Interviewed by: Taylor Scheib Edited by: Katrina Villareal
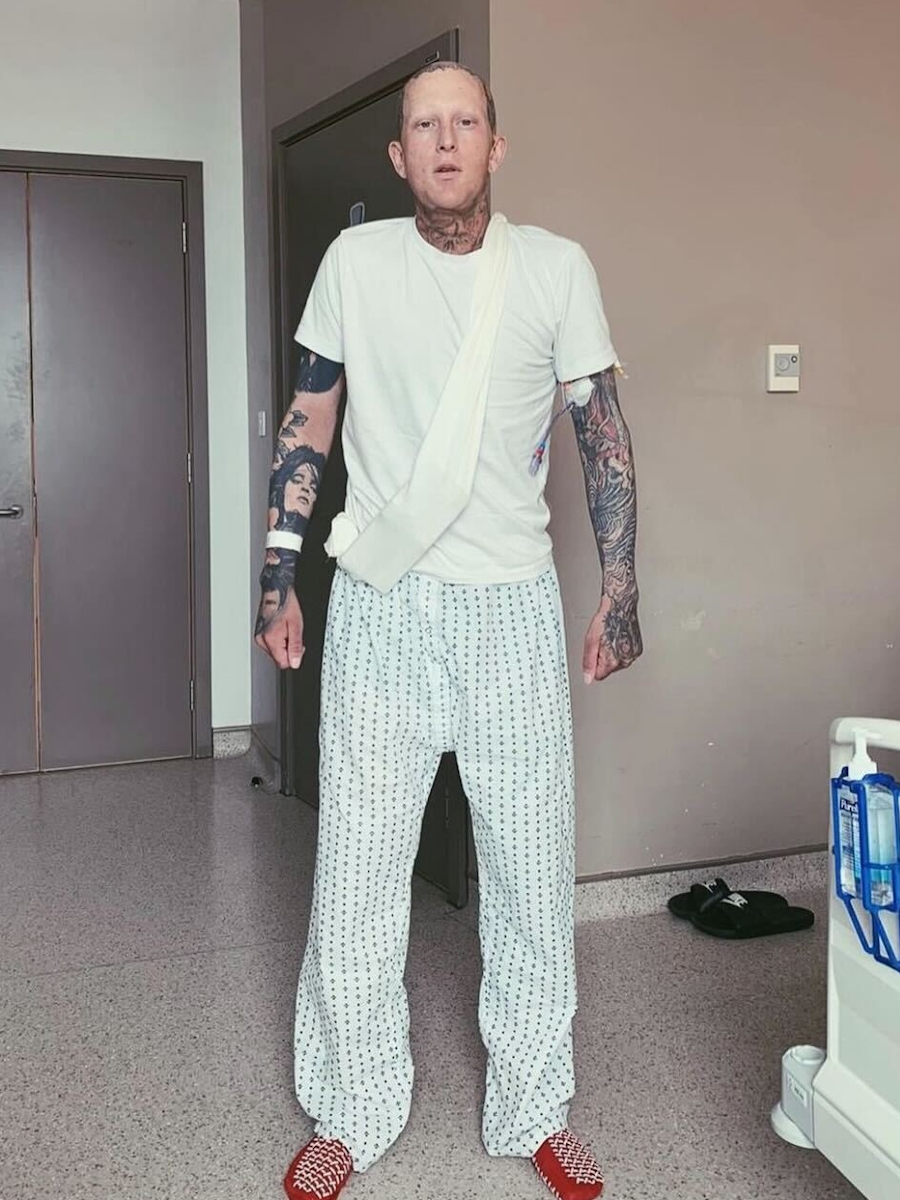
Before his stage 3 testicular cancer diagnosis, Callan was actively engaged in mixed martial arts and Brazilian jiu-jitsu, maintaining a rigorous fitness regime. Upon discovering a lump in his right testicle, Callan immediately suspected cancer, a diagnosis that was confirmed after a series of medical consultations.
Initially, Callan underwent multiple chemotherapy treatments and one surgery, but the cancer recurred within six months. He subsequently tried a low-level chemotherapy regimen, which proved ineffective. Recently, Callan began participating in a clinical trial for a targeted treatment designed to attack the remaining tumor in his lung.
Throughout his treatment journey, Callan faced significant physical and emotional challenges. He experienced severe side effects from various chemotherapy regimens, including BEP (bleomycin, etoposide phosphate, cisplatin), cisplatin, and the high-dose TopCaT (topotecan, carboplatin, thiotepa) treatment with blood stem cells. These treatments caused debilitating symptoms such as extreme weight loss, nerve damage, temporary blindness, and a plethora of other health issues. Despite these setbacks, Callan remained determined, continuing to engage in physical activities whenever possible.
Callan’s resilience is evident in his ability to maintain a positive outlook and a sense of normalcy amid ongoing treatments. He has found solace in helping others by sharing his experiences and supporting fellow cancer patients. His participation in the trial, which targets a specific protein in his tumor, represents a glimmer of hope though it also comes with risks as his liver has recently been affected by the treatment.
Callan’s story is one of tenacity and hope, as he navigates the complexities of cancer treatment while striving to lead a meaningful life and support others facing similar battles.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Lexie’s High-Grade Endometrial Stromal Sarcoma Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Lexie’s life changed dramatically when she was diagnosed with cancer three times. Her symptoms started with a prolonged period and severe cramps. Initially misdiagnosed, she eventually discovered she had cancer. The first treatment involved surgery, but subsequent relapses required more aggressive treatments.
During her first relapse, severe cramps led to the discovery of a softball-sized mass. She underwent surgery and chemotherapy, maintaining a positive attitude with support from her husband and family.
Later, respiratory issues revealed another mass in her chest. Proton beam radiation followed by chemotherapy initially seemed successful, but cancer spread to her lung lining, necessitating further treatments.
Throughout her journey, Lexie faced severe side effects from chemotherapy. She learned the importance of self-advocacy in medical care and relied on her strong support system and medical team. She focuses on controlling what she can, finding silver linings, and encouraging others to seek support.
Thank you to Karyopharm for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I had a period that lasted over a month. I kept thinking that it was normal and that it was going to stop.
Introduction
I live in Scottsdale, Arizona, but I grew up in a small town in Minnesota.
I love going to different coffee shops and checking out the vibe and the coffee. I love hiking and being out in nature during the day. I did a lot of camping growing up. That was usually our vacation.
I love to travel and go to different places. It’s fun to see different cultures. I love to spend time with friends and family.
I have been diagnosed with cancer three times. What I have now is high-grade endometrial stromal sarcoma. It was low-grade at first, then it became high-grade.
Initial Cancer Diagnosis
One time, I experienced intense cramps but I knew they weren’t period cramps. I know my body very well and I knew that something was off, so I went to the emergency room. They gave me Midol and sent me home.
Another time, I had a period that lasted over a month. I kept thinking that it was normal and that it was going to stop, but my sister told me I needed to get checked so she scheduled an appointment for me.
I was eventually diagnosed with low-grade endometrial cancer, but I didn’t do chemotherapy or radiation. I felt I got off a little easier, having to undergo surgeries and then continue living my life.
A doctor came in and said, ‘You’ve got a huge mass the size of a softball that’s pushing up on stuff.’ I asked, ‘When are we going to find out if it’s cancer?’ He said, ‘It is.’
First Relapse
Symptoms
I experienced very similar symptoms and I was still being so ignorant of it. I didn’t think of cancer, which was crazy to me, but that’s how I live my life. I don’t try to allow those thoughts to come in too often.
At the time, my husband was traveling for work. I was walking with a friend and I was a little bit hunched over because I was having a lot of intense cramp-like feelings. I kept telling her I thought it was my appendix, thinking it was appendicitis.
I went to the ER and that was pretty tough because I was by myself. After they ran all the tests, a doctor came in and said, “You’ve got a huge mass the size of a softball that’s pushing up on stuff.” I asked, “When are we going to find out if it’s cancer?” He said, “It is. We can tell,” so that was tough.
Reaction to the Relapse
I was overwhelmed, but I never felt like my life was over. I thought it was another fight I was going to have to fight. It was more about putting my game face on. It was another obstacle in front of me that I had to conquer.
It was tough to make the phone call to my husband. I told him I was going to the ER and he knew the entire time what it could be. When I called, I could barely get words out. He said, “I’m on my way.” It’s so good to have such a good support system, so that was tough, but we got through it.
They all came to the same conclusion. Chemotherapy was necessary knowing that I already had cancer once before.
Treatment
I ended up going through surgery to get the mass out and then I had to decide whether I was going to do chemotherapy or not to make sure that we got rid of all cancer cells.
Make sure that you get a second opinion so that you’re as informed as possible before making a treatment decision. I ended up getting the opinion of a few different doctors. I gave them all of my test results and they all came to the same conclusion. Chemotherapy was necessary knowing that I already had cancer once before and it came back and is now high-grade.
Side Effects of Chemotherapy
Chemotherapy was intense. I also got pneumonia during treatment. There was one point when I was lying on the floor and, in that moment, I felt like my life was over because I was so done that I could not fight anymore.
Chemotherapy was brutal on me. The fatigue was pretty intense. The brain fog was pretty bad too. I had hair loss, but it never mattered to me, which is crazy because I was so superficial growing up.
Since the first time I got cancer, one of the silver linings is my priorities changed. It wasn’t about making sure my hair or makeup was perfect. I couldn’t care less. There was hair loss, but I never cared about wearing a wig. The only time I wear a head cover is to protect myself from the sun, but otherwise, it’s part of my journey, so I go with it.
I was exhausted. I’ve already done this twice. I didn’t want to do this again, but I wasn’t ready to give up.
Second Relapse
Symptoms
I’ve gone through cancer twice and I thought a cold was going to knock me out because, at the time, I couldn’t breathe very well and I was fatigued. I thought it was COVID.
I went to the ER because I also couldn’t breathe. They ran a test and said I didn’t have COVID. They ran a few tests to make sure and did a scan. The doctor came in and said, “You have a big mass in your chest that is pushing up on all of the important tubes that help you breathe.”
Treatment Decision-Making
I thought that they could remove the mass and then we were good, but the mass was next to some important organs. At that moment, I was exhausted. I’ve already done this twice. I didn’t want to do this again, but I wasn’t ready to give up.
After my first relapse and going through chemotherapy, I told my family that if it happened again, we’d be waving the white flag. I couldn’t go through the treatments again. It was too much. That was a hard pill for my family to swallow because it could cut my life short.
But when I was put in the actual situation, I decided I wasn’t done yet. I still had too much to do in my life. It was difficult because I had to think through. Was this something I wanted to do? Did I want to go through the different treatment options? Is this going to affect my quality of life? That’s how I choose to make my decisions these days.
When I looked at my PET scans, it looked like everything was gone. The only thing that was showing was a little bit of red near the scar tissue.
We ended up not doing surgery. We did proton beam radiation, which is different from the traditional one. I was so grateful to be able to go to a facility that had that available because that’s not very common everywhere. It has fewer short-term and long-term side effects.
After radiation, I did three cycles of chemotherapy. The radiation seemed to work, so that was great news.
When I looked at my PET scans, it looked like everything was gone. The only thing that was showing was a little bit of red near the scar tissue. According to my radiologist and doctor, they were pretty sure it was scarring, so I should be good to go and continue to live my life. We could do a couple more rounds, but ultimately, it was my decision. I weighed the pros and cons, and I felt good that it was gone.
Cancer Spread
I was able to live my life normally for a couple of months, so it was a nice little reprieve from a mental health standpoint. I needed it because I was tired of fighting.
I did my follow-up PET scan a couple of months later, which showed it had spread. It’s in the lining of my lungs. I don’t say I regretted my decision, but it was the decision I made.
Treatment
I had to do a lung surgery. I’ve been doing chemotherapy. I’m cautiously optimistic. I hope that the PET scan will show that it worked because I had to make another hard decision of what type of treatment plan I wanted to go with for this next round.
I had three different options. I took some time to think. I was tired of it. I wanted to move on with my life. I went with the most aggressive options, which also had the highest risk. If the PET scan doesn’t show what I hope and believe it will show, then I don’t have a whole lot of options.
I have a decent amount of anxiety, but I’ve been raised to focus on what I can control and then let the rest go.
Having a Strong Support System
With the medical team that I have, it’s a collaboration. They keep me informed and give me all the options. If they believe an option to be better than the others, they’re going to voice their expert opinion. One thing that I like about where I go now is they have a tumor board. As we talk about self-advocacy and getting second opinions, they’ve already integrated those into their model, which is so reassuring.
If they come across unique cases that they’re not as exposed to, they bring the case to the tumor board, so they can weigh in. They bring the information back to the patient to help the patient make an informed decision.
Because of that collaboration, I don’t feel like I’m on an island. All of my family members rally together during these times. They try to get as much information as they can and filter what’s valuable to help me make an informed decision. It’s a lot of weight to be the sole decider, but I guess that’s part of life. We have to make decisions all the time. How do you do that successfully? It’s a team effort.
Living Life
I’m like a duck where I’m calm on top of the water and swimming for my life underneath. I have a decent amount of anxiety, but I’ve been raised to focus on what I can control and then let the rest go.
There’s a lot in my life that I cannot control and this is one of those things. I remind myself that I’m doing everything that I can and I have to be okay with it. Then let the rest be what it is.
I didn’t understand that I could advocate for myself. You know what’s best for you, so it’s important to push for what you know is right.
Importance of Self-Advocacy
Self-advocacy is so important to be able to make an informed decision. You can’t do that without getting all of the information and advocating for what you feel is right. The reason why I think it’s so important to push for what you feel is right is because of my situation. They kept telling me that it was just period cramps when I knew it wasn’t, but they’re the experts and so I felt a little bit defeated and didn’t necessarily know what direction to take.
I needed my sister to advocate for me because I didn’t know what self-advocacy was. It was my first time going through cancer, so I didn’t understand that I could advocate for myself. You know what’s best for you, so it’s important to push for what you know is right.
Words of Advice
Live positively because the opposite sounds so miserable. Of course, we all have our moments. I’m not saying I’m positive 24/7; that’s unrealistic. I have days when I feel down. You need to have more up days than down days. I choose to be positive.
Go big or go home because life is too short. Take full advantage of your situation and find the silver lining.
You’re not alone. I don’t want people to ever feel like they’re alone. There are communities and resources out there to help you.
Life is too short. Take full advantage of your situation and find the silver lining.
Special thanks again to Karyopharm for its support of our independent patient education content. The Patient Story retains full editorial control.
Don’s Relapsed Diffuse Large B-cell Lymphoma (DLBCL) Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Don was 1 of nearly 70,000 Americans diagnosed with non-Hodgkin lymphoma in 2013. Unfortunately, Don fell into the 20-50% of patients whose non-Hodgkin lymphoma came back 8 years later. But still, it wasn’t over. After a second round of chemo, within one year, the non-Hodgkin lymphoma came back.
Don underwent chemotherapy regimens twice. The third time doctors found his cancer, his treatment options were limited. The conversation became more difficult.
This is Don’s story of how he got diagnosed with cancer 3 times and the decisions that led him to no evidence of disease.
Thank you to Genmab for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I was losing weight, didn’t feel good, and was always tired. I was admitted to the hospital for three weeks to run tests and they discovered I had lymphoma.
Introduction
I grew up in Connecticut and then in 1979, I moved to North Carolina where I live with my wife. We’ve been married for over 20 years.
I worked for IBM for 25 years and while there, I got my master’s degree in electrical engineering from Syracuse University. I retired in the ‘90s and started my own computer business. I did that for another 20 years and then retired for good.
I used to race sailboats, but I’ve aged out of that and now I’m into golf.
Non-Hodgkin’s Diagnosis
In 2013, I was losing weight, didn’t feel good, and was always tired. I was admitted to the hospital for three weeks to run tests and they discovered I had lymphoma. Dr. Favaro was the on-call doctor then. I went with him when I got out and I’ve been with him ever since.
Eight years later, it came back and this time, it was the lymph nodes in my neck. We did treatment again but no radiation this time.
Less than a year later, it was back for a third time. The glands in my neck got swollen, so I knew something wasn’t right. I thought it might go away, but it never did, so I went to see my oncologist again.
Dr. Favaro said, “We have to do something different.” I looked into CAR T-cell therapy, but the problem was it required 24/7 care. My wife was still working, so we couldn’t do that. We then looked at Epkinly and we’ve been doing that since February.
The regimen for Epkinly initially starts with three weeks of low doses… it may be possible that after a year or two, I won’t even need to go once a month.
Making Treatment Decisions Together
Dr. Favaro set me up with another doctor in Charlotte. I went to see her and discovered that it was going to be more intense than we were able to do. Dr. Favaro said he could do the Epkinly. I got all the booklets and we read all about it. As it turns out, I’m his first patient with Epkinly and it’s gone very well.
Treatment Timeline
The regimen for Epkinly initially starts with three weeks of low doses. It becomes a full dose for about two months, every other week for another two months, and then once a month from then on.
Epkinly has been around since 2018. As they get more and more data, it may be possible that after a year or two, I won’t even need to go once a month.
Starting on a Newly Approved Treatment
Initially, you go in for a shot once a week. It goes in the stomach. It’s an easy pinch. You don’t feel anything and it takes less than 30 seconds. A rash will show up and I use medication on that, so that fixes that itch.
In addition to that, you get steroids. They do blood lab work to make sure everything’s going okay. You get fluids. Since I was on clopidogrel, a blood thinner, they couldn’t put a port in, so they put a PICC line in. The bad news is it has to be flushed every day and that was a challenge because my oncologist’s office isn’t open on weekends. My wife could do them, but when she went on a week-long vacation, I had to go to the local hospital.
I’ve got side effects, but they don’t last very long and for the most part, I can take medication and then I’m okay.
Getting Through Side Effects
I was on steroids and sleeping was very difficult.
I was pretty hungry all the time, even though I lost weight because of cancer.
One weekend, I had hot flashes. I’d have upset stomachs, but after taking ondansetron, within 15 minutes, I would get relieved.
I’ve got side effects, but they don’t last very long and for the most part, I can take medication and then I’m okay. A lot of people I know who have cancer have side effects that are difficult to handle, so I’m lucky.
Finally… Some Good News!
I went in for a PET scan and the results came out clean. No more cancer! The Epkinly works and I’ve stayed in remission so far.
My neck glands have gone down and haven’t enlarged. Dr. Favaro and I both think that Epkinly is working.
Importance of Having a Care Partner
Without my wife Chris, I don’t know if I could have gone through all of this. When I get my Epkinly shots, we text back and forth. The shot only takes 20 seconds, but we do lab work, so I’m there for maybe an hour plus a 45-minute drive.
Chris has a distribution list that goes to all the kids. We’ve got six kids between us and only one is within a half hour; everybody else is further away. When I was in the hospital, Chris would send daily messages to the kids.
My sister lives in the Charlotte area, so she’s kept in the loop and has become a mentor. She says, “Did you tell the doctor this? Did you tell the doctor that?” She’s in constant contact.
Planning Ahead
We could always do CAR T-cell therapy in the future since Chris will retire soon, but if Epkinly continues to work, I’ll stay with it. It’s easy. You go in for a shot once a week and it takes 20 seconds.
Without my wife Chris, I don’t know if I could have gone through all of this.
The Biggest Difference: Finding the Right Doctor
The best thing that’s happened to me is my oncologist, Dr. Favaro. He’s on top of his game. I trust him wholeheartedly and he cares. He has a lot of patients but when I go into the exam room, he’s there for me. We talk and he listens. If you’re not happy with who you’re going to, find another one.
Special thanks again to Genmab for its support of our independent patient education content. The Patient Story retains full editorial control.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Nick’s symptoms began a year or two before his diagnosis, including changes in bowel habits, size, and consistency, blood in the stool, and abdominal pain, which he initially attributed to aging or irritable bowel syndrome. After experiencing fatigue and escalating pain, he went to the ER where he was diagnosed with diverticulitis and sepsis. Despite initial treatment, he required a laparoscopic washout due to a perforated colon and subsequent complications, including an abscess.
During a follow-up colonoscopy, doctors found a mass, which was later confirmed as adenocarcinoma. He underwent a sigmoid resection, removing part of his colon. While clear margins were achieved, 19 of 49 lymph nodes tested positive for cancer.
Nick began CAPOX chemotherapy, experiencing severe side effects like fatigue, neuropathy, and an acne rash due to the addition of Avastin (bevacizumab). When they noticed an elevation in his tumor marker and growth in his lymph nodes, he was switched to Keytruda (pembrolizumab), an immunotherapy, to reduce the cancer to a manageable level.
Nick emphasizes the importance of mental health support to manage anxiety. He advises listening to your body, advocating for yourself, and using support systems. He encourages seeking thorough medical evaluation for unexplained symptoms and finding strength in support groups, hobbies, and loved ones, stressing perseverance and finding reasons to keep fighting.
Name: Nick S.
Diagnosis:
Colorectal Cancer
Staging:
Stage 4A
Initial Symptoms:
Change in bowel habits, size & consistency
Blood in stool
Abdominal pain
Fatigue
Treatment:
Surgery: sigmoid colectomy
Chemotherapy: CAPOX (capecitabine & oxaliplatin),
Immunotherapy: bevacizumab, pembrolizumab
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
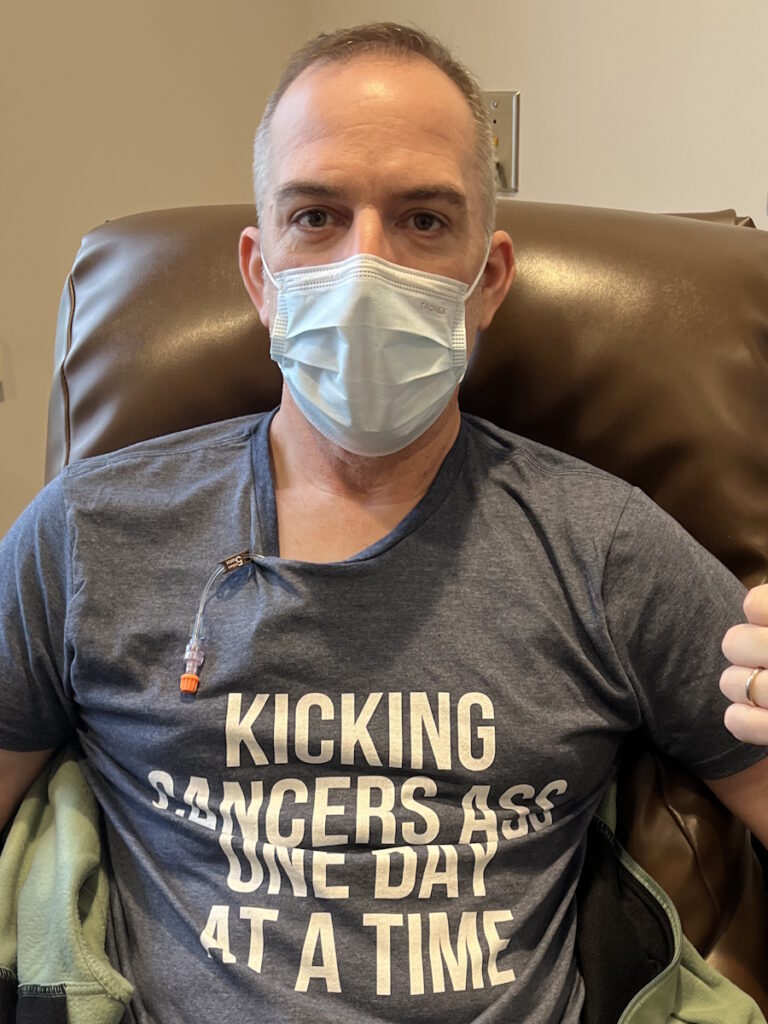
My symptoms started a year or two before diagnosis. It started with a change in bowel habits, size, consistency, some blood in the stool, and abdominal pain.
Introduction
I’m a stage 4A colorectal cancer fighter. My wife and I live in Chippewa Falls, Wisconsin. We have a wonderful 28-year-old daughter.
I’m a full-time firefighter and critical care paramedic. I’ve been doing firefighting for about 16 years and paramedicine for about 13 of those 16 years.
Pre-diagnosis
Initial Symptoms
My symptoms started a year or two before diagnosis with stage 4A colorectal cancer. It started with a change in bowel habits, size, consistency, some blood in the stool, and abdominal pain. I had some acid reflux type of reactions that my wife and I chalked up to aging and not being as healthy as I could be. My wife has irritable bowel syndrome and I thought some of it was IBS because some foods would trigger some reactions in me.
I was working full-time for the department for about a decade and a couple of years later, I decided to change over to a neighboring department. For these jobs, we have to pass a physical agility test.
I have been working by myself daily. I was in pretty good shape. The test is a pretty rigorous test to be able to do what we do. I was 48. I was doing this at an older age than the 20-year-olds they were usually hiring.
I was diagnosed with diverticulitis and sepsis, so they started me on antibiotics right away.
A couple of months later, we responded to a house fire. At some point, my battalion chief pulled me off the line and said, “You look wiped out. I’m going to sit you out for a little bit to catch your breath.” I felt a little tired, but, again, I was getting a little older.
I sat out and went back in for another round. This time, the chief was on the scene and said, “Nick, take your gear off. You don’t look good. Go back to the ambulance. You’re going to be doing rehab, making sure everyone else is doing okay, but we don’t want you going back in.” I thought something was weird.
I called my wife to meet me in the ER. I didn’t know what was going on. I’ve got bad abdominal pain. I haven’t slept. I’m going to go get checked out.
Diverticulitis & Sepsis
I was diagnosed with diverticulitis and sepsis, so they started me on antibiotics right away. They weren’t sure if surgery was going to be necessary, but they transferred me to another hospital. At that point, I was stable.
When I got transferred, I met with a thoracic surgeon and started to realize that things were serious. He said, “We’re not going to go in right away. We’re going to keep an eye on you tonight. Hopefully, things will subside with some more antibiotics and some steroids, if we have to. But we’re going to keep an eye on you and evaluate you. We’d like to avoid surgery.”
The next day, when they were getting my vitals, the nurses said, “We see you’re slated for surgery.” That turned into a laparoscopic washout. They found that I had a perforated colon in the sigmoid area, the area right before the rectum, but that had healed itself.
All of a sudden, I heard the doctors say, ‘That’s not good.’ I remember seeing a black mass on the screen.
They went in through a couple of small incisions, washed everything out to make sure there was no fecal matter, and stitched me back up. I had a couple of surgical drains. I was in the hospital for five or six days and then I was sent home to heal.
I ended up getting readmitted a couple of days later because I had some drainage coming from my drain sites. After a CT scan, they found I had an abscess. I believe E coli was one of the culprits. There was something else too, so they needed heavy-hitter antibiotics.
After another two weeks of antibiotics, the PICC line was removed. I met with the surgeon and everything was looking great. He said, “Let’s do a follow-up colonoscopy to check how the diverticulitis is.”
Colonoscopy
I wanted to sleep through it. I was joking with them and we were all relaxed when all of a sudden, I heard the doctors say, “That’s not good.” I remember seeing a black mass on the screen. He tried advancing past it and I said, “Ow,” but I didn’t feel it. I said “ow” instinctively. He said, “We can’t get past this mass. We’re going to pull out.” The tone changed. You could have heard a needle drop in that procedure room.
They wheeled me back into the recovery room where my wife was waiting. On the way there, one of the nurses handed me a polished stone that had the word “hope” stamped on it. I didn’t think that choked me up, but I carry it wherever I go. In hindsight, it meant a lot and drove home the seriousness of the situation. We didn’t know exactly what was going on, but something wasn’t right. I have enough medical training and field experience to read the room and know it wasn’t good.
The doctor eventually came back in and said they couldn’t diagnose it yet. They took a small sample to send off for testing to confirm what they thought it was. He wouldn’t say whether it was cancer or not.
The good news was they got the tumor with clear margins. They felt it hadn’t spread far…
Diagnosis
Getting the Biopsy Results
I was waiting for the results at home. When I finally got the notification on my phone, I checked it and it said adenocarcinoma. Now we know what we’re dealing with. It’s cancer of some sort. I never thought about it as a possibility.
Treatment
Sigmoid Colectomy
During the colonoscopy, he said we were going to have surgery because what it was had to come out. He referred me to surgery right away. Luckily, it was the same surgeon who performed my earlier surgery who I trusted with my life.
I met with him about a week later. They were going to do an exploratory surgery until they knew exactly what it was in there and then do their thing.
I remember being in the room when my mother-in-law came out too. My wife was there, of course. They wheeled me in, put in the IVs, and told me to start counting back from 100. I don’t think I hit 95. Hours later, I woke up in my hospital room with a slightly sore throat. They performed a sigmoid resection. I can’t remember how much of my colon they took out, but I didn’t require an ostomy, thankfully. They were able to resect it and reconnect it right away.
The good news was they got the tumor with clear margins. They felt it hadn’t spread far, at least in the tissue of the colon. But the surgeon sampled some lymph nodes right next to the tumor site. They took out 49 and 19 of them tested positive for cancer.
I stayed positive. The whole reason I’m in this fight is my family.
CAPOX Chemotherapy
At that point, I was referred to oncology. I met with my oncologist. His nurse was a former ER nurse who I was familiar with and seeing a familiar face went a long long way.
He explained what he planned on doing based on the CT scans. They saw some inflammation in other lymph nodes and they weren’t sure if that was post-surgical. They wanted to do another CT scan to check, but they were happy about the margins being clear. I was staged at 3C then. It metastasized a little bit past the point of origin but not very far.
The first day of chemo was going to include labs and a CT scan to see where we were at. The plan was to do CAPOX: capecitabine, an oral medication, and oxaliplatin, an IV medication. I would do the oral chemo for two weeks and then on the third week, I would go in for the IV chemo. They would do labs on those days to make sure everything was okay.
Unfortunately, the doctor didn’t like what he saw on the CT. He wanted to get a little more defined imaging, so he set me up for a PET scan and delayed the chemo. A couple of days later, we came back to start chemo again and get the PET scan read.
The doctor confirmed that it had spread to the lymph nodes in the abdominal area, along my aorta, and up to my left shoulder. It had spread a lot further than we thought it had.
I felt like every time we made a plan to move forward, we were getting kicked back a couple of steps, but I stayed positive. The whole reason I’m in this fight is my family. I believe that someday, this cancer will get me, but I’m not going down without a fight. I’m stubborn, so it’s going to be a long fight. I won’t go down without swinging.
I have a four-day weekend so I tried to time my infusion, so I had a couple of days to recover post-infusion and feel somewhat human before returning to work.
Side Effects of CAPOX Chemotherapy
Chemo wasn’t fun. It knocks you out. I felt fatigued on the first day. For probably a week and a half, when you start getting the infusion, you can’t drink cold drinks. It felt like swallowing glass shards. A lot of fatigue and neuropathy kicked in.
I didn’t like being out in the cold and I love ice fishing. You’ll catch me outside at -20°F on a normal day, but with chemo, not a chance. I had to be bundled all the time.
My eyes were always drying out, so they hurt a lot. I had insomnia, joint pain, and muscle pain.
They added Avastin (bevacizumab), which is an immunotherapy, to my chemo routine. That caused a bad acne rash on my back from the waistline up to my neck. The doctor had never seen nor heard of it, but we can only attribute it to Avastin.
Working While in Treatment
I was able to go back to work full-time as a firefighter. I have a four-day weekend so I tried to time my infusion, so I had a couple of days to recover post-infusion and feel somewhat human before returning to work.
My work was very accommodating. We’re firefighters, so we don’t sleep all day, but the chief said if I needed to rest, I could go to the dorm, which I appreciate. I never took him up on it. I tried to stay with my brothers and sisters training or doing calls, and that worked great.
I was going to be on treatment for the rest of my life. I might get some time off if we get no evidence of disease at any point, but it will come back at some point and I’ll have to go back on treatment.
Switching to Immunotherapy
The initial plan was for six months or eight cycles of chemo and Avastin. Unfortunately, because of the restaging, I was going to be on treatment for the rest of my life. I might get some time off if we get no evidence of disease at any point, but it will come back at some point and I’ll have to go back on treatment.
My tumor marker was through the roof when this all started and it was dropping with chemo. We were seeing shrinkage in the lymph nodes. Chemo sucks, but it’s doing what it’s doing, so we stayed very positive.
When we got to cycle six, we noticed my CEA was going up a little bit. We were doing CT scans every three months and we noticed some growth in the lymph nodes. The doctor said, “We’re going to stop the chemo. It’s not working. You can only receive so much oxaliplatin before it becomes completely ineffective. This saves us a couple of cycles where if we need to go back to it, we can go back to it. We’re going to switch over to an immunotherapy called Keytruda (pembrolizumab).”
The side effects of immunotherapy are supposed to be much less than chemo and I’m all for that. I switched from chemotherapy to immunotherapy in August 2023. I still have very slight neuropathy every now and then in my toes and my fingertips. Nothing debilitating but a reminder that I was on chemo at one point and that probably won’t get any better or any worse, hopefully.
Keytruda is a half-hour infusion. Side effects are minimal. Between cycles two and three, while we were camping, I noticed that my resting heart rate was higher than it should be. I was not exercising as much and a little out of shape, but I shouldn’t have a resting heart rate of 130-140 beats a minute. I was sweating a lot without doing anything, so I couldn’t figure it out. I talked to the oncologist and they ran some thyroid tests.
One of the known side effects of Keytruda is thyroid burn. It’ll cause hyperthyroidism until the thyroid burns out and then it’ll cause hypothyroidism.
The support of my family, my work family, and my friends is what gets me through this.
Treatment Plan
We want to do Keytruda for 18 more months. It’s a two-year plan. We’ll see what it does and go from there. Hopefully, the response brings everything down to normal levels, I won’t have evidence of disease, and I can ride that out for a while.
Fingers crossed, maybe Keytruda is the cure for colon cancer, but realistically, I don’t think so. I think it’ll be a lifetime battle, but it’s going to be a long life. The support of my family, my work family, and my friends is what gets me through this.
Managing Scanxiety
As a paramedic, I’ve dealt with patients with panic attacks and anxiety. Anxiety’s a real thing. A lot of times, it doesn’t seem like it with the patients you’re dealing with, but now that I’m put in that position, it’s a real thing. I’ve dealt with it even before cancer through another set of unfortunate circumstances and luckily, I have a great support group in place.
We see a lot of things as paramedics and firefighters, so after a while, you realize things aren’t normal. I had to start paying closer attention to my mental health. I started seeing a therapist and she’s great. She taught me how to deal with stress, anxiety, and my feelings.
What we go through as cancer patients is not something most people go through nor is it something they understand.
Stay strong and recognize that the stress is real. What we go through as cancer patients is not something most people go through nor is it something they understand. Take a deep breath. Listen to what your mind and body are telling you.
Your feelings are valid. Don’t try to brush it off and try to be strong by pushing your way through it. Rely on your support team. If you have a therapist, talk to that therapist.
Most oncology teams come with a social worker. Use that resource. Rely on your family for strength. Tell your spouse what you’re feeling even when you don’t want to. Sometimes talking about it gets it out there and puts it away, as opposed to it weighing you down.
What helps me is retreating home, spending time with family, or staying busy with work. Rely on your hobbies if you have any. If you don’t, find some. I’m a big fisherman. I love fishing. You could put me on a lake and even if I couldn’t catch a fish for days, I would be in my happy place. Find something that helps you disconnect from the cancer and what you’re going through.
Words of Advice
For anyone who might be experiencing symptoms that you’re not quite sure of, listen to your body. Talk to your doctor. Advocate for yourself. If you feel something’s not right, push for tests to try and figure out what’s going on. The answer, “We don’t know what’s wrong with you,” is not acceptable. Push to find answers.
For cancer warriors who are going through this, keep going. You’re not alone. There’s support beyond your family, friends, and coworkers. There are a ton of support groups online. There are social workers available. There are platforms like The Patient Story.
You’re not in this alone. Some days, it may feel like it. Some days, I get down in the dumps, but I find something to get me back up. I find a reason to keep going. There are a million reasons to keep going and even if you find just one, that’s all it takes.
Listen to your body. Talk to your doctor. Advocate for yourself.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Meghan’s journey began with symptoms that are all too familiar to both Crohn’s disease and colorectal cancer patients: persistent diarrhea, blood in the stool, and severe stomach pain. Initially dismissed as stress-related by her doctor, it wasn’t until her condition worsened that another doctor suspected a more serious issue—possibly Crohn’s disease or colitis. This overlap in symptoms between inflammatory bowel disease (IBD) and colorectal cancer underscores the importance of thorough medical evaluation and early diagnosis.
After her diagnosis, Meghan tried various treatments. Initial oral medications didn’t work, so she switched to Remicade (infliximab), which put her in remission. Despite the medication’s risks, her symptoms improved and she was able to resume a normal life.
Five years later, her symptoms returned and after trying different medications, Entyvio (vedolizumab) helped manage her symptoms. In 2016, a routine colonoscopy revealed precancerous tissue, leading to the recommendation for a permanent ileostomy. Initially resistant, Meghan decided to proceed with the surgery after a pivotal conversation with her surgeon about her future. Despite initial concerns, she had two complication-free pregnancies and successful vaginal births.
Meghan’s husband has been incredibly supportive throughout her journey. She emphasizes the importance of finding a supportive community, maintaining a sense of humor, and living without regrets.
Name: Meghan B.
Diagnosis:
Crohn’s disease (a type of Inflammatory Bowel Disease or IBD)
Initial Symptoms:
Persistent diarrhea
Blood in stool
Stomach pain
Treatment:
Remicade (infliximab)
Humira (adalimumab)
Methotrexate
Entyvio (vedolizumab)
Surgery: proctocolectomy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
When I was in eighth grade, I started having diarrhea and it happened every single time I went to the bathroom.
Introduction
I’m from Charlottesville, Virginia. I love to travel. I love going to the beach, going on hikes, and being outside in general. I love spending time with my family.
I have Crohn’s disease as well as a permanent ileostomy. My biggest passion is disease advocacy and awareness.
Pre-diagnosis
Initial Symptoms
As a child, I was extremely active. I was an avid softball and basketball player, constantly going to camp. I spent tons of time outside. I was very active and very social.
When I was in eighth grade, I started having diarrhea and it happened every single time I went to the bathroom. Thankfully, my mom was very aware and thought it wasn’t normal. She told me we would go to the doctor because it was getting progressively worse.
I didn’t have any other symptoms. I went to the doctor and she said, “There’s nothing wrong with her. She’s just nervous and that’s why she’s having diarrhea.”
It felt like a punch to the gut because I never felt like a nervous child. It didn’t seem to be a good enough answer for what was happening. Thankfully, both of my parents advocated for me. They felt it didn’t sound right so we sought a second opinion.
I was in so much pain and my body was so weak. I was in and out of the hospital all the time.
Symptoms Worsen
I started having blood in my stool and horrible stomach pain. I went to see another doctor and at that point, they weren’t sure if I had Crohn’s or colitis. I continued to get worse. When I was a freshman in high school, I had to be homeschooled. I was too sick to get out of bed. It’s crazy to look back to see the 180 my life took. I was in so much pain and my body was so weak. I was in and out of the hospital all the time.
Diagnosis
I ended up having a colonoscopy and got diagnosed with Crohn’s disease. After getting a formal diagnosis, I began treatment. Compared to other people, I got diagnosed pretty quickly, but my health was rapidly declining.
Getting Diagnosed as a Teen
I turned lemons into lemonade. This was in 2006, so it was before social media and texting, but I could text 50 words a month. I was isolated from my friends. It was hard. I was homeschooled and a lot of people didn’t know where I was. All these rumors spread about me that I had died or had gotten pregnant and was sent away.
Meanwhile, I was in and out of the hospital and horribly sick, so it was hard. That was where the isolation came in plus not knowing anyone else going through this.
I started various oral medications, but I wasn’t digesting them. I would take these medications, but they would go straight through me that I would see them in the toilet. Since the medications weren’t working, my symptoms weren’t getting better.
Remicade (infliximab)
I started taking infusion medications and went on a drug called Remicade (infliximab). By the time I started my sophomore year of high school, I was in remission. I was on monthly infusions, but I was well enough to go to school. I was so excited to find some type of normalcy and feel good for the first time in a long time.
Everything was going great. My symptoms, for the most part, were at bay. The next question was: what do we do now? The infusions were eight-hour-long sessions. I would go to the hospital and stay for eight hours to get my medication.
I made it through high school and the beginning of college with symptoms at bay. Then in my sophomore year, I started to go downhill drastically.
Before I started treatment, while driving to the hospital, I could hear my parents whispering about how they were going to have to sign a waiver saying that they would not sue the hospital if I died by taking this drug. It was that serious, but they didn’t want to freak me out.
Remicade was a scary drug. When I was responding to it and doing well, they had to decide if they wanted to keep me on it. It’s a harsh drug and I was so young. We decided to get off of it.
Going Off Treatment
I went the homeopathic route for around five years. I took different supplements and probiotics. Those bought me five years.
Recurrence
Symptoms Return
I made it through high school and the beginning of college with symptoms at bay. Then in my sophomore year, I started to go downhill drastically. College is stressful and stress is one of my big triggers.
New Treatment
It was time to return to my doctor and go back on medication. I tried Remicade again because it worked well for me in the past. Unfortunately, I could no longer take it this time, so I went on a trial-and-error phase.
I tried taking Humira (adalimumab), which I didn’t respond to. I also tried methotrexate, which was a weekly injection that I had to administer myself. I drove home every weekend from college to give myself these shots.
Finally, after a lot of trial and error, I responded to a drug called Entyvio (vedolizumab). It didn’t necessarily send me back into remission, but my symptoms were kept at bay. Entyvio worked until I ended up having my colon removed.
My doctor said, ‘There is precancerous tissue deep within your colon. There’s a high chance that you’re going to need surgery.’
Getting a Colonoscopy
The conversation of having my colon removed was something I never had with my doctors. I didn’t know what an ostomy bag was when I was told that I needed one. It had never been mentioned, I had never heard of it, and I never thought I would be living with one.
At this point, I had graduated. I met my husband in college. We dated and right after graduating, we got engaged and got married at 23.
Eight months after we got married, in July, I went in for a routine colonoscopy. I had been feeling fine. There was nothing drastic or new. My symptoms had pretty much stayed the same. They were present but not how I had previously been in the past. I was able to function and have a life.
I went into this appointment excited because I thought they were going to tell me I was doing well. After all, I felt like I had been doing well. At the appointment, they came out and said, “We saw a few things. We’re sending a few biopsies off to make sure everything is fine.”
Getting the Biopsy Results
A week later, while I was home alone and my husband was at work, I got a phone call and my doctor said, “There is precancerous tissue deep within your colon. There’s a high chance that you’re going to need surgery.”
I vividly remember that moment. I collapsed in my kitchen crying because even though my colon was precancerous, all I could hear was the word “cancer.” Immediately, all I thought was I didn’t want to die. I was terrified.
I couldn’t believe this was happening to me. I was angry and upset. There was a lot of dwelling and processing.
Treatment-Decision Making
My surgeon and I talked about the different options I had. He said, “We can do nothing and hope for the best. We can remove part of your colon, but you’re going to have to come in for routine monitoring probably every three months or so, possibly have colonoscopies to check for any progression and make sure nothing is happening. Or we can remove your colon and your rectum, you will have a permanent ostomy bag, but you will never have the chance of colon cancer.” I left that appointment thinking, There’s no way I’m getting an ostomy bag. I’m not doing that. I’m not having surgery. I absolutely refuse that.
A week later, my husband had to deploy and I moved back home with my parents. I had a month to make this decision if I was going to have ostomy surgery or not. In the meantime, we went for a second opinion, which I always highly suggest because it never hurts. Unfortunately, it was the same response. This is what needed to happen.
I was still adamantly against it. I’m 24 years old. I’m not going to ruin my body. Thinking back, it’s wild that I was willing to live with the threat of cancer to have this unscathed body for the aesthetic side of it. I was willing to possibly have cancer and that blows my mind today that I would feel like that.
I fell into a dark tunnel. I don’t think it was depression, but I fell into a dark space. I couldn’t believe this was happening to me. I was angry and upset. There was a lot of dwelling and processing until finally, I went to my next surgery appointment where I was going to have to give my decision.
We had a conversation that changed my mind forever… He said to me, ‘Imagine being a young mom and finding out you have cancer.’
Deciding to Have a Proctocolectomy
I was ready to go into the appointment to say, “I will have part of my colon removed with the monitoring, but I’m not doing an ostomy bag.” That’s where I was at, even though my parents didn’t agree. They wanted me to do the ostomy bag because they thought this wasn’t something to joke with and we needed to be serious about this. I wasn’t ready to do that. My surgeon knew how horrified I was and how adamantly against it I was.
We had a conversation that changed my mind forever. I still get chills and goosebumps and tear up whenever I think of it. He said to me, “Imagine being a young mom and finding out you have cancer.” That put everything into perspective for me because he knew how important having a family and having children was to me. I left that appointment with my surgery booked to have my colon and rectum removed with a permanent ileostomy bag.
That conversation made me stop and realize that this wasn’t just about me. It’s also about my family. I want to be around for my husband and my parents. At that point, I didn’t have children, so it was also for my future children. I want to be able to have children, be there to watch them grow up, and be a significant part of their lives.
It made me realize it was worth it. It was worth it to have an ostomy bag to be able to be here with my children for every milestone and witness everything. It put everything into perspective. That’s a conversation I will never forget. I think about it every single day. That’s what led me to get my ostomy bag.
Going into it with an open mind, a more positive mindset, a willingness to learn, and a willingness to educate made a huge difference in my situation.
Mentally Preparing for a Permanent Ileostomy
There are two avenues to getting an ostomy bag: either it’s an emergency or it’s a planned surgery. I felt lucky because mine was planned so I had time to process beforehand. Even though I only had a month to figure everything out, I did what everyone else does: I went online.
This was 2016 and I was trying to find anything. There was social media, but I didn’t see a lot of ostomy on social media. I read a couple of blogs and there was one called The Stolen Colon, which offered more information and insight. Everything else I saw was the ostomy being associated with older generations. No one in their 20s had an ostomy bag.
All of the negative stigmas were popping up as well as the negative sides of having an ostomy bag. I tried to research and educate myself as much as I could beforehand. What helped was going into it with the mindset that it could only get better. I had been sick for so long. At that point, it’s been 10 years and my colon turned precancerous because of the intense scarring from Crohn’s disease. It could only get better, so why not try? It couldn’t get worse than it already is.
Going into it with an open mind, a more positive mindset, a willingness to learn, and a willingness to educate made a huge difference in my situation. Before having surgery, I felt very negative towards an ostomy bag. But as soon as I was rolled out after surgery, I never had any negative, upset, or harsh feelings. I always felt this was my second chance at life, so I’ll figure it out and get going. I felt like I missed out on so much when I was a teenager and in college. Now it’s time to make up for that.
What is an Ostomy Bag?
I always tell everyone that, essentially, my ileostomy bag is how I go number two. I have a stoma, which is a little round, fleshy pink-looking thing that sticks out of the skin on my abdomen, and it’s part of my intestines. My surgeons created a hole through my abdomen and brought a little piece of my intestines out. I wear an ostomy bag over it so you don’t see it and that’s what collects my stool.
I have to wear an ostomy bag at all times because I have no control. I don’t know when I’m going to the bathroom. It happens all the time. I have no urge to go.
I also don’t have a rectum. I had my rectum removed and that means I will have my ostomy bag forever because there’s no possible way to reconnect anything down there.
I always tell everyone to try everything. Once you find what works for you, it will be so much easier.
Ostomy Care
I’m biased because I’ve had this for almost eight years. At first, it’s very difficult to figure out. Once you get the hang of it and find the appliance that works best for you, it’s so much easier.
Overall maintenance is not too terrible. I change the complete system every three or four days. You buy an ostomy bag from the distributors and you get a prescription for ostomy bags sent to your house. You take it off and clean the skin around it. A lot of times, people will tell you not to use any soaps or perfumes because you can have issues with the adhesive sticking to your skin or an allergic reaction.
You have to empty your ostomy bag daily. I got into the habit of emptying it every time I use the bathroom even if it’s not full yet. I don’t like walking around with a full ostomy bag because it’s not comfortable.
There are certain factors that people have to deal with, especially if you have skin irritation. You can get skin irritation if your ostomy bag leaks because sometimes your stool can seep through under the wafer and it can sit on your skin. When that happens, it’s essentially burning your skin until you clean it off and change it. It hurts so bad because you have this rash. It’s difficult to get it to heal because you’re constantly covering it up.
They have different products to help treat different rashes. There are different adhesives because people may have an adhesive allergy. That’s where the trial and error comes in and that can be frustrating in the beginning when you’re trying to find out what works best for you. It can be very overwhelming, but I always tell everyone to try everything. Once you find what works for you, it will be so much easier.
Tips and tricks for ostomy bags change. Everyone asks, “How are you not pooping everywhere when you change your ostomy bag? You always have clean bag changes.” A big part of that is being mindful of when you last ate. I’ve had my ostomy for almost eight years. I have learned my body and my ostomy. I know that if I eat lunch at noon, I’m probably going to have output at around 1:00 or 1:30 PM, so I’m not going to change my ostomy bag after I eat.
I had my ostomy bag for a year and on the first anniversary, I posted a picture. I wouldn’t say I was hiding, but I wasn’t public about it.
A lot of times, people would change it first thing in the morning because you’ve been asleep all night and things have slowed down.
Another tip that I love and I’m always so surprised that more ostomates have not heard of this is eating marshmallows before doing bag changes. Marshmallows, bananas, and bread can slow down your output so you can have a small window to have a clean bag change.
Knowing how to have a clean bag change is important because, a lot of times, people are horrified to have a messy one. It sounds gross, but if you get output on your hands, it’s not a big deal. It happens. You can wash it off. Also, I have two kids, so it’s nothing.
Being Comfortable with Having an Ostomy Bag
I had my ostomy bag for a year and on the first anniversary, I posted a picture. I wouldn’t say I was hiding, but I wasn’t public about it. My husband and I saw it, but that’s it. I didn’t want to talk about it. That was my year to process and figure it out. I wasn’t trying to hide it, but I wasn’t the proudest of it.
A year into it, I made an Instagram account and made a post. I had come to terms with it and a big part of me said, “When I went through this, I didn’t see anyone else my age, so I want to put this out there.”
I had no idea what the response was going to be, but I felt okay and safe because I did this on Instagram. None of these people knew me. I had no idea who these people were. All I knew was they were people on the internet. To my surprise, I got an overwhelmingly positive response and that fueled the fire.
Having an ostomy bag did not take away from me as a person. Having that positivity helped me to become more comfortable.
Social media was a coping mechanism for me because it allowed me to express myself. I love to write. Before Instagram reels, Instagram was about posting pictures with captions, so I would post a picture and pour my heart out. That allowed me to cope.
The biggest thing was that it allowed me to accept myself and my body because other people were so accepting of it. I didn’t know any of these people. They were random people on the Internet, but people were so kind and genuinely wanted to know more. Having an ostomy bag did not take away from me as a person. Having that positivity helped me to become more comfortable.
I kept sharing and reached more people. People then started coming to me, asking for tips and advice. It quickly became my passion. That’s honestly how I became more comfortable with it. Finally, after seven years, I wore my ostomy bag out at the beach for the very first time. It was amazing.
I’m learning not to worry about what other people think and having the mindset that life is too short. Ostomy surgery was a huge experience. It made me realize that I don’t want to grow old and look back having these regrets that I didn’t do what I wanted to do because I was worried about what other people would think about me. It’s weird and funny, but I always tell people that I feel more confident with an ostomy than I did without because I had that life-changing experience that put everything into perspective.
Being Pregnant with an Ostomy Bag
I had no idea what it was going to be like to be pregnant with an ostomy. There’s not a lot of research out there. With my first pregnancy, there weren’t a lot of other people who had been pregnant who were sharing their experiences. I was going to have to figure it out.
My doctors never said I wouldn’t be able to get pregnant, but I was concerned that it would be difficult because I had this massive surgery. I was worried there could be a lot of scar tissue. We tried for a year and a half, and while my husband was on his second deployment, I went to the fertility doctor to find out what was going on.
Thankfully, I only had a hormonal imbalance. It wasn’t ostomy-related at all. My husband had a short deployment, so he was gone for five months only. I did one round of Clomid (clomiphene) and got pregnant with our daughter.
On the ostomy side, there were a few changes but nothing crazy or out of the ordinary. As my belly grew, I had to switch ostomy appliances. I typically wear a convex wafer that helps push my stoma out, but because my belly was big and round, that wouldn’t fit anymore, so I had to wear flat wafers.
Everyone has a different situation and a different story, but pregnancy with an ostomy is possible.
My biggest concern was childbirth. Because I don’t have a rectum, I was scared to death that I was going to tear, which would cause issues with my rectum removal. My worst nightmare was having a baby and then going through “Barbie butt surgery” again and having to be stitched back up down there because that was by far more difficult than the ostomy recovery, in my opinion. I didn’t do the two surgeries at the same time.
Another concern I had was automatically assuming I was going to undergo a C-section, but thankfully, I had an incredible doctor who advocated for me. Dr. Bearling at Fort Carson was amazing. She asked, “Why do you think you’re going to have to have a C-section?” I said, “I don’t have a rectum and I have an ostomy.” She checked to make sure I still had muscle function down there and I did. I was still able to push, so she said, “You’re going to have a vaginal birth. You’re fine. You can do this.”
I am so glad I had that conversation with her. At the initial appointment when I first found out I was pregnant with my son, I gave them my history and told them that story. They said, “I’m glad you shared that because if you hadn’t, we were going to schedule a C-section for you.” There’s a difference in care.
Overall, I felt lucky with childbirth. I didn’t have any complications with my ostomy or during pregnancy. I’ve heard stories of people having stomach blockages and issues where they had to go in for surgery or deliver their baby early. People have said that the baby can kick inside where your stoma is located and that can be painful. Thankfully, my babies never did that. Overall, I had a great experience.
Postpartum with my son, our second-born, was wild. My hormones went crazy and, as a result, my skin broke out. Suddenly, I was reacting to the adhesive of ostomy appliances that I’d been wearing for five to six years at that point. My skin was an absolute nightmare. I had a 2-year-old and a two-week-old, and I am trying to get an ostomy bag to stick to my body. It wasn’t very pleasant.
My hormones readjusted after giving birth and the hormonal storm ended. My skin calmed back down and I was able to wear my appliance. Everyone has a different situation and a different story, but pregnancy with an ostomy is possible. It’s wonderful, it’s beautiful, and I’m lucky that I got to experience it twice.
I always think back to the conversation that I had with my surgeon because I’m at that age now. I’m that mom with young children. What if I did not have ostomy surgery? I could potentially have colon cancer right now with two young children. I’m so thankful every day that I made the hardest decision of my life to have surgery.
Ostomy surgery did not faze him. I’m sure he was freaked out and probably scared inside, but he didn’t let that show. He’d always been extremely supportive.
Having a Supportive Husband
Thankfully, I have a very wonderful and accepting husband. Before my ostomy, he had only ever known me as being sick. He’d never seen me healthy. I knew he was a keeper because I was sick all the time. There were numerous occasions where we’d been driving and we’d have to pull over to the side of the road because I was in excruciating pain and needed to use the bathroom or lay down in the car. He never batted an eye. He was always there to take care of me and help me with anything I needed.
Ostomy surgery did not faze him. I’m sure he was freaked out and probably scared inside, but he didn’t let that show. He’d always been extremely supportive. He fought tooth and nail to come home when I had surgery. They told him he couldn’t go home from deployment unless a close family member passed away. I don’t know how he did it, but he did and went back before I was discharged.
When he returned from his deployment, we had to navigate each other. We had been married, but it was like we were dating again. We had to relearn each other. He’d always been supportive, but deep down, I had these fears of being a different person compared to when he left. He took it with grace.
With intimacy, the best tip I can give is to have a sense of humor. Laugh it off. He’s my best friend and, thankfully, we can joke and laugh about things. Laughter and a sense of humor can be a great coping mechanism; it’s the best medicine. Nothing’s ever going to be perfect. Funny things are going to happen. They happen even to people who don’t have an ostomy bag.
He’s been so supportive since day one. Now he knows how to change my ostomy bag and we posted a video of him changing my ostomy bag. It’s so important to teach someone you know how to change your ostomy bag. If something ever happened to you or you were physically unable to do it, having someone close to you who knows how to take care of you and help you in that way is extremely important.
You can still live a long, beautiful, happy, healthy life with an ostomy bag. Try to keep a positive mindset and view this as your second chance in life.
Words of Advice
Finding a community is incredibly important. I turned to social media to find my ostomy community. You would be surprised at how many people in the world have an ostomy bag. People you know may have one, but you wouldn’t know it. Put yourself out there and be willing to find community.
I have made so many lifelong friends through social media. I’ve had the pleasure of meeting a couple of them in person. Being able to connect with someone who has gone through a situation like yours is earth-shattering. Someone could have all the empathy in the world, but it’s truly difficult to understand unless you have been through it. Having a community where you can talk about these things with other people who have similar experiences makes such a huge difference.
Ostomies save lives! You can still live a long, beautiful, happy, healthy life with an ostomy bag. Try to keep a positive mindset and view this as your second chance in life. You can do things that you didn’t get to do. This is what helped me and made me into the person that I am today. I’m a changed person since having an ostomy bag, but I’m so happy with where I am.
An ostomy bag is not the end. It’s all about how you perceive it and how you decide to live with it. I’ve grown to love and appreciate it. You can do everything with an ostomy bag. You can do anything that you want to do. It’s all about the decisions you make and how you decide to live with it.
Living with the Mental Health Aspects of Waldenström Macroglobulinemia (WM)
Edited by: Katrina Villareal
WM patient advocate Pete DeNardis leads the discussion as two experts in the field of cancer care, Dr. Jonas Paludo from the Mayo Clinic and Dr. Shayna Sarosiek from Dana-Farber Cancer Institute, dive deep into the crucial topics of watch and wait and mental health. Gain insights that could transform your understanding and approach to cancer treatment.
Thank you to Blood Cancer United for their support of our patient education program. The Patient Story retains full editorial control over all content
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang: I’m the founder of The Patient Story after my non-Hodgkin lymphoma diagnosis. The goal of our platform is to help patients, care partners, and anyone in the support circle navigate life after a diagnosis. The Patient Story does this primarily through in-depth patient stories and educational programs.
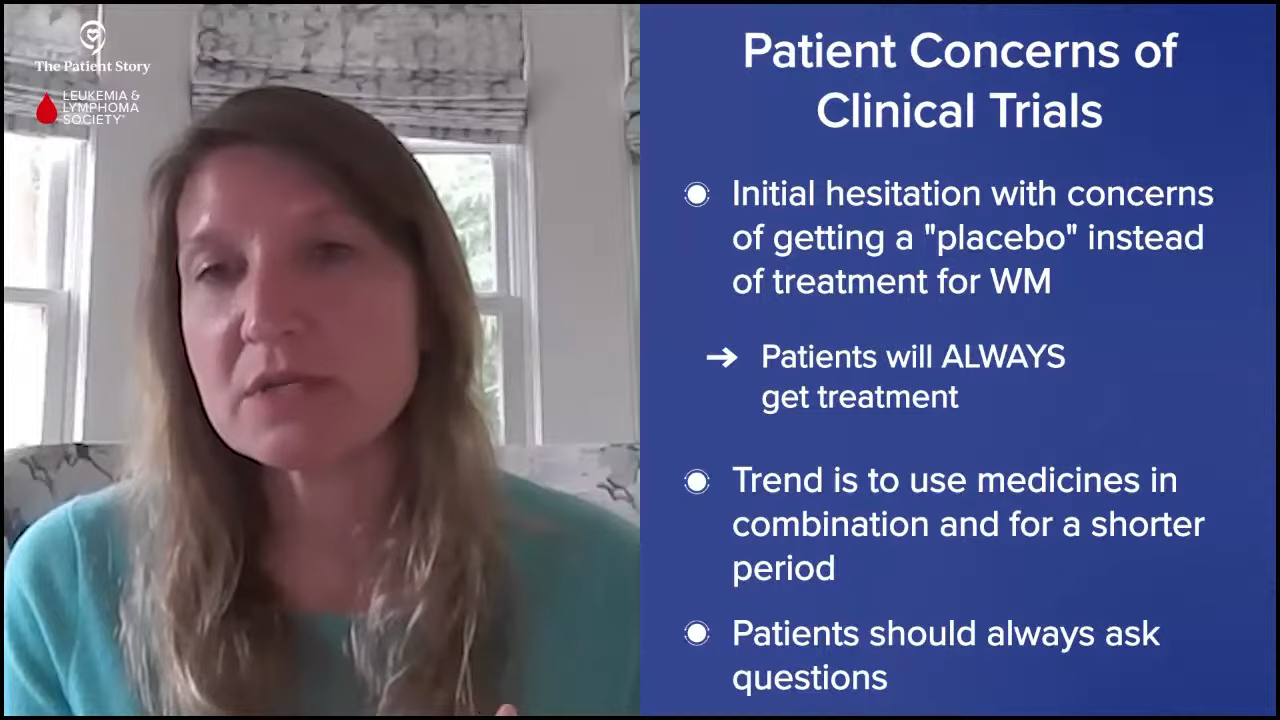
It’s especially important in a space like Waldenstrom’s where patients and families are told many times that there will be no immediate treatment and that they’ll enter a period known by most as watch and wait. This discussion is all about support and getting through something as difficult as hearing that.
We want to thank The Leukemia & Lymphoma Society for supporting this independent educational program, which helps us host more of these and always for free for our audience. The LSS has invested over $1.5 billion in blood cancer research and provides free educational resources and support, like information specialists on hand who provide one-on-one support on everything from questions about treatment to social and financial challenges.
While we hope you walk away with more knowledge, this discussion is not meant to be a substitute for medical advice. Please speak with your medical team about important decisions.
Stephanie: I’m lucky to know Pete DeNardis, who has been an incredible part of the IWMF as someone who was diagnosed with Waldenström’s and an advocate. Pete, thank you for taking the time.
Pete DeNardis, WM Patient Advocate
Pete DeNardis: I’m a WM patient myself. I was diagnosed in 2003 at the age of 43. I’ve been a volunteer for the International Waldenstrom’s Macroglobulinemia Foundation (IWMF) since 2005 and have been a board member for a long time and currently serving as the chair of the board of trustees.
I’ve been in multiple periods of treatment and watch and wait, so I understand the physical and mental impact of Waldenstrom’s when you’re navigating through those various periods.
Dr. Jonas Paludo, Hematologist-Oncologist
Pete: Dr. Jonas Paludo is a hematologist-oncologist at the Mayo Clinic and part of their lymphoma group, including Waldenstrom’s Macroglobulinemia. He also investigates the effectiveness of various treatments for WM, examines the outcomes of patients with the disease, and studies the genetic mechanisms associated with the development of this malignancy. Dr. Paludo, what drew you to becoming a doctor?
Dr. Jonas Paludo: I had the first-hand opportunity to experience the difference that a good doctor can make in the lives of patients and families when they go through a cancer diagnosis. I thought my calling was to help patients and people when they’re struggling with a difficult diagnosis. I always thought I was going to be an electric engineer because I enjoyed math and physics. I changed my mind, applied to medical school, and never looked back.
Dr. Shayna Sarosiek, Hematologist-Oncologist
Pete: Dr. Shayna Sarosiek is a hematologist-oncologist at Dana-Farber Cancer Institute, specifically at The Bing Center for Waldenström’s Macroglobulinemia, the largest center in the world dedicated to the study and development of new targeted therapies for Waldenstrom’s. She’s involved in clinical research focused on the use of immunotherapies and antibody treatments. She also sees patients on a day-to-day basis and deals with patients who have both WM and amyloidosis. Dr. Sarosiek, what drew you to becoming a doctor?
Dr. Shayna Sarosiek: I was very young when I decided I wanted to be a doctor. I was interested in biology. Instead of pictures of bands on my bedroom wall, I had a poster of every system in the body. I had anatomy setups around my room so that I could study the human body. I also had a close family member with cancer when I was a child and that’s what drew me to cancer care specifically. I’m very happy that I’m in this field.
Understanding Waldenström Macroglobulinemia
What is Waldenstrom’s Macroglobulinemia?
Pete: Let’s talk about understanding WM. Dr. Paludo, can you describe Waldenstrom’s Macroglobulinemia?
Dr. Paludo: Waldenstrom’s is a type of lymphoma. There are many different types of lymphomas, several dozen to be honest, and they behave in different ways. They come from different cell types and different classifications. Waldenstrom’s belongs to the non-Hodgkin’s lymphoma category, which has several dozen different lymphoma subtypes.
Waldenstrom is also sometimes called lymphoplasmacytic lymphoma as it involves the bone marrow of the patients. This type of cancer comes from B cells or B lymphocytes that are part of our immune system. For reasons that we don’t understand exactly why or how, when one of those normal B cells or B lymphocytes becomes a cancer cell, it starts to grow and take up space in the bone marrow.
But it does grow very slowly and that’s why we also classify Waldenstrom’s as indolent lymphoma or slow-growing lymphoma. It’s an indolent lymphoma that comes from B cells and belongs to the category of non-Hodgkin’s lymphoma.
Waldenstrom’s is very unique in that not only is the cancer cell in the bone marrow, but these cancer cells can go to other organs, like lymph nodes and the spleen. It also produces a protein called IgM protein that can circulate in the blood and can cause different types of symptoms along the way.
Most Common Symptoms of Waldenstrom’s Macroglobulinemia
Pete: Dr. Sarosiek, we know that WM is rare as Dr. Paludo just mentioned, but what are common ways people find out that they have Waldenstrom’s and what are the symptoms when they’re diagnosed?
Dr. Sarosiek: Patients find out that they have Waldenstrom’s in a multitude of different ways, but a lot of patients don’t have any symptoms and it’s picked up incidentally when they have other testing done.
One of the most common things I see in my clinic is that during normal primary care follow-up, patients are noted to have a high total protein on routine blood tests. The IgM antibody that you heard from Dr. Paludo is made in Waldenstrom’s and is a type of protein. Often, the protein level in a patient’s blood might be high if they’re making a lot of IgM.
For some patients, it’s picked up because they had an MRI done for other reasons and the bone marrow looks active or looks like it has some changes.
Some patients are noted to have anemia in routine labs. Even if they don’t have symptoms, their doctor notices that their hemoglobin or red blood cell level is a little below normal. Sometimes it’s picked up incidentally; other times, patients have symptoms.
The most common symptoms we see with Waldenstrom’s, both at the time of diagnosis and the time of treatment, are symptoms of anemia. Some patients notice that they’re feeling tired, weak, or getting short of breath doing their usual activities. More commonly, patients attribute their symptoms to aging when in reality, it’s because they’ve developed anemia and their disease has progressed. When symptoms of anemia are present, it might be a cause for a workup.
Another symptom that isn’t as common is hyperviscosity or thickened blood. They might have frequent nosebleeds or visual changes and their eye doctor notices some bleeding in the blood vessels in the back of the eye. Sometimes, they might have symptoms from thickened blood, but it can be a variety of different things that happen and lead to the diagnosis.
Pete: My diagnosis came as a result of a blood test I had for another reason. The doctor said I had elevated protein levels and I thought I needed to cut back on my red meat to lower the protein level. I didn’t know anything about it.
Watch and Wait Process
What is Watch and Wait?
Pete: I’ve had Waldenstrom’s for almost 20 years now, so the definition of watch and wait has evolved and continues to evolve depending on the stage of the disease that I’m at. Initially, it was to see how well the treatments were working but in between treatment periods, watch and wait turns more into a waiting process.
Each time there’s a blood test, you have a little bit of anxiety as to what the results will be. I learned over the years to watch the trends and not focus so much on one blip up or down and that’s helped me relax a little bit. It’s not easy and it can lead to a lot of anxiety on the part of the patient and the caregiver. It’s important to watch those trends and stay in close contact with your doctor.
From the doctor’s perspective, can you describe the watch and wait process?
Dr. Paludo: The watch-and-wait process is the time between diagnosis and when we have to do something or start treatment. It’s the period when you’re monitoring the disease and waiting for symptoms or changes that would require treatment.
Pete, as you mentioned, you were diagnosed when they found an abnormal protein level in your blood. I’m assuming you weren’t having any symptoms at that time and that’s the case for a good number of patients diagnosed with Waldenstrom’s. As Dr. Sarosiek mentioned, a patient could have a test done that eventually led to a Waldenstrom’s diagnosis, but they were feeling well and not having symptoms at that time. Because Waldenstrom’s is a very slow-growing disease, we know that a lot of patients can go for many, many years without having any symptoms from this disease.
During watch and wait, we are keeping an eye on things and monitoring labs, like the trends of the protein level, hemoglobin, and platelet count. Some people call it active monitoring because we’re doing frequent follow-ups with labs and doctor visits, looking for symptoms or changes that would suggest treatment has to be done.
Dr. Sarosiek: I agree with everything you said. Generally, the process of watch and wait, active surveillance, or active monitoring is keeping an eye on a few key things, most importantly patient symptoms. Often, symptoms will align with a patient’s lab results or physical exam, but sometimes they don’t.
We’re trying to maintain a patient’s quality of life, so during that period, we’re monitoring the patient’s symptoms and blood work because if there are changes that are concerning or could become dangerous, then that’s the other thing we want to watch. Sometimes patients develop enlarged lymph nodes or an enlarged spleen.
Pete, you hit the nail on the head by saying that watching the trend is important because there can be some natural fluctuations. The IgM might increase or decrease a little bit. If a patient had a viral infection, it could affect the lab results. It’s more about the trend over the course of time rather than one lab value.
The same thing is true for symptoms. If a patient is sick, they might feel more fatigued but feel better the following week. We like to see the trend over some time during watch and wait.
Pete: I used to keep a spreadsheet to track the trends. My doctor used to expect that and wait for me to hand the sheet that I put together so we could look at the trends together. Thanks to technological advancements, I don’t have to do that anymore.
How Often Do Patients See Their Doctors?
Pete: When someone is in watch and wait, is there a standard frequency of doing blood tests or does it vary?
Dr. Sarosiek: It varies from patient to patient. On average for most of my patients, we follow up every three months. A lot of patients have a very slow progression of the disease, but it depends on the patient. Sometimes we have patients who have been stable for years, so we might extend that follow-up to align with what we know is happening with their disease.
In the beginning, patients are adjusting to their diagnosis and learning more about the disease and probably have more questions, so more frequent follow-up sometimes happens. Even if we don’t feel like we need it from a lab perspective, more frequent follow-ups allow us to check in with patients and allow them to ask questions and get used to having this disease. It can be important from a mental health perspective.
I don’t want any of my patients to be at home thinking they wanted to check at two months and spending the last month of the three-month period waiting anxiously. Sometimes, we’ll check in a little more frequently, especially around the time of a new diagnosis, but on average, it’s every three months.
Dr. Paludo: We have a very similar schedule. We tend to follow up with watch-and-wait patients approximately every three months, especially at the beginning as we have a better idea of how the disease is changing and what the trends look like initially. Assuming that everything is stable or mostly stable, then we start to space those visits about every six months, sometimes even a little longer depending on the patient, what they might be experiencing, and where they’re coming from.
Pete: I hadn’t considered the mental aspect behind the timing. You’re not just focused on the physical aspects of what the patient’s going through but also mentally. Looking back, I guess that did happen to me also. I appreciate that that’s part of the art of being a doctor as it’s not just science, so I compliment both of you on your ability to do that.
Top Tips for Getting Through Watch and Wait
Pete: Are there mental health issues surrounding being on watch and wait? I’ve been in various phases of watch and wait as I’ve been through multiple rounds of treatment. Fortunately, I have a strong support network with my wife, my kids, and my family. Through my involvement with the IWMF, I’ve talked to a lot of patients and not every patient has that support. Patient support is important. Talking to other patients and being part of a support group helps.
All that being said, there are still periods where you have rough patches. You don’t know what’s going to happen next and you’re either anxious about where your disease is heading or when the other shoe is going to drop. It’s important to take advantage of your support network, talk to your doctors, and seek mental help if you need it. There’s no shame in seeking help. You’re to be commended for doing so because you’re taking active control of your disease and your condition.
Doctors, what are the most common questions and concerns you get from your patients when it comes to watching and waiting? What are the top tips you provide them when they’re going through that process?
Dr. Sarosiek: Mentally, for a patient who has cancer, something changes in terms of the way that you think about new symptoms that come up. If you don’t have cancer or haven’t had a major medical issue and you have a little bit of back pain, you might think you hurt your back and move on with your day. But once you have an underlying diagnosis, you start to interpret symptoms differently. I see that very commonly and it’s very normal for that to happen with patients with Waldenstrom’s and other cancers. You start to see your symptoms through a new eye.
From my perspective, it’s important to have an open line of communication with your provider to relieve your anxiety, especially at the beginning when you don’t know exactly what to expect. Many patients will reach out to me and say, “I know this probably isn’t related, but I want to reassure myself. I have this new pain or new symptom. Do you think it’s part of the Waldenstrom’s or something bigger to worry about?”
The important part of active monitoring and surveillance is having that open line of communication to be able to ask questions to put into the context of your Waldenstrom’s, which otherwise you might have ignored. Don’t be afraid to ask to allay your anxieties and be able to enjoy your quality of life without having to worry every day about the small things.
Dr. Paludo: Another common thing is being concerned about watching and waiting. A patient is told they have Waldenstrom’s and now that patient is told that we’re not going to do anything about it. I discuss the rationale and the quality of life component, and reinforce that we do not forget about it. We’re going to have frequent regular time points to check and monitor things.
As Dr. Sarosiek mentioned, have an open line of communication and tell the patients to ask questions. If you have any concerns, contact your doctor to discuss them because there could be a great deal of anxiety, especially at the beginning as patients are getting used to living with Waldenstrom’s and not starting treatment right away.
Dr. Sarosiek: It’s important to find support and resources that work best for you. A lot of people have families and friends to support them and though some patients don’t have that, they might find support in other places. A lot of institutions have great social work care or psycho-social teams that can help deal with anxieties and mental health issues surrounding a cancer diagnosis. There are resources like the IWMF.
Some patients benefit from talking with other patients and being active participants on online forums. Other patients may find that overwhelming and don’t want to necessarily get all that information in the beginning. They might want to learn on their own through patient-directed education. Patients should use the resources available to them and find support in ways that they find most helpful. They don’t need to feel like they have to use everything available. It’s about finding a balance of what they feel most comfortable in.
Pete: Those are very insightful responses and hopefully, people find some help and guidance. I’ve been on this journey for a long time and I’m at a point where my disease is behaving itself and has been so for a while. I’m at the point where I’m worried more about my children and my grandchildren. If they have a bruise or some strange thing, I think, Could it be Waldenstrom’s or something related? It’s a different level of anxiety and I hate to admit that, but it’s true.
What Factors Impact the Watch-and-Wait Process?
Pete: Do different patient profiles, like age, gender, geographic location, and other considerations, impact how you work with patients on the watch-and-wait process? Does it matter where they are in terms of what type of patient they are or even where they live?
Dr. Paludo: They certainly influence the approach to a certain degree. I think about the interaction of Waldenstrom’s and other medical problems patients may have. For example, am I concerned about a potential kidney problem in a specific patient because they may have other risk factors for kidney problems or am I concerned about something else, like a big spleen?
Depending on how a patient presents, depending on what other medical problems they may have that could interfere with Waldenstrom’s, I may look at that and adjust a little bit of how we watch and wait. At the end of the day, it’s all about the trends in their labs and how the patient is feeling, but depending on other medical issues they may have, we may keep a closer eye or adjust the watch and wait period.
Dr. Sarosiek: You mentioned urban versus rural in terms of where a patient resides. That also can impact continued care. Dr. Paludo and I are both very fortunate to work at larger academic centers where we get to have more experience with specific diseases. If a patient is in a rural area, their local doctor might not see as much Waldenstrom’s.
Connecting with someone at a larger academic center could be helpful in terms of continuing to follow the disease. I work with a lot of local oncologists in terms of developing watch-and-wait plans and seeing what they’re comfortable with and what the patient is comfortable with. In some settings, in terms of developing a plan for active monitoring, it’s not just me and the patient, but it’s me, the patient, and their local oncologist.
Approaching the Mental Challenges of Watch and Wait
Pete: If a patient’s going through a mentally difficult time, do you do anything different in the treatment? How do you work through that process when they’re on watch and wait and they’re particularly anxious?
Dr. Paludo: A component of our discussions at patient visits is talking about stressors and anxiety symptoms. I tend to meet more often with patients who may have a higher anxiety level, which is not uncommon. The shorter intervals between appointments allow us to monitor labs a little closer. I found that usually helps a lot with those patients.
More important than that, we’re fortunate to have a very large group of psychologists and psychiatrists at Mayo who are experts in cancer patients. We tend to make a referral earlier in the disease process, so patients would have other professionals to speak with. We also share the different resources available outside of our institution.
Dr. Sarosiek: Part of the beauty of Waldenstrom’s is since our patients do well and we get to know them very well, we can have open conversations when they’re feeling more anxious or when they would like to be connected to more support systems. Based on our conversations, if they have anxiety about specific things happening with the disease, we can connect them to resources or see them more often.
I have many patients who I would feel comfortable seeing less often from a medical perspective, but the mental health perspective is also very important, so I continue to follow them a little bit more closely to manage that part. Keeping both mental and physical health in mind is an important part of the follow-up.
Importance of WM Caregivers
Pete: I’m a patient, but I also happen to be a caregiver. My wife has a related blood cancer and it’s strange to find myself wearing the caregiver hat. Do you work with caregivers in this regard? Do you have advice for them, specifically when a patient is going through the watch and wait period?
Dr. Sarosiek: Caregivers carry a big portion of the burden of the disease. We have a great social work team and they’re quite wonderful in terms of working with the families and seeing what needs the caregiver or the family member might have.
A patient needs to bring someone to an appointment. I always try to address if the family member or caregiver has other questions too because they’re quite involved. They’re often an extra set of ears, help quell anxieties the patient may have later, and can report back information that might have been too overwhelming at the time of the appointment.
A key part of caring for the patient during a visit is whoever they bring along is someone important and involved in their care, so I make sure their questions are answered too.
Dr. Paludo: Caregivers are very important, especially in Waldenstrom’s. I include them and check with them because they might be experiencing different types of anxieties and concerns. Caregivers are also looking for other things that we may not discuss, like family, work, and finances, which are important topics that don’t take center stage in the discussions but are important to address. They provide a lot of support to the patient, so it’s important to make sure they’re supported as well.
Pete: Having to wear the caregiver hat, I had a newfound respect for what my wife had been through for years. In some respects, it’s harder than being the patient. I have a lot of appreciation for all the caregivers and physicians who are working with us, trying to help during these difficult periods, whether we’re in treatment or watch and wait.
Latest Treatment Options for Waldenström Macroglobulinemia
Pete: We want to touch on the current treatment landscape or what treatment is like for Waldenstrom’s patients and where we might be headed. When I was diagnosed in 2003, Rituxan (rituximab) was a fairly new treatment paradigm and there were concerns about whether it was safe to take long-term. We know much better now, but back then, we weren’t sure.
One of my initial treatments, which was fludarabine, cytoxan, and rituximab, isn’t used anymore. I have an unusual disease course, so I’ve had different courses of treatment. I’m currently on a BTK inhibitor, which is working well for me. Because I have a different manifestation of the disease, I also get monthly IVIG.
Every patient is different. What are the current treatment options for patients? If they’re newly diagnosed, what do they have to look forward to in terms of options?
Dr. Sarosiek: Over time, if a patient’s disease progresses or comes back, we have a lot of different treatment options, which is wonderful. Most commonly for a treatment-naïve patient, which means they’ve never had treatment for their Waldenstrom’s, we think of two big categories for first-line therapies.
We often think about BTK inhibitors, like zanubrutinib, ibrutinib, and acalabrutinib. There’s also chemotherapy with rituximab. There are quite a few different chemotherapies. Fludarabine is one of the older ones, but we don’t use that as frequently anymore. In the US, we often use bendamustine with rituximab, but there’s also another chemo called Cytoxan (cyclophosphamide) that can be combined with rituximab. I would say the two most common are rituximab with chemotherapy or BTK inhibitor.
There is another class of drugs called proteasome inhibitors, like bortezomib, or related drugs that we can also use. I tend to use those in younger patients. A lot of patients with Waldenstrom’s have neuropathy, so we don’t use those drugs as frequently because neuropathy can happen with that group of drugs.
There are other oral therapies like venetoclax or the newer BTK inhibitor ibrutinib. There are also different options available as well for patients who have had their disease come back. Clinical trials are also an option, which is the way that we move therapies forward.
We have so many different options and we’re lucky enough to have a conversation with our patients about what might fit their disease and their preferences. Some patients don’t want to take a pill every day, some people don’t want chemotherapy. In most cases, we can tailor therapies to patient preferences and what we might expect to be best for their disease.
Pete: Dr. Paludo, can you talk about fixed-duration therapy versus continuous therapy? What are the differences and what are the advantages and disadvantages?
Dr. Paludo: As Dr. Sarosiek mentioned, we are very lucky to have so many different options, a lot more options than we had 20 years ago, Pete, when you were diagnosed. We can divide the different treatments into fixed-duration treatments and continuous treatments.
With fixed-duration treatment, there’s a start date and an end date. Those include chemoimmunotherapy regimens, like bendamustine and rituximab, and cyclophosphamide, rituximab, and steroids. Treatment is usually given at frequent intervals for a specific amount of time.
Continuous treatments include newer drugs, like targeted therapy. They have a start date but they don’t have a predefined end date. Treatment is continued for as long as it’s working and not causing side effects that require us to stop treatment. That’s where BTK inhibitors come into play, like the one you’re currently taking, Pete. You’re going to continue on it for as long as it’s working and not causing enough side effects to impact your quality of life to justify stopping treatment.
We usually think of fixed-duration treatments as having more side effects at a higher intensity and that’s why they’re given for a certain duration. Continuous therapy tends to have a lower level of side effects so patients can continue on treatment for a long time. Patients can choose what fits them better, whether it’s fixed-duration treatment or continuous treatment.
Promising Clinical Trials in Waldenström Macroglobulinemia
Pete: What’s always interested me was when it was time to decide, the doctor would tell me my options and ask which one I wanted. We’re fortunate as WM patients to have so many different options available regarding treatment, which is a testament to the amazing research being done to move the ball forward.
We look forward to the newer agents down the road and better treatments in the future for improved quality of life for all. With that in mind and looking at the future of treatments, what’s exciting at this point? What are some of the studies you’re most interested in, and why should patients and care partners be interested in participating in a clinical trial specifically?
Dr. Sarosiek: Clinical trials are how we move forward in the field. We’re in an exciting time with the number of clinical trials that we have available for Waldenstrom’s and there are quite a few that I’m interested in. When I bring up Waldenstrom’s clinical trials to patients, there’s an initial hesitance because of concern that a patient would get a placebo and not get treatment for their disease.
An important thing to remember is that we’re certainly treating our patients and what the trials do is try some of the treatments in a new way. Maybe a specific treatment was effective for other types of lymphomas and we’re seeing if it would work in Waldenstrom’s or if a combination of two effective therapies has been used before, we’re studying if we could use both for a shorter duration.
Patients should always be open to asking questions about clinical trials if they have any hesitancy, are worried that they’re not going to get active therapy, or are worried about side effects. Some trials offer an opportunity to get something new and different that might be more effective based on some encouraging background data.
We have a couple of ongoing clinical trials for patients with Waldenstrom’s, a precursor of Waldenstrom’s, or who don’t quite meet the criteria for Waldenstrom’s but have an abnormal IgM antibody. Patients can develop neuropathy that affects the lining of the nerves We have a clinical trial open for exploring that neuropathy differently by treating the underlying abnormal IgM and then following the patient’s nerve damage over time and hoping to find something that’s effective. That trial used rituximab with acalabrutinib to see if that regimen can protect the patient’s nerves.
Another clinical trial we have is using a drug called loncastuximab tesirine, an antibody that delivers a toxin to the site where the abnormal cells are, and that’s a limited-time therapy of six months. The trial is ongoing and it’s for patients who have had at least two other types of therapy in the past.
We have another clinical trial that’s using two oral therapies, venetoclax and pirtobrutinib. We know both of those drugs are effective in Waldenstrom’s on their own, but this trial is using a combination of both for two years in hopes of deepening or getting better control of Waldenstrom’s, and also in hopes of allowing patients to come off treatment after two years.
I could go on and on about many other clinical trials available for Waldenstrom’s, but those are some of the more exciting ones that we’re talking about. Dr. Paludo, do you have other thoughts about clinical trials for patients with Waldenstrom’s?
Dr. Paludo: Participating in clinical trials is very important for patients and the community. Participating helps patients have new and other different treatment options available and that’s how we got where we are right now. Often, the first patients to benefit from a new treatment are the ones in the clinical trials, so the ones in the ibrutinib clinical trial are the first ones to benefit from that drug and become the standard of care. Hopefully, loncastuximab will become part of the standard treatment in those patients in clinical trials who are the first ones to benefit from that.
There are several clinical trials available for Waldenstrom’s. There are a few that are very interesting and seeing results and I hope they will be available soon. There are some trials comparing differences in the treatment regimens and classes that we were talking about earlier, trying to see if one is better than the other, or which situation to use one or the other.
We don’t have the specific trials yet, but I’m looking forward to seeing what novel types of immunotherapy drugs will bring to Waldenstrom’s field. I’ll be very curious to see what we’re going to find with bispecific antibodies in Waldenstrom’s. We have seen excellent results in different lymphomas similar to Waldenstrom’s and I’m hoping that we’ll have clinical trials soon that will be able to investigate if those treatments are helpful in Waldenstrom’s as well.
Pete: With the clinical trials, what it comes down to is that it’s an opportunity to be on the cutting edge in a sense of what treatments are out there and find something that will work well for you.
Correct me if I’m wrong, but the thing that people should take away is that if you are in a position where you need treatment, you will get treatment whether it’s from a clinical trial drug or another treatment.
Dr. Sarosiek: That’s correct. No matter what, patients need to understand that if their disease needs treatment, they will get treatment for their disease. If they qualify for a trial and want to participate, they can do that. We would never advocate for a clinical trial that wouldn’t provide the treatment that the patient needed.
Dr. Paludo: We also look for clinical trials that make sense for the patient. If the patient needs treatment, do the new drugs in clinical trials make sense for that patient or do they have potential side effects that will cause more trouble? If so, we would avoid those clinical trials. When looking for a clinical trial or treatment, it has to fit the patient.
Pete: Patients could always ask if there’s a clinical trial that they can participate in. Depending on where they’re located, they may have to reach out to people, like at Mayo Clinic and Dana-Farber, to see if there are trials available. They may have to travel, but they have an option. I encourage patients to always look at clinical trials and see if any of them are the right fit for them because you help yourself and you also help other Waldenstrom patients in the process. It’s a win-win situation.
Final Takeaways
Pete: Dr. Paludo, as a final message to any patient who’s in watch and wait, what would you tell them to alleviate their anxiety and mentally dealing with being on watch and wait?
Dr. Paludo: I always try to convey to my patients that being able to watch and wait is very positive. It’s an excellent situation to be in where you don’t need treatment. You want to kick that can down the road only when you have symptoms. Work with your hematologist. You need to follow up. Despite all the anxiety that comes with it, being on watch and wait is an excellent position to be in.
Dr. Sarosiek: Watch and wait or active monitoring is a personalized process. It can be adjusted and will be adjusted as needed for each patient in terms of what to follow up on and how often to follow up. I encourage everyone to find a physician who they’re comfortable with, who they can go through that process with, and who they feel is supporting them.
Pete: As a patient myself, I always appreciate my doctor and the advice that he gives me. Having a good working relationship with your doctor and having your caregiver involved is important, so make sure to have someone come to your appointments with you.
It’s okay to let your emotions out. Be upset, yell, and cry if you need to. Don’t hold it in. But if you find that that doesn’t help, reach out to your doctor, to your care professionals, to social workers, and to whatever support is available to you. Take advantage of that support network. You don’t have to suffer alone. There are people who can help you through the process.
The Leukemia & Lymphoma Society
Stephanie: Before we wrap up this discussion, I’d like to spend time on a very great hands-on resource at your fingertips, The LLS’ Information Resource Center, which features specialists who work with people one-on-one. Joining us is Jennifer Wilson, a senior information specialist with The LLS. Jennifer, can you share the basics of how you are helping patients and care partners in general?
Jennifer Wilson: We want to make sure that whether someone calls us for the first time or the 40th time that we hear what they need. Sometimes people can identify it, but sometimes they can’t. We want to make sure that they have good, up-to-date information on their disease and treatment options and how to get support because we know that what your needs are from day one can be very different over time.
Stephanie: For Waldenstrom’s patients and care partners in particular, what are some of the common questions and topics that come up, and how do you help the people who approach you?
Jennifer: When someone is newly diagnosed, oftentimes they may be told that Waldenstrom’s is a chronic illness so they’re going to watch and wait, but to hearing that can be completely overwhelming. We prefer to use the phrase “active surveillance” because that indicates that they’re keeping an eye on things. They’re not waiting to see what happens. They’re very deliberately monitoring to manage the disease.
Then we look at what supports are available. We have the First Connection® Program, a peer-to-peer program so that someone with Waldenstrom’s would have the opportunity to speak with someone else who has been in watch and wait to find out what that felt like and how to communicate with their friends and family.
A lot of times, we help patients figure out what they need to ask at their next appointment to ensure that when they leave the doctor’s office, their top five questions have been answered.
Conclusion
Pete: Thank you again to both of you, Drs. Paludo and Sarosiek. We look forward to future discussions and further advancements in the clinical trials and the future of Waldenstrom’s research.
Stephanie: Thank you, Jennifer, for the work that you’re doing to help patients and families everywhere, including those who are dealing with Waldenstrom’s. We want to thank both Blood Cancer United and the IWMF for being incredible partners.
Thank you, Pete, for leading an incredible discussion, spending the time, and your advocacy in general. You have made an immeasurable impact in this space.
Thank you, Dr. Sarosiek and Dr. Paludo, for the work that you’re doing both in the clinic with the people you’re helping directly in Waldenstrom’s and beyond, and also all the research that you’ve contributed to lifting the possibilities for everybody with Waldenstrom’s.
I hope that this discussion was helpful and that you walk away feeling more confident. We hope to see you at a future program.
If you read and/or watched our program, we encourage you to take our program survey to help us improve future programs and answer your questions.
Gigi’s Stage 1A, High-Grade Serous HER2+, PR+, ER- Endometrial Cancer Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Gigi’s initial symptoms included hiccup-like sensations behind her sternum, gastrointestinal issues, and spotting. An ultrasound showed a thickened endometrial lining, and a biopsy confirmed her diagnosis – endometrial cancer. A month later, she underwent a radical hysterectomy.
Initially, Gigi thought a hysterectomy would suffice, but further testing revealed a more serious condition. Her tumor had 25% mixed undifferentiated cells, placing her in the top 1-2% for her cancer type.
Although additional tests showed no spread of the cancer, her oncologist recommended chemotherapy. Gigi enrolled in a clinical trial, receiving six rounds of carboplatin and paclitaxel every three weeks.
Alongside chemotherapy, Gigi took dexamethasone, anti-nausea medication, antihistamines, and gabapentin. She found chemotherapy more manageable over time, despite side effects like facial redness, dry skin, nausea, bone pain, restless leg syndrome, neuropathy, and tinnitus. Fortunately, her blood work stayed stable, allowing continuous treatment without delays.
Gigi adopted a plant-based, low-inflammatory diet and explored alternative therapies to support her body during treatment. She now has CT scans every nine weeks and follow-ups with labs every 12 weeks.
Inspired by resilient patients, Gigi actively participates in her care and treatment decisions, collaborating with respected care providers, asking tough questions, and balancing being well-informed with learning to let go.
Name: Gigi D.
Diagnosis:
Endometrial Cancer
HER2+
PR+
ER-
Staging:
1A High-Grade Serous
Initial Symptoms:
Hiccup-like sensations behind the sternum
Gastrointestinal issues
Spotting
Treatment:
Clinical trial: chemotherapy (carboplatin and paclitaxel)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Samantha’s Stage 4 ER+ PR+ HER2+ IDC Breast Cancer Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Samantha’s journey with stage 4 breast cancer began in March 2019 when she was 22. Living in Virginia with her husband and young daughter, she first noticed a lump in her breast. Initially dismissed by her primary care physician and an ultrasound tech as an infection, a biopsy eventually confirmed her cancer diagnosis. Despite the initial belief that her cancer was at stage 1, further tests revealed it had spread, making it stage 4 breast cancer.
Her treatment plan involved chemotherapy, which she had to stop early due to severe neuropathy, followed by a lumpectomy, radiation, hormone therapy, and targeted therapy. Despite significant side effects, she managed to maintain no evidence of disease (NED) for some time. After two years of hormone therapy, Samantha decided to take a break to try for a baby, which led to a successful pregnancy in April 2022.
However, during her pregnancy, she and her family moved to Alaska. While there, Samantha’s cancer recurred, causing severe back pain due to lesions in her spine and pelvis. Unable to travel back to Virginia without stabilizing her spine, she underwent surgery and later radiation before returning to her oncologist for a new treatment plan. She joined a clinical trial involving a new radium drug for bone metastases but had to leave it due to mixed results.
Samantha then resumed hormone therapy and targeted therapy with different drugs than before. Throughout her treatment, she emphasized the importance of careful decision-making, the support of her family, and maintaining a positive outlook.
Name: Samantha L.
Diagnosis:
Breast Cancer
Invasive ductal carcinoma (IDC)
ER+
PR+
HER2+
Staging:
Stage 4
Initial Symptom:
Lump in breast
Treatment:
Chemotherapy
Surgeries: Surgery: lumpectomy, spinal surgery (fractured vertebrae)
Radiation
Hormone therapy: anastrozole & letrozole
Targeted therapy: abemaciclib & ribociclib
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I went to my regular doctor who said it was nothing. I was so young that it couldn’t be breast cancer.
Introduction
My husband and I live in Virginia and have a 1-½-year old daughter. I was diagnosed with stage 4 breast cancer at 22 in March 2019.
Pre-diagnosis
Initial Symptoms
It was the day after Valentine’s Day. My husband and I weren’t married yet. He was my boyfriend at the time. My mom loves to celebrate Valentine’s with the family. The celebration had ended and we were watching TV. He hugged me from behind and squeezed me tight. When he did, I felt some pain in my left breast. I realized there was a lump.
PCP Appointment
I went to my regular doctor who said it was nothing. I was so young that it couldn’t be breast cancer. They told me to put a warm compress on it, but that didn’t do anything. They put me on antibiotics thinking it was an infection and, of course, that didn’t help.
They finally sent me for an ultrasound and the ultrasound tech looked at it and said, “This looks like an infection. You’re 22 and I’ve never seen breast cancer in a 22-year-old, so that’s not what it is. But just in case, you can get a biopsy if you want.”
Getting a Biopsy
I almost left the hospital and went home without doing anything about it. He said it wasn’t urgent, but there was an opening so I got the biopsy done.
When you’re 22 and recently graduated college, cancer is not on your mind at all.
Diagnosis
Biopsy Results
The results revealed abnormal cells, so I had to go in for a second biopsy. That was the one that told us that I had breast cancer.
Reaction to the Diagnosis
When you’re 22 and recently graduated college, cancer is not on your mind at all.
My breast surgeon called me on the day the abnormal cells came back and said, “You need to come in again.” I went in and that’s when she started to prepare me that it could be cancer. She ended up calling me when she found out that it was.
She told me she cleared out an appointment for me at the end of the day and that we should get more information about the hormone receptors at that point. She scheduled an appointment so that I could talk to my family and get all of our questions written down before the appointment.
Treatment
Discussing the Treatment Plan
I didn’t know anything. I thought it was stage 1. I went through it in stages, always thinking that it was the least concerning thing. I don’t think there’s a big shock. It came about over time as we had more questions and learned more about it.
She was suspicious right when I walked in. She wanted to check the lymph nodes under my arm because that’s the first place cancer spreads. My boyfriend, my parents, and a friend who’s a doctor came to the appointment with me. They all had questions and wanted to help me and know everything. They went into a separate room and she took me back and did the biopsy under my arm.
When we went back, she laid out a plan. It was March and she said we should be done with all active treatment by Christmas. She said the standard is chemotherapy and then surgery, which was going to be a lumpectomy or a mastectomy, and then radiation. Since my cancer was hormone-positive, I would be on hormone therapy for some years after.
The spot was more contained. They said it was probably cancer because the chemo shrunk it. Then we realized I was stage 4 breast cancer.
Chemotherapy
There were a few hiccups. I had to stop chemo early because Taxol (paclitaxel) was causing neuropathy in my fingers. It got too bad and my oncologist didn’t want permanent nerve damage to happen. I was a little bummed about stopping Taxol early because it made me feel like I wasn’t doing everything that I could, but it’s what happens when your side effects get too bad.
Originally, all of my doctors wanted me to do a double mastectomy because I was young. Younger women tend to choose a double mastectomy because it gives people peace of mind to make sure all of the breast tissue is removed and there’s no place for cancer to grow.
I had a scan where they saw a spot in one of my ribs. They weren’t positive it was cancer and it was in a weird location that they wouldn’t be able to biopsy it. We talked to neurosurgeons about removing it, but we weren’t sure if it was cancer.
When I had chemo and scans again, the spot was more contained. They said it was probably cancer because the chemo shrunk it. Then we realized I was stage 4 breast cancer.
Lumpectomy
At this point, mastectomy isn’t going to matter too much because the cancer has already spread past the breasts. If I do a lumpectomy, the recovery time is shorter so I could get started with radiation immediately after. They wanted to do radiation on the rib to target the spot that was seen in the scan since it couldn’t be removed with surgery.
I ended up doing a lumpectomy, which is weird because when you think about cancer when you don’t have it, you think you’d do the most drastic option possible. But when you’re faced with your options, you’re not always picking that for yourself and your situation.
Radiation
After the lumpectomy, I did radiation and finished that in November.
My case wasn’t as bad of a stage 4 breast cancer case, so we were hopeful that I was cured at that point and that getting pregnant would be fine.
Hormone Therapy & Targeted Therapy
I started hormone therapy and targeted therapy after radiation and did that for two years. Since I had radiation on that tiny spot on my rib, I had no evidence of disease (NED) on scans.
I was having a lot of side effects with hormone therapy and targeted therapy. Being NED for so long, I didn’t even know if these therapies were doing anything or just making me miserable. It was causing a lot of physical and mental side effects that were the hardest time in my life so far. Way harder than chemo, radiation, and the rest of it.
I wanted to stop early. My oncologist wanted me to get to three years, but I could only make it two.
Fertility Post-Treatment
I wanted to try having a baby so I asked him. He cited some recent studies about women who had breast cancer, stopped hormone therapy after two years, took a break, got pregnant, and then went back on treatment. The chances of their cancer reoccurring didn’t increase. Some people had their cancer come back and some people didn’t, but getting pregnant didn’t affect that.
However, the study was for stage 3 and below and not stage 4 breast cancer. Since I only had a tiny spot of cancer and it wasn’t in multiple places throughout my body, my case wasn’t as bad of a stage 4 breast cancer case, so we were hopeful that I was cured at that point and that getting pregnant would be fine.
I got off hormone therapy and targeted therapy. I started in November 2019 and ended in October 2021. I wasn’t having periods the whole time and then my cycles returned to normal. I felt amazing. I think it was because I wasn’t on hormones anymore. Then I got pregnant in April 2022.
You can’t let the fear of cancer coming back control your life. You can’t make every decision based on whether your cancer comes back or not.
Pregnancy was great. I still had all of the same pregnancy side effects, like nausea, but I was so used to being nauseous from treatment that it didn’t affect me. I just felt good that I wasn’t on medication. There were lingering side effects from both chemotherapy and targeted therapy. I still have hot and cold sensitivity in my fingers, toes, ears, and teeth. I have dry eyes.
It can be difficult because people don’t want their cancer to come back. They don’t want their child to be left without a mother. That’s the main worry people have. My philosophy on it is that you’re not a statistic. You don’t know what could happen in your life and you can’t let the fear of cancer coming back control your life. You can’t make every decision based on whether your cancer comes back or not.
If I can, then I will. If I feel good, then I’m going to do this or that. It’s not a decision that I made easily. My husband and I talked through it and we spoke to our doctor about it. We did what was best for him and what was best for our family specifically. It’s not for everybody. You have to figure it out for yourself.
There are all these medical questions that you need to ask your doctor, but it can be a good thing and possible. There’s a lot of new research coming out. You don’t have to be afraid of having hormones in your body after having hormone-positive cancer.
Moving to Alaska
In the middle of my pregnancy, we moved to Alaska, so we were away from my oncologist for a while. I was still keeping in touch with him, but we were hopeful that I was cured since I had scans that showed no evidence of disease for so long after my daughter was born. I was breastfeeding, so we didn’t do a lot of monitoring because I was still feeling good and there were no new symptoms.
Several lesions throughout my spine and pelvis were found on the MRI.
Cancer Recurs
We were on a mountain one day taking family photos when I collapsed to the ground. My back hurt so bad that I couldn’t get up. Five guys had to carry me to the car. I went to the ER that day and eventually had a scan. The results showed a fracture in my spine because there was cancer growing in it, crushing the vertebrae, and causing the pain. Several lesions throughout my spine and pelvis were found on the MRI as well.
I couldn’t get on a plane to fly back to Virginia because they were worried that if something shifted, I could be paralyzed, so I needed to have surgery to stabilize my spine before moving back. We couldn’t even think about treating the cancer until that happened. It was scary because we weren’t doing anything to address the cancer.
I had surgery in the middle of August followed by a very painful recovery. I was already in a lot of pain beforehand, but I needed two weeks of recovery. When we got to Virginia, I met with my oncologist and came up with a new plan.
New Treatment Plan
They thought I needed radiation on the vertebra that had the fracture because there were other spots throughout my spine and pelvis, but that was the biggest and causing the most problems. We did three rounds of radiation on that first.
My oncologist knew that hormone therapy and targeted therapy made me miserable, so he gave me three options. He said I could go on hormone-targeted therapy, I could take a chemo pill called Xeloda (capecitabine), or I could get on a clinical trial.
I couldn’t start the trial until 14 days after my last radiation, so for two weeks, I wasn’t doing anything and I could feel things getting worse.
Joining the Clinical Trial
He was excited about the clinical trial because it used a new radium drug targeting bone metastases. It was already an approved treatment for prostate cancer with lots of success and this trial was testing it on metastatic breast cancer patients. We went with that because he said it could eliminate what’s in my bones.
The problem was that I didn’t know which group I would be in. They were going to tell me, but I was either going to be in the group getting chemo or in the group getting chemo and the radium drug.
That was a stressful time because there was a period when I had to wait to get approved for the trial. I couldn’t start the trial until 14 days after my last radiation, so for two weeks, I wasn’t doing anything and I could feel things getting worse.
I ended up in the radium arm of the trial, which was good, and I did that for a while. It helped with my pain a lot and decreased some of the markers in my body.
I ended up having to go off the trial because my scan showed mixed results. Some areas were better, but some areas were worse. I think it’s because my original scan was in September and not right before I started the trial. There was that two-week period when things got worse, but there’s no way of knowing if that was it or not.
Hormone Therapy & Targeted Therapy
After the trial, I talked with my husband and my family and decided that I was going to give hormone therapy and targeted therapy another try. My oncologist recommended trying a different drug than what I was on before, so that’s what I’m doing now. I’m on anastrozole and abemaciclib, which is slightly different from the letrozole and ribociclib that I did in 2019.
The whole point of stage 4 treatment is to find a treatment that you can tolerate for the rest of your life.
Treatment Decision-Making
People don’t realize how much thought is put into treatment-decision making. You think about it for days, weeks, and months, talking it through and talking to doctors. I think that experience was good because it led me to my decision and made me realize that I’m exactly where I should be.
Having a Strong Support System
I have a supportive husband and family who help talk through things with me. I think about things a lot, pray all the time, and try to get the wisdom to make all these decisions in a way that’s going to be the best for myself, my husband, and my daughter.
It’s not just about patience. It takes a lot of work and it’s not something that you make a split-second decision about. There’s a lot of thinking and praying.
The whole point of stage 4 breast cancer treatment is to find a treatment that you can tolerate for the rest of your life. When we went to a new center, found out all the information, and talked with my oncologist more about whether this was realistically going to be the best option for me, that’s what made us think that this is what’s going to be good.
It wasn’t just me. My husband was so afraid of me being on it again. He knew how much I suffered when I was on it. It affects both of us. Going on it for the second time around was nice. It was working better. I don’t know if it’s because I went through a pregnancy, I’m older, it’s a different drug than before, or if I have a different mental attitude towards it.
If I didn’t have a baby who was so dependent on me, I don’t think I would’ve even considered going back on hormone therapy.
Everything happens for a reason. Some people thought it was a dumb decision for me to get pregnant, but having her is what made me do this treatment in the first place. If I didn’t have a baby who was so dependent on me, I don’t think I would’ve even considered going back on hormone therapy. I would’ve done the chemo pill. It could have worked, but it could not have worked. Having her around gave me this huge drive to live for as long as possible. It’s what made me even try it again in the first place. I wouldn’t have even known that it would be better this time around.
A cancer diagnosis is harder on the family than on the person going through it. Your family loves you. A lot of family members feel like they’re being pushed away and that they’re not wanted. My instinct is to do that because I don’t want to put a burden on them. But at the end of the day, it’s important that they’re there. The best thing that a family member can do is be there and listen. What to say and do is going to be different for everybody, but being there is a good place to start.
Words of Advice
Don’t wait. If you want to do something, do it. You never know when your life is going to dramatically change. I didn’t realize how much I enjoyed picking up my baby and rocking her to sleep then all of a sudden, it’s taken away from me.
When we moved to Alaska, people asked why we were going. We had an opportunity, so we’re going to move to Alaska for a year. We probably could never do that again because now I need all this treatment so I’m back in Virginia where my original team is.
If you want to do something, do it while you can because you never know when you’re physically not going to be able to do it.
Don’t wait. If you want to do something, do it. You never know when your life is going to dramatically change.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Amy initially noticed a slight change in her stool consistency, which persisted despite normal test results. After a year-long delay due to the COVID-19 pandemic, a colonoscopy revealed a 6-cm mass in her colon. Although the initial biopsy showed no cancer, surgery confirmed cancer in the tumor center and 11 out of 21 lymph nodes. It was stage 4 colon cancer.
She began treatment with FOLFOX, experiencing severe side effects like jaw pain, cold sensitivity, and neuropathy. Despite completing the regimen, a slight increase in CEA levels prompted further tests. A CT scan and MRI revealed cancer in her liver, leading to a relapse diagnosis. Unhappy with her initial oncologist’s pessimism, she sought a second opinion and switched to a more supportive doctor.
Her new oncologist initiated FOLFOXIRI, which shrank the tumors but wasn’t enough to eradicate the cancer, leading to surgery and an ablation. When the cancer resurfaced, she joined an immunotherapy clinical trial. The difference between chemotherapy and immunotherapy was substantial, providing her with a significantly improved quality of life.
Throughout her stage 4 colon cancer journey, Amy emphasized the importance of a supportive medical team, listening to her body, advocating for her health, and maintaining movement and proper nutrition during treatment. She also stressed the need for open communication with healthcare providers about side effects and health concerns.
Name: Amy L.
Diagnosis:
Colon Cancer
Staging:
4
Symptoms:
Slight change in stool consistency
Treatments:
Chemotherapy: FOLFOX, FOLFOXIRI
Clinical trial: immunotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
What might be normal for somebody else might not be for you. If there’s a change, it’s important to talk to your doctor about it.
Introduction
I’m from the Seattle Pacific Northwest area and I was diagnosed with stage 4 colon cancer.
Pre-diagnosis
Initial Symptoms
I only had one symptom, which was a very small change in my stool. It became slightly looser, but it wasn’t consistent. For most people, that might not be a big deal, but I hadn’t changed my diet. The first time I noticed it was when I had just come back from Spain and I thought it was from traveling. I gave it a few weeks, but it wasn’t getting better.
PCP Appointment
I listened to my body and talked to my doctor about it within a month of this first symptom. My doctor at the time thought it was food sensitivity. They did autoimmune testing for Crohn’s and celiac disease, but those came up negative. They did an allergy panel to see if I developed any new food allergies. That came back normal. I also had my first CEA test, but I had no idea what that was and that also came back normal.
I was blessed to have a doctor who was very proactive and didn’t ignore my symptoms. They knew that I knew my body. What might be normal for somebody else might not be for you. If there’s a change, it’s important to talk to your doctor about it.
Unfortunately, they couldn’t get me in for a colonoscopy. They did the fecal immunochemical test (FIT) test. They did all these tests and everything was coming back normal.
He recommended me to a dietician who started looking at what I was eating and what we could change that might explain the stool change. My doctor said that since everything’s coming back normal, he wanted to do due diligence to make sure that there’s nothing they might be missing. He said, “Let’s get you in for a colonoscopy.” That was in the end of 2019.
They called in and said my procedure was non-essential and not COVID-related, so I needed to be put on hold… Unfortunately, I ended up waiting for a whole year.
Getting a Colonoscopy
They were booked back a few months. I wasn’t considered urgent. Nobody thought I had cancer. I was 39. They said they’ll get to me at the end of January or early February 2020. Then the COVID pandemic happened.
A week before my appointment, they called in and said my procedure was non-essential and not COVID-related, so I needed to be put on hold. They would call when they could make it happen again. Unfortunately, I ended up waiting for a whole year.
During that year, I was furloughed, so I was staying at home. My symptoms went away, which confirmed to me that maybe it was something I was eating since I wasn’t eating out.
By January 2021, I got a phone call asking if I wanted to schedule my colonoscopy again. I almost said no and that I didn’t need it anymore because the problem had gone away, but a little voice inside me told me to go ahead and do it. The “worst” thing that they could tell me is that nothing’s going on. I had nothing to lose, so I told them to go ahead and schedule it. They scheduled me for the first week of February 2021.
I didn’t have any other symptoms, like pencil-thin stools, bloating, or pain. Nobody was looking for cancer, especially colon cancer. Most people who get colon cancer are in their 70s and 80s. The first oncologist I had even told me that I was the youngest patient he ever had. Most of his patients were 60 and older, so it wasn’t on anyone’s mind that I could have cancer.
When I did the prep for my first colonoscopy, it was worse than the colonoscopy itself, but it’s a small drop in the bucket out of all the days in my life. On the day I came in, everything proceeded as normal. I got onto the table and they told my husband that the procedure could take up to 30 to 45 minutes. He couldn’t stay with me, so he dropped me off and left.
They put me in twilight sedation so I’m out of it, but the doctor’s voice and tone cut through. She turned to her nurses and said, “Where is her husband? Get him back here right now. Call him. We need him back here right now.”
She didn’t say anything, but because of her tone, I knew something was wrong. I felt my heart dropped to my stomach. I was half awake and the anesthesiologist was trying to put me back to sleep because my eyes were open and I was starting to ask questions. I didn’t feel anything, so it wasn’t traumatic.
The biopsy results showed there was cancer in the center of the tumor and 11 of 21 lymph nodes.
Diagnosis
Biopsy
When they wheeled me back into a curtained area, my husband was already there waiting for me. The doctor came and said they found a 6-cm mass in my colon.
I waited for the biopsy results to come back and when she finally called, she said they biopsied the tumor, but there was no cancer. However, they were extremely concerned given the size. It was either going to turn into cancer soon or there would be cancer in the center and not on the outside, so they wanted to get me in quickly. Everything was indicating that they had “caught this in time” and that I would just need surgery and might not even need chemo.
Surgery
They scheduled the surgery within three weeks of that conversation. They were on top of it and wanted to get it out.
The surgeon came in to talk to me. The biopsy results showed there was cancer in the center of the tumor and 11 of 21 lymph nodes. The tumor hadn’t broken through the colon, like they usually see with more advanced cancer, so they were not expecting to see cancer in my lymph nodes. He was very shocked it was stage 4 colon cancer.
I made an appointment with a doctor at Fred Hutchinson Cancer Center to get a second opinion because I wanted to know more.
Oncologist Appointment
My mom was an ER nurse. She also has leukemia, so she hasn’t worked while dealing with that. My mother-in-law is a hematology-oncology nurse at the Mayo Clinic. I’m fortunate to have knowledgeable people who helped me through the next process.
They referred me to my regular oncologist and said he’d go through my stage 4 colon cancer treatment plan. I had a meeting with him and it went okay, but I ended up switching. He told me that I would need clean-up chemo or adjuvant chemotherapy. Everything looked fine. He wasn’t hugely concerned.
Treatment
FOLFOX Chemotherapy
They said I was going to do FOLFOX (folinic acid, fluorouracil, and oxaliplatin) and then we would do a CT scan. They did a CT scan right after the colonoscopy where they found the mass, but they didn’t find anything else. He said it’ll be good.
Getting a Second Opinion
I made an appointment with a doctor at Fred Hutchinson Cancer Center to get a second opinion because I wanted to know more. I knew nothing. Is FOLFOX the standard treatment? What were my treatment options for stage 4 colon cancer?
Different doctors have different preferences and I wanted to ensure I was getting all the information. I made an appointment and brought all of my medical records to make sure. The doctor said they would do the same treatment.
I had a very rare side effect where I had jaw pain… This was a rare side effect of oxaliplatin.
Side Effects of FOLFOX
I did 12 and it was terrible. Before my second round, I had a very rare side effect where I had jaw pain. It was the most excruciating pain I’d ever experienced in my entire life. It radiated from my jaw back up around my neck and felt like somebody had put my head into a vice.
They didn’t know what was going on. I didn’t find out until I switched oncologists that this was a rare side effect of oxaliplatin. They sent me to a jaw specialist to make sure there wasn’t something else going on. I spent the rest of my treatment switching back and forth between morphine and oxycodone because the pain was so horrific.
On top of the nausea and hair loss, the cold sensitivity was bad. I like my drinks either really hot or cold. I don’t like lukewarm drinks. Chemo, especially oxaliplatin, made everything taste like pennies and dirt. I’m a big water drinker and I couldn’t drink water because the taste would make me gag. I started drinking electrolyte drinks to mask the taste. I don’t like sugary drinks, but I needed to get fluids in me so I don’t end up in the hospital. You have to do what you have to do to survive, I guess.
I also developed bad neuropathy in my hands and feet, and that came on suddenly. I was doing fine, but by cycle 10, the pain in my feet started to get bad. I was having trouble gripping things. I couldn’t wash the dishes. I would pick something up and drop it.
When the CT scan results came back, they found something in my liver… they didn’t think the cancer had come back, even though my CEA was up to 5 or 5.5.
Post-Treatment Follow-Up
After they finished, they did my scan and didn’t notice anything, so they sent me on my way and said they’d see me in six months. I wanted to see him in three, but he said he didn’t think that was necessary. I said I did, so he scheduled me for a three-month visit, which ended up being fine.
During my six-month visit, my CEA went up to 2 and that was my first flag. My CEA was still perfectly normal, but my CEA had never gone above 1.7. When I had the appointment with my oncologist, I told him this was concerning for me and he said it was a little concerning for him too. It’s a little bit of an increase, but it could still be normal, so he scheduled a blood draw after four weeks.
In four weeks, my CEA was 4.6 and that was abnormal for me. It was still within the normal range because anything under 5 is still normal, but I thought it was concerning. He said we could do another blood draw in four weeks.
By this time, it was around July and he said I wasn’t due for my CT until October. I said I didn’t want to wait until then.
Relapse
When the CT scan results came back, they found something in my liver. They thought it was a lesion because they said cancer usually looks like billiard balls but this looked like a zucchini. At that point, they didn’t think the cancer had come back, even though my CEA was up to 5 or 5.5, so something was going on.
They did an MRI and the results looked more like cancer. When they did a PET scan, the results looked even more like cancer. The biopsy confirmed it.
He said, “It’s looking more like it could be cancer.” They hadn’t done the biopsy yet at this point. He said, “If it’s cancer, there’s only a 20% chance you’ll make it to old age. That’s what the statistics tell us.”
I needed a doctor who I felt was on my side. I needed someone who I felt was going to fight for me.
Reaction to the Relapse
I walked out, got in my car, closed the door, and broke down crying. I was done with this oncologist. This is a horrific journey in itself. I needed a doctor who I felt was on my side. I needed someone who I felt was going to fight for me. I don’t care what the statistics say. There’s always somebody that’s on one side or the other.
Looking at Statistics
When you get these statistics, they mean something to doctors and researchers, but they don’t mean anything to people personally because you don’t know which side of that line you’re going to fall on. You could have the worst diagnosis and still survive.
I didn’t want to hear the statistics not because I was blind to it but because I knew it didn’t matter to me. The doctors are guessing which side of the line I’m going to end up on and I don’t want to hear their guess. I wanted to know if my treatment was working and if not, what my next steps would be.
She noticed the lymphatic system near my kidneys was getting larger so they thought that there was cancer there.
Switching Oncologists
I went back to the oncologist from whom I got a second opinion and she’s fantastic. She’s the best decision I ever made. One of the first things she did was get all of my scan results. She called my former doctor, requested all of my scan results, and sent them to a couple of different specialists so they could look at all of them. My new oncologist is on top of it and doing CT scans every eight weeks.
She noticed the lymphatic system near my kidneys was getting larger so they thought that there was cancer there. My first oncologist hadn’t even looked at that and it was one of the first things she noticed. It confirmed to me that I made a good decision.
I have this bad luck of getting things that look favorable but don’t end up being favorable. When I had my relapse, they looked at it and said I had a single liver lesion, which isn’t common. At that point, I was still considered curable.
Relapse Treatment
FOLFOXIRI Chemotherapy
She put me on FOLFOXIRI (folinic acid, fluorouracil, oxaliplatin, and irinotecan). I did FOLFOX a few times, but it wasn’t shrinking, so they added irinotecan and it started to shrink.
I went back on the full treatment for six months with very low node shrinkage but with slow growth.
Side Effects of FOLFOXIRI
I was miserable on oxaliplatin. It was terrible. I was sick all the time. The neuropathy in my hands had gotten better, but my feet had gotten worse. I could still do stuff with my hands, but my feet are pretty bad. I also had cold sensitivity, like not being able to eat cold food. Breathing in cold air was like breathing in shards of glass. My oncologist said they didn’t see any shrinkage with oxaliplatin, so she decided to remove it.
I had treatment until February 2023. It was shrinking and looking good, but it wasn’t going away, so they wanted to do surgery to remove the lymph system that had cancer in it. They did an ablation on one spot.
My oncologist wanted to do the ctDNA test to see if I had circulating tumor DNA in my blood. Four weeks later, that came out positive.
She said they usually wait 8 to 10 weeks before doing the first scan post-treatment, but she wanted to go ahead and do an MRI six weeks after surgery. She wanted to make sure because it looked like there was residual cancer.
Unfortunately, my liver lit up. They did a PET scan and there are a couple of spots now. I went back on the full treatment for six months with very low node shrinkage but with slow growth.
The difference between immunotherapy and chemotherapy is like night and day.
Joining a Clinical Trial
I started with an immunotherapy clinical trial in December 2023. The difference between immunotherapy and chemotherapy is like night and day. I’m not sick and tired all the time, so I’m able to go out and do normal activities. I feel like I’m able to have more of a normal life. It’s been fantastic, but I’m still fighting.
This is why it’s important to have a doctor who’s on your side. As soon as my recurrence happened, she went ahead and signed me up for every single trial that they offered. She didn’t ask me because she knew that these trials could have a year’s wait list. She figured that wherever I was, at least I was on the wait list. If a spot opened up, we could have a conversation about it.
When it comes to treatment, you do have a say. Your doctor may have a recommendation, but you have a say in what your treatment plan is going to be. You can tell them if you want an alternative.
A lot of people are intimidated, so they don’t want to tell their doctor what to do. It’s important to remember that your doctor is working for you. Find someone who’s working for you. My oncologist definitely was working for me.
Future Treatment Plans
My cancer is still growing. At any time, I can say I want to try something different. My oncologist and I have had those conversations. Because I’m on a trial, it’s not going to last forever. Unfortunately, I can’t be on this for the next five years. Having been off chemo, I’m hesitant about going back to it. I wanted to find out if there were non-chemo options we could explore, so we’ve talked about other options that are on the table.
With cancer, a lot of times, people sit and suffer in silence so by the time symptoms start rearing their big ugly heads, it’s often in the advanced stages.
Words of Advice
Know your body and trust your body. If something changes and there’s no warrant for that change, talk to your doctor. Don’t talk to your friends. Don’t go to social media. For everyone else, it might be normal, but if it’s not normal for you, it does warrant a conversation with your doctor. If it turns out to be nothing, you’re not out that much. I don’t think any doctor’s going to be mad that you wasted their time coming to them with your concern. Get rid of that fear. Know your body and know what’s normal for your body.
If anything comes up abnormal, don’t be afraid to go to your doctor and advocate for yourself. Tell them you want to find out what’s going on. With cancer, a lot of times, people sit and suffer in silence so by the time symptoms start rearing their big ugly heads, it’s often in the advanced stages.
People ignore the early symptoms. Maybe they’re busy, maybe they’re afraid, but I think primarily it’s because people think it’s not a big enough issue to warrant seeing a doctor. If it’s not normal for you, speak up and say something. The best thing that could happen is they tell you it’s nothing. The worst thing that could happen is they tell you it’s something, but maybe they found it before it’s something big and problematic.
Leah’s Stage 4 Non-Small Cell Lung Cancer with EGFR exon 19 Deletion Story
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Leah was diagnosed with stage 4 non-small-cell lung cancer (NSCLC) with EGFR exon 19 deletion at 43. Initially misdiagnosed with a post-viral cough and exercise-induced asthma, her persistent symptoms led to multiple doctor visits and treatments. Despite these efforts, her condition worsened, culminating in a CT scan that revealed metastatic cancer with a bone biopsy confirming stage 4 NSCLC.
Leah began treatment with Tagrisso (osimertinib), a targeted therapy that significantly shrank her primary tumor and healed bone metastases, and also underwent SBRT radiation. Although she faced side effects like gastrointestinal issues, a rash, skin and nail issues, and mouth sores, she remains stable with no progression in her lungs and continues her treatment at Vanderbilt-Ingram Cancer Institute.
Emphasizing the importance of self-advocacy and seeking second opinions, Leah recounts her insistence on further testing and comprehensive care. Her husband’s previous cancer diagnosis highlighted the necessity of thorough medical evaluation. She stresses the importance of enjoying daily life and finding inspiration and new beginnings even after a terminal diagnosis.
Name: Leah P.
Diagnosis:
Lung Cancer
Mutation:
EGFR exon 19 deletion (E19del)
Staging:
Stage 4
Symptoms:
Persistent dry cough
Shortness of breath
Heaviness in the chest
Coughing up blood
Weight loss
Right rib pain
Right shoulder pain
Treatments:
Chemotherapy
Targeted therapy
Radiation: stereotactic body radiation therapy (SBRT)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
I was born and raised in Louisville, Kentucky, but now live right outside of Louisville. I’ve been a stay-at-home mom for 19 years now. My oldest is 19 and I also have a 17 ½-year-old daughter and an almost 14-year-old son.
In December 2019 at 43 years old, I was diagnosed with stage 4 non-small-cell lung cancer (NSCLC) with a driving mutation of EGFR exon 19.
Pre-diagnosis
Initial Symptoms
In mid-September 2019, I started having persistent dry cough. I didn’t think anything of it, but after about two weeks, I went to my primary care physician because the cough wouldn’t go away. She diagnosed me with what she called a post-viral cough and put me on a steroid. In about a week or so, I started feeling better.
‘I’m feeling worse. Now I’m feeling tired. I’m still coughing, I have a heaviness in my chest, and I feel as if I may have pneumonia.’
Symptoms Worsen
A few weeks later, the cough came back. I also started having shortness of breath. I was a distance runner for many years and I would run 8.5-minute miles with my running group while talking the entire time. I started noticing that I could keep up my pace, but I couldn’t keep up the conversation without feeling winded.
When I went back to the clinic, I saw a different doctor and told him I felt a heaviness in my chest, especially when running. He told me that I had exercise-induced asthma. I know my body and I’ve never had this issue before, so why is this suddenly an issue?
I saw an allergist and he said it wasn’t asthma. I went back to the same doctor, who wasn’t my first choice but was the one available, and said, “I’m feeling worse. Now I’m feeling tired. I’m still coughing, I have a heaviness in my chest, and I feel as if I may have pneumonia. Can I have a chest X-ray?” He said I didn’t need it because I sounded like I was breathing fine. I asked him to do it to make me feel better.” He said, “I’ll do it, but I’m going to call you in 45 minutes and tell you it’s negative for pneumonia. This is either allergies or asthma.”
Forty-five minutes later, he called me and said, “You know what, I can’t believe I’m admitting this, but you have consolidation in your right lung, which means you have pneumonia.” He put me on a Z-Pak and a steroid.
Halfway through the Z-Pak, while at my daughter’s swim meet, I kept feeling worse and worse. When we got back home that night, I started coughing up blood. I thought this wasn’t right. On Monday morning, I called the doctor to let him know what was going on. He thought I needed a stronger antibiotic and more steroids. Every time I was on steroids, I felt better, but I still thought this wasn’t right.
I could hardly walk up the steps without having to sit down because I couldn’t breathe.
Hospitalized for Pneumonia
About mid-November, I went back to the doctor and said, “Can you please do another X-ray? Clearly, this pneumonia is not going away.” They did and it still showed right lung consolidation. They admitted me to the hospital for 4 days to be on round-the-clock IV infusion, high-powered antibiotics, and steroids. By the time I left, I felt pretty good because I had been on steroids through IV.
While I was there, the pulmonologist came in and said, “I’m going to do a bronchoscopy. We’re going in through your nose, down through your throat, and into your lung to look around with a camera and flush it with saline. If I see any masses or nodules, we’ll go ahead and biopsy them.” He did that and everything looked great.
He said, “There’s consolidation in your right lung. It’s residual pneumonia. Pneumonia can hang around for several weeks. I didn’t see anything unusual.”
Seeing a Nurse Practitioner
I could hardly walk up the steps without having to sit down because I couldn’t breathe. I was having right rib pain and right shoulder pain. I was coughing, lost weight, and looked awful.
I called the doctor’s office and they said they didn’t have any appointments, so I drove there and cried to the ladies at the front desk. I told them there was something seriously wrong with me and I needed someone to see me. They ignored me a bit, so I said, “I’m not leaving until someone sees me.”
They sent the nurse practitioner out, but that was more for a mental wellness check because I think they thought I was losing it. She sat down and listened to everything I had been through. I had written down dates and times. She said, “Something’s not right about this. You know your body. I’m going to send you to the hospital for an outpatient CT scan.”
She said, ‘There are some things on your CT that are a little concerning… we need you to go to the emergency room to be admitted to do further testing.’
Getting the CT Scan Results
I got a CT scan while I was in the hospital. After I got home, my original primary care physician called me and kept asking, “Are you having any back pain?” I said no. She asked a few other questions and I explained I had a cough, heaviness in my chest, and shortness of breath.
She said, “There are some things on your CT that are a little concerning. I’m not that worried, but we need you to go to the emergency room to be admitted to do further testing.”
Going to the Emergency Room
My mom and I went to the emergency room. After waiting for my husband to get there, we saw the doctor, who said, “Have you seen your CT results?” This was before test results arrived in real time on MyChart. He showed me the computer screen and said, “This is what we’re concerned about.” It said, “Lytic lesions present on T4 and T5. Highly concerning for metastatic cancer.”
I read that to my husband and mom, looked at the doctor, and said, “That means cancer that spread from where it started.” He said, “Yes, ma’am, you’re correct.” I said, “I don’t understand. What’s going on?” He said, “I don’t know, but we’re going to admit you and figure out where this cancer is coming from.”
They admitted me to the hospital and called in a pulmonologist because I had fluid in my right lung. They said that could be a sign of breast cancer or ovarian cancer, given my age, health, and that I had never smoked.
None of us knew that you could get lung cancer without smoking.
Getting a Thoracentesis
The hospitalist came in and called the pulmonologist to do a thoracentesis to remove some of the fluid from my lung to test for malignancy. Within 24 hours, the test came back as malignant, but it didn’t indicate where it was coming from.
Spinal Biopsy
They sent an oncologist over and he opted to do a bone biopsy of my spine because it was the easiest place to reach.
Diagnosis
Official Diagnosis
When the bone biopsy came back a day or so later, it said stage 4 non-small-cell lung cancer. You could have knocked us over with a feather because none of us knew that you could get lung cancer without smoking.
The oncologist told me that I had 6 to 12 months to live and that I needed to get my affairs in order. I was 43 with young kids. My husband asked him to leave the room, never come back, and to send a different oncologist.
Biomarker Testing
The second oncologist that came in was one of my husband’s fraternity brothers. He said, “I’m not going to say 6 to 12 months yet because you’ve never smoked and you’re healthy. You may have a biomarker or a gene driving this lung cancer, so we need to do biomarker testing.” It was the first time we ever heard of that. I tested positive for the EGFR exon 19 deletion mutation.
How can you tell me that I have metastatic cancer and I’m going to die?
Reaction to the Diagnosis
I burst into tears, thinking this couldn’t be happening. Metastatic cancer is what you die from. I ran the morning that I was admitted to the ER. Even though my breathing was so bad, I still ran 3 miles, so how can you tell me that I have metastatic cancer and I’m going to die when I’m still doing these things? I remember sitting there and crying, “My job is not done here. My job cannot be done here. I still have life to live. I still have kids to raise.”
Treatment
Tyrosine Kinase Inhibitor
I went to see the local oncologist and was prescribed Tagrisso, which is a targeted therapy (tyrosine kinase inhibitor) for my genetic marker. He had a sample, so I was able to start immediately.
The only places my cancer had spread was to my spine and pelvis. I had one primary tumor in my right middle lobe and about 13 bone metastases in my spine and pelvis. About a year into my treatment, all those bone metastases were sclerotic, meaning they were healing, and my primary tumor had shrunk by 70%.
SBRT Radiation
We wanted to be aggressive and asked what else we could do. They introduced us to a radiation oncologist at the end of November 2021. In the beginning of December, I had eight sessions of SBRT radiation, which is strong, high-powered, and precise, to the primary tumor in my right lung.
About a year into my treatment, all those bone metastases were sclerotic, meaning they were healing, and my primary tumor had shrunk by 70%.
Side Effects of Tagrisso
When you’re prescribed Tagrisso, they give you a laundry list of possible side effects. The most common are gastrointestinal, which is diarrhea, and what they call the Tagrisso rash. You can get it anywhere, but it’s primarily on your face and looks like bad acne.
The next most common side effects are skin and nail issues around nail beds because Tagrisso is so drying. You get splits around your nails and they become paper thin. You get little paper cuts, but they hurt worse in the fingers and toes. They also told me to expect some nausea.
When I first started taking Tagrisso, I didn’t have diarrhea as much as I got the rash. I also had zero appetite. Food didn’t taste right, so I was forcing myself to eat. That lasted about two weeks.
Another possible side effect but not as common are mouth sores. For whatever reason, those came with a vengeance. The first time I got them, they were everywhere in my mouth and on my lips. Some of them were the size of a quarter. They prescribed a specific mouthwash, but I met an oncology dermatologist who is amazing and gets things under control.
Importance of Self-Advocacy
When I was admitted to the floor, I was still in a state of shock, saying the same things over and over, and crying. The nurse practitioner who was getting me situated broke into tears. She apologized and said, “I’m so sorry. I’m being unprofessional. I have kids your age and I understand what you are going through. I must leave the room.” She came back and said, “I’m so proud of you for standing up to these doctors.”
In some ways, I was so disappointed in the medical community. What if I wasn’t educated? What if I didn’t stand up for myself? What if I didn’t have the financial means or the insurance to keep coming back? Those are the people my heart breaks for.
Advocate for yourself and if you don’t feel like you can, find somebody who will advocate for you.
Being dismissed has never been my style. I’m not confrontational, but once I’m passionate about something, I will stand up for what I believe in.
I knew I deserved better care than what I was getting. I knew there was something wrong and we were going to get to the bottom of it.
It’s very easy to put your head in the sand because you don’t want to hear the real story and get the diagnosis. You have to advocate for yourself and if you don’t feel like you can, find somebody who will advocate for you.
Importance of Getting a Second Opinion
My husband was diagnosed with prostate cancer 18 months before I was diagnosed. That cancer has been taking men in his family for years. Todd’s been cancer-free for 6 years now and he’s great. We knew the importance of seeking a second opinion when he was diagnosed. A second opinion is not a luxury. It’s not a maybe. We didn’t even have a conversation; we knew that was what we needed to do.
As soon as I was diagnosed, my husband was emailing and calling people he knew in the medical field. He doesn’t work in the medical field, but he was asking, “Where do we need to go? What is the best place? We don’t care if it’s international; tell us and we’re going.” That’s how we ended up at Vanderbilt-Ingram Cancer Institute.
I could sit here and dwell on the fact that more than likely, this will end my life earlier than it should or I can choose to live my best life one day at a time.
I’m not going to be in remission. I will never be cured. If you look at lung cancer statistics, 5% of people are still living in 5 years. From day one, I said I will be one of the 5%. Somebody has got to be one of them. Those statistics are so outdated and so skewed. There’s a whole new population of younger lung cancer patients who are being diagnosed under age 50 with genetically-driven mutations and have never smoked.
This puts us in a totally different ballgame than people who are at an average age of 65 with a history of smoking. That’s not to say that I’m any better or my lung cancer is more important. It’s just different. It’s like comparing BRCA breast cancer with HER2 breast cancer. They’re two different types of cancer and we must treat them differently.
Saying I’m not a smoker is not to isolate or make someone feel guilty for the choices they made. No one deserves cancer. I don’t care if they’ve smoked a thousand cigarettes. No one deserves this, but it does put us in a different position for treatment. Everyone should get a second opinion on something this important.
Living a Day at a Time
This is a cruddy hand to be dealt. I could sit here and dwell on the fact that more than likely, this will end my life earlier than it should or I can choose to live my best life one day at a time. That has always been my motto. Every day can be your best day. Some days are better than others, but enjoy the simple things, whether it’s getting to watch your child play a sport or simply having 45 minutes to yourself to read a book.
If I’m going to go through this, I want to be able to help the people behind me. A good friend and I were talking about this and we agreed that it’s always good to have someone ahead of you that you can look to for what’s coming down the road. It’s always good to have someone walking the path next to you who understands what you’re going through. It’s always good to have somebody behind you who you can help lead.
It’s not a matter of if I progress; it’s a matter of when… I’m still getting a response, so I’m technically on borrowed time.
Current Status
Since I started treatment, I’ve had four thoracenteses done to drain fluid. I’ve had numerous PET scans and CTs of my chest and abdomen, which I do every 3 months. I also switched my primary care to Vanderbilt University because it’s a comprehensive care center.
I have remained stable with no progression in my lungs at any of the sites where I had metastases. I take Tagrisso every day and I’m staying on that protocol until I progress. It’s not a matter of if I progress; it’s a matter of when. The average patient can take Tagrisso for 2-3 years with a response. I have been on it for 4 ½ years and I’m still getting a response, so I’m technically on borrowed time.
There’s no official next step. They would redo biomarker testing to make sure I did not develop any other mutations or it hasn’t changed to small cell lung cancer. At that point, we would discuss our next options. Do we radiate depending on how many spots I progress in? Do we add IV infusion chemotherapy to the oral targeted therapy? Do we add another targeted therapy? What we would do is unclear because lung cancer is ever-changing.
Words of Advice
Statistics are not always right and just because it statistically says something does not mean that you’re going to be that statistic.
I firmly believe in alternative modalities to help with the emotional, mental, and physical side effects. I see a Reiki therapist every eight weeks. I get a therapeutic massage every other month. I listen to sound bowls. Maybe they’re working, maybe they’re not. If it’s not going to interfere with your treatment and makes you feel better and live a better life, then it’s worth trying.
Second opinions are priceless. I’m trying to honor each day as a new day and a new gift. No one is guaranteed to live forever. For some of us, it’s going to be sooner than others. We need to remember that, enjoy the small things, and try not to sweat the little things.
Life is not over when they tell you that you have a terminal diagnosis. It’s just the beginning.
We taught our kids that there’s a difference between a small problem and a big problem. A small problem is when they forgot to put ketchup on your burger. A big problem is cancer. A small problem is being disappointed that you didn’t get an A on a test and you got a B; a big problem is cancer.
There are a lot of life lessons that come along with a cancer diagnosis. As many bad things come with this, there are some very good things. You find out there are some good people out there. You make new friends. You become an inspiration to people. Life is not over when they tell you that you have a terminal diagnosis. It’s just the beginning.