic colorectal cancer, potentially leading to more personalized and effective treatment plans. Discover emerging therapies and the most promising clinical trials available, offering new hope and options for patients. Equip yourself with the knowledge to collaborate effectively with your medical team, ensuring the best possible outcomes and quality of life.
We’d like to thank our promotional partners for their continued support of our programs. Please visit the Colon Cancer Coalition and Colontown to learn more about the important work they are doing.
The Patient Story retains full editorial control over all content. This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang: I’m a blood cancer survivor and the founder of The Patient Story, which I started out of my own experience. I had so many questions and all I found was medical jargon and outdated statistics.
Our goal at The Patient Story is to help patients and care partners navigate life after a diagnosis. What does this mean in human terms? We do this primarily through in-depth patient stories and educational programs. We hope to help connect patients and families to information about topics like self-advocacy and the latest treatment options, which is especially important in colorectal cancer. It makes a difference how early someone can get a diagnosis, how much people know about what’s available to them, and what questions they can ask their healthcare providers.
The Patient Story retains full editorial control of the content. We also want to thank our promotional partner, the Colon Cancer Coalition.
While we hope you walk away with more knowledge, this discussion is not a substitute for medical advice so please consult with your healthcare team.
It’s my pleasure to introduce Allison Rosen, a very well-known and respected individual in the colorectal cancer advocacy space and someone I’m lucky to call a friend. Thank you so much, Allison, for joining us.
Allison Rosen, Patient Advocate
Allison Rosen: I’m a 12-year stage 2C colorectal cancer survivor and a very passionate patient advocate. My treatment consisted of surgery, radiation, chemotherapy, more surgery, and ultimately, a permanent ostomy.
I wanted to meet other young people like me who were diagnosed with colorectal cancer because I felt very alone when I was first diagnosed. When I was being treated at MD Anderson, I asked to talk to another young adult. She was very active in advocacy and introduced me to the advocacy space. Now I volunteer with a lot of national and local advocacy organizations. I get to work with amazing clinicians, researchers, and doctors to help provide the patient perspective.
Dr. Cathy Eng: You are so fortunate to be diagnosed with stage 2 because, unfortunately, most young adults are diagnosed with a much more advanced stage. Stage 2 is a very unique setting because it’s extremely early with regard to prognosis. For the majority of patients, surgical resection is curative. I’m so glad to have you here with us today.
Allison: Thank you. It’s interesting because the reason why I’m so active is because I’m alive. I have a purpose and my mission is to be a part of things like this educational program to talk about what is out there, so people who may not have access to what I had access to can get current information and the best possible treatment.
Dr. Cathy Eng, Medical Oncologist
Allison: Dr. Cathy Eng is the David H. Johnson Endowed Chair in Surgical and Medical Oncology at the Vanderbilt-Ingram Cancer Center. She’s also the co-leader of the Gastrointestinal Cancer Research Program, co-director of GI Oncology at Vanderbilt, the executive director of the Young Adults Cancers Program, and co-chair of the NCI GI Steering Committee. Dr. Eng, what drew you to this field?
Dr. Eng: What drew me is individuals like yourself. I had a very, very large clinic when I used to work at MD Anderson and I was seeing patients as young as 16. These patients do not have an inherited form of colorectal carcinoma. The majority have sporadic colorectal cancer and, unfortunately, they were showing up in my clinic with very advanced diseases, stages 3 and 4. It’s hard not to be able to appreciate all the hurdles that a young adult has to go through in order to go through their treatment with success and hopefully few toxicities. It’s that communication with the patient and that lives with you as a physician.
Allison: I know many people who are part of the Young Adult Cancers Program and many people who have gone through it. I appreciate everything you’re doing for the young adults who are going through treatment and, unfortunately, the future young adults who will go through treatment. You have to treat the patient as a whole. Things like fertility and body image are so important along with chemotherapy and radiation.
Dr. Eng: Thank you. I want to thank you also for helping promote education and awareness. We don’t know the exact etiology of why this is happening, but in the interim, we can continue to promote awareness so people can be diagnosed earlier.
Allison: Awareness is key.
You don’t need to remove your primary tumor to improve overall survival. In fact, it does not improve overall survival and that’s important to keep in mind.
Dr. Cathy Eng
Latest Treatment Options for Metastatic Colorectal Cancer
Allison: As an advocate, I’ve seen that progress is being made in treating metastatic colorectal cancer, but it’s still challenging. What are the latest treatment options?
Dr. Eng: Oxaliplatin-based and irinotecan-based treatments are still commonly utilized for patients who don’t have a particular molecular marker. We have to recognize that it’s still important to be in contact with the patient because in combination with a fluorouracil-based therapy, those regimens are still the foundation of basic treatment.
Over the past two years, one thing that came out was looking at tumor-sidedness. A patient with a left-sided tumor has a better prognosis overall than a right-sided tumor for a non-inherited form of colorectal cancer. If the patient is RAS wild-type, the data shows that you would probably benefit from anti-EGFR therapy in combination if you’re considering irinotecan- or oxaliplatin-based therapy and that has been shown to improve overall survival. Not everybody loves EGFR therapy because it causes a significant rash, but there are benefits to considering that type of treatment.
A RAS mutation is very common in up to 60% of all colorectal cancer patients. We’re getting so specific that we’re asking what type of RAS mutation you have with regard to KRAS.
Patients ask if they need to have their primary tumor removed because they have metastatic disease. It’s not like breast cancer where you need to have your primary tumor removed to reduce your tumor burden. That doesn’t benefit a colorectal cancer patient with metastatic disease.
A pooled analysis came out in the Journal of Clinical Oncology. Three presentations from countries all across the world indicated that you don’t need to remove your primary tumor to improve overall survival. In fact, it does not improve overall survival and that’s important to keep in mind.
Sometimes we hear from patients that they’re told they have to remove their primary tumor. You shouldn’t have to unless you have uncontrolled bleeding, near obstruction, or a high risk of perforation. We don’t encourage that for all comers in general. For a rectal cancer patient, if you’re having symptoms, we can give short-course radiation therapy to help alleviate some of those symptoms despite having metastatic disease.
HER2-Targeted Therapy Combination
Dr. Eng: Tucatinib is the most recent drug that has been approved, which is an oral tyrosine kinase inhibitor of HER2 that prevents downstream phosphorylation and involves the EGFR pathway. These are for patients with RAS wild-type and most often have left-sided tumors.
The best part about the tucatinib study, which shows the relevance of having a rare mutation, is it got FDA-approved based on a small phase 2 study. It wasn’t a giant phase 3 study and that’s important to keep in mind. It showed that these patients, despite heavily being heavily pre-treated, had a great response rate. Progression-free survival was excellent and the overall survival was close to two years.
HER2 testing is one of the newest things to be considered. We’re very familiar with it in gastric cancer and breast carcinoma, but this is the first time looking at it in metastatic colorectal cancer and making sure that all patients get tested for HER2. It’s extremely important to look at the role of HER2. We have seen that looking at HER2 amplification, which is present in approximately 4% of our patient population, is very, very important.
Looking at HER2 amplification, which is present in approximately 4% of our patient population, is very, very important.
Dr. Cathy Eng
Fam-Trastuzumab Deruxtecan-nxki (ENHERTU)
Dr. Eng: The new drug deruxtecan is an antibody-drug conjugate. It isn’t necessarily new with regard to its presentation but in the sense that it just received tumor-agnostic approval, so it’s approved for colorectal cancer and other tumor types.
It does best in the IHC 3+ patient population, but it has a benefit with regard to progression-free survival and overall survival. What’s unique about deruxtecan is that the original study that resulted in its approval allowed patients who received prior HER2-based therapy. You could have had tucatinib, pertuzumab, or lapatinib, but you can receive deruxtecan as a single agent.
They’re moving the G12C inhibitors in combination with chemotherapy to the front-line setting.
KRAS G12C inhibitors don’t work by themselves. They were evaluated by themselves with a less than 10% response rate. In combination with anti-EGFR (epidermal growth factor receptor) therapy, the combination resulted in an improved benefit for patients. Although it’s not FDA-approved at this time, if you’ve been previously treated, you can inquire about receiving it in combination with anti-EGFR therapy.
They’re moving the G12C inhibitors in combination with chemotherapy to the front-line setting. In the HER2 setting with newly diagnosed patients, they’re also looking at tucatinib in combination with oxaliplatin-based therapy. The fact that we’ve found molecular alterations that have been positive studies in the refractory setting is exciting. We’re now moving into front-line therapy to see if that is more advantageous for our patient population.
BREAKWATER Trial
Dr. Eng: BREAKWATER is a phase 3 trial for BRAF V600E mutation tumor types, which is about 9% of all of our patients. Encorafenib and cetuximab were approved in the previously treated setting and are now being moved up to the front-line setting in combination with oxaliplatin-based therapy. I’m one of the investigators on that trial and there’s another arm that’s open, which is in combination with irinotecan-based therapy.
I hope that we will continue to move these rare molecular alteration subtypes earlier on in development because we can get greater outcomes. We hope to improve and break the barrier of overall survival, which is currently about 35 to 37 months for the majority of our patients.
For any metastatic patient, the very first thing they need to ask is their molecular sequencing. It’s critical because it helps create a treatment plan.
Dr. Cathy Eng
Trending to More Personalized Treatment
Allison: You talked about the KRAS, HER2, and BRAF mutations, and about treatment being driven by a particular mutation. Why is biomarker testing important? What would you tell a patient if their doctor hasn’t necessarily brought it up?
Dr. Eng: For any metastatic patient, the very first thing they need to ask is their molecular sequencing. It’s critical because it helps create a treatment plan. Previously, we would look at all metastatic colorectal cancer patients as the same and that’s not the case. Having a molecular marker can make a big difference because it can prevent you from receiving unnecessary toxicities and costs.
KRAS- and EGFR-Targeted Therapy
Dr. Eng: The most pivotal one was looking at KRAS and anti-EGFR therapy, such as panitumumab and cetuximab. That class of drugs causes a rash in 80 to 90% of patients and depending on where you live, you’re also at a higher risk for having an allergic hypersensitivity reaction to cetuximab.
Bevacizumab
Dr. Eng: Bevacizumab is an IV drug that’s involved in anti-angiogenic therapy. Anti-angiogenesis or anti-VEGF (vascular endothelial growth factor) therapy means it’s working on the blood supply. Our goal for this class of drugs is to reduce the development of metastatic disease because a tumor needs a blood supply to survive and thrive.
FRESCO-2 Trial
Dr. Eng: When we designed FRESCO-2, it allowed almost all comers. Patients were allowed to have received prior TAS-102 (trifluridine/tipiracil) and that was before the approval with bevacizumab in combination. They also could have received regorafenib, which has been approved for quite a while now. Patients may have been exposed to either or both of the drugs. It was a trial that allowed almost all patients to participate with the median line of four prior lines of therapy.
Fruquintinib was compared to a placebo. It was a 2-to-1 randomization. Some people criticize the fact that there was a placebo arm, but there’s no standard of care for fourth-line or fifth-line therapy, so there was nothing to compare it to. Some people say, “Can’t you go back to 5-FU (fluorouracil)?” But the reality is patients have already progressed through 5-FU, so they’re not going to be receptive to 5-FU.
The primary endpoint was met with an improvement in overall survival as well as progression-free survival.
The FDA approval allows patients to receive oral fruquintinib as a potential option for third-line therapy and beyond.
Dr. Cathy Eng
Fruquintinib (FRUZAQLA) Approved by FDA
Allison: With the recent FDA approval of fruquintinib, how can it help address an unmet need in the metastatic colorectal cancer treatment landscape?
Dr. Eng: It’s a drug that I helped bring to the United States. I was involved in the original trial as the senior investigator. This drug is an oral agent, which specifically blocks receptors 1, 2, and 3 of the VEGF pathway. It was originally approved in China in the third-line setting based on a phase 3 trial called FRESCO that was conducted overseas.
FRESCO-2 is specifically trying to address the practice patterns of what we are doing in the United States, which is continuing bevacizumab for front-line and second-line therapy but also trying to ensure the majority of patients had received anti-VEGF therapy as part of treatment, which was the case in 97-98% of patients who participated in FRESCO-2.
Based on the results of both FRESCO and FRESCO-2, the FDA approval allows patients to receive oral fruquintinib as a potential option for third-line therapy and beyond.
Overall, it was tolerated fairly well. Hypertension is an issue with this class of drugs, but it’s treatable. It got approved in November and we are very pleased to see the FDA approved it. It’s pending the European Medicines Agency’s approval as well as approval in Japan. After that, hopefully, it will be approved internationally so all patients can get access.
At the end of the day, the reality is you need to make sure you have drugs available to the patient. When you ask, “Do you prefer FOLFIRI (folinic acid, fluorouracil, and irinotecan) or FOLFOX (folinic acid, fluorouracil, and oxaliplatin)?” The reality is you’re going to get both regimens. What matters is how well you tolerate the treatment and how you derive the best benefit.
I try not to make it very competitive. I don’t think it benefits anybody. It’s important to recognize that there’s a new drug on the market, it’s available for patients, and it does not require IV therapy.
In a prior study, it was seen that if you have the RAS mutation and receive anti-EGFR therapy, it’s no better than receiving a placebo.
Dr. Cathy Eng
Biomarkers (“Molecular Markers”)
Dr. Eng: There’s a lot of interest with regard to other molecular markers, like a patient’s KRAS status and mutation. KRAS G12C inhibitors are further along in development than G12D. Granted, G12C in colorectal carcinoma is less than 5% of our patient population, but once those patients are identified, they may benefit from therapy.
Importance of Biomarkers
Dr. Eng: The KRAS mutation is in about 30 to 60% of all colorectal cancer patients. In a prior study, it was seen that if you have the RAS mutation and receive anti-EGFR therapy, it’s no better than receiving a placebo. Why would you want to subject your patient to toxicity, a potential allergic reaction, and extreme financial costs if it doesn’t benefit them?
Different Biomarkers
Dr. Eng: KRAS was just the beginning. We are now identifying all these new molecular subgroups, such as HER2, BRAF, and microsatellite instability-high (MSI-H), which is extremely important with regard to the role of immunotherapy. That’s another small patient population, less than 5% of our patients, but that’s where immunotherapy may benefit our MSI-high or mismatch repair protein deficiency (MMR-d) patient population where immunotherapy can have a significant role in potentially curing them.
Tissue molecular sequencing can look at hundreds and hundreds of various molecular alterations, mutations, or amplifications… Information from the blood can be critical in identifying a suitable clinical trial.
Dr. Cathy Eng
Tissue vs. Blood Samples in Biomarker Testing
Dr. Eng: Molecular sequencing can be obtained from tissue and blood. If you’re newly diagnosed, it’s important to send off that tissue as soon as possible before it gets sent off to some warehouse because it can’t sit in the pathology department forever.
Depending on which panel you use, tissue molecular sequencing can look at hundreds and hundreds of various molecular alterations, mutations, or amplifications. Blood sequencing is quicker. You can get it back within less than two weeks, but you’re only looking at 100 different mutations relative to the 500 or so plus potential molecular alterations.
Some places still do it in-house, but the majority of institutions send it out to a third party. Ask for tissue and blood to be sent off because the information from the blood can be critical in identifying a suitable clinical trial for the patient as well. I cannot emphasize enough the importance of participating in clinical trials.
Allison: I’m very, very passionate about access to clinical trials, education for clinical trials, not being scared, and not thinking that a clinical trial means you’re going to die.
Dr. Eng: Every single FDA-approved drug came from a clinical trial.
Allison: Exactly. It’s the point that I make as an advocate all the time.
Choosing Among Different Treatment Options
Allison: Where do you see fruquintinib fitting in with the current therapies available for metastatic colorectal cancer? Is there a potential for it to be used as a maintenance therapy?
Dr. Eng: My understanding is it’s being investigated as a maintenance therapy. It makes a lot of sense since the majority in the United States use capecitabine, bevacizumab, or 5-FU with bevacizumab for maintenance therapy, so it would make sense to consider this as a potential maintenance therapy.
When thinking about it relative to other agents, such as regorafenib and TAS-102 plus bevacizumab, I talk to the patient. I utilize TAS-102 plus bevacizumab quite a bit. However, some patients are tired of coming in every two weeks for bevacizumab. They want a break and that’s very reasonable.
With TAS-102, they’re at risk for myelosuppression, so their white blood cell count can drop. That’s a known side effect of that class of drugs, so the patient has to be compliant and not take medications incorrectly. You don’t want a neutropenic patient walking around at risk for other infections.
I don’t offer TAS-102 to certain patients. I had an elderly patient whose platelet count was never above 100,000. He had been on a lot of therapies and came to me for a second opinion. I would be hesitant to give him TAS-102 because I know that his platelet count is going to be a problem, so I chose fruquintinib for him first. Once again, I don’t try to choose one versus the other. I talk to the patient about the potential side effects and see what they’re willing to endure.
Allison: It’s all about shared decision-making. You know about what’s going on and having that conversation with your physician is very, very important.
Emerging Clinical Trials for Metastatic Colorectal Cancer Patients
Dr. Eng: For the MSI-high patient population, there should be some updates soon regarding NIVO+IPI (nivolumab and ipilimumab). They presented their data at the 2024 ASCO GI (American Society of Clinical Oncology Gastrointestinal Cancers Symposium) looking at NIVO+IPI in combination versus chemotherapy and that was superior, but it was a very rapid abstract presentation, so we don’t have further details. I think there’s going to be an update at the 2024 ASCO, so I look forward to that. Are two immunotherapies better than one for this patient population? What about toxicities? It will be interesting to see.
The CodeBreaK 301 trial is looking at the role of sotorasib, a first-generation KRAS G12C inhibitor, in the upfront setting. Sometimes the next generation may be even better, so I’m looking forward to those trials as well.
EA2222 (PUMP) Trial
Dr. Eng: The PUMP trial is a new NCI-sponsored study specific for newly diagnosed patients. They will get randomized to having the PUMP versus continuing chemotherapy.
This is an important trial that will answer that question. We know all the data from Memorial Sloan Kettering, but can we validate and replicate that data outside of that institution, especially in an earlier line setting?
ERASur Trial
Dr. Eng: The ERASur trial is another NCI-sponsored study that looks at the role of stereotactic radiation therapy, ablation, or some type of liver-directed intervention to improve overall survival.
MOUNTAINEER-03 Trial
Dr. Eng: The MOUNTAINEER-03 trial is looking at tucatinib with trastuzumab in the front-line setting.
We cannot make breakthroughs until we get trials completed. It’s very, very important to keep in mind that not all trials involve a placebo.
Dr. Cathy Eng
Importance of Participating in Clinical Trials
Allison: We touched on the importance of clinical trials, but do you have any message about the importance of participating in clinical trials?
Dr. Eng: Focusing on metastatic disease, I encourage all patients to consider participating in a clinical trial. Currently, enrollment across the United States is about 7% for non-NCI cancer centers and up to 20% for NCI-designated cancer centers. We cannot make breakthroughs until we get trials completed. It’s very, very important to keep in mind that not all trials involve a placebo.
All patients should consider getting a second opinion if they haven’t been offered a clinical trial. There are some selective settings where there is no clinical trial available, but you should have that discussion with your provider on your first or second meeting.
It doesn’t take that long to get a second opinion. You want to look at all your options and feel informed. That’s extremely important as a patient and the best way to optimize your care. As a medical oncologist, it’s very, very distressing when I meet a patient who received one cycle of chemotherapy before they walked into my office and find out they would have been a perfect candidate for a clinical trial but now they’re automatically disqualified.
Allison: Knowledge is power. There are so many amazing trials and the first step is educating yourself on clinical trials. There are a lot of advocacy groups and organizations that are trying to educate patients on what a trial is and having that conversation with their doctors. It’s so important because the last thing you want to do is disqualify yourself for a trial because you did something here versus going there.
Because of my age, I got three different opinions before I decided on where I was going to get treated. For the younger people especially, talk to as many people as you can and educate yourself as much as you possibly can. This program is an amazing start for people to better understand that there are options.
Get a second or a third opinion. I’m not telling you to delay your treatment by months, but give yourself 2 to 3 weeks to make an informed decision by getting another opinion.
Dr. Cathy Eng
Final Takeaways
Allison: What message do you have for metastatic colorectal cancer patients? I always tell them that their lives aren’t over. There are treatment options available. I know quite a few people who were stage 4 who are now in remission.
Dr. Eng: I hear time and time again that they’ve been given a poor prognosis of 6 to 8 months to live; that’s very discouraging and not the right approach. We have so many new options available. Science has advanced so much. If you hear that kind of negative attitude at your first meeting with your physician, you need to go get a second or a third opinion. I’m not telling you to delay your treatment by months but give yourself 2 to 3 weeks to make an informed decision by getting another opinion.
Allison: I agree. The relationship you have with your care team is important. It can spell the difference between a lot of different things that can happen along a journey.
Dr. Eng: It’s also important for people to keep in mind that there’s always hope.
Allison: I was originally diagnosed with stage 3 and they said it was about to break through my colon wall. There’s so much going on and so much information you’re getting when you’re first diagnosed. Talking to someone else who’s gone through it gave me hope. It differs with every stage. I know people who are 20-year stage 4 colorectal cancer survivors. That’s the hope that someone needs.
Dr. Eng: Your medical oncologist is key. Your radiation oncologist and surgical oncologist are always there, but the captain of your ship, besides your primary care doctor, is your medical oncologist.
Allison: You are an amazing captain of the ship. I know this from hearing from many people and knowing you for as long as I have. Thank you so much for your time and for sharing invaluable information.
Stephanie: Thank you so much, Dr. Eng, for what you do in terms of research, which is critical to advancing care, and the way you’re thinking about patients. Thank you also to Allison for the work you do in advocacy and leading this program, which wouldn’t be the same without the patient perspective.
Thank you to our promotional partner the Colon Cancer Coalition, which was founded by someone who lost her sister to stage 4 colorectal cancer. The Colon Cancer Coalition is celebrating its 20th Get Your Rear in Gear fundraiser in the Twin Cities in Minnesota with other rides and fundraisers happening across the country as well. These fundraisers highlight the need to screen and raise awareness of colorectal cancer. The organization gives more than $1 million every year to local community programs to help fill that need.
We hope that you walk away with a better understanding of what’s out there and something to talk to your own healthcare team about. We hope to see you at a future program.
If you read and/or watched our program, we encourage you to take our program survey to help us improve future programs and answer your questions.