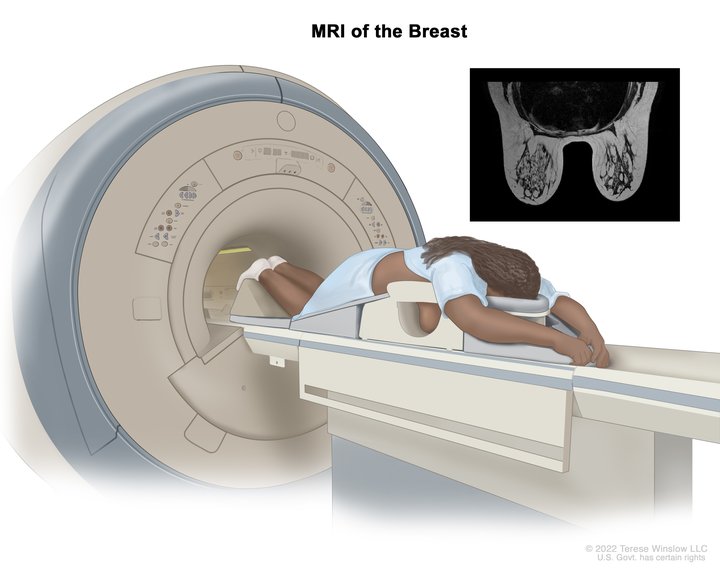
Sandy was diagnosed with stage 4 non-Hodgkin lymphoma in 2024. Her initial symptoms included persistent coughing, weakness, and shortness of breath. After weeks of worsening symptoms and ineffective treatments, an MRI revealed a large mass in her chest, which eventually led to the collapse of her left lung due to a massive tumor. A biopsy confirmed the diagnosis of lymphoma, a cancer that Sandy later described as a blessing in disguise due to its responsiveness to chemotherapy.
Treatment began immediately, consisting of six intense rounds of chemotherapy, each lasting five days in the hospital followed by two weeks of recovery at home. The process was physically and emotionally grueling, marked by extreme fatigue, weight loss, and hair loss. Despite these challenges, Sandy focused on mental resilience, which she believes was critical to her survival. She emphasized the importance of maintaining movement, even during the most debilitating moments.
To cope mentally with stage 4 non-Hodgkin lymphoma, Sandy turned to spirituality, meditation, and writing. She frequented a meditation garden where she found solace. Writing became a therapeutic outlet, leading to the creation of her book, Cancer Ramblings. Writing helped her process her experience and turn her pain into purpose.
Sandy celebrated her remission as a profound moment of liberation and gratitude, describing it as a second chance at life. She plans to monitor her health closely while maintaining a conscious lifestyle. She views sharing her story as a way to inspire others, providing hope and comfort to those facing similar challenges. Her key advice is to visualize a positive outcome and hold onto it as a guiding light through the darkest moments. Sandy’s enduring image was of herself running on the beach—a vision she ultimately realized.
Name: Sandy D.
Age at Diagnosis:
45
Diagnosis:
Non-Hodgkin lymphoma
Staging:
Stage 4
Symptoms:
Persistent coughing
Weakness
Shortness of breath
Treatment:
Chemotherapy (six rounds)
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: Severe fatigue, deep shoulder pain, ear pain with inflammation, abdominal and pelvic pain, bloating, early fullness, nausea, difficulty eating, inability to urinate despite feeling an urgent need, internal bleeding, delayed period/bleeding, intense whole‑body pain leading to collapse
Treatments: Surgeries (emergency laparoscopic surgery with left ovary removal), chemotherapy (R‑CODOX‑M/IVAC), immunotherapy, hormonal therapy (to protect the remaining ovary)
...
Symptoms: Feeling like holding breath when bending down or picking up objects from the floor, waking abruptly at night feeling “off,” one episode of fainting (syncope), presence of a large mass in the breast
Treatments: Chemotherapy, bridge therapy of chemotherapy and radiation, CAR T-cell therapy
...
Symptoms: Constant fatigue, tongue deviated to the left, abscess in right breast, petechiae on legs, night sweats, nausea and vomiting, persistent cough
Amrit was diagnosed with appendix cancer, or appendiceal adenocarcinoma (ApAC), in 2022 after enduring a series of vague and confusing symptoms. Initially attributing her severe migraines, abdominal bloating, skin changes, and irregular menstrual cycles to perimenopause, she delayed seeking medical attention. However, persistent bloating prompted her to visit her general practitioner, who conducted further tests. A scan revealed a mass on her ovary, leading to a referral to the fast-track cancer pathway. Further imaging uncovered a ruptured appendix and mucin accumulation throughout her peritoneal cavity.
Amrit underwent a grueling 9.5-hour surgery involving extensive procedures: the removal of her appendix, spleen, gallbladder, omentum, ovaries, and visible mucin deposits. This was followed by heated intraperitoneal chemotherapy (HIPEC) to address any residua cancer cells. Post-surgery, she learned her condition was malignant, requiring additional chemotherapy. Amrit described the physical toll of treatment, including neuropathy, extreme fatigue, and other side effects.
Throughout her appendix cancer experience, Amrit confronted significant mental health challenges, including post-traumatic stress disorder (PTSD). She found coping mechanisms in running, advocating for women’s health, and compartmentalizing for her children’s sake. She emphasized the importance of women advocating for themselves, recognizing symptoms, and prioritizing their health over societal and familial pressures.
Amrit now monitors her condition under a 10-year surveillance program. While her latest scans show no active disease, the possibility of recurrence remains. She continues to process her trauma, engage in physical activities like marathons, and share her story to inspire others to take control of their health.
Name: Amrit R.
Age at Diagnosis:
46
Diagnosis:
Appendiceal Adenocarcinoma (ApAC)
Symptoms:
Persistent migraines
Severe bloating
Rapid weight loss elsewhere but abdominal enlargement
Irregular menstrual cycles with heavy bleeding
Facial rash and skin changes
Treatments:
Surgeries: cytoreductive surgery with heated intraperitoneal chemotherapy (HIPEC); removal of the appendix, spleen, gallbladder, ovaries, and omentum
Chemotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Jessica was diagnosed with stage 2 Hodgkin lymphoma at 26. Before her diagnosis, she led an active and healthy lifestyle, enjoying time at the gym and with her fiancé. Her first symptom was a recurring red lump on her leg, which she initially dismissed. After the lump persisted and caused pain, she visited her general practitioner, who first changed her contraceptive pill. When the lump returned, her GP ordered a chest X-ray, revealing a mass in her chest.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Further testing, including biopsies and bronchoscopy, failed to confirm lymphoma until February 2024, when a video-assisted thoracic surgery provided a definitive diagnosis of stage 2 Hodgkin lymphoma. Jessica had no classic symptoms of lymphoma, such as night sweats or significant weight loss, and was shocked to learn she had a 19 cm tumor in her chest and surrounding areas.
Her treatment plan involved fertility preservation, followed by four rounds of intense chemotherapy. The physical and emotional toll was significant, including nausea, hair loss, and isolation due to her young age in the treatment unit. Despite these challenges, Jessica found support through social media, sharing her experiences to demystify cancer treatment and connect with others.
Now in remission, Jessica reflects on how the experience reshaped her perspective, emphasizing gratitude, resilience, and the importance of seeking medical advice for unexplained symptoms. She continues to advocate for awareness and hopes her story inspires others to face cancer with courage.
Name: Jessica H.
Age at Diagnosis:
26
Diagnosis:
Hodgkin lymphoma
Staging:
Stage 2
Symptom:
Recurring red lump on the leg (painful, swollen, hot to touch)
Treatment:
Chemotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
In 2020, at the age of 33, Calvin was diagnosed with stage 1 lung cancer after enduring four years of misdiagnosed symptoms, including frequent illness and breathing difficulties. His initial symptoms began in 2016, with a severe bout of illness in Germany leading to a pneumonia diagnosis. Subsequent cycles of sickness and treatments yielded no lasting improvement, and he was misdiagnosed with adult asthma. Despite consulting various specialists, it wasn’t until 2020 that further tests, including X-rays and pulmonology consultations, revealed a potential cancer diagnosis.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
A biopsy confirmed a mass in his left lung, necessitating immediate surgery. In September 2020, his left lung was removed entirely via pneumonectomy. Recovery was arduous, requiring relearning basic functions such as walking and urination. The emotional toll on his family, particularly his wife who assumed caregiving responsibilities, was profound. Determined to recover for his two-year-old daughter, he sought trauma therapy to navigate the psychological challenges.
Living with one lung transformed his life. He now prioritizes low-altitude, climate-controlled environments to manage breathing and accommodate his family’s activities. He has since welcomed a second child and adjusted to his new reality with resilience. His advice underscores the importance of self-advocacy in medical care, urging others to trust their instincts, persist through diagnostic hurdles, and seek second opinions when necessary.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I was diagnosed with stage 1 lung cancer in 2020 at the age of 33.
Initial Symptoms
In 2016, I was traveling quite a bit for work. After a long flight to Germany, I wasn’t feeling too well and ended up bedridden for four days in a hotel room. When I arrived home, I immediately went to the doctor with the medication they gave me in Germany. My doctor in Denver looked at it and said, “It looks like you had pneumonia. Let’s treat you for that and run some tests.” After the tests, she said, “You have adult asthma. You had asthma as a kid, now you have adult asthma.”
In 2017, I kept traveling. I continuously went through a three-month cycle. I would get sick for a week or so in the first month. In the second month, we would change medications. In the third month, I’d feel okay. I kept traveling for work until COVID hit.
We went up to somewhere above Vail where the elevation was around 7,000 feet and I couldn’t breathe.
Calvin, Stage 1 Lung Cancer Patient
In April 2020, we were at an allergy and asthma center getting my daughter tested because she’s allergic to peanuts. I asked her doctor, “Can I get a meeting with you? I supposedly have had adult asthma for the last few years, but it’s not getting better. We’re not doing anything because of COVID and I’m still getting sick.” She ordered an allergy test, some asthma tests, and X-rays, and then told me to go to a pulmonologist.
After the pulmonologist ran some tests, she said, “You have one of three things. You have a fatal lung disease and you’ve got 6 to 12 months to live, you have cauliflower lung, which is what a lot of people get from vaping, or you have lung cancer. It’s the most probable option, so we have to do some tests.” This was around April and May 2020, so it wasn’t the easiest time to get in and out of medical centers. It took a while, but I was able to do all these different tests.
We went camping because that’s what we did during COVID. Since I lived in Denver, we went up to somewhere above Vail where the elevation was around 7,000 feet and I couldn’t breathe. I thought, “How is this possible? I’m not sick. I don’t have COVID.” We were testing all the time since we had a two-year-old then. We came back down and they said they needed to do a biopsy of my lung.
Diagnosis
They scheduled the biopsy for an hour and five minutes. As soon as they put the camera in, they saw a mass sitting over my left lung, so they stopped and pulled the camera out of my throat. The next thing they said was, “You have to come back in tomorrow. We have to remove this mass. We’ve done this a bunch, so we know what it is. We can’t tell you officially, but based on the color and the type, it looks exactly like cancer. We’ll have to take it out tomorrow. We weren’t prepared for this mass. We thought we were going to do a biopsy.”
The next day, they removed the mass and said they would get back to me within 7 to 10 days. The next Friday was the Friday before Labor Day weekend. My wife and I were sitting at home, twiddling our thumbs. It was the eighth day and we hadn’t gotten the test results back. We’re hammering our pulmonologist and everyone else to give us answers. At 5:07 p.m., the chief of surgeons called and said, “Hey, I’m sorry that it’s so late. We have the results. You have stage 1 cancer, but it’s the best outcome and it’s the easiest thing for us to treat.”
‘In 13 days, your life will never be the same. You need to grab your family, go wherever you want… you’re never going to be able to breathe this way again.’
Discussing the Treatment Plan
When we walk into his clinic, he has everything decked out. He said, “Here’s the deal. In 13 days, you’re going to have surgery. We’re taking out your entire left lung. Here’s what we’re going to do,” and he mapped it all out. We asked, “Do we have a second opinion on this?” He said, “Look, I’m on the board of Colorado with your oncologist and pulmonologist. We’re the team. This is what you’re going to do. I got you booked in because I’m the chief of surgeons here and I own the books. This is your appointment time. I’ll see you in 13 days on Thursday.”
Then he asked, “Where do you work?” I told him where I work and he asked, “They’re not going to shut down without you, are they?” I told them that they’d be fine. He said, “Here’s what you’re going to do. You’re going to walk out of this office. You’re going to call your boss and say, ‘I’ll see you in six months,’ or whatever time you can do because in 13 days, your life will never be the same. You need to grab your family, go wherever you want, see the leaves change, and go to altitude because you’re never going to be able to breathe this way again.” The mass was moved so I could breathe.
I was at the point that a lot of people go through, which is, “Wait, I feel amazing. You removed the mass. Can I wait for science? Can I wait for something to come in and fix this?” I asked him that and he said, “If you do, you’ll end up with stage 3 or 4 cancer and you will die. Don’t be an idiot.”
My wife went into full caregiver mode. It’s missed how much caregivers give, how much they put in, and what they’re going through.
Calvin, Stage 1 Lung Cancer Patient
Reaction to the Diagnosis
At the time, our daughter was two. My immediate thought was: what are the next steps? Lung cancer is thought of as fatal. In the lung cancer community, we talk a lot about the stigma that comes with it. I’ve never smoked. Then my thoughts went to, “What did I do wrong? What did I do to cause this? How do I stop it?” You can’t. At that point, it’s done. Finally, it came down to, “Is my wife going to be stuck raising our daughter by herself?”
There’s a seven-month part of my life that is completely blacked out, especially after surgery and the meds I was on. I don’t remember a lot of it, but I was in a lot of shock. One of the first things I did was to reach out and find a trauma therapist to get ahead of it because I knew it was going to be bad. My wife went into full caregiver mode. It’s missed how much caregivers give, how much they put in, and what they’re going through.
I’ve never only lived with one lung. I don’t know what the reality of that is.
Calvin, Stage 1 Lung Cancer Patient
Pneumonectomy
They took out my entire lung. I’m knocked out and my wife had to go through all of these emotions, which is way worse than anything in the moment. It was rough for her. They put me in the ICU for a day and a half and then I was in a regular room for five days.
I didn’t know what to expect as a young 30-year-old athlete who played sports his entire life. You get through injuries and it hurts, but you know you’ll get through it. I’ve never had major surgery. I’ve never only lived with one lung. I don’t know what the reality of that is.
Recovering from Surgery
I had to relearn how to walk, to urinate, and to do everything. Nothing was working. It was difficult having to relearn those, but not being able to see anyone else, particularly my daughter, was more difficult. My mom sat in the parking lot because she couldn’t come in since they only allowed one person.
If I had known four years prior when I first was getting sick, if they had immediately diagnosed and figured it out, I don’t know if I would have cared as much because I didn’t have my daughter then. Recovering from surgery was all about needing to get back to as best as I could be because I’m her dad. I’m the one that she plays with. I needed to be able to still do these things.
If you believe something is wrong, if you listen to your body and something is different, go through every process to figure it out.
Calvin, Stage 1 Lung Cancer Patient
Living with One Lung
Vacations are different. Getting to sea level is always amazing. We plan our trips based on where I can operate well. For example, I can’t go to Mexico anymore because I can’t breathe. I need to sit in an air-conditioned room because that’s where I can breathe.
I have a one-and-a-half-year-old son now. I can sit and throw a ball with him and play horse, but it comes with a lot of breaks. We make sure that what we do is essentially climate-controlled. It’s different and you have to work through it.
Words of Advice
If you believe something is wrong, if you listen to your body and something is different, go through every process to figure it out. Don’t be arrogant or cocky about where you believe you are and don’t blindly trust every medical professional you find. Some rules and things get in the way of how you can get the testing you need. Don’t go through the course because that’s what they tell you to do. Get hungry. Find the information. Advocate for yourself.
From Hospice to Hope: Eugenia’s Fight Against Stage 4 Lung Cancer
Eugenia was diagnosed with poorly differentiated stage 4 non-small cell lung cancer at the age of 46. Her symptoms began around Christmas 2018 with a lingering illness, followed by chest tightness and coughing up blood. She initially dismissed her symptoms, but after experiencing significant bleeding, she sought medical attention in February 2019. Despite her concerns, her doctor initially attributed her symptoms to anxiety. However, blood tests indicated abnormalities, prompting further scans that revealed a 5 cm mass at the apex of her right lung and another tumor compressing her bronchi.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Initially skeptical of the non-curative treatment options presented to her, Eugenia sought alternative medical opinions. When her condition worsened, she finally met an oncologist who admitted her for further evaluation. A biopsy was performed but was later deemed ineffective due to an error in sampling. By this time, her tumor had expanded, obstructing 95% of her trachea, leading to severe respiratory distress.
Doctors started her on chemotherapy in June 2019, administering small doses due to concerns that the tumor might break apart and cause fatal complications. Despite the treatments, her condition continued to deteriorate, culminating in respiratory failure by mid-July. She was transferred to a higher-level care center where she underwent brachytherapy, external radiation, repeated cryotherapy, and CyberKnife treatment. These interventions successfully removed the tumor after nine days of intensive procedures.
During her recovery, another setback emerged: a bowel obstruction that required emergency surgery. The obstruction turned out to be cancerous, escalating her condition to stage 4 non-small cell lung cancer. Following this diagnosis, her treatment plan was abruptly halted, and she was placed in hospice care. Despite this, she remained determined to fight for her life.
Eugenia learned about an immunotherapy drug and insisted on trying it, despite her oncologist’s reluctance due to her frail condition. With limited time left, she convinced her doctor to administer the treatment, starting the immunotherapy on August 29, 2019. Over time, this treatment proved to be the key factor in her survival. Five years later, Eugenia remains alive, defying the terminal prognosis she was given. She challenges the notion of “incurable” cancer and shares her experience to inspire others to advocate for their care.
Surgeries: tracheostomy & emergency bowel obstruction surgery
Immunotherapy
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Adenoid Cystic Carcinoma: The Rare Cancer That Almost Went Undiagnosed
Alyssa was diagnosed with adenoid cystic carcinoma in September 2024. Her diagnosis followed months of unrelenting jaw pain that was repeatedly dismissed as a TMJ disorder or stress. Alyssa’s first symptoms emerged during her third pregnancy, but the pain persisted postpartum. Being a dental hygienist, she knew her symptoms did not align with a TMJ disorder. Despite her advocacy, she encountered multiple misdiagnoses and ineffective treatments until she insisted on specific imaging, which revealed a tumor in her parotid gland.
Alyssa underwent a biopsy, which was inconclusive, prompting her to proceed with surgery. The operation lasted over four hours as the surgeon carefully removed the 3 cm tumor entangled with her facial nerve, preserving nerve function. Post-surgery, Alyssa faced radiation therapy, undergoing 20 sessions at Huntsman Cancer Institute. The treatment, though effective, caused side effects like dry mouth, taste changes, sore throat, and significant skin irritation.
Her experiences with adenoid cystic carcinoma were mentally taxing, intensified by anxiety stemming from prior health challenges, including a near-fatal postpartum infection and a life-saving hysterectomy. Alyssa leaned on therapy, visualization techniques, and her faith to navigate the isolation of radiation and the emotional toll of her journey.
She emphasizes trusting one’s instincts and knowing one’s body while advocating for persistence in seeking answers. Despite challenges, Alyssa remains resilient, finding strength in her family, faith, and the hope of inspiring others to persevere.
Name: Alyssa N.
Age at Diagnosis:
31
Diagnosis:
Adenoid Cystic Carcinoma
Symptoms:
Persistent jaw pain
Lightning-like facial pain during the first bite of meals
Treatments:
Surgery: tumor removal
Radiation
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Symptoms: Sore on the tongue, which caused pain during eating and speaking; changes in the color and texture of the tissue where the sore was located Treatments: Surgery (partial glossectomy, radical neck dissection, reconstruction), radiation
...
Thriving with Multiple Myeloma: Bispecific Treatment Options
Multiple myeloma patient advocate Kenny Capps speaks with multiple myeloma expert Dr. Carl Ola Landgren of the University of Miami Sylvester Comprehensive Cancer Center as he shares actionable insights on the latest treatments, effective side effect management, and innovative therapies. Gain the knowledge you need to thrive with multiple myeloma and take charge of your journey.
Learn about treatments like CAR T-cell therapy and bispecific antibodies. Discover effective strategies for managing treatment side effects to improve your quality of life. Get expert tips for living well and staying active while managing multiple myeloma. Understand how to tailor your treatment journey with the latest medical advancements and expert advice.
Tiffany Drummond: I’m a patient advocate with over 20 years of experience in cancer research. My journey as a caregiver began when my mother was diagnosed with endometrial cancer in 2014. I quickly realized the challenges of finding resources, support, and shared experiences, and I’m committed to helping others avoid similar difficulties, no matter the condition.
At The Patient Story, we create programs to help you figure out what comes next. Think of us as your go-to guide for navigating not only the cancer journey but your overall health journey. From diagnosis to treatment, we’ve got you covered with real-life patient stories and educational programming with subject matter experts. I’m here to help you and your loved ones best communicate with your healthcare team as you go from diagnosis through treatment and survivorship.
We want to thank our promotional partners for their support. Because of you, our programming reaches the audience who needs it. I hope you all find this program helpful, but please keep in mind that the information provided is not a substitute for medical advice.
We have two amazing guests that I want to introduce as we talk about the latest treatment options for multiple myeloma. Dr. Carl Ola Landgren is a hematologist and oncologist, professor of medicine, and division chief of myeloma in the Department of Medicine. He is the director of the Sylvester Myeloma Institute at the Sylvester Comprehensive Cancer Center and co-leader of the Translational and Clinical Oncology Program at the University of Miami. We are so happy to have you, Dr. Landgren. Thank you so much for taking the time to be with us. Our moderator will be Kenny Capps, a multiple myeloma survivor and thriver.
Kenny Capps: Thanks, Tiffany, I’m honored to be your moderator. I’m the executive director of Cancer Active, a nonprofit organization dedicated to empowering those affected by cancer to live active and fulfilling lives. I’ve been on my journey with multiple myeloma since 2014. I understand many of the challenges that patients must navigate.
I was diagnosed relatively young at the age of 42 and have lots of bone involvement, spinal compression, fractures, and lesions. I’ve undergone infusions and a bone marrow transplant. I’ve lost count of how many bone marrow biopsies I’ve had. In 2023, I relapsed, changed therapies, and added radiation treatment to the list of things I’ve never done before.
I did all this while raising three kids, training 30 to 70 miles a week, running 1,200 miles across the state of North Carolina, and experiencing all the celebrations and heartbreaks that come with life, regardless of whether you’re treating cancer or not. I’ve had many experiences and a lot of education as an athlete, a coach, an attorney, and a father, and 10 years ago, I combined all of those experiences to become a patient advocate and a Cancer Active leader.
We’re fortunate to have one of the leading voices in multiple myeloma research and treatment with us. Dr. Landgren is not only a pioneer in advancing care for this disease but also deeply committed to translating cutting-edge science into real, human-centered solutions for patients like you and me. His work has helped reshape how we understand and treat multiple myeloma, giving us more options and more hope than ever before.
This conversation is all about you. We’ll explore the latest in multiple myeloma treatment and emerging research, and, most importantly, answer your questions in a way that makes this topic understandable and actionable. It’s my privilege to introduce our distinguished guest, Dr. Carl Ola Lindgren.
Dr. Carl Ola Landgren: Thank you very much for having me. It’s a great pleasure and a great honor.
What Does Relapsed/Refractory Mean in Multiple Myeloma?
Kenny: Our audience is pretty savvy, but for those unfamiliar with the term relapsed or refractory in the multiple myeloma setting, could you break down what that means?
Dr. Landgren: Relapsed and refractory refers to the multiple myeloma disease becoming active again. Someone who is newly diagnosed would typically receive combination therapy with or without transplant and with continued therapy, which we also call maintenance therapy. Over time, unfortunately, the majority of patients will have the disease become active again and this is because we do not have an established cure for the disease.
In 2025 and onwards, many patients can live for 10 to 20-plus years and there will be patients who will not have their lifespans shortened, which is what the field is going for. For the most part, the disease will be managed as a chronic disease as we try to develop definitive cures.
If there is reappearance of rising levels of proteins in the blood, if other clinical suspicions are going on that would trigger additional radiological assessments, like PETs, PET/CTs, or MRIs, or if we do bone marrow biopsies and see that there is more disease, then that would be consistent with the disease becoming active again.
When we do clinical trials, we have rule books for what is what. We have a rule book for what’s called a partial response, what’s a complete response, what MRD negativity is, and we also have rules for what progressive disease is and how to capture that. If you don’t have a common language, we cannot compare the results across different trials, so that’s very important. We worked on that as a community for over 20 years.
In the setting of those rules, a relapsed/refractory disease refers to a situation when a patient has rising levels of markers by these definitions we have, either while being on a given therapy or if it happens within 60 days after stopping therapy, then that would also count as a relapsed/refractory state.
We looked at drugs that had a good benefit, were not too toxic for the patient, had no other contraindications, and tried to see how we can partner them with other drugs than we did the previous time we gave them.
Dr. Landgren
Kenny: About refractory, does that mean that they are unable to continue along that line of treatment?
Dr. Landgren: The word refractory carries probably more focus on things that are not true, which is that you cannot go back and use that treatment. In reality, what it means is that right now, it is not the optimal therapy to use going forward. You can revisit and use that drug in the future, maybe in combination with other drugs at a later time point as what we very frequently do. We recycle the drugs.
An example could be you use a proteasome inhibitor, an IMiD (immunomodulatory drugs), and a steroid with a CD38-targeted antibody as a combination therapy and you give that for a certain number of cycles. You may collect stem cells, give more cycles, do a transplant or not, and go to a maintenance therapy. You may have an IMiD at a lower dose with the CD38-targeted antibody and eventually, you may step down to a single drug IMiD.
Many years later, there’s a reappearance of protein in the blood. Could you go back and use a proteasome inhibitor? Yes, you can. Could you go back and use the CD38-targeted antibody? Yes, you can. Is it the best thing to use that same IMiD at the same dose level? Probably not because the disease was able to grow through that. What about increasing the dose? Probably not the best option right now, so maybe switch to another IMiD or some other drug. Then you can overcome this reappearance or relapse and get many more years with the same benefit. You get rid of the disease and keep the disease from becoming active.
If the disease comes back again, could you not ask the same question? Could you go back to those same drugs, including the first IMiD? I would think yes. You could think about using the same drugs over and over again, but there are so many new drugs coming to the field. Many times, we are going to new mechanisms of action as the next step forward.
At some point, when we have used all the different mechanisms of action, we will go back, recycle, and use them in different combinations. We looked at drugs that had a good benefit, were not too toxic for the patient, had no other contraindications, and tried to see how we can partner them with other drugs than we did the previous time we gave them.
Kenny: When you’re saying that, what I think about is lenalidomide, bortezomib, and dexamethasone, and then a maintenance therapy after a bone marrow transplant, but a patient might stop responding to 5 or 10 mg of lenalidomide at some point in the future. You’re saying that they could switch over, so maybe pomalidomide at some point as a substitute, but that doesn’t discount the possibility that lenalidomide might be a solution for them in the future.
Dr. Landgren: That’s exactly right. If you look at how these drugs were developed, they were developed for certain indications. You mentioned pomalidomide as the next move and that’s the example I gave between the lines. I didn’t mention the drugs, but you filled in the blanks and the drugs you gave were probably the drugs that, for the most part, would fit with the example I gave.
We do not have an established cure, so if you look at the population databases that are currently available, unfortunately, the majority of patients will have the disease become active again at some point.
Dr. Landgren
Pomalidomide was developed in 2006 and was given to a patient that lenalidomide failed and that’s how the FDA approval was granted. It’s a logical thing to do. What hasn’t been done in a trial is to go back and revisit lenalidomide at a later time point. Why is that? Once the drugs are approved, they are commercially available and we can prescribe them.
It addresses an important topic of the so-called real-world evidence and that’s where people like me come into play. I have been a doctor for 29 years. I’ve treated probably thousands of patients and used all the FDA-approved drugs. I’ve worked on very many clinical trials, phase 1 and phase 2 studies, and also some of the phase 3 trials. I have a lot of experience with these drugs.
When people like me use the drugs every day in our clinics, we learn how to use them in a recycled manner for patients who have the disease coming back. Sometimes we document and many times, we talk about it. When I’m at meetings, many colleagues who may see fewer patients could come up and get the advice. We try to share our experiences with each other and that’s how we help each other as a community.
What Percentage of Multiple Myeloma Patients Experience Relapse or Become Refractory to Initial Therapy?
Kenny: Given the evolving landscape of myeloma treatment, what are the current estimates for the percentage of patients who experience relapse or become refractory to initial therapy? How do factors, such as patient age, disease stage, and genetic risk profile, influence these rates?
Dr. Landgren: We do not have an established cure, so if you look at the population databases that are currently available, unfortunately, the majority of patients will have the disease become active again at some point. There’s a small group of patients whose disease doesn’t come back and that’s an important piece to point out that the disease is curable.
The problem is that the disease is very different from patient to patient. We call it genomically heterogeneous, which means it’s not the same disease in every patient. When we profile the disease, we can see that if we perform whole genome sequencing, the average patient has a few thousand mutations and you can also see alterations in the immune system. With a disease that is so different from patient to patient, it’s not surprising that when you give the same therapy to everyone, the outcome would be different and that’s why we say there are different prognoses.
As the treatment gets better and better, more and more patients could benefit from the therapies, so there will be fewer patients who will have the disease return sooner.
Dr. Landgren
People have talked about high risk or standard risk in this very setting. The concept of high-risk disease is a moving target. If you have a weaker treatment and you treat 1,000 patients, more patients will not benefit from that treatment because the disease biology could be stronger than the therapy over time and it will come back sooner.
As the treatment gets better and better, more and more patients could benefit from the therapies, so there will be fewer patients who will have the disease return sooner. For that reason, the so-called high-risk group is shrinking and it’s always in the light of how you treat. Ultimately, with the best available therapy, there is no high-risk disease and we could envision a scenario of a cure.
The rate of relapse is in the light of how we treat, but we still don’t have a definitive cure, so statistically, the majority of patients will have their disease coming back. What’s different at this time compared to 10 or 20 years ago is the duration of the benefit of therapy is drastically different.
The disease will probably come back for the majority of patients, so we are trying to develop curative strategies that are definitively curative.
Dr. Landgren
When I was in fellowship 25 years ago, the time from diagnosis to a patient passing away from the disease could be only one or two years. I have many patients who are 20 years out and doing great, and many of those patients will not die due to myeloma. We will all die at some point, but many people will probably die with myeloma not from myeloma, which is a huge change.
Kenny: Yeah, and that’s a phrase I hear more and more, which is good to hear.
Dr. Landgren: If we can keep the disease away and people can have a good quality of life and no shortening of lifespan, that’s a huge deliverable. For many patients, we’re already at that point, but there may have to be changes in treatment. The disease will probably come back for the majority of patients, so we are trying to develop curative strategies that are definitively curative.
Does Traditional Chemotherapy Still Play a Role in the Relapsed/Refractory Setting?
Kenny: You mentioned quality of life and that’s impacted by the progression of the disease, side effects from treatment, or the psychosocial challenges that patients have to deal with day-to-day that negatively impact how they feel and what their life is. As you mentioned, the treatments over the past decades have changed dramatically. In the context of relapsed/refractory multiple myeloma, does traditional chemotherapy still have a role to play in the world of IMiDs, CD38 treatment, bone marrow transplants, and CAR T-cell therapy?
Dr. Landgren: We don’t want to stop using drugs that we know work until we have a definitive cure. You want to keep all the different options. We want to have all the doors open. But the order and the priority of the different therapies will probably continue to change.
When I was in fellowship, the therapies were very, very inferior. The overall survival was one to two years. The remission rates were in the single digits. These days, if I treat, I would achieve remission rates of 90 to 95-plus percent. I have MRD negativity rates in my newly diagnosed patients of over 70%.
Will that mean that chemotherapies will go away? I don’t think so. Not until we have a cure. Potentially, the role for these therapies will shift that they will be options if patients have later line relapses.
Dr. Landgren
For the majority of my patients, I don’t use any chemotherapy. For many years, we have also explored harvesting the stem cells and holding them, so you could also not go for a transplant. Transplant is chemotherapy. In the United States, it’s called transplant, but in Europe, it’s called high-dose chemotherapy and it is chemotherapy because it’s melphalan chemotherapy. The stem cells are not part of the treatment. They’re a way to recover from the chemotherapy.
There will be a shift away from chemotherapy as we see more and more immunotherapies coming. The CD38-targeted antibodies are coming at full speed, but there are also new antibodies with new targets coming. In 2024, the FDA approved CAR T-cell therapy for the first relapse.
Will that mean that chemotherapies will go away? I don’t think so. Not until we have a cure. Potentially, the role for these therapies will shift that they will be options if patients have later line relapses. If you have immunotherapies upfront and if there is recurrence, there are more immunotherapies. If there is a recurrence again, there are more immunotherapies. Eventually, maybe the chemotherapies will be part of it.
There will be patients who will be outliers from this principle. Chemotherapy drugs are the most tumor-sensitive drugs. Some patients to whom we give immunotherapies don’t do as well. Those patients are a minority, but there are patients like that, so it’s good to have options.
Bispecific Antibodies vs. CAR T-cell Therapy
Kenny: Could you discuss further the differences between bispecific antibodies and CAR T-cell therapy?
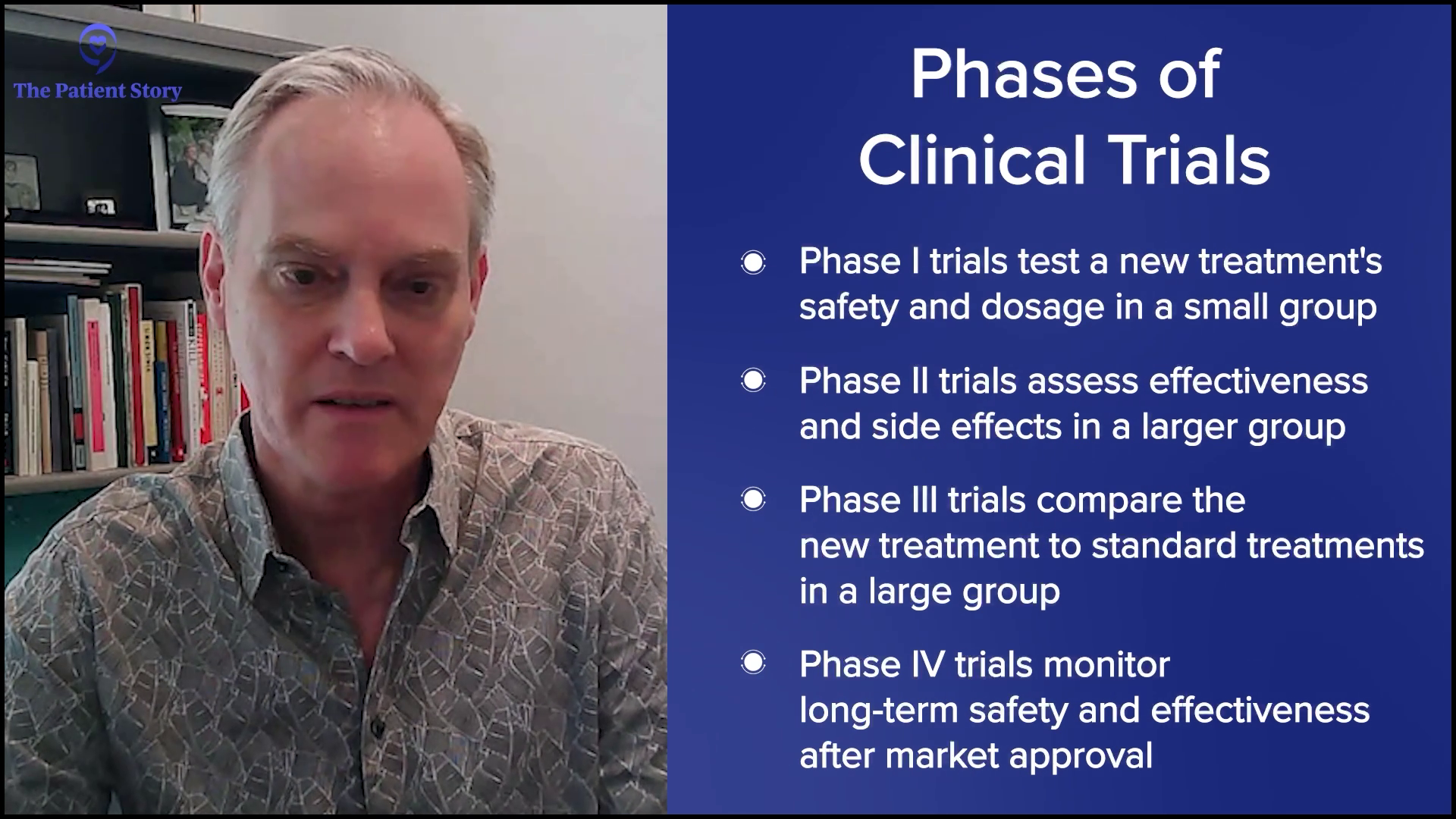
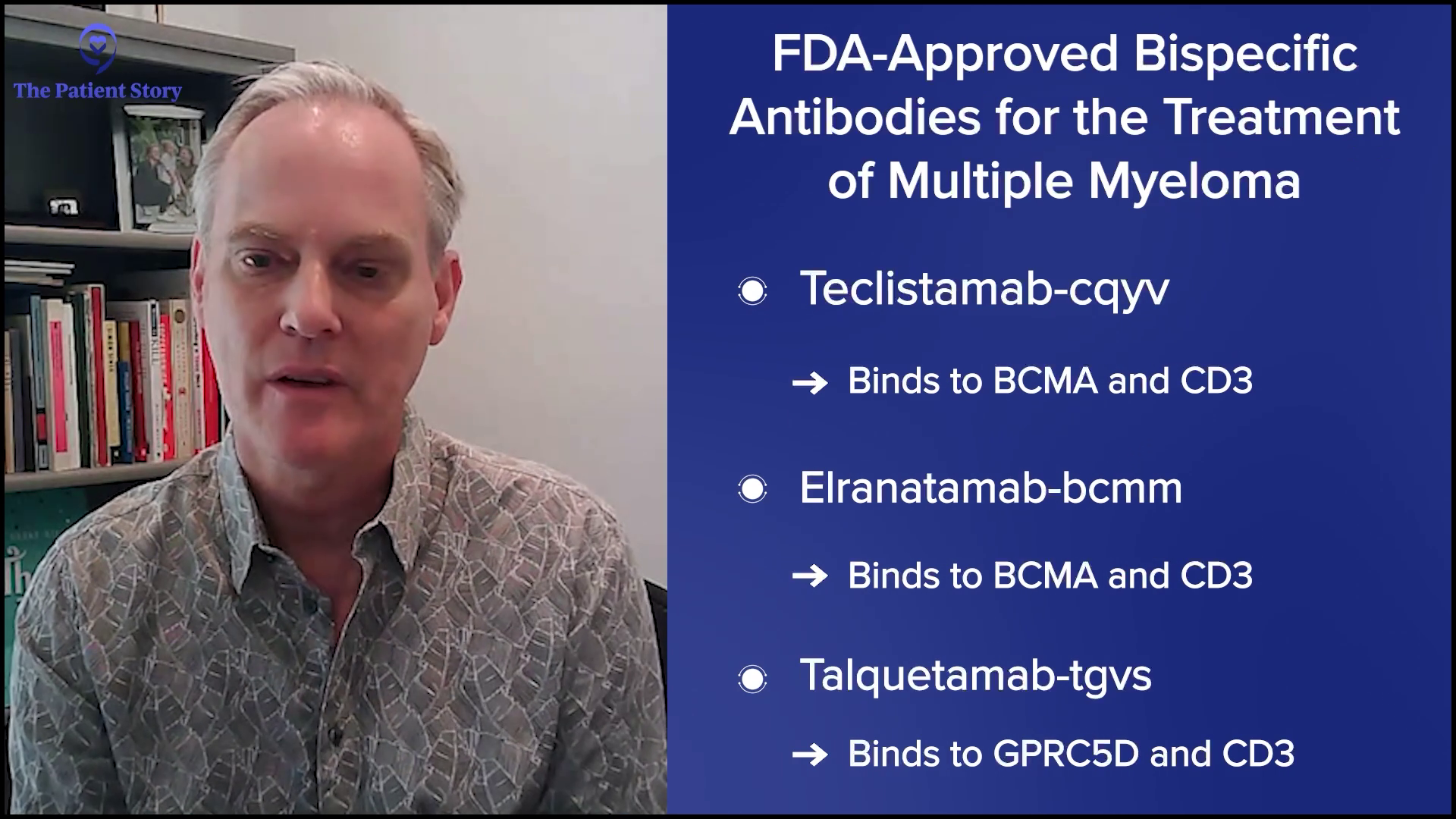
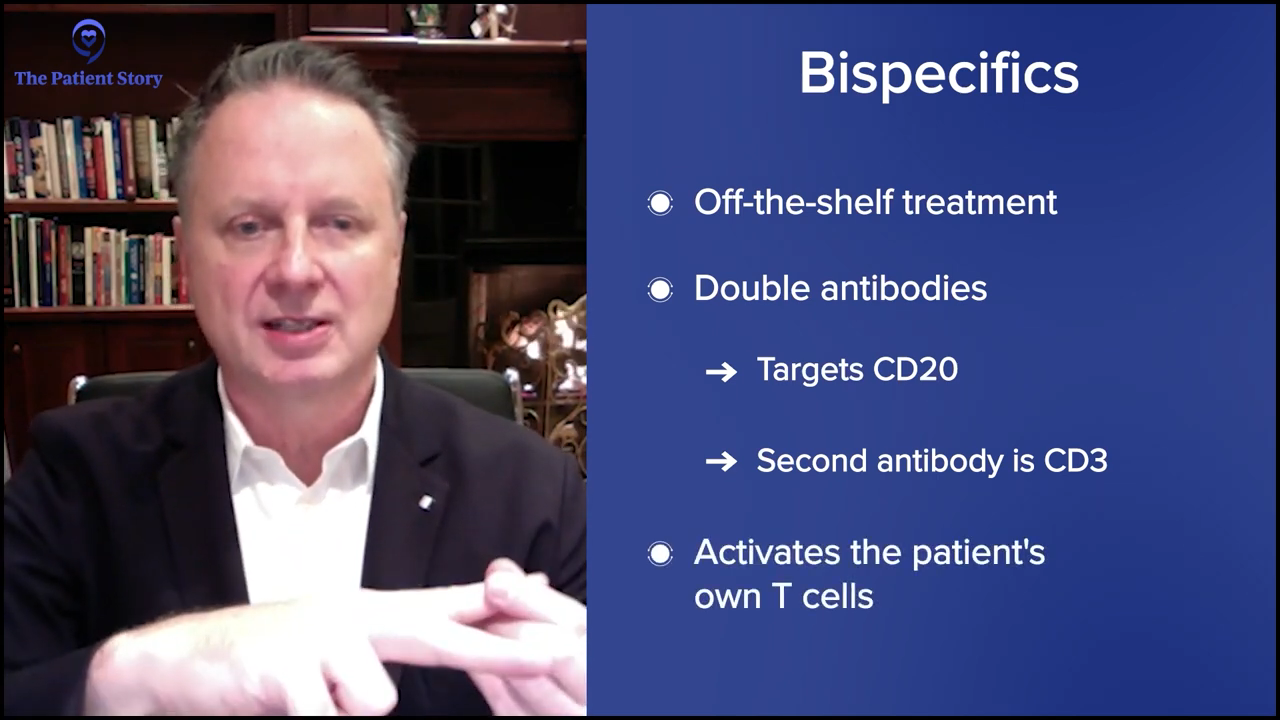
Dr. Landgren: A bispecific antibody is exactly what the name tells you: it’s bi, so it’s two, and it’s specific, so it’s specific in the sense that it goes for myeloma and it’s linked towards immune cells, T cells. The way these antibodies are engineered is they have two heads. One head binds to a protein on the surface of the myeloma cells and the other head binds to a surface marker on the T cell. On the T cell, the marker is CD3. For the myeloma cells, there are currently two approved antibodies that have two different targets: BCMA (B-cell maturation agent) and GPRC5D.
A bispecific antibody is exactly what the name tells you… One head binds to a protein on the surface of the myeloma cells and the other head binds to a surface marker on the T cell.
Dr. Landgren
There are three bispecific antibodies approved for multiple myeloma. All of these antibodies bind to CD3. They bring the T cells to the antibody, so they hold on to the T cell, and when they grab the myeloma cell with the other marker, the myeloma cell is now neighbors with a T cell and the T cell will then do its job of killing the myeloma cell. That’s how bispecific antibodies work.
CAR T cells is an acronym for chimeric antigen receptor T cells. T cells circulate in the blood and you can take them out from the blood of a person. They are not stem cells. They’re not the type of cells you would collect for a transplant. These are circulating immune T cells. You can take them out and send them to an approved facility. They will do a transduction of these T cells, which means they are being exposed to a genomic vector that will change the DNA in these cells. They will insert certain information that contains instructions for these T cells to do things that they normally wouldn’t do, which is to develop an antenna on their surface and that is what the receptor is. They are the same T cells plus the instruction that says to make this receptor on their surface. Other than that, they do the same job they normally would do. You feed them with glucose and nutrients and keep them warm.
In a way, bispecific antibodies and CAR T cells do the same thing. They take advantage of T cells.
Dr. Landgren
In the current development setting, about four to six weeks later, you give the CAR T cells to the patient. When they reenter the body, they will be let in because the body will recognize them as their own T cells. When they come in, they are now programmed with receptor-like antennae on the surface to bind to something that fits, which is the BCMA protein. When they bind to it, same as the bispecific antibodies, now a T cell is neighbor to a myeloma cell and when it sees the myeloma cell, it will kill it.
In a way, bispecific antibodies and CAR T cells do the same thing. They take advantage of T cells. In one setting, you keep the T cells in the body and give a matchmaker, which is the antibody. In the other example, you take out the T cells, modify them, and give them back.
There are other ways of doing it. You can have donors give blood where you can make something called allogeneic CAR T cells, which is a mass-produced CAR T cell that comes from a pool of donors, and you give that to multiple patients. The idea here is that you can give them immediately because there is no need to harvest them, manufacture them, and give them back. You have donor-derived T cells. Unfortunately, there are none yet approved for myeloma.
There are also other technologies where you can insert mRNA-made T cells and bispecific antibodies. Similar to how the COVID vaccines were developed, you can use mRNA infusions to synthesize these types of products within the body. That has not yet happened in humans, but there are a lot of animal models. We’ll see how these mRNA-based technologies will speed up the development of immunotherapies. This is going to be very, very exciting.
The jury is still out on the right sequence, whether you should do CAR T-cell therapy first and then at a later time point, bispecific antibodies or vice versa.
Dr. Landgren
Are There Specific Patients Populations More Likely to Benefit from Bispecific Antibody Therapy?
Kenny: Are there specific patient populations that are most likely to benefit from bispecific antibody therapy?
Dr. Landgren: Currently, there is no head-to-head randomized study that has compared patients given a bispecific antibody and patients given CAR T-cell therapy. All the studies have compared CAR T-cell therapy with older combination therapies or bispecific antibodies compared with older combination therapies.
What we do know is if a patient has an activation of the disease or there is a relapse, the majority of patients have a slower evolution of the disease. The disease usually shows up as increasing protein markers in a blood test and it can go on for many weeks or even months before you start making decisions to change the therapy, so you have some time to make treatment decisions.
But for some patients, the disease becomes active in a short timeframe, so you cannot wait to collect the T cells, send them for manufacturing, keep the disease under control with bridge therapy, and then give back the CAR T cells. In their case, a bispecific antibody is the better option.
If you have patients where the disease is moving more slowly, you have two options. You could argue which is better and I would say different experts would have different opinions. In my experience, different patients will have different opinions.
The jury is still out on the right sequence, whether you should do CAR T-cell therapy first and then at a later time point, bispecific antibodies or vice versa. There are so many details when it comes to this and we don’t have the data to fully answer.
If you started with a bispecific antibody, could you do CAR T-cell therapy in the future?
Dr. Landgren
If you treat someone with CAR T-cell therapy, on average, it would last for many years. But if a patient, God forbid, has a shorter benefit, let’s say 6 or 12 months, going right to a bispecific antibody with the same target usually doesn’t work because the time in between is too tight. But if you go to another therapy with another target with another mechanism of action, could you revisit that same target using a bispecific? I would say the answer is yes for the most part. It comes back to recycling drugs or targets.
If you started with a bispecific antibody, could you do CAR T-cell therapy in the future? Yes, with the same target, but if you do them back to back, that may not be optimal. If the cells build up some form of resistance to the same mechanism of action, you want to distract the cells by doing something else to bring down the disease. If you get good mileage out of that and need to switch again, that could be the time to go back to the same target.
Common Side Effects: Bispecific Antibodies and CAR T-cell Therapy
Kenny: For patients treated with bispecific antibodies, could you discuss the most common side effects and how they are managed?
Dr. Landgren: Compared to bone marrow transplants, CAR T-cell therapy is way less toxic, so the patient experience is much easier. I’ve seen patients who were transplanted years ago and got CAR T-cell therapy and they said this was not even comparable. My oldest patient who turned 87 years old underwent CAR T-cell therapy when he was 86. We would not transplant an 86-year-old, but you could give CAR T cells. I have also treated patients in that age category with bispecific antibodies. I have many patients who have done that and they do extremely well. On average, both CAR T-cell therapy and bispecific antibodies are very, very well-tolerated overall, but everything has some form of side effect. If there is no side effect, usually there is no effect, unfortunately.
On average, both CAR T-cell therapy and bispecific antibodies are very, very well-tolerated overall, but everything has some form of side effect.
Dr. Landgren
When you give a CAR T cell product, you would expect to see cytokine release syndrome (CRS), which means the immune system gets triggered by this immunotherapy and releases substances that the immune system uses to communicate with different immune cells and other surrounding cells. These are the cytokines and chemokines. When they get released, it leads to an immune reaction. It’s a ramped-up version of a person getting sick from an infection or inflammation. Patients get a fever, they don’t feel well, and they could have organs responding to it, like blood pressure going down and things like that.
There are two approved CAR T cell products. When you give cilta-cel, CRS usually takes about a week to kick in. Presumably, that’s the time it takes for the CAR T cell product to amplify, expand, and become fully active. But if you look at the alternative protocol ide-cel, usually the same phenomenon with CRS happens sooner, around the next day. The time windows are different for these different products for reasons we don’t completely understand.
The duration of CRS is usually one to a few days. If the patient has a fever, we can treat it with acetaminophen or we can also give steroids. If it’s a little bit stronger, we would give IL-6 (interleukin-6) receptor inhibitors. There’s a drug called tocilizumab that we use quite frequently and usually, that takes the edge off it. We may have to give IV fluids if the blood pressure goes down a little bit.
Unfortunately, some patients get a little bit sicker and we may have to give them additional drugs. But for the most part, CRS is very manageable and the majority of patients don’t have severe side effects. When this has leveled off, the patient would leave the hospital if the patient was admitted.
Many institutions, including ours in Miami, can administer CAR T-cell therapy outpatient. We have the patient come in, give the CAR T cells, and have the patient stay in close proximity to our institution. If the patient were to develop CRS, we would treat it along the lines of what I said. We may have to admit the patient after a week for one, two, or three nights, and then we can discharge them.
For a few weeks, we would do labs once a week to make sure blood counts are stable and then we would do them once a month and eventually, every three months. We would keep the patient on prophylactic medications with antivirals and antibiotics. We usually give IVIG infusion, which means that we supplement immunoglobulin G levels to keep the patient free from infections. Over time, all these things will be taken off. The average patient could be off therapy for many years and do blood tests every three months.
For the most part, CRS is very manageable and the majority of patients don’t have severe side effects.
Dr. Landgren
For bispecific antibodies, you see the same CRS phenomenon. If you look at the registrational trials that led to the approval of these drugs, the rates are quite high with over 70 or up to 80 percent of patients developing CRS. Most of them are less intense. They are also along the lines of what I said, like fever and drops in blood pressure.
Nevertheless, the FDA has put in the USPI (United States Prescribing Information) saying that the first few doses should be done inpatient to monitor and see if the patient develops CRS, which the majority of patients do if you follow the standard trajectory of the standard recommendations.
Our group at the University of Miami has used premedication with a single dose of IL-6 receptor inhibitors. We give one dose one hour before the very first dose of a bispecific antibody. We presented this at ASH 2024 in San Diego, showing that you can decrease that rate of CRS to 10% and they virtually are always the lowest grade.
This is a huge step forward and sets the stage for thinking about doing this outpatient. If you can premedicate and avoid 9 in 10 patients from having any side effects or if the patient has CRS symptoms and you could guide them on the phone to come in for monitoring or do some intervention overnight, that’s a huge improvement. Premedications should be part of the next step and we are working on that with other groups. I hope in 2025 that these therapies could also be given outpatient.
It’s very important for physicians who treat patients with bispecific antibodies to keep an eye on immunoglobulin G levels and use proper antibiotic and antiviral medications, so patients don’t run into opportunistic infections
Dr. Landgren
An important side effect profile for bispecific antibodies is infection. I have seen this firsthand because I’ve been involved with drug development for a very long time. When I worked in Miami, I was the chief of the Memorial Sloan Kettering myeloma program for many years, so we were involved a lot in these early developments. We don’t want to develop great drugs that hold the myeloma away and allow patients to have a good quality of life but have other problems arising, such as infections.
It’s very important for physicians who treat patients with bispecific antibodies to keep an eye on immunoglobulin G levels and use proper antibiotic and antiviral medications, so patients don’t run into opportunistic infections, which could be very dangerous. This is very important to emphasize. We can premedicate the immediate side effects, but the doctors need to stay on top of it. Patients also need to know that if they develop an infection, they should always alert their doctor.
Clinical Research and Development
Kenny: When it comes to discussing clinical trials and patient support, what do you see as the most promising areas of investigation in terms of bispecific antibody development?
Dr. Landgren: We will see more and more trials with bispecific antibodies that will be used in combinations. At ASH 2024, we saw combinations of two bispecific antibodies: BCMA-CD3 and GPRC5D-CD3. This is the REDIRECT trial, which has been discussed at prior meetings. There were more patients this time and you see very high rates of response. You also see BCMA-CD3 partnered with lenalidomide or carfilzomib, a proteasome inhibitor, in the MagnetisMM-20 study. There are many other studies as well.
What I’m talking about are combinations of bispecific antibodies and other drugs. Eventually, that’s probably what these drugs will fit in with the best. What we will learn, hopefully very fast, is which are the better options to partner them with, the optimal dosing schedules, and the optimal duration of therapy. Can you step down the dose? Can you give it less often? Can you even stop some of these therapies over time?
I don’t have the evidence to prove this, so don’t take this 100% for sure, but based on my looking at data, I project that patients who have been treated with bispecific antibodies, if they have been successfully treated for an extended period or for whatever defined window of time, they may be able to go off therapy.
The missing piece that we are trying to develop is a blood-based MRD test. If you could give treatment and prove that there is no detectable disease, if you could reliably check every three months and make sure there is no disease, many patients could potentially be off therapy for extended periods. It’s an important piece that’s currently missing and we are working on that together with other groups to move that forward.
What Should Patients Consider When Deciding on Bispecific Clinical Trial Participation?
Kenny: For patients who might be considering a clinical trial involving bispecific antibodies, what factors should they consider when making the decision?
Dr. Landgren: The field is moving forward so fast. At this time, bispecific antibodies are only FDA-approved for patients who have failed four or more prior lines. We see from all these trials that they seem to work very well for patients who had their first, second, or third relapse, but that’s only available in trials at the current time.
Getting a second opinion is very well-invested time.
Dr. Landgren
I mentioned combinations with IMiDs and proteasome inhibitors, but there are other drugs as well. I mentioned two bispecific antibodies, but you also have naked antibodies like daratumumab being combined with bispecific antibodies.
If someone is looking for a trial in the space of one to three prior lines, you have to determine what’s available, where you live, what’s feasible to do, what are the different options, what are the dosing schedules, and what are the safety profiles. The side effects always should be looked at in combination with efficacy. It’s a balance between the two. Look at what’s available and make wise decisions. If you’re not sure, go for a second opinion. Getting a second opinion is very well-invested time.
What Makes a Cancer Center Comprehensive?
Kenny: Could you tell us more about the oncology social work service at the Sylvester Comprehensive Cancer Center? What makes it truly comprehensive?
Dr. Landgren: We have a very strong team for multiple myeloma. We have doctors, nurse practitioners, nurses, pharmacists, social workers, patient coordinators, navigators, and researchers. We have a very, very comprehensive program.
Many times, patients ask about the cost and implications of the drugs due to insurance. People are changing from one insurance to another or someone is switching to Medicare and wants to know how that works. We have people dedicated to our program. If I get asked this, which I very frequently do, I will always involve my social worker and finance people to help guide the patient. As a doctor, I don’t have access to all this information, but I have a very strong team that will always help me.
If they come to us for help, we want to make sure that we can give every patient the same high level of knowledge, experience, and care that they deserve.
Dr. Landgren
Overcoming Barriers to Patient Engagement
Kenny: One of the challenges is getting some patients to the clinic because I have a feeling that some of them feel like it’s overwhelming. It’s beyond them either because of the cost or the amount of effort on their part to understand. There’s a base layer of knowledge and there’s a language that they have to learn to speak. Sometimes I have a feeling that the patients feel like they don’t belong in this world. How do you navigate that with a patient? Sometimes you have limited time yourself to engage with them. You can’t solve all the problems, like psychosocial issues, mental wellness issues, diet and nutrition issues, and so forth. All of those things are not where you are, but they’re still your patient.
Dr. Landgren: I serve as the chief of the program, so I’ve thought about these things a lot and how we can scale this up and give the ultimate quality for every patient. How can we treat every patient and provide VIP medical care and support?
The way I try to build our program is to build multidiscipline cells of professionals. Every doctor works with a nurse practitioner, a nurse, and a patient coordinator. That’s the backbone of the little group that we have. We have been growing quite fast with an increase in patients of over 20% every year. If the patient volume goes up, when the group gets too busy, then we hire another doctor, nurse, nurse practitioner, and patient coordinator.
At this point, we have close to 10 of those cells. The right size for our program is somewhere between 15 and 20, but right now, 10 is a good number. We will probably hire another one or two and keep on going as our needs grow because there are a lot of patients who need our help. We don’t wish anyone to have myeloma, but if they come to us for help, we want to make sure that we can give every patient the same high level of knowledge, experience, and care that they deserve, and we are very committed to doing that.
Our program is very active when it comes to different patient organizations… I work with anyone who reaches out to us and I always dedicate my time and attention.
Dr. Landgren
On top of that, we have pharmacists, dietitians, finance, and social workers who support all these groups. The model we have is to build a very small group of experts that hold everything together, where everyone knows the patient and the patient knows them. You don’t call a 1-800 number; you call directly or send a message and we will respond usually within an hour if you send a message through our portal. We will be very, very responsive.
We also organize patient seminars. We have programs where patients can volunteer if they want to be part of that. They can talk to other patients. Some patients like that, some patients don’t, but we have that as an option. Our program is very active when it comes to different patient organizations. I’m very inclusive as a person. I welcome all the different organizations and I’ve done so for a long, long time.
Finding More Information About the Latest Relapsed/Refractory Treatment Options
Kenny: What advice would you give to patients and caregivers who are seeking more information about the latest treatment options for relapsed/refractory myeloma?
Dr. Landgren: If you have a doctor who you trust and things are going well, work with that doctor and follow that doctor’s recommendations. If you want to have a second opinion, it’s very easy these days to get one. You can travel or if you’re within the States, for the most part, telemedicine visits are available and it’s very important to be able to continue that.
After COVID, I know that there have been some discussions about whether telemedicine should remain or not. All the patient organizations should band together and make sure politicians will never be able to change that because that is going to create barriers for patient access.
If you live in a big city, you have access. If you live in a smaller town, you don’t have access if you have to travel long distances, if you are older, or if you’re frail. Telemedicine breaks down all these barriers. In my opinion, the number one priority for all patient organizations is to make sure that no politician will ever change that because that’s going to cause a lot of patient suffering. In the end, it’s going to take people’s lives and have a lot of negative impact.
Conclusion
Kenny: I love it. Thank you, Dr. Landgren, for taking the time to speak to The Patient Story.
Dr. Landgren: Thank you very much for having me. It was a great pleasure.
Tiffany: What an engaging conversation. Thank you again, Kenny and Dr. Landgren, for taking the time to dive deep into the latest treatment options for relapsed/refractory multiple myeloma patients. If you are a patient advocate, patient, or caregiver, consider being a voice leader in your community or with The Patient Story.
It’s important to be empowered so that you and your caregivers can make informed decisions about your care and that includes being educated about the latest treatment options. Until next time, I’m Tiffany Johnson signing off and on behalf of The Patient Story, thank you for watching.
Symptom: None; found through blood tests Treatments: Total Therapy Four, carfilzomib + pomalidomide, daratumumab + lenalidomide, CAR T-cell therapy, selinexor-carfilzomib
Overcoming Racial Barriers in Clinical Trials from a Lung Cancer Oncologist
Marjory Charlot, MD, MPH, MSc, is a medical oncologist and health services researcher at UNC Lineberger Comprehensive Cancer Center. She primarily specializes in people who have lung cancer. Her research focuses on increasing awareness and access to clinical trials among Black communities and communities with low-income or persistent poverty.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
Dr. Marjory Charlot: I’m a medical oncologist and health services researcher. I work at UNC Lineberger Comprehensive Cancer Center and primarily specialize in lung cancer patients. Part of my work is working in the hospital for patients who either have a suspicion of cancer or have a cancer diagnosis but are hospitalized for symptoms of their cancer or side effects from their treatment. As a health services researcher, my research focuses on increasing awareness and access to clinical trials among Black communities and communities with low-income or persistent poverty.
Outside of medicine, I’m a wife and a mom. I have two children, one in elementary school and one in middle school. I recently completed an aquathlon, a swim-run competition, which is a big deal for me because I don’t have a great relationship with swimming. I learned to swim as an adult, so it was a big accomplishment for me to be able to complete this duathlon, so that was exciting. I also love to travel and visit different places across the US or abroad. I also love to eat. I love various types of foods.
When I completed my medical training, I knew that I wanted to be an oncologist. There was no question about that.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
A Winding Path to Medicine
Nikki: What was your number one driver to becoming a doctor?
Dr. Charlot: I knew from a young age that I wanted to become a doctor. I grew up in Mattapan, a neighborhood in Boston, and I was privileged enough to have a Haitian pediatrician who had his practice in the community and did house visits. The Haitian community where I grew up was tight-knit and it was informative for me to be able to see someone who shared my heritage be a physician and be one with the community, so I wanted to be exactly like him.
My path to becoming a doctor was not straight and narrow. After I graduated from college, I spent a couple of years working in different types of advocacy work related to education and moved on to teaching middle school students about health professional careers. After that, I got my degree in public health and then after that, I went to medical school. It was a winding path to medicine, but I knew that’s where I would end up eventually.
Why Oncology Became Her Calling
Nikki: How did you end up specializing in lung cancer?
Dr. Charlot: When I completed my medical training, I knew that I wanted to be an oncologist. There was no question about that. I felt like it was the field where you develop close-knit relationships with your patients, so that was a no-brainer. Oncology was the way that I wanted to go.
Concerning lung cancer, I was influenced by my mentor. When I started my training, there weren’t that many options for lung cancer. There was chemotherapy and that was pretty much it. However, during my training, there were a lot of new therapies coming up, like immunotherapy and targeted therapy. The excitement in the field drew me to want to be a part of this growing field concerning options for our patients. The field was getting to a place where we had more options to offer our patients other than chemotherapy itself and that’s where my love and compassion towards lung cancer grew.
It was ingrained in me that we needed to think about the community and the circumstances that people are born in or the conditions they live in for the healthcare system to work.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
Growing Up in Mattapan
Nikki: What motivated you to go above and beyond and focus on helping an entire community get better access to health care and treatment options, including clinical trials?
Dr. Charlot: Mattapan is a predominantly Black community and interestingly enough, my street and pretty much my whole block were folks that immigrated to Boston. I have a Haitian background, so my interest in terms of thinking about communities draws from that experience.
I lived in two different worlds. I had the world where I grew up in Mattapan, but I also always went to Catholic school, which was outside of our neighborhood. I saw the dichotomy between the school in terms of the affluence of the area and some of the students who attended that school and my neighborhood where we’re very rich in culture and pride, and hardworking, but we didn’t have the same resources.
When I became a doctor, I did all of my training at a safety net hospital, so we cared primarily for people who were underinsured or had no insurance. It was the hospital where I was born, so it was ingrained in me that we needed to think about the community and the circumstances that people are born in or the conditions they live in for the healthcare system to work.
That’s where my whole approach comes from in terms of thinking about Black communities and the importance of ensuring that they have the knowledge and the awareness of all the resources available to ensure that they have access to care and can improve their outcomes through those connections. As a physician, I think about the Black community and understand ways how we need to make those connections together for us to thrive, do better, and live healthy lives.
I used my background concerning patient and community engagement to improve access to clinical trials, cancer care, and high-quality cancer care.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
Developing the CREATE Initiative
Nikki: How did you end up at UNC?
Dr. Charlot: I was recruited to UNC primarily to work as a thoracic oncologist, so my specialty in lung cancer, as well as develop a program that was focused on clinical trials and increasing equity in clinical trials. As a result of my research and clinical background, I ended up starting the CREATE initiative, which is Cancer Research, Equity, and Advocacy Through Engagement. This initiative speaks to the strong community focus and the work that we do with our community partners for the healthcare system to work and for the treatments to get to the people that they were designed to treat. I used my background concerning patient and community engagement to improve access to clinical trials, cancer care, and high-quality cancer care.
Most Common Lung Cancer Symptoms
Nikki: We understand that there’s a wide range of symptoms, but what are the most common symptoms of lung cancer? And what should people never ignore?
Dr. Charlot: Screening in general is meant to detect cancers early, before they cause symptoms. But generally speaking, by the time a patient is diagnosed with cancer, medical oncologists see patients after the cancer has spread or advanced and not in a stage where it could be cured with surgery. However, things have changed with cancer where we’re using chemotherapy and immunotherapy even for earlier cancer stages.
Common symptoms are generally related to shortness of breath, coughing (particularly coughing up blood), and sometimes weight loss. Those are the top three that patients describe in terms of things that they’ve noticed when they’re diagnosed with cancer.
If the cancer has spread, they could present with various symptoms, like a headache if the cancer has spread to the brain or pain in various areas, like in the bones or the joints. There could be a wide range of symptoms depending on where the cancer is.
The most important thing is to be aware that cancer screening is an option, particularly for people who have had a long history of smoking. Twenty pack-years is the recommendation. Screening is for those who don’t have symptoms, but if they do have symptoms, it’s another reason to see their doctors so they can get examined and evaluated for potential cancer.
It’s important to be able to test these drugs on a variety of people and understand how these treatments impact various groups.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
Demystifying Clinical Trials
Nikki: We know that trials aren’t for everyone. What would you say specifically to Black and African Americans to convince them to learn about clinical trials?
Dr. Charlot: Clinical trials are an opportunity to get access to new treatments that are not currently available. For the Black community in particular, we know that outcomes are worse when it comes to cancer survival and mortality rates. Clinical trials provide an opportunity to get access to new drugs, which ideally will prolong life.
It’s important for all patients, regardless of background, to have access. We don’t know how these drugs are going to affect people, whether it’s based on their environment, socioeconomic status, or race. It’s important to be able to test these drugs on a variety of people and understand how these treatments impact various groups.
A Patient’s Clinical Trial Success Story
Nikki: Can you think of a specific story that shows how impactful a trial can be for someone?
Dr. Charlot: I started the CREATE initiative at Lineberger and we’re in the process of completing a research grant that I have, which is building a mobile app for Black women with breast cancer to see if it can help increase discussions about clinical trials with their providers. One of our patient research partners shared her story about participating in a trial where the trial led to her being cancer-free for a very long time in that she’s been able to see this drug become a standard of care for breast cancer treatment.
It’s important to acknowledge the historical past and some of the mistreatment that Black communities and individuals often get within the medical care system.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
This goes to show that when going into a trial, we don’t know whether or not these drugs are going to work. What we do know is that when you’re in a clinical trial, you’re under such close follow-up, which gives you even an extra layer of eyes of people who are watching how you’re doing. If these drugs prove to be better than the standard of care, these drugs end up helping people live longer.
It’s fascinating and wonderful to be able to work with someone who’s been through this whole process of participating in a clinical trial and seeing that her participation led to the approval of a new drug that is now being used for breast cancer patients. There’s no better story than to live through the process of being in a clinical trial and to see how that participation led to the approval of a drug that more women and other people with breast cancer can benefit from.
Overcoming Barriers in Black Communities
Nikki: What would your message be to the Black and African-American community who are fearful of clinical trials?
Dr. Charlot: We know that our healthcare system and our research enterprise in this country have not been the best, particularly for our Black communities. At the same time, it’s important to acknowledge the historical past and some of the mistreatment that Black communities and individuals often get within the medical care system. Acknowledgment is at the forefront.
It’s also important to know that there are safeguards in place with clinical trials. It’s important for us, specifically as Black individuals, to be a part of clinical trials because it gives us opportunities that we would potentially not have to access newer drugs. Acknowledge the past and understand that we have a part and the right to have access to newer treatments and interventions.
We need to understand where our patients are coming from, know what their needs are, and partner with them.
Marjory Charlot, MD, MPH, MSc at UNC Lineberger Comprehensive Cancer Center
The Role of Black Physicians in Healthcare
Nikki: What do you think healthcare professionals can do better when building trust with the Black and African American community?
Dr. Charlot: As a Black physician and even for healthcare providers who are not Black, we need to be one with our community. We need to understand where our patients are coming from, know what their needs are, and partner with them. If we do these separately in our silos, it doesn’t help improve access to care. It doesn’t help our communities thrive and live healthy lives. Making connections is what’s helped me in the work that I do and hopefully helping the patients that I’ve had the privilege to take care of over these past couple of decades as a physician.
An internal medicine physician discusses healthcare access, preventative care, patient trust, and how both doctors and patients can improve relationships for better outcomes.
The Future of Lymphoma Therapy: Expert Perspectives After ASH
Treatment News Coming Out of the American Society of Hematology Annual Conference
We’re talking about the two most common subtypes of non-Hodgkin lymphoma: diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma. We recently had a meeting of minds from all over the world at the 2024 American Society of Hematology (ASH) annual meeting, where doctors and researchers present the latest updates on treatments and potential treatments with the most promise.
Explore advancements in non-Hodgkin lymphoma treatments with cancer experts, Dr. Andrew Evens from the Rutgers Cancer Institute and Dr. Tycel Phillips from City of Hope, and Stephanie Chuang, a non-Hodgkin lymphoma survivor and founder of The Patient Story. Dive into the latest research, treatments, and strategies to empower patients and caregivers. Gain valuable insights including promising clinical trial results, breakthrough therapies, and personalized treatment options.
Discover breakthrough treatments reshaping care for DLBCL and follicular lymphoma. Understand cutting-edge combinations like CAR T-cell therapy, antibody-drug conjugates, and bispecific antibodies. Learn to balance effectiveness and quality of life with insights into side effects and survivorship. Access guidance on clinical trials, emerging therapies, and personalized medicine. Hear directly from leading experts about what’s next in lymphoma research and care.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make treatment decisions.
Stephanie Chuang: Hi, everyone! We’re talking about the two most common subtypes of non-Hodgkin lymphoma: diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma. We recently had a meeting of minds from all over the world at the 2024 American Society of Hematology (ASH) annual meeting, where doctors and researchers present the latest updates on treatments and potential treatments with the most promise.
Our goal is that you, as patients, caregivers, and partners, walk away with a better understanding of how to approach your own decision-making with your medical team, specifically how to understand the options and balance effective treatment and quality of life.
We want to thank the LLS for its partnership. If you don’t know already, the LLS offers great free resources, like their Information Specialists and the Clinical Trial Support Center, which is staffed to provide one-on-one support in different areas for the blood cancer community.
The Patient Story retains full editorial control over all of this content as always. While we hope that this is helpful, keep in mind this is not a substitute for medical advice. Consult with your team about treatment decisions.
We have an incredible panel of experts to discuss the latest advancements in the field. Dr. Tycel Phillips is a hematologist-oncologist from the City of Hope National Cancer Center in Southern California. He’s an associate professor in the Department of Hematology and focused on treating patients with lymphomas, both Hodgkin and non-Hodgkin. Dr. Phillips lost his grandmother to pancreatic cancer and his mother to breast cancer while he was studying to become a doctor, and I’m sure that informs the way Dr. Phillips practices as a doctor.
Dr. Andrew Evens is a physician-scientist and clinical expert in lymphoid malignancies at the Rutgers Cancer Institute in New Jersey. He serves as associate director for clinical services and the associate vice chancellor for clinical innovation and data analytics at Rutgers Biomedical and Health Sciences. Over the past two decades, he’s been the principal investigator of more than 80 cancer clinical trials from phase 1 through phase 3 studies.
Our audience is cancer patients and the people around them. The goal is to translate for our audience what matters to them. The two of you are dedicated to the patients you see in your clinic and to the research happening in lymphoma. You go above and beyond outside the clinic walls, so thank you so much for that, especially as a former diffuse large B-cell lymphoma patient.
We’re covering two types of non-Hodgkin lymphoma: one is the most common aggressive form, which is diffuse large B-cell lymphoma, and the other is slow-growing or indolent and the most common form of that, follicular lymphoma. We often see a lot of research in these areas. Let’s go into DLBCL first.
Latest DLBCL Advancements in Front-Line Therapy Options
Stephanie: Dr. Evens, what’s been the standard of care for front-line therapy for DLBCL? What’s happening now with front-line therapy options after we have the POLARIX trial where, for the first time in decades, the FDA approved a new option for patients?
Dr. Andrew Evens: It’s evolved and you said it. R-CHOP chemotherapy had been the standard of care for more than 15 years after rituximab broke through around 2005, but it wasn’t for lack of trying. A multitude of randomized phase 3 studies over the ensuing 15 years tried to knock R-CHOP off the top of the hill.
Finally, one at least had some benefit. In a head-to-head study, polatuzumab vedotin replaced the O in CHOP and garnered FDA approval after a phase 3 randomized trial, which was POLARIX, and pola-R-CHP has broken through. Is it used in all patients? That’s open for discussion. It’s FDA-approved for patients who have a certain clinical risk score.
Ongoing DLBCL Studies in First-Line Treatments
Stephanie: Dr. Phillips, ASH is a big conference. What excited you the most about the ongoing studies for first-line treatments, specifically with R-CHOP and novel treatments?
Dr. Tycel Phillips: Surprisingly, a whole section was dedicated to R-CHOP plus X. The POLARIX study invigorated the field to explore more options to improve the front-line setting because, after so many negative studies, we had hit a point where there was very little interest in exploring a way to improve R-CHOP.
In the 2024 ASH meeting, there were a few studies. Venetoclax was added to pola-R-CHP for patients with aggressive B-cell features and this was presented by Dr. Diefenbach. This study looked at venetoclax at a dose of 800 mg given for five days, which indicated a very high response rate across the board, even in those with triple- and double-hit lymphoma, albeit only seven patients. It’s still a very short follow for all of these, but in this situation, a way to move the needle. Some drawbacks were higher rates of neutropenia and grade 5 CRS events. If that were to move forward, there may be some dose reductions to venetoclax because they went up to 800 mg. The question is whether it’s necessary.
Moving along the theme of adding a small molecule to a chemotherapy backbone, there was a study looking at parsaclisib, which is a PI3Kδ (PI3 kinase delta) inhibitor in patients with R-CHOP, which was presented by Dr. Yucai Wang from Mayo Clinic. Surprisingly, this showed a very high overall response rate for the patients enrolled. It’s a small study and didn’t appear to be subtype-specific, so it’s a little bit agnostic. But as Dr. Evens can tell you, the delta inhibitors have become a dirty word in our industry, so how that moves forward will be very interesting considering that for the most part, outside of CLL, these drugs have pretty much been killed off by the FDA.
Additionally, there was golcadomide plus R-CHOP in patients with large-cell lymphoma. This was presented by Dr. Jason Westin from MD Anderson. Again, this compared to lenalidomide, which is built off of, supposedly keeps cereblon in a more closed configuration, so more inhibition of Ikaros and Helios and more T-cell activity than what we saw with lenalidomide. This also had a very encouraging high overall response rate. We can all agree we can’t hang our hats on phase 2 studies anymore, but this one will move forward into a randomized phase 3 trial to try to see if this can improve on the R-CHOP backbone.
Dr. Lorenzo Falchi presented a study with epcoritamab, which is a bispecific antibody, and R-CHOP. Again, a very high overall response rate. We all suspect bispecifics will move forward in this space. There will be a phase 3 study looking at epcoritamab in this patient population.
Lastly, we had the COALITION study, which looked at glofitamab and R-CHOP or glofitamab and pola-R-CHP. Again, a high response rate in the phase 2 studies, very impressive complete response rates, and a high short-term duration of response; but again, more follow-up. As Dr. Evens can attest to, there’s a third bispecific. The OLYMPIA study is looking at odronextamab in this patient population.
It’s going to be a very, very difficult next couple of years teasing out the new standard of care for front-line large cell lymphoma if any of these phase 3 trials are positive. There are several ones that we didn’t even mention that will likely read out in that time frame. We’re in interesting times, but again, there’s a bit of confusion based on the backbone that’s being used — R-CHOP, pola-R-CHP — and the partner drug.
Stephanie: Dr. Phillips, thank you so much for going over all of that. You could characterize that as difficult and confusing because there are so many options now in a space that you’re looking at.
At the end of the day, whatever gets approved will be great for patients and that will be up to the providers, together with patients, to say what’s best for them.
Dr. Andrew Evens
How Long Until We See These Options? How Do We Choose?
Stephanie: Dr. Evens, how long until people could potentially see some of these treatment options? Let’s say they all get approved at some point. How would you decide for individual patients on recommendations for which way to go?
Dr. Evens: It’s a lot to digest and Dr. Phillips did a great job as he alluded to the tip of the iceberg, but it’s confusing. We say it’s a competitive landscape, but through the lens of the patient, it’s fantastic because it means we have a certain standard and a certain cure rate, and we’re trying to do better.
At the end of the day, whatever gets approved will be great for patients and that will be up to the providers, together with patients, to say what’s best for them. We always desire what’s called biomarkers to try to predict personalized therapy. Can we find a treatment or a regimen for particular patients? We’re certainly not there yet but that’s hopefully along with, in parallel, or, at worst, in sequence. We have a regimen approved for a large general patient population. Can we start to figure out who it works in?
To your point, the question always is how effective it is. It’s not just the initial response, but we want it to be stable and stay in remission. How is it tolerated? If it is as good or better tolerated, then that’s fantastic. If there are different or unique toxicities, is it balanced out by the efficacy? Then we think about the cost of care. We want to make sure it can be affordable for patients.
At the end of the day, whatever is approved down the road that builds upon R-CHOP and pola-R-CHP is all good news. Patient by patient, we’ll have to make smart, informed, personalized decisions.
Dr. Phillips: ASH in 2026 and 2027 will be quite interesting.
Dr. Evens: There’s going to be a lot. You know how it goes, Tycel. Most won’t break through, but maybe I’m wrong. As you mentioned, the bispecifics have the best chance.
With the bispecifics, part of the belief in how they will be upwardly mobile is that they’re built off the backbones of monoclonal antibodies, which have revolutionized how we treat patients with lymphoma.
Dr. Tycel Phillips
Questions for Patients to Ask Their Doctors
Stephanie: Bispecifics look like they might rise to the top. Can you share more about why that is? You talked about more personalized medicine. We’re certainly not there yet with biomarkers, but it’s a conversation that’s very hot for patient advocates as well. What guidance do you have for patients to ask their doctors? What can they ask about these different options?
Dr. Phillips: With the bispecifics, part of the belief in how they will be upwardly mobile is that they’re built off the backbones of monoclonal antibodies, which have revolutionized how we treat patients with lymphoma. As Dr. Evens mentioned, the major improvement was the addition of rituximab to a chemo backbone in CHOP. Ideally, if we look at glofitamab, epcoritamab, odronextamab, and mosunetuzumab, they’re still built off that same paradigm. In this sense, we’re encouraging the patient’s immune system to take more part in trying to fight off these cancers with the addition of chemotherapy drugs that are not necessarily immunotoxic.
In that sense, the combined ability and safety of these medications, especially when the patients get a few cycles of chemo first, support their addition to the front-line regimen. It’s that balance. If you have all these different options, we’re going to start going into the weeds and figuring out if there are any things that separate these regimens, like the safety, tolerability, and convenience of giving these to patients.
Is it more convenient to come in for an injection or infusion every couple of weeks or have to take a pill for a certain number of days? We already know that compliance with oral medications is not great. While you may get surveillance and pharmacovigilance on clinical trials, that doesn’t happen outside of a clinical trial setting. Quite frequently, patients will not be as adherent to these medications as they should be and that may impact clinical outcomes.
Echoing Dr. Evens again, it’s an exciting time. Another part we also want to look at is how they may impact certain subsets. With POLARIX, there’s the issue of subtype specificity, but do we have other treatments that may be agnostic to subtype? If we start getting more of these molecular tests that will divide patients into certain subtypes, how do these treatments broadly apply across the board? Do we need to play mix and match based on a person’s genomic profile? We’re still away from that, but that’s a place where everybody is trying to get to where it’s more individualized for the patient versus everybody who walks in gets the same treatment even though they’re not the same.
Dr. Evens: Dr. Phillips summed it up greatly. Clinical trials can be overwhelming. There’s not a better or the best clinical trial. To me, they’re all good options and that is one thing I would ask your doctor. What’s currently FDA-approved for my condition? Are there any new treatments? For newly diagnosed, there are very mature clinical trials taking the standard of treatment, like R-CHOP or pola-R-CHP, and trying to do better and looking at safety.
Long-Term Benefits/Risks of Bispecifics
Stephanie: There are clinical trials where we’re studying all these possibilities and then there are the approved options. The Patient Story set this conversation up backward in terms of clinical trials in that much of it is done for relapsed/refractory patients first and then works its way up to earlier lines of treatment.
We’re going to talk about bispecifics for relapsed/refractory patients. Dr. Evens, you talked about bispecifics rising to the top. Is there anything else in terms of long-term benefits and risks for what we understand so far when it comes to everything presented at ASH?
Dr. Evens: What about after treatment? Survivorship is very important. Yes, we want to cure with minimal side effects and fairly cost-effective treatment, but there are late effects that remain to be determined. Since these agents are not classical cytotoxic chemotherapy or radiation for the most part, the hope is that they’re going to have less late effects, whether it’s cardiac, pulmonary, or infections. But at the same time, we can’t assume anything. It needs to be studied.
My hope is that, whether through the pharmaceutical companies or academic institutions, it will be bolted on in some form or fashion to these studies to follow clinical trial participants for late effects whether it’s five or 10 years later because we certainly don’t want to cause harm down the road.
Dr. Phillips: When you have options, you could be a little bit more stringent about what’s the best thing moving forward. The more options there are, the better it is for our patients.
Dr. Evens: Tycel, I’m sure you have survivorship expertise at City of Hope.
Dr. Phillips: Yes, there is a survivorship clinic.
Dr. Evens: In the past, I wouldn’t say we minimized it, but maybe we didn’t appreciate or have the science associated with survivorship after treatment, so that’s also a valid question for your oncologist whether it’s two years or five years later. Can we talk more about my individualized survivorship? In most academic centers, even in some non-academic centers, there is survivorship expertise. Whether it’s led by nurse practitioners or physicians, it’s all good as we get into that important part of the rest of life.
Dr. Phillips: Yes, life after chemo.
Stephanie: I can’t tell you both how much I appreciate that you brought that up. I love how survivorship is becoming much more of a focal point. I went through hundreds of hours of chemo. I had dose-adjusted R-EPOCH in 2017 and the thought of being able to focus on survivorship and the things that I need to look out for because my body went through this is wonderful.
Dr. Evens: You look great and I’m hopeful you’re doing well, but it’s something to bring up. I don’t want to make it seem like it’s an epidemic or malady of late effects. They’re slight and subtle, but they’re real and we’re still learning a lot about them. We’ve learned a lot from Hodgkin’s lymphoma, which was one of the first curable cancers in man that we learned in the 1970s. But a lot of the medications, in particular anthracyclines, the vinca alkaloids, the alkylators they’re called, whether dacarbazine or cytoxan, are very similar, so they’re probably more similar than not and, frankly, regardless of age.
One other important pin to put in this point is when we hear about late effects, we sometimes think that’s 20 to 30 years down the road. What we’re learning, at least in Hodgkin’s and it’s probably true in large cell lymphoma if we take a close look, is within a few years and for sure by five and 10 years after treatment, we’re already seeing some of these late effects. It’s important to get that understanding from your local oncologist or survivorship expert.
Dr. Phillips: With anthracycline, a lot of times, we didn’t look and when you looked, you’d see a lot of cardiac effects, even within a year after completion of treatment.
Dr. Evens: You do. Now, it’s always tough. What do you do about it? But at a minimum, controlling your risk factors, like hypertension and cholesterol, certainly can’t hurt. It’s only going to do the body good.
Dr. Phillips: A lot of sites have cardiologists now that have taken an interest in oncology-related events. There are a lot of processes and steps, cardiac rehab per se, that have helped ejection fractions for a lot of patients.
Dr. Evens: There’s more funding. I’m working with a cardiologist at Tufts Medical Center who’s going to Beth Israel in Boston. She’s a cardio-oncologist and got a big grant funded to look at some cardioprotective agents early on, so thankfully, hopefully, they’ll be some resources.
It’s always hard, Stephanie. Whenever we talk about doing research, as you can imagine, you need funding and there tends to be a lot more from the pharmaceutical companies, which is understandable with the medications. With survivorship, there aren’t as many companies there, so we rely on the government through the National Institutes of Health or National Cancer Institute and philanthropy. There might be some other ways, but it’s such an important part of cancer care.
Stephanie: A hundred percent. Let’s get more funding for studying survivorship because that is so impactful for people.
With various agents, there’s always a small risk of secondary cancers that come from chemotherapy drugs. Whether you receive radiation or not is also a very important concern.
Dr. Tycel Phillips
Treatment Side Effects
Stephanie: Are there other late-term effects that people should be thinking about if they’ve undergone chemoimmunotherapy? Based on what you’re talking about from the R-CHOP plus X from ASH, is there anything else to call out specifically? People might think you’re adding a new drug, so does that mean they’re going to experience more side effects?
Dr. Phillips: It depends on the drug. With various agents, there’s always a small risk of secondary cancers that come from chemotherapy drugs. Whether you receive radiation or not is also a very important concern. We’ve learned long-term that some radiation risk factors don’t plateau and rather age with the patient. Those are all things to keep in consideration with some of these other drugs.
Thankfully, even with vincristine, which is a microtubule inhibitor, the biggest thing is neuropathy. The risk is the nerve damage is unpredictable and you may not get a resolution, so there’s always that concern and trying to prevent that from happening.
With some of the newer drugs, depending on their class, they all have unique side effect profiles. In the front-line setting, they’re given for a more limited time, which would hopefully prevent some of the side effects that we see in the relapsed/refractory setting, especially for drugs that are given until intolerance or progression, which is always a concern.
Looking at delta inhibitors in the relapsed/refractory setting, with indefinite use, you worry about liver irritation in some situations, diarrhea, and infection risk. With golcadomide, which is like a lenalidomide analog, reproductive risk is always a concern with that class, so if you’re a young woman, that’s always a concern in handling that medication. It can cause neutropenia, which may increase your infection risk when given with chemotherapy.
With the bispecifics, cytokine release syndrome is the biggest concern. Depending on when you give the chemo, you may mitigate a lot of higher-grade CRS, so you can potentially make that a bit easier to tolerate and less risky if you give a little chemotherapy to debulk the tumor and maybe blunt the immune response a bit.
Recent Data About Current FDA-Approved Bispecifics
Stephanie: Let’s move to relapsed/refractory DLBCL. There are two approved bispecifics for DLBCL: glofitamab and epcoritamab. Dr. Evens, can you talk about the most recent data? What’s relevant to patients about the two of them and the differences?
Dr. Evens: Generally speaking, it dovetails off of a lot of what we’ve already said. They’re very active. There are side effects, thankfully less than CAR T-cell therapy but similar, which is called cytokine release syndrome. Patients experience almost flu-like symptoms and some neurologic side effects as well. Thankfully, it’s less common, but it can still happen, so there certainly needs to be caution.
When we’re meeting a patient who received front-line therapy, whether it’s R-CHOP, R-pola-CHP, or dose-adjusted EPOCH and there’s a relapse, the historic standard was an autologous stem cell transplant. That’s gone down, but not away, with CAR T-cell therapy, commercial CD19.
I know your question was about bispecific antibodies, but there is a multitude of new CAR constructs. The current commercial CARs are CD19. More often than not, that’s the treatment of choice for many patients who relapse the first time, especially if it happens within 12 months, because bispecific antibodies for diffuse large B-cell have been after that. Not that it would be wrong to do it instead of CAR T-cell therapy; we just haven’t seen as much of the data. In some ways, that’s where bispecifics have tried to leapfrog and go to the front-line setting.
Whether it’s used in second-line or third-line, the bottom line is both medications are very active. They’re more similar than different, although there are some key differences. One is given intravenously, the other is given subcutaneously, and one has a few more doses than the other, but they’re largely much more similar than they are different.
Tycel, you don’t ever use standard before CAR, do you, in someone who can take CAR, right?
Dr. Phillips: That was a bridge.
Dr. Evens: Are you doing bispecifics as a bridge to CAR sometimes?
Dr. Phillips: Only in patients whose diseases rapidly progress and we need to stabilize before we can get them to the CAR product. But I agree with you. CAR equals cure. With bispecifics, we guess, but we don’t know for sure. Until we can be 100% certain, you’d be very hard-pressed to put a bispecific before a CAR in the second-line space.
Dr. Evens: Part of that is time. CARs have a several-year lead time and to say “cure,” two years in remission is a pretty good point. After five years, you feel good. That’s where we see CAR T-cell therapies. We saw some data at the meeting settling out around the 30% to maybe 40% range. We’re hopeful that we can say cure. We don’t have that lead time with bispecifics, although we’ll see over the next couple of years where those land.
Stephanie: CAR T-cell therapy came out first in research, so there’s more data and real-world evidence about how they perform. With clinical trials, it’s a different population, so it’s nice to be able to see what happens.
Dr. Phillips: CAR T-cell therapy has remained reproducible in the real-world space as it has in clinical trials, which is not the same as a lot of other drugs where you typically see a decline in efficacy once you move out of the clinical trial space. That hasn’t happened with CAR T-cell therapy.
Dr. Evens: Clinical trials are real world. Real world is a lingo that we use, meaning all comers, regardless of kidney function, age, etc., and not like the qualifications you need to join a clinical trial. He’s exactly right.
To put an extra point on that, for CAR T-cell therapy and bispecifics, there’s almost no upper age limit. With autologous stem cell transplant, you can do it up to patients in their 70s, maybe up to 80, but it gets a little tricky. Not to say CAR T-cell therapy and bispecifics in older age groups are a walk in the park, but they’re very manageable and doable.
Another part of science we hope to understand: which treatment works in which type of patient.
Dr. Andrew Evens
Bispecifics vs. CAR T-cell Therapy Mechanism of Action
Stephanie: Dr. Evens, could you summarize the mechanisms between CAR T-cell therapy and bispecifics in a way patients can understand?
Dr. Evens: It can be confusing for sure. I would frame them both under the rubric of immunotherapy. We talked about autologous stem cell transplant, which is also a fancy word. It’s not like getting a new liver or kidney; that’s called an allogeneic. Autologous transplant is one cycle: a very high-dose chemotherapy blasting hopefully the lymphoma away. But what about blasting your cells? We know that one of the most powerful anti-cancer agents is your immune system — your T cells in particular. We don’t know why, but in some cancer patients, lymphoma patients, they’re not doing what they’re supposed to.
CAR T-cell therapy cell is filtering out your T cells, sending them to a company, and over about a 3 to 4, sometimes five-week period, they’re re-engineering it by doing two things. They’re transfecting an antibody to tell it where to go when you put it back in and then in some ways, you supercharge it or activate it. When you re-inject it, it’s a one-time treatment several weeks later. It not only rapidly expands, but hopefully, it goes this supercharged T cell with the CD19 attached to it wherever the lymphoma is in the body.
What are bispecifics? It’s similar in concept in that it’s the patient’s immune system, but it’s an off-the-shelf treatment. The way to think about it most simply is a double antibody. It’s a CD20, which interestingly is rituximab. If rituximab in most patients stops working, why would this? Because the second antibody is CD3. When it’s off the shelf and injected, CD20 goes to where the lymphoma is, but the CD3 has T cells attached to it, so it delivers the patient’s endogenous or in vivo T cells to where the lymphoma is.
It’s remarkable. I’ve had a multitude of patients, as I’m sure Dr. Phillips has, where CAR T-cell therapy is given, it doesn’t work and we don’t honestly know why, but we’re thrilled when it happens, then you give bispecifics, and the lymphoma completely goes away. This is someone who has already failed regular CD20 single antibody, CD19 CAR, and then a different immunotherapy for one reason or another is effective. That’s another part of science we hope to understand: which treatment works in which type of patient.
Stephanie: There’s a lot of science to wrap up into this very abridged version, but I know the goal here is this more targeted. It’s engineered and using your immune system and it’s targeted with the goal being that we feel fewer side effects than blasting the whole body with chemoimmunotherapy. Dr. Phillips, is that how people can think about that?
Dr. Phillips: When I try to find the easiest way to compare chemotherapy to other treatments, I go back to the military where chemo is like napalm. It’s going to kill anything that’s growing rapidly because that’s what it’s designed to do. It isn’t specific for anything, one way or the other. A lot of these targeted treatments, such as bispecifics and CAR T-cell therapy, are more focused on directing your treatment toward the problem, which is, in essence, a malignant B cell.
There is still some ambiguity because normal B cells will be impacted. After all, we’re still targeting CD20. Hopefully, in the future, we’ll have some cancer-specific markers that may even spare normal immune cells. But to this point, we’re sparing a lot of other tissue because it’s directed toward a malignant B cell, which chemotherapy can’t do.
The closest we can get to that is antibody-drug conjugates, which will deliver a toxic drug directly to the tumor. The drug isn’t active until it’s internalized and then it can kill the tumor off. But even in that sense, you will get some spillage. As the cancer cells die and open up, that drug is also free to kill other bystander tumors but also any normal tissue that’s in the area, which explains some of the side effects we see.
Stephanie: I love it when there’s real-world verbiage so people can understand better.
Cytokine Release Syndrome
Stephanie: Dr. Evens, cytokine release syndrome was mentioned as a monitored side effect when it comes to immunotherapy. What does that look like in patients and what are the differences between what you’ve seen in the responses with CRS from CAR T-cell therapy versus bispecific?
Dr. Evens: It’s very similar as to when it happens. Thankfully, with bispecifics, it’s usually less frequent and less severe, although not zero, so you still have to have some caution. We don’t like to talk about it, but whenever we mention grade 5, that’s a fatal side effect and thankfully, it’s very uncommon, but we want to keep that 0%, as long as there’s the right training and the right medication on the shelves.
When I say the right training, it’s not the oncologists, doctors, nurses, and pharmacists. It’s making sure your emergency room and intensive care unit know. Like for many things in life, you’re preparing for the worst in case it happens.
For example, I gave a patient a bispecific antibody on a Friday. By Wednesday night, that patient had a very high fever, so he was experiencing a delayed cytokine release. He went to the emergency room. We have a protocol, so they know what to look for. We had a conversation and were able to mitigate it. The patient did not need to be admitted to the hospital. The fever quickly came down and he felt fine.
It’s a team sport as we’re managing some of the side effects and thankfully, almost always, it’s very manageable but it’s important to have that communication and collaboration across all specialties.
If a patient has cytokine release syndrome, the earlier you intervene, the better because you can mitigate and stop it from escalating to a higher grade, but your team has to be aware of what to look out for.
Dr. Tycel Phillips
Monitoring Side Effects
Stephanie: A huge topic for patients is the logistics side and considering what they have access to. Dr. Phillips, can you paint that picture for those considerations when it comes to patients? Do they have to be monitored? How long do they have to be monitored for potential CRS after CAR T-cell therapy and bispecifics? How can that impact the choices that they may have depending on where they live?
Dr. Phillips: In essence, CAR T-cell therapy is a little different. We typically think that the patient will be in and around the cancer center for about 30 days. You also are required to have a caregiver with you almost 24/7. Even in institutions where we can move patients to outpatient for CAR T-cell therapy, that still requires you to be on campus, have a caregiver, and go back and forth to the hospital. It requires more logistical hurdles to get over.
In some sense, CAR T-cell therapy is also akin to transplant centers. A lot of these things are in place as far as the inpatient portion because instead of admitting somebody for high-dose chemotherapy and then a stem cell rescue, you’re giving them CAR T-cell therapy with inpatient monitoring and very close follow-up. When you’re in the hospital, they’ll be monitoring you for neurological changes and vitals will be taken to monitor for any signs of cytokine release syndrome. These are done very closely.
Bispecifics, on the other hand, as Dr. Evens has eloquently elucidated, can be given in a community setting. The only real thing you need to have is education for the patient and the staff about what may happen if bad things happen. If a patient has cytokine release syndrome, the earlier you intervene, the better because you can mitigate and stop it from escalating to a higher grade, but your team has to be aware of what to look out for.
Normally, when a patient is on any oncologic treatment and they come in with a fever, you reflexively think it’s an infection and you give antibiotics and draw blood cultures. You don’t necessarily think cytokine release syndrome. With bispecifics, you need to think of cytokine release syndrome. Even if you are working up for an infection, you need to be putting those things in place to mitigate cytokine release syndrome.
Having certain medications on the formulary, like tocilizumab, can be difficult because it is cost-prohibitive, to be honest, so every hospital system doesn’t want to keep this on, especially if they’re not using it. These need to be in place. Most centers that have incorporated bispecifics have a designated champion, which is somebody who plays quarterback to organize the rest of the team. We have plans in place when patients come in. We have contact information and if anything goes awry, they’re there to fix and get everybody realigned, so when the next patient comes in, it doesn’t happen.
The timing depends on what you receive. IV medications tend to have an early onset of cytokine release syndrome with bispecific. With these subcutaneous formulations, sometimes these things happen at home, at which patient education becomes very important.
Make sure you have a thermometer at home to monitor for fevers. Some people have blood pressure monitors. Some people have advocated for other things to self-help. Make sure you have antipyretics at home, like acetaminophen or ibuprofen. Some physicians send patients home with a pill in a pocket, which is steroids, which in some situations can mitigate cytokine release syndrome or at least keep things stable until they can get to the hospital.
Can CAR T-cell Therapy Cure Some Patients?
Stephanie: Dr. Evens, you mentioned the word “cure,” but we need data. There was the five-year data for ZUMA and TRANSCEND trials. From a quick glance at that, is there anything more you want to add to this general feeling about CAR T-cell therapy and its ability to be curative? I know you talked again about needing more time.
Dr. Evens: It is time, though, Stephanie. It comes down to that. In the pre-CAR era, we tell patients that hopefully it doesn’t come back. In the minority of cases when it does, it most commonly happens in the first two years and then a little bit through years three, four, and five. It’s uncommon after five years with chemotherapy, but never impossible.
We expect that that dynamic should be the same because it is an aggressive cancer. How can it live around for five-plus years? These numbers we’re seeing at five years is what we call the plateau in the curve. It looks pretty darn flat once you’re getting out to three, four, and especially five years. I feel pretty confident we can use the word cure.
Anytime you have a treatment primarily anchored around academic medical centers when we know that over 80% of cancer care happens at nonacademic centers or community centers, there’s going to be a problem and a problem related to access.
Dr. Andrew Evens
Community Access to Treatments
Stephanie: Dr. Evens, widely discussed in patient groups is accessibility to CAR T-cell therapy. You both are at major academic centers. You’ve got all the tools and the latest, but for a lot of people who live in the community, this doesn’t seem to be very feasible.
Dr. Evens: That’s a major issue and Dr. Phillips aptly alluded to this. Depending on which data set you look at, in some cases, only 20 to 25% of patients who should receive it are receiving it. It will never be 100%, but it certainly should be more than 20. Anytime you have a treatment primarily anchored around academic medical centers when we know that over 80% of cancer care happens at nonacademic centers or community centers, there’s going to be a problem and a problem related to access.
What are ways to circumvent that? We don’t want to do anything haphazardly with any treatment. Can we try with certain community centers in collaboration with academic centers or maybe on their own and working with pharmaceutical companies or even foundations to be able to do it? You bet. In New Jersey, some strong, non-academic medical centers are giving CAR T-cell therapy carefully, so it definitely can be done. Better knowledge and prophylactic treatments, like steroids or tocilizumab. There was some data on this at the 2024 ASH meeting.
Maybe we can get to second- and third-generation CAR T-cell therapies that are engineered in a way that rapid overexpansion of T cells, which is driving a lot of the side effects, is more predictable or doesn’t happen. I’m hopeful that we’ll get there, but that’s part of the reason why bispecific antibodies have become a little easier.
Assuming the patients have access, some can’t wait four or five weeks. They don’t have enough time. It’s a big issue, but it’s top of mind and we’re thinking about all of these issues and how to remedy them. You guys have community centers don’t you, Tycel, not just in Duarte, right?
Dr. Phillips: We have a lot of community sites. They’re not doing CAR though.
Dr. Evens: They’re not? You know what we’re starting to do? We’re segmenting it. We loosened it to a little less than 30, but what we’re doing is having them do the pheresis. We have the New York Blood Center. It’s going to be tough with the current commercial CAR. Maybe in a bigger community, but it’s going to be tough in a small one.
We’ve had several data sets that show that you can still successfully harvest and administer CAR T-cell therapy in patients who’ve been exposed to bispecifics.
Dr. Tycel Phillips
Choosing Bispecifics vs. CAR T-cell Therapy
Stephanie: With bispecifics being more accessible in the community and in terms of wait time, when would you want to give bispecifics versus CAR T-cell therapy? Let’s say a patient has both as an option.
Dr. Evens: We’re not sure bispecifics are as effective as CAR T-cell therapy in the second-line setting. Let’s say for one reason or another, you can’t get CAR T-cell therapy. I don’t know what you think, Tycel. It wouldn’t be wrong to give bispecifics.
The only mild note of caution would be it’s not like rituximab. Even though most patients do well, you have to have some structure and organization in place before you even give the bispecific antibodies. They’re more doable for community oncology for sure than CAR T-cell therapy, but there still needs to be that note of caution.
Dr. Phillips: Thankfully, we know that limited use of bispecifics doesn’t appear to impact the efficacy of CAR T-cell therapy. We’ve had several data sets that show that you can still successfully harvest and administer CAR T-cell therapy in patients who’ve been exposed to bispecifics. That was a big concern that everyone had. But so far, based on a French and a US study, it doesn’t seem like that is much of an issue in that patient population.
Because they’re off the shelf, the accessibility of bispecifics is there. As these drugs move into other disease settings, such as solid tumors, you’ll likely see wider adoption and more incentive for community sites to use them because they won’t be doing them for the limited number of lymphoma patients. If they’re giving it for lung cancer, breast cancer, and prostate cancer, there are far more patients in that sense. Financially, it gives them more of a reason to have a structure in place for bispecifics and also the medication they need in case things go wrong.
Dr. Evens: There are two off-the-shelf CAR T-cell therapies in clinical trials, which are the so-called allo-CARs. The current agents we have FDA-approved are good, but there are still barriers and we need them to transcend more throughout the community for our cancer treatment.
Stephanie: For clarification, Dr. Phillips, there was some concern about bispecifics impacting the efficacy of CAR T-cell therapy given after, but that hasn’t proved to be the case. You were talking about bridging as well. What I’m hearing is it’s looking promising in terms of the optionality that is here at the fingertips and in research. Is that right?
Dr. Phillips: At this point, especially for the patients who Dr. Evens has talked about and those who maybe can’t get to CAR T-cell therapy for whatever reason, at least with these, we can maybe stabilize the disease enough to allow them the opportunity to get the CAR T-cell therapy if it’s feasible. In some patients, they won’t be able to get to CAR T-cell therapy because they need a lot more support than other treatments so that all has to be in place.
Latest Treatments in Follicular Lymphoma
Stephanie: Follicular lymphoma is very different in that it’s a slow-growing, indolent disease. Let’s start with the relapsed/refractory follicular lymphoma patient population. Can we set the stage by going over what’s available right now and some of the updates?
Dr. Phillips: In the relapsed/refractory phase, most people will use R2 (Revlimid and rituximab) based on the AUGMENT study, which showed a significant improvement over rituximab in this patient population. A lot of us are very comfortable with the use of that medication, and the efficacy and tolerability seem to justify it in the second-line space.
After that, it gets a little bit more variable. You have bispecific antibodies approved: mosunetuzumab and epcoritamab. CAR T-cell therapy is available in follicular lymphoma, albeit a little bit of a different argument. CAR T-cell therapy doesn’t necessarily have that curative label as it does in large cell lymphoma, so there’s a lot more variability about what you use in that space.
Recently, we had zanubrutinib and obinutuzumab based on the ROSEWOOD study, which is the first time a BTK inhibitor has shown any benefit for follicular lymphoma. Then there’s tazemetostat, which is an oral EZH2 inhibitor for patients with an EZH2 mutation or those who are deemed to be unfit for other agents, which are all approved in the relapsed/refractory follicular lymphoma space.
Top Developments in Relapsed/Refractory Follicular Lymphoma
Stephanie: Dr. Evens, there was a late-breaking abstract at the 2024 ASH meeting from the phase 3 InMIND study, which looked at tafasitamab plus lenalidomide and rituximab for the relapsed/refractory situation. Can you provide highlights from this and why patients should pay attention?
Dr. Evens: This was an important presentation and abstract, which was presented by Dr. Laurie Sehn from BC Cancer. It was built off the R2, Revlimid (lenalidomide) in combination with rituximab, which is commonly used in the second-line setting. It was a placebo-controlled study of R2 plus or minus tafasitamab, a CD19 antibody that is already FDA-approved for relapsed/refractory diffuse large B-cell and looking at its entry into follicular lymphoma. It was relapsed/refractory follicular lymphoma, so you had to at least have received rituximab therapy, second line, some somewhere beyond.
It was very effective. There are certain things we look at called hazard ratios and percentage points. Relatively speaking, there was a 57% improvement in progression-free survival, which was pretty significant. If you want to look at it by absolute months, it was on the median of about 12 months, a little bit less than 12 months benefit. This is a presentation. It doesn’t mean it’s FDA-approved although it’s pretty encouraging. I would hope and expect that soon, it will be submitted and eventually be an FDA-approved option for patients.
Dr. Phillips: I was surprised when I saw it and even more surprised about the results.
Dr. Evens: I like tafasitamab. There are no side effects and sometimes it works, but obviously, it’s a tougher patient population than diffuse large B-cell lymphoma. But it had very impressive efficacy and tolerability. We’ve known through the diffuse large B-cell approval that it’s a pretty tolerable medication.
Dr. Phillips: One key point also is that the standard of care arm performed worse than the AUGMENT study, but they enrolled patients with worse disease burden than AUGMENT did. It was a harder-to-treat patient population and they still had very good results that look better than what we got on AUGMENT, so hats off to them because they addressed the elephant in the room ahead of time and had data to support it.
How Should Patients Interpret the Results?
Stephanie: Compared to what’s approved for relapsed/refractory follicular lymphoma, Dr. Evens, how would you explain to patients one side’s already approved and the other side we’re talking about is promising data in research?
Dr. Evens: Like many clinical trials, it’s more than encouraging. It was a phase 3 head-to-head study and you’re not sure of the comparison. It’s a little bit of a waiting game. Sometimes what happens in the United States is there’s a panel called the National Comprehensive Cancer Network (NCCN) that will sometimes list it on its site before FDA approval, although usually they like to see a peer-reviewed manuscript and FDA approval. It emboldens the point of how important clinical trials are. For all of non-Hodgkin’s lymphoma and Hodgkin’s lymphoma for that matter, there are so many new and exciting treatments, but they have to be done with caution on a controlled clinical trial.
Bispecifics and Follicular Lymphoma
Stephanie: We talked extensively about bispecifics in DLBCL. What has the response been in follicular lymphoma and relapsed/refractory follicular lymphoma?
Dr. Phillips: It’s been good. The data has been very impressive. They have longer follow-up mosunetuzumab compared to epcoritamab, but that’s because it was approved sooner. I would think most people would prefer a bispecific over CAR T-cell therapy in a very similar patient.
There are some caveats. Some patients have more aggressive disease and more concerning features where you would probably go to CAR T-cell therapy. The safety of these drugs and lack of hospitalization are important. None of the ones approved in follicular lymphoma require patients to be hospitalized for observation and have very low rates of CRS. Mostly the ones that we see are grade 1, very few grade 2, and again, high overall response rate, high complete response rate, and very impressive durability of response.
Pending how things appear when the patient relapses, like if they still express CD20, it does offer the opportunity to retreat these patients with a bispecific, which is some of the stuff that future research is looking to determine whether they can still get very durable responses on second treatment. There have been very small data sets so far about the retreatment aspect, but that’s the opportunity that bispecifics can offer patients, even in a community setting without having to travel far from home.
Dr. Evens: Sometimes these diseases, even follicular lymphoma or other indolent lymphomas, can pick up ahead of steam and cause symptoms and that usually is where it gets large or becomes a trigger to start treatment. It’s treatable. We know now through randomized trials that life is extended with many of these therapies.
Generally speaking, it’s still not curable. We’re going to keep doing clinical trials and shooting for that cure. Not that quality of life is not important in diffuse large B-cell, but it’s ultra-important in follicular lymphoma. Hopefully, most if not all of these trials have some embedded quality-of-life measures to make sure that not only is the treatment effective, but it also allows patients to maintain their quality of life.
Over a 20-or 30-year period, some patients with follicular lymphoma may go through six, seven, or eight different treatments. Our hope is during that length of life, a good chunk of it is off-treatment and that’s why so many of these studies, thankfully, are being done with time-limited treatment. You treat for six months, a year, or even 18 months, pause, and hopefully patients can enjoy that remission off-treatment for as long as possible.
Dr. Phillips: He summarized the dilemma in follicular. You’re less willing to take toxicity because longevity and quality of life are paramount.
Dr. Evens: We presented a poster at ASH. Dr. Vaishalee Kenkre at the University of Wisconsin was the lead author. We have the Big Ten Cancer Research Consortium where we’re able to study. A study that Dr. Kenkre brought up is a common treatment, bendamustine-rituximab, in the front-line setting, given usually for six months. She brought tazemetostat, one of the medications Dr. Phillips mentioned, to the front-line setting and only gave three cycles of bendamustine-rituximab. There was a very early, response rate of 100% so far. But again, every trial in many ways is a good clinical trial. Hopefully, we can shift many of these novel and targeted treatments to the frontline that are more tolerable and time-limited, and garner long remissions without cytotoxic chemotherapy.
Dr. Phillips: Tazemetostat is one of the more tolerable oral medications I’ve ever seen.
Dr. Evens: It is and it’s remarkable. It’s very early. It was only 12 or 13 patients, but it’s a lead-in study, so you get tazemetostat and then concurrent taz-BR. It’s agnostic of the EZH2 mutation. We’ll have to see how that pans out, whether it matters or not in the front-line setting.
Dr. Phillips: The big point you said is no added toxicity, which we saw with a lot of other drugs. Lenalidomide is toxic with bendamustine. Even BTK inhibitors can cause some problems with bendamustine.
Dr. Evens: That’s right. It was investigator-initiated and thankfully, we were able to convince the company not to add it on to six of bendamustine-rituximab, but let’s try and do a short course of bendamustine. We’ll see how that pans out. Almost all of the medications in some form or fashion are being looked at in clinical trials in the front-line setting and that’s what we want — super-targeted, effective, incredibly well-tolerated, yet time-limited therapy for follicular lymphoma and other indolent lymphomas.
Key Takeaways
Stephanie: We’ve talked a lot about the research that’s happening and what’s already out there. What would you say to patients and their care partners in terms of the landscape over the next few years, both in DLBCL and in follicular? What are the trends and what are you excited by for patients and care partners?
Dr. Phillips: In large cell lymphoma, we are moving towards more personalized care. Even though we’re adding extra medications, it doesn’t necessarily mean we’re adding extra toxicity, which hopefully gives more efficacies without impacting quality of life or even adding long-term side effects to the patient profile. It’s all good news for the patients because everything for the most part is a specifically targeted treatment and not necessarily as generalized and causing a lot of side effects.
I’m excited to see where front-line large-cell lymphoma goes. Even in the relapsed/refractory space, as Dr. Evens alluded to, there are more and more treatments coming along. We are incrementally increasing the number of patients we’re curing from this cancer. The fewer patients there are in the relapsed/refractory space, the fewer patients we lose to this cancer, which is important and a big leap. Five years ago, you could routinely say that about 35% of patients would probably have very bad outcomes and there wasn’t much we could do about it.
Follicular lymphoma has become like what we see with Hodgkin’s without the ability to cure, but we’re trying to improve what we’re doing for patients with a very high recognition of tolerability. Anything moving up and being added are drugs that are safe and effective. Safety is paramount, so the quality of life that patients deserve and the extended survival will be time that they can enjoy with their family without worrying about side effects that come from these treatments.
We’ve already talked about tafasitamab, lenalidomide, and rituximab. We’ll have the bispecifics. Tazemetostat is being explored with R2. Eventually, some of these things may move into the front-line space and we can re-challenge the role of where chemotherapy fits in our patient population, even with time-limited therapies without cytotoxic drugs. It’s a very exciting time as we move forward. It may be more confusing for us as physicians because we’ll have more options, but that usually always equals good outcomes for patients.
Dr. Evens: Tycel did an amazing job of giving a summary, so I’m going to put a pin in a word he said: exciting. It’s an exciting time for investigators, like Dr. Phillips and myself, but also for patients and caregivers. There are a multitude of novel, targeted treatment options. We talked a lot about immunotherapy but also even some oral, targeted therapies that are on our shelves now as we speak and probably 100-plus new ones coming down the pipeline. What does that mean for patients? It hopefully means a lot of good things and a lot of more effective and tolerated therapy.
For patients and caregivers, always ask questions. Please never be hesitant to ask your oncologist a question. What are all of my treatment options, whether on the shelf or on a clinical trial? Never hesitate to bring up a side effect you have, whether it’s numbness, tingling, fever, or something more significant. Open lines of communication are paramount.
Patients have their family members and doctors, but there are so many good societies and foundations out there that can be a great anchor for patients to talk to other patients and get information. There’s a lot of great information in a fast-moving field but in all great directions.
Conclusion
Stephanie: Thank you so much, Drs. Evens and Phillips, for being here, for the work that you do, and for going way above and beyond treating your patients. We look forward to featuring you again soon.
With that, we wrap up another wonderful discussion at The Patient Story. I appreciate these doctors who take time out of their busy schedules to provide great insights for us in a way that we can understand better. It’s so important to be empowered, to lean into this communication, and to have more conversations about what’s impacting your quality of life so that you as patients, caregivers, and care partners can work together with the medical teams to stay on treatments that are effective and live life the way that you want to.
Thank you again to our partner, The Leukemia & Lymphoma Society. Check out the links to the LLS’ different parts of their website for their resources, like the information resource center, which provides free one-to-one support with questions across the board, and their Clinical Trial Support Center, where clinical trial nurses help you find trials, stay on trials, and answer all the questions in between.
We hope that this was helpful to you. Thank you so much for joining and we hope to see you at another program soon. Take good care.
Thank you to The Leukemia & Lymphoma Society for their partnership. The Leukemia & Lymphoma Society is here for you with information about clinical trials, resources, and support.
How I Learned to Live with CLL—And Stop Letting It Control Me
Margie was diagnosed with a type of blood cancer that affects the bone marrow and blood. One day, she noticed a swollen lymph node she had never seen before. Doctors ordered a scan and biopsy of the lump. That’s when she got the news no one wanted to hear: she had a rare blood cancer called chronic lymphocytic leukemia, or CLL.
Interviewed by: Taylor Scheib Edited by: Katrina Villareal
Margie’s diagnosis was a rare blood cancer, chronic lymphocytic leukemia (CLL). There’s no official cure but there are a lot of treatment options.
Name: Margie H.
Diagnosis:
Chronic lymphocytic leukemia (CLL)
Symptoms:
Large lymph node in her neck
Fatigue as the disease progressed
Treatment:
Targeted therapy
Thank you to AbbVie for supporting our patient education program. The Patient Story retains full editorial control over all content
I live in Southern California. I had a lymph node in my neck that was enlarged. I was diagnosed with chronic lymphocytic leukemia (CLL) in 2019. They gave it a little positive spin and told me that if I had to have cancer, it was the best kind to have.
How She Found Out She Had Cancer
I noticed a lump in my neck, so I went to my primary doctor. She didn’t know what it was, so she sent me for a CAT scan. I had a biopsy and that’s how it was diagnosed.
I didn’t have any other symptoms, so it was quite a shock. I’m relatively healthy, so to have someone say that I had cancer, I thought, “That can’t be,” but it was.
It’s very scary. One of the hardest things for me was telling my kids. It’s hard to tell your kids that you have cancer, but they were very supportive. I noticed the lump in September and was diagnosed in November, so it was very quick.
Finding the Right Doctor
Kaiser was willing to send my information for a second opinion. I ended up with the head of the department of chronic lymphocytic leukemia (CLL) at Dana-Farber Cancer Institute in Boston and I thought that was God’s doing. He was even involved in the research of the medication that I eventually took. Before he looked at my information, he said, “What’s your plan? What’s your goal? Do you want to have more life in your life or do you want to have a longer life?”
My daughter got a list of all the treatments and medications from a niece who’s a doctor. When I was with my family, we went through everything. We had a couple of nurses in the family, so we had some medical knowhow. Because I had high blood pressure and was taking blood thinners, we found all the ones that I was eligible for and talked about the side effects.
The specialist said, “I looked at everything. You need one more test and if you don’t have a mutation, then this is exactly what you should take. If you come out mutated, this is what you should take.” I took his report to my oncologist and that’s the way we went.
Because the side effects of the medication can be bad, they don’t want to start treatment until your symptoms are much more severe
Learning She Wouldn’t Get Treatment Right Away
I was on watch and wait. Some people call it watch and worry. Because the side effects of the medication can be bad, they don’t want to start treatment until your symptoms are much more severe, so I wasn’t treated until June 2021.
I came up with an idea during watch and wait. Think of it as boot camp. When you go to boot camp, they get you physically strong and when you’re physically strong, you do exercises to keep it that way. If you’re not, then you start.
Next, they teach you what you need to do if you have to go into battle, which is what you need to learn about chronic lymphocytic leukemia. The next thing they do is build a community around you. I didn’t recognize it at the time, but those were the steps I took. If a person would use watch and wait as a boot camp rather than as a time to worry, it would make a difference.
Noticing More Symptoms from the Cancer
After a year and a half, I developed more lymph nodes. A lot of them were on my stomach, so they were concerned about crowding the main organs. Other than that, they wouldn’t have started treatment.
You’re supposed to watch out for fatigue and night sweats. I didn’t have night sweats, but I experienced fatigue by early spring of 2021. I measured how I was doing by how I fared when I hiked. If I could still hike as far as I could or as fast as I could, if I could get up the hill, then I was still okay. However, I noticed a difference in late spring that year.
We had a family meeting after my grandson’s wedding and we decided that I should do the targeted, time-limited medication.
Fatigue was the only thing that I felt that made a difference. Eventually, I told a couple of my hiking friends. I also put in a prayer request at church, so my church family knew.
I see myself as a strong person. When something happens to you, you think that will diminish your strength and people will start looking at you differently because you aren’t as strong as you thought you were.
There are several types of treatments. I didn’t qualify for some because I’m taking blood pressure medication and blood thinners. There’s time-limited therapy and medication that you’re on for life or until it quits working and then they put you on a different one. We had a family meeting after my grandson’s wedding and we decided that I should do the targeted, time-limited medication.
Her Treatment Experience
I was a textbook case. It was fantastic. I had no side effects. I had six infusions in the beginning. One month after I started my infusions, I started my oral medication.
There are serious side effects to the oral medication. Tumor lysis syndrome is very dangerous. It can affect your kidneys. They put you in the hospital for the oral medication. I was in the hospital for three days as they put me on step-up dosing. It couldn’t have gone more perfect, so I’m very blessed.
Why worry about the things that we can’t change? If it comes back, I’ll be treated again.
Being Off-Treatment
I have blood tests every three months and see the oncologist every six months. I have no symptoms. Everything’s good. I couldn’t ask for anything better.
I don’t even think about it anymore. Before treatment, it used to be like having a time bomb that you’re waiting to go off. But since I’ve had treatment, I rarely even think about it — only when I have my blood test or oncologist appointment. I’m a very positive person.
I listen to a Christian radio station in my car and I heard something that said, “Change the things you can and adjust your attitude to the things you can’t.” Why worry about the things that we can’t change? If my chronic lymphocytic leukemia comes back, I’ll be treated again. It’s likely to come back. I’m not cured. I’m in remission or what they call undetectable minimal residual disease (uMRD).
Words of Advice
CLL isn’t a death sentence. Be your own advocate. Go and find the information. I know there are other sources, but HealthUnlocked was so fantastic for me. Build a good support system.
I want people to be encouraged and not discouraged. There are so many diseases out there that are so much worse than what I have and what I went through. We have to count our blessings when we can.
Special thanks again to AbbVie for supporting our independent patient education content. The Patient Story retains full editorial control.