Our “Office Hours” bridge the gap between clinical expertise and lived experience. In this program, we tackle the topics that matter most to your daily life:
Understanding Your Diagnosis: Learn exactly what CLL is—a cancer of the immune system—and why it often acts more like a lymphoma than a traditional leukemia.
The “Watch and Wait” Strategy: Get an expert explanation on why “active surveillance” (monitoring without immediate treatment) is often the safest, most effective path forward.
Daily Living & Wellness: Discover how simple lifestyle adjustments, from vitamin D to regular exercise, can help manage common symptoms like fatigue and keep you “treatment-ready.”
The Power of Second Opinions: Understand why seeing a CLL specialist—especially when transitioning from surveillance to treatment—is a vital step in your advocacy toolkit.
Your Actionable Roadmap: Walk away with a “Shower Check” routine for monitoring lymph nodes and a clear understanding of the genetic tests (like FISH and IGHV) that define your personalized care plan.
Expert Panel:
Dr. Adam Kittai, MD Associate Professor of Medicine and Hematology/Oncology; Assistant Director of Lymphoma Clinical Research Icahn School of Medicine at Mount Sinai, New York
Strategies for Treatment, Trials, and Team Building
Watch the Replay ON DEMAND
Chronic lymphocytic leukemia (CLL) care is getting more personalized than ever.
CLL patient advocate Jeff Folloder and expert hematologist-oncologist Dr. Nicole Lamanna (Columbia University Irving Medical Center) explain how today’s innovative targeted therapies, time-limited treatment options, and emerging clinical trials can help patients craft a care strategy that truly fits their needs. The conversation dives into how to assemble a strong, collaborative medical team, at both local hospitals and major centers, so patients and families feel empowered at every step.
Program Topics
Set Your Treatment Strategy: Understand targeted therapies (BTK and BCL-2 inhibitors), their benefits, and when time-limited options fit your journey
Explore Clinical Trials: Discover how and where clinical trials fit in the CLL landscape, plus how to find the right match—whether at a major center or community clinic
Build an Empowered Team: Learn how to connect with local doctors and specialists from top centers for a coordinated plan, and what roles nurses, advocates, and social workers play
Get Organized: Practical tips for tracking labs, sharing results, and communicating with your care team
Prioritize Quality of Life: Find resources to manage daily challenges like fatigue, infection risk, and stress, while keeping your goals central to treatment talks
Join Your CLL Community: How support groups and partnerships can boost health literacy, advocacy, and your decision-making power
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Thank you to AbbVie for its support of our independent patient education program. The Patient Story retains full editorial control over all content.
Building a CLL Game Plan: Strategies for Treatment, Trials, and Team Building
Hosted by The Patient Story Team
Chronic lymphocytic leukemia (CLL) care is more personalized than ever. Patient advocate Jeff Folloder and expert hematologist-oncologist Dr. Nicole Lamanna (Columbia University Irving Medical Center) explain how today’s innovative targeted therapies, time-limited treatment options, and emerging clinical trials can help patients craft a care strategy that truly fits their needs.
ASH Update on CLL Treatment Advances: Moving from Research to Reality
Experts Attending the American Society of Hematology Discuss Targeted Therapies, Breakthrough Combinations, and Minimal Residual Disease (MRD)
Each year, there are several meetings where we discuss the latest in research in CLL, but the big meeting in December 2024 was the American Society of Hematology meeting or ASH. The impression I had was we have several approved therapies that are waiting in the wings for CLL. Let’s get into the details.
The world of CLL treatment is evolving fast, with new breakthroughs offering more options and greater precision than ever before.
This program brings together expert Dr. Jeff Sharman and patient advocate Andrew Schorr to break down the most important updates from recent research and clinical trials. Learn what’s changing, how it impacts treatment decisions, and what it all means for patients today.
New Treatment Advances: Get the latest updates on targeted therapies, combination approaches, and next-generation treatments.
Understanding MRD: Learn how minimal residual disease (MRD) testing is shaping treatment strategies.
Clinical Trials & Personalized Care: Discover how biomarkers and ongoing research are changing the CLL treatment landscape.
Expert Insights & Patient Focus: Hear from Dr. Jeff Sharman and Andrew Schorr on what this means for patients now and in the future.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang: Welcome to “CLL Treatment Advances: Moving from Research to Reality,” a program focused on all of the latest in research and clinical trials in the world of CLL treatment. It’s a space that we know has experienced so much development in the last few years especially. While that’s incredible news, it also means that there might be more questions about CLL treatment options. We are featuring some incredible CLL advocates on the topic from both the specialist side and the patient side.
I’m the founder of The Patient Story and I was diagnosed with a different kind of blood cancer, an aggressive form of non-Hodgkin lymphoma. While I was undergoing hundreds of hours of chemo, the idea for The Patient Story came up. I thought that other people would want humanized information the way that I did and that’s what we try to do. We help people navigate life at and after diagnosis in human terms and build community through in-depth patient stories and educational discussions.
I want to stress that, as always, The Patient Story retains full editorial control over all content. While we hope that this is helpful, keep in mind that this is not a substitute for medical advice so still consult with your health team about your decisions.
There’s so much to get through, so I will hand it over to someone many of you are very familiar with and who I’m proud to say has become a friend of mine, Andrew Schorr.
Andrew Schorr: Hello and welcome to this program. We’re going to discuss the latest in CLL, particularly based on one of the big medical meetings that happened not too long ago where a lot of studies came out. What does it mean for all of us? I’m in San Diego and I’ve been living with CLL since 1996.
Dr. Jeff Sharman: It’s great to be back with you, Andrew. Thanks for having me.
What Happens After a CLL Diagnosis?
Andrew: Jeff, I’ve been living with CLL for many years. Some people who will watch this program are newly diagnosed. I went through all the stages and I’m sure you see it in your practice daily. “What the hell is this? I’m scared. I have a blood cancer. Will my life be shorter? Am I going to die anytime soon? What do you have that’s effective to treat me? If that doesn’t work, do you have something else?” We’re going to get into all that, but at a high level, Jeff, how do you feel for today’s patient?
As a doctor, one of the things is figuring out how to administer the most unique medicine we give, which is the medicine of hope
Dr. Jeff Sharman
Dr. Sharman: I have a very large practice. I take care of about 400 CLL patients and for many of them, I’ve been their first doctor. That’s the nature of my practice. For a lot of folks I take care of, I’m their first contact in terms of understanding CLL.
What you highlighted is something I see time and time again, which is a very understandable fear patients come in with. It’s very common. You say leukemia and you see their eyes widen and see them sit up a little straighter. What you recognize is a great deal of distress that any cancer would cause. As a doctor, one of the things is figuring out how to administer the most unique medicine we give, which is the medicine of hope, and communicate that with patients in the midst of some of the worst days of their lives.
I do reference quite frequently a study done in the Italian group, which showed that if you’re age 65 and above diagnosed with CLL, you can’t measure a statistical impact on survival. Most patients are going to outlive their diagnosis and that’s an optimistic message. Most patients aren’t going to pass away from their disease and that bears out from my experience. The number of patients who die from complications of CLL is a very small fraction. Even in my large CLL practice, it’s only a small number; two or three per year might be the case. We have a lot of treatment options for CLL apart from the traditional chemotherapy. We have targeted agents, immunotherapy, and so forth.
Most patients are going to outlive their diagnosis and that’s an optimistic message.
Dr. Jeff Sharman
Andrew: The bottom line is most of us are going to live a pretty normal life. We may need to take medicines along the way, but we have more effective medicines than ever before and others that are very promising.
The Latest Treatment Options for CLL
Andrew: I was diagnosed in 1996, but I wasn’t treated until 2000. At that time, the feeling was that treatment might be more harmful than waiting and seeing what happens. There’s still a percentage of patients who never need treatment.
I was in a clinical trial of fludarabine and cyclophosphamide with rituximab. It led to a 17-year remission, but it had the chemo component. I had a treatment that sometimes comes into play years later, which was high-dose methylprednisolone with obinutuzumab. That was about seven years ago and I’ve never had any treatment since then.
Each year, there are several meetings where you discuss the latest in research in CLL, but the big meeting in December 2024 was the American Society of Hematology meeting or ASH. The impression I had, Jeff, was we have several approved therapies, but we have what looks like planes circling the airport at different altitudes — stage 1, stage 2, stage 3 — that are very promising and are waiting in the wings for CLL. We will get into the details, but am I right that we have a lot coming?
Dr. Sharman: A lot is coming, Andrew. At these meetings, we get to see a cross-section of development. We see all those airplanes in various stages of flight. Some are coming in for landing, some are still on the assembly line, some are mid-flight, and so forth. There are severeal reasons to be optimistic about what’s out there.
Andrew: Let’s understand where we are with approved therapy. I had some chemo years ago, but you mentioned that people aren’t going to need chemo. We have this whole class of medicines — BTK inhibitors — and even new generations of that we can talk about. With the approved therapies, you have quite an arsenal now where you can use drugs either by themselves or together.
Dr. Sharman: There are three main classes of drugs. You mentioned BTK inhibitors. I would add BCL-2 inhibitors and immunotherapy, particularly obinutuzumab, which goes by the commercial name Gazyva. It took a lot of work to get each of these drugs approved. Right now, we’ve learned how to combine these drugs in terms of what we call doublet therapy, where we use two of those drugs together, and even triplet therapy, where we put three of them together. What the field is trying to figure out is the best combination and the best sequence.
The good news is these drugs are FDA-approved and available to patients. When most patients think about chemotherapy, they think of the traditional drugs developed from the 1950s through the year 2000. Those are drugs that typically damage DNA and cause cells to die as a result of damaging DNA.
What’s different now is we have these targeted therapies, which have no DNA-damaging component but instead exploit certain vulnerabilities of the cancer cell. There’s an enzyme sequence or a signaling mechanism inside a cell. I like to think of it as an electrical current, which needs to keep going to keep the CLL cell alive. What BTK inhibitors do is cause a short circuit in that electrical circuit, so the cancer cells die as a result. It turns out that the cancer cells are more sensitive to it than normal healthy B cells. It’s a targeted therapy. It doesn’t damage DNA. It exploits a certain vulnerability.
BCL-2 inhibitors are similar in that the cancer cells are dependent upon this enzyme called BCL-2, which helps keep the cell alive. If we disrupt BCL-2, it’s almost like taking off the fence from around the Grand Canyon — they fall in and the cancer cells die as a result. It gets rid of the safety mechanism for the cells.
With obinutuzumab, what we’re doing is recruiting the immune system to fight off the cancer of the immune system. It’s as though we’re giving the immune system the tools it needs to fight off the cancer that’s already there.
Each of these drugs has its side effects. There’s no such thing as a drug that doesn’t have side effects, but in contrast to traditional chemotherapy, it’s not the same type of patient experience. These aren’t nausea-provoking drugs and they certainly don’t cause hair loss. In a lot of cases, these drugs are pretty easy to take side by side with the rest of your medications and you might not necessarily know there’s something unique about it, if that makes sense.
Andrew: As far as BTKs, we have ibrutinib (Imbruvica), acalabrutinib (Calquence), zanubrutinib (Brukinsa), and pirtobrutinib (Jaypirca). For BCL-2, we have venetoclax (Venclexta) and others in development. Many people are taking BTKs now. How do you determine who gets what?
Dr. Sharman: There’s a lot of terminology around first-generation, second-generation, and third-generation. We’re researching fourth-generation BTK inhibitors.
The very first BTK inhibitor to come about was ibrutinib, which turns off the BTK enzyme in a unique way. It forms a bond with the BTK molecule, which we call an irreversible inhibitor or covalent inhibitor. It forms a permanent attachment to the BTK enzyme so that particular enzyme will never work again until the cancer cell makes a new one. Cancer cells make new ones and in about 24 hours, they’re starting to wake up their BTK, which is why ibrutinib is taken once a day. The new enzyme needs to be shut down, just like the old enzyme was.
There are some unique side effects with ibrutinib. We see an increased rate of bruising and bleeding, which tends to be mild arm bruising. For most patients, it doesn’t prove to be all that much, but a lot of our patients are already on blood thinners so if you start adding them together, the risk of bleeding goes up. We see some joint aches and muscle cramps happen. Occasionally, patients can have an abnormal heart rhythm called atrial fibrillation. Originally, we didn’t know if that came from the drug, but we’ve largely concluded now that it does.
That left room for the second-generation BTK inhibitors, acalabrutinib and zanubrutinib. These medications underwent more rigorous pre-clinical development of medicinal chemistry to try to dial out some of those side effects. In fact, acalabrutinib and zanubrutinib have been compared head to head against ibrutinib in various studies and have shown fewer side effects for most patients and some increased efficacy. Within the field, most doctors who follow this area closely tend to start patients on either acalabrutinib or zanubrutinib.
How do we pick? Sometimes it’s an insurance issue. Sometimes you might have some bias. The cardiac differentiation is a bit in favor of acalabrutinib. In the head-to-head study where zanubrutinib was compared to ibrutinib, there may be a signal of higher efficacy. If you’re going to combine it with obinutuzumab, you go with acalabrutinib. There are various reasons you might pick one over the other. Sometimes it comes down to insurance, but I view acalabrutinib and zanubrutinib as more similar than different.
What is Pirtobrutinib?
Andrew: You used the term covalent. I understand there are non-covalent BTKs and I believe pirtobrutinib is one of those. What’s the difference?
Dr. Sharman: We talked about acalabrutinib and zanubrutinib as second-generation BTK inhibitors because they differentiate from ibrutinib. We consider pirtobrutinib a third-generation BTK inhibitor.
When we talk about the different generations, what’s the main difference? It’s a non-covalent inhibitor. Over time, patients can develop resistance to the first- and second-generation BTK inhibitors and the most common way they do that is by modifying the exact spot on the BTK enzyme where the first- and second-generation BTK inhibitors bind. There’s an amino acid in position 481 called cysteine that can get mutated. All of a sudden, those drugs don’t work. There are other mutations, but that’s the most common one.
Pirtobrutinib does not require forming a bond. It stays in the system a little bit longer, fits into the binding pocket more easily, and doesn’t require that irreversible bond. Pirtobrutinib has been shown to work even after patients have developed resistance to the first- and second-generation BTK inhibitors and that’s what differentiates it as a third-generation BTK inhibitor.
Another one in late development is called nemtabrutinib, which may or may not get approved — I suspect it will. It may still be a little ways away and has flown under the radar a little bit. The distinct advantage of non-covalent inhibitors is they can continue to inhibit the BTK enzyme even after the first- and second-generation BTK inhibitors have stopped working.
What is a Degrader?
Andrew: Some of our patients are like mini scientists and are asking about degraders. What are degraders? I know we don’t have them approved yet, but where are they going to fit in?
Dr. Sharman: They would be a fourth-generation BTK inhibitor. I’ll take the cloud-level view. One paradigm in all of oncology is that when you find a good target, a good enzyme to inhibit, or a good surface target, there are always efforts to continue to exploit the therapeutic opportunity of going after that target in new and improved ways. Clearly, one of the improved ways is to work when the other drugs stop working.
BTK degraders get rid of the BTK enzyme completely instead of turning it off.
Dr. Jeff Sharman
The concept of degraders is a lot like pirtobrutinib, although it does it through a different mechanism. It’s designed to inhibit BTK even when the BTK inhibitors have stopped working. Within any cell — cancer cell or regular cell — there is trash disposal for old broken-down proteins. We are constantly synthesizing new proteins and getting rid of the old ones. Degraders glue a couple of molecules together — one that goes after BTK and then the other one designates the protein for the trash heap — and tags the BTK molecule to dispose of this enzyme. Instead of inhibiting BTK, it’s degrading BTK, which is very different. BTK degraders get rid of the BTK enzyme completely instead of turning it off.
BTK degraders are a very active area of research right now. These would be the airplanes that aren’t necessarily coming in for a landing or even mid-flight. They are still getting manufactured and haven’t taken off from the ground.
CLL Treatments Being Studied Now
Andrew: Venetoclax is a BCL-2 inhibitor, which is a different mechanism of action. There are other BCL-2s in development as well. What are some of the names?
Dr. Sharman: Sonrotoclax is probably the one that’s farthest along. There have been a handful of other BCL-2 inhibitors that have gotten out there. Venetoclax is an incredibly effective drug. In fact, it’s so effective that its effectiveness may almost be its biggest liability. It can literally kill cancer cells so fast that the consequences of that can be some electrolyte abnormalities and disturbances that can be life-threatening, which is what we call tumor lysis syndrome where you’re killing cancer cells too quickly. The inside of cancer cells has a lot of potassium and uric acid.
Andrew: Your kidneys can’t keep up.
Dr. Sharman: You can’t keep up. It can clog up the kidneys, cause heart arrhythmias, and so forth. With venetoclax, we start with a very low dose of 20 mg for a week. The following week, we go up to 50 mg. The week after, we go up to 100 mg. Then 200 mg. Patients generally go on 400 mg.
It also has some drug interactions, more for our patients who have acute myelogenous leukemia (AML) or patients on cardiac medications. What we have to do is check labs frequently. We stratify the risk for these patients. Are they low risk, intermediate risk, or high risk? That has to do with how high their white blood cell count is, how big their lymph nodes are, and how their kidneys function, so we follow these patients closely. For a lot of patients, it’s a month with a lot of lab visits. Sometimes, we even put patients in the hospital when we start the medication because we want to be able to jump into gear if they’re high risk.
It has logistical challenges. It’s not used quite as frequently in the front-line setting as BTK inhibitors, which are oftentimes quite simple to give, but it’s a very effective drug. One of the big advantages is it gives very deep remissions. Oftentimes, we’re able to give patients the drug for one year in the front-line setting, two years in the relapse setting, and then stop the medicine. Patients can have remissions that can last multiple years without requiring ongoing therapy. Whereas with BTK inhibitors, once we start them, patients always ask, “Am I going to be on this forever?” I say, “You’re going to be on it as long as it’s working for you.” For many patients, it can be from five to 10 years, which feels like a long time to be on an anti-cancer medicine for patients.
Patients can have remissions that can last multiple years without requiring ongoing therapy.
Dr. Jeff Sharman
Deciding When to Use a Combination of Drugs for Treatment
Andrew: Let’s tie this together. We have BTK inhibitors that work for most people and depending on the side effects you might experience, the health of your heart, or other issues you might have, your doctor would work with you to choose one that’s the kindest on your body. You might combine it with another drug. You talked about doublets or even triplets, so somebody might receive one of these drugs with obinutuzumab. Would somebody get a BTK and a venetoclax?
Dr. Sharman: That leads us to some of the discussions at the 2024 ASH meeting. If we go back in time to a couple of meetings ago, we saw data for the combination of ibrutinib and venetoclax that was compared against one of the standards at that time, which included obinutuzumab with a chemotherapy drug that’s not used much anymore called chlorambucil. The ibrutinib-venetoclax clearly beat obinutuzumab-chlorambucil and interestingly, we had a different opinion depending on where you are in the world as to whether or not it could be approved. That combination was approved in most of Europe and is reimbursed by insurance in several jurisdictions. In fact, ibrutinib-venetoclax is a very common regimen utilized in Europe.
The combination of acalabrutinib-venetoclax or the triplet acalabrutinib-venetoclax with obinutuzumab was compared against two of the harder chemoimmunotherapy regimens.
Dr. Jeff Sharman
Interestingly, there was a different take on the US regulatory environment. There were some technical reasons that had to do with some of the side effects of combining ibrutinib with venetoclax. Diarrhea was considerably more common and this was in an older population. It was a harder regimen in older patients. The US did not approve it.
You have this difference between the US and Europe. The combination of ibrutinib-venetoclax is not used much in the United States outside of some studies. It does have an endorsement by the National Comprehensive Cancer Network (NCCN). Oftentimes, you could get it, but it leaves a window of opportunity for other BTK inhibitors, which gets us into some of the discussion at the 2024 ASH meeting.
The combination of acalabrutinib-venetoclax or the triplet acalabrutinib-venetoclax with obinutuzumab was compared against two of the harder chemoimmunotherapy regimens, either fludarabine, cyclophosphamide, and rituximab (FCR) or bendamustine-rituximab (BR). In both experimental arms, the doublet (acalabrutinib-venetoclax) and the triplet (acalabrutinib-venetoclax with obinutuzumab) beat chemoimmunotherapy.
Within the field, there’s an expectation that there will be approval fairly soon for acalabrutinib-venetoclax with or without obinutuzumab, which is attractive to patients because it’s an all-oral regimen. You take the acalabrutinib for a while before you start the venetoclax. It cuts down on the risk of tumor lysis quite a bit. It’s convenient, effective, and fixed duration, so patients don’t take it until it stops working. There are a lot of advantages to that combination and it’s one of the things that we’re expecting to get an approval by the FDA sometime in 2025.
Andrew: To be clear though, obinutuzumab is an infused therapy.
Dr. Sharman: Yes, obinutuzumab is an infused therapy. The triplet includes obinutuzumab, which is an infused therapy.
Andrew: Jeff, it sounds like we’ve got lines of therapy. We have people who you might start on a single drug. You might have a discussion with a patient about fixed duration, putting two drugs together, taking them for a while, and if you can get their disease undetectable or very low, they can stop and see how long that goes. That might be attractive.
Dr. Sharman: We haven’t talked about obinutuzumab-venetoclax as another doublet. We’ve talked about BTK inhibitors. We’ve talked about venetoclax. Most of the time, once somebody starts a BTK inhibitor, they stay on it until it stops working.
Obinutuzumab-venetoclax is generally considered a one-year therapy. Patients start with obinutuzumab, get a sequence of several infusions, and continue on it for a total of six months. We start venetoclax somewhere around month two and go through a careful ramp-up. For those patients, we generally can stop at 12 months. For the molecularly favorable, they may not need therapy for another five, six, or seven years. For some of the higher risk, like the IGHV unmutated population, those remissions might not last quite as long. But one of the big things in the field right now is: what’s the optimal doublet?
Most of the time, once somebody starts a BTK inhibitor, they stay on it until it stops working.
Dr. Jeff Sharman
We have obinutuzumab-venetoclax. We’re likely going to have the approval of acalabrutinib-venetoclax. Which of the two would you rather do? There might be different reasons for different patients. I’m excited about the MAJIC study, which we helped design and lead. The study directly compares obinutuzumab-venetoclax to acalabrutinib-venetoclax. We’re going to learn a lot from that. Do you take it for one year or two years? All oral or IV? That’s one of the big questions in the field. If I’m going to pick a doublet, which two do I pick?
What is CAR T-cell Therapy?
Andrew: Some people will progress and there’s one kind of treatment we haven’t talked about yet: CAR T-cell therapy. Where do we stand with that? My friend Dr. Brian Koffman, who’s gone through many different therapies, had CAR T-cell therapy. It’s a big gun. Where does that fit in for people who don’t do so well on some of these other drugs?
Dr. Sharman: CAR T is an amazing science, Andrew. It’s so amazing to see. The concept here is that we have a patient go through a one-day procedure that is conceptually like dialysis. We take out and isolate their T cells then ship those T cells to a lab. They get reprogrammed in part by the use of a virus that’s been engineered to give the cell different instructions. The cells get manufactured, expanded, and infused back into the patient. It’s amazing, Andrew. The CLL cells get destroyed by these reprogrammed T cells and patients can get very deep remissions.
Now, this is a technology that’s not unique to CLL. In fact, it was first used in CLL and acute lymphoblastic leukemia (ALL). The development in CLL stalled a little bit. But in other diseases, such as diffuse large B-cell lymphoma (DLBCL) and ALL, we feel very comfortable as a field saying that CAR T-cell therapy can be curative in those settings. It is too early to say whether it can be curative in CLL or not. My professional opinion is that for some patients, it could be.
Right now, [CAR T-cell therapy]’s only approved for patients who’ve had both a BTK inhibitor and a BCL-2 inhibitor, but it’s been an effective therapy for a number of my patients.
Dr. Jeff Sharman
The clinical trial that led to the approval of CAR T-cell therapy took the worst of the worst patients who were extraordinarily sick. The data that led to the approval wasn’t the most impressive or compelling; it limped across the finish line. That said, sometimes we design studies to get a drug approved by the FDA and then how we use them in the real world can differ. The opportunity with CAR T-cell therapy may exceed the perception from the study that led to its approval.
Who’s it right for? The reality is a lot of older patients with CLL may not ever need it. Give them a pill, send them on their way, and they’re going to be fine. But the younger they are, the more aggressive the disease, or the combination of young patients with aggressive disease, CAR T-cell therapy is something that needs to be factored into their thinking earlier on. Right now, it’s only approved for patients who’ve had both a BTK inhibitor and a BCL-2 inhibitor, but it’s been an effective therapy for a number of my patients.
We think about treatment sequencing… You need to almost have a game plan in mind for somebody from the outset.
Dr. Jeff Sharman
Working with Your Doctor to Decide on a Treatment
Andrew: In 1996, when I started talking to Dr. Kanti Rai, one of the grandfathers in CLL in clinical research, there wasn’t much to talk about. I said, “Dr. Rai, it seems like you have a lot of furniture in the room and you’re trying to figure out where to put the couch, where to put the easy chair, and how to move things around.” It sounds like that’s where you are now, except you have more furniture.
Dr. Sharman: We’ve lived in the house longer, so it’s more cluttered, and we’ve upgraded the couch.
Andrew: I’m sure there are patients whose heads are spinning. Not all CLL patients are the same and treatment is an individualized choice.
Dr. Sharman: Absolutely. There are some patients who, from the physician’s perspective, I would say, “Oh, this is what we’re doing.” Then there are other patients who are very involved in their care and want to be involved in the decision-making. That’s great and they should be involved.
A patient might have preferences, but I may have different preferences based on how I’m thinking. Sometimes it’s a matter of calling to attention some of the potential side effects in a certain circumstance. Maybe somebody wants to do a fixed duration, but their kidneys aren’t doing well, they have bulky disease, or other reasons why we might pick one over the other.
We think about treatment sequencing. If we’re going to pick this first, what’s the patient going to look like five to seven years from now when we might need to do a second therapy? You need to almost have a game plan in mind for somebody from the outset.
When Do Doctors Decide to Start Treatment?
Andrew: I went four and a half years without treatment and felt pretty good. Then I started to develop some lymph nodes and my white blood count fueled by lymphocytes went up to about 283,000. My friend Dave has a white blood count that’s even higher than that, but he hasn’t had treatment and feels fine. When do you start treatment for a new patient?
Dr. Sharman: Back in the 1950s, steroids were a new thing. This was a byproduct of World War II and we were giving steroids to patients with CLL. In some original manuscripts, patients were getting white blood cell counts of 1.5 million, a number we would never see today. Patients always want to know: At what white count do I need to intervene? The answer is: There isn’t a white count where you need to intervene.
We look at the lymphocyte doubling time (LDT). When that number goes up more than twofold in less than six months, that’s our clue that we need to do something.
Dr. Jeff Sharman
You see doctors get squeamish at different thresholds. If you’re a non-CLL doc, you start to get squeamish around 100,000. If you’re a CLL doc, 200,000 or 300,000 will start to make you nervous. If you’ve been around the block a long time, you have patients who come into your clinic with a white count of 600,000 who are stable. You get desensitized to it.
It’s not a number; it’s a rate of change. It’s not about whether you hit 100, 200, 400, or 600; it’s how quickly your numbers are increasing. For a patient who’s climbing quite rapidly, we look at the lymphocyte doubling time (LDT). When that number goes up more than twofold in less than six months, that’s our clue that we need to do something.
There are other reasons we might treat somebody. When they have bulky lymph nodes, start developing marrow dysfunction, get anemic or their platelets are starting to go down, those can be reasons to intervene. If you treat a lot of CLL, you see some weird ones. I had a patient who had direct kidney involvement with the CLL and had significant kidney problems; that’s not a very common one.
What comes up periodically is fatigue. Some patients have disabling fatigue. They might be 55 years old. They’re not depressed. Their thyroid is fine. They’re not iron-deficient. But they can only go to work for four hours before they have to come home. Disabling fatigue is a reason to treat. These are all pretty well spelled out in the iwCLL criteria: rate of change, symptomatic, bulky lymph nodes, marrow dysfunction, and others. Those are the reasons we treat patients.
I have had some young women, one or two in particular, who were diagnosed at childbearing potential. It’s fine to have kids.
Dr. Jeff Sharman
CLL and Fertility Concerns in Younger Women
Andrew: Another thing that people wonder about is if they’re told they’re diagnosed with CLL and they’re younger and female, would you tell them not to get pregnant?
Dr. Sharman: It hasn’t come up all that much because most women, if they’re going to have kids, will do so before their mid-40s or even younger. The typical age of diagnosis of CLL is 72 with the first line of therapy typically at 74, so it’s not a common scenario. That said, I have had some young women, one or two in particular, who were diagnosed at childbearing potential. It’s fine to have kids. It doesn’t come up often, but it’s not a contraindication.
Addressing Side Effects with Your Doctor
Andrew: We had people who wrote that they had a back rash, a migraine, or this or that. Is it because of the drug they’re taking for CLL, is it the CLL, or is it something else? How do you determine if it’s the drug, the illness, or something else?
Dr. Sharman: There’s obviously no uniform answer to all of that. It’s going to take a close relationship with your oncologist. I always invite my patients to ask questions and do my best as a clinician to say, “Yep, I own that one,” or, “Nope, I don’t think that’s me,” and call balls and strikes. I figure if I’m honest with it and own up to something, then they’ll believe me when I say it’s not on me.
As doctors, we don’t always know. Sometimes it takes working it out together with your patient about how you solve this.
Dr. Jeff Sharman
Even if I’ve done this for a long time, there are times when we don’t know. Sometimes you have to hold the drug for a little while, see if it gets better, restart it, and see if it comes back. You can do that with side effects that are of lower consequence. If it’s a major side effect, like a hemorrhage, that’s a different story altogether. As doctors, we don’t always know. Sometimes it takes working it out together with your patient about how you solve this.
What is Richter’s Transformation?
Andrew: Jeff, there’s a small percentage of patients where you talked about aggressive disease and there’s something called Richter’s Transformation. Could you explain that? One of the patients who wrote in is worried about that.
Dr. Sharman: Richter’s Transformation is a potential complication of CLL that is definitely more concerning. It’s generally when the CLL cell acquires a more aggressive behavior and becomes DLBCL, which is a different entity altogether. It requires a different treatment approach. Generally speaking, we reach for more traditional chemotherapy in that setting. In some cases, it can be fairly resistant to therapy. It’s a disease that can move very quickly.
Richter’s Transformation is rare… But if you’ve had the disease for 20 years, that risk starts to build up.
Dr. Jeff Sharman
If it’s suspected, the clinician has to jump into gear quickly. It requires a biopsy because you have to get a biopsy and prove that it’s not Richter’s Transformation quickly. Most often, you see a lymph node that’s swelling very quickly and disproportionate to the others. If you’re going to get a PET scan, it’s oftentimes bright on a PET scan. These are the things we’re thinking of as a clinician.
Fortunately, Richter’s Transformation is rare. It’s seen in about 1% of patients per year. But if you’ve had the disease for 20 years, that risk starts to build up. It probably hits a plateau at around 15 to 20%.
Sometimes, Richter’s Transformation is misdiagnosed. If you stop somebody on a BTK inhibitor, oftentimes their nodes will increase pretty quickly thereafter and in that circumstance, I’ve seen cases where Richter’s may have been inaccurately diagnosed. It requires a certain degree of suspicion if you’ve got a biopsy right after starting BTK inhibitors.
How Do Doctors Treat Younger Patients with CLL?
Andrew: I know this is complicated for people. We discussed that if you haven’t had treatment, you don’t treat the number; you look at the overall patient. You have a variety of medicines. BTK inhibitors are used by themselves or in combination, and there are different generations. We have clinical trials for some of these treatments mentioned at the 2024 ASH meeting. There are phase 1 trials for BTK degraders. CAR T-cell therapy is for people with more aggressive disease, although we’ll see if that creeps up a little earlier for younger patients.
Some people on Facebook, for instance, are under 50 with CLL and I know it’s not the most common. Is their age of diagnosis a bad thing? Are they going to have a rougher time with CLL because they’re diagnosed younger? Will they not live as long? What do you tell a younger patient based on their age?
Our therapies are as effective in younger individuals as they are in older individuals… we need to come up with something that’s going to keep this disease in control for quite a bit longer.
Dr. Jeff Sharman
Dr. Sharman: For these patients, we have to plan not only for the next 10 to 15 years but also for the next 30 years. To some degree, we celebrate that we have a lot of new tools to control the disease. It is a reasonable question to ask: Can you use these tools to control it for twice as long or three times as long as somebody who’s diagnosed at age 80? It’s a different game plan.
Our therapies are as effective in younger individuals as they are in older individuals and in some cases, maybe even more effective in younger individuals. But it does require some thoughtfulness to think about the fact that we need to come up with something that’s going to keep this disease in control for quite a bit longer.
The field is moving so fast that the tools we’ll be using five to seven years from now may not even have been conceived of at this point. If somebody’s diagnosed younger, it’s fair to assume that there will be more tools in the tool shed down the road.
There’s a general misperception that you would only do a clinical trial if you’re running out of options but it’s not the case at all.
Dr. Jeff Sharman
Considering a Clinical Trial for CLL
Andrew: Some of your patients are on clinical trials. When someone meets with their CLL doctor, should clinical trials be part of the discussion? Do you lay all this stuff out and then say what are in trials that they should consider as well?
Dr. Sharman: Andrew, we treated the very first CLL patient in the world with ibrutinib in my clinic and I’ve been a believer ever since. In many cases, we’re so grateful for patients who’ve volunteered for studies in the past because they’re the ones who’ve moved this field forward.
Clinical trials are not a one-size-fits-all scenario. There’s a general misperception that you would only do a clinical trial if you’re running out of options but it’s not the case at all. There are great studies for previously untreated patients, patients on first relapse, and patients who are resistant to certain treatments. In many cases, for the last 15 to 20 years, some of our best options have only been available in research studies.
It calls for a unique answer for every patient and what sort of studies might be available and accessible to them, but I would definitely like to dispel the notion that it’s only a therapy for patients who’ve run out of options.
Andrew: I was in a phase 2 trial in 2000 for FCR and it led to a 17-year remission, for which I’m very grateful. Would I have had that otherwise?
Concerns About Funding for CLL Research
Andrew: There are challenges about funding for research and researchers are worried. From the point of view of a CLL patient or CLL researcher, do you have a concern where that throws cold water on progress for CLL?
Dr. Sharman: It’s a great question and a sensitive discussion. People are going to have different opinions on this. The funding environment is shifting and I don’t know if we totally understand all the implications. It is worth noting that many studies are supported by the pharmaceutical industry. I know that the pharmaceutical industry is oftentimes considered a bad word, but they’ve been the friends that have brought us a lot of progress in the last handful of years.
The funding environment is shifting and I don’t know if we totally understand all the implications.
Dr. Jeff Sharman
For studies that are sponsored by pharmaceutical companies, these are oftentimes trying to develop a new drug or getting a new drug approved, so I don’t see much impact there. But when it comes to academic, university-based exploratory studies that are grant-funded, some of those will be impacted and some of the basic science research is up in the air right now. People don’t know if grants are going to be renewed or not. Amongst my academic colleagues, there is a great deal of concern and consternation about what the funding changes will mean. The whole story hasn’t been written yet, but like anything, it’s a nuanced answer where some areas will be affected more than others.
Andrew: How many years have you been at it, Jeff? How many years have you been in practice and seeing CLL patients?
Dr. Sharman: I finished my fellowship in 2008 at Stanford and I’ve been in practice in Eugene, Oregon, since then. Fellowship, residency, med school, and undergraduate studies all take a while. I don’t know where you start the clock, but I’m getting gray. How’s that?
Is There a Cure for CLL in Sight?
Andrew: I used to ask Dr. Keating, one of the grandfathers in Seattle, about this. Will we see a cure for CLL in your lifetime? Dr. Sharman, do you have hope for a cure?
Dr. Sharman: Unequivocally yes.
Andrew: I like that answer.
Dr. Sharman: I’ll leave it simple.
The world has changed in the last decade for what it means to be a patient with CLL and it is an area where I think hope is very reasonable.
Dr. Jeff Sharman
Andrew: I like that. When you put it all together, we have a variety of treatments that you can choose from with your patient based on their preference, your recommendations, and their clinical situation. We had some early- and later-stage research at the 2024 ASH meeting in December. Other meetings will happen during the year and then we’ll have ASH again, so we’ll get to talk again. You have different doublets and triplets, and even different ways of doing it. It sounds like there’s great hope for people.
Dr. Sharman: I couldn’t agree more, Andrew. I feel like the world has changed in the last decade for what it means to be a patient with CLL and it is an area where I think hope is very reasonable.
Conclusion
Andrew: Like you, I’ve been at this a while. I was diagnosed in 1996. I’ve seen some sick people, people who’ve been on clinical trials like me, and people on newer medicines. Most people are doing well. My CLL is at a very low level. You may be in long-term remission and though we may not be cured, go live your life. With Dr. Sharman and his colleagues doing the research and the studies that keep coming out, we have every reason to think that we can do that for a long time. Dr. Sharman, thank you so much for being with us and explaining all this.
Dr. Sharman: It’s my pleasure. Thank you so much, Andrew, and I look forward to future conversations.
Andrew: Remember: knowledge — and we’ve been getting some today — can be the best medicine of all.
Stephanie: Thank you, Andrew and Dr. Sharman, for leading this wonderful and very educational discussion at The Patient Story and taking the time out of your very busy schedules to provide such great insights.
As always, we retain full editorial control. We want to point out some incredible resources from our friends at partner organizations, like The Leukemia & Lymphoma Society and the CLL Society.
The LLS has a community section for people to meet and chat with other blood cancer patients and care partners; in this case, in CLL. The LLS offers many things, but one of the free resources is the Clinical Trial Support Center. It’s free, one-on-one personal guidance throughout the process before, during, and after clinical trials, which, as we know, can be a lot.
The CLL Society has a lot of great programs, too. It’s dedicated to the CLL community and offers programs like Expert Access™, connecting patients to world-renowned CLL experts for a free virtual second opinion, which is so important, especially with all the things that are going on, as you can see from this discussion.
I hope this program was helpful and that you walk away with more knowledge and questions to ask your doctors. Thank you for coming and we hope to see you at another program. Take good care.
CLL 360°: It’s Time for Treatment – Making the Right Decision for Me
Edited by: Katrina Villareal
Learn how shared treatment decision-making—a collaborative process where patients and doctors work together to make healthcare decisions—can help you navigate the rapidly evolving landscape of CLL treatment options.
Discover what shared decision-making means and how it can empower you in your treatment journey. Get insights into the latest advancements in CLL therapy and how to choose the best treatment plan for you. Learn how to weigh the potential benefits of treatment against its impact on your daily life. Gain strategies for discussing your preferences and concerns with your healthcare team.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang: The goal of our program is for patients and care partners to walk away with a better understanding of how to approach decision-making with their medical team with all these options. There’s so much rapid change happening with continuous therapy and time-limited treatment. The ultimate question is: what is the best for you and or your loved one?
My name is Stephanie Chuang. I’m also a blood cancer patient advocate. I was diagnosed with non-Hodgkin lymphoma and that experience is how I decided to start The Patient Story, a platform that aims to help people navigate life before and after diagnosis in human terms. We do this through in-depth patient stories as well as educational discussions, which we know is especially important for those who are dealing with CLL and SLL wanting to empower themselves continuously throughout treatment.
We also want to give a shout-out to our friends over at The CLL Support Group on Facebook led by our friends, including our moderator Michele Nadeem-Baker. They offer ongoing virtual support for folks dealing with a CLL diagnosis.
Michele Nadeem-Baker, Patient Advocate
Michele Nadeem-Baker: I was diagnosed in 2012 and by the time I needed treatment, it was the end of 2015. I had a simple choice: standard of care or go on a clinical trial. I chose to join a clinical trial and luckily, it gave me part of the standard of care in combination with the future of treatment. I discussed all of this with my CLL specialist and we came to a shared decision for my treatment.
When I relapsed a few years ago, I had to make a decision once again. There were so many choices at that point, which was fantastic for patients but made it a little more difficult to make the decision.
Dr. Nicole Lamanna, Hematologist-Oncologist
Michele: Dr. Nicole Lamanna is the director of chronic lymphocytic leukemia and professor of medicine at Columbia University Medical Center. Dr. Lamanna, what drew you to specializing in CLL?
Dr. Nicole Lamanna: When I was a resident at NYU at Bellevue, we used to rotate at Memorial Sloan Kettering for our oncology experience. As an intern and then as a resident, they put me on the leukemia service every year.
When I became a third year, one of the leukemia docs kept in touch with me and said, “Nicole, what are you thinking about doing?” I was into taking care of the whole patient, so I said, “I’m going to be an internist or a primary care physician. I love taking care of every part of the patient.” He said, “Didn’t we do that on leukemia when you were in the inpatient unit? Don’t you remember we took care of infection, kidney failure, and heart attacks?”
The more I thought about it, the more I thought about applying to an oncology fellowship. Sure enough, that little push and having good mentors did that for me. I decided to apply for a fellowship and went to Sloan Kettering. While I did my fellowship, I did my research with one of the leukemia guys, was taken under their wing, and started working with a CLL mentor. I wouldn’t be doing this if it wasn’t for them. I give them lots of credit.
Dr. Charles Farber, Hematologist-Oncologist
Michele: Dr. Charles Farber is a board-certified oncologist and medical director of oncology research network development for Atlantic Health System. He also serves as a clinical assistant professor at Rutgers Cancer Institute of New Jersey. Dr. Farber, what drew you to specializing in CLL?
Dr. Charles Farber: When I was a college student, I was working in a laboratory and doing structural activity relationships. I got into an MD/PhD program at NYU and was slated to go there and start research with Eric Simon who coined the term endorphin.
Right before I got there, he moved to Columbia, so I had to find someone with a research interest that would overlap with mine. I looked at the faculty at NYU and Robert Silber was doing cutting-edge work in CLL. I ended up joining his laboratory and I’ve kept up my interest in CLL throughout my career.
Treatment Advances in CLL
Michele: Doctors, the world of CLL has changed tremendously with so many more treatment options. Dr. Lamanna, can you give us a summarized update on the current CLL treatment landscape and how it’s changed, especially in the last couple of years?
Dr. Lamanna: To allude to what Michele was saying, back in the day, we had chemoimmunotherapy regimens like fludarabine, cyclophosphamide, and rituximab or FCR, or bendamustine-rituximab intravenous therapies. These were standard of care. We didn’t have as many choices.
Now we have more of these targeted small molecule inhibitors. The two big classes we have are BTK or Bruton tyrosine kinase inhibitors and BCL2 inhibitors. These oral therapies have become the standard of care. Patients can either take a chronic therapy with one of these oral BTK inhibitors or you can get a time-limited approach with a BCL2 inhibitor.
The only one we have currently approved is venetoclax in combination with a CD20 monoclonal antibody, which is rituximab or obinutuzumab. We’ve moved away from chemotherapy and now people are on either BTK inhibitors or some sort of venetoclax-based therapy.
Shared decision-making is a collaborative process where patients—often with their family members—and their doctors sit down, communicate, and come up with a plan.
Dr. Charles Farber
What is Shared Treatment Decision-Making?
Michele: I’m extremely thankful for all of these new treatments, but this means choices, and choices mean decisions need to be made. Many patients are hearing the term shared decision-making. What does that mean?
It’s understood that doctors are the experts from a medical and clinical standpoint, and patients are the experts on themselves and what matters most. Dr. Farber, please explain in simple terms what shared decision-making means when it comes to treatment and what the process typically involves.
Dr. Farber: Shared decision-making is a collaborative process where patients—often with their family members—and their doctors sit down, communicate, and come up with a plan. It’s not limited to a choice of treatment or duration of treatment. With CLL in particular, most patients don’t need treatment, so we observe them. We do watchful waiting or as my patients refer to it, watchful worrying.
The first decision is what criteria need to be met before a treatment is offered. Then we discuss what treatment options are available, what are they, and what’s best for the particular patient. It’s individualized, so it relies on two-way communication where the doctor may have in mind what’s best for the patient, but the doctor doesn’t make the decisions for you.
We do share in the decision-making where it’s appropriate. It boils down to trying to communicate and impart important information to our patients and their loved ones to determine what’s best. It’s interactive. It’s a dialogue. The doctor with their experience and knowledge has to work with the patient with what they desire.
What Factors Guide Shared Decision-Making?
Michele: Dr. Lamanna, what factors guide you in making treatment decisions?
Dr. Lamanna: This has become more complicated and part of it is because shared decision-making has become more present because we have more options. When there was only one option, the choices were whether the patient was going to do treatment or not. With all these options, it becomes a conversation.
We do shared decision-making because these treatment options are slightly different… what may be relevant for them at this particular moment in their life may be different later on down the road.
Dr. Nicole Lamanna
We think about the genetics and the disease itself. What is going on with the patient? What are the features of their disease? Are their blood counts bad? Do they have big bulky lymph nodes? Do they have genetic features? Do they have chromosomal abnormalities? Do they have high-risk disease? You might hear about 17p deletion, TP53 mutation, or even multiple chromosomal abnormalities.
What other medical problems does the patient have? What other comorbidities do they have? How is their kidney function? What are their social circumstances? Can they get back and forth to the clinic or the hospital frequently or not? Do they need extra support? Are we looking at therapies that might be easier for that patient?
We take all of those into consideration and that’s where shared decision-making comes into play when we talk about either BTK inhibitors or venetoclax-based therapy. What are the choices in that person’s life at that particular time? Some people might have little kids and are busy and active, so they need something simple and not going to be too labor intensive. Other people may choose something different and go for more intensive therapy because they can put in the time.
We do shared decision-making because these treatment options are slightly different. They’re both great treatment options. Even though many people will wind up potentially using both of these options during their lifetime, what may be relevant for them at this particular moment in their life may be different later on down the road. That’ll come up again when you talk about relapse or needing more therapy.
Balancing Treatment and Quality of Life
Michele: Dr. Farber, quality of life is an important factor for all patients when considering treatment options. How do you balance the potential benefits of treatment with the impact on a patient’s daily life?
Dr. Farber: It’s a very complex equation. I saw a physician newly diagnosed with a low-grade lymphoma. I asked him if he was retired, about his personal life, and what he enjoys doing. He was with his wife and family. The wife interrupted and asked, “Why are you asking these questions?”
I told her it’s very relevant in terms of the big picture. What are the goals of treatment? What’s the lifestyle of the patient? What are they willing to tolerate? How temporary is the initial treatment? Is it a phase? Some of the medicines require more intensive monitoring before things get better, so the questions are very important.
Quality of life is a very important issue and one of the more important variables in the treatment equation.
Dr. Charles Farber
Quality of life is life. Whether someone is willing to sacrifice, people want to live longer and better, and what they’re willing and able to tolerate and for how long has to be assessed. It’s a very complex equation and with these many variables, it needs to be explored.
What are the goals of therapy? Is it to make you live longer? Is it to make you live better? What are we trying to achieve? What are the treatment options? What are the side effects? Quality of life is a very important issue and one of the more important variables in the treatment equation. Shared decision-making is critical where you can’t do for the patient what you think is important. It has to be a dialogue.
Michele: All this is music to my ears because when I was on frontline treatment, my quality of life wasn’t so great, but at that point, there were no choices. We are so fortunate to have these choices now and that we can have a better quality of life as CLL patients.
Approaches to Treatment
Michele: Dr. Lamanna, what are the potential advantages and disadvantages of a fixed-duration treatment versus a continuous treatment?
Dr. Lamanna: Both treatment options are great and because we have these excellent options, we talk about the logistics, the advantages and disadvantages of going for either approach, and then we align that with what’s going on with the patient at the time in their life.
Unless there’s something glaring, like a comorbidity or medical problem where I think one drug might be better than another, then I’ll still discuss both agents, but I’ll bring up my concerns and what I think they should do. You have these discussions and factor in what their wishes are.
We teach everybody that if you’re taking BTK inhibitors continuously, some of these nagging side effects can occur later because you’re taking this indefinitely unless you have a side effect or your disease progresses. The downside is you could have some uncomfortable side effects, like diarrhea, GI issues, cardiac issues, bleeding, and bruising.
The benefit of venetoclax-based combinations is that it’s time-limited. It’s very similar to what we used to do with chemoimmunotherapy where you’re getting a short duration of therapy and hopefully won’t need to be on treatment until many years down the road.
The downside is that it’s more labor-intensive in the beginning. There’s a lot of monitoring because your blood counts can fluctuate a little bit more commonly with the combination. Sometimes you need extra help.They might have dose modifications. There are different logistics with a time-limited approach that people have to be willing to commit to, but the advantage is you get a break from therapy.
I have both of these conversations with patients because it is rare to say that somebody is precluded from one regimen versus another and that’s why most patients have an option. There might be some circumstances based on comorbidity, cytogenetics, or other issues that I’m concerned about with where I might recommend one approach versus another, but we have that dialogue.
Michele Baker: Dr. Farber, is your approach different and if so, how?
Dr. Farber: No, it’s very much in line with Dr. Lamanna’s. I would echo what she said that BTK inhibitors are very easy to start and hard to continue whereas the BCL2 inhibitor venetoclax is very cumbersome to start and requires a lot of initial monitoring. The patient has to come in very frequently for lab work and hydration as we’re ramping up, but it’s easy to continue.
Treatment has to be individualized. There may not be a perfect treatment, but one clearly may be better than another.
Dr. Charles Farber
With ongoing treatment versus finite treatment, the majority of people would like to be treated with finite therapy for one or two years, but that’s not for everyone. It’s a little counterintuitive, but some people feel very comfortable being treated with ongoing therapy because they feel like they’re proactively being monitored and treated.
A lot of people panic when it comes to the end of the year or two years on venetoclax and they become concerned about what we’re going to do next. It’s not broken. Why do we want to fix this? What’s wrong with continuing with venetoclax?
Shared treatment decision-making is individualized. Comorbidities, age, and ability to come in frequently in those first few weeks may dampen my enthusiasm for venetoclax in certain individuals. If they’re on an anticoagulant or blood thinner, I worry about that with BTK inhibitors.
It’s truly a situation where the treatment has to be individualized. There may not be a perfect treatment, but one clearly may be better than another. There’s a lot of information. CLL patients tend to be older and have comorbidities, so Michele, you are quite the exception. But you do the best you can. It requires a lot of patience, but it’s very gratifying.
We’ve had amazing treatments historically. If you look back 10 or 15 years ago, it was prehistoric, particularly for patients at higher risk with unmutated, immunoglobulin-heavy chains or TP53. We had no treatment until the advent of ibrutinib. It’s a very gratifying time to be in practice where we have options and we can talk to patients about what may be better for them.
Bridging the Gap: When Patients and Doctors Disagree on Treatment
Michele: What happens when a patient and their doctor have differing views on a treatment plan’s next steps? What do you do?
Dr. Farber: To some degree, the patient’s always right. If you feel they’re taking a misstep and if it’s not a horrible misstep, you voice your concern. If it’s something terrible to you, tell them you’re not willing to do it or perhaps they should seek an additional opinion. You try to resolve it.
The C in CLL is chronic. If they want to take ivermectin or something unproven, you try to educate them. You try to intellectualize. But it could be difficult because some patients get an idea and it may not be a good idea, but they feel very strongly about it.
If it’s something you’re uncomfortable doing, you can try to excuse yourself and offer a second opinion. It could be challenging and some patients get offended when you don’t do exactly what they’d like you to do. They could come at you with something from Dr. Google that isn’t necessarily appropriate. You have to be calm and try to explain the rationale for why you think it may not be a great idea.
Michele: What you would say to someone exactly if they brought up ivermectin?
Dr. Farber: I tell them that there have been anecdotal reports of patients doing well with various diseases, but that’s not scientific and doesn’t prove that ivermectin is effective in a given setting. I explain about randomized prospective trials. The best way that this is done scientifically is to take a group of patients and divide them into two or more groups. One group is treated with the test agent and the other is treated with standard therapy, placebo, or under observation. The true scientific way is if the group that gets ivermectin does better, lives longer, has a better quality of life, and has objective improvements in their labs or radiographs, that is scientific.
Sometimes in CLL and other diseases, there are spontaneous remission improvements. Single cases of patients getting better is akin to snake oil where someone comes up and endorses a treatment. That’s what I would I would try to explain. I try to explain that individuals getting better on ivermectin is not akin to a randomized prospective trial showing clinical benefit.
Michele: You’re very polite with your explanation and what you would say to someone about ivermectin. I appreciate that. Dr. Lamanna, what would you do if you and a patient disagree about what their treatment plan will be and their next steps?
Dr. Lamanna: To be fair, it is a dialogue. I’ve been fortunate that there aren’t many patients who I’ve had real troubles with. Thankfully, many patients either want to hear the whole discussion or read and bring up their questions with me and that helps the dialogue because you hear where they’re coming from.
If people bring up things that are completely not standard of care, then I have a discussion with them on the standard of care and about supplements or alternative medicines and how to integrate those into current practices or therapies that might be needed for their leukemia.
If somebody doesn’t want to take any standard of care treatment, then I’m probably the wrong person for them. It’s not difficult to have that conversation because either the patient is a right fit and doesn’t want to have anything, is afraid to take any kind of standard of care therapy for CLL, and that’s very easy to have the discussion and see where they want to take that.
Another conversation is when people get multiple opinions from different doctors. We see patients who talk about different therapies and they’re usually talking about all the standard of care therapies. The discussion now shifts to treatment sequencing. Should they do this one first or that one first?
Another discussion is talking about the different clinical trials and that’s great because that’s an open dialogue and right up my alley. I’m happy to talk about any of that, share my knowledge and expertise, and come to a mutual agreement if they want to do one or another, whether with me or someone else. I’ve never had too many difficulties where we’ve disagreed or where it’s been not approachable. It’s something that we have a conversation about.
You want to partner with a doctor and a team that fits you. I may not be the right person for that person all the time and that’s okay. I respect that.
Dr. Nicole Lamanna
I always say to patients that because CLL is a journey, you need to find somebody that you feel comfortable partnering with. That may not be me and that’s okay. It’s a long journey and they’re with you for a lifetime. You hope that they’re with you for 20-plus years or more. Hopefully, they will have a normal lifespan. That’s what we’re shooting for with all our research. You want to partner with a doctor and a team that fits you. I may not be the right person for that person all the time and that’s okay. I respect that.
Michele: It’s a long-term relationship and it’s important that you and your doctor gel. I always say it’s almost like dating, trying to figure out who’s right. My relationship with my CLL specialist is probably one of the longest I’ve had; not quite as long as with my husband but almost.
Beyond Initial (Frontline) Treatment
Michele: Let’s move forward to second-line and third-line therapy. Dr. Lamanna, what factors do you consider? Are they different when selecting a second-line therapy and planning for future treatment options?
Dr. Lamanna: This is a journey. Although most patients are focused on their first treatment and what they’re getting at that moment, I’m always thinking about their next lines. The goal is to try to think ahead.
What they got in the frontline and what their response duration was to that therapy will play a role in what they’re going to be recommended in the second or third line.
Dr. Nicole Lamanna
In the second or third line, you consider several factors. What did they get in the frontline? Have the genetics of their disease changed? Were they once a favorable risk and now changed to 17p deletion or TP53 mutation? How did they tolerate their first regimen? Do they have new comorbidities or new medications that we have to be concerned about? What they got in the frontline and what their response duration was to that therapy will play a role in what they’re going to be recommended in the second or third line.
If they got a time-limited approach with a venetoclax-based regimen, like venetoclax-obinutuzumab, how long did that last? Was it short? Was it long? Did they tolerate the regimen? Is that something we can reconsider? If they were on a BTK inhibitor for their frontline treatment, then we’re not going to offer them another covalent because most people at this point have gotten covalent BTK inhibitors in the frontline.
How to sequence these drugs is still being evaluated. The point is it’s important to know what they had for frontline therapy.
Dr. Nicole Lamanna
If they’re continuously taking a medicine, you’re not going to switch them to the same class of covalent BTK inhibitor. You’ll likely go to a venetoclax-based regimen. We have a non-covalent BTK inhibitor, pirtobrutinib, which recently got approved. How to sequence these drugs is still being evaluated.
The point is it’s important to know what had for frontline therapy, whether their genetics changed, if they have any new comorbidity, what their response was, and if they had any major side effects. All of those play a role in determining second and third-line therapy.
The Role of Genetics in CLL
Michele: Dr. Farber, this is something that CLL patients are always asking. I had my test when I was first diagnosed and this is what it showed, but now they’re showing something else. What happens to our genetics? Is it from treatment?
Dr. Farber: Yes, genetics can change. If you look at newly diagnosed patients who’ve never been treated, perhaps 5% or 7% will have a TP53 mutation or 17p deletion whereas if you look at populations of patients who were very heavily treated, particularly with chemotherapy drugs, up to 50% of those patients will have the dreaded TP53 mutation or 17p deletion.
If a patient needs a new line of treatment or is having progressive disease, if they haven’t had genetic testing, they should be checked
Dr. Charles Farber
By treating, you do one of several things. You can introduce new mutations or at least select a population of cells that have that mutation. What’s very important is if a patient needs a new line of treatment or is having progressive disease, if they haven’t had genetic testing, they should be checked again because there may be something emerging that was not there or not recognized earlier. There are a variety of different assays used, like FISH and next-generation sequencing.
It’s not the same biology through the course of the disease in a given patient. It can sincerely change in part through treatment and that’s one of the reasons in general that we tend to try not to treat patients until they need treatment. The International Workshop on Chronic Lymphocytic Leukemia (iwCLL) has criteria for who needs treatment and not everyone needs treatment.
They say there’s no benefit to treating early. I would take it a step further. There may be a detriment to treating a patient before they need treatment. It’s like shooting off your ammunition before the war begins. Some are seldom accused of starting treatment before an individual needs treatment. If a patient hasn’t had a genetic profile of their disease done in recent times and they progress, they should be checked out again.
Key Takeaways
Michele: What is your advice to patients? How can they most effectively advocate for themselves and have shared treatment decision-making conversations with their doctors, especially when they’re so overwhelmed with the amount of information they’re getting? How can they advocate for themselves when their doctor is not looking at newer therapies, like if they’re in a rural community and don’t have that advantage?
Dr. Farber: The patient needs to bring their spouse, a relative, or a loved one to review what the doctor’s saying at one of these critical junctures. It’s important to write things down.
When all is said and done, the patient can come up with a little chart where they can see the pros and cons of a treatment. You might have one for each different treatment being offered to you. Listen carefully to the doctor.
Come up with very focused questions. Write things down before you go in rather than having a free-for-all discussion.
Dr. Charles Farber
Ask their opinion. What do you think? Do you think one is better than the other? Do you think they’re equivalent? What aspects of one treatment would be better than another treatment? What aspects would be inferior? Are there any nuances to my current medical state that might make one treatment better than another? Come up with very focused questions.
Write things down before you go in rather than having a free-for-all discussion. Back in the day, we didn’t have options. There was one best treatment and we could change the dosing and the schedule to try and finesse it, but now we have different options. We have different agents within a given class. The doctor and the patient must come up with a good plan for the individual.
Dr. Lamanna: It’s often good for patients to bring somebody to their appointments because it’s hard to hear everything with one set of ears. Sometimes what the patient might be focusing on is different from what their loved one or friend might be. They may hear other aspects of the conversation.
The beauty of CLL compared to other cancers is we can have multiple conversations when we’re gearing somebody up for treatment. I often encourage them to write down questions and bring them to their next visit or message us. Thankfully, we have the leeway and flexibility of doing this at multiple sessions to try to answer their questions more thoroughly. That’s very rare. That’s not to say it never happens in CLL because sometimes it happens, but often, you have that luxury of time.
Thankfully, we have the leeway and flexibility of doing this at multiple sessions to try to answer their questions more thoroughly.
Dr. Nicole Lamanna
We also try to set up educational visits to go over the drugs and their side effects. There are a lot of good support groups for CLL where they can go over questions. I hook patients up early when I first meet them. I give them a book from The LLS talking about CLL and then I give them websites that they can visit. I say to patients that not everybody’s ready to go online and look at their disease. Dr. Google can be a problem, but for those who want to, I want them to go to reputable sites that talk about the disease.
Conclusion
Michele: This has been wonderful. I’ve learned so much from you. Thank you, doctors, for your devotion and dedication to helping CLL and SLL patients. We all better understand shared treatment decision-making and how important it is in our journeys.
Stephanie: Thank you so much, Michele. Thank you to Dr. Lamanna and Dr. Farber for all the work that you are doing with your patients and patients everywhere in CLL and SLL. It’s so important to be empowered again, especially in the space of this disease, which requires a lot of engagement and understanding because there’s so much rapid development happening with different therapies.
I hope that you learned something from the program, that it spurred some thoughts, and that you can walk away with some actionable items on your list of things to do. We hope to see you at a future program. Take good care.
CLL 360°: Navigating Side Effects with the Experts
Edited by: Katrina Villareal
Hosted by CLL patient advocate Jeff Folloder, this crucial discussion on chronic lymphocytic leukemia (CLL) with Dr. Matthew Davids from the Dana-Farber Cancer Institute and Dr. Kerry Rogers from The Ohio State University Comprehensive Cancer Center will equip you with the knowledge to manage CLL treatment side effects better and improve communication with your healthcare team.
Understand the latest advancements in CLL therapy and their impact on patients. Gain practical advice on managing the side effects of CLL treatments, including BTK inhibitors. Learn how to balance treatment efficacy with tolerability to improve your daily life. Discover ways to communicate your concerns and treatment preferences with your healthcare providers.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang: As part of our CLL 360° series, this topic is navigating side effects with the experts, both on the patient side as well as the medical side. The goal is for you to walk away with a better understanding of what side effects are commonly driven by CLL treatments and how to help manage them, including how to have conversations with your medical team about them.
This program is hosted by The Patient Story. Our multi-platform organization aims to help people navigate life before and after diagnosis through in-depth patient stories and educational discussions, which we understand is especially important for a community like CLL where you’re all so engaged and want to empower yourselves continuously.
We want to thank The Leukemia & Lymphoma Society for its partnership. The LLS offers incredible free resources, like their Information Specialists who provide one-on-one support in different areas for blood cancer. We also want to thank The CLL Support Group on Facebook led by our friends, including our moderator Jeff Folloder. They provide virtual support anytime for folks dealing with a CLL diagnosis.
We want to thank our sponsors for their support, which helps us to host more of these programs for free to our audience. The Patient Story retains full editorial control over all the content. While we hope this will be very helpful and that you walk away with a better understanding of this topic, this is not meant to be a substitute for your own medical advice.
Now we get to the great discussion ahead and I’ll send it to Jeff.
Jeff Folloder, CLL Patient Advocate
Jeff Folloder: I am a passionate patient care advocate. Why am I an advocate? Because I know that it is truly possible to live a great life with a CLL diagnosis.
I went through a clinical trial many years ago. I experienced side effects, which were quite profound. I know so much has changed. There are still side effects, but we take care of them differently.
We have two fantastic medical experts to join us. Dr. Matthew Davids is an associate professor of medicine at the Division of Lymphoma of the Harvard Medical School. He’s a hematologist-oncologist at the Dana-Farber Cancer Institute where he serves as director of clinical research and associate director of the Center for Chronic Lymphocytic Leukemia. Dr. Davids, why CLL?
Dr. Matthew Davids, Hematologist-Oncologist
Dr. Matthew Davids: I was very fortunate to grow up in the era when we were starting to transition away from chemotherapy to targeted therapies. We could begin to develop drugs with fewer side effects and more effective than chemotherapy. I was inspired by that and the relationships with my patients, and I haven’t looked back.
Dr. Kerry Rogers, Hematologist-Oncologist
Jeff: Also joining us is Dr. Kerry Rogers. She’s the assistant professor in the Division of Hematology at The Ohio State College of Medicine and a hematologist-oncologist and researcher at The Ohio State University. Dr. Rogers, why did you choose CLL?
Dr. Kerry Rogers: When I was doing my fellowship in hematology and medical oncology, I had the privilege of taking care of patients in some of the original ibrutinib clinical trials who had been living with CLL for over a decade or two and had experienced a lot of chemoimmunotherapy treatment. They said ibrutinib was the best that they’d ever had in terms of how it impacted their daily lives and so I thought that was intriguing. Now we know that these drugs are not only generally more tolerable but also more effective than chemoimmunotherapy.
I like the long-term relationships you can have with patients and the variety of experiences with CLL. You have people who are quite ill, who have experienced a lot of treatment, may have had CLL that’s become resistant to some of those treatments, and need to do a lot of things to manage the CLL. You also see people who are living with it who currently do not have symptoms or do not need treatment.
I also like the fact that there are some people you encourage to do what they want with their lives and not focus on having cancer. Mostly, I’d like all my patients to be bothered by CLL as little as possible, but you do get people in a variety of situations and I appreciate that about working in CLL.
Everyone reacts completely differently to the treatments. For most patients, treatment side effects are common and can be impactful. Some of them are temporary, but some of them are more severe.
Impact of Recent Treatment Advancements on Side Effects
Jeff: I participated in a clinical trial where I received intravenous monoclonal antibodies. Like everyone who participates in a clinical trial, I received a stack of informed consent papers that looked to be about a foot and a half thick and described every single side effect that might happen with the administration of that drug.
The first time that I went to get the infusion, I was told to expect that it was going to take four to six hours. Unfortunately, it took 23 1/2 hours for me because I experienced pretty much every single one of its side effects. We got through them all. When the side effects happened, they were treated and we’d hit the reset button and start over again. As I progressed through the clinical trial, the side effects were minimized.
We’re in a different world now. Everyone reacts completely differently to the treatments. For most patients, treatment side effects are common and can be impactful. Some of them are temporary, but some of them are more severe. Sometimes treatment or even hospitalization is required. And then some people, for whatever reason, never have a single side effect.
Dr. Davids, the treatment landscape for CLL patients has truly evolved in the past couple of years. Could you discuss these advancements and how the side effects of CLL therapy, more specifically the BTK inhibitors, have changed over time?
Dr. Davids: To contrast with the older chemotherapy-based approaches, I told patients, “We’re going to start treatment. You’re going to need to take probably 6 to 12 months off from work and go on disability. Your whole life is going to change over this timeframe, but eventually, you’ll get better and get back to what you’re doing.”
When BTK inhibitors like ibrutinib first entered into trials, we quickly realized that these drugs are much better tolerated than the older chemotherapy-based regimens. There may be some side effects that arise, but we’ll deal with them. We’ll use various supportive care measures. We may need to reduce the dose, but you should be able to keep doing the things you want to be doing. You can usually keep working while on treatment.
We have venetoclax, which we usually give in a time-limited fashion for one or two years, and it has a different side effect profile than the BTK inhibitors. The nice thing about that is with a time-limited treatment, when we stop the treatment, usually the side effects go away or are minimized at least. There are lots of different options.
Jeff: When we first started treating CLL, the treatments were pretty drastic and the side effects were pretty intense for the majority of people. Now, with the new treatments, specifically the BTK inhibitors and drugs like venetoclax, the side effects aren’t as intense and are usually easier to treat. Is that a fair statement?
Dr. Davids: Yeah, that’s a fair statement. There are rare situations where you can have more severe side effects, but for the most part, most of our patients are doing very well with these new targeted therapies.
Relationship Between Side Effects and Quality of Life for CLL Patients
Jeff: For me as a patient, quality of life is at the top of my list. If I can’t do the things that I want, we’re going to have a conversation and figure out how to get there. Quality of life is a complex and personal concept, but it’s directly intertwined with cancer treatment side effects. Dr. Rogers, how do you define the quality of life for a CLL patient and how do the side effects of treatment impact this in your experience?
Understanding what matters most to the patient or what’s going to have the least impact on their enjoyment of their life is what we do.
Dr. Rogers: If we’re trying to decide between two targeted agents that are both good options with different side effects, understanding what matters most to the patient or what’s going to have the least impact on their enjoyment of their life is what we do and it can be different for different people.
With a BTK inhibitor, some of the common side effects are bleeding, bruising, joint pains, and abnormal heart rhythms like atrial fibrillation. I have a few patients where atrial fibrillation has been much harder for them than the CLL was at any point. If you’ve had someone who’s experienced atrial fibrillation before and it was bothersome to them, they’re going to try to avoid that treatment.
Treatment Side Effects vs. Treatment Schedule
Dr. Rogers: Meanwhile, for venetoclax, quality of life isn’t treatment side effects but also treatment schedule. When given as a first treatment, venetoclax is given for a year with obinutuzumab, which is a monoclonal antibody, and that requires an eight-week start-up. It was very striking what Dr. Davids said that we try hard now to make it clear to patients that we don’t want them to be disabled by the treatment they’re going through, even temporarily.
We mostly want you to be able to live your life and do what you want.
People have told me they worry about their lives being over and not being able to do anything when they do treatment. I usually tell them that some people get severe side effects that have to be dealt with, but we mostly want you to be able to live your life and do what you want. That’s how I define quality of life as a physician. I want my patients to be living their lives and doing the things they enjoy with minimal impact from their treatment.
These days, one of the biggest impacts can be the treatment schedule. You can continue to work or play golf, but you still have to come for visits and that’s the biggest thing that changes with treatment. The venetoclax and obinutuzumab regimen requires an eight-week start-up, which can be intense. I’ve had patients who choose not to do that because they don’t want to take time off work to go to infusion visits.
I’ve also had patients take online meetings during infusion visits, which I’m fine with as long as they’re still engaged in their medical care. I don’t tell anyone they have to work during treatment but some people love their job and don’t want to step away from it.
Quality of life is defined by the person and I try to minimize the impact of what we’re doing for CLL on people’s enjoyment of their life, whatever that is. Something that isn’t talked about a lot is trying to minimize the psychological impact of starting treatment. We make sure people know that treatment doesn’t mean that they won’t get to do the things they like, even though scheduling is something they’re going to have to deal with for the most part.
Dr. Davids: If they do want to do the venetoclax-based regimen, it’s a bit disruptive to their schedule. When patients aren’t on a clinical trial, I try to have some flexibility so that if they have an important event, we can delay by a day or two, but I try to keep them on schedule. It can be a little more challenging when patients are on a clinical trial because we need to rigorously adhere to a specific schedule.
For some patients, it doesn’t make sense to invest eight weeks or so in coming in for frequent visits. A lot of our patients are used to being seen every three to six months. If we tell them to come in once or twice a week for a couple of months, that can be challenging. Some of our older patients don’t drive anymore and need to get rides or live far from the center.
One of the beauties of the CLL treatment setting right now is that we have other options. Patients like that can go on BTK inhibitors. They require minimal monitoring and for some patients, that’s nice for their quality of life. They come in a couple of times early on to make sure everything’s going well and they can get back to their three- to six-month interval schedule.
Having different options for different patients is great. We’re on the precipice of having a new regimen approved in the US, which is a combination of acalabrutinib, one of the BTK inhibitors, with venetoclax. That’s going to be a nice advance because it will offer the opportunity for an all-oral, time-limited regimen.
One of the beauties of the CLL treatment setting right now is that we have other options… Having different options for different patients is great.
Right now, if you want all-oral therapy, you have to go with a BTK inhibitor and take it long-term for many years or you can go with obinutuzumab and venetoclax and have that opportunity for the one-year, time-limited therapy.
If approved, which we think it likely will be, acalabrutinib with venetoclax will be two pills. It’s a time-limited treatment of about 14 months or so and then you’re done. You don’t need to go through obinutuzumab infusions and that’s going to be a nice option to have for patients as well.
Dealing with Side Effects
Jeff: Whether you’re being treated, waiting for treatment, relapsed, or in remission, all CLL patients are dealing with some kind of symptom. It’s a fact of life, whether we call it fatigue, low platelets that make people bleed easily, joint pain, or AFib. Dr. Davids, what kind of practical advice do you give patients for dealing with those symptoms?
Dr. Davids: The disease itself can cause a lot of symptoms. There’s an interesting study where they took CLL patients who didn’t need treatment and randomized them to an early intervention approach with ibrutinib versus a placebo. It’s a rare opportunity in CLL to see what happens in a population being treated with a placebo.
As they stay on therapy longer and the CLL gets into a better remission, they tend to start to feel better overall.
In that study, there was a 90% rate of side effects in the patients on ibrutinib and a 90% rate of side effects in the patients on placebo. It was the same in both arms. That speaks to how the disease itself can cause a lot of issues, like fatigue, unintentional weight loss, sweats, and joint aches.
I counsel my patients that as they stay on therapy longer and the CLL gets into a better remission, they tend to start to feel better overall. They’ll develop better energy, their appetite may come back, they may gain some weight back if they’ve lost weight, and sweats can go away.
One of the more challenging periods is getting started on treatment because that’s when you have some side effects from the drugs and there’s still a lot of CLL around, so they may not be feeling great. As they get a few months into treatment, the CLL starts to get better. It involves counseling and coaching them through that. Hold out and be optimistic. It’s going to get better with time. For most patients, they may start feeling better pretty quickly, even within a few weeks of starting on therapy, because of disease control.
We have a very good multidisciplinary team. We have a great nurse practitioner who’s seeing the patients often more frequently than I do. We have pharmacists who help and look for issues with the drugs and side effects. The caregivers for the patient are a key part as well. It’s a team effort, but we do a pretty good job of getting patients through that more difficult period and to a better place where they’re feeling better.
How Can Patients Actively Participate in Their Care?
Jeff: Dr. Rogers, it’s hard for a doctor and the care team to know how to guide a patient through their side effects if they don’t know they exist. How do we do this? What does a patient have to do to get the best possible side-effect care from you and your team?
Dr. Rogers: One thing Dr. Davids said that’s important is I’m not the only person. Different members of the team are asking about side effects. Nurses, nurse practitioners, and physician assistants help too.
The nurse practitioner I primarily work with is a man and sometimes, patients tell him things that they won’t tell me or vice-versa. Sometimes the gender of the care provider or the care team member can make a difference in people disclosing side effects.
Asking about specific side effects that we know are common can help because I find people disclose more. If there’s one that they perceive is ruining their quality of life, we ask about it so we can get the spectrum.
Sometimes there are side effects that are bothersome to one person that aren’t to somebody else, like joint pain. We ask about it, learn about it, and suggest pain medication. But if the person’s happier living with it than trying any sort of intervention, I’m okay with that.
Effective Patient-Physician Communication
Jeff: Dr. Davids, it sounds like in the current landscape, most side effects are fairly easily managed for CLL patients. Let’s talk about how you deal with these side effects.
Dr. Davids: Every drug is different. Every side effect is different. Every patient is different. Sometimes we see more significant side effects with BTK inhibitors where we run into issues with bleeding and that can be serious.
Being very proactive and communicating with your doctor about what’s going on is important.
One thing that’s very important for patients on BTK inhibitors is to know that if they need any kind of surgical procedure, they need to stop taking their BTK inhibitor before and after the procedure. It’s helpful for patients to check in with us because every procedure is different and may require a different length of hold.
I have seen some patients run into issues where they forgot to call and ask us. They were taking their BTK inhibitor and had pretty serious bleeding issues after surgery. It’s about communication and anticipation. We’ve had situations where we’ve had to postpone surgeries. Being very proactive and communicating with your doctor about what’s going on is important.
Another common one that I see with venetoclax and BTK inhibitors is diarrhea or loose stools when patients are first getting started on these drugs. There’s a period when your body needs to adapt to the drug.
If it’s pretty significant diarrhea, we usually want to do some testing first before we do interventions. We’ll look for certain infections, like C. diff, which can be a more serious infection. It’s usually not there, but we like to make sure that’s not there before we recommend things like loperamide, which slows down the bowels.
There are little tricks as well. Sometimes taking the pill at a different time of day or with a different type of food can be helpful.With venetoclax, I’ve had luck with patients taking it with a fatty meal at night and when they wake up, they feel better and not having diarrhea during the day.
Sometimes we need to reduce the dose of the drug. I do find that it settles within the first couple of months. Most patients can then back off on loperamide and get back up to the full dose of venetoclax.
Overcoming the Fear of Dose Reduction
Jeff: Dr. Rogers, for whatever reason, a lot of patients are uncertain and fearful regarding dose reduction because it introduces a cloud of uncertainty to what’s going on.
Dr. Rogers: This is true across other cancers as well. People worry about dose reduction largely because they worry that the treatment will stop being effective if the dose is reduced.
With venetoclax, for example, the target dose for most people who don’t have drug interactions with it is 400 mg a day. However, when people have been on it for a while, there’s an efficacy at 300 mg or even 200 mg. If you’re taking 100 mg twice a week, you start to worry that it’s not going to work. There’s a point where you get to a dose where most people think that’s not going to be effective or with BTK inhibitors, you’re not going to have occupancy or the inhibitory action.
There’s a lot of room for dose reduction before you get to a point where the drug isn’t going to work. For people with side effects, maybe the target dose isn’t the right dose for them. When we do studies to design dosing of drugs, they look at drug levels in the blood, biological outcomes, and how much of that BTK protein is occupied with different dosing schedules. But that’s in a group of people and individuals can have different experiences.
There’s a lot of room for dose reduction before you get to a point where the drug isn’t going to work.
There’s some thought and some data to support this that people with side effects might naturally have different drug metabolism and maybe what’s needed is a different dose. With BTK inhibitors, there’s some scientific evidence that early in the disease, the drug is cleared by the amount of BTK in the body, which is a lot when there’s a lot of CLL, and further in is not a lot and the protein production is downregulated.
It’s quite possible that a lower dose is necessary to maintain that response after beginning treatment. Some of these side effects improve over time. People have a lot of CLL in their bodies. They see things improve every time they come for a visit. But a year in, when you’re looking at joint pain that’s interfering with your pickleball game when your blood counts look good, maybe it’s time to think about dose reduction. It’s also a time when the CLL is in a different spot and dose reduction might be more reasonable.
It’s quite possible that a lower dose is necessary to maintain that response after beginning treatment.
There are even some studies looking at databases of people using these drugs through insurance claims showing that reducing the dose did not result in a sooner time being prescribed a new treatment. It looked like it might even be going better for people probably because they were able to tolerate and stay on this drug.
It’s always worth asking your physician anything you’re worried about. If dose reduction is suggested, talk to them about whether they expect this will change your treatment outcome, but there are plenty of reasons to think that in most cases it will not. There’s a lot of room for dose reduction in a way that we know is not going to compromise how well the treatment works.
Fostering Effective Provider Communication
Jeff: We’ve talked about side effects. We’ve talked about the difference between male and female patients and how they communicate these side effects to their care team. Is there a way that you prefer patients to communicate with you?
Dr. Davids: I encourage patients to make a list of their issues ahead of time before coming to the visit. When you get to a visit, sometimes you’re like a deer caught in the headlights. Sometimes people don’t think of the things that have been occurring to them.
Keep a little notebook over the months in between the visits and jot stuff down. I find it most efficient to go through all those things in person together with the patient and counsel them through each one. I don’t mind if it’s a long visit.
A challenging mechanism that has developed is using a patient gateway to communicate, which has its pros and cons. It’s good for patients to be able to access their care team. But sometimes, over three months, patients send a message every time they think of a question, so they may be sending 15 to 20 messages in between their three-month visits.
It takes a lot of time on our end. We try to be as responsive as we can. We’ve hired additional staff to manage the volume of messages that come in because as you can imagine, if you have 10 or 15 messages from 200 or 300 of your patients, that’s a lot. I’m not saying that’s a bad thing, but we need to rethink how we do that.
If patients are having more acute side effects, I encourage them to page us directly. We’re available to call back and have teams to help support us as well. If you’re sitting on a more serious side effect, that’s not good. Communication is key, but be smart about how to communicate.
A challenging mechanism that has developed is using a patient gateway to communicate, which has its pros and cons.
Dr. Rogers: If there are things you want to discuss, make a list. I’ve had a couple of people who send a list of questions a week before their appointment through the patient portal. We have a list now so that they know what it is and I can read what it is. Some people take physical notes, some people have them on their phones. If there’s something that they want to discuss, decide ahead and use your visit time to do it.
The patient portal is an excellent communication tool, but you can’t be doing that every day, asking something new. We do those during business hours. I tell my patients that they’re welcome to write a note at 2 a.m., but we will not be replying until the next business day. Sometimes, you get people who send a bunch of concerns and I tell them that we can’t answer all of these on the phone and that we’re going to schedule a visit. Occasionally, we’ll provide education. This is a concern. This is something that should be handled by the phone, so we can call and get it sorted out.
I have some patients who don’t use MyChart and they have a different way to communicate with us. It’s good to have multiple approaches. In terms of making lists of questions and sending them ahead, whatever helps you stay organized so that you get the answers you need.
Something that has been very helpful for us is open notes. We have been required to provide all test results to patients and provide notes. Some people like reading them but some people don’t. Some patients couldn’t remember something I said so they went back and looked at what I wrote and that helped. They didn’t have to call because they saw my notes. Some people know how to look at those. Some people don’t. They’re not written in patient-friendly language.
Patients will get their blood test results before they even come to see me, so they can think of questions about their results and I can address that during the visit.
Think through if you want to open your test results on a weekend and do what’s right for you.
Overall, it’s good to allow people access to their health information immediately. But I’ve had a few patients who call us up very angry that we released imaging results on a weekend. We didn’t do that; radiology did. Then they thought they had no way to reach out to us about something they were terrified about, which is also not true.
We have a 24-hour answering service if people are extremely worried about a test result that was released to them by the system on a weekend. Understand the process and the value in it but also think through if you want to open your test results on a weekend and do what’s right for you.
Dr. Davids: I feel very similarly about test results. It’s great to have access to all your data, but you have to know yourself. If you’re the type of person who’s going to freak out if you see something strange in a report and it’s a Friday evening and no one’s going to be able to get back to you for a few days, don’t open the report.
I see our job as looking at those reports, filtering out the things that aren’t worrisome, and telling you what’s important. Patients will be very worried about a tiny little lung nodule that wasn’t described before. If it’s 2 mm, I’ll say that they don’t have to worry about it, but if you see that result first and I’m not immediately available, you may be worried for days. It doesn’t bother some people and if you’re one of them, look right away. You have to know yourself and what you’re comfortable with.
If you’re the type of person who’s going to freak out if you see something strange in a report… don’t open the report.
Dr. Rogers: We have a system where if it’s a result that needs emergent action, which rarely happens in my clinic, the radiologist will call me so I can contact the patient. We don’t release test results with emergent findings without anyone on the healthcare team being notified, which I think some people don’t know.
Jeff: For the past couple of years, as I sat in the waiting room after having my blood work done, I have a very distinctive alert from my phone as my test results start coming in. I’m one of those people who are face down on the phone almost instantly because I want to know what questions to ask my doctor when I go in to review those results.
I’m coming up on 15 years of living with CLL and I’ve learned that the most important thing is not one test result; it’s the trend of the test results and how things are going over time. Not everyone is there yet and this is part of how we communicate with our care providers. This is how we work with our team.
Clinical Trials in CLL
Jeff: We’ve been talking about BTK inhibitors and it seems like the drugs keep on coming, one after the other after the other. When I started, it was pretty much FCR (fludarabine, cyclophosphamide, and rituximab) or nothing.
Let’s talk about how we got here. We’ve been doing all this research. We have CLL patients participating in clinical trials. We have the data coming back. How do you anticipate these advancements and how they’re going to impact treatment decisions? Are people going to put off starting treatment because something new is right around the corner?
Dr. Davids: We wouldn’t have all these great new drugs if patients didn’t go on clinical trials. The patients who came before helped bring these drugs to the patients of today. Patients of today also should consider clinical trials because you can help to develop the next wave of drugs for the next wave of patients. Patients deserve a ton of credit for making all this possible.
We wouldn’t have all these great new drugs if patients didn’t go on clinical trials.
Ibrutinib was a huge advancement. When I heard about a new BTK inhibitor coming along, acalabrutinib, I was skeptical at first. We already have a great drug with ibrutinib. Why do we need a second BTK inhibitor? Acalabrutinib turned out to be as equally effective as ibrutinib but with fewer side effects. It was a big innovation that acalabrutinib came along.
Then zanubrutinib came along and I said the same thing. Why do we need another, more selective BTK inhibitor? It turned out that in one study, zanubrutinib is better than ibrutinib in terms of how well it controls the CLL and is better tolerated.
Pirtobrutinib works very differently from the three BTK inhibitors and it can work even after all three of those other drugs stop working, so that’s a big advance. I’ve been proven wrong at each step along the way.
It’s helpful to have four different BTK inhibitors. I’m trying not to make the same mistake with a new class of drugs called BTK degraders, which are in early-phase clinical trials. This is another way to target BTK and they’re showing some significant promise.
It’s possible and very likely that eventually, we’ll have at least a fifth BTK inhibitor approved for this disease. It’s not what we’d call me-too drugs where it’s the same drug with a different label. These are all different drugs. They all have pros and cons and there’s a role for each of them in the treatment of CLL. It’s exciting times and continues to be exciting for patients to have all these options continuing to evolve.
It takes some courage to try new combinations or schemes for giving them.
Dr. Rogers: I completely agree. The only reason that we have these drugs is because people were willing to participate in clinical trials. I also see people who are afraid of participating in a clinical trial for fear of getting a placebo. Some of the lack of understanding of what research participation is a barrier to people doing it. It takes a lot of courage to do something where we don’t have all the information about how this particular treatment scheme is going to work.
A study we have right now for people going through their first treatment is a combination of currently approved drugs. Mostly, when people hear what it is, they say, “Okay, neat. These are drugs that you’re talking about as a standard of care.” It takes some courage to try new combinations or schemes for giving them. I always try to remember to cover that people will not be getting a placebo because we don’t have that in any of our current CLL trials.
Someone said once that participating in a clinical trial is like getting tomorrow’s treatment today. For people who are worried or don’t want to take an investigational drug, I remind them that these currently approved drugs were drugs that people got as research participants before they were on the market. They were able to benefit from what is a highly effective therapy before it was commercially available. This can directly improve the type of treatment people are getting, even though there’s some element of unknown because it’s a research study and we’re trying to learn more about these drugs.
For anyone considering research participation, definitely asking what’s known about the drug, where it is in development, and what the goal of this study is can help people understand better. When people are excited about approved drugs, we were able to treat people with those same drugs before they were commercially available because they participated in research.
These currently approved drugs were drugs that people got as research participants before they were on the market.
I would never suggest a clinical trial that I didn’t think was going to be highly beneficial to the person who was going to take that treatment. We’ve talked about choices for taking a first targeted agent, but there are people who have had CLL that’s now become resistant to several targeted agents. That’s where drugs we have under investigation are much more likely to be effective for their CLL than drugs that are currently on the market and a huge reason for people to consider research participation. At that point, you’re going to get something that we know is very likely to be better than commercially available drugs.
Shared Decision-Making in Your Care
Jeff: What you were saying got me thinking about this process as a collaborative process. It used to be like it or not. The paradigm was a patient presented with an illness, they saw the doctor, the doctor did an evaluation, the doctor prescribed a course of treatment, and the patient took the treatment. Things have changed now.
We have a lot of options. There are four BTK inhibitors. There’s venetoclax. There are monoclonal antibodies. There’s no treatment. I would like to think that we’re moving closer to a collaborative environment where the care team does the decision matrix with the patient. Dr. Rogers, how do you foster that environment with the patient?
We’ll discuss the treatments and by the time we’re done talking, it’ll be clear what to do and we can decide together.
Dr. Rogers: I strive to make my clinic a collaborative environment. When the venetoclax and obinutuzumab regimen was approved, you have BTK inhibitors versus venetoclax and obinutuzumab. I had a lot of consultations with people considering their options for the first treatment and asking me what they should do. Until I get to know you, I can’t help you. I can’t tell you what to do.
Usually, I say, “Why don’t we talk? I have some questions for you. You probably have some questions for me. We’ll discuss the treatments and by the time we’re done talking, it’ll be clear what to do and we can decide together.” That’s the best approach.
Some people don’t want to get options. They’re very overwhelmed by the options, so they want a recommendation. After a discussion, they say, “I don’t want to think about this. Ask me what you need to know to make the best recommendation for me, but I don’t want options. I want you to tell me what I should do.”
I find it difficult to pick for someone. I have to ask enough questions so that I can make the recommendation for what I think will be best. I respect the fact that some people get overwhelmed by the choices, don’t want to have options, and want to be told what to do. That’s not the way I prefer to do things, but if that’s what the person who I’m taking care of wants, then I try to do that.
I try to narrow it down. Often, there will be 1 or 2 options that I would prefer for the patient.
Dr. Davids: I have a very similar approach, I would say. Some patients prefer to be told what to do and it’s important to ask what their preference is upfront about how they want to approach it.
Another scenario is completely leaving it up to the patient. Present the options as all being equal and let the patient choose. I tend not to do that so much either, so I try to narrow it down. Often, there will be 1 or 2 options that I would prefer for the patient.
Sometimes you get the dreaded question: what would you do if this was your sister or your mother? I would recommend to a patient anything that I would for a family member because I believe in it no matter who I’m recommending it for.
There are scenarios where we’ve gotten down to maybe two or three options and the patient will say, “I would lean more toward this one based on what you’ve told me, but these other choices are reasonable too, so think it over.” Ultimately, it’s the patient’s choice. I see my role as guiding them to that choice and sometimes it does help if I express what my thought is for a particular patient. A lot of patients find that helpful.
Final Takeaways
Jeff: If a brand new CLL patient comes into your clinic and you’ve got 60 seconds to give them one message, what do you tell them?
Dr. Rogers: I usually tell people that we expect them to live with this for a very long time. The goal is to help them live as well as possible and be the least bothered as possible by CLL.
Dr. Davids: Depending on their age, for patients diagnosed with CLL in their 70s and 80s, I always say to them that our goal is to have them live whatever their normal life expectancy would be otherwise. We have very effective treatments and it’s unlikely that CLL is going to shorten your lifespan.
For younger patients, I don’t feel as confident saying that yet because if you’re diagnosed with CLL in your 50s, we don’t know what happens with these targeted therapies 30 years from now. I tell those patients that we already have a lot of good treatments, but over the next few years, we expect even more good treatments to be developed. The longer you live with CLL, the longer you’re going to live with CLL because we’ll have more and more treatments available. I also try to be optimistic.
Jeff: I was diagnosed with CLL at 46 and I’m now 60. Currently, I’m knocking out between 40 and 55 miles every week speed walking. I’m eating well and drinking well. I’m being a good father and husband. I’m doing all the things that I would want to do if I didn’t have CLL. I’m living a good life. It’s my mission as a patient advocate to make sure that it is possible to live a very good life, even with a CLL diagnosis.
I take an active role in my care. I listen to my care team when they say I need to do this, this, and this. I do what I need to do to present my body to my care team in the best possible shape so that when it is time to treat, we get to pick the right treatment plan so that I can live my best life. That is literally what I want for every single patient and caregiver. You can live a very long, very good life with CLL.
Conclusion
Stephanie: Thank you so much, Jeff, for your guidance in the conversation and for your perspective. We always want to make sure that we are emphasizing what that patient and care partner voice is. It is critical obviously beyond the education here.
Thank you so much, Dr. Rogers and Dr. Davids, for not only being incredible as CLL specialists but also for providing so much more time and extra time to help the community beyond the people and the patients you see in the clinic.
Patients, care partners, and a panel of CLL experts including Dr. William Wierda, MD, Ph.D. from MD Anderson, Dr. Nicole Lamanna, MD from the Columbia University Medical Center, Dr. Adam Kittai, MD from the Ohio State University, and Jackie Broadway-Duren, PhD, DNP, APRN, FNP-BC from MD Anderson gather to share the latest in CLL research, clinical trials, treatments, and comprehensive care strategies.
Guided by the insights of patient advocate moderator Jeff Folloder, the discussion will bridge the gap between medical expertise and patient perspectives, creating a truly comprehensive dialogue.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Updated October 9, 2023. Originally broadcast September 20, 2023.
Quality of life and precision are top of mind for chronic lymphocytic leukemia (CLL) patients. Understanding the complexities of available treatments can help you optimize your CLL care and prioritize the questions to ask your doctor.
During this live conversation, panelists Dr. M. Yair Levy, director of hematologic malignancies research at Texas Oncology, and Dr. Catherine Coombs, a hematologist oncologist at UCI Health who specializes in CLL, discussed the latest in CLL care. The discussion was hosted by CLL patients, advocates, and administrators of the CLL Support Facebook group Michele-Nadeem Baker and Jeff Folloder.
This discussion covers the current landscape of CLL treatment and care options, as well as new CLL treatments awaiting FDA approval, factors doctors consider when starting or switching a patient’s treatment, encouragement for CLL patients to advocate for themselves, and each doctor’s outlook on CLL treatment and patient quality of life.
There is hope. Hope to live a normal life, and hope to see your kids and your grandkids grow up. There’s always hope on the horizon, in my opinion.
Dr. Catherine Coombs
Thank you to AbbVie and BeiGene for their support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Michele-Nadeem Baker: I’m Michele-Nadeem Baker. I’m a medical and health journalist, but in addition to that, I am also a patient. I started advocating for other patients on my first day of treatment when I realized that there was so much unknown out there and to demystify things for my fellow patients and help them through their journey.
Jeff Folloder: My name is Jeff Folloder. I am a passionate patient advocate. I am now in year 14 of my little journey with CLL and I am living a great life. That’s why I became a patient advocate because I want to make sure that everyone knows that it is possible to live a great life with CLL.
First up, I get to introduce Dr. Catherine Coombs. She is a hematologist oncologist with UCI Health and she specializes in chronic lymphocytic leukemia. She also helps lead clinical trials, trying to find better ways to treat CLL. Dr. Coombs, tell me what drew you to specializing in CLL. We don’t hear that a lot.
Dr. Catherine Coombs: It was a long road. I went into medical school knowing I wanted to be a cancer doctor. I didn’t have any doctors in my family, but I do have a lot of family members with cancer. It always inspired me to be on the patient end of the oncologic relationship. That’s always what I thought I would do.
Now, I didn’t decide on CLL until my residency years. I looked for a research project right away, because that’s the only way to get into a good fellowship program is by doing research. It always was something I wanted to do regardless. I found a wonderful mentor in my time at Duke University as a resident, Mark Llaneza, where I focused on the underlying genetic risk of CLL as my residency project. That drew me to the field right away.
Then I saw all these other benefits of being a CLL-focused clinician, which is that the patients do really well and they live a long time. I love having that long-term relationship with my patients. I love blood cancers in general, but I would say the acute leukemias, which I had focused on a bit earlier on in my time as a faculty when I was doing a bit of both were hard because there are a lot of patients that we lose and I really admire the docs that do it. But I think for my long-term well-being, I know that it’s just so much more gratifying and less emotionally traumatic to be able to have patients that thrive for so many years and be able to really enjoy those relationships as the added benefit.
The therapeutics have just continued to improve over the 13 years since I first graduated medical school and started doing research.
Michele: We need more doctors like you. Dr. Coombs, thank you so much. I’d also like to introduce Dr. Levy, who is a hematologist oncologist at Texas Oncology. He is the director of Hematologic Malignancies Research and specializes in CLL. He’s also helped lead clinical trials in CLL. Dr. Levy, what drew you to CLL?
Dr. Yair Levy: Before moving to Texas, I actually did mostly chronic lymphocytic leukemia, but I’m a little older than Dr. Coombs. So back when I was doing it, it was still a relatively better outcome for this cancer, but we still lost some folks to chronic lymphocytic leukemia. However, if I reflect on my current experience, I don’t believe that I have lost a patient to chronic lymphocytic leukemia in the past decade. This is not because I have a shortage of patients. I’ve probably accumulated about 150. I’m not saying that the patients don’t die, but they don’t die of CLL.
So to live a normal life is the goal. Even though we still think of CLL as a treatable but incurable malignancy, for the most part, people are doing relatively well. Not to mention, not only are our treatments better in terms of efficacy, but they’re so much better tolerated.
If I reflect on my current experience, I don’t believe that I have lost a patient to chronic lymphocytic leukemia in the past decade. This is not because I have a shortage of patients. I’ve probably accumulated about 150. I’m not saying that the patients don’t die, but they don’t die of CLL.
Dr. Yair Levy
Jeff: We have an interesting topic for today’s program, Shared Treatment Decision Making: How To Be An Empowered Patient. This is something that strikes me right in my heart. I am a firm believer that patients who take an active role in their own care tend to have better outcomes, and this is actually borne out of clinical research.
I took an active role in my own care. I chose not to go in the specific direction that my first doctor wanted to go in, and I wound up at a large research hospital participating in a clinical trial. I’ve been living a great life as a result.
Michele: For me, treatment decision-making also came down to becoming an empowered patient and becoming health literate in CLL. The more I could learn from credible sources, for me, was better. I realized all patients are different and doctors, you can probably relate to this more than anyone but the world has changed quickly and pretty drastically for clinicians, researchers, and those of us who are patients.
I was diagnosed 11 years ago, not quite as long ago as Jeff, but still a long time ago. My frontline treatment started in 2015 and things were even different back then. I was on a trial that combined ibrutinib, which at the time was not approved yet for frontline treatment. It had been for relapsed and refractory but not frontline treatment. It was combined with FCR, the standard at the time, fludarabine, cyclophosphamide, and rituximab. Things have changed so quickly even since then. In my frontline treatment, I’m now on a different treatment. I had relapsed in between.
Dr. Coombs, could you tell us how the landscape of treatments for patients has vastly changed over the last couple of years?
BTK Inhibitors
Dr. Catherine Coombs: Over the past decade, but even over the past few years, we’re seeing advances. When I first got into the field, yes, it was chemoimmunotherapy for patients fit enough to receive it like FCR and BR. With the introduction of targeted agents, largely chemoimmunotherapy is not widely used. However, we still do see about a third of uptake looking at these large-scale studies across the country.
I’d say that doctors who are focused on CLL realize that chemoimmunotherapy is not worth the toxicity. Its efficacy is also inferior to these novel drugs that are more efficacious, so more likely to put the CLL at bay, in remission, and delay time until ultimate progression, but also hugely safer. That was first ibrutinib, as you wisely know from your own personal experience and your knowledge over the time of your journey as a patient. But now we have a lot of newer and better drugs. Ibrutinib has been amazing and revolutionary, but it does have some side effects. Fortunately, they’re not so common, but they still can be clinically significant.
The first category of drugs that have really changed in the past few years is newer generation BTK inhibitors. Ibrutinib was the first in class. It inhibits this critical protein that’s part of CLL cell machinery, BTK, but it’s not totally selective for its target. We now have 2 additional drugs that inhibit BTK – acalabrutinib and the most recent addition, zanubrutinib which was FDA-approved in January.
The advantage of both of these drugs is that they’re more selective for their target, BTK. That, fortunately, has translated to improved safety, where both drugs have been compared head to head with ibrutinib and they demonstrate improved tolerability, specifically lower rates of atrial fibrillation for both drugs. Acalabrutinib also has the advantage of lower rates of hypertension.
What we don’t know is whether zanubrutinib is better than acalabrutinib or acalabrutinib is better than zanubrutinib, because we don’t have that comparison. But I think they’re both excellent options and both offer advantages over the ibrutinib days when we were dealing with a lot of atrial fibrillation. There’s a lot less in the way of that.
The other huge class of drugs that I haven’t mentioned is a completely different way of treating CLL, so I’ll mention it briefly. I don’t know if we’re going to get more into the nitty gritty on this, but these BTK inhibitors work wonderfully at controlling CLL, but they’re considered as treat-to-progression regimens, meaning that patients go on and stay on as long as they’re, number one, tolerating it and their CLL is responding favorably.
Some patients don’t like the idea of being on a drug indefinitely, so the other huge therapeutic advance over the past few years that’s been widely available is the drug venetoclax. This is typically combined with another drug called obinutuzumab when used in the frontline setting. Because it can so effectively kill off the CLL to very deep levels, patients are able to completely stop treatment after one year and then eventually relapse, but it can take a long time. That’s one of the other major, major changes in CLL just over these past 5 years or so.
I’d say that doctors who are focused on CLL realize that chemoimmunotherapy is not worth the toxicity. Its efficacy is also inferior to these novel drugs that are more efficacious, so more likely to put the CLL at bay, in remission, and delay time until ultimate progression, but also hugely safer.
Dr. Catherine Coombs
Michele: Dr. Levy, what else would you add?
Dr. Yair Levy: Dr. Coombs, you hit the nail on the head. It’s a dramatic change from chemoimmunotherapy. In the chemoimmunotherapy era, our high unmet need was what we considered high risk which were ones that harbor a 17p deletion, or a mutation in this TP53 tumor suppressor protein, or these cells of origin that are called pre-germinal cells of origin. So a more immature cell that had gone bad, and we’ve known that they have done historically quite poorly with chemoimmunotherapy.
As Dr. Coombs mentioned, the biggest improvement that we saw was when we actually recognized druggable targets within the B-cell receptor pathway. The first such drugs were actually not Bruton’s tyrosine kinase (BTK) inhibitors, and they are largely relegated to the history of the B-cell receptor pathway now. But these were the PI3K delta inhibitors. Those worked irrespective of cell of origin, and they also worked in the 17p deletion. So again, they did certainly have some tolerability issues and the efficacy was not comparable to those of Bruton’s tyrosine kinase inhibitors, which is one of the big reasons that those have really fallen out of favor.
As Dr. Coombs mentioned, the BCL2 inhibitor venetoclax has also been a game changer. We’ve been utilizing these agents, either alone or in combination with CD20 monoclonal antibodies. Now, the European Medical Association has even approved the combination of a BCL2 and a BTKi. This is something that we’re doing further studies on within the United States as well because we’re seeing that people achieve very impressively high rates of response. More importantly, very deep responses can allow, hopefully, a very long treatment-free interval, and perhaps even in some cases, a functional cure.
So, in the beginning, we were saying that CLL is largely treatable but incurable, but we put an asterisk on that. Even with chemoimmunotherapy, there was a subset of CLL that may have been cured by chemoimmunotherapy, or at least a functional cure. I think we’re going to see the same thing with these other combinations as well.
We’re seeing that people achieve very impressively high rates of response. More importantly, very deep responses that can allow, hopefully, a very long treatment-free interval, and perhaps even in some cases, a functional cure.
Dr. Yair Levy
How CLL doctors are providing CLL patients with precision care
Jeff: This is exciting stuff. We’re talking about an awful lot of options for patients, but before we can get to those options, we need to figure out how we get to that point. So let’s chat a little bit about the tests that are needed to diagnose and then accurately inform those potential treatments.
A lot of us in the support groups and on social media love tossing around the cute names, the FISH test, the flow test. Not a lot of people truly understand what’s going on with those tests. They don’t understand the concept of chromosomal abnormalities that may be going on with a patient at the time of diagnosis. Dr. Coombs, can you briefly give us a top line as to what these tests are doing and more importantly, what they’re telling you in terms of prognostics?
Dr. Catherine Coombs: Absolutely. Before the advent of all these, let’s call them sophisticated tests, we would stage patients. That’s always what I think cancer patients think of, what stage am I? We do have a staging system called the Rai Staging System that we use in the US. In Europe, they use this Binet Staging System. But the idea is, how much is this really affecting me? Rai stage 0 is when it’s just a high white count to Rai stage 4 when you have low platelets from the CLL.
I’m taking a step back because there were, for decades, ways of saying this a good or a bad CLL. However, what we’ve learned over the years is that there are some patients with really early-stage disease that would follow very aggressive clinical courses and then some that may have been technically a Rai stage 4 that were totally stable for decades. The goal with all these more sophisticated tests was to better predict, how is this person’s CLL going to behave, which then helps us as clinicians know what to expect. It helps the patient as far as what he or she should expect.
So taking a step back, we now have a lot of advanced testing that we can send. The good news is that these can be sent on the peripheral blood so it’s not necessary to get a bone marrow biopsy early on. Of course, we do consider these at the time of therapy, but we can send these tests in the blood because the CLL, by its nature, is circulating in the blood. So we can pick up different abnormalities that can tell us, this is a good or a bad CLL or maybe somewhere in the middle to help us, number one, know if we should follow this person more closely. Number two, is this someone that perhaps it’s less likely to cause more trouble than not?
The categories of tests are looking at the DNA, which is either via a FISH test which uses fluorescent probes to find common abnormalities that are known to be seen in CLL. The most adverse is the 17p deletion. On the other spectrum, the most favorable is an isolated 13a deletion.
However, what we’ve learned is that this is only looking at certain probes. Sometimes you can have other abnormalities that aren’t present as part of the FISH panel. In my own practice, I also send a karyotype test which looks for the same thing, abnormal chromosomes. Instead of using a preselected panel of common abnormalities in CLL, it just looks at all the chromosomes. The chromosomes, just for the patient’s knowledge, are just the big chunks of DNA that live inside every one of our cells. We’re focusing on what these abnormalities are in the cells because there are common patterns. There are good patterns and bad patterns.
It’s also bad to have a complex karyotype, meaning 3 or more abnormalities in any given cell, so that’s one category. The 17p deletion I mentioned is known to behave more aggressively. It’s still a chronic disease, but those are often the bad actors, especially back in the chemo days when chemo doesn’t work well at all. It does do better with our new drugs, but that is a particular problem because it deletes a copy of this very important gene called TP53.
We used to think the only way of losing that gene was by completely deleting the part of the chromosome where it’s contained. What has been learned over the past 10 to 15 years now in CLL, is that it may not be deleted, but it could be mutated. That’s another test that I think is very wise to send, especially in patients who are going to need treatment because a TP53 mutation is largely the same as a 17p deletion. There are a little bit of nuances there, but these are 2 separate tests. They both give similar information because those 2 abnormalities are treated as one and the same as far as their impact on prognosis.
The next category of testing is looking at the immunoglobulin heavy chain status, so a normal B-cell over its life. CLL is a cancer of B-cells that undergoes a process of somatic hypermutation where it just acquires mutations. It’s actually good to have a mutated, immunoglobulin-heavy chain. The bad finding is for that to be unmutated, which suggests this is a bit more primitive of a cell. And what’s been borne out through a lot of studies is that patients with unmutated are the ones who need therapy quicker and they don’t respond as well to certain therapies. Now, again, the negative predictive impact of some of these abnormalities is somewhat outdated. Sometimes they do just as well with our new treatments, but they definitely don’t do as well with the old treatments.
The other test I always send is the beta-2 microglobulin (B2M), mainly because that goes into our scoring system for CLL, the CLL International Prognostic Index, but it’s an adverse finding to have that elevated. I think that wraps up the bulk of all the prognostic tests that I send at the time of meeting a new patient and trying to help understand what is our future going to be like.
The goal with all these more sophisticated tests was to better predict, how is this person’s CLL going to behave, which then helps us as clinicians know what to expect. It helps the patient as far as what he or she should expect.
Dr. Catherine Coombs
Jeff: Let me play that back for just a second and put it in terms that are not quite so technical. You have a toolbox, and that toolbox has a lot of really nifty tools in it, where instead of saying you have leukemia or you have chronic lymphocytic leukemia or you have one of these genetic abnormalities, you’re able to hone down to a very precise level of differentiation. That’s where the term personal and precision care comes in. Correct?
Dr. Catherine Coombs: Excellent explanation. Yes.
Michele-Nadeem Baker: I love this term and how that is happening more and more for patients. Dr. Levy, before planning treatment, what do you like to understand from your patients so that you can learn more about them when it comes to prescribing their treatment?
We need to speak with the patient and find out what is most important to them and explain everything about the treatment, including side effects, logistics, expected outcomes if you choose one route versus another, and the cost of travel. There are a lot of things that go into everything.
Dr. Yair Levy
Dr. Yair Levy: We’re all different and everybody’s cancer is also different. The reason that we have jobs as oncologists is because, I’m not sure that’s true here, but hopefully we know more about CLL and the treatment options than the patients. It’s our job to explain to them all their various options and then help them arrive at a choice that makes the most sense for them.
I think Dr. Coombs mentioned that we have a lot of options, but they haven’t necessarily been compared head to head. So we can’t tell you prospectively how treatment A compares to treatment B or treatment C. There are certain guidelines of what’s called preferred therapies and other alternative therapies that are also acceptable. We need to speak with the patient and find out what is most important to them and explain everything about the treatment, including side effects, logistics, expected outcomes if you choose one route versus another, and the cost of travel. There are a lot of things that go into everything. This is our job to get them to ask the right questions and then answer those questions.
The role of patient comorbidities in CLL care
Michele: And what about comorbidities? Is it important for patients to discuss their other health issues with you, such as cardiac issues? There’s a myriad of so many other types.
Dr. Yair Levy: Absolutely. This is what we were saying is, we’re all different, we all have different things that matter, and we are all in a different place in our lives. We take all of that into consideration, there’s no question about it.
The comorbidities are incredibly important, but we certainly advanced past where we were 15 or 20 years ago when we were looking at whether patients are fit enough to take therapy versus not because right now we’re not necessarily looking at fitness for therapy as much as we’re looking at what is the optimal therapy for them.
Many of the therapies that we have, if you take a look at what’s called the Preferred Category 1 recommendations from the NCCN Panel, were all studied in what we would have technically called a non-fit population before. It’s wonderful that we have all these highly effective therapies that we can give to people, even if their fitness is not optimal.
The benefits of watch and wait
Jeff: We’ve been talking about a whole bunch of novel therapies, stuff that has really impressive outcomes these days. Michele and I will both be able to tell you without hesitation, that the first thing that most patients encounter is not treatment. It’s this thing that we call watch and worry. You guys call it watch and wait. CLL does not always need to be treated right away. Your medical team is going to work with you to decide when it’s best to start treatment. In the meantime, the patient’s worry. Did I sum that up correctly, Michele?
Michele: We sure do, even though we tell everyone not to and to take a breath when they’re first diagnosed. Jeff, you and I both know that we still go through that when we’re back in that time period. It’s just so counterintuitive to not be treated right away when the disease has not progressed where it ends up going when you do get treated.
Dr. Coombs, what are you looking for when it’s time to treat? You go through years, hopefully, during watch and wait. Worry and wait, as patients call it. But what is it that you’re looking for and is there any benefit to treating it sooner as with some of the other cancers out there?
Dr. Catherine Coombs: I’m coming straight from my clinic. I’m in a clinic room. I just had this conversation with a patient who is newly diagnosed about watchful waiting, which I totally understand why it’s watchful worrying for many. I always see it as my duty to help them understand why this is our approach. I acknowledge this is not what we do for many other cancers where you hear, find it early, treat it early. I wish our treatments were so good that treating it early would knock it out and you’d never have to worry about it again. In 2023, we haven’t been smart enough to come up with something that will do that for CLL.
The way that I help put that in context for my patients is this disease can be so indolent that maybe up to 1 in 3 patients never need treatment in their lifetime. So if we treated everyone, inherently we’re over-treating people. I hate giving people things they don’t need because every treatment comes with a cost, whether it’s financial or side effects. That’s my one very strong argument for not over-treating. But also, none of the early treatments that we have tried and done clinical trials on have been shown to make patients live any longer. That is just where we are.
I definitely could understand the frustration on the part of patients because that leaves you with these worries. I do see those getting better in patients as time goes on. There’s this initial period of uncertainty, but then as you see what your pattern is, that either tells us, maybe we are approaching the time for therapy or nothing’s really changing, I feel fine, and this is something I can accept.
Now, obviously, we never know which camp a patient is going to fall into in these prognostic tests. They help us have a general sense of, maybe this will be a super slow CLL versus one that progresses more rapidly, but nothing is certain. I do personally have enthusiasm for making this change.
There is an ongoing countrywide clinical trial looking at early intervention for patients with high risk. That is open at my own institution and across many, many institutions in the country. I really hope things will change so we can improve patients with early disease. I don’t think it’s going to be every patient because of this third that never needs treatment. I don’t ever see a reason to just treat everyone, but the trial specifically is focusing on high-risk patients. Maybe there will be some movement there. It’ll probably take about 10 years to find the results of the study because you have to follow patients for a really long time.
For now, my job is to not over-treat and not make people who are feeling good feel worse. If you’re asymptomatic, then the best I can do is leave you alone, but hopefully calm some of whatever natural anxieties come about with what is a life-changing diagnosis.
This disease can be so indolent that maybe up to 1 in 3 patients never need treatment in their lifetime. So if we treated everyone, inherently we’re over-treating people.
Dr. Catherine Coombs
Michele: We have some questions coming in from our audience. Dr. Levy, here’s one of the questions for those of us with liver enlargement. Should we watch and wait?
Dr. Yair Levy: I completely understand the anxiety that comes along with this. I’ve been treating indolent lymphomas for a couple of decades now, and I’ve got the same experience. You talk with patients, you tell them they have cancer, and then they’re saying, “You tell me I have cancer, but you’re not going to treat me now. Are you sure you went to medical school?” I had that come up several times.
By the way, we don’t do watchful waiting anymore. We call it active surveillance. Nobody likes watchful waiting, but if we’re saying we’re actively surveilling you, that sounds certainly a lot better.
The way that I explain it is, that there are really only two good reasons to treat you for anything. This isn’t just an oncologist, it’s in all of medicine. My wife is a real doctor, she’s an internist. She has the same parameters for treatment. So, number one, if you can make somebody feel better, that’s absolutely a great reason to treat them. Number two, if you can make them live longer.
What we’ve seen, as Dr. Coombs was saying in chronic lymphocytic leukemia, as well as a variety of other indolent non-Hodgkin’s lymphomas is that early treatment does not confer a benefit in survival. In other words, if we treat you when you’re asymptomatic, you’re not going to live any longer than if we wait to treat you when you are symptomatic. This is important because as we were talking before, our treatments are changing and changing for the better.
The treatments are becoming more effective and better tolerated. And remember, something is only incurable until we’re able to cure it. So there are a lot of good reasons to wait. Dr. Coombs mentioned this as well. If I can’t make you live longer by treating you earlier with our current therapeutics, the question is, can I make you feel better? If you’re asymptomatic, I can’t make you feel better. I can make you feel worse. I can spend a lot of your money, but I’m not helping you. You are the most important part of that equation.
If somebody has liver enlargement, the question is, are they symptomatic? Are they having pain? Are they having any other symptoms from their liver involvement? If they’re asymptomatic, I would not necessarily treat them just for liver enlargement. The same thing is true with spleen enlargement as well, which is a far more common finding in chronic lymphocytic leukemia.
If we treat you when you’re asymptomatic, you’re not going to live any longer than if we wait to treat you when you are symptomatic.
Dr. Yair Levy
Michele: I experienced that when I relapsed, but along with other things as well, which led to my going back into treatment. Dr. Levy, thank you. You brought up a lot of great reasons why people are not rushed into treatment which also hints at all the things that you do look at when it is time for treatment, which we’ll continue to talk about as we go through with our program today. Thank you very much.
Considering the duration of treatment for CLL patients
Jeff: We spoke earlier about a bunch of the newer options that are available. We know that the treatment landscape is changing by the minute. I’m going to tee this up in terms that forum participants and our support group participants, they all had the same questions.
Yeah, the drugs are great. Am I going to have to take them for the rest of my life, or is there a chance that I can do it for a fixed duration? Dr. Levy, let’s break down what those current treatments are, what baskets they fall into and is this a lifetime activity or could we end it in 6 months? Could we end it in one year? You’ve got a lot of stuff that ends in -ibs, and -tas, and -mabs, and all that. Explain to us what’s going on.
Dr. Yair Levy: Again, this treatment progression model is a relatively new phenomenon for us in the treatment of malignancies. We used to treat with a fixed duration of therapy when all we had was chemoimmunotherapy. You can understand why. Once we give chemo, we can’t take it back. Certainly, the effects of cytotoxic chemotherapy are not something that you want in a cumulative manner.
Because of the logistics of how cytotoxic chemotherapy works, we could not give that till progression because that would be a very difficult life. Everybody thinks that the worst thing in the world is dying, and no, the worst thing in the world is not dying. The worst thing is a long, crappy life. That’s what we would assure we would do to people if we continued them on chemoimmunotherapy.
If you take a look at our approved therapies right now, basically it’s two categories. Bruton’s tyrosine kinase inhibition, BCL2 inhibitors, and monoclonal antibodies, can be sprinkled on any of these regimens. In terms of approved fixed durations of therapy, it’s only with the BCL2 inhibitors. The reason for that is that’s the most ideal drug that we have seen in the treatment of chronic lymphocytic leukemia. What I mean by that is it is a killing machine. It kills so well that we had to attenuate the dose because if you kill things too quickly, that can also become a problem.
We’re able to get those very, very deep responses. These deep responses, even if they’re what’s called MRD, which stands for minimal residual disease, really should be measurable residual disease. Even if people achieve a level of disease below where we can measure it, we know that in many cases it still returns. We really need to get that logarithmic killing. We really need to reduce their tumor burden by many zeroes in order to give them that long treatment-free interval. Currently, that’s possibly more likely with a BCL2 inhibitor venetoclax.
As we were alluding to before, we are seeing combinations of Bruton’s tyrosine kinase inhibitors like ibrutinib, acalabrutinib, or zanubrutinib in combination with venetoclax. Again, this was based on these laboratory models in which they actually saw whether or not these cells were primed for death with this combination. They actually saw synergy, meaning that the drugs worked better together than the sum of their parts.
As we mentioned, this is a fixed duration of therapy that’s actually approved in Europe right now, but not here in the United States. In the United States, we certainly can give a fixed duration of therapy with venetoclax and a CD20 monoclonal antibody. I can tell you that anecdotally, I’ve also done that with Bruton’s tyrosine kinase inhibitor and a monoclonal antibody if I can achieve that very deep response.
In terms of approved fixed durations of therapy, it’s only with the BCL2 inhibitors. The reason for that is that’s the most cidal drug that we have seen in the treatment of chronic lymphocytic leukemia.
Dr. Yair Levy
Factors in choosing a first-line treatment for CLL
Jeff: Excellent. Lonnie’s got a great question. Since we’re now considering treatments, he wants to know what are the primary factors to consider in choosing a first-line treatment. Dr. Coombs How do doctors and patients make that call? How do you choose which drugs are up on deck first?
Dr. Catherine Coombs: I think there are disease-related factors and patient-specific factors. We tackle those one at a time. I think there is an important role in knowing what an individual’s CLL risk findings are because those can help inform how likely a treatment is to lead to prolonged remission. Specific to a venetoclax-based approach in the front line, what we do know is that there are shorter remissions in patients with the 17p deletion or TP53 mutation and also shorter remissions for individuals with unmutated IGHV.
I tend to be an optimist and so my view is that these therapies, venetoclax-based, work way better than chemotherapy ever did for patients with these high-risk features. We can still see lengthy remissions on the order of a little over 4 years for the 17p patients for progression-free survival or around 5 some years for the unmutated IGHV. That is shorter than if you don’t have those markers.
I do think it helps weigh expectations on what to expect from a time-limited regimen. If you have high-risk markers, if you have all favorable markers, venetoclax also works really well and it just works longer than if you had negative markers.
Now, Bruton’s tyrosine kinase inhibitors as a class that have really leveled the playing field. If we divvy up patients with the unmutated and the mutated IGHV and the chemo days, the unmutated would relapse years faster than the mutated. There’s not much of a difference, and so those drugs work really for everyone. Now, they’re just so different conceptually and side effect-wise, which is why it is so important to weigh the patient’s comorbidities.
In addition to these disease-related factors that could help gauge the relative success of any given therapeutic approach, there are patient-specific factors. That’s why it’s so important for me to know, not only the details of the CLL but also the details of your specific comorbidities. Do you have a high degree of cardiac comorbidities where maybe we might be a little bit nervous about the BTK inhibitors, which can have cardiac side effects?
I will say the newer drugs are much better than ibrutinib, but it is something I weigh whether you have significant kidney disease, which might be a little bit risky. When we think of a drug like venetoclax that causes tumor lysis syndrome – none of these are complete no-goes, but they help tip the scale of which one are we favoring a bit more.
Then, of course, I want to know what other medications you’re taking, because a lot of medications can interact. That’s something we have to make sure of. Often that’s not a big deal, we just switch one out, but we have to know.
Lastly is social factors. What are your preferences? Are you the type of person who wants to do everything and doesn’t mind a frequent schedule, but wants that payoff of then being done with treatment in a year, where we might lean more towards venetoclax-obinutuzumab? Or are you someone who wants to spend as little time at a doctor’s office as possible and is okay with indefinite treatment where we may lean more towards BTKi? Those are the 3 major categories I think of – disease factors, patient comorbidity, specific factors, and then social and preference.
My view is that these therapies, venetoclax-based, work way better than chemotherapy ever did for patients with these high-risk features.
Dr. Catherine Coombs
The benefits of monoclonal antibodies for some CLL patients
Michele: Dr. Coombs, thank you for talking about the biomarkers that might indicate someone is a high risk, such as 17p or TP53. I am high-risk, but I don’t have either of those. I have the other that you had discussed being unmutated IGHV, and that actually impacted my treatment decision when I relapsed. I just finished. I am on acalabrutinib and was on a blinatumomab until a couple of weeks ago. It was obinutuzumab for 6 months along with the acalabrutinib.
Now, I will be staying on acalabrutinib indefinitely because I am considered high-risk. I had originally stated before that I started on ibrutinib. BTK inhibitors work for me and I just had adverse events initially and that’s why I went off. I had a couple of years of a drug holiday and then my doctor decided that while BTK inhibitors were still working, let’s go for it. I would still have another option with venetoclax.
Dr. Levy, why does a monoclonal antibody help? What does it add to the one-two punch? I know you talked about the different things that they’re addressing and being a killing machine, but why is it only for some patients? For example, what I’m on, acalabrutinib and obinutuzumab trials have shown that it specifically works the best. One trial was presented at ASH this past year for people like me who were unmutated. So, why only for some patients is it a benefit?
Dr. Yair Levy: Well, that’s a great question. The CD20 monoclonals were our first immunotherapy in the treatment of many B-cell malignancies. When we combined them with some of the targeted therapies, we didn’t necessarily see what we were expecting. In all of the trials with chemoimmunotherapy, adding a CD20 monoclonal improved progression-free survival. But interestingly, when we took a look at some of the studies that had arms that contained both ibrutinib, our first, covalent Bruton’s tyrosine kinase inhibitor in combination with a CD20 monoclonal or without those progression-free survival curves were superimposable. I think we were really surprised by that.
By the way, I need a button that says “I agree with Dr. Coombs.” Dr. Coombs was actually mentioning the fact that there are differences among these covalent Bruton’s tyrosine kinase inhibitors, and our first one had a less focused kinase profile. In other words, it hit other kinases, not just Bruton’s tyrosine kinase that we were trying to inhibit. One of the other kinases that it inhibited was something called ITK or IL-2-inducible tyrosine kinase. This led to antagonism of the CD20 monoclonal, which is why we got no benefit from the addition of the CD20 monoclonal.
This is not true for the other covalent BTKi, zanubrutinib and acalabrutinib. However, you’re seeing the combination with acala because that is FDA-approved and zanubrutinib does not have an FDA label in combination with a CD20 monoclonal. Do I have any reason to think that it wouldn’t work as well? I do not. There’s certainly data that supports that as well, that there are differences in terms of PFS for folks receiving the combination of zanubrutinib with a CD20 as well as without.
Now you can say, so why doesn’t everybody get a CD20 monoclonal? The answer is that there are trade-offs. Everything in life is a risk-benefit ratio. We know that, for example, there is this virus here in Texas, I don’t know if you guys have it too, called COVID. We know that for COVID, the CD20 monoclonal certainly antagonized an immune response to vaccination, as do the BCL2s and Bruton’s tyrosine kinase inhibitors.
Certainly, you are at more risk for adverse events and complications when you add additional drugs, so everything is a trade-off. We’re getting additional efficacy but at a cost. Our job is not to tell patients what to do. Our job is to have a discussion and come up with a solution that works best for them after we have a discussion and they are fully informed.
Now you can say, so why doesn’t everybody get a CD20 monoclonal? The answer is that there are trade-offs. Everything in life is a risk-benefit ratio.
Dr. Yair Levy
What CLL doctors consider before ramping up treatment and dosing
Michele: Thank you. Dr. Coombs, let’s talk about ramping up treatment. When you start treatments such as with venetoclax or even obinutuzumab, you start with smaller amounts and then ramp up to full dosing. Why is that?
Dr. Catherine Coombs: It’s different based on the drug. Let’s tackle obinutuzumab first. Obinutuzumab is the monoclonal antibody that can be paired with either venetoclax or acalabrutinib. It can also be used by itself less often. It’s a hugely effective drug, and it doesn’t really have that many side effects except for one that’s almost universal, which is these infusion-related reactions. Of course, it has other side effects such as impaired vaccine efficacy infections. It can cause low blood counts, but the one that’s universal is infusion-related reactions.
Instead of just giving patients their full dose of 400 mg daily, we…slowly introduce it so we’re more slowly killing off the cells in a way that’s friendly to the kidney and friendly to the rest of the body to minimize any potential risks from all this dead cancer cell debris.
Dr. Catherine Coombs
What they’ve learned over the course of developing this drug in clinical trials is that, instead of blasting patients with the full dose on the first day, the reaction seemed to be more manageable if you split the dose. The traditional way of administering obinutuzumab, the full dose is 1000 mg.
Instead of doing that all at once, which would make for a very colorful reaction in the infusion suite that no one nurse nor patient wants to be involved with is giving 100 mg on day one and then the other 900 mg on day two. Then of course you follow along with the rest of the schedule. The reactions, fortunately, are almost always on the first 1 or 2 days and then not long-lasting except for rare exceptions. That’s the reason for ramping up obinutuzumab, to make the reactions more manageable.
Venetoclax is a different story. As Dr. Levy mentioned, this drug is remarkably effective at annihilating CLL cells. But it’s not a good idea to kill any cancer just too quickly, because when you kill a cancer cell, all this dead cancer cell debris gets released into our bloodstream and our kidneys can’t handle that, even the best kidney in the world.
Instead of killing cancer rapidly by administering the full dose, it’s been learned through very well thought out and designed clinical trials that patients tolerate it better with less chance for dangerous tumor lysis syndrome, which is the term for complications from cancer dying too quickly, is to ramp it up. Instead of just giving patients their full dose of 400 mg daily, we give them a little whiff of venetoclax in week one, 20 mg, a little whiff the next week, 50 mg, and slowly introduce it so we’re more slowly killing off the cells in a way that’s friendly to the kidney and friendly to the rest of the body to minimize any potential risks from all this dead cancer cell debris.
Considering the side effects of CLL treatments
Jeff: Dr. Levy, I love the fact that you used the term risk management because that’s pretty much how I approached my entire journey, with risk management. We know that for most people there are going to be some side effects. There’s going to be some challenges when they start treatment. Can you give us a minute on, are they all going to happen upfront? And how do you manage them?
Dr. Yair Levy: That’s a great question. As Dr. Coombs mentioned, for the CD20 monoclonals, most of the reactions occur early and typically improve as you receive more of the drug. This is also true for the oral medications that we have. Most of the side effects, if you look at what’s called adjusted incidence, meaning how likely is it to happen per amount of time, it’s more likely to happen in the beginning. However, as we talked about, some of these therapies are indefinite progression or intolerance.
If you take a look at the cumulative incidence of events that continue to go up, there are certainly some events that are much more difficult to come back from. One that we worry about in particular is what’s called ventricular tachyarrhythmias, so getting a funny heart rhythm can actually lead to sudden death. It’s tough to come back from sudden death, isn’t it? One person’s done it right. They wrote a book about Him. One Person came back from the dead. A very popular book, but nobody else has done it since so we want to make sure that we give patients the safest possible therapeutics that we can.
Reasons to switch a CLL patient’s inhibitor
Jeff: Sometimes patients are told that they need to switch out their BTK inhibitor. There are a lot of reasons why this could be done. Dr. Coombs, can you tell us what’s going on with this?
Dr. Catherine Coombs: That is a common question, and that’s something that’s evolved over the years from having one option, just ibrutinib, to now having multiple options. In my own practice, I actually have switched patients for a number of reasons. I would say the reason that I consider switching a patient off of a BTK inhibitor to a different BTK inhibitor is if they’re having some side effect that’s negatively impacting their quality of life. I have switched patients from ibrutinib to acalabrutinib with very good success. I’ve also switched patients from ibrutinib to zanubrutinib, and I’ve even switched patients from acalabrutinib to zanubrutinib.
There have been studies looking at switching for side effects. About 70% of the time, the patients have improved tolerability on one of the newer drugs. There have been studies looking at switching to both acalabrutinib from ibrutinib and then switching to zanubrutinib from both ibrutinib and acalabrutinib and it seems to be a pretty uniform result where more often than not, the newer drugs are better tolerated than our oldest drug, specifically ibrutinib. I think that’s a very valid reason to switch.
The education point is, I would not switch in the setting of progression. That just is not a strategy that works more than a month or two and it isn’t really worth it. If you’re progressing on a BTK inhibitor of these FDA-approved ones, again, not speaking to switching from any of the approved ones, ibrutinib, acalabrutinib, or zanubrutinib, that is not recommended.
Now, I’ve heard of some occasional doctors just switching everyone off of ibrutinib. I’d say I talk to a lot of the community. I think most of us don’t do that because the side effects that occur most of the time are early on. I don’t use ibrutinib for my new starts, but I definitely have patients in my clinic who have been on it for years and they’re doing well. The old expression is if it ain’t broke, don’t fix it. Some people think, well, let’s just switch everyone. I don’t think that’s wrong, but it’s just not something that I’ve done for the reason I mentioned.
Jeff: Thank you for that. Makes complete sense.
I would not switch in the setting of progression. That just is not a strategy that works more than a month or two and it isn’t really worth it.
Dr. Catherine Coombs
New CLL treatments awaiting FDA approval
Michele: Doctors, there are so many types of treatment and clinical trials. Dr. Coombs, which ones are you most excited about that are getting closer to FDA approval?
Dr. Catherine Coombs: There are two that I’m going to mention. I’m excited about a lot of things, but the ones that I think are the closest to being approved potentially, I have no window into when the FDA actually approves things. One is a drug called pirtobrutinib. This is a drug that inhibits the same target as ibrutinib, acalabrutinib, zanubrutinib, and BTK, but instead of inhibiting it irreversibly, it is a reversible inhibitor.
The reason that that’s important is that when patients develop resistance to ibrutinib, acalabrutinib, and zanubrutinib, the resistance is shared by all of these drugs. So you can’t switch from acalabrutinib to zanubrutinib or ibrutinib to zanubrutinib, etc., if your patient is resistant because they develop most commonly mutations where the drugs bind. Pirtobrutinib binds at a different mechanism. It’s in a different part of the BTK molecule protein and it has shown very excellent efficacy in a very large study. I do think that that may attain FDA approval for CLL in the coming days.
It’s already FDA-approved for mantle cell lymphoma as of January, so there are ways to get it off-label, but I would much rather see it get full FDA approval to help with insurance paying for the drug when it’s needed. It fills a huge unmet need for patients who have progressed on covalent BTKis, especially after patients who have progressed following venetoclax where we don’t really have good options.
The other big category that Dr. Levy has alluded to is the combination of a BTKi plus venetoclax. Europe approved the combination of ibrutinib with venetoclax, which did not get approved in the United States. I can’t really speak about the reasons because I’m not involved with those discussions. I do wonder if some of it may be the toxicity of that regimen, which can be somewhat hard to tolerate, especially for older adults.
But what we know is that we have better BTK inhibitors with respect to tolerability. So there are a couple of trials that are looking at the combination of acalabrutinib and venetoclax that I do think hopefully will be positive trials that lead to FDA approval. That’s the other major category that I’m looking forward to. Those would be frontline treatment. You would use that combination as your first treatment. Whereas pirtobrutinib, if it gets approved, would be a relapsed treatment, at least for now. Things obviously change as time goes on.
It fills a huge unmet need for patients who have progressed on covalent BTKis, especially after patients who have progressed following venetoclax where we don’t really have good options.
Dr. Catherine Coombs
Michele: So your top two are pirtobrutinib and the combination of–.
Dr. Catherine Coombs: A BTKi plus venetoclax.
Michele-Nadeem Baker: Dr. Levy?
Dr. Yair Levy: I agree once again. There are other small molecule inhibitors, again, targeting that B-cell receptor pathway, which has really revolutionized the way that we treat a lot of these B-cell NHLs. In addition, the bispecifics, are certainly working their way into our armamentarium for non-Hodgkin’s lymphomas as well as CAR Ts.
Interestingly, one of the first articles that came out about CAR T was in chronic lymphocytic leukemia, despite the fact that our current constructs, these current autologous derived products are certainly not showing the same level of efficacy in chronic lymphocytic leukemia as they are in diffuse large B-cell lymphoma, for example. Nevertheless, I think that we are going to see some tremendous improvements in terms of the CAR Ts in chronic lymphocytic leukemia as well as the Bispecifics.
CLL doctors’ top takeaways
Jeff: So, Dr. Levy, I’m going to put you on the spot. What is the number one takeaway that patients should be grabbing from this discussion that we’re having today? What’s the top of the list?
Dr. Yair Levy: We’re doing so much better. As I mentioned at the beginning of the conversation, I have not had a patient die of CLL in the past decade. When we take a look at the high unmet need and again, Dr. Coombs was alluding to that. Folks who have progressed on a Bruton’s tyrosine kinase inhibitor and a BCL2 inhibitor are certainly the unmet need. We have a tough time finding those folks.
We’ve had some studies that have been languishing for accrual because it required folks to become double refractory. Again, we have a tough time finding those patients, which is wonderful. I don’t want to find those patients. I’ve put 2 people on in the past 5 years, and one of them was actually not even really refractory. He just wasn’t taking his medication. With CAR T, once I give it to him, he can’t take it, so this was more of me being paternalistic.
We’re doing so much better. As I mentioned at the beginning of the conversation, I have not had a patient die of CCL in the past decade.
Dr. Yair Levy
Jeff: Dr. Coombs, what is the single most important thing that you want patients and their caregivers to take away from this discussion?
Dr. Catherine Coombs: Jeff, we are friends now. It’s going to be hard to narrow down one thing, but I think if I have to say one thing, it’s there is hope. Leukemia is a horrifically scary word to hear for the first time, or maybe even after years of knowing that this is what you have. But all the treatments work extremely well and they work for an extremely long time. There is hope. Hope to live a normal life, and hope to see your kids and your grandkids grow up. There’s always hope on the horizon, in my opinion.
Encouragement for CLL patients to advocate for themselves
Jeff: What can patients and their caregivers do or ask if their local hematologist-oncologist isn’t quite looking at this new wonderful stuff that’s on the plate right now? What if they’re just going with the old stuff?
Dr. Catherine Coombs: That’s such an important question. And, you know, I think it’s tricky. I think it depends on what your personality type is. My personality is that I want to make everyone happy. I never want to offend anyone. I certainly understand the hesitation to question your doctor. But I think in the end, you just have to realize this is your life. If your doctor is not sounding up to date or if you’re just not getting your questions answered, then you deserve more than that.
I just think it’s so important to advocate for yourself or advocate for your loved ones if things aren’t adding up. I think our community docs are amazing. The ones that I interact with, I have no idea how they keep up with everything they keep up with. To put things into context, there are around 20,000 cases of CLL diagnosed a year.
When you think about the common cancers that have a majority of patients, they’re seeing lung cancer, breast cancer – those are like 200,000 plus cases. CLL ends up just being a much smaller slice of what they’re seeing every day, and it’s just very hard to keep up. I would say most community docs I work with very much welcome the second opinion because I can teach them something and then we now have a relationship where they’ll ask me questions and we can work together.
So, number one, don’t be worried about offending your doctor. Number two, most doctors aren’t going to be offended. Number three, if they are, well, I don’t know what to say about that, but I don’t get offended. Back when I was at UNC, I had patients go to Duke and the Duke patients would come to me. Sometimes it’s just good to hear things twice. I think if your doctor is offended, that’s a red flag on their own ego. I think all that we should want as your doctors is for you to get the information you need. That is your job to advocate for yourself, and almost all doctors are going to be totally happy with it. We can learn something from each other as we share in your care journey going forward.
There is hope. Hope to live a normal life, and hope to see your kids and your grandkids grow up. There’s always hope on the horizon.
Dr. Catherine Coombs
Jeff: Thank you for that and I love the way you put it. Patients should not be concerned about asking questions. They shouldn’t be concerned about saying, why not? If they’re having trouble getting along with their doctor, like you said, that’s a red flag.
Navigating what symptoms you should share with your doctor
Michele: We have some more patient questions, so here’s one of them. Sara N. asks, “How do I know when I should contact my doctor between visits? Do they need to know about every infection or just about CLL symptoms?”
Dr. Catherine Coombs: Sara, that’s a great question. I think in the digital age, we certainly can let doctors know about every single detail, but I think it’s good to set up expectations. I try to do this on my first visit or maybe my second visit if we don’t have time to cover it.
But what things do I always want to know about, and then what goes into the other category? I always educate my patients on red-flag symptoms. Things that for my patients on watch and wait, watch and worry, active surveillance, things that make me think, we need to get you in right away. Unintentional weight loss, drenching night sweats, fevers. I go through the list of the things I always want to know about – a rapidly enlarging lymph node, etcetera.
Then there may be other symptoms, and the ones I want to know about are the ones that are worrying you. I don’t want you to go to bed freaking out about something that may be nothing. Just send me a message and I’ll tell you, that’s nothing or I need more information. Maybe let’s have you come in. I’d say, it’s never wrong if it’s something worrying you. But of course, we all have to acknowledge it could get to be a lot of messages if it’s every single thing. I think you just learn that over time as you establish with a doctor, but I think it’s good to go through what things should I let you know about right away, and what things can wait. Then obviously there’s some gray zone where it doesn’t hurt to just pass the info along and then you can get back a message and not worry about that.
Michele: In looking at a patient holistically, so to speak, regarding these little things that we may not think are important, such as all these various infections – I keep getting sinus infections. I’m trying to think of some other types of infections. Maybe you could list those for patients, some of the ones that they might be seeing that you want to know about.
Dr. Catherine Coombs: We do see an increase in infections in our patients with CLL. I do like to get a general sense of how often patients are getting infections. If they have a primary care doctor who’s very responsive, I’m okay with them treating these infections. I’m also okay taking the lead, whatever works best.
But when they become really frequent, especially if it ends up with the patient landing in the hospital, I absolutely do want to know about that. There are some strategies we have to lessen the incidence of these infections.
Patients with CLL, a proportion of them, don’t make enough immunoglobulins. If you’re landing in a situation where you’re having a lot of severe infections, meaning pneumonia that you’re in the hospital for, or terrible sinus infections, etc., that may be a reason to consider this intervention called immunoglobulin infusions.
I definitely like to know about things that I can fix. I’m okay knowing about things I can’t fix too. The ones where it’s like, this would change what we do, those are especially important. The patients may not know that before messaging me, and that’s okay. It’s okay to just message because you don’t know and then I’ll tell you there’s nothing to do or let’s bring you in and talk about X, Y, Z.
I always educate my patients on red-flag symptoms…Unintentional weight loss, drenching night sweats, fevers.
Dr. Catherine Coombs
Jeff: Fantastic. I’m going to make this a little bit personal as far as what I hope people are taking away from this discussion. When I was first diagnosed with CLL, my doctor told me straight up that I was going to die in about 6 years, and that doctor got fired. My next doctor told me, “Don’t worry, we’ve got this. You might die with this, but you’re not going to die from this.”
Listening to both of you fantastic doctors talk about the landscape of CLL and even use the 4 letter word “cure,” I am convinced that I am going to be able to continue doing everything that I want to do, and I want to do an awful lot of things at some point. If my daughters’ are cooperative, maybe I’ll become a grandfather, but I’m going to continue knocking out half-marathons. I’m going to continue knocking out full marathons. I’m going to drink good wine and good whiskey. I’m going to eat well. I’m going to laugh a lot. I’m going to smile a lot and I’m going to share my story so that patients and their caregivers know that that can be their life, too. Michele, how about you?
Michele: I agree some of my key takeaways are that there are so many things in research and we have the potential of being approved in the somewhat near future, which is yet another option for us. As you had explained, it does work in a different way than the traditional types of BTK inhibitors we now have. I think this is fabulous to have yet another option for patients.
Also, I love what you said about what you really need to look for in your own doctor and not be worried about offending your doctor. This is so vital for patients. I ask a million questions and I encourage patients to do so so that they can become more empowered for their own care and self-advocate for themselves.
It’s been so great hearing you and Dr. Levy both talk about patients asking questions and encouraging them so that patients are not afraid of this. This is again, one of the things I had started doing to try to get rid of the mystique around care and treatment with people’s doctors. I continue to do that.
In addition with Jeff – and we’ll be toasting soon, hopefully in person about this with something more than water, which we’ve been drinking during the program – and that is to live life to its fullest and to live a normal expected life span thanks to doctors like you, Dr. Coombs and Dr. Levy. I thank you so much for joining us, both of you and I thank all of our audience members watching us.
Dr. Catherine Coombs: And thank you both for all the work you do in patient advocacy. Like 10, 15 years ago when the Internet wasn’t available, I think there’s so much more fear. To be able to bring light in a way that patients can understand is so hugely important. So thanks for what you do as well and for having me.
Special thanks again to AbbVie and BeiGene for their support of our patient education program all about building shared treatment decision-making! The Patient Story retains full editorial control.
How to Work with a CLL Specialist and Build a Strong Team
Are you or someone you know navigating the complexities of chronic lymphocytic leukemia (CLL) treatment? We understand the importance of building a strong support system and collaborating effectively with multiple doctors. The Patient Story features a panel of experts and individuals with firsthand experience.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang: I’m Stephanie Chuang, founder of The Patient Story and a blood cancer survivor. It’s another edition of CLL Conversations and our topic is how to build a strong CLL team. We have an incredible group of people to help [give] some guidance, sharing their own experiences from the patient’s perspective as well as from the physician’s perspective.
Our goal at The Patient Story is for patients, by patients and to help those who have been diagnosed with cancer or those around them navigate life after that diagnosis. Our tagline is Humanize Cancer. We specialize in in-depth conversations with patients, care partners, and cancer specialists. Our goal is to help people through a really tough time.
Michele Nadeem-Baker: Thank you so much, Stephanie, for ensuring that the CLL and SLL communities are spoken to here at The Patient Story. I’m Michele Nadeem-Baker, a medical and health journalist and also a CLL patient.
When I was first diagnosed in 2012, things were so different in the CLL landscape. Once I started treatment, I made a vow to try to help other patients. Since then, I’ve been growing my patient advocacy and patient leadership and one of the people I do that with is Jeff.
Jeff Folloder: Hi, I’m Jeff Folloder, a passionate patient advocate. I really take this seriously because it’s really, really important for me to share that you can live a great life with CLL. Not just a good life; a great life.
I just entered my 14th year of dealing with CLL and it seems like yesterday I got the diagnosis. But what I’m really excited about right now is introducing you to Lisa, someone I met years ago in a waiting room and I’m so glad that she’s going to share her story.
Groups like this are so helpful so I’m very grateful, especially when you’re new and don’t know what lies ahead. There’s so much information.
Lisa P.
Lisa P.: I’m Lisa. I was diagnosed in 2012. I just went for a routine physical and got the diagnosis, which came as a surprise, but it doesn’t define who I am.
I’m a mom of three grown children. I’m a yoga instructor. I actually went to yoga after my diagnosis to help deal with it. I used to go to yoga as a workout and once I was diagnosed, yoga became much more than that to me. It became a mental practice that helped me not to spin the stories in a scary direction, but to stay grounded and focused on what was going on without being so fearful.
I was very grateful to have someone like Jeff to talk to; really comforting. I remember meeting in that waiting room after meeting online. Groups like this are so helpful so I’m very grateful, especially when you’re new and don’t know what lies ahead. There’s so much information.
Jeff: This is going to be a fantastic discussion. We also have two world-class medical experts joining us. Dr. Nicole Lamanna is a hematologist-oncologist at Columbia University.
Dr. Nicole Lamanna: I’ve been doing this for a long time. I started at Memorial Sloan Kettering and was there for 12 years. I’ve now been at Columbia University since we set up a leukemia service. I’m also a staunch CLL patient advocate as well as a CLL physician.
I had an interest in leukemia when I was in my early days of training. I found it a very complex and unique disease. I was very fascinated by the immunologic things that can happen with CLL patients. I had a mentor who did CLL and I decided I would continue research. I’ve been doing that ever since. Twenty years of doing CLL, at least.
It’s a disease that you live with for a prolonged period of time. I like taking care of other aspects also, not just CLL. Folks have been with me for 20 years so it’s almost like a primary care internal medicine clinic. I enjoy building relationships that last a lifetime so that has also been a very important aspect of my practice and one of the other things I like about treating patients with this disease.
Michele: Dr. Lamanna, it’s always such a joy to see you and to also be with you on these programs. You are such an advocate for all of us and what a specialist you are. It’s a delight to have you with us.
Dr. Spencer Bachow: I knew I didn’t want to do internal medicine; I wanted to be a subspecialist. It wasn’t until I did my malignant hematology rotations as an internal medicine resident that I had role models. These were the types of doctors that I always dreamed of. The way they thought about patients was very different and I knew this was the type of doctor I wanted to be.
I got into it from great role models and the same with CLL. Dr. Lamanna was my fellowship mentor and you could really feel the excitement she and everybody else had in this field.
A lot of the cancer advances that we’ve seen in CLL are some of the biggest. The transformation of the treatment of CLL is one of the biggest cancer advances of the 21st century.
Finally, like what Dr. Lamanna said, it’s a very heterogeneous disease where a lot of patients do well long term. You could establish long-term relationships with them. You get a chance to help people during some of the most difficult stages of their lives.
Finding a CLL specialist
Jeff: One of the things that Michelle and I constantly hear, constantly see, especially in online groups, is the recommendation to get a CLL specialist. It’s almost always the first thing that’s tossed out to someone new who shows up. Go get a CLL specialist.
I’m fortunate I live in a metro area. Michele’s fortunate she lives in a metro area. Getting access to a CLL specialist is not very difficult for us. We have them around.
Not everybody who gets diagnosed with CLL has that access. Or maybe they do. How do you build a strong CLL team when you might not necessarily have one in your hip pocket?
My first doctor wanted to start a treatment program that was ancient by CLL standards and I quickly learned that it wasn’t right for me. I had to make changes. I had to get a CLL expert on the team. I did just that and here I am 14 years down the road, doing great because I built a good team.
Michele: Jeff is the second CLL patient I ever met and that was probably a year or so into knowing I had CLL. He came up to Boston and we both spoke at an event. It has been wonderful having Jeff as my CLL buddy and all the things that we’ve been doing together. We are both so passionate about this.
I didn’t even know what a CLL specialist was. I did know there was such a thing as a hematologist-oncologist, but just because I knew one personally doesn’t mean I really knew exactly what all this meant. I think that’s how a lot of us are when we’re first diagnosed.
I was first diagnosed while I was working in South Florida. I had the job of my dreams. I was at the C-level of a major international company with a corner office overlooking Biscayne Bay.
I was diagnosed by someone at a hospital nearby except they didn’t explain anything about CLL. They told me to come back in four months. They had nothing to give me when I asked. But again, this is back in 2012. Things have come a long way since then, thank goodness.
I left everything behind; I really didn’t have to. I quit my job. I was living between Boston and there. I moved back north because I knew Boston has a plethora of healthcare.
When I was diagnosed, I didn’t even know there was such a thing as a CLL specialist. I didn’t even know what CLL stood for. I started seeing a CLL specialist once I heard about one and that’s how I started building my medical team.
Since then, I have been a huge proponent of having a CLL specialist on your team. You don’t have to have one to see all the time if you don’t live near one. Jeff and I were very blessed in that we happen to have centers near us.
Jeff, when you heard about specialists, did you get to one right away or did you take your time in seeing one?
Jeff Folloder: For me, it was right away. I did not feel comfortable with the advice that I was getting. I leaned on a family member who worked at a large research facility in Houston and they got me hooked up.
What you and I have been doing over the past years is encouraging people to get in touch with a CLL specialist, no matter where they are. That’s actually something that Lisa was encouraged to do.
How CLL specialists work with local hematologist-oncologists
Jeff: I want to toss this to Dr. Lamanna. How do you work with a local hematologist-oncologist? How does this whole concept of having a CLL expert quarterback actually work in real life?
Dr. Lamanna: You both have been blessed by being in cities that have major academic centers that have CLL specialists.
CLL is not a common disease like breast cancer or colon cancer. CLL is relatively small when we compare them to solid tumor cancers. Most oncologists might see a little bit of this and a little bit of that, and that’s fair.
Although I would love for every CLL folk to come and see me in New York, we know that’s not feasible or possible. Oftentimes, folks will come for an opinion, to discuss their disease, or at a crux where they might need treatment.
I will communicate via phone, email, or message and start a relationship with their local person to help guide them, particularly if this is not a disease they typically treat.
As Dr. Bachow alluded to, there’s such an explosion of treatment options. Depending on other factors, navigating these treatments and choosing between different drugs can seem a little daunting. I’ll try to communicate with their local physician to see if I can help them, guide them, and be a link between the patient and their local physician.
Sometimes it’s extremely easy because their physicians are very willing to have that extra specialist help them in an area that they’re less familiar with. Sometimes it doesn’t go as quite smoothly as I’d like.
My patients know me. Oftentimes, if I think something’s a red flag, I will speak honestly about that. I need them to find somebody that I think is going to be in their best interest. This isn’t about egos. I know many patients actually feel uncomfortable about having a team because they don’t want to upset their local physician.
Remember, this is all for you. This isn’t for me. This isn’t for your local physician. This is really about you getting the best care that you need for your CLL. If you’re uncomfortable talking about that with your physician, that could be a problem.
You want to be able to communicate with your physician and the physician team about your needs and any issues that arise. You’re going to build a long-term relationship so you want to find a local physician that you can trust, that you can work with throughout the years, and then if advice is needed from somebody like myself, they’re willing to take it because the likelihood is I probably see more CLL patients than they do.
Most of the time, it works well. Occasionally, there may be some issues that need a little bit of hand-holding until they smooth out over time so that you can also include the specialist, particularly at certain cruxes that might come along on your CLL journey.
Dr. Bachow: Echoing what Dr. Lamanna said, the CLL specialist is very important. There’s a huge landscape of all kinds of different treatment options that we didn’t have several years ago. Knowing when to use them and how to safely use them can be tough for anybody. Employing the CLL specialist is very, very, very helpful as a local CLL doctor and a local hematologist-oncologist.
A lot of times, we don’t have access to certain clinical trials that our patients may be candidates for and may be interested in and that is a huge plus you can get when you have your patient meet with a CLL specialist. The local doctor is still important because things happen. Complications happen, hospitalizations sometimes occur, and if you don’t live near your CLL specialist, having somebody there who knows your care is very important.
Additionally, a lot of the CLL treatments these days can be very labor-intensive and require very frequent follow-up. Unless you’re planning on moving to where your specialist is, having a local person that you can trust, that your CLL specialist trusts and that can work together as a team is so important.
Lisa’s CLL story
Michele: I met Lisa about four years ago. We’ve been buddies virtually but she lives near where I used to live in Florida. We even know some of the same people.
I was really touched by how you educated yourself on CLL. You learned a lot. You were able to be your own advocate, which is so important, and I’ve always noted that. Could you share when you were diagnosed, your experience, and how you ended up being educated and advocating?
Lisa: I was diagnosed during a routine physical with my primary care doctor. She re-did the blood work, thinking it was a machine glitch, and it wasn’t.
I was immediately sent to this wonderful local doctor at the time and I adored him. He gave me some information, but he wasn’t a CLL specialist by any means and he was very open to me going to other places.
It was really the resources online, support groups that I found, and Jeff that I got directed, speaking to people who had already lived this experience. They pointed me to the current treatments. Oral BTK inhibitors were just starting to explode at that time. Infusions were more common back then.
How to find a CLL specialist
Michele: How did you find your eventual specialist?
Lisa: Once I was diagnosed and starting to get thrown into the trenches of what the reality of this was, I became very involved online, met Jeff, met some other people that had been dealing with CLL for longer, and you hear, “Find a specialist.”
There is a lot of information out there. I would watch Patient Power videos. The Leukemia & Lymphoma Society offers a lot of panels of doctors’ discussions. I would listen to them and listen to the new research. All these specialists are generous, giving their time, and that is how I found both specialists that I went to just by watching videos and being my own patient advocate.
Dr. Lamanna sits on a lot of panels. I would watch these videos and hear her on these panels. On some of them, she was sitting right next to my other specialist. He was getting older and was going to retire, too.
I was just drawn to her. I loved how she spoke and how she relayed information. I loved her personality. I said to my husband, “I really like her. I want to go have drinks with her.” That’s how I felt watching the videos.
It was a small world. I had a visit with my local doctor at the time and I mentioned Dr. Lamanna to him. He literally looked at me and said, “I don’t know why I didn’t think of this before.” They knew each other very well. He texted her and said, “I have a patient and I’m sending her to you.”
My daughter was moving to New York. She was just graduating college. You have to find what’s going to work in your life and it makes sense. I was going to New York anyway so why not have a specialist there?
The puzzle pieces came together and I had this wonderful team. I felt that my local doctor had a better means of communication now. I love and trust my specialist and my local doctor. They communicate well.
Scott’s CLL Story
Michele: We have Scott who talks about how he found a CLL specialist and his path to getting one.
Scott W.: Hi, Michele. My name is Scott. I’m a news photographer in Cincinnati, Ohio, and I was diagnosed in November 2019.
Finding a CLL specialist
Scott: At first, I didn’t know what a specialist was. I was assigned a hematologist at one of the hospitals here in town. It was a shock to find out that there’s this thing called watch and wait, which just didn’t make sense to me, as I’m sure it didn’t make sense to a lot of other first-time folks diagnosed.
I started doing some research and found that there’s some controversy, I guess, and some progress being made on whether watch and wait is appropriate or not. I started questioning my hematologist-oncologist about it and he didn’t really have any answers for me.
I sought out another hematologist, still didn’t know what a specialist was, and was getting sort of the same thing. “Well, you’ve got about five years to live, but you’re not sick enough to have treatment.”
I got frustrated and, by good fortune, my general practice doc said that one of the premier specialists in the world was coming to Cincinnati and that he is accepting patients for CLL.
I signed up and was one of his first patients here in Cincinnati. Within five minutes of our first meeting, he said, “Yes, we can start you on treatment right away. And I can say with 95% certainty that we can put you in remission and reset your lifespan to pre-diagnosis limits.”
How to find the right CLL specialist
Michele: Dr. Lamanna, how can anyone find the right specialist? Is there a list? Lisa had one, but this is a long-term relationship. This is probably the person you’re going to be with for the rest of your life so it’s really important that it works.
At what point do you need to bring a CLL specialist onto your medical team? Do you do it just after you were diagnosed? Do you wait until it’s time for treatment? How do you even know?
We want to ask the doctors because we all seem to have our own opinions as patients. This is not meant to take the place of someone’s local hematologist-oncologist who works in conjunction with them.
Dr. Lamanna: You all have already mentioned a couple of areas. One is these online forums, The Leukemia & Lymphoma Society, Patient Power, and the CLL Society. There are lists of CLL specialists in states all across the country so that might provide a starting point, depending on where you live.
You might be restricted because you need to see someone in the area where you live because of your circumstances and so you want to do local. You have to do what fits you. There are people like Lisa who can travel to another state to see a specialist.
Ultimately, your personality and the personality of another physician have to jive, too. Not everybody may jive with a particular person so that’s another layer to add in.
When to see a CLL specialist
Depending on when someone’s initially diagnosed, if you’re not receiving the information so you understand the disease and where you’re at, having that first consultation is very helpful.
If the local physician isn’t spending enough time to explain things because you don’t need treatment and they’re rushing you out the door and saying, “You have a good cancer. You don’t need to see us. You’re great,” that’s not really satisfying to many patients when they’re first diagnosed with any cancer. Sometimes that initial consultation is important.
Another very important time, which Dr. Bachow brought up, is when you’re told you might need therapy. The question is: do you need therapy? What kind of treatment is being recommended? There are new agents and each patient might have a little bit of a different nuance to their disease so that’s really another key point to see a specialist.
Then there are clinical trials. There might be some options that could be really important as well.
Certainly, any time is a good answer, but if you don’t have the ability to do it very frequently, those key time points might be important.
Dr. Bachow: As Dr. Lamanna said, a good time is if you’re at diagnosis and you don’t feel like you’re getting all the information that you need to feel comfortable with the diagnosis.
One time that you really should it’s when you’re going to need treatment, but you can also take it a step further — you don’t want to wait too long.
In some cases for patients with very high-risk disease, their disease can grow exponentially and it may be tough to get in to see a CLL specialist. They’re all so great that they’re booked out weeks and weeks and weeks and they’re doing favors all the time, double-booking patients to bring them in.
I wouldn’t necessarily say just when you’re told that you need treatment. You and your doctor should try to talk together. “Am I more likely to need treatment in the future rather than not need treatment?”
Maybe now’s the time to go get more information, hear what trials are out there, and hear what the treatment landscape looks like now. If the time does come, you’re not rushing to see somebody.
Michele: That’s such an important point, Dr. Bachow. You want to have that established relationship in case it is more of an emergent time.
My CLL relapsed really quickly and I was looking for a second opinion because I was given so many choices. That’s the beauty of research right now. We have so many choices between what’s been approved and what’s in a trial. I didn’t have time to find someone. I had to start treatment the next week.
Thankfully, I had a great relationship and established one with Dr. Lamanna. Knowing you, it’s not like I had to wait months to get to see you so it was wonderful. There can be challenges in getting in to see one.
Patient’s perspective working with a local oncologist & a CLL specialist
Michele: What are the challenges and workarounds of working with different teams in different healthcare systems? Lisa, what did you experience here? You were working with different healthcare systems.
Lisa: The biggest challenge with the first CLL specialist I went to was communication as well as changing doctors when my first doctor suddenly left for a different facility.
My local doctor struggled with getting calls and emails returned. He would voice a little bit of frustration when I would come in for appointments. He hadn’t gotten the information he needed and if I could call and see if I could get things sent. That was the biggest challenge and part of what made me feel I didn’t quite have my right team yet.
One thing I always heard was to go to one of the world-renowned places for leukemia and lymphomas. My local doctor at the time encouraged me because he was also looking forward to having this be a learning experience for him. I went and it was great. They were wonderful.
I don’t have anything bad to say about my experience there other than it wasn’t the right place for me. It was difficult to travel to and I was hearing frustration from my local doctor. When I first went, I didn’t need treatment. After all the testing they did, I was told I’d probably need treatment in about three years and they were absolutely right.
The first doctor I saw was lovely. Shortly after my first appointment, I ended up getting a letter that she was no longer there and had moved to a different facility in California. Then I was on my second doctor so the next time I went, I was meeting a new doctor again.
I started my treatment there. I did my first course then they sent the protocol home so I could finish here. He was frustrated with the lack of communication. It’s a very big, well-known hospital and doctors are busy so he wasn’t getting responses to emails in a timely manner. You can’t expect anything right away.
What was frustrating to me was that he was frustrated. We ended up finishing after three rounds because that treatment didn’t really work well for me.
Dr. Bachow wasn’t my original local doctor. He came into the picture later. Unfortunately, my local doctor passed away unexpectedly so I was left with this situation where now I didn’t have my team.
The first time I ever went to Dr. Lamanna, Dr. Bachow happened to be her fellow. When we met him, we adored him. We thought he was great. We both went to the University of Florida. We knew he was moving back to Florida.
When I was in this position, I called Dr. Lemanna and she said he was in Boca Raton. I was really lucky. He’s just as wonderful. You need to have trust in both your doctors. To me, the biggest thing is communication.
Nowadays, we have telemedicine visits. If you can’t travel as much, it’s really important to try to get in the system with a specialist so that when they are needed, if your disease does accelerate, you’re already in the system.
I can see Dr. Bachow here and if we have questions, if there’s an unknown, or if we’re unsure, I can see Dr. Lamanna via telemedicine visit through Columbia Health. We can send my lab reports.
It’s the communication, the ease of appointments whether you’re traveling or doing virtual, trusting both doctors and the doctors willing to have a shared patient relationship with each other. That’s what I have been fortunate to find, not once but twice and I feel so grateful for that.
Jeff: I would love to tie two thoughts together. You went through a lot in the beginning. You had to deal with different doctors. You had to deal with travel. You had to deal with different levels of comfort. Ultimately, it was your comfort, your ability to mesh well with the doctor as opposed to being abrasive that guided your decisions. That’s really, really important.
We’ve got two doctors who are enthusiastic and their personalities are top of the scale. That doesn’t always happen with every patient relationship. The goal is a long-term relationship so you have to be comfortable with the team that’s taking care of you.
Communication between a local oncologist & CLL specialist
Jeff: How do you coordinate between a local oncologist and a CLL specialist at a distance? This can be a lot of heavy lifting.
Dr. Lamanna: As long as the CLL specialist and the local physician communicate, there are lots of different ways that they can build a relationship. Phone, messaging, and texting are one way of getting records seamlessly. Sometimes via email attachments and faxes.
Remember, different physicians may want to communicate in different fashions, but as long as you can make a connection between the two and they figure out which way works best for them, that’s fine.
Again, as Lisa noted, if there seems to be a struggle, then obviously something’s not working well and that needs to be addressed. You want records and things to be done in a decent time frame, especially if it impacts you.
There are many different varieties to establish that communication given the technology that we have today so it’s not difficult. Technology has gotten better. It’s become easier to communicate so there are a variety of different ways that two physicians and the patient can do that.
Jeff: Dr. Bachow, how do you keep everyone in the loop when everybody’s using different medical record systems? I know we’d like to think that everybody’s on the same page, but that’s not always the case. How do you guide patients? Can you tell us some of your experiences when the platforms don’t sync up quite perfectly?
Dr. Bachow: Office notes and consultations should be faxed back and forth. As Dr. Lamanna said, every doctor is different. The best way of communicating is probably more direct: email and cell phone.
Do the two doctors have a prior relationship together? Do they see each other at national meetings? Luckily, the hematology and CLL world is somewhat small and people do know each other quite a bit. The two doctors having a prior relationship is important but that doesn’t always happen.
You have to recognize that doctors are busy. Discuss with your local hematologist-oncologist what kind of changes would really warrant us reaching out to the CLL specialist sooner rather than later. We’re sending office notes, letting them know the most recent CBC results or physical exam, etc. What kind of changes would warrant us to pick up the phone and call them?
Working with other CLL doctors around the country, I also found that not all of them are like that and that’s okay. Everybody’s extremely busy, but some of them are very busy. They’re running a lab or traveling all the time and getting access to them is not always very easy. Sometimes you do have some important questions for them.
I’ve had an experience where I learned that it doesn’t matter how much you email or if you happen to get their cell phone; I’m just not going to be able to talk to this doctor. But I’ve learned to build relationships with that doctor’s staff — the nurse practitioners, physician assistants, advanced clinic nurses — who have direct access to the CLL specialist and they’ve been able to convey information. I feel comfortable with that and as long as the patient feels comfortable with that, then it turns out to be okay.
Michele: Thank you, doctors, for those answers because that is something we all worry about.
Jeff: One of the bright faces that we have on the support group on Facebook is a young lady by the name of Christy and she’s got a story that she would like to tell.
Christy’s CLL story
Christy V.: Thanks, Jeff. I was diagnosed with CLL in 2017 and that’s when I was referred to an oncologist. From that point, I started considering seeing a CLL specialist based on things that I had seen online from other CLL patients who said that that made a world of difference in their treatment.
Getting pushback from the oncologist
Christy V.: When I asked my oncologist at the time about seeing a CLL specialist, he pushed back a little bit. He seemed to think that it would be fine to proceed with just my local primary oncologist.
I was a little bit concerned about that because I feel that any patient, regardless of their disease or their diagnosis, should be able to seek a second opinion, especially in this case because CLL is a potentially serious diagnosis. Based on what I have been reading in CLL patient forums and support groups, it’s vital to seek the opinion of a CLL specialist.
Finding a new oncologist & a CLL specialist
Christy V.: Based on the hesitancy of my first oncologist to “allow” me to see a CLL specialist, I determined that it was probably better that I find a local oncologist who is a better fit for me and is more open to working with the CLL specialist.
At that point, I found a local oncologist that’s actually closer to me. I also found a CLL specialist within about three hours so that was very helpful. That got me started and feeling a little bit more confident about my diagnosis and that I was going to get good information.
My CLL specialist works very well with my local oncologist. I have some complicating factors with my diagnosis. I have rheumatoid arthritis and it can get a little bit tricky managing both. It was really important for me that my oncologist, my rheumatologist, and my CLL specialist work together to make sure that we are treating both while not harming one or the other.
Finding a CLL specialist
Christy V.: It’s very important to find the right fit for you. Don’t feel intimidated or feel guilty for switching oncologists or deciding that you need to find somebody who you trust. Not only do they need to have the knowledge to treat your disease, but you also have to be able to trust them. For me, that’s really important.
I have to be able to speak to them, feel comfortable speaking with them, and feel comfortable that they are considering my best interests so that’s why I made the switch.
This is a lifelong illness and sometimes people spend more time studying about a new car they’re going to buy than researching the doctor that they have. I did some research and found a CLL specialist that I like and that my oncologist was comfortable working with and that’s worked out very well.
Different opinions among doctors
Michele: What do you do if your two doctors disagree or have differing opinions on the next steps for you? Talk about stress for a patient, right?
Lisa: Honestly, I haven’t had that happen. Should it happen, as the patient, we ultimately have the final say so.
Right now, I have two doctors that I love and trust so much. I would just have to go with my gut and trust in myself. Maybe bring in a third opinion, but sometimes too many cooks… I’d have to see because I have not experienced that.
Jeff: Way back, my first doctor wanted to start treatment immediately and aggressively. My CLL specialist was literally putting up the stop sign and saying, “No. Don’t do that. I helped invent that. It’s old. We’re going to do nothing,” which is a completely different program to talk about.
But, yes, sometimes doctors are going to disagree and like what Lisa said, this is when the patient has to take a deep breath and figure out which voice resonates best with them.
Michele: What do you do when you get two completely different recommendations from two CLL specialists? Dr. Bachow, what happens if doctors have varying opinions about the next steps for approach and care? How can patients and caregivers understand the right way to go? I know this is similar to the last, but it has a little bit of a different nuance.
Dr. Bachow: If you’re going to have more than one CLL specialist — and some people get multiple opinions or have multiple people weighing in — there is a good chance that, at some point, there’s going to be a difference in opinion on how you’re treated and that’s not necessarily a bad thing.
The treatment for CLL has become very nuanced and sometimes there’s more than one right answer. If you put yourself in the patient’s shoes, it can be very frustrating and anxiety-provoking.
Speak to each doctor and be frank with them. Say, “I’ve seen other doctors and they’re recommending this. Why would you not recommend that and you’re recommending this instead?”
Something else you can do is if you develop analysis paralysis, if you have so many different opinions and you’re not sure what to do with them, use your local doctor to help bridge them all together. Weigh the pros and cons of each one to help yourself make an informed decision.
It’s a tough situation, but it’s also a fortunate situation in that you have the ability to have multiple opinions from multiple CLL doctors. It can be very frustrating, but it can be managed.
Michele: And local doctors generally see you more so they might know you better.
Dr. Lamanna: It’s very true. There are circumstances when there’s more than one drug that could be totally applied to a particular individual, which is a good thing because it means they have a lot of different therapeutics they can use. There are situations that might be a little different and we have different opinions about that.
Sometimes, there isn’t a particular right answer. But other times, if there’s more than one answer, then from a patient perspective, you’re also looking at other things like side effects of the therapy, social circumstances, and your ability to go to and from the clinic. One therapy might require hospitalization or more frequent monitoring and maybe that doesn’t work with your lifestyle right now.
There’s more than one thing that might also go into choosing an agent. If there’s more than one being offered, the decision will perhaps be more personal and not necessarily due to the specifics of your disease.
There’s no doubt that you can certainly get another opinion but sometimes, that can be a little bit limiting, too, because then it becomes a little bit difficult. As Dr. Bachow noted, that can be challenging sometimes.
When you’re getting five different opinions, then what do you choose? You’re the one who’s faced with that. Usually, it’s not that many differences of opinion, but it does occasionally happen.
Sitting down and talking about the different options with somebody who will be more than willing to go through all those options is important. You can level out the playing field and see where the differences really are and that will help guide you to choose something that works for you.
Hematologist-oncologist vs. CLL specialist
Stephanie: Dr. Bachow, you’re in a different kind of group. You’re really working as a CLL specialist. A lot of the local hematologist-oncologists aren’t. There was a question referencing how long someone’s been a hematologist-oncologist and how close they would be to the research.
Dr. Bachow is young and closer to being a fellow at a time when there was a lot of research happening. There were some differences people were seeing locally, depending on if their local doctor was older and more set in their ways and maybe less open to the idea of clinical trials or new methods. Have either of you heard anything about that before?
Dr. Lamanna: To be honest, the relationship that Dr. Bachow and I have is a unique one so that’s a little unfair. He is closer to somebody who’s a true academic than not. He has access to clinical trials and things like that.
You’re talking about folks that are dealing with hematology-oncologists who also treat lung cancer and other things and one or two CLL folks. There’s no doubt that could be more of a challenge.
What it boils down to is having a good doctor who you can communicate with and who takes good and loving care of you. Then a CLL specialist can guide them in terms of the treatment options and help with the management of certain toxicities and issues with drugs that they need to look out for while they’re treating somebody.
They can have a very good physician who’s willing to talk with somebody, who has more experience treating CLL than they do, and really willing to hear them out.
I’m not expecting them to know the data. Somebody willing to understand certain things that I’m looking for or what they need to pay attention to versus somebody who really doesn’t, who is irritated by me calling, who doesn’t want to hear me, who doesn’t want to hear that I’m a specialist, let alone a female because they’re somebody who’s really stuck in their ways and they don’t want to deal with it, that’s a red flag to me.
Unfortunately, I don’t mind telling the patient that I have a problem with that. It’s up to them to choose whether they want to stay with that physician or not; that’s not my call. But if they don’t want to work with me and I’m trying to help the person, then that tells me that there’s a problem, right?
Sometimes we’ll use a call as a vetting, particularly if it’s somebody I don’t know, that I haven’t worked with before, just to see if they’re somebody that’s willing to work with a specialist if the patient needs it. As somebody who does this all the time, I can get a sense that that person is somebody I can work with.
Jeff: The CLL specialist as champion is very, very important for patients to hear. Patients need to know that they have someone in their corner who’s going to work towards their best care.
Dr. Lamanna: That’s what you want to do. I know that doesn’t always happen in practice. Some of us are more willing to do that than others.
To be fair, I’m sure not every CLL specialist wants to do that either because that’s a lot of extra work. I don’t want to say that all of my colleagues will be willing to do that, but I do think that most of us who love taking care of CLL patients want the best.
When people come and see me, I don’t stress that they need to stay with me, especially if they’re coming from far away. If they have future questions, they can email me. I recognize that they can’t always make that same connection so I’m really there for them and I’m willing to help. Everybody is a little different.
Dr. Bachow: Dr. Lamanna and I have a unique relationship with regard to CLL. I’m in a community setting where I can’t only see CLL patients, but I’ve been able to develop a reputation and build up my practice where I’m only seeing blood cancers for the most part.
For instance, multiple myeloma, which I’ve had to learn. I’ve had to learn how to reach out and find out who is big in the multiple myeloma field and what are some of the new things. Who can I contact to run cases by, especially for patients who have very aggressive managed care plans that can’t go for second opinions? I have a lot of patients that can’t go for a second opinion. Who can I run the cases by?
My perspective really is finding good people to run cases by, not just send patients for a second opinion. Those that can’t go and have an established specialist, at least. Being able to run new situations by them, they can give you advice on them off the cuff.
Dr. Lamanna: That happens, too, where doctors will just call because they know so-and-so treats this cancer or so-and-so treats that cancer and we have those relationships so they’ll email or just call us. We’ll be helping them and we know that their patients aren’t going to be seeing us. We’re just trying to help them because they need advice on a particular case. Many of us do that as well.
Limited options due to HMO restrictions
Jeff: What we’ve been talking about is something that’s actually a luxury. A lot of people have really great insurance that will allow this second opinion, that will allow the consultation with the CLL specialist. And if that doesn’t work, maybe a third, fourth, or, as you said, even a fifth consult.
What happens if you’re in a tightly managed HMO-style program? You’ve been assigned to a hematologist-oncologist at best, but more likely, you’re with a generalist who’s seeing everything from solid tumors to hematology patients.
Barbara, a care partner to her husband who’s had CLL for more than a dozen years, asks, “We are members of a closed healthcare system and are assigned an oncologist. Who needs to be on the CLL team? How do we get them on that team?”
Do you have any words of advice on how to navigate that?
Dr. Lamanna: You might be able to get a free consultation through some of the panels if you’re really strapped and not able to go for a second opinion somewhere due to insurance limitations. There are different ways through different patient advocacy groups to have access to CLL specialists like myself to go over your case for free.
We also take calls from local physicians without having seen a patient because of our relationships with physicians across the country. We’re willing to talk to them and help advise the physician about their patient who’s having issues.
Michele: There are programs to help access a specialist and one that a lot of patients we know have been using is the CLL Society’s Expert Access™, an innovative program offering free consultation to patients, providing them with expert opinions to share with their local treatment team. We urge any patient to consider using this service when they are unsure of their disease status or their treatment plan.
Jeff: It’s a really great program that we recommend quite a lot on social media.
Living your life with CLL
Jeff: When I was first diagnosed, my CLL specialist told me that I wasn’t going to die from this disease, I was going to die with this disease and that was actually very comforting to hear. You hear the word cancer and you immediately think death sentence.
Here we are, more than a decade past that, and I had the opportunity to be with my first CLL specialist again. When he gave me a great big hug, he said, “You’re not going to die from this. You’re not going to die with this. You’re going to die from something else,” and it was really, really cool. That’s been like guidance for me.
Go live your life. Go live a great life. What kind of guidance can you give patients and their caregivers as far as living that great life?
Dr. Bachow: Live your life to the fullest. Stay in close touch with your family. If you’re working, continue to work. If you’re still able to, continue with your usual activities of daily living.
The CLL Society, The Leukemia & Lymphoma Society, and different social media networks are involved with CLL. Reaching out to other CLL patients is very important so you can learn that other people are living their best lives with CLL and you can, too.
Dr. Lamanna: I’ve always taught people that this is a chronic disease. People live with many other medical problems on a daily basis, like diabetes, heart disease, and hypertension. Some people take medications every day for some of their other medical problems.
You need to understand that this is a chronic medical condition, you’re living with this like other medical problems, and you move on. This doesn’t mean that this isn’t an important part of your life, but you need to live your life. This is a chronic condition that you can live with and that we can manage.
Lisa: Live your life. Enjoy. Do things that bring you joy, that relieve your stress levels, and then just be confident in the team you create once you find it and that can be a journey.
I’m lucky I am able to travel to New York, but I’m also lucky that I have Dr. Bachow here. I can honestly say I’ll be seeing more of Dr. Bachow and not necessarily as much of Dr. Lamanna because of the ease, my trust level in him, and knowing that he’s also well on his way to becoming a CLL specialist. How lucky am I? But I love traveling to New York so I’ll check in with Dr. Lamanna.
Find doctors you trust. Trust in yourself. Advocate for yourself, whether it be insurance, your treatment, or whatever comes up in your health care. Do the best you can.
I had two children get engaged four weeks apart so I’ve been planning weddings. In the midst of all that, we’re building our dream home. We just had wedding one, moved into our dream home, and now I’m well into planning bridal shower two, wedding two, and just enjoying all of it.
What I really find amazing is that 11 years ago, I wasn’t sure I’d be able to do these things. I didn’t know I’d be here. How lucky am I that I am? Hopefully, in the next few years, I’ll be able to say, I’m a grandma.
Jeff: Outstanding. That is the stuff that I love to hear. People aren’t just saying words, not just parroting things. They’re having those moments. Lisa, I am so glad that you are living well. I remember meeting you in that waiting room and it seems like a world away, but so much has changed for the better.
Lisa: We all are.
Jeff: We’re doing that and it’s a great story to tell.
Lisa: And through this pandemic. It was scary for us to get through these last few years and still is. We’re doing it.
Jeff: We’ve got hope for a cure for some of us. We’ve got great treatment programs. We can do this.
Conclusion
Jeff: We honestly hope that each of you has taken away useful tips, some clarity, and guidance on how to build a great CLL team and how to work with different physicians on your team. It makes a big impact.
We are so glad that you joined us today and we hope that you’ll look for more programs with more content.
Stephanie: Thank you to all who participated. It was really amazing to hear what everybody had to say.
Doctors Lamanna and Bachow, thank you so much for your time and your dedication to patients and their families. Lisa, hearing about all that you’ve been able to do; really appreciate you sharing your story. And, of course, Michele and Jeff, always a pleasure to work with you, and excited about more collaborations.
When you get the chance, don’t forget to sign up for our newsletter list so you don’t miss any of the content and the latest in these programs. Wishing you all the very best and really hope to see you at our next program and discussion. Thank you!
Watch-and-wait strategies can be confusing for both cancer patients and their care partners. The Leukemia and Lymphoma Society defines this approach as “closely monitoring a patient’s condition without administering any treatment until symptoms appear or change.”
But how does this approach affect the day-to-day life of a cancer patient? In this live discussion held in May 2023, we explore everything you need to know about the watch-and-wait strategy, including red-flag symptoms, safe activities, and tips for maintaining good health.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Michele Nadeem-Baker: I am a CLL patient, but I’m also a medical journalist and a really passionate CLL patient advocate trying to help all of us understand better just what CLL is and SLL in everyday language.
So probably like the majority of you, I was pretty surprised when I was diagnosed with CLL and thrown into something called watch-and-wait, which made absolutely no sense to me. It was pretty illogical. The doctor walked in. I had no clue there was anything wrong with me and he said, “You have the C word, but it’s the best you can have.” Doesn’t that kill you when they say that? Nothing made sense to me. How anything with cancer could be the best. And then he told me that he’d see me in four months and then I’d be fine. So all of this was pretty illogical to me, having to grasp all of this at once and understand.
But during this time of watch-and-wait, what I did is I got a second opinion and then I started what you would call front-loading information. I was trying to find out the most credible places to go for information, but also the most current. And that’s something we have to watch out for with Dr. Google. So I learned Dr. Google is not necessarily the doctor, you want to listen to and also to go to find where we can find some credible answers. And so in that time, I also found great CLL specialists, the latest in treatment, and it’s good to stay on top of what those treatments are.
I made sure that I took a lot of stress out of my life. My job was a 24/7 job and when I tell you that, that’s not an exaggeration. I slept 2-4 hours a night — Dr. Rogers, can you believe this? — for years because that was my job. I thought, “I think I need to get a little healthier.” I upped my game on working out and on eating healthy and I started doing yoga and meditating and trying to do everything I could to be the healthiest I could be for when it was time to start treatment. And in treatment didn’t happen for some years.
Jeff Folloder: I am a passionate patient advocate. And there’s a reason for that. The reason is I am living an excellent life with CLL. And my goal, my mission is to make sure that others know it is possible to live a great life with CLL. A little bit about me. I love fast red cars, I love expensive whiskey, and I love sharing stories and learning about this ugly journey of cancer that I’m dealing with and helping people figure out better ways to deal with it.
Catherine Ferguson: My name is Catherine Ferguson.
I live just outside of Boston and am a retired college professor. I’m a vet tech and I work in surgery. And I’m also a CLL thriver — not only surviving but thriving.
Dr. Kerry Rogers: I just love doing this type of thing and I really enjoy talking to my patients in the clinic and I enjoy talking about CLL in general. I’m a hematologist, I’m a physician-scientist, and I’m an associate professor in the Division of Hematology at the Ohio State University. I see people with both CLL and hairy cell leukemia in my clinic and do research mainly in investigational therapeutics. And I enjoy talking about CLL with people, but I also really enjoy college football and was just reminded it’s only three and a half months or so until we have college football back.
Why is watch-and-wait used for CLL Treatment?
Dr. Kerry Rogers: The majority of people diagnosed with CLL won’t need treatment right away. And, in fact, with people getting routine blood work now so often, the most common way to be diagnosed is getting a blood test and then finding out you have CLL without any symptoms. It is very confusing for people when you’re told you have a cancer and most of the things you hear about all forms of cancer is that you have to treat it, catch it early, and be aggressive with treatment, and that’s not really the scheme in CLL.
The reason for that is that we know that treating it earlier doesn’t help people live any longer or any better. So way back when we used to use chemotherapy to treat CLL, there was more than one randomized study where they took people who were recently diagnosed with CLL that did not have any of the traditional reasons to treat it, like symptomatic lymph nodes or blood counts that were abnormal enough to need treatment. So they took people who were asymptomatic or minimally symptomatic with no issues that required treatment and randomized them to either be observed and then get treatment when they needed it or to get treatment right away with chemotherapy. And there was more than one study and this is, again, back when chemotherapy was the thing we used.
Does immediate treatment for CLL/SLL improve overall survival compared to the watch-and-wait approach?
Dr. Kerry Rogers: And, actually, there was no difference in overall survival, which is how long people were living between the two groups. People treated when they needed it or people treated immediately had the same survival so we know it doesn’t help you live longer. And, actually, it looked like there was a slight trend towards shorter survival in people treated immediately because chemotherapy is not overly good for people and they got chemotherapy they didn’t need yet.
The way I like to view it is CLL is not something that we can currently cure with conventional treatments. We expect people to live a very long and rich lifespan with it. And so given that, why expose someone to side effects from treatment earlier? Because the sooner you take it, the sooner you get side effects from treatment. And why expose he CLL cells earlier to agents they could become resistant to, shortening the amount of someone’s lifespan, where they might be expected to have their CLL controlled by targeted agents?
So if you think about it, there are a couple of reasons not to do early treatment because of side effects and the risk of resistance to the treatment. And we know it doesn’t help people live any longer in fact, it might help them live worse if they’re getting side effects. So that’s the rationale on the science side behind watch-and-wait, which I like to call observation.
Is there a percentage of patients that go immediately into treatment?
Dr. Kerry Rogers: That’s a good question. I do think that percentage is probably decreased over the years so I’m sure someone has looked at that as a straight percentage, but I’m not sure that really applies anymore. But it is really the vast majority of people that are in watch-and-wait, at least for some time. It’s a much, much less common thing to need treatment immediately.
Are there ongoing studies with newer drugs to determine if treating early improves survival?
Dr. Kerry Rogers: As a scientific question, they are repeating some of these studies with the newer drugs to see if this is still true, that it doesn’t improve survival for people, which is how long they live with their CLL, to treat early. Those studies are being done. The German CLL study group has one with ibrutinib as an early intervention. And then there’s one that’s occurring in the United States called EVOLVE that’s looking at venetoclax-obinutuzumab either immediately or delayed. We will get more information about that. Because people live so long, it will take over a decade or more to see if there’s a survival difference because people don’t die, which is great. I think that when you think about other types of cancers, like colon cancers or breast cancers, the reason to find them early is that you can cure them. And if you don’t find them and treat them earlier, people die of them.
When you’re looking at CLL, you’ve got a lot of people who, even though they have it, are unlikely to die of it — that’s not everybody, but a lot of people are unlikely to die of it — and we can’t cure it so you don’t get to do treatment and go back to whatever indefinitely, right? If you do treatment now, even with our newer drugs, these still have side effects.
What are the potential risks and drawbacks of treating CLL/SLL early with targeted treatment?
Dr. Kerry Rogers: Anyone that thinks they’re getting treatment with no side effects, you never get anything for free, right? Why expose someone to risks of high blood pressure, diarrhea? And then also we know that once you start exposing CLL cells to these targeted agents we use, there’s an amount of time that the disease will respond before the cells become resistant and their CLL comes back. If you start treatment 5 years before you had to, that’s 5 fewer years where someone’s CLL could be controlled by that drug so you might actually shorten someone’s lifespan by giving them a drug that you didn’t have to by either causing a severe side effect or causing their cancer cells to become resistant earlier.
Understanding the challenges of diagnosing and treating CLL/SLL
Dr. Kerry Rogers: And those schemes for screening, treat early — and I get asked this all the time, “But what if my cancer has spread? What if the CLL has spread? How will I know if it’s spread?” And I’m like, “Okay, this is really hard because it’s a blood cancer, right? So it goes everywhere the blood goes.” And they’re like, “Well, that’s everywhere.” And I was like, “I know,” and it’s so upsetting to think that. I can just see how upset people are by this idea. But for CLL, it’s actually okay. We expect it to be everywhere the blood can go and that doesn’t make it any less treatable or make our therapies any less effective.These conventional things that apply to solid tumors are not really the same as applied to these blood cancers and then there’s a huge difference between aggressive cancers that can be cured or cause symptoms immediately and some of these cancers.
And just for context, I have some patients that were diagnosed with CLL when I was in high school and have never needed treatment and it’s been over 20 years — actually over 25 now; I’m getting old.It’s hard to say that you can improve someone’s life by treating early and aggressively when the last two-plus decades have been them living their lives without anything hurting them from the CLL. So when you see that, then you think. it’s not a good idea to expose these people to things they don’t need. You can’t improve on feeling well, right?
Mental and emotional health effects
Jeff Folloder: The most debilitating part of CLL for me is the mental burden of this. We can be candid with each other. watch-and-wait is not a normal thing for anyone. And when you’re told you have cancer and you’re told you’re going to watch, you’re going to wait, you’re going to have to be vigilant, you’re going to have to go into observation mode, that becomes a mental burden. I will admit that I did not deal with that mental burden very well when I first went through watch-and-wait.
Michele Nadeem-Baker: Jeff had been through treatment. I’m like, “How did you do this? I didn’t have control over what my own body was doing and that is really difficult, especially for someone like myself who really likes to be in control of things. I think I’m doing everything I can. Is there anything more I can do? No, there really isn’t and it just doesn’t matter and that is so difficult.
And also my dad passed away from mesothelioma, a lung cancer. He was diagnosed and in two weeks, he died. So it’s just like, to me, that’s like, “You don’t treat? Oh my gosh, that’s what happens.”I got all worked up there from when I was going through it the first time because you really don’t know what it looks like. You don’t know what it’s like.
Catherine’s experience before front-line treatment
Catherine Ferguson: I dealt with it about the same as you guys initially. When I was diagnosed, I was at one of the top hospitals in Boston, but when they said they weren’t going to treat it, I was like, “Oh my God, I’m going to have to go to Dana-Farber.” So I went for a second opinion over to Dana-Farber and they told me pretty much the same thing.
My personality is I’m a go-getter. I want the plan. I want to get it done. I want to get it started and I want to get it ended. So for the first couple of weeks, it was probably all-consuming for me, honestly. I could have gone down the rabbit hole really quickly.
I look at my dogs and I’d think, “Am I going to outlive them or are they going to outlive me?” But pretty soon thereafter, I had an epiphany where one day, I thought,” I could go walk off the curb tomorrow and get hit by a car,” and then I spent my last days on this earth worrying about when I might die somewhere down the line.
For me, that set something off in my head that life is for living right now and none of us know what tomorrow brings. It’s not a guarantee for anybody. So for me, I try and just live my life. I’m basically an optimistic person in general, by nature. So for me, I try and just believe that] I do the things that I can do for myself and stuff like that. I take care of myself. I listen to the doctors. I get my screenings. I do all the things I’m supposed to do in watch-and-wait. And then I just continue to live my life. I have to say, the second time around, it’s been much better.
How did you cope with the emotional toll?
Catherine Ferguson: When I was first diagnosed, I was diagnosed with intermediate markers. I wasn’t high risk, I was intermediate on the genetic markers and so I knew I was going to likely need treatment. What the doctor couldn’t tell me is when. So I knew that sooner or later, I wasn’t going to be one of those people that was going to go forever without needing treatment.
And so around the 4-year mark, I started to get really anemic. I started getting really, really tired. I had a couple of nodes that were big, but that was it. Everything else — my platelets, my white blood count — was perfectly fine. We found out I was iron deficient so I did iron infusions. It helped initially, but when we rechecked it again two months later, it had dropped again.
Because I didn’t have any other symptoms other than I was anemic, we kind of assumed that it might be the CLL progressing at that point. I had a bone marrow biopsy done and it came back as Hodgkin’s lymphoma from a Richter’s transformation. So Richter’s transformation is when the CLL transforms into something much more aggressive. Usually, it’s not a Hodgkin’s, usually it’s something worse so I actually got the better of the two, if you want to see that. See, that’s the optimism.
I had to do a regular six months of chemo every other week. High-dose chemos. And for me, I’ve been in remission since I finished that chemo and that was five years ago. I have never had any more issues with the Hodgkins or the Richters.
What are some tips for guys dealing with watch-and-wait and how can they learn to talk to people about it?
Jeff Folloder: We’re at a point where I’m supposed to give some pro tips about how guys deal with watch-and-wait. And we’re going to go straight to a poll that Stephanie’s going to introduce in just a second. I’m going to give you a sliver of the pro tip because it’s part of dealing with this whole mental health aspect that we’re going to be focusing on a bit here.
Michele talked about it. She talked about being in control.] Guys, we all try to be type A and we try to always be in control. The answer is not always, “I’m fine.” The answer is not always, “I’m good.” You’re going to need to learn how to talk to people.
How do patients and care partners cope with watch-and-wait from an emotional and mental health standpoint?
Dr. Kerry Rogers: As you were saying that don’t just say, “Oh, I’m okay,” I have people’s partners all the time say, “Will you just go ahead and tell her what’s on your mind? You need to actually tell people what’s happening.” And I was like, “I’m here to listen to you about what’s happening.” I observe that quite a bit. We get so many people now diagnosed at a time when they have no symptoms — their blood tests are abnormal, they get diagnosed with CLL, they don’t need treatment, and they had no symptoms and say they felt perfectly fine and had no idea something was wrong until this happened —for this group of people, sometimes I think the hardest aspect of having CLL is knowing that they have it.
I see people where the worst part of it for them is not physical symptoms, but it’s living with knowing you have it. And I try to tell people, “You’re feeling well from this.” I’ve said, “Based on the disease features, I don’t expect this to be something that shortens your lifespan, even though you might need treatment at some point. Please don’t let knowing you have this ruin your life] Don’t let just knowing you have this fear in your life.”
We have great programs here at Ohio State at the James, like psychosocial oncology, which is mental health professionals that can help with this. I try to offer what I can, but this is something that I don’t have formal training in helping people cope with some of these aspects, which really can be much more impactful on their lives than the physical symptoms of CLL.
I think people knowing they have it can actually be much harder for them than any physical symptoms they’re experiencing. I can see sometimes people that have spouses or partners or caregivers or people in their lives that come to the clinic with them, it’s really helpful because sometimes, something, their friends, family, or loved ones are observing is something they choose to share during the visit and that helps me know that there’s something else that needs to be addressed.I think sometimes it can be hard for other people to know how to support their loved one that has CLL. I find that the majority of people help facilitate some of the communication in clinic and have been good.
Jeff’s experience with watch-and-wait: learning to communicate with healthcare team
Jeff Folloder: I want to share just a little bit about my experience with watch-and-wait I learned through going through all the questions and answers at the hospital that I chose that I wasn’t being candid with my healthcare team. I believe the military says I was exhibiting a lack of candor.
Well, the problem was I didn’t know how to answer their questions. I didn’t know what was important when they said, “So what’s going on? How are you dealing with things? Is there anything that we need to know about?” Things like night sweats. I associated it with my love of Thai food. You eat too much hot chili, you’re going to sweat at night, right? No. Going through all of this watch-and-wait was learning how to communicate with my healthcare team and not knowing what was going to be the tripwire for treatment meant that I was learning new things about communication.
I started treatment when my doctors discovered that my fatigue had become so debilitating that I couldn’t do the normal things I needed to do in my daily life. I couldn’t lift certain things. I couldn’t stay awake long enough. I couldn’t do this. I couldn’t do that. That was the tripwire for, “Okay, watch-and-wait is now over. Now it’s time to move into treatment.”
Dr. Rogers, explain to us what you’re doing with all these questions and answers. What are you looking for? What is happening during this period? And what should the patients and their caregivers be looking out for?
How to determine symptom severity and potential causes
Dr. Kerry Rogers: There are a few things that we always look for. We always check people’s lymph nodes. But just because we found some lymph nodes, it’s okay. It doesn’t mean you need treatment. But if people notice a bunch of lymph nodes everywhere that’s bothering them and keep getting bigger, then that might be important that we should do something to improve that for them. And then we look at the blood counts, which people don’t usually see their blood counts between visits that often and so that’s something that’s really important.
But in terms of what people tell us, it’s always good to hear about how people are functioning. If they have things that are interfering with their professional, leisure, or preferred activities, if it’s fatigue, if it’s something else, we always ask about night sweats. And then if someone’s like, “Yeah, I’m going through menopause,” I’m like, “Right, so that’s cool.”
The difference between normal night sweats and abnormal night sweats
Dr. Kerry Rogers: There are people with night sweats where everyone in bed with them is wet. They’re wet, their wife is wet, and the dog is wet. They had to change all the sheets. That’s actually a problem. And it’s hard because people don’t know that that we think there’s a difference between, “Oh, yeah, my neck got sweaty at night,” because they got hot versus, “Everyone in the entire bed with me is soaked because I’m so sweaty.” Those are the things we try to figure out by asking questions when people like to come to see us. Finding out about night sweats is fine and we can help people determine what might be normal like you were saying, the Thai food versus not really normal, right?
The significance of reporting severe fatigue and sleep issues
Dr. Kerry Rogers: Fatigue is the hardest because there are so many things that can add to someone’s fatigue. Every once in a while, we get someone that has fatigue that’s really quite severe and it’s actually sleep apnea. So we get their sleep apnea treated and they’re like, “Oh, I feel like a million bucks.” And you’re like, “I’m glad we didn’t treat your CLL because of that,” because that’s not going to fix your sleep apnea, right?
Part of what we do when symptoms are reported is not like, “Oh, you have fatigue, you need treatment,” but have more questions about what’s going on, and what might be causing that. One patient I talked to said, “I have fatigue, but I haven’t slept.” She only slept 2 to 4 hours a night. People are tired when they’re busy and they have something going on. A lot of the stuff we look for is not only asking those questions but severity and follow-up questions about some of those symptoms.
What is the average watch-and-wait period for intermediate and high-risk CLL/SLL patients, and does it vary by mutation type?
Dr. Kerry Rogers: The answer is yes, there is. This has been done in more than one study where they’ve looked at the time from diagnosis to first treatment. It’s hard to pinpoint from these studies what will happen to any one person though. So these are studies that look at a group of people diagnosed with CLL and how long between the time they are diagnosed and treated. Then they look at different disease features — so high-risk features like deletion 17p in the CLL,ow-risk features like IgHV mutated status, and then they look at the median. You can think of the median as a little bit like the average. It’s not exactly the same thing, but the median number of times for the 100 people in that group to start treatment.
Dr. Kerry Rogers: For things like deletion 17p, the median in one study was around a year and a half between diagnosis and needing treatment. But within that group, some people needed treatment right away, some people didn’t need treatment for five years. There’s a staging system called Rai staging that can help predict the time to the first treatment. But you never know what’s going to happen for an individual person so I try not to get people too wrapped up in that because you don’t know how it’s going to turn out for them.
Activities, supplements, and exercise
What activities can you do during watch-and-wait?
Dr. Kerry Rogers: I’m going to go with all of them that are recommended for people. People ask me this all the time, “Can I do this? Can I do that? Can I do the other thing?” I’m like, “Yeah, do all of it.” And then they’re like, “Can I do something crazy that really nobody should be doing?” I’m like, “No, don’t do that.”
“Can I drink beer because I have CLL? I like drinking beer and watching football.” I’m like, “Me too. That’s the best.” And they say, “I want to drink one beer watching football.” I’m like, “Okay.” Or they say, “Sometimes I like to drink two beers while watching football.” I’m like, “Yeah, that’s fine. Really just don’t get drunk every day and that’s not because of the CLL, that’s just general advice.”
If you think of someone with CLL, people in observation do live with a higher risk of infection and other forms of cancer. So I do think the COVID-19 pandemic was much more limiting for people with CLL in observation than for the rest of the public so there are a few things like that. But aside from going somewhere where you can’t access medical care if you’re about to need treatment or some really dangerous activities that are not recommended for anybody, I tell people to just go ahead, enjoy their lives, and do whatever they want to do.
How can we extend the watch-and-wait period and slow down CLL or SLL progression?
Dr. Kerry Rogers: Not that I’m aware of. There are a couple of things, right? There’s a study with green tea extract tablets like a high dose that can lower the white count, but I don’t know that there’s any data that really help people live longer or really prolonged watch-and-wait.
There are things that I’m sure help people in general. You were saying you did some things to make sure you’re fit and rested and eating healthier. Those things can make people feel better and be better with their overall health. But I don’t know of anything people can do specifically to increase the amount of time before they need treatment.
Matcha green tea and supplements: Are they effective in managing CLL or SLL?
Dr. Kerry Rogers: Not that I know of for CLL. Vitamin D does have a variety of health benefits. If you’re deficient, getting that replaced is important for other health metrics. But I don’t know of anything specific that will help the CLL. [Supplmenents] aren’t regulated so it’s helpful to go on the Internet and look at some of the companies that rate the quality of supplements before you buy them.
Green tea, it was an extract used in a study. You’d have to drink more than one can physically drink in a day to get the same benefit if you’re going to drink the tea. So if someone wants to try that, I strongly recommend finding a high-quality green tea supplement because it’s just physically not possible to drink that much green tea in a day.
Can jumping rope be beneficial for managing CLL/SLL?
Dr. Kerry Rogers: Exercise is good for people, right? But there’s no data that jump rope actually helps CLL. Probably won’t help your joint health but will help your cardiovascular health. But it doesn’t do anything to impact the CLL specifically.
Managing CLL/SLL Comorbidities
Jeff Folloder: One of the things that I have learned through my 13 years of dealing with CLL, I finally believe my first CLL specialist. He said, “I’m more worried about the comorbidities than I am about the CLL. If you will actually put time and effort into taking care of those comorbidities, you’ll actually make my job easier.” So I have embraced that.
I know it’s going to sound pedantic, but you can exercise more, you can eat better, you can eat less, and you can do all the things that you need to do to reduce your comorbidities. And, truthfully, there is no upper ceiling for it. I’m currently training for a marathon. I’m relapsed and training for a marathon, so yay.
Dr. Kerry Rogers: Modifying your other risk factors for your other health conditions because that is something everybody can do in watch-and-wait. And I would say more people with CLL my clinic die of heart attacks than die of CLL. So just please keep that in mind. And, of course, keeping up with cancer screenings and vaccines is very important.
When to start treatment for CLL/SLL
What are the indicators that it’s time to end watch-and-wait and start treatment for CLL/SLL?
Dr. Kerry Rogers: There’s a group of people where they have no symptoms, lymph nodes aren’t big, blood counts look fine, and you say absolutely there’s no reason whatsoever to treat this person. There is no cut-off on white blood cell count where you need to do treatment. I do think if you get above 400 or 500, usually other reasons develop and it’s about time, but there’s no cutoff like, “Oh no, my white count hit 50. We need treatment.” That’s not a thing. And yes, there is a thing with doubling, but that’s only with higher white counts. So it’s not like, “Oh, it went from 10 to 20, I need treatment.” That’s not a thing. You can actually be very flexible with the white blood cell count. Don’t think of a hard number there.
There are people who I think could be ready for treatment.] The blood counts are going in the wrong direction so you can see the hemoglobin and platelets are dropping, white counts going up, and lymph nodes are getting big, but they’re not actually really problematic for the person. Maybe they’re having some fatigue so there’s a window where you could say like treatment’s reasonable.
The span from, “We shouldn’t do treatment,” to “We should have done this sooner,” especially for a first treatment can be over a year. You’ve got a very long window and that gives you some time to decide, along with your doctor, what treatment’s best for you and things like that. It’s uncommon that you hit something and you need treatment tomorrow. It’s more like an ongoing discussion for a while.
The things I see that I notice sometimes are, “The white count shooting up pretty fast, along with the hemoglobin and platelets kind of dropping.” Or every time people come back, there are more lymph nodes and they’re losing some weight. There are a lot more lymph nodes and you see this trend happening. And then I do see some people that develop a lot of fatigue that suddenly starts to interfere with their personal and professional activities and that would be a reason to say, “We should really do something before this really impairs your life more.”
Are there any specific signs to watch for?
Dr. Kerry Rogers: Every once in a while, I have a patient who develops a significant health concern that they think is in another area, like severe diarrhea or chest pain, that’s not addressed by going to like their cardiologist or something else. When people develop health concerns, weird symptoms — and not like, “Oh, my toe is itchy one day and then it’s not the next day,” that’s fine; that happens to everybody – something significant, impacting their life, weird that maybe other doctors they thought might help them with this can’t figure it out, that is always something to check in and ask, “Hey, could this be related to CLL?”
Because there are some weird things that happen to people with CLL and certainly the physician caring for anyone with CLL should be able to figure it out. If anyone develops weird health concerns that are really symptomatic or problematic that other doctors can’t figure out, always a good chance that it could be CLL related and you should check in.
Does CLL increase the risk of other cancers?
Dr. Kerry Rogers: Yes, it is true. CLL is a cancer of immune system cells called B lymphocytes so it changes the way the immune system works because the CLL cells are there. By the way, treatment to reduce the CLL cells doesn’t fix this — only makes the problem worse. Your immune system is what protects you from other cancers by killing abnormal cells that your body forms as it makes new cells over time so cancer screening is important.
The top ones we see are actually skin cancers and, of course, lymphomas, as was pointed out earlier, do occur in people with CLL but those are kind of related types of cancers. But skin cancer’s actually one of the top ones so I try to get everyone’s skin cancer screening.
Side effects of treatments
Fatigue caused by CLL treatment
Catherine Ferguson: That was the worst part of it for me, honestly. I could deal with any of the other side effects even when I just finished a clinical trial a year ago. I’ve been undetectable MRD and in remission now for a year and I feel so much better. But that fatigue, even during treatment. Everybody said once you start treatment, the fatigue goes away, but I still had the fatigue even during treatment till I got off of the meds.
I work out a lot and I went to the gym every day and I tried to just keep up my routines. I’m generally an active person anyhow so I try not to give into it.
For a time period there, I would fall asleep while I was working on the computer with my hand on the mouse and my wife would look over and say, “Cathy,” and then I just wake up and I’d start to keep on moving again like I didn’t do anything. But I didn’t decide I was going to take a nap; I would just fall asleep. It’s just really hard.
How do new CLL/SLL treatments differ from traditional ones and what are some of the latest options available?
Dr. Kerry Rogers: I like to say that about a decade and a half before this kind of chemotherapy or chemoimmunotherapy, which is chemotherapy with an antibody works real well. In last decade and a half have been all about targeted agents. We actually no longer use chemotherapy to treat CLL. We do use it to treat other lymphoma successfully, but the whole name of the game is oral targeted agents and these are drugs that interfere with proteins in the CLL cells that make them behave like cancer cells.
The two main classes of drugs are something called BTK inhibitors and venetoclax, and they are extremely successful with virtually everyone achieving a remission, and just work very well.
The field is currently looking at newer generation agents of these different dosing schemes or different combinations to try to make treatment more effective but also easier to do for people and to have fewer side effects.
Is it crucial to see a CLL specialist immediately after diagnosis, or can it wait?
Dr. Kerry Rogers: It’s actually an individual decision. There are some reasons that people actually definitely need to see a CLL specialist. One is just if things aren’t going well, right? So not responding to treatment, developing side effects, not being offered acceptable options from your general hematologist oncologist — things aren’t going well, always see an expert.
Some other good times are planning a treatment, any treatment, because, usually, the CLL specialist will be able to have a good and, hopefully, more detailed discussion about treatment options or even offer participation in a clinical trial, which has a lot of advantages. But this doesn’t always have to be done at the time people are diagnosed just because if you’re in watch-and-wait and you’re happy with what’s going on,] it doesn’t mean you have to run out and see a CLL specialist right away, especially if you don’t live near a CLL specialist.
If you live in Boston, it’s very easy to go see one of my colleagues at Dana-Farber and other excellent doctors in that area. But if you live in rural Ohio or West Virginia, we get people that come from West Virginia. It’s like a three-hour drive so it’s a big burden to do that right away
And then I guess at diagnosis, one of the main reasons to see a CLL specialist is to get questions answered and to learn about CLL, which I think benefits all people. Most people do want to learn more about it, but there’s] a group of people that cope by putting CLL from their mind and they can certainly delay seeing a CLL specialist until there’s a reason like needing treatment.
Featuring: CLL Patient & Advocate Michele Nadeem-Baker Dr. Nicole Lamanna, Columbia Univ. Medical Center Dr. William Wierda, MD Anderson
There are so many exciting developments in chronic lymphocytic leukemia or CLL treatment. But there is so much to wade through, how do we know what’s right for us and what we should be asking our doctors?
CLL patient and advocate, Michele Nadeem-Baker, guides us through the most promising trends in CLL treatment, spotlighting the voices of top CLL specialists who cover everything from new oral combinations to new drugs (pirtobrutinib) and so much more.
Michelle Nadeem-Baker: I’m Michele Nadeem-Baker, your Chronic Lymphocytic Leukemia Reporter for The Patient Story and a CLL Patient. There is so much happening in terms of new treatment research for us! There are more choices than ever for when it’s time to be treated and more in the pipeline. But how do you know what they are, how they’re different and which is best for you?
Our program will help new and not so new CLL patients learn today’s treatment landscape and the hottest drug trials from two leading CLL Specialists, Dr. Bill Wierda at MD Anderson in Houston and Dr. Nicole Lamanna at Columbia University Medical.
First, many patients think they need to start on chemotherapy. This is old school thinking.
Small molecular inhibitors > chemotherapy and chemoimmunotherapy
William Wierda, MD, Ph.D:: The targeted therapies BTKi, BCL-2 are superior to chemo and chemoimmunotherapy, so I don’t like to think about, or talk about, or plan for chemoimmunotherapy any longer because I think it’s inferior treatment for our patients and much more aligned with giving small molecule inhibitor based therapy.
I think for patients and moving that discussion a little bit further, what patients need to think about and have a discussion with their physician about is:
Do I want fixed duration or finite duration treatment?
Do I want to get in remission and get off treatment and have a reasonable period of time to expect off treatment in remission?
Or do I want to go on a maintenance and have medication that I take every day that is extremely effective at controlling the disease? But I continue on it and there are side effects associated with all treatments, including the continuous treatment.
Chemotherapy outcomes or outcomes with chemotherapy were inferior to outcomes for treatment with small molecule inhibitors, whether we’re talking about venetoclax-based therapy or BCL-2 inhibitor based therapy, or we’re talking about BTK-inhibitor based therapy or drugs.
Small molecule inhibitors
BCL-2 inhibitors
William Wierda, MD, Ph.D:: The small molecule inhibitors that we have are oral agents, and there are two category, three categories right now that we have of drugs that fall into the small molecule inhibitor category:
BCL2 inhibitors, we have one. There are several that are in clinical trial. The one that we have is called venetoclax. Very potent at eliminating disease, very potent at getting deep remissions. It’s the type of treatment that we give with the expectation of giving it for a set period of time and then stopping treatment once patients are in remission.
BTK inhibitors
William Wierda, MD, Ph.D:: The next category is BTK inhibitors. Those have been around longer than BCL-2 inhibitors. Examples of this drug that we currently have available are acalabrutinib and ibrutinib.
Ibrutinib has the most experience associated with it, and we have the most data and most patients treated so far on clinical trials with Ibrutinib. Acalabrutinib, though, is approved.
Zanubrutinib is not yet approved, but perhaps will be in the next within the next year probably. Those are drugs that are extremely effective at controlling the disease, but not as effective as, for example,
Venetoclax is in terms of getting the amount of disease down to the point where we’re comfortable with stopping treatment. So the best response, the lowest level of disease is usually still measurable with the BTK inhibitors like Ibrutinib or Acalabrutinib. So patients go on those medicines and they stay on them until they don’t work any longer. It’s more of a maintenance type treatment.
PI3K inhibitors
William Wierda, MD, Ph.D:: Third category of drugs are the P-I-3-Kinase-inhibitors. There’s two that we have currently available. One is called idelalisib. The other is called duvelisib. Those have a bit more side effects and toxicities associated with them, particularly Idelalisib and are used less frequently these days.
Ibrutinib and the BTK-inhibitors and the venetoclax or BCL-two inhibitors, are extremely effective and give very good and durable disease control. You can switch between those two if you develop resistance. So if you develop resistance to venetoclax, for example, you can switch to the BTK-inhibitors, one of the BTK-inhibitors, and expect a response and vice versa.
New BTKis
Michelle Nadeem-Baker: There’s another generation and category of BTKis – a new type – reversible and non-covalent. One of them in trial and getting much attention is pirtobrutinib. Until this trial, patients, and this includes me currently on one, hadn’t known about these BTKi differentiators – reversible and irreversible and non-covalent and covalent.
Pirtobrutinib is looking very promising.
William Wierda, MD, Ph.D
Pirtobrutinib
William Wierda, MD, Ph.D: So there’s a lot of things happening in CLL. There are a lot of new and exciting drugs that we’re studying that are in early development. There’s a drug called pirtobrutinib, which is a reversible inhibitor of BTK, which you would consider giving in a patient who has developed resistance to one of the irreversible inhibitors, such as ibrutinib, zanubrutinib or acalabrutinib.
Pirtobrutinib is looking very promising. It’s active in patients who are resistant to irreversible inhibitors, and those remissions are lasting a reasonable amount of time. It also is working in patients who are resistant to ibrutinib and venetoclax. So we’re excited about that.
Nicole Lamanna, MD: There are reversible and irreversible inhibitors. And so what’s different about pirtobrutinib or these non-covalent BTK inhibitors is that what we started to notice is that as patients who were on the covalent BTK inhibitors, such as ibrutinib or acalabrutinib, that there is no doubt that over time, some patients can develop resistant mutations to this class.
We can actually test for that in the lab so we can send somebody’s blood or their bone marrow sample and see that they might have, they might be starting to develop some resistance to the drug that they’re on, and we’ve identified some of these mutations.
Looking at pirtobrutinib, that certainly is a drug that might be able to reverse or overcome the resistant mutation that patients have developed on the other BTK inhibitors. And that may be useful to have another medicine. We know Venetoclax works for these individuals, but having yet another BTK inhibitor that works slightly differently may also be helpful.
Combination therapies
Acalabrutinib + ibrutinib + obinutuzumab (AVO)
Michele Nadeem-Baker: Combination therapies – means giving 2 or more treatments concurrently. Combining for treatment isn’t new – FCR, the former CLL go to treatment, was 3 drugs given all together: 2 chemotherapies: fludarabine and cyclophosphamide plus monoclonal antibody rituxan (rituximab).
Today, many CLL clinical trials are testing various drug combinations of individually approved drugs, such as acalabrutinib plus venetoclax plus obinutuzumab, AVO.
All eyes are on this important triplet trial as it could lead to more combination trials being approved. It’s currently in a trial and if approved, doctors say it will be “practice changing.”
Ibrutinib + venetoclax VS. chlorambucil + obinutuzumab
CLL trials are also comparing drug combinations with other drug combinations. A highly anticipated trial pitted ibrutinib plus venetoclax against chlorambucil plus obinutuzumab.
Ibrutinib plus venetoclax has better results giving a nice durable remission with the possibility of going treatment free for a while.
Nicole Lamanna, MD: So then can we take two orals – a BTK inhibitor and BCL-2 inhibitor and then do more of what they call a time limited approach, right? So then taking both of these oral agents for a period of time and then stopping, so, then they would be not, that you wouldn’t then be taking the BTK inhibitor chronically indefinitely. And so there were many trials producing very exciting results. The responses are very good with the oral-oral combinations, but we need longer follow up.
The role of venetoclax in combinations
Michele Nadeem-Baker: Both of these trials include venetoclax and many other trials using it are having great results.
William Wierda, MD, Ph.D: Right now, we’re seeing good responses for all patients independent of their risk features. If they have an unmutated immunoglobulin gene, their response is similar. If they have a 17p deletion, their response is similar to the non 17p. The challenge for the high risk is showing that they remain in remission and that their disease doesn’t come back and grow.
If we’re talking about achieving an undetectable-MRD state, venetoclax-based therapy is what we need to give to do that. Whether it’s the standard treatment which is venetoclax plus obinutuzumab, which is a CD20 antibody or a newer combination venetoclax plus ibrutinib, venetoclax plus acalabrutinib – those combinations, all of which include venetoclax, are intended to get into a deep remission, undetectable MRD and time off treatment.
Other CLL treatments
Michele Nadeem-Baker: And there are other types of treatments being studied for CLL patients.
Nicole Lamanna, MD: There are definitely some bispecific monoclonal antibodies that are also being looked at that also target the CLL cells. And so they’re early in development. And so that’s something that we’re going to see. Stay tuned.
CAR T Cell Therapy
And of course, many of us have also always talked about CAR T-cell therapy. So looking at different forms of immunotherapy to try to target the CLL cells in a different way. Manipulating the cells to then stay stimulated so that they attack your CLL cells. And so certainly there’s longer follow up on the CAR T-cell data as well.
Dr. William Wierda, MD, Ph.D: CAR T is an exciting topic. It’s an area that I’ve been involved in in development, and we will hear more about CAR T.
I have had many patients who have been treated with CAR T and who were resistant to standard treatments, who have had very durable remissions and who are doing very well. So for me, that holds a lot of promise for our patients.
Having multiple choices and having these conversations with your physician and team is great because there’s more than one option that is really good therapy for your disease
Nicole Lamanna, MD
Can treatments prevent relapse?
Michele Nadeem-Baker: Are there any treatments that can keep you from Relapsing?
Nicole Lamanna, MD: We know that patients can relapse even after these more aggressive therapies like CAR-T and allogeneic stem cell transplant. I think that it’s appropriate those conversations about where you are in your journey and your therapy and what you might need in the future are really good conversations to have with your physician team, for sure.
Having multiple choices and having these conversations with your physician and team is great because there’s more than one option that is really good therapy for your disease, which is very hopeful and great that you can. I think that the field has come a long way. Stay tuned. We’re doing a lot more, but there’s lots of lots of good things to look forward to.
Are we close to a cure?
Michele Nadeem-Baker: With so much research, are we close to a cure?
William Wierda, MD, Ph.D: In order for a patient to be cured, meaning no more leukemia period ever to be seen, they have to be undetectable MRD, whether that’s at the end of treatment or it’s three years or five years later.
I’m optimistic that we are curing some patients currently with our non-chemo treatment. Certainly, we know patients are being cured with chemo options. The problem is that chemo has side effects and toxicities associated with it, and we have exceptionally good treatments now with small molecule inhibitors to the point where I think despite the fact that we are able to cure some patients with with chemo, it doesn’t justify giving every patient who potentially could be cured the chemo because it’s only about half of those patients.
Nicole Lamanna, MD: I think that we’re going to need a lot more long term follow up to show that something is potentially curative in CLL. So stay tuned because some of this combination data, I think in some subgroups might render somebody with undetectable MRD for a really, really long time and albeit perhaps even cured.
But I never use that word. I use that word very cautiously. But I think that therapies have gotten so great that there’s no doubt a potential for some individuals. I think that we’re getting to a very good point, but we still have a lot of work to do.
Clinical trials
Michele Nadeem-Baker: Clinical trials are a great way to get tomorrow’s treatment today. If you’re interested in finding out more, ask your CLL team if they have any open trials or any in the future that would be a good match for you and for more trial information checkout clinicaltrials.gov
William Wierda, MD, Ph.D: I think clinical trials are important. They’re the only way that we’re going to make progress in the disease. They’re the only way we’ve made progress in treating the disease, and they’re very, very important.
Conclusion
I’m driven to share it to help you better advocate for yourself and to gain hope.
Michele Nadeem-Baker: Promising ongoing research continues producing more treatments for CLL patients with more on the way.
In the near term be on the lookout for news on potential FDA Approvals for:
Zanabrutinib (BTKi)
Ibrutinib and Venetoclax in combination
Importance – “could be practice changing – could lead to more combination approvals
Keep an eye on updates for pirtobrutinib and others in this new class of BTK inhibitors, as well as CAR T-cell therapy and the latest generations of BCL-2 drugs like venetoclax, and so much more.
As a CLL patient, seeing so much ongoing research and drug discoveries gives me so much hope! And I’m driven to share it to help you better advocate for yourself and to gain hope.






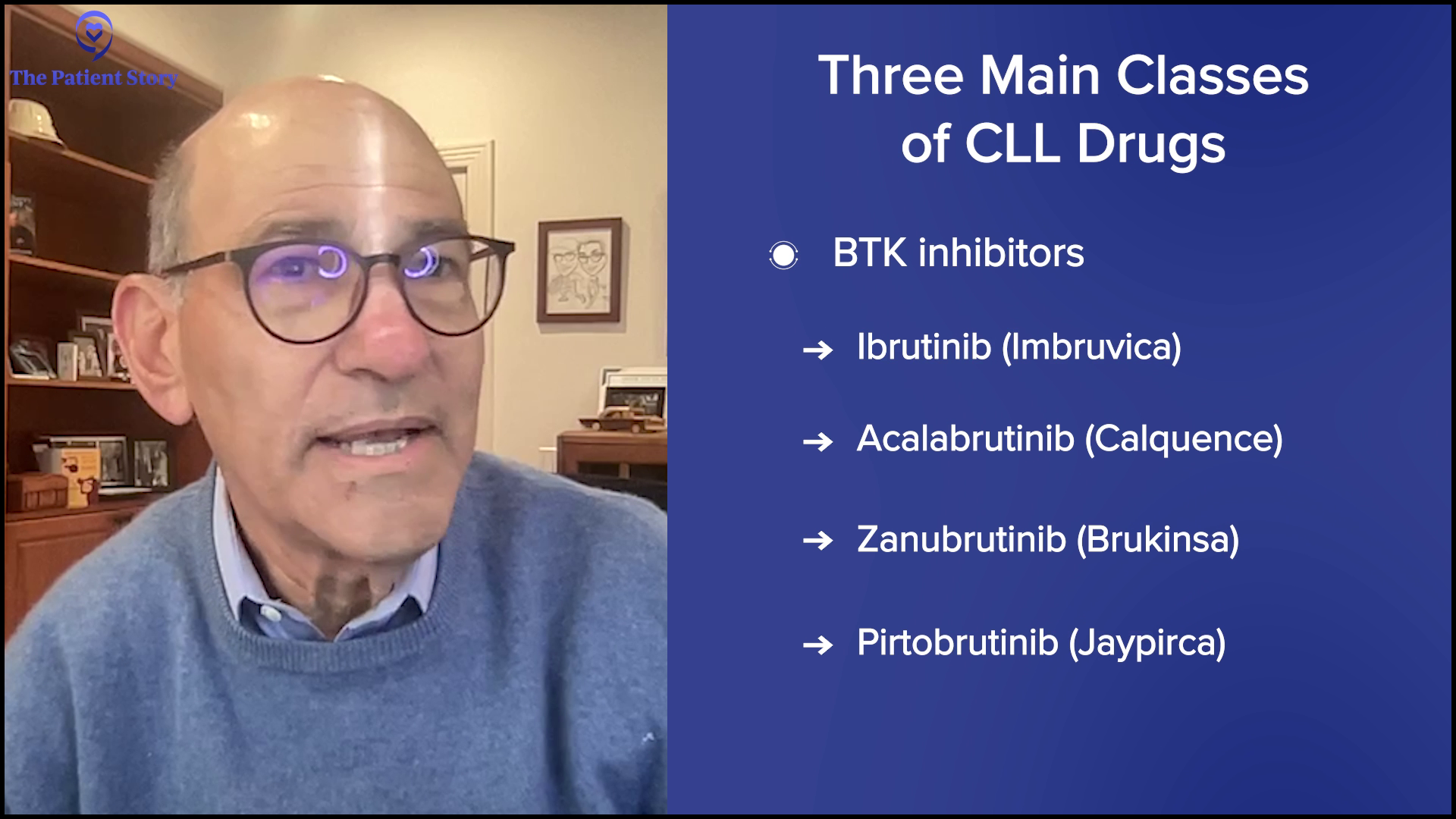
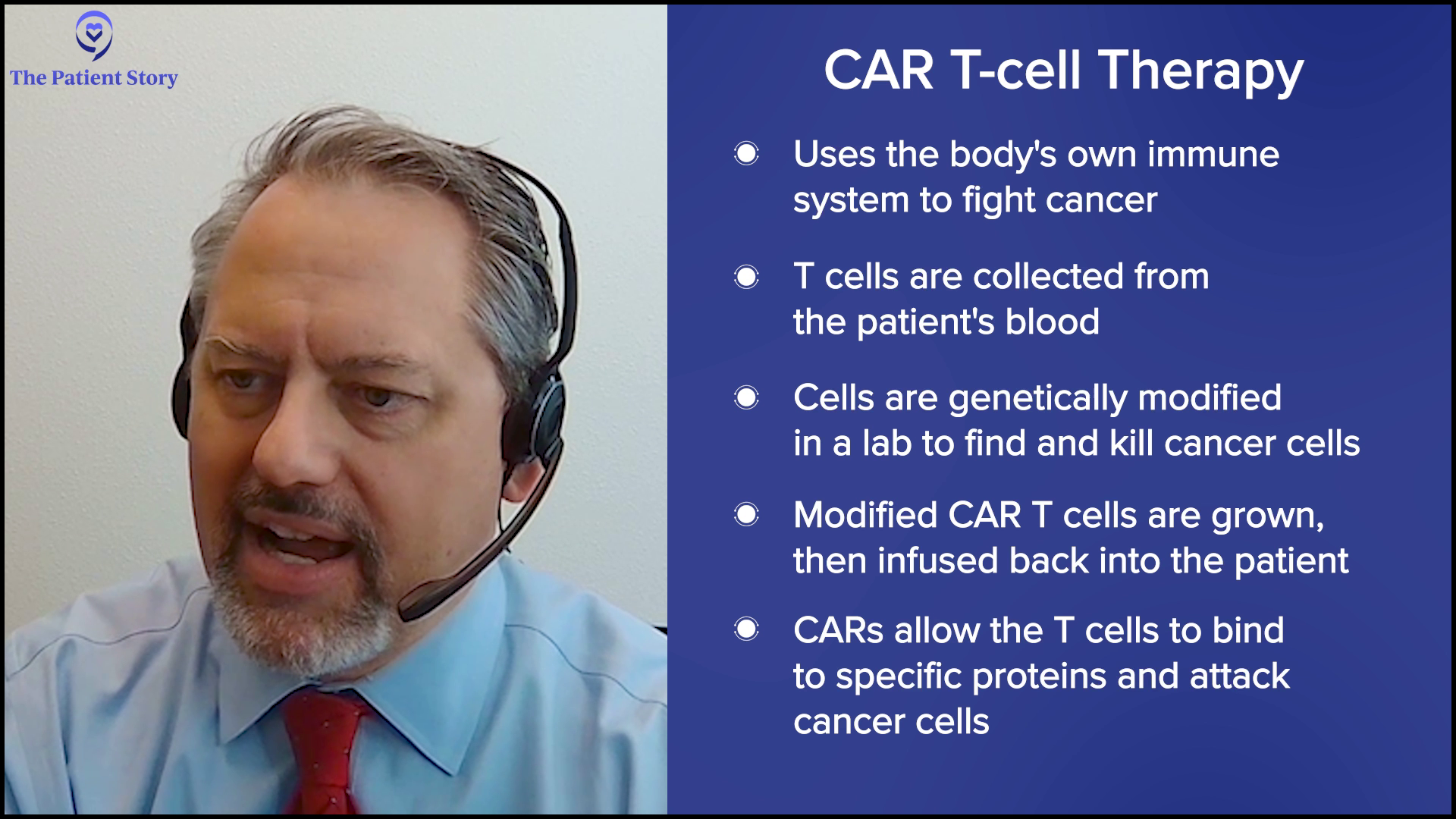
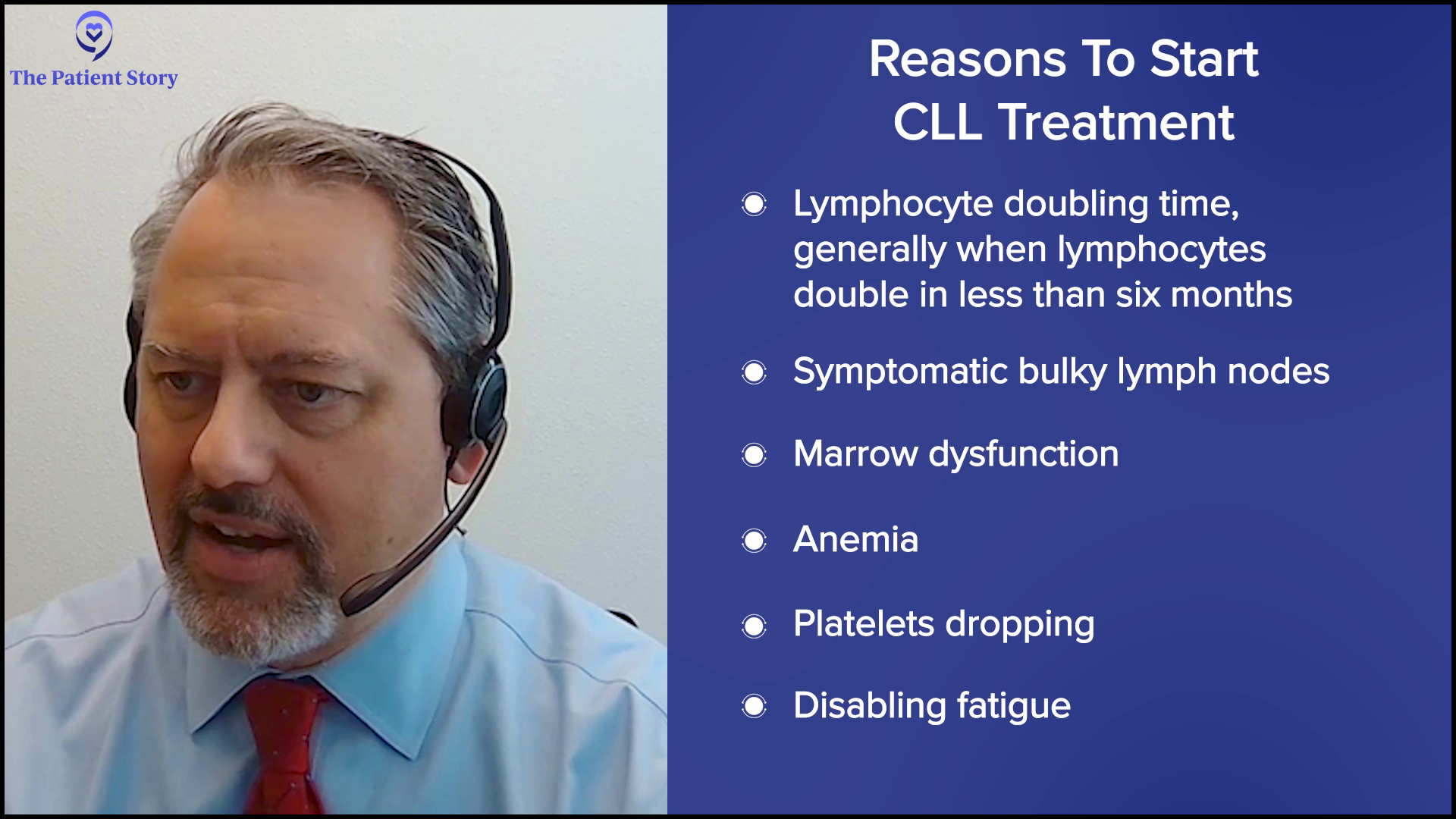











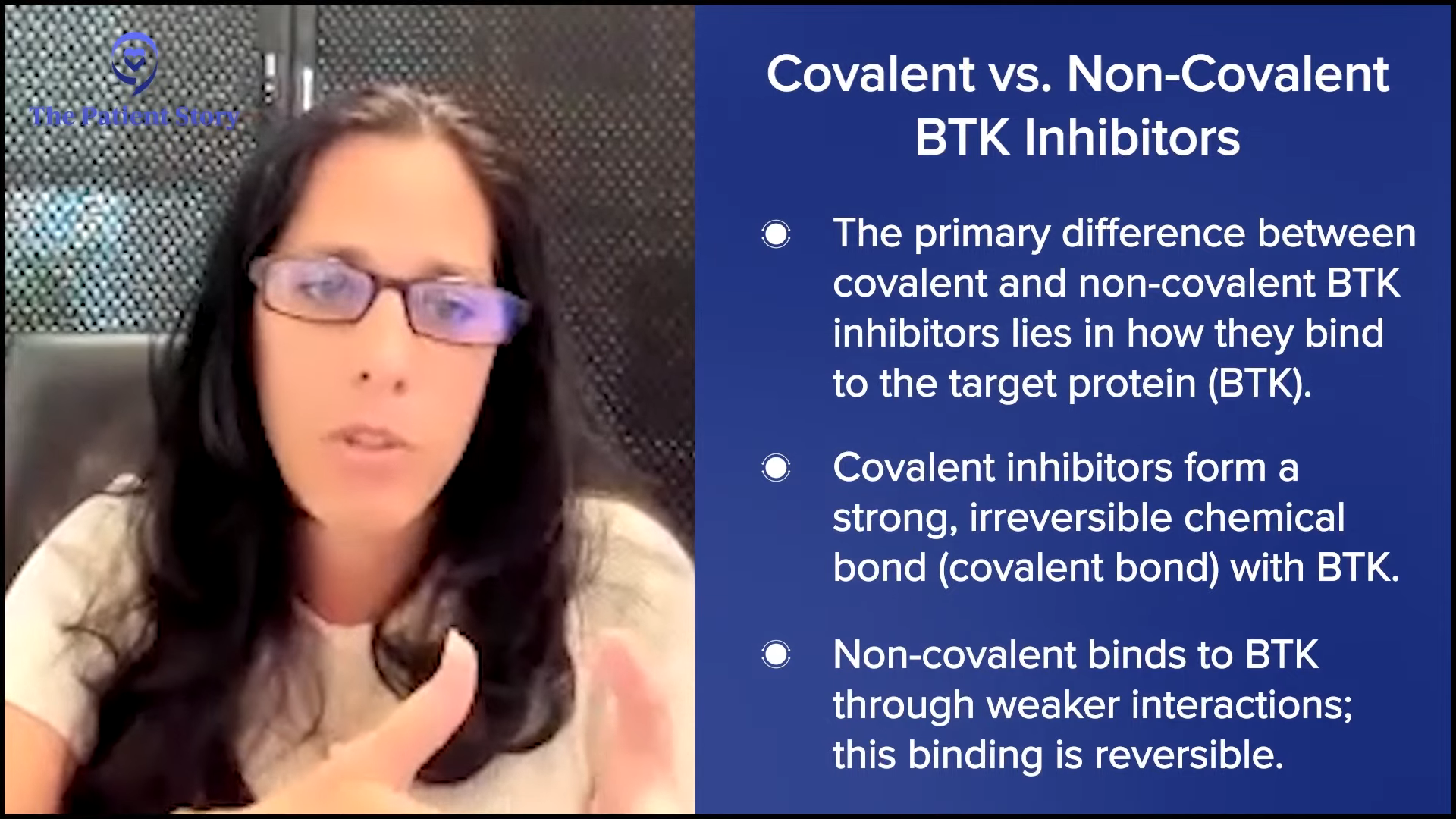







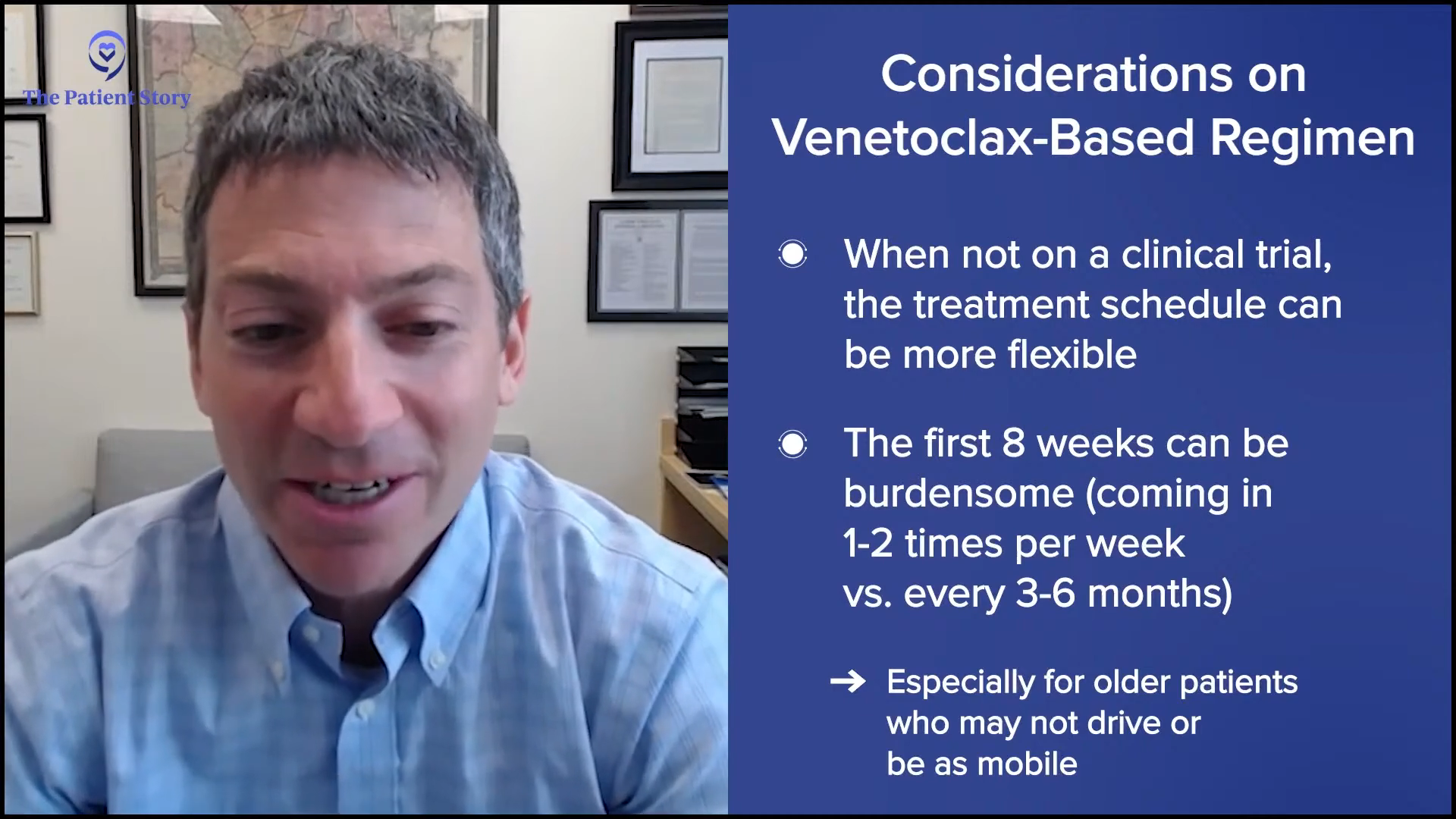









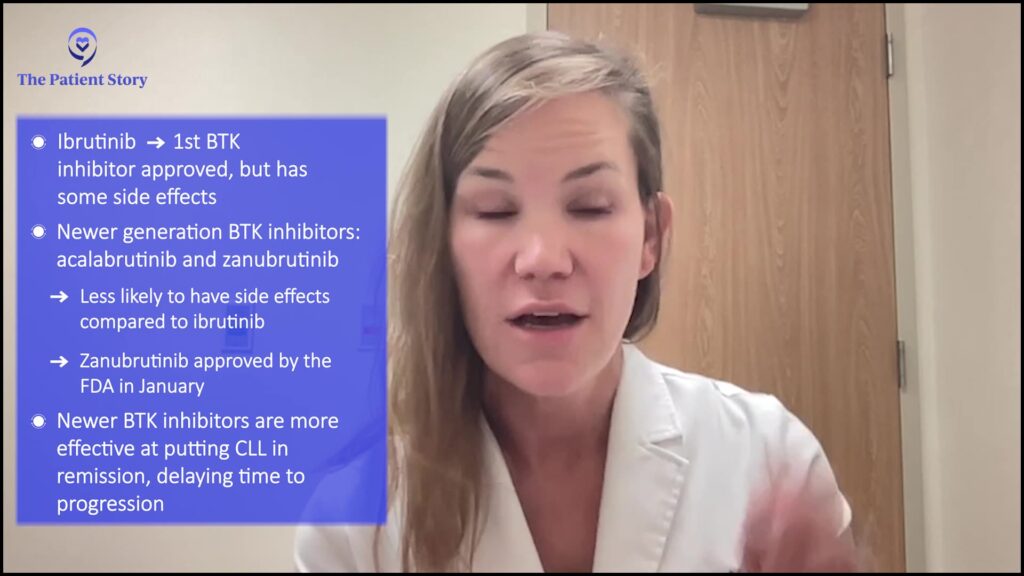
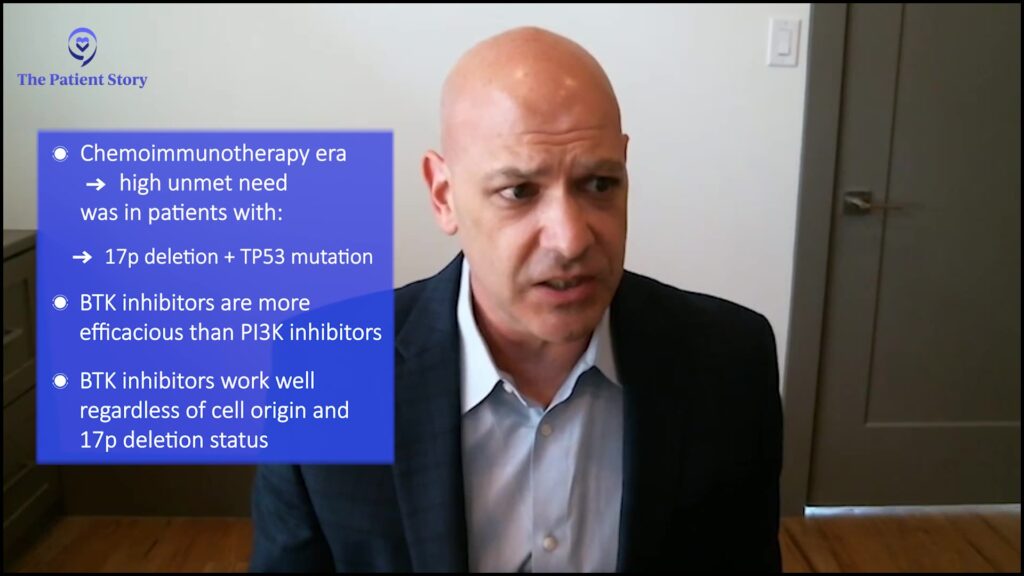



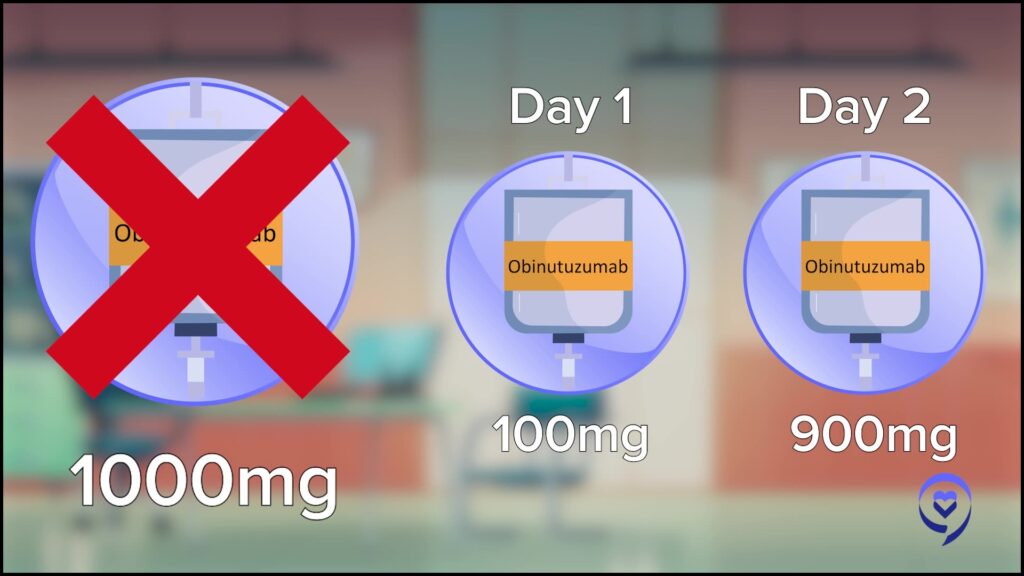




























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}