The Patient Story’s series “Cancer Friends” features Andrew and Esther Schorr. They co-founded PatientPower.info, a resource for other cancer patients and caregivers to help them through their diagnosis and treatment.
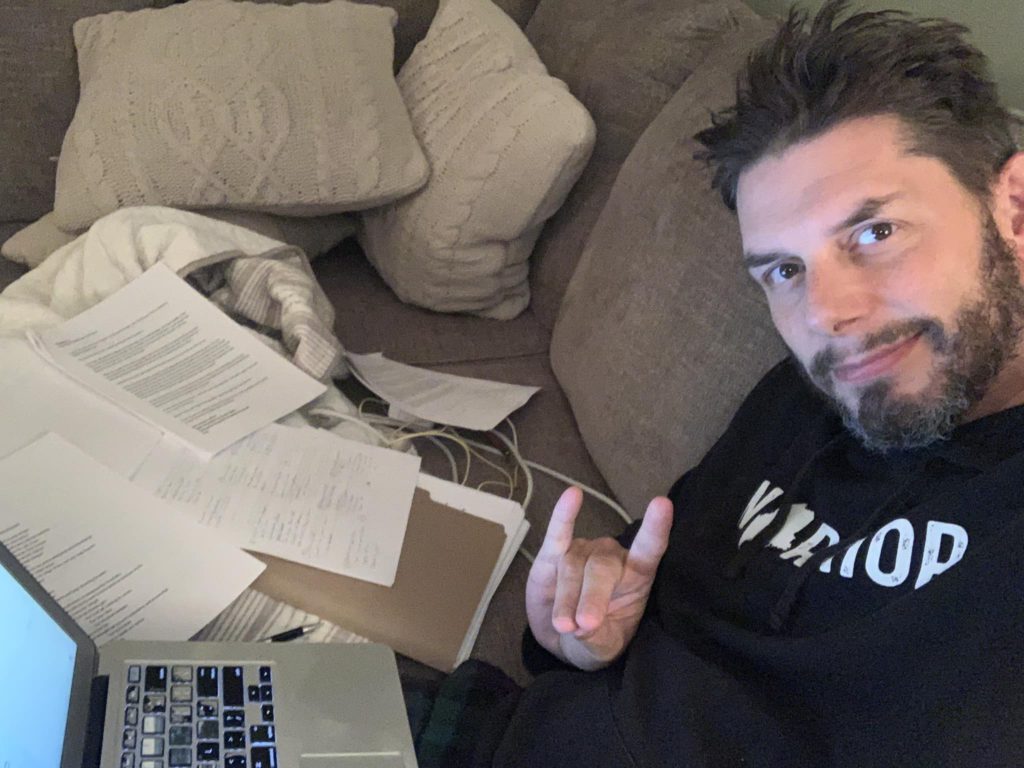
This segment focuses on Trevor Maxwell, the founder of Man Up to Cancer. After being diagnosed with colon cancer, Trevor went to a dark place. Support from his family led him to seeking help. Trevor noticed how few men were engaging in online support groups, so he created Man Up to Cancer.
Trevor shares his journey, how he started a group for men to be vulnerable and how the experience has changed him. He also details how cancer has given him a more present and grateful mindset.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Introduction to Trevor Maxwell
Andrew Schorr, The Patient Story: Hello, It’s Andrew Schorr with another edition of our Cancer Friends series. I’m in San Diego, but joining us from Cape Elizabeth, Maine, is my friend Trevor Maxwell. Trevor, thanks for joining us.
Trevor Maxwell: Pleasure’s all mine, Andrew. So great to see you. Thanks for having me.
Andrew, TPS: It’s great to see you. Trevor, I’m really delighted that we can tell your story, which has been quite a journey.
You have really been a pioneer in giving voice to men like you and me, living with cancer, and saying that it may be a little different or that men maybe didn’t speak up so much. Maybe we were keeping a lot inside. I’m sure you’ve seen it all, but it started with you. We should also mention that you have a new book. What’s the name of the book?
Andrew, TPS: It is coming out to the world now in December 2022, and people can get it through Amazon, etc. The book is just an example of where you’ve come. Let’s back up. You’ve been a newspaper reporter in Portland in New England. You’ve been in public relations. [You have a] wife of many years now, and you’ve been together 30 years, married 20. You had 2 little girls.
1st Symptoms
Andrew, TPS: What happened? You had a cancer diagnosis. Tell us how this happened.
Trevor: In the spring or late winter — this would have been right around January [or] February 2018 — I started to just get super, super fatigued. As I look back on it, I know that I was getting more and more fatigued throughout 2017, but I was 40 years old [and] working full-time as a public relations and freelance writer. My wife was working full-time as a teacher, and our daughters were 12 and 10 at the time.
As I started to get more and more tired, I just chalked it up to midlife fatigue. I had had some bouts of depression [and] anxiety prior to cancer, so I just said, “Well, this is mental health.” We were just kind of cruising through life.
The biggest things I identified mostly as [were] being a husband, dad, also a writer, and someone who enjoyed writing about others and putting the spotlight on other people.
Then this fatigue just kept creeping more and more. I’d walk up the stairs, and my heart is just kind of pounding out of my chest. I was 41 and I had not seen my primary care doctor in several years. I wasn’t doing check-ins at that point or annual physicals because I didn’t really feel like I had a need to.
I did finally call my primary care [physician], and she said, “We need to do some blood work. [We’ve] got to figure this out.” [They] did some blood work. [It] turned out I was super anemic [and] hardly had any iron in my blood. She said, “We need to get you a colonoscopy. Have you noticed any bleeding anywhere?” I had not.
Trevor Maxwell with his family (l-r): daughter Elsie, wife Sarah, and daughter Sage outside the family’s home in Cape Elizabeth, Maine. For Cancer Today Magazine. Photos by Brian Fitzgerald.
Colon Cancer Diagnosis
Trevor: Iwent in for a colonoscopy. Even at that time, between my primary care doctor and the gastroenterologist, no one was thinking [it was] cancer. I had looked it up, like, “What are the causes of blood loss?” You know, a couple of things. Cancer, of course, is on there, but it certainly was not on the radar.
March 22, 2018, I went in for a colonoscopy and had the procedure. Afterwards, the nurse took my wife and I and said, “You need to see the doctor.” I went into the doctor’s office, and he said, “I’m sorry to tell you this, but you have a pretty large mass in your ascending colon.”
At the time, I couldn’t tell you much about where the colon was or what it did. He said, “You have a mass. It’s about 9 or 10 centimeters, [about] 4 inches plus. We’re going to need to refer you to a surgical oncologist, and we’re sending off tissue samples for pathology.”
He didn’t say the word, but I’m hearing all this stuff like “oncologist.” I’m just like, “Are you saying that I have cancer?” He looks at me and says, “Until the tests come back, I can’t tell you 100%, but I’m 99% certain that you have colon cancer.”
When I use the phrase “life asteroid,” that’s really what it was. You’re just going along through your life and then this asteroid comes and just blows everything up. That was the day everything changed for us.
Processing the Diagnosis
Andrew, TPS: Wow. So there you are. You have 2 little kids. Your wife. You’ve been healthy. You mentioned you had some bouts of depression and anxiety before. Did this send you into a tailspin?
Trevor: Yeah, absolutely. The first period after a diagnosis, you really are in a physiological shock state. I remember the first week, [I was] reaching out to people, calling people, and [saying] “I have cancer. We’re going to do what we need to do.” But it was kind of dreamlike. It was very surreal.
Then after that, I was thrust into this very unfamiliar chute. You’re down the chute into this cancer land. You need to have surgery. You’ve got to talk about chemo. You’re trying to learn all the stuff.
It’s just so overwhelming and scary. We have little kids. I had no frame of reference that this was going to happen in my life, so it was crushing. Then my mental health really started to go to some very dark places.
During 2018, I had colon surgery [and] started on chemo. We thought I was stage 3 early on, but right away, we did a scan after chemo. It showed a lesion in my liver, a metastatic tumor, and they could see that it was there prior to [chemo]. They just didn’t see it on the first scan.
There I was, a stage 4 metastatic cancer patient. In terms of survival, when you’re looking at colorectal cancer, if your stage is 1 through 3, you’re looking at 70+% survival, depending on your stage.
It’s a very good prognosis if you get it early. But once it spreads to other organs — often the liver, lungs, and other places — then the 5-year overall survival rate goes down to less than 15%.
Trevor: Just crippling anxiety and depression. Very clinical. I thought I was going to have to go into an inpatient hospital for my mental health, not even my cancer. I had the first surgery, chemotherapy, and then I went for my first liver resection in the fall of 2018.
I was just at my lowest point. I was in a very dark place. I was checked out, isolated, couldn’t make a phone call, [and] couldn’t even talk to people about it. I just thought, “I’m going to die. I’m going to leave my kids behind. I’m a failure.”
By accepting help and getting out there and saying that I couldn’t do this on my own, I started to get better. All of a sudden, I was meeting people that were helping me. I wasn’t alone.
Just all this crushing emotional burden came down on me because I had always viewed myself as a very capable, strong person who was there for his wife and kids. Now I was facing this life-threatening illness with really a terminal diagnosis and I didn’t know how to handle it.
My first instinct was to just leave. I wanted to just go into the woods and say, “I don’t want to be a burden.” That’s a theme that comes up a lot in managing cancer. We don’t want to be burdens to our family. Sometimes when you get a diagnosis like this, that’s how you feel. That first stretch was a very tough place to be.
Finding Purpose Again
Andrew, TPS: Somewhere along the line, Trevor, you found purpose to dig yourself out of the hole. Tell us about that and what you noticed about yourself as a guy and then how it could relate to others.
Trevor: I’m really, really lucky because I have a wife and kids and family and friends who [are supportive]. I told them, “I don’t want to burden you anymore. I just want to leave.” My wife is like, “Hell, no, you’re not leaving. We’re going to love you through this and you’re going to get better.”
I say I’m lucky because a lot of men that I know don’t have that support system. When they want to run away, they just run away. My family was like, “Whatever we need to do to get through this, we’ll do.” My wife really gave me that tough love conversation.
One night [I was] talking to my wife. It’s around Christmas 2018. [I] just had my liver surgery. I had drain tubes. I was a mess. She was just encouraging me to somehow get out of this mental health pit.
I said, “I just can’t get over the idea of the kids remembering me as sick, being on the couch, being on the bed.” She said, “I’m not afraid they’re going to remember you as sick. I’m afraid they’re going to remember you as sad.”
In the book, I say this is [the] kind of conversation that puts you on a different path. I call that my Shawshank moment. Get busy living or get busy dying. Because I knew at that point I’m not a sad person. I never was.
It was just that cancer had taken me into a very depressed and anxious place. I couldn’t snap my fingers and just crawl out of that pit at that moment. But I heard what she said and it kind of cracked me open to the place where I could be like, “All right, I can’t do this by myself. I need to get help.”
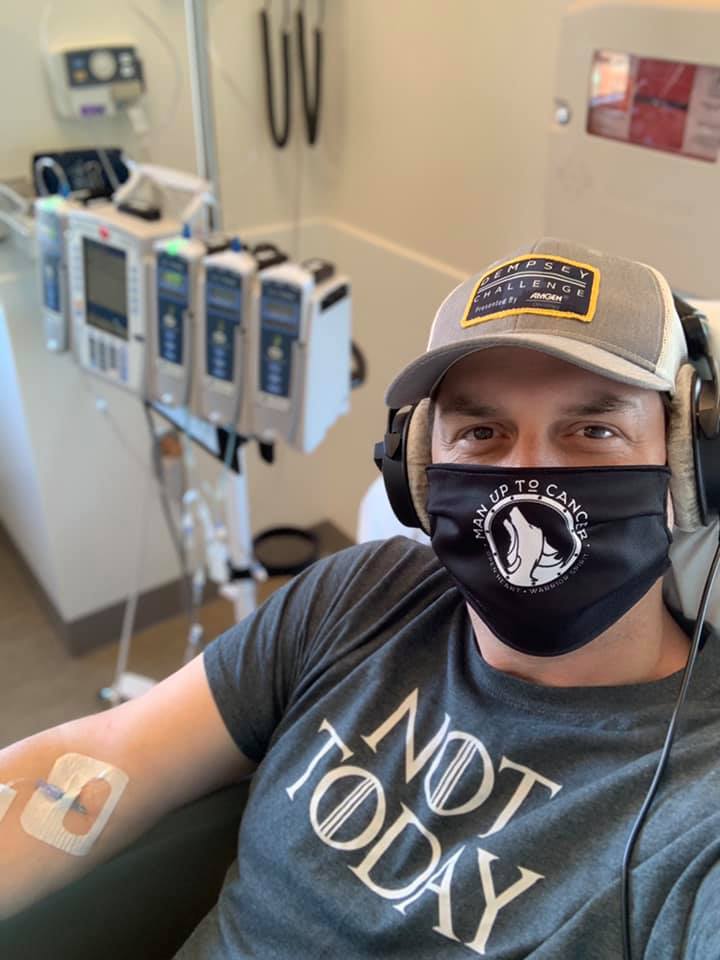
That was the turning point. I started asking for help everywhere. I went to the Dempsey Center here in Maine. I got individual counseling [and] group counseling. I started reaching out to groups online, especially COLONTOWN and the Colon Club.
By accepting help and getting out there and saying I couldn’t do this on my own, I started to get better. All of a sudden, I was meeting people that were helping me. I wasn’t alone. I realized that so many people are going through this challenge. So many people with kids and people at my age and even earlier.
That was really the turning point that started leading me towards my purpose. How I finally really got revved up about my purpose was as my mental health got better, I started seeing what I call the 3-to-1 rule in cancer land.
In all these cancer support communities, whether it be the Dempsey Center or COLONTOWN or places online, usually it’s at least 3 women to 1 man. Women are much more comfortable in general accessing these supports that are out there, networking, being out there, having conversations with other patients, getting second opinions, [and] all this stuff.
Where are the men at in these support spaces? Is it possible that I’m one of the only few men who is getting crushed by this and needs help? I knew there were other guys out there struggling like me and who could use the benefits of these support places.
Maybe these places, for whatever reason, just weren’t connecting with the men. There were barriers. Men needed the help, but they’re not accessing it. That was the issue. I was looking for a place to give back and I was coming out of this mental health pit.
That really was the genesis of the Man Up to Cancer movement and mission. [It] was to say, “Let’s build something specifically for men who are out there struggling.”
By supporting them, we can also support their partners, spouses, families, and communities. [In] Man Up to Cancer, we inspire men to avoid isolation during the journey. In doing that, we also help everyone around them. That’s the background.
Man Up to Cancer
Andrew, TPS: January 2020, you launch Man Up to Cancer, not quite 2 years after you were diagnosed. How did you start?
Trevor: I knew the idea was going to be Man Up to Cancer because we want to take back that phrase. To me, “man up” means bringing your toughness, because you’re going to need every bit of your toughness to get through cancer — but also being willing to accept help, having the bravery and courage to accept help along the way, and then give it when you can.
I said, “I’m going to do something called Man Up to Cancer, but I don’t exactly know what it’s going to be yet.” I knew I wanted to have a group, and I knew I wanted to do a podcast and have a website with resources. I actually started putting up a Facebook group and I developed the framework.
Everything about Man Up to Cancer uses the wolf and the wolf pack theme. The whole idea behind that was we need to be wolves for one another going through cancer. Wolf packs are very social. If there’s a sick or injured wolf, the pack is going to take care of that wolf.
They’re not going to just abandon them. If that wolf dies, they have a ceremony. They remember that wolf. I thought, “As men going through cancer, why aren’t we together like this? We need a pack.” I had fun with it. I just started putting wolf stuff everywhere and being like, “Hey, be part of the cancer Wolfpack.”
Then one really important thing happened. Anyone can have an idea like this, but you need people to buy in and help spread it. My buddy Joe Bullock from Durham, North Carolina, was that first follower who came in and was like, “This is exactly what I’m looking for. Can I help you build this and spread the word?”
I was like, “Yeah, come on board.” To this day, Joe has been the lead administrator of the Facebook group. We have the private Facebook group for Man Up to Cancer, the Howling Place, which is for male patients, survivors, caregivers, any type of cancer, any age, any background, [and] anywhere in the world.
We have about 2,000 men in that group now. Joe has been critical to building that up and really facilitating the community piece of it so that I could do the podcast, the website, fundraising, all these other components of Man Up to Cancer, and writing the book.
The two of us have worked really well to grow the community and to facilitate it. Then I’ve also been able to do these other pieces along the way. It started with the Facebook group. Then I started the podcast. I’ve done 68 episodes. [I’m] on a little break right now.
Of course, all through this, though, I’m going through cancer. I still have active cancer. I’ve now had 5 major surgeries. I’ve gone through a bunch of chemo, so I haven’t really had a break from the physical treatments of cancer.
My mental health has been a lot better. I still have my days, of course, where I have ups and downs. I throw a pity party occasionally, but I just don’t dwell there like I did.
We sort of had to grow organically and slowly, which is good. That’s the way a community like this should grow. A piece of that has just been because I’ve been in the trenches with the treatments I’ve been going through, so I’ve needed and I’ve really wanted Man Up to Cancer to just kind of slowly grow.
We’re not about numbers. Yes, we want to help the guys out there who need it, but to me it’s about the quality of the relationships and the quality of the people who come into the group.
We have a lot of other leaders now in the group who are ambassadors for Man Up to Cancer. It’s not just me out here saying a message. We have a pretty large group of ambassadors who believe in this mission of not isolating and who are out there talking about it.
Stuffing Emotion Down
Andrew, TPS: What is it, Trevor, about men, where without your organization, we tend to stuff it? I’ve been that way. I’ve been living with leukemia for 26 years. Little kids, duties as a father, a breadwinner, just try to push on and not talk about it much.
Trevor: Absolutely. A couple of things come to mind. Number one — and I talk about this a lot in the book — is cultural conditioning. We are conditioned as men in America and in many other cultures to when a challenge comes along in life, that we’re supposed to be able to fix it or solve it, that we are supposed to be strong and tough, and that we can handle our business.
For a lot of things, that rugged individualism is a positive. But with cancer, it’s not.
Men who isolate going through cancer have worse problems with mental health, anxiety, depression, all that stuff, and more substance abuse. They are more apt to have broken relationships, and they have worse medical outcomes. There’s real consequences here.
To your question, I think a lot of men just have that instinct that is like, “Well, this is a problem. [I’m] not going to burden others. I just need to focus on somehow I’m going to fix this on my own, and I shouldn’t need help.” That is a killer. That’s a killer. If you think like that going into cancer, it’s going to be a really tough road.
Then number two is the environment. [In] these support communities, a lot of men were trying to meet men where they are. A lot of men don’t feel comfortable going into a co-ed environment or an environment where it’s 75% women, 25% men, and being vulnerable with sharing about the struggles they’re going through.
That is meeting men where they’re at. It’s 2022. We’d love it if everything could be coed and not have genders assigned to it, but that’s not the reality on the ground. The reality on the ground is that many men just don’t feel comfortable. They don’t want to be perceived as weak. They don’t want to be seen in those groups as struggling.
This is the environment piece of it, because I think we have these stereotypes around men. People are like, “You can create whatever group you want, but the men aren’t going to be willing to share. They’re not going to be vulnerable.”
I’ll tell you what, you give them a platform and have it be just guys and the sharing is just like [boom]. I think some of it is, some of these men hadn’t had a support environment that they felt comfortable in.
Man Up to Cancer gives them a place to start being more vulnerable, sharing some of the struggle, [and] sharing what it’s really like to go through this cancer without those feelings of feeling shameful or that they’re going to be judged.
We put up the walls and started inviting people to do that, and some of our role models started sharing their vulnerabilities and how bad it sucks to go through cancer. All of a sudden, all these men just started opening up.
We’ll have people every week that’ll be like, “I haven’t really shared about this. I’ve been going through cancer for a couple of years, and I haven’t shared about this part of it, but man, I’m really struggling with X.”
Other guys will come in and be like, “Yeah, man, I’ve been struggling with that, too. You’re not alone in that.” That is the heart of what happens in the group — that kind of just bonding and open sharing [with] no judgment [and] all love.
Group for All Cancers
Andrew, TPS: One of the things I wanted to ask you about is “cancer land.” You used that term earlier. So much in cancer land has been driven by treatment and specific diseases.
Trevor: Correct.
Andrew, TPS: Your organization is talking to men no matter what cancer [they have]. It seems like that was maybe a real gap not just for men, but across cancer land. [It was] not so much about treatment, but about being a man with cancer.
Trevor: Yeah, you nailed it. That, from day 1, has been built into the recipe. We are not a treatment group. We have more than 20 types of cancer represented in our group.
From the beginning, I didn’t want [it] to be a treatment group because there’s tons of those. I wanted to be the emotional support, like the guys lodge. You’ve had a day of being out in the woods, and now you just kick back in the lodge and [socialize].
We talk about cancer. We vent about it. We share about it. It, of course, is a central theme in our group and what connects us as that shared experience and challenge. But we’re just a social group at the heart of it. We talk about our pets, cars, and favorite drinks. It’s the social isolation, too, that is not being addressed by some of these other groups.
There are great groups for treatment out there. What we can do is act as a bridge. Let’s say someone comes in, and they have colorectal cancer. We’re not going to sit there talking about all the treatments at all.
We’ll say, “Hey, come here for your emotional support and your brotherhood, but if you want to learn about your treatment options, go connect with these people at COLONTOWN, Fight CRC, Colorectal Cancer Alliance, or all these groups that are out there that do these different things. If you want to learn about advocacy, here’s the places where you can go.”
We find that most of our core members, people who are really into it will go to these different groups based on their cancer type to talk about those treatment options and then they’ll come to The Howling Place to get the emotional support, joke around and all that stuff.
I’m really proud of that because I don’t know of any pan-cancer groups for men that cross. We have guys with all these different types of cancer. Because of the shared experience and hearing these words, “You have cancer,” we have so much that binds us together emotionally.
Andrew, TPS: You’ve seen people change. We’re going to talk about how you’ve changed, but you’ve had these thousands of men who participate. Tell me a couple stories about the guy who was all bottled up who maybe isn’t now. Can you think of some stories?
Trevor: I think of Mike Reilly. Mike is a young colorectal cancer survivor, diagnosed at 31, with a wife. He lives near Buffalo. His story is really inspiring in that he was told, “You only have a couple of months to live. Wrap up your affairs. There’s nothing we can do for you.”
Then through COLONTOWN, he was able to find out that’s not necessarily true. I’m going to go over here to this other hospital, and they gave him a different plan. Now he has the HAI pump, and he’s been NED, no evidence of disease, for a year and a half.
Huge difference in his treatment plan, but that leads into then our movement with Man Up to Cancer. Then I saw him in COLONTOWN. I connected with him. We kind of became friends. He came into Man Up to Cancer, and then I saw him change as a leader.
He had been someone who didn’t talk. He was one of those guys who was in isolation. He wasn’t really talking about it. He wasn’t a leader at that point. He was someone who was struggling emotionally. Then through the friendships in Man Up to Cancer and through that empowerment, he has really established himself as this voice for men’s health and getting screened. [He’s] also in the group encouraging people to avoid isolation.
He’s just out there doing his thing. He’s covered with tattoos. Handsome young guy, covered in tattoos. He hauls cars for a living.
Then at the end of the day, he’s posting about, “Hey, make sure if you’re struggling, reach out to us or see a counselor.” I love role models like that who are complex. We can’t put them in a box. You can be a guy’s guy and a tough guy and all these things, but you can also take care of your mental health. Especially during cancer, taking care of your mental health [and] emotional health is part of how you get through this.
As you know, finding male role models in cancer land in all these support groups and everyone else is difficult. To have men who are willing to put themselves out there in public to speak, to write about it, to share — every time a guy does that, some other guy is out there being like, “Oh man, thank goodness I’m not the only one feeling these things.”
Personal Changes from Man Up to Cancer
Andrew, TPS: Trevor, I want to ask about how this has changed you. We should mention you’ve gone through 5 surgeries. I think you may have a 6th one coming up. You’re going through all the treatment stuff, and thank God, now you’re here. You’re going into your 6th year. Is that right?
Trevor: I will be at my 5-year mark in March of 2023. I’m 4.5 years right now, coming up on 5 years real quick.
Andrew, TPS: How has this changed you?
Trevor: It’s a great question. I don’t spend a lot of time thinking too much about my own evolution because I’m living it day to day. When I step back, I guess I could say that for me, doing Man Up to Cancer, I have more support now than I’ve ever had.
I have this Wolfpack. I have these guys that if I’m having a rough day, I can go online and get all this love and support, which is huge for me. I’m just so grateful for that. I’m grateful for the men in the Wolfpack and others that I’ve met through this Man Up to Cancer journey who support me and my family.
That’s number one. The second thing I really wanted to do was get redemption. I felt when I checked out from my family and when I was going through all that depression and anxiety, I let them down. I know they don’t look at it that way and I don’t either.
I don’t look back and get upset with myself for the way I was, because I needed to go through that dark place to do the work that I do now. I wouldn’t have this purpose without going through that hell. I’m thankful for it now.
As I started to get out of it and improve my mental health, I wanted to show my daughters especially that life is going to knock you down. Life is going to get you to your knees, whether it’s cancer or something else. You don’t have a choice. That’s what’s going to happen. But you do have a choice on how you respond to that.
I wanted to show them that life knocked me down, but that I could get up, and I could do something with that pain. That I could make some change in the world that’s positive, that’s loving, and that’s helpful so that no matter how long I live — because my prognosis is still not good.
If I have another year or 2, or whether I get through this and live another 40, that I can on that day, whenever that is, say, “You know what? I got up and did something to give them that example,” so that when the hard times come in their life, they can look to me as a role model, too, and say, “Look what Dad did.”
How You View Every Day Now
Andrew, TPS: Trevor, there’s uncertainty in all our lives, and there certainly is uncertainty in yours with advanced colon cancer. The 6th surgery [is] coming up, but happily, the book [is] coming out. How do you view every day now as you are propelled by Man Up to Cancer?
Trevor: Again, I have my normal ups and downs, and I have my appropriate emotions for what I’m facing — going through a life-threatening illness when you have a family like this. Our girls are 17 and 15 now. I’m so grateful to be here with them. I guess what I’m saying is it’s not all sunshine and rainbows.
It’s hard. It’s really hard, and we can’t ignore that. At the same time, I think my heart and my spirit and my mind have all kind of evolved to live with this and to accept it. If I progress and pass away soon, of course that’s never going to be okay. It’s all going to be grief for the people left behind.
What I want everyone to know and feel hopefully is that the joy of having me in their lives outweighs the sadness of having to say goodbye to me. For me personally, I have adopted a very present mindset. I am very in the here and now, and I am grateful for every day.
I’m grateful for all the blessings we have in our lives, and I feel like I’m on bonus time. There were plenty of times in the past 5 years that I did not think that I would be here in 2022, so I’m very grateful for that. I’m grateful to just keep doing what I’m doing, first and foremost with my family, Sarah and the girls, and how wonderful our family is.
Sage is applying for colleges, and I’m teaching Elsie how to drive now. I already taught Sage how to drive. These are things that every dad wants to do. These [are] milestones. Every time that something like this happens, I just give myself that smile and be like, “Look how amazing this is.”
It’s a very present, grateful mindset. Again, that’s not all the time. You can’t live with that kind of mindset all the time. I’ll get pissed off. I’ll get sad. I’ll get upset. But for the most part, I’m much more present and grateful than I was. I’ve always been a grateful person, but now it’s even more so.
I’m out walking the dog and just wondering at nature and being here. You think those big thoughts and big feelings when you’re living stage 4. I’m grateful for that. All these silver linings, which there are many, I didn’t see early on in cancer.
I would have said, “Don’t even talk to me about the gifts of cancer.” But now that I’m almost 5 years in, I’m definitely accepting of them. I think I’m in a good place. I think I’m doing the best that I can. I think our family is doing the best that we can with a really tough situation.
Doing Man Up to Cancer and being able to have those relationships and being able to bring something positive in some lives out there in cancer land, outside of my family, is something that I’m most proud of, and it’s an honor and a privilege to do it.
Conclusion
Andrew, TPS: Just as you say you’ve received gifts, though, with Man Up to Cancer, you’ve given us a gift. I want to thank you as a guy living with cancer, and I know I speak for many, Trevor.
We all have our journeys. You’ve had your own personal journey. The fact that you have found purpose and then reached out to all of us. Thank you, my friend. I really appreciate it.
The Patient Story’s series “Cancer Friends” features Andrew and Esther Schorr. They co-founded PatientPower.info, a resource for other cancer patients and caregivers to help them through their diagnosis and treatment.
Join us every Sunday for a new “Cancer Friends” episode, airing on our video channel here!
This segment focuses on Christy and Vince Vaal. A month before their wedding, Christy was diagnosed with chronic lymphocytic leukemia (CLL). Christy and Vince discuss how they reconnected decades after being prom dates, the importance of support through cancer, and how love helped Christy through her cancer journey.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Everybody’s future is uncertain… She needed support. I loved her. I was hoping if the same thing happened to me, she would do the same thing I would.
Vince Vaal
Introduction
Andrew Schorr, The Patient Story: Hello and welcome to another edition of Cancer Friends with Andrew Schorr and Esther Schorr.
We’re joined by new friends from Jasper, Indiana, south of Indianapolis or north of Kentucky. Christy and Vince Vaal, thanks for joining us.
Vince: Thanks for having us.
Andrew, TPS: This is in part a love story, and it’s a love story that does really warm your heart. Christy, you’ve been living for a number of years with chronic lymphocytic leukemia like me, and you’re doing okay?
Christy: Yes, for the most part. Still in watch and wait, technically.
Beginning of your love story
Andrew, TPS: We’re going to talk about your illness as well, but we want to talk about your love story. Let’s go way back. This guy was your date at your Jasper High School senior prom. Most people would say you went to the senior prom, eventually kept in touch, and got married. But it wasn’t so simple, was it, Christy?
Christy: No, it wasn’t. That’s not how our story went.
Esther Schorr, The Patient Story: How did it go? What happened?
Christy: We went to my senior prom, and that summer we just hung out with friends. We had mutual friends, and we would just drive around and do things you do in small towns. Then that August, I left for college and went to Purdue, and then he moved to Bloomington.
Andrew, TPS: You went two different directions. Christy, you’re a clinical social worker. Vince, you have a family farm. Dairy farmer for many years. You’re in the construction business with concrete and trucks and all that kind of stuff.
Each of you got married and eventually divorced. Each of you had children — two for Christy, one for Vince.
Reconnecting after 28 years
Andrew, TPS: Let’s flash-forward 28 years later. You’re both divorced by then. Christy, what happened?
Christy: In 2016, it was nighttime. My kids had gone to bed. I was just thumbing through Facebook, scrolling, and he came up as a suggested friend. I couldn’t believe it because I hadn’t seen him in 28 years.
I thought, “Oh, it’d be fun to just say hi or connect on Facebook.” I clicked Add Friend, and he accepted pretty quickly. I think it was the same night. It was pretty quickly.
Vince: That was probably the first month I had Facebook. I’m not into computers or iPhones.
Andrew, TPS: You get this message, Vince, from your prom date. What was your reaction?
Vince: I really couldn’t believe it. I didn’t know where she was. I hadn’t talked to her in 28 years. I drove by her home place the past 20 years. I never even thought she would move back to Jasper after moving away, but here she was at Jasper.
Christy and Vince at their wedding.
Andrew, TPS: Your work took you to Jasper. What happened?
Vince: I was telling the guys I work with about it. They said, “Well, hell, you’re over here. You might as well give her a call. What’s the worst that can happen?”
I said, “Nothing bad’s going to happen.” I texted her and said, “Do you want to meet? Do you want to go eat somewhere or maybe just get a drink?”
The first date
Vince: We decided to meet at the ice cream place on the square. I pulled up. I haven’t seen her in 28 years.
She pulls up and gets out of the car, and when she smiled, she has a gap between her teeth. I always remembered that gap. I love that gap. She goes, “Well, I’m not really hungry, and I’m not really thirsty.”
I said, “Well, you want to go to the river walk and walk and talk?” We walked to a bridge. We sat in the bridge and talked for about 3 [or] 4 hours. Then [we] went our separate ways, and two days later we went out.
The proposal
Andrew, TPS: That is so cute. We should mention now, Christy, you were already living with a diagnosis of a chronic illness: rheumatoid arthritis.
Christy: Correct, yes.
Andrew, TPS: You were getting medicine for that. Now you’re dating. [Vince], you at some point then say, “I’m going to propose.” That was a big deal.
Esther, TPS: How did that happen?
Vince: I went down and bought a ring, and I had the ring for a while. I kept waiting, and she kept going, “I need to get my nails done. I need to get my nails done.”
Finally, one day we were standing outside. I said, “You need to get your nails done. Then it hit her, and she was like, “Okay, I’ll go get my nails done.” I proposed to her the next day.
Andrew, TPS: You didn’t do it on the bridge, did you?
Vince: No. That’s where we got married.
1st symptoms and diagnosis
Andrew, TPS: Something intervened. Christy, after you were already together with Vince and were making plans for a wedding, you’d been losing weight rapidly. Your voice was kind of getting shaky. You’re having swallowing issues. You go to the doctor, you have blood tests, and you get a phone call. You’re home alone. What did they say?
Christy: I started having symptoms in December. That weight loss, the swallowing issues, the voice. My voice was almost completely gone. It took 3 months for them to actually run blood work. I had all kinds of other tests done, but the blood work wasn’t run until March. A nurse called me when I was home alone and told me I have leukemia.
Esther, TPS: This was just before you two were going to get married, right?
Vince: The wedding was planned for April.
Andrew, TPS: You were crying, totally devastated. Vince isn’t there. You’re distraught. Vince, on your side, here’s the woman who you’re supposed to marry in a month. She’s diagnosed with cancer with an uncertain future. Not everybody would go through with it. Tell me about your line of thinking.
Christy during treatment.
Vince: Everybody’s future is uncertain. Nobody sees it that way. We were committed. We were dating. We were going to get married. We had it planned. I always tell people I’m too fat to run, so I just stay there and take it. She needed support. I loved her. I was hoping if the same thing happened to me, she would do the same thing I would.
Overcoming the guilt of a diagnosis
Andrew, TPS: Christy, did you have any doubt about whether he would want to continue?
Christy: No, I didn’t have any doubt about him continuing. I felt bad. I felt guilty that here we were, looking forward to getting married, and we had finally found each other. I wanted to be a good wife to him, and I wanted us to have a fun, adventurous life and do things. Just what anybody expects. It didn’t go that way, and I felt guilt.
Esther, TPS: How did you get past that? That’s an understandable feeling. Individuals always have this vision of what it’s going to look like and what we’re going to do. It sounds like Vince had already made peace that, okay, this is a curve ball, and it’s going to go the way it’s going to go because you love each other. You’re still married, and you have a life together. How did you get past how you were feeling?
Christy: [It was him]. He was there every single day. He never, ever made me feel like he went through with the marriage because he felt a sense of obligation or anything like that. He acted the day after I was diagnosed the exact same way he acted towards me every day before that.
He was there for every appointment. I was very sick at that time, and I had lots of procedures that were scary and uncomfortable. He was there every single [time]. [He] took off work. Never batted an eye. Then I also had the support of my kids. That’s how I got through.
Andrew, TPS: Christy’s first husband, the father of her two children, became sick with cancer as well, advanced colon cancer, after [you] were married. You still were, of course, in touch with [him]. I understand you also knew him, Vince.
You wanted to support him, Christy. Vince, you wanted to support Christy as she supported her ex-husband, the father of her children.
Vince: And her kids. I was supporting her kids, too. He was a nice guy. I never had any trouble with him. We talked. He would come over, we’d talk, and he’d just run into bad luck. He had no family around here that I knew of, except his two kids.
Christy: He actually was at our wedding.
Parenting with cancer
Esther, TPS: How old were [your kids] when all this was happening, and what was their role in supporting either one or both of you?
Christy: My son was 16 when I was diagnosed. My daughter was about to turn 14. His daughter is the same age as my son, so she was about to turn 16 at that time. They all handled it pretty gracefully.
We were very honest with them because they had already been through something very similar to this with their father. They watched him get diagnosed, and he had multiple major surgeries that we would travel to Indianapolis for. They were very well versed in sleeping in waiting rooms and just being through all of those types of things.
I knew I couldn’t hide it from them even if I wanted to. I was losing about 7 pounds a week. It was very clear, very obvious. I couldn’t talk. I was very clearly sick, and there was no way to hide that from them. They’re strong. Kids are so much more resilient than I think we give them credit for.
Vince: There was a stint that she had to stay in the hospital, and Greg would come and visit because he was feeling better.
She called me at work and goes, “I’m going to the ER.” I said, “I’ll be home in an hour,” and I hung up the phone. We shut everything down. I called my boss (the owner of the company), and I said, “My wife’s going into the emergency room. I’ll be back when she gets out of the hospital.”
There were nine days she was in there. Greg would come and see her, come talk to me while she was in there, and bring the kids sometimes. He supported her, she supported him, and I’m just here. It’s just a fact of life for me. This stuff’s going to happen to everyone.
Andrew, TPS: You say you’re just here, but Vince, you impressed me as sort of [being] a rock in all this.
Vince: I don’t get excited about too much. This is just a fact of life. It happens. I grew up on the farm. There’s life and death. That’s pretty much it.
Christy getting her first dose of Rituxan through a PICC line.
How do you feel about the future?
Andrew, TPS: Christy, your CLL seems to be pretty well controlled now, right? Your RA is pretty well controlled, right?
Christy: Yeah.
Andrew, TPS: How do you see the future?
Christy: I think I would have a more clear answer if it wasn’t for COVID. Being immunosuppressed, I’m isolated. We used to go out to eat every Saturday. We would just do the normal couple of things and things with our kids. It’s really hard to predict what the future looks like as far as that type of thing, because we’re still isolated. He stays relatively isolated because of me, too. He goes to work and things. I find it more difficult these days to predict what the future is.
Andrew, TPS: But you’re hopeful?
Christy: Hopeful, yes, and you adapt. We adapt. We’ve adapted as much as we can, and we try to do as many things as we can safely.
Esther, TPS: Vince, what about you?
Vince: The future is what it is. We’re going to be together through it all. Now we’re trying to get a house built out in the country. She’s isolated, so she might as well be able to go outside and see the country. [We] just live and do whatever we can. Once the COVID clears up, maybe we’ll go on trips. Have a good time. We missed 28 years of the good times, so we might as well have it now.
How COVID affects life
Esther, TPS: With COVID, I think it depends on where you’re living in the country at the moment. I’m interested that you’ve made the choice to remain very isolated. Does it feel as though that’s what’s needed given what’s going on in your area?
Vince: She goes to places more than I do. It’s for the simple fact I’d rather just go to work, go to the farm, and come home.
Christy: This area of the country is a heavily, heavily Catholic population. A lot of the generations before us had a lot of children. We have a big family between the both of us. He has five siblings.
We have family gatherings and that’s been difficult to navigate, to try to stay connected to the family but not put myself at risk. Yes, it’s been difficult.
Christy with her infusion nurse.
Importance of seeking out support
Andrew, TPS: Christy, there you are, a social worker, but I know you’ve told me previously it’s meant a lot to you to connect with other patients, particularly online in a virtual support group. I’m sure a lot of these people will hear your love story. It’ll make them feel great.
Why do you think it’s so important for people to seek out support? First, of course, from a close relationship like you have with Vince, but also even people who may be far away?
Christy: First of all, I always say to my patients, “Whatever your illness is, whatever your issue is, try to find a support group that is comprised of people that are going through exactly what you’re going through, that have your diagnosis, or whatever it is.”
There’s just nothing quite like being able to talk to people who know exactly what you’re going through and are going through it themselves. It’s been very important to me to have family support. I was very fortunate to have that.
The group of ladies that I’m in the virtual support group with, they have just helped me feel [normal]. It’s hard to feel normal when you have CLL, especially during COVID. They kind of normalize it in a way for me and make me feel not so different.
Sharing information with peers
Christy: We share information. We all go to various specialists and things, and we’re all at various stages of our disease. There’s a lot of information I’ve gained from talking to them, because some of them are farther along than I am. It gives me an idea of what to expect possibly.
We support each other. We know exactly what it feels like when you get bad news [or] when you’ve gone to your doctor and your labs aren’t great. It’s just so helpful and so important to have that. It’s validation. Sometimes you can feel when you’re chronically ill like you’re a burden or like you’re always kind of preoccupied with your illness. When you talk to other people who are going through it, you realize they feel the same way, and it’s validating.
Helpful support for care partners
Esther, TPS: Vince, I’m in sort of the same position as you are, being the person along for the ride for the long term. From the standpoint of support that you’ve needed or you’ve gotten, [is there] anything you would say has been helpful to you or that you would say other care partners would want to have?
Vince: My biggest relief is when I go to the farm and work. It’s just like the world’s lifted off my shoulders. Nobody bothers me. I can do what I want. I get to spend time with my mom and dad. They’re getting up in age. A lot of kids don’t get that. For the past 25 years, I’ve got to see him every day, except the past 2 years. I don’t make it down there every day like I used to, but I try to make it about 3 or 4 times a week.
Andrew, TPS: Good for you.
Vince: I just love it out there in the country. Nobody bothers you. No neighbors. My mom and dad got a little dog. I got friends.
Love being more powerful than cancer
Vince: When this all first started, my friends were like, “You could have run.” I said, “Yeah, but you know me. I like to take the difficult path. I’ve been doing it my whole life. You can’t run.” That’s just kind of being a coward to me.
I loved her. It’s been different. I’ve learned a lot. My great uncles and stuff, they got cancer, and we took care of them. But they were 78 years old. It’s different when they’re young like that, and it’s different when you’re side by side with them. My only prom I ever went to, this is my date.
Andrew, TPS: Christy, would you say that from your experience, love can have a power over cancer?
Christy: Yes. It obviously can’t cure it, but it sure can make it a lot easier to live with and to make it through it. It gives you the strength, I think, that you need to make it day to day and to just not give up. That support is everything. Just knowing that no matter what happens, he’s right by me. That really helped me get through it.
Going to all the appointments
Vince: To be honest with you, I never thought I’d be going to a cancer treatment unless it was my own until I went with her. Knock on wood, I haven’t had to go through any yet.
It’s like I told her, “I’ve been around chemicals my whole life. I used to drink, party like hell. I actually made it through it all, and I’m still in decent health.”
Christy: The farmers around here don’t like to go to doctors, and they fix themselves. He’s stitched himself up; he’s set his own bones. For him, to be at a doctor’s office every month with me is totally new.
It’s a totally different environment. When he goes with me, he can’t help but look through the cabinets until the doctor gets in, and he just kind of snoops.
Vince supporting Christy during treatment.Holding hands at an appointment.Vince snooping in cabinets.
Vince: I have to sit in the doctor’s chair.
Christy: It’s become fun. We kind of make it a joke, and we make it funny. It was a totally different experience for him because he’s just never been a person to go to the doctor or anything like that.
Vince: When she first started going through treatment, I would go in there. It was taking 6 to 8 hours. The nurses are like, “We can call you when it’s done.” I said, “What if something happens in between to her? What if something happens to her, and I’m not here?”
I said, “Hell, I took off work. They’re paying me. I can sit in here and grunt through it with her.” I sat through every treatment just in case, because her body’s wacky. Stuff happens to her that doesn’t happen to the normal person.
Christy and Vince holding hands at their wedding.
Being hopeful for the future of medical progress
Andrew, TPS: Are you hopeful? With CLL, there’s been a lot of progress. Are you hopeful for yourself?
Christy: Yes. I’m just shocked all the time about how fast progress is being made. It seems like every other month, there’s a new drug that they’re talking about that they’re doing trials on. Listening to my friends, the support group, and some of the new drugs and the clinical trials that they’re in, it’s just amazing. Yes, absolutely I have hope, and I don’t think it’s false hope.
Vince: The medicine is amazing. The stuff they do is just unreal.
Andrew, TPS: Esther and I, as we hope to have many years together, wish you many, many years together.
Thank you for joining us from Jasper, Indiana. Christi and Vince Vaal, we wish you great time together. Thank you for being our friends here in honor of our Cancer Friends program. We really enjoy it. Andrew and Esther, Christy and Vince, all together with love.
The Patient Story’s new series “Cancer Friends” features Andrew and Esther Schorr. They co-founded PatientPower.info, a resource for other cancer patients and caregivers to help them through their diagnosis and treatment.
Join us every Sunday for a new “Cancer Friends” episode, airing on our video channel here!
This segment focuses on Alan Stephenson, who was diagnosed with multiple myeloma in 2016. Alan had never heard of this rare cancer, and he didn’t know the long journey ahead of him when he went to University of Arkansas Medical Sciences (UAMS) for treatment. Through this experience, he believes he became a better person, a better husband and a better father.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
At the end of the day, I wouldn’t change any of this, as hard as it’s been. Some days it’s easier to say that than others, but I wouldn’t change it. In many ways, [it’s] one of the best things that ever happened to me.
Alan Stephenson
Introduction
Andrew Schorr, The Patient Story: Hello and welcome to Cancer Friends. I’m Andrew Schorr. Joining me is a new friend from Monroe, Louisiana, in northeastern Louisiana, and that’s Alan Stephenson. Alan, welcome.
Alan: Thank you for having me.
Andrew, TPS: Alan, let me tell the folks a little bit about you. As I understand, you’ve been in the investment business for years. You’re a financial planner and have been investing in stocks since you were a kid. You’re a businessman and active in your community.
[You have]3 children, 2 grandchildren, and [your wife] Miriam of more than 30 years. But cancer intervened in your life. But before cancer, were you a pretty healthy guy, a pretty active guy?
Alan: Oh, yeah. Very active. Hunting, fishing, shooting archery tournaments, scuba diving, spearfishing. Just very active. I like being outdoors.
Andrew, TPS: How would you describe your personality, growing up and being in business? Were you an easygoing guy?
Alan: I would say in some ways, yes. For the most part, type A, fairly aggressive personality, very driven. I think most people would say I was a really nice guy and fairly generous, but a little bit of a light-switch-type personality, I guess you would say.
Andrew, TPS: Temperamental sometimes?
Alan: Sometimes. When I was young, I had a very bad temper. The good Lord’s been working on me over the years.
1st symptoms
Andrew, TPS: In 2015, you sneezed. That’s not a big deal, but what happened to you?
Alan: It was a big deal for me. I was standing in my kitchen and watching television while I was grabbing a bite to eat. I sneezed, and it put me on the floor. It injured my back, and I was pretty sure I had fractured some ribs. I’ve had fractured ribs before. I’ve been kind of hard on my body over the years. I could hardly breathe. It hurt so bad.
Andrew, TPS: You were having other back problems, and you were telling your wife you’re probably a candidate for back surgery, right?
Alan: Right. Back problems were not really new to me because I grew up being pretty hard on my body. When I was young, I thought I was 9 feet tall and bulletproof. I grew up riding motocross bikes and survived a lot of things I probably shouldn’t have. It took a toll on my body. Even though I was very healthy, I’d had a lot of old injuries, and I just thought it was old injuries coming back to haunt me. I told her in late 2015 that I just couldn’t keep living like I was, because I was in so much pain.
Andrew, TPS: But it wasn’t only the pain. You were having chest congestion, and you were sick.
Alan: For the most part, I just didn’t have any energy. I thought that was because of the pain I was in, just wearing me down. I do have a very high pain tolerance. I didn’t go to the doctor. I was kind of raised where you don’t go to the doctor unless the bone’s showing.
Even after I sneezed and injured myself, I didn’t go to the doctor. I kept getting sick with chest congestion and fever. [It] seemed like every 2 or 3 months, I would get really sick and I’d have a hard time shaking it. I just never put two and two together.
Going to the doctor
Andrew, TPS: How did you eventually get to a doctor? Tell us what happened.
Alan: Well, two and two came together on March 30th of 2016. I was sick once again [with] really bad chest congestion [and a] fever. I was sleeping in our upstairs bedroom so that I didn’t get my wife sick. I got in the shower, and the steam made me start coughing. The pain was indescribable. Every time I coughed, it just seemed like my back was just about to break in half.
I actually got on my hands and knees in the shower right before my L5 vertebra collapsed. For those [who] don’t know, multiple myeloma is a cancer of the blood that makes your bones basically disintegrate and become brittle. That’s why my back broke.
Andrew, TPS: Right, but this is before you even knew you had multiple myeloma or knew anything about this. You went to the local doctor or local hospital, I imagine.
Alan: I was at home alone. I have been blessed, like I said, with a pretty high pain tolerance, so I was able to turn the water off. Eventually, I was able to stand up and dry off. I got dressed and had to crawl down my stairs. I went and drove myself.
I drive a 4-wheel-drive truck that’s fairly high off the ground, and I had to drag myself into the truck. I went to work, so my assistant had to come outside and help me out of my truck. I couldn’t get out, and I was walking like I’d had a stroke. I couldn’t pick my feet up. I was having to shuffle them across the ground.
I stayed at work that day, and that night I spent most of the night in tears. The next day I went to see my primary care doctor, and he wanted me to go to the emergency room. I wouldn’t go. I basically walked around for a week and a half on a collapsed vertebra, waiting to get [the MRI] done and get the results.
Results and diagnosis
Andrew, TPS: The results come. What happened?
Alan: They did the MRI on a Friday. It was funny because as I was walking out of the doctor’s office — he’s a buddy of mine — I asked him, “What are the chances you think I have bone cancer?”
He just looked at me funny. He said, “You know, I wasn’t even thinking that way until you said that.” Anyway, they did the test on a Friday. He called me on Monday morning, and he said, “You were right. It’s cancer, and it’s bad. I’ve got you a room reserved. You need to be there either today or in the morning at the latest.”
I said, “All right, I’ll be there in the morning. I’ve got some work I’ve got to finish up.” Anyway, they put me in my local hospital, and that’s when the adventure started.
Andrew, TPS: Let’s carry on from there. Clearly, what you described, you were a type A guy, for sure. Driven by work. Typical man. Not all men are this way, but trying to ignore the pain, push forward, not wanting to go to the doctor until maybe the very 11th hour. Now you’re in the local hospital. They tell you they think it’s this cancer, multiple myeloma. Do they tell you that?
Alan: Yes. But I had a bad reaction to some pain meds when they first put me in the hospital. I woke up the next day running a fever of 103, with the room spinning and nauseous, and I was shaking like I was having seizures.
Basically, the pain meds had shut down my digestive system. I don’t really remember much of those first few days, but during that time, they were able to do a bone marrow biopsy. They told my wife that it looked like it was multiple myeloma and they wanted me to go to UAMS.
How did you feel seeking treatment for an unfamiliar illness?
Andrew, TPS: Let’s talk about that, too. First of all, I would think you hadn’t heard of multiple myeloma. It’s not uncommon, but it’s not common. It’s often in people older than you. How old were you?
Alan: I was almost 49.
Andrew, TPS: You would have been a younger myeloma patient, probably not familiar with it. They tell you that you need to go to a special center for it — not in Louisiana, but in Little Rock, Arkansas. How did you feel about that? You had to go somewhere to deal with this illness that you’d probably never heard of.
Alan: You’re right. I had never heard of it. Like I said, I don’t really remember a lot about those first few days, but I remember they said, “Don’t Google it.” For once in my life, I actually did what I was told, and I didn’t Google it. My wife did, so she knew how serious things were.
Because I hadn’t heard of multiple myeloma, I was thinking, “Oh, that’s just a junior league cancer. It’s not pancreatic cancer. It’s not brain cancer. I’ll be all right.” As far as going out of state, the fear of the unknown is probably as bad as anything else.
I went in the hospital on a Tuesday, and of course, on Wednesday I woke up sick and couldn’t eat. They had to do a vertebroplasty to rebuild my L5 vertebra. That’s where they go in and inject cement and rebuild the vertebra. They were just trying to do that just to get me to Little Rock.
I didn’t really have a lot of time to think about it during those first few days. I got out of the hospital. I went on Tuesday; I got out on Sunday. I lied to them and told them I could eat. Finally, about Thursday, I got to where I could eat. From Tuesday until Thursday, I’d lost 18 pounds.
UAMS called me on Friday and said, “When can you be here?” I said, “Well, it doesn’t really matter. As soon as possible.” They said, “Be here Monday.” I said okay and hung up the phone. I didn’t ask him, “Am I going to be doing testing? How long am I going to be there? Am I going to start treatments?”
We went to UAMS with absolutely no knowledge of how long we were going to be there or what to expect, and that was terrifying. It really was. I am fortunate that that’s only about a 3.5-hour drive from my house.
Andrew, TPS: People want to feel like they can get expert care close to home. You were in not a rural area, but not a big city area. We should say that UAMS, or University of Arkansas Medical Sciences, is one of the foremost places in the world for the treatment of multiple myeloma. Renowned world experts [are] there. You go there, not knowing if you’ll be there an hour or a month. How long were you there?
Alan: Four days. We check in. We go into the waiting room and sit down. We’re just waiting for them to come out and have that initial meeting with us. This man walks up to us and he says, “Are you new here?”
I said, “Yeah.” He said, “Multiple myeloma?” “Yes, sir.” He said, “Man, you’re in the best place in the world to be treated for multiple myeloma. When I came here 7 years ago, I was in a wheelchair. Everybody thought I was a dead man. Now I’m back working my cattle in Oklahoma, and I’m doing great. I just come here once a year for a checkup.”
I was like, “Oh, congratulations. That’s awesome. I’m so happy for you. Thank you for sharing that.” Then he said, “Yeah, but it took a while, so I just moved my camper here and lived here for 2 years while they treated me.”
I will tell you, at that moment, my world stopped. It hit me that I had no clue what we were in for. He just kept talking. I looked over at my wife and the look on her face just broke my heart.
Treatment at UAMS
Andrew, TPS: Alan, you went through a broad range of treatments: two transplants, lots of meds. Over the course of the treatment, how long was that time with University of Arkansas?
Alan: I went through two really hard rounds of chemo. We’d go up for a few days of testing, come home for 2 days or 3 days, and then go back up since it was close to home. I was there for about a month for each of those treatments, with about a month break in between.
Then I went back and did my first stem cell transplant. [For] the stem cell transplant, I was up there for 3 or 4 weeks, came home for 2 months, went back, did another stem cell transplant and had about a 2-month break. I went back for a checkup. They said I was doing really well, so then they started another treatment.
Basically, it took about a year of being treated up there to get me in remission. Then I started maintenance treatments locally and going back to UAMS every quarter in the beginning for testing, but I was doing treatments locally. I did a total of 4 years of treatments.
Andrew, TPS: Now, as we do this interview, you are in remission, right?
Alan: I am.
Andrew, TPS: I think you still take some maintenance medicine.
Alan: No, actually, the last treatment I had was April of 2020. I do have some medications that I still have to take because my immune system probably won’t ever be quite right. I take some antivirals and things, but that’s really it now.
How did this change you?
Andrew, TPS: Let’s talk about how this changed you. Here’s the guy in the shower enduring tremendous pain. He literally had to be dragged to the doctor. I see you driving in your truck to work when you should be in the hospital. We talked about being a type A person, driven, dedicated to your clients, financial planning, and your family. What changed you?
Alan: I changed a lot. There are those defining moments in your life that when we look back on our lives, [we] say, “This one instance changed us in some way.” I have quite a few of those. For me, I can really pinpoint it down to one moment: that day that we had our encounter with Camper Man.
We were just on this emotional roller coaster because it hit us. When he was talking, I was sitting next to my wife. I sent her a text, and it said, “This just got real.” We were on this emotional roller coaster. One minute I’m thinking I’ll be all right. The next minute we’re like, “Oh my gosh, what are we going to do? I’ve got a business. I’ve got a daughter.”
My daughter was 13 or 14 at the time. My sons were older. I had no clue what we were going to do. I had no clue how I was going to provide for my family. Luckily, being in the financial industry, I can work from anywhere as long as I have an internet connection and a phone.
Anyway, I had to go for a bone marrow biopsy and the doctor doing it said, “I’m going to give you a local anesthetic, and I’m going to drill a hole in your hip bone and open that enclosed cavity to air. I’m going to stick a needle in there and draw fluid out.”
He said, “The pain is going to be off the charts and there’s nothing we can do about it. The good news is it will be over really quick.” I was a little bit nervous. They’d already done one on me, but they knocked me out for that one.
He started talking to me and he said, “What do you do for a living?” “I’m a financial advisor. I’m a lot smarter than I look.” He started laughing, and we kind of hit it off.
Anyway, after it was all over with, I was getting dressed, pulling my pants up over this big diaper-sized bandage on my hip and he said, “Before you go, here’s my name and number. I want you to call me so we can discuss you being my financial advisor.”
At that very moment, my life changed. I had a peace wash over me that is really hard to explain. I knew it was God telling me everything was going to be all right.
I knew that he was telling me, “Hey, your business might even grow because of this. You don’t need to worry about taking care of your family.” I know a lot of people don’t understand this, but from that moment forward, I didn’t worry about whether I was going to live or die. I didn’t worry about providing for my family. I didn’t worry about the treatments.
I just didn’t worry. I had peace for probably the first time in my life. I changed at that very moment. I’ve actually shared the story with that doctor. He and I became friends. I think it had an impact on him, too. I found peace for the first time in my life.
I had somebody ask me one time, “When this is all said and done, what do you want to take away with it? What was important to you?” I wouldn’t change that peace for anything. Because I got that peace and because I’ve been through this, I’m a lot more thoughtful of others. I am so much more appreciative of my family and friends.
When I was going through treatments, my phone would start going off at 6:30 in the morning from people all over the country, just telling me that they love me. They were praying for me. They were wishing me the best. They were thinking about me.
I was in so much pain. I had so much damage to my body. I don’t care how sick you are, because that chemo was strong. It was so strong. I didn’t have a hair left on my body. I don’t care how sick you are. I don’t care how much you hurt.
It’s hard to have a bad day when you start your day off like that [with those messages]. I saw so many good things coming out of all of this that it encouraged me and it strengthened me. When you see good coming out of bad situations, it makes them not seem quite so bad.
Damage to your body
Andrew, TPS: You said you did a lot to your body, so you’re probably not the same guy physically that you were before. How are you doing physically?
Alan: To understand what I mean by the damage to my body — I found out the reason I had been in so much pain was I had fractures in almost every vertebra. I had clusters of fractures, like spider webs, through my ribs on both sides. I had close to 150 lesions, holes on my bones from my thighs to my skull, and 60% of the cells in my bone marrow was cancerous.
I asked my doctor, “If I refuse treatments, how long do you think I have? He said, “Maybe 3 months.” I was right there at the end. They did the vertebroplasty on my L5. They did kyphoplasty on the vertebra between my shoulder blades.
The fractures were so bad they were afraid I would get pneumonia because I was breathing so shallowly. I could feel my vertebrae separating when I would take a breath. When I rolled over the bed or had to get up out of a chair, I had to hold my ribs or I had to keep them wrapped up to keep them from moving around.
That’s pretty uncomfortable. I had a lot of damage to my body. They did a really good job of patching me up, though. I’m in pain all the time — I can’t lie about that — but it’s tolerable.
Sometimes it wears me down, but I live a very normal life. I’m mowing a yard, doing things I didn’t feel like doing is what helped me recover. I actually started shooting archery tournaments again while I was still going through chemo. Right after they patched me up, I couldn’t shoot any of my bows.
My daughter had one, and so I got it. I was used to shooting these super high-powered compound bows [that] throw arrows like lightning bolts. I was at the archery tournaments, shooting arrows that look like a rainbow. Once again, my archery friends took good care of me.
Andrew, TPS: Hunting and fishing — are you back to that?
Alan: Yeah. I’ve been working a little bit more than I probably should be. I’ve got about 5 acres of land. I keep that up and a few weeks ago, I was running a chainsaw. I went scuba diving last month.
Having a second life
Andrew, TPS: Did you ever think when you were lying there in the hospital that you would have this second life?
Alan: I didn’t know for certain that it would happen, but I knew if it didn’t happen, I’d go down swinging. I’ve got a lot of fight in me.
Andrew, TPS: You do. You mentioned about the businesses, but you also said you’ve become closer to your family. You’ve started some additional businesses with your boys, and it brought you closer to them.
Alan: In 2018, my oldest son and I and a friend of mine started a professional handyman and remodeling business. I’m just the business guy. We actually bought my partner out earlier this year, so it’s just me and my oldest son [who] have the handyman business.
Then in 2019, me and my youngest son partnered in his air conditioning business. Then in January of 2020, he and I bought an air conditioning duct cleaning business. I didn’t think I’d be working this hard at this age.
Faith for having life after cancer
Andrew, TPS: I imagine you now more relaxed than the person I envisioned before that. Maybe I’m right.
Alan: I am.
Andrew, TPS: It seems like you are. Let me ask you this. Monroe, Louisiana, is not a big place. I think if you stop people on the street and ask people, “If somebody’s diagnosed with cancer…?” The typical media thing has usually been, “That person’s going to die.”
For people who knew you, they knew you were a really sick puppy. But now you’re out and about, whether archery, hunting, fishing, doing business, working with your clients, working with your family. Do you feel that just you being there gives other people faith that there’s been progress in cancer and that there can be for not everyone, but for many people, life after cancer?
Alan: Without a doubt. I get a lot of people referred to me because, as you said, a lot of people haven’t heard about multiple myeloma. When I was diagnosed, I did not know anybody that had it.
I [now] get a lot of people referred to me from around the country through various friends and organizations. I always try to have this conversation with them to tell them what to expect and to give them hope.
I’ll do some public speaking. I’ve been sent to some events and things, but the message that I try to give people and leave them with is that we have a conscious decision to make. It is our decision on how we’re going to deal with the tragedies and the difficulties that come along in our lives.
It might be health. It may be marriage. It might be whatever business. We have to make that conscious decision of who we’re going to be and how people are going to remember us, whether we die tomorrow or 30 years from now.
What is our legacy going to be? Was my family going to remember a guy that was angry or felt sorry for himself? Or was my family going to remember the guy that laughed when all of his hair fell out and half his mustache fell out, and the other side was still there like normal? That actually happened twice.
It’s changed me in many ways, and I try to help others any time I can.
How do you view the future?
Andrew, TPS: You’ve had all this treatment. Right now, you’re not having any treatment. The medical team has kind of rebuilt your body. You still have the reminder with the pain, but you go on in a very positive way. How do you view the future?
Alan: I know the chances of multiple myeloma coming back are pretty high. I don’t think the good Lord is done with me yet. I’m just trying to do a little good while I’m here, whether it be a short time or a long time.
I’ve got a lot of young people around me that are just amazing that I try to mentor, and I love seeing them grow in business and then their confidence and their abilities. I try to help people that are fighting this multiple myeloma.
I don’t know what it’s like to have prostate cancer. I don’t know what it’s like to have breast cancer or lung cancer. I know what it’s like to have multiple myeloma, and that’s maybe 1% of all cancer diagnoses. I can help those people, and I want to in any way that I can.
I’m going to have some fun while I’m here. [I’ll] deal with the things that aren’t fun to the best of my ability. I’m a better husband. I’m a better father. I’m a better friend. I’m more spiritual. I’m Christian, and I’m closer to God than I’ve ever been.
At the end of the day, I wouldn’t change any of this, as hard as it’s been. Some days it’s easier to say that than others, but I wouldn’t change it. In many ways, [it’s] one of the best things that ever happened to me.
Conclusion
Andrew, TPS: That’s quite a statement. Alan, you’ve had this tremendous change. Medically, you’ve been through quite a valley, and you’ve come through that with the help of medical science. I think your faith as well, for sure, and the support of your family. You’re giving back. I want to thank you for visiting with us.
Thank you for being with us on our Cancer Friends program. Alan Stephenson, joining us from Louisiana, as we get to know someone in this case with multiple myeloma, but also with some inspiration and lessons for anybody who is affected by cancer. Thanks for joining us.
The Patient Story’s series “Cancer Friends” features Andrew and Esther Schorr. They co-founded PatientPower.info, a resource for other cancer patients and caregivers to help them through their diagnosis and treatment.
Join us every Sunday for a new “Cancer Friends” episode, airing on our video channel here!
This segment focuses on Sonya Lea and Richard Bandy, who share their incredible experience of learning to love each other again. Richard’s surgery to remove his pseudomyxoma peritonei (PMP) was successful, but he was left with a major complication: memory loss.
Richard and Sonya discuss finding each other again, writing about the experience, and the importance of grieving who someone used to be.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
It’s phenomenal to be able to share life, period, after something that takes you so close to death.
Sonya Lea
She found that she fell in love with the new person, the new Richard, as much as I fell in love with her.
Richard Bandy
Introduction
Andrew Schorr, The Patient Story: Hello, I’m Andrew Schorr. Welcome to Cancer Friends. Here’s my very best friend —
Esther Schorr, The Patient Story: Esther Schorr.
Andrew, TPS: We’ve been married 37 years now and really enjoy the people we meet. We thought it would be important, related to cancer, to talk about love. It’s helped me, Esther.
Esther, TPS: It’s helped me, too.
Andrew, TPS: We want you to meet a couple we’ve come to know from Banff, Alberta, Canada, Richard Bandy and Sonya Lea. They’ve been married for how long?
Richard: 41 years.
Esther, TPS: Congratulations.
Andrew, TPS: You’re so young looking!
Sonya: Thank you. We were young and foolish when we got married.
Esther, TPS: Aren’t we all?
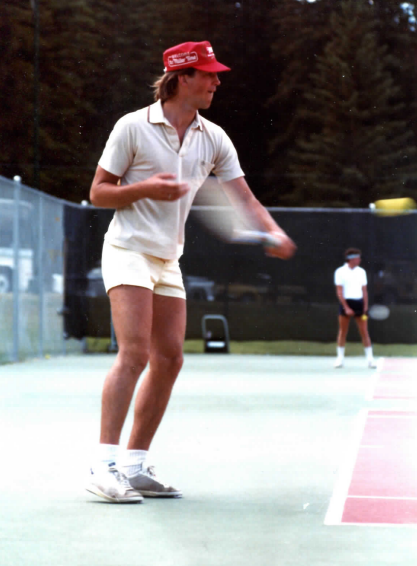
Andrew, TPS: We have a lot to talk about. They were living in Seattle. Richard, in 2000, was diagnosed with a very rare cancer, with “jelly belly,” mucus all through his abdomen, and he ended up having surgeries and experimental surgery as well.
But it also led to a complication where he lost his memory. Imagine that.
What was the impact as a care partner?
Esther, TPS: As I understand it, Richard came out of the trauma of all of this and didn’t remember anything. You had been married for a while already. As his partner and care partner, how did that impact you?
Sonya: I think we’d been married for 19 or 20 years when he had the surgery that caused the anoxic insult due to a bleed, which then caused traumatic brain injury. Initially, when he was in the hospital, I would ask the doctors and nurses about what was going on, and they thought that it was just the medication that he was taking.
That’s reasonable. We have pain medications that are kind of diluting our ability to stay in touch with reality. But then after a period of a week, maybe even less than a week, it started to be clear to me that something was really different in his personality.
He was extroverted and very verbal before the operation. He was really withdrawn, really emotional, and had — I know this sounds strange to say —kind of an angelic sense around him. He was very innocent, almost like he’d been moved back to a childlike state.
That’s when I started to ask lots of questions. I realized that it wasn’t just the drugs that were operating on him.Something else was happening. It set us out on a really different trajectory to find a neuropsychologist, get some testing done, go to a neurologist, see if we could find anything physical that was happening, and then eventually get this diagnosis.
He had had both long-term and short-term issues with memory, meaning that he didn’t remember a good majority of our past. I would say maybe 1 or 2 things was all that he remembered from before. Then he also had a difficult time creating memory and holding on to it.
We were in a really completely different situation without understanding how long it was going to take to resolve initially. Of course, I’m completely innocent also at that time, [thinking], “Well, maybe this will just take a year to come back from.” [I was] not realizing the extent of the damage or what a real recovery was going to be like.
Finding each other again
Esther, TPS: In all of that, this is the man that you loved and love. I’d love to hear what the two of you have to say about the bond you had. Now you’re going to go through this other journey of essentially finding each other again.
Richard: I will say that initially the first 6 months, even the first year, I was such a neophyte, such a newborn sort of person. I think I just kind of imprinted on Sonya as the person that loves me, and so I love her. There was very much that little baby bird sort of idea right at the start, and that continued for quite a while for me.
Sonya was completely responsible for my care. For me, she was everything to me. It was years before I kind of had more of my independent thought and was able to actually rebel against some of the things that I didn’t agree with at the time. For years, it was just a matter of… I don’t know. She was everything for me.
Andrew, TPS: She probably still is everything for you. I know for Esther, when I was diagnosed with leukemia, that was pretty devastating. When I was diagnosed with the second cancer, that added insult to injury.
Coping with your partner’s memory loss
Andrew, TPS: How did you cope, and how would you say love propelled you to stay in the game? Let’s face it, there are people affected by cancer where someone leaves. You dove in.
Sonya: In brain injury, those statistics are fairly high. I think that 60% of people where brain injury happens leave within the first year afterwards. There’s just so much to cope with in terms of the personality changes.
I remember running across a man who said his former wife left because he was breathing differently. Absolutely everything about the person changes. You’re having a relationship with a completely new person. We’ve talked with lots of people, lots of couples who’ve experienced brain injury in this regard.
I do think that love is the foundation that has to happen. It has to be present to some degree in order to make that journey a sustainable one. I think for me, particularly after I wrote a book about my experiences — I wrote a memoir about what it’s like to be in a relationship where this kind of thing can happen.
I think the thing that was most relevant for me was curiosity. In other words, I wasn’t staying to be the good wife or to fulfill some type of a role of the caregiver. I was actually really authentically curious about who this person was, and I turned everything over to that curiosity.
We’d had some good therapy training before Richard got a cancer diagnosis. I had had experiences of my own identity changing radically in some ways throughout my life. But this was really such a fundamental change to the relationship.
I think it was good to have some of that grounding, to know how to work out conflict with each other, and how to turn towards each other and be curious about each other. We just started from that place and worked from there.
I also think, secondly, it was really fundamental for me to grieve in front of Richard, in front of this body of Richard, for the former man, and to not have that grief be personal to the new him. In other words, grief is real.
He couldn’t experience it because he didn’t know his former identity, but he could feel compassion for me and also our children, who were having the experience of relating to a different person and feeling loss. We all just agreed in our family to tell the truth about these experiences. I think that mattered a great deal.
There was love and there was honesty at the same time. We kind of created this network, at least in our home, of us as kin, able to re-knit together through expressing what we knew to be true about the situation.
Awareness of grief and acceptance
Andrew, TPS: Richard, what awareness have you had of this process at the beginning?
Richard: Nothing initially.
Andrew, TPS: Then as time went on, here Sonya was doing a lot of work, and it sounds like the kids, too, trying to recapture a relationship with you. How did it become apparent to you that you had work to do, and it was based on a long-term relationship?
Richard: I would say that there were issues that came up over the course of the years after the surgery, but the big thing was me reading her book. I read it before it got published, obviously, and I read every chapter [as it] came in.
There were so many things that I had no idea that she had been involved with that I was just totally clueless about. [There were] even some of the past historical details from our early relationship that I had completely forgotten about. I
It was amazing to me to read the story and get an insight into what had actually gone on for us in years gone by and what was going on for us currently at the time of the writing. That was amazing to me.
Esther, TPS: I have read it. I can imagine how that would happen for you, Richard. In just listening to the 2 of you, I realize that while absolutely not as traumatic a change in the relationship as you guys had, the evolution of any loving relationship as you get older, as there is a diagnosis — Andrew’s had 2 of them — that I think you’re right, Sonya, that there’s a measure of grieving that goes on for former self or selves.
I think the way that love plays into all of that is if there’s truly this loving relationship between two people, you have to be honest about how you feel about that loss. It’s not a personal thing.
Andrew, TPS: The story, Richard, you told about reading the book, where you’re like one of the main characters —
Esther, TPS: He was the main character.
Andrew, TPS: It’s like, “Who is this guy?”
Sonya: We would give him passages in the book, and he would cry every time. I’m like, “This is your story.” Following the brain injury, he had such a beautiful sensitivity about him. It was so endearing to really not just me or the kids, just so many people. That was part of it. He was discovering his story for the first time, and that’s an absolutely magnificent thing to be able to watch.
I had a background in this also because I got sober 25 years ago. Part of that kind of recovery is you become aware of all the ways your identity is radically changing, and he had to get used to that at that point. There were just lots of changes that came about as a result of healing, but also writing about the book, sharing the book, and getting a sensibility about what really happened here.
The other strange thing I just want to say is that it was very unusual for me to see how he reacted to the book and what his awareness was about his own story.
Then I had a later reaction, which was, “Oh my gosh, what would have happened if I wouldn’t have told him his story?”
He then attached to the memories, and then that’s what becomes our personality, right? That kind of capsule of our identity that we show to the world. I became curious about what he would have been like if I had never shared that part of him.
In brain injury, you do have to rebuild a personality, or else you don’t know how to engage with the world. Richard very much wanted to re-engage with the world afterwards. I felt a loss there, too. We encourage that side of him to come forward as much as possible — the story that wasn’t given to him, but the story that’s emerging nonetheless.
I think that’s a real gift in any relationship where there’s a disease process and the healing process happening. Give someone space to be who they are, even though you don’t recognize where that history or where that shape of that story is coming from.
Sharing life again
Andrew, TPS: In a separate interview that I’ve done with Richard, he describes how he’s gotten back to a lot of the physical activity he loves to do, some with you. Hiking, biking, [skiing]. What’s it like now to have this man back — or even a little different man — when you’re out there doing one of these physical activities in such a beautiful setting, where you live in Banff?
Sonya: It’s phenomenal to be able to share life, period, after something that takes you so close to death. I do think that Richard died on the table. I kind of woke up out of that thinking that [with] the way that he is now… every day is a bonus day. It doesn’t really matter what it is that we’re doing. It really is something. Even if it’s a really crappy time, we get to have it together, and that feels huge to me.
Living that close to the wilderness, being able to be in nature is really critical to my writing [and] critical to who I am as a human being. We share probably so many more activities that we never shared before because we had really busy lives. This has involved a lot of slowing down and paying attention.
Esther, TPS: I think we’re doing some of that, too.
Accepting love and giving back
Andrew, TPS: Richard, as you become aware over the years, this devoted relationship from your wife — as the cancer survivor, you have to kind of accept the love.
Richard: Yes.
Andrew, TPS: How did you get to that, from being childlike almost to being accepting and giving back?
Richard: It took me a lot of years. I would say, 10 years after the surgery. I can’t say exactly, but there was a point at which our relationship actually became mature enough again, where I could be curious about whether I loved Sonya as much as I’d loved her before. And I did.
The love was obviously a little different, but there’s no question that the curiosity actually became important to me as well. I think Sonya would say the same thing [about] her curiosity. She found that she fell in love with the new person, the new Richard, as much as I fell in love with her. I think that that’s been marvelous.
I would say that we probably have had 4 different marriages over the course of our lives together in terms of our personality changes and things that we’ve been through over the course of the numbers of years that we’ve been together.
Andrew, TPS: Maybe you need a new wedding celebration sometime.
Richard: We actually redid our vows a couple of years ago. We went up on a hike [by] a lake and redid our vows just to kind of recommit ourselves to each other.
Andrew, TPS: How beautiful. Love, we believe, plays a role. Sonya, you said [for] some people, [it] doesn’t work when they’re challenged with cancer in the family. I’m so glad it has worked for you. Thank you, Esther. [I’m glad] that it works in ours.
Hopefully, this has been a story that people will remember. They’ll look up your book. Now they know the main character, Richard. It’s really fascinating. We wish you well as you go on with your life that you have now. Maybe different in some ways, different people in some ways, but still with love as a tremendous bond. It’s really beautiful.
Esther, TPS: It is.
Andrew, TPS: Sonya and Richard, cancer friends in Banff, Canada, and moving on with their life. Andrew and Esther here in San Diego, tied with love as well, and we hope that’s true for you.
The Patient Story’s series “Cancer Friends” features Andrew and Esther Schorr. They co-founded PatientPower.info, a resource for other cancer patients and caregivers to help them through their diagnosis and treatment.
Join us every Sunday for a new “Cancer Friends” episode, airing on our video channel here!
This segment focuses on Susan Hartman, a survivor of acute lymphoblastic leukemia (ALL). Susan details her first symptoms, dealing with isolation during diagnosis and treatment, and how she gives back to the community now.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Remember you are stronger than your situation. You are never alone. There are many people and many ways that people will help to lift up others.
Susan Hartman
Introduction
Andrew Schorr, The Patient Story: Hello and welcome to Cancer Friends.
Esther Schorr, The Patient Story: One of the ways that I communicate with cancer patients and with their families is through Facebook groups of patients and care partners. I was fortunate a couple of weeks ago to connect with our guest, Susan Hartman, who was actively participating in one of those groups.
Andrew, TPS: Susan is our newest cancer friend. Susan, welcome. Thank you for being with us.
Susan and Gene, her husband, sailing before she was diagnosed with cancer.
Susan: Thanks so much. I appreciate you having me.
Andrew, TPS: You have been an ALL (acute lymphoblastic leukemia) patient. That’s a big deal. We’re going to learn about that in your journey, but let’s start before you were diagnosed with a blood cancer. What was life like for you in Cranston, Rhode Island?
Susan: Good. Very good. One of the things that I have always appreciated is that I’ve always felt very blessed that I had so many friends and family that were close by. [There are] a lot of things that my husband and I like to do together. [We’re] very active. We spend as much time outdoors with every season that we have. We’re in New England, so we have a nice changing weather pattern.
I had been moving into my own consultancy practice, and that was starting to get going. We were having a good time. We sail and bicycle. I swam.
In my mind, I always used to say to people that I felt like I had a charmed existence and I was very healthy. I took a vitamin. I might take an aspirin once in a while. That was it.
Symptoms and diagnosis
Andrew, TPS: What changed?
Susan: Back in 2020, coming into March, I was finding that I was having some difficulty doing [my] lap swimming. I was having trouble with really getting a good full breath, but it wasn’t slowing me down completely.
We also knew things were starting to get a little bit squirrelly. We were hearing a lot about COVID. We were listening to different broadcasts and we decided to take a real cautionary approach to everywhere we went and everything we did.
It didn’t matter, because what ended up taking place is that rolling into May, really the end of that April, I suddenly was at the point where I couldn’t get a good breath. I couldn’t manage to lie down to sleep, I couldn’t bicycle and breathe and I couldn’t make the bed.
My husband said, “You really have to get to the doctor.” Of course, I knew that he was right. It was all of a sudden. Over the course of maybe 4 weeks, it just accelerated. I thought, this is seriously wrong.
[I went] to the doctor. I figured maybe I’ve got [a] virus and I’ll get something that’ll get me over the hump. I should have probably known. When I went in, she had me go in to take scans in the same building and said, “Let’s take some scans. We’ll take a look.”
Kismet, Susan and Gene’s boat.
The radiologist came out, handed me a disk, and said, “I think you should hang on to this. You’re going to need it.” It never dawned on me that there should be a reason that she would do that. I just assumed it was a health care privacy thing. I took the disk, and I managed to get myself back into the car.
I’m sitting there, trying to catch my breath, when she called me. She said, “Are you in the building?” I said no. She said, “Can you come back in the building?” I said, “I really don’t think so.” She said, “You need to go to the hospital right now. You need to go to the emergency room. We’re calling ahead to let them know you’re coming.”
My husband was just down the street because and [he] picked me up. Thankfully, the hospital is very close to where we are. He dropped me off at the ER. It was a really strange time and things started rolling forward at that point.
Gene, Susan and her brothers.
Being in the ER and hospital during the COVID pandemic
Esther, TPS: Susan, all of that happened shockingly all at once. You acknowledged we were right at the lockdown stage of COVID. How did that impact what happened to you next and how it happened?
Susan: When he dropped me off, the exterior of the ER was tented. They would only allow me to go in. He couldn’t come with me. He drops me off. I go in. They check me. I then proceeded to sit in an emergency room cubicle for about 5 hours, waiting for something to happen.
The place was just bonkers. This is Rhode Island Hospital, which is one of the best hospitals in the region. It has an alliance with Brown University Medical School. For oncology, they have a very close alliance with Dana-Farber out of Boston.
I waited and waited until finally they could put me into a room, and they still didn’t know what this was. I was hearing from different people, asking me different questions and trying to understand what was wrong, what was happening, what had I done, and where had I been?
At that point, they decided to keep me overnight. I’ve never been in a hospital in my life. I didn’t have children. I married a man with two sons and that’s great. That’s instant family. Not having ever been in a hospital, even to have children, I didn’t have a clue what this was going to be about.
The first night, I remember waking up at about 1:00 in the morning because I couldn’t sleep. I just sat there, and I thought, “What’s happening? What does this mean? What do I do? I don’t understand how to deal with this, and I don’t know what’s going on.”
You always feel like the people that are supposed to be there in your life show up when you need them the most. The next day, there was a doctor who came in, this woman full of energy and very positive. She said to me, “You need to do your biopsy tomorrow, but this is what we think you have.” She alluded to ALL.
I’m thinking, “I have no idea what that is.” Of course, I’m online Googling this. I still was having trouble breathing, but I said, “Look, I have a biopsy scheduled tomorrow morning. I will be here, but I need to go home tonight. I need to go home and be in my house. I need to see my husband.”
She agreed to that and I came back the next morning. I don’t know whether that would have changed certain pieces of this or not. When I came back in that next morning, they did the biopsy. They did a procedure that removed the fluid in my right lung. At that point, I needed to wait until I had a full diagnosis and I was introduced to an oncologist.
Then I had to take a COVID test. Before they could admit anybody, everyone had to have a COVID test.The bizarre thing that happened is that my COVID test came back positive. I was more aggravated about that than anything else, because we had worked so hard to be so careful. I couldn’t understand how it was possible.
Susan with her mom.
The hospital was in chaos because everybody was moved around. They had taken over floors of the hospital to care for all the COVID patients. Everybody’s walking around in full garb. They couldn’t come in and out of rooms without all of the gear that they had on.
In the meantime, they’re waiting to see if I present any symptoms. The odd thing is I never presented symptoms. That is a blessing. The oncology team was extremely concerned because they had [never] seen that together. I was only the second patient that had shown up that had the two things happening potentially at once.
I spent about 10 days floating around in those rooms until they finally felt that I was free and clear. I had to do a double test negative. They moved me into the oncology space, which strangely was still not the normal oncology floor, because they didn’t have room there. I ended up in the children’s oncology department.
Andrew, TPS: Because of COVID, nobody could visit you.
Susan: Nobody could visit me. This entire time that I’ve now been back in the hospital again, I’m by myself. Any conversations I have, it’s just me. My husband would be on the phone when we talked to the doctors. If they had anything serious they needed to discuss and any process, plan, or any outcomes, they would bring him in on the phone. The entire time I was there, I was by myself. That started, I think, May 4th, and I finally came out on May 27th.
Coping with isolation while at the hospital
Esther, TPS: During that time, Susan, how did you cope with that? Tell us how you managed that isolation and confusion about what was going on.
Susan: I’m sure anyone who might hear this and has gone through this knows what I mean when you say it’s totally surreal. You’re just not believing that this is all what you’re hearing or what you know. It’s kind of an odd thing that throws you off. It makes you feel very insecure [and] makes you feel shaky.
Several people have said to me, “It’s a good idea to journal things. Write things down because you won’t be able to keep track of things, and it’ll be a good way to know the details.” That’s a really important and [something] I started to do. I did a lot of journaling.
I also leaned on a lot of the things that I’ve done in the past through yoga practice, through meditation, through listening to music or sounds of nature. Whatever it is that soothes you, I would spend a lot of time with that. I found that that was how I was able to calm my mind, relax and get some sleep at night.
Your head is whirring around, and you’re having all kinds of crazy dreams. You’re awake in the middle of the night for various reasons. This was how I would manage all of that.
Then the other side of it was – I kept in touch with very select people, namely my family. I spoke to them. I had a regular pattern of when I would speak to them, so they knew they would hear from me. I knew that I would talk to them or FaceTime with them.
My husband would send things to the hospital for me. He became really good at baking these phenomenal pound cakes that were one of the few things that I could eat and that I loved. He would have pound cakes delivered, candy, or more clean pajamas and socks. You can’t have enough good socks, I have to say.
Because he was trying to deal with all of this himself, he started biking more actively. What I would do is tell him where I was in the hospital, which room I was in, and I’d say, “Okay, this tree, that park, whatever.” He would come.
At the appointed time, I knew he was down there. I’d have my tea, and he’d bring his coffee. We’d chat on the phone, and I could look at him. We had a regular schedule of visitation that way.
Gene visiting Susan at the hospital.
Undergoing treatment
Andrew, TPS: Susan, the good news is [you were] treated successfully with this acute blood cancer. You were in the hospital [for] how long?
Susan: That first visit was probably 24 [or] 25 days. Then the cycle that I was on is called a hyper-CVAD treatment. Because of my age and the level of invasiveness that I had — which wasn’t extreme, it wasn’t full on into my marrow — they said, “Okay, these are the drugs that we’re going to work with. This is the methodology. This is the process.”
Susan and Gene biking.
It meant I was home for two weeks, then I’d come in for a week, home for two weeks, and so forth for 8 cycles. From May until the end of November of 2020, I was in and out of the hospital for that whole duration.
Andrew, TPS: Just to be clear, at what age were you diagnosed?
Susan: I would be 58. Then I started the maintenance cycles after that, and I’m still finishing the maintenance.
How are you doing now?
Andrew, TPS: How are you today as far as ongoing treatment, and how do you feel?
Susan: It’s a world of difference this time this year than it was even last year. This is the second year of the maintenance. I’m scheduled to finish in December. I asked my doctor, “You can tell me the details later, but how do we close this out? Are we going to break up?” She said, “It’s going to be cold turkey. That’s it.” I had to laugh because I thought, “What a great expression.”
Susan banging the end-of-chemo gong.
Then I finish taking the outpatient medicines and that’ll be done in December. I feel immensely better. I have highs and lows based on any of the extra things they might need to give me along the way. They’re part of this process, but I usually know when I’m having a low, I’m going to come back up again.
It’s cyclical. Just have the patience, have belief and trust in the process and just roll with it. Just keep going. You’re going to be okay. It’s going to be okay.
You just keep moving through that. That’s that whole fierceness I had. I’m like, “I’m going to just keep pushing and pushing and pushing.” I wasn’t going to stop pushing. We just kept on going. So far, the care they’ve given me is incredible. They’ve been an amazingly great team.
Writing as catharsis
Esther, TPS: You’re over that initial very intense treatment crisis. How are you living your best life now? What are the things that you’ve incorporated back into your life that give you pleasure?
Andrew, TPS: What’s the through line with that writing you started during COVID? Tell us how this has propelled you.
Susan: I’ve said this to several friends of mine who have been diagnosed with different cancers over the past two years.
I said, “Write this stuff down. If nothing else, it’ll help you to remember what’s going on, what’s being said, and who you saw. But the other thing is it’s a safe place. Get it out of your head, take it out of your body, and put it on that piece of paper. It’s there for safekeeping.”
I started writing every day for the last three years. As a result, I started to put some of my writing into blogs and that was the site I started, called FierceWithJoy.com. I started writing my stories and experiences.
Susan celebrating the New Year.
Incorporating activities back into life
Susan: Gardening is very big for me. In fact, I’m hoping to complete a Master Gardener program this winter, which would be really exciting, so I can help to do different gardening programs in the community afterwards. Playing in the dirt is great. I highly recommend it.
I did finally find a dog. I was very excited. We finally were able to find one. During COVID, pets were being scooped up, and we couldn’t have a pet at that time. When we found this little dog — or he found us, one or the other. That’s been a lot of fun.
Andrew, TPS: What’s his name?
Susan: His name’s Cormac. It’s a funny little Irish name, and he’s a funny little dog. He’s a mix of a bunch of things. When people look at him, they think he’s either a corgi, an Australian shepherd, or all of those smushed together. He’s quite the character. He’s very cute.
We’ve also gotten back on the boat. The boat didn’t go in the water in 2020, and we really didn’t get out to the boat much last year. But this summer, we’ve had better opportunities to go and do overnight or day sails, and we’ve brought the dog. That’s been really nice. It’s an amazing feeling to be out on the water, just feel the sun and the wind, and be a part of all of that again.
Susan’s “Pain Cave.”
I’ve been doing a lot of water rowing. I have a water rower. I started building in some exercise elements because the treatments really decimate you physically. “I’ve got to get some strength back, if nothing else,” I thought. I’m building it up, and then eventually I’ll get back out on my bike.
Not knowing if life would continue
Andrew, TPS: How would you describe the fullness of your life now, given that when you were in the hospital, you didn’t know if you’d pass on?
Susan: Where that hit me the most was, when I really thought, “Is this it? Is this going to be it?” It’s amazing where your head goes. That’s why I was so grateful that this doctor came in, and she just was like, “Nope, this is what I think we’ve got. We have great success, and I’m going to connect you to this other woman oncologist.”
I’ve had all women caring for me. This has been spectacular and unusual.
I feel like I always appreciated my life. I never took it for granted. I never took any days for granted. But I feel like I have a different approach to how I want to spend my time and where. I have always been one to contribute to my community and donate time.
Giving back to the community
Esther, TPS: That’s what I was going to ask about, Susan. You’ve mentioned your master gardening and that you wanted to give back to the community. Can you talk a little bit about this idea of giving back and what that means for you?
Susan with Dr. Egan.
Susan: We live in a historic community, actually. One of the houses that I grew up in is a 1700s house. We have a very old community and a lot of tradition and activities. I like giving to that community in terms of helping with whatever we’re working on in the town.
The other thing that I do is to support the gardening elements, which I really wanted to expand out. [I want to] help move into communities and areas where people are doing more with gardening, or they want to understand more about how they can do it and have access to it.
The incorporation of nature has a very soothing effect for a lot of people, and it makes a big difference. We’re not terribly connected to nature. I think this would be something I could help to bring into some areas, and they seem to be interested. The program itself seems to be looking for that.
Living a full life
Andrew, TPS: [How] you would describe this, Susan? A, do you feel like you’re living a second life? B, is it a full life?
Susan: I would say it’s a new life, and it’s a full life. [I’m ] working on it. I don’t have all the answers yet. I haven’t figured it all out yet. I’m sure there are other things I’m going to want to do and ways I’ll give back. I figured I needed to get through all of what I’ve done and be past that a little bit, and then determine how it fits or where my contribution is wanted and how I can help.
In doing this site that I built, one of the big elements of this is that I really wanted to help other people to get through this process and to assist them. Not in the counseling way, but connect the dots, get people to the resources they need, help them to understand they’re not alone, and offer support and encouragement.
It’s so important, and it’s so important to stay positive through all of this as best you can. There is another side that is a great side. You can feel that change once you get through it.
Advice for others with a recent diagnosis
Esther, TPS: You’ve given some advice already by just talking about your story to other people who have gone or are going to go through this, unfortunately, at some point. What would be your advice to them [about recapturing zest for life]?
Susan: Remember you are stronger than your situation. You are never alone. There are many people and many ways that people will help to lift up others. One of the things that was the most remarkable, enlightening thing I found — and this was even while I was in the hospital — is the humanity is just incredible.
You end up being handed the grace from other people for them to want to help you as a perfect stranger. That humanity is so incredible. You can’t deny that that’s a part of what this is about. I don’t know what the reason is that I got through all of this, but I knew I was going to get through all of this.
I really felt like being positive and moving forward and doing all of the things that you need to do. Trust the process and be your own advocate. Those were like the key things that just kept popping into my head. All of those things, I felt, were just really important. Partly because I thought it, and partly because people said that to me.
They would send me messages, and they would forward texts to me. I’d wake up every morning, and I’d have a bunch of texts from people. My West Coast people would be in touch with me later, and then my East Coast people would get me in the early part of the day.
It was like this continuum of connecting with people, which was really key. I don’t think it was because of the pandemic. I think it was largely because that’s the nature of what this is about. Very few people are not touched by this or haven’t had a family member touched by it in some way. We need to lift each other up. I think it’s important.
Conclusion
Andrew, TPS: I think you said it just now, but also what I read into it is you were touched by the human-to-human connection of other people, people who never met you before. What it sounds like you’re doing now with the gardening, with the writing, with the dedication to your community, is you’re in touch with that humanity within you and now paying it forward, if you will.
Susan with her brother.Susan with her brother.
Andrew, TPS: I think that’s a beautiful, beautiful thing. Even after a very potentially fatal condition like ALL, an acute condition, with the right care hopefully, there is life afterwards. You can get back to giving. You get up in the morning. Sounds like with all the things you listed, you say, “It’s another day. Let’s go.”
Susan: Yeah, absolutely. Absolutely. I do. I always joke that I’m the busiest unemployed person I know.
Esther, TPS: There’s no such thing as retirement.
Susan: I have so many things I want to do.
Gene crossing the finish line of the Pan-Mass Challenge.Cormac the sailor.Cormac and Gene on the boat.
Andrew, TPS: We’re so delighted that Esther connected with you cross-country, San Diego to Cranston, to bring this story to others. Susan Hartman, we wish you all the best as you continue your recovery. Thank you for being with us.
Susan: Thank you both. I really appreciate that. It was great to talk to you.
Andrew, TPS: This is what Esther and I do with our Cancer Friends series, and we’re delighted that we’ve connected with Susan Hartman. We look forward to more Cancer Friends stories. We always welcome suggestions. Thanks for [reading].
Esther, TPS: Remember, knowledge can be the best medicine of all.
The Patient Story’s new series “Cancer Friends” features Andrew and Esther Schorr. They co-founded PatientPower.info, a resource for other cancer patients and caregivers to help them through their diagnosis and treatment.
Join us every Sunday for a new “Cancer Friends” episode, airing on our video channel here!
This segment focuses on Richard Bandy, a physical therapist who was diagnosed with a rare cancer in 2000. He then had to have a major surgery to remove the pseudomyxoma peritonei (PMP) which resulted in almost complete memory loss. Richard discusses relearning his life and passions.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I just wake up happy to be here. Happy to be here at all. Happy to be anywhere.
Introduction
Andrew Schorr, The Patient Story: Hello and welcome to Cancer Friends. I’m Andrew Schorr in San Diego, and joining me from Banff, Alberta, Canada is Richard Bandy. Hi, Richard.
Richard: Hello, Andrew. It’s good to be here.
Andrew, TPS: Thank you. Richard has an incredible story, which I think will inspire many people. He was diagnosed with a rare cancer. Some people have heard of it: “Jelly Belly.” What’s the official name of it, Richard?
Richard: Pseudomyxoma peritonei, PMP, is what it’s called. If you look it up on Google, it’s PMP.
Andrew, TPS: [A] rare cancer, where your abdomen kept filling with mucus. That’s pretty scary. We’re going to talk with Richard about what his life was like before, how he got through this very serious cancer — and quite frankly, almost died — and how he’s put a life back together for himself in Banff, where he’s a pretty active guy.
Richard, let’s start at the beginning. You were for many years in physical therapy. Were you a physical guy? Did you do sports? What did you do?
Richard: Actually, I did a lot of sports. I was Athlete of the Year at my high school. I played basketball, volleyball, tennis, skiing, biking, hiking, badminton, and ping pong, and I played pretty much any sport with a racquet and a ball.
Then I became a physical therapist. I actually went to school on a phys ed program, graduated, did a master’s in exercise physiology. [We] got married, got pregnant, moved to Banff, then lived there for 8 years, and then moved down to the States to become a physical therapist.
Andrew, TPS: Being physical, both with your patients and yourself and all your interests, that was a basic part of you.
Richard: No question. Yes, I was always very active and enjoyed physical activity very much.
PMP diagnosis and surgery
Andrew, TPS: But then, kind of a bomb hits. I understand you had a TB test. When was that? What happened, and what eventually became your diagnosis?
Richard: It was in late spring of 2000. Because I was a physical therapist, we had to do annual TB tests at the time, and so I did a TB test. It came back positive. [It] ended up being a false positive. They went in and did a chest X-ray on me the next day, and it turned out that I had some fluid in my lungs.
[I] went to the hospital. They biopsied the fluid, found this mucus, and came up with this diagnosis of pseudomyxoma peritonei. It is a mucus-producing tumor that comes off your appendix, and your body fills up with mucus until you die from it.
I had surgery there in June of 2000. They took a gallon of mucus out of me, took my appendix, and sewed me back up. I was back at work 10 days later and continued on, although I got regular checkups every year.
After three years, the cancer came back. The oncologists in Seattle were telling me I could just do debulking every 2 or 3 years to try and rid myself of the mucus. Eventually, it would scar down to the point where they couldn’t do surgery, and I would eventually die from the disease.
I looked around to find if there was some other place that I could go, found a place, and had the big surgery. [It was] 12-hours. [They] cut me from xiphoid to pubis, took all my organs out, scraped all the mucus off by hand, sewed me back up, put heated chemotherapy into me 12 hours a day for 5 days, and then sent me on my way.
Andrew, TPS: This is a major abdominal surgery for a rare cancer, and it’s delicate. You had a complication where you were bleeding with a nicked artery, and that affected the oxygen to your brain. What effect did that have?
Richard: I woke up with basically no memory of my life. You know what my first memory was coming back from the hospital? I remember walking down the hallway towards the window with my IV pole in my hand.
That was the first memory I had after the surgery and Sonya, my wife, later told me that it was two weeks after the surgery. That’s my first memory of anything in the hospital. I didn’t really have any memory of my activities before, although since then, some stuff has certainly come back. It was pretty dramatic.
I didn’t really say more than two or three words to anybody for the first year after the surgery. I could speak, but I just didn’t really have anything to say, or I was unable to initiate thoughts. I just had no idea what to say to people.
Andrew, TPS: Language, memory. You did get to go home, but you had to work with an expert and your wife to try to get your life back. That’s taken years, right?
Richard: Yes. I tell people that physically it was probably 5 – 7 years before I was able to do like 80% of the stuff I was able to do before the surgery. Mentally, I still have issues.
I still do accommodation strategies for things that I forget, and I still don’t remember anything from really much before we were even married. I don’t remember the birth of my kids. There are still some things that I don’t remember that I wish I remembered.
For the most part, I’m functional. I can go to the grocery store, I can drive, and I can do a lot of things that people have difficulty doing regardless. I’m very grateful to be here.
Becoming active again
Andrew, TPS: You retired professionally from physical therapy. Let’s talk about your activities. There you are, having been a very active guy physically. You go through this very rare cancer, major surgery, and complications. You lose your memory, and you can’t speak, really. How have you put things back together to be a physically active guy? That seems to give you joy.
Richard: It does. It gives me a lot of joy, especially living in Banff. It’s such a magnificent place in terms of its surroundings. The mountains are just spectacular around here. I started pretty easily. Walking to the end of the driveway and back was enough for the first couple of months.
Then eventually we got into walking and then hiking. Biking took a while. I eventually got a little mountain bike and started doing some trails around where we were living. Skiing was a real challenge. I came back up to bat for the first time maybe 10 years after the surgery and had not skied in the meantime since before the surgery. I’d skied 100 days one year when I worked up at Sunshine Village, one of the ski resorts locally.
I was a good skier, but I was really freaked out about being on the slopes with my head above my skis. I was really fearful the first few times that I went out, but now I’m back to skiing pretty good blue runs. I skied 60 days this last year, which was obviously wonderful.
What gives you a zest for life?
Andrew, TPS: Richard, what gets you up in the morning? As I hear it, you’re leading a second life. You fortunately survived. You’ve put your life back together pretty well.
When you wake up in the morning with this beautiful setting — you’re in Banff, the Rocky Mountains there, these beautiful mountains, the ski areas, the hiking trails, and you being a physical guy. What gives you a zest for life?
Richard: I will tell you that the natural surroundings that we live in really engage me. I love just waking up in the morning and looking out at the mountains first thing. I don’t have a lot of commitments right now, which is really good for me, because I’m retired.
I’ll have some chores to do around the house, grocery shopping, or activities that keep us busy, but I don’t really have many constraints on me right now, which I’m very, very grateful for. I just wake up happy to be here. Happy to be here at all. Happy to be anywhere.
Andrew, TPS: I want an image of that. Maybe you went down the double diamonds years ago, but when you go down that blue run now, is there sort of an exhilaration that happens?
Richard: There’s no question. It’s one of the most exhilarating experiences that I have currently in my life. Skiing is this controlled falling sort of thing. You’re just kind of falling, falling, falling and just experiencing the snow and the wind and the sky. It really is very thrilling to me. I enjoy it very much.
Andrew, TPS: You said you also do biking.Where you live, you can go biking on a trail, and you could meet a bear, which could be another challenge to your life. You like that kind of exploring as well? You have thousands and thousands of acres to explore there.
Richard: Yes. Sonya and I bought e-bikes a year ago to try them out. It’s been a game changer for us because there are so many miles of trails around us that we’ve kind of explored a little bit, and Sonya had not been on a bike in like 35 years before last year.
When we started riding again, it was just a marvelous experience. We take books, and we go out by the river and sit at the beach, sit at the side of the river and read books for a little bit, or we’ll travel around and go to different trails.
Actually, when we were in Utah vacationing earlier this year, we took our bikes, rode through the national parks, hooked them up, then went for a hike, came back to the bikes, and then rode back to the car. It was just magnificent.
Finding ways to still do the things you’d like to do
Andrew, TPS: Let’s talk about that. E-bikes are a good example. Trying to ride a standard bike, there are people [who] may be huffing and puffing, and it may be difficult. There are adaptive ways of living now. E-bike are an example.
What would you say to cancer survivors who maybe aren’t back to 100%, but there’s a world out there, and there are things they’re interested in? [What is your advice] to find ways to do it, even if it’s different or more limited?
Richard: I would say that it’s definitely worthwhile. It’s worth investigating what is available out there, because there are some different technologies and different adaptive devices that are out there for walking, hiking, biking, swimming, or boating. There are just lots of different things out there.
I think the focus for me was concentrating on what I could do, because there were so many things that I couldn’t do for a number of years after the surgery. I couldn’t walk more than a mile. I couldn’t run at all. My thinking was still pretty wobbly in the first couple of years.
For me, I concentrated on the little things that I could do, [like] the first time I went to the grocery store by myself. This was after I’d become certified to be able to drive again, which is about maybe a year after the surgery. I went to the grocery store, and I was just kind of overwhelmed by the numbers of things on the shelves. [I] just kind of went down two or three aisles, left and went back home, and got maybe half the stuff I was supposed to get.
But that in itself was very thrilling for me because I was able to do something on my own, and it was just a great sense of accomplishment. Finding things that I could do on my own and just little progressions that I made week after week or month after month was very important to me.
Andrew, TPS: There are people, though, who have limitations. They used to lead a more active life. Now they’re struggling to get back to some of it, and it’s depressing, quite frankly. I imagine you had to work through that, too. A sense of loss. How have you gotten past that to celebrate what you can do?
Richard: That took some time. There’s no question about it. Initially, after the surgery, I was actually at such a low state of thought processing [that] I didn’t really feel sorry for myself at all. I was just kind of surviving. That went on for a number of months to the point where, again, maybe a year out, I started thinking about things that I couldn’t do, things that I was trying to be able to do.
One of the big things for me was becoming a physical therapist again, because my neuropsychologist told me I probably could not do it because [of] the amount of thought processing and cognitive processing that it required.
I told him that I was going to do it regardless. [It] became my full-time job [to] read orthopedic manual therapy textbooks. I’d read a chapter and I’d forget 80% of it, and read it and forget 80% of it. I just kept doing it and doing it.
Perseverance was a big thing for me. I eventually became a physical therapist, returned to physical therapy, and worked at it for another 10 years after the surgery. I thought that was pretty good.
Looking forward to the future
Andrew, TPS: No kidding. How do you see the rest of your life now, as far as hopefully continued recovery and enjoying life and those activities?
Richard: I’m very much looking forward to what’s ahead of us. Hopefully, we’re going to be able to travel a little bit over the course of the next few years, COVID notwithstanding. I’m hopeful about traveling and experiencing some different parts of the world that I’ve never seen before.
The other thing is just the accommodation strategies, because sometimes I’ll forget that I actually have a brain injury. It does happen. I’ll be in a store, and I’ll try to remember something. I haven’t written it down, and I forget. I’m always conscious of the fact that I’m not quite where I need to be.
I’m always working a little bit to try and shore up my accommodation strategies, put myself through some paces, or do some little mental mind games on my phone, [like] things to try and keep my memory going. I’m really optimistic that we have a fairly long life ahead of us, health notwithstanding, but I’m hopeful.
Andrew: I hope so. Like so many people who’ve been treated for cancer, there can be life after cancer. It may be different. It may not be 100% of what it was before. I really wish you well.
You’re in a beautiful setting in Banff. You have the natural beauty all around you, and it sounds like you’re taking advantage of that. Richard, I just see you biking and going down those ski runs, and your heart beating fast and just really enjoying it. That’s a great image for me.
Changes from having a brain injury
Richard: There are two changes that occurred. I used to get really bad motion sickness before the cancer, and after the surgery, I haven’t had a single bout of motion sickness since. It’s been almost 20 years and I’ve been in boats and planes. I would have thrown up multiple times on some of these things, and it never happened, which is really strange for me.
The second thing is that I went from being a visual learner to a kinesthetic learner. When I returned to physical therapy, I returned in a volunteer capacity with a friend of the neuropsychologist that was treating me at the time.
Once I got my hands on patients, my hands started doing things my brain really wasn’t connected to. [They] just started working on their own. That’s kind of how I relearned my physical therapy, and that was kind of interesting as well.
Andrew TPS: It’s an adventure. Life can be different, but it can be fascinating.
Richard: For me, it’s been a real adventure afterward, trying to figure out what’s different and what’s the same.
Andrew, TPS: We’ll continue that adventure, Richard Bandy. Thank you so much for being with us. I know your story, incredible as it is, can give people a lot of hope that you can have a pretty full life after even being treated very aggressively for cancer. Thanks for being with us.
Richard: Thank you, Andrew. My pleasure.
Andrew, TPS: I’m Andrew Schorr. Thanks for joining us, and my cancer friend, Richard Bandy.
The Patient Story’s new series “Cancer Friends” features Andrew and Esther Schorr. They co-founded PatientPower.info, a resource for other cancer patients and caregivers to help them through their diagnosis and treatment.
Join us every Sunday for a new “Cancer Friends” episode, airing on our video channel here!
This segment focuses on Shellie Oakley, who was diagnosed with breast cancer in 2008. She underwent a mastectomy and reconstruction. Shellie shares how she returned to her active life after treatment, as well as being a hands-on grandmother.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
One of my things in terms of embracing life has been always looking for a sense of awe in the world.
Shellie Oakley
Introduction and diagnosis
Esther Schorr, The Patient Story: This is Esther Schorr with another edition of our Cancer Friends series. Today I feel very, very fortunate to have one of my dearest friends, Shellie Oakley from Bellevue, Washington, who is a breast cancer survivor of many years.
Shellie went through a mastectomy, reconstruction and a number of complications and additional things that happened to her. She is one of the most stick-to-it, can-do people that I know, an incredible outdoors woman and has a partner who equally has a love of outdoors and activities.
We want to talk today about her determination to return to the things that she loves: hiking, biking, kayaking, active grandparenting and so many other things. Shellie, thank you for being here and for being willing to have this conversation with me. It’s good to see you.
Shellie: Thanks for asking me to do it.
Esther, TPS: I gave the 30,000-foot view of your cancer journey, but can you talk about when you were diagnosed and then the steps that happened up until now?
Shellie: January 2008, I had gotten into the habit of going and doing a lot of diagnostics, my usual mammogram, etc. Right at the beginning of the year, [I] started out. Because I have a family history of breast cancer, [I] wanted to take care of it. Somehow I thought I was going to beat that bullet.
It was a routine mammogram and ultrasound. The doctor [was] like, “Hmm. Well, I think maybe we should do a biopsy.” It went on from there. Luckily, it was discovered early. It was small. They framed it [as] the kind of cancer you want to have if you’re going to have breast cancer.
I called you and Andrew pretty early on. It was a hard weekend waiting, but once I was diagnosed, it was moving forward to, “Okay, what are the next steps? What do I need to do?”
I really wasn’t liking the answer that I was getting at first, which was they couldn’t do lumpectomy or anything else. It had to be a mastectomy, even though it was very early and small. I went and got 3 different opinions from 3 different hospital systems because they each have their own way of doing things. Everybody gave me the same answer.
I was coming to terms with that and had a little bit of time to prepare myself. [I] had a mastectomy and reconstruction. I actually feel like I was very fortunate because I did not need chemo and I did not need radiation. They could surgically feel like they safely did take care of it, and then [treated with] drugs as well. It was a series of surgeries.
That was my main treatment. Because of some problems, it turned into many more surgeries than I ever thought it was going to be. I remained grateful that I was alive, that I was going to stay alive and that [I] could move on. It’s a major thing for your body not just to have surgery, but to have it altered by something like a mastectomy.
Where are you now in terms of treatment and maintenance?
Esther, TPS: Where are you now, Shellie, just from the standpoint of treatment and maintenance?
Shellie: I did a lot of follow-up. It was every year. I’m now 14 and a half years out. I have awareness. I still go get my annual mammogram and ultrasound. The biggest thing that still stays with me is [that] it changes. For me, it changed a certain trust in one’s body. I could feel fine, but there could be something else going on.
Esther, TPS: How do you deal with that?
Shellie: I am aware of it. I do the best I can to take as good of care of myself as I can. I like certain alternative stuff and I work also with a functional medicine doctor. When I feel like there’s something going on, they’re looking at root causes, not just symptoms.
I have that awareness and in some ways it woke me up, because nothing changed. That reality existed before. I’m just more aware of it. There are no guarantees for anybody, any day of their life, so let’s make the most of whatever time we have.
How did you get back into your passions?
Esther, TPS: That is a great attitude and I’ve seen it. I’ve seen that that’s the way you live your life now. Let’s talk a little bit about incrementally returning to the things that you’re passionate about.
Obviously, when you’re recovering from surgery and all of that, some of that wasn’t happening the way you’d like. What are the things you’re passionate about and how did you get back to those things? How did that happen?
Shellie: While I was lying there waiting for the biopsy, I had just said yes to a new job that was going to be 60 hours a week and very stressful. The way I decided to interpret this diagnosis was, “Yeah, that’s my body telling me.” I was doing it interim, so I was already [stressed]. I don’t need to do that and I chose not to. I hung in there until they found somebody and then I took time off.
We’re now [in] summertime. This was my dear husband encouraging me or being willing to do it. We had planned on doing something called Cycle Oregon, which is a weeklong biking group trip. We switched to a tandem, really with no training and giving myself a lot of permission and we took an extra bike. If there was a day I didn’t want to bike, he could still bike and I could do the sag wagon.
[The sag wagon will] pick you up if you tire out or you can ride. In retrospect, Randy pulled me up so many of those mountains. That I was kind of like, “I’m not going to stop living.” Going ahead and doing that and then I ended up having more surgery afterwards. That first year was up and down and then there was a pretty long period because I had multiple surgeries. I would go do things, but at a lower level.
Esther, TPS: What were some of those things? Obviously biking. What were some of the other things? I know I mentioned at the beginning, but talk to me about how those came back into your life.
Shellie: Certainly always making sure we get out for walks and just to keep my body moving. Once winter came, I think we probably did a little bit of cross-country skiing, just gentle, flat [and] short. I am very grateful that I have a husband who is always willing to do it at whatever level I can do it at.
Esther, TPS: Bless his heart.
Shellie: Bless his heart. He is hardcore. He does go off with other people and do really hardcore stuff. Just to be able to be together, he’s willing. More recently, when I got down to downhill skiing. You only want to go for an hour. We’ll drive almost an hour, go for an hour, come home. No problem.
Being able to listen to my body and listen to my mind as well [is important]. There’s a certain fear factor of getting back into downhill skiing at my age. Taking things slow, but doing it. Doing something.
Esther, TPS: I know you love to travel, and I know that there is a member of your family named Pokey. Can you talk a little bit about that adaptation of travel in and of itself?
Shellie: After Randy retired and after we came back from New York… we decided that we wanted to be able to go at our own pace to be off-grid some of the time. We were looking and looking, [and] he bought a very old, fairly funky, beloved RV. Fairly funky. It’s very funky.
It turned into a project, so we didn’t get off on the road nearly as quickly as we thought we were going to. A lot of months were spent with him working on it and me working on being patient. Then we took off and took our time going down the coast. This is a 28-foot ’92 RV. 28 feet, so big but not crazy big. We had put in solar, and then we went into Baja.
One of my [bucket-type things] was going down [to] bays in Baja where in the late winter/spring, the whales are there. They give birth. They do the initial raising of the young ones before they start migrating back. There’s something about these bays that over time, they have learned they’re curious about people. It’s very well regulated and restricted, but you can go out in these little boats and the whales come up to the boat and want to be touched.
It is an incredible experience. One of my things in terms of embracing life has been always looking for a sense of awe in the world. That can be a flower in somebody’s front yard that you really look [at] the detail of. Touching these whales was definitely awe.
Esther, TPS: I can definitely understand that.
Shellie: That was a big highlight. Then we just spent time in Baja and then very slowly worked our way back when the RV wasn’t working well.
Esther, TPS: Having Pokey the RV clearly let you travel, very much on your own terms, at your own pace, with the partner you love. That’s a cool adaptation of, “Oh, I got to get on a plane, and I got to do the hotel thing, and what am I going to eat, and where am I going to sleep?” It’s just cool.
Shellie: It was, and we found that — this is maybe not true for everybody — but we actually did really well together in 150 square feet. You can’t take very much with you. It takes a lot of everyday-life stress issues that can come up. Who’s doing what? Who’s taking care of what? Just go out on the road and take it as it comes, meet people, and be in beautiful places. Go off the grid to places where you can’t find places to stay. It was wonderful.
Spending time with grandkids
Esther, TPS: Let’s pivot for a second. There is another great love and passion in your life: your kids and your grandchildren. Can you talk a little bit about how that has filled a very big part of being active now as an amazing survivor and thriver?
Shellie: It is. I feel such gratitude to be able to be close and have these relationships. We have 3 grandchildren. We have 3 children, and now we have 3 grandchildren from our oldest son and his wife. They had a little boy and then when he was about a year old, they discovered they were having twins. [There are] 19 months between them.
For me, it was actually a spiritual process. If you had a year to live, what choices would you make in your life? Even though at that point I did have a job that I liked a lot, I retired from that, and we moved to Harlem in New York City. [It was] never a place that we anticipated or desired to live, but they needed help.
We wanted to be close. We wanted to have that kind of relationship with all of them. We lived there for 2 years, helping take care of these 3 babies. Then even after we came back, every 6 or 8 weeks, we would fly back to give them a break. It’s a lot.
Esther, TPS: Now you’re still involved.
Shellie: We are super involved because the silver lining of the pandemic for us was they moved here to Bellevue. They live less than a mile from us. We see them regularly. We are able to not only help schlep and drive and help with whatever is needed, but to play with them.
What do we want to make today be? Some days it won’t be a lot, and that’s okay, too.
The beautiful thing about Washington is the easy access to the outdoors. I have woods to hike in a mile and a half from my house and a lake about the same distance to put a kayak in. I can take them out kayaking, which I do, and hiking. We call it walks. They are New York City kids. They haven’t fully embraced the hiking thing.
Esther, TPS: They’ll get there.
Shellie: We did a bicycle camping trip with Micah one of the years before they had actually even moved here. [We] toured with him [and] went over to one of the islands. We did stuff with our kids, but it’s a different joy with grandkids. We’re very involved. We’re happy to be very involved and really happy that we get to share what we love with them.
Esther, TPS: My guess is that you and Randy are going to be the grandparents that those grandchildren will actually still talk to when they’re teenagers.
Shellie: We hope so. We’re here, and hopefully we haven’t become too much associated with day-to-day parenting. So far, there are those moments to be able to be that extra adult and take them up on a lap and just listen and talk. It’s pretty precious.
Advice for recapturing life and passions
Esther, TPS: What advice would you give to other patients, [as well as] their care partners, who are trying to recapture their own zest for life, their own passions? Fortunately, as you said, for you [it] was up and down. It didn’t destroy your spirit.
You figured out how to move on and do the things you love. How would you advise people who are just starting on that journey of trying to get back to whatever it is that they love?
Shellie: First, there’s that level of acceptance. First, you have to really go through with what is. This is the journey you’re on, and it’s not what you hoped for or expected. Go through it, and when ready, be willing to take it slow. Maybe it’s not exactly how you did it before. Maybe it’s even better. Know what your passions are.
Maybe some of that has changed. Maybe what you thought you enjoyed doing, not so much anymore, and something else has taken its place. In general, kindness to oneself in going back and doing things, and just that little reminder of gratitude. What do we want to make today be? Some days it won’t be a lot, and that’s okay, too. I think that that’s a really important one.
Esther, TPS: Shellie, I really appreciate you sharing this story, not just with me, but with our other friends who are going to be hopefully listening and appreciating your story.
For those of you who are listening in, I hope that the stories that Andrew and I tell and that our friends like Shellie tell are helpful to you in navigating your own journey. We’ll look forward to having you join us for other stories with our Cancer Friends.
Abigail was a busy lawyer and mom of 2 when she found a lump in her breast. After her first mammogram and a biopsy, she was diagnosed with breast cancer.
What was originally thought to be stage 2A turned out to be stage 4 metastatic, meaning it had spread throughout her body.
Abigail talks about parenting with cancer, the transition from a busy career to going through treatment, patient advocacy, and the exciting breakthroughs in treatment.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
1st Symptoms and Testing
Introduction and Symptoms
Who are you outside of cancer?
I style myself a recovering lawyer. I have had a legal license for 20 years. I’m a mom. I have 2 boys — they are now 7 and 9 — and a husband as well.
I have a very supportive husband. He’s had to make a whole heck of a lot of adjustments since [I went] from healthy to not so healthy. He has weathered all of those adjustments with a lot of grace, which I appreciate.
I love the Enneagram. It’s is a personality type [or] way of understanding motivations. I very much resonate with type 8, which is sometimes called the challenger. I tend to challenge systems and definitely have learned a lot in the last 20 years about being an advocate. It’s kind of in my DNA. If something is wrong, I have to fix it, which is challenging at times with the amount of energy I have during the day.
Justice is something that’s very important to me. It’s probably why I ended up going to law school. My husband is black. He’s from Jamaica, so I’m understanding a whole lot more about the experience of people who are marginalized. That really pisses me off. I tend to get into the weeds with people about fixing those things.
What led to that first diagnosis?
I was 38 when I was diagnosed. Typically they don’t begin mammograms until 40. Because my mother is a breast cancer survivor, I could have gotten mammograms beginning at 36, but I was pregnant and nursing.
The mammogram itself doesn’t see as well into the breast when the milk is there. It clouds the image, so it wasn’t recommended by my primary care physician. Looking back, in 2016 I began having a lot of pain in my back and in my legs. Now I understand that was the metastasis that had spread to my bones.
I was a mom. I was tandem breastfeeding at that point. My kids were 1 and 3. I had a million things going on. I was running my law firm. You don’t prioritize yourself, I think, as a mom. [You don’t prioritize] your health, that sort of thing. It’s so important for us moms to listen to our bodies, to go to the doctor when things are wrong, and to ask the questions that need to be asked.
I don’t know if things would have been different if I had been diagnosed sooner. Certainly, by the time I was diagnosed, it had progressed to a very significant disease load. I don’t know if things would be different if I had said something sooner. Anyway, at the end of 2016, I was in a fair amount of pain.
Finding a lump in the breast
Then in January 2017, I felt a lump in my left breast. Because I was tandem nursing and pumping every 2 to 3 hours and had been doing that for 4 years, I was certainly very familiar with my breast tissue. But because of all of the nursing, I also had more tissue than I would normally. Even though the lump was relatively close to the surface, I didn’t really fully grasp what was going on.
I thought it was a clog and went to my lactation consultant. Interestingly enough, the cancer in my body happened in my breast exactly where I’d had clogs, and the same thing happened to my mom. The areas where the tumors were that they found when she had her DCIS diagnosis almost 20 years ago now were exactly in the places where she had clogs.
Definitely something to think about if you’re a nursing mom. Pay attention to those areas of your body and make sure that your doctors are paying attention to them as well. No one really treats your breast when you’re breastfeeding.
Your PCP might know something. The pediatrician knows some things. The OB-GYN knows some things. There’s not somebody who’s really talking about your breasts, especially when you’re nursing, except for lactation consultants. Not every medical practice has those.
Testing for Cancer
Is there a way to have a baseline to understand changes happening?
Absolutely. It’s so important to understand that. With lactation consultants, you would want to see an IBCLC, International Board-Certified Lactation Consultant. There are different certifications, but that’s the most important one that has the most medical knowledge.
Those professionals are so important, even with things like latching and different things as you go through your breastfeeding journey. Having that resource is so important. I had that.
We were also part of a milk-sharing organization, so we were able to share about 25,000 ounces during the 4 years that I was nursing and pumping. Ironically, the very first person that got milk from us was someone who had been diagnosed with breast cancer while pregnant. She literally had her baby and was wheeled into the chemo suite. She was unable to breastfeed, and everything just came full circle.
What was that feeling of being able to help someone who wasn’t able to breastfeed?
We had to go through fertility treatment to get pregnant. In a lot of ways, my breasts did what they were supposed to do when the rest of my body didn’t want to. I had a lot of hormonal imbalances that we were able to correct with medications. We didn’t have to get IVF or any of those things, but we struggled to get pregnant.
In a lot of ways, my breastfeeding experience was really redeeming in that my body was doing what it was supposed to do, and it was really doing what it was supposed to do. I had an overabundance of milk, and it was something that was a huge part of parenting. We had to adjust once they were weaned because everything could be fixed by saying, “Let’s nurse.” While tandem nursing, I got to see my boys just bond so tightly because they were nursing at the same time.
I don’t know [if] there’s any experience as good as meeting somebody who was just so grateful for the gift of something that was easy for me. A lot of the children that got the milk from our organization were children who were adopted. A lot of them were drug addicted at birth, and that nutrition — what we called “liquid gold” — was still very important to them.
We didn’t supply the NICUs because we didn’t pasteurize or do any of the things that the larger organizations do. I would take my bags and hand them to someone else. It was an amazing time. I was so grateful to be able to help as many people as we were able to during that time.
What happened at the lactation consultant?
She touched the area and said, “It’s probably nothing.” This is something that was consistent across the medical providers that I saw. “But I’d really like you to just go to your primary care physician and ask her.”
I had actually picked a primary care physician who not only personally tandem breastfed her children, but also had an extra lactation certification. Again, there aren’t those doctors that treat you when you are nursing. It took a bit for me to find somebody, but I had.
This was literally my second appointment with this particular doctor. She said, very similarly to the lactation consultant, “95% sure this is absolutely nothing, but since you’ve never had a mammogram…” Because of my mother’s history of cancer, she sent me for my very first mammogram.
How genetic testing for cancer has changed
My mother had breast cancer when they really only knew about the BRCA1 and 2. She did genetic testing immediately because [she was very concerned about her daughters]. I’m the oldest of 6, and there’s 3 girls. Because she was BRCA negative, we thought, “Oh, we’re in the clear.”
In 2013, they updated the panel of genes that they know to look for to 40. Now, almost 10 years later, we’re at 92. If anybody has had genetic testing prior to 2013, you really should get it redone. Honestly, my mother doesn’t remember being prompted to redo it in 2013, [so] she didn’t.
We later found out in my breast cancer experience that we carry a germline mutation ATM, literally like you get money from the ATM. ATM is part of your DNA that’s responsible for repair. If there’s a mutation in the part of your DNA that’s supposed to repair mutations, clearly that can be an issue. We didn’t find that out until later.
I am so grateful. For a lot of young women under 40, their doctors say, “You’re too young to get breast cancer. It’s probably a cyst; it’s probably this. Don’t worry about it.” Instead, my doctor said, “Let’s double-check.”
Mammogram appointment
I went for that very first mammogram appointment. They were very unhappy with me because, of course, as soon as they squished my breast, milk went everywhere. The machine [was] covered in milk. They did a mammogram, and they did a diagnostic ultrasound.
I didn’t really connect to how serious it was. The radiologist came in and wanted to do a biopsy right then. To me, I was like, “Oh, you just want to follow up right now.” My doctor had said that she wanted me to go to a specialist if they wanted to do a biopsy. The specialist that ended up doing my biopsy was both a breast surgeon and a radiologist. She was able to do all of it and then did my surgery.
That was my first experience leaving somewhere against medical advice. Looking back, the social worker came in to talk to me, [and] there were like 12 people that talked to me before they let me leave. I think they thought I wasn’t going to follow up on it. I think they thought maybe I wouldn’t take it seriously.
I’m pretty sure they knew pretty definitively right then that it was something very serious. I was just like, “No, my doctor told me to do something different.” Because I tend to be a bit stubborn when I decide I’m going to do something, I left.
That was a Thursday. The following Monday, I was in the surgeon’s office getting a biopsy, which was a very interesting experience. I’m very thankful my husband went with me.
I got a primary care physician [right] after we got married. I’d never had a primary care physician. I went to urgent care if I had something serious, and I had my OB-GYN that I went to every year. I really just didn’t engage with the medical system all that much. Thank God I was healthy.
My first introduction to medical things was the fertility experience, which was terrible because it was so emotional. It was invasive, and having vaginal ultrasounds every other day for weeks on end was so not fun.
I think one of the big things that was interesting about the biopsy experience is it was done in my doctor’s office, so I didn’t have to go to a surgery center or anything like that. It was ultrasound guided, so I was lying on the table fully exposed, which then was kind of an issue. Now it’s totally not an issue.
There was a person holding the ultrasound wand, and then the doctor had [something] like a long needle with a little grabber thing on the end, where it sounds like a click when they grab the piece of tissue. There was some pain. They used lidocaine to numb the area, and lidocaine shots are not fun to get either.
I felt so vulnerable, probably for one of the first times. [I was] in a doctor’s office, doing [the] procedure right there, where I hadn’t had time to prepare. All of the other testing that I had, somebody explained it to me, and then I made the appointment. I had time to assimilate to what was happening.
This was like, “No, we need to do this biopsy right now.” Oh, okay. Then I leaked milk and blood from the site of the biopsy for about a week afterwards. She had to biopsy a couple of my lymph nodes. The lymph nodes turned out to be full of milk. Not cancer, just milk.
I got to watch on the ultrasound screen as she was doing it and she narrated. It was a very different experience, different from anything that I had ever experienced previous to that. I think I was still in denial at that moment.
My father-in-law just passed away, but my husband and I had cared for him. On our third date, I met him in the nursing home. He had just transitioned into a nursing home. My husband had been his caregiver as a young professional for about 10 years before he went into the nursing home. He had 3 strokes.
I’m so thankful that my husband was much more in tune with, “Okay, this is serious. Yes, we need to do this right now.” I had meetings. I had client meetings, and I wanted to leave. He was like, “No, no, we have to do this now.”
He was very good at knowing that it was serious enough to do something. I think I was a little emotionally disconnected from the experience at that point. Mostly because I had no idea what was going on.
Breast Cancer Diagnosis
Testing Results
Insurance issues and waiting for results
This was all [of] January, February, but it was April 8th of 2017 when I went back to get the results of the biopsy and they confirmed that it was breast cancer.
Yes, it took a while. One of the reasons it did was because my insurance company was only contracted with one lab, and they were significantly backed up. It was across the state, so there was mailing things back and forth and all of that.
One of the very big lessons I learned right at the beginning was it is not our doctors that run our medical care; it is the insurance companies. [I had to understand] early on what my insurance covered, what it didn’t, and how we had to handle the things that insurance didn’t cover. Fighting with my insurance company — it seems like that’s a full-time job in and of itself, because insurance is ridiculous.
When did you realize this was something more serious?
April 8th of 2017 was when we found out it was breast cancer. I think then, we still thought [I would] go through treatment and be done. I had my mother’s experience to compare with. She is amazing and worked all the way through chemo and radiation and everything else. She had a double mastectomy and did all the things that you need to do.
My mother still [has] no evidence of disease now, almost 20 years later. I had her experience to think about. We really thought in April of 2017 that it was going to be a situation where I went through treatment, and then we could put breast cancer in the rearview mirror.
When we found out it was cancer, I left that appointment with an appointment with the medical oncologist, an appointment with the radiation oncologist and plastic surgeon, etc. I had all these appointments to learn about [and] all of the people who were going to be on my team.
I am so thankful that my introduction to this whole experience was [with] someone who said, “I have other doctors I work with very closely. We text each other.” She was texting different doctors to get me in the next day and to talk about treatment options. How amazing!
Genetic testing
The only fly in the ointment, looking back at that initial experience, is that we did genetic testing, but she only did BRCA1 and 2. Here we go again. My mother didn’t get retested, and then this surgeon was only looking at BRCA1 and 2 [and] did not do the full genetic panel.
I understand that it is hard sometimes to get those things covered by insurance, especially when you’re at the very beginning of these breast cancer experiences. Now when I talk to newly diagnosed people or people who are beginning the process, [I tell them] to insist on the full genetic panel, because BRCA1 and 2 are not the only genes that are associated with breast cancer. There are now 93 that they look at and that can change your treatment.
There’s literally an algorithm where they plug in all the different details. Your risk changes when you have cancer that’s associated with a genetic mutation, which is still only 12% of breast cancer. The vast, vast, vast majority of breast cancer has no genetic or discernible basis for it. Our genes just go haywire, or our cells go haywire at some point.
Being connected to other patients
We went into all of the appointments. I remember the radiation oncologist literally spent 2 hours with us, [and] the medical oncologist spent about an hour. All the doctors were so kind and caring, and it was a good introduction to something terrible.
I had my lumpectomy. We decided on a lumpectomy versus a mastectomy. Legally, an insurance company is required to cover a mastectomy if the patient wants it, as well as reconstruction. No insurance company can refuse to cover those things. My doctor was like, “All of these options are yours.”
She also connected me with a couple of her patients who had different surgeries, which I thought was amazing. I haven’t heard of other doctors doing this, but she connected me with somebody who had a lumpectomy, somebody who had a mastectomy, and somebody who had a double mastectomy. That was very helpful because I could compare and contrast their different experiences.
How did you decide which option to pursue?
There’s always pros and cons. Everybody is an individual. My mother had a double mastectomy and then did reconstruction. She had a couple of issues where they had to go back and redo things. One was a whole surgery where she got the scar tissue tightened up, and they had to go in and loosen it.
Honestly, my biggest issue at that point in time was recovery time. I didn’t want to have to have multiple procedures. Typically, when you have reconstruction, they put an expander in. Then you go in over time, and they inject more and more saline into that expander. You’re actually stretching out the skin to make room for the implant. Then you have surgery to put the implant in. The whole reconstruction process can take up to a year.
At the time, I opted for an oncoplastic reduction because we didn’t know I was stage 4 and we thought this was going to be an experience [of] go through it, be done, and it would be in our rearview mirror.
They did the lumpectomy to remove the cancer. They took tissue from my right breast to fill in the hole, or the divot, because it was a pretty big area that they had to remove. Then I got a lift and all of those fun, good, nice things to have everything look aesthetically the same.
That was important to me then: the aesthetic, how much I would have to be in various surgeries, how long it would take. I really wanted to be finished as soon as humanly possible with the medical side of things, because I thought, “Hey, I got to go back to work. I got to get back to doing the things that we’re doing.”
Preparing for the lumpectomy
I had my lumpectomy in June of 2017. It was pushed off a little bit because that particular surgery, there were only 2 plastic surgeons that knew how to do it with my surgeon, and I had to dry out my milk. My doctor handed me a paper with 2 or 3 things to do, and she said, “In about a week, you’ll have no more milk.”
I had been nursing and pumping every 2 to 3 hours for 4 years straight, and it took a lot longer than 1 week for my milk to dry up. One of the things that they needed to do was do an MRI to be sure that there was no cancer in my right breast. We had to get the milk out of the way so those images would be effective and reliable.
Scans and recovery from lumpectomy
I hadn’t had a lot of scanning, but I get PET scans every 3 months. I’m radioactive for at least 24 hours, depending on which isotope and the half-life and all of that. I typically have to stay away from my kids overnight after a PET scan because they don’t know how radiation affects a growing body.
[According to] the picture that they pulled out, the lumpectomy went great. It was a 7-hour or something surgery. I got to go home the same day. It was a great recovery. It was a big change. I went from DD to A. That was a very big change. I was normally an A, almost a B cup. Nursing definitely gave me more tissue than I had normally.
That was a big adjustment, too. Clothes fit differently. You have to wear those awful compression garments for the first [couple of] weeks. It was a big adjustment, but I was still working, still trying to have as much normalcy as possible.
Receiving the Diagnosis
When you received the diagnosis, what staging and details were you given?
My doctor was perfect for me because she was very direct. There wasn’t a whole lot of packaging or hemming and hawing. It was, “Okay, it came back. It’s breast cancer. It’s hormone positive, strongly hormone positive.” At that point, we didn’t have the HER2 status because they had to do the extra testing.
I still have the paper where she drew where it was. I had a tumor and then an empty spot, and then it would look like the cancer was developing a second tumor. It was kind of this weird, almost 2 tumors. At that point, she said most likely I was stage 2 because of the size of the tumor.
At that point, I had not talked about any of the other symptoms I was having. There wasn’t any sense that it had spread anywhere at that point. When we did the lumpectomy, they took 4 lymph nodes.
This is one thing that I learned from my mother. When they do lymph node dissections and they take 26 or 30 lymph nodes out of your body, that compromises your lymphatic system in such huge ways. My mom is a physical therapist. At that point, they were already going to do chemo, and she said, “If you take all those lymph nodes, will that change my treatment plan?” They said no, and she said, “No, thank you.”
Node negative
They injected dye around the nipple in the 4 quadrants. I think it was an ultrasound, or it might have been a different type of imaging. They watch to see the first 4 lymph nodes that the dye went to. Those are called sentinel nodes. Those are the first lymph nodes that would be processing any kind of fluid that came from the breast area.
They took those 4 during my surgery, tested them, and they were determined to be node negative. The typical spread of cancer is from the breast through the lymphatic system into other areas of the body. In about 5% of us — of course, I always fall in these weird percentages — it has spread through the blood before it ever really recruits the lymphatic system. Nobody knows why that is.
Statistically and generally, if you are node negative, [typically] doctors then say, “Okay, you don’t have to worry about the cancer having metastasized.” Because I was node negative, they initially staged me at 2A.
Then they sent off the tumor cancer tissue from my lumpectomy to have genomic testing done. I talked about genetic testing. That’s your DNA, your blood, and what you get from your family. Genomic testing is to look at the characteristics of the cancer to see what kind of mutations it has, etc.
Oncotype test results
It’s called an Oncotype test. There’s Oncotype and MammaPrint. They’re basically the same thing, just 2 different companies. They’re able to score, based on your different markers, your risk of recurrence.
My risk of recurrence came back in the gray area, which is super weird, knowing now that I was already stage 4 at that point. At the time, the gray area for me at my age was 27, and 25 to 30 was the gray area. That’s no longer the gray area. Now over 25 is recommended for chemo. They keep learning, which is so good.
My doctor said I wasn’t at 30, which would have made me in the high-risk area, but his personal, “definitely get chemo recommendation” began at 25. Because I was 27, he said, “You should consider chemo.” The report that we got said if I did chemotherapy, it would reduce my risk of recurrence by a little over 20%. For my husband and I, that was enough of a percentage that it made sense to go through chemo.
We scheduled chemo, and that was Adriamycin and Cytoxan. Adriamycin is often called “the Red Devil.” I would do 4 rounds of Adriamycin and Cytoxan and 12 rounds of Taxol and then radiation. That was the treatment plan.
The nurse in my doctor’s office made a mistake and checked the box for them to check my tumor markers at my first chemo session. Tumor markers are various proteins that are given off and are in the blood when cancer is spreading. It was a mistake. It’s not standard of care. A lot of doctors don’t even look at tumor markers.
In June, I had my first chemo session. My doctor called me the day after and said, “There’s something amiss with your blood work. We want you to do a bone scan and a CT scan.” I was hopped up on Benadryl and all of the other pre-meds they give you. Again, I didn’t freak out. I was like, “Okay, sure. More tests. More scans.”
I had asked about the PET scan. He said, “It’s hard to get them approved by insurance, but we’ll do it if you want it.” He didn’t seem very concerned about doing scanning, so I was like, “Oh, okay,” and didn’t push it. I don’t not push it anymore, because I think my intuition was telling me we needed to get more information.
I went in for the bone scan and the CT scan. It was a whole day at the hospital. I vividly remember having client consults, drafting pleadings, and doing all these things from the waiting area. Then we got the call June 22nd of 2017, and the nurse who called said, “You just need to come in. It doesn’t matter when. Just come.”
I was in the middle of preparing for a hearing and was totally distracted. I called my husband and said, “I had a weird phone call. They’re not even making me make an appointment. You don’t need to go. I’m sure it’s nothing.”
Thank God my husband had the presence of mind, because of his experiences with his father. [He said], “Doctors don’t say, ‘Just come whenever you can get here. We’ll see you.'”
Receiving the stage 4 diagnosis
My husband took me to the last hearing that I conducted as a practicing attorney, and I won. Of course, you have to include that. My husband took me to the hearing, and then we drove up to my doctor’s office.
What’s funny is I didn’t really like the medical oncologist the first time we met him. He has a daughter that’s very close to my age, and he was just very paternalistic. [It was different] going from my breast surgeon, who was like, “Let’s talk about it. All the details. Let’s make the best decision.”
He was very like, “You’re going to do X; you’re going to do Y.” I kind of bristled at that. It’s kind of like, “What, you’re going to tell me what to do?” In hindsight, he was the perfect doctor to have broken that news to us.
He brought us back into his office. He put his hand on my knee. We were talking about how breast cancer was going to be something that was going to be an experience, a season, and you would die of something else. He said, “You’re stage 4. This is going to kill you.”
That was extremely sobering. It was totally out of the blue. Totally not expecting that. I had a 5-centimeter tumor in the middle of my right femur. My breast tumor was only about 2.4 centimeters. It was bigger in my leg than it was in my breast. They were worried that my bone was going to shatter.
Processing the Diagnosis
Initial response to the diagnosis
My first thought after he said this was, “My kids aren’t going to remember me.” They had turned 2 and 4 at that point. He started giving some statistics, and he was very careful to say, “You are not a statistic. Statistics are not everything. I have patients that have been living for 10, 15 years with metastatic disease. But this is a serious situation.”
I had bone-only metastases at that point; it only spread to the bones. There was some data that was a longer life expectancy than if cancer was in your organs. He shared that with us. He was very kind, and he let us ask all the questions.
Of course, I tried to pin him down onto, “What is the timeline? I get 10 years, right?” He’s like, “Well, some people do.” It was a very good balance of hope and reality. He was going to manage me being on tamoxifen, which is typically a hormonal medication that you’re on after you finish chemotherapy when you have early-stage breast cancer. He said, “Now, we’re going to be talking about totally different medications.”
How did you process your second diagnosis?
I think partly because of my training and partly because of my personality, I tend to think about something first, and then the feelings come later. At the time, it was much more of a project management type of, “Okay, how are we going to fit all this in?” I was thinking much more about the nitty-gritty. “This was going to be the plan, but now that’s all blown out of the water.”
It was a lot of trying to assimilate and understand what’s going to happen now. I vividly remember he sent in his social worker, who was 22, right out of college, and she was trying to talk to us about how we felt about things. We were both just like, “Now is not the time. We’re overwhelmed with all of this.”
We got into the car. I told my husband, “I can’t drive. You have to drive.” My brain was just whirling, and we both cried all the way home. A lot of it was about the kids. A lot of it was that they’re going to lose their mom at such a young age. One of my first thoughts was, “I have to protect them against the crazy stepmother that my husband is going to marry, this other woman, and there’s going to be other kids.”
Your brain goes to so many weird places when you have a trauma like that. I don’t think that my executive functioning was fully online. I think [I was] just kind of bouncing all over the place. It took about a week, I think, for things to really marinate and for us to really wrap our heads around things.
Of course, I was in surgery within a week to get titanium rods put in both femurs, and so there were a ton of appointments as well. We had a business, my law firm. We had employees. I had a roster of clients. There was a lot of, “Okay, I have to take care of all these different pieces before I can even focus on what’s going on with me.”
It was about a week or so, maybe 2 weeks after the diagnosis. I started seeing a psychiatrist because I realized very quickly that the coping mechanisms that I had developed over my 38 years of living were not up to the task of dealing with this huge diagnosis.
[I] sought out mental health treatment and got on medication pretty much right away to manage anxiety. There was depression, those dark nights of the soul, when you are just thinking about the end of your life. That’s what I obsessed over for the first couple of weeks.
Getting all those different pieces of support. My parents came up. We lived in Orlando when I was diagnosed. My parents were in Miami, so they came up. My mom was with me in the hospital, spending the night after surgeries.
Realizing how serious things were?
I didn’t fully grasp how serious things were. I did on some level, but it became so real when we were in the orthopedic surgeon’s office. He pulled up my scans. I had not looked at my scans. Now, I look at everything, but at that point, I was relying on the doctors to tell me what was going on and what was in the scans. He pulled it up, and it was a picture of my right femur.
On an X-ray, your bone is supposed to be white. That’s the color it’s supposed to be. Mine was mostly black, or it looked that way to me, because there was so much cancer. If you think about your bone being round or 3-dimensional, much of the bone was full of cancer. In that area where the tumor was concentrated, it looked like there was only really one area of the bone that was still solid.
Reacting to the X-ray
One of the nurses wouldn’t make eye contact with me through the whole appointment. She told me later that it was because, of course, I had started chemo. I was bald. I did not look healthy. She told me later that it was just really triggering for her because her sister had just been diagnosed with cancer. She made me this bracelet. It was very kind.
I did not fully connect with how serious it was really until that moment. I didn’t fully understand even some of the conversations that were going on among my doctors. One of my friends actually saw my radiation oncologist recently, and she expressed some amount of surprise that I was still alive.
I think [it was because of] the disease load. It was in every bone, and every bone was liberally sprinkled with cancer: all through my spine, it was in [my humeri], but my legs were the worst. Obviously, you need your femurs to walk and to remain upright. Those are kind of important bones. That was the focus.
I found out on a Friday about my diagnosis. The following Friday, I was in surgery to have the titanium rods put in both femurs. We decided to finish the Adriamycin and Cytoxan, save the Taxol for later, and then we scheduled my hysterectomy, too.
Processing Cancer and Finding Community
Processing the Diagnosis
When did you allow yourself to grieve?
There’s a lot of grief when it comes to any cancer diagnosis. I think that you go from being a healthy person generally. It’s a betrayal, right? Your body has betrayed you in a lot of ways. I think that really resonated with me a lot at the beginning.
I did what a lot of people tell you not to do, which is I went online. Certainly there was Google, but then through some of the ladies that I talked to that my surgeon had sent me to — and my mom because she had been through treatment as well — [I found] different support groups and other people to talk to.
[There was] one thing that was extremely traumatizing. One of the support groups I joined probably 2 or 3 weeks after I found out I was stage 4, 3 of their members died in the week that I joined. That was so sobering and overwhelming. I don’t know that I really did process things very well initially. It was not until things died down a little bit.
We transitioned my clients and a lot of my staff to the firm of some dear friends of mine. It was a good transition. They practiced very similarly to me. It was a lot to undo all of the contracts. We had actually just signed a contract to move into a new office.
Once the logistical stuff was done — because again, I think first and feel second. I focused on doing all of that. I had so much downtime. [I went] from working at a million miles an hour with my hair on fire to having all that downtime. My kids were in a Montessori school, so I had all that time during the day.
What helped with your emotions?
That is when a lot of the emotions started coming, and I found a lot of relief in writing. I have a literature undergraduate degree, so writing, journaling, and that sort of thing has always been something that has been helpful for me. I found a lot [of] release there. The psychiatrist that I saw did talk therapy, as well as the medication. That was helpful, certainly.
Connecting with other people who are going through the same thing, I think, has probably been the number one thing to alleviate some of the intensity of those feelings. The ability to say, “I’m going through X,” and there’ll be 20 people who respond, “I’m going through the exact same thing.”
That was such a weirdly comforting thing that we’re all going through something so awful at the same time, but it was. It was really helpful outside of the place where all the people were dying. I got out of that group because that was too much at the beginning for me.
I now moderate a Facebook group that is specifically geared toward the newly diagnosed. We take the people in the first 2 years of MBC diagnosis and really mentor and model for them. We’re kind of onboarding them into the MBC community, and then we get them into other groups and let them graduate. [We do this] because of those initial experiences that a lot of us have had, because death is such a constant in the MBC community.
Coping with cancer and loss
Finding the coping skills and finding the ability to handle that, I’m still not good at it. It’s been 5 years. I’m still not good at it, but I have more coping skills now. A lot of it has to do with these key people that have the same disease that we can really just talk frankly about what’s going on. Support groups where that’s facilitated [have] helped, in addition to the direct connection.
I started CaringBridge sites pretty early on just to keep everybody informed. Things were changing every day, and that made a lot of sense to keep everybody informed that way. I think writing and talking with other people have really been the best things.
All of them understand. It seems like the intensity happens at night. The amount of times that I’ve texted friends of mine in the MBC community — I’m always thankful for people in different time zones because it’s not the middle of the night for them.
[I’m thankful for] being able to talk things through and just really say that this what I’m feeling at this moment instead of stuffing it. I was a very good stuffer before this. Again, coping mechanisms that do not work for a terminal diagnosis. Stuffing is not good. That’s not a good thing.
Parenting while dealing with cancer
Being open with your children
Our parenting style has always been to be as open and honest as possible with our kids on the correct developmental level. One of the things has just been to talk to them, to make sure that they’re equipped with information generally. We’ve done a lot around helping them to name their emotions.
We have a whole lot of books that we read. “The Invisible String” is a big favorite, talking just about how whether you’re at school or somebody is not around anymore, that love connects you to the person that you are connected to.
I think that one of the things that I read when I was a new mom was just this concept of how we’re always the ones behind the camera. We’re always taking the pictures, so we’re not often in the pictures. That’s for a lot of different reasons.
I have prioritized having regular professional photoshoots. We do one for Christmas cards every year. Then I’ve told my husband, “I don’t want all the stuff for Mother’s Day. I just want a photoshoot so that we have that record of them, of me being in their life.”
Both of them are very active children. They’re both boys. I was always very active with them prior to my diagnosis. That was a huge change because I was on crutches and then a walker and wheelchair, especially after my leg surgery.
Energy is something that is in short supply when you’re in treatment and radiation. It makes you so tired as well.. I had radiation to my legs and to my back. [I had] to adjust to not being active with them, but finding other times of connection with them.
All the parenting stuff talks about how you’re not going to be in your children’s memories if you’re not in their lives today. Because I’ve had the ability to have more time with them, because I’m not working and running around and having a million to-do’s, I’ve been able to be a lot more intentional in spending individual time with them, putting the electronics away.
I do a date with each of them once a week, where we go out. It’s usually for ice cream because of course they want ice cream, although my older son is now quite obsessed with the French bakery and croissants and lava cakes and all of that.
Every week, and now we’ve done this for years, I’ve taken them out and just had an individual conversation with them about whatever it is that comes to their mind. I’m just trying to be very intentional about being in the moment with them, about listening to them, trying to consider very carefully the lessons that I want to pass on to them. I also have memory boxes for them.
Leaving letters for the future
Our niece got married. Her husband was there dancing with his mom, and I about lost it. Of course, I immediately thought, “I’m not going to be able to do that.” The likelihood of me being here, although we hope so, when they get married is low. I’m not going to be able to have that dance with my son at his wedding, either of them.
What I have tried to do in terms of channeling that emotion, channeling that energy, is I sit down and write them a letter to open on their wedding day. I have a box full of letters for different times. I don’t even know where I came across it, but I came across a list of all the times that you want to hear from your mom.
You come back home after your first binge drinking or wake up with your first hangover, break up with your girlfriend for the first time, buy your first car — all those milestones and moments that it is unlikely that I’ll be here for. I’m trying to have a card for them to open with my handwriting, with my reassurances and those kinds of things.
Saying the important things while you can
I have realized over the last 5 years — not just with my kids, but with everybody — that you have to say the things that are important. You have to say that you love people. You have to say that you care for them. You have to verbalize those things because we have no idea what’s going to happen tomorrow.
For so many of my friends in the MBC community, once the cancer gets out of control, it’s a very short time period between finding out there are no more treatments and death. We typically don’t get a lot of time in hospice. I have friends in the last month that passed away, and they literally went out of the hospital into home hospice and died the next day. That is the trajectory of this disease.
This is my legal training. I try to look at the worst possible thing that could happen, plan for that, and then everything else is taken care of. We tried to look at those kinds of things unflinchingly, but saying the things that you need to get off of your heart, I think, is one of the big things that we’ve tried to do with the kids.
I’ve just tried to do with relationships in general because you don’t know what’s going to happen. I think those of us dealing with a serious illness, we have a little bit more of a sense of that, just because we have a serious diagnosis. Somebody can die at any point.
Preparing financially
We also redid our trust. I am thankful that as a young professional, I got a good private disability policy. I also signed up for probably more life insurance than I really needed to because I practiced a little bit in personal injuries, so people who get into car accidents.
Ever since then, even though I despise insurance companies, I have every type of insurance you can think of because I’ve seen what happens when you don’t have the coverage. It’s a domino effect of losing things — your house, your car, your job, etc. — when something serious happens.
Thankfully, we had planned for that. We redid the trust that we have set up for the boys. One, I was trying to protect the money from the evil stepmother. See, it’s still a theme. It’s still something I think about. Also, just thinking I’m not going to be around to help them figure out what to do with money with these kinds of decisions.
My husband’s a banker. He’s obviously very well equipped with that. We have a few more restrictions on what they’re going to be able to do with that money, like not being able to get the principal until they’re at least 30. I just tried to be very intentional about those things, about my legacy, and about what I’m going to leave behind.
Living with Cancer
Jolting changes to life
I think the average age of breast cancer diagnoses is still 60. It’s still mostly people who are either retired or heading in that direction. But when you’re diagnosed in the middle of your career, the middle of what’s supposed to be your productive years, it’s jolting on so many different levels.
I talked about all that time that I had on my hands after things got wrapped up with the firm. When you have a career versus just a job — maybe it’s not as much for women as it is for men — I think a lot of our identity becomes wrapped up in what we do for a living.
I love the spoon theory, where we wake up with less energy or less spoons than a healthy person. We can’t just drink a cup of coffee and get more energy. Once the energy is gone, it is gone.
For me, anyway, the idea of advocacy has always been something that permeated my entire life. I think I identified with helping people and advocating for people. That sort of thing is a big part of who I am. When you are deprived of that purpose or the thing that gave your life purpose, then you start looking around and saying, “What am I supposed to do now?”
For me, it was a lot of boredom. You can only read so many books and watch so many videos or movies on Netflix. I very quickly found that sense of restlessness. Certainly, I also had a lot of physical impairments, having to really work at getting mobile and being able to walk better. At the beginning, there are cognitive deficits that come about because of chemo.
Managing self-expectations with low energy
A lot of what I struggled to figure out was, okay, I have these expectations of myself. I have this knowledge of myself as a healthy person. What is this now? What can I do now? That was where I found my way into patient advocacy. I’m not just advocating for myself, but working with nonprofits to advocate for others in the community.
[I] very quickly found that there is a hole when it comes to the people getting good legal advice. I had great legal advice because all my friends are attorneys, and all I had to do was call up a friend of mine and ask a legal question. Most people don’t have that access.
[I] started to delve into the ability to use my experience and use the things that I had already done to do that, but then still struggling with this adjustment of, “I can’t think of the word.” I love the spoon theory, where we wake up with less energy or less spoons than a healthy person. We can’t just drink a cup of coffee and get more energy. Once the energy is gone, it is gone. I would literally sit there and fall asleep sitting talking to somebody.
That’s a huge adjustment from being very high functioning. I think that those of us who go from a 90-miles-an-hour career to a cancer diagnosis, that’s a much bigger change than those people who are either already retired or kind of winding down in terms of the things that they’re doing. Plus, I have young kids, versus people who have adult children.
Being diagnosed with cancer at a young age
I think the younger breast cancer experience is very different. I think that a lot of hospital systems and survivorship clinics don’t often remember that it is very different for us. That has been a bone of contention between myself and every single one of my doctors about how the general rule just doesn’t apply to me. You can’t just make an appointment for me during school pickup, because DCF gets a little upset if I leave my children at school. A lot of that has been something that I’ve had to educate people about.
Social media has allowed me to connect with other younger women with breast cancer, because our experience is so different. We’re a minority still, but the under-40 population is the only segment of the population where diagnoses of breast cancer are growing and continuing to grow. In all other segments of age ranges, it’s declining. I don’t know why that is.
In some ways, it’s kind of a double-edged sword, but it’s kind of good that more of us are educating our doctors because I think they will be more sensitive to our experiences. It’s obviously a terrible thing to be diagnosed at a young age with something so serious.
Complete overhaul of life
Because mine was a de novo diagnosis, I was not given the opportunity to go through treatment, have some years of no evidence of disease — and you notice that I’m not saying cured because there is no cure for cancer — and then have a stage 4 diagnosis.
I find that the people who go through that trajectory in terms of their disease just have a very different experience. It was just a complete overhaul of our entire lives from the very beginning. Not that I think that that’s necessarily a bad thing overall.
I think we can learn a lot from people who have serious diagnoses because we have a whole different perspective on the things that matter. How often do we get so focused on things that don’t matter in our lives because we’re just caught up in whatever it is?
Community
The importance of finding support and community
First, let me talk about finding people. Most cancer centers and doctor’s offices have either a support group that’s managed by a social worker or peer support groups. COVID changed a lot of that in terms of in-person groups, although I still think that meeting with people in person is so very important.
Social media has become a really good way of connecting to people that have a similar disease experience. Even the people who don’t have children, I find that sometimes I can’t even connect with them as much. Yes, we can connect on the disease level or on health care experiences and insurance. But when it comes to the lived experience, the people who have young kids are probably the people that I end up connecting to the most.
I don’t think I’ve ever met somebody who has been diagnosed with cancer who doesn’t have a story of healthy people ghosting us. What I mean is when you have somebody who has been in your life in one way or another, you have a serious diagnosis, and they do not engage in any way. They completely leave.
Over the last 5 years, that’s happened to me. It’s happened to me with family. There were people who just couldn’t handle things. I have mostly gotten to the point of understanding and remembering and reminding myself that this is not about me. It’s about them. There are those people who don’t have the capacity to enter into the suffering of somebody else.
I have found over the last 5 years that when we do enter in, when we sit with people, there is this whole concept of holding space and just being with people. [We’re] not trying to fix anything, not trying to change anything; we’re just connecting and being with someone else in a space, whether it’s virtually or in person.
The connections that I have made in the MBC community are the deepest that I’ve ever had in my entire life, and I mean people even that I’ve known for decades, sometimes even more than my husband. It’s because we get each other’s suffering on such a deep level.
I hear from various people that people in other cancer communities are often jealous of how in the breast cancer community we do this community thing pretty well. Yes, there are still disagreements and whatever, but we do this connection thing in a way that I’ve never experienced in any other segment of my life.
Making deep connections in the MBC community
Acute vs. chronic trauma
I have continued to be connected to people who don’t have cancer, but the vast majority of the people who have stuck around are the people who’ve been through trauma themselves. We have a great group of friends from Miami, where we lived for a bit, where each of them has a child with a very serious diagnosis, whether it’s autism or strokes or other syndromes.
They get on a different level what it’s like to be in a trauma. [It’s not like] you get a diagnosis, you go through treatment, and maybe you’ve got some side effects that last. I don’t want to discount the fact that there are side effects that last after chemo. The people who are in the trauma for life, you’re in that trauma over and over and over again for the rest of your life. There’s a sense of community, and there’s a sense of connection. There’s a sense of going deep really fast that happens in no other area.
You remember the emotions. You remember the connections with these people or with people that have made an impact on you.
The price of that is that when the people you have gotten that close to and you have connected that much to, when they die because they have a terminal diagnosis like mine, a piece of your heart goes with them. There have been several times where I’ve gotten very close to somebody, and they died. I said, “Well, forget this advocacy stuff. I don’t want to be connected to it.”
But I keep coming back because of the genuine connection. I read a meme, something about how amazing it is when you’ve got somebody who has gone through the fire, and they’re handing buckets of water to the people entering into that same fire. That is a good visual for me of what we do in the MBC community. Sometimes well, sometimes not so well. There’s a connection there that’s just like no other connection.
Disenfranchised grief
Some of these people I’ve never even met in person, which is a weird thing and does lead to some of the concept of disenfranchised grief, where it’s not normal or mainstream grief. You talk a lot about miscarriages or the death of a pet or somebody you’ve never met online that you’re grieving for. There aren’t great grief rituals in those contexts. You can’t necessarily go to a funeral and have the expected support and things that would happen [if] you lost your parent.
My husband just lost his father, so we just went through this. It’s that sense of being disconnected at that last piece so that you don’t get a chance to do the grief rituals. A lot of families do their funeral. It’s not necessarily public, where they invite people from the community to attend those things. It’s weird, and it’s a strange, great space to be in. That’s something that we talk a lot about, just developing grief rituals that help us.
There are 3 deaths. One is when your physical body ceases to function, the second is when your physical body is buried, and the third death is when people stop saying your name.
One of mine — I’ll grab my bowl over here — is for the people who I’ve gotten very close with, I have a rock with their names on them. I keep it in my space. That’s part of how I remember them. I sit down, and I decorate a rock after they’ve passed.
I’m not very artistic, so I can do little flowers. That’s pretty much the extent of some of my creativity. Some of them just have the name and a heart on them.
We’ve done a fair amount of grief circles, where we get together and talk about and memorialize that person. I keep close to me the things that people have given me. I have various little notes and a stack of cards that I’ve gotten from various people who have since passed away.
Every now and again, especially on the anniversary of their deaths, I go back through that and just remember the things that were good about that relationship, remember the things that I’ve gotten from that, and remember that connection and that love. Because that’s what keeps bringing me back to the community.
What do you feel when you are holding the rocks with their names?
I remember them. I remember the times that we had together. There’s that saying that people don’t remember what you said, but they remember how you made them feel. You remember the emotions. You remember the connections with these people or with people that have made an impact on you.
One of the things that we talk about our kids quite a bit about is when they’ve had different experiences with different people — especially the ones that we’ve lost, like my husband’s father — we talk about that person. I have learned over time to not stuff (because that was one of my coping mechanisms before cancer), but talk about the people.
On Twitter and other places on social media, we talk about these people a lot. I still tag people who have passed in some of my posts when we’re talking about various things that remind us of that person. In our support groups, we talk about these people.
I don’t remember what tradition it’s in, but I read somewhere that there are 3 deaths. One is when your physical body ceases to function, the second is when your physical body is buried, and the third death is when people stop saying your name. I think one of the things that we do in our community for each other is that we say each other’s names.
We talk about the impact that those people have made, especially the ones who have been advocates and who have been very public in what they’ve accomplished. We’re just honoring their accomplishments and honoring what they were able to do with the time that they had.
It all helps. None of it’s easy. None of it is simple. I think everybody has different things that help them process.
Remembering as a way to heal
There’s a podcast, Our MBC Life, that is specifically for the MBC community and is created by the MBC community. It’s through SHARE Cancer Support. Every year, we have a memorial episode, and everybody calls in to say the names of the people that we’ve lost in the last year.
It’s a very difficult, but a very healing time to really focus on the positive impact and the things that people did that touched us. Those are the things that I want people to remember about me.
Having that as part of the routine is helpful, and I think it’s helpful to begin talking about that with my kids. They dealt with their grandfather’s death, I think, better than they would have if we had not been doing a lot of this, talking about what happens when people die. “Yes, that’s Grandpa’s physical body, but that’s not Grandpa anymore. His spirit, the thing that makes him him is not here anymore.”
I’m hopeful that doing some of that and having that be very natural, matter of fact — this is the part of life, birth, death, and all of that — will help my kids make that transition after my passing as well. I’m trying to be very intentional even about prepping them for that.
Undergoing Treatment
Different Treatment Options
What were your side effects from treatment, and how did you manage them?
The way I’ve learned to look at treatment is that the more information we know, the better the doctors can prescribe the right treatment. One of the challenges that we had in the first about 4 and a half years of my treatment was because I only had bone mets. It’s very difficult to get information about the metastases.
Stage 4 is when the cancer has left the original site and gone somewhere else. For me, I think about 60% of the cancer went from my breast to my bones. When you try to get a biopsy of a met that’s in a bone, you have to decalcify it before you can actually look at it under the microscope. That process of decalcification often destroys the cancer. We had not been able to see how the cancer was mutating.
In a metastatic cancer diagnosis, we’re basically on treatment until the cancer mutates around the treatment. Knowing what treatment to be able to target something in the cancer, to stop it and to deprive it of fuel, is why I had the oophorectomy to check out my ovaries, because that’s the main source of estrogen.
For those of us with estrogen-positive breast cancer, that’s typically the strongest receptor, so that’s the main thing you want to take away. The cancer in my body is now resistant to a lot of the hormonal medication because it has learned, because cancer is always learning and mutating around.
CDK4/6 inhibitors
We’re testing what we can through liquid biopsies. In January, the cancer spread to my liver, so for the first time we were able to get a met and look at it and see how it had so fundamentally changed. Unfortunately, cancer treatment is a lot about chasing. Not chasing but staying ahead of the cancer, because we don’t want to chase the cancer. Once we’re chasing it, it’s gotten out of control. We want to control it as much as possible.
The good thing for me was that going through Adriamycin, kind of the big chemo, meant that I could stay on targeted therapy for 4 and a half years. My first line of treatment in 2017 was Ibrance, which was approved by the FDA in 2015. I was able to be on a medication that had just recently been approved by the FDA, which is huge.
That line or that class of drugs, the CDK4/6 inhibitors, has really changed the landscape of breast cancer. Starting in 2015 with Ibrance, and then there’s now a fourth one that’s being added to that class. People are living a whole lot longer with far less side effects. My first line of treatment after I finished chemo was Ibrance and letrozole, and I was able to be on that for 2 years.
There were very low side effects. Most targeted therapy affects the bone marrow, so we had to watch for low white blood cells, or neutropenia. I was always immunocompromised and having to be careful. The main side effects were the blood counts and some fatigue.
Switching to Piqray
The value, I think, of having gone through that misdiagnosis was that I got the big guns, Adriamycin, and then I was able to get 2 years of stability on Ibrance. Then in August of 2019, the cancer mutated, but it was still in my bone. We switched to a different targeted therapy, Piqray.
Ibrance works by disrupting the CDK4/6 pathway, and that’s how cancer grows or can grow with the pathway that cancer often uses to grow. Piqray was targeting a very specific mutation called PIK3CA, which is actually present in about 80% of people with breast cancer. It’s pretty significant.
In 2019, it was approved by the FDA in May, and I started it in August. I try to have those dates because that is research benefiting people directly. Now, it typically takes about 10 years for medication [to go] from concept to actually get in the clinic, although there are some new ways that drugs can be fast-tracked, and things like that that have helped. It takes a long time for medication to get from concept to actually be given to the patient.
Research and fundraising
It’s so significant. Research advocacy has been something that I’ve gotten really involved in. I go to all the big conferences. I think my medical oncologist was a little surprised, and I was like, “Hi, I’m here at the conference for all the doctors.”
It gives me a little bit of a sense of control. You’re so vulnerable, and you are so out of control when you are in the health care system, that having even a little bit helps me. It helps me cope with the uncertainty by learning as much as I possibly can about the drugs that are in the pipeline, about what trends are we seeing (you see that in the big conferences), and where the drug companies are reporting about their data.
One thing that has been a huge part of that is participating in the GRASP poster sessions. GRASP stands for Guiding Scientists and Advocates to Scientific Partnerships. They pick the big posters or the significant posters. I’m talking [about] an actual poster, a gigantic thing that’s full of words and really, really confusing graphs.
We have these small groups, and it’s all on Zoom. After each of the big conferences, we have these small groups, where we talk to the poster author, we have a clinician there, and then we have patient advocates. We talk about what is happening in the science.
Why is this thing important? When I went to the big San Antonio Breast Cancer Symposium in December of 2018, that’s when [everybody was all excited about] Piqray, which I eventually was able to be on.
The future of treatment
At the most recent conference for the American Society of Clinical Oncologists, there was a standing ovation at the news about a medication that just got approved by the FDA recently for treatment of HER2-low, and that’s [the] first one. In the last 5 years, I have seen these drugs that come [that are] the first in their class.
They’re the first way of identifying and of attacking certain pathways in your body. It’s immunotherapy, where we’re teaching the body how to attack the cancer, which I think is the future. I think that’s the future of precision medicine, teaching our body how to deal with it versus having to stay on this treadmill of medications.
Being in the room and hearing about these things and just hearing the excitement in terms of that. San Antonio was like 40,000 people that come to this from all over the world. These people have made breast cancer their life, their everything. They are in the lab 24/7 trying to figure these things out.
One of the really key things that has given me a lot of hope is that there are all these really, really, really smart people who are giving their lives to figure this out, for one reason or another. For most of them, it’s not a profession. It is their life. Seeing that dedication and seeing that energy put towards finding medications…
Unfortunately, I think breast cancer is too complicated to find a cure, but we are getting so much better at treating different subtypes. People are living so much longer. Like I said, the CDK4/6 inhibitors really changed the landscape. That’s the first line of treatment that everybody gets now, a CDK4/6 inhibitor almost exclusively.
Patient advocacy
Over the last five years, I have seen how patient advocates can fuel and push research during the time that I’ve been diagnosed. It used to be that if you had brain meds, you couldn’t participate in clinical trials at all. Now, most clinical trials will accept you so long as the brain meds are stable.
That has been something that has been fueled and pushed by the doctors, but also by patients speaking up and saying, “Hey, wait a minute, you’re excluding me just because of this one thing. Otherwise, I fit perfectly in your trial.”
I think as a lawyer, I get a lot more of the limitations of our system. There are all these regulations. The drug companies have to fit in this box, which is there for a reason. We don’t want to repeat all of the horrific things that happened in Tuskegee and with all of the things that a lot of doctors did for a long time, especially in minority communities.
The importance of clinical trials
It’s still only about 3 to 5% of us that participate in trials. One area where I try to educate people a lot is the only way that we will have more medication is if people participate in trials. Trials are not for the end. It’s not for when there’s nothing else. I’ve already participated in 4 trials, and none of them have been about medication.
It’s all been about improving algorithms to look at liquid biopsies, where we can see things in the blood without having to look at a soft tissue met. Actually, the very first genomic testing I had, which was looking at the mutations that the cancer had acquired, was done through a study.
It’s so important that we participate in this research for the scientists to be able to discover and understand things. The fact that we enroll so few minority populations in these trials means that they’re only testing stuff on middle-aged white women. I am a middle-aged white woman, so I’m happy that they’re testing things on something that most likely would work for me.
But then how do we know if it is going to work for somebody who’s from the islands or somebody who’s from Africa or somebody who’s from an Asian country? It’s so hard for scientists to be able to tease out all the different specifics about our bodies without having people to test it on.
What are the differences between genetic and genomic testing?
Genetic testing is the stuff that changes in your DNA, so what you get from your parents. Obviously, you get half of your copy from mom, half the copy from dad. Sometimes, if there are DNA mutations on both sides, that creates something entirely different, and they learn so much all the time.
I do want to say one thing about genetic testing. 23andMe or Color Testing or Ancestry.com is not genetic testing. That’s information that’s available to the public. The genetic testing I’m talking about is through a lab that is FDA approved. You’re not going to get the same information from something that’s like, “Hey, do you have more susceptibility for cholesterol?” That’s different from the genetic mutations that I’m talking about.
Like I said, now the panel is 93 genes that they’re looking at that have to do with breast cancer. I’m just talking about breast cancer. There are so many different genes that are associated with all kinds of other things. I don’t have mutations anywhere other than in this ATM gene. That has to do with breast cancer, ovarian cancer, prostate cancer and colorectal cancer. That’s the makeup of your DNA. That doesn’t change. That’s static.
Then the cancer, as it mutates, acquires somatic mutations. That just means in the body. Genomic testing or tissue, with the cancer that they’re looking at under the microscope, gives you the genomic data, and that typically (hopefully) perfectly gives you targets. I talked about the PIK3CA mutation. That’s a target, where we have a medication that targets that.
Using genomic testing to plan for progression
One of the things that came up on my recent genomic testing is that the cancer has acquired the PD-L1 somatic mutation, which is an indication of sensitivity to immunotherapy. This is the knowledge that the doctors have [to use] to then build out options. I always insist that my doctors give me plan A, B, C, D, E, F, G, H, all the way down the alphabet, because I want to know all the different things.
When there’s the progression and you have to change the medication, if you haven’t already selected or pre-selected some options, it’s chaos. You’re overwhelmed, and you’re having to make really big decisions. I like to make sure that I have the list ready. If there’s a big progression, we’re going to go this way. If there’s a more minor progression, we’re going to go that way.
That genomic testing can give doctors the building blocks to be able to put together a treatment plan. That’s the science part. I’ve also been so blessed to be with doctors who have been doing this for so long that their clinical knowledge, their gut, because they’ve just absorbed all this data for all these years — and we as individuals are not statistics — that they can look at us and draw on that experience.
That’s what I call the art of practicing medicine. You have to have both. You have to have the scientific data, the scientific research, the peer-reviewed studies, and the understanding of what kind of side effects you might be experiencing when you’re going into something, But then you also have these doctors who have this more intuitive feel.
Experimenting with treatment
One of the things that’s happened since I’ve changed teams, since I moved from Miami to Orlando, is a lot of my new doctors are looking at my treatment plans and saying, “Oh, you did things very differently.” And we did. My doctor and I experimented.
I talked a little bit before about Piqray. I had a PET scan after I had been on Piqray for about 6 months. All the cancer was becoming more metabolically active, meaning I was about to have a progression. We added a third drug. I was on Piqray and on Faslodex, which is the hormone suppressor, and then we added Kisqali, which is another CDK4/6 inhibitor similar to Ibrance.
There was a study on that particular combination, or an arm of a study on that particular combination, and no one was able to stay on that combination. I was on that combination for 2 and a half years. You don’t know how your body is going to respond until you try. Some people have no side effects on particular medication.
Piqray is known to cause hyperglycemia, so I was on glucose drugs for the entire time that I was on Piqray. Not a super easy drug, but I got 2 and a half years off of that particular rather aggressive combination. I think one thing that I’ve done in my treatment is that I have not been afraid to try something that may or may not work.
How Treatment Affects Life
Why is Piqray a hard drug to be on, and how did you deal with that?
Hyperglycemia — people mostly associate that with diabetes — can cause a whole lot of things in your body. There’s a rash that Piqray often causes as well. You have an allergic response to it, but hyperglycemia is probably the biggest thing. Pricking my finger every day and having to be on medication to manage the hyperglycemia.
That is probably the biggest challenge that most people face on Piqray, especially just because hyperglycemia is one of those things that affects your whole body. It affects everything. Managing the hyperglycemia can actually be a really, really big lift.
Oncologists go to school for oncology. They don’t go to school to manage hyperglycemia. The endocrinologists know how to treat diabetes, but it’s not diabetes. It’s medication-induced hyperglycemia. People were finding themselves in this very big gray area.
I’m extremely proud to say that I’ve been working with Novartis, who is the drug company that produces Piqray. Anyway, we have a poster coming out at the ASCO session that’s coming up, and it’s all about teaching the doctors how to manage the hyperglycemia. Literally, you have a patient that comes in with this, do this. If a patient comes in with that, do this. [It has] preferred drugs and dosages and everything like that.
This has been a huge labor of love in a lot of ways. I’m the only patient advocate on the panel. I think there were 12 or 15 doctors, endocrinologists and a medical oncologist. We had a pharmacist. That’s probably one of the most amazing things I’ve ever done, because I brought the patient experience to the table.
Plus, I moderate a Facebook group for people on Piqray, and we have hundreds of people in the group. I was able to do some polling of the people in the group to bring some real-time data to these discussions. This is where patients can help educate, because all the doctors on this panel are all at major academic centers. The vast majority of people being treated for cancer are in rural settings, not a major academic center.
Some of the doctors that treat you in the community are not maybe a breast specialist. You may see an endocrinologist who’s not an oncology endocrinologist or [doesn’t have] some of that specific training or experience.
The doctors didn’t know what to do, and that was such a huge issue for so many patients that Novartis put their money where their mouth is and invested in coming up with these guidelines [from] discussion and consensus among all the different specialties.
Yes, I was very proud to participate in that, and part of it was because I was harassing Novartis about all the things that people were talking about in the group and referring them to the patient advocacy program. Their doctors were trying to figure things out. I think they finally said, “I think we need to give this person a job.”
Treatment affecting quality of life
Grade 3 diarrhea means you’re in the bathroom like 10 times a day. If you’re only doing that for a couple of days, okay. You deal with it, maybe take some medication, whatever. Then the rest of the time between treatments is not so bad.
The difference with these oral meds is that that’s the side effect that you have every day, 24/7, for all the time that you’re on the drug. I have seen a shift in the last 5 years of researchers really beginning to understand that. You start looking at it really closely when it’s about grade 3. Grade 5 is death, just to put it in perspective.
They’re paying a lot more attention to that and understanding that with these oral meds, you can’t live if you’re in the bathroom 10 times a day. We talk to people about literally not being able to make it to the bathroom. As an adult, actually having an accident is not something that is okay.
We had several advocates talk about, “I think I need to wear a diaper to go to the conference because I don’t know if I’m going be able to get to the bathroom in time.” That’s the kind of quality of life stuff that I am seeing be much more focused on, thank God. Not that they didn’t want to, but I think that they needed the push, and I think they needed incentives. I’m also seeing much more of the patient voice being included in these trials.
Designing trials with patient input
The piece that I think needs to change is getting the patient advocates involved at the time of the design of the trial. So many times the trials are designed in such a way, whether it’s transportation or parking or having to be at the doctor 3 times a week. There are things that they design that make sense to them from a gathering data perspective. It’s just not livable.
This idea is of having trials where you don’t have to go to one place or don’t have to go to the major academic center. Maybe there’s more places, or you can get blood work yourself and bring it. COVID has helped this, too.
They’re becoming much more aware. There are things we can relax in terms of the structure that are not meaningful overall, but it means everything to the patient. That’s huge, getting the patients in at the beginning.
HER2-low medication approval and its impact
Everybody has HER2. It’s a biomarker that everybody has. For some people who are HER2-positive, it is overexpressed. When I talked about how estrogen is the strongest receptor for people who are HER2-positive, that’s the receptor to target.
Herceptin has been out 15, 20 years now. That was a game changer for people who are HER2-positive because that HER2-positive overexpression means that the cancer was so much more aggressive. The life expectancy of somebody who was HER2-positive was very low.
That is about 25%-ish of the total breast cancer diagnoses, so it’s a pretty significant group. About a fourth of people are diagnosed HER2-positive. It used to be negative or positive. You either had an overexpression, which would be 6 plus, or you were zero.
But then they started seeing that those of us — because I’m now HER2-low in my last genomic testing — that there can be zero, or you can be in this 2 to 3 category, meaning you have some HER2 expression, but it’s not overexpressed.
Because Herceptin was such a huge game changer, a lot of the research started looking at maybe that type. If you look at your cell, you’ve got receptors, and they’re like little antennae. They’re looking for the thing that will feed them.
What Herceptin does is it blocks that receptor and says, “Nope, you can’t get in.” Once there’s something that blocks that receptor, it’s no longer able to help fuel the cancer or help the cancer proliferate. That is my very non-scientific explanation.
Antibody-drug conjugates
Because Herceptin was such a game changer, there’s been a lot of people who have been starting to look at that thought process of targeting that particular receptor. Maybe that would be helpful [to focus on] the people who have a smaller expression of HER2, not quite to the 6 plus. That’s where Enhertu came from.
Enhertu is an ADC, which is an [antibody]-drug conjugate. That’s the new class. The antibody-drug conjugates is the new thing that everybody is super excited about, because it is a chemotherapy in the sense that you get it through an IV, but it is targeted like an oral so that you theoretically don’t have so many of the side effects. It goes to the cancer versus just killing all the active cells.
Adriamycin, taxane, Taxol and Abraxane kill all the good cells and the bad cells at the same time, anything that’s fast growing. My hair is growing back. I just finished Taxol here in May. That’s why you lose your hair, because your hair is a fast-growing area of your body. So is all the good bacteria in your gut. There are so many things. Your white blood cells and your bone marrow are affected because it just carpet bombs your body.
Being able to be more targeted, you don’t have the same overall effect. Theoretically, you don’t have the terrible blood counts, and you don’t have all of the other side effects that come along with chemo, like nausea and everything else.
I’m not saying Enhertu is an easy drug, because I know quite a few people who have really struggled on Enhertu. Everybody’s different, and you don’t know how your body is going to react until you’re on it.
Cumulative effect of treatment
When you’ve had multiple lines of treatment, your body just gets depleted. I’m on my fourth line of treatment right now in 5 years, and that’s partially because I had multiple progressions here recently and had to change medications quickly. Once your body has been what they call heavily pretreated, your body just doesn’t respond as well.
Those of us who are younger, sometimes we’re able to handle some of the harsher medications. It’s a double-edged sword because our immune systems are actually better, and it takes a little while for your body to adjust to some of the immunosuppressive activity of some of the medications.
We just did an amazing presentation from Paolo Tarantino, who is at Dana-Farber in Boston, on what HER2-low means. He did a whole hour and had these amazing slides. That is something that’s available through Project Life. I’m still wrapping my head around it. He talked for like 20 minutes, and my brain started hurting.
Reflections
What is your last message to others?
When I was practicing law, I always told my clients they brought the facts, I brought the law, and we couldn’t do the case by ourselves. We had to do it together. That’s the thing that I think we all have to look at with our team. We’re on the team, because our doctors have no idea what’s going on at home.
They don’t live in our bodies. Many of the things that we deal with on a day-to-day basis, they had a day or an hour or a little bit of continuing education about. Really understanding that when we walk into our doctor’s office, we are there to be a partner with them. We need to be an active partner in that.
My husband, as a minority, as a black man, he’s always more worried than I am about asking questions, speaking up and challenging the doctors. I obviously have no problem with that. I think that you don’t have to do it in an aggressive or in a challenging-type way, although sometimes I get that way with my doctors.
Understanding that they don’t know what they don’t know, that you know the things. You’re an expert in your body. You bring your body to the table. They bring the scientific knowledge, plus that experiential art piece. It doesn’t work if you’re not telling your doctor what’s going on and if you’re not saying, “That doesn’t work for me,” when they run over you, as so many doctors do.
Being an active part of the team
In our support groups, we often talk to each other about, “Ask your doctor this. Ask your doctor that.” I think a secondary thing would be making friends in the community who can help coach you on the questions that you’re not even seeing. It can be huge.
There are all kinds of people where research advocacy is their lifeblood, their thing. They’re not doing this alone. The whole idea of no man is an island, right? We cannot do this thing by ourselves. As just a consumer, we can’t just receive what the doctors are saying. We have to be active in that discussion or in that partnership.
I think doctors are getting better about that. They’re not always great about that, but they are getting better and understanding that we patients have the same access to clinicaltrials.gov, and we have the same access to the papers and all of that, as long as they’re not behind a paywall.
We have access to those things, and we can read. We can bring in things and say, “Well, hey, what about this?” or “I heard this thing in a seminar.” That is what gives me, again, a little bit back of that sense of control, as well as the hope of, “I’m going to take some responsibility for this.”
This is also on me. It’s not just on my doctors, in terms of them figuring out what happens next. I’m going to take some of that responsibility, because that makes me feel empowered. That makes me feel more of an active member of the team.
Margo never expected to develop bladder cancer, let alone two versions at the same time.
When Margo noticed something was off, she visited her OB/GYN, then a urologist and urologist oncologist. If she hadn’t advocated for herself, she would not have gone to MD Anderson and discovered a second diagnosis of plasmacytoid, a rare and often deadly form of bladder cancer.
Margo underwent intense chemotherapy and a radical cystectomy to save her life. Margo shares her story of dealing with loss and isolation during treatment, finding humor and the sliver linings in life, and writing a book about her incredible journey.
Name: Margo W.
1st Symptoms:
Blood in urine
Diagnosis (DX):
Stage 1 bladder cancer
Plasmacytoid
Tests for DX:
Cystoscopy
TURBT
Treatment:
Chemotherapy
Methotrexate, vinblastine, doxorubicin and cisplatin
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
1st Symptoms and Self-Advocacy
Introduction
Tell us about yourself
I am a seize-the-day, make-the-most-of-life, passion-for-life kind of a gal, and I pretty much always have been. For example, we go on family dive trips. I got my children certified to dive when they were 13, the earliest age that you could do it. We like to travel. We love our dogs. We love spending time together. I’m married to a great guy and I consider myself very fortunate.
You noticed something wasn’t right in November 2019. What happened?
I think one of the things that is very common for cancer patients is that we don’t feel anything. Nothing’s up. We don’t have any pain symptoms or discomfort or anything like that. It was the same for me, except for that one day late in November, I noticed that my urine was the color of rosé, like a deep rosé.
I thought, “Well, that’s not right.” I’m old enough that menstruation could not have anything to do with it, but women are often kind of swept under the rug when it comes to things like that. At any rate, it stopped. The afternoon was clear. Then the next morning, it happened again. A little bit of blood in the urine. Then I never had it again. That’s the only symptom I had.
I consulted Dr. Google, which is both a good and a bad thing. I immediately went to a lab and did a UTI test. Now you can get them over the counter, which is awesome. I was on extra alert and a little concerned.
I have developed over the years a way of saying to myself, “I don’t have that information. If it is worst-case scenario, I will have plenty of time to stress and worry and fret over it. If it’s not worst-case scenario, why put myself through that in the meantime?” I tried very hard to hang on to that. The lab called and said, “Great news, it’s not a UTI.” I was like, “No, that is not great news. UTI would be so much better.”
Margo and her husband celebrating their 4th wedding anniversary.
OB-GYN appointment
I called the OB-GYN. I treat her very much like my GP. A lot of us do, I think, especially if your GP retires, and you’re like, “Yeah, she knows me. We had babies together.” I called the nurses there, got a hold of one of them, and I told her what had happened. She said, “Well, let’s just keep an eye on it.”
I thought to myself, “Nope, I’m not doing that, because nothing good happens from waiting.” What’s the worst thing that happens if I go right away to a urologist and find out that it is nothing? I don’t know what it could have been that was nothing, but it might have been.
What am I? I’m not a doctor, so I don’t know. That information can only help me. Waiting cannot at all help me. That would absolutely make things worse, especially given that it was actually something nefarious.
I immediately started looking for a urologist, and for one that I could get in to see pretty quickly. It was 2 weeks out, so I made the appointment with the urologist, who had a good reputation.
How did you research and make decisions?
First, I call my friends. I say, “Do we have a urologist in the stable of providers?” We do the same thing with shoes. “I need silver platform shoes for a dance. Does anybody have one?” Nobody had a urologist. I did do some research and looked for health grades and a couple other things like that, and I did what I could for due diligence. He had a good reputation, and everybody seemed to love him.
Cystoscopy and TURBT
In mid-December, you find a urologist. What happened at the appointment?
I don’t know the outcome, and I’m doing the discovery. I’m getting the answers. It’s very scary. We could very easily go to DEFCON 5. What good is that going to do? I can’t operate at my best abilities to make decisions and continue self-care and advocating for myself if I’m just freaked out.
I kept doing that, but it’s beginning to take more effort at this point. But I did that, and we went in. That was early mid-December. A little nervous, not too bad. Went in, did the cystoscopy, and I actually could see it. You could look over on the monitor and see this little soft cauliflower wafting. It looks kind of pretty.
Did you know you were going to have a cystoscopy before the appointment?
Actually, I just collapsed 2 appointments together. I went into the first appointment with the urologist. He said, “Yes, we should do some looking around. Go get an MRI, and let’s meet back here for an appointment.” The MRI had showed nothing.
Margo and family hiking the Appalachian Trail in October 2020.
I actually tried to cancel the cystoscopy because I was like, “Since there’s nothing on the MRI, I guess we can go ahead and say that it’s all fine.” They were like, “Sometimes it doesn’t show everything.” Then we ended up with a cystoscopy. That was after Christmas. That was actually a day before my birthday, on the 27th.
What was the cystoscopy like?
What I will tell you is that men complain about this a lot more than women do. It’s a little more complicated. There’s more acreage that has to be covered with a man, but they’re basically slipping a tiny tube with a camera through your urethra to head on into the bladder and have a look-see around. That’s being shown on a screen. It might have an easier term than that, but that’s what’s happening.
Margo as a baby.
Did you have localized anesthesia or a painkiller?
They said it’s not necessary. I said, “Well, maybe for you. Can I please have a Xanax at least? Or I’m going to have 2 margaritas before I come in here. Either one.” They gave me a Xanax.
Your urethra is one of the several areas that is designed to be a one-way street. It is not comfortable. It was worth the discussion. If you’re a doctor and you’re doing 20 of these a day or something, it’s nothing to you, but it’s not nothing to the patients.
Results of the cystoscopy
[The doctor] said, “Oh, yeah, that’s a lesion.” That was his less scary word for a tumor. I learned that that’s what he meant when I had coffee with a good friend of mine who shares the same birthday as me the next day. I said, “Oh, I’m not really worried about it because he said it was just a lesion.”
She said, “Yeah, that’s a nice word for a tumor.” She’s a doctor. I thought, and then I said, “Yeah, but at that point, I’m still feeling pretty positive because it could be a tumor. It could still be benign. Those happen as well.” The next step was to schedule the transurethral resection of the bladder tumor.
Transurethral resection of the bladder tumor (TURBT)
They again go in through the urethra and use whatever tools that they use to remove tumors. I imagine there’s cutting things involved. Then they send that off for biopsy to find out what’s going on with it.
Managing scanxiety while waiting for results
I focused on that I still had my kids at home and family to enjoy and everything else I could think of. I also had work, so I just focused on everything else that I could think of. Again, I’m flexing that muscle more and more and strengthening it to be able to put it off and say, “I’ll wait till I have more information before I freak out or get concerned.” I also discontinued Googling all this stuff at that point, which is what I advise.
6 days later, I still had a catheter, which is just no fun. You’re carrying a bag around. 6 days later, I was in the office. They remove the catheter, and they go, “Okay, so you have stage 1 highly aggressive bladder cancer.” That’s staggering.
I thought I had a contract with cancer. I will do the lifestyle things over here, and you leave me alone. I thought that I had made that arrangement. Cancer didn’t sign that contract, so it was void.
Then he drew a crude picture, just like a basic picture of, “Here’s a bladder; here’s the ureters.” He said, “Here’s what’s going on. Stage 1 means it’s only in the bladder. It hasn’t crept through to some of the other layers — 2, 3, 4 and so on. The good news about that is that we can treat this with BCG.” I don’t remember what that stands for, but it’s related to what they use to treat tuberculosis.
Immunotherapy in this case would be inconvenient, not very pleasant. Again, it’s going through the urethra to deliver immunotherapy to the bladder. At this point, I’m just thinking, “Ugh, okay, so now I’ve got to do this every 6 weeks. Then I’ve got to have another cystoscopy, so I’ve got to do this for the next 2 years.” I’m making peace with that. That’s what’s happening in that doctor visit.
How were you feeling?
I think this is probably the case for a lot of us. You’re thinking, “This cannot be. This doesn’t make any sense to me. Nothing about this makes sense to me. This couldn’t be more out of the blue.” Zero kind of cancer runs in my family. Lots of other stuff, but just not that.
Smokers are associated with many kinds of cancer, and actually, bladder cancer is one of the things. So I’m like, “It’s not that.” Because in the meantime, I had done research on causes, trying to understand how we got here? I gave up sodas. I eat clean. I drink a lot of water. I exercise. I do all those things.
I thought I had a contract with cancer. I will do the lifestyle things over here, and you leave me alone. I thought that I had made that arrangement. Cancer didn’t sign that contract, so it was void, and you just never know. I’m told by doctors that sometimes you can figure it out, and sometimes you can’t. Sometimes it’s just random, which is 100% unsatisfying.
All of that’s going on in your head at one time. How did this happen? How can this be true? Come on, universe, higher being. I have enough character. I feel like now I am hogging the character. Somebody else wants to have a shot at going through something difficult. I’d been through a lot already in life. That’s what I thought. Really, another thing that’s really hard? All of that was going on through my head at the time, and it’s frightening.
How did you break the news to the rest of the family?
My hubby was with me the whole time for all of that, which was really great. His name is Coleman, and he’s unbelievable. I think that caregivers have a whole different set of needs than patients. They go through all of it with us, just not the physical part of it. They can’t lean on us as patients to be there for them, so they definitely need to have resources and support.
It was wonderful that he was able to be that support for me. With me, I could squeeze his hand as tight as I needed to, and he could handle that. Then we just looked at each other like, “Okay, well, we’re going to get through this somehow, some way. We don’t need to know all of the ways and the details and what comes. We don’t need to know all those things. We just know we’re going to get through this.”
My kids at this point are 19 and 21. They’re adults. One’s in town. One is not in town. This is not news you like to break over the phone to people.
Part of what made this hard for me telling my kids is that I’m their only living parent. When they were in middle school, their father died. I was not married to him at the time, but he died. There wasn’t a reason that he should have died, but he did. He basically died from alcoholism. He drank himself to death.
That was a terrible experience for me to have to come home and tell them that their father had died. Not only was I thinking I don’t want to worry them because I am their only parent. Even though they’re 19 and 21, they still need parents and family. That was the biggest concern I had. How do I make sure that I explain this to them in a way that doesn’t feel as scary and life-threatening and doesn’t freak them out?
I don’t want to mince words either. I don’t want to mislead them. I don’t want to sugarcoat it. Kind of choosing the right way to communicate with each of them. Now, at this point, that’s all I know about my cancer. I’m still thinking it’s garden variety, essentially, and this is going to be really inconvenient. That’s what I understood at that point.
Is there anything you learned in terms of guidance for other people on how to navigate that?
Yes, there is. I learned that the best way to do this, at least for me and definitely for them, is to go right to it and to say, “Reed, we just got home from the doctor, and it does turn out that this is cancer. It is stage 1, and here’s what we’re going to do about it.”
Right to the point. Don’t go heavy into details. In this case, I just said, “Here’s the therapy.” They’re grown, so they can understand it, but that’s not the point of the conversation. Then follow it up right away with, “And we’re going to get through this.”
Getting a Second Opinion
Why did you get a second opinion?
Actually, it’s my job. I sell health insurance policies for self-employed people, like realtors. I had learned a lot about what most policies do and don’t include. Second opinion is really, really important. I’d learned that the data shows the number of misdiagnoses is really high. I didn’t know how high. For cancer, it’s actually 70%. That’s what my oncologist told me.
I said, “How many of the cases you see are wrong, or it’s an incomplete diagnosis?” They all said 70% in separate appointments. I knew to take advantage of a second opinion service, which I did. The second opinion service was an oncologist urologist.
Back up for a second. I went to see a urologist. At this point, what do I know? Do I know that there’s a urologist oncologist in the world? I know nothing of this world. I don’t know that I should be seeing an oncologist urologist. Who tells you that? Not your urologist.
There’s a lot of this seeking information, gathering it real time while you’re experiencing it, trying to process it, trying to hold it together and figuring out what’s the best path forward. It, as you know, is a mind-numbing experience. It’s a soul-numbing experience.
Without this experience, you may not have known to ask for a second opinion
I may not have. I’d kind of like to think I would, but I can’t say for a fact that I would. You don’t know what you don’t know. If you are aware and then you choose to not get that information, that’s on you. But if you don’t even know, it’s tough to say, “Oh, I should have gone and done that.” I’m really glad I did go get that second opinion from a specialist, who was a urologist oncologist.
Seeing the urologist oncologist
He said, “About 20 or 30% of the time” — this was his number — “stage 1 bladder cancer is actually stage 2 bladder cancer. Completely different treatment regimen. I want you to go get a blue light cystoscopy.”
I thought, “Oh, that sounds almost fun.” The blue light picks up on cancer cells that aren’t visible to the naked eye. Okay, that sounds like a good thing to do. I hung up the phone. Actually, it was a virtual visit.
Then I called my urologist office, and he said, “Oh, I don’t have the equipment to do that. It’s a good test. I believe in it, and one day we’ll all use it. But right now, nobody in Austin does it.”
Going to MD Anderson
I did my own research. I live in Austin, Texas. MD Anderson is right down the road in Houston, 3 hours away. I’m aware of them and their reputation, and I thought, “Well, I’m stage 1, garden variety bladder cancer. I don’t need to go to MD Anderson.” Why did I think that? I have no idea. That’s kind of the bias that you have — it’s not that serious. I so wanted to cling to that.
At any rate, when the second MD recommended the blue light, I couldn’t find one here. I had to start doing research, and I found that there were 3 places nearby. One was San Antonio, and 2 were in Houston. What I did — and I think this is really smart — is always ask the people who know more than you do and ideally who know the most of any one thing.
What did I do? I sent those names to the urologist oncologist, who was the specialist in my second opinion. I said, “What do you think of these?” He goes, “I can vouch for these 2 cases. I’m just saying, don’t go to the one in San Antonio.” He didn’t vouch for that one.
Then I basically figured out how you open up records and let hospitals see your records and start the process. You don’t know how any of that works, and so you’re figuring that out as you go. How do you get an appointment? I went through the process of getting the documents in my records and everything to them.
Within days, appointments started showing up on my calendar. MD Anderson — you’re going to have a blood test; you’re going to have all these different things. I thought, “Okay, I guess I’m going to MD Anderson.” They’re one of the best. They’re rated the top all the time. I felt confident about that and good that I’d found one that was highly [recommended]. I was, at this point, still hopeful that this was just mainly super inconvenient and uncomfortable.
Seeing Dr. Ashish Kamat
He’s a superhero. He’s amazing. I had an occasion to see him at a bladder cancer event recently, where I was one of the 3 patients that shared their stories. We just hugged. I had sent him the first chapter of my book and said, “I don’t know if you feel like saying anything.”
The second kind is lethal. It is very rare, it’s fatal, and it always comes back. We have to do everything. If we do everything, we throw the kitchen sink at it, we can save your life.
Dr. Ashish Kamat
I didn’t know if he was going to read this email or not. He replied back through one of his assistants. “Here’s what I think.” He said these glowing, wonderful things. 2 years to the month later, he told me in person at this event, “I want the whole book, and I want it signed by you.” Okay, I’ll do that for you.
Second Diagnosis
Receiving an additional diagnosis
[Seeing him]would save my life. I did a bunch of breathing exercises while we sat in the room waiting for him to come in. I’d done blood work and X-rays and things, but I’m still thinking that he’s going to go, “Yep, we need to do immunotherapy.” But I also know there’s a chance that it could be something else.
It takes forever. There’s so much waiting. The good news about all that waiting is not that you’re waiting with your thoughts to yourself, but it is that when it’s your turn, they’re there for you. I used all of my best coping skills to get through the [waiting]. It felt like an hour. It probably was 30 minutes. Breathing in and out, and just trying to stay calm.
When he came in and talked to us, he got right to the point. He said, “We’re not going to do a blue light cystoscopy tomorrow, or at all. Because looking at your slides, at the images from your biopsy, you have not 1, but 2 forms of cancer in your bladder.”
I’m thinking, “Yet another thing I had no idea was possible.” What’s the limit? How many is the most you can have in one place? 2? He said, “The first kind that you already know about will respond to BCG. The second kind is lethal. It is very rare, it’s fatal, and it always comes back. We have to do everything. If we do everything, we throw the kitchen sink at it, we can save your life.”
Processing the plasmacytoid diagnosis
That is the hardest thing I’ve ever had to hear. You don’t even know how to react when that’s what you hear. Save my life? I’m fine. Look at me. I’m healthy. I don’t feel anything.
He went on to explain that this second form is a plasmacytoid, and it does sinister things like cloak itself and make itself look like bladder cells to the other bladder cells. That’s very sneaky. That is one of the reasons it’s so hard to treat.
Throwing the kitchen sink at it in this case was 4 kinds of chemo every other week for 8 weeks, followed by a radical cystectomy. That is the removal of the bladder and usually some other things along the way.
What were you feeling?
It was indescribable. It felt like my throat, my stomach, all just dropped. I thought, “I’m going to black out.” I really thought I was going to just pass out. My husband’s with me, thank goodness, and so I held his hand. He listened for both of us, which is great because in some ways, I did black out.
No one knows us like we do. I think it’s really important to listen to our instincts, to listen to our gut.
Margo W.
I was conscious, but I don’t recall the conversation after that. My husband will say, “Remember when he said blah, blah, blah, and you said yada, yada, yada?” And I’m like, “No, I don’t. I don’t remember that.” I don’t. I remember the part I just shared with you, and really nothing after that.
It’s impossible [to process in the moment]. I agree with using the phone to record. I found that later on that was very useful, and they were always really open to it. You can’t necessarily process everything. You’re like, “I’m sitting up, right? I’m looking at you. Not on the floor, so that’s good. That’s all I got. That’s all I can deliver right now.”
The importance of self-advocacy and getting additional opinions
As individuals who need to have access to health care, the best thing we can do is advocate for ourselves all along the way. That doesn’t mean yelling and screaming and saying, “Get somebody in here.”
I think we almost have a passive acceptance and total trust of anybody in a white coat. Doctors are amazing, and I have huge respect for them and nurses and everybody who does all that work. But they don’t know each of us individually, and no one knows us like we do. I think it’s really important to listen to our instincts, to listen to our gut.
I joked it was my spidey sense. [It] was like, “Oh, this doesn’t feel right.” Listening to that and then just keep getting information. Don’t accept no answers when you can get answers. Then always go to the very best that you can get your hands on, because they’ve seen the most cases.
Dr. Kamat asked me, “Who were you seeing in Austin?” Austin has almost 2 million people. It’s not a little podunk town. This doctor had a good reputation, but when I said his name, he goes, “I don’t know him.” I thought, “Well, that’s bad, if you haven’t heard of him.” I don’t know how big the world of urologists is, but he wasn’t a urologist oncologist. He doesn’t see as many cases as they do.
You want that. You want literal volume. Let’s take a look at what the Austin doctor and Austin pathologist had versus MD Anderson doctors and MD Anderson pathologists. They had the same images, same exact data. It was really important to get the best eyes on it. They already knew before I got there what the diagnosis was and what they were going to need to tell me.
They knew that because they see so many more. This is so rare. It’s like 1%, 2% of bladder cancer patients, but they see 4 or 5 of them a month. Which is just so many, relatively speaking, and there are very few survivors of plasmacytoid. They don’t often get to save their lives, because it’s also asymptomatic.
Sneaky, asymptomatic, and 100% fatal and recurring. If you don’t know you have it, by the time you do, you typically don’t have much time left. I can thank the first kind for giving me the flowy tumor that there was to see to take me to the doctor, and then thank of myself for continuing to advocate and go to the best doctors I could find.
Don’t worry about hurting doctors’ feelings
Don’t rest if there’s something I’m thinking needs to be addressed or seen. That’s just so important for all of us. We can advocate for ourselves without offending doctors. This is something I want to mention. I feel like it’s really common that we don’t want to hurt their feelings. Some people will say, “Well, shame on you for worrying about hurting their feelings.”
Well, maybe you don’t care about other people’s feelings, but I do. This is a real thing for a lot of people. I did take into account my doctor’s feelings. I did feel like I was being disloyal to get a second opinion. It didn’t change my behavior. It didn’t change that I did go get that second opinion, and in fact, saved my life. But it is a real thing that people go through.
Let me shine a light on that and say that’s pretty common. You can feel a little bit like you’re being disloyal to your doctor, and they’re going to have their feelings hurt or be offended. Just acknowledge you might feel that way if you have to go get the second opinion, and that’s okay. Do it anyway.
Many doctors say, “It’s your prerogative, and you go do what’s best for you.”
That’s actually what my doctor said. It was a good thing. I would have done it anyway. That just would have been more uncomfortable. Probably most of them will say that. It’s important to not have an expectation that we’re not going to feel that.
We’re thinking, “I’ve got a diagnosis.” The next thing needs to be to get a second, maybe a third opinion. If you feel this reticence or concern about how you’re going to leave the doctor feeling, that’s okay. Do it anyway.
Treatment
Chemotherapy
What was the plan going forward?
The plan going forward was to start radical chemo. It was 4 kinds of chemo. It required a 3-night stay in the hospital to have all of that chemo. I didn’t get a port. Sometimes that’s what you get, but I had a PICC line instead. I don’t know why. It was fine. It doesn’t matter. That’s the least of the concerns.
It’s like going to college when you go to a place like MD Anderson. You have all these classes. You don’t know where they are or where this lab is. Where is that [department]? Okay, go get a CT scan there. But I could go get it there, too. You just have to pay attention and ask for help along the way.
That meant checking in the following week to MD Anderson on, I think, the 12th of March. My husband could come with me for that. Anyway, we knew that I would have 3 nights of chemo every other week for 8 weeks, followed by a 6-week break, and then a radical mastectomy in June.
The chemo plan was methotrexate, vinblastine, doxorubicin and cisplatin. What were the major side effects, and what helped with them?
They are so great at handing you resources. I got a book this thick with what to expect when you’re having chemo. You read through it, and you go, “What, my fingernails could fall out? My hair is absolutely going to fall out, and there’s nothing we can do?”
I’m a gal who has always had long hair, and I associated with me and part of my femininity — right, wrong or indifferent. Having it just taken away all of a sudden… Most of us don’t welcome that. When I see teenage girls shaving their heads for no reason, I’m like, “Don’t do it.”
At any rate, it was so overwhelming to read all those potential side effects. I couldn’t really handle it. Most of that didn’t sink in. I remember sitting there with the oncologist March 2nd, that day that we got the news that this was big and bad, and we had to do everything. Another oncologist said we need to do [methotrexate, vinblastine, doxorubicin and cisplatin].
It’s a common MVAC, I think, for bladder cancer. It’s different. She’s telling me all these things. Tears are rolling down my face. I couldn’t process it, yet you can’t say, “Hold on a minute. I need to go collect myself.” This is what they do. They need to see patients.
Fortunately, I had my husband with me for that appointment. We just got through. We got through learning about what the chemo was going to do. I didn’t really know what I was in for.
What was it about that moment in particular where you felt this eruption of all this emotion?
Wow, that’s a great question. I don’t know if I can answer it. My immediate response was that was just the icing on the cake. To hear her talking about the chemo treatment and the hair loss, and maybe the fingernails are going to fall out. Just the stream of all these things, because that’s when we dug into what the treatment was going to look like.
Self-care isn’t selfish.
Margo W.
Dr. Kamat laid out the strategy. Now we’re into the tacticals of what it’s going to look like. I compartmentalize pretty well, and that’s handy. I know that it’s really important to not compartmentalize so much that you don’t deal with stuff. Part of it was that.
Some of it s because I’ve been compartmentalizing, and now the greatest fear was in fact what was happening. Then the gates unloaded. If it is really terrible news, I will have time to grieve and be angry and sort through it and process it. That’s what I started doing right then and there.
Giving yourself grace to grieve
I don’t want it to seem like I was able to actively make that choice. By that time, I was just so overwhelmed I could no longer keep it at bay. Self-care is not something we heard about until, for me, like the last 5 years. It was selfish and indulgent if I did hear about it.
Self-care isn’t selfish. Listening to our instincts, listening to what our needs are — whether they are medical, whether they are emotional, all of the needs — is really important. Allowing ourselves to process all this stuff is really key. It’s going to look the way it’s going to look.
I think one thing we know, a lot of us know anyway, is that grief is very personal. It looks different for everybody. Because it looked like this for me doesn’t mean that’s going to be somebody else’s path, even if they have the same exact diagnosis. Whatever the path is is fine. There’s zero judgment on what it should or shouldn’t look like. We need no more “shoulds.”
Undergoing chemo during the pandemic
The first chemo treatment was in early March. That’s the last time anybody could come into the hospital with me, because we were in full quarantine after that. Every day, the nurses and providers were wearing more stuff, more masks, more plastic, all of that. It was just changing.
I don’t know if anybody remembers. It’s hard to go back to that. The president was talking about it, and they were trying to figure it out. That was the last time he came into the hospital with me. Every single other time — there were 3 other rounds of chemo for 3 nights, and then the surgery — he had to drop me at the door and leave.
That’s really not fun at all, because when you have the 4 kinds of chemo, they get progressively more uncomfortable. The first one, you’re like, “That’s fine.” The second one, you’re like, “Oh, I have a headache.” Then you start feeling just like living hell, and your face is puffy, and you look and feel terrible, and that’s hard.
You have to leave when it’s your turn to leave, even after that fourth round of chemo — which, by the way, they call the red devil, and they were wearing literal hazmat suits to handle it. I thought, “Okay, you’re wearing a hazmat suit to handle it, and then you’re dripping it right into my veins. This definitely feels like poisoning me within an inch of my life.” [That] is essentially what chemo is.
How were you able to manage the extra isolation?
I have a few things to be grateful for. First of all, my husband and I both were working remotely already, so there was no change there. Literally no change there. I had the love and support of my husband. I had the love and support of 2 amazing kids.
Then I had the love and support of my extended family, who were here to do what they could, like leaving food at the door. This is how we did it during quarantine. You couldn’t come in and heat it up. People would just take a whole cooler and drop it off.
I just would accept the help. Accepting the love and support from the people whose love and support I had was essential. We had dogs, and so lots of loving on the dogs. There would be a time after at least a week that I would start to feel like maybe I could take a little walk around the neighborhood. I would do that if at all possible, and try to do as many normal things as I could think of to do.
Radical Cystectomy
Undergoing a radical cystectomy (removal of the bladder) for 7-8 hours
Well, it is figure-changing. Again, an unwelcome result. Not happy about that. I’d already been concerned about my waistline, but it’s vanity weight. It’s 10 or 15 pounds that I’d rather not have. For health reasons, it wasn’t an issue.
Now, I knew that I was going to have a forever-changed body. I chose the ostomy bag solution. Think of an oblong, elliptical-shaped Ziploc stuck to your belly 100% of the time. That’s pretty much what you got going on. They’ve done some things to make it a little more comfortable. There’s little fabric; it’s not just plastic on your skin. But not fun.
Nobody wants to have this at all, although I will say — and here’s me doing my little humor thing. I will say that when I was hiking in the Appalachian Mountains with my family, I could tell [I] needed to empty the bag. I stood up like a guy in the woods. It was so cool. I was like, “This is great.” That’s the only good thing that came from it.
Margo recovering from surgery.
Finding the silver linings
Sometimes it’s so slim. It’s helpful, and looking for, “What do I have to be grateful for?” is a big part of how I have gotten through difficult times in the past. I called it the grateful game way back in the 90s, when I’d be like, “Okay, I feel like hell. I’m so depressed and frustrated. What can I think about that’s positive? What can I feel grateful for?”
That’s a baseline, the core framework for how I navigate through the tough times. Also core to how I do that is to embrace what’s actually happening. I don’t try to stuff it, pretend like it’s not happening or “should” it somehow.
What were your options after the radical cystectomy?
The options presented to me were I could have a neobladder, or I could have the ostomy, so that’s 2. When we were with Dr. Kamat in that first meeting and he explained those to me, I said, “What about a pig bladder? Come on, we’ve got lots of different organs we can borrow from animals. Surely those would work.”
He said, “No, those don’t work.” I said, “Okay, can you 3D print one?” Can we not use technology here? Of course, we’re not ready. We don’t have 3D printed full bladders, and maybe one day we will. Once I exhausted all the other ideas, I had to accept that these were my 2 options.
I said, “Well, tell me about the neobladder.” It’s pretty tempting to think of. Basically what they do is take a part of your intestine — I don’t recall which one — and they make a new bladder out of it, which is pretty fancy. It’s not shaped the right way, so it’s pretty creative.
It doesn’t have muscles, so you have to train it. But if it doesn’t have muscles, how do you train it? Leaking is a common problem. He said, “It can take a year to train it.” I thought, “Oof.” He seemed to think that the ostomy was the better path as well, so I took that.
Anxiety surrounding the neobladder
This is an embarrassing problem to deal with. Nobody wants to have issues with any kind of fluids or matter that our body gets rid of. We don’t want to deal with that. It’s inherently embarrassing, so adding to that embarrassment. It might be a year before you can get it to work.
Well, I can’t stay at home and not live my life. I have jobs and things to do. Those question marks definitely weighed in on that. When [the practical side of me is] deciding something big like that, the emotional side of me says, “Hey, I have an opinion about this.”
The [practical] side says, “That’s great. We’re going to hear about that later. That’s valid. We thank you for that, but we’re going to just make a practical decision here. We’ll talk about how you feel later.” It’s kind of how I ended up managing making that decision.
What guidance do you have for someone getting a radical cystectomy?
First of all, I think it’s personal. However other people are experiencing it is fine. I’m doing my path. You do you. I’ll do me. I think having conversations with other people who’ve gone through similar things.
For example, I know there’s women on Tik Tok who show off their ostomy bags, and good for them. I’m not going to do that. Do not look for me to do that on Tik Tok. It’s not happening. Good for them, and I like that they’re doing what they feel comfortable. Or maybe they’re pushing themselves, and they don’t feel comfortable.
It doesn’t have to look a certain way for any one of us. For me, I have what I call a love/hate relationship with my ostomy. I would like to be less disdainful. Last night, we were watching a show. I have very sensitive skin, and it’s got adhesive on it all the time. Sometimes it’s very raw, and it itches.
I can’t not have anything on it, because here’s what happens: what they do is take a little part of your intestine. They create a little conduit. They reroute the ureters to connect from your kidneys to this little tube instead of to the bladder. Then the tube just gets rid of the urine, and it goes straight into the back.
I can’t control that. I can’t just take it off for a while and walk around. You can’t. It’s not an option. I get very frustrated when that happens. I try to be kind to myself, and that’s how I feel. When I’m feeling up and good, I’m grateful.
Changing perspective
The night before the surgery, I had a lot of feelings. I looked at my body, and I thought, “I’m never going to look down and see this again. It’s going to look totally different.” That made me sad.
My brother said, “Well, think of it as getting rid of a body part that’s no longer serving you. This is your metamorphosis.” I thought, “Oh, that sounds a lot better than what I’m imagining, so I’ll go with that.”
Talking to others who have been through it
I think talking to people who’ve been through it [helps]. There are support groups on Facebook. The hospitals do a lot of things now. I couldn’t tap into any of the support because it was all shut down for quarantine, so I don’t know how good it is. I wasn’t able to use it.
Tap into all the things that are useful and have conversations with people. Some people you’ll connect with, and others you won’t. I wanted to talk to a woman who had been through what I’d been through. I was scared. I didn’t know what was going to be left. I didn’t know a lot of things. I talked to a woman who had had the radical cystectomy 10 years before.
I said, “Kind of a tough subject, but sexually, how were you after this thing?” She goes, “Well, I wasn’t interested in sex, and my partner wasn’t that excited about that.” I thought, “No, that is not what I want to hear.”
I’d been married to my husband for 5 whole years at that point. We’d just found each other finally, so I wasn’t ready to go to, “Octogenarian, we don’t have intimacy anymore.” I was not prepared for that. Fortunately, that doesn’t have to be the answer.
There may be some other things going on with her besides that, but that’s the problem with talking to people. Sometimes you hear things that upset you, or you think, “I don’t know if I can live with that.”
Just keep talking to other people, and keep going back to your doctors and asking them what’s physiologically going to be intact or not intact to understand. Allowing ourselves to be assertive and ask those questions, even if they’re a little uncomfortable, is well worth it. It’s our lives.
Hair Loss
Dealing with hair loss
I guess one of the things that’s good to know is what you can and can’t control. I couldn’t control that it was going to come out or when. By the way, it’s day 14, so that’s what I learned. That is when my hair follicles started hurting.
I likened it to when you have your hair in a bun or in a ponytail for a really long time, then you take it down. It’s like the follicles go, “Oh no!” Only it felt like that a lot of the time, and clumps are falling out, so it’s different. I felt nothing the first week, hair-wise. But on day 14, when we were checking back in, a whole bunch came out.
My daughter was at home. Her hair was, I think, purple at the time. [Knowing that it was going to come out,] I said, “Hey, let’s just make it whatever. What’s the wildest color? It’s all going away anyway, so let’s just go be wild.”
I have a professional job. I can’t have pink hair most days, but I thought, “Why not? Why not?” She dyed my hair bright pink. We had kind of fun doing it. It was a way for us to enjoy doing a little fun mother-daughter activity.
The reason that we were doing it wasn’t fun. I think there was a really therapeutic thing going on. [For me, it was] accepting her help, even if it’s just this light little color happening. For her, it was understanding what it’s like for me to go through this. She’s seen her mom always have long hair, and now all of a sudden, we’re going to have to cut it off, which we did days later.
She helped me with that. I said, “If it’s not too much for you, will you help me cut it all off and shave it down?” She said, “I’d be honored.” We went outside, put the iPhone up on the fence, and let it run. Fast-forward, because that’s a slow process. I still have a hard time watching that today because it’s just such a shift. We would love to say the hair doesn’t matter that much, but it does.
What comes up for you when you’re watching that video?
Part of who we are is how we look. We could comment on whether that should or shouldn’t be, maybe especially even more so for women. You see part of yourself that you expect to see and you define yourself as, “Okay, I am a tall woman with blonde hair that is long, and I can wear it in a braid or ponytail.”
Then you see that it is gone. Now I’ve got to figure out a new way to look at myself, but I feel like part of me and my sense of self. That’s a blow, even though I know intellectually it’s just hair. What does it matter? Everybody loves me. Who still loves me? Who’s important? Nothing about that has changed.
I get both how unimportant it seems, and yet I felt that it was very much a loss at the time. Also, I’m a woman in my 50s, and we’re doing everything we can to try to look as nice as we can and keep the gray and the wrinkles and all that at bay. A bald head is not a good way to do that.
It’s rough. I think it was the emotions of seeing that happening and seeing the hair coming off. It’s a very literal vision of me losing part of myself. I was able to learn down the road how to keep myself intact as a result. But at that moment, that’s not how I felt.
Your brother had the longest hair at one point
I never imagined this day would ever come. My brother’s always had super short hair. I laughingly refer to him as my baby brother. He’s 8 years younger than I am, but he’s a foot taller than I am. He’s 6’6″. He’s this huge guy, and he wears his hair short. After my hair was just starting to grow back a little bit, for some reason, my sister had super short hair at that time. His hair was actually longer than both his sisters’ hair. We thought that was a really funny thing.
Can you describe the importance of singling out these moments of humor?
I had to. That is part of my coping skill. I have gallows humor, because sometimes you’re in the freaking gallows, and that’s all you have to work with. A little bit of humor is a great way for me to help get through impossibly difficult times.
My mother, may her soul rest in peace, would say to me, “Sometimes you make a joke of everything.” And I’m like, “Hmm, well, sometimes I have to just to get through everything.” If you can find humor in any little thing, then I think it’s a very helpful way to get through, because then you’re like, “Well, at least 1% of that wasn’t terrible.”
Reflections
Normalizing the conversation about sexual health effects
It isn’t comfortable to talk about for me, and I do want to help normalize this conversation. One of the things that we talked about at the Bladder Cancer Advocacy Network Think Tank ‘22 was that this is one of those cancers that’s below the belt.
It’s a little bit embarrassing to talk about, a little personal and all that kind of stuff. That just makes it worse. That makes it harder if we feel like there’s shame involved with talking about the kind of cancer. I didn’t choose this. Nobody chooses this.
We’re all putting ourselves out there and pushing our comfort level to help bring that conversation along. I was on a panel with 2 other men, and what I can share with you is a woman’s perspective and a man’s perspective. There’s more cancer, more bladder cancer in men than women.
Both of them said that there was sexual dysfunction as a result of going through the treatment and also the surgery. One of them still had his bladder, and he said that that was the most important thing to him. I thought, “Yes, as it was to me.”
But if they say you’re going to die if you keep your bladder, then you take it out. That’s what happens. Specifically, they were able to get erections. They were able to have orgasms. There were a couple of other [things], but it wasn’t 100%. Everything wasn’t 100% the way they’d like it to be. That was interesting to hear.
Physical effects of treatment
When you’re removing the bladder, the urethra, the whole geography down there is pretty important. I don’t know where all the important bits and pieces and nerves are. I literally didn’t know whether I was going to be able to have fun or not. But everything’s still intact — the parts that matter are.
One of the things that goes along with a radical cystectomy is that often the way our bodies are shaped, they have to take some of the vagina. They didn’t in my case. That can mean that you now have a shortened vagina, and intercourse can be uncomfortable.
There are things that can be done to address that. Just go figure it out. There are all kinds of things. Go find out ways to do that and get the life you had back as much as you can. It just depends on your situation.
Emotional effects of treatment
I would say for me, it was more emotional than it was physiological. I didn’t like being bald, and I didn’t like having a bag on my front of my body. Now I’m no longer in shape either because I’ve been through all this stuff. I feel like I’ve been run over by dump trucks.
It’s hard to re-access the feelings of intimacy and the feelings of your sexual self. I think that’s been a longer journey than I would have liked. I think it’s personal. Again, grace. Give yourself self-grace. Part of me goes, “Well, there’s no time for that because now I’m 59 years old, and who knows how long I have? I just want to go ahead and hurry up and enjoy everything.”
I think that the whole accepting of where we are — which varies maybe day by day, hour by hour — is really key. Very clear and candid conversations with my husband have been good. That’s been enlightening. We’ve had to push the boundaries on what we’re comfortable talking about. That’s a good thing.
Ask the questions and understand what is and isn’t going to be in place, and what you might expect. Then I think what’s important is to look for what’s the highest and best potential outcome that I can have with this cancer, with what’s left of my body as a result of it, and what’s left of my life as a result of it. Then go make the very most that we can out of all of those things.
What other losses did you experience around this time?
I definitely had the, “I can’t take one single more thing,” because [I was] fighting this cancer alone in the hospital by myself. The week in the hospital after the surgery, tubes coming out of me all over the place, and people come in to poke and prod and all of that. The worst beds, the food’s terrible, the TV’s worse, and there’s nothing.
I had my phone, but it was really hard. I really did think, “Okay, well, that’s it,” but that wasn’t it. The blows kept coming. It was like it was bad writing. This is not all going to happen to one person in one year. But it did.
The next thing that happened that was a blow was the loss of my mother. I was sitting in the office by myself, waiting to see Dr. Kamat to find out if the chemo and the surgery had worked. This was 6 weeks after the surgery. I was waiting to see the doctor, so alone in the office by myself.
I looked down at my phone, which I had on silent but not turned all the way off. It was ringing, and it said St. Vincent’s Hospital in Jacksonville, Florida. It’s actually the hospital I was born in. I thought, “That’s not good. That’s either my sister or my mother.”
The doctor wasn’t there, so I answered the phone, which is not what you want to be doing when you’re waiting for the doctor to come in. First of all, it’s rude, and second of all, you need to be alert and paying attention. But I thought maybe it’s an emergency, and it was.
The last time Margo saw her mother.Margo’s mom and dad.Margo and her siblings where their mother is buried.
Losing your mom
It was St. Vincent’s saying, “Your mother is here. She is dying from dementia. She has a few days to live. She can’t stay here. Also, by the way, she tested positive for COVID. She doesn’t have any of the symptoms, but she can’t go to a regular hospice place, and she can’t go to her nursing home.”
So right now she’s homeless on a gurney, essentially, in the hospital, and I’ve got to deal with that right now. I couldn’t process that. I could not. I thought, “Really? Ridiculous.” I couldn’t process it, so I just was sort of stunned. I did my kind of compartmentalizing thing.
I got that phone call, and that meant I had a lot to deal with all of a sudden. I had to deal with the fact that my mother was dying in a few days, and that meant I would never see her again because we were in quarantine, and she had COVID. That was a lot to process.
I was her power of attorney, medical power. I forget what that’s called, but I was the one in charge. It was up to me to make those calls. I had the tactical thing of this list of really hard things I needed to do right then, which I couldn’t because I was waiting for the doctor to come in.
Taking time to celebrate remission
I reached for my husband’s hand to comfort me, but it wasn’t there because he wasn’t there, because we were still in lockdown. I was like, “Oh, that’s right. I’m by myself.” I had to just sit there and wait. The doctor finally did come in, and great news! You’re cancer-free.
Oh, my gosh. That is amazing news. Also, at the same exact time, my mother is dying, I can’t go see her, and I have to figure out where to even put her for the next few days. All at the same time. Insane breadth of different emotions and feelings all at one time. After we had the good news, I had the phone on the table [to record] so that I can share that with my husband.
When he picked me up, I said, “Let’s do this. We have a 3-hour drive ahead of us. We’re going to take 2 hours, the first 2 of 3 hours, and we’re going to celebrate that I’m cancer-free. We’re going to drive through Chick-Fil-A and get a milkshake and some French fries. Then the third hour, I will get on the phone, and I will start making calls and finding things out.”
That’s what we did. As we’re driving home and talking about celebrating that I’m cancer-free, we felt like we could finally exhale. For 6 months, we’ve been trying to save my life here. We didn’t know we were going to need to do that. Here we are doing that.
Now we’ve done that. What, it’s over? It’s over, more or less. We wanted to give ourselves time to celebrate. We gave ourselves 2 hours to celebrate. Of course, there were times besides that.
Experiencing more loss
Then I had to get on the phone and start finding special COVID hospice locations that I couldn’t go visit. None of us got to see her again alive, ever. The last time I saw her was the December before that August that she died, and that was impossibly hard. Then there was processing that grief and dealing with really tough things to manage logistically during the stupid lockdown.
Reagan, Margo’s dog.
Then a month later, the family dog died. This was the dog that raised my kids with me. She was 14 and a half, which is really old for a big dog. I feel like she made it through the death of my mom. I feel like she hung on to get me through. That was really hard, and then that wasn’t the last one.
Then my father-in-law died the following month, and we couldn’t go. My husband couldn’t go see him before either, so it had been January. We each had lost a parent after 8 months of not being able to see them, and we couldn’t see them before. We both had to do those absurd Zoom funerals, and you do the best you can.
Getting through so much loss
It felt like I just kept posting, “Here’s another dead person. Here’s another terrible thing,” on Facebook. One of my friends is like, “Dear God, what is happening?” I’m like, “I have no idea, but it just keeps coming.”
But here I am to live and tell about it. It turns out we can get through pretty much anything. I did tell myself at times, “Okay, you don’t live in a concentration camp, so it could actually always be worse.”
I’ll share something else for all the parents out there. If your kid had cancer, what parent wouldn’t say, “Give it to me; I’d rather have it”? It was me, and I was really grateful that it was me and not my kids.
They still have a life ahead of them, and I do too now, as a matter of fact. It could have been worse. It really could. I’m glad that it wasn’t them. I’m glad it was me and that I’m here to tell about it.
You filmed a video as Wonder Woman. What did that mean to you?
https://www.instagram.com/p/CgxqyJNvIjZ
I realized when I was lying down in the bed at the hospital after this cystectomy. I felt just terrible. Pain and discomfort. Now we’re in the day and age where they don’t give you pain meds anymore. They’re like, “Here’s the Tylenol,” but [it] hardly helps. I know why we do it. I couldn’t have a Vicodin or anything, so I was uncomfortable.
I was tired, and I couldn’t sleep. I’m lonely; I’m depressed. I just thought, “You know what? For the first time in my life, I actually feel a little bit like giving up and feeling like I just could go to sleep, and then that would be it. Then all of this would stop.” That is so not like me, but it’s pretty brutal.
What I told myself in that moment was, “Well, you can’t do that. You can’t do that to your kids. You can’t do that to your husband and the other people who love you. Actually, all you have to do right now is not die. You don’t have to get up and fight or feel brave or energized. You don’t need to feel anything. You can feel like crap, which is how I felt. You can feel empowered. You can feel sorry for yourself. Feel whatever you feel. Not dying today is enough to keep fighting.”
Later, when I was reflecting back on that, I thought, “Yeah, you know, I think we have this perception that fighting, whether it’s cancer or another illness or another difficult chapter in life. Persevering has to look like this superhuman, like a Marvel character persona, who’s just big and strong and has all of the energy and the strength in the world to take on these battles.”
In fact, we don’t. It doesn’t have to look like that for it to be legitimate and enough. I have focused on that. I think that being able to laugh at the idea that we need to be Thor or somebody else in order to fight whatever battles that are ahead of us is — I think that is something we need to maybe leave behind us and accept a wider view of what courage looks like.
I feel like courage is not that you feel like fighting, that you feel like continuing to go on and do whatever the hard thing is that you’ve got to do. Courage is doing it anyway. Being brave is one thing, but having courage?
That’s when the rubber hits the road and you don’t feel like doing anything, and you grab yourself by the scruff of the neck. You get yourself up or crawl, whatever you have to do.
I just wanted to expand our view of what being brave and courageous and fighting can look like, and it can look like you’re lying in bed feeling like dying. Actually, that still counts. I still didn’t die. Good for me.
It didn’t come to me right away. Again, I think I mentioned that I work for a company, and we sell health insurance plans for self-employed people. As part of my job, I present to groups and teams, both virtually — well, at that point, it was still virtually.
Here’s the overview of the plans. Here’s what you do if you want to access them. Here’s what one of the plans looks like when you need it. Here’s my story, and I shared. I’m on the plans that we sell. I shared my story, and I was really surprised by the response. It’s the only story I had, so at first I couldn’t, but then I did.
I thought, “Well, maybe this will help me process it, and maybe it will be helpful, because here’s a real person who’s actually needed to use it and what it looks like when you need to.”
I was really surprised by how emotional people felt as a result of hearing me tell this story. That really took me aback, and how caring and loving. To this day, 2 years later, I still tell the story, and they still respond in the same encouraging way, saying, “Thank you for sharing that with us. It’s inspiring.”
I thought, “If that is inspiring to the handfuls of people that I’m presenting to, maybe I could put it in a book and share it with even more people. That might be helpful for them as well.” My goal was to write a book that was easy to read and that would show people how I personally [got through it].
It’s just one way to get through all this stuff, but it has the little tips and tricks that I used to get myself through this really tough time. [My goal was to] give people hope that they can get through it, even when it looks like it’s insurmountable and impossible. Okay, feel that way. It feels that way. It does, and you can get through it. The book came out in July, and I couldn’t be happier.
The Patient Story’s new series “Cancer Friends” features Andrew and Esther Schorr. They co-founded PatientPower.info, a resource for other cancer patients and caregivers to help them through their diagnosis and treatment.
Join us every Sunday for a new “Cancer Friends” episode, airing on our video channel here!
This segment focuses on Valarie, who was diagnosed with multiple myeloma in 2015. Valarie shares learning to accept help, the support that helped her, and now giving back to the community.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I didn’t lose my independence. I learned how to live with help, which we all need.
Valarie T.
Introduction
Esther Schorr, The Patient Story: Greetings. I’m Esther Schorr, and welcome to Cancer Friends. This series is an ongoing conversation with patients and care partners, those who love and care for cancer patients, about the journey we take together. We talk about issues and obstacles that we face, and share collective wisdom with each other.
This month’s series is focused on the uncertainty that a cancer diagnosis brings and how both patients and care partners can deal with it. We’ll also discuss some ways to get support and talk about the role that giving support can play in helping further overcome the shock of diagnosis.
Diagnosis and getting support
Esther, TPS: My terrific guest today is Valarie Traynham. You live outside Chicago, you’re active in your church, and you’re definitely someone who’s figured out that getting and giving support go hand in hand in managing a cancer journey. At least, that’s what I gather about you. Tell me a little bit about your diagnosis and where you went for support. Did that help initially?
Valarie: I was diagnosed with multiple myeloma back in 2015. You know, very shocking diagnosis, obviously. Never heard of it before. Never heard of the disease before. It was really hard for me because when I think of support, I’m thinking, “Okay, well, my family.” You think of your friends and your family. I didn’t live near my family. My family lives out on the East Coast, and they were not able to be with me throughout the treatment there.
So I reached out to my church family. I like to call them my chosen family. These are the people that we get to choose if we want to bring them along on the journey or not. I chose people in my church family and my church circle, my friends that had been a part of my life before the cancer diagnosis came along. But I must say that it was very hard.
When I got the cancer diagnosis, I almost looked at it as stealing my independence. Being a single woman, working on a career, and then to have a cancer diagnosis come out of nowhere, it’s like, “What’s going on?” Am I going to be able to do the things that I used to do? I was very put off by that at first because I’m like, “This is taking away my independence.” I’m going, “I’m not going to be able to do the things that I used to do.”
Esther, TPS: Valarie, did that keep you from looking for support within your church family, or how did that work?
Valarie: At the beginning, it was hard to accept help because I had not needed it before. I had been, as you say, the independent person. But as time went on, I realized that this cancer was not something that I could do on my own. I needed support.
I also came to find out that the support that I was receiving from my friends and church family as well — it was such a blessing to me, and it was also a blessing for them to be able to help. That’s one big takeaway that I take away from this whole situation. I didn’t lose my independence. I learned how to live with help, which we all need.
What support helped you?
Esther, TPS: Can you talk a little bit about what that support and help looked like, that was helpful to you initially?
Valarie: Initially, I didn’t know what kind of support that I would need. Obviously, going back and forth to the doctor for your chemo appointments and treatment. I originally thought I was going to be able to do it. I’m like, “You know what? It’s not going to be that bad. I can drive. It’ll give me time to think before the appointment and think on my way home about everything that’s going on.”
But my friends were like, “Absolutely not. You will not do that.” I’m glad that they kind of persuaded me not to do that, because it helped build some even stronger friendships. What that looked like — I had a very good friend. Her name is Karen. She lived in a city that was not very close to me. She was about 30 or 40 miles away, but she would drive to my home, pick me up and then drive me to my appointments.
She did it because she wanted to be a source of support for me. It was not out of obligation or anything of that nature. She was like, “This is what you do when someone you love is going through something. You stand by them; you support them.” She would take me to my appointments.
Another thing that I learned is when it came to support, knowing what kind of support each person was best at giving. You have those that can really give good emotional support, and then you have those that are doers. They’re the ones that you can give them a list and say, “Hey, go to the grocery store and get me this, this, this and this,” and they’ll bring it back.
They will bring back everything. Brand, everything that you wanted. Those were doers, so I learned to accept that support from my doers. When I needed more emotional support, I figured out who exactly I could go to to get that emotional support.
It took me a while to figure that out. I would send somebody that’s really good with emotional support to the store and say, “I want some Greek yogurt.” They would come back with the wrong stuff. I’d be like, “Oh, that’s not what I wanted, but yogurt’s yogurt, right?” So I learned that. Then once I figured out who was a doer and who’s going to be there for emotional support, it just helped things so much more. It just grew my support team to an even greater level.
Esther, TPS: You use the word “team,” and you’re really talking about with a diagnosis, you need to build a team. It’s like building, in a sense, the way you build a business. What are the skills you need? What are the things people like to do and are good at doing? You match them up, and then it turns out that that’s the best help for you. It’s kind of unfortunate. It almost sounds like as a patient, you have to be a manager.
What prompted you to give back, and what does that look like?
Esther, TPS: In the end, I think the way you’ve described building that team is it also gives those people the greatest satisfaction at being able to give back, which kind of leads me to my next question for you. What prompted you to give back, and what does that look like? Because I know that you balance being the patient and accepting support, but now a lot of your time is giving back. What does that look like?
Valarie: Giving back is just something that I really enjoy. I find that with giving back, I lead a myeloma support group. I’m also a myeloma coach. I do some mentoring with Imerman Angels, Cancer Fighters, organizations like that that provide one-on-one support to newly diagnosed patients or patients that are a little bit further down the line who still have questions. They need somebody that they can connect with, shared experiences and things of that nature.
I really enjoy that because it gives me the opportunity to give help. When I was first diagnosed, I didn’t have all of that help. I know what it’s like to be in that need, where you are not sure who to reach out to. You’re not comfortable talking to certain people simply because they may not be able to relate. I do it because it brings me joy just to be able to help somebody, to be able to guide somebody along their journey.
But I also do it because it’s just a need, or it’s just something that’s lacking within the community. People are scared to reach out. They are scared to talk to other people because of whatever reason — fear of being judged or fear of just being rejected, or things of that nature. I do it for those reasons.
I also do it because it takes the focus off of me. When I’m talking to somebody else, I don’t have to worry about the disease. I don’t have to worry about myeloma and what’s going on with me and the disease. It just brings me so much joy to be able to do that.
How did you find the organizations you help through?
Esther, TPS: I know, from your describing, bringing your support team together. But now as you turn the focus to, “How can I help other people?” How did you find the organizations that plugged you into being able to give back?
Valarie: Most of it was done online. A lot of it was social media. When I was early on in my diagnosis, I just knew that I needed to connect with other myeloma patients. I just knew it. I still had my great support team, but they just couldn’t relate. If I said, “Hey, it’s 1 in the afternoon. I’m sorry, I just need to go take a nap. I’m feeling very fatigued.” They didn’t understand that. It’s 1 in the afternoon. Why would you need to lay down?
I found that when I got with other myeloma patients and I said that, it was like, “Oh yeah, I do it all the time.” Because it comes with the disease. When you’re with others like that, they understand what you’re going through. But I found a support group early on, which made a tremendous difference in my life because, like I said, they were like-minded individuals. They were individuals that had been through what I was going through or getting ready to go through, so they could guide me along that process there. That was just so eye-opening for me.
That support group provided patient education and just resources and things that I would not have known about. Various workshops and patient seminars and things of that nature, which really got me connected. The more I did that, the more I really enjoyed it. I really like this, making people aware, helping people along their journey.
Then I got into coaching, the one-on-one mentorship with the different organizations, which eventually led to what I do as an Black Myeloma Health Community mentor. Really, the focus kind of shifted there, because I saw that there was an unmet need within the African American community in bringing support, resources and patient education to that community. That’s kind of how it’s all unfolded with receiving support and jumping into giving support. It’s really trying to fill that unmet need that we have.
Utilizing support to help others
Esther, TPS: It sounds to me like it’s kind of a cycle. First, you need your own support to understand, “How am I going to cope?” Then you learn these coping skills and what kind of support you need, so then you can, like you said, stop focusing just on what’s happening for you. By giving back, it reaffirms that you’re in a better place. It sounds like a give and take.
I see that with my experience as a care partner. My partner, Andrew, is a cancer survivor. I see it with him as well. You go through the initial shock. We both needed a lot of support. Then as time goes on, there are moments where we each need some kind of support. But the giving back part takes the focus off of immediate, “What’s actually going to happen or is happening?” We’re in a community of people who can support each other. It’s really helpful.
What do you see happening next? You’re doing all this work supporting others. Is there some specific thing where you think you’ll focus your energies going forward? Other than staying healthy, of course.
Valarie: Well, staying healthy. I really believe that this is my purpose. This is why I have been through this myeloma — to be able to help others along. My goal is really to work more in the patient advocacy role. Just build that role and go from there. The possibilities are endless in that area.
Esther, TPS: Valarie, it’s really delightful to get to talk to you, and it’s very inspirational for me to hear that there are people in the world who take care of themselves, and then what gives them pleasure is to help others take care of themselves as well. I really appreciate you taking the time to speak with me.
Thank you for sharing your experience as both a taker and a giver in the most wonderful sense of the word. I’m Esther Schorr with Cancer Friends, and I hope that our series on dealing with uncertainty of a cancer diagnosis is helpful to you as you move through your journey.