Embracing Life with Chronic Lymphocytic Leukemia (CLL): Serena’s Empowering Story
Serena shares her experience of living with chronic lymphocytic leukemia (CLL). At just 26, she started to experience strange and worrisome health issues, including severe leg cramps, ovarian cramps, strange knots on her body, hormonal acne, night sweats, and extreme fatigue. She first thought that these were signs of benign conditions like ovarian cysts or perhaps a blood clot. Despite feeling something was off, she had to deal with skepticism from healthcare professionals due to her youth, which only added to her distress.
Interviewed by: Taylor Scheib Edited by: Chris Sanchez
Seeking answers, Serena struggled with a convoluted healthcare journey that included financial burdens and dismissals due to her insurance struggles. After months of elevated white blood cell counts and persistent advocacy for herself, she finally went to The James Cancer Hospital and Solove Research Institute. Her diagnosis of CLL came unexpectedly and left her to process the emotional impact of having a treatable yet incurable disease.
Serena’s treatment approach, “watch and wait,” seemed strange at first but was necessary. Her medical team decided against immediate treatment, as early intervention does not extend the lifespan of CLL patients. Despite the idea of waiting for her condition to progress, Serena found comfort and strength in the support network provided by the hospital, which connected her with resources to ease her financial and emotional burdens.
Throughout her experience, Serena has remained proactive and optimistic. She had neck surgery to remove lymph nodes when faced with the possibility of Richter’s syndrome, a more aggressive lymphoma transformation. This successful surgery brought her relief and renewed hope.
Serena’s strength and resilience are deeply inspiring. Her advice to others about navigating cancer is to live life fully and focus on joy and self-advocacy. She now knows that it’s crucial to listen to your body and trust your instincts. Even though she isn’t currently on active treatment, she has still made herself part of the CLL community. By joining clinical trials, she also helps contribute to future treatments.
Watch Serena’s video and read this story to learn about:
How she defies expectations by advocating for her health.
The “watch and wait” approach to cancer treatment.
Finding strength in community and support.
Inspirational insights on living fully in the face of adversity.
Groundbreaking highlights on CLL from the world’s largest gathering of blood cancer and disease experts.
Name:
Serena V.
Age at Diagnosis:
26
Diagnosis:
Chronic Lymphocytic Leukemia (CLL)
Symptoms:
Night sweats
Extreme fatigue
Severe leg cramps
Ovarian cramps
Appearance of knots on body
Hormonal acne
Treatment:
Surgery: lymphadenectomy
Thank you to AbbVie for supporting our patient education program. The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Focus on living. It’s way better than to focus on dying.
Introduction
Serena V.: Hi, I’m Serena. I live in Columbus, OH.
I have CLL, which is chronic lymphocytic leukemia.
Before My Diagnosis
Serena V.: In the summer before I was diagnosed, I kept getting cramps in my legs and ovarian cramps, and I also kept getting these knots all over my body. My complexion was off, and although I didn’t realize it until later, I was also having horrible hormonal acne on my chin. I was in a lot of pain, too, and I was sleeping all the time and having night sweats. I thought I might have a cyst — a lot of friends had had ovarian cysts and things like that. I also wondered if I was getting a blood clot or something like that because of the knots. It all got me thinking: am I a hypochondriac?
So, I got medical help. The urgent care that I went to said that I might have some sort of mass or something internal and sent me to my gynecologist. But at the time, I didn’t have good insurance, so my gynecologist deferred me. I ended up having to go to the emergency room (ER) instead.
At the ER, they did an internal and external ultrasound, but it didn’t find anything wrong. The only thing the visit turned up was a slightly elevated white blood cell count. The ER then referred me to primary care, but I didn’t have one at the time. So we called a family friend who was a nurse practitioner. She found out that my white blood cell count was elevated, too.
All in all, it took six months for me to get referred to a cancer hospital because my white blood cell count just kept being elevated. I did have health insurance, but it didn’t really help me with my payments — for instance, I would get a $5,000 bill for the ER — and that stressed me out. And especially since I was just 26, people kept gaslighting me and doubting that I could be seriously ill. They would say, OK, there might be something off, but you’re fine. But I did know that something was wrong with my body. I mean, because of the cramps, I would be lying in bed all day with a heating pad because if I moved, I would be in awful pain.
So I didn’t really know what answers I was seeking, but I was afraid. I think what added to my fear was the fact that my brother had Hodgkin’s lymphoma at 22, and he had fortunately beat it, but it was still scary.
Even when I finally did end up going to a cancer hospital and seeing a hematologist, she literally told me that I was pretty healthy. A person only has a 2% chance of getting a blood cancer, and she told me that she thought I would be one of the 98% who wouldn’t get one. Plus, there’s a lot of uncertainty that comes with my age because most people who do get CLL are much older, and there’s just not much data about patients my age.
… since I was just 26, people kept gaslighting me and doubting that I could be seriously ill. They would say, OK, there might be something off, but you’re fine. But I did know that something was wrong with my body.
My CLL Diagnosis
Serena V.: So I was working at a career fair at a school and was driving back to my office, and I had to pull over because my doctor called all of a sudden. I thought, oh, she’s probably calling to tell me I’m fine. But she went, “Hey, Serena, we got your blood results back a day ago. However, I had my coworker double-check my work, which took an extra day. I’ve never seen this in my entire career.” And my stomach dropped.
The doctor said, “You have a disease called chronic lymphocytic leukemia or CLL.” And even now, I remember how I reacted at that moment. Your body doesn’t forget how you feel at a moment like that. My chest tightened up. And I asked her, “What is CLL?” And my next question was — “Am I going to die?”
She replied, “CLL is the most common type of leukemia. It’s treatable but incurable. But I will say that the average age of patients with CLL is 72.” I was so much younger than that.
My Search for the Right Doctor and Treatment
Serena V.: I got transferred to The James Cancer Hospital and Solove Research Institute, where we took things forward. I was expecting to start chemotherapy right away because my other doctor said, “We’re probably going to have to start treatment soon because you’re young, and we don’t want your CLL to get worse.” But when I got to James, they found that my counts were great, and they also told me that for CLL, early treatment doesn’t help with the disease and doesn’t increase the longevity of CLL patients’ lives.
They told me, “We’re going to put you on watch and wait”, which is a treatment approach under which my doctors would watch my condition but not treat me just yet unless and until my condition changes for the worse.
I remember feeling like that was the weirdest thing, because not only was I diagnosed with incurable cancer, but my medical team and I would need to wait and watch for it to get worse before I would start getting treated. Moreover, I was still experiencing those debilitating symptoms. So I was quite anxious.
I was grateful, though, that in the first year of my treatment, I was able to go to James every three months, and they also gave me access to some incredible resources. For example, James linked me up with a young adult cancer social worker who helped me connect with The Leukemia & Lymphoma Society for grants — which was massive considering the financial stress I had been under from the start. And she also gave me some important “cancer 101” tips regarding how to prepare for my appointments.
Overall, I’m optimistic. I think the science is really there, and my doctors are here for me — and they are optimistic about my lifespan.
My Reaction
Serena V.: I had so many questions for the social worker and in general. Since I’m so young, will I need to be treated multiple times? What does treatment look like for me? What would remission mean for someone like me who has an incurable cancer when “remission” means that there’s no more cancer in your body? So, things like that confuse me sometimes. But I do find a lot of hope in going in this direction.
Last year, I had neck surgery to remove five lymph nodes because we thought I was transitioning into Richter’s syndrome, which is a rare complication of CLL in which it quickly transforms into a more aggressive form of lymphoma. That was a horrifying experience. I thought, “Oh, what does my future look like now?” I thought I was going to die. But the operation was successful. My hematologist, for instance, is extremely optimistic that I’m not going to need treatment for a while, especially after that surgery.
Overall, I’m optimistic. I think the science is really there, and my doctors are here for me — and they are optimistic about my lifespan. I did have that question for them, too: since I found out I had CLL at 26, will I die in 20 years or just five? Or will I live longer and die at 80? That’s a question that none of them can answer with any certainty, and of course, I can’t answer it either.
But what I found works is focusing on life, on what I have, on what I can do, and on what I’m in control of, instead of just focusing on the fear of death. Those fears and thoughts are obviously still present. But being able to focus on the good things and on what I already have has really helped me.
What I Think About Clinical Trials
Serena V.: I opted into Ohio State’s research when I was first diagnosed with CLL. They have a program that entails taking an extra tube or two of blood for research. I do think clinical trials are amazing. I was open to whatever I could find because I was desperate for a solution. I was thinking, “What’s going to help me? Are you guys going to do it for me?” It’s nerve-wracking because I’m putting all my eggs in one basket, so to speak. “Do you think this is going to make me better or will it make things worse?”
I do realize there is some uncertainty with clinical trials. It’s obviously a trial you’re undergoing. But you do have to have that trust in your doctors that it might be the right thing for you and your condition.
Serena’s CLL Story Continues Below
CLL Program Highlight
The ASH (American Society of Hematology) Annual Meeting is the world’s leading conference on blood cancers and disorders, like leukemia, lymphoma, and multiple myeloma where top doctors and researchers share the latest breakthroughs. The below program excerpt if from our recent discussion with CLL expert, Dr. Jeff Sharman on news that came out of that meeting that could impact CLL patients like Serena.
CLL patient advocate and long-time health journalist Andrew Schorr sat down with Dr. Sharman to break down the most important updates for you.
Insights on CLL Treatment Advances
Andrew Schorr: So, Jeff, I’ve been living for many years with CLL. Some people who will watch this program are newly diagnosed. I went through all the stages you go through, and I’m sure you see it every day in your practice. What is this? I’m really scared. I have a blood cancer. Will my life be shorter? Am I going to die anytime soon? Please, doctor, what do you have that’s effective to treat me? And if that doesn’t work, do you have something else? We’re going to get into all that, but just at a high level, Jeff, how do you feel for today’s patients?
Dr. Jeff Sharman: You know, Andrew, it’s a great question and I have a very large practice of CLL patients. I take care of about 400 CLL patients and meet each of them. For many of them, I’ve been their first doctor. That’s the nature of my practice. So, for a lot of folks I take care of, I’m their first contact with the medical system in terms of understanding CLL. And I think what you highlight is something I see time and time again, which is a very understandable fear patients come in with.
It’s very common, you say “leukemia” and you see their eyes widen, you see them sit up a little straighter, and what you recognize under there is just a great deal of distress that any cancer would cause.
That’s a really optimistic message that most patients aren’t going to pass away from their disease.
And I think that one of the things we do as a doctor is figuring out how to measure out and administer the unique medicine we give, which is the medicine of hope. And how do you communicate that to patients in the midst of some of the worst days of their lives where they’re like, oh my God, I’ve been diagnosed with cancer? And I do reference quite frequently; there’s a study done in the Italian group that showed that if you’re age 65 and above and have been diagnosed with chronic lymphocytic leukemia, they have demonstrated that you really can’t measure a statistical impact on survival, that most patients are going to outlive their diagnosis. And I think that’s a really optimistic message that most patients aren’t going to pass away from their disease. And my own experience bears that out. The number of patients that I can think of who die of complications of CLL is really a very small fraction even in my large CLL practice — only a small number, maybe two or three per year.
So, a lot of it is communicating that there’s a lot that we’ve got for you. And it’s not the traditional chemotherapy you used to have. We’ve got targeted agents, immunotherapy, and so forth.
Andrew: You already mentioned that sort of people aren’t going to need chemo. We’ve got this whole class of medicines, BTK inhibitors, and even new generations of that which we can talk about. So, first of all, the approved therapies. You have quite an arsenal now, where you can use drugs either by themselves or together, maybe for a bigger impact, right?
Dr. Sharman: Right. You know, I think the way I look at this is that there are three main classes of chronic lymphocytic leukemia drugs. You mentioned BTK inhibitors. I would add to that BCL-2 inhibitors, and then I would add immunotherapy to that.
I think the status of the field right now is trying to figure out the best combination and the best sequence, and those are the big questions shaping the field right now. But the good news is, of course, these drugs are FDA-approved and they’re available to patients. So those are the kind of core questions.
Andrew: So, I’m sure there are patients listening, and their heads are spinning. And they’re saying, well, the different BTKs or a next-generation BTK, with or without venetoclax, with or without obinutuzumab. And I guess what I know is not all CLL patients are the same.
Dr. Sharman: Yeah.
Andrew: This is an individualized choice, right?
Dr. Sharman: Yeah, absolutely. Some patients take the physician’s perspective. Others are involved in their care and want to take an active part in the decision-making. I think that’s great. They should play an active role in it. And there are times when a patient might have their own preferences, but I may have different preferences based on how I’m thinking about their treatment. And sometimes, it’s a matter of calling to attention some of the potential side effects in a certain circumstance. Maybe somebody wants to do fixed duration, but their kidneys aren’t working too well any longer, or they’ve got a really bulky disease, or there could be various reasons why we might pick one over the other. Or even just how we think about, if we’re going to do this first, what do we do second? What’s going to be third? And if we’re going to pick this first, what’s the patient going to look like five to seven years from now when we might need to do the second therapy? So, you have to have a game plan in mind for somebody from the outset.
Andrew: Yeah, that is really well said. Now, I want to back up for a minute. We’ve got several questions from patients. One of them is like me. I said I went four and a half years without treatment. I felt pretty good. Then, I started to develop some lymph node issues, and my white blood count, fueled by lymphocytes, rose to about 283,000. My friend Dave is even higher than that. He hasn’t had treatment, and he feels fine. So, when should a new patient start treatment?
Dr. Sharman: So, for a chronic lymphocytic leukemia patient who’s climbing quite rapidly, what we talk about is the lymphocyte doubling time. Generally, when that number is going up more than twofold in less than six months, that’s our clue that we need to do something. But there are other reasons we might treat decide to somebody, such as bulky lymph nodes, if they start developing marrow dysfunction, if they’re getting anemic, or if their platelets are starting to go down — those can be reasons.
The one that does come up periodically is fatigue. Some patients have disabling fatigue. They might be 55 years old, they’re not depressed, their thyroid is fine, they’re not iron deficient, but they can only go to work for four hours before they have to come home.
So, disabling fatigue, that’s a reason to treat it, but these are all pretty well spelled out in what we call the iwCLL criteria. Rate of change, symptomatic bulky lymph nodes, marrow dysfunction, and others as well. Those are the reasons we treat patients.
… our therapies are just as effective for younger individuals than for older individuals, and in some cases, maybe even more effective for younger individuals.
Andrew: Some people on Facebook, for instance, are under 50 with chronic lymphocytic leukemia. And I know it’s not all that common, but there are people like that. And they say, well, is my age of diagnosis a bad thing? In other words, am I going to have a rougher time with CLL because I’m diagnosed younger? Would I not live as long? What do you tell a younger patient based on their age?
Dr. Sharman: Yeah, that’s a great question. I like to think of these patients in terms of having to plan not for the next 10 to 15 years but for the next 30 years. And I think that, to some degree, we celebrate that we have a lot of these new tools to control the disease. But I think it is a reasonable question to say, can you use these tools to control it for twice as long or three times as long as somebody who’s diagnosed, maybe at age 80? So, it requires a different game plan. And yes, our therapies are just as effective for younger individuals than for older individuals, and in some cases, maybe even more effective for younger individuals. But I think it does require some thoughtfulness to consider that we need to come up with something that’s going to keep this disease in control for quite a bit longer.
Now, the other thing is, this field is moving so fast that those tools that we’ll be using five to seven years from now may not even have been conceived of yet. And we don’t have a ton of time to talk about bispecific antibodies or other drug targets and so on. But to benefit those who are diagnosed younger, I think it’s fair to assume that there will be more tools in the tool shed down the road.
For the rest of this interview, watch our program replay ON DEMAND.
Learn what’s changing, how it impacts treatment decisions, and what it all means for patients today.
Webinar: CLL Treatment Advances: Moving From Research to Reality
Hosted by The Patient Story
The world of CLL treatment is evolving fast, with new breakthroughs offering more options. This program breaks down the most important updates from recent research and clinical trials.
… what I found works is focusing on life, on what I have, on what I can do, and on what I’m in control of, instead of just focusing on the fear of death.
My Life on Watch and Wait
Serena V.: How do I live on watch and wait? I just live. I live life as much as I can, and that’s the advice I can offer people facing chronic lymphocytic leukemia, or similar situations.
Find something that brings you joy and focus on that. Focusing on watching and waiting — well, it just makes you wait and watch. Even worse, it really makes you hyper fixate on your condition.
And, while you’re at it, listen to your body, too. If you’re feeling off, advocate for yourself with your doctor. In my case, I did realize that for the first year, I felt bad the whole time, and I wasn’t communicating this because I didn’t realize that some of what I was doing, like going home and napping so much, wasn’t normal.
I also realized that my fatigue was keeping me from spending time with family and friends. And later on, those were things that I was told to look out for as symptoms. But I didn’t process that something was actually wrong with me — and I was gaslit about my condition, too. And that’s how it was until I finally listened to my body and realized that something was wrong.
So I say, trust your body, find something that brings you joy, and focus on it. Focus on living. It’s way better than to focus on dying.
Special thanks again to AbbVie for supporting our patient education program. The Patient Story retains full editorial control over all content.
Patients, care partners, and a panel of CLL experts including Dr. William Wierda, MD, Ph.D. from MD Anderson, Dr. Nicole Lamanna, MD from the Columbia University Medical Center, Dr. Adam Kittai, MD from the Ohio State University, and Jackie Broadway-Duren, PhD, DNP, APRN, FNP-BC from MD Anderson gather to share the latest in CLL research, clinical trials, treatments, and comprehensive care strategies.
Guided by the insights of patient advocate moderator Jeff Folloder, the discussion will bridge the gap between medical expertise and patient perspectives, creating a truly comprehensive dialogue.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Updated October 9, 2023. Originally broadcast September 20, 2023.
Quality of life and precision are top of mind for chronic lymphocytic leukemia (CLL) patients. Understanding the complexities of available treatments can help you optimize your CLL care and prioritize the questions to ask your doctor.
During this live conversation, panelists Dr. M. Yair Levy, director of hematologic malignancies research at Texas Oncology, and Dr. Catherine Coombs, a hematologist oncologist at UCI Health who specializes in CLL, discussed the latest in CLL care. The discussion was hosted by CLL patients, advocates, and administrators of the CLL Support Facebook group Michele-Nadeem Baker and Jeff Folloder.
This discussion covers the current landscape of CLL treatment and care options, as well as new CLL treatments awaiting FDA approval, factors doctors consider when starting or switching a patient’s treatment, encouragement for CLL patients to advocate for themselves, and each doctor’s outlook on CLL treatment and patient quality of life.
There is hope. Hope to live a normal life, and hope to see your kids and your grandkids grow up. There’s always hope on the horizon, in my opinion.
Dr. Catherine Coombs
Thank you to AbbVie and BeiGene for their support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Michele-Nadeem Baker: I’m Michele-Nadeem Baker. I’m a medical and health journalist, but in addition to that, I am also a patient. I started advocating for other patients on my first day of treatment when I realized that there was so much unknown out there and to demystify things for my fellow patients and help them through their journey.
Jeff Folloder: My name is Jeff Folloder. I am a passionate patient advocate. I am now in year 14 of my little journey with CLL and I am living a great life. That’s why I became a patient advocate because I want to make sure that everyone knows that it is possible to live a great life with CLL.
First up, I get to introduce Dr. Catherine Coombs. She is a hematologist oncologist with UCI Health and she specializes in chronic lymphocytic leukemia. She also helps lead clinical trials, trying to find better ways to treat CLL. Dr. Coombs, tell me what drew you to specializing in CLL. We don’t hear that a lot.
Dr. Catherine Coombs: It was a long road. I went into medical school knowing I wanted to be a cancer doctor. I didn’t have any doctors in my family, but I do have a lot of family members with cancer. It always inspired me to be on the patient end of the oncologic relationship. That’s always what I thought I would do.
Now, I didn’t decide on CLL until my residency years. I looked for a research project right away, because that’s the only way to get into a good fellowship program is by doing research. It always was something I wanted to do regardless. I found a wonderful mentor in my time at Duke University as a resident, Mark Llaneza, where I focused on the underlying genetic risk of CLL as my residency project. That drew me to the field right away.
Then I saw all these other benefits of being a CLL-focused clinician, which is that the patients do really well and they live a long time. I love having that long-term relationship with my patients. I love blood cancers in general, but I would say the acute leukemias, which I had focused on a bit earlier on in my time as a faculty when I was doing a bit of both were hard because there are a lot of patients that we lose and I really admire the docs that do it. But I think for my long-term well-being, I know that it’s just so much more gratifying and less emotionally traumatic to be able to have patients that thrive for so many years and be able to really enjoy those relationships as the added benefit.
The therapeutics have just continued to improve over the 13 years since I first graduated medical school and started doing research.
Michele: We need more doctors like you. Dr. Coombs, thank you so much. I’d also like to introduce Dr. Levy, who is a hematologist oncologist at Texas Oncology. He is the director of Hematologic Malignancies Research and specializes in CLL. He’s also helped lead clinical trials in CLL. Dr. Levy, what drew you to CLL?
Dr. Yair Levy: Before moving to Texas, I actually did mostly chronic lymphocytic leukemia, but I’m a little older than Dr. Coombs. So back when I was doing it, it was still a relatively better outcome for this cancer, but we still lost some folks to chronic lymphocytic leukemia. However, if I reflect on my current experience, I don’t believe that I have lost a patient to chronic lymphocytic leukemia in the past decade. This is not because I have a shortage of patients. I’ve probably accumulated about 150. I’m not saying that the patients don’t die, but they don’t die of CLL.
So to live a normal life is the goal. Even though we still think of CLL as a treatable but incurable malignancy, for the most part, people are doing relatively well. Not to mention, not only are our treatments better in terms of efficacy, but they’re so much better tolerated.
If I reflect on my current experience, I don’t believe that I have lost a patient to chronic lymphocytic leukemia in the past decade. This is not because I have a shortage of patients. I’ve probably accumulated about 150. I’m not saying that the patients don’t die, but they don’t die of CLL.
Dr. Yair Levy
Jeff: We have an interesting topic for today’s program, Shared Treatment Decision Making: How To Be An Empowered Patient. This is something that strikes me right in my heart. I am a firm believer that patients who take an active role in their own care tend to have better outcomes, and this is actually borne out of clinical research.
I took an active role in my own care. I chose not to go in the specific direction that my first doctor wanted to go in, and I wound up at a large research hospital participating in a clinical trial. I’ve been living a great life as a result.
Michele: For me, treatment decision-making also came down to becoming an empowered patient and becoming health literate in CLL. The more I could learn from credible sources, for me, was better. I realized all patients are different and doctors, you can probably relate to this more than anyone but the world has changed quickly and pretty drastically for clinicians, researchers, and those of us who are patients.
I was diagnosed 11 years ago, not quite as long ago as Jeff, but still a long time ago. My frontline treatment started in 2015 and things were even different back then. I was on a trial that combined ibrutinib, which at the time was not approved yet for frontline treatment. It had been for relapsed and refractory but not frontline treatment. It was combined with FCR, the standard at the time, fludarabine, cyclophosphamide, and rituximab. Things have changed so quickly even since then. In my frontline treatment, I’m now on a different treatment. I had relapsed in between.
Dr. Coombs, could you tell us how the landscape of treatments for patients has vastly changed over the last couple of years?
BTK Inhibitors
Dr. Catherine Coombs: Over the past decade, but even over the past few years, we’re seeing advances. When I first got into the field, yes, it was chemoimmunotherapy for patients fit enough to receive it like FCR and BR. With the introduction of targeted agents, largely chemoimmunotherapy is not widely used. However, we still do see about a third of uptake looking at these large-scale studies across the country.
I’d say that doctors who are focused on CLL realize that chemoimmunotherapy is not worth the toxicity. Its efficacy is also inferior to these novel drugs that are more efficacious, so more likely to put the CLL at bay, in remission, and delay time until ultimate progression, but also hugely safer. That was first ibrutinib, as you wisely know from your own personal experience and your knowledge over the time of your journey as a patient. But now we have a lot of newer and better drugs. Ibrutinib has been amazing and revolutionary, but it does have some side effects. Fortunately, they’re not so common, but they still can be clinically significant.
The first category of drugs that have really changed in the past few years is newer generation BTK inhibitors. Ibrutinib was the first in class. It inhibits this critical protein that’s part of CLL cell machinery, BTK, but it’s not totally selective for its target. We now have 2 additional drugs that inhibit BTK – acalabrutinib and the most recent addition, zanubrutinib which was FDA-approved in January.
The advantage of both of these drugs is that they’re more selective for their target, BTK. That, fortunately, has translated to improved safety, where both drugs have been compared head to head with ibrutinib and they demonstrate improved tolerability, specifically lower rates of atrial fibrillation for both drugs. Acalabrutinib also has the advantage of lower rates of hypertension.
What we don’t know is whether zanubrutinib is better than acalabrutinib or acalabrutinib is better than zanubrutinib, because we don’t have that comparison. But I think they’re both excellent options and both offer advantages over the ibrutinib days when we were dealing with a lot of atrial fibrillation. There’s a lot less in the way of that.
The other huge class of drugs that I haven’t mentioned is a completely different way of treating CLL, so I’ll mention it briefly. I don’t know if we’re going to get more into the nitty gritty on this, but these BTK inhibitors work wonderfully at controlling CLL, but they’re considered as treat-to-progression regimens, meaning that patients go on and stay on as long as they’re, number one, tolerating it and their CLL is responding favorably.
Some patients don’t like the idea of being on a drug indefinitely, so the other huge therapeutic advance over the past few years that’s been widely available is the drug venetoclax. This is typically combined with another drug called obinutuzumab when used in the frontline setting. Because it can so effectively kill off the CLL to very deep levels, patients are able to completely stop treatment after one year and then eventually relapse, but it can take a long time. That’s one of the other major, major changes in CLL just over these past 5 years or so.
I’d say that doctors who are focused on CLL realize that chemoimmunotherapy is not worth the toxicity. Its efficacy is also inferior to these novel drugs that are more efficacious, so more likely to put the CLL at bay, in remission, and delay time until ultimate progression, but also hugely safer.
Dr. Catherine Coombs
Michele: Dr. Levy, what else would you add?
Dr. Yair Levy: Dr. Coombs, you hit the nail on the head. It’s a dramatic change from chemoimmunotherapy. In the chemoimmunotherapy era, our high unmet need was what we considered high risk which were ones that harbor a 17p deletion, or a mutation in this TP53 tumor suppressor protein, or these cells of origin that are called pre-germinal cells of origin. So a more immature cell that had gone bad, and we’ve known that they have done historically quite poorly with chemoimmunotherapy.
As Dr. Coombs mentioned, the biggest improvement that we saw was when we actually recognized druggable targets within the B-cell receptor pathway. The first such drugs were actually not Bruton’s tyrosine kinase (BTK) inhibitors, and they are largely relegated to the history of the B-cell receptor pathway now. But these were the PI3K delta inhibitors. Those worked irrespective of cell of origin, and they also worked in the 17p deletion. So again, they did certainly have some tolerability issues and the efficacy was not comparable to those of Bruton’s tyrosine kinase inhibitors, which is one of the big reasons that those have really fallen out of favor.
As Dr. Coombs mentioned, the BCL2 inhibitor venetoclax has also been a game changer. We’ve been utilizing these agents, either alone or in combination with CD20 monoclonal antibodies. Now, the European Medical Association has even approved the combination of a BCL2 and a BTKi. This is something that we’re doing further studies on within the United States as well because we’re seeing that people achieve very impressively high rates of response. More importantly, very deep responses can allow, hopefully, a very long treatment-free interval, and perhaps even in some cases, a functional cure.
So, in the beginning, we were saying that CLL is largely treatable but incurable, but we put an asterisk on that. Even with chemoimmunotherapy, there was a subset of CLL that may have been cured by chemoimmunotherapy, or at least a functional cure. I think we’re going to see the same thing with these other combinations as well.
We’re seeing that people achieve very impressively high rates of response. More importantly, very deep responses that can allow, hopefully, a very long treatment-free interval, and perhaps even in some cases, a functional cure.
Dr. Yair Levy
How CLL doctors are providing CLL patients with precision care
Jeff: This is exciting stuff. We’re talking about an awful lot of options for patients, but before we can get to those options, we need to figure out how we get to that point. So let’s chat a little bit about the tests that are needed to diagnose and then accurately inform those potential treatments.
A lot of us in the support groups and on social media love tossing around the cute names, the FISH test, the flow test. Not a lot of people truly understand what’s going on with those tests. They don’t understand the concept of chromosomal abnormalities that may be going on with a patient at the time of diagnosis. Dr. Coombs, can you briefly give us a top line as to what these tests are doing and more importantly, what they’re telling you in terms of prognostics?
Dr. Catherine Coombs: Absolutely. Before the advent of all these, let’s call them sophisticated tests, we would stage patients. That’s always what I think cancer patients think of, what stage am I? We do have a staging system called the Rai Staging System that we use in the US. In Europe, they use this Binet Staging System. But the idea is, how much is this really affecting me? Rai stage 0 is when it’s just a high white count to Rai stage 4 when you have low platelets from the CLL.
I’m taking a step back because there were, for decades, ways of saying this a good or a bad CLL. However, what we’ve learned over the years is that there are some patients with really early-stage disease that would follow very aggressive clinical courses and then some that may have been technically a Rai stage 4 that were totally stable for decades. The goal with all these more sophisticated tests was to better predict, how is this person’s CLL going to behave, which then helps us as clinicians know what to expect. It helps the patient as far as what he or she should expect.
So taking a step back, we now have a lot of advanced testing that we can send. The good news is that these can be sent on the peripheral blood so it’s not necessary to get a bone marrow biopsy early on. Of course, we do consider these at the time of therapy, but we can send these tests in the blood because the CLL, by its nature, is circulating in the blood. So we can pick up different abnormalities that can tell us, this is a good or a bad CLL or maybe somewhere in the middle to help us, number one, know if we should follow this person more closely. Number two, is this someone that perhaps it’s less likely to cause more trouble than not?
The categories of tests are looking at the DNA, which is either via a FISH test which uses fluorescent probes to find common abnormalities that are known to be seen in CLL. The most adverse is the 17p deletion. On the other spectrum, the most favorable is an isolated 13a deletion.
However, what we’ve learned is that this is only looking at certain probes. Sometimes you can have other abnormalities that aren’t present as part of the FISH panel. In my own practice, I also send a karyotype test which looks for the same thing, abnormal chromosomes. Instead of using a preselected panel of common abnormalities in CLL, it just looks at all the chromosomes. The chromosomes, just for the patient’s knowledge, are just the big chunks of DNA that live inside every one of our cells. We’re focusing on what these abnormalities are in the cells because there are common patterns. There are good patterns and bad patterns.
It’s also bad to have a complex karyotype, meaning 3 or more abnormalities in any given cell, so that’s one category. The 17p deletion I mentioned is known to behave more aggressively. It’s still a chronic disease, but those are often the bad actors, especially back in the chemo days when chemo doesn’t work well at all. It does do better with our new drugs, but that is a particular problem because it deletes a copy of this very important gene called TP53.
We used to think the only way of losing that gene was by completely deleting the part of the chromosome where it’s contained. What has been learned over the past 10 to 15 years now in CLL, is that it may not be deleted, but it could be mutated. That’s another test that I think is very wise to send, especially in patients who are going to need treatment because a TP53 mutation is largely the same as a 17p deletion. There are a little bit of nuances there, but these are 2 separate tests. They both give similar information because those 2 abnormalities are treated as one and the same as far as their impact on prognosis.
The next category of testing is looking at the immunoglobulin heavy chain status, so a normal B-cell over its life. CLL is a cancer of B-cells that undergoes a process of somatic hypermutation where it just acquires mutations. It’s actually good to have a mutated, immunoglobulin-heavy chain. The bad finding is for that to be unmutated, which suggests this is a bit more primitive of a cell. And what’s been borne out through a lot of studies is that patients with unmutated are the ones who need therapy quicker and they don’t respond as well to certain therapies. Now, again, the negative predictive impact of some of these abnormalities is somewhat outdated. Sometimes they do just as well with our new treatments, but they definitely don’t do as well with the old treatments.
The other test I always send is the beta-2 microglobulin (B2M), mainly because that goes into our scoring system for CLL, the CLL International Prognostic Index, but it’s an adverse finding to have that elevated. I think that wraps up the bulk of all the prognostic tests that I send at the time of meeting a new patient and trying to help understand what is our future going to be like.
The goal with all these more sophisticated tests was to better predict, how is this person’s CLL going to behave, which then helps us as clinicians know what to expect. It helps the patient as far as what he or she should expect.
Dr. Catherine Coombs
Jeff: Let me play that back for just a second and put it in terms that are not quite so technical. You have a toolbox, and that toolbox has a lot of really nifty tools in it, where instead of saying you have leukemia or you have chronic lymphocytic leukemia or you have one of these genetic abnormalities, you’re able to hone down to a very precise level of differentiation. That’s where the term personal and precision care comes in. Correct?
Dr. Catherine Coombs: Excellent explanation. Yes.
Michele-Nadeem Baker: I love this term and how that is happening more and more for patients. Dr. Levy, before planning treatment, what do you like to understand from your patients so that you can learn more about them when it comes to prescribing their treatment?
We need to speak with the patient and find out what is most important to them and explain everything about the treatment, including side effects, logistics, expected outcomes if you choose one route versus another, and the cost of travel. There are a lot of things that go into everything.
Dr. Yair Levy
Dr. Yair Levy: We’re all different and everybody’s cancer is also different. The reason that we have jobs as oncologists is because, I’m not sure that’s true here, but hopefully we know more about CLL and the treatment options than the patients. It’s our job to explain to them all their various options and then help them arrive at a choice that makes the most sense for them.
I think Dr. Coombs mentioned that we have a lot of options, but they haven’t necessarily been compared head to head. So we can’t tell you prospectively how treatment A compares to treatment B or treatment C. There are certain guidelines of what’s called preferred therapies and other alternative therapies that are also acceptable. We need to speak with the patient and find out what is most important to them and explain everything about the treatment, including side effects, logistics, expected outcomes if you choose one route versus another, and the cost of travel. There are a lot of things that go into everything. This is our job to get them to ask the right questions and then answer those questions.
The role of patient comorbidities in CLL care
Michele: And what about comorbidities? Is it important for patients to discuss their other health issues with you, such as cardiac issues? There’s a myriad of so many other types.
Dr. Yair Levy: Absolutely. This is what we were saying is, we’re all different, we all have different things that matter, and we are all in a different place in our lives. We take all of that into consideration, there’s no question about it.
The comorbidities are incredibly important, but we certainly advanced past where we were 15 or 20 years ago when we were looking at whether patients are fit enough to take therapy versus not because right now we’re not necessarily looking at fitness for therapy as much as we’re looking at what is the optimal therapy for them.
Many of the therapies that we have, if you take a look at what’s called the Preferred Category 1 recommendations from the NCCN Panel, were all studied in what we would have technically called a non-fit population before. It’s wonderful that we have all these highly effective therapies that we can give to people, even if their fitness is not optimal.
The benefits of watch and wait
Jeff: We’ve been talking about a whole bunch of novel therapies, stuff that has really impressive outcomes these days. Michele and I will both be able to tell you without hesitation, that the first thing that most patients encounter is not treatment. It’s this thing that we call watch and worry. You guys call it watch and wait. CLL does not always need to be treated right away. Your medical team is going to work with you to decide when it’s best to start treatment. In the meantime, the patient’s worry. Did I sum that up correctly, Michele?
Michele: We sure do, even though we tell everyone not to and to take a breath when they’re first diagnosed. Jeff, you and I both know that we still go through that when we’re back in that time period. It’s just so counterintuitive to not be treated right away when the disease has not progressed where it ends up going when you do get treated.
Dr. Coombs, what are you looking for when it’s time to treat? You go through years, hopefully, during watch and wait. Worry and wait, as patients call it. But what is it that you’re looking for and is there any benefit to treating it sooner as with some of the other cancers out there?
Dr. Catherine Coombs: I’m coming straight from my clinic. I’m in a clinic room. I just had this conversation with a patient who is newly diagnosed about watchful waiting, which I totally understand why it’s watchful worrying for many. I always see it as my duty to help them understand why this is our approach. I acknowledge this is not what we do for many other cancers where you hear, find it early, treat it early. I wish our treatments were so good that treating it early would knock it out and you’d never have to worry about it again. In 2023, we haven’t been smart enough to come up with something that will do that for CLL.
The way that I help put that in context for my patients is this disease can be so indolent that maybe up to 1 in 3 patients never need treatment in their lifetime. So if we treated everyone, inherently we’re over-treating people. I hate giving people things they don’t need because every treatment comes with a cost, whether it’s financial or side effects. That’s my one very strong argument for not over-treating. But also, none of the early treatments that we have tried and done clinical trials on have been shown to make patients live any longer. That is just where we are.
I definitely could understand the frustration on the part of patients because that leaves you with these worries. I do see those getting better in patients as time goes on. There’s this initial period of uncertainty, but then as you see what your pattern is, that either tells us, maybe we are approaching the time for therapy or nothing’s really changing, I feel fine, and this is something I can accept.
Now, obviously, we never know which camp a patient is going to fall into in these prognostic tests. They help us have a general sense of, maybe this will be a super slow CLL versus one that progresses more rapidly, but nothing is certain. I do personally have enthusiasm for making this change.
There is an ongoing countrywide clinical trial looking at early intervention for patients with high risk. That is open at my own institution and across many, many institutions in the country. I really hope things will change so we can improve patients with early disease. I don’t think it’s going to be every patient because of this third that never needs treatment. I don’t ever see a reason to just treat everyone, but the trial specifically is focusing on high-risk patients. Maybe there will be some movement there. It’ll probably take about 10 years to find the results of the study because you have to follow patients for a really long time.
For now, my job is to not over-treat and not make people who are feeling good feel worse. If you’re asymptomatic, then the best I can do is leave you alone, but hopefully calm some of whatever natural anxieties come about with what is a life-changing diagnosis.
This disease can be so indolent that maybe up to 1 in 3 patients never need treatment in their lifetime. So if we treated everyone, inherently we’re over-treating people.
Dr. Catherine Coombs
Michele: We have some questions coming in from our audience. Dr. Levy, here’s one of the questions for those of us with liver enlargement. Should we watch and wait?
Dr. Yair Levy: I completely understand the anxiety that comes along with this. I’ve been treating indolent lymphomas for a couple of decades now, and I’ve got the same experience. You talk with patients, you tell them they have cancer, and then they’re saying, “You tell me I have cancer, but you’re not going to treat me now. Are you sure you went to medical school?” I had that come up several times.
By the way, we don’t do watchful waiting anymore. We call it active surveillance. Nobody likes watchful waiting, but if we’re saying we’re actively surveilling you, that sounds certainly a lot better.
The way that I explain it is, that there are really only two good reasons to treat you for anything. This isn’t just an oncologist, it’s in all of medicine. My wife is a real doctor, she’s an internist. She has the same parameters for treatment. So, number one, if you can make somebody feel better, that’s absolutely a great reason to treat them. Number two, if you can make them live longer.
What we’ve seen, as Dr. Coombs was saying in chronic lymphocytic leukemia, as well as a variety of other indolent non-Hodgkin’s lymphomas is that early treatment does not confer a benefit in survival. In other words, if we treat you when you’re asymptomatic, you’re not going to live any longer than if we wait to treat you when you are symptomatic. This is important because as we were talking before, our treatments are changing and changing for the better.
The treatments are becoming more effective and better tolerated. And remember, something is only incurable until we’re able to cure it. So there are a lot of good reasons to wait. Dr. Coombs mentioned this as well. If I can’t make you live longer by treating you earlier with our current therapeutics, the question is, can I make you feel better? If you’re asymptomatic, I can’t make you feel better. I can make you feel worse. I can spend a lot of your money, but I’m not helping you. You are the most important part of that equation.
If somebody has liver enlargement, the question is, are they symptomatic? Are they having pain? Are they having any other symptoms from their liver involvement? If they’re asymptomatic, I would not necessarily treat them just for liver enlargement. The same thing is true with spleen enlargement as well, which is a far more common finding in chronic lymphocytic leukemia.
If we treat you when you’re asymptomatic, you’re not going to live any longer than if we wait to treat you when you are symptomatic.
Dr. Yair Levy
Michele: I experienced that when I relapsed, but along with other things as well, which led to my going back into treatment. Dr. Levy, thank you. You brought up a lot of great reasons why people are not rushed into treatment which also hints at all the things that you do look at when it is time for treatment, which we’ll continue to talk about as we go through with our program today. Thank you very much.
Considering the duration of treatment for CLL patients
Jeff: We spoke earlier about a bunch of the newer options that are available. We know that the treatment landscape is changing by the minute. I’m going to tee this up in terms that forum participants and our support group participants, they all had the same questions.
Yeah, the drugs are great. Am I going to have to take them for the rest of my life, or is there a chance that I can do it for a fixed duration? Dr. Levy, let’s break down what those current treatments are, what baskets they fall into and is this a lifetime activity or could we end it in 6 months? Could we end it in one year? You’ve got a lot of stuff that ends in -ibs, and -tas, and -mabs, and all that. Explain to us what’s going on.
Dr. Yair Levy: Again, this treatment progression model is a relatively new phenomenon for us in the treatment of malignancies. We used to treat with a fixed duration of therapy when all we had was chemoimmunotherapy. You can understand why. Once we give chemo, we can’t take it back. Certainly, the effects of cytotoxic chemotherapy are not something that you want in a cumulative manner.
Because of the logistics of how cytotoxic chemotherapy works, we could not give that till progression because that would be a very difficult life. Everybody thinks that the worst thing in the world is dying, and no, the worst thing in the world is not dying. The worst thing is a long, crappy life. That’s what we would assure we would do to people if we continued them on chemoimmunotherapy.
If you take a look at our approved therapies right now, basically it’s two categories. Bruton’s tyrosine kinase inhibition, BCL2 inhibitors, and monoclonal antibodies, can be sprinkled on any of these regimens. In terms of approved fixed durations of therapy, it’s only with the BCL2 inhibitors. The reason for that is that’s the most ideal drug that we have seen in the treatment of chronic lymphocytic leukemia. What I mean by that is it is a killing machine. It kills so well that we had to attenuate the dose because if you kill things too quickly, that can also become a problem.
We’re able to get those very, very deep responses. These deep responses, even if they’re what’s called MRD, which stands for minimal residual disease, really should be measurable residual disease. Even if people achieve a level of disease below where we can measure it, we know that in many cases it still returns. We really need to get that logarithmic killing. We really need to reduce their tumor burden by many zeroes in order to give them that long treatment-free interval. Currently, that’s possibly more likely with a BCL2 inhibitor venetoclax.
As we were alluding to before, we are seeing combinations of Bruton’s tyrosine kinase inhibitors like ibrutinib, acalabrutinib, or zanubrutinib in combination with venetoclax. Again, this was based on these laboratory models in which they actually saw whether or not these cells were primed for death with this combination. They actually saw synergy, meaning that the drugs worked better together than the sum of their parts.
As we mentioned, this is a fixed duration of therapy that’s actually approved in Europe right now, but not here in the United States. In the United States, we certainly can give a fixed duration of therapy with venetoclax and a CD20 monoclonal antibody. I can tell you that anecdotally, I’ve also done that with Bruton’s tyrosine kinase inhibitor and a monoclonal antibody if I can achieve that very deep response.
In terms of approved fixed durations of therapy, it’s only with the BCL2 inhibitors. The reason for that is that’s the most cidal drug that we have seen in the treatment of chronic lymphocytic leukemia.
Dr. Yair Levy
Factors in choosing a first-line treatment for CLL
Jeff: Excellent. Lonnie’s got a great question. Since we’re now considering treatments, he wants to know what are the primary factors to consider in choosing a first-line treatment. Dr. Coombs How do doctors and patients make that call? How do you choose which drugs are up on deck first?
Dr. Catherine Coombs: I think there are disease-related factors and patient-specific factors. We tackle those one at a time. I think there is an important role in knowing what an individual’s CLL risk findings are because those can help inform how likely a treatment is to lead to prolonged remission. Specific to a venetoclax-based approach in the front line, what we do know is that there are shorter remissions in patients with the 17p deletion or TP53 mutation and also shorter remissions for individuals with unmutated IGHV.
I tend to be an optimist and so my view is that these therapies, venetoclax-based, work way better than chemotherapy ever did for patients with these high-risk features. We can still see lengthy remissions on the order of a little over 4 years for the 17p patients for progression-free survival or around 5 some years for the unmutated IGHV. That is shorter than if you don’t have those markers.
I do think it helps weigh expectations on what to expect from a time-limited regimen. If you have high-risk markers, if you have all favorable markers, venetoclax also works really well and it just works longer than if you had negative markers.
Now, Bruton’s tyrosine kinase inhibitors as a class that have really leveled the playing field. If we divvy up patients with the unmutated and the mutated IGHV and the chemo days, the unmutated would relapse years faster than the mutated. There’s not much of a difference, and so those drugs work really for everyone. Now, they’re just so different conceptually and side effect-wise, which is why it is so important to weigh the patient’s comorbidities.
In addition to these disease-related factors that could help gauge the relative success of any given therapeutic approach, there are patient-specific factors. That’s why it’s so important for me to know, not only the details of the CLL but also the details of your specific comorbidities. Do you have a high degree of cardiac comorbidities where maybe we might be a little bit nervous about the BTK inhibitors, which can have cardiac side effects?
I will say the newer drugs are much better than ibrutinib, but it is something I weigh whether you have significant kidney disease, which might be a little bit risky. When we think of a drug like venetoclax that causes tumor lysis syndrome – none of these are complete no-goes, but they help tip the scale of which one are we favoring a bit more.
Then, of course, I want to know what other medications you’re taking, because a lot of medications can interact. That’s something we have to make sure of. Often that’s not a big deal, we just switch one out, but we have to know.
Lastly is social factors. What are your preferences? Are you the type of person who wants to do everything and doesn’t mind a frequent schedule, but wants that payoff of then being done with treatment in a year, where we might lean more towards venetoclax-obinutuzumab? Or are you someone who wants to spend as little time at a doctor’s office as possible and is okay with indefinite treatment where we may lean more towards BTKi? Those are the 3 major categories I think of – disease factors, patient comorbidity, specific factors, and then social and preference.
My view is that these therapies, venetoclax-based, work way better than chemotherapy ever did for patients with these high-risk features.
Dr. Catherine Coombs
The benefits of monoclonal antibodies for some CLL patients
Michele: Dr. Coombs, thank you for talking about the biomarkers that might indicate someone is a high risk, such as 17p or TP53. I am high-risk, but I don’t have either of those. I have the other that you had discussed being unmutated IGHV, and that actually impacted my treatment decision when I relapsed. I just finished. I am on acalabrutinib and was on a blinatumomab until a couple of weeks ago. It was obinutuzumab for 6 months along with the acalabrutinib.
Now, I will be staying on acalabrutinib indefinitely because I am considered high-risk. I had originally stated before that I started on ibrutinib. BTK inhibitors work for me and I just had adverse events initially and that’s why I went off. I had a couple of years of a drug holiday and then my doctor decided that while BTK inhibitors were still working, let’s go for it. I would still have another option with venetoclax.
Dr. Levy, why does a monoclonal antibody help? What does it add to the one-two punch? I know you talked about the different things that they’re addressing and being a killing machine, but why is it only for some patients? For example, what I’m on, acalabrutinib and obinutuzumab trials have shown that it specifically works the best. One trial was presented at ASH this past year for people like me who were unmutated. So, why only for some patients is it a benefit?
Dr. Yair Levy: Well, that’s a great question. The CD20 monoclonals were our first immunotherapy in the treatment of many B-cell malignancies. When we combined them with some of the targeted therapies, we didn’t necessarily see what we were expecting. In all of the trials with chemoimmunotherapy, adding a CD20 monoclonal improved progression-free survival. But interestingly, when we took a look at some of the studies that had arms that contained both ibrutinib, our first, covalent Bruton’s tyrosine kinase inhibitor in combination with a CD20 monoclonal or without those progression-free survival curves were superimposable. I think we were really surprised by that.
By the way, I need a button that says “I agree with Dr. Coombs.” Dr. Coombs was actually mentioning the fact that there are differences among these covalent Bruton’s tyrosine kinase inhibitors, and our first one had a less focused kinase profile. In other words, it hit other kinases, not just Bruton’s tyrosine kinase that we were trying to inhibit. One of the other kinases that it inhibited was something called ITK or IL-2-inducible tyrosine kinase. This led to antagonism of the CD20 monoclonal, which is why we got no benefit from the addition of the CD20 monoclonal.
This is not true for the other covalent BTKi, zanubrutinib and acalabrutinib. However, you’re seeing the combination with acala because that is FDA-approved and zanubrutinib does not have an FDA label in combination with a CD20 monoclonal. Do I have any reason to think that it wouldn’t work as well? I do not. There’s certainly data that supports that as well, that there are differences in terms of PFS for folks receiving the combination of zanubrutinib with a CD20 as well as without.
Now you can say, so why doesn’t everybody get a CD20 monoclonal? The answer is that there are trade-offs. Everything in life is a risk-benefit ratio. We know that, for example, there is this virus here in Texas, I don’t know if you guys have it too, called COVID. We know that for COVID, the CD20 monoclonal certainly antagonized an immune response to vaccination, as do the BCL2s and Bruton’s tyrosine kinase inhibitors.
Certainly, you are at more risk for adverse events and complications when you add additional drugs, so everything is a trade-off. We’re getting additional efficacy but at a cost. Our job is not to tell patients what to do. Our job is to have a discussion and come up with a solution that works best for them after we have a discussion and they are fully informed.
Now you can say, so why doesn’t everybody get a CD20 monoclonal? The answer is that there are trade-offs. Everything in life is a risk-benefit ratio.
Dr. Yair Levy
What CLL doctors consider before ramping up treatment and dosing
Michele: Thank you. Dr. Coombs, let’s talk about ramping up treatment. When you start treatments such as with venetoclax or even obinutuzumab, you start with smaller amounts and then ramp up to full dosing. Why is that?
Dr. Catherine Coombs: It’s different based on the drug. Let’s tackle obinutuzumab first. Obinutuzumab is the monoclonal antibody that can be paired with either venetoclax or acalabrutinib. It can also be used by itself less often. It’s a hugely effective drug, and it doesn’t really have that many side effects except for one that’s almost universal, which is these infusion-related reactions. Of course, it has other side effects such as impaired vaccine efficacy infections. It can cause low blood counts, but the one that’s universal is infusion-related reactions.
Instead of just giving patients their full dose of 400 mg daily, we…slowly introduce it so we’re more slowly killing off the cells in a way that’s friendly to the kidney and friendly to the rest of the body to minimize any potential risks from all this dead cancer cell debris.
Dr. Catherine Coombs
What they’ve learned over the course of developing this drug in clinical trials is that, instead of blasting patients with the full dose on the first day, the reaction seemed to be more manageable if you split the dose. The traditional way of administering obinutuzumab, the full dose is 1000 mg.
Instead of doing that all at once, which would make for a very colorful reaction in the infusion suite that no one nurse nor patient wants to be involved with is giving 100 mg on day one and then the other 900 mg on day two. Then of course you follow along with the rest of the schedule. The reactions, fortunately, are almost always on the first 1 or 2 days and then not long-lasting except for rare exceptions. That’s the reason for ramping up obinutuzumab, to make the reactions more manageable.
Venetoclax is a different story. As Dr. Levy mentioned, this drug is remarkably effective at annihilating CLL cells. But it’s not a good idea to kill any cancer just too quickly, because when you kill a cancer cell, all this dead cancer cell debris gets released into our bloodstream and our kidneys can’t handle that, even the best kidney in the world.
Instead of killing cancer rapidly by administering the full dose, it’s been learned through very well thought out and designed clinical trials that patients tolerate it better with less chance for dangerous tumor lysis syndrome, which is the term for complications from cancer dying too quickly, is to ramp it up. Instead of just giving patients their full dose of 400 mg daily, we give them a little whiff of venetoclax in week one, 20 mg, a little whiff the next week, 50 mg, and slowly introduce it so we’re more slowly killing off the cells in a way that’s friendly to the kidney and friendly to the rest of the body to minimize any potential risks from all this dead cancer cell debris.
Considering the side effects of CLL treatments
Jeff: Dr. Levy, I love the fact that you used the term risk management because that’s pretty much how I approached my entire journey, with risk management. We know that for most people there are going to be some side effects. There’s going to be some challenges when they start treatment. Can you give us a minute on, are they all going to happen upfront? And how do you manage them?
Dr. Yair Levy: That’s a great question. As Dr. Coombs mentioned, for the CD20 monoclonals, most of the reactions occur early and typically improve as you receive more of the drug. This is also true for the oral medications that we have. Most of the side effects, if you look at what’s called adjusted incidence, meaning how likely is it to happen per amount of time, it’s more likely to happen in the beginning. However, as we talked about, some of these therapies are indefinite progression or intolerance.
If you take a look at the cumulative incidence of events that continue to go up, there are certainly some events that are much more difficult to come back from. One that we worry about in particular is what’s called ventricular tachyarrhythmias, so getting a funny heart rhythm can actually lead to sudden death. It’s tough to come back from sudden death, isn’t it? One person’s done it right. They wrote a book about Him. One Person came back from the dead. A very popular book, but nobody else has done it since so we want to make sure that we give patients the safest possible therapeutics that we can.
Reasons to switch a CLL patient’s inhibitor
Jeff: Sometimes patients are told that they need to switch out their BTK inhibitor. There are a lot of reasons why this could be done. Dr. Coombs, can you tell us what’s going on with this?
Dr. Catherine Coombs: That is a common question, and that’s something that’s evolved over the years from having one option, just ibrutinib, to now having multiple options. In my own practice, I actually have switched patients for a number of reasons. I would say the reason that I consider switching a patient off of a BTK inhibitor to a different BTK inhibitor is if they’re having some side effect that’s negatively impacting their quality of life. I have switched patients from ibrutinib to acalabrutinib with very good success. I’ve also switched patients from ibrutinib to zanubrutinib, and I’ve even switched patients from acalabrutinib to zanubrutinib.
There have been studies looking at switching for side effects. About 70% of the time, the patients have improved tolerability on one of the newer drugs. There have been studies looking at switching to both acalabrutinib from ibrutinib and then switching to zanubrutinib from both ibrutinib and acalabrutinib and it seems to be a pretty uniform result where more often than not, the newer drugs are better tolerated than our oldest drug, specifically ibrutinib. I think that’s a very valid reason to switch.
The education point is, I would not switch in the setting of progression. That just is not a strategy that works more than a month or two and it isn’t really worth it. If you’re progressing on a BTK inhibitor of these FDA-approved ones, again, not speaking to switching from any of the approved ones, ibrutinib, acalabrutinib, or zanubrutinib, that is not recommended.
Now, I’ve heard of some occasional doctors just switching everyone off of ibrutinib. I’d say I talk to a lot of the community. I think most of us don’t do that because the side effects that occur most of the time are early on. I don’t use ibrutinib for my new starts, but I definitely have patients in my clinic who have been on it for years and they’re doing well. The old expression is if it ain’t broke, don’t fix it. Some people think, well, let’s just switch everyone. I don’t think that’s wrong, but it’s just not something that I’ve done for the reason I mentioned.
Jeff: Thank you for that. Makes complete sense.
I would not switch in the setting of progression. That just is not a strategy that works more than a month or two and it isn’t really worth it.
Dr. Catherine Coombs
New CLL treatments awaiting FDA approval
Michele: Doctors, there are so many types of treatment and clinical trials. Dr. Coombs, which ones are you most excited about that are getting closer to FDA approval?
Dr. Catherine Coombs: There are two that I’m going to mention. I’m excited about a lot of things, but the ones that I think are the closest to being approved potentially, I have no window into when the FDA actually approves things. One is a drug called pirtobrutinib. This is a drug that inhibits the same target as ibrutinib, acalabrutinib, zanubrutinib, and BTK, but instead of inhibiting it irreversibly, it is a reversible inhibitor.
The reason that that’s important is that when patients develop resistance to ibrutinib, acalabrutinib, and zanubrutinib, the resistance is shared by all of these drugs. So you can’t switch from acalabrutinib to zanubrutinib or ibrutinib to zanubrutinib, etc., if your patient is resistant because they develop most commonly mutations where the drugs bind. Pirtobrutinib binds at a different mechanism. It’s in a different part of the BTK molecule protein and it has shown very excellent efficacy in a very large study. I do think that that may attain FDA approval for CLL in the coming days.
It’s already FDA-approved for mantle cell lymphoma as of January, so there are ways to get it off-label, but I would much rather see it get full FDA approval to help with insurance paying for the drug when it’s needed. It fills a huge unmet need for patients who have progressed on covalent BTKis, especially after patients who have progressed following venetoclax where we don’t really have good options.
The other big category that Dr. Levy has alluded to is the combination of a BTKi plus venetoclax. Europe approved the combination of ibrutinib with venetoclax, which did not get approved in the United States. I can’t really speak about the reasons because I’m not involved with those discussions. I do wonder if some of it may be the toxicity of that regimen, which can be somewhat hard to tolerate, especially for older adults.
But what we know is that we have better BTK inhibitors with respect to tolerability. So there are a couple of trials that are looking at the combination of acalabrutinib and venetoclax that I do think hopefully will be positive trials that lead to FDA approval. That’s the other major category that I’m looking forward to. Those would be frontline treatment. You would use that combination as your first treatment. Whereas pirtobrutinib, if it gets approved, would be a relapsed treatment, at least for now. Things obviously change as time goes on.
It fills a huge unmet need for patients who have progressed on covalent BTKis, especially after patients who have progressed following venetoclax where we don’t really have good options.
Dr. Catherine Coombs
Michele: So your top two are pirtobrutinib and the combination of–.
Dr. Catherine Coombs: A BTKi plus venetoclax.
Michele-Nadeem Baker: Dr. Levy?
Dr. Yair Levy: I agree once again. There are other small molecule inhibitors, again, targeting that B-cell receptor pathway, which has really revolutionized the way that we treat a lot of these B-cell NHLs. In addition, the bispecifics, are certainly working their way into our armamentarium for non-Hodgkin’s lymphomas as well as CAR Ts.
Interestingly, one of the first articles that came out about CAR T was in chronic lymphocytic leukemia, despite the fact that our current constructs, these current autologous derived products are certainly not showing the same level of efficacy in chronic lymphocytic leukemia as they are in diffuse large B-cell lymphoma, for example. Nevertheless, I think that we are going to see some tremendous improvements in terms of the CAR Ts in chronic lymphocytic leukemia as well as the Bispecifics.
CLL doctors’ top takeaways
Jeff: So, Dr. Levy, I’m going to put you on the spot. What is the number one takeaway that patients should be grabbing from this discussion that we’re having today? What’s the top of the list?
Dr. Yair Levy: We’re doing so much better. As I mentioned at the beginning of the conversation, I have not had a patient die of CLL in the past decade. When we take a look at the high unmet need and again, Dr. Coombs was alluding to that. Folks who have progressed on a Bruton’s tyrosine kinase inhibitor and a BCL2 inhibitor are certainly the unmet need. We have a tough time finding those folks.
We’ve had some studies that have been languishing for accrual because it required folks to become double refractory. Again, we have a tough time finding those patients, which is wonderful. I don’t want to find those patients. I’ve put 2 people on in the past 5 years, and one of them was actually not even really refractory. He just wasn’t taking his medication. With CAR T, once I give it to him, he can’t take it, so this was more of me being paternalistic.
We’re doing so much better. As I mentioned at the beginning of the conversation, I have not had a patient die of CCL in the past decade.
Dr. Yair Levy
Jeff: Dr. Coombs, what is the single most important thing that you want patients and their caregivers to take away from this discussion?
Dr. Catherine Coombs: Jeff, we are friends now. It’s going to be hard to narrow down one thing, but I think if I have to say one thing, it’s there is hope. Leukemia is a horrifically scary word to hear for the first time, or maybe even after years of knowing that this is what you have. But all the treatments work extremely well and they work for an extremely long time. There is hope. Hope to live a normal life, and hope to see your kids and your grandkids grow up. There’s always hope on the horizon, in my opinion.
Encouragement for CLL patients to advocate for themselves
Jeff: What can patients and their caregivers do or ask if their local hematologist-oncologist isn’t quite looking at this new wonderful stuff that’s on the plate right now? What if they’re just going with the old stuff?
Dr. Catherine Coombs: That’s such an important question. And, you know, I think it’s tricky. I think it depends on what your personality type is. My personality is that I want to make everyone happy. I never want to offend anyone. I certainly understand the hesitation to question your doctor. But I think in the end, you just have to realize this is your life. If your doctor is not sounding up to date or if you’re just not getting your questions answered, then you deserve more than that.
I just think it’s so important to advocate for yourself or advocate for your loved ones if things aren’t adding up. I think our community docs are amazing. The ones that I interact with, I have no idea how they keep up with everything they keep up with. To put things into context, there are around 20,000 cases of CLL diagnosed a year.
When you think about the common cancers that have a majority of patients, they’re seeing lung cancer, breast cancer – those are like 200,000 plus cases. CLL ends up just being a much smaller slice of what they’re seeing every day, and it’s just very hard to keep up. I would say most community docs I work with very much welcome the second opinion because I can teach them something and then we now have a relationship where they’ll ask me questions and we can work together.
So, number one, don’t be worried about offending your doctor. Number two, most doctors aren’t going to be offended. Number three, if they are, well, I don’t know what to say about that, but I don’t get offended. Back when I was at UNC, I had patients go to Duke and the Duke patients would come to me. Sometimes it’s just good to hear things twice. I think if your doctor is offended, that’s a red flag on their own ego. I think all that we should want as your doctors is for you to get the information you need. That is your job to advocate for yourself, and almost all doctors are going to be totally happy with it. We can learn something from each other as we share in your care journey going forward.
There is hope. Hope to live a normal life, and hope to see your kids and your grandkids grow up. There’s always hope on the horizon.
Dr. Catherine Coombs
Jeff: Thank you for that and I love the way you put it. Patients should not be concerned about asking questions. They shouldn’t be concerned about saying, why not? If they’re having trouble getting along with their doctor, like you said, that’s a red flag.
Navigating what symptoms you should share with your doctor
Michele: We have some more patient questions, so here’s one of them. Sara N. asks, “How do I know when I should contact my doctor between visits? Do they need to know about every infection or just about CLL symptoms?”
Dr. Catherine Coombs: Sara, that’s a great question. I think in the digital age, we certainly can let doctors know about every single detail, but I think it’s good to set up expectations. I try to do this on my first visit or maybe my second visit if we don’t have time to cover it.
But what things do I always want to know about, and then what goes into the other category? I always educate my patients on red-flag symptoms. Things that for my patients on watch and wait, watch and worry, active surveillance, things that make me think, we need to get you in right away. Unintentional weight loss, drenching night sweats, fevers. I go through the list of the things I always want to know about – a rapidly enlarging lymph node, etcetera.
Then there may be other symptoms, and the ones I want to know about are the ones that are worrying you. I don’t want you to go to bed freaking out about something that may be nothing. Just send me a message and I’ll tell you, that’s nothing or I need more information. Maybe let’s have you come in. I’d say, it’s never wrong if it’s something worrying you. But of course, we all have to acknowledge it could get to be a lot of messages if it’s every single thing. I think you just learn that over time as you establish with a doctor, but I think it’s good to go through what things should I let you know about right away, and what things can wait. Then obviously there’s some gray zone where it doesn’t hurt to just pass the info along and then you can get back a message and not worry about that.
Michele: In looking at a patient holistically, so to speak, regarding these little things that we may not think are important, such as all these various infections – I keep getting sinus infections. I’m trying to think of some other types of infections. Maybe you could list those for patients, some of the ones that they might be seeing that you want to know about.
Dr. Catherine Coombs: We do see an increase in infections in our patients with CLL. I do like to get a general sense of how often patients are getting infections. If they have a primary care doctor who’s very responsive, I’m okay with them treating these infections. I’m also okay taking the lead, whatever works best.
But when they become really frequent, especially if it ends up with the patient landing in the hospital, I absolutely do want to know about that. There are some strategies we have to lessen the incidence of these infections.
Patients with CLL, a proportion of them, don’t make enough immunoglobulins. If you’re landing in a situation where you’re having a lot of severe infections, meaning pneumonia that you’re in the hospital for, or terrible sinus infections, etc., that may be a reason to consider this intervention called immunoglobulin infusions.
I definitely like to know about things that I can fix. I’m okay knowing about things I can’t fix too. The ones where it’s like, this would change what we do, those are especially important. The patients may not know that before messaging me, and that’s okay. It’s okay to just message because you don’t know and then I’ll tell you there’s nothing to do or let’s bring you in and talk about X, Y, Z.
I always educate my patients on red-flag symptoms…Unintentional weight loss, drenching night sweats, fevers.
Dr. Catherine Coombs
Jeff: Fantastic. I’m going to make this a little bit personal as far as what I hope people are taking away from this discussion. When I was first diagnosed with CLL, my doctor told me straight up that I was going to die in about 6 years, and that doctor got fired. My next doctor told me, “Don’t worry, we’ve got this. You might die with this, but you’re not going to die from this.”
Listening to both of you fantastic doctors talk about the landscape of CLL and even use the 4 letter word “cure,” I am convinced that I am going to be able to continue doing everything that I want to do, and I want to do an awful lot of things at some point. If my daughters’ are cooperative, maybe I’ll become a grandfather, but I’m going to continue knocking out half-marathons. I’m going to continue knocking out full marathons. I’m going to drink good wine and good whiskey. I’m going to eat well. I’m going to laugh a lot. I’m going to smile a lot and I’m going to share my story so that patients and their caregivers know that that can be their life, too. Michele, how about you?
Michele: I agree some of my key takeaways are that there are so many things in research and we have the potential of being approved in the somewhat near future, which is yet another option for us. As you had explained, it does work in a different way than the traditional types of BTK inhibitors we now have. I think this is fabulous to have yet another option for patients.
Also, I love what you said about what you really need to look for in your own doctor and not be worried about offending your doctor. This is so vital for patients. I ask a million questions and I encourage patients to do so so that they can become more empowered for their own care and self-advocate for themselves.
It’s been so great hearing you and Dr. Levy both talk about patients asking questions and encouraging them so that patients are not afraid of this. This is again, one of the things I had started doing to try to get rid of the mystique around care and treatment with people’s doctors. I continue to do that.
In addition with Jeff – and we’ll be toasting soon, hopefully in person about this with something more than water, which we’ve been drinking during the program – and that is to live life to its fullest and to live a normal expected life span thanks to doctors like you, Dr. Coombs and Dr. Levy. I thank you so much for joining us, both of you and I thank all of our audience members watching us.
Dr. Catherine Coombs: And thank you both for all the work you do in patient advocacy. Like 10, 15 years ago when the Internet wasn’t available, I think there’s so much more fear. To be able to bring light in a way that patients can understand is so hugely important. So thanks for what you do as well and for having me.
Special thanks again to AbbVie and BeiGene for their support of our patient education program all about building shared treatment decision-making! The Patient Story retains full editorial control.
Watch-and-wait strategies can be confusing for both cancer patients and their care partners. The Leukemia and Lymphoma Society defines this approach as “closely monitoring a patient’s condition without administering any treatment until symptoms appear or change.”
But how does this approach affect the day-to-day life of a cancer patient? In this live discussion held in May 2023, we explore everything you need to know about the watch-and-wait strategy, including red-flag symptoms, safe activities, and tips for maintaining good health.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Michele Nadeem-Baker: I am a CLL patient, but I’m also a medical journalist and a really passionate CLL patient advocate trying to help all of us understand better just what CLL is and SLL in everyday language.
So probably like the majority of you, I was pretty surprised when I was diagnosed with CLL and thrown into something called watch-and-wait, which made absolutely no sense to me. It was pretty illogical. The doctor walked in. I had no clue there was anything wrong with me and he said, “You have the C word, but it’s the best you can have.” Doesn’t that kill you when they say that? Nothing made sense to me. How anything with cancer could be the best. And then he told me that he’d see me in four months and then I’d be fine. So all of this was pretty illogical to me, having to grasp all of this at once and understand.
But during this time of watch-and-wait, what I did is I got a second opinion and then I started what you would call front-loading information. I was trying to find out the most credible places to go for information, but also the most current. And that’s something we have to watch out for with Dr. Google. So I learned Dr. Google is not necessarily the doctor, you want to listen to and also to go to find where we can find some credible answers. And so in that time, I also found great CLL specialists, the latest in treatment, and it’s good to stay on top of what those treatments are.
I made sure that I took a lot of stress out of my life. My job was a 24/7 job and when I tell you that, that’s not an exaggeration. I slept 2-4 hours a night — Dr. Rogers, can you believe this? — for years because that was my job. I thought, “I think I need to get a little healthier.” I upped my game on working out and on eating healthy and I started doing yoga and meditating and trying to do everything I could to be the healthiest I could be for when it was time to start treatment. And in treatment didn’t happen for some years.
Jeff Folloder: I am a passionate patient advocate. And there’s a reason for that. The reason is I am living an excellent life with CLL. And my goal, my mission is to make sure that others know it is possible to live a great life with CLL. A little bit about me. I love fast red cars, I love expensive whiskey, and I love sharing stories and learning about this ugly journey of cancer that I’m dealing with and helping people figure out better ways to deal with it.
Catherine Ferguson: My name is Catherine Ferguson.
I live just outside of Boston and am a retired college professor. I’m a vet tech and I work in surgery. And I’m also a CLL thriver — not only surviving but thriving.
Dr. Kerry Rogers: I just love doing this type of thing and I really enjoy talking to my patients in the clinic and I enjoy talking about CLL in general. I’m a hematologist, I’m a physician-scientist, and I’m an associate professor in the Division of Hematology at the Ohio State University. I see people with both CLL and hairy cell leukemia in my clinic and do research mainly in investigational therapeutics. And I enjoy talking about CLL with people, but I also really enjoy college football and was just reminded it’s only three and a half months or so until we have college football back.
Why is watch-and-wait used for CLL Treatment?
Dr. Kerry Rogers: The majority of people diagnosed with CLL won’t need treatment right away. And, in fact, with people getting routine blood work now so often, the most common way to be diagnosed is getting a blood test and then finding out you have CLL without any symptoms. It is very confusing for people when you’re told you have a cancer and most of the things you hear about all forms of cancer is that you have to treat it, catch it early, and be aggressive with treatment, and that’s not really the scheme in CLL.
The reason for that is that we know that treating it earlier doesn’t help people live any longer or any better. So way back when we used to use chemotherapy to treat CLL, there was more than one randomized study where they took people who were recently diagnosed with CLL that did not have any of the traditional reasons to treat it, like symptomatic lymph nodes or blood counts that were abnormal enough to need treatment. So they took people who were asymptomatic or minimally symptomatic with no issues that required treatment and randomized them to either be observed and then get treatment when they needed it or to get treatment right away with chemotherapy. And there was more than one study and this is, again, back when chemotherapy was the thing we used.
Does immediate treatment for CLL/SLL improve overall survival compared to the watch-and-wait approach?
Dr. Kerry Rogers: And, actually, there was no difference in overall survival, which is how long people were living between the two groups. People treated when they needed it or people treated immediately had the same survival so we know it doesn’t help you live longer. And, actually, it looked like there was a slight trend towards shorter survival in people treated immediately because chemotherapy is not overly good for people and they got chemotherapy they didn’t need yet.
The way I like to view it is CLL is not something that we can currently cure with conventional treatments. We expect people to live a very long and rich lifespan with it. And so given that, why expose someone to side effects from treatment earlier? Because the sooner you take it, the sooner you get side effects from treatment. And why expose he CLL cells earlier to agents they could become resistant to, shortening the amount of someone’s lifespan, where they might be expected to have their CLL controlled by targeted agents?
So if you think about it, there are a couple of reasons not to do early treatment because of side effects and the risk of resistance to the treatment. And we know it doesn’t help people live any longer in fact, it might help them live worse if they’re getting side effects. So that’s the rationale on the science side behind watch-and-wait, which I like to call observation.
Is there a percentage of patients that go immediately into treatment?
Dr. Kerry Rogers: That’s a good question. I do think that percentage is probably decreased over the years so I’m sure someone has looked at that as a straight percentage, but I’m not sure that really applies anymore. But it is really the vast majority of people that are in watch-and-wait, at least for some time. It’s a much, much less common thing to need treatment immediately.
Are there ongoing studies with newer drugs to determine if treating early improves survival?
Dr. Kerry Rogers: As a scientific question, they are repeating some of these studies with the newer drugs to see if this is still true, that it doesn’t improve survival for people, which is how long they live with their CLL, to treat early. Those studies are being done. The German CLL study group has one with ibrutinib as an early intervention. And then there’s one that’s occurring in the United States called EVOLVE that’s looking at venetoclax-obinutuzumab either immediately or delayed. We will get more information about that. Because people live so long, it will take over a decade or more to see if there’s a survival difference because people don’t die, which is great. I think that when you think about other types of cancers, like colon cancers or breast cancers, the reason to find them early is that you can cure them. And if you don’t find them and treat them earlier, people die of them.
When you’re looking at CLL, you’ve got a lot of people who, even though they have it, are unlikely to die of it — that’s not everybody, but a lot of people are unlikely to die of it — and we can’t cure it so you don’t get to do treatment and go back to whatever indefinitely, right? If you do treatment now, even with our newer drugs, these still have side effects.
What are the potential risks and drawbacks of treating CLL/SLL early with targeted treatment?
Dr. Kerry Rogers: Anyone that thinks they’re getting treatment with no side effects, you never get anything for free, right? Why expose someone to risks of high blood pressure, diarrhea? And then also we know that once you start exposing CLL cells to these targeted agents we use, there’s an amount of time that the disease will respond before the cells become resistant and their CLL comes back. If you start treatment 5 years before you had to, that’s 5 fewer years where someone’s CLL could be controlled by that drug so you might actually shorten someone’s lifespan by giving them a drug that you didn’t have to by either causing a severe side effect or causing their cancer cells to become resistant earlier.
Understanding the challenges of diagnosing and treating CLL/SLL
Dr. Kerry Rogers: And those schemes for screening, treat early — and I get asked this all the time, “But what if my cancer has spread? What if the CLL has spread? How will I know if it’s spread?” And I’m like, “Okay, this is really hard because it’s a blood cancer, right? So it goes everywhere the blood goes.” And they’re like, “Well, that’s everywhere.” And I was like, “I know,” and it’s so upsetting to think that. I can just see how upset people are by this idea. But for CLL, it’s actually okay. We expect it to be everywhere the blood can go and that doesn’t make it any less treatable or make our therapies any less effective.These conventional things that apply to solid tumors are not really the same as applied to these blood cancers and then there’s a huge difference between aggressive cancers that can be cured or cause symptoms immediately and some of these cancers.
And just for context, I have some patients that were diagnosed with CLL when I was in high school and have never needed treatment and it’s been over 20 years — actually over 25 now; I’m getting old.It’s hard to say that you can improve someone’s life by treating early and aggressively when the last two-plus decades have been them living their lives without anything hurting them from the CLL. So when you see that, then you think. it’s not a good idea to expose these people to things they don’t need. You can’t improve on feeling well, right?
Mental and emotional health effects
Jeff Folloder: The most debilitating part of CLL for me is the mental burden of this. We can be candid with each other. watch-and-wait is not a normal thing for anyone. And when you’re told you have cancer and you’re told you’re going to watch, you’re going to wait, you’re going to have to be vigilant, you’re going to have to go into observation mode, that becomes a mental burden. I will admit that I did not deal with that mental burden very well when I first went through watch-and-wait.
Michele Nadeem-Baker: Jeff had been through treatment. I’m like, “How did you do this? I didn’t have control over what my own body was doing and that is really difficult, especially for someone like myself who really likes to be in control of things. I think I’m doing everything I can. Is there anything more I can do? No, there really isn’t and it just doesn’t matter and that is so difficult.
And also my dad passed away from mesothelioma, a lung cancer. He was diagnosed and in two weeks, he died. So it’s just like, to me, that’s like, “You don’t treat? Oh my gosh, that’s what happens.”I got all worked up there from when I was going through it the first time because you really don’t know what it looks like. You don’t know what it’s like.
Catherine’s experience before front-line treatment
Catherine Ferguson: I dealt with it about the same as you guys initially. When I was diagnosed, I was at one of the top hospitals in Boston, but when they said they weren’t going to treat it, I was like, “Oh my God, I’m going to have to go to Dana-Farber.” So I went for a second opinion over to Dana-Farber and they told me pretty much the same thing.
My personality is I’m a go-getter. I want the plan. I want to get it done. I want to get it started and I want to get it ended. So for the first couple of weeks, it was probably all-consuming for me, honestly. I could have gone down the rabbit hole really quickly.
I look at my dogs and I’d think, “Am I going to outlive them or are they going to outlive me?” But pretty soon thereafter, I had an epiphany where one day, I thought,” I could go walk off the curb tomorrow and get hit by a car,” and then I spent my last days on this earth worrying about when I might die somewhere down the line.
For me, that set something off in my head that life is for living right now and none of us know what tomorrow brings. It’s not a guarantee for anybody. So for me, I try and just live my life. I’m basically an optimistic person in general, by nature. So for me, I try and just believe that] I do the things that I can do for myself and stuff like that. I take care of myself. I listen to the doctors. I get my screenings. I do all the things I’m supposed to do in watch-and-wait. And then I just continue to live my life. I have to say, the second time around, it’s been much better.
How did you cope with the emotional toll?
Catherine Ferguson: When I was first diagnosed, I was diagnosed with intermediate markers. I wasn’t high risk, I was intermediate on the genetic markers and so I knew I was going to likely need treatment. What the doctor couldn’t tell me is when. So I knew that sooner or later, I wasn’t going to be one of those people that was going to go forever without needing treatment.
And so around the 4-year mark, I started to get really anemic. I started getting really, really tired. I had a couple of nodes that were big, but that was it. Everything else — my platelets, my white blood count — was perfectly fine. We found out I was iron deficient so I did iron infusions. It helped initially, but when we rechecked it again two months later, it had dropped again.
Because I didn’t have any other symptoms other than I was anemic, we kind of assumed that it might be the CLL progressing at that point. I had a bone marrow biopsy done and it came back as Hodgkin’s lymphoma from a Richter’s transformation. So Richter’s transformation is when the CLL transforms into something much more aggressive. Usually, it’s not a Hodgkin’s, usually it’s something worse so I actually got the better of the two, if you want to see that. See, that’s the optimism.
I had to do a regular six months of chemo every other week. High-dose chemos. And for me, I’ve been in remission since I finished that chemo and that was five years ago. I have never had any more issues with the Hodgkins or the Richters.
What are some tips for guys dealing with watch-and-wait and how can they learn to talk to people about it?
Jeff Folloder: We’re at a point where I’m supposed to give some pro tips about how guys deal with watch-and-wait. And we’re going to go straight to a poll that Stephanie’s going to introduce in just a second. I’m going to give you a sliver of the pro tip because it’s part of dealing with this whole mental health aspect that we’re going to be focusing on a bit here.
Michele talked about it. She talked about being in control.] Guys, we all try to be type A and we try to always be in control. The answer is not always, “I’m fine.” The answer is not always, “I’m good.” You’re going to need to learn how to talk to people.
How do patients and care partners cope with watch-and-wait from an emotional and mental health standpoint?
Dr. Kerry Rogers: As you were saying that don’t just say, “Oh, I’m okay,” I have people’s partners all the time say, “Will you just go ahead and tell her what’s on your mind? You need to actually tell people what’s happening.” And I was like, “I’m here to listen to you about what’s happening.” I observe that quite a bit. We get so many people now diagnosed at a time when they have no symptoms — their blood tests are abnormal, they get diagnosed with CLL, they don’t need treatment, and they had no symptoms and say they felt perfectly fine and had no idea something was wrong until this happened —for this group of people, sometimes I think the hardest aspect of having CLL is knowing that they have it.
I see people where the worst part of it for them is not physical symptoms, but it’s living with knowing you have it. And I try to tell people, “You’re feeling well from this.” I’ve said, “Based on the disease features, I don’t expect this to be something that shortens your lifespan, even though you might need treatment at some point. Please don’t let knowing you have this ruin your life] Don’t let just knowing you have this fear in your life.”
We have great programs here at Ohio State at the James, like psychosocial oncology, which is mental health professionals that can help with this. I try to offer what I can, but this is something that I don’t have formal training in helping people cope with some of these aspects, which really can be much more impactful on their lives than the physical symptoms of CLL.
I think people knowing they have it can actually be much harder for them than any physical symptoms they’re experiencing. I can see sometimes people that have spouses or partners or caregivers or people in their lives that come to the clinic with them, it’s really helpful because sometimes, something, their friends, family, or loved ones are observing is something they choose to share during the visit and that helps me know that there’s something else that needs to be addressed.I think sometimes it can be hard for other people to know how to support their loved one that has CLL. I find that the majority of people help facilitate some of the communication in clinic and have been good.
Jeff’s experience with watch-and-wait: learning to communicate with healthcare team
Jeff Folloder: I want to share just a little bit about my experience with watch-and-wait I learned through going through all the questions and answers at the hospital that I chose that I wasn’t being candid with my healthcare team. I believe the military says I was exhibiting a lack of candor.
Well, the problem was I didn’t know how to answer their questions. I didn’t know what was important when they said, “So what’s going on? How are you dealing with things? Is there anything that we need to know about?” Things like night sweats. I associated it with my love of Thai food. You eat too much hot chili, you’re going to sweat at night, right? No. Going through all of this watch-and-wait was learning how to communicate with my healthcare team and not knowing what was going to be the tripwire for treatment meant that I was learning new things about communication.
I started treatment when my doctors discovered that my fatigue had become so debilitating that I couldn’t do the normal things I needed to do in my daily life. I couldn’t lift certain things. I couldn’t stay awake long enough. I couldn’t do this. I couldn’t do that. That was the tripwire for, “Okay, watch-and-wait is now over. Now it’s time to move into treatment.”
Dr. Rogers, explain to us what you’re doing with all these questions and answers. What are you looking for? What is happening during this period? And what should the patients and their caregivers be looking out for?
How to determine symptom severity and potential causes
Dr. Kerry Rogers: There are a few things that we always look for. We always check people’s lymph nodes. But just because we found some lymph nodes, it’s okay. It doesn’t mean you need treatment. But if people notice a bunch of lymph nodes everywhere that’s bothering them and keep getting bigger, then that might be important that we should do something to improve that for them. And then we look at the blood counts, which people don’t usually see their blood counts between visits that often and so that’s something that’s really important.
But in terms of what people tell us, it’s always good to hear about how people are functioning. If they have things that are interfering with their professional, leisure, or preferred activities, if it’s fatigue, if it’s something else, we always ask about night sweats. And then if someone’s like, “Yeah, I’m going through menopause,” I’m like, “Right, so that’s cool.”
The difference between normal night sweats and abnormal night sweats
Dr. Kerry Rogers: There are people with night sweats where everyone in bed with them is wet. They’re wet, their wife is wet, and the dog is wet. They had to change all the sheets. That’s actually a problem. And it’s hard because people don’t know that that we think there’s a difference between, “Oh, yeah, my neck got sweaty at night,” because they got hot versus, “Everyone in the entire bed with me is soaked because I’m so sweaty.” Those are the things we try to figure out by asking questions when people like to come to see us. Finding out about night sweats is fine and we can help people determine what might be normal like you were saying, the Thai food versus not really normal, right?
The significance of reporting severe fatigue and sleep issues
Dr. Kerry Rogers: Fatigue is the hardest because there are so many things that can add to someone’s fatigue. Every once in a while, we get someone that has fatigue that’s really quite severe and it’s actually sleep apnea. So we get their sleep apnea treated and they’re like, “Oh, I feel like a million bucks.” And you’re like, “I’m glad we didn’t treat your CLL because of that,” because that’s not going to fix your sleep apnea, right?
Part of what we do when symptoms are reported is not like, “Oh, you have fatigue, you need treatment,” but have more questions about what’s going on, and what might be causing that. One patient I talked to said, “I have fatigue, but I haven’t slept.” She only slept 2 to 4 hours a night. People are tired when they’re busy and they have something going on. A lot of the stuff we look for is not only asking those questions but severity and follow-up questions about some of those symptoms.
What is the average watch-and-wait period for intermediate and high-risk CLL/SLL patients, and does it vary by mutation type?
Dr. Kerry Rogers: The answer is yes, there is. This has been done in more than one study where they’ve looked at the time from diagnosis to first treatment. It’s hard to pinpoint from these studies what will happen to any one person though. So these are studies that look at a group of people diagnosed with CLL and how long between the time they are diagnosed and treated. Then they look at different disease features — so high-risk features like deletion 17p in the CLL,ow-risk features like IgHV mutated status, and then they look at the median. You can think of the median as a little bit like the average. It’s not exactly the same thing, but the median number of times for the 100 people in that group to start treatment.
Dr. Kerry Rogers: For things like deletion 17p, the median in one study was around a year and a half between diagnosis and needing treatment. But within that group, some people needed treatment right away, some people didn’t need treatment for five years. There’s a staging system called Rai staging that can help predict the time to the first treatment. But you never know what’s going to happen for an individual person so I try not to get people too wrapped up in that because you don’t know how it’s going to turn out for them.
Activities, supplements, and exercise
What activities can you do during watch-and-wait?
Dr. Kerry Rogers: I’m going to go with all of them that are recommended for people. People ask me this all the time, “Can I do this? Can I do that? Can I do the other thing?” I’m like, “Yeah, do all of it.” And then they’re like, “Can I do something crazy that really nobody should be doing?” I’m like, “No, don’t do that.”
“Can I drink beer because I have CLL? I like drinking beer and watching football.” I’m like, “Me too. That’s the best.” And they say, “I want to drink one beer watching football.” I’m like, “Okay.” Or they say, “Sometimes I like to drink two beers while watching football.” I’m like, “Yeah, that’s fine. Really just don’t get drunk every day and that’s not because of the CLL, that’s just general advice.”
If you think of someone with CLL, people in observation do live with a higher risk of infection and other forms of cancer. So I do think the COVID-19 pandemic was much more limiting for people with CLL in observation than for the rest of the public so there are a few things like that. But aside from going somewhere where you can’t access medical care if you’re about to need treatment or some really dangerous activities that are not recommended for anybody, I tell people to just go ahead, enjoy their lives, and do whatever they want to do.
How can we extend the watch-and-wait period and slow down CLL or SLL progression?
Dr. Kerry Rogers: Not that I’m aware of. There are a couple of things, right? There’s a study with green tea extract tablets like a high dose that can lower the white count, but I don’t know that there’s any data that really help people live longer or really prolonged watch-and-wait.
There are things that I’m sure help people in general. You were saying you did some things to make sure you’re fit and rested and eating healthier. Those things can make people feel better and be better with their overall health. But I don’t know of anything people can do specifically to increase the amount of time before they need treatment.
Matcha green tea and supplements: Are they effective in managing CLL or SLL?
Dr. Kerry Rogers: Not that I know of for CLL. Vitamin D does have a variety of health benefits. If you’re deficient, getting that replaced is important for other health metrics. But I don’t know of anything specific that will help the CLL. [Supplmenents] aren’t regulated so it’s helpful to go on the Internet and look at some of the companies that rate the quality of supplements before you buy them.
Green tea, it was an extract used in a study. You’d have to drink more than one can physically drink in a day to get the same benefit if you’re going to drink the tea. So if someone wants to try that, I strongly recommend finding a high-quality green tea supplement because it’s just physically not possible to drink that much green tea in a day.
Can jumping rope be beneficial for managing CLL/SLL?
Dr. Kerry Rogers: Exercise is good for people, right? But there’s no data that jump rope actually helps CLL. Probably won’t help your joint health but will help your cardiovascular health. But it doesn’t do anything to impact the CLL specifically.
Managing CLL/SLL Comorbidities
Jeff Folloder: One of the things that I have learned through my 13 years of dealing with CLL, I finally believe my first CLL specialist. He said, “I’m more worried about the comorbidities than I am about the CLL. If you will actually put time and effort into taking care of those comorbidities, you’ll actually make my job easier.” So I have embraced that.
I know it’s going to sound pedantic, but you can exercise more, you can eat better, you can eat less, and you can do all the things that you need to do to reduce your comorbidities. And, truthfully, there is no upper ceiling for it. I’m currently training for a marathon. I’m relapsed and training for a marathon, so yay.
Dr. Kerry Rogers: Modifying your other risk factors for your other health conditions because that is something everybody can do in watch-and-wait. And I would say more people with CLL my clinic die of heart attacks than die of CLL. So just please keep that in mind. And, of course, keeping up with cancer screenings and vaccines is very important.
When to start treatment for CLL/SLL
What are the indicators that it’s time to end watch-and-wait and start treatment for CLL/SLL?
Dr. Kerry Rogers: There’s a group of people where they have no symptoms, lymph nodes aren’t big, blood counts look fine, and you say absolutely there’s no reason whatsoever to treat this person. There is no cut-off on white blood cell count where you need to do treatment. I do think if you get above 400 or 500, usually other reasons develop and it’s about time, but there’s no cutoff like, “Oh no, my white count hit 50. We need treatment.” That’s not a thing. And yes, there is a thing with doubling, but that’s only with higher white counts. So it’s not like, “Oh, it went from 10 to 20, I need treatment.” That’s not a thing. You can actually be very flexible with the white blood cell count. Don’t think of a hard number there.
There are people who I think could be ready for treatment.] The blood counts are going in the wrong direction so you can see the hemoglobin and platelets are dropping, white counts going up, and lymph nodes are getting big, but they’re not actually really problematic for the person. Maybe they’re having some fatigue so there’s a window where you could say like treatment’s reasonable.
The span from, “We shouldn’t do treatment,” to “We should have done this sooner,” especially for a first treatment can be over a year. You’ve got a very long window and that gives you some time to decide, along with your doctor, what treatment’s best for you and things like that. It’s uncommon that you hit something and you need treatment tomorrow. It’s more like an ongoing discussion for a while.
The things I see that I notice sometimes are, “The white count shooting up pretty fast, along with the hemoglobin and platelets kind of dropping.” Or every time people come back, there are more lymph nodes and they’re losing some weight. There are a lot more lymph nodes and you see this trend happening. And then I do see some people that develop a lot of fatigue that suddenly starts to interfere with their personal and professional activities and that would be a reason to say, “We should really do something before this really impairs your life more.”
Are there any specific signs to watch for?
Dr. Kerry Rogers: Every once in a while, I have a patient who develops a significant health concern that they think is in another area, like severe diarrhea or chest pain, that’s not addressed by going to like their cardiologist or something else. When people develop health concerns, weird symptoms — and not like, “Oh, my toe is itchy one day and then it’s not the next day,” that’s fine; that happens to everybody – something significant, impacting their life, weird that maybe other doctors they thought might help them with this can’t figure it out, that is always something to check in and ask, “Hey, could this be related to CLL?”
Because there are some weird things that happen to people with CLL and certainly the physician caring for anyone with CLL should be able to figure it out. If anyone develops weird health concerns that are really symptomatic or problematic that other doctors can’t figure out, always a good chance that it could be CLL related and you should check in.
Does CLL increase the risk of other cancers?
Dr. Kerry Rogers: Yes, it is true. CLL is a cancer of immune system cells called B lymphocytes so it changes the way the immune system works because the CLL cells are there. By the way, treatment to reduce the CLL cells doesn’t fix this — only makes the problem worse. Your immune system is what protects you from other cancers by killing abnormal cells that your body forms as it makes new cells over time so cancer screening is important.
The top ones we see are actually skin cancers and, of course, lymphomas, as was pointed out earlier, do occur in people with CLL but those are kind of related types of cancers. But skin cancer’s actually one of the top ones so I try to get everyone’s skin cancer screening.
Side effects of treatments
Fatigue caused by CLL treatment
Catherine Ferguson: That was the worst part of it for me, honestly. I could deal with any of the other side effects even when I just finished a clinical trial a year ago. I’ve been undetectable MRD and in remission now for a year and I feel so much better. But that fatigue, even during treatment. Everybody said once you start treatment, the fatigue goes away, but I still had the fatigue even during treatment till I got off of the meds.
I work out a lot and I went to the gym every day and I tried to just keep up my routines. I’m generally an active person anyhow so I try not to give into it.
For a time period there, I would fall asleep while I was working on the computer with my hand on the mouse and my wife would look over and say, “Cathy,” and then I just wake up and I’d start to keep on moving again like I didn’t do anything. But I didn’t decide I was going to take a nap; I would just fall asleep. It’s just really hard.
How do new CLL/SLL treatments differ from traditional ones and what are some of the latest options available?
Dr. Kerry Rogers: I like to say that about a decade and a half before this kind of chemotherapy or chemoimmunotherapy, which is chemotherapy with an antibody works real well. In last decade and a half have been all about targeted agents. We actually no longer use chemotherapy to treat CLL. We do use it to treat other lymphoma successfully, but the whole name of the game is oral targeted agents and these are drugs that interfere with proteins in the CLL cells that make them behave like cancer cells.
The two main classes of drugs are something called BTK inhibitors and venetoclax, and they are extremely successful with virtually everyone achieving a remission, and just work very well.
The field is currently looking at newer generation agents of these different dosing schemes or different combinations to try to make treatment more effective but also easier to do for people and to have fewer side effects.
Is it crucial to see a CLL specialist immediately after diagnosis, or can it wait?
Dr. Kerry Rogers: It’s actually an individual decision. There are some reasons that people actually definitely need to see a CLL specialist. One is just if things aren’t going well, right? So not responding to treatment, developing side effects, not being offered acceptable options from your general hematologist oncologist — things aren’t going well, always see an expert.
Some other good times are planning a treatment, any treatment, because, usually, the CLL specialist will be able to have a good and, hopefully, more detailed discussion about treatment options or even offer participation in a clinical trial, which has a lot of advantages. But this doesn’t always have to be done at the time people are diagnosed just because if you’re in watch-and-wait and you’re happy with what’s going on,] it doesn’t mean you have to run out and see a CLL specialist right away, especially if you don’t live near a CLL specialist.
If you live in Boston, it’s very easy to go see one of my colleagues at Dana-Farber and other excellent doctors in that area. But if you live in rural Ohio or West Virginia, we get people that come from West Virginia. It’s like a three-hour drive so it’s a big burden to do that right away
And then I guess at diagnosis, one of the main reasons to see a CLL specialist is to get questions answered and to learn about CLL, which I think benefits all people. Most people do want to learn more about it, but there’s] a group of people that cope by putting CLL from their mind and they can certainly delay seeing a CLL specialist until there’s a reason like needing treatment.
Stephen Brown’s Chronic Lymphocytic Leukemia Story
Stephanie Chuang Interviewed July 9, 2021 Updated September 18, 2025
Stephen Brown was 45 years old when he felt his first symptoms that sent him to the doctor. After seeing specialists and undergoing several scans, he was diagnosed with chronic lymphocytic leukemia or CLL.
Now on ongoing targeted therapy, Stephen shares the details of his CLL diagnosis story to help others go through their own CLL treatment and experience.
From being a very fit and active triathlete, Stephen started feeling the first symptoms of what changed his life forever – getting diagnosed with CLL.
Explore his story below and hear about his experience, including some very important messages to the patient-caregiver community.
Life Before Cancer
I am a very multi-faceted guy. I’m 61 years old, a happily married father of two girls, and grandfather of four kids aged 2 to 11.
I reside in suburban Philadelphia, work for a Wells Fargo bank. That’s my professional side.
My passion side has always revolved around multi-sport racing, triathlon, marathoning, multi-sport activities, and things like that, including having been a running coach and a triathlon coach for many years before that.
I come from a soccer background, went to a local college on a soccer scholarship, and then continued to play high-caliber soccer for several years until I discovered the beauty of multi-sport racing and marathon.
Some people would have a real problem with me calling that beautiful because most people look at me and say, ‘Why in God’s name do you do what you do?’
But for me, that’s my passion. That’s fun for me.
First Symptoms
It was late 2005. I was experiencing several symptoms, including fatigue. The most prominent one was a difficulty in swallowing. I was just feeling generally crumbled. But here’s the backstory:
2005 was a horrible year for our family. My father had been hospitalized, had a near-football size tumor removed from his pleural cavity, never made it out of intensive care, and passed away a few months later.
I was registered to race a full distance Iron Man triathlon that July 2005, which I had a whole lot of trouble getting to, but my family insisted that I go to. That was kind of contributing to my overall fatigue.
So when I talked to doctors and describe the fatigue, they asked me what my lifestyle is. And they said, “Well, you just went out for a hundred-mile bike ride. You’re going to feel a little fatigued.”
But to me, I knew something was off. Something was just not quite right.
So like many guys who maybe are not quite as diligent as they should be with keeping up on appointments, as long as they’re feeling okay. Maybe I was not ahead of some blood work the way it should have been. I wasn’t ahead of some preventative appointments and things like that.
First doctor appointments
When it came time to try to figure out why I was having this difficulty swallowing, it took several phone calls to my primary care physician. And we tried chasing the symptoms, not thinking it was anything evil; thinking it was something simple.
We tried antibiotics, steroids, or anti-inflammatories, just trying to figure out what was going on. Finally, none of that work. He referred me to an ear, nose, and throat specialist.
The ENT specialist took a look at my throat. Granted I’m 45 years old at the time, the ear nose, and throat doctor said, “Those tonsils are the worst things I’ve ever seen in my life. We would have gotten them removed yesterday.” Which made sense why I was having difficulty swallowing if I’ve got these two large things in the back of my throat.
I scheduled pre-admission blood work for the surgery for the tonsillectomy. And I got a call that nobody ever wants to get from the surgeon saying, “We came across a little bit of a problem with your blood work. We’d like to refer you to an oncologist before we proceed. Do you have an oncologist?”
I’m looking at the phone and thought, why in God’s name would I have an oncologist? I’m the healthiest person on the planet.
One thing led to the next. My wife was a nurse in a local practice. She knew how to get us to the front of the line of a preferred practice. And then we asked for the first available physician within that practice and met the guy.
I can remember the dates like my own birthday.
I met him for the first time, February 17th, 2006, at which point it was more of a consult. He said, “Let’s review the original blood work, consider some possibilities. And then let’s order every test under the sun to try to figure out what’s happening.”
So from February 17 to February 24, I had everything you could possibly imagine doing. And then February 24, 2006, I received my official diagnosis.
Breaking the news to the family
My wife and I obviously were fully engaged in every conversation with any medical professional.
My initial reaction and what I told my wife was, “These people are crazy. Something’s not right. And it has nothing to do with oncology. Somebody is just not looking at the right chart.”
I was convinced that the diagnosis isn’t right. The patient chart is not right. There’s something that doesn’t add up. It has to be as simple as an infection that they’re missing. Somebody’s missing something.
I guess you can call it denial, but I was convinced that I’m right, and everyone else is wrong and there’s no way this could possibly be oncology. But I agreed to play the game, to check all the boxes and rule everything out, which is why we had the conversations that we had. Thankfully we had the conversations that we had.
You know your body more than any other doctor is gonna know your body. You, we, the patient community just need to be fully dialed into what you’re feeling, to any changes in routines, any changes in diet, any weight changes, any changes in anything. You’ll know because you’ll feel it.
One of the first things my oncologist asks me when I check in every three months and we draw blood and I immediately want to know what he’s looking at.
He says, “No, timeout, tell me how you’re feeling.” Because that’s such an important indicator of your overall patient health. So I think it’s really important to pay attention, to listen to your body.
One of the things my oncologist told me was, “As you’re going through treatment, be smart. Listen to your body. If you feel that you can carry on with a run or with a workout, do it. But if you wake up one morning and you’re fatigued, pull the plug, go home, get some rest.”
I think people don’t put enough trust or faith in their interpretation of their own body and their symptoms.
They tend to want to put everything on the shoulders of the medical experts who, yes, can look at the diagnostics, can evaluate you, in some cases, in meeting you for the first time. They’re going to know something, but you’re going to have a lot of the missing information.
You’re going to have a lot of missing pieces and you need to speak up. You need to be that advocate for yourself to say, “Nope, something doesn’t sound right with what you’re saying because it’s not jiving with what I’m feeling.”
CLL Diagnosis
Diving deeper into his story, Stephen shares his insights about patient self-advocacy, and how he managed processing the news of cancer with himself and loved ones.
First oncology appointment
That was a very powerful first meeting with that doctor.
At that first appointment, he ordered for me a CT scan, a PET scan and a bone marrow biopsy, more blood work, and X-ray in the course of a week, and said, “Let’s get you back here this time, next week.”
He was ready for me to walk out but I said, “Hold on, I need to know what are we chasing? What are we ruling out? What’s the game plan here?”
And that’s the very first time I heard the words chronic lymphocytic leukemia.
I knew of leukemia. I knew of lymphoma as blood cancers but I did not know the different types of nuances. I had never heard of chronic lymphocytic leukemia.
So that was the first time that I’d heard and explained to me a little bit about what it was. But truthfully, even he, at that stage of the game was saying, “I don’t think that’s what we’re dealing with, but we need to cover all our bases and we need to make sure that we can rule that out.”
I’m getting ready to walk out of the office and my wife says, “Well, maybe we should let the doctor know a little bit about your lifestyle in case he wants to make any limitations or changes.”
I looked at her andtold her I don’t want to tell him anything. Because what if he ended up taking something away from me and I don’t want that. But I did and I told them what I do for fun.
I told him that I’m an endurance athlete. I race marathons, triathlons, and Iron Mans, and this is what I do for fun. And this is what I do to feed my soul. And his first reaction was, “It’s probably a good idea to give that stuff arrest for now until we figured this stuff out.”
I was ready to walk right out because I just didn’t think that that was the right approach or the right doc. But we talked through it some more.
That’s when we reached the middle agreement and said, “Again, if you’re feeling fatigued, I don’t want you to do anything. If you’re feeling good, you have some energy, then, go for it. So it was a little bit interesting.”
Navigating the conversation with your doctor
I think it comes down to this: if you are not your advocate, no one’s going to be your advocate.
You have to know what your passions are and you have to know what drives you, what’s important to you. And if someone’s going to say to you, “don’t do any of that anymore while I figure this out,” it needs to be a conversation.
You need to remain true to yourself. You need to remain true to your own spirit and your own soul and figure out.
You should be able to say, “If you’re really telling me this, let’s understand why, and let’s figure out if there’s a middle ground.” And that’s what we ended up doing.
I understood where he’s coming from having. He didn’t know me. He was taking the ultra-conservative route but I’m not an ultra-conservative person. So I said, “Let’s align ourselves here and figure out what we can do.”
Fast forward many years after, at the time he thought I was completely out of my mind because of my lifestyle. But today, he’s a runner and he blames me for that.
Every time I go in for my appointment, one of the first things we talk about is how our runs have been going.
I just think it’s the coolest thing because we’ve both come full circle—I’ve become kind of a CLL expert, he’s become a little bit of an athlete, and that doesn’t happen every day. I think that was a cool exchange of whatever that we had.
Understanding your diagnosis
I made the mistake after that first appointment of going home, opening my laptop, and Googling CLL.
Another key piece of advice to never ever do is don’t just blindly Google your disease because for every one good resource website out there, there are going to be fifteen garbage ones.
That’s going to ultimately steer you down the wrong path and give you some wrong information and can really wreak havoc on your confidence and your psyche.
The first couple of hits that I came up with were memorial pages that were set up by loved ones who lost someone to CLL. That was my first foray into CLL.
So I closed the laptop and thought I was going to die. I walked away. I thought this isn’t going to be good.
After the fact, I said to him, “Can you give me some reputable sources? Can you give me some good links, some good organizations that I can stay connected with, that I can do my own research, my own homework, that I can understand more about my disease?” That’s a key takeaway for everybody.
You have to, you have to learn about it, but you can’t just do it blindly. You need to ask for trusted resources.
Managing “scanxiety”
A test is a test. It’s not always the be-all, end-all to anything.
You need to have those scans and tests to help paint the picture. It contributes to the information. It helps with the ultimate decision-making. It’s really important that they get evaluated appropriately, and properly by the right people, and discussions are had around those two.
In other words, if your PET scan showed this, let’s talk about that a little bit more. Feel free to say, “Tell me what you saw in that scan that was frightening or concerning, and what are some other possible things that might present that same type of concern.”
I also understand that at that point, I still thought everyone else was crazy. So I was just going through the motions, satisfying everyone else. And I thought at the end of the day, I would come back with getting an apology from everyone and say, “Oh my gosh, we’re so sorry to alarm you. Take two of these and you’ll be fine in a month.”
But that wasn’t the case. I think the big thing for me was having to take it in stride. You can’t overreact to any single test.
It’s just one piece of the puzzle. And it’s a puzzle that might have several different ways of coming together. You just need to maintain a sense of being open, a sense of positivity and a sense of hope.
Processing the news of cancer with the family
Dr. Shore had all the results right there in front of them. He ran through the different results saying conclusively, everything confirmed the same thing. That hunch that we had from the elevated white count from the ear, nose, and throat tonsillectomy guy—everything else painted a similar picture.
That’s when he said, “There’s little doubt that I was looking at anything other than chronic lymphocytic leukemia. This presents itself as a classic case of CLL for a number of reasons.”
And he talked about the size of the lymph nodes, the white count. Little did I know that I felt the tonsils, but the rest of my lymphatic system, like my spleen, was enlarged. All my unseen lymph nodes were also oversized. And my white count was up around 70 or 80,000.
It was what it was. You listen, you hear the plan, you hear the protocol.
And he said I’m welcome to talk to any number of other people, which I did. But I also didn’t want to waste time. So I moved ahead with his plan of treatment, at least, getting that stuff scheduled.
I then quickly ran home, reached out to some other folks, to a doc in the University of Pennsylvania, to another doc I knew and I was close friends with within the multi-sport triathlon world.
I sent them my results, talked about protocols, and standard care for CLL. Without even seeing them, I kind of rallied my team that way. And they were all on board with a diagnosis and the plan of attack.
It’s hard to just give examples of when it might be warranted and when it might not be. But I would say, in most cases, it definitely warrants a second opinion.
As much as I love my doctor, he’s human. And I was meeting him for the first time. So there are good auto mechanics and there are bad auto mechanics.
There are physicians who might be really good at diagnosing this kind of thing. And there might be guys who are not. So it was critical that I had a conversation with multiple physicians
If the doctor has your best interest, first and foremost, and if the doctor is what he should be, he would embrace that. He would welcome that.
In fact, he would even help facilitate that and will potentially give you some names and some contacts for you to reach out to have that second opinion.
And if he’s really good, he’s not only going to help facilitate the conversation, you will allow those two physicians to get on the same page. And if it’s a matter of hashing something out medically, they will do that.
I had that happen personally. If my primary guy needs to recommend or refer something, he’ll say to me, “I don’t want him to do that until we talked to Dr. Porter who was in a totally different network but is very much an expert in this field. They would often bounce ideas off of one another in terms of my treatment and care.
1st Line Treatment
With a positive outlook, and by taking it moment by moment, Stephen was able to get through longer-term treatment, including two years of rituxan.
Undergoing Chemotherapy
What I learned was it’s a very cyclical process. And it builds a cumulative effect on your body.
I remember the first couple of days of treatment walking away thinking nothing. In fact, I felt so good early on in the first couple of days of each cycle that I would run home for my chemotherapy treatments.
And I did it for a number of reasons. It made me feel good. It made me feel physically and mentally good. I thought it showed my loved ones that I must be okay if I’m still doing the things that I love to do.
But as the week wore on and the toxins accumulated in my body, by that Thursday/Friday, I was pretty beat up. All it took was one cycle to realize that Monday, Tuesday, Wednesday are kind of scratch days; Thursday, Friday, I’m out. The weekends not great, but up by Monday, the following week, I’m not bad again.
So once I was able to digest that fact and I knew what was probably to be expected and I can predict and plan on that, I was able to do that.
I didn’t overthink the days. I felt bad because I knew I was going to rebound and I knew that it was cyclical.
And I also knew that they do such a great job of pre-treating with a number of different cocktails, supplements, and other things to help offset anything that you might be experiencing.
I think people have this image of a chemo suite as this dark dungeon of hell but I had the exact opposite experience. It was upbeat. It was positive.
The oncology nurses that I worked with were saints. They did everything humanly possible to keep my spirits up, to keep me feeling good physically, to make sure I didn’t need something to drink or eat.
It made all the difference in the world. I just had a pretty positive experience throughout the whole thing. I had my moments, but for the most part, it was good.
I knew about that. And truthfully, the idea was a little daunting for me in the beginning.
I could wrap my head around the initial four rounds of treatment. That seemed moderately tolerable for me to comprehend. But when I thought of two years of follow-up every six months, getting five more doses of toxin, that set me back a little bit.
That took some time to wrap my head around. But at the same time, I didn’t need to think about it until six months after I was done that last round.
I didn’t overthink it until it was time to go back in.
Truthfully, by that time, I felt great again. I was hundred percent of my own self again. I understood what the Rituxan was going to do and how I was going to respond and how my body would cycle through it. So I became okay with it.
You just have to be patient and just work through it and you’ll get there. You get through it.
The smiles on some of my pictures are not anomalies. That is pretty much the approach I tried to take throughout any treatment when I was in the chemo suite.
In fact, if the nurses didn’t see me smiling or making a joke about something, or if they saw a serious look on my face, they’d come over and they’d want to know what’s wrong.
That became an indicator that I might be tanking because I’m being serious. I tried to be as upbeat as I could throughout.
Long-term Treatment
He didn’t put a timeline on it, but he did say that this is going to buy us a whole lot of time.
If we’re really lucky, it’s going to buy us a whole lot of time, but it’s not going to buy us forever.
It’s a chronic condition that it’s incurable. There’s no known fix for it today. So at some point, we’re going to have to revisit it. But the hope and the goal were to be as definitive as we can with the initial sweep of therapy to really knock it way back, down, and off the radar as far as possible so that we don’t have to have this conversation again in the near future.
While staying focused and positive, and with the support of his family, Stephen confronts relapse and moves on from one treatment to another.
Follow up Protocol
Visits to Oncologist
I see my oncologist every three months for the last 15 years, as long as things were okay. But anytime there was, at least, a little bit of a hiccup, it could be a month. It could be six weeks when he’d say, “I want to check your blood again in one month, come back.”
Three months is what we hope for. It’s never any longer than that. I think every once in a while, I’ll bargain for four months.
He’ll joke with me when I leave. When he asks when do I want to come back, I’ll say, six months. And he’ll say, “Okay, I’ll see you in three.” It’s not a negotiation but he says it anyway.
Second Line Treatment
Steroids (dexamethasone or prednisone) were always the go-to bandaid when things would start to escalate a little bit. But not to the point of needing a full-blown treatment.
If the white count is elevated, or the lymph nodes are starting to flare up again, I’d take that. If we got some swelling, we’d do an MRI, and if we’re seeing some things but not worth going through putting the body through the full treatment, we’ll try to get a handle on it with some high doses of prednisone, or Decadron, on the interim basis.
And hopefully, that’ll knock it off the grid or, or just see how we do from there. I’ve been through several rounds of both of those drugs over time.
And I’ve developed a love-hate relationship with both of them; probably hate Decadron and love prednisone more, but that’s just me. The love-hate part is where I totally recognize the benefit and I see how well it works.
When I’m on Decadron for a couple of days, I’m awake throughout the night with enough energy to build a house. And then at some point during the day, I start to bunk and I don’t know what to do with myself. And then I’ll crash and I’m all mixed up. My cycles are mixed up. I get a little cranky.
They all come with a price tag. But they work tremendously well. So you have to just accept the whole package. If you’re going to accept the treatment, you need to accept what comes along with it.
Dealing with Steroids
Stick with “eating chocolate.” And by that, I mean those things in life that make you feel really good and make your eyes roll and back your head, and you say that’s delicious.
Whatever that is for you, if it’s needlepoint, gardening, birdwatching, or running marathons, if you can keep up some level of something that makes you feel really good about yourself, that’s going to help offset any kind of emotional stress that any of this stuff is putting on you.
As far as the physical stuff goes, again, it’s a cycle. You’re going to stay awake.
One thing I learned very early on in my triathlon and marathon-running days is that you’re probably not going to sleep very well the night before a race.
It’s just a given. So stop putting pressure on yourself that you need to fall asleep immediately. You’re going to stare at the ceiling and you’re going to toss and turn.
It’s the same thing on Decadron. I’m not going to sleep tonight so I’m going to rest, have my feet up, and just relax. I will read and put on some relaxing music. I will do something that will help level me out, even if I don’t sleep soundly.
That’s typically the kind of rest that will, at least, get you through for a little while anyway.
Getting Through It for the Long-Term
It sounds like a negative thing that one has to get over. How about we flip it and say, “I’m fortunate enough to be tightly tethered to my oncologist that every three months I know the state of my health. Not everybody walking the planet can say that.”
That’s how I chose to view that. I’m safe. And if the doctor were to say to me that I should just come back next year, I would say, “Wait, what? No, I need to see you sooner than that because I need you to tell me that I’m okay.”
Addressing the Relapse
Symptoms started to reappear. Same types of problems—difficulty swallowing, swollen lymph nodes.
This time I was experiencing some night sweats, and other classic symptoms.
But he just didn’t want to venture down the same path because he felt like we had already gotten our money’s worth out of that previous treatment. There were so many other really good things in the pipeline and already in-flight that he wanted to venture down that road.
So he was the first person to bring up Bendeka.
Every appointment, we will talk about what’s in the pipeline. Like, “Have you heard about the next generation of this drug?” So I have a little bit of an understanding of some of the things that are coming.
When he said Bendeka is probably the next logical path, I had full faith in him at this point and I was willing to take the leap with him.
It wasn’t even a full year that I was on Bendeka. It was four-weekly cycles. We didn’t even get all the way through the fourth because my blood work overall had plummeted after about three and a half. So we ended up not finishing that fourth.
But I think in many cases that the fourth cycle is at the oncologist’s discretion. Based on what are the results, how the patient’s feeling, what we are seeing. And he had seen enough.
The results were pretty definitive that we’re getting the response we need. He said, “There’s no need to put you through this for another few sessions. Let’s just pull the plug now.”
I kept the port in for a couple of months while we made sure that it was gonna remain at bay, which it did for a few months. And then I was the first one to say, “Can we please take this thing out?” Because I was conscientious about it.
It doesn’t look exceptionally big, but you know, it’s there and it doesn’t belong there. It just made me feel kind of awkward.
I was on the operating table, having it removed. The same doctor who put it in took it out.
At the time I felt, “Hey, this little device that’s inside me was very powerful. It delivered what it needed to deliver and helped put me in a good place.” So I was in a mild twilight for this procedure. Just local anesthesia or some numbing on my chest.
As the doctor’s getting ready to go in, I said, “I have a favor. Can I have that when you take it out?” And he said, “What? You want your dirty port from inside your body?”
And I said, “I want to take it home and put it in my trophy cabinet. And he said, “There are strict hospital policies about that.”
The next thing I know, as he’s finishing up, I hear him turn to one of the nurses in the room and said, “Would you please take this thing, go clean it up over there, put it in this vial, slide it under his sheet.” And he mums the word.
I have my port in my cabinet. I just thought there was another chapter of the story. When I can do little crazy things like that, it makes me feel as though I’m one step ahead of the disease, because I’m almost mocking it.
Having Support and Caregivers
It was critical. For me, it was important that I had loved ones nearby.
You might not get the same answer from everybody because some people just prefer to live this more privately. I’m not advocating anyone to go through it in a complete vacuum, a hundred percent by themselves.
But I’m one end of the spectrum.
I was very public about this. And I continued to be very public about it. I will climb to the highest mountain and preach about what I went through, how I did it, how we can advocate together, and how I can help others.
But then there are some people who will say, “Look, I just want to show up, get my treatment, go home, not talk about it.” And you have to be respectful of that, too.
I don’t think there’s any standard formula for how this all has to work. But I think it’s really important that everyone at least has someone that they can talk to.
Maybe it’s family, maybe it’s a professional. Maybe it’s a faceless person through one of the organizations that partner patients and mentors because then they become faceless and they can offer some advice and some help in that respect.
But again, everybody needs somebody, but to varying levels. No two people are on the same level.
It felt different only that it was a different method.
I just feel like it was a different chapter of the story.
I don’t think my body necessarily felt any difference or responded differently. Maybe the whole routine became different, but I just thought that was part of the evolution of treatment.
This Bendeka wasn’t an option when I was diagnosed, then it was, so we moved on to that. And then at some point, we move onto the next thing and the time is right.
Targeted Therapy
Learning to value the here and now, Stephen lends his experiences and insights to getting ahead of his cancer, saying yes to a newer treatment, how he managed the side effects, and why he finds it so important to use his voice to help others.
Pursuing More Treatment
Even though I was living my thing, feeling good and all systems were normal and go again, I was still having those appointments every three months just to confirm that I’m okay. I needed it.
But my doctor and I have always had those conversations—about what’s next. Even if the topic of conversation isn’t, we would.
We’re going to have the conversation anyway because that’s just the way it is. That’s the nature of the beast with a disease like this.
My doctor said, “I’ve got several people or a lot of people on this. The practice has had great luck with it. I think if and when the time is right, that’s probably going to be what’s next for you. But I have to warn you, it’s a little pricey. So we’re going to have to work through all that if and when the time comes.”
That’s how we framed it for me. But it wasn’t until several months, a year, or maybe even longer before he said, “I think it’s time because symptoms have come back. CT scan revealed more lymph node movement from the prior and white count was on the climb.”
I look at it like this: you keep going to the same restaurant. And every time you go in there, there’s a new menu, which is pretty cool. It keeps things fresh and you’re not going to get sick of the same food because you’re looking at something different every time you go in there.
That’s been the options whenever I walk into the oncology office and I need treatment. Like, “What is the special of the day?”
And by day, I mean, what’s the protocol for this period of time? And at this time it was Imbruvica. That was the hot drug. And we took a shot at it.
Going into it, at the back of my head, I’m thinking, I don’t know what this is going to feel like.
I read the potential side effects. As with any medication, like when you watch a TV, any ad that you see on TV, you’d hear the disclaimers and you think, “Oh my God, I’m never going to take that! The side effects are going to kill me before whatever I’m being treated for kills me.”
I was a little concerned about some of the side effects that I have read about but they were the standard cookie-cutter type.
But I experienced basically none of them and I was extremely happy about it. I was able to maintain my lifestyle and keep going with what I was doing. It was literally a good call.
There was literally one small pill taken once in the morning. There was only one other supplemental drug I would take with it called Allopurinol. And all that does is help the body rid some of the toxins that accumulate, similarly to a patient with gout or with some other disease where they need to rid the system of that stuff.
Now it’s three years in and it’s just been a very positive experience.
I filled the prescription right there in my oncologist’s office. I can run down to pick it up and run back home again, which gives the ultimate feeling of empowerment.
Okay, yeah, maybe I have leukemia. Maybe I had to go pick up my targeted therapy drug, but you know what, I’m kicking its butt because now I’m running home from picking out my drug. And now I’m just going to settle back into my lifestyle.
More Treatments on the Horizon
His hunch was by the time we need to have that conversation for real, whatever we talk about now, it’s going to be yesterday’s news. There’s going to be something else that’s more relevant.
I’ve done a lot of work aligned with leukemia and lymphoma society. So I see a lot of those announcements of things that have been passed and funding that has taken place.
I thank God every day that I am where I am at this point because there have been so many options available. Maybe you don’t have the solution that you need today but you’re going to have your solution.
Every day that I’m not being treated or every day I’m in remission and not in need or not in a dire situation is me winning.
Six months, a year, or two years from now, you might have to go back into that same restaurant. But when you open that menu, you’ll be like, “oh my God, where all this stuff comes from?”
And that’s just going to be the way it is.
Things continue to evolve. Things get perfected. Research gets better. Funding gets better. Solutions get better. It’s an okay time to have blood cancer from my perspective.
When my doctor and I first started talking about Imbruvica, he did mention to me that it can be costly. But I was fortunate that the stars aligned in that by the time I really needed it.
It had become more mainstream. Insurances started to pick it up and it became the perfect storm for me. Essentially, it was fully covered by my insurance program.
But I also learned that if you’re on any kind of high-end, very expensive medication, many of the manufacturers themselves have different co-pay programs.
Typically, you’re not eligible if you’re on any kind of Medicaid or Medicare insurance. But if you’re on conventional insurance, whether it be subsidized through your work or private pay, there are organizations that facilitate these programs.
You have to apply for it and meet certain criteria, but essentially you can be qualified for a copay plan of your medication, which I didn’t know existed.
I actually signed up for that with the urging of the team at my doctor’s office. They’re the ones who made me aware of it. They said, “We’re going to sign you up for this. And then we’re just going to wait and see, who’s going to offer the best coverage.”
We actually used that to now with my wife on a different medication. They’re offering the same thing but not oncology-related. Just search co-pay for that drug, and you will ultimately find it.
Dealing with the Side Effects
Don’t overthink what you read and communicate what’s real.
They have to give you a warning of what might happen. But that’s for a fractionally small amount of time in a very small population of patients. They just have to go on record. They have to document and publish them.
My doc said, “If you start feeling anything that makes you feel uncomfortable, come back to me and we’ll talk about it. We’ll figure out if it is temporary, long-term, or a showstopper. Is whatever you’re experiencing bad enough to pull the plug on this? Isn’t it worth it?” Because that possibility exists with anything.”
I think people are afraid to take a chance on a drug for fear of what might be without ever giving it a shot. What matters is how are you personally going to respond.
Again, no two patients are going to respond the same to any of this stuff. So give it a shot and see what happens. You can always redirect, go a different direction and call it off and then try something different.
I think it has changed me and it hasn’t changed me.
How it hasn’t changed me is that I’ve been able to do exactly what we’re looking at right now. I’ve been able to continue with my lifestyle and continue doing the things that I love doing.
How it has changed me is looking at me crossing that finish line. And I cherish that just a little bit more.
I know and value the here and now.
I treasure the time spent with my wife, kids and grandkids. And I look at things through a happier lens. And I’ve always been optimistic, but this forces me to live it a little bit more.
It’s hard to explain but I felt ever more grateful for the little things in life. Whereas before, I would often think that I’ve got tomorrow, the next day or the next month.
I still have that. But the brutal reality is that we’re all mortal.
We’re never sure how many tomorrows, next month, or next year that we have. So it’s important that you really take care of the things you need to take care of in your here and now so that you can appreciate them. Then you can really just live in love at the moment.
Sharing my story through writing
I never set out with the intention of needing to write a book. What I set out with was needing a way to get the thoughts out of my head and out of my heart.
I needed to find a way to purge some things and keep myself fluid in what I was doing.
A lot of what you’re reading started as blog posts, where I would chronicle my day in treatment, or I would start with the beginning of my journey. And then I’ll throw in a random thought or a short story about something.
It was really just more for my benefit than anything. To get things out of my head and keep it as a creative outlet for me.
What I learned in the process was it helped a whole lot of other people because those who read it have really positive things to say. And I think it’s helped more people than I ever would have imagined possible.
That was never the goal. That was never my point.
In terms of advice or suggestions, this book fits into that category of “don’t let go of the things that make you feel good.”
In some cases, for me, that’s running, hopping on a bike and working out. But it’s also being reflective.
It’s putting your thoughts down on paper, or putting on headphones and getting lost on your favorite album or whatever it might be. It helped me as much as it has helped others. And I am proud of it.
I mean, it’s a thing. I’ve got a few of them sitting in the bookcase.
I don’t expect everyone to go out and write a book. Some people might not want to talk to an actual person, but some people might be very good at writing their own thoughts down. So that might be their own support.
Maybe they go home after a tough day of chemo and they just want to chronicle their thoughts. Maybe when they first sit down, they’re feeling overwhelmed. But when they get done writing for a half-hour or an hour, they would feel a little lighter and better. And that was part of the process for me.
Finding my voice
I look at myself as a people-broker in life in general. There’s so many people out there doing all kinds of different things, and there’s so many commonalities in what they do. And sometimes it’s hard to put all the pieces together and to figure out who’s connected to whom.
That’s another reason why I put myself out there and that makes the oncology patient-caregiver community much stronger. What has happened by me doing that and by you (Stephanie) doing that is why we are having this conversation right now. You’re going to post this and it’s going to reach many people.
I won’t say it’s our obligation, but I think, it’s a real added benefit that we are able to improve the landscape just by living our life and story, which is pretty cool.



































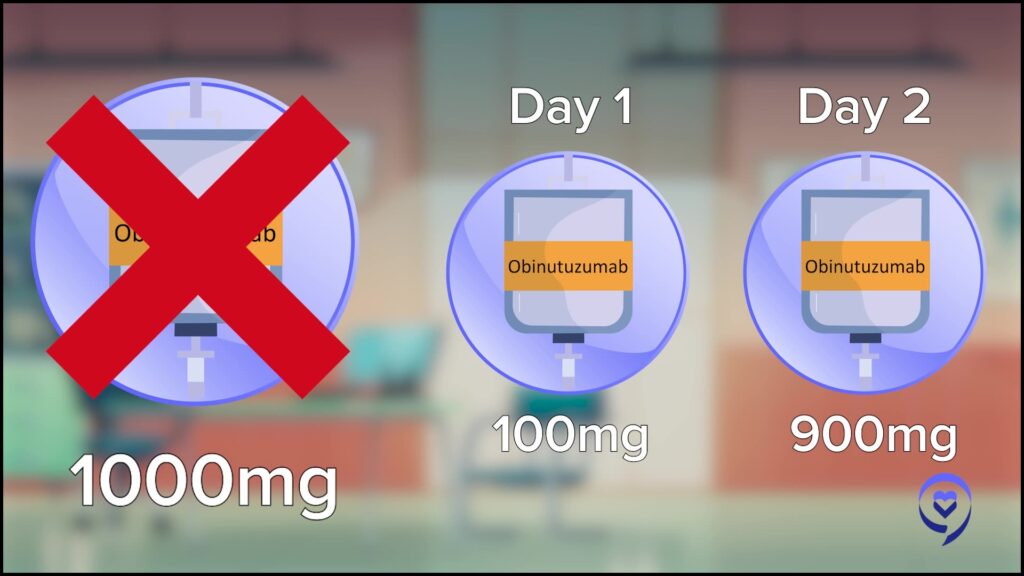













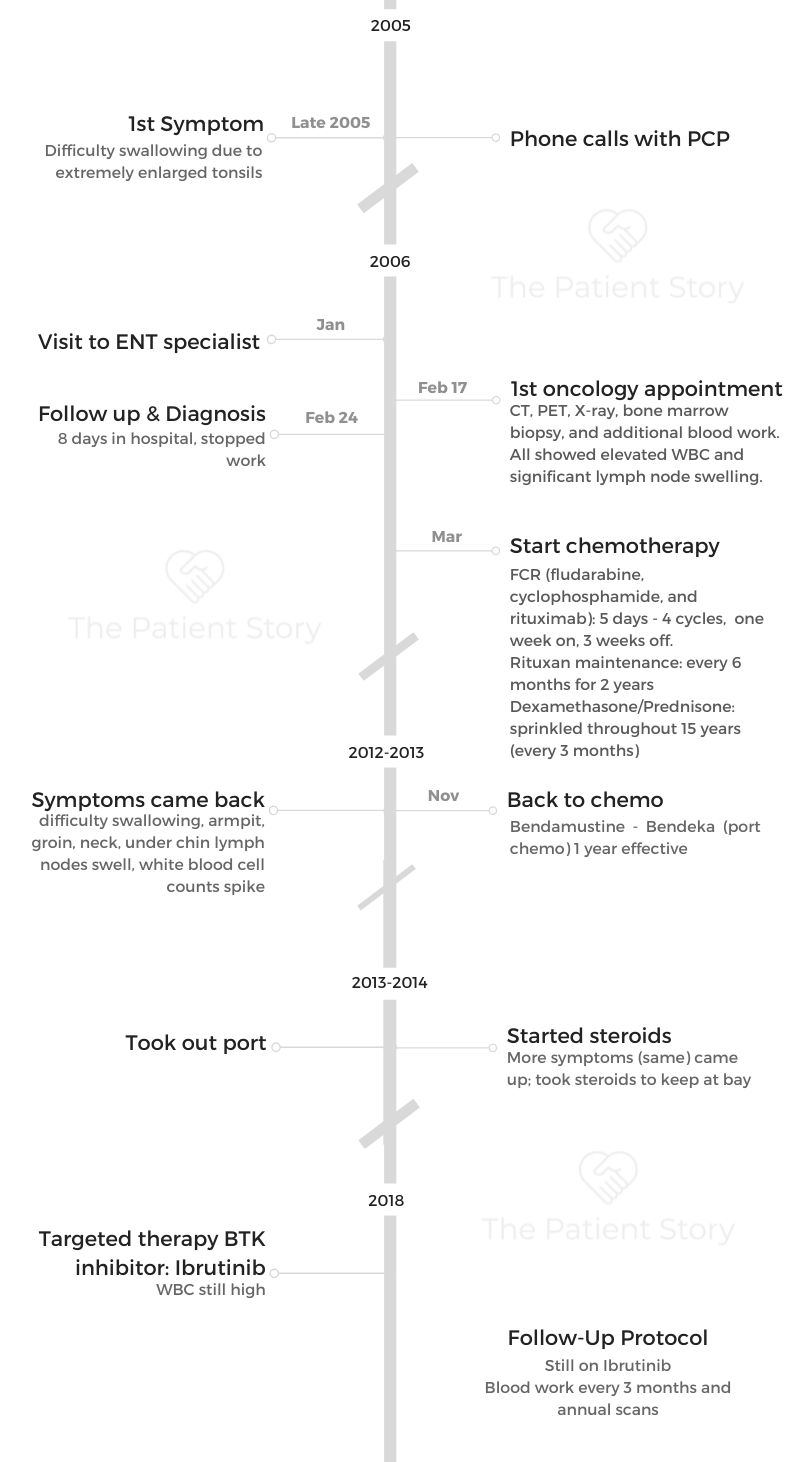












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}