

Stephanie Chuang: I’m the founder of The Patient Story. More importantly, as someone who’s dealt with her own blood cancer diagnosis, I have spent a lot of time talking with patients, care partners, and doctors about how we can make the best treatment decisions, including figuring out when clinical trials enter the conversation, especially in multiple myeloma where so much development has happened. I know firsthand how confusing and overwhelming it can be trying to navigate those options. We’re here to try and give you the information and, hopefully, the confidence that you need to have those important conversations with your care team.
Before we dive in, I want to give a big shout-out to our friends at Blood Cancer United (formerly The Leukemia & Lymphoma Society). As you probably know, they offer so many fantastic resources, including the free one-on-one support in navigating clinical trials through their Clinical Trial Support Center. I have the pleasure of speaking with many of their nurses who are there for you on the other end of that line and they are fantastic. It’s clear that not only do they know about clinical trials and how to navigate them, but they also care about these relationships and the people they connect with.
For this discussion, we teamed up with Blood Cancer United, which supported and sponsored this program, and also one of its community outreach managers, to bring you a special conversation. You’re going to hear from Bryon Daily, who was diagnosed with multiple myeloma in 2018. He had a basketball injury that then led to the diagnosis. After years of navigating treatment, Bryon has been dedicating his time to helping other people find their way after diagnosis.

He’s going to sit down with Dr. Ajai Chari, one of the leading experts in multiple myeloma. Dr. Chari is from the University of California San Francisco (UCSF), which is where I got my care in lymphoma. They’re going to talk about the latest in treatments, research happening through clinical trials, and why knowing your clinical trial options matters so much for us as patients and care partners. It’s not a last resort. It can bring tomorrow’s treatment to you today and it’s about figuring out if this is the right trial for you.
While we hope that you find this discussion to be helpful, it is not a substitute for medical advice, so please talk with your healthcare team about what’s right for you.
Bryon Daily: Our discussion will be on treatment options for patients with multiple myeloma and the importance of clinical trials in battling this disease. I’m the National Community Outreach Manager for Blood Cancer United’s Myeloma Link initiative. I’m also a six-year survivor of multiple myeloma, having been diagnosed back in 2018.
I have no history of cancer in my family that I’m aware of, so, needless to say, it was a surprise when I was diagnosed. The diagnosis was a result of my primary care physician being very diligent in following certain trends in my labs. I had escalating protein over the course of several months, but it wasn’t until about the sixth month when, while I was playing basketball at the gym, I caught the ball wrong, which hit my finger. I went home thinking it was a simple sprain.
Two weeks later, it didn’t heal; it was still as if it happened the day before, so I went to my doctor. We did imaging and it turned out to be a fracture. The fracture, paired with the escalating levels of protein, was a red flag for my primary care physician. Fortunately, he was able to refer me to several specialists.
About a month later, we ultimately went to see an oncologist who ordered a biopsy and I turned out to have myeloma. I went through several months of chemotherapy and, ultimately, had an autologous bone marrow transplant, which was successful. After several months of being out of the public domain, I began to recover.
I’m joined by Dr. Ajai Chari, a hematologist-oncologist at the University of California San Francisco. He is the Director of the Multiple Myeloma Program and Professor of Clinical Medicine. His research interests include the development of novel chemotherapy regimens, including phase 1 and 2 studies.

Bryon: Dr. Chari, our audience includes patients, caregivers, and partners. What is the number one takeaway you hope that they walk away with before we dive into details?
Dr. Ajai Chari: Thank you, Bryon, for having me. It’s a pleasure to be with you and thanks for sharing your story. The number one thing that patients are looking for is hope. They want to know that they’re going to be able to live as long as they want to live and with a good quality of life.
Bryon: Doctor, what is multiple myeloma and how do we treat it?
Dr. Chari: Myeloma is a cancer of the plasma cells. The hallmark of any cancer is that one cell in the body grows out of control and when it’s myeloma, it’s a plasma cell. They live in the marrow, so we call it a bone marrow disorder, but the manifestations can be in the blood and outside the bone marrow.
The symptoms of myeloma, when those plasma cells grow too much, are often summarized by CRAB: high calcium (C), renal failure (R) or kidney dysfunction, anemia (A), and bone disease (B).
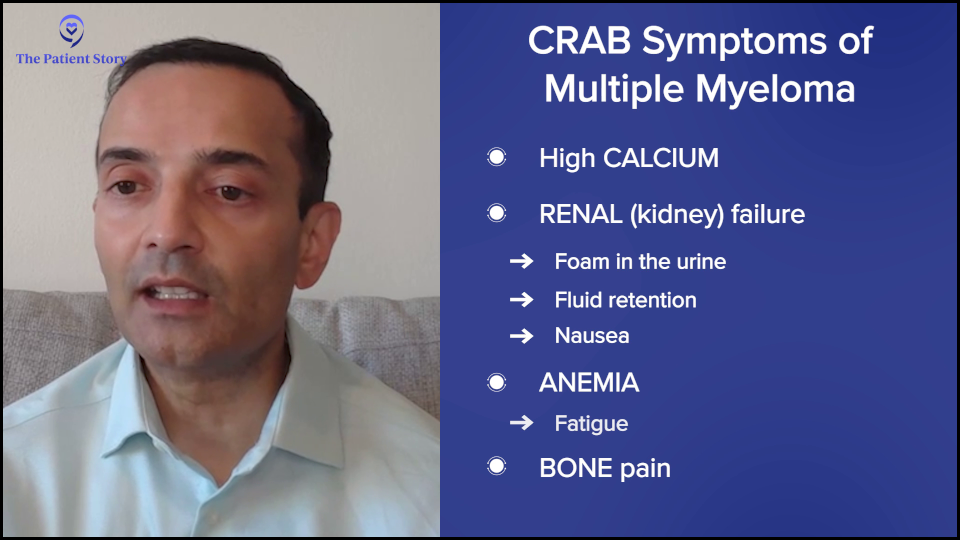
If they’re hypercalcemic, they can present with confusion or bone pain. Kidney failure can often be subtle. They may see foam in the urine. In advanced kidney failure, they may see fluid retention or nausea. Anemia often presents with fatigue, which is one of the more common symptoms.
Because it’s usually a slow-growing condition, it’s not something that pops up right away, but patients may gradually notice that they’re not able to walk as briskly or go up hills or stairs as readily. Everybody can have bone pain, especially as we get older, but it’s persistent, severe bone pain, and not something that comes and goes or fractures.
Bryon: Dr. Chari, how do we treat it?
Dr. Chari: At a high level, cancers can be treated theoretically by chemotherapy, radiation, or surgery. In myeloma, there’s not a role for surgery other than to fix a fracture because it’s a bone marrow cancer. Radiation can be used for spot welding of pain at a particular site. But the mainstay of therapy is systemic or whole-body therapies.
Sometimes, people get concerned about the terms chemotherapy and immunotherapy. I would say any drug that’s used to kill cancer theoretically could be called chemotherapy because it’s killing cancer. A good example of that is steroids, everybody’s least favorite drug. Dexamethasone technically kills myeloma.
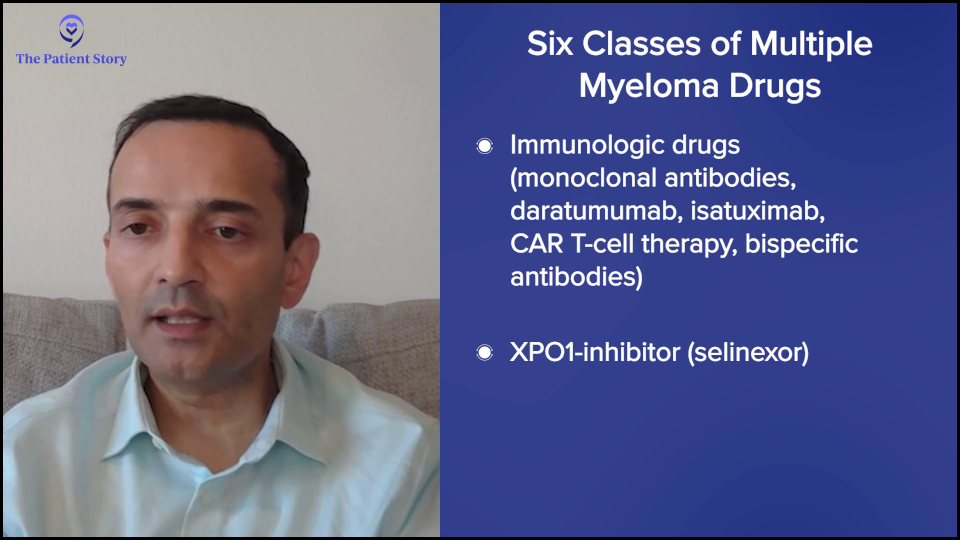
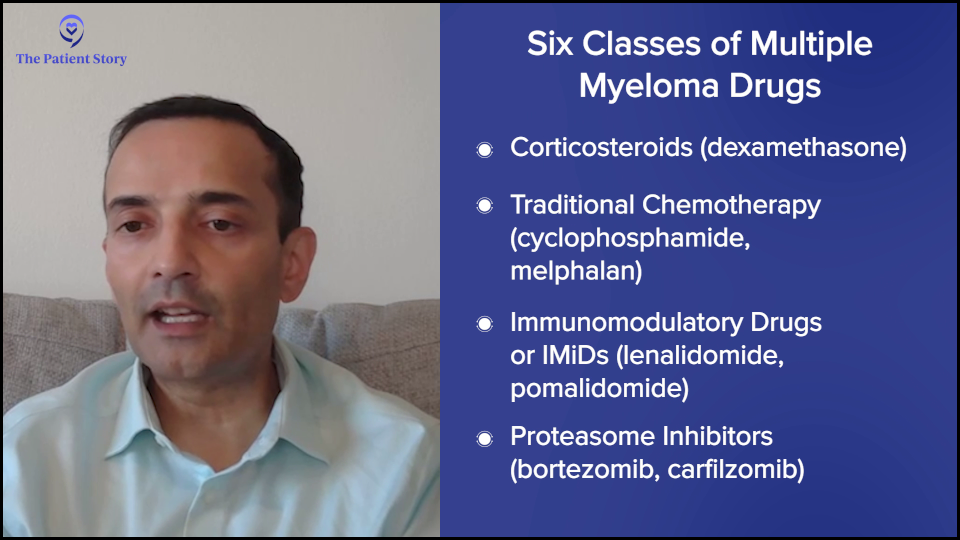
The classes of drugs in myeloma, which we can use in a newly diagnosed patient, are steroids, conventional chemotherapy (cyclophosphamide or Cytoxan, melphalan or Alkeran), immunomodulatory drugs (lenalidomide or Revlimid, pomalidomide or Pomalyst), proteasome inhibitors (bortezomib or Velvade, carfilzomib or Kyprolis), immunologic drugs (naked monoclonal antibodies, daratumumab or Darzalex, isatuximab or Sarclisa, CAR T-cell therapy, bispecific antibodies), and an XPO1 inhibitor (selinexor or Xpovio).
Those are the six classes of drugs and we can mix and match these based on efficacy and safety data, and how they will work and combine. For a newly diagnosed patient, the field has moved to, at a minimum, three drugs. Everybody gets steroids, at least at the beginning. Most people get lenalidomide (Revlimid), which is an oral drug, and CD38 antibodies, such as daratumumab (Darzalex) or isatuximab (Sarclisa).
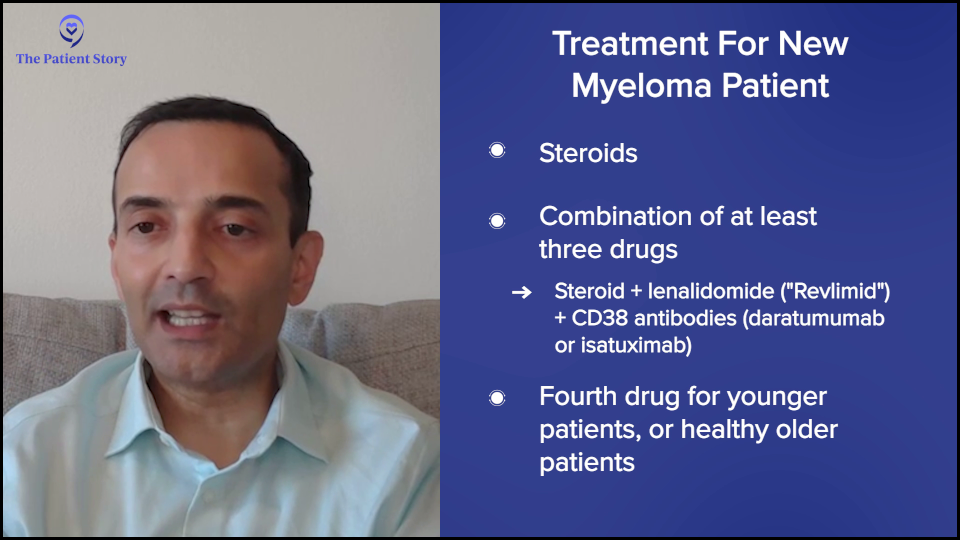
There’s now a movement for younger patients and now even older patients to also get a fourth drug, which is a proteasome inhibitor, either bortezomib (Velcade) or carfilzomib (Kyprolis). The challenge there is that daratumumab (Darzalex), lenalidomide (Revlimid), and dexamethasone, which is called DRd or MAIA, is projected to give a five-year remission for the typical older patient even without a transplant.
To me, it’s not clear that every patient needs an extra drug because the fourth drug can come with additional side effects. But if it’s a fit older patient, certainly four drugs can be done. The other question is how long you need to continue. There are these movements of “down with dex.” Get the myeloma under control, but then drop it off, and then similarly drop the proteasome inhibitor.

For younger patients, there’s the question of whether or not to do the transplant. It’s not wrong to do the transplant, particularly for high-risk patients. The value added is even higher. For the typical patient, transplant adds about 16 months of remission. For high risk, it can be even up to three years.
Some people have an aversion to transplant and are more interested in CAR T-cell therapy, but we need those data sets to read out that CAR T-cell therapy’s better than transplant. Whether or not you do transplant, you go to maintenance therapy typically of three to four drugs. Lenalidomide (Revlimid) is the easiest drug to maintain because it’s a pill. Some people also get daratumumab (Darzalex). Very rarely, we also do the other drugs.
We hope these remissions last a long time. Some of the quadruplets are now projected to last, believe it or not, 90 or 100 months, so eight to nine years, which is amazing.
But unfortunately, many patients will relapse. When a patient relapses, you could go back to any of those drugs on that six classes, except you can’t go to drugs that the patient’s no longer responding to. For example, if somebody was on lenalidomide (Revlimid) maintenance, you wouldn’t use that. If somebody was on lenalidomide (Revlimid) and daratumumab (Darzalex), you wouldn’t use those.
There are a lot of options and it’s impossible to go through them in a short time, but at a high level, the more high-risk the patient is, meaning the earlier or the more aggressive the relapse, the more you might want to consider CAR T-cell therapy because it’s now approved for one to three lines of prior therapy.
The slower and more well-behaved a myeloma is, you may be able to get away, for example, with a combination a CD38 monoclonal antibody, carfilzomib (Kyprolis), and dexamethasone, like daratumumab (Darzalex), carfilzomib (Kyprolis), and dexamethasone (DKd), or isatuximab (Sarclisa), carfilzomib (Kyprolis), and dexamethasone (Isa-Kd). You could also use the other drugs that we mentioned, like pomalidomide (Pomalyst). At a high level, that would be the first relapse. There’s now data to even potentially use belantamab (Blenrep), but it’s not yet approved. It’s an antibody-drug conjugate that could also be used in this space.
Lastly, for those who’ve had more than one relapse — they’ve had initial therapy, first-line therapy, and they’re now in second line and beyond — it’s the same principle. You can’t use drugs that the patient’s no longer responding to and, of course, you wouldn’t use drugs that the patient didn’t tolerate in the past. Beyond that, you could come up with any other combination. For example, you could do carfilzomib (Kyprolis), pomalidomide (Pomalyst), and dexamethasone (KPd) if you haven’t had those drugs before. You use all the drugs that you can.
Currently, bispecific antibodies, which are also exciting, require four or more lines of prior therapy, so that’s how the sequencing works. If you’re going to consider CAR T-cell therapy, it needs to be done before bispecific antibodies and antibody-drug conjugates because those will adversely affect the CAR T-cell therapy outcome. That’s a high-level overview of how we approach myeloma therapy.
Bryon: What role do demographics like age, gender, and race play in treatment?
Dr. Chari: We would love to personalize myeloma. Our closest example is translocation t(11;14), which was targetable by venetoclax (Venclexta, Venclyxto), but it was very complicated. Part of the reason is that even though patients did better with that drug, the studies were not always clear and I think it has to do with how complex myeloma is. It’s not just the genetic component. There are also a lot of important patient factors.
One of the unmet needs in myeloma is for the frail elderly patients, people who are 70-plus with a lot of medical problems. We have to do better for them. It’s great to have all of these amazing regimens, but if you can’t give them safely, then that’s a problem. Younger patients typically do better.
Concerning gender, we’ve seen pretty balanced outcomes. One thing is that CAR T-cell therapy with the rare Parkinsonism seems to be seen more in men than women, but that’s also because that’s where the demographics of Parkinson’s are, in that men get it more than women.
With race, the biggest thing is disparities in outcomes. Not everybody’s getting access to therapy. For example, when you look at the veterans’ hospital where everybody has access to therapy, you don’t see the differences in race-based outcomes. It’s when you take away equal access that you start to see differences. There are some studies suggesting that African-Americans may have better disease biology, so they may even have better outcomes with the same therapies if everybody’s getting access equally.
I would add that not just race, but anybody underserved, which includes economically disadvantaged and people in rural communities. We’re such a large country and if you live in a rural part of the country, you may not have access to some of the novel, exciting therapies. We have a lot of work to do in transposing all of these amazing outcomes and exciting drugs to all patients in the U.S. with myeloma and, honestly, globally, too.
Bryon: Doctor, when I was diagnosed, I had a sit-down visit with my oncologist to discuss next steps. We talked about clinical trials, of course, but that’s not always the case. I decided at the time that I didn’t know enough to decide on the spot, so I said, “What is the standard line of treatment? I prefer to follow that and then see what happens.” How do you decide what treatment options are best for a patient?
Dr. Chari: Myeloma is not one of the most common tumors. The most common cancers are breast, colon, prostate, and lung. If you’re a patient who’s diagnosed in the community, chances are your oncologist is very experienced with those cancers, but possibly not as much with myeloma.
Studies show that outcomes are better for patients who are affiliated in some way with an academic center. I always tell my patients that they don’t get points for suffering. You don’t need to drive hours to come see me or get the same treatment you’re going to get close to home.
However, you should have a connection with an academic doctor who knows and keeps up with the latest data. Myeloma publications are like drinking from a fire hydrant. Every year, there are multiple, high-impact publications. As a community oncologist who’s treating all those other cancers, how can you possibly expect one person to be an expert at everything?
If you’re a patient, you want expert opinion, but the convenience of getting it close to home. At a minimum, get that academic opinion, hear about the options that are being proposed, which may or may not include clinical trials, and then make a decision.
Remember that today’s clinical trials are tomorrow’s standard of care. Every treatment that you’re getting today was because people like you did studies before you. We found that these newer therapies often displace the older therapies. It’s important to get your options, but also to recognize that some patients may not be eligible. If you have kidney failure or your counts are too low, you may not be eligible for studies, but it never hurts to have the options.
Bryon: A lot of your research has been focused on CAR T-cell therapy. Can you explain how it works and some of the challenges with T-cell therapies?
Dr. Chari: People ask why they got myeloma. The short answer is we don’t know, but the fact that most people get it in their 60s and 70s suggests that perhaps the immune system gets lazy as we get older. Maybe we all have a little bit of cancer when we’re younger, but our immune system gets rid of it. As the immune system gets lazy, we can lose that ability.
One way to deal with that is you can take somebody’s T cells out, genetically modify them, and put them in the patient. Essentially, these supercharged T cells can then kill the myeloma.
Initially, I have to say we were not too excited about this. As with all clinical trials of new therapies, we typically test them in people who have exhausted all available options because that’s the only way to do it. If you don’t know the side effects of something, you first start with patients who have very limited options.
When you take patients who are older and have been treated with many chemotherapy regimens, you don’t necessarily think the new therapies are going to work, but guess what? These CAR T-cell therapies are working like gangbusters.
When we put these supercharged T cells into patients, we’re getting responses of 80 to 90% lasting from one to three years in patients where you would historically expect — at best — a new exciting therapy to give a 20 to 30% response rate lasting from three to four months.
It’s a paradigm-shifting time. CAR T-cell therapies have taken patients who are almost hospice-bound and now put them in stringent complete remission, off therapy, and enjoying their lives.
Bryon: Another area of research is bispecific antibodies. What advantages do bispecific antibodies offer over CAR T-cell therapies?
Dr. Chari: CAR T-cell therapy has to be very personalized. You have to collect T cells, genetically modify them, and put them back, so it’s personalized therapy. There’s what’s called vein-to-vein time, which is the time from collection to administration, and that can be anywhere from four to six weeks.
I would add that there’s also a brain-to-vein time. It’s from the day patients who are in the community are evaluated by their doctor and referred to an academic center, to when they get insurance approval and have their T cells collected.
The problem is that some patients don’t have the luxury of time. Whether it’s four to six weeks or several months, if your myeloma is taking off, you don’t have the luxury of waiting, so you need an off-the-shelf product that’s ready to go and this is where bispecific antibodies come in.
Bispecifics are like all other myeloma medications. If there’s a side effect, you can stop the drug and wait for the side effect to get better.
With CAR T-cell therapy, you administer it once it’s manufactured and after you put it all in, you don’t have control. You can’t take it back. If somebody has severe side effects, you just have to manage them. You can’t pause or reverse the process. In patients who have a lot of medical problems, you have a little bit more control over bispecifics than you do with CAR T-cell therapy.
Those are the two main differentiations: off-the-shelf and the ability to stop the therapy.
Bryon: Can you elaborate on the development and potential impact of trispecific antibodies in multiple myeloma patients?
Dr. Chari: CAR T-cell therapies and bispecific antibodies have historically targeted one antigen or one protein, which is ideally overexpressed on myeloma and not on other cells. The reason you want to do that is if you’re going to activate your T cell, whether with a CAR or bispecific, you don’t want them to attack your heart, kidneys, lungs, or normal parts of your body. You want those T cells to be like snipers and go after the cancer. We do that by selecting proteins that are overexpressed in myeloma but not in normal body parts.
Bispecifics bind your T cell, which is your immune cell, and your myeloma cell. With CAR T-cell therapy, the T cells are supercharged to kill one protein. Trispecifics are saying, “Why do we have to stick with one protein? Why not have the snipers go after two different proteins to increase the specificity?”
Even though we try to pick proteins that are overexpressed in myeloma, some of the other cells that express these will also be hit. For example, many people know about BCMA or B-cell maturation antigen. When you target that protein, you kill the myeloma cell, but you also kill some other immune cells, which can then increase the risk of infections.
The other big protein that we target is GPRC5D, which stands for G protein-coupled receptor class C group 5 member D. A mouthful, but it’s basically a protein that’s overexpressed on myeloma. But this protein can also be overexpressed in tissues that have a lot of keratin, like the nails and skin, so you see some of those side effects. It also causes oral side effects, like affecting taste and weight loss.
The trispecific is saying, “What if we target both? Let’s take the T cells and attack GPRC5D and BCMA at the same time. Will that decrease some of these side effects? Can you get even better responses?” It’s a nuclear war. When we go after one protein, the myeloma cell stops making that protein. By targeting two at the same time, it’s harder for the myeloma cell to bypass that.
Those are some of the theoretical benefits, which are possibly fewer side effects and hopefully more efficacy and better activity, but we’ll have to see. Preliminary data will be presented at the 2025 American Society of Clinical Oncology (ASCO) meeting and there’s a lot of excitement about this approach.
Another difference is when you give bispecifics and CAR T-cell therapy, after the first dose, sometimes you have massive T-cell activation. We call that cytokine release syndrome (CRS), which can present with fever and low blood pressure, often requiring hospital admission. By doing this dual targeting, will that make the safety profile better?
Bryon: These novel innovative treatments that you mentioned have emerged over the past few years at a rapid pace. Let’s talk about clinical trials. There have been a few trials recently looking at different combination therapies, such as the AURIGA trial, MajesTEC-5 trial, and DREAMM-7 trial. What are researchers hoping to understand about these treatment options?
Dr. Chari: When we start with the patient journey, most people are getting an initial therapy of a combination of three drugs, now often four, then many people get a transplant. What happens after a transplant?
Dr. Chari: If you’ve gone through initial chemotherapy and transplant and you’re still not what I call the A+ of myeloma — which means not only have we eradicated all the myeloma in the blood, the urine, and the bone marrow, but even the minimal residual disease — can we improve your outcome to get you to an A+?
In the AURIGA study, you had to be MRD positive after a transplant and could not have had a CD38 monoclonal antibody, like daratumumab (Darzalex) or isatuximab (Sarclisa), in your initial therapy. You could have had chemotherapy and a transplant, and you were still MRD positive. In the study, half of the patients got lenalidomide (Revlimid) alone and the other half had the addition of daratumumab (Darzalex) as a shot.
What that study showed is that the A+ conversion was improved, so more patients got MRD negativity, which, more importantly, translated into doubling of the remission duration. That’s now a strategy that could be used. Although it’s a randomized phase 2, not a phase 3, there’s a lot of excitement about trying to improve outcomes.
Dr. Chari: Similarly, the MajesTEC-5 trial takes patients who are post-transplant and asks, rather than just doing lenalidomide (Revlimid) maintenance as a minimum, can you do better than that? One of the ways they’re trying to do that is by incorporating a BCMA bispecific known as teclistamab (Tecvayli), which is why it’s called MajesTEC-5. The TEC in MajesTEC refers to teclistamab.
This is not a randomized study. It’s a small study of only about 30 patients in two different arms, but it showed dramatic responses where the MRD negativity achieving A+ was markedly increased. Pretty much everybody achieved MRD negativity in this study.
Now, of course, we haven’t talked a lot about side effects, but these bispecifics can increase the risk of infections when you’re targeting BCMA. We’re going to need larger data sets to understand how to put getting an A+ into context with the potential risk of infections and needing preventative drugs and intravenous immunoglobulin (IVIG). It’s hard to argue against an A+ for 100 % of patients and so I think that’s where a lot of excitement is.
Dr. Chari: With the DREAMM-7 trial, patients have had an initial therapy, they may or may not have had a transplant, and they may or may not have had maintenance, but now the myeloma has come back. What can you do?
Historically, because a lot of patients are getting lenalidomide (Revlimid) maintenance after transplant, you can’t use lenalidomide (Revlimid) anymore. You have to move on. We could use daratumumab (Darzalex) and bortezomib (Velcade), and dexamethasone (DVd), but can we do better than that?
In this study, they took bortezomib (Velcade) and dexamethasone, but swapped out the daratumumab (Darzalex) with a new BCMA antibody-drug conjugate known as belantamab mafodotin (Blenrep), or bela for short. Basically, it’s a three-drug versus three-drug combination and everybody got Velcade-dex. The question being asked is belantamab (Blenrep) versus daratumumab (Darzalex). What that study showed was, surprisingly, belantamab (Blenrep) beat the pants off daratumumab (Darzalex). This was a marked improvement in the remission duration.
Now, this drug does come with eye side effects. It can cause dryness of the eye, irritation, and blurry vision. Most of them are reversible and sometimes they can hold the belantamab (Blenrep). This is a great option because if you can beat daratumumab (Darzalex), then why not?
The only limitation is that very few people will be in this population. These are typically going to be older patients. For most people who are younger with relapsed myeloma, you’re going to want to think about CAR T-cell therapy. If you give drugs, like belantamab (Blenrep) or BCMA bispecifics, you’re going to impair the CAR T-cell therapy outcomes down the road, which we know from some clinical trials.
For example, cilta-cel (Carvykti) gives a three-year remission. If you give a bispecific that goes to five months and an antibody-drug conjugate that goes to nine months, we don’t want to impair that amazing CAR T-cell therapy outcome.
For those who may not be eligible for CAR T-cell therapy— either they don’t want to do it, or they’re perhaps old and have a lot of medical problems — DREAMM-7 could be a good and exciting option. The other big difference is that it could be done in the community. You don’t need to go to an academic center to get belantamab mafodotin (Blenrep).
Bryon: Why should a patient consider a clinical trial?
Dr. Chari: I was in New York for about 18 years, including the time when CAR T-cell therapy and bispecific antibodies came. I remember patients had exhausted all the therapies at that point. They’ve had the big five: lenalidomide (Revlimid), pomalidomide (Pomalyst), bortezomib (Velcade), carfilzomib (Kyprolis), and daratumumab (Darzalex). What do you do for someone like that?
We’ve had hospice conversations with some people, but let’s try this study. Those patients are now in their deepest and most durable remissions in their entire myeloma journey, despite having had all those drugs, which is a clear example. If you’ve run out of options, then you should be looking for new strategies. Many people would understand the need for clinical trials there. Even if you’re newly diagnosed or have had an early relapse, it’s also important to think about a clinical trial.
Back when I was a fellow, our initial therapy was two drugs, lenalidomide (Revlimid) and dexamethasone. How would we know that we need to do three drugs, then four drugs, a transplant, and maintenance? That’s been incremental learning from every clinical trial and that’s how medicine progresses. It’s always good to think about how you can get the best care for yourself and how you can advance the science for everybody.
Bryon: The results of those clinical trials helped to determine what’s best for any given patient based on the data that comes out of trials. There are a lot of myths about clinical trials, as you know. One of the concerns we address with Myeloma Link is the fear that people will be receiving a placebo and getting no treatment or that the participants will become guinea pigs. Think about the Tuskegee syphilis study or the harvesting of Henrietta Lacks’ cells. What do you tell patients about these fears?
Dr. Chari: Fear is understandable, especially when you’re dealing with a diagnosis of cancer. When I was a medical student, we had a class called “Is It Cancer and Can I Still Have Sex: The Two Questions Patients Had, But Were Afraid to Ask.” What you learn is that 50% of the information during that first cancer visit goes in one ear and out the other because not only are they dealing with the diagnosis and the intellectual questions, but also the emotional aspect. It’s always good to have a family member or friend with you to listen in on all of your conversations, so that they can help catch some of the things you might have missed or record the visit, if your provider allows.
It’s also important to understand that because of the Tuskegee syphilis study, Henrietta Lacks, and all of these other stories, there are a lot of protections built in. As an investigator, you can’t simply say that you want to test a new drug.
You have to write a protocol. You have to write a consent form, which independent doctors review on several committees. The FDA has to oversee it. If it’s sponsored by a company, the company has to oversee it. There are a lot of checks and balances within the institution, the pharmaceutical company, and the FDA. There are three different major stakeholders.
As a patient, you have to ask: What’s the question being asked? For example, it’s unethical to take somebody with advanced myeloma, who has active disease, and assign them to a placebo. That would never pass all of those various committees.
Where you might see a placebo is if you’re not sure if you need an extra drug. If the combination of three drugs is doing pretty well and you want to add a fourth drug, you might have to do a placebo arm. There is a placebo effect. When people take a drug, they’re going to feel better and think they’re getting a better outcome.
In my experience with myeloma, the placebo-based studies are very few and far between. Probably the only time you see that is in maintenance, where you don’t know if you should be doing something preventively or wait for the cancer to act up. Or perhaps in smoldering myeloma, where you don’t have symptoms and you’re trying to prevent the cancer, you might think about doing something like that. But even with those, the field is moving.
In cancer, the concern that you’re going to be a guinea pig is typically because of an admitted lack of knowledge. Otherwise, if we knew the answer, we wouldn’t be doing it, so there is an inherent unknown. We put a lot of safeguards in to mitigate that.
Bryon: Let’s talk about managing treatment side effects. What are some of the common side effects people experience from treatment and what can be done to mitigate them?
Dr. Chari: This is a complicated question because it is very drug-specific and therapy-specific.
If we’re talking about steroids, everybody’s least favorite drug, the possible side effects include irritability, sleep, heartburn, and fluid retention. You can try to lower the dose and, if possible, even stop it. You could also take a sleep medication.
Conventional chemotherapies often cause a lowering of blood counts because they kill the myeloma cells. We’re talking about drugs like melphalan (Alkeran), which is part of the transplant. There’s some interest in cooling caps for reducing hair loss that are showing some activity at our institution.
For the IMiDs (immunomodulatory drugs), like thalidomide (Thalomid), lenalidomide (Revlimid), and pomalidomide (Pomalyst), they typically increase the risk of blood clots, so it’s important to take an aspirin to prevent those. If you’re on certain other drugs, have a history, or have a high risk, you might want to take something stronger.
With proteasome inhibitors like bortezomib (Velcade), carfilzomib (Kyprolis), and ixazomib (Ninlaro), there’s a risk of shingles, so you would want to take a preventative pill. Sometimes, bortezomib (Velcade) can cause neuropathy, and carfilzomib (Kyprolis) can cause heart issues, so you have to monitor blood pressure. Immunotherapy drugs can also increase the risk of infection, so you have to monitor that.
CAR T-cell therapy and bispecific antibodies can cause cytokine release syndrome, which has to be monitored and treated. With bispecifics, there is also the risk of infections and oral toxicity, which you have to do supportive care, like IVIG, or modify the dose.

Bryon: At what point would side effects lead to considering switching a patient from one treatment to another?
Dr. Chari: This is always a balance between efficacy and safety. What kind of myeloma is this? How well is it controlled? How bad are the side effects? If somebody has very favorable myeloma with very little disease, you’re not going to tolerate many side effects. If you have very difficult-to-control myeloma or very high-risk myeloma with multiple genetic abnormalities, there might be more willingness to take on side effects.
Ultimately, you have to give it a shot. This is why oncology is a specialty. You have to know this kind of risk-benefit balance and walk this tightrope. That’s why we have frequent visits and labs so that you can make treatment decisions. Am I happy with the myeloma control? How bad are the side effects that this patient’s having? Is the patient willing to continue with some modifications of dose and schedule or medications to offset side effects?
Bryon: Multiple myeloma is generally diagnosed in older patients. What are some of the quality of life considerations that you discuss with patients who are younger than 50?
Dr. Chari: My youngest patient was diagnosed below 18 and the oldest is over 100. It’s a very heterogeneous disease, so it’s hard to do a one-size-fits-all. There’s a movement in all of medicine, specifically in oncology, to not use a chronological age and to focus on how healthy that person is. Some 70-year-olds are going to be way healthier than 50-year-olds who might have multiple other medical problems.
For older patients, you have to look at their other medical issues. For young patients, you’re trying to walk that tightrope between preventing the disease from coming back and allowing them to live their lives. It’s important to talk about fertility preservation, maybe banking sperm or freezing eggs and embryos if possible, understanding what may or may not be feasible depending on the pace of the disease. Ultimately, it’s what we do in oncology. You have to personalize the therapy for each patient.
Bryon: What are the most promising developments in multiple myeloma treatment that you foresee in the next few years?
Dr. Chari: The first is moving therapies that are currently in advanced myeloma to earlier and earlier lines of therapy. Initially, CAR T-cell therapy was for heavily treated patients; now it’s approved for patients who have had one to three prior lines. There are clinical trials that may lead to their approval in newly diagnosed patients and perhaps even smoldering myeloma. Similarly, bispecific antibodies are making their way up, showing 100% response rates and MRD negativity in earlier lines of therapy.
We also need new combination therapies. Let’s say somebody has had CAR T-cell therapy and bispecific antibodies. What do we do then? When you beat up all the T cells with all these therapies, you need non-T-cell-dependent strategies. Some new targets are promising, like bromodomain inhibitors and trispecifics that target different antigens.
Then we talked about dual CARs, triple CARs, and newer CARs that don’t have the same safety issues, some data that maybe we don’t see Parkinsonism, improving on existing therapies and moving them earlier, and having new targets.
Bryon: How do you envision the integration of novel immunotherapies into standard treatment protocols for multiple myeloma?
Dr. Chari: Thankfully, the health authorities across the Atlantic, both our FDA and Europe, have allowed MRD negativity. The MAIA study had a median age of 73, who received daratumumab (Darzalex), lenalidomide (Revlimid), and dexamethasone (DRd). If you start at 73, those patients are going to get a five-year remission. If you’re going to try to improve on that combination, imagine how long you’re going to have to wait before hundreds of patients are accrued and randomized before we find out if they’re better.
The MRD negativity is a huge advancement in earlier lines of therapy because then, MRD negativity should translate into progression-free survival, which is how long the remission lasts. Ideally, that could lead to living longer. Sometimes people are looking for overall survival improvement, but as you get to newer and newer diagnoses of myeloma or less heavily treated, the number of drugs that we have to rescue myeloma can make it very difficult to show that the initial therapy is going to translate into living longer. MRD negativity is going to be a big one.

Honestly, we need these clinical trials, like CAR T-cell therapy versus transplant, which I think is super exciting. I don’t think anybody wants to go through a transplant voluntarily. If we can do new therapies that don’t cause hair loss, nausea, vomiting, diarrhea, weight loss, and fatigue, by all means, we should get rid of it.
But we need studies to show not just that they’re better, but remember, we also need to think about long-term side effects. Because myeloma patients are living longer, there’s an increased risk of getting other cancers, so we need to follow patients long enough to know that not only is the initial benefit there, but there are no unexpected longer-term side effects.
Bryon: Dr. Chari, as we wrap up, if there’s one thing you want someone newly diagnosed with multiple myeloma to know about their treatment options, what would it be?
Dr. Chari: My passion is the personalization of therapy. No two patients are alike. You can read about a clinical trial, you can go to a patient support group, and you can talk to a friend, but that doesn’t mean that’s the right treatment for you.
There are patient factors to consider, like age, kidney function, heart history, diabetes, and neuropathy. There’s the disease, like your ISS stage and genetics. Do you have myeloma coming out of the bone marrow or extramedullary disease (EMD)? There are treatment considerations. What side effects are you willing to accept? Can you take time off work? Do you have a caregiver? What therapies have you had?
I see a lot of patients who come in the door so anxious that they just want me to give an immediate answer as to what I would recommend. You have to put all of those factors that I mentioned together. I need to know your medical history, your cancer, and what you want as a patient. Then I can give you an answer. But if you’re just asking for an answer, you’re not getting the best care, and that includes the options for clinical trials.
I would encourage everybody to speak to a myeloma consultant at an expert medical center and make sure that all of these factors are being considered to personalize a therapy for you.

Bryon: Dr. Chari, thank you so much for sharing your insights.
We hope this discussion has provided you with valuable information. We encourage you to follow or continue following the latest advancements in the field and to discuss your options with your healthcare providers. Please check out Blood Cancer United’s Myeloma initiatives and support for patients and caregivers.
Stephanie: Thank you so much, Bryon and Dr. Chari, for leading this incredible conversation. We’re so glad that you could be a part of this discussion about promising clinical trials in multiple myeloma. We hope that this leaves you with new information, fresh hope, and a reminder that you are not alone as you’re dealing with this.
Every patient and care partner deserves to understand all of their options. Clinical trials are not just for someone else. They’re not a last resort. They can open doors to the latest in treatments and care. It’s all about having the conversation with your team to know your options. It may not be the right one for you, but at least you have that at your fingertips.
If you need any support, don’t hesitate to reach out to The Patient Story or Blood Cancer United. They have a Clinical Trial Support Center that offers free one-on-one support for clinical trial navigation, which happens even before the clinical trial. They can help you figure out the questions beforehand, including which clinical trial might be the right one for you. They also have a patient community and peer-to-peer support.
Remember, your voice and story matter. Keep advocating for yourself. Don’t be afraid to ask questions. Do your research. Talk openly with your team. Be curious. We hope to see you again at another conversation. Take good care.





Multiple myeloma advocate Valarie Traynham is joined by Donna Catamero, Associate Director of Myeloma Research at the Icahn School of Medicine at Mount Sinai and a nurse practitioner specializing in the treatment of multiple myeloma patients, and Abbey Reiser, a dietitian/nutritionist and board-certified specialist in oncology nutrition from the Ruttenberg Treatment Center The Tisch Cancer Institute, to share practical strategies for handling side effects, optimizing nutrition, and improving quality of life.
Interviewed by: Tiffany Drummond
Edited by: Katrina Villareal
Tiffany Drummond: I’m a patient advocate with over 20 years of experience in cancer research. My journey began as a caregiver when my mother was diagnosed with endometrial cancer in 2014. I quickly realized the challenges of finding resources, support, and shared experiences, and now I’m committed to helping others, no matter the condition.
At The Patient Story, we create programs to help you figure out what comes next. Think of us as your go-to guide for navigating not only the cancer journey but your overall health journey. From diagnosis to treatment, we’ve got you covered with real-life patient stories and educational programming with subject matter experts. I’m your personal cheerleader to help you and your loved ones best communicate with your healthcare team as you go from diagnosis through treatment and survivorship.

The Patient Story retains full editorial control over all content. We want to thank all of our promotional partners for their support. Because of them, our programming reaches the audience who needs it. I hope that you find this program helpful, but please keep in mind that while the information provided is encouraging, engaging, and insightful, it is not a substitute for medical advice.



We are joined by two experts from The Tisch Cancer Institute at Mount Sinai in New York. First up is Donna Catamero, Associate Director of Myeloma Research at the Icahn School of Medicine at Mount Sinai and a nurse practitioner specializing in the treatment of multiple myeloma patients. We also have Abbey Reiser, who has a unique role as part of the multidisciplinary team at the cancer institute’s Ruttenberg Treatment Center. She is a dedicated dietitian/nutritionist and is also board-certified as a specialist in oncology nutrition. Valarie Traynham, a multiple myeloma survivor and thriver and an inspiration to many, will moderate this conversation. Your journey is one of inspiration. I’m excited about this engaging discussion.
Valarie Traynham: I’m a myeloma and breast cancer thriver. I’ve been on the myeloma journey for about nine years and the breast cancer journey for about five years. I can understand the issues when it comes to treatment side effects, so I am so excited to be here and have this conversation with these two ladies.
Valarie: Donna, can you explain the difference between relapsed and refractory disease? I get this question a lot and it can be confusing to some of the patients.
Donna Catamero: Most patients are both relapsed and refractory. Relapsed is when a patient has an initial response to therapy, so they’re either in complete remission, partial remission, or very good remission, and then their disease starts coming back, which means they’re relapsing from their response.
Refractory is when patients are on therapy and start to relapse, so that means they’re refractory to that therapy. Most myeloma patients are on continuous therapy, so when they start to relapse, they’re going to be a relapsed patient and then refractory to the current treatment thereon. Most patients past their first line of therapy are going to be relapsed/refractory.
Valarie: When we think of relapsed/refractory, what are some of the common symptoms? Is it just like when we are first diagnosed with myeloma? Is it some of those same symptoms or is it totally different when it comes to the relapsed/refractory setting?
Donna: Patients fall into two categories. Some patients have a biochemical relapse, which means only their numbers are going up. We monitor myeloma patients through their labs. We look at their protein levels and see an increase, but otherwise, the patient feels fine. On paper, we see that their cancer is coming back.
On the other hand, a patient can have a symptomatic relapse, so they’re either more anemic (A), have new bone disease (B), new renal (R) insufficiency or kidney disease, or elevated calcium (C) in their blood. These are the typical CRAB symptoms of myeloma, so they either have those or none at all and we’re seeing the cancer in their blood work.
Valarie: What are some of the current treatment options for relapsed and refractory multiple myeloma?
Donna: The landscape of treating relapsed/refractory myeloma is so quickly evolving. We have so many new therapies. In the past five years, we’ve had so many approvals for multiple myeloma patients in the relapsed setting, so it’s a very exciting time.
We have more targeted approaches with proteasome inhibitors, like kyprolis and bortezomib, that we can use in the relapse setting. We have more novel mechanisms of action, so more targeted towards the immune system, like bispecific antibodies for patients who’ve had four prior lines of therapy and then CAR T-cell therapy, another immunotherapy, which is very exciting for patients. It was initially approved for patients who had four prior lines of therapy, but now we can use CAR T-cell therapy in patients after one prior line of therapy.
Valarie: That’s awesome. I always get excited when I think of the therapies that we have since I’ve been diagnosed and even the therapies in the pipeline. It’s given us so much hope as patients.
Valarie: Abbey, how can a well-balanced diet specifically benefit multiple myeloma patients undergoing treatment?
Abbey Reiser: Diet recommendations often change throughout treatment based on how patients feel and if they experience any side effects that affect their appetite and/or their ability to eat. For multiple myeloma patients who are feeling an eating well, the nutrition recommendations are the same for most other cancers, which is also consistent with the recommendations for the general population.
Plant foods, like fruits, vegetables, whole grains, beans, nuts, and seeds, contain a variety of cancer fighters, including vitamins, minerals, fiber, and phytochemicals. Phytochemicals are naturally occurring compounds in plants that have the potential to stimulate the immune system, reduce inflammation, and fight infection, making these foods especially beneficial for patients to consume while undergoing treatment.

Protein can also help to boost the immune system, promote healing, and build cells, tissues, and muscles. We encourage choosing a variety of lean, animal-based and plant-based proteins, including chicken, fish, turkey, tofu, beans, and nuts. The current plant-based eating model recommends filling two-thirds or more of your plate with plant-based foods and one-third or less of your plate with animal protein to create a well-balanced meal.
Valarie: Are there certain nutrients or dietary patterns that can help manage side effects like fatigue and anemia?
Abbey: Definitely. Patients who experience side effects from treatment may find it difficult to follow a plant-based diet to a tee. Fatigue is one of the most common symptoms among myeloma patients and one of the most common side effects of treatments. I typically recommend staying as active as you can, eating often, and adequately drinking plenty of fluids. Try planning ahead by asking for help with meal prep, trying meal delivery services, and keeping ready-to-eat snacks on hand, like nuts, granola bars, or pre-made protein shakes.

Anemia is commonly caused by the disease, treatments, or kidney dysfunction caused by multiple myeloma and cannot be improved by diet. However, nutritional deficiencies such as iron, B12, or folic acid can also be a cause, and this can be improved by supplementation either orally or by injection. It also couldn’t hurt for patients with these deficiencies to increase their intake of foods rich in these vitamins and minerals, such as turkey, sardines, lentils, and beans for iron, lentils, beans, and spinach for folate, and fish and dairy for B12.
Typically, I encourage patients to talk to their doctor about the cause of and plan of care for anemia before making any significant changes to the diet or starting a new supplement.
Valarie: As a patient, we’re often told to eat the rainbow. Is that something you recommend?
Abbey: Yes. If their appetite is good, they’re feeling well, and they can eat a variety of fruits and vegetables, I’m all for it because they’re going to get different nutrients from different colors. That’s definitely a recommendation that’s still staying strong to this day.
Valarie: We often hear about the role of hydration. Can you discuss that role in managing side effects of multiple myeloma treatment, such as kidney function and even oral health?
Abbey: Staying hydrated during myeloma treatment is essential, especially because dehydration can worsen kidney function, which is a common concern due to the disease’s impact on the kidneys. Drinking sufficient fluids helps to flush out waste products and manage potential complications, like high calcium levels, which can occur with myeloma. Bispecific treatments, like talquetamab, can cause oral toxicities including dry mouth, mucositis, and taste changes, and good fluid intake plays an important role in managing these side effects.
I recommend aiming for at least 8 to 10 8-ounce glasses of low-sugar fluids per day. Plain water is the gold standard and the preferred beverage for hydration, but other beverages such as seltzer, decaf tea, coconut water, and lower-sugar electrolyte drinks can also promote adequate hydration. Caffeinated beverages, like coffee, tea, and colas, as well as alcohol may worsen side effects like dry mouth, so I recommend limiting those.
Valarie: Are there any specific dietary considerations or restrictions that myeloma patients should be aware of? You mentioned alcohol and caffeine, but are there certain foods or drinks that they should strictly avoid?
Abbey: A couple of limitations apply to every type of cancer. We recommend limiting red meat, such as beef and pork, to less than 18 ounces per week, and avoiding processed meats, like bacon and sausage, as much as possible.
I also recommend limiting processed foods that are high in fat, starches, or sugars, such as chips, cookies, candies, cakes, and sugary cereals. Patients should also limit sugar-sweetened beverages, like juice and soda, and avoid or limit alcohol. General guidelines recommend no more than two alcoholic beverages per day for men and one drink per day for women, but I typically defer questions regarding alcohol to the doctor.
Multiple myeloma and its treatments can weaken the immune system and increase the risk of infection, which can make patients more susceptible to foodborne illness, which we often call food poisoning. Therefore, it’s important to follow food safety guidelines while on treatment in an effort to reduce infection risk. General tips include washing your hands well, separating ready-to-eat food and raw meats, checking expiration dates, refrigerating leftovers immediately, and avoiding high-risk places, like salad bars and buffets, and high-risk foods, like raw and rare meats, runny eggs, unpasteurized dairy, sushi, and unwashed fruits and vegetables.
I also discourage the use of supplements, unless you have a deficiency or are told otherwise by your medical team. Supplements don’t offer the same benefits as eating whole foods. They’re typically not regulated by the FDA, and research tends to be limited in terms of how they may interact with treatment. For patients who are hoping to start taking a supplement, make sure to check with your doctor before doing so.

Valarie: What advice can you provide about green tea? With some treatments, they say to avoid green tea on the day that you’re getting treatment and a few days after. Is there anything you can say about that?
Abbey: That’s usually discussed if they’re on bortezomib. Donna, you and I talked about this before. I believe it’s the green tea supplement that they need to avoid entirely.
Donna: It’s the high-dose green tea extract that’s available as a supplement, which is contraindicated when on a regimen containing bortezomib. I advise patients who love green tea to not consume it on treatment days. The beverage itself is fine for patients. It’s the supplement that can get patients into trouble.
Valarie: How can a nutritionist help patients manage weight changes? I experienced a lot of weight gain taking steroids. Some patients deal with weight loss, which can be a common side effect of treatment. What can we do from a nutrition standpoint?
Abbey: Treatment side effects, especially oral toxicities, often lead to decreased appetite and weight loss. If a patient is experiencing unintentional weight loss, I recommend having small, frequent meals every 2 to 3 hours and choosing high-calorie foods as tolerated. I will emphasize healthy fat sources, like nuts and nut butters, avocado, and olive oil, because fat contains more calories per gram than proteins and carbs. I also encourage them to make homemade smoothies and shakes, and to drink oral nutrition supplements because sometimes it is easier to drink your calories than eat them when your appetite is low.
Low-impact physical activity as tolerated can also help to increase appetite and maintain muscle mass. For patients who are struggling to eat and whose appetite has been consistently low, it could be worth asking the doctor if starting an appetite stimulant is appropriate.

On the other hand, I also see patients experience weight gain while in treatment. Oftentimes, this is in part due to steroids or fluid retention. To maintain a healthy weight, we recommend following a Mediterranean-style, plant-based diet, which emphasizes having lots of fruits and vegetables, lean proteins, whole grains, and legumes. We also emphasize watching calorie intake, monitoring portion sizes, and eating slowly and mindfully. It takes 20 minutes for your brain to get the message that your body is getting food before you stop feeling hungry. The slower and more mindfully you eat, the sooner you should realize that you’re full.

I also recommend being physically active as tolerated, specifically to engage in at least 150 minutes of moderate-intensity physical activity per week, which can equate to 30 minutes, five days per week. Moderate-intensity physical activity could be a brisk walk or biking.
Valarie: I’ve dealt with severe dry skin and hyperpigmentation. What are some of the common skin conditions that multiple myeloma patients experience as a result of treatments?
Donna: A lot of multiple myeloma treatments are subcutaneous injections, which means they go right underneath the skin, so we often will see injection site reactions. Around the area where we administered the medication, it gets inflamed, red, and itchy.
Another side effect we see is dry skin. For patients who experience this and if I know a regimen will cause dry skin, I tell patients to use heavy barrier moisturizing creams at the initiation of therapy, especially during long winter months. Our skin dries out fairly quickly with the heat. You want to use heavy barrier creams to help retain the moisture and start at the initiation of therapy.

When we see on-target, off-tumor side effects with talquetamab, for example, the skin on the palms of the hands and the soles of the feet start to peel. These side effects can be self-limiting and we can manage them well. We use lotions, like ammonia lactate, on the area. We’ll do that twice a day and this typically will resolve in 2 to 3 weeks for patients.
We also see nails that get brittle and peel. Unfortunately, there isn’t something we can give patients to eliminate brittle, peeling nails, but we can suggest nail polish hardener lacquers to make the nails stronger so they’re less likely to break. We recommend cuticle oil around the cuticle bed. We look for signs and symptoms of infection because we don’t want to have any nail infections.
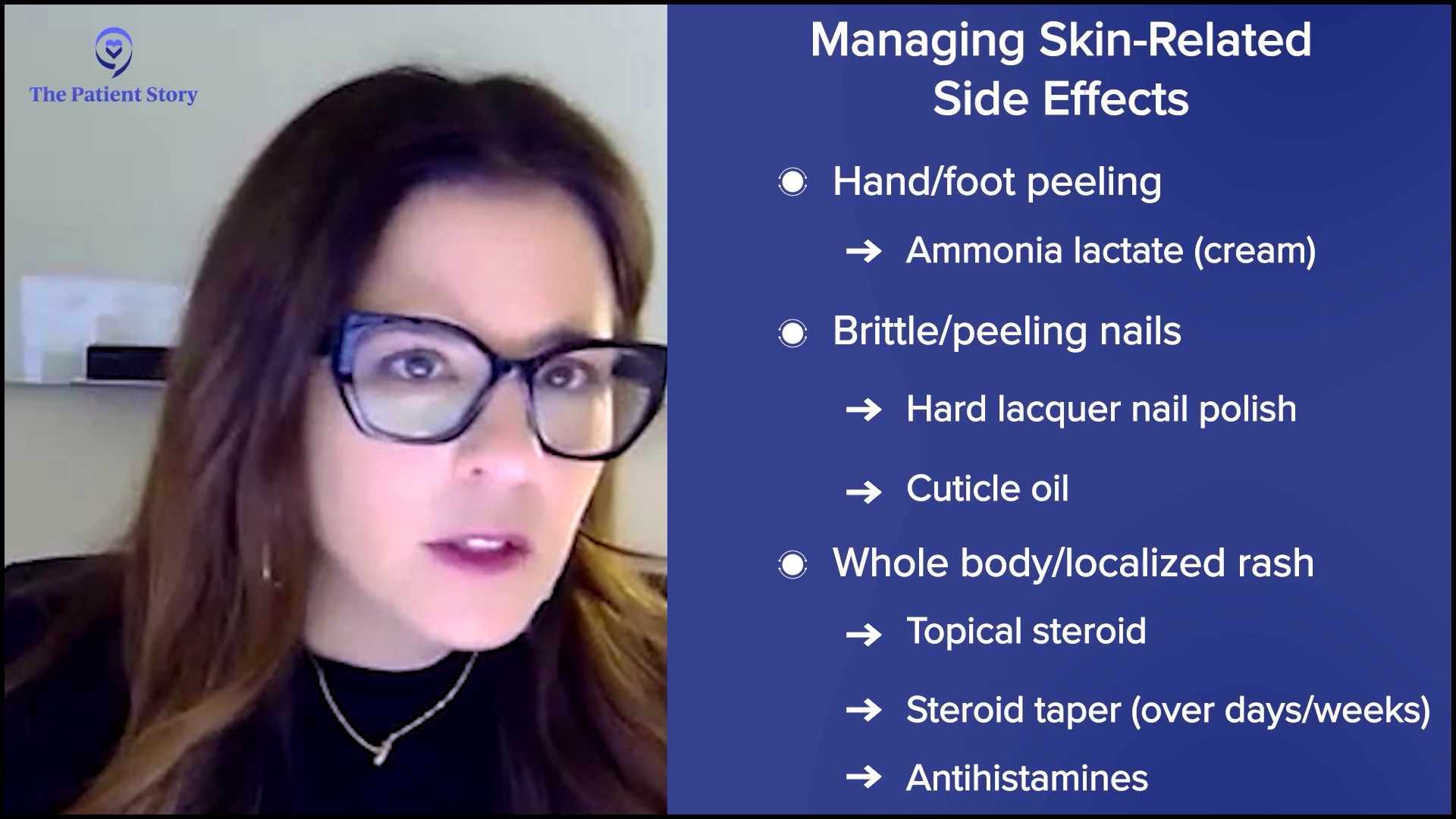
Another side effect that patients can experience is a whole-body rash or a localized rash. Depending on the size of the rash, we can manage it quite well with topical steroids or lotions. If a rash is more generalized, we’ll add a steroid taper. A course of steroids over several days will tamper down the whole-body rash, which will typically be resolved in several days.
A rash can be itchy or a patient could feel itchy in general, so we can use antihistamines for several days to help with any itchiness. If the itchiness is drug-induced and depending on the severity of the skin reaction, I’m going to hold off on the medication until these symptoms resolve before resuming therapy. If the rash is severe enough, I would consider either a dose reduction or a look at how frequently treatment is administered.

Valarie: Do you often refer to a dermatologist or treat them within your cancer center?
Donna: Early on, when we look at these new treatment modalities, we weren’t typically seeing these side effects. We work very closely with our dermatology colleagues, but we can manage these side effects quite well. I will definitely refer to our colleagues in dermatology, but for the most part, we can manage these symptoms quite well within our own practice.
Valarie: Bispecific antibodies are emerging as a promising treatment option for relapsed/refractory myeloma. Donna, can you explain how these antibodies work? Have you seen an increase in this approach with patients?
Donna: This is a new and very exciting treatment modality. We had several drug approvals within the past few years with this new class of drugs. It’s similar to daratumumab where it will bind to a receptor on the myeloma cell. One arm of the bispecific antibody will grab the myeloma cell and the other arm will grab the receptor of a T cell.
Our T cells are little soldiers of our immune system. T cells will do surveillance and get rid of anything that looks bad in our system, so that includes infections and cancer cells. What a bispecific antibody does is grab onto the myeloma cell, grab onto the T cell, and bring that T cell close to the myeloma cell so that the T cell can recognize the myeloma cell and kill it
In essence, it mimics the mechanism of action of CAR T-cell therapy, but the benefit of a bispecific antibody is it’s off the shelf, so there’s no downtime unlike waiting for manufacturing CAR T cells. If I need to start a patient tomorrow, we can initiate therapy quickly. We’re harvesting the patient’s immune system to attack the myeloma cells. This is an exciting new treatment approach.
Valarie: As a patient, I’m very excited to hear about bispecific antibodies. What are some of the common side effects associated with these newer targeted therapies?
Donna: We’re activating that immune system, so the immune system gets revved up and what happens is it releases cytokines. Cytokines are little immune substances that can cause havoc. It can affect everybody’s system. Typically, when a patient gets a bispecific antibody, they’ll have a fever. This can progress to low blood pressure or difficulty with breathing, but these are so well-managed now.
The patient will typically complain of a fever, almost like when we get our flu shots where we feel a little achy and get a low-grade fever. As a provider, I know this patient is probably having cytokine release syndrome (CRS). The immune system is getting revved up, so I will tap the brakes. We have treatments that will simmer down the immune system and within 24 to 48 hours, the patient’s symptoms will resolve and allow us to continue treatment.
We try to mitigate this side effect by giving premedication, so we’ll give acetaminophen, diphenhydramine, and some steroids, but the majority of patients are going to experience CRS. Typically, we manage this inpatient, but more and more institutions are learning to manage these side effects as outpatients. We monitor patients very closely by checking their vital signs and intervening at the first sign of a fever. If a patient has a drop in their blood pressure or difficulty with breathing, we intervene very quickly.
The majority of patients will have cytokine release syndrome and to a much, much lesser extent, we see neurotoxicity. If patients have cytokine release syndrome, typically we see neurotoxicity immediately after. A patient might present with some confusion and maybe a little disoriented. They can name the hospital and their name, but instead of saying that it’s winter, they’ll tell you it’s spring.
Also, we see patients with a change in their handwriting and this can be quite drastic. Before starting these therapies, we obtain a handwriting sample and monitor the handwriting sample throughout treatment. We’ll see a change from one 12-hour shift to the next where a patient will write a beautiful sentence and then a few hours later, will scribble across the paper. This patient is experiencing a neuro event. This can be scary, but this is reversible. We manage this very well. This is self-limiting, so it won’t reappear.
Care partners are very important when we give these types of treatment because if the patient is at home, they might not understand that they’re confused. It’s very important to have a care partner to monitor the patient to see if there’s any alteration in their mental status. We manage this quite well with steroids.
Valarie: Are there specific strategies for managing cytokine release syndrome and neurological side effects?
Donna: To mitigate some of these potential side effects, like cytokine release and neurotoxicity, we do two things. First, we’re going to do a step-up dosing approach. We’re going to give a small dose for that first dose, a slightly higher dose for that second dose, and then the full dose. We ease the patient into that medication.
The second thing we do is to have premedication on board to mitigate the severity. Most patients are going to have cytokine release syndrome, but it’s typically mild like a fever, which we can manage quite well. Neurotoxicity happens in a very low percentage. Less than 7% of patients will have this neurological event. Step-up dosing and medications can help, but that’s something we will manage when the symptoms arise.
Valarie: Abbey, we talked about diets and how having healthy snacks can help manage the side effects. For patients experiencing loss of taste, how can they change their diet to help manage that particular side effect?
Abbey: Taste change is one of the most common side effects that I talk about and it’s definitely one of the most difficult to manage. There’s no one-size-fits-all approach, not one miracle food that everyone enjoys, and no medication that provides total relief. It’s tough for patients to find foods they enjoy, let alone tolerate.

Something I emphasize to everyone, regardless of their experience, is good oral hygiene. Patients are often prescribed a mouth rinse, but if this doesn’t help, I recommend trying a homemade rinse made with baking soda, salt, and water, or an over-the-counter, alcohol-free mouthwash. Brushing the tongue and teeth after meals and before bed is also important to keep the mouth clean. It also doesn’t hurt to try sugar-free gums or mints to see if that improves any unpleasant taste in the mouth.

When patients describe taste changes, I hear a wide range of statements, including everything tastes too bitter, too sweet, too metallic, has no taste, tastes like cardboard, or everything tastes bad. If food tastes too bitter or too sour, I recommend adding something sweet to food, like honey or fruit. Or, if food tastes too sweet, try adding an acid, such as vinegar, lemon, or other tart, tangy, or acidic flavors. If everything tastes metallic, I recommend using nonmetal utensils and cookware, such as plastic, glass, or ceramic. Try fresh or frozen foods over canned and serving meat cold or at room temperature.

For bispecific therapies, the most common statement is everything tastes bad or has no taste. For this, I emphasize the importance of experimenting with different flavors, textures, temperatures, herbs, spices, seasonings, and sauces because you never know what might work for you. I often hear that adding acids like lemon, lime, vinegar, and tomato can make foods more enjoyable. I’ll often recommend adding fresh lemon or lime juice during and after cooking, and adding citrus to water, such as lemon packets or sliced lemons and oranges, if plain water tastes unpleasant.
Taste is the combination of not only the taste but also the smell and touch of food. If you can’t get any pleasure from taste, don’t underestimate the power of texture and smell. Soft, moist foods like oatmeal, soups, and mashed potatoes are usually more tolerable since they’re easier to chew and swallow, which means they spend less time in your mouth.
Smoothies and oral nutrition supplements are my go-to recommendations because they’re quick and easy ways to get in calories. Protein and smoothies allow a patient to experiment. Fruit is one of those foods that are often tolerable, so I recommend blending different fruits into smoothies to see if that makes them easier to get down. Animal proteins tend to be tough for patients to tolerate, so I typically recommend choosing softer animal proteins, like egg salad or fish, or marinating and cooking meats in acidic dressings or sweet juices.
Many patients report that they maintain their sense of smell despite losing their taste. I’ve had a patient say that certain foods, like cucumbers, cantaloupe, and coffee smelled good, which helped them taste good too, so it’s definitely worth experimenting in this way.
An important point that patients should take away when it comes to taste changes is that everyone is different. A recommendation that works for one person may not work for the other, so it’s important to keep trying and retrying foods because you never know what may end up working for you. Even though everyone is different, if patients are experiencing these side effects, they should know that they’re common and they’re not alone.
Valarie: Let’s talk about the emotional side, such as anxiety and depression. Donna, how can patients cope with these types of challenges?
Donna: In the relapsed/refractory setting, every relapse causes a lot of anxiety and fear. When starting a new treatment, there’s a lot of fear, which can then increase anxiety and can lead to depression. Having a good support network is important for patients. We’re very fortunate in my institution to have a wonderful social work team that can help patients. We have support groups. Support groups work for some patients but not for others, so have care partners on your team to help patients through these challenging times. Each relapse becomes challenging for patients. The good news is that we do have great therapies for patients to provide support for patients to get through their therapies.
Abbey: From a nutrition standpoint, a patient experiencing side effects from treatment that affect their ability to eat can significantly impact a patient’s quality of life. It can cause patients to feel isolated because it’s hard for anyone to fully understand what they’re going through. On top of that, they might feel pressure from family and friends to eat more even when they don’t feel well and I’ve seen that cause resentment. Eating is such a social and cultural activity, and many patients feel like they don’t have a place at the table to help cope with these challenges.
I encourage patients to ask for a referral to a dietitian. Our job is to provide tips and tricks to help patients eat despite these side effects. I also encourage them to try to continue living their lives as much as possible, to go out to eat, and to attend social events when they have the energy and when it is safe for them to do so. When people are experiencing side effects and they go out to eat, they feel embarrassed or afraid to advocate for themselves. I encourage them not to hesitate to ask for their food to be prepared a certain way if it makes it easier for them to eat. If they want to bring their own food when they go out, that’s completely okay. I’m sure their friends and family would prefer to see them enjoying their meal and feeling supported, rather than feeling embarrassed or ashamed.
Valarie: As a patient and as somebody who’s been on that side of it, you have to look out for yourself. If that means taking something to a restaurant to spend time with your loved ones and be able to enjoy a meal, then do it.
Support groups are not for everyone, but there’s also one-to-one support available. You can talk with a myeloma coach or a mentor angel in various programs. Know that you’re not alone as you’re dealing with these side effects. Others are going through them as well and you always have someone to support you.

Valarie: Thank you, Donna and Abbey, for taking the time to speak with me and The Patient Story audience. Do you have any final remarks?
Donna: We have some great therapies we can offer patients. The important thing is getting patients through that therapy. There are side effects, but we’re going to help manage those so that patients can have the best possible outcomes.
Abbey: I encourage patients who are experiencing any side effects to speak up, advocate for themselves, and let their teams know. The sooner their team is aware, the sooner they can provide supportive care or treatment to help manage those side effects. If the side effects they experience make it difficult to eat, don’t hesitate to ask for a referral to a dietitian if their team has not referred them to one already.
Valarie: Yes, I agree with you wholeheartedly. Speak up and don’t suffer in silence. There’s no need for that.
Tiffany: Thank you again, Donna, Abbey, and our patient moderator and advocate Valarie, for taking the time to discuss mitigating side effects, especially to Valarie for sharing her myeloma experience. I am grateful that she shared her story with us. It takes a village and I know that your story, Valarie, will resonate.
It is important to be empowered so that you and your caregivers can make informed decisions about your care. That includes being educated on the latest on the side effects, mitigating those side effects, and getting the support that you need.





Multiple myeloma patient advocate Kenny Capps speaks with multiple myeloma expert Dr. Carl Ola Landgren of the University of Miami Sylvester Comprehensive Cancer Center as he shares actionable insights on the latest treatments, effective side effect management, and innovative therapies. Gain the knowledge you need to thrive with multiple myeloma and take charge of your journey.
Learn about treatments like CAR T-cell therapy and bispecific antibodies. Discover effective strategies for managing treatment side effects to improve your quality of life. Get expert tips for living well and staying active while managing multiple myeloma. Understand how to tailor your treatment journey with the latest medical advancements and expert advice.
Edited by: Katrina Villareal
Tiffany Drummond: I’m a patient advocate with over 20 years of experience in cancer research. My journey as a caregiver began when my mother was diagnosed with endometrial cancer in 2014. I quickly realized the challenges of finding resources, support, and shared experiences, and I’m committed to helping others avoid similar difficulties, no matter the condition.
At The Patient Story, we create programs to help you figure out what comes next. Think of us as your go-to guide for navigating not only the cancer journey but your overall health journey. From diagnosis to treatment, we’ve got you covered with real-life patient stories and educational programming with subject matter experts. I’m here to help you and your loved ones best communicate with your healthcare team as you go from diagnosis through treatment and survivorship.
We want to thank our promotional partners for their support. Because of you, our programming reaches the audience who needs it. I hope you all find this program helpful, but please keep in mind that the information provided is not a substitute for medical advice.
We have two amazing guests that I want to introduce as we talk about the latest treatment options for multiple myeloma. Dr. Carl Ola Landgren is a hematologist and oncologist, professor of medicine, and division chief of myeloma in the Department of Medicine. He is the director of the Sylvester Myeloma Institute at the Sylvester Comprehensive Cancer Center and co-leader of the Translational and Clinical Oncology Program at the University of Miami. We are so happy to have you, Dr. Landgren. Thank you so much for taking the time to be with us. Our moderator will be Kenny Capps, a multiple myeloma survivor and thriver.


Kenny Capps: Thanks, Tiffany, I’m honored to be your moderator. I’m the executive director of Cancer Active, a nonprofit organization dedicated to empowering those affected by cancer to live active and fulfilling lives. I’ve been on my journey with multiple myeloma since 2014. I understand many of the challenges that patients must navigate.
I was diagnosed relatively young at the age of 42 and have lots of bone involvement, spinal compression, fractures, and lesions. I’ve undergone infusions and a bone marrow transplant. I’ve lost count of how many bone marrow biopsies I’ve had. In 2023, I relapsed, changed therapies, and added radiation treatment to the list of things I’ve never done before.
I did all this while raising three kids, training 30 to 70 miles a week, running 1,200 miles across the state of North Carolina, and experiencing all the celebrations and heartbreaks that come with life, regardless of whether you’re treating cancer or not. I’ve had many experiences and a lot of education as an athlete, a coach, an attorney, and a father, and 10 years ago, I combined all of those experiences to become a patient advocate and a Cancer Active leader.

We’re fortunate to have one of the leading voices in multiple myeloma research and treatment with us. Dr. Landgren is not only a pioneer in advancing care for this disease but also deeply committed to translating cutting-edge science into real, human-centered solutions for patients like you and me. His work has helped reshape how we understand and treat multiple myeloma, giving us more options and more hope than ever before.
This conversation is all about you. We’ll explore the latest in multiple myeloma treatment and emerging research, and, most importantly, answer your questions in a way that makes this topic understandable and actionable. It’s my privilege to introduce our distinguished guest, Dr. Carl Ola Lindgren.
Dr. Carl Ola Landgren: Thank you very much for having me. It’s a great pleasure and a great honor.
Kenny: Our audience is pretty savvy, but for those unfamiliar with the term relapsed or refractory in the multiple myeloma setting, could you break down what that means?
Dr. Landgren: Relapsed and refractory refers to the multiple myeloma disease becoming active again. Someone who is newly diagnosed would typically receive combination therapy with or without transplant and with continued therapy, which we also call maintenance therapy. Over time, unfortunately, the majority of patients will have the disease become active again and this is because we do not have an established cure for the disease.
In 2025 and onwards, many patients can live for 10 to 20-plus years and there will be patients who will not have their lifespans shortened, which is what the field is going for. For the most part, the disease will be managed as a chronic disease as we try to develop definitive cures.
If there is reappearance of rising levels of proteins in the blood, if other clinical suspicions are going on that would trigger additional radiological assessments, like PETs, PET/CTs, or MRIs, or if we do bone marrow biopsies and see that there is more disease, then that would be consistent with the disease becoming active again.
When we do clinical trials, we have rule books for what is what. We have a rule book for what’s called a partial response, what’s a complete response, what MRD negativity is, and we also have rules for what progressive disease is and how to capture that. If you don’t have a common language, we cannot compare the results across different trials, so that’s very important. We worked on that as a community for over 20 years.
In the setting of those rules, a relapsed/refractory disease refers to a situation when a patient has rising levels of markers by these definitions we have, either while being on a given therapy or if it happens within 60 days after stopping therapy, then that would also count as a relapsed/refractory state.
We looked at drugs that had a good benefit, were not too toxic for the patient, had no other contraindications, and tried to see how we can partner them with other drugs than we did the previous time we gave them.
Dr. Landgren
Kenny: About refractory, does that mean that they are unable to continue along that line of treatment?
Dr. Landgren: The word refractory carries probably more focus on things that are not true, which is that you cannot go back and use that treatment. In reality, what it means is that right now, it is not the optimal therapy to use going forward. You can revisit and use that drug in the future, maybe in combination with other drugs at a later time point as what we very frequently do. We recycle the drugs.
An example could be you use a proteasome inhibitor, an IMiD (immunomodulatory drugs), and a steroid with a CD38-targeted antibody as a combination therapy and you give that for a certain number of cycles. You may collect stem cells, give more cycles, do a transplant or not, and go to a maintenance therapy. You may have an IMiD at a lower dose with the CD38-targeted antibody and eventually, you may step down to a single drug IMiD.
Many years later, there’s a reappearance of protein in the blood. Could you go back and use a proteasome inhibitor? Yes, you can. Could you go back and use the CD38-targeted antibody? Yes, you can. Is it the best thing to use that same IMiD at the same dose level? Probably not because the disease was able to grow through that. What about increasing the dose? Probably not the best option right now, so maybe switch to another IMiD or some other drug. Then you can overcome this reappearance or relapse and get many more years with the same benefit. You get rid of the disease and keep the disease from becoming active.
If the disease comes back again, could you not ask the same question? Could you go back to those same drugs, including the first IMiD? I would think yes. You could think about using the same drugs over and over again, but there are so many new drugs coming to the field. Many times, we are going to new mechanisms of action as the next step forward.
At some point, when we have used all the different mechanisms of action, we will go back, recycle, and use them in different combinations. We looked at drugs that had a good benefit, were not too toxic for the patient, had no other contraindications, and tried to see how we can partner them with other drugs than we did the previous time we gave them.
Kenny: When you’re saying that, what I think about is lenalidomide, bortezomib, and dexamethasone, and then a maintenance therapy after a bone marrow transplant, but a patient might stop responding to 5 or 10 mg of lenalidomide at some point in the future. You’re saying that they could switch over, so maybe pomalidomide at some point as a substitute, but that doesn’t discount the possibility that lenalidomide might be a solution for them in the future.
Dr. Landgren: That’s exactly right. If you look at how these drugs were developed, they were developed for certain indications. You mentioned pomalidomide as the next move and that’s the example I gave between the lines. I didn’t mention the drugs, but you filled in the blanks and the drugs you gave were probably the drugs that, for the most part, would fit with the example I gave.
We do not have an established cure, so if you look at the population databases that are currently available, unfortunately, the majority of patients will have the disease become active again at some point.
Dr. Landgren
Pomalidomide was developed in 2006 and was given to a patient that lenalidomide failed and that’s how the FDA approval was granted. It’s a logical thing to do. What hasn’t been done in a trial is to go back and revisit lenalidomide at a later time point. Why is that? Once the drugs are approved, they are commercially available and we can prescribe them.
It addresses an important topic of the so-called real-world evidence and that’s where people like me come into play. I have been a doctor for 29 years. I’ve treated probably thousands of patients and used all the FDA-approved drugs. I’ve worked on very many clinical trials, phase 1 and phase 2 studies, and also some of the phase 3 trials. I have a lot of experience with these drugs.
When people like me use the drugs every day in our clinics, we learn how to use them in a recycled manner for patients who have the disease coming back. Sometimes we document and many times, we talk about it. When I’m at meetings, many colleagues who may see fewer patients could come up and get the advice. We try to share our experiences with each other and that’s how we help each other as a community.
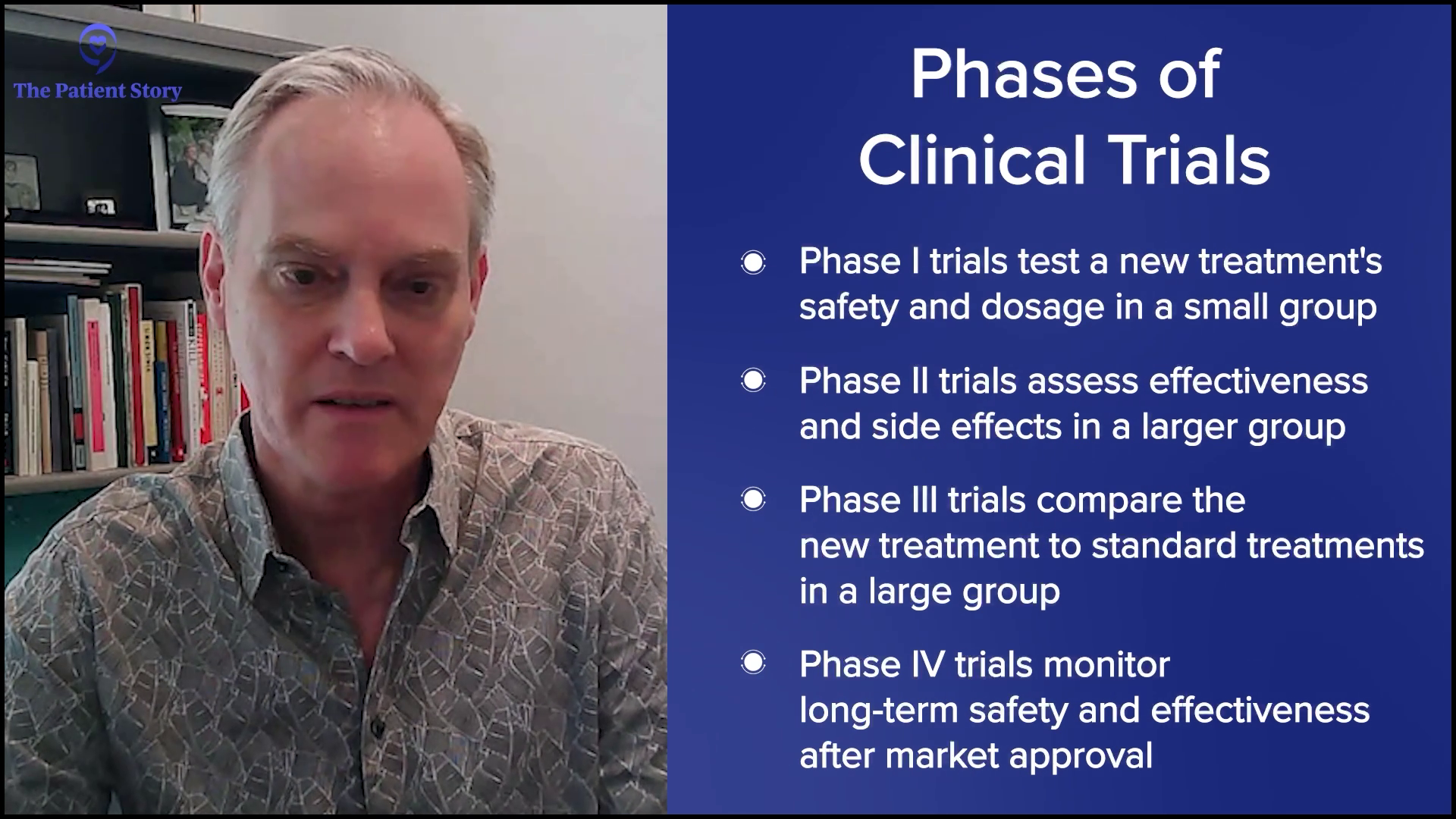
Kenny: Given the evolving landscape of myeloma treatment, what are the current estimates for the percentage of patients who experience relapse or become refractory to initial therapy? How do factors, such as patient age, disease stage, and genetic risk profile, influence these rates?
Dr. Landgren: We do not have an established cure, so if you look at the population databases that are currently available, unfortunately, the majority of patients will have the disease become active again at some point. There’s a small group of patients whose disease doesn’t come back and that’s an important piece to point out that the disease is curable.
The problem is that the disease is very different from patient to patient. We call it genomically heterogeneous, which means it’s not the same disease in every patient. When we profile the disease, we can see that if we perform whole genome sequencing, the average patient has a few thousand mutations and you can also see alterations in the immune system. With a disease that is so different from patient to patient, it’s not surprising that when you give the same therapy to everyone, the outcome would be different and that’s why we say there are different prognoses.
As the treatment gets better and better, more and more patients could benefit from the therapies, so there will be fewer patients who will have the disease return sooner.
Dr. Landgren
People have talked about high risk or standard risk in this very setting. The concept of high-risk disease is a moving target. If you have a weaker treatment and you treat 1,000 patients, more patients will not benefit from that treatment because the disease biology could be stronger than the therapy over time and it will come back sooner.
As the treatment gets better and better, more and more patients could benefit from the therapies, so there will be fewer patients who will have the disease return sooner. For that reason, the so-called high-risk group is shrinking and it’s always in the light of how you treat. Ultimately, with the best available therapy, there is no high-risk disease and we could envision a scenario of a cure.
The rate of relapse is in the light of how we treat, but we still don’t have a definitive cure, so statistically, the majority of patients will have their disease coming back. What’s different at this time compared to 10 or 20 years ago is the duration of the benefit of therapy is drastically different.
The disease will probably come back for the majority of patients, so we are trying to develop curative strategies that are definitively curative.
Dr. Landgren
When I was in fellowship 25 years ago, the time from diagnosis to a patient passing away from the disease could be only one or two years. I have many patients who are 20 years out and doing great, and many of those patients will not die due to myeloma. We will all die at some point, but many people will probably die with myeloma not from myeloma, which is a huge change.
Kenny: Yeah, and that’s a phrase I hear more and more, which is good to hear.
Dr. Landgren: If we can keep the disease away and people can have a good quality of life and no shortening of lifespan, that’s a huge deliverable. For many patients, we’re already at that point, but there may have to be changes in treatment. The disease will probably come back for the majority of patients, so we are trying to develop curative strategies that are definitively curative.
Kenny: You mentioned quality of life and that’s impacted by the progression of the disease, side effects from treatment, or the psychosocial challenges that patients have to deal with day-to-day that negatively impact how they feel and what their life is. As you mentioned, the treatments over the past decades have changed dramatically. In the context of relapsed/refractory multiple myeloma, does traditional chemotherapy still have a role to play in the world of IMiDs, CD38 treatment, bone marrow transplants, and CAR T-cell therapy?
Dr. Landgren: We don’t want to stop using drugs that we know work until we have a definitive cure. You want to keep all the different options. We want to have all the doors open. But the order and the priority of the different therapies will probably continue to change.
When I was in fellowship, the therapies were very, very inferior. The overall survival was one to two years. The remission rates were in the single digits. These days, if I treat, I would achieve remission rates of 90 to 95-plus percent. I have MRD negativity rates in my newly diagnosed patients of over 70%.
Will that mean that chemotherapies will go away? I don’t think so. Not until we have a cure. Potentially, the role for these therapies will shift that they will be options if patients have later line relapses.
Dr. Landgren
For the majority of my patients, I don’t use any chemotherapy. For many years, we have also explored harvesting the stem cells and holding them, so you could also not go for a transplant. Transplant is chemotherapy. In the United States, it’s called transplant, but in Europe, it’s called high-dose chemotherapy and it is chemotherapy because it’s melphalan chemotherapy. The stem cells are not part of the treatment. They’re a way to recover from the chemotherapy.
There will be a shift away from chemotherapy as we see more and more immunotherapies coming. The CD38-targeted antibodies are coming at full speed, but there are also new antibodies with new targets coming. In 2024, the FDA approved CAR T-cell therapy for the first relapse.
Will that mean that chemotherapies will go away? I don’t think so. Not until we have a cure. Potentially, the role for these therapies will shift that they will be options if patients have later line relapses. If you have immunotherapies upfront and if there is recurrence, there are more immunotherapies. If there is a recurrence again, there are more immunotherapies. Eventually, maybe the chemotherapies will be part of it.
There will be patients who will be outliers from this principle. Chemotherapy drugs are the most tumor-sensitive drugs. Some patients to whom we give immunotherapies don’t do as well. Those patients are a minority, but there are patients like that, so it’s good to have options.
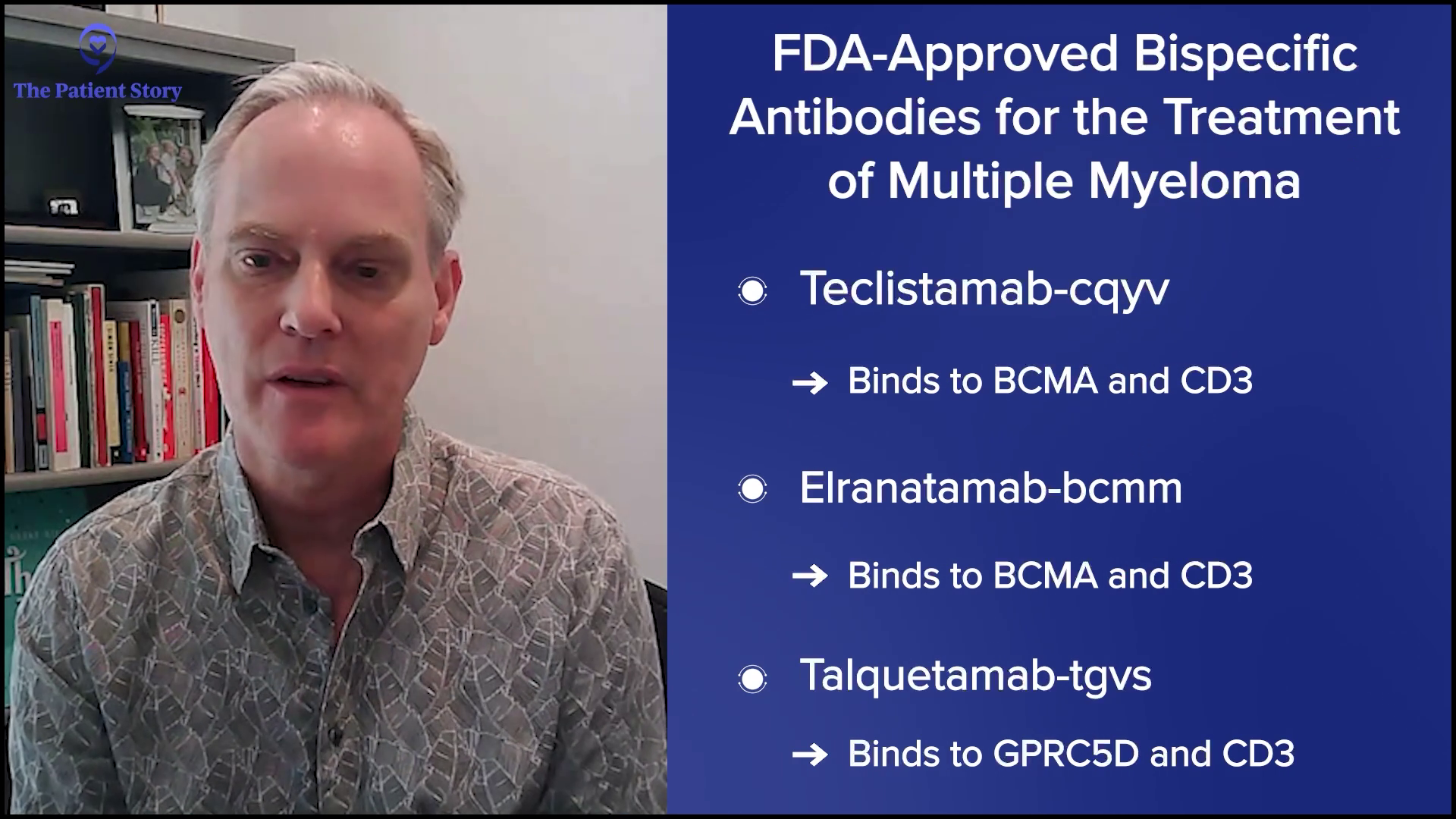
Kenny: Could you discuss further the differences between bispecific antibodies and CAR T-cell therapy?
Dr. Landgren: A bispecific antibody is exactly what the name tells you: it’s bi, so it’s two, and it’s specific, so it’s specific in the sense that it goes for myeloma and it’s linked towards immune cells, T cells. The way these antibodies are engineered is they have two heads. One head binds to a protein on the surface of the myeloma cells and the other head binds to a surface marker on the T cell. On the T cell, the marker is CD3. For the myeloma cells, there are currently two approved antibodies that have two different targets: BCMA (B-cell maturation agent) and GPRC5D.
A bispecific antibody is exactly what the name tells you… One head binds to a protein on the surface of the myeloma cells and the other head binds to a surface marker on the T cell.
Dr. Landgren
There are three bispecific antibodies approved for multiple myeloma. All of these antibodies bind to CD3. They bring the T cells to the antibody, so they hold on to the T cell, and when they grab the myeloma cell with the other marker, the myeloma cell is now neighbors with a T cell and the T cell will then do its job of killing the myeloma cell. That’s how bispecific antibodies work.
CAR T cells is an acronym for chimeric antigen receptor T cells. T cells circulate in the blood and you can take them out from the blood of a person. They are not stem cells. They’re not the type of cells you would collect for a transplant. These are circulating immune T cells. You can take them out and send them to an approved facility. They will do a transduction of these T cells, which means they are being exposed to a genomic vector that will change the DNA in these cells. They will insert certain information that contains instructions for these T cells to do things that they normally wouldn’t do, which is to develop an antenna on their surface and that is what the receptor is. They are the same T cells plus the instruction that says to make this receptor on their surface. Other than that, they do the same job they normally would do. You feed them with glucose and nutrients and keep them warm.
In a way, bispecific antibodies and CAR T cells do the same thing. They take advantage of T cells.
Dr. Landgren
In the current development setting, about four to six weeks later, you give the CAR T cells to the patient. When they reenter the body, they will be let in because the body will recognize them as their own T cells. When they come in, they are now programmed with receptor-like antennae on the surface to bind to something that fits, which is the BCMA protein. When they bind to it, same as the bispecific antibodies, now a T cell is neighbor to a myeloma cell and when it sees the myeloma cell, it will kill it.
In a way, bispecific antibodies and CAR T cells do the same thing. They take advantage of T cells. In one setting, you keep the T cells in the body and give a matchmaker, which is the antibody. In the other example, you take out the T cells, modify them, and give them back.
There are other ways of doing it. You can have donors give blood where you can make something called allogeneic CAR T cells, which is a mass-produced CAR T cell that comes from a pool of donors, and you give that to multiple patients. The idea here is that you can give them immediately because there is no need to harvest them, manufacture them, and give them back. You have donor-derived T cells. Unfortunately, there are none yet approved for myeloma.
There are also other technologies where you can insert mRNA-made T cells and bispecific antibodies. Similar to how the COVID vaccines were developed, you can use mRNA infusions to synthesize these types of products within the body. That has not yet happened in humans, but there are a lot of animal models. We’ll see how these mRNA-based technologies will speed up the development of immunotherapies. This is going to be very, very exciting.
The jury is still out on the right sequence, whether you should do CAR T-cell therapy first and then at a later time point, bispecific antibodies or vice versa.
Dr. Landgren
Kenny: Are there specific patient populations that are most likely to benefit from bispecific antibody therapy?
Dr. Landgren: Currently, there is no head-to-head randomized study that has compared patients given a bispecific antibody and patients given CAR T-cell therapy. All the studies have compared CAR T-cell therapy with older combination therapies or bispecific antibodies compared with older combination therapies.
What we do know is if a patient has an activation of the disease or there is a relapse, the majority of patients have a slower evolution of the disease. The disease usually shows up as increasing protein markers in a blood test and it can go on for many weeks or even months before you start making decisions to change the therapy, so you have some time to make treatment decisions.
But for some patients, the disease becomes active in a short timeframe, so you cannot wait to collect the T cells, send them for manufacturing, keep the disease under control with bridge therapy, and then give back the CAR T cells. In their case, a bispecific antibody is the better option.
If you have patients where the disease is moving more slowly, you have two options. You could argue which is better and I would say different experts would have different opinions. In my experience, different patients will have different opinions.
The jury is still out on the right sequence, whether you should do CAR T-cell therapy first and then at a later time point, bispecific antibodies or vice versa. There are so many details when it comes to this and we don’t have the data to fully answer.
If you started with a bispecific antibody, could you do CAR T-cell therapy in the future?
Dr. Landgren
If you treat someone with CAR T-cell therapy, on average, it would last for many years. But if a patient, God forbid, has a shorter benefit, let’s say 6 or 12 months, going right to a bispecific antibody with the same target usually doesn’t work because the time in between is too tight. But if you go to another therapy with another target with another mechanism of action, could you revisit that same target using a bispecific? I would say the answer is yes for the most part. It comes back to recycling drugs or targets.
If you started with a bispecific antibody, could you do CAR T-cell therapy in the future? Yes, with the same target, but if you do them back to back, that may not be optimal. If the cells build up some form of resistance to the same mechanism of action, you want to distract the cells by doing something else to bring down the disease. If you get good mileage out of that and need to switch again, that could be the time to go back to the same target.
Kenny: For patients treated with bispecific antibodies, could you discuss the most common side effects and how they are managed?
Dr. Landgren: Compared to bone marrow transplants, CAR T-cell therapy is way less toxic, so the patient experience is much easier. I’ve seen patients who were transplanted years ago and got CAR T-cell therapy and they said this was not even comparable. My oldest patient who turned 87 years old underwent CAR T-cell therapy when he was 86. We would not transplant an 86-year-old, but you could give CAR T cells. I have also treated patients in that age category with bispecific antibodies. I have many patients who have done that and they do extremely well. On average, both CAR T-cell therapy and bispecific antibodies are very, very well-tolerated overall, but everything has some form of side effect. If there is no side effect, usually there is no effect, unfortunately.
On average, both CAR T-cell therapy and bispecific antibodies are very, very well-tolerated overall, but everything has some form of side effect.
Dr. Landgren
When you give a CAR T cell product, you would expect to see cytokine release syndrome (CRS), which means the immune system gets triggered by this immunotherapy and releases substances that the immune system uses to communicate with different immune cells and other surrounding cells. These are the cytokines and chemokines. When they get released, it leads to an immune reaction. It’s a ramped-up version of a person getting sick from an infection or inflammation. Patients get a fever, they don’t feel well, and they could have organs responding to it, like blood pressure going down and things like that.
There are two approved CAR T cell products. When you give cilta-cel, CRS usually takes about a week to kick in. Presumably, that’s the time it takes for the CAR T cell product to amplify, expand, and become fully active. But if you look at the alternative protocol ide-cel, usually the same phenomenon with CRS happens sooner, around the next day. The time windows are different for these different products for reasons we don’t completely understand.
The duration of CRS is usually one to a few days. If the patient has a fever, we can treat it with acetaminophen or we can also give steroids. If it’s a little bit stronger, we would give IL-6 (interleukin-6) receptor inhibitors. There’s a drug called tocilizumab that we use quite frequently and usually, that takes the edge off it. We may have to give IV fluids if the blood pressure goes down a little bit.
Unfortunately, some patients get a little bit sicker and we may have to give them additional drugs. But for the most part, CRS is very manageable and the majority of patients don’t have severe side effects. When this has leveled off, the patient would leave the hospital if the patient was admitted.
Many institutions, including ours in Miami, can administer CAR T-cell therapy outpatient. We have the patient come in, give the CAR T cells, and have the patient stay in close proximity to our institution. If the patient were to develop CRS, we would treat it along the lines of what I said. We may have to admit the patient after a week for one, two, or three nights, and then we can discharge them.
For a few weeks, we would do labs once a week to make sure blood counts are stable and then we would do them once a month and eventually, every three months. We would keep the patient on prophylactic medications with antivirals and antibiotics. We usually give IVIG infusion, which means that we supplement immunoglobulin G levels to keep the patient free from infections. Over time, all these things will be taken off. The average patient could be off therapy for many years and do blood tests every three months.
For the most part, CRS is very manageable and the majority of patients don’t have severe side effects.
Dr. Landgren
For bispecific antibodies, you see the same CRS phenomenon. If you look at the registrational trials that led to the approval of these drugs, the rates are quite high with over 70 or up to 80 percent of patients developing CRS. Most of them are less intense. They are also along the lines of what I said, like fever and drops in blood pressure.
Nevertheless, the FDA has put in the USPI (United States Prescribing Information) saying that the first few doses should be done inpatient to monitor and see if the patient develops CRS, which the majority of patients do if you follow the standard trajectory of the standard recommendations.
Our group at the University of Miami has used premedication with a single dose of IL-6 receptor inhibitors. We give one dose one hour before the very first dose of a bispecific antibody. We presented this at ASH 2024 in San Diego, showing that you can decrease that rate of CRS to 10% and they virtually are always the lowest grade.
This is a huge step forward and sets the stage for thinking about doing this outpatient. If you can premedicate and avoid 9 in 10 patients from having any side effects or if the patient has CRS symptoms and you could guide them on the phone to come in for monitoring or do some intervention overnight, that’s a huge improvement. Premedications should be part of the next step and we are working on that with other groups. I hope in 2025 that these therapies could also be given outpatient.
It’s very important for physicians who treat patients with bispecific antibodies to keep an eye on immunoglobulin G levels and use proper antibiotic and antiviral medications, so patients don’t run into opportunistic infections
Dr. Landgren
An important side effect profile for bispecific antibodies is infection. I have seen this firsthand because I’ve been involved with drug development for a very long time. When I worked in Miami, I was the chief of the Memorial Sloan Kettering myeloma program for many years, so we were involved a lot in these early developments. We don’t want to develop great drugs that hold the myeloma away and allow patients to have a good quality of life but have other problems arising, such as infections.
It’s very important for physicians who treat patients with bispecific antibodies to keep an eye on immunoglobulin G levels and use proper antibiotic and antiviral medications, so patients don’t run into opportunistic infections, which could be very dangerous. This is very important to emphasize. We can premedicate the immediate side effects, but the doctors need to stay on top of it. Patients also need to know that if they develop an infection, they should always alert their doctor.
Kenny: When it comes to discussing clinical trials and patient support, what do you see as the most promising areas of investigation in terms of bispecific antibody development?
Dr. Landgren: We will see more and more trials with bispecific antibodies that will be used in combinations. At ASH 2024, we saw combinations of two bispecific antibodies: BCMA-CD3 and GPRC5D-CD3. This is the REDIRECT trial, which has been discussed at prior meetings. There were more patients this time and you see very high rates of response. You also see BCMA-CD3 partnered with lenalidomide or carfilzomib, a proteasome inhibitor, in the MagnetisMM-20 study. There are many other studies as well.
What I’m talking about are combinations of bispecific antibodies and other drugs. Eventually, that’s probably what these drugs will fit in with the best. What we will learn, hopefully very fast, is which are the better options to partner them with, the optimal dosing schedules, and the optimal duration of therapy. Can you step down the dose? Can you give it less often? Can you even stop some of these therapies over time?
I don’t have the evidence to prove this, so don’t take this 100% for sure, but based on my looking at data, I project that patients who have been treated with bispecific antibodies, if they have been successfully treated for an extended period or for whatever defined window of time, they may be able to go off therapy.
The missing piece that we are trying to develop is a blood-based MRD test. If you could give treatment and prove that there is no detectable disease, if you could reliably check every three months and make sure there is no disease, many patients could potentially be off therapy for extended periods. It’s an important piece that’s currently missing and we are working on that together with other groups to move that forward.
Kenny: For patients who might be considering a clinical trial involving bispecific antibodies, what factors should they consider when making the decision?
Dr. Landgren: The field is moving forward so fast. At this time, bispecific antibodies are only FDA-approved for patients who have failed four or more prior lines. We see from all these trials that they seem to work very well for patients who had their first, second, or third relapse, but that’s only available in trials at the current time.
Getting a second opinion is very well-invested time.
Dr. Landgren
I mentioned combinations with IMiDs and proteasome inhibitors, but there are other drugs as well. I mentioned two bispecific antibodies, but you also have naked antibodies like daratumumab being combined with bispecific antibodies.
If someone is looking for a trial in the space of one to three prior lines, you have to determine what’s available, where you live, what’s feasible to do, what are the different options, what are the dosing schedules, and what are the safety profiles. The side effects always should be looked at in combination with efficacy. It’s a balance between the two. Look at what’s available and make wise decisions. If you’re not sure, go for a second opinion. Getting a second opinion is very well-invested time.
Kenny: Could you tell us more about the oncology social work service at the Sylvester Comprehensive Cancer Center? What makes it truly comprehensive?
Dr. Landgren: We have a very strong team for multiple myeloma. We have doctors, nurse practitioners, nurses, pharmacists, social workers, patient coordinators, navigators, and researchers. We have a very, very comprehensive program.
Many times, patients ask about the cost and implications of the drugs due to insurance. People are changing from one insurance to another or someone is switching to Medicare and wants to know how that works. We have people dedicated to our program. If I get asked this, which I very frequently do, I will always involve my social worker and finance people to help guide the patient. As a doctor, I don’t have access to all this information, but I have a very strong team that will always help me.
If they come to us for help, we want to make sure that we can give every patient the same high level of knowledge, experience, and care that they deserve.
Dr. Landgren
Kenny: One of the challenges is getting some patients to the clinic because I have a feeling that some of them feel like it’s overwhelming. It’s beyond them either because of the cost or the amount of effort on their part to understand. There’s a base layer of knowledge and there’s a language that they have to learn to speak. Sometimes I have a feeling that the patients feel like they don’t belong in this world. How do you navigate that with a patient? Sometimes you have limited time yourself to engage with them. You can’t solve all the problems, like psychosocial issues, mental wellness issues, diet and nutrition issues, and so forth. All of those things are not where you are, but they’re still your patient.
Dr. Landgren: I serve as the chief of the program, so I’ve thought about these things a lot and how we can scale this up and give the ultimate quality for every patient. How can we treat every patient and provide VIP medical care and support?
The way I try to build our program is to build multidiscipline cells of professionals. Every doctor works with a nurse practitioner, a nurse, and a patient coordinator. That’s the backbone of the little group that we have. We have been growing quite fast with an increase in patients of over 20% every year. If the patient volume goes up, when the group gets too busy, then we hire another doctor, nurse, nurse practitioner, and patient coordinator.
At this point, we have close to 10 of those cells. The right size for our program is somewhere between 15 and 20, but right now, 10 is a good number. We will probably hire another one or two and keep on going as our needs grow because there are a lot of patients who need our help. We don’t wish anyone to have myeloma, but if they come to us for help, we want to make sure that we can give every patient the same high level of knowledge, experience, and care that they deserve, and we are very committed to doing that.
Our program is very active when it comes to different patient organizations… I work with anyone who reaches out to us and I always dedicate my time and attention.
Dr. Landgren
On top of that, we have pharmacists, dietitians, finance, and social workers who support all these groups. The model we have is to build a very small group of experts that hold everything together, where everyone knows the patient and the patient knows them. You don’t call a 1-800 number; you call directly or send a message and we will respond usually within an hour if you send a message through our portal. We will be very, very responsive.
We also organize patient seminars. We have programs where patients can volunteer if they want to be part of that. They can talk to other patients. Some patients like that, some patients don’t, but we have that as an option. Our program is very active when it comes to different patient organizations. I’m very inclusive as a person. I welcome all the different organizations and I’ve done so for a long, long time.
I work with the Multiple Myeloma Research Foundation, the International Myeloma Foundation, the HealthTree Foundation, The Leukemia & Lymphoma Society, and The Patient Story. I work with anyone who reaches out to us and I always dedicate my time and attention. If they have in-person meetings or virtual meetings, we always try to help. That’s how we want to share our expertise and our knowledge to help the community.
Kenny: What advice would you give to patients and caregivers who are seeking more information about the latest treatment options for relapsed/refractory myeloma?
Dr. Landgren: If you have a doctor who you trust and things are going well, work with that doctor and follow that doctor’s recommendations. If you want to have a second opinion, it’s very easy these days to get one. You can travel or if you’re within the States, for the most part, telemedicine visits are available and it’s very important to be able to continue that.
After COVID, I know that there have been some discussions about whether telemedicine should remain or not. All the patient organizations should band together and make sure politicians will never be able to change that because that is going to create barriers for patient access.
If you live in a big city, you have access. If you live in a smaller town, you don’t have access if you have to travel long distances, if you are older, or if you’re frail. Telemedicine breaks down all these barriers. In my opinion, the number one priority for all patient organizations is to make sure that no politician will ever change that because that’s going to cause a lot of patient suffering. In the end, it’s going to take people’s lives and have a lot of negative impact.

Kenny: I love it. Thank you, Dr. Landgren, for taking the time to speak to The Patient Story.
Dr. Landgren: Thank you very much for having me. It was a great pleasure.
Tiffany: What an engaging conversation. Thank you again, Kenny and Dr. Landgren, for taking the time to dive deep into the latest treatment options for relapsed/refractory multiple myeloma patients. If you are a patient advocate, patient, or caregiver, consider being a voice leader in your community or with The Patient Story.
It’s important to be empowered so that you and your caregivers can make informed decisions about your care and that includes being educated about the latest treatment options. Until next time, I’m Tiffany Johnson signing off and on behalf of The Patient Story, thank you for watching.

Edited by: Katrina Villareal
The relationship between a patient and their doctor can make all the difference. A strong partnership leads to more informed decisions, personalized care, and a greater sense of control. Myeloma patient advocate Michelle and her doctor and myeloma expert Dr. Caitlin Costello discuss what makes their patient-doctor teamwork truly effective.
Learn how to build trust and open communication with your healthcare team. Understand the role of shared decision-making in multiple myeloma care. Hear first-hand experiences of navigating a chronic cancer with your doctor by your side. Discover practical tips for advocating for yourself or a loved one in the treatment process. Explore how teamwork fosters a supportive environment for long-term care.
We would like to thank The Leukemia & Lymphoma Society for its partnership.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.

Tiffany Drummond: I’m an advocate who has worked in cancer research for 20 years, but more importantly, I became a care partner advocate when my mom was diagnosed with endometrial cancer in 2014. Her journey led me to find out as much as I could to help with her care. Information wasn’t easy to find, so I’m honored to join The Patient Story in putting on programs to help people navigate life after diagnosis.
This program is hosted by The Patient Story, where we aim to help people navigate life before, at, and after diagnosis through empowering patient stories and educational discussions where we focus on how patients, caregivers, and their partners can best communicate with their doctors as they go from diagnosis through treatment with myeloma.

We want to thank The Leukemia & Lymphoma Society for its partnership. The LLS offers incredible free resources, like their Information Specialists, to help you communicate with members of your healthcare team and provide information about treatment options.
The Patient Story retains full editorial control over all content. I hope you find this information helpful, but please keep in mind that this program is not a substitute for medical advice.
We have two special guests from whom we can learn more about the patient-physician partnership. We have Dr. Caitlin Costello, an associate professor of medicine at UC San Diego Health and a hematologist-oncologist specializing in blood cancers, including myeloma, lymphoma, and leukemia. We also have our patient advocate, Michelle, who is a multiple myeloma fighter and a survivor.

Tiffany: Let’s start back to your initial diagnosis. What was that experience like for you?
Michelle: I was diagnosed in 2016 at the age of 35. I had a five-year-old and a one-year-old at the time. The year leading up to my diagnosis, I had on-and-off back pain, which they said was because my muscles weren’t strong after having a baby. I was starting to lose weight, which they attributed to breastfeeding. I ended up having other symptoms that led me to go to the doctor more.
But then I ended up having severe stomach pain, which at times made me want to drive myself to the ER. I also ended up having itchy scabs all over my body. I went to the dermatologist and my general physician. They both started digging, and my general physician started ordering lab work, which eventually led to the diagnosis of multiple myeloma.
Tiffany: You knew in your gut that something wasn’t right. What did it take for you to advocate for yourself? And when you were referred to a specialist or a hematologist-oncologist, what was your initial experience like?
Michelle: My husband travels for work. was at home with my one-year-old and five-year-old when I was having stomach pains. I didn’t know what to do. I almost drove myself to the ER one day. I took a breath, pulled over, and the pain stopped. I called my doctor and told him he needed to see me the following day. I had already seen the dermatologist about the scabs all over my body. She looked into things and I didn’t know if any of my symptoms were related.
The doctor called and said, “You need to come in right now.” My husband was home, so we picked up our one-year-old and drove to the doctor’s office. My husband stayed with our one-year-old so I could listen to what the doctor was saying.

When we got home, we started making calls…. They all led us to Dr. Caitlin Costello… She fit me in right away, and we never looked back.
Michelle
He said, “You have multiple myeloma.” I asked, “Is that cancer?” He said yes, explained what it was, and sent me to a hematologist-oncologist in their group, who was not at UCSD then. They got me in that day, and the hematologist-oncologist did a bone marrow biopsy.
When we got home, we started making calls. I called my boys’ pediatrician, who I loved and whose opinion I valued, and we reached out to several other people. They all led us to Dr. Caitlin Costello, so we gave her a call. She fit me in right away, and we never looked back.

Tiffany: Doctors all explain myeloma differently, so Dr. Costello, how do you explain myeloma to your patients?
Dr. Caitlin Costello: For many people, when they hear of and think of cancer, they think of a lump, like breast cancer, or there are symptoms associated with a tumor. But when you’re talking about blood cancers, no tumor can be picked up on routine screening tests, of which there aren’t any for myeloma.
With more “typical cancers,” we’re so used to having public health initiatives for screenings like mammograms and colonoscopies. Multiple myeloma, however, while it’s the third most common blood cancer, doesn’t come anywhere near number-wise in terms of how many patients are affected in the United States each year. For that reason, for better or for worse, I don’t think we have good epidemiologic advances to say that everyone should have a blood test screening looking for this.
There’s ongoing interest in screening wide groups of populations. In Iceland, they’re screening the entire country for all patients over the age of 40 to see if they can figure out how many patients have what looks like the beginnings of multiple myeloma. And if they’re not myeloma at that point, they want to understand if it makes sense to screen patients.
Patients are going to live with this for the rest of their lives, so there’s no greater importance than understanding and knowledge.
Dr. Caitlin Costello
For the most part, that means that most patients are diagnosed with multiple myeloma when they develop a symptom of some sort. Many people have not heard of myeloma. When a doctor says to a patient that they have multiple myeloma, they ask, “What does that mean?”
When I describe multiple myeloma to a patient, I say, “What we have identified is a form of a blood cancer called multiple myeloma based on your blood tests and your bone marrow tests.” A lot of my consultations with patients are to explain that diagnosis because.
We have a wonderful problem with myeloma. This has turned into a chronic illness. Patients are going to live with this for the rest of their lives, so there’s no greater importance than understanding and knowledge so that patients know what it is that we’re talking about, know how to follow their blood tests, understand the successes of therapy or perhaps early signs of failures of therapy, and advocate for themselves.
There’s so much to say of the educated patient, which doesn’t mean Doctor Google. There are very good patient advocacy groups and platforms like The Patient Story, where patients can get great information to help them understand their disease and their journey with it.

When I explain myeloma, I explain that it’s a form of blood cancer that comes from a plasma cell, which is part of your immune system. The plasma cell is designed to produce the weapons needed to protect our body. The bone marrow is like the armed forces. We have an army, a navy, an air force, and all these different branches with different weapons designed to protect you. One branch went rogue when one plasma cell went rogue and started producing extra bad guy weapons that don’t work well and cannot protect the body and cause damage.
Bones are the most common way that myeloma can affect a person’s body, and therefore, that’s one of the most common ways that patients are eventually diagnosed because they come seeking help for pain. As Michelle experienced, back pain is one of the most common ones. We think the bones in the middle of our body are more often affected than elsewhere. The classic story is someone had back pain, their doctor did X-rays, but they didn’t see anything, or they were referred to physical therapy, but the pain got worse.
Everyone’s allowed to hurt, but pain that doesn’t go away, came on for no good reason, and is persistent needs to be evaluated. Michelle did all the right things because she had what we can say are typical symptoms with pain, some atypical symptoms with the skin and the belly discomfort, but she asked all the right questions to get her to the right people who could help her.

Tiffany: I love that you talk about patient education. I believe that part of patient education is learning all the medical terms you probably weren’t familiar with before. How receptive are your patients in terms of wanting to learn all that? What are the top three common questions you get after someone is diagnosed with myeloma?
Dr. Costello: The top three questions are: How did I get this? What can I do to make it go away? Is it genetic?
Everyone wants to feel empowered that they can make some lifestyle change, for example, to make things better or help rationalize this to some degree to say X caused Y. It would be fair if there was some culprit, but it’s unfair because there is no culprit. We think this is a random thing that happened for no good reason, by no fault of anybody’s. Nature changed the makeup of your bone marrow and the part of your immune system.
Tiffany: Michelle, when you first met with Dr. Costello and as she was explaining your treatment options, how involved were you in the decision-making process? What did that experience look like?
Michelle: Dr. Costello presented me with what the standard of care was for multiple myeloma at the time. I was very receptive. I sought a second opinion and reached out to another multiple myeloma specialist in the vicinity. She confirmed the same thing, so we went with what everyone was recommending.
Tiffany: Dr. Costello, when you approach your patients about their treatment options, what are your thoughts? How do you approach shared decision-making with your patients? What factors do you consider to help them come to that process with you?

Dr. Costello: Every person is different. People process information differently. People hear information differently. Some people want to know more, and some people don’t want to know more.
An important part of any conversation is to level set and say, “What do you want to get out of this conversation? What is it that you want to know?” More often than not, the patient has something in mind, and the family members have something different in mind. It’s important to gauge the group to determine what it is that they’re hoping to get out of the appointment so that I’m not overstepping boundaries.
Once we are able to establish how much will be shared, my job is to give the information. What is the standard of care? What is the typical approach? Once we’ve laid the groundwork, then we can determine treatment recommendations based on the patient and the details of their health, caregiver support, and the biology of their disease. Very specific details can make treatment recommendations slightly nuanced for any individual person.
My job is to help them be as informed as possible so that they can make the best decision for themselves.
Dr. Caitlin Costello
I love that Michelle got a second opinion. I have no ego. When you are diagnosed with something life-changing, you need to feel very confident in what your next approach is going to be. The more people think about you, the better. Like many myeloma specialists, this is what we do day in and day out, but it’s nice to have a fresh set of eyes so nothing’s missed. Yesterday’s information may have been different from a month ago’s research.
The approach is standard, but the shared decision-making is where things may be slightly different. I can make all of my recommendations and say, “This is what’s standard. These are the slight modifications I would make for you.” Sometimes, the patients will take that information and say, “I’ll get back to you.” Some people will say, “Let’s do this. Whatever you say, doc.” Some people will say, “No.”
I’m not in their body. I’m not making decisions for them. My job is to help them be as informed as possible so that they can make the best decision for themselves. I may not agree with their decision, but that’s not my job. My job is to help them arrive at the best decision that’s for them.

Tiffany: You said everything that I wanted to hear personally, especially when it comes to seeking a second opinion. For a lot of patients, especially if they like their physician in the first meeting, they feel like they’re turning their back on their physician. Thank you so much for encouraging patients to seek a second opinion.
Tiffany: Michelle, where are you in your treatment journey?
Michelle: I did four months of the initial treatment regimen and went into an autologous stem cell transplant. Unfortunately, it wasn’t successful and the myeloma returned within the 100-day mark. We regrouped, went back on one treatment for the summer, regrouped again, and did a more aggressive approach.
The MRD testing at the beginning of 2024 showed that the myeloma was slightly coming back. It was affecting my quality of life and I was ready for something different, so we regrouped again. The doctors agreed that I could take the summer off. We did a repeat bone marrow biopsy, so I would have some initial data to compare against when I start my new treatment plan.
Tiffany: Did the pandemic affect your treatment at all?
Michelle: It gave me a lot of anxiety, but I had to be persistent. Even when everything closed down initially, we were on the phone asking, “Am I coming in?” She said yes, so I went in. I went in every other week all through the pandemic.
Tiffany: When it comes to cancer, you have more than one healthcare provider. Your healthcare team is very vast. Is that specific to UC San Diego or do you have local providers that you also go to? You’re always receiving a lot of information, so how do you coordinate that among yourself and your medical team?
Michelle: I don’t live in San Diego anymore, so I have a local hematologist-oncologist in Sacramento where I now live. This is my disease and my choice. I’ve always sought second opinions, especially when making big decisions about changing treatment plans and what to do next.
Thankfully, the multiple myeloma world is small, so they all know each other. I’ve always been able to discuss with each physician. Even if I don’t agree with a treatment plan, I can seek a different opinion. They have been very kind and take into account my quality of life and what I would like.
Getting the information is best. I seek opinions, weigh out what I want to do and how the treatment is going to affect my life, especially with raising two active boys, what I can handle as far as raising them and having a great quality of life, and then make my decision of how I want to proceed based on their recommendations.

Tiffany: Dr. Costello, for someone like Michelle who doesn’t live in your area, how do you approach seeing patients from afar? Is that something that you do? I had a conversation recently about how large academic centers are more specialized and how you share information with local providers who may not have the same knowledge that you would have. How does that work for you?
Dr. Costello: I don’t feel like Michelle gives herself enough credit. From everything that she said, while raising two young children amid a pandemic, I told her to jump, and she said, “How high?” She has such a commitment to her health and her family.
She got her care at UCSD where we have myeloma-dedicated physicians, but most myeloma patients are taken care of in the community. They see an oncologist, who is possibly a general oncologist who’s seeing them right after they see someone with breast cancer and right before they see someone with lung cancer. Often, they’re good with myeloma, but it’s hard to be a jack of all trades also, and that’s where the importance of a myeloma specialist comes in. I don’t know how they do what they do, seeing so many different cancers. I have difficulty keeping track of one, let alone all of them.
The importance of the connection between the community oncologist and the academic myeloma specialists can’t be underlined enough because we have different tools at our disposal.
Dr. Caitiln Costello
Myeloma is a team sport. Your team includes the patient, myeloma specialist, general oncologist, nurse navigator, nurse, and social worker. There’s a whole team of people who are trying to come together to hold hands with our patients to get them through this whole process.
I can’t speak for other places, but a lot of that can be a little insurance-driven, especially in California. Some insurers will require you to stay with your community oncologist and if that’s the case, the patients get referred for their stem cell transplant, CAR T-cell therapy, or whatever treatment we have to offer at the academic center that perhaps the local oncologist cannot offer. That allows us to maintain that relationship with our patients as well. I have a list of phone numbers of all my local community oncologists down here because we are constantly talking about our patients behind the scenes.

The importance of the connection between the community oncologist and the academic myeloma specialists can’t be underlined enough because we have different tools at our disposal. Myeloma is complicated. There are so many drugs, which is a wonderful problem, but that means that it can be complicated to understand which drug to use and in what order. The connection between the oncologist in the community and the myeloma specialist is absolutely paramount to navigate this whole thing.
I want to be well and healthy to see my boys’ future, and I want to do that with a great quality of life.
Michelle
Tiffany: I used to be a caregiver, so I understand the importance of quality of life. Michelle, you were able to take some time off treatment. How important was your quality of life in driving treatment decisions?
Michelle: I want to be around for my children. That’s my top priority and however I’m going to get there, I will get there. I will cross that finish line no matter what it takes. I want to be well and healthy to see my boys’ future, and I want to do that with a great quality of life.
I started not feeling well after treatments. I was dragging myself and making myself nauseous before even getting to treatment. It was psychosomatic. I realized this wasn’t good and I needed to switch things.
I’m very fortunate where I have a lot of flexibility in my time, so I’m able to make doctor’s appointments and do my treatments during the day when my boys are at school. I try to lead my life in a way that doesn’t affect my children. I’m not in the infusion center when they’re home and going to bed, and I’m very blessed to have that opportunity.
Tiffany: Dr. Costello, is there increasing data that looks at quality of life when it comes to myeloma and treatment options?
Dr. Costello: I don’t even know how to emphasize quality of life enough. People ask, “Is it quantity of life? Is it quality of life? Is it both?” I ask that to some degree to find out about their goals. People’s goals are different. It’s realistic though to say that some of our treatments are not that great. They’re inconvenient and take up a lot of time even though they work. We need to have a conversation to find out their deal breakers. Some patients don’t want to be in an infusion center and only want to take a pill, even if it means it’s not as effective because that’s what’s meaningful to them.
As far as research goes, fortunately, a lot of different studies are looking at new drugs or new drug combinations, including what we call patient-related outcomes. People may hate it because there’s a lot of surveys that happen in the midst of clinical trials asking them, “How’s today? How’s your body image? How do you feel like this? Are you content with this treatment? How do you perceive the side effects of treatment? How much time has this taken out of your day to do this?”
There is more interest in expanding on what we’ve always relied on to evaluate the safety and efficacy of drugs, to incorporate how these drugs can change people’s lives positively and negatively, and to help guide doctors in making treatment decisions and help patients understand if that’s a deal breaker.

Tiffany: You brought up clinical trials, which is one of my favorite topics. Oftentimes, I’ll hear patients say they don’t want to go on a clinical trial because they think that’s the last resort. Dr. Costello, how do you approach the clinical trial conversation with your patients?
Dr. Costello: I first dispel the myth that placebos still exist. Some people still have it embedded in their mind. I always say that it isn’t ethical. We don’t do that anymore. Clinical trials are designed to give you what we consider the best available treatment right now and/or compare it to something that we think is as good or potentially better. I tell patients they’re potentially getting the best of both worlds no matter what they get assigned to at clinical trials.
Part of clinical trials is to help patients understand that there are various phases. Some are randomized where we don’t get to say in what treatment the patient will get. They get assigned to one or the other, but both are great options. There’s an earlier phase trial, which evaluates the safety or efficacy of these treatments and every patient will get the exact same treatment.
There are great benefits that can be reaped by participating in trials, which include getting access to cutting-edge therapies.
Dr. Caitlin Costello
There’s a thought that participating in a clinical trial is purely altruism and to some degree, yes. You are helping the future of myeloma therapies, but you’re getting the benefit yourself from it. Clinical trials are not always designed to be testing the next best thing when a patient has no other options. It’s improving all the steps of treatment that currently exist because we can always do better.
When the conversation about clinical trials comes up, a lot of it is dispelling myths and helping people recognize that it’s not just for others. There are great benefits that can be reaped by participating in trials, which include getting access to cutting-edge therapies that I otherwise cannot write a prescription for.
Seek other opinions and make the best informed decision for yourself.
Michelle
Tiffany: Michelle, what would you tell a patient who is newly diagnosed? Honestly, it seems like you did everything right, so I want to commend you.
Michelle: You are your best advocate. Do your research. Seek other opinions and make the best informed decision for yourself.
Tiffany: Dr. Costello, how do you help a provider to be an active participant and proponent of informed decision-making and shared decision-making, especially junior providers who are coming into the fold? What advice would you give providers to be the kind of person who has relationships with their patients like you and Michelle have?

Dr. Costello: Thank goodness that the paternalistic approach to medicine is a thing of the past. While there may still be a bit of it out there, there has been such an important message about customer service with medicine. You have to understand that this is a give-and-take relationship to some degree. The patient deserves to hear all the information and it’s the physician’s role to give all that information.
There’s been such an important emphasis on compassion and communication. If the physician can put themselves in the shoes of a 35-year-old newly diagnosed mom walking into a cancer center, we can all step out of our bodies and our egos to understand that there is more that can be improved in terms of developing that relationship and the importance of communication. We need to understand that we have much to offer, but our patients have so much to offer us as well.

Tiffany: Thank you, Michelle and Dr. Costello, for such an engaging and empowering conversation. I learned a lot about both of you personally and professionally. What you’ve had to say is going to resonate with our audience.
Dr. Costello is truly a testament to what makes a great physician partner. Witnessing her and Michelle interact was refreshing since we know the patient-physician conversation isn’t always light-hearted when it comes to cancer care. It is important to be empowered so that you and your caregivers can make informed decisions about your care.
Thanks again to our partner The Leukemia & Lymphoma Society. Check out the links on their website, including their information resource center, which provides free one-on-one support.
Special thanks to The Leukemia & Lymphoma Society for its partnership.
The relationship between a patient and their doctor can make all the difference. A strong partnership leads to more informed decisions, personalized care, and a greater sense of control. Multiple myeloma patient advocate Cyndie Dunlap and her doctor Dr. James Berenson, president and medical director of the Berenson Cancer Center, discuss what makes their patient-doctor teamwork truly effective.
Learn how to build trust and open communication with your healthcare team. Understand the role of shared decision-making in multiple myeloma care. Hear first-hand experiences of navigating chronic cancer with your doctor by your side. Discover practical tips for advocating for yourself or a loved one during the treatment process. Explore how teamwork fosters a supportive environment for long-term care.
We would like to thank Blood Cancer United for its partnership.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Edited by: Katrina Villareal
Tiffany Drummond: I’m an advocate who has worked in cancer research for 20 years, but more importantly, I became a care partner advocate when my mom was diagnosed with endometrial cancer in 2014. Her journey led me on a quest to find out as much as I could to help with her care. Information wasn’t easy to find, that’s why we at The Patient Story put on programs to help people navigate life after diagnosis.
This program is hosted by The Patient Story. Our multi-platform organization aims to help people navigate life before, at, and after diagnosis in human terms through empowering patient stories and educational discussions focused on how patients, caregivers, and their partners can best communicate with their doctors as they go from diagnosis through treatment with myeloma.
We want to thank Blood Cancer United for its partnership. They offer incredible free resources, like their Information Specialists, to help you communicate with members of your healthcare team and provide information about treatment options.
The Patient Story retains full editorial control over all content. Please keep in mind this program is not a substitute for medical advice.
I have two exceptional guests. Cyndie, a multiple myeloma patient, and her wonderful doctor, Dr. James Berenson, a hematologist-oncologist at the Berenson Cancer Center in West Hollywood, California, and the president and CEO of the Institute of Myeloma and Bone Cancer Research.

Tiffany: Cyndie, what were your symptoms leading up to seeing a hematologist-oncologist?
Cyndie Dunlap: I was having a little bit of back pain, but I was prompted when I got a routine DEXA scan and was told to take Fosamax (alendronate). I decided to see a bone specialist and instead of going on Fosamax, the bone specialist found myeloma.
Tiffany: Take me through that. What made you decide to talk to someone else?
Cyndie: My first career was as a critical care dietician, so I had some hospital experience and I also had a sister who had a lifelong illness. I realized to trust my gut. I knew that I wanted to see a specialist.
Tiffany: How did you get to the Berenson Cancer Center, which is in a whole other state from where you live?
Cyndie: I started at a top 10 cancer hospital. I was diagnosed at the beginning of the pandemic, so I didn’t have an option. I did the standard treatment that every myeloma patient gets put on and had a transplant.
I always knew that I would get a second opinion when things opened up. I started researching and Dr. Berenson’s name kept coming up over and over and over again, so I decided he was where I was going to start.
The Berenson team absolutely fought for my treatment to get covered. They’re very skilled in navigating insurance.
Cyndie Dunlap
Tiffany: Was it an issue having to go to a different state? Did that affect your insurance at all or was it more seamless for you?
Cyndie: It was fairly seamless. My insurance is national and Dr. Berenson accepts different kinds of insurance, so that was not an issue at all. I’ve had a great coordinator in case I had any issues.
Not that you don’t have to fight. The Berenson team absolutely fought for my treatment to get covered. They’re very skilled in navigating insurance as well, so I appreciate the teamwork on that end.
Tiffany: Dr. Berenson, can you explain in basic terms what multiple myeloma is?
Dr. James Berenson: Multiple myeloma is a form of blood cancer, but it’s bone marrow-based and it involves a type of white cell called a plasma cell. The job of a plasma cell is to make antibodies. Normally, one plasma cell makes one antibody. About a half percent of the cells in your bone marrow are plasma cells and each one makes a different antibody.
What happens in myeloma is it starts with one cell that keeps dividing and dividing. Eventually, there are billions of these cells in the bone marrow, so the protein in the blood—the antibody—sticks out like a sore thumb and tells the patient there’s a marker for myeloma.
Myeloma can cause bone destruction, blood count problems because it’s in the bone where you make all your blood cells, kidney problems, or high calcium from the calcium leaching out of your bones. However, myeloma patients are doing much better because of all the new treatments.
Tiffany: It seems very complex as opposed to a solid tumor, so thank you so much for explaining that.
Tiffany: You get patients pretty much from all over the country. How do you approach your patients? In Cyndie’s instance when she already saw someone, what was your initial consultation like? What general questions are asked and what general information do you give at the initial consult when you meet a patient?
Dr. Berenson: I saw a new patient who came in from a kidney doctor because his kidneys were a little off. The big thing here is to make sure that you take the whole patient into account. A lot of things are blamed on myeloma. A patient who’s anemic could probably be iron deficient. Kidneys don’t quite work right, but that may be from diabetes and not myeloma.
I’ve seen this all the time. What happens many times is patients have a blinder-on type of doctor that blames everything on myeloma, they throw everything but the kitchen sink, and the patient just has iron deficiency. He doesn’t even need treatment for myeloma. They have kidney disease maybe because they took too much medication, from diabetes, or high blood pressure. When you see a patient, you have to think about the whole patient and not just the myeloma.
Take into account: what are their goals for treatment? How old are they? What’s their quality of life? What are their expectations? Do they want to travel? Do they want to stay local? All these things come into account. It’s not just myeloma.
He looked at me as a whole patient and explained things incredibly thoroughly. I’d had myeloma for two years, but he described the plan that he wanted to put me on and why he wanted to and it’s been amazing.
Cyndie Dunlap
Tiffany: Cyndie, when you wanted a second opinion, you knew you wanted to go to Dr. Berenson’s cancer center where you’re getting treatment. How did that look for you? Did you already have in mind what your quality of life needed to be in order for you to sustain yourself? Or did you say you want to see what Dr. Berenson had to say first and go from there?
Cyndie: With my previous experience, I was put through some pretty hardcore treatment. It was very fear-based and not quite as helpful. I’m a very positive person, but that was probably the biggest difference when I went into Dr. Berenson’s office. We discussed. He looked at me as a whole patient and explained things incredibly thoroughly. I’d had myeloma for two years, but he described the plan that he wanted to put me on and why he wanted to and it’s been amazing.
Honestly, I’m doing things that I didn’t think I’d be able to do and I have no hesitancy doing them. One of the things that I appreciate is that I am youngish to have this disease and I live a very carefree life. I have virtually no side effects from the treatment I’m on. He had me in complete remission within, I would say, two months of starting this treatment and I had not achieved that after all the hardcore chemo.
One time, I asked him if I could go down on steroids and we discussed it and what my goals were. Ultimately, I trust his judgment. He’s one of, if not the best, in the world, but I appreciate that he takes the time to explain why he does or does not want to do something.
The goal here is to give patients a long life that they can have with great quality.
Dr. James Berenson
Tiffany: Dr. Berenson, you have this novel approach to the way you do care. Do you find that most of your patients are open to that? How do you approach that when the actual treatment plan isn’t something that is a standard?
Dr. Berenson: I have the outcome data now to say we’re doing well. Our patients are living longer. As my daughter said, “They’re living better and they’re living longer.” When you walk into our clinic, you don’t even know anybody has myeloma or is sick because we don’t make them sick with treatment and yet they do well. There’s nothing better.
What Cyndie’s getting isn’t approved as a single agent, but we’ve published it works great. There’s another antibody in the company that makes it and another drug said you have to use them together. My 90-year-old, who’s been in complete remission for five years, would disagree. I won’t say everything works for every patient because it doesn’t. I’d rather start slowly and give drugs in a way that people don’t get sick.
Most oncologists don’t understand that the goal here is to give patients a long life that they can have with great quality. If people are living with better quality, they’re going to live longer and that’s shown in the results from our patients over the last 20 years.
Part of the story is our hands-on approach. Everybody has my cellphone number… We respond immediately and that makes a huge difference in outcomes.
Dr. James Berenson
Tiffany: You both are the epitome of a patient-physician partnership. You’re communicating with each other and very trusting of each other. You know that this plan is what works for you. Like you said, it doesn’t work for everyone, but your data is clearly showing that, which is promising.
Dr. Berenson: Part of the story is our hands-on approach. Everybody has my cellphone number. I don’t care when they call me, day or night. It doesn’t bother me. My daughter had a problem that a GI doctor helped with and we were all over it within an hour or two. That’s how I respond to my patients.
Cyndie: In fact, I had a GI problem and Dr. Berenson had me on the phone with the same GI doctor.
Dr. Berenson: Being available is such a big thing. I had a patient who came in with neck pain and had cord compression lower down. I got his MRI that same afternoon. Thank God he didn’t have anything on his neck, but if he did, we would have been all over it that afternoon with the surgeon and the radiotherapist. We respond immediately and that makes a huge difference in outcomes. It’s not just throwing the right brews and cocktails together of drugs, but also being available for all these other things and trying to sort them out so they don’t become major problems for the patient.
When you talk to him, you realize that he has an understanding of this disease like no one else.
Cyndie Dunlap
Tiffany: Cyndie, how often do you have to travel to see Dr. Berenson and what does that look like? Do you have a local healthcare team that communicates with him and shares your medical information? How does that work?
Cyndie: My treatment is every two weeks. Up until recently, I traveled every 4 to 10 days. We’ve created a special arrangement where Dr. Berenson is my primary and does all of my oncology and myeloma blood work. I receive one treatment a month locally and then I go to California for a week once every four weeks. I appreciate that he’s willing to talk to my local oncologist if I need to, but honestly, he has me in such good shape.
If anything changed and, for some reason, I needed a different treatment, I would go to California more frequently. It’s a hands-on approach. When you talk to him, you realize that he has an understanding of this disease like no one else. My kids and I all want me in his care.
Tiffany: Dr. Berenson, can you talk to me about monitoring from afar? Has the pandemic even changed how you do that? Is telehealth part of your care now? What’s that like for you when you have patients who don’t live in your local area?
Dr. Berenson: I had a consult with a guy from another country and his doctor’s the head of their myeloma unit. I wanted to give a drug that Cyndie’s on with another one because he has a very specific genetic marker. Sometimes, it’s hard to deal with other countries because they don’t have approvals and these people can’t get drugs. It’s very frustrating. I do telehealth with people all over the country and around the world, and I’m aghast at some of the care.
I have a patient in Nelson, British Columbia, who’s getting his care for his myeloma from a primary care doctor. There’s an incredible myeloma doctor I know well in Calgary, 150 miles east, but he can’t go there because it’s outside the province. He’s got a marker in which he would do beautifully on what Cyndie’s on, but he can’t go. This is frustrating for me because you know what to do, but your hands are tied.
I appreciate the way that he practices medicine and the thought behind how he approaches his patients in the clinic is filled with hope.
Cyndie Dunlap
Tiffany: Your relationship is one that a lot of patients want to have with their physician. Cyndie, what makes your relationship with Dr. Berenson so successful?
Cyndie: He’s a very unique physician as well as an outstanding human being. There was another patient that I know who said this is a passion and not just his profession. I do believe that I am positive because I had a different experience. I appreciate the way that he practices medicine and the thought behind how he approaches his patients in the clinic is filled with hope. I appreciate the way that he treats me holistically. It’s not fear-based. I’m positive and I respond to that. I’m not alone in this feeling about him. You could survey his patients and I think you’d get similar responses over and over again.
Tiffany: Dr. Berenson, what makes you so successful that your patients travel hundreds and thousands of miles to see you and want to keep coming back? What do you think it is that makes that relationship so special where they feel that they’re getting the best care?
Dr. Berenson: We have the best survival rate in the entire world by far. We’ll be publishing that, so I can’t say what it is right now. Let’s not let facts get in the way of opinion. If I were a patient, show me the data. Let me look at it. Let me peruse it. That will not tell you the quality of life data, but I always say if you’re feeling better, you’re probably living longer.
I don’t think very many oncologists give their cellphone numbers, but I do. Everybody has it. I don’t care when you call me. I had a patient who was worried that she had dents in her skull, which turned out to be nothing. But she was freaking out, so I said, “Come in tomorrow morning. I’ll get X-rays in the clinic.” Then I can reassure her that she’s fine. You don’t want that anxiety. You want to get rid of it with reassurance.
For example, like what happened with Cyndie, I got her to the guy who knows. I don’t know about her gut, but I know the guy to deal with it. Figure out a triage. Figure out what you don’t know. Don’t pretend you know everything. Know your limitations. All of that comes into play, but the big thing is availability, willingness to think outside the box, and not being afraid to try things.
I use drugs in more combinations to treat myeloma than any oncologist in the world. I’m not afraid. Sometimes you blow it and it doesn’t work, but I’m also quick to respond. We have a new marker that’s allowing us to respond. You can respond quickly if something’s going awry and that’s cool. I have a patient who’s the first person in the world going on a trial using that marker to make a clinical decision, so we’re very excited about that.
I’m more interested in trying to figure out how to use fewer drugs so we have less cost to the system and fewer side effects for patients.
Dr. James Berenson
Tiffany: Dr. Berenson, do you conduct clinical trials at the Berenson Cancer Center or do you keep it more investigator-initiated where you’re developing it yourself?
Dr. Berenson: We try to spread the love. Sometimes, we start on a whim and we’ll try a drug that may be approved for something else, repurpose it, we’ll get an activity, and then we’ll go to the company to spread the love and do it with other sites around the country. Sometimes we’ll piggyback on larger drug company-sponsored trials.
I’m more interested in trying to figure out how to use fewer drugs so we have less cost to the system and fewer side effects for patients. Perhaps, we’re going to be able to intermittently treat with some of the newer drugs and the better markers we’re going to have to track myeloma.
I tell people that no matter where they are in the country, they should at least try to get a consultation from Dr. Berenson before they start treatment.
Cyndie Dunlap
Tiffany: This conversation has been great. It’s going to be evident to anyone how this patient-partner relationship works. Cyndie, if you could advise someone who may be newly diagnosed or even relapsed/refractory, what is something that you wish you knew?
Cyndie: I would have asked my initial oncologist: what are the other options? It was very directly said to me that my treatment was the only way to go. I tell people that no matter where they are in the country, they should at least try to get a consultation from Dr. Berenson before they start treatment. If not for the pandemic, that’s the way I would have gone. I wish that I had started with him. It would have saved me from getting a transplant and all kinds of chemo.
Tiffany: I’m pretty sure there are some people out there who feel that they’re stuck in one place. There’s no one replacing Dr. Berenson, but there may be someone close to him in your local community. Find that person if you can’t get to Dr. Berenson.
We shouldn’t allow this hands-off and less involved approach to occur… To me, it’s individualized care and getting to know everything about your patient and their life. Only then can you personalize care.
Dr. James Berenson
Dr. Berenson: You have to try to push what people should be doing. What should be the norm? The norm should be availability. The norm should be that you touch a patient and examine them. The norm should be that you spend enough time to find out whether their eyes, ears, nose, throat or something else is going on. That should be what we allow.
We shouldn’t allow this hands-off and less involved approach to occur. People are talking about personalized medicine. I find it rather ironic at a time when medicine is so much more depersonalized and I don’t think that’s the idea of personalization. To me, it’s individualized care and getting to know everything about your patient and their life. Only then can you personalize care.
Tiffany: Especially for my loved one that I was caregiving for, their care team became our family. I looked at them like I would look at family and wanted the best for them like I would family as well.

Tiffany: Thank you, Cyndie and Dr. Berenson, for a great discussion. Dr. Berenson is such a colorful character and brings humanization to cancer that we at The Patient Story continuously strive for. It is important to be empowered so that you and your caregivers can make informed decisions about your care.
Thanks again to our partner Blood Cancer United. Check out the links on their website and also check out their information resource center, which provides free one-on-one support. Until next time.
Special thanks to Blood Cancer United for its partnership.

Edited by:
Katrina Villareal
Multiple Myeloma:
Symptoms & Signs
PERSEUS Trial
IsKia Trial
Quadruplet Therapy
MAIA Trial
CAR T-Cell Therapy
Bispecific Antibodies
BLENREP (Belantamab Mafodotin)
Impact of Dexamethasone (Dex) Dose
In this discussion, patient advocates Cindy Chmielewski and Jack Aiello speak with multiple myeloma experts, Dr. Rafael Fonseca with Mayo Clinic and Dr. Susan Bal with University of Alabama at Birmingham. They discuss the latest coming out of the 2023 American Society of Hematology meeting and share the latest multiple myeloma clinical trials and treatment options.
Learn about new multiple myeloma treatment options, including triplet and quadruplet combination therapies, CAR T-cell therapy, bispecific antibodies, and trispecifics. Find out about the future of belantamab mafodotin (BLENREP), dose reduction of dexamethasone, and the introduction of sonrotoclax, dubbed as the next-generation venetoclax.
Stephanie Chuang: I’m the founder of The Patient Story and, more importantly, I also got a blood cancer diagnosis of non-Hodgkin lymphoma a few years ago.
We have so many shared experiences in what we’re looking for and that’s what The Patient Story is all about.
We try to help patients and care partners navigate a cancer diagnosis primarily through in-depth conversations with patients, care partners, and top cancer specialists.
We want to note that The Patient Story retains full editorial control of this entire program and this is not meant to be a substitute for medical advice.
Our patient moderators Cindy Chmielewski and Jack Aiello will lead this conversation. Cindy and Jack, can you share a little bit more about your own stories and how you became such passionate advocates in this space?


Cindy Chmielewski: I’ve been living with multiple myeloma since 2008. What brought me to the doctor was very debilitating back pain. The pain was so bad that it affected my job. I was having a hard time standing up to teach. I wasn’t able to take my class to the playground for recess. I had to have other teachers do that.
I went to an orthopedic doctor who, unfortunately, I think was unfamiliar with the symptoms of multiple myeloma because he diagnosed me with degenerative disc disease. It took an additional two years to get the correct diagnosis.
Since then, I’ve had several treatments and I’m now doing very, very well. I’m excited because I’m hearing all these new therapies that will be available to me if and when I relapse.
Jack Aiello: I was diagnosed with multiple myeloma at the beginning of 1995.
It started with a backache but MRIs and X-rays didn’t show anything wrong according to a specialist I went to see. I ended up taking a blood test and that showed an elevated protein. The specialist said I likely have multiple myeloma and that was the start of about eight years of significant treatment.
Back then, the average life span for myeloma patients with treatment was only 2 to 3 years. I was fortunate to respond to a third transplant except that I used donor stem cells after a couple of earlier transplants and clinical trials didn’t work for me.
I’m extremely appreciative to be alive 29 years later. I think this discussion is awfully important as all of these webinars are for myeloma. In particular, we focus on what happened at the 2023 American Society of Hematology meeting that will affect patients immediately as well as where the research is going. I’m always in favor of making sure I understand what’s going on so that I can help myself if my disease comes back and I can help others when I’m leading our support group or talking with other patients.


Cindy: Dr. Rafael Fonseca is a hematologist-oncologist at Mayo Clinic with a special interest in multiple myeloma. He also participates in and leads clinical trials that have led to the approval of various drugs for the treatment of myeloma
Dr. Fonseca, what drew you to multiple myeloma, and what drives you most to continue to work in helping myeloma patients?
Dr. Rafael Fonseca: The way I got into myeloma is a little bit of luck but mainly because I had great mentors. The late Dr. Philip Greipp was a wonderful influence. I wanted to do lymphoma, but he steered me into myeloma without knowing what would happen. Those were the days of melphalan and prednisone, which links exactly to what drives me now.
We are very fortunate to be living through these times when so many things are happening in the treatment of myeloma. One of my colleagues, Dr. Ruben Mesa, told me a few years back that we are either a drug away or a combination away from being able to cure a significant fraction of patients. We’re shuffling the pieces on the table, but I think we’re there so that keeps us going every day.

Jack: Dr. Susan Bal is a hematologist-oncologist with the University of Alabama at Birmingham with a special interest in myeloma and CAR T-cell therapies. In fact, at the recent American Society of Hematology meeting, I was fortunate to see Dr. Bal as a primary investigator present phase 1 findings for the clinical trial of BMS-986393, which is a GPRC5D CAR T-cell therapy.
Dr. Bal, what drew you to myeloma, and what drives you most to continue your work to help patients?
Dr. Susan Bal: Myeloma was always very exciting to me personally. I started my fellowship the year that we saw the first results from daratumumab come about.
Other than the excitement in the field and the possibility of a cure, one thing that drives me most is the meaningful relationships that you can continue to build because our patients live for so long and do so well.
I’m so delighted to be able to work with a great group here and across the country. The myeloma community is strong and we forge onward in our path to curing this condition.

Patients can come to us from any of these avenues and that’s what makes it interesting… It’s a very heterogeneous disease, certainly in terms of presentation and how people do overall.
Dr. Susan Bal
Cindy: Briefly, what is multiple myeloma and what are some of the first signs and symptoms?
Dr. Bal: Multiple myeloma is a plasma cell disorder so it’s plasma cells that have become cancerous. We have white cells, red cells, and platelets. White cells fight infections, red cells carry oxygen, and platelets stop us from bleeding.
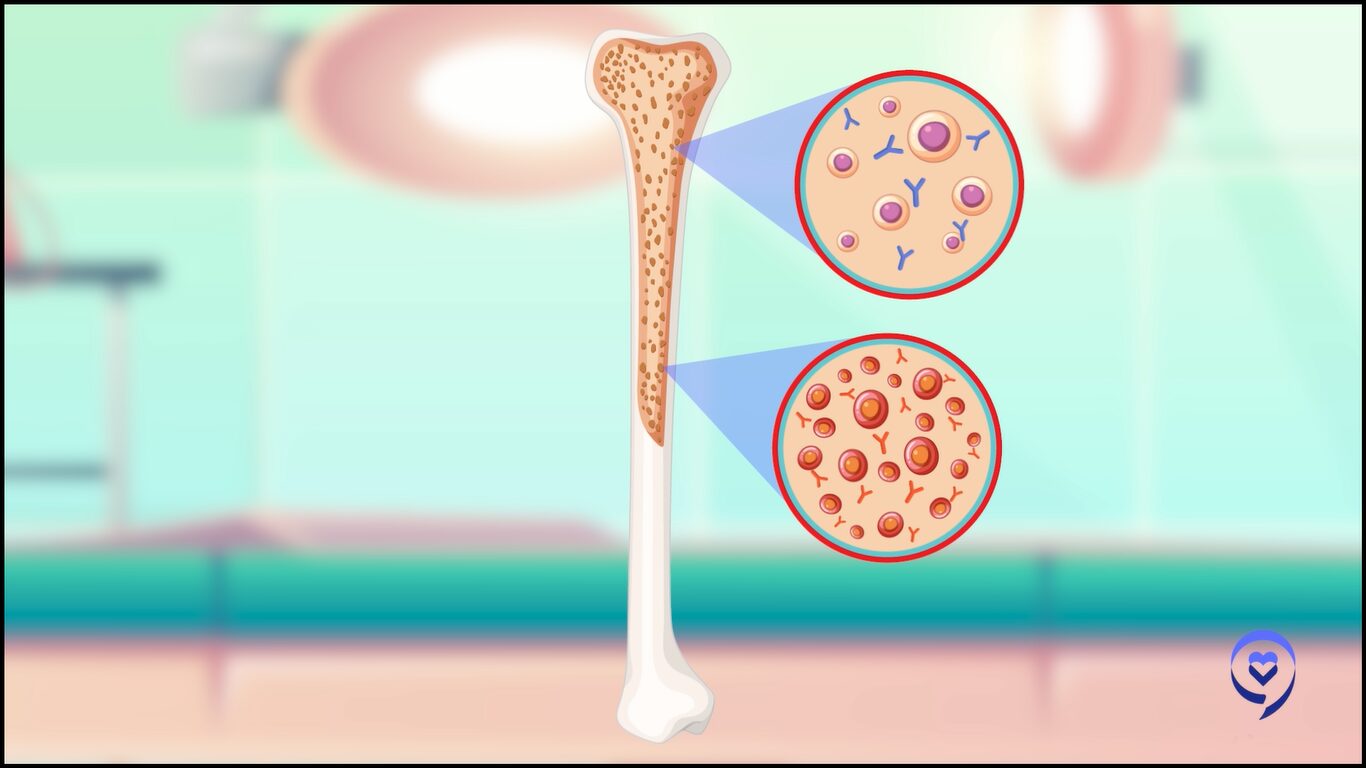
Dr. Bal: One of the types of white cells that help us fight infection is the plasma cell. The plasma cell is responsible for making antibodies that normally help us fight infection.
Sometimes when these plasma cells go awry and become cancerous, they can crowd out the bone marrow, resulting in symptoms such as elevated calcium levels, bone breakage, and bone damage. It can affect our kidney function, causing renal dysfunction. It can also cause low blood counts because of crowding out of the marrow.
Because it’s a part of the immune system and its job is to prevent infections, oftentimes, patients can present with recurrent infections as a presenting feature as well.
Patients can come to us from any of these avenues and that’s what makes it interesting. We see patients who are simply diagnosed because they had an astute primary care physician who picked up on a protein gap. We have patients presenting on the other end of the spectrum with the plethora of all symptoms that we know as CRAB symptoms, presenting with very disabling features. It’s a very heterogeneous disease, certainly in terms of presentation and how people do overall.
As is true with everything else in medicine, the availability of additional information has allowed us to narrow down the best options for patients.
Dr. Rafael Fonseca
Cindy: Dr. Fonseca, we’re lucky now that there are so many treatments available. When I was diagnosed back in 2008, the treatment arsenal was not nearly as filled as it is now.
What are some of the considerations you think about when choosing treatments for different groups, like transplant-eligible versus transplant-ineligible and newly diagnosed and high-risk? What goes through your mind?
Dr. Fonseca: That’s the essence of everything we do in the practice. All of those considerations and how we present them and share them with patients as options for their treatments.
When we started seeing all these drugs come forward and being approved, my first reaction was, “Boy, this is going to get complicated. How are we going to choose? We have all these treatments. My appointments may have to be two hours long because I have to present everything to patients.”
As is true with everything else in medicine, the availability of additional information has allowed us to narrow down the best options for patients. Even though we have many more drugs, we still have 1, 2, or 3 options that are probably the best for a person at a given step. That has allowed us to work more on our messaging and the rationale of what we do.
The considerations you mentioned are critical. We always want to look at, first of all, the patient as a person with their preferences and goals, as well as some other health issues or comorbidities.
One of the critical aspects — and one we can’t modify though I know many wish we could — is our age. Age is a major determinant of how well you’re going to be able to tolerate treatment or not.
Some treatments become quite a bit toxic as we take them later on in life. A great example of this is the stem cell transplant. As physicians and clinical teams, we have to tailor our approach to patients as we start proposing the various treatments.
The second consideration is whether the patient is newly diagnosed or someone who, unfortunately, has myeloma that’s coming back or what we call recurrent myeloma. If we think about that, then we say: which stage is this? Is this an early recurrence or is this someone who has already received 3 or 4 prior lines of therapy?
Then we bring other factors that are important for patients to know about and we discuss them with the patients. We test the myeloma cells for genetic makeup. When we talk about genetics in myeloma, we’re mostly talking about the changes that occur in the myeloma cells, not the genetics that a person may have in the rest of their body and, very importantly, not genetic things that are passed on from generation to generation.
Those are things that play into our decision-making process. Some patients have markers that would make us more concerned, something we call high-risk myeloma. With that in mind, we put together treatment plans that we propose to our patients.
We’re moving forward with a more unified approach to goals. If you go back 15 years or certainly, in 1995, our goal was to control. Can we do something that will put the myeloma at bay that would allow us to gain time?
Many of us feel like the pendulum has swung completely in the other direction. Many individuals, myself included, think that we should aim to eradicate all myeloma cells and, ultimately, produce cures for patients. How you phrase that and plan for that becomes important. Behind that, there’s a whole set of other principles. Those are some of the overriding things we think about but always starting with the patient.
We were lucky to have two major presentations at the meeting, including a plenary session where we saw results from the IsKia trial, as well as a late-breaking session where we saw results from the PERSEUS trial.
Dr. Susan Bal
Jack: Dr. Bal, can you explain the importance of the American Society of Hematology meeting and what, from your standpoint, were the biggest takeaways?
Dr. Bal: The American Society of Hematology meeting is a key event for hematologists. It’s where we expect to see some of the latest and greatest of science and all the discoveries and innovations that are occurring within the field. It’s a one-stop shop where we get to see some of the best data so it’s a very looked forward to event in the community.
This ASH was no different. We were lucky to have two major presentations at the meeting, including a plenary session where we saw results from the IsKia trial, as well as a late-breaking session where we saw results from the PERSEUS trial.
The PERSEUS study was perhaps one of the most awaited trials in the sense that this was a randomized phase 3 trial evaluating a quadruplet regimen of daratumumab, bortezomib, lenalidomide, and dexamethasone versus the same combination without daratumumab in patients with newly-diagnosed, transplant-eligible multiple myeloma. For many in the field, we have moved towards using these quadruplets based on an earlier phase 2 randomized GRIFFIN trial. This was practice-affirming and perhaps practice-changing for a small proportion of patients in the community.
What this trial did was take patients who were transplant-eligible — who are fit and in the European and Australian countries where this was predominantly performed — and were randomized into receiving four drugs versus three drugs followed by stem cell transplant and then a doublet maintenance following consolidation therapy with the same regimen.
Overall, what we saw was with a close to four-year follow-up, patients who received this four-drug regimen did a lot better and had longer progression-free survival at the four-year time point. Patients had a very deep response with this regimen achieving measurable residual disease negativity, both using very sensitive markers and sustaining over prolonged periods, which has been shown to be hopefully a surrogate for improved patient outcomes overall.
Within the US, many in the field have already taken up the practice of adopting this four-drug regimen based on the prior GRIFFIN study, but I think this was confirming and affirming for those of us who are doing that and practice-changing for those who were still using the triplet combination. This was perhaps one of the most exciting things to come out of this trial, among other things.
Jack: That’s fantastic. Dr. Fonseca, what about you? Can you describe an outcome you saw from ASH that was so important to the myeloma community?
Depending on how you measure and what the threshold is, we have studies showing that somewhere between 60 and 80% of patients can get into minimal residual disease.
Dr. Rafael Fonseca
Dr. Fonseca: What Dr. Bal described is the crux of what we saw at the 2023 ASH meeting. This is our key meeting where we see all this data.
No one would be surprised if we tell you we actually have a lot of fun being at that meeting because we’re with friends. We work the longest hours that we work in the year. Sometimes it’s hard to convince our family that it’s work because we’re all smiling, talking, and exchanging ideas, and then we go for dinner and discuss further.
It’s a wonderful time for us and more so given the progress we’re seeing in myeloma. The fact that we now have very strong data for what needs to be done in the front line is very important for patients.
At this moment, it’s beyond any doubt that we need to use the best treatments up front. For now, that means the incorporation of anti-CD38 monoclonal antibodies. Dr. Bal mentioned the use of daratumumab. We also have a similar molecule, isatuximab.
The clinical trials point to outstanding results, which could not be seen ever before in the treatment of myeloma. The results are so good that they’re now going to start challenging some of our assumptions.
We had the meta-analysis for the maintenance strategy for myeloma, where patients go through induction, get the transplant, and are placed on maintenance. But Dr. Luciano Costa has pointed out repeatedly that those maintenance studies were done where we could achieve a complete response in about 30 to 40% of patients, minimal MRD negativity, and sometimes patients were getting two drugs as induction.
One would say it was no surprise that more treatment was effective. Whether we call it maintenance or consolidation is semantics. Now we’re getting to the point where many patients have a complete response. Depending on how you measure and what the threshold is, we have studies showing that somewhere between 60 and 80% of patients can get into minimal residual disease.
We’re starting to ask: do you even need maintenance in those patients? I don’t claim in any way that we have the answers, but it reflects how fast things are moving forward. Breaking it down, as Dr. Bal did, is critical.
For some people, we were practicing this, but for other people, either they need this for regulatory purposes across the globe or their reading of the medical literature is such that they want to have that phase 3 trial before they change clinical practice.
Right now, it would be rare that a patient would not be offered induction therapy with something, as we were describing. A lot of things are getting simplified. In a conversation with colleagues, I said the treatment of myeloma should always start with something like daratumumab, lenalidomide, and dexamethasone.
The secondary question is whether the patient needs to get a proteasome inhibitor, like bortezomib or carfilzomib, and whether they need to get a transplant. But then things get simplified because the best players rise to the very top of what we’re doing so I’m excited for what this means for patients.
Dr. Bal: I completely agree with Dr. Fonseca. I feel like some things are almost becoming cleaner as we go. I remember this discussion about three years ago where everybody wanted to know: would you give daratumumab to a transplant-eligible patient? The answer is becoming clearer and clearer that you want to use your best drugs upfront and make that first cut your deepest.
Recently, somebody asked me, “Is there a patient whom you would not give daratumumab to?” I said, “I don’t know who that would be because it’s such a well-tolerated, effective therapy.” Now I’m thinking more like what Dr. Fonseca said about which of the other agents you could potentially get rid of or improve upon, rather than the daratumumab.
I’m not saying we’re ready to dispense with transplants, but the data continues to show that deep responses, no matter how you get there, will result in better outcomes.
Dr. Rafael Fonseca
Jack: Dr. Fonseca, one of the important trials — and Dr. Bal referred to it earlier as having been given special recognition at ASH as a plenary session — was the IsKia clinical trial, which compared carfilzomib, lenalidomide, and dexamethasone, adding isatuximab to it or not as front-line therapy for transplant-eligible patients. Isatuximab is like daratumumab in that they’re both CD38 monoclonal antibodies. It was another four-drug trial. Can you talk a little bit about that?
Dr. Fonseca: The reason something is given that plenary status is when the reviewers and the reviewing committee feel that there is something of such high value that reaches the high standards of evidence or that even potentially becomes immediately practice-changing.
This particular clinical trial was one more point in that direction where they started looking at the response rate and the MRD negativity rate for those patients. MRD negativity refers to measurable residual disease or minimal residual disease, which is nothing different than saying we have better markers to assess the depth of a response through mechanisms such as genetic testing.
It’s becoming increasingly clear and very well-documented that achieving the status where you can no longer find measurable disease — using very sensitive tools where some can go at the level of detecting one cell out of a million — becomes a harbinger of great outcomes for patients, of durable responses, and ultimately improvements in the various metrics that we call survival. The IsKia trial shows that.
It’s very interesting to me for a couple of reasons. This is a different antibody, a different molecule than daratumumab, but the presumption by those in the field has been that we should see similar results. These antibodies carry nothing of what we call a payload. They’re a naked antibody so they go and bind to those cells. By doing that, they unleash our immune response to those cells. They’re able to kill more cells. We know that because the responses are better and the MRD is better.
In that particular trial, we have to wait a little bit longer to see over time what the outcomes will be on those metrics that people hear about, like progression-free survival and overall survival. But given what I said about MRD, all the indicators are that this will be a very useful approach for the treatment of patients.
Everyone should get a CD38, like lenalidomide and dexamethasone, at least for the time being. But then the question is: what about these drugs that we call proteasome inhibitors? In this particular trial, they used carfilzomib. For me, that’s very interesting because that’s what I do in my clinical practice.
When we make decisions in our clinical practice, there are trade-offs. Carfilzomib is a sister medication of bortezomib. They’re both proteasome inhibitors, but each one has different toxicities.
There’s no clear-cut evidence that one is better than the other, but I don’t like the enduring toxicity that occurs with some of the other drugs, like bortezomib. That’s where we will be spending our time, talking about those types of drugs. Should we use bortezomib or carfilzomib? Both are standard of care and excellent treatment. There are nuances of why we choose one or the other.
There will be the question of transplant, too. If you have these regimens that can make patients have such a great response that they become “MRD negative,” the question will come forward: do you even need a transplant?
I’m not saying we’re ready to dispense with transplants, but the data continues to show that deep responses, no matter how you get there, will result in better outcomes. Maybe some patients will elect to say, “I’m going to collect cells and think about a transplant later.” That’s a very long, nuanced conversation but a reflection of the progress we’re making with this type of combination.
In terms of which proteasome inhibitor is the right choice, some of that depends on the patient’s profile, comorbidities that they already have, and age.
Dr. Susan Bal
Cindy: Dr. Bal, you were saying that things are becoming cleaner, but now, we’re thinking about four drugs upfront, but which four drugs? Dr. Fonseca was alluding to it, but are there any considerations that you take into whether your proteasome inhibitor is going to be bortezomib or carfilzomib, or what CD38 monoclonal antibody to use? What goes through your mind now that you’re picking four drugs?
Dr. Bal: As Dr. Fonseca mentioned, the patient in front of you helps determine some of that. As you know, daratumumab and isatuximab are both anti-CD38 monoclonal antibodies. They are both very effective drugs.
However, one is subcutaneous so administration is a little bit easier with daratumumab, which is given as a short injection underneath the skin. The other one requires an IV. For now at least, until we have the subcutaneous version for isatuximab, I do believe that reduces share time and and patient inconvenience very much.
In terms of which proteasome inhibitor is the right choice, some of that depends on the patient’s profile, comorbidities that they already have, and age.
For example, with bortezomib, we’re aware that the risk of peripheral neuropathy is significant and can be quite disabling even at lower grades. However, with carfilzomib, we have seen cardiac and renal toxicities. Even more than just objective data, a lot of people complain of subjective dyspnea and subjective shortness of breath, which can make it challenging for them to feel good during treatment.
Young, very robust, and perhaps high-risk patients are best stratified into the carfilzomib arms, and older patients, depending on their fitness, would then get either no proteasome inhibitor or a bortezomib-based option.
That part is rather individualized, without any clear data of one being overly more efficacious than the other, at least based on the data that we do have in front of us.
In very elderly, very frail patients, daratumumab is exceedingly both efficacious and quite safe, as long as you provide them with appropriate antibiotic coverage, close monitoring, vaccination, and perhaps even IVIG use to protect them from infections.
Dr. Susan Bal
Cindy: Are there particular patients that you would not give the quadruplet regimen to, where you would probably go back to triplet therapy or maybe even doublets?
Dr. Bal: Incorporating frailty assessment and assessment of the patient’s overall performance status going beyond the eyeball test that we do is going to be critical in determining who is not fit to receive a quad.
In cases where there are concerns about the use of a proteasome inhibitor, particularly bortezomib, due to underlying diabetes or other comorbidities or the patient’s age and you’re concerned about cardiopulmonary toxicity with carfilzomib, as Dr. Fonseca also mentioned, daratumumab with lenalidomide and dexamethasone is an excellent option with high-level evidence of benefit.
I would say for very old patients who are in their high 80s, even 90s, I would consider a doublet. What’s interesting is that the doublet I would consider would be a dara-dex type of combination or even single-agent dara because IMiDs require hematopoietic monitoring or blood work closely checked for low blood counts. The proteasome inhibitors carry all the concerns that we mentioned.
In very elderly, very frail patients, daratumumab is exceedingly both efficacious and quite safe, as long as you provide them with appropriate antibiotic coverage, close monitoring, vaccination, and perhaps even IVIG use to protect them from infections.
Does everyone need maintenance? I don’t know what the answer to that is yet, but I know that the question is very relevant.
Dr. Rafael Fonseca
Cindy: Dr. Fonseca, do you have anything to add to what Dr. Bal said? What about maintenance? Are you seeing single-drug or double-drug maintenance?
Dr. Fonseca: I want to emphasize one of the points that Dr. Bal made. If you asked me two years ago what I would do with a frail patient who has newly diagnosed myeloma, my response would have been lenalidomide and dexamethasone. However, we saw with the subset analysis in the context of the MAIA clinical trial that the addition of daratumumab significantly improved outcomes for these patients.
I’m glad we have the data because we would be at significant risk of shortchanging patients in the line of thinking of beneficence. Let’s be kind. Let’s use mild treatments. But it turns out that the survival numbers are not as good.
Now, whenever we add a drug, we have to think whether we’re adding toxicity, but the reality is these antibodies are incredibly well-tolerated. It’s different to propose adding carfilzomib or not versus adding daratumumab. Today, I would say the vast majority of patients, even if they’re frail, should get something like daratumumab upfront.
Maintenance is really, really interesting. I’m hoping and I think we’re going to get there soon. Studies, like the ones done by the group of Dr. Bal, are using these adaptive strategies to look at whether we can stop therapy, which naturally leads to the next question. Does everyone need maintenance? I don’t know what the answer to that is yet, but I know that the question is very relevant.
We’re going to get to the point where we’re going to think of maintenance like people think of adjuvant therapy for breast cancer. You complete the surgery. They look at the lymph nodes and the genetic makeup of breast cancer and say whether you need chemotherapy or not. As we incorporate our genetic knowledge, the status of response after induction plus or minus transplant, then we are going to ask those questions.
Does everyone need maintenance? I think it’s going to diverge a little bit more to the extremes. There’s going to be greater contrast. For patients who have standard risk genetic factors, are able to complete induction therapy, have a transplant, and have MRD negativity 10-6, it’s going to be hard to prove that maintenance would have an added benefit. If so, hopefully something that’s better tolerated because, as we know, lenalidomide has significant burden toxicities for patients.
On the other hand, if the patient has residual disease, I don’t think there’s a good enough reason to say that’s what we do. That’s standard. I’m going to cross my fingers and wish that this is not going to come back. I think those are patients for whom we’re going to provide additional treatment for no other reason than to try to get rid of all residual myeloma cells.
I think that’s where we’re going to go with maintenance. I don’t foresee that maintenance, as we have it right now, where everyone gets lenalidomide. You get it until you can tolerate it and hopefully not have side effects or no disease progression. I think that has to change.
If you can eradicate evidence of disease, you can improve your outcomes significantly.
Dr. Susan Bal
Dr. Bal: I couldn’t agree more. We certainly share our opinions regarding the use of measurable residual disease. It’s become the single most important prognostic marker, one that is not defined at all when you’re first diagnosed but comes into play after therapy.
If you can eradicate evidence of disease, you can improve your outcomes significantly. Whether you’re starting as a high-risk patient or a standard-risk patient, getting to that milestone and, more importantly, maintaining that milestone can improve outcomes.
I think maintenance as we know it today will soon cease to exist, hopefully, but mostly because we’re either giving them more therapy, getting them where they need to be, or they’ve done so well because of the excellent therapies we have that we don’t need to continue suboptimal treatments that have other toxicities and risks associated with them.
In the lab, we essentially teach these cells using a viral vector to express receptors on their surface that can target cancer antigens within a patient’s body.
Dr. Susan Bal
Jack: As effective as the treatments are, myeloma still often comes back and one of the exciting new treatments going forward is CAR T-cell therapy. Dr. Bal, can you explain what CAR T-cell therapy is in conjunction with what you presented at ASH?
Dr. Bal: CAR T-cell therapy stands for chimeric antigen receptor T-cell therapy. Within our bodies, there are immune cells and one of those subtypes is T cells, which are normally working to keep our cancers in check. The thought is that these T cells are not working as well as they need to be and the cancer itself is finding mechanisms to evade our immune system, which is what results in disease relapse.
CAR T-cell therapy is a revolutionary therapy. We take out a patient’s T cells by apheresis, very similar to a procedure that patients go through when they do stem cell collection. In the lab, we essentially teach these cells using a viral vector to express receptors on their surface that can target cancer antigens within a patient’s body.
Thereafter, we provide the patients with lymphodepletion chemotherapy, which is essentially chemotherapy that’s given to reduce the number of T cells which are within the patient’s body. We then infuse these chimeric antigen receptor T cells, which go and interact with the antigen, using their CAR receptor, and cause cancer killing or tumor death.
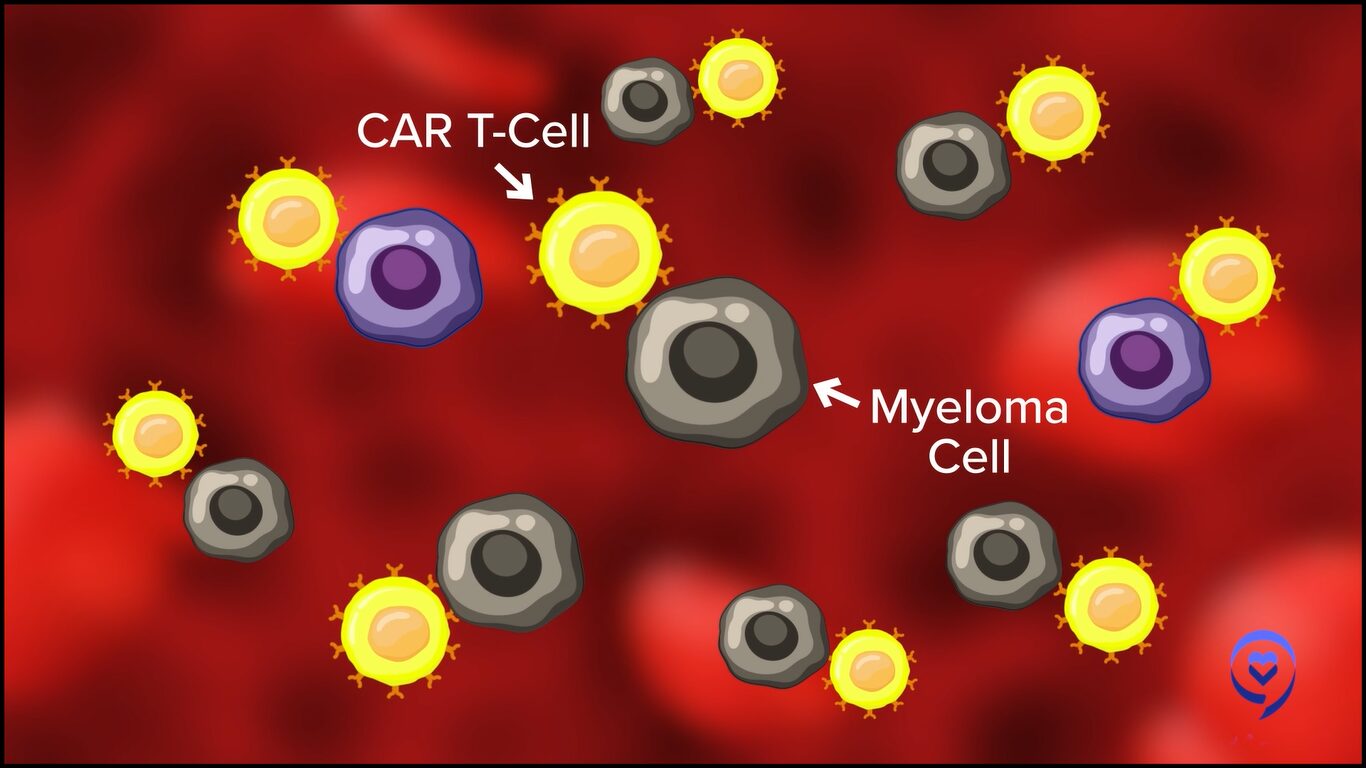
This has been shown to be a very effective modality, particularly in patients who previously haven’t had very good treatment options after they’ve been through the three main pillars of therapy, like CD38 monoclonal antibodies, immunomodulatory agents, and proteasome inhibitors. These patients previously had dismal outcomes measured in single-digit months. Now with these therapies, they’re living longer and having excellent responses, including several that are MRD negative even in late-line disease settings.
At this time, there is FDA approval for two chimeric antigen receptor therapies in myeloma that target the B-cell maturation antigen. This is an antigen that is present on the surface of plasma cells in general and more on the surface of malignant plasma cells or cancer cells. Using this target, we have seen very impressive responses of up to 98% overall responses with one of the FDA-approved agents, known as cilta-cel. This is shown to be an effective avenue.

What we presented at the 2023 ASH meeting is a chimeric antigen receptor T-cell therapy that targets a different antigen known as GPRC5D. This antigen is also one that is expressed preferentially on the surface of these cancer cells and has limited expression across normal tissues, although we do see some expression on tissues such as heart keratinized tissues, on the skin, on nail beds, and in hair follicles. We see some typical side effects, including dyskinesia, with treatments that target this therapy.
Overall, GPRC5D has been shown to be a promising therapeutic target in myeloma. We already have a different immune strategy that’s working against this and is FDA-approved.
In this phase 1 study, we evaluated a CAR T cell that is targeting GPRC5D in patients with relapsed myeloma. What we saw is that in a heavily pre-treated patient population who have received a median of five prior lines of therapy, this was associated with deep responses overall. In about 73 patients who were efficacy available, meaning were available for response assessment, we saw that 88% of the patients had a response.
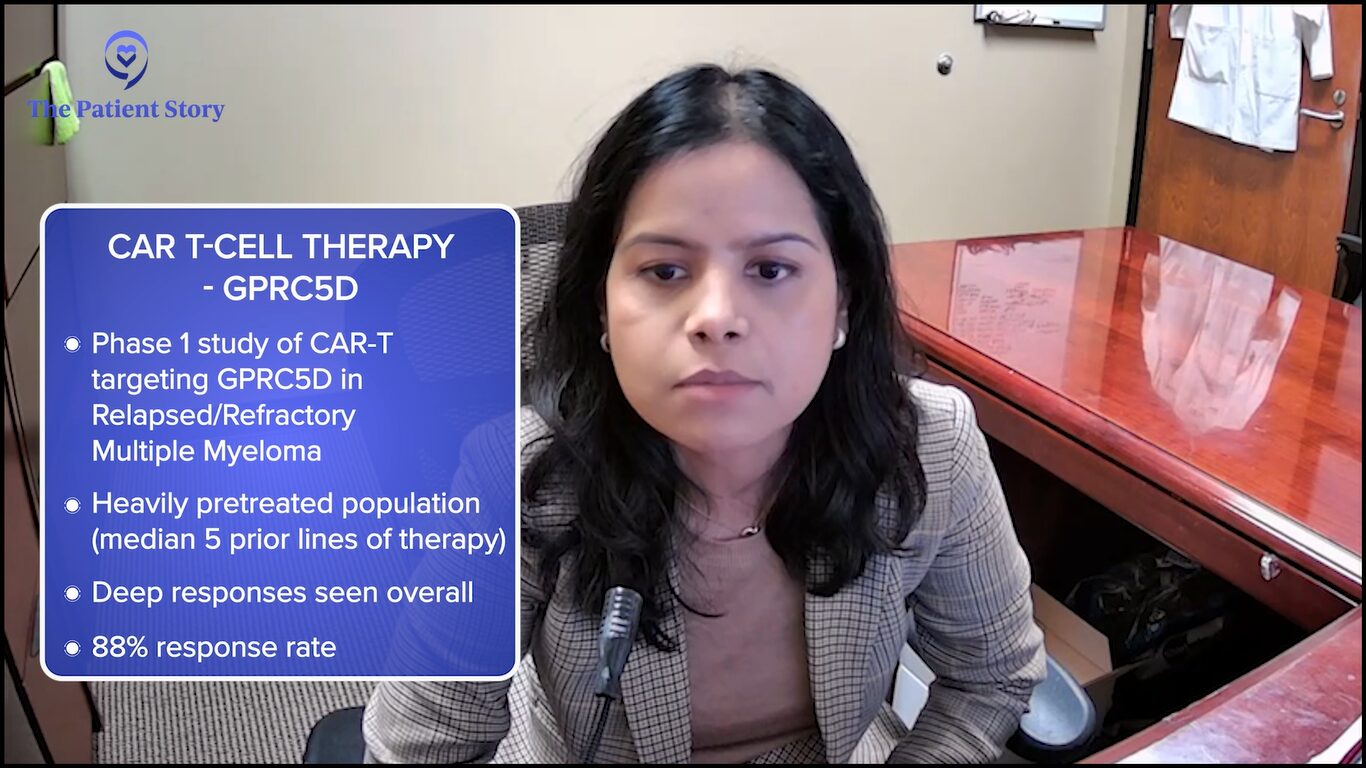
For the first time, we shared the recommended phase 2 dose, which is the dose that’s going to be moving forward. It was determined at about 150 million CAR T cells. What was encouraging was that the response rate for this recommended phase 2 dose was 91%. At that dose level, we saw low-grade CRS. No patient had grade 3 or higher CRS. There were no cases of other serious toxicities, such as macrophage activation syndrome, etc. This dose was efficacious.
So far, the follow-up for this dose cohort is relatively short so we don’t know what the long-term progression-free survival and overall survival are going to be. But the responses are deep. We need to follow the study longer to understand the more important and relevant outcomes, like progression-free survival and overall survival.
If they work well downstream, as is true for every single myeloma drug, we keep bringing them towards the forefront. The results are quite remarkable.
Dr. Rafael Fonseca
Jack: Dr. Bal mentioned that there are a couple of approved CAR Ts available for patients now, except for the fact that they require four-plus lines of prior therapy.
There are trials and announcements of results from those trials, like CARTITUDE-4 and KarMMa-3, that are testing these same CAR T-cell therapies in earlier lines of treatment. Can you talk about the results in relation to a patient’s quality of life?
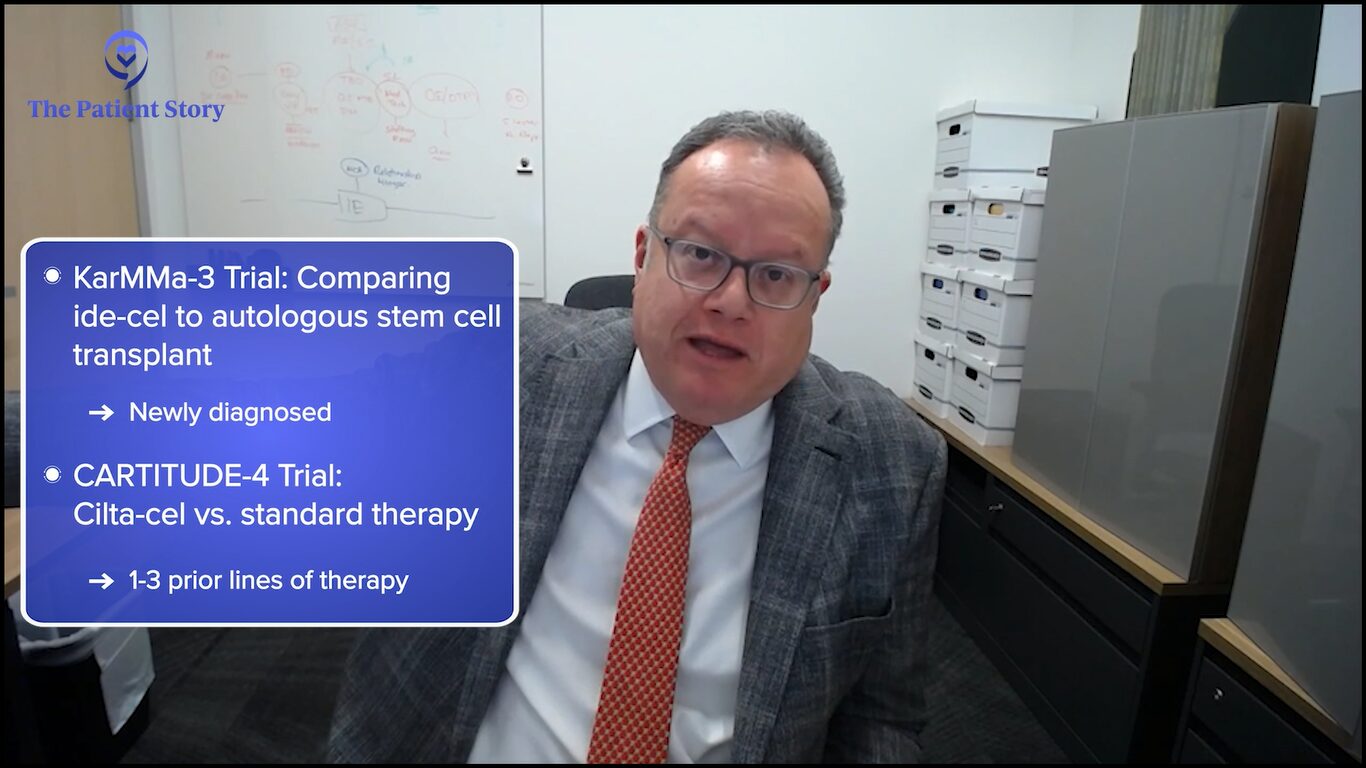
Dr. Fonseca: I think that is probably the key aspect of all of this. As you mentioned, two trials are looking at CAR T-cell therapy earlier on: KarMMa-3 with 2 to 4 prior lines of therapy and CARTITUDE-4 with 1 to 3.
What they explored is if they work well downstream, as is true for every single myeloma drug, we keep bringing them towards the forefront. The results are quite remarkable. Many of you saw the presentations and ultimately the publication of the CARTITUDE-4, which was presented at ASCO as well as EHA and published in the New England Journal.
What we’re seeing is this treatment can provide very durable responses that can go on for years for some patients. Then, of course, the natural question is: how does this compare to other treatments? We have effective treatments that can work very well in someone who is experiencing a first relapse, such as the combination of daratumumab, carfilzomib, and dexamethasone or isatuximab, carfilzomib, and dexamethasone.
But the one big advantage of CAR T-cell therapy is that it’s “one and done.” We’re seeing patients who are reporting very high levels of quality of life and making statements like, “I haven’t felt this well in such a long time.” It’s not because CAR T-cell therapy gives you superpowers. It gets rid of all of the side effects that come with treatment.
Even the most benign of treatments involves logistics, medications, blood draws or venipuncture, and some have side effects that come from the chemicals or the biologics that are used. Even in the best-case scenario, it’s something that the patient has to do. The idea that you’re done and all that needs to be done is occasional labs to monitor becomes very appealing.
I think that’s probably going to be the number one driver. Of course, we’re very excited. We’re hoping to see these treatments have very, very long-lasting benefits for some patients. But even if they were not, for some, the ability to be treatment-free would be beautiful.
I always quote our colleague, Dr. Amrita Krishnan from City of Hope. She said that one of the unmet needs in myeloma is to stop therapy so even if it’s temporary, for some hopefully more durable, this would be a way to achieve that.
Jack: I have patients in my support group who say exactly what you say. Some are without treatment three years after their CAR T-cell therapy but even those who relapsed sooner, like within six or ten months, say they would do it all over again because they had that drug-free period that they were so appreciative of.
We know that patients, after having the CAR Ts, can sometimes have prolonged periods of low blood counts and no one really knows why.
Dr. Rafael Fonseca
Jack: That said, Dr. Fonseca, I want to ask another question about a specific CAR T-cell therapy side effect having to do with secondary myeloid cancers, like acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS). I’m hearing some concerns about that and wonder what your take is on what’s out there.
Dr. Fonseca: First of all, I’m going to say that we don’t completely understand this and many other factors may come into play.
The FDA recently put an announcement that a fraction of patients, up to 10% in the series that was reported, could develop secondary myeloid malignancies. These are the cells that produce your regular white cells and the conditions that follow from that are either leukemia, acute leukemia, or the preceding stage, which we call myelodysplasia, which is concerning as well to us as physicians.
There are many reasons why this could be nothing more than the reflection of patients living longer and patients who have had exposure before to a number of agents and drugs that are clearly known to cause this. This could include things such as melphalan, which is used for stem cell transplant, but also some of the drugs that are used for the priming of the body for CAR T cells, including fludarabine.
On the other hand, there might be other reasons why this could be linked to CAR T-cell therapy. You’re going to hear more about this as people do the research. For instance, we know that patients, after having the CAR Ts, can sometimes have prolonged periods of low blood counts and no one really knows why.
For instance, in the case of BCMA. BCMA is predominantly expressed in B cells, not in these myeloid cells. How come we have myelosuppression? We don’t know for sure. But if you have that, then there are a lot of hypotheses that can come forward. Does that create an environment that maybe selects for clones that are going to do this? Does that create an inflammatory situation that maybe allows for the progression of some of those pre-malignant clones?
The threat is much greater from unattended myeloma. While we want to have perfect treatments with no side effects, for someone who’s considering CAR T-cell therapy, it’s much better to get it than not, despite these considerations.
Dr. Rafael Fonseca
Our audience is familiar with the term MGUS (monoclonal gammopathy of undetermined significance). As you know, we have myeloma and you have MGUS, and this is a prototype of this stepwise progression. It turns out there’s a similar thing that happens for myeloid cells that there’s something called CHIP (clonal hematopoiesis of indeterminate potential) and it turns out to be very common. It’s one of the things that happens to all of us in life as we age. You develop these premalignant states and CHIP is very common. It can be seen in up to 40% of people.
The question is: what are the CAR Ts doing that maybe makes some of this CHIP grow more or the CHIP cells be favored? We don’t know, but this is an important question.
But practically speaking, as of now, the threat is much greater from unattended myeloma. While we want to have perfect treatments with no side effects, for someone who’s considering CAR T-cell therapy, it’s much better to get it than not, despite these considerations.
Jack: They have other options, like bispecific antibodies.
One of the best parts about bispecific antibodies is the fact that you don’t have this lag time or delay that comes with manufacturing associated with CAR T cells.
Dr. Susan Bal
Cindy: Dr. Bal, I hear patients sometimes refer to bispecific antibodies as off-the-shelf CAR Ts and I know they’re not. Can you explain the difference between a bispecific antibody and a CAR T?
Dr. Bal: Bispecific antibodies are antibody fragments. I typically describe them to my patients as a little Y-shaped linker. This is an antibody with two prongs if you will. On one hand, it uses the CD3 molecule to catch the T cell and on the other hand, it has an antigen receptor for one of the myeloma targets.
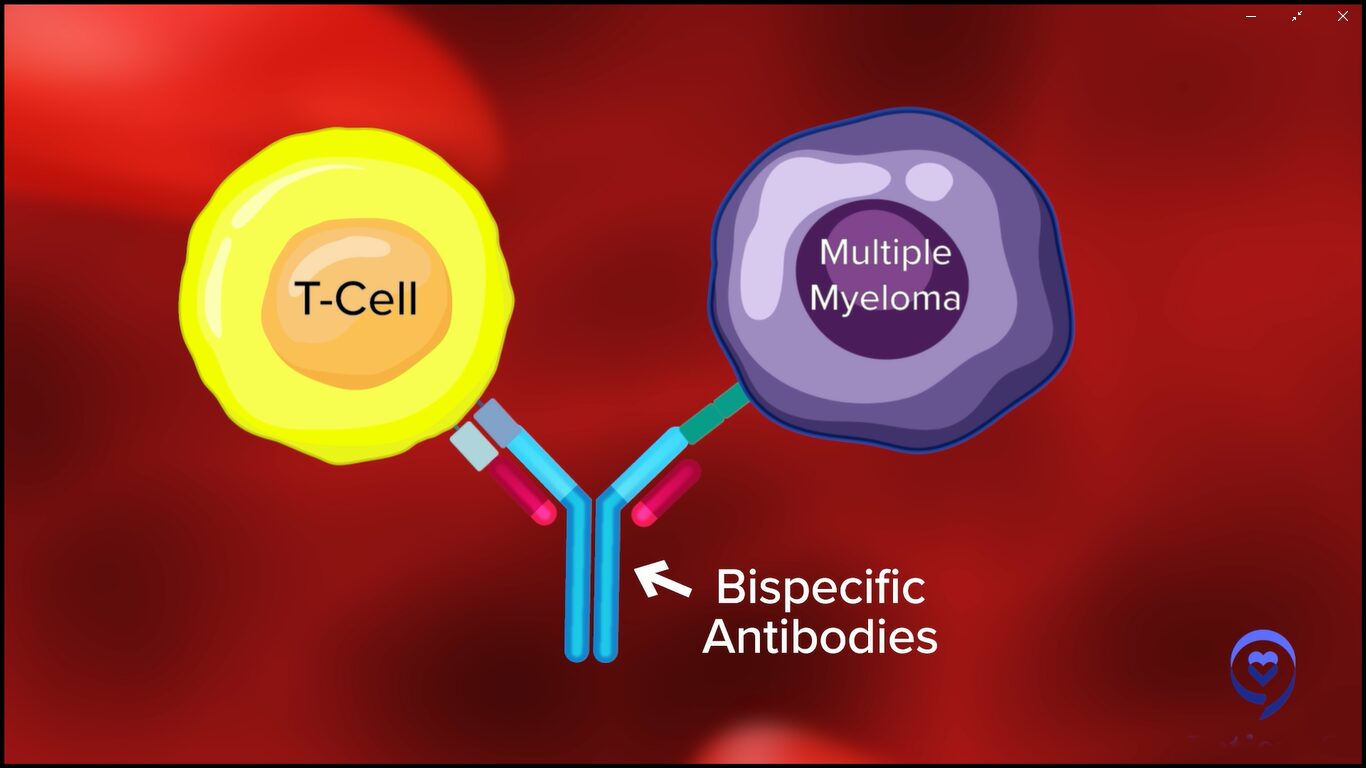
Currently, we have bispecific antibodies that target cancer cells using the same antigens that we talked about for CAR T-cell therapy, such as B-cell maturation antigen (BCMA) or GPRC5D. They target the cancer cell using one of these antigens and bring the two close so that cancer cell killing by the immune system can occur.
One of the best parts about bispecific antibodies is the fact that you don’t have this lag time or delay that comes with manufacturing associated with CAR T cells. These therapies are off the shelf. They utilize the patient’s own T cells, bring them close to the cancer cells, and result in cancer cell killing.
Oftentimes, where we don’t have the time or the manufacturing capability or the slot allocation, or all of those patients who are not necessarily being treated at a large center with CAR T-cell capabilities, this provides an avenue to use new immune treatments and immunotherapies for a wider range of patients. It has the potential to reach many more patients, given the current state of affairs, at least in 2023 and 2024, and so presents a very exciting option for our patients.
Some could argue they don’t have as of yet the same horsepower as some of the CAR Ts. Many of us are thinking of using them down the line, but some of them in combination are incredibly, incredibly active.
Dr. Rafael Fonseca
Cindy: Dr. Fonseca, were there any major updates on bispecifics at ASH 2023 that we should know about?
Dr. Fonseca: We had a number of updates from some of the longer-term outcomes and some of the studies that are looking at bispecifics in various combinations, including with some of the traditional agents. I’m very interested to see how this plays out.
What we’re seeing is that bispecifics, first of all, are very active. Some could argue they don’t have as of yet the same horsepower as some of the CAR Ts. Many of us are thinking of using them down the line, but some of them in combination are incredibly, incredibly active.
There are clinical trials looking at bispecifics in combination with pomalidomide, bispecifics between themselves, and bispecifics with daratumumab in combination. There’s a trial that combines talquetamab and teclistamab, the RedirecTT-1 trial.
We have new constructs that are being developed. We saw a presentation about something called a trispecific so instead of having one side that a bispecific can attach to, there are bispecifics that could attach to two different anchor points that these myeloma cells have.
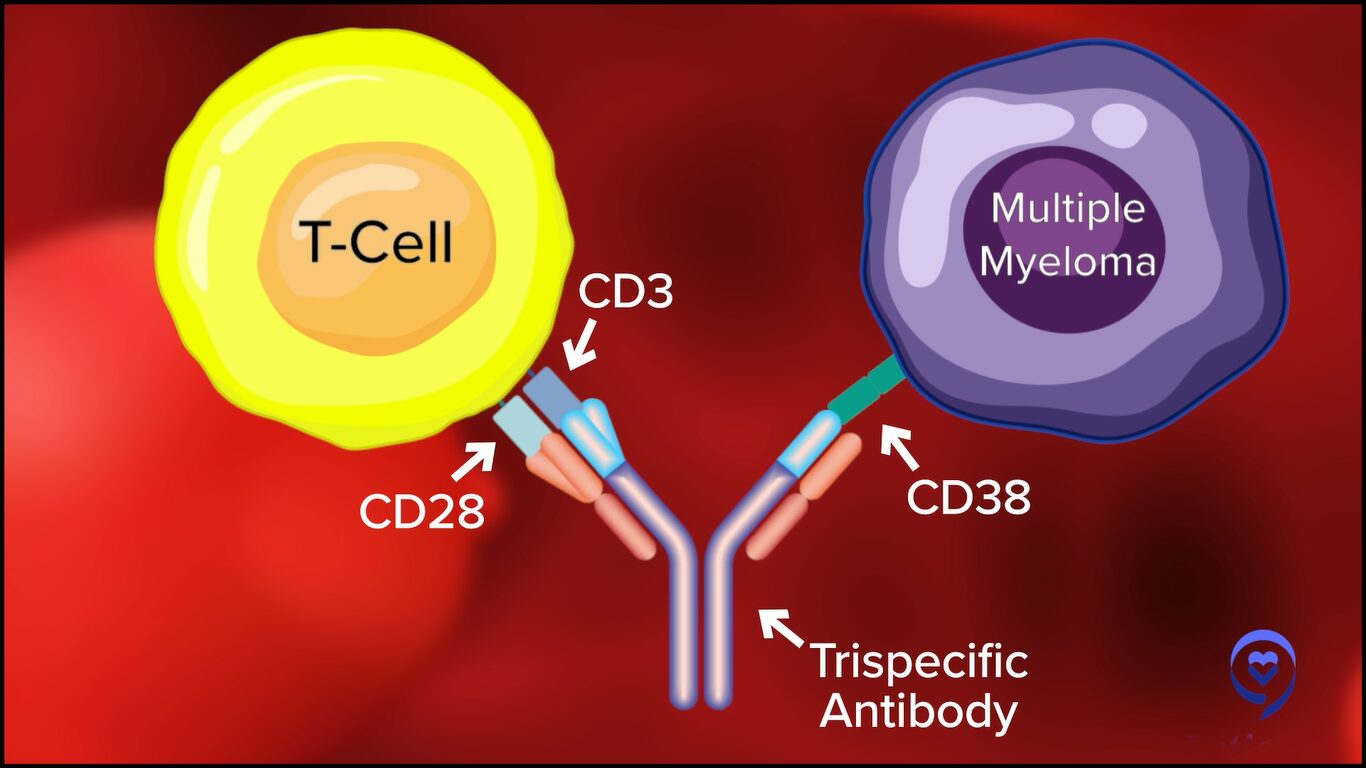
Now, I’m particularly interested in bispecifics because the possibility that many more patients be treated is there for bispecifics than for CAR T-cell therapy. CAR T-cell therapy requires centers of excellence and referral patterns, and there are wait times for cell production. Whereas with the bispecifics, they’re “off the shelf.”
It’s going to take some time. People have to become familiarized with this, but in the future, we’ll see community hospitals and mid-sized hospitals administering these bispecifics, which in my mind is wonderful because many more patients will derive benefit from this type of therapy.
This is the beginning of a new era in cancer treatment because solid tumors are being explored for bispecifics so lung cancer might be treated with this. Oncologists in the future will certainly need to be facile and comfortable with the use of bispecific antibodies.
There’s a lot of push for fixed-duration therapy. One of the greatest reasons, beyond patients having to come to the hospital or clinic and the treatment and travel burden, is the side effect profile.
Dr. Susan Bal
Cindy: Dr. Bal, can you talk about the dosing and schedule of bispecifics?
Dr. Bal: Currently, three FDA-approved bispecific antibodies are on the market. We have two agents targeting BCMA: teclistamab and elranatamab. Both target the B-cell maturation antigen. As of right now, these drugs are typically given on an ongoing basis until disease progression or unacceptable toxicity.
Typically, these start in the hospital with a small portion of inpatient hospitalization. Patients receive step-up dosing to minimize the risk of certain side effects. Afterward, they go on to weekly or every two weeks. In this fashion, they go on until the patients continue to respond or come off due to side effects.
However, patients take a median of a little over a month to respond to these agents and up to about six months to get into a complete response. Often, these responses are very deep. In patients who go off treatment because of side effects, we see that some of these patients can maintain their response for years without treatment.
There’s a lot of push for fixed-duration therapy. One of the greatest reasons, beyond patients having to come to the hospital or clinic and the treatment and travel burden, is the side effect profile. These B-cell maturation antigen-directed bispecific antibodies have a lot of infection risk.
Seventy-plus percent of patients get infections and 40 to 50% of these can often be grade 3 or higher, which can be quite serious. These infection risks, particularly oftentimes infection with unusual things that we don’t typically see in myeloma patients, have also enhanced some of our concerns about using these agents on a prolonged basis in patients whose disease may be controlled.
Multiple factors are at play so there’s a lot of interest in studying fixed-duration therapy of these agents to tailor it to a patient’s response and be able to discontinue these therapies once they’re responding to optimize their risk and benefit profiles.
We know that when we use several agents that target the same anchor, there is a possibility that you could develop resistance so we’ll have to wait and see.
Dr. Rafael Fonseca
Cindy: Dr. Fonseca, we talked about CAR T-cell therapy and bispecific antibodies. Let’s talk about antibody-drug conjugates. We had one that was approved through accelerated approval and then taken off the market but now it may be back. Could you talk about BLENREP (belantamab mafodotin)?
Dr. Fonseca: Antibody-drug conjugates are antibodies that carry a payload. There’s usually a chemical entity attached to an antibody. In general, what happens is the antibodies bind to the cell surface and go inside the cell. They’re eaten into the cell where they release that chemical structure.
One of those antigens is belantamab. When it first started, it showed very, very high rates of response. Quite promising responses. It went through regulatory approval for a fast-track approval.
Unfortunately, there had to be a confirmatory phase 3 trial that did not meet the endpoint. That means that the data for the trial would not support the complete approval by the FDA. The product has been since withdrawn from the market but is available on a compassionate basis.
This is a highly active compound. It comes with some baggage. One of the main baggage is toxicity to the eyes. Something we call keratopathy and that’s inflammation of the outside layer of the eye, the cornea. As we’re learning how to use it in better doses, that has been a little bit better tolerated. It’s not to say it doesn’t exist, but people are understanding better how to use this.
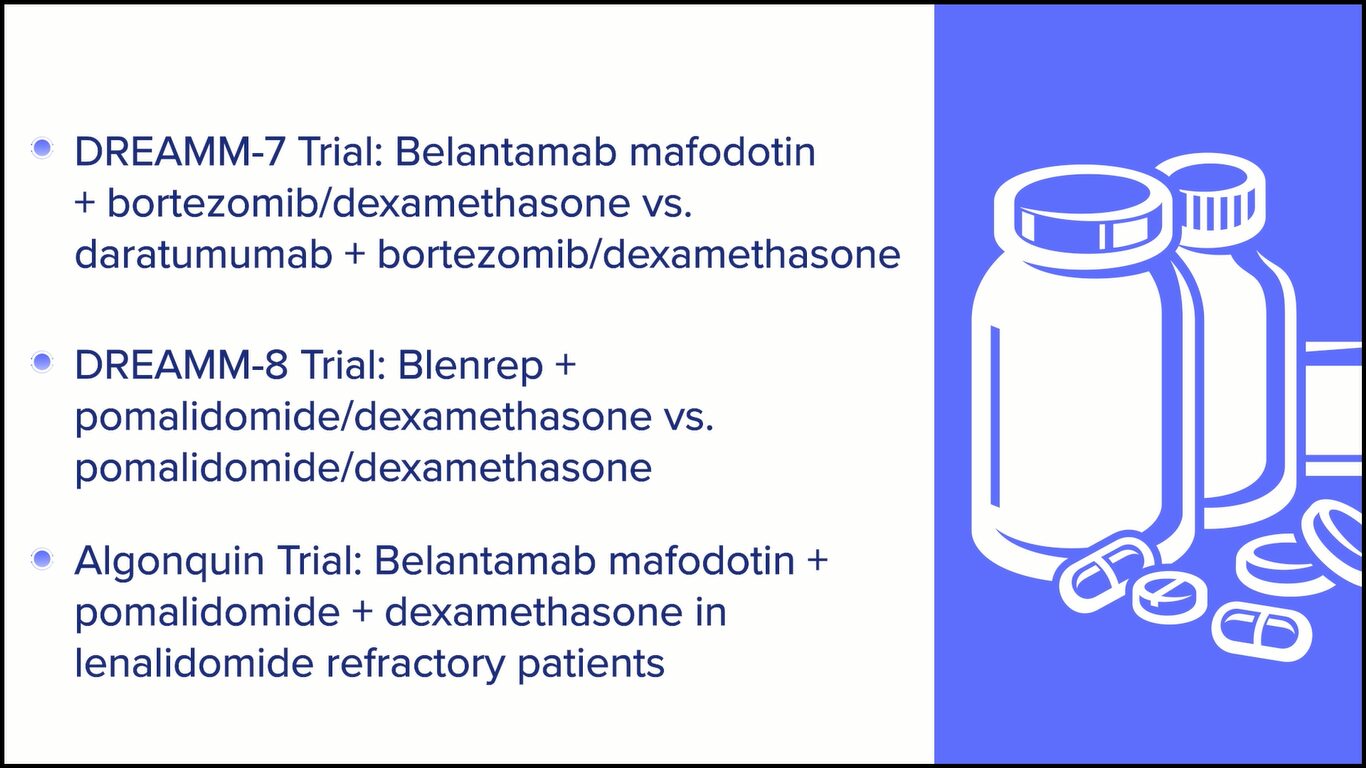
We learned about two very exciting trials. One of them is the DREAMM-7 trial, which was belantamab, lenalidomide, and dexamethasone versus daratumumab, lenalidomide, and dexamethasone. We’re told the trial is positive meaning there are favorable effects of the belantamab. We’ll have to see what the actual numbers show.
There’s another one that was recently published called the ALGONQUIN clinical trial, which is a combination of belantamab, pomalidomide, and dexamethasone, which has pretty interesting results.
The question is going to be: how do we time all of this? Belantamab targets BCMA as well, too, so that means it could compete with bispecifics and CAR Ts. We know that when we use several agents that target the same anchor, there is a possibility that you could develop resistance so we’ll have to wait and see.
ADCs are one of the hottest things right now in biotech and development for solid tumors as well, too. I heard from people who were at one of those recent conferences that a lot of companies are interested in them. I think we’ll see a comeback of ADCs in myeloma and in other diseases as well, too.
I have patients right now who are still enjoying the benefits of the prior administration of belantamab.
Dr. Rafael Fonseca
Cindy: Do you think Blenrep will be coming back on the market?
Dr. Fonseca: It’s interesting. I’m not currently up to date on what the regulatory pathway will be for that to occur. I think it will, but the results are exciting. The question is how this will compare to some of the other things that I’m mentioning with bispecifics.
I have patients right now who are still enjoying the benefits of the prior administration of belantamab. They have since resolved the eye toxicity. In all cases, with time, the eye toxicity improves. These are patients that may have gotten a short course of treatment with belantamab and remain under excellent control right now.
It’s always better to have more options. I don’t think I would venture out to say exactly how we’re going to sequence this because of the issues of resistance, but I certainly would welcome having that back in our toolkit.
Cindy: I agree. More options are better because we’re also unique and what works for one person may not work for somebody else so I’m glad to have as many bullets in our arsenal as possible.
BCL2 inhibition has a place and hopefully, we’ll find FDA approval soon so we can use it more freely and benefit this unique subset of patients.
Dr. Susan Bal
Jack: Dr. Bal, venetoclax is well-known out there. It’s an approved drug for chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL), but it gets used off-label in myeloma patients who have a translocation called t(11;14). At ASH, something called sonrotoclax was introduced as the next-generation venetoclax. Do you have any comments about that particular new drug?
Dr. Bal: Translocation t(11;14) myeloma is a subtype of myeloma that’s a little bit of a different disease itself. It’s a distinct entity and a distinct subtype of myeloma, which responds a little bit differently to different agents. It has a higher dependency on BCL2 inhibition, which is a key part of what drives this myeloma and, therefore, inhibiting it in this space helps drive treatment responses.
We know venetoclax is an effective therapy. Unfortunately, the randomized trials have not worked very much in favor of it. However, those of us who use it and single-arm studies have shown impressive responses in this subset of myeloma patients.
At the ASH 2023 meeting, we looked at a novel BCL2 inhibitor, which is supposed to be at least 10 times more effective and more selective for BCL2 inhibition. It’s called sonrotoclax and they are studying it in a phase 1 setting in several countries. They’re looking to first get the right dose and then expand it in combination with carfilzomib to best understand how these patients respond.
We know venetoclax is an effective therapy. Unfortunately, the randomized trials have not worked very much in favor of it.
Dr. Susan Bal
What we have seen at ASH 2023 was a result from about 19 patients, 10 of whom got the recommended phase 2 dose, which is going to move forward in studies. What we saw was very impressive single-agent activity in combination with dexamethasone at the recommended phase 2 dose of 70%.
What was even more impressive to me was the complete lack of dose-limiting toxicities. There were really minimal side effects that would prevent dose-finding and dose escalation, and a very low risk of low blood counts, which was something that we thought we would see.
The drug was very, very well tolerated. I recall maybe a single patient with high-grade diarrhea and maybe a COVID-19 infection, which was ongoing during the study. Overall, the safety profile is very impressive with responses in combination with dexamethasone of 70% at the recommended phase 2 dose. As the study accrues more patients and studies combinations with carfilzomib, I think it will be exciting.
I will also touch on some of the data that was presented by Dr. Bahlis, which was venetoclax in combination with daratumumab, which showed very impressive responses. Although the patient population was less heavily pre-treated and mostly daratumumab-naive, response rates and measurable residual disease negative states were very, very impressive. BCL2 inhibition has a place and hopefully, we’ll find FDA approval soon so we can use it more freely and benefit this unique subset of patients.
The long-term use of dexamethasone is not contributing much to the control of the disease and we know for sure it’s contributing to the burden of side effects.
Dr. Rafael Fonseca
Jack: Dr. Fonseca, we patients always appreciate it when we learn that doses can be reduced. When we hear that dexamethasone dosing can be reduced, we get giddy about it.
At ASH 2023, there was a presentation that looked retrospectively at a couple of SWOG trials, S0777 and S1211, which looked at patients who had lower dex dosage. Can you talk about that and what that might mean for patients going forward?
Dr. Fonseca: Whenever we discuss treatments with a patient, I usually emphasize that the hardest part is probably going to be the dexamethasone, for reasons you know better than I do. It all started several years ago with a patient, Michael Katz, who said, “We get too much dexamethasone. What can you do about that?” That led to the design of E4A03, which changed our paradigm that we now use dexamethasone at what we call “low doses.”
When my endocrinology friends see those doses, they tell us, “What are you doing? This is a massive dose of dexamethasone.” That was a significant change. We used to use 12 days per cycle, that is 12 out of 28 days at 40 mg of dexamethasone.
We’ve moved forward but have not completely gotten rid of it. From what we know now, as you go on with treatment, as shown by the studies mentioned, as the patient gets stabilized, it becomes increasingly clear that the long-term use of dexamethasone is not contributing much to the control of the disease and we know for sure it’s contributing to the burden of side effects. It should be noted that several studies are showing that. Clinicians need to be cautious and need to adjust the doses of dexamethasone.
In the beginning, most of us feel that patients need a little bit of dexamethasone to “jump start” a good response. But even then, you can do some dose adjustments. In patients of more advanced age, we often will use 20 mg instead of 40 mg. As well, in patients who have amyloidosis, we’ll make adjustments like that.
Is there a way by which we can tell who is going to benefit from the addition of the steroids?
Dr. Rafael Fonseca
It’s important to be mindful of this because patients should not be on 40 mg of dexamethasone once a week for a long time. In general, this is not something that we should be using long-term for maintenance. It can be used short-term for consolidation or other reasons.
The field continues to move in that direction. One patient once asked me, “You always talk about lenalidomide resistance, but you never say dexamethasone resistance. How do you know if it’s contributing down the line?” That is one question that we need to go back and address.
At the beginning of myeloma drug development, there were a lot of people who were interested in resistance to steroids, like Dr. Steve Rosen from City of Hope, and we abandoned that line of thinking. We need to go back and say: is there a way by which we can tell who is going to benefit from the addition of the steroids?
Sometimes, myeloma is very aggressive and very difficult to control. But please don’t assume that because you’re facing this diagnosis, there’s an imminent threat that for sure will be life-limiting because the treatments continue to get better.
Dr. Rafael Fonseca
Cindy: If you had one key takeaway that you want patients to hear, what would it be?
Dr. Bal: For me, the most exciting thing in myeloma right now is immunotherapy. The prospect of these new agents that use our immune system to kill cancer cells is really innovative and exciting. I can’t wait to understand how best we can use these strategies to provide fixed-duration treatment and lead to the longest possible remission in a low or undetectable cancer state, such that our patients can have an excellent quality of life.
Dr. Fonseca: We’re very excited and positively so because of the developments in myeloma. We fully realize it would be better to meet you in social circumstances or at coffee somewhere else. But right now, if you’re diagnosed with myeloma, for many, many patients, there are options such that myeloma should not be an immediate threat.
In fact, for many patients, we develop this relationship, as Dr. Bal was saying, and then we track along with you for years and even decades for some patients. It’s not unusual for us to see patients in the clinic well beyond 10 years, sometimes 15 and 20-plus years. I am convinced some of those patients have been cured because of effective frontline therapy. But even for those who haven’t, there are often times options for treatment.
Unfortunately, I know this is not a reality for everyone. Sometimes, myeloma is very aggressive and very difficult to control. But please don’t assume that because you’re facing this diagnosis, there’s an imminent threat that for sure will be life-limiting because the treatments continue to get better.

Jack: For any myeloma patient and care partner, stay educated. There are so many new treatments coming so quickly for myeloma and they are for different target audiences: newly diagnosed as well as relapse patients.
One way to stay educated is to listen to programs like this. Check out the myeloma advocacy websites that offer webinars and videos. Join a support group and make sure to understand the best questions to ask your doctor.
Cindy: It’s important for patients to be seen by a myeloma specialist. Anytime a patient has to have a treatment decision to make, it’s imperative that they get guidance from a myeloma specialist. There are so many new treatments available, new data being presented on different treatments that are now coming to market, and clinical trials so it’s overwhelming.
Stephanie: Thank you so much, Jack and Cindy, for being our incredible patient advocates and moderators. Also to Drs. Fonseca and Bal for the work and research you do to help move the landscape of treatment options in multiple myeloma.
We hope that you walk away with a better understanding of the latest treatments and clinical trials in myeloma. They may or may not be right for you, but it is our goal to make sure you feel empowered to make a decision for yourself.
Thank you and we hope to see you again at a future program at The Patient Story.





Edited by:
Katrina Villareal
Led by patient advocate Cindy Chmielewski, this enlightening session features experts Dr. Carl Ola Landgren (Sylvester Comprehensive Cancer Center, University of Miami) and Dr. Caitlin Costello (University of California San Diego). Together with Clinical Trial Nurse Christen Hawthorne (The Leukemia & Lymphoma Society), they will uncover groundbreaking insights
Learn about new multiple myeloma treatment classes and combinations, including advances in BCMA-targeted therapies, like CAR T-cell therapy and bispecific antibodies. Find out the future of belantamab mafodotin combinations in relapsed/refractory multiple myeloma. Acquire clinical trial knowledge and bust common misconceptions about clinical trials.
Brought to you in partnership with The Leukemia & Lymphoma Society and its Clinical Trial Support Center.
Stephanie Chuang, The Patient Story: My name is Stephanie Chuang, founder of The Patient Story. A few years ago, I had a diagnosis of non-Hodgkin lymphoma, but we have so many shared experiences in what we’re looking for.
The Patient Story tries to help both patients and care partners navigate life after a cancer diagnosis and we do this primarily through in-depth conversations with patients, care partners, caregivers, and top specialists across cancers.
We believe it’s especially important to have these educational programs specifically for patients, family members, and supporters when it comes to topics like clinical trials, which can sound daunting and have lots of jargon so our goal is to humanize your options.
We’re so proud to be co-hosting this with The Leukemia & Lymphoma Society, a great partner of ours. It’s the world’s largest nonprofit health organization dedicated to funding blood cancer research that is so critical as well as offers patient services and education.
They have great resources, including information specialists who are a phone call away to help answer your cancer questions. We’ll be highlighting the LLS’ Clinical Trial Support Center or CTSC, which is a huge free resource that offers one-on-one support to enroll and stay in clinical trials.
We want to note that The Leukemia & Lymphoma Society and The Patient Story retain full editorial control of this entire program.
This is not meant to be a substitute for medical advice. We want you to walk away and be able to go to your own medical team with questions and more knowledge to make more empowered decisions.

Stephanie: Our first incredible panelist, a myeloma patient voice, and leader in the community, Cindy Chmielewski, will be leading this conversation from this point forward.
Cindy, I know you’re going to share more about your own story and how you became such a passionate advocate, but we would love to learn more about you because as we know, we are so much more than a diagnosis.
Cindy Chmielewski: Hi, everyone! My name is Cindy Chmielewski and I’ve been living with multiple myeloma since 2008. Prior to my myeloma diagnosis, I was a fifth-grade teacher.
Since being diagnosed with myeloma, I realized how important it is for patients to be part of their care and educated so they can be part of the decision-making process. Now I’m using my teaching skills to help myeloma patients learn more about myeloma so they can engage in discussions with their doctors.
Cindy: We have Dr. Caitlin Costello, a hematologist-oncologist and associate professor of medicine at the University of California San Diego. She specializes in treating blood cancers with a focus on multiple myeloma. She also participates in a number of clinical trials that offer cutting-edge treatment strategies and therapies for myeloma.
Dr. Costello, what drew you to myeloma and what’s your passion for helping patients?

Dr. Caitlin Costello: It’s people like you who draw us into the things we love. Multiple myeloma satisfied a lot of my interests. The science of myeloma exploded during the course of my career, which really satisfies the academic side of my brain.
I didn’t want to go into oncology when I was doing my training. I find such passion and reward in connecting with my patients. At the very beginning of my training, I felt like cancer oncology was not going to allow me to have long-standing relationships with patients because of the biology of the disease and the outcomes associated with it.
I found myeloma and it satisfied both. It let me find that scientific side and let me have enduring relationships with patients as myeloma patients live long with this cancer. Sometimes things fall into place and I’m so grateful for that.
Cindy: I’m so glad that we are living much longer. We do develop relationships with our doctors because we’re in ongoing treatment so we’re seen for a very, very long period of time.
Cindy: Dr. Carl Ola Landgren is a hematologist-oncologist at the University of Miami Sylvester Comprehensive Care Center. He is a professor of medicine, chief of the myeloma division, and co-leader of the Translational and Clinical Oncology Program. He also has a strong interest in the development of early treatment clinical trials.
Dr. Landgren, what drew you to myeloma, and what drives you most to continue your work with helping patients?
Dr. Carl Ola Landgren: I’ve been in the field for quite a few years; almost 30 years since I started my career.
When I was in fellowship, the senior doctors were saying there are two diseases you should stay away from, chronic lymphocytic leukemia and multiple myeloma, because there had been so little development in those disease areas.
I thought, That sounds like a really great opportunity. We need to go there. We need to do more investigation and see if we can change that. I was drawn to that and initially started working on both. Over time, I picked multiple myeloma as the disease that I was most interested in.
It’s been spectacular to be part of this journey together with so many other colleagues and friends around the world, with all the development of new drugs, and all the new technologies.
Over three decades, we are at a very different place. I’m very, very happy about it. All my research is centered on patient needs. I’m dedicated to driving the research forward.
Cindy: Thank you for choosing myeloma. We’re very lucky to have you because I’ve seen all the work that you do.
Cindy: I would like to introduce Christen Hawthorne from The Leukemia & Lymphoma Society, a nurse navigator with the Clinical Trial Support Center. Christen, share a little bit about yourself and what made you become a clinical trial nurse navigator.

Christen Hawthorne: I’m originally from northern New York, but moved to Denver, Colorado, in 2015 to pursue a career in cancer care. Since then, I’ve specialized in the area of bone marrow transplants and worked with patients who have a blood cancer diagnosis at different stages in their treatment plan.
My grandfather, unfortunately, passed away from cancer. I was so inspired by the holistic care that he received not only when he was in the hospital but also from my grandmother, who’s a retired registered nurse. Seeing that care and devotion, both professionally and personally, inspired me to pursue a specialty that allowed me to care for people beyond the clinical landscape and really focus on them as a person.
I’ve volunteered for The Leukemia & Lymphoma Society since 2015, fundraising for Light The Night and as an advocate with their Office of Public Policy. Seeing the many different pillars at LLS and how they support patients and families inspired me to pursue a position within the organization, joining the CTSC team in 2022.
Clinical trials and research are critical pillars of cancer care. They are how efficacious treatments are developed with the hope of fewer side effects and better outcomes. I hope I’m able to shed some light on their importance, dispel myths, and share additional resources.
Cindy: The myeloma landscape has changed over the last decade or two for clinicians, researchers, and patients.
When I was diagnosed in 2008, there were very, very few treatment options. Most of what’s available today were not available. Induction therapy was normally a doublet. Eventually, it became a triplet. Now we have quadruplets.
Back in 2015, there was something called the November to Remember and it was in that November when three myeloma drugs got approved within weeks of each other. We had our first two monoclonal antibodies and an oral proteasome inhibitor. It seemed like a great time.
But since then, we’ve had so many more drug approvals that I can’t even keep track of them — CAR T cells, bispecific antibodies, and the next generations of some of our other drugs. It really is an exciting time.
With all these drugs coming into the market, it’s so important that myeloma patients work with the myeloma specialists because there are so many combinations. How do you sequence them? What’s best for you? Are there any biomarkers that will help predict what would be a better outcome for you?
The landscape is changing, which is exciting, but we have a lot of work to do to figure out the best combination for each patient.
Multiple myeloma is technically a cancer of a cell called a plasma cell, which is an important part of your immune system.
Dr. Caitlin Costello
Cindy: Dr. Costello, can you briefly describe what multiple myeloma is and some of the signs and symptoms of multiple myeloma?
Dr. Costello: It’s so important to do myeloma 101. Patients can advocate for themselves if they understand the basics of the disease.
Multiple myeloma is technically a cancer of a cell called a plasma cell, which is an important part of your immune system.

When they do that, they don’t work like they’re supposed to either. Now you have cancerous plasma cells that are not working the way they’re supposed to and they start producing abnormal proteins.
Your body, your immune system, and your plasma cells are supposed to produce a variety of different proteins or antibodies to fight the bad guys. But when one plasma cell goes rogue and starts copying itself, it starts prioritizing to make one form of those antibodies relative to the rest of them. Those bad antibodies get produced and find a way to run around the body and wreak havoc a bit.
Significant fatigue, shortness of breath, and lightheadedness are some of the most common symptoms that patients come to get medical help for when they’re first diagnosed with myeloma.
Dr. Caitlin Costello
Dr. Costello: Myeloma can affect your body in a variety of ways, one of which is having an interest in the bones. There are a couple of different ways it affects the bones. I like to think of it as a little Pac-Man. It takes little bites out of the bones or can almost form little tumors within the bones and that can hurt.
A lot of patients who are first diagnosed with myeloma say, “I have this pain. I don’t know why it’s there and it’s not going away,” and they seek care for that. Sometimes it can take a while to get to a diagnosis of multiple myeloma, but bone pain is a common presenting symptom.
Another common presentation is fatigue and this is hard because we’re all tired; life is hard sometimes. Fatigue can happen because of anemia.
Multiple myeloma is a problem in your bone marrow, which is the factory not only of your immune system but also of your blood. If your bone marrow is busy making cancerous cells, there’s not enough room to make the normal blood you need. That decreased production known as anemia can really produce symptoms of significant fatigue, shortness of breath, and lightheadedness.

Those are some of the most common symptoms that patients come to get medical help for when they’re first diagnosed with myeloma.
Cindy: They were the two symptoms that brought me to the doctor. I had terrible back pain and I was so tired and out of breath.
A big step forward in the field has been the evolution of all the different options. It’s no longer a matter of picking A or B. We pretty much have the whole alphabet to present.
Dr. Carl Ola Landgren
Cindy: We’ve had a slew of new treatments. When you think about what treatments a person should be on, what are some considerations that you weigh? What do you think about when they’re transplant eligible or ineligible, newly diagnosed versus relapsed/refractory?

Dr. Landgren: A big step forward in the field has been the evolution of all the different options. It’s no longer a matter of picking A or B. We pretty much have the whole alphabet to present.
There are very many options and it starts in the newly diagnosed setting. If someone has a recurrence, there are many options looking at the guidelines that dictate what we’re allowed to prescribe. Based on the NCCN Guidelines, there are over 40 different combinations in the setting of relapsed/refractory disease.
When I have a newly diagnosed patient, I have to think if this person is a potential transplant candidate or not. That has also shifted over the years because we can technically transplant many more patients than we could before. We can transplant people who are older and even those with comorbidities.
On the flip side, I personally think that the need for transplants has probably gone down. There are so many new treatments so we could do more. But in reality, I think we do less and I think the numbers point in that direction as well.
Cindy: I’m glad you include the patient. Shared decision-making is always the best.
We have to understand the difference between a long, durable remission, which means it goes away and stays away for some great period of time, versus a cure, which means it ain’t ever coming back, which is what we’re all aspiring to.
Dr. Caitlin Costello
Cindy: Is there a treatment that can cure myeloma or put myeloma in a really deep remission? A few years ago, doctors were very hesitant to use the word cure. They were talking about controlling myeloma and keeping it at bay for several years, but I never heard the word cure. But more recently, I’ve heard the word cure and doctors are thinking that maybe we are curing some patients.
I talked to lots of patients and one of the most common questions I hear is what treatment works the best. Should I be on three drugs? Should I be on four drugs? What should I have? They also want to know: is there a cure for myeloma?
The words myeloma and cure were never used in the same sentence by myeloma specialists, but things began to change. I started hearing myeloma doctors say, “Yes, I think we may be curing some patients and maybe in 10 years, we’ll be curing more patients.”
Dr. Costello, can you talk about your perspective on a cure for myeloma?
Dr. Costello: This is the other C word. The big C we think about is cancer, but the cure word is becoming something we’re really starting to flirt with. Over the last couple of years, we’ve seen this explosion of new medications.
In the last two decades or so, we have seen the number of options for treatment go from a few to a wide variety of options that let people get into remission and stay in remission for very durable long periods of time. We’re starting to see that happening for such long periods of time that we’re saying, “Is it ever coming back?”
We have to understand the difference between a long, durable remission, which means it goes away and stays away for some great period of time, versus a cure, which means it ain’t ever coming back, which is what we’re all aspiring to.

I think we’re getting there. I always tell my patients, “In my lifetime, we’re going to do this. We absolutely are going to do this.” We’ve seen too much change in the last decade or two decades to not reach that point.
This is not a one-size-fits-all type of cancer. Although multiple myeloma is grouped together as one form of blood cancer, there are very different subtypes and very different forms of myeloma that act differently. Some are easier to treat and may go away, others can be a little bit more stubborn.
When we’re thinking about ideal treatments for any individual person, we have to look at you as a person, your health, your social situation, and your support. Then we have to look at the biology of the disease and put all of that together to figure out the best means of achieving a cure.
With more and more of these drugs delivering great, deep, durable responses, it’s natural for the field to talk about it.
Dr. Carl Ola Landgren
Dr. Landgren: I do think we are heading towards a cure. There are multiple reasons that the field has not talked about that cure for myeloma in the past. Quite frankly, the drugs were not good enough. We used to have 1 or 2 drugs for many years, way before I started practicing.
Then there was the emergence of high-dose chemotherapy with melphalan, the so-called transplant. Then there was the rediscovery of IMiDs with Dr. Bart Barlogie’s discovery of thalidomide that led to lenalidomide and pomalidomide. We had proteasome inhibitors coming around. Then we had all the immunotherapy.
The field has evolved. We see many patients achieving remissions and minimal residual disease (MRD) negativity so there is no detectable disease. When you don’t have those perspectives, it’s not really something brought up frequently with cure. With more and more of these drugs delivering great, deep, durable responses, it’s natural for the field to talk about it.

There is really no definition in the literature. What is the definition of cure? It’s true for any disease. If you were to survey myeloma experts and ask how they define cure, you would probably get very different answers.
If you ask me what I think, someone who has been treated with effective therapy and repeatedly shows no detectable disease is, at some point, probably cured.
If you put me on the spot and say how long that window is, then I will start going back and forth but maybe five years or so is a reasonable endpoint. Can you be 100% sure that the disease will never come back? Probably not, but life is filled with a lot of unknowns.
Many patients in my clinic are cured. Many of those patients come from Dr. Barlogie, who used to treat a lot of patients in Arkansas. He gave every drug under the sun. When he moved to New York, I was the chief of the Sloan Kettering myeloma program then he retired. When he retired, many of those patients were looking for another doctor and came to me. Then I moved to Florida. Many of those patients followed me to Miami.
I had many of his former patients who were treated for five years and then stopped treatment. I have patients who have been off treatment for 20 years. They remain off treatment and are doing very, very well.
Cindy: Thanks for giving me hope that you think there’ll be a cure in my lifetime so that makes me smile.
All drugs have to move through steps or phases to ultimately be approved by the FDA.
Christen Hawthorne
Cindy: We have a new section called Trial Knowledge where we’re going to give you some knowledge about clinical trials and maybe do some myth-busting of things we’ve heard.
Christen, there are different phases of clinical trials. Can you talk about what happens in each of those phases?
Christen: I like to think of clinical trials as steps to drug approval. All drugs have to move through steps or phases to ultimately be approved by the FDA. If drugs are studied in new combinations or in diseases outside of the approved indication of the drug, they still have to go through these phases.
In phase 1, we’re investigating the safety, side effects, dosing, and best way to administer treatment. This is usually in 20 to 100 patients.
In phase 2, we’re determining the effectiveness and safety of the study drug in about 100 to 300 patients.
In phase 3, we’re looking at the effectiveness, side effects, and safety of the study drug in comparison with other treatments. This includes anywhere from a few hundred to a couple thousand patients.
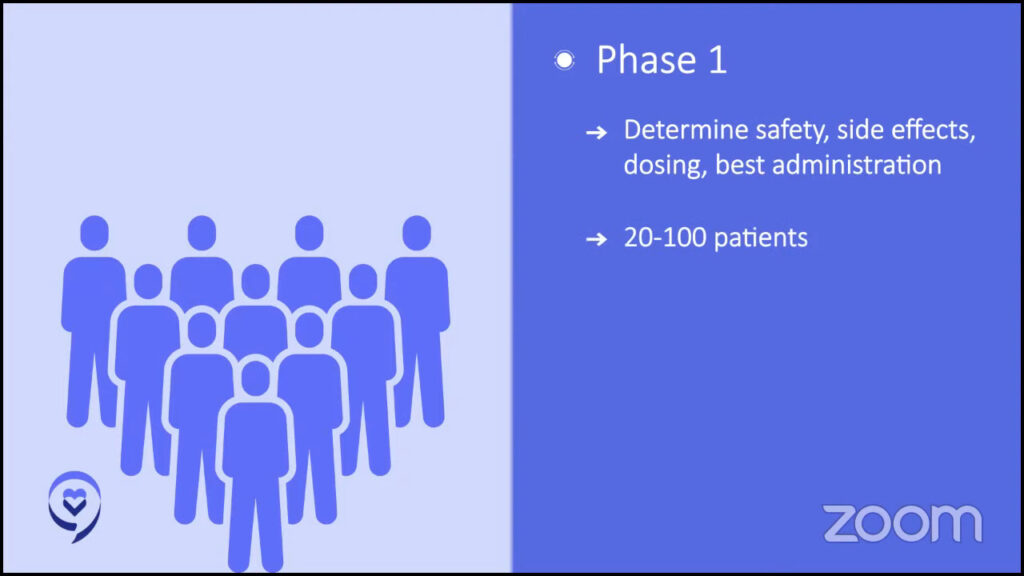
No one with active cancer would be treated with only a placebo as that is unethical.
Christen Hawthorne
Cindy: One thing I hear from lots of patients and care partners is that they really don’t want to consider clinical trials because they’re afraid that they’re going to be given a placebo. With cancer, you don’t want to be given a placebo. Can you talk about placebos and how they are used in cancer trials?
Christen: It’s definitely a common one that we get from our patients.
Federal regulations require patients to know if a placebo or a substance that looks the same as the one used in the treatment but is inactive will be used in a trial. Placebos are not typically used with patients in cancer care trials. The decision of whether to use a placebo in a clinical trial is based on how serious the illness is or if the disease is life-threatening.
Patients with these types of diseases are given the best available treatment or standard of care instead of a placebo. If used in cancer clinical trials, the placebo will be in combination with active drugs so you’re at least receiving the standard of care. No one with active cancer would be treated with only a placebo as that is unethical.
Cindy: It’s good to know that if there is a placebo, it’s in addition to the standard of care that you normally would be receiving. You will never be given just a placebo alone.
Clinical trials are a very complicated care landscape to navigate. The mission of the Clinical Trial Support Center is to help patients and caregivers identify potential clinical trials and overcome the barriers to enrollment.
Christen Hawthorne
Cindy: Christen, how do patients find clinical trials? I know there’s ClinicalTrials.gov, but it’s not the most user-friendly. You might end up with hundreds of trials when you search for them and you won’t know what’s right for you. Can you talk about how The Leukemia & Lymphoma Society can help?
Christen: Clinical trials are a very complicated care landscape to navigate between understanding what institutions are participating in certain trials, their inclusion and exclusion criteria, and what might be the best match for your unique profile. It can be really overwhelming.
The national average of cancer clinical trial enrollment is only between 5 and 10%. We found that, on average, our team has 22 interactions on behalf of a patient from the initial assessment to the time of enrollment — that’s 22 potential holes in the road where patients or caregivers could fall through. We’re able to fill those holes in 23% of eligible patients that we work with enroll in a clinical trial.
Resources within the LLS, including the Clinical Trial Support Center, collaborate with your care team, helping equip you with the knowledge to support you and to help you feel confident in making an informed decision about your care.
Our support center is a team of nurses and nurse practitioners who work one-on-one with you and your family to understand your unique clinical situation while getting to know you as a human, providing support that aligns with your goals of care.
Our mission is to help patients and caregivers identify potential clinical trials and overcome the barriers to enrollment.
We start with an initial conversation to learn more about you, your goals of care, your treatment plan, and your past medical history. From there, we begin a search based on the information provided, including ability and willingness to travel, insurance concerns, and any other factors specific to you.
Once our search is complete, we provide a comprehensive but easy-to-digest list of potential trials and resources to review with your care team. If there is an appropriate trial to pursue, we can reach out to the clinical trial sponsor or specific site with any questions or find out the next steps to enroll on your behalf. Throughout this process, we remain available to support you and answer questions along the way.
You can connect with one of our information resource specialists. They are happy to assist you in filling out the form and we can connect to get to know you and do a thorough assessment.
Cindy: Sometimes staying on a clinical trial may be difficult. Can you explain some of the things that the LLS can do to help patients stay on a trial?
Christen: In the Clinical Trial Support Center, we’re able to understand your unique clinical situation before providing a comprehensive list of trials to review with your care team. We also provide continuity of care by working with you and your family throughout your diagnosis and this could be months to years long. We continue to understand your evolving goals and tailor our support to meet them.
We do have regular meetings with sponsors of clinical trials to understand patient requirements of the trial and if there are additional support opportunities for patients or families to cover travel and lodging expenses associated with trial participation.
While we provide education and resources to our patients within the CTSC, we also have an incredible network of information resource specialists, the financial assistance department, and patient and community outreach managers who can help support patients throughout their care plans in unique ways.
Clinical trials exist at every part of the journey with myeloma and they really offer opportunities for patients.
Dr. Caitlin Costello
Cindy: A newly diagnosed patient is someone who’s just starting treatment. In my mind, I always thought that clinical trials would be for later down the line when you’re running out of treatment options.
Dr. Costello, can you talk about trials for newly diagnosed patients?
Dr. Costello: Clinical trials exist at every part of the journey with myeloma and they really offer opportunities for patients. Like Christen beautifully said, you’re either getting the standard of care or you’re getting something that might be better so it gives patients opportunities for the next new and cutting-edge treatments.
In the last few years, we’ve had the outcomes of some of these newly diagnosed trials, particularly the ones that finally are getting published. One was the GRIFFIN study. As Cindy mentioned previously, two drugs are good, three drugs look better so maybe four is the best.
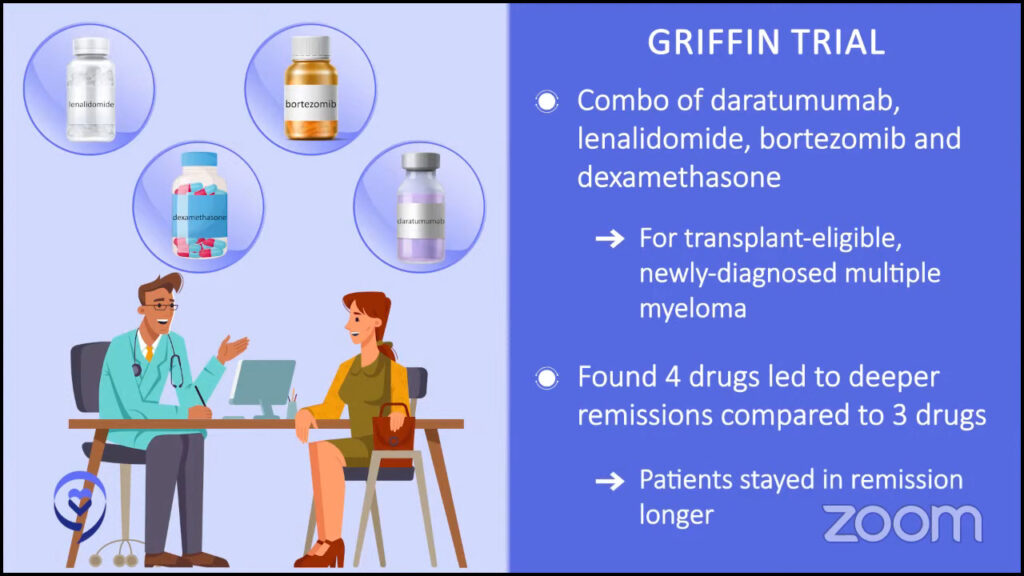
When someone’s newly diagnosed, our usual cocktail is three different drugs together. But what if we give them four? Does that have better outcomes and more likelihood of achieving remission? Does it get us more durable remissions where people are staying in remission longer?
We have the final analysis published that showed us that those patients who get four drugs when they’re first diagnosed have deeper and more durable remissions than those who get standard of care. Our standard of care of three drugs now seemed outdated.
It’s in recent years that we’ve said four drugs are the way to go. This is specific to younger and/or healthier patients. Age is just a number. The reality is some intensive therapies may be too much for a patient depending on their health or other medical issues that they may have.
If we find the next new and exciting thing for someone younger and/or healthier, the next question is: what about someone who may not be as young or as fit or possibly more frail?
The triplet combination that came out of the MAIA study combined three different drugs, which we proved was better than two different drugs. To say that, though, that cocktail truly has exceedingly, exceedingly effective outcomes for patients who may be older or more frail, for example.
There’s a lot of work that’s been done to get us to this point. We’re so glad that we finally have a new standard of care that we can have future trials use as a baseline to compare to for the next steps to get us to that cure.
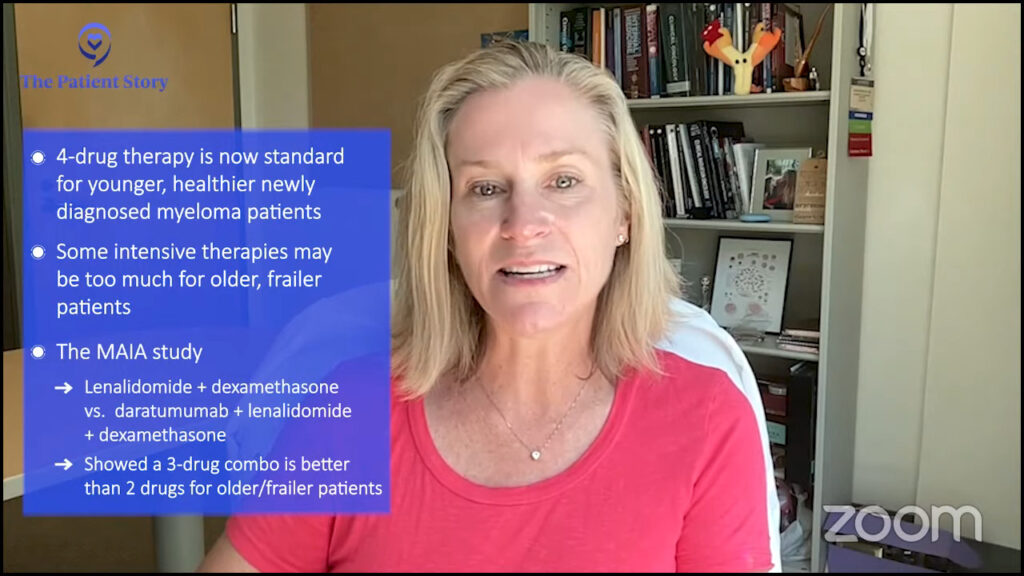
Cindy: We’re in exciting times. If you ask different myeloma specialists, they would have different answers about what a cure is. The same holds true for patients. If you ask what they expect in a cure, you might come up with different answers. But to me, it sounds wonderful being treated for a set period of time and then being off drugs for an extended period of time; that would be my definition of a cure.
We need more classes of drugs because if you treat the patient and it works, that’s fantastic. But if the therapy stops working, we need to have other classes of drugs.
Dr. Carl Ola Landgren
Cindy: We’ve been talking about how things have changed. I know when I was diagnosed back in 2008, induction therapy was a doublet. Now, the standard of care is a triplet, but it seems to be moving towards quadruplets.
Before we start talking about quads and the benefits of some of these four-drug combinations, can we focus on some of the clinical trials that are triplet combinations and which ones have been gaining your attention and why?
Dr. Landgren: The bigger triplets that I pay attention to are the RVd or VRd regimen. This is bortezomib, lenalidomide, and dexamethasone. This was initially developed by Paul Richardson and the group at Dana-Farber. It was presented at ASH 2008 and it was published in a small study in 2010 that became the standard in the US, based on a little bit more than 50 patients treated.
Eventually, it was published as a randomized study compared to lenalidomide and dexamethasone. The randomized evidence came many, many years after this had already become a standard of care. That is one of the three-drug combinations that I think are important. They pushed the field forward.
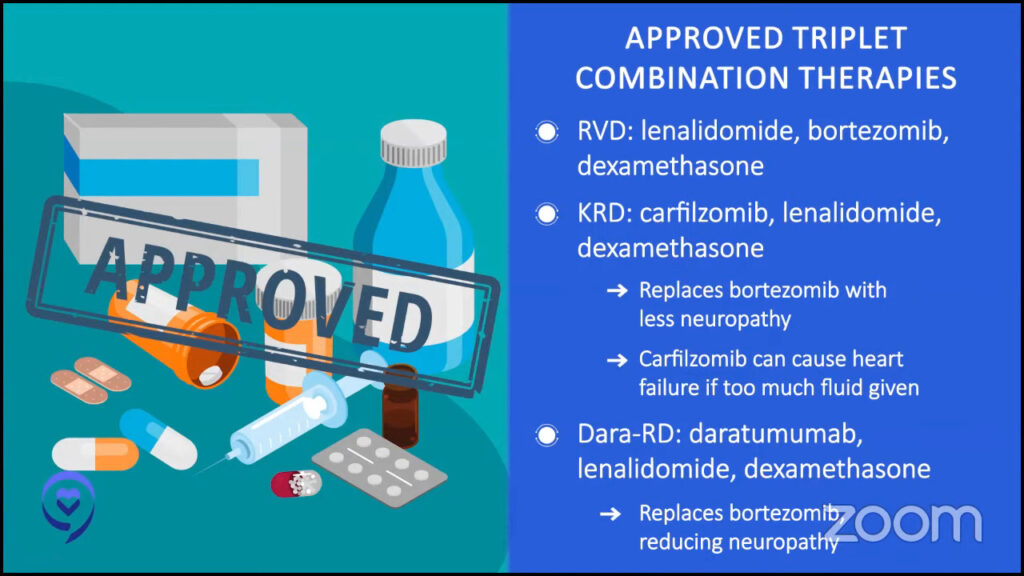
I was involved in the development of the KRd regimen with carfilzomib, lenalidomide, and dexamethasone. The difference between these two regimens is that the proteasome inhibitors are different. You have no added neuropathy with carfilzomib, which you have with bortezomib.
But if you give carfilzomib to a patient with underlying cardiovascular disease, you could push that patient into congestive heart failure. What has been found also is that a lot of this is due to giving too much fluid. But that’s a great, great combination. For patients who are otherwise fit, that would be my go-to therapy.
Then you have the DRd, which is daratumumab or DARZALEX with lenalidomide and dexamethasone. That was approved in 2019. That has been a game-changer. It takes away all the problems with bortezomib’s neuropathy. You replace the proteasome inhibitor with an antibody. Giving a CD38-targeted antibody with lenalidomide and dexamethasone has really changed the field.
It has also erased some of the age discrimination that’s been in the field for a long time where younger patients could get more effective therapies while patients who were older and more frail have very few options. You had only two drugs.
With daratumumab coming, the difference between patients that are frailer, older, or have other issues and patients who are younger and more fit became smaller in terms of efficacious drugs. The addition of immunotherapy has really, really made a huge step forward.
Cindy: How about your thoughts on the trials that are doing selinexor, pomalidomide, and dexamethasone against elotuzumab, pomalidomide, and dexamethasone? Any thoughts on that trial?
Dr. Landgren: Those are combinations in trials for patients who have relapsed/refractory disease. Elotuzumab is a drug that binds to a protein called CS1 or SLAMF7, and it was discovered many years ago.
In the laboratory, this antibody bound to myeloma cells and they died. However, in patients, elotuzumab alone has not been found to have any clinical benefit.
Elotuzumab has been partnered either with lenalidomide or pomalidomide. Given in combination, it has been found to be more efficacious than lenalidomide with dexamethasone alone or pomalidomide with dexamethasone alone. Elotuzumab adds to these backbones.
Selinexor can be used in different combinations. It has been approved with bortezomib and for patients with a first, second, or third relapse. There are other combinations as well with pomalidomide and also with carfilzomib.
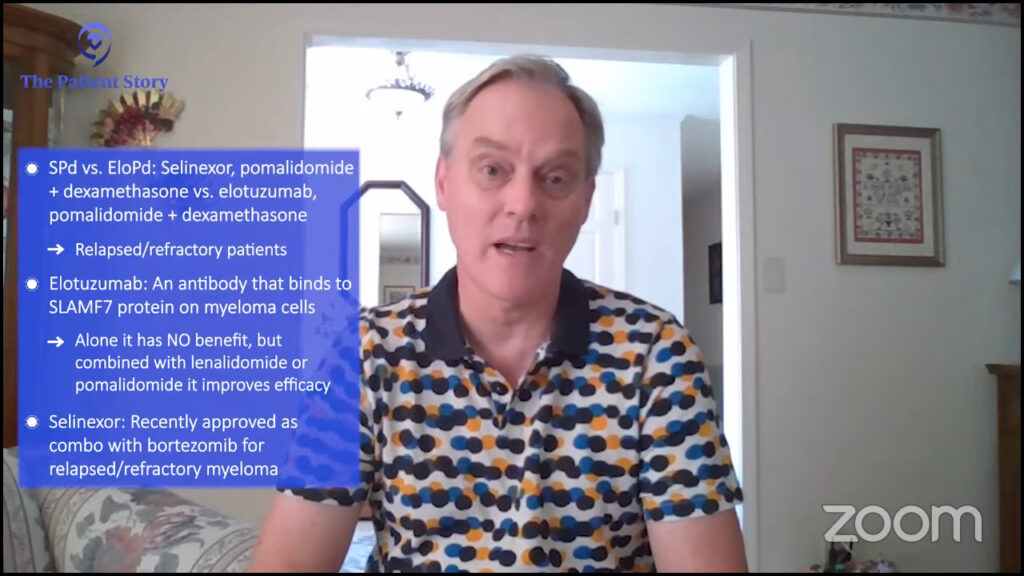
Selinexor is a new class of drugs. It binds to a protein that is sent into the center of the tumor cells, the nucleus, so it’s a blocker of certain proteins that go in and out of the nucleus and has been found to work very well in myeloma.
We need more classes of drugs because if you treat the patient and it works, that’s fantastic. But if the therapy stops working, we need to have other classes of drugs.
Cindy: Before we move on to the four-drug combinations, let’s talk about BLENREP or belantamab mafodotin. We had it on the market for a bit and then it was pulled because it didn’t meet one of its primary endpoints, but it’s still in trials, like the DREAMM 8 trial, using BLENREP in combination.
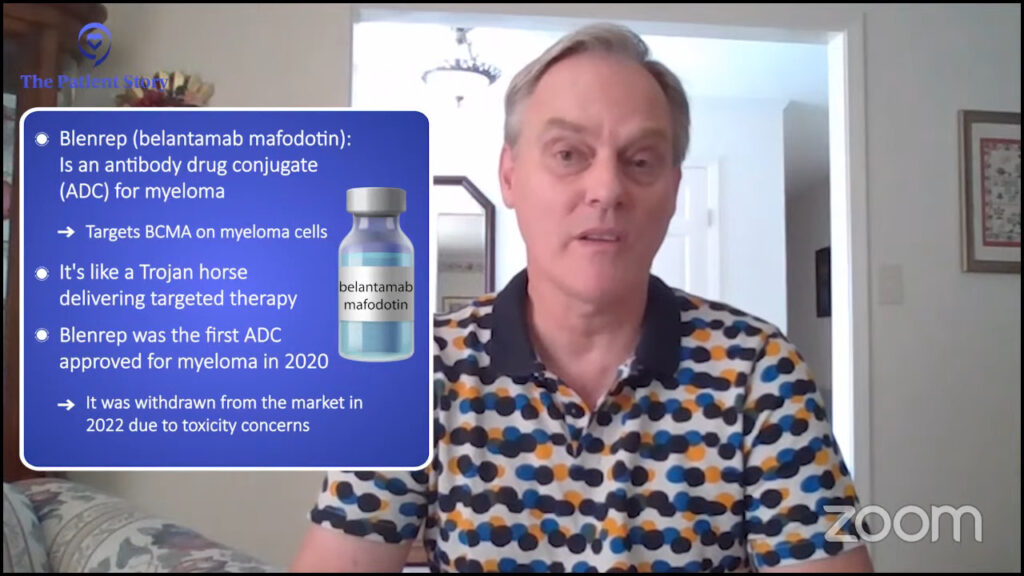
Dr. Landgren: Belantamab mafodotin is an antibody-drug conjugate. It’s a small molecule, a toxin similar to lenalidomide or carfilzomib that can have an anti-myeloma effect. The difference between belantamab mafodotin and these other drugs is the way it’s delivered.
The drug is not given as a tablet, an injection, or an infusion; it’s bound to an antibody and that antibody is infused into the vein. When the antibody comes into the human body, it looks for the corresponding protein that this antibody’s been designed to bind to and that is the BCMA protein that’s widely expressed on the surface of myeloma cells.
When these antibodies find the myeloma cells, they bind to the BCMA protein. Once they have, the myeloma cell lets this antibody in and once it’s in there, it releases this toxin that will kill the myeloma cells. It’s like a Trojan horse.
This is the first and so far only antibody-drug conjugate developed for myeloma. It was approved in 2020 and then pulled from the market in 2022. What happened?
The FDA has a fast track for drug development, which is great for patients. That will speed up the availability of new drugs. A drug company can do all the safety and toxicity data pre-clinically. They can open a phase 1 study and identify the right dose, then you can have an expansion cohort or a phase 2 study and treat a number of patients per agreement with the FDA.
If the right proportion of patients responds to the drug, if the FDA agrees, then an accelerated approval will happen. That’s what happened to most of the drugs. All the drugs we currently have in more recent times have been approved based on this mechanism; that happened to belantamab mafodotin.
When belantamab mafodotin was compared to its control arm, the drug belantamab mafodotin was not superior. When the FDA reviewed the data, they said this study did not live up to its endpoint.
FDA did not stop the drug. GSK, who owns the drug, took it off the market before the FDA made that decision. There was nothing for the FDA to stop because they already took it off the market.
However, in agreement with the FDA, the drug is available for compassionate use. The fact is that the drug works for many patients. If there is a doctor who thinks this is the best option for a given patient here and now, that doctor can reach out to the FDA and get permission to use it.
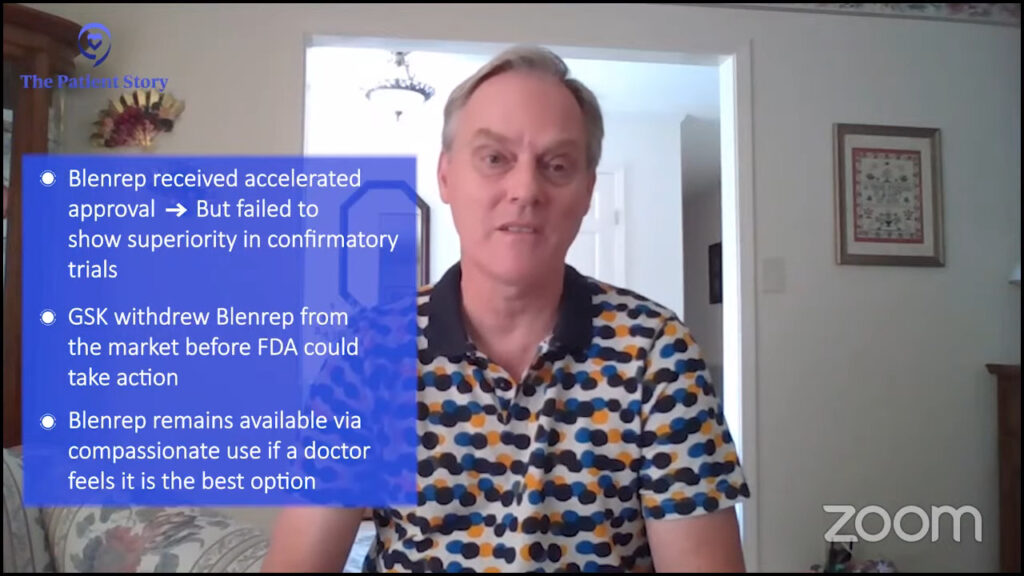
The FDA has the next rule in place. Once you’re given accelerated approval, you have to design a randomized study where you prove that this drug is superior to a control arm. A randomized study has to be written, launched, and concluded, and the data has to be handed to the FDA.
There are other trials that they had already launched in combination with belantamab mafodotin and there are two of them ongoing. There is a control arm and now it’s belantamab mafodotin in combination.
The study that failed was belantamab mafodotin as a single drug versus a control arm. There are two ongoing trials that use combination therapies versus control arms. When they are done, the data will be handed back to the FDA.
It’s very likely that those trials, one or both of them, may read out with the drug being superior and that could reintroduce the drug and they could get the full approval. We have to just wait and see.
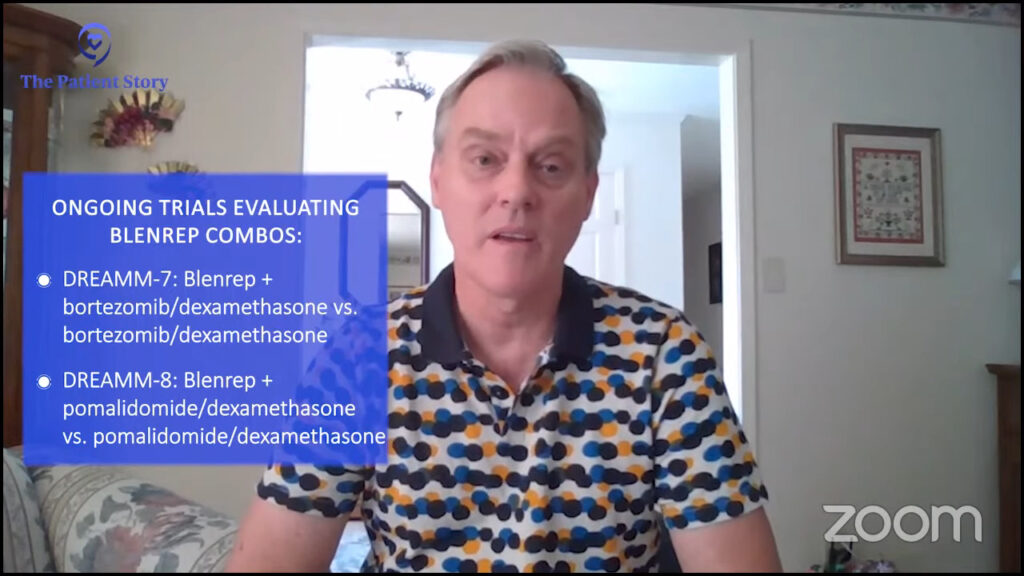
They are part of the DREAMM program. Belantamab mafodotin was initially developed in DREAMM 1 and then there’s been 2, 3, and 4, and so forth. Now we’re up to DREAMM 7 and DREAMM 8.
The trials use belantamab mafodotin. One of them uses it with bortezomib and dexamethasone and the control arm is bortezomib and dexamethasone. The other one uses it with pomalidomide and dexamethasone and the control arm is pomalidomide and dexamethasone.
With all things being equal, I do think that four drugs are here to stay. The GRIFFIN study showed us that it is better than three.
Dr. Caitlin Costello
Cindy: Do you think the four-drug combinations are going to be the new standard of care for newly diagnosed myeloma? If so, which four drugs do you envision to be used as part of induction therapy? How do you weigh the risks and benefits of adding that other drug with the side effects it may cause? Would there be some patients that maybe could still use three?
Dr. Costello: Four drugs are definitely here to stay but not for everyone. We talked about the importance of personalizing this approach and how we take into consideration so many different aspects of you, your health, and your myeloma when we make these decisions.
With all things being equal, I do think that four drugs are here to stay. The GRIFFIN study showed us that it is better than three.
There are more trials coming out. GRIFFIN was a phase 2 trial, which showed us important things, but we want to extrapolate that data to use it in several hundred different patients to prove what was shown in the GRIFFIN study.
The next studies that are coming along, like the PERSEUS phase 3 trial, are going to show us how we can get the durability of response and prove that the initial study, GRIFFIN, was right and is proof that quadruplet or four drugs is here to stay.
Dr. Landgren: Similar to most things in life, there will be early adopters and people who will be the very last people to change their minds. Some people build their career on saying no, no, no all the time and that’s how the field goes.
The three-drug combinations I mentioned before are proteasome inhibitors with IMiDs and steroids, and the evolution has also been CD38-targeted antibodies with IMiDs and steroids.
When we talk about four-drug combinations, it’s basically a merge of those so that means that you add a CD38-targeted monoclonal antibody. For the most part, the studies out there are using daratumumab added to a proteasome inhibitor, IMiD, and steroid. In plain language, you’re talking about Dara-RVd or Dara-KRd; those are the two that have been presented.
There are three trials that have been published so far using those combinations. The first was the Dara-RVd randomized phase 2 study that was published about three years ago in the Blood journal. They wrote the protocol and the lead author is Peter Voorhees.
That had about 100 patients with daratumumab with RVd and about 100 patients just with RVd. Patients receive four cycles of either of the regimens. They were all transplanted then they got two more cycles with the same regimen that they started off with.
After completing the sixth cycle, the study looked to see if there was an improvement in the stringent complete response rate. There was a slightly higher stringent complete response rate if you add the daratumumab therefore the study was deemed successful. Clinically, you could argue: is that really meaningful? But that’s how the study was designed.
Patients who got dara-RVd continued on daratumumab with lenalidomide maintenance for two years. The patients who got RVd got lenalidomide maintenance.
What the study continued to show is that the rate of MRD negativity is much, much higher in the group that started and continued on daratumumab. They have plotted out the progression-free survival curves. The progression-free survival seems to be way superior in the four-drug combination.
But it’s not only the four-drug combination upfront that’s different between the two arms. It’s not four versus three. It’s also the maintenance being very, very different. You could ask the question: what would happen if you gave everybody three drugs to begin with and had a two-drug or one-drug maintenance, would that make a difference? That study has not been done so we don’t know the answer to that.
The other combination is Dara-KRd and I was the lead investigator in the first trial to be published called the MANHATTAN study. I did that when I was at Sloan Kettering. We gave Dara-KRd for eight cycles and patients were not transplanted in that study.
After four cycles of treatment, a patient had the option of collecting their stem cells or not, and after eight cycles, they had the option of being transplanted or not. Some patients were MRD negative and they chose to go for transplant.
The majority of patients who were MRD negative chose not to be transplanted so they kept their stem cells in the freezer. We have kept on following these patients. So far, we have not really seen any significant difference in whether you were transplanted or not, but the study was not designed to fully answer this question.
The third study that used Dara-KRd is the MASTER trial, which was developed by Luciano Costa. He treated a smaller number of patients. Patients got four cycles of Dara-KRd, were transplanted, and if they were MRD negative after each of these two steps, were taken off therapy
If they turned MRD negative, they got another four cycles of Dara-KRd and, again, if they were negative two times in a row, they were taken off therapy. They could get an additional four cycles so they could end up with a total of 12 cycles. Every patient was transplanted in this study.
He has shown that with a relatively short follow-up, patients who didn’t have adverse cytogenetics continued to be free from disease after 1 or 2 or so years, while patients who had more aggressive disease would have their disease flare back again if you take them off therapy. That’s where the field is right now.
From what we’ve seen so far, it’s been a new, wonderful treatment option for myeloma patients.
Dr. Caitlin Costello
Cindy: When I first heard about CAR T-cell therapy, it was when the University of Pennsylvania and CHOP had their first CAR T-cell patient and how well that response was. Can you talk about what CAR T-cell therapy is and some of the benefits of using this type of immunotherapy in treating myeloma? What could some of the challenges be?
Dr. Costello: This has been one of the single most exciting treatments I have seen in my career. They were developing CAR Ts for other kinds of cancer patients and none of us really knew what to expect. But over the course of the last decade or so, we’ve learned so much.
CAR T stands for chimeric antigen receptor T-cell therapy. Your T cells are part of your immune system. They are these fighter cells that are designed to look for bad guys that come into your presence, whatever that may be.
What if there was an opportunity to train your T cells to specifically look for your myeloma? Speaking of personalized medicine, it doesn’t get much better than this. This is your own immune system fighting your own cancer.
Every myeloma cell has little tags on it that identify it as a myeloma cell. There’s a tag called BCMA, B-cell maturation antigen, on the myeloma cell. CAR T cell is a way that we can train your T cells to look for that tag.
The logistics of it can be a little overwhelming and it’s one of the challenges of CAR T. If you’ve ever undergone a stem cell transplant or have heard of it, it feels very similar.
Your T cells are removed from your body, similar to a blood donation. They’re sent off to a specific company that re-engineers them in order to create and train the T cell to look for that tag we talked about.

The CAR T cells are mailed back and, with some additional logistics, your doctor will put them right back into your body. Your immune system is now trained to look for your myeloma cells.
There are two different CAR Ts that were approved by the FDA in 2023 for treating relapsed or relapsed/refractory multiple myeloma. It’s approved for patients who have had four or more different treatments.
The benefit of it is that it is a one-and-done treatment. Myeloma patients have probably been on myeloma treatments for a very long time. They keep a lid on everything. Maybe it can delay it from coming back. But with that comes cost, time, side effects, and a lot of additional challenges.
When you receive CAR T-cell therapy, that is the treatment, and your immune system is now trained to go to war against your myeloma and knock everything down. It’s a very exciting opportunity to allow patients to have a treatment-free interval where they’ve done their treatment and can enjoy years without any additional therapy.
Unfortunately, it’s not curing everybody yet, but it’s buying us time, which is what we really do with myeloma treatments. We kick the can down the road until the next treatment comes.
There are lots of exciting benefits. With new drugs come new side effects that your doctor and you need to learn about and figure out how to manage to keep you safe. With new exciting options, there’s a lot of popularity around them.
There are a lot of logistics involved in getting the T cells out of you, engineering them, sending them back to you, having the manufacturing capabilities to do that, and that is time, money, and accessibility.
There is still not enough access for everybody who needs it to have it. We’re going to continue to fine-tune and hone this. But from what we’ve seen so far, it’s been a new, wonderful treatment option for myeloma patients.
Cindy: Patients were so excited when we had our first approved CAR T-cell therapy. It prolonged life. People who were out of options were given an option. That’s what we do in myeloma. We just keep on treating ’til the next new thing.
These CARTITUDE studies are looking to see if CAR T-cell therapy is at least as good, if not better, than our standards of care.
Dr. Caitlin Costello
Cindy: The CARTITUDE trials talked about cilta-cel or CARVYKTI. Can you talk a little bit about what we found out from the CARTITUDE trials and maybe specifically CARTITUDE-4 and what’s happening in CARTITUDE-5 and 6?
Dr. Costello: The CARTITUDE trials are looking at how can we use cilta-cel, which is one of the two CAR T products targeting BCMA.
Drugs get approved on the basis of safety and effectiveness from the very get-go. Truly, and maybe unfortunately, this is oftentimes studied with patients who have no other options.
Once we prove it works and that it is safe, then we can cast a wider net. If it works at that point in the disease, could we potentially study it in patients who have been diagnosed with myeloma more recently or have had fewer than four treatments or maybe even when they were first diagnosed?
The CARTITUDE trials, and there are a lot of them, are looking at exactly this. It’s a randomized trial that gives one set of patients the standard of care, what I know works, and another set of patients CAR T cells. These CARTITUDE studies are looking to see if CAR T-cell therapy is at least as good, if not better, than our standards of care.
We’ve been doing bone marrow transplants for a very long time and it has been great in the sense that it works. It has its issues, it has its side effects, and there are parts of it that are no fun. But everyone’s starting to say: can we compare that to CAR T instead?
We’re going to see more and more data coming out about some of these CARTITUDE studies. There’s the KarMMa study, which is evaluating the other BCMA CAR T cell with ide-cel, asking the age-old question: do we still need a transplant?
As a disclaimer, I’m a transplanter. I believe in transplants. Until someone shows me it’s better, there’s still a great role for transplant, but I can’t wait to see how those results turn out.
Cindy: I’m excited about that, too, because I haven’t had CAR T cell. I’ve had a transplant and from everyone I’ve talked to who’s had both, they had an easier time going through the CAR T-cell therapy.
The other more exciting thing is trying to put CAR T cells closer to the front line. As patients, we hear that sometimes CAR T cells aren’t working as great as they can because of exhausted T cells so if we did them sooner, they might not be exhausted. I’m hoping to see if that might be true and if we use some of these CAR T cell therapies upfront, maybe they’ll be closer to being curative than they are later on down the road.
The only way we’re going to find these answers is from clinical trials so we need them, we need patients to enroll in them, we need them to answer these questions, and we need those answers fast because patients are waiting.
We give an antibody that links the T cells to the myeloma cells. We are trying to engage the T cells so the T cells can act as the treatment for myeloma.
Dr. Carl Ola Landgren
Cindy: Bispecific antibodies are a new type of immunotherapy, too. Can you talk about what bispecific antibodies are, their mechanism of action, and some of the side effects that we’re seeing?
Dr. Landgren: From a development point of view, bispecific antibodies are very different from other antibodies. We talked about daratumumab and elotuzumab before they were developed back in 2015. The first bispecific antibody that came to myeloma was at the end of October 2022. We have additional two bispecifics in August 2023.
Bispecific antibodies bind to the surface of the myeloma cells and to the surface of T cells. They bring these two cells to sit next to each other. When a T cell sits next to the myeloma cell, it will kill the myeloma cell.
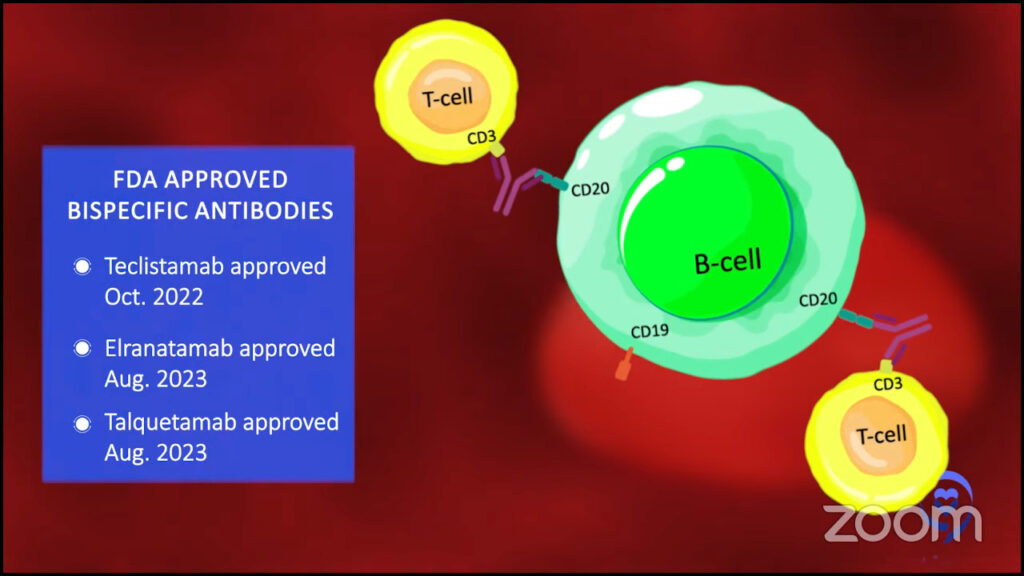
When we talk about CAR T-cell therapy, what does that mean? We take out the T cells, make them into CAR T cells, and those T cells bind to myeloma cells. You could say it’s very similar.
Instead of taking out the T cells, we keep the T cells in the body, but we give an antibody that links the T cells to the myeloma cells. We are trying to engage the T cells so the T cells can act as the treatment for myeloma.
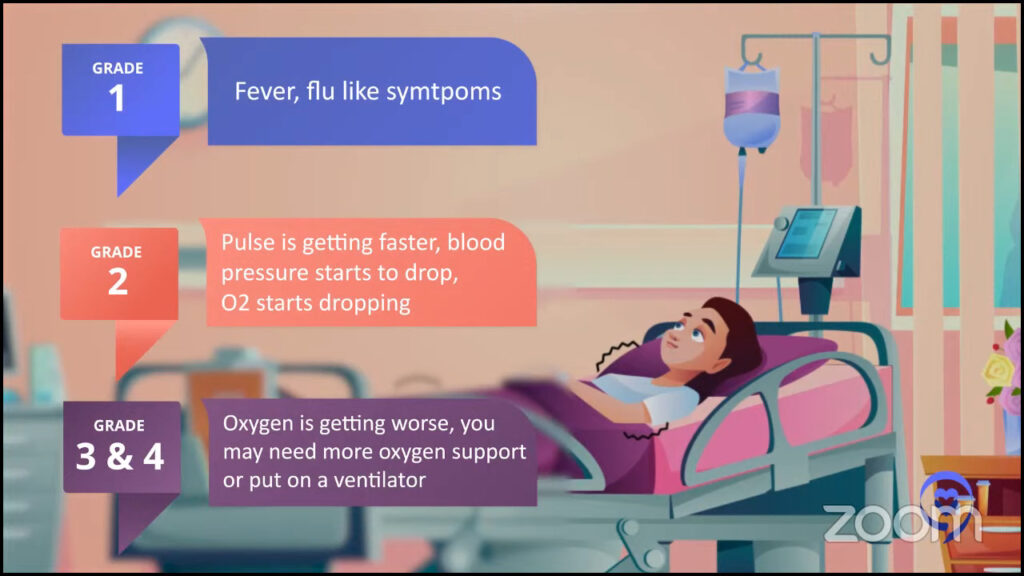
The side effects of bispecific antibodies are quite similar to CAR T cells in that you could have cytokine release syndrome and these immune cell-mediated neurological syndromes with neurological side effects.
But usually with bispecific antibodies, you have less profound, less severe reactions. Most of the cytokine release syndrome we see are grade 1 or grade 2, but we very seldom or almost never see higher grades. But with CAR T cells, you could see grade 3 or grade 4.
There is some continued immunosuppression and patients seem to be more able to capture infections over time with bispecific antibodies.
Dr. Carl Ola Landgren
Cindy: Do bispecifics have higher rates of infection?
Dr. Landgren: Infections can happen both with CAR T cells and bispecific antibodies. I spent a lot of time going through the literature, trying to understand the dynamics of these types of immune cells and the side effects from both short- and long-term perspectives. I continuously go through the literature and talk to other investigators.
What I’ve seen is that the infections are more likely to happen earlier on with CAR T cells because you have more profound suppression. With the antibodies, the way they are developed is you keep on giving them. You not only hit the myeloma if it’s there or keep the myeloma away, but you also keep on hitting the immune system. You will see there is some continued immunosuppression and patients seem to be more able to capture infections over time with bispecific antibodies.
There are ways to prevent this and this all comes back to the physicians. Every time I talk about this, I always emphasize that doctors have to know exactly how to manage this.
These antibodies bind to markers, like BCMA and GPRC5D, which are widely expressed on myeloma cells. Unfortunately, these can be also expressed on normal plasma cells, which means that the patient would make fewer immunoglobulins. Low IgG in the body is called hypogammaglobulinemia and that could increase the risk for capturing infections. It could also be more severe infections.
A way to prevent these infections is to give intravenous immunoglobulin or IVIg. I always say to check your IgG levels. If they go under 400, you have to give IVIg. I would give it, check the next month, give it, and check the next month. If it goes into the normal range, then you can hold off, but you have to keep on checking it. If it starts drifting down again, you have to give it.
You can see with these combinations that you can bump up response rates from 60 to 70 to 80 to 90 to 95%.
Dr. Carl Ola Landgren
Cindy: The bispecifics that are currently approved are approved as monotherapy or just by themselves. There are some trials that are doing some combinations. Can you talk about those trials?
Dr. Landgren: The field is moving forward very fast and there is a whole range of combinations.
Damian Green of the Fred Hutch Cancer Center in Seattle found that myeloma cells can protect themselves by chopping off BCMA from their surface, the target for many of these bispecific antibodies and the currently available CAR T cells.
The drug binds to the target, but the target gets chopped off so it’s circulating free in the blood. The cancer cells are swimming by, waving to these receptors and the drug. That’s not a good scenario. How could you prevent that from happening?
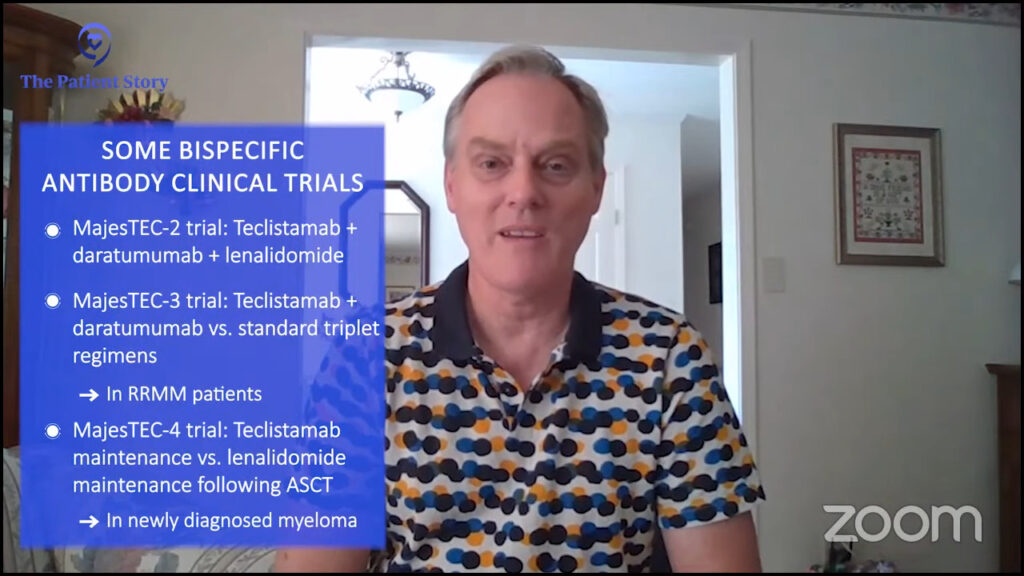
Dr. Green and his colleagues found that this happens when the cells release γ (gamma) secretase. They used γ-secretase inhibition to stop this from happening. There are newer developments now and we have been part of this as well.
It’s probably overkill to give every patient this. For some patients, it may be the right thing to do, but in general, it’s probably not needed. That’s one line of investigation. We are not yet done, but that seems to be the way the field is going.
Then you could increase the efficacy of it. You could use other antibodies. You could use daratumumab in combination with bispecifics.
People have daratumumab and teclistamab. Let’s put them together and see what happens. People have used teclistamab with lenalidomide or elranatamab, which is also an approved BCMA bispecific antibody, together with lenalidomide and pomalidomide. You can start using it also with proteasome inhibitors, carfilzomib, or other drugs.
Why not take two of these bispecifics at the same time? You could take a BCMA and GPRC5D-targeted bispecific antibody and use that together. There is data coming out and ASH 2023 will present a lot of this data.
The bottom line is that these single drugs are amazing. About 60% of patients respond to bispecifics. To put it in context, when daratumumab was approved in 2015, it was 30%.
Patients today have been treated with many more drugs when they go on trials. Almost 10 years ago, there were virtually no drugs around. You could argue and say patients today are sicker than they were 10 years ago and it still delivers over 60% so that’s amazing.
You can see with these combinations that you can bump up response rates from 60 to 70 to 80 to 90 to 95%. There are some studies treating 28 patients and 27 of them respond. It makes me wonder how we can learn from that so we can take the last person over the goal line.
We will probably have, I would say, 95 to 100% response rates in later lines. These drugs will probably become part of front-line therapy. What we have known for a long time is that what works in later lines usually works better in earlier lines. If we have this discussion in five years, everything will have probably changed.
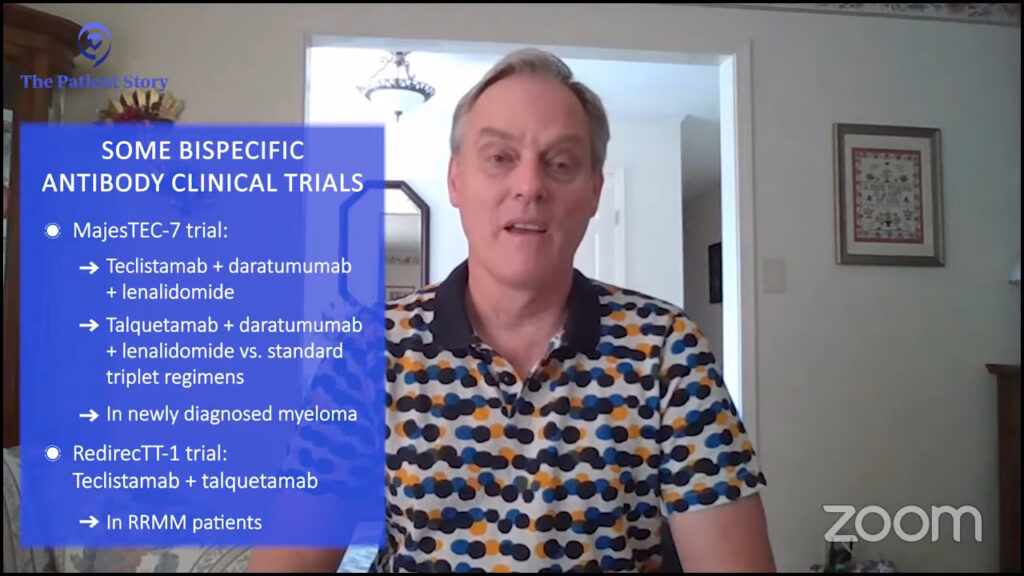
Cindy: Exciting times. I’m very, very hopeful. I hope to be here five years from now. When I was newly diagnosed, five years from now was really scary to me. Now with all these new drugs, I’m counting on being here and having a discussion with you in five years.
It scientifically makes sense for me to put CAR before BiTE, but I do think we have the reality of challenges with CAR T that don’t allow us to sequence it the way we would want to.
Dr. Caitlin Costello
Cindy: How do I know whether or not I should be looking for a bispecific antibody or a CAR T-cell therapy? Dr. Costello, how do you have that discussion with your patients? I know it’s probably going to be very specific, but what are some of your guiding principles?
Dr. Costello: We have to break this down into the ideal world and the real world.
In an ideal world, everyone has access to everything. We are sitting in front of our patients, say A or B, and we can do A or B soon but that is not the real world.
The real world makes that difference for usually at least two reasons. People relapse differently. Some people have myeloma that grows back very slowly so we have time to organize the next treatment and think through the logistics. We can prepare ourselves or get on waitlists for CAR T because that’s the reality of CAR T.
However, other patients have myeloma that relapses very quickly. We may not have the benefit of time to think about our next steps, pursue treatments that may not be locally available, or be on a CAR T-cell therapy waitlist. We have to consider all these different scenarios to help make that decision.
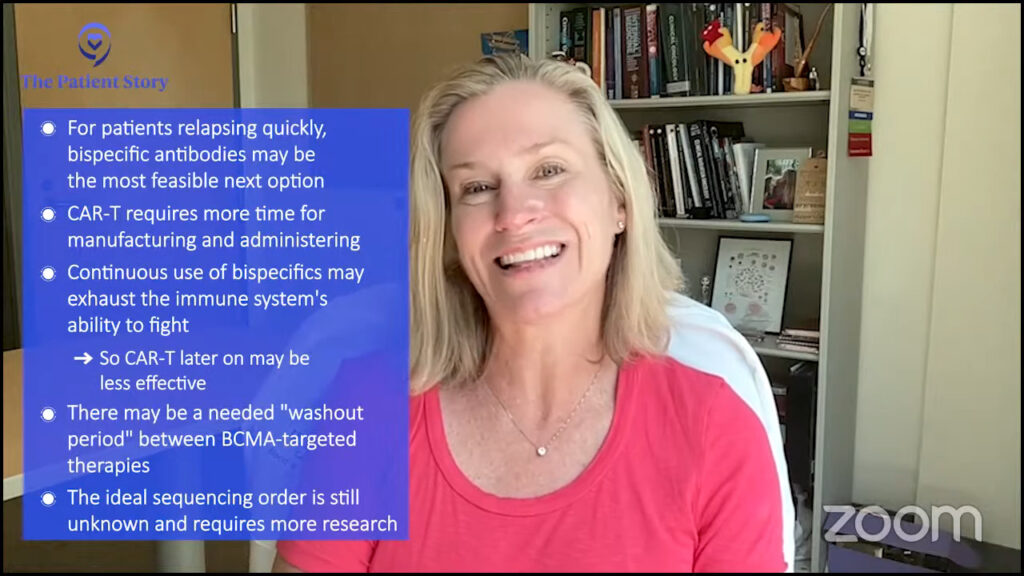
In an ideal world, I like the idea of starting with CAR T. I would love for patients to have time to get off treatment and enjoy treatment-free intervals.
Bispecific therapies are a great way to keep using the immune system to keep pushing against the cancer cells, but they’re going to get tired, too.
If we continuously ask the immune system to fight, fight, fight, and then we try to take those immune system cells out and re-engineer them and ask them to go to a whole ’nother battle, they may not be as effective.
It scientifically makes sense for me to put CAR before BiTE, but I do think we have the reality of challenges with CAR T that don’t allow us to sequence it the way we would want to.
The other thing worth mentioning is that there’s this concept of a waiting period because we have different ways to attack the BCMA tag. As we attack it, we can see that the tag level in your bloodstream goes down as your myeloma gets killed.
At some point, it may regrow as your myeloma grows and we may need that BCMA to start growing back so we can attack it again. I don’t know if we know the answer yet about the ideal waiting period between doing sequential BCMA-targeted therapies, but it also does rationally make sense to me.
I think CAR T buys us more time to allow the T cells to do their thing then allow the BCMA to redevelop to allow us to target it again. It’s a little complicated because we don’t know.
No one really knows for sure. The jury is still out. There are so many questions that we don’t really have the answer to when it comes to this.
Dr. Carl Ola Landgren
Cindy: We could have a whole discussion on BCMA treatment, sequencing, and waiting periods. There’s so much going on.
Dr. Landgren: We talk about it at conferences. It always comes up and people talk about it internally. I get phone calls from private practice doctors asking for advice on how to think about it.
The short version is no one really knows for sure. The jury is still out. There are so many questions that we don’t really have the answer to when it comes to this.
If you look at the trials that use bispecific antibodies, some of those trials have allowed patients with prior exposure to BCMA-targeted therapies, like belantamab mafodotin or CAR T-cell therapy. If you look at the overall results, the numbers are not significantly different.
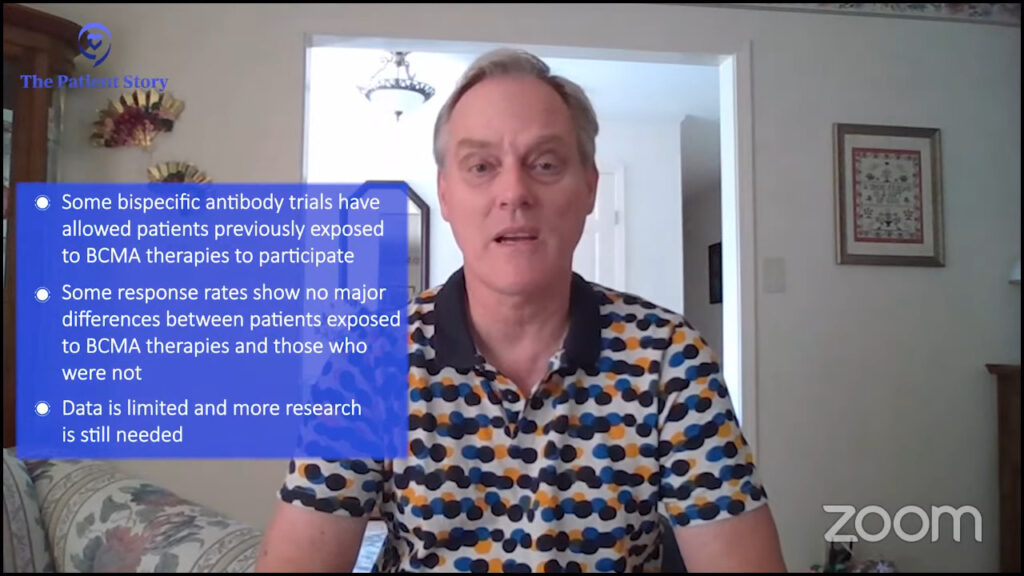
Similarly, there are CAR T cell studies that have been done that allowed people who have been exposed to prior BCMA-targeted therapy. Again, if you look at these response rates, they don’t look that different.
Based on the small numbers from available studies, if you do these so-called stratifications — you look at one study whether they have prior exposure or not, or do another study and flip it around from CAR T cell to bispecific or bispecific to CAR T cell — it doesn’t look that drastically different. There is no significant P value. There is no definitive answer. That’s why I started off by saying we really don’t know.
We have to be open-minded and we have to involve the patient. Every patient will have his or her own perspective.
Dr. Carl Ola Landgren
Cindy: With all these newer treatment options, is a stem cell transplant still necessary?
Dr. Landgren: That is a very difficult question to answer because it is all about what you have as alternatives.
In a broader context, if you think about the whole world, transplant has been proven for a very long time. It was initially developed in 1983 for a very old treatment that is a spinoff of mustard gas, which is what melphalan is. It was mustard gas discovered taken in to become melphalan chemotherapy; that is the so-called transplant. It has been implemented around the world for all these years.

In many countries, there is limited access. There are very few treatment options for patients. Transplant remains a very, very good alternative. In many parts of the world, in 2023, this remains one of the most, if not the most, powerful therapies widely available so to take that away would be the wrong thing.
If you look at the United States, we are very lucky. We have so many treatment options. Is it the ultimate therapy for every patient? Do you have to have to do it? The answer is more complicated. It’s probably more towards maybe not.
If you ask someone who is a transplant specialist, that person will say, “It’s been around for a long time. I use it all the time. It’s a great therapy. It’s not a big deal. You should really do it.” I have respect for that and I see where they come from.
There are other people who will say, “There are so many new treatments. We have CAR T cells and bispecifics. There are so many alternatives. The patient is already MRD negative. Why don’t you keep the cells in the freezer and give the patient the option of doing a delayed transplant if needed?” I would agree with that, too. I have great respect for that opinion.
We have to be open-minded and we have to involve the patient. Every patient will have his or her own perspective.
Cindy: That’s why it’s so important to have educated patients who could be part of that conversation and make the decision about what they feel is best for them.
We don’t have a cure yet, but we can control the disease and provide a very good quality of life for many, many patients with these drugs.
Dr. Carl Ola Landgren
Cindy: Thank you all for such a wonderful and incredible discussion. If you had to leave our audience with one takeaway message, what would that be?
Dr. Costello: Advocate for yourself. There is so much that you need to understand about your cancer so that you can find your best, personalized pathway forward. With all these resources, you have no excuse to not do that.
Dr. Landgren: Myeloma is at a tipping point as a disease. If I put all my years of experience into perspective, it used to be a disease that was almost like a kiss of death. Now it’s a disease where the lifespan for many patients is getting very close to, if not identical, to the general population.
We don’t have a cure yet, but we can control the disease and provide a very good quality of life for many, many patients with these drugs.

Seek advice from experts. If you choose to be treated locally, the expert can always be looped in and give advice if there needs to be some changes and strategic considerations. Involve an expert when you’re newly diagnosed or if there are new decisions to be made. The future is very bright and we are always here to help you.
Cindy: I’m glad there’s a bright future. You just made this girl’s day because that’s not what I was told in 2008 so I’m glad times have changed.
Christen: I hope that you feel less intimidated by the clinical trial landscape and are encouraged to reach out to support teams like the Clinical Trial Support Center. We’re here to support you through your journey, whatever it may look like.
Cindy: It’s so important to be involved in your care. When I was newly diagnosed, I blindly followed my doctor’s orders. I grew up in that age of doctor knows best so whatever the doctor told me to do, that’s what I did without asking questions, without being part of that decision-making process. I’ve learned how it feels to be educated and empowered and part of that decision-making process.
Stephanie: Thank you so much, Cindy, for being our incredible patient advocate and moderator.
Thank you also to Drs. Landgren and Costello for the work that you do in the clinic and in research to help move the landscape of myeloma options and treatment forward, and for helping patients and families who are trying to navigate a multiple myeloma diagnosis and treatment.
Thank you to our LLS clinical trial nurse, Christen Hawthorne, for being there for people who are overwhelmed by approaching clinical trials.
We really hope that you walk away with a better understanding of clinical trials, specifically in multiple myeloma. Again, they may or may not be right for you, but our goal is to make sure you feel empowered to make a decision for yourself. We hope to see you at a future program.