Accessing the Best Care for You or a Loved One
Understanding New Options for Non-Hodgkin Lymphoma
Edited by:
Katrina Villareal
Dr. Kulsum Bano and Dr. Nilanjan Ghosh from Atrium Health Levine Cancer Center, along with Dr. Justin Favaro from Oncology Specialists of Charlotte, discuss with 3-time DLBCL survivor and patient advocate Dr. Robyn Stacy-Humphries the latest advancements in non-Hodgkin lymphoma treatment, including DLBCL and follicular lymphoma.
Key topics include emerging treatments and clinical trials, care collaboration, symptoms and side effect management, and optimizing sequencing.
This program is brought to you by The Patient Story in partnership with The Leukemia & Lymphoma Society, the American Cancer Society, the Lymphoma Coalition, and LIVESTRONG® at the YMCA.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider to make informed treatment decisions.
The views and opinions expressed in this interview do not necessarily reflect those of The Patient Story.
- Introduction
- Diffuse Large B-cell Lymphoma (DLBCL)
- Follicular Lymphoma
- Bispecific Antibodies
- CAR T-cell Therapy
- Cancer Clinical Trials
- Treatment Sequencing
- Possibility of Chemo-Free Cancer Treatment
- Improving Access to Cancer Care
- Final Takeaways
- Q&A
- Getting a Second Opinion
- Epcoritamab vs. CAR T-cell Therapy
- Remission After Bendamustine & Rituximab (BR)
- Possibility of a Repeat Transformed Follicular Lymphoma (tFL)
- B-cell-based Immunotherapy
- Post-CAR T-cell Therapy
- Second CAR T-cell Therapy
- Newer Monoclonal Antibodies
- Cannabis & Non-Hodgkin’s Lymphoma
- Keto Diet
- Intermittent Fasting
- R-EPOCH vs. R-CHOP for Triple-Hit DLBCL
- Patient Group That Benefits More from CAR T-cell Therapy
- CLL vs. Follicular Lymphoma
- Conclusion
Introduction
Stephanie Chuang, The Patient Story Founder
Stephanie Chuang: My name is Stephanie Chuang. I’m the founder of The Patient Story. The genesis of The Patient Story was my non-Hodgkin lymphoma diagnosis at 31 years old. I remember how overwhelmed I felt and didn’t even know what questions to ask my doctor. What do I do? Where do I go? But it was more like what do we do? Where do we go? Because as we all know, a cancer diagnosis impacts so much more than the patient.
We know there are so many things to consider, but I believe the core of what can make a difference is empowering ourselves to be more active in our care. I’m so thankful for advocates in every form, including other patients, care partners, and healthcare providers who invest so much time and energy in ensuring that we get the best care and know what clinical trials may be an option for us and not as a last resort.
This program is produced by The Patient Story in collaboration with The Leukemia & Lymphoma Society, an incredible advocacy organization that has free resources for patients and care partners in blood cancers, and an organization that has supported more than 85% of blood cancer treatments approved by the FDA to date.

As with all our programs, The Patient Story retains full editorial control over the content.
While we hope you learn a lot, it is important to note that these discussions are not a substitute for seeking medical advice, so please speak with your own medical team about what’s most appropriate for you.
Our patient moderator is Dr. Robyn Stacy-Humphries. Not only is she a long-time respected physician in the Charlotte area, but she is a three-time DLBCL patient and survivor, and someone I’m lucky to consider a friend. I admire her so much for the advocacy work that she does as a physician and now as a patient advocate. Robyn, thank you so much for joining us and leading our discussion.

Robyn Stacy-Humphries, 3x DLBCL Survivor
Dr. Robyn Stacy-Humphries: I’m Robyn Stacy-Humphries, a three-time diffuse large B-cell lymphoma survivor. I’m one of the first patients in the United States who received CAR T-cell therapy in 2016.
Nilanjan Ghosh, MD, PhD
Dr. Nilanjan Ghosh: I’m Nilanjan Ghosh, the head of hematology at Levine Cancer Institute at Atrium Health. I also lead the lymphoma division. It’s a real pleasure to be here to discuss DLBCL as well as follicular lymphoma with my colleagues.
Kulsum Bano, MD
Dr. Kulsum Bano: I’m Kulsum Bano, a community oncologist who works at Levine Cancer Institute. It’s a privilege to take care of patients with lymphoma and an honor to be here to talk to everyone. Thank you.
Justin Favaro, MD, PhD
Dr. Justin Favaro: I’m Justin Favaro, a physician, medical oncologist, and hematologist in Charlotte, North Carolina. I’ve been in private practice for 18 years. I see a wide spectrum of different types of cancer, with a special interest in malignant hematology, lymphoma, and leukemia. I love the science of this disease and the technology, and I love to learn more from you all as we try to tell you what we know about this disease. It’s a pleasure to be here.
Diffuse Large B-cell Lymphoma (DLBCL)
Robyn: Diffuse large B-cell lymphoma is the most common of the non-Hodgkin lymphoma types. It is very aggressive and, without treatment, most people’s survival rate is only one year.
We are also going to talk about follicular lymphoma. There is some overlap, but follicular is an indolent lymphoma. People may present or be asymptomatic. It can progress rapidly or it can last for years. DLBCL and follicular lymphoma are managed differently.
First, we’re going to talk about diffuse large B-cell lymphoma. Dr. Favaro, what are the current treatment options for diffuse large B-cell lymphoma when a patient is first diagnosed? What you do with your patients?
Current Treatment Options for DLBCL
Dr. Favaro: Before I talk about this disease, try to imagine a cancer cell as a ball. It’s a little simplistic, but if you think about a ball, in the middle of the ball is where all the DNA is. The DNA is the recipe for what makes a cancer cell what it is. There are 30,000 genes. This DNA in the middle of that cell is making all these proteins that make that cancer cell grow and make it do what it does in your body.
On the inside part of that ball are all these proteins. We’re going to talk about some of these proteins. These proteins circulate around the inside of that cell and make the cancer cell grow.
On the outside of that ball are spikes. There are different types of spikes on the outside of the cell. They’re called receptors. We can use those spikes and target cancer cells with our treatments.
CHOP
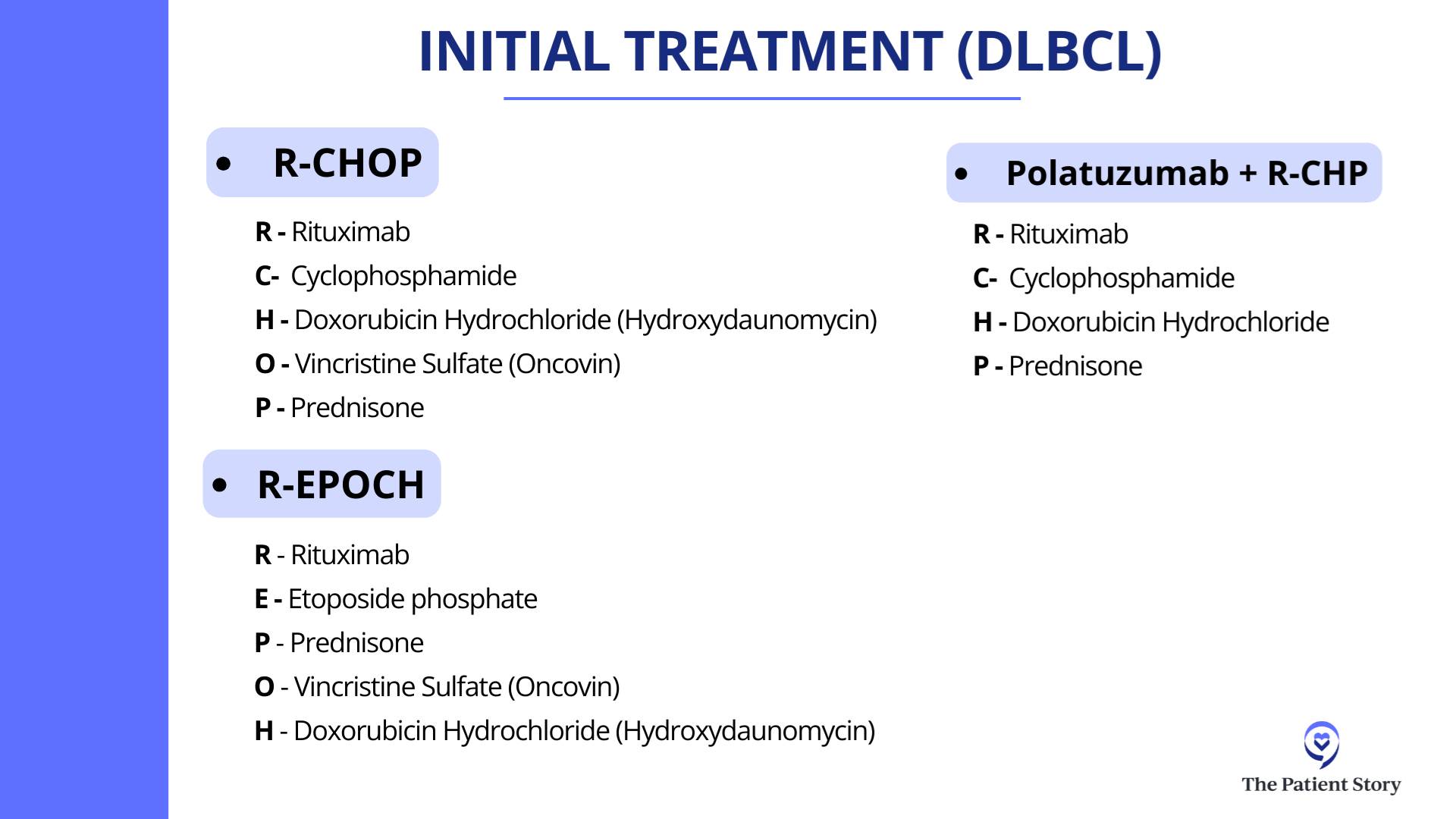
Dr. Favaro: The initial treatment for lymphoma goes back to 1976 when a combination of different chemotherapy drugs was first approved. CHOP is a combination of three different chemotherapy drugs (cyclophosphamide, doxorubicin hydrochloride, and vincristine sulfate) along with prednisone. Back in the 1970s, we were giving chemotherapy that attacked and killed all these fast-growing cells. It wasn’t targeted to spikes or proteins.
R-CHOP
Dr. Favaro: About 20 years ago, we discovered rituximab, which is a targeted therapy. It’s an antibody, a Y-shaped molecule that targets CD20, which is one of the spikes on the outside of the cell. We found that this is a great advance in cancer treatment.
If we added rituximab to all that chemotherapy, patients did better. They lived longer and had a much better chance of going into remission. R-CHOP has been the standard first-line treatment for diffuse large B-cell lymphoma for over the last 20 years.
pola-R-CHP
Dr. Favaro: Finally now, we have a new drug called polatuzumab vedotin, another targeted treatment and Y-shaped molecule. This time, it binds to CD79.
Polatuzumab vedotin added to rituximab, which hits CD20, and two different chemotherapy drugs plus prednisone (pola-R-CHP) is the new standard of care for the treatment of diffuse large B-cell lymphoma. Studies have shown that the response rate and survival is about the same versus the old regimen, but it looks like at two years, the remission rate is better if you take the new regimen of pola-R-CHP. This is the newest treatment for this disease.
Treatment Options for Relapsed Patients
Robyn: Unfortunately, even with these advances and the durable remission rate of 80% or so with the current therapy, there’s 20% where it doesn’t work. Patients will relapse very quickly. Dr. Ghosh, what happens in these patients whose initial therapy fails? What do we have to offer them now?
Autologous Stem Cell Transplant
Dr. Ghosh: In the past, the standard for patients who are eligible for an autologous transplant would be to get salvage chemotherapy, like RICE (rituximab, ifosfamide, carboplatin, and etoposide), R-DHAP (rituximab, cisplatin, cytarabine or cytosine arabinoside, and dexamethasone), or R-GDP (rituximab, gemcitabine, dexamethasone, and cisplatin).
If they are chemosensitive, meaning the tumor shrunk with chemotherapy, then they would go for an autologous stem cell transplant, which is high-dose chemotherapy followed by giving them their own stem cells back.
CAR T-cell Therapy
Dr. Ghosh: As immunotherapy advanced and as we learned more about ways to harness the immune system to fight against cancers, this was applied to diffuse large B-cell lymphoma and a novel treatment came about: CAR T-cell therapy.
Initially, it was approved after two prior lines of therapy. Patients would have had to gone through a transplant and if the transplant failed, they would get CAR T-cell therapy, or if they got chemo and then got CAR T-cell therapy as the third-line treatment. But then knowing that it was very powerful even in the third-line setting, there were some randomized clinical trials directly comparing it with transplant.
In the second-line setting, we are thinking a lot in terms of CAR T-cell therapy, reserving transplant for patients who relapsed late but are transplant candidates.
Dr. Nilanjan Ghosh
There were three large, randomized phase 3 studies that compared efficacy and toxicity of CAR T-cell therapy with that of autologous transplant. Two of those trials were positive in terms of ensuring that the primary endpoint, which was free of disease, progression-free, or event-free survival, was better compared to transplant. One of those studies actually showed overall survival was also better compared to transplant.
The current standard of care if somebody was refractory to front-line chemotherapies, like R-CHOP, pola-R-CHP, or R-EPOCH, or if they have relapsed within one year, the second-line therapy would be CAR T-cell therapy.
One of the CAR T-cell therapies called liso-cel was also used for patients who were not eligible for transplant, like older patients. Patients could get liso-cel as a second-line therapy if they had late relapse but were not considered to be transplant candidates, like if they had some organ dysfunction which would preclude them from getting a transplant.
In the second-line setting, we are thinking a lot in terms of CAR T-cell therapy, reserving transplant for patients who relapsed late but are transplant candidates. They could get salvage chemotherapy. If chemosensitive, go for transplant; if not, then still go for CAR T-cell therapy.
Follicular Lymphoma
Current Treatment Options for Follicular Lymphoma
Robyn: Follicular lymphoma is actually very common. It’s managed in the outpatient setting and Dr. Bano has seen quite a few of these cases. How do you manage these patients in your clinic?
Dr. Bano: I agree, it’s very common to see follicular lymphoma. It’s a different kind of disease process compared to DLBCL in the ways that patients present. It’s not the typical storm of symptoms that you expect with DLBCL. Follicular lymphoma tends to be slower-growing and presents in a way where most patients are even asymptomatic on initial presentation. They’ll have scans for something else, we’ll find enlarged lymph nodes, they’ll have biopsies, and that’s how we find it a lot of the time.
The way to approach treatment is a little bit different when you compare it to a more aggressive lymphoma like DLBCL. Sometimes, we’re thinking about stages like we generally do with lymphoma. The treatment differs based on what stage you are.
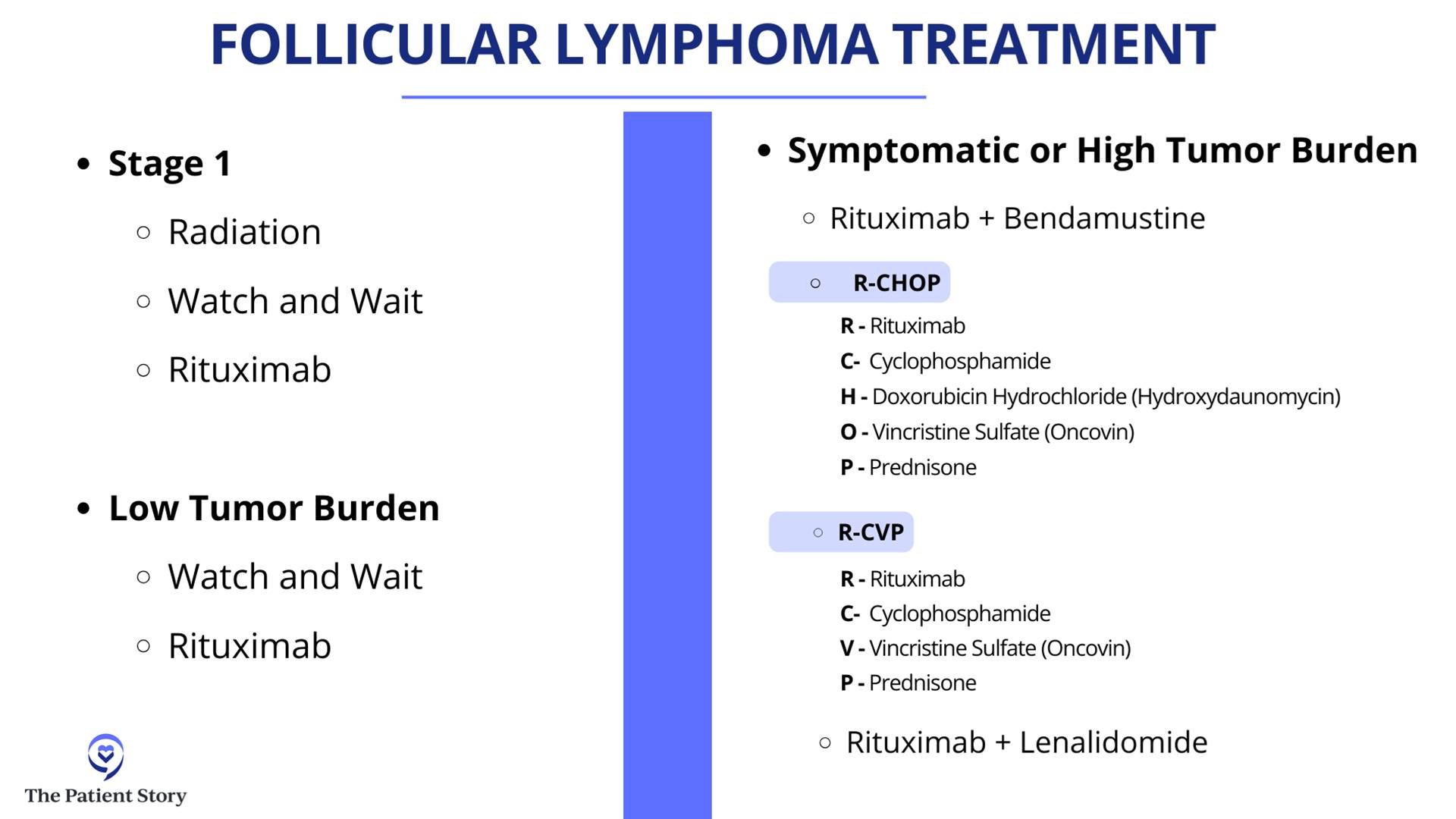
If you have a localized group of lymph nodes that are involved, a lot of times, if patients are asymptomatic, we watch and wait. Sometimes, if they have symptoms from a bulky lymph node enlargement, they can get radiation. A lot of times, we’ll combine that with CD20 monoclonal antibodies, as Dr. Favaro very nicely explained, that target these lymphoma cells directly. That is usually the option in limited stages of disease, like stage 1 and stage 2.
As we approach further spread out disease like stage 3 or stage 4, a lot of folks are asymptomatic and have a low burden of disease. We tend to watch and wait. That’s still an option.
Because of the indolent nature of follicular lymphoma, there’s a chance that it may come back, but we try to treat it and keep it in under control for as long as possible with milder therapies.
Dr. Kulsum Bano
Broadly, follicular lymphoma also is divided based on its grade. Not all follicular lymphoma comes equally. Some of the cases are lower grade, meaning the cells that are involved are not as actively dividing and do not appear as aggressive. For those patients, we tend to steer more toward the watch and wait and low tempo of therapy.
The more aggressive varieties, like the grade 3s, which is divided into 3A and 3B, we look more toward the DLBCL kind of treatment because these tend to act like a more aggressive lymphoma. In that scenario, we look more at chemotherapy plus immunotherapy, like R-CHOP. That usually tends to be the front line of therapy for follicular lymphoma.
It’s very varied. It’s a broad spectrum depending on stage as well as grade, but it tends to be a slow-growing disease in general. For those who get front-line treatment, some get even rituximab with bendamustine. Not everyone needs multi-agent chemotherapy.
A lot of times, we do a finite amount of chemo and follow it up with rituximab maintenance for up to two years. Every eight weeks, they get a rituximab infusion and that keeps patients in remission for a long, long time.
But as we talk about the difference in the nature of the two diseases, follicular versus DLBCL, there is also a difference in the treatment goals for these diseases. DLBCL is more aggressive and, as we were discussing earlier, we talk about a curative approach. Because of the indolent nature of follicular lymphoma, there’s a chance that it may come back, but we try to treat it and keep it in under control for as long as possible with milder therapies.
Treatment Options for Transformed Follicular Lymphoma (tFL)
Robyn: As a radiologist, there are a lot of CT scans and PET/CT involved where you monitor the lymph nodes. Unfortunately, even when someone’s in remission for two years, even after 10 years, it can come back aggressively. Dr. Ghosh, what do you do with a follicular lymphoma that is aggressive, has failed all treatments, and has transformed into diffuse large B-cell?
Dr. Ghosh: The first thing to think about when follicular lymphoma comes back is when it comes back. If it comes back within two years of front-line chemo-immunotherapy, then it’s considered to be progression of disease in 24 (POD24). Even if it has come back as follicular lymphoma, it’s a more aggressive variant. In long-term studies, the survival for that type has not been good. Many research studies have focused on this POD24 group to see what treatments would be effective.
The second thing to think about is: what does it come back as? As we discussed, follicular lymphoma can come back as low-grade follicular lymphoma, so grade 1, grade 2, or grade 3A.
Robyn: That’s based on pathology or the way it looks under a microscope.
If it’s aggressive B-cell lymphoma, then the treatment would be more like DLBCL. If it’s low-grade follicular lymphoma, you would treat more like the low grades.
Dr. Nilanjan Ghosh
Dr. Ghosh: When it comes back, it’s important to get a PET/CT scan and try to biopsy the most aggressive lymph node. A person might have multiple lymph nodes and if you only biopsy one, it could be low-grade follicular lymphoma. You don’t want to miss another lymph node with a high grade because the treatment would differ.
Convenience is important and sometimes a very bright lymph node may be in an inaccessible site, which makes it challenging. Try to biopsy the most active lymph node. If it’s aggressive B-cell lymphoma, then the treatment would be more like DLBCL. If it’s low-grade follicular lymphoma, you would treat more like the low grades.
PET scans are good, but the biopsy is where the money is, so put it under the microscope. Let the pathologist tell us what it looks like and then we can decide what to do.
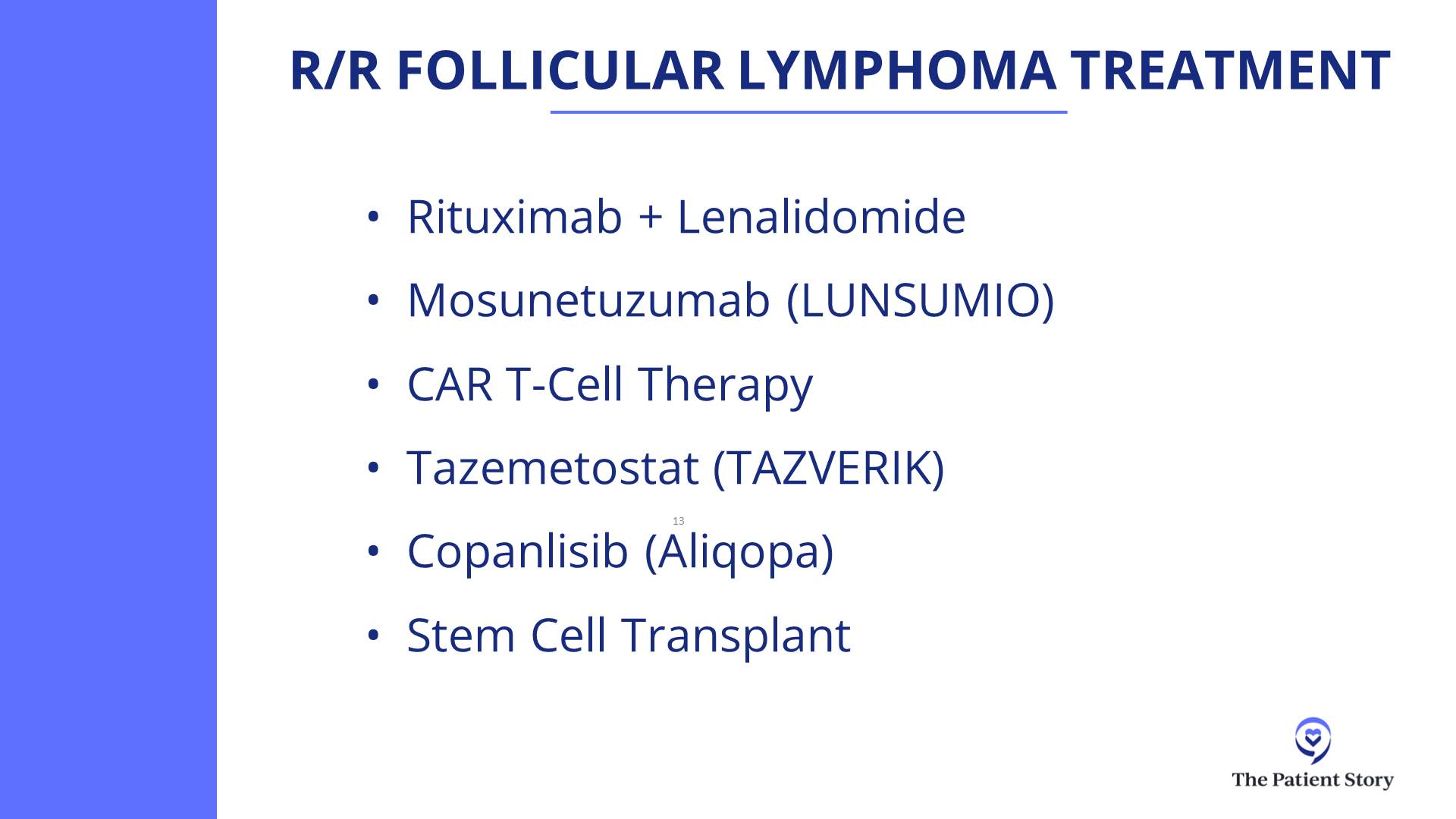
In general, if it is follicular lymphoma, there are many treatment options in the second-line setting. Our commonly used one, if rituximab plus chemotherapy has been used before, is a lenalidomide-based treatment in combination with a monoclonal antibody like rituximab or obinutuzumab.
Subsequently, CAR T-cell therapy has been very effective in follicular lymphoma. Bispecific antibodies are also approved and very effective in follicular lymphoma.
In follicular lymphoma, the disease can relapse 10 or 12 years later… CAR T-cell therapy has not been around for that long.
Dr. Nilanjan Ghosh
CAR T-cell Therapy for Follicular Lymphoma
Robyn: Follicular lymphoma traditionally has been viewed as incurable. But with CAR T-cell therapy, there is now possibility of a cure. Is that correct?
Dr. Ghosh: Yes, there is a possibility. The only long-term follow ups we have with follicular lymphoma being curative is allogeneic transplant, which have been around for decades. Follicular lymphoma can come back. DLBCL typically doesn’t have late relapses. There can be some, but usually relapses occur early. In follicular lymphoma, the disease can relapse 10 or 12 years later. What that implies is that you would have to follow people for more than a decade or perhaps even two decades to be sure that the disease doesn’t come back.
CAR T-cell therapy has not been around for that long, so we don’t know for sure, but there are hints though. We now have data that patients who were POD24 (patients who had front-line chemotherapy and their disease came back within 24 months) got CAR T-cell therapy and their disease hasn’t come back even beyond two years, which means the second-line treatment was more effective than the front-line treatment. This typically doesn’t happen in cancer. If that is there, then you’re overcoming the bad disease biology.
If it doesn’t come back after 5 years, after 10 years, and after 15 years, with follicular lymphoma, that’s when we’ll know. With DLBCL, you can have quicker readouts because if it doesn’t come back in two, three, or five years, then you’re likely cured.
Robyn: We have a CAR T-cell therapy online support group and we have several patients who had follicular lymphoma and who are 4-5 five years out from CAR T-cell therapy and in remission, so it’s very encouraging.
Bispecific Antibodies
Robyn: Moving on to exciting new treatments, Dr. Favaro, would you talk about bispecifics? What’s been approved and how do they work?
Dr. Favaro: Bispecifics are a fascinating field of medicine. The first bispecific that was approved was blinatumomab, which was approved for acute lymphocytic leukemia (ALL).
It’s a very small, V-shaped molecule. One part of the V would attach to your T cell, the other part of the V would attach to your cancer cell, and it will bring them together so the T cell can kill the cancer cell. If you flood your body with these, you can bring all the cancer cells next to your T cells and get a lot of death of the cancer cells.
We still use it for acute lymphoblastic leukemia. The problem with that molecule is that it has a very short half-life. It’s a small molecule and it would be degraded quickly, so you have to use continuous infusion and treatments in the hospital.
Over the last few years, they’ve developed better molecules that are more stable. Instead of a V shape, it’s actually a Y shape. The long part of the Y stabilizes that protein so it doesn’t degrade so quickly. These Y-shaped proteins still do the same thing, bringing the cancer cell next to the T cells, and they are now available for patients with lymphoma.
Epcoritamab
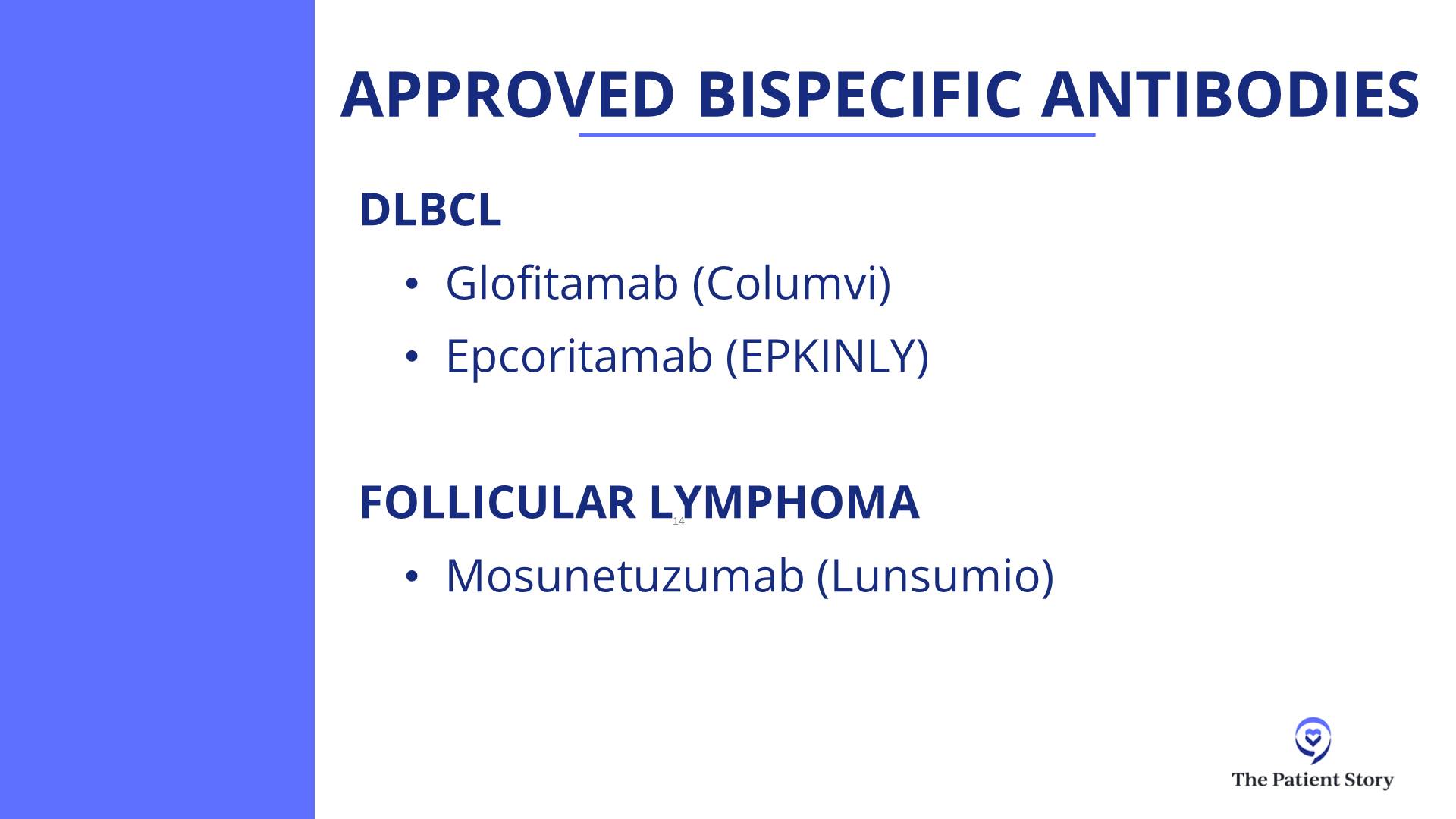
Dr. Favaro: There are two that are approved for diffuse large B-cell lymphoma patients who have had at least two prior treatments. One is called epcoritamab (EPKINLY). It’s a subcutaneously administered drug that attaches to the T cell and the cancer cell, bringing them together.
They’re seeing very high response rates in the 60% range and almost 80% in some cases, where for 80% of the patients that take this drug, their lymphoma shrinks down and up to 60% will have a complete response where their lymphoma completely goes away.
It’s a great new treatment. However, when you do this, you get a lot of release of cytokines and proteins in the body and they can cause side effects, almost like you have the flu or a fever, and can even get worse. Sometimes, you can have low blood pressure. We have to be very careful about how we dose these treatments.
We start with a low dose once a week and gradually bring the dose up. The side effects usually happen in the first month or so. Once you get to the higher dose level, then you’re basically taking an injection once a month.
Glofitamab
Dr. Favaro: There’s another drug called glofitamab. It’s a very similar molecule that does the very same thing, except it’s given intravenously. We step up the dose of the treatment over a period of a month and then the patient gets IV therapy every three weeks. It’s a limited duration of treatment. For that particular drug, it’s about 12 cycles or eight months of therapy.
The results we’re seeing with these two drugs are that most patients will have a complete response and you can see that being a long, durable, complete response.
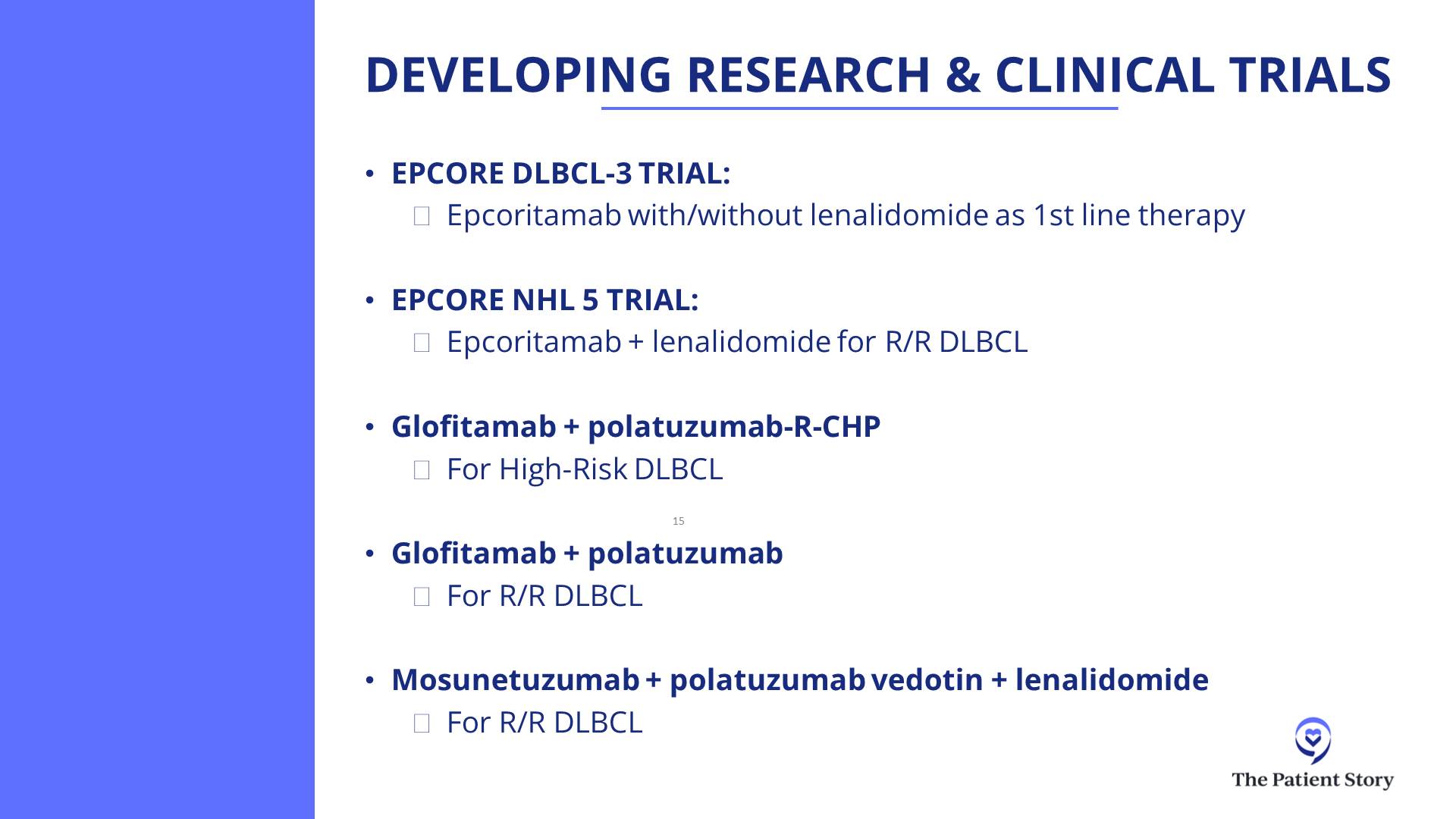
Mosunetuzumab
Dr. Favaro: There’s also a BiTE (bispecific T-cell engager) therapy that’s approved for follicular lymphoma as well. This is a drug called mosunetuzumab and is given intravenously in a similar step-up dosage. This is given for a total of either eight cycles if you go into complete response or 17 cycles if you have partial response. We’re seeing great results with that as well in patients who have had at least two prior treatments for either diffuse large B-cell lymphoma or follicular lymphoma.
Robyn: Is this performed as an outpatient?
Dr. Favaro: It’s outpatient. There’s a risk of a severe reaction. In the early onset of the trials, most patients had to be admitted in the hospital after their second treatment or so because when you step the dose up, that’s when these side effects can happen.
The other two drugs can be given completely in the outpatient setting. We have a protocol set up for epcoritamab. You take the injection once a week for the step-up dose of that first month. As the dose is increased, you get steroids before getting the treatment and for three days afterwards. That seems to really reduce the side effects.
There’s a whole lot of education and prevention that goes into preventing and treating side effects immediately.
Dr. Justin Favaro
Side Effects of Bispecific Antibodies
Dr. Favaro: You have to understand these side effects and how to manage them, so we do a lot of education for our patients. Again, most of these side effects happen within the first month.
CRS (Cytokine Release Syndrome)
Dr. Favaro: There are three major side effects of those treatments. One is called CRS (cytokine release syndrome) and that’s where a lot of cytokines are released as the dose is increased. There are certain stages. CRS can manifest as a fever or if it gets worse, you can get low blood pressure and sometimes have to be admitted to the hospital.
We give steroids and, when needed, a drug called tocilizumab. Almost always, we’re able to reverse those side effects, but it’s something we do educate patients about and keep a close eye on.
ICANS (Immune Effector Cell-Associated Neurotoxicity Syndrome)
Dr. Favaro: The second side effect, which is much less common, is called ICANS (immune effector cell-associated neurotoxicity syndrome). You can have neurologic changes, difficulty with thinking or decreased mentation, and some weakness of the muscles. Again, this is very rare, but it’s all about education, watching for that, and treating appropriately.
Infection
Dr. Favaro: The third big one is infection. We do treat with prophylactic antibiotics to prevent infection and sometimes we give IVIG to boost the patient’s immune system if needed.
There’s a whole lot of education and prevention that goes into preventing and treating side effects immediately. It’s amazing to have these drugs as options now for our patients.
With glofitamab and epcoritamab, as more time goes, we are starting to see a flattening of the curve for some patients… we’ll know over time how that looks, but it’s remarkable progress.
Dr. Nilanjan Ghosh
Success Rate of Bispecific Antibodies
Robyn: Dr. Ghosh, what bispecifics are you using and what kind of success have you seen?
Dr. Ghosh: We have all the bispecifics that are approved as well as those in clinical trials. We’ve been using mosunetuzumab for follicular lymphoma and glofitamab and epcoritamab for DLBCL.
For DLBCL, we usually do CAR T-cell therapy as second line. Studies have shown that even if CAR T-cell therapy has failed, patients have a very good response with both epcoritamab and glofitamab. These were phase 2 studies and remarkably had the same complete response rate. Epcoritamab showed about a 40% complete response rate and glofitamab also had a similar complete response rate.
Epcoritamab is subcutaneous, glofitamab is IV. Epcoritamab is given indefinitely until progression or if someone has bad side effects so they stop. Glofitamab, as Dr. Favaro mentioned, is given for 12 cycles.
I wouldn’t say choosing between the two can be tricky. Both have very similar efficacy, but you have to decide which one is going to work for somebody who lives far away and who wants limited-duration therapy.
Rather than focusing on the differences, the 40% complete response rate is the most important thing to take home. CAR T-cell therapy failed many of these patients. We don’t have very long-term data for the high-risk population in these studies who were refractory to previous treatments and yet did well.
With glofitamab and epcoritamab, as more time goes, we are starting to see a flattening of the curve for some patients. There are patients who got complete remission. They may still relapse, but there are some patients who will get into longer remission. We don’t have five-year data from either of the two, so we’ll know over time how that looks, but it’s remarkable progress.
In general, mosunetuzumab has lesser CRS compared to glofitamab and epcoritamab, but is also used more commonly in follicular lymphoma. Again, all these are done in the outpatient setting.
We have been involved in clinical trials combining mosunetuzumab and polatuzumab. A very effective strategy and though not yet approved, many other studies are ongoing.
The other thing we’ve done is combined bispecific antibodies with front-line treatment. We did a clinical trial of taking glofitamab and R-CHOP in the front line and we’ve seen remarkable remission rates.
Robyn: 80%?
Dr. Ghosh: Higher. When you combine glofitamab with R-CHOP in the front-line setting, the complete response rates are in the 80%. In DLBCL, we focus more on complete responses. Partial responses are okay to mention, but they are very temporary, so we want to focus on complete responses. Sometimes a partial response may turn into a complete response.
Clinical Trials of Bispecific Antibodies
Robyn: There are so many new exciting therapies and our panel has submitted some trials for bispecifics that they’re particularly excited about. What are some of these new trials that are revolutionizing treatment for lymphoma?
EPCORE DLBCL-3
Dr. Ghosh: The EPCORE DLBCL-3 clinical trial is looking at patients who are in the front-line setting and are not eligible for anthracycline-based treatments. They would get either epcoritamab or epcoritamab plus lenalidomide. If somebody has congestive heart failure or some cardiac problems that will preclude them from getting anthracycline-based chemotherapy, then instead of doing R-mini-CHOP or R-CHOP, they could get onto this study.
If bispecifics are moved up from more advanced relapsed/refractory treatments to earlier, can we get chemo-free front-line treatments? That is an effort with the EPCORE DLBCL-3 study.
EPCORE NHL-5
Dr. Ghosh: The EPCORE NHL-5 clinical trial is looking at epcoritamab plus lenalidomide in relapsed/refractory DLBCL. It has shown remarkable activity. It has not been directly compared with epcoritamab alone in the same study, but we have results from epcoritamab alone and that is a complete response rate of 40%. With epcoritamab plus lenalidomide, I believe the complete response rate goes up to the 50s and close to 60%.
Lenalidomide is an immunomodulatory drug. Combining an immunomodulatory drug with an antibody, which is also a kind of immunotherapy, we’re trying to focus on harnessing the immune system to fight against the lymphoma.
Glofitamab + Pola-R-CHP
Dr. Ghosh: Another powerful combination is glofitamab plus polatuzumab-R-CHP. As Dr. Favaro mentioned, pola-R-CHP showed improvement over R-CHOP. That has become a new standard. It showed improvement in progression-free survival compared to R-CHOP. If that is the backbone, can we further improve on that? That’s how we have made improvements over time.
CHOP came in the 70s. R-CHOP was approved in 2006 and showed improvement over CHOP. Pola-R-CHP showed improvement over R-CHOP. If we add a bispecific antibody to pola-R-CHP, can it show improvement over pola-R-CHP?
Glofitamab and pola-R-CHP is a study which we have done at the Levine Cancer Institute as well and it’s been done worldwide and has shown amazing effects. I saw one of my patients very recently who was in this study. He had an extremely explosive DLBCL about two years ago and he’s still in remission.
There are a lot of trials for diffuse large B-cell lymphoma that are moving a little bit more away from chemo and going toward these targeted therapies.
Dr. Justin Favaro
Glofitamab + Polatuzumab
Dr. Ghosh: Glofitamab and polatuzumab is another ongoing study. Taking polatuzumab, a CD79b antibody drug conjugate, and combining it with glofitamab showed high complete response rates. Similar studies have been done for mosunetuzumab plus polatuzumab as well.
A lot of these combinations are being done with the common theme being chemo-free. Some have chemo. CHP is chemo and antibody-drug conjugates are also chemo, but antibody-drug conjugates are very targeted chemo. It targets only the cells where the antibody binds to those spikes, so there is much less collateral damage.
The focus is trying to do less in terms of lowering the side effects, improving the efficacy, and improving quality of life and quantity of life. When you put that all together, the field is moving very well toward immunotherapies. I think these are all really good clinical trials.
Robyn: It’s very exciting. For the audience, the most common used anthracycline is doxorubicin, which is also known as the Red Devil. It can cause cardiotoxicity even in young people, who can end up with congestive heart failure at a young age. Other medications used, like cyclophosphamide, can cause neuropathy, which in some cases is irreversible. To move away from these medications and have the same results or better is great for quality of life and very, very encouraging.
Dr. Favaro: These are all great trials. There are a lot of trials for diffuse large B-cell lymphoma that are moving a little bit more away from chemo and going toward these targeted therapies.
Zanubrutinib + Tafasitamab + Lenalidomide + Rituximab
Dr. Favaro: There’s another interesting trial combining four different drugs and none of them are really chemotherapy. There’s an oral drug that’s a BTK inhibitor called zanubrutinib, another monoclonal antibody called tafasitamab (MONJUVI), plus lenalidomide and rituximab. Of the four different drugs, two of them are targeting the spikes, one of them is targeting a protein inside the cell, and the lenalidomide is there to stimulate the immune system, the T cells, to grow and attack the cancer.
A newly diagnosed patient with no prior chemotherapy is seeing a very nice response rate. In this particular trial, they started with this and if they went into a complete response, then they got two cycles of chemotherapy and went back on the targeted therapy.
I like the idea of targeting some of these molecules on the outside or the inside, combining it with something that turns the immune system on as a way to eliminate some of those long-term potential side effects from chemotherapy. I think that’s the theme that we’re seeing here.
CAR T-cell Therapy
Robyn: I’m one of the first patients to get CAR T-cell therapy. I’m going to have the experts explain it, but as a patient, I compare it to Pac-Man. You put the T cells in and the little Pac-Man goes over and eats the cancer cells.
CAR T-cell therapy is new. I received tisagenlecleucel in 2016 as a phase 2 trial. It’s been very successful for me and I’m very, very grateful. I was able to go back to work as a physician. I have a great quality of life. Most of my side effects are from the chemotherapy, which did save my life but I wish I hadn’t had those.
This is a great therapy and now, not only is CAR T-cell therapy used for blood cancers, but it’s also being used in trials for solid tumors and autoimmune diseases, such as lupus, scleroderma, and glioblastoma.
Dr. Favaro, can you explain CAR T-cell therapy?
Dr. Favaro: T cells are part of your white blood cells that circulate around your body. They’re constantly looking to treat infection or try to treat cancer and that’s part of their job. Why can’t they kill cancer cells on their own? Because cancer cells learn how to hide. There are certain proteins they can take away from their surface, so your normal T cells can’t find the cancer cells sometimes and that’s part of the reason why cancer cells can grow in your body.
How do we stimulate those T cells and make them angrier and more attracted to kill and attack those cancer cells? In my mind, that’s what CAR T-cell therapy is.
The whole process starts by taking out your T cells. We do that as a part of an apheresis process that happens in the clinic or in the hospital. Those T cells are sent off to a company that will take those T cells and reengineer them in the lab to become CAR T cells. Those T cells that are now transformed will attach to a CD19 spike on a lymphoma cell.
The whole process takes about two weeks. The CAR T cells are infused back into the body. They have this new protein on the outside of their cell called chimeric antigen receptors (CARs). They go into the body and attack the lymphoma cells. It’s pretty amazing technology.
The data shown with diffuse large B-cell is that you can get a 40% long-term remission rate in patients who have had prior treatment but now the lymphoma has come back. Those are amazing results and Robyn is a testimony to that.
The downside is it takes a long time. This is a process and you have to wait. There’s also the issue of insurance authorization. Medicare pays for these treatments, but insurance companies take a long time. You have lymphoma that’s growing in your body and we have to wait to get this whole process done.
It requires you to take other treatments, like lymphodepleting chemotherapy, to control the lymphoma before we can get the CAR T-cell process done. Once you collect the cells, it takes about two weeks to get them back. It could take up to six weeks from the time you meet until infusion day.
There’s a lot of thought about how we can make this process better. The companies that make these products are telling us that 8 out of 10 patients who are eligible aren’t getting CAR T-cell therapy. Maybe they don’t live close to a big academic hospital center or it takes too long and their cancer is growing too quickly.
A lot of the research is focused on making the process faster. Can we create CAR T cells in the lab so we don’t have to go through this whole process? That’s what we’re looking to talk about down the road.
The goal has also been to see if we can lower the intensity and the incidence of CRS and neurologic toxicities.
Dr. Nilanjan Ghosh
Side Effects of CAR T-cell Therapy
Robyn: Dr. Ghosh, you have spearheaded CAR T-cell therapy in Charlotte, did the first cases, and have a lot of experience. I would love to have you talk about the side effects of CAR T-cell therapy.
Patients are terrified of the CRS and ICANS. Meanwhile, they’re not as terrified of a stem cell transplant, which has more side effects. How you do you manage the side effects? What kind of results have you seen with CAR T-cell therapy?
Dr. Ghosh: We have had significant experience with CAR T-cell therapy at our center because we participated in some of the clinical trials, which led to the approval of CAR T-cell therapy. It’s certainly a learning curve on how to manage CRS and ICANS.
When we think about CRS, these are serious side effects, but what’s important is these are reversible for the most part. Some clinical trials report very high rates of CRS and some even with ICANS. Most of these happen early on and within a few days of receiving CAR T-cell therapy.
They are managed with a team of physicians, nurse practitioners, nurses, and pharmacists who are very, very in tune with how to manage these side effects. We also have help from ICU doctors, neurologists, and infectious disease specialists, so it’s a team approach.
Each grade of CRS and ICANS has its own treatment. As the grade goes higher, treatments can intensify. The mortality from CRS and ICANS is extremely low. The reversibility is extremely high.
CAR T-cell therapy is underutilized because of the fear of side effects, but the potency which it has far outweighs the risks associated with it
Dr. Nilanjan Ghosh
CAR T-cell therapy has a 40% long-term remission rate and, more importantly, it’s a one-time treatment. You come in, get three days of lymphodepleting chemotherapy followed by a couple of days rest, get the CAR T cells, and then a week of monitoring for CRS or neurologic side effects. If nothing happens, then you remain outpatient. If they happen, then we treat them and reverse them, then monitor for infection risk after.
The treatments can include acetaminophen, fluids, oxygen, steroids, and other drugs, like tocilizumab and anakinra. What we have seen is by doing these measures and being aggressive in terms of treatment, these side effects are reversible.
The goal has also been to see if we can lower the intensity and the incidence of CRS and neurologic toxicities. There are drugs which can be used. For example, prophylactic steroids can sometimes lower the intensity of CRS and that has already been approved. There are multiple ways, but if you have a team who has been doing it for a while and can react immediately, the side effects can be managed.
Another side effect, which is not very common but very important to address, is macrophage activation syndrome or HLH (hemophagocytic lymphohistiocytosis). Again, that is also managed with medications. We are able to recognize it early by monitoring things like ferritin and other markers as well.
I feel that CAR T-cell therapy is underutilized because of the fear of side effects, but the potency which it has far outweighs the risks associated with it, especially now that it’s been so long and we’ve been able to manage the risks in a relatively protocolized manner.
Be aware of side effects, but don’t be freaked out by them.
Dr. Nilanjan Ghosh
Robyn: My therapy was pretty much outpatient. I think that some of the treatments are drifting toward outpatient until you actually need to be inpatient, which decreases your risk of infection and increases your quality of life. My understanding is that a lot of hospitals are trying to move toward that, but it depends on the type of CAR T and also the patient.
Dr. Ghosh: The patient and caregiver. Another very important thing for CAR T-cell therapy is you need to have a caregiver. If someone is having confusion, you need a caregiver if you’re outpatient to be able to call and say that there’s something wrong.
Even in an outpatient setting, for the initial part, there are very frequent follow-ups, almost daily, so distance from the center can be an issue. If someone lives close by, you can do it outpatient. If someone lives far, it may be hard to go back and forth. We are working very hard to try to overcome barriers to CAR T-cell therapy.
Be aware of side effects, but don’t be freaked out by them. If CAR T-cell therapy is right for you, go for CAR T-cell therapy at a place where they know how to manage these side effects and get the benefits.
Cancer Clinical Trials
Robyn: One of our co-presenters is The Leukemia & Lymphoma Society. They have a Clinical Trial Support Center with nurse navigators who can help patients look for trials because it can be overwhelming.
The first person to ask about trials would be your physician, but no matter how good the physician, they won’t know about all the trials in the United States and the world. Another resource is ClinicalTrials.gov, which is what my husband and I utilized when we were looking for a trial though it’s a little bit harder to navigate. Trials are accessible, but you have to be your own advocate to some degree.
Dr. Ghosh: For anyone who has barriers to clinical trials, remember that we would not be here today if not for clinical trials. Even CHOP came through a clinical trial, which was started in the early 70s. Everything came through clinical trials.
Robyn: Again, I’m an example. I was one of the first who got CAR T-cell therapy through a clinical trial. I’ve told other patients that sometimes, the best treatment you can receive is through a clinical trial.
Dr. Ghosh: Cancer clinical trials don’t compare a cancer drug and a placebo. They have a well-established cancer regimen and may add one drug to it, but those who are not getting the study drug get the best established cancer regimen. Unlike other diseases where you can get a placebo versus the study drug, this is a serious, life-threatening disease so you’re either getting the standard of care or the new promising drug. If it’s a phase 1 or phase 2 study, everybody gets the same treatment.
Robyn: In a lot of trials, patients have been through all these standard treatments. They may have had CAR T-cell therapy or BiTE therapy then the lymphoma comes back. What do you do? That’s where these companies are on the cutting edge of developing newer treatments.
Cancer clinical trials don’t compare a cancer drug and a placebo. They have a well-established cancer regimen and may add one drug to it, but those who are not getting the study drug get the best established cancer regimen.
Dr. Nilanjan Ghosh
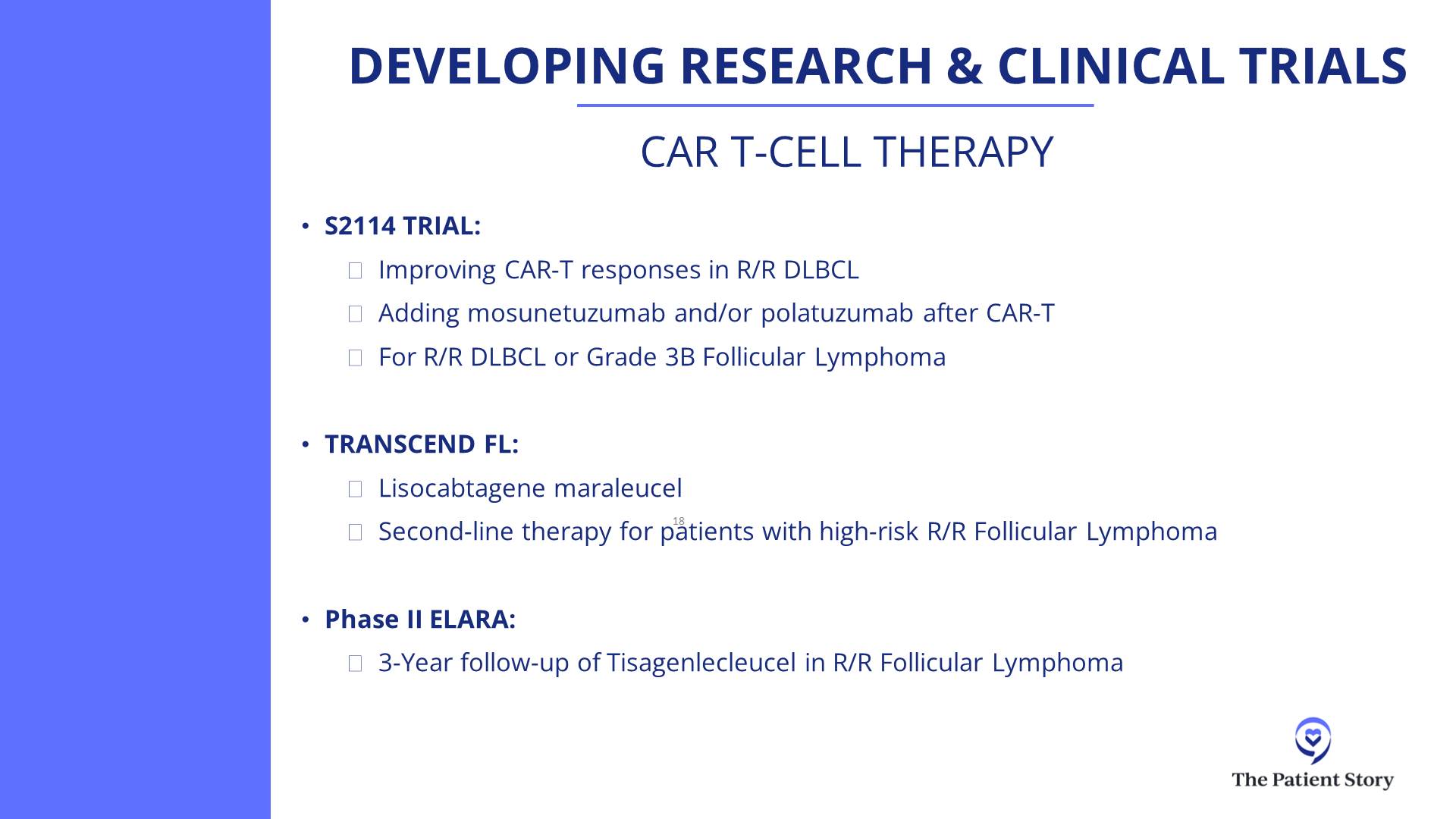
TRANSCEND FL
Robyn: I know some people who are in the TRANSCEND trial for follicular lymphoma. There’s a lot of people enrolled in that. From what I’ve seen from the data from ASCO, it looks like it’s very successful.
Dr. Ghosh: TRANSCEND FL took patients with relapsed/refractory follicular lymphoma and treated them with liso-cel. It’s been reported and has fantastic efficacy with very high complete response rates in the 90s.
The follow-up is not very long, so that’s one downside, but the FDA is doing a priority review to see if this is good enough that it should get approval in follicular lymphoma. It also has been done as second-line treatment and that has very, very good activity in the second-line setting.
SWOG S2114
Dr. Ghosh: Remember we said that 40% patients with large B-cell lymphoma will get long-term remission after CAR T-cell therapy. What about the other 60%? We always have to think about the people who didn’t benefit. We have a great example of benefit right here, Robyn, but there are others who didn’t.
Complete remission is the most important thing for diffuse large B-cell lymphoma. What about people who get partial remission or stable disease and it didn’t grow? That’s not good enough because within a few months, many of those patients will progress. What if you can intervene before that with bispecific antibodies and polatuzumab?
This S2114 study is a trial which is trying to improve the outcome of patients who are in partial remission or have stable disease by adding drugs post CAR T-cell therapy and trying to see if they would benefit and convert them into complete remission. This is a national trial and we have it open at our site as well.
ELARA
Dr. Ghosh: The ELARA study is looking at tisagenlecleucel for relapsed/refractory follicular lymphoma. This is showing high response rates, low CRS, low neurotoxicity, and durable remissions. Now with three-year follow-up and showing that nearly close to 60% of patients are in remission.
This is a one-time treatment given three years ago and patients are still in remission. Many of those patients are in that POD24 group, where they had progressed within 24 months, so their first remission was two years and now the second remission has been lasting for three years. I hope the remission will last for 5, 7, 10, 15 years, but only time will tell. That’s where whether it’s curable or not will come in for follicular lymphoma.
A lot of companies are developing CAR T cells in the lab that are engineered so they can go in and attack the lymphoma cells, but the body’s immune system won’t attack them and kill them.
Dr. Justin Favaro
Other Clinical Trials
Dr. Favaro: It’s exciting to see CAR T-cell therapy patients in follicular lymphoma and seeing long-term responses. That’s a disease that tends to relapse over and over.
Robyn: People can go on with their life.
Dr. Favaro: The other trials I do like are looking at CAR T-cell therapy patients who don’t have a complete response. Let’s bring in BiTE therapy for those patients as well to try to get them into complete response.
We’re part of a national network of cancer clinics called OneOncology and some of our clinic sites are looking at doing outpatient CAR T-cell therapy. There are different products that are now approved. Liso-cel is one that has the least side effects and is the most predictable.
In outpatient clinics in the OneOncology network, we’re doing CAR T-cell therapies and watching them as an outpatient. They can be watched for four days. It’s pretty predictable that at day four is when a lot of the side effects happen for that particular product.
That’s one example of how we’re moving things more toward the outpatient by monitoring patients while they’re at home. If it’s day four and the patient is starting to have side effects, we bring them in, keep an eye on them for a few days, take care of the side effects, and send them home.
There are a lot of companies developing new CAR T-cell therapies. Why do we need to take the T cells from the patient, reengineer them, and put them back? What about taking regular cells? You can take a culture of human cells and, believe it or not, take stem cells and turn them into T cells in the lab.
A lot of companies are developing CAR T cells in the lab that are engineered so they can go in and attack the lymphoma cells, but the body’s immune system won’t attack them and kill them because these are foreign cells to the body.
One of the other trials happening in the OneOncology network is using allogeneic CAR T cells, meaning they come from a different person. They’re engineered in a way to help your body accept them and see if you can get a response.
Multiple companies are doing this and, in some cases, these are patients who have been through everything. We get a response and a reduction in their lymphoma by using these foreign cells created in a lab. To me, that’s where the future is: looking at this in the outpatient setting and having it ready for the person when they need it.
Robyn: It’s also less costly because it’s technically off the shelf, which should be excellent.
Treatment Sequencing
Robyn: At some of the meetings, people still talk about bispecifics versus CAR T-cell therapy and in which order. We talked about bispecifics after CAR T-cell therapy. Some people are saying bispecifics should be done before CAR T-cell therapy.
Dr. Ghosh: CAR T-cell therapy came first. Outside of blinatumomab, which was for ALL, most of our DLBCL and follicular bispecifics came later. Naturally, by the time bispecifics were available in trials, CAR T-cell therapy had already been around. We know that after CAR T-cell therapy, bispecifics are very active, but what we didn’t know was the reverse.
Recently, a European study was presented and showed that if you use bispecifics before CAR T-cell therapy, you can still get really good activity from CAR Ts. On that study, bispecifics failed a lot of patients so they went on to get CAR T-cell therapy, which was then effective.
In the United States, bispecifics are not approved in the second-line setting, while CAR T-cell therapy is, so undergoing CAR T-cell therapy before bispecifics makes a lot of sense. We don’t have long-term data for bispecifics in the second line but we do have data saying that if it didn’t work, at least CAR T-cell therapy may be able to rescue those patients.
That was a very good study. Overall, we do great in oncology in terms of getting new drugs approved, but we don’t do a great job in sequencing them. That’s left a lot to the physician in discussion with the patient because not everything from the menu is going to be available or accessible right away.
With disease, you may have to do something right away because you can’t wait for six weeks or so to get CAR T-cell therapy. If CAR T-cell therapy is available, then you may want to wait and do the bispecifics later.
In DLBCL right now, I would do front-line treatment of CAR T-cell therapy and bispecific antibodies. In follicular lymphoma, you could do the reverse. It’s a more indolent disease. We don’t know about curability as much. We know that mosunetuzumab works well in relapsed/refractory follicular lymphoma. You have long-term remissions and you could save exa-cel or tisa-cel and, if liso-cel does get approved, then liso-cel for later.
As we are seeing longer data, you have to think: do you want to be on a treatment where you are coming in frequently versus getting a one-time treatment? The treatment where you’re coming in frequently has lesser side effects than the one-time treatment, so it’s a discussion.
Will clinical trials ever be done to answer the sequencing question? I don’t know. I think we’ll learn over time. What will matter is the side effects and the durability of the response. Any response which is durable will be higher in the flowchart compared to the ones where relapse will happen sooner.
Folks who’ve gotten chemotherapy upfront are often left with life-limiting or daily activity-limiting side effects, like neuropathy, so it’s extremely exciting to have this option of chemo-free treatment without long-lasting side effects.
Dr. Kulsum Bano
Possibility of Chemo-Free Cancer Treatment
Robyn: I’ve been in medicine for a long time. When I trained in medicine, oncology was still relatively barbaric, I would say. Chemotherapy and cancer treatments involved cutting, burning, and poisoning. Way back in the 80s, they didn’t even have antiemetics or ports, so giving people doxorubicin was difficult to say the least.
We’ve progressed dramatically. Oncologists have found ways to decrease nausea and take care of neuropathy, but the side effects are still there. Do you see chemo-free treatment of cancer in the future? Perhaps in the next 10 to 15 years?
Dr. Bano: I think that’s the direction we’re slowly heading in. A lot of these trials are slowly moving treatments that were thought to be more exciting and more novel approaches from the fourth to the third, to the second, and then slowly into the front-line setting. That happens over time because the more we learn, the more experience we have with all of these wonderful patients who’ve been on trials and given us this knowledge.
As a community oncologist, that’s extremely exciting because I hope to see patients for years to come who are going to be disease-free and who’ll just be monitored. Folks who’ve gotten chemotherapy upfront are often left with life-limiting or daily activity-limiting side effects, like neuropathy, so it’s extremely exciting to have this option of chemo-free treatment without long-lasting side effects. People are going to live longer with these disease-free intervals. It’s very exciting and hopefully that’s where we’re headed.
Dr. Favaro: I think it’s a combination of things. If you look at chemotherapy, these are chemicals that kill fast-growing cells and that’s pretty good against lymphoma. These often are fast growing, especially diffuse large B-cell lymphoma, so it’s been very active treatments that have put people into long-term remission. But the downside of chemotherapy is the potential long-term side effects plus it’s harder to go through, so what can we do?
Cancer cells are complicated. We’ve got the DNA inside the cell, which has 30,000 genes and over 100 probable mutations in those genes. You’ve got all these crazy proteins in the cell. A lot of them are active and helping the cell grow. Then there are the different spikes outside of the cell.
You have to think about how you attack not just one protein or one spike but multiple targets. A trial I mentioned took a BTK inhibitor and attacked the protein inside and had a couple of drugs attacking the spikes on the outside. That’s probably where we’re going to head to avoid treatments that are so toxic.
Multiple targeted agents is the way to go. For example, with BiTE therapy, we know what happens with those patients. It’s very effective pretty early, but what’s going to happen down the road? Will there be a potential risk of the cancer coming back?
You’re taking the T cell, bringing it to the cancer cell, turning that T cell on, and killing the cancer cell. But over time, those T cells get tired, which is something called T-cell exhaustion, and don’t want to work as well. Sometimes it’s as simple as giving people a break from treatment to let their T cells recover.
But the other thing I think that we’re going to head toward down the road is limited duration therapy but baking something in. You give BiTE therapy, but because we know the T cells can get exhausted, we need to add in another targeted therapy to kill some of those proteins and give 2 or 3 of those for a limited duration. I hope that’s where we end up to finally wipe out the disease for good.
Improving Access to Cancer Care
Robyn: One of the things that all of us as doctors are focused on is access to care. In my case, there was no CAR T-cell therapy offered nearby. My oncologist here had to coordinate with an oncologist who was in a trial in Ohio and my team in Charlotte did a fantastic job. Dr. Ghosh, what do you do in the academic center to reach out to community doctors? How do we improve access to care?
Dr. Ghosh: Late 2017 is when we moved forward with signing up for the TRANSCEND study, which eventually led to approval. Once we signed up for the study, we were the only center in all of North and South Carolina to offer CD19 CAR T-cell therapy before any other center. We got patients from everywhere in that study.
Access is certainly a very, very big issue for CAR T-cell therapy. It becomes even bigger because you need a caregiver. How do we overcome some of the socioeconomic barriers? The caregiver would have to take some time off. Typically, we need patients to be within a one-hour radius, so they would need local housing.
The first part of access is providing education and understanding the benefits of CAR T-cell therapy and referring the patients in a timely manner. It could take up to 6 to 8 weeks to get CAR T-cell therapy, so if you wait for the referral, then it may not be doable because the disease will take off. Early referral is extremely essential for CAR T-cell therapy.
There’s a lot of fine-tuning involved, so the team together with the patient decide what’s best. We try to do this in a really timely manner.
Dr. Nilanjan Ghosh
Patient navigation can be very helpful to help find resources, whether it’s local housing or any type of support. I think that’s essential.
Insurance can be a barrier, especially in terms of single-case agreements, but we are trying very hard. We have a study in which we are looking at the effect of these insurance problems on patient outcomes, so that is a barrier we’d like to overcome. Some barriers are within our control, some are not.
There are ways to control the disease. Giving the right treatment is very important. For example, we have learned that if you give bendamustine, then that can mess up your CAR T-cell therapy. Bendamustine kills T cells, so if you kill T cells before you collect them, then those T cells aren’t going to work. Either you won’t have much or if you have enough, they may not be as functional and not be able to do the job.
What is the right treatment to use if you’re planning to do CAR T-cell therapy? There are so many available. Do you want to modify your regimen somewhere so that you can control the disease but perhaps not kill all your T cells before you collect them? Do you want to wait? But if you wait, then the disease may take off and that may not work.
There’s a lot of fine-tuning involved, so the team together with the patient decide what’s best. We try to do this in a really timely manner. We coordinate very well with all our regional sites within the Levin Cancer Institute as well as beyond.

The bigger challenge is those who live far away. Do they want to come to Charlotte to get CAR T-cell therapy or would they rather not do it because it’s not feasible to come? That’s where eventually having outpatient CAR T-cell therapy done locally comes in and having the expertise to manage the side effects if they happen.
We have more CAR T-cell therapy centers today than two years ago. I hope it keeps getting better and better so that more patients all over get access to this treatment.
We also don’t want to have the treatments in an environment where there isn’t the expertise to manage the side effects because then it becomes very hard. Somebody who came in for a potential curative disorder and perhaps were going to be cured succumbed to the side effect because the team was not able to manage them. That wouldn’t be right either.
The other part of it is coming up with protocols to lower the incidence of side effects without compromising efficacy. This is where the clinical trials of some of the products that have less CRS and less ICANS come in. Not zero, unfortunately. I don’t think we’re going to get there.
Infections can be there, but we know how to manage them. Please communicate quickly so that they can be managed appropriately.
Dr. Nilanjan Ghosh
Robyn: Zero is impossible. What if there are trials at Memorial Sloan Kettering in New York or MD Anderson in Texas? The idea is that people can follow up with their local oncologists.
Dr. Ghosh: After the CAR T-cell therapy. It’s a one-time treatment.
Robyn: That’s what happened in my case. Sometimes you have to go somewhere else for treatment or to join a trial and then do follow-up blood work and scans locally to make it more convenient for the patient.
Dr. Ghosh: The most important thing for CAR T-cell therapy is that there are two side effects that can persist after being discharged.
One thing to watch out for is low blood counts, which is an important one and can persist for a little bit of time. For the most part, that’s because of the lymphodepleting chemotherapy given prior. But sometimes, if patients have had many prior treatments, low blood counts can also be because now they’ve developed MDS (myelodysplastic syndrome) or a pre-leukemia situation.
It’s important to pay attention to the low blood counts to see if it’s getting better or persisting for a very long time, then looking at the bone marrow to see if they have developed something else because there are other reasons for low blood counts other than CAR T-cell therapy.
Second is infection risk. CAR T-cell therapy takes out the B cells because normal B cells also express CD19. You can check immunoglobulin levels and give IVIG. Vaccine responses also go down, so if someone had a vaccine for flu or COVID, they may not be able to respond well, so people become prone to infections.
Patient education is very important as well as letting your doctors know. I always advise patients that if they have a cold or something, reach out to their doctors first. Many times, we would react to it faster. We won’t give a Z pack for a cold. We’ll get them in, get a swab, check what virus is there, and check the immunoglobulin level.
Give them antivirals, if antivirals are available. Give them IVIG, if the IgG is low to help them overcome that infection. Get some imaging needed to see if there’s pneumonia. When the immune system is low and you get a virus and sit on it for some time taking an antibacterial, which is not going to work because it’s not a bacterial infection, it can get worse.
We educate our patients that infections can be there, but we know how to manage them. Please communicate quickly so that they can be managed appropriately compared to some other person who is not as immunocompromised.

Final Takeaways
Robyn: This has been a great discussion. If there’s something you would like to tell the people about diffuse large B-cell lymphoma and follicular lymphoma, treatments, and the future, what final statements would you like to give?
Dr. Favaro: There is so much to learn for patients and doctors. These new treatments come out and it’s our job to learn about them. CHOP came out in 1976. It was our job to learn how to give it and also how to manage any side effects that come up. That’s the same with CAR T-cell therapy.
Quite frankly, 4,000 papers come out every day in health care. There’s a ton of information coming out. We are constantly learning and educating patients about these new treatments.
The cooperation that we have as a community practice with academic centers is very important. When we see patients who need CAR T-cell therapy, we refer them and take them back to help manage potential side effects. The technology that’s advancing to make these treatments less toxic is key. We used to have to admit patients overnight for epcoritamab, for BiTE therapy; now we can do it all as an outpatient. That’s the type of thing that’s happening on a daily basis.
Physicians will never go away. We are here because we know you. We take care of you as a person, but we are going to see more and more about artificial intelligence coming into health care. It’s happening. We do need to look at that and embrace that.
Somebody comes in with lymphoma. What should their treatment be? There are so many different factors: age, personal health, disease, potential treatments, and side effects. It takes a good physician to understand the data. But over time, there probably will be the development of assistance to doctors with artificial intelligence and neural networks that I think will help. There are journals about AI in oncology and I think this is going to be the future for health care as well.
Dr. Bano: None of us in medicine work in a vacuum. It’s a concerted effort getting these patients to the most advanced treatments out there. In the community, our responsibility is to know that these even exist and to maintain that chain of communication with the academic centers to get our patients the care that they need, but we always serve as home base. We give patients the feeling that, yes, we’re sending you away, but you’re always going to come back and we are here to take care of you for years to come.
It’s always been a great collaboration between community and academics, getting that relationship established, and always having that chain of communication to ask questions and get opinions. It doesn’t always have to be advanced therapy. Sometimes you get a challenging case that you want to discuss with someone who has seen something like this before.
It’s very exciting to see what’s on the horizon. It’s exciting to see what we can do for our patients. It’s a learning process. Every day, we learn something new.
In the community, our responsibility is to know that these even exist and to maintain that chain of communication with the academic centers to get our patients the care that they need, but we always serve as home base.
Dr. Kulsum Bano
Dr. Ghosh: I cherish the community-academic partnership. I’ve cherished that over the years. That helps patients to get their treatment locally but also get access to a specialist who treats that disease. When I started, lymphoma treatments were not as effective but were simple. You get the first line, another option for the second line, then after that, there were 1 or 2 options and that’s it.
Now, there are a lot of options. When you have so many options, each with their unique side effects and sequencing is not worked out, how do you know which is best for you? There are so many intricacies. If you use this, then the next treatment could be a problem.
Trying to find the right option, keeping abreast of what comes out, and keeping pace with how this is moving along can be challenging. That’s where the academic-community collaboration can be very good. Patients can always go back to the community to get their treatments, have access to a new clinical trial or the latest treatment, and have really good care.
I encourage participation in clinical trials, knowing that these are ethical and vetted by institutional review boards. That is how we have come to where we are and I hope that we get into more chemo-free treatment options.
Some chemo is still very effective. I would not say anthracyclines have saved many lives. They have been around for 50 years, but if we can achieve our goal with less toxicity and by harnessing the immune system, that would be fantastic.
Robyn: I’m honored to be here. Shout out to The Patient Story and the unique ability of patients to get their voice out and for people to do their research online. As a physician and a former patient, it’s very important to be your own advocate, to research, to ask questions, and to keep your mind open. Sometimes clinical trials are the best treatment, so do consider them.
Consult with your doctor. It’s okay to get a second opinion at some points. Medicine has come a long way. When I first started, there was not much available. The survival rate for non-Hodgkin’s was about 30-40%.
I hope that everyone gets treatment and gets in remission like myself. At that point, you need to live your life. Enjoy your family, travel, work, stay healthy, and exercise. Don’t let cancer define you. It’s part of you, but there’s much more to you, so enjoy life.
You need to be your own advocate. If you feel like something that’s been recommended is not working for you, you have all the right to get a second opinion.
Dr. Kulsum Bano
Q&A
Getting a Second Opinion
Robyn: Joan asks, “What is the polite way to get a second opinion without being rude?”
Dr. Bano: Very rarely are there egos in medicine. As a physician, you try to make the best decision for your patient knowing that there may be something out there that is newer or better. Everyone is entitled to a second opinion and that’s how we learn more.
If somebody comes back to me with a different treatment approach and says somebody else recommended this, that’s something I would definitely encourage. You need to be your own advocate. If you feel like something that’s been recommended is not working for you, you have all the right to get a second opinion. You’re not being rude at all. You’re entitled to that and it’s actually encouraged if that’s what you feel is right for you.
Robyn: I agree. Even in radiology, we get asked for second opinions all the time. Doctors are human. We are not perfect. We can look at the same case and have different opinions. We’re not insulted. We’ve all been trained to work together and I would say that happens 99% of the time. There are always exceptions.
If you look at the commonly used CAR T-cell therapy, the complete response rate is much higher than the complete response rate for epcoritamab.
Dr. Nilanjan Ghosh
Epcoritamab vs. CAR T-cell Therapy
Robyn: Don asks, “I’m on epcoritamab. We considered CAR T-cell therapy, but wouldn’t be able to provide the 24/7 care required. So far, it’s working very well. How does it stack up compared to CAR T-cell therapy?”
Dr. Ghosh: They have never been compared head to head, so there is currently no clinical trial which takes half the patients and gives them epcoritamab and half the patients get CAR T-cell therapy. The best way to compare two groups of patients is if they were randomized on a clinical trial, had similar characteristics, and then followed over time to find out the effectiveness of one versus the other.
If not, you’re comparing across trials and when you do, it’s flawed because the patients who went for epcoritamab may have very different characteristics than the patients who went for CAR T-cell therapy. In fact, many patients who went for epcoritamab on a clinical trial already had CAR T-cell therapy, so how could you compare the effect of CAR T-cell therapy with a drug used for post-CAR T-cell therapy failures?
Having said that, we are left with no choice but to compare across trials. I will say that if you look at the commonly used CAR T-cell therapy, the complete response rate is much higher than the complete response rate for epcoritamab. Epcoritamab is around 40%. CAR T-cell therapy complete response rates are usually in the 50s to 60s.
That being said, it comes down to the 40% number because even if CAR T-cell therapy gets a higher complete response, some people will start relapsing despite getting a complete response. We know that with CAR T-cell therapy, about 35 to 40% people will have long-term remission.
We don’t have long-term data yet with epcoritamab. The complete response rate is 40%, but some of those will progress over time. We don’t know whether it will go down to 30% or 25% as we go up to five years, but we will find out over time.
At this point in time for DLBCL, we feel that CAR T-cell therapy is better, but if it’s not feasible, bispecific antibodies would be the next best option. The important thing is: are you getting complete remission or not? If it’s complete remission, we see long-term sustainability. If it’s not complete remission, then we start seeing early progression.
Epcoritamab is targeting CD20 and CAR T-cell therapy is targeting CD19 — two very different ways of attacking the lymphoma. CAR T-cell therapy is still a great option for those who choose epcoritamab for whatever reason.
Dr. Justin Favaro
Dr. Favaro: Another point is that a lot of patients on the epcoritamab trial had CAR T-cell therapy before. If you have somebody who’s never had CAR T-cell therapy and you had the option of CAR T-cell therapy or BiTE therapy, which one do you choose if you’re eligible for both?
It comes down to logistics and what’s going to be a good fit for you. Keep in mind that if you would need CAR T-cell therapy later, you can still get it because a study at ASH 2023 showed that if even if you had BiTE therapy before, you’re still eligible to get CAR T-cell therapy later.
Epcoritamab is targeting CD20 and CAR T-cell therapy is targeting CD19 — two very different ways of attacking the lymphoma. CAR T-cell therapy is still a great option for those who choose epcoritamab for whatever reason. You can still have a great outcome. It doesn’t necessarily matter how you sequence it.
The hope is that whatever treatment you’re getting works for you and you won’t need anything else. But if you do, there are options available and there will be even better treatments in a few years.
Dr. Nilanjan Ghosh
Robyn: If for some reason this doesn’t work and you decide to get CAR T-cell therapy, a lot of the hospitals have come a long way with helping people get 24/7 care. There are options. Hopefully you won’t need them since epcoritamab is working well, but know that there are things that the hospitals are now aware of and they’re trying to assist patients with those.
Dr. Ghosh: There are many devices coming out for 24/7 monitoring, especially in the outpatient setting. Companies are coming up with devices to monitor your oxygen level, heart rate, and temperature then feed them back to the electronic medical record and create alerts. At least from the standpoint of vital sign monitoring, people are trying to overcome this barrier.
Understand that 24/7 support, even if it is for a short time, is a lot for a caregiver, especially if the caregiver has to work. You can rotate caregivers. You don’t need to have just one. Most places will allow multiple caregivers.
Epcoritamab is a good option if you’re not able to do CAR T-cell therapy. You can still have very long remission and perhaps not need further treatment ever again. The hope is that whatever treatment you’re getting works for you and you won’t need anything else. But if you do, there are options available and there will be even better treatments in a few years. Maybe allogeneic CAR Ts will hit a big wave. We don’t know yet, but we’ll find out.
Dr. Favaro: That’s the advantage of getting BiTE therapy upfront. If you need something later, it may be a lot easier with a lot fewer side effects and it can be done as an outpatient. With epcoritamab, you can get steroids and don’t need to be in the hospital. As we make more progress with CAR T-cell therapy, maybe we can do that as an outpatient to reduce severe side effects. Sometimes there’s an advantage to waiting as the technology advances.
Dr. Ghosh: If it’s accessible, knowing the track record of CAR T-cell therapy and that now we have five-year data, we still like to sequence CAR T-cell therapy before bispecific antibodies. Over time, we’ll find out if things change and do it in reverse.
Remission After Bendamustine & Rituximab (BR)
Robyn: Diana asks, “What is the median length of remission after the first B&R treatment”
Dr. Ghosh: For which disease?
Robyn: I would assume it’s follicular lymphoma, but we don’t know what stage. Let’s assume it’s stage 2.
Dr. Bano: If it’s stage 2 follicular lymphoma, generally you have a sustained response after B&R treatment. We’re looking at about five years or so. We need more information to answer that question appropriately.
Dr. Ghosh: It may also depend on whether rituximab maintenance was used. It could be a little bit different with maintenance versus without. I’ve even seen patients who are 10 years out after bendamustine and have not relapsed. Some people will relapse, so it’s a whole spectrum.
There are treatments now that will attack both follicular lymphoma and the transformed lymphoma, so sometimes you want to harness that.
Dr. Nilanjan Ghosh
Possibility of a Repeat Transformed Follicular Lymphoma (tFL)
Robyn: “If you have follicular lymphoma that transformed into diffuse large B-cell, went into remission after treatment, but a few years later, the follicular lymphoma came back, what is the probability that this will transform again?”
Dr. Ghosh: With indolent follicular lymphoma, there’s a small percentage of transforming every year. As more years go by, that risk accumulates. If it’s already happened, will a second transformation happen? It’s possible, but the likelihood goes down because it’s a random event.
Is it a relapse of the previously transformed follicular lymphoma? That’s hard to sort out, but usually what happens with the transformed disease, if the transformed disease has been in remission for a long time, that’s an aggressive lymphoma and usually, aggressive transformers respond well to whatever the treatments were given to them, especially since long-term remission was achieved.
The likelihood of what comes back is often the indolent lymphoma and we see this sometimes with transplant. I had a patient who had follicular lymphoma, had treatment, had a relapse of the follicular lymphoma, had another treatment, then her lymphoma transformed, and we gave her transplant for that. Years later, the aggressive transformed lymphoma went away and she had a relapse again, but this time, it was back to follicular. The aggressive lymphoma never came back. What we did at the time was CAR T-cell therapy for the follicular lymphoma.
There are treatments now that will attack both follicular lymphoma and the transformed lymphoma, so sometimes you want to harness that. For example, axi-cel is approved for follicular lymphoma and for DLBCL. When you use a treatment like CAR T-cell therapy, you are basically killing both. Ultimately, it’s all coming from one B cell. It may be transformed, but if you attack that B cell clone, then both the low-grade and the high-grade can go away. Similar with bispecific antibodies. They attack both. Many of the treatments we use now, especially some of the more modern treatments, have activity against both follicular lymphoma as well as the transformed component.
The fortunate part about lymphoma is that you can target lymphoma cells. You will deplete your own B cells, but we can mitigate that.
Dr. Justin Favaro
B-cell-based Immunotherapy
Robyn: “CAR T-cell therapy is a great new treatment, but as I understand, it targets all B cells and not just the cancerous ones, leading to a depleted immune system that can last a long time. Is there any current research on a similar immunotherapy treatment than can identify and attack the cancer cells and not the normal B cells?”
Dr. Ghosh: That would be something we would love to have. We are fortunate that we have been able to identify antigens. Dr. Favaro mentioned those spikes. Imagine if those spikes were not only in B cells but in liver cells, heart cells, and kidney cells, then CAR T-cell therapy would go and kill all of those.
Fortunately, this is what we can get away with as CD19 is expressed only in B cells but not in other normal tissues — not even on T cells or other parts of the immune system. Many other diseases don’t have that. We are starting to work with some solid tumors which have these, but it’s been difficult. Even in diseases like acute myeloid leukemia, you don’t have things that are specific to that cell.
With B cells, you’re more prone to infections, but you can still get IVIG, which is a immunoglobulin supplementation to help reduce your risk for infections. We currently don’t have spikes on the surface of just cancerous B cells but are absent on normal B cells, but that would be something which I hope the future researchers can identify.
Robyn: I believe there are studies that show B cell recovery over time. A lot of people will gradually recover and it doesn’t affect their remission rate. Everyone is unique. Some people with low IgG can get infections, some people do fine. There are patients who haven’t had CAR T-cell therapy who have primary B-cell aplasia and do fine and a lot of them don’t need IVIG. It’s a case-by-case situation. Most people have had some infection, but most people have been fine and living a normal life even without IVIG.
Dr. Favaro: The challenge with the solid tumor CAR Ts that they’re trying to make right now is finding the antigen on the lung cancer, for example, that won’t damage or destroy the lung. The fortunate part about lymphoma is that you can target lymphoma cells. You will deplete your own B cells, but we can mitigate that with prophylactic antibiotics, IVIG if needed, and taking precautions so you can still live your life.
Masking, especially if you’re in a crowded area, and frequent hand washing would be advisable. As more time passes, those restrictions start coming down a lot.
Dr. Nilanjan Ghosh
Post-CAR T-cell Therapy
Robyn: Michael asks, “What are the overall risks as far as activities, food, etc., for post-CAR T-cell therapy patients?”
I have not been avoiding anything for many years, but I’m eight years out at this point. There are initial precautions because a lot of people have low ANC (absolute neutrophil count) and some other depletion.
Dr. Ghosh: Right after CAR T-cell therapy, blood counts are low. Sometimes we even need to give growth factors to improve blood counts. The risk is going to be higher in terms of infections initially than a few months out. If the blood counts recover, especially neutrophil counts, then certain infection risks go down.
B cells always take time to recover. As the lymphocyte count recovery takes longer, your immune system is compromised and that’s where the possibility of viral infections happen. Masking, especially if you’re in a crowded area, and frequent hand washing would be advisable. As more time passes, those restrictions start coming down a lot.
Ultimately, you have to live your life, but still be cautious. If you do get an infection, then alert your providers so they can do some tests to find out if it’s a mild infection or something that needs to be worked up or treated.
In terms of food, you have to take certain precautions in terms of raw food while your neutrophil count is low, but that typically happens in the immediate post-CAR T-cell therapy phase. As more time goes, those usually are not an issue.
Robyn: You need to have a team take care of you. Your oncologist will move out of your realm because they have people who are very sick to take care of. I do encourage everyone to get an internist or an immunologist who can take care of the day-to-day.

Second CAR T-cell Therapy
Robyn: “Does CAR T-cell therapy work a second time if it didn’t keep the complete response the first time?” Can you have a second CAR T?
Dr. Ghosh: Not commercially. CAR Ts are approved once in the commercial setting, but we have clinical trials which will allow a second CAR T. For example, there’s a clinical trial using natural killer cells that are modified to become CARs or chimeric antigen receptor expressing cells. In that clinical trial, we allow patients who have had a commercial CAR T but it failed. Some of the allogeneic CAR T-cell therapy trials will allow patients who have had a previous CAR T-cell therapy.
There are other CAR Ts coming out. For example, we have a CD19/CD20 bispecific CAR T trial, which we are about to open. In that clinical trial, if someone had commercial CAR T, that is probably not allowed because the CD19 CAR T had already failed. But let’s say you have another clinical trial targeting CD22 and people have had the traditional CAR T, now you are using CAR T again but it’s different spikes. If you’re going against a different spike with a clinical trial, that would be doable. But if it’s the same one, then likely not.
The second time will be in a trial unless a CAR T-cell therapy gets approved that allows previous CAR T treatments.
Newer Monoclonal Antibodies
Robyn: Mike asks, “I’m still unsure about some of the things I’ve heard more recently because I don’t know if I have access to them. What about newer monoclonal antibodies? Do they still play a role?”
Dr. Favaro: There are definitely other options out there. Monjuvi is a monoclonal antibody against CD19 that has been looked at in relapsed lymphoma in combination with lenalidomide. Loncastuximab, which is one of these antibody-drug conjugates, is an anti-CD19 with a chemotherapy payload. It’s going to attach to your CD19 spike and internalize the chemotherapy right into that cell. It’s given via IV every three weeks.
These are two really good options for patients who, for whatever reason, CAR T-cell therapy or BiTE are not working or not available. These easily given off-the-shelf and approved by insurance.
When your blood counts are low and you’ve gone through therapy, there’s a risk of fungal infection as well.
Dr. Kulsum Bano
Cannabis & Non-Hodgkin’s Lymphoma
Robyn: “Cannabis and non-Hodgkin’s lymphoma. Are there any benefits?”
Dr. Bano: It’s a question that comes up pretty frequently. There may be some misinformation out there and some misconceptions of prevention of cancer with cannabis, and I don’t think there’s any founded data.
Certainly, people think about it in terms of symptom control. We do have medications that use the cannabinoid derivatives in a medical form, such as dronabinol, that we use for nausea and appetite stimulation for patients who have gone through chemotherapy.
Generally, we discourage smoking of cannabis only because there are a lot of additives that could be associated with it. When your blood counts are low and you’ve gone through therapy, there’s a risk of fungal infection as well.
There’s a lot of unregulated things that we don’t know what we’re dealing with. I don’t think there are any recommendations that can be definitely given. I don’t know that there are benefits per se, but it’s a discussion to have with your physician about what works for you and what doesn’t.
You need a small amount of protein, usually seafood, mostly vegetables on your plate, and some whole grains for carbohydrates. All these things are important.
Dr. Justin Favaro
Keto Diet
Robyn: “Can you speak about the keto diet? Is it effective against cancer? Is it helpful in any way?”
Dr. Favaro: It’s probably the most common question we get as oncologists every day. What can I eat? What should I eat?
My general recommendation is the Mediterranean diet. If you talk to nutritionists and look at the studies, you need several components to your diet. You need a small amount of protein, usually seafood, mostly vegetables on your plate, and some whole grains for carbohydrates. All these things are important.
I believe the keto diet takes out all carbohydrates, so you’re dealing with a lot of protein and a lot of fat. There are downsides of that for the rest of your body. Your cholesterol could go up and that could be damaging to your heart. Your body needs sugar and glucose.
For example, let’s look at a PET scan. What’s lighting up on the PET scan? Besides the lymphoma, it’s your heart and your brain. They need sugar to work. You don’t need sweets all the time, but you need complex carbohydrates. Maybe switch to whole grains and whole wheat pasta instead of white pasta. That’s only a portion of your diet, about 25%. The majority is vegetables and lean protein.
If you look at some of the recent studies that have come out that have looked at who lives the longest with cancer and what diet they follow, the winner seems to be the vegan diet in terms of cancer survival and decreasing risk of recurrence. This is cancer broadly and not lymphoma. But sometimes that’s a hard diet to follow, so a Mediterranean diet is a reasonable diet for most people to follow.
Robyn: Everybody wants control. You want control of your disease.
I have to add: Exercise helps. Studies in breast cancer and prostate cancer — because they’re so much more common and easy to study — showed that even for people who have never exercised before, if they walked 30 minutes a day, they had a longer remission rate and cure rate.
I encourage everyone to exercise. That doesn’t mean you have to do CrossFit because that may lead to shoulder injuries; we see that in radiology. You can do any type of walking or cycling. If you look at other studies, it’s not only the diet. People are active. Get yourself moving.
There have been studies done, not particularly in cancer, that show that insulin resistance is improved with intermittent fasting.
Dr. Kulsum Bano
Intermittent Fasting
Robyn: “Does intermittent fasting help patients with follicular lymphoma or any cancer? Does sugar play any part?”
Dr. Bano: There have been studies done, not particularly in cancer, that show that insulin resistance is improved with intermittent fasting. At any point, when you have dysregulation in your blood sugar control, that tends to lead to other medical complications. There is some role to play in improvement in outcomes. I don’t know that it’s been studied particularly.
Robyn: There are studies with BMI. People who are obese have a higher incidence of all sorts of cancers and have poorer outcomes. There are a lot of reasons for that. It’s multifactorial, but eating healthy and exercise make sense.
R-EPOCH vs. R-CHOP for Triple-Hit DLBCL
Robyn: “Is there any strong evidence that R-EPOCH is better than R-CHOP for triple-hit diffuse large B-cell?”
Dr. Ghosh: This type of aggressive lymphoma is one of the most aggressive variants. R-EPOCH is still considered as the standard of care for this disease based on a lot of retrospective data. There is no clinical trial taking patients with double-hit or triple-hit lymphomas and giving half of them R-CHOP and half of them R-EPOCH.
However, there was a large clinical trial which took all patients with diffuse large B-cell lymphoma and gave half of them R-CHOP and half of them R-EPOCH, and R-EPOCH was not shown to have a better efficacy. They were similar, but it was not really better.
That study was inconclusive in terms of the improvement for double-hit patients. If you ask most doctors, double-hit patients will still be getting R-EPOCH because there’s a lot of good retrospective data showing better long-term responses with R-EPOCH compared to R-CHOP.
We have an ongoing study where we are monitoring different types of cells post-CAR T-cell therapy.
Dr. Nilanjan Ghosh
Patient Group That Benefits More from CAR T-cell Therapy
Robyn: John asks, “We’ve talked about complete response rates and durable remission rates following CAR T-cell therapy. With the much larger patient population, have you seen any trends emerge as to which patients tend to do better in terms of a better response rate, a better complete response rate, as well as a more durable remission with CAR T-cell therapy?”
Dr. Ghosh: People have tried to figure it out. Before you start any treatment, you want to know if this treatment is going to give long-term remission for this person versus someone else. We are not there yet, but we have some ideas. It’s not perfect.
With CAR T-cell therapy, we know that if someone has very bulky disease and fast-growing bulky disease, CAR T-cell therapy will not give great outcomes. Unfortunately, nothing else does so people still go for it, but sometimes you want to debulk while waiting because CAR T-cell therapy is a weeks-long process.
For example, if there’s one site of bulk, we often can do radiation. There are new radiation techniques. One is called “boom boom” where short, very effective radiation is done to shrink the tumors, perhaps even express all these antigens, and have a better kill.
Bulky tumors can often cause T-cell exhaustion quickly so if they get overwhelmed with the tumor, then those T cells can get immune tolerance. There is also a subpopulation of these T cells that can cause immune suppression.
We have an ongoing study where we are monitoring different types of cells post-CAR T-cell therapy and checking them multiple times to see if we can identify patients who might have relapsed and had one type of immune repertoire versus those who had long-term remission and have a different type of immune repertoire.
We presented the initial data at ASH 2023, but hopefully, we’ll do a little bit more analysis on that and try to understand it better. We have samples taken pre-CAR T-cell therapy to see what may be the characteristics of a person that could predict long-term response.
We also have a study with BiTE. We are doing it for patients who are getting mosunetuzumab. We are collecting samples before and after treatment, and trying to identify which type of T cells may be associated with a better response versus a not-so-durable response.
CLL vs. Follicular Lymphoma
Robyn: Tim asks, “Can you define CLL and how it complements follicular lymphoma?”
Dr. Ghosh: CLL is chronic lymphocytic leukemia, which is under non-Hodgkin lymphoma. CLL is circulating disease in the blood. There is a lymphoma component to it called SLL, small lymphocytic lymphoma. It’s essentially the same disease. SLL is in the lymph nodes, CLL is in the blood. If there are more than 5,000 circulating lymphocytes, then it is a definition for CLL. If it’s below that, it’s called MBL, monoclonal B-cell lymphocytosis.
CLL is an indolent form of lymphoma circulating in the blood but could also be in the lymph nodes, spleen, and bone marrow. Like follicular lymphoma, it belongs to the same indolent non-Hodgkin lymphoma group considered as less aggressive.
CLL has tremendous progress where we have given up chemotherapy, so that’s where it’s a little bit different. You heard about R-bendamustine. We used to use that in CLL. In the past, we used to think we could use the same treatment for all indolent lymphoma.
We have relied on targeted treatment, like BTK inhibitors — ibrutinib was the first generation, then acalabrutinib and zanubrutinib, now pirtobrutinib — and then BCL2 inhibitors like venetoclax (VENCLEXTA). These have all come either in sequence or in combination.
Liso-cel got approved very recently for CLL, so now you have CAR T-cell therapy available as well. Chemotherapy was FCR and BR. We don’t really use those anymore. They’ve been shown to be inferior compared to these newer drugs that we have.
Conclusion
Robyn: We want to give special thanks to Atrium Health Levine Cancer Center and Oncology Specialists of Charlotte, and our partners The Leukemia & Lymphoma Society, the American Cancer Society, Lymphoma Coalition, and LIVESTRONG® at the YMCA.
More Medical Expert Interviews

What’s New in Metastatic Breast Cancer Treatment

Using AI to Detect Lung Cancer Risks With Dr. Lecia Sequist

Trends in Cancer Research 2022

The Role of Bispecific Antibodies in the Treatment of Multiple Myeloma
