How CT, PET/CT, MRI and Ultrasound Guide Blood Cancer Care
Watch a replay ON DEMAND
Let’s make scans less scary (and less painful) together!
Scans can bring a lot of worry. Join expert radiologists Dr. Robyn Stacy Humphries (Charlotte Radiology) and Dr. David Prologo (Winship Cancer Institute of Emory University) to learn what each imaging test really shows and how to stay calm before, during, and after your appointment.
They’ll both share how CT, PET/CT, MRI, and ultrasound help diagnose and monitor blood cancers such as lymphoma, CLL, and myeloma. Learn more about what each test shows and what results may mean for treatment.
Program Topics
Imaging 101: Ultrasound, CT, PET/CT, and MRI—what each shows and when it’s used
Image-Guided Biopsies: How radiologists target tissue safely and why repeat biopsies matter
Ports vs. Central Lines: Options for easier chemotherapy, blood draws, and comfort
Managing Scanxiety: Coping strategies while waiting for imaging or results
Teamwork in Care: How radiologists, oncologists, and tumor boards coordinate decisions
Blood Work Basics: Making Sense of Your Test Results
Watch ON DEMAND
What does your cancer blood test results really mean — and how do they help doctors detect or monitor cancer?
Listen in as hematopathologist Dr. Kamran Mirza and cancer advocate Stephanie Chuang to break down the most common diagnostic cancer blood tests, including the CBC. Learn how pathologists interpret results, what those ranges mean, and how small changes in your numbers can offer big insights into your health.
Key Topics:
Why doctors order cancer blood tests: What they’re looking for and how to prepare.
Making sense of the CBC: Understand what each number represents — and what it doesn’t.
How blood results guide treatment: From diagnosis to tracking remission or recurrence.
Should I be worried?: When out-of-range numbers matter and when they don’t.
What’s next in the series: Learn how this session leads into condition-specific follow-ups for 6 different blood cancers.
The LLS offers free resources like its Information Specialists, who are one free call away for support in different areas of blood cancer.
Register now to get notified about the follow-up program tailored to your cancer type.
Blood Work Basics: Making Sense of Your Test Results
Hosted by The Patient Story
What do your blood test results really mean — and how do they help doctors detect or monitor cancer? Learn about the most common diagnostic tests, including the CBC and the CMP.
Graft-versus-host disease is a potentially life-threatening condition affecting an estimated 50% of blood cancer patients who receive stem cell transplants from a donor. Transplant experts explain GVHD risks, how to watch for symptoms, the current treatments available, and new clinical trials aimed at prevention and treatment.
Watch the Full Webinar
In addition to our summary from this empowering webinar, watch the full video replay and catch every word from the experts and patient advocate!
Patient advocate and GVHD Alliance co-founder Meredith Cowden shares her experiences with GVHD. Experts from UChicago Medicine, Roswell Park Comprehensive Cancer Center, and The Leukemia & Lymphoma Society who are on the front lines of GVHD research and treatment discuss the role clinical trials play in advancing the treatment landscape and what it could mean for you. Discover how to take steps to learn more about clinical trials from a clinical trial nurse navigator.
Stephanie Chuang: I’m a blood cancer survivor myself and started The Patient Story out of my own experience. I felt so alone. I wanted to know what it meant after diagnosis and how we could get through it. As we know, a diagnosis is just the beginning of figuring things out. Our goal at The Patient Story is to help patients and care partners navigate life after a cancer diagnosis, primarily through in-depth conversations with patients, care partners, and top cancer specialists.
We are so proud to partner with The Leukemia & Lymphoma Society, the largest nonprofit dedicated to creating a world without blood cancers. For decades, they have invested almost $2 billion in groundbreaking research and pioneering so many approaches. On top of that, they also support patients and families with programs like the Clinical Trial Support Center, which provides free one-on-one support with nurse navigators.
This program is not meant to be a substitute for medical advice, although we hope that you walk away feeling like you have more to ask your own medical team.
Satyajit Kosuri, MD
Stephanie: Dr. Satyajit Kosuri is a hematologist-oncologist with the University of Chicago Medicine. He is an expert in stem cell transplantation and leads the Graft-Versus-Host-Disease Clinic and the research in trying to improve patient access to transplants. Dr. Kosuri, what drew you to this field of medicine and specifically GVHD?
Dr. Satyajit Kosuri: When I started my oncology fellowship, I was going to be a genitourinary oncologist and I was very much set. When I did my transplant rotation, what drew me was that it spanned all fields of medicine, so you had to continue to have a pretty good breadth of knowledge. The immunology was very, very intriguing. We’re dealing with very complex diseases as well as the transplant itself, which is basically an immune system transplant.
When I tell patients, family members, fellows, and trainees about the field of transplant, I tell them, number one, I’m an immunologist, number two, I become an infectious disease doctor, and then, number three, oncology comes in as part of the triad. That’s what drew me to the field and what I find very interesting. Graft-versus-host disease is part of the entire picture that we’re trying to improve upon within the context of transplant.
Shernan Holtan, MD
Stephanie: Dr. Shernan Holtan is a hematologist-oncologist with Roswell Park Comprehensive Cancer Center in Buffalo, New York. She is the chief of the Blood and Marrow Transplantation and has led so many clinical trials in GVHD. Her research has led to the discovery of the amphiregulin (AREG) biomarker for monitoring graft-versus-host-disease. Dr. Holtan, what drew you to medicine and specifically focus on graft-versus-host disease?
Dr. Shernan Holtan: My story is a lot like Dr. Kosuri’s. In medical school, I was most interested in rheumatology, infectious disease, cancer medicine, critical care medicine, dermatology, and plastic surgery. I thought, How am I ever going to pick between these different specialties? I loved cancer reconstruction and the connection with patients going through cancer and giving them hope after a devastating diagnosis.
On a whim, I took a rotation on the BMT service, in part because it sounded cool. The other part of it is you didn’t have to work weekends and as a very tired fourth year med student, I was excited about that. I was stunned. It was every great aspect of medicine rolled in one specialty, so I was sold and never looked back.
Meredith Cowden, Patient Advocate
Stephanie: Meredith Cowden is a chronic GVHD patient advocate and co-founder of the GVHD Alliance. Why did you decide to dedicate your life to advocating for so many other people with GVHD?
Meredith Cowden: I had acute myelogenous leukemia (AML) at 19. Chemotherapy wouldn’t completely work, so I needed a bone marrow transplant. Shortly after, I developed acute graft-versus-host disease and then I developed chronic graft-versus-host disease, which I’ve had since April 2002.
Graft-versus-host disease is rare and we’re spread out all over the place, so it’s isolating and hard to find resources, information, and even the appropriate treatment team.
I originally wasn’t into the patient advocacy world. I didn’t want to deal with it anymore, but I didn’t want anyone else to have to deal with it. I got angry and frustrated, and frustration is one of the greatest motivators for me. When I would talk to other patients, there was a sense of relief and comfort they felt in talking with somebody who could understand their experience. From that point, I thought that this is where I need to be.
Ashley Giacobbi: I am a nurse navigator with The Leukemia & Lymphoma Society’s Clinical Trial Support Center. We provide individualized clinical trial searches and clinical trial resources to patients with blood cancers or patients who have had blood cancer in the past but may be managing long-term effects of their disease or treatment.
We provide one-on-one connection with patients, caregivers, and their healthcare providers. We take the time to learn about a patient’s diagnosis, past treatment, and other medical conditions that could play a role in their eligibility for clinical trials. Most importantly, we take the time to learn about patient and caregiver preferences and any unique obstacles that may hinder or support their participation in a clinical trial, so that we can target the support that we’re able to offer and give personalized resources.
When immune systems grow suspicious, they’re programmed to do one thing and that is to attack. This new immune system can attack the recipient from the inside.
Dr. Satyajit Kosuri
Understanding Graft-Versus-Host Disease (GVHD)
Stephanie: Dr. Kosuri, what is GVHD?
Dr. Kosuri: When we’re doing a stem cell transplant or bone marrow transplant, we’re doing an immune system transplant. When we’re healthy, the immune system protects us, whether it’s getting rid of bad cells or protecting us from various infections. It considers the body that it’s growing up in as its neighborhood, so it has an inherent desire to protect its neighborhood and recognizes the body that it’s in as being part of itself. When there are things that are not supposed to be there, it recognizes them and gets rid of them.
We’re taking the stem cells from a person with a healthy immune system and putting them into the transplant recipient, so this immune system is growing inside of a new neighborhood. For the most part — and this is where matching comes into play — it recognizes its new neighborhood as its own and leaves it alone. It takes up the mantle of, “I’m going to protect this body and eradicate any leukemia cells,” and that’s the graft-versus-leukemia effect.
But sometimes, there are parts of the new neighborhood that are not what it’s used to, so it starts to grow a little bit suspicious. When immune systems grow suspicious, they’re programmed to do one thing and that is to attack. This new immune system can attack the recipient from the inside, which can lead to some inflammatory physical damage to the patient or the recipient of the stem cell transplant.
Types of GVHD
Stephanie: Dr. Holtan, what are the main types of GVHD? How do they differ and what are some of the common symptoms?
Dr. Holtan: We mainly think of graft-versus-host disease in two phase although there can be some overlap between the two.
Acute graft-versus-host disease happens within weeks to the first few months post-transplant and that has a particular pattern. Most of the time, it’s a red skin rash, but sometimes it can also lead to nausea, vomiting, diarrhea, and liver abnormalities that we might see on blood tests. There’s a very clear time during which this develops and a pretty clear clinical presentation, so it’s pretty easy to determine what it is.
Chronic graft-versus-host disease typically happens later in the months to years after transplant. It can be more subtle and difficult to diagnose. As Dr. Kosuri was saying, this is primarily an inflammatory reaction at the beginning, which ultimately will gradually lead to scar tissue.
Think of a wound that is having some difficulty healing. There’s a lot of inflammation and the body tries to stop that inflammation by putting a scar on top of it. This can happen in almost any organ in the body. Usually, the skin is involved, but it can also cause dry eyes, dry mouth, mouth sores, difficulty breathing, difficulty swallowing, changes with the muscle tissue fascia, and making people feel stiff and have muscle cramps. Any organ can be involved with chronic graft-versus-host disease.
Even though we think about chronic manifestations as a later problem after transplant, we can see some of those changes even within the first few weeks.
Dr. Shernan Holtan
Stephanie: Dr. Holtan, when does it technically turn from acute to chronic? Is there an official time where now we know it’s chronic? Is there a general time frame?
Dr. Holtan: There isn’t an official rule. When Dr. Kosuri and I were in training, we were taught that acute graft-versus-host disease happens before Day 100 and chronic GVHD happens after Day 100, but that’s not really true. The biologic processes can happen at any time post-transplant. Acute GVHD usually happens in the first few weeks to months, but we have even seen acute manifestations of GVHD happen much later.
Even though we think about chronic manifestations as a later problem after transplant, we can see some of those changes even within the first few weeks. The lines are blurred now, so we describe graft-versus-host disease based on its symptoms and appearance rather than time frame post-transplant.
It took a while before my doctors said I had GVHD because they were thinking it was something else. Over the years, I’ve had a variety of different manifestations of chronic GVHD.
Meredith Cowden
Meredith’s GVHD Story
Stephanie: Meredith, what was it for you in terms of those first symptoms? At what point did you realize that this was not going away?
Meredith: In the beginning, I noticed that I had a couple of different things going on at the same time. My stomach started to bother me a lot and I got very nauseous. It was hard to find food that I could tolerate and that was appetizing. I had some gastrointestinal issues going on. I also developed a rash. I’m naturally a pasty pink person, but my skin got red and burned, so it was hard to wear clothing.
When I received treatment, the issues started to get resolved, but then it started to transition. The GI issues didn’t necessarily go away but they changed and my skin got a little bit different.
I had musculoskeletal involvement. I developed polymyositis, so there was a lot of pain. I was very weak and couldn’t move around a lot. I lost muscle mass. It took a while before my doctors said I had GVHD because they were thinking it was something else. Over the years, I’ve had a variety of different manifestations of chronic GVHD.
Dr. Kosuri: Chronic graft-versus-host disease can affect multiple sites in a way that may be difficult to initially pick up. I’ve gotten feedback from patients that what they’ve found helpful is when I describe chronic GVHD prior to the transplant.
I ask them to imagine taking all the autoimmune conditions and rolling them into one and putting them inside a human body. Those are ways that chronic GVHD can manifest, whether it’s dry eyes, a scleroderma type presentation, or pulmonary fibrosis. It’s a great mimicker.
Stephanie: It sounds like it might be hard to identify quickly if people aren’t speaking up too and share the different things that you’re experiencing and communicating openly with your doctor.
There are many different types of complications, but infection comes to the forefront.
Dr. Satyajit Kosuri
Severe Complications in GVHD
Stephanie: I don’t know if there’s difficulty in noticing what the severe complications are, but, Dr. Kosuri, are there any that you’d like to highlight?
Dr. Kosuri: There are complications of the entity itself and then there are complications that will arise from the treatment or the way we try to treat the disease. GVHD in and of itself is an immune dysregulation. The immune system that’s supposed to behave in a certain way is misbehaving or it might be turned on and can’t really control itself. What happens in this state?
There are many different types of complications, but infection comes to the forefront. We prioritize monitoring patients who have graft-versus-host disease not only from the GVHD itself but also from the medications that we use to try to quell the inflammation and calm things down. Both can lead down the pathway of bringing down the level of protection that the human body has as it’s starting or trying to recover from the stem cell transplant.
One of the things that we emphasize for patients is if they’re feeling unwell in any way, shape, or form, they have to let their transplant providers know very quickly. That way, whatever suspicion we may have, we can diagnose and take care of it very quickly. If it’s a small infection, we can treat it and it doesn’t become a big infection.
Be very proactive and very compliant with the medications. Patients take 20 different medications after a transplant and sometimes it’s hard to take all of them, especially when the pills are big. We hear that as one of the main complaints. We make sure that patients are on antiviral medications, antifungal medications, and a medication to protect them from PJP (pneumocystis jiroveci) pneumonia. These help protect and almost substitute in a way because the immune system is not online early on and when you have graft-versus-host disease, it’s not behaving the way that it’s supposed to.
Dr. Holtan: We certainly know that graft-versus-host disease can affect different organs and tissues, and that the treatment can have just as many toxicities as GVHD itself. Some of the most challenging issues we run into are malnutrition, straight-up difficulty eating, all the way to impaired organ function.
What Dr. Kosuri mentioned is key about notifying for changes in symptoms with chronic graft-versus-host disease. You want to intervene before there’s permanent damage. The longer the inflammation and scar tissue goes, the more difficult it is or it might even become impossible to reverse. Early intervention is necessary to try to avoid permanent damage.
If there’s anything that seems even a little bit wacky, ask. There’s no harm in asking. It’s one of the best ways to take care of yourself.
Meredith Cowden
Stephanie: From your own patient experience, did you know that you could bring these up to your doctor? Do you feel that patients you talk to know that they can do that? What do we need to do to make sure that this is happening?
Meredith: I was diagnosed at 19. I was young and there were things I learned over the years. This might sound naive and silly, but there were things that I thought were completely normal but were actually symptoms of GVHD.
Over time, I’ve developed strong relationships with each member of my care team, so I’m very comfortable saying, “This feels weird. I don’t know about this. Can you look at that? Check me out please.” To have that kind of conversation, you have to build that relationship so that everyone is comfortable and can have a discussion with one another even when they have differing opinions. You can get more out of that conversation than if a typical patient-doctor exchange. Oftentimes, things get missed that way.
For patients, treat your doctors like people. Be friends with them. You’re going to be with them for a long time. They want to help you. If there’s anything that seems even a little bit wacky, ask. There’s no harm in asking. It’s one of the best ways to take care of yourself. For the providers, it’s a good idea to ask patients to do a quick scan of their body to get the whole picture because it’s easy to forget stuff. Is there anything that’s going on that we haven’t touched on that you noticed?
The backbone of therapy for both acute and chronic GVHD is corticosteroids.
Dr. Satyajit Kosuri
Current GVHD Treatments
Stephanie: Dr. Kosuri, what are the current standard treatments for GVHD?
Dr. Kosuri: The keyword is current because this is something that’s changing and we hope will continue to change as we go through the years.
The backbone of therapy for both acute and chronic GVHD is corticosteroids. Many patients and their family members will have heard of the medication called prednisone or various types of the steroid.
The degree of the GVHD matters. If you have a mild, acute graft-versus-host disease, this could be potentially managed with topical corticosteroid. As it becomes more severe or involves more organ systems or more of the skin, we start graduating from topical steroids to systemic steroids.
Depending on where we are in the transplant process, our patients will already have been on another immunosuppressive agent, like tacrolimus, sirolimus, or cyclosporine. The goal is to treat with steroids plus or minus this other agent and then taper them off once we have a response.
With steroids, over a period of time, you can accumulate some of those side effects that we don’t like to see in patients, like insomnia, jitteriness, and fluid retention. Those are for people who are in the category of steroid-responsive.
Another category of patients are those who are steroid-refractory, which is where the graft-versus-host disease may be a little bit more sticky and not respond to steroids, or steroid-dependent, where patients are unable to get off steroids. In those cases, we go further down on immune suppression choices. There are other medications available. One that’s FDA-approved and works for both is ruxolitinib. There are also other various options. That becomes more of a longer term treatment.
There isn’t a blood test that can diagnose graft-versus-host disease right now, but we can use biomarkers to help us understand the severity of the immunologic reaction and how much damage has been done.
Dr. Shernan Holtan
Challenges of Existing Options for Managing GVHD
Stephanie: Dr. Holtan, what are some of the key limitations or challenges with the existing options for managing GVHD?
Dr. Holtan: The greatest challenge is understanding how much therapy to give for graft-versus-host disease. We base our treatment upon the severity of symptoms, but that isn’t adequate. There are still some patients that we are over-treating and some patients we are under-treating.
This is where the role of biomarkers can come in. There isn’t a blood test that can diagnose graft-versus-host disease right now, but we can use biomarkers to help us understand the severity of the immunologic reaction and how much damage has been done internally that we can’t detect clinically. This is a huge challenge because even though we examine patients fully and they reveal all their symptoms, we still can’t know how bad things are, so biomarkers can support us in helping to guide that therapy.
This is particularly under investigation right now using biomarkers such as ST2 (suppressor of tumorigenesis 2), REG3α (regenerating islet-derived 3-alpha) known as the MAGIC (Mount Sinai Acute GVHD International Consortium) biomarkers, and then the one that we developed at the University of Minnesota, amphiregulin or AREG. Both of these biomarkers can be used to understand how severe the graft-versus-host disease is.
I have patients who have had severe infections of the GI tract, like C. difficile colitis or viral gastroenteritis such as adenovirus gastroenteritis. An allogeneic transplant recipient might have these infections and we’ll treat the infections, but they’ll have persistent severe diarrhea so you won’t know if you’re still dealing with the infectious process and the healing that has to occur or if graft-versus-host disease developed as a result of the immune system trying to target the infections. Even a biopsy can’t always tell you this, but we can use biomarkers, especially amphiregulin, to help sort this out.
When we’re treating patients with these symptoms, it’s almost like it’s graft-versus-host disease until proven otherwise.
Dr. Satyajit Kosuri
I had a gentleman who had severe adenovirus gastroenteritis and was having 15 to 20 bowel movements a day. We used an amphiregulin test to know if this could be graft-versus-host disease. The result was normal. It was not elevated. I continued to check every week because his gastroenteritis went on for a long time, even though we treated it.
Clinically, he had weeks of diarrhea, but we followed that test every week and the number was always low, so we never gave him prednisone. If I didn’t have this reassurance, someone might say it’s GVHD. It took some time, but he made a full recovery. This is how we can use these biomarkers to help support our clinical decision-making. We need more trials along these lines because the real world is messy.
Dr. Kosuri: I can’t emphasize how important what Dr. Halton is mentioning because oftentimes in transplant medicine, we’re operating in the gray and we have to make guesses. Sometimes when we’re treating patients with these symptoms, it’s almost like it’s graft-versus-host disease until proven otherwise. When you have that type of thought process, it can be difficult and we can actually hurt the patient with the GVHD management in and of itself.
The example that Dr. Holtan mentioned, most transplant physicians would say, “This has to be GVHD and we have to give them prednisone,” and that could lead to other infections or it can worsen the infection the patient already has. We get into these situations that are difficult to manage and if we have something like these biomarkers, it can make our lives as well as the patient’s life much easier and with less toxicity than what we would say is the normal kind of approach.
We had no human data to support how we manage steroid-refractory GVHD. Out of decades worth of work, there were no studies.
Dr. Shernan Holtan
Stephanie: A lot of this is addressing the symptoms that come with GVHD. This may be a rookie question, but I’m trying to understand. Is there research going into how to address the drivers of what’s happening with GVHD?
Dr. Holtan: We know what causes graft-versus-host disease. The donor T cells are attacking tissues and organs. However, we can’t always tell when that attack is over. The whole field of steroid-refractory graft-versus-host disease has developed out of an assumption that the T cell-mediated attack is still happening, so all trials for steroid-refractory GVHD involve intensification of immunosuppression without actual knowledge that there are T cells still causing damage.
This was something that bothered me. These are things that drive you crazy about the field and want to change it. I realized that we had no human data to support how we manage steroid-refractory GVHD. Out of decades worth of work, there were no studies that justified that this is the right path.
I performed a study where we had rectal biopsies of patients with grades 3 to 4 gastrointestinal GVHD. They were steroid-refractory and received other therapy. I wanted to look at the biopsies for a sign that it was the donor immune system still doing the damage to prove what we’re doing is right and I found absolutely no evidence to support our practices. There was no increase in T cell infiltration. There was no immune signature at all that suggested that it was out of control T cell-mediated damage in the steroid-refractory patients. All we saw were signs of tissue damage.
I’m hoping that the field will evolve. Instead of intensifying immunosuppression, give something more immunomodulatory, support immune tolerance, and give something to help heal the damaged organ. Change the paradigm. That was a huge frustration that I had as a fellow and I hope more people read that paper now.
Clinical Trials for GVHD
Stephanie: We’ve talked about the current landscape of GVHD and treatments, and some gaps of need. Before we go into them, what are clinical trials?
Ashley: Clinical trials are carefully controlled research studies that may be conducted by scientists, doctors, or researchers to either test new treatments or test treatments that have been used in the past in a potentially different way. Trials can also compare new treatments to existing treatments or to various combinations of treatments to find out which treatment might work best or which would be better tolerated, all with the goal of improving care and treatment for patients.
BMT CTN 1703 Clinical Trial
Stephanie: Dr. Holtan, can we talk about one of the trials that you helped lead? What’s the potential and the excitement about that?
Dr. Holtan: An ounce of prevention is worth a pound of cure. The theme in these studies is prevention of graft-versus-host disease. Our field is in the midst of an important era. We have very effective prevention for acute and chronic graft-versus-host disease with multiple modalities that we have not had in the past.
The BMT CTN 1703 study was repurposing a chemotherapy agent called cyclophosphamide to prevent acute and chronic graft-versus-host disease by giving it after transplant in the setting of reduced-intensity transplants, so patients who are typically older. The median age of the trial was 66, going through transplant, and would receive this chemotherapy after the transplant. That initially sounds crazy to do. Why would you give chemo after the transplant?
We’re learning how this works, but it helps to deplete allo-reactive T cells. The good cells that we want to persist are completely immune to cyclophosphamide, so regulatory T cells, which are T cell peace mediators, and stem cells themselves are resistant to this chemotherapy. It eliminates the cells we don’t want and preserves the cells we do.
This modality was compared against the standard, which was a calcineurin inhibitor (CNI) plus methotrexate (MTX), and that’s been the standard since 1986. Our field hasn’t undergone a major change where we saw that the new treatment arm was superior. We haven’t had this kind of change since the mid-80s.
We did a similar study in Minnesota looking at post-transplant cyclophosphamide in the myeloablative setting. We saw remarkably low rates of acute and chronic GVHD using this platform. The rates of grade 3 to 4 acute GVHD were 5%. The rates of chronic GVHD requiring immunosuppression were also about 5%. It’s not a randomized nor a phase 3 study, so we haven’t done that comparison. I have a lot of conflicts of interest, so I don’t want to do that study because the results of phase 2 are so good. I wonder what Dr. Kosuri thinks about that.
Dr. Kosuri: Dr. Holtan’s work with 1703 is one of the more important studies that we’ve had recently in the field of stem cell transplant. When we look at our field and the studies that we conduct, having a randomized study in such a large manner is very, very rare, so this was a big deal. It’s not just the findings, but the way that the study was conducted.
The study went through other randomized trials and the two best options went into 1703. As Dr. Holtan mentioned, the results are very, very important and being adapted in a widespread manner amongst many of the transplant centers not only in the United States but even abroad, so it’s a very, very impactful piece of work.
The important thing, as she highlighted, is that these are for older patients who have had multiple lines of therapy and may be coming into transplant in a more frail physiologic manner than someone who is in their 20s, 30s, or 40s. The reduced-intensity aspect is very, very important.
I agree that the post-transplant side has had such an impact on the incidence of acute and chronic GVHD. The other thing that I’ve noticed is the nature of the graft-versus-host disease that could develop. Even if someone were to receive post-transplant cyclophosphamide as a GVHD prevention strategy or what we call T cell-depleting methods, there are other ones also.
When we’re giving higher-intensity conditioning, the amount of initial damage and inflammation that occurs is higher and the risk of developing both acute and eventually chronic GVHD can also be higher.
Dr. Satyajit Kosuri
When we compare it to the standard of care, if they were to develop graft-versus-host disease, there is the potential that it may be more responsive to current treatment modalities. You can treat it and it can potentially go away versus you trying to treat it and patients may become more steroid-refractory or steroid-dependent. Incidence is important and the incidence is much lower. My opinion is that the nature of the GVHD that may happen is also different.
As far as myeloablative conditioning, if we think it works in one setting with a group of patients who may be a little bit more sensitive to the toxicities of transplant, as a transplant physician, we want to try to apply it to the younger, fitter patient population who are receiving myeloablative transplants or the higher-intensity transplant.
The important point there also is when we’re giving higher-intensity conditioning, the amount of initial damage and inflammation that occurs is higher and the risk of developing both acute and eventually chronic GVHD can also be higher.
If we can take this modality, use it in the myeloablative setting, and decrease the incidence of both acute and chronic GVHD, that’s something I think that we’re all very supportive of. As transplant centers are changing their standard approaches, we ourselves at the University of Chicago are figuring out a way to standardize our myeloablative transplants using PTCy (post-transplantation cyclophosphamide), even though we don’t have a randomized, large randomized study.
VIC-1911 Clinical Trial
Stephanie: Speaking of higher-intensity transplant groups, that’s also for VIC-1911, right, Dr. Holtan? What’s exciting about that and who’s going to benefit from that potentially?
Dr. Holtan: This is a new clinical trial looking to improve on the post-transplant cyclophosphamide platform. Now that we’ve nearly eliminated severe acute and chronic graft-versus-host disease, our unmet need is addressing relapse.
We’re looking to see if we could do something different within the GVHD prophylaxis platform that not only keeps GVHD rates low but also directly reduces the risk of relapse. We took away one of the drugs in the platform called mycophenolate mofetil (MMF). We don’t think that MMF probably does very much to be honest. The heavy lifting is done by cyclophosphamide in combination with whatever we partner it with, tacrolimus or sirolimus.
We took MMF out and put in a drug called VIC-1911, an Aurora kinase A inhibitor (AURKA). That drug is known in preclinical testing to keep GVHD rates low, but it also has direct anti-leukemia effects. It helped to kill leukemia cells in the test tube and in mice. Mice who received this combination had better survival overall due to less graft-versus-host disease and less relapse.
We’re testing a platform to see: does it protect people from graft-versus-host disease and can it also protect from relapse? We have two primary endpoints in this study: GVHD and relapse. If we can move the needle with relapse, we will have evolved the platform even further.
This trial is ongoing right now only for the myeloablative or high-intensity conditioning regimen, but we hope to complete the study, learn the results, and, if successful, expand it to other platforms. It’s currently in phase 1. We have just found the dose that we want to test going forward.
Stephanie: That’s great context. Some trials are further along. People are always wondering, “Oh, that sounds so promising! But when are we actually going to see that in the real-world setting?” It’s great to know that the research is happening, but we’ve got a ways to go with that one.
Dr. Kosuri, you talked about PTCy and this trial is about lowering the dose. Can you talk more about that and who will benefit?
Dr. Kosuri: In Dr. Holtan’s 1703 study, we were looking at patients who have fully matched donors or what we call well-matched donors. Well-matched donors could also mean having a single-antigen mismatch. This is coming off post-transplant cyclophosphamide.
For patients who have haploidentical donors or half-matched donors, we’ve been able to successfully use that platform with very comparable and good rates of graft-versus-host disease reduction. The idea is if you can use it in a half-matched or half-mismatch, you can also use it in well-matched patients. We call that 7/8.
There are two studies. OPTIMIZE is coming after another study called ACCESS, which is looking at the same dose of post-transplant cyclophosphamide that we used in haploidentical transplants and reducing the dose a little bit.
Post-transplant cyclophosphamide is given on days 3 and 4 after a transplant at 50 mg each day. Data in the haploidentical transplant setting suggests that if we’re able to reduce the dose a little bit, a couple of things can happen along the lines of toxicity. One of the things that interests us is how quickly someone may engraft after a transplant, meaning how quickly their white blood cells come back and how quickly their hemoglobin and platelets recover.
If we reduce the dose a little bit, are we able to maintain graft-versus-host disease prevention, efficacy, or advantage? Maybe we’re able to improve a little bit with regard to the time it takes for the graft to come in. It’s a phase 2 study looking at patients who are 18 and older, who have a 7/8 donor, and both reduced-intensity as well as the myeloablative condition transplants.
We can find a list of clinical trials that will be open for consideration for a particular patient based on prior treatments and any conditions they may have.
Ashley Giacobbi
Enrolling in GVHD Clinical Trials
Finding a Clinical Trial
Stephanie: Finding clinical trials and enrolling in them is very difficult. We know ClinicalTrials.gov is available but may not be the most user-friendly. Can you walk us through the steps of how a patient could find a clinical trial that’s right for them?
Ashley: ClinicalTrials.gov is an amazing resource. It’s a database of all active and ongoing clinical trials, but it can be very challenging to use. This database contains all clinical trials for all conditions. It’s not exclusive to cancer clinical trials. Although cancer clinical trials make up a large portion of the clinical trials conducted in the United States, there are so many other clinical trials that are ongoing that it can be challenging to find one that’s right for you.
As a representative of the LLS and the Clinical Trial Support Center, we always encourage people to reach out. We hone in and find clinical trials that are most appropriate for the individual in whatever situation they are in. As opposed to having to filter through ClinicalTrials.gov, we can find a list of clinical trials that will be open for consideration for a particular patient based on prior treatments and any conditions they may have.
Types of Clinical Trials
Stephanie: We also understand that there are different kinds of trials available, like prevention, treatment, quality of life, and observational. Can you take us through what they mean in the context of GVHD?
Ashley: There are a lot of ongoing clinical trials for GVHD as this is an area of need. There’s a lot of ongoing research and that falls into different buckets.
Prevention clinical trials may look at altering the regimen prior to transplant or the medications taken after the transplant in an effort to prevent the development of acute or chronic GVHD.
Another type is treatment trials and these may include specific medications or investigational therapies that would manage acute or chronic GVHD if it’s already present.
Quality of life clinical trials are so important. There are a lot of clinical trials investigating symptoms that people with GVHD may experience. There may be behavioral interventions being investigated, such as exercise or even the use of an app to provide support. Some clinical trials offer social support or dietary recommendations in an effort to reduce symptom burden and really improve quality of life.
Finally, there are observational or natural history trials. These would be less involved as patients wouldn’t have to participate as much. These trials collect information either from the patient’s medical record or prior testing that’s been done to learn more about GVHD, who might develop GVHD, or how they might respond to specific treatments. These are important in the information gathering phase, but they might not require as much involvement from the patient perspective.
Eligibility criteria help determine the group of patients who will potentially receive the most benefit from the therapy being investigated.
Ashley Giacobbi
Qualifying for a Clinical Trial
Stephanie: You may find a trial that seems great, but there are eligibility criteria and screening processes that you may have to go through. What does that typically look like for patients?
Ashley: History, previous treatment received, and other factors play a role in the eligibility criteria, but those help determine the group of patients who will potentially receive the most benefit from the therapy being investigated. These criteria are also there to help reduce any unnecessary risk by preventing those who have underlying conditions that could be made worse by the treatment from participating in that clinical trial.
Those criteria may include things like the type of GVHD, acute versus chronic, which body systems are being affected, as well as any prior treatment received for the management of GVHD. Very often, steroids are used and some of these clinical trials will require that people have already attempted the use of steroids. Those eligibility criteria help us to find appropriate clinical trials for the individual.
Stephanie: You have touched on what you at the Clinical Trial Support Center in terms of helping people with a personalized trial list, going off of ClinicalTrials.gov and making sure it’s more tailored to them. Is there anything else you’d like to share about what they could expect?
Ashley: Patients can be referred to the Clinical Trial Support Center either by a healthcare provider or they can get in touch directly themselves. Very often, we connect with caregivers of patients.
Initially, we take the time to learn about the patient, what’s important to them, and their history. Those details are so important when looking for clinical trials and that’s usually via phone call.
Beyond that, we take the time to go through and review clinical trials. We’re very fortunate to have a unique database that looks at clinical trials in ClinicalTrials.gov but also stores information that we receive from investigators and sponsors of clinical trials so that we’re able to provide the most up-to-date information to patients when they’re considering clinical trial options.
Once we’ve generated a list, we’re able to send that to the patient, caregiver, or healthcare provider and share the clinical trials that we’ve found for that particular person. They can then take back that list to review with their healthcare team and see if any of those trials is a potential option for them to explore.
A lot of emerging data suggests that preservation of muscle mass actually helps reduce the risk of relapse, so this is not just cosmetic. It is about quality of life, but it’s also about the efficacy of the therapy itself.
Dr. Shernan Holtan
Nutrition & Exercise When You Have GVHD
Stephanie: Dr. Holtan, what specific nutritional and exercise interventions are being investigated to support muscle health during and after transplant?
Dr. Holtan: This is a substantial topic. I always tell my patients that if I could give a pill that could keep their muscles strong, I’d be the richest woman in the world. Having the ability to maintain muscle mass throughout chemotherapy of any kind is important. We need to do more in this area not just for transplant but for all cancer therapy.
There are multiple studies going on around the world that are looking at different types of nutritional supplements to maintain muscle mass and help promote intestinal healing. There’s some interesting research going on out of Italy using a nutritional supplement that has a growth factor that can help the gut heal itself.
There might be different nutritional approaches based on infection profiles. For example, we want to avoid a certain type of bacteria growing in the intestinal tract and avoid something in the diet that might help prevent that from growing. Those types of studies are important and we need to be able to expand them so that more patients can participate because, in reality, we don’t know what the best diet really is. We want people to get calories and protein in.
The same thing goes for exercise. We need to do more to facilitate exercise, especially resistance training. A lot of emerging data suggests that preservation of muscle mass actually helps reduce the risk of relapse, so this is not just cosmetic. It is about quality of life, but it’s also about the efficacy of the therapy itself. There’s a lot of work we need to keep doing in this space, so stay tuned. Obviously, this is the most important thing that we can work on besides improving the toxicities of the treatment itself. Supportive care is so important. We have a lot more work to do.
It’s on us to educate both referring providers as well as patients to understand that things have improved over time both from an access standpoint as well as supportive care standpoint.
Dr. Satyajit Kosuri
Areas Requiring More Research & Gaps in Transplants & GVHD
Stephanie: Dr. Holtan, you did mention that only a fraction of potential transplant candidates even get referred. What is contributing to this under-utilization? How can we address those barriers?
Dr. Holtan: We have an educational gap. The transplant field is vastly different in 2024 than it was even in 2021 and certainly way different than it was in the ‘80s or ‘90s, so we have to do a better job of communicating. What have been the advancements in care? How have we improved on the availability of donors? We no longer need a perfect match. How have we reduced graft-versus-host disease and improved other toxicities so that more patients are able to be reached?
There’s a lack of referral and also fear from the patient’s side as well. We have a lot of education to do to share that it is different today, much safer, and hopefully we can be able to take care of a lot more patients in the future.
Dr. Kosuri: Many of the old thoughts that we have about transplant are that you have to be a certain age or how scary it is and things of that nature. It’s on us to educate both referring providers as well as patients to understand that things have improved over time both from an access standpoint as well as supportive care standpoint.
The supportive care has changed over the last decade significantly and that’s why we’re able to take patients who previously the field would not consider, even if they were in good shape.
There can be a patient who is 50-some-odd years old but has been beaten up because of the disease or the treatment, so transplant would be very difficult for them, whereas we can have a 70-year-old who is running a half marathon. It’s not just numerical age; it’s the physiology of what the patient’s body is at the time that we’re considering transplant.
I totally echo what Dr. Holtan’s saying. It’s about education and casting our net very wide with regard to patients and patient advocacy groups as well as physicians or the referring providers.
We’re seeing so much change because of our understanding of the biology of the diseases that we’re dealing with coming into transplant, the technical aspects of the transplant, and GVHD prevention.
Dr. Satyajit Kosuri
GVHD Treatments Final Takeaways
Ashley: There are resources and support available. It’s never too early or too late to explore clinical trials when you’re talking about GVHD and clinical trial options during the transplant process.
Dr. Kosuri: Over the last decade, I have had more hope as a clinician in the field of transplant. Even though it’s trying to move, the field has been set in its ways for a very long period of time. But within the last 5 to 7 years, we’re seeing so much change because of our understanding of the biology of the diseases that we’re dealing with coming into transplant, the technical aspects of the transplant, and GVHD prevention, like the 1703 study.
There are many trials looking at the initial treatment of graft-versus-host disease and how to get patients off of steroids quicker. With chronic graft-versus-host disease that is far off, more severe, and more fibrotic, there are ways to manage that.
I want to emphasize Dr. Holton’s work regarding biomarkers. For a long period of time, our approach when it comes to GVHD was if we try something and it fails, we try another agent and provide more immune suppression. We’re hoping to minimize that approach where you throw something at a wall and see what sticks. It may be different for each patient. Do we need GVHD treatment in patients who have certain symptoms? If it is graft-versus-host disease, how do we know when to come off therapy or how to add therapy? That’s where the biomarker becomes very, very important.
I can’t emphasize enough how nutrition, exercise, and sleep are key to help recovery and resilience. I want people to know that they have more control than they think.
Dr. Shernan Holtan
Dr. Holtan: I want patients and their families to know that they have a lot of control in these processes. I believe very much in the principle of self-efficacy. Yes, this is a medical treatment that we are delivering, but there’s a lot a person can do for themselves and that their family can do together to help make the process easier.
I can’t emphasize enough how nutrition, exercise, and sleep are key to help recovery and resilience. I want people to know that they have more control than they think and look for ways that they can help build up their strength and resilience, lean on their network, and use these tools and resources to help build up the spirit and body to be able to withstand the trials and tribulations that certainly lie ahead. The medical advancements are real, but people also have a lot of control and they should know that.
Meredith: Hope is incredibly important. Recognition that you do have control is imperative. Be selfish and put yourself first. Don’t try to take care of all the people around you to the detriment of yourself. If you don’t want to do something or can’t meet with somebody, don’t do it.
Continue to find meaningful and fulfilling activities so that the illness doesn’t become your identity. You have an illness, but you’re not defined by that illness.
The LLS, being a partner of ours on this program, is such a great resource. The CTSC provides amazing one-on-one support in terms of understanding clinical trials, finding, enrolling, and even staying on them.
We hope that this program was empowering and that you’re able to take away not just from this program but from the many stories that we have.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Stephanie Chuang: My name is Stephanie Chuang. I’m the founder of The Patient Story. The genesis of The Patient Story was my non-Hodgkin lymphoma diagnosis at 31 years old. I remember how overwhelmed I felt and didn’t even know what questions to ask my doctor. What do I do? Where do I go? But it was more like what do we do? Where do we go? Because as we all know, a cancer diagnosis impacts so much more than the patient.
We know there are so many things to consider, but I believe the core of what can make a difference is empowering ourselves to be more active in our care. I’m so thankful for advocates in every form, including other patients, care partners, and healthcare providers who invest so much time and energy in ensuring that we get the best care and know what clinical trials may be an option for us and not as a last resort.
This program is produced by The Patient Story in collaboration with The Leukemia & Lymphoma Society, an incredible advocacy organization that has free resources for patients and care partners in blood cancers, and an organization that has supported more than 85% of blood cancer treatments approved by the FDA to date.
As with all our programs, The Patient Story retains full editorial control over the content.
While we hope you learn a lot, it is important to note that these discussions are not a substitute for seeking medical advice, so please speak with your own medical team about what’s most appropriate for you.
Our patient moderator is Dr. Robyn Stacy-Humphries. Not only is she a long-time respected physician in the Charlotte area, but she is a three-time DLBCL patient and survivor, and someone I’m lucky to consider a friend. I admire her so much for the advocacy work that she does as a physician and now as a patient advocate. Robyn, thank you so much for joining us and leading our discussion.
Robyn Stacy-Humphries, 3x DLBCL Survivor
Dr. Robyn Stacy-Humphries: I’m Robyn Stacy-Humphries, a three-time diffuse large B-cell lymphoma survivor. I’m one of the first patients in the United States who received CAR T-cell therapy in 2016.
Nilanjan Ghosh, MD, PhD
Dr. Nilanjan Ghosh: I’m Nilanjan Ghosh, the head of hematology at Levine Cancer Institute at Atrium Health. I also lead the lymphoma division. It’s a real pleasure to be here to discuss DLBCL as well as follicular lymphoma with my colleagues.
Kulsum Bano, MD
Dr. Kulsum Bano: I’m Kulsum Bano, a community oncologist who works at Levine Cancer Institute. It’s a privilege to take care of patients with lymphoma and an honor to be here to talk to everyone. Thank you.
Justin Favaro, MD, PhD
Dr. Justin Favaro: I’m Justin Favaro, a physician, medical oncologist, and hematologist in Charlotte, North Carolina. I’ve been in private practice for 18 years. I see a wide spectrum of different types of cancer, with a special interest in malignant hematology, lymphoma, and leukemia. I love the science of this disease and the technology, and I love to learn more from you all as we try to tell you what we know about this disease. It’s a pleasure to be here.
Diffuse Large B-cell Lymphoma (DLBCL)
Robyn: Diffuse large B-cell lymphoma is the most common of the non-Hodgkin lymphoma types. It is very aggressive and, without treatment, most people’s survival rate is only one year.
We are also going to talk about follicular lymphoma. There is some overlap, but follicular is an indolent lymphoma. People may present or be asymptomatic. It can progress rapidly or it can last for years. DLBCL and follicular lymphoma are managed differently.
First, we’re going to talk about diffuse large B-cell lymphoma. Dr. Favaro, what are the current treatment options for diffuse large B-cell lymphoma when a patient is first diagnosed? What you do with your patients?
Current Treatment Options for DLBCL
Dr. Favaro: Before I talk about this disease, try to imagine a cancer cell as a ball. It’s a little simplistic, but if you think about a ball, in the middle of the ball is where all the DNA is. The DNA is the recipe for what makes a cancer cell what it is. There are 30,000 genes. This DNA in the middle of that cell is making all these proteins that make that cancer cell grow and make it do what it does in your body.
On the inside part of that ball are all these proteins. We’re going to talk about some of these proteins. These proteins circulate around the inside of that cell and make the cancer cell grow.
On the outside of that ball are spikes. There are different types of spikes on the outside of the cell. They’re called receptors. We can use those spikes and target cancer cells with our treatments.
CHOP
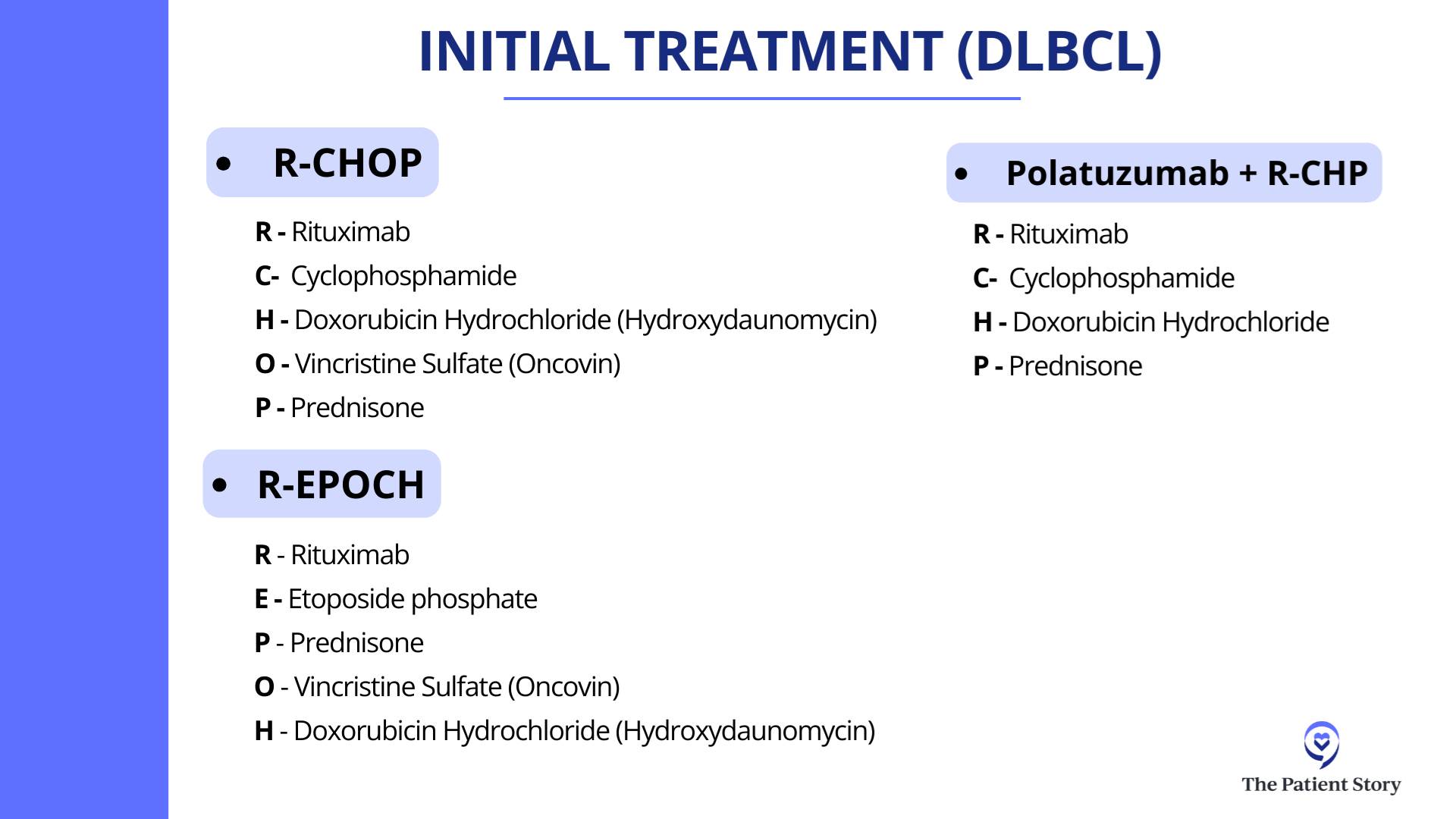
Dr. Favaro: The initial treatment for lymphoma goes back to 1976 when a combination of different chemotherapy drugs was first approved. CHOP is a combination of three different chemotherapy drugs (cyclophosphamide, doxorubicin hydrochloride, and vincristine sulfate) along with prednisone. Back in the 1970s, we were giving chemotherapy that attacked and killed all these fast-growing cells. It wasn’t targeted to spikes or proteins.
R-CHOP
Dr. Favaro: About 20 years ago, we discovered rituximab, which is a targeted therapy. It’s an antibody, a Y-shaped molecule that targets CD20, which is one of the spikes on the outside of the cell. We found that this is a great advance in cancer treatment.
If we added rituximab to all that chemotherapy, patients did better. They lived longer and had a much better chance of going into remission. R-CHOP has been the standard first-line treatment for diffuse large B-cell lymphoma for over the last 20 years.
pola-R-CHP
Dr. Favaro: Finally now, we have a new drug called polatuzumab vedotin, another targeted treatment and Y-shaped molecule. This time, it binds to CD79.
Polatuzumab vedotin added to rituximab, which hits CD20, and two different chemotherapy drugs plus prednisone (pola-R-CHP) is the new standard of care for the treatment of diffuse large B-cell lymphoma. Studies have shown that the response rate and survival is about the same versus the old regimen, but it looks like at two years, the remission rate is better if you take the new regimen of pola-R-CHP. This is the newest treatment for this disease.
Treatment Options for Relapsed Patients
Robyn: Unfortunately, even with these advances and the durable remission rate of 80% or so with the current therapy, there’s 20% where it doesn’t work. Patients will relapse very quickly. Dr. Ghosh, what happens in these patients whose initial therapy fails? What do we have to offer them now?
Autologous Stem Cell Transplant
Dr. Ghosh: In the past, the standard for patients who are eligible for an autologous transplant would be to get salvage chemotherapy, like RICE (rituximab, ifosfamide, carboplatin, and etoposide), R-DHAP (rituximab, cisplatin, cytarabine or cytosine arabinoside, and dexamethasone), or R-GDP (rituximab, gemcitabine, dexamethasone, and cisplatin).
If they are chemosensitive, meaning the tumor shrunk with chemotherapy, then they would go for an autologous stem cell transplant, which is high-dose chemotherapy followed by giving them their own stem cells back.
CAR T-cell Therapy
Dr. Ghosh: As immunotherapy advanced and as we learned more about ways to harness the immune system to fight against cancers, this was applied to diffuse large B-cell lymphoma and a novel treatment came about: CAR T-cell therapy.
Initially, it was approved after two prior lines of therapy. Patients would have had to gone through a transplant and if the transplant failed, they would get CAR T-cell therapy, or if they got chemo and then got CAR T-cell therapy as the third-line treatment. But then knowing that it was very powerful even in the third-line setting, there were some randomized clinical trials directly comparing it with transplant.
In the second-line setting, we are thinking a lot in terms of CAR T-cell therapy, reserving transplant for patients who relapsed late but are transplant candidates.
Dr. Nilanjan Ghosh
There were three large, randomized phase 3 studies that compared efficacy and toxicity of CAR T-cell therapy with that of autologous transplant. Two of those trials were positive in terms of ensuring that the primary endpoint, which was free of disease, progression-free, or event-free survival, was better compared to transplant. One of those studies actually showed overall survival was also better compared to transplant.
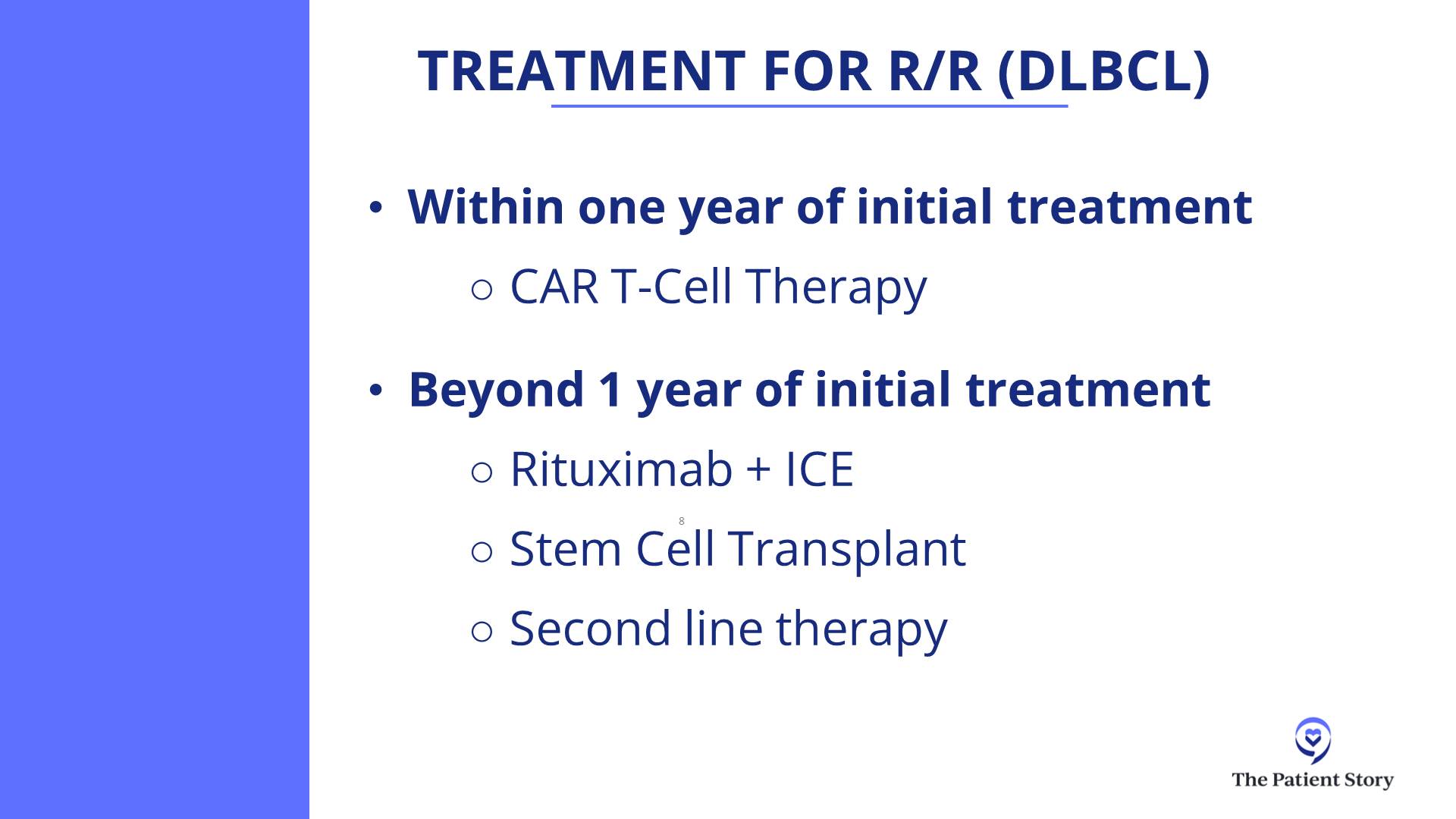
The current standard of care if somebody was refractory to front-line chemotherapies, like R-CHOP, pola-R-CHP, or R-EPOCH, or if they have relapsed within one year, the second-line therapy would be CAR T-cell therapy.
One of the CAR T-cell therapies called liso-cel was also used for patients who were not eligible for transplant, like older patients. Patients could get liso-cel as a second-line therapy if they had late relapse but were not considered to be transplant candidates, like if they had some organ dysfunction which would preclude them from getting a transplant.
In the second-line setting, we are thinking a lot in terms of CAR T-cell therapy, reserving transplant for patients who relapsed late but are transplant candidates. They could get salvage chemotherapy. If chemosensitive, go for transplant; if not, then still go for CAR T-cell therapy.
Follicular Lymphoma
Current Treatment Options for Follicular Lymphoma
Robyn: Follicular lymphoma is actually very common. It’s managed in the outpatient setting and Dr. Bano has seen quite a few of these cases. How do you manage these patients in your clinic?
Dr. Bano: I agree, it’s very common to see follicular lymphoma. It’s a different kind of disease process compared to DLBCL in the ways that patients present. It’s not the typical storm of symptoms that you expect with DLBCL. Follicular lymphoma tends to be slower-growing and presents in a way where most patients are even asymptomatic on initial presentation. They’ll have scans for something else, we’ll find enlarged lymph nodes, they’ll have biopsies, and that’s how we find it a lot of the time.
The way to approach treatment is a little bit different when you compare it to a more aggressive lymphoma like DLBCL. Sometimes, we’re thinking about stages like we generally do with lymphoma. The treatment differs based on what stage you are.
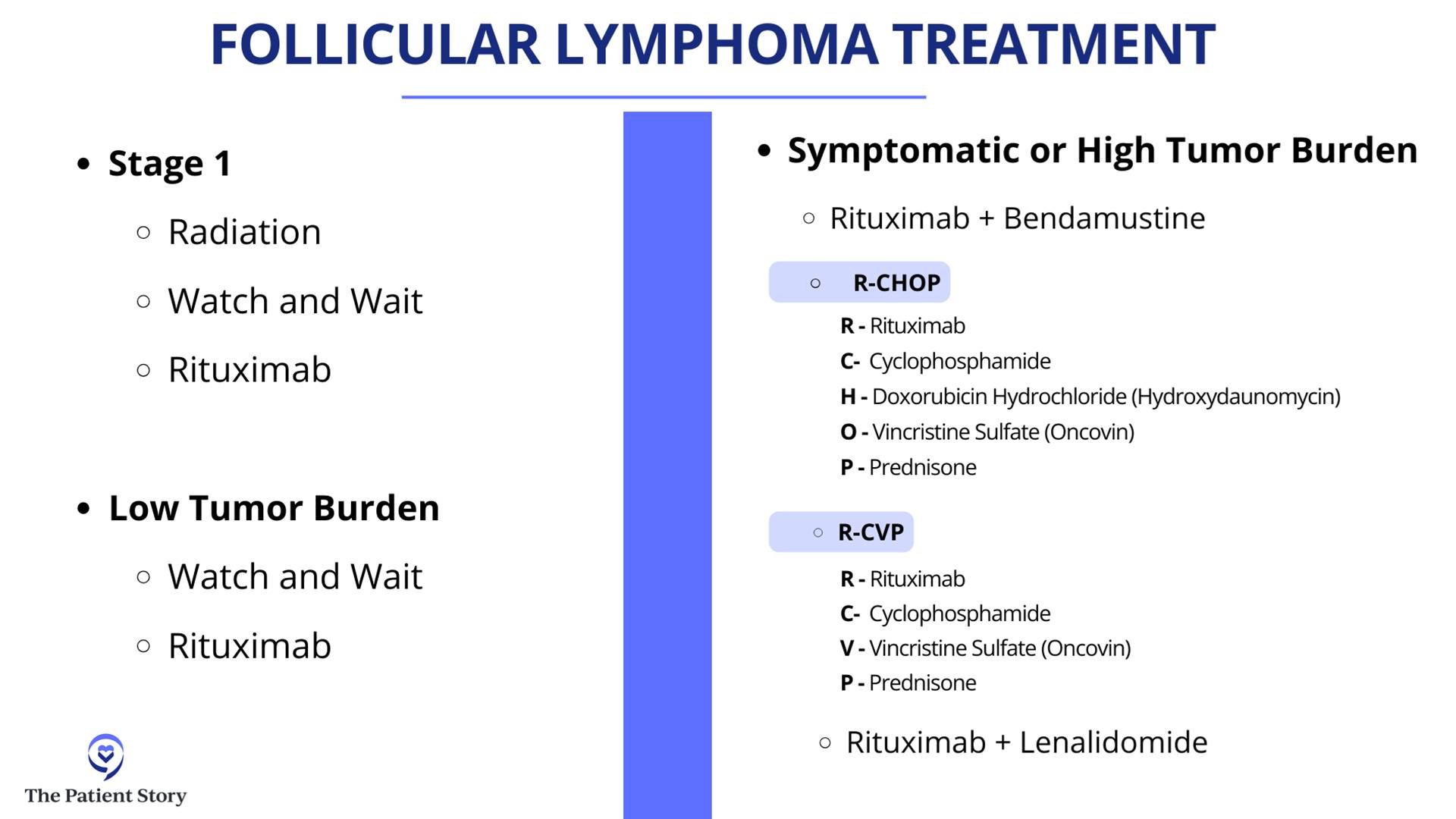
If you have a localized group of lymph nodes that are involved, a lot of times, if patients are asymptomatic, we watch and wait. Sometimes, if they have symptoms from a bulky lymph node enlargement, they can get radiation. A lot of times, we’ll combine that with CD20 monoclonal antibodies, as Dr. Favaro very nicely explained, that target these lymphoma cells directly. That is usually the option in limited stages of disease, like stage 1 and stage 2.
As we approach further spread out disease like stage 3 or stage 4, a lot of folks are asymptomatic and have a low burden of disease. We tend to watch and wait. That’s still an option.
Because of the indolent nature of follicular lymphoma, there’s a chance that it may come back, but we try to treat it and keep it in under control for as long as possible with milder therapies.
Dr. Kulsum Bano
Broadly, follicular lymphoma also is divided based on its grade. Not all follicular lymphoma comes equally. Some of the cases are lower grade, meaning the cells that are involved are not as actively dividing and do not appear as aggressive. For those patients, we tend to steer more toward the watch and wait and low tempo of therapy.
The more aggressive varieties, like the grade 3s, which is divided into 3A and 3B, we look more toward the DLBCL kind of treatment because these tend to act like a more aggressive lymphoma. In that scenario, we look more at chemotherapy plus immunotherapy, like R-CHOP. That usually tends to be the front line of therapy for follicular lymphoma.
It’s very varied. It’s a broad spectrum depending on stage as well as grade, but it tends to be a slow-growing disease in general. For those who get front-line treatment, some get even rituximab with bendamustine. Not everyone needs multi-agent chemotherapy.
A lot of times, we do a finite amount of chemo and follow it up with rituximab maintenance for up to two years. Every eight weeks, they get a rituximab infusion and that keeps patients in remission for a long, long time.
But as we talk about the difference in the nature of the two diseases, follicular versus DLBCL, there is also a difference in the treatment goals for these diseases. DLBCL is more aggressive and, as we were discussing earlier, we talk about a curative approach. Because of the indolent nature of follicular lymphoma, there’s a chance that it may come back, but we try to treat it and keep it in under control for as long as possible with milder therapies.
Treatment Options for Transformed Follicular Lymphoma (tFL)
Robyn: As a radiologist, there are a lot of CT scans and PET/CT involved where you monitor the lymph nodes. Unfortunately, even when someone’s in remission for two years, even after 10 years, it can come back aggressively. Dr. Ghosh, what do you do with a follicular lymphoma that is aggressive, has failed all treatments, and has transformed into diffuse large B-cell?
Dr. Ghosh: The first thing to think about when follicular lymphoma comes back is when it comes back. If it comes back within two years of front-line chemo-immunotherapy, then it’s considered to be progression of disease in 24 (POD24). Even if it has come back as follicular lymphoma, it’s a more aggressive variant. In long-term studies, the survival for that type has not been good. Many research studies have focused on this POD24 group to see what treatments would be effective.
The second thing to think about is: what does it come back as? As we discussed, follicular lymphoma can come back as low-grade follicular lymphoma, so grade 1, grade 2, or grade 3A.
Robyn: That’s based on pathology or the way it looks under a microscope.
If it’s aggressive B-cell lymphoma, then the treatment would be more like DLBCL. If it’s low-grade follicular lymphoma, you would treat more like the low grades.
Dr. Nilanjan Ghosh
Dr. Ghosh: When it comes back, it’s important to get a PET/CT scan and try to biopsy the most aggressive lymph node. A person might have multiple lymph nodes and if you only biopsy one, it could be low-grade follicular lymphoma. You don’t want to miss another lymph node with a high grade because the treatment would differ.
Convenience is important and sometimes a very bright lymph node may be in an inaccessible site, which makes it challenging. Try to biopsy the most active lymph node. If it’s aggressive B-cell lymphoma, then the treatment would be more like DLBCL. If it’s low-grade follicular lymphoma, you would treat more like the low grades.
PET scans are good, but the biopsy is where the money is, so put it under the microscope. Let the pathologist tell us what it looks like and then we can decide what to do.
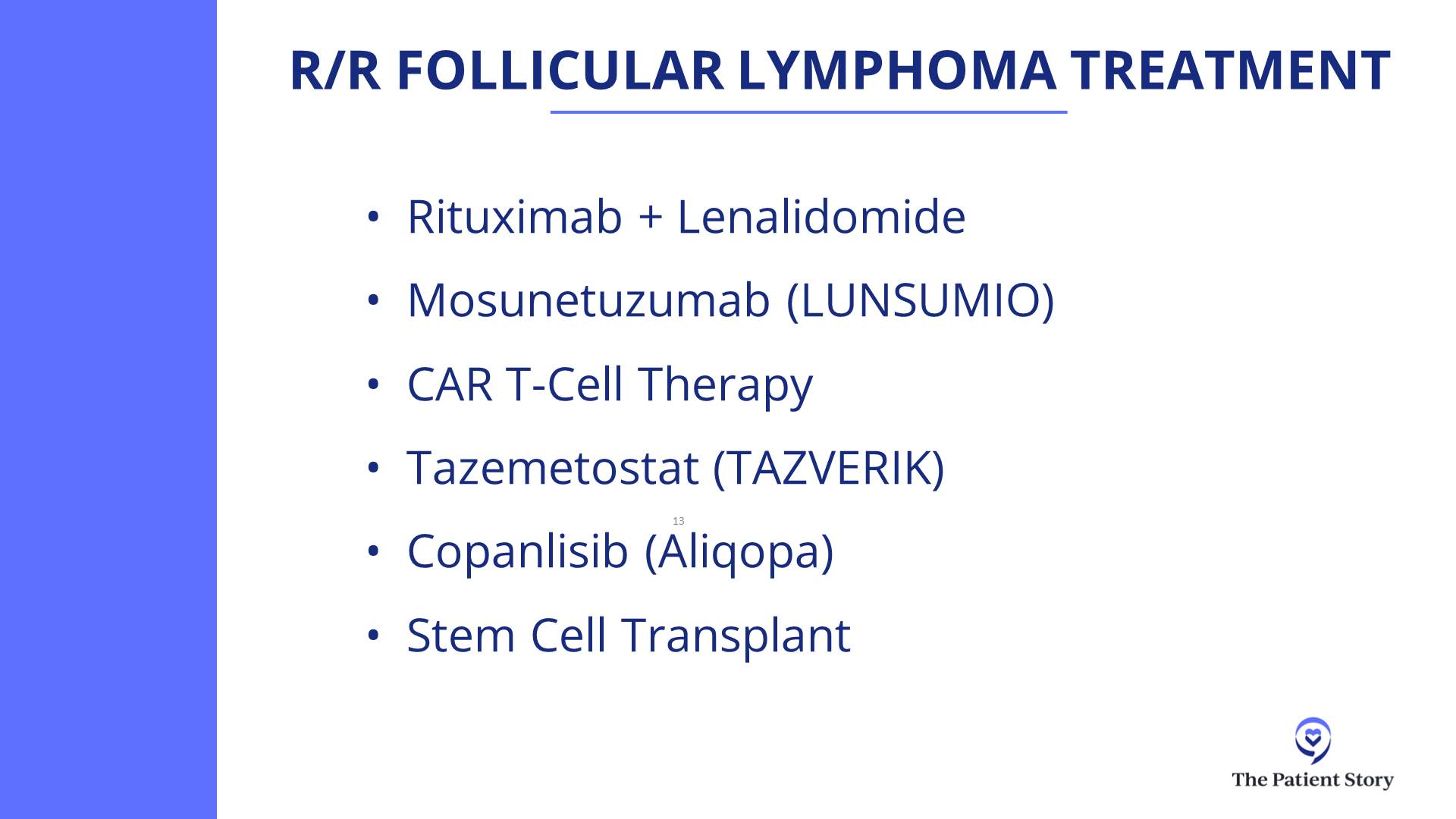
In general, if it is follicular lymphoma, there are many treatment options in the second-line setting. Our commonly used one, if rituximab plus chemotherapy has been used before, is a lenalidomide-based treatment in combination with a monoclonal antibody like rituximab or obinutuzumab.
Subsequently, CAR T-cell therapy has been very effective in follicular lymphoma. Bispecific antibodies are also approved and very effective in follicular lymphoma.
In follicular lymphoma, the disease can relapse 10 or 12 years later… CAR T-cell therapy has not been around for that long.
Dr. Nilanjan Ghosh
CAR T-cell Therapy for Follicular Lymphoma
Robyn: Follicular lymphoma traditionally has been viewed as incurable. But with CAR T-cell therapy, there is now possibility of a cure. Is that correct?
Dr. Ghosh: Yes, there is a possibility. The only long-term follow ups we have with follicular lymphoma being curative is allogeneic transplant, which have been around for decades. Follicular lymphoma can come back. DLBCL typically doesn’t have late relapses. There can be some, but usually relapses occur early. In follicular lymphoma, the disease can relapse 10 or 12 years later. What that implies is that you would have to follow people for more than a decade or perhaps even two decades to be sure that the disease doesn’t come back.
CAR T-cell therapy has not been around for that long, so we don’t know for sure, but there are hints though. We now have data that patients who were POD24 (patients who had front-line chemotherapy and their disease came back within 24 months) got CAR T-cell therapy and their disease hasn’t come back even beyond two years, which means the second-line treatment was more effective than the front-line treatment. This typically doesn’t happen in cancer. If that is there, then you’re overcoming the bad disease biology.
If it doesn’t come back after 5 years, after 10 years, and after 15 years, with follicular lymphoma, that’s when we’ll know. With DLBCL, you can have quicker readouts because if it doesn’t come back in two, three, or five years, then you’re likely cured.
Robyn: We have a CAR T-cell therapy online support group and we have several patients who had follicular lymphoma and who are 4-5 five years out from CAR T-cell therapy and in remission, so it’s very encouraging.
Bispecific Antibodies
Robyn: Moving on to exciting new treatments, Dr. Favaro, would you talk about bispecifics? What’s been approved and how do they work?
Dr. Favaro: Bispecifics are a fascinating field of medicine. The first bispecific that was approved was blinatumomab, which was approved for acute lymphocytic leukemia (ALL).
It’s a very small, V-shaped molecule. One part of the V would attach to your T cell, the other part of the V would attach to your cancer cell, and it will bring them together so the T cell can kill the cancer cell. If you flood your body with these, you can bring all the cancer cells next to your T cells and get a lot of death of the cancer cells.
We still use it for acute lymphoblastic leukemia. The problem with that molecule is that it has a very short half-life. It’s a small molecule and it would be degraded quickly, so you have to use continuous infusion and treatments in the hospital.
Over the last few years, they’ve developed better molecules that are more stable. Instead of a V shape, it’s actually a Y shape. The long part of the Y stabilizes that protein so it doesn’t degrade so quickly. These Y-shaped proteins still do the same thing, bringing the cancer cell next to the T cells, and they are now available for patients with lymphoma.
Epcoritamab
Dr. Favaro: There are two that are approved for diffuse large B-cell lymphoma patients who have had at least two prior treatments. One is called epcoritamab (EPKINLY). It’s a subcutaneously administered drug that attaches to the T cell and the cancer cell, bringing them together.
They’re seeing very high response rates in the 60% range and almost 80% in some cases, where for 80% of the patients that take this drug, their lymphoma shrinks down and up to 60% will have a complete response where their lymphoma completely goes away.
It’s a great new treatment. However, when you do this, you get a lot of release of cytokines and proteins in the body and they can cause side effects, almost like you have the flu or a fever, and can even get worse. Sometimes, you can have low blood pressure. We have to be very careful about how we dose these treatments.
We start with a low dose once a week and gradually bring the dose up. The side effects usually happen in the first month or so. Once you get to the higher dose level, then you’re basically taking an injection once a month.
Glofitamab
Dr. Favaro: There’s another drug called glofitamab. It’s a very similar molecule that does the very same thing, except it’s given intravenously. We step up the dose of the treatment over a period of a month and then the patient gets IV therapy every three weeks. It’s a limited duration of treatment. For that particular drug, it’s about 12 cycles or eight months of therapy.
The results we’re seeing with these two drugs are that most patients will have a complete response and you can see that being a long, durable, complete response.
Mosunetuzumab
Dr. Favaro: There’s also a BiTE (bispecific T-cell engager) therapy that’s approved for follicular lymphoma as well. This is a drug called mosunetuzumab and is given intravenously in a similar step-up dosage. This is given for a total of either eight cycles if you go into complete response or 17 cycles if you have partial response. We’re seeing great results with that as well in patients who have had at least two prior treatments for either diffuse large B-cell lymphoma or follicular lymphoma.
Robyn: Is this performed as an outpatient?
Dr. Favaro: It’s outpatient. There’s a risk of a severe reaction. In the early onset of the trials, most patients had to be admitted in the hospital after their second treatment or so because when you step the dose up, that’s when these side effects can happen.
The other two drugs can be given completely in the outpatient setting. We have a protocol set up for epcoritamab. You take the injection once a week for the step-up dose of that first month. As the dose is increased, you get steroids before getting the treatment and for three days afterwards. That seems to really reduce the side effects.
There’s a whole lot of education and prevention that goes into preventing and treating side effects immediately.
Dr. Justin Favaro
Side Effects of Bispecific Antibodies
Dr. Favaro: You have to understand these side effects and how to manage them, so we do a lot of education for our patients. Again, most of these side effects happen within the first month.
CRS (Cytokine Release Syndrome)
Dr. Favaro: There are three major side effects of those treatments. One is called CRS (cytokine release syndrome) and that’s where a lot of cytokines are released as the dose is increased. There are certain stages. CRS can manifest as a fever or if it gets worse, you can get low blood pressure and sometimes have to be admitted to the hospital.
We give steroids and, when needed, a drug called tocilizumab. Almost always, we’re able to reverse those side effects, but it’s something we do educate patients about and keep a close eye on.
Dr. Favaro: The second side effect, which is much less common, is called ICANS (immune effector cell-associated neurotoxicity syndrome). You can have neurologic changes, difficulty with thinking or decreased mentation, and some weakness of the muscles. Again, this is very rare, but it’s all about education, watching for that, and treating appropriately.
Infection
Dr. Favaro: The third big one is infection. We do treat with prophylactic antibiotics to prevent infection and sometimes we give IVIG to boost the patient’s immune system if needed.
There’s a whole lot of education and prevention that goes into preventing and treating side effects immediately. It’s amazing to have these drugs as options now for our patients.
With glofitamab and epcoritamab, as more time goes, we are starting to see a flattening of the curve for some patients… we’ll know over time how that looks, but it’s remarkable progress.
Dr. Nilanjan Ghosh
Success Rate of Bispecific Antibodies
Robyn: Dr. Ghosh, what bispecifics are you using and what kind of success have you seen?
Dr. Ghosh: We have all the bispecifics that are approved as well as those in clinical trials. We’ve been using mosunetuzumab for follicular lymphoma and glofitamab and epcoritamab for DLBCL.
For DLBCL, we usually do CAR T-cell therapy as second line. Studies have shown that even if CAR T-cell therapy has failed, patients have a very good response with both epcoritamab and glofitamab. These were phase 2 studies and remarkably had the same complete response rate. Epcoritamab showed about a 40% complete response rate and glofitamab also had a similar complete response rate.
Epcoritamab is subcutaneous, glofitamab is IV. Epcoritamab is given indefinitely until progression or if someone has bad side effects so they stop. Glofitamab, as Dr. Favaro mentioned, is given for 12 cycles.
I wouldn’t say choosing between the two can be tricky. Both have very similar efficacy, but you have to decide which one is going to work for somebody who lives far away and who wants limited-duration therapy.
Rather than focusing on the differences, the 40% complete response rate is the most important thing to take home. CAR T-cell therapy failed many of these patients. We don’t have very long-term data for the high-risk population in these studies who were refractory to previous treatments and yet did well.
With glofitamab and epcoritamab, as more time goes, we are starting to see a flattening of the curve for some patients. There are patients who got complete remission. They may still relapse, but there are some patients who will get into longer remission. We don’t have five-year data from either of the two, so we’ll know over time how that looks, but it’s remarkable progress.
In general, mosunetuzumab has lesser CRS compared to glofitamab and epcoritamab, but is also used more commonly in follicular lymphoma. Again, all these are done in the outpatient setting.
We have been involved in clinical trials combining mosunetuzumab and polatuzumab. A very effective strategy and though not yet approved, many other studies are ongoing.
The other thing we’ve done is combined bispecific antibodies with front-line treatment. We did a clinical trial of taking glofitamab and R-CHOP in the front line and we’ve seen remarkable remission rates.
Robyn: 80%?
Dr. Ghosh: Higher. When you combine glofitamab with R-CHOP in the front-line setting, the complete response rates are in the 80%. In DLBCL, we focus more on complete responses. Partial responses are okay to mention, but they are very temporary, so we want to focus on complete responses. Sometimes a partial response may turn into a complete response.
Clinical Trials of Bispecific Antibodies
Robyn: There are so many new exciting therapies and our panel has submitted some trials for bispecifics that they’re particularly excited about. What are some of these new trials that are revolutionizing treatment for lymphoma?
EPCORE DLBCL-3
Dr. Ghosh: The EPCORE DLBCL-3 clinical trial is looking at patients who are in the front-line setting and are not eligible for anthracycline-based treatments. They would get either epcoritamab or epcoritamab plus lenalidomide. If somebody has congestive heart failure or some cardiac problems that will preclude them from getting anthracycline-based chemotherapy, then instead of doing R-mini-CHOP or R-CHOP, they could get onto this study.
If bispecifics are moved up from more advanced relapsed/refractory treatments to earlier, can we get chemo-free front-line treatments? That is an effort with the EPCORE DLBCL-3 study.
EPCORE NHL-5
Dr. Ghosh: The EPCORE NHL-5 clinical trial is looking at epcoritamab plus lenalidomide in relapsed/refractory DLBCL. It has shown remarkable activity. It has not been directly compared with epcoritamab alone in the same study, but we have results from epcoritamab alone and that is a complete response rate of 40%. With epcoritamab plus lenalidomide, I believe the complete response rate goes up to the 50s and close to 60%.
Lenalidomide is an immunomodulatory drug. Combining an immunomodulatory drug with an antibody, which is also a kind of immunotherapy, we’re trying to focus on harnessing the immune system to fight against the lymphoma.
Glofitamab + Pola-R-CHP
Dr. Ghosh: Another powerful combination is glofitamab plus polatuzumab-R-CHP. As Dr. Favaro mentioned, pola-R-CHP showed improvement over R-CHOP. That has become a new standard. It showed improvement in progression-free survival compared to R-CHOP. If that is the backbone, can we further improve on that? That’s how we have made improvements over time.
CHOP came in the 70s. R-CHOP was approved in 2006 and showed improvement over CHOP. Pola-R-CHP showed improvement over R-CHOP. If we add a bispecific antibody to pola-R-CHP, can it show improvement over pola-R-CHP?
Glofitamab and pola-R-CHP is a study which we have done at the Levine Cancer Institute as well and it’s been done worldwide and has shown amazing effects. I saw one of my patients very recently who was in this study. He had an extremely explosive DLBCL about two years ago and he’s still in remission.
There are a lot of trials for diffuse large B-cell lymphoma that are moving a little bit more away from chemo and going toward these targeted therapies.
Dr. Justin Favaro
Glofitamab + Polatuzumab
Dr. Ghosh: Glofitamab and polatuzumab is another ongoing study. Taking polatuzumab, a CD79b antibody drug conjugate, and combining it with glofitamab showed high complete response rates. Similar studies have been done for mosunetuzumab plus polatuzumab as well.
A lot of these combinations are being done with the common theme being chemo-free. Some have chemo. CHP is chemo and antibody-drug conjugates are also chemo, but antibody-drug conjugates are very targeted chemo. It targets only the cells where the antibody binds to those spikes, so there is much less collateral damage.
The focus is trying to do less in terms of lowering the side effects, improving the efficacy, and improving quality of life and quantity of life. When you put that all together, the field is moving very well toward immunotherapies. I think these are all really good clinical trials.
Robyn: It’s very exciting. For the audience, the most common used anthracycline is doxorubicin, which is also known as the Red Devil. It can cause cardiotoxicity even in young people, who can end up with congestive heart failure at a young age. Other medications used, like cyclophosphamide, can cause neuropathy, which in some cases is irreversible. To move away from these medications and have the same results or better is great for quality of life and very, very encouraging.
Dr. Favaro: These are all great trials. There are a lot of trials for diffuse large B-cell lymphoma that are moving a little bit more away from chemo and going toward these targeted therapies.
Dr. Favaro: There’s another interesting trial combining four different drugs and none of them are really chemotherapy. There’s an oral drug that’s a BTK inhibitor called zanubrutinib, another monoclonal antibody called tafasitamab (MONJUVI), plus lenalidomide and rituximab. Of the four different drugs, two of them are targeting the spikes, one of them is targeting a protein inside the cell, and the lenalidomide is there to stimulate the immune system, the T cells, to grow and attack the cancer.
A newly diagnosed patient with no prior chemotherapy is seeing a very nice response rate. In this particular trial, they started with this and if they went into a complete response, then they got two cycles of chemotherapy and went back on the targeted therapy.
I like the idea of targeting some of these molecules on the outside or the inside, combining it with something that turns the immune system on as a way to eliminate some of those long-term potential side effects from chemotherapy. I think that’s the theme that we’re seeing here.
CAR T-cell Therapy
Robyn: I’m one of the first patients to get CAR T-cell therapy. I’m going to have the experts explain it, but as a patient, I compare it to Pac-Man. You put the T cells in and the little Pac-Man goes over and eats the cancer cells.
CAR T-cell therapy is new. I received tisagenlecleucel in 2016 as a phase 2 trial. It’s been very successful for me and I’m very, very grateful. I was able to go back to work as a physician. I have a great quality of life. Most of my side effects are from the chemotherapy, which did save my life but I wish I hadn’t had those.
This is a great therapy and now, not only is CAR T-cell therapy used for blood cancers, but it’s also being used in trials for solid tumors and autoimmune diseases, such as lupus, scleroderma, and glioblastoma.
Dr. Favaro, can you explain CAR T-cell therapy?
Dr. Favaro: T cells are part of your white blood cells that circulate around your body. They’re constantly looking to treat infection or try to treat cancer and that’s part of their job. Why can’t they kill cancer cells on their own? Because cancer cells learn how to hide. There are certain proteins they can take away from their surface, so your normal T cells can’t find the cancer cells sometimes and that’s part of the reason why cancer cells can grow in your body.
How do we stimulate those T cells and make them angrier and more attracted to kill and attack those cancer cells? In my mind, that’s what CAR T-cell therapy is.
The whole process starts by taking out your T cells. We do that as a part of an apheresis process that happens in the clinic or in the hospital. Those T cells are sent off to a company that will take those T cells and reengineer them in the lab to become CAR T cells. Those T cells that are now transformed will attach to a CD19 spike on a lymphoma cell.
The whole process takes about two weeks. The CAR T cells are infused back into the body. They have this new protein on the outside of their cell called chimeric antigen receptors (CARs). They go into the body and attack the lymphoma cells. It’s pretty amazing technology.
The data shown with diffuse large B-cell is that you can get a 40% long-term remission rate in patients who have had prior treatment but now the lymphoma has come back. Those are amazing results and Robyn is a testimony to that.
The downside is it takes a long time. This is a process and you have to wait. There’s also the issue of insurance authorization. Medicare pays for these treatments, but insurance companies take a long time. You have lymphoma that’s growing in your body and we have to wait to get this whole process done.
It requires you to take other treatments, like lymphodepleting chemotherapy, to control the lymphoma before we can get the CAR T-cell process done. Once you collect the cells, it takes about two weeks to get them back. It could take up to six weeks from the time you meet until infusion day.
There’s a lot of thought about how we can make this process better. The companies that make these products are telling us that 8 out of 10 patients who are eligible aren’t getting CAR T-cell therapy. Maybe they don’t live close to a big academic hospital center or it takes too long and their cancer is growing too quickly.
A lot of the research is focused on making the process faster. Can we create CAR T cells in the lab so we don’t have to go through this whole process? That’s what we’re looking to talk about down the road.
The goal has also been to see if we can lower the intensity and the incidence of CRS and neurologic toxicities.
Dr. Nilanjan Ghosh
Side Effects of CAR T-cell Therapy
Robyn: Dr. Ghosh, you have spearheaded CAR T-cell therapy in Charlotte, did the first cases, and have a lot of experience. I would love to have you talk about the side effects of CAR T-cell therapy.
Patients are terrified of the CRS and ICANS. Meanwhile, they’re not as terrified of a stem cell transplant, which has more side effects. How you do you manage the side effects? What kind of results have you seen with CAR T-cell therapy?
Dr. Ghosh: We have had significant experience with CAR T-cell therapy at our center because we participated in some of the clinical trials, which led to the approval of CAR T-cell therapy. It’s certainly a learning curve on how to manage CRS and ICANS.
When we think about CRS, these are serious side effects, but what’s important is these are reversible for the most part. Some clinical trials report very high rates of CRS and some even with ICANS. Most of these happen early on and within a few days of receiving CAR T-cell therapy.
They are managed with a team of physicians, nurse practitioners, nurses, and pharmacists who are very, very in tune with how to manage these side effects. We also have help from ICU doctors, neurologists, and infectious disease specialists, so it’s a team approach.
Each grade of CRS and ICANS has its own treatment. As the grade goes higher, treatments can intensify. The mortality from CRS and ICANS is extremely low. The reversibility is extremely high.
CAR T-cell therapy is underutilized because of the fear of side effects, but the potency which it has far outweighs the risks associated with it
Dr. Nilanjan Ghosh
CAR T-cell therapy has a 40% long-term remission rate and, more importantly, it’s a one-time treatment. You come in, get three days of lymphodepleting chemotherapy followed by a couple of days rest, get the CAR T cells, and then a week of monitoring for CRS or neurologic side effects. If nothing happens, then you remain outpatient. If they happen, then we treat them and reverse them, then monitor for infection risk after.
The treatments can include acetaminophen, fluids, oxygen, steroids, and other drugs, like tocilizumab and anakinra. What we have seen is by doing these measures and being aggressive in terms of treatment, these side effects are reversible.
The goal has also been to see if we can lower the intensity and the incidence of CRS and neurologic toxicities. There are drugs which can be used. For example, prophylactic steroids can sometimes lower the intensity of CRS and that has already been approved. There are multiple ways, but if you have a team who has been doing it for a while and can react immediately, the side effects can be managed.
Another side effect, which is not very common but very important to address, is macrophage activation syndrome or HLH (hemophagocytic lymphohistiocytosis). Again, that is also managed with medications. We are able to recognize it early by monitoring things like ferritin and other markers as well.
I feel that CAR T-cell therapy is underutilized because of the fear of side effects, but the potency which it has far outweighs the risks associated with it, especially now that it’s been so long and we’ve been able to manage the risks in a relatively protocolized manner.
Be aware of side effects, but don’t be freaked out by them.
Dr. Nilanjan Ghosh
Robyn: My therapy was pretty much outpatient. I think that some of the treatments are drifting toward outpatient until you actually need to be inpatient, which decreases your risk of infection and increases your quality of life. My understanding is that a lot of hospitals are trying to move toward that, but it depends on the type of CAR T and also the patient.
Dr. Ghosh: The patient and caregiver. Another very important thing for CAR T-cell therapy is you need to have a caregiver. If someone is having confusion, you need a caregiver if you’re outpatient to be able to call and say that there’s something wrong.
Even in an outpatient setting, for the initial part, there are very frequent follow-ups, almost daily, so distance from the center can be an issue. If someone lives close by, you can do it outpatient. If someone lives far, it may be hard to go back and forth. We are working very hard to try to overcome barriers to CAR T-cell therapy.
Be aware of side effects, but don’t be freaked out by them. If CAR T-cell therapy is right for you, go for CAR T-cell therapy at a place where they know how to manage these side effects and get the benefits.
The first person to ask about trials would be your physician, but no matter how good the physician, they won’t know about all the trials in the United States and the world. Another resource is ClinicalTrials.gov, which is what my husband and I utilized when we were looking for a trial though it’s a little bit harder to navigate. Trials are accessible, but you have to be your own advocate to some degree.
Dr. Ghosh: For anyone who has barriers to clinical trials, remember that we would not be here today if not for clinical trials. Even CHOP came through a clinical trial, which was started in the early 70s. Everything came through clinical trials.
Robyn: Again, I’m an example. I was one of the first who got CAR T-cell therapy through a clinical trial. I’ve told other patients that sometimes, the best treatment you can receive is through a clinical trial.
Dr. Ghosh: Cancer clinical trials don’t compare a cancer drug and a placebo. They have a well-established cancer regimen and may add one drug to it, but those who are not getting the study drug get the best established cancer regimen. Unlike other diseases where you can get a placebo versus the study drug, this is a serious, life-threatening disease so you’re either getting the standard of care or the new promising drug. If it’s a phase 1 or phase 2 study, everybody gets the same treatment.
Robyn: Ina lot of trials, patients have been through all these standard treatments. They may have had CAR T-cell therapy or BiTE therapy then the lymphoma comes back. What do you do? That’s where these companies are on the cutting edge of developing newer treatments.
Cancer clinical trials don’t compare a cancer drug and a placebo. They have a well-established cancer regimen and may add one drug to it, but those who are not getting the study drug get the best established cancer regimen.
Dr. Nilanjan Ghosh
TRANSCEND FL
Robyn: I know some people who are in the TRANSCEND trial for follicular lymphoma. There’s a lot of people enrolled in that. From what I’ve seen from the data from ASCO, it looks like it’s very successful.
Dr. Ghosh: TRANSCEND FL took patients with relapsed/refractory follicular lymphoma and treated them with liso-cel. It’s been reported and has fantastic efficacy with very high complete response rates in the 90s.
The follow-up is not very long, so that’s one downside, but the FDA is doing a priority review to see if this is good enough that it should get approval in follicular lymphoma. It also has been done as second-line treatment and that has very, very good activity in the second-line setting.
SWOG S2114
Dr. Ghosh: Remember we said that 40% patients with large B-cell lymphoma will get long-term remission after CAR T-cell therapy. What about the other 60%? We always have to think about the people who didn’t benefit. We have a great example of benefit right here, Robyn, but there are others who didn’t.
Complete remission is the most important thing for diffuse large B-cell lymphoma. What about people who get partial remission or stable disease and it didn’t grow? That’s not good enough because within a few months, many of those patients will progress. What if you can intervene before that with bispecific antibodies and polatuzumab?
This S2114 study is a trial which is trying to improve the outcome of patients who are in partial remission or have stable disease by adding drugs post CAR T-cell therapy and trying to see if they would benefit and convert them into complete remission. This is a national trial and we have it open at our site as well.
ELARA
Dr. Ghosh: The ELARA study is looking at tisagenlecleucel for relapsed/refractory follicular lymphoma. This is showing high response rates, low CRS, low neurotoxicity, and durable remissions. Now with three-year follow-up and showing that nearly close to 60% of patients are in remission.
This is a one-time treatment given three years ago and patients are still in remission. Many of those patients are in that POD24 group, where they had progressed within 24 months, so their first remission was two years and now the second remission has been lasting for three years. I hope the remission will last for 5, 7, 10, 15 years, but only time will tell. That’s where whether it’s curable or not will come in for follicular lymphoma.
A lot of companies are developing CAR T cells in the lab that are engineered so they can go in and attack the lymphoma cells, but the body’s immune system won’t attack them and kill them.
Dr. Justin Favaro
Other Clinical Trials
Dr. Favaro: It’s exciting to see CAR T-cell therapy patients in follicular lymphoma and seeing long-term responses. That’s a disease that tends to relapse over and over.
Robyn: People can go on with their life.
Dr. Favaro: The other trials I do like are looking at CAR T-cell therapy patients who don’t have a complete response. Let’s bring in BiTE therapy for those patients as well to try to get them into complete response.
We’re part of a national network of cancer clinics called OneOncology and some of our clinic sites are looking at doing outpatient CAR T-cell therapy. There are different products that are now approved. Liso-cel is one that has the least side effects and is the most predictable.
In outpatient clinics in the OneOncology network, we’re doing CAR T-cell therapies and watching them as an outpatient. They can be watched for four days. It’s pretty predictable that at day four is when a lot of the side effects happen for that particular product.
That’s one example of how we’re moving things more toward the outpatient by monitoring patients while they’re at home. If it’s day four and the patient is starting to have side effects, we bring them in, keep an eye on them for a few days, take care of the side effects, and send them home.
There are a lot of companies developing new CAR T-cell therapies. Why do we need to take the T cells from the patient, reengineer them, and put them back? What about taking regular cells? You can take a culture of human cells and, believe it or not, take stem cells and turn them into T cells in the lab.
A lot of companies are developing CAR T cells in the lab that are engineered so they can go in and attack the lymphoma cells, but the body’s immune system won’t attack them and kill them because these are foreign cells to the body.
One of the other trials happening in the OneOncology network is using allogeneic CAR T cells, meaning they come from a different person. They’re engineered in a way to help your body accept them and see if you can get a response.
Multiple companies are doing this and, in some cases, these are patients who have been through everything. We get a response and a reduction in their lymphoma by using these foreign cells created in a lab. To me, that’s where the future is: looking at this in the outpatient setting and having it ready for the person when they need it.
Robyn: It’s also less costly because it’s technically off the shelf, which should be excellent.
Treatment Sequencing
Robyn: At some of the meetings, people still talk about bispecifics versus CAR T-cell therapy and in which order. We talked about bispecifics after CAR T-cell therapy. Some people are saying bispecifics should be done before CAR T-cell therapy.
Dr. Ghosh: CAR T-cell therapy came first. Outside of blinatumomab, which was for ALL, most of our DLBCL and follicular bispecifics came later. Naturally, by the time bispecifics were available in trials, CAR T-cell therapy had already been around. We know that after CAR T-cell therapy, bispecifics are very active, but what we didn’t know was the reverse.
Recently, a European study was presented and showed that if you use bispecifics before CAR T-cell therapy, you can still get really good activity from CAR Ts. On that study, bispecifics failed a lot of patients so they went on to get CAR T-cell therapy, which was then effective.
In the United States, bispecifics are not approved in the second-line setting, while CAR T-cell therapy is, so undergoing CAR T-cell therapy before bispecifics makes a lot of sense. We don’t have long-term data for bispecifics in the second line but we do have data saying that if it didn’t work, at least CAR T-cell therapy may be able to rescue those patients.
That was a very good study. Overall, we do great in oncology in terms of getting new drugs approved, but we don’t do a great job in sequencing them. That’s left a lot to the physician in discussion with the patient because not everything from the menu is going to be available or accessible right away.
With disease, you may have to do something right away because you can’t wait for six weeks or so to get CAR T-cell therapy. If CAR T-cell therapy is available, then you may want to wait and do the bispecifics later.
In DLBCL right now, I would do front-line treatment of CAR T-cell therapy and bispecific antibodies. In follicular lymphoma, you could do the reverse. It’s a more indolent disease. We don’t know about curability as much. We know that mosunetuzumab works well in relapsed/refractory follicular lymphoma. You have long-term remissions and you could save exa-cel or tisa-cel and, if liso-cel does get approved, then liso-cel for later.
As we are seeing longer data, you have to think: do you want to be on a treatment where you are coming in frequently versus getting a one-time treatment? The treatment where you’re coming in frequently has lesser side effects than the one-time treatment, so it’s a discussion.
Will clinical trials ever be done to answer the sequencing question? I don’t know. I think we’ll learn over time. What will matter is the side effects and the durability of the response. Any response which is durable will be higher in the flowchart compared to the ones where relapse will happen sooner.
Folks who’ve gotten chemotherapy upfront are often left with life-limiting or daily activity-limiting side effects, like neuropathy, so it’s extremely exciting to have this option of chemo-free treatment without long-lasting side effects.
Dr. Kulsum Bano
Possibility of Chemo-Free Cancer Treatment
Robyn: I’ve been in medicine for a long time. When I trained in medicine, oncology was still relatively barbaric, I would say. Chemotherapy and cancer treatments involved cutting, burning, and poisoning. Way back in the 80s, they didn’t even have antiemetics or ports, so giving people doxorubicin was difficult to say the least.
We’ve progressed dramatically. Oncologists have found ways to decrease nausea and take care of neuropathy, but the side effects are still there. Do you see chemo-free treatment of cancer in the future? Perhaps in the next 10 to 15 years?
Dr. Bano: I think that’s the direction we’re slowly heading in. A lot of these trials are slowly moving treatments that were thought to be more exciting and more novel approaches from the fourth to the third, to the second, and then slowly into the front-line setting. That happens over time because the more we learn, the more experience we have with all of these wonderful patients who’ve been on trials and given us this knowledge.
As a community oncologist, that’s extremely exciting because I hope to see patients for years to come who are going to be disease-free and who’ll just be monitored. Folks who’ve gotten chemotherapy upfront are often left with life-limiting or daily activity-limiting side effects, like neuropathy, so it’s extremely exciting to have this option of chemo-free treatment without long-lasting side effects. People are going to live longer with these disease-free intervals. It’s very exciting and hopefully that’s where we’re headed.
Dr. Favaro: I think it’s a combination of things. If you look at chemotherapy, these are chemicals that kill fast-growing cells and that’s pretty good against lymphoma. These often are fast growing, especially diffuse large B-cell lymphoma, so it’s been very active treatments that have put people into long-term remission. But the downside of chemotherapy is the potential long-term side effects plus it’s harder to go through, so what can we do?
Cancer cells are complicated. We’ve got the DNA inside the cell, which has 30,000 genes and over 100 probable mutations in those genes. You’ve got all these crazy proteins in the cell. A lot of them are active and helping the cell grow. Then there are the different spikes outside of the cell.
You have to think about how you attack not just one protein or one spike but multiple targets. A trial I mentioned took a BTK inhibitor and attacked the protein inside and had a couple of drugs attacking the spikes on the outside. That’s probably where we’re going to head to avoid treatments that are so toxic.
Multiple targeted agents is the way to go. For example, with BiTE therapy, we know what happens with those patients. It’s very effective pretty early, but what’s going to happen down the road? Will there be a potential risk of the cancer coming back?
You’re taking the T cell, bringing it to the cancer cell, turning that T cell on, and killing the cancer cell. But over time, those T cells get tired, which is something called T-cell exhaustion, and don’t want to work as well. Sometimes it’s as simple as giving people a break from treatment to let their T cells recover.
But the other thing I think that we’re going to head toward down the road is limited duration therapy but baking something in. You give BiTE therapy, but because we know the T cells can get exhausted, we need to add in another targeted therapy to kill some of those proteins and give 2 or 3 of those for a limited duration. I hope that’s where we end up to finally wipe out the disease for good.
Improving Access to Cancer Care
Robyn: One of the things that all of us as doctors are focused on is access to care. In my case, there was no CAR T-cell therapy offered nearby. My oncologist here had to coordinate with an oncologist who was in a trial in Ohio and my team in Charlotte did a fantastic job. Dr. Ghosh, what do you do in the academic center to reach out to community doctors? How do we improve access to care?
Dr. Ghosh: Late 2017 is when we moved forward with signing up for the TRANSCEND study, which eventually led to approval. Once we signed up for the study, we were the only center in all of North and South Carolina to offer CD19 CAR T-cell therapy before any other center. We got patients from everywhere in that study.
Access is certainly a very, very big issue for CAR T-cell therapy. It becomes even bigger because you need a caregiver. How do we overcome some of the socioeconomic barriers? The caregiver would have to take some time off. Typically, we need patients to be within a one-hour radius, so they would need local housing.
The first part of access is providing education and understanding the benefits of CAR T-cell therapy and referring the patients in a timely manner. It could take up to 6 to 8 weeks to get CAR T-cell therapy, so if you wait for the referral, then it may not be doable because the disease will take off. Early referral is extremely essential for CAR T-cell therapy.
There’s a lot of fine-tuning involved, so the team together with the patient decide what’s best. We try to do this in a really timely manner.
Dr. Nilanjan Ghosh
Patient navigation can be very helpful to help find resources, whether it’s local housing or any type of support. I think that’s essential.
Insurance can be a barrier, especially in terms of single-case agreements, but we are trying very hard. We have a study in which we are looking at the effect of these insurance problems on patient outcomes, so that is a barrier we’d like to overcome. Some barriers are within our control, some are not.
There are ways to control the disease. Giving the right treatment is very important. For example, we have learned that if you give bendamustine, then that can mess up your CAR T-cell therapy. Bendamustine kills T cells, so if you kill T cells before you collect them, then those T cells aren’t going to work. Either you won’t have much or if you have enough, they may not be as functional and not be able to do the job.
What is the right treatment to use if you’re planning to do CAR T-cell therapy? There are so many available. Do you want to modify your regimen somewhere so that you can control the disease but perhaps not kill all your T cells before you collect them? Do you want to wait? But if you wait, then the disease may take off and that may not work.
There’s a lot of fine-tuning involved, so the team together with the patient decide what’s best. We try to do this in a really timely manner. We coordinate very well with all our regional sites within the Levin Cancer Institute as well as beyond.
The bigger challenge is those who live far away. Do they want to come to Charlotte to get CAR T-cell therapy or would they rather not do it because it’s not feasible to come? That’s where eventually having outpatient CAR T-cell therapy done locally comes in and having the expertise to manage the side effects if they happen.
We have more CAR T-cell therapy centers today than two years ago. I hope it keeps getting better and better so that more patients all over get access to this treatment.
We also don’t want to have the treatments in an environment where there isn’t the expertise to manage the side effects because then it becomes very hard. Somebody who came in for a potential curative disorder and perhaps were going to be cured succumbed to the side effect because the team was not able to manage them. That wouldn’t be right either.
The other part of it is coming up with protocols to lower the incidence of side effects without compromising efficacy. This is where the clinical trials of some of the products that have less CRS and less ICANS come in. Not zero, unfortunately. I don’t think we’re going to get there.
Infections can be there, but we know how to manage them. Please communicate quickly so that they can be managed appropriately.
Dr. Nilanjan Ghosh
Robyn: Zero is impossible. What if there are trials at Memorial Sloan Kettering in New York or MD Anderson in Texas? The idea is that people can follow up with their local oncologists.
Dr. Ghosh: After the CAR T-cell therapy. It’s a one-time treatment.
Robyn: That’s what happened in my case. Sometimes you have to go somewhere else for treatment or to join a trial and then do follow-up blood work and scans locally to make it more convenient for the patient.
Dr. Ghosh: The most important thing for CAR T-cell therapy is that there are two side effects that can persist after being discharged.
One thing to watch out for is low blood counts, which is an important one and can persist for a little bit of time. For the most part, that’s because of the lymphodepleting chemotherapy given prior. But sometimes, if patients have had many prior treatments, low blood counts can also be because now they’ve developed MDS (myelodysplastic syndrome) or a pre-leukemia situation.
It’s important to pay attention to the low blood counts to see if it’s getting better or persisting for a very long time, then looking at the bone marrow to see if they have developed something else because there are other reasons for low blood counts other than CAR T-cell therapy.
Second is infection risk. CAR T-cell therapy takes out the B cells because normal B cells also express CD19. You can check immunoglobulin levels and give IVIG. Vaccine responses also go down, so if someone had a vaccine for flu or COVID, they may not be able to respond well, so people become prone to infections.
Patient education is very important as well as letting your doctors know. I always advise patients that if they have a cold or something, reach out to their doctors first. Many times, we would react to it faster. We won’t give a Z pack for a cold. We’ll get them in, get a swab, check what virus is there, and check the immunoglobulin level.
Give them antivirals, if antivirals are available. Give them IVIG, if the IgG is low to help them overcome that infection. Get some imaging needed to see if there’s pneumonia. When the immune system is low and you get a virus and sit on it for some time taking an antibacterial, which is not going to work because it’s not a bacterial infection, it can get worse.
We educate our patients that infections can be there, but we know how to manage them. Please communicate quickly so that they can be managed appropriately compared to some other person who is not as immunocompromised.
Final Takeaways
Robyn: This has been a great discussion. If there’s something you would like to tell the people about diffuse large B-cell lymphoma and follicular lymphoma, treatments, and the future, what final statements would you like to give?
Dr. Favaro: There is so much to learn for patients and doctors. These new treatments come out and it’s our job to learn about them. CHOP came out in 1976. It was our job to learn how to give it and also how to manage any side effects that come up. That’s the same with CAR T-cell therapy.
Quite frankly, 4,000 papers come out every day in health care. There’s a ton of information coming out. We are constantly learning and educating patients about these new treatments.
The cooperation that we have as a community practice with academic centers is very important. When we see patients who need CAR T-cell therapy, we refer them and take them back to help manage potential side effects. The technology that’s advancing to make these treatments less toxic is key. We used to have to admit patients overnight for epcoritamab, for BiTE therapy; now we can do it all as an outpatient. That’s the type of thing that’s happening on a daily basis.
Physicians will never go away. We are here because we know you. We take care of you as a person, but we are going to see more and more about artificial intelligence coming into health care. It’s happening. We do need to look at that and embrace that.
Somebody comes in with lymphoma. What should their treatment be? There are so many different factors: age, personal health, disease, potential treatments, and side effects. It takes a good physician to understand the data. But over time, there probably will be the development of assistance to doctors with artificial intelligence and neural networks that I think will help. There are journals about AI in oncology and I think this is going to be the future for health care as well.
Dr. Bano: None of us in medicine work in a vacuum. It’s a concerted effort getting these patients to the most advanced treatments out there. In the community, our responsibility is to know that these even exist and to maintain that chain of communication with the academic centers to get our patients the care that they need, but we always serve as home base. We give patients the feeling that, yes, we’re sending you away, but you’re always going to come back and we are here to take care of you for years to come.
It’s always been a great collaboration between community and academics, getting that relationship established, and always having that chain of communication to ask questions and get opinions. It doesn’t always have to be advanced therapy. Sometimes you get a challenging case that you want to discuss with someone who has seen something like this before.
It’s very exciting to see what’s on the horizon. It’s exciting to see what we can do for our patients. It’s a learning process. Every day, we learn something new.
In the community, our responsibility is to know that these even exist and to maintain that chain of communication with the academic centers to get our patients the care that they need, but we always serve as home base.
Dr. Kulsum Bano
Dr. Ghosh: I cherish the community-academic partnership. I’ve cherished that over the years. That helps patients to get their treatment locally but also get access to a specialist who treats that disease. When I started, lymphoma treatments were not as effective but were simple. You get the first line, another option for the second line, then after that, there were 1 or 2 options and that’s it.
Now, there are a lot of options. When you have so many options, each with their unique side effects and sequencing is not worked out, how do you know which is best for you? There are so many intricacies. If you use this, then the next treatment could be a problem.
Trying to find the right option, keeping abreast of what comes out, and keeping pace with how this is moving along can be challenging. That’s where the academic-community collaboration can be very good. Patients can always go back to the community to get their treatments, have access to a new clinical trial or the latest treatment, and have really good care.
I encourage participation in clinical trials, knowing that these are ethical and vetted by institutional review boards. That is how we have come to where we are and I hope that we get into more chemo-free treatment options.
Some chemo is still very effective. I would not say anthracyclines have saved many lives. They have been around for 50 years, but if we can achieve our goal with less toxicity and by harnessing the immune system, that would be fantastic.
Robyn: I’m honored to be here. Shout out to The Patient Story and the unique ability of patients to get their voice out and for people to do their research online. As a physician and a former patient, it’s very important to be your own advocate, to research, to ask questions, and to keep your mind open. Sometimes clinical trials are the best treatment, so do consider them.
Consult with your doctor. It’s okay to get a second opinion at some points. Medicine has come a long way. When I first started, there was not much available. The survival rate for non-Hodgkin’s was about 30-40%.
I hope that everyone gets treatment and gets in remission like myself. At that point, you need to live your life. Enjoy your family, travel, work, stay healthy, and exercise. Don’t let cancer define you. It’s part of you, but there’s much more to you, so enjoy life.
You need to be your own advocate. If you feel like something that’s been recommended is not working for you, you have all the right to get a second opinion.
Dr. Kulsum Bano
Q&A
Getting a Second Opinion
Robyn: Joan asks, “What is the polite way to get a second opinion without being rude?”
Dr. Bano: Very rarely are there egos in medicine. As a physician, you try to make the best decision for your patient knowing that there may be something out there that is newer or better. Everyone is entitled to a second opinion and that’s how we learn more.
If somebody comes back to me with a different treatment approach and says somebody else recommended this, that’s something I would definitely encourage. You need to be your own advocate. If you feel like something that’s been recommended is not working for you, you have all the right to get a second opinion. You’re not being rude at all. You’re entitled to that and it’s actually encouraged if that’s what you feel is right for you.
Robyn: I agree. Even in radiology, we get asked for second opinions all the time. Doctors are human. We are not perfect. We can look at the same case and have different opinions. We’re not insulted. We’ve all been trained to work together and I would say that happens 99% of the time. There are always exceptions.
If you look at the commonly used CAR T-cell therapy, the complete response rate is much higher than the complete response rate for epcoritamab.
Dr. Nilanjan Ghosh
Epcoritamab vs. CAR T-cell Therapy
Robyn: Don asks, “I’m on epcoritamab. We considered CAR T-cell therapy, but wouldn’t be able to provide the 24/7 care required. So far, it’s working very well. How does it stack up compared to CAR T-cell therapy?”
Dr. Ghosh: They have never been compared head to head, so there is currently no clinical trial which takes half the patients and gives them epcoritamab and half the patients get CAR T-cell therapy. The best way to compare two groups of patients is if they were randomized on a clinical trial, had similar characteristics, and then followed over time to find out the effectiveness of one versus the other.
If not, you’re comparing across trials and when you do, it’s flawed because the patients who went for epcoritamab may have very different characteristics than the patients who went for CAR T-cell therapy. In fact, many patients who went for epcoritamab on a clinical trial already had CAR T-cell therapy, so how could you compare the effect of CAR T-cell therapy with a drug used for post-CAR T-cell therapy failures?
Having said that, we are left with no choice but to compare across trials. I will say that if you look at the commonly used CAR T-cell therapy, the complete response rate is much higher than the complete response rate for epcoritamab. Epcoritamab is around 40%. CAR T-cell therapy complete response rates are usually in the 50s to 60s.
That being said, it comes down to the 40% number because even if CAR T-cell therapy gets a higher complete response, some people will start relapsing despite getting a complete response. We know that with CAR T-cell therapy, about 35 to 40% people will have long-term remission.
We don’t have long-term data yet with epcoritamab. The complete response rate is 40%, but some of those will progress over time. We don’t know whether it will go down to 30% or 25% as we go up to five years, but we will find out over time.
At this point in time for DLBCL, we feel that CAR T-cell therapy is better, but if it’s not feasible, bispecific antibodies would be the next best option. The important thing is: are you getting complete remission or not? If it’s complete remission, we see long-term sustainability. If it’s not complete remission, then we start seeing early progression.
Epcoritamab is targeting CD20 and CAR T-cell therapy is targeting CD19 — two very different ways of attacking the lymphoma. CAR T-cell therapy is still a great option for those who choose epcoritamab for whatever reason.
Dr. Justin Favaro
Dr. Favaro: Another point is that a lot of patients on the epcoritamab trial had CAR T-cell therapy before. If you have somebody who’s never had CAR T-cell therapy and you had the option of CAR T-cell therapy or BiTE therapy, which one do you choose if you’re eligible for both?
It comes down to logistics and what’s going to be a good fit for you. Keep in mind that if you would need CAR T-cell therapy later, you can still get it because a study at ASH 2023 showed that if even if you had BiTE therapy before, you’re still eligible to get CAR T-cell therapy later.
Epcoritamab is targeting CD20 and CAR T-cell therapy is targeting CD19 — two very different ways of attacking the lymphoma. CAR T-cell therapy is still a great option for those who choose epcoritamab for whatever reason. You can still have a great outcome. It doesn’t necessarily matter how you sequence it.
The hope is that whatever treatment you’re getting works for you and you won’t need anything else. But if you do, there are options available and there will be even better treatments in a few years.
Dr. Nilanjan Ghosh
Robyn: If for some reason this doesn’t work and you decide to get CAR T-cell therapy, a lot of the hospitals have come a long way with helping people get 24/7 care. There are options. Hopefully you won’t need them since epcoritamab is working well, but know that there are things that the hospitals are now aware of and they’re trying to assist patients with those.
Dr. Ghosh: There are many devices coming out for 24/7 monitoring, especially in the outpatient setting. Companies are coming up with devices to monitor your oxygen level, heart rate, and temperature then feed them back to the electronic medical record and create alerts. At least from the standpoint of vital sign monitoring, people are trying to overcome this barrier.
Understand that 24/7 support, even if it is for a short time, is a lot for a caregiver, especially if the caregiver has to work. You can rotate caregivers. You don’t need to have just one. Most places will allow multiple caregivers.
Epcoritamab is a good option if you’re not able to do CAR T-cell therapy. You can still have very long remission and perhaps not need further treatment ever again. The hope is that whatever treatment you’re getting works for you and you won’t need anything else. But if you do, there are options available and there will be even better treatments in a few years. Maybe allogeneic CAR Ts will hit a big wave. We don’t know yet, but we’ll find out.
Dr. Favaro: That’s the advantage of getting BiTE therapy upfront. If you need something later, it may be a lot easier with a lot fewer side effects and it can be done as an outpatient. With epcoritamab, you can get steroids and don’t need to be in the hospital. As we make more progress with CAR T-cell therapy, maybe we can do that as an outpatient to reduce severe side effects. Sometimes there’s an advantage to waiting as the technology advances.
Dr. Ghosh: If it’s accessible, knowing the track record of CAR T-cell therapy and that now we have five-year data, we still like to sequence CAR T-cell therapy before bispecific antibodies. Over time, we’ll find out if things change and do it in reverse.
Remission After Bendamustine & Rituximab (BR)
Robyn: Diana asks, “What is the median length of remission after the first B&R treatment”
Dr. Ghosh: For which disease?
Robyn: I would assume it’s follicular lymphoma, but we don’t know what stage. Let’s assume it’s stage 2.
Dr. Bano: If it’s stage 2 follicular lymphoma, generally you have a sustained response after B&R treatment. We’re looking at about five years or so. We need more information to answer that question appropriately.
Dr. Ghosh: It may also depend on whether rituximab maintenance was used. It could be a little bit different with maintenance versus without. I’ve even seen patients who are 10 years out after bendamustine and have not relapsed. Some people will relapse, so it’s a whole spectrum.
There are treatments now that will attack both follicular lymphoma and the transformed lymphoma, so sometimes you want to harness that.
Dr. Nilanjan Ghosh
Possibility of a Repeat Transformed Follicular Lymphoma (tFL)
Robyn: “If you have follicular lymphoma that transformed into diffuse large B-cell, went into remission after treatment, but a few years later, the follicular lymphoma came back, what is the probability that this will transform again?”
Dr. Ghosh: With indolent follicular lymphoma, there’s a small percentage of transforming every year. As more years go by, that risk accumulates. If it’s already happened, will a second transformation happen? It’s possible, but the likelihood goes down because it’s a random event.
Is it a relapse of the previously transformed follicular lymphoma? That’s hard to sort out, but usually what happens with the transformed disease, if the transformed disease has been in remission for a long time, that’s an aggressive lymphoma and usually, aggressive transformers respond well to whatever the treatments were given to them, especially since long-term remission was achieved.
The likelihood of what comes back is often the indolent lymphoma and we see this sometimes with transplant. I had a patient who had follicular lymphoma, had treatment, had a relapse of the follicular lymphoma, had another treatment, then her lymphoma transformed, and we gave her transplant for that. Years later, the aggressive transformed lymphoma went away and she had a relapse again, but this time, it was back to follicular. The aggressive lymphoma never came back. What we did at the time was CAR T-cell therapy for the follicular lymphoma.
There are treatments now that will attack both follicular lymphoma and the transformed lymphoma, so sometimes you want to harness that. For example, axi-cel is approved for follicular lymphoma and for DLBCL. When you use a treatment like CAR T-cell therapy, you are basically killing both. Ultimately, it’s all coming from one B cell. It may be transformed, but if you attack that B cell clone, then both the low-grade and the high-grade can go away. Similar with bispecific antibodies. They attack both. Many of the treatments we use now, especially some of the more modern treatments, have activity against both follicular lymphoma as well as the transformed component.
The fortunate part about lymphoma is that you can target lymphoma cells. You will deplete your own B cells, but we can mitigate that.
Dr. Justin Favaro
B-cell-based Immunotherapy
Robyn: “CAR T-cell therapy is a great new treatment, but as I understand, it targets all B cells and not just the cancerous ones, leading to a depleted immune system that can last a long time. Is there any current research on a similar immunotherapy treatment than can identify and attack the cancer cells and not the normal B cells?”
Dr. Ghosh: That would be something we would love to have. We are fortunate that we have been able to identify antigens. Dr. Favaro mentioned those spikes. Imagine if those spikes were not only in B cells but in liver cells, heart cells, and kidney cells, then CAR T-cell therapy would go and kill all of those.
Fortunately, this is what we can get away with as CD19 is expressed only in B cells but not in other normal tissues — not even on T cells or other parts of the immune system. Many other diseases don’t have that. We are starting to work with some solid tumors which have these, but it’s been difficult. Even in diseases like acute myeloid leukemia, you don’t have things that are specific to that cell.
With B cells, you’re more prone to infections, but you can still get IVIG, which is a immunoglobulin supplementation to help reduce your risk for infections. We currently don’t have spikes on the surface of just cancerous B cells but are absent on normal B cells, but that would be something which I hope the future researchers can identify.
Robyn: I believe there are studies that show B cell recovery over time. A lot of people will gradually recover and it doesn’t affect their remission rate. Everyone is unique. Some people with low IgG can get infections, some people do fine. There are patients who haven’t had CAR T-cell therapy who have primary B-cell aplasia and do fine and a lot of them don’t need IVIG. It’s a case-by-case situation. Most people have had some infection, but most people have been fine and living a normal life even without IVIG.
Dr. Favaro: The challenge with the solid tumor CAR Ts that they’re trying to make right now is finding the antigen on the lung cancer, for example, that won’t damage or destroy the lung. The fortunate part about lymphoma is that you can target lymphoma cells. You will deplete your own B cells, but we can mitigate that with prophylactic antibiotics, IVIG if needed, and taking precautions so you can still live your life.
Masking, especially if you’re in a crowded area, and frequent hand washing would be advisable. As more time passes, those restrictions start coming down a lot.
Dr. Nilanjan Ghosh
Post-CAR T-cell Therapy
Robyn: Michael asks, “What are the overall risks as far as activities, food, etc., for post-CAR T-cell therapy patients?”
I have not been avoiding anything for many years, but I’m eight years out at this point. There are initial precautions because a lot of people have low ANC (absolute neutrophil count) and some other depletion.
Dr. Ghosh: Right after CAR T-cell therapy, blood counts are low. Sometimes we even need to give growth factors to improve blood counts. The risk is going to be higher in terms of infections initially than a few months out. If the blood counts recover, especially neutrophil counts, then certain infection risks go down.
B cells always take time to recover. As the lymphocyte count recovery takes longer, your immune system is compromised and that’s where the possibility of viral infections happen. Masking, especially if you’re in a crowded area, and frequent hand washing would be advisable. As more time passes, those restrictions start coming down a lot.
Ultimately, you have to live your life, but still be cautious. If you do get an infection, then alert your providers so they can do some tests to find out if it’s a mild infection or something that needs to be worked up or treated.
In terms of food, you have to take certain precautions in terms of raw food while your neutrophil count is low, but that typically happens in the immediate post-CAR T-cell therapy phase. As more time goes, those usually are not an issue.
Robyn: You need to have a team take care of you. Your oncologist will move out of your realm because they have people who are very sick to take care of. I do encourage everyone to get an internist or an immunologist who can take care of the day-to-day.
Second CAR T-cell Therapy
Robyn: “Does CAR T-cell therapy work a second time if it didn’t keep the complete response the first time?” Can you have a second CAR T?
Dr. Ghosh: Not commercially. CAR Ts are approved once in the commercial setting, but we have clinical trials which will allow a second CAR T. For example, there’s a clinical trial using natural killer cells that are modified to become CARs or chimeric antigen receptor expressing cells. In that clinical trial, we allow patients who have had a commercial CAR T but it failed. Some of the allogeneic CAR T-cell therapy trials will allow patients who have had a previous CAR T-cell therapy.
There are other CAR Ts coming out. For example, we have a CD19/CD20 bispecific CAR T trial, which we are about to open. In that clinical trial, if someone had commercial CAR T, that is probably not allowed because the CD19 CAR T had already failed. But let’s say you have another clinical trial targeting CD22 and people have had the traditional CAR T, now you are using CAR T again but it’s different spikes. If you’re going against a different spike with a clinical trial, that would be doable. But if it’s the same one, then likely not.
The second time will be in a trial unless a CAR T-cell therapy gets approved that allows previous CAR T treatments.
Newer Monoclonal Antibodies
Robyn: Mike asks, “I’m still unsure about some of the things I’ve heard more recently because I don’t know if I have access to them. What about newer monoclonal antibodies? Do they still play a role?”
Dr. Favaro: There are definitely other options out there. Monjuvi is a monoclonal antibody against CD19 that has been looked at in relapsed lymphoma in combination with lenalidomide. Loncastuximab, which is one of these antibody-drug conjugates, is an anti-CD19 with a chemotherapy payload. It’s going to attach to your CD19 spike and internalize the chemotherapy right into that cell. It’s given via IV every three weeks.
These are two really good options for patients who, for whatever reason, CAR T-cell therapy or BiTE are not working or not available. These easily given off-the-shelf and approved by insurance.
When your blood counts are low and you’ve gone through therapy, there’s a risk of fungal infection as well.
Dr. Kulsum Bano
Cannabis & Non-Hodgkin’s Lymphoma
Robyn: “Cannabis and non-Hodgkin’s lymphoma. Are there any benefits?”
Dr. Bano: It’s a question that comes up pretty frequently. There may be some misinformation out there and some misconceptions of prevention of cancer with cannabis, and I don’t think there’s any founded data.
Certainly, people think about it in terms of symptom control. We do have medications that use the cannabinoid derivatives in a medical form, such as dronabinol, that we use for nausea and appetite stimulation for patients who have gone through chemotherapy.
Generally, we discourage smoking of cannabis only because there are a lot of additives that could be associated with it. When your blood counts are low and you’ve gone through therapy, there’s a risk of fungal infection as well.
There’s a lot of unregulated things that we don’t know what we’re dealing with. I don’t think there are any recommendations that can be definitely given. I don’t know that there are benefits per se, but it’s a discussion to have with your physician about what works for you and what doesn’t.
You need a small amount of protein, usually seafood, mostly vegetables on your plate, and some whole grains for carbohydrates. All these things are important.
Dr. Justin Favaro
Keto Diet
Robyn: “Can you speak about the keto diet? Is it effective against cancer? Is it helpful in any way?”
Dr. Favaro: It’s probably the most common question we get as oncologists every day. What can I eat? What should I eat?
My general recommendation is the Mediterranean diet. If you talk to nutritionists and look at the studies, you need several components to your diet. You need a small amount of protein, usually seafood, mostly vegetables on your plate, and some whole grains for carbohydrates. All these things are important.
I believe the keto diet takes out all carbohydrates, so you’re dealing with a lot of protein and a lot of fat. There are downsides of that for the rest of your body. Your cholesterol could go up and that could be damaging to your heart. Your body needs sugar and glucose.
For example, let’s look at a PET scan. What’s lighting up on the PET scan? Besides the lymphoma, it’s your heart and your brain. They need sugar to work. You don’t need sweets all the time, but you need complex carbohydrates. Maybe switch to whole grains and whole wheat pasta instead of white pasta. That’s only a portion of your diet, about 25%. The majority is vegetables and lean protein.
If you look at some of the recent studies that have come out that have looked at who lives the longest with cancer and what diet they follow, the winner seems to be the vegan diet in terms of cancer survival and decreasing risk of recurrence. This is cancer broadly and not lymphoma. But sometimes that’s a hard diet to follow, so a Mediterranean diet is a reasonable diet for most people to follow.
Robyn: Everybody wants control. You want control of your disease.
I have to add: Exercise helps. Studies in breast cancer and prostate cancer — because they’re so much more common and easy to study — showed that even for people who have never exercised before, if they walked 30 minutes a day, they had a longer remission rate and cure rate.
I encourage everyone to exercise. That doesn’t mean you have to do CrossFit because that may lead to shoulder injuries; we see that in radiology. You can do any type of walking or cycling. If you look at other studies, it’s not only the diet. People are active. Get yourself moving.
There have been studies done, not particularly in cancer, that show that insulin resistance is improved with intermittent fasting.
Dr. Kulsum Bano
Intermittent Fasting
Robyn: “Does intermittent fasting help patients with follicular lymphoma or any cancer? Does sugar play any part?”
Dr. Bano: There have been studies done, not particularly in cancer, that show that insulin resistance is improved with intermittent fasting. At any point, when you have dysregulation in your blood sugar control, that tends to lead to other medical complications. There is some role to play in improvement in outcomes. I don’t know that it’s been studied particularly.
Robyn: There are studies with BMI. People who are obese have a higher incidence of all sorts of cancers and have poorer outcomes. There are a lot of reasons for that. It’s multifactorial, but eating healthy and exercise make sense.
R-EPOCH vs. R-CHOP for Triple-Hit DLBCL
Robyn: “Is there any strong evidence that R-EPOCH is better than R-CHOP for triple-hit diffuse large B-cell?”
Dr. Ghosh: This type of aggressive lymphoma is one of the most aggressive variants. R-EPOCH is still considered as the standard of care for this disease based on a lot of retrospective data. There is no clinical trial taking patients with double-hit or triple-hit lymphomas and giving half of them R-CHOP and half of them R-EPOCH.
However, there was a large clinical trial which took all patients with diffuse large B-cell lymphoma and gave half of them R-CHOP and half of them R-EPOCH, and R-EPOCH was not shown to have a better efficacy. They were similar, but it was not really better.
That study was inconclusive in terms of the improvement for double-hit patients. If you ask most doctors, double-hit patients will still be getting R-EPOCH because there’s a lot of good retrospective data showing better long-term responses with R-EPOCH compared to R-CHOP.
We have an ongoing study where we are monitoring different types of cells post-CAR T-cell therapy.
Dr. Nilanjan Ghosh
Patient Group That Benefits More from CAR T-cell Therapy
Robyn: John asks, “We’ve talked about complete response rates and durable remission rates following CAR T-cell therapy. With the much larger patient population, have you seen any trends emerge as to which patients tend to do better in terms of a better response rate, a better complete response rate, as well as a more durable remission with CAR T-cell therapy?”
Dr. Ghosh: People have tried to figure it out. Before you start any treatment, you want to know if this treatment is going to give long-term remission for this person versus someone else. We are not there yet, but we have some ideas. It’s not perfect.
With CAR T-cell therapy, we know that if someone has very bulky disease and fast-growing bulky disease, CAR T-cell therapy will not give great outcomes. Unfortunately, nothing else does so people still go for it, but sometimes you want to debulk while waiting because CAR T-cell therapy is a weeks-long process.
For example, if there’s one site of bulk, we often can do radiation. There are new radiation techniques. One is called “boom boom” where short, very effective radiation is done to shrink the tumors, perhaps even express all these antigens, and have a better kill.
Bulky tumors can often cause T-cell exhaustion quickly so if they get overwhelmed with the tumor, then those T cells can get immune tolerance. There is also a subpopulation of these T cells that can cause immune suppression.
We have an ongoing study where we are monitoring different types of cells post-CAR T-cell therapy and checking them multiple times to see if we can identify patients who might have relapsed and had one type of immune repertoire versus those who had long-term remission and have a different type of immune repertoire.
We presented the initial data at ASH 2023, but hopefully, we’ll do a little bit more analysis on that and try to understand it better. We have samples taken pre-CAR T-cell therapy to see what may be the characteristics of a person that could predict long-term response.
We also have a study with BiTE. We are doing it for patients who are getting mosunetuzumab. We are collecting samples before and after treatment, and trying to identify which type of T cells may be associated with a better response versus a not-so-durable response.
CLL vs. Follicular Lymphoma
Robyn: Tim asks, “Can you define CLL and how it complements follicular lymphoma?”
Dr. Ghosh: CLL is chronic lymphocytic leukemia, which is under non-Hodgkin lymphoma. CLL is circulating disease in the blood. There is a lymphoma component to it called SLL, small lymphocytic lymphoma. It’s essentially the same disease. SLL is in the lymph nodes, CLL is in the blood. If there are more than 5,000 circulating lymphocytes, then it is a definition for CLL. If it’s below that, it’s called MBL, monoclonal B-cell lymphocytosis.
CLL is an indolent form of lymphoma circulating in the blood but could also be in the lymph nodes, spleen, and bone marrow. Like follicular lymphoma, it belongs to the same indolent non-Hodgkin lymphoma group considered as less aggressive.
CLL has tremendous progress where we have given up chemotherapy, so that’s where it’s a little bit different. You heard about R-bendamustine. We used to use that in CLL. In the past, we used to think we could use the same treatment for all indolent lymphoma.
We have relied on targeted treatment, like BTK inhibitors — ibrutinib was the first generation, then acalabrutinib and zanubrutinib, now pirtobrutinib — and then BCL2 inhibitors like venetoclax (VENCLEXTA). These have all come either in sequence or in combination.
Liso-cel got approved very recently for CLL, so now you have CAR T-cell therapy available as well. Chemotherapy was FCR and BR. We don’t really use those anymore. They’ve been shown to be inferior compared to these newer drugs that we have.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Ruth Fein Revell: Hi and welcome to our program, Clinical Trials Update: What to Know in Myelofibrosis Care. My name is Ruth Fein Revell and I’ve lived with a myeloproliferative neoplasm (MPN) for nearly 30 years.
I was diagnosed with essential thrombocythemia in 1995, polycythemia vera about 20 years later, and myelofibrosis in 2018. I’ve also lived with a number of complications from dangerous blood clots and hemorrhages that put me in the ICU to debilitating headaches, bone pain, and extreme fatigue.
I’m a health and science writer and very fortunate to be in a clinical trial for the last four years with amazing results, eliminating my symptoms, and significantly reducing my bone marrow.
We want to note that The Patient Story retains full editorial control of this entire program. This is not meant to be a substitute for medical advice.
Joining us is Dr. Naveen Pemmaraju, a top expert in MPNs and myelofibrosis from MD Anderson. Dr. Pemmaraju, it’s so nice to see you. Thanks for joining us and for being a part of this program. Can you tell us more about yourself and what drew you to MPNs?
Naveen Pemmaraju, MD
Dr. Naveen Pemmaraju: Thanks for having me. I’m a professor of leukemia at MD Anderson in Houston, Texas. I serve as the executive director for cancer medicine and as the director for our rare disease program, including blastic plasmacytoid dendritic cell neoplasm (BPDCN).
Ruth: It’s always great to see you and to speak to you. You offer so much to the MPN community and we really thank you.
JAK inhibitors are not JAK2 mutant-specific inhibitors, so that’s why they work in patients whether they’re JAK, MPL, CALR, triple-negative, or have no mutations.
Dr. Naveen Pemmaraju
Standard of Care: JAK Inhibitors
Ruth: We now have four JAK inhibitors and one one of them was just approved. Walk us through this. First of all, how does a JAK inhibitor work?
Dr. Pemmaraju: The basic premise is that MPN cells signal through a specific pathway called the JAK/STAT pathway.
A regular cell uses the JAK/STAT pathway for normal blood cell growth, differentiation, and lifespan. Now take an MPN cell and that pathway is hijacked and used in a malignant way, so those cells keep growing and dividing. It’s like a light switch that’s turned on that doesn’t go off.
Interestingly, the JAK inhibitors are not JAK2 mutant-specific inhibitors, so that’s why they work in patients whether they’re JAK, MPL, CALR, triple-negative, or have no mutations.
JAK inhibitors are based on the principle that the JAK/STAT pathway and the cells are overactive and not working properly. JAK inhibitors aim to block that malignant activity and restore normal growth.
Ruxolitinib was the first-ever approved JAK inhibitor. Since 2011, three JAK inhibitors have been US FDA-approved: fedratinib in 2019, pacritinib in 2022, and momelotinib in 2023. The four currently approved JAK inhibitors have some interesting similarities and differences.
[Ruxolitinib] works very quickly in relieving the symptom burden for our patients with MPNs.
Dr. Naveen Pemmaraju
Ruxolitinib
Dr. Pemmaraju: Ruxolitinib, the first and longest in class, is a JAK1/JAK2 inhibitor. This drug was simply amazing in the original clinical trials, which were COMFORT-I and COMFORT-II, led by Serge Verstovsek and Professor Claire Harrison.
In those studies, we learned a few things about ruxolitinib. One is that it works very quickly in relieving the symptom burden for our patients with MPNs. It can shrink the spleen rather quickly as well, so quickly that the hallmark ended up being at week 24 by six months.
Some side effects to look out for over time in this otherwise well-tolerated drug have been the development in some patients of opportunistic infections, such as herpes zoster or shingles, weight gain, and non-melanoma skin cancers.
Basal cell and squamous cell cancers of the skin are already common in our patient population, so a lot of our patients end up seeing a dermatologist. Most of our patients don’t necessarily discontinue for those side effects, but we need to watch out for them.
All patients who are going to get treated with fedratinib should have their thiamine level checked.
Dr. Naveen Pemmaraju
Fedratinib
Dr. Pemmaraju: Fedratinib improves symptoms and decreases spleen size, but it has a very notable toxicity or side effect, which garnered an FDA black box warning. It’s a very serious potential side effect called encephalopathy. Some have seen it to be Wernicke’s encephalopathy, but on later analysis, not exactly.
Wernicke’s encephalopathy is a name for a syndrome that can cause problems with thinking and even balance and can result from severe nutritional deficiencies. For fedratinib, it appears that it displaces vitamin B1 (thiamine) so what we see is the linking of those. All patients who are going to get treated with fedratinib should have their thiamine level checked because the encephalopathy can be related to that.
Patients can have GI side effects with fedratinib, like nausea, vomiting, and diarrhea, so we have to watch out for that, particularly in our older and more frail patients.
The unique thing with pacritinib is for several years, it was being watched for the development of cardiac and/or bleeding signals.
Dr. Naveen Pemmaraju
Pacritinib
Dr. Pemmaraju: Pacritinib is an interesting agent. Again, all these are trying to hit the JAK/STAT pathway, but this hits other pathways outside of that and that may be part of its benefits and toxicities.
It helps to shrink down the spleen and improve the symptom burden of patients, but the unique thing with pacritinib is for several years, it was being watched for the development of cardiac and/or bleeding signals.
I and others have done a lot of evaluation and analysis, including post-approval. We’re not seeing a high signal for that, but that’s something you have to be aware of if the patient is on a blood thinner, having chest pain, or having heart surgery.
Not only did [momelotinib] show improvement in the spleen size and symptoms, but what’s interesting — and pacritinib is showing this as well — is having an improvement in anemia.
Dr. Naveen Pemmaraju
Momelotinib
Dr. Pemmaraju: Momelotinib is the most recently approved JAK inhibitor. Again, not only did it show improvement in the spleen size and symptoms, but what’s interesting — and pacritinib is showing this as well — is having an improvement in anemia. Now that’s important.
Ruxolitinib and fedratinib don’t necessarily do that and, in some cases, it can make it transiently worse. Momelotinib has ACVR1 inhibition. Pacritinib also showing that as well unleashes a new era for our patients of JAK inhibitors having beneficial side effects, such as improvement of anemia and potentially, thrombocytopenia.
You have to watch out for GI side effects with fedratinib, pacritinib, and even momelotinib. In the earlier studies of momelotinib, there was a signal for peripheral neuropathy. I want to put those forward as an overview. There are some subtleties and differences, if one reads further.
Ruth: Thanks for that explanation. I’ve heard a lot of people say that they have a different mutation, so a JAK inhibitor isn’t going to help them, but we know that that’s not the case, so thanks for your explanation of how they work.
There isn’t a single molecular test. The decision is based on clinical factors and the art of medical decision-making.
Dr. Naveen Pemmaraju
Switching JAK Inhibitors
Ruth: How do you know which JAK inhibitor might or might not work and which one to try first? How is that decision made?
Dr. Pemmaraju: The decision to switch JAK inhibitors is not scientific. We’re not there yet. At some point, I envision that we’ll have a decision tree, like our colleagues in CML. But right now, there’s no molecular test, so it is the art of medicine. It is clinical decision-making.
There are some factors, if one looks up in the NCCN and other guidelines. One is platelet count. Ruxolitinib and fedratinib should be given to patients who have a certain amount of platelets and that’s where pacritinib was able to get its approval.
Pacritinib is specifically approved in the front-line setting for patients whose platelet count is less than 50, for example. The NCCN guidelines and other groups say that once you use pacritinib in later lines, maybe you don’t have to pay attention to the platelet as much, but that’s obviously for debate.
Another factor is the GI signal. If you have someone who has a known encephalopathy syndrome or thiamine deficiency, then fedratinib is not going to be one that you would choose.
Finally, you have to look at some of these subtle side effects that we mentioned earlier, such as GI and neuropathy, to help you choose.
The bottom line is there isn’t a single molecular test. The decision is based on clinical factors and the art of medical decision-making.
Switching can have financial cost repercussions, new toxicities when a patient was otherwise doing ‘okay,’ problems with access to the drug, and could uncover idiosyncratic side effects that may be specific to that patient and weren’t seen in the studies.
Dr. Naveen Pemmaraju
Ruth: So it’s possible that somebody could start on one JAK inhibitor and at some point switch to another. Is that an issue if you change?
Dr. Pemmaraju: This is a great important point about switching JAK inhibitors and what are the indications. There are several buckets here.
First is clear disease progression in terms of the spleen. If you have a patient who’s been on a certain JAK inhibitor for a sufficient amount of time and you have a spleen that previously shrunk but now starting to rise again, that could be considered disease progression and an indication to switch.
Second is worsening MPN symptom burden to the point where the patient’s quality of life is affected.
Third is blast count, peripheral blasts or bone marrow blasts, going up.
Fourth is the progression of the disease to an outright higher level of disease, what we call an accelerated blast phase.
The development of these clinical factors, such as the platelet count, may matter if you have a patient who’s on ruxolitinib, for example, and you consistently have platelets below 50, then that’s an indication to switch, for example, to pacritinib. If you have a patient who has anemia, you may think about momelotinib.
These are some of the reasons to think about switching. But again, there isn’t a molecular test or a definitive moment to switch. Switching can have financial cost repercussions, new toxicities when a patient was otherwise doing “okay,” problems with access to the drug, and could uncover idiosyncratic side effects that may be specific to that patient and weren’t seen in the studies.
Finally, you have a question about withdrawal and overlap, so these are things I think we’ll all work out together over the coming years as we have these JAK inhibitors in the clinic.
The story of JAK inhibitors is an evolving story and it’s evolving at three levels.
First is the science of it alone. In 2005, I was at Johns Hopkins with Alison Moliterno and Jerry Spivak, and I remember the day that the JAK2 mutation V617F was elucidated. From that time to now, we have JAK inhibitors that are amazing, so science is still evolving.
Second is the clinical part, as we’ve discussed. When to switch, how to switch, what are the factors, etc.
Third is the future. How do we combine these drugs with a second agent and potentially a third agent? What are those cross-reactivities? How does that benefit the patient to start those upfront rather than later on? You have this evolving area that’s quite exciting but also quite daunting not only for the patients and the clinic but for researchers.
This is preliminary data, but it was so encouraging that they are now moving on to a phase 3 randomized global study.
Dr. Naveen Pemmaraju
Clinical Trials: Combination Therapy
Selinexor & Ruxolitinib
Ruth: We’re seeing some really exciting updates as far as combination therapy. Let’s talk about clinical trials, starting with selinexor plus a JAK inhibitor and then move on to other combinations.
Dr. Pemmaraju: At ASH 2023, Dr. Sri Tantravahi from Utah presented the first public data of front-line combination, updated I should say, of selinexor with ruxolitinib. This is untreated patients with myelofibrosis, intermediate to high risk, who were given the combination rather than ruxolitinib, which would be considered the standard or JAK inhibitor.
Although it was early on and only a few patients, very surprisingly and amazingly, the group showed that there’s a high rate of activity in spleens being reduced as well as symptom burden being increased.
Now, this is preliminary data, but it was so encouraging that they are now moving on to a phase 3 randomized global study. The combination selinexor-ruxolitinib, so the XPO1 inhibitor plus JAK inhibitor, versus JAK inhibitor alone. Those data will be eagerly awaited.
This is also, if I may say, a fascinating study.
Dr. Naveen Pemmaraju
Navitoclax & Ruxolitinib
Ruth: What about the BCL inhibitor navitoclax?
Dr. Pemmaraju: A second combination is that of the BCL-XL inhibitor navitoclax with ruxolitinib, which I presented as an oral presentation at ASH on behalf of my colleagues. This is also, if I may say, a fascinating study.
We globally enrolled 252 patients into a randomized, double-blind, placebo-controlled study of ruxolitinib plus navitoclax, which is not yet approved for any indication, versus ruxolitinib alone. Again, we had intermediate to high-risk patients, around 80-plus percent of intermediate-2 patients.
What we found is a very outstanding rate of 60-plus percent of patients in the combination arm having an SVR35 at week 24, so spleen volume reduction of 35% or more, versus only 30-plus percent in the control arm, which was ruxolitinib alone. The waterfall plot showed that almost all patients benefited from the combination.
In terms of statistical analysis, the primary endpoint of spleen reduction was met with a high statistical significance, but the symptom burden difference was not yet found to be statistically significant. Both groups had reductions, so there was a numerical reduction of the symptoms in both the combination and the ruxolitinib alone, but there was no statistical difference.
The study is ongoing for collecting for maturity and overall survival duration, so this was a preliminary presentation at 15 months follow-up. We’ll stay tuned to see how it gets updated over the next congresses.
Great safety, but you have to watch out for thrombocytopenia, which is low platelets, and watch for that signal very closely.
Luspatercept & Ruxolitinib
Ruth: Another combination being investigated is the use of a shot called luspatercept to boost hemoglobin or fight anemia, and that also is being used with ruxolitinib. Can you tell us more about that one?
Dr. Pemmaraju: Luspatercept is a fascinating molecule. It’s already FDA-approved in the myelodysplastic syndrome setting. In the MPN setting, we think it has a similar activity to improve hemoglobin and anemia, which is an urgent, unmet medical need.
The initial studies have shown positive data, which is either luspatercept by itself, usually given every three weeks, or in combination with the JAK inhibitor ruxolitinib. Those studies are ongoing and we eagerly await those results in the coming year or two.
When the group looked back at certain subsets, including the intermediate-1 patients and others, it appeared that there was a benefit in both spleen size and symptoms.
Dr. Naveen Pemmaraju
Pelabresib & Ruxolitinib
Ruth: We’ve also had the MANIFEST trial, which is the trial that I happen to have been on for the last four years, and that’s a different drug, s pelabresib. Could you talk about that combination and what you think the potential is?
Dr. Pemmaraju: Another exciting combination presented at ASH 2023 was that of the MANIFEST-2, which is ruxolitinib plus a new agent pelabresib, a bromodomain or BET inhibitor, which is not yet FDA-approved for any indication.
This encouraging data set was presented by Dr. Raajit Rampal from Memorial Sloan Kettering. It’s the second-largest study ever conducted in the myelofibrosis front-line space, which included 430 patients. They also randomized ruxolitinib-pelabresib versus ruxolitinib alone in the control, mostly intermediate-1 to intermediate-2 patients, so a slightly different population.
They showed a very similar profile. A highly statistically significant primary endpoint was met, which is SVR35 at week 24. The symptoms in all comers, although showing a numerical decrease in both groups, did not quite meet statistical significance.
When the group looked back at certain subsets, including the intermediate-1 patients and others, it appeared that there was a benefit in both spleen size and symptoms.
The supposition is the same as navitoclax. These two are the first ever in our field, resulting in phase 3 global, double-blind, placebo-controlled, front-line, untreated myelofibrosis patients with a novel combination of pelabresib and navitoclax, neither of which are FDA-approved for any indication.
I would say my editorial comment is super exciting for the field that we even did it. Both were international studies largely conducted during the pandemic and involved lots of patients and investigators.
The primary endpoint was met for both of them. The symptoms were not quite met in either study in terms of statistical significance so the question asked is three-fold.
What is the utility of following the symptom burden scale in combination studies, something that was designed 15 years ago for a single-agent JAK inhibitor?
Do we expect a combination to improve symptoms over ruxolitinib alone, or because you’re introducing a second drug, you’re going to introduce new toxicity?
On behalf of my colleagues, maybe it’s time to reevaluate: what are the endpoints for our patients with myelofibrosis? Perhaps in addition to reducing spleen size and improving symptoms, we should be factoring in overall survival, progression-free survival, and bridging to stem cell transplant. This is the time to talk about it because these combination studies are difficult, if not impossible, to judge based on the COMFORT-I and COMFORT-II studies.
Imetelstat is in an ongoing phase 3 trial, which is in the second-line setting and beyond, against the best available therapy (BAT).
Dr. Naveen Pemmaraju
Telomerase Inhibitors
Ruth: Let’s go beyond JAK inhibitors. There are other drugs being studied. Can you help us understand other approaches?
Dr. Pemmaraju: There’s an exciting alphabet soup of clinical trials and drug molecules out there. It’s exciting for our patients to know that there are people around the world who care about MPNs, so it’s good to know that despite COVID, we have a lot of innovation.
We’re adding a new trial once a week, so it’s almost impossible to keep up, but I do want to give some sampling of what’s going on.
Imetelstat is very important for everyone to know. It’s a first-in-class telomerase inhibitor. Some people have heard of telomeres. They are the little ends on the ends of chromosomes that help to determine aging and possibly even cancer biology.
Imetelstat is in an ongoing phase 3 trial, which is in the second-line setting and beyond, against the best available therapy (BAT). I praised this trial because it’s the first and, to my knowledge, only phase 3 trial that has overall survival as its primary endpoint. Hopefully, it will give us a readout in the next year or two.
MDM2 Inhibitors
Dr. Pemmaraju: MDM2 inhibitors have gotten a lot of press in all MPNs. This is a key pathway that has to do with guarding the cell TP53. It’s an oral drug that has been studied before. As a class of drugs, there may be some GI side effects to watch out for, but in the later trials we’ve seen, the groups have figured out a way to address that by either adjusting the dosing schedule or dosing frequency.
I’m excited to see where that area goes. Right now, the lead trials are MDM2 inhibitors with ruxolitinib as an add-on approach or a suboptimal approach. You’re already on a JAK inhibitor. You have an okay response, not a great one, but not quite ready to come off of it, and then you add the MDM2 inhibitor. Those studies are actively ongoing and I think we’ll be excited to see those results.
The good thing about myelofibrosis is whether you’re JAK, CALR, MPL, or triple negative, you respond to JAK inhibitors and novel agents alike.
Dr. Naveen Pemmaraju
Genetic Mutations in Myelofibrosis
Ruth: What if someone’s myelofibrosis isn’t driven by a JAK mutation but a different mutation, is there a different approach? We’ve also been hearing about a cancer vaccine related to CALR, so could you walk us through both?
Dr. Pemmaraju: There’s a two-part answer to the question of molecular mutation targeting in MPNs. Historically and in the clinic right now, there is no difference at the moment.
The good thing about myelofibrosis is whether you’re JAK, CALR, MPL, or triple negative, you respond to JAK inhibitors and novel agents alike. That’s an interesting thing that suggests that there’s a common pathway.
But for the future, yes. Already in the clinic in 2024, we expect a new era to begin, which is, for the first time, to have mutant-specific approaches for both JAK2 and CALR. I expect that we’ll see multiple different drugs targeting mutant JAK2 specifically. The hypothesis is: could that be better and more specific than targeting the whole pathway? Let’s see. You’ll see phase 1 trials there.
CALR turns out to be a really good target, especially for immune therapy targeting. That’s only new science in the last five years. There are vaccine approaches either by themselves or with other immune drugs, such as ipilimumab. There’s an exciting bispecific molecule, which is a mutant CALR x CD3 bispecific antibody that I and others will be working on.
There are also going to be other ways to target CALR. You have multiple different ways of targeting mutant-specific approaches, but let me highlight these are phase 1 clinical trials. They’re backed by animal preclinical data. Now we need to see how they do in the initial trials.
For the first time, I’m seeing sustained improvement in the anemia of MPN, specifically myelofibrosis. We have three different categories trying to address this for our patients.
Dr. Naveen Pemmaraju
Anemia in Myelofibrosis
Ruth: Dr. Pemmaraju, you mentioned that many people suffer from anemia when hemoglobin is low. We know they can feel extremely fatigued so much that it interferes with their quality of life, which I know from personal experience, unfortunately. With what you’ve described, do you feel like we’re getting better tools to fight anemia and hopefully avoid people needing more frequent transfusions?
Dr. Pemmaraju: Yes. For the first time, I’m seeing sustained improvement in the anemia of MPN, specifically myelofibrosis. We have three different categories trying to address this for our patients and it’s simply exciting.
First is the JAK inhibitors themselves. As we mentioned earlier, the first initial ones did not improve and may have worsened the anemia transiently in some patients. Now these second- and third-generation JAK inhibitors are improving the anemia and possibly through the inhibition of ACVRL1, so that’s exciting.
Second is the additional agents, such as luspatercept. You can add on an agent that works outside of the JAK inhibitor that aims to stimulate the hemoglobin and improve the anemia.
Third is these novel agents. When you look closely at the navitoclax and pelabresib data sets, in those two particular instances, you have some people who get anemia as toxicity, but you also have patients who have anemia improvement with the combination, maybe better than with ruxolitinib alone. These three approaches, we’re already seeing in the clinic in phase 1, 2, and 3 clinical trials.
Out of all of these theoretical things, a lot of times what our patients are suffering from is anemia. When the hemoglobin gets below 7, 6, 5, or 4, it’s not even compatible with life, much less quality of life. Anything we can do to reduce the burden of getting transfusions, missing appointments, and missing life events is going to be a big breakthrough, and I’m starting to see that.
If a transplant is available and indicated, it is the only curative approach for myelofibrosis.
Dr. Naveen Pemmaraju
Role of Stem Cell Transplant in the Treatment of Myelofibrosis
Ruth: Typically, a doctor will tell a patient that the only cure for myelofibrosis is having a stem cell transplant. With these new medical therapies, my question is always the same: do you see a changing role for transplants?
Dr. Pemmaraju: The role of stem cell transplant in myelofibrosis is one of great importance still. While I’m personally excited about all of these drugs in development, two things are important.
First, none of these have been shown to create a long-term cure in and of themselves for myelofibrosis. Second, if a transplant is available and indicated, it is the only curative approach for myelofibrosis.
Having said that, the realistic problem with allogeneic transplants is that it’s not available for everyone because of their comorbidities, how frail versus how fit they are, matching, the infection rate, and the mortality rate. As patients get older, it may be tougher at some centers and for some folks to do it. There are some real limitations.
The other problem is that out of all of our patients, the vast majority are not going to transplant. Improvements are being made with transplants every day. Haploidentical transplant, which is a half match, is becoming more of a standard, so that gives the donor pool exponentially more options.
Trying to reduce graft versus host disease, which are complications after the transplant, with medicines are revolutionizing the field.
As I’ve traveled all over the world, people can do stem cell transplants in economically diverse situations. The transplant procedure itself can be highly expensive. Interestingly, even though cost-effectiveness is an issue, in some locales, if you can do a transplant and potentially cure the disease, it can lead to an improvement in socioeconomic status overall.
There are some cool, important things happening. But it’s an important point that even with all the excitement of these medicines and medicine combos, we’re still not at the point where we’re talking about a cure, so if you have the availability and indication for transplant, you have to pursue that consideration.
We have brand new approaches that we didn’t have a few years ago. There is a lot of data and science, so there’s hope.
Dr. Naveen Pemmaraju
Final Takeaways
Ruth: Let’s put all of this together. For those of us living with myelofibrosis or others who are concerned about progressing to myelofibrosis, what do you want to leave them with? When you total up everything we’ve talked about, how do you want to leave the conversation?
Dr. Pemmaraju: This discussion was very exciting because it left me with even more hope than when I started the day. I would leave our patients, caregivers, family members, advocates, and stakeholders with a message of hope and positivity. It’s not blind hope and positivity. It’s not based on hunches or ideas. It’s based on data.
The last three years in particular, I would call it — and I do not use this phrase lightly — a golden era for research for the MPN, specifically including myelofibrosis.
There are four areas to highlight and to be very excited about for our patients and families. First is the development of new JAK inhibitors. We mentioned the four that are already approved in the US, so let’s get them available all over the world. There are several more in clinical development.
Second is the JAK inhibitor combinations. Very exciting data from ASH. Let’s see the new combinations. Maturing data for navitoclax, pelabresib, and selinexor.
A third area of excitement and hope is that of anemia-improving agents.
Finally, the delineation, description, and demonstration of brand-new molecular pathways inside the cells that were never known before. New insights and ways of approaching. We mentioned potential immune therapy approaches, like the CALR mutation. It’s exciting that we have brand new approaches that we didn’t have a few years ago. There is a lot of data and science, so there’s hope.
Ruth: Dr. Pemmaraju, thanks so much for being with us today. You’re always a pleasure to talk to and so informative to our guests. We really appreciate your time.
Dr. Pemmaraju: Thank you so much for having me. This was a very thought-provoking and stimulating discussion.
Where is Hodgkin lymphoma headed in 2024? Two-time Hodgkin’s lymphoma survivor Dr. Sam Siegel discusses with top lymphoma experts, Dr. Natalie Grover of UNC Health and Dr. Stephen Ansell of Mayo Clinic, as they break down what patients and caregivers need to know!
Key topics include the latest treatment options and clinical trials, reducing toxicity from treatments, advances in post-transplant relapse, and the roles of CAR T-cell therapy and bispecific antibodies in the treatment of Hodgkin lymphoma.
Stephanie Chuang, The Patient Story: My name is Stephanie Chuang, the founder of The Patient Story. I also got a blood cancer diagnosis a few years ago. Mine was non-Hodgkin lymphoma, but we have so many shared experiences in what we’re looking for and that’s what The Patient Story is all about.
We help both patients and care partners navigate a cancer diagnosis. We do this primarily through in-depth conversations with patients, care partners, and top cancer specialists.
We want to note that The Patient Story retains full editorial control of this entire program and that this is not meant to be a substitute for medical advice.
Our patient moderator, Dr. Sam Siegel, will be leading the conversation from this point forward.
Sam Siegel, MD, Patient Advocate
Dr. Sam Siegel: Thanks, Stephanie! I’m a two-time Hodgkin’s lymphoma survivor, bone marrow transplant survivor, and primary care physician doing survivorship medicine. I’m here to have this wonderful conversation with Dr. Natalie Grover and Dr. Stephen Ansell about Hodgkin lymphoma updates.
Natalie Grover, MD
Sam: Dr. Natalie Grover is a hematologist-oncologist at the UNC School of Medicine. She’s the clinical director of the cellular therapy program, leads several CAR T-cell therapy clinical trials in lymphoma, and strives to improve treatment options and quality of life for lymphoma patients.
Dr. Grover, can you tell us a little bit about yourself, what drew you to lymphoma, and about your approach to patients and how you care for them?
Dr. Natalie Grover: I was drawn to oncology as a maternal medicine resident. Much of it was based on my relationship with patients whom I saw in the inpatient oncology ward. When I saw those patients, I always wanted to go back and find out more about what happened to them and form connections with them.
There were so many discoveries and new treatments available. Even during residency, the treatment landscape was changing so much and that drove me to oncology.
I like how heterogeneous lymphoma is and how it involves a wide patient population of both young and older patients. It’s truly a systemic disease. There are so many different types of lymphoma so my clinic is a very heterogeneous mix of different patients and I enjoy that.
Sam: That makes a lot of sense. Lymphoma is the umbrella, but it’s a lot of different diseases that can affect multiple parts of the body. I could see how that’s interesting.
Stephen Ansell, MD, PhD
Sam: Dr. Stephen Ansell is a hematologist-oncologist at the Mayo Clinic who studies and specializes in Hodgkin’s lymphoma. His research has led to the use of immune checkpoint therapy in lymphomas, which is a very exciting development. His goal is to translate his research into new treatment approaches.
Dr. Ansell, can you tell us about your path into lymphoma, what drew you to the field, and your approach to patients?
Dr. Stephen Ansell: I trained in South Africa. I was very focused on internal medicine, but they needed someone to do some work temporarily in oncology and assigned me.
When I got there, similar to Dr. Grover, I was excited about the opportunity, the disease, the patients, and how we could make a difference based on the fact that treatments were highly effective and beneficial. Patients benefited substantially even from initial treatments back in the day of more chemotherapy.
What has been exciting for me throughout my career has been to see how we can change treatments by increasing the number of people who benefit and hopefully get cured, and decreasing the side effects and toxicities by being able to find effective therapies that aren’t that hard on patients.
Sam: Your areas of interest and passion are so personally meaningful to me and my lymphoma journey, and I think will resonate with a lot of people.
Even though I had some side effects from the brentuximab at the highest dose that I first started it on, it still felt like a cakewalk compared to my initial drug regimen.
Dr. Sam Siegel
Sam’s Hodgkin Lymphoma Story
Sam: I was diagnosed with stage 2AE Hodgkin’s lymphoma and the reason that 2AE is important is because E means extranodal manifestations. I had some lung involvement and it was confusing whether or not I was a stage 2 with right around the lymph nodes in that lung or stage 4. That was going to impact how many months of chemotherapy I would have.
I started with ABVD chemotherapy. Within two months, the initial cough that I had at the time of diagnosis improved pretty quickly. Towards the end of those two months, I started getting a cough again. My PET scan looked good so the thought was that bleomycin was probably to blame for that cough.
We dropped bleomycin and it felt pretty okay making that decision. I suspected that something else was going on, but because the scan had come back clean, we decided to watch and wait.
About a month or two after that, I developed symptoms that were eerily reminiscent of my initial diagnosis, such as wheezing in the upper left side of my chest, which I knew wasn’t normal, and a pea-sized lump above my collarbone in a very similar location to where the initial lump was.
I suspected that those were Hodgkin lymphoma symptoms and sought care right away. The PET scan showed that I was most likely having a relapse.
It was a process to get the tissue to confirm the relapse. I had to have three biopsies, with the third one involving a thoracic surgery to get a lymph node right near my heart.
By that time, I felt so beaten up by traditional cytotoxic chemotherapy. New information was coming around about salvage therapy, which is the therapy after a person has relapsed from initial therapy. At that time, I didn’t feel that I could go through another few months of multi-drug traditional cytotoxic chemotherapy.
Data was coming out about brentuximab, an antibody-drug conjugate, and using that as a bridge to autologous bone marrow transplant. My oncologist said, “These trials showed that this could be an effective bridge to transplant. What do you think?” I said yes because I wanted to go for the therapy with the least amount of toxicity.
Even though I had some side effects from the brentuximab at the highest dose that I first started it on, it still felt like a cakewalk compared to my initial drug regimen.
That goes to show how important the science is and the clinical trials that inform oncologists how to adjust therapies, especially therapies that were traditionally pretty toxic in terms of long-term and late-term effects.
There are always ways in which we’re trying to make treatment better… we’re trying to replace radiation therapy by utilizing new agents.
Dr. Stephen Ansell
Standard of Care: First-Line Treatments
Sam: Dr. Ansell, can you tell us about the current standard first-line treatments and their efficacy for Hodgkin lymphoma?
Dr. Ansell: In many respects, we think about it in two buckets: people who have more limited-stage disease (only on one side of the diaphragm, either above or below) or advanced-stage disease (both sides of the diaphragm, in the bone marrow, or other tissues).
With limited-stage disease, we again think of two buckets. These are different symptoms and other tests to determine prognostic factors. If you have favorable prognostic factors, we treat you with very minimal chemotherapy. If you have more symptoms and unfavorable factors, we will treat you with a little bit more treatment. If you have advanced disease, we give you more treatment yet again.
There are always ways in which we’re trying to make treatment better, but the most standard way is if you have very limited disease with good favorable factors, we often will give two rounds of chemotherapy treatment and then consider consolidation radiation treatment.
If you have a more advanced disease, still limited to one side of the diaphragm but with more unfavorable factors, we would give more chemotherapy and more radiation treatment. Then for advanced-stage disease, we would give chemotherapy and no radiation treatment.
However, we’re trying to replace radiation therapy by utilizing new agents. We’ve used PET scans to tell us who might need extra treatment or not. I have to hedge a little bit because a lot of it is individualized and that’s the most important thing.
It’s so important to raise awareness about the importance of being involved in clinical trials and knowing that you don’t have to have failed multiple lines of therapy before you consider them.
Dr. Sam Siegel
Sam: Absolutely. How do you decide? There are different prognostic systems so if somebody is unfavorable in one and favorable in others, how do you factor that in?
Dr. Ansell: Pick one system and utilize the data supported by that system. The German Hodgkin Study Group has done a lot of work in this space. In our practice, we tend to use the prognostic system that they use because that helps us standardize treatment.
What we want to do is always push the envelope. We encourage people to participate in clinical trials that are testing new ways compared to the standard ways to see if we can optimize treatment even further.
Sam: I love that. Thank you for bringing up clinical trials. It’s so important to raise awareness about the importance of being involved in clinical trials and knowing that you don’t have to have failed multiple lines of therapy before you consider them.
Clinical trials can be for everyone and there are so many different types of situations where somebody could need a clinical trial. We’re looking at things to de-escalate therapy or alter treatments based on a patient’s situation.
Dr. Ansell: I would say you’re exactly right. The most impressive and important data that has come out on Hodgkin lymphoma is in the front line based on recent clinical trials. Everyone needs to remember that what we do currently is based on people who have participated in clinical trials that have changed how we practice.
Standardly, we utilize new agents, like PD-1 blocking antibodies or brentuximab vedotin plus chemotherapy, rather than chemotherapy alone because that’s improved the outcome of patients. Especially in advanced-stage patients, that’s now the standard of care.
The two biggest drugs that have transformed the care for Hodgkin lymphoma in the past 5 to 10 years are brentuximab vedotin… and checkpoint inhibitors.
Dr. Natalie Grover
Latest Advancements in Treatments
Sam: Dr. Grover, what are some of the newest and hottest treatments for Hodgkin lymphoma?
Dr. Grover: I think the hottest advances in Hodgkin lymphoma are related to incorporating some of these new treatments into earlier lines of therapy to try to both improve outcomes so increase the chance of cure and reduce long-term toxicities.
The two biggest drugs that have transformed the care for Hodgkin lymphoma in the past 5 to 10 years are brentuximab vedotin, which is an antibody-drug conjugate. It delivers chemotherapy specifically to the cancer cells.
The cancer cells in Hodgkin lymphoma have a marker on them—CD30—that’s pretty much universally seen in all the Reed-Sternberg cells, the cancer cells in Hodgkin lymphoma. Brentuximab specifically targets those.
The other drugs are what people may have heard of called checkpoint inhibitors. These immunotherapies help the immune system fight Hodgkin’s lymphoma.
When they incorporated these drugs—nivolumab, pembrolizumab, and brentuximab—they were successful in relapsed/refractory disease. Now they’re being moved to earlier lines of therapy to try to reduce the amount of chemotherapy that we’re giving patients and hopefully to enhance care in these patients.
By limiting chemotherapy and radiation, can you improve patient outcomes?
Dr. Natalie Grover
Sam: How about some recent clinical trials for reducing toxicity? I heard about AHOD2131.
Dr. Grover: There’s a clinical trial for pediatric and adult patients looking at whether we can incorporate these newer treatments, brentuximab and checkpoint inhibitors, in newly diagnosed Hodgkin lymphoma patients.
Everyone gets two cycles of standard chemotherapy then patients get randomized to either getting these new treatments, brentuximab and nivolumab, or continuing to standard chemotherapy.
The question is: by limiting chemotherapy and radiation, can you improve patient outcomes? One thing they want to look at is cure rates and long-term survival from a Hodgkin’s standpoint, but they’re also collecting data looking at quality of life patient-reported outcomes.
The top priority is curing their lymphoma, but we also want to think about the quality of life for patients moving forward and making sure that they live long lives.
Dr. Natalie Grover
Sam: That’s incredible. When you’re talking about late-term effects or reducing toxicities, what are some of the things that we’re trying to reduce long-term?
Dr. Grover: One of the chemotherapy drugs that we give patients can affect their heart function so some of the things that we think about are the risk of heart disease down the line.
One of the drugs that we’re using a lot less often now can affect lung function so we look at issues with lung function past therapy.
With some of these drugs and using more brentuximab, another thing that we’re thinking about is neuropathy. Patients can have some nerve damage and issues with pain, numbness, and tingling or doing different functions, like texting, typing, or writing.
With young patients, another thing we think about is fertility. Even though many of these patients can have children in the future as a lot of these earlier treatments don’t have as big an effect on fertility, it’s still something we think about, especially if we need to escalate people who have a disease that relapses or need more aggressive therapies.
We also think of secondary cancers. Some chemotherapy and radiation may increase the risk of having other cancers.
The positive is that most of these patients live long enough for us to focus on that and think about these effects. The top priority is curing their lymphoma, but we also want to think about the quality of life for patients moving forward and making sure that they live long lives.
Checkpoint inhibitors help the immune system fight the cancer. Some of these patients may stop responding to checkpoint inhibitors so there’s interest in using other types of treatments in combination.
Dr. Natalie Grover
Sam: What about trials to re-sensitize to PD-1 drugs? What does that mean?
Dr. Grover: Checkpoint inhibitors are effective in Hodgkin lymphoma. Right now, we’re moving them to earlier lines of therapy but these are treatments that can also work well for relapsed and refractory patients.
Hodgkin lymphoma is unique because, compared to other lymphomas, there aren’t that many cancer cells in these patients. When pathologists look at cells, there are a lot of immune cells around the cancer cells so there aren’t that many lymphoma cells. A lot of it is your immune reaction to the lymphoma.
Checkpoint inhibitors help the immune system fight the cancer. Some of these patients may stop responding to checkpoint inhibitors so there’s interest in using other types of treatments in combination. If a patient progresses on pembrolizumab or nivolumab, can you combine them with other treatments and re-sensitize your immune system so they can be sensitive again to these treatments? There’s some research looking into that.
We’ve also seen patients get the reverse. These treatments may reset the patients in some way. Patients may get checkpoint inhibitors and then after that may respond better to other treatments. There have been some studies showing that after checkpoint inhibitors, even if they progress on those drugs, patients potentially respond better to chemotherapy or other treatments.
Sam: We’re still learning how these drugs impact the immune system and how they might make you respond better to traditional chemotherapies, even if you didn’t initially. That’s incredible.
Dr. Grover: The current biggest advances are in advanced-stage Hodgkin lymphoma. More recently, brentuximab was incorporated in addition to chemotherapy. Dr. Ansell was part of that study. That improved overall survival in advanced-stage Hodgkin lymphoma patients compared to standard of care.
We can see the progression from old-style chemotherapy to immune checkpoint plus chemotherapy as the front-line treatment.
Dr. Stephen Ansell
Early vs. Advanced Stage Advancements
Sam: Dr. Ansell, can you tell us about the SWOG S1826 trial and what that showed?
Dr. Ansell: Picking up again on the theme of better therapies getting better outcomes and using some of the new drugs that we’ve touched on, as Dr. Grover said, the management of advanced-stage patients has moved over time.
Back in the day, we gave ABVD chemotherapy and tried to leave out bleomycin, which causes lung toxicity, if patients were doing well based on PET scans.
These new drugs, brentuximab vedotin being the first one, were brought into the combination in place of bleomycin. It’s now brentuximab with AVD. When compared head to head, it showed that brentuximab improved the outcome of patients—not only their likelihood of staying in remission but their overall survival.
It was then compared as the standard to nivolumab, the PD-1-directed therapy, plus AVD chemotherapy in place of bleomycin. That then showed progression-free survival at a one-year follow-up. We don’t have mature data yet, but it seemed better already than the brentuximab-AVD chemotherapy and, as Dr. Grover touched on, less in the way of side effects and better tolerated.
That’s likely to become the new standard for advanced-stage patients. We want to see a little bit more mature data. But certainly, in elderly patients where toxicity is a real challenge, this has become a standard for many. We can see the progression from old-style chemotherapy to immune checkpoint plus chemotherapy as the front-line treatment.
Sam: These are exciting times. It’s wild because, for decades and decades, it seemed like we were doing the same thing for Hodgkin patients. Even if I were diagnosed with the same clinical scenario now compared to when I was first diagnosed in 2021, I would be treated differently.
There is still a subset of people where the disease proves to be very challenging and keeps relapsing… We still see patients who have gone through this standard treatment using these new drugs and then the disease comes back yet again.
Dr. Stephen Ansell
Gaps Clinical Trials are Filling
Sam: Can you tell us about these clinical trials and what gaps they fill?
Dr. Ansell: You heard us talk about two new drugs. They came from the relapsed setting but have moved up to front-line treatments. The gaps are for patients, heaven forbid, who have gone through these new therapies.
There is still a subset of people where the disease proves to be very challenging and keeps relapsing. That group’s getting to be smaller and smaller so that’s the good news. The challenging point is that it’s never good enough until there’s nobody in that group. We still see patients who have gone through this standard treatment using these new drugs and then the disease comes back yet again.
Things that are becoming exciting and that we need to do better on is what to do for those patients. Additional treatments that target these other immune checkpoints aside from PD-1 and other ways to make the immune system wake up and do its job are being tested.
The work that Dr. Grover and her team do is taking your immune cells, sending them to “training camp” to get a little docking site on them so they can detect the cancer in a much better way, and then unleashing them on the cancer. That’s proving exciting.
Finally, what we call bispecific antibodies. Those are also being tested and are some of the exciting opportunities in the future.
One arm of the antibody is directed to CD30, but the other arm grabs onto CD3 in the T cells.
Dr. Stephen Ansell
Bispecific Antibodies
Sam: Can you tell us about bispecific antibodies?
Dr. Ansell: This is an area that’s growing fast in Hodgkin lymphoma. Dr. Grover talked about CD30, which is on the cancer cells. One arm of the antibody is directed to CD30, but the other arm grabs onto CD3 in the T cells.
Bispecific antibodies bring those cells into very close proximity to each other. Like your kids in the back of the car who don’t like to sit next to each other and keep poking each other, this causes those cells to be grumpy with each other. The T cells, your immune cells, will then fight the cancer. That’s really what you want to see.
We talked about immune checkpoints that make T cells do a better job. One of the ways we’re doing that is on one arm, PD-1, which is an established immune checkpoint, but on the other, something like TIM-3, which is another immune checkpoint.
Other ways in which T cells are being switched off are now protected so it’s making those cells even more efficient. Those are two of the main ways bispecific antibodies are being tested right now.
With CAR T-cell therapy, we have seen some nice responses in patients whose disease has progressed after many different therapies, but there’s still work to do to improve these therapies.
Dr. Natalie Grover
CAR T-cell Therapy
Sam: Dr. Grover, how about CAR T-cell therapy and post-transplant relapses? Can you tell us about that and where CAR T-cell therapy might play a role?
Dr. Grover: As Dr. Ansell briefly mentioned, CAR T-cell therapy involves taking a patient’s T cells, sending them off, and re-engineering them so they can specifically target the CD30 protein on the cancer cell.
We have a CAR T-cell therapy trial at UNC and at the Baylor College of Medicine. There are two academic trials where we’re studying these CAR T cells in patients with Hodgkin lymphoma. There are also a few international trials. I know there’s a group in Spain and China.
Unfortunately, there isn’t a company-sponsored trial. They’re exciting treatments, but they’re not as easily accessible. Patients do need to travel for these for these treatments.
The big thing is long waiting lists, but we are hoping to get more patients treated more quickly because it still shows that there is an unmet need. Some patients have not responded, progressed after brentuximab, progressed after checkpoint inhibitors, progressed after transplant, and need additional options for treatment.
With CAR T-cell therapy, we have seen some nice responses in patients whose disease has progressed after many different therapies, but there’s still work to do to improve these therapies.
Right now, we have some patients who have been in remission for many years—five-plus years after getting CAR T cells. Many patients get the CAR T cells and have a great response, but their disease relapses afterward. We’re trying to figure out why that’s happening and how we can improve the CAR T cells and improve outcomes for patients.
Patients who relapse can have more aggressive disease as opposed to some other more aggressive types of lymphoma, but with Hodgkin, patients who have relapsed oftentimes can live a long time even with the disease.
Dr. Natalie Grover
Dr. Ansell: There’s one other option that takes both bispecifics and cellular therapies and combines those strategies. That’s taking the natural killer cells from cord blood and using a bispecific antibody that targets CD30 and a protein called CD16 on the NK cell. It sticks this bispecific antibody to the NK cell.
They pre-treat the NK cells before they give them to the patient and then infuse them. You activate the cells outside the body, add the bispecific antibody so that it’s already stuck to the NK cells, and infuse them. Those also have been effective therapies.
Dr. Grover’s right. We’re still learning about how many treatments you need to get. They’re getting high response rates, but the durability is still in question. But I think that’s another exciting strategy of taking cellular therapies and bispecifics and using them together.
Dr. Grover: I think that’s the LuminICE trial, which will be open at several different sites across the country.
Sam: That’s great. That’s an important point. It’s part of the issue of Hodgkin lymphoma compared to non-Hodgkin’s. It’s not nearly as common in terms of the number of people that will qualify for these trials so that may be why there are less commonly offered.
Dr. Grover: Hodgkin lymphoma has higher cure rates and is less common. A lot of times, patients who relapse can have more aggressive disease as opposed to some other more aggressive types of lymphoma, but with Hodgkin, patients who have relapsed oftentimes can live a long time even with the disease.
I’ve seen patients in my trials who have relapsed and have not even been in remission but have been living for many, many years with relapsed disease. A lot of times, these patients may not be as sick, which is a good thing, so they’re able to travel and participate in these trials. Many of these patients may be alive and doing well even though they’re going through treatment or have some disease left.
An allogeneic transplant is still a curative option and something that we would always consider.
Dr. Stephen Ansell
Transplant
Sam: Where is all this in relation to allogeneic transplants for people who are relapsing after transplant? Allogeneic, meaning the donor is somebody else, as opposed to autologous, which is more common in Hodgkin.
Dr. Ansell: To be honest, an allogeneic transplant is still a curative option and something that we would always consider. It’s a little bit high-risk because of the potential for longer-term toxicities.
With a lot of these novel treatments, many of which have been very successful in the past, people delayed allogeneic transplants a little bit. There are some challenges now as patients are having their disease come back after standard treatment so there is a subset of patients for whom that needs to be considered. That’s a very individualized discussion between patients and their doctors to weigh the risks versus the benefits.
One of the key questions to ask is what treatment somebody got as their first line because that impacts what you would do in the second line.
Dr. Stephen Ansell
Developments in Salvage Therapy
Sam: Dr. Ansell, what are some of the developments in salvage therapy, which is given when somebody has their initial relapse?
Dr. Ansell: It’s moving pretty fast right now. Novel drugs are being used in the front line so one of the key questions to ask is what treatment somebody got as their first line because that impacts what you would do in the second line.
However, based on where most patients are right now, not very many have had an immune checkpoint treatment, which is the nivolumab and pembrolizumab that Dr. Grover spoke about. Not too many people have had that as their front-line treatment and using those in combination with standard chemotherapies, like ICE chemotherapy or GVD chemotherapy. In the majority of particularly younger patients, going to more intensive treatment and a stem cell transplant using your own cells is very much the standard management.
Some interesting recent data compared where that was used to standard chemotherapy or the use of brentuximab and chemotherapy then a transplant and then looked at outcomes. The patients with the best outcome got a PD-1 antibody before they got their transplant.
Dr. Grover touched on this, which is an important point. The PD-1 blocking antibody team seems to change the immune system a bit and make patients more sensitive to some of the chemotherapies after the fact so that’s why it seems like it makes a difference. We tend to favor chemotherapy with immune checkpoint therapy as a treatment approach before going to transplant.
We want to see people cured. Heaven forbid that it comes back the first time, but if it does, all the gloves are off. Now we’re going at it as hard as we possibly can.
Dr. Stephen Ansell
Sam: That’s interesting because I know in other cancers, people will save therapies or not want to expose them because the body will learn them. What you’re saying is that the same principle may not apply in Hodgkin. These therapies may sensitize to other therapies or make people respond better so you don’t necessarily need to leave them until later when you’ve burned through other options.
Dr. Ansell: Correct. We want to see people cured. Heaven forbid that it comes back the first time, but if it does, all the gloves are off. Now we’re going at it as hard as we possibly can and we want to utilize all the effective tools that we have so that we can truly beat it into the ground. That’s what I would recommend. Different from other cancers where you might want to string things along in a palliative approach. With Hodgkin, you want to go after it with curative intent.
Sam: It’s wild to think how quickly things evolve and how important it is for patients to seek out providers or treatment at cancer centers who have some connection with the trials and know the latest updates.
How can we advise patients to seek out that kind of care? How can they ask for that from their oncologist if they’re getting treatment in the community?
Dr. Ansell: Be an informed patient. Ask questions and be a strong advocate for yourself. There are excellent resources, like The Leukemia & Lymphoma Society, which have good information related to many of these topics. Being informed about the best way to be managed is useful.
When your doctor sees you and goes through things, asking questions relative to the information that you have helps you feel reassured that you’re on the right track. Most of us are quite okay with patients getting second opinions from other colleagues.
Second opinions help people reinforce the messages you’re already giving. People will be more comfortable doing what needs to be done if they’re hearing the same thing from more than one person. All of that pertains to a good outcome. If you ask questions, make sure you get your questions answered.
Sam: Thanks for empowering patients because it’s so hard to make these decisions even when you have a lot of resources and education. It could be such an emotional time, in addition to not feeling well, and it’s helpful to hear that you expect people to want other opinions and be informed.
Dr. Ansell: To be honest, a lot of patients come in and get so much information that it’s pretty challenging to retain them. I always tell people to bring friends or family. Have other sets of ears that can help reinforce some of the messages so that when your brain is locked down and you can’t think straight, they hear things that you might have missed.
The treatments are getting better all the time so there’s a lot of hope. I’m hoping that in the not-very-distant future, every patient with Hodgkin lymphoma can be cured with front-line treatment.
Dr. Stephen Ansell
Final Messages
Sam: Dr. Grover, can you give us some final points or takeaway messages?
Dr. Grover: I’m excited about improving earlier therapies and moving these newer therapies to the front line both to hopefully enhance cure to prevent patients from relapsing again and reduce long-term toxicities and improve quality of life.
There’s still an unmet need for patients who are refractory to PD-1 inhibitors, brentuximab, and chemotherapy. I’m hoping that over the next few years, we will have more clinical trials and more developments for that patient population.
For patients, ask questions of your provider. Don’t be shy about getting a second opinion. I’m never offended if a patient goes for a second opinion.
Sam: How about you, Dr. Ansell?
Dr. Ansell: If you’re a patient with Hodgkin lymphoma, there are unique and novel treatments that are making a big difference to patient outcomes. The treatments are getting better all the time so there’s a lot of hope. I’m hoping that in the not-very-distant future, every patient with Hodgkin lymphoma can be cured with front-line treatment.
Sam: Thank you so much for that. I remember initially being scared about death and dying. I think that’s what a lot of people think about when they hear the word cancer. Once it began to move away from that and began to become living with cancer or living life after a cancer diagnosis, I thought, I’d like to jog, paint, play guitar, hold my kids, and be able to think as well as possible.
These trials to improve quality of life while simultaneously improving outcomes are so meaningful personally. I know it means a lot to our patient population that you took the time to have this conversation with us. Thank you so much.
Dr. Ansell: My pleasure.
Dr. Grover: Thanks so much for having us.
Stephanie: Thank you so much, Sam, for being our incredible patient advocate and moderator. Also, thank you to Dr. Grover and Dr. Ansell, for the work and research you do to help move the landscape of treatment options in Hodgkin lymphoma.
We hope that you walk away with a better understanding of the latest treatments and clinical trials in Hodgkin lymphoma. They may or may not be right for you, but our goal is to make sure you feel empowered to make a decision for yourself.
Thank you and we hope to see you again at a future program at The Patient Story.
Learn about success stories, dispel myths about experimental drugs, and understand the broader impact of trial participation on advancing MPN treatments.
Find out about the latest options for myelofibrosis patients, how to deal with myelofibrosis symptoms, and how factors like age, mutation status, treatment history, and personal preferences inform your treatment.
Learn about how the latest advancements may affect your care and get updates on exciting news about the pace and progress of myelofibrosis treatments.
The myelofibrosis panelists discuss momelotinib, fedratinib, selinexor, pelabresib, navitoclax, and other myelofibrosis treatments.
Thank you to GSK and Karyopharm for their support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Stephanie Chuang: I’m the founder of The Patient Story and, more importantly, I also got a blood cancer diagnosis of non-Hodgkin lymphoma a few years ago.
We have so many shared experiences in what we’re looking for and that’s what The Patient Story is all about.
We try to help patients and care partners navigate a cancer diagnosis primarily through in-depth conversations with patients, care partners, and top cancer specialists, like the ones you’ll hear from today.
We do want to note The Patient Story retains full editorial control of this entire program. A quick reminder that this is not meant to be a substitute for medical advice.
Our patient moderator is Ruth Fein Revell. Ruth, can you share a little bit more about your story and how you became such a passionate advocate in this space?
Ruth Fein Revell, MPN Patient Advocate
Ruth Fein Revell: Welcome, and thank you for joining us. I’m Ruth Fein, a health and science writer. I’m also a patient and a patient advocate who’s been living with a myeloproliferative neoplasm of one type or another for almost 30 years.
I was diagnosed with essential thrombocythemia when I was 38 years old and raising two young boys. I had had symptoms for many years, but they were disregarded or misdiagnosed. The most troublesome of which was severe, debilitating headaches with blind spots where I literally couldn’t work for hours at a time. I also had bone pain that I experienced for years.
What started as essential thrombocythemia transitioned to polycythemia vera and then progressed to myelofibrosis, which is where I am now. I’m very fortunate to be on a clinical trial that’s working so well that my life is wonderful. I also recognize that everyone isn’t in the same position as I am as there are a lot of people who suffer greatly from myelofibrosis.
I’m speaking with two world-renowned experts in MPNs, Dr. Raajit Rampal of Memorial Sloan Kettering Cancer Center and Dr. Gabriela Hobbs of Dana-Farber/Harvard Cancer Center. Both of you are very, very involved in the patient community and giving back through your knowledge and also taking time to do interviews like this so thank you for that.
We’ll dig into what’s been reported recently at ASH, the annual meeting of the American Society of Hematology where a lot of reports come out. Some of them are quite exciting.
Raajit K. Rampal, MD, PhD
Ruth: Dr. Rampal, give us a little bit of your background, why and how you became interested in MPNs, as well as what your practice looks at.
Dr. Raajit Rampal: I’m a physician-scientist and I lead the MPN program at MSK.
My interest came from the biology side. I’ve been working with Ross Levine for a number of years on the lab side. It became clinically interesting based on what I was learning in the lab so I’ve taken on clinical practice and doing clinical trials for patients in MPN.
This is a field with such an unmet need for effective therapies. Wanting to be at the forefront of that and trying to deliver change where it’s needed have always driven what I want to do. This was the perfect intersection of my scientific and clinical interests.
Gabriela S. Hobbs, MD
Ruth: Dr. Hobbs, would you tell us a little bit about yourself and how your interest in MPNs began?
Dr. Gabriela Hobbs: I am the clinical director of the leukemia service as well as the MPN program at Massachusetts General Hospital in Boston. I’ve always been interested in hematology as far as I can remember, and I was very fortunate to do fellowship training with Dr. Rampal.
For me, myeloproliferative neoplasms in particular are such a rewarding group of patients to take care of. It merges everything that I love about being a physician. I can have very longitudinal as well as very intimate patient relationships with the patients whom I take care of. From the clinical perspective, I found taking care of patients incredibly rewarding and also very varied.
From the scientific perspective, when I was an undergraduate student, we started seeing some of these oral-targeted agents being approved and I knew that was something I wanted to be involved in for my career.
Being a clinical investigator who’s able to see clinicians like Raajit Rampal doing investigations in the lab, finding new targets and new drugs, and being the person who helps take that to clinical trials to the patients is incredibly rewarding.
The most common symptom of patients with myelofibrosis is fatigue, which is probably one of the reasons why myelofibrosis and the other MPNs sometimes take a while to get diagnosed.
Dr. Gabriela Hobbs
Symptoms of Myelofibrosis
Ruth: Myelofibrosis is rare. Some practitioners don’t see very many MF patients. Some patients who are diagnosed with myelofibrosis don’t have enough information or are misguided at times. What do you each see as the major symptoms of myelofibrosis?
Dr. Hobbs: Myelofibrosis is a disease that can present in many different ways. I certainly see completely asymptomatic patients. Their doctor noticed that they had some abnormalities in their blood counts or maybe the patient themself noted that their abdomen felt a little bit different. Patients are on the spectrum of either not having a lot of symptoms or having lots and lots of symptoms.
I would say the most common symptom of patients with myelofibrosis is fatigue, which is probably one of the reasons why myelofibrosis and the other MPNs sometimes take a while to get diagnosed. Other symptoms that we see a lot of are itching, night sweats, fevers, and unintentional weight loss.
Dr. Rampal: Part of the challenge is whether those symptoms are communicated in visits with physicians. Part of that involves us asking the right questions or, at least, training our colleagues to ask the right questions because not everybody is forthcoming about their symptoms. The alternative is that they get so used to their symptoms that it’s the new normal for them and that is sometimes the tougher part of trying to understand how somebody is doing.
Dr. Hobbs: Occasionally, there may be some patients who feel like there are certain symptoms that they wouldn’t bring up to an oncologist. When I meet a patient for the first time and go down my checklist of MPN symptoms, I’ll ask them about itching and they’d say, “How did you know?” We’re fortunate in the MPN world to have these forms that have been validated to help us ask about symptoms that we know are very common in patients with MPN so that we don’t miss anything.
There’s a whole spectrum of symptoms patients can experience.
Dr. Raajit Rampal
Dr. Rampal: Myelofibrosis is a disease of the bone marrow where you have mutated cells that start to grow and take over the bone marrow. They cause inflammation and we think the inflammation causes scarring in the bone marrow. As that happens, the bone marrow starts to contract and is unable to make blood cells. Blood cells start to go into the liver and the spleen to try to produce blood so those organs get larger and cause symptoms.
The inflammation that causes the scarring and damage in the bone marrow also causes people to have symptoms. Those include getting fatigued, losing weight unexpectedly, and having bone pain and aches. There’s a whole spectrum of symptoms patients can experience, but those are among the most common.
That’s how we think about myelofibrosis and how we think about the disease getting worse. We look at blood counts. If people’s blood counts are getting worse, that’s a sign of disease progression. If their spleens or livers are getting larger or they’re feeling worse, all of those are signs of the disease progressing.
There were two phase 3 studies presented about myelofibrosis, the navitoclax and pelabresib studies.
Dr. Gabriela Hobbs
ASH 2023 Updates on Myelofibrosis Treatments
Ruth: We all know there’s been such an explosion in advances in myelofibrosis in recent years. Dr. Hobbs, what came out of ASH 2023 that you’re most excited about?
Dr. Hobbs: It’s exciting. I can’t remember participating in an ASH conference where there were two phase 3 studies presented about myelofibrosis, the navitoclax and pelabresib studies. That in and of itself was a reflection of how far the field has come. We’re now presenting phase 3 studies on drugs that may get approved.
Dr. Rampal: I totally agree. When have we had two phase 3 studies read out? I can’t remember if that’s ever even been the case simultaneously. Thinking about this in the context of our patient audience, this is a clear sign of progress in the field.
Let’s separate that idea from what happens from a regulatory standpoint. You have to get to this point. This is where the finish line is. It is incredibly encouraging that we’ve got drugs to this point of phase 3 where we may have definitive results that could lead to approvals.
What we can probably say, at least with both drugs, is that they have activity in the disease. There’s no question. What happens from here, of course, is up to the FDA. But I’m encouraged by this. I think these drugs have the potential to make a difference for patients so this is exciting.
The combination (ruxolitinib and navitoclax) led to a very dramatic improvement in spleen volume reduction in patients compared to patients who were treated with ruxolitinib alone.
Dr. Gabriela Hobbs
Dr. Hobbs: Both of these studies were phase 3 studies, as Dr. Rampal mentioned. The navitoclax study was the TRANSFORM study that compared ruxolitinib alone to ruxolitinib and navitoclax. They wanted to see if the combination of the two drugs was more effective at improving spleen volume response as well as improving the symptoms of myelofibrosis patients.
They found that the combination led to a very dramatic improvement in spleen volume reduction in patients compared to patients who were treated with ruxolitinib alone. The symptom endpoint was more difficult, as it seemed like symptom improvement was similar with the combination of navitoclax and ruxolitinib compared to ruxolitinib alone.
My take on that is it’s not entirely surprising that a drug like navitoclax would not improve the symptoms, but it certainly didn’t make patients feel worse. I think that’s important when you think about combination therapy as well. I wouldn’t consider that an entirely negative endpoint.
Why should patients care about how big the spleen is and how much it shrinks? That is one of the few things we know that correlates with survival.
Dr. Raajit Rampal
Dr. Rampal: Let me build off of something that Dr. Hobbs said. Symptoms are important to patients and that has to be part of any of our treatment arsenals. But as you said, we want to get drugs that alter the trajectory of the disease and not simply focus on symptom reduction. That has to be part of the conversation going forward as we think about new drugs in this space.
How much weight do we put on symptom reduction as something that we, as a community or the FDA, should fixate on? As long as the drug is not making people feel worse, if it’s doing other things for patients, then maybe that’s where the win is if you will.
About pelabresib, this is a study of the combination of pelabresib, which is a BET inhibitor, plus ruxolitinib versus ruxolitinib alone. The study looked at whether patients had a greater degree of spleen shrinkage with the combination or ruxolitinib alone.
The answer was unequivocally yes. Patients who got the combination had a much greater spleen response, 65% versus 30%.
Why is that important? Why should patients care about how big the spleen is and how much it shrinks? That is one of the few things we know that correlates with survival. We’ve known from the time of ruxolitinib. Spleen shrinkage correlates with overall survival, which is something we all care about deeply.
There was a trend toward the symptoms getting better with the combination. It wasn’t quite statistically significant, but it was certainly a trend that favored the combination.
Importantly, it didn’t add toxicity. We didn’t see that there were any new major signs of toxicity with the two drugs versus one. In oncology, we worry about that all the time. If you add another drug, you may add toxicity, but that wasn’t the case here. From that standpoint, I’m very encouraged by both data sets.
A big takeaway from having all these drugs is that we shouldn’t wait for people to get that sick. We should treat earlier on.
Dr. Raajit Rampal
Treatment Sequencing
Ruth: Dr. Rampal, as we talk about more options available both today and in the future, one of the things that comes up often, especially for higher-risk MF, is sequencing. What are we learning about optimizing the new drugs and combination drug therapies, including determining when and how to switch therapies?
Dr. Rampal: The answer is we don’t know. The broader context of this is that we have more options so that has two implications.
Historically, there’s been a reluctance to start therapy because you didn’t have anything else. If you were in a world where there was only ruxolitinib and it stopped working, what were you going to do? That’s not true anymore.
A big takeaway from having all these drugs is that we shouldn’t wait for people to get that sick. We should treat earlier on. What is earlier on? There’s some ambiguity there, but I think that is one of the implications of having a lot more drugs.
The reality is we’re going to learn how to use these drugs as we go along. There isn’t a great deal of data. We have data on switching from ruxolitinib to fedratinib. We know what happens and how people do when you do that, but do we have data for the other drugs?
If we start going from momelotinib to ruxolitinib, we don’t have the granular data for that. Those are things we’re going to figure out in practice, probably over the next 1 to 2 years, I’d say.
Now that we have four approved JAK inhibitors, there’s no reason to feel like somebody needs to wait for symptoms from their spleen or their disease.
Dr. Gabriela Hobbs
Dr. Hobbs: The point that Dr. Rampal made is so important, especially when we think about what he said about one of the things that we know in myelofibrosis, which is a smaller spleen equals better outcomes.
An important message for patients is exactly what Dr. Rampal said. Now that we have four approved JAK inhibitors, there’s no reason to feel like somebody needs to wait for symptoms from their spleen or their disease because we do have a lot of options.
Now that we have a lot of options, it became a situation where all of us are calling each other and asking, “How do you switch from this one to the other? Have you had a good experience?”
Sometimes, the clinical trials don’t necessarily translate to what we do in clinical practice. Many clinical trials require that patients be completely off of a JAK inhibitor before they switch to the other, which is something that, in practice, probably neither of us would ever really feel like doing. Over the next year, it’s something that we’re going to have some publications about to help guide the broader community to do that safely.
What these data have shown with the FREEDOM trials is that you can better manage gastrointestinal toxicity and that it does get better over time.
Dr. Raajit Rampal
ASH 2023 Updates on Fedratinib
Ruth: Dr. Rampal, what did we learn about fedratinib at ASH 2023?
Dr. Rampal: The most updated data was the FREEDOM2 study, which looked at fedratinib in patients who have been on ruxolitinib. There were earlier trials that looked at the same question, like the JAKARTA2 trial.
When fedratinib was being studied early on, it was seen that there was a lot of gastrointestinal toxicity, like nausea, vomiting, and diarrhea, which was experienced by the majority of patients.
There have been two subsequent trials with fedratinib, the FREEDOM trials, where they aggressively tried to manage the symptoms from the get-go. They didn’t wait for people to get sick or have nausea or diarrhea. When they prescribe the drug, they say, “When you start the drug, if you start to feel nausea, you’re going to take this medication or if any diarrhea starts, you’re going to take this medication.” You don’t let these symptoms get out of control.
What these data have shown with the FREEDOM trials is that you can better manage gastrointestinal toxicity and that it does get better over time. Is that still a side effect that we have to be concerned about? Yes, but it is something that we can manage in most cases if we’re aggressive about doing that upfront and the expectation is that it will get better over time.
The data (on selinexor) is still in earlier stages so I’m waiting to see if this agent is well-tolerated by patients.
Dr. Gabriela Hobbs
ASH 2023 Updates on Selinexor
Ruth: Dr. Hobbs, what about selinexor?
Dr. Hobbs: Selinexor has been interesting as well. This is a newer agent that we’ve started to see some preliminary results on and they presented their data also in combination with ruxolitinib. This agent seems to have very impressive responses in terms of shrinking the spleen and improving symptoms as well.
The data is still in earlier stages so I’m waiting to see if this agent is well-tolerated by patients. We’ll have to see how the later studies will pan out, but it’s still exciting.
Having this fourth agent will be very helpful in the management of patients with MF, especially patients who have anemia and aren’t able to get a bone marrow transplant.
Dr. Gabriela Hobbs
ASH 2023 Updates on Momelotinib
Ruth: There’s an unmet need for the treatment of anemia for patients with MPN, specifically myelofibrosis, which brings us to momelotinib and a few others.
Dr. Hobbs: We’ve mentioned that there are now four JAK inhibitors that are approved for the treatment of myelofibrosis. We have pacritinib, ruxolitinib, fedratinib, and momelotinib, which was approved at the end of September 2023.
Momelotinib is a JAK inhibitor that was approved a little bit differently than the others. Its main indication is for patients who have myelofibrosis and anemia. Anemia has been an unmet need in the management of myelofibrosis so it’s exciting to have a drug like momelotinib that can help anemia and also a drug like pacritinib that can also help anemia in a subset of patients.
In my practice, I’ve noticed that since the approval of this agent, there have been many patients, especially those who are active online, in their communities, and in patient advocacy organizations, who have been excited or eager to switch to this medication.
I do think that having this fourth agent will be very helpful in the management of patients with MF, especially patients who have anemia and aren’t able to get a bone marrow transplant.
When we have patients with myelofibrosis who have anemia, it’s important to consider if a bone marrow transplant is the right therapy. But for those who can’t receive that therapy, momelotinib takes care of a lot of the parts of the disease that we worry about, like the symptoms, the spleen, and the low red blood cell numbers.
In some cases, they take patients who are relying on transfusions and convert them to not needing a transfusion, which is important in terms of survival.
Dr. Raajit Rampal
Dr. Rampal: There is so much going on in anemia in this disease, it’s remarkable. It’s a problem for which we had no good solutions until very recently.
As you mentioned, momelotinib and pacritinib also seem to have an effect in a proportion of patients where they can increase the hemoglobin. In some cases, they take patients who are relying on transfusions and convert them to not needing a transfusion, which is important in terms of survival.
We know that that correlates with survival, but it’s also quality of life. If you have a patient who’s getting stuck in the transfusion chair for 4 to 6 hours a week or more and that is no longer an issue, that is immensely important to their quality of life. It’s an important problem.
There are some other drugs in development and that includes a drug called luspatercept, which is FDA-approved for myelodysplastic syndrome. There are also some other drugs from a few other companies that are anemia-specific and there was some data presented at ASH on them. There are early signs of efficacy. Too early to say anything definitively, but at least it looks like these are drugs that will be studied further.
What’s been practice-changing is having the approval of the last JAK inhibitor, which is momelotinib.
Dr. Gabriela Hobbs
Practice-Changing Updates
Ruth: We talked about what’s happened in the lab, what’s in the drug approval process, what’s recently been approved, and where our needs still are. What came out of ASH that you think is truly practice-changing immediately or in the near future?
Dr. Hobbs: What was very exciting was seeing the two phase 3 studies. Although those two drugs, pelabresib and navitoclax, are still not approved, they are potentially closer to our doorstep and something that we will have to have conversations about how to use.
Do we use them in combination with the JAK inhibitor that they were studied with? Do we use them with other JAK inhibitors? How do we think about sequencing when we’re talking about combination? Although neither of these agents is approved, these are questions that need to be discussed.
What’s been practice-changing is having the approval of the last JAK inhibitor, which is momelotinib. We now have four drugs that we can prescribe to our patients when we see them in the clinic, especially those who have anemia.
There are so many drugs coming down the pipeline and showing interesting activity, especially some of those showing activity by themselves.
Dr. Gabriela Hobbs
Personalizing Myelofibrosis Treatment
Ruth: The drugs and the studies we’ve talked about are all very exciting, but what other treatments are you excited to share with patients to help you personalize treatment?
Dr. Hobbs: We’ve discussed the MANIFEST and TRANSFORM studies looking at combination studies in phase 3. There are so many drugs that are being evaluated and it’s been very exciting to be at an ASH where we hear about so many different mechanisms of action being explored. Many of those are by themselves and some of them are now getting to the point where they’re used in combination.
To mention a few, there was a compound called a PIM1 kinase inhibitor, another one that inhibits lysyl oxidase, which is a group of enzymes that have to do with making fibrosis or scarring happen in the bone marrow, and an LSD1 inhibitor called bomedemstat.
There are so many drugs coming down the pipeline and showing interesting activity, especially some of those showing activity by themselves. Generally speaking, when we have new drugs that are not JAK inhibitors used by themselves, we rarely see a lot of clinical activity so I thought that that was exciting.
Individualized medicine is the holy grail and there’s a lot of different ways to think about it. There’s how we use the drugs we have now and what some of the newer drugs may be able to do for us.
Dr. Raajit Rampal
Dr. Rampal: There is this whole pipeline of things coming forward, which is amazing for this field. We spent some time talking about the top-line phase 3. But as Dr. Hobbs mentioned, there are all of these drugs that are in early development that are showing us that they may be able to do something. Even beyond what we have, some things are part of the big picture here.
Individualized medicine is the holy grail and there’s a lot of different ways to think about it. There’s how we use the drugs we have now and what some of the newer drugs may be able to do for us.
A key example of this is calreticulin. There’s been a focus on this. There are drugs in investigation that are specific antibodies that target calreticulin. That could be a game-changer if those things work. Pre-clinically, there’s good rationale. Imagine a future where if those drugs are effective, then for calreticulin-mutant patients, this is what we use. We have a drug that targets your mutation. That is where we want to be.
Of course, other mutations occur in the disease and we’ve already started trying to do personalized medicine for patients. Some patients have an IDH mutation that occurs typically in people with more advanced diseases.
We’ve completed a trial where we used a JAK inhibitor plus an IDH inhibitor. IDH inhibitors are FDA-approved for people with leukemia and we’ve combined those drugs and seen very good results. That’s an example of genetically-informed personalized medicine, but there’s also how you use the drugs we have in practice.
Dr. Hobbs: We’ve mentioned a few times that we have four different JAK inhibitors and it’s important to know which patients those are going to help. Are there certain situations where we should use one JAK inhibitor versus another?
At ASH 2023, we saw an update on a similar study that was published recently by the folks who looked at pacritinib. They found that patients who have a symptom improvement of greater than 10% had an improvement in survival, which is similar to what they showed recently with patients on pacritinib having a survival benefit if they also had a spleen volume reduction.
Again, that goes to the theme that we were saying. It’s important to use these drugs and make sure that those drugs are doing what they’re supposed to be doing for the patient. We have endpoints that help patients not only to live better but hopefully to live longer. That can also help the practicing doctor to say this drug is not meeting those endpoints. It’s not helping my patient have an improvement in their spleen or their symptoms. We have other drugs that we should we should think about switching to.
One of the areas where there’s a lot of interest is looking at pre-fibrotic myelofibrosis or early myelofibrosis to see if we can get to the disease earlier before a lot of scarring develops.
Dr. Gabriela Hobbs
ASH 2023 Updates on Interferon
Ruth: There was an interesting study presented at ASH about interferon-α versus hydroxyurea, which is the oldest of the drugs still used for myelofibrosis or MPNs. This study was in untreated MPN patients who were unable to take ruxolitinib. What did we learn?
Dr. Hobbs: Several abstracts were presented with interferon. One was the updated results of the DALIAH study comparing pegylated interferon to hydroxyurea for patients with earlier disease essential thrombocythemia and polycythemia vera. There was also another study looking at earlier myelofibrosis, like pre-fibrotic myelofibrosis.
There’s been a lot of interest in looking at interferons in general across the spectrum of the disease. One of the areas where there’s a lot of interest is looking at pre-fibrotic myelofibrosis or early myelofibrosis to see if we can get to the disease earlier before a lot of scarring develops.
If we look at all the characteristics of the patients who had stable disease for years versus those who progressed, is there a difference that AI can say if you look at these particular parameters, this is a warning sign?
Dr. Raajit Rampal
Artificial Intelligence in Hematology
Ruth: There was a fascinating presentation on the use of artificial intelligence, specifically to differentiate between essential thrombocythemia and pre-fibrotic primary myelofibrosis. Is that something that you see coming into practice or are we way off on that?
Dr. Rampal: We’ll level set by talking about what we mean by AI, which neither of us are experts in. One of the powers of AI is to take broad sets of data and identify patterns. That is a very simplistic way of thinking about the many things that AI can do and is built to do. It can take thousands of variables and find patterns that humans aren’t going to be able to find in real time.
This is an example of what you’re talking about. If you took thousands of bone marrow samples and you said that clinically, these people look like ET, but based on the other parameters that we have, these people look like myelofibrosis. Is AI going to be able to better discriminate versus a human and say this pattern better fits the ET pattern and that pattern better fits the MF pattern?
It will help us refine some of the key characteristics of the disease. The hope is that it may also give us some clues for things like progression if you look at the pattern of a lot of patients. We’re talking about thousands of patients and if we look at all the characteristics of the patients who had stable disease for years versus those who progressed, is there a difference that AI can say if you look at these particular parameters, this is a warning sign? That I think is part of where we think this is going to go.
There are lots of great resources online where, as a patient, you can advocate for yourself to recommend different treatments to your provider to make sure that you’re getting the most updated care.
Dr. Gabriela Hobbs
How Patients Can Be More Proactive in Their Treatment
Ruth: Now that we’ve heard updates out of ASH 2023, what can a patient bring to their community hematology-oncologist as opposed to waiting for it to trickle down? What are some of the ways that a patient can be more proactive with knowing what we now know?
Dr. Hobbs: If you’re a patient or a family member of a patient, you’re already taking those steps that are so important. It’s important to remember that myeloproliferative neoplasms are rare diseases so not everybody has access to subspecialized care.
What’s incredible about the MPN community is that the group of clinicians who treat MPN and are doing research in MPN are extremely committed and passionate about treating these diseases. We’re excited to work with industry partners who are similarly very passionate about finding new therapies for these diseases.
There are lots of great resources online where, as a patient, you can advocate for yourself to recommend different treatments to your provider to make sure that you’re getting the most updated care.
It’s worth asking your physician: when is it time for me to get started on treatment? If you are at the point of needing treatment, it may be worth getting a consultation in a center where there’s a lot of experience.
Dr. Raajit Rampal
Dr. Rampal: If you’re a patient who’s being cared for in the community, it’s worth asking your physician: when is it time for me to get started on treatment? This is an evolving space. We’re more and more convinced that earlier may be more beneficial, but there is a danger in waiting too long.
If you are at the point of needing treatment, it may be worth getting a consultation in a center where there’s a lot of experience. We, who are focused on this, have the forefront of the developments at our fingertips. Doctors in the community setting are busy seeing a lot of different types of cancers. They have to keep up on all of this and they may not have immediate access to that information.
If it is time to get treated, it may be worth a consultation at least to say, “Is this the right thing? Or is there a compelling clinical trial that maybe may make more sense right in the current era?”
We’re bringing back hope. We’ve seen more developments at ASH 2023 than in maybe any prior in the last ten years that I can think of. That’s not unimportant.
Ruth: That’s a very hopeful message. We seem to say that every year but maybe now even more than ever.
Conclusion
Ruth: From a patient perspective, one of the themes that came out of ASH 2023 is all these new approaches to old diseases. It’s not that we’ve discovered new diseases. It’s that these are diseases and patients who have not had solutions for so long or our options have been so limited and now there are more and more options.
Thank you both so much for your time, Dr. Hobbs and Dr. Rampal. Always my pleasure.
Stephanie: Thank you so much, Ruth, for being our incredible patient advocate and moderator. Also to Drs. Hobbs and Rampal for the work and research you do to help move the landscape of myelofibrosis options.
We hope that you walk away with a better understanding of the latest treatments and clinical trials in myelofibrosis. They may or may not be right for you, but it is our goal to make sure you feel empowered to make a decision for yourself.
Thank you and we hope to see you again at a future program at The Patient Story.
Special thanks again to GSK and Karyopharm for their support of our independent patient education content. The Patient Story retains full editorial control.
A Practical Approach to Disputing Cancer Care Expenses, Backed by Experts and Real Patient Experiences
Edited by: Katrina Villareal
Navigating the costs of cancer treatment can be overwhelming. This live conversation provides practical tips from experts and real cancer patients on understanding your health insurance, finding financial assistance programs, knowing your rights to appeal insurance decisions, and reducing financial toxicity.
In this conversation, we’ll explore the fundamentals of health insurance, emphasizing the importance of reading and understanding your policy, including basic insurance terms. Discover your rights as a cancer patient, learn strategies for appealing insurance decisions, and explore avenues for applying for financial assistance.
Hear from Abigail Johnson, a stage 4 metastatic breast cancer patient advocate, and attorney, Gregory Proctor, a multiple myeloma patient advocate, and Monica Fawzy Bryant, a cancer rights attorney and co-founder of Triage Cancer, as they share real-world experiences, health insurance tips, and strategies for tackling financial toxicity to help you navigate the financial aspects of cancer treatment. This live conversation took place in November 2023.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Abigail Johnson: Hello, everyone, and welcome to a discussion of how to dispute cancer care costs sponsored by The Patient Story and including representatives of patients experiencing this individually, as well as a representative from Triage Cancer.
The Patient Story’s tagline is Human Answers to Your Cancer Questions. Founded by a cancer survivor who took her love of storytelling and producing videos, they assist people in the cancer community to get that all-important peer support and information about how other people have handled something that you as an individual might be facing yourself.
Without further ado, I want to get to the amazing people that we have talking about this very human issue, which is getting your cancer care costs covered.
Gregory Proctor: My name is Gregory Proctor. I’m a multiple myeloma survivor diagnosed back in July 2021. In the early stages, it was very overwhelming and very impactful not only emotionally but physically. Coming from a project management background, one of the things was trying to figure out how to navigate.
Information is not easily found in a lot of cases because if you Google things, you tend to get the bad before you get the good. But overall, my professional experience as well as having friends and family to help me move this forward has provided an overall successful outcome.
I’m proud to say that I’m still MRD negative, thriving, in remission, and continuing to flourish and be an advocate.
Monica Bryant: My name is Monica Bryant. I’m a cancer rights attorney and co-founder and chief operating officer for Triage Cancer, which is a national nonprofit dedicated to providing free education on legal and practical issues that arise after a cancer diagnosis. We provide education to the individuals who have been diagnosed, their caregivers, and healthcare professionals who are often on the front lines of getting these questions.
Abigail: Thank you, Monica. Y’all wrote the book on cancer and the law. What’s the name of that again?
It isn’t written for lawyers because we wanted to make sure that it was written in a way that was accessible for anybody to be able to access it — whether it’s the person who’s been diagnosed, their caregivers, lawyers who are trying to help out, or healthcare professionals. It’s written in a way that anybody should be able to pick it up, regardless of whether or not they have a law degree.
Abigail: I enjoyed reading it very much.
Like Monica, I’m also a lawyer, and in 2017, I was diagnosed with stage 4 metastatic breast cancer. I was 38 and it was, to put it nicely, a bombshell that went off in our lives and has changed everything since that has happened.
I’m working on getting into a clinical trial, which will be my sixth line of treatment. With breast cancer, because it’s a solid tumor, we don’t go into remission. That’s not necessarily a status or a goal for us. It doesn’t necessarily apply to our experience.
There can be no evidence of disease or, in my case, no evidence of active disease. I have been able to get to that point at least once in the last six years but I’m back getting a new treatment. For us with metastatic breast cancer, we go from treatment to treatment to treatment. There are a few that can go off treatment for some time.
I’m learning to adjust to being a professional patient, I like to call myself, because managing cancer itself can be a full-time job and that’s why discussions like this are very important because our quality of life, and Gregory alluded to this, is very much tied to not just how the cancer cells are being controlled in our bodies by the medication but also impacted by how we can get to that treatment, whether it’s literal transportation to get to that treatment or being able to afford cancer treatment.
Here in the US, cancer is quite the machine in a lot of ways. There are a lot of different players and moving parts. Our goal is hopefully to illuminate some of those moving parts, at least when it comes to covering the cost of cancer care.
Managing cancer itself can be a full-time job.
Abigail Johnson
Health Insurance
Abigail: This concept of covering cancer care a lot of times boils down to insurance. In my experience, being on a private insurance plan through my husband’s employment as well as Medicare, the first thing that I always talk to people about is getting a copy of the insurance contract. That can be daunting for a lot of people because these contracts can be 200 or 300 pages long. They are written by lawyers and many clauses can be super complicated.
If this seems daunting, intimidating, and confusing, it is. It absolutely is. It is for the professionals that are working in this arena. Getting your insurance contract, whether you have a government-sponsored insurance policy, whether you’re working with the Veterans Affairs and have coverage there, whether it’s Medicare, some documents explain what is covered.
When it’s private insurance, it is a literal contract between you and the insurance company, and it spells out what they’re going to do and not do. In my experience, there are about 10 pages that are vital for me to know out of the 300-page long contract. I have those pages highlighted, bookmarked, saved, and written all over.
I continually go back to those pages to see the clauses and the language that govern what my insurance company is supposed to do. I set my expectations based on what my insurance company is supposed to do, and then I know if they have or not.
It’s important to know what tier your medication falls in because that impacts the cost of your copay.
Abigail Johnson
Many times, a medication, a surgery, or a procedure has to have prior authorization. The medical professional has to get with the insurance company and say, “We want to do X,” and the insurance company has to look over that and opine whether or not that is medically necessary. I won’t get started about how that is practicing medicine on the part of the insurance company, but that’s the system that we have.
My insurance company has 24 hours to respond to a prior authorization request from my medical team. That’s important for me to know because if there’s a delay, I can call the insurance company and say, “My doctor sent you a fax 48 hours ago. You had 24 hours to respond. This needs to rise to the top. You need to deal with this right away because you’ve not responded in the timeline that we anticipate.”
That’s one example of how knowing what my policy says, who’s supposed to do what, and when they’re supposed to do that helps me set my expectations. I’m not fussing at my doctor’s office if it’s not their responsibility and I’m not fussing at the insurance company if my doctor hasn’t done what they’re supposed to do. Knowing when they have not done what they’re supposed to do, I can bring that to their attention and that means that will become more of a priority for my insurance company.
It’s important to know what tier your medication falls in because that impacts the cost of your copay. These are examples of things that are important to know about your insurance policy so that you know how to navigate that.
Gregory: I’ve worked with a lot of attorneys in my professional career, but I’m not one. I have always been a professional. I make my premium payment and expect that coverages are going to be there when I need them. Until something traumatic or something like cancer knocks on your door, you don’t realize the implications that you’re faced with.
We contacted my insurance company and they said, “Okay, we’re going to be able to help you move and navigate through this,” with all of the empathy and compassion that they try to give.
I’m 2 ½-3 months into treatment. I’m paying my $1,000 premium and doing everything I need to do, but I’m burning $22,500 a week. The billing department for my oncologist calls and says, “Mr. Proctor, we’re at a point where you’re a quarter of $1 million. We’re going to have to stop your treatment. Your insurance company hasn’t paid.”
I’m sitting here flabbergasted. I’m trying to fight for my life. I’m several months into my treatment and my doctor hasn’t received a single dollar from my private healthcare insurance. At that moment, I realized it wasn’t just about me fighting cancer. Now I’ve got to engage in something that you expect would be covered.
For me and my family, we had to turn the switch on and get laser-focused. Now it’s not just about the financial implications, insurance, and survival. We’ve got to look at all three with a critical eye.
Having the knowledge and knowing what to do with that knowledge to be able to save your life, save money, and avoid some of those pitfalls is extremely important.
Gregory Proctor
I had to contact the insurance company and say, “I need to see the full contract. I need to understand why you guys are not paying my doctor.” Their reason at that time was, “We have to go through an audit, Mr. Proctor. You’ve been healthy. You’ve never had any type of circumstance like this come along and then all of a sudden, now you go from 0 to $22,500 a week.”
To me, that wasn’t an excuse. I said, “I’ve never missed a premium. I’ve never missed a payment. I need this to occur for me on my behalf because I’ve done what I needed to do.”
Everyone comes from a different walk of life and sometimes knowing what to do as well as knowing how to do it becomes extremely important. One of the things that was formidably important for my wife and me was taking all of my project management experience and applying it to myself as the project so that we could cover all of the gaps.
As they always say, knowledge is power. In this particular case, having the knowledge and knowing what to do with that knowledge to be able to save your life, save money, and avoid some of those pitfalls is extremely important.
In most cases, those are not things that you think about when you’re thrown into the tsunami of cancer. You’re thinking how to get from day to day, from week to week. There’s a lot more involved and it all embodies getting yourself educated.
Abigail: Thank you for all of that, Gregory. You’re coming to this with all of the information and experience that you have. You’re going to do it as a project manager because that’s your background. Who you are, your strengths, and how you solve problems is going to be key.
Understanding Insurance Terms
Abigail: Monica, what are the top things that patients need to know when they’re looking at their insurance contract or how to get cancer care covered?
Monica: There are some things that people really should understand about their insurance long before there’s ever a diagnosis or a serious medical situation. But the unfortunate reality is that in this country, health insurance is confusing. There are going to be differences depending on the source of that insurance, whether that’s government insurance, through an employer, or a policy someone purchased on their own.
Based on studies that have been done, only about 4% of Americans understand the four most common terms used in health insurance policies. People don’t even understand the words. We’re not even talking about complex legalese here. We’re talking about the basic words because we’re never taught what those words mean.
There is an amount someone pays monthly to have health insurance and that’s the monthly premium. They’re going to pay that amount whether they go to the doctor or not. It’s like having car insurance all year but never getting into an accident.
Once someone starts utilizing their health care, there are going to be some additional costs and those costs are going to depend on the policy. Most policies have an annual deductible, a fixed dollar amount that someone has to pay before health insurance kicks in. Someone could have a $500 deductible or a $5,000 deductible. It’s all going to depend on the plan.
Once they’ve met that deductible, insurance kicks in and pays a percentage. That percentage is referred to as the cost share or the coinsurance. Here’s where it gets tricky because we have multiple names for the same thing. Cost share and coinsurance are the same thing, and that’s a percentage. If someone has an 80/20 plan, once they meet their deductible, insurance kicks in at 80%, but they’re still responsible for 20%. And when the treatment is expensive, 20% is still a huge dollar figure.
Based on studies that have been done, only about 4% of Americans understand the four most common terms used in health insurance policies.
Monica Fawzy Bryant
In addition to that percentage, many plans have copayments, which is a fixed dollar amount that is going to depend on the policy and also potentially on the service. Someone could have a $25 copayment to see the doctor, a $35 copayment to see a specialist, or a $250 copayment to go to the E.R. Figuring that out could be complicated.
The most important thing for every single person to know about their health insurance policy is if there’s an out-of-pocket maximum and what is it. Because in theory, that’s the most that someone is going to pay out of pocket for their care if they go to in-network providers for the year.
Understanding that allows us to figure out what you are going to have to be responsible for out of pocket in a worst-case scenario. The way you get to your out-of-pocket maximum depends on the plan, but often it involves adding up everything you’re paying towards your deductible, your copayments, and your coinsurance. It’s everything you’re paying out of pocket except the monthly premiums.
The reason this is so important on the front end is when people are making choices around their health insurance. We have the opportunity to do that every single year now, thanks to the Affordable Care Act and a whole bunch of other laws.
To be an effective shopper and consumer of health insurance, you have to understand those terms and be able to do the math concerning your out-of-pocket maximum.
Gregory: For me, that’s key. I always maintain a pretty healthy lifestyle. I don’t want to have to come up with $15,000 as a deductible. If I’m healthy and I still feel pretty good, I can go with a little less coverage. You take a little bit more risk.
I was diagnosed at the age of 50, which was not the best year to be diagnosed with multiple myeloma. The older I got, I began to get laser-focused in my mindset as it relates to my family of four and my insurance.
At the age of 50, I’m more susceptive to all of these things that maybe I don’t want to think about, but I need to be in a position to ensure that I’m covered holistically without any repercussions.
Abigail: It’s amazing how expensive everything is. One of the things about cancer treatment is the medication and prescription drug costs, which can be complicated. When you’re put on medication by your doctor, they don’t always tell you the price tag upfront. In the breast cancer world, many of the medications that we take will cost our insurance companies between $14,000 and $20,000 per month.
Copay Assistance Programs
Abigail: In the context of private insurance, there are often copay assistance programs, which pharmacists will often help patients apply for. These programs are offered by the drug manufacturers or pharmaceutical companies. They will also have foundations sometimes. But depending on your insurance, these programs apply differently.
For myself, having a private policy means I’m eligible for copay assistance programs. Those copays go from hundreds of dollars a month to zero, oftentimes depending on which tier of medication you’re on.
My friends who transitioned to Medicare are surprised to notice that those copay assistance programs are not always possible when you’re on Medicare and that’s where those foundations do come into play as well.
Gregory, how has that affected you in terms of paying for your medication and working with the VA, where your primary insurance is?
Gregory: I was in a unique category. I had private healthcare insurance with a national provider when I was first diagnosed. I had been away from the government programs for many years. Since I’d gotten out of the Navy, I hadn’t utilized any of their benefits.
I started going through this process and all of this funding that you don’t account for starts to show up at my doorstep. Blood work for $16,000, a test for $15,000, and I wondered what insurance is truly covering if these bills are showing up.
I was very lethargic and incoherent for five days a week for three and a half months because I was on chemo for five days a week, 6 to 8 hours per day, which was tough.
Once I finally got to the point of reckoning and saying it was time to get a hold of this situation, I found out that there are subsidy programs. Sometimes they’re publicly known, other times they’re not, particularly if you don’t ask. We started pulling our energy into how could we tap into maybe a program to be able to give us a grant and move forward.
On record today, I’ve spent $2.65 million. Navigating that journey was not easy… It’s overwhelming. You’ve got to get other people involved to help be your eyes and ears
Gregory Proctor
With private healthcare, there’s a little bit of leniency. By the time I was approved for government healthcare being a prior veteran, I couldn’t utilize those programs. It was a very delicate balancing act to ensure that going forward, I would be able to reap all of the potential benefits that I could not afford out of my pocket to maximize my overall primary care going forward.
Because on record today, I’ve spent $2.65 million. Navigating that journey was not easy. But certainly, you have to get laser-focused because no one is going to do it for you.
It’s overwhelming. You’ve got to get other people involved to help be your eyes and ears, to help address the questions of who, what, where, when, and how. Sometimes when you’re getting information from the doctors, you don’t want to accept the reality. Acceptance is always the key to making the first step in the progress of being able to battle and weather the storm.
Abigail: You have personally spent $2.65 million or your insurance company has spent that?
Gregory: I love to throw that number out there because people always say, “Oh my, what happened?” For clarification, that’s the running total. When you think about that number and go back to what Monica said. Whether you’re 70/30, 80/20, or 60/40, part of that expense is coming from you as the patient.
When you step into the throes of dealing with cancer, these are the things that you have to get laser-focused on very early on. Are you going to be successful coming out of the back side of this? Are you going to be bankrupt or dealing with the overall financial toxicity of what it does to you and how it changes your life?
Abigail: Thank you for that. Those are big numbers. Mine’s a little over $3 million so I’m tracking with you. I have not spent $3 million keeping me alive, but certainly between my family and the insurance company.
Monica: Thank you for your service, Gregory. I’m glad that the VA was helpful in this process for you because it’s deserved.
Financial Assistance for Cancer Patients
Abigail: Monica, would you like to talk a little bit more about financial assistance and how patients can go about getting help to cover their portion of these costs?
Monica: With respect to getting financial assistance, I would say don’t start there. That should not be step one when you see the big bills come in because there isn’t a whole lot to go around. As you both alluded to, there are some barriers depending on the type of insurance that somebody has.
Before someone goes down the path of trying to apply for financial assistance, there are some steps to take. Did the insurance company cover what they’re supposed to cover? That requires making sure you’ve waited until you’ve gotten your explanation of benefits, which is the letter from the health insurance saying this is what we’re going to cover and this is what you potentially owe. It’s about keeping track of your out-of-pocket maximums.
If someone understands what their out-of-pocket maximum is and what’s included in their out-of-pocket maximum, it can help them figure out how much they need from financial assistance. A lot of times, people get those prescription drug bills and don’t realize the prescription drug benefits are included. It doesn’t matter what their insurance company will pay or not. If you’ve hit your out-of-pocket maximum, they’re responsible for 100% of it.
Unfortunately, some additional steps fall into the laps of patients and family members before getting financial assistance.
Do a deep dive into what’s out there and what’s available. Even among the pharmaceutical companies, there might be different programs.
Monica Fawzy Bryant
With financial assistance, oftentimes people get tunnel vision when they’re thinking about sources of help. Abigail, you mentioned how expensive your monthly prescription drug is.
How am I going to get money? How am I going to get assistance to pay for that prescription drug? I’m on Medicare so I don’t have access to the same pharmaceutical programs that I did. What am I going to do now?
Are there other places you could potentially get help? Could you get mortgage assistance, utility assistance, or other types of financial assistance and then shift the money around? Anything that you set aside to pay for the mortgage or student loans can get shifted to help pay for prescription drugs.
Do a deep dive into what’s out there and what’s available. Even among the pharmaceutical companies, there might be different programs. Some companies can provide free drugs, some companies can provide assistance to pay copays. They all have different programs. Figuring that out is daunting.
AtTriageCancer.org, we have a chart that lists most of the major cancer drugs, the pharmaceutical companies that make those drugs, and the various programs that they have to try to make it a little less daunting to go down the Google rabbit hole because that is stressful by itself.
You can look for other types of financial assistance or grants that might be out there based on the type of cancer you’ve been diagnosed with. Sometimes there’s even financial assistance for family members who might be acting as caregivers. We have a tool called Cancer Finances that has pulled those resources from trusted sources to make it a little easier. It’s still not easy but a little easier for people who are trying to seek out those sources of financial support.
Abigail: Great resources. I have sent so many people to Triage Cancer. If you have a Sam’s or a Costco membership, you don’t even use insurance when you go to your wholesale clubs. For a medication that I was previously on, my copay was $15, but if I got it without using my insurance company, it was $20, which boggled my mind. Unfortunately, that puts a whole lot of burden on the family to figure out some of those things.
Gregory, did you ever get assistance from a social worker to help you figure some of these things out? Was that something that was offered in your oncologist’s office?
The life that you know before and after cancer is totally different. Asking questions could be the differentiator in a lot of the things that we’re talking about.
Gregory Proctor
Gregory: Not in my oncologist’s office but as I was getting prepped for a stem cell transplant. As a patient, it is important for you to ask.
Seek out and ask as many questions as possible. What do I need to do? How do I need to do it? What resources? What assets? Even if your doctor doesn’t want to give you the answers, you need to continue to perpetuate that going forward because it’s your life. The importance of survival doesn’t have a price tag.
I looked at everything. My wife and I flipped everything upside down because, at that point in time, your life is already flipped upside down. The life that you know before and after cancer is totally different. Asking questions could be the differentiator in a lot of the things that we’re talking about.
Abigail: Thank you for saying that. I talk to so many patients all the time who are worried that asking questions might be offensive or upset their healthcare providers. While that is certainly a good human thing to think about, in a situation like cancer, it’s your life on the line so ruffling a few feathers doesn’t seem to be as important as getting the answers.
Appealing Insurance Decisions
Abigail: I want to talk more about denials or when the insurance company is asking for your doctor to jump through some hoops. I talked about prior authorizations. What happens when an insurance company says, “No, we don’t think that that is medically necessary,” or like in Gregory’s situation, “We need to examine this a little bit more,” that sort of thing?
I want to throw out a couple of things that I’ve learned along the way in dealing with private insurance. Typically, when a doctor gets prior authorization, the insurance company says no. Usually, you, as the insured, get a letter that says why they denied it. Your doctor typically gets the same letter. And then what?
Besides changing your mind and doing something different that your insurance company goes along with, in my experience, what’s next is your doctor has the opportunity to do a peer-to-peer discussion. This is covered in all the insurance contracts that I have seen, along with the definition of what a peer is.
Very early on in my cancer treatment, my doctor wanted to do a PET scan. For those of us with solid tumor cancers, PET scans are often the gold standard in terms of seeing where the cancer is and how metabolically active it is. This is a tool that doctors need to be able to make good decisions.
A doctor employed by my insurance company, who was a family doctor about five years out of medical school, deemed the PET scan not medically necessary.
By looking at my insurance policy, I learned that my insurance company was required, upon my asking, to provide a peer to my doctor. I realized that somebody who’s five years out of medical school, who has a small amount of experience, and who is in a specialty that has nothing to do with oncology does not meet the definition of a peer.
I learned that I could say to my insurance company, “I require you to provide a peer to talk to my doctor.” That conversation took five minutes.
In the first conversation where it was denied, my doctor spent 40 minutes trying to convince this doctor employed by the insurance company that what she was doing was standard of care. When she was able to talk to an oncologist — not an oncologist that had 30-plus years of experience, but somebody in the cancer world — it was a five-minute conversation and it was approved.
The first person that my doctor talked to was looking at a chart and the wrong category. She was looking at somebody who was stage 3 versus stage 4.
I’ve let my doctor’s offices and their staff know as they are scheduling that they can ask for a peer. Make sure it’s a peer who’s talking to your doctor.
By looking at my insurance policy, I learned that my insurance company was required, upon my asking, to provide a peer to my doctor.
Abigail Johnson
By looking at your insurance policy and understanding the definition of a peer, that one small thing can save your doctor time. That 40-minute conversation took my doctor away from seeing patients. The five-minute conversation was a whole lot more effective and efficient.
As an insured, you also have the option of filing an appeal. It can get involved and it’s a really heavy lift when it comes to attempting to explain to your insurance company why they are not following the contract.
Gregory, what experiences have you had in getting something covered, especially when you got that initial no?
Gregory: After burning $22,500 a week and hitting a cap, hearing the words, “We will cover this, but we won’t cover that,” meant, “We’ll cover you for the period of your transplant. However, if there are any complications, then that’s on you, Mr. Proctor.”
Going from my private healthcare and trying to get the VA to pick me up had already been denied by the VA. It was very frustrating very early on knowing that I would want it to go through the VA from the beginning, but I was denied and that’s just how the system works.
Their rationale was there was no service-related tie that could tie back to me being diagnosed with cancer. I had to get attorneys involved and justify what my job and MOS (military occupational specialty) was in the military. Going through that took a tremendous amount of time.
You can’t ever give up. You have to continue to push.
Gregory Proctor
For me, one of the things that I had to sink into throughout this whole journey is don’t ever give up. Find a will. Find a way to navigate. I had to go back through all of the tests to prove that I had multiple myeloma.
Once we proved that, I was able to get 100% coverage but that took approximately five months from the time that I was diagnosed up until I was getting ready to go into a stem cell transplant.
The best Christmas gift that my wife and I could have ever received in December 2021 was that letter from the VA saying they are now my primary healthcare provider and they will cover not only my stem cell transplant but all post-maintenance costs. We’re talking, “Hallelujah!”
That was well worth all of the effort, the headache, the anxiety, the concerns, and the worries to get to that point. But like I said, you can’t ever give up. You have to continue to push.
Abigail: Thank you for those reminders. It’s easy to give up, especially when there are a lot of roadblocks. I love how you mentioned that you realized you needed help and that getting a professional involved was important.
Legal Rights as Insurance Consumers
Abigail: Monica, would you talk a little bit about the legal rights that we each have as consumers and talk about those appeals and what services might be available to patients?
Monica: Gregory did a little bit of my job for me in that we don’t have to take no for an answer. The details around that will certainly depend on the type of insurance we’re talking about, whether it’s the VA, Tricare, Medicare, or Medicaid.
If we’re talking about private insurance, at the bare minimum, every single consumer is entitled to at least two levels of appeal. The first level is an internal appeal and that’s essentially where we go back to the insurance company and say we’d like you to reconsider.
The internal appeal can take a couple of different forms. It could be a written internal appeal where you’re providing documentation. It could also be what Abigail was referring to, which is a peer-to-peer conversation between two healthcare providers.
There are time limitations on when we as consumers get to file internal appeals. We usually get 180 days. Then there are time limitations on the insurance company to give a response depending on where somebody is.
In Abigail’s example, it was a denial of a prior authorization so the insurance company has to answer within 30 days. If you’ve already received the service and they’ve come back and said, “Nope, we’re not covering that,” then they get 45 days.
Here’s the problem. When we’re talking about cancer care specifically, a lot of times we don’t have 30 or 45 days to wait for an answer. What we as consumers need to understand is that we have the right to ask for an expedited appeal when the need for care is urgent, which it is in most cases when we’re talking about cancer care. The insurance company then has to answer within 72 hours. But people don’t know this. People don’t understand that they have this right.
If the insurance company ultimately comes back and still says no, we have the right to an external appeal and that’s where we go to an independent entity. It’s going to vary from state to state, but an independent entity will look at all the facts and all the medical evidence, and then make a decision as to whether or not the care is medically necessary.
People need to understand those words, medically necessary, are the legal standard on which the appeals will be decided. Is it medically necessary for you to get that service? The decision of the independent entity at these external appeals is binding on the insurance company.
We don’t have to take no for an answer. The details around that will certainly depend on the type of insurance we’re talking about
Monica Fawzy Bryant
I made it overly simplistic for this session. I understand that requires a lot of legwork and effort to get the doctors involved. I’m not minimizing any of that, but here’s what we know to be true.
Of the millions of claims that are denied every single year, 99.9% of them are never appealed. Yet we also know that when people do appeal, somewhere between 40 and 60% of the time is decided in favor of the patient.
When we’re talking about how to help people afford cancer care, I want to talk about appeals long before we get to financial assistance. If insurance is coming back and saying, “We’re not going to cover that,” for whatever reason, “You’ve hit your max,” “We think you’re too expensive,” “We don’t think you need your PET scan,” if you’re not appealing those denials, you’re essentially leaving money on the table.
Abigail: That is such a great point. When your insurance company knows that you will appeal and will not take their decision lying down, in my experience, they’re much less likely to deny things in the future. It’s really important to make it hurt and make it difficult for them.
I’m not talking about doing anything drastic. Take up a lot of their time. Be bold in saying what you need and in filing those appeals. In my experience, they typically won’t be as likely to deny something in the future.
Thank you for giving us those numbers, Monica, because those are shocking numbers, like the millions of dollars that Gregory and I were talking about earlier.
I’m going to do whatever it takes because I’m all about living. I still have a lot more life to live than to let cancer dictate and determine how that’s going to be for me.
Gregory Proctor
Monica: It’s also helpful to put into context for people who are already overwhelmed. They’re reaching capacity in what they can handle. They’re trying to survive. Now the lawyer is saying to go through this burdensome appeals process. The numbers are helpful, particularly around the number of successful stories, to make that additional burden almost worthwhile, so to speak.
Gregory: That’s the main reason why my mantra going through this was don’t ever give up. There’s got to be a will. There’s got to be a way. It may not be door A, it may be door B or door C, but you’ve got to keep asking those questions and ensure that you’re getting the answer that you need to move forward.
When my life’s at stake, it doesn’t matter to me if it’s $1 billion. I’m going to do whatever it takes because I’m all about living. I still have a lot more life to live than to let cancer dictate and determine how that’s going to be for me.
Financial Toxicity
Abigail: I want to talk about financial toxicity. We’ve thrown that word around a couple of times. I didn’t realize this, but in 2013, it was researchers at Duke University that coined the term financial toxicity to describe the financial hardship and distress that can result from the high cost of cancer treatment.
Their research showed how the burdensome out-of-pocket expenses associated with cancer care, such as copays and deductibles, can negatively impact a patient’s mental health and quality of life, leading to increased anxiety, stress, and depression.
We hear all the time that stress is not good for patients. Stress is not good because it changes chemical things in your body. It makes your quality of life more difficult when you are stressed out. Then here comes our medical system that causes stress on us.
Gregory, how have you handled the mental toll of those bills and the financial stress? How do you handle that emotionally, too?
At one point in my life, I was questioning whether or not I would be able to afford groceries that week. That’s when you know the toxicity has gotten hold of you.
Gregory Proctor
Gregory: You’ve got to be willing to accept that this is your reality. That’s the first step in going forward with any type of traumatic or life-altering things that are happening.
The other aspect that became very, very important for me personally was stepping away from the notion of dealing with cancer 24 hours a day, seven days a week. One of the most therapeutic things that I did during my cancer battle was getting out in nature, walking on the trails, and separating my mind from the overall objective of having this wreak havoc on me.
With all of the debt and bills coming in, your life still goes on. You still have your normal expenses and now you’ve got cancer expenses and all these other things that happen. At one point in my life, I was questioning whether or not I would be able to afford groceries that week. That’s when you know the toxicity has gotten hold of you. You’ve got to navigate and weather the storm to figure out how to maneuver and move forward.
I’ve done a lot of things to get through that and find assets and various other elements in my life that I could move forward without having so much of the burden of the debt wreak havoc on me.
Abigail: Thank you for sharing that. I tell my medical teams all the time that I have to fit cancer care into my life not fit my life into cancer care. It’s a paradigm or a different way of looking at things that I think makes us as patients address some of these things a little bit differently.
Monica, would you talk a little bit about resources that Triage Cancer has or strategies for managing medical bills and finances so that people can have a good quality of life?
Monica: It’s at the core of what Triage Cancer is about. We have tons of educational resources in a variety of formats because we’re trying to meet people where they are and how they learn. Some people are big readers and that’s how they’re going to absorb information so we have quick guides and longer practical guides that can be downloaded and read off our websites.
We have live events that people can join for free, both in person and virtually. We also have worksheets, animated videos, and other materials to help people with things that can contribute to financial toxicity.
Health insurance status and navigation are only one piece of the puzzle. Certainly, employment changes that can occur after a diagnosis are going to impact somebody’s finances. Everything that normally happens in life that impacts finances keeps happening. You don’t get a pause button on paying the mortgage.
When you look at TriageCancer.org, you will see a variety of topics around health insurance, employment, and disability insurance to address holistically the financial impact that cancer and cancer care can have on people. When thinking about how to maximize health insurance, people need to remember a couple of things.
Every single year, we have the opportunity to make choices. If someone is experiencing high out-of-pocket expenses due to their insurance this year, there may be opportunities to pick a different source of insurance for the coming year.
Open enrollment for Medicare is coming up at the end of the year and that’s an opportunity to make some different choices — whether that’s finding a plan with a lower out-of-pocket maximum, a plan that has more of your providers in their network so they’re being covered at higher rates, or has a different prescription drug formulary so any prescription drugs you’re taking may be covered at a better rate.
You may be experiencing high financial toxicity right now based on the type of insurance you have, but there may be opportunities to make those changes for the coming year. We have resources at Triage Cancer to help you make those determinations.
When you look at TriageCancer.org, you will see a variety of topics around health insurance, employment, and disability insurance to address holistically the financial impact that cancer and cancer care can have on people.
Monica Fawzy Bryant
We also have a legal and financial navigation program where people can fill out a form and they’ll get a calendar link where they can schedule a call with one of our staff. We’ll talk through their situation and the sources of financial toxicity. We’ll try to provide them with personalized education and information about what they need to know and understand, point them in the right direction, and give them action steps. You can read quick guides all day long, but you may still have questions about your situation.
Abigail: Those are wonderful resources. I’ve sent all kinds of people to Triage Cancer and they’ve helped them figure things out and navigate those things.
Since Monica was talking about open enrollment and the possibility of adjusting your coverage, working with a good insurance broker can also be a tremendous help, especially when you’re going on Medicare. There are all these supplements and different options. Working with somebody who can take your situation, your doctors, your medication, and your diagnosis, and help you back into those policies that would meet some of those needs.
Typically, brokers are paid by the companies so you are not out of pocket any amount of money when you work with an insurance broker. That’s one thing that I suggest to a lot of people, especially those transitioning from private insurance to Medicare because it can be complicated with all of the different supplements.
Monica: I actually would give the opposite advice to somebody and that’s based on reports that have come out of the U.S. General Accountability Office. Over the last several years, many insurance agents and brokers have misbehaved in several ways. Now, certainly, that is not all of them. There are wonderful insurance agents and brokers out there so I’m not disparaging the profession as a whole by any stretch of the imagination.
Oftentimes, people can be led down a path that may not be the best for them. Those agents and brokers are paid by the insurance companies so they have a vested interest in enrolling people in specific insurance policies, even if those aren’t the best policies for that patient.
For the cancer community, where there is a heightened importance of making sure they are in the right plan for them, we would suggest unbiased sources of support and there are different places that people could go.
You might get a very different answer from an insurance broker versus a social worker who is employed by your cancer center. Getting different input can be important.
Abigail Johnson
If someone is transitioning to Medicare for the first time, every single state has a SHIP program, which is the State Health Insurance Assistance Program. They’re called different things in every single state. They are trained to help people navigate their Medicare options and they are unbiased. They do not get paid by enrolling people in one plan over the other.
For people who are buying insurance in the marketplace, there is a similar entity called In-Person Assistors. Again, they are paid by the government not by the insurance companies so they don’t have any bias as to putting people in one plan over the other. I agree with your sentiment about seeking help and support in picking those plans, but I’m not sure that’s the place I would send someone for support.
Abigail: That’s why we’re having this conversation to talk about different perspectives. I work with a handful of insurance brokers who I have personally vetted and are now familiar with metastatic breast cancer because they’ve assisted a lot of people that I have worked with. Having those connections and knowing if there are people in your community who are doing some of these things can be key.
But thank you for that caution, Monica, because that’s also important to remember who you’re talking to and who they’re employed by. You might get a very different answer from an insurance broker versus a social worker who is employed by your cancer center. Getting different input can be important.
Gregory: You have to educate yourself. You have to go through due diligence to ensure that you understand your situation. I’m more aware of my needs now going forward as opposed to before because it was something that I wasn’t interested in. Make sure that you educate yourself and do your due diligence because those two things can save you thousands of dollars going forward.
As we’re navigating this system, how we embody that power can make a big difference in navigating cancer treatment.
Abigail Johnson
Empowerment
Abigail: The word empowerment gets thrown around a lot. We need to understand how we’re looking at empowerment because there are multiple definitions of empowerment.
One definition, that makes me itchy, is that somebody is giving you power. The second definition, which doesn’t make me as itchy, is that we all have inherent power as people and as patients. As we’re navigating this system, how we embody that power can make a big difference in navigating cancer treatment.
Gregory, how do you look at empowerment? How have you gotten in touch with your power as an individual and as a patient?
Gregory: When I was diagnosed, I realized the importance of my purpose in life and the importance of rekindling my faith in the Lord Jesus Christ. My empowerment came back through not only my connectivity to my spirituality but also through my family, friends, and the congregation of people who follow me on social media who were there to lift me.
I took that empowerment and tried to be a beacon of hope and inspiration, uplifting people’s minds and souls when they go through a horrific experience, and letting them know that they’re not in this alone. There’s unconditional love out there, even if you get that unconditional love from a stranger who gives you power and uplifts you to be able to weather the storm and be able to move forward.
Abigail: Thank you for that, Gregory, that was beautiful. Monica, would you like to chime in on this whole idea of empowerment and how that fits in with what Triage Cancer does?
Monica: It’s not my job as a cancer rights attorney to give somebody else power because that power is theirs. But what I can hopefully give people is the knowledge that they need. Knowledge is power.
You shouldn’t have to have a law degree, a project management background, or a million people surrounding you and lifting you to be able to survive this disease with your homes intact, your jobs intact, your insurance, and overall financial health. Yet, unfortunately, because of our system, sometimes that is what’s needed. We want to walk side by side with people and support them through education and providing information so that they can then take that and use their power.
I took that empowerment and tried to be a beacon of hope and inspiration, uplifting people’s minds and souls when they go through a horrific experience, and letting them know that they’re not in this alone.
Gregory Proctor
Gregory: That’s very, very powerful. As we talk about education, you need to seek others who have endured and weathered the same storm that you’ve gone through. A lot of times, people say that may not be a good idea or maybe that is a good idea.
For me, that became one of the circumstances that my wife and I were able to glean from others who are five-year survivors, 10-year survivors, and 20-year survivors and understand how they made it that far. Of course, now drugs and everything has changed, but knowing how they weathered the storm became a tremendous, valuable lesson for us.
Abigail: That’s a wonderful comment, Gregory, this idea of seeing examples of other people, which is what we’re doing and what The Patient Story does all the time as well.
Key Takeaways
Abigail: Know who you are. Allow your strategies and how you figure out how to pay for cancer to flow from who you are. You’re doing something that’s not you. It’s not going to work so well so know who you are.
Knowledge is power. Knowing how to navigate things, knowing the right things, and sticking to your guns in that context can be extremely helpful.
Don’t take no for an answer. Keep going. Keep pushing. Keep asking questions.
Don’t forget to ask for help and collect those people who you can ask so make sure that you’re saving the link to Triage Cancer, which is TriageCancer.org.
Watch for other patients who are navigating this, jot their names down, and know that you might be able to reach out to those people for help. That list can include social workers, nurse navigators, and professionals who do these things that you’re trying to do.
Vote with your feet. When your insurance policy doesn’t cover what you need, vote with your feet. If your doctor is not going to bat for you and not going to do that peer-to-peer discussion, vote with your feet. If you know that medication is way too costly and there’s an alternative, vote with your feet.
We have these choices and to vote with our feet can be extremely helpful and maintain that quality of life to fit cancer care into our lives versus the other way around.
Knowledge is power. Knowing how to navigate things, knowing the right things, and sticking to your guns in that context can be extremely helpful.
Myelofibrosis experts Dr. John Mascarenhas (Mount Sinai) and Dr. Tania Jain (Johns Hopkins Medicine), and Clinical Trial Nurse Ashley Giacobbi (The Leukemia & Lymphoma Society) explain cutting-edge therapies. Hosted by The Patient Story Founder Stephanie Chuang and featuring insights from patient advocate Mary Linde, this empowering discussion will help you navigate all aspects of clinical trials.
The myelofibrosis panelists discuss momelotinib, navtemadlin, selinexor, pelabresib, navitoclax, imetelstat, and other myelofibrosis treatments.
I had a different blood cancer, non-Hodgkin lymphoma, and I went through treatment a few years ago, but I’m so passionate about these discussions. So many things are happening in the landscape of changing treatment options and they start with clinical trials.
We hear about clinical trials but the term is so daunting and overwhelming. Our goal is for you to have a much better understanding of what they are in human terms. Maybe some might be right for you that you can ask your own doctors about.
The Patient Story features hundreds of in-depth, authentic patient stories across cancers and we also feature top cancer specialists. Our goal is to humanize cancer and help you navigate life after a diagnosis, whether you’re a patient or a caregiver. You can join our community and you’ll get first access to programs like these with new updates and new stories.
We’re so proud to be co-hosting this with The Leukemia & Lymphoma Society. It is the world’s largest nonprofit health organization dedicated to funding blood cancer research as well as offering patient services and education.
They have great resources if you haven’t checked them out yet. Their information specialists are just a phone call away to help you answer some cancer questions. They also offer help to pay for cancer costs through a co-pay assistance program, like travel to CAR T-cell therapy or clinical trials.
Dr. Mascarenhas, really appreciate you being here. I heard you describe yourself as being tireless and working nights and weekends to help patients in this space. We really want to understand what drew you to MPNs and to continue to do this work for patients.
Dr. John Mascarenhas: Thanks for having me join you. My interest began in the laboratory doing leukemia research many years ago. It evolved over time into clinical research in which I was introduced to MPNs and I really gravitated towards it. This was at a point where we didn’t have JAK inhibitors.
I was at the right time when the discovery of the JAK2 mutation came out. I got involved in the early development of JAK inhibitors and watched the field blow up. It’s been really exciting and rewarding to see this transition from how we used to treat patients with myelofibrosis and other related MPNs to what it looks like today so I’m very enthusiastic and optimistic about the future.
Stephanie: Thank you, Dr. Mascarenhas. We know that the landscape has shifted very quickly in a short amount of time. Excited to talk about it.
Dr. Tanya Jain
Stephanie: We’re also really excited to have Dr. Tanya Jain here tonight, another MPN specialist. She is an assistant professor of oncology at Johns Hopkins Medicine and director of the Adult CAR-T Cell Therapy Program at the Sidney Kimmel Comprehensive Cancer Center with myeloproliferative disorders as a top area of interest and studying newer drugs in the early phase of development.
Dr. Jain, thank you for joining our discussion. We’d also love to understand what drew you to the MPN space. What’s the driver of doing this work for patients and their families?
Dr. Tania Jain: Thank you so much for having me. I’m absolutely delighted to be a part of this panel.
I don’t think it was a specific event. It was a natural transition during my fellowship under the mentorship of Dr. Ruben Mesa and Dr. Jeanne Palmer, who’ve obviously done a lot of work and continue to do so.
How that transitioned me was to recognize the significant unmet need in the space and the opportunity that existed to contribute to improve outcomes for patients and to improve the lives of patients and their families so that’s what we try to do.
Stephanie: Thank you so much. That means a lot for all of us who’ve gone through cancer.
Ashley Giacobbi
Stephanie: Speaking of incredible work, we have Ashley Giacobbi representing The Leukemia & Lymphoma Society’s Clinical Trial Support Center. It’s a really great resource because as we know, clinical trials can be very daunting and seem like a lot to wade through.
Ashley, thank you for being here. I have such a special place in my heart for nurses. I remember going through my treatment and nurses being such a lifeline so I really appreciate the work that you do. We’d love to understand more about yourself and what drew you to this calling.
Ashley Giacobbi: Thank you so much. I’m really honored to be here.
I have been a nurse for almost 20 years now and have enjoyed all of my time at the bedside.
I get extra excited when talking about new changes and how much has changed in the world of oncology over the last 20 years. It’s exciting to be able to help patients find clinical trials when they’re seeking the newest and next level of care and some of these new developments and advancements that we’ve had.
Stephanie: Thank you, Ashley. We’ll be talking about some of the top topics you’re getting from patients and care partners who are calling you and asking for your help in the clinical trial space.
Mary Linde
Stephanie: Finally, we’ve got Mary Linde, who I’m really blessed to be able to call a friend now. Mary, you’re a myelofibrosis patient advocate. You lead a group on Facebook with myelofibrosis patients and care partners. We’re so lucky to have you share your perspective as well. Can you describe yourself a little bit outside of cancer? As we know, we are so much more than a diagnosis.
Mary Linde: Thank you for that. I’m almost 61 years old. I’m a nurse as well and have both a bachelor’s and a master’s degree in nursing. I stopped clinical nursing for 25 years.
I’m currently the CEO of a small nonprofit foundation that mostly runs a retirement community here in San Francisco. I have always had a heart to serve the elderly.
I’m a mom to two amazing adult sons who are launched and living on their own. One is married and one is about to get married. I’m really hoping for grandchildren soon and to live long enough to really enjoy those grandchildren.
I have a three-year-old Coton de Tulear puppy who gets me out and moving. I walk 3 or 4 miles a day with him.
Mary’s myelofibrosis diagnosis
Stephanie: Like so many of us experience, a diagnosis changes our lives. What led you to figure out that something wasn’t right and how did you get your primary myelofibrosis diagnosis?
Mary: It wasn’t easy. I was about 54 1/2 when I started with vague symptoms. I had fatigue, dizziness, and sometimes vertigo to the tune of whoosh and then I fell. I felt like I needed to nap more frequently. I felt like if I walked up any incline, I needed to rest.
I knew something was wrong. I thought I had mono or Lyme disease. I kept complaining to my primary physician about these symptoms. He kept telling me I had menopause, which had long been through at that point.
I would repeatedly go back to my primary physician and say, “Please, let’s investigate what this is,” and even told him that my father had a rare blood cancer at around this same age.
Finally, six months into begging, I reached out my arm to the doctor and said, “I’m not leaving your office till you do a chem 7 and a CBC,” and he did.
Three days later, I got the results that I had platelets in the 800,000. Of course, Google became my friend. I called the doctor and he refused to talk to me. He said, “I’m sending your blood off for special testing. I don’t want to tell you because I don’t want to scare you.”
I started Googling and I was pretty certain I had an MPN. Three months later, I found out that I had the JAK2 mutation. I didn’t find out from my primary care physician; I found out when I got a call from the oncology center admitting me to services.
When I walked into the oncology center, I had a very strange experience. The introductory oncologist said to me, “I know you’re probably really afraid of the C-word so we’re not going to talk about it. Let’s talk about it like a blood disease.” I told her that I was a nurse so she didn’t have to do this. Then she said, “The other C word is an evil drug so we’re not going to talk about that either.”
I kindly asked her to get me another doctor and then sought a second opinion. At that time, I wasn’t so afraid of dying as much as I was afraid of not having the information I needed to live well. I didn’t know if my life was going to be shortened and I wanted as much information as I could get.
Stephanie: I really appreciate you sharing all that, Mary. I also love the message of self-advocacy and empowerment. It’s your life, you know your body, and you certainly didn’t let that fall through the cracks.
What is myelofibrosis?
Stephanie: Dr. Jain, what is myelofibrosis in layman’s terms? What are some of the more common first signs or symptoms?
Dr. Jain: What we heard from Mary’s story is something that I hear in the clinic fairly commonly. Having that fatigue and tiredness is something that often takes people to physicians to get tested. Delays are not uncommon either because fatigue or tiredness have several possible reasons. Some may be more common than others.
Mary also mentioned the JAK2 mutation, which is of relevance here. The premise of myelofibrosis starts with the overactivation of the JAK/STAT pathway, which is supposed to be a normal functional pathway that’s supposed to do regular stuff and make blood cells.
When it’s over-activated or activated without any restrictions, that’s when undesirable things happen, which can include affecting the bone marrow function in a negative way.
You could be making too many cells or you could alter the bone marrow function in the way that there is more scarring in the bone marrow, which is the fibrosis in the term myelofibrosis, which again affects the ability of the bone marrow to function normally whose job is to make a normal quantity and quality of blood cells.
As a result, patients can get anemic or have low hemoglobin, which can cause tiredness, fatigue, difficulty breathing, and related symptoms.
By virtue of the JAK/STAT pathway activation, this systemic or generalized inflammation that we often notice or patients leads them to a workup. What that results in is what we in our clinic call constitutional symptoms or symptoms that could be nonspecific or vague as sometimes labeled.
Those can include things like night sweats, low appetite, or other symptoms resulting from an enlarged spleen like abdominal discomfort, which are other symptoms that can sometimes lead to further investigations clinically.
Stephanie: Thank you. I know that’s a lot to cover in a short amount of time. We do hear lots of stories about how long it can take to figure out a myelofibrosis diagnosis so that’s not unique to Mary’s situation.
Landscape shifts in myelofibrosis treatments
Stephanie: Dr. Mascarenhas, you alluded to how optimistic you are because there are so many developments happening. How would you describe the landscape shifts that have happened in myelofibrosis treatments, especially in just the last few years?
Dr. Mascarenhas: Myelofibrosis is a stem cell-derived blood cancer and it could affect people in different ways. You don’t meet two people that walk the same path. They all come in different forms and fashions. Their clinical picture can be really varied and their course can be quite heterogeneous and variable, too. You have to understand the patient that you’re dealing with and the patient-specific goals of therapy.
For some patients, it could be alleviation of anemia. For other patients, it could be systemic symptoms like fevers, night sweats, weight loss, bone pain, and profound fatigue that can be quite debilitating. For many patients, it can be an enlarged spleen or liver that’s causing a lot of discomfort and challenging normal activities like bending over and doing things that would be normally easy to do.
Knowing how the disease is affecting the patient really informs and dictates how best to approach the patient. It’s typically trying to alleviate the symptomatology and reduce the spleen, and that’s usually using JAK inhibitors.
JAK inhibitors
Dr. Mascarenhas: Over the years, we’ve grown to have three clinically or commercially available JAK inhibitors: ruxolitinib since 2011, fedratinib since 2019, and pacritinib since 2022. And a fourth one, momelotinib, later in 2023.
This provides a lot of opportunities to try to address those symptoms. Those cytokine-driven symptoms that Dr. Jain explained are a result of this JAK/STAT pathway. These drugs are great in reducing a lot of that inflammatory cue that makes patients feel terrible, improving their sense of well-being and functionality, and reducing their spleen.
In doing so, patients have a better quality of life and, by virtue in most cases, will live longer because they can do the simple things that we need to do. They can move and eat. People who move and eat will simply live longer and do better than patients who cannot and that’s just generally true in oncology.
They have really revolutionized the quality of life aspect. As Dr. Jain pointed out, she worked with Dr. Mesa who was really instrumental in measuring quality of life and making that an endpoint for clinical trials and bringing attention to symptomatology and quality of life.
We have a great armamentarium that covers lots of different types of patients to improve their symptoms and quality of life.
We are developing drugs that are looking to try to improve anemia. Historically, we use drugs like epoetin alfa or darbepoetin alfa, which are erythropoiesis-stimulating agents, to try to improve hemoglobins, get patients out of the transfusion suite, and give them some more energy back, or drugs like danazol, a synthetic male androgen.
There are drugs that we repurpose, which is a common theme in oncology, from other diseases like multiple myeloma. We use drugs called IMiDs or immunomodulatory drugs like thalidomide, lenalidomide, or pomalidomide. These can all be used in myelofibrosis off-label to improve hemoglobin with responses of about 20 to 30%.
The reality is we can improve hemoglobin in some patients, we can improve symptoms in the spleen, but there’s still really a lot left to do.
How JAK inhibitors work
Mary: Dr. Mascarenhas, could you tell us how JAK inhibitors work? What are their benefits and limitations?
Dr. Mascarenhas: JAK inhibitors are a class of agents interestingly invented in the setting of this disease and now have applications to a lot of different diseases that are not even malignant.
They intermittently reduce the JAK/STAT pathway that is inappropriately activated in the bone marrow cells. This pathway is responsible for causing the proliferation of blood cells and elaborating inflammatory mediators.
JAK inhibitors intermittently quell this cascade of events. That reduces the propensity to have this inflammatory state, this overproduction of blood cells, and seems to improve symptoms by reducing cytokines, which are inflammatory byproducts.
Patients feel better and can move and eat. It restores vitality for reasons that I personally don’t understand and I’ve never seen a good explanation for.
It also reduces the spleen. It’s a phenomenon I don’t really understand. It’s an interesting aspect of the drug. It reduces symptoms by reducing the activity of this pathway.
Unfortunately, these drugs don’t induce remissions. They don’t kill what I would call the maternal stem cell that gives rise to all of these abnormal cells. It doesn’t get rid of that cell.
It quiets down what’s happening in the bone marrow and the spleen allows for some degree of normalcy. The malignant cell population still remains in the body, in the bone marrow, and in the organs.
Unfortunately, we don’t see changes in the bone marrow that would lead us to believe that we’ve remitted the disease. Myelofibrosis is in the name. You have scarring in the bone marrow that typically remains even while patients enjoy the clinical benefits of the drug.
Then there’s the potential for downsides of the drugs. They often will exacerbate cytopenia or low blood count. Anemia and thrombocytopenia (low hemoglobin and low platelet) count can often get lower with these drugs.
We’ve pivoted to try to develop drugs that may not be as myelosuppressive, as count reducing and may even improve some of the blood counts.
Pacritinib can be delivered in patients with low blood counts and can improve hemoglobin in about 25% of patients. Momelotinib has also been associated with improvements in blood counts.
What we now know, which we didn’t know when we started off in all of this, is these drugs are not just JAK inhibitors. They interfere with a lot of different pathways that may be relevant and irrelevant and cause toxicity.
For example, inhibiting ACVR1, which is another pathway that’s important for iron availability, might explain why pacritinib and momelotinib improve hemoglobins and why maybe ruxolitinib and fedratinib.
There are a lot of nuances with these drugs that help us understand why they may fit niches and help certain people in certain ways and why you can provide serial JAK inhibitors.
If you fail one, it doesn’t necessarily mean that you wouldn’t enjoy some response to another. You can go from one to the other. The tailoring of the JAK inhibitor is somewhat of an art more than a science in some cases and requires knowing the patient, what the goals are, and trying to match the potential goals and potential toxicities to that patient.
Mary: Thank you for that. I’ve often heard that we’re not getting rid of our JAK2 but maybe turning the volume down on it a bit with the use of these drugs.
Determining the sequence of treatment
Mary: Dr. Jain, how do you know which JAK inhibitor might or might not work and which one to try first for a patient?
Dr. Jain: I’m going to piggyback on what Dr. Mascarenhas said and emphasize the point that no two patients with myelofibrosis will be the same. Everybody will have their own presentation or different things that you need to address.
Everybody will have a different trajectory in terms of their disease course and that’s what’s important to recognize as you’re thinking about what you’re going to start a patient on in terms of your choice of JAK inhibitor. We don’t have the same treatment for everyone. We’re looking at what we need to address in you as a patient.
If we’re trying to address high counts, a JAK inhibitor makes sense. If they have a big spleen and/or symptoms that will need to be addressed in combination with that, a JAK inhibitor would make sense based on the fact that we have the longest experience with it.
Ruxolitinib has been our first go-to. It was the first approved and we feel more comfortable with it. We know how to adjust the dose and move things around with it. If that doesn’t work, then the go-to next step in an ideal world would be a clinical trial.
If we don’t have one that would fit, it would either be fedratinib or pacritinib. The choice would depend on where the blood counts stand. If the platelets or the cell counts are on the lower side, pacritinib would probably be a better choice.
There are patients who have anemia as a major presenting symptom. In those situations, options such as epoetin alfa, danazol, pacritinib to some extent, and hopefully momelotinib in the future are some of the options. Luspatercept is in clinical trials; we’ll see how that pans out. Those will be some of the options.
The third set of patients is those who come with more advanced disease in the way of more excess or a higher fraction of blasts or leukemic cells or very, very early cells in the bone marrow that indicate that these patients are headed towards the pathway of a more aggressive pattern of disease like leukemia.
In those situations, either in combination with JAK inhibitors or without something like hypomethylating agents could be considered usually en route to a bone marrow transplant, if that makes sense in terms of eligibility.
Stephanie: What’s clear is this is very individualized. There are so many considerations.
What are clinical trials?
Stephanie: Mary, can you bring us back to the day when you got the diagnosis? What was that like for you learning about cancer?
Mary: When I was initially diagnosed, it was over a long period of time so it wasn’t shocking exactly as I grew into it.
I thought back to my own father, who had a rare blood cancer in the late 1980s, had it for five years, and died at age 60. In fact, we were both diagnosed at age 55. I felt like I was somewhat prepared for how to manage this because I’m in the health field.
I had a bird’s eye view of it with my own father and I knew how to advocate for myself, especially since my dad had to advocate at a time when there really weren’t a lot of options for this cancer.
There’s a lot of fear and a lot of wondering. Will I be around to see my grandchildren? Will I finish my career? Will I make the contribution to society that I had hoped? Will I have a painful death?
I’m grateful over the years to have learned that I have so many treatment options available to me that I don’t look at the future as something grim at all. I just see it as my normal life.
I’m so grateful to learn of combination therapies because not all of us can make it to stem cell transplant, which is ultimately our cure.
There’s a whole lot more hope on the horizon for us with MPNs, particularly primary myelofibrosis. I’m just grateful for the research and the amount of research that’s being churned out these days, the clinical trials, and the combination therapies.
I’m so excited to be able to talk to experts in the industry about research and development towards not only treatment but cure for myelofibrosis.
Stephanie: We’ve talked a little bit about some of the drugs and combinations that are being studied now.
The first time I heard the term clinical trials, it felt a little daunting. There are lots of misconceptions about clinical trials. We do know that different stakeholders are trying to research what can be better to improve the standard of care for different patients and patient groups. One of the challenges is that people view clinical trials as a last resort.
Ashley, we know clinical trials might not be right for everybody, but they are an access to tomorrow’s treatment today. We’re sure you get lots of questions in your role at the LLS. What are clinical trials in layman’s terms and what are some of the top questions and misconceptions you hear from people?
Ashley: Clinical trials are carefully controlled research studies, which are conducted by doctors, researchers, and scientists. They may be investigating new therapies or therapies used in the past in a slightly different way or in combination with other therapies to find out which works better or might have fewer side effects. They’re looking at both tolerability as well as effectiveness of the treatments.
There are so many misconceptions out there, but one of the largest is that it’s for patients who have exhausted all options. That’s simply not the case. There are clinical trial options at all stages of diagnosis.
There are interventional trials, which test treatment options, as well as observational or registry trials, which help us learn more about myelofibrosis as a diagnosis but may not involve specific treatments.
Another concern that we regularly hear about is the use of placebos. Placebos have definitely gotten a bad rap. A placebo can be known as a sugar pill. They’re not very commonly used in cancer clinical trials because it just wouldn’t be right for us to use a sugar pill in place of somebody who needed active therapy for a serious or life-threatening disease.
When placebos are used, it would be in a setting where a patient doesn’t require any type of treatment at that particular moment or in combination with another therapy so that the patient is continuing to receive active therapy for the disease that they have.
Logistical concerns may come up as well. We always like to chat with patients about travel for clinical trials and what that might entail. We’ve talked about some of the academic medical centers and how important it is to have an MPN specialist.
Very often, investigators who are looking at clinical trials for myelofibrosis are in academic centers. We’re always encouraging and pushing for those clinical trials to be available in the community setting because traveling to and from those academic centers can be a real challenge for patients.
In addition to the logistical travel considerations, there are some misconceptions that clinical trial participation is free or that patients may even receive money for participating. Unfortunately, that’s not always the case. It’s really important that we explain that to patients.
Parts of the clinical trial that are investigational or are not approved will be provided by the clinical trial. Physician visits and lab work are things that we would expect patients to undergo if they were receiving standard care. Those will still get billed back to the insurance company or may have to be paid for in another manner.
Each clinical trial is structured a little bit differently and it’s hard to know from an overview, but really it’s important to have a general understanding before diving into the specifics of any clinical trial.
If you are participating in a clinical trial, occasionally, there can be stipends available to support the patient or caregiver and that’s why it’s so important to reach out and find out more and make sure that you have all the information you need as you make a decision about participating.
Mary: Thank you, Ashley. It’s so important to hear that we do have access to medication, not necessarily the placebo. A lot of us do worry about that. We also need to check in to find out what is available to us in terms of financing.
Momelotinib, a new drug
Mary: Dr. Mascarenhas, let’s talk about single-drug therapy. There’s a new drug that was recently FDA-approved, momelotinib. What patient might it benefit?
Dr. Mascarenhas: Momelotinib is a JAK inhibitor so it’s much like ruxolitinib except as I mentioned before, there are some nuances that make these drugs a little bit different. It also inhibits ACVR1, which is another pathway that regulates iron availability for red blood cell production. In its long development history, it’s differentiated itself from other drugs in large part by its ability to improve hemoglobins in a subset of patients.
It went to the FDA based on a study called MOMENTUM. The expected approval was in late June. It was delayed by the FDA, which is not uncommon, to September for re-review. My expectation is it will probably be commercially available in the pharmacies and available for prescription likely by mid to late September.
I encourage patients to discuss with their physicians if that drug might make sense for them or any of the other drugs that we’ve talked about, whether it’s fedratinib, ruxolitinib, or pacritinib. As we’ve said, it really has to be tailored to the patient.
I’m excited to see momelotinib come up. For a physician, it’s great because it gives us different options and allows us to tailor the treatment for each patient. That might be a great opportunity for some patients to either embark on that therapy or switch.
The clinical trials set the tone for the interactions with the FDA about what that label would look like based on the way the clinical trial was designed and run. We can only guess that there may be stipulations.
It may only be available after the use of a first-line JAK inhibitor or it might have to have certain requirements for depth of anemia level. There are some nuances that sometimes play into the decision-making and these are based on the clinical trials that led to the approval.
Best drug combination therapies
Mary: Dr. Jain, there’s combination therapy to think about. June F. asks, “What are the best drug combinations at present?” Can you introduce us to combination therapies?
Dr. Jain: I’m not sure if I can answer what the best drug combination is right now, but hopefully that is a question we will learn more about and address in the future.
There are drug combinations that are promising. It brings options that we can offer to patients. They’re mostly in clinical trials but hopefully, some will move the field forward.
Historically, we addressed the JAK/STAT pathway, which we have learned the most about in the last couple of decades. That is the primary pathway involved in the occurrence of myelofibrosis.
As we have learned more over the years, there are other pathways that are critical to the development of myelofibrosis and that is where the rationale for drug combinations comes in.
We’ve seen several clinical trials that have addressed that or used combination therapy in patients who don’t have a good response to ruxolitinib itself and need more than that. Many of those drugs have been tested in the first-line setting to see if patients would do better with combinations upfront rather than ruxolitinib alone, which has been the long-standing go-to first-line treatment for over a decade now.
Some of the drugs that you’ll hear about are navtemadlin, for example, which is an MDM2 inhibitor. Dr. Mascarenhas presented data at EHA that showed a 35% spleen reduction in about one-third of patients in patients who weren’t responding to ruxolitinib itself.
There are BET inhibitors like pelabresib that I heard Dr. Mascarenhas talk about at ASH, which also is being tested in the first line in patients who are starting upfront treatment.
There are BCL-xL inhibitors like navitoclax, which have shown some improvement in the second-line setting. We’re awaiting a public announcement on the data for the first-line trial.
The premise is that you’re combining two mechanisms that have shown to work such that you do not have overlapping toxicities. That’s an important piece to remember.
JAK inhibitors can cause some decrease in blood counts; we’ve seen that with ruxolitinib. You want to add a drug that may not do that as much or may not do that to an extent that makes it prohibitive of a combination.
With pacritinib, for example, patients often would get gastrointestinal toxicity so don’t combine a drug that may also have gastrointestinal toxicity. That’s important to remember as we think about combinations, which we will see more and more in the future.
Logistics are certainly important to consider as we’re thinking about clinical trials, what the trial offers, the frequency of visits to the center, and whether that makes sense in terms of continuing to be on it or not.
When to consider combination therapy
Mary: Dr. Mascarenhas, what should patients ask when considering a combination therapy like Dr. Jain just talked about? How do we know when it’s right or the right time to start one?
Dr. Mascarenhas: The first question to ask is: Why is this combination for me? What would be the advantage in my case in terms of addressing my goals of therapy? Importantly, what are the potential risks?
As physicians—and I’m definitely included when I say this—we often focus on what we think is going to be the advantage of participating in a clinical trial. The reality is there are disadvantages sometimes. There can be toxicity associated with approved drugs and unapproved drugs that are in clinical trials.
Patients want to understand expectations of results and the potential toxicities that one could incur. What does the patient need to be aware of in terms of mitigating and reporting?
A trial is not really a passive experience. Patients are active participants. They’re not simply receiving a drug. They have to be very willing and engaged to report all symptoms and not just what they think might be important. They need to report everything to the study team.
That might involve calling ahead of their visit to let the team know what’s going on, making sure that all their medications are accounted for, and they’re following up. It’s an opportunity to assess whether a drug is active and adequately characterize the toxicities of a drug. As the drug moves along, it’s optimized in the delivery for future patients.
There are two objectives. How is this drug going to help me and what is my role in this whole process? It really should be a joint venture. It’s not a one-sided experience. We learn from the patients. Hopefully, the patient community learns from what we’re doing and everyone benefits.
Stephanie: Dr. Jain had set up the landscape of combination therapies and talked about different options. Dr. Mascarenhas, it’d be great to run through a few specific combinations.
Dr. Mascarenhas: Clinical trials today to a large degree are unlike what clinical trials were historically. These drugs are all rational with supporting pre-clinical data. People don’t always realize that they go through enormous amounts of testing through various aspects before they ever enter a human being.
There’s an enormous amount of regulatory burden that exists that’s really annoying but really important because it provides that sense of confidence in the investigators but also in the patients that what we’re introducing makes sense. We’re not just taking something off the counter and saying, “I wonder if this is going to work,” and throwing it into a clinical trial. These are rationally developed drugs.
An example is selinexor. Selinexor is a really interesting drug. It’s already approved for blood cancers that are not myeloid cancer like multiple myeloma and other B-cell lymphomas. This drug affects the shuttling of proteins in different compartments in the blood cell, in the nucleus, and in the cytoplasm.
Why does that matter? Because if you can affect where proteins are in a cell, you can ultimately affect the functioning of these proteins. Selinexor inhibits this shuttling protein and affects the way certain proteins exert their function, which might be important to the pathophysiology of the disease. This might even turn on other proteins and put them in an area where they can actually induce a good effect.
For example, there is probably a multitude of different changes when you use a drug like selinexor that shifts the cell’s functioning from one in which it’s acting inappropriately and nefariously into one in which you try to induce it to die through normal mechanisms.
There are normal mechanisms that are built into our cells that if they get corrupted by a virus or by cancer, they turn on this mechanism called apoptosis and undergo programmed cell death. Cancer cells have ingeniously figured out ways to get around that. We struggle each day to figure out ways to get them back on track, to encourage them to recognize that they’re inappropriate and to undergo this programmed death.
Selinexor is a great example of a drug that affects multiple pathways and induces myelofibrosis, perhaps even the primordial cells, to undergo this process of death. It works best in combination with ruxolitinib and that’s a common theme that we’ve seen.
In oncology, it’s very rare, except for maybe CML or some other diseases, that we use monotherapies. In most of oncology, we use combination therapies to synergize together to get deeper responses and avoid overlapping toxicities.
That’s what we’re seeing with drugs like selinexor or navtemadlin, which has a great wealth of data at this point. These drugs are active as single agents, but they seem to be even more active in combination.
This is supported by studies that are done in mice that are engineered to have myelofibrosis with primary cells from people who have been generous enough to donate their blood cells. We experiment and figure out how we are going to make better drugs in the future.
I thank those patients. Seems like a small thing, but it’s a huge, huge aspect of how we move this whole machine forward in clinical research. All of that information allows us to say this combination really looks effective.
We’ve got JAK inhibitors that are commercially available. We’re going to add this drug that synergizes nicely in preclinical models and cells in the dish. We think it’s going to work better than each drug alone and we’ll figure out how to dose them and schedule them to minimize toxicity. That’s really where we’re seeing it.
Selinexor, navtemadlin, pelabresib (BET inhibitor), and navitoclax (BCL-xL inhibitor) all look good in combination with ruxolitinib. As Dr. Jain said, ruxolitinib has been around the longest and that’s the go-to drug that we combine drugs with.
We’re not even waiting anymore for patients to have failed the first line of therapy. We’re introducing the drugs earlier on. We get confidence in their ability and their toxicity profile. Why wait for patients to do worse? Why not try to get deeper responses earlier on?
The deeper we can reduce the disease burden, we believe that the better the patient will be overall. They will not simply feel better but have smaller spleens, which is important. Fewer disease cells in their body will hopefully mean longer progression-free survival.
Navtemadlin, selinexor, pelabresib, navitoclax, imetelstat — there’s a whole host of drugs that are aiming to really hit the clone and induce deeper responses.
Second-line treatment after Jakafi
Mary: For people who have been on ruxolitinib and, for whatever reason, the treatment wasn’t effective, what treatment options are available?
Dr. Jain: That’s a common situation we run into because as Dr. Mascarenhas pointed out, ruxolitinib has a very strong role. There are a lot of things that it does do, but there are a few things that it doesn’t do. Based on registration studies and clinical practice, if it works, it works for a few years and then we start losing that response.
A clinical trial available that would be a combination of a JAK inhibitor with something else or something added to ruxolitinib itself would be my go-to to consider. There are several of those going on at this time. There are also trials with single-agent drugs.
The way drug development goes is there’s testing of efficacy by using the drug alone. Then once we are comfortable with their efficacy and safety profile, we add it onto a ruxolitinib or a JAK inhibitor backbone.
If we see efficacy and safety in that combination, we move it up the ladder a little bit more and try to investigate if that would be a better option in the front line compared to ruxolitinib itself.
There are non-JAK inhibitor combinations that get added to ruxolitinib. Navtemadlin, an MDM2 inhibitor, has data. It restores the natural cell-killing pathway that should happen but is not working very well for some reason. We’ve seen patients respond in a post-ruxolitinib setting in terms of their spleen and symptoms.
There are other drugs like navitoclax, a BCL-xL inhibitor, that show responses in about one-third of the patients who were not having a good response to ruxolitinib by itself.
Pelabresib is a BET inhibitor. There are other BET inhibitors in the pipeline that are being developed with slightly different nuances to their conformation and how they inhibit the pathway. These are some of the categories of drugs that look promising and worth looking forward to.
Imetelstat has emerging data. It’s slightly different in the way it works. It inhibits the telomerase activity. It’s one of what we think happens in myelofibrosis or leads to that, even though the telomerase length may be not as long or in fact short. The telomerase activity tends to be high and that’s what imetelstat inhibits.
I’m sure I’m missing some here and that’s not for the lack of preference. Selinexor is another one that Dr. Mascarenhas already mentioned.
I would tell my patients that if we can get our hands on one of these combination clinical trials at that time, that would be my first go-to option.
If for any reason there are no clinical trial options available after ruxolitinib, then obviously there are other JAK inhibitors like fedratinib, pacritinib, and hopefully soon momelotinib. Patients may still benefit even though they stopped responding to or did not achieve benefit from ruxolitinib as a front-line JAK inhibitor.
When to get a second opinion
Mary: When is it right for a patient to seek a second opinion during this time of figuring out the right treatment options?
Dr. Mascarenhas: The right answer always is now. I don’t think it ever hurts to seek a second opinion at the time of diagnosis to confirm the diagnosis. There is a lot of heterogeneity in the way these diseases can present. There are overlaps and nuances.
It’s important to seek a second opinion because you may be a patient who should be considered for a bone marrow transplant, which is the only curative option we have. Sometimes that’s delayed too late and the patient misses the window of opportunity. For some patients, that may not be on their plate but having that discussion is really important.
I don’t recommend seeing lots of different people; that can be problematic. Getting a second opinion at each stage never hurts — at the time of diagnosis, if you’re not doing well on your first therapy, and when there’s consideration of second therapy.
If you have a physician who gives you pushback about getting a second opinion or comes across negatively, you might want to find another physician because it shouldn’t be an ego thing.
It’s your life. You’re dealing with cancer. You should feel free and confident that a second opinion is not a reflection of your treating physician. It’s getting more information and the more information you have, the better the outcome.
Dr. Jain: I agree with that 100%. The MPN community is small but also very well knit and I think we work very closely together. I’ve asked my patients to get second opinions and I’ve set them up for them if they need to go. I’ve sent patients to Dr. Mascarenhas and to others if there is, for example, a clinical trial opportunity that we may not have and they may have.
Sometimes it’s better for them to hear it from more than one person. We do a lot of things similarly, but there are some that we may have different perspectives about.
A common joke is if you ask 10 MPN experts, you’ll get 12 different opinions, and not because anything is right or wrong. There just may be a slight difference in our prior experience with a particular strategy or what our perspective about a particular strategy may be. All those are important things.
The role and timing of the transplant may benefit from a second opinion. Get another perspective as to what their center’s experience has been and how they may do something different. There are nuances to every transplant center and some of it may be more beneficial to you. Geography obviously plays a big role.
How to look for myelofibrosis clinical trials
Stephanie: We’ve talked about treatment options in myelofibrosis, but when you actually come down to needing to find one or stay on one, there are so many questions that we all encounter. We know that ClinicalTrials.gov is out there, but it’s a little bit difficult to navigate and that’s why the LLS’ Clinical Trial Support Center is so important. Ashley, what are your top recommendations in terms of looking for clinical trials?
Ashley: Often, people try to go about it on their own. ClinicalTrials.gov is the most comprehensive database of all clinical trials. In addition to cancer clinical trials, there are also clinical trials for all types of disorders and diagnoses.
It’s not always easy to hone in on what you need depending on past treatments you’ve had or medical history so it can be a challenging situation to find clinical trials that are actually applicable to you as an individual.
It’s a free service staffed by nurses who have expertise in blood cancers and clinical trials. Nurse navigators connect one-on-one with patients, caregivers, or even other healthcare providers who may need to learn more about potential clinical trial options.
We find out more about the patient’s diagnosis. We learn about any past treatments they may have had and find out about their medical history because all of those factors will play into a patient’s eligibility to participate in a clinical trial.
We also take a long time to find out about patient preferences and any unique obstacles that could hinder or drive participation in clinical trials. We help tailor some of the support and resources that we’re able to provide so that patients can overcome some of those barriers that may be in place.
After we’ve generated all of that information and really taken the time to get to know the patients, we produce an individualized clinical trial search. That could be related to geography and preferences. What matters most to the patient? Is this something that they’re really not interested in spending a long time in the hospital if they can avoid it?
We definitely look at all of those and produce a list that can be taken back and reviewed with their treatment team so that that can be part of the informed decision-making with the patient’s next steps.
We are available for all blood cancers, including myelofibrosis and other MPNs. It’s important to know that patients can reach out.
Half of the ongoing clinical trials are cancer clinical trials, but sadly, only about 5% of cancer patients actually enroll or participate. There’s so much opportunity out there and we’d really love to help overcome any barriers that patients might have so that they can consider participating.
The role of stem cell transplant
Stephanie: Transplant is such a huge topic for so many people and they hear so much about it. In the context of the landscape changing so quickly, do you feel that you and other specialists in the field will be recommending transplants less to people? This is probably a very individual response, but with everything happening, what’s the trend?
Dr. Jain: I actually think of it the other way. By virtue of having more effective treatment strategies to improve the spleen and symptoms, and get a disease response, we may be able to take more patients to transplant as a curative therapy.
A lot of times, lack of spleen response, poor performance by virtue of a lot of symptoms, or disease advancement into a more aggressive disease pattern become barriers to transplant. Having more options in the future will allow us to take more of these patients to transplant.
We’ve seen a lot of advances with a lot of these options. What we have not seen so far is the curative potential. Hopefully, we will in the future. All of these drugs have a lot of advantages in terms of improving spleen symptoms and cytopenias but we have not had definitive improvement or getting rid of the abnormal stem cell clone. That’s something that at least so far we’ve only achieved with a stem cell transplant.
At some point, as long as patients are eligible for transplant and that is something that would fit their life wishes in general, that would be a curative option to consider. Better non-transplant treatments will only get more patients to something more curative like a transplant.
Dr. Mascarenhas: I couldn’t have said it better myself.
Final takeaways
Stephanie: We’ve covered a lot of ground in a short amount of time. If there’s one thing you’d like for our audience of patients and care partners to walk away with, what would that be?
Dr. Mascarenhas: I hope to share my enthusiasm and optimism that we are making advances. There is a brighter future and I’m really genuinely excited about that.
Embrace the opportunity of clinical trials. Clinical trials are looked at for other people, but they may be important for you. Talk to your physicians. You may not go through with it but learning about it and exploring it is important for each patient.
Dr. Jain: It’s never a wrong time to see a specialist or to see someone else if something is not working out. Some symptoms are nonspecific. Never hesitate to be an advocate for yourself, to get things done, and to seek a second opinion.
As a transplanter, I’m obliged to pitch in that getting an opinion about transplant and at what course in your disease that makes sense is important to address. You don’t have to wait until you’re progressing or not responding to drugs. That needs to be addressed and outlined in an early appointment rather than waiting for too long.
Ashley: I really want to echo what’s already been said. It’s so important to consider clinical trials as part of the treatment plan. Even if they may not be an option at that particular moment, it’s important to be informed and look at all of those components as you’re making an informed decision about the treatment plan with your providers.
As a representative of The Leukemia & Lymphoma Society, I would really encourage any patient with myelofibrosis or any MPN to reach out. The Leukemia & Lymphoma Society has so many resources available, including clinical trial support but also so many others that we would really enjoy the opportunity to connect and provide those resources to patients.
Mary: Continue to have hope. Continue to want to thrive and live.
At the beginning of my journey with myelofibrosis six years ago, I was told I’d be dead by 72. Now they’re saying you could outlive this. You could die with this, not of it. Hearing both Dr. Jain and Dr. Mascarenhas talk about all these combination therapies and how they actually might get us to the cure was very exciting.
Conclusion
Stephanie: Thank you so much, Mary. Your story is so powerful. It’s also on our platform so feel free to check out Mary’s story.
Thank you to Ashley from The Leukemia & Lymphoma Society and to Dr. Jain and Dr. Mascarenhas for the work that you’re doing to push forward research and help patients and family members better understand their options in myelofibrosis and MPNs altogether.
I hope you’re able to take away something that was really key for you, because that’s our goal, to empower you in your own care. We look forward to seeing you at a future program.
Sharing from real-life experience, the panelists were Stephanie Chuang, founder of The Patient Story and non-Hodgkin lymphoma survivor, Dr. Matthew Matasar, Hodgkin lymphoma specialist at Rutgers Cancer Institute, Dr. Samantha Siegel, both a doctor and Hodgkin lymphoma patient, and Chelsey Gomez, Hodgkin lymphoma patient advocate and artist behind Ohyouresotough.
The discussion covered an overview of Hodgkin lymphoma, standard, and emerging first-line treatments, options for relapsed/refractory patients including immunotherapy and stem cell transplants, managing side effects, the importance of doctor-patient relationships and shared decision-making, and key takeaways about community support and focusing on the quality of life during and after cancer treatment.
I’m a non-Hodgkin lymphoma survivor, founder of The Patient Story, and first and foremost, a patient advocate. The Patient Story was born out of my own experience with cancer. At the time, as a patient, I was looking for humanized answers for what my life with cancer would look like.
We’re proud to partner with The Leukemia & Lymphoma Society or the LLS, which is the world’s largest nonprofit health organization dedicated to funding blood cancer research. They also provide a lot of education and services and that includes their information specialists who are just one call away to help with your questions. They also have financial scholarships and we’ll talk about that at the very end as well.
Last but not least is Imerman Angels, a wonderful peer-to-peer support group program. I used Imerman while I was a cancer patient and they will connect cancer patients and caregivers with mentor angels. They will use things like age, gender, where you live, and experiences to try and make that match.
We also want to give a special thanks to Seagen for supporting our educational program and allowing us to really do the work that we want to do in true patient education, connection, and space and provide it for free; that’s really important to us.
We want to stress that The Patient Story, The Leukemia & Lymphoma Society, and Imerman Angels all retain full editorial control of the entire program. A reminder that this is not meant to be medical advice or a substitute for medical advice. It is educational and we’re hoping that you’re able to take away great information tonight back to your own doctors and healthcare team.
Introduction
Stephanie: First up, Dr. Matthew Matasar, someone we’ve been able to work with before. He’s the chief of the Division of Blood Disorders at Rutgers Cancer Institute. He’s been a medical oncologist specializing in lymphoma for more than 25 years and leads clinical trials to try and find new and better ways to treat diseases like Hodgkin lymphoma.
Dr. Matasar, what drew you to lymphoma? What inspires you to do the research that you do and dedicate yourself to patient care?
Dr. Matthew Matasar: First of all, thanks for having me. I’m really thrilled to have this opportunity. What we’re doing together really matters and makes a big difference so thanks for making this happen.
I started out as a philosophy major back when I was in college, wanted to go into medical ethics, and then got sucked into oncology.
I saw oncology in general and lymphoma, especially as a place where I could make a difference, where being a really good doctor or being a crummy doctor makes a difference. I wanted to be the kind of doctor who listens to his patients, works with them as individuals, and understands that when they’re coming to me, they’re having the worst day of their life. I want to try to make it a little bit better using my brain and my heart as best I can.
If I do my job well, it’ll be better than if I don’t. These things matter and what I do matters. I feel this pride in knowing that what I’m doing is making a difference for people in my clinic, individual by individual, and by trying to develop newer, more effective, and less toxic treatments.
Maybe I could leave a little bit broader mark on the world. Trying to make a difference. What we’re doing here is trying to make a difference.
Stephanie: Yes, and you’ve been doing that and we really appreciate that you go above and beyond to help patients and their families.
Next up, from one doctor to another, Dr. Samantha Siegel, both a doctor and a patient, which is a really interesting perspective. Sam, I’m really, really grateful to have you here and lucky to get to know you. Thank you for all that you do.
We will get into your Hodgkin lymphoma story shortly but, first, we’d love to hear more about you outside of the cancer diagnosis because as we know, we are so much more than that.
Dr. Sam Siegel: Thanks for having me. I’m so excited to be here and to connect with you and all of the patients, caregivers, and community members.
I am one-half of a sandwich. I’m married to another doctor named Sam, but we got married before med school. Sam squared, Samwich, he Sam she Sam — a lot of iterations of that that are fun and interesting.
I’m a proud mom of three kids. They’re my best teachers in this world. They’re so incredible. Parenting them through cancer and through medicine has been very interesting. It’s always exciting. Our house is never boring.
I love jogging, painting, and playing guitar. I’ve recently become an enthusiast of ecstatic dance. It’s like a nightclub but during the day. No booze and kids are allowed. It’s just freestyle dancing.
I used to dance growing up and I’ve gotten back into it lately as a way to connect with myself and my body. I found it really helpful in healing from chemo and chemo treatment. I love dancing, music, moving through music, cooking, and food.
I’m hoping to unify how other people enjoy aspects of being alive and how we can talk to our doctors about how to tailor our cancer treatment to what matters most to us. That’s really important to me because if I couldn’t jog, play my guitar, paint, or work with my hands anymore, that would be pretty devastating to me.
All of that matters when it comes to talking with my doctor. I’m excited to be here as a doctor, as a patient, as a person, as a human being, first and foremost so thank you.
Stephanie: Thank you, Sam. I couldn’t have put it better myself. It’s not just about extending life, it’s the quality of life and even after treatment.
We will talk about the long-term side effects because we all want to live and get back to living the way that we know how and maybe better.
Up next, another awesome rock star. You may know her as the genius behind Ohyouresotough, which is amazing artwork. Chelsea Gomez, thank you for being here tonight. As a patient advocate, you’ve grown such a community yourself. Can you also tell us more about you outside of the diagnosis?
Chelsey Gomez: Hi, everyone! I’m so happy to be here.
I’m from Florida. I just turned 33 and have a daughter.
I’m a professional artist. I own my own cancer awareness brand named Ohyouresotough. If you ever see anything of mine, you’ll see that I like to cope with hard things with humor. It’s really important to see the lighter side because a lot of the cancer world is not so fun.
I love all things art. I use clay, I paint, and I do digital art. When I’m not doing art, I’m running after my daughter to do whatever she wants to do, like play Barbies. I’m really excited to be here. Thank you for giving me the opportunity to share my story, too.
Stephanie: We appreciate it. Without voices like yours and Sam’s, we wouldn’t have the platform that we have today. Both of your stories are on The Patient Story so thank you for being here and for sharing your voice to help other people.
What is Hodgkin lymphoma?
Stephanie: Let’s get down to business. We’re going to try to avoid medical terminology as best as possible. Dr. Matasar, what is Hodgkin lymphoma?
Dr. Matasar: Working through things without terminology is theoretically what we’re supposed to be doing all day any day. When we’re talking to patients, families, and caregivers, we try to help people make sense of their illness.
What is lymphoma? Lymphomas are types of cancer. They’re cancers of cells called lymphocytes or immune cells. Lymphomas collectively are cancers that come from and are of the immune system.
That’s not to say somebody who has a lymphoma has a bad immune system — far from it. In fact, most people diagnosed with Hodgkin lymphoma have perfectly fine immune systems. They’re not constantly sick with infections.
For whatever reason, some cells mutate or change in a way that makes them live too long and start making copies of themselves. Then those copies live too long and they copy and the copies copy.
Compounding that, your body sees these cells that are copying that don’t belong there and views them as foreign or not right. In a similar way to an oyster that has a little grain of sand in it, it starts making a pearl around it. The body reacts to these cells and causes inflammation and scarring to try to wall off these weird cells causing even more swelling typically in lymph nodes, although that swelling can happen outside of lymph nodes in other parts of the body as well. It’s that swelling that usually leads to people being diagnosed with this type of specific cancer.
Sam’s Hodgkin lymphoma diagnosis
Stephanie: Sam and Chelsey, you had symptoms and red flags that helped you figure out something’s not right. Sam, what was your experience?
Sam: I wasn’t feeling right. In hindsight, it’s interesting to go back and piece things together, but I felt this vague sense of tiredness. I didn’t have enough gas in my tank. I was still running 10 miles on the weekends, but coughing a lot.
I didn’t have the steam for my usual level of physical exercise. I was coughing a lot, particularly at night. There were a lot of California wildfires at that time so I thought it was the air.
And, of course, I’m tired. Every parent during the pandemic is tired, especially with our kids doing homeschooling. It’s a whole different world. Then being a doctor at that time was very hard.
But then I got a rock-hard lump that appeared above my collarbone. It was painless and rapidly growing. As a doctor, I knew that I had cancer.
I got a scan and mine said something about possibly metastatic lung cancer or breast cancer. They weren’t sure so I needed to get a tissue biopsy. A little bit of time transpired between noticing the symptoms and getting the tissue biopsied.
Once that came back as Hodgkin’s lymphoma, I knew what the path ahead would be like. Around the time I was diagnosed in 2021, there was this big change that started happening with immunotherapy. It was the standard of what had been happening for a really long time, which is ABVD or a combination of four drugs.
I got on the eve of my 30th birthday. Then I started ABVD.
There was a question about my staging, whether I was stage 2AE or stage 4 because there was some lung infiltration. Long story short, that meant that I was going to get six months of ABVD.
After a month or two, the coughing went away and I started feeling better. My cough came back at about month 2 to 3. We thought it was the bleomycin. I’m a runner and that’s very, very bad. We ended up dropping the bleomycin and I continued on AVD alone for the remaining four months.
Coincidentally, there had been a trial around that time to say that that’s okay, the de-intensification of therapy. Dropping the bleomycin became a standard thing, if people got a scan after a couple of months that showed that the body was responding.
My PET scan after two months looked really good. My cancer was responding and I was having that cough. We dropped the bleo and then I did four more months of AVD and boy, was it hard. It was really, really hard.
I had a lot of side effects. I struggled a lot and I struggled with that feeling. I hear people say about Hodgkin’s that this is the good one. It certainly didn’t feel that way. It felt really hard.
Stephanie: I hate when I hear whenever people say you got the good one.
Chelsey’s Hodgkin’s lymphoma diagnosis
Stephanie: Chelsey, how about you? What were the first symptoms for you or the red flags?
Chelsey: I was first diagnosed with Hodgkin’s in 2018 when I was 28. I was working a lot of hours so I was very tired, but I didn’t think much of it.
I had weight loss. I was trying, but it never worked before and then I suddenly started losing weight. I had shortness of breath and, at one point, I almost crashed my car because I had a vertigo episode. I ended up going to the doctor and they told me it was just stress.
The only reason I got diagnosed with Hodgkin’s was I eventually had a lump come up on the left side of the base of my neck. I went to urgent care. They told me that I just needed antibiotics, but there was something in their eyes that told me that wasn’t all I needed.
Eventually, my family forced me to go to the ER and we got a full biopsy done. I was in the hospital for the first time. Long story short, I had stage 2 Hodgkin’s and I also had ABVD. About halfway through, we had to drop below because I had toxicity.
I was re-diagnosed with Hodgkin’s in 2019 as well.
Dr. Matasar: First, hearing Chelsey, how you knew better, listened to your body, didn’t take no for an answer, and saw something that made more sense to you. The importance of that just can’t be overstated.
I meet so many patients who say, “Well, they told me not to worry,” or “My doctor told me to come back in six months and I was getting worse and worse, but I was told not to worry. I was told it was something else.” Congratulations on knowing better and I hope that people take heed and learn from the example that you set.
Chelsey: Especially when you’re young. It’s hard sometimes to speak up. But even if you’re young, you know your body.
Dr. Matasar: Maybe even especially if you’re young. We all know that old doctors sometimes don’t have the best reputation for listening to young people, trusting them, or taking them as seriously as they ought to be taken. Doubly so because of your youth at the time.
Changes in the treatment of Hodgkin lymphoma
Stephanie: Dr. Matasar, the treatment landscape in Hodgkin lymphoma has been changing quickly. Can you share about the evolution that’s been going on?
Dr. Matasar: Back in the ’80s, ’90s, and 2000s, clinical trials to try to make Hodgkin lymphoma better were all about intensification. How can I ratchet the treatment up to make it even stronger, even more toxic, but even stronger against lymphoma?
We were climbing that mountain of pushing to see just how much chemo we could cram into someone’s gullet in pursuit of a cure. All we had was chemo so what you want to do is more.
We’ve come over the other side of the mountain now and we’re in a very different place. As a discipline and lymphoma experts in the field, we’ve moved away from intensification.
We’re into de-intensification, personalization, and leveraging treatments other than chemotherapy as we try to help both maximize the chances of cure and minimize the short- and long-term risks of our treatment.
We’ve gone away from uniformly using ABVD, which remains a very good treatment and a very commonly used treatment.
More often, we’re now using other adjunctive treatments like brentuximab vedotin or ADCETRIS in lieu of bleomycin, which both Chelsey and Sam talked about potentially injuring their lungs, leading to cough or shortness of breath.
We’re finding ways to cure more people and, at the same time, cause less harm along the way and that’s really where the future of Hodgkin’s lymphoma is going to take us. We try to make even more progress on this mission towards more effective and less toxic treatments.
Stephanie: I love that that’s the trend and that we can continue going down that path.
First-line treatment for Hodgkin lymphoma
Stephanie: We’ll talk about some of these newer promising treatments and new directions, but can you tell us a little bit more about the standard first-line treatment for Hodgkin lymphoma?
Dr. Matasar: As oncologists, when we meet a Hodgkin’s patient for the first time and we work through their treatment choices, we think through those choices together with our patients and their families.
We split people into different categories as we understand the risk of their disease and the options that are presented because of that.
One first way to try to put people into categories to help them think through their choices together is based on stage. We talk about early-stage Hodgkin lymphoma and advanced-stage Hodgkin lymphoma.
People will often ask, “What’s my numerical stage? Is it stage 1, stage 2, stage 3, stage 4?” We heard from Sam that sometimes, it’s not even clear to us as oncologists exactly what the stage is. Is it a stage 2E or is it a stage 4?
The staging exercise, which sometimes feels very black and white, can have shades of gray. We do our best to try to put people into risk categories informed by their stage and then think through the treatments that we know are best for that stage of illness.
Early-stage Hodgkin lymphoma treatment
Dr. Matasar: For the vast majority of people with early-stage Hodgkin lymphoma, the standard of care remains to be ABVD. It’s been around longer than I’ve been a doctor. It’s an oldie but a goodie and it still will cure the vast majority of patients.
Sometimes we think about radiation therapy as part of that treatment and sometimes not. However, ABVD for early-stage Hodgkin lymphoma remains the standard of care.
Advanced-stage Hodgkin lymphoma treatment
Dr. Matasar: For most patients with advanced-stage Hodgkin lymphoma, we’ve moved away from ABVD. This is based on really powerful clinical research comparing ABVD to a program where the bleomycin was swapped out in lieu of this newer immunotherapy called brentuximab vedotin, which is a type of drug called an antibody-drug conjugate.
An antibody is a protein that binds onto the surface of a cell and stapled to that is a toxin so this conglomerate attaches onto the Hodgkin cell, the Hodgkin cell absorbs it, and then the toxin is released inside the cell — like a Trojan horse sneaking into the city and releasing the soldiers inside.
This newer program where bleomycin was swapped out for brentuximab — so BV-AVD instead of ABVD — not only got more people into remission and kept them in remission longer, but actually led to a higher cure rate, people living longer, and everything good that we as doctors want for our patients.
Because of this important research, we really now use brentuximab plus AVD as our traditional standard of care treatment for patients with advanced-stage Hodgkin lymphoma in pursuit of a cure.
Role of radiation in Hodgkin lymphoma treatment
Stephanie: You mentioned radiation therapy as well and that has been its own sort of beast, if you will. There are a lot of considerations about long-term side effects and where the mass is located. What role do you think radiation therapy has been playing? What are your thoughts about whether it should still be used and in what situation?
Dr. Matasar: It’s a great question and you’re right, it is sort of its own beast. Back in the ’80s and early ’90s, almost everybody with early-stage Hodgkin lymphoma got radiation treatment as part of their care.
We knew then and now that using radiation therapy would cure a few more patients than not, but that slight improvement in cure rate never translated to people living longer.
It’s a trade-off. You may do a little bit better with Hodgkin lymphoma in some situations but you’re paying a steep price oftentimes in terms of long-term effects, late effects, and risks of health problems later in life.
That includes radiation therapy putting patients at a higher risk for other cancers later in their life, particularly younger women who need radiation therapy to the chest. If that radiation touches the chest wall and breast tissue, particularly for women under the age of 35 or especially under 30, it really does heighten the risk of breast cancer later in life.
Your heart also doesn’t like radiation therapy much more than the rest of you. We know that radiation therapy to the heart can lead to a higher risk of heart disease later in life.
There are all these consequences of the decisions that we make together in our pursuit of a cure. Because we know so well about these late effects of radiation therapy, increasingly, we try to be ultra choosy with whom we use radiation therapy.
We really restrict its use for what we think we really need to get a cure. For most patients, we can cure them just fine without using radiation therapy and putting people at risk for health problems later in life because of that treatment.
Use radiation therapy if you need to; it’s a great treatment. It can be life-saving when you need it but don’t use it willy-nilly.
Side effects of Hodgkin lymphoma treatment
Chelsey’s side effects of bleomycin
Stephanie: Chelsey, you experienced the toxicity and side effects of bleomycin. Can you talk to us about what that reaction was and what you did about it?
Chelsey: I had my fifth chemo right before New Year. I had chemo four other times, but I went home and spiked a really high fever all of a sudden. As a cancer patient, if it’s 100.4°F, you have to go. Mine was 102 and my husband said, “We’re getting in the car.” I was very lethargic and just not feeling well.
We ended up in the ER and they told me I was septic. Of course, my mom heard that as well. She was watching my daughter and she’s freaking out because it’s not good when you’re septic. They put me in the ICU and I was in the ICU for at least two days.
The symptoms dissipated after a few hours. I was feeling better, not 100%, but they started giving me antibiotics around the clock.
I had a feeling that it had something to do with bleomycin. I’ve researched what can happen with bleomycin because I have asthma and that was something I had to consider going into the treatments.
Everything I was seeing was adding up to it being toxicity, but there was nobody at that hospital who really treated cancer patients. They came in and out, but they weren’t there all the time.
It took about four days for my oncologist to actually come and see me. At that time, I pretty much diagnosed myself with bleomycin toxicity. I also stopped accepting the antibiotics because it wasn’t an infection. It was a reaction to this drug and it was confirmed later on.
I also had a pulmonary function test and I had a 30-point drop or something. I’m happy to report that I have regained a lot of my pulmonary function now many years out. For a lot of people, I know that’s something scary when you do go through this.
This was a local hospital and they had never seen this before. The doctor was saying, “You need to advocate for yourself, especially when you’re in a situation where you know your cancer probably better than the people that are there. It’s not your regular care team.” I had to speak up for myself and it was hard, but I did it.
Stephanie: I really appreciate that you spelled that out. Dr. Matasar talked about it earlier, too, and I know Sam’s a huge proponent of that as well.
You said it was hard and I think we’ve all experienced that as patients where you want to advocate for yourself. You hear it from other people. It can be a little bit difficult to speak up. Do you have any other tips for people who are on the fence about it, who aren’t sure if they’re supposed to speak up?
Chelsey: I wasn’t a great advocate for myself when I first got sick. The oncologist I ended up with was the one who was just walking by when I was in the ER initially and I thought it was fate. It wasn’t. Immediately upon meeting him in his office, he told me it was the good cancer.
I was like a unicorn of the Hodgkin’s. Nothing went how it was supposed to go. It wasn’t good at all. Sometimes I was quiet about it. I didn’t know what to do because I always look things up and he would call me Dr. Google but not in a nice way. I was scared to bring up a lot of things.
If you’re young and you’re scared or sometimes it’s when you’re female and you have a male doctor, it can be intimidating. Bring your family with you or somebody else you trust and have them speak up for you if you are scared to do it. I know a lot of people do that and it’s helpful.
When you’re inside that room, your mind goes fuzzy and you don’t even know what’s going on half the time. It can be the difference between having a good result or ending up pretty much needing a transplant like I did. I truly believe that if I had been a better advocate, I might have not needed one.
Stephanie: Thank you for going into all that. I can completely attest to blanking out in the doctor’s office and not hearing the same thing that my family heard. I appreciate that tip about bringing people in if you can.
Sam’s side effects
Stephanie: In terms of side effects, you worked with your doctor to manage them. Can you share anything that was helpful there?
Sam: I had a lot of side effects. I had a lot of nausea and vomiting, yet I gained a ton of weight during AVD from all the steroids and I was developing a lot of problems from that. My glucose and liver enzymes were increasing. I had inflammation in various organs.
In hindsight, I think that was also making my neuropathy really bad because once my glucose got better and I lost weight, my pain and my nerves got better, too, despite the fact that I was getting more medicine that theoretically should have been impacting the nerves.
All your systems can be impacted. Taking care of the whole body is really important. I talked to my doctor about diet, lifestyle, and supportive therapy. What are some complementary therapies that I could try while getting my traditional medicines?
I also took a lot of medicine at the time. I needed pain medicine. I needed nausea medicine. I needed all the tools in the toolbox to cope with living day-to-day because it was just really hard.
The medicines caused a lot of mood and neuropsychiatric side effects. I had problems thinking. At some points, I had problems driving or following a list of simple items and that was really tough for me. That was a really far fall in terms of functioning, going from being a doctor to having trouble shopping a grocery list of five items so that was pretty devastating.
When I found out that I could do brentuximab as therapy leading up to the transplant, that gave me a huge quality of life back. As those other drugs cleared out and my body healed, I could think again and started feeling myself in here again. I’m not gone, I’m still there, and that mattered so much to me. It was a huge gift.
Stephanie: I really appreciate you bringing that to life because sometimes, we feel lost in that fog and how important it is to get any semblance of that quality of life back of ourselves. Your story shares that so powerfully.
Immunotherapy for Hodgkin lymphoma
Stephanie: We’re going to shift to combination therapy for the front line. Patient Matthew S. asks, “How successful have immunotherapy trials been in regard to Hodgkin lymphoma?” Dr. Matasar, can you explain the idea behind combination drug approaches and for whom would this benefit?
Dr. Matasar: We’ve talked about the progress that we’ve made with swapping brentuximab vedotin for bleomycin.
Matthew’s question about immunotherapy is a really valuable one. This idea of immunotherapy has really been a revolution in a lot of different forms of cancer, but nowhere has it been more impactful than in Hodgkin lymphoma.
When we talk about immunotherapy in Hodgkin lymphoma, what we’re generally speaking about is a class of medicines called checkpoint inhibitors.
One of the ways that these Hodgkin’s cells survive in our body is they are able to effectively shield themselves from our normal healthy immune system cells. They put up these barricades and ways of shielding themselves or hiding or preventing our immune system from doing the trash.
There are two checkpoint inhibitors that are approved for Hodgkin lymphoma, which are very similar medicines truthfully: one called nivolumab and one called pembrolizumab — we’ll call them nivo and pembro for short. These medicines are able to strip those shields off of the Hodgkin lymphoma cells and allow your immune system to see what it was otherwise blind to.
The treatment itself does nothing to the cancer cells. It does not kill a single cell all by itself. What it does is re-enable your own body’s immune system to do the work. It’s a game-changer.
When we use these medicines by themselves and use them as a treatment for a patient who’s been failed by many different prior chemotherapies, they’re able to put people into remission more than half the time.
They’re actually able to cure some patients. Despite chemotherapy having failed again and again and again, this medicine is able to eradicate the lymphoma. It goes away and never comes back. That’s amazingly powerful to be able to say and it’s an amazingly powerful treatment modality for patients with Hodgkin lymphoma.
The more we learn about how good these medicines work, the more we want to use them for more patients to try to help cure more people. It went from being a last-ditch effort after everything else has failed to be part of the treatment when it comes back. Using it in that situation was able to help more patients.
We’re now seeing the initial results of our first trials of using it as part of the first treatment. Instead of ABVD or brentuximab plus AVD, we’re combining nivo or pembro with chemotherapy like AVD and we’re starting to see very promising early results.
BV-AVD vs. ABVD as first-line treatment
Stephanie: How much is brentuximab and AVD being used? Is it standard of care or does it just vary depending on the hospital system or the healthcare provider versus going to ABVD first-line?
Dr. Matasar: It’s a little bit hard. Everybody’s situation is a little bit different. There are standards of care, which means that all things being equal, it’s sort of a one-size-fits-all approach.
Medicine is never that clean or that easy. There are times when ABVD would be a standard for early-stage disease, but we have to use brentuximab instead of bleo. There are people with advanced-stage disease who even if BV-AVD would be the standard, I still want to use ABVD for this individual patient.
This happens because doctors listen to our patients and we take into account their personal priorities, preferences, and individual risk profile. All of these medicines have their own pros and cons and their own risks and rewards.
A treatment program is best when it’s personalized and done in the context of a doctor and a patient having meaningful and valuable conversations about what matters to that person. Is it just a cure regardless of side effects? Is it being able to play the guitar and run? What is it about the treatment that we need to take into account as we map a path toward cure?
Stephanie: Any idea of when we could see the FDA approval of checkpoint inhibitors in the front line?
Dr. Matasar: Certainly not anytime soon. The first results that we had were read out at major conferences. This is still very early data.
When it comes to Hodgkin lymphoma, doctors were very conservative. We don’t want to mess this up. We know that the stakes are high and that many people will be cured with traditional treatments. We don’t want to change gears until we’re really confident that we’re not hurting people in the process.
The initial safety readout of this combination using the checkpoint inhibitors in the first treatment looked better than any of us expected. There are a lot fewer immune-related side effects than we’re accustomed to seeing when using these immunotherapies. They do have their own immune-related side effects.
We want to see the data mature, as we say. We want to see how people do over time and make sure that there are no dangerous signals about increased late effects or late side effects happening as we gain more experience with this treatment approach.
Long story short, we don’t want to change anytime immediately soon. We’re probably looking a couple of years down the road.
Treatment for relapsed/refractory Hodgkin lymphoma
Stephanie: Dr. Matasar, how have the standard of care treatments for relapsed/refractory Hodgkin lymphoma patients been changing?
Dr. Matasar: Historically, when chemo failed, we would use other chemotherapy programs that use different chemotherapy medicines than the first cocktail. The most commonly used in America historically was a program called ICE: ifosfamide, carboplatin, etoposide. Different than ABVD because they’re different medicines, but still chemo.
We’ve moved away from ICE being the only standard of care and we’re using more of those other medicines — brentuximab, the checkpoint inhibitors. You can use one of them all by itself or in combination.
It’s informed, of course, by what we did the first time. If patients get brentuximab as part of their first treatment, we’re not going to rush into doing it a second time and want to do something a little different. Maybe we would use checkpoint inhibitors alone or combined with some milder chemotherapy programs.
This is the art of medicine. Trying to pick amongst a number of very effective choices and determining how to leverage those medicines and combine them to achieve our patient’s goals. Always with this view of maximizing the good and minimizing the bad.
Sam’s Hodgkin lymphoma relapse
Stephanie: Sam, you relapsed a month after finishing your first-line treatment. I can’t even imagine what a gut punch it was to go through all that and then find out that news. What was that conversation like about where you were going to go next?
Dr. Siegel: Gut punch is a really great way to put it because it was. I finished six months of ABVD, which then went down to AVD. Despite a scan saying that I had no evidence of disease, I felt pretty awful.
At that point, I wasn’t sure. Am I just feeling awful because this is just what a body feels like after you’ve had six months of this poison? Something in my gut was telling me that something wasn’t right yet, but my scan was clean so I just focused on recovery for a little bit.
Within a month, I started having symptoms that were eerily reminiscent of my initial symptoms — a wheeze only in the left upper part of my chest and a little pea-sized lump. That time around, I thought, Okay, I think I’m pretty clear what’s happening here.
I got a scan, which led to some biopsies and a diagnosis of a relapse. I’m already researching on Google the next treatment regimen that I’m going to have to go through. The whole while, I’m preparing myself that I’m going to have to go through ICE.
I’m thinking for sure I’m going to have to go through something called ICE, DHAP, or one of these other regimens that have been used longer term for relapsed/refractory Hodgkin’s or salvage therapy.
When the relapse was confirmed, my doctor said, “There’s this drug now, a targeted therapy called brentuximab. Instead of doing ICE, would you be open to trying that alone for a couple of months and then repeating a PET scan to see where we’re at?”
There was a pretty decent chance that if the brentuximab didn’t get me into remission before the transplant, I would have to get ICE, a multi-drug, more traditional chemo. I was willing to take that chance because I felt so beaten up by having to get all those months of traditional cytotoxic chemotherapy and all the side effects.
The decision made sense to me at that time whereas maybe other people may have been, “No, I want to hit it hard and do that right away.” For me, I was going to take the least amount of poison possible to get me into remission before transplant.
It worked. I got a strong remission before my transplant. I went on to get the bone marrow transplant then I took brentuximab. I did almost a year of post-transplant consolidation treatment.
Because those studies and the data were just coming through, my doctor said, “You know, this is kind of becoming a thing now based on the research and this seems like it might really fit you based on how bad you’re feeling,” so that was perfect for me. I was so grateful.
Stephanie: The timing matters, right? It just happened.
Stem cell transplant
Dr. Matasar: The first thing to say is that there are two types of transplants. What we’re talking about so far is a treatment called autologous, or from yourself, stem cell transplant.
To call it a transplant is actually wrong. There’s no transplantation going on; it’s just a word that we use. This treatment that you’re hearing from Chelsey and Sam is basically just a trick. It’s a way of letting us give a round of super strong treatment.
With regular strength treatment like ABVD or ICE, we give those treatments and then let people recover. Sometimes if the chemo is stronger, you might need to boost the recovery.
Here, we’re talking about a single course of treatment, usually six days, that is so strong that if I gave it to my patient, gave them a hug, and said, “I’ll see you later,” I wouldn’t see you later. It’s too strong.
We need a very powerful antidote for such a powerful treatment. The antidote that we use is actually a person’s own stem cells, these special Adam and Eve progenitor cells that live in our bodies and let us heal.
We filter the blood ahead of time with a process like a mini dialysis where we filter out a few of those special stem cells. We put them in the freezer, give people six days of chemotherapy, thaw out those cells, and give them back as an antidote.
The course of the six days of treatment and the stem cell re-infusion as a little mini transfusion, that’s the antidote. That is we are calling a transplant.
That’s different than an allogeneic or donor stem cell transplant where there really is transplantation going on. Your immune system is being put to sleep and a new immune system from a sibling or a stranger is put into your body to give you a new immune system. We then task that new immune system with attacking your cancer. For us, that’s a very different ball of yarn.
Chelsey’s Hodgkin lymphoma relapse
Stephanie: Patient Caitlin M. asks, “For relapsed/refractory patients, are there other options aside from chemo to get into remission before a stem cell transplant?”
Chelsey, you went through immunotherapy, but unlike Caitlin, you didn’t respond. After three cycles, your PET scan showed disease progression. I can’t imagine what that was like.
It would be great to understand more about your experience in terms of the conversation you were having with your doctor ahead of the transplant. Are there questions you wish you’d ask your doctor?
Chelsey: I relapsed in the latter part of 2019. I switched to the Mayo Clinic for my care. I had been researching through the relapsed/refractory Hodgkin’s groups on Facebook. I saw nivolumab, brentuximab, and all of those things, and they were a lot less harsh.
I asked about it when I went there and it was a newer thing at that time. My oncologist said, “Yeah, we can give it a try. It’s had really good results.”
Sam mentioned that the side effects of ICE and the side effects of brentuximab are a night-and-day difference. I don’t think anybody wouldn’t want to try the less harsh one leading up to the transplant.
I had three of those treatments, had a scan, and my cancer progressed. My oncologist was honestly shocked as well that it didn’t respond whatsoever and that made me actually ineligible for maintenance, like what Sam had.
We switched to ICE. ICE was the first chemo where I had to be inpatient for three days every time. It was intense.
When your hair falls out on ABVD, for the most part, it’s slowly coming out. With ICE, it was clumps of hair coming out. I was very sick. It was very, very harsh chemo.
Chemotherapy & immunotherapy pre-transplant
Stephanie: Dr. Matasar, for relapsed/refractory patients, can you explain this combination of chemo and immunotherapy in the context of a transplant, hopefully, what this might lead to?
Dr. Matasar: Up until now, the goal for patients who have their disease come back despite good first treatment is to get their disease into remission and then into a round of high-dose therapy or autologous transplant in an attempt to maximize the chances of cure.
Can we cure people reliably and consistently without a transplant by leveraging these immunotherapies either alone or in combination with chemotherapy? This remains a clinical trial-type question; this is not a DIY thing.
My hope for the future is to use these treatments, particularly immunotherapies, to really limit our need to take people through the rigors of high-dose chemotherapy, cure more people, and cause fewer problems.
Determining the sequence of treatment
Stephanie: If the ABVD didn’t work, there’s a relapsed/refractory situation. Maybe there’s some radiation that’s been involved. You have studies about brentuximab, nivolumab, or pembrolizumab alone or in combination. How are doctors having that conversation about the right thing to do next? What is the most promising next course of option?
Dr. Matasar: This is the art standing next to the science. There is some artistry to what we try to do to figure out the right lid for each pot and how to help a patient navigate the course of their illness.
There is no one-size-fits-all anymore. It used to be ICE; that’s all we did. It worked well and it was awful. Now we have a range of choices.
You have to sit with a patient and think through it. How much disease is there that I’m trying to shrink away? How quickly is it growing? How do you feel? How sick is it making you? How quickly do we need to get you better? What was your first treatment? How well did it work? How badly did it not work?
Take all of these factors, try to cram it into your doctorly brain, and try to give some reasonable recommendations. Sometimes you’re going to be as gentle as brentuximab all by itself. Sometimes you’ll want to give more chemo. Sometimes you want to give checkpoint inhibitors alone or with BV. Sometimes you want to do checkpoint inhibitors plus chemo. These are all reasonable courses.
Ideally, what you’re doing as a doctor is working with your patient as a person, as an individual, and charting a course that makes sense for them, for their illness, and for their life.
Stephanie: It’s a really thoughtful response. Are some of the considerations the treatments you had before, how successful they were, what’s already been done… What about things like age or comorbidities or those kinds of factors?
Dr. Matasar: We try not to be ageist, but, truthfully, taking care of a 30-year-old is different than taking care of a 90-year-old and to not recognize that would be silly.
That being said, it’s always a matter of individualization — understanding an individual person’s goals, their preferences, what risks they’re willing to take, what matters to them, and then trying to figure out the best treatment for that person, given everything you know about them, about their value system, and about their goals of care.
Stephanie: Wonderful. I wish every doctor thought like you.
Long-term post-treatment side effects
Stephanie: We’ve talked a little bit about long-term or late-term side effects. Patient Ariadne J. asks, “What is known about long-term post-treatment side effects?”
Sam: I love this question because now I can plug survivorship, which is basically my newfound life passion as a patient-doctor. Cancer survivorship, even though a lot of people don’t necessarily identify with the word survivor, is an important thing to keep your finger on the pulse.
Survivorship applies to this area of medicine that’s changing and evolving. It’s anybody living after a cancer diagnosis and that could be during treatment if you’re on long-term treatment and that could be after your treatment is over.
There are a lot of ways that the cancer experience, even if the treatment goes perfectly, makes you question your life when you’re in your 30s and have your fertility changed. There are all these things that get impacted once you hear that big C word.
Survivorship is an evolving area in medicine that is trying to address all of that. For me, there was a lot. There was identity. There was this existential crisis. Death and dying and making sense of all of that.
The steroids and the other medicine that I had to take impacted my thinking and my emotions. I’m usually a pretty balanced, even person so that was a very hard roller coaster.
There’s some cardiac stuff for some people. Doxorubicin, which is part of the initial treatment, is something that we really need to be thinking about. We’re giving people this medicine that’s toxic to the heart in their 20s, 30s, and 40s. We need to talk about intensive lifestyle interventions like a healthy diet and cardiovascular exercise.
An overall program that focuses on wellness is hugely important in managing long-term side effects and integrative medicine. I’m doing an integrative medicine fellowship. I’m trying to unify everything that I learned in medical school with everything I needed as a patient to get better from cancer and cancer treatment and hoping to offer that to other people.
Those are practitioners that you could consider going to or looking up. Make sure that you communicate everything you’re trying and doing with all of the people who are in charge of your care, including yourself. You’re an important part of that conversation. Cancer survivorship is important for managing long-term side effects.
Stephanie: Chelsey, what were the long-term side effects for you? You talked about going into menopause, for instance.
Chelsey: The main thing I struggle with that is the most apparent in my everyday life is the cognitive side effects of all the different treatments. I honestly think it was from the extreme stress that I was under for so long.
I was on this job in an insurance company and I had to balance things with legal documents. I know that if I were to go back to that job, I would not be able to do it now and that’s taken me a long time to see that that’s okay. I’m still me and I just have to work with things differently.
I have fatigue a lot of times and joint pain. I often joke that inside, I’m 80 years old but on the outside, I’m in my 30s so it feels like that.
As Sam mentioned, there’s a lot of identity crisis that you have as a cancer patient. Who am I now? What happened to the old me? What can I do?
I really want to encourage people to seek community. Even just hearing from Sam, I’m sure some people will say, “Oh, other people feel like that?” That’s definitely what inspired me to start making art and connecting with others. It can truly make a difference in your long-term mental health in survivorship.
Stephanie: Thank you so much, Chelsey. You capture a lot of that in your artwork.
Stephanie: Dr. Matasar, with the newer therapies that are either just approved or in the pipeline, are we addressing some of these long-term/late-term side effects that hopefully people can avoid even years later after treatment ends?
Dr. Matasar: We are. A lot of the drive to develop these newer treatments has been informed by our understanding of late effects, cancer survivorship, and the risks that survivors of Hodgkin lymphoma treated with more traditional treatments go on to face.
We still need to follow with these newer treatments to watch for the possibility of late effects. We don’t believe that they’re going to cause as many or as severe, but part of the work of survivorship is learning from our survivors and walking that path with them as we see how their lives unfold over the years and decades to come.
The number one thing that I would encourage survivors to do is to work with your care teams on developing a survivorship care plan. It can be a paper document or a digital document. It should be something that lives with you that says what your diagnosis was, what your treatments were, and what our understanding is of what you can be doing to safeguard your health in the years to come.
That’s informed by understanding the possible long-term consequences of the treatments that you received, how doctors think you’re best served by taking care of yourself, and what doctors can do to prevent or reduce the risk of those problems as you go on to live your lives.
Stephanie: Wonderful. That’s a great tip. It’s great that the trend of more focus on survivorship after treatment is going to do wonders for so many people.
Shared treatment decision-making
Stephanie: We all want to be more empowered in our care to be able to ask doctors the questions, to feel that we can, and to ask ones that will be impactful.
Dr. Matasar, you talked about how the right treatment for each patient depends on different things like age, health, transplant eligibility, and goals of therapy. How can a patient find out the best treatment options for them and in what order? From a doctor’s perspective, what should that conversation be to elicit the best response for patients and their family members?
Dr. Matasar: I was really disheartened, Chelsey, to hear your story of your doctor disparagingly calling you Dr. Google. Nobody should have to deal with this stuff anymore. We’ve got to be better than that.
Everybody should be empowered to come into a conversation with a doctor as an equal partner in this process. I tell my patients, “This is about you. It’s not about me. I’ve got no ego in this. This is your mountain that you’re climbing. I’m not climbing the mountain. I’m the Sherpa. I’m dragging your bags alongside you. But this is your climb and I’m here to help.”
As patients or as caregivers, if you aren’t feeling valued and heard, then you may not have found the right fit for you in terms of your care team. Everybody should always feel free to be getting a second opinion. I Not enough people take advantage of this sometimes. They don’t want to insult their doctor. I don’t want to be that guy or that gal and I don’t want to be a pain in the ass. Be a pain in the ass.
I like nothing more than when my patients are pains in the ass and they come in with lots of questions. It means they’re doing their homework and they’re really invested. They want to learn and take advantage of whatever I’ve got up in my brain. I love nothing more and any doctor should love nothing more than a patient who’s all in on partnering with me on making this thing work.
Be vocal. Do your research if you want to. You don’t have to. You shouldn’t have to. But if you want to and if it’s something that you value, then that should be celebrated by your care team and never put down.
Chelsey: Have open discussions with your oncologist. If you do find other studies or other treatments, they should be open to answering your questions about it and not being dismissive, even if it’s not an option for you. They should be able to explain to you why or why not.
If you’re a young person about to have a transplant, even if you’re not but if you’re in childbearing age, please ask about fertility. I’m now in menopause at 33 years old.
It was explained to me and I understood. We didn’t really have time to waste to get me to transplant. That’s a conversation you should bring up not only when you’re going into a transplant but also when you first get diagnosed with cancer.
Stephanie: Thank you, Chelsey, those are very important questions. I was lucky to have first-line treatment and be okay, but I asked that question before my intensive chemotherapy. It’s great whenever we’re reminded: advocate for yourself depending on what you want your life to look like.
Finding a Hodgkin lymphoma specialist
Stephanie: Dr. Matasar, it’s clear that for relapsed/refractory patients, and if people are experiencing multiple relapses, it’s hard to find one answer from one doctor. They seek different opinions or get different responses. It’s a very personal discussion to be had.
Is there a right time to find a Hodgkin lymphoma specialist? When should that happen? How can you have that conversation?
Dr. Matasar: It’s tough because it’s very personal. My general philosophy is that people deserve to have expertise in their corner. I also recognize that people want to receive care close to home and they should be able to receive good care close to home.
In an ideal world, everybody would have an oncologist who lives close to them and everybody would have access to an expert to support the decision-making and to support the care journey. Sometimes that would be the same person.
If you lived near an expert, perfect. If you don’t have an expert in your neck of the woods and you want it, then you should have the opportunity to seek out that expert as a consultant and as a backup.
That doctor would work collaboratively with your local oncologist as a team to make sure that they’re doing everything to the best of their ability. You have the expert on standby in case things go sideways. In my mind, that’s the ideal.
If patients aren’t comfortable with what they’re hearing, even from me as an expert, go see somebody else. Hear from another set of lips. Get a fresh perspective. Maybe there will be a better fit in terms of that critical doctor-patient relationship.
Any doctor who doesn’t want you to get a second opinion doesn’t deserve to be your first opinion. Find the care that feels right to you. Trust your gut. The importance of the doctor-patient relationship is too great. It’s too critical in a relationship to settle for anything less than the best.
Stephanie: It’s so resonant and it’s powerful to hear from someone like you, Dr. Matasar. If the doctor doesn’t support you getting a second opinion, they’re not worthy of being your first opinion. I really love that.
Final takeaways
Stephanie: If there’s anything else you want to add, what would you really want people to take away from this discussion?
Dr. Matasar: I’m just bringing it back to The Patient Story. What you’re doing, what we’re doing together is where modern medicine should be. We should be building community. We should be sharing experiences and stories and supporting one another.
Every patient’s journey is unique and yet we don’t walk these paths alone. If you can find ways to build community and be supported by various communities, it makes the journey a little bit less painful.
Chelsey: He said it really well. When I went to my second doctor, I felt comfort and care that I hadn’t gotten before. Make sure that you are having a good relationship with your doctor.
A sense of community is very important because a lot of society puts a little bit of an expectation on our shoulders to always be brave, positive, and strong warriors, and not everyone feels that way.
I just want you to know that’s okay. It’s okay to authentically be yourself and talk about the hard parts of cancer, not just the smiling, ringing the bells, and all of that. There’s a lot more to cancer than that. It’s okay for you to feel the way that you feel, however that is.
Sam: Having lots of questions doesn’t make you anxious so it’s okay to have lots of questions and concerns and to look things up. It’s okay to reject that label because you’re just appropriately concerned about your life and the quality of your life.
Some doctors may be more attuned to knowing to ask about what’s really important to you in your life. Some people may be really busy that they forget that. As patients, it’s up to us to tell our doctors what’s really important to us and things that we like doing.
Share with your doctor what’s really important to you. Not only will it help them to know you as a human being, but it will help inform treatment decisions.
There were times during my treatment and I’ve heard from other patients where it felt like to want anything more than not dying was greedy. We’re beyond that now in medicine.
We are in the era of personalization, community, and individualized care within the guidelines of all the new things that are being discovered. It’s not greedy to want to keep exercising to some degree or keep doing your art or whatever defines the quality of life for you.
Tell your doctor what’s important to you. Reject the anxiety label. Let’s shift the focus from mortality to vitality in cancer. It’s so much more than just not dying. It’s the living part.
Stephanie: You both have exemplified that so much. I’m really grateful to have had you, Chelsey, and Dr. Matasar doing your work in research and helping patients and families holistically. Thank you for the work that all three of you are doing as advocates.