How CT, PET/CT, MRI and Ultrasound Guide Blood Cancer Care
Watch a replay ON DEMAND
Let’s make scans less scary (and less painful) together!
Scans can bring a lot of worry. Join expert radiologists Dr. Robyn Stacy Humphries (Charlotte Radiology) and Dr. David Prologo (Winship Cancer Institute of Emory University) to learn what each imaging test really shows and how to stay calm before, during, and after your appointment.
They’ll both share how CT, PET/CT, MRI, and ultrasound help diagnose and monitor blood cancers such as lymphoma, CLL, and myeloma. Learn more about what each test shows and what results may mean for treatment.
Program Topics
Imaging 101: Ultrasound, CT, PET/CT, and MRI—what each shows and when it’s used
Image-Guided Biopsies: How radiologists target tissue safely and why repeat biopsies matter
Ports vs. Central Lines: Options for easier chemotherapy, blood draws, and comfort
Managing Scanxiety: Coping strategies while waiting for imaging or results
Teamwork in Care: How radiologists, oncologists, and tumor boards coordinate decisions
Blood Work Basics: Making Sense of Your Test Results
Watch ON DEMAND
What does your cancer blood test results really mean — and how do they help doctors detect or monitor cancer?
Listen in as hematopathologist Dr. Kamran Mirza and cancer advocate Stephanie Chuang to break down the most common diagnostic cancer blood tests, including the CBC. Learn how pathologists interpret results, what those ranges mean, and how small changes in your numbers can offer big insights into your health.
Key Topics:
Why doctors order cancer blood tests: What they’re looking for and how to prepare.
Making sense of the CBC: Understand what each number represents — and what it doesn’t.
How blood results guide treatment: From diagnosis to tracking remission or recurrence.
Should I be worried?: When out-of-range numbers matter and when they don’t.
What’s next in the series: Learn how this session leads into condition-specific follow-ups for 6 different blood cancers.
The LLS offers free resources like its Information Specialists, who are one free call away for support in different areas of blood cancer.
Register now to get notified about the follow-up program tailored to your cancer type.
Blood Work Basics: Making Sense of Your Test Results
Hosted by The Patient Story
What do your blood test results really mean — and how do they help doctors detect or monitor cancer? Learn about the most common diagnostic tests, including the CBC and the CMP.
The Patient Exchange: Improving Clinical Trial Diversity
Edited by: Katrina Villareal
The Patient Exchange: Improving Diversity in Clinical Trials
Hosted by The Patient Story
Take part in a transformative conversation with five Black patients as they share their personal journeys navigating clinical trials. This program tackles cultural and social barriers head-on, offering insights on starting discussions with your doctor, understanding enrollment, and overcoming mistrust and misinformation. Learn why cancer clinical trials are not so much about placebos but about “getting tomorrow’s medicine today,” and gain the knowledge to make informed decisions for your health.
Take part in a transformative conversation with six Black patients as they share their journeys navigating clinical trials. This program tackles cultural and social barriers head-on, offering insights on starting discussions with your doctor, understanding enrollment, and overcoming mistrust and misinformation. Learn why cancer clinical trials are not so much about placebos but about “getting tomorrow’s medicine today” and gain the knowledge to make informed decisions for your health.
Know how to bring up clinical trials with your doctor. Understand the screening and enrollment process. Listen to real patients discuss their clinical trial experiences. Help dispel the myth of placebos in cancer clinical trials. Overcome mistrust, lack of info, and other traditional cultural barriers.
Thank you to Johnson & Johnson for supporting our patient education program. The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
This great conversation is a true discussion where we can talk about barriers in the African American and Black community and the hesitation that some of us often feel when we want to go on a clinical trial.
Tiffany Drummond
Introduction
Tiffany Drummond: I’m a patient advocate with over 20 years of experience in cancer research. My journey as a care partner began when my mother was diagnosed with endometrial cancer in 2014. I quickly realized the challenges of finding reliable information to support her care, so I am committed to helping others avoid similar difficulties.
At The Patient Story, we create programs to help you figure out what comes next. Think of us as your go-to guide for navigating not only the cancer journey but your overall health journey. From diagnosis to treatment, we have you covered with real-life patient stories and educational programs with subject matter experts and inspirational patient advocates and guests. I truly am your personal cheerleader here to help you and your loved ones best communicate with your healthcare team as you go from diagnosis through treatment and survivorship.
Before we get to our speakers, we want to thank all of our promotional partners for their support, allowing our programs to reach the audience who needs them. I hope you’ll find this program helpful, but please keep in mind that the information provided is not a substitute for medical advice.
You may be wondering: what exactly is diversity in clinical research and why is this so important? Diversity in and of itself is vast in terms of what it means in specific settings. We’re going to focus on the experiences of Black patients. For instance, when we look at cancer and chronic conditions that increase the risk of developing cancer, Black people, who make up 14% of the US population, have a higher incidence and mortality rate.
Research is going to be paramount in understanding and eliminating this disparity, yet only 5 to 7% of Black patients are clinical trial participants. The panel you’re about to meet is representative of those who go on clinical trials. The conversation is going to be one that I hope resonates with everyone within and outside the Black and African-American community to help move research and development forward and be made accessible to all.
This great conversation is a true discussion where we can talk about barriers in the African American and Black community and the hesitation that some of us often feel when we want to go on a clinical trial. This conversation is going to resonate with us, especially in the Black and African American community because we don’t often talk about it, except when we’re thinking about the mistrust and other things that we’re going to get into throughout this conversation.
I had a bad taste in my mouth about clinical trials because my dad joined them and they didn’t work for him.
Gwen
I have with me current and former clinical trial participants, incredible panelists, and patient advocates. I also have with me Tony Williams, who is with The Patient Story as our head of diversity and inclusion and also a diffuse large B-cell lymphoma survivor. We also have Gwendolyn, a cervical cancer survivor, and Shyreece, a non-small cell lung cancer survivor. Because not all clinical trials are cancer-based, I have LaTisha, Latasha, and Cayla who were on clinical trials or at least screened for clinical trials for uterine fibroids, a chronic condition.
Clinical Trials Knowledge
Tiffany: If you’re familiar with The Patient Story, often we talk about the medical aspect of the patient story and experience, but what I want to talk about is getting to the point of clinical trials.
Cayla, how did you first learn about clinical trials? Was it through a healthcare provider or were you already well-versed in this space? What was that experience like for you?
Cayla: My mom was diagnosed with uterine fibroids and she learned from her gynecologist about a clinical trial that was going on. I didn’t even know I had fibroids. I was diagnosed at the trial and followed up with my healthcare provider, so it opened my eyes to my diagnosis.
Tiffany: Tony, what about you? Were you familiar with clinical trials before you started this journey?
When I was diagnosed in 2021 with stage 4 DLBCL, my front-line treatment was R-CHOP, which wasn’t as successful as we needed it to be so I relapsed. At the time, CAR T-cell therapy was being developed, but it wasn’t available for my type of cancer, so I waited about 4 or 5 months before CAR T-cell therapy became available for me. Participating in that clinical trial was a giving back and a next stage for me. My first and second line of treatments failed and that’s how I fell into it.
Tiffany: Shyreece, what about you? Were you always familiar with clinical trials or was this something that happened when you started your cancer journey?
Shyreece: I was ignorant about what cancer was and what clinical trials were. It wasn’t my world when I was first diagnosed in 2014, but I’m happy to be living now for over 10 years with active cancer.
I first heard about the clinical trial through a team of doctors when I was initially diagnosed. One oncologist said you need resources to have clinical trials in your local clinic. She didn’t have access to it. I needed to accept my diagnosis and the intravenous chemo that was given to me. I stayed one month with her and then decided to get a second opinion from the University of Michigan, where I had more options.
I moved to California and in 2022 at Stanford University, I had no idea that the mutations from the targeted therapy would no longer respond to any treatment, so they started popping up and growing. My doctor, whom I greatly respect and trust, said for two years that he looked out for a trial for me. They worked to get it to their hospital so that I could try it. I’m currently on it and I’m doing well. The tumors are disappearing. I’m excited to look at possibly another 10 years of living with a deadly cancer.
Tiffany: That is a perfect story to share because you went from not knowing what a clinical trial was to knowing medical terms and things that you didn’t know before, and that is inspirational at best. Gwen, did you know what a clinical trial was? How did this come into your purview?
Gwen: My father was diagnosed with lung cancer. I had a bad taste in my mouth about clinical trials because my dad joined them and they didn’t work for him.
Going into any treatment, you’re always going to have apprehension, but it’s the next step and you’ve come this far. Participating in a trial was a no-brainer for me.
Tony Williams
Clinical Trial Screening Process
Tiffany: Tony, can you share your experience about the screening process itself? Was it stressful for you? Did you feel supported?
Tony: My first two lines of treatments failed. Because I was at UNC Chapel Hill Medical Center, they offer a lot of different types of screenings and trials, so I was part of a university program that they were working on. UNC is a teaching hospital and because my oncologist was heading that up, it was easy for me to be screened. I didn’t have to go through anything. It was a matter of deciding if I wanted to participate. It was that easy.
You always have that anxiety because you never know. Whatever you’re participating in, you want to see the desired result at the end, which is to be made whole and healed. Going into any treatment, you’re always going to have apprehension, but it’s the next step and you’ve come this far. Participating in a trial was a no-brainer for me.
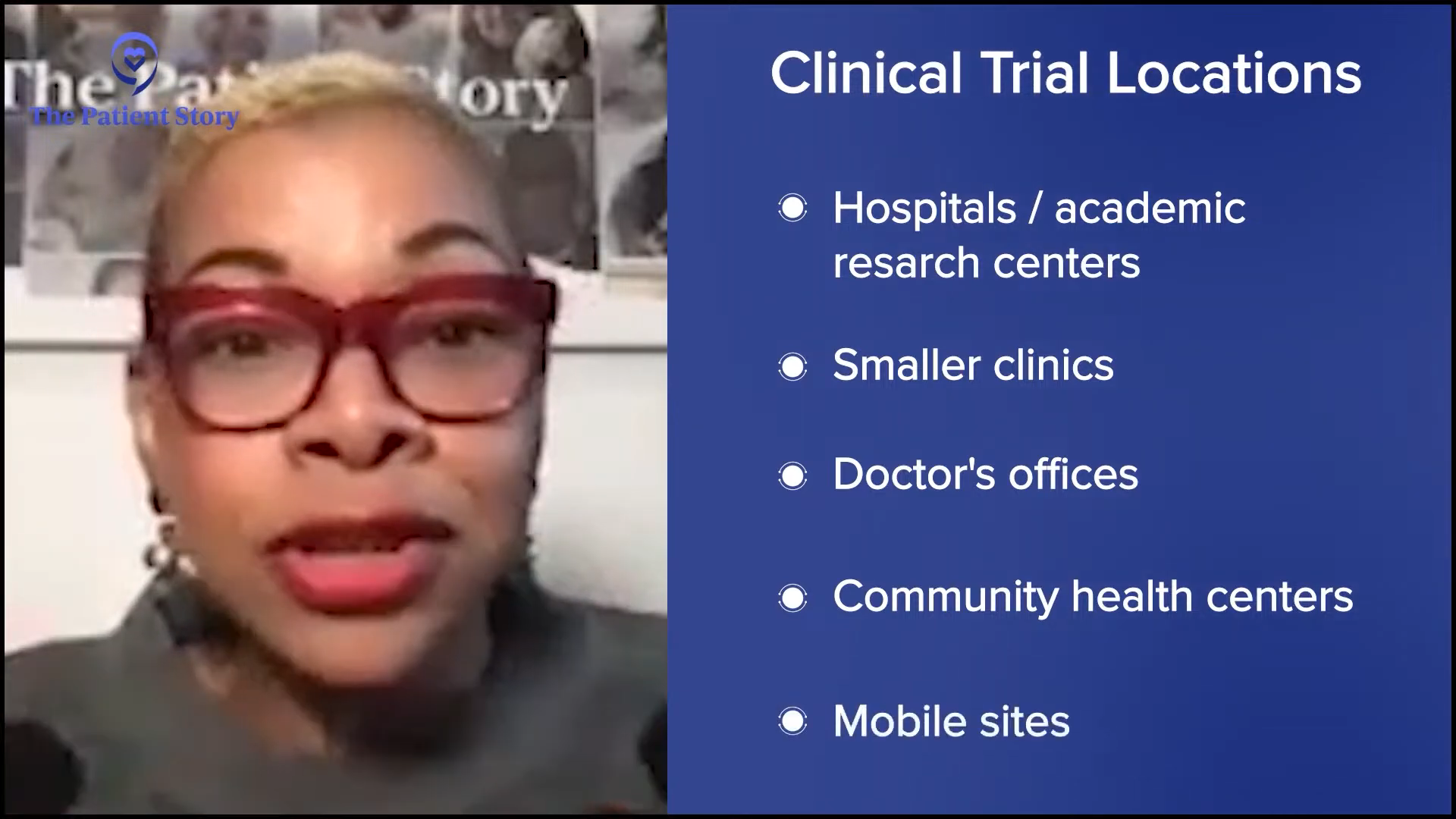
Tiffany: That brings up a point about where to go to access clinical trials. Oftentimes, it is going to be a large academic research center, but not everybody has access to that. There are local sites as well. We have to get that knowledge to the community about where these sites exist. Going to a larger research center like UNC, you will get comprehensive care.
LaTisha, when you were going through the screening process, did you have any hesitancy? More importantly, were there any barriers for you, like with transportation? Did you have to travel far? What was the experience like for you?
LaTisha: I’m in the hospitality industry, so it was hard to sync my schedule. I had to wait a little longer than anticipated to go to my first appointment to get the initial information on everything I needed to do, so that was pretty hard. It was around 15 miles away and I don’t drive, so those were barriers for me when I first started the screening process.
Tiffany: Thank you for being transparent. Those are barriers that exist and can prevent you from going on a clinical trial. Maybe you are eligible, but you can’t get there. With trials, you tend to have to go more often than you would for your standard care because it’s more comprehensive and they’re doing a lot of data collection. I know the medical community, especially the research community, is looking into how they can build in these added costs that affect participants’ ability to join the trial.
Receiving Treatment on a Clinical Trial
Tiffany: This conversation is specific to the Black and African American community participating in clinical trials, so hesitations and mistrust come into the intervention itself. For participants who received an investigational drug, starting with Shyreece, what can you tell me about the information you received when you were told about the clinical trial and what your treatment was going to be? Did you feel like you were a test subject or guinea pig when they were giving you the information?
Shyreece: ALKOVE-1 is a clinical trial studying NVL-655 for patients with advanced ALK-positive non-small cell lung cancer, which I’ve had for over 10 years. For someone to come and tell me after fighting that long that they’ve got something for me is incredible.
My doctor said, “I’ve been watching your cancer. I’ve been watching you and getting to know you, so I think that this is good for you.” The doctor-patient trust was already there because I trusted him along the journey through other things that he was doing. He said, “We’re going to counteract your cancer this way. We’re going to try this, slow it down, but the resistant mutations are always going to pop up, but I got something for you. We’re going to wait.”
He was trying to get his clinic ready to receive all of the resources needed to accommodate me in that trial as much as they could. I asked about transportation and all those barriers because I would have to go every week. It was an investigational drug, but I’m a power horse, so if there’s hope attached to it, then I’m going to try it. I’m not influenced by culture. I’m influenced by my trust in God and my doctor.
I can’t speak for everybody. If you don’t have that connection and trust with your doctor, I say find another one. I had no problem with going into the NVL-655 clinical trial because it was fully explained to me. I knew what the risks were. They sent the information to me by email and I had a month before I signed the consent form. I was very well informed and I knew that he was waiting on that trial for me. When the study coordinator gave me her cell phone number, I knew I was going to be in good hands.
It was an investigational drug, but I’m a power horse, so if there’s hope attached to it, then I’m going to try it.
Shyreece
Placebo-Controlled Clinical Trials
Tiffany: Here’s the question that’s going to need some unpacking, especially in the Black and African American community. When it comes to treatment, we don’t understand placebo, especially when it comes to cancer and chronic conditions. Before I get into that, to clarify, what are your thoughts on placebo-controlled clinical trials?
Gwen: After someone tells you that you have 15 months to live, you’re at the point where you accept whatever you can do to stay alive and to see your grandchildren grow up. You’re going to do whatever you have to do. I knew I had some more living to do. She said, “You have to trust the team. You have to trust God first and then you have to trust the medical team,” and I trusted MD Anderson.
I met my doctor at a retreat by a cervical cancer organization called Cervivor. She was a doctor at MD Anderson and I was going to another hospital at the time. I used to be a case manager, but I was having so many issues as a case manager that I needed a case manager.
At the retreat, I was crying to her. I said, “They don’t care about Black women. They don’t care about the women in my community.” She looked at me and said, “I care. Call me when you get back.” She has been true to her word. I reached out to her and said, “I need to know some things about clinical trials.” Her team reached out to me. It’s all about trust.
Tiffany: What often happens is when you go on a clinical trial, you get more comprehensive care. They want to know if the study drug or new combination is working for you. Maybe it doesn’t, but it may work for the next person. These experiences are what this program is about because when it comes to clinical trials, we don’t often get to see that experience. We only get to read about it or hear about the bad things that happen. Cayla, do you have any thoughts on placebo-controlled clinical trials?
Please note that the use of placebos in cancer clinical trials is very uncommon. In nearly every case, cancer clinical trials compare a new treatment or combination of therapies to the existing standard of care, rather than a placebo.
The Patient Story
Cayla: Automatically, you go in and say, “I’m going to try this and I’m going to be healed.” That’s the positive aspect, but not everyone is getting the medication. You don’t understand that a placebo has to be in effect. Try to do as much research as you can and reach out to the staff or someone you have a rapport with on the team. They can’t tell you if you’re getting a placebo because you might drop out. You should go in there knowing that you might receive the placebo and the next person next to you might receive the medication. Who knows? The person may receive the treatment and yet not have it work for them.
The Patient Exchange: Improving Diversity in Clinical Trials
Hosted by The Patient Story
Take part in a transformative conversation with five Black patients as they share their personal journeys navigating clinical trials. This program tackles cultural and social barriers head-on, offering insights on starting discussions with your doctor, understanding enrollment, and overcoming mistrust and misinformation. Learn why cancer clinical trials are not so much about placebos but about “getting tomorrow’s medicine today,” and gain the knowledge to make informed decisions for your health.
For anyone on a clinical trial, you will never not get anything. That is unethical. If you go on a clinical trial, you are at least going to get the standard of care for your condition.
Tiffany Drummond
It’s all about research and trying to understand as much as you can. There’s a lot of information out there and it discourages everyone from trying to be a part of the trials. People use verbiage that a lot of the people in the community don’t understand. Instead of explaining in-depth, the staff members look at us wondering why we don’t know. I’m a little 50-50 with the placebo. I’m proud of the trial, but I understand why the placebo is needed.
Tiffany: I’m glad you said that. This is what I always drive home. For anyone on a clinical trial, you will never not get anything. That is unethical. If you go on a clinical trial, you are at least going to get the standard of care for your condition. You’re never not going to get that.
What may happen is they give you the standard treatment in addition to whatever investigational drug they’re researching or a placebo. Oftentimes in our community, we think that they’re not giving us anything. This is the last resort, so we’re getting a placebo. This isn’t true.
You can ask. If you’re going into an office and they’re offering you a clinical trial, ask, “What’s the minimum I’m going to get? Am I going to get treated for my condition?” No matter what it is, whether it’s a headache or diabetes. “What is my alternative?” They should tell you in the consenting process what your alternatives are and the options that you’re going to be getting on the trial.
I didn’t want to have surgery. I wanted the bleeding to slow down or stop. That was what I was going to the trial for.
LaTisha
Measuring Expectations on a Clinical Trial
Tiffany: LaTisha, when you went on the clinical trial, what were your expectations? What were your thoughts on what you wanted to happen? Were you realistic about whether or not it will work?
LaTisha: I wanted to be more informed. I knew I had had fibroids for a long time. I was trying to figure out what my other options were. I didn’t want to do the surgery at all, so this would have been an option to not have surgery. However, they didn’t have the resources to see where my fibroids were, so she wasn’t able to see exactly where they were. I didn’t know they could be in multiple places. I didn’t want to have surgery. I wanted the bleeding to slow down or stop. That was what I was going to the trial for. I did not want to have the surgery at all.
Tiffany: Did you enroll or were you considered a screening failure?
LaTisha: I was enrolled. I had to do samples. They kept trying to do the ultrasound. They would tell me to come at different times of the month, but she could only do the vaginal ultrasound. She couldn’t send me for an MRI or anything that wasn’t part of the screening process. I probably went for about three months. When they couldn’t get the imaging that they needed to get, then that’s when I had to stop.
Tiffany: What about you, Latasha? Are you still on a clinical trial or are you done? Would you consider going on another one?
Latasha: I’m at the beginning of a clinical trial. When I started my endometriosis journey a couple of years ago, my fibroids were small. Then it got to a point where they started to bother me so much and I was hurting, so I had them removed.
I didn’t want to have surgery either, but when they say they need to remove something that’s not supposed to be there, I’m all for it. It gives me a better chance to regroup and allows the researchers to see how fast the tissue is growing or how much the lining of the uterus is accumulating each month. They’re able to start tracking what they couldn’t see before the fibroids started growing or the uterus started thickening. It’s hard to go by what everybody else says because they have some good points about the placebo.
Side Effects on Clinical Trials
Tiffany: Oftentimes, we’re afraid of the unknown and when I say we, I’m talking about the Black and African American community and with valid reasons. Tony, when you were on a clinical trial, did you experience any adverse effects? How did the side effects differ than when you were on standard therapy?
Tony: Anytime you’re diagnosed with cancer or any other disease, there’s a level of faith that you have to have and that will be activated during your journey. You’re going to believe in God, but you’re also going to believe in the medicine that God can work through.
Undergoing CAR T-cell therapy was terrible. I had a very aggressive chemotherapy regimen, but CAR T-cell therapy was worse because it was coming off a clinical trial and I was getting that as a second-line defense. The procedure that I had to go through was a lot of trauma to the body, with the extracting of my blood, taking it to a lab to get it re-engineered, and giving it back to me. I have received the worst chemotherapy that they have and that didn’t solve this, but I kept my faith knowing that at the end, I’m going to see this through.
One thing I never asked during my journey and until now was why. Why not me?
Tony Williams
When I did CAR T-cell therapy, that previous six-month period when I got chemo, they gave me that in three days. I felt like I was seeing death. Darkness came over me because it was so aggressive. My body was in shock. I recall the first day that happened, I was out of sorts. The second day, I passed the chapel and said, “I can’t do this,” but I knew I could and I did.
It was very hard, but one thing I never asked during my journey and until now was why. Why not me? Why can’t I be the one to help somebody get through this? I made it through the chemo on CAR T-cell therapy, but it was unknown. I was afraid, even though I didn’t admit it.
You have to exist in a reality that’s not there for you but where you’re going to exist because if you exist in the right now, you will not get through it. You have to exist in a realm that’s beyond where you are. It was very challenging and tough. Not knowing if it was going to work was even more excruciating because you knew what you had already been through.
I never felt like a guinea pig. I felt like it was necessary. The way that drugs come to the market now is not like it was back in the time of Tuskegee or Henrietta Lacks. They have to do what they can to bring the drug to the market. When you join a clinical trial, like Tiffany said, you are getting the best of what they have because they want that to succeed. You are a frontline participant of the best of what they have.
It was traumatizing. It was excruciating and painful. Parts of me wanted to doubt, but when you’ve come this far, what do you have to lose? God has already proven that He’s with you. When they give you a ticking clock and say you have one to three years left and you passed that, what do you have to lose except to continue to believe? That was my mentality.
Tiffany: As a caregiver to someone who did not go on a clinical trial but knew about clinical trials, I understand that some of these drugs are toxic, whether they come to the market or not. Gwendolyn, when you go through that on a clinical trial, does it make you doubt? Am I doing the right thing or is it like Tony said, like you know it’s going to be hard, but you’re going to push through? What was your experience?
If you want to send somebody to talk about clinical trials, send me. I’m alive today first because of God, but second because of the clinical trials.
Gwen
Gwen: So much of what Tony said is so true. Radiation and chemo kicked my butt. I had every side effect on the list. I knew I was a fighter, but I was leaning against the ropes and I wasn’t standing anymore. I want to live.
I tried everything. When you’re fighting stage 4, all of your family and friends have the remedy. Everybody called me saying, “Eat right. Don’t eat meat. Juice. Do nothing but herbs.” I was everybody’s guinea pig. In the Black community, everybody has a remedy, so I said let’s go. If you’re stage 4, you’re already getting a beating, so let’s try something new.
The crazy part about it is when I tried clinical trials, they put me on steroids too because mine was in my bones, so I gained weight and got stronger. I tell people all the time that I’m a walking billboard now. I’m alive because of a clinical trial. If you want to send somebody to talk about clinical trials, send me. I’m alive today first because of God, but second because of the clinical trials. I was dying from radiation and chemo. I had three strokes and two heart attacks. I’m on team clinical trial. You can’t tell me anything different.
Tiffany: Experiencing side effects when you go on these trials isn’t talked about a lot, not realizing that you can have these same side effects with drugs that are on the market as well. Shyreece, I want to hear your experience as well. When you were going through your treatment on the clinical trial, did you ever reach a point when you thought about whether this was the right thing to do or you should think about going off? What was that like for you?
Shyreece: Muscle myalgia was big for me in the initial stage of my diagnosis. It was so bad that I had cramping and abdominal pain. I even got C. diff at one stage of my journey. It was so bad that on Christmas day, I had to go into the hospital for two weeks to be treated.
I love mustard greens. Thanksgiving was coming up and I cooked some ahead. I ate a couple of bowls and it tore me up. I had to lay down, cramped. Sometimes you have to change some of the natural things that you’ve been doing every year. The side effects can come out of the blue. You don’t even know when they’re going to hit you. I nurtured myself until I felt better. That’s how I roll when it comes to side effects.
I’m at a place where I stay surrendered. If I’m going to do the trials and treatments, I have to stay surrendered and resilient. I’ve always believed in God. I’ve always believed in Jesus. But when I got diagnosed with cancer, I thought, “What did I do wrong? Oh, I need to forgive somebody.”
When I went to Stanford, they issued an NCCN Distress Thermometer, a survey that assesses your well-being from week to week by the time you come into your clinical appointment to see where your psychological state of mind is at. Fighting cancer is as much mental as it is physical. How did a cough turn into stage 4 lung cancer? When I cough now and clear my throat, I say, “Wait a minute.” I’ll cough and then tell myself, “Self, don’t you over cough. Self, cough just enough. Self, get you some water.” I have to talk to myself like that. It may sound crazy, but it works for me.
I also tell myself that I was created. I had to read the Word for myself. I love everybody in my faith community, but I had to get deeper into finding a purpose as to why I’m still here. I’m not going anywhere until I have done everything that my Creator has prepared for me to do.
With that being said, I take that power and mental state of mind, get to know my team, and pray. What should I be doing? Who should I be doing it with and where? I’m at Stanford. The people who I’m working with are those particular people. I am present. I am all in. If and when I do decide whatever treatment I’m going to do, I don’t attach any cultural baggage to it because I know it comes from a place of fear and I can’t live in fear. I have to trust today. I have to trust God today and the people of today. If I don’t trust who I’m around, it’s not going to work anyway.
Tiffany: Cayla, LaTisha, and Latasha, for your clinical trials, what did they tell you was your intervention?
Cayla: They had to confirm that I had fibroids to be on the trial. They asked a set of questions to see if I qualify. I got to a certain point and they told me there was nothing they could do. They needed more resources.
An MRI confirms how big the fibroids are and their location. Fibroids can enlarge the uterus and it can be on the uterus, behind the uterus, and in different locations, so they weren’t too sure. They knew I had them, the size, and how many, but they didn’t know where they were. They told me to count how many sanitary napkins I was going through. I kept a log of how often I had to change and how often I had to take anything for pain management. They wanted to make sure before they gave an intervention.
You had to see them more. They had to collect samples. My intervention was to make sure I controlled it. With any disease, diet is important. Are you exercising? Are you a smoker? Do you drink alcohol? These have an effect. I would say they contributed to the intervention as well. I didn’t take medication to assist me. I did the non-pharmacological method.
Tiffany: What this shows is that when we say intervention, people automatically think it’s a drug and that’s not true. They could be collecting data. Oftentimes, what we don’t understand collectively as a community is that the data that we’re looking at is not representative of the people who it affects the most. With conditions that disproportionately affect Black and African Americans in high incidence and mortality, we’re never going to find an answer about why it’s happening if we don’t get data from the people it’s happening to.
Go to where we are. Use layman’s terms, simple language in a nice brochure, and put them in common places
Shyreece
Bridging the Clinical Trials Gap
Tiffany: You all have been passionate in your answers and that spreads more message than someone reading something that they don’t understand. These are shared experiences. What can we do to bridge the gap to make clinical trials less fearful?
Shyreece: We’re the ones who can best spread the message. Go to where we are. Use layman’s terms, simple language in a nice brochure, and put them in common places, like supermarkets, churches, and predominantly underserved schools, where the demographic is mostly Black. Leave some literature with visual representation so they can be easily read. Include information about the screening. Don’t be afraid to speak a little faith language to get on the inside and let them know that you care.
Tiffany: I believe that our life experience is our expertise and sharing that is going to make the difference. I talk about clinical research to anyone. If they’re listening, I want to promote it. These are things that we want to understand because we’re always asking why. Why us? Why are we always getting this? No one can ever give us an answer. The only way we’re going to get that is to look at data.
I believe that we as African American people have a lack of awareness overall about our health.
Tony Williams
Tony: What I have found over my travels with The Patient Story and being the head of diversity is to stress overall health awareness. When you go to the places that Shyreece mentions — our churches and civic centers, where we gather — cancer is not the one single modality. There is always something attached to it, like high blood pressure, high cholesterol, or diabetes.
I believe that we as African American people have a lack of awareness overall about our health. Cancer manifests itself, but something else is manifesting. If we can get to the root that, we take care of ourselves overall and you will not see the manifestation of a lot of these things.
Everything is tied to what you put into your body. Limit exposure to garbage. Overall awareness and pushing that initiative is the first place to start. Cancer is one of many. We all have that in common, but that’s not the only thing. We’re being taken out by heart attacks and other health issues too. Cancer didn’t have a chance to pop up because the heart attack got you first.
Tiffany: Usually, you’re seeing your primary care for everything and that’s the person who’s going to give you the workup that’s going to say something’s not right. How can we be more self-aware and advocate for ourselves to say, “Doc, what else is out there?” We know there will be barriers, like transportation, childcare, and having to leave work, which is a deal breaker for many people because they don’t have the means to do that.
I had to put myself out there and start a fundraiser… If I’m doing this and willing to do this, how can I encourage someone who may not have the skill set?
Shyreece
Shyreece: When I realized that, I had to put myself out there and start a fundraiser. It’s so humbling and so vulnerable, but I wanted to do it and I had to go first. I couldn’t wait for the reimbursement from the sponsor, so I had to put a plan together and execute the plan.
There’s so much preparation involved. If I’m doing this and willing to do this, how can I encourage someone who may not have the skill set? Let’s talk about that and be very transparent. Everybody may not have the skill set and the resources. How do you encourage them? Where can we have a list of resources? Where are these places to get support? How do you handle rejection? I powered through it. Everybody doesn’t have that support system. How do we encourage those things first?
I tell my story because this is my community and where I grew up. Start where you are.
Gwen
Gwen: Cervivor trains us. Even though I have cervical cancer, that doesn’t mean that I’m trained to speak to the community. Before I can do that, I have to know the facts and when I’m speaking, I have to give them the truth. I can’t talk off the top of my head.
Before I even knew I had cancer, I started a cancer organization in memory of my father. I go around the low-income Black and Hispanic communities. I go with MD Anderson now because now we have a relationship. I tell them to leave their white coats at home and be in jeans and tennis shoes. We want them to have a comfortable conversation where they’ll open up to you.
When I go out there, I bring in resources because I can’t go in there and tell you to get screening and not have help for you. I can’t leave you out there by yourself. We have to have more of that going on. We have to get out there.
I tell my story because this is my community and where I grew up. Start where you are. Cervivor told me that my story matters. They gave me confidence, so I’m out there now telling my story and we can have that conversation. I partner with schools, business owners, and churches. We need to go to the important places in the community.
Shyreece: Amen. I wrote my book for that reason. I started in my church. Start where you are.
Conclusion
Tiffany: I want to thank every single one of you. You all have made an impact in this conversation. I’ve learned about things that I did not know, so thank you so much for being willing to share with me and The Patient Story. Your experiences are going to resonate with a lot of people.
If you’re in medical school, you’re seeing the same stats that we’re seeing. You’re reading it, but we’re living it. You can understand better and get a bigger picture about why it’s so important that we participate in these clinical trials that can literally save lives.
What an electric and energizing conversation for sure. It doesn’t take much for me to talk about clinical research. Sharing the room with Tony, Gwendolyn, Shyreece, LaTisha, Cayla, and Latasha was icing on the cake. It is important to be empowered so that you and your caregivers can make informed decisions about your care.
Thanks again to our promotional partners.
The Patient Exchange: Improving Diversity in Clinical Trials
Hosted by The Patient Story
Take part in a transformative conversation with five Black patients as they share their personal journeys navigating clinical trials. This program tackles cultural and social barriers head-on, offering insights on starting discussions with your doctor, understanding enrollment, and overcoming mistrust and misinformation. Learn why cancer clinical trials are not so much about placebos but about “getting tomorrow’s medicine today,” and gain the knowledge to make informed decisions for your health.
Background: Chris' wife Keasha passed away from stage 4 lung cancer one month after they married. He's been a passionate lung cancer advocate ever since. Focus: Leading with love, making connections to grow lung cancer community, NFL liaison
Background: Jeff was diagnosed with stage 4 lung cancer and given months to live, but his wife, Rhonda, fought for a specialist that led to biomarker testing and better treatment options Focus: Education of biomarker testing for driver mutations, patient and caregiver self-advocacy
Graft-versus-host disease is a potentially life-threatening condition affecting an estimated 50% of blood cancer patients who receive stem cell transplants from a donor. Transplant experts explain GVHD risks, how to watch for symptoms, the current treatments available, and new clinical trials aimed at prevention and treatment.
Watch the Full Webinar
In addition to our summary from this empowering webinar, watch the full video replay and catch every word from the experts and patient advocate!
Patient advocate and GVHD Alliance co-founder Meredith Cowden shares her experiences with GVHD. Experts from UChicago Medicine, Roswell Park Comprehensive Cancer Center, and The Leukemia & Lymphoma Society who are on the front lines of GVHD research and treatment discuss the role clinical trials play in advancing the treatment landscape and what it could mean for you. Discover how to take steps to learn more about clinical trials from a clinical trial nurse navigator.
Stephanie Chuang: I’m a blood cancer survivor myself and started The Patient Story out of my own experience. I felt so alone. I wanted to know what it meant after diagnosis and how we could get through it. As we know, a diagnosis is just the beginning of figuring things out. Our goal at The Patient Story is to help patients and care partners navigate life after a cancer diagnosis, primarily through in-depth conversations with patients, care partners, and top cancer specialists.
We are so proud to partner with The Leukemia & Lymphoma Society, the largest nonprofit dedicated to creating a world without blood cancers. For decades, they have invested almost $2 billion in groundbreaking research and pioneering so many approaches. On top of that, they also support patients and families with programs like the Clinical Trial Support Center, which provides free one-on-one support with nurse navigators.
This program is not meant to be a substitute for medical advice, although we hope that you walk away feeling like you have more to ask your own medical team.
Satyajit Kosuri, MD
Stephanie: Dr. Satyajit Kosuri is a hematologist-oncologist with the University of Chicago Medicine. He is an expert in stem cell transplantation and leads the Graft-Versus-Host-Disease Clinic and the research in trying to improve patient access to transplants. Dr. Kosuri, what drew you to this field of medicine and specifically GVHD?
Dr. Satyajit Kosuri: When I started my oncology fellowship, I was going to be a genitourinary oncologist and I was very much set. When I did my transplant rotation, what drew me was that it spanned all fields of medicine, so you had to continue to have a pretty good breadth of knowledge. The immunology was very, very intriguing. We’re dealing with very complex diseases as well as the transplant itself, which is basically an immune system transplant.
When I tell patients, family members, fellows, and trainees about the field of transplant, I tell them, number one, I’m an immunologist, number two, I become an infectious disease doctor, and then, number three, oncology comes in as part of the triad. That’s what drew me to the field and what I find very interesting. Graft-versus-host disease is part of the entire picture that we’re trying to improve upon within the context of transplant.
Shernan Holtan, MD
Stephanie: Dr. Shernan Holtan is a hematologist-oncologist with Roswell Park Comprehensive Cancer Center in Buffalo, New York. She is the chief of the Blood and Marrow Transplantation and has led so many clinical trials in GVHD. Her research has led to the discovery of the amphiregulin (AREG) biomarker for monitoring graft-versus-host-disease. Dr. Holtan, what drew you to medicine and specifically focus on graft-versus-host disease?
Dr. Shernan Holtan: My story is a lot like Dr. Kosuri’s. In medical school, I was most interested in rheumatology, infectious disease, cancer medicine, critical care medicine, dermatology, and plastic surgery. I thought, How am I ever going to pick between these different specialties? I loved cancer reconstruction and the connection with patients going through cancer and giving them hope after a devastating diagnosis.
On a whim, I took a rotation on the BMT service, in part because it sounded cool. The other part of it is you didn’t have to work weekends and as a very tired fourth year med student, I was excited about that. I was stunned. It was every great aspect of medicine rolled in one specialty, so I was sold and never looked back.
Meredith Cowden, Patient Advocate
Stephanie: Meredith Cowden is a chronic GVHD patient advocate and co-founder of the GVHD Alliance. Why did you decide to dedicate your life to advocating for so many other people with GVHD?
Meredith Cowden: I had acute myelogenous leukemia (AML) at 19. Chemotherapy wouldn’t completely work, so I needed a bone marrow transplant. Shortly after, I developed acute graft-versus-host disease and then I developed chronic graft-versus-host disease, which I’ve had since April 2002.
Graft-versus-host disease is rare and we’re spread out all over the place, so it’s isolating and hard to find resources, information, and even the appropriate treatment team.
I originally wasn’t into the patient advocacy world. I didn’t want to deal with it anymore, but I didn’t want anyone else to have to deal with it. I got angry and frustrated, and frustration is one of the greatest motivators for me. When I would talk to other patients, there was a sense of relief and comfort they felt in talking with somebody who could understand their experience. From that point, I thought that this is where I need to be.
Ashley Giacobbi: I am a nurse navigator with The Leukemia & Lymphoma Society’s Clinical Trial Support Center. We provide individualized clinical trial searches and clinical trial resources to patients with blood cancers or patients who have had blood cancer in the past but may be managing long-term effects of their disease or treatment.
We provide one-on-one connection with patients, caregivers, and their healthcare providers. We take the time to learn about a patient’s diagnosis, past treatment, and other medical conditions that could play a role in their eligibility for clinical trials. Most importantly, we take the time to learn about patient and caregiver preferences and any unique obstacles that may hinder or support their participation in a clinical trial, so that we can target the support that we’re able to offer and give personalized resources.
When immune systems grow suspicious, they’re programmed to do one thing and that is to attack. This new immune system can attack the recipient from the inside.
Dr. Satyajit Kosuri
Understanding Graft-Versus-Host Disease (GVHD)
Stephanie: Dr. Kosuri, what is GVHD?
Dr. Kosuri: When we’re doing a stem cell transplant or bone marrow transplant, we’re doing an immune system transplant. When we’re healthy, the immune system protects us, whether it’s getting rid of bad cells or protecting us from various infections. It considers the body that it’s growing up in as its neighborhood, so it has an inherent desire to protect its neighborhood and recognizes the body that it’s in as being part of itself. When there are things that are not supposed to be there, it recognizes them and gets rid of them.
We’re taking the stem cells from a person with a healthy immune system and putting them into the transplant recipient, so this immune system is growing inside of a new neighborhood. For the most part — and this is where matching comes into play — it recognizes its new neighborhood as its own and leaves it alone. It takes up the mantle of, “I’m going to protect this body and eradicate any leukemia cells,” and that’s the graft-versus-leukemia effect.
But sometimes, there are parts of the new neighborhood that are not what it’s used to, so it starts to grow a little bit suspicious. When immune systems grow suspicious, they’re programmed to do one thing and that is to attack. This new immune system can attack the recipient from the inside, which can lead to some inflammatory physical damage to the patient or the recipient of the stem cell transplant.
Types of GVHD
Stephanie: Dr. Holtan, what are the main types of GVHD? How do they differ and what are some of the common symptoms?
Dr. Holtan: We mainly think of graft-versus-host disease in two phase although there can be some overlap between the two.
Acute graft-versus-host disease happens within weeks to the first few months post-transplant and that has a particular pattern. Most of the time, it’s a red skin rash, but sometimes it can also lead to nausea, vomiting, diarrhea, and liver abnormalities that we might see on blood tests. There’s a very clear time during which this develops and a pretty clear clinical presentation, so it’s pretty easy to determine what it is.
Chronic graft-versus-host disease typically happens later in the months to years after transplant. It can be more subtle and difficult to diagnose. As Dr. Kosuri was saying, this is primarily an inflammatory reaction at the beginning, which ultimately will gradually lead to scar tissue.
Think of a wound that is having some difficulty healing. There’s a lot of inflammation and the body tries to stop that inflammation by putting a scar on top of it. This can happen in almost any organ in the body. Usually, the skin is involved, but it can also cause dry eyes, dry mouth, mouth sores, difficulty breathing, difficulty swallowing, changes with the muscle tissue fascia, and making people feel stiff and have muscle cramps. Any organ can be involved with chronic graft-versus-host disease.
Even though we think about chronic manifestations as a later problem after transplant, we can see some of those changes even within the first few weeks.
Dr. Shernan Holtan
Stephanie: Dr. Holtan, when does it technically turn from acute to chronic? Is there an official time where now we know it’s chronic? Is there a general time frame?
Dr. Holtan: There isn’t an official rule. When Dr. Kosuri and I were in training, we were taught that acute graft-versus-host disease happens before Day 100 and chronic GVHD happens after Day 100, but that’s not really true. The biologic processes can happen at any time post-transplant. Acute GVHD usually happens in the first few weeks to months, but we have even seen acute manifestations of GVHD happen much later.
Even though we think about chronic manifestations as a later problem after transplant, we can see some of those changes even within the first few weeks. The lines are blurred now, so we describe graft-versus-host disease based on its symptoms and appearance rather than time frame post-transplant.
It took a while before my doctors said I had GVHD because they were thinking it was something else. Over the years, I’ve had a variety of different manifestations of chronic GVHD.
Meredith Cowden
Meredith’s GVHD Story
Stephanie: Meredith, what was it for you in terms of those first symptoms? At what point did you realize that this was not going away?
Meredith: In the beginning, I noticed that I had a couple of different things going on at the same time. My stomach started to bother me a lot and I got very nauseous. It was hard to find food that I could tolerate and that was appetizing. I had some gastrointestinal issues going on. I also developed a rash. I’m naturally a pasty pink person, but my skin got red and burned, so it was hard to wear clothing.
When I received treatment, the issues started to get resolved, but then it started to transition. The GI issues didn’t necessarily go away but they changed and my skin got a little bit different.
I had musculoskeletal involvement. I developed polymyositis, so there was a lot of pain. I was very weak and couldn’t move around a lot. I lost muscle mass. It took a while before my doctors said I had GVHD because they were thinking it was something else. Over the years, I’ve had a variety of different manifestations of chronic GVHD.
Dr. Kosuri: Chronic graft-versus-host disease can affect multiple sites in a way that may be difficult to initially pick up. I’ve gotten feedback from patients that what they’ve found helpful is when I describe chronic GVHD prior to the transplant.
I ask them to imagine taking all the autoimmune conditions and rolling them into one and putting them inside a human body. Those are ways that chronic GVHD can manifest, whether it’s dry eyes, a scleroderma type presentation, or pulmonary fibrosis. It’s a great mimicker.
Stephanie: It sounds like it might be hard to identify quickly if people aren’t speaking up too and share the different things that you’re experiencing and communicating openly with your doctor.
There are many different types of complications, but infection comes to the forefront.
Dr. Satyajit Kosuri
Severe Complications in GVHD
Stephanie: I don’t know if there’s difficulty in noticing what the severe complications are, but, Dr. Kosuri, are there any that you’d like to highlight?
Dr. Kosuri: There are complications of the entity itself and then there are complications that will arise from the treatment or the way we try to treat the disease. GVHD in and of itself is an immune dysregulation. The immune system that’s supposed to behave in a certain way is misbehaving or it might be turned on and can’t really control itself. What happens in this state?
There are many different types of complications, but infection comes to the forefront. We prioritize monitoring patients who have graft-versus-host disease not only from the GVHD itself but also from the medications that we use to try to quell the inflammation and calm things down. Both can lead down the pathway of bringing down the level of protection that the human body has as it’s starting or trying to recover from the stem cell transplant.
One of the things that we emphasize for patients is if they’re feeling unwell in any way, shape, or form, they have to let their transplant providers know very quickly. That way, whatever suspicion we may have, we can diagnose and take care of it very quickly. If it’s a small infection, we can treat it and it doesn’t become a big infection.
Be very proactive and very compliant with the medications. Patients take 20 different medications after a transplant and sometimes it’s hard to take all of them, especially when the pills are big. We hear that as one of the main complaints. We make sure that patients are on antiviral medications, antifungal medications, and a medication to protect them from PJP (pneumocystis jiroveci) pneumonia. These help protect and almost substitute in a way because the immune system is not online early on and when you have graft-versus-host disease, it’s not behaving the way that it’s supposed to.
Dr. Holtan: We certainly know that graft-versus-host disease can affect different organs and tissues, and that the treatment can have just as many toxicities as GVHD itself. Some of the most challenging issues we run into are malnutrition, straight-up difficulty eating, all the way to impaired organ function.
What Dr. Kosuri mentioned is key about notifying for changes in symptoms with chronic graft-versus-host disease. You want to intervene before there’s permanent damage. The longer the inflammation and scar tissue goes, the more difficult it is or it might even become impossible to reverse. Early intervention is necessary to try to avoid permanent damage.
If there’s anything that seems even a little bit wacky, ask. There’s no harm in asking. It’s one of the best ways to take care of yourself.
Meredith Cowden
Stephanie: From your own patient experience, did you know that you could bring these up to your doctor? Do you feel that patients you talk to know that they can do that? What do we need to do to make sure that this is happening?
Meredith: I was diagnosed at 19. I was young and there were things I learned over the years. This might sound naive and silly, but there were things that I thought were completely normal but were actually symptoms of GVHD.
Over time, I’ve developed strong relationships with each member of my care team, so I’m very comfortable saying, “This feels weird. I don’t know about this. Can you look at that? Check me out please.” To have that kind of conversation, you have to build that relationship so that everyone is comfortable and can have a discussion with one another even when they have differing opinions. You can get more out of that conversation than if a typical patient-doctor exchange. Oftentimes, things get missed that way.
For patients, treat your doctors like people. Be friends with them. You’re going to be with them for a long time. They want to help you. If there’s anything that seems even a little bit wacky, ask. There’s no harm in asking. It’s one of the best ways to take care of yourself. For the providers, it’s a good idea to ask patients to do a quick scan of their body to get the whole picture because it’s easy to forget stuff. Is there anything that’s going on that we haven’t touched on that you noticed?
The backbone of therapy for both acute and chronic GVHD is corticosteroids.
Dr. Satyajit Kosuri
Current GVHD Treatments
Stephanie: Dr. Kosuri, what are the current standard treatments for GVHD?
Dr. Kosuri: The keyword is current because this is something that’s changing and we hope will continue to change as we go through the years.
The backbone of therapy for both acute and chronic GVHD is corticosteroids. Many patients and their family members will have heard of the medication called prednisone or various types of the steroid.
The degree of the GVHD matters. If you have a mild, acute graft-versus-host disease, this could be potentially managed with topical corticosteroid. As it becomes more severe or involves more organ systems or more of the skin, we start graduating from topical steroids to systemic steroids.
Depending on where we are in the transplant process, our patients will already have been on another immunosuppressive agent, like tacrolimus, sirolimus, or cyclosporine. The goal is to treat with steroids plus or minus this other agent and then taper them off once we have a response.
With steroids, over a period of time, you can accumulate some of those side effects that we don’t like to see in patients, like insomnia, jitteriness, and fluid retention. Those are for people who are in the category of steroid-responsive.
Another category of patients are those who are steroid-refractory, which is where the graft-versus-host disease may be a little bit more sticky and not respond to steroids, or steroid-dependent, where patients are unable to get off steroids. In those cases, we go further down on immune suppression choices. There are other medications available. One that’s FDA-approved and works for both is ruxolitinib. There are also other various options. That becomes more of a longer term treatment.
There isn’t a blood test that can diagnose graft-versus-host disease right now, but we can use biomarkers to help us understand the severity of the immunologic reaction and how much damage has been done.
Dr. Shernan Holtan
Challenges of Existing Options for Managing GVHD
Stephanie: Dr. Holtan, what are some of the key limitations or challenges with the existing options for managing GVHD?
Dr. Holtan: The greatest challenge is understanding how much therapy to give for graft-versus-host disease. We base our treatment upon the severity of symptoms, but that isn’t adequate. There are still some patients that we are over-treating and some patients we are under-treating.
This is where the role of biomarkers can come in. There isn’t a blood test that can diagnose graft-versus-host disease right now, but we can use biomarkers to help us understand the severity of the immunologic reaction and how much damage has been done internally that we can’t detect clinically. This is a huge challenge because even though we examine patients fully and they reveal all their symptoms, we still can’t know how bad things are, so biomarkers can support us in helping to guide that therapy.
This is particularly under investigation right now using biomarkers such as ST2 (suppressor of tumorigenesis 2), REG3α (regenerating islet-derived 3-alpha) known as the MAGIC (Mount Sinai Acute GVHD International Consortium) biomarkers, and then the one that we developed at the University of Minnesota, amphiregulin or AREG. Both of these biomarkers can be used to understand how severe the graft-versus-host disease is.
I have patients who have had severe infections of the GI tract, like C. difficile colitis or viral gastroenteritis such as adenovirus gastroenteritis. An allogeneic transplant recipient might have these infections and we’ll treat the infections, but they’ll have persistent severe diarrhea so you won’t know if you’re still dealing with the infectious process and the healing that has to occur or if graft-versus-host disease developed as a result of the immune system trying to target the infections. Even a biopsy can’t always tell you this, but we can use biomarkers, especially amphiregulin, to help sort this out.
When we’re treating patients with these symptoms, it’s almost like it’s graft-versus-host disease until proven otherwise.
Dr. Satyajit Kosuri
I had a gentleman who had severe adenovirus gastroenteritis and was having 15 to 20 bowel movements a day. We used an amphiregulin test to know if this could be graft-versus-host disease. The result was normal. It was not elevated. I continued to check every week because his gastroenteritis went on for a long time, even though we treated it.
Clinically, he had weeks of diarrhea, but we followed that test every week and the number was always low, so we never gave him prednisone. If I didn’t have this reassurance, someone might say it’s GVHD. It took some time, but he made a full recovery. This is how we can use these biomarkers to help support our clinical decision-making. We need more trials along these lines because the real world is messy.
Dr. Kosuri: I can’t emphasize how important what Dr. Halton is mentioning because oftentimes in transplant medicine, we’re operating in the gray and we have to make guesses. Sometimes when we’re treating patients with these symptoms, it’s almost like it’s graft-versus-host disease until proven otherwise. When you have that type of thought process, it can be difficult and we can actually hurt the patient with the GVHD management in and of itself.
The example that Dr. Holtan mentioned, most transplant physicians would say, “This has to be GVHD and we have to give them prednisone,” and that could lead to other infections or it can worsen the infection the patient already has. We get into these situations that are difficult to manage and if we have something like these biomarkers, it can make our lives as well as the patient’s life much easier and with less toxicity than what we would say is the normal kind of approach.
We had no human data to support how we manage steroid-refractory GVHD. Out of decades worth of work, there were no studies.
Dr. Shernan Holtan
Stephanie: A lot of this is addressing the symptoms that come with GVHD. This may be a rookie question, but I’m trying to understand. Is there research going into how to address the drivers of what’s happening with GVHD?
Dr. Holtan: We know what causes graft-versus-host disease. The donor T cells are attacking tissues and organs. However, we can’t always tell when that attack is over. The whole field of steroid-refractory graft-versus-host disease has developed out of an assumption that the T cell-mediated attack is still happening, so all trials for steroid-refractory GVHD involve intensification of immunosuppression without actual knowledge that there are T cells still causing damage.
This was something that bothered me. These are things that drive you crazy about the field and want to change it. I realized that we had no human data to support how we manage steroid-refractory GVHD. Out of decades worth of work, there were no studies that justified that this is the right path.
I performed a study where we had rectal biopsies of patients with grades 3 to 4 gastrointestinal GVHD. They were steroid-refractory and received other therapy. I wanted to look at the biopsies for a sign that it was the donor immune system still doing the damage to prove what we’re doing is right and I found absolutely no evidence to support our practices. There was no increase in T cell infiltration. There was no immune signature at all that suggested that it was out of control T cell-mediated damage in the steroid-refractory patients. All we saw were signs of tissue damage.
I’m hoping that the field will evolve. Instead of intensifying immunosuppression, give something more immunomodulatory, support immune tolerance, and give something to help heal the damaged organ. Change the paradigm. That was a huge frustration that I had as a fellow and I hope more people read that paper now.
Clinical Trials for GVHD
Stephanie: We’ve talked about the current landscape of GVHD and treatments, and some gaps of need. Before we go into them, what are clinical trials?
Ashley: Clinical trials are carefully controlled research studies that may be conducted by scientists, doctors, or researchers to either test new treatments or test treatments that have been used in the past in a potentially different way. Trials can also compare new treatments to existing treatments or to various combinations of treatments to find out which treatment might work best or which would be better tolerated, all with the goal of improving care and treatment for patients.
BMT CTN 1703 Clinical Trial
Stephanie: Dr. Holtan, can we talk about one of the trials that you helped lead? What’s the potential and the excitement about that?
Dr. Holtan: An ounce of prevention is worth a pound of cure. The theme in these studies is prevention of graft-versus-host disease. Our field is in the midst of an important era. We have very effective prevention for acute and chronic graft-versus-host disease with multiple modalities that we have not had in the past.
The BMT CTN 1703 study was repurposing a chemotherapy agent called cyclophosphamide to prevent acute and chronic graft-versus-host disease by giving it after transplant in the setting of reduced-intensity transplants, so patients who are typically older. The median age of the trial was 66, going through transplant, and would receive this chemotherapy after the transplant. That initially sounds crazy to do. Why would you give chemo after the transplant?
We’re learning how this works, but it helps to deplete allo-reactive T cells. The good cells that we want to persist are completely immune to cyclophosphamide, so regulatory T cells, which are T cell peace mediators, and stem cells themselves are resistant to this chemotherapy. It eliminates the cells we don’t want and preserves the cells we do.
This modality was compared against the standard, which was a calcineurin inhibitor (CNI) plus methotrexate (MTX), and that’s been the standard since 1986. Our field hasn’t undergone a major change where we saw that the new treatment arm was superior. We haven’t had this kind of change since the mid-80s.
We did a similar study in Minnesota looking at post-transplant cyclophosphamide in the myeloablative setting. We saw remarkably low rates of acute and chronic GVHD using this platform. The rates of grade 3 to 4 acute GVHD were 5%. The rates of chronic GVHD requiring immunosuppression were also about 5%. It’s not a randomized nor a phase 3 study, so we haven’t done that comparison. I have a lot of conflicts of interest, so I don’t want to do that study because the results of phase 2 are so good. I wonder what Dr. Kosuri thinks about that.
Dr. Kosuri: Dr. Holtan’s work with 1703 is one of the more important studies that we’ve had recently in the field of stem cell transplant. When we look at our field and the studies that we conduct, having a randomized study in such a large manner is very, very rare, so this was a big deal. It’s not just the findings, but the way that the study was conducted.
The study went through other randomized trials and the two best options went into 1703. As Dr. Holtan mentioned, the results are very, very important and being adapted in a widespread manner amongst many of the transplant centers not only in the United States but even abroad, so it’s a very, very impactful piece of work.
The important thing, as she highlighted, is that these are for older patients who have had multiple lines of therapy and may be coming into transplant in a more frail physiologic manner than someone who is in their 20s, 30s, or 40s. The reduced-intensity aspect is very, very important.
I agree that the post-transplant side has had such an impact on the incidence of acute and chronic GVHD. The other thing that I’ve noticed is the nature of the graft-versus-host disease that could develop. Even if someone were to receive post-transplant cyclophosphamide as a GVHD prevention strategy or what we call T cell-depleting methods, there are other ones also.
When we’re giving higher-intensity conditioning, the amount of initial damage and inflammation that occurs is higher and the risk of developing both acute and eventually chronic GVHD can also be higher.
Dr. Satyajit Kosuri
When we compare it to the standard of care, if they were to develop graft-versus-host disease, there is the potential that it may be more responsive to current treatment modalities. You can treat it and it can potentially go away versus you trying to treat it and patients may become more steroid-refractory or steroid-dependent. Incidence is important and the incidence is much lower. My opinion is that the nature of the GVHD that may happen is also different.
As far as myeloablative conditioning, if we think it works in one setting with a group of patients who may be a little bit more sensitive to the toxicities of transplant, as a transplant physician, we want to try to apply it to the younger, fitter patient population who are receiving myeloablative transplants or the higher-intensity transplant.
The important point there also is when we’re giving higher-intensity conditioning, the amount of initial damage and inflammation that occurs is higher and the risk of developing both acute and eventually chronic GVHD can also be higher.
If we can take this modality, use it in the myeloablative setting, and decrease the incidence of both acute and chronic GVHD, that’s something I think that we’re all very supportive of. As transplant centers are changing their standard approaches, we ourselves at the University of Chicago are figuring out a way to standardize our myeloablative transplants using PTCy (post-transplantation cyclophosphamide), even though we don’t have a randomized, large randomized study.
VIC-1911 Clinical Trial
Stephanie: Speaking of higher-intensity transplant groups, that’s also for VIC-1911, right, Dr. Holtan? What’s exciting about that and who’s going to benefit from that potentially?
Dr. Holtan: This is a new clinical trial looking to improve on the post-transplant cyclophosphamide platform. Now that we’ve nearly eliminated severe acute and chronic graft-versus-host disease, our unmet need is addressing relapse.
We’re looking to see if we could do something different within the GVHD prophylaxis platform that not only keeps GVHD rates low but also directly reduces the risk of relapse. We took away one of the drugs in the platform called mycophenolate mofetil (MMF). We don’t think that MMF probably does very much to be honest. The heavy lifting is done by cyclophosphamide in combination with whatever we partner it with, tacrolimus or sirolimus.
We took MMF out and put in a drug called VIC-1911, an Aurora kinase A inhibitor (AURKA). That drug is known in preclinical testing to keep GVHD rates low, but it also has direct anti-leukemia effects. It helped to kill leukemia cells in the test tube and in mice. Mice who received this combination had better survival overall due to less graft-versus-host disease and less relapse.
We’re testing a platform to see: does it protect people from graft-versus-host disease and can it also protect from relapse? We have two primary endpoints in this study: GVHD and relapse. If we can move the needle with relapse, we will have evolved the platform even further.
This trial is ongoing right now only for the myeloablative or high-intensity conditioning regimen, but we hope to complete the study, learn the results, and, if successful, expand it to other platforms. It’s currently in phase 1. We have just found the dose that we want to test going forward.
Stephanie: That’s great context. Some trials are further along. People are always wondering, “Oh, that sounds so promising! But when are we actually going to see that in the real-world setting?” It’s great to know that the research is happening, but we’ve got a ways to go with that one.
Dr. Kosuri, you talked about PTCy and this trial is about lowering the dose. Can you talk more about that and who will benefit?
Dr. Kosuri: In Dr. Holtan’s 1703 study, we were looking at patients who have fully matched donors or what we call well-matched donors. Well-matched donors could also mean having a single-antigen mismatch. This is coming off post-transplant cyclophosphamide.
For patients who have haploidentical donors or half-matched donors, we’ve been able to successfully use that platform with very comparable and good rates of graft-versus-host disease reduction. The idea is if you can use it in a half-matched or half-mismatch, you can also use it in well-matched patients. We call that 7/8.
There are two studies. OPTIMIZE is coming after another study called ACCESS, which is looking at the same dose of post-transplant cyclophosphamide that we used in haploidentical transplants and reducing the dose a little bit.
Post-transplant cyclophosphamide is given on days 3 and 4 after a transplant at 50 mg each day. Data in the haploidentical transplant setting suggests that if we’re able to reduce the dose a little bit, a couple of things can happen along the lines of toxicity. One of the things that interests us is how quickly someone may engraft after a transplant, meaning how quickly their white blood cells come back and how quickly their hemoglobin and platelets recover.
If we reduce the dose a little bit, are we able to maintain graft-versus-host disease prevention, efficacy, or advantage? Maybe we’re able to improve a little bit with regard to the time it takes for the graft to come in. It’s a phase 2 study looking at patients who are 18 and older, who have a 7/8 donor, and both reduced-intensity as well as the myeloablative condition transplants.
We can find a list of clinical trials that will be open for consideration for a particular patient based on prior treatments and any conditions they may have.
Ashley Giacobbi
Enrolling in GVHD Clinical Trials
Finding a Clinical Trial
Stephanie: Finding clinical trials and enrolling in them is very difficult. We know ClinicalTrials.gov is available but may not be the most user-friendly. Can you walk us through the steps of how a patient could find a clinical trial that’s right for them?
Ashley: ClinicalTrials.gov is an amazing resource. It’s a database of all active and ongoing clinical trials, but it can be very challenging to use. This database contains all clinical trials for all conditions. It’s not exclusive to cancer clinical trials. Although cancer clinical trials make up a large portion of the clinical trials conducted in the United States, there are so many other clinical trials that are ongoing that it can be challenging to find one that’s right for you.
As a representative of the LLS and the Clinical Trial Support Center, we always encourage people to reach out. We hone in and find clinical trials that are most appropriate for the individual in whatever situation they are in. As opposed to having to filter through ClinicalTrials.gov, we can find a list of clinical trials that will be open for consideration for a particular patient based on prior treatments and any conditions they may have.
Types of Clinical Trials
Stephanie: We also understand that there are different kinds of trials available, like prevention, treatment, quality of life, and observational. Can you take us through what they mean in the context of GVHD?
Ashley: There are a lot of ongoing clinical trials for GVHD as this is an area of need. There’s a lot of ongoing research and that falls into different buckets.
Prevention clinical trials may look at altering the regimen prior to transplant or the medications taken after the transplant in an effort to prevent the development of acute or chronic GVHD.
Another type is treatment trials and these may include specific medications or investigational therapies that would manage acute or chronic GVHD if it’s already present.
Quality of life clinical trials are so important. There are a lot of clinical trials investigating symptoms that people with GVHD may experience. There may be behavioral interventions being investigated, such as exercise or even the use of an app to provide support. Some clinical trials offer social support or dietary recommendations in an effort to reduce symptom burden and really improve quality of life.
Finally, there are observational or natural history trials. These would be less involved as patients wouldn’t have to participate as much. These trials collect information either from the patient’s medical record or prior testing that’s been done to learn more about GVHD, who might develop GVHD, or how they might respond to specific treatments. These are important in the information gathering phase, but they might not require as much involvement from the patient perspective.
Eligibility criteria help determine the group of patients who will potentially receive the most benefit from the therapy being investigated.
Ashley Giacobbi
Qualifying for a Clinical Trial
Stephanie: You may find a trial that seems great, but there are eligibility criteria and screening processes that you may have to go through. What does that typically look like for patients?
Ashley: History, previous treatment received, and other factors play a role in the eligibility criteria, but those help determine the group of patients who will potentially receive the most benefit from the therapy being investigated. These criteria are also there to help reduce any unnecessary risk by preventing those who have underlying conditions that could be made worse by the treatment from participating in that clinical trial.
Those criteria may include things like the type of GVHD, acute versus chronic, which body systems are being affected, as well as any prior treatment received for the management of GVHD. Very often, steroids are used and some of these clinical trials will require that people have already attempted the use of steroids. Those eligibility criteria help us to find appropriate clinical trials for the individual.
Stephanie: You have touched on what you at the Clinical Trial Support Center in terms of helping people with a personalized trial list, going off of ClinicalTrials.gov and making sure it’s more tailored to them. Is there anything else you’d like to share about what they could expect?
Ashley: Patients can be referred to the Clinical Trial Support Center either by a healthcare provider or they can get in touch directly themselves. Very often, we connect with caregivers of patients.
Initially, we take the time to learn about the patient, what’s important to them, and their history. Those details are so important when looking for clinical trials and that’s usually via phone call.
Beyond that, we take the time to go through and review clinical trials. We’re very fortunate to have a unique database that looks at clinical trials in ClinicalTrials.gov but also stores information that we receive from investigators and sponsors of clinical trials so that we’re able to provide the most up-to-date information to patients when they’re considering clinical trial options.
Once we’ve generated a list, we’re able to send that to the patient, caregiver, or healthcare provider and share the clinical trials that we’ve found for that particular person. They can then take back that list to review with their healthcare team and see if any of those trials is a potential option for them to explore.
A lot of emerging data suggests that preservation of muscle mass actually helps reduce the risk of relapse, so this is not just cosmetic. It is about quality of life, but it’s also about the efficacy of the therapy itself.
Dr. Shernan Holtan
Nutrition & Exercise When You Have GVHD
Stephanie: Dr. Holtan, what specific nutritional and exercise interventions are being investigated to support muscle health during and after transplant?
Dr. Holtan: This is a substantial topic. I always tell my patients that if I could give a pill that could keep their muscles strong, I’d be the richest woman in the world. Having the ability to maintain muscle mass throughout chemotherapy of any kind is important. We need to do more in this area not just for transplant but for all cancer therapy.
There are multiple studies going on around the world that are looking at different types of nutritional supplements to maintain muscle mass and help promote intestinal healing. There’s some interesting research going on out of Italy using a nutritional supplement that has a growth factor that can help the gut heal itself.
There might be different nutritional approaches based on infection profiles. For example, we want to avoid a certain type of bacteria growing in the intestinal tract and avoid something in the diet that might help prevent that from growing. Those types of studies are important and we need to be able to expand them so that more patients can participate because, in reality, we don’t know what the best diet really is. We want people to get calories and protein in.
The same thing goes for exercise. We need to do more to facilitate exercise, especially resistance training. A lot of emerging data suggests that preservation of muscle mass actually helps reduce the risk of relapse, so this is not just cosmetic. It is about quality of life, but it’s also about the efficacy of the therapy itself. There’s a lot of work we need to keep doing in this space, so stay tuned. Obviously, this is the most important thing that we can work on besides improving the toxicities of the treatment itself. Supportive care is so important. We have a lot more work to do.
It’s on us to educate both referring providers as well as patients to understand that things have improved over time both from an access standpoint as well as supportive care standpoint.
Dr. Satyajit Kosuri
Areas Requiring More Research & Gaps in Transplants & GVHD
Stephanie: Dr. Holtan, you did mention that only a fraction of potential transplant candidates even get referred. What is contributing to this under-utilization? How can we address those barriers?
Dr. Holtan: We have an educational gap. The transplant field is vastly different in 2024 than it was even in 2021 and certainly way different than it was in the ‘80s or ‘90s, so we have to do a better job of communicating. What have been the advancements in care? How have we improved on the availability of donors? We no longer need a perfect match. How have we reduced graft-versus-host disease and improved other toxicities so that more patients are able to be reached?
There’s a lack of referral and also fear from the patient’s side as well. We have a lot of education to do to share that it is different today, much safer, and hopefully we can be able to take care of a lot more patients in the future.
Dr. Kosuri: Many of the old thoughts that we have about transplant are that you have to be a certain age or how scary it is and things of that nature. It’s on us to educate both referring providers as well as patients to understand that things have improved over time both from an access standpoint as well as supportive care standpoint.
The supportive care has changed over the last decade significantly and that’s why we’re able to take patients who previously the field would not consider, even if they were in good shape.
There can be a patient who is 50-some-odd years old but has been beaten up because of the disease or the treatment, so transplant would be very difficult for them, whereas we can have a 70-year-old who is running a half marathon. It’s not just numerical age; it’s the physiology of what the patient’s body is at the time that we’re considering transplant.
I totally echo what Dr. Holtan’s saying. It’s about education and casting our net very wide with regard to patients and patient advocacy groups as well as physicians or the referring providers.
We’re seeing so much change because of our understanding of the biology of the diseases that we’re dealing with coming into transplant, the technical aspects of the transplant, and GVHD prevention.
Dr. Satyajit Kosuri
GVHD Treatments Final Takeaways
Ashley: There are resources and support available. It’s never too early or too late to explore clinical trials when you’re talking about GVHD and clinical trial options during the transplant process.
Dr. Kosuri: Over the last decade, I have had more hope as a clinician in the field of transplant. Even though it’s trying to move, the field has been set in its ways for a very long period of time. But within the last 5 to 7 years, we’re seeing so much change because of our understanding of the biology of the diseases that we’re dealing with coming into transplant, the technical aspects of the transplant, and GVHD prevention, like the 1703 study.
There are many trials looking at the initial treatment of graft-versus-host disease and how to get patients off of steroids quicker. With chronic graft-versus-host disease that is far off, more severe, and more fibrotic, there are ways to manage that.
I want to emphasize Dr. Holton’s work regarding biomarkers. For a long period of time, our approach when it comes to GVHD was if we try something and it fails, we try another agent and provide more immune suppression. We’re hoping to minimize that approach where you throw something at a wall and see what sticks. It may be different for each patient. Do we need GVHD treatment in patients who have certain symptoms? If it is graft-versus-host disease, how do we know when to come off therapy or how to add therapy? That’s where the biomarker becomes very, very important.
I can’t emphasize enough how nutrition, exercise, and sleep are key to help recovery and resilience. I want people to know that they have more control than they think.
Dr. Shernan Holtan
Dr. Holtan: I want patients and their families to know that they have a lot of control in these processes. I believe very much in the principle of self-efficacy. Yes, this is a medical treatment that we are delivering, but there’s a lot a person can do for themselves and that their family can do together to help make the process easier.
I can’t emphasize enough how nutrition, exercise, and sleep are key to help recovery and resilience. I want people to know that they have more control than they think and look for ways that they can help build up their strength and resilience, lean on their network, and use these tools and resources to help build up the spirit and body to be able to withstand the trials and tribulations that certainly lie ahead. The medical advancements are real, but people also have a lot of control and they should know that.
Meredith: Hope is incredibly important. Recognition that you do have control is imperative. Be selfish and put yourself first. Don’t try to take care of all the people around you to the detriment of yourself. If you don’t want to do something or can’t meet with somebody, don’t do it.
Continue to find meaningful and fulfilling activities so that the illness doesn’t become your identity. You have an illness, but you’re not defined by that illness.
The LLS, being a partner of ours on this program, is such a great resource. The CTSC provides amazing one-on-one support in terms of understanding clinical trials, finding, enrolling, and even staying on them.
We hope that this program was empowering and that you’re able to take away not just from this program but from the many stories that we have.
A Practical Approach to Disputing Cancer Care Expenses, Backed by Experts and Real Patient Experiences
Edited by: Katrina Villareal
Navigating the costs of cancer treatment can be overwhelming. This live conversation provides practical tips from experts and real cancer patients on understanding your health insurance, finding financial assistance programs, knowing your rights to appeal insurance decisions, and reducing financial toxicity.
In this conversation, we’ll explore the fundamentals of health insurance, emphasizing the importance of reading and understanding your policy, including basic insurance terms. Discover your rights as a cancer patient, learn strategies for appealing insurance decisions, and explore avenues for applying for financial assistance.
Hear from Abigail Johnson, a stage 4 metastatic breast cancer patient advocate, and attorney, Gregory Proctor, a multiple myeloma patient advocate, and Monica Fawzy Bryant, a cancer rights attorney and co-founder of Triage Cancer, as they share real-world experiences, health insurance tips, and strategies for tackling financial toxicity to help you navigate the financial aspects of cancer treatment. This live conversation took place in November 2023.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Abigail Johnson: Hello, everyone, and welcome to a discussion of how to dispute cancer care costs sponsored by The Patient Story and including representatives of patients experiencing this individually, as well as a representative from Triage Cancer.
The Patient Story’s tagline is Human Answers to Your Cancer Questions. Founded by a cancer survivor who took her love of storytelling and producing videos, they assist people in the cancer community to get that all-important peer support and information about how other people have handled something that you as an individual might be facing yourself.
Without further ado, I want to get to the amazing people that we have talking about this very human issue, which is getting your cancer care costs covered.
Gregory Proctor: My name is Gregory Proctor. I’m a multiple myeloma survivor diagnosed back in July 2021. In the early stages, it was very overwhelming and very impactful not only emotionally but physically. Coming from a project management background, one of the things was trying to figure out how to navigate.
Information is not easily found in a lot of cases because if you Google things, you tend to get the bad before you get the good. But overall, my professional experience as well as having friends and family to help me move this forward has provided an overall successful outcome.
I’m proud to say that I’m still MRD negative, thriving, in remission, and continuing to flourish and be an advocate.
Monica Bryant: My name is Monica Bryant. I’m a cancer rights attorney and co-founder and chief operating officer for Triage Cancer, which is a national nonprofit dedicated to providing free education on legal and practical issues that arise after a cancer diagnosis. We provide education to the individuals who have been diagnosed, their caregivers, and healthcare professionals who are often on the front lines of getting these questions.
Abigail: Thank you, Monica. Y’all wrote the book on cancer and the law. What’s the name of that again?
It isn’t written for lawyers because we wanted to make sure that it was written in a way that was accessible for anybody to be able to access it — whether it’s the person who’s been diagnosed, their caregivers, lawyers who are trying to help out, or healthcare professionals. It’s written in a way that anybody should be able to pick it up, regardless of whether or not they have a law degree.
Abigail: I enjoyed reading it very much.
Like Monica, I’m also a lawyer, and in 2017, I was diagnosed with stage 4 metastatic breast cancer. I was 38 and it was, to put it nicely, a bombshell that went off in our lives and has changed everything since that has happened.
I’m working on getting into a clinical trial, which will be my sixth line of treatment. With breast cancer, because it’s a solid tumor, we don’t go into remission. That’s not necessarily a status or a goal for us. It doesn’t necessarily apply to our experience.
There can be no evidence of disease or, in my case, no evidence of active disease. I have been able to get to that point at least once in the last six years but I’m back getting a new treatment. For us with metastatic breast cancer, we go from treatment to treatment to treatment. There are a few that can go off treatment for some time.
I’m learning to adjust to being a professional patient, I like to call myself, because managing cancer itself can be a full-time job and that’s why discussions like this are very important because our quality of life, and Gregory alluded to this, is very much tied to not just how the cancer cells are being controlled in our bodies by the medication but also impacted by how we can get to that treatment, whether it’s literal transportation to get to that treatment or being able to afford cancer treatment.
Here in the US, cancer is quite the machine in a lot of ways. There are a lot of different players and moving parts. Our goal is hopefully to illuminate some of those moving parts, at least when it comes to covering the cost of cancer care.
Managing cancer itself can be a full-time job.
Abigail Johnson
Health Insurance
Abigail: This concept of covering cancer care a lot of times boils down to insurance. In my experience, being on a private insurance plan through my husband’s employment as well as Medicare, the first thing that I always talk to people about is getting a copy of the insurance contract. That can be daunting for a lot of people because these contracts can be 200 or 300 pages long. They are written by lawyers and many clauses can be super complicated.
If this seems daunting, intimidating, and confusing, it is. It absolutely is. It is for the professionals that are working in this arena. Getting your insurance contract, whether you have a government-sponsored insurance policy, whether you’re working with the Veterans Affairs and have coverage there, whether it’s Medicare, some documents explain what is covered.
When it’s private insurance, it is a literal contract between you and the insurance company, and it spells out what they’re going to do and not do. In my experience, there are about 10 pages that are vital for me to know out of the 300-page long contract. I have those pages highlighted, bookmarked, saved, and written all over.
I continually go back to those pages to see the clauses and the language that govern what my insurance company is supposed to do. I set my expectations based on what my insurance company is supposed to do, and then I know if they have or not.
It’s important to know what tier your medication falls in because that impacts the cost of your copay.
Abigail Johnson
Many times, a medication, a surgery, or a procedure has to have prior authorization. The medical professional has to get with the insurance company and say, “We want to do X,” and the insurance company has to look over that and opine whether or not that is medically necessary. I won’t get started about how that is practicing medicine on the part of the insurance company, but that’s the system that we have.
My insurance company has 24 hours to respond to a prior authorization request from my medical team. That’s important for me to know because if there’s a delay, I can call the insurance company and say, “My doctor sent you a fax 48 hours ago. You had 24 hours to respond. This needs to rise to the top. You need to deal with this right away because you’ve not responded in the timeline that we anticipate.”
That’s one example of how knowing what my policy says, who’s supposed to do what, and when they’re supposed to do that helps me set my expectations. I’m not fussing at my doctor’s office if it’s not their responsibility and I’m not fussing at the insurance company if my doctor hasn’t done what they’re supposed to do. Knowing when they have not done what they’re supposed to do, I can bring that to their attention and that means that will become more of a priority for my insurance company.
It’s important to know what tier your medication falls in because that impacts the cost of your copay. These are examples of things that are important to know about your insurance policy so that you know how to navigate that.
Gregory: I’ve worked with a lot of attorneys in my professional career, but I’m not one. I have always been a professional. I make my premium payment and expect that coverages are going to be there when I need them. Until something traumatic or something like cancer knocks on your door, you don’t realize the implications that you’re faced with.
We contacted my insurance company and they said, “Okay, we’re going to be able to help you move and navigate through this,” with all of the empathy and compassion that they try to give.
I’m 2 ½-3 months into treatment. I’m paying my $1,000 premium and doing everything I need to do, but I’m burning $22,500 a week. The billing department for my oncologist calls and says, “Mr. Proctor, we’re at a point where you’re a quarter of $1 million. We’re going to have to stop your treatment. Your insurance company hasn’t paid.”
I’m sitting here flabbergasted. I’m trying to fight for my life. I’m several months into my treatment and my doctor hasn’t received a single dollar from my private healthcare insurance. At that moment, I realized it wasn’t just about me fighting cancer. Now I’ve got to engage in something that you expect would be covered.
For me and my family, we had to turn the switch on and get laser-focused. Now it’s not just about the financial implications, insurance, and survival. We’ve got to look at all three with a critical eye.
Having the knowledge and knowing what to do with that knowledge to be able to save your life, save money, and avoid some of those pitfalls is extremely important.
Gregory Proctor
I had to contact the insurance company and say, “I need to see the full contract. I need to understand why you guys are not paying my doctor.” Their reason at that time was, “We have to go through an audit, Mr. Proctor. You’ve been healthy. You’ve never had any type of circumstance like this come along and then all of a sudden, now you go from 0 to $22,500 a week.”
To me, that wasn’t an excuse. I said, “I’ve never missed a premium. I’ve never missed a payment. I need this to occur for me on my behalf because I’ve done what I needed to do.”
Everyone comes from a different walk of life and sometimes knowing what to do as well as knowing how to do it becomes extremely important. One of the things that was formidably important for my wife and me was taking all of my project management experience and applying it to myself as the project so that we could cover all of the gaps.
As they always say, knowledge is power. In this particular case, having the knowledge and knowing what to do with that knowledge to be able to save your life, save money, and avoid some of those pitfalls is extremely important.
In most cases, those are not things that you think about when you’re thrown into the tsunami of cancer. You’re thinking how to get from day to day, from week to week. There’s a lot more involved and it all embodies getting yourself educated.
Abigail: Thank you for all of that, Gregory. You’re coming to this with all of the information and experience that you have. You’re going to do it as a project manager because that’s your background. Who you are, your strengths, and how you solve problems is going to be key.
Understanding Insurance Terms
Abigail: Monica, what are the top things that patients need to know when they’re looking at their insurance contract or how to get cancer care covered?
Monica: There are some things that people really should understand about their insurance long before there’s ever a diagnosis or a serious medical situation. But the unfortunate reality is that in this country, health insurance is confusing. There are going to be differences depending on the source of that insurance, whether that’s government insurance, through an employer, or a policy someone purchased on their own.
Based on studies that have been done, only about 4% of Americans understand the four most common terms used in health insurance policies. People don’t even understand the words. We’re not even talking about complex legalese here. We’re talking about the basic words because we’re never taught what those words mean.
There is an amount someone pays monthly to have health insurance and that’s the monthly premium. They’re going to pay that amount whether they go to the doctor or not. It’s like having car insurance all year but never getting into an accident.
Once someone starts utilizing their health care, there are going to be some additional costs and those costs are going to depend on the policy. Most policies have an annual deductible, a fixed dollar amount that someone has to pay before health insurance kicks in. Someone could have a $500 deductible or a $5,000 deductible. It’s all going to depend on the plan.
Once they’ve met that deductible, insurance kicks in and pays a percentage. That percentage is referred to as the cost share or the coinsurance. Here’s where it gets tricky because we have multiple names for the same thing. Cost share and coinsurance are the same thing, and that’s a percentage. If someone has an 80/20 plan, once they meet their deductible, insurance kicks in at 80%, but they’re still responsible for 20%. And when the treatment is expensive, 20% is still a huge dollar figure.
Based on studies that have been done, only about 4% of Americans understand the four most common terms used in health insurance policies.
Monica Fawzy Bryant
In addition to that percentage, many plans have copayments, which is a fixed dollar amount that is going to depend on the policy and also potentially on the service. Someone could have a $25 copayment to see the doctor, a $35 copayment to see a specialist, or a $250 copayment to go to the E.R. Figuring that out could be complicated.
The most important thing for every single person to know about their health insurance policy is if there’s an out-of-pocket maximum and what is it. Because in theory, that’s the most that someone is going to pay out of pocket for their care if they go to in-network providers for the year.
Understanding that allows us to figure out what you are going to have to be responsible for out of pocket in a worst-case scenario. The way you get to your out-of-pocket maximum depends on the plan, but often it involves adding up everything you’re paying towards your deductible, your copayments, and your coinsurance. It’s everything you’re paying out of pocket except the monthly premiums.
The reason this is so important on the front end is when people are making choices around their health insurance. We have the opportunity to do that every single year now, thanks to the Affordable Care Act and a whole bunch of other laws.
To be an effective shopper and consumer of health insurance, you have to understand those terms and be able to do the math concerning your out-of-pocket maximum.
Gregory: For me, that’s key. I always maintain a pretty healthy lifestyle. I don’t want to have to come up with $15,000 as a deductible. If I’m healthy and I still feel pretty good, I can go with a little less coverage. You take a little bit more risk.
I was diagnosed at the age of 50, which was not the best year to be diagnosed with multiple myeloma. The older I got, I began to get laser-focused in my mindset as it relates to my family of four and my insurance.
At the age of 50, I’m more susceptive to all of these things that maybe I don’t want to think about, but I need to be in a position to ensure that I’m covered holistically without any repercussions.
Abigail: It’s amazing how expensive everything is. One of the things about cancer treatment is the medication and prescription drug costs, which can be complicated. When you’re put on medication by your doctor, they don’t always tell you the price tag upfront. In the breast cancer world, many of the medications that we take will cost our insurance companies between $14,000 and $20,000 per month.
Copay Assistance Programs
Abigail: In the context of private insurance, there are often copay assistance programs, which pharmacists will often help patients apply for. These programs are offered by the drug manufacturers or pharmaceutical companies. They will also have foundations sometimes. But depending on your insurance, these programs apply differently.
For myself, having a private policy means I’m eligible for copay assistance programs. Those copays go from hundreds of dollars a month to zero, oftentimes depending on which tier of medication you’re on.
My friends who transitioned to Medicare are surprised to notice that those copay assistance programs are not always possible when you’re on Medicare and that’s where those foundations do come into play as well.
Gregory, how has that affected you in terms of paying for your medication and working with the VA, where your primary insurance is?
Gregory: I was in a unique category. I had private healthcare insurance with a national provider when I was first diagnosed. I had been away from the government programs for many years. Since I’d gotten out of the Navy, I hadn’t utilized any of their benefits.
I started going through this process and all of this funding that you don’t account for starts to show up at my doorstep. Blood work for $16,000, a test for $15,000, and I wondered what insurance is truly covering if these bills are showing up.
I was very lethargic and incoherent for five days a week for three and a half months because I was on chemo for five days a week, 6 to 8 hours per day, which was tough.
Once I finally got to the point of reckoning and saying it was time to get a hold of this situation, I found out that there are subsidy programs. Sometimes they’re publicly known, other times they’re not, particularly if you don’t ask. We started pulling our energy into how could we tap into maybe a program to be able to give us a grant and move forward.
On record today, I’ve spent $2.65 million. Navigating that journey was not easy… It’s overwhelming. You’ve got to get other people involved to help be your eyes and ears
Gregory Proctor
With private healthcare, there’s a little bit of leniency. By the time I was approved for government healthcare being a prior veteran, I couldn’t utilize those programs. It was a very delicate balancing act to ensure that going forward, I would be able to reap all of the potential benefits that I could not afford out of my pocket to maximize my overall primary care going forward.
Because on record today, I’ve spent $2.65 million. Navigating that journey was not easy. But certainly, you have to get laser-focused because no one is going to do it for you.
It’s overwhelming. You’ve got to get other people involved to help be your eyes and ears, to help address the questions of who, what, where, when, and how. Sometimes when you’re getting information from the doctors, you don’t want to accept the reality. Acceptance is always the key to making the first step in the progress of being able to battle and weather the storm.
Abigail: You have personally spent $2.65 million or your insurance company has spent that?
Gregory: I love to throw that number out there because people always say, “Oh my, what happened?” For clarification, that’s the running total. When you think about that number and go back to what Monica said. Whether you’re 70/30, 80/20, or 60/40, part of that expense is coming from you as the patient.
When you step into the throes of dealing with cancer, these are the things that you have to get laser-focused on very early on. Are you going to be successful coming out of the back side of this? Are you going to be bankrupt or dealing with the overall financial toxicity of what it does to you and how it changes your life?
Abigail: Thank you for that. Those are big numbers. Mine’s a little over $3 million so I’m tracking with you. I have not spent $3 million keeping me alive, but certainly between my family and the insurance company.
Monica: Thank you for your service, Gregory. I’m glad that the VA was helpful in this process for you because it’s deserved.
Financial Assistance for Cancer Patients
Abigail: Monica, would you like to talk a little bit more about financial assistance and how patients can go about getting help to cover their portion of these costs?
Monica: With respect to getting financial assistance, I would say don’t start there. That should not be step one when you see the big bills come in because there isn’t a whole lot to go around. As you both alluded to, there are some barriers depending on the type of insurance that somebody has.
Before someone goes down the path of trying to apply for financial assistance, there are some steps to take. Did the insurance company cover what they’re supposed to cover? That requires making sure you’ve waited until you’ve gotten your explanation of benefits, which is the letter from the health insurance saying this is what we’re going to cover and this is what you potentially owe. It’s about keeping track of your out-of-pocket maximums.
If someone understands what their out-of-pocket maximum is and what’s included in their out-of-pocket maximum, it can help them figure out how much they need from financial assistance. A lot of times, people get those prescription drug bills and don’t realize the prescription drug benefits are included. It doesn’t matter what their insurance company will pay or not. If you’ve hit your out-of-pocket maximum, they’re responsible for 100% of it.
Unfortunately, some additional steps fall into the laps of patients and family members before getting financial assistance.
Do a deep dive into what’s out there and what’s available. Even among the pharmaceutical companies, there might be different programs.
Monica Fawzy Bryant
With financial assistance, oftentimes people get tunnel vision when they’re thinking about sources of help. Abigail, you mentioned how expensive your monthly prescription drug is.
How am I going to get money? How am I going to get assistance to pay for that prescription drug? I’m on Medicare so I don’t have access to the same pharmaceutical programs that I did. What am I going to do now?
Are there other places you could potentially get help? Could you get mortgage assistance, utility assistance, or other types of financial assistance and then shift the money around? Anything that you set aside to pay for the mortgage or student loans can get shifted to help pay for prescription drugs.
Do a deep dive into what’s out there and what’s available. Even among the pharmaceutical companies, there might be different programs. Some companies can provide free drugs, some companies can provide assistance to pay copays. They all have different programs. Figuring that out is daunting.
AtTriageCancer.org, we have a chart that lists most of the major cancer drugs, the pharmaceutical companies that make those drugs, and the various programs that they have to try to make it a little less daunting to go down the Google rabbit hole because that is stressful by itself.
You can look for other types of financial assistance or grants that might be out there based on the type of cancer you’ve been diagnosed with. Sometimes there’s even financial assistance for family members who might be acting as caregivers. We have a tool called Cancer Finances that has pulled those resources from trusted sources to make it a little easier. It’s still not easy but a little easier for people who are trying to seek out those sources of financial support.
Abigail: Great resources. I have sent so many people to Triage Cancer. If you have a Sam’s or a Costco membership, you don’t even use insurance when you go to your wholesale clubs. For a medication that I was previously on, my copay was $15, but if I got it without using my insurance company, it was $20, which boggled my mind. Unfortunately, that puts a whole lot of burden on the family to figure out some of those things.
Gregory, did you ever get assistance from a social worker to help you figure some of these things out? Was that something that was offered in your oncologist’s office?
The life that you know before and after cancer is totally different. Asking questions could be the differentiator in a lot of the things that we’re talking about.
Gregory Proctor
Gregory: Not in my oncologist’s office but as I was getting prepped for a stem cell transplant. As a patient, it is important for you to ask.
Seek out and ask as many questions as possible. What do I need to do? How do I need to do it? What resources? What assets? Even if your doctor doesn’t want to give you the answers, you need to continue to perpetuate that going forward because it’s your life. The importance of survival doesn’t have a price tag.
I looked at everything. My wife and I flipped everything upside down because, at that point in time, your life is already flipped upside down. The life that you know before and after cancer is totally different. Asking questions could be the differentiator in a lot of the things that we’re talking about.
Abigail: Thank you for saying that. I talk to so many patients all the time who are worried that asking questions might be offensive or upset their healthcare providers. While that is certainly a good human thing to think about, in a situation like cancer, it’s your life on the line so ruffling a few feathers doesn’t seem to be as important as getting the answers.
Appealing Insurance Decisions
Abigail: I want to talk more about denials or when the insurance company is asking for your doctor to jump through some hoops. I talked about prior authorizations. What happens when an insurance company says, “No, we don’t think that that is medically necessary,” or like in Gregory’s situation, “We need to examine this a little bit more,” that sort of thing?
I want to throw out a couple of things that I’ve learned along the way in dealing with private insurance. Typically, when a doctor gets prior authorization, the insurance company says no. Usually, you, as the insured, get a letter that says why they denied it. Your doctor typically gets the same letter. And then what?
Besides changing your mind and doing something different that your insurance company goes along with, in my experience, what’s next is your doctor has the opportunity to do a peer-to-peer discussion. This is covered in all the insurance contracts that I have seen, along with the definition of what a peer is.
Very early on in my cancer treatment, my doctor wanted to do a PET scan. For those of us with solid tumor cancers, PET scans are often the gold standard in terms of seeing where the cancer is and how metabolically active it is. This is a tool that doctors need to be able to make good decisions.
A doctor employed by my insurance company, who was a family doctor about five years out of medical school, deemed the PET scan not medically necessary.
By looking at my insurance policy, I learned that my insurance company was required, upon my asking, to provide a peer to my doctor. I realized that somebody who’s five years out of medical school, who has a small amount of experience, and who is in a specialty that has nothing to do with oncology does not meet the definition of a peer.
I learned that I could say to my insurance company, “I require you to provide a peer to talk to my doctor.” That conversation took five minutes.
In the first conversation where it was denied, my doctor spent 40 minutes trying to convince this doctor employed by the insurance company that what she was doing was standard of care. When she was able to talk to an oncologist — not an oncologist that had 30-plus years of experience, but somebody in the cancer world — it was a five-minute conversation and it was approved.
The first person that my doctor talked to was looking at a chart and the wrong category. She was looking at somebody who was stage 3 versus stage 4.
I’ve let my doctor’s offices and their staff know as they are scheduling that they can ask for a peer. Make sure it’s a peer who’s talking to your doctor.
By looking at my insurance policy, I learned that my insurance company was required, upon my asking, to provide a peer to my doctor.
Abigail Johnson
By looking at your insurance policy and understanding the definition of a peer, that one small thing can save your doctor time. That 40-minute conversation took my doctor away from seeing patients. The five-minute conversation was a whole lot more effective and efficient.
As an insured, you also have the option of filing an appeal. It can get involved and it’s a really heavy lift when it comes to attempting to explain to your insurance company why they are not following the contract.
Gregory, what experiences have you had in getting something covered, especially when you got that initial no?
Gregory: After burning $22,500 a week and hitting a cap, hearing the words, “We will cover this, but we won’t cover that,” meant, “We’ll cover you for the period of your transplant. However, if there are any complications, then that’s on you, Mr. Proctor.”
Going from my private healthcare and trying to get the VA to pick me up had already been denied by the VA. It was very frustrating very early on knowing that I would want it to go through the VA from the beginning, but I was denied and that’s just how the system works.
Their rationale was there was no service-related tie that could tie back to me being diagnosed with cancer. I had to get attorneys involved and justify what my job and MOS (military occupational specialty) was in the military. Going through that took a tremendous amount of time.
You can’t ever give up. You have to continue to push.
Gregory Proctor
For me, one of the things that I had to sink into throughout this whole journey is don’t ever give up. Find a will. Find a way to navigate. I had to go back through all of the tests to prove that I had multiple myeloma.
Once we proved that, I was able to get 100% coverage but that took approximately five months from the time that I was diagnosed up until I was getting ready to go into a stem cell transplant.
The best Christmas gift that my wife and I could have ever received in December 2021 was that letter from the VA saying they are now my primary healthcare provider and they will cover not only my stem cell transplant but all post-maintenance costs. We’re talking, “Hallelujah!”
That was well worth all of the effort, the headache, the anxiety, the concerns, and the worries to get to that point. But like I said, you can’t ever give up. You have to continue to push.
Abigail: Thank you for those reminders. It’s easy to give up, especially when there are a lot of roadblocks. I love how you mentioned that you realized you needed help and that getting a professional involved was important.
Legal Rights as Insurance Consumers
Abigail: Monica, would you talk a little bit about the legal rights that we each have as consumers and talk about those appeals and what services might be available to patients?
Monica: Gregory did a little bit of my job for me in that we don’t have to take no for an answer. The details around that will certainly depend on the type of insurance we’re talking about, whether it’s the VA, Tricare, Medicare, or Medicaid.
If we’re talking about private insurance, at the bare minimum, every single consumer is entitled to at least two levels of appeal. The first level is an internal appeal and that’s essentially where we go back to the insurance company and say we’d like you to reconsider.
The internal appeal can take a couple of different forms. It could be a written internal appeal where you’re providing documentation. It could also be what Abigail was referring to, which is a peer-to-peer conversation between two healthcare providers.
There are time limitations on when we as consumers get to file internal appeals. We usually get 180 days. Then there are time limitations on the insurance company to give a response depending on where somebody is.
In Abigail’s example, it was a denial of a prior authorization so the insurance company has to answer within 30 days. If you’ve already received the service and they’ve come back and said, “Nope, we’re not covering that,” then they get 45 days.
Here’s the problem. When we’re talking about cancer care specifically, a lot of times we don’t have 30 or 45 days to wait for an answer. What we as consumers need to understand is that we have the right to ask for an expedited appeal when the need for care is urgent, which it is in most cases when we’re talking about cancer care. The insurance company then has to answer within 72 hours. But people don’t know this. People don’t understand that they have this right.
If the insurance company ultimately comes back and still says no, we have the right to an external appeal and that’s where we go to an independent entity. It’s going to vary from state to state, but an independent entity will look at all the facts and all the medical evidence, and then make a decision as to whether or not the care is medically necessary.
People need to understand those words, medically necessary, are the legal standard on which the appeals will be decided. Is it medically necessary for you to get that service? The decision of the independent entity at these external appeals is binding on the insurance company.
We don’t have to take no for an answer. The details around that will certainly depend on the type of insurance we’re talking about
Monica Fawzy Bryant
I made it overly simplistic for this session. I understand that requires a lot of legwork and effort to get the doctors involved. I’m not minimizing any of that, but here’s what we know to be true.
Of the millions of claims that are denied every single year, 99.9% of them are never appealed. Yet we also know that when people do appeal, somewhere between 40 and 60% of the time is decided in favor of the patient.
When we’re talking about how to help people afford cancer care, I want to talk about appeals long before we get to financial assistance. If insurance is coming back and saying, “We’re not going to cover that,” for whatever reason, “You’ve hit your max,” “We think you’re too expensive,” “We don’t think you need your PET scan,” if you’re not appealing those denials, you’re essentially leaving money on the table.
Abigail: That is such a great point. When your insurance company knows that you will appeal and will not take their decision lying down, in my experience, they’re much less likely to deny things in the future. It’s really important to make it hurt and make it difficult for them.
I’m not talking about doing anything drastic. Take up a lot of their time. Be bold in saying what you need and in filing those appeals. In my experience, they typically won’t be as likely to deny something in the future.
Thank you for giving us those numbers, Monica, because those are shocking numbers, like the millions of dollars that Gregory and I were talking about earlier.
I’m going to do whatever it takes because I’m all about living. I still have a lot more life to live than to let cancer dictate and determine how that’s going to be for me.
Gregory Proctor
Monica: It’s also helpful to put into context for people who are already overwhelmed. They’re reaching capacity in what they can handle. They’re trying to survive. Now the lawyer is saying to go through this burdensome appeals process. The numbers are helpful, particularly around the number of successful stories, to make that additional burden almost worthwhile, so to speak.
Gregory: That’s the main reason why my mantra going through this was don’t ever give up. There’s got to be a will. There’s got to be a way. It may not be door A, it may be door B or door C, but you’ve got to keep asking those questions and ensure that you’re getting the answer that you need to move forward.
When my life’s at stake, it doesn’t matter to me if it’s $1 billion. I’m going to do whatever it takes because I’m all about living. I still have a lot more life to live than to let cancer dictate and determine how that’s going to be for me.
Financial Toxicity
Abigail: I want to talk about financial toxicity. We’ve thrown that word around a couple of times. I didn’t realize this, but in 2013, it was researchers at Duke University that coined the term financial toxicity to describe the financial hardship and distress that can result from the high cost of cancer treatment.
Their research showed how the burdensome out-of-pocket expenses associated with cancer care, such as copays and deductibles, can negatively impact a patient’s mental health and quality of life, leading to increased anxiety, stress, and depression.
We hear all the time that stress is not good for patients. Stress is not good because it changes chemical things in your body. It makes your quality of life more difficult when you are stressed out. Then here comes our medical system that causes stress on us.
Gregory, how have you handled the mental toll of those bills and the financial stress? How do you handle that emotionally, too?
At one point in my life, I was questioning whether or not I would be able to afford groceries that week. That’s when you know the toxicity has gotten hold of you.
Gregory Proctor
Gregory: You’ve got to be willing to accept that this is your reality. That’s the first step in going forward with any type of traumatic or life-altering things that are happening.
The other aspect that became very, very important for me personally was stepping away from the notion of dealing with cancer 24 hours a day, seven days a week. One of the most therapeutic things that I did during my cancer battle was getting out in nature, walking on the trails, and separating my mind from the overall objective of having this wreak havoc on me.
With all of the debt and bills coming in, your life still goes on. You still have your normal expenses and now you’ve got cancer expenses and all these other things that happen. At one point in my life, I was questioning whether or not I would be able to afford groceries that week. That’s when you know the toxicity has gotten hold of you. You’ve got to navigate and weather the storm to figure out how to maneuver and move forward.
I’ve done a lot of things to get through that and find assets and various other elements in my life that I could move forward without having so much of the burden of the debt wreak havoc on me.
Abigail: Thank you for sharing that. I tell my medical teams all the time that I have to fit cancer care into my life not fit my life into cancer care. It’s a paradigm or a different way of looking at things that I think makes us as patients address some of these things a little bit differently.
Monica, would you talk a little bit about resources that Triage Cancer has or strategies for managing medical bills and finances so that people can have a good quality of life?
Monica: It’s at the core of what Triage Cancer is about. We have tons of educational resources in a variety of formats because we’re trying to meet people where they are and how they learn. Some people are big readers and that’s how they’re going to absorb information so we have quick guides and longer practical guides that can be downloaded and read off our websites.
We have live events that people can join for free, both in person and virtually. We also have worksheets, animated videos, and other materials to help people with things that can contribute to financial toxicity.
Health insurance status and navigation are only one piece of the puzzle. Certainly, employment changes that can occur after a diagnosis are going to impact somebody’s finances. Everything that normally happens in life that impacts finances keeps happening. You don’t get a pause button on paying the mortgage.
When you look at TriageCancer.org, you will see a variety of topics around health insurance, employment, and disability insurance to address holistically the financial impact that cancer and cancer care can have on people. When thinking about how to maximize health insurance, people need to remember a couple of things.
Every single year, we have the opportunity to make choices. If someone is experiencing high out-of-pocket expenses due to their insurance this year, there may be opportunities to pick a different source of insurance for the coming year.
Open enrollment for Medicare is coming up at the end of the year and that’s an opportunity to make some different choices — whether that’s finding a plan with a lower out-of-pocket maximum, a plan that has more of your providers in their network so they’re being covered at higher rates, or has a different prescription drug formulary so any prescription drugs you’re taking may be covered at a better rate.
You may be experiencing high financial toxicity right now based on the type of insurance you have, but there may be opportunities to make those changes for the coming year. We have resources at Triage Cancer to help you make those determinations.
When you look at TriageCancer.org, you will see a variety of topics around health insurance, employment, and disability insurance to address holistically the financial impact that cancer and cancer care can have on people.
Monica Fawzy Bryant
We also have a legal and financial navigation program where people can fill out a form and they’ll get a calendar link where they can schedule a call with one of our staff. We’ll talk through their situation and the sources of financial toxicity. We’ll try to provide them with personalized education and information about what they need to know and understand, point them in the right direction, and give them action steps. You can read quick guides all day long, but you may still have questions about your situation.
Abigail: Those are wonderful resources. I’ve sent all kinds of people to Triage Cancer and they’ve helped them figure things out and navigate those things.
Since Monica was talking about open enrollment and the possibility of adjusting your coverage, working with a good insurance broker can also be a tremendous help, especially when you’re going on Medicare. There are all these supplements and different options. Working with somebody who can take your situation, your doctors, your medication, and your diagnosis, and help you back into those policies that would meet some of those needs.
Typically, brokers are paid by the companies so you are not out of pocket any amount of money when you work with an insurance broker. That’s one thing that I suggest to a lot of people, especially those transitioning from private insurance to Medicare because it can be complicated with all of the different supplements.
Monica: I actually would give the opposite advice to somebody and that’s based on reports that have come out of the U.S. General Accountability Office. Over the last several years, many insurance agents and brokers have misbehaved in several ways. Now, certainly, that is not all of them. There are wonderful insurance agents and brokers out there so I’m not disparaging the profession as a whole by any stretch of the imagination.
Oftentimes, people can be led down a path that may not be the best for them. Those agents and brokers are paid by the insurance companies so they have a vested interest in enrolling people in specific insurance policies, even if those aren’t the best policies for that patient.
For the cancer community, where there is a heightened importance of making sure they are in the right plan for them, we would suggest unbiased sources of support and there are different places that people could go.
You might get a very different answer from an insurance broker versus a social worker who is employed by your cancer center. Getting different input can be important.
Abigail Johnson
If someone is transitioning to Medicare for the first time, every single state has a SHIP program, which is the State Health Insurance Assistance Program. They’re called different things in every single state. They are trained to help people navigate their Medicare options and they are unbiased. They do not get paid by enrolling people in one plan over the other.
For people who are buying insurance in the marketplace, there is a similar entity called In-Person Assistors. Again, they are paid by the government not by the insurance companies so they don’t have any bias as to putting people in one plan over the other. I agree with your sentiment about seeking help and support in picking those plans, but I’m not sure that’s the place I would send someone for support.
Abigail: That’s why we’re having this conversation to talk about different perspectives. I work with a handful of insurance brokers who I have personally vetted and are now familiar with metastatic breast cancer because they’ve assisted a lot of people that I have worked with. Having those connections and knowing if there are people in your community who are doing some of these things can be key.
But thank you for that caution, Monica, because that’s also important to remember who you’re talking to and who they’re employed by. You might get a very different answer from an insurance broker versus a social worker who is employed by your cancer center. Getting different input can be important.
Gregory: You have to educate yourself. You have to go through due diligence to ensure that you understand your situation. I’m more aware of my needs now going forward as opposed to before because it was something that I wasn’t interested in. Make sure that you educate yourself and do your due diligence because those two things can save you thousands of dollars going forward.
As we’re navigating this system, how we embody that power can make a big difference in navigating cancer treatment.
Abigail Johnson
Empowerment
Abigail: The word empowerment gets thrown around a lot. We need to understand how we’re looking at empowerment because there are multiple definitions of empowerment.
One definition, that makes me itchy, is that somebody is giving you power. The second definition, which doesn’t make me as itchy, is that we all have inherent power as people and as patients. As we’re navigating this system, how we embody that power can make a big difference in navigating cancer treatment.
Gregory, how do you look at empowerment? How have you gotten in touch with your power as an individual and as a patient?
Gregory: When I was diagnosed, I realized the importance of my purpose in life and the importance of rekindling my faith in the Lord Jesus Christ. My empowerment came back through not only my connectivity to my spirituality but also through my family, friends, and the congregation of people who follow me on social media who were there to lift me.
I took that empowerment and tried to be a beacon of hope and inspiration, uplifting people’s minds and souls when they go through a horrific experience, and letting them know that they’re not in this alone. There’s unconditional love out there, even if you get that unconditional love from a stranger who gives you power and uplifts you to be able to weather the storm and be able to move forward.
Abigail: Thank you for that, Gregory, that was beautiful. Monica, would you like to chime in on this whole idea of empowerment and how that fits in with what Triage Cancer does?
Monica: It’s not my job as a cancer rights attorney to give somebody else power because that power is theirs. But what I can hopefully give people is the knowledge that they need. Knowledge is power.
You shouldn’t have to have a law degree, a project management background, or a million people surrounding you and lifting you to be able to survive this disease with your homes intact, your jobs intact, your insurance, and overall financial health. Yet, unfortunately, because of our system, sometimes that is what’s needed. We want to walk side by side with people and support them through education and providing information so that they can then take that and use their power.
I took that empowerment and tried to be a beacon of hope and inspiration, uplifting people’s minds and souls when they go through a horrific experience, and letting them know that they’re not in this alone.
Gregory Proctor
Gregory: That’s very, very powerful. As we talk about education, you need to seek others who have endured and weathered the same storm that you’ve gone through. A lot of times, people say that may not be a good idea or maybe that is a good idea.
For me, that became one of the circumstances that my wife and I were able to glean from others who are five-year survivors, 10-year survivors, and 20-year survivors and understand how they made it that far. Of course, now drugs and everything has changed, but knowing how they weathered the storm became a tremendous, valuable lesson for us.
Abigail: That’s a wonderful comment, Gregory, this idea of seeing examples of other people, which is what we’re doing and what The Patient Story does all the time as well.
Key Takeaways
Abigail: Know who you are. Allow your strategies and how you figure out how to pay for cancer to flow from who you are. You’re doing something that’s not you. It’s not going to work so well so know who you are.
Knowledge is power. Knowing how to navigate things, knowing the right things, and sticking to your guns in that context can be extremely helpful.
Don’t take no for an answer. Keep going. Keep pushing. Keep asking questions.
Don’t forget to ask for help and collect those people who you can ask so make sure that you’re saving the link to Triage Cancer, which is TriageCancer.org.
Watch for other patients who are navigating this, jot their names down, and know that you might be able to reach out to those people for help. That list can include social workers, nurse navigators, and professionals who do these things that you’re trying to do.
Vote with your feet. When your insurance policy doesn’t cover what you need, vote with your feet. If your doctor is not going to bat for you and not going to do that peer-to-peer discussion, vote with your feet. If you know that medication is way too costly and there’s an alternative, vote with your feet.
We have these choices and to vote with our feet can be extremely helpful and maintain that quality of life to fit cancer care into our lives versus the other way around.
Knowledge is power. Knowing how to navigate things, knowing the right things, and sticking to your guns in that context can be extremely helpful.