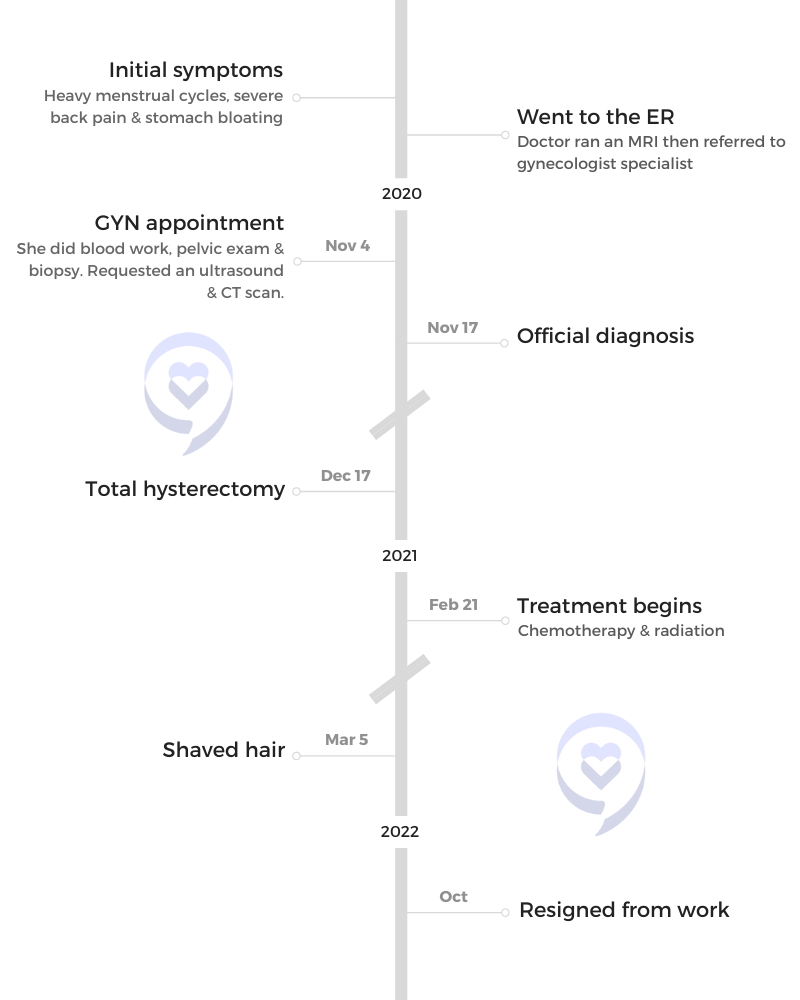
Gwendolyn Jackson initially experienced heavy menstrual cycles, back pain, and bloating, which her doctor suspected to be fibroids. Despite regular tests, including an HPV test and ultrasound, her symptoms persisted. Later, clear fluid leakage led to an ER visit where an MRI and biopsy confirmed cervical cancer.
She underwent a hysterectomy, followed by chemotherapy and radiation, but further tests revealed the cancer had spread, drastically changing her prognosis. Severe side effects from treatment, including weakness, nausea, multiple strokes, and heart attacks due to dehydration, required intensive therapy. Despite initial hesitation, she joined a clinical trial at MD Anderson, which has helped manage her condition more effectively than traditional chemotherapy.
Throughout her journey, Gwendolyn faced misconceptions about clinical trials and the stigma of cervical cancer within the African-American community. Financial challenges resulted in losing her job, insurance, and assets. She found crucial support through Cervivor, an online community for women with cervical cancer.
Gwendolyn’s experience highlights the importance of self-advocacy in healthcare, the life-saving potential of clinical trials, and the need for greater awareness and support for cancer patients.
Name: Gwendolyn J.
Diagnosis:
Cervical Cancer
Staging:
Stage 4
Initial Symptoms:
Heavy menstrual cycles
Severe back pain
Stomach bloating
Treatments:
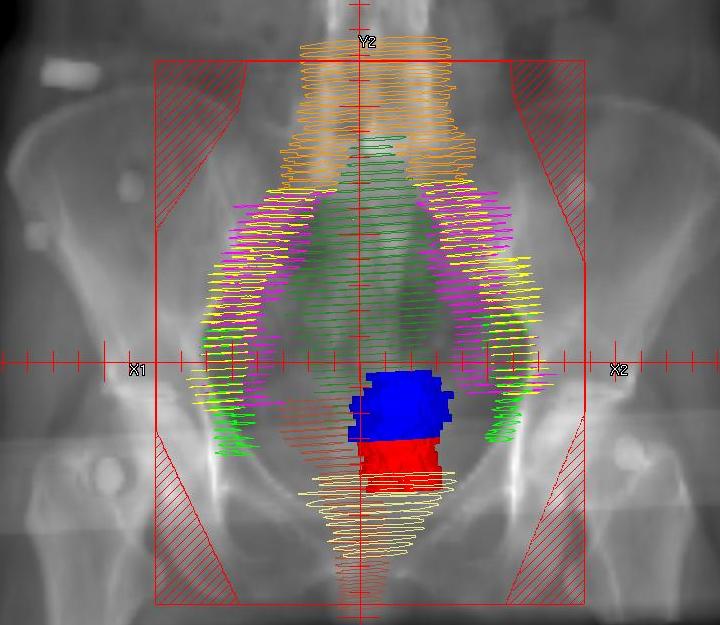
Chemotherapy
Radiation
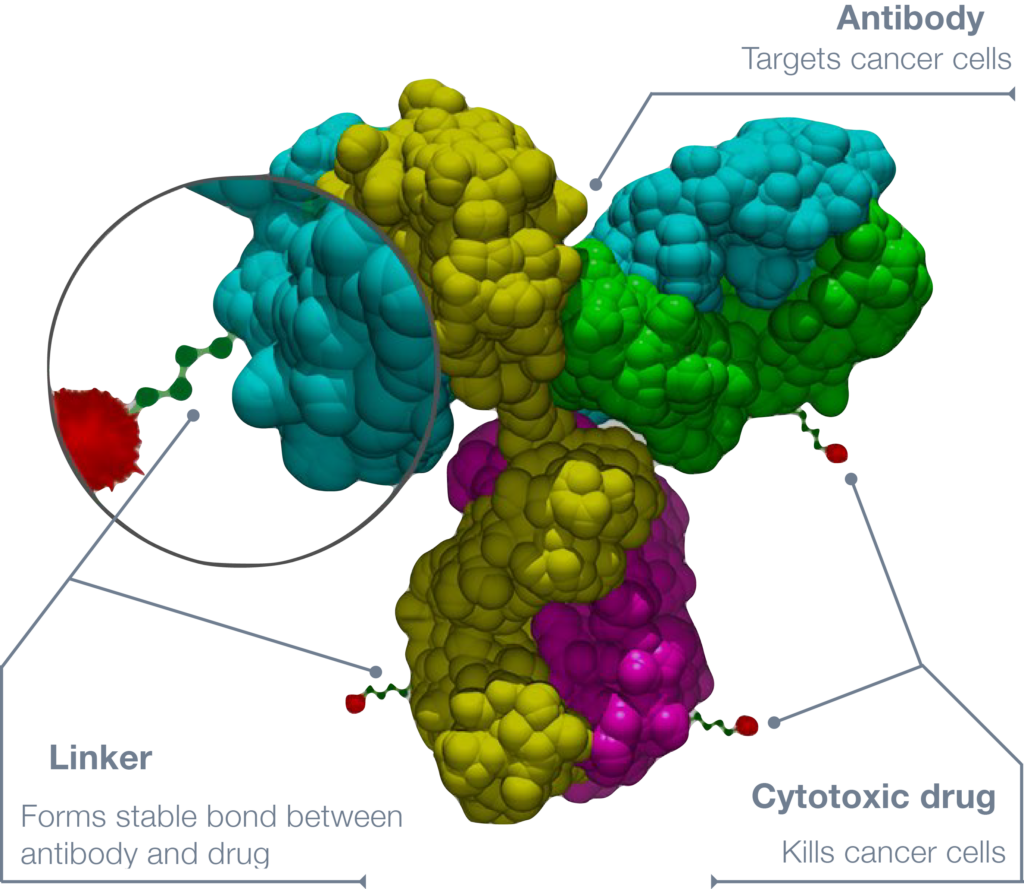
Tisotumab vedotin (innovaTV 301 clinical trial)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I started having heavy cycles, severe back pain, and bloating in the stomach.
I went to the doctor regularly. When I went for my well-woman exam, I told my doctor. He said, “I think you have fibroids. It’s very common in the African-American community.” That’s what it sounded like to me. “We’ll run some more tests.”
My symptoms persisted, so I went to my mother because I’m that girl who thinks mom can fix everything. I told her, “I’m having very heavy cycles. I don’t know what’s going on. The doctor said he was going to run some tests. They haven’t called me back yet.” She said, “You’re going through pre-menopause. I went through the same thing at the same age. It’s just pre-menopause.”
My cycle wasn’t getting any better. I finally went back to my doctor and he ran some tests. He did the HPV test and it came back negative. I was still having symptoms, so he said, “I’m going to do an ultrasound.” He did and said, “I see fibroids, so we might have to do a hysterectomy.”
In October 2020, while I was at work, I started leaking clear fluid from my vagina. I knew I wasn’t pregnant, but it felt like my water bag had burst. I said, “Okay, this is not good.”
When I saw cervical cancer written on that paper, I lost it. He wrote it down before they even found out I had it.
Going to the ER
I wish I could remember the name of the doctor who saved my life. I don’t know what would’ve happened if it wasn’t for him and that MRI.
When I went to the emergency room, a younger doctor who looked like he had just become a doctor said, “I want to run some more tests on you. I don’t feel comfortable with everything you told me. What can we lose? Let’s do an MRI.”
After the MRI, he came back and said, “I see fibroids, but I see something under the fibroid, so I’m going to send you to a gynecologist specialist, so they can run more tests because I’m not sure,” but he put “cervical cancer” on my paperwork.
I went home and did the worst thing I could do. I went online and searched “cervical cancer.” My father passed away from cancer, so when I saw cervical cancer written on that paper, I lost it. He wrote it down before they even found out I had it.
Diagnosis
Seeing a Specialist
I went to the specialist who said, “We have to run a biopsy. Calm down. Don’t worry. You’re pretty healthy. I see all the tests they’ve done. I don’t think you have cervical cancer. It might just be fibroids.”
Getting the Official Diagnosis
I was diagnosed during the COVID pandemic, so I had to go by myself. On the way, I talked to my mother and my sisters. Everybody said it was just fibroids. My sister said, “We have fibroids. We had to have a hysterectomy too.” They were reassuring me, so that’s what I thought.
I went in thinking I had fibroids and left finding out I had cancer. You will never forget the day. I was diagnosed on November 17, 2020.
I started treatment right after I recovered from the hysterectomy. I thought it was just a preventative measure to make sure I was okay.
Reaction to the Diagnosis
When you first hear, “You have cancer,” it doesn’t register. For some reason, I thought I was exempt because I was helping people with cancer. I started my nonprofit in memory of my father who died from lung cancer. I thought, I eat right. I run five miles every morning. I don’t smoke. I don’t drink. What did I miss?
Cervical cancer has this stigma that people who get it are either prostitutes, have a high sexual drive, or don’t go for their well-woman exam. That’s not me. On the way home, I thought it was something I did wrong.
I wanted to find out for sure first. The doctor put it on the chart and then gave me paperwork for the referral. I was left alone not knowing if this really was true. That two-week wait was difficult mentally.
Treatment
Hysterectomy
They said, “We’re going to go in and remove the whole tumor. After, you’ll do radiation and that’s it. Your life will be back to the way it was,” so that’s what I thought.
I had a full hysterectomy on December 17, 2020. The tumor was 9 centimeters. Before I went in, they were telling me, “You’ll be fine. After we remove the tumor, radiation will take care of everything else.”
After 6 to 8 weeks, I went for radiation. My doctor did some blood work and he was concerned with the results. He said, “The blood work didn’t change. Something isn’t right. I’m going to do an MRI and a PET scan. We have to see what’s going on.”
After I had the hysterectomy, they said, “We’re going to do radiation and you’ll take a chemo pill. That’s just protocol.” I started treatment right after I recovered from the hysterectomy. I thought it was just a preventative measure to make sure I was okay. They were thinking they got everything not knowing that it was spreading.
The chemo was so hard on me. Some days, you can’t get out of bed. Some days, you don’t have an appetite.
Cancer Spread
They found out that my cancer had spread to my hip bone, my legs, and my spine. Imagine going from everything is going to be okay to find out you have 16 months to live.
I said, “God, I don’t want to die. I just had grandchildren. I just turned 49. I haven’t hit 50 yet. I’ve been waiting to be 50 all my life. Please give me more time.”
When they realized it spread, my team had to come back together and treat me differently. They were going to try a bone marrow transplant, but they couldn’t do it because of how mine spread. My insurance would no longer approve it.
Knowing that was all they could do, I got scared. I have anxiety and depression, and I take medication for them now. I’ve never had depression before, but because of all of this, I take medication for it.
Chemotherapy & Radiation
I didn’t want a port. I asked, “Can we figure out something? Is there a way that I can take pills?” I took chemo pills and did radiation.
Side Effects of Chemotherapy & Radiation
The chemo was so hard on me. Some days, you can’t get out of bed. Some days, you don’t have an appetite. You don’t want to eat. You look at food and get nauseous. People don’t understand that. It’s not that we don’t want to. I’m trying. I’m showing up every day and doing the best I can. I used to tell my dad, “Come on, you can eat. Come on, you can get out of bed.” Now, I understand.
The radiation that targeted my cervical cancer was terrible. It burned the lining of my stomach and I kept getting infections.
I used to help my dad button and zip his clothes. I have the same issues now. I can’t button or zip. These are everyday things that we take for granted. I also felt numbness in my fingers and my feet.
I couldn’t keep anything in my stomach. I was vomiting and had diarrhea. They were giving me medication for everything, but nothing was working.
I feel so weak and cold all the time. I always have a heater with me, but I was so, so weak that I didn’t think I was going to make it. My daughter and the guy I was dating at the time were very helpful. They would bathe me and help me get up.
Because I lost so much weight and wasn’t strong, even my doctor was saying, “You’re getting weaker and weaker.” He kept prescribing me medication for nausea. They finally found a prescription that worked for me and that I love.
Radiation burned my face. It was burning and itching at the same time. My face swelled up and blistered. My doctor told me about a cream I could use, which cleared up my face.
The radiation that targeted my cervical cancer was terrible. It burned the lining of my stomach and I kept getting infections. I never want to do that again ever.
Strokes & Heart Attacks
When I went to the hospital, the ER doctor said, “She has high blood pressure.” I said, “No, I don’t have high blood pressure.” When he checked, my blood pressure was very low. When they ran tests, he said, “You’re having a stroke and a heart attack, and it’s because you are severely dehydrated. You need fluids in the body to make all the organs work.” I didn’t even know you could have a stroke or a heart attack from being severely dehydrated.
I had to stop treatment temporarily because I was in inpatient therapy for 14 days.
Recovering from the Strokes & Heart Attacks
I couldn’t walk, so I was in a wheelchair. I had to stop treatment temporarily because I was in inpatient therapy for 14 days and then I went to the Centre for Neuro Skills in Webster, Texas. I always speak so highly of them because they gave me my life back.
When I came in, I felt so helpless. I wouldn’t use the restroom, even though I was there from 9 to 2 o’clock. I didn’t want anyone to take me. I ended up getting a UTI and people there had to tell me, “We’re here to help. We want to make you better. You have to allow us to help you. You’re still the same person.”
I had three mild strokes. They didn’t understand the last one I had. They said, “Usually when you have a transient ischemic attack, you bounce right back.” I didn’t, so he said the last one wasn’t a TIA. It was a regular stroke because I had all the symptoms. I had to go from a wheelchair to a walker to a cane.
Because of the strokes, I can’t remember exactly what chemo I was on.
Joining a Clinical Trial
I met a doctor at one of Cervivor’s retreats. She was different if that makes sense. I knew that she cared about people. She said, “When you get back to Houston, let’s stay in touch,” because she worked at MD Anderson. I said, “My treatments are not at MD Anderson.” She said, “Let’s just stay in touch.”
My doctor never brought up clinical trials. I was doing some research. I kept hearing other patients talk about clinical trials when I went to the doctor. I decided I was going to ask my doctor, but I want to have information before I go in. I wanted to educate myself.
My doctor said, ‘This is great, but these clinical trials are at MD Anderson. If you can get in, go there. I’ll send your medical records over.’
I reached out to the doctor at MD Anderson and asked about clinical trials. She gave me all the information, told me which ones she recommended, and sent an email right away. It was after hours and she was volunteering her hours to help me. She’s still a big supporter of mine. She still checks on me and asks how I’m doing.
I took the information to my doctor and my doctor said, “This is great, but these clinical trials are at MD Anderson. If you can get in, go there. I’ll send your medical records over.”
My dad enrolled in clinical trials at the end and I said, “Y’all not helping him. This is not helping him.” My dad was such a great guy. He said, “This is how they’ll find out if it works for someone else. If it doesn’t work for me, they know it doesn’t work. If I can help someone, that’s what I want to do. I want to help someone.”
I didn’t understand at that time because I wasn’t a patient. But when you become a patient, you feel that way. If it doesn’t work for me, we know we have to try something else. If it works for me, that means this could be it. If I have to go through all of this to make sure it can save me and someone else, it’s so worth it.
When I went to MD Anderson, they had to do all the scans themselves. Their team comes in and speaks with you, and they have a team for everything. Even though I had cervical cancer, they also had a bone cancer specialist.
They redid all the tests I already had to make sure what they had in the file matched. Once they did everything over and made sure I was good to go, they started talking about treatment.
The clinical trial I’m on is called innovaTV 301. It’s a phase 3 study of tisotumab vedotin.
I like tisotumab vedotin better than traditional chemotherapy. It’s not so hard on my body.
Side Effects of Tisotumab Vedotin
They gave me medication for nausea and vitamin B12. So far, so good. The steroids are putting weight on me. I was a little nauseous at first, but the pill helped with that.
I lost my hair. I went bald when I first started and then it started growing back.
With bone cancer, being cold is a no-no for me. It’s very painful, so I wear a lot of warm-ups or layers to try and stay warm. Even in the summer, when I feel cold, I’ll be in warm-ups. I tell people all the time to be nice to people in warm-ups because you never know why they’re wearing them even when it’s warm out.
I noticed my appetite was not the same. I’ll crave something because of the steroids, but when I get it in front of me, I might take one or two bites and then I don’t want it anymore.
I like tisotumab vedotin better than traditional chemotherapy. It’s not so hard on my body. Do we know if it’s working? I don’t know if they think it’ll work. They’re buying me more time, so if that’s what it can do, I’m okay with that.
In the African-American community, clinical trials are frowned upon…In our mind, we still think we are being experimented on.
Misconceptions
In the African-American community, clinical trials are frowned upon. I think it goes back to when they were using African Americans for experiments and being the guinea pigs. In our mind, we still think we are being experimented on. If you tell anybody you’re doing clinical trials, they think you’re being a guinea pig.
I didn’t have the support. Everybody supports you when you’re going through chemo, but when it comes to clinical trials, they think you’re letting them experiment on you. They don’t care. I have to keep it to myself. I’ll tell people who are battling cancer that I’m in clinical trials, but other people, I don’t.
When it comes to the medical team, sometimes we feel like we’re not being heard. At first, I felt like my doctor wasn’t hearing me when I said it wasn’t fibroids and that something was going on, but they kept brushing me off.
I thought it was just Black women who go through that. Being in the teal and white community and the Cervivor community, I found out that it’s women as a whole. They are not listening to us.
Insurance Coverage
People think that if you want to be a patient at MD Anderson, you can just show up. It doesn’t work like that. When I first found out I had cancer, I wanted to go to MD Anderson because they’re number one. My insurance wasn’t in their network so they couldn’t take me.
While I was going through all of this, I still had insurance because I was still employed. They took excellent care of me during that time, but they could only take me so far. I was getting temporary disability, but my doctor put “permanently disabled” on my paperwork, so I had to resign from my job. They knew I wasn’t coming back, so they said, “You’re going to have to figure out your insurance yourself.”
Even with insurance, I was paying $2,000 to $3,000 for treatment. I lost everything. I lost my cars and my townhouse. The clinical trial was free for me, so that was good. They just had to make sure everything lined up.
I needed people who understood what I was going through, the stigma that comes with it, and that we have a voice. We didn’t do anything wrong.
Finding Support Online
I felt like nobody understood what I was feeling or going through. My mother kept saying, “It’s going to be okay,” but I told her, “What if it’s not? What if I die? What if this is my story?” But, of course, she didn’t want to hear that. “No, you’re going to be okay.”
My sisters were supportive, but nobody knew what I was going through. The only person that I felt I could talk to was deceased. My father would be the only one that would know what I was going through.
I went online and found Cervivor. I needed them more than they probably knew. I needed people who understood what I was going through, the stigma that comes with it, and that we have a voice. We didn’t do anything wrong.
I went to a retreat because I needed to be around these women. I needed them to love on me and I needed to love on them. They gave me hope. They said, “You can do this. You can fight this. Don’t give up. We support you.” They have a group chat where they talk about whatever they’re going through. If somebody doesn’t respond, they all get nervous.
Words of Advice
Cancer taught me to slow down because I was always on the go. I never slowed down to notice anything. Now I would stop and notice things. “Did you know mom has roses in front of her house?” And then I would stop and smell them.
Everything matters to me now because I don’t know how long I have. When I had my stroke, I couldn’t walk and we take that for granted. Even going to the restroom, I needed someone to help me and I appreciate that so much now.
Clinical trials can save us. I’m doing pretty well. It’s working for me. I’m still alive because of the clinical trial. My brother, who has cancer, is on a clinical trial and doing well too.
A doctor told me, “When you go into the doctor’s office, they are working for you. You are not working for them.” When you have that in mind as you’re going in, it’s different.
If you feel like something is not right, speak up. If there’s a treatment that you don’t want to do, say it. We get so nervous when we go in that we freeze up. Use your voice.
Cancer taught me to slow down because I was always on the go… Everything matters to me now.
In addition to Gwendolyn’s narrative, The Patient Story offers a diverse collection of cervical cancer stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
Symptoms: Heavy periods, abnormal bleeding, large blood clots, severe cramping, severe abdominal pain, pain radiating down the left leg, loss of mobility in the left leg, loss of appetite, fatigue
Shyreece’s story began with an unexpected onset of symptoms. After experiencing sudden shortness of breath, she was soon diagnosed with advanced-stage cancer following a series of hospital visits and tests. Visit her first in-depth patient story here.
She underwent various treatments, including chemotherapy and clinical trials, experiencing both successes and setbacks. While some treatments provided relief, others led to significant side effects and the progression of her cancer.
Her cancer journey is marked not only by the challenges of the disease and its treatments but also by her resilience and determination. She stresses the importance of self-advocacy, informed decision-making, and community support. She also became an advocate for understanding biomarker testing and exploring every possible avenue for treatment, including participation in clinical trials for new therapies.
Despite the challenges, Shyreece remained steadfast in her faith and determination to live fully. She shares her story through writing and mentoring, offering hope and encouragement. As she continues her fight, she approaches each day with unwavering resolve and a commitment to living without fear.
In addition to Shyreece’s narrative, The Patient Story offers a diverse collection of non-small cell lung cancer stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
Such heaviness and shortness of breath came over me out of nowhere. I thought, What is this? From that moment, I knew something was wrong
Introduction
It’s been 10 years for me. Before the cancer diagnosis, my answer was, “I’m Shyreece. I’m a teacher and I love kids. I’m so glad to have overcome so many obstacles to teach and do wonderful things.”
When cancer hit me, I thought, Who am I? Where do I go from here? What do I take from this battle that I’m in and can’t seem to get out of? On any given day, I could be floored on my back and the next moment, I’ll be coaxing myself to get up and go to the bathroom.
Pre-diagnosis
Initial Symptoms
My students and I were getting prepared for spring assessments. After they came in from lunch, I said, “Let’s get ourselves ready and do a little brain break dance,” and then everything got heavy. The kids were moving, wiggling their arms, having a good time, and, for whatever reason, I couldn’t do it with them anymore.
I said, “Kids, you guys are going to have to sit down.” I had to hurry and sit down. Such heaviness and shortness of breath came over me out of nowhere. I thought, What is this? From that moment, I knew something was wrong, but I kept pushing past it. That’s what superheroes do, that’s what super teachers do. We push through it. We keep going.
That weekend, my boss came in and said, “We’re moving you to a more administrative role.” I said, “This is great. Now I’m excited again.” But when Monday came, I couldn’t carry my book bags into the office. It was such a short distance from the parking lot to the front door of the school, but I couldn’t do it. When I finally got in and started trying to catch my breath, somebody heard me wheezing and said, “Shyreece, you need to go to the ER.”
I didn’t know what was going on, but that started a two-week journey to being diagnosed.
Going to the ER
My husband picked me up from work at about 7:00 pm and took me to the ER. The doctor said, “You’re not going anywhere. You’re in such a state that we don’t even trust your husband to take you to the hospital. We’re going to take you by ambulance.”
I didn’t know what was going on, but that started a two-week journey to being diagnosed with stage 4 ALK-positive lung cancer. We didn’t even know what ALK meant. I learned that along the 10-year journey.
Diagnosis
Five doctors were standing in my room and they were as confused as I was. The hospitalist said, “We don’t know what’s going on on the surface, but I’m going to send this to the University of Michigan.”
He waited for the results to come back and when he got them, he said, “Oh my goodness.” He came in, held my hand, and told me, “You have cancer,” and then called the local cancer clinic.
Something in my gut said to go to the University of Michigan. When I got there, they said, ‘We have an inhibitor we want you to try. It’s promising.’
Treatments
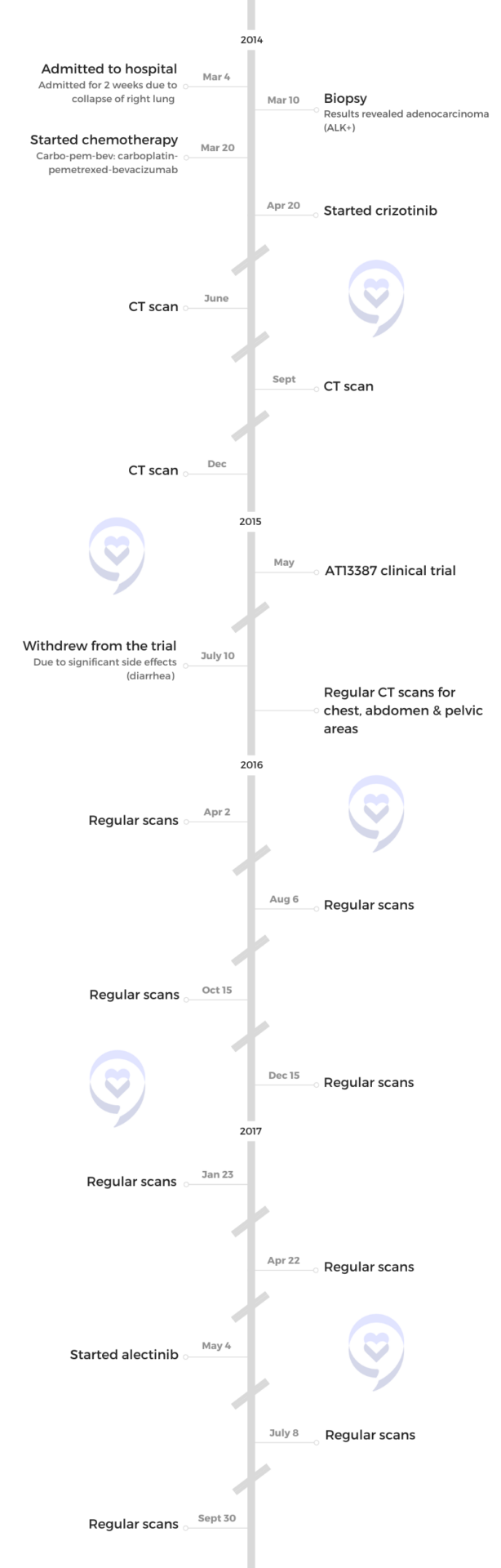
Carbo-Pem-Bev
They had no idea what to do next, but she said, “Shyreece, I’m going to go ahead and load you up with the best chemotherapy mix that we can possibly give you right now.” I said, “Okay, let’s do it,” so I started with carbo-pem-bev (carboplatin-pemetrexed-bevacizumab) at the local clinic.
I didn’t know what I was asking for. We had to do it overnight. It was a long night, but I took it like a champ. I had the most angelic nurse that night. She was amazing. It was her first time treating me and it was my first time going through such an ordeal.
Crizotinib
Something in my gut said to go to the University of Michigan. When I got there, they said, “We have an inhibitor we want you to try. It’s promising and we want you to start that in April.” That’s when I started crizotinib.
AT13387 Clinical Trial
I joined a clinical trial of AT13387 (HSP90 inhibitor) times two cycles with concurrent crizotinib. I didn’t feel right with that one. I did everything that I was asked to do during the trial, but I withdrew due to significant diarrhea.
In the middle of the night, I would have to drink oral electrolytes quickly enough to stop the spasms. They were out of control. It was a couple of days or so after the cycle. I lived through that and didn’t like it at all. It didn’t give me a good quality of life. After I came off of it, I felt a little bit better, so I was able to enjoy my anniversary around that time.
After withdrawing and feeling a little bit better from the nausea and cramping, according to some scans around the time, there were improvements in some areas. For example, I used to have to do an abdominal CT scan, but I didn’t have to do that anymore, so something got better there, but I didn’t know what. I didn’t have to focus on getting some of the areas scanned.
After the trial, there was some metastasis. The University of Michigan said, “You can’t use crizotinib anymore, so you can stop taking it.”
Alectinib
I waited and had to fight for alectinib. I had to get it approved by insurance so that I could start taking it. The doctor said he was fighting behind the scenes with me to get the insurance to approve it so that I could start taking it. Even though I started panicking, he said, “Shyreece, it’ll be worth the wait.”
Everybody needs to understand what biomarker testing is and how to read certain test results when they come back.
Treatment Decision-Making
When I hear clinical trials, I hear another opportunity to step out in faith. At first, I didn’t want another clinical trial. I would have to be on my deathbed and have 24 hours to live before I do another clinical trial, but that’s not where I’m at right now. I’ve changed. I’m thankful I’ve had 10 years and kept up with enough.
Whatever decision I make, I’m not going to waver on it. I’m solid in my faithfulness. I’m going to make it knowing that this is what I’m choosing today. I hope that this encourages somebody else to live their best life with no fear. I’m not going into any trials with fear. It’s another opportunity to live my life with faith.
Somebody can benefit from me. I need them as much as they need me. I give love to people who need it and the relationship that they have with me, so I’m going to be present and I’m going to live.
Let the medicine do what it’s going to do, but know that it’s not everything. Whatever regimen I’m doing at the moment is what works best. That’s what I keep telling myself.
Biomarker Testing
Something told me that I did not have regular lung cancer. Nothing made sense to me and yet I was this close to dying. Everybody needs to understand what biomarker testing is and how to read certain test results when they come back. When I looked into it, I learned that there were different types of lung cancer. It opened up a whole new window of options.
In my situation, it seemed like biomarker testing was already done but the results weren’t disclosed to me. The test that the hospitalist sent out had some information in there. Stanford didn’t do a repeat biopsy. They trusted all the records from the University of Michigan. When they looked at them, they highlighted: stage 4 ALK, rearranged bronchogenic. That’s when I first heard those terms.
Six years went by before I found out what biomarker testing was. I learned that through LUNGevity, who heard about me through an ALK-positive online cancer group. The doctor at Stanford said, “Shyreece, have you heard of the ALK Positive group? Look them up. I heard that they just had their first summit.”
I started digging. Then-president Gina Hollenbeck and I started conversing. Sad to say, she’s no longer here. She lived eight years with the same cancer that I have. I have a lot of stories about the loss of friends with the same biomarker. That’s how I started talking about biomarker testing and doing a lot of the advocacy work that I’m doing now.
We have to be empowered. For patients who are getting these diagnoses, self-advocacy is a must.
Message to Other Patients & Care Partners
We have to be careful with the words we use regarding remission. The CT scan showed no evidence of disease. Friends and family even thought I was healed because I looked good and didn’t look like I had cancer. I’m so sick of hearing that. I don’t even have the energy for it anymore.
We have to be empowered. For patients who are getting these diagnoses, self-advocacy is a must. If you’ve been shy all your life, then you better grow out of it. I had to grow out of it and quickly.
I moved around all these clinics and doctors, and all of them didn’t want to have a meeting to see what was going on and what was best. I had to piece everything together. Advocate for yourself. You become a self-advocate when the flame of other voices lights you. What are you advocating? Who are you advocating for? What gives you strength and power? Nine times out of ten, it will come from something else that motivates you.
This is the time to just really lock in and go all in. This is war.
Advocating for Yourself
I always say when you’re advocating, get yourself locked arms. I love watching some war movies, like the movie called, “300.” I love it when they get ready to go to battle. Come on, they lock…formation, and then you can see them taking their shields. It’s in front of them. They locked in and they’re ready to go.
When you get ready to advocate, who are you locked in with? Find a group of folks who you can lock in with. This is not for the faint of heart. This is the time to just really lock in and go all in. This is war.
I have made it no secret in my faith. Now, there were some people in the beginning. They knew me as Sister Pompey, Sunday School teacher, and all this. But when I got a diagnosis, they were like,”Where is your faith now?”
I did take a tumble. I did take a hit, but I’m gonna tell you right now, I wouldn’t take [anything else] for my journey now. Look, if I die, I am the Lord’s and if I live, I am the Lord’s, so whether I live or die, I am the Lord’s. I’m going from life to life. I’m going to live my life.
I know this is not Scripture, but Gandhi said learn as if you’ll live forever, so maybe that’s why I keep reading all these reports and stuff. I’m going to learn as if I’ll live forever, but I’m going to live as if I’ll die tomorrow.
I’m living it all. I’m leaving it all out on the field today. Everything that was ever given to me, I’m giving it all, give it all, give it all. I’m not holding nothing. When I go to bed tonight and I’m [worn] out and I’m tired, I don’t have time for depression. I’m too tired.
You’ve got to connect to something bigger than yourself. That’s all I’m saying.Let the medicine do what it’s going to do, but you just know it’s not everything.
I do want to say for you or anybody else who’s watching, please, one of the things that I look for, I love giving back and I love sharing my story and my journey. [Here’s] a link to my book. It’s on Amazon — Fruititude: Growing Spiritual Virtues Through Adversity. I’m always giving back to children and families, so any way that you can support, that would be great and I would really appreciate it.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Stephanie Chuang: My name is Stephanie Chuang. I’m the founder of The Patient Story. The genesis of The Patient Story was my non-Hodgkin lymphoma diagnosis at 31 years old. I remember how overwhelmed I felt and didn’t even know what questions to ask my doctor. What do I do? Where do I go? But it was more like what do we do? Where do we go? Because as we all know, a cancer diagnosis impacts so much more than the patient.
We know there are so many things to consider, but I believe the core of what can make a difference is empowering ourselves to be more active in our care. I’m so thankful for advocates in every form, including other patients, care partners, and healthcare providers who invest so much time and energy in ensuring that we get the best care and know what clinical trials may be an option for us and not as a last resort.
This program is produced by The Patient Story in collaboration with The Leukemia & Lymphoma Society, an incredible advocacy organization that has free resources for patients and care partners in blood cancers, and an organization that has supported more than 85% of blood cancer treatments approved by the FDA to date.
As with all our programs, The Patient Story retains full editorial control over the content.
While we hope you learn a lot, it is important to note that these discussions are not a substitute for seeking medical advice, so please speak with your own medical team about what’s most appropriate for you.
Our patient moderator is Dr. Robyn Stacy-Humphries. Not only is she a long-time respected physician in the Charlotte area, but she is a three-time DLBCL patient and survivor, and someone I’m lucky to consider a friend. I admire her so much for the advocacy work that she does as a physician and now as a patient advocate. Robyn, thank you so much for joining us and leading our discussion.
Robyn Stacy-Humphries, 3x DLBCL Survivor
Dr. Robyn Stacy-Humphries: I’m Robyn Stacy-Humphries, a three-time diffuse large B-cell lymphoma survivor. I’m one of the first patients in the United States who received CAR T-cell therapy in 2016.
Nilanjan Ghosh, MD, PhD
Dr. Nilanjan Ghosh: I’m Nilanjan Ghosh, the head of hematology at Levine Cancer Institute at Atrium Health. I also lead the lymphoma division. It’s a real pleasure to be here to discuss DLBCL as well as follicular lymphoma with my colleagues.
Kulsum Bano, MD
Dr. Kulsum Bano: I’m Kulsum Bano, a community oncologist who works at Levine Cancer Institute. It’s a privilege to take care of patients with lymphoma and an honor to be here to talk to everyone. Thank you.
Justin Favaro, MD, PhD
Dr. Justin Favaro: I’m Justin Favaro, a physician, medical oncologist, and hematologist in Charlotte, North Carolina. I’ve been in private practice for 18 years. I see a wide spectrum of different types of cancer, with a special interest in malignant hematology, lymphoma, and leukemia. I love the science of this disease and the technology, and I love to learn more from you all as we try to tell you what we know about this disease. It’s a pleasure to be here.
Diffuse Large B-cell Lymphoma (DLBCL)
Robyn: Diffuse large B-cell lymphoma is the most common of the non-Hodgkin lymphoma types. It is very aggressive and, without treatment, most people’s survival rate is only one year.
We are also going to talk about follicular lymphoma. There is some overlap, but follicular is an indolent lymphoma. People may present or be asymptomatic. It can progress rapidly or it can last for years. DLBCL and follicular lymphoma are managed differently.
First, we’re going to talk about diffuse large B-cell lymphoma. Dr. Favaro, what are the current treatment options for diffuse large B-cell lymphoma when a patient is first diagnosed? What you do with your patients?
Current Treatment Options for DLBCL
Dr. Favaro: Before I talk about this disease, try to imagine a cancer cell as a ball. It’s a little simplistic, but if you think about a ball, in the middle of the ball is where all the DNA is. The DNA is the recipe for what makes a cancer cell what it is. There are 30,000 genes. This DNA in the middle of that cell is making all these proteins that make that cancer cell grow and make it do what it does in your body.
On the inside part of that ball are all these proteins. We’re going to talk about some of these proteins. These proteins circulate around the inside of that cell and make the cancer cell grow.
On the outside of that ball are spikes. There are different types of spikes on the outside of the cell. They’re called receptors. We can use those spikes and target cancer cells with our treatments.
CHOP
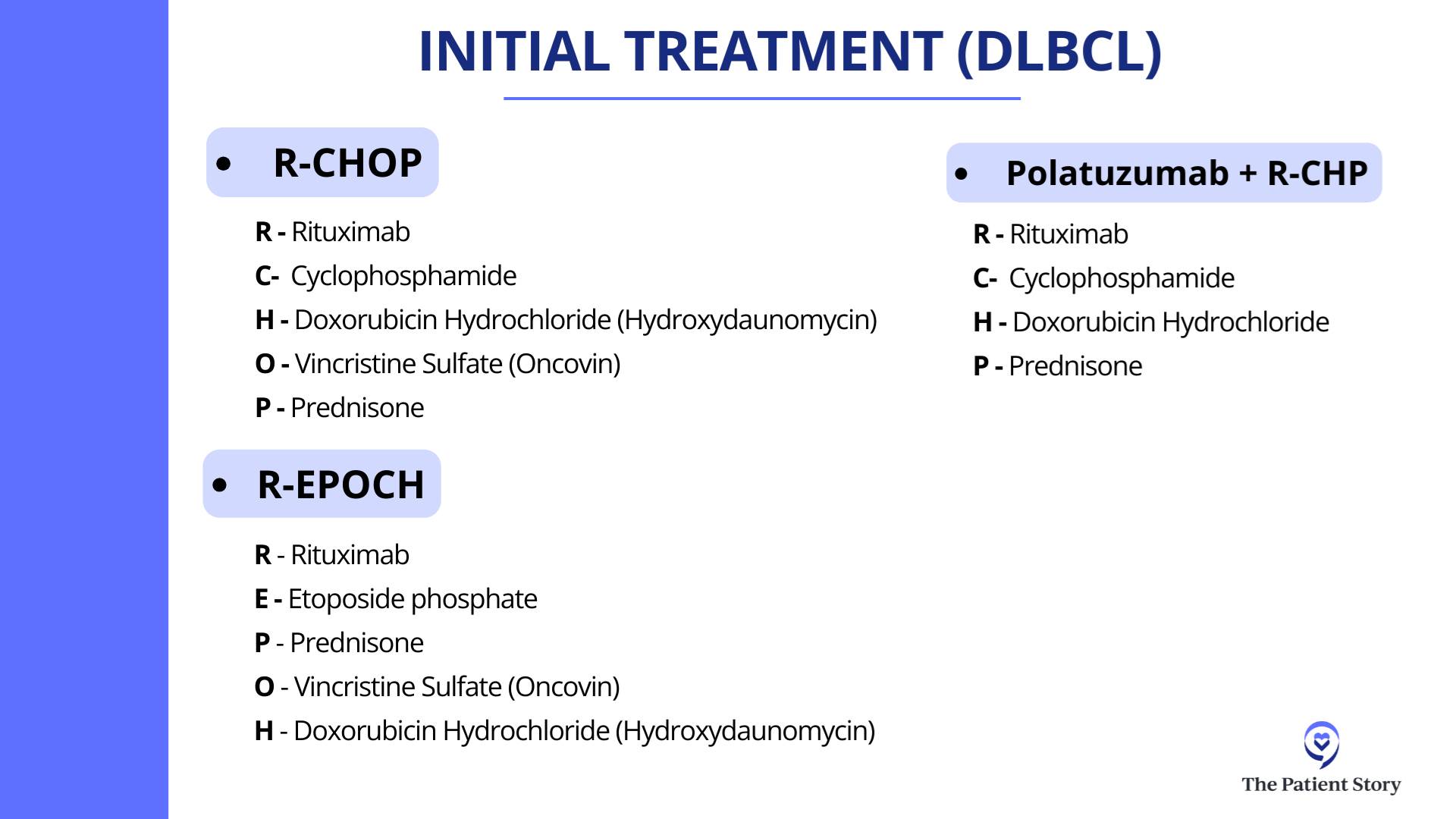
Dr. Favaro: The initial treatment for lymphoma goes back to 1976 when a combination of different chemotherapy drugs was first approved. CHOP is a combination of three different chemotherapy drugs (cyclophosphamide, doxorubicin hydrochloride, and vincristine sulfate) along with prednisone. Back in the 1970s, we were giving chemotherapy that attacked and killed all these fast-growing cells. It wasn’t targeted to spikes or proteins.
R-CHOP
Dr. Favaro: About 20 years ago, we discovered rituximab, which is a targeted therapy. It’s an antibody, a Y-shaped molecule that targets CD20, which is one of the spikes on the outside of the cell. We found that this is a great advance in cancer treatment.
If we added rituximab to all that chemotherapy, patients did better. They lived longer and had a much better chance of going into remission. R-CHOP has been the standard first-line treatment for diffuse large B-cell lymphoma for over the last 20 years.
pola-R-CHP
Dr. Favaro: Finally now, we have a new drug called polatuzumab vedotin, another targeted treatment and Y-shaped molecule. This time, it binds to CD79.
Polatuzumab vedotin added to rituximab, which hits CD20, and two different chemotherapy drugs plus prednisone (pola-R-CHP) is the new standard of care for the treatment of diffuse large B-cell lymphoma. Studies have shown that the response rate and survival is about the same versus the old regimen, but it looks like at two years, the remission rate is better if you take the new regimen of pola-R-CHP. This is the newest treatment for this disease.
Treatment Options for Relapsed Patients
Robyn: Unfortunately, even with these advances and the durable remission rate of 80% or so with the current therapy, there’s 20% where it doesn’t work. Patients will relapse very quickly. Dr. Ghosh, what happens in these patients whose initial therapy fails? What do we have to offer them now?
Autologous Stem Cell Transplant
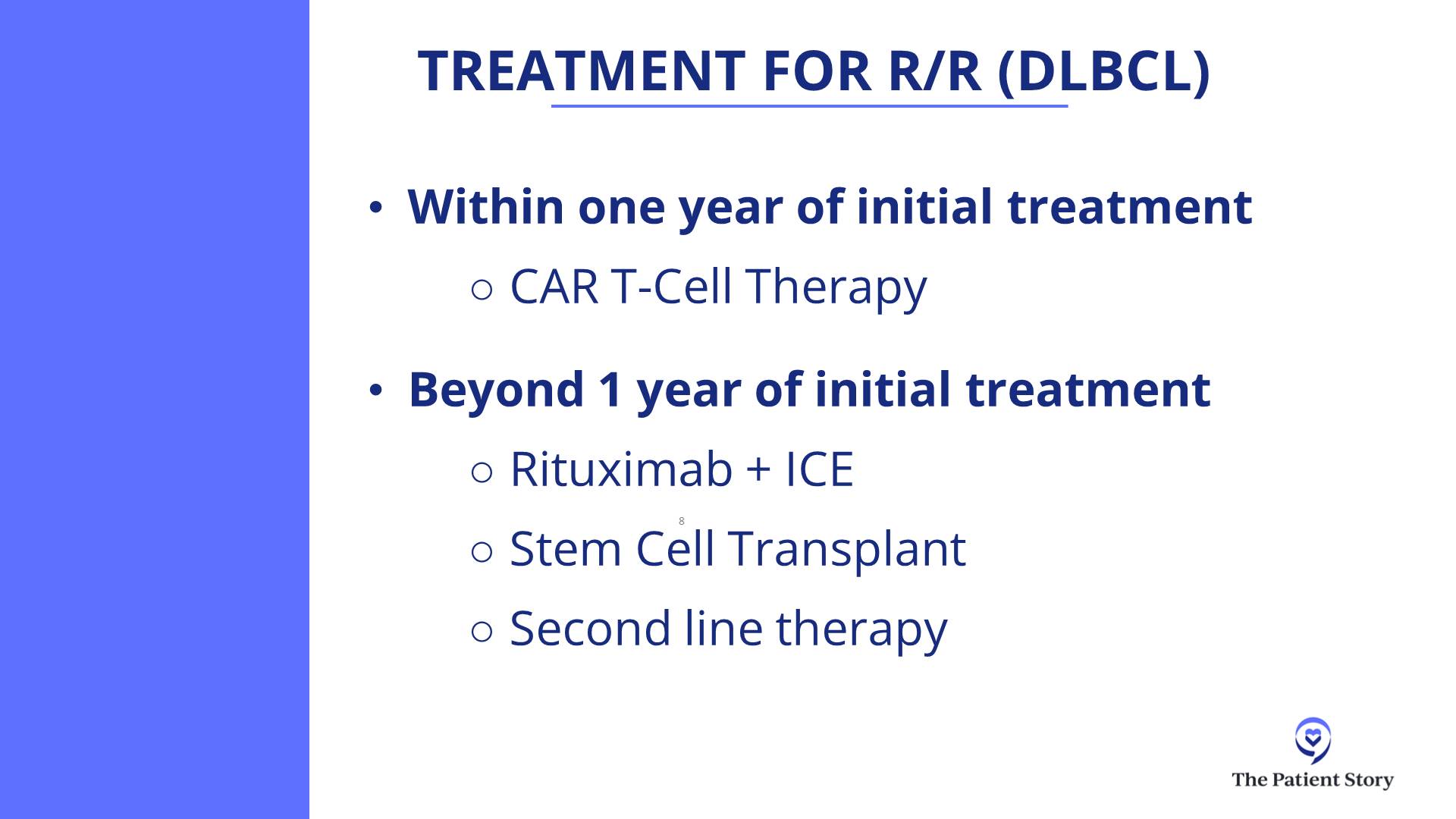
Dr. Ghosh: In the past, the standard for patients who are eligible for an autologous transplant would be to get salvage chemotherapy, like RICE (rituximab, ifosfamide, carboplatin, and etoposide), R-DHAP (rituximab, cisplatin, cytarabine or cytosine arabinoside, and dexamethasone), or R-GDP (rituximab, gemcitabine, dexamethasone, and cisplatin).
If they are chemosensitive, meaning the tumor shrunk with chemotherapy, then they would go for an autologous stem cell transplant, which is high-dose chemotherapy followed by giving them their own stem cells back.
CAR T-cell Therapy
Dr. Ghosh: As immunotherapy advanced and as we learned more about ways to harness the immune system to fight against cancers, this was applied to diffuse large B-cell lymphoma and a novel treatment came about: CAR T-cell therapy.
Initially, it was approved after two prior lines of therapy. Patients would have had to gone through a transplant and if the transplant failed, they would get CAR T-cell therapy, or if they got chemo and then got CAR T-cell therapy as the third-line treatment. But then knowing that it was very powerful even in the third-line setting, there were some randomized clinical trials directly comparing it with transplant.
In the second-line setting, we are thinking a lot in terms of CAR T-cell therapy, reserving transplant for patients who relapsed late but are transplant candidates.
Dr. Nilanjan Ghosh
There were three large, randomized phase 3 studies that compared efficacy and toxicity of CAR T-cell therapy with that of autologous transplant. Two of those trials were positive in terms of ensuring that the primary endpoint, which was free of disease, progression-free, or event-free survival, was better compared to transplant. One of those studies actually showed overall survival was also better compared to transplant.
The current standard of care if somebody was refractory to front-line chemotherapies, like R-CHOP, pola-R-CHP, or R-EPOCH, or if they have relapsed within one year, the second-line therapy would be CAR T-cell therapy.
One of the CAR T-cell therapies called liso-cel was also used for patients who were not eligible for transplant, like older patients. Patients could get liso-cel as a second-line therapy if they had late relapse but were not considered to be transplant candidates, like if they had some organ dysfunction which would preclude them from getting a transplant.
In the second-line setting, we are thinking a lot in terms of CAR T-cell therapy, reserving transplant for patients who relapsed late but are transplant candidates. They could get salvage chemotherapy. If chemosensitive, go for transplant; if not, then still go for CAR T-cell therapy.
Follicular Lymphoma
Current Treatment Options for Follicular Lymphoma
Robyn: Follicular lymphoma is actually very common. It’s managed in the outpatient setting and Dr. Bano has seen quite a few of these cases. How do you manage these patients in your clinic?
Dr. Bano: I agree, it’s very common to see follicular lymphoma. It’s a different kind of disease process compared to DLBCL in the ways that patients present. It’s not the typical storm of symptoms that you expect with DLBCL. Follicular lymphoma tends to be slower-growing and presents in a way where most patients are even asymptomatic on initial presentation. They’ll have scans for something else, we’ll find enlarged lymph nodes, they’ll have biopsies, and that’s how we find it a lot of the time.
The way to approach treatment is a little bit different when you compare it to a more aggressive lymphoma like DLBCL. Sometimes, we’re thinking about stages like we generally do with lymphoma. The treatment differs based on what stage you are.
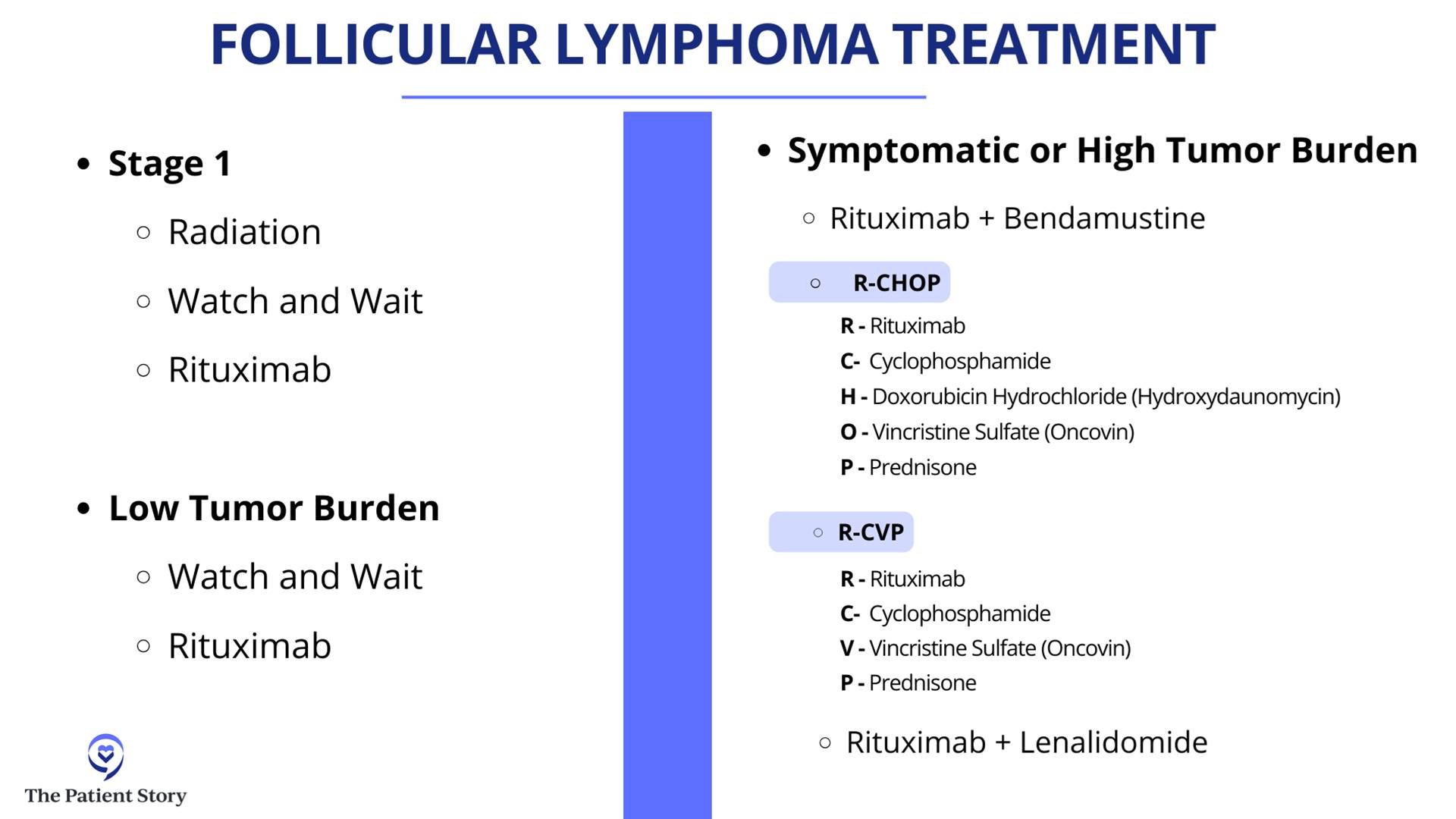
If you have a localized group of lymph nodes that are involved, a lot of times, if patients are asymptomatic, we watch and wait. Sometimes, if they have symptoms from a bulky lymph node enlargement, they can get radiation. A lot of times, we’ll combine that with CD20 monoclonal antibodies, as Dr. Favaro very nicely explained, that target these lymphoma cells directly. That is usually the option in limited stages of disease, like stage 1 and stage 2.
As we approach further spread out disease like stage 3 or stage 4, a lot of folks are asymptomatic and have a low burden of disease. We tend to watch and wait. That’s still an option.
Because of the indolent nature of follicular lymphoma, there’s a chance that it may come back, but we try to treat it and keep it in under control for as long as possible with milder therapies.
Dr. Kulsum Bano
Broadly, follicular lymphoma also is divided based on its grade. Not all follicular lymphoma comes equally. Some of the cases are lower grade, meaning the cells that are involved are not as actively dividing and do not appear as aggressive. For those patients, we tend to steer more toward the watch and wait and low tempo of therapy.
The more aggressive varieties, like the grade 3s, which is divided into 3A and 3B, we look more toward the DLBCL kind of treatment because these tend to act like a more aggressive lymphoma. In that scenario, we look more at chemotherapy plus immunotherapy, like R-CHOP. That usually tends to be the front line of therapy for follicular lymphoma.
It’s very varied. It’s a broad spectrum depending on stage as well as grade, but it tends to be a slow-growing disease in general. For those who get front-line treatment, some get even rituximab with bendamustine. Not everyone needs multi-agent chemotherapy.
A lot of times, we do a finite amount of chemo and follow it up with rituximab maintenance for up to two years. Every eight weeks, they get a rituximab infusion and that keeps patients in remission for a long, long time.
But as we talk about the difference in the nature of the two diseases, follicular versus DLBCL, there is also a difference in the treatment goals for these diseases. DLBCL is more aggressive and, as we were discussing earlier, we talk about a curative approach. Because of the indolent nature of follicular lymphoma, there’s a chance that it may come back, but we try to treat it and keep it in under control for as long as possible with milder therapies.
Treatment Options for Transformed Follicular Lymphoma (tFL)
Robyn: As a radiologist, there are a lot of CT scans and PET/CT involved where you monitor the lymph nodes. Unfortunately, even when someone’s in remission for two years, even after 10 years, it can come back aggressively. Dr. Ghosh, what do you do with a follicular lymphoma that is aggressive, has failed all treatments, and has transformed into diffuse large B-cell?
Dr. Ghosh: The first thing to think about when follicular lymphoma comes back is when it comes back. If it comes back within two years of front-line chemo-immunotherapy, then it’s considered to be progression of disease in 24 (POD24). Even if it has come back as follicular lymphoma, it’s a more aggressive variant. In long-term studies, the survival for that type has not been good. Many research studies have focused on this POD24 group to see what treatments would be effective.
The second thing to think about is: what does it come back as? As we discussed, follicular lymphoma can come back as low-grade follicular lymphoma, so grade 1, grade 2, or grade 3A.
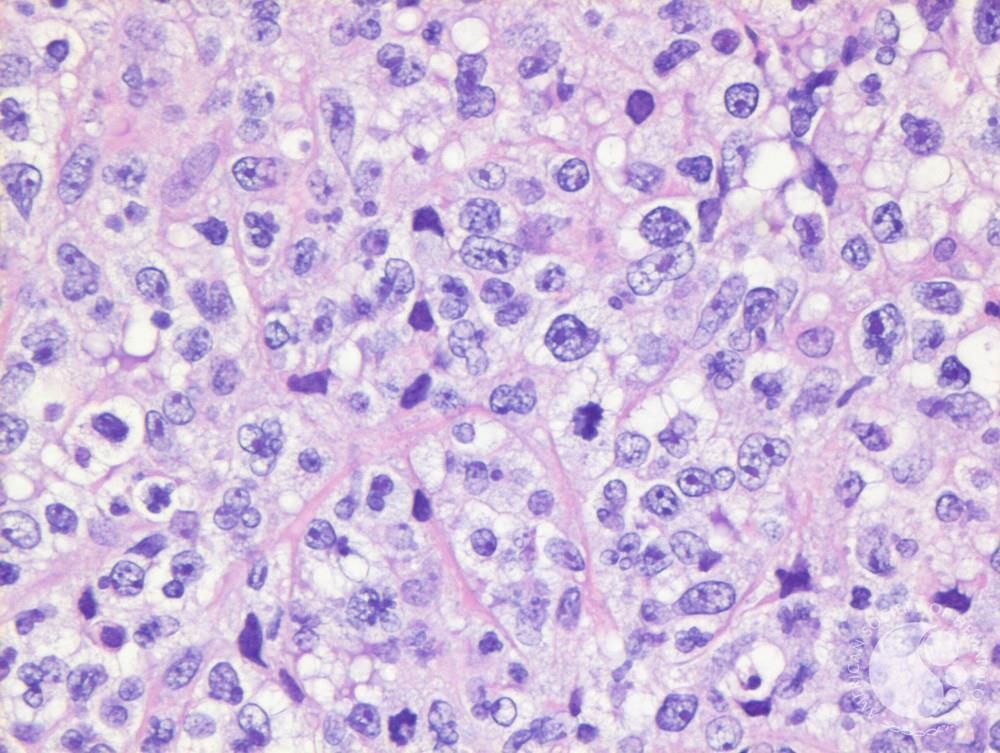
Robyn: That’s based on pathology or the way it looks under a microscope.
If it’s aggressive B-cell lymphoma, then the treatment would be more like DLBCL. If it’s low-grade follicular lymphoma, you would treat more like the low grades.
Dr. Nilanjan Ghosh
Dr. Ghosh: When it comes back, it’s important to get a PET/CT scan and try to biopsy the most aggressive lymph node. A person might have multiple lymph nodes and if you only biopsy one, it could be low-grade follicular lymphoma. You don’t want to miss another lymph node with a high grade because the treatment would differ.
Convenience is important and sometimes a very bright lymph node may be in an inaccessible site, which makes it challenging. Try to biopsy the most active lymph node. If it’s aggressive B-cell lymphoma, then the treatment would be more like DLBCL. If it’s low-grade follicular lymphoma, you would treat more like the low grades.
PET scans are good, but the biopsy is where the money is, so put it under the microscope. Let the pathologist tell us what it looks like and then we can decide what to do.
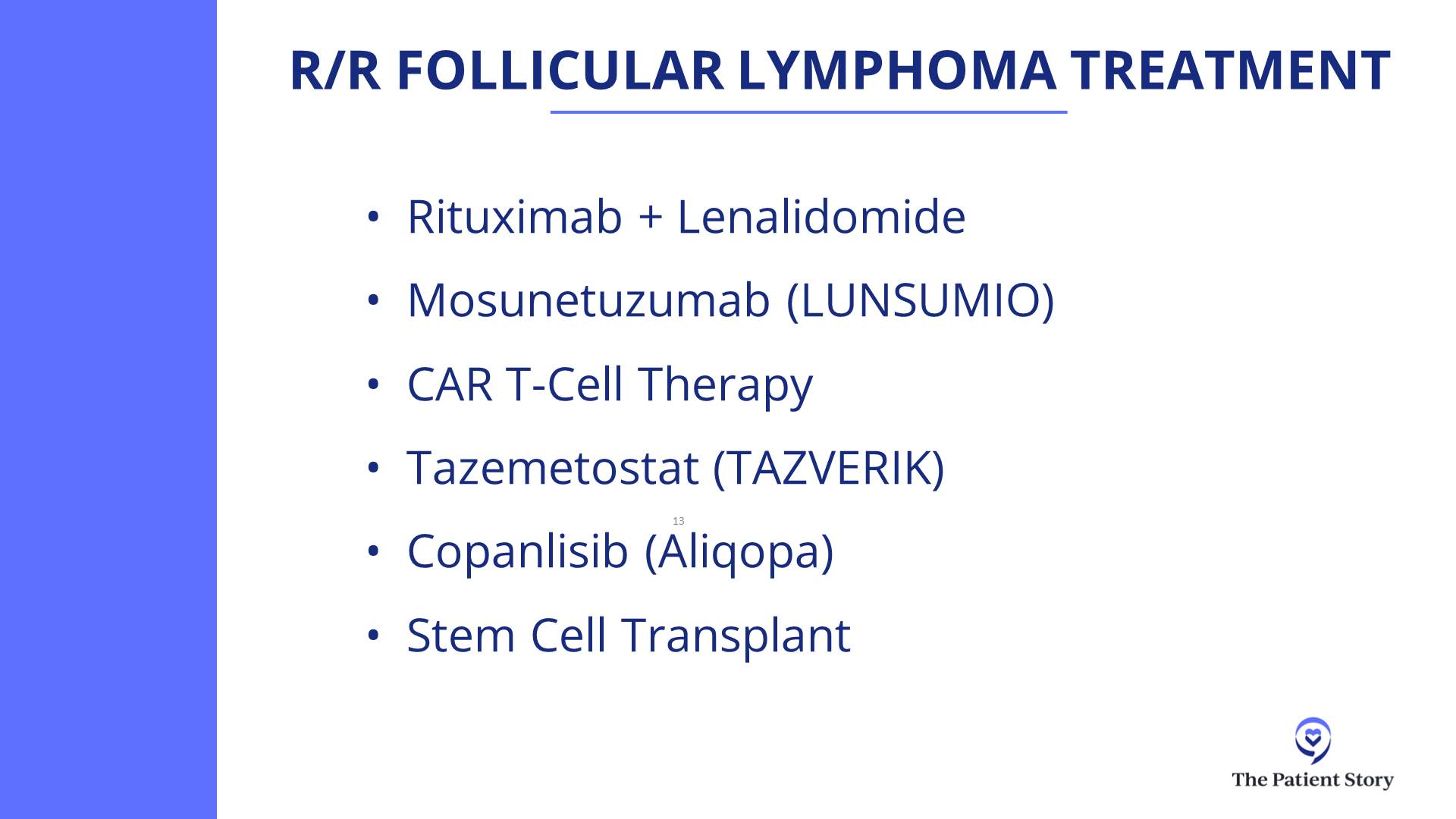
In general, if it is follicular lymphoma, there are many treatment options in the second-line setting. Our commonly used one, if rituximab plus chemotherapy has been used before, is a lenalidomide-based treatment in combination with a monoclonal antibody like rituximab or obinutuzumab.
Subsequently, CAR T-cell therapy has been very effective in follicular lymphoma. Bispecific antibodies are also approved and very effective in follicular lymphoma.
In follicular lymphoma, the disease can relapse 10 or 12 years later… CAR T-cell therapy has not been around for that long.
Dr. Nilanjan Ghosh
CAR T-cell Therapy for Follicular Lymphoma
Robyn: Follicular lymphoma traditionally has been viewed as incurable. But with CAR T-cell therapy, there is now possibility of a cure. Is that correct?
Dr. Ghosh: Yes, there is a possibility. The only long-term follow ups we have with follicular lymphoma being curative is allogeneic transplant, which have been around for decades. Follicular lymphoma can come back. DLBCL typically doesn’t have late relapses. There can be some, but usually relapses occur early. In follicular lymphoma, the disease can relapse 10 or 12 years later. What that implies is that you would have to follow people for more than a decade or perhaps even two decades to be sure that the disease doesn’t come back.
CAR T-cell therapy has not been around for that long, so we don’t know for sure, but there are hints though. We now have data that patients who were POD24 (patients who had front-line chemotherapy and their disease came back within 24 months) got CAR T-cell therapy and their disease hasn’t come back even beyond two years, which means the second-line treatment was more effective than the front-line treatment. This typically doesn’t happen in cancer. If that is there, then you’re overcoming the bad disease biology.
If it doesn’t come back after 5 years, after 10 years, and after 15 years, with follicular lymphoma, that’s when we’ll know. With DLBCL, you can have quicker readouts because if it doesn’t come back in two, three, or five years, then you’re likely cured.
Robyn: We have a CAR T-cell therapy online support group and we have several patients who had follicular lymphoma and who are 4-5 five years out from CAR T-cell therapy and in remission, so it’s very encouraging.
Bispecific Antibodies
Robyn: Moving on to exciting new treatments, Dr. Favaro, would you talk about bispecifics? What’s been approved and how do they work?
Dr. Favaro: Bispecifics are a fascinating field of medicine. The first bispecific that was approved was blinatumomab, which was approved for acute lymphocytic leukemia (ALL).
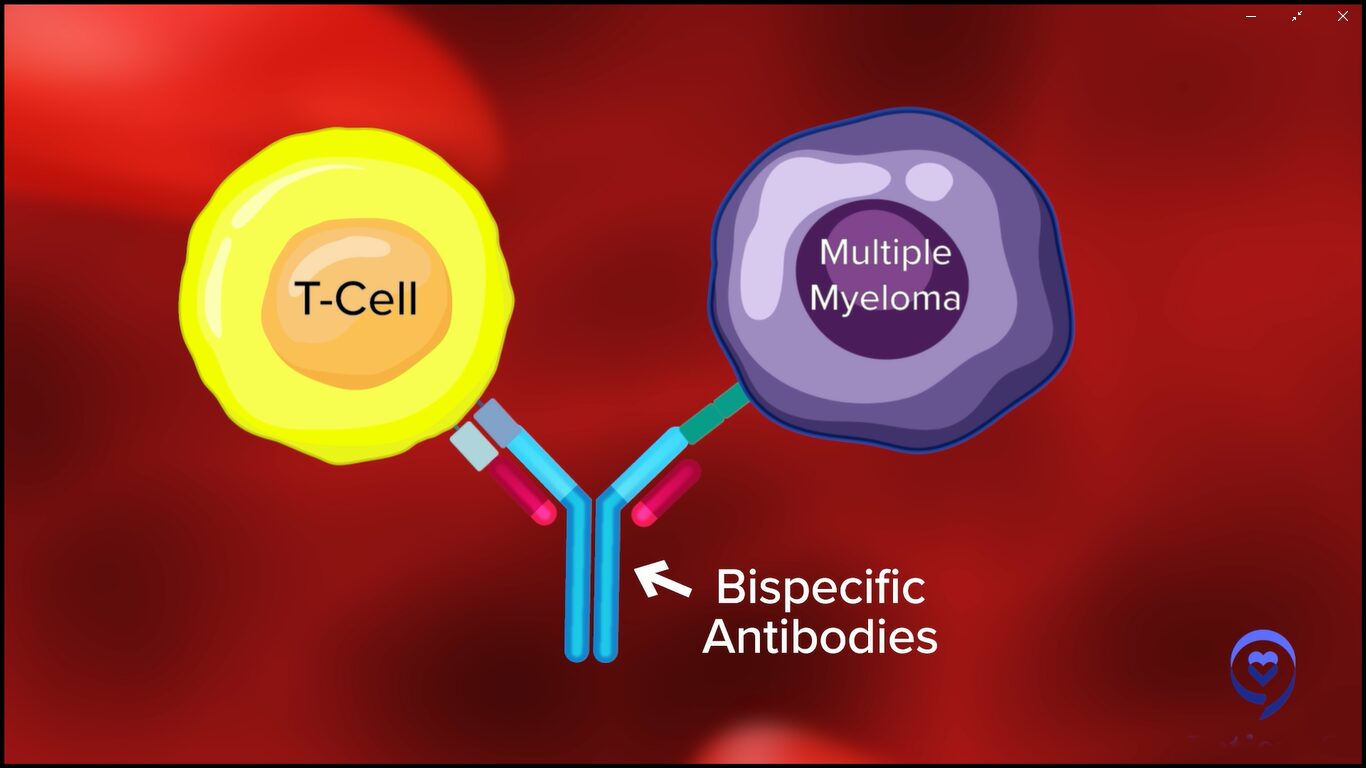
It’s a very small, V-shaped molecule. One part of the V would attach to your T cell, the other part of the V would attach to your cancer cell, and it will bring them together so the T cell can kill the cancer cell. If you flood your body with these, you can bring all the cancer cells next to your T cells and get a lot of death of the cancer cells.
We still use it for acute lymphoblastic leukemia. The problem with that molecule is that it has a very short half-life. It’s a small molecule and it would be degraded quickly, so you have to use continuous infusion and treatments in the hospital.
Over the last few years, they’ve developed better molecules that are more stable. Instead of a V shape, it’s actually a Y shape. The long part of the Y stabilizes that protein so it doesn’t degrade so quickly. These Y-shaped proteins still do the same thing, bringing the cancer cell next to the T cells, and they are now available for patients with lymphoma.
Epcoritamab
Dr. Favaro: There are two that are approved for diffuse large B-cell lymphoma patients who have had at least two prior treatments. One is called epcoritamab (EPKINLY). It’s a subcutaneously administered drug that attaches to the T cell and the cancer cell, bringing them together.
They’re seeing very high response rates in the 60% range and almost 80% in some cases, where for 80% of the patients that take this drug, their lymphoma shrinks down and up to 60% will have a complete response where their lymphoma completely goes away.
It’s a great new treatment. However, when you do this, you get a lot of release of cytokines and proteins in the body and they can cause side effects, almost like you have the flu or a fever, and can even get worse. Sometimes, you can have low blood pressure. We have to be very careful about how we dose these treatments.
We start with a low dose once a week and gradually bring the dose up. The side effects usually happen in the first month or so. Once you get to the higher dose level, then you’re basically taking an injection once a month.
Glofitamab
Dr. Favaro: There’s another drug called glofitamab. It’s a very similar molecule that does the very same thing, except it’s given intravenously. We step up the dose of the treatment over a period of a month and then the patient gets IV therapy every three weeks. It’s a limited duration of treatment. For that particular drug, it’s about 12 cycles or eight months of therapy.
The results we’re seeing with these two drugs are that most patients will have a complete response and you can see that being a long, durable, complete response.
Mosunetuzumab
Dr. Favaro: There’s also a BiTE (bispecific T-cell engager) therapy that’s approved for follicular lymphoma as well. This is a drug called mosunetuzumab and is given intravenously in a similar step-up dosage. This is given for a total of either eight cycles if you go into complete response or 17 cycles if you have partial response. We’re seeing great results with that as well in patients who have had at least two prior treatments for either diffuse large B-cell lymphoma or follicular lymphoma.
Robyn: Is this performed as an outpatient?
Dr. Favaro: It’s outpatient. There’s a risk of a severe reaction. In the early onset of the trials, most patients had to be admitted in the hospital after their second treatment or so because when you step the dose up, that’s when these side effects can happen.
The other two drugs can be given completely in the outpatient setting. We have a protocol set up for epcoritamab. You take the injection once a week for the step-up dose of that first month. As the dose is increased, you get steroids before getting the treatment and for three days afterwards. That seems to really reduce the side effects.
There’s a whole lot of education and prevention that goes into preventing and treating side effects immediately.
Dr. Justin Favaro
Side Effects of Bispecific Antibodies
Dr. Favaro: You have to understand these side effects and how to manage them, so we do a lot of education for our patients. Again, most of these side effects happen within the first month.
CRS (Cytokine Release Syndrome)
Dr. Favaro: There are three major side effects of those treatments. One is called CRS (cytokine release syndrome) and that’s where a lot of cytokines are released as the dose is increased. There are certain stages. CRS can manifest as a fever or if it gets worse, you can get low blood pressure and sometimes have to be admitted to the hospital.
We give steroids and, when needed, a drug called tocilizumab. Almost always, we’re able to reverse those side effects, but it’s something we do educate patients about and keep a close eye on.
Dr. Favaro: The second side effect, which is much less common, is called ICANS (immune effector cell-associated neurotoxicity syndrome). You can have neurologic changes, difficulty with thinking or decreased mentation, and some weakness of the muscles. Again, this is very rare, but it’s all about education, watching for that, and treating appropriately.
Infection
Dr. Favaro: The third big one is infection. We do treat with prophylactic antibiotics to prevent infection and sometimes we give IVIG to boost the patient’s immune system if needed.
There’s a whole lot of education and prevention that goes into preventing and treating side effects immediately. It’s amazing to have these drugs as options now for our patients.
With glofitamab and epcoritamab, as more time goes, we are starting to see a flattening of the curve for some patients… we’ll know over time how that looks, but it’s remarkable progress.
Dr. Nilanjan Ghosh
Success Rate of Bispecific Antibodies
Robyn: Dr. Ghosh, what bispecifics are you using and what kind of success have you seen?
Dr. Ghosh: We have all the bispecifics that are approved as well as those in clinical trials. We’ve been using mosunetuzumab for follicular lymphoma and glofitamab and epcoritamab for DLBCL.
For DLBCL, we usually do CAR T-cell therapy as second line. Studies have shown that even if CAR T-cell therapy has failed, patients have a very good response with both epcoritamab and glofitamab. These were phase 2 studies and remarkably had the same complete response rate. Epcoritamab showed about a 40% complete response rate and glofitamab also had a similar complete response rate.
Epcoritamab is subcutaneous, glofitamab is IV. Epcoritamab is given indefinitely until progression or if someone has bad side effects so they stop. Glofitamab, as Dr. Favaro mentioned, is given for 12 cycles.
I wouldn’t say choosing between the two can be tricky. Both have very similar efficacy, but you have to decide which one is going to work for somebody who lives far away and who wants limited-duration therapy.
Rather than focusing on the differences, the 40% complete response rate is the most important thing to take home. CAR T-cell therapy failed many of these patients. We don’t have very long-term data for the high-risk population in these studies who were refractory to previous treatments and yet did well.
With glofitamab and epcoritamab, as more time goes, we are starting to see a flattening of the curve for some patients. There are patients who got complete remission. They may still relapse, but there are some patients who will get into longer remission. We don’t have five-year data from either of the two, so we’ll know over time how that looks, but it’s remarkable progress.
In general, mosunetuzumab has lesser CRS compared to glofitamab and epcoritamab, but is also used more commonly in follicular lymphoma. Again, all these are done in the outpatient setting.
We have been involved in clinical trials combining mosunetuzumab and polatuzumab. A very effective strategy and though not yet approved, many other studies are ongoing.
The other thing we’ve done is combined bispecific antibodies with front-line treatment. We did a clinical trial of taking glofitamab and R-CHOP in the front line and we’ve seen remarkable remission rates.
Robyn: 80%?
Dr. Ghosh: Higher. When you combine glofitamab with R-CHOP in the front-line setting, the complete response rates are in the 80%. In DLBCL, we focus more on complete responses. Partial responses are okay to mention, but they are very temporary, so we want to focus on complete responses. Sometimes a partial response may turn into a complete response.
Clinical Trials of Bispecific Antibodies
Robyn: There are so many new exciting therapies and our panel has submitted some trials for bispecifics that they’re particularly excited about. What are some of these new trials that are revolutionizing treatment for lymphoma?
EPCORE DLBCL-3
Dr. Ghosh: The EPCORE DLBCL-3 clinical trial is looking at patients who are in the front-line setting and are not eligible for anthracycline-based treatments. They would get either epcoritamab or epcoritamab plus lenalidomide. If somebody has congestive heart failure or some cardiac problems that will preclude them from getting anthracycline-based chemotherapy, then instead of doing R-mini-CHOP or R-CHOP, they could get onto this study.
If bispecifics are moved up from more advanced relapsed/refractory treatments to earlier, can we get chemo-free front-line treatments? That is an effort with the EPCORE DLBCL-3 study.
EPCORE NHL-5
Dr. Ghosh: The EPCORE NHL-5 clinical trial is looking at epcoritamab plus lenalidomide in relapsed/refractory DLBCL. It has shown remarkable activity. It has not been directly compared with epcoritamab alone in the same study, but we have results from epcoritamab alone and that is a complete response rate of 40%. With epcoritamab plus lenalidomide, I believe the complete response rate goes up to the 50s and close to 60%.
Lenalidomide is an immunomodulatory drug. Combining an immunomodulatory drug with an antibody, which is also a kind of immunotherapy, we’re trying to focus on harnessing the immune system to fight against the lymphoma.
Glofitamab + Pola-R-CHP
Dr. Ghosh: Another powerful combination is glofitamab plus polatuzumab-R-CHP. As Dr. Favaro mentioned, pola-R-CHP showed improvement over R-CHOP. That has become a new standard. It showed improvement in progression-free survival compared to R-CHOP. If that is the backbone, can we further improve on that? That’s how we have made improvements over time.
CHOP came in the 70s. R-CHOP was approved in 2006 and showed improvement over CHOP. Pola-R-CHP showed improvement over R-CHOP. If we add a bispecific antibody to pola-R-CHP, can it show improvement over pola-R-CHP?
Glofitamab and pola-R-CHP is a study which we have done at the Levine Cancer Institute as well and it’s been done worldwide and has shown amazing effects. I saw one of my patients very recently who was in this study. He had an extremely explosive DLBCL about two years ago and he’s still in remission.
There are a lot of trials for diffuse large B-cell lymphoma that are moving a little bit more away from chemo and going toward these targeted therapies.
Dr. Justin Favaro
Glofitamab + Polatuzumab
Dr. Ghosh: Glofitamab and polatuzumab is another ongoing study. Taking polatuzumab, a CD79b antibody drug conjugate, and combining it with glofitamab showed high complete response rates. Similar studies have been done for mosunetuzumab plus polatuzumab as well.
A lot of these combinations are being done with the common theme being chemo-free. Some have chemo. CHP is chemo and antibody-drug conjugates are also chemo, but antibody-drug conjugates are very targeted chemo. It targets only the cells where the antibody binds to those spikes, so there is much less collateral damage.
The focus is trying to do less in terms of lowering the side effects, improving the efficacy, and improving quality of life and quantity of life. When you put that all together, the field is moving very well toward immunotherapies. I think these are all really good clinical trials.
Robyn: It’s very exciting. For the audience, the most common used anthracycline is doxorubicin, which is also known as the Red Devil. It can cause cardiotoxicity even in young people, who can end up with congestive heart failure at a young age. Other medications used, like cyclophosphamide, can cause neuropathy, which in some cases is irreversible. To move away from these medications and have the same results or better is great for quality of life and very, very encouraging.
Dr. Favaro: These are all great trials. There are a lot of trials for diffuse large B-cell lymphoma that are moving a little bit more away from chemo and going toward these targeted therapies.
Dr. Favaro: There’s another interesting trial combining four different drugs and none of them are really chemotherapy. There’s an oral drug that’s a BTK inhibitor called zanubrutinib, another monoclonal antibody called tafasitamab (MONJUVI), plus lenalidomide and rituximab. Of the four different drugs, two of them are targeting the spikes, one of them is targeting a protein inside the cell, and the lenalidomide is there to stimulate the immune system, the T cells, to grow and attack the cancer.
A newly diagnosed patient with no prior chemotherapy is seeing a very nice response rate. In this particular trial, they started with this and if they went into a complete response, then they got two cycles of chemotherapy and went back on the targeted therapy.
I like the idea of targeting some of these molecules on the outside or the inside, combining it with something that turns the immune system on as a way to eliminate some of those long-term potential side effects from chemotherapy. I think that’s the theme that we’re seeing here.
CAR T-cell Therapy
Robyn: I’m one of the first patients to get CAR T-cell therapy. I’m going to have the experts explain it, but as a patient, I compare it to Pac-Man. You put the T cells in and the little Pac-Man goes over and eats the cancer cells.
CAR T-cell therapy is new. I received tisagenlecleucel in 2016 as a phase 2 trial. It’s been very successful for me and I’m very, very grateful. I was able to go back to work as a physician. I have a great quality of life. Most of my side effects are from the chemotherapy, which did save my life but I wish I hadn’t had those.
This is a great therapy and now, not only is CAR T-cell therapy used for blood cancers, but it’s also being used in trials for solid tumors and autoimmune diseases, such as lupus, scleroderma, and glioblastoma.
Dr. Favaro, can you explain CAR T-cell therapy?
Dr. Favaro: T cells are part of your white blood cells that circulate around your body. They’re constantly looking to treat infection or try to treat cancer and that’s part of their job. Why can’t they kill cancer cells on their own? Because cancer cells learn how to hide. There are certain proteins they can take away from their surface, so your normal T cells can’t find the cancer cells sometimes and that’s part of the reason why cancer cells can grow in your body.
How do we stimulate those T cells and make them angrier and more attracted to kill and attack those cancer cells? In my mind, that’s what CAR T-cell therapy is.
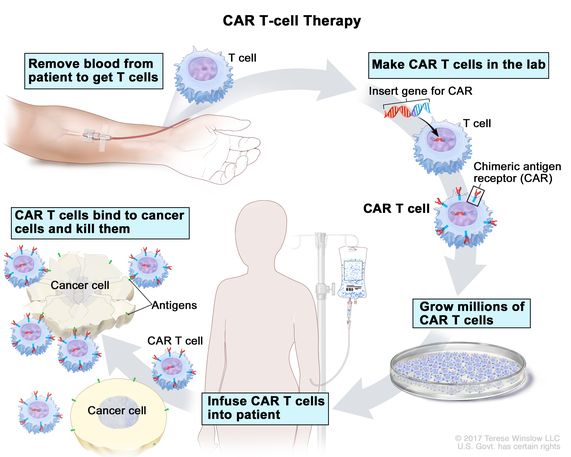
The whole process starts by taking out your T cells. We do that as a part of an apheresis process that happens in the clinic or in the hospital. Those T cells are sent off to a company that will take those T cells and reengineer them in the lab to become CAR T cells. Those T cells that are now transformed will attach to a CD19 spike on a lymphoma cell.
The whole process takes about two weeks. The CAR T cells are infused back into the body. They have this new protein on the outside of their cell called chimeric antigen receptors (CARs). They go into the body and attack the lymphoma cells. It’s pretty amazing technology.
The data shown with diffuse large B-cell is that you can get a 40% long-term remission rate in patients who have had prior treatment but now the lymphoma has come back. Those are amazing results and Robyn is a testimony to that.
The downside is it takes a long time. This is a process and you have to wait. There’s also the issue of insurance authorization. Medicare pays for these treatments, but insurance companies take a long time. You have lymphoma that’s growing in your body and we have to wait to get this whole process done.
It requires you to take other treatments, like lymphodepleting chemotherapy, to control the lymphoma before we can get the CAR T-cell process done. Once you collect the cells, it takes about two weeks to get them back. It could take up to six weeks from the time you meet until infusion day.
There’s a lot of thought about how we can make this process better. The companies that make these products are telling us that 8 out of 10 patients who are eligible aren’t getting CAR T-cell therapy. Maybe they don’t live close to a big academic hospital center or it takes too long and their cancer is growing too quickly.
A lot of the research is focused on making the process faster. Can we create CAR T cells in the lab so we don’t have to go through this whole process? That’s what we’re looking to talk about down the road.
The goal has also been to see if we can lower the intensity and the incidence of CRS and neurologic toxicities.
Dr. Nilanjan Ghosh
Side Effects of CAR T-cell Therapy
Robyn: Dr. Ghosh, you have spearheaded CAR T-cell therapy in Charlotte, did the first cases, and have a lot of experience. I would love to have you talk about the side effects of CAR T-cell therapy.
Patients are terrified of the CRS and ICANS. Meanwhile, they’re not as terrified of a stem cell transplant, which has more side effects. How you do you manage the side effects? What kind of results have you seen with CAR T-cell therapy?
Dr. Ghosh: We have had significant experience with CAR T-cell therapy at our center because we participated in some of the clinical trials, which led to the approval of CAR T-cell therapy. It’s certainly a learning curve on how to manage CRS and ICANS.
When we think about CRS, these are serious side effects, but what’s important is these are reversible for the most part. Some clinical trials report very high rates of CRS and some even with ICANS. Most of these happen early on and within a few days of receiving CAR T-cell therapy.
They are managed with a team of physicians, nurse practitioners, nurses, and pharmacists who are very, very in tune with how to manage these side effects. We also have help from ICU doctors, neurologists, and infectious disease specialists, so it’s a team approach.
Each grade of CRS and ICANS has its own treatment. As the grade goes higher, treatments can intensify. The mortality from CRS and ICANS is extremely low. The reversibility is extremely high.
CAR T-cell therapy is underutilized because of the fear of side effects, but the potency which it has far outweighs the risks associated with it
Dr. Nilanjan Ghosh
CAR T-cell therapy has a 40% long-term remission rate and, more importantly, it’s a one-time treatment. You come in, get three days of lymphodepleting chemotherapy followed by a couple of days rest, get the CAR T cells, and then a week of monitoring for CRS or neurologic side effects. If nothing happens, then you remain outpatient. If they happen, then we treat them and reverse them, then monitor for infection risk after.
The treatments can include acetaminophen, fluids, oxygen, steroids, and other drugs, like tocilizumab and anakinra. What we have seen is by doing these measures and being aggressive in terms of treatment, these side effects are reversible.
The goal has also been to see if we can lower the intensity and the incidence of CRS and neurologic toxicities. There are drugs which can be used. For example, prophylactic steroids can sometimes lower the intensity of CRS and that has already been approved. There are multiple ways, but if you have a team who has been doing it for a while and can react immediately, the side effects can be managed.
Another side effect, which is not very common but very important to address, is macrophage activation syndrome or HLH (hemophagocytic lymphohistiocytosis). Again, that is also managed with medications. We are able to recognize it early by monitoring things like ferritin and other markers as well.
I feel that CAR T-cell therapy is underutilized because of the fear of side effects, but the potency which it has far outweighs the risks associated with it, especially now that it’s been so long and we’ve been able to manage the risks in a relatively protocolized manner.
Be aware of side effects, but don’t be freaked out by them.
Dr. Nilanjan Ghosh
Robyn: My therapy was pretty much outpatient. I think that some of the treatments are drifting toward outpatient until you actually need to be inpatient, which decreases your risk of infection and increases your quality of life. My understanding is that a lot of hospitals are trying to move toward that, but it depends on the type of CAR T and also the patient.
Dr. Ghosh: The patient and caregiver. Another very important thing for CAR T-cell therapy is you need to have a caregiver. If someone is having confusion, you need a caregiver if you’re outpatient to be able to call and say that there’s something wrong.
Even in an outpatient setting, for the initial part, there are very frequent follow-ups, almost daily, so distance from the center can be an issue. If someone lives close by, you can do it outpatient. If someone lives far, it may be hard to go back and forth. We are working very hard to try to overcome barriers to CAR T-cell therapy.
Be aware of side effects, but don’t be freaked out by them. If CAR T-cell therapy is right for you, go for CAR T-cell therapy at a place where they know how to manage these side effects and get the benefits.
The first person to ask about trials would be your physician, but no matter how good the physician, they won’t know about all the trials in the United States and the world. Another resource is ClinicalTrials.gov, which is what my husband and I utilized when we were looking for a trial though it’s a little bit harder to navigate. Trials are accessible, but you have to be your own advocate to some degree.
Dr. Ghosh: For anyone who has barriers to clinical trials, remember that we would not be here today if not for clinical trials. Even CHOP came through a clinical trial, which was started in the early 70s. Everything came through clinical trials.
Robyn: Again, I’m an example. I was one of the first who got CAR T-cell therapy through a clinical trial. I’ve told other patients that sometimes, the best treatment you can receive is through a clinical trial.
Dr. Ghosh: Cancer clinical trials don’t compare a cancer drug and a placebo. They have a well-established cancer regimen and may add one drug to it, but those who are not getting the study drug get the best established cancer regimen. Unlike other diseases where you can get a placebo versus the study drug, this is a serious, life-threatening disease so you’re either getting the standard of care or the new promising drug. If it’s a phase 1 or phase 2 study, everybody gets the same treatment.
Robyn: Ina lot of trials, patients have been through all these standard treatments. They may have had CAR T-cell therapy or BiTE therapy then the lymphoma comes back. What do you do? That’s where these companies are on the cutting edge of developing newer treatments.
Cancer clinical trials don’t compare a cancer drug and a placebo. They have a well-established cancer regimen and may add one drug to it, but those who are not getting the study drug get the best established cancer regimen.
Dr. Nilanjan Ghosh
TRANSCEND FL
Robyn: I know some people who are in the TRANSCEND trial for follicular lymphoma. There’s a lot of people enrolled in that. From what I’ve seen from the data from ASCO, it looks like it’s very successful.
Dr. Ghosh: TRANSCEND FL took patients with relapsed/refractory follicular lymphoma and treated them with liso-cel. It’s been reported and has fantastic efficacy with very high complete response rates in the 90s.
The follow-up is not very long, so that’s one downside, but the FDA is doing a priority review to see if this is good enough that it should get approval in follicular lymphoma. It also has been done as second-line treatment and that has very, very good activity in the second-line setting.
SWOG S2114
Dr. Ghosh: Remember we said that 40% patients with large B-cell lymphoma will get long-term remission after CAR T-cell therapy. What about the other 60%? We always have to think about the people who didn’t benefit. We have a great example of benefit right here, Robyn, but there are others who didn’t.
Complete remission is the most important thing for diffuse large B-cell lymphoma. What about people who get partial remission or stable disease and it didn’t grow? That’s not good enough because within a few months, many of those patients will progress. What if you can intervene before that with bispecific antibodies and polatuzumab?
This S2114 study is a trial which is trying to improve the outcome of patients who are in partial remission or have stable disease by adding drugs post CAR T-cell therapy and trying to see if they would benefit and convert them into complete remission. This is a national trial and we have it open at our site as well.
ELARA
Dr. Ghosh: The ELARA study is looking at tisagenlecleucel for relapsed/refractory follicular lymphoma. This is showing high response rates, low CRS, low neurotoxicity, and durable remissions. Now with three-year follow-up and showing that nearly close to 60% of patients are in remission.
This is a one-time treatment given three years ago and patients are still in remission. Many of those patients are in that POD24 group, where they had progressed within 24 months, so their first remission was two years and now the second remission has been lasting for three years. I hope the remission will last for 5, 7, 10, 15 years, but only time will tell. That’s where whether it’s curable or not will come in for follicular lymphoma.
A lot of companies are developing CAR T cells in the lab that are engineered so they can go in and attack the lymphoma cells, but the body’s immune system won’t attack them and kill them.
Dr. Justin Favaro
Other Clinical Trials
Dr. Favaro: It’s exciting to see CAR T-cell therapy patients in follicular lymphoma and seeing long-term responses. That’s a disease that tends to relapse over and over.
Robyn: People can go on with their life.
Dr. Favaro: The other trials I do like are looking at CAR T-cell therapy patients who don’t have a complete response. Let’s bring in BiTE therapy for those patients as well to try to get them into complete response.
We’re part of a national network of cancer clinics called OneOncology and some of our clinic sites are looking at doing outpatient CAR T-cell therapy. There are different products that are now approved. Liso-cel is one that has the least side effects and is the most predictable.
In outpatient clinics in the OneOncology network, we’re doing CAR T-cell therapies and watching them as an outpatient. They can be watched for four days. It’s pretty predictable that at day four is when a lot of the side effects happen for that particular product.
That’s one example of how we’re moving things more toward the outpatient by monitoring patients while they’re at home. If it’s day four and the patient is starting to have side effects, we bring them in, keep an eye on them for a few days, take care of the side effects, and send them home.
There are a lot of companies developing new CAR T-cell therapies. Why do we need to take the T cells from the patient, reengineer them, and put them back? What about taking regular cells? You can take a culture of human cells and, believe it or not, take stem cells and turn them into T cells in the lab.
A lot of companies are developing CAR T cells in the lab that are engineered so they can go in and attack the lymphoma cells, but the body’s immune system won’t attack them and kill them because these are foreign cells to the body.
One of the other trials happening in the OneOncology network is using allogeneic CAR T cells, meaning they come from a different person. They’re engineered in a way to help your body accept them and see if you can get a response.
Multiple companies are doing this and, in some cases, these are patients who have been through everything. We get a response and a reduction in their lymphoma by using these foreign cells created in a lab. To me, that’s where the future is: looking at this in the outpatient setting and having it ready for the person when they need it.
Robyn: It’s also less costly because it’s technically off the shelf, which should be excellent.
Treatment Sequencing
Robyn: At some of the meetings, people still talk about bispecifics versus CAR T-cell therapy and in which order. We talked about bispecifics after CAR T-cell therapy. Some people are saying bispecifics should be done before CAR T-cell therapy.
Dr. Ghosh: CAR T-cell therapy came first. Outside of blinatumomab, which was for ALL, most of our DLBCL and follicular bispecifics came later. Naturally, by the time bispecifics were available in trials, CAR T-cell therapy had already been around. We know that after CAR T-cell therapy, bispecifics are very active, but what we didn’t know was the reverse.
Recently, a European study was presented and showed that if you use bispecifics before CAR T-cell therapy, you can still get really good activity from CAR Ts. On that study, bispecifics failed a lot of patients so they went on to get CAR T-cell therapy, which was then effective.
In the United States, bispecifics are not approved in the second-line setting, while CAR T-cell therapy is, so undergoing CAR T-cell therapy before bispecifics makes a lot of sense. We don’t have long-term data for bispecifics in the second line but we do have data saying that if it didn’t work, at least CAR T-cell therapy may be able to rescue those patients.
That was a very good study. Overall, we do great in oncology in terms of getting new drugs approved, but we don’t do a great job in sequencing them. That’s left a lot to the physician in discussion with the patient because not everything from the menu is going to be available or accessible right away.
With disease, you may have to do something right away because you can’t wait for six weeks or so to get CAR T-cell therapy. If CAR T-cell therapy is available, then you may want to wait and do the bispecifics later.
In DLBCL right now, I would do front-line treatment of CAR T-cell therapy and bispecific antibodies. In follicular lymphoma, you could do the reverse. It’s a more indolent disease. We don’t know about curability as much. We know that mosunetuzumab works well in relapsed/refractory follicular lymphoma. You have long-term remissions and you could save exa-cel or tisa-cel and, if liso-cel does get approved, then liso-cel for later.
As we are seeing longer data, you have to think: do you want to be on a treatment where you are coming in frequently versus getting a one-time treatment? The treatment where you’re coming in frequently has lesser side effects than the one-time treatment, so it’s a discussion.
Will clinical trials ever be done to answer the sequencing question? I don’t know. I think we’ll learn over time. What will matter is the side effects and the durability of the response. Any response which is durable will be higher in the flowchart compared to the ones where relapse will happen sooner.
Folks who’ve gotten chemotherapy upfront are often left with life-limiting or daily activity-limiting side effects, like neuropathy, so it’s extremely exciting to have this option of chemo-free treatment without long-lasting side effects.
Dr. Kulsum Bano
Possibility of Chemo-Free Cancer Treatment
Robyn: I’ve been in medicine for a long time. When I trained in medicine, oncology was still relatively barbaric, I would say. Chemotherapy and cancer treatments involved cutting, burning, and poisoning. Way back in the 80s, they didn’t even have antiemetics or ports, so giving people doxorubicin was difficult to say the least.
We’ve progressed dramatically. Oncologists have found ways to decrease nausea and take care of neuropathy, but the side effects are still there. Do you see chemo-free treatment of cancer in the future? Perhaps in the next 10 to 15 years?
Dr. Bano: I think that’s the direction we’re slowly heading in. A lot of these trials are slowly moving treatments that were thought to be more exciting and more novel approaches from the fourth to the third, to the second, and then slowly into the front-line setting. That happens over time because the more we learn, the more experience we have with all of these wonderful patients who’ve been on trials and given us this knowledge.
As a community oncologist, that’s extremely exciting because I hope to see patients for years to come who are going to be disease-free and who’ll just be monitored. Folks who’ve gotten chemotherapy upfront are often left with life-limiting or daily activity-limiting side effects, like neuropathy, so it’s extremely exciting to have this option of chemo-free treatment without long-lasting side effects. People are going to live longer with these disease-free intervals. It’s very exciting and hopefully that’s where we’re headed.
Dr. Favaro: I think it’s a combination of things. If you look at chemotherapy, these are chemicals that kill fast-growing cells and that’s pretty good against lymphoma. These often are fast growing, especially diffuse large B-cell lymphoma, so it’s been very active treatments that have put people into long-term remission. But the downside of chemotherapy is the potential long-term side effects plus it’s harder to go through, so what can we do?
Cancer cells are complicated. We’ve got the DNA inside the cell, which has 30,000 genes and over 100 probable mutations in those genes. You’ve got all these crazy proteins in the cell. A lot of them are active and helping the cell grow. Then there are the different spikes outside of the cell.
You have to think about how you attack not just one protein or one spike but multiple targets. A trial I mentioned took a BTK inhibitor and attacked the protein inside and had a couple of drugs attacking the spikes on the outside. That’s probably where we’re going to head to avoid treatments that are so toxic.
Multiple targeted agents is the way to go. For example, with BiTE therapy, we know what happens with those patients. It’s very effective pretty early, but what’s going to happen down the road? Will there be a potential risk of the cancer coming back?
You’re taking the T cell, bringing it to the cancer cell, turning that T cell on, and killing the cancer cell. But over time, those T cells get tired, which is something called T-cell exhaustion, and don’t want to work as well. Sometimes it’s as simple as giving people a break from treatment to let their T cells recover.
But the other thing I think that we’re going to head toward down the road is limited duration therapy but baking something in. You give BiTE therapy, but because we know the T cells can get exhausted, we need to add in another targeted therapy to kill some of those proteins and give 2 or 3 of those for a limited duration. I hope that’s where we end up to finally wipe out the disease for good.
Improving Access to Cancer Care
Robyn: One of the things that all of us as doctors are focused on is access to care. In my case, there was no CAR T-cell therapy offered nearby. My oncologist here had to coordinate with an oncologist who was in a trial in Ohio and my team in Charlotte did a fantastic job. Dr. Ghosh, what do you do in the academic center to reach out to community doctors? How do we improve access to care?
Dr. Ghosh: Late 2017 is when we moved forward with signing up for the TRANSCEND study, which eventually led to approval. Once we signed up for the study, we were the only center in all of North and South Carolina to offer CD19 CAR T-cell therapy before any other center. We got patients from everywhere in that study.
Access is certainly a very, very big issue for CAR T-cell therapy. It becomes even bigger because you need a caregiver. How do we overcome some of the socioeconomic barriers? The caregiver would have to take some time off. Typically, we need patients to be within a one-hour radius, so they would need local housing.
The first part of access is providing education and understanding the benefits of CAR T-cell therapy and referring the patients in a timely manner. It could take up to 6 to 8 weeks to get CAR T-cell therapy, so if you wait for the referral, then it may not be doable because the disease will take off. Early referral is extremely essential for CAR T-cell therapy.
There’s a lot of fine-tuning involved, so the team together with the patient decide what’s best. We try to do this in a really timely manner.
Dr. Nilanjan Ghosh
Patient navigation can be very helpful to help find resources, whether it’s local housing or any type of support. I think that’s essential.
Insurance can be a barrier, especially in terms of single-case agreements, but we are trying very hard. We have a study in which we are looking at the effect of these insurance problems on patient outcomes, so that is a barrier we’d like to overcome. Some barriers are within our control, some are not.
There are ways to control the disease. Giving the right treatment is very important. For example, we have learned that if you give bendamustine, then that can mess up your CAR T-cell therapy. Bendamustine kills T cells, so if you kill T cells before you collect them, then those T cells aren’t going to work. Either you won’t have much or if you have enough, they may not be as functional and not be able to do the job.
What is the right treatment to use if you’re planning to do CAR T-cell therapy? There are so many available. Do you want to modify your regimen somewhere so that you can control the disease but perhaps not kill all your T cells before you collect them? Do you want to wait? But if you wait, then the disease may take off and that may not work.
There’s a lot of fine-tuning involved, so the team together with the patient decide what’s best. We try to do this in a really timely manner. We coordinate very well with all our regional sites within the Levin Cancer Institute as well as beyond.
The bigger challenge is those who live far away. Do they want to come to Charlotte to get CAR T-cell therapy or would they rather not do it because it’s not feasible to come? That’s where eventually having outpatient CAR T-cell therapy done locally comes in and having the expertise to manage the side effects if they happen.
We have more CAR T-cell therapy centers today than two years ago. I hope it keeps getting better and better so that more patients all over get access to this treatment.
We also don’t want to have the treatments in an environment where there isn’t the expertise to manage the side effects because then it becomes very hard. Somebody who came in for a potential curative disorder and perhaps were going to be cured succumbed to the side effect because the team was not able to manage them. That wouldn’t be right either.
The other part of it is coming up with protocols to lower the incidence of side effects without compromising efficacy. This is where the clinical trials of some of the products that have less CRS and less ICANS come in. Not zero, unfortunately. I don’t think we’re going to get there.
Infections can be there, but we know how to manage them. Please communicate quickly so that they can be managed appropriately.
Dr. Nilanjan Ghosh
Robyn: Zero is impossible. What if there are trials at Memorial Sloan Kettering in New York or MD Anderson in Texas? The idea is that people can follow up with their local oncologists.
Dr. Ghosh: After the CAR T-cell therapy. It’s a one-time treatment.
Robyn: That’s what happened in my case. Sometimes you have to go somewhere else for treatment or to join a trial and then do follow-up blood work and scans locally to make it more convenient for the patient.
Dr. Ghosh: The most important thing for CAR T-cell therapy is that there are two side effects that can persist after being discharged.
One thing to watch out for is low blood counts, which is an important one and can persist for a little bit of time. For the most part, that’s because of the lymphodepleting chemotherapy given prior. But sometimes, if patients have had many prior treatments, low blood counts can also be because now they’ve developed MDS (myelodysplastic syndrome) or a pre-leukemia situation.
It’s important to pay attention to the low blood counts to see if it’s getting better or persisting for a very long time, then looking at the bone marrow to see if they have developed something else because there are other reasons for low blood counts other than CAR T-cell therapy.
Second is infection risk. CAR T-cell therapy takes out the B cells because normal B cells also express CD19. You can check immunoglobulin levels and give IVIG. Vaccine responses also go down, so if someone had a vaccine for flu or COVID, they may not be able to respond well, so people become prone to infections.
Patient education is very important as well as letting your doctors know. I always advise patients that if they have a cold or something, reach out to their doctors first. Many times, we would react to it faster. We won’t give a Z pack for a cold. We’ll get them in, get a swab, check what virus is there, and check the immunoglobulin level.
Give them antivirals, if antivirals are available. Give them IVIG, if the IgG is low to help them overcome that infection. Get some imaging needed to see if there’s pneumonia. When the immune system is low and you get a virus and sit on it for some time taking an antibacterial, which is not going to work because it’s not a bacterial infection, it can get worse.
We educate our patients that infections can be there, but we know how to manage them. Please communicate quickly so that they can be managed appropriately compared to some other person who is not as immunocompromised.
Final Takeaways
Robyn: This has been a great discussion. If there’s something you would like to tell the people about diffuse large B-cell lymphoma and follicular lymphoma, treatments, and the future, what final statements would you like to give?
Dr. Favaro: There is so much to learn for patients and doctors. These new treatments come out and it’s our job to learn about them. CHOP came out in 1976. It was our job to learn how to give it and also how to manage any side effects that come up. That’s the same with CAR T-cell therapy.
Quite frankly, 4,000 papers come out every day in health care. There’s a ton of information coming out. We are constantly learning and educating patients about these new treatments.
The cooperation that we have as a community practice with academic centers is very important. When we see patients who need CAR T-cell therapy, we refer them and take them back to help manage potential side effects. The technology that’s advancing to make these treatments less toxic is key. We used to have to admit patients overnight for epcoritamab, for BiTE therapy; now we can do it all as an outpatient. That’s the type of thing that’s happening on a daily basis.
Physicians will never go away. We are here because we know you. We take care of you as a person, but we are going to see more and more about artificial intelligence coming into health care. It’s happening. We do need to look at that and embrace that.
Somebody comes in with lymphoma. What should their treatment be? There are so many different factors: age, personal health, disease, potential treatments, and side effects. It takes a good physician to understand the data. But over time, there probably will be the development of assistance to doctors with artificial intelligence and neural networks that I think will help. There are journals about AI in oncology and I think this is going to be the future for health care as well.
Dr. Bano: None of us in medicine work in a vacuum. It’s a concerted effort getting these patients to the most advanced treatments out there. In the community, our responsibility is to know that these even exist and to maintain that chain of communication with the academic centers to get our patients the care that they need, but we always serve as home base. We give patients the feeling that, yes, we’re sending you away, but you’re always going to come back and we are here to take care of you for years to come.
It’s always been a great collaboration between community and academics, getting that relationship established, and always having that chain of communication to ask questions and get opinions. It doesn’t always have to be advanced therapy. Sometimes you get a challenging case that you want to discuss with someone who has seen something like this before.
It’s very exciting to see what’s on the horizon. It’s exciting to see what we can do for our patients. It’s a learning process. Every day, we learn something new.
In the community, our responsibility is to know that these even exist and to maintain that chain of communication with the academic centers to get our patients the care that they need, but we always serve as home base.
Dr. Kulsum Bano
Dr. Ghosh: I cherish the community-academic partnership. I’ve cherished that over the years. That helps patients to get their treatment locally but also get access to a specialist who treats that disease. When I started, lymphoma treatments were not as effective but were simple. You get the first line, another option for the second line, then after that, there were 1 or 2 options and that’s it.
Now, there are a lot of options. When you have so many options, each with their unique side effects and sequencing is not worked out, how do you know which is best for you? There are so many intricacies. If you use this, then the next treatment could be a problem.
Trying to find the right option, keeping abreast of what comes out, and keeping pace with how this is moving along can be challenging. That’s where the academic-community collaboration can be very good. Patients can always go back to the community to get their treatments, have access to a new clinical trial or the latest treatment, and have really good care.
I encourage participation in clinical trials, knowing that these are ethical and vetted by institutional review boards. That is how we have come to where we are and I hope that we get into more chemo-free treatment options.
Some chemo is still very effective. I would not say anthracyclines have saved many lives. They have been around for 50 years, but if we can achieve our goal with less toxicity and by harnessing the immune system, that would be fantastic.
Robyn: I’m honored to be here. Shout out to The Patient Story and the unique ability of patients to get their voice out and for people to do their research online. As a physician and a former patient, it’s very important to be your own advocate, to research, to ask questions, and to keep your mind open. Sometimes clinical trials are the best treatment, so do consider them.
Consult with your doctor. It’s okay to get a second opinion at some points. Medicine has come a long way. When I first started, there was not much available. The survival rate for non-Hodgkin’s was about 30-40%.
I hope that everyone gets treatment and gets in remission like myself. At that point, you need to live your life. Enjoy your family, travel, work, stay healthy, and exercise. Don’t let cancer define you. It’s part of you, but there’s much more to you, so enjoy life.
You need to be your own advocate. If you feel like something that’s been recommended is not working for you, you have all the right to get a second opinion.
Dr. Kulsum Bano
Q&A
Getting a Second Opinion
Robyn: Joan asks, “What is the polite way to get a second opinion without being rude?”
Dr. Bano: Very rarely are there egos in medicine. As a physician, you try to make the best decision for your patient knowing that there may be something out there that is newer or better. Everyone is entitled to a second opinion and that’s how we learn more.
If somebody comes back to me with a different treatment approach and says somebody else recommended this, that’s something I would definitely encourage. You need to be your own advocate. If you feel like something that’s been recommended is not working for you, you have all the right to get a second opinion. You’re not being rude at all. You’re entitled to that and it’s actually encouraged if that’s what you feel is right for you.
Robyn: I agree. Even in radiology, we get asked for second opinions all the time. Doctors are human. We are not perfect. We can look at the same case and have different opinions. We’re not insulted. We’ve all been trained to work together and I would say that happens 99% of the time. There are always exceptions.
If you look at the commonly used CAR T-cell therapy, the complete response rate is much higher than the complete response rate for epcoritamab.
Dr. Nilanjan Ghosh
Epcoritamab vs. CAR T-cell Therapy
Robyn: Don asks, “I’m on epcoritamab. We considered CAR T-cell therapy, but wouldn’t be able to provide the 24/7 care required. So far, it’s working very well. How does it stack up compared to CAR T-cell therapy?”
Dr. Ghosh: They have never been compared head to head, so there is currently no clinical trial which takes half the patients and gives them epcoritamab and half the patients get CAR T-cell therapy. The best way to compare two groups of patients is if they were randomized on a clinical trial, had similar characteristics, and then followed over time to find out the effectiveness of one versus the other.
If not, you’re comparing across trials and when you do, it’s flawed because the patients who went for epcoritamab may have very different characteristics than the patients who went for CAR T-cell therapy. In fact, many patients who went for epcoritamab on a clinical trial already had CAR T-cell therapy, so how could you compare the effect of CAR T-cell therapy with a drug used for post-CAR T-cell therapy failures?
Having said that, we are left with no choice but to compare across trials. I will say that if you look at the commonly used CAR T-cell therapy, the complete response rate is much higher than the complete response rate for epcoritamab. Epcoritamab is around 40%. CAR T-cell therapy complete response rates are usually in the 50s to 60s.
That being said, it comes down to the 40% number because even if CAR T-cell therapy gets a higher complete response, some people will start relapsing despite getting a complete response. We know that with CAR T-cell therapy, about 35 to 40% people will have long-term remission.
We don’t have long-term data yet with epcoritamab. The complete response rate is 40%, but some of those will progress over time. We don’t know whether it will go down to 30% or 25% as we go up to five years, but we will find out over time.
At this point in time for DLBCL, we feel that CAR T-cell therapy is better, but if it’s not feasible, bispecific antibodies would be the next best option. The important thing is: are you getting complete remission or not? If it’s complete remission, we see long-term sustainability. If it’s not complete remission, then we start seeing early progression.
Epcoritamab is targeting CD20 and CAR T-cell therapy is targeting CD19 — two very different ways of attacking the lymphoma. CAR T-cell therapy is still a great option for those who choose epcoritamab for whatever reason.
Dr. Justin Favaro
Dr. Favaro: Another point is that a lot of patients on the epcoritamab trial had CAR T-cell therapy before. If you have somebody who’s never had CAR T-cell therapy and you had the option of CAR T-cell therapy or BiTE therapy, which one do you choose if you’re eligible for both?
It comes down to logistics and what’s going to be a good fit for you. Keep in mind that if you would need CAR T-cell therapy later, you can still get it because a study at ASH 2023 showed that if even if you had BiTE therapy before, you’re still eligible to get CAR T-cell therapy later.
Epcoritamab is targeting CD20 and CAR T-cell therapy is targeting CD19 — two very different ways of attacking the lymphoma. CAR T-cell therapy is still a great option for those who choose epcoritamab for whatever reason. You can still have a great outcome. It doesn’t necessarily matter how you sequence it.
The hope is that whatever treatment you’re getting works for you and you won’t need anything else. But if you do, there are options available and there will be even better treatments in a few years.
Dr. Nilanjan Ghosh
Robyn: If for some reason this doesn’t work and you decide to get CAR T-cell therapy, a lot of the hospitals have come a long way with helping people get 24/7 care. There are options. Hopefully you won’t need them since epcoritamab is working well, but know that there are things that the hospitals are now aware of and they’re trying to assist patients with those.
Dr. Ghosh: There are many devices coming out for 24/7 monitoring, especially in the outpatient setting. Companies are coming up with devices to monitor your oxygen level, heart rate, and temperature then feed them back to the electronic medical record and create alerts. At least from the standpoint of vital sign monitoring, people are trying to overcome this barrier.
Understand that 24/7 support, even if it is for a short time, is a lot for a caregiver, especially if the caregiver has to work. You can rotate caregivers. You don’t need to have just one. Most places will allow multiple caregivers.
Epcoritamab is a good option if you’re not able to do CAR T-cell therapy. You can still have very long remission and perhaps not need further treatment ever again. The hope is that whatever treatment you’re getting works for you and you won’t need anything else. But if you do, there are options available and there will be even better treatments in a few years. Maybe allogeneic CAR Ts will hit a big wave. We don’t know yet, but we’ll find out.
Dr. Favaro: That’s the advantage of getting BiTE therapy upfront. If you need something later, it may be a lot easier with a lot fewer side effects and it can be done as an outpatient. With epcoritamab, you can get steroids and don’t need to be in the hospital. As we make more progress with CAR T-cell therapy, maybe we can do that as an outpatient to reduce severe side effects. Sometimes there’s an advantage to waiting as the technology advances.
Dr. Ghosh: If it’s accessible, knowing the track record of CAR T-cell therapy and that now we have five-year data, we still like to sequence CAR T-cell therapy before bispecific antibodies. Over time, we’ll find out if things change and do it in reverse.
Remission After Bendamustine & Rituximab (BR)
Robyn: Diana asks, “What is the median length of remission after the first B&R treatment”
Dr. Ghosh: For which disease?
Robyn: I would assume it’s follicular lymphoma, but we don’t know what stage. Let’s assume it’s stage 2.
Dr. Bano: If it’s stage 2 follicular lymphoma, generally you have a sustained response after B&R treatment. We’re looking at about five years or so. We need more information to answer that question appropriately.
Dr. Ghosh: It may also depend on whether rituximab maintenance was used. It could be a little bit different with maintenance versus without. I’ve even seen patients who are 10 years out after bendamustine and have not relapsed. Some people will relapse, so it’s a whole spectrum.
There are treatments now that will attack both follicular lymphoma and the transformed lymphoma, so sometimes you want to harness that.
Dr. Nilanjan Ghosh
Possibility of a Repeat Transformed Follicular Lymphoma (tFL)
Robyn: “If you have follicular lymphoma that transformed into diffuse large B-cell, went into remission after treatment, but a few years later, the follicular lymphoma came back, what is the probability that this will transform again?”
Dr. Ghosh: With indolent follicular lymphoma, there’s a small percentage of transforming every year. As more years go by, that risk accumulates. If it’s already happened, will a second transformation happen? It’s possible, but the likelihood goes down because it’s a random event.
Is it a relapse of the previously transformed follicular lymphoma? That’s hard to sort out, but usually what happens with the transformed disease, if the transformed disease has been in remission for a long time, that’s an aggressive lymphoma and usually, aggressive transformers respond well to whatever the treatments were given to them, especially since long-term remission was achieved.
The likelihood of what comes back is often the indolent lymphoma and we see this sometimes with transplant. I had a patient who had follicular lymphoma, had treatment, had a relapse of the follicular lymphoma, had another treatment, then her lymphoma transformed, and we gave her transplant for that. Years later, the aggressive transformed lymphoma went away and she had a relapse again, but this time, it was back to follicular. The aggressive lymphoma never came back. What we did at the time was CAR T-cell therapy for the follicular lymphoma.
There are treatments now that will attack both follicular lymphoma and the transformed lymphoma, so sometimes you want to harness that. For example, axi-cel is approved for follicular lymphoma and for DLBCL. When you use a treatment like CAR T-cell therapy, you are basically killing both. Ultimately, it’s all coming from one B cell. It may be transformed, but if you attack that B cell clone, then both the low-grade and the high-grade can go away. Similar with bispecific antibodies. They attack both. Many of the treatments we use now, especially some of the more modern treatments, have activity against both follicular lymphoma as well as the transformed component.
The fortunate part about lymphoma is that you can target lymphoma cells. You will deplete your own B cells, but we can mitigate that.
Dr. Justin Favaro
B-cell-based Immunotherapy
Robyn: “CAR T-cell therapy is a great new treatment, but as I understand, it targets all B cells and not just the cancerous ones, leading to a depleted immune system that can last a long time. Is there any current research on a similar immunotherapy treatment than can identify and attack the cancer cells and not the normal B cells?”
Dr. Ghosh: That would be something we would love to have. We are fortunate that we have been able to identify antigens. Dr. Favaro mentioned those spikes. Imagine if those spikes were not only in B cells but in liver cells, heart cells, and kidney cells, then CAR T-cell therapy would go and kill all of those.
Fortunately, this is what we can get away with as CD19 is expressed only in B cells but not in other normal tissues — not even on T cells or other parts of the immune system. Many other diseases don’t have that. We are starting to work with some solid tumors which have these, but it’s been difficult. Even in diseases like acute myeloid leukemia, you don’t have things that are specific to that cell.
With B cells, you’re more prone to infections, but you can still get IVIG, which is a immunoglobulin supplementation to help reduce your risk for infections. We currently don’t have spikes on the surface of just cancerous B cells but are absent on normal B cells, but that would be something which I hope the future researchers can identify.
Robyn: I believe there are studies that show B cell recovery over time. A lot of people will gradually recover and it doesn’t affect their remission rate. Everyone is unique. Some people with low IgG can get infections, some people do fine. There are patients who haven’t had CAR T-cell therapy who have primary B-cell aplasia and do fine and a lot of them don’t need IVIG. It’s a case-by-case situation. Most people have had some infection, but most people have been fine and living a normal life even without IVIG.
Dr. Favaro: The challenge with the solid tumor CAR Ts that they’re trying to make right now is finding the antigen on the lung cancer, for example, that won’t damage or destroy the lung. The fortunate part about lymphoma is that you can target lymphoma cells. You will deplete your own B cells, but we can mitigate that with prophylactic antibiotics, IVIG if needed, and taking precautions so you can still live your life.
Masking, especially if you’re in a crowded area, and frequent hand washing would be advisable. As more time passes, those restrictions start coming down a lot.
Dr. Nilanjan Ghosh
Post-CAR T-cell Therapy
Robyn: Michael asks, “What are the overall risks as far as activities, food, etc., for post-CAR T-cell therapy patients?”
I have not been avoiding anything for many years, but I’m eight years out at this point. There are initial precautions because a lot of people have low ANC (absolute neutrophil count) and some other depletion.
Dr. Ghosh: Right after CAR T-cell therapy, blood counts are low. Sometimes we even need to give growth factors to improve blood counts. The risk is going to be higher in terms of infections initially than a few months out. If the blood counts recover, especially neutrophil counts, then certain infection risks go down.
B cells always take time to recover. As the lymphocyte count recovery takes longer, your immune system is compromised and that’s where the possibility of viral infections happen. Masking, especially if you’re in a crowded area, and frequent hand washing would be advisable. As more time passes, those restrictions start coming down a lot.
Ultimately, you have to live your life, but still be cautious. If you do get an infection, then alert your providers so they can do some tests to find out if it’s a mild infection or something that needs to be worked up or treated.
In terms of food, you have to take certain precautions in terms of raw food while your neutrophil count is low, but that typically happens in the immediate post-CAR T-cell therapy phase. As more time goes, those usually are not an issue.
Robyn: You need to have a team take care of you. Your oncologist will move out of your realm because they have people who are very sick to take care of. I do encourage everyone to get an internist or an immunologist who can take care of the day-to-day.
Second CAR T-cell Therapy
Robyn: “Does CAR T-cell therapy work a second time if it didn’t keep the complete response the first time?” Can you have a second CAR T?
Dr. Ghosh: Not commercially. CAR Ts are approved once in the commercial setting, but we have clinical trials which will allow a second CAR T. For example, there’s a clinical trial using natural killer cells that are modified to become CARs or chimeric antigen receptor expressing cells. In that clinical trial, we allow patients who have had a commercial CAR T but it failed. Some of the allogeneic CAR T-cell therapy trials will allow patients who have had a previous CAR T-cell therapy.
There are other CAR Ts coming out. For example, we have a CD19/CD20 bispecific CAR T trial, which we are about to open. In that clinical trial, if someone had commercial CAR T, that is probably not allowed because the CD19 CAR T had already failed. But let’s say you have another clinical trial targeting CD22 and people have had the traditional CAR T, now you are using CAR T again but it’s different spikes. If you’re going against a different spike with a clinical trial, that would be doable. But if it’s the same one, then likely not.
The second time will be in a trial unless a CAR T-cell therapy gets approved that allows previous CAR T treatments.
Newer Monoclonal Antibodies
Robyn: Mike asks, “I’m still unsure about some of the things I’ve heard more recently because I don’t know if I have access to them. What about newer monoclonal antibodies? Do they still play a role?”
Dr. Favaro: There are definitely other options out there. Monjuvi is a monoclonal antibody against CD19 that has been looked at in relapsed lymphoma in combination with lenalidomide. Loncastuximab, which is one of these antibody-drug conjugates, is an anti-CD19 with a chemotherapy payload. It’s going to attach to your CD19 spike and internalize the chemotherapy right into that cell. It’s given via IV every three weeks.
These are two really good options for patients who, for whatever reason, CAR T-cell therapy or BiTE are not working or not available. These easily given off-the-shelf and approved by insurance.
When your blood counts are low and you’ve gone through therapy, there’s a risk of fungal infection as well.
Dr. Kulsum Bano
Cannabis & Non-Hodgkin’s Lymphoma
Robyn: “Cannabis and non-Hodgkin’s lymphoma. Are there any benefits?”
Dr. Bano: It’s a question that comes up pretty frequently. There may be some misinformation out there and some misconceptions of prevention of cancer with cannabis, and I don’t think there’s any founded data.
Certainly, people think about it in terms of symptom control. We do have medications that use the cannabinoid derivatives in a medical form, such as dronabinol, that we use for nausea and appetite stimulation for patients who have gone through chemotherapy.
Generally, we discourage smoking of cannabis only because there are a lot of additives that could be associated with it. When your blood counts are low and you’ve gone through therapy, there’s a risk of fungal infection as well.
There’s a lot of unregulated things that we don’t know what we’re dealing with. I don’t think there are any recommendations that can be definitely given. I don’t know that there are benefits per se, but it’s a discussion to have with your physician about what works for you and what doesn’t.
You need a small amount of protein, usually seafood, mostly vegetables on your plate, and some whole grains for carbohydrates. All these things are important.
Dr. Justin Favaro
Keto Diet
Robyn: “Can you speak about the keto diet? Is it effective against cancer? Is it helpful in any way?”
Dr. Favaro: It’s probably the most common question we get as oncologists every day. What can I eat? What should I eat?
My general recommendation is the Mediterranean diet. If you talk to nutritionists and look at the studies, you need several components to your diet. You need a small amount of protein, usually seafood, mostly vegetables on your plate, and some whole grains for carbohydrates. All these things are important.
I believe the keto diet takes out all carbohydrates, so you’re dealing with a lot of protein and a lot of fat. There are downsides of that for the rest of your body. Your cholesterol could go up and that could be damaging to your heart. Your body needs sugar and glucose.
For example, let’s look at a PET scan. What’s lighting up on the PET scan? Besides the lymphoma, it’s your heart and your brain. They need sugar to work. You don’t need sweets all the time, but you need complex carbohydrates. Maybe switch to whole grains and whole wheat pasta instead of white pasta. That’s only a portion of your diet, about 25%. The majority is vegetables and lean protein.
If you look at some of the recent studies that have come out that have looked at who lives the longest with cancer and what diet they follow, the winner seems to be the vegan diet in terms of cancer survival and decreasing risk of recurrence. This is cancer broadly and not lymphoma. But sometimes that’s a hard diet to follow, so a Mediterranean diet is a reasonable diet for most people to follow.
Robyn: Everybody wants control. You want control of your disease.
I have to add: Exercise helps. Studies in breast cancer and prostate cancer — because they’re so much more common and easy to study — showed that even for people who have never exercised before, if they walked 30 minutes a day, they had a longer remission rate and cure rate.
I encourage everyone to exercise. That doesn’t mean you have to do CrossFit because that may lead to shoulder injuries; we see that in radiology. You can do any type of walking or cycling. If you look at other studies, it’s not only the diet. People are active. Get yourself moving.
There have been studies done, not particularly in cancer, that show that insulin resistance is improved with intermittent fasting.
Dr. Kulsum Bano
Intermittent Fasting
Robyn: “Does intermittent fasting help patients with follicular lymphoma or any cancer? Does sugar play any part?”
Dr. Bano: There have been studies done, not particularly in cancer, that show that insulin resistance is improved with intermittent fasting. At any point, when you have dysregulation in your blood sugar control, that tends to lead to other medical complications. There is some role to play in improvement in outcomes. I don’t know that it’s been studied particularly.
Robyn: There are studies with BMI. People who are obese have a higher incidence of all sorts of cancers and have poorer outcomes. There are a lot of reasons for that. It’s multifactorial, but eating healthy and exercise make sense.
R-EPOCH vs. R-CHOP for Triple-Hit DLBCL
Robyn: “Is there any strong evidence that R-EPOCH is better than R-CHOP for triple-hit diffuse large B-cell?”
Dr. Ghosh: This type of aggressive lymphoma is one of the most aggressive variants. R-EPOCH is still considered as the standard of care for this disease based on a lot of retrospective data. There is no clinical trial taking patients with double-hit or triple-hit lymphomas and giving half of them R-CHOP and half of them R-EPOCH.
However, there was a large clinical trial which took all patients with diffuse large B-cell lymphoma and gave half of them R-CHOP and half of them R-EPOCH, and R-EPOCH was not shown to have a better efficacy. They were similar, but it was not really better.
That study was inconclusive in terms of the improvement for double-hit patients. If you ask most doctors, double-hit patients will still be getting R-EPOCH because there’s a lot of good retrospective data showing better long-term responses with R-EPOCH compared to R-CHOP.
We have an ongoing study where we are monitoring different types of cells post-CAR T-cell therapy.
Dr. Nilanjan Ghosh
Patient Group That Benefits More from CAR T-cell Therapy
Robyn: John asks, “We’ve talked about complete response rates and durable remission rates following CAR T-cell therapy. With the much larger patient population, have you seen any trends emerge as to which patients tend to do better in terms of a better response rate, a better complete response rate, as well as a more durable remission with CAR T-cell therapy?”
Dr. Ghosh: People have tried to figure it out. Before you start any treatment, you want to know if this treatment is going to give long-term remission for this person versus someone else. We are not there yet, but we have some ideas. It’s not perfect.
With CAR T-cell therapy, we know that if someone has very bulky disease and fast-growing bulky disease, CAR T-cell therapy will not give great outcomes. Unfortunately, nothing else does so people still go for it, but sometimes you want to debulk while waiting because CAR T-cell therapy is a weeks-long process.
For example, if there’s one site of bulk, we often can do radiation. There are new radiation techniques. One is called “boom boom” where short, very effective radiation is done to shrink the tumors, perhaps even express all these antigens, and have a better kill.
Bulky tumors can often cause T-cell exhaustion quickly so if they get overwhelmed with the tumor, then those T cells can get immune tolerance. There is also a subpopulation of these T cells that can cause immune suppression.
We have an ongoing study where we are monitoring different types of cells post-CAR T-cell therapy and checking them multiple times to see if we can identify patients who might have relapsed and had one type of immune repertoire versus those who had long-term remission and have a different type of immune repertoire.
We presented the initial data at ASH 2023, but hopefully, we’ll do a little bit more analysis on that and try to understand it better. We have samples taken pre-CAR T-cell therapy to see what may be the characteristics of a person that could predict long-term response.
We also have a study with BiTE. We are doing it for patients who are getting mosunetuzumab. We are collecting samples before and after treatment, and trying to identify which type of T cells may be associated with a better response versus a not-so-durable response.
CLL vs. Follicular Lymphoma
Robyn: Tim asks, “Can you define CLL and how it complements follicular lymphoma?”
Dr. Ghosh: CLL is chronic lymphocytic leukemia, which is under non-Hodgkin lymphoma. CLL is circulating disease in the blood. There is a lymphoma component to it called SLL, small lymphocytic lymphoma. It’s essentially the same disease. SLL is in the lymph nodes, CLL is in the blood. If there are more than 5,000 circulating lymphocytes, then it is a definition for CLL. If it’s below that, it’s called MBL, monoclonal B-cell lymphocytosis.
CLL is an indolent form of lymphoma circulating in the blood but could also be in the lymph nodes, spleen, and bone marrow. Like follicular lymphoma, it belongs to the same indolent non-Hodgkin lymphoma group considered as less aggressive.
CLL has tremendous progress where we have given up chemotherapy, so that’s where it’s a little bit different. You heard about R-bendamustine. We used to use that in CLL. In the past, we used to think we could use the same treatment for all indolent lymphoma.
We have relied on targeted treatment, like BTK inhibitors — ibrutinib was the first generation, then acalabrutinib and zanubrutinib, now pirtobrutinib — and then BCL2 inhibitors like venetoclax (VENCLEXTA). These have all come either in sequence or in combination.
Liso-cel got approved very recently for CLL, so now you have CAR T-cell therapy available as well. Chemotherapy was FCR and BR. We don’t really use those anymore. They’ve been shown to be inferior compared to these newer drugs that we have.
Daniella recounts her journey through a stage 2 PMBCL diagnosis. She underwent chemotherapy and CAR T-cell therapy, and ultimately achieved remission. Initially attributing her symptoms to allergies, she experienced a persistent cough that worsened over time, accompanied by night sweats and low-grade fevers. Concerned by her symptoms, she sought medical attention and underwent various tests, leading to a diagnosis of primary mediastinal B-cell lymphoma (PMBCL).
Facing the shock of her diagnosis as a 28-year-old with no prior health issues, Daniella embarked on a treatment journey that included chemotherapy, fertility preservation, CAR T-cell therapy, and radiation. Throughout her treatment, she experienced side effects such as hair loss, fatigue, nausea, and fever, but she found strength in focusing on the present moment and relying on her support system, including family, friends, and medical professionals.
Despite setbacks and challenges, including a bout of COVID-19 and the discovery of residual disease after chemotherapy, Daniella remained resilient. She underwent CAR T-cell therapy, navigating delays and side effects, and ultimately achieved remission.
She acknowledges the ongoing emotional and psychological impact of her cancer journey, emphasizing the importance of taking things day by day, seeking support, and connecting with others facing similar experiences. As she continues to navigate survivorship, she encourages others facing cancer to lean on their support networks, seek professional assistance when needed, and remain resilient in the face of adversity.
In addition to Daniella’s narrative, The Patient Story offers a diverse collection of primary mediastinal B-cell lymphoma (PMBCL) stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
Name: Daniella S.
Diagnosis:
Primary Mediastinal B-Cell Lymphoma (PMBCL)
Staging:
2
Symptoms:
Prolonged cough
Low-grade fever
Night sweats
Treatments:
Chemotherapy (R-EPOCH)
Radiation
CAR T-cell therapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I grew up in the Tri-State area. I work for a large communications firm in New York City and live in Jersey City with my fiancé and dog.
Pre-diagnosis
Initial Symptoms
The journey started in the summer of 2022. It began with a tickle in my throat, which was very vague, and I attributed it to either allergies or the dry air in my apartment.
After a while, that tickle turned into a cough, which didn’t go away. After a few weeks of having that cough, I decided to go to urgent care. They thought I had bronchitis, which I thought was likely. I figured whatever I had probably turned into bronchitis. I was working a very high-paced job, was very career-oriented, and dismissed a lot of my initial symptoms.
The doctor said it was the night sweats that concerned him the most. I don’t think that he thought of a potential cancer diagnosis because I was otherwise healthy.
Symptoms Worsening
My symptoms got worse. When I went to urgent care, I was diagnosed with bronchitis and they treated me with steroids. My cough improved, which was great, but when I went off the steroids, my cough came back immediately. I went back to urgent care and they thought I had pneumonia.
The cough lasted four weeks before I thought it seemed like a long time to be going through it. I also started to develop a low-grade fever in the evenings. Even further along, I started to have night sweats, which I later learned was one of the symptoms of lymphoma.
The night sweats became apparent to me because they came with low-grade fevers. That’s when I thought I needed to see a doctor urgently because I knew that I was sick.
The doctor said it was the night sweats that concerned him the most. I don’t think that he thought of a potential cancer diagnosis because I was otherwise healthy. He was ticking off other things that it could be, but he called out the night sweats as concerning.
The night sweats got progressively uncomfortable to the point where I was waking up in the middle of the night to change my clothes. But I attributed that to some infection that had gone on for too long and now becoming severe. I didn’t even consider cancer.
My mom pushed me to ask for a chest X-ray from the urgent care doctor. The radiologist thought it was pneumonia, but the doctor scared me when I was told that it could be tuberculosis. I decided to get a second opinion.
Getting a Second Opinion
I sent the X-ray to my cousin, who’s a radiologist. She said the X-ray would be a lot worse if I had pneumonia. She pushed me to get a CT scan. I went to my primary care doctor and got a CT scan, which immediately revealed a large mass in the center of my chest.
My cousin prepared us for the different possibilities, but it was still very much a shock.
Diagnosis
This was something that we were anticipating at this point. My cousin prepared us for the different possibilities, but it was still very much a shock. I was an otherwise healthy 28-year-old with no prior history of anything and no history of lymphoma.
My primary care doctor asked me, “Do you work around any chemicals?” I said, “Unless you’re talking about the chemicals from the New York City subway, I don’t. I work in an office. I work on the computer.”
It was a huge shock when I was initially diagnosed. Upon receiving the results of the CT, we immediately went to the ER. From there, the process started in terms of finalizing my diagnosis.
Reaction to the Diagnosis
It was a crazy out-of-body experience for me. I would say I was somewhat primed for it. I was with my fiancé at the time, but I don’t know how primed he was for it. I remember seeing his face and the color draining from it. I immediately had an out-of-body experience and emotionally shut down in a way.
I knew that I needed to go to the ER so I didn’t have time to process what it all meant. The moment I received the news, I was shaking.
From that point on until the day I heard I was in remission, every moment of my life was lived minute by minute. I remember thinking to myself, I’m going to the ER. I’m going to the front desk. I’m telling them what’s going on. I’m sitting in my chair, waiting. They’re going to take me back to the ER.
I was living moment to moment, doing my best to not anticipate what was next. My life went from everything being planned to getting through by the minute, by the hour, or by the day. It was a big mindset shift for me.
In the initial moments of my diagnosis, I distinctly remember thinking that this couldn’t be happening to me. This is too insane. I was supposed to get married in seven months.
I thought that I couldn’t do this. I have an extreme fear of needles. How am I going to make it through knowing that they’re going to need blood work? I actively avoided needles for a long time and any blood work that wasn’t necessary. That’s how bad my phobia was so that was one of the main things that I discussed with everybody because that was tough for me.
The interventional radiology team that did the biopsy was wonderful in keeping me calm throughout the process. They were so confident in what they were doing that it made me feel more relaxed and very well taken care of.
Doing the Biopsy
I was admitted upon going to the ER. They had my CT results. From there, there were various consultations with doctors and potential surgeons to understand what we should be doing about the mass, considering that it was pushing on my chest and my heart, causing me to cough and some fluid to build up in my lungs. There was a lot of discussion on what we should be doing at this point.
They ultimately decided that they didn’t need to do anything urgently, but they scheduled a biopsy for me. They went back and forth to decide what type of biopsy to do. Ultimately, they went with a needle biopsy to get pieces of the tumor in my chest to be able to do the diagnosis and staging.
They wanted to do the biopsy before the weekend. I wanted to be knocked out during the whole process, but unfortunately, I had breakfast that morning before I knew that they were going to do the biopsy. To do the biopsy under anesthesia, I wasn’t supposed to eat, so they had to do the biopsy while I was awake. Luckily, they gave me lorazepam (Ativan) via IV so I was able to calm down before the biopsy.
Honestly, that experience went well and opened my eyes to a lot in terms of how this medical process works. The interventional radiology team that did the biopsy was wonderful in keeping me calm throughout the process. They were so confident in what they were doing that it made me feel more relaxed and very well taken care of. It was the first procedure that happened to me in my journey that made me feel like I could do it. That was the first moment of encouragement for me, knowing I could get through this.
Additional Testing
Following the biopsy, I had to have additional CT scans of my head, neck, and stomach. I also had to have a bone marrow biopsy to confirm the staging to see if the lymphoma was anywhere else.
The bone marrow biopsy was done under anesthesia. I was a little sore afterward and a little nauseous from the anesthesia, but otherwise, it was fine.
Getting the Official Diagnosis
After all of that testing, I got my final diagnosis a few days later. It was confirmed that I had stage 2 PMBCL or primary mediastinal B-cell lymphoma.
I started the fertility preservation process while I was still in the hospital.
Fertility Preservation
I was lucky to be able to do fertility preservation before starting chemotherapy, which I realized after my treatment was very rare. There were a lot of things that lined up that allowed me to do fertility preservation.
The fertility clinic is inside the hospital. When I was diagnosed, they kept me in the hospital for 10 days while they were doing all the procedures and monitoring. During that time, my doctor consulted with the fertility doctor at the clinic and she was able to come down to see me and talk to me about my options.
I started the fertility preservation process while I was still in the hospital. Had the clinic not been in the hospital building itself, they probably wouldn’t let me be discharged to undergo fertility preservation. When I decided to move forward, I was able to go to the clinic and do the tests that they needed. Otherwise, I don’t know if they would have let me so I was very fortunate in that sense.
Honestly, it took me a while to figure out that this was even going to be a part of the journey, but upon hearing what my options were, I was firm in my decision. That being said, I was also very scared because I knew it involved a lot more needles. Of course, that wasn’t fun, but I was no longer operating in what I wanted, but more so what I needed to do.
I went to the fertility clinic every day for blood work. They would monitor me and how my eggs were growing because they gave me hormones to stimulate my eggs so they could retrieve them.
I was doing hormone shots in the evening and going to the clinic so they could check on how my eggs were growing. After the clinic visit, I would go down to the cancer clinic where the doctor would check me. They were afraid that my cancer would grow since it’s a very aggressive lymphoma, that my symptoms would get bad again, and that I would need to start chemotherapy immediately.
I would go to the fertility clinic and then the cancer clinic every morning to see my doctor and get checked out. Then I would get myself an emotional support bagel and lay around all day and think about what was going on.
The fertility preservation process was not that bad. Besides some minor discomfort and minor bloating, it was very manageable.
They were able to retrieve seven eggs. My fiancé and I decided to fertilize all seven eggs in the hope of creating healthy embryos.
Egg Retrieval
Upon my egg retrieval, my doctor warned me that my body was fighting something so there was a chance that they might not be able to get any eggs. I went in understanding that it might not turn out how we wanted, but they were able to retrieve seven eggs. The procedure was done under anesthesia, which was something I was very familiar with at the time. The egg retrieval process itself was fine.
I had the egg retrieval done in the morning. I was out of there probably by noon or 1 o’clock. After they did the retrieval, they brought me to the recovery area. When I woke up from anesthesia, they wanted me to walk around a little bit before sending me home. That evening, I was admitted to the hospital for my first round of chemotherapy.
Embryo Freezing
They were able to retrieve seven eggs. My fiancé and I decided to fertilize all seven eggs in the hope of creating healthy embryos because that’s what my doctor recommended. If I were to freeze seven unfertilized eggs, they might not survive the thawing process. Embryos are a little more robust. They’re a little tougher so my doctor recommended trying to fertilize all seven eggs.
We had to wait a few days to find out how many of those eggs were fertilized and how many of those fertilized eggs turned into big enough embryos for us to freeze. We ended up being able to freeze five embryos, which is pretty good when you consider that we fertilized only seven eggs to get five good-quality embryos. That was a success.
Truthfully, I was so happy with how the experience went. Knowing that I had five embryos in storage was a big motivator for me and gave me a lot of hope that even beyond surviving cancer, I would still be able to have a family. I was thankful to be able to have that possibility.
If your fertility doctor can talk to your oncologist and make a plan, there can be workarounds that would allow you to do it.
Everybody’s scenario is different, but if it’s important to you, definitely explore every resource and avenue that you can to do it. It’s not easy, but it’s not too difficult if you want it and if it’s really important to you.
I’m a huge proponent of doing everything you can, advocating for yourself, and asking how you can get fertility preservation done. If your fertility doctor can talk to your oncologist and make a plan, there can be workarounds that would allow you to do it.
I had to be on blood thinners during the whole process. I gave myself blood thinner shots every morning while going through fertility preservation. My doctor was afraid that I would develop blood clots, especially considering the hormones. There were risks, but there are also ways to mitigate those risks and work around them. Advocate for fertility preservation, if it’s important to you.
Treatment
Discussing the Treatment Plan
Everything was moving pretty fast. I celebrated my birthday in the hospital. I was diagnosed on September 29th and turned 29 on October 1st, which was a very surreal experience to celebrate my birthday in the hospital during this time.
My doctor was very communicative about my treatment options, even though we were still confirming what type of lymphoma I had and what the staging was. He went through the options of either doing R-EPOCH chemotherapy or R-CHOP chemotherapy, both of which are similar to each other.
R-EPOCH is what he was leaning towards. He explained that R-EPOCH was going to be done inpatient at the hospital for five days. I would get chemo for five days, wait for three weeks, go back for the next round, and do that cycle for six rounds. R-CHOP would be outpatient.
After receiving my diagnosis, he said that I was going to do six rounds of R-EPOCH chemotherapy, which equated to about six months of treatment. I would be in the hospital receiving chemotherapy, come in to see him a few days later, and then two weeks after that, be back in the hospital for my next round of chemo.
The anticipation of side effects was worse than any side effects that I felt. I had a lot of anxiety about what I would feel and what I would be going through.
Side Effects of Chemotherapy
My oncologist explained what I could expect from the chemo, the first one being hair loss. He noted that I would be fatigued and that I could be nauseous. He was very good. He wrote down everything for me. He also drew pictures of where the lymphoma was. It was very helpful in those moments for him to write everything down for me.
He explained to me that I should expect to feel pretty crappy the week after chemotherapy and have a good week during that second-week break before I would be in for my next round.
The anticipation of side effects was worse than any side effects that I felt. I had a lot of anxiety about what I would feel and what I would be going through, but none of my worst nightmares came true except one.
The side effects were quite manageable. The hair loss was something I knew was a given upon diagnosis, so I tried my best to not focus on it. I didn’t want to give the thought of losing my hair power. What I was most concerned about was losing my eyebrows, which was tough.
After the first round of chemotherapy, I started to lose my hair, which was traumatic — I don’t think there’s any way that it can’t be. I cut my hair short before starting chemotherapy with the hope that it wouldn’t be as apparent when it did fall out, but it fell out in clumps in the shower. It was constant. I woke up with hair on my pillow. It was very hard to go through that process.
Once I was able to shave my head, it felt so much better because then I wasn’t constantly dealing with hair falling out in clumps. I bought a lot of head wraps and wore a lot of beanies. I was going through treatment during the winter time mainly, so I was able to do that. I tried to not give it so much power and kept telling myself that it would come back.
The side effects compounded as I got more and more chemo. As I went through the rounds, the side effects got a little tougher.
I struggled with fatigue and some nausea. The nausea wasn’t overwhelming and I was able to take ondansetron (Zofran) to handle it, but it was mainly overwhelming fatigue and an overall feeling of malaise. I would explain to my friends that it was like a bad hangover, a feeling of not having any energy and can’t get out of bed.
I stayed with my parents because they lived close to the hospital. There were days when I only stayed on one floor because I was afraid that if I went down the stairs, I wouldn’t have the strength to come back up or I would lose my balance.
There was always a general feeling of unwellness between cycles. My body would rebound in the last week and I would start to feel a little bit better and have a little bit more energy.
The side effects compounded as I got more and more chemo. As I went through the rounds, the side effects got a little tougher. Overall, I considered myself pretty lucky in the way that my body was able to handle all of the chemotherapy.
I had to deal with one bout of COVID during my second cycle of chemo, which was awful. My symptoms weren’t awful, but getting COVID set off a bunch of logistical headaches with my chemotherapy that were tough to deal with and manage. I had to advocate hard for myself. That was a tough roadblock, but we got through it.
Post-Treatment Scans
I finished treatment in February 2023. We were feeling very confident about how things were and how the treatment went. I had a good midway scan. They saw that the mass in my chest was shrinking a lot. Everything was moving back into place, as my doctor said. Things were clearing up so it was a good sign that the chemotherapy was working, which was great.
When I received the news that there was still residual disease, that was truly crushing not only for me but for my family and my fiancé who were on their own journeys considering my cancer diagnosis.
I had to wait a month after I finished my last day of chemotherapy to have my last PET scan where two spots lit up. That was tough because we weren’t expecting it. There’s a 50% chance there could be inflammation and a 50% chance that it could be residual disease.
We had to do another biopsy, which was a little bit more invasive. They put me under for that one because they needed to get samples to see if it was residual disease, which it was.
Truthfully, those weeks were the toughest. After my diagnosis, I was able to tell myself that it was just six months of my life. I was going to be able to get through this and then everything’s going to go back to normal. I was going to get my life back. That’s what got me through the six rounds of intense chemotherapy, saying that it was only six months and that I could do this.
Since I had residual disease, I was going to be on this ride for a lot longer and I didn’t know what to expect. My doctors were very encouraging. Considering that I was so young, didn’t have a prior history, could handle the chemotherapy, and that it would probably work, I had a good chance of being cured.
We were holding on to that hope, but when I received the news that there was still residual disease, that was truly crushing not only for me but for my family and my fiancé who were on their own journeys considering my cancer diagnosis. It was heartbreaking news for all of us. There were definitely a lot of tears.
My team very quickly referred me to a larger cancer hospital and connected me with the CAR T team there. They had already gotten the ball rolling for me to do CAR T-cell therapy.
There were a lot of questions about whether or not I needed CAR T-cell therapy or additional radiation to clear up the small spots that were left over. There was a lot of back and forth.
CAR T-cell Therapy
I knew about CAR T-cell therapy because I read stories on The Patient Story about other patients who had lymphoma and have gone through CAR T-cell therapy. I understood the basics and what patients can expect to go through. My family had a lot of learning to do. But again, I was still living moment to moment, day by day. What were the next steps? Who do I need to talk to about CAR T-cell therapy?
While I knew about it, it was still very scary to me. Mentally, I was at a point where I didn’t want more treatment, but, at the same time, I knew that I had to steel myself for additional treatment.
Once I met with my CAR T-cell therapy team, I felt like I was in very good hands. There were a lot of questions about whether or not I needed CAR T-cell therapy or additional radiation to clear up the small spots that were left over. There was a lot of back and forth.
My case was presented to a lymphoma tumor board where multiple doctors weighed in. I also got second and third opinions on CAR T-cell therapy from other oncologists. After speaking to the other doctors, I felt very confident in moving forward with CAR T-cell therapy because there was a consensus that it was the next step for me, with some radiation in between.
Once I knew that CAR T-cell therapy was the best next step, I mentally was ready for it. You don’t have a choice, so you have to be ready. I felt very confident going into it.
All’s well that ends well. I was focused on the mission and the mission was to get my T cells and send them out.
Process of CAR T-cell Therapy
My team went over in detail what the process entailed, so that made me feel a lot better because I was prepared for what to expect. They gave me resources and booklets. They connected me with a resource that will help sponsor hotel stays close to the hospital because you have to stay close to the hospital when you receive CAR T-cell therapy.
There was a little bit of a wait of a few weeks to a month between the first meeting with my team and cell collection day.
The first step is collecting the T cells. They do that by putting your blood through a machine that separates your T cells, which are then sent to the manufacturer of the CAR T that you’re going to be receiving. I received liso-cel (Breyanzi).
If you have good veins, they can do it through the peripheral veins in your arms. I have small veins that are very hard to access, which is why I have needle phobia. They had to put a catheter in my neck. It’s not comfortable. However, I was given lorazepam and I told myself that I could get through this. They put the catheter in my neck specifically for T-cell collection and then immediately after, they would take it out.
We hit our first stumbling block. My neck catheter wasn’t working so they had to stick my veins. Luckily, I had a good team of people who were able to find a vein and complete the T-cell collection.
The T-cell collection day is pretty long. You’re sitting in a chair and can’t move because you’re connected to the machine. My advice is to bring snacks, your tablet or laptop, and be prepared to watch a lot of Netflix. I was living day to day, so I knew I could get through it.
I didn’t experience any side effects after the T-cell collection other than being a little bit tired. During the collection, you might feel that your body or lips are tingling, which has something to do with the calcium level in your body, so they will give you some calcium to help supplement but it’s not uncomfortable or painful. It’s just a weird feeling.
It was a little bit crazy for me but, again, through the journey and the experience, I told myself I could get through this. All’s well that ends well. I was focused on the mission and the mission was to get my T cells and send them out.
[I had] to get special permission from the drug manufacturer to use my T cells, which put my CAR T-cell therapy in jeopardy of being pushed back.
CAR T-cell Infusion
CAR T-cell infusion day came. Unfortunately, there were some delays in the schedule, which was very stressful. The drug manufacturer has to test your T cells. My T cells were considered too robust or too healthy and were labeled as out of range so that required me to get special permission from the drug manufacturer to use my T cells, which put my CAR T-cell infusion in jeopardy of being pushed back.
They were able to have a meeting and they approved for me to use my T cells. But then they were mislabeled so during the shipping process, they had to be sent back and then re-shipped, which was very stressful because my CAR T-cell infusion date was pushed back. I was very worried because this was happening in May. I wanted to at least have a summer and go to the beach so I wanted my CAR T-cell treatment over and done with as soon as possible.
Mentally, I was prepared for the process, but I didn’t prepare myself for the potential setbacks. While that was very stressful at the moment and I advocated a lot for myself to make sure that everything was going to turn out okay, I eventually ended up getting my CAR T-cell infusion done at the beginning of June.
You first receive three days of lymphodepleting chemotherapy, which is a low-dose chemotherapy done in the hospital as an outpatient. I was able to go back to the hotel that I was staying at nearby.
After three days of chemo, they gave me two days to rest before the infusion. I felt crappy after. It made me much more nauseous. I did not feel good. At points, I thought I could faint or lose consciousness. I felt pretty crappy during those two days that I wasn’t receiving anything. They do their best to give you what you need, such as anti-nausea drugs.
When they were pushing the CAR T cells in, I felt a garlicky or cream corn taste in my mouth, which is something that happens.
By the time infusion day came around, I was feeling much better. I went to the infusion center and the CAR T cells were brought in a little cooler. It wasn’t an infusion bag that they held. It was a syringe.
I had a PICC line where they would give me chemo through so they pushed the CAR T cells through my PICC line for about five minutes. They monitor you very closely in terms of your vitals. Beforehand, they pre-medicate you with diphenhydramine (Benadryl) to prevent any allergic reaction.
When they were pushing the CAR T cells in, I felt a garlicky or cream corn taste in my mouth, which is something that happens. It was fine though. I didn’t mind or anything.
Overall, the CAR T-cell infusion was not a big deal. They monitor you for the rest of the day. The infusion itself took less than 30 minutes. They monitored me for a few hours and upon discharge, I went back to the nearby hotel that I was staying at.
You have to come back to the hospital every day for regular blood work. They’ll ask you a bunch of questions because CAR T-cell therapy has two main side effects: cytokine release syndrome (CRS) and neurotoxicity.
CRS is noted by high fevers and other symptoms. Neurotoxicity is when your handwriting gets messed up, you’re not able to answer questions, your speech is jumbled, etc., so they were testing me for those things.
While it certainly wasn’t easy, I wouldn’t say that anything that happened was unexpected. They prepared us for the side effects that I could experience.
Side Effects of CAR T-cell Therapy
When I went into the hospital on day one, I was fine. They did blood work. I looked okay, so I went back to the hotel. I couldn’t be out in public, but we were able to take a walk outside and get fresh air.
That evening, I started to develop a fever, which they expected. I went to the ER and they put me in a room where I spent about five days dealing with high fevers and a general feeling of unwellness. I was weak and tired
My main side effect from the CAR T-cell therapy was on-and-off fever. I received a few doses of tocilizumab, which is what they give to control CRS, and one dose of steroid. The steroid knocked me out. I took the best nap of my life. For four hours, I was finally able to sleep. I was struggling with the fevers so with the help of the medications, I was able to recover.
After five days in the hospital, they were able to discharge me. I went back to the hotel because I still had to be monitored closely before I could be sent home.
While it certainly wasn’t easy, I wouldn’t say that anything that happened was unexpected. They prepared us for the side effects that I could experience. The most anxiety-inducing was waiting, being in the hospital, and not knowing how bad it was going to get.
I remember focusing hard on the tests that they would give me in terms of assessing my mental status because I was really scared that, at any minute, I could be losing it. But they assured me that I would be okay and, luckily, everything was so.
The first thing my fiancé and I did coming from the doctor’s office was go to the beach. It was a wonderful moment and a real first moment of victory where we were able to breathe for the first time in a little bit.
Radiation
After the T-cell collection, I immediately went to radiation, which is a whole other process. They had to do a CT scan of my chest to understand where they had to radiate. They gave me tiny little tattoos that nobody else would notice except me to mark the areas.
During radiation, I was doing breath holds to lift the area that they had to radiate. I needed to lift it away from my lungs and my heart as much as I could so that there was no scatter to my other organs, which is something that they tried to avoid. They want to do their best to radiate just the area that they have to.
The breath holds were tougher than I thought because you have to hold your breath exactly right for them to radiate the exact spots. It felt like a hard yoga class where you have to breathe a certain way and hold your breath. It was tougher than I initially imagined.
I did ten rounds of radiation and ten rounds of radiation with those breath holds made me very tired. Honestly, I wasn’t expecting to be so tired from radiation. Luckily, I didn’t have any other side effects.
Follow-up Protocol
After my CAR T-cell therapy, which was a month total from the time I got my infusion to when I was allowed to go home and started seeing the doctor on a less frequent basis, they determined that I was safe to go home. I took it easy and took things day by day.
I had a PET scan scheduled at the 60-day mark. The results showed that I was 100% in remission. There was no evidence of disease.
The first thing my fiancé and I did coming from the doctor’s office was go to the beach. It was a wonderful moment and a real first moment of victory where we were able to breathe for the first time in a little bit. We were sitting by the ocean, having lunch, and then we saw dolphins jumping. You don’t see that often in New Jersey, so we took it as a good omen for things to come.
It was a turning point and the biggest moment for my mom, honestly, who was my main caregiver during the entire time. She said the last time she was this happy was the day that she gave birth to me, so it was an emotional moment.
I didn’t know who I was anymore. I was still me in many ways, but in other ways, I wasn’t.
Cancer Survivorship
Survivorship is honestly very difficult. In a way, it’s more difficult than going through cancer. Once you’re able to pick your head up, everything else starts to come into focus again. That’s tough sometimes because you finally start to take stock and understand what was lost in a way. For me, a big part of it was my identity.
I didn’t know who I was anymore. I was still me in many ways, but in other ways, I wasn’t. Honestly, I don’t know if I’ve found myself again even at this point, but it’s a continuing journey and I’m still on the ride.
Words of Advice
Honestly, what helped me was taking things day by day, moment by moment, whatever time increment to get through difficult moments. I would tell myself, “I just need to get through these 10 minutes. If I can get through 10 minutes, I can get through 20 minutes. If I can get through 20 minutes, I can get through the next hour.” During those tough times, when I was in pain and wasn’t feeling well, and when I was struggling, that’s what helped me get through.
It’s important to have a good support system. I had a lot of cheerleaders in my corner, mainly my family, my fiancé, and my fiancé’s family. They were there for every step of the way. Being able to lean on those who are there to support you is huge.
If you don’t have people close to you to support you, definitely lean into the resources that are provided to you. There are a lot of cancer centers that provide free social workers for cancer patients. I saw a social worker and she was very helpful. She had a lot of experience and, based on her experience with cancer patients, understood what I was going through. She helped me through some of the tougher moments as well.
Connect with others who are going through the same experience as you. It doesn’t have to happen all at once. It’s certainly a journey. Upon diagnosis, I wasn’t ready to talk to anyone, do anything, or reach out to anyone. But as I went through the process, I became more and more comfortable about reaching out and it was a huge help to me. Don’t be afraid to reach out and ask for help where you need it.
Being able to lean on those who are there to support you is huge. If you don’t have people close to you to support you, definitely lean into the resources that are provided to you.
Role: Hematologist-Oncologist Focus: chronic lymphocytic leukemia (CLL) & leukemia and lymphoma | CAR T, targeted therapy Provider: Medical College of Wisconsin
...
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Ruth Fein Revell: Hi and welcome to our program, Clinical Trials Update: What to Know in Myelofibrosis Care. My name is Ruth Fein Revell and I’ve lived with a myeloproliferative neoplasm (MPN) for nearly 30 years.
I was diagnosed with essential thrombocythemia in 1995, polycythemia vera about 20 years later, and myelofibrosis in 2018. I’ve also lived with a number of complications from dangerous blood clots and hemorrhages that put me in the ICU to debilitating headaches, bone pain, and extreme fatigue.
I’m a health and science writer and very fortunate to be in a clinical trial for the last four years with amazing results, eliminating my symptoms, and significantly reducing my bone marrow.
We want to note that The Patient Story retains full editorial control of this entire program. This is not meant to be a substitute for medical advice.
Joining us is Dr. Naveen Pemmaraju, a top expert in MPNs and myelofibrosis from MD Anderson. Dr. Pemmaraju, it’s so nice to see you. Thanks for joining us and for being a part of this program. Can you tell us more about yourself and what drew you to MPNs?
Naveen Pemmaraju, MD
Dr. Naveen Pemmaraju: Thanks for having me. I’m a professor of leukemia at MD Anderson in Houston, Texas. I serve as the executive director for cancer medicine and as the director for our rare disease program, including blastic plasmacytoid dendritic cell neoplasm (BPDCN).
Ruth: It’s always great to see you and to speak to you. You offer so much to the MPN community and we really thank you.
JAK inhibitors are not JAK2 mutant-specific inhibitors, so that’s why they work in patients whether they’re JAK, MPL, CALR, triple-negative, or have no mutations.
Dr. Naveen Pemmaraju
Standard of Care: JAK Inhibitors
Ruth: We now have four JAK inhibitors and one one of them was just approved. Walk us through this. First of all, how does a JAK inhibitor work?
Dr. Pemmaraju: The basic premise is that MPN cells signal through a specific pathway called the JAK/STAT pathway.
A regular cell uses the JAK/STAT pathway for normal blood cell growth, differentiation, and lifespan. Now take an MPN cell and that pathway is hijacked and used in a malignant way, so those cells keep growing and dividing. It’s like a light switch that’s turned on that doesn’t go off.
Interestingly, the JAK inhibitors are not JAK2 mutant-specific inhibitors, so that’s why they work in patients whether they’re JAK, MPL, CALR, triple-negative, or have no mutations.
JAK inhibitors are based on the principle that the JAK/STAT pathway and the cells are overactive and not working properly. JAK inhibitors aim to block that malignant activity and restore normal growth.
Ruxolitinib was the first-ever approved JAK inhibitor. Since 2011, three JAK inhibitors have been US FDA-approved: fedratinib in 2019, pacritinib in 2022, and momelotinib in 2023. The four currently approved JAK inhibitors have some interesting similarities and differences.
[Ruxolitinib] works very quickly in relieving the symptom burden for our patients with MPNs.
Dr. Naveen Pemmaraju
Ruxolitinib
Dr. Pemmaraju: Ruxolitinib, the first and longest in class, is a JAK1/JAK2 inhibitor. This drug was simply amazing in the original clinical trials, which were COMFORT-I and COMFORT-II, led by Serge Verstovsek and Professor Claire Harrison.
In those studies, we learned a few things about ruxolitinib. One is that it works very quickly in relieving the symptom burden for our patients with MPNs. It can shrink the spleen rather quickly as well, so quickly that the hallmark ended up being at week 24 by six months.
Some side effects to look out for over time in this otherwise well-tolerated drug have been the development in some patients of opportunistic infections, such as herpes zoster or shingles, weight gain, and non-melanoma skin cancers.
Basal cell and squamous cell cancers of the skin are already common in our patient population, so a lot of our patients end up seeing a dermatologist. Most of our patients don’t necessarily discontinue for those side effects, but we need to watch out for them.
All patients who are going to get treated with fedratinib should have their thiamine level checked.
Dr. Naveen Pemmaraju
Fedratinib
Dr. Pemmaraju: Fedratinib improves symptoms and decreases spleen size, but it has a very notable toxicity or side effect, which garnered an FDA black box warning. It’s a very serious potential side effect called encephalopathy. Some have seen it to be Wernicke’s encephalopathy, but on later analysis, not exactly.
Wernicke’s encephalopathy is a name for a syndrome that can cause problems with thinking and even balance and can result from severe nutritional deficiencies. For fedratinib, it appears that it displaces vitamin B1 (thiamine) so what we see is the linking of those. All patients who are going to get treated with fedratinib should have their thiamine level checked because the encephalopathy can be related to that.
Patients can have GI side effects with fedratinib, like nausea, vomiting, and diarrhea, so we have to watch out for that, particularly in our older and more frail patients.
The unique thing with pacritinib is for several years, it was being watched for the development of cardiac and/or bleeding signals.
Dr. Naveen Pemmaraju
Pacritinib
Dr. Pemmaraju: Pacritinib is an interesting agent. Again, all these are trying to hit the JAK/STAT pathway, but this hits other pathways outside of that and that may be part of its benefits and toxicities.
It helps to shrink down the spleen and improve the symptom burden of patients, but the unique thing with pacritinib is for several years, it was being watched for the development of cardiac and/or bleeding signals.
I and others have done a lot of evaluation and analysis, including post-approval. We’re not seeing a high signal for that, but that’s something you have to be aware of if the patient is on a blood thinner, having chest pain, or having heart surgery.
Not only did [momelotinib] show improvement in the spleen size and symptoms, but what’s interesting — and pacritinib is showing this as well — is having an improvement in anemia.
Dr. Naveen Pemmaraju
Momelotinib
Dr. Pemmaraju: Momelotinib is the most recently approved JAK inhibitor. Again, not only did it show improvement in the spleen size and symptoms, but what’s interesting — and pacritinib is showing this as well — is having an improvement in anemia. Now that’s important.
Ruxolitinib and fedratinib don’t necessarily do that and, in some cases, it can make it transiently worse. Momelotinib has ACVR1 inhibition. Pacritinib also showing that as well unleashes a new era for our patients of JAK inhibitors having beneficial side effects, such as improvement of anemia and potentially, thrombocytopenia.
You have to watch out for GI side effects with fedratinib, pacritinib, and even momelotinib. In the earlier studies of momelotinib, there was a signal for peripheral neuropathy. I want to put those forward as an overview. There are some subtleties and differences, if one reads further.
Ruth: Thanks for that explanation. I’ve heard a lot of people say that they have a different mutation, so a JAK inhibitor isn’t going to help them, but we know that that’s not the case, so thanks for your explanation of how they work.
There isn’t a single molecular test. The decision is based on clinical factors and the art of medical decision-making.
Dr. Naveen Pemmaraju
Switching JAK Inhibitors
Ruth: How do you know which JAK inhibitor might or might not work and which one to try first? How is that decision made?
Dr. Pemmaraju: The decision to switch JAK inhibitors is not scientific. We’re not there yet. At some point, I envision that we’ll have a decision tree, like our colleagues in CML. But right now, there’s no molecular test, so it is the art of medicine. It is clinical decision-making.
There are some factors, if one looks up in the NCCN and other guidelines. One is platelet count. Ruxolitinib and fedratinib should be given to patients who have a certain amount of platelets and that’s where pacritinib was able to get its approval.
Pacritinib is specifically approved in the front-line setting for patients whose platelet count is less than 50, for example. The NCCN guidelines and other groups say that once you use pacritinib in later lines, maybe you don’t have to pay attention to the platelet as much, but that’s obviously for debate.
Another factor is the GI signal. If you have someone who has a known encephalopathy syndrome or thiamine deficiency, then fedratinib is not going to be one that you would choose.
Finally, you have to look at some of these subtle side effects that we mentioned earlier, such as GI and neuropathy, to help you choose.
The bottom line is there isn’t a single molecular test. The decision is based on clinical factors and the art of medical decision-making.
Switching can have financial cost repercussions, new toxicities when a patient was otherwise doing ‘okay,’ problems with access to the drug, and could uncover idiosyncratic side effects that may be specific to that patient and weren’t seen in the studies.
Dr. Naveen Pemmaraju
Ruth: So it’s possible that somebody could start on one JAK inhibitor and at some point switch to another. Is that an issue if you change?
Dr. Pemmaraju: This is a great important point about switching JAK inhibitors and what are the indications. There are several buckets here.
First is clear disease progression in terms of the spleen. If you have a patient who’s been on a certain JAK inhibitor for a sufficient amount of time and you have a spleen that previously shrunk but now starting to rise again, that could be considered disease progression and an indication to switch.
Second is worsening MPN symptom burden to the point where the patient’s quality of life is affected.
Third is blast count, peripheral blasts or bone marrow blasts, going up.
Fourth is the progression of the disease to an outright higher level of disease, what we call an accelerated blast phase.
The development of these clinical factors, such as the platelet count, may matter if you have a patient who’s on ruxolitinib, for example, and you consistently have platelets below 50, then that’s an indication to switch, for example, to pacritinib. If you have a patient who has anemia, you may think about momelotinib.
These are some of the reasons to think about switching. But again, there isn’t a molecular test or a definitive moment to switch. Switching can have financial cost repercussions, new toxicities when a patient was otherwise doing “okay,” problems with access to the drug, and could uncover idiosyncratic side effects that may be specific to that patient and weren’t seen in the studies.
Finally, you have a question about withdrawal and overlap, so these are things I think we’ll all work out together over the coming years as we have these JAK inhibitors in the clinic.
The story of JAK inhibitors is an evolving story and it’s evolving at three levels.
First is the science of it alone. In 2005, I was at Johns Hopkins with Alison Moliterno and Jerry Spivak, and I remember the day that the JAK2 mutation V617F was elucidated. From that time to now, we have JAK inhibitors that are amazing, so science is still evolving.
Second is the clinical part, as we’ve discussed. When to switch, how to switch, what are the factors, etc.
Third is the future. How do we combine these drugs with a second agent and potentially a third agent? What are those cross-reactivities? How does that benefit the patient to start those upfront rather than later on? You have this evolving area that’s quite exciting but also quite daunting not only for the patients and the clinic but for researchers.
This is preliminary data, but it was so encouraging that they are now moving on to a phase 3 randomized global study.
Dr. Naveen Pemmaraju
Clinical Trials: Combination Therapy
Selinexor & Ruxolitinib
Ruth: We’re seeing some really exciting updates as far as combination therapy. Let’s talk about clinical trials, starting with selinexor plus a JAK inhibitor and then move on to other combinations.
Dr. Pemmaraju: At ASH 2023, Dr. Sri Tantravahi from Utah presented the first public data of front-line combination, updated I should say, of selinexor with ruxolitinib. This is untreated patients with myelofibrosis, intermediate to high risk, who were given the combination rather than ruxolitinib, which would be considered the standard or JAK inhibitor.
Although it was early on and only a few patients, very surprisingly and amazingly, the group showed that there’s a high rate of activity in spleens being reduced as well as symptom burden being increased.
Now, this is preliminary data, but it was so encouraging that they are now moving on to a phase 3 randomized global study. The combination selinexor-ruxolitinib, so the XPO1 inhibitor plus JAK inhibitor, versus JAK inhibitor alone. Those data will be eagerly awaited.
This is also, if I may say, a fascinating study.
Dr. Naveen Pemmaraju
Navitoclax & Ruxolitinib
Ruth: What about the BCL inhibitor navitoclax?
Dr. Pemmaraju: A second combination is that of the BCL-XL inhibitor navitoclax with ruxolitinib, which I presented as an oral presentation at ASH on behalf of my colleagues. This is also, if I may say, a fascinating study.
We globally enrolled 252 patients into a randomized, double-blind, placebo-controlled study of ruxolitinib plus navitoclax, which is not yet approved for any indication, versus ruxolitinib alone. Again, we had intermediate to high-risk patients, around 80-plus percent of intermediate-2 patients.
What we found is a very outstanding rate of 60-plus percent of patients in the combination arm having an SVR35 at week 24, so spleen volume reduction of 35% or more, versus only 30-plus percent in the control arm, which was ruxolitinib alone. The waterfall plot showed that almost all patients benefited from the combination.
In terms of statistical analysis, the primary endpoint of spleen reduction was met with a high statistical significance, but the symptom burden difference was not yet found to be statistically significant. Both groups had reductions, so there was a numerical reduction of the symptoms in both the combination and the ruxolitinib alone, but there was no statistical difference.
The study is ongoing for collecting for maturity and overall survival duration, so this was a preliminary presentation at 15 months follow-up. We’ll stay tuned to see how it gets updated over the next congresses.
Great safety, but you have to watch out for thrombocytopenia, which is low platelets, and watch for that signal very closely.
Luspatercept & Ruxolitinib
Ruth: Another combination being investigated is the use of a shot called luspatercept to boost hemoglobin or fight anemia, and that also is being used with ruxolitinib. Can you tell us more about that one?
Dr. Pemmaraju: Luspatercept is a fascinating molecule. It’s already FDA-approved in the myelodysplastic syndrome setting. In the MPN setting, we think it has a similar activity to improve hemoglobin and anemia, which is an urgent, unmet medical need.
The initial studies have shown positive data, which is either luspatercept by itself, usually given every three weeks, or in combination with the JAK inhibitor ruxolitinib. Those studies are ongoing and we eagerly await those results in the coming year or two.
When the group looked back at certain subsets, including the intermediate-1 patients and others, it appeared that there was a benefit in both spleen size and symptoms.
Dr. Naveen Pemmaraju
Pelabresib & Ruxolitinib
Ruth: We’ve also had the MANIFEST trial, which is the trial that I happen to have been on for the last four years, and that’s a different drug, s pelabresib. Could you talk about that combination and what you think the potential is?
Dr. Pemmaraju: Another exciting combination presented at ASH 2023 was that of the MANIFEST-2, which is ruxolitinib plus a new agent pelabresib, a bromodomain or BET inhibitor, which is not yet FDA-approved for any indication.
This encouraging data set was presented by Dr. Raajit Rampal from Memorial Sloan Kettering. It’s the second-largest study ever conducted in the myelofibrosis front-line space, which included 430 patients. They also randomized ruxolitinib-pelabresib versus ruxolitinib alone in the control, mostly intermediate-1 to intermediate-2 patients, so a slightly different population.
They showed a very similar profile. A highly statistically significant primary endpoint was met, which is SVR35 at week 24. The symptoms in all comers, although showing a numerical decrease in both groups, did not quite meet statistical significance.
When the group looked back at certain subsets, including the intermediate-1 patients and others, it appeared that there was a benefit in both spleen size and symptoms.
The supposition is the same as navitoclax. These two are the first ever in our field, resulting in phase 3 global, double-blind, placebo-controlled, front-line, untreated myelofibrosis patients with a novel combination of pelabresib and navitoclax, neither of which are FDA-approved for any indication.
I would say my editorial comment is super exciting for the field that we even did it. Both were international studies largely conducted during the pandemic and involved lots of patients and investigators.
The primary endpoint was met for both of them. The symptoms were not quite met in either study in terms of statistical significance so the question asked is three-fold.
What is the utility of following the symptom burden scale in combination studies, something that was designed 15 years ago for a single-agent JAK inhibitor?
Do we expect a combination to improve symptoms over ruxolitinib alone, or because you’re introducing a second drug, you’re going to introduce new toxicity?
On behalf of my colleagues, maybe it’s time to reevaluate: what are the endpoints for our patients with myelofibrosis? Perhaps in addition to reducing spleen size and improving symptoms, we should be factoring in overall survival, progression-free survival, and bridging to stem cell transplant. This is the time to talk about it because these combination studies are difficult, if not impossible, to judge based on the COMFORT-I and COMFORT-II studies.
Imetelstat is in an ongoing phase 3 trial, which is in the second-line setting and beyond, against the best available therapy (BAT).
Dr. Naveen Pemmaraju
Telomerase Inhibitors
Ruth: Let’s go beyond JAK inhibitors. There are other drugs being studied. Can you help us understand other approaches?
Dr. Pemmaraju: There’s an exciting alphabet soup of clinical trials and drug molecules out there. It’s exciting for our patients to know that there are people around the world who care about MPNs, so it’s good to know that despite COVID, we have a lot of innovation.
We’re adding a new trial once a week, so it’s almost impossible to keep up, but I do want to give some sampling of what’s going on.
Imetelstat is very important for everyone to know. It’s a first-in-class telomerase inhibitor. Some people have heard of telomeres. They are the little ends on the ends of chromosomes that help to determine aging and possibly even cancer biology.
Imetelstat is in an ongoing phase 3 trial, which is in the second-line setting and beyond, against the best available therapy (BAT). I praised this trial because it’s the first and, to my knowledge, only phase 3 trial that has overall survival as its primary endpoint. Hopefully, it will give us a readout in the next year or two.
MDM2 Inhibitors
Dr. Pemmaraju: MDM2 inhibitors have gotten a lot of press in all MPNs. This is a key pathway that has to do with guarding the cell TP53. It’s an oral drug that has been studied before. As a class of drugs, there may be some GI side effects to watch out for, but in the later trials we’ve seen, the groups have figured out a way to address that by either adjusting the dosing schedule or dosing frequency.
I’m excited to see where that area goes. Right now, the lead trials are MDM2 inhibitors with ruxolitinib as an add-on approach or a suboptimal approach. You’re already on a JAK inhibitor. You have an okay response, not a great one, but not quite ready to come off of it, and then you add the MDM2 inhibitor. Those studies are actively ongoing and I think we’ll be excited to see those results.
The good thing about myelofibrosis is whether you’re JAK, CALR, MPL, or triple negative, you respond to JAK inhibitors and novel agents alike.
Dr. Naveen Pemmaraju
Genetic Mutations in Myelofibrosis
Ruth: What if someone’s myelofibrosis isn’t driven by a JAK mutation but a different mutation, is there a different approach? We’ve also been hearing about a cancer vaccine related to CALR, so could you walk us through both?
Dr. Pemmaraju: There’s a two-part answer to the question of molecular mutation targeting in MPNs. Historically and in the clinic right now, there is no difference at the moment.
The good thing about myelofibrosis is whether you’re JAK, CALR, MPL, or triple negative, you respond to JAK inhibitors and novel agents alike. That’s an interesting thing that suggests that there’s a common pathway.
But for the future, yes. Already in the clinic in 2024, we expect a new era to begin, which is, for the first time, to have mutant-specific approaches for both JAK2 and CALR. I expect that we’ll see multiple different drugs targeting mutant JAK2 specifically. The hypothesis is: could that be better and more specific than targeting the whole pathway? Let’s see. You’ll see phase 1 trials there.
CALR turns out to be a really good target, especially for immune therapy targeting. That’s only new science in the last five years. There are vaccine approaches either by themselves or with other immune drugs, such as ipilimumab. There’s an exciting bispecific molecule, which is a mutant CALR x CD3 bispecific antibody that I and others will be working on.
There are also going to be other ways to target CALR. You have multiple different ways of targeting mutant-specific approaches, but let me highlight these are phase 1 clinical trials. They’re backed by animal preclinical data. Now we need to see how they do in the initial trials.
For the first time, I’m seeing sustained improvement in the anemia of MPN, specifically myelofibrosis. We have three different categories trying to address this for our patients.
Dr. Naveen Pemmaraju
Anemia in Myelofibrosis
Ruth: Dr. Pemmaraju, you mentioned that many people suffer from anemia when hemoglobin is low. We know they can feel extremely fatigued so much that it interferes with their quality of life, which I know from personal experience, unfortunately. With what you’ve described, do you feel like we’re getting better tools to fight anemia and hopefully avoid people needing more frequent transfusions?
Dr. Pemmaraju: Yes. For the first time, I’m seeing sustained improvement in the anemia of MPN, specifically myelofibrosis. We have three different categories trying to address this for our patients and it’s simply exciting.
First is the JAK inhibitors themselves. As we mentioned earlier, the first initial ones did not improve and may have worsened the anemia transiently in some patients. Now these second- and third-generation JAK inhibitors are improving the anemia and possibly through the inhibition of ACVRL1, so that’s exciting.
Second is the additional agents, such as luspatercept. You can add on an agent that works outside of the JAK inhibitor that aims to stimulate the hemoglobin and improve the anemia.
Third is these novel agents. When you look closely at the navitoclax and pelabresib data sets, in those two particular instances, you have some people who get anemia as toxicity, but you also have patients who have anemia improvement with the combination, maybe better than with ruxolitinib alone. These three approaches, we’re already seeing in the clinic in phase 1, 2, and 3 clinical trials.
Out of all of these theoretical things, a lot of times what our patients are suffering from is anemia. When the hemoglobin gets below 7, 6, 5, or 4, it’s not even compatible with life, much less quality of life. Anything we can do to reduce the burden of getting transfusions, missing appointments, and missing life events is going to be a big breakthrough, and I’m starting to see that.
If a transplant is available and indicated, it is the only curative approach for myelofibrosis.
Dr. Naveen Pemmaraju
Role of Stem Cell Transplant in the Treatment of Myelofibrosis
Ruth: Typically, a doctor will tell a patient that the only cure for myelofibrosis is having a stem cell transplant. With these new medical therapies, my question is always the same: do you see a changing role for transplants?
Dr. Pemmaraju: The role of stem cell transplant in myelofibrosis is one of great importance still. While I’m personally excited about all of these drugs in development, two things are important.
First, none of these have been shown to create a long-term cure in and of themselves for myelofibrosis. Second, if a transplant is available and indicated, it is the only curative approach for myelofibrosis.
Having said that, the realistic problem with allogeneic transplants is that it’s not available for everyone because of their comorbidities, how frail versus how fit they are, matching, the infection rate, and the mortality rate. As patients get older, it may be tougher at some centers and for some folks to do it. There are some real limitations.
The other problem is that out of all of our patients, the vast majority are not going to transplant. Improvements are being made with transplants every day. Haploidentical transplant, which is a half match, is becoming more of a standard, so that gives the donor pool exponentially more options.
Trying to reduce graft versus host disease, which are complications after the transplant, with medicines are revolutionizing the field.
As I’ve traveled all over the world, people can do stem cell transplants in economically diverse situations. The transplant procedure itself can be highly expensive. Interestingly, even though cost-effectiveness is an issue, in some locales, if you can do a transplant and potentially cure the disease, it can lead to an improvement in socioeconomic status overall.
There are some cool, important things happening. But it’s an important point that even with all the excitement of these medicines and medicine combos, we’re still not at the point where we’re talking about a cure, so if you have the availability and indication for transplant, you have to pursue that consideration.
We have brand new approaches that we didn’t have a few years ago. There is a lot of data and science, so there’s hope.
Dr. Naveen Pemmaraju
Final Takeaways
Ruth: Let’s put all of this together. For those of us living with myelofibrosis or others who are concerned about progressing to myelofibrosis, what do you want to leave them with? When you total up everything we’ve talked about, how do you want to leave the conversation?
Dr. Pemmaraju: This discussion was very exciting because it left me with even more hope than when I started the day. I would leave our patients, caregivers, family members, advocates, and stakeholders with a message of hope and positivity. It’s not blind hope and positivity. It’s not based on hunches or ideas. It’s based on data.
The last three years in particular, I would call it — and I do not use this phrase lightly — a golden era for research for the MPN, specifically including myelofibrosis.
There are four areas to highlight and to be very excited about for our patients and families. First is the development of new JAK inhibitors. We mentioned the four that are already approved in the US, so let’s get them available all over the world. There are several more in clinical development.
Second is the JAK inhibitor combinations. Very exciting data from ASH. Let’s see the new combinations. Maturing data for navitoclax, pelabresib, and selinexor.
A third area of excitement and hope is that of anemia-improving agents.
Finally, the delineation, description, and demonstration of brand-new molecular pathways inside the cells that were never known before. New insights and ways of approaching. We mentioned potential immune therapy approaches, like the CALR mutation. It’s exciting that we have brand new approaches that we didn’t have a few years ago. There is a lot of data and science, so there’s hope.
Ruth: Dr. Pemmaraju, thanks so much for being with us today. You’re always a pleasure to talk to and so informative to our guests. We really appreciate your time.
Dr. Pemmaraju: Thank you so much for having me. This was a very thought-provoking and stimulating discussion.
Doug shares his myelofibrosis journey after being diagnosed in 2016. He initially experienced fatigue, leading to a series of tests, which included a bone marrow biopsy that led to his diagnosis.
After following a watchful waiting approach, he started treatment with ruxolitinib. However, he continued to experience fatigue and platelet issues.
After extensive reading, he discovered a clinical trial for selinexor. Despite initial hesitation from his local doctor, he joined the trial in November 2019, experiencing positive results. Despite some side effects, like loss of appetite and weight as well as temporarily feeling off, the overall impact on his health has been significant.
Doug, now well beyond the initial life expectancy range, maintains a stable condition, visiting the Huntsman Cancer Institute every three months for follow-up. He emphasizes the importance of being proactive in exploring new treatments and encourages others to explore clinical trials for potential advancements in cancer care.
In addition to Doug’s narrative, The Patient Story offers a diverse collection of myeloproliferative neoplasm (MPN) stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
I was born and raised in Illinois and moved to Idaho for work in the early ‘70s. I love living in Idaho. Before I retired, I was working in Eastern Washington. My wife and I moved back to Idaho to be with family and we live outside of Boise.
I was having trouble with fatigue… When I mowed the lawn, I had to stop and rest because I was getting exhausted.
Pre-diagnosis
Initial Symptoms
I mentioned to my doctor that I was having trouble with fatigue. I noticed that when I mowed the lawn, I had to stop and rest because I was getting exhausted. At first, I didn’t notice it, but it got to a point where I was doing that every time.
I can’t remember what steps he went through with me, but after two or three different tries, he ended up referring me to a hematologist.
Diagnosis
Seeing a Hematologist
When I went to a hematologist in Washington, we went through a series of tests, including a bone marrow biopsy. That’s how I got my diagnosis in May 2016.
It was a shock. It was made doubly so because my wife was diagnosed with breast cancer a couple of weeks away from my diagnosis.
Learning About Myelofibrosis
I knew absolutely nothing. It took me a while to remember the name. They call it a rare disease. You don’t know people who have myelofibrosis. It’s not like breast cancer. Everybody knows somebody who had breast cancer so that’s familiar.
Reaction to the Diagnosis
It was a shock. It was made doubly so because my wife was diagnosed with breast cancer a couple of weeks away from my diagnosis. We were a year into my retirement and getting going with traveling when all of a sudden, both of us had cancer.
Her breast cancer was treatable. It was one of the less aggressive ones so after she had two surgeries and radiation treatment, she hasn’t had to do anything since. She’s clean every time she goes in for an examination.
Learning to live with the idea that I had cancer took a while. Through my reading and thinking about it, somehow your mind comes to terms with it. You can’t have a big open issue like that. You resolve it a little bit at a time. It comes down to it’ll be what it’ll be, but it isn’t necessarily what I would like it to be.
I was not doing that well on ruxolitinib. I had a lot of fatigue. I felt like I was going downhill.
Treatment
Watch and Wait
My disease wasn’t that far along so we decided to do what he called watchful waiting. At the time, there was only one medication, ruxolitinib, and it was not a cure. As long as I didn’t have symptoms that we were going to try to treat, we would wait.
That went on for the better part of a year. In the middle of all that, we moved back to Boise. When I found a new hematologist in town, he prescribed ruxolitinib right away.
Starting Treatment on Ruxolitinib
I was a fairly typical patient. I went through a period where I had very low platelet counts. We had to keep adjusting my dosage because at one point, I went well below 50 and I was having trouble with it. I also had anemia and it had gotten worse. I was on ruxolitinib for probably a year and a half, no more than two years.
I was not doing that well on ruxolitinib. I had a lot of fatigue. I felt like I was going downhill and my platelet counts continued to be a problem.
I wanted to find a clinical trial that I could buy into the idea of what the drug was.
Learning About a Selinexor Clinical Trial
Early on after my diagnosis, I started doing a lot of reading. I subscribed to Google Alerts where you provide keywords and it sends you links to articles with those keywords.
An article showed up from The Salt Lake Tribune and it was from the Huntsman Cancer Institute at the University of Utah. The doctor in the article had a new FDA study that he and his team were initiating. The drug was called selinexor and they saw good results in their clinical studies so they were ready to start a human trial. They described in layman’s terms how the drug worked and what it did.
It was interesting because it was unique and completely different from ruxolitinib. It had been FDA-approved and was used as a treatment for multiple myeloma. It was just a matter of trying to see if it had efficacy with myelofibrosis.
I’ve been grateful for the good fortune I had to read that article. It was a shot in the dark. Something I say to anybody is you don’t know where the answers will come from.
It always amazes me that myelofibrosis is a rare disease. Not many people have it, but it amazes me the amount of effort that the pharmaceutical community is putting into developing treatments. I don’t see how they can come out ahead financially, but I’m grateful for it. I’m all for it. If they’re willing to go for it, I’m willing.
I had gotten familiar enough with my reading. I knew there was only one approved drug that I could have prescribed for me. Now, there are four, but they’re all somewhat similar. They have different characteristics, but they’re all JAK inhibitors. If you’re going to get anything different, it’s going to have to go through a clinical trial first. I wanted to find a clinical trial that I could buy into the idea of what the drug was.
There was another drug in the trial phase with a very different mode of operation. I went to Oregon Health & Science University and interviewed with them at the same time as the selinexor clinical trial. I was considering it, but at that point, I had some issues going on with my kidneys and they wouldn’t accept me because of my kidney function.
As far as trials are concerned, if you want to get the latest and greatest technology, it’s probably the best way to do it. You have to accept that there’s a certain amount of risk. With selinexor, after you’ve been on the drug for a year, nobody knows what the effects are. That’s what they’re trying to find out.
My doctor wasn’t enthusiastic about the idea (of a clinical trial) so that put me in a quandary because I didn’t want to get in a situation where I was running contrary to my doctor’s advice.
Joining the Selinexor Clinical Trial
There was a name and a phone number so I contacted them. They invited me to Salt Lake, which was a six-hour drive. One of the problems I had when I was doing my reading was every time I came across a new drug that was in a trial, it was always in some place like Los Angeles, Houston, or New York. Travel was always a big bugaboo for me, but Salt Lake was doable. I could do a six-hour drive or a one-hour plane flight and be there.
They evaluated me and extended an offer. The doctor said that he could tell that my spleen was large. I didn’t have that much information about my spleen at that point, but his take on the whole thing was that ruxolitinib was not effective for me and the outward evidence was my enlarged spleen.
Oftentimes, we hear people say you need to be your own advocate. It’s not just up to the doctor. It’s up to you to take care of things.
I went back to my doctor and said, “There’s this drug trial that they’re starting at Huntsman and I’ve been invited. What do you think?” He wasn’t enthusiastic about the idea so that put me in a quandary because I didn’t want to get in a situation where I was running contrary to my doctor’s advice.
After a week or two, I got a call from the doctor in Salt Lake and he said, “Doug, are you going to come on the program or not?” I explained to him about my doctor being reluctant about it and he said, “Let me talk to him.” They talked on the phone and after their conversation, my doctor was enthusiastic about it so I said, “Let’s go do it.”
This was in November 2019. I had to get off of ruxolitinib for a couple of weeks before I started. That was an ordeal for me because I quit cold turkey and it was like the worst flu I ever had. I felt bad for a couple of weeks. I felt like I was sinking, but I got through that.
I was feeling the results of the drug and it was all good.
Effects of Selinexor
Within a month or two after starting selinexor, I was feeling the results of the drug and it was all good. I wasn’t keeping a journal but over time, my platelet counts started stabilizing and went up.
My hemoglobin was increasing. I was at 7.8 and my doctor told me that when a patient is 7.5 or less, they start doing transfusions. A lot of myelofibrosis patients live on transfusions. I was steadily getting closer to the territory where I would have to get transfusions.
My blood count took off from 8.7 and after a year or two, my blood count is now 12.5. It’s almost at the low end of the normal range. My platelets are in the 250 range. My hemoglobin varies somewhere between 12 and 12.5.
My white blood cell count was one of the early indicators at the very beginning. The counts were high and in the normal range, but they were at the high end of the range. The doctor noticed that they were consistently high.
White blood cell counts vary quite a bit in normal people, but mine were always at the high end of the range. I never go out of the range, but the white blood cell counts for me are high.
My anemia has been solved in the last two years that I’ve been on the drug. When I do monthly blood draws, my hemoglobin and my red blood cell counts are in the normal range, my white blood cell counts are at the high end of the normal range, and my platelet counts are in the middle of the normal range.
Before I started the selinexor clinical trial, I bought a walker because I was having so much trouble with fatigue that I wasn’t taking walks. I didn’t want to go on a walk somewhere and be exhausted. She suggested I get a walker with a seat. That way, I could park myself for a time and get my energy back.
I haven’t used that walker ever since I started the selinexor clinical trial. I’ve loaned it out to friends a couple of times. I can’t say that my energy level is the same as it was before I received my diagnosis. It’s not quite the same, but I still can go out to take a half-hour walk and it’s not a big deal for me to do that.
Because the anemia went down, my energy levels have gone up. I take selinexor once a week. We’ve adjusted the dosage. When I first was on the selinexor clinical trial, I was taking 80 mg. Now that the initial trial period is over, the doctor adjusted my dosage to 40 mg.
What’s different about being on a trial is you don’t know what to expect over time.
Side Effects of Selinexor
The problem I have gotten into with selinexor is my appetite and maintaining my weight. I’ve lost 85 or 90 lbs. It was over a year or two, but it was still a significant weight loss. It was due almost entirely to the fact that selinexor took away my appetite.
The doctor gave me different medicines to try to counteract that problem. I still take one pill daily. Food doesn’t appeal to me like it used to. When I sit down at dinner, I invariably look at my plate of food and think I don’t want to eat, but once I get started, I can finish my meal. This comes from my experience and dealing with the change.
That’s been the only hard part of being on selinexor. My doctor tried to find a dose where I would quit losing weight and maintain a stable weight. I’ve been at this dosage level for a long time. I seem to be in a place where it’s still effective but I’ve stopped losing weight and can better maintain it.
I weigh myself every day. I have heart failure and they want me to weigh myself every morning. They’re looking for weight loss as an indicator of an event, but that’s been pretty stable for a long time.
Another thing that I have to put up with is selinexor puts me in a mode where I feel off. I take the drug on a Wednesday and it’s not until Saturday or Sunday before I feel completely right again. Sometimes it’s like having the blues. Sometimes it’s not feeling quite right, but it’s never intolerable. It isn’t like I lay around and writhe. No pain goes along with it, but it’s part of what I have to put up with.
What’s different about being on a trial is not knowing what to expect over time. The doctor and I have talked a couple of times about that. I was the fourth person on the selinexor clinical trial so nobody with my disease has been on the drug for that long. The doctor said at the end of the day, maybe the main thing that comes out of this is that we’ll have a drug that will arrest the progress of the disease.
I got something that works and it doesn’t seem to be fading out on me.
Current Status
I don’t feel like I’m gaining or losing. I know that my status has improved greatly. I don’t seem to be going any further up but neither am I going down. I’m maintaining a good normal.
There’s not a lot you can do. I was first diagnosed in 2016. I’m already beyond the range of what they say the life expectancies are, which is often a mid-range of about 5 to 5 1/2 years. I’m already beyond that and I feel good.
I know that a lot of cancer treatments only last for a time. Somehow, the cancer adjusts to them and they lose their efficacy. I had a sister-in-law who had breast cancer. She came in and moved in with us in her final year. They were constantly coming up with a new treatment. But 3 or 4 months later, she’s right back where she was again until she finally got to the point where she said no more and she passed.
Cancer treatments tend to have a limited period of effectiveness. But this one, because it has such a unique method of operating, doesn’t seem to have that same life expectancy so I’m grateful for that. I got something that works and it doesn’t seem to be fading out on me.
It was my good fortune that the selinexor clinical trial worked out well for me and was doable from the standpoint of the travel.
Traveling to Clinical Trials
The biggest bugaboo in the clinical trial process is the fact that it’s such an isolated condition. There are a handful of hospitals, most of which are associated with a university. It logically makes sense that that’s where these trials would be centered, but it sure leaves a lot of people out.
I’ve talked to a number of people over time. Somebody who lives in Idaho, Montana, or somewhere similar doesn’t have any way to commit to the travel. I know people who get on a plane to go to Los Angeles because that’s where the trial is.
I get a certain amount of reimbursement for travel down to Huntsman from the University of Utah. As I recall, their accounting people figured out a rate per mile. I get a check for a little over $200. But all of that is predicated on the fact that Salt Lake is relatively close to where I live.
For me, driving down to Salt Lake was doable. One way or another, I was going to make it happen. It’s a few hundred bucks to go down there, spend the night, and come back the next day. I’ve since found that it costs me about the same to take a plane because I can go in the morning, come back in the afternoon, and I don’t have to stay overnight.
They reimburse me based on the mileage of driving back and whether I drove or not. Flying is a little more expensive. But at the end of the day, it’s a difference of a couple hundred bucks. It’s not that big of a deal. It was my good fortune that the selinexor clinical trial worked out well for me and was doable from the standpoint of the travel that was required over three months.
Follow-up Protocol
I go once every three months. I do blood tests and sampling. They take a certain amount of blood for research and a certain amount for monitoring my health. I visit with a nurse and doctor. They’ve been good people to work with.
I encourage people to be open and moderately aggressive in looking for new things that are out there.
Words of Advice
Cancer is a nasty animal. We’re learning more and more about it all the time. It’s more and more getting to be a condition that can be solved. I look at selinexor knowing that it’s not a cure, but it seems to be holding me steady enough that over time, maybe there will be a cure.
I would expect there will be one at some point in time. Somebody will figure something out. If I die two months before that gets decided, it doesn’t do me any good, but this way, at least I give myself a chance to take advantage of new developments.
I encourage people to be open and moderately aggressive in looking for new things that are out there. There are new trials that are starting all the time.
There’s a new selinexor clinical trial that’s going into phase 3, I think, which means it’s well on its way to being an approved drug. They’re doing it in combination with ruxolitinib. I’m on selinexor alone. I don’t know what ruxolitinib adds to it, but if it works, it works.
Based on my experience, there’s a lot of safety built into the process. I had the benefit of selinexor being tested for other cancers before it came to me. Some questions on safety had already been answered with other drug trials. It made it a little bit easier for me to make a decision.
Don’t think that it’s dangerous and you’re out there all by yourself. There’s a whole network of knowledgeable people who are supporting and running these programs. They don’t want to have a failure in me any more than I want one.
Theresa’s myeloma journey is one marked by resilience, determination, and a profound sense of hope. Her life took an unexpected turn when she began experiencing severe hip pain in 2012. Despite numerous tests and consultations, it took several months to arrive at a diagnosis of IgG kappa light chain multiple myeloma.
The initial shock of the diagnosis was met with a steely resolve to confront the disease head-on. Supported by her husband Tom and guided by her medical team, Theresa embarked on a treatment journey that included RVd chemotherapy, which initially showed promising results but eventually led to relapse. Undeterred, she enrolled in a clinical trial for CAR T-cell therapy, becoming one of the first recipients of this innovative treatment.
While the CAR T-cell therapy initially induced remission, the cancer eventually recurred, prompting Theresa to explore further treatment options. She participated in another CAR T-cell therapy trial and subsequently underwent treatment with selinexor, carfilzomib, and dexamethasone (XKd), which has been effective in managing the multiple myeloma.
Throughout her journey, Theresa has remained optimistic, actively participating in her treatment decisions, and advocating for herself. Her story is a testament to the power of resilience, hope, and the relentless pursuit of innovative treatments in the face of adversity. As she continues her journey with multiple myeloma, Theresa’s unwavering spirit serves as an inspiration to others facing similar challenges.
In addition to Theresa’s narrative, The Patient Story offers a diverse collection of multiple myeloma stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
It gives me hope that there are more treatment options out there. There are so many people working at different levels to help folks with myeloma be better-taken care of. They’re looking for a cure, so that’s very exciting. They’re getting closer than they have ever been.
Theresa: I was born in New York City, grew up primarily in Connecticut, and currently live in San Francisco. I went to college in Boston, moved to San Francisco a month after graduating, and I’ve been here ever since.
I had a great career in human resources. I loved that because I love helping and training people. That helped me a lot in my myeloma journey. I’ve been able to talk to other people who have myeloma, help them, and provide information. It’s always good to extend a helping hand to other people. People have done that to me as well, so I want to give back.
I have three brothers and two sisters. It was great growing up with great siblings. We all get along, which is wonderful. I love my brothers and sisters.
I used to be a lot more active. I love to swim. I love to go to the beach. I wish it was a little bit warmer, but it’s close.
I’m full of energy, loving, funny, sometimes smart, and strong, which is interesting. It’s sometimes hard to take that compliment when you go through cancer. People say, “Oh, you’re so strong. I admire you.” Meanwhile, inside, you’re freaking out.
I’ve had people say that to me a lot, so I guess it’s true. I think it comes from being from a long line of strong women in my family. I have good role models. I don’t know any other way to be.
Pre-diagnosis
Initial Symptoms
Theresa: Around February 2012, I started having bad pain in my right hip, which kept getting worse and worse.
I went to my primary care physician who took blood tests and X-rays but didn’t find anything. We kept digging further. We didn’t know what was going on. It was rough, but I kept going. I probably had 6 or 7 different kinds of blood panels to try and figure out what was going on.
For a period of about 3 to 4 months, she went from working out once a week to being unable to walk on level ground without a cane.
Tom
Scans
Theresa: She sent me to an orthopedic surgeon for a spinal X-ray. He’s the one who suggested that I get an MRI, which revealed lytic lesions. Myeloma tends to create lytic lesions. It’s a cancer of the bone marrow, so it eats away at the insides of your bones.
Between mid-February to the end of June is how long it took to get a real diagnosis. In the meantime, my pain kept getting worse and worse. I was using a cane and on pain relievers. It was frustrating to not know what was going on.
Tom: It was unpleasant and worrisome. We didn’t know what it was. For a period of about 3 to 4 months, she went from working out once a week to being unable to walk on level ground without a cane.
Diagnosis
Getting the Official Diagnosis
Theresa: I had an appointment set up at the end of June with my primary care physician. I had seen her several times since February to try to figure out what was going on.
The day before my appointment, I got an email from the doctor’s office referring me to a hematologist-oncologist. I was in denial as to what that meant. It was pretty shocking, but I wanted to wait until I saw my doctor.
They set up an appointment with the hematologist-oncologist for me to talk to. He was a lovely man and was very good. I got one of my first bone marrow biopsies. At the end of June, it was confirmed that I had multiple myeloma.
Tom: He said, “As far as survival is concerned, five years is easy.” My jaw dropped.
It was going to be a big part of her life from here on out, which meant it was also going to be a big part of my life from here on out.
Tom
Reaction to the Diagnosis
Theresa: My myeloma story started when there were a lot of emerging therapies for myeloma. I had always been pretty much healthy and didn’t have anything wrong with me specifically. I led a fairly healthy lifestyle while enjoying life, but I was shocked to get this diagnosis.
Tom: It happened pretty fast. I knew what it meant for her and it was going to be a big part of her life from here on out, which meant it was also going to be a big part of my life from here on out.
Theresa: I left his office better informed. It took me a while to absorb everything. I didn’t completely freak out. I was still in a bit of a denial.
As I talked to them, did more research, and got information about what the treatment was going to be, it slowly seeped in that I had cancer.
Theresa
Discussing the Treatment Plan
Theresa: When they discussed setting up the appointment for the first treatment, I said, “Maybe we’ll wait a few weeks.” He said, “Why are we waiting? We should do this right away.” I didn’t understand the impact of it right away.
As I talked to them, did more research, and got information about what the treatment was going to be, it slowly seeped in that I had cancer. It’s not the worst cancer, but it’s not good because it doesn’t have a cure, so that was a little shocking.
I came back the following week with Tom. The doctor very patiently and thoroughly went through what this disease was, what the treatment protocols were, and what we would do next. The good thing is they’ve developed new therapies.
RVd Chemotherapy
Theresa: The oncologist had a very specific treatment plan. He said, “The initial treatment you get is RVd (lenalidomide, bortezomib, and dexamethasone). This is the standard of care. This is the best that we can do for you.” At that time, there wasn’t a good alternative.
Tom and I talked about it. One thing that I appreciate he always says is, “It’s your body. You have to make the ultimate decision.” Over the years, we’ve talked about different treatment plans, what they’re going to involve, timing, and everything. But in the beginning, the timing was as soon as possible.
Subconsciously, I was doing things often because I couldn’t control this part of my life, so I would try to overcorrect by controlling other parts of my life.
Theresa
Side Effects of RVd Chemotherapy
Theresa: I had a fever. After my second infusion appointment, the fever got worse. They took me to the hospital, which at the time was at CPMC (California Pacific Medical Center). I stayed overnight for observation to make sure I was okay.
When you start a new therapy, your body tends to be shocked and you often have adverse reactions. Luckily, they didn’t continue.
My first reaction was itching. A couple of months later, I had a little rash, but it went away. It was nothing awful.
I had a lot of fatigue. I wasn’t sure if I was going to take time off of work. I took time off for all the appointments, but after that, I took a three-month leave of absence.
After about six months, my numbers went down. I have IgG kappa light chain myeloma. There are different kinds of myeloma. It’s so varied that it’s hard to pinpoint sometimes. I found out that what works for one person may not work for the next person.
I was on and off treatment for a while. That’s my story. It’s been a roller coaster ever since, going up and down, having longer stretches of relapse or shorter stretches of relapse depending on what’s going on.
I’ve gotten upset a lot during these 10 years, especially when I didn’t have control. That’s what affected me more than the why.
I don’t have any control over this disease. I can’t control the effects of the treatment. Even subconsciously, I was doing things often because I couldn’t control this part of my life, so I would try to overcorrect by controlling other parts of my life.
I ask questions and follow orders, so he thought I would be a very good candidate for the CAR T-cell therapy trial.
Theresa
CAR T-cell Therapy Clinical Trial
Theresa: [My disease] became refractory towards my line of treatment. It stopped working. They had a clinical trial available and he thought I was a good candidate. I asked him why he thought that and he said, “You’re in otherwise pretty good shape. You’re doing well. I know you pay attention.” I ask questions and follow orders, so he thought I would be a very good candidate for the CAR T-cell therapy trial.
I was enrolled in the bb2121 trial, which led to the very first FDA-approved CAR T-cell treatment [in myeloma]. I know my number is in there somewhere about my survival with that treatment, so that’s fun.
Clinical trials are a lot. You have to be dedicated. I remember talking to somebody who said, “Why are you doing this trial?” I said, “I want to help other people. Besides, I think it’s going to help me. It sounds really good.” You’ve got to do what you’ve got to do.
Deciding to Participate in a Clinical Trial
Theresa: I had been reading about CAR T-cell therapy and learned they had amazing results. People thought that this might be the cure for myeloma that everybody’s been frantically searching for, so it seemed like a good idea at the time.
There was a lot of paperwork to go through. There were 55 pages of study material that you had to sign your name on about 20-some-odd times, but it’s so worth it.
I trusted my doctor, Dr. Thomas Martin, who is a world-renowned myeloma specialist. I trusted his opinion and read everything.
I had some hesitation because it was still a trial, but the safety and efficacy had been already dealt with. This was a matter of figuring out the dosage, I believe. I felt it was safe and a good idea. I trusted the doctors and trusted what I read.
Within 30 days, I had a complete response. There was no myeloma detected in my system. That lasted for about 18 months.
Theresa
CAR T-cell Therapy Process
Theresa: First, they take your cells out. They had to send them to New Jersey and then back to California. Before that, there were three days of chemo. To get the CAR T cells, you have to go to the hospital. It’s like a short infusion.
I got them on a Monday and then I had what we like to call Loopy Tuesday. I did have cytokine release syndrome. I don’t remember most of that day at all. I said some strange things when they asked me questions.
After that, they hooked me up. They did so many things to make sure I was okay. I felt okay. They did tests. Doctors came every five minutes. They wouldn’t leave me alone. Everything was fine, except for that 12- to 18-hour stretch. It was otherwise being bored in the hospital.
Luckily, within 30 days, I had a complete response. There was no myeloma detected in my system. That lasted for about 18 months, which is better than the average of about a year or 13 months. I beat the odds, but it came back.
JCAR CAR T-cell Therapy Clinical Trial
Theresa: We talked about options. I didn’t go on treatment right away when I started relapsing. There was another trial that he wanted to try, which had a different target. I tried that, but only for a month. It didn’t do any good and it was hard.
Dr. Martin said, “I’ve got another CAR T trial we could try. It’s got a little bit of a different target, so maybe it’ll work.” I went on the second CAR T-cell therapy clinical trial. I did not have the bad CRS I had with the first one. I was only in remission for three months, so it wasn’t effective. That’s when we decided to go on selinexor.
Know that it could get better. If it’s your first treatment, give your body time. Talk to the doctors and the nurses. Ask them what to expect and what’s normal. Don’t be afraid to ask what’s going on. “What can I expect from this? What can I do to change this? Can I change the dosage? Can I change the timing?”
Selinexor, Carfilzomib, and Dexamethasone (XKd)
Theresa: I’m taking selinexor in combination with carfilzomib and dexamethasone (XKd). In the beginning, it was three weeks straight of carfilzomib infusions and selinexor every other week.
They said it would make me nauseous, so they gave me two anti-nausea drugs while I was getting the carfilzomib. I had two kinds of pills to take at home: one at night for three days and then another to take any other day that I felt nauseated.
It did usually present with some nausea for about three days. I experienced extreme fatigue, although we found out that it was due to the anti-nausea medicine that I was taking at night, so we changed it.
I take three pills in the morning before I get my infusion and on selinexor days. Five or six hours after I get my infusion, I take dexamethasone.
I’m very lucky to have responded to a lot of different treatments. Most of my treatments have been pretty good.
Theresa
Adjusting to New Treatments
Theresa: Know that it could get better. If it’s your first treatment, give your body time. Talk to the doctors and the nurses. Ask them what to expect and what’s normal. Don’t be afraid to ask what’s going on. “What can I expect from this? What can I do to change this? Can I change the dosage? Can I change the timing?”
With dexamethasone, sometimes, it depends on the dosing schedule because it can keep you awake. Work with your body to know the best time to take it and if you can make adjustments. Ask the doctor, “What else can I do?”
This is one mistake that I made in the beginning. I thought if I said something to my doctor, they would address it, but they don’t always do that. If you say something, they’ll listen and write it down, so you have to specifically ask them.
I’ve been on this regimen since September 2021. Again, beating those odds.
One thing I know is that I’m very lucky to have responded to a lot of different treatments. Most of my treatments have been pretty good. Maybe a quarter to a third of them didn’t work, but others have, so I’ve been very lucky to have that percentage work for me.
Future Treatments
Theresa: I don’t think about them specifically. I’ve already discussed what my next treatments would probably be. I have a choice between a bispecific antibody trial or another kind of CAR T-cell therapy clinical trial on a completely different target.
It’s likely that within some amount of time, maybe 3 to 6 months even, I’ll have to go on another treatment. Selinexor has worked for way longer than expected and it’s been well-tolerated.
I have hope. I’ll still be around. I still have stuff to do. I’m not ready to go yet.
Theresa
Words of Advice
Tom: When we got the diagnosis, I said, “Okay, we’re on our way. We got a name. We can pin this sucker down.” We’re getting closer to 10. Median survival rate was 7 ½ years and she’s beaten the hell out of that.
Theresa: I have hope. I’ll still be around. I still have stuff to do. I’m not ready to go yet. It gives me hope that there are more treatment options out there. There are so many people working at different levels to help folks with myeloma be better-taken care of. They’re looking for a cure, so that’s very exciting. They’re getting closer than they have ever been.
It’s about survival, doing the right things, getting support, and being tough.
Symptom: None; found through blood tests Treatments: Total Therapy Four, carfilzomib + pomalidomide, daratumumab + lenalidomide, CAR T-cell therapy, selinexor-carfilzomib
Relapsed/refractory Hodgkin’s thriver Sam Siegel and Dr. Andy Evens from Rutgers Cancer Institute discuss the latest in Hodgkin’s lymphoma treatments and how to reduce the toxicity of treatments so patients can live their best lives after cancer.
Get updates on recent and upcoming clinical trials, how to manage treatment side effects, and new approaches to mitigate chemo toxicity.
Know more about the role of stem cell transplant and radiation in the treatment of Hodgkin lymphoma, and how to create personalized Hodgkin treatment plans.
Learn what questions to discuss with your care team, lifestyle changes to improve quality of life, and how to have a holistic approach to your care.
Dr. Sam Siegel: I’m a relapsed/refractory Hodgkin’s thriver, mom of three, loving wife, primary care provider, and survivorship medicine practitioner. I’m here to talk about Hodgkin’s lymphoma, the latest treatments focusing on reduced side effects, and a holistic approach to care.
We want to note that The Patient Story retains full editorial control of this entire program and that this is not meant to be a substitute for medical advice.
I’m excited for this conversation with Dr. Andrew Evens from Rutgers Cancer Institute to talk about the latest trials in Hodgkin’s lymphoma and how to reduce the toxicity of treatments so that we can live our best lives after surviving cancer.
Andrew Evens, DO, MBA, MSc
Sam: I have the privilege of being with Dr. Andrew Evens, a specialist in Hodgkin’s lymphoma at Rutgers, leading clinical trials for more than 20 years, and also the medical director of RWJBarnabas Health.
Dr. Evens, can you tell us more about your path into Hodgkin’s lymphoma treatments and all of the amazing things that you do for the lymphoma community?
Dr. Leo Gordon, who was and is still the director of the lymphoma program, Dr. Jane Winter, one of our recent American Society of Hematology (ASH) presidents, Dr. Martin Tallman, and Dr. Steve Rosen—stalwarts in the field of hematologic malignancies.
I had an early interest. This was over 20 years ago and at the time, we knew that Hodgkin lymphoma was pretty curable. We’ve known that since the 1980s, but nothing’s 100%.
Sometimes, it doesn’t always work or there are side effects. Even though we have known for a few decades that it’s very treatable and curable, we’re always trying to do better and do so with more tolerable targeted treatments. It’s an active area of study.
I was finishing my training with a global network of Hodgkin lymphoma experts. There are many different meetings and conferences we all go to. There’s one in particular in Cologne, Germany, that they’ve had for over 20 years. They’ve been amongst the world’s leaders in Hodgkin lymphoma research, clinical research, and basic science research.
At the time, Hodgkin lymphoma experts across the world met there every three years. Now, it’s every two years. When I say all of the experts, it’s not just clinicians. It’s soup to nuts Hodgkin lymphoma. It’s epidemiology. What causes it? It’s etiology. What’s in the microbiology and genomics? It’s diagnosis, treatment, and, importantly, post-treatment survivorship. It’s an incredible meeting.
When I went to that first meeting as a young whippersnapper hematology-oncology fellow, I knew that was for me. Something called to me about it. Knowing that so many different aspects related to Hodgkin lymphoma, I’ve been fortunate to be involved in the field for over 20 years now.
Sam: I did a lot of hematology-oncology in my internal medicine residency. I started as a hospitalist where I did a lot of hematology-oncology and had that lens with end-stage pathology where people come into the hospital very sick and then to outpatient medicine, seeing people sooner and trying to get them diagnosed sooner. Then I got cancer.
Sam’s Hodgkin Lymphoma Story
Sam: My story began in 2021 when I began feeling super exhausted. I thought I was just tired like every other doctor-parent was during the pandemic. A lot of people I knew were tired. I had a lot of justifications for why I was feeling that way.
I started coughing, but there were some wildfires in California so I thought maybe that was it. Maybe I was getting asthma.
When I developed a rapidly growing, rock-solid, painless lump above my collarbone, I thought, Oh, gosh. I have cancer. Once that showed up, I was no longer in denial and got a whole series of tests that ultimately led to a diagnosis of stage 2AE Hodgkin’s.
In the beginning, there was some controversy about my staging. I had some lung involvement and my understanding at the time was if there’s lung involvement but it’s connected to the major tumors that are there, it’s still stage 2 with extranodal (outside of the lymph nodes) manifestations versus stage 4. That was the first decision-making point. What’s my stage and how would that impact my treatment?
It was a complete shock. I was a marathon-running doctor mom, minding my own business, doing life, and then boom—Hodgkin’s diagnosis. I believed myself to be healthy, even though I was feeling symptomatic.
I started what was considered back then the standard upfront treatment called ABVD chemotherapy. My cough went away with my initial chemotherapy and after about two months, the cough came back.
Around that time, I had a scan that showed that my disease was responding well so we decided to drop the bleomycin. We thought I was developing a bleomycin-related cough after the initial cough had gone away.
I continued the next four months with AVD. I got a scan at the end of six months and had no evidence of disease. That was very exciting but also troubling because I felt bad and I wasn’t sure why. Do I feel bad because this is how a body feels after having a multiple-drug regimen for six months or is there something else going on?
I had another PET scan after developing symptoms of relapse and that showed that I had most likely developed a relapse. I had to undergo various procedures to get a tissue sample to confirm. Within a month, I was diagnosed.
What started as a seemingly “simple cancer” or “winning the cancer lottery” as some people are told, I realized very quickly that the treatments are hard, especially some of the older treatments before you get to the immunotherapy and the newer discoveries. Even if you get cured or have no evidence of disease, it can come at a great cost.
Cancer Survivorship
Sam: I found my way to the field of cancer survivorship and I’m super pumped about that and to talk to you about holistic health and your role at RWJBarnabas Health. Because I’m also doing an integrative medicine fellowship, I realized how incomplete our medicine is.
Allopathic Western medicine saved my life, but it also decimated my health at various points so I realized we need other tools. We need to embrace this other field of medicine to complement that, to help people withstand the toxicity of treatment, and to recover and rehabilitate from it when they’re done. I’d love to hear your thoughts.
Dr. Evens: There are so many good clinical trials happening across the world. Every clinical trial asks a slightly different question. At the end of the day, however good clinical that trial is, how is that applied at the bedside?
Sometimes, for better or for worse, treatment ideations and recommendations end up becoming one size fits all and we know every patient is different. I always say that there are a lot of commonalities between Hodgkin lymphoma and non-Hodgkin lymphoma, but each patient is unique and different.
How do we take large amounts of data, amalgamate it, and apply it to the patient? It’s difficult because we have lots of data and there are recommendations and certain guidelines.
But what about you, Dr. Sam? For an individual patient with your stage, your albumin, and your lymphocyte count, there might not be one best therapy. There might be treatment options A, B, or C. But are there data or algorithms that I can put my characteristics, desires, hopes, and patient preferences to say if I go with A, B, or C, here’s what I would expect in acute within 1 or 2 years, and here’s what I would expect moreover 30 years down the road?
Sam: My mindset shifted. In the beginning, I was so afraid. I’m a young mom with my whole life ahead of me. I was so afraid of dying so I thought, Let’s hit it hard. Let’s do everything. Let’s get the strongest therapy.
As I began to move through treatment and experience, there were some pretty devastating adverse effects that I wasn’t sure how long they would last. As a doctor, I was primarily concerned with the cognitive impairment. I experienced severe chemo-related cognitive impairment, which is the worst form of chemo brain.
I gained 40 lbs from steroids and became severely metabolically ill. I got the rash that people get when they are going to develop diabetes called acanthosis nigricans. My glucose was high and my cravings changed. I wasn’t sure that life as I knew it would ever return.
When I developed symptoms of a relapse, my mindset was different, even just one month later. Let’s not give it everything we’ve got. Let’s make some decisions about how I can take the least amount of therapy to get me into remission and then to transplant.
New Targeted Therapies
Sam: Right around that time, science had shown that people were doing single-agent brentuximab as a bridge to transplant. If that didn’t work, then you could get ICE or some of the other stronger therapies. But there was science to support that single-agent brentuximab was a reasonable thing to do and had lesser toxicity than some of the old bridge therapies.
I was so grateful because I could not psychologically, mentally, and physically handle the more traditional, cytotoxic chemotherapies that I had upfront and that were previously used as part of salvage regimens.
I took brentuximab, initially at the exact dosing used in the trials. Then I developed a strange, rheumatoid arthritis-type illness—bad morning stiffness, joint swelling, pains, and these crazy rashes. Those got better with dose reduction.
Individualizing Hodgkin’s Lymphoma Treatments for Patients
Sam: We’re starting to talk about individualizing therapy for the person, for their circumstances, for their medical comorbid conditions, and to make decisions that way.
Dr. Evens: It sounds like you had a tough time and that’s where everyone is so different. Some patients do relatively well with chemotherapy. Then there are weird side effects that pop up. You went through that roller coaster and were able to course-correct where needed with the dosing.
There have been two big therapeutic breakthroughs in the last 10 years for Hodgkin lymphoma in particular.
We figured out over 20 years ago that one of the antigens that sticks out of a Hodgkin lymphoma cell is called CD30. Brentuximab vedotin, which was first approved in 2018, is an antibody-drug conjugate that attaches to the Hodgkin lymphoma cell, has a little bit of chemotherapy attached to it, and then gets inside the Hodgkin lymphoma cell.
Immunotherapy
Dr. Evens: After that came checkpoint inhibitors or immunotherapy that aren’t just approved for Hodgkin lymphoma, but also for more than 12 different cancers, like melanoma, lung cancer, and renal cancer.
It’s a fascinating science and, in a way, it’s the antithesis to chemotherapy. How does chemotherapy work? It kills cells that grow fast. Not very specific in the body. You hope it knocks out lymphoma cells, but the side effect is it affects anything that grows fast. What are some of our fastest-growing cells? The hair and the immune system. Though chemotherapy is not so targeted, we still use it.
Current and future medicine is more about targeted therapy. How do checkpoint inhibitors work? It reinvigorates the patient’s immune system, the T cells in particular. Simplistically, there are some cancers like Hodgkin lymphoma that have receptors that don’t allow the patient’s immune system to engage with the Hodgkin lymphoma cell. It’s almost like creating a force field.
What these inhibitors do is take down the force field and let the patient’s immune system go after and take down the lymphoma. We’ve learned how to use these medications when the disease relapses, but also for newly diagnosed patients as well through clinical trials.
Sam: I’m so excited because within the last 5 to 10 years, things have changed so much. If I was diagnosed with the same clinical situation as I was back in 2021, my treatment now might be different. That’s pretty crazy to think about because, for so many decades, it was the same: ABVD and possibly radiation.
Decreasing the Toxicity of Therapy
Role of Radiation in Hodgkin’s Lymphoma Treatments
Sam: Where does radiation fit in all this? I haven’t even heard much about radiation lately.
Dr. Evens: It still fits for early-stage or limited-stage disease. Yours was a tricky one. We still have to figure out the stage Es. If it’s disseminated extranodal involvement, it’s stage 4. If it’s a lymph node extending towards the lung, that’s more extranodal, but there can be some grey zones. It can be tricky.
Radiation still has a role in limited-stage disease, especially stage 1. For stage 2, the question there is: do I give less chemotherapy and low-dose radiation or more chemotherapy? There’s absolutely no right answer. There’s more disease control. It’s more effective to receive radiation. We always debate the trade-off. What about some of those late consequences? Can radiation contribute to that?
Late-Term Side Effects of Treatment
Sam: Can you mention some of those?
Dr. Evens: It partly depends on the treatment, whether chemotherapy or radiation.
One is arterial disease. Now it depends on location. Radiation techniques have gotten much better over the years. If there’s any scatter of radiation, there could be some carotid involvement or if there’s radiation in the chest area, there’s cardiac involvement. It’s not like there’s an incredible risk. The risk of arterial disease is a little bit increased.
That’s not to say there aren’t risks from chemotherapy, by the way. When we look at chemotherapy alone, there is an increased risk of myocardial infarction later in life because adriamycin can irritate the heart not just acutely but later in life. It rarely happens but it still does.
Another secondary or late consequence we think about, unfortunately, can be second cancers. It’s hard enough to have one, but sometimes, 10, 20, or 30 years later, there can be secondary breast or thyroid cancer. Those are more serious late effects.
Other still serious but maybe not life-threatening late side effects could be hypothyroidism, fatigue, or neuropathy.
At the end of the day, clinical trials are important as they’ve been able to show how to get these novel agents approved and how to bring them to the front line, but we also need to study those late consequences.
Clinical Trials in Hodgkin Lymphoma
Targeted Therapy
Sam: Can you mention clinical trials concerning targeted therapy and immunotherapy?
Dr. Evens: Many of the ones that garnered its approval for relapse don’t have an acronym or a name because they’re often phase 2 trials. We think treatments need phase 3 studies to garner approval. But in uncommon diseases like Hodgkin’s, which affects about 8,000 patients a year in the United States versus 90,000 with non-Hodgkin’s, it’s hard to have randomized data. With a rigorous, large phase 2 study, it can garner approval.
Thankfully, there have been a couple of phase 3 studies. One of them that garnered the approval of brentuximab vedotin in the maintenance after a transplant was called AETHERA. It was a phase 3 blinded randomized study.
The standard of care for relapsed Hodgkin’s is usually some form of therapy, whether chemotherapy or brentuximab, then a transplant. AETHERA added one time a month for a year of maintenance therapy and showed a pretty significant benefit that garnered that approval. But why do we have to wait for a relapse? What if we do it in the beginning?
An important global study called ECHELON-1 was published and has been republished a couple of times in the New England Journal of Medicine. It showed replacing bleomycin with brentuximab vedotin (BV-AVD) compared to ABVD.
The real landmark breakthrough in that study was not just showing progression-free survival, but an overall survival benefit, which we had never seen in the field. You want an overall survival benefit and some of the updated analyses of ECHELON-1 showed that, so that’s great but we’re not done yet.
BV-AVD might be the new king of the hill. How can we knock you off? The most recent phase 3 randomized trial was conducted in the US by our cooperative groups. It was called SWOG S1826. All the groups, including the pediatric oncology group, participated in this study. That’s another important point. We’re working with our pediatric colleagues to go after Hodgkin lymphoma.
That study compared nivolumab, one of the checkpoint inhibitors, and AVD (N-AVD) to brentuximab vedotin and AVD (BV-AVD). It hasn’t been published yet. It’s been presented a couple of times. Long story short, at least at one year, checkpoint chemotherapy looked to have a higher progression-free survival than BV-AVD.
As we go through these studies, we’re trying to not only get better but also get better and have fewer side effects.
Progression-Free Survival vs. Overall Survival
Sam: Could you explain the difference between progression-free survival and overall survival and why that’s exciting?
Dr. Evens: Progression-free survival means the length of life might not be different, but I’m progression-free or in remission longer.
When we first looked at ECHELON-1, we saw that progression-free survival was improved by about 10%. Another way to say that is, for example, for patients treated with BV-AVD, at three years, around 80% of patients were still in remission versus 70%, or maybe it was 85 and 75. That’s good. I’d rather be in remission longer, but I’d also like to live longer. That’s overall survival.
Before ECHELON-1, there had never been a study showing better, longer overall survival compared with classic ABVD. Part of the reason is that if you have a good second therapy, even though there can be side effects, it’s easier to modulate overall survival.
What they showed when they looked at six years for BV-AVD was overall survival improvements. That’s a game-changer in the field. It was already FDA-approved based on progression-free survival, but I think it became more common in use after the overall survival data.
Sam: These are exciting times. I hope to never need the services of a hematologist ever again, but I do have hope that should I experience another relapse, heaven forbid, there are good treatments out there to provide remission and quality of life.
Pembrolizumab
Sam: Tell us about pembrolizumab.
Dr. Evens: Pembrolizumab is another checkpoint inhibitor. Nivolumab and pembrolizumab are much more similar than different. A lot of their studies are keynote studies from that company and it has a number. In particular, Hodgkin’s was KEYNOTE-087. They keep adding numbers throughout all the different cancers. That was initially approved as nivolumab for relapsed Hodgkin lymphoma. That garnered that approval, one of the keynote studies, like nivolumab.
SWOG S1826 was for advanced-stage disease, so stages 3 and 4. When something gets approved for a certain situation, a certain stage, and for certain ages, what about for limited stage or early stage?
For many patients, a common treatment modality for early stage is six months of chemotherapy. Others might receive four cycles of chemotherapy and radiation. We were planning this study for the United States through the US cooperative groups. This study involves the pediatric oncology and adult groups. The Children’s Oncology Group is leading it, but we’re all working together.
There is a new national, high-priority study called AHOD2131. It’s comparing the standard of care that we talked about for early-stage disease versus everybody on the new arms of two cycles of chemo and the rest, targeted therapy: a combination of brentuximab vedotin and a checkpoint inhibitor.
The hypothesis is it’ll be more effective and likely better tolerated. That’s an ongoing study. It opened in the summer of 2023 and is planning to enroll over the next couple of years.
What’s great about that study is not that it incorporates novel therapeutic agents in place of cytotoxic chemotherapy, but over 10 to 12 years, it’s going to study some of the late-term effects and that’s sometimes a gap with clinical trials.
They’re great in the first couple of years then they fall off and don’t have the resources or funding to study late-term effects. In great collaboration with the National Cancer Institute and CTEP (Cancer Therapy Evaluation Program), they are providing resources not just to study the initial 3, 4, or 5 years, but extend beyond 10 years, which is fantastic.
Understanding Clinical Trials
Sam: You brought up some great points and I want to highlight this for patients because I don’t even think I felt empowered to think these things or ask some of these questions with the initial shock of the diagnosis.
Clinical trials are not just for people who have failed multiple lines of therapy. Clinical trials could be for multiple situations. How do we de-intensify therapy? How do we make different therapeutic decisions? How do we start using therapies that were used in a very specific situation, like only for relapsed/refractory, and use them for early-stage patients upfront? That’s what some of these trials are showing.
What advice could you give to patients?
Dr. Evens: Be an advocate for yourself or your family member because this is your life. Not to minimize it, but there should be no intimidation or concern of talking to the oncologist.
99.9% of oncologists want the best for their patients. Sometimes, the provider might not always bring up a clinical trial because they might not have access. But I would encourage you to ask if a clinical trial is right for you.
I wish we had a clinical trial for every condition. There’s always a semi-standard of care. We’re always trying to do better or if not do better, do the same with fewer side effects. The only way you can do that is ultimately in a clinical trial.
These are very sophisticated studies where we’re hopeful. Of course, we have to prove it in that clinical trial. The vast majority of clinical trials are with targeted agents or immunotherapy agents. I would implore the patients and patient family members to, if not self-advocate, reach out to other foundations.
Sam: On that note, if you have any questions regarding how to look up and navigate through clinical trials, The Leukemia & Lymphoma Society has a clinical trial support center with free access to experts who can guide you through that process.
Dr. Evens: The best outcomes are usually with the most informed patients who know the different options. In Hodgkin lymphoma, very, very often, there’s not one right way to treat it. There are different options. There shouldn’t be anything scary or wrong with getting second opinions. We’re often happy to help.
Sometimes we won’t have anything different to offer or it might not even be a clinical trial, but a little nuance on dosing or something based on patient characteristics or comorbidity. We might want to make a certain adjustment a priori to a treatment. When that’s all you do for 20 years, you’ve seen it all and every condition, and we’re happy to lend any advice we can.
Role of Stem Cell Transplant in the Treatment of Hodgkin Lymphoma
Sam: Where does transplant fit in all of this? I had an autologous stem cell transplant. I’m so grateful for it, but it was tough. I had beam therapy as a conditioning regimen because I had hemorrhagic cystitis from cyclophosphamide when I was mobilizing my stem cells.
Dr. Evens: You had almost every side effect.
Sam: I did and then I had pneumonitis from carmustine. I believe that I had this cancer at this time in my life and had such a tough course so that I could learn about these things, be an advocate, and go into longitudinal survivorship.
I know now some of the questions to ask, some of the things that can happen, and how hard it can be, even when it’s the “good cancer.” I did just like AETHERA—I had one year of post-transplant brentuximab.
Dr. Evens: Did you do okay with it?
Sam: I did. I ended up getting a dose reduction because we learned before I had a transplant that I needed the dose-reduced brentuximab as well. I had some neuropathy, which wasn’t just pain. It was falls, clumsiness, and dropping things.
Dr. Evens: It was affecting your function.
Sam: It was. I do a lot of procedures so for people like me who work with their hands or do a lot of things with their hands or feet, it could be important. The neuropathy is still there, but it’s recovering.
Autologous vs. Allogeneic
Dr. Evens: For over 30 years, transplant has been the standard for Hodgkin lymphoma in younger patients. When we say younger, we mean less than age 70. The patient receives some new treatment, gets back in remission, and then a one-time transplant.
When we say transplant, it’s an autologous transplant, which uses your own cells so it’s not a transplant. It’s one cycle of high-dose chemotherapy followed by a rescue using your own stem cells so you bounce back after the chemotherapy. We do an immune system transplant or allogeneic transplant, but we rarely have to do this for Hodgkin’s.
As much of a standard of care as it’s been, we’re revisiting everything and asking: does everybody need a transplant? Now that we have brentuximab vedotin and checkpoint inhibitors, can we lean on these targeted therapies for certain patients?
Studies take months and sometimes a couple of years to plan because you want to get it right and have the latest treatment and data. We’ve been talking about it and planning it to ultimately prove it because it can’t just be an idea. We have to prove it. It would have to be a clinical trial where there’s some randomization to the standard transplant or no transplant.
It’s not done yet, but I’m hopeful that is something we can explore and that we can cure relapsed Hodgkin lymphoma without a transplant. But right now, that’s not the standard of care. It would still be a transplant.
Continued Monitoring
Sam: How are we monitoring patients with Hodgkin’s lymphoma?
Dr. Evens: There are different practice styles and part of the reason is it also comes back to data. We don’t want to do a scan just to do a scan. Is it helpful? Does it tell us information?
What had been standard for a while, whether for initially diagnosed or for relapsed, is when there’s a transplant, the vast majority of the time, we count two years from diagnosis.
During that two-year time mark counting from the initial diagnosis or the initial relapse, some of us will usually see patients in the office every three months for a physical exam, history physical, maybe some blood tests, and sometimes a CT scan every six months.
Not everyone does scans. They think there’s lead time bias and it only maybe helps you pick it up a little bit earlier but doesn’t improve survival. But if someone does scans, they should not do it past the two-year mark.
There’s radiation with CT scans. We don’t think of it, but for many types of CT scans, that’s equal in radiation to 500 chest X-rays. Imagine getting 500 chest X-rays. It’s something we want to use if it’s helpful, but not too much.
But what about after two years? What about after five years? Ten years? That’s where I think we need a greater focus and an opportunity on bonafide survivorship clinics.
There are some good algorithms. I know our pediatric oncology group at the Rutgers Cancer Institute has a computer program where they can put in the patient’s age, treatment, and whether they’ve undergone radiation, then based on the best available data, it will generate your primary care follow-up.
None of the recommendations are likely, but they’re usually evidence-based to show that there’s some impact on that. I would say individualized, but it’s something that we need to make sure, as a community, our patients know that the survivorship aspects are still very important.
It’s not just about breast cancer screening, heart screening, etc. What about chronic fatigue? What about anxiety and other emotional disturbances that can happen? In a survivorship clinic, like what we have at the Rutgers Cancer Institute, you have experts like physicians, nurses, and social workers surrounding the patient throughout the life-long care continuum.
Sam: I love that and I love that you made the distinction between surveillance and survivorship because I think surveillance is a big part of survivorship, but it’s not all of survivorship.
My understanding in speaking with people from the NCI Office of Cancer Survivorship is that a hot topic within the survivorship research community right now is what is a mutually agreed upon definition. It includes surveillance. But it’s also cancer-surviving mindsets and how we plan for life after a cancer diagnosis, including oncofertility, social-emotional well-being, family planning, and reintegration in work life, society, or family. How do you live your life after you’ve had a cancer diagnosis, regardless of your remission status or where you’re at and all that, including making sure that you get your scans and your bloodwork and all that?
I think a lot of people in the community are starting to realize that it’s so much more. I’m hoping that, ultimately, it’ll be a board-certified fellowship in the next five years or so with core competencies like this is what a survivorship clinician should know and be able to talk to patients about.
Dr. Evens: Absolutely. We talked a little bit about the HoLISTIC Consortium and that’s one of our goals. Despite the commonality in terms of the number of diagnoses, it’s remarkable that we’ve come together under this consortium and have done so in the last few years and that’s to gather the world’s data of clinical trials.
In many of those clinical trials we talked about, this is individual patient-level data. It’s de-identified, careful individual patient data put into a huge master database with a common data model and data dictionary so they all come in a readable and harmonized fashion.
We’ve also knitted together and synthesized large amounts of clinical trial data. There are survivorship clinics and survivorship cohorts out there across the world collecting data over decades at Princess Margaret in Toronto, BC Cancer Vancouver, Stanford in California, Australia, the Netherlands, and Denmark.
Over the last few years, we have put together 20,000 cases of patients in clinical trials and survivorship registry cohorts to give objective information. If you did A, B, or C, here are your expected efficacy and side effects based on your individual characteristics.
But also to simulate, as best as we can tell, based on this treatment and at this point in your cancer journey, what we estimate to be your 10-, 20-, and 30-year late consequences to make a more personalized survivorship plan and not just an initial treatment plan. The way we’re going to do that is through large amounts of big data and data analytics with some machine learning mixed in.
Sam: That’s exciting because one of my big aha moments with starting to participate in the survivorship community is that survivorship is defined as anybody living after a cancer diagnosis, but it doesn’t seem to be routinely delivered that way. It seems that it’s piecemeal and it’s focused on a couple of cancers.
I believe that longitudinal survivorship is the way. We should deliver survivorship from the time of diagnosis, in parallel with oncology care that’s delivered by the oncologist. If we know we’re going to give a person cardiotoxic chemotherapy, let’s not wait until they develop heart disease 20 years down the road to start paying attention to heart disease risk. We could put people through intensive lifestyle medicine therapies where we talk about diet and exercise, check their A1C and cholesterol levels, monitor their blood pressure, and talk about heart health in the beginning.
Dr. Evens: We have some patient advocates and we’d love for you to become involved to some degree as a patient advocate and a physician expert as part of HoLISTIC. We’re still gathering and building data, but we’re looking forward to starting how we best apply this to patients and the medical community.
Final Takeaways
Sam: This has been just such an exciting conversation. What are some final takeaway messages that you have for patients, providers, and advocates?
Dr. Evens: It starts with an informed provider and informed patients. Is Hodgkin lymphoma treatable and curable? Yes, whether it’s newly diagnosed or stage 4, even if it comes back once or twice, but there are different treatment options.
When it comes to treatment options, how effective are they? How will the patient tolerate it in the moment and later in life? The number one goal is to cure but do so with minimal side effects. It comes back to personalized cancer care.
There has been great progress over the last few decades. We still have room to have treatments that are better tolerated. We’re thankful to have well-informed patients, patient advocates, scientists, clinicians, epidemiologists, and survivorship experts. Everyone is coming together, laser-focused on Hodgkin lymphoma to continue to advance the field.
Sam: I agree. I think that there’s a palpable shift in cancer culture. We need to do more than just focus on not dying. Let’s focus on the living part. How do we help people fully live after facing a cancer diagnosis? This is a really exciting time. I’m grateful to have had this conversation with you and can’t thank you enough for your time.
Initially misdiagnosed due to overlapping symptoms with his existing condition, Matthew experienced concerning symptoms such as dark urine, pale stool, and intense itching. Eventually diagnosed with metastatic pancreatic cancer, Matthew underwent different combination chemotherapy treatments, including FOLFIRINOX (leucovorin calcium or folinic acid, fluorouracil, irinotecan hydrochloride, and oxaliplatin) and GAP (gemcitabine, nab-paclitaxel, and cisplatin).
Despite setbacks and the grim prognosis associated with pancreatic cancer, Matthew’s tumor responded positively to the new chemotherapy regimen, leading to tumor shrinkage and the disappearance of metastases in the liver. Following a successful Whipple procedure, Matthew emphasizes the importance of not being defined by statistics and advises others facing similar challenges to live life to the fullest while also taking their health seriously.
His story highlights the unpredictable nature of cancer treatment, the importance of advocating for oneself in medical settings, and the significance of cherishing each moment, even in the face of adversity.
In addition to Matthew’s narrative, The Patient Story offers a diverse collection of cancer stories. These empowering stories provide real-life experiences, valuable insights, and perspectives on symptoms, diagnosis, and treatment options for cancer.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I live in Hazel Park, Michigan, with my girlfriend Natalie and our pug Monique. Because of the nature of my illness, I haven’t had a job in three years, but in my former life, I was finishing a PhD. I was going to be an academic.
Pre-diagnosis
Initial Symptoms
The most popular narrative surrounding pancreatic cancer is that not only is it very lethal but also very difficult to diagnose. The pancreas is deep in the body. The earlier symptoms are very nuanced, can go unnoticed, and can also be misdiagnosed as a multitude of other things. By the time you’re experiencing symptoms, the cancer has spread outside of the pancreas. I don’t want to say it’s too late, but that’s what conventional wisdom is.
I was diagnosed with Crohn’s disease when I was 25. Gastrointestinal distress, which is one of the more perceptible symptoms of pancreatic cancer, was par for the course for me. I probably wouldn’t have noticed even if I didn’t have Crohn’s. I lost some weight over the months, but it wasn’t until late January 2021 that I started to experience starkly distinct symptoms.
It was the COVID pandemic. I lost my job and moved to a different city to help my friend with his business. His business closed and he moved away, so I was alone when all this started.
I had dark urine and bone-white stool. I didn’t even notice the stool color for a while. At first, I thought I was hungover. I had a few beers the night before so I drank some Gatorade and lay in bed, but the urine did not get lighter.
My skin started to itch. The bathroom symptoms were pretty jarring, seeing urine that dark and poop that pale, but the itching was probably the worst. The palms of my hands and the bottoms of my feet itch. It was worse at night. I never felt anything like it before and those are hard places to scratch.
After a whole night of itching, I put my hands and feet in the tub under hot water to numb the sensation. In retrospect, it’s jarring to think about burning my hands and feet to alleviate the pain, but the itching was that significant.
Not everyone gets the itchiness. There seems to be some controversy because not every pancreatic cancer awareness campaign includes itchiness. I experienced it and it was horrible.
When something started to happen, I sat on it for 48 hours before I finally told someone. It wasn’t the most responsible, but in retrospect, not that bad. I was in a long-distance relationship with a woman I knew from graduate school. I told her and she said, “You should go to the doctor.”
I have a lot of medical anxiety. I have never been a good patient. For someone with such anxiety about doctors and hospitals, I needed someone to tell me.
Going to Urgent Care
I had recently moved to Durham and didn’t even have health insurance, but I went to an urgent care center. My blood test results showed that my bilirubin was high. We get some more tests back. The nurse said, “You don’t have a doctor here yet and these test results are troubling. You should go to the ER.”
Going to the Emergency Room
I went home to sleep because I hadn’t slept in three nights. I was so tired that despite the itching, I passed out. Early the next morning, I went to the ER and that was the beginning of my journey.
They admitted me to the hospital and ran some more blood tests to see what was going on with my liver enzymes. They did an ultrasound and an endoscopic ultrasound.
Bile Duct Stricture
They found that there was a stricture in my bile duct. Your liver produces bile, a digestive enzyme stored in your gallbladder and then released into your small intestine to digest fats and other foods. The tube that brings the bile down goes through the head of your pancreas. That tube had a stricture, so it was closed off. When bile can’t be distributed normally, you end up depositing it in your blood and your flesh, and that causes jaundice and elevated liver enzymes.
With the endoscopic ultrasound, they were able to place a stent in my bile duct in the hope that it would stretch it out. They told me to come back in a few weeks to have another endoscopy and remove the stent.
There was no sense of urgency. I was an otherwise healthy person with a history of colitis. They didn’t think that this was anything scary.
After they removed the stent, the symptoms came back, so they decided that it was my gallbladder causing the symptoms. With pancreatic cancer, it’s very common for people to assume that it’s a gallbladder issue. They decided to take my gallbladder out. After the surgery, the symptoms return.
It was late April. I went to my gastroenterologist’s office, who was the one who did the endoscopy. She said, “I don’t know what’s happening, but you for sure don’t have cancer. We have done so many brushings and you definitely don’t have cancer. If you have cancer, I will roll over in my grave.” I left her office feeling pretty confident.
Diagnosis
Getting the Official Diagnosis
Three hours later, I got an automatic notification on my phone from MyChart. One of my cytology reports came back. It said adenocarcinoma. I didn’t know what that meant, but I knew it wasn’t good.
I sat with that for about two hours. Then the surgical oncologist who did my gallbladder surgery called me. My case got automatically referred back to him. He was out of town and called me using his personal cell phone.
I told him, “This lady told me I definitely did not have cancer and now I do so I’m freaked out,” and he apologized. My surgeon is the salt of the earth. He calmed me down. I don’t know if he remembers it this way, but I’ll never forget this conversation. He said, “If this is cancer, the tumor’s very small and I should be able to get this. I’m confident.”
The area in which they found the adenocarcinoma is called the ampulla of Vater. Everything in this part of the body is pretty small and overlapping so pancreatic cancer could be an explanation. But given my age and, let’s face it, the taboo around death, no one was talking about that.
When pressed, the doctor told me ampullary cancer, which has a higher survival rate and is still incredibly rare for someone my age but less rare than pancreatic cancer in the same age category.
Treatment
Discussing the Treatment Plan
Because of the size and the layout of this part of the body, they do the Whipple procedure, also called the pancreaticoduodenectomy. They do the same surgery for ampullary cancer as they do for pancreatic cancer.
Five days after the phone call, I was in his office and he said, “I’m going to remove part of your pancreas and part of your small intestine.” I didn’t have a gallbladder, but that also would have gone including part of my stomach.
My surgeon told me that they cut me open and, contrary to what they thought, found a tumor on the head of my pancreas that had spread outside of the pancreas. Metastatic pancreatic cancer is considered inoperable so when they saw that, they closed me up.
Because of my age and because they suspect that I’m a BRCA2 mutation carrier, the surgeon said, “We have to confirm with genetic tests, but I’m pretty sure you have this particular genetic abnormality. If that’s the case, then there are targeted therapies that might work for you.”
He said, “This is a mean cancer. But because of your particular situation, after treatment, we might be able to try the surgery again in a year.” For pancreatic cancer, surgery is the only long-term survival solution. Chemotherapy and radiation are life-extending, but they’re not curative. He was pretty confident, at least in the context of a lethal diagnosis.
Later that day, he introduced me to my oncologist. He was not as confident. When pressed, he said, “With treatment, you might have 1 to 3 good years left, but that’s it.”
FOLFIRINOX Chemotherapy
This was at the beginning of May 2021. My wound had to heal. Three weeks later, I started chemotherapy. Like a lot of other people with metastatic pancreatic cancer, I was given FOLFIRINOX, which is five different drugs. It’s awful. Chemo combinations are all awful, but FOLFIRINOX was really, really abrasive.
I had a scan after three months on FOLFIRINOX. The oncologist said, “Your tumor shrank a little bit,” but you can tell from the way he’s telling me that it could be an imaging error or a minute retreat that it’s barely perceptible.
At my next CT and MRI three months later, the tumor grew. It had metastasized to my liver so things were not looking good. At this point, I was not confident that I would be a special case or a miracle. I thought this was it.
Switching Chemotherapy Regimens
My oncologist switched me to a different chemotherapy combination. He told me there was a combination that some researchers found was promising for people in my situation. It was gemcitabine, nab-paclitaxel, and cisplatin (GAP).
I was honestly relieved because after being on FOLFIRINOX for almost six months, the neuropathy had gotten so bad that I couldn’t get out of a chair by myself. I needed someone to hoist me up. I was pretty thin at this point. It was miserable.
On the new chemotherapy regimen, my quality of life improved dramatically. By the time my first set of scans came around three months in, some of the spots on my liver had started to disappear. I did three more months of chemo and made it through.
I didn’t lose my hair. I’m six feet tall. I was 215 lbs when I was diagnosed and miraculously maintained a healthy weight so I’m very thankful for that. At this point, I thought I was still dying sooner rather than later so I was trying to have fun and it certainly made having fun a lot easier.
Post-Treatment Scans
In March 2021, he looked at my scans and, if memory serves, they could not identify cancer outside of the tumor.
Almost a year to the day, they attempted to do the Whipple and, this time, it was successful. When Dr. Allen came into my hospital room, he said all of my margins were good and the lymph nodes they tested were negative.
Before this, they couldn’t see any cancer on the CT or MRI, but that didn’t mean that my peritoneum wasn’t covered in cancer. That just meant that they wouldn’t be able to tell until they got in there. They were pleasantly surprised that things had worked.
Follow-up Protocol
The last scan was a lot smoother than the others, but they’re incredibly difficult. I get a scan every three months for the next six years, but the chances of me living out those six years are astronomically small. Pancreatic cancer has a remarkably low five-year survival rate. It’s unlikely that I will see all of that time, at least on paper.
Words of Advice
It’s important to remember that you are not a statistic. I was diagnosed with something I wasn’t supposed to have at my age. It was very unlikely. It was supposed to kill me and I didn’t die so, in a sense, I beat the odds not once, but twice.
People think that pancreatic cancer is an old person’s disease. I think that’s why no one ever looked because no one ever even thought that I could have pancreatic cancer. I’ve heard over and over again that I’m too young. Statistically speaking, they’re correct. For people under 35, it’s incredibly rare, but there is a difference between statistical analysis and what statistics are for, and encountering a patient one-on-one.
Treatment is not linear. Pancreatic cancer is often thought of in linear terms as a quick, short trajectory to death. We assume that if treatment will work, it will work immediately. You don’t take one step back and one step forward. In my experience, that’s not true. Sometimes things get worse before they get better and it’s not a reason to lose heart.
Have a drink, eat the cheeseburger, and live your life to the extent that you can. That’s how I lived. Take your health seriously but also meet yourself where you are.
In this discussion, patient advocates Cindy Chmielewski and Jack Aiello speak with multiple myeloma experts, Dr. Rafael Fonseca with Mayo Clinic and Dr. Susan Bal with University of Alabama at Birmingham. They discuss the latest coming out of the 2023 American Society of Hematology meeting and share the latest multiple myeloma clinical trials and treatment options.
Learn about new multiple myeloma treatment options, including triplet and quadruplet combination therapies, CAR T-cell therapy, bispecific antibodies, and trispecifics. Find out about the future of belantamab mafodotin (BLENREP), dose reduction of dexamethasone, and the introduction of sonrotoclax, dubbed as the next-generation venetoclax.
Stephanie Chuang: I’m the founder of The Patient Story and, more importantly, I also got a blood cancer diagnosis of non-Hodgkin lymphoma a few years ago.
We have so many shared experiences in what we’re looking for and that’s what The Patient Story is all about.
We want to note that The Patient Story retains full editorial control of this entire program and this is not meant to be a substitute for medical advice.
Our patient moderators Cindy Chmielewski and Jack Aiello will lead this conversation. Cindy and Jack, can you share a little bit more about your own stories and how you became such passionate advocates in this space?
Cindy Chmielewski, Patient Advocate
Cindy Chmielewski: I’ve been living with multiple myeloma since 2008. What brought me to the doctor was very debilitating back pain. The pain was so bad that it affected my job. I was having a hard time standing up to teach. I wasn’t able to take my class to the playground for recess. I had to have other teachers do that.
I went to an orthopedic doctor who, unfortunately, I think was unfamiliar with the symptoms of multiple myeloma because he diagnosed me with degenerative disc disease. It took an additional two years to get the correct diagnosis.
Since then, I’ve had several treatments and I’m now doing very, very well. I’m excited because I’m hearing all these new therapies that will be available to me if and when I relapse.
Jack Aiello, Patient Advocate
Jack Aiello: I was diagnosed with multiple myeloma at the beginning of 1995.
It started with a backache but MRIs and X-rays didn’t show anything wrong according to a specialist I went to see. I ended up taking a blood test and that showed an elevated protein. The specialist said I likely have multiple myeloma and that was the start of about eight years of significant treatment.
Back then, the average life span for myeloma patients with treatment was only 2 to 3 years. I was fortunate to respond to a third transplant except that I used donor stem cells after a couple of earlier transplants and clinical trials didn’t work for me.
I’m extremely appreciative to be alive 29 years later. I think this discussion is awfully important as all of these webinars are for myeloma. In particular, we focus on what happened at the 2023 American Society of Hematology meeting that will affect patients immediately as well as where the research is going. I’m always in favor of making sure I understand what’s going on so that I can help myself if my disease comes back and I can help others when I’m leading our support group or talking with other patients.
Rafael Fonseca, MD
Cindy: Dr. Rafael Fonseca is a hematologist-oncologist at Mayo Clinic with a special interest in multiple myeloma. He also participates in and leads clinical trials that have led to the approval of various drugs for the treatment of myeloma
Dr. Fonseca, what drew you to multiple myeloma, and what drives you most to continue to work in helping myeloma patients?
Dr. Rafael Fonseca: The way I got into myeloma is a little bit of luck but mainly because I had great mentors. The late Dr. Philip Greipp was a wonderful influence. I wanted to do lymphoma, but he steered me into myeloma without knowing what would happen. Those were the days of melphalan and prednisone, which links exactly to what drives me now.
We are very fortunate to be living through these times when so many things are happening in the treatment of myeloma. One of my colleagues, Dr. Ruben Mesa, told me a few years back that we are either a drug away or a combination away from being able to cure a significant fraction of patients. We’re shuffling the pieces on the table, but I think we’re there so that keeps us going every day.
Dr. Bal, what drew you to myeloma, and what drives you most to continue your work to help patients?
Dr. Susan Bal: Myeloma was always very exciting to me personally. I started my fellowship the year that we saw the first results from daratumumab come about.
Other than the excitement in the field and the possibility of a cure, one thing that drives me most is the meaningful relationships that you can continue to build because our patients live for so long and do so well.
I’m so delighted to be able to work with a great group here and across the country. The myeloma community is strong and we forge onward in our path to curing this condition.
Patients can come to us from any of these avenues and that’s what makes it interesting… It’s a very heterogeneous disease, certainly in terms of presentation and how people do overall.
Dr. Susan Bal
Overview of Multiple Myeloma
What is Multiple Myeloma?
Cindy: Briefly, what is multiple myeloma and what are some of the first signs and symptoms?
Dr. Bal: Multiple myeloma is a plasma cell disorder so it’s plasma cells that have become cancerous. We have white cells, red cells, and platelets. White cells fight infections, red cells carry oxygen, and platelets stop us from bleeding.
Symptoms of Multiple Myeloma
Dr. Bal: One of the types of white cells that help us fight infection is the plasma cell. The plasma cell is responsible for making antibodies that normally help us fight infection.
Sometimes when these plasma cells go awry and become cancerous, they can crowd out the bone marrow, resulting in symptoms such as elevated calcium levels, bone breakage, and bone damage. It can affect our kidney function, causing renal dysfunction. It can also cause low blood counts because of crowding out of the marrow.
Because it’s a part of the immune system and its job is to prevent infections, oftentimes, patients can present with recurrent infections as a presenting feature as well.
Patients can come to us from any of these avenues and that’s what makes it interesting. We see patients who are simply diagnosed because they had an astute primary care physician who picked up on a protein gap. We have patients presenting on the other end of the spectrum with the plethora of all symptoms that we know as CRAB symptoms, presenting with very disabling features. It’s a very heterogeneous disease, certainly in terms of presentation and how people do overall.
As is true with everything else in medicine, the availability of additional information has allowed us to narrow down the best options for patients.
Dr. Rafael Fonseca
Considerations When Choosing Treatments for Different Patient Groups
Cindy: Dr. Fonseca, we’re lucky now that there are so many treatments available. When I was diagnosed back in 2008, the treatment arsenal was not nearly as filled as it is now.
What are some of the considerations you think about when choosing treatments for different groups, like transplant-eligible versus transplant-ineligible and newly diagnosed and high-risk? What goes through your mind?
Dr. Fonseca: That’s the essence of everything we do in the practice. All of those considerations and how we present them and share them with patients as options for their treatments.
When we started seeing all these drugs come forward and being approved, my first reaction was, “Boy, this is going to get complicated. How are we going to choose? We have all these treatments. My appointments may have to be two hours long because I have to present everything to patients.”
As is true with everything else in medicine, the availability of additional information has allowed us to narrow down the best options for patients. Even though we have many more drugs, we still have 1, 2, or 3 options that are probably the best for a person at a given step. That has allowed us to work more on our messaging and the rationale of what we do.
The considerations you mentioned are critical. We always want to look at, first of all, the patient as a person with their preferences and goals, as well as some other health issues or comorbidities.
One of the critical aspects — and one we can’t modify though I know many wish we could — is our age. Age is a major determinant of how well you’re going to be able to tolerate treatment or not.
Some treatments become quite a bit toxic as we take them later on in life. A great example of this is the stem cell transplant. As physicians and clinical teams, we have to tailor our approach to patients as we start proposing the various treatments.
The second consideration is whether the patient is newly diagnosed or someone who, unfortunately, has myeloma that’s coming back or what we call recurrent myeloma. If we think about that, then we say: which stage is this? Is this an early recurrence or is this someone who has already received 3 or 4 prior lines of therapy?
Then we bring other factors that are important for patients to know about and we discuss them with the patients. We test the myeloma cells for genetic makeup. When we talk about genetics in myeloma, we’re mostly talking about the changes that occur in the myeloma cells, not the genetics that a person may have in the rest of their body and, very importantly, not genetic things that are passed on from generation to generation.
Those are things that play into our decision-making process. Some patients have markers that would make us more concerned, something we call high-risk myeloma. With that in mind, we put together treatment plans that we propose to our patients.
We’re moving forward with a more unified approach to goals. If you go back 15 years or certainly, in 1995, our goal was to control. Can we do something that will put the myeloma at bay that would allow us to gain time?
Many of us feel like the pendulum has swung completely in the other direction. Many individuals, myself included, think that we should aim to eradicate all myeloma cells and, ultimately, produce cures for patients. How you phrase that and plan for that becomes important. Behind that, there’s a whole set of other principles. Those are some of the overriding things we think about but always starting with the patient.
We were lucky to have two major presentations at the meeting, including a plenary session where we saw results from the IsKia trial, as well as a late-breaking session where we saw results from the PERSEUS trial.
Dr. Bal: The American Society of Hematology meeting is a key event for hematologists. It’s where we expect to see some of the latest and greatest of science and all the discoveries and innovations that are occurring within the field. It’s a one-stop shop where we get to see some of the best data so it’s a very looked forward to event in the community.
This ASH was no different. We were lucky to have two major presentations at the meeting, including a plenary session where we saw results from the IsKia trial, as well as a late-breaking session where we saw results from the PERSEUS trial.
The PERSEUS study was perhaps one of the most awaited trials in the sense that this was a randomized phase 3 trial evaluating a quadruplet regimen of daratumumab, bortezomib, lenalidomide, and dexamethasone versus the same combination without daratumumab in patients with newly-diagnosed, transplant-eligible multiple myeloma. For many in the field, we have moved towards using these quadruplets based on an earlier phase 2 randomized GRIFFIN trial. This was practice-affirming and perhaps practice-changing for a small proportion of patients in the community.
What this trial did was take patients who were transplant-eligible — who are fit and in the European and Australian countries where this was predominantly performed — and were randomized into receiving four drugs versus three drugs followed by stem cell transplant and then a doublet maintenance following consolidation therapy with the same regimen.
Overall, what we saw was with a close to four-year follow-up, patients who received this four-drug regimen did a lot better and had longer progression-free survival at the four-year time point. Patients had a very deep response with this regimen achieving measurable residual disease negativity, both using very sensitive markers and sustaining over prolonged periods, which has been shown to be hopefully a surrogate for improved patient outcomes overall.
Within the US, many in the field have already taken up the practice of adopting this four-drug regimen based on the prior GRIFFIN study, but I think this was confirming and affirming for those of us who are doing that and practice-changing for those who were still using the triplet combination. This was perhaps one of the most exciting things to come out of this trial, among other things.
Jack: That’s fantastic. Dr. Fonseca, what about you? Can you describe an outcome you saw from ASH that was so important to the myeloma community?
Depending on how you measure and what the threshold is, we have studies showing that somewhere between 60 and 80% of patients can get into minimal residual disease.
Dr. Rafael Fonseca
Dr. Fonseca: What Dr. Bal described is the crux of what we saw at the 2023 ASH meeting. This is our key meeting where we see all this data.
No one would be surprised if we tell you we actually have a lot of fun being at that meeting because we’re with friends. We work the longest hours that we work in the year. Sometimes it’s hard to convince our family that it’s work because we’re all smiling, talking, and exchanging ideas, and then we go for dinner and discuss further.
It’s a wonderful time for us and more so given the progress we’re seeing in myeloma. The fact that we now have very strong data for what needs to be done in the front line is very important for patients.
At this moment, it’s beyond any doubt that we need to use the best treatments up front. For now, that means the incorporation of anti-CD38 monoclonal antibodies. Dr. Bal mentioned the use of daratumumab. We also have a similar molecule, isatuximab.
The clinical trials point to outstanding results, which could not be seen ever before in the treatment of myeloma. The results are so good that they’re now going to start challenging some of our assumptions.
We had the meta-analysis for the maintenance strategy for myeloma, where patients go through induction, get the transplant, and are placed on maintenance. But Dr. Luciano Costa has pointed out repeatedly that those maintenance studies were done where we could achieve a complete response in about 30 to 40% of patients, minimal MRD negativity, and sometimes patients were getting two drugs as induction.
One would say it was no surprise that more treatment was effective. Whether we call it maintenance or consolidation is semantics. Now we’re getting to the point where many patients have a complete response. Depending on how you measure and what the threshold is, we have studies showing that somewhere between 60 and 80% of patients can get into minimal residual disease.
We’re starting to ask: do you even need maintenance in those patients? I don’t claim in any way that we have the answers, but it reflects how fast things are moving forward. Breaking it down, as Dr. Bal did, is critical.
For some people, we were practicing this, but for other people, either they need this for regulatory purposes across the globe or their reading of the medical literature is such that they want to have that phase 3 trial before they change clinical practice.
Right now, it would be rare that a patient would not be offered induction therapy with something, as we were describing. A lot of things are getting simplified. In a conversation with colleagues, I said the treatment of myeloma should always start with something like daratumumab, lenalidomide, and dexamethasone.
The secondary question is whether the patient needs to get a proteasome inhibitor, like bortezomib or carfilzomib, and whether they need to get a transplant. But then things get simplified because the best players rise to the very top of what we’re doing so I’m excited for what this means for patients.
Dr. Bal: I completely agree with Dr. Fonseca. I feel like some things are almost becoming cleaner as we go. I remember this discussion about three years ago where everybody wanted to know: would you give daratumumab to a transplant-eligible patient? The answer is becoming clearer and clearer that you want to use your best drugs upfront and make that first cut your deepest.
Recently, somebody asked me, “Is there a patient whom you would not give daratumumab to?” I said, “I don’t know who that would be because it’s such a well-tolerated, effective therapy.” Now I’m thinking more like what Dr. Fonseca said about which of the other agents you could potentially get rid of or improve upon, rather than the daratumumab.
I’m not saying we’re ready to dispense with transplants, but the data continues to show that deep responses, no matter how you get there, will result in better outcomes.
Dr. Rafael Fonseca
Front-Line Therapy for Transplant-Eligible Patients
Jack: Dr. Fonseca, one of the important trials — and Dr. Bal referred to it earlier as having been given special recognition at ASH as a plenary session — was the IsKia clinical trial, which compared carfilzomib, lenalidomide, and dexamethasone, adding isatuximab to it or not as front-line therapy for transplant-eligible patients. Isatuximab is like daratumumab in that they’re both CD38 monoclonal antibodies. It was another four-drug trial. Can you talk a little bit about that?
Dr. Fonseca: The reason something is given that plenary status is when the reviewers and the reviewing committee feel that there is something of such high value that reaches the high standards of evidence or that even potentially becomes immediately practice-changing.
This particular clinical trial was one more point in that direction where they started looking at the response rate and the MRD negativity rate for those patients. MRD negativity refers to measurable residual disease or minimal residual disease, which is nothing different than saying we have better markers to assess the depth of a response through mechanisms such as genetic testing.
It’s becoming increasingly clear and very well-documented that achieving the status where you can no longer find measurable disease — using very sensitive tools where some can go at the level of detecting one cell out of a million — becomes a harbinger of great outcomes for patients, of durable responses, and ultimately improvements in the various metrics that we call survival. The IsKia trial shows that.
It’s very interesting to me for a couple of reasons. This is a different antibody, a different molecule than daratumumab, but the presumption by those in the field has been that we should see similar results. These antibodies carry nothing of what we call a payload. They’re a naked antibody so they go and bind to those cells. By doing that, they unleash our immune response to those cells. They’re able to kill more cells. We know that because the responses are better and the MRD is better.
In that particular trial, we have to wait a little bit longer to see over time what the outcomes will be on those metrics that people hear about, like progression-free survival and overall survival. But given what I said about MRD, all the indicators are that this will be a very useful approach for the treatment of patients.
Everyone should get a CD38, like lenalidomide and dexamethasone, at least for the time being. But then the question is: what about these drugs that we call proteasome inhibitors? In this particular trial, they used carfilzomib. For me, that’s very interesting because that’s what I do in my clinical practice.
When we make decisions in our clinical practice, there are trade-offs. Carfilzomib is a sister medication of bortezomib. They’re both proteasome inhibitors, but each one has different toxicities.
There’s no clear-cut evidence that one is better than the other, but I don’t like the enduring toxicity that occurs with some of the other drugs, like bortezomib. That’s where we will be spending our time, talking about those types of drugs. Should we use bortezomib or carfilzomib? Both are standard of care and excellent treatment. There are nuances of why we choose one or the other.
There will be the question of transplant, too. If you have these regimens that can make patients have such a great response that they become “MRD negative,” the question will come forward: do you even need a transplant?
I’m not saying we’re ready to dispense with transplants, but the data continues to show that deep responses, no matter how you get there, will result in better outcomes. Maybe some patients will elect to say, “I’m going to collect cells and think about a transplant later.” That’s a very long, nuanced conversation but a reflection of the progress we’re making with this type of combination.
In terms of which proteasome inhibitor is the right choice, some of that depends on the patient’s profile, comorbidities that they already have, and age.
Dr. Susan Bal
Triplet and Quadruplet Regimens
Cindy: Dr. Bal, you were saying that things are becoming cleaner, but now, we’re thinking about four drugs upfront, but which four drugs? Dr. Fonseca was alluding to it, but are there any considerations that you take into whether your proteasome inhibitor is going to be bortezomib or carfilzomib, or what CD38 monoclonal antibody to use? What goes through your mind now that you’re picking four drugs?
Dr. Bal: As Dr. Fonseca mentioned, the patient in front of you helps determine some of that. As you know, daratumumab and isatuximab are both anti-CD38 monoclonal antibodies. They are both very effective drugs.
However, one is subcutaneous so administration is a little bit easier with daratumumab, which is given as a short injection underneath the skin. The other one requires an IV. For now at least, until we have the subcutaneous version for isatuximab, I do believe that reduces share time and and patient inconvenience very much.
In terms of which proteasome inhibitor is the right choice, some of that depends on the patient’s profile, comorbidities that they already have, and age.
For example, with bortezomib, we’re aware that the risk of peripheral neuropathy is significant and can be quite disabling even at lower grades. However, with carfilzomib, we have seen cardiac and renal toxicities. Even more than just objective data, a lot of people complain of subjective dyspnea and subjective shortness of breath, which can make it challenging for them to feel good during treatment.
Young, very robust, and perhaps high-risk patients are best stratified into the carfilzomib arms, and older patients, depending on their fitness, would then get either no proteasome inhibitor or a bortezomib-based option.
That part is rather individualized, without any clear data of one being overly more efficacious than the other, at least based on the data that we do have in front of us.
In very elderly, very frail patients, daratumumab is exceedingly both efficacious and quite safe, as long as you provide them with appropriate antibiotic coverage, close monitoring, vaccination, and perhaps even IVIG use to protect them from infections.
Dr. Susan Bal
Possibility of Quadruplet Treatment as Standard of Care
Cindy: Are there particular patients that you would not give the quadruplet regimen to, where you would probably go back to triplet therapy or maybe even doublets?
Dr. Bal: Incorporating frailty assessment and assessment of the patient’s overall performance status going beyond the eyeball test that we do is going to be critical in determining who is not fit to receive a quad.
In cases where there are concerns about the use of a proteasome inhibitor, particularly bortezomib, due to underlying diabetes or other comorbidities or the patient’s age and you’re concerned about cardiopulmonary toxicity with carfilzomib, as Dr. Fonseca also mentioned, daratumumab with lenalidomide and dexamethasone is an excellent option with high-level evidence of benefit.
I would say for very old patients who are in their high 80s, even 90s, I would consider a doublet. What’s interesting is that the doublet I would consider would be a dara-dex type of combination or even single-agent dara because IMiDs require hematopoietic monitoring or blood work closely checked for low blood counts. The proteasome inhibitors carry all the concerns that we mentioned.
In very elderly, very frail patients, daratumumab is exceedingly both efficacious and quite safe, as long as you provide them with appropriate antibiotic coverage, close monitoring, vaccination, and perhaps even IVIG use to protect them from infections.
Does everyone need maintenance? I don’t know what the answer to that is yet, but I know that the question is very relevant.
Dr. Rafael Fonseca
Cindy: Dr. Fonseca, do you have anything to add to what Dr. Bal said? What about maintenance? Are you seeing single-drug or double-drug maintenance?
Dr. Fonseca: I want to emphasize one of the points that Dr. Bal made. If you asked me two years ago what I would do with a frail patient who has newly diagnosed myeloma, my response would have been lenalidomide and dexamethasone. However, we saw with the subset analysis in the context of the MAIA clinical trial that the addition of daratumumab significantly improved outcomes for these patients.
I’m glad we have the data because we would be at significant risk of shortchanging patients in the line of thinking of beneficence. Let’s be kind. Let’s use mild treatments. But it turns out that the survival numbers are not as good.
Now, whenever we add a drug, we have to think whether we’re adding toxicity, but the reality is these antibodies are incredibly well-tolerated. It’s different to propose adding carfilzomib or not versus adding daratumumab. Today, I would say the vast majority of patients, even if they’re frail, should get something like daratumumab upfront.
Maintenance is really, really interesting. I’m hoping and I think we’re going to get there soon. Studies, like the ones done by the group of Dr. Bal, are using these adaptive strategies to look at whether we can stop therapy, which naturally leads to the next question. Does everyone need maintenance? I don’t know what the answer to that is yet, but I know that the question is very relevant.
We’re going to get to the point where we’re going to think of maintenance like people think of adjuvant therapy for breast cancer. You complete the surgery. They look at the lymph nodes and the genetic makeup of breast cancer and say whether you need chemotherapy or not. As we incorporate our genetic knowledge, the status of response after induction plus or minus transplant, then we are going to ask those questions.
Does everyone need maintenance? I think it’s going to diverge a little bit more to the extremes. There’s going to be greater contrast. For patients who have standard risk genetic factors, are able to complete induction therapy, have a transplant, and have MRD negativity 10-6, it’s going to be hard to prove that maintenance would have an added benefit. If so, hopefully something that’s better tolerated because, as we know, lenalidomide has significant burden toxicities for patients.
On the other hand, if the patient has residual disease, I don’t think there’s a good enough reason to say that’s what we do. That’s standard. I’m going to cross my fingers and wish that this is not going to come back. I think those are patients for whom we’re going to provide additional treatment for no other reason than to try to get rid of all residual myeloma cells.
I think that’s where we’re going to go with maintenance. I don’t foresee that maintenance, as we have it right now, where everyone gets lenalidomide. You get it until you can tolerate it and hopefully not have side effects or no disease progression. I think that has to change.
If you can eradicate evidence of disease, you can improve your outcomes significantly.
Dr. Susan Bal
Dr. Bal: I couldn’t agree more. We certainly share our opinions regarding the use of measurable residual disease. It’s become the single most important prognostic marker, one that is not defined at all when you’re first diagnosed but comes into play after therapy.
If you can eradicate evidence of disease, you can improve your outcomes significantly. Whether you’re starting as a high-risk patient or a standard-risk patient, getting to that milestone and, more importantly, maintaining that milestone can improve outcomes.
I think maintenance as we know it today will soon cease to exist, hopefully, but mostly because we’re either giving them more therapy, getting them where they need to be, or they’ve done so well because of the excellent therapies we have that we don’t need to continue suboptimal treatments that have other toxicities and risks associated with them.
In the lab, we essentially teach these cells using a viral vector to express receptors on their surface that can target cancer antigens within a patient’s body.
Dr. Susan Bal
CAR T-cell Therapy
Jack: As effective as the treatments are, myeloma still often comes back and one of the exciting new treatments going forward is CAR T-cell therapy. Dr. Bal, can you explain what CAR T-cell therapy is in conjunction with what you presented at ASH?
Dr. Bal: CAR T-cell therapy stands for chimeric antigen receptor T-cell therapy. Within our bodies, there are immune cells and one of those subtypes is T cells, which are normally working to keep our cancers in check. The thought is that these T cells are not working as well as they need to be and the cancer itself is finding mechanisms to evade our immune system, which is what results in disease relapse.
CAR T-cell therapy is a revolutionary therapy. We take out a patient’s T cells by apheresis, very similar to a procedure that patients go through when they do stem cell collection. In the lab, we essentially teach these cells using a viral vector to express receptors on their surface that can target cancer antigens within a patient’s body.
Thereafter, we provide the patients with lymphodepletion chemotherapy, which is essentially chemotherapy that’s given to reduce the number of T cells which are within the patient’s body. We then infuse these chimeric antigen receptor T cells, which go and interact with the antigen, using their CAR receptor, and cause cancer killing or tumor death.
This has been shown to be a very effective modality, particularly in patients who previously haven’t had very good treatment options after they’ve been through the three main pillars of therapy, like CD38 monoclonal antibodies, immunomodulatory agents, and proteasome inhibitors. These patients previously had dismal outcomes measured in single-digit months. Now with these therapies, they’re living longer and having excellent responses, including several that are MRD negative even in late-line disease settings.
At this time, there is FDA approval for two chimeric antigen receptor therapies in myeloma that target the B-cell maturation antigen. This is an antigen that is present on the surface of plasma cells in general and more on the surface of malignant plasma cells or cancer cells. Using this target, we have seen very impressive responses of up to 98% overall responses with one of the FDA-approved agents, known as cilta-cel. This is shown to be an effective avenue.
What we presented at the 2023 ASH meeting is a chimeric antigen receptor T-cell therapy that targets a different antigen known as GPRC5D. This antigen is also one that is expressed preferentially on the surface of these cancer cells and has limited expression across normal tissues, although we do see some expression on tissues such as heart keratinized tissues, on the skin, on nail beds, and in hair follicles. We see some typical side effects, including dyskinesia, with treatments that target this therapy.
Overall, GPRC5D has been shown to be a promising therapeutic target in myeloma. We already have a different immune strategy that’s working against this and is FDA-approved.
In this phase 1 study, we evaluated a CAR T cell that is targeting GPRC5D in patients with relapsed myeloma. What we saw is that in a heavily pre-treated patient population who have received a median of five prior lines of therapy, this was associated with deep responses overall. In about 73 patients who were efficacy available, meaning were available for response assessment, we saw that 88% of the patients had a response.
For the first time, we shared the recommended phase 2 dose, which is the dose that’s going to be moving forward. It was determined at about 150 million CAR T cells. What was encouraging was that the response rate for this recommended phase 2 dose was 91%. At that dose level, we saw low-grade CRS. No patient had grade 3 or higher CRS. There were no cases of other serious toxicities, such as macrophage activation syndrome, etc. This dose was efficacious.
So far, the follow-up for this dose cohort is relatively short so we don’t know what the long-term progression-free survival and overall survival are going to be. But the responses are deep. We need to follow the study longer to understand the more important and relevant outcomes, like progression-free survival and overall survival.
If they work well downstream, as is true for every single myeloma drug, we keep bringing them towards the forefront. The results are quite remarkable.
Dr. Rafael Fonseca
Jack: Dr. Bal mentioned that there are a couple of approved CAR Ts available for patients now, except for the fact that they require four-plus lines of prior therapy.
There are trials and announcements of results from those trials, like CARTITUDE-4 and KarMMa-3, that are testing these same CAR T-cell therapies in earlier lines of treatment. Can you talk about the results in relation to a patient’s quality of life?
Dr. Fonseca: I think that is probably the key aspect of all of this. As you mentioned, two trials are looking at CAR T-cell therapy earlier on: KarMMa-3 with 2 to 4 prior lines of therapy and CARTITUDE-4 with 1 to 3.
What they explored is if they work well downstream, as is true for every single myeloma drug, we keep bringing them towards the forefront. The results are quite remarkable. Many of you saw the presentations and ultimately the publication of the CARTITUDE-4, which was presented at ASCO as well as EHA and published in the New England Journal.
What we’re seeing is this treatment can provide very durable responses that can go on for years for some patients. Then, of course, the natural question is: how does this compare to other treatments? We have effective treatments that can work very well in someone who is experiencing a first relapse, such as the combination of daratumumab, carfilzomib, and dexamethasone or isatuximab, carfilzomib, and dexamethasone.
But the one big advantage of CAR T-cell therapy is that it’s “one and done.” We’re seeing patients who are reporting very high levels of quality of life and making statements like, “I haven’t felt this well in such a long time.” It’s not because CAR T-cell therapy gives you superpowers. It gets rid of all of the side effects that come with treatment.
Even the most benign of treatments involves logistics, medications, blood draws or venipuncture, and some have side effects that come from the chemicals or the biologics that are used. Even in the best-case scenario, it’s something that the patient has to do. The idea that you’re done and all that needs to be done is occasional labs to monitor becomes very appealing.
I think that’s probably going to be the number one driver. Of course, we’re very excited. We’re hoping to see these treatments have very, very long-lasting benefits for some patients. But even if they were not, for some, the ability to be treatment-free would be beautiful.
I always quote our colleague, Dr. Amrita Krishnan from City of Hope. She said that one of the unmet needs in myeloma is to stop therapy so even if it’s temporary, for some hopefully more durable, this would be a way to achieve that.
Jack: I have patients in my support group who say exactly what you say. Some are without treatment three years after their CAR T-cell therapy but even those who relapsed sooner, like within six or ten months, say they would do it all over again because they had that drug-free period that they were so appreciative of.
We know that patients, after having the CAR Ts, can sometimes have prolonged periods of low blood counts and no one really knows why.
Dr. Rafael Fonseca
Side Effects of CAR T-cell Therapy
Jack: That said, Dr. Fonseca, I want to ask another question about a specific CAR T-cell therapy side effect having to do with secondary myeloid cancers, like acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS). I’m hearing some concerns about that and wonder what your take is on what’s out there.
Dr. Fonseca: First of all, I’m going to say that we don’t completely understand this and many other factors may come into play.
The FDA recently put an announcement that a fraction of patients, up to 10% in the series that was reported, could develop secondary myeloid malignancies. These are the cells that produce your regular white cells and the conditions that follow from that are either leukemia, acute leukemia, or the preceding stage, which we call myelodysplasia, which is concerning as well to us as physicians.
There are many reasons why this could be nothing more than the reflection of patients living longer and patients who have had exposure before to a number of agents and drugs that are clearly known to cause this. This could include things such as melphalan, which is used for stem cell transplant, but also some of the drugs that are used for the priming of the body for CAR T cells, including fludarabine.
On the other hand, there might be other reasons why this could be linked to CAR T-cell therapy. You’re going to hear more about this as people do the research. For instance, we know that patients, after having the CAR Ts, can sometimes have prolonged periods of low blood counts and no one really knows why.
For instance, in the case of BCMA. BCMA is predominantly expressed in B cells, not in these myeloid cells. How come we have myelosuppression? We don’t know for sure. But if you have that, then there are a lot of hypotheses that can come forward. Does that create an environment that maybe selects for clones that are going to do this? Does that create an inflammatory situation that maybe allows for the progression of some of those pre-malignant clones?
The threat is much greater from unattended myeloma. While we want to have perfect treatments with no side effects, for someone who’s considering CAR T-cell therapy, it’s much better to get it than not, despite these considerations.
Dr. Rafael Fonseca
Our audience is familiar with the term MGUS (monoclonal gammopathy of undetermined significance). As you know, we have myeloma and you have MGUS, and this is a prototype of this stepwise progression. It turns out there’s a similar thing that happens for myeloid cells that there’s something called CHIP (clonal hematopoiesis of indeterminate potential) and it turns out to be very common. It’s one of the things that happens to all of us in life as we age. You develop these premalignant states and CHIP is very common. It can be seen in up to 40% of people.
The question is: what are the CAR Ts doing that maybe makes some of this CHIP grow more or the CHIP cells be favored? We don’t know, but this is an important question.
But practically speaking, as of now, the threat is much greater from unattended myeloma. While we want to have perfect treatments with no side effects, for someone who’s considering CAR T-cell therapy, it’s much better to get it than not, despite these considerations.
Jack: They have other options, like bispecific antibodies.
One of the best parts about bispecific antibodies is the fact that you don’t have this lag time or delay that comes with manufacturing associated with CAR T cells.
Dr. Susan Bal
Bispecific Antibodies
Cindy: Dr. Bal, I hear patients sometimes refer to bispecific antibodies as off-the-shelf CAR Ts and I know they’re not. Can you explain the difference between a bispecific antibody and a CAR T?
Dr. Bal: Bispecific antibodies are antibody fragments. I typically describe them to my patients as a little Y-shaped linker. This is an antibody with two prongs if you will. On one hand, it uses the CD3 molecule to catch the T cell and on the other hand, it has an antigen receptor for one of the myeloma targets.
Currently, we have bispecific antibodies that target cancer cells using the same antigens that we talked about for CAR T-cell therapy, such as B-cell maturation antigen (BCMA) or GPRC5D. They target the cancer cell using one of these antigens and bring the two close so that cancer cell killing by the immune system can occur.
One of the best parts about bispecific antibodies is the fact that you don’t have this lag time or delay that comes with manufacturing associated with CAR T cells. These therapies are off the shelf. They utilize the patient’s own T cells, bring them close to the cancer cells, and result in cancer cell killing.
Oftentimes, where we don’t have the time or the manufacturing capability or the slot allocation, or all of those patients who are not necessarily being treated at a large center with CAR T-cell capabilities, this provides an avenue to use new immune treatments and immunotherapies for a wider range of patients. It has the potential to reach many more patients, given the current state of affairs, at least in 2023 and 2024, and so presents a very exciting option for our patients.
Some could argue they don’t have as of yet the same horsepower as some of the CAR Ts. Many of us are thinking of using them down the line, but some of them in combination are incredibly, incredibly active.
Dr. Rafael Fonseca
ASH 2023 Updates on Bispecific Antibodies
Cindy: Dr. Fonseca, were there any major updates on bispecifics at ASH 2023 that we should know about?
Dr. Fonseca: We had a number of updates from some of the longer-term outcomes and some of the studies that are looking at bispecifics in various combinations, including with some of the traditional agents. I’m very interested to see how this plays out.
What we’re seeing is that bispecifics, first of all, are very active. Some could argue they don’t have as of yet the same horsepower as some of the CAR Ts. Many of us are thinking of using them down the line, but some of them in combination are incredibly, incredibly active.
There are clinical trials looking at bispecifics in combination with pomalidomide, bispecifics between themselves, and bispecifics with daratumumab in combination. There’s a trial that combines talquetamab and teclistamab, the RedirecTT-1 trial.
We have new constructs that are being developed. We saw a presentation about something called a trispecific so instead of having one side that a bispecific can attach to, there are bispecifics that could attach to two different anchor points that these myeloma cells have.
Now, I’m particularly interested in bispecifics because the possibility that many more patients be treated is there for bispecifics than for CAR T-cell therapy. CAR T-cell therapy requires centers of excellence and referral patterns, and there are wait times for cell production. Whereas with the bispecifics, they’re “off the shelf.”
It’s going to take some time. People have to become familiarized with this, but in the future, we’ll see community hospitals and mid-sized hospitals administering these bispecifics, which in my mind is wonderful because many more patients will derive benefit from this type of therapy.
This is the beginning of a new era in cancer treatment because solid tumors are being explored for bispecifics so lung cancer might be treated with this. Oncologists in the future will certainly need to be facile and comfortable with the use of bispecific antibodies.
There’s a lot of push for fixed-duration therapy. One of the greatest reasons, beyond patients having to come to the hospital or clinic and the treatment and travel burden, is the side effect profile.
Dr. Susan Bal
Dosage & Administration of Bispecific Antibodies
Cindy: Dr. Bal, can you talk about the dosing and schedule of bispecifics?
Dr. Bal: Currently, three FDA-approved bispecific antibodies are on the market. We have two agents targeting BCMA: teclistamab and elranatamab. Both target the B-cell maturation antigen. As of right now, these drugs are typically given on an ongoing basis until disease progression or unacceptable toxicity.
Typically, these start in the hospital with a small portion of inpatient hospitalization. Patients receive step-up dosing to minimize the risk of certain side effects. Afterward, they go on to weekly or every two weeks. In this fashion, they go on until the patients continue to respond or come off due to side effects.
However, patients take a median of a little over a month to respond to these agents and up to about six months to get into a complete response. Often, these responses are very deep. In patients who go off treatment because of side effects, we see that some of these patients can maintain their response for years without treatment.
There’s a lot of push for fixed-duration therapy. One of the greatest reasons, beyond patients having to come to the hospital or clinic and the treatment and travel burden, is the side effect profile. These B-cell maturation antigen-directed bispecific antibodies have a lot of infection risk.
Seventy-plus percent of patients get infections and 40 to 50% of these can often be grade 3 or higher, which can be quite serious. These infection risks, particularly oftentimes infection with unusual things that we don’t typically see in myeloma patients, have also enhanced some of our concerns about using these agents on a prolonged basis in patients whose disease may be controlled.
Multiple factors are at play so there’s a lot of interest in studying fixed-duration therapy of these agents to tailor it to a patient’s response and be able to discontinue these therapies once they’re responding to optimize their risk and benefit profiles.
We know that when we use several agents that target the same anchor, there is a possibility that you could develop resistance so we’ll have to wait and see.
Dr. Rafael Fonseca
Antibody-Drug Conjugates
Cindy: Dr. Fonseca, we talked about CAR T-cell therapy and bispecific antibodies. Let’s talk about antibody-drug conjugates. We had one that was approved through accelerated approval and then taken off the market but now it may be back. Could you talk about BLENREP (belantamab mafodotin)?
Dr. Fonseca: Antibody-drug conjugates are antibodies that carry a payload. There’s usually a chemical entity attached to an antibody. In general, what happens is the antibodies bind to the cell surface and go inside the cell. They’re eaten into the cell where they release that chemical structure.
One of those antigens is belantamab. When it first started, it showed very, very high rates of response. Quite promising responses. It went through regulatory approval for a fast-track approval.
Unfortunately, there had to be a confirmatory phase 3 trial that did not meet the endpoint. That means that the data for the trial would not support the complete approval by the FDA. The product has been since withdrawn from the market but is available on a compassionate basis.
This is a highly active compound. It comes with some baggage. One of the main baggage is toxicity to the eyes. Something we call keratopathy and that’s inflammation of the outside layer of the eye, the cornea. As we’re learning how to use it in better doses, that has been a little bit better tolerated. It’s not to say it doesn’t exist, but people are understanding better how to use this.
We learned about two very exciting trials. One of them is the DREAMM-7 trial, which was belantamab, lenalidomide, and dexamethasone versus daratumumab, lenalidomide, and dexamethasone. We’re told the trial is positive meaning there are favorable effects of the belantamab. We’ll have to see what the actual numbers show.
There’s another one that was recently published called the ALGONQUIN clinical trial, which is a combination of belantamab, pomalidomide, and dexamethasone, which has pretty interesting results.
The question is going to be: how do we time all of this? Belantamab targets BCMA as well, too, so that means it could compete with bispecifics and CAR Ts. We know that when we use several agents that target the same anchor, there is a possibility that you could develop resistance so we’ll have to wait and see.
ADCs are one of the hottest things right now in biotech and development for solid tumors as well, too. I heard from people who were at one of those recent conferences that a lot of companies are interested in them. I think we’ll see a comeback of ADCs in myeloma and in other diseases as well, too.
I have patients right now who are still enjoying the benefits of the prior administration of belantamab.
Dr. Rafael Fonseca
Cindy: Do you think Blenrep will be coming back on the market?
Dr. Fonseca: It’s interesting. I’m not currently up to date on what the regulatory pathway will be for that to occur. I think it will, but the results are exciting. The question is how this will compare to some of the other things that I’m mentioning with bispecifics.
I have patients right now who are still enjoying the benefits of the prior administration of belantamab. They have since resolved the eye toxicity. In all cases, with time, the eye toxicity improves. These are patients that may have gotten a short course of treatment with belantamab and remain under excellent control right now.
It’s always better to have more options. I don’t think I would venture out to say exactly how we’re going to sequence this because of the issues of resistance, but I certainly would welcome having that back in our toolkit.
Cindy: I agree. More options are better because we’re also unique and what works for one person may not work for somebody else so I’m glad to have as many bullets in our arsenal as possible.
BCL2 inhibition has a place and hopefully, we’ll find FDA approval soon so we can use it more freely and benefit this unique subset of patients.
Dr. Susan Bal
BCL2 Inhibitors for Myeloma
Jack: Dr. Bal, venetoclax is well-known out there. It’s an approved drug for chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL), but it gets used off-label in myeloma patients who have a translocation called t(11;14). At ASH, something called sonrotoclax was introduced as the next-generation venetoclax. Do you have any comments about that particular new drug?
Dr. Bal: Translocation t(11;14) myeloma is a subtype of myeloma that’s a little bit of a different disease itself. It’s a distinct entity and a distinct subtype of myeloma, which responds a little bit differently to different agents. It has a higher dependency on BCL2 inhibition, which is a key part of what drives this myeloma and, therefore, inhibiting it in this space helps drive treatment responses.
We know venetoclax is an effective therapy. Unfortunately, the randomized trials have not worked very much in favor of it. However, those of us who use it and single-arm studies have shown impressive responses in this subset of myeloma patients.
At the ASH 2023 meeting, we looked at a novel BCL2 inhibitor, which is supposed to be at least 10 times more effective and more selective for BCL2 inhibition. It’s called sonrotoclax and they are studying it in a phase 1 setting in several countries. They’re looking to first get the right dose and then expand it in combination with carfilzomib to best understand how these patients respond.
We know venetoclax is an effective therapy. Unfortunately, the randomized trials have not worked very much in favor of it.
Dr. Susan Bal
What we have seen at ASH 2023 was a result from about 19 patients, 10 of whom got the recommended phase 2 dose, which is going to move forward in studies. What we saw was very impressive single-agent activity in combination with dexamethasone at the recommended phase 2 dose of 70%.
What was even more impressive to me was the complete lack of dose-limiting toxicities. There were really minimal side effects that would prevent dose-finding and dose escalation, and a very low risk of low blood counts, which was something that we thought we would see.
The drug was very, very well tolerated. I recall maybe a single patient with high-grade diarrhea and maybe a COVID-19 infection, which was ongoing during the study. Overall, the safety profile is very impressive with responses in combination with dexamethasone of 70% at the recommended phase 2 dose. As the study accrues more patients and studies combinations with carfilzomib, I think it will be exciting.
I will also touch on some of the data that was presented by Dr. Bahlis, which was venetoclax in combination with daratumumab, which showed very impressive responses. Although the patient population was less heavily pre-treated and mostly daratumumab-naive, response rates and measurable residual disease negative states were very, very impressive. BCL2 inhibition has a place and hopefully, we’ll find FDA approval soon so we can use it more freely and benefit this unique subset of patients.
The long-term use of dexamethasone is not contributing much to the control of the disease and we know for sure it’s contributing to the burden of side effects.
Dr. Rafael Fonseca
Dexamethasone Dose Reduction
Jack: Dr. Fonseca, we patients always appreciate it when we learn that doses can be reduced. When we hear that dexamethasone dosing can be reduced, we get giddy about it.
At ASH 2023, there was a presentation that looked retrospectively at a couple of SWOG trials, S0777 and S1211, which looked at patients who had lower dex dosage. Can you talk about that and what that might mean for patients going forward?
Dr. Fonseca: Whenever we discuss treatments with a patient, I usually emphasize that the hardest part is probably going to be the dexamethasone, for reasons you know better than I do. It all started several years ago with a patient, Michael Katz, who said, “We get too much dexamethasone. What can you do about that?” That led to the design of E4A03, which changed our paradigm that we now use dexamethasone at what we call “low doses.”
When my endocrinology friends see those doses, they tell us, “What are you doing? This is a massive dose of dexamethasone.” That was a significant change. We used to use 12 days per cycle, that is 12 out of 28 days at 40 mg of dexamethasone.
We’ve moved forward but have not completely gotten rid of it. From what we know now, as you go on with treatment, as shown by the studies mentioned, as the patient gets stabilized, it becomes increasingly clear that the long-term use of dexamethasone is not contributing much to the control of the disease and we know for sure it’s contributing to the burden of side effects. It should be noted that several studies are showing that. Clinicians need to be cautious and need to adjust the doses of dexamethasone.
In the beginning, most of us feel that patients need a little bit of dexamethasone to “jump start” a good response. But even then, you can do some dose adjustments. In patients of more advanced age, we often will use 20 mg instead of 40 mg. As well, in patients who have amyloidosis, we’ll make adjustments like that.
Is there a way by which we can tell who is going to benefit from the addition of the steroids?
Dr. Rafael Fonseca
It’s important to be mindful of this because patients should not be on 40 mg of dexamethasone once a week for a long time. In general, this is not something that we should be using long-term for maintenance. It can be used short-term for consolidation or other reasons.
The field continues to move in that direction. One patient once asked me, “You always talk about lenalidomide resistance, but you never say dexamethasone resistance. How do you know if it’s contributing down the line?” That is one question that we need to go back and address.
At the beginning of myeloma drug development, there were a lot of people who were interested in resistance to steroids, like Dr. Steve Rosen from City of Hope, and we abandoned that line of thinking. We need to go back and say: is there a way by which we can tell who is going to benefit from the addition of the steroids?
Sometimes, myeloma is very aggressive and very difficult to control. But please don’t assume that because you’re facing this diagnosis, there’s an imminent threat that for sure will be life-limiting because the treatments continue to get better.
Dr. Rafael Fonseca
Final Takeaways
Cindy: If you had one key takeaway that you want patients to hear, what would it be?
Dr. Bal: For me, the most exciting thing in myeloma right now is immunotherapy. The prospect of these new agents that use our immune system to kill cancer cells is really innovative and exciting. I can’t wait to understand how best we can use these strategies to provide fixed-duration treatment and lead to the longest possible remission in a low or undetectable cancer state, such that our patients can have an excellent quality of life.
Dr. Fonseca: We’re very excited and positively so because of the developments in myeloma. We fully realize it would be better to meet you in social circumstances or at coffee somewhere else. But right now, if you’re diagnosed with myeloma, for many, many patients, there are options such that myeloma should not be an immediate threat.
In fact, for many patients, we develop this relationship, as Dr. Bal was saying, and then we track along with you for years and even decades for some patients. It’s not unusual for us to see patients in the clinic well beyond 10 years, sometimes 15 and 20-plus years. I am convinced some of those patients have been cured because of effective frontline therapy. But even for those who haven’t, there are often times options for treatment.
Unfortunately, I know this is not a reality for everyone. Sometimes, myeloma is very aggressive and very difficult to control. But please don’t assume that because you’re facing this diagnosis, there’s an imminent threat that for sure will be life-limiting because the treatments continue to get better.
Jack: For any myeloma patient and care partner, stay educated. There are so many new treatments coming so quickly for myeloma and they are for different target audiences: newly diagnosed as well as relapse patients.
One way to stay educated is to listen to programs like this. Check out the myeloma advocacy websites that offer webinars and videos. Join a support group and make sure to understand the best questions to ask your doctor.
Cindy: It’s important for patients to be seen by a myeloma specialist. Anytime a patient has to have a treatment decision to make, it’s imperative that they get guidance from a myeloma specialist. There are so many new treatments available, new data being presented on different treatments that are now coming to market, and clinical trials so it’s overwhelming.
Conclusion
Stephanie: Thank you so much, Jack and Cindy, for being our incredible patient advocates and moderators. Also to Drs. Fonseca and Bal for the work and research you do to help move the landscape of treatment options in multiple myeloma.
We hope that you walk away with a better understanding of the latest treatments and clinical trials in myeloma. They may or may not be right for you, but it is our goal to make sure you feel empowered to make a decision for yourself.
Thank you and we hope to see you again at a future program at The Patient Story.