Living Well with ALK+ Lung Cancer
Finding the Balance with Treatment & Side Effects
Living with ALK+ lung cancer means constantly weighing what your treatment can do against what it does to your body. Side effects are real, dose adjustments feel scary, and it’s hard to know when to speak up.
We meet with a leading oncologist on ALK lung cancer, D. Ross Camidge, MD, PhD, from the University of Colorado, who’s also a stage 4 lung cancer patient himself. Along with Dr. Camidge, we are joined by Nancee Pronsati, a stage 4 ALK+ NSCLC patient advocate with ALK Positive diagnosed in 2016, who has helped author a research paper on this exact topic. Between them, you get the clinical expertise and the lived reality in one conversation.
Program Topics
- Why ALK+ cancer spreads to the brain and which treatments are designed to stop it
- How oncologists choose between today’s first-line options and what to do when one stops working
- Which side effects to watch for on each TKI and when to call your care team
- Why a dose reduction is a strategy, not a treatment failure
- What questions to ask your oncologist about brain protection and clinical trials
- How care partners can help catch early warning signs
Program Panel

Visit Our Partner
Thank you to ALK Positive for their partnership. ALK Positive is a patient-driven organization that seeks a cure for ALK+ cancer and works to improve patients’ quality of life and life expectancy worldwide. Their mission goes well-beyond raising awareness by driving research, funding clinical trials, and demanding better treatment options.
Program Sponsor

Thank you to our sponsor for their support of our independent patient education program. The Patient Story retains full editorial control over all content.
This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
We’ll send you the replay link after the program airs.
- Introduction
- Meet our experts
- What it was like for Nancee to hear “ALK-positive”
- The initial questions after diagnosis and what your doctor is looking for
- How targeted therapy works and what is happening in your body
- Tyrosine kinase inhibitors (TKIs) and what knowing your marker changes
- First-line treatment decision: Lorlatinib, alectinib, and the CROWN trial
- What you need to know about brain metastases in ALK-positive lung cancer
- First-line treatment guidelines and the “Big Three”
- Managing the side effects of lorlatinib: What to expect and what to do
- Speaking up about side effects: Why it matters and how to do it
- Why side effects happen and the science behind them
- How Nancee and Dr. Camidge had the dose reduction conversation
- What’s next: New therapies, second drivers, and rebiopsy
- When to ask about getting rebiopsied and why it matters
- Key takeaways: What to walk away with
- Conclusion
- Hear from people living with ALK-positive cancer
Edited by: Katrina Villareal
Introduction
Stephanie Chuang: Hi, everyone. Welcome to “Living Well with ALK Positive Lung Cancer: Finding the Balance with Treatment and Side Effects.” There is a balance to strike when considering treatment strategy while also considering quality of life during treatment. We have two incredible guests to speak on this who are great voices in the lung cancer patient advocacy space.
I’m Stephanie Chuang, a cancer survivor and patient advocate in blood cancer. I feel like there are common threads to the patient experience. I felt incredibly alone when I was diagnosed with a lot of medical jargon to navigate through. I started The Patient Story to help connect people to other voices and to education with top cancer specialists through our video stories and educational discussions to humanize this conversation.
I want to thank our sponsor, Pfizer, for supporting this independent patient education program, which allows us to put on more of these for our communities. I want to note that The Patient Story maintains full editorial control over all content. And while I hope you walk away with a better understanding of this topic and questions you can ask your own doctor, this is not a substitute for medical advice, so please still consult with your healthcare team.
Finally, we want to hear from you because your voices matter. How did we do? What other topics might you be interested in? Who else do you want to hear from?
Meet our experts
Stephanie: Let’s meet today’s panel, thoracic oncologist Dr. Ross Camidge and patient advocate Nancee Pronsati. They will bridge clinical expertise with lived experience to navigate treatment paths and treatment decision-making that happens in ALK-positive lung cancer care, and navigate life while on treatment.
Dr. Ross Camidge is a professor of medicine in medical oncology, a Joyce Zeff Chair in Lung Cancer Research, and the director of the Thoracic Oncology Clinical Program and Clinical Research Program at the University of Colorado. In 2022, Dr. Camidge himself was diagnosed with stage 4 EGFR-positive non-small cell lung cancer, and he was gracious enough to tell his story on our platform. It was an incredible privilege to have that conversation with Dr. Camidge.
We also have an incredible patient advocate, Nancee Pronsati, who is a stage 4 ALK-positive non-small cell lung cancer patient and patient advocate. She was diagnosed in 2016 after a couple of years of not receiving the correct diagnosis. She’s been on a tyrosine kinase inhibitor (TKI) therapy for a decade, helped author a research paper in 2025 focused on the very topic we’re tackling, and has been a big part of the ALK Positive advocacy group. She’s been on the board, having previously held a vice president role. It’s a great organization that helps patients and families who are dealing with an ALK-positive diagnosis.

I’m so excited about the guests we have for this conversation who are experts in their own right. Dr. Camidge, you have all this expert knowledge, but bringing a patient perspective is going to be amazing. And, Nancee, we’d love to understand more about bridging between the things that we hear as patients from the doctor’s side and the actual impact and what questions we wish we had asked. The goal is to talk about targeted therapy, but when we’re talking about the best path forward, it’s not just about living longer but also about the quality of life.
I had been having recurrent bronchitis for a couple of years. My general practitioner kept saying I was fine and gave me an inhaler and some antibiotics. Finally, I got an X-ray, which showed innumerable nodules in both lungs.
Nancee Pronsati, Stage 4 ALK+ NSCLC Patient Advocate
What it was like for Nancee to hear “ALK-positive”
Stephanie: Before we dive into the conversation, I’d like to ask you, Nancee, to bring us back to when you were first getting the diagnosis. Had you heard about ALK-positive before? Do you remember the moment when doctors told you? How did that change how you saw what your patient experience might be like?
Nancee Pronsati: When I was diagnosed almost 10 years ago, I had never heard of ALK-positive lung cancer. Frankly, I was one of the people who lived in an ignorant bubble, thinking that only people who smoked got lung cancer. At that time, I was under 50 years old. I had been having recurrent bronchitis for a couple of years. My general practitioner kept saying I was fine and gave me an inhaler and some antibiotics. Finally, I got an X-ray, which showed innumerable nodules in both lungs. At that time, I was in New York City at Memorial Sloan Kettering Cancer Center, and Dr. Greg Riely was the person who diagnosed me.
I had a bronchoscopy, but it came back with no driver. I had no idea what that meant. He said, “I know you have one. I know you do,” so we did another biopsy and it came back ALK-positive. I still had no idea what that meant, but Dr. Riely said, “This is good,” and I was started on crizotinib (Xalkori) right away.
I was extremely unknowledgeable. My family did not have any history of cancer and even in my friend group, there hadn’t been a lot. I was starting from square one in terms of knowledge, but I have since learned a lot from understanding other people’s perspectives from this. We jumped right in and, miraculously, crizotinib (Xalkori) started to impact me within a matter of days. It was interesting because it wasn’t something that I even knew was possible with cancer, wherein pills could do that for you.
Stephanie: Thank you for sharing that. You say unknowledgeable, but I also think: How would we know? Are we reading textbooks about biomarkers on the side? Like with everybody’s experience, you’re thrown into this. And that’s the direction I’d like to go.
When someone emails me and says, ‘My relative has just been diagnosed with lung cancer,’ there are three questions that I need the answers to before I can offer any kind of opinion.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
The initial questions after diagnosis and what your doctor is looking for
Stephanie: Dr. Camidge, it’s incredible to have you for many reasons. You have the lens of an expert in lung cancer and have helped countless people, but you have your personal experience as well. You knew much more than the average patient. What are the questions that surface when people are told that they’ve just been diagnosed with lung cancer? Here’s why we’re going to do this. There are questions of “Why would I wait or pause? Why do I need this?” What are the questions you hope patients might learn to ask their doctors at that time?
Dr. Ross Camidge: When someone emails me and says, “My relative has just been diagnosed with lung cancer,” there are three questions that I need the answers to before I can offer any kind of opinion. Those are the questions that you, as the patient, need to know.
The first question is: Has someone done a biopsy? Does it fall into non-small cell lung cancer or small cell lung cancer? Then, under non-small cell, is it squamous cancer or adenocarcinoma? Those are the most common ones. Then what it looks like under the microscope gives us some clues.
The second question is: How far has the cancer spread? That tells you the stage of the cancer, which is usually determined by a PET scan and an MRI of the brain. If the cancer hasn’t spread very far, maybe surgery is on the horizon. If it has spread a little bit more, maybe radiation is on the horizon. Unfortunately, for something like two-thirds of people, the cancer has already spread beyond that phase when they’re first diagnosed.
The third question is: Have you had any molecular testing done? Honestly, that’s the bit that you mentioned about having to wait. That test takes the longest to come back, sometimes as long as two weeks, depending on where they do the testing. You’re going to have a biopsy and scans, which will tell you that you have lung cancer and the stage. But before you jump into your first-line treatment, if you can, you’re going to wait for the molecular test results to come back. That’s the information that Nancee mentioned, telling her she was ALK positive.
Nancee and I have had to enter this world where we’re not actively dying from it, but we’re not cured either… that does take a little while to get your head around.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Stephanie: You have had so many patients, care partners, and family members go through your office, Dr. Camidge. When you heard Nancee describe herself as being unknowledgeable and having no idea what this was, I want to get a reaction from you because I’m sure you get similar comments and reactions from people when you hear this. What crosses your mind? What are you hoping to get through to people, especially in the first couple of visits?
Dr. Camidge: The first thing is not to panic, which is easier said than done. Your mind tends to go to dark places and fill in the gaps with the worst possible scenario, which is usually balanced by your relative or friend who’s trying to fill you with the most positive things. You have to sit in this area of unknowing until you have all of the facts.
Then most people, once they have the facts, can get their heads around it. It might take them a little while, but they have to get their head around it. The first question that goes through everybody’s head is whether this is curable or not, because when you hear the word cancer, the next word that you want to hear is cure. You know that you’ll go through hell to be cured. But Nancee and I have had to enter this world where we’re not actively dying from it, but we’re not cured either, so there’s this third area, and that does take a little while to get your head around.
When I was first diagnosed and I was looking online, there wasn’t a lot of information about ALK-positive. It was all about lung cancer in general.
Nancee Pronsati, Stage 4 ALK+ NSCLC Patient Advocate
Stephanie: Nancee, I heard some affirmation. You have your patient-doctor relationship with Dr. Camidge, who has multiple perspectives. What resonated with you when he was saying that?
Nancee: It’s definitely the response to not panic. But as many people do, you either panic or become numb. I want to go to a whole other place that I can hardly even describe. I thought, “Okay, I have to give money to my children. I have to write letters to people. I have to do all these things.”
But once I learned I had ALK-positive lung cancer and Dr. Riely was very calm, and then I eventually transitioned to Dr. Camidge, who was equally calm. There is something to be said for the oncologist that you see. Maybe they’re all calm and maybe I’ve just been lucky, but that helps a lot. Becoming as knowledgeable as you can helps too. When I was first diagnosed and I was looking online, there wasn’t a lot of information about ALK-positive. It was all about lung cancer in general.
Stephanie: Not panicking is hard. It’s a very tall order.
What results in probably as many as 40% of cases of lung cancer is that there’s a specific gene in that cell which has gone wrong.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
How targeted therapy works and what is happening in your body
Stephanie: We’re going to talk about targeted therapy and quality of life. Before we dive in, it would be great to understand the science. What does it mean? Why have we been able to target these different drivers? Can you humanize the science for us on what’s happening in our bodies and how these targeted therapies work?
Dr. Camidge: The big change over the last 15 years is recognizing that lung cancer is not a uniform entity and that different forms of lung cancer are caused on a molecular level by different things. Now, I don’t mean cause in the sense of what started them, but what results in probably as many as 40% of cases of lung cancer is that there’s a specific gene in that cell which has gone wrong. You’re not born with it, so your other cells are fine, but it’s an abnormal gene in those cells that turns them into cancer.
What causes that change in the gene? Most of the time, it’s not smoking. These things are not enriched in smokers. Smokers tend to have much more complex cancers with multiple different mutations. It’s not 100% true, but it’s certainly broadly true. But if you’re a never-smoker and you get lung cancer, you tend to have a simpler cancer. You tend to have one where a single thing has gone wrong. People argue that maybe it’s caused by air pollution or radon gas. We don’t know because most of our studies of what causes things are looking at lung cancer in general. They’re not looking at ALK-positive lung cancer or EGFR-mutant lung cancer.
For ALK-positive lung cancer, what happens is that there’s a gene that is involved in your development when you were still a little ball of cells inside your mummy’s tummy, and that gene is involved in moving cells around, forming your organs, and everything that happens before you even look like an embryo. Then it gets turned off as it’s done its job.
What happens is that when this thing that causes the cancer occurs, that gene wakes up again. The way it wakes up is you break off the sleeping bit and attach another bit to it that’s actually already awake, so it’s actually a fusion between two genes: one that is awake, most commonly something called EML4, and then the sleeping bit, the ALK, is now also dragged out of its bed. They’re called ALK fusions or ALK rearrangements, but they’re all ways of waking up that ALK gene and saying to go move cells around and make things grow. This is fine when you’re trying to create an embryo, but not when you’re an adult. That turns it into a cancer.
Tyrosine kinase inhibitors (TKIs) and what knowing your marker changes
Stephanie: We’re talking about TKIs. People typically think that, historically, with advanced-stage cancer, you attack it right away. How does that change now that you know your marker and how your disease is behaving? How does that conversation change? Can you give us some comparison, Dr. Camidge?
Dr. Camidge: When you know what’s driving the cancer, if you know the ringleader of that particular group of cancer cells, you can personalize the therapy. We have developed treatments that can specifically silence the orders or the noise shouted out by that aberrant gene. It’s not a cure, but it can make the cells die off. The vast majority of the cells die off and there’s a dramatic response, often very quickly. Nancee said she felt better within days, and that’s true.
Some oncologists, rather unfortunately, I think, will say, “Oh, you won the lottery. You’ve got ALK-positive lung cancer.” You’ve still got lung cancer, so we have to rein in what we mean by good news. Amongst the bad news lottery, maybe you got a slightly less bad ticket, but no one should pretend that this is good news. Nancee, is that okay to say that?
There are many people whose diseases don’t respond as mine did, who also got the ‘lucky’ ALK-positive biomarker
Nancee Pronsati, Stage 4 ALK+ NSCLC Patient Advocate
Nancee: Oh, I’m grateful to hear you say that. Daily, I would hear, “You won the lottery,” directed at somebody who was diagnosed with ALK-positive lung cancer. My husband says, “Well, you could look at it like you’re the luckiest unlucky person.” Maybe that’s a different way of putting it.
I would never say that I’m not grateful that I had a mutation and that there were treatments. After all this time, I’m still here. But to Dr. Camidge’s point, it’s still lung cancer and there’s still such a long way to go. And there are many people whose diseases don’t respond as mine did, who also got the “lucky” ALK-positive biomarker, but they’re short responders. So it’s not quite winning the lottery, I guess.
Stephanie: This conversation matters. I’m so happy that Dr. Camidge brought it up and that, Nancee, you shared what you hear on a daily basis because it invalidates people’s experiences and their feelings, and it’s not helpful.
What changed in the last few years is that a single dominant first-choice pill has emerged.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
First-line treatment decision: Lorlatinib, alectinib, and the CROWN trial
Stephanie: Dr. Camidge, when you have a patient who you’ve determined has ALK-positive lung cancer, what’s the conversation you have with them about treatment options and why you would recommend one? What factors do you consider?
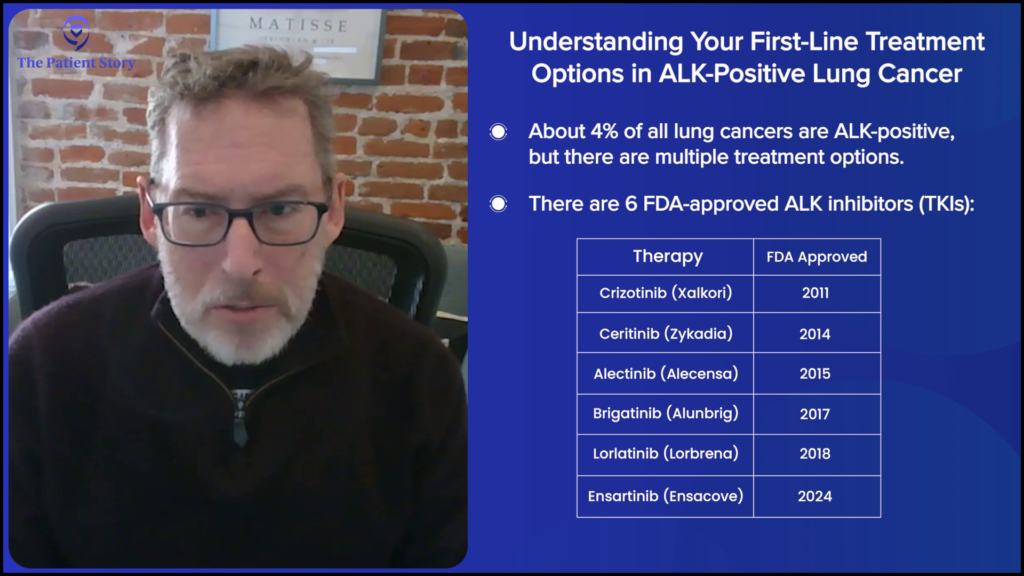
Dr. Camidge: The discussion has gotten easier. Around 40% of people have a specific genetic change in their cancer. Of those, maybe 10% have ALK, which means 4% of lung cancers have ALK. You’re special if you have ALK, but you’re also special if you have EGFR, BRAF, or RET. These things are all individualized. Most of the ones where we can identify a specific genetic change, there is a targeted therapy available, which is usually a pill. Certainly, in the world of ALK-positive lung cancer, we have an embarrassment of riches. We have five or more different ALK inhibitors.
What changed in the last few years is that a single dominant first-choice pill has emerged. The reason it took a while is that you don’t know who’s going to win the marathon in the first 10 minutes of the race. You have to see who has got the legs and who can control the disease the longest. That took something like five years of follow-up in that clinical trial to see that one particular pill, in this case, a drug called lorlatinib (Lorbrena), could actually control the disease longer than anything else. As of about 2024, most people would recommend starting on lorlatinib (Lorbrena) if you have advanced ALK-positive lung cancer.
After about five years of follow-up, the number of patients whose cancer was progressing started to plateau after two or three years, and it stayed there.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Stephanie: Thank you. I appreciate that. You have the clinical trial data, but then you have the years out there, actually seeing how people’s diseases respond to the therapy. It took another five years before you could say this had emerged as a pretty good winner.
Dr. Camidge: When the first data came out, it looked about the same as the other stuff and it had more side effects. I was certainly one of the people who said, “I don’t know that this is any better. You can show me all the preclinical science, but maybe we’re getting a little ahead of ourselves.” But then, when I saw data with five years of follow-up, I realized that this is better than using this drug sequentially. I changed my tune when I saw the data.
Stephanie: Since you’re talking about the data, are you talking about the CROWN trial? If so, let’s get into it. Nancee, I certainly want to get your perspective on this as well. What is it that you were looking at? Tell us about the update and what was such a headline.
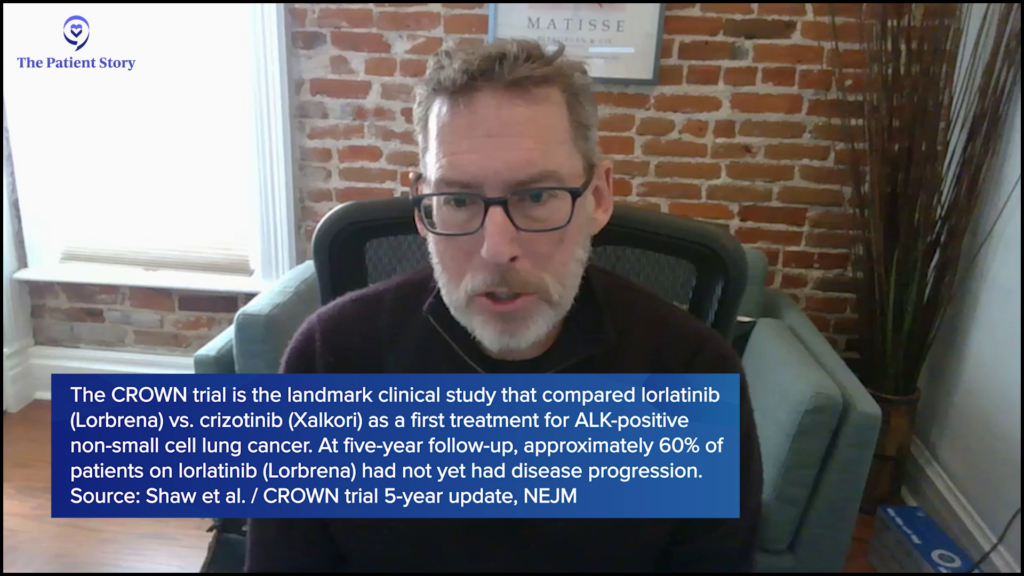
Dr. Camidge: We look at progression-free survival (PFS), which is the time it takes for the patient’s cancer to either grow or for the patient to pass on. In other words, survival is in there. What we saw is that after about five years of follow-up, the number of patients whose cancer was progressing started to plateau after two or three years, and it stayed there. Now, for something like 60% of people, their cancer has not yet progressed on the drug. It’s quite incredible. There’s a bit more in the way of side effects that you have to manage, but they’ve become “acceptable” because of the benefit that we’re seeing.
Stephanie: The cost versus benefit of how much you’re giving for what you’re getting in return, and that’s something people have to decide whether it’s worth it for them or not. Is that right?
Dr. Camidge: Yeah. You walk through the door and don’t know if you’re going to be in the 60% or not, but those are the best odds you’re going to get. There’s a 60% chance that in five years, your cancer is still going to be controlled.
I had an MRI where they found brain metastases, so the cancer progressed… My choices were more driven by what was available.
Nancee Pronsati, Stage 4 ALK+ NSCLC Patient Advocate
Stephanie: There’s so much development happening. Nancee, you can give such a great perspective because you’ve been on multiple therapies since being diagnosed in 2016. Can you give that patient perspective? How did the conversation shift? What matters to you as a patient when all this development is happening?
Nancee: When I was diagnosed in 2016, the only TKI that was available for first-line was crizotinib (Xalkori). There weren’t any options like there are today, where people sit down and talk through all the pros and cons. There were some clinical trials, though. The other alternative was to do chemotherapy first, but my oncologist at that time suggested that I try crizotinib (Xalkori).
In about a year, I had an MRI where they found brain metastases, so the cancer progressed, which was common, but I did not realize that. At that point, the choices were alectinib (Alecensa) or ceritinib (Zykadia), so I was in a different place compared to people who are more recently diagnosed. My choices were more driven by what was available, but I’ve been very lucky on alectinib (Alecensa).
I’ve now been on alectinib (Alecensa) for nine years. When the cancer had progressed, in my mind, I thought I had brain cancer, which, of course, I know now is not the case. I had lung cancer that metastasized to my brain. I was still flying from Denver to New York. Dr. Riely said, “You’re still my patient, but we have the best ALK specialist in Denver and you live in Denver.” He was so gracious and modest. That was when I switched and was lucky enough to be Dr. Camidge’s patient. I haven’t had progression, so I’ve been lucky to remain on alectinib (Alecensa).
I will say that my side effects are increasing dramatically, so I would be interested at some point in talking about other options as they come down the pike. I don’t know what that would be, like whether it would be lorlatinib (Lorbrena) for me.
Dr. Camidge: We talked about what a patient would start with if they walked through the door today. But when you have someone like Nancee who’s on a different drug and doing great, that doesn’t mean you have to change because you’ve already declared that’s the right drug. You are in your own personal plateau of no progression, so you don’t need to jump.
Nancee: If someone went in today with my exact diagnosis, they would probably start with lorlatinib (Lorbrena). What we see in our group is a lot of people who, if they started on alectinib (Alecensa) within the last six months, are switching to lorlatinib (Lorbrena), hoping to take advantage of that great progression-free survival. Most people are trying to make their best bet and go with lorlatinib (Lorbrena).
If you’re on a drug and you’re doing great, you don’t need to change.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Dr. Camidge: There’s a tail in the alectinib (Alecensa) curve, too. There’s a plateau at a slightly lower level, but you’re on that plateau. For me, it’s within the first two years when you haven’t declared that you’re on that plateau of it being the best drug for you.
Stephanie: Dr. Camidge, does that mean that, generally speaking, it takes about one to two years to see if this is going to stick and make an impact, which is why someone would stay on alectinib (Alecensa)?
Dr. Camidge: Yeah. If you look at a population of people, you can very simplistically put people into one of two buckets: those who will have disease progression within the first couple of years (or what we uncharitably call bad ALKs) and the group of people who hit that plateau where, year after year, they can stay on the same drug, whatever that drug is. There’s a plateau with crizotinib (Xalkori), too, but it’s the number of people in those plateaus. If you’re on a drug and you’re doing great, you don’t need to change.
Nancee: I met someone recently who’s been on crizotinib (Xalkori) for 12 years.
Your cancer can take a left turn and then you’ll need something other than just an ALK inhibitor.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Stephanie: That’s why this is great nuance, because this is about each individual and how their disease is responding to different treatments. It’s not to generalize for everybody, but it’s good to understand. To summarize, you wait to see if a person is within the two-year range and if they haven’t hit that plateau or not, then it’s open. If someone has responded well, like Nancee, you keep them on the same therapy until something changes, and then switch.
Dr. Camidge: Essentially, yes. We might play around with the dose to manage side effects. But I want to pick up on something: We’re not waiting for somebody to be within the two-year range. They are wherever they are when this new drug comes along. If somebody is already one to two years out and doing well, you don’t need to change. But if they have just started and a new development comes out tomorrow, you can say that the new development looks better and the odds are you’ll stay on it longer, so you could change.
Stephanie: I asked because something that’s come up in multiple conversations is how many tools we have in the toolkit. I’ve heard some patients say, “I want to try this until I know I absolutely can’t, because then at least I have something else to go to and I want to preserve that option.”
Dr. Camidge: Yeah. That gets into a whole interesting area of whether everybody goes from A to B to C to D, and the answer is no. Your cancer can take a left turn and then you’ll need something other than just an ALK inhibitor.
Stephanie: Got it. We will also get into other considerations, including second drivers.
There is a certain tendency for ALK-positive lung cancer to go to the brain more than other forms.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
What you need to know about brain metastases in ALK-positive lung cancer
Stephanie: Nancee, the cancer spread to the brain and now there’s this whole other set of questions. By the way, I think it’s very natural to think that you now have brain cancer.
Nancee: Right? It doesn’t seem natural, but it did at the time.
Stephanie: I’d like to zoom out there. Dr. Camidge, there’s a higher tendency for ALK-positive lung cancer to cross the blood-brain barrier. How do you describe that?
Dr. Camidge: Yeah, there is. It all depends on how you do the calculation. You have to factor in that if you live longer with a particular subtype of disease, you have more time for it to spread, so you do the calculation when you’re first diagnosed. What proportion of people with ALK-positive lung cancer versus other types of lung cancer has spread to the brain? Assuming everybody gets a brain scan and you’re comparing like with like, it’s over 30%, which is probably 10% higher than most forms of lung cancer. There is a certain tendency for ALK-positive lung cancer to go to the brain more than other forms.
We’re still grateful for crizotinib (Xalkori), the drug that Nancee first started on, because there are people alive today who wouldn’t be without it, but nobody starts on that now. One of its Achilles’ heels was that it was very bad at getting into the brain, so it left that area unprotected.
Now all of the new drugs have activity in the brain. Lorlatinib (Lorbrena), for reasons that are still debated, has incredible activity not just in treating disease within the brain but also in protecting the brain. I believe that’s separate from its ALK activity. It has activity against NTRK, which I believe is the key to protecting the brain.
Every one of these targeted therapies, despite calling them targeted therapies, hits more than one thing inside your cells. It’s more like a Swiss Army knife and slightly less like the key in the lock that we like to pretend it is. Lorlatinib (Lorbrena) hits ALK, but it also hits ROS1 and NTRK, which are forms of lung cancer. But there’s also a normal form of NTRK in our bodies and when that normal NTRK is inhibited by this drug, it can cause a whole bunch of side effects. People tend to think of that as unnecessary baggage that lorlatinib (Lorbrena) drags along, although I think there’s some increasing data that there’s some benefit from inhibiting NTRK as well.
I want people to realize that if it does metastasize to your brain, it’s not the death sentence or the horrible outcome that I thought it was.
Nancee Pronsati, Stage 4 ALK+ NSCLC Patient Advocate
Stephanie: Nancee, as you’re hearing all this, is there anything you wish you had known back when you were first told the cancer had spread to your brain — things you hope that other patients and families can take away?
Nancee: I want people to realize that if it does metastasize to your brain, it’s not the death sentence or the horrible outcome that I thought it was. I thought that was the end. I had had no symptoms. The metastases were very tiny, but it still felt so profound because there was cancer in my brain. I want people to understand that there are many ways to treat it, like with stereotactic body radiotherapy (SBRT), surgical treatment, and powerful TKIs. It’s been nine years since alectinib (Alecensa) inhibited those in my brain; fingers crossed for a little bit longer. It isn’t that different from progression somewhere else, I would say.
Dr. Camidge: When I first looked at my scans, I saw a 2-centimeter lesion in my brain stem. For those who don’t know, your brain stem is only about 3 centimeters across. When I looked at it, I thought, “I shouldn’t be alive with that.”
Stephanie: I remember you mentioned that when we were talking about your patient story. Dr. Camidge, with your perspective on top of being an expert in this space, is there anything you now say to people, understanding where they are mentally and emotionally, that’s different from before?
Dr. Camidge: I don’t know if it’s different from before, but I’ve been doing it for a while. Since 2018 and every year since then, we’ve taken a picture of all of the people who are at least five years out from their diagnosis. We get them all in a room together, give them a birthday cake, take a picture, and stick it up in the clinic. When I’m talking to patients who are newly diagnosed, I see that panic and withdrawal on their faces. At some point, I break the fourth wall and say, “Can I borrow you for a second?” I take them to the corridor, show them the pictures, and say, “I’m not guaranteeing that this is going to be you, but I am showing you that it’s possible. There are real people, not just statistics, who do it.” And you can see people gather themselves together and say, “Okay, that’s the challenge. I can do this.”
Stephanie: I love that you have the wherewithal to understand the impact of why that’s so necessary. I hear sometimes that we can’t share this story because it’s giving false hope. When people are thrust into this, there’s only one way forward. By showing them the pictures, the message is: I’m not guaranteeing this will be you, but here’s what we’re working towards and here’s what’s possible.
My attitude is: I don’t care about how easy your conversation is in the second line. You should do the right thing for the patient.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
First-line treatment guidelines and the “Big Three”
Stephanie: There are NCCN Guidelines and ASCO Guidelines on first-line options. We’ve talked a lot about lorlatinib (Lorbrena) and alectinib (Alecensa). Dr. Camidge, is it true that there’s a big three? How would you characterize that conversation on first-line treatments?

Dr. Camidge: The third one is brigatinib (Alunbrig). In terms of where people are in the big three, it depends on what country they’re in. There are some countries where brigatinib (Alunbrig) dominates over alectinib (Alecensa). In most of the world, alectinib (Alecensa) was the dominant drug. Then, in the last two years, lorlatinib (Lorbrena) has started to take over in terms of new prescriptions.
But there are still people who are starting patients on alectinib (Alecensa). I think they’re probably wrong. Those are well-meaning oncologists who may not be 100% up to speed and are saying, “I want to save my conversation about what to give in the second line and I’ll know what to do. I can give them lorlatinib (Lorbrena) second line.” My attitude is: I don’t care about how easy your conversation is in the second line. You should do the right thing for the patient. Sorry to be blunt.
Stephanie: No, please be blunt. That’s exactly when you need to be blunt.
Managing the side effects of lorlatinib: What to expect and what to do
Stephanie: Let’s get into side effects. Nancee, you authored this paper. Dr. Camidge, when you’re talking to patients about lorlatinib (Lorbrena), how do you navigate that conversation? Here’s how it’s effective and also, here’s how you might prepare for X, Y, and Z. What does that conversation look like?
Dr. Camidge: It varies depending on the drug. You have to explain that even though it’s a pill, it’s not benign. It’s a powerful medicine that happens to be available in pill form. For lorlatinib (Lorbrena), there are several different things that will affect your life. Something like 80% of people will end up having to go on medications to lower their cholesterol, triglycerides, or other fats in the bloodstream. That’s coming. You don’t feel any different; it simply shows up in the blood tests.
Probably the biggest thing in the short term is that it can affect your thinking in the broadest possible way. It can affect your mood, your memory, your speech, and your sleep. When the drug first came out, oncologists didn’t know the right questions to ask and most people don’t volunteer that they’re feeling different. Sometimes we have to learn what questions to ask. Over time, you could see that the percentage of people with these types of neurological side effects went up because we learned what questions to ask and to ask the caregiver who came with them.
The company says that when side effects arise, a way of managing them is to reduce the dose. The trouble is, if you look at clinical trials, the dose reduction rate is 20%, but the frequency of neurological side effects is 60%, so most people are not getting their doses reduced.
What many of my colleagues and I do is we start at a dose that’s lower than the prescribed dose, and then we increase as tolerated. The company isn’t doing that because they didn’t do the trials that way. The starting dose is 100 mg, but I actually start patients on 50 mg. Many of my colleagues start at 75 mg. Then you escalate. But it can take some time for these neurological side effects to manifest, so you don’t escalate quickly. People are going to be on this for years, so there’s no rush. I take at least six weeks before I even think about escalating the dose. When you do that, it’s much easier for someone to determine if they felt different when the dose was increased and you’re able to find the sweet spot for that individual.
Don’t be afraid to go down on the dose. This isn’t supposed to be punishment.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Stephanie: What do you recommend for patients whose doctors start at the full company-prescribed dose? Do you have guidance for patients on how to advocate for a different approach?
Dr. Camidge: Dose reduction is not compromising efficacy. It’s a very real part of managing long-term side effects associated with these drugs. Don’t be afraid to go down on the dose. This isn’t supposed to be punishment. Our aspirational goal is perfect control of the cancer and perfect quality of life. Maybe we don’t achieve either of those, but that’s still what we should aim for.
Stephanie: Thank you, Dr. Camidge. Nancee, what resonates with you on this? Not only are you an ALK-positive lung cancer patient, but also an advocate. What bubbles to the surface when talking about managing side effects of treatment?
Talk to your doctor about modifying your dose. It’s so important for people to take that seriously and watch what’s happening in their bodies.
Nancee Pronsati, Stage 4 ALK+ NSCLC Patient Advocate
Nancee: I hate to speak to it since I’m not on lorlatinib (Lorbrena) myself. However, we as an organization have done focus groups that I helped moderate, and they were talking about exactly what Dr. Camidge was saying. A lot of them were experiencing cognitive effects. The word “rage” came up many times on the 100 mg dose.
Interestingly, the other thing is weight gain. I know it sounds great to say, “Oh, I’m alive. It’s fine if I’m fat.” It’s hard. For people to gain 40 or 50 pounds very quickly is very emotionally distressing. In the paper I co-authored, they made me the lead author as a gesture, as I’m a patient, but I did participate in it. The paper discussed the timing of when these events tend to happen within the CROWN trial. The patients could understand that, typically, people go through this stage at 180 days.
Pfizer put in conversations about dose reductions, which I thought was impressive given that they tell people to start at 100 mg. They opened that as a recommendation in a patient guide: Talk to your doctor about modifying your dose. It’s so important for people to take that seriously and watch what’s happening in their bodies. Talk to your doctor, whether it means palliative care or something else. You hear about these side effects impacting people’s relationships, which is a high price to pay when it can be managed.
When you first analyze studies after a relatively short period of time, your cancer is shrinking, but you don’t see some of these long-term side effects.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Dr. Camidge: Can we talk about the weight gain? I think that’s insidious because it’s slow and cumulative. We talked about how long it took for the penny to drop once we were looking at efficacy. You need to be on it long enough. When you first analyze studies after a relatively short period of time, your cancer is shrinking, but you don’t see some of these long-term side effects.
Weight gain is a big deal. But my issue with the companies that make these drugs is that they need to start to own the management strategies, too. They shouldn’t just say, “Let’s get some experts in the room and ask, ‘What did you do to manage?’” It should be, “Did it work?” There are weight loss drugs and we have many of them now. Do a study and show that they work. Anecdotally, we believe that they work, but I believe the people who make these drugs should own that responsibility, too.
Nancee: I agree. I heard about a potential trial related to GLP-1s with TKIs. It’s so important because I’ve seen presentations where they talk about diet and exercise as the solution for weight gain, but that isn’t what’s causing it. People can watch what they eat and still gain weight. There are financial aspects too. Maybe they can’t afford to pay $500 a month for GLP-1s. How can we pair lorlatinib (Lorbrena), for example, with a GLP-1 prescription if that turns out to be viable?
Dr. Camidge: Yeah. We now know, because now we’ve studied it, that there’s some weight gain with alectinib (Alecensa), too.
Nancee: There is, yes, and it finally shows up in the list of side effects. I don’t know when it did, but it didn’t at first. People kept saying it wasn’t real. It is. And I believe that it is.
Stephanie: Is there anything we can simply explain about why the weight gain is happening on these TKIs?
Dr. Camidge: For alectinib (Alecensa), I can’t explain it yet. For lorlatinib (Lorbrena), it’s the NTRK again, the other target it hits. We know that NTRK is involved in controlling hunger or satiety, which makes you feel full. If you inhibit it, you feel hungry.
Stephanie: So maybe GLP-1s can come in and address that?
Dr. Camidge: Yeah, so it makes perfect sense.
Speaking up about side effects: Why it matters and how to do it
Stephanie: I want to dive more into the real-life experiences of why people would or wouldn’t want to mention side effects to their oncologist. Some people might be concerned that if I say this, they would be taken off the drug. What’s your guidance to people on speaking up?
Dr. Camidge: Can I put a little pin that we should talk about the side effects of alectinib (Alecensa) too, since we have Nancee here?
It’s incredibly important to volunteer that information to your doctor. The caregiver, relative, or friend who comes with you is also an important voice because they can give a different perspective. Some people may be intimidated by doctors, so it slips their mind. Before you go, write a list of things to discuss or questions to ask. Other people, particularly if they’re in a clinical trial, might be worried they’ll be taken off the trial. Sometimes it’s cultural. They think that they shouldn’t worry the doctor with those things.
But honestly, if we don’t hear, we don’t know. I’ll give you an example. There’s a drug we are using increasingly to control nausea called olanzapine, which is used as an antipsychotic at higher doses. One of the side effects of olanzapine is sexual dysfunction. Imagine how embarrassing it would be to come in and tell people that. You think it’s just you or because you’ve got cancer. When you form a close relationship with your patient, they start to tell you these things. And we only know because people have had the guts to stand up and volunteer this information.
There are probably other people like me who try to be grateful that their disease is stable.
Nancee Pronsati, Stage 4 ALK+ NSCLC Patient Advocate
Stephanie: Nancee, marrying that with your own experience, how have you approached this? What side effects have you had to deal with? Has it been easy to engage in conversation about them with Dr. Camidge?
Nancee: To start with, I have not been the greatest about sharing side effects along the way. I have shared some, but in part I think it’s because I think, “My cancer’s not growing. I need to be more grateful. These are minor things in the big picture.” And when I compare myself, which I know is the thief of joy, to others who are doing so much worse and struggling so much more, I feel like a whiner. There are probably other people like me who try to be grateful that their disease is stable.
That said, I’ve had side effects, but not the same as some have had. Some people on alectinib (Alecensa) have crippling fatigue, which I don’t have, but I have terrible neuropathy. I would say that over time, now that I’ve been on these drugs for this long, it’s so much worse. I’ve had periods when it wasn’t as bad. I did have a dose reduction a few years ago, which helped for a little while. The pretty common side effects are aching legs and neuropathy. For me, it now goes from my feet all the way to my hips. With the fatigue, I’ve convinced myself that it’s just 10 years later and that’s all it is.
I would think, “Should I be doing something different?” I feel like there’s some cumulative effect of this medicine over this time. I have a great quality of life, but there are certainly some side effects that wear you out a little on some days. It was easy to talk to Dr. Camidge. Over the years, he has had several fellows who are very curious young people who ask a lot of questions and are always great at coming up with helpful solutions.
There clearly are cumulative effects over time.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Dr. Camidge: Nancee, you raise a very interesting point, which is that there clearly are cumulative effects over time. When they follow up with people in trials, one of the expressions that people use, which I hate, is that they say there are “no new safety signals.” What they mean is that there are no brand-new side effects that no one had seen before. That doesn’t tell you that among the safety signals we already had, they’re increasing in frequency, so it’s a very misleading statement. You could say the neuropathy rate is 5%, but now it’s 20% if you’ve been on it this long. There’s a lot of potential to improve what we record and how we present it.
Nancee: Yes, I agree with that. I wonder what will change that, whether it’s time and researchers talking about it as we go forward or maybe the data will start to bubble up the longer we live on these drugs.
Dr. Camidge: No new safety signal sounds like nobody’s doing anything different. But it’s not. I think it’s inappropriately used to reassure people and is actually misleading. I hope that, in the future, there will be certain expressions that will be called out as inappropriate language to use in publications.
Nancee: Yeah, that makes sense. I hope so.
Stephanie: It’s actually detrimental to patients if that language continues and people don’t understand what’s actually happening. I appreciate you raising that, Dr. Camidge.
Why side effects happen and the science behind them
Stephanie: It’s helpful for people to understand why these side effects are happening, so it’s not in a vacuum. Could you go through some of these? Nancee’s talked about fatigue. We’ve talked about brain fog.
Dr. Camidge: When people are looking at the next ALK inhibitor to develop, I’ve tried to dial out activity against the NTRK pathway, as it’s the guilty party for many of the side effects of lorlatinib (Lorbrena). The N in NTRK stands for neurotrophic, so it’s involved in the development of our nervous system. To be honest, we’re learning its function by interfering with it. It’s clearly involved in how we think, how we process mood, and how we do all of these other things, so it’s a direct side effect of this other tool in the Swiss Army knife of lorlatinib (Lorbrena).
On the other hand, alectinib (Alecensa) doesn’t affect your thinking, but fatigue is an interesting thing because it’s common with many anti-cancer treatments. Nancee, how does fatigue manifest in you or in the people that you’ve spoken to?
Nancee: I’m used to being able to get up and go and feel very energetic and light. But there’s almost like this feeling of heaviness and feeling like I need to take a nap. I feel so heavy on my feet, like I’m drudging through.
Dr. Camidge: So it’s like a physical heaviness?
Nancee: Maybe it’s more mental. It seems physical to me as I say those words, but I think it’s more mental fatigue.
Fatigue is a very simplistic umbrella term… If you got people in a room and talked about it, I feel there are different types of fatigue.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Dr. Camidge: Mine manifests as a screensaver function. If you’re interesting, I’m perky as anything. If you’re not, I will fall asleep.
Nancee: You know what, that might be what mine is too. Before this talk, I was tired. Now I’m here and I’m not, so maybe mine is similar in a way.
Dr. Camidge: There’s a movie titled “Crank,” where you have to keep your heart rate up. That’s what life is like.
Nancee: That’s a great analogy. I’m going to have to remember that one. That’s very close to what mine is like.
Stephanie: Also, it’s a lot of pressure. Now anytime we engage with Dr. Camidge, we’d think, “How close did he get to falling asleep on us?”
Dr. Camidge: No, you’re safe. You’re good.
Stephanie: It’s interesting to describe fatigue because it’s not just tiredness. I had a different cancer, but my fatigue was taking five times longer to do something that was earlier classified as simple. Putting on my socks felt like such a laborious thing to do.
Dr. Camidge: I feel like fatigue is a very simplistic umbrella term. It’s a bit like the Eskimos having multiple names for snow. If you got people in a room and talked about it, I feel there are different types of fatigue.
Stephanie: That’s interesting. We should do a focus group or a panel discussion on that. I’ve never thought about that. I love that.
Effects on the liver usually just show up in blood tests. Most people don’t have any symptoms from that.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Nancee: I agree. That’d be interesting because it’s not fatigue like you imagine when you run a race. It’s a different fatigue.
Stephanie: Is there anything else in terms of explaining why some of these things happen? I think on alectinib (Alecensa) and brigatinib (Alunbrig), something I saw in the research was the impact on the muscle and liver.
Dr. Camidge: Effects on the liver usually just show up in blood tests. Most people don’t have any symptoms from that. Concerning the muscle, there’s a breakdown product of your muscle called creatinine kinase or creatinine phosphokinase that goes up in the blood. Most people don’t have any symptoms, but if people are very physically active, like going to the gym, the achiness that they get the following day becomes exaggerated. If you measure, there are even higher levels in the blood. It’s mostly subclinical and just shows up in the blood test, but some people can actually get that achiness, which is different from the generalized achiness that you can get on alectinib (Alecensa), which isn’t directly related to muscle breakdown.
It’s not unusual for me to raise the issue of dose reduction, but we don’t put it into action straight away.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
How Nancee and Dr. Camidge had the dose reduction conversation
Stephanie: You two had the dose reduction conversation for Nancee. Can you bring us through it? Nancee, how did you feel? Were you tentative about going to Dr. Camidge? You talked about gratefulness and not wanting to complain. Was the conversation hard or easy?
Nancee: It’s not hard for me to be open and share, but it’s always hard for me to sound like I’m complaining. It wasn’t hard to bring it up, though. Every time I saw him, I’d say, “Oh, my legs hurt.” We had tried some medicines and other things, like gabapentin, but it made me so tired and miserable. He proactively suggested the dose reduction and I have been on it since. I didn’t question it. I question a lot of things, but I was very comfortable with that suggestion. The dose reduction helped. The side effects have ramped back up again over the last year or so, but it helped a lot at the time.
Dr. Camidge: It’s not unusual for me to raise the issue of dose reduction, but we don’t put it into action straight away. I seed the idea in someone’s head; they go away and think about their side effects, and then maybe they come back in three or six months and say, “Let’s try it.”
Nancee: Yeah, you were very much like that. We would talk about it. I jumped on it because I wanted to try something different, because it had been quite a few years of that. But yeah, you were always saying, “What do you think? You can think about it.” I don’t even think you reduced my prescription right away.
It’s taking a long time for us to get people to the point of understanding that the dosage was part of the trial, but it does have equal efficacy at a lower dose and it’s safe to try.
Nancee Pronsati, Stage 4 ALK+ NSCLC Patient Advocate
Dr. Camidge: It’s easy for alectinib (Alecensa). Four pills twice a day is the full dose, so you’re on eight pills a day. So telling a patient to reduce it to six isn’t hard; you don’t have to change the prescription. Whereas for lorlatinib (Lorbrena), you need to have a new prescription with smaller-dose pills.
Nancee: Yeah, it was easy and that conversation was as well. I understand that for some people, it’s not easy. There are people who have been very afraid and nervous about lowering the dose, particularly of lorlatinib (Lorbrena), when they’re starting. They feel like they need the full 100 mg. It’s taking a long time for us to get people to the point of understanding that the dosage was part of the trial, but it does have equal efficacy at a lower dose and it’s safe to try.
Dr. Camidge: What’s important is exposure or the levels in your blood, which isn’t the same as the dose you put in your mouth because it has to be absorbed, metabolized, and excreted. All three of us could take the same size pill, but the levels in our blood might be different. Maybe the person with more side effects is absorbing more and not metabolizing as much. If you bring the dose down, you can get them into the same range as other people and that’s why they don’t have side effects. Sometimes what the side effects are doing is telling you that you already have too much in your blood.
Some [side effects] are reversible and that’s where it’s easy to experiment: go down on the dose and see if they feel better.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Stephanie: I love that framework. To wrap this piece, Dr. Camidge, what is your message to other treating oncologists on tips for having that dose reduction conversation?
Dr. Camidge: It depends on the side effects. Some of them are reversible and that’s where it’s easy to experiment: go down on the dose and see if they feel better. Some of them aren’t, like neuropathy, which is probably damage to the nerves. You go down on the dose and slow the rate of decline, but it doesn’t automatically reverse what’s already happened, so that’s a slightly harder message to get across. But, Nancee, did you say your neuropathy got better, or did it not get worse as much?
Nancee: I felt a little better. Maybe it was even fatigue as well. And then it came back. It never went away throughout this.
What’s next: New therapies, second drivers, and rebiopsy
Stephanie: We have new things happening in the context of efficacy, quality of life, clinical trials, and new breakthroughs. Dr. Camidge, is there anything you want to highlight?
Dr. Camidge: As people move through therapies, one of the things to realize is that their cancer can evolve in different ways. The cancer doesn’t always stay driven by just one pathway. There’s a phenomenon called second drivers, where, in this case, ALK is joined by something else that can drive the cancer: MET activation, EGFR activation, or KRAS activation. There, changing the ALK inhibitor isn’t going to get your cancer under control if it was growing back.
The trouble is there’s no drug company selling a combination of drugs. As these drug companies get better, we will start to see them defining populations in which their drug doesn’t work. When that happens, we should applaud those companies as they’re leading the way in how these drugs should be developed.
Stephanie: Are there any specific ones you want to call out that are exciting? And also the limitations you’re talking about.
Dr. Camidge: I do a lot of second opinions around the country and the world. If I see somebody progressing on an ALK inhibitor and through whatever the next ALK inhibitor is, I suspect there might be a second driver. When I’ve done the testing, more often than not, you can find one. The MET pathway activation is in probably 20 to 30% of cases. I’m prepared to bet that for most next-generation drugs, if you looked at MET activation and found it in some people, they would have zero benefit from these drugs. As we start to test for that and present that data, that becomes informative. You don’t waste their time with a treatment that isn’t going to work and send them in another direction.
Stephanie: You’re saying that in a large number of patients, a second driver has happened, especially in later lines of therapy. If we can’t develop therapies that address that, the value proposition for later-line drugs is lower.
Dr. Camidge: Let’s say we develop a new ALK or ROS1 inhibitor. We do it in a later line and get a 50% response rate. My first reaction is: That’s great, but what about the other 50%? It’s not acceptable to say that this is Russian roulette. I can probably tell if you’re going to be in the wrong 50% by doing a rebiopsy and appropriate testing. Let’s say you have a MET driver. Then you’d need to be on an ALK inhibitor plus something directed against MET, either a MET inhibitor or a MET-directed antibody-drug conjugate. That’s going to be the future.
The goal of academic centers is to export that knowledge. It should be the tide that floats all boats and not keep everything hidden in the ivory towers.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
Stephanie: The combinations are going to be more targeted in every single case. How long till we get there, and what’s preventing us?
Dr. Camidge: It comes back to the idea that not everybody can reasonably stay up to speed with everything, especially a general oncologist. The goal of academic centers is to export that knowledge. It should be the tide that floats all boats and not keep everything hidden in the ivory towers. But what we’re talking about and what seems like science fiction is actually going on day to day. Rebiopsying, reanalyzing, and redirecting people to something personalized to them has been going on in expert centers for many years.
Stephanie: Wonderful. Nancee, is there anything that’s caught your eye? How do you approach what’s happening in developments and what matters to you when you’re looking ahead?
Nancee: As I observe other people and eventually myself too, I agree with what Dr. Camidge is saying about continuously doing biopsies and testing and making sure that we’re addressing the actual drivers at progression. I was interested in the mRNA vaccine data for pancreatic cancer that just came out and whether we will have something similar to that, not just for ALK but for lung cancer. I know that there are things that are happening, but I’m wondering if those are hopeful or science fiction. I find those interesting to hear about.
Dr. Camidge: For me, that was exciting because my concern about vaccine approaches has always been: They’re very good at showing immune response going up in the blood, but nobody shows that it matters. That pancreatic cancer study was the first I’ve seen to correlate stuff going up in the blood with how long the cancer was controlled. I took that as very promising evidence that maybe stuff going on with the blood could be a reasonable surrogate of benefit.
Nancee: Because that seemed like all they were looking at, right? And then after six years, most of them had not progressed. For pancreatic cancer, that seemed quite astounding.
Dr. Camidge: To be clear, those people had early-stage pancreatic cancer that was resected. They walk through the door, get the vaccine, and technically don’t have any evidence of disease at that point, so you’re looking at relapse rate. Classically, that’s where vaccines work best, where there’s minimal burden of disease. But where they’re going to come in with ALK-positive lung cancer is during the TKI, when you get to minimal burden of disease. That’s where you come in with your vaccine.
The proactive way is you get rebiopsied, they see the information, and try to send you down the right pathway initially. The reactive way is when you try something and it doesn’t work, and that’s when someone is rebiopsied.
Dr. Ross Camidge, Thoracic Oncologist and Stage 4 Lung Cancer Patient
When to ask about getting rebiopsied and why it matters
Stephanie: Since you talked about second drivers, how often should patients be asking about getting rebiopsied? What are the signals? How does that happen?
Dr. Camidge: You can do it one of two ways: proactively or reactively.
In academic centers, the proactive way is you get rebiopsied, they see the information, and try to send you down the right pathway initially. The reactive way is when you try something and it doesn’t work, and that’s when someone is rebiopsied. You assumed that if you switched someone from alectinib (Alecensa) to lorlatinib (Lorbrena), it was going to work, but it didn’t. That’s telling you something and makes the case that you need to figure out what’s going on in that person’s cancer.
Proactively, I rebiopsy, reanalyze, and then don’t just try them on lorlatinib (Lorbrena). I already know what’s going on. Maybe I put them on a combination from the get-go.
Key takeaways: What to walk away with
Stephanie: Dr. Camidge, if people watching this could walk away with one thing on TKI therapies and managing quality of life, what do you hope they walk away with? And then the same question for you, Nancee.
Dr. Camidge: I want people to be able to go to their doctor with the expectation that they should have perfect quality of life. If they don’t, they need to write it down and remember to tell their doctor. Maybe the doctor can do nothing about it, but it’s like the Billy Joel song: Tell her about it.
Stephanie: Love it. Nancee, how about you?
Nancee: Oh, I can’t add to that because quality of life is my number one desire through this path. But I would say: Try to learn as much as you can, so that you know the right questions to ask. If your oncologist is not testing for another driver or not talking about second drivers when you have progression, try to be aware so you can bring it up. Local oncologists aren’t going to know every single thing there is to know about ALK-positive lung cancer.
Conclusion
Stephanie: Amazing. Thank you both so much for this incredible conversation. I learned a lot, and I know many people in our communities will too, so thank you.
Dr. Camidge: Thanks for having me.
Nancee: Thank you for having us.
Stephanie: I’m so grateful for both of you being here. Thank you again to Dr. Ross Camidge. He’s the person at the University of Colorado who leads the thoracic oncology program and clinical research, so not only is he taking care of patients, but he’s spent many years trying to further treatment options and the understanding of different spaces in lung cancer, including ALK-positive. Also, a shout-out to Nancee herself for all the dedicated work that she’s committed to patient advocacy and to their organization, ALK Positive Inc., which features great resources for patients and families, because as we know, it’s so much more than one person who’s impacted by a diagnosis.
I want to highlight again the second opinion program from ALK Positive Inc. that Nancee has mentioned. Dr. Camidge is featured on that, and what they do is help connect you to a second opinion with a specialist. It’s an amazing program to take advantage of.
Again, I want to thank our sponsor, Pfizer, for supporting this independent patient education program. That support is critical as it allows us to do more of these educational programs for our patient and care partner communities. Remember, this is not a substitute for medical advice, so please still talk to your doctor and healthcare team about treatment decision-making.
The Patient Story has countless stories across lung cancer, both ALK-positive and others, and I hope that is helpful for so many of you and for those you love.
It’s important to us to hear your voice and your opinions as they impact what we focus on next, like topics and people to interview. Please take the opportunity to tell us what you think.
I hope you learned as much as I did and walk away with great questions after this program. For now, I’m Stephanie Chuang with The Patient Story, and I hope to see you again. Take good care.
Program Sponsor
Thank you to our sponsor for their support of our independent patient education program. The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story. This content does not replace professional medical advice.
Hear from people living with ALK-positive cancer
Real experiences with diagnosis, treatment choices, side effects, and life beyond ALK+ lung cancer — in their own words.







